4/11/2016 MethotrexateLoaded Solid Lipid Nanoparticles for Topical Treatment of Psoriasis: Formulation & Clinical Implications | Articles | drug development and delivery back issues | Drug Development & Delivery http://www.drugdev.com/Main/BackIssues/MethotrexateLoadedSolidLipidNanoparticlesforT89.aspx?format=2 1/14 Issue: Vol. 4 No. 8 October 2004, Posted Date: 3/27/2008 MethotrexateLoaded Solid Lipid Nanoparticles for Topical Treatment of Psoriasis: Formulation & Clinical Implications ABSTRACT Purpose: The purpose of these studies was to prepare Methotrexate (MTx) loaded solid lipid nanoparticles (SLN), incorporate it in suitable gel base, and evaluate it in vitro and clinically to justify the role of the developed gel in treatment of psoriasis. Method: MTxloaded SLN were prepared by hot microemulsion congealing technique. A Taguchi orthogonal experimental design was used to establish optimum combination of lipid, drug:lipid molar ratio, concentration of surfactant, and type of cosurfactant to achieve maximum percent drug entrapment (PDE) and particle size. The mean diameter of MTxSLN and surface morphology were evaluated using laser light diffractometry and scanning electron microscopy (SEM), respectively. The unentrapped drug was separated by dialysis. The PDE of prepared MTxSLN was estimated, and SLN were incorporated in Carbopol 934p (1% w/w) gel base. In vitro skin deposition studies were carried on human cadaver skin (HCS). Doubleblind clinical studies of potential batches were conducted on 24 mildtomoderate psoriasis patients. Results: Type of lipid, drug:lipid molar ratio, and concentration of surfactant were found to be critical variables influencing particle size and PDE (P < 0.05). However, concentration of cosurfactant was observed as noninfluencing parameter. The optimized MTxSLN was smooth, spherical with average diameter about 123 nm, and PDE of 52.16%. In vitro skin deposition studies showed significantly higher (P < 0.05) deposition of MTx from MTxSLN gel. Clinical studies have demonstrated improvement in therapeutic response (P < 0.01) at all evaluation time points and reduction in local side effects. Conclusion: Findings of the studies suggest that there is significant improvement in therapeutic index in treatment of psoriasis by MTxSLN incorporated gel base developed in this investigation over plain drug gel currently available in the market. INTRODUCTION Psoriasis is a quintessential chronic skin disease prevalent from 0.12% to 8% in the general population throughout the world. It is clinically characterized by erythematous, sharply demarcated papules and rounded plaques, and covered by silvery micaceous scale, epidermal hyper proliferation overlying immunemediated dermal inflammation. 1 Psoriasis is a T cellmediated disorder in which a particular set of cytokines released from activated T cells enhances keratinocyte proliferation and

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
4/11/2016 MethotrexateLoaded Solid Lipid Nanoparticles for Topical Treatment of Psoriasis: Formulation & Clinical Implications | Articles | drug development and delivery back issues | Drug Development & Delivery
http://www.drugdev.com/Main/BackIssues/MethotrexateLoadedSolidLipidNanoparticlesforT89.aspx?format=2 1/14
Issue: Vol. 4 No. 8 October 2004, Posted Date: 3/27/2008
MethotrexateLoaded Solid Lipid Nanoparticles for Topical Treatment ofPsoriasis: Formulation & Clinical Implications
ABSTRACT
Purpose: The purpose of these studies was to prepare Methotrexate (MTx) loaded solid lipid nanoparticles (SLN), incorporate it in suitable gel base, and evaluate it invitro and clinically to justify the role of the developed gel in treatment of psoriasis.
Method: MTxloaded SLN were prepared by hot microemulsion congealing technique. A Taguchi orthogonal experimental design was used to establish optimumcombination of lipid, drug:lipid molar ratio, concentration of surfactant, and type of cosurfactant to achieve maximum percent drug entrapment (PDE) and particle size. Themean diameter of MTxSLN and surface morphology were evaluated using laser light diffractometry and scanning electron microscopy (SEM), respectively. Theunentrapped drug was separated by dialysis. The PDE of prepared MTxSLN was estimated, and SLN were incorporated in Carbopol 934p (1% w/w) gel base. In vitroskin deposition studies were carried on human cadaver skin (HCS). Doubleblind clinical studies of potential batches were conducted on 24 mildtomoderate psoriasispatients.
Results: Type of lipid, drug:lipid molar ratio, and concentration of surfactant were found to be critical variables influencing particle size and PDE (P < 0.05). However,concentration of cosurfactant was observed as noninfluencing parameter. The optimized MTxSLN was smooth, spherical with average diameter about 123 nm, and PDEof 52.16%. In vitro skin deposition studies showed significantly higher (P < 0.05) deposition of MTx from MTxSLN gel. Clinical studies have demonstrated improvement intherapeutic response (P < 0.01) at all evaluation time points and reduction in local side effects.
Conclusion: Findings of the studies suggest that there is significant improvement in therapeutic index in treatment of psoriasis by MTxSLN incorporated gel basedeveloped in this investigation over plain drug gel currently available in the market.
INTRODUCTION
Psoriasis is a quintessential chronic skin disease prevalent from 0.12% to 8% in the general population throughout the world. It is clinically characterized by erythematous,sharply demarcated papules and rounded plaques, and covered by silvery micaceous scale, epidermal hyper proliferation overlying immunemediated dermalinflammation.1 Psoriasis is a T cellmediated disorder in which a particular set of cytokines released from activated T cells enhances keratinocyte proliferation and
4/11/2016 MethotrexateLoaded Solid Lipid Nanoparticles for Topical Treatment of Psoriasis: Formulation & Clinical Implications | Articles | drug development and delivery back issues | Drug Development & Delivery
http://www.drugdev.com/Main/BackIssues/MethotrexateLoadedSolidLipidNanoparticlesforT89.aspx?format=2 2/14
promotes granulocyte accumulation.2 Management of this disease requires knowledge regarding its occurrence, causative factors, and behavior of disease in differentindividuals, aggravating factors; efficacy, availability, and cost of different therapies on a longterm basis.3 For practical purposes, patients with less than 15% body surfaceinvolvement can be treated effectively with topical agents like coal tar, calcipotriene, anthralin, tazarotene, MTx, topical glucocorticoids, etc.
MTx is a folic acid antagonist with antineoplastic activity. It is also effective in controlling recalcitrant psoriasis when administered by the oral or parenteral route longterm.It has been shown to selectively inhibit DNA synthesis in psoriatic epidermal cells, thus decreasing mitotic activity.4 However, the systematic use of this drug may provokeany of a number of side effects, notably hepatotoxic effects. To reduce these effects, clinical studies have been done with topical MTx. It is useful in treating a number ofcutaneous conditions, including psoriasis, pityriasis, lichenoids, lymphomatoid papulosis, pemphigus vulgaris, lupus erythematosis, and dermatomyositis, and wasapproved by the FDA in 1971 for treating severe psoriasis.1 A major problem in topical administration of MTx currently available in market is that the drug is hydrosolubleand is mostly in the dissociated form at physiological pH. Its capacity for passive diffusion is thus limited.5 Localization of MTx in effected layers of skin is likely to improvethe role of topical dosage form of the drug as a supplementary to oral therapy for treatment of psoriasis. In addition, the aforementioned cure of the disease requires longerduration of treatment, and in many cases, the lesions are not responsive to plain drug therapy beyond a certain percent reduction in skin lesions. One of the possibilitiesfor increasing the penetration of drugs through the skin is the use of solid lipid nanoparticles.
During recent years, SLN have been used in topical drug formulations and cosmetic products. Small particle size ensures close contact to the stratum corneum, and drugencapsulated in lipid improves selective drug delivery to skin layers.6,7 SLN possess a solid matrix, which has the potential to modulate the drug release over a prolongedperiod with a reduced rate of systemic absorption.8,9 Another benefit of SLN for topical delivery of active compounds is that the timetomarket is very short for theseproducts.6,10,11 Hence, the purpose of these studies was to develop an MTxloaded SLN topical gel to improve therapeutic index of MTx compared to topical formulationscurrently available in market in the treatment of psoriasis.
MATERIALS & METHODS
Chemicals & ReagentsMethotrexate and Compritol 888 were gifted by Dabur Research Foundation Gaziabad and Colorcon Asia Pvt. Ltd., Mumbai, respectively. Cetyl Alcohol, Stearic acid, andTween 80 were purchased from S.D. Fine Chem. Ltd., Boisar. Dialysis Bag (mol. Cut off weight 10,000), Poloxamer 188, Sodium tauroglycocholate, and Human cadaverskin were obtained from Sigma Chemicals Co., St.Louis, BASF, Frankfurt, Loba Chemie Mumbai, and S.S.G. Hospital, Vadodara, respectively. All chemicals wereanalytical grade or spectroscopic grade.
Reagents
Water: Purified Water I.P.12Phosphate buffer pH 7.4: Prepared as per the procedure given in the Indian Pharmacopoeia.12Dialysis Medium: A mixture of Propylene Glycol (PG) and phosphate buffer pH 7.4 (2:8) at 4°C.
Preparation of skin for diffusion studies: Human cadaver skin (HCS), from elbow regions of the bodies of either sex (aged between 25 to 35 years), was obtained usingHumby's knife from autopsy at S.S.G. Hospital (Vadodara, India). The skin was washed thoroughly with water, and subcutaneous fat was removed. The skin was thenstored at 4°C. Full thickness HCS membrane was prepared by shaving the skin, punching out a disc of approximately 2.5 cm2 in area and slicing to a 500mm thicknessusing a Davis Dermatome 7. These slices were hydrated with diffusion medium for 24 hours at room temperature prior to use.
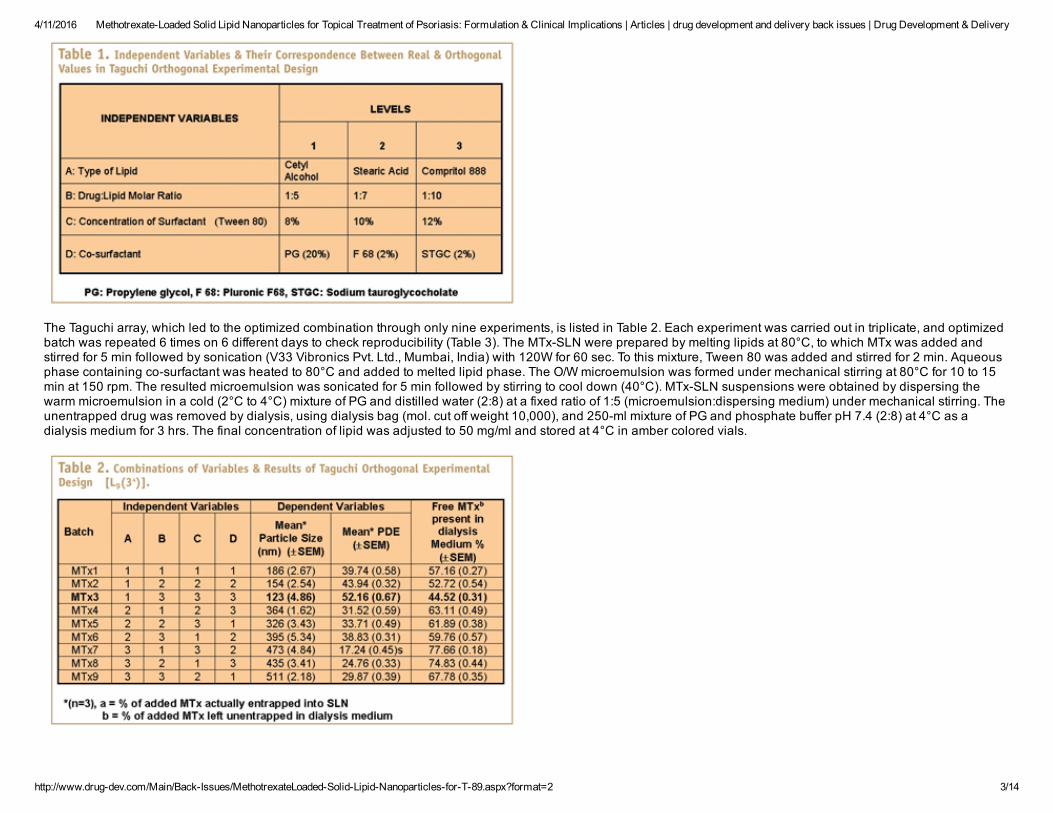
Preparation of MTxSLNMTxloaded SLN were prepared by hot microemulsion congealing technique reported by Gasco et al.13,14 The optimum combination of four independent variables, suchas type of lipid, drug:lipid molar ratio, concentration of surfactant, and type of cosurfactant were varied at three levels by Taguchi orthogonal experimental design toachieve maximum PDE and optimum particle size (Table 1).15
4/11/2016 MethotrexateLoaded Solid Lipid Nanoparticles for Topical Treatment of Psoriasis: Formulation & Clinical Implications | Articles | drug development and delivery back issues | Drug Development & Delivery
http://www.drugdev.com/Main/BackIssues/MethotrexateLoadedSolidLipidNanoparticlesforT89.aspx?format=2 3/14
The Taguchi array, which led to the optimized combination through only nine experiments, is listed in Table 2. Each experiment was carried out in triplicate, and optimizedbatch was repeated 6 times on 6 different days to check reproducibility (Table 3). The MTxSLN were prepared by melting lipids at 80°C, to which MTx was added andstirred for 5 min followed by sonication (V33 Vibronics Pvt. Ltd., Mumbai, India) with 120W for 60 sec. To this mixture, Tween 80 was added and stirred for 2 min. Aqueousphase containing cosurfactant was heated to 80°C and added to melted lipid phase. The O/W microemulsion was formed under mechanical stirring at 80°C for 10 to 15min at 150 rpm. The resulted microemulsion was sonicated for 5 min followed by stirring to cool down (40°C). MTxSLN suspensions were obtained by dispersing thewarm microemulsion in a cold (2°C to 4°C) mixture of PG and distilled water (2:8) at a fixed ratio of 1:5 (microemulsion:dispersing medium) under mechanical stirring. Theunentrapped drug was removed by dialysis, using dialysis bag (mol. cut off weight 10,000), and 250ml mixture of PG and phosphate buffer pH 7.4 (2:8) at 4°C as adialysis medium for 3 hrs. The final concentration of lipid was adjusted to 50 mg/ml and stored at 4°C in amber colored vials.

4/11/2016 MethotrexateLoaded Solid Lipid Nanoparticles for Topical Treatment of Psoriasis: Formulation & Clinical Implications | Articles | drug development and delivery back issues | Drug Development & Delivery
http://www.drugdev.com/Main/BackIssues/MethotrexateLoadedSolidLipidNanoparticlesforT89.aspx?format=2 4/14
CHARACTERIZATION OF MTxSLN
Particle Size DistributionThe particle size distribution of MTxSLN were carried out by laser light diffractometry, using Malvern MasterSizer SM 2000K (Malvern Instruments Inc.,Worcestershire,UK).Samples were prepared by dispersing MTxSLN with sufficient amount of water to achieve obscuration between 10% to 20%. The samples were stirred using a bladestirrer at 1000 rpm to keep MTxSLN in suspended form.
Surface MorphologySurface morphology of MTxSLN were studied by SEM (JSM5610LV, JEOL, Japan). The scanning electron microphotographs were taken using a double adhesive tapeapplied on the aluminium dies and MTxSLN were spread uniformly on it.
Encapsulation EfficiencyThe drugloading and entrapment efficiency of MTxSLN were determined by using dialysis bag (mol. cut off weight 10,000, Sigma Chemicals Co., St.Louis, USA) and 250ml mixture of PG and phosphate buffer pH 7.4 (2:8) at 4°C as dialysis medium for 3 hrs. PDE in the SLN was determined by UV spectrophotometric method in methanol asdescribed by Klaus Florey.16 Briefly, 0.1 ml of MTxSLN suspension was dissolved by adding 1.0 ml of methanol (chloroform in case of Compritol 888 SLN) into a 25mlvolumetric flask, and volume was made up to 25 ml with methanol. The resulting solution was diluted suitably if necessary, and the MTx content was analyzed bymeasuring the absorbance at lmax 306 nm against reagent blank. Similarly, unentrapped drug in dialysis medium was estimated by transferring 0.5 ml of the dialysismedia into a clean and dry 10ml volumetric flask, and volume was made up to 10 ml with methanol. The resulting solution was further diluted if necessary, and the MTxcontent was analyzed by measuring the absorbance at lmax 306 nm against the reagent blank.
PREPARATION & EVALUATION OF GELS
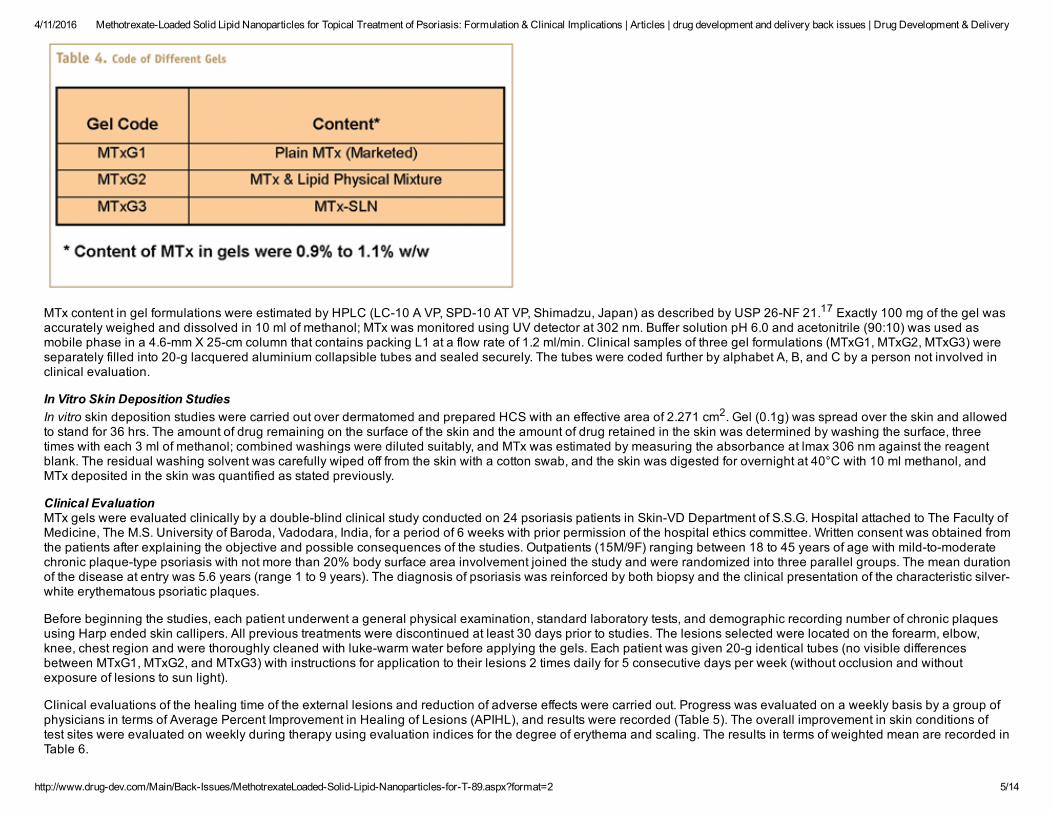
The MTxSLN gel was prepared by dispersing required quantity of Carbopol 934p (1% w/w) in small quantity of distilled water to prepare an aqueous dispersion andallowed to hydrate for 4 to 5 hrs. Propylene glycol (10% w/w) and glycerol (30% w/w) were added subsequently to the aqueous dispersion, and 0.5 ml of triethanolaminewas added under gentle stirring to avoid the inclusion of air.7 Equivalent amount of MTxSLN suspension containing 1 g of drug was centrifuged, and the pellets obtainedwere incorporated. The dispersion was neutralized with 1% w/v NaOH to pH 6.0, and final weight was adjusted to 100 g with distilled water (MTxG3). The gel was allowedto stand overnight to remove entrapped air. Gel containing physical mixture of drug and lipid was prepared by incorporating equivalent amount of drug and cetyl alcoholinto Carbopol base gel (MTxG2). Gel containing plain MTx (marketed formulation) was acquired from the local market. The various gels prepared are enlisted in the Table4.
4/11/2016 MethotrexateLoaded Solid Lipid Nanoparticles for Topical Treatment of Psoriasis: Formulation & Clinical Implications | Articles | drug development and delivery back issues | Drug Development & Delivery
http://www.drugdev.com/Main/BackIssues/MethotrexateLoadedSolidLipidNanoparticlesforT89.aspx?format=2 5/14
MTx content in gel formulations were estimated by HPLC (LC10 A VP, SPD10 AT VP, Shimadzu, Japan) as described by USP 26NF 21.17 Exactly 100 mg of the gel wasaccurately weighed and dissolved in 10 ml of methanol; MTx was monitored using UV detector at 302 nm. Buffer solution pH 6.0 and acetonitrile (90:10) was used asmobile phase in a 4.6mm X 25cm column that contains packing L1 at a flow rate of 1.2 ml/min. Clinical samples of three gel formulations (MTxG1, MTxG2, MTxG3) wereseparately filled into 20g lacquered aluminium collapsible tubes and sealed securely. The tubes were coded further by alphabet A, B, and C by a person not involved inclinical evaluation.
In Vitro Skin Deposition StudiesIn vitro skin deposition studies were carried out over dermatomed and prepared HCS with an effective area of 2.271 cm2. Gel (0.1g) was spread over the skin and allowedto stand for 36 hrs. The amount of drug remaining on the surface of the skin and the amount of drug retained in the skin was determined by washing the surface, threetimes with each 3 ml of methanol; combined washings were diluted suitably, and MTx was estimated by measuring the absorbance at lmax 306 nm against the reagentblank. The residual washing solvent was carefully wiped off from the skin with a cotton swab, and the skin was digested for overnight at 40°C with 10 ml methanol, andMTx deposited in the skin was quantified as stated previously.
Clinical EvaluationMTx gels were evaluated clinically by a doubleblind clinical study conducted on 24 psoriasis patients in SkinVD Department of S.S.G. Hospital attached to The Faculty ofMedicine, The M.S. University of Baroda, Vadodara, India, for a period of 6 weeks with prior permission of the hospital ethics committee. Written consent was obtained fromthe patients after explaining the objective and possible consequences of the studies. Outpatients (15M/9F) ranging between 18 to 45 years of age with mildtomoderatechronic plaquetype psoriasis with not more than 20% body surface area involvement joined the study and were randomized into three parallel groups. The mean durationof the disease at entry was 5.6 years (range 1 to 9 years). The diagnosis of psoriasis was reinforced by both biopsy and the clinical presentation of the characteristic silverwhite erythematous psoriatic plaques.
Before beginning the studies, each patient underwent a general physical examination, standard laboratory tests, and demographic recording number of chronic plaquesusing Harp ended skin callipers. All previous treatments were discontinued at least 30 days prior to studies. The lesions selected were located on the forearm, elbow,knee, chest region and were thoroughly cleaned with lukewarm water before applying the gels. Each patient was given 20g identical tubes (no visible differencesbetween MTxG1, MTxG2, and MTxG3) with instructions for application to their lesions 2 times daily for 5 consecutive days per week (without occlusion and withoutexposure of lesions to sun light).
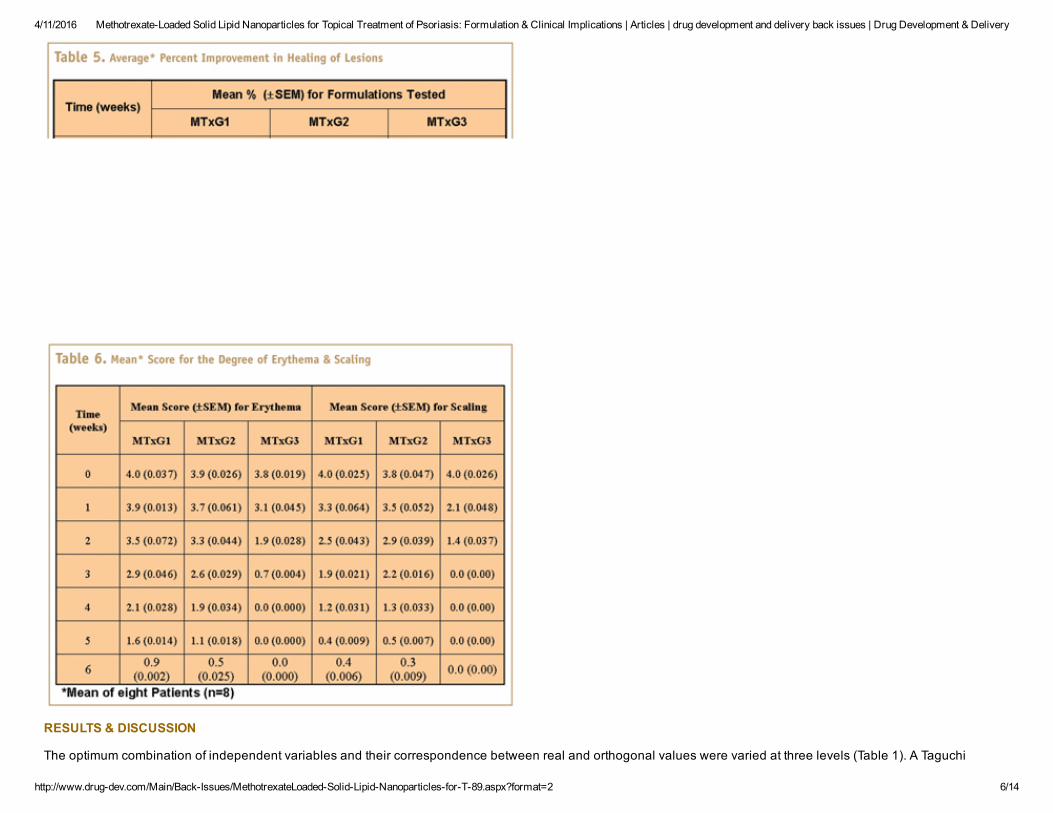
Clinical evaluations of the healing time of the external lesions and reduction of adverse effects were carried out. Progress was evaluated on a weekly basis by a group ofphysicians in terms of Average Percent Improvement in Healing of Lesions (APIHL), and results were recorded (Table 5). The overall improvement in skin conditions oftest sites were evaluated on weekly during therapy using evaluation indices for the degree of erythema and scaling. The results in terms of weighted mean are recorded inTable 6.
4/11/2016 MethotrexateLoaded Solid Lipid Nanoparticles for Topical Treatment of Psoriasis: Formulation & Clinical Implications | Articles | drug development and delivery back issues | Drug Development & Delivery
http://www.drugdev.com/Main/BackIssues/MethotrexateLoadedSolidLipidNanoparticlesforT89.aspx?format=2 6/14
RESULTS & DISCUSSION
The optimum combination of independent variables and their correspondence between real and orthogonal values were varied at three levels (Table 1). A Taguchi

4/11/2016 MethotrexateLoaded Solid Lipid Nanoparticles for Topical Treatment of Psoriasis: Formulation & Clinical Implications | Articles | drug development and delivery back issues | Drug Development & Delivery
http://www.drugdev.com/Main/BackIssues/MethotrexateLoadedSolidLipidNanoparticlesforT89.aspx?format=2 7/14
orthogonal experimental design [L9(34)] was used to investigate the influence of critical variables by performing only 9 experiments. The optimum setting of variables andtheir levels were found to be A1 (Type of lipid, Cetyl alcohol), B3 (Drug:Lipid molar ratio, 1:10), C3 Concentration of Surfactant, 12%), and D3 (Concentration of cosurfactant, 2%) with regard to least particle size 123 nm and maximum PDE of 52.16% (batch MTx3) (Table 2). The batch MTx3 was further evaluated for reproducibility,and results were recorded in Table 3. Differences in particle size and PDE within and among the batches were observed to be insignificant (P <0.05). Increase in theconcentration of surfactant was found to decrease in MTxSLN size significantly (P < 0.05), while type of lipid used and drug:lipid molar ratio decided the fate of PDE ofMTxSLN (P < 0.05). However, type of cosurfactant used did not show any significant effect on the MTxSLN formation. Cetyl alcohol was found to influence PDE of MTxSLN maximum, followed by stearic acid and compritol 888, respectively. This is in consistence with the findings that the chemical and physical structure of solid lipid matrixdetermines the loading capacity of drug in the SLN.1820 Smaller particle size of cetyl alcohol SLN might be due to the shorter fatty chain length and bearing of surfaceactive properties.21,22 PDE increases as drug:lipid molar ratio increases due to increased amount of dissolved drug in melted lipids.20 The choice of the surfactant and itsconcentration had a great impact on the particle size of the SLN.23,24 The decrease in particle size during microemulsion formation is associated with increase in surfacearea. The excessive surfactant molecules present rapidly cover the new surfaces, which reduce the surface tension and thereby facilitate the particle partition duringemulsification.25 Hence, an increase in surfactant concentration results in decrease in particle size of the SLN. SEM revealed that the MTxSLN were smooth andspherical as shown in Figure 1, no free drug crystals are visible under the SEM in all the SLN preparations indicating that dialysis technique was an efficient means ofseparating the unentrapped drug from dispersions of SLN. Content of MTx in gels (Table 4) were found to be between 90% and 110% of the labelled amount, ie, 0.9% to1.10% w/w.
In vitro skin deposition studies revealed significantly higher deposition of MTx from MTxG3 (P < 0.05) in the skin (74.52±1.13%) than MTxG1 (36.48±0.96%) and MTxG2(39.11±0.85%), (Table 7). The procedure used for washing the skin surface was found to be effective in removing > 99% of the residual drug. Mass balance data fromdeposition studies accounted for high recovery of the applied drug dose. The results of these studies support that encapsulation of MTx into SLN enhances the drugdeposition into the HCS and supports mechanism of formation of cetyl alcohol reservoir containing MTx in the skin layers.7,26,27 Hence, MTxG3 was chosen for clinicalevaluation, and its efficacy was compared with that of MTxG1 and MTxG2.

4/11/2016 MethotrexateLoaded Solid Lipid Nanoparticles for Topical Treatment of Psoriasis: Formulation & Clinical Implications | Articles | drug development and delivery back issues | Drug Development & Delivery
http://www.drugdev.com/Main/BackIssues/MethotrexateLoadedSolidLipidNanoparticlesforT89.aspx?format=2 8/14
Plain drug MTx is known to be effective in topical treatment of psoriasis; however, physicochemical properties of drug limits the capacity for passive diffusion. Hence, itwas thought worthwhile to investigate localization of MTx in effected layers of skin with view to improving therapeutic response and reducing possible side effects.
Clinical efficacy and tolerability of the trial preparations were ascertained by physical inspection and overall general response of patients at each scheduled weekly visits.At each clinic visit, used tubes were replaced with fresh coded tubes. The progress of treatment was evaluated on a weekly basis by a group of physicians in terms ofAPIHL, representing combined decrease in dimension and elevation of the lesions. The measurement of dimension and elevation was made using vernier callipers (leastcount = 0.01 cm) by the physicianincharge before starting the treatment and later on weekly basis after commencement of treatment. Because the lesions wereasymmetrical, the measurements of dimension of lesions were made, and the average values were taken for calculation. Average of the three of four crosssectionallengths of all the lesions were summed up and divided by number of lesions (8 patients in each treatment group) yield the average length of lesions (Figure 2). Similarly,average of three measurements at different places of lesions were summed up and divided by the number of lesions (8 patients in each treatment group) yield the averagethickness of lesions. The study lasted for 6 weeks, and the patients thereafter were followed up on a monthly basis for 2 months. Patients who showed progressiveremission of lesions, desquamation, followed by decreased erythema and infiltration were considered effectively treated. The results of the studies obtained with MTxSLNgels were compared with those obtained with plain drug gel and druglipid physical mixture gels using analysis of variance (ANOVA); differences greater than p < 0.01were considered significant.

4/11/2016 MethotrexateLoaded Solid Lipid Nanoparticles for Topical Treatment of Psoriasis: Formulation & Clinical Implications | Articles | drug development and delivery back issues | Drug Development & Delivery
http://www.drugdev.com/Main/BackIssues/MethotrexateLoadedSolidLipidNanoparticlesforT89.aspx?format=2 9/14
In addition, the test sites were evaluated weekly during therapy for the degree of erythema and scaling on a scale of 0 to 4+ (0, clear; 1+, mild; 2+, moderate; 3+, severe;and 4+, extreme). The findings were duly filled in the datasheet of the patients.
The lesions located in the forearm, elbow, knee, and chest regions were selected for the study because the physician could count them easily. The patients wereinstructed to avoid contact of formulation with nose, eye, and mucous membrane because of possible irritant effects.
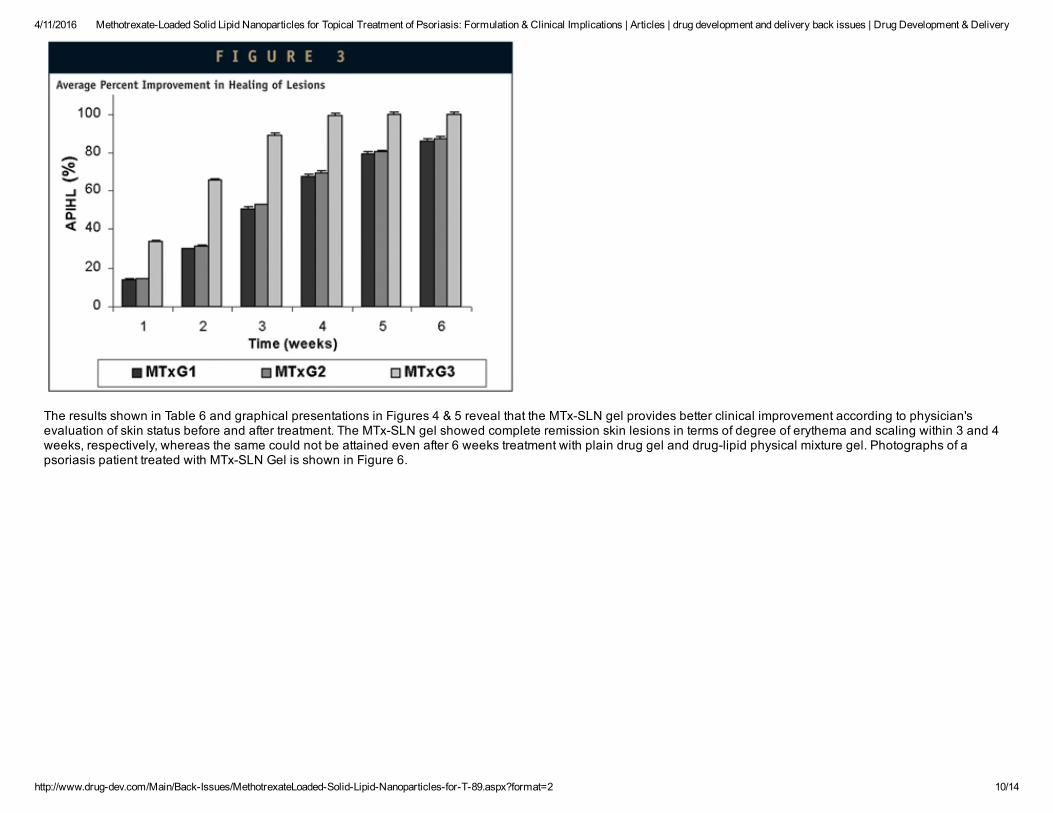
It is evident from the results shown in Table 5 manifestations of psoriasis are equally responsive to marketed plain drug gel and MTxlipid physical mixture gel. However,MTxSLN gel showed significant (approx.1.7fold) (P < 0.01) improvement in therapeutic response at all evaluation time points. In addition to the MTxSLN, almostcomplete cures (99.4 % improvement in healing of lesions) within 4 weeks, whereas 86.1% and 86.9% reduction in skin lesions was achieved with the plain drug gel andlipid physical mixture gel, respectively even after prolonging the application of preparations for up to 6 weeks. The results in terms of weighted means are shown in Figure3. Cure of the disease required longer duration of treatment, and in many cases, the lesions are not responsive to plain drug therapy beyond a certain percent reduction inskin lesions. The results clearly suggest that MTxSLN gel requires shorter duration of therapy and achieves complete remission of symptoms, perhaps due to higher skindeposition with cetyl alcohol reservoir as previously reported.7,26,27
4/11/2016 MethotrexateLoaded Solid Lipid Nanoparticles for Topical Treatment of Psoriasis: Formulation & Clinical Implications | Articles | drug development and delivery back issues | Drug Development & Delivery
http://www.drugdev.com/Main/BackIssues/MethotrexateLoadedSolidLipidNanoparticlesforT89.aspx?format=2 10/14
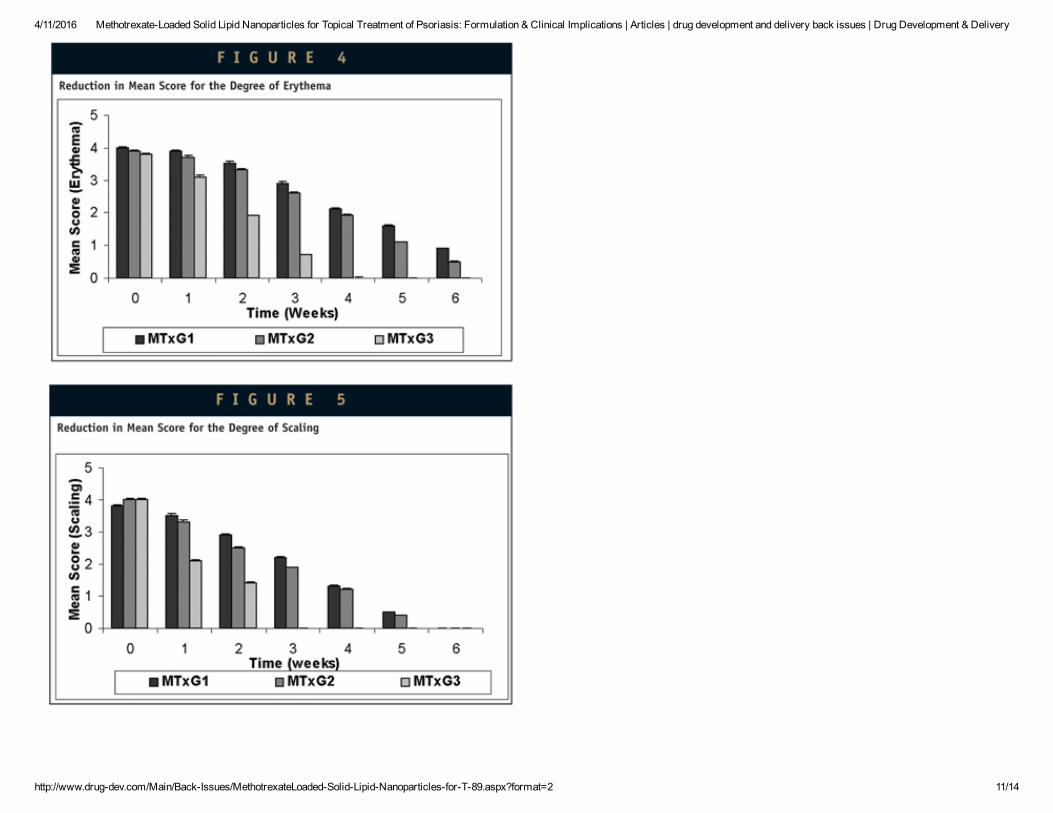
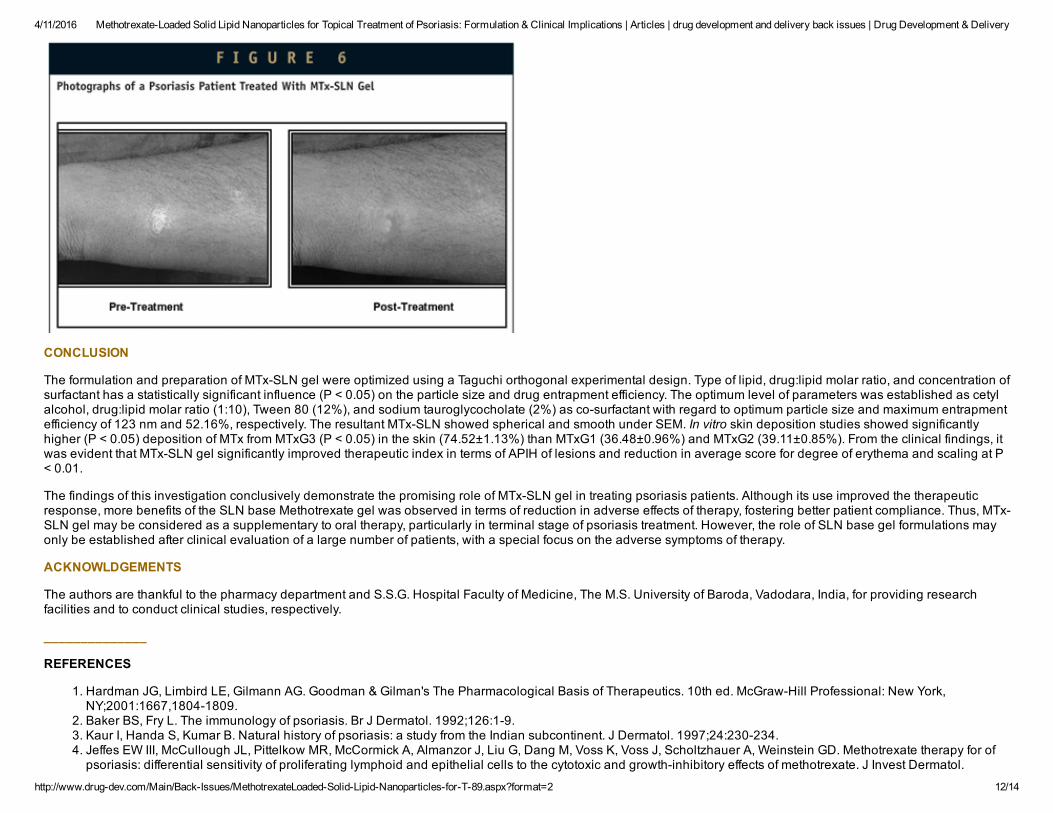
The results shown in Table 6 and graphical presentations in Figures 4 & 5 reveal that the MTxSLN gel provides better clinical improvement according to physician'sevaluation of skin status before and after treatment. The MTxSLN gel showed complete remission skin lesions in terms of degree of erythema and scaling within 3 and 4weeks, respectively, whereas the same could not be attained even after 6 weeks treatment with plain drug gel and druglipid physical mixture gel. Photographs of apsoriasis patient treated with MTxSLN Gel is shown in Figure 6.
4/11/2016 MethotrexateLoaded Solid Lipid Nanoparticles for Topical Treatment of Psoriasis: Formulation & Clinical Implications | Articles | drug development and delivery back issues | Drug Development & Delivery
http://www.drugdev.com/Main/BackIssues/MethotrexateLoadedSolidLipidNanoparticlesforT89.aspx?format=2 11/14
4/11/2016 MethotrexateLoaded Solid Lipid Nanoparticles for Topical Treatment of Psoriasis: Formulation & Clinical Implications | Articles | drug development and delivery back issues | Drug Development & Delivery
http://www.drugdev.com/Main/BackIssues/MethotrexateLoadedSolidLipidNanoparticlesforT89.aspx?format=2 12/14
CONCLUSION
The formulation and preparation of MTxSLN gel were optimized using a Taguchi orthogonal experimental design. Type of lipid, drug:lipid molar ratio, and concentration ofsurfactant has a statistically significant influence (P < 0.05) on the particle size and drug entrapment efficiency. The optimum level of parameters was established as cetylalcohol, drug:lipid molar ratio (1:10), Tween 80 (12%), and sodium tauroglycocholate (2%) as cosurfactant with regard to optimum particle size and maximum entrapmentefficiency of 123 nm and 52.16%, respectively. The resultant MTxSLN showed spherical and smooth under SEM. In vitro skin deposition studies showed significantlyhigher (P < 0.05) deposition of MTx from MTxG3 (P < 0.05) in the skin (74.52±1.13%) than MTxG1 (36.48±0.96%) and MTxG2 (39.11±0.85%). From the clinical findings, itwas evident that MTxSLN gel significantly improved therapeutic index in terms of APIH of lesions and reduction in average score for degree of erythema and scaling at P< 0.01.
The findings of this investigation conclusively demonstrate the promising role of MTxSLN gel in treating psoriasis patients. Although its use improved the therapeuticresponse, more benefits of the SLN base Methotrexate gel was observed in terms of reduction in adverse effects of therapy, fostering better patient compliance. Thus, MTxSLN gel may be considered as a supplementary to oral therapy, particularly in terminal stage of psoriasis treatment. However, the role of SLN base gel formulations mayonly be established after clinical evaluation of a large number of patients, with a special focus on the adverse symptoms of therapy.
ACKNOWLDGEMENTS
The authors are thankful to the pharmacy department and S.S.G. Hospital Faculty of Medicine, The M.S. University of Baroda, Vadodara, India, for providing researchfacilities and to conduct clinical studies, respectively.
______________
REFERENCES
1. Hardman JG, Limbird LE, Gilmann AG. Goodman & Gilman's The Pharmacological Basis of Therapeutics. 10th ed. McGrawHill Professional: New York,NY;2001:1667,18041809.
2. Baker BS, Fry L. The immunology of psoriasis. Br J Dermatol. 1992;126:19.3. Kaur I, Handa S, Kumar B. Natural history of psoriasis: a study from the Indian subcontinent. J Dermatol. 1997;24:230234.4. Jeffes EW III, McCullough JL, Pittelkow MR, McCormick A, Almanzor J, Liu G, Dang M, Voss K, Voss J, Scholtzhauer A, Weinstein GD. Methotrexate therapy for ofpsoriasis: differential sensitivity of proliferating lymphoid and epithelial cells to the cytotoxic and growthinhibitory effects of methotrexate. J Invest Dermatol.
4/11/2016 MethotrexateLoaded Solid Lipid Nanoparticles for Topical Treatment of Psoriasis: Formulation & Clinical Implications | Articles | drug development and delivery back issues | Drug Development & Delivery
http://www.drugdev.com/Main/BackIssues/MethotrexateLoadedSolidLipidNanoparticlesforT89.aspx?format=2 13/14
1995;104:183188.5. Trotta M, Peira E, Carlotti ME, Gallarate M. Deformable liposomes for dermal administration of methotrexate. Int J Pharm. 2004;270:119125.6. Feste JV. Lipid nanopartikel ais tragersystem for die dermale Applikation von retinol. PhD Thesis. Free University of Berlin;1999.7. Maia SC, Mehnert W, SchaferKorting M. Solid lipid nanoparticles as drug carriers for topical glucocorticoids. Int J Pharm. 2000;196:165167.8. Muller RH, Dingler A. Faste lipidnanopartikel (LipopearlsTM) alsneuartiger carrier fur kosmetische und dermatologische Wirkstoffe. Pharmazeutische ZeitungDermopharmazie. 1998:1115.
9. Muller RH, Dingler A. The next generation after the liposomes: solid lipid nanoparticles (SLNTM, LipopearlsTM) as dermal carrier in cosmetics. Eurocosmetics.1998;7/8:1926.
10. Jeffes EW III, McCullough JL, Pittelkow MR, McCormick A, Almanzor J, Liu G, Dang M, Voss K, Voss J, Scholtzhauer A, Weinstein GD. Methotrexate therapy for ofpsoriasis: differential sensitivity of proliferating lymphoid and epithelial cells to the cytotoxic and growthinhibitory effects of methotrexate. J Invest Dermatol.1995;104:183188.
11. Ball MA, McCullough JL,Weinstein GD. Percutaneous absorption of methotrexate: effect on epidermal DNA synthesis in hairless mice. J Invest Dermatol.1982;79(1) :710.
12. Indian Pharmacopoeia 1996. Controller of Publications, Delhi.13. Gasco MR. Method for producing solid lipid microspheres having a narrow size distribution. US Patent No. 5250236 (1993).14. Utreja S, Khopade AJ, Jain NK. Lipoproteinmimicking biovectorized systems for methotrexate delivery. Pharm Acta Helv. 1999;73:275279.15. Taguchi G. Taguchi Method: Design of Experiments; Quality Engineering Series; 1993, Vol. 4.16. Chamberlin AC, Andrew PK, Cheung, Peterlin, Florey K. Analytical Profiles of Drug Substances. Vol. 5. Academic Press, Inc.: New York;1976:283306.17. USP 26NF 21. The United States Pharmacopeial Convention, Inc., Rockville, Maryland; 2003.18. Franz T J. Percutaneous absorption on the relevance of in vitro data. J Invest Dermatol. 1975;67:190196.19. Washington C. Drug release from microdisperse system: a critical review. Int J Pharm. 1990;58:112.20. Muller RH, Mader K, Gohla S. Solid lipid nanoparticles (SLN) for controlled drug delivery a review of the state of the art. Eur J Pharm Biopharm. 2000;50:161177.21. Siekmann B, Westensen K. Submicron sized parenteral carrier systems based on solid lipid. Pharm Pharmacol Lett. 1992;1:123126.22. Ahlin P, Kristl J. Optimization of procedure parameters and physical stability of solid lipid nanoparticles in dispersions. Acta Pharm. 1998;48:257267.23. Muller RH, Mehnert W, Lucks JS, Schwarz C, zurMuhlen A, Weyhers H, Freitas C, Ruhl D. Solid lipid nanoparticles (SLN) an alternative colloidal carrier system for
controlled drug delivery. Eur J Pharm Biopharm. 1995;45:6269.24. zurMuhlen A. Feste lipidnanopartikel mit prolongierter wirkstoffliberation: herstellung, langzeitstabilitat, charakterisierung, freisetzungsverhalten und
mechanismen. PhD Thesis, Free University of Berlin;1996.25. Mehnert W, Mader K. Solid lipid nanoparticles: production, characterization, and applications. Adv Drug Del Rev. 2001;47:165196.26. Jenning V, SchaferKorting M, Gohla S. Vitamin A loaded solid lipid nanoparticles for topical application: drug release properties. J Control Rel. 2000;66(23):115
126.27. Hand Book of Pharmaceutical Excipients. 1986:6366.
BIOGRAPHIES
4/11/2016 MethotrexateLoaded Solid Lipid Nanoparticles for Topical Treatment of Psoriasis: Formulation & Clinical Implications | Articles | drug development and delivery back issues | Drug Development & Delivery
http://www.drugdev.com/Main/BackIssues/MethotrexateLoadedSolidLipidNanoparticlesforT89.aspx?format=2 14/14
Dr. Ambikanandan Misra is currently Head, Pharmacy Department, The Maharaja Sayajirao University of Baroda, India. With more than 25 years of both academic andindustrial experience in the field of Drug Delivery Research, he has more than 50 research publications and several formulation patents to his credit. He was accreditedthe national award on Liposomal Dry Powder Inhalation and is a major contributor to the pharmaceutical industry in the field of Pulmonary and Transdermal Drug Delivery.He earned his MPharm in Pharmaceutics from University of Sagar, Sagar, India, and his PhD in Controlled Drug Delivery Systems from The M.S. University of Baroda,Vadodara, India.
Mr. Mayur Kalariya is currently working for Sun Pharmaceuticals Advanced Research Centre, Vadodara, India. He earned his MPharm from The M.S. University ofBaroda, Vadodara, India.
Mr. Bijay Kumar Padhi is a Research Scholar in the Pharmacy Department, The M.S. University of Baroda, Vadodara, India. He earned his MPharm from the Rajiv GandhiTechnological University, Bhopal, India.
Mr. Mahavir Chougule is a Research Scholar in the Pharmacy Department, The M.S. University of Baroda, Vadodara, India. He earned his MPharm from The M.S.University of Baroda, Vadodara, India.
Popularity:This record has been viewed 105 times.
Related Documents










![Therapy treatment options for psoriasis: topical and … 321 Therapy treatment options for psoriasis – REVIEW areas [9]. In extensive cases of psoriasis requiring large amounts of](https://static.cupdf.com/doc/110x72/5b0a88b87f8b9a0b0f8bd4bc/therapy-treatment-options-for-psoriasis-topical-and-321-therapy-treatment-options.jpg)
