Understanding and Fighting Understanding and Fighting Methicillin Methicillin - - Resistant Staphylococcus Aureus Resistant Staphylococcus Aureus “ “ MRSA MRSA ” ” This program was supported by an educational grant provided by PFIZER Pharmaceuticals. PharmCon is accredited by the Accreditation Council for Pharmacy Education as a provider of continuing pharmacy education. Michael E. Barton, M.D. Michael E. Barton, M.D. Emergency Medicine Emergency Medicine Pittsburgh, Pennsylvania Pittsburgh, Pennsylvania

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Understanding and Fighting Understanding and Fighting MethicillinMethicillin--Resistant Staphylococcus AureusResistant Staphylococcus Aureus
““MRSAMRSA””
This program was supported by an educational grant provided by PFIZER Pharmaceuticals.
PharmCon is accredited by the Accreditation Council for Pharmacy Education as a provider of continuing pharmacy education.
Michael E. Barton, M.D.Michael E. Barton, M.D.Emergency MedicineEmergency MedicinePittsburgh, PennsylvaniaPittsburgh, Pennsylvania
Speaker: Michael Barton, MD
has served as the chairman of the Infection Control Committee at a community hospital in Pittsburgh for the past 2 years. While continuing to care for patients in the emergency department, he has developed a fascination for community-associated MRSA and a growing concern over the rapid spread of this "superbug". Dr. Barton is a graduate of The Pennsylvania State University with a B.S. in Biology and earned his medical degree at Temple University School of Medicine. His post-graduate training was in Emergency Medicine at Allegheny General Hospital in Pittsburgh.
Understanding and Fighting MethicillinUnderstanding and Fighting Methicillin-- Resistant Staphylococcus Aureus Resistant Staphylococcus Aureus ““MRSAMRSA””
Speaker Disclosure: Dr. Barton has no actual or potential conflicts of interest in relation to this program
PharmCon is accredited by the accreditation counsel for Pharmacy Education as a provider of continuing pharmacy education
Legal Disclaimer: The material presented here does not necessarily reflect the views of Pharmaceutical Education Consultants (PharmCon) or the companies that support educational programming. A qualified healthcare professional should always be consulted before using any therapeutic product discussed. Participants should verify all information and data before treating patients or employing any therapies described in this educational activity.
Accreditation:
Pharmacists 798-000-08-049-L01-P
Pharmacy Technicians 798-000-08-049-L01-T
Nurses N-081308-314-L01
Physicians
Target Audience: Pharmacists, Pharmacy Technicians, Nurses, and Physicians
Understanding and Fighting MethicillinUnderstanding and Fighting Methicillin--Resistant Staphylococcus Aureus Resistant Staphylococcus Aureus ““MRSAMRSA””
CE Credits:
1.0 Continuing Education Credit or 0.1 CEU for pharmacists/technicians
Expiration Date: 5/11/2011
Program Overview: In the battle of man vs. bacteria, a new enemy has emerged as the most feared “superbug” of 2008. Forget West Nile and bird flu – Methicillin Resistant Staphylococcus Aureus (MRSA) is suddenly all over the media. This well deserved media spotlight highlights the increasing danger associated with MRSA infections. This program will review the most recent guidelines for the diagnosis and management of pneumonia and skin and skin-structure infections caused by MRSA. The program includes information on pharmacological treatments, patient counseling, and a question/ answer period.
Objectives:1. Identify the epidemiology and differences between CA-MRSA and HA-MRSA, including virulence
factors and antibiotic susceptibilities.2. Outline the virulence mechanism of methicillin resistance in Staphylococcus aureus.3. Explain the modes of action, efficacy, and advantages and disadvantages of currently available
pharmacological therapies for both HA-MRSA and CA-MRSA.4. Review the conventional actions necessary to prevent MRSA infections in both the clinical and
community settings.This program has been supported by an educational grant from Pfizer Pharmaceuticals
Understanding and Fighting MRSAUnderstanding and Fighting MRSA
1.1. What is MRSA?What is MRSA?2.2. Why is it such a problem today?Why is it such a problem today?3.3. What is CommunityWhat is Community--associated MRSA?associated MRSA?4.4. Is it really that serious?Is it really that serious?5.5. How is it treated?How is it treated?6.6. How can we prevent it?How can we prevent it?

What is MRSA?What is MRSA?
MethicillinMethicillin--resistant Staphylococcusresistant Staphylococcus aureusaureus
Staph aureusStaph aureus
Transient skin floraTransient skin floraMost common cause of skin infectionsMost common cause of skin infectionsVarious strains with variety of virulence factorsVarious strains with variety of virulence factors–– Encoded by phages,Encoded by phages, plasmidsplasmids,, pathogenicitypathogenicity islands islands
and SCCand SCC
Virulence factorsVirulence factors–– LeukocidinLeukocidin (kills WBC)(kills WBC)–– ExfoliatinsExfoliatins (scalded skin syndrome)(scalded skin syndrome)–– Toxic shock toxin TSS T1 (Toxic shock syndrome)Toxic shock toxin TSS T1 (Toxic shock syndrome)–– EnterotoxinsEnterotoxins (food borne illness)(food borne illness)
History of S.History of S. aureusaureus ResistanceResistance
1941 1941 -- Introduction of Penicillin into Introduction of Penicillin into treatment of infectious diseasetreatment of infectious disease1944 1944 -- S.S. aureusaureus becomes Pen resistantbecomes Pen resistant1959 1959 -- Methicillin introducedMethicillin introduced19601960’’s s -- MRSA strains emergeMRSA strains emerge1968 1968 -- First case found USAFirst case found USA1970/801970/80’’s s -- Problem in hospitals (ICU, Problem in hospitals (ICU, burn units)burn units)

History of S.History of S. aureusaureus ResistanceResistance
1988 2% MRSA1988 2% MRSA1991 29% MRSA1991 29% MRSAToday ~ 70% of S.Today ~ 70% of S. aureusaureus in USA is MRSAin USA is MRSA
010203040506070
1960 1967 1974 1981 1988 1995 2002
% R
esist
ant
USA
Prevalence of MRSA ColonizationPrevalence of MRSA Colonization
Carriage rates in the general population Carriage rates in the general population range from 2 to 10%range from 2 to 10%Recent pediatric study: 36% s.Recent pediatric study: 36% s. aureusaureus ininnaresnares (9% were MRSA)(9% were MRSA)Higher rates among certain populationsHigher rates among certain populations–– Old (nursing home residents)Old (nursing home residents)–– Sick (hospitalized, dialysis)Sick (hospitalized, dialysis)–– Health care workers (ICU, surgical wards)Health care workers (ICU, surgical wards)
One study showed up to 70% colonizedOne study showed up to 70% colonized

Prevalence of MRSA InfectionPrevalence of MRSA Infection
1818--25 cases/100,000 noted in 2001/02 25 cases/100,000 noted in 2001/02 study from CA, GA, and MNstudy from CA, GA, and MN–– MajorityMajority SSTIsSSTIs (77%)(77%)–– 73% resistant to initial antibiotics73% resistant to initial antibiotics
Proportion of PostProportion of Post--op infections with op infections with MRSA from 1992 to 2002 increased from MRSA from 1992 to 2002 increased from 9.2% to 49.3% (NNSI/CDC)9.2% to 49.3% (NNSI/CDC)
Invasive MRSA Infection IncidenceInvasive MRSA Infection Incidence
For every 100,000 people living in the U.S. For every 100,000 people living in the U.S. there were 32 cases of invasive MRSA in there were 32 cases of invasive MRSA in 2005 2005 MRSA was responsible for an estimated MRSA was responsible for an estimated 94,000 life94,000 life--threatening infections and threatening infections and 18,650 deaths in 2005 18,650 deaths in 2005
(CDC report; Oct 17, 2007 (CDC report; Oct 17, 2007 The Journal of The Journal of the American Medical Association)the American Medical Association)
What happened?What happened?
CommunityCommunity--associated associated MRSAMRSA
CA vs. HA MRSACA vs. HA MRSA
CDC definitionsCDC definitions–– ““CommunityCommunity--associatedassociated””
In prior year no hospitalizations, NH, dialysis, In prior year no hospitalizations, NH, dialysis, surgery, or permanent indwelling devicessurgery, or permanent indwelling devices
–– ““associatedassociated”” vs. vs. ““acquired/onsetacquired/onset””CommunityCommunity--acquired = diagnosed in outpatient acquired = diagnosed in outpatient setting or w/in 48hrs of staysetting or w/in 48hrs of stay
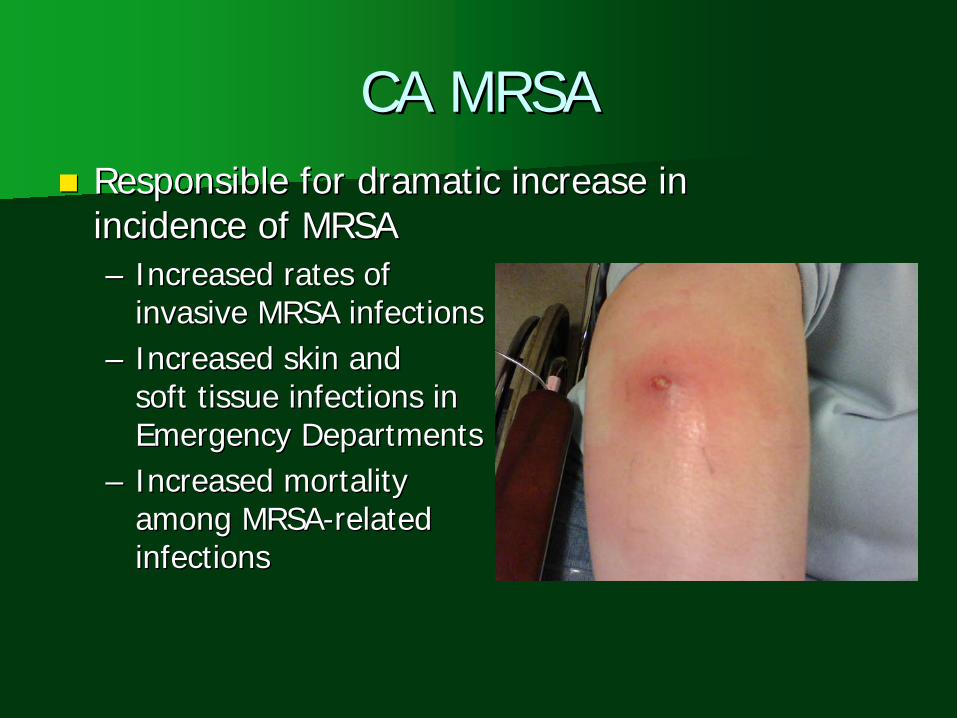
CA MRSACA MRSAResponsible for dramatic increase in Responsible for dramatic increase in incidence of MRSA incidence of MRSA –– Increased rates of Increased rates of
invasive MRSA infectionsinvasive MRSA infections–– Increased skin and Increased skin and
soft tissue infections in soft tissue infections in Emergency DepartmentsEmergency Departments
–– Increased mortality Increased mortality among MRSAamong MRSA--related related infectionsinfections
CA MRSACA MRSA
““Four Pediatric Deaths from CommunityFour Pediatric Deaths from Community--Acquired Acquired MethicillinMethicillin--Resistant Resistant StaphylococcusStaphylococcus aureusaureus ---- Minnesota and North Dakota, 1997Minnesota and North Dakota, 1997--19991999””

The Culprit!The Culprit!
USA300USA300
CA MRSA OutbreaksCA MRSA Outbreaks
Saint Louis Rams in 2003Saint Louis Rams in 2003Fencers in ColoradoFencers in ColoradoPrison inmates (MS, GA, TX)Prison inmates (MS, GA, TX)Children in TennesseeChildren in TennesseeGay men in CaliforniaGay men in California

USA 300 MRSA StrainUSA 300 MRSA Strain
Originated in the communityOriginated in the community““A single clone of CA MRSA accounts A single clone of CA MRSA accounts for the majority of infectionsfor the majority of infections””
Huang,H., et.al. Journal of Clinical Microbiology, July 2006, p.2423-2427 “Comparisons of Community-Associated Methicillin- Resistant Staphylococcus aureus (MRSA) and Hospital- Associated MRSA Infections in Sacramento, California”


CA vs. HA MRSA GeneticsCA vs. HA MRSA Genetics
Community AssociatedCommunity Associated–– USA300 and USA400 USA300 and USA400
PFPF--typestypes–– CarryCarry SCCmecSCCmec IV gene IV gene
Healthcare AssociatedHealthcare Associated–– USA100 and USA200 USA100 and USA200
PFPF--typestypes–– Carry theCarry the SCCmecSCCmec types types
II and IIIII and III
Huang, et al. J. Clin. Microbiol. July 2006, 44:2423-2427

CA vs. HA CharacteristicsCA vs. HA Characteristics
CA MRSACA MRSA–– ““multimulti--drug susceptibledrug susceptible””–– Produce superProduce super--antigens antigens
(SEB, SEC, and TSST(SEB, SEC, and TSST--1)1)
HA MRSAHA MRSA–– ““multimulti--drug resistantdrug resistant””–– Fewer toxins producedFewer toxins produced

CA MRSA in the hospitalCA MRSA in the hospital
Seybold et al. Clin Inf Dis 2006;42:647-56 “Emergence of CA- MRSA USA300 Genotype as a Major Cause of Health Care- Associated Blood Stream Infections”
USA300 accounted for 34% of MRSA BSI over a 7 mo period in 2004 at Grady Memorial Hospital in Atlanta
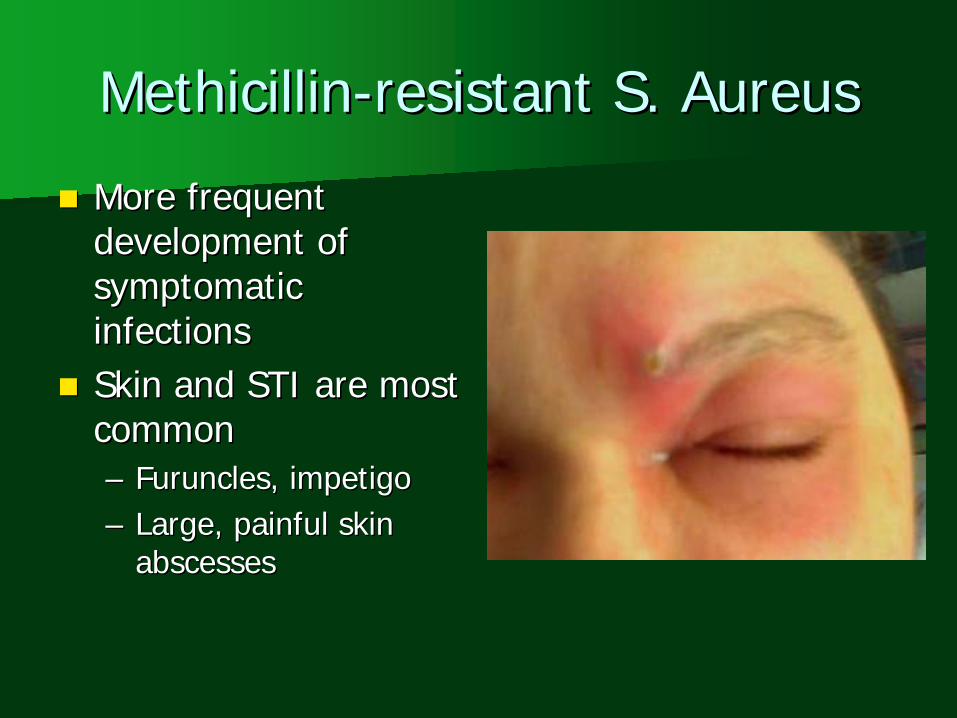
MethicillinMethicillin--resistant S. Aureusresistant S. Aureus
More frequent More frequent development of development of symptomatic symptomatic infectionsinfectionsSkin and STI are most Skin and STI are most commoncommon–– Furuncles, impetigo Furuncles, impetigo –– Large, painful skin Large, painful skin
abscessesabscesses
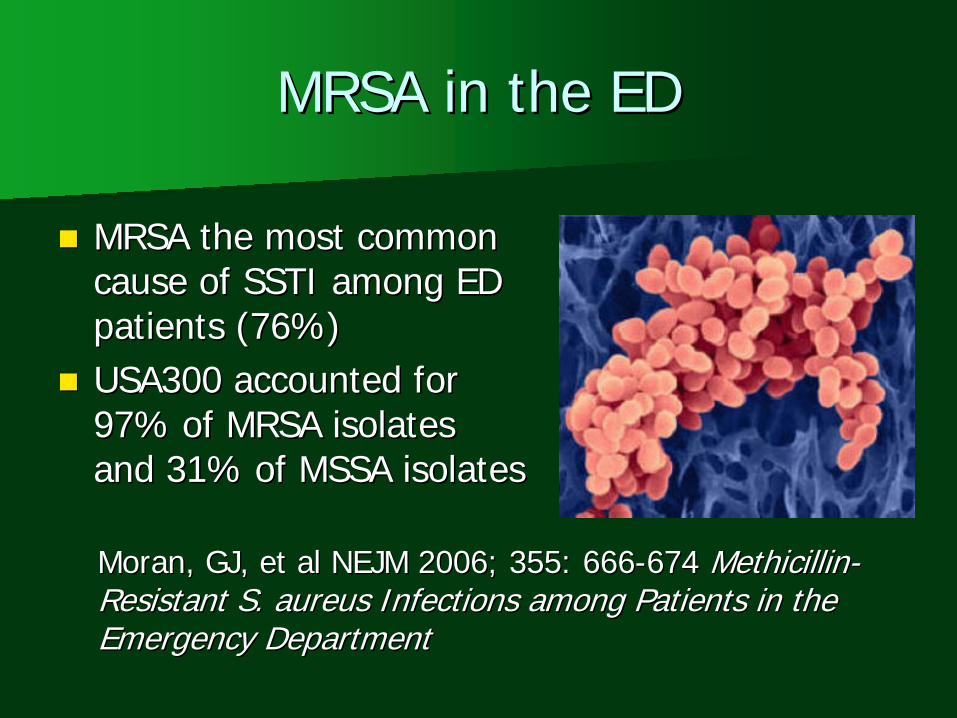
MRSA in the EDMRSA in the ED
MRSA the most common MRSA the most common cause of SSTI among ED cause of SSTI among ED patients (76%)patients (76%)USA300 accounted for USA300 accounted for 97% of MRSA isolates 97% of MRSA isolates and 31% of MSSA isolatesand 31% of MSSA isolates
Moran, GJ, et al NEJM 2006; 355: 666Moran, GJ, et al NEJM 2006; 355: 666--674 674 MethicillinMethicillin-- Resistant S.Resistant S. aureusaureus Infections among Patients in the Infections among Patients in the Emergency DepartmentEmergency Department
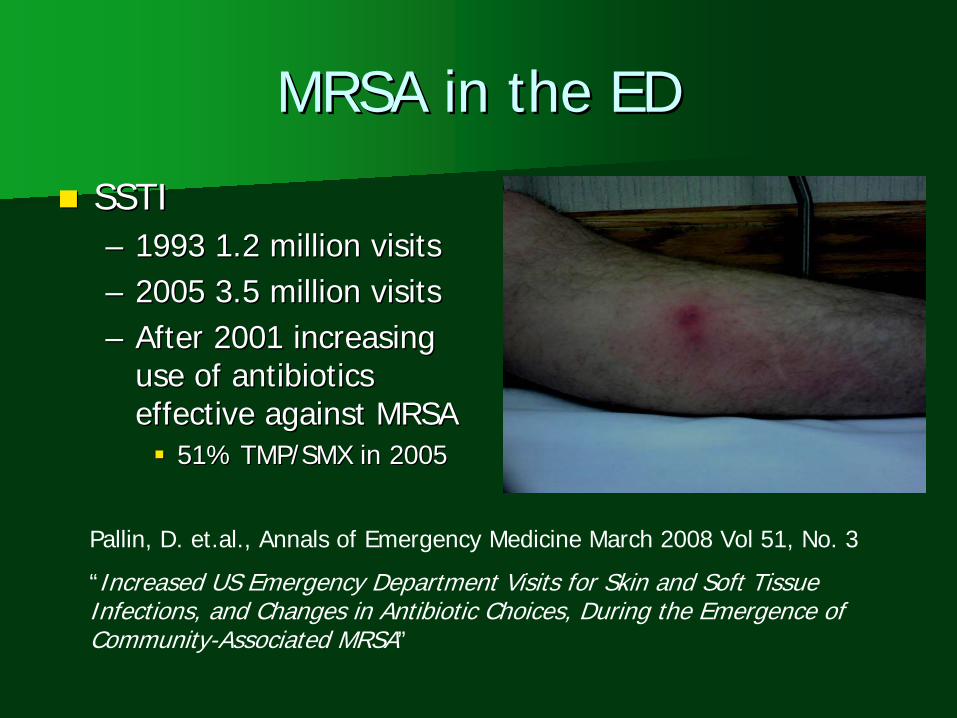
MRSA in the EDMRSA in the ED
SSTI SSTI –– 1993 1.2 million visits1993 1.2 million visits–– 2005 3.5 million visits2005 3.5 million visits–– After 2001 increasing After 2001 increasing
use of antibiotics use of antibiotics effective against MRSAeffective against MRSA
51% TMP/SMX in 200551% TMP/SMX in 2005
Pallin, D. et.al., Annals of Emergency Medicine March 2008 Vol 51, No. 3
“Increased US Emergency Department Visits for Skin and Soft Tissue Infections, and Changes in Antibiotic Choices, During the Emergence of Community-Associated MRSA”
How bad can it get?How bad can it get?
Higher fatality ratesHigher fatality rates–– 2X more likely to die from MRSA than MSSA2X more likely to die from MRSA than MSSA
PyomyositisPyomyositis,, necrotizing fasciitisnecrotizing fasciitis, septic, septicthrombophlebitisthrombophlebitisNecrotizingNecrotizing pneumoniapneumonia–– Lung necrosis,Lung necrosis, empyemaempyema–– Rapid progression to death within 48 to 72 Rapid progression to death within 48 to 72
hourshours
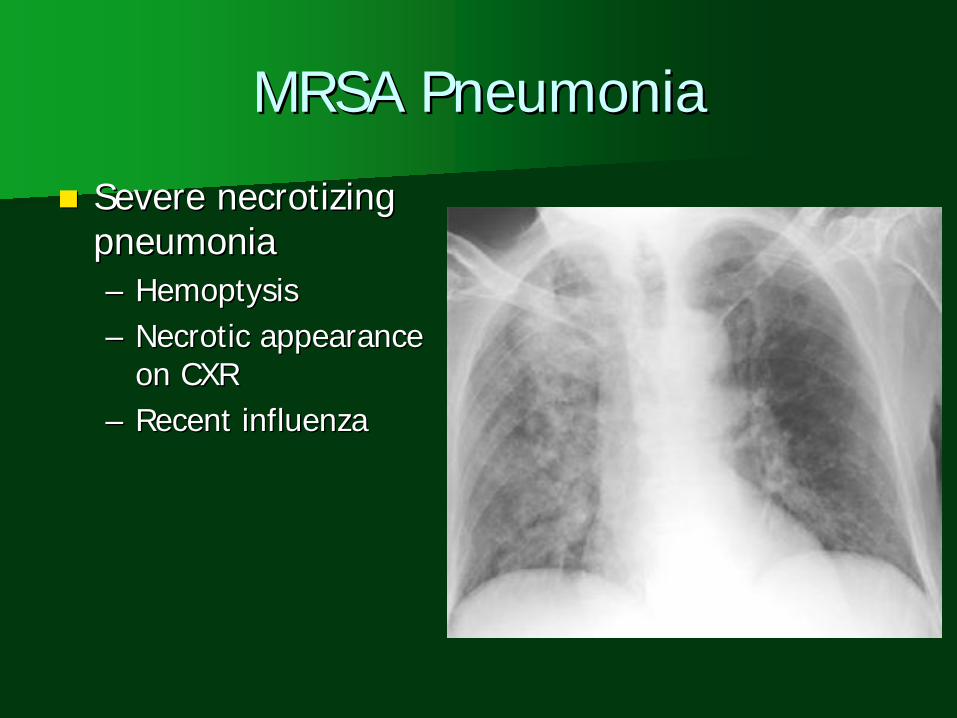
MRSA PneumoniaMRSA Pneumonia
SevereSevere necrotizingnecrotizingpneumoniapneumonia–– HemoptysisHemoptysis–– Necrotic appearance Necrotic appearance
on CXRon CXR–– Recent influenzaRecent influenza
MRSA PneumoniaMRSA Pneumonia
S.S. aureusaureus is most is most common cause of common cause of HospitalHospital--acquired acquired pneumoniapneumoniaMRSAMRSA nosocomialnosocomialpneumonia has been pneumonia has been associated with associated with significantly poorer significantly poorer outcomes than MSSA outcomes than MSSA pneumoniapneumonia

Treatment of MRSA PneumoniaTreatment of MRSA Pneumonia
Antibiotic OptionsAntibiotic Options–– vancomycinvancomycin–– quinupristinquinupristin//dalfopristindalfopristin–– linezolidlinezolid–– daptomycindaptomycin–– tigecyclinetigecycline
Treatment of MRSA PneumoniaTreatment of MRSA Pneumonia
VancomycinVancomycin–– 2g/day (15mg/kg q12hr)2g/day (15mg/kg q12hr)
Goal is trough concentration 15Goal is trough concentration 15--20 mcg/20 mcg/mLmL
–– Poor lung perfusionPoor lung perfusion–– Failure rates up to 40% reportedFailure rates up to 40% reported

Treatment of MRSA PneumoniaTreatment of MRSA Pneumonia
LinezolidLinezolid ((ZyvoxZyvox))–– OxazolidinoneOxazolidinone–– 100 %100 % bioavailabilitybioavailability–– Epithelial lining fluid levels Epithelial lining fluid levels
exceed plasma exceed plasma concentrationsconcentrations
May benefit those withMay benefit those withempyemaempyema//loculationsloculations/abscess/abscess
–– Aerobic gram positive Aerobic gram positive organismsorganisms
Treatment of MRSA PneumoniaTreatment of MRSA Pneumonia
No definite superiority toNo definite superiority to vancomycinvancomycin in in studies to datestudies to dateSide effectsSide effects–– SerotoninSerotonin syndrome (weak MOA inhibitor)syndrome (weak MOA inhibitor)–– thrombocytopeniathrombocytopenia–– neuropathiesneuropathies
Management of MRSA InfectionsManagement of MRSA Infections
Consider in all cases of skin and soft tissue Consider in all cases of skin and soft tissue infections infections –– esp. abscesses and esp. abscesses and ““spider bitesspider bites””Consider in sepsis,Consider in sepsis, osteomyelitisosteomyelitis, septic , septic arthritis, severe pneumonia,arthritis, severe pneumonia, necrotizing necrotizing fasciitisfasciitisCulture all pus!Culture all pus!Blood cultures?Blood cultures?–– Severe disease (sepsis,Severe disease (sepsis, lymphangitislymphangitis))
Management of SSTI InfectionsManagement of SSTI Infections
RecommendationsRecommendations::–– Culture all wounds!Culture all wounds!–– I&D alone may be adequate. Consider I&D alone may be adequate. Consider
antibiotics on individual basis:antibiotics on individual basis:severity and rapidity of progressionseverity and rapidity of progressionsurroundingsurrounding cellulitiscellulitis (>5cm(>5cm diamdiam))signs/symptoms of systemic illnesssigns/symptoms of systemic illnessCoCo--morbidities (DM, malignancy, HIV)morbidities (DM, malignancy, HIV)extremes of ageextremes of ageunable to drain completelyunable to drain completely

Antibiotic OptionsAntibiotic Options
BactrimBactrim–– Not FDA approved for use inNot FDA approved for use in staphstaph but it but it
works.works.–– GAS commonly resistant (consider adding GAS commonly resistant (consider adding
BetaBeta--lactamlactam ifif cellulitiscellulitis))Tetracycline/Tetracycline/minocyclineminocycline//doxycyclinedoxycycline–– Limited studies to support efficacy in invasive Limited studies to support efficacy in invasive
infectionsinfections–– Not in children/pregnancyNot in children/pregnancy–– Also need double coverage forAlso need double coverage for StrepStrep

Antibiotic OptionsAntibiotic Options
ClindamycinClindamycin–– High level of resistance in HA strainHigh level of resistance in HA strain–– Increased incidence of C. diff colitisIncreased incidence of C. diff colitis
LevaquinLevaquin–– High prevalence of resistanceHigh prevalence of resistance–– Not recommended first lineNot recommended first line
VancomycinVancomycin
For severe infections requiring For severe infections requiring hospitalizationhospitalizationMust be given IVMust be given IV““Red man syndromeRed man syndrome””OtotoxicOtotoxicThrombophlebitisThrombophlebitis
Newer AgentsNewer Agents
LinezolidLinezolid ((ZyvoxZyvox))–– VERY effective, but VERY expensiveVERY effective, but VERY expensive–– Available orallyAvailable orally–– Resistance has been reportedResistance has been reported–– MyelosuppressionMyelosuppression with prolonged usewith prolonged use
TigecyclineTigecycline ((TygacilTygacil))–– glycylcyclineglycylcycline–– FDA approved for complicated SSTI andFDA approved for complicated SSTI and intraabd intraabd
infxnsinfxns (not pneumonia)(not pneumonia)–– Active against MRSA and VREActive against MRSA and VRE

Newer AgentsNewer Agents
QuinupristinQuinupristin--dalfopristindalfopristin ((SynercidSynercid))–– Not approved for MRSA infectionsNot approved for MRSA infections–– Poor tolerability profile (Poor tolerability profile (arthralgiasarthralgias,, myalgiasmyalgias,,
thrombophlebitisthrombophlebitis))–– Need central lineNeed central lineDaptomycinDaptomycin ((CubicinCubicin))–– FDA approved in 2003 for MRSA FDA approved in 2003 for MRSA –– bactericidalbactericidal–– Dose dependant myopathyDose dependant myopathy–– Not for pneumonia, CNS or boneNot for pneumonia, CNS or bone
Newer AgentsNewer Agents
CeftobiproleCeftobiprole–– ““fifth generationfifth generation””–– Phase III trials for treatment of Phase III trials for treatment of nosocomialnosocomial
pneumoniapneumonia–– Phase II trials for complicated STTIPhase II trials for complicated STTI–– BacteriocidalBacteriocidal
Clin Infect Dis 2008;46:647-655, 656-658

The ProblemThe Problem
CA MRSA isCA MRSA isspreading fast!spreading fast!
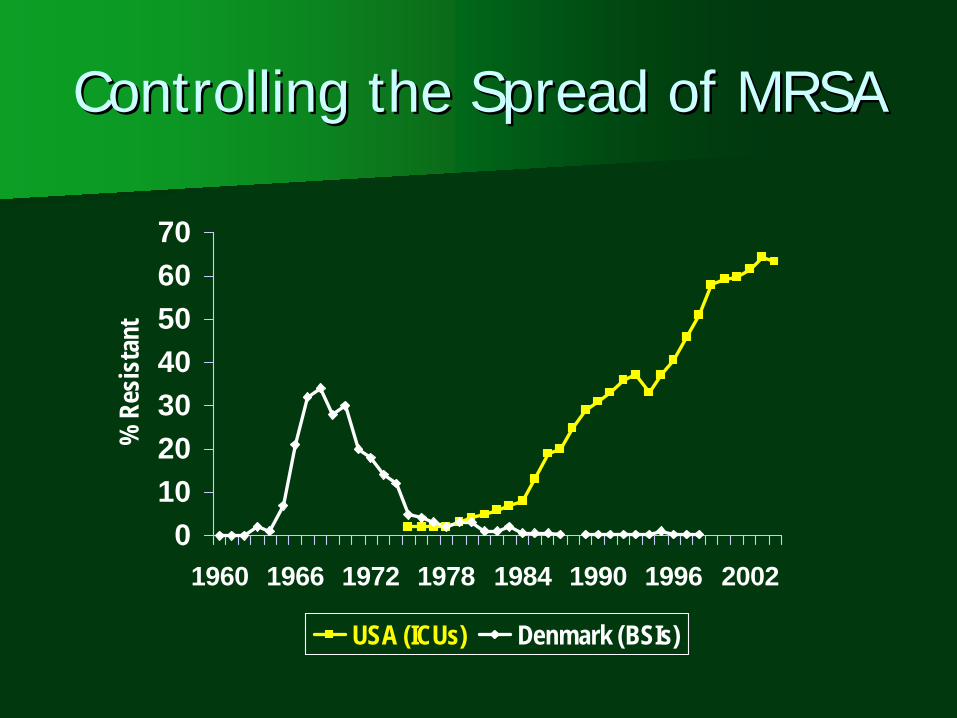
Controlling the Spread of MRSAControlling the Spread of MRSA
010203040506070
1960 1966 1972 1978 1984 1990 1996 2002
% R
esis
tant
USA (ICUs) Denmark (BSIs)
CA MRSA Risk FactorsCA MRSA Risk Factors
Crowding Crowding Person to person contact (athletes)Person to person contact (athletes)Contact with woundsContact with woundsPoor hygienePoor hygieneLow socioeconomic statusLow socioeconomic statusIVDAIVDAHomosexualsHomosexualsPrisonersPrisoners
HA MRSA Risk FactorsHA MRSA Risk Factors
Previous antibiotic usePrevious antibiotic use>8.4 days in hospital>8.4 days in hospitalIndwelling catheters/IVsIndwelling catheters/IVsSurgical proceduresSurgical proceduresDialysisDialysisDiabetesDiabetesNursing Home ResidentsNursing Home Residents

The SolutionThe Solution
Hygiene!Hygiene!Antibiotic stewardship!Antibiotic stewardship!
Education!Education!

Questions?Questions?
Related Documents











