Mike Malone, D.D.S. & Assoc. Mike Malone, D.D.S., F.A.G.D. 300 Doucet Road Lafayette, Louisiana 70503 phone: (337) 989-1268 fax: (337) 989-1324 www.mikemalonedds.com mike@mikemalonedds.com A Commitment to Excellence How to Achieve Predictable Excellence in Cosmetic Dentistry

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Mike Malone, D.D.S. & Assoc.
Mike Malone, D.D.S., F.A.G.D.300 Doucet Road
Lafayette, Louisiana70503
phone: (337) 989-1268fax: (337) 989-1324
A Commitment to Excellence
How to Achieve Predictable Excellence in Cosmetic Dentistry
Mike Malone, D.D.S. & Associates
300 Doucet Rd.● Lafayette ● Louisiana ● 70503 ● 337-989-1268 ● www.mikemalonedds.com
OUR MISSION STATEMENT
We believe that every patient should be offered the highest quality of dental health care that is consistent with their dental needs and values.
The compelling principles for which we stand are service, quality and commitment to excellence.
Our goal is simply to help our patients retain their teeth all of their lives if possible…in maximum comfort, function, health and esthetics…and to accomplish this appropriately.
OUR PATIENTS:Our practice will offer general dentistry of the highest quality for the entire family. We strive to
provide cosmetic and restorative dentistry at a level that equals or surpasses the best available in the world.
STAFF:The employment of the highest caliber people is of utmost importance to our purpose. They
must always be willing to strive to improve technical skills, interpersonal communications, and team interactions. These are people who are excited about what they are doing, are motivated to achieve results, and have high standards of quality and integrity.
CONTINUING EDUCATION:A commitment to excellence in patient care is the key to our mission. Attending continuing
education courses is essential to develop every team member to their highest potential. The journey towards excellence requires growth and openness to change.
BUSINESS GROWTH:A profitable business will allow everyone to concentrate on delivering superior dental care. A
fair fee is one that the patient will pay with gratitude for the care, skill and judgment necessary to deliver the appropriate service.
LEADERSHIP:The practice will provide support, feedback, and appreciation to promote growth and long-term
commitment from each employee.Our standards will always be set high so that our employees can achieve higher levels of
expertise and self-esteem. We will strive to make our employees happy with their jobs and attempt to help them end each day feeling like a winner.
Mike
2
Telephone Script
MAKE APPOINTMENT
Go to initial report form. “In order for me to make………………”
Answer Phone: “Good Morning/Good Afternoon, Dr. Mike Malone and Associates. This is ____________, how may I help you?
“How long has it been since you were seen in our office?” “So you would be a new patient in our practice. We offer General Dentistry for all ages with a special emphasis on preventive, as well as cosmetic and restorative dentistry. Our #1 priority is excellent and affordable dental care in a relaxed and comfortable environment. Is this the type of dental practice you are looking for?” “That’s great! For our adult new patients we dedicate your entire appointment with the doctor. You will start with a one-on-one discussion with the doctor about what your needs and expectations are, followed by a very thorough comprehensive examination. Is that the type of care you were looking for?
“Dr. Malone’s practice is limited to patients requiring cosmetic or complex restorative care.” “Dr. _________ sees patients of all ages for comprehensive general dentistry.” “Would you like to schedule with Dr. Malone or Dr. _________? “The fee for your comprehensive examination, including all necessary X-rays, other records, and the follow up consultation appointment is $_______. For your convenience we accept all Major Credit Cards, Cash, or Check. Would you prefer morning or afternoon?”
“You only want your teeth cleaned? We can do that for you. I would be happy to make an appointment for you with the dental hygienist for what we call an adult prophylaxis. This is a dental cleaning above the gumline for patients who have no signs or symptoms of gum disease. The fee for that type of appointment is $________. Would you prefer morning or afternoon?”
“If you are not certain what your dental needs are, I would be happy to schedule a complimentary consultation with either Dr. Malone or Dr. ________.”
“We would be happy to help you by collecting your portion of the dental cost at the time of the visit and bill your insurance for their portion, however our system does not allow us to do that on the initial visit only. The fee for that appointment will be $________. For your convenience we accept all Major Credit Cards, Cash, or Check.
Mike
3
Date Called Appointment Date Doctor Initials
� Comprehensive Exam � Hygiene � Consultation � Emergency
1. “In order for me to make the proper appointment for you, may I ask you a few questions?”
Name Pronounced/Preferred NameAddressHome Phone Work Phone DOB:Chief concern
Referred By; Fee Quoted:Initial Reaction to Patient:� Fearful � Talkative � Quiet � Aggresive � Polite
2. “Are there other family members you would like me to schedule an appointment for?”� Yes � No If so, who?
3. “Is there anything else that we should know that would make your visit more comfortable?” (Medicalconditions that may require antibiotic premedication?)
4. “In order to save you valuable time, I will mail your dental and medical forms to you. Please complete andbring them with you. Remember that your appointment with Dr. will last 1-2 hours and weusually start right on time! If something should occur that would prevent you from keeping yourappointment, please let me know in advance so I can give the time to another patient.
� Welcome Letter/Packet Sent � New Patient Chart Made
5. Tell me about yourself?
6. Chief Concern:
7. Dental History:
8. Medical History:
9. Is there anything else?
10. Have your thought about your budget?
11. Personality type: � Amiable � Analytic � Expressive � Driver
12. Dental IQ: � High � Average � Low
13 Obstacles: � Fear � Time � Budget
INITIAL REPORT
Mike
4
Patient Information Date
Name Home Phone BirthdateAddress City State ZipSocial Security #: E-mailCheck Appropriate Box ❑ Minor ❑ Single ❑ Married ❑ Divorced ❑ Widowed ❑ SeparatedPatient’s Employer Work PhoneBusiness Address City State ZipSpouse or Parent’s Name Employer Work PhoneWho May We Thank for Referring You?Person to Contact in Case of Emergency Phone
Responsible PartyRelationship
Name of Person Responsible for this Account to PatientAddress Home PhoneSocial Security # BirthdateEmployer Work PhoneOccupationIs This Person Currently a Patient in our Office? ❑Yes ❑No
Dental Insurance InformationRelationship
Name of Insured to PatientBirthdate Social Security #Name of Employer Work PhoneAddress of Employer City State ZipInsurance Company Group # PhoneIns. Co. Address City State Zip
I authorize my insurance company to pay the dentist all insurance benefits otherwise payable to me for services rendered. I authorize theuse of this signature on all insurance submissions. I authorize the dentist to release all information necessary to secure the payment ofbenefits. I understand that I am financially responsible for all charges whether or not paid by insurance.
Insurance Authorization Signature Date
Payment is due in full at time of treatment.
Please indicate preferred method of payment:
❑ Cash or Check at time of appointment
❑ Visa, Discover, Mastercard, or American Express
General Dentistry • Cosmetic Dentistry • Restorative Dentistry • Implant Dentistry
300 Doucet Road, Ste. A • Lafayette, Louisiana 70503 • (337) 989-1268over
Mike Malone, D.D.S. & Assoc.
Mike Malone, D.D.S., F.A.G.D.Accredited by The American Academy of Cosmetic DentistryFellow of the Academy of General Dentistry
A Commitment to Excellence
Mike
5
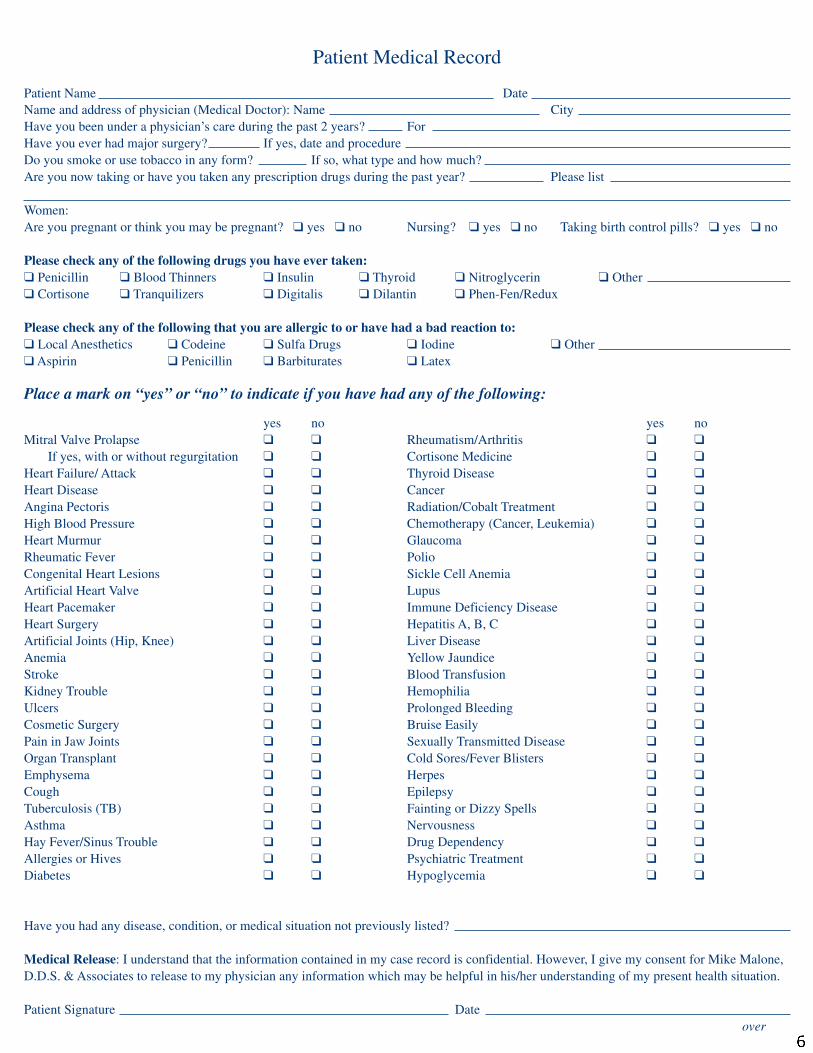
Patient Medical Record
Patient Name DateName and address of physician (Medical Doctor): Name CityHave you been under a physician’s care during the past 2 years? ForHave you ever had major surgery? If yes, date and procedureDo you smoke or use tobacco in any form? If so, what type and how much?Are you now taking or have you taken any prescription drugs during the past year? Please list
Women:Are you pregnant or think you may be pregnant? ❑ yes ❑ no Nursing? ❑ yes ❑ no Taking birth control pills? ❑ yes ❑ no
Please check any of the following drugs you have ever taken:❑ Penicillin ❑ Blood Thinners ❑ Insulin ❑ Thyroid ❑ Nitroglycerin ❑ Other❑ Cortisone ❑ Tranquilizers ❑ Digitalis ❑ Dilantin ❑ Phen-Fen/Redux
Please check any of the following that you are allergic to or have had a bad reaction to:❑ Local Anesthetics ❑ Codeine ❑ Sulfa Drugs ❑ Iodine ❑ Other❑ Aspirin ❑ Penicillin ❑ Barbiturates ❑ Latex
Place a mark on “yes” or “no” to indicate if you have had any of the following:
yes no yes noMitral Valve Prolapse ❑ ❑ Rheumatism/Arthritis ❑ ❑
If yes, with or without regurgitation ❑ ❑ Cortisone Medicine ❑ ❑
Heart Failure/ Attack ❑ ❑ Thyroid Disease ❑ ❑
Heart Disease ❑ ❑ Cancer ❑ ❑
Angina Pectoris ❑ ❑ Radiation/Cobalt Treatment ❑ ❑
High Blood Pressure ❑ ❑ Chemotherapy (Cancer, Leukemia) ❑ ❑
Heart Murmur ❑ ❑ Glaucoma ❑ ❑
Rheumatic Fever ❑ ❑ Polio ❑ ❑
Congenital Heart Lesions ❑ ❑ Sickle Cell Anemia ❑ ❑
Artificial Heart Valve ❑ ❑ Lupus ❑ ❑
Heart Pacemaker ❑ ❑ Immune Deficiency Disease ❑ ❑
Heart Surgery ❑ ❑ Hepatitis A, B, C ❑ ❑
Artificial Joints (Hip, Knee) ❑ ❑ Liver Disease ❑ ❑
Anemia ❑ ❑ Yellow Jaundice ❑ ❑
Stroke ❑ ❑ Blood Transfusion ❑ ❑
Kidney Trouble ❑ ❑ Hemophilia ❑ ❑
Ulcers ❑ ❑ Prolonged Bleeding ❑ ❑
Cosmetic Surgery ❑ ❑ Bruise Easily ❑ ❑
Pain in Jaw Joints ❑ ❑ Sexually Transmitted Disease ❑ ❑
Organ Transplant ❑ ❑ Cold Sores/Fever Blisters ❑ ❑
Emphysema ❑ ❑ Herpes ❑ ❑
Cough ❑ ❑ Epilepsy ❑ ❑
Tuberculosis (TB) ❑ ❑ Fainting or Dizzy Spells ❑ ❑
Asthma ❑ ❑ Nervousness ❑ ❑
Hay Fever/Sinus Trouble ❑ ❑ Drug Dependency ❑ ❑
Allergies or Hives ❑ ❑ Psychiatric Treatment ❑ ❑
Diabetes ❑ ❑ Hypoglycemia ❑ ❑
Have you had any disease, condition, or medical situation not previously listed?
Medical Release: I understand that the information contained in my case record is confidential. However, I give my consent for Mike Malone,D.D.S. & Associates to release to my physician any information which may be helpful in his/her understanding of my present health situation.
Patient Signature Dateover
Mike
6

Mike Malone, D.D.S. & Associates
Mike Malone, D.D.S.Accredited by The American Academy of Cosmetic DentistryFellow of the Academy of General Dentistry
A Commitment to Excellence
General Dentistry • Cosmetic Dentistry • Restorative Dentistry • Implant Dentistry
300 Doucet Road, Ste. A • Lafayette, Louisiana 70503 • (337) 989-1268w w w. m i k e m a l o n e d d s . c o m • i n f o @ m i k e m a l o n e d d s . c o m
DENTAL HEALTHWhen was your last dental visit? How often did you see the dentist?Are you having any dental problems that require immediate attention?Do any of the following cause tooth discomfort? Hot Cold Sweets ChewingHow often do you brush your teeth? Floss? Medicated rinse?Do your gums bleed while cleaning? Do your gums ever feel tender or swollen?Have you had periodontal gum treatment? When?Do you clench or grind your teeth? Do your jaws ever feel tired or ache? Click or pop?Can you chew on both sides of your mouth? Comfortable?Do you have frequent headaches? Earaches? Neck or shoulder pain?Have you had orthodontic treatment (braces)? When?Do you usually have many cavities? Do you lose fillings or break fillings?Do you have any loose teeth? Cracked or broken teeth?Do you have any noticeable wear on your teeth? Food traps?Do you have any missing teeth? Have they been replaced?If so, how? Fixed bridge Removable partial Full denture Dental implantAre you comfortable with the replacement? Please describe
Have you ever had an unpleasant dental experience?
CIRCLE CORRECT ANSWER(S):1. My mouth is A) very comfortable 5. I have A) always done the best that was
B) moderately comfortable recommended for my dental healthC) uncomfortable I B) have not done what dentists have
recommended for my mouth2. I A) think the appearance of my mouth C) rarely go, and don’t care much
is excellent about having any dental workB) am satisfied with the appearance completed.
of my mouthC) am dissatisfied with the appearance 6. I have A) put dentistry for myself and my
of my mouth family high on my priority listB) put dentistry for myself and my
3. I A) will do anything to keep my family low on my priority listnatural teeth C) it’s on my list but hard to find
B) want to keep my teeth, but have acertain budget of time and money 7. I think my present state of dental health is:that I am willing to spend on them A) Excellent
B) Good4. I A) have set goals for my oral health C) Poor
with a previous dentistB) have never set goals 8. I would like a mouth with:
concerning my oral health A) Excellent healthC) want to set goals concerning B) Good health
my dental health C) Poor health
What are some questions about dentistry and oral health that you have never had adequately answered?
(over)
Mike
7
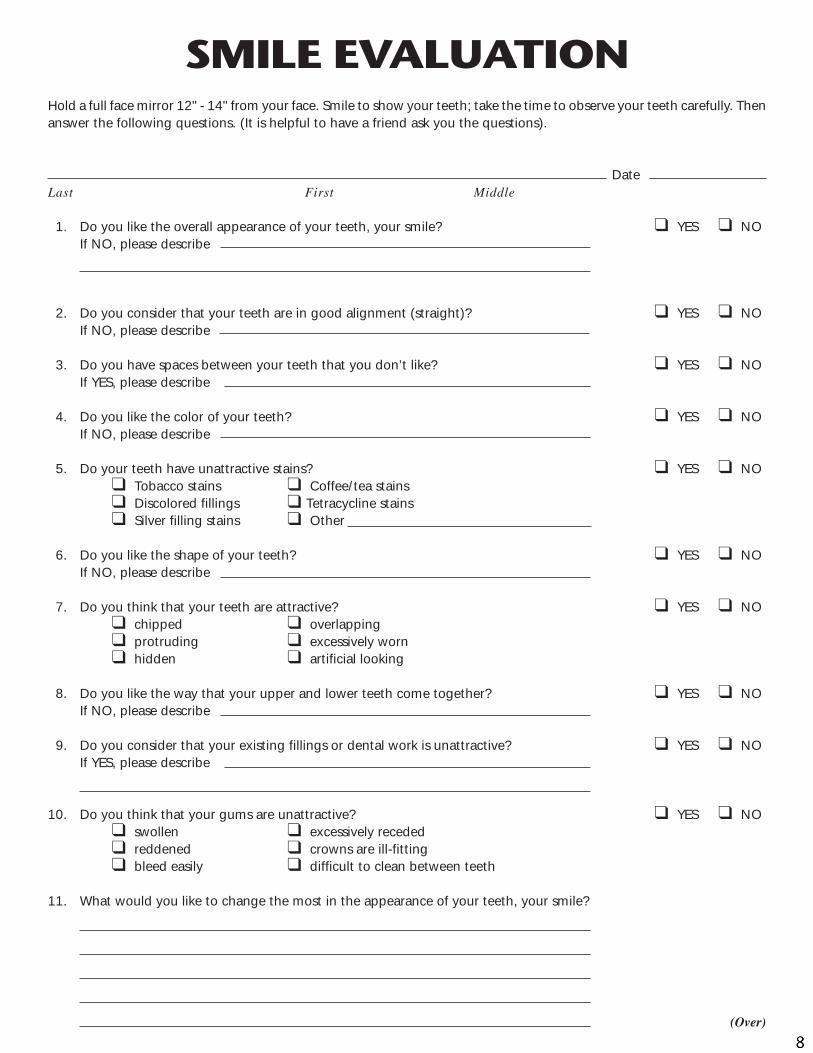
SMILE EVALUATIONHold a full face mirror 12" - 14" from your face. Smile to show your teeth; take the time to observe your teeth carefully. Thenanswer the following questions. (It is helpful to have a friend ask you the questions).
DateLast First Middle
1. Do you like the overall appearance of your teeth, your smile? ❑ YES ❑ NOIf NO, please describe
2. Do you consider that your teeth are in good alignment (straight)? ❑ YES ❑ NOIf NO, please describe
3. Do you have spaces between your teeth that you don’t like? ❑ YES ❑ NOIf YES, please describe
4. Do you like the color of your teeth? ❑ YES ❑ NOIf NO, please describe
5. Do your teeth have unattractive stains? ❑ YES ❑ NO❑ Tobacco stains ❑ Coffee/tea stains❑ Discolored fillings ❑ Tetracycline stains❑ Silver filling stains ❑ Other
6. Do you like the shape of your teeth? ❑ YES ❑ NOIf NO, please describe
7. Do you think that your teeth are attractive? ❑ YES ❑ NO❑ chipped ❑ overlapping❑ protruding ❑ excessively worn❑ hidden ❑ artificial looking
8. Do you like the way that your upper and lower teeth come together? ❑ YES ❑ NOIf NO, please describe
9. Do you consider that your existing fillings or dental work is unattractive? ❑ YES ❑ NOIf YES, please describe
10. Do you think that your gums are unattractive? ❑ YES ❑ NO❑ swollen ❑ excessively receded❑ reddened ❑ crowns are ill-fitting❑ bleed easily ❑ difficult to clean between teeth
11. What would you like to change the most in the appearance of your teeth, your smile?
(Over)
Mike
8
Mike
9

Mike Malone, D.D.S. & Assoc.
Mike Malone, D.D.S., D.D.S.Accredited by The American Academy of Cosmetic DentistryFellow of the Academy of General Dentistry
A Commitment to Excellence
G e n e r a l D e n t i s t r y • C o s m e t i c D e n t i s t r y • R e s t o r a t i v e D e n t i s t r y • I m p l a n t D e n t i s t r y
3 0 0 D o u c e t R o a d , S uite A • L a f a y e t t e , L o u i s i a n a 7 0 5 0 3 • (337) 989-1268
TODAY’S DENTAL EXAMINATION INCLUDED
� Dental History
� Medical History� Discussion of Practice Philosophy� Oral Cancer Examination� Soft Tissue Examination� DENTAL HEALTH EVALUATION
� Periodontal Examination (attachment level measurement)� Plaque Score� Bleeding Score
� State of Existing Repair Evaluation� Occlusal Evaluation� Tooth by Tooth Examination� Complete Series of X-rays� Panoramic X-ray� T.M.J. X-ray� Study Models� Face-Bow for Articulator Mounting� Bite Records - to Evaluate Bite Relationship
YOUR NEXT APPOINTMENT will include a discussion of our examination findingsand recommendations for preventive and corrective treatment to return yourdental condition to a state of OPTIMUM DENTAL HEALTH.
Mike
10
Mike Malone, D.D.S. & Associates
300 Doucet Rd.● Lafayette ● Louisiana ● 70503 ● 337-989-1268 ● www.mikemalonedds.com
REVIEW OF FINDINGS FOR JILL SWITZER
The most important service any dentist or physician can offer is a thorough examination, a diagnosis of the existing conditions, and a treatment plan that serves the short-range and long-range needs of his patients. An understanding of the existing conditions provides the patient with the knowledge and information to make proper choices that suit his or her individual wants and needs.
In the past, most dental treatment was carried out without a plan, (“patchwork” or “maintenance” dentistry). Today, our goal of optimum dental health can be achieved because we now understand the causes of dental disease and the objectives for controlling them.
In order to help you keep your teeth all of your life, we take a great deal of time and effort to help you understand your present conditions and develop a MASTER PLAN of treatment. Once our MASTER PLAN is completed, it will be your responsibility to complete the plan in a time period that works for you, and meets the objectives for your dental health. Quality is the constant ... time is the variable.
The following is a written resume of the existing findings that are present at this time, and the recommendations for corrective treatment. While you are reading it, questions may arise in your mind. Write them down, because I want to discuss your concerns with you.
YOUR PRIORITIES:During our examination you told me your priorities are:1. Straighter teeth2. Replace missing tooth on upper right3. Sensitive teeth
*If you have additional concerns or priorities, please let me know.
Mike
11
PRESENT CONDITIONS
Tooth Decay – There are 4 areas of tooth decay.
Periodontal Disease – Your Plaque Control Index of 80% and Periodontal Bleeding Index of 63% indicate that there is some active gum disease at the Stage 2 level. Please review your Dental Health Report for a more detailed explanation.
State of Existing Dentistry –. Large silver-mercury fillings in the back teeth; some defective and failing.
Bite Relationship – Jaw relationship and tooth position are adequate, but large silver-mercury fillings are wearing, causing some shifting of the teeth and an unstable bite.
DIAGNOSIS SUMMARY: My findings are that you have periodontal disease (periodontitis), tooth decay, defective fillings, missing teeth, and an abscessed tooth.
TREATMENT RECOMMENDATIONS
Our goal is simply to help you keep your teeth all of your life if possible…in maximum comfort, function, health and esthetics…and to accomplish this appropriately. Suggestions for your master plan of treatment are listed below.
Phase I - Multiple appointments to initiate the correction of your periodontal problems.Phase II -Treat abscessed teeth.Phase III - Restore the teeth with appropriate restorations for optimum cosmetics, longevity, and bite stability.Phase IV - InvisalignPhase V - Whitening of the teeth..Phase VI - Active involvement in our Dental Health Program to maintain excellent oral health for a lifetime.
01/12/03
Mike
12
PATIENT’S NAME ______________________________________________________ DATE DUE FOR REVIEW ________________________________________________
DEFINITIONS
Tooth Decay: _______ Periodontal Disease: Plaque _______% Bleeding _______% Category _______. Existing Dentistry: _______ Adequate _______ Large silver-mercury fillings in the back teeth; some defective and failing. _______ Discolored and defective composite resin fillings in the front teeth. _______ Defective crowns. ________________________________________________________________________ ________________________________________________________________________ Bite Relationship: _______ Adequate _______ Excessive wear of the teeth and fillings has resulted in an unstable bite relationship and tooth mobility. _______ Multiple missing teeth have caused some tooth shifting , resulting in an unstable bite and excessive force on the remaining teeth. _______ Deep overbite and poor jaw relationship have resulted in an unstable bite and tooth mobility. _______ Jaw relationship and tooth position are adequate , but large silver-mercury fillings are wearing, causing some shifting of the teeth and an unstable bite. ________________________________________________________________________ ________________________________________________________________________
Mike
13
Diagnosis: _______ Periodontal disease (gingivitis) _______ Periodontal disease (periodontitis) _______ tooth decay _______ defective fillings _______ defective crown (crowns) _______ missing teeth _______ fractured teeth _______ abscessed tooth (teeth) _______ discolored teeth _______ unstable bite _______ TMJ symptoms ________________________________________________________________________ ________________________________________________________________________ Treatment recommendations: _______ Multiple appointments to initiate the correction of your periodontal problems. _______ Bite correction. _______ Treat abscessed teeth. _______ Remove wisdom teeth. _______ Restore the teeth with appropriate restorations for optimum cosmetics, longevity, and bite stability. _______ Active involvement in our Dental Fitness Program to maintain excellent oral health for a lifetime. _______ Whitening of the teeth. ________________________________________________________________________ ________________________________________________________________________
Mike
14
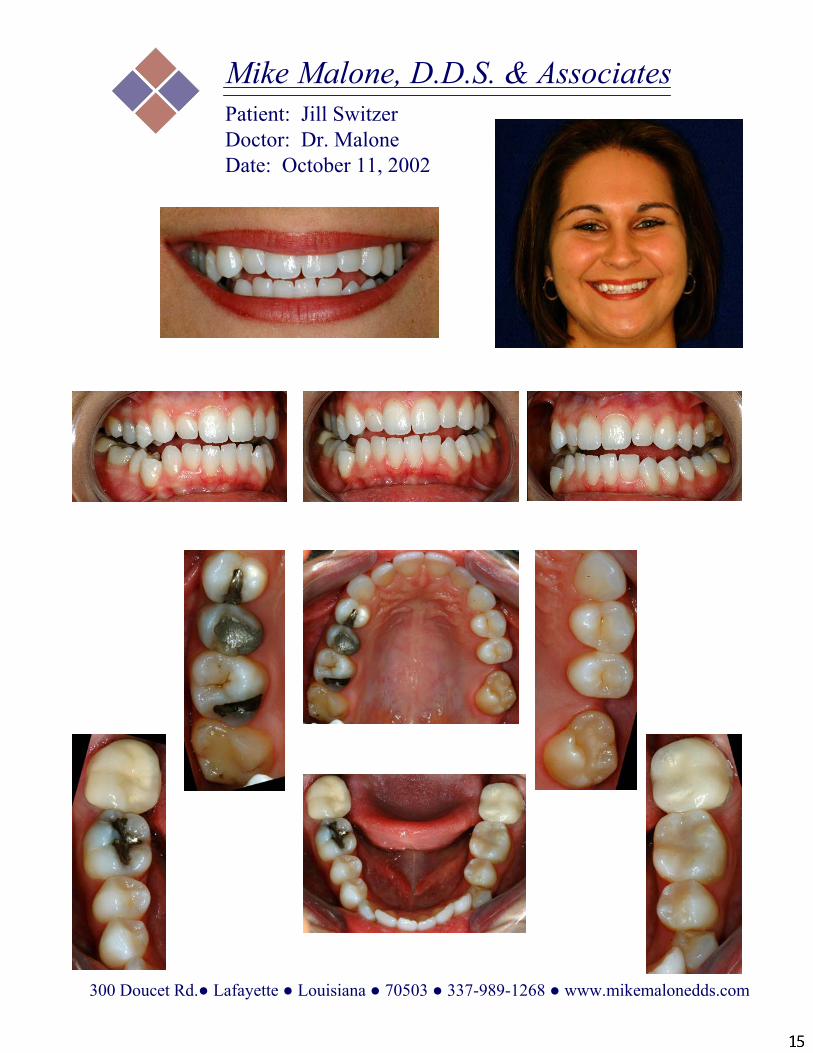
Mike Malone, D.D.S. & AssociatesPatient: Jill SwitzerDoctor: Dr. MaloneDate: October 11, 2002
300 Doucet Rd.● Lafayette ● Louisiana ● 70503 ● 337-989-1268 ● www.mikemalonedds.com
Mike
15
General Dentistry • Cosmetic Dentistry • Restorative Dentistry • Implant Dentistry
300 Doucet Road, Ste. A • Lafayette, Louisiana 70503 • (337) 989-1268
w w w. m i k e m a l o n e d d s . c o m • i n f o @ m i k e m a l o n e d d s . c o m
Mike Malone, D.D.S. & Associates
Mike Malone, D.D.S.Accredited by The American Academy of Cosmetic DentistryFellow of the Academy of General Dentistry
A Commitment to Excellence
For:Date:
Today’s Score Previous Score
Plaque Score:Bleeding Score:Fitness Category:
Plaque Score - The number of surfaces of plaqueat the gumline are counted and converted to apercentage of fitness.
92% - 100% - Excellent Fitness87% - 91% - Marginal Fitness86% and lower - Active Gum Disease
Bleeding Score - Gums that bleed afterattachment level measurement are unhealthy.Bleeding areas are counted and converted into apercentage of fitness.
92% - 100% - Excellent Fitness87% - 91% - Marginal Fitness86% and lower - Active Gum Disease
Fitness Categories - Optimum Dental Health isthe ideal - the absence of disease.There are five stages of gum disease determinedprimarily by the gum attachment level.
Recommendations for Optimum Dental Health:
DENTAL HEALTHREPORT
FITNESS CATEGORIES(Stages of Health and Gum Disease)
Optimum Dental Health- Minimal or no plaque, calculus, or bleeding.- Attachment level 3 mm or less.
Stage One (Gingivitis)- Plaque, some calculus, and bleeding gums.- Attachment level 1-4 mm.
Stage Two (Early Periodontitis)- Plaque, calculus, swollen and bleeding gums.- Attachment level 3-5 mm.- Beginning bone loss.
Stage Three (Moderate Periodontitis)- Plaque, calculus, swollen and bleeding gums.- Attachment level 5-7 mm.- Moderate bone loss, beginning tooth mobility.
Stage Four (Advanced Periodontitis)- Plaque, calculus, swollen and bleeding gums.- Attachment level 7-9 mm.- Advanced bone loss and increased tooth
mobility.
Stage Five (Refractory Periodontitis)- Plaque, calculus, swollen and bleeding gums.
- Attachment level 10 mm or more.- Advanced bone loss that does not respond
to therapy, severe mobility, often hopelessprognosis.
Mike
16
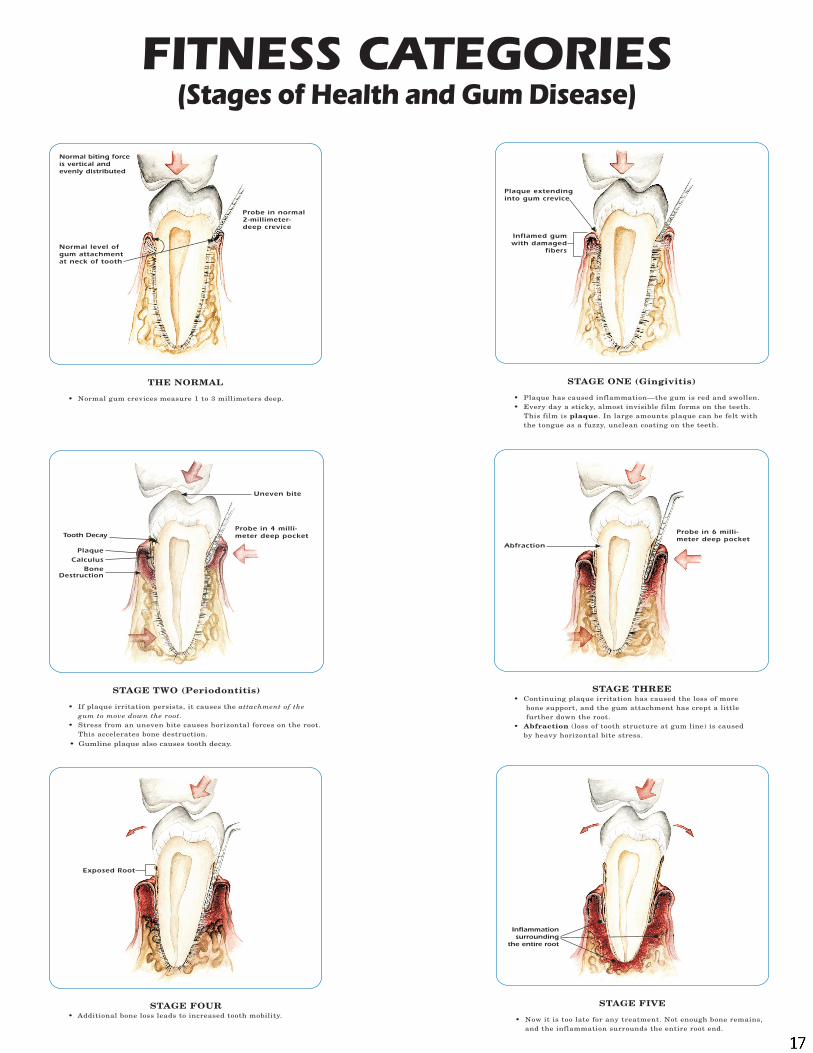
FITNESS CATEGORIES(Stages of Health and Gum Disease)
Mike
17
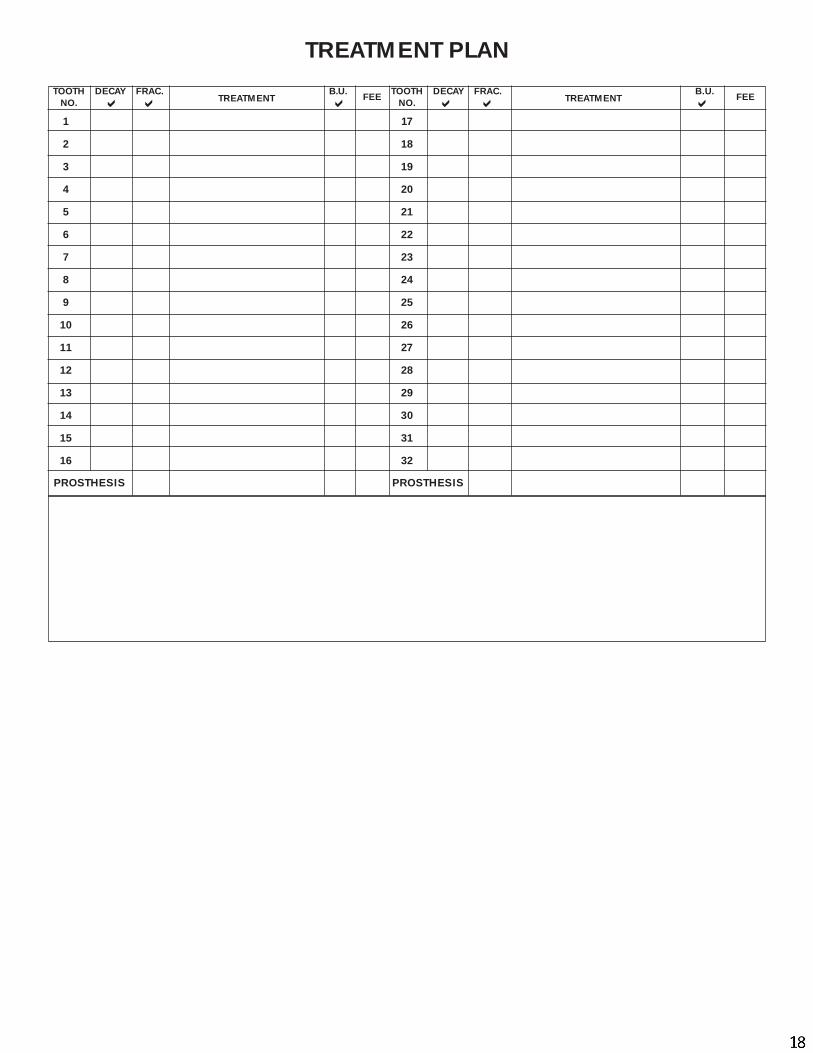
TOOTH DECAY FRAC. B.U. TOOTH DECAY FRAC. B.U.NO. NO.
1 17
2 18
3 19
4 20
5 21
6 22
7 23
8 24
9 25
10 26
11 27
12 28
13 29
14 30
15 31
16 32
PROSTHESIS PROSTHESIS
TREATMENT PLAN
TREATMENT TREATMENT� � � �
FEE��
FEE
Mike
18
Mike
Mike Malone, D.D.S. & Associates
300 Doucet Rd.● Lafayette ● Louisiana ● 70503 ● 337-989-1268 ● www.mikemalonedds.com
Treatment Proposal
PatientName:______________________________________Date:_________________
The following is your treatment proposal with estimated fees. It is not a binding contract. You should be aware that clinical findings might necessitate a change in the treatment plan, with a possible change in cost. For your benefit, we would like to make definite financial arrangements before treatment starts. This treatment proposal will remain valid for 90 days.
Area of Mouth Treatment Fee
_____________________________________________________________________
_____________________________________________________________________
_____________________________________________________________________
_____________________________________________________________________
_____________________________________________________________________
_____________________________________________________________________
_____________________________________________________________________
Total Fee_________________
__________________ _________________________For Dr. Mike Malone Patient Signature
Mike
19
Smile Design - Mike Malone D.D.S.
Review of Smile Design Review of Smile Design ConceptsConcepts
Jeff Morley, DDS, Jimmy Eubank, DDSJeff Morley, DDS, Jimmy Eubank, DDSRonald Goldstein, DDS, David Garber, DMDRonald Goldstein, DDS, David Garber, DMDMaurice Salama, DDSMaurice Salama, DDSAACD AACD –– Guide to Accreditation CriteriaGuide to Accreditation Criteria
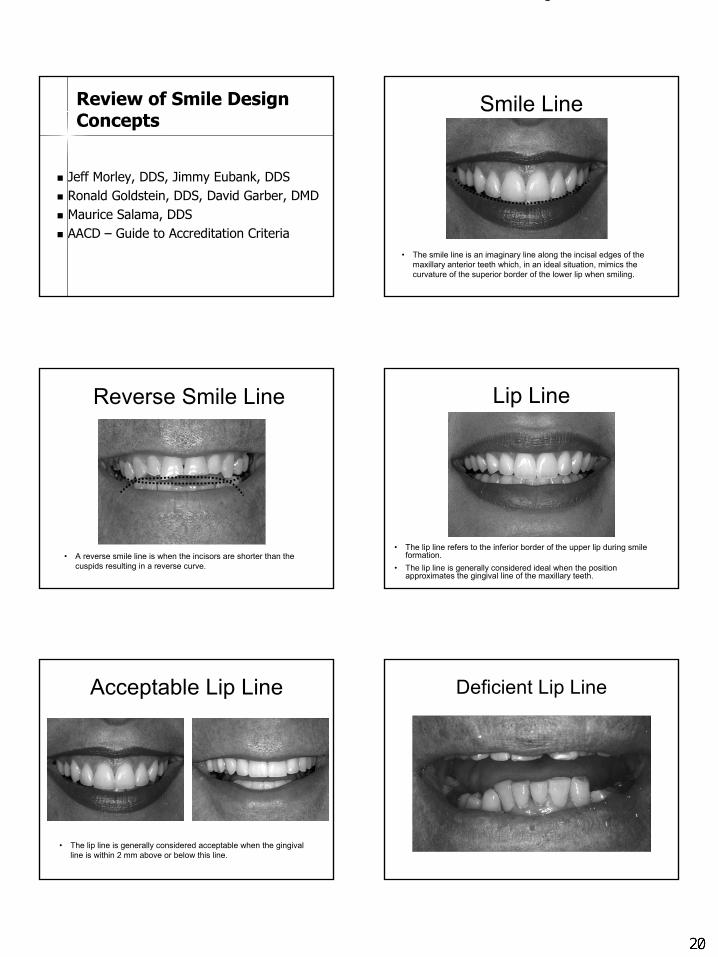
Smile Line
• The smile line is an imaginary line along the incisal edges of the maxillary anterior teeth which, in an ideal situation, mimics the curvature of the superior border of the lower lip when smiling.
Reverse Smile Line
• A reverse smile line is when the incisors are shorter than the cuspids resulting in a reverse curve.
Lip Line
• The lip line refers to the inferior border of the upper lip during smile formation.
• The lip line is generally considered ideal when the position approximates the gingival line of the maxillary teeth.
Acceptable Lip Line
• The lip line is generally considered acceptable when the gingival line is within 2 mm above or below this line.
Deficient Lip Line
Operatory 3
20
Smile Design - Mike Malone D.D.S.
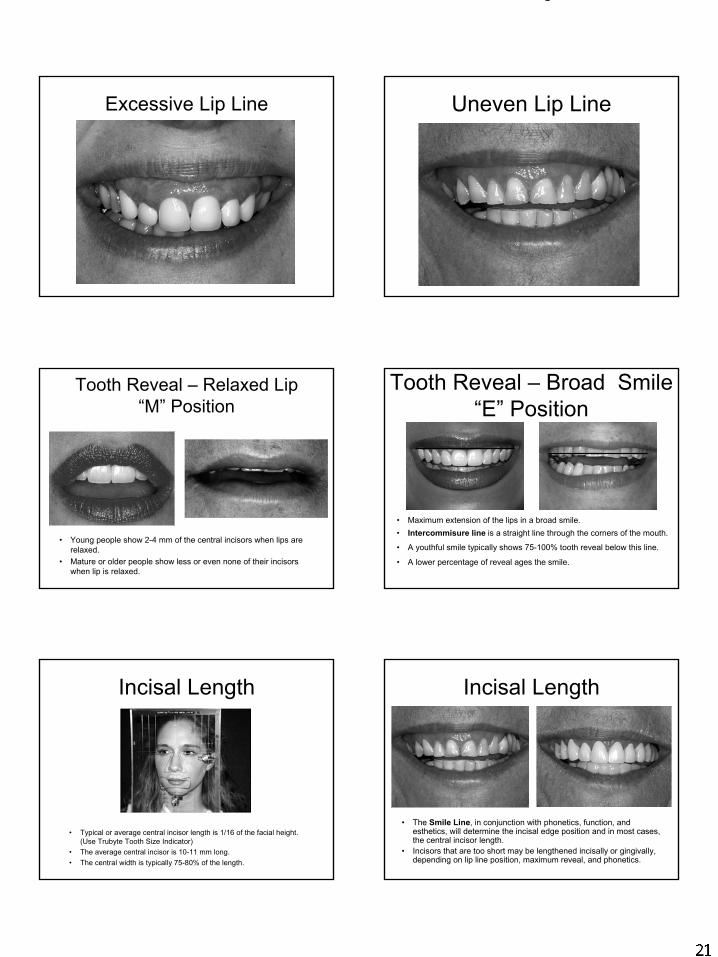
Excessive Lip Line Uneven Lip Line
Tooth Reveal – Relaxed Lip “M” Position
• Young people show 2-4 mm of the central incisors when lips are relaxed.
• Mature or older people show less or even none of their incisors when lip is relaxed.
Tooth Reveal – Broad Smile “E” Position
• Maximum extension of the lips in a broad smile.• Intercommisure line is a straight line through the corners of the mouth.
• A youthful smile typically shows 75-100% tooth reveal below this line.
• A lower percentage of reveal ages the smile.
Incisal Length
• Typical or average central incisor length is 1/16 of the facial height. (Use Trubyte Tooth Size Indicator)
• The average central incisor is 10-11 mm long.• The central width is typically 75-80% of the length.
Incisal Length
• The Smile Line, in conjunction with phonetics, function, and esthetics, will determine the incisal edge position and in most cases, the central incisor length.
• Incisors that are too short may be lengthened incisally or gingivally, depending on lip line position, maximum reveal, and phonetics.
Operatory 3
Operatory 3
Operatory 3
21
Smile Design - Mike Malone D.D.S.
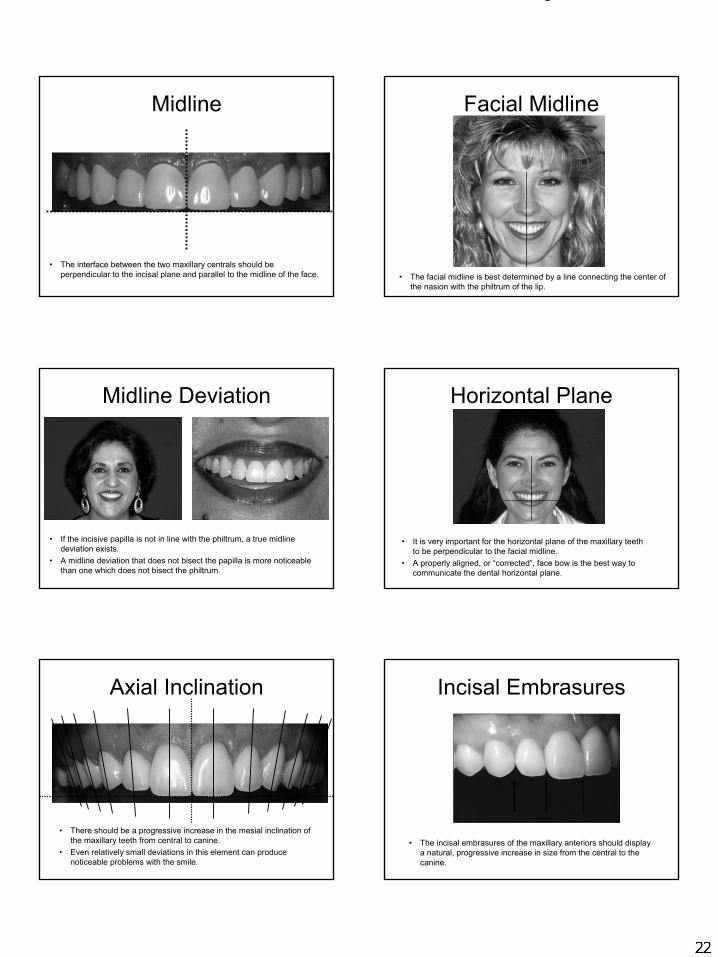
Midline
• The interface between the two maxillary centrals should be perpendicular to the incisal plane and parallel to the midline of the face.
Facial Midline
• The facial midline is best determined by a line connecting the center of the nasion with the philtrum of the lip.
Midline Deviation
• If the incisive papilla is not in line with the philtrum, a true midline deviation exists.
• A midline deviation that does not bisect the papilla is more noticeable than one which does not bisect the philtrum.
Horizontal Plane
• It is very important for the horizontal plane of the maxillary teeth to be perpendicular to the facial midline.
• A properly aligned, or “corrected”, face bow is the best way to communicate the dental horizontal plane.
Axial Inclination
• There should be a progressive increase in the mesial inclination of the maxillary teeth from central to canine.
• Even relatively small deviations in this element can produce noticeable problems with the smile.
Incisal Embrasures
• The incisal embrasures of the maxillary anteriors should displaya natural, progressive increase in size from the central to the canine.
Operatory 3
Operatory 3
22
Smile Design - Mike Malone D.D.S.
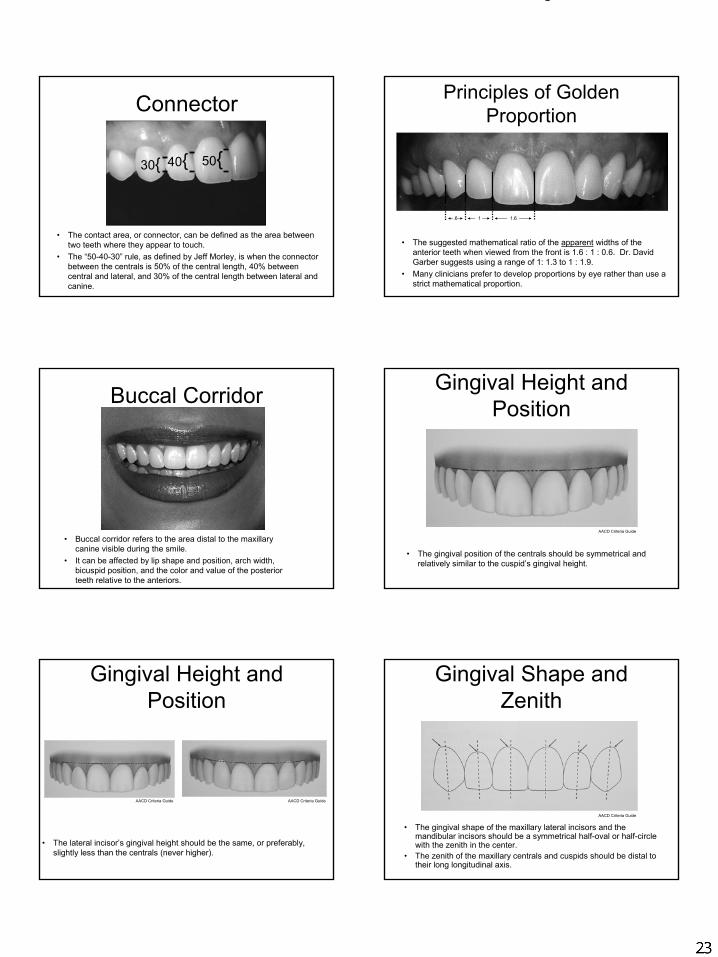
Connector
• The contact area, or connector, can be defined as the area between two teeth where they appear to touch.
• The “50-40-30” rule, as defined by Jeff Morley, is when the connector between the centrals is 50% of the central length, 40% between central and lateral, and 30% of the central length between lateral and canine.
50{40{30{
Principles of Golden Proportion
• The suggested mathematical ratio of the apparent widths of the anterior teeth when viewed from the front is 1.6 : 1 : 0.6. Dr. David Garber suggests using a range of 1: 1.3 to 1 : 1.9.
• Many clinicians prefer to develop proportions by eye rather than use a strict mathematical proportion.
.6 1 1.6
Buccal Corridor
• Buccal corridor refers to the area distal to the maxillary canine visible during the smile.
• It can be affected by lip shape and position, arch width, bicuspid position, and the color and value of the posterior teeth relative to the anteriors.
Gingival Height and Position
• The gingival position of the centrals should be symmetrical and relatively similar to the cuspid’s gingival height.
AACD Criteria Guide
Gingival Height and Position
• The lateral incisor’s gingival height should be the same, or preferably, slightly less than the centrals (never higher).
AACD Criteria Guide AACD Criteria Guide
Gingival Shape and Zenith
• The gingival shape of the maxillary lateral incisors and the mandibular incisors should be a symmetrical half-oval or half-circle with the zenith in the center.
• The zenith of the maxillary centrals and cuspids should be distal to their long longitudinal axis.
AACD Criteria Guide
Operatory 3
Operatory 3
23
Smile Design - Mike Malone D.D.S.
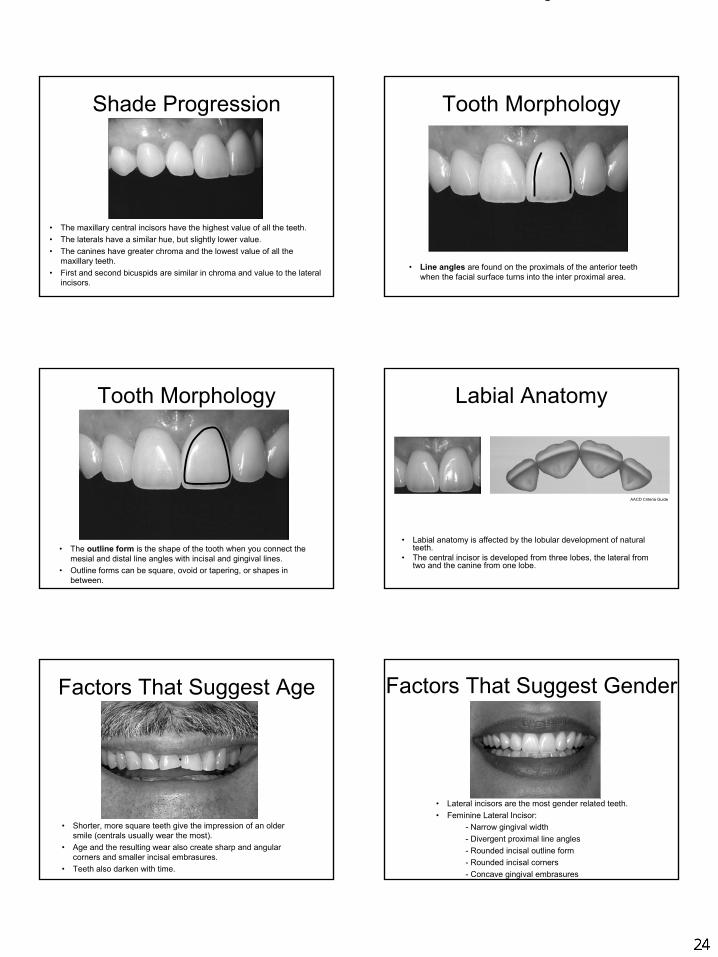
Shade Progression
• The maxillary central incisors have the highest value of all the teeth.• The laterals have a similar hue, but slightly lower value.• The canines have greater chroma and the lowest value of all the
maxillary teeth.• First and second bicuspids are similar in chroma and value to the lateral
incisors.
Tooth Morphology
• Line angles are found on the proximals of the anterior teeth when the facial surface turns into the inter proximal area.
Tooth Morphology
• The outline form is the shape of the tooth when you connect the mesial and distal line angles with incisal and gingival lines.
• Outline forms can be square, ovoid or tapering, or shapes in between.
Labial Anatomy
• Labial anatomy is affected by the lobular development of naturalteeth.
• The central incisor is developed from three lobes, the lateral from two and the canine from one lobe.
AACD Criteria Guide
Factors That Suggest Age
• Shorter, more square teeth give the impression of an older smile (centrals usually wear the most).
• Age and the resulting wear also create sharp and angular corners and smaller incisal embrasures.
• Teeth also darken with time.
Factors That Suggest Gender
• Lateral incisors are the most gender related teeth.• Feminine Lateral Incisor:
- Narrow gingival width- Divergent proximal line angles- Rounded incisal outline form- Rounded incisal corners- Concave gingival embrasures
Operatory 3
24
Smile Design - Mike Malone D.D.S.
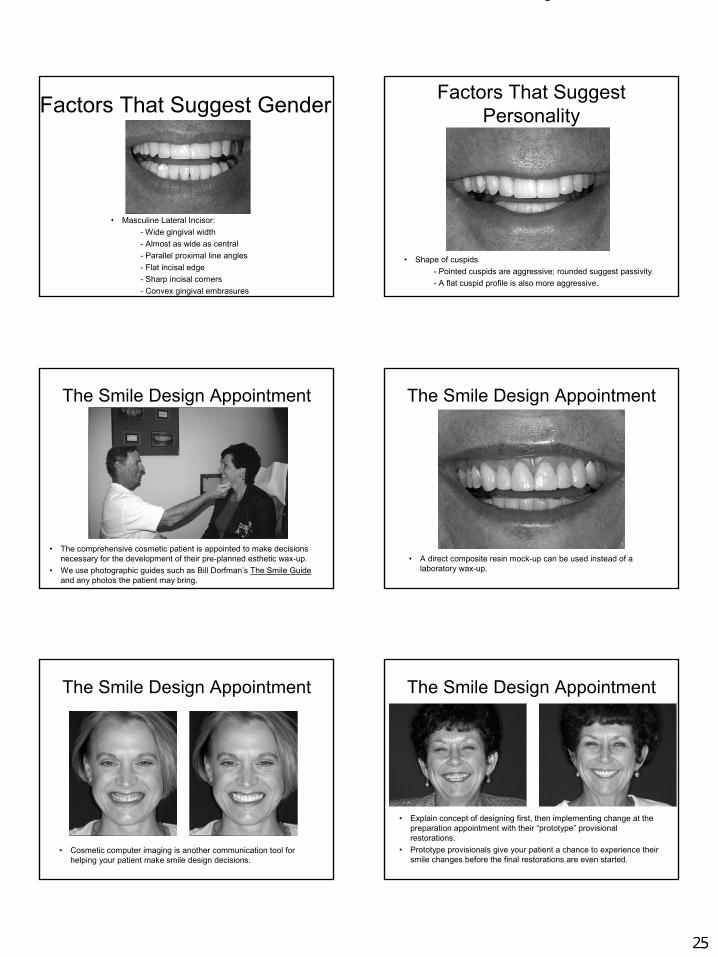
Factors That Suggest Gender
• Masculine Lateral Incisor:- Wide gingival width- Almost as wide as central- Parallel proximal line angles- Flat incisal edge- Sharp incisal corners- Convex gingival embrasures
Factors That Suggest Personality
• Shape of cuspids- Pointed cuspids are aggressive; rounded suggest passivity.- A flat cuspid profile is also more aggressive.
The Smile Design Appointment
• The comprehensive cosmetic patient is appointed to make decisions necessary for the development of their pre-planned esthetic wax-up.
• We use photographic guides such as Bill Dorfman’s The Smile Guideand any photos the patient may bring.
The Smile Design Appointment
• A direct composite resin mock-up can be used instead of a laboratory wax-up.
The Smile Design Appointment
• Cosmetic computer imaging is another communication tool for helping your patient make smile design decisions.
The Smile Design Appointment
• Explain concept of designing first, then implementing change at the preparation appointment with their “prototype” provisional restorations.
• Prototype provisionals give your patient a chance to experience their smile changes before the final restorations are even started.
Operatory 3
25
Thirteen procedures to insure an ideal restoration‐Dawson
1. Do a thorough examination.
2. Visualize your end result.
3. Outline the treatment in the proper sequence.
4. Make sure the tissues are healthy before beginning final restorative procedures.
5. Prepare the teeth meticulously.
6. Magnify your vision.
7. Verify the accuracy of your impression.
8. Verify the accuracy of your dies.
9. Verify bite records, both in the mouth and on the models.
10. Fabricate good temporaries.
11. Provide the technician with all the information he or she needs to make a masterpiece.
12. Verify the accuracy of lab procedures.
13. Check the accuracy of the restorations before placing them in the mouth.
Billy Malone
26
ESTHETIC WAX-UP CHECK LIST
Mike Malone, DDS, FAGD 300 Doucet Rd. Lafayette, LA 70503 Patient _________________________________ Date _________________________________________ Due date ________________________________________
Tooth Numbers Type of Restoration
1. Central incisor size. Length ____mm. Width____ mm.
2. Move the midline____ align ______mm Right ______mm Left
3. Free gingival line. ___Maintain position. ___Modify position ____mm apically.
4. Incisor shape or Smile Guide___________________.
5. Horizontal plane. ____Change to coincide with desktop (mounted models).
____Leave as is.
____Other modifications______________________________.
6.Occlusal plane. ____Develop ideal plane with plane analyzer.
____Leave as is.
7. Vertical dimension. _ __Position at the level of centric occlusion.
__ __Open vertical ____mm __ anteriorly, or ___posteriorly.
8. Buccal corridor. _ _ __Change to idealize. ____Leave as is.
9. Photos included: ___Face ___1:2 Smile ___1:2 Retracted ___Imaged
10.Other:_______________________________________________________________
Billy Malone
27

Mike Malone, D.D.S. & Associates
Prototype Approval Formyp pp
Patient Name: ____________________________________________ Date: ________________________
Approval of Prototype RestorationsI have had the opportunity to view the final shape of the prototype restorations. With the exception of the requested modifications noted below, if any, I approve the restoration giving the lab permission to proceed with the fabrication of the final restorations. Any changes in the porcelain material after the final restorations are completed will require an additional fee for remaking the restorations.
Patient Signature:____________________________Guardian (if under 18)_______________________
Additional Requested ModificationsAdditional requested modifications, if any, are noted as follows: _______________________________
___________________________________________________________________________________
___________________________________________________________________________________
300 Doucet Rd.● Lafayette ● Louisiana ● 70503 ● 337-989-1268 ● www.mikemalonedds.com
Billy Malone
28
Mike Malone, D.D.S. & Associates
Trial Approval Formpp
Patient Name: ____________________________________________ Date: ________________________
Approval of Trial VeneerI have had the opportunity to view the color and shape of the trial porcelain restoration under different lighting conditions, including natural sunlight. With the exception of the requested modifications noted below, if any, I approve the restoration giving the lab permission to proceed with the fabrication of the final restorations. Any changes in color or porcelain material after the final restorations are completed will require an additional fee for remaking the restorations.will require an additional fee for remaking the restorations.
Patient Signature:____________________________Guardian (if under 18)_______________________
Additional Requested ModificationsAdditional requested modifications, if any, are noted as follows: _______________________________
___________________________________________________________________________________
___________________________________________________________________________________
300 Doucet Rd.● Lafayette ● Louisiana ● 70503 ● 337-989-1268 ● www.mikemalonedds.com
Billy Malone
29
Mike Malone, D.D.S. & Associates
Patient Approval Form
Patient Name: ____________________________________________ Date: ________________________
Approval For Placement
I have had the opportunity to view the color and shape of the porcelain restorations under different
lighting conditions, including natural sunlight. With the exception of the requested modifications noted
below, if any, I approve the restorations to be bonded in place. I understand that certain bite
adjustments will likely need to be made after bonding in the teeth, but that other changes (e.g., relating
to the color and the shape) after the bonding process would likely require cutting off the restorations,
which may result in further reduction in tooth structure and an additional full fee under our then current
fee structure.
Patient Signature:____________________________Guardian (if under 18)_______________________
300 Doucet Rd.● Lafayette ● Louisiana ● 70503 ● 337-989-1268 ● www.mikemalonedds.com
Additional Requested Modifications
Additional requested modifications, if any, are noted as follows: _______________________________
___________________________________________________________________________________
___________________________________________________________________________________
Mike
30
Billy Malone
31

Smile Design & Advanced Cosmetic Provisional Fabrication
Mike Malone, DDS, FAGD
Crown Form Fabrication
• Paint mock-up model with Liquid Foil Separator and blow dry
• Place Copyplast material in MiniStar Machine
• Turn on heating element and wait until light turns green
• Place model of mock-up in lead beads approximately 3 mm from gingival line
• Pull heating element down over Copyplast material and heat for 60 seconds
• Pull heating element up, quickly place softened Copyplast onto model and engage
lever. Let cool for 60 seconds
• Remove Copyplast from model and trim with scissors, leaving 2-3 mm.beyond
gingival margin
• Place trimmed Copyplast back onto model and place into beads, leaving only
teeth exposed (leave tissue stops for full arch cases)
• Remove blue film from 2.5 mm Splint Biocryl and place on MiniStar machine
• Turn on heating element, wait until light turns green
• Pull heating element over Biocryl and heat for 75 seconds
• Pull up heating element and quickly place softened Biocryl onto model with
Copyplast, engage lever and cool down for 120 seconds
• Remove Copyplast from inside Biocryl
• Trim Biocryl with the Almore Soft Line Trimmer and an acrylic bur to the
gingival margin
Operatory 3
Operatory 3
32
Operatory 3

Smile Design & Advanced Cosmetic Provisional Fabrication
Mike Malone, DDS, FAGD
Triad Advanced Provisionals
• Take bonding hydrocolloid/alginate impression of prepared teeth.
• Pour up impression with Snap Stone. Allow to set for five minutes.
• Remove the model from the alginate.
• Clean up and try crown form on model. Draw red pencil line at crown form margin.
• Paint two coats of Rubber Sep onto preps, drying each layer (should look like die spacer).
• Coat entire model with thin layer of Liquid Foil Separator and dry.
• Place Triad enamel, light, and medium into crown form for desired result.
• Place loaded crown form in Zip-Lock bag and place in hot water bath at 175 degrees for two
minutes.
• Place loaded crown form (with Biocryl reinforcement) onto prep model. Press all the way to red
line.
• Secure with rubber band and cure in Triad oven for four minutes.
• Separate provisionals between cuspids and first bicuspids on both sides with diamond disk (for
full arch provisionals).
• Gently remove provisional from model, being careful not to break the provisional. (You must
trim excess from lingual of veneers before removal)
• Cure in Triad oven for 2-4 minutes after painting inside of temps with glycerin (air barrier).
• Trim excess material close to margins on the facial and lingual using preferred acrylic burs.
• Trim and remove excess interproximal from the gingival embrasures using modified green wheel.
• Refine margins using favorite burs.
• Remove internal flash and any existing bubbles.
• Place back on model and repair any deficient margins.
• Transfer to the patient adjusting any other undercuts as necessary.
• Refine facial and incisal embrasures using the Vision Flex 140.
• Polish with medium pumice and Shurshine on the lathe or paint with Palaseal and light cure.
• Polish interproximals and embrasures with a Robinson wheel and Shurshine.
Operatory 3
33
Operatory 3

Smile Design & Advanced Cosmetic Provisional Fabrication
Mike Malone, DDS, FAGD
Radica Advanced Provisionals
• Take bonding hydrocolloid/alginate impression of prepared teeth.
• Pour up impression with Snap Stone. Allow to set for five minutes.
• Remove the model from the alginate.
• Clean up and try crown form on model. Draw red pencil line at crown form margin.
• Paint two coats of Rubber Sep onto preps, drying each layer (should look like die spacer).
• Coat entire model with thin layer of Liquid Foil Separator and dry.
• Place Radica incisal into crown form and shape for mamelon effect with wax pencil.
• Place Radica body shade into crown form and quickly place into prep model. Press all the way
to the red line and hold until cool.
• Place in Enterra curing unit and cure for recommended time.
• Repair any voids or discrepancies with Radica body placed with wax pencil and cure.
• Separate provisionals between cuspids and first bicuspids on both sides with diamond disk (for
full arch provisionals).
• Gently remove provisional from model, being careful not to break the provisional. (You must
trim excess from lingual of veneers before removal)
• Cure in Enterra oven for 2-4 minutes after painting inside of temps with glycerin (air barrier).
• Trim excess material close to margins on the facial and lingual using preferred acrylic burs.
• Trim and remove excess interproximal from the gingival embrasures using modified green wheel.
• Refine margins using favorite burs.
• Remove internal flash and any existing bubbles.
• Place back on model and repair any deficient margins.
• Transfer to the patient adjusting any other undercuts as necessary.
• Refine facial and incisal embrasures using the Vision Flex 140.
• Paint all exterior surfaces with Radica Sealer and cure at the sealer setting.
• Cement with appropriate temporary cement.
Operatory 3
34
LA Academy of Continuing Dental Education in cooperation with
LSU School of Dentistry
Cosmetic Dentistry Continuum – Level I
BONDING SEQUENCE By Dr. Jimmy Eubank
1.) Clean tooth – Remove prototype cement and sandblast while protecting the tissue and
adjacent teeth. Rinse and remove all grit. 2.) Apply superoxyol with microbrush to stop tissue seepage and clean tooth, leave 10 to 15
seconds – then rinse. 3.) Etch – 37% Phosphoric – scrub with microbrush for 10 to 15 seconds 4.) Rinse and dry – Verify proper etch pattern. 5.) Apply Liner Bond 2V (A & B Primer) – (add Activator if bonding to composite build-up)
scrub with microbrush for 20 seconds then let set for 20 seconds. 6.) Gently air dry until nothing wiggles – this will leave isolated surface areas that are not
glossy. 7.) Apply Photo Bond plus Activator to tooth and blow off excess (no pooling) - establishes
a uniform glossy surface (mix catalyst and activator first). 8.) Light cure 10 – 40 seconds depending upon light source. 9.) Apply Photo Bond mixture to sandblasted, etched restoration and blow off excess. 10.) Place restoration with the appropriate resin cement, verify seat and light cure.
Billy Malone
35
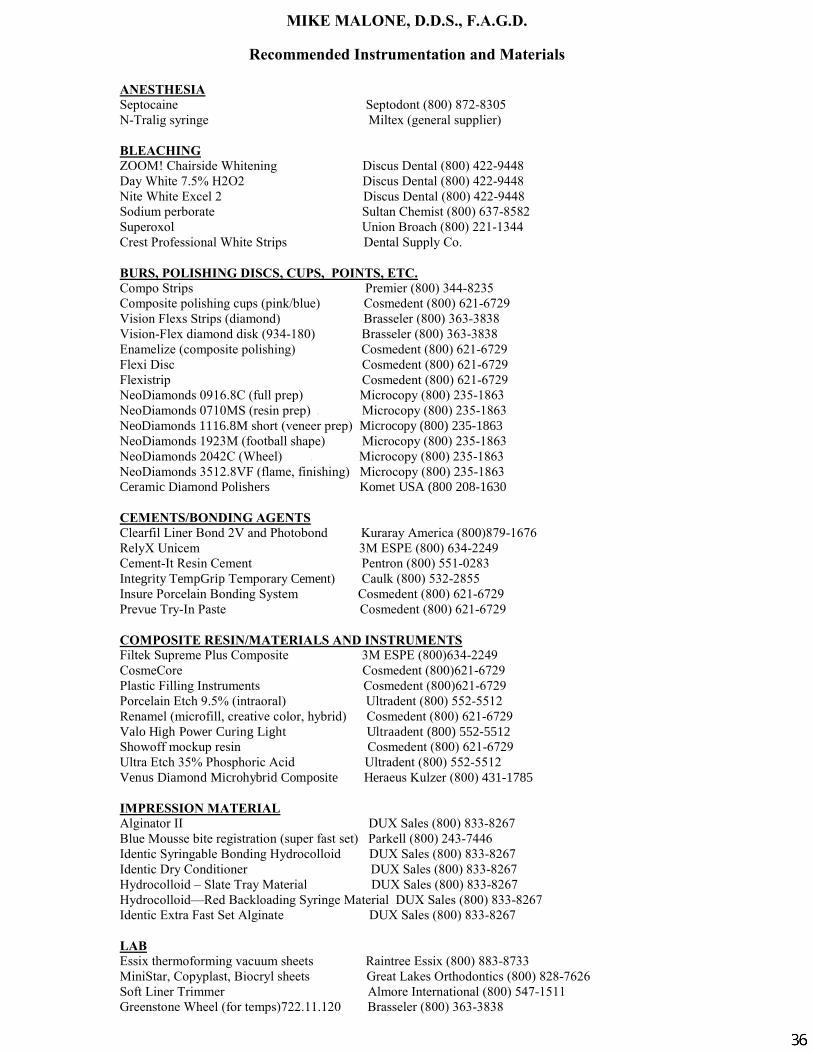
MIKE MALONE, D.D.S., F.A.G.D.
Recommended Instrumentation and Materials
ANESTHESIA
Septocaine Septodont (800) 872-8305
N-Tralig syringe Miltex (general supplier)
BLEACHING
ZOOM! Chairside Whitening Discus Dental (800) 422-9448
Day White 7.5% H2O2 Discus Dental (800) 422-9448
Nite White Excel 2 Discus Dental (800) 422-9448
Sodium perborate Sultan Chemist (800) 637-8582
Superoxol Union Broach (800) 221-1344
Crest Professional White Strips Dental Supply Co.
BURS, POLISHING DISCS, CUPS, POINTS, ETC. Compo Strips Premier (800) 344-8235
Composite polishing cups (pink/blue) Cosmedent (800) 621-6729
Vision Flexs Strips (diamond) Brasseler (800) 363-3838
Vision-Flex diamond disk (934-180) Brasseler (800) 363-3838
Enamelize (composite polishing) Cosmedent (800) 621-6729
Flexi Disc Cosmedent (800) 621-6729
Flexistrip Cosmedent (800) 621-6729
NeoDiamonds 0916.8C (full prep) Microcopy (800) 235-1863
NeoDiamonds 0710MS (resin prep) O Microcopy (800) 235-1863
NeoDiamonds 1116.8M short (veneer prep) Microcopy (800) 235-1863 NeoDiamonds 1923M (football shape) Microcopy (800) 235-1863 NeoDiamonds 2042C (Wheel) O O Microcopy (800) 235-1863
NeoDiamonds 3512.8VF (flame, finishing) Microcopy (800) 235-1863
Ceramic Diamond Polishers Komet USA (800 208-1630
CEMENTS/BONDING AGENTS Clearfil Liner Bond 2V and Photobond Kuraray America (800)879-1676
RelyX Unicem 3M ESPE (800) 634-2249
Cement-It Resin Cement Pentron (800) 551-0283
Integrity TempGrip Temporary Cement) Caulk (800) 532-2855 Insure Porcelain Bonding System Cosmedent (800) 621-6729
Prevue Try-In Paste Cosmedent (800) 621-6729
COMPOSITE RESIN/MATERIALS AND INSTRUMENTS Filtek Supreme Plus Composite 3M ESPE (800)634-2249
CosmeCore Cosmedent (800)621-6729
Plastic Filling Instruments Cosmedent (800)621-6729
Porcelain Etch 9.5% (intraoral) Ultradent (800) 552-5512
Renamel (microfill, creative color, hybrid) Cosmedent (800) 621-6729
Valo High Power Curing Light Ultraadent (800) 552-5512 Showoff mockup resin Cosmedent (800) 621-6729
Ultra Etch 35% Phosphoric Acid Ultradent (800) 552-5512
Venus Diamond Microhybrid Composite Heraeus Kulzer (800) 431-1785
IMPRESSION MATERIAL Alginator II DUX Sales (800) 833-8267
Blue Mousse bite registration (super fast set) Parkell (800) 243-7446
Identic Syringable Bonding Hydrocolloid DUX Sales (800) 833-8267
Identic Dry Conditioner DUX Sales (800) 833-8267
Hydrocolloid – Slate Tray Material DUX Sales (800) 833-8267
Hydrocolloid—Red Backloading Syringe Material DUX Sales (800) 833-8267
Identic Extra Fast Set Alginate DUX Sales (800) 833-8267
LAB
Essix thermoforming vacuum sheets Raintree Essix (800) 883-8733
MiniStar, Copyplast, Biocryl sheets Great Lakes Orthodontics (800) 828-7626
Soft Liner Trimmer Almore International (800) 547-1511
Greenstone Wheel (for temps)722.11.120 Brasseler (800) 363-3838
Mike
36
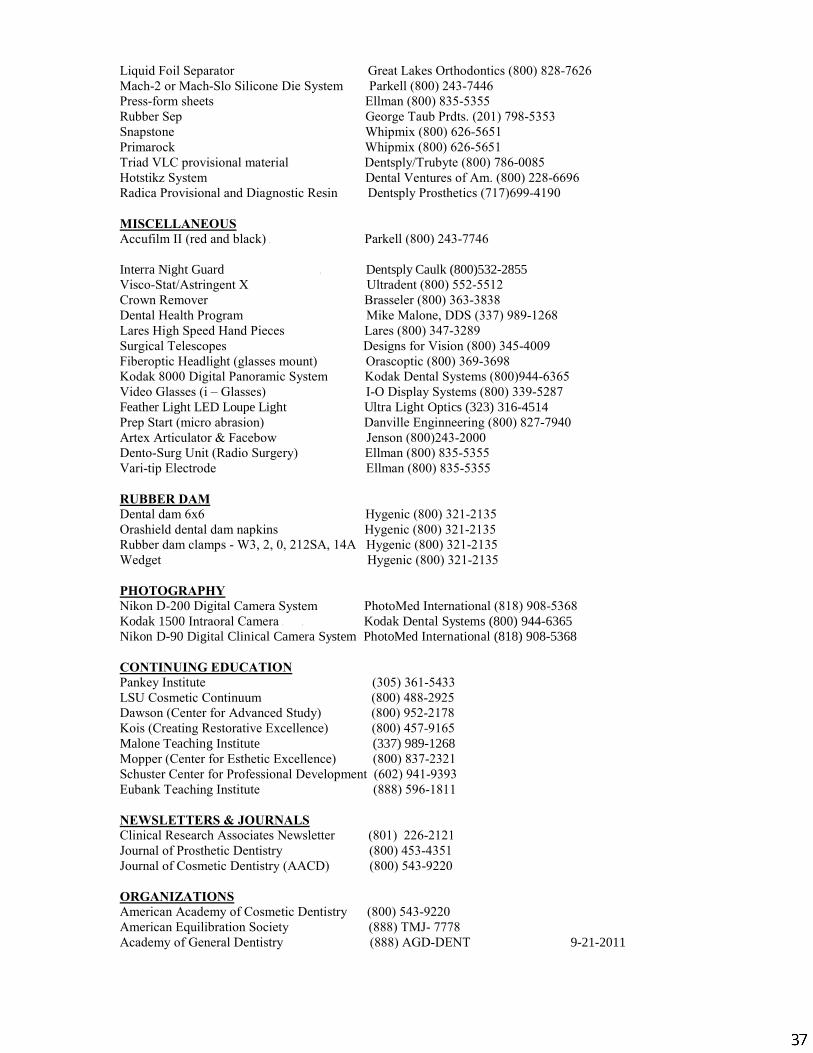
Liquid Foil Separator Great Lakes Orthodontics (800) 828-7626
Mach-2 or Mach-Slo Silicone Die System Parkell (800) 243-7446
Press-form sheets Ellman (800) 835-5355
Rubber Sep George Taub Prdts. (201) 798-5353
Snapstone Whipmix (800) 626-5651
Primarock Whipmix (800) 626-5651
Triad VLC provisional material Dentsply/Trubyte (800) 786-0085
Hotstikz System Dental Ventures of Am. (800) 228-6696
Radica Provisional and Diagnostic Resin Dentsply Prosthetics (717)699-4190
MISCELLANEOUS Accufilm II (red and black) O Parkell (800) 243-7746
Interra Night Guard O Dentsply Caulk (800)532-2855 Visco-Stat/Astringent X Ultradent (800) 552-5512
Crown Remover Brasseler (800) 363-3838
Dental Health Program Mike Malone, DDS (337) 989-1268
Lares High Speed Hand Pieces Lares (800) 347-3289
Surgical Telescopes Designs for Vision (800) 345-4009
Fiberoptic Headlight (glasses mount) Orascoptic (800) 369-3698
Kodak 8000 Digital Panoramic System Kodak Dental Systems (800)944-6365
Video Glasses (i – Glasses) I-O Display Systems (800) 339-5287
Feather Light LED Loupe Light Ultra Light Optics (323) 316-4514 Prep Start (micro abrasion) Danville Enginneering (800) 827-7940
Artex Articulator & Facebow Jenson (800)243-2000
Dento-Surg Unit (Radio Surgery) Ellman (800) 835-5355
Vari-tip Electrode Ellman (800) 835-5355
RUBBER DAM Dental dam 6x6 Hygenic (800) 321-2135
Orashield dental dam napkins Hygenic (800) 321-2135
Rubber dam clamps - W3, 2, 0, 212SA, 14A Hygenic (800) 321-2135
Wedget Hygenic (800) 321-2135
PHOTOGRAPHY Nikon D-200 Digital Camera System PhotoMed International (818) 908-5368
Kodak 1500 Intraoral Camera O O Kodak Dental Systems (800) 944-6365 Nikon D-90 Digital Clinical Camera System PhotoMed International (818) 908-5368
CONTINUING EDUCATION
Pankey Institute (305) 361-5433
LSU Cosmetic Continuum (800) 488-2925
Dawson (Center for Advanced Study) (800) 952-2178
Kois (Creating Restorative Excellence) (800) 457-9165
Malone Teaching Institute (337) 989-1268 Mopper (Center for Esthetic Excellence) (800) 837-2321
Schuster Center for Professional Development (602) 941-9393
Eubank Teaching Institute (888) 596-1811
NEWSLETTERS & JOURNALS
Clinical Research Associates Newsletter (801) 226-2121
Journal of Prosthetic Dentistry (800) 453-4351
Journal of Cosmetic Dentistry (AACD) (800) 543-9220
ORGANIZATIONS
American Academy of Cosmetic Dentistry (800) 543-9220
American Equilibration Society (888) TMJ- 7778
Academy of General Dentistry (888) AGD-DENT 9-21-2011
Mike
37
Mike
Mike
Name: ____________________________________________________________________________
Member Number: ___________________________________________________________________
Address: ___________________________________________________________________________
__________________________________________________________________________________
City: __________________________________ State:____________ Zip:___________________
Phone: _______________________________ Fax: _____________________________________
E-mail: ____________________________________________________________________________
❏ Check Enclosed ❏ MasterCard ❏ Visa ❏ American Express
Credit Card # ______________________________________________________________________
Card Security Code #__________________ Exp. Date _______________________
Signature __________________________________________________________________________MM '05
American Academy of Cosmetic Dentistry®
5401 World Dairy Drive • Madison, WI 53718608.222.8583 • 800.543.9220 • Fax 608.222.9540 • www.aacd.com
AACD CREDENTIALING GUIDESChoose one of the following 3 options:
Special Offer!Purchase the AACD's A Guide to Accreditation Criteria today and receive a complimentary copy of A Guide to Accreditation Photography Cost: $30.00 ea. (USD) for AACD Members $60.00 ea. (USD) for Non-Members
Quantity Ordered: _______ Total $__________________
A Guide to Accreditation PhotographyDesigned and produced specifically to give you guidance relating to photographic requirements for an AACD Accreditation exam presentation. Cost: $15.00 ea. (USD) for AACD Members $25.00 ea. (USD) for Non-Members
Quantity Ordered: _______ Total $__________________
A Guide to Accreditation CriteriaA valuable resource for anyone interested in a better understanding of the components of fine smile design and improved ability to self-critique their clinical casework. Cost: $30.00 ea. (USD) for AACD Members $60.00 ea. (USD) for Non-Members
Quantity Ordered: _______ Total $__________________
International shipping charges will be calculated at time of shipping. All orders will ship the fastest and most cost effective way, unless requested otherwise on this order form.
Please allow 2 weeks for processing and shipping within the United States.
Operatory 3
38
Related Documents











