MHFA Sally Trembath Manager, Mental Health & Safer Community Programs Health Wellbeing & Development

MHFA Sally Trembath Manager, Mental Health & Safer Community Programs Health Wellbeing & Development.
Dec 18, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

MHFA
Sally TrembathManager, Mental Health & Safer Community Programs
Health Wellbeing & Development

Aims of introducing Mental Health First Aid (MHFA) at Monash
Reducing stigma associated with mental health
Increasing mental health literacy and confidence in order to reduce anxiety when dealing with mental health issues
Promoting pro-active and early intervention strategies
Building capacity to respond in crisis situations
Promoting culture of care and safer community

Summary of Feedback Overall themes
Change in attitude
Reducing stigma
Building capacity
Change in behaviour
Early interventions
Improved communication
Improved workplace outcomes

Tracking these aims …Survey Monkey demographics
Composition of staffn = 145
Numbers
Academic Staff 19
Professional Staff 79
Student 19
Monash Residential Services
39
Campusn = 146
Numbers
Berwick 8
Caulfield 26
Clayton 83
Gippsland 16
Peninsula 12
Malaysia 1
South Africa 0

Changing attitudeSince completing MHFA, do you believe you are:
n = 141
Response percent
Response count
More able to recognise mental health problems
34.8% 49
More confident in offering help 39.7% 56
More inclined to actively engage with those effected by mental illness
25.5% 36
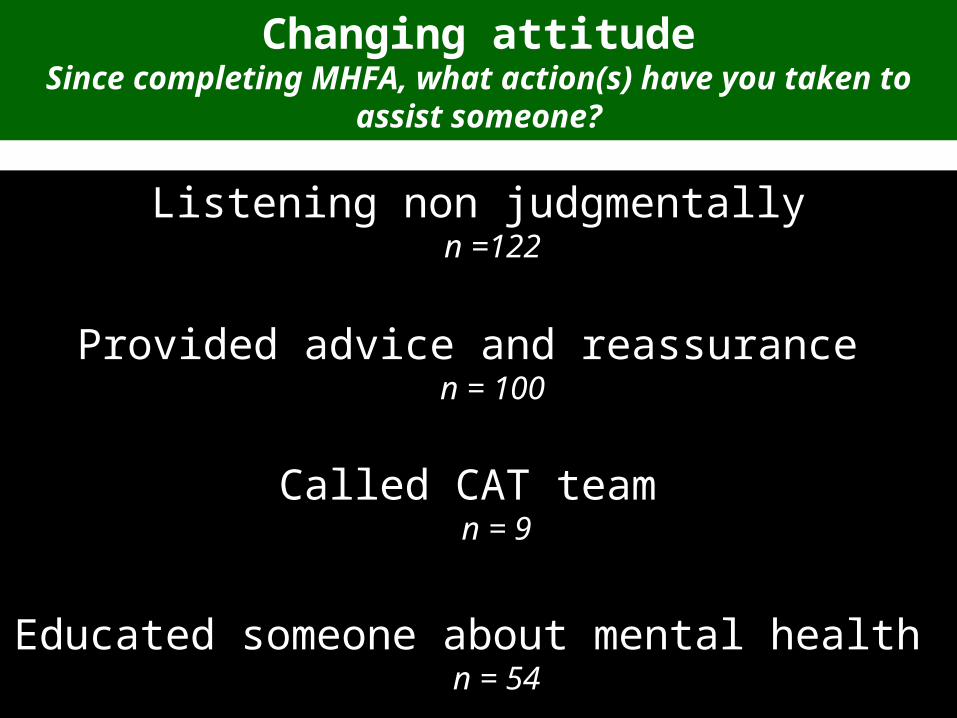
Changing attitudeSince completing MHFA, what action(s) have you taken to
assist someone?
Listening non judgmentallyn =122
Provided advice and reassurance n = 100
Called CAT team n = 9
Educated someone about mental health n = 54

• Avoid engaging in mental debate with those having a mental health illness.
• Increased awareness has helped boost my confidence and tips about how to communicate and respond have helped.
• Very positive experience, will be useful in my role as a First Aid/Safety Officer and in my life outside of work.
• I have changed my approach to people since the workshop. I am much more understanding of those with depression and anxiety.
• Has given me practical advice for dealing with people who suffer from mental illness.
Feedback from respondents Reducing stigma & building capacity

Change in behaviourQ: Since completing MHFA, have you done anything differently to help
others?
0
10
20
30
40
50
60
Assisting others post MHFA training (n = 119)
Family (n=45)
Colleague (n=39)
Student (n=61)
Friend (n=59)

0
10
20
30
40
50
60
70
80
90
Specific interventions post MHFAtraining (n = 110)
Panic/Anxiety attack(n=40)
Suicidal thoughts/threats (n=25)
Psychotic episode(n=7)
Depression (n=94)
Threats to inflict selfinjury (n=10)
Change in behaviour Q: Since completing MHFA, have you helped someone with:

0
20
40
60
80
100
120
140
Specific interventions post MHFAtraining (n=134)
Listened nonjudgmentally (n=122)
Provided advice andreassurance (n=100)
Referred forprofessional help(n=63)
Called CAT team(n=9)
Consulted auniversity counsellor(n=36)
Educated someoneabout mental health(n=54)
Change in behaviourQ: Since completing MHFA, what action(s) have you taken to assist
someone?

• Helped to have strategies for dealing with panic attacks – I actually helped someone while they were having an attack.
• I had to call a CAT team and I was more confident in dealing with them because of the training.
• I dealt with a student suffering severe depression, including being suicidal and was able to convince them to see a professional.
• A staff member was suffering an anxiety attack and after having attended the workshop I was able to suggest methods of getting them through the anxiety episode.
• As a member of the Halls of Residence, I have found MHFA to be the single most beneficial professional development activity I have ever participated in.
Feedback from respondents Early interventions, Improved communication & workplace outcomes
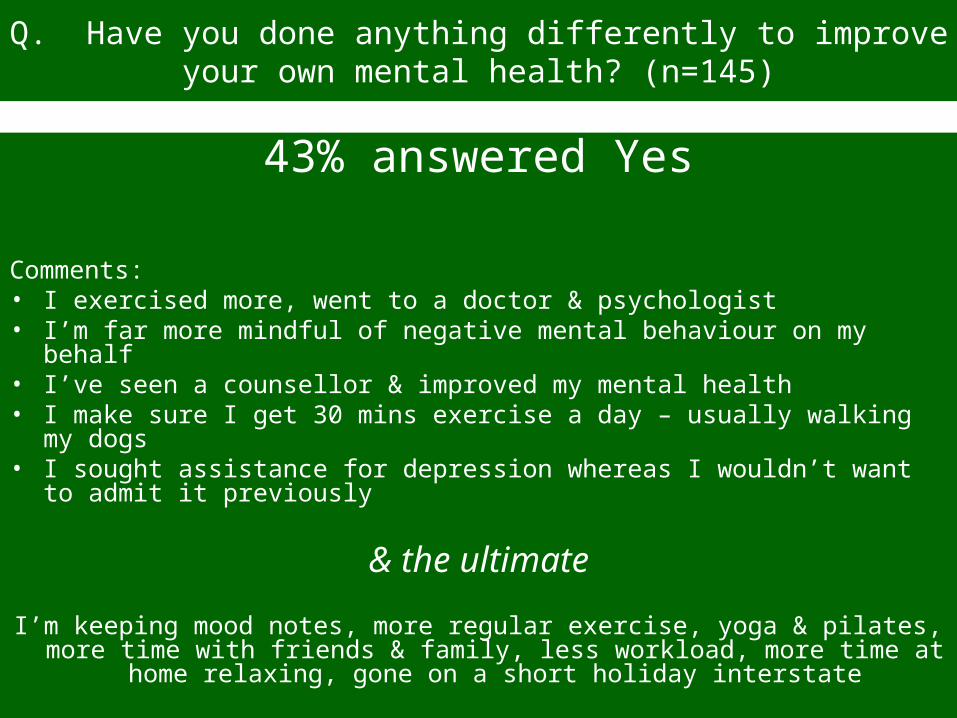
Q. Have you done anything differently to improve your own mental health? (n=145)
43% answered Yes
Comments:• I exercised more, went to a doctor & psychologist• I’m far more mindful of negative mental behaviour on my behalf• I’ve seen a counsellor & improved my mental health• I make sure I get 30 mins exercise a day – usually walking my dogs• I sought assistance for depression whereas I wouldn’t want to admit it
previously
& the ultimate
I’m keeping mood notes, more regular exercise, yoga & pilates, more time with friends & family, less workload, more time at home relaxing, gone on a short
holiday interstate

Reducing staff stress Testimonial
I feel more able to deal with any unexpected mental health problems that I may be
confronted with in my daily working with students. Coming to work in the morning is
less stressful because I know that when there is a problem I will be able to help in a constructive and safe manner. I have recommended to my colleagues that they should attend the course
as well.

General concerns and recommendations…
• MHFA is a fair introduction into mental health but it only scrapes the surface. I worry that it may make the trainees feel overly confident in dealing with people who have mental health issues that are not as mild as those portrayed in the training.
• Very useful and I think all those dealing with students should attend this program. Further, it might be useful to run a refresher program (half day) each year for those who have done it.
• Whilst MHFA is valuable, I have found getting management to understand and acknowledge things is the greatest challenge. … The failure to acknowledge changing situations and symptoms seems to be common and managers being older or more experienced overrides their willingness to listen to the advice of a mental health first aider.
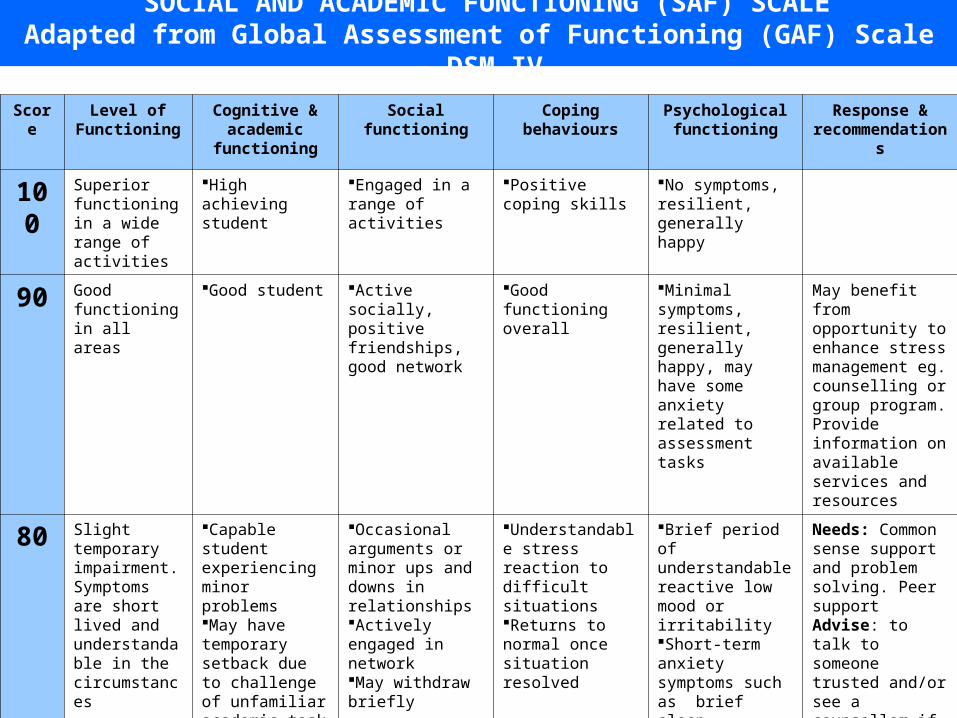
SOCIAL AND ACADEMIC FUNCTIONING (SAF) SCALEAdapted from Global Assessment of Functioning (GAF) Scale – DSM IV
Score Level of Functioning
Cognitive & academic
functioning
Socialfunctioning
Copingbehaviours
Psychologicalfunctioning
Response & recommendation
s
100 Superior functioning in a wide range of activities
High achieving student
Engaged in a range of activities
Positive coping skills
No symptoms, resilient, generally happy
90 Good functioning in all areas
Good student Active socially, positive friendships, good network
Good functioning overall
Minimal symptoms, resilient, generally happy, may have some anxiety related to assessment tasks
May benefit from opportunity to enhance stress management eg. counselling or group program.Provide information on available services and resources
80 Slight temporary impairment.Symptoms are short lived and understandable in the circumstances
Capable student experiencing minor problemsMay have temporary setback due to challenge of unfamiliar academic task
Occasional arguments or minor ups and downs in relationshipsActively engaged in networkMay withdraw briefly
Understandable stress reaction to difficult situationsReturns to normal once situation resolved
Brief period of understandable reactive low mood or irritabilityShort-term anxiety symptoms such as brief sleep disturbance
Needs: Common sense support and problem solving. Peer supportAdvise: to talk to someone trusted and/or see a counsellor if no improvement after 2 weeks
SOCIAL AND ACADEMIC FUNCTIONING (SAF) SCALEAdapted from Global Assessment of Functioning (GAF) Scale – DSM IV
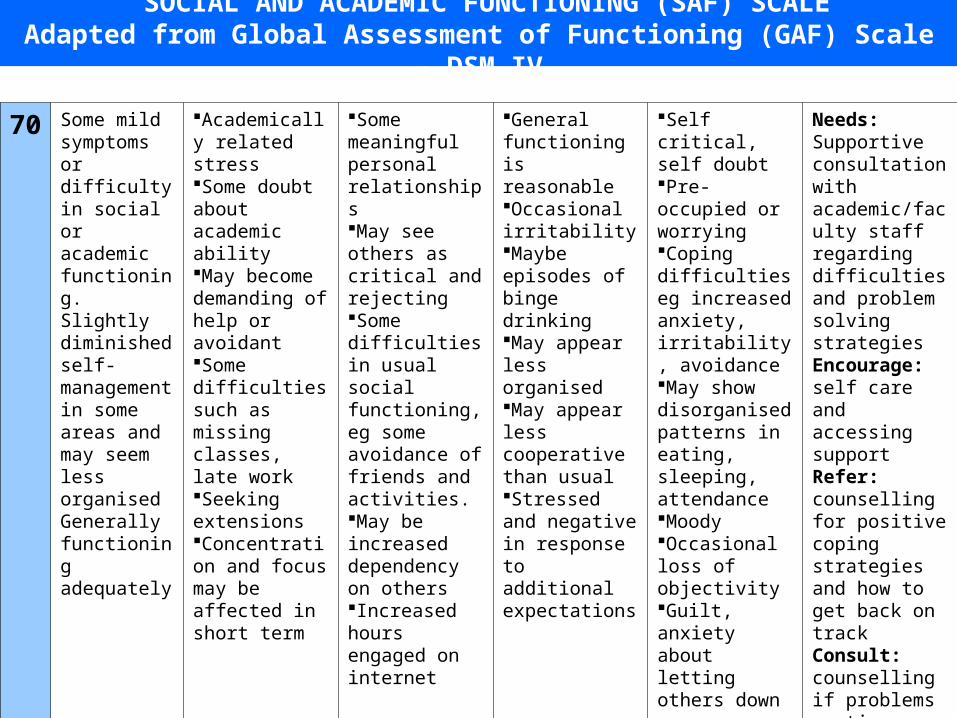
70 Some mild symptoms or difficulty in social or academic functioning.Slightly diminished self-management in some areas and may seem less organisedGenerally functioning adequately
Academically related stressSome doubt about academic abilityMay become demanding of help or avoidant Some difficulties such as missing classes, late workSeeking extensionsConcentration and focus may be affected in short term
Some meaningful personal relationshipsMay see others as critical and rejectingSome difficulties in usual social functioning, eg some avoidance of friends and activities.May be increased dependency on othersIncreased hours engaged on internet
General functioning is reasonableOccasional irritabilityMaybe episodes of binge drinkingMay appear less organisedMay appear less cooperative than usualStressed and negative in response to additional expectations
Self critical, self doubtPre-occupied or worryingCoping difficulties eg increased anxiety, irritability, avoidanceMay show disorganised patterns in eating, sleeping, attendanceMoodyOccasional loss of objectivityGuilt, anxiety about letting others down
Needs: Supportive consultation with academic/faculty staff regarding difficulties and problem solving strategiesEncourage: self care and accessing supportRefer: counselling for positive coping strategies and how to get back on trackConsult: counselling if problems continue
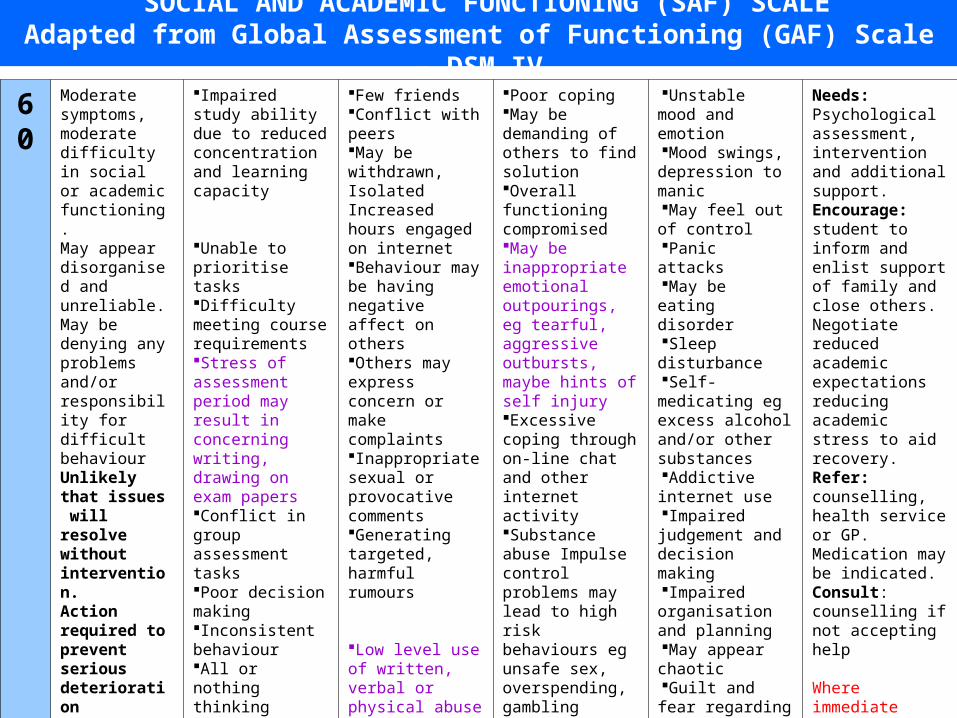
SOCIAL AND ACADEMIC FUNCTIONING (SAF) SCALEAdapted from Global Assessment of Functioning (GAF) Scale – DSM IV
60 Moderate symptoms, moderate difficulty in social or academic functioning.May appear disorganised and unreliable.May be denying any problems and/or responsibility for difficult behaviourUnlikely that issues will resolve without intervention. Action required to prevent serious deterioration
Impaired study ability due to reduced concentration and learning capacity
Unable to prioritise tasksDifficulty meeting course requirementsStress of assessment period may result in concerning writing, drawing on exam papersConflict in group assessment tasksPoor decision making Inconsistent behaviourAll or nothing thinkingRuminating/circular worrying
Few friendsConflict with peersMay be withdrawn,IsolatedIncreased hours engaged on internetBehaviour may be having negative affect on othersOthers may express concern or make complaintsInappropriate sexual or provocative commentsGenerating targeted, harmful rumours
Low level use of written, verbal or physical abuse eg pushing, shoving
Concerning unwelcome relationship seeking
Poor copingMay be demanding of others to find solution Overall functioning compromisedMay be inappropriate emotional outpourings, eg tearful, aggressive outbursts, maybe hints of self injuryExcessive coping through on-line chat and other internet activitySubstance abuse Impulse control problems may lead to high risk behaviours eg unsafe sex, overspending, gamblingIntentional theftDamage to propertyThreatening communications (non-violent)Sleeping on campusPornography use contravening Monash IT policy and/or affecting othersPersistent complaining
Unstable mood and emotionMood swings,
depression to manicMay feel out of
controlPanic attacksMay be eating
disorder Sleep disturbanceSelf-medicating eg
excess alcohol and/or other substancesAddictive internet
useImpaired judgement
and decision makingImpaired
organisation and planningMay appear chaoticGuilt and fear
regarding poor performance, letting others downThought sof
escaping situation, possibly of suicideNon suicidal self
injury
Needs: Psychological assessment, intervention and additional support. Encourage: student to inform and enlist support of family and close others.Negotiate reduced academic expectations reducing academic stress to aid recovery.Refer: counselling, health service or GP. Medication may be indicated. Consult: counselling if not accepting help
Where immediate threat call security ext 333
Where risk of harm to others consult community care on 9905 1599.A safety plan may be recommended

SOCIAL AND ACADEMIC FUNCTIONING (SAF) SCALEAdapted from Global Assessment of Functioning (GAF) Scale – DSM IV
50Serious impairment in a number of areas of functioning.May be avoiding reality of situation.May have high investment in staying a student and gaining degree.despite reduced capacityIssues will not resolve without intervention. Action required to prevent further serious deterioration
Unable to focus on academic tasks eg in tutorialsMissed classes and deadlinesConfused, ineffective decision making and communicationConcerning written, drawn material on exam papers
No friendship groupUnresolved conflicts interfere with daily functioningOthers may express concern or make complaintsPoor self- care in decisions regarding social group and activitiesUnresponsive to efforts to supportMight be very demanding of others Isolated and withdrawnOverly dependent on friendsRepeated episodes of physical aggression Physical attackStalking behaviourThreats of violence and/or suicideUnwanted attention: physical, written, verbal
Serious strugglingIf faced with seriousness of situation may become very demanding of solution or threaten self injuryLikelihood of alcohol or other substance abuse, self-medicatingnon suicidal self injuryCompromised self-carePossibly eating disorderCompulsive behaviour eg hand washing,cleaning, use of pornographyObscene exposure
Thoughts of suicide and may have plan and meansSuicide attemptFeeling hopelessIneffective problem solvingVulnerable and withdrawnExtreme emotional pain eg possibly severe eating problemsSevere depressionImpaired self controlExcessive hours sleepingUnable to sleepShame and guilt regarding perceived failure and letting others downFeelings may be masked by addictive behaviours such as excessive internet use, alcohol, drugs
Needs : Assessment and treatment with psychiatrist, possible specialist forensic assessment. Reduced stressors so reduction or removal of academic expectations while recovering.Recommend: University Community Care-line and counselling services to be involved in developing a coordinated intervention to facilitate assessment and care of the person and safety of community.A behaviour contract may be recommended including informing parents should an emergency occur.If not accepting recommendations Statute 6.3 exclusion on health grounds may be indicated Inform: parentsAction: consult community care-line or community care drop-in on your campus for advice.Where immediate threat call security ext 333
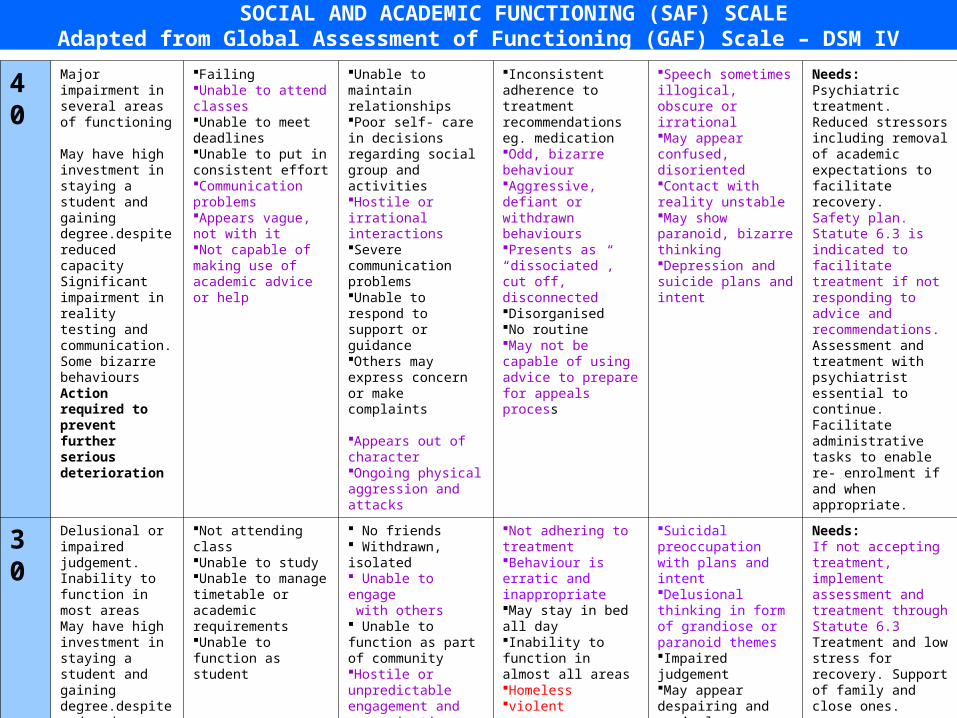
SOCIAL AND ACADEMIC FUNCTIONING (SAF) SCALEAdapted from Global Assessment of Functioning (GAF) Scale – DSM IV
40 Major impairment in several areas of functioning May have high investment in staying a student and gaining degree.despite reduced capacitySignificant impairment in reality testing and communication.Some bizarre behavioursAction required to prevent further serious deterioration
FailingUnable to attend classesUnable to meet deadlinesUnable to put in consistent effortCommunication problemsAppears vague, not with itNot capable of making use of academic advice or help
Unable to maintain relationshipsPoor self- care in decisions regarding social group and activitiesHostile or irrational interactionsSevere communication problemsUnable to respond to support or guidanceOthers may express concern or make complaints Appears out of characterOngoing physical aggression and attacks
Inconsistent adherence to treatment recommendations eg. medicationOdd, bizarre behaviourAggressive, defiant or withdrawn behavioursPresents as “dissociated”, cut off, disconnectedDisorganisedNo routineMay not be capable of using advice to prepare for appeals process
Speech sometimes illogical, obscure or irrationalMay appear confused, disorientedContact with reality unstableMay show paranoid, bizarre thinking Depression and suicide plans and intent
Needs: Psychiatric treatment. Reduced stressors including removal of academic expectations to facilitate recovery. Safety plan.Statute 6.3 is indicated to facilitate treatment if not responding to advice and recommendations. Assessment and treatment with psychiatrist essential to continue.Facilitate administrative tasks to enable re- enrolment if and when appropriate.
30 Delusional or impaired judgement.Inability to function in most areasMay have high investment in staying a student and gaining degree.despite reduced capacityAction required to prevent further serious deterioration
Not attending classUnable to studyUnable to manage timetable or academic requirementsUnable to function as student
No friends Withdrawn, isolated Unable to engage with others Unable to function as part of communityHostile or unpredictable engagement and communicationsOngoing physical aggression and attacks
Not adhering to treatmentBehaviour is erratic and inappropriateMay stay in bed all dayInability to function in almost all areasHomelessviolent
Suicidal preoccupation with plans and intentDelusional thinking in form of grandiose or paranoid themes Impaired judgementMay appear despairing and cynical
Needs: If not accepting treatment, implement assessment and treatment through Statute 6.3Treatment and low stress for recovery. Support of family and close ones. Facilitate administrative tasks to enable re- enrolment if and when appropriate.Where immediate threat call security ext 333

SOCIAL AND ACADEMIC FUNCTIONING (SAF) SCALEAdapted from Global Assessment of Functioning (GAF) Scale – DSM IV
20 Danger of hurting self or others.Gross impairment in communication and interaction
Not attending classUnable to function as student
Friends and peers alienated, unable to understand the person, may feel afraidUnable to function as part of communityDisorganised lack of boundaries
Not adhering to treatmentLargely incoherentNeglects basic self care, eg poor hygiene, poor diet
Psychotic thinking: delusions and hallucinationsChaoticSuicide attempts
Needs: Hospitalisation for assessment and treatment. Low stress for recovery.Support of family and close ones.Facilitate administrative tasks to enable re- enrolment if and when appropriate.
Where immediate threat call security ext 333
10 Persistent danger of severely hurting self or others Persistent inability to maintain hygiene. Serious suicidal act with clear expectation of death
Unable to function as a student
UnsafeDanger to self or othersUnable to function independently
Behaviour is unsafeNot adhering to treatment Suicidal or violentUnable to function independently
Serious suicidal act with a clear expectation of deathNo attachment or concern for othersRecurrent violence
Needs: Hospitalisation, case management. Facilitate appropriate administrative tasks to enable re- enrolment if and when appropriate
Where immediate threat call security ext 333

INTRODUCING COMMUNITY CARE-LINE Community Care-line: 990 51599
Email: [email protected]
Community Care-line is not an emergency response.For emergency response phone security on ext 333
Community Care-line is a new service providing a central point of enquiry by phone or email to Community Care staff
who will provide advice and support for managing concerning or threatening behaviour and situations
within the Monash University community.
Students and staff are encouraged to ask for assistance if they:
Feel threatened or unsafe Have concerns about someone else’s behaviour Are worried about someone harming themselves or someone else Wish to clarify issues of responsibility, confidentiality or duty of care

INTRODUCING COMMUNITY CARE-LINE Community Care-line: 990 51599
Email: [email protected]
The Co-ordinator Community Care programs will provide leadership and support at all stages of responding to complex and sensitive
situations.
At all times the welfare of both the individual and the Monash community will be considered and all recommended action will be in
accordance with university statutes and policies.
Community care drop-in times for your campus in HWD
Berwick (Monday & Friday) 10.00-11.00am HWD Hub Bldg 930
Caufield (Wednesday) 9.00-9.30am HWD Hub Level 1 Bldg B
Clayton (Daily) 9.00-9.30am HWD Hub Western end Campus Centre
Gippsland (Monday) 10.30–11.30am HWD Hub Room 102 Bldg 3N
Parkville (Monday) 10.00-10.30am HWD Hub Ground Floor, Sissons Bldg
Peninsula (Tuesday & Thursday) 10.00-11.00am HWD Hub Level 1 Bldg A

Future directions …
• Tutor training
• MHFA for students
• Speakers on mental health issues during mental health week
• Health Wellbeing & Development webpage MHFA@Monash
Related Documents











