1301 Fifth Avenue, Suite 3800 Seattle, WA 98101 USA Tel +1 206 624 7940 Fax +1 206 447 6909 milliman.com Milliman Client Report Electronic Transactions Between Payors and Providers: Pathways to Administrative Cost Reductions in Health Insurance May 6, 2010 John L. Phelan, Ph.D. Milliman, Inc. john.phelan@milliman,com DISCLAIMER AND THIRD PARTY USE: This report was prepared by Milliman, Inc. for NaviNet, Inc. We understand that NaviNet may wish to distribute it publicly and it is intended for public distribution. The report, however, should be distributed only with the permission of Milliman. In addition, the study may be distributed to third parties only so long as it is distributed in its entirety and Milliman makes no warranties to those parties of its accuracy or any other aspect of the study. Milliman does not intend for this information to benefit any third party even if it permits the distribution of this work product to such third party.. Further, any results presented in this report represent an analysis of typical administrative processes. Industry averages may vary and may not apply to a specific circumstance, healthcare payor, or point in time. They are not a guarantee of savings in a specific situation.

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
1301 Fifth Avenue, Suite 3800 Seattle, WA 98101 USA Tel +1 206 624 7940 Fax +1 206 447 6909
milliman.com
Milliman Client Report
Electronic Transactions Between Payors and Providers: Pathways to Administrative Cost Reductions in Health Insurance
May 6, 2010
John L. Phelan, Ph.D. Milliman, Inc. john.phelan@milliman,com
DISCLAIMER AND THIRD PARTY USE: This report was prepared by Milliman, Inc. for NaviNet, Inc. We understand that NaviNet may wish to distribute it publicly and it is intended for public distribution. The report, however, should be distributed only with the permission of Milliman. In addition, the study may be distributed to third parties only so long as it is distributed in its entirety and Milliman makes no warranties to those parties of its accuracy or any other aspect of the study. Milliman does not intend for this information to benefit any third party even if it permits the distribution of this work product to such third party.. Further, any results presented in this report represent an analysis of typical administrative processes. Industry averages may vary and may not apply to a specific circumstance, healthcare payor, or point in time. They are not a guarantee of savings
in a specific situation.
Administrative Cost Reduction Opportunities in the U.S. Health Insurance Industry through Use of Electronic Transactions between Payers and Providers
February 23, 2010
Milliman White Paper
Table of Contents
Executive Summary ................................................................................................................... 1
Background ............................................................................................................................... 3
Methods ..................................................................................................................................... 5
Covered Transactions ................................................................................................................................... 5 Data Sources .................................................................................................................................................. 6 Calculations for Costs and Savings ............................................................................................................. 7
Survey Findings ......................................................................................................................... 8
Additional Opportunities to Leverage Electronic Transactions ............................................. 11
Electronic Fund Transfers ......................................................................................................................... 11 Internet-based Patient Responsibility Estimation for Providers .......................................................... 12 Real-time Claim Adjudication .................................................................................................................... 12 Clinical Messaging ....................................................................................................................................... 13
Strategies for Change............................................................................................................... 14
About Milliman ........................................................................................................................ 15
1
Milliman White Paper
Administrative Cost Reduction Opportunities in the U.S. Health Insurance Industry through Use of Electronic Transactions between Payers and Providers
May 6, 2010
Executive Summary Milliman conducted a survey examining the current state of electronic transaction adoption and savings estimates for specific transactions among healthcare payors such as government entities, health plans, and health insurance companies. From our findings, we estimate that one half of the total savings opportunity available through the use of electronic transactions has already been achieved. Most of this has been driven by electronic claim submissions, with a somewhat smaller portion driven by electronic eligibility verification. At this time, efforts to increase use of electronic eligibility verification and prior authorization would seem to hold the greatest promise for industry-wide savings in the future. Milliman estimates that, for an average healthcare plan with 500,000 commercial members, using standard electronic transactions to communicate with providers, as defined in the Health Insurance Portability and Accountability Act of 1996 (HIPAA), could result in annual administrative savings of over $23 million. When extrapolated to the entire U.S. healthcare payor market, this represents up to $19 billion in possible administrative savings annually over manual transactions if all transactions were conducted electronically. We estimate that the industry has already achieved about $9.2 billion of those savings. For this study, Milliman looked closely at the five most common transactions involving healthcare payors and providers: 1) claim submission (including attachments), 2) eligibility verification, 3) prior authorization/referral certification, 4) claim status inquiries, and 5) remittance advice. Other uses of electronic transactions between healthcare payors and providers that may reduce administrative expense were considered as well, including use of electronic fund transfers (EFTs) for claim payment, eligibility estimation, real-time claim adjudication, and clinical messaging. While the study did not quantify the benefits from these activities, innovations such as these appear to hold significant promise for future additional savings. For all the potential it offers to reduce costs, implementation of electronic transactions between payors and providers remains fraught with challenges. While often compared to the retail sector, where very high levels of penetration have been achieved, use of electronic transactions in healthcare is lagging with only approximately half of the basic transactions described in HIPAA conducted electronically. This may be due in significant part to the complexity of the required transactions and the lack of strong incentives among all stakeholders to drive adoption. In addition to savings from increasing use of standardized electronic transactions, healthcare payors have other opportunities to drive administrative savings through promotion of other types of electronic transactions, such as use of EFTs for payments, providing estimates of patient responsibility, real-time adjudication of claims, and use of electronic clinical messaging to physicians. Health plans clearly have a significant incentive to drive adoption of electronic transactions. Even small gains in use of electronic transactions result in material financial benefits. These incentives are somewhat diminished for providers, especially smaller provider practices, where the return on

2
Milliman White Paper
Administrative Cost Reduction Opportunities in the U.S. Health Insurance Industry through Use of Electronic Transactions between Payers and Providers
May 6, 2010
investment is smaller or more difficult to actually realize through staff reductions. Several different strategies are now available to payors and regulators for increasing adoption rates, including:
Establishing additional financial incentives for providers
Identifying and leveraging vendor programs that support electronic transactions and communications, such as multi-payor portals, clearinghouses, electronic networks and other electronic communications services
Offering several options to providers for conducting transactions. These options can support variations among payor information needs in certain transactions that cannot be resolved through regulation alone, such as unique benefit designs
Improving existing standards in areas such as claim formats and coding of certain key elements
Establishing standards for interoperability among electronic medical records
Implementing mandates for providers to use electronic transactions
3
Milliman White Paper
Administrative Cost Reduction Opportunities in the U.S. Health Insurance Industry through Use of Electronic Transactions between Payers and Providers
May 6, 2010
Background Achieving greater administrative expense efficiencies through electronic transactions has been a stated public policy goal since the 1980s. The 1996 enactment of the Health Insurance Portability and Accountability Act (HIPAA) provided further impetus for widespread use of electronic transactions. This legislation included a major focus on developing standards to reduce healthcare administrative costs through greater use of electronic transactions as well as mandates to protect the security and confidentiality of electronic information. The Department of Health and Human Services (DHHS) estimated that as a result of greater adoption of electronic transactions “[t]he total net savings for the period 2002-2011 will be … $13.1 billion for health plans, and … $16.7 billion for health care providers.”1 This white paper focuses on quantifying the financial savings that may accrue to healthcare payors through adoption of certain types of electronic transactions. Almost 10 years after adoption of the HIPAA standards, the DHHS estimate appears to represent only a portion of total possible savings from using electronic instead of manual transactions. Unfortunately, no methodology can isolate the impact of regulatory changes for causing a specific level of savings, especially because a number of other factors contributed concurrently to increasing use of electronic transactions across the industry. What can be accomplished in looking at healthcare payor administrative savings, and is the focus of this white paper, is to examine the extent to which savings appear to result from use of electronic transactions compared to a more labor-intensive approach to the same transactions. More traditional transaction methods involve telephone conversations and paper-based methods such as faxes and mail. Healthcare payors may also reasonably expect transaction savings to have a proportionately greater impact on their operations than on those of providers. This is because conducting transactions is a core function of healthcare payor operations. That is, as risk-bearing entities, one of the primary responsibilities of a healthcare payor or health insurer is the receipt of funds from individuals and organizations and the disbursement of those funds among medical providers for services rendered. By contrast, the primary function of healthcare providers is to deliver medical services, with transactions serving in a secondary role to provide funding for performance of these services. In other analyses that examine the pace of the healthcare sector’s adoption of electronic transactions, the industry often shows poorly when compared to the retail and financial sectors, in which electronic transactions have been widely embraced for some time. There are a number of reasons that account for the slower pace of adoption in the healthcare industry, such as:
Need for greater detail in the transaction data for identifying the nature of the service delivered. This may be in large part because a third-party payor, which cannot directly
1 Federal Register 65 Fed. Reg. 50351, August 17, 2000.
4
Milliman White Paper
Administrative Cost Reduction Opportunities in the U.S. Health Insurance Industry through Use of Electronic Transactions between Payers and Providers
May 6, 2010
observe the service that is being provided, must evaluate the appropriateness and payment levels for the service. As a result, the healthcare system maintains a relatively complex system of service coding and must work to assure that it is consistently applied. This has been a problem for many years, especially given the regional diversity of healthcare. These coded service explanations need to be part of the electronic transaction. HIPAA’s rules specifically included setting standards for such codes, although the regulations for the codes are only five years old and there is a continued effort to further refine this coding.
Final service pricing often lacks transparency and immediacy. Unlike typical retail sales in which there may be one product price or limited pricing variations based on purchase quantity, healthcare service pricing may involve a wide variety of ways to bundle and discount services and payments. Further, each of these ways may differ based on payor and service provider. As a result, not only may uniform service coding be problematic, but electronic transaction benefits may be less immediate because the final service price may require multiple input variables before performing the payment calculation. For example, some payments may bundle several different services.
Standard transaction formats may not provide sufficient detail. Benefit designs, in particular may vary significantly from payor to payor with unique characteristics that, such as exceptions, exclusions and incentives that are difficult to capture in standard fields.
Healthcare is seller-driven, not buyer-driven as in retail sales. Healthcare providers, in many ways, determine the nature, prices, and availability of services. There is limited comparison shopping. Therefore, there are fewer incentives for service providers to implement technologies and service features that tend to have greater value for payors, who are in the primary business of conducting transactions.
Despite these impediments, both government and private sector initiatives have long supported a transition to greater use of electronic transactions in principle if not in practice; and, over the last decade, there has been especially significant progress. Incentives for this, essentially a sea change in payor and provider communications, include:
Greater efficiency. Electronic communications, and especially transactions, generally require substantially less staff time than the alternatives. This applies to both preparation of the information for transmission and the transmission process itself. Human resources over time tend to be significantly more expensive than electronic resources. This report will address this issue specifically and evaluate payor savings potential from use of electronic communications and transactions.
Greater accuracy. A common source of errors in communications and transactions comes with human involvement, for example, transcription errors. Computer software programs increasingly support a capacity to access the critical information directly from source files and transmit it to destination files with minimal or no human intervention, thus minimizing the likelihood of errors.
Increasing standardization of transaction formats. The healthcare service industry has shown increasing support for standard electronic transaction formats. HIPAA reinforced this trend by mandating common formats and coding for many transactions. The actions and
5
Milliman White Paper
Administrative Cost Reduction Opportunities in the U.S. Health Insurance Industry through Use of Electronic Transactions between Payers and Providers
May 6, 2010
proposals of industry trade groups and healthcare payors, providers, and industry vendors have also helped significantly accelerate this trend.
The growth of electronic transaction communication networks. Multi-payor portals, clearinghouses, and other forms of electronic networks support an efficient communications infrastructure among healthcare participants. They permit both the growth of standard transactions as well as allow for payers and providers to communicate through more customized messages, in the latter case for example, as clinical messages or unique patient benefit features.
Decreasing costs for technology. There continue to be dramatic technological innovations that permit wider access to computer technology at lower costs than ever before. In addition, access to high speed connectivity is increasingly prevalent and affordable so the benefits of adopting technological processes increasingly outweigh the costs.
The remainder of this white paper will focus in more detail on estimating the financial savings that may accrue to healthcare payors through use of electronic transactions. The following sections will describe the methodology for evaluating savings, provide results from the study, and analyze these findings.
Methods The purpose of the study was to identify potential administrative savings that may accrue to healthcare payors from the use of electronic means compared to “manual” or “paper” means for typical transactions between payors and providers. Historically, the U.S. health insurance industry has relied on paper (by fax and mail) and telephones calls for communications between payors and providers. In recent years, industry and government initiatives have driven adoption of electronic options for many transactions.
Covered Transactions
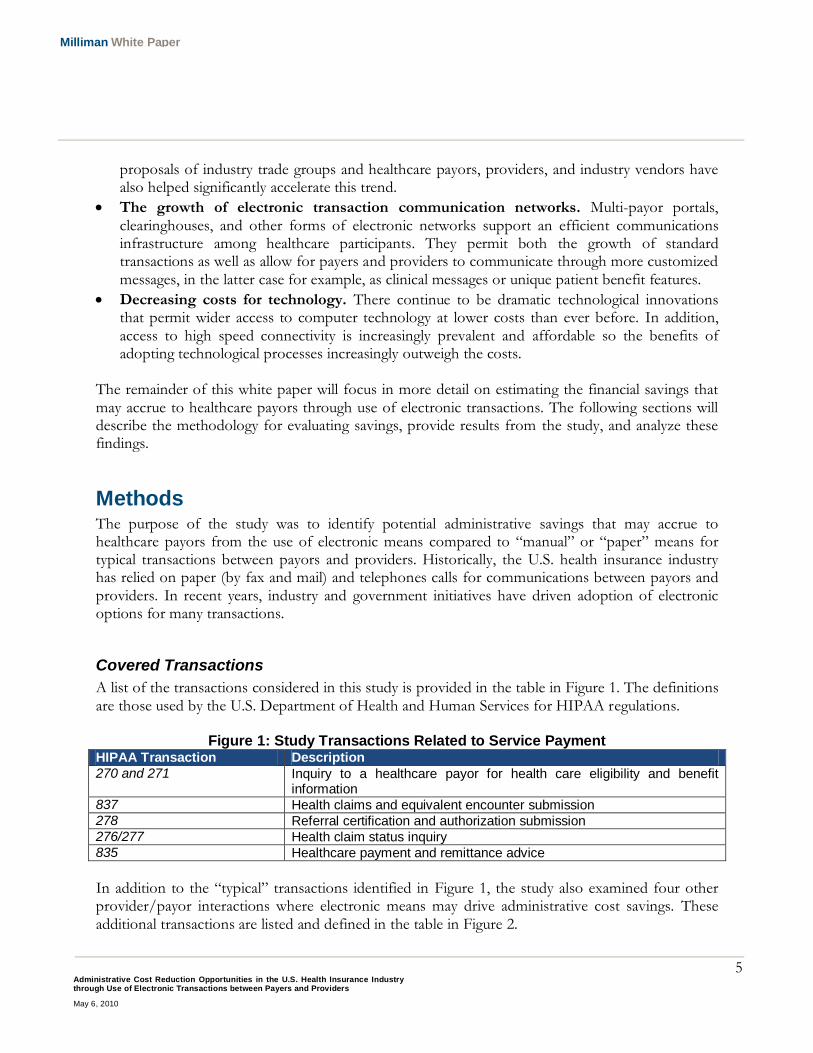
A list of the transactions considered in this study is provided in the table in Figure 1. The definitions are those used by the U.S. Department of Health and Human Services for HIPAA regulations.
Figure 1: Study Transactions Related to Service Payment HIPAA Transaction Description
270 and 271 Inquiry to a healthcare payor for health care eligibility and benefit information
837 Health claims and equivalent encounter submission 278 Referral certification and authorization submission 276/277 Health claim status inquiry 835 Healthcare payment and remittance advice
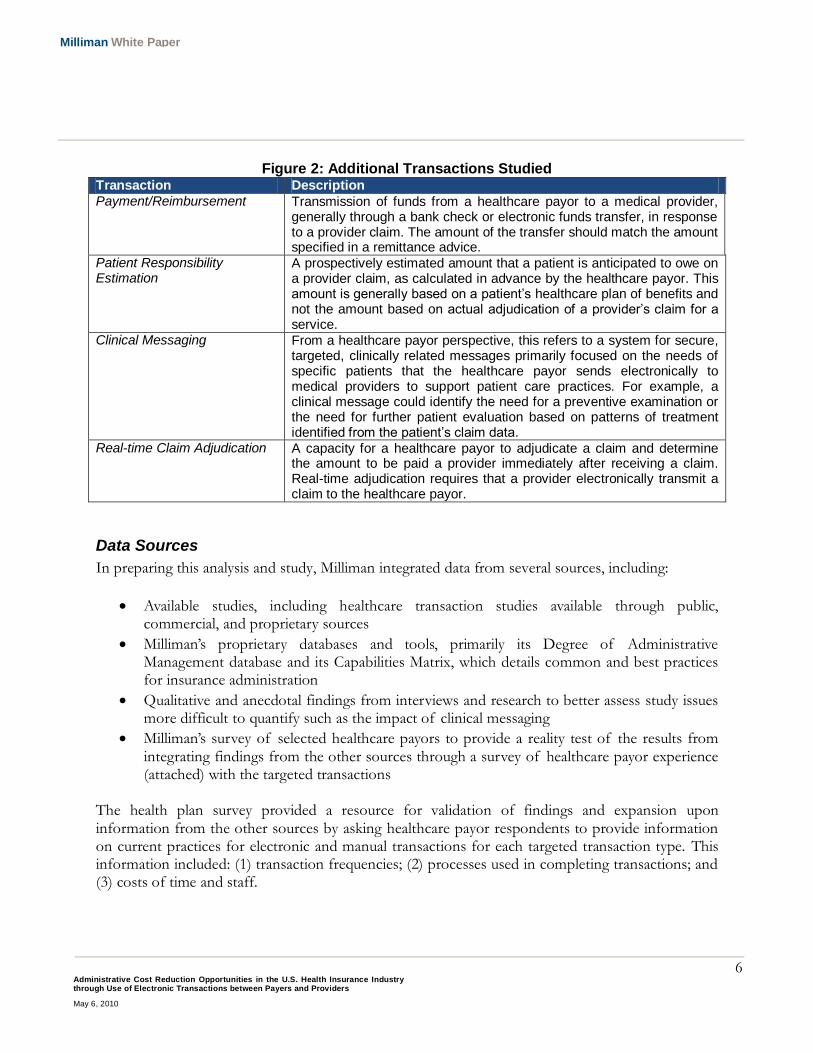
In addition to the “typical” transactions identified in Figure 1, the study also examined four other provider/payor interactions where electronic means may drive administrative cost savings. These additional transactions are listed and defined in the table in Figure 2.
6
Milliman White Paper
Administrative Cost Reduction Opportunities in the U.S. Health Insurance Industry through Use of Electronic Transactions between Payers and Providers
May 6, 2010
Figure 2: Additional Transactions Studied Transaction Description
Payment/Reimbursement
Transmission of funds from a healthcare payor to a medical provider, generally through a bank check or electronic funds transfer, in response to a provider claim. The amount of the transfer should match the amount specified in a remittance advice.
Patient Responsibility Estimation
A prospectively estimated amount that a patient is anticipated to owe on a provider claim, as calculated in advance by the healthcare payor. This amount is generally based on a patient’s healthcare plan of benefits and not the amount based on actual adjudication of a provider’s claim for a service.
Clinical Messaging From a healthcare payor perspective, this refers to a system for secure, targeted, clinically related messages primarily focused on the needs of specific patients that the healthcare payor sends electronically to medical providers to support patient care practices. For example, a clinical message could identify the need for a preventive examination or the need for further patient evaluation based on patterns of treatment identified from the patient’s claim data.
Real-time Claim Adjudication A capacity for a healthcare payor to adjudicate a claim and determine the amount to be paid a provider immediately after receiving a claim. Real-time adjudication requires that a provider electronically transmit a claim to the healthcare payor.
Data Sources
In preparing this analysis and study, Milliman integrated data from several sources, including:
Available studies, including healthcare transaction studies available through public, commercial, and proprietary sources
Milliman’s proprietary databases and tools, primarily its Degree of Administrative Management database and its Capabilities Matrix, which details common and best practices for insurance administration
Qualitative and anecdotal findings from interviews and research to better assess study issues more difficult to quantify such as the impact of clinical messaging
Milliman’s survey of selected healthcare payors to provide a reality test of the results from integrating findings from the other sources through a survey of healthcare payor experience (attached) with the targeted transactions
The health plan survey provided a resource for validation of findings and expansion upon information from the other sources by asking healthcare payor respondents to provide information on current practices for electronic and manual transactions for each targeted transaction type. This information included: (1) transaction frequencies; (2) processes used in completing transactions; and (3) costs of time and staff.

7
Milliman White Paper
Administrative Cost Reduction Opportunities in the U.S. Health Insurance Industry through Use of Electronic Transactions between Payers and Providers
May 6, 2010
Calculations for Costs and Savings
Cost and savings estimates were developed based on operations for a 500,000-commercial member health plan and then extrapolated to estimate potential savings for all health plans nationally. The steps involved in developing the cost of time transactions were:
Delineate tasks and estimate time in minutes required for tasks. Milliman used survey data and professional experience in working with health plan clients to identify tasks involved in completing both manual and electronic transactions and the time required for completing those tasks. The study made allowances for instances in which a manual intervention might be required to complete an electronic transaction, for instance in manual adjudication of a portion of a claim that could not be processed electronically or for medical review of prior authorization requests.
Identify number of transaction-related tasks performed in a day by a single staff member. Milliman estimated that the average staff member had six and a half hours, or 390 productive minutes, in one day. In some instances, transactions may have involved several different staff such as mailroom and customer service staff.
Develop fully loaded cost estimates per staff member minute: Milliman used survey data and additional resources to estimate average wages for staff performing these tasks. Milliman estimated fully loaded costs by multiplying estimated average employee salaries times estimates of employee benefits and general and administrative cost that accounted for such overhead factors as management and IT support and amortized equipment and facility costs.
Calculate composite cost per transaction considering all staff contributions. This calculation combined and weighed the contributions of different staff that may have completed specific tasks that are part of the transaction, such as mailroom costs and claim processer costs in paying a paper claim. In addition, the calculations weighed the proportional contribution of certain specialized staff, such as nursing staff, that are likely to become involved in only a portion of certain transactions.
Validate calculations based on research findings. Milliman compared its findings to other published studies, such as those by the Centers for Medicare and Medicaid Services (CMS). Generally, findings were close, and Milliman selected its estimates over those of other studies. In a few instances, where the variances between other studies and Milliman’s results appeared significant, the cause was explainable, such as use of different methods for calculating overheads or the evaluation of different staff inputs to a task. In these cases, we selected the most appropriate estimates.
Estimate transaction frequencies: Milliman found significant variance in comparative transaction frequencies among surveyed healthcare payors. After reviewing other research, Milliman decided to develop frequencies for health plans based on findings in other research, most notably the study “Overhauling the US health care payment system,” McKinsey Quarterly, June 2007. Milliman used as a model a health plan with approximately 500,000 commercial members generating approximately 7 million claims per year.
8
Milliman White Paper
Administrative Cost Reduction Opportunities in the U.S. Health Insurance Industry through Use of Electronic Transactions between Payers and Providers
May 6, 2010
Calculate savings. Savings calculations represent the differences between the estimated fully loaded administrative costs for manual transactions and the fully loaded costs if those transactions were conducted through primarily electronic means.
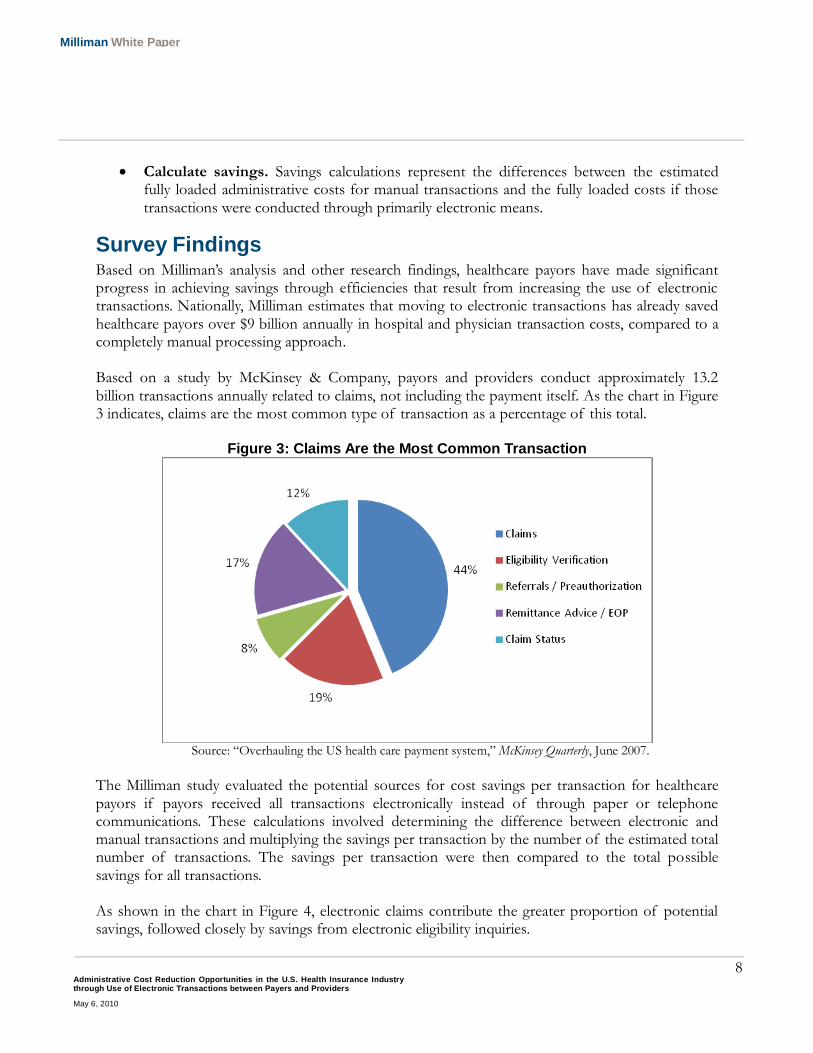
Survey Findings Based on Milliman’s analysis and other research findings, healthcare payors have made significant progress in achieving savings through efficiencies that result from increasing the use of electronic transactions. Nationally, Milliman estimates that moving to electronic transactions has already saved healthcare payors over $9 billion annually in hospital and physician transaction costs, compared to a completely manual processing approach. Based on a study by McKinsey & Company, payors and providers conduct approximately 13.2 billion transactions annually related to claims, not including the payment itself. As the chart in Figure 3 indicates, claims are the most common type of transaction as a percentage of this total.
Figure 3: Claims Are the Most Common Transaction
Source: “Overhauling the US health care payment system,” McKinsey Quarterly, June 2007.
The Milliman study evaluated the potential sources for cost savings per transaction for healthcare payors if payors received all transactions electronically instead of through paper or telephone communications. These calculations involved determining the difference between electronic and manual transactions and multiplying the savings per transaction by the number of the estimated total number of transactions. The savings per transaction were then compared to the total possible savings for all transactions. As shown in the chart in Figure 4, electronic claims contribute the greater proportion of potential savings, followed closely by savings from electronic eligibility inquiries.
9
Milliman White Paper
Administrative Cost Reduction Opportunities in the U.S. Health Insurance Industry through Use of Electronic Transactions between Payers and Providers
May 6, 2010
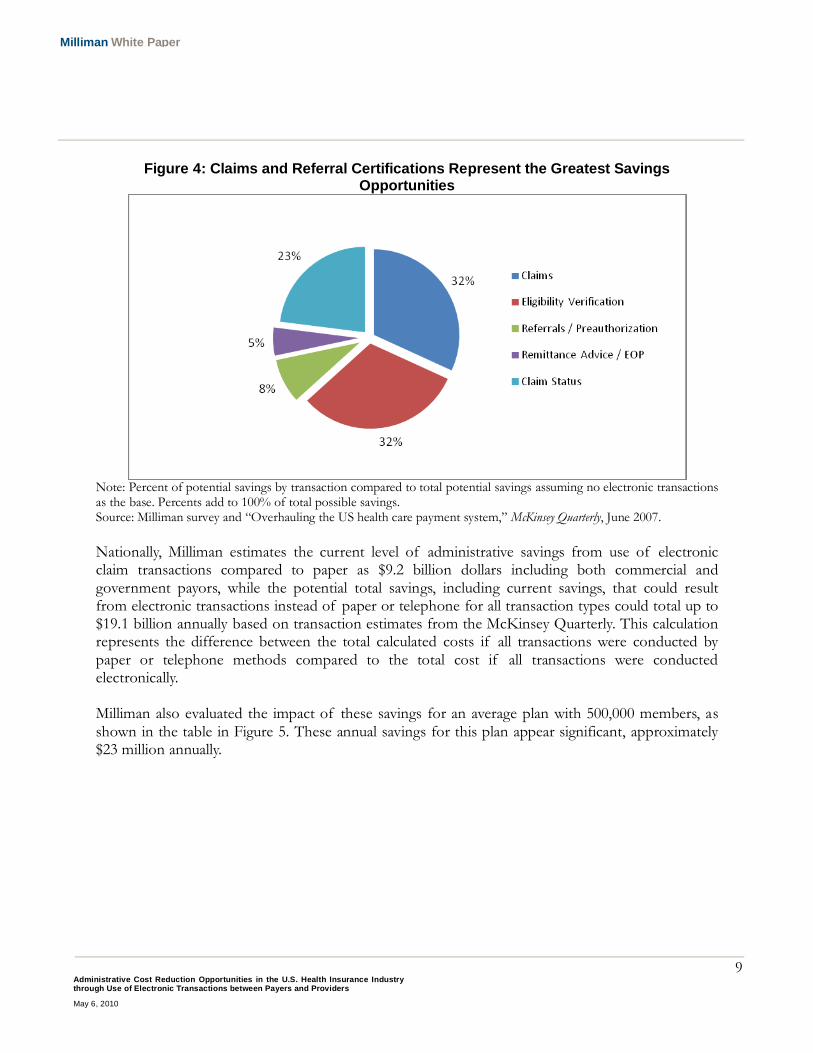
Figure 4: Claims and Referral Certifications Represent the Greatest Savings Opportunities
Note: Percent of potential savings by transaction compared to total potential savings assuming no electronic transactions as the base. Percents add to 100% of total possible savings. Source: Milliman survey and “Overhauling the US health care payment system,” McKinsey Quarterly, June 2007.
Nationally, Milliman estimates the current level of administrative savings from use of electronic claim transactions compared to paper as $9.2 billion dollars including both commercial and government payors, while the potential total savings, including current savings, that could result from electronic transactions instead of paper or telephone for all transaction types could total up to $19.1 billion annually based on transaction estimates from the McKinsey Quarterly. This calculation represents the difference between the total calculated costs if all transactions were conducted by paper or telephone methods compared to the total cost if all transactions were conducted electronically. Milliman also evaluated the impact of these savings for an average plan with 500,000 members, as shown in the table in Figure 5. These annual savings for this plan appear significant, approximately $23 million annually.
10
Milliman White Paper
Administrative Cost Reduction Opportunities in the U.S. Health Insurance Industry through Use of Electronic Transactions between Payers and Providers
May 6, 2010
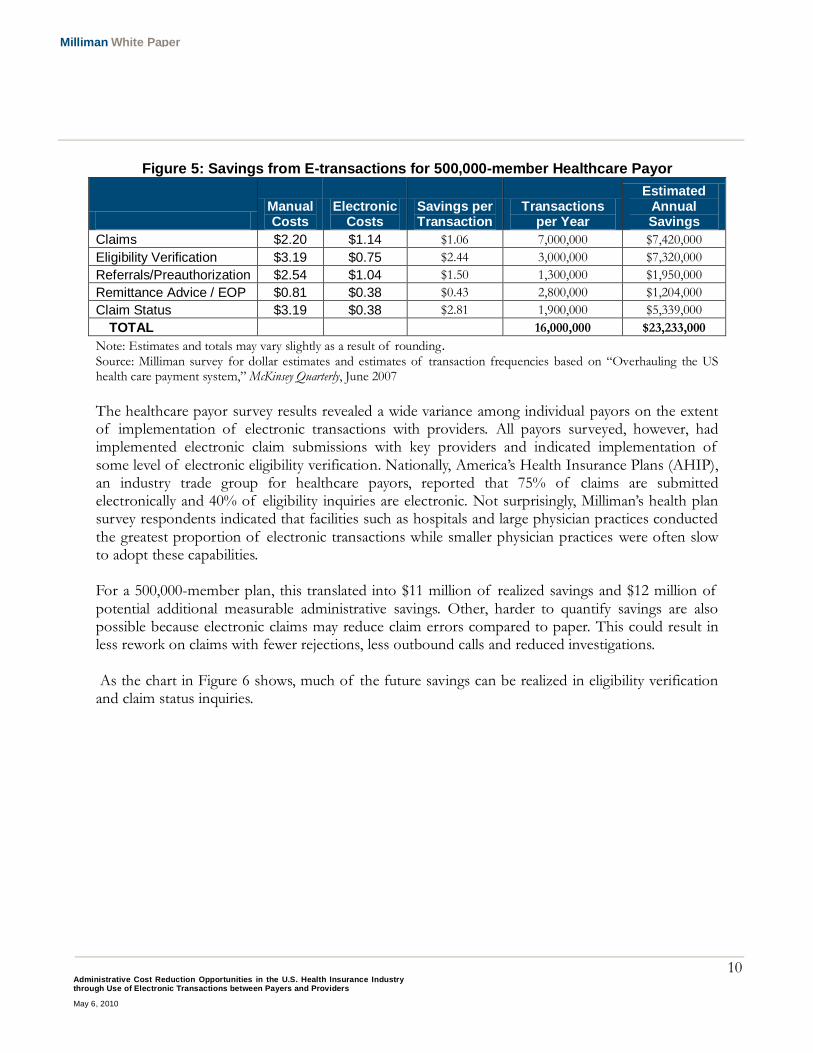
Figure 5: Savings from E-transactions for 500,000-member Healthcare Payor
Manual Costs
Electronic Costs
Savings per Transaction
Transactions per Year
Estimated Annual Savings
Claims $2.20 $1.14 $1.06 7,000,000 $7,420,000
Eligibility Verification $3.19 $0.75 $2.44 3,000,000 $7,320,000
Referrals/Preauthorization $2.54 $1.04 $1.50 1,300,000 $1,950,000
Remittance Advice / EOP $0.81 $0.38 $0.43 2,800,000 $1,204,000
Claim Status $3.19 $0.38 $2.81 1,900,000 $5,339,000
TOTAL 16,000,000 $23,233,000
Note: Estimates and totals may vary slightly as a result of rounding. Source: Milliman survey for dollar estimates and estimates of transaction frequencies based on “Overhauling the US health care payment system,” McKinsey Quarterly, June 2007
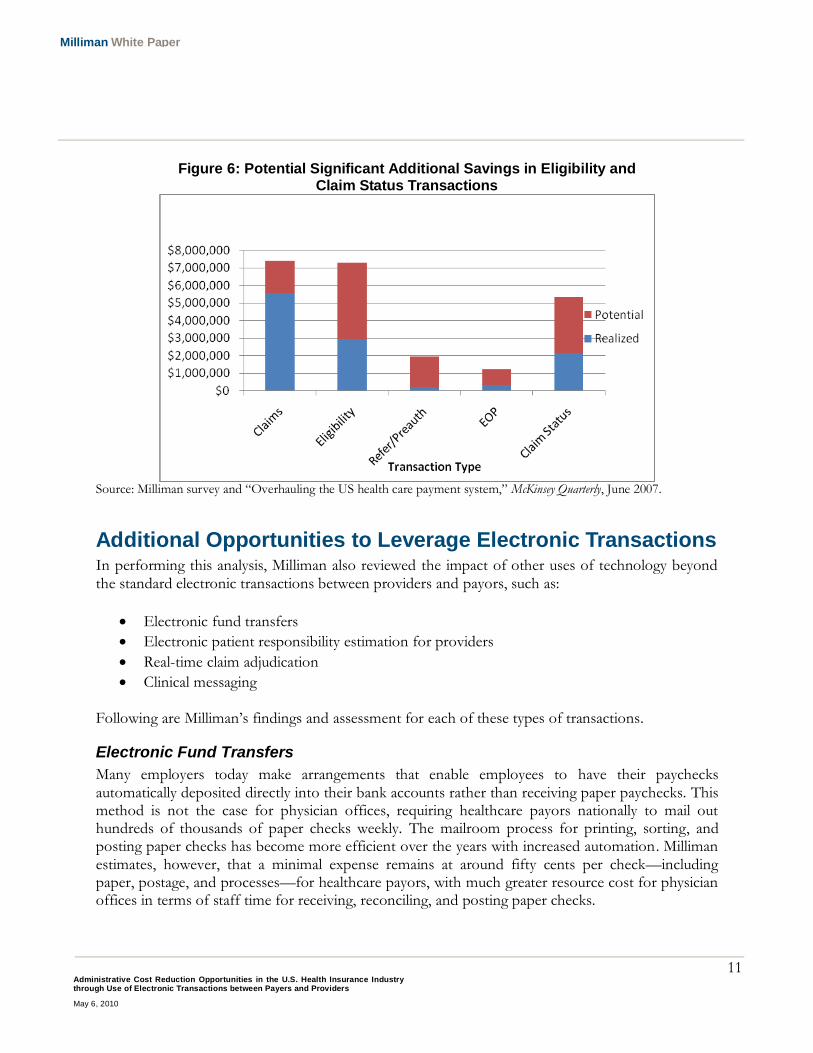
The healthcare payor survey results revealed a wide variance among individual payors on the extent of implementation of electronic transactions with providers. All payors surveyed, however, had implemented electronic claim submissions with key providers and indicated implementation of some level of electronic eligibility verification. Nationally, America’s Health Insurance Plans (AHIP), an industry trade group for healthcare payors, reported that 75% of claims are submitted electronically and 40% of eligibility inquiries are electronic. Not surprisingly, Milliman’s health plan survey respondents indicated that facilities such as hospitals and large physician practices conducted the greatest proportion of electronic transactions while smaller physician practices were often slow to adopt these capabilities. For a 500,000-member plan, this translated into $11 million of realized savings and $12 million of potential additional measurable administrative savings. Other, harder to quantify savings are also possible because electronic claims may reduce claim errors compared to paper. This could result in less rework on claims with fewer rejections, less outbound calls and reduced investigations. As the chart in Figure 6 shows, much of the future savings can be realized in eligibility verification and claim status inquiries.
11
Milliman White Paper
Administrative Cost Reduction Opportunities in the U.S. Health Insurance Industry through Use of Electronic Transactions between Payers and Providers
May 6, 2010
Figure 6: Potential Significant Additional Savings in Eligibility and Claim Status Transactions
Source: Milliman survey and “Overhauling the US health care payment system,” McKinsey Quarterly, June 2007.
Additional Opportunities to Leverage Electronic Transactions In performing this analysis, Milliman also reviewed the impact of other uses of technology beyond the standard electronic transactions between providers and payors, such as:
Electronic fund transfers
Electronic patient responsibility estimation for providers
Real-time claim adjudication
Clinical messaging Following are Milliman’s findings and assessment for each of these types of transactions.
Electronic Fund Transfers
Many employers today make arrangements that enable employees to have their paychecks automatically deposited directly into their bank accounts rather than receiving paper paychecks. This method is not the case for physician offices, requiring healthcare payors nationally to mail out hundreds of thousands of paper checks weekly. The mailroom process for printing, sorting, and posting paper checks has become more efficient over the years with increased automation. Milliman estimates, however, that a minimal expense remains at around fifty cents per check—including paper, postage, and processes—for healthcare payors, with much greater resource cost for physician offices in terms of staff time for receiving, reconciling, and posting paper checks.
12
Milliman White Paper
Administrative Cost Reduction Opportunities in the U.S. Health Insurance Industry through Use of Electronic Transactions between Payers and Providers
May 6, 2010
Milliman estimates that, nationally, healthcare payors could save over $1 billion annually from use of electronic explanations of benefits (EOBs) or remittances. If healthcare payors must continue mailing paper checks to providers, the potential savings from electronic remittances is less, because many payors mail both payment checks and remittances together. Therefore, to realize the full savings, both the remittance and payment need to become electronic, thereby coupling an electronic remittance with an EFT payment. Federal policy initiatives that will eventually require physicians to accept EFT payments for Medicare would appear to offer significant hope in encouraging physician offices to accept EFTs for all payments.
Internet-based Patient Responsibility Estimators and Accumulators for Providers
Obtaining patient responsibility estimations and accumulated deductibles and spending over the Internet permits providers to receive real-time information on patient eligibility and an estimate of financial obligations. This capability allows providers to determine patient copayment and deductible obligations and collect these revenues at the time of service. Patient responsibility estimation improves on the copayment information that insurers may include on a patient’s insurance card by providing more specific coverage detail by procedure, and tracking the level of a patient’s remaining deductible—especially critical for patients who are paying for care through a Health Savings Account. It does not provide adjudication results for a specific claim but considers the patient’s benefit design to provide an estimate with reasonable likelihood the amount of patient responsibility for coinsurance and deductibles. It is also a relatively low-cost service that healthcare payors can offer network providers. Providers benefit from real-time patient responsibility estimators and accumulators that enable accurate collection of patient responsibility amounts (copayments, coinsurance, deductible amounts, etc.) at the time of service, reducing expenses associated with attempting to collect from the patient after the fact, and reducing uncollectible amounts. For healthcare payors, benefits may include reductions in call volumes to determine patient responsibility, although there is a lack of data currently available to clearly determine this impact. Other, less tangible benefits involve reduced levels of claim appeals and improved provider and potentially health plan participant relationships as a result of higher and more immediate settlement of patient financial obligations and an improved position in negotiating provider rates because patient responsibility estimation should reduce provider need for allowances for uncollected debt in provider payment rate determination.
Real-time Claim Adjudication
Real-time claim adjudication allows a provider to submit a claim for a service and receive a fully adjudicated response to that claim before the patient leaves the office or facility. The technology permits a provider to receive a payment response that displays total and allowable charges, as well as the patient's responsibility, including coinsurance, deductible, and copayment. Real-time claim adjudication is already in widespread use for prescription drug claims.
13
Milliman White Paper
Administrative Cost Reduction Opportunities in the U.S. Health Insurance Industry through Use of Electronic Transactions between Payers and Providers
May 6, 2010
In real-time adjudication, provider claim information is entered either through a Web portal or uploaded through the provider’s practice management system to the payor’s adjudication system. Actual reimbursement for the adjudicated amount occurs through normal payment process such as checks or electronic fund transfers. Real-time adjudication is an improvement from a provider perspective over Web-based claim estimation because the provider can have relative certainty over the amount that the healthcare payor will reimburse and may receive the reimbursement itself more quickly. Real-time claim adjudication would make the process of payment for healthcare services comparable to retail purchase in which payment is resolved at the point of service. From the patient and provider perspective it would mean transparency in service pricing and it would reduce disputes on patient out-of-pocket responsibilities. While the technical capabilities exist for real-time adjudication, a number of barriers exist that impede rapid growth. These include:
Provider delays in assembling all the information necessary for claim submission. This is especially true for claims that may involve charges from multiple sources, such as with an inpatient stay in which charges from more than one department may be part of a claim, or in which payment levels depend on a patient diagnosis.
Healthcare payor reimbursement practices that bundle payments for more than one service into a single payment, for example a surgical procedure and post-operative care. Therefore payors need information on all these components before determining a payment amount.
Provider management systems that lack the capability for processing a single claim in real time.
Lack of clearinghouse capabilities for transmission and management of real-time claims.
Provider ambivalence toward technology investments to provide real-time claim submission capabilities, especially because real-time adjudication may require a change in work flow from current batch processing to claim-by-claim transactions.
Need for improvements in coding and common claim formats, including implementing the X12 version of the 5010 claim transactions with ICD-10 coding.
Thus, while real-time electronic claim adjudication may in many ways represent the Holy Grail for healthcare electronic transactions, bringing healthcare in line with retail services, the barriers for widespread adoption in the near future are significant.
Clinical Messaging
Clinical messaging involves healthcare payors delivering clinical information on patient healthcare needs to providers along with other electronic patient information such as eligibility status. This information is then immediately available to physicians while providing patient care. An example of a clinical message would be notification of a patient’s need for a routine mammogram, or providing
14
Milliman White Paper
Administrative Cost Reduction Opportunities in the U.S. Health Insurance Industry through Use of Electronic Transactions between Payers and Providers
May 6, 2010
a physician with comparative effectiveness guidelines supporting physical therapy over surgery for treatment of back pain. As a result of the healthcare payor’s claim processing role, a healthcare payor can maintain a relatively comprehensive picture of a patient’s health, especially as it relates to the combination of information from multiple providers. Healthcare payors can use clinical messaging to take advantage of this information to improve the quality of care available through provider networks and to minimize potential conflicts arising from utilization and quality management guidelines. The federal government is also looking at the potential of linking clinical messages to electronic medical record content. These messages could support implementation of comparative effectiveness guidelines as part of implementing national healthcare reform. While some healthcare payors are beginning to experiment with clinical messaging, issues that need to be addressed include:
Healthcare payor capabilities to communicate directly with providers through secure channels, such as through secure e-mail or as part of other transactions such as eligibility look-up
Healthcare payor capabilities to effectively assess patient medical needs through the application of clinical guidelines
Provider acceptance of clinical direction from healthcare payors
Strategies for Change Both economic and clinical needs support greater use of electronic transactions and communications among healthcare payors and providers. Healthcare payor practices and government policies can take additional steps to reinforce efforts among the nation’s hundreds of thousands of healthcare service providers to speed implementation. Potential actions include:
Establishing additional financial incentives for providers to use electronic transactions, such as higher payment levels for providers that submit electronic claims and accept EFT payments.
Identifying and taking advantage of vendor programs that support electronic transactions and communications, such as multi-payor portals, clearinghouses and other electronic networks that improve on transaction capabilities or that improve on real-time claim adjudication.
Promulgating improved transaction standards though both private and public venues. More work needs to done to improve on the transaction standards originally promulgated through HIPAA in such areas as claim formats, coding of certain key elements (for example denial codes), interfaces for eligibility look-ups, and so on.
Seeking more creative solutions for payor and provider communications that support efficient electronic communications where there is a need for transactional information in

15
Milliman White Paper
Administrative Cost Reduction Opportunities in the U.S. Health Insurance Industry through Use of Electronic Transactions between Payers and Providers
May 6, 2010
which it is difficult to establish a single standard or in which the standard is still evolving. Payor portals, for example, are evolving to meet these more cutting edge transaction needs.
Establishing electronic medical record standards that will support long-term provider implementation of electronic offices and interoperability of electronic standards.
Contractual and government mandates for providers to use electronic transactions. For example, Medicare has moved aggressively in this direction with mandates and some payors that are dominant in certain geographic regions have insisted that network providers use electronic claim submission in provider contract provisions
The goal of achieving near universal adoption of electronic transaction format appears achievable but not likely to happen quickly given the diverse provider priorities and resource capabilities. It will require continued and focused efforts on behalf of healthcare payors and government to keep implementation on track.
About Milliman Milliman, Inc (formerly Milliman and Robertson, Inc) is a leading international consulting and actuarial firm serving healthcare payors, service providers, and consumer organizations for over half a century. The firm is especially well-known and trusted for its quantitative analyses. It has established substantial practice expertise in healthcare technology applications and in evaluating the benefits of those applications. For more information about the study, or about Milliman, please contact the study authors, John Phelan at [email protected] or Andrew Naugle at [email protected].
Related Documents











