Microvascular decompression of cranial nerves David B. MacDonald Nothing to declare

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Microvascular decompression of cranial nervesDavid B. MacDonald
Nothing to declare

Objectives
• Summarize the indications
• Describe the procedure
• Apply established monitoring techniques
• Consider investigational methods

Indications for microvascular decompression
• Medically intractable paroxysmal cranial nerve disorders attributable to compression by an aberrant blood vessel loop
• Mainly hemifacial spasm or trigeminal neuralgia
• Rarely glossopharyngeal neuralgia, paroxysmal vertigo or tinnitus
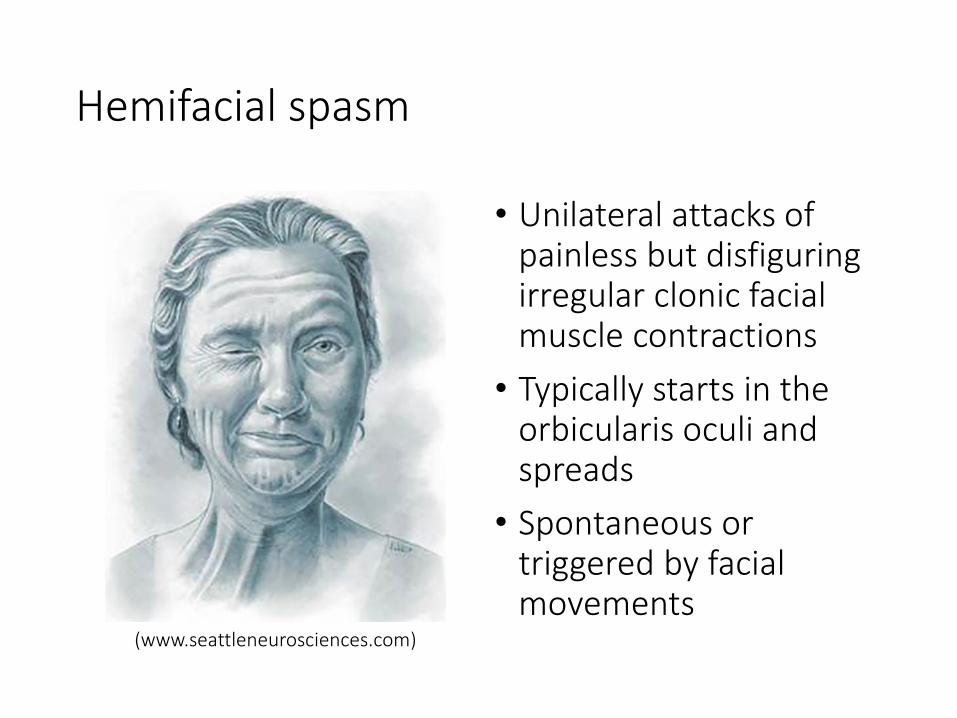
Hemifacial spasm
(www.seattleneurosciences.com)
• Unilateral attacks of painless but disfiguring irregular clonic facial muscle contractions
• Typically starts in the orbicularis oculi and spreads
• Spontaneous or triggered by facial movements

Trigeminal neuralgia
• Unilateral attacks of severe lancinating facial pain
• Often V2 or V3 distributions
• Spontaneous or triggered by facial touch, chewing, or brushing the teeth
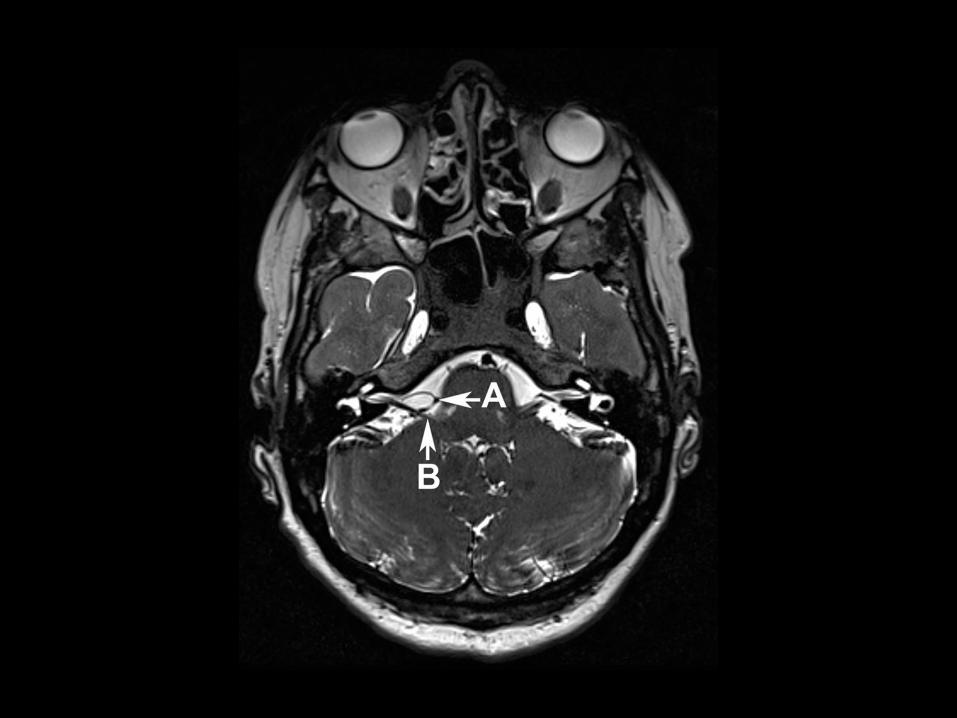
Pathology and pathophysiology
• Usually due to focal nerve compression and demyelination near the root entry zone, but may be caused by central demyelination instead
• Most often attributed to a tortuous artery or vein after excluding aneurysm, tumor, and multiple sclerosis
• Pathophysiologic theories:• Ephaptic transmission between demyelinated axons
• Nuclear hyperexcitability
• Spontaneous ectopic firing of injured axons
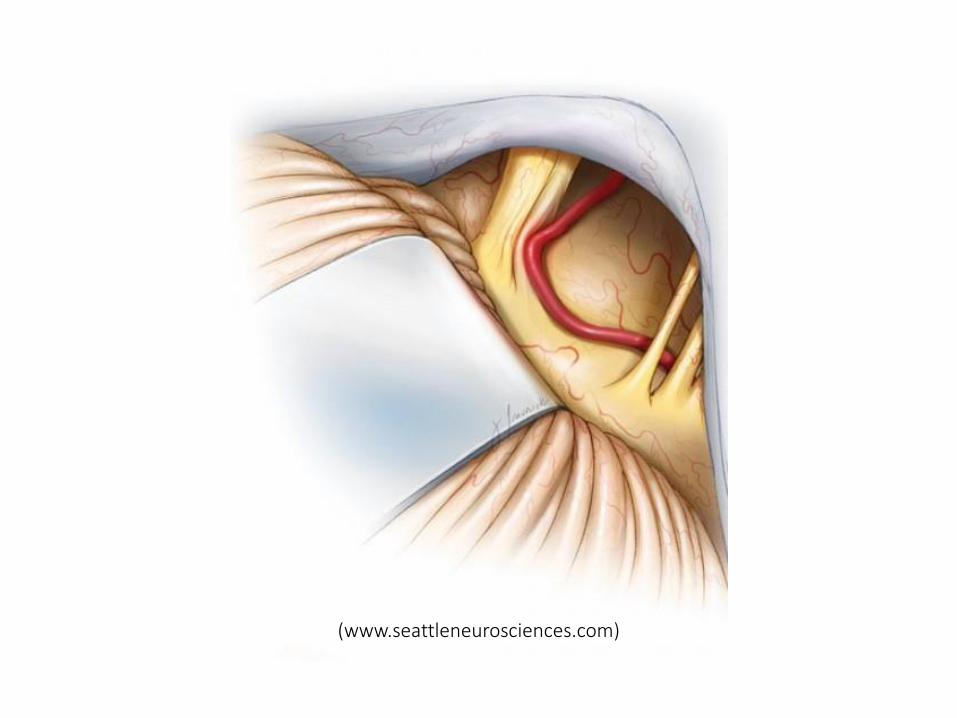
(www.seattleneurosciences.com)

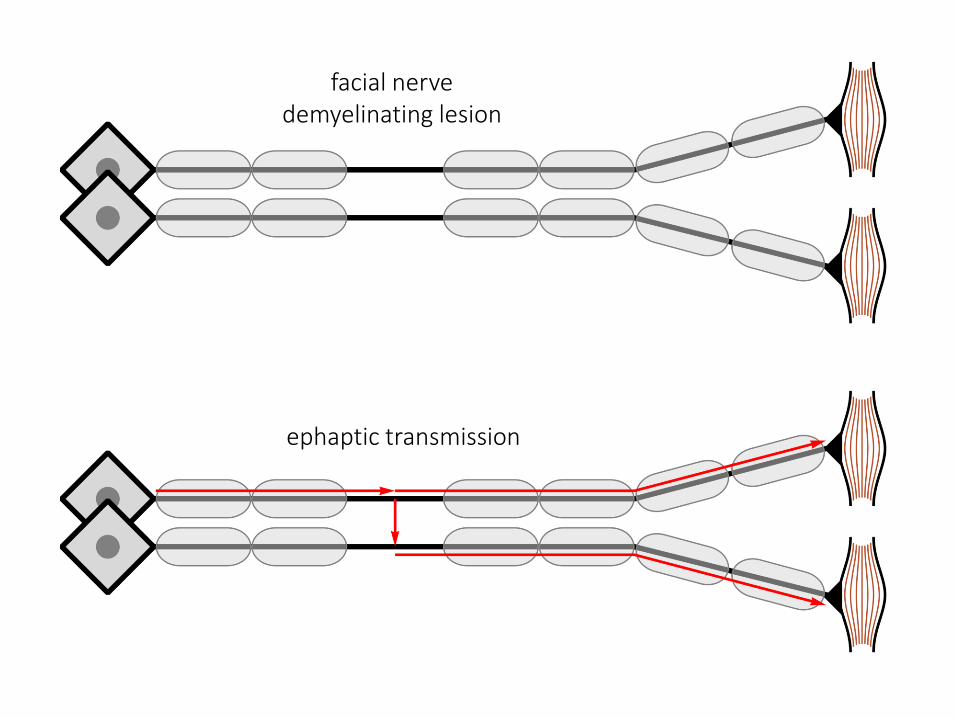
facial nervedemyelinating lesion
ephaptic transmission

ectopic axonal firing
hyperexcitable nucleus
Treatment
• Medical• Carbamazepine, baclofen, gabapentin
• Botulinum toxin injections
• Can be sufficient
• Surgery if intractable

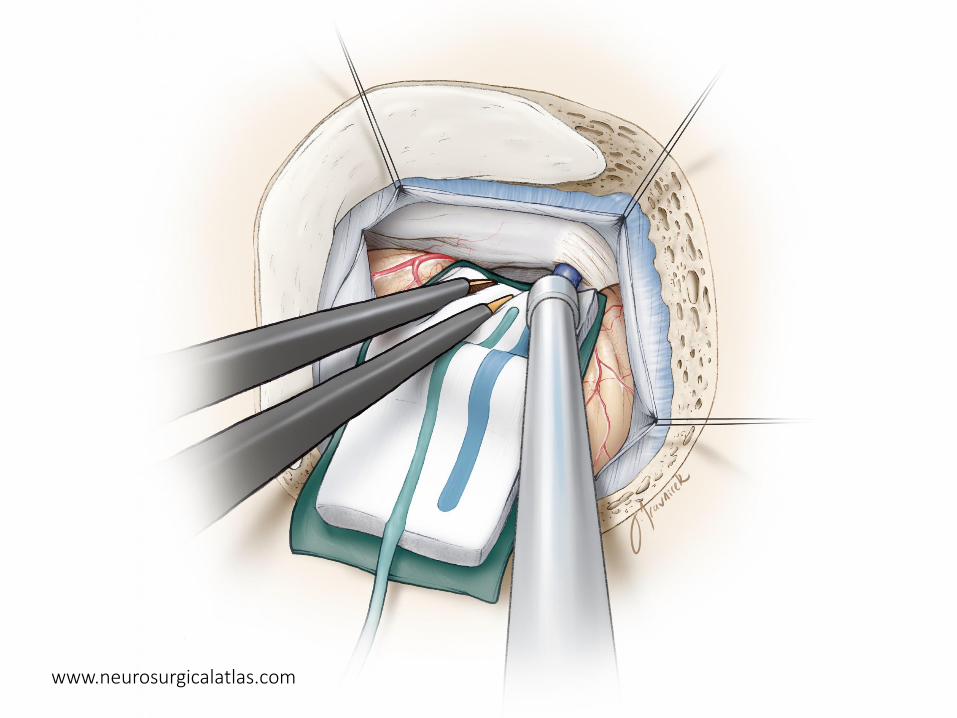
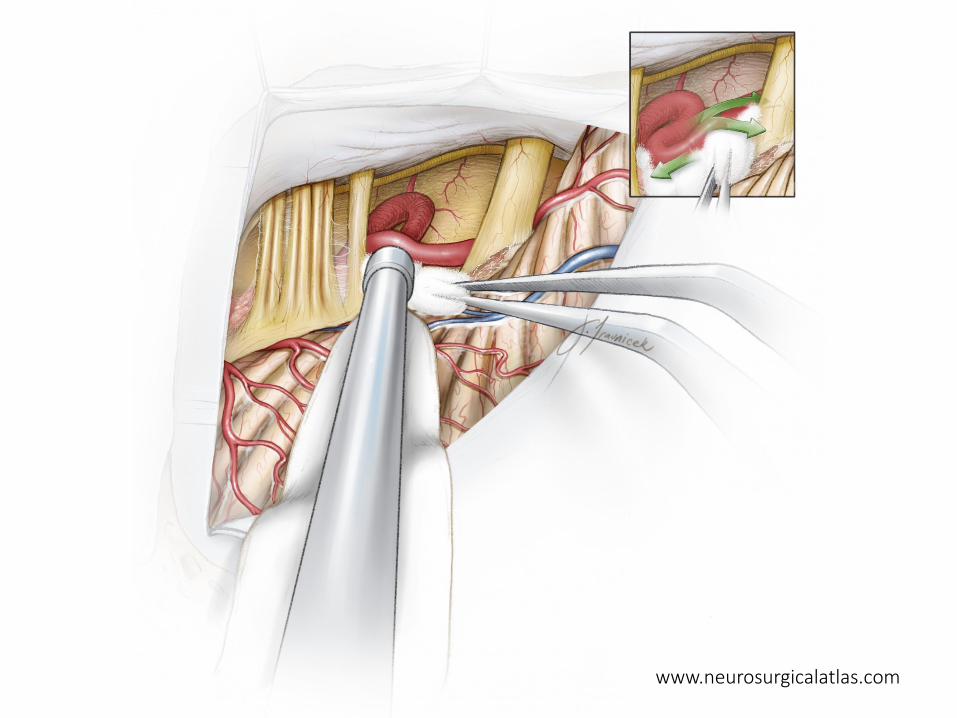
Microvascular decompression
• “Jannetta procedure”
• Retromastoid craniectomy
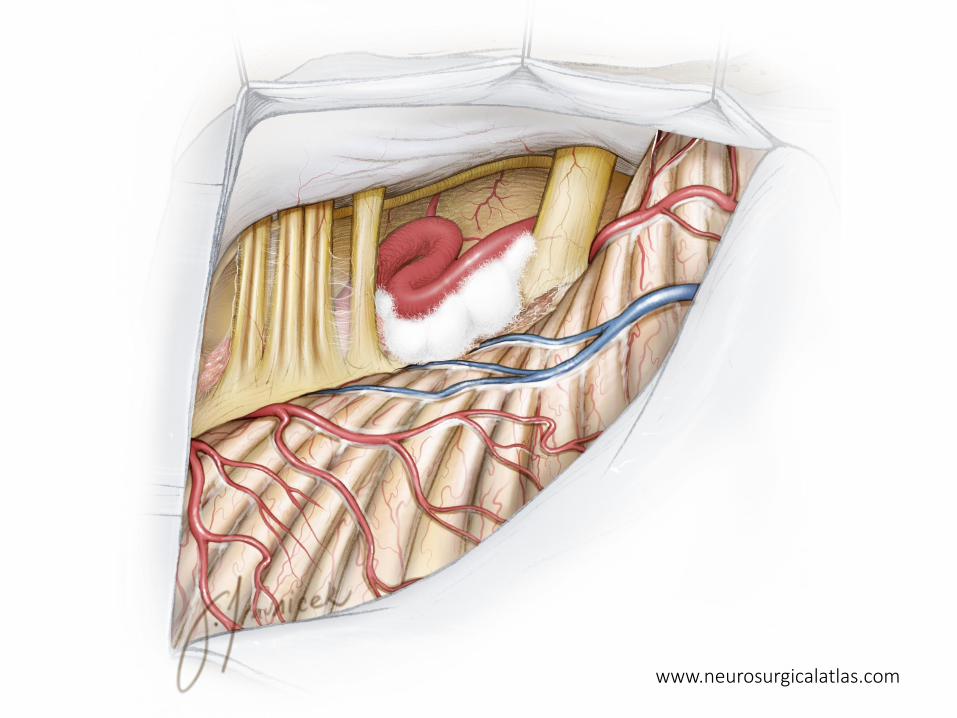
• Microsurgical dissection to expose the nerve and identify the offending vessel
• Mobilize the vessel and insert Teflon pads between it and the nerve
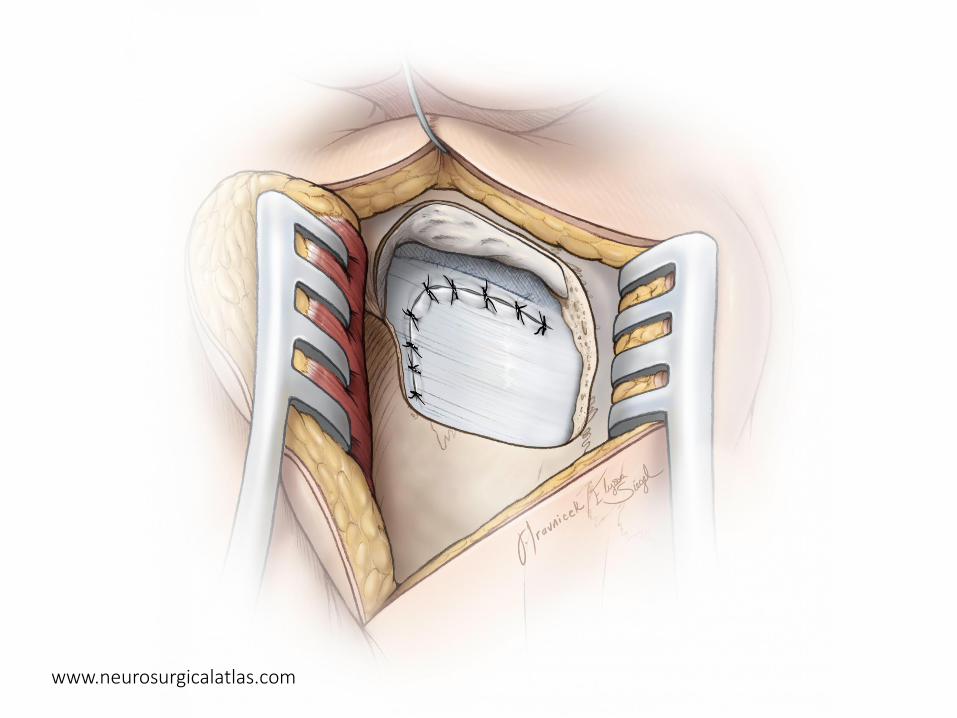
• Hemostasis and closure

www.neurosurgicalatlas.com
www.neurosurgicalatlas.com

www.neurosurgicalatlas.com

www.neurosurgicalatlas.com

www.neurosurgicalatlas.com

www.neurosurgicalatlas.com

www.neurosurgicalatlas.com
www.neurosurgicalatlas.com
www.neurosurgicalatlas.com
www.neurosurgicalatlas.com

Success rates
• Hemifacial spasm: 70–97% long-term cure. Some early residual spasms resolve.
• Trigeminal neuralgia: 70% long-term cure. Some early successes relapse.
trigeminal neuralgia
(Barker, et. al, NEJM 1996;334:1078–83)

Neurological complications
• Cranial nerve injury• Facial numbness
• Facial paralysis
• Hearing loss
• Extraocular muscle palsy
• Rare• Brainstem or cerebral infarction
• Death

Intraoperative monitoring
• Cranial nerve protection• Brainstem auditory evoked potentials (BAEPs)
• May reduce hearing loss from 8–20% to <2%
• Free-running and triggered EMG• Corticobulbar MEPs• Possibly blink reflexes, trigeminal SEPs
• Optimize facial nerve decompression• Lateral spread response (LSR)• Investigational methods
• Facial MEPs• Other techniques
Lateral spread response (LSR)
• Developed by Møller and Jannetta
• Stimulate one facial nerve branch• Normal direct muscle response
• Abnormal muscle response from another branch
• Ephaptic transmission or nuclear hyperexcitability
• Usually present before and absent after surgery
• Can acutely disappear during surgery• May identify the offending blood vessel(s)
• May signify successful decompression
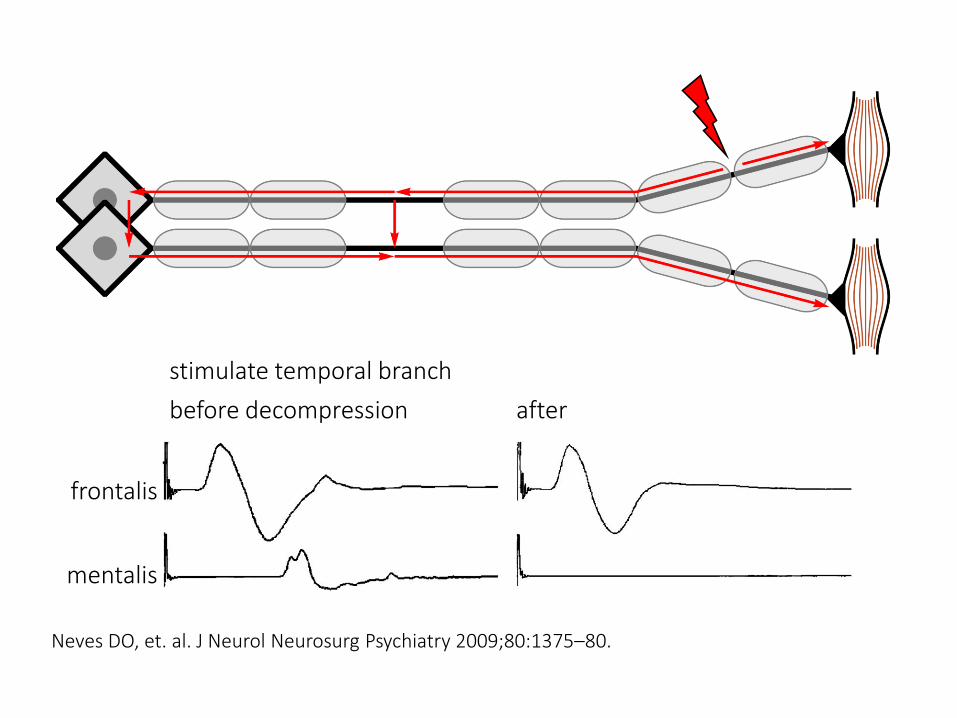
frontalis
mentalis
stimulate temporal branch
before decompression after
Neves DO, et. al. J Neurol Neurosurg Psychiatry 2009;80:1375–80.
Møller A. In: Nuwer M, ed. Intraoperative Monitoring of Neural Function 2008, pp. 547–55.
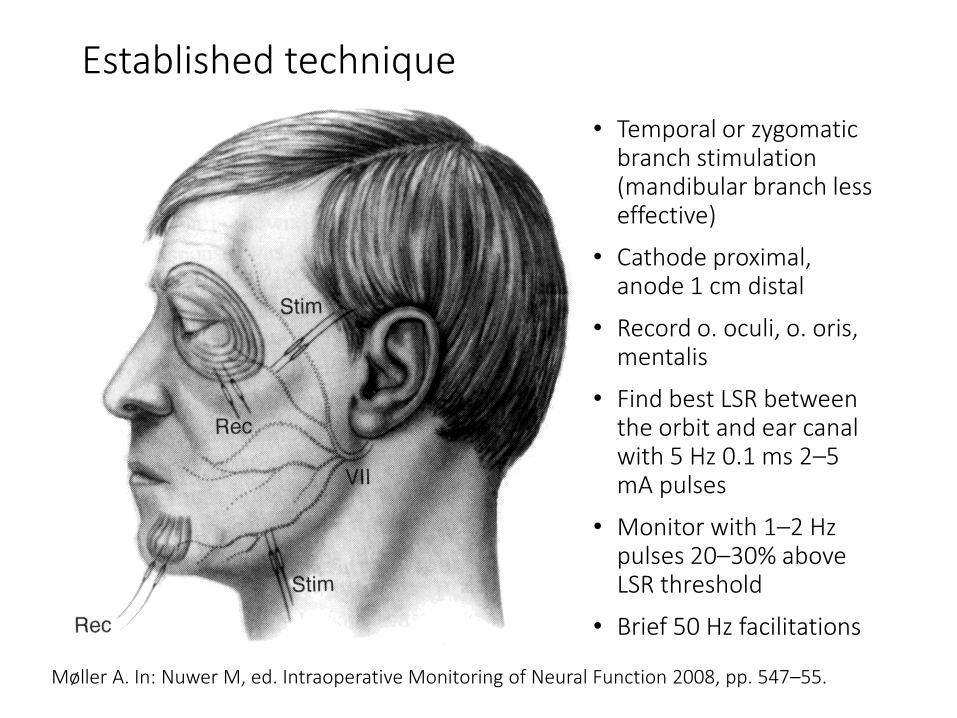
Established technique
• Temporal or zygomatic branch stimulation (mandibular branch less effective)
• Cathode proximal, anode 1 cm distal
• Record o. oculi, o. oris, mentalis
• Find best LSR between the orbit and ear canal with 5 Hz 0.1 ms 2–5 mA pulses
• Monitor with 1–2 Hz pulses 20–30% above LSR threshold
• Brief 50 Hz facilitations
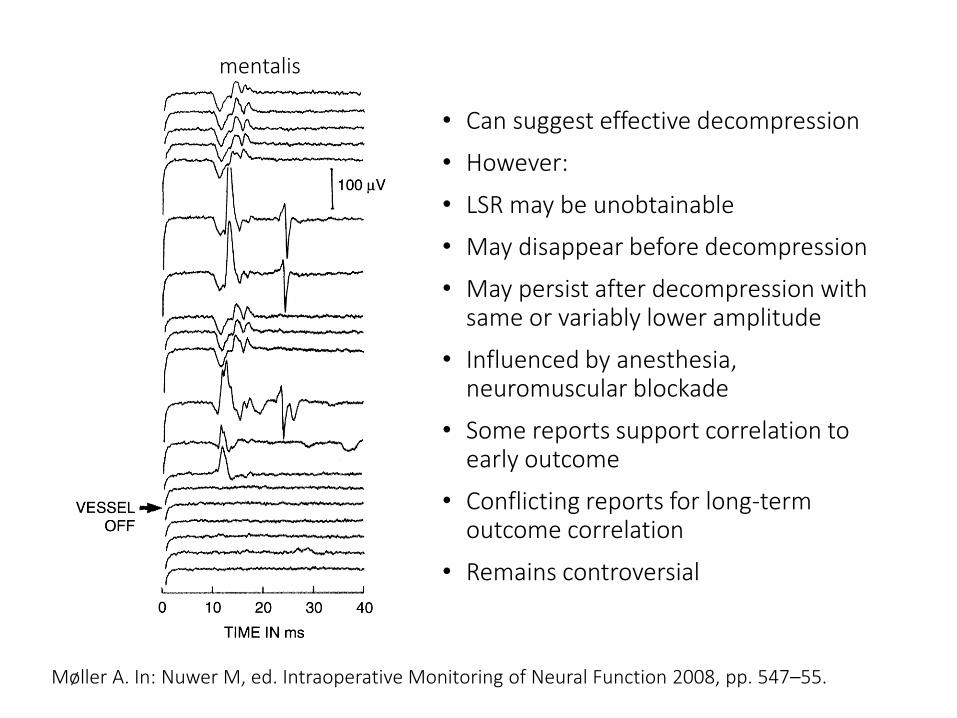
mentalis
Møller A. In: Nuwer M, ed. Intraoperative Monitoring of Neural Function 2008, pp. 547–55.
• Can suggest effective decompression
• However:
• LSR may be unobtainable
• May disappear before decompression
• May persist after decompression with same or variably lower amplitude
• Influenced by anesthesia, neuromuscular blockade
• Some reports support correlation to early outcome
• Conflicting reports for long-term outcome correlation
• Remains controversial

Possible improvement
• Preoperative facial nerve mapping to find best LSR (usually the temporal branch)
• Cathode distal, anode proximal at mandibular fossa (‘centrifugal’)
• 0.3 ms 5–25 mA pulses
• Record frontalis, o. oculi, o. oris, mentalis
• Initial report suggests greater success and outcome correlation
Lee S, et al. Clin Neurophysiol 2018;129:1490–5
Facial MEPs
• Presumably due to facial nucleus hyperexcitability:• Lower MEP threshold than the non-spasm side
• Single-pulse MEPs can occur
• Possibly signifying adequate decompression:• Threshold elevation?
• Amplitude reduction?
• Single-pulse MEP disappearance?
• Needs further study
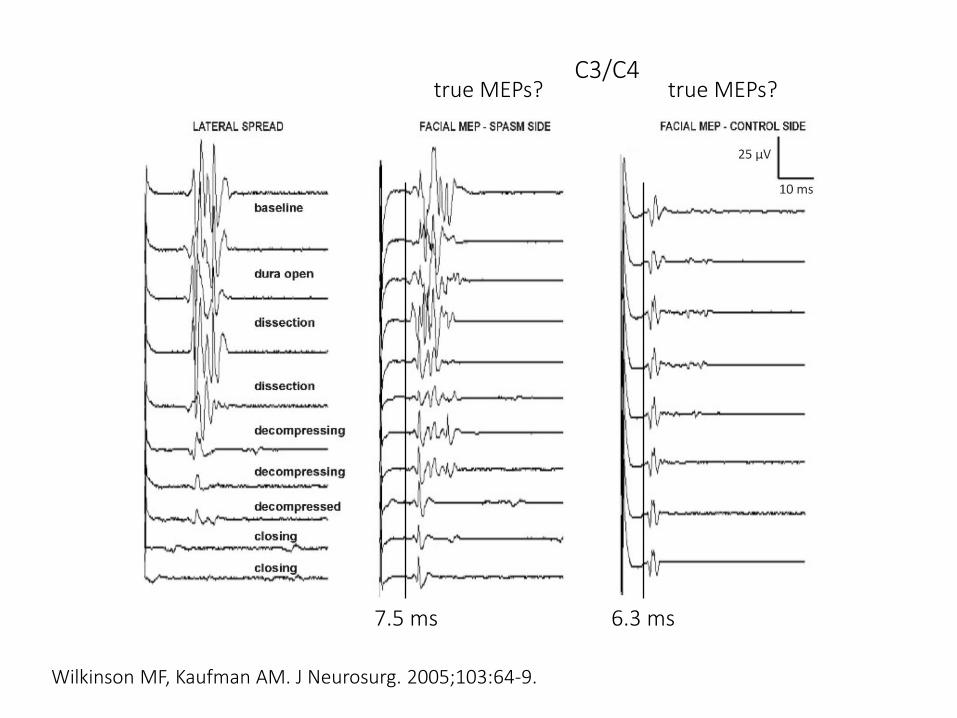
Wilkinson MF, Kaufman AM. J Neurosurg. 2005;103:64-9.
true MEPs? true MEPs?
7.5 ms 6.3 ms
C3/C4
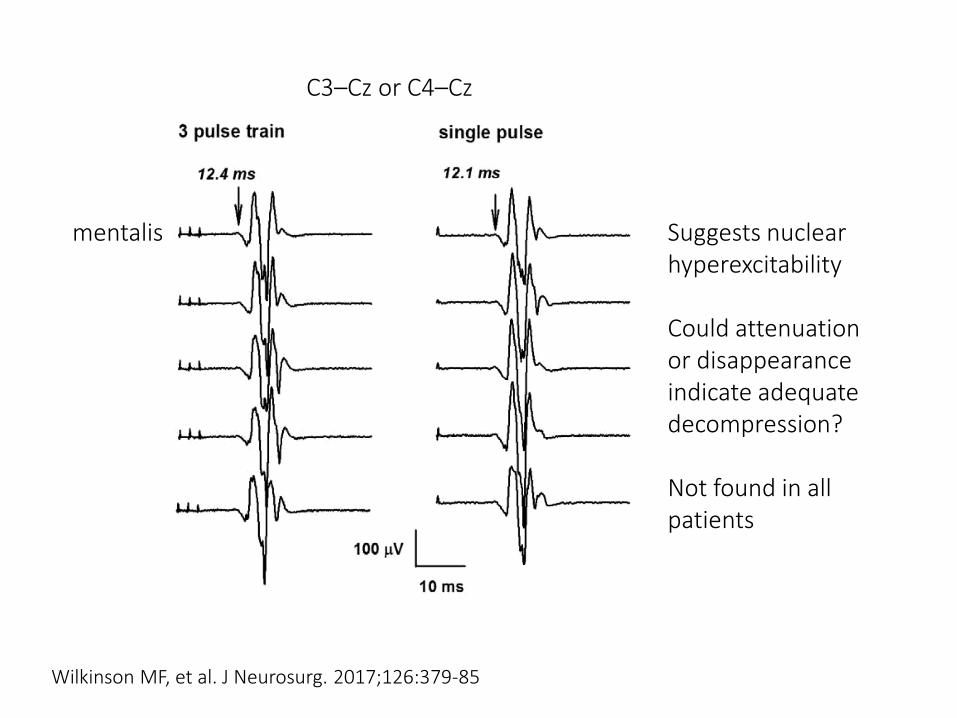
Wilkinson MF, et al. J Neurosurg. 2017;126:379-85
mentalis
C3–Cz or C4–Cz
Suggests nuclear hyperexcitability
Could attenuation or disappearance indicate adequate decompression?
Not found in all patients

before decompression after
Fukuda M, et al. J Neurol Neurosurg Psychiatry 2009;81:519–23
true decrease?
C3–Cz or C4–Cz

Other investigational techniques
• Blink reflex• Pulse trains can elicit blink reflexes under anesthesia
• Could be exaggerated with hemifacial spam
• Might attenuate or disappear with decompression
• Blink reflex synkinesis• Abnormal lower facial muscle response
• Might attenuate or disappear with decompression
• Facial F-waves• Could be exaggerated with hemifacial spasm
• Might attenuate or disappear with decompression
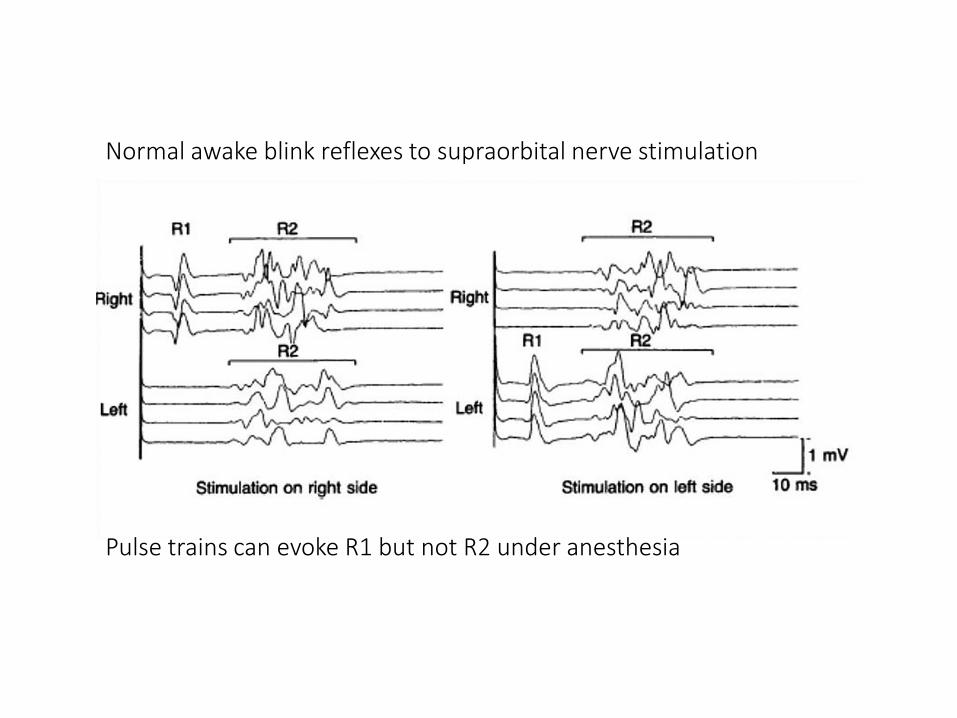
Normal awake blink reflexes to supraorbital nerve stimulation
Pulse trains can evoke R1 but not R2 under anesthesia

Blink reflex synkinesis with hemifacial spasm
Kim P, Fukushima T. J. Neurosurg 1984;60:821–7
R1 R2
During surgery:
Would pulse trains evoke R1 synkinesis in o. oris or mentalis muscles?
If so, might synkinesis disappearance signify decompression?
Before surgery
o. oculi
o. oris
After surgery

Objectives
• Summarize the indications
• Describe the procedure
• Apply established monitoring techniques
• Consider investigational methods
Related Documents











