Review Meta-review of depressive subtyping models Baumeister Harald a, b, ⁎, Parker Gordon a, c a Black Dog Institute, Prince of Wales Hospital, Randwick, Australia b Department of Rehabilitation Psychology and Psychotherapy, Institute of Psychology, University of Freiburg, Germany c School of Psychiatry, University of New South Wales, Sydney, Australia article info abstract Article history: Received 2 March 2011 Received in revised form 11 May 2011 Accepted 15 July 2011 Available online 1 September 2011 Background: Increasing dissatisfaction with the non-specificity of major depression has led many to propose more specific depressive subtyping models. The present meta-review seeks to map dominant depressive subtype models, and highlight definitions and overlaps. Methods: A database search in Medline and EMBASE of proposed depressive subtypes, and limited to reviews published between 2000 and 2011, was undertaken. Of the more than four thousand reviews, 754 were judged as potentially relevant and provided the base for the present selective meta-review. Results: Fifteen subtype models were identified. The subtypes could be divided into five molar categories of (1) symptom-based subtypes, such as melancholia, psychotic depression, atypical depression and anxious depression, (2) aetiologically-based subtypes, exemplified by adjustment disorders, early trauma depression, reproductive depression, perinatal depression, organic depression and drug-induced depression, (3) time of onset-based subtypes, as illustrated by early and late onset depression, as well as seasonal affective disorder, (4) gender-based (e.g. female) depression, and (5) treatment resistant depression. An overview considering definition, bio- psycho-social correlates and the evidence base of treatment options for each subtype is provided. Limitations: Despite the large data base, this meta-review is nevertheless narrative focused. Conclusions: Subtyping depression is a promising attempt to overcome the non-specificity of many diagnostic constructs such as major depression, both in relation to their intrinsic non-specificity and failure to provide treatment-specific information. If a subtyping model is to be advanced it would need, however, to demonstrate differential impacts of causes and treatments. © 2011 Elsevier B.V. All rights reserved. Keywords: Subtypes of depression Melancholia Atypical depression Psychotic depression Aetiology Contents 1. Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 127 2. Methods . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 127 3. Results . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 128 3.1. Symptom-based subtypes of depression . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 128 3.1.1. Melancholia . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 128 3.1.2. Psychotic (delusional) depression . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 128 3.1.3. Atypical depression . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 130 3.1.4. Anxious depression . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 130 Journal of Affective Disorders 139 (2012) 126–140 ⁎ Corresponding author at: University of Freiburg, Institute of Psychology, Department of Rehabilitation Psychology and Psychotherapy, Engelbergerstr. 41, D-79085 Freiburg, Germany. Tel.: +49 761 203 3044; fax: +49 761 203 3040. E-mail address: [email protected] (H. Baumeister). 0165-0327/$ – see front matter © 2011 Elsevier B.V. All rights reserved. doi:10.1016/j.jad.2011.07.015 Contents lists available at ScienceDirect Journal of Affective Disorders journal homepage: www.elsevier.com/locate/jad

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Journal of Affective Disorders 139 (2012) 126–140
Contents lists available at ScienceDirect
Journal of Affective Disorders
j ourna l homepage: www.e lsev ie r.com/ locate / j ad
Review
Meta-review of depressive subtyping models
Baumeister Harald a,b,⁎, Parker Gordon a,c
a Black Dog Institute, Prince of Wales Hospital, Randwick, Australiab Department of Rehabilitation Psychology and Psychotherapy, Institute of Psychology, University of Freiburg, Germanyc School of Psychiatry, University of New South Wales, Sydney, Australia
a r t i c l e i n f o
⁎ Corresponding author at: University of Freiburg,D-79085 Freiburg, Germany. Tel.: +49 761 203 3044
E-mail address: [email protected]
0165-0327/$ – see front matter © 2011 Elsevier B.V.doi:10.1016/j.jad.2011.07.015
a b s t r a c t
Article history:Received 2 March 2011Received in revised form 11 May 2011Accepted 15 July 2011Available online 1 September 2011
Background: Increasing dissatisfaction with the non-specificity of major depression has ledmany to propose more specific depressive subtyping models. The present meta-review seeks tomap dominant depressive subtype models, and highlight definitions and overlaps.Methods: A database search in Medline and EMBASE of proposed depressive subtypes, andlimited to reviews published between 2000 and 2011, was undertaken. Of the more than fourthousand reviews, 754 were judged as potentially relevant and provided the base for thepresent selective meta-review.Results: Fifteen subtype models were identified. The subtypes could be divided into five molarcategories of (1) symptom-based subtypes, such as melancholia, psychotic depression, atypicaldepression and anxious depression, (2) aetiologically-based subtypes, exemplified by adjustmentdisorders, early trauma depression, reproductive depression, perinatal depression, organicdepression and drug-induced depression, (3) time of onset-based subtypes, as illustrated by earlyand late onset depression, as well as seasonal affective disorder, (4) gender-based (e.g. female)depression, and (5) treatment resistant depression. An overview considering definition, bio-psycho-social correlates and the evidence base of treatment options for each subtype is provided.Limitations: Despite the large data base, this meta-review is nevertheless narrative focused.Conclusions: Subtyping depression is a promising attempt to overcome thenon-specificity ofmanydiagnostic constructs such as major depression, both in relation to their intrinsic non-specificityand failure to provide treatment-specific information. If a subtyping model is to be advanced itwould need, however, to demonstrate differential impacts of causes and treatments.
© 2011 Elsevier B.V. All rights reserved.
Keywords:Subtypes of depressionMelancholiaAtypical depressionPsychotic depressionAetiology
Contents
1. Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1272. Methods . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1273. Results . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 128
3.1. Symptom-based subtypes of depression . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1283.1.1. Melancholia . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1283.1.2. Psychotic (delusional) depression . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1283.1.3. Atypical depression . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1303.1.4. Anxious depression . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 130
Institute of Psychology, Department of Rehabilitation Psychology and Psychotherapy, Engelbergerstr. 41,; fax: +49 761 203 3040.urg.de (H. Baumeister).
All rights reserved.

127Baumeister, H., Parker, G. / Journal of Affective Disorders 139 (2012) 126–140
3.2. Aetiologically-based subtypes of depression . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1303.2.1. Adjustment disorder with depressed mood . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1313.2.2. Early trauma depression . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1313.2.3. Reproductive depression . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1323.2.4. Perinatal depression . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1323.2.5. Organic and drug induced depression . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 133
3.3. Time of onset based subtypes of depression . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1333.3.1. Early vs. late onset depression . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1333.3.2. Seasonal affective disorder . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 133
3.4. Female depression . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1343.5. Treatment resistant depression . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 134
4. Discussion . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 134Role of funding source . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 135Conflict of interest . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 135Appendix A . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 135References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 137
1. Introduction
The current classification of unipolar depression essen-tially relies on the presence of a defined number of clinicalfeatures and a time period over which these symptoms needto be present (Paykel, 2008), as well as by identification ofimpairment (Baumeister, 2010; Wakefield et al., 2010). Themost prominent candidate is DSM-defined major depressionwith 12-month prevalence rates between 6.3% and 10.3%across western societies (Baumeister and Härter, 2007).Major depression is commonly contrasted with a set of‘minor’ depressions (dysthymia, depressive disorder NOS)and extended to include sub-threshold or sub-clinicaldepressive states with even fewer depressive symptoms(Baumeister and Morar, 2008; Parker and Manicavasagar,2005). This model can be viewed as a variant of the former‘unitarian’ model of depression, which viewed depressionas a single condition varying by severity. Due to the highprevalence of clinical depression — as well as its associateddisability and burden (Baumeister et al., in press, 2011;Hutter et al., 2010; WHO, 2008), it has generated the mostresearch and clinical focus of all psychiatric disorders.
However, after two decades of extensive research effortsconsidering major depression, dissatisfaction with its non-specificity is increasingly evident (Ghaemi, 2008; Luyten et al.,2006; Parker, 2005, 2006). There are 227 possible symptomconstellations of a DSM-IV-defined major depression episode(APA, 2000). Further, latent class analyses have indicated sub-stantial heterogeneity in depressive symptomatology (Carragheret al., 2009; Sullivan et al., 2002), so that a diagnosis of majordepression effectively risks ‘homogenising’ constituent types orconditions, in the sameway that a diagnosis of ‘major dyspnoea’might homogenise constituent conditions such as asthma,pneumonia or a pulmonary embolus. The clinical presentationof major depression is even more heterogeneous if course andseverity – as well as possible aetiological explanations – aretaken into account (Keller et al., 2007b; Luyten et al., 2006;Parker, 2005). As a consequence of its heterogeneity, there is apredictable lack of consistent genetic and neurobiologicalfindings validating major depression as a distinct or even cleardiagnostic entity (Antonijevic, 2006, 2008; Krishnan andNestler,
2010; Shyn and Hamilton, 2010). Finally, and most importantly,the comparable efficacy of psychotherapies and antidepressantmedication treatments (Baumeister et al., 2011, in press;Cuijpers et al., 2010; Ghaemi, 2008; Kirsch et al., 2008; Pigottet al., 2010; Turner et al., 2008) does not allow us to deducespecific treatment strategies for those receiving a diagnosisof major depression. Such limitations presumably reflectmajor depression being a non-specific domain diagnosis thatsubsumes numerous conditions, potentially differing (tosome degree) by their clinical picture, causes and differentialcapacities to respond to differing interventions.
As a consequence, many writers have advanced alternatedepressive subtyping models. Any qualitative review of suchwritings indicates considerable variation in both the definitionand separation of subtypes, and risks subjective and idiosyncraticinterpretation. The present meta-review (review of reviews)therefore seeks to map subtypes of depression, and highlightdefinitions, overlaps and idiosyncrasies of each subtype, as wellas consider their empirical evidence in termsof bio-psycho-socialcorrelates and interventions. The meta-review has the potentialto advance more refined and applied research.
2. Methods
To identify current subtype models of depression, weconducted a database search in Medline and EMBASE (from2000 to Jan. 5th 2011; limited to English or German reviewswith an abstract), and with the detailed search strategypresented in Appendix A. The time period sought ensuresonly recently published reviews rather than providing ahistoric overview about earlier hypotheses and multiplesubtype models, often weighted to idiosyncratic formula-tions. The iterative search process commenced with subtypesdefined by other reviews (Baumeister and Parker, 2010; Bech,2010; Benazzi, 2006; Lichtenberg and Belmaker, 2010;Paykel, 2008; Rush, 2007). Additional subtypes identifiedduring that process were added to the search strategy andthe database search was repeated. Excluded from the searchwere depressive conditions defined by illness course (single,recurrent, or chronic major depression, dysthymic disorder)or by disorder severity, being viewed as more modifiers of

128 Baumeister, H., Parker, G. / Journal of Affective Disorders 139 (2012) 126–140
depression rather than distinct subtypes. The final databasesearch yielded 4594 potentially relevant reviews. Afterscreening all titles and abstracts, we judged 754 as relevantto this meta-review. From this database we selected recentgeneral overviews as well as reviews on specific topics oneach subtype for inclusion in our meta-review.
3. Results
The search process revealed 15 frequently proposed depres-sive subtypes (Fig. 1), now consolidated as (1) symptom-based,(2) aetiologically-based, and (3) time of onset-based subtypes,as well as (4) female depression as a gender-based subtypeand (5) treatment resistant depression (TRD) as a treatmentresponse-based subtype. These categories are not assumed asnecessarily distinct from each other, but rather representdifferent starting points for subtyping. As a result, there issubstantial overlap across the five categories (e.g. a patientmight fulfil criteria for early trauma depression, early-onsetdepression and atypical depression).
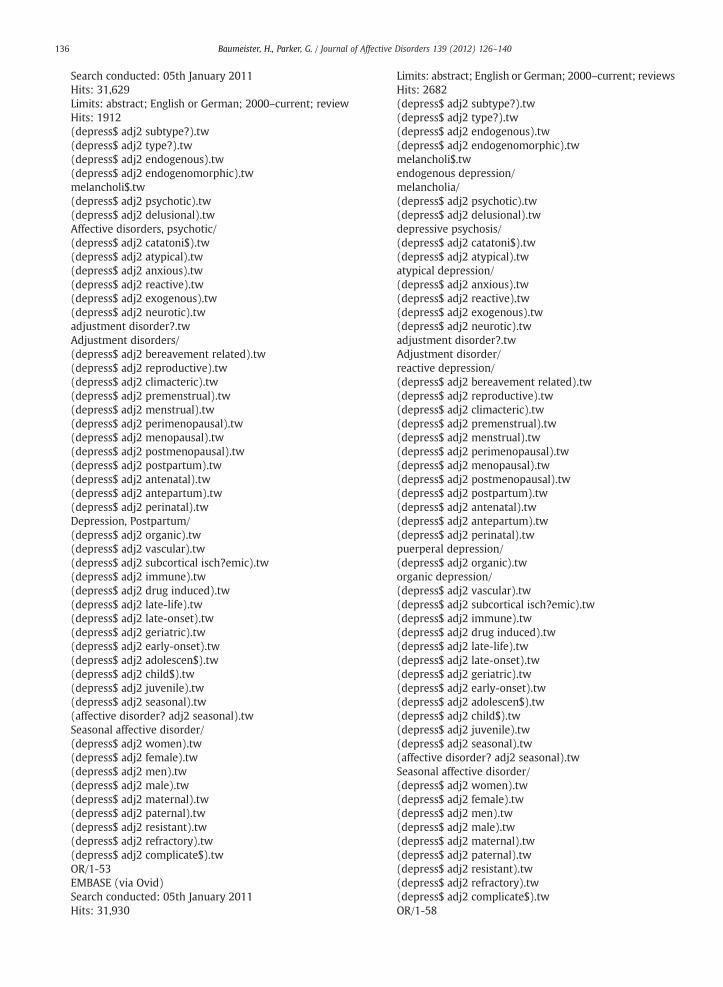
Table 1 summarises details on the definition, bio-psycho-social correlates and evidence base of subtype specifictreatment options for each subtype, to some degree simplifyingthe complex research on each model. While we discuss theprincipal aspects and controversies surrounding each subtype,the overall cited literature offers a comprehensive overviewabout aspects and current hypotheses in relation to thepostulated subtype models.
3.1. Symptom-based subtypes of depression
The four principal symptom-based subtypes of depression –
melancholia, psychotic depression, atypical depression andanxious depression – are characterised by specified clusters ofdiffering or differentially represented depressive symptoms.While latent class and factor analyseshave frequentlymodelledmelancholia and atypical depression as subtypes of depressionas a higher ‘class’ (Biro and Till, 1989; Marcos and Salamero,1990; Sullivan et al., 2002), psychotic depression and anxiousdepression tend to be more positioned as distinct subtypes onthe basis of respective core symptoms of psychotic features andcomorbid anxiety being dominant.
3.1.1. Melancholia
3.1.1.1. Definition.Melancholia is oneof sixDSM-IV specifiers ofmajor depression disorder (i.e. MD with melancholic features)(APA, 2000). However, the DSM diagnostic criteria areviewed as too non-specific to be able to delineate melancholiafrom other subtypes of depression and even from majordepression itself (Parker et al., 2010a; Taylor and Fink, 2008).Beyond DSM-IV, there are several conceptualisations ofmelancholia and similar concepts such as ‘endogenous’,‘endogenomorphic’, ‘autonomous’, ‘vital’, ‘Type A’ and ‘typical’depression (Leventhal and Rehm, 2005; Parker et al., 2010a),complicating the integration of the empirical evidence as itis not necessarily clear that such terms always refer to aputative nuclear melancholic ‘type’. Current proposals for adistinctmelancholia disorder weight (1) a disturbance in affectmarked by apprehension and morbid statements, bluntedemotional response, nonreactive mood, and pervasive anhe-
donia, (2) psychomotor disturbance expressed as retardationor agitation, and (3) vegetative and cognitive signs of interruptedsleep, loss of appetite, reduced libido, diurnal variation withmood and energy generally worse in the morning, as well asimpaired concentration and working memory (Parker et al.,2010a; Taylor and Fink, 2008).
3.1.1.2. Correlates. Core biological correlates which have beenproposed to delineate melancholia from non-melancholicdepression are hypercortisolemia, psychomotor disturbanceand specific sleep patterns — characterised by reduced REMlatency, increased REM time, and reduced deep sleep(Antonijevic, 2008; Armitage, 2007; Buyukdura et al., 2011;Dinan and Scott, 2005; Gold and Chrousos, 2002; Heim et al.,2004; Leventhal and Rehm, 2005; Parker et al., 2010a; Taylorand Fink, 2008). Psycho-social correlates are more elusive,but include fewer distal and proximal adverse life events, alower likelihood of personality disorder and parasuicide aswell as a higher likelihood of actual suicide (Coryell, 2007;Leventhal and Rehm, 2005).
3.1.1.3. Treatment. Based on preliminary evidence, researchdata suggest that patients with melancholia might respondbetter to broad-action tricyclic antidepressants (TCAs) thanto narrow-action antidepressants (e.g. selective serotoninuptake inhibitors (SSRI)), and well to electroconvulsivetherapy (ECT) (Parker et al., 2010a; Taylor and Fink, 2008).Moreover, melancholia appears to predict a poor response toplacebo, psychotherapy and social interventions (Brown,2007; Leventhal and Rehm, 2005; Malhi et al., 2005; Thaseand Friedman, 1999).
3.1.2. Psychotic (delusional) depression
3.1.2.1. Definition. DSM-IV allows for specification of severemajor depressionwith psychotic features,marked by delusionsor hallucinations. Since psychotic features have been reportedin those with mild to moderate major depression, anydiagnostic weighting to severity has been questioned (Kelleret al., 2007a; Lykouras and Gournellis, 2009). Specific symp-toms that appear to be more pronounced in psychotic than innon-psychotic depression are, by definition, psychotic featuresas well as over-valued feelings of guilt and worthlessness,severe psychomotor disturbance and cognitive symptoms,characterised by deficits in attention, psychomotor speed,executive functioning andmemory (Fleming et al., 2004; Kelleret al., 2007a; Lykouras and Gournellis, 2009; Rothschild, 2003).In line with these core features, some conceptualise psychoticdepression parsimoniously as melancholia with additionalpsychotic features (Malhi et al., 2005; Taylor and Fink, 2008).
3.1.2.2. Correlates. Similar to melancholia, core biologicalcorrelates are hypercortisolemia and reduced REM latency(Keller et al., 2007a; Lykouras and Gournellis, 2009; Rothschild,2003). In relation to healthy control subjects, a decrease inserum dopamine-beta-hydroxylase activity (the enzyme thatconverts dopamine to norepinephrine) compared to an in-creased activity in non-psychotic depressed patientswas shown(Keller et al., 2007a; Lykouras and Gournellis, 2009; Rothschild,2003). Moreover, enlarged cerebral ventricles and paralimbicabnormalities have been reported (Keller et al., 2007a; Lykouras
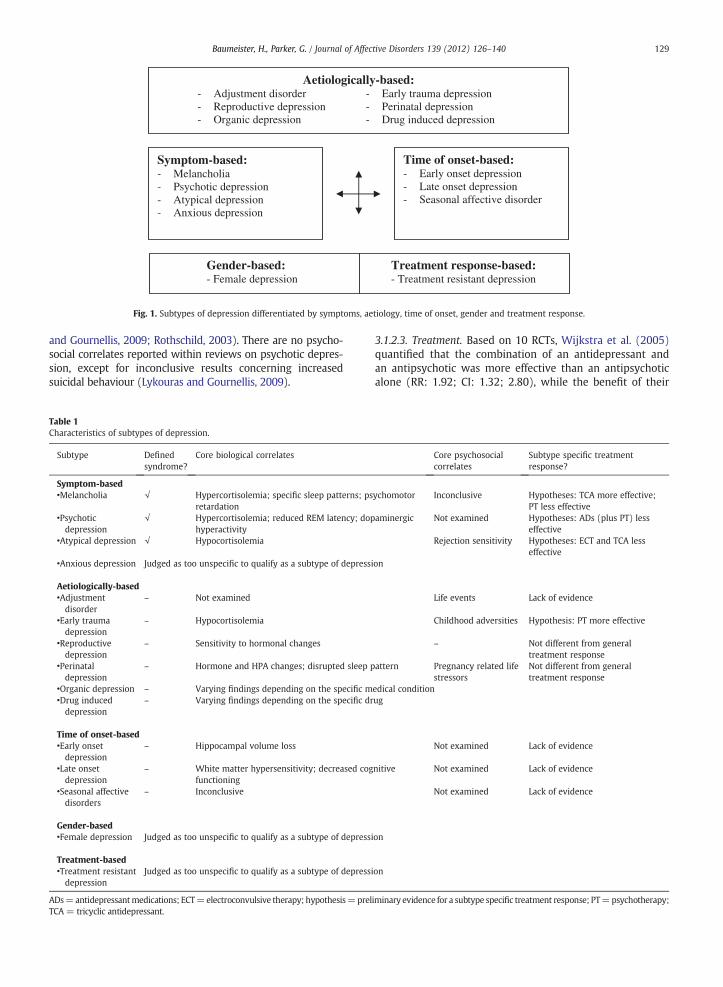
Aetiologically-based: - Adjustment disorder - Early trauma depression - Reproductive depression - Perinatal depression - Organic depression - Drug induced depression
Symptom-based: - Melancholia - Psychotic depression - Atypical depression - Anxious depression
Time of onset-based: - Early onset depression - Late onset depression - Seasonal affective disorder
Gender-based: Treatment response-based: - Female depression - Treatment resistant depression
Fig. 1. Subtypes of depression differentiated by symptoms, aetiology, time of onset, gender and treatment response.
129Baumeister, H., Parker, G. / Journal of Affective Disorders 139 (2012) 126–140
and Gournellis, 2009; Rothschild, 2003). There are no psycho-social correlates reported within reviews on psychotic depres-sion, except for inconclusive results concerning increasedsuicidal behaviour (Lykouras and Gournellis, 2009).
Table 1Characteristics of subtypes of depression.
Subtype Definedsyndrome?
Core biological correlates
Symptom-based•Melancholia √ Hypercortisolemia; specific sleep patterns; ps
retardation•Psychoticdepression
√ Hypercortisolemia; reduced REM latency; dophyperactivity
•Atypical depression √ Hypocortisolemia
•Anxious depression Judged as too unspecific to qualify as a subtype of depressi
Aetiologically-based•Adjustmentdisorder
– Not examined
•Early traumadepression
– Hypocortisolemia
•Reproductivedepression
– Sensitivity to hormonal changes
•Perinataldepression
– Hormone and HPA changes; disrupted sleep p
•Organic depression – Varying findings depending on the specific m•Drug induceddepression
– Varying findings depending on the specific dr
Time of onset-based•Early onsetdepression
– Hippocampal volume loss
•Late onsetdepression
– White matter hypersensitivity; decreased cogfunctioning
•Seasonal affectivedisorders
– Inconclusive
Gender-based•Female depression Judged as too unspecific to qualify as a subtype of depressi
Treatment-based•Treatment resistantdepression
Judged as too unspecific to qualify as a subtype of depressi
ADs=antidepressantmedications; ECT=electroconvulsive therapy; hypothesis=prelTCA = tricyclic antidepressant.
3.1.2.3. Treatment. Based on 10 RCTs, Wijkstra et al. (2005)quantified that the combination of an antidepressant andan antipsychotic was more effective than an antipsychoticalone (RR: 1.92; CI: 1.32; 2.80), while the benefit of their
Core psychosocialcorrelates
Subtype specific treatmentresponse?
ychomotor Inconclusive Hypotheses: TCA more effective;PT less effective
aminergic Not examined Hypotheses: ADs (plus PT) lesseffective
Rejection sensitivity Hypotheses: ECT and TCA lesseffective
on
Life events Lack of evidence
Childhood adversities Hypothesis: PT more effective
– Not different from generaltreatment response
attern Pregnancy related lifestressors
Not different from generaltreatment response
edical conditionug
Not examined Lack of evidence
nitive Not examined Lack of evidence
Not examined Lack of evidence
on
on
iminary evidence for a subtype specific treatment response; PT=psychotherapy;

130 Baumeister, H., Parker, G. / Journal of Affective Disorders 139 (2012) 126–140
combination over an antidepressant alone did not reachsignificance (RR: 1.44; CI: .86; 2.41). An earlier meta-analysisof a larger sample of clinical studies, however, indicated that acombination was significantly more effective than bothantipsychotic and antidepressant medication alone (Parkeret al., 1992). Within the class of antidepressants, TCAs havebeen suggested as superior to SSRIs (Wijkstra et al., 2005).ECT has been shown to be at least as effective as pharmaco-logical treatment (Keller et al., 2007a; Tyrka et al., 2006; Vegaet al., 2000). Compared with non-psychotic depressedpatients, those with psychotic depression appear to show apoorer response to antidepressant medications alone as wellas to combined antidepressant medication and psychother-apy treatment (Gaudiano et al., 2005). The latter findings,however, have been viewed as based only on limited data(Gaudiano et al., 2005, 2007).
3.1.3. Atypical depression
3.1.3.1. Definition. As defined by DSM-IV, the main criterionfor atypical depression is mood reactivity in combinationwith two or more of the following secondary symptoms:weight gain or increased appetite, hypersomnia, leadenparalysis, and long-standing vulnerability to rejection. Basedon this definition, atypical depression is a rather prevalentdepressive condition, estimated as present in 15%–50% of alldepressed patients (depending on criteria, method andsetting) (Thase, 2007) and to be two to three times morelikely in women than in men (Halbreich and Kahn, 2007;Parker, 2007). However, there is an ongoing debate about thebest criteria to delineate atypical depression from melancho-lia and other depressive conditions. Controversy concerns thevalidity of mood reactivity as the main criterion, rejectionsensitivity as an alternative core feature, and of anxiety andsomatic complaints as additional criteria as well as earlyonset and chronic course being necessary criteria (Paing et al.,2008; Parker, 2007; Parker et al., 2002; Stewart et al., 2007;Stewart et al., 2009; Thase, 2007; Thase, 2009).
3.1.3.2. Correlates. Diametrically differing to melancholia andpsychotic depression, and different fromother non-melanchol-ic depressive conditions as well, atypical depression appears tobe associatedwith abnormally decreasedHPAaxis function andhypocortisolemia, at least in a subsample of atypical depressionin those with an early-onset and chronic course (Posternak,2003; Thase, 2009). The finding of hypocortisolemia has ledsome to propose a link between atypical depression andboth the chronic fatigue syndrome and post-traumatic stressdisorder, for which hypocortisolemia was shown as well(Juruena and Cleare, 2007; Thase, 2009), but we do notconsider that sufficient support to include those latter statesin any sub-typing model of clinical depression. Moreover,abnormally increased right hemispheric processing wasreported, delineating atypical depression from bothmelancho-lia and other depressive conditions (Thase, 2009). There are nopsycho-social correlates reported within reviews on atypicaldepression, except for rejection sensitivity being proposed as acentral criterion of this diagnosis (Pae et al., 2009; Parker,2007).
3.1.3.3. Treatment. The term ‘atypical’ originated from ahistorically reported poor treatment response to TCAs and asuperior response to monoamine oxidase inhibitors (MAOIs)in patients with atypical depression (Davidson, 2007). Ameta-analysis of antidepressant medication treatmentsshowed, based on a limited evidence base, that MAOIs areindeed superior to TCAs and placebo, but only comparableeffective to SSRIs (Henkel et al., 2006). ECT is assumed to beineffective for patients with atypical depression, however,evidence for this assumption is lacking (Stewart et al., 2009).Psychotherapeutic intervention remains mostly unmen-tioned in reviews of atypical depression, despite its provenefficacy against MAOIs in one RCT comparing cognitivebehaviour therapy and phenelzine (response rate being 58%for both active treatments compared to 28% for placebo;while 92% of those receiving phenelzine had marked side-effects) (Pae et al., 2009; Stewart and Thase, 2007). Thus, theearlier suggested specificity of response to an MAOI has notbeen sustained, an issue of importance in and of itself inrelation to subtype definition but also important in cost–benefit treatment considerations.
3.1.4. Anxious depressionAnxious depression has been suggested as a specific
subtype, but has not as yet been included as DSM-IV specifierof major depression (Rao and Zisook, 2009; Silverstone andvon Studnitz, 2003). Most writers conceptualise it reflectingmajor depression with a distinct comorbid anxiety disorderor as major depression with a high level of anxiety (Rao andZisook, 2009; Silverstone and von Studnitz, 2003). Alterna-tively, anxious depression might be conceptualised as majordepressionwith anxiety beingmore distinctive or severe thanthe depression, or with anxiety being the antecedent driverfor the depression (Parker and Manicavasagar, 2005). Basedon these definitions, anxious depression risks overlap withmelancholia, psychotic depression and atypical depression,which frequently manifest comorbid anxiety disorders, atleast during an episode but not necessarily as an antecedentcause. The present review failed to identify any evidence forspecific biological and psycho-social correlates of anxiousdepression other than an early age of onset (Rao and Zisook,2009; Silverstone and von Studnitz, 2003). While treatmentof complex patients in terms of multimorbidity needs specialattention, no evidence has been provided of specific treat-ment effects in patients with anxious depression comparedto patients with major depression in general (Diefenbach andGoethe, 2006; Panzer, 2005; Rao and Zisook, 2009; Silverstoneand von Studnitz, 2003). Thus, based on its present con-ceptualisation, there is no evidence to argue for anxiousdepression qualifying as a specific subtype of depression.
3.2. Aetiologically-based subtypes of depression
The political drive to move psychiatry away from itspsychoanalytic weighting (Nesse, 2007) as well as inconclu-sive results examining for differential associations betweenlife stressors and both non-melancholic reactive and melan-cholic depression (Paykel, 2008; Shorter, 2007) led to DSM-IIIexcluding ‘causes’ for mental disorders, including the depres-sive conditions. As depression is commonly viewed accordingto a diathesis–stress model (Goldberg, 2006; Hammen, 2005;

131Baumeister, H., Parker, G. / Journal of Affective Disorders 139 (2012) 126–140
Uher, 2008), each attempt to reduce the psychopathology to asingle cause runs the risk of confounding the identification ofother important determinants (Pies, 2009). On the otherhand, ignoring aetiology means ignoring important diagnos-tic information for validly assessing depressive disorders(Nesse, 2007). It might be that aetiologically defined subtypesof depression were, in fact, never completely abandoned inDSM as a consequence of the latter factor — as evidenced bythe DSM-IV categories of adjustment disorders, mood dis-orders due to a general medical condition, substance-inducedmood disorders and postpartum depression. Further, fre-quently considered aetiologically-defined subtypes of de-pression include early trauma depression as well as antenataldepression and reproductive depression.
3.2.1. Adjustment disorder with depressed mood
3.2.1.1. Definition. Adjustment disorder with depressed moodis defined by DSM-IV as a disorder characterised by de-pressive symptoms in response to an identifiable stressor,but not fulfilling the criteria of another specific mood dis-order. As such, it replaced the former diagnosis of reactivedepression, except for its limitation to subthreshold depres-sion (Baumeister et al., 2009). In clinical practice, however,this diagnosis is also frequently used for patients fulfilling thecriteria for major depression, making an adjustment disorderwith depressed mood one of the most frequent diagnoses inclinical practice (Casey, 2009). Against this background, itseems surprising that adjustment disorders are neglected byresearchers (Baumeister et al., 2009; Baumeister and Kufner,2009; Casey, 2009; Laugharne et al., 2009; Strain et al., 2011).Such neglect is likely to reflect multiple reasons – includingthe lower scientific appeal of minor disorders – but is mostcommonly viewed as reflecting inadequate operationalisa-tion of adjustment disorders and poor delineation of adjust-ment disorders from normal stress responses and from otherspecific disorders (Baumeister et al., 2009; Baumeister andKufner, 2009; Laugharne et al., 2009; Semprini et al., 2010).
3.2.1.2. Correlates. There is no evidence for specific biologicalcorrelates (Laugharne et al., 2009). In regard to psycho-socialcorrelates, the core question is whether or not there is a causallink between the stressor and depressive symptomatology orwhether antecedent stressors are non-causal epiphenomena oreven consequences of the depressed mood state. While ageneral linear association between both severity and numberof negative events and the probability of depression has beenreported (Hammen, 2005; Tennant, 2002), current researchweights a complex diathesis–stress interaction, with geneticcontributions (e.g. neuroticism) and developmental factors(e.g. early adversity) moderating vulnerability to depression,which in turn increases the likelihood of experiencing stressfullife events and reduces the threshold at which stressorsprecipitate depression (Hammen, 2005; Heim et al., 2008;Risch et al., 2009; Uher, 2008).
3.2.1.3. Treatment. There is almost no evidence supportingany treatment of adjustment disorders with depressed moodhaving specific benefit, which both reflects the limitedresearch attention and the high spontaneous remission ratein such states. Expert recommendations, however, advocate
brief psychological interventions and stepped care modelsstarting with close monitoring and counselling (Casey, 2009;Laugharne et al., 2009; Strain et al., 2011).
3.2.2. Early trauma depression
3.2.2.1. Definition. Childhood adversities such as sexual andphysical abuse, emotional abuse and neglect – as well asparental loss – have consistently been quantified as strongpredictors of depression in adulthood (Hammen, 2005; Heimet al., 2008, 2010; Maniglio, 2010; Neigh et al., 2009). Owingto increasing evidence of specific biological correlates andtreatment effects in depressed patients with a history ofchildhood trauma, early trauma depression has been sug-gested as a specific depressive subtype (shaped by geneticand other risk factors for depression) (Heim et al., 2008,2010). A definition of this subtype in terms of expressions andonset of childhood adversities or traumata as well asassociated symptoms has, however, not yet been provided.
3.2.2.2. Correlates. Research on childhood adversity suggeststhat several of the biological changes reported for depressionmight be secondary to childhood adversity itself (Heim et al.,2008). These changes include the increased probability of along-term disturbance of the HPA axis as well as a decreasedhippocampal volume following childhood adversity (Binderand Nemeroff, 2010; Heim et al., 2008, 2010). Certainly,hypocortisolemia, as reported for atypical depression, hasbeen shown in women with a history of childhood abuse(Heim et al., 2008). As indicated by the diagnostic label, thecore psycho-social correlate is childhood adversity. A ques-tion of interest is whether specific adversities (e.g. sexualabuse) are particularly predictive of subsequent depression.This would offer one explanation for the increased risk ofnon-melancholic depression in women (Heim et al., 2010;Young and Korszun, 2009) as, while childhood adversities aresimilarly prevalent in girls and boys, girls are more frequentlyvictims of sexual abuse (Heim et al., 2010; Young andKorszun, 2009). Another explanation for gender differencesin the prevalence of depression is that girls and boys differ intheir biological response to childhood adversity, with girlsshowing greater reactivity to stress (Heim et al., 2010; Youngand Korszun, 2009).
3.2.2.3. Treatment. Research on this subtype has beenstimulated in particular by findings of a secondary analysisof an RCT comparing psychotherapy (Cognitive BehavioralAnalysis System of Psychotherapy; CBASP), psychopharma-cological treatment (nefazodone) or the combination of both(Nemeroff et al., 2003). While combination treatment wasmost effective in depressed patients without a history ofchildhood trauma, psychotherapy was as effective as combi-nation treatment and significantly superior to nefazodonein depressed patients with a history of childhood trauma.While still requiring replicationwith varying psychotherapiesand pharmacotherapies (especially other antidepressantdrug classes), such findings support a pluralistic treatmentapproach in depressed patients with childhood adversities incomparison to some depressive conditions where evidenceweights a monotherapy (e.g. antidepressant drug therapyfor melancholia, counselling and supportive therapy for

132 Baumeister, H., Parker, G. / Journal of Affective Disorders 139 (2012) 126–140
adjustment disorders). Besides these specific findings, earlytrauma depression seems to be associatedwith higher relapserates and a treatment-resistant outcome (Heim et al., 2010).
3.2.3. Reproductive depression
3.2.3.1. Definition. Depression is twice as common inwomen asin men (Accortt et al., 2008; Noble, 2005). The increased risk isparticularly pronounced from early adolescence to the end ofthe fifth decade, corresponding to women's reproductive yearswith inherent hormonal changes (Deecher et al., 2008; Soaresand Zitek, 2008). While this increased risk might also beattributable to genetic and psychosocial aspects such as rolestress, childhood adversities and gender-specific emotionalreactivity and cognitive style (Accortt et al., 2008; Hyde et al.,2008; Noble, 2005; Wilhelm et al., 2008), many propose that asubgroup of women develops ‘reproductive depression’ as aspecific subtype of depression in response to a susceptibilityto hormonal changes (Deecher et al., 2008; Halbreich, 2010;Payne et al., 2009; Soares and Zitek, 2008; Ter Horst et al.,2009).More precisely, reproductive depression is positioned asreflecting the effects of drastically changing levels of estradioland progesterone during the premenstrual, postpartum andperimenopausal phases in women with a vulnerability tohormonal changes (Freeman, 2010; Halbreich, 2010; Payneet al., 2009; Soares and Zitek, 2008). Close timing between suchhormonal changes and the onset of depression has beenproposed (e.g. four weeks after delivery) (Payne et al., 2009)as a criterion. This is of particular importance to delineatereproductive depression (i.e. due to a vulnerability to hor-monal changes) from other depressive episodes present duringa reproductive event (e.g. adjustment disorder) (Payne et al.,2009). Subtype-specific associated symptoms have not as yetbeen identified, perhaps reflecting the clinical picture ofreproductive depression being described as diverse amongwomen (Halbreich, 2010).
3.2.3.2. Correlates. Preliminary genetic and correlation studiessuggest that sensitivity to hormonal changes is a stable traitthat persists across women's reproductive years, with adepressive episode during one reproductive event increasingthe likelihood of depressive episodes during subsequentreproductive events (Payne et al., 2009). While the biologicalpathway from sensitivity to hormonal changes to depressionremains open, some evidence indicates an impact of thissensitivity on the serotonergic system, as well as on sleepand other biological rhythms such as melatonin and cortisol(Deecher et al., 2008; Parry et al., 2006a,b; Payne et al.,2009).
3.2.3.3. Treatment. A specific responsiveness to oestrogen andother hormonal treatments as well as to SSRIs in reproductivedepression has been proposed (Payne et al., 2009). Findings,however, are inconclusive (Ancelin et al., 2007; Dennis et al.,2008; Howland, 2010; Soares and Zitek, 2008), with only afew reviews providing support for such hypotheses (Payneet al., 2009; Studd and Panay, 2009). Despite the provenefficacy of psychotherapeutic interventions for postpartumandperi-menopausal depression (Cuijpers et al., 2008;DennisandHodnett, 2007; Gyllstromet al., 2007),most reviews focussolely on drug treatments.
3.2.4. Perinatal depression
3.2.4.1. Definition. Perinatal depression refers to depressivesyndromes during pregnancy (antenatal) or within the firstfour weeks to 12 months after delivery (postpartum; post-natal) (Leung and Kaplan, 2009; Lusskin et al., 2007). DSM-IVallows for the diagnosis of postpartum depression if theonset of the major depression episode is within four weekspostpartum, while there is no specific antenatal depressioncategory. The narrower DSM-IV definition of postpartumdepression might substantially overlap with the concept ofreproductive depression. Usually, the term perinatal depres-sion is only used for mothers (also maternal depression),while the risk of developing perinatal depression, as well asits negative impact on child development, has been shown forboth mothers and fathers (Grote et al., 2010; Leung andKaplan, 2009; Lusskin et al., 2007; Paulson and Bazemore,2010; Schumacher et al., 2008; Wilson and Durbin, 2010). Nosubtype-specific symptomatology has been described, andthere is a risk of misattributing the neurovegetative symp-toms (e.g. sleep and appetite disturbances, low energy, poorconcentration) to the normative changes of pregnancy andthe postpartum period (Lusskin et al., 2007; Pearlstein et al.,2009; Riecher-Rossler and Hofecker Fallahpour, 2003).
3.2.4.2. Correlates. During pregnancy and postpartum periods,changes in gonadal hormones and the HPA axis are distinctive(Brummelte and Galea, 2010; Corwin and Pajer, 2008;Kammerer et al., 2006; Zonana and Gorman, 2005). Increasesin cortisol during pregnancy reach levels reported in Cushing'ssyndrome and for those with melancholia (Kammerer et al.,2006). Postpartum findings of altered cortisol levels are in-conclusive, with decreased levels of cortisol in at least asubsample of depressed women (Brummelte and Galea, 2010;Corwin and Pajer, 2008; Kammerer et al., 2006). The suddendrop of gonadal hormones after delivery might contribute tothe postpartum blues (temporary depressive mood whichoccurs in thefirstweek after delivery),whichmight in turn be arisk factor for developing postpartum depression (see alsoreproductivedepression) (Brummelte andGalea, 2010; Lusskinet al., 2007; Riecher-Rossler and Hofecker Fallahpour, 2003).Sleep patterns remain disrupted until about three monthspostpartum and may also contribute to the increased risk ofdeveloping such depressive states (Parry et al., 2006b; Rosset al., 2005). In regard to psycho-social correlates, life stressorssuch as unplanned pregnancy, ambivalence about the preg-nancy, relationship problems and biographical adverse lifeevents, as well as domestic violence and lack of social support,are associated with a greater likelihood of perinatal depression(Lancaster et al., 2010; Lusskin et al., 2007).
3.2.4.3. Treatment. Treatment recommendations for perinataldepression are generally the same as for depression treat-ment in general. There is, however, a special emphasis onpotential side-effects of antidepressant medications, sincelong term side-effects cannot be safely excluded (Freeman,2007; Pariante et al., 2011; Yonkers et al., 2009). Furthermore,mothers are understandably ambivalent about taking anti-depressant medications during pregnancy and while lactat-ing, as well as being reluctant to stop breastfeeding (Pearlsteinet al., 2009; Riecher-Rossler and Hofecker Fallahpour, 2003).

133Baumeister, H., Parker, G. / Journal of Affective Disorders 139 (2012) 126–140
Psychotherapy and antidepressant medication are effectivetreatment options for postpartum depression (Cuijpers et al.,2008; Dennis and Hodnett, 2007; Di Scalea and Wisner,2009; Ng et al., 2010). There is only inconclusive evidence,however, regarding the efficacy of psychotherapy and antide-pressant medication for antenatal depression and preventionof perinatal depression (Dennis et al., 2007; Howard et al.,2005; Yonkers et al., 2009) as well as for hormone, comple-mentary and alternative medicine treatments for perinataldepression (Borja Hart and Marino, 2010; Daley et al., 2009;Dennis et al., 2008; Dennis and Allen, 2008; Freeman, 2009;Jans et al., 2010).
3.2.5. Organic and drug induced depression
3.2.5.1. Definition. A range of somatic diseases as well asseveral medications is viewed as capable of inducing depres-sive syndromes— and classifiable as a DSM-IV mood disorderdue to a generalmedical conditionwith depressive features ora substance-induced mood disorder with depressive features.These comprise infectious conditions, rheumatoid arthritis,cancer, Alzheimer's disease, multiple sclerosis and otherneurodegenerative diseases, vascular depression, post-strokedepression, and Cushing's syndrome as somatic conditions(Baldwin, 2005; Pucak et al., 2007; Pucak and Kaplin, 2005;Robinson and Spalletta, 2010; Samaras et al., 2010; Schieperset al., 2005; Sonino et al., 2010; Tharwani et al., 2007) aswell as medications, such as some β-blockers (propranolol,sotalol), corticosteroids, contraceptive implants, gonadotropin-releasing hormone antagonists, interferon-α, interleukin-2, 5-alpha-reduced steroids and mefloquine (Kotlyar et al., 2005;Patten and Barbui, 2004; Pucak and Kaplin, 2005; Römer andGass, 2010; Schiepers et al., 2005). Depending on the particularcondition or medication, the clinical presentation, psychopath-ological pathways and treatment options vary widely andpartly differ from other subtypes of depression. Since thesesubtypes comprise a very heterogeneous class of depressivesyndromes themselves, it would be beyond the scope of thismeta-review to discuss the various forms of organic and drug-induced depressive disorders in greater detail.
3.3. Time of onset based subtypes of depression
Early and late onset depression, aswell as seasonal affectivedisorders, are subtypes of depression primarily defined by thespecific time of depression onset.
3.3.1. Early vs. late onset depression
3.3.1.1. Definition. Early onset depression (EOD) has beendefined as a first episode occurring before age 18 years (Rush,2007), and late onset depression (LOD) as a first episodeoccurring from 45 to 65 years (Herrmann et al., 2007; Panza etal., 2010). The clinical pictures of EODandLODhavenot yet beendescribed in detail (Boyd et al., 2000; Rush, 2007), but proved tobe similar in an original study undertaken at our institute(Brodaty et al., 2001). Overall, the evidence of differential EODand LOD depressive subtypes is rather weak due to themethodological problemsof recall bias, the need for longitudinalstudies and the challenges of determining the first (especiallyminor) depression episode (Alexopoulos, 2005). Some evidence
has been deduced from research on childhood and adolescentdepression on the one hand (Andersen and Teicher, 2008;Goodyer, 2008; Miller, 2007; Rao and Chen, 2009) and late-life(geriatric) depression on the other hand (Alexopoulos, 2005;Butters et al., 2008; Crocco et al., 2010; Panza et al., 2010).Therefore, it would appear important to delineate LOD moreclearly from late-life depression (Baumeister and Parker, 2010).The latter comprises both EOD and LOD, with biological (e.g.genetics, biological changes due to diseases), psychological (e.g.cognitive style, self-efficacy, neuroticism) and social origins(e.g. childhood adversities, bereavement, role changes due toretirement and disease-caused disability) of depression in laterlife (Alexopoulos, 2005; Blazer and Hybels, 2005). In contrast,LOD might be more indicative of a prominent biologicalpathology reflecting medical and neurological causes andcomorbidities (Alexopoulos, 2005).
3.3.1.2. Correlates. There is evidence that patients with LODhave a lower family history rate of depression and a higherprevalenceof dementia andcerebrovascular conditions (see alsoorganic depression) (Alexopoulos, 2005; Baldwin and O'Brien,2002; Herrmann et al., 2007; Panza et al., 2010). LOD has beenassociatedwith a greater enlargement in lateral brain ventricles,and more white matter hyperintensities (Alexopoulos, 2005;Herrmann et al., 2007, 2008; Vaishnavi and Taylor, 2006), whileEOD has been associated with hippocampal volume loss,presumably due to recurrence of depression (Herrmann et al.,2007). Moreover, patients with LOD in comparison to patientswith EOD show a decrease in cognitive executive function andprocessing speed (Herrmann et al., 2007).
3.3.1.3. Treatment. As yet, there is no evidence for specificresponsiveness to different treatments for EOD versus LOD(Rush, 2007).
3.3.2. Seasonal affective disorder
3.3.2.1. Definition. In DSM-IV, seasonal affective disorder (SAD)is classified as major depressive disorder with a seasonalpattern, with such seasonality marked by a regular temporalrelationship between the onset of the depressive episode and aparticular time of the year (Howland, 2009). Full remission hasto occur at another time of the year. The disorder has beenlinked to a specific responsiveness to light therapy. Until now,there has been substantial debate as to whether SAD is adistinct depressive subtype or rather only a pronouncedseasonality trait of patients with fluctuating minor and majordepression (Hansen et al., 2008; Rosenthal, 2009; Westrin andLam, 2007). The core symptom patterns are conceptualised asto be the same as for non-seasonal major depression, althoughhypersomnia, hyperphagia, irritability and loss of energy aremore likely to be reported (Howland, 2009). These latterclinical features are linked more with atypical depression thanwith melancholia (Howland, 2009; Juruena and Cleare, 2007),as considered earlier.
3.3.2.2. Correlates. Biological research on SAD was stimulatedby circadian rhythm theories, especially ones proposing thatSAD is caused by shorter winter photoperiod or by internalcircadian rhythms that are phase delayed relative to theexternal clock or to other rhythms (e.g. sleep–wake) (Levitan,

134 Baumeister, H., Parker, G. / Journal of Affective Disorders 139 (2012) 126–140
2007; Rohan et al., 2009; Sohn and Lam, 2005). Both hypoth-eses are still controversial with conflicting results (Levitan,2007; Rohan et al., 2009; Sohn and Lam, 2005). For example,there seems to be no meaningful correlation betweenprevalence rates of SAD and latitude (Sohn and Lam, 2005).SAD has further been linked to neurotransmitter alterations,and particularly to serotonin and norepinephrine (Rohanet al., 2009). The main obstacle to research on SAD as adistinct subtype of depression, however, is the lack of studiescomparing patients with and without SAD in terms of aspecific clinical picture, bio-psycho-social correlates andspecific treatment responsiveness.
3.3.2.3. Treatment. Light therapy has been proven as aneffective treatment option in SAD (Golden et al., 2005).Moreover, psychotherapy, dawn simulation, exercise andantidepressant medication have been held to be effective inSAD (Howland, 2009; Westrin and Lam, 2007). However,light therapy has also been proven as effective in non-SADdepressive conditions (Even et al., 2008; Golden et al., 2005).Overall, there is a lack of clinical trials providing evidence fora subtype specific responsiveness to either of the aforemen-tioned therapies.
3.4. Female depression
More narrowly, this subtype is used synonymously withreproductive depression, which is the more specific term fordepression reflecting women's mood perturbations associat-ed with their reproductive life cycle. More broadly defined, itrefers to all social, psychological, and biological aspects ofdepression, which are different to male depression such assex-specific socialisation, internalising coping style, temper-ament and hormonal differences (Accortt et al., 2008; Hydeet al., 2008; Noble, 2005; Parker et al., 2011a; Wilhelm et al.,2008). Defined in this way, female depression less reflects aspecific subtype of depression and more refers to a variety ofpossible overrepresented subtypes of depression in females.The same would apply to male depression as counterpart offemale depression, but depression in males has generatedlittle research (Wilhelm, 2009).
3.5. Treatment resistant depression
Treatment resistant depression (TRD) has most frequentlybeen operationalised as being non-responsive to one, two ormore than two antidepressants with or without a change ofantidepressant classes (Berlim and Turecki, 2007; Rush et al.,2003). The origin of this proposed subtype appears to datefrom awareness of the unsatisfying effectiveness of antide-pressant medication, with only about half those with majordepression responding to an antidepressant (NICE, 2009;Pigott et al., 2010). Accordingly, literature on TRD focusesmainly on treatment options such as augmentation strategies,dose escalation, switching between antidepressants, thesequential integration of psychotherapy and more invasivesomatic therapies (i.e. repetitive transcranial magneticstimulation, vagus nerve stimulation, deep brain stimulation)for patients not responding to one or several antidepressantmedications (Adli et al., 2005; Bauer et al., 2010; Blomstedtet al., 2011; Bschor and Baethge, 2010; Carvalho et al., 2009;
Croxtall and Scott, 2010; Fava, 2010; Guidi et al., 2011;Obrocea et al., 2008; Philip et al., 2010; Shelton et al., 2010).From a conceptual point of view, however, TRD remainsrather weakly defined and presumably reflecting intrinsicheterogeneity of cause and constituent disorders (Fagiolini andKupfer, 2003; Fava, 2003;Wijeratne and Sachdev, 2008)— and‘condition persistence’ rather than necessary treatment resis-tance. Thereby, the term ‘treatment resistant’ seems inappro-priate, since antidepressant medication is only one first-linetreatment option next to psychotherapy proven to be (to somedegree) effective in depression (Fava, 2003; NICE, 2009). Amore appropriate conceptualisation of TRD would thereforeeither refer to patients who are non-responsive to all first-lineinterventions or specify resistance to the specific treatments(e.g. SSRI-TRD). Finally, TRD has been shown to be present inthe previously overviewed subtypes of depression, which(might) have differential responsiveness to different antide-pressant interventions. Accordingly, TRD is not a specificsubtype of depression and might be better conceptualisedand understood in the context of the natural and treatmentoutcomes of the respective subtypes of depression (Wijeratneand Sachdev, 2008).
4. Discussion
Based on the assumption of major depression as a non-specific class comprising numerous depressive conditions,several subtypes of depression have been proposed. Thesesubtypes have never been shown to be absolutely distinctfrom one other, with substantial overlaps across symptoms,aetiologies and time of onset. Thereby, the preliminaryevidence suggests that any subtyping model must respectinterdependency as against pristine independency (Fig. 2).
More specifically, melancholic and psychotic depressionshow both overlap and independent categorical features,with some conceptualising psychotic depression as melan-cholia with additional psychotic features (Malhi et al., 2005;Taylor and Fink, 2008). Both subtypes are marked bypsychomotor retardation and hypercortisolemia. Genderdifferences in prevalence rates are not as pronounced as innon-melancholic or non-psychotic depression (Khan et al.,2006; Lykouras and Gournellis, 2009). In terms of treatmenteffects, rates of spontaneous improvement and placeboresponses are lower than in non-melancholic and non-psychotic depression (Malhi et al., 2005). A commonalternative explanation for the latter finding is that melan-cholia is correlated with severe depression (Khan et al.,2006), which in turn has been associated with non-respon-siveness to placebo (Kirsch et al., 2008). In a recent study,however, we did not identify any greater depression severityin melancholia (Parker et al., 2010b) than in non-melancholicdepression.
Secondly, and in contrast to the aforementioned subtypes,atypical depression and early trauma depression have beenassociated with hypocortisolemia. Moreover, atypical depres-sion, early trauma depression, adjustment disorder, perinataldepression and reproductive depression have been associatedwith an increased reactivity to stress (rejection sensitivity,reactivity to adverse childhood events and other life stressorssuch as unplanned pregnancy or chronic diseases, sensitivity to

Unipolar depression
Late onsetdepression
Psychotic depression
Melancholia Organicdepression
Atypical depression
Early onset depression
Early trauma depression
Adjustment disorder
Reproductive depression
Perinatal depression
Drug induced depression
Seasonal affective disorder
Fig. 2. Integrating findings on subtypes of depression.
135Baumeister, H., Parker, G. / Journal of Affective Disorders 139 (2012) 126–140
hormonal changes). In regard to treatment effects, psychother-apy has been proven to be more salient to the latter types.
Thirdly, organic depression and late onset depression bothmight be attributable to biological changes due to neurolog-ical and medical conditions. Most prominently, this has beendiscussed in the context of depression in patients withcerebrovascular disease. Overall, patients with both cerebro-vascular disease and depression seem to be more resistant toantidepressants therapies (Baumeister et al., in press, 2011;Hackett et al., 2008). Secondary analyses of recent trials andlongitudinal studies, however, indicate that such patientswith new-onset depression are more likely to be nonrespon-sive to antidepressant medication and psychotherapy, andshow an increased mortality risk (Carney and Freedland,2009; Parker et al., 2008, 2011b). These patients might morefrequently present with cerebrovascular brain lesions indic-ative of ‘vascular depression’ as a specific, frequently treat-ment refractory, organic depression (Carney and Freedland,2009; Samaras et al., 2010).
Besides the discussed similarities between some subtypes,however, there are several conflicting and inconclusiveresults leaving many questions unanswered. One reason forconflicting results in research considering subtypes might bethat subtypes rarely occur in pure form. For example, vasculardepression might be over-represented in patients with lateonset depression but also occur in patients with a history ofmelancholia or early trauma depression. Another reasonmight be that some subtypes reflect differential rather thanabsolute weightings emerging from differing causes. Forexample, the clinical picture of childhood and adolescentdepression differs between those with and without a historyof childhood adversities (Kaufman et al., 2001). Hence,findings on early onset depression might be blurred bydifferent pathological pathways, increasing the varianceof the clinical picture, and also by the bio-psycho-socialcorrelates and treatment outcomes of early onset depression.Similarly, perinatal depression could basically be a subtypeof reproductive depression (depression due to sensitivity tohormonal changes) caused by pregnancy-related life stressorsor again represent a combination of both.
Taken together, research on subtypes of depression wouldbenefit from a more integrative approach, examining the‘thick description’ pattern of the overall research rather thanelecting one or more models as necessarily superior. Yet,some ‘unpacking’ and comparative analyses examining eachmodel should be undertaken. One example of an integrativeapproach is our structural and functional models of depres-
sion (Parker and Manicavasagar, 2005), which positionsclinical depression as comprising three depressive subtypes:(i) melancholia marked by depressive symptoms and thespecific presence of psychomotor disturbance; (ii) psychoticdepression, akin to melancholic depression but with thespecific feature of delusions and/or hallucinations, and (iii) aheterogeneous and residual set of non-melancholic disordersreflecting a primary contribution of stressor and/or predispos-ing personality style. The three depressive subtypes arepositioned to differ functionally by differential contributionsby serotoninergic, noradrenergic and dopaminergic neuro-transmitter circuits (Malhi et al., 2005), allowing anaetiologicalmodel to be derived with treatment specificity implications.
As noted at the beginning of this review, themost importantargument for research on subtypes of depression is the non-specific response of major depression to quite differingtreatmentmodalities. Thereby, delineating subtypes of depres-sion that showdifferential treatment response should be one ofthe main objectives when conducting and interpreting clinicaltrials of differing treatments. The current weighting to domaindiagnoses such as major depression and dysthymia preventssuch analyses. Another challenge might be to cope with thediscomfort of more difficult sampling procedures and small-scale trials as a result of splitting the broad category ofdepression into several more or less infrequent subtypes. Onthe positive side, however, shifting to subtype specific researchwould prevent us from merely seeking to develop furthertreatment options for homogenised entities such as majordepression, when acceptance of potential depressive subtypesmight identify quite type-specific treatments.
Role of funding sourceFunding for this review was provided by the German Research
Foundation (DFG; Ref.: BA3407/2-1). The DFG had no further role in studydesign, in the collection, analysis and interpretation of data, in the writing ofthe report, and in the decision to submit the paper for publication.
Conflict of interestHarald Baumeister has no conflict of interest. Gordon Parker has been a
consultant, had advisory Board memberships, and spoken at or chairedmeetings for the following pharmaceutical companies: Astra Zeneca, Eli Lilly,Lundbeck, Pfizer, Servier and Wyeth.
Appendix A
Supplement document: Search strategies for MEDLINEand EMBASE
MEDLINE (via Ovid)
136 Baumeister, H., Parker, G. / Journal of Affective Disorders 139 (2012) 126–140
Search conducted: 05th January 2011Hits: 31,629Limits: abstract; English or German; 2000–current; reviewHits: 1912(depress$ adj2 subtype?).tw(depress$ adj2 type?).tw(depress$ adj2 endogenous).tw(depress$ adj2 endogenomorphic).twmelancholi$.tw(depress$ adj2 psychotic).tw(depress$ adj2 delusional).twAffective disorders, psychotic/(depress$ adj2 catatoni$).tw(depress$ adj2 atypical).tw(depress$ adj2 anxious).tw(depress$ adj2 reactive).tw(depress$ adj2 exogenous).tw(depress$ adj2 neurotic).twadjustment disorder?.twAdjustment disorders/(depress$ adj2 bereavement related).tw(depress$ adj2 reproductive).tw(depress$ adj2 climacteric).tw(depress$ adj2 premenstrual).tw(depress$ adj2 menstrual).tw(depress$ adj2 perimenopausal).tw(depress$ adj2 menopausal).tw(depress$ adj2 postmenopausal).tw(depress$ adj2 postpartum).tw(depress$ adj2 antenatal).tw(depress$ adj2 antepartum).tw(depress$ adj2 perinatal).twDepression, Postpartum/(depress$ adj2 organic).tw(depress$ adj2 vascular).tw(depress$ adj2 subcortical isch?emic).tw(depress$ adj2 immune).tw(depress$ adj2 drug induced).tw(depress$ adj2 late-life).tw(depress$ adj2 late-onset).tw(depress$ adj2 geriatric).tw(depress$ adj2 early-onset).tw(depress$ adj2 adolescen$).tw(depress$ adj2 child$).tw(depress$ adj2 juvenile).tw(depress$ adj2 seasonal).tw(affective disorder? adj2 seasonal).twSeasonal affective disorder/(depress$ adj2 women).tw(depress$ adj2 female).tw(depress$ adj2 men).tw(depress$ adj2 male).tw(depress$ adj2 maternal).tw(depress$ adj2 paternal).tw(depress$ adj2 resistant).tw(depress$ adj2 refractory).tw(depress$ adj2 complicate$).twOR/1-53EMBASE (via Ovid)Search conducted: 05th January 2011Hits: 31,930
Limits: abstract; English or German; 2000–current; reviewsHits: 2682(depress$ adj2 subtype?).tw(depress$ adj2 type?).tw(depress$ adj2 endogenous).tw(depress$ adj2 endogenomorphic).twmelancholi$.twendogenous depression/melancholia/(depress$ adj2 psychotic).tw(depress$ adj2 delusional).twdepressive psychosis/(depress$ adj2 catatoni$).tw(depress$ adj2 atypical).twatypical depression/(depress$ adj2 anxious).tw(depress$ adj2 reactive).tw(depress$ adj2 exogenous).tw(depress$ adj2 neurotic).twadjustment disorder?.twAdjustment disorder/reactive depression/(depress$ adj2 bereavement related).tw(depress$ adj2 reproductive).tw(depress$ adj2 climacteric).tw(depress$ adj2 premenstrual).tw(depress$ adj2 menstrual).tw(depress$ adj2 perimenopausal).tw(depress$ adj2 menopausal).tw(depress$ adj2 postmenopausal).tw(depress$ adj2 postpartum).tw(depress$ adj2 antenatal).tw(depress$ adj2 antepartum).tw(depress$ adj2 perinatal).twpuerperal depression/(depress$ adj2 organic).tworganic depression/(depress$ adj2 vascular).tw(depress$ adj2 subcortical isch?emic).tw(depress$ adj2 immune).tw(depress$ adj2 drug induced).tw(depress$ adj2 late-life).tw(depress$ adj2 late-onset).tw(depress$ adj2 geriatric).tw(depress$ adj2 early-onset).tw(depress$ adj2 adolescen$).tw(depress$ adj2 child$).tw(depress$ adj2 juvenile).tw(depress$ adj2 seasonal).tw(affective disorder? adj2 seasonal).twSeasonal affective disorder/(depress$ adj2 women).tw(depress$ adj2 female).tw(depress$ adj2 men).tw(depress$ adj2 male).tw(depress$ adj2 maternal).tw(depress$ adj2 paternal).tw(depress$ adj2 resistant).tw(depress$ adj2 refractory).tw(depress$ adj2 complicate$).twOR/1-58

137Baumeister, H., Parker, G. / Journal of Affective Disorders 139 (2012) 126–140
References
Accortt, E.E., Freeman, M.P., Allen, J.J., 2008. Women and major depressivedisorder: clinical perspectives on causal pathways. J. Women's Health 17,1583–1590.
Adli, M., Baethge, C., Heinz, A., Langlitz, N., Bauer, M., 2005. Is dose escalationof antidepressants a rational strategy after a medium-dose treatment hasfailed? A systematic review. Europ. Arch. Psychiatry Clin. Neurosci. 255,387–400.
Alexopoulos, G.S., 2005. Depression in the elderly. Lancet 365, 1961–1970.Ancelin, M.L., Scali, J., Ritchie, K., 2007. Hormonal therapy and depression: are
we overlooking an important therapeutic alternative? J. Psychosom. Res.62, 473–485.
Andersen, S.L., Teicher, M.H., 2008. Stress, sensitive periods andmaturationalevents in adolescent depression. Trends Neurosci. 31, 183–191.
Antonijevic, I.A., 2006. Depressive disorders — is it time to endorse differentpathophysiologies? Psychoneuroendocrinol. 31, 1–15.
Antonijevic, I., 2008. HPA axis and sleep: identifying subtypes of majordepression. Stress 11, 15–27.
APA, 2000. Diagnostic and Statistical Manual of Mental Disorders, TextRevision, 4th Edition. American Psychiatric Association, Washington, DC.
Armitage, R., 2007. Sleep and circadian rhythms in mood disorders. ActaPsychiatry Scand. Suppl. 433, 104–115.
Baldwin, R.C., 2005. Is vascular depression a distinct sub-type of depressivedisorder? A review of causal evidence. Int. J. Geriat. Psychiatry 20, 1–11.
Baldwin, R.C., O'Brien, J., 2002. Vascular basis of late-onset depressivedisorder. Br. J. Psychiatry 60.
Bauer, M., Adli, M., Bschor, T., Pilhatsch, M., Pfennig, A., Sasse, J., Schmid, R.,Lewitzka, U., 2010. Lithium's emerging role in the treatment of refractorymajor depressive episodes: augmentation of antidepressants. Neurop-sychobiol. 62, 36–42.
Baumeister, H., 2010. A clinical significance criterion is essential fordiagnosing subthreshold depression. Am. J. Psychiatry 167, 866.
Baumeister, H., Härter, M., 2007. Prevalence of mental disorders based ongeneral population surveys. Soc. Psychiatry Psychiatry Epidemiol. 42,537–546.
Baumeister, H., Kufner, K., 2009. It is time to adjust the adjustment disordercategory. Curr. Opin. Psychiatry 22, 409–412.
Baumeister, H., Morar, V., 2008. The impact of clinical significance criteria onsubthreshold depression prevalence rates. Acta Psychiatr. Scand. 118,443–450.
Baumeister, H., Parker, G., 2010. A second thought on subtyping majordepression. Psychother. Psychosom. 79, 388–389.
Baumeister, H., Maercker, A., Casey, P., 2009. Adjustment disorders withdepressed mood: a critique of its DSM-IV and ICD-10 conceptualizationand recommendations for the future. Psychopathology 42, 139–147.
Baumeister, H., Hutter, N., Bengel, J., Härter, M., 2011. Quality of life inmedically ill persons with comorbid mental disorders: a systematicreview and meta-analysis. Psychother. Psychosom. 80, 275–286.
Baumeister, H., Hutter, N., Bengel, J., in press. Psychological and pharmaco-logical interventions for depression in patients with coronary arterydisease. Cochrane Database Syst. Rev.
Bech, P., 2010. Struggle for subtypes in primary and secondary depressionand their mode-specific treatment or healing. Psychother. Psychosom.79, 331–338.
Benazzi, F., 2006. Various forms of depression. Dialog. Clin. Neurosci. 8, 151–161.Berlim, M.T., Turecki, G., 2007. What is the meaning of treatment resistant/
refractory major depression (TRD)? A systematic review of currentrandomized trials. Europ. Neuropsychopharmacol. 17, 696–707.
Binder, E.B., Nemeroff, C.B., 2010. The CRF system, stress, depression andanxiety: insights from human genetic studies.Mol. Psychiatry 15, 574–588.
Biro, M., Till, E., 1989. Factor analytic study of depressive disorders. J. Clin.Psychol. 45, 369–373.
Blazer, D., Hybels, C.F., 2005. Origins of depression in later life. Psychol. Med.35, 1241–1252.
Blomstedt, P., Sjoberg, R.L., Hansson, M., Bodlund, O., Hariz, M.I., 2011. Deepbrain stimulation in the treatment of depression. Acta Psychiatr. Scand.123, 4–11.
Borja Hart, N.L., Marino, J., 2010. Role of omega-3 fatty acids for prevention ortreatment of perinatal depression. Pharmacother. 30, 210–216.
Boyd, J.,McKiernan, F.,Waller, G., 2000. Early-onset and late-onsetdepression inolder adults: psychological perspectives. Rev. Clin. Gerontol. 10, 149–159.
Brodaty, H., Luscombe, G., Parker, G., Wilhelm, K., Hickie, I., Austin, M.P.,Mitchell, P., 2001. Early and late onset depression in old age: differentaetiologies, same phenomenology. J. Affect. Disord. 66, 225–236.
Brown, W.A., 2007. Treatment response in melancholia. Acta PsychiatryScand. Suppl. 433, 125–129.
Brummelte, S., Galea, L.A., 2010. Depression during pregnancy andpostpartum: contribution of stress and ovarian hormones. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 34, 766–776.
Bschor, T., Baethge, C., 2010. No evidence for switching the antidepressant:systematic review and meta-analysis of RCTs of a common therapeuticstrategy. Acta Psychiatry Scand. 121, 174–179.
Butters, M.A., Young, J.B., Lopez, O., Aizenstein, H.J., Mulsant, B.H., Reynolds,C., DeKosky, S.T., Becker, J.T., 2008. Pathways linking late-life depressionto persistent cognitive impairment and dementia. Dialog. Clin. Neurosci.10, 345–357.
Buyukdura, J.S., McClintock, S.M., Croarkin, P.E., 2011. Psychomotor retarda-tion in depression: biological underpinnings, measurement, and treat-ment. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 35, 395–409.
Carney, R.M., Freedland, K.E., 2009. Treatment-resistant depression andmortality after acute coronary syndrome. Am. J. Psychiatry 166, 410–417.
Carragher,N., Adamson,G., Bunting,B.,McCann, S., 2009. Subtypesofdepression ina nationally representative sample. J. Affect. Disord. 113, 88–99.
Carvalho, A.F., Machado, J.R., Cavalcante, J.L., 2009. Augmentation strategiesfor treatment-resistant depression. Curr. Opin. Psychiatry 22, 7–12.
Casey, P., 2009. Adjustment disorder: epidemiology, diagnosis and treat-ment. CNS Drugs 23, 927–938.
Corwin, E.J., Pajer, K., 2008. The psychoneuroimmunology of postpartumdepression. J. Women's Health 17, 1529–1534.
Coryell, W., 2007. The facets of melancholia. Acta Psychiatry Scand. 433,31–36.
Crocco, E.A., Castro, K., Loewenstein, D.A., 2010. How late-life depressionaffects cognition: neural mechanisms. Curr. Psychiatry Rep. 12, 34–38.
Croxtall, J.D., Scott, L.J., 2010. Olanzapine/fluoxetine: a review of its use inpatients with treatment-resistant major depressive disorder. CNS Drugs24, 245–262.
Cuijpers, P., Brannmark, J.G., van Straten, A., 2008. Psychological treatment ofpostpartum depression: a meta-analysis. J. Clin. Psychol. 64, 103–118.
Cuijpers, P., van Straten, A., Bohlmeijer, E., Hollon, S.D., Andersson, G., 2010.The effects of psychotherapy for adult depression are overestimated: ameta-analysis of study quality and effect size. Psychol. Med. 40, 211–223.
Daley, A., Jolly, K., MacArthur, C., 2009. The effectiveness of exercise in themanagement of post-natal depression: systematic review and meta-analysis. Fam. Pract. 26, 154–162.
Davidson, J.R., 2007. A history of the concept of atypical depression. J. Clin.Psychiatry 68, 10–15.
Deecher, D., Andree, T.H., Sloan, D., Schechter, L.E., 2008. From menarcheto menopause: exploring the underlying biology of depression inwomen experiencing hormonal changes. Psychoneuroendocrinol. 33,3–17.
Dennis, C.L., Allen, K., 2008. Interventions (other than pharmacological,psychosocial or psychological) for treating antenatal depression.Cochrane Database Syst. Rev. CD006795.
Dennis, C.L., Hodnett, E., 2007. Psychosocial and psychological interventionsfor treating postpartum depression. Cochrane Database Syst. Rev.CD006116.
Dennis, C.L., Ross, L.E., Grigoriadis, S., 2007. Psychosocial and psychologicalinterventions for treating antenatal depression. Cochrane Database Syst.Rev. CD006309.
Dennis, C.L., Ross, L.E., Herxheimer, A., 2008. Oestrogens and progestins forpreventing and treating postpartum depression. Cochrane Database Syst.Rev. CD001690.
Di Scalea, T.L., Wisner, K.L., 2009. Pharmacotherapy of postpartum depres-sion. Expert. Opin. Pharmacother. 10, 2593–2607.
Diefenbach, G.J., Goethe, J., 2006. Clinical interventions for late-life anxiousdepression. Clin. Intervent. Aging 1, 41–50.
Dinan, T.G., Scott, L.V., 2005. Anatomy of melancholia: focus on hypothalamic–pituitary–adrenal axis overactivity and the role of vasopressin. J. Anat. 207,259–264.
Even, C., Schroder, C.M., Friedman, S., Rouillon, F., 2008. Efficacy of light therapy innonseasonal depression: a systematic review. J. Affect. Disord. 108, 11–23.
Fagiolini, A., Kupfer, D.J., 2003. Is treatment-resistant depression a uniquesubtype of depression? Biol. Psychiatry 53, 640–648.
Fava, M., 2003. Diagnosis and definition of treatment-resistant depression.Biol. Psychiatry 53, 649–659.
Fava, M., 2010. Switching treatments for complicated depression. J. Clin.Psychiatry 71, e04.
Fleming, S.K., Blasey, C., Schatzberg, A.F., 2004. Neuropsychological correlatesof psychotic features in major depressive disorders: a review and meta-analysis. J. Psychiatr. Res. 38, 27–35.
Freeman, M.P., 2007. Antenatal depression: navigating the treatmentdilemmas. Am. J. Psychiatry 164, 1162–1165.
Freeman, M.P., 2009. Complementary and alternative medicine for perinataldepression. J. Affect. Dis. 112, 1–10.
Freeman, E.W., 2010. Associations of depression with the transition tomenopause. Menopause 17, 823–827.
Gaudiano, B.A., Beevers, C.G., Miller, I.W., 2005. Differential response tocombined treatment in patients with psychotic versus nonpsychoticmajor depression. J. Nervous Ment. Dis. 193, 625–628.

138 Baumeister, H., Parker, G. / Journal of Affective Disorders 139 (2012) 126–140
Gaudiano, B.A., Miller, I.W., Herbert, J.D., 2007. The treatment of psychoticmajor depression: is there a role for adjunctive psychotherapy?Psychother. Psychosom. 76, 271–277.
Ghaemi, S.N., 2008. Why antidepressants are not antidepressants: STEP-BD,STAR*D, and the return of neurotic depression. Bipolar Dis. 10, 957–968.
Gold, P.W., Chrousos, G.P., 2002. Organization of the stress system and itsdysregulation in melancholic and atypical depression: high vs. low CRH/NE states. Mol. Psychiatry 7, 254–275.
Goldberg, D., 2006. The aetiology of depression. Psychol. Med. 36,1341–1347.
Golden, R.N., Gaynes, B.N., Ekstrom, R.D., Hamer, R.M., Jacobsen, F.M., Suppes,T., Wisner, K.L., Nemeroff, C.B., 2005. The efficacy of light therapy in thetreatment of mood disorders: a review and meta-analysis of theevidence. Am. J. Psychiatry 162, 656–662.
Goodyer, I.M., 2008. Emanuel Miller Lecture: early onset depressions —
meanings, mechanisms and processes. J. Child Psychol. Psychiatry AlliedDiscipl. 49, 1239–1256.
Grote, N.K., Bridge, J.A., Gavin, A.R., Melville, J.L., Iyengar, S., Katon, W.J., 2010.A meta-analysis of depression during pregnancy and the risk of pretermbirth, low birth weight, and intrauterine growth restriction. Arch. Gen.Psychiatry 67, 1012–1024.
Guidi, J., Fava, G.A., Fava, M., Papakostas, G.I., 2011. Efficacy of the sequentialintegration of psychotherapy and pharmacotherapy in major depressivedisorder: a preliminary meta-analysis. Psychol. Med. 41, 321–331.
Gyllstrom, M.E., Schreiner, P.J., Harlow, B.L., 2007. Perimenopause anddepression: strength of association, causal mechanisms and treatmentrecommendations. Best Pract. Res. Clin. Obstet. Gynaecol. 21, 275–292.
Hackett, M.L., Anderson, C.S., House, A., Xia, J., 2008. Interventions for treatingdepression after stroke. Cochrane Database Syst. Rev. CD003437.
Halbreich, U., 2010.Women's reproductive related disorders (RRDs). J. Affect.Disord. 122, 10–13.
Halbreich, U., Kahn, L.S., 2007. Atypical depression, somatic depression andanxious depression in women: are they gender-preferred phenotypes?J. Affect. Dis. 102, 245–258.
Hammen, C., 2005. Stress and depression. Ann. Rev. Clin. Psychol. 1, 293–319.Hansen, V., Skre, I., Lund, E., 2008. What is this thing called “SAD”? A critique
of the concept of Seasonal Affective Disorder. Epidemiologia e PsichiatriaSociale 17, 120–127.
Heim, C., Plotsky, P.M., Nemeroff, C.B., 2004. Importance of studying thecontributions of early adverse experience to neurobiological findings indepression. Neuropsychopharmacol 29, 641–648.
Heim, C., Newport, D.J., Mletzko, T., Miller, A.H., Nemeroff, C.B., 2008. The linkbetween childhood trauma and depression: insights from HPA axisstudies in humans. Psychoneuroendocrinol. 33, 693–710.
Heim, C., Shugart, M., Craighead, W.E., Nemeroff, C.B., 2010. Neurobiologicaland psychiatric consequences of child abuse and neglect. Dev..Psychobiol. 52, 671–690.
Henkel, V., Mergl, R., Allgaier, A.K., Kohnen, R., Moller, H.J., Hegerl, U., 2006.Treatment of depression with atypical features: a meta-analyticapproach. Psychiatry Res. 141, 89–101.
Herrmann, L.L., Goodwin, G.M., Ebmeier, K.P., 2007. The cognitive neuropsy-chology of depression in the elderly. Psychol. Med. 37, 1693–1702.
Herrmann, L.L., Le, M., Ebmeier, K.P., 2008. White matter hyperintensities inlate life depression: a systematic review. J. Neurol. Neurosurg. Psychiatry79, 619–624.
Howard, L.M., Hoffbrand, S., Henshaw, C., Boath, L., Bradley, E., 2005.Antidepressant prevention of postnatal depression. Cochrane DatabaseSystem. Rev. CD004363.
Howland, R.H., 2009. An overview of seasonal affective disorder and itstreatment options. Physician Sportsmed. 37, 104–115.
Howland, R.H., 2010. Use of endocrine hormones for treating depression.J. Psychosoc. Nurs. Ment. Health Serv. 48, 1–4.
Hutter, N., Schnurr, A., Baumeister, H., 2010. Health care costs in personswithdiabetes mellitus and comorbid mental disorders — a systematic review.Diabetol. 53, 2470–2479.
Hyde, J.S., Mezulis, A.H., Abramson, L.Y., 2008. The ABCs of depression: integratingaffective, biological, and cognitive models to explain the emergence of thegender difference in depression. Psychol. Rev. 115, 291–313.
Jans, L.A., Giltay, E.J., van derDoes, A.J., 2010. The efficacy of n−3 fatty acids DHAand EPA (fish oil) for perinatal depression. Br. J. Nutr. 104, 1577–1585.
Juruena, M.F., Cleare, A.J., 2007. Overlap between atypical depression,seasonal affective disorder and chronic fatigue syndrome. Rev. Bras.Psiquiatr. 29, S19–S26.
Kammerer, M., Taylor, A., Glover, V., 2006. The HPA axis and perinataldepression: a hypothesis. Arch. Women's Ment. Health 9, 187–196.
Kaufman, J., Martin, A., King, R.A., Charney, D., 2001. Are child-, adolescent-,and adult-onset depression one and the same disorder? Biol. Psychiatry49, 980–1001.
Keller, J., Schatzberg, A.F., Maj, M., 2007a. Current issues in the classificationof psychotic major depression. Schizophr. Bull. 33, 877–885.
Keller, M.C., Neale, M.C., Kendler, K.S., 2007b. Association of different adverselife events with distinct patterns of depressive symptoms. Am. J.Psychiatry 164, 1521–1529.
Khan, A.Y., Carrithers, J., Preskorn, S.H., Lear, R., Wisniewski, S.R., Rush, A.J.,Stegman, D., Kelley, C., Kreiner, K., Nierenberg, A.A., Fava, M., 2006.Clinical and demographic factors associated with DSM-IV melancholicdepression. Ann. Clin. Psychiatry 18, 91–98.
Kirsch, I., Beacon, B.J., Huedo-Medina, T.B., Scoboria, A., Moore, T.J., Johnson,B.T., 2008. Initial severity and antidepressant benefits: a meta-analysis ofdata submitted to the food and drug administration. PLoS Med. 5, e45.
Kotlyar, M., Dysken, M., Adson, D.E., 2005. Update on drug-induceddepression in the elderly. Am. J. Geriat. Pharmacother. 3, 288–300.
Krishnan, V., Nestler, E.J., 2010. Linking molecules to mood: new insight intothe biology of depression. Am. J. Psychiatry 167, 1305–1320.
Lancaster, C.A., Gold, K.J., Flynn, H.A., Yoo, H., Marcus, S.M., Davis, M.M., 2010.Risk factors for depressive symptoms during pregnancy: a systematicreview. Am. J. Obstet. Gynecol. 202, 5–14.
Laugharne, J., van der Watt, G., Janca, A., 2009. It is too early for adjusting theadjustment disorder category. Curr. Opin. Psychiatry 22, 50–54.
Leung, B.M., Kaplan, B.J., 2009. Perinatal depression: prevalence, risks, andthe nutrition link — a review of the literature. J. Am. Dietetic Assoc. 109,1566–1575.
Leventhal, A.M., Rehm, L.P., 2005. The empirical status of melancholia:implications for psychology. Clin. Psychol. Rev. 25, 25–44.
Levitan, R.D., 2007. The chronobiology and neurobiology of winter seasonalaffective disorder. Dial. Clin. Neurosci. 9, 315–324.
Lichtenberg, P., Belmaker, R.H., 2010. Subtyping major depressive disorder.Psychother. Psychosom. 79, 131–135.
Lusskin, S.I., Pundiak, T.M., Habib, S.M., 2007. Perinatal depression: hiding inplain sight. Can. J. Psychiatry 52, 479–488.
Luyten, P., Blatt, S.J., van Houdenhove, B., Corveleyn, J., 2006. Depressionresearch and treatment: are we skating to where the puck is going to be?Clin. Psychol. Rev. 26, 985–999.
Lykouras, L., Gournellis, R., 2009. Psychotic (delusional) major depression:new vistas. Curr. Psychiatry Rev. 5, 1–28.
Malhi, G.S., Parker, G.B., Greenwood, J., 2005. Structural and functionalmodels of depression: from sub-types to substrates. Acta Psychiatr.Scand. 111, 94–105.
Maniglio, R., 2010. Child sexual abuse in the etiology of depression: asystematic review of reviews. Depress. Anxiety 27, 631–642.
Marcos, T., Salamero, M., 1990. Factor study of the Hamilton Rating Scale forDepression and the Bech Melancholia Scale. Acta Psychiatry Scand. 82,178–181.
Miller, A., 2007. Social neuroscience of child and adolescent depression. BrainCogn. 65, 47–68.
Neigh, G.N., Gillespie, C.F., Nemeroff, C.B., 2009. The neurobiological toll ofchild abuse and neglect. Trauma Violence Abuse 10, 389–410.
Nemeroff, C.B., Heim, C.M., Thase, M.E., Klein, D.N., Rush, A.J., Schatzberg, A.F.,Ninan, P.T., McCullough, J.P., Weiss, P.M., Dunner, D.L., Rothbaum, B.O.,Kornstein, S., Keitner, G., Keller, M.B., 2003. Differential responses topsychotherapy versus pharmacotherapy in patients with chronic formsof major depression and childhood trauma. PNAS 100, 14293–14296.
Nesse, R.M., 2007. Evolution is the scientific foundation for diagnosis:psychiatry should use it. World Psychiatry 6, 160–161.
Ng, R.C., Hirata, C.K., Yeung, W., Haller, E., Finley, P.R., 2010. Pharmacologictreatment for postpartum depression: a systematic review. Pharmac-other. 30, 928–941.
NICE, 2009. Depression: the treatment and management of depression inadults. National Clinical Practice Guideline 90. http://guidance.nice.org.uk/CG90. Accessed Feb. 10th 2011.
Noble, R.E., 2005. Depression in women. Metabol. Clin. Exp. 54, 49–52.Obrocea, G.V.,Margolin, R.A., Yoo, T.P., 2008. Thyroid hormone augmentation in
treatment-refractory depression. Clin. Psychopharmacol. Neurosci. 6, 3–10.Pae, C.U., Tharwani, H., Marks, D.M., Masand, P.S., Patkar, A.A., 2009. Atypical
depression: a comprehensive review. CNS Drugs 23, 1023–1037.Paing, W.W., Weller, R.A., Brennan, L., Weller, E.B., 2008. Atypical depression
in children and adolescents. Curr. Psychiatry Rep. 10, 130–133.Panza, F., Frisardi, V., Capurso, C., D'Introno, A., Colacicco, A.M., Imbimbo, B.P.,
Santamato, A., Vendemiale, G., Seripa, D., Pilotto, A., Capurso, A., Solfrizzi,V., 2010. Late-life depression, mild cognitive impairment, and dementia:possible continuum? Am. J. Geriat. Psychiatry 18, 98–116.
Panzer, M.J., 2005. Are SSRIs really more effective for anxious depression?Ann. Clin. Psychiatry 17, 23–29.
Pariante, C.M., Seneviratne, G., Howard, L., 2011. Should we stop usingtricyclic antidepressants in pregnancy? Psychol. Med. 41, 15–17.
Parker, G., 2005. Beyond major depression. Psychol. Med. 35, 467–474.Parker, G., 2006. Through a glass darkly: the disutility of the DSM nosology of
depressive disorders. Can. J. Psychiatry 51, 879–886.Parker, G., 2007. Atypical depression: a valid subtype? J. Clin. Psychiatry 68,
e08.

139Baumeister, H., Parker, G. / Journal of Affective Disorders 139 (2012) 126–140
Parker, G., Manicavasagar, V., 2005. Modelling and Managing the DepressiveDisorders. A Clinical Guide. Cambridge University Press, Cambridge.
Parker, G., Roy, K., Hadzi-Pavlovic, D., Pedic, F., 1992. Psychotic (delusional)depression: ameta-analysis ofphysical treatments. J. Affect.Disord. 24, 17–24.
Parker, G., Roy, K., Mitchell, P., Wilhelm, K., Malhi, G., Hadzi-Pavlovic, D.,2002. Atypical depression: a reappraisal. Am. J. Psychiatry 159,1470–1479.
Parker, G., Hilton, T.M., Walsh, W.F., Owen, C.A., Heruc, G.A., Olley, A.,Brotchie, H., Hadzi-Pavlovic, D., 2008. Timing is everything: the onset ofdepression and acute coronary syndrome outcome. Biol. Psychiatry 64,660–666.
Parker, G., Fink, M., Shorter, E., Taylor, M.A., Akiskal, H., Berrios, G., Bolwig, T.,Brown, W.A., Carroll, B., Healy, D., Klein, D.F., Koukopoulos, A., Michels,R., Paris, J., Rubin, R.T., Spitzer, R., Swartz, C., 2010a. Issues for DSM-5:whither melancholia? The case for its classification as a distinct mooddisorder. Am. J. Psychiatry 167, 745–747.
Parker, G., Fletcher, K., Barrett, M., Synnott, H., Breakspear, M., Rees, A.-M.,Hadzi-Pavlovic, D., 2010b. Inching toward Bethlehem: mapping melan-cholia. J. Affect. Disord. 123, 291–298.
Parker, G., Blanch, B., Crawford, J., 2011a. Does gender influence response todiffering psychotherapies by those with unipolar depression? J. Affect.Disord. 130, 17–20.
Parker, G., Hyett, M., Walsh, W., Owen, C., Brotchie, H., Hadzi-Pavlovic, D.,2011b. Specificity of depression following an acute coronary syndrometo an adverse outcome extends over five years. Psychiatry Res. 185,347–352.
Parry, B.L., Fernando, M., Maurer, E.L., Lopez, A.M., Sorenson, D., Meliska, C.J.,2006a. Sleep, rhythms and women's mood. Part II. Menopause. SleepMed. Rev. 10, 197–208.
Parry, B.L., Martinez, L.F., Maurer, E.L., Lopez, A.M., Sorenson, D., Meliska, C.J.,2006b. Sleep, rhythms and women's mood. Part I. Menstrual cycle,pregnancy and postpartum. Sleep Med.Rev. 10, 129–144.
Patten, S.B., Barbui, C., 2004. Drug-induced depression: a systematic reviewto inform clinical practice. Psychother. Psychosom. 73, 207–215.
Paulson, J.F., Bazemore, S.D., 2010. Prenatal and postpartum depression infathers and its association with maternal depression: a meta-analysis.JAMA 303, 1961–1969.
Paykel, E.S., 2008. Basic concepts of depression. Dialog. Clin. Neurosci. 10,279–289.
Payne, J.L., Palmer, J.T., Joffe, H., 2009. A reproductive subtype of depression:conceptualizing models and moving toward etiology. Harvard Rev.Psychiatry 17, 72–86.
Pearlstein, T., Howard, M., Salisbury, A., Zlotnick, C., 2009. Postpartumdepression. Am. J. Obstet. Gynecol. 200, 357–364.
Philip, N.S., Carpenter, L.L., Tyrka, A.R., Price, L.H., 2010. Pharmacologicapproaches to treatment resistant depression: a re-examination for themodern era. Expert. Opin. Pharmacother. 11, 709–722.
Pies, R.W., 2009. Depression and the pitfalls of causality: implications forDSM-V. J. Affect. Disord. 116, 1–3.
Pigott, H.E., Leventhal, A.M., Alter, G.S., Boren, J.J., 2010. Efficacy andeffectiveness of antidepressants: current status of research. Psychother.Psychosom. 79, 267–279.
Posternak, M.A., 2003. Biological markers of atypical depression. HarvardRev. Psychiatry 11, 1–7.
Pucak, M.L., Kaplin, A.I., 2005. Unkind cytokines: current evidence for thepotential role of cytokines in immune-mediated depression. Int. Rev.Psychiatry 17, 477–483.
Pucak, M.L., Carroll, K.A., Kerr, D.A., Kaplin, A.I., 2007. Neuropsychiatricmanifestations of depression in multiple sclerosis: neuroinflammatory,neuroendocrine, and neurotrophic mechanisms in the pathogenesis ofimmune-mediated depression. Dialog. Clin. Neurosci. 9, 125–139.
Rao, U., Chen, L.-A., 2009. Characteristics, correlates, and outcomes of childhoodand adolescent depressive disorders. Dialog. Clin. Neurosci. 11, 45–62.
Rao, S., Zisook, S., 2009. Anxious depression: clinical features and treatment.Curr. Psychiatry Rep. 11, 429–436.
Riecher-Rossler, A., Hofecker Fallahpour, M., 2003. Postpartum depression: do westill need this diagnostic term? Acta Psychiatr. Scand Suppl. 418, 51–56.
Risch, N., Herrell, R., Lehner, T., Liang, K.Y., Eaves, L., Hoh, J., Griem, A., Kovacs,M., Ott, J., Merikangas, K., 2009. Interaction between the serotonintransporter gene (5-HTTLPR), stressful life events, and risk of depres-sion: a meta-analysis. JAMA 301, 2462–2471.
Robinson, R.G., Spalletta, G., 2010. Poststroke depression: a review. Can. J.Psychiatry 55, 341–349.
Rohan, K.J., Roecklein, K.A., Haaga, D.A., 2009. Biological and psychologicalmechanisms of seasonal affective disorder: a review and integration.Curr. Psychiatry Rev. 5, 37–47.
Römer, B., Gass, P., 2010. Finasteride-induced depression: new insights intopossible pathomechanisms. J. Cosmetic Dermatol. 9, 331–332.
Rosenthal, N.E., 2009. Issues for DSM-V: seasonal affective disorder andseasonality. Am. J. Psychiatry 166, 852–853.
Ross, L.E., Murray, B.J., Steiner, M., 2005. Sleep and perinatal mood disorders:a critical review. J. Psychiatry Neurosci. 30, 247–256.
Rothschild, A.J., 2003. Challenges in the treatment of depression withpsychotic features. Biol. Psychiatry 53, 680–690.
Rush, A.J., 2007. The varied clinical presentations of major depressivedisorder. J. Clin. Psychiatry 68.
Rush, A.J., Thase, M.E., Dube, S., 2003. Research issues in the study of difficult-to-treat depression. Biol. Psychiatry 53, 743–753.
Samaras, N., Rossi, G., Giannakopoulos, P., Gold, G., 2010. Vasculardepression. An age-related mood disorder. Eur. Geriatr. Med. 1, 220–225.
Schiepers, O.J., Wichers, M.C., Maes, M., 2005. Cytokines and majordepression. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 29, 201–217.
Schumacher, M., Zubaran, C., White, G., 2008. Bringing birth-related paternaldepression to the fore. Women Birth 21, 65–70.
Semprini, F., Fava, G.A., Sonino, N., 2010. The spectrum of adjustmentdisorders: too broad to be clinically helpful. CNS Spectr 15, 382–388.
Shelton, R.C., Osuntokun, O., Heinloth, A.N., Corya, S.A., 2010. Therapeuticoptions for treatment-resistant depression. CNS Drugs 24, 131–161.
Shorter, E., 2007. The doctrine of the two depressions in historicalperspective. Acta Psychiatry Scand. Suppl. 433, 5–13.
Shyn, S.I., Hamilton, S.P., 2010. The genetics of major depression: moving beyondthe monoamine hypothesis. Psychiatry Clin. North Am. 33, 125–140.
Silverstone, P.H., von Studnitz, E., 2003. Defining anxious depression: goingbeyond comorbidity. Can. J. Psychiatry 48, 675–680.
Soares, C.N., Zitek, B., 2008. Reproductive hormone sensitivity and risk fordepression across the female life cycle: a continuum of vulnerability?J. Psychiatry Neurosci. 33, 331–343.
Sohn, C.H., Lam, R.W., 2005. Update on the biology of seasonal affectivedisorder. CNS Spectr. 10, 635–646.
Sonino, N., Fallo, F., Fava, G., 2010. Psychosomatic aspects of Cushing'ssyndrome. Rev. Endocr. Metab. Disord. 11, 95–104.
Stewart, J.W., Thase, M.E., 2007. Treating DSM-IV depression with atypicalfeatures. J. Clin. Psychiatry 68, e10.
Stewart, J.W., McGrath, P.J., Quitkin, F.M., Klein, D.F., 2007. Atypicaldepression: current status and relevance to melancholia. Acta PsychiatryScand. Suppl. 433, 58–71.
Stewart, J.W., McGrath, P.J., Quitkin, F.M., Klein, D.F., 2009. DSM-IVdepression with atypical features: is it valid? Neuropsychopharmacol.34, 2625–2632.
Strain, J.J., Klipstein, K.G., Newcorn, J.H., 2011. Adjustment disorders, In:Hales, R.E., Yudofsky, S.C., Gabbard, G.O. (Eds.), Essentials of Psychiatry,3rd ed. American Psychiatric Publishing, Arlington, VA, pp. 255–270.
Studd, J., Panay, N., 2009. Are oestrogens useful for the treatment ofdepression in women? Best Pract. Res. Clin. Obstet. Gynaecol. 23, 63–71.
Sullivan, P.F., Prescott, C.A., Kendler, K.S., 2002. The subtypes of majordepression in a twin registry. J. Affect. Disord. 68, 273–284.
Taylor, M.A., Fink, M., 2008. Restoring melancholia in the classification ofmood disorders. J. Affect. Disord. 105, 1–14.
Tennant, C., 2002. Life events, stress and depression: a review of recentfindings. Aust. N. Z. J. Psychiatry 36, 173–182.
Ter Horst, G.J., Wichmann, R., Gerrits, M., Westenbroek, C., Lin, Y., 2009. Sexdifferences in stress responses: focus on ovarian hormones. Physiol.Behav. 97, 239–249.
Tharwani, H.M., Yerramsetty, P., Mannelli, P., Patkar, A., Masand, P., 2007.Recent advances in poststroke depression. Curr. Psychiatry Rep. 9,225–231.
Thase, M.E., 2007. Recognition and diagnosis of atypical depression. J. Clin.Psychiatry 68.
Thase, M.E., 2009. Atypical depression: useful concept, but it's time to revisethe DSM-IV criteria. Neuropsychopharmacol. 34, 2633–2641.
Thase, M.E., Friedman, E.S., 1999. Is psychotherapy an effective treatment formelancholia and other severe depressive states? J. Affect. Disord. 54,1–19.
Turner, E.H., Matthews, A.M., Linardatos, E., Tell, R.A., Rosenthal, R., 2008.Selective publication of antidepressant trials and its influence onapparent efficacy. N. Engl. J. Med. 358, 252–260.
Tyrka, A.R., Price, L.H., Mello, M.F., Mello, A.F., Carpenter, L.L., 2006. Psychoticmajor depression: a benefit-risk assessment of treatment options. DrugSafety 29, 491–508.
Uher, R., 2008. The implications of gene–environment interactions indepression: will cause inform cure? Mol. Psychiatry 13, 1070–1078.
Vaishnavi, S., Taylor, W.D., 2006. Neuroimaging in late-life depression. Int.Rev. Psychiatry 18, 443–451.
Vega, J.A., Mortimer, A.M., Tyson, P.J., 2000. Somatic treatment of psychoticdepression: review and recommendations for practice. J. Clin. Psycho-pharmacol. 20, 504–519.
Wakefield, J.C., Schmitz, M.F., Baer, J.C., 2010. Does the DSM-IV clinicalsignificance criterion for major depression reduce false positives?Evidence from the National Comorbidity Survey Replication. Am. J.Psychiatry 167, 298–304.

140 Baumeister, H., Parker, G. / Journal of Affective Disorders 139 (2012) 126–140
Westrin, A., Lam, R.W., 2007. Seasonal affective disorder: a clinical update.Ann. Clin. Psychiatry 19, 239–246.
WHO, 2008. The Global Burden of Disease: 2004 Update. http://www.who.int/healthinfo/global_burden_disease/GBD_report_2004update_full.pdf.Accessed Feb. 10th 2011.
Wijeratne, C., Sachdev, P., 2008. Treatment-resistant depression: critique ofcurrent approaches. Aust. N. Z. J. Psychiatry 42, 751–762.
Wijkstra, J., Lijmer, J., Balk, F., Geddes, J., Nolen, W.A., 2005. Pharmacologicaltreatment for psychotic depression. Cochrane Database Syst. Rev.CD4044.
Wilhelm, K., 2009. Men and depression. Austral. Fam. Physician 38, 102–105.Wilhelm, K., Parker, G., Geerligs, L., Wedgwood, L., 2008. Women and
depression: a 30 year learning curve. Austral. New Zeal. J. Psychiatry 42,3–12.
Wilson, S., Durbin, C.E., 2010. Effects of paternal depression on fathers'parenting behaviors: a meta-analytic review. Clin. Psychol. Rev. 30,167–180.
Yonkers, K.A., Wisner, K.L., Stewart, D.E., Oberlander, T.F., Dell, D.L., Stotland,N., Ramin, S., Chaudron, L., Lockwood, C., 2009. The management ofdepression during pregnancy: a report from the American PsychiatricAssociation and the American College of Obstetricians and Gynecolo-gists. Gen. Hosp. Psychiatry 31, 403–413.
Young, E., Korszun, A., 2009. Sex, trauma, stress hormones and depression.Mol. Psychiatry 15, 23–28.
Zonana, J., Gorman, J.M., 2005. The neurobiology of postpartum depression.CNS Spectr. 10, 792–799.
Related Documents