Minerals Trace Elements R. C. Gupta M.D. (Biochemistry) Jaipur (Rajasthan), India

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

MineralsTrace Elements
R. C. GuptaM.D. (Biochemistry)
Jaipur (Rajasthan), India

Some minerals essential for human beingsare required in minute quantities
These are known as trace elements
These are also known as micro-nutrients
The trace elements includeː
1. Iron
2. Iodine
3. Copper
4. Zinc
5. Cobalt
6. Manganese
7. Molybdenum
8. Chromium
9. Selenium
10. Fluorine

Iron
Total amount of iron in an adult humanbeing is 3.5-4.5 gm
Blood and blood-forming organs are thelargest reservoirs of iron
But small amounts of iron are present innearly every tissue

Important iron-containing compounds are:
• Haemoglobin
• Myoglobin
• Ferritin
• Haemosiderin
• Transferrin
• Cytochromes
• Iron-containing enzymes

About 70% of the body iron is present inhaemoglobin and 5% in myoglobin
Ferritin and haemosiderin, which are storageforms of iron, contain about 20% of the body iron
Transferrin, an iron carrier protein present inplasma, contains 0.1% of the body iron
The remaining iron is present in cytochromes andenzymes

Haem
Haemoglobin
Each subunit contains one iron atom
Haemoglobin is a tetramer made up of
four subunits
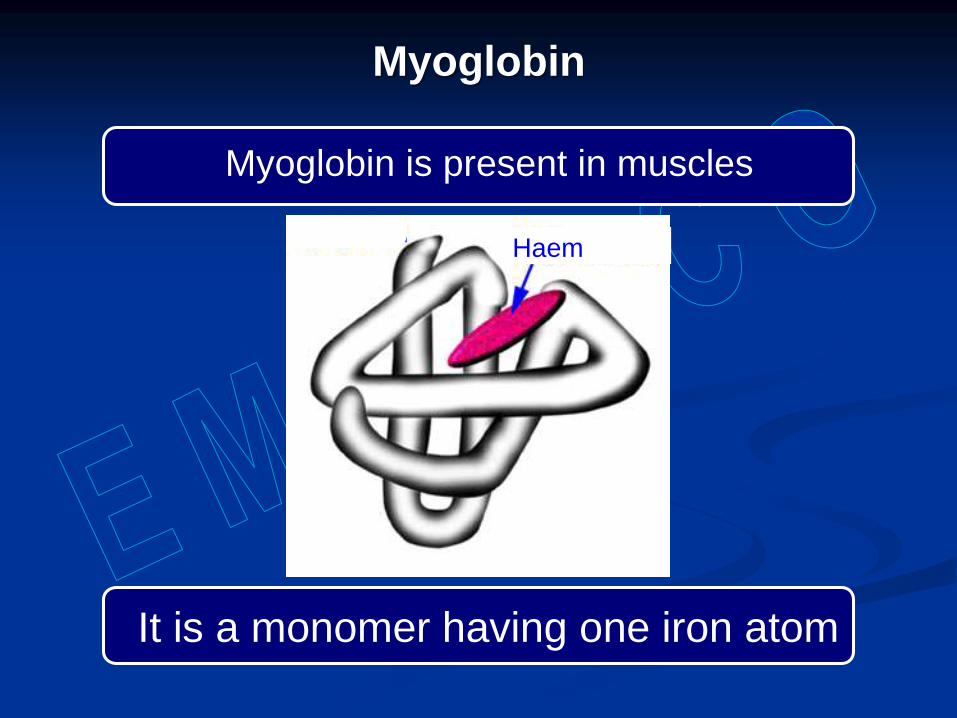
Myoglobin
Haem
Myoglobin is present in muscles
It is a monomer having one iron atom

Cytochromes
Cytochromes are present in respiratorychain, and support tissue respiration
Cytochrome P-450 and cytochrome b5
are components of microsomal hydroxy-lase system
Ferritin
Ferritin is one of the storage forms of iron
The protein portion of ferritin is known asapoferritin
Apoferritin combines with iron to formferritin

Ferritin is present in:
• Liver
• Spleen
• Bone marrow
• Brain
• Kidneys
• Intestine
• Placenta
The first step in the synthesis of ferritin isformation of apoferritin
Synthesis of apoferritin is induced by theentry of ferrous iron in the cell
This is followed by oxidation of ferrousiron to the ferric form
Ferric iron forms ferric hydrophosphatemicelles

Apo-ferritin Ferritin
80 Å
Ferric hydro-phosphate micelles
Ferric hydrophosphate micelles enter the protein shell to form ferritin
120 Å

Apoferritin is made up of 24 subunits oftwo types – H and L
Molecular weight of H subunits is 21,000and that of L subunits is 19,000
The proportion of H and L subunits inapoferritin differs in different tissues
The subunits are joined together to forma hollow sphere
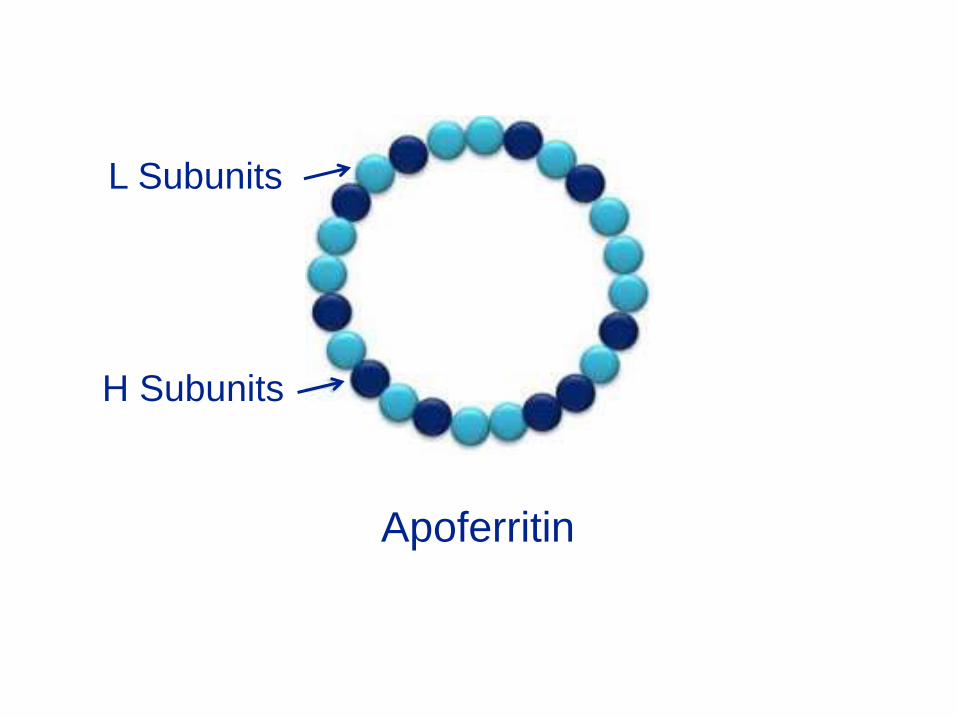
Apoferritin
L Subunits
H Subunits
Ferric hydrophosphate micelles are
present in the hollow space in ferritin
When fully saturated, a molecule offerritinː
Contains 4,500 atoms of iron
Has a molecular weight of 900,000

Iron stored
inside ferritin

Haemosiderin is a granular iron-rich protein
Unlike ferritin, it is insoluble in water
The exact structure of haemosiderin is not known
Haemosiderin

Iron is first stored in the body in the form offerritin
As the iron stores increase, older ferritinmolecules aggregate to form haemosiderin
Some of the protein is degraded in thisprocess
Therefore, percentage of iron in haemo-siderin is higher than in ferritin
Normally, two-thirds of stored iron is inthe form of ferritin
The remaining one-third is stored in theform of haemosiderin

Transferrin is a carrier protein which transports iron in circulation
Free iron is toxic, and has a tendency to precipitate
These problems are overcome by combining iron with transferrin
Transferrin
Transferrin is a glycoprotein with a molecular weight of about 80,000
It is made up of a single polypeptide chain
One molecule of transferrin can transport up to two ferric atoms

Transferrin(By Emw - Own work, CC BY-SA 3.0,
https://commons.wikimedia.org/w/index.php?curid=9444665)

Transferrin present in plasma may be:
Diferric transferrin (carrying two ferric ions)
Monoferric transferrin (carrying one ferric ion)
Apotransferrin (carrying no ferric ions)

Transferrin carries iron to and fromvarious tissues through circulation
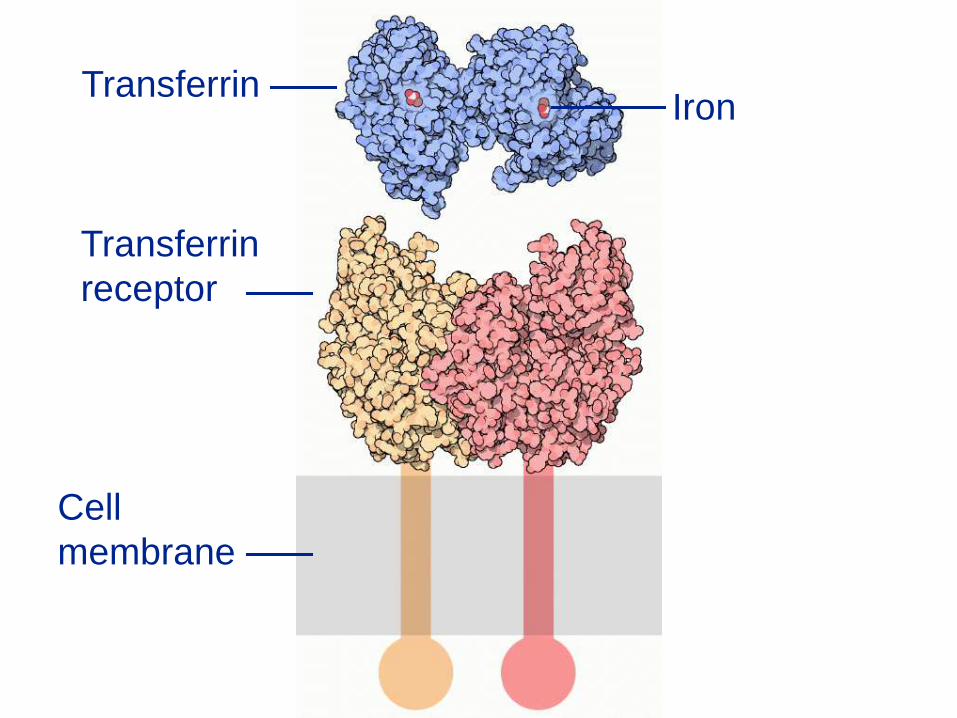
There are specific receptors for trans-ferrin on the cell membrane
The receptors are transferrin receptor 1(TfR1) and transferrin receptor 2 (TfR2)

TfR1 is synthesised by all iron-
requiring cells
It is present in high numbers on:
Immature erythroid cells
Rapidly dividing cells
Placental cells
TfR2 is synthesised by:
Liver cells
Haematopoietic cells
Duodenal crypt cells

TfR is a transmembrane glycoprotein madeup of two polypeptide chains
The polypeptide chains are joined by twodisulphide bonds
Each polypeptide possesses one bindingsite for transferrin
TfR has greater affinity for diferric transferrin than for monoferric or iron-free transferrin
Transferrin
Transferrin
receptor
Iron
Cell
membrane

Binding of iron-carrying transferrin to itsreceptor results in endocytosis of both,forming an endosome
Proton pumping into endosome changesthe conformation of transferrin and itsreceptor
The conformational change results inrelease of iron
Fe3+ is reduced to Fe2+ by ferrireductase
Iron is transported across the membraneof endosome into the cytoplasm

Transferrin receptor and apotransferrinare returned to the cell surface
Apotransferrin is released in plasma to becharged with iron again
Transferrin, once formed, can participatein 100-200 cycles of iron transport

Normal concentration of transferrin inplasma is 200-400 mg/dl
This amount of transferrin is capable ofcarrying 250-400 mg of iron/ dl of plasma
This is known as the total iron bindingcapacity of plasma

Normal plasma iron level is 50-175 µg/dl
This means that the iron binding capacityof plasma is nearly 30% saturated inhealthy subjects
Several enzymes require iron for theircatalytic activity
In some cases, iron forms an integral part of the enzyme molecule
In others, presence of iron is required forthe catalytic activity of the enzymes
Iron-containing enzymes

The iron-containing enzymes are mostlyconcerned with biological oxidation
Examples of such enzymes are catalase,peroxidase, aconitase, xanthine oxidase,succinate dehydrogenase etc
Iron is a transition metal, and can exist intwo redox states: Fe2+ and Fe3+
At the oxygen concentrations prevailing inthe body, the stable state of iron is Fe3+
But reduction of Fe3+ to Fe2+ is importantbecause most of the functions of irondepend upon the ferrous form
Functions of iron
Moreover, Fe2+ is the only form that canbe transported across membranes
Fortunately, the two forms are readilyinter-convertible

Functions
Transport of oxygen
Oxidative reactions
Tissue respiration
The most important function of iron is totransport oxygen in the body
This function is performed by haemo-globin
A similar function is performed in musclesby myoglobin
Transport of oxygen

Iron is a component of various oxido-reductase enzymes
As such, it plays a role in a number ofoxidative reactions
Oxidative reactions

As a component of cytochromes in theelectron transport chain, iron is involvedin tissue respiration
It is the iron component of cytochromes that accepts and donates electrons
Tissue respiration

Iron status depends upon the relative ratesof iron absorption and iron excretion
Iron absorption is the major mechanism formaintaining normal iron balance
Iron balance

Iron metabolism is said to occur within a closedsystem in the body
There is hardly any exchange of iron betweenman and his environment
The iron present in the body is continuouslyreutilized
Only a minute amount of iron is lost everydayfrom the body in the form of exfoliated cells

The faecal iron loss in 0.4-0.5 mg a day
The urinary iron loss is about 0.1 mg a day
About 0.2-0.3 mg of iron is lost daily from the skinalong with the exfoliated cells
Thus, the total iron loss is just under one mg aday

In premenopausal women, there are twoadditional routes of iron loss
About 20-25 mg of iron is lost withmenstrual blood in each cycle
This is equivalent to a daily loss of 0.7-0.8mg of iron


Iron balance is maintained by intestinalabsorption of iron
Iron lost is replenished by intestinal ironabsorption
Intestinal absorption of iron is affected by:
• Body iron stores
• Erythropoietic activity
• Degree of saturation of plasma transferrin
• The amount of dietary iron
• Valency of ingested iron (Fe+2 or Fe+3)
• Presence of other substances in the food
More iron is absorbed when:
• Body iron stores are low
• Erythropoietic activity is high
• Saturation of plasma transferrin is low
• Iron is ingested in ferrous form
Presence of the following in food increases iron absorption:
• Ascorbic acid
• Succinic acid
• Histidine
• Cysteine
Presence of the following in food decreases iron absorption:
• Phytates
• Phosphates
Iron can be absorbed from all segmentsof the small intestine
But presence and normal functioning ofstomach are essential
Achlorhydric and gastrectomized personsabsorb less iron as compared to normalpersons

Gastric enzymes and hydrochloric acid:
Release iron from iron-containing foods
Reduce ferric iron to the ferrous form

Enterocytes (mucosal cells of intestine) possess channels for:
Entry of iron on the luminal side
Exit of iron on the basolateral side

Iron is present in food as either inorganiciron or haem iron
Inorganic iron is about 90% of the totaland haem contains the remaining 10%

Bioavailability of haem iron is very high; itsabsorption is not hampered by other foodconstituents
Intact haem moiety is absorbed by entero-cytes via haem-carrier protein 1 (HCP1)
In the cells, iron is released from the proto-porphyrin ring by haem oxygenase-1

Inorganic iron is present in the diet mostlyin ferric form
It is reduced to ferrous form by duodenalcytocrome B (DcytB)
DcytB is present on the brush borderepithelium
Ascorbate may be an electron donor forthis reaction

Ferrous ions are transported into cells viadivalent metal transporter 1 (DMT1)
DMT1 is present on luminal membrane ofduodenal enterocytes
DMT1 is not a specific iron transporter
It also mediates transport of other divalentmetal cations such as Zn+2, Mn+2 and Cu+2
DMT1 is also present on the membrane of endosomes
It mediates iron transport from endosomes into the cytoplasm of the cell
The iron absorbed by the enterocyte, canbe stored within the cell as ferritin
Or it can be transported into circulationacross the basolateral membrane
Iron is transported across the basolateralmembrane via a specific transporter,ferroportin

Transport across basolateral membranerequires a change in redox state of iron
The intracellular Fe2+ form has to changeinto extracellular Fe3+ form
This conversion is brought about byhephaestin, a ferroxidase

All the iron that enters circulation is boundto transferrin
Affinity of transferrin for iron at normal pHof blood is extremely high
Transferrin delivers iron to the cells thatneed it
The main iron consumers are red cellprecursors

Iron homeostasis is maintained by regulating its absorption
It is believed that ferritin content of entero-cytes determines the absorption of iron
These cells are formed in the crypts ofLeiberkuhn
Regulation of iron absorption

Goblet cells
EnterocytesCrypt of
Leiberkuhn
Villus
Tip of villus
The enterocytes reach the tip of the villiand are shed off into the intestinal lumen
Their average life-span is three days
The function of ferritin in these cells is toblock the absorption of iron
The enterocytes formed during a period ofiron sufficiency are rich in ferritin
These cells will absorb very little iron duringtheir life-span
Moreover, when these are shed off, theiriron content will also be lost in faeces

Conversely, the cells formed during aperiod of iron deficiency are poor in ferritin
These cells absorb more iron and transfer itinto the plasma
Homeostatic mechanisms ensure that:
Systemic iron stores in the body areadequate
Each cell has an adequate amountof iron

The main sources of iron for cells are:
Iron absorbed by enterocytes
Iron stored in liver cells
Iron present in reticuloendothelial macrophages

Enterocytes, liver cells and macrophagesrelease iron through ferroportin
Ferroportin is the sole iron export channel
Iron export requires a change in the redoxstate of iron by ferroxidase
The ferroxidase is hephaestin in theduodenum and ceruloplasmin elsewhere

Macrophages are an important source ofiron for erythropoiesis
The macrophages obtain iron from agederythrocytes
Aged erythrocytes are engulfed by macro-phages in the reticulo-endothelial system
Their haemoglobin is broken up into haemand globin

The iron present in haem is released byhaem oxygenase-1
It is either stored within the macrophagesor is released into circulation
The iron released into plasma is taken upby transferrin
Most of the iron used for erythropoiesiscomes from haemoglobin recycling
The amount of iron recycled every day is10-20 times the amount absorbed by theintestine

Hepcidin is a peptide hormone synthesised in liver
Action of hepcidin is targeted at ferroportin
Hepcidin is a negative regulator of ferro-portin
Besides being an iron export channel,ferroportin also acts as hepcidin receptor
Role of hepcidin in iron homeostasis
Hepcidin binding to ferroportin causes itsinternalisation and lysosomal degradation
Loss of ferroportin decreases iron effluxfrom the cell
This leads to intracellular iron retention
As a result, plasma iron is decreased
Requirement
Only a small proportion of the dietary ironis normally absorbed
Hence, much larger amounts have to beprovided in diet than the requirement

Age and sex Requirement
Infants 6-10 mg/day
Children 10 mg/day
Adolescents 12 mg/day
Adult men and postmenopausal
women 10 mg/day
Premenopausal and lactating
women 15 mg/day
Pregnant women 30 mg/day
EMB-RCG

Iron is present in animal as well as plantfoods
Iron absorption from animal foods muchmore efficient than that from plant foods
On a mixed diet, healthy subjectsabsorb 5-10% of the dietary iron
Dietary sources

Animal sources of iron
Eggs FishMeat
Liver Kidney Heart

Plant sources of iron
Whole wheat Figs Dates
Beans SpinachNuts

Iron deficiency is widespread both in poor and in affluent countries
Iron deficiency is the commonest causeof anaemia throughout the world
Iron deficiency
Iron deficiency can result from:
Inadequate intake
Malabsorption
Blood loss

Inadequate intake is likely when the requirement is high e.g. in:
Infancy
Adolescence
Pregnancy

Malabsorption can be due to:
Steatorrhoea
Coeliac disease
Gastrectomy

Persistent blood loss can occur from:
Genital tract
Gastrointestinal tract
Hookworm infestation

The earliest change in iron deficiency is adepletion of body iron stores
Other changes follow progressively
Plasma transferrin saturation is decreased
Plasma iron is decreased
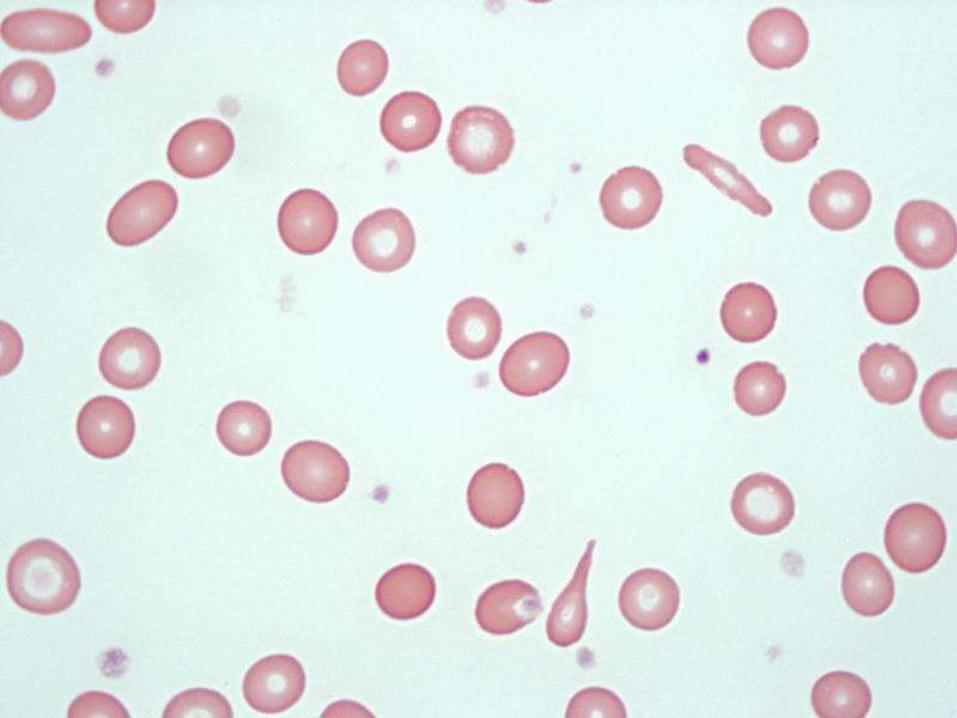
Microcytic hypochromic anaemia develops
Hemoglobin level falls
Poikilocytosis becomes evident

Severe and prolonged deficiency leads to:
Koilonychia
Angular stomatitis
Glossitis
Pharyngeal and oesophageal webs
Atrophic gastritis
Partial villus atrophy
Iron overload
Iron overload is much less common thaniron deficiency
Two types of iron overload syndromes areknown:
Haemosiderosis
Haemochromatosis
The excess iron is deposited in reticulo-endothelial cells
There is no tissue damage
Excess iron enters via parenteral route
This can be due to repeated bloodtransfusions e.g. in thalassaemia
Haemosiderosis

Haemochromatosis
Haemochromatosis can be primary or secondary
Primary haemochromatosis is genetic
The genes implicated in primary haemochromatosis are:
Hepcidin gene
Ferroportin gene
TfR2 gene
The genetic defect leads to excessiveintestinal absorption of iron
Excess iron is deposited in liver, heart,skin, pancreas and other endocrine glands
The condition is also known as bronzediabetes
The clinical abnormalities in haemochromatosis are:
• Hepatomegaly
• Cardiomegaly
• Congestive heart failure
• Hypogonadism
• Diabetes mellitus
• Bronze-coloured pigmentation of skin
Serum iron, ferritin and saturation of iron-binding capacity are increased in haemo-chromatosis
Phlebotomy and iron-chelating agentse.g. desferrioxamine are used to removeexcess iron

Secondary haemochromatosis may occur inalcoholic liver disease
Iron deposition is usually confined to hepatictissue
South African Bantus are known to develophaemochromatosis
It is due to heavy intake of iron present in analcoholic beverage brewed in iron vessels

Total iodine in an adult is 45-50 mg
About 10-15 mg is present in the thyroidgland
Muscles contain about 25 mg
About 5 mg is present in skin, 3 mg in the skeleton and 2 mg in liver
Iodine

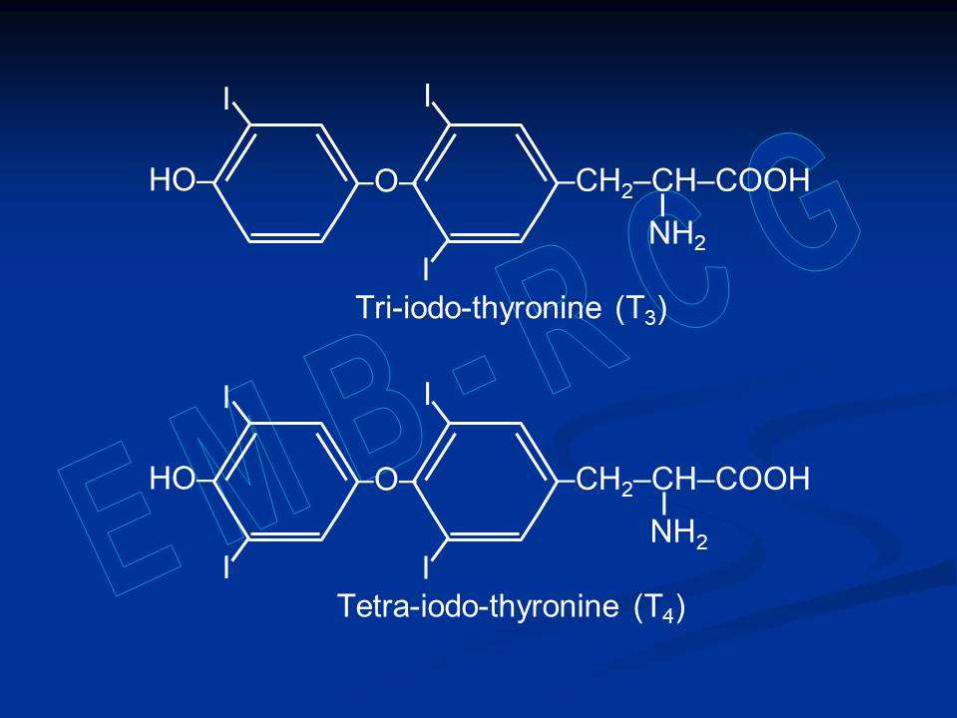
The only known function of iodine is in thesynthesis of thyroid hormones
The thyroid gland synthesizes tri-iodo-thyronine (T3) and tetra-iodothyronine (T4)
These two are synthesized from iodineand tyrosine residues of thyroglobulin
Functions

The thyroid gland:
Actively takes up iodide ions from plasma
Oxidizes iodide to iodine
Incorporates iodine into tyrosine residues of thyroglobulin
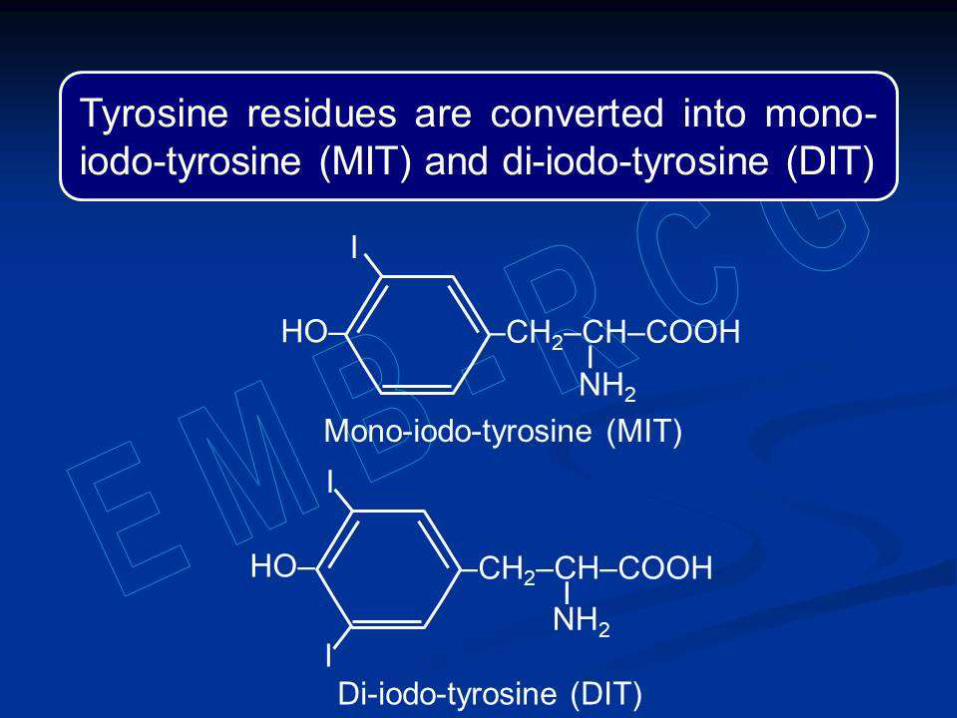
Two DIT residues combine with each
other to form thyroxine (T4)
One MIT and one DIT residues combine to
form tri-iodo-thyronine (T3)

Iodine is absorbed from entire alimentarytract, particularly from small intestine
Iodine and iodate are converted intoiodide prior to absorption
Other mucous membranes and skin canalso absorb iodine
Absorption

Iodide absorbed from alimentary tract andelsewhere enters the circulation
About one third is taken up by the thyroidgland
The remainder is excreted, mainly by thekidneys
Small amounts of iodide are excreted insaliva, bile, milk, sweat and expired air

Plasma iodine level is 4-10 mg/dl
Only 10% of it is inorganic iodide
Organic iodine is present mostly in theform of thyroid hormones
Thyroid hormones are bound to someproteins (called protein bound iodine)

Daily requirement
Infants 40–50 µg/day
Children 70–120 µg/day
Adults 150 µg/day
Pregnant women 200 µg/day
Lactating women 250 µg/day

Iodine is present in water and soil
Foods, both animal and plant, obtainiodine from water and soil
Iodine content of foodstuffs depends
upon iodine content of water and soil
Dietary sources
Sea water is rich in iodine
Sea foods, e.g. fish, oysters, lobsters etc,are the best sources of iodine
As we go away from the sea, the iodinecontent of water and soil, and hence thatof the foodstuffs, decreases

Iodine deficiency is common in certainareas of the world
These areas constitute the so-calledgoitre belt
Sub-Himalayan region of India is a part ofgoitre belt since the iodine content of soiland water is poor in this region
Iodine deficiency
Iodine deficiency results in goitre(enlargement of thyroid gland)
Thyroid gland becomes hypertrophic in order to produce enough hormones from
the available iodine
The goitre is generally non-toxic (symptomless)

Goitre is endemic in the goitre belt areas
Goitre →
A severe deficiency of iodine can producehypothyroidism
Endemic goitre can be prevented byproviding iodized salt in the goitre belt
Iodized salt is prepared by addingpotassium iodate to common salt
Its iodine content should be 30 ppm (partsper million) at the manufacturing stage
It is supposed to be at least 15 ppm whenit reaches the consumer

Govt. of India has made iodisation of salt compulsory
About 60-100 mg of copper is present inan average adult
Relatively large amounts of copper arepresent in muscles (30-50 mg), bones(12-20 mg) and liver (9-15 mg)
Copper
Plasma copper level is 100-200 mg/dl
Nearly 90% of the plasma copper istightly bound to ceruloplasmin
The rest is loosely attached to albumin
Albumin is the major carrier of copper asit can easily release copper
Copper performs its functions in the formof copper-containing enzymes
These include cytochrome oxidase, super-oxide dismutase, monoamine oxidase,tyrosinase, dopamine b-hydroxylase etc
Ceruloplasmin also functions as ferro-xidase which oxidises Fe+2 to Fe+3
Functions
Copper is also required for:
Synthesis of haemoglobin
Formation of bones
Maintenance of myelin sheath of nerves

One third of dietary copper is normallyabsorbed, mainly from small intestine
Copper-binding P-type ATPase transferscopper from the lumen of the gut intoportal circulation
Copper-binding P-type ATPase is presentin intestinal mucosa and many other cells
Absorption

Albumin carries copper to liver
A different copper-binding P-type ATPaseis present in liver
This ATPase incorporates copper intoapo-ceruloplasmin

Adults require about 2.5 mg of copperdaily
Infants and children require about 0.05mg/kg of body weight
Daily requirement
Dietary sources of copper
Liver Kidney Meat
Nuts Legumes Raisins

Disorders of copper metabolism
Inherited disorders include:
Wilson’s disease
Menkes’ disease

Wilson’s disease is also known ashepato-lenticular degeneration
It is an autosomal recessive disease
Synthesis of ceruloplasmin is impaired inWilson’s disease
Wilson’s disease

There is no defect in the gene for cerulo-plasmin
Apoceruloplasmin is synthesized normally
The genetic defect involves incorporationof copper into apoceruloplasmin
There is congenital deficiency of copper-binding P-type ATPase in liver
This causes copper toxicity by impairing:
Incorporation of copper into apo-ceruloplasmin
Biliary excretion of copper

Large amounts of copper are deposited inliver, basal ganglia and around cornea
Serum copper and ceruloplasmin levelsare very low
Urinary excretion of copper is increased

This is an X-linked recessive disease
Copper-binding P-type ATPase isdeficient in intestinal mucosa and mostother tissues but not in liver
Copper accumulates in intestinal mucosa;it cannot be released into circulation
Menkes’ disease
Lack of absorption leads to deficiency ofcopper in the tissues
The deficiency causes:
Cerebral degeneration
Hypochromic microcytic anaemia
Steely and kinky hair

Serum copper and ceruloplasminlevels are elevated in:
• Pregnancy
• Infections
• Leukaemia
• Collagen diseases
• Myocardial infarction
• Cirrhosis of liver

The total amount of zinc in an averageadult is 1.3-2.1 gm
Its tissue distribution is very wide
Prostate, liver, kidneys, muscles, heart,skin, bones and teeth have zinc in highquantities
Zinc

Plasma zinc level is 50-150 µg/dl
Erythrocytes and leukocytes have ahigher concentration of zinc than plasma
Zinc is essential for normal growth andsexual development
It is required for synthesis of nucleic acids,which is essential for cell division andgrowth
In the form of zinc fingers, it is a part ofsome proteins which regulate transcription
Functions

Many enzymes require zinc for their catalytic activity such as:
• Alkaline phosphatase
• Carbonic anhydrase
• Carboxypeptidase
• Glutamate dehydrogenase
• Lactate dehydrogenase
• Malate dehydrogenase
• Alcohol dehydrogenase etc
Zinc is present in the b-cells of the isletsof Langerhans
It is required for the storage and releaseof insulin

Zinc is absorbed from the small intestine
Copper, cadmium and calcium interferewith the absorption of zinc
Phytates also retard zinc absorption byforming an insoluble complex with zinc
Absorption

Daily requirement
Age and sex Requirement
Infants 2-3 mg/day
Children 5-8 mg/day
Adult men 12 mg/day
Adult women 10 mg/day
Pregnant women 12 mg/day
Lactating women 12 mg/day

Meat
Dietary sources of zinc
Liver Kidney
Fish Eggs
Milk
Fish
Yeast
Whole grain cereals
Dietary zinc deficiency may occur invegetarians taking refined wheat flour astheir staple diet
It can also occur in acrodermatitis entero-pathica
Zinc deficiency
Zinc deficiency causes:
• Retardation of growth
• Dwarfism
• Delayed puberty
• Hypogonadism
A milder deficiency may
cause:
• Poor wound healing
• Impaired perception of taste

About one mg of cobalt is present in anaverage adult
It is distributed chiefly in liver, kidneys andbones
Cobalt is present almost entirely as aconstituent of vitamin B12
Cobalt

Inorganic cobalt doesn’t perform anyfunction in human beings
Inorganic cobalt is not absorbed from thegut; injected cobalt is rapidly excreted
Cobalt functions solely as a component ofvitamin B12
It must be provided in the diet as vitaminB12
About 12-20 mg of manganese is presentin an average adult
Liver, pancreas and kidneys containrelatively more manganese than othertissues
Manganese

Manganese is present mainly in themitochondria and nuclei of the cells
Manganese is absorbed from the smallintestine
Less than 5% of the ingested manganeseis normally absorbed

Manganese is required for:
• Formation of matrix of bones and cartilages
• Normal reproduction
• Normal functioning of central nervous system
• Stabilizing the structure of nucleic acids

A number of enzymes require manganese as a cofactor such as:
• Superoxide dismutase
• Arginase
• Acetylcholine esterase
• RNA polymerase
• Carboxylases
• Glycosyl transferases
The daily requirement of manganese is2-5 mg
Whole-grain cereals, legumes, nuts,green vegetables and fruits are goodsources of manganese

Molybdenum is present in very smallamounts in human beings, mainly in liverand kidneys
It is a component of xanthine oxidase,aldehyde oxidase and sulphite oxidase
Sulphite oxidase converts sulphite andsulphur dioxide into sulphate
Molybdenum

The exact requirement for molybdenum isunknown
An average diet provides 75-100 µg ofmolybdenum a day
Molybdenum deficiency is unknown inhuman beings
Excessive intake of molybdenum maycause copper deficiency
The total amount of chromium in anaverage adult is about 6 mg
It is widely distributed in the body
Chromium is a constituent of glucosetolerance factor (GTF)
Chromium
GTF is a low molecular weight peptide
GTF binds to insulin receptor andpotentiates the actions of insulin
A relationship has been shown betweenchromium deficiency and glucoseintolerance

Absorption of chromium is less than 1%
Stainless steel utensils contain chromiumwhich can be absorbed
Chromium intake is about 0.35 mg/day inmen and 0.25 mg/day in women which isadequate
Excess chromium can be toxic

Selenium content of normal adult humansvaries widely
Values from 3 mg to 15 mg have beenreported in different geographical areas
About 30% of the total body selenium ispresent in the liver, 30% in muscles, 15%in kidneys, and 10% in blood
Selenium

Most of the selenium present in tissues ispresent in proteins (selenoproteins)
Selenium performs its functions in theform of selenoproteins, many of whichare enzymes
Four different glutathione peroxidaseshave been identified, all of which containselenium

Glutathione peroxidase (GPx) is a part ofthe anti-oxidant defence system
GPx can break down hydrogen peroxideand fatty acid hydroperoxides
Both these are toxic compounds


Thus, the major role of selenium is as ananti-oxidant
In this function, it complements the role of vitamin E

Another role of selenium is in iodinemetabolism
Three different iodo-thyronine deiodinaseshave been identified
These convert thyroxine (T4) into the moreactive tri-iodo-thyronine (T3)
All the three are selenium-containingenzymes
The two major forms of selenium in foodare selenomethionine and selenocysteine
Selenomethionine is found mainly in plant foods and selenocysteine in animal foods
Their absorption is highly efficient
The main site of absorption is duodenum
Absorption and excretion

Selenium homeostasis is maintainedprimarily through excretion
Selenium is excreted via urinary andalimentary tracts
Urinary excretion is the primary route ofregulation under normal conditions

Different selenium requirements havebeen recommended in different countries
In India, the recommended intake is 40μg/day for adults of both sexes

The role of selenium deficiency in humanbeings came to the fore in 1979
Selenium deficiency was correlated withKeshan disease and Kashin-Beck diseasein China
These diseases were found in areas wheresoil is severely deficient in selenium

Keshan disease results in cardiomegaly,congestive heart failure and cardiacnecrosis
Kashin-Beck disease results in severeosteoarthritis, and degeneration ofchondrocytes and nerves
Selenium supplementation was found toprotect people from these diseases

Fluorine naturally occurs as thenegatively charged fluoride ion
Only small amounts are present inhuman beings (about 2.5 gm in adults)
More than 95% of fluoride is present inbones and teeth
Fluorine
Fluoride is not physiologically essentialbecause it doesn’t perform any function
Still, it is considered as essential becauseof its role in prevention of dental caries
Dental caries is a chronic disease causedby cariogenic bacteria

Cariogenic bacteria are naturally presentin the oral cavity
They metabolize carbohydrates intoorganic acids (pyruvic and lactic acids)
These acids can dissolve tooth enamel
This produces cavities in teeth (dentalcaries)

Dental caries
Teeth are made up mainly of calciumhydroxyapatite
Fluoride ions displace the hydroxyl ionsforming fluoroapatite
This hardens the tooth enamel, andmakes it resistant to dissolution
Fluoride ions also decrease acidproduction by inhibiting bacterial enzymes

The fluoride content of most foods is verylow
Exceptions are tea, grape juice andmarine fish
Some fruits and vegetables may acquirefluoride from fluoride-based pesticides
Main source of fluoride is drinking water
In tropical countries like India, waterintake is relatively high
Drinking water provides enough fluoride ifits fluoride content is 0.5-0.8 ppm (partsper million)

If fluoride content of water is low, dentalcaries becomes a public health problem
In such areas, fluoride must be added tothe source of drinking water (fluoridation)
The aim is to raise the fluoride content to0.5-0.8 ppm

Excess of fluoride in drinking water isharmful
If the fluoride content of water exceeds1.5 ppm, it can cause fluorosis
If the excess is mild, only the teeth areaffected (dental fluorosis)
If the excess is severe, the bones areaffected (skeletal fluorosis)
In early stage, the teeth appear mildlydiscoloured
Later on, stains ranging in colour fromyellow to dark brown appear on teeth
The surface of teeth becomes irregularwith noticeable pits
Dental fluorosis

Moderate fluorosis Severe fluorosis
Dental fluorosis
Normal teeth Mild fluorosis

Prolonged intake of excessive fluorideaffects the bones
The bones of vertebral column, pelvis andlimbs get deformed
There is calcification of ligaments andtendons, immobility and muscle wasting
Skeletal fluorosis
Skeletal fluorosis can also result inneurological problems
Neurological problems are caused byspinal cord compression

Skeletal fluorosis

Fluorosis occurs in certain areas where fluoride content of water is high
There are several such areas in the world

There are some high-
fluoride areas in India also
Defluoridationof drinking
water is required in such areas
Related Documents