
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Systemic Metronidazole i n Periodontal Therapy
Usama M. madanyProfessor, Department of Oral Medicine
Periodontology, Diagnosis and Oral Radiology, Faculty of Dental Medicine , Al-Azhar University

- Commonly used antibiotics in periodontal therapy :
Tetrayclines (doxycycline) MetronidazoleClindamycin Penicillins (amoxicillin)Erythromycins (azithromycin, clarithromycin)Ciprofloxacin
The microbial etiology of inflammatory periodontal diseases provides the rationale for the local and systemic use of different antibiotics in periodontal therapy.
-Systemic antibiotic therapy in periodontics should be reserved to the following:
A. Prophylaxis for patients with medical problems requiring antibiotic coverage.
B. Patients with systemic manifestations associated with
acute periodontal infections (ANUG and acute periodontal abscess) .
C. As an adjunct to surgical and non surgical periodontal therapy.
D. Patients who undergo continued periodontal breakdown in spite of thorough debridement and excellent home care .

Metronidazole
Pharmacology and spectrum:
-It is a nitroimidazole compound mainly active against protozoal infections.
-It is very effective in low reduction potential areas, and bactericidal to anaerobes through inhibition of DNA synthesis.
-It can readily attain effective antibacterial concentration in gingival tissue, saliva and crevicular fluid.
-It is effective against the microorganism strongly associated with and implicated in pathogenesis of periodontal disease.

% Absorption after Peak serum level Serum half-life
Antibiotic oral adminestration (µg/ml) (hours)
Metronidazole 90 20-25 6-14
Tetracyclines 93 2- 4 18
(Doxycyline)
Clindamycin 90 5 2.4
Penicillins 75 5- 8 1.2
(Amoxicillin)
Ciprofloxacine 70 1.5 4
Erythromycines 37-50 0.4-3 5-12
Selected pharmacological features of common antibiotics in use for periodontics
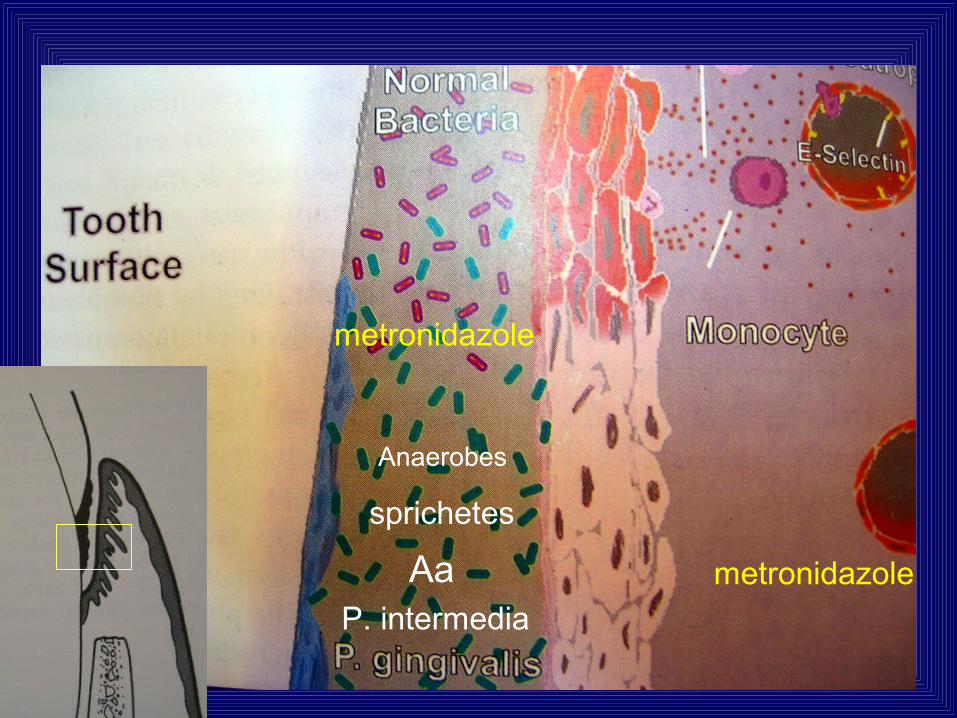
•metronidazole
metronidazole
metronidazole
AaP. intermedia
sprichetes
Anaerobes

Metronidazole
Spirochetes
P. gingivalis
P. intermedia
A.actinomycetemcomitansHydroxy metaolites of nitroimidazole
+ other antibiotics
tissues

Clinical use of systemic metronidazole:
If to be used, metronidazole should not be administered as monotherapy.
Alone
1- Treatment of ANUG 2- Treatment of periodontitis
250-500 mg/ tid/ 3-5 days 750-1000 mg /day for 7-14 days*
- growth of anaerobic bacteria.
- histopathological and Clinical
signs of periodontitis.
- the need for surgery.
-Recommended doses :
250 mg/ tid/ 7 days (Greenstien, 1993).
500 mg/ tid/ 8 days (Slots and Ting,
2002)
Loesche 1992; Nieminen et al.1996; Soder 1999.

Combined with other antibiotics -Complexity of periodontal pathogens in dental biofilm (dental plaque).-Considerable variation of sensitivity of these bacteria to different antibiotics.Treatment of periodontitis:
1- Metronidazole + amoxiciilin 250 mg/ tid/ 8 days of each drug. 2- Metronidazole 250 mg + amoxycillin-clavulanate potassium (augmentin) 375 mg / tid/ 8 days.3- Metronidazole + ciprofloxacin 500 mg/ bid/ 8 days of each drug.
-These regimens resulted in improved clinical status and suppression and/or elimination of Aa and Pg in aggressive and recurrent forms of periodontitis ( Slots and Ting 2002, AAP position paper 2004).

Adsverse reactios and side effects:
-Nausia/vomiting
-Unpleasant (metallic) taste.
-Pregnancy: Possible risk of teratogenicity.
Drug Interactions*:
1-Metronidazole metabolism of warfarin prolonged prothrombin time bleeding tendency (definite action).
2-Metronidazole + Ethanol disulfiram-like reaction:
nausia, vomiting, severe cramps, flushing, sweating, hypotension, palpitation and headache (probable action).
*Yagiela, 1999, Horn et al.2004

3-Metronidazole metabolism of oral hypoglycemic drugs Hypoglycemia (probable) .
5-Metronidazole may inhibit the action of estrogen components of oral contraceptives unexpected pregnancies ( Hersh 1999).
6-Barbiturates effectiveness of metronidazole (probable).
Precautions on prescription
1-Metronidazole should be avoided in patients undergoing warfarin therapy.
2-Alcohol containing products should be avoided during metronidazole therapy and for at least one day after therapy is discontinued.
3-Metronidazole is better to be avoided for diabetics on oral hypoglycemic drug.
4-It should be avoided during pregnancy especially in the first trimester, and also for females on oral contraceptives.
5-In patients with impairment of liver functions, metronidazole is better to be avoided or its dose to be decreased.
6-Dose for children should by properly adjusted according to body weight (7.5 mg/kg 8 hourly).
