351 SECTION 5 PULMONARY DISORDERS 45 APPROACH TO THE PATIENT WITH PULMONARY SYMPTOMS ............................................................. 353 Chest Pain ................................................................. 355 Cough ...................................................................... 355 Dyspnea .................................................................... 357 Hemoptysis ................................................................ 359 Solitary Pulmonary Nodule ............................................. 361 Stridor ...................................................................... 363 Wheezing .................................................................. 363 46 TESTS OF PULMONARY FUNCTION ............................. 364 Flow Rates, Lung Volumes, and Flow-Volume Loops ............... 364 Measurement of Gas Exchange ......................................... 369 Tests of Respiratory Muscle Function ................................. 372 Exercise Testing .......................................................... 373 47 DIAGNOSTIC AND THERAPEUTIC PULMONARY PROCEDURES .......................................................... 374 Chest Imaging............................................................. 374 Electrocardiography ...................................................... 375 Bronchoscopy ............................................................. 375 Mediastinoscopy and Mediastinotomy ................................ 377 Physiotherapy ............................................................. 377 Pleural Biopsy ............................................................ 377 Pulmonary Rehabilitation ............................................... 378 Thoracentesis.............................................................. 378 Thoracoscopy and Video-Assisted Thoracoscopic Surgery ......... 379 Thoracotomy .............................................................. 379 Transthoracic Needle Biopsy ........................................... 380 Tube Thoracostomy ...................................................... 380 48 ASTHMA.................................................................. 381 Allergic Bronchopulmonary Aspergillosis ............................ 398 49 CHRONIC OBSTRUCTIVE PULMONARY DISEASE ........... 400 α 1 -Antitrypsin Deficiency ............................................... 410 50 PULMONARY EMBOLISM .......................................... 412 045_062PUL Page 351 Tuesday, November 8, 2005 10:54 AM

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

351
SECTION 5
PULMONARY DISORDERS
45 APPROACH TO THE PATIENT WITH PULMONARY SYMPTOMS ............................................................. 353
Chest Pain
................................................................. 355
Cough
...................................................................... 355
Dyspnea
.................................................................... 357
Hemoptysis
................................................................ 359
Solitary Pulmonary Nodule
............................................. 361
Stridor
...................................................................... 363
Wheezing
.................................................................. 363
46 TESTS OF PULMONARY FUNCTION............................. 364
Flow Rates, Lung Volumes, and Flow-Volume Loops
............... 364
Measurement of Gas Exchange
......................................... 369
Tests of Respiratory Muscle Function
................................. 372
Exercise Testing
.......................................................... 373
47 DIAGNOSTIC AND THERAPEUTIC PULMONARY PROCEDURES .......................................................... 374
Chest Imaging
............................................................. 374
Electrocardiography
...................................................... 375
Bronchoscopy
............................................................. 375
Mediastinoscopy and Mediastinotomy
................................ 377
Physiotherapy
............................................................. 377
Pleural Biopsy
............................................................ 377
Pulmonary Rehabilitation
............................................... 378
Thoracentesis
.............................................................. 378
Thoracoscopy and Video-Assisted Thoracoscopic Surgery
......... 379
Thoracotomy
.............................................................. 379
Transthoracic Needle Biopsy
........................................... 380
Tube Thoracostomy
...................................................... 380
48 ASTHMA.................................................................. 381
Allergic Bronchopulmonary Aspergillosis
............................ 398
49 CHRONIC OBSTRUCTIVE PULMONARY DISEASE........... 400
α
1
-Antitrypsin Deficiency
............................................... 410
50 PULMONARY EMBOLISM .......................................... 412
045_062PUL Page 351 Tuesday, November 8, 2005 10:54 AM
352
SECTION 5 PULMONARY DISORDERS
51 ACUTE BRONCHITIS.................................................. 423
52 PNEUMONIA............................................................ 423
Community-Acquired Pneumonia
..................................... 424
Hospital-Acquired Pneumonia
......................................... 430
Nursing Home–Acquired Pneumonia
................................. 432
Pneumonia in the Immunocompromised Host
....................... 434
Pneumocystis jiroveci
Pneumonia
...................................... 435
Aspiration Pneumonitis and Pneumonia
.............................. 436
53 LUNG ABSCESS ....................................................... 437
54 BRONCHIECTASIS..................................................... 439
55 INTERSTITIAL LUNG DISEASES................................... 443
Idiopathic Interstitial Pneumonias
..................................... 443
Idiopathic Pulmonary Fibrosis
.......................................... 444
Desquamative Interstitial Pneumonia
................................... 448
Respiratory Bronchiolitis-Associated Interstitial Lung Disease
...... 448
Acute Interstitial Pneumonia
............................................ 449
Bronchiolitis Obliterans Organizing Pneumonia
...................... 449
Nonspecific Interstitial Pneumonia
..................................... 450
Drug-Induced Pulmonary Disease
..................................... 450
Eosinophilic Pulmonary Diseases
...................................... 450
Chronic Eosinophilic Pneumonia
....................................... 452
Acute Eosinophilic Pneumonia
......................................... 452
Löffler’s Syndrome
....................................................... 453
Hypersensitivity Pneumonitis
........................................... 453
Lymphangioleiomyomatosis
............................................ 457
Lymphoid Interstitial Pneumonia
...................................... 459
Pulmonary Alveolar Proteinosis
........................................ 460
Pulmonary Langerhans’ Cell Granulomatosis
........................ 461
56 SARCOIDOSIS........................................................... 462
57 ENVIRONMENTAL PULMONARY DISEASES.................. 469
Air Pollution–Related Illness
........................................... 469
Asbestos-Related Disorders
............................................. 470
Beryllium Disease
........................................................ 472
Building-Related Illnesses
.............................................. 473
Byssinosis
................................................................. 474
Coal Workers’ Pneumoconiosis
......................................... 475
Occupational Asthma
.................................................... 476
Silicosis
.................................................................... 477
Toxic Inhalation Injury
.................................................. 480
58 PULMONARY HYPERTENSION ................................... 481
Portopulmonary Hypertension
.......................................... 484
Hepatopulmonary Syndrome
........................................... 484
045_062PUL Page 352 Tuesday, November 8, 2005 10:54 AM

45 APPROACH TO THE PATIENT WITH PULMONARY SYMPTOMS
353
59 DIFFUSE ALVEOLAR HEMORRHAGE AND PULMONARY-RENAL SYNDROMES ......................485
Diffuse Alveolar Hemorrhage Syndrome
..............................485
Pulmonary-Renal Syndrome
.............................................486
Goodpasture’s Syndrome
.................................................486
60 MEDIASTINAL AND PLEURAL DISORDERS....................488
Mediastinal Masses
.......................................................488
Mediastinitis
...............................................................488
Pleural Effusion
...........................................................489
Pleural Fibrosis and Calcification
.......................................495
Pneumomediastinum
.....................................................496
Pneumothorax
.............................................................496
Viral Pleuritis
..............................................................498
61 SLEEP APNEA...........................................................499
Obstructive Sleep Apnea
.................................................499
Central Sleep Apnea
......................................................502
62 TUMORS OF THE LUNGS ............................................503
Lung Carcinoma
...........................................................503
Airway Tumors
............................................................509
Bronchial Carcinoid
......................................................510
Chest Wall Tumors
........................................................510
45
APPROACH TO THE PATIENT WITH PULMONARY SYMPTOMS
Key components in the evaluation of pa-tients with pulmonary symptoms are the his-tory, physical examination, and, in most cases,a chest x-ray. These components establish theneed for subsequent testing, including pul-monary function testing and ABG analysis(see p. 364), CT scan and other imaging tests(see p. 374), and bronchoscopy (see p. 375).
History
The history can often establish whethersymptoms of dyspnea, chest pain, wheezing,stridor, hemoptysis, and cough are likely to bepulmonary in origin. The history should focuson which symptom is primary when more thanone occurs concurrently and whether consti-tutional symptoms, such as fever, weight loss,and night sweats, also occur. Other importantinformation includes occupational and envi-ronmental exposures; family, travel, and con-tact history; previous illnesses and use of med-ications or illicit drugs; and previous test re-sults (eg, tuberculin skin test, chest x-rays).
Physical Examination
Physical examination starts with assess-ment of general appearance. Discomfortand anxiety, habitus, and the effect of talking ormovement on symptoms all can be assessedwhile greeting the patient and taking a historyand may provide useful information relevant to
045_062PUL Page 353 Tuesday, November 8, 2005 10:54 AM

354
SECTION 5 PULMONARY DISORDERS
pulmonary status. Next comes inspection, aus-cultation, and chest percussion and palpation.
Inspection:
Inspection should focus onsigns of respiratory difficulty and hypoxemia,such as restlessness, cyanosis, and accessorymuscle use, and of possible chronic pulmo-nary disease, such as clubbing or pedal edema.
Cyanosis is bluish discoloration of the lips,face, or nail beds, signifying low arterial O
2
saturation (
<
85%).Accessory muscle use is defined as use of in-
tercostal, sternocleidomastoid, and/or scalenemuscles to breathe. Intercostal retractions (in-ward movement of the rib interspaces) are com-mon in infants and in patients with severe air-flow limitation; paradoxical breathing (inwardmotion of the abdomen during inspiration)signifies respiratory muscle fatigue or weakness.
Clubbing is enlargement of the fingertips(or toes) due to proliferation of connectivetissue between the fingernail and the bone.Diagnosis is based on an increase in the pro-file angle of the nail as it exits the finger (to
>
176
°
) or on an increase in the phalangealdepth ratio (to
>
1) (see F
IG
. 45–1). “Spongi-ness” of the nail bed beneath the cuticle alsosuggests clubbing. Clubbing is most com-monly observed in lung cancer but is an im-portant sign of chronic pulmonary disease,such as cystic fibrosis and idiopathic pulmo-nary fibrosis; it occurs less commonly in cy-anotic heart disease, chronic infection (eg, in-fective endocarditis), stroke, inflammatorybowel disease, and cirrhosis. Clubbing occa-sionally occurs with osteoarthropathy andperiostitis (primary or hereditary hyper-trophic osteoarthropathy); in this instance,clubbing may be accompanied by skinchanges, such as hypertrophied skin on thedorsa of the hands (pachydermoperiostosis),seborrhea, and coarse facial features. Digitalclubbing can also occur as a benign heredi-
tary abnormality; benign clubbing can be dis-tinguished from pathologic clubbing by theabsence of pulmonary symptoms or diseaseand by patient report of clubbing from anearly age.
Chest wall deformities, such as pectus ex-cavatum and kyphoscoliosis, may restrictrespirations and exacerbate symptoms ofpreexisting pulmonary disease.
Respiratory rate should be assessed andcounted for 1 min to account for fluctuations inrate attributable to abnormal breathing patterns.
Cheyne-Stokes respiration (periodic breath-ing) is a cyclic fluctuation of respiratory rate anddepth. From periods of brief apnea, patientsbreathe progressively faster and deeper (hy-perpnea), then slower and less deeply untilthey become apneic and repeat the cycle.Cheyne-Stokes respiration is most often causedby heart failure, neurologic disease (eg, stroke,advanced dementia), or medications. The pat-tern in heart failure is probably attributable to de-lays in cerebral circulation; respiratory centerslag in recognition of systemic acidosis/hypoxia(causing hyperpnea) and of alkalosis/hypocap-nia (causing apnea).
Biot’s respiration is an uncommon variantof Cheyne-Stokes respiration in which irreg-ular periods of apnea alternate with periods inwhich 4 or 5 deep, equal breaths are taken. Itdiffers from Cheyne-Stokes respiration inthat it is characterized by abrupt starts andstops and lacks periodicity. It results from in-jury to the CNS and occurs in such disordersas meningitis.
Kussmaul’s respirations are deep, regularrespirations caused by metabolic acidosis.
Jugular venous distention is usually a signof volume overload or right heart failure(see p. 574).
Auscultation:
Auscultation is arguablythe most important component of the physical
Fig. 45–1. Measuring finger clubbing.
The ratio of the anteroposterior diameter of the fin-ger at the nail bed (a–b) to that at the distal interphalangeal joint (c–d) is a simple measurement offinger clubbing. It can be obtained readily and reproducibly with calipers. If the ratio is
>
1, club-bing is present. Finger clubbing is also characterized by loss of the normal angle at the nail bed.
160°
a
b
Normal finger Clubbed finger
c
d
>180°
045_062PUL Page 354 Tuesday, November 8, 2005 10:54 AM
45 APPROACH TO THE PATIENT WITH PULMONARY SYMPTOMS
355
examination. All fields of the chest should belistened to, including the flanks, to detect ab-normalities associated with each lobe of thelung. Features to listen for include the characterand volume of breath sounds, the presence orabsence of vocal sounds, pleural friction rubs,and ratio of inspiration to expiration (I:E ratio).
Vesicular breath sounds are the normalsounds heard over most lung fields. Bronchialbreath sounds are slightly louder, harsher, andhigher pitched. They normally can be heardover the trachea and over areas of lung consol-idation, such as pneumonia. Adventitioussounds are abnormal sounds, such as crackles,rhonchi, wheezes, and stridor.
Crackles, previously called rales, are discon-tinuous adventitious breath sounds. Fine crack-les are short high-pitched sounds; coarse crack-les are longer-lasting low-pitched sounds.Crackles have been compared to the sound ofcrinkling plastic wrap and can be simulated byrubbing strands of hair together between 2 fin-gers near one’s ear. They occur most commonlywith atelectasis and alveolar filling processes,such as pulmonary edema, and interstitial lungdisease; they signify distention of fibrotic lungtissue or opening of collapsed alveoli.
Rhonchi are low-pitched respiratory soundsthat can be heard during inspiration or expira-tion. They occur in a variety of conditions, in-cluding chronic bronchitis. The mechanismmay relate to variations in obstruction as air-ways distend with inhalation.
Wheezes are a whistling, musical breathsound worse during expiration than inspira-tion. Wheezing can be a physical finding or asymptom usually associated with dyspnea.
Stridor is a high-pitched, predominantlyinspiratory sound formed by extrathoracicupper airway obstruction. It usually can beheard without a stethoscope. Stridor is usu-ally louder than wheezing, is predominantlyinspiratory, and is heard loudly over the lar-ynx. It should trigger a concern for life-threatening upper airway obstruction.
Decreased breath sounds signify poor airmovement in airways, as occurs with asthmaand COPD where bronchospasm or othermechanisms limit airflow. Breath sounds mayalso be decreased in the presence of a pleuraleffusion or pneumothorax.
Bronchophony is clear transmission of thepatient’s spoken voice through the chest wall.It results from alveolar consolidation, such asin pneumonia.
Egophony is said to occur when a patientsays the letter “e” and the examiner hears the
letter “a” on auscultation. It is heard in anycondition that results in pulmonary consoli-dation, such as pneumonia.
Whispered pectoriloquy is transmissionof the patient’s whispered voice through thechest wall at an increased volume. It is mostoften heard in pneumonia.
Friction rubs are grating or creakingsounds that fluctuate with the respiratory cy-cle and sound like skin rubbing against wetleather. They are a sign of pleural inflamma-tion and are heard in pleurisy, after thoracot-omy, and with empyema.
I:E ratio is normally 1:2 but is prolonged to≥ 1:3 when airflow is limited, such as in asthmaand COPD, even in the absence of wheezing.
Cardiac auscultation may reveal signs ofpulmonary hypertension, such as a loud P2(pulmonic 2nd heart sound), and of rightheart failure, such as a right ventricular S4(4th heart sound—see p. 578) and tricuspidregurgitation.
Percussion and palpation: Percussion isthe primary physical maneuver used to detect thepresence and level of pleural effusion. Findingson percussion of areas of dullness signify under-lying fluid or, less commonly, consolidation. Pal-pation includes tactile fremitus, vibration of thechest wall felt when a patient is asked to speak;it is decreased in pleural effusion and pneu-mothorax and increased in pulmonary consoli-dation. Point tenderness on palpation may signalunderlying rib fracture or pleural inflammation.
In cor pulmonale (see p. 664), a right ven-tricular impulse at the left lower sternal bor-der may become evident and may be increasedin amplitude and duration (right ventricularheave).
CHEST PAINPulmonary and pleural diseases cause chest
pain; examples include pneumonia, pulmo-nary embolism, pleuritis, lung cancer, and ribfractures. Cardiac causes of chest pain requireurgent evaluation and treatment (see p. 580).
COUGHCough is an explosive expiratory maneuver
that is reflexively or deliberately intended toclear the airways. Coughing is a normal re-sponse to the presence of mucus or other for-eign material in the airway or upper airway,but persistent coughing is annoying and gen-erally indicates irritation of the pulmonaryairways. It is the 5th most common symptom
045_062PUL Page 355 Tuesday, November 8, 2005 10:54 AM

356 SECTION 5 PULMONARY DISORDERS
prompting patients to visit their physician.Awareness of cough varies considerably. Acough that appears suddenly, interferes withsleep, or causes musculoskeletal chest wallpain can be distressing. A cough that developsover decades (eg, in a smoker with mildchronic bronchitis) may be hardly noticeableor may be considered normal by the patient.
EtiologyLikely etiologies of cough differ depend-
ing on whether the symptom is acute (< 3 wk)or chronic.
Acute cough is most often caused by a URI,especially the common cold. Other causes in-clude pneumonia; postnasal drip resultingfrom rhinitis or sinusitis that can be allergic,viral, or bacterial in origin; and COPD exac-erbations. Cough may rarely be the only pre-senting symptom of pulmonary embolus. Inthe elderly, acute cough may signify aspira-tion or heart failure.
Chronic cough in smokers is most oftencaused by chronic bronchitis, defined as thepresence of productive cough over ≥ 3 mo for> 2 yr consecutively. Compression of upperairways by tumor is much less common butshould always be considered. The most com-mon causes regardless of smoking history in-clude postnasal drip syndrome, gastroesoph-ageal reflux disease (GERD), asthma (cough-variant asthma), and use of ACE inhibitors.Less common causes include eosinophilicbronchitis (characterized by sputum eosino-philia without airway hyperresponsiveness)and bronchiectasis. The causes of chroniccough in children are similar to those ofadults, but aspiration and pertussis must alsobe considered. Tracheobronchitis after a URIis a common cause of cough but rarely lasts >3 mo after the infection. Rarely, impactedcerumen or a foreign body in the external au-ditory canal triggers reflex cough throughstimulation of the auricular branch of the va-gus nerve. Psychogenic cough is even rarerand is a diagnosis of exclusion.
EvaluationHistory: URI and sinus symptoms suggest
postnasal drip syndrome, but postnasal dripoften causes cough without other symptoms.Heartburn, hoarseness, and chronic nocturnalor early morning cough, especially if no othersymptoms are present, suggests GERD. Coughafter exposure to dusts or allergens suggestscough-variant asthma. Chronic cough withproduction of purulent sputum in smokers sug-
gests chronic bronchitis. A change in cough inthese patients may, however, be an early man-ifestation of lung cancer. Cough productive ofgritty sputum may signify broncholithiasis.Copious volumes of sputum suggest alveolarcell carcinoma.
Physical examination: Physical exam-ination should focus on signs of sinusitis,rhinitis, and postnasal drip. Lung ausculta-tion during cough may help detect lungsounds suggestive of asthma (wheezing) orbronchiectasis (rhonchi). Examination of theears can detect triggers of reflex cough.
Testing: Most patients with acute or chroniccough without clear etiology by history and ex-amination can be treated empirically for post-nasal drip syndrome, GERD, or asthma basedon clinical judgment; an adequate response tothese therapeutic interventions precludes theneed for further testing. A chest x-ray can beperformed but usually is not helpful. Patientswith chronic cough and inadequate responsesto interventions can undergo more extensivetesting for asthma (pulmonary function testswith methacholine challenge, sinus disease[sinus CT], or GERD [esophageal pH moni-toring]). Bronchoscopy should be performedin selected patients in whom lung cancer orother bronchial tumor is suspected.
TreatmentTreatment is management of the underlying
cause. Little evidence exists to support the useof cough suppressants or mucolytic agents forcough, but patients often expect or requestsuch treatment, and multiple options exist.Coughing is an important mechanism forclearing secretions from the airways and canassist in treating respiratory infections. There-fore, cough suppression in infectious condi-tions should be done with caution. Nonspe-cific treatments for cough should be reservedas much as possible for patients with a URI andfor those receiving therapy for the underlyingcause but for whom cough is still troubling.
Antitussives depress the medullary coughcenter (dextromethorphan and codeine) oranesthetize stretch receptors of vagal afferentfibers in bronchi and alveoli (benzonatate).Dextromethorphan, a congener of the nar-cotic levorphanol, is effective as a tablet orsyrup at a dose of 15 to 30 mg 1 to 4 times/dayfor adults or 0.25 mg/kg qid for children. Co-deine has antitussive, analgesic, and sedativeeffects, but dependence is a potential prob-lem, and nausea, vomiting, constipation, andtolerance are common adverse effects. Usual
045_062PUL Page 356 Tuesday, November 8, 2005 10:54 AM

45 APPROACH TO THE PATIENT WITH PULMONARY SYMPTOMS 357
doses are 10 to 20 mg po q 4 to 6 h as neededfor adults and 0.25 to 0.5 mg/kg qid for chil-dren. Other opioids (eg, hydrocodone, hydro-morphone, methadone, morphine) have anti-tussive properties but are avoided because ofhigh potential for dependence and abuse.Benzonatate, a congener of tetracaine in liq-uid-filled capsules, is effective at a dose of100 to 200 mg po tid. Inhaled ipratropium isnot generally considered an antitussive butmay be of use in some patients with acutecough due to URI.
Expectorants are thought to decrease vis-cosity and facilitate expectoration, or cough-ing up, of secretions, but are of limited ben-efit. Guaifenesin (200 to 400 mg po q 4 h insyrup or tablet form) is most commonly usedbecause it has no serious adverse effects, butmultiple expectorants exist, including brom-hexine, ipecac, saturated solution of potas-sium iodide (SSKI), and domiodol. Aero-solized expectorants, which include isopro-terenol, beclomethasone, N-acetylcysteine,and deoxyribonuclease (DNase), are gener-ally reserved for hospital-based treatment ofcough in patients with bronchiectasis orcystic fibrosis. Ensuring adequate hydrationmay facilitate expectoration, as may inhala-tion of steam, although neither has been rig-orously tested.
Topical treatments, such as acacia, lico-rice, glycerin, honey, and wild cherry coughdrops or syrups (demulcents), are locally andperhaps emotionally soothing but are notsupported by scientific evidence.
Protussives, which stimulate cough, areindicated for such disorders as cystic fibrosisand bronchiectasis, in which a productivecough is thought to be important for airwayclearance and preservation of pulmonaryfunction. DNase or hypertonic saline is givenin conjunction with chest physical therapyand postural drainage to promote cough andexpectoration. This approach seems to bebeneficial in cystic fibrosis but not in mostother causes of chronic cough.
Bronchodilators, such as albuterol andipratropium or inhaled corticosteroids, canbe effective for cough after URI and in cough-variant asthma.
DYSPNEADyspnea is unpleasant or uncomfortable
breathing. It has multiple components and isexperienced and described differently de-pending on the cause.
Dyspnea has multiple pulmonary, cardiac,and other causes (see TABLE 45–1). Often,more than one mechanism underlies thesensation.
The basis for the sensation of discomfort ofdyspnea is unclear but may be a centrallyperceived discrepancy between respiratorymuscle tension (the need to take a deepbreath) and length (the ability to take a deepbreath). This mechanism partially explainswhy some forms of breathlessness and hyper-pnea, such as with metabolic acidosis (Kuss-maul’s respirations), in CNS disease (Biot’sand Cheyne-Stokes respirations), and during
TABLE 45–1. CAUSES OF DYSPNEA
Acute onset (within minutes)Pulmonary
PneumothoraxPulmonary embolismBronchospasm
Asthma (with previous history)Reactive airway disease (with previous exposure)
Foreign bodyToxic inhalation (eg, chlorine, hydrogen sulfide)
CardiacAcute myocardial ischemia or infarction
Papillary muscle dysfunction or ruptureVentricular dysfunction
Cardiogenic pulmonary edemaOther
Diaphragmatic paralysisAnxiety disorder—hyperventilation
Subacute onset (within hours or days)Same as acute onset, with addition of:
PneumoniaAcute bronchitisPoisoning
SalicylateEthylene glycol
Nonacute onset (hours–years)Pulmonary
Obstructive lung diseaseRestrictive lung diseaseInterstitial lung diseasePleural effusion
CardiacVentricular dysfunctionPericardial effusion and tamponade
Other AnemiaPhysical deconditioning
045_062PUL Page 357 Tuesday, November 8, 2005 10:54 AM

358 SECTION 5 PULMONARY DISORDERS
exercise among trained athletes, are not ex-perienced as dyspnea.
EvaluationHistory: Reports of shortness of breath or of
being unable to take a deep breath are morecommon among patients with COPD exacer-bation. Chest tightness or increased effort tobreathe suggests asthma or an obstructive ven-tilatory disorder. A feeling of suffocation ischaracteristic of pulmonary edema. Heavybreathing on exertion is common in physicaldeconditioning, whereas air hunger, or an ur-gent sense of a need to breathe in more air, hasbeen linked to hypercapnia, restricted chestwall excursions, and pulmonary edema.Phrases such as “out of breath” and “hard tobreathe” are nonspecific.
Abrupt onset of dyspnea with or withoutsharp chest pain suggests spontaneous pneu-mothorax or pulmonary embolism; concom-itant leg pain and swelling or recent immobil-ity support pulmonary embolism. Abrupt on-set of productive cough and fever suggestsbacterial pneumonia, particularly that causedby Streptococcus pneumoniae if it is accom-panied by pleuritic chest pain. Severe dyspneathat appears 1 to 2 h after falling asleep (par-oxysmal nocturnal dyspnea) is pathogno-monic for left ventricular dysfunction, but itmust be distinguished from nocturnal awak-ening by cough from asthma or mucus hyper-secretion. Dyspnea while recumbent (ortho-pnea) also implies left ventricular dysfunc-tion or, less commonly, pericardial effusion,respiratory muscle weakness, or diaphrag-matic paralysis. Dyspnea that worsens whensitting upright and resolves when recumbent(platypnea) is unusual and suggests pulmo-nary arteriovenous malformation or thehepatopulmonary syndrome; it may also oc-cur after pneumonectomy, in recurrent pul-monary embolism, and in chronic pulmonarydiseases that preferentially affect the lowerlobes, such as aspiration pneumonia and α1-antitrypsin deficiency. Dyspnea accompa-nied by paresthesias in the fingers or aroundthe mouth suggests hyperventilation. Exer-tional dyspnea in the absence of objectivefindings on examination or testing may indi-cate anemia, primary pulmonary hyperten-sion (if it occurs in a young woman), or, morelikely, physical deconditioning.
Physical examination: Absent or mark-edly diminished breath sounds on only one sidesuggest pneumothorax or pleural effusion;these can be distinguished by increased res-
onance and dullness to percussion, respec-tively. Wheezing (see p. 363) suggests asthmaor COPD. Stridor (see p. 363) suggests extra-thoracic airway obstruction (eg, foreign body,epiglottitis, vocal cord dysfunction). Crack-les in the dyspneic patient suggest left heartfailure or interstitial lung disease. Rhonchisuggest COPD.
Testing: A chest x-ray should be taken inmost patients. Acute dyspnea also warrantspulse oximetry, which provides a noninvasivemeasure of O2 saturation. An ECG to detectcardiac ischemia is mandatory unless cardiacischemia can be excluded clinically. In pa-tients with severe or deteriorating respiratorystatus, an ABG should be performed to moreprecisely quantify hypoxemia, measure PCO2,and measure any acid-base disorders stimulat-ing hyperventilation and to calculate the alve-olar-arterial gradient (see p. 370). Patients sus-pected of having pulmonary embolism shouldundergo ventilation/perfusion scanning or CTangiography.
Chronic dyspnea may warrant additionaltests, such as CT scan, pulmonary functiontests, echocardiography, and bronchoscopy.
TreatmentTreatment is correction of the underlying
cause. Hypoxemia is addressed with sup-plemental O2 as needed to maintain SaO2 ≥88% or PaO2 > 55 mm Hg as levels abovethese thresholds provide adequate O2 deliv-ery to tissues. Levels below these thresholdsare on the steep portion of the O2-Hb disso-ciation curve, in which small declines in ar-terial O2 tension result in large declines inHb saturation (see FIG. 46–4 on p. 371). O2saturation should be maintained at > 93% ifmyocardial or cerebral ischemia is a con-cern. Morphine 0.5 to 5 mg IV helps reduceanxiety and the discomfort of dyspnea invarious conditions, including MI, pulmo-nary embolism, and the dyspnea that com-monly accompanies terminal illnesses (seep. 2765). However, opioids can be deleteri-ous in patients with acute airflow limitation(eg, asthma, COPD) because they suppressthe ventilatory drive and worsen respiratoryacidemia.
HYPERVENTILATION SYNDROMEHyperventilation syndrome is anxiety-relateddyspnea and tachypnea often accompaniedby systemic symptoms.
045_062PUL Page 358 Tuesday, November 8, 2005 10:54 AM

45 APPROACH TO THE PATIENT WITH PULMONARY SYMPTOMS 359
Hyperventilation syndrome is common inyoung women but can affect either sex at anyage. It is sometimes precipitated by emotion-ally stressful events. Hyperventilation syn-drome is separate from panic disorder (see p.1674), although the 2 conditions overlap;about 1⁄2 of patients with panic disorder havehyperventilation syndrome and 1⁄4 of patientswith hyperventilation syndrome have panicdisorder.
History: Patients with acute hyperventila-tion syndrome present with dyspnea some-times so severe as to feel like suffocation. Itis accompanied by agitation and a sense ofterror or by somatic symptoms of chest pain,paresthesias (peripheral and perioral), pe-ripheral tetany, and presyncope or syncope orsometimes by a combination of all of these.Tetany occurs because respiratory alkalosiscauses both hypophosphatemia and hypocal-cemia. Patients with chronic hyperventila-tion syndrome present far less dramaticallyand often escape detection; they sigh deeplyand frequently and often have nonspecific so-matic symptoms in the context of mood andanxiety disorders and emotional stress.
Physical examination: Physical exam-ination is normal in both acute and chronichyperventilation syndrome, although patientsmay be tachypneic and appear anxious oragitated.
Testing: Hyperventilation syndrome is adiagnosis of exclusion; the challenge is touse tests and resources judiciously to distin-guish this syndrome from more serious di-agnoses. Basic testing includes pulse oxim-etry, chest x-ray, and ECG. Pulse oximetry inhyperventilation syndrome shows O2 satu-ration at or close to 100%. Chest x-ray is nor-mal. ECG is performed to detect cardiac is-chemia, although hyperventilation syndromeitself can cause ST-segment depressions, T-wave inversions, and prolonged QT intervals.ABGs are needed when other causes of hy-perventilation are suspected, such as meta-bolic acidosis. Occasionally, acute hyper-ventilation syndrome is indistinguishablefrom acute pulmonary embolism, and testsfor pulmonary embolism (eg, D-dimer, ven-tilation/perfusion scan, helical CT) may benecessary.
TreatmentTreatment is reassurance. Some physicians
advocate teaching the patient maximal exhala-tion and diaphragmatic breathing. Most pa-tients require treatment for underlying mood or
anxiety disorders that includes cognitive ther-apy, stress reduction techniques, and/or drugs(anxiolytics, antidepressants, or lithium).
HEMOPTYSISHemoptysis is coughing up of blood from
the respiratory tract. Most of the lung’s blood(95%) circulates through low-pressure pul-monary arteries and ends up in the pulmonarycapillary bed, where gas is exchanged; about5% of the blood supply circulates throughhigh-pressure bronchial arteries, which origi-nate at the aorta and supply major airways andsupporting structures. The blood in hemopty-sis generally arises from this bronchial circu-lation, except when pulmonary arteries aredamaged by trauma, by erosion of a granulo-matous or calcified lymph node or tumor, or,rarely, by pulmonary arterial catheterizationor when pulmonary capillaries are affected byinflammation. Blood-streaked sputum is com-mon in many minor respiratory illnesses, suchas URI and viral bronchitis. Massive hemop-tysis is production of 600 mL of blood (abouta full kidney basin’s worth) within 24 h.
The differential diagnosis is broad (seeTABLE 45–2). Bronchitis, bronchiectasis,TB, and necrotizing pneumonia or lung ab-scess account for 70 to 90% of cases. CavitaryAspergillus infection is being increasinglyrecognized as a cause but is not as commonas malignancy; hemoptysis in smokers ≥ 40yr triggers suspicion of primary lung cancer.Metastatic cancer rarely causes hemoptysis.Pulmonary-renal and diffuse alveolar hem-orrhage syndromes (see p. 485), pulmonaryembolism and infarction (see p. 412), and leftventricular failure (especially secondary tomitral stenosis) are less common causes ofhemoptysis. Hemoptysis in heart failure isunusual but occurs as a result of pulmonaryvenous hypertension from left ventricularfailure. Primary bronchial adenoma and ar-teriovenous malformations are rare but tendto cause severe bleeding. Rarely, hemoptysisoccurs during menstruation (catamenial he-moptysis) because of intrathoracic endo-metriosis.
EvaluationHistory: A key objective is to distinguish
hemoptysis from hematemesis and from na-sopharyngeal or oropharyngeal bleeding. Thisdistinction can generally be accomplishedwith history and physical examination. An
045_062PUL Page 359 Tuesday, November 8, 2005 10:54 AM

360 SECTION 5 PULMONARY DISORDERS
extensive smoking history suggests malig-nancy. A patient’s sensation of where thebleeding may be coming from may help iden-tify its origin if it is emanating from one of theupper lobes.
Physical examination: Examination fo-cuses on ruling out upper airway sites of bleed-ing and on listening over the lungs for focal ab-normalities that may indicate the area wherebleeding may be occurring. Unfortunately,blood originating from any area can be aspi-rated throughout the lung.
Testing: Patients with minor hemoptysiscan undergo testing on an outpatient basis. Achest x-ray is mandatory. Patients with nor-mal results, a consistent history, and nonmas-sive hemoptysis can undergo empirical treat-ment for bronchitis. Those with abnormal re-sults and those without a supporting historyshould undergo CT and bronchoscopy. CTmay reveal pulmonary lesions that are not ap-parent on the chest x-ray and can help locate
lesions in anticipation of bronchoscopy andbiopsy. A ventilation/perfusion scan or CTangiogram can confirm the diagnosis of pul-monary embolism; CTs and pulmonary an-giography can also detect pulmonary arteri-ovenous fistulas. When the etiology is ob-scure, fiberoptic inspection of the pharynx,larynx, esophagus, and/or airways may beindicated to distinguish hemoptysis fromhematemesis and from nasopharyngeal ororopharyngeal bleeding.
Patients with massive hemoptysis requiretreatment and stabilization before testing.The cause of hemoptysis remains unknown in30 to 40% of cases. The prognosis for patientswith cryptogenic hemoptysis is generally fa-vorable, usually with resolution of bleedingwithin 6 mo of evaluation.
TreatmentThe two objectives of treatment are to pre-
vent aspiration of blood to the uninvolved
TABLE 45–2. DIFFERENTIAL DIAGNOSIS OF HEMOPTYSIS
Larynx and pharynxCarcinomaLymphomaTuberculous ulceration
Trachea and large bronchiBenign or malignant primary tumor
(carcinoma and adenoma)Bronchogenic cystBroncholithiasisErosion by an aortic aneurysmErosion by a caseocalcific nodeErosion by a tumor from nodes, esophagus, or
other mediastinal structuresSevere acute bronchitisTelangiectasiaTrauma
Smaller bronchial structuresAcute bronchitis Adenoma (carcinoid or cylindromatous)BronchiectasisBronchopulmonary sequestrationCarcinomaChronic bronchitisTrauma
Pulmonary parenchymaAbscess Active granulomatous disease (tuberculous, fungal, parasitic, syphilitic)
Acute pneumoniaFungus ball (aspergilloma) in an
old cavityGoodpasture’s syndrome or variantsIdiopathic hemosiderosisInfarctPrimary or metastatic tumorTrauma
Heart and blood vesselsAortic aneurysm with leakage into the
pulmonary parenchymaAtrial myxomaFibrous mediastinitis with pulmonary vein
obstructionLeft ventricular failureMitral stenosisPulmonary arteriovenous malformationPulmonary embolism/infarctPrimary pulmonary hypertension
Bleeding diathesisAnticoagulant therapy Deficiency of vitamin K–dependent
factors: prothrombin (II), Stuart factor (X), factor VII, Christmas factor (IX)
Disseminated intravascular coaulationFibrinolytic therapy: urokinase, streptokinaseMiscellaneous congenital coagulation defectsThrombocytopenia
045_062PUL Page 360 Tuesday, November 8, 2005 10:54 AM

45 APPROACH TO THE PATIENT WITH PULMONARY SYMPTOMS 361
lung (which can cause asphyxiation) andto prevent exsanguination from ongoingbleeding.
Protection of the uninvolved lung can bedifficult because the site of bleeding often isunclear. Strategies include positioning ma-neuvers (eg, having the patient lie with thebleeding lung in a dependent position) andselective intubation and obstruction of thebronchus going to the bleeding lung.
Prevention of exsanguination involves re-versal of any bleeding diathesis and direct ef-forts to stop the bleeding. Clotting deficien-cies can be reversed with fresh-frozen plasmaand factor-specific or platelet transfusions.Laser therapy, cauterization, or direct injec-tion with epinephrine or vasopressin can beperformed bronchoscopically.
Massive hemoptysis is one of the few in-dications for rigid bronchoscopy, which pro-vides control of the airway, allows for a largerfield of view than flexible bronchoscopy, al-lows better suctioning, and is more suited totherapeutic interventions, such as laser ther-apy. Embolization of a pulmonary segment isbecoming the preferred method with whichto stop massive hemoptysis, with reportedsuccess rates of up to 90%. Emergency sur-gery is indicated for massive hemoptysis notcontrolled by rigid bronchoscopy or embo-lization and is generally considered a last re-sort.
Early resection may be indicated forbronchial adenoma or carcinoma. Bron-cholithiasis (erosion of a calcified lymphinto an adjacent bronchus) may require pul-monary resection if endobronchial removalof the stone via rigid bronchoscopy cannotbe performed. Bleeding secondary to heartfailure or mitral stenosis usually responds tospecific therapy for heart failure, but in rarecases, emergency mitral valvulotomy isnecessary for life-threatening hemoptysisdue to mitral stenosis. Bleeding from a pul-monary embolism is rarely massive and al-most always stops spontaneously. If embolirecur and bleeding persists, anticoagulationmay be contraindicated, and placement of aninferior vena cava filter is the treatment ofchoice.
Because bleeding from bronchiectatic ar-eas usually results from infection, treatmentof the infection with appropriate antibioticsand postural drainage is essential.
Sedatives and opioids suppress the venti-latory drive and should be avoided.
SOLITARY PULMONARY NODULE
A solitary pulmonary nodule is defined asa discrete lesion < 3 cm in diameter that iscompletely surrounded by lung parenchyma,does not touch the hilum or mediastinum, andis without associated atelectasis or pleural ef-fusion (for evaluation of a mediastinal mass,see p. 505).
Solitary pulmonary nodules are most oftendetected incidentally when a chest x-ray istaken for other reasons.
The differential diagnosis of a solitarypulmonary nodule is extensive. Malignantcauses are primary lung cancer (usually ade-nocarcinoma or small cell carcinoma) andmetastatic cancer (breast melanoma; colon,renal, and testicular carcinoma; sarcoma; andhead and neck cancer). The likelihood of ma-lignancy increases with age.
Nonmalignant causes are granulomatousinfection (TB, atypical mycobacterial infec-tion, histoplasmosis, coccidioidomycosis,blastomycosis), benign tumors (hamartoma,lipoma), connective tissue disease (RA, We-gener’s granulomatosis), parasitic infection(dirofilariasis [dog heartworm]), ascariasis,infection with Pneumocystis jiroveci (for-merly called P. carinii), and pulmonary arte-riovenous malformations. Nonpulmonarysoft-tissue densities caused by nipple shad-ows, warts, cutaneous nodules, and bone ab-normalities are often confused for a noduleon chest x-ray.
EvaluationThe primary goal of evaluation is to detect
malignancy and active infection.History: Older age, current or past ciga-
rette smoking, and a history of malignancy allincrease the probability of malignancy.These risk factors (plus nodule size) havebeen used to estimate likelihood ratios formalignant disease (see TABLE 45–3). Historymay reveal other information that suggests anunderlying etiology (eg, a history of treatedcolon, breast, or renal cell carcinoma) but,in general, is not helpful in determining acause when the major risk factors have beenexcluded.
Physical examination: A thorough phys-ical examination may uncover findings thatsuggest an underlying etiology for a pulmo-nary nodule but usually does not help deter-mine a cause.
045_062PUL Page 361 Tuesday, November 8, 2005 10:54 AM

362
SECTION 5 PULMONARY DISORDERS
Testing:
Four radiographic characteris-tics help narrow the differential diagnosis ofa solitary pulmonary nodule: growth rate;pattern of calcification, if present; margins;and size. These characteristics are sometimesevident on the original plain film but usuallyrequire a CT scan. CT can also distinguishpulmonary from pleural radiopacities. CThas a sensitivity of 70% and a specificity of60% for detecting malignancy.
Growth rate is determined by comparisonwith previous chest x-ray or CT, if available.
A lesion that has not enlarged in
≥
2 yr sug-gests a benign etiology. Tumors that have vol-ume doubling times from 21 to 400 days arelikely to be malignant. Small nodules shouldbe monitored every year for 2 yr.
Calcification suggests benign disease,particularly if it is central (tuberculoma, his-toplasmoma), concentric (healed histoplas-mosis), or in popcorn configuration (ham-artoma). CT scanning is often necessary todetect these patterns. Margin patterns arealso suggestive. Spiculated or irregular
TABLE 45–3. ESTIMATING THE PROBABILITY OF MALIGNANCY OF A SOLITARY PULMONARY NODULE
I. Establish likelihood ratios (LRs)* for malignancy with the following table:
FindingLikelihood Ratio for Malignancy Finding
Likelihood Ratio for Malignancy
Diameter of nodule (cm) Current smoker or quit within past 9 yr
<
1.5 0.11.5–2.2 0.5 Average number of
cigarettes per day:2.3–3.2 1.73.3–4.2 4.3 1–9 0.34.3–5.2 6.6 10–20 1.05.3–6.0 29.4 21–40 2.0
Patient’s age (yr)
≥
41 3.9
≤
35 0.136–44 0.3
Quit smoking (yr)
45–49 0.7
≤
3 1.450–59 1.5 4–6 1.060–69 2.1 7–12 0.570–83 5.7
≥
13 0.1
Smoking history
Never smoked 0.15
Overall prevalence
Pipe or cigar only 0.3 Clinical settings 0.7Ex-cigarette smoker 1.5 Community surveys 0.1
II. Multiply the LRs for nodule diameter, patient’s age, smoking history, and cancerprevalence to obtain an estimate of the odds of malignancy in a solitary pulmo-nary nodule (Odds CA);
That is, OddsCA
=
LR Size
×
LR Age
×
LR Smoking
×
LR Prev
III. Convert the odds into a probability of cancer:
Probability of cancer (PCA)
=
OddsCA / (1 + OddsCA)
So for a 65-yr-old patient who smokes a pack of cigarettes (20) daily and who has a 2.0 cm nodule:
II. OddsCA
=
(1.5
×
2.1
×
1.0
×
0.7) / 1
=
2.21:1
III. PCA (as %)
=
2.21/(1+ 2.21)
×
100
=
69%I. LR Size
=
1.5; LR Age
=
2.1;LR Smoking
=
1.0; LR Prev
=
0.7
*The LR is a measure of how predictive a finding is of disease and is defined as the probability of thefinding being present in a patient with disease divided by the probability of the finding being present in apatient without disease; ie, it is the ratio of true positives to false positives or of sensitivity to 1- specificity.
Adapted from Cummings, SR, Lillington, GA, Richard, RJ: Estimating the probability of malignancyin solitary pulmonary nodules. A Bayesian approach.
The American Review of Respiratory Disease
134(3):449–452, 1986.
045_062PUL Page 362 Monday, November 21, 2005 11:37 AM

45 APPROACH TO THE PATIENT WITH PULMONARY SYMPTOMS 363
(scalloped) margins are more indicative ofmalignancy. Diameter < 1.5 cm stronglysuggests a benign etiology; diameter > 5.3cm strongly suggests malignancy.
PET scanning has an uncertain role in eval-uation. It has a sensitivity > 90% and a spec-ificity of about 78% for detecting malig-nancy, but it is relatively new, and its role inevaluating pulmonary nodules is still beingdeveloped. False-negative PET scans canresult from metabolically inactive tumors, andfalse-positive results can occur in a variety ofinfectious and inflammatory conditions.
When historical information or radio-graphic appearance is not diagnostic, biopsyand culture may be useful, but usually onlywhen history supports TB or coccidioidomy-cosis as possible diagnoses. Although can-cers can be diagnosed by biopsy, definitivetreatment is resection, and so invasive testingshould be reserved for patients in whom non-malignant causes are a possibility.
TreatmentIf the suspicion of malignancy is very low,
the lesions are very small (< 1 cm), or the pa-tient refuses or is not a candidate for surgicalintervention, observation is reasonable.Monitoring with follow-up at 3 mo, 6 mo, andthen yearly for 2 yr is recommended. If the le-sion has not grown for > 2 yr, it is likely be-nign. When cancer is the most likely cause orwhen nonmalignant causes are unlikely, pa-tients should undergo resection unless sur-gery is contraindicated due to poor pulmo-nary function, comorbidities, or withholdingof consent.
STRIDORStridor is a high-pitched, predominantly
inspiratory sound formed by extrathoracicupper airway obstruction. The most commoncause in children is epiglottitis, croup, or for-eign body aspiration. Common causes inadults include vocal cord dysfunction, post-extubation vocal cord edema or paralysis, la-ryngeal tumors, allergic reactions, aspiratedforeign body, and retropharyngeal abscess.
EvaluationHistory: Sore throat and fever suggest ab-
scess; sore throat, fever, and drooling sug-gest epiglottitis. Preceding URI symptomsand cough suggest croup. Dysphonia sug-gests laryngeal tumor. Abrupt onset sug-gests acute allergic reaction or aspirated for-eign body.
Physical examination: Examination fo-cuses initially on determining the patency ofthe airway. Examination includes measuringvital signs and determining if the patient is inacute distress as evidenced by use of acces-sory muscles and intercostal retractions. In-spiratory stridor suggests obstruction of thetrachea, larynx, or epiglottis and is usually amedical emergency, whereas expiratory stri-dor suggests bronchial obstruction.
Testing: Testing should include pulseoximetry and chest and neck x-rays. Lateralsoft-tissue x-rays of the neck can be diagnos-tic of epiglottitis. X-rays can also identify for-eign objects in the neck or chest. Confirma-tion of the cause of stridor may require directlaryngoscopy to detect vocal cord abnormal-ities and tumors. In more chronic cases of stri-dor, flow-volume loops can help distinguishextrathoracic from intrathoracic causes.
TreatmentDefinitive treatment of stridor is treatment
of the underlying cause. Helium-O2 (heliox)improves airflow and reduces stridor in dis-orders of the large airways, such as postextu-bation laryngeal edema, croup, and laryngealtumors; mechanism of action is thought to bereduced flow turbulence as a result of lowerdensity of helium compared with O2.
VOCAL CORD DYSFUNCTIONParadoxical movement of the vocal cords
is adduction of the true vocal cords on inspi-ration and abduction on expiration; it causesinspiratory functional airway obstructionand stridor that is often mistaken for asthma.This disorder commonly occurs in patientswith mental disease. Diagnosis is made byobserving inspiratory closure of the vocalcords with direct laryngoscopy. Treatmentinvolves educating the patient about the na-ture of the problem; counseling from a speechtherapist on special breathing techniques,such as panting, which can relieve episodesof stridor and obstruction; and avoidance ofasthma misdiagnosis and treatment.
WHEEZINGWheezing is a symptom as well as a physical
finding. Wheezing occurs as a result of airwaynarrowing. Asthma is the most classic cause ofwheezing, but wheezing may be part of COPD,heart failure exacerbation (cardiac asthma),bronchiolitis in children, anaphylaxis, toxicinhalation, foreign body aspiration, tracheo-malacia, or vocal cord dysfunction.
045_062PUL Page 363 Tuesday, November 8, 2005 10:54 AM

364 SECTION 5 PULMONARY DISORDERS
EvaluationHistory: Wheezing in a patient with
known asthma or COPD is usually presumedto represent an exacerbation. A history ofcough, postnasal drip, exposure to allergens,or toxic or irritant gases may suggest a trigger.Acute onset without a history of lung diseasesuggests allergic reaction or impending ana-phylaxis. Worsening with cold air, dust, to-bacco smoke, perfumes, or other factors sug-gests asthma.
Physical examination: Localized wheez-ing suggests focal bronchial obstruction bytumor or foreign body. Diffuse wheezing in-dicates that all airways are involved or that thesite of airway narrowing is in the trachea orat the level of the vocal cords. Urticaria or an-gioedema suggests an allergic reaction. Fe-ver and URI symptoms suggest infection,especially bronchiolitis in children < 2 yr.Crackles, distended neck veins, and periph-eral edema suggest heart failure.
Testing: A pulse oximetry reading and achest x-ray should be taken. Segmental orsubsegmental atelectasis or infiltrate sug-gests an obstructing endobronchial lesion.
Radio-opacity in the airways or focal areas ofhyperinflation suggests a foreign body.
Spirometry (see Ch. 46, below) canconfirm airflow limitation and quantify itsreversibility and severity. Flow-volumeloops can help diagnose large airwayobstructions, such as those caused bytumors or vocal cord dysfunction, and candifferentiate extrathoracic from intratho-racic sites of obstruction. Extrathoracicvariable obstruction causes flattening ofthe inspiratory limb of the flow-volumeloop, whereas intrathoracic variable ob-structions cause flattening of the expira-tory limb (see FIG. 46–3E and 3F on p. 369).Fixed lesions affect both limbs.
TreatmentDefinitive treatment of wheezing is treat-
ment of underlying causes. Wheezing itselfcan be relieved with inhaled bronchodilators(eg, albuterol 2.5 mg nebulized solutionor 180 µg metered dose inhalation) exceptin the case of foreign body or vocal cordabnormalities.
46TESTS OF PULMONARY FUNCTION
Pulmonary function tests provide mea-sures of flow rates, lung volumes, gas ex-change, and respiratory muscle function. Ba-sic pulmonary function tests available in theambulatory setting include spirometry andpulse oximetry; these tests provide physio-logic measures of pulmonary function andcan be used to quickly narrow a differentialdiagnosis and suggest a subsequent strategyof additional testing or therapy. More com-plicated testing includes esophageal pressuremeasurement to determine pressure-volumerelationships and exercise testing. These pro-vide a more detailed description of physio-logic abnormalities and the likely underlying
pathology. The choice and sequence of test-ing are guided by information from the his-tory and physical examination.
FLOW RATES, LUNG VOLUMES, AND
FLOW-VOLUME LOOPSFlow rate and lung volume measurements
can be used to differentiate obstructive fromrestrictive pulmonary disorders, to charac-terize disease severity, and to measure re-sponses to therapy. Measurements are typi-cally reported as absolute flows and volumesand as percentages of predicted values de-rived from large populations of people pre-sumed to have normal lung function. Vari-ables that help predict normal values includeage, sex, ethnicity, and height.
Flow rates: Quantitative measures of in-spiratory and expiratory flow are obtained byforced spirometry. Nose clips are used to oc-clude the nares.
045_062PUL Page 364 Tuesday, November 8, 2005 10:54 AM
46 TESTS OF PULMONARY FUNCTION 365
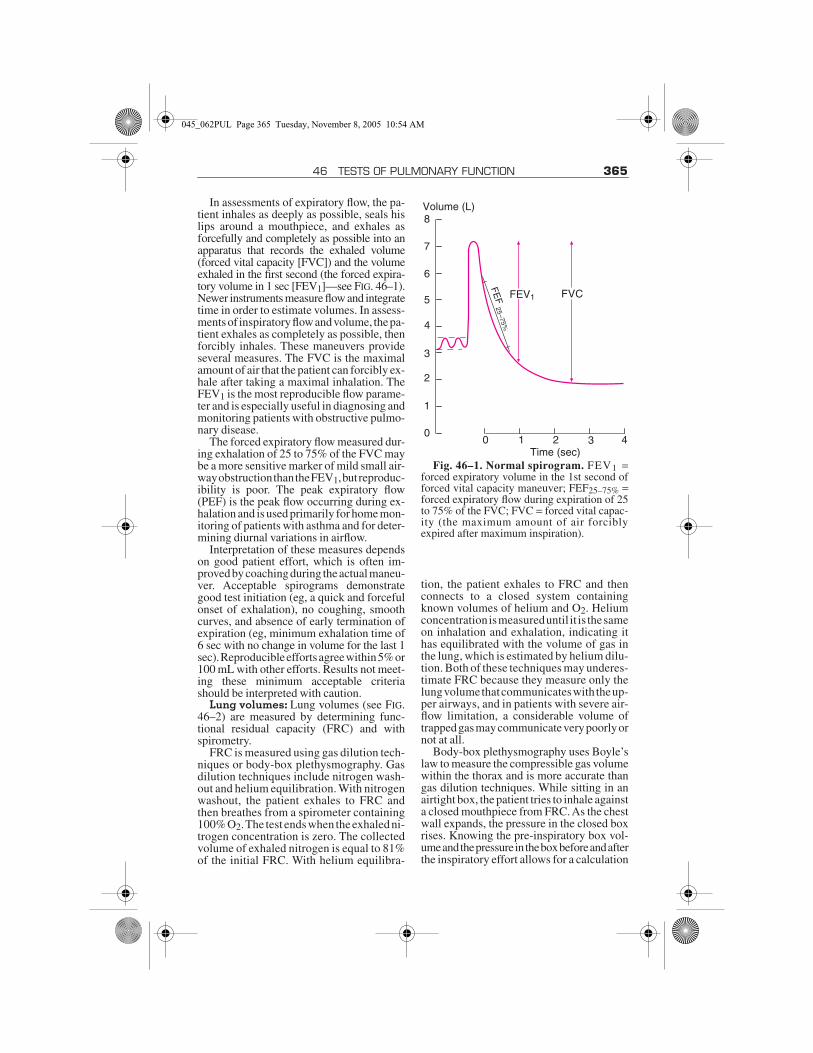
In assessments of expiratory flow, the pa-tient inhales as deeply as possible, seals hislips around a mouthpiece, and exhales asforcefully and completely as possible into anapparatus that records the exhaled volume(forced vital capacity [FVC]) and the volumeexhaled in the first second (the forced expira-tory volume in 1 sec [FEV1]—see FIG. 46–1).Newer instruments measure flow and integratetime in order to estimate volumes. In assess-ments of inspiratory flow and volume, the pa-tient exhales as completely as possible, thenforcibly inhales. These maneuvers provideseveral measures. The FVC is the maximalamount of air that the patient can forcibly ex-hale after taking a maximal inhalation. TheFEV1 is the most reproducible flow parame-ter and is especially useful in diagnosing andmonitoring patients with obstructive pulmo-nary disease.
The forced expiratory flow measured dur-ing exhalation of 25 to 75% of the FVC maybe a more sensitive marker of mild small air-way obstruction than the FEV1, but reproduc-ibility is poor. The peak expiratory flow(PEF) is the peak flow occurring during ex-halation and is used primarily for home mon-itoring of patients with asthma and for deter-mining diurnal variations in airflow.
Interpretation of these measures dependson good patient effort, which is often im-proved by coaching during the actual maneu-ver. Acceptable spirograms demonstrategood test initiation (eg, a quick and forcefulonset of exhalation), no coughing, smoothcurves, and absence of early termination ofexpiration (eg, minimum exhalation time of6 sec with no change in volume for the last 1sec). Reproducible efforts agree within 5% or100 mL with other efforts. Results not meet-ing these minimum acceptable criteriashould be interpreted with caution.
Lung volumes: Lung volumes (see FIG.46–2) are measured by determining func-tional residual capacity (FRC) and withspirometry.
FRC is measured using gas dilution tech-niques or body-box plethysmography. Gasdilution techniques include nitrogen wash-out and helium equilibration. With nitrogenwashout, the patient exhales to FRC andthen breathes from a spirometer containing100% O2. The test ends when the exhaled ni-trogen concentration is zero. The collectedvolume of exhaled nitrogen is equal to 81%of the initial FRC. With helium equilibra-
tion, the patient exhales to FRC and thenconnects to a closed system containingknown volumes of helium and O2. Heliumconcentration is measured until it is the sameon inhalation and exhalation, indicating ithas equilibrated with the volume of gas inthe lung, which is estimated by helium dilu-tion. Both of these techniques may underes-timate FRC because they measure only thelung volume that communicates with the up-per airways, and in patients with severe air-flow limitation, a considerable volume oftrapped gas may communicate very poorly ornot at all.
Body-box plethysmography uses Boyle’slaw to measure the compressible gas volumewithin the thorax and is more accurate thangas dilution techniques. While sitting in anairtight box, the patient tries to inhale againsta closed mouthpiece from FRC. As the chestwall expands, the pressure in the closed boxrises. Knowing the pre-inspiratory box vol-ume and the pressure in the box before and afterthe inspiratory effort allows for a calculation
Fig. 46–1. Normal spirogram. FEV1 =forced expiratory volume in the 1st second offorced vital capacity maneuver; FEF25–75% =forced expiratory flow during expiration of 25to 75% of the FVC; FVC = forced vital capac-ity (the maximum amount of air forciblyexpired after maximum inspiration).
0 1 2 3 4Time (sec)
0
1
2
3
4
5
6
7
8Volume (L)
FEV1 FVC
FEF
25–75%
045_062PUL Page 365 Tuesday, November 8, 2005 10:54 AM

366 SECTION 5 PULMONARY DISORDERS
of the change in box volume, which mustequal the change in lung volume.
Knowing FRC allows the lung to be dividedinto subvolumes that are either measured withspirometry or calculated (see FIG. 46–2). Nor-mally the FRC represents about 40% of totallung capacity (TLC).
Flow-volume loop: In contrast to thespirogram, which displays flow (in L) overtime (in sec), the flow-volume loop (see FIG.46–3) displays flow (in L/sec) as it relates tolung volume (in L) during maximal inspira-tion from complete exhalation (residual vol-ume [RV]) and during maximum expirationfrom complete inhalation (TLC). The prin-cipal advantage of the flow-volume loop isthat it can show whether flows are appropri-ate for a particular lung volume. For exam-ple, flow is normally slower at low lungvolumes. Because patients with pulmonaryfibrosis have low lung volumes, flow ap-pears to be decreased if measured alone.However, when flow is measured againstlung volumes, it becomes apparent that flowis actually higher than normal because of theincreased elastic recoil characteristic offibrotic lungs.
Flow-volume loops require that absolutelung volumes be measured. Unfortunately,many laboratories simply plot flow againstthe FVC; the flow-FVC loop does not have aninspiratory limb and therefore does not pro-vide as much information.
Patterns of AbnormalitiesMost common respiratory disorders can be
categorized as obstructive or restrictive onthe basis of flow rates and lung volumes (seeTABLE 46–1).
Obstructive disease: Obstructive dis-ease is a reduction in flow rates, particularlythe FEV1 and the FEV1 as a percentage of theFVC (FEV1/FVC). The reduction in FEV1determines the degree of the obstructive de-fect (see TABLE 46–2). Obstructive defectsare caused by increased resistance to flowfrom abnormalities within the airway lumen(eg, tumors, secretions, mucosal thickening);changes in the wall of the airway (eg, contrac-tion of smooth muscle, edema); or elastic re-coil (eg, the parenchymal destruction that oc-curs in emphysema). With decreased flowrates, expiratory times are longer than usual,and air may become trapped in the lungs fromincomplete emptying and increased lung vol-umes (eg, TLC, RV).
Improvement of FEV1 and FEV1/FVC by≥ 12% or 200 mL with the administration ofa bronchodilator confirms the diagnosis ofasthma or airway hyperresponsiveness.However, some patients with asthma canhave normal pulmonary function and normalspirometric parameters between exacerba-tions. When suspicion of asthma remainshigh despite normal spirometry, provocativetesting with methacholine, a synthetic analogof acetylcholine that is a nonspecific bron-
Fig. 46–2. Normal lung volumes. TLC = total lung capacity; VT = tidal volume; ERV =expiratory reserve volume; IRV = inspiratory reserve volume; FRC = functional residual capac-ity; IC = inspiratory capacity; VC = vital capacity; RV = residual volume; FRC = RV + ERV;IC = VT + IRV; VC = VT + IRV + ERV.
Time0
TLC
FRCERV
ICIRV
VT VC
RV
045_062PUL Page 366 Tuesday, November 8, 2005 10:54 AM

46 TESTS OF PULMONARY FUNCTION 367
chial irritant, is indicated to detect or excludebronchoconstriction. In a methacholine chal-lenge test, spirometric parameters are mea-sured at baseline and after inhalation of in-creasing concentrations of methacholine.Laboratories have different definitions of air-way hyperreactivity, but in general a provoc-ative concentration of methacholine thatcauses a 20% drop in FEV1 from baseline(PC20) of < 1 mg/mL is considered diagnosticof asthma, whereas a PC20 > 16 mg/mL ex-cludes the diagnosis. PC20 values between1 and 16 mg/mL are inconclusive.
Exercise testing may be used to detectexercise-induced bronchoconstriction but is
less sensitive than methacholine challengetesting for detecting general airway hyper-responsiveness. The patient performs aconstant level of work on a treadmill or cy-cle ergometer for 6 to 8 min at an intensityselected to produce a heart rate of 80% ofpredicted maximum heart rate. The FEV1and FVC are measured before and 5, 15, and30 min after exercise. Exercise-inducedbronchospasm reduces FEV1 or FVC ≥ 15%after exercise.
Restrictive disease: Restrictive diseaseis a reduction in lung volume, specifically,a TLC < 80% of the predicted value. The de-crease in TLC determines the severity of
TABLE 46–1. CHARACTERISTIC PHYSIOLOGIC CHANGES ASSOCIATED WITH PULMONARY DISORDERS
MEASUREOBSTRUCTIVE
DISORDERSRESTRICTIVE
DISORDERSMIXED
DISORDERS
FEV1/FVC Decreased Normal or increased Decreased
FEV1 Decreased Decreased, normal, or increased
Decreased
FVC Decreased or normal Decreased Decreased
TLC Normal or increased Decreased Decreased
RV Normal or increased Decreased Decreased, normal, or increased
FEV1 = forced expiratory volume in 1 sec; FVC = forced vital capacity; TLC = total lung capacity; RV = residual volume.
TABLE 46–2. SEVERITY OF OBSTRUCTIVE AND RESTRICTIVE LUNG DISEASES
OBSTRUCTIVE RESTRICTIVE
SEVERITY* FEV1/FVC (% predicted)
FEV1 (% predicted)
TLC (% predicted)
Normal ≥ 70 ≥ 80 ≥ 80
Mild < 70 ≥ 80 70–79
Moderate < 70 50 ≤ FEV1 < 80 50–69
Severe < 70 30 ≤ FEV1 < 50 < 50
Very severe < 70 < 30 or < 50 with chronic respiratory
failure
—
*Criteria vary by guideline.FEV1 = forced expiratory volume in 1 sec.
045_062PUL Page 367 Tuesday, November 8, 2005 10:54 AM

368 SECTION 5 PULMONARY DISORDERS
Fig. 46–3. Flow-volume loops. (A) Normal. Inspiratory limb of loop is symmetric andconvex. Expiratory limb is linear. Flow rates at the midpoint of the inspiratory and expiratorycapacity are often measured. Maximal inspiratory flow at 50% of forced vital capacity (MIF50%FVC) is greater than maximal expiratory flow at 50% FVC (MEF 50%FVC) becausedynamic compression of the airways occurs during exhalation. (B) Obstructive disease (eg,emphysema, asthma). Although all flow rates are diminished, expiratory prolongation pre-dominates, and MEF < MIF. Peak expiratory flow is sometimes used to estimate degree of air-way obstruction but is dependent on patient effort. (C) Restrictive disease (eg, interstitiallung disease, kyphoscoliosis). The loop is narrowed because of diminished lung volumes, butthe shape is generally the same as in normal volume. Flow rates are greater than normal atcomparable lung volumes because the increased elastic recoil of lungs holds the airwaysopen. (D) Fixed obstruction of the upper airway (eg, tracheal stenosis, goiter). The top andbottom of the loops are flattened so that the configuration approaches that of a rectangle.Fixed obstruction limits flow equally during inspiration and expiration, and MEF = MIF. (E)Variable extrathoracic obstruction (eg, unilateral vocal cord paralysis, vocal cord dysfunc-tion). When a single vocal cord is paralyzed, it moves passively with pressure gradients acrossthe glottis. During forced inspiration, it is drawn inward, resulting in a plateau of decreasedinspiratory flow. During forced expiration, it is passively blown aside, and expiratory flow isunimpaired. Therefore, MIF 50%FVC < MEF 50%FVC. (F) Variable intrathoracicobstruction (eg, tracheomalacia). During a forced inspiration, negative pleural pressure holdsthe “floppy” trachea open. With forced expiration, loss of structural support results in trachealnarrowing of the trachea and a plateau of diminished flow. Flow is maintained briefly beforeairway compression occurs.
MEF50% FVC
RV
PEF
TLC
Inspiration
6 5 4 3 2 1 0
10.0
7.5
5.0
2.5
0
2.5
5.0
7.5
Volume (L)
Flo
w (
L/se
c)
MIF50% FVC
Expiration
BA
Normal
RV
PEFMEF
50% FVC
TLC
6 5 4 3 2 1 0
10.0
7.5
5.0
2.5
0
2.5
5.0
7.5
Volume (L)
Flo
w (
L/se
c)
MIF50% FVC
Normal
RV
PEFMEF
50% FVC
TLC MIF50% FVC
6 5 4 3 2 1 0
10.0
7.5
5.0
2.5
0
2.5
5.0
7.5
Volume (L)
Flo
w (
L/se
c)
MEF50% FVC
RV
PEF
TLC
7 6 5 4 3 2 0
10.0
7.5
5.0
2.5
0
2.5
5.0
7.5
Volume (L)
Flo
w (
L/se
c)
MIF50% FVC
1
Normal
C D
045_062PUL Page 368 Tuesday, November 8, 2005 10:54 AM

46 TESTS OF PULMONARY FUNCTION 369
restriction (see TABLE 46–2). The decreasein lung volumes produces a decrease in flowrates (reduced FEV1 and FVC—see FIG.46–3B). However, the airflow relative to thespecific volume is increased, so the FEV1/FVC ratio is normal or increased. Restric-tive defects are caused by a loss in lung vol-ume (eg, lobectomy), abnormalities of struc-tures surrounding the lung (eg, pleural dis-ease, kyphosis, obesity), weakness of theinspiratory muscles of respiration (eg, neu-romuscular disease), or abnormalities of thelung parenchyma (eg, pulmonary fibrosis).The feature common to all is a decrease inthe compliance of the lungs, the chest wall,or both.
MEASUREMENT OF GAS EXCHANGE
The diffusing capacity for carbon monox-ide (DLCO) is a measure of the ability of gasto transfer from alveoli to RBCs across the al-veolar epithelium and the capillary endothe-lium. The DLCO depends not only on the areaand thickness of the blood-gas barrier butalso on the volume of blood in the pulmonarycapillaries. The distribution of alveolar vol-ume and ventilation also affects the measure-ment. DLCO is measured by sampling end-expiratory gas for carbon monoxide (CO)after a patient inspires a small amount of CO,holds his breath, and exhales. Measured DLCO
should be adjusted for alveolar volume (whichis estimated from dilution of helium) and thepatient’s Hct. DLCO is reported as mL/min/mm Hg and as a percentage of a predictedvalue.
Conditions that primarily affect the pul-monary vasculature, such as primary pulmo-nary hypertension and pulmonary embolism,decrease DLCO. Conditions that affect thelung diffusely, such as emphysema and pul-monary fibrosis, decrease both DLCO and al-veolar ventilation (VA). Reduced DLCO alsooccurs in patients with past lung resection be-cause total lung volume is smaller, but DLCOcorrects to or even exceeds normal when ad-justed for VA because increased additionalvascular surface area is recruited in the re-maining lung. Anemic patients often havelower DLCO values that correct when adjustedfor Hb. DLCO may be higher than predicted inpatients with heart failure, presumably be-cause the increased pulmonary venous andarterial pressure results in recruitment of ad-ditional pulmonary microvessels. DLCO isalso increased in patients with polycythemia,in part because of increased Hct and becauseof the vascular recruitment that occurs withincreased pulmonary pressures due to in-creased viscosity. DLCO is increased in pa-tients with alveolar hemorrhage becauseRBCs in the alveolar space can also bind CO.DLCO is also increased in patients withasthma. Although this increase is attributed topresumed vascular recruitment, the actualmechanism is unknown.
Fig. 46–3. Continued.
Normal
RVRV
PEF
MEF50% FVCTLC
MIF50% FVC
6 5 4 3 2 1 0
10.0
7.5
5.0
2.5
0
2.5
5.0
7.5
Volume (L)
Flo
w (
L/se
c)
MIF50% FVC
MEF50% FVC
NormalPEF
TLC
Inspiration
6 5 4 3 2 1 0
10.0
7.5
5.0
2.5
0
2.5
5.0
7.5
Volume (L)
Flo
w (
L/se
c)
Expiration
E F
045_062PUL Page 369 Tuesday, November 8, 2005 10:54 AM

370 SECTION 5 PULMONARY DISORDERS
PULSE OXIMETRYTranscutaneous pulse oximetry esti-
mates O2 saturation (SpO2) of capillaryblood based on the absorption of light fromlight-emitting diodes positioned in a fingerclip or adhesive strip probe. The estimatesare generally very accurate and correlate towithin 5% of measured atrial O2 saturation(SaO2). Results may be less accurate in pa-tients with highly pigmented skin, thosewearing nail polish, and those with ar-rhythmias or hypotension, in whom theamplitude of the signal may be dampened.Also, pulse oximetry is only able to detectoxyhemoglobin or reduced Hb; other typesof Hb (eg, carboxyhemoglobin, methemo-globin) are assumed to be oxyhemoglobinand falsely elevate the SpO2 measurement.
ARTERIAL BLOOD GAS SAMPLINGABG sampling is performed to obtain ac-
curate measures of PaO2, PaCO2, and bloodpH; these variables combined with the pa-tient’s temperature allow for calculation ofHCO3 level (which can also be measured di-rectly from venous blood) and SaO2. ABGsampling can also accurately measure car-boxyhemoglobin and methemoglobin.
The radial artery is usually used. Becausearterial puncture in rare cases leads tothrombosis and impaired perfusion of distaltissue, Allen’s test is first performed to en-sure adequate collateral circulation. Withthis maneuver, the radial and ulnar pulsesare simultaneously occluded until the handbecomes pale. The ulnar pulse is then re-leased while the pressure on the radial pulseis maintained. A blush across the entirehand within 7 sec of release of the ulnarpulse suggests adequate flow through theulnar artery.
Under sterile conditions, a 22- to 25-gauge needle attached to a heparinized sy-ringe is inserted just proximal to the maxi-mal impulse of the radial arterial pulse andadvanced slightly distally into the artery un-til pulsatile blood is returned. Systolic BPoften pushes back the syringe plunger. After3 to 5 mL of blood is collected, the needle isquickly withdrawn, and firm pressure is ap-plied to the puncture site to facilitate hemo-stasis. Simultaneously, the ABG specimenis placed on ice to reduce O2 consumption
and CO2 production by WBCs and is sent tothe laboratory.
OxygenationHypoxemia is a decrease in PO2 in arterial
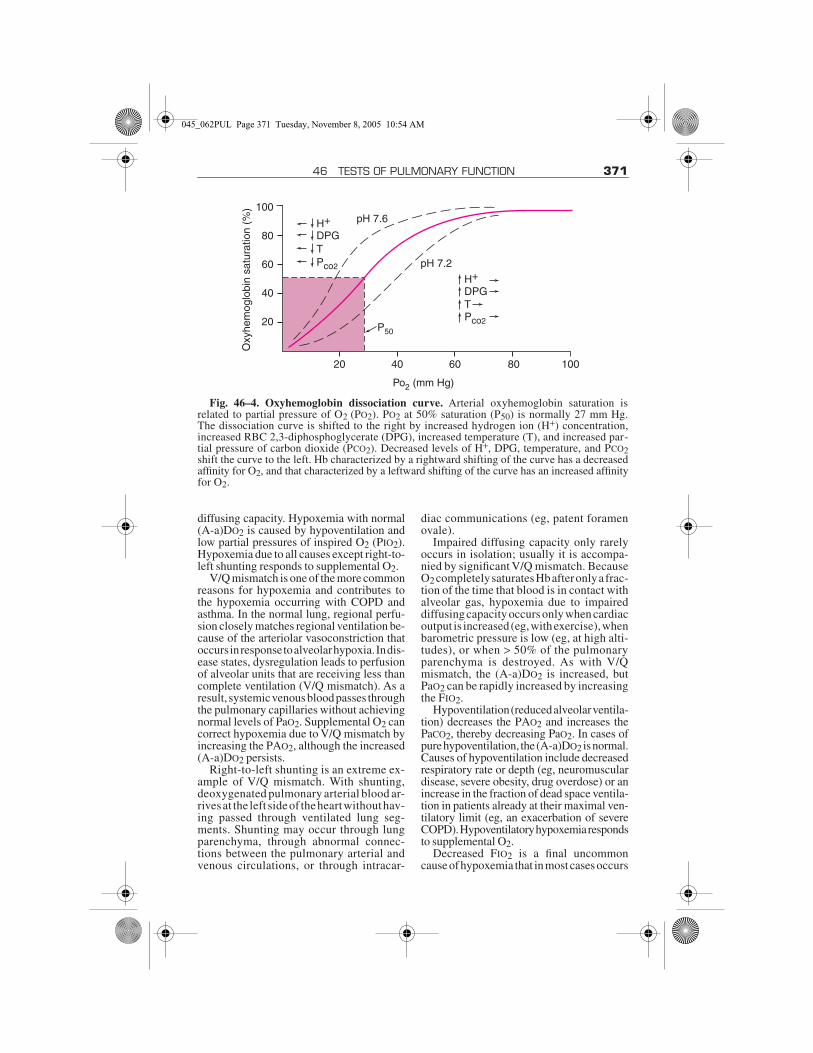
blood; hypoxia is a decrease in the PO2 in thetissue. ABGs accurately assess the presenceof hypoxemia, which is generally defined asa PaO2 low enough to reduce the SaO2 below90% (ie, PaO2 < 60 mm Hg). Abnormalitiesin Hb (eg, methemoglobin), higher tempera-tures, lower pH, and higher levels of 2,3-diphosphoglycerate reduce Hb O2 saturationdespite an adequate PaO2, as predicted bythe oxyhemoglobin dissociation curve (seeFIG. 46–4).
Causes of hypoxemia can be divided intothose with elevated or normal alveolar-arterial PO2 gradients [(A-a)DO2], defined asthe difference between alveolar O2 tension(PAO2) and PaO2. PAO2 is calculated asfollows:
where FIO2 is the fraction of inspired O2(eg, 0.21 at room air), Patm is the ambientbarometric pressure (eg, 760 mm Hg at sealevel), PH2O is the partial pressure of watervapor (eg, usually 47 mm Hg), PaCO2 is themeasured partial pressure of arterial CO2,and R is the respiratory quotient, which isassumed to be 0.8 in a resting patient on anormal diet.
At sea level and on room air, FIO2 = 0.21,and the (A-a)DO2 can be simplified as follows:
where (A-a)DO2 is typically < 20 but in-creases with age (because of age-related de-cline in pulmonary function) and with in-creasing FIO2 (because, although Hb becomes100% saturated at a PaO2 of about 150 mm Hg,O2 is soluble in blood, and the O2 content ofplasma continues to increase at increasingFIO2). Estimations of normal (A-a)DO2 val-ues as < (2.5 + [FIO2 × age in years]) or as lessthan the absolute value of the FIO2 (eg, < 21on room air; < 30 on 30% FIO2) correct forthese effects.
Hypoxemia with increased (A-a)DO2 iscaused by ventilation-perfusion (V/Q) mis-match, right-to-left shunting, and impaired
PAO2 FIO2 Patm PH2 O– × PaCO2/R,–=
A a–( )DO2 150 PaCO2/0.8– PaO2,–=
045_062PUL Page 370 Tuesday, November 8, 2005 10:54 AM
46 TESTS OF PULMONARY FUNCTION 371
diffusing capacity. Hypoxemia with normal(A-a)DO2 is caused by hypoventilation andlow partial pressures of inspired O2 (PIO2).Hypoxemia due to all causes except right-to-left shunting responds to supplemental O2.
V/Q mismatch is one of the more commonreasons for hypoxemia and contributes tothe hypoxemia occurring with COPD andasthma. In the normal lung, regional perfu-sion closely matches regional ventilation be-cause of the arteriolar vasoconstriction thatoccurs in response to alveolar hypoxia. In dis-ease states, dysregulation leads to perfusionof alveolar units that are receiving less thancomplete ventilation (V/Q mismatch). As aresult, systemic venous blood passes throughthe pulmonary capillaries without achievingnormal levels of PaO2. Supplemental O2 cancorrect hypoxemia due to V/Q mismatch byincreasing the PAO2, although the increased(A-a)DO2 persists.
Right-to-left shunting is an extreme ex-ample of V/Q mismatch. With shunting,deoxygenated pulmonary arterial blood ar-rives at the left side of the heart without hav-ing passed through ventilated lung seg-ments. Shunting may occur through lungparenchyma, through abnormal connec-tions between the pulmonary arterial andvenous circulations, or through intracar-
diac communications (eg, patent foramenovale).
Impaired diffusing capacity only rarelyoccurs in isolation; usually it is accompa-nied by significant V/Q mismatch. BecauseO2 completely saturates Hb after only a frac-tion of the time that blood is in contact withalveolar gas, hypoxemia due to impaireddiffusing capacity occurs only when cardiacoutput is increased (eg, with exercise), whenbarometric pressure is low (eg, at high alti-tudes), or when > 50% of the pulmonaryparenchyma is destroyed. As with V/Qmismatch, the (A-a)DO2 is increased, butPaO2 can be rapidly increased by increasingthe FIO2.
Hypoventilation (reduced alveolar ventila-tion) decreases the PAO2 and increases thePaCO2, thereby decreasing PaO2. In cases ofpure hypoventilation, the (A-a)DO2 is normal.Causes of hypoventilation include decreasedrespiratory rate or depth (eg, neuromusculardisease, severe obesity, drug overdose) or anincrease in the fraction of dead space ventila-tion in patients already at their maximal ven-tilatory limit (eg, an exacerbation of severeCOPD). Hypoventilatory hypoxemia respondsto supplemental O2.
Decreased FIO2 is a final uncommoncause of hypoxemia that in most cases occurs
Fig. 46–4. Oxyhemoglobin dissociation curve. Arterial oxyhemoglobin saturation isrelated to partial pressure of O2 (PO2). PO2 at 50% saturation (P50) is normally 27 mm Hg.The dissociation curve is shifted to the right by increased hydrogen ion (H+) concentration,increased RBC 2,3-diphosphoglycerate (DPG), increased temperature (T), and increased par-tial pressure of carbon dioxide (PCO2). Decreased levels of H+, DPG, temperature, and PCO2shift the curve to the left. Hb characterized by a rightward shifting of the curve has a decreasedaffinity for O2, and that characterized by a leftward shifting of the curve has an increased affinityfor O2.
100
80O
xyhe
mog
lobi
n sa
tura
tion
(%)
60
40
20
20 40 60
Po2 (mm Hg)
80 100
pH 7.6
pH 7.2
H+
DPG
H+
DPG
P50
TPco2
Pco2
T
045_062PUL Page 371 Tuesday, November 8, 2005 10:54 AM
372 SECTION 5 PULMONARY DISORDERS
only at high altitude. Although FIO2 does notchange with altitude, ambient air pressuredecreases exponentially; thus, PIO2 decreasesas well. For example, PIO2 is only 43 mmHg at the summit of Mt. Everest (altitude,29,028 ft). (A-a)DO2 remains normal. Hy-poxic stimulation of respiratory drive in-creases alveolar ventilation and decreasesPaCO2 level.
Carbon DioxidePCO2 normally is maintained between 35
and 45 mm Hg. A dissociation curve similarto that for O2 exists for CO2 but is nearly lin-ear over the physiologic range of PaCO2. Ab-normal PCO2 is always linked to disorders ofventilation and is always associated withacid-base changes.
Hypercapnia is PCO2 > 45 mg Hg. Causesof hypercapnia are the same as those of hy-poventilation (see p. 371). Hypocapnia is PCO2< 35 mm Hg. Hypocapnia is always caused byhyperventilation due to pulmonary (eg, pul-monary edema or embolism), cardiac (eg,heart failure), metabolic (eg, acidosis), drug-induced (eg, aspirin, progesterone), CNS (eg,infection, tumor, bleeding, increased intra-cranial pressure) or physiologic (eg, pain,pregnancy) disorders or conditions. Hypo-capnia is thought to directly increase bron-choconstriction and lower the threshold forcerebral and myocardial ischemia, perhapsthrough its effects on acid-base status.
Carboxyhemoglobinemia and Methemoglobinemia
CO binds to Hb with an affinity 210 timesthat of O2 and prevents O2 transport. Clini-cally toxic carboxyhemoglobin levels aremost often the result of exposure to exhaustfumes or from smoke inhalation, althoughcigarette smokers have detectable levels. Pa-tients with CO poisoning may present withnonspecific symptoms such as malaise, head-ache, and nausea. Because poisoning oftenoccurs during colder months (because of in-door use of combustible fuel heaters), symp-toms may be confused with a viral syndromesuch as influenza. Clinicians must be alert tothe possibility of CO poisoning and measurelevels of carboxyhemoglobin when indi-cated; COHb can be directly measured froman arterial sample.
Treatment is the administration of 100%O2 (which shortens the half-life of carboxy-
hemoglobin) and/or the use of a hyperbaricchamber.
Methemoglobin is Hb in which the iron isoxidized from its ferrous (Fe2+) to its ferric(Fe3+) state. Methemoglobin does not carryO2 and shifts the normal HbO2 dissociationcurve to the left, thereby limiting the releaseof O2 to the tissues. Methemoglobinemia iscaused by certain drugs (eg, dapsone, localanesthetics, nitrates, primaquine, sulfona-mides) or, less commonly, by certain chemi-cals (eg, aniline dyes, benzene derivatives).Methemoglobin level can be directly mea-sured by co-oximetry (which emits 4 wave-lengths of light and is capable of detectingmethemoglobin, COHb, Hb, and HbO2) ormay be estimated by the difference betweenthe O2 saturation calculated from the mea-sured PaO2 and the directly measured SaO2.Patients with methemoglobinemia most of-ten have asymptomatic cyanosis. In severecases, O2 delivery is reduced to such a degreethat symptoms of tissue hypoxia result, suchas confusion, angina, and myalgias. Stoppingthe causative drug or chemical exposure isoften sufficient. Rarely, methylene blue (areducing agent) or exchange transfusion isneeded.
TESTS OF RESPIRATORY MUSCLE FUNCTION
Maximal inspiratory pressure (MIP) andmaximal expiratory pressure (MEP) mea-surements may aid in evaluating respiratorymuscle weakness. MIP is the pressure gener-ated during maximal inspiratory effortagainst a closed system. It is usually measuredat residual volume (RV) because inspiratorymuscle strength is inversely related to lungvolume. MEP is measured during a similarmaneuver at total lung capacity (TLC) be-cause expiratory muscle strength is directlyrelated to lung volume. The informationavailable from these maneuvers is nonspe-cific, however, and cannot distinguish be-tween insufficient effort, muscle weakness,and neurologic disease.
The maximal voluntary ventilation(MVV) is another combined measure of theneuromuscular and respiratory systems. TheMVV is the total volume of air exhaled during12 sec of rapid, deep breathing. It can also beestimated as the forced expiratory volume in
045_062PUL Page 372 Tuesday, November 8, 2005 10:54 AM

46 TESTS OF PULMONARY FUNCTION 373
1 sec (FEV1) × 35 or 40. A significant differ-ence between the predicted and measuredMVV may indicate insufficient neuromus-cular reserve, abnormal respiratory mechanics,or an inadequate effort. Progressive reduc-tion of tidal volumes during the test is sugges-tive, but rarely diagnostic, of neuromuscularabnormalities.
The sniff test is sometimes used in sus-pected cases of diaphragmatic paralysis orparesis. During continuous fluoroscopic ex-amination, the patient makes a quick, short,strong inspiratory effort (“sniff ”). This ma-neuver minimizes the contribution of theother muscles of respiration (eg, intercos-tals). A weakened hemidiaphragm may havedecreased excursion compared with the con-tralateral diaphragm or may move upwardparadoxically. Occasionally, electromyo-graphic interrogation of the diaphragm andphrenic nerve is performed but is of uncertaindiagnostic accuracy. Muscle and nerve biop-sies may be helpful in selected cases.
EXERCISE TESTINGThe two most common forms of exercise
testing used to evaluate pulmonary diseaseare the 6-min walk test and full cardiopulmo-nary exercise testing.
Six-minute walk test: This simple testmeasures the maximal distance that a patientcan walk at his own pace in 6 min. The test glo-bally assesses functional capacity but doesnot provide specific information on the mul-tiple systems (cardiac, pulmonary, hemato-logic, musculoskeletal) involved in exercise,nor does it assess patient effort. This test isused for preoperative and postoperative eval-uation of lung transplantation and lung vol-ume reduction surgery, to monitor responseto therapeutic interventions and pulmonaryrehabilitation, and to predict mortality andmorbidity in patients with cardiac and pul-monary vascular disease.
Cardiopulmonary exercise testing(CPET): This computerized test provides abreath-by-breath analysis of respiratory gas
exchange at rest and during a period of exer-cise, the intensity of which is increased incre-mentally until symptoms limit testing or thepatient reaches maximal levels. Informationon airflow, O2 consumption, CO2 produc-tion, and heart rate are collected and used forcomputation of other variables; ABGs mayalso be sampled. Exercise is performed on atreadmill or on a bicycle ergometer; the er-gometer may be preferable because work ratecan be directly measured.
CPET primarily determines if the patienthas normal or reduced maximal exercise ca-pacity (VO2max). Reduced VO2max can fur-ther suggest probable causes. CPET is usedto define which organ systems contribute toa patient’s symptoms of exertional dyspneaand exercise intolerance and to what extent.The test is also more sensitive for detectingearly or subclinical disease than are less com-prehensive tests that are done at rest. Exam-ples of applications include assessment of ex-ercise capacity for disability evaluation, pre-operative assessment, determining whethersymptoms of dyspnea are the result of cardiacor pulmonary problems in patients who havedisorders of both organ systems, selection ofcandidates for cardiac transplantation, andassessing prognosis in selected diseases,such as heart disease, pulmonary vasculardisease, and cystic fibrosis. CPET can alsohelp gauge responses to therapeutic interven-tions and guide prescription of exercise in re-habilitation programs. In following the re-sponse to therapy or disease progression, asteady-state CPET involving at least 6 min ofconstant work at 50 to 70% of the maximalwork rate achieved during a maximal CPETmay be more useful than an incremental,maximal CPET. Repeated evaluation at thiswork rate over time provides comparabledata and is sensitive to improvement or de-cline in cardiopulmonary function.
Multiple variables are assessed duringCPET, and no single one is diagnostic of acause for exercise limitation. Instead, an in-tegrative approach using clinical data, trendsduring exercise, and recognition of underly-ing patterns of physiologic responses is used.
045_062PUL Page 373 Tuesday, November 8, 2005 10:54 AM

374
47DIAGNOSTIC AND THERAPEUTIC PULMONARY PROCEDURES
Diagnostic tests besides pulmonary func-tion testing (see p. 364) include a variety oftypes of chest imaging, electrocardiography,and ventilation/perfusion (V/Q) scanning.Diagnostic procedures include bronchos-copy, mediastinoscopy and mediastinot-omy, pleural biopsy, thoracentesis, thora-coscopy and video-assisted thoracoscopicsurgery (VATS), thoracotomy, transthoracicneedle biopsy, and tube thoracostomy; pul-monary artery catheterization is discussed inCRC01. Therapeutic procedures includechest physiotherapy and pulmonary rehabil-itation.
CHEST IMAGINGThere are no absolute contraindications to
undergoing noninvasive imaging proce-dures.
Chest x-ray: Plain chest x-rays provideimages of structures in and around the thoraxand are most useful for identifying abnormal-ities in the heart, lung parenchyma, pleurae,chest wall, diaphragm, mediastinum, andhilum. They are usually the initial test per-formed to evaluate the lungs. The standardchest x-ray is taken from back to front (pos-teroanterior view) to minimize x-ray scatterthat could artifactually enlarge the cardiac sil-houette and from the side of the thorax (lateralview). Lordotic or oblique views can be ob-tained to evaluate pulmonary nodules or toclarify abnormalities that may be due tosuperimposed structures, though chest CTprovides more information and has largelysuperseded these views. Lateral decubitusviews may be used to distinguish free-flowingfrom loculated pleural effusion, but again,CT provides more information. End-expiratoryviews are used to detect pneumothoraces.
Screening chest x-rays are often performedbut are almost never indicated; one exceptionis in the asymptomatic patient with a positivetuberculin skin test, in whom a single poster-oanterior chest x-ray without a lateral view isused to make decisions regarding treatmentfor pulmonary TB. Portable (usually antero-posterior) chest x-rays are almost always sub-optimal and should be used only when a pa-tient is too ill to be transported to the radiologydepartment.
Chest fluoroscopy is the use of a continuousx-ray beam to image movement. It is useful fordetecting unilateral diaphragmatic paralysis.During a sniff test, in which the patient is in-structed to forcibly inhale through the nose (orsniff), a paralyzed hemidiaphragm moves cra-nially (paradoxically) while the unaffectedhemidiaphragm moves caudally.
Computed tomography: CT defines in-trathoracic structures and abnormalitiesmore clearly than does a chest x-ray. Con-ventional (planar) CT provides multiple 10mm-thick cross-sectional images of thechest. Its main advantage is wide availabil-ity. Disadvantages are motion artifact andlimited detail from volume averaging of tis-sue within each 10-mm slice.
High-resolution CT (HRCT) provides1-mm-thick cross-sectional images; this isparticularly helpful in evaluation of intersti-tial lung diseases (eg, lymphangitic carcino-matosis, sarcoid, fibrosing alveolitis) andbronchiectasis.
Helical (spiral) CT provides multiplanarimages of the entire chest as patients holdtheir breath for 8 to 10 sec while being movedcontinuously through the CT gantry. HelicalCT is thought to be at least equivalent to con-ventional CT for most purposes. Its main ad-vantages are speed, less radiation exposure,and an ability to construct 3-dimensional im-ages. Software can also generate images ofbronchial mucosa (virtual bronchoscopy). Itsmain disadvantages are less availability andthe requirement for breath-holding, whichcan be difficult for patients with symptomaticpulmonary disease.
CT angiography uses a bolus of IV contrastto highlight the pulmonary arteries, which isuseful in diagnosis of pulmonary embolism.Dye load is comparable to conventional an-giography, but the test is quicker and lessinvasive.
Magnetic resonance imaging: MRIhas a relatively limited role in pulmonary
045_062PUL Page 374 Tuesday, November 8, 2005 10:54 AM
47 DIAGNOSTIC AND THERAPEUTIC PULMONARY PROCEDURES 375
imaging but is preferred over CT in specificcircumstances (eg, for assessment of superiorsulcus and other tumors that abut the chestwall). In patients with suspected pulmonaryembolism in whom IV contrast cannot beused, MRI can sometimes identify largeproximal emboli but usually is limited in thisdisorder.
Advantages include absence of radiationexposure, excellent visualization of vascularstructures, lack of artifact from bone, andexcellent soft-tissue contrast. Disadvantagesinclude respiratory and cardiac motion andthe time it takes to do the procedure.
Ultrasonography: Ultrasonography is pri-marily used to facilitate such procedures asthoracentesis and central venous catheter in-sertion. Endobronchial ultrasound is some-times used in conjunction with fiberopticbronchoscopy.
V/Q scanning: V/Q scanning uses radio-nuclides to detect areas of the lung where sup-ply of O2 (ventilation) and blood (perfusion)are mismatched. Areas of ventilation with-out perfusion, perfusion without ventilation,or matched increases and decreases in bothcan be detected with 6 to 8 views of the lung.V/Q scanning is used almost exclusively fordiagnosis of pulmonary embolism. Split-function ventilation scanning, in which thedegree of ventilation is quantified for eachlobe, is used to predict the effect of lobar orlung resection on pulmonary function; post-surgical forced expiratory volume in 1 sec(FEV1) is the percentage of uptake of venti-lation tracer in the healthy fraction of thelungs multiplied by preoperative FEV1 (in li-ters). A value of < 0.8 L (or < 40% of that pre-dicted for the patient) indicates limited pul-monary reserve and the likelihood of unac-ceptably high perioperative morbidity andmortality.
Positron emission tomography scan-ning: PET scanning uses radioactively la-beled glucose (fluorodeoxyglucose) to mea-sure metabolic activity in tissues. It is used inpulmonary medicine to determine if lungnodules and mediastinal lymph nodes har-bor tumor (metabolic staging) and if canceris recurrent in previously irradiated, scarredareas of the lung. PET is superior to CT scan-ning for mediastinal evaluation for stagingbecause PET can identify tumor in normal-sized lymph nodes and at extrathoracic sites,thereby decreasing the need for invasive pro-cedures such as mediastinoscopy and needle
biopsy. Current spatial resolution of PET is 7to 8 mm; thus the test is not useful for lesions< 1 cm. PET reveals metastatic disease in upto 14% of patients in whom it would not oth-erwise be suspected. The sensitivity of PET(80 to 95%) is comparable to that of histologictissue examination. False-positive resultshave been reported; slowly growing tumors(eg, bronchoalveolar carcinoma, carcinoidtumor, some metastatic malignancies) maycause false-negative results. A new genera-tion of combined CT-PET scanners may be-come the most cost-effective technology forlung cancer diagnosis and staging.
ELECTROCARDIOGRAPHYElectrocardiography is a useful adjunct
to other pulmonary tests because it providesinformation about the right heart (see alsop. 593).
Chronic pulmonary hypertension leadingto chronic right atrial and ventricular hyper-trophy may manifest as prominent P waves(P pulmonale) and ST-segment depressionin leads II, III, and aVF; rightward shift inQRS axis; and decreased progression of Rwaves in precordial leads. COPD patientscommonly have low voltage due to interpo-sition of hyperexpanded lungs between theheart and ECG electrodes.
Acute right ventricle overload or failure, asoccurs in submassive or massive pulmonaryembolism, manifests as right axis deviation(R > S in V1), with S-wave deepening in leadI, Q-wave deepening in lead III, and ST-segment elevation and T-wave inversion inlead III and the precordial leads (S1Q3T3 pat-tern). Right bundle branch block also some-times occurs.
BRONCHOSCOPYBronchoscopy is introduction of an endo-
scope into the airways. Flexible fiberopticbronchoscopy has replaced rigid bronchos-copy for virtually all diagnostic and most ther-apeutic indications. Rigid bronchoscopy isnow used only when a wider aperture and chan-nels are required for better visualization and in-strumentation. Examples include active vigor-ous pulmonary hemorrhage, in which the rigidbronchoscope can better identify the bleeding
045_062PUL Page 375 Tuesday, November 8, 2005 10:54 AM

376 SECTION 5 PULMONARY DISORDERS
source and, with its larger suction channel, canbetter suction blood and prevent asphyxiation;aspirated foreign bodies in young children; andobstructive endobronchial lesions that requirelaser debulking or stent placement. Nearly allflexible bronchoscopes are color video–compatible, facilitating airway visualizationand documentation of findings.
Diagnostically, flexible fiberoptic bron-choscopy allows for direct airway visualiza-tion down to and including subsegmentalbronchi; sampling of respiratory secretionsand cells via bronchial washings, brushings,and lavage of peripheral airways and alve-oli; and biopsy of endobronchial, parenchy-mal, and mediastinal structures. Therapeuticuses include suctioning of retained secretions.
Absolute contraindications include un-treatable life-threatening arrhythmia, inabil-ity to adequately oxygenate the patient duringthe procedure, and acute respiratory failurewith hypercapnia (unless the patient is endo-tracheally intubated and ventilated). Relativecontraindications include an uncooperativepatient, recent MI, high-grade tracheal ob-struction, and uncorrectable coagulopathy.Transbronchial biopsy should be performedwith caution in patients with uremia, superiorvena cava obstruction, or pulmonary hyper-tension because of increased risk of bleedingand pneumothorax. Inspection of the airwaysis safe in these patients, however.
Bronchoscopy should be performed onlyby a pulmonologist or trained surgeon in amonitored setting, typically a bronchoscopysuite, operating room, or ICU (for ventilatedpatients).
The patient should receive nothing bymouth for at least 4 h before bronchoscopyand have IV access, intermittent BP monitor-ing, continuous pulse oximetry, and cardiacmonitoring; supplemental O2 should beavailable. Premedication with atropine 0.01mg/kg IM or IV to decrease secretions and va-gal tone is common, although this practicehas been questioned in recent studies. Short-acting benzodiazepines, opioids, or both maybe given to patients before the procedure todecrease anxiety, discomfort, and cough.
The pharynx and vocal cords are anesthe-tized with nebulized or aerosolized (1 or 2%)lidocaine (maximum, 250 to 300 mg for a70-kg patient). The bronchoscope is lubri-cated with lidocaine jelly and passed throughthe nostril or through the mouth with an oralairway or bite block. After inspection of thenasopharynx and larynx, the scope is passed
through the vocal cords during inspirationand into the trachea and upper airways.
Several ancillary procedures can be per-formed as needed with or without fluoro-scopic guidance. In bronchial washing, sa-line is sprayed in and aspirated from theairways. In bronchial brushing, a brush isadvanced through the bronchoscope andused to abrade suspicious lesions to obtaincells. In bronchoalveolar lavage, 50 to 200mL of sterile saline is infused into the distalbronchoalveolar tree; aspiration of the fluidretrieves cells, protein, and microorganismslocated at the alveolar level. Local areas ofpulmonary edema created by lavage maycause transient hypoxemia. In transbronchialbiopsy, forceps are advanced through thebronchoscope and airway to biopsy one ormore sites in the lung parenchyma. Trans-bronchial biopsy can be performed withoutx-ray guidance, but evidence supports in-creased diagnostic yields and lower inci-dence of pneumothorax when fluoroscopicguidance is used.
Patients are typically observed 2 to 4 h afterthe procedure on supplemental O2. Return ofa gag reflex and maintenance of O2 saturationoff O2 are the two primary indices of recov-ery. Standard practice is to obtain an expiratoryposteroanterior chest x-ray after transbron-chial lung biopsy to exclude pneumothorax.
Serious complications are uncommon; mi-nor bleeding from a biopsy site and fever occurin 10 to 15%. Premedication can cause over-sedation with respiratory depression, hy-potension, and cardiac arrhythmias. Rarely,topical anesthesia causes laryngospasm,bronchospasm, seizures, methemoglobine-mia with refractory cyanosis, or cardiac ar-rhythmias or arrest. Bronchoscopy itself maycause minor laryngeal edema or injury withhoarseness, hypoxemia in patients with com-promised gas exchange, arrhythmias (mostcommonly premature atrial contractions,ventricular premature beats, or bradycardia),and, very rarely, transmission of infectionfrom suboptimally sterilized equipment.Transbronchial biopsy can cause pneu-mothorax (2 to 5%) and significant hemor-rhage (1 to 1.5%). Mortality is 1 to 4/10,000patients. The elderly and others with seriouscomorbidities (severe COPD, coronary ar-tery disease, pneumonia with hypoxemia, ad-vanced neoplasia, mental dysfunction) are atgreatest risk. Transbronchial biopsy increasesmortality to 12/10,000 patients but can pre-clude the need for thoracotomy.
045_062PUL Page 376 Tuesday, November 8, 2005 10:54 AM
47 DIAGNOSTIC AND THERAPEUTIC PULMONARY PROCEDURES 377
MEDIASTINOSCOPY AND MEDIASTINOTOMY
Mediastinoscopy is introduction of an en-doscope into the mediastinum. Mediastinot-omy is surgical opening of the mediastinum.The two are complementary procedures;mediastinotomy gives direct access to aor-topulmonary window lymph nodes, whichare inaccessible to mediastinoscopy. Bothprocedures are performed to evaluate orexcise mediastinal lymphadenopathy ormasses and to stage cancers (eg, lung andesophageal cancer), though PET scan is de-creasing the need for the procedures in thelatter indication.
Contraindications include superior venacava syndrome; previous mediastinal irradi-ation, mediastinoscopy, median sternotomy,or tracheostomy; and aneurysm of the aorticarch.
Mediastinoscopy and mediastinotomy areperformed by surgeons in an operating roomusing general anesthesia. For mediastinos-copy, neck soft tissue is bluntly dissecteddown to the trachea and distally to the carinathrough an incision in the suprasternal notch.A mediastinoscope is inserted into the space,allowing access to paratracheal, tracheo-bronchial, azygous, and subcarinal nodes andto the superior posterior mediastinum. Ante-rior mediastinotomy (Chamberlain proce-dure) is surgical entry to the mediastinumthrough a parasternal 2nd left intercostalspace incision, allowing access to anteriormediastinal and aortopulmonary windowlymph nodes, common sites of metastases forleft upper lobe lung cancers.
Complications occur in < 1% of patientsand include bleeding, infection, vocal cordparalysis from recurrent laryngeal nervedamage, chylothorax from duct injury, andpneumothorax.
PHYSIOTHERAPYChest physiotherapy consists of external
mechanical maneuvers, such as chest percus-sion, postural drainage, and vibration, to aug-ment mobilization and clearance of airwaysecretions. It is indicated for patients inwhom cough is insufficient to clear thick, te-nacious, or loculated secretions. Examplesinclude cystic fibrosis, bronchiectasis, lungabscess, neuromuscular diseases, and pneu-monias in dependent lung regions.
Contraindications are relative and in-clude discomfort from physical positions ormanipulations, anticoagulation, rib or ver-tebral fractures or osteoporosis, and recenthemoptysis.
Chest physiotherapy may be administeredby a respiratory therapist, although the tech-niques can often be taught to family membersof patients. The most common proceduresused are postural drainage and chest percus-sion, in which the patient is rotated to facili-tate drainage of secretions from a specificlobe or segment while being clapped withcupped hands to loosen and mobilize retainedsecretions that can then be expectorated ordrained. The procedure is somewhat uncom-fortable and tiring for the patient. Alterna-tives to chest percussion, the benefits ofwhich remain unproven, include mechanicalvibrators, inflatable vests, controlled patternsof breathing, positive expiratory pressure de-vices to maintain airway patency, and ultra-low-frequency airway oscillation devices tomobilize sputum.
Complications are unusual but includeposition-related hypoxia and aspiration ofsecretions in other lung regions.
PLEURAL BIOPSYPleural biopsy is performed to determine
the underlying cause of an exudative pleuraleffusion when repeated thoracenteses arenondiagnostic. Improved laboratory tech-niques, newer diagnostic tests for pleuralfluid (eg, adenosine deaminase levels, inter-feron-γ, PCR studies for suspected tubercu-losis), and more widespread availability ofthoracoscopy have made the procedure lessnecessary.
Percutaneous pleural biopsy should bedone only by a pulmonologist or surgeontrained in the procedure. Technique is essen-tially the same as that for thoracentesis andcan be done at the bedside; no specific pa-tient preparation is necessary. At least 3specimens obtained from one skin location,with 3, 6, and 9 o’clock positioning of theneedle-cutting chamber, are needed for his-tology and culture.
Chest x-ray should be performed afterbiopsy because of increased risk of com-plications, which are the same as those forthoracentesis but with higher incidence ofpneumothorax and hemorrhage.
045_062PUL Page 377 Tuesday, November 8, 2005 10:54 AM
378 SECTION 5 PULMONARY DISORDERS
PULMONARY REHABILITATION
Pulmonary rehabilitation is the use of exer-cise, education, and behavioral intervention toenhance quality of life. It is indicated for anycondition in which respiratory symptoms causeactivity restriction—eg, COPD, interstitiallung disease, neuromuscular disease causingchest wall weakness—and for respiratory re-training after prolonged ventilator dependence.Contraindications are relative and include co-morbidities that could complicate attempts toincrease a patient’s level of exercise, such as un-treated angina or left ventricular dysfunction.These do not preclude application of other com-ponents of pulmonary rehabilitation programs,however.
For many patients with chronic respiratorydisease, medical therapy only partially allays thesymptoms and complications of their illness. Acomprehensive program of pulmonary rehabil-itation may lead to significant clinical improve-ment by reducing shortness of breath, increasingexercise tolerance, and, to a lesser extent, de-creasing the number of hospitalizations. How-ever, these programs do not improve survival.
Pulmonary rehabilitation is best adminis-tered as part of an integrated program of exer-cise training, education, and psychosocial andbehavioral intervention by a team of physi-cians, nurses, respiratory therapists, physicaland occupational therapists, and psycholo-gists or social workers. Exercise training in-volves aerobic exercise and respiratory mus-cle and extremity strength training; lower ex-tremity strength training may be particularlyimportant for patients with COPD. Educationinvolves smoking cessation; teaching breath-ing strategies (such as pursed-lip breathing, inwhich exhalations are begun against closedlips to splint open airways before breathingout); principles of conserving physical en-ergy; treatment options, including drug ther-apy; and advanced-care planning. Psychoso-cial interventions involve counseling andfeedback for the depression, anxieties, andfear that obstruct the patient’s full participa-tion in activities.
THORACENTESISThoracentesis is chest wall puncture for as-
piration of pleural fluid. It is used to determinethe etiology of a pleural effusion (diagnosticthoracentesis), to relieve dyspnea caused by
pleural fluid (therapeutic thoracentesis), and,occasionally, to perform pleurodesis.
Relative contraindications include uncer-tain fluid location by examination; minimalfluid volume; altered chest wall anatomy; pul-monary disease severe enough to make com-plications life threatening (see p. 379); bleedingdiatheses; uncontrolled coughing; and coagu-lopathy. No absolute contraindications to tho-racentesis exist except refusal or inability toconsent to the procedure.
Thoracentesis can be safely performed atthe patient’s bedside or in an outpatient setting.Presence and location of pleural fluid is veri-fied by physical examination (chest percus-sion) or by imaging techniques. Ultrasonog-raphy, CT, or both may be useful if chest x-raysare equivocal, if prior thoracentesis attemptswere unsuccessful, or if the fluid is loculated.
Thoracentesis is best performed with thepatient sitting upright and leaning slightly for-ward with arm support. Recumbent or supinethoracentesis (eg, in a ventilated patient) ispossible but best done with ultrasound or CTguidance. Only unstable patients and those athigh risk of decompensation from complica-tions require monitoring (eg, pulse oximeter,ECG).
Under sterile conditions, 1 to 2% lidocaineis injected with a 25-gauge needle to anesthe-tize the skin. A larger (20- or 22-gauge) nee-dle with anesthetic is then inserted at the upperborder of the rib one intercostal space belowthe fluid level in the midscapular line. Theneedle is advanced with periodic aspiration(to avoid inadvertent insertion into a bloodvessel and intravascular injection), and anes-thetic is injected at progressively deeper lev-els. The most painful level after the skin is theparietal pleura, which should be infiltratedthe most. The needle is then advanced beyondthe parietal pleura until pleural fluid is aspi-rated, at which point the depth of the needleshould be noted. A large-bore (16- to 19-gauge) thoracentesis needle-catheter deviceis then attached to a 3-way stopcock, whichis connected to a 30- to 50-mL syringe andtubing that drains into a container. The tho-racentesis needle is passed through the skinand subcutaneous tissue along the upper bor-der of the rib into the effusion at about thesame depth noted during anesthesia. Thecatheter is inserted through the needle, andthe needle is withdrawn to decrease the riskof pneumothorax. Pleural fluid can then beaspirated and, with a turn of the stopcock, col-lected in tubes or bags for further evaluation.
045_062PUL Page 378 Tuesday, November 8, 2005 10:54 AM

47 DIAGNOSTIC AND THERAPEUTIC PULMONARY PROCEDURES 379
Fluid should be removed in stages not to ex-ceed 1.5 L/day; hypotension and pulmonaryedema may occur with removal of > 1.5 L offluid at one sitting or with rapid evacuation ofthe pleural space using a vacuum or suctionbottle. When large volumes of fluid must beremoved, blood pressure should be moni-tored continuously.
It has been standard practice to obtain achest x-ray after thoracentesis to rule outpneumothorax, document the extent of fluidremoval, and view lung fields previouslyobscured by fluid, but evidence suggeststhat routine chest x-ray is not necessary inasymptomatic patients.
Coughing is common as the lung re-ex-pands; it does not signify pneumothorax. If thepleural process is inflammatory, pleuritic pain,an audible pleural rub, or both may develop asfluid is removed because of approximation ofinflamed visceral and parietal pleura. Whensubstantial volumes of fluid are removed fromthe pleural space, the plunger on the syringeshould be released periodically midway dur-ing an aspiration. If the fluid in the syringe isdrawn back into the pleural space when nega-tive pressure on the syringe is decreased, pleu-ral pressure may be too negative, and the lungmay be restricted from re-expanding becauseof enveloping adhesions or tumor.
Complications include pneumothorax, he-moptysis from lung puncture, re-expansionpulmonary edema or hypotension after rapidremoval of large volumes of fluid, hemothoraxfrom damage to intercostal vessels, punctureof the spleen or liver, and vasovagal syncope.Bloody fluid that does not clot in a collectingtube indicates that blood in the pleural spacewas not iatrogenic, because free blood in thepleural space rapidly defibrinates.
THORACOSCOPY AND VIDEO-ASSISTED
THORACOSCOPIC SURGERYThoracoscopy is introduction of an endo-
scope into the pleural space. Thoracoscopycan be used for visualization (pleuroscopy)or for surgical procedures. Surgical thoracos-copy is more commonly referred to as video-assisted thoracoscopic surgery (VATS).Pleuroscopy can be performed with con-scious sedation in an endoscopy suite,whereas VATS requires general anesthesiaand is usually performed in the operating
room. Both procedures induce a pneumotho-rax to create a clear view.
Thoracoscopy is used to evaluate exuda-tive effusions and various pleural and lunglesions when noninvasive testing is incon-clusive. The diagnostic accuracy for malig-nant and tuberculous disease of the pleura is95%. The procedure is also used for pleu-rodesis in patients with recurrent malignanteffusions and to break up loculations in pa-tients with empyema.
Indications for VATS include correctionof spontaneous primary pneumothorax, bul-lectomy and lung volume reduction surgeryin emphysema, wedge resection, and, insome medical centers, lobectomy and evenpneumonectomy. Less common indicationsare excision of benign mediastinal masses,biopsy and staging of esophageal cancer,sympathectomy for severe hyperhidrosis orcausalgia, and repair of traumatic injuries tothe lung, pleura, and diaphragm.
Contraindications are the same as those forthoracentesis; adhesive obliteration of thepleural space is an absolute contraindication.Biopsy is contraindicated in patients withhighly vascular cancers, severe pulmonary hy-pertension, and severe bullous lung disease.
Though some pulmonologists performpleuroscopy, VATS is performed by thoracicsurgeons. Both procedures are similar tochest tube insertion; a trocar is inserted intoan intercostal space through a skin incision,through which a thoracoscope is inserted.Additional incisions permit the use of videocameras and accessory instruments.
After thoracoscopy, a chest tube is usuallyrequired for 1 to 2 days. Complications aresimilar to those of thoracentesis. Postproce-dural fever is common (16%); pleural tearscausing air leak and/or subcutaneous emphy-sema are less common (2% each). Hemor-rhage, lung perforation, and gas embolismare serious but rare.
THORACOTOMYThoracotomy is surgical opening of the
chest. It is performed to evaluate and treatpulmonary problems when noninvasive pro-cedures are nondiagnostic or unlikely to bedefinitive.
Contraindications are those general to sur-gery and include coagulopathy that cannot becorrected and instability or insufficiency ofmajor organ systems.
045_062PUL Page 379 Tuesday, November 8, 2005 10:54 AM

380 SECTION 5 PULMONARY DISORDERS
Three basic approaches are used. In limitedanterior or lateral thoracotomy, a 6- to 8-cmintercostal incision is made to approach ante-rior structures. A posterolateral thoracotomygives access to pleurae, hilum, mediastinum,and the entire lung. When access to both lungsis desired, as in lung volume reduction sur-gery, a sternal splitting incision (median ster-notomy) may be used.
Patients undergoing limited thoracotomyrequire a chest tube for 1 to 2 days and in manycases can leave the hospital in 3 to 4 days. Theprincipal indications for thoracotomy todayare lobectomy and pneumonectomy (eg, lungcancer surgery). Video-assisted thoraco-scopic surgery has replaced thoracotomy foropen pleural and lung biopsies.
Complications are greater than those forany other pulmonary biopsy procedure be-cause of the risks of general anesthesia, sur-gical trauma, and a longer hospital stay withmore postoperative discomfort. Hemor-rhage, infection, pneumothorax, broncho-pleural fistula, and reactions to anestheticsare the greatest hazards. Mortality for explor-atory thoracotomy ranges from 0.5 to 1.8%.
TRANSTHORACIC NEEDLE BIOPSY
Transthoracic needle biopsy of thoracic ormediastinal structures uses a cutting needleto aspirate a core of tissue for histologic anal-ysis. Transthoracic needle biopsy is per-formed to evaluate peripheral lung nodules ormasses; hilar, mediastinal, and pleural ab-normalities; and undiagnosed infiltrates orpneumonias when bronchoscopy is contra-indicated or nondiagnostic. When performedwith CT guidance and with a skilled cyto-pathologist in attendance, transthoracic nee-dle biopsy confirms the diagnosis of malig-nancy with > 95% accuracy. Needle biopsyyields an accurate diagnosis in benign pro-cesses only 50 to 60% of the time.
Contraindications are similar to those ofthoracentesis. Additional contraindicationsinclude mechanical ventilation, contralateralpneumonectomy, suspected vascular lesions,putrid lung abscess, hydatid cyst, pulmonaryhypertension, bullous lung disease, intractablecoughing, coagulopathy, and platelet count< 50,000/µL and other bleeding diatheses.
Transthoracic needle biopsy is usually per-formed by an interventional radiologist, often
with a cytopathologist present. Under sterileconditions, local anesthesia, and imaging guid-ance—usually CT but sometimes ultrasoundfor pleural-based lesions—a biopsy needle ispassed into the suspected lesion while the pa-tient holds his breath. The lesion is aspiratedwith or without saline; 2 or 3 samples are col-lected for cytologic and bacteriologic process-ing. After the procedure, fluoroscopy and chestx-rays are used to rule out pneumothorax andhemorrhage. Core needle biopsies are used toobtain a cylinder of tissue suitable for histo-logic examination.
Complications include pneumothorax (10to 37%), hemoptysis (10 to 25%), parenchy-mal hemorrhage, air embolism, and subcuta-neous emphysema.
TUBE THORACOSTOMYTube thoracostomy is insertion of a tube
into the pleural space. It is used to drain air orfluid from the chest (eg, for large or recurrenteffusion refractory to thoracentesis, pneu-mothorax, complicated parapneumonic ef-fusions, empyema, and hemothorax) and toperform pleurodesis or fibrinolytic adhesi-olysis.
Chest tube insertion is best performed by aphysician trained in the procedure. Other phy-sicians can handle emergency situations us-ing a needle and syringe. Tube insertion re-quires one or two hemostats or Kelly clamps,a silk suture, gauze dressing, and a chest tube.Recommended tube sizes are 16 to 24 French(F) for pneumothorax; 20 to 24 F for malignantpleural effusion; 28 to 36 F for bronchopleu-ral fistula, complicated parapneumonic effu-sions, and empyema; and 32 to 40 F for he-mothorax.
The insertion site and patient position de-pend on whether air or fluid is being drained.For pneumothorax, the tube is usually in-serted in the 4th intercostal space and forother indications in the 5th or 6th intercostalspace, in the midaxillary line with the ipsilat-eral arm abducted above the head.
No specific patient preparation is neces-sary except, in some cases, conscious seda-tion. Under sterile conditions, the skin, sub-cutaneous tissue, rib periosteum, and parietalpleura are locally anesthetized, more gener-ously than with thoracentesis (see p. 378).Proper location is confirmed by return of airor fluid in the anesthetic syringe. A purse-string suture can be placed but not yet tied
045_062PUL Page 380 Tuesday, November 8, 2005 10:54 AM

48 ASTHMA 381
around the site while the anesthetic takes ef-fect. A 2-cm skin incision is made, and the in-tercostal soft tissue down to the pleura is thenbluntly dissected by advancing a clampedhemostat or Kelly clamp and opening it; thepleura is then perforated with the clamped in-strument and opened in the same way. A fin-ger can be used to widen the tract and confirmentry into the pleural space. The chest tube,with a clamp grasping the tip, is insertedthrough the tract and directed inferoposteri-orly for effusions or apically for pneumotho-rax until all of the tube’s holes are inside thechest wall. The purse-string suture is closed,the tube is sutured to the chest wall, and a ster-ile dressing with petroleum gauze to help sealthe wound is placed over the site.
The tube is connected to water seal to pre-vent air from entering the chest through thetube and to allow drainage without suction(for effusions or empyema) or with suction(for pneumothorax). A posteroanterior andlateral chest x-ray is obtained after insertionto check the tube’s position.
The tube is removed when the conditionfor which it was placed resolves. In the caseof pneumothorax, suction is stopped and thetube is placed on water seal for several hoursto ensure that the air leak has stopped and thatthe lung remains expanded. At the moment ofremoval, the patient is asked to take a deepbreath and then to forcibly exhale; the tube isremoved during exhalation and the site is cov-ered with petroleum gauze, a sequence thatreduces the chance of pneumothorax duringremoval. For effusions or hemothorax, thetube is typically removed when the drainageis < 100 mL/day.
Complications include malpositioning ofthe tube in the lung parenchyma, in the lobarfissure, under the diaphragm, or subcutane-ously; clotting, kinking, or dislodgement ofthe tube, requiring replacement; re-expansionpulmonary edema; subcutaneous emphy-sema; infection of residual pleural fluid or re-current effusion; pulmonary or diaphragmaticlaceration; and, rarely, perforation of otherstructures.
48ASTHMA
Asthma is a disease of diffuse airway inflam-mation caused by a variety of triggeringstimuli resulting in partially or completelyreversible bronchoconstriction. Symptomsand signs include dyspnea, chest tightness,and wheezing. The diagnosis is based on his-tory, physical examination, and pulmonaryfunction tests. Treatment involves control-ling triggering factors and drug therapy,most commonly with inhaled β-agonists andinhaled corticosteroids. Prognosis is goodwith treatment.
EpidemiologyThe prevalence of asthma appears to have
increased continuously since the 1970s, andasthma now affects an estimated 4 to 7% ofpeople worldwide. About 12 to 17 millionpeople in the US have asthma; from 1982 to1992, the prevalence increased from 34.7 to49.4 per 1000. Prevalence is higher for people< 18 yr (6.1%) than for those 18 to 64 yr(4.1%) and is higher in males before puberty
and in females after puberty. It is also higherin urban populations and among blacks andsome Hispanic groups. Asthma mortality hasalso increased, and about 5000 deaths occurfrom asthma annually in the US. The deathrate is 5 times higher for blacks than forwhites. Asthma is the leading cause of hospi-talization for children and is the number onechronic condition causing elementary schoolabsenteeism. In 2002, the total cost of asthmacare was $14 billion.
EtiologyDevelopment of asthma is multifactorial
and depends on interactions between multi-ple susceptibility genes and environmentalfactors.
Susceptibility genes are thought to includethose for T-helper 2 (TH2) cells and their cy-tokines (IL-4, -5, -9, and -13) and the recentlyidentified ADAM33 gene, which may stimu-late airway smooth muscle and fibroblast pro-liferation or regulate cytokine production.
Evidence clearly implicates household(dust mite, cockroach, pet) and other environ-mental (pollen) allergens in disease develop-ment in older children and adults. Endotoxin
045_062PUL Page 381 Tuesday, November 8, 2005 10:54 AM

382 SECTION 5 PULMONARY DISORDERS
infection or exposure early in life can inducetolerance and may be protective. Air pollutionis not definitively linked to disease develop-ment, though it may trigger exacerbations.Diets low in vitamins C and E and in ω–3 fattyacids have been linked to asthma, as has obe-sity. Asthma has also been linked to peri-natal factors, such as young maternal age,poor maternal nutrition, prematurity, lowbirthweight, and lack of breastfeeding. Therole of childhood exposure to cigarette smokeis controversial, with some studies finding acontributory and some a protective effect.
Indoor exposures to nitrogen oxide andvolatile organic compounds are implicated inthe development of the reactive airways dys-function syndrome (RADS), a syndrome ofpersistent reversible airway obstruction inpeople with no history of asthma (see alsop. 476). Whether RADS is separate fromasthma or a form of occupational asthma iscontroversial, but the two conditions havemany similarities (eg, wheezing, dyspnea,cough) and respond to corticosteroids.
Pathophysiology and Classification
Genetic and environmental componentsmay interact by determining the balance be-tween T-helper 1 (TH1) and TH2 cell lineages.Experts believe that infants are born with a dis-position toward pro-allergic and pro-inflam-matory TH2 immune responses, characterizedby growth and activation of eosinophils andIgE production, but that early childhood expo-sure to bacterial and viral infections and en-dotoxins shifts the body to TH1 responses,which suppresses TH2 cells and induces toler-ance. Trends in developed countries towardsmaller families with fewer children, cleanerindoor environments, and early use of vacci-nations and antibiotics may deprive childrenof these TH2-suppressing, tolerance-inducingexposures and may partly explain the contin-uous increase in asthma prevalence in devel-oped countries (the hygiene hypothesis).
In asthmatics, these TH2 cells and othercell types—notably, eosinophils and mastcells, but also other CD4+ subtypes and neu-trophils—form an extensive inflammatoryinfiltrate in airway epithelium and smoothmuscle, leading to desquamation, subepithe-lial fibrosis, and smooth muscle hypertro-phy. Hypertrophy of smooth muscle narrowsthe airway and increases reactivity to aller-gens, infections, irritants, parasympatheticstimulation (which causes release of pro-
inflammatory neuropeptides, such as sub-stance P, neurokinin A, and calcitonin gene-related peptide), and other bronchoconstric-tive triggers. Additional contributors to air-way hyperreactivity include loss of inhibitorsof bronchoconstriction (epithelium-derivedrelaxing factor, prostaglandin E2) and othersubstances that metabolize endogenousbronchoconstrictors (endopeptidases) as aresult of desquamated epithelium and mu-cosal edema. Mucus plugging and peripheralblood eosinophilia are additional classicfindings in asthma and may be epiphenomenaof airway inflammation.
Common triggers of an asthma attack in-clude environmental and occupational aller-gens; infections (respiratory syncytial virusand parainfluenza infection in young chil-dren, URIs and pneumonia in older childrenand adults); exercise, especially in cold or dryenvironments; inhaled irritants (air pollu-tion); and anxiety, anger, and excitement. As-pirin is a trigger in up to 30% of older or moresevere asthmatics and is typically accompa-nied by nasal polyps with nasal and sinus con-gestion. Gastroesophageal reflux disease(GERD) has recently been recognized as acommon trigger of asthma, possibly viaesophageal acid-induced reflex bronchocon-striction or by microaspiration of acid. Aller-gic rhinitis often coexists with asthma; it isunclear whether the two are different mani-festations of the same allergic process orwhether rhinitis is a discrete asthma trigger.
In the presence of triggers, the pathophys-iologic changes characteristic of asthmacause reversible airway obstruction and non-uniform lung ventilation. Relative perfusionexceeds relative ventilation in obstructed ar-eas, and alveolar O2 tensions fall and alveolarCO2 tensions rise as a result. Most patientscan compensate by hyperventilating, therebymaintaining PaCO2 below normal levels. Butin severe exacerbations, diffuse bronchocon-striction causes severe gas trapping, the res-piratory muscles are put at a profound me-chanical disadvantage and become incapableof generating inspiratory force, and the workof breathing increases. Under these condi-tions, hypoxemia and hyperexertion worsenand PaCO2 rises. Respiratory and metabolicacidosis may result and, if left untreated, re-sult in respiratory and cardiac arrest.
Asthma is classified into 4 categories—mild intermittent, mild persistent, moderatepersistent, and severe persistent—accordingto symptoms (see TABLE 48–1). Because the
045_062PUL Page 382 Tuesday, November 8, 2005 10:54 AM

48 ASTHMA 383
course of asthma varies, a patient may moveamong categories. Regardless of the cate-gory, a patient may have mild, moderate, orsevere exacerbations. For example, somepatients with mild intermittent asthma havesevere, life-threatening exacerbations sepa-rated by long periods of no or mild symptomsand normal pulmonary function. The termstatus asthmaticus describes severe, intense,prolonged bronchospasm that is resistant totreatment.
Asthma and COPD are sometimes easilyconfused; they cause similar symptoms andsimilar results on pulmonary function testsbut differ in important biologic ways that arenot always clinically apparent.
Symptoms and SignsPatients with mild intermittent or mild per-
sistent asthma are typically asymptomaticbetween exacerbations. Those with more se-vere disease or those with exacerbations ex-perience dyspnea, chest tightness, audiblewheezing, and coughing; coughing may bethe only symptom in some patients (cough-variant asthma). Symptoms can follow a cir-cadian rhythm and worsen during sleep, oftenaround 4 AM. Many patients with more severedisease suffer nocturnal awakenings (noctur-nal asthma).
Signs are wheezing, pulsus paradoxus (fallof systolic BP > 10 mm Hg during inspiration—see p. 573), tachypnea, tachycardia, and vis-ible efforts to breathe (use of neck and su-prasternal [accessory] muscles, upright pos-ture, pursed lips, inability to speak). The ex-piratory phase of respiration is prolonged,with an inspiratory:expiratory ratio of at least1:3. Wheezes can be present through bothphases or just on expiration. A patient with se-vere bronchoconstriction may have no audi-ble wheezing because of markedly limitedairflow.
A patient with a severe exacerbation andimpending respiratory failure typically hassome combination of altered consciousness;cyanosis; pulsus paradoxus > 15 mm Hg; O2saturation (O2sat) < 90%; PaCO2 > 45 mm Hg(sea level); and hyperinflation. Rarely, pneu-mothorax or pneumomediastinum is seen onchest x-ray.
Symptoms and signs disappear betweenacute asthma attacks, although soft wheezesmay be audible during forced expiration, afterexercise, and at rest in some asymptomatic pa-tients. Hyperinflation of the lungs may alter
the chest wall in patients with long-standinguncontrolled asthma, producing a barrel-shaped thorax.
All symptoms and signs are nonspecific,are reversible with timely treatment, and typ-ically are brought on by exposure to one ormore triggers.
DiagnosisDiagnosis is based on history and physical
examination and is confirmed with pulmo-nary function tests. Diagnosis of underlyingcauses and the exclusion of diseases thatcause wheezing are also important.
Pulmonary function tests: Patients sus-pected of having asthma should undergopulmonary function testing to confirm andquantify the severity and reversibility of air-way obstruction. Pulmonary function dataquality is effort-dependent and requires pa-tient education before the test. If it is safe todo so, bronchodilators should be stopped be-fore the test: 6 h for short-acting β-agonists,such as albuterol; 8 h for ipratropium; 12 to36 h for theophylline; 24 h for long-acting β-agonists, such as salmeterol and formoterol;and 48 h for tiotropium.
Spirometry (see Ch. 46 on p. 364) shouldbe obtained before and after inhalation of ashort-acting bronchodilator. Signs of airwayobstruction before bronchodilator inhalationinclude reduced forced expiratory volume inthe first second (FEV1) and a reduced ratio ofFEV1 to forced vital capacity (FEV1/FVC).The FVC may also be decreased. Lung vol-ume measurements may show an increase inthe residual volume and/or the functionalresidual capacity because of air trapping. Animprovement in FEV1 of > 12% or > 0.2 L inresponse to bronchodilator treatment con-firms reversible airway obstruction, al-though absence of this finding should notpreclude a therapeutic trial of bronchodila-tors. Spirometry should be repeated at leastyearly in known asthmatics to monitor dis-ease progression.
Flow-volume loops should also be re-viewed to diagnose or exclude vocal corddysfunction, a common cause of upper air-way obstruction that mimics asthma.
Provocative testing, in which inhaledmethacholine (or alternatives, such as in-haled histamine, adenosine, bradykinin, orexercise testing) is used to provoke broncho-constriction, is indicated for suspected asth-matics with normal findings on spirometry
045_062PUL Page 383 Tuesday, November 8, 2005 10:54 AM

384 SECTION 5 PULMONARY DISORDERS
TABLE 48–1. CLASSIFICATION AND MANAGEMENT OF CHRONIC ASTHMA
CATEGORY SYMPTOMS*PULMONARY FUNCTION* TREATMENT
Mild intermittent
Daytime symptoms ≤ 2 days/wk or no symptoms and nor-mal PEF between exacerbations
Nighttime symp-toms ≤ 2 times/mo
Exacerbations brief (from a few hours to a few days); intensity may vary
FEV1 ≥ 80% predicted
PEF ≥ 80% personal best
PEF variability < 20%
All patients:No daily drugs required;
rescue β-agonist as needed for symptoms; systemic corticosteroids if needed for exacerbations
Mild persistent
Daytime symptoms > 2 times/wk but not daily
Nighttime symp-toms > 2 times/mo
Exacerbations that sometimes limit activity
FEV1 ≥ 80% predicted
PEF ≥ 80% personal best
PEF variability 20–30%
Children ≤ 5 yr:Preferred: Low-dose ICS
via nebulizer, MDI with holding chamber, or DPI
Alternative: Mast cell stabi-lizers or leukotriene recep-tor antagonist
Children > 5 yr and adults:Preferred: Low-dose ICSAlternative: Mast cell stabi-
lizers, leukotriene modifi-ers (≥ 12 yr), or theophyl-line
ANDRescue β-agonist
Moderate persistent
Daily daytime symp-toms
Nighttime symp-toms > 1 time/wk
Daily use of inhaled short-actingβ-agonist
Exacerbations that limit activity
Exacerbations ≥ 2 times/wk; may last days
FEV1 60–80% predicted
PEF 60–80% personal best
PEF variability > 30%
Children ≤ 5 yr:Preferred: Low-to-medium-
dose ICS plus long-acting β-agonist, or medium-dose ICS
Alternatives: Low-dose ICS plus either leukotriene receptor antagonist or theophylline
If needed (eg, for patients with recurring severe exacerbations):
Preferred: Medium-dose ICS plus long-actingβ-agonist
Alternatives: Medium-dose ICS plus either leukotriene receptor antagonist or theophylline
Children > 5 yr and adults:Preferred: Low-to-medium-
dose ICS plus long-acting β-agonist
045_062PUL Page 384 Tuesday, November 8, 2005 10:54 AM

48 ASTHMA 385
and flow-volume testing, suspected cough-variant asthma and no contraindications. Con-traindications include FEV1 < 1 L or < 50%,recent MI or stroke, and severe hypertension(systolic BP > 200 mm Hg; diastolic BP > 100mm Hg). A decline in FEV1 of > 20% sup-ports the diagnosis of asthma. However,FEV1 may decline in response to these drugsin other diseases, such as COPD.
Other tests: Other tests may be helpful insome circumstances.
Diffusing capacity for carbon monoxide(DLCO) testing can help distinguish asthmafrom COPD. Values are normal or elevated in
asthma and usually reduced in COPD, partic-ularly in the setting of emphysema.
A chest x-ray may help exclude underlyingcauses of asthma or alternative diagnoses,such as heart failure or pneumonia. The chestx-ray in asthma is usually normal but mayshow hyperinflation or segmental atelectasis,a sign of mucous plugging. Infiltrates, espe-cially those that come and go and that areassociated with findings of central bron-chiectasis, suggest allergic bronchopulmo-nary aspergillosis (see p. 398).
Allergy testing is indicated for all childrenwhose history suggests allergic triggers
Alternatives: Low-to-medium-dose ICS plus either leukotriene modi-fier or theophylline; increase ICS within medium-dose range
ANDRescue β-agonistIf needed (eg, for patients
with recurring severe exacerbations):
Preferred: Increase ICS within medium-dose range and add long-acting β-agonist
Alternatives: Increase ICS within medium-dose range and add eitherleukotriene modifier or theophylline
Severe persistent
Continual symptomsFrequent nighttime
symptomsLimited physical
activityFrequent
exacerbations
FEV1 ≤ 60% predicted
PEF ≤ 60% personal best
PEF variability > 30%
All patients:Preferred: High-dose ICS
plus long-acting β-agonist and, if needed, corticoste-roid tablets or syrup (1–2 mg/kg/day, not to exceed 60 mg/day)
Symptom relief
All patients: Short-acting β-agonist, 2–4 puffs
PEF = peak expiratory flow; FEV1 = forced expiratory volume in 1 sec; ICS = inhaled corticoste-roid; MDI = metered dose inhaler; DPI = dry-powder inhaler.
*Patient is assigned to most severe category in which any feature occurs; pulmonary function typi-cally not available for children < 5 yr.
Modified from the National Asthma Education and Prevention Program, Expert Panel Report II,National Heart, Lung, & Blood Institute, 1997.
TABLE 48–1. CLASSIFICATION AND MANAGEMENT OF CHRONIC ASTHMA—Continued
CATEGORY SYMPTOMS*PULMONARY FUNCTION* TREATMENT
045_062PUL Page 385 Tuesday, November 8, 2005 10:54 AM

386 SECTION 5 PULMONARY DISORDERS
(because all children are potentially eligible forimmunotherapy). It should be considered foradults whose history indicates relief of symp-toms with allergen avoidance and for those inwhom a trial of therapeutic anti-IgE antibodytherapy (see p. 393) is being considered. Skintesting and measurement of allergen-specificIgE via radioallergosorbent testing (RAST)can identify specific allergic triggers (seepp. 1354–1355). Elevated blood eosinophils(> 400 cells/µL) and nonspecific IgE (>150 IU)are suggestive but not diagnostic of allergicasthma because they can be elevated in a va-riety of other conditions.
Sputum evaluation for eosinophils is notcommonly practiced; finding large numbersof eosinophils is suggestive of asthma but isneither sensitive nor specific.
Peak expiratory flow (PEF) measurementswith inexpensive handheld flow meters arerecommended for home monitoring of dis-ease severity and for guiding therapy.
Evaluation of exacerbations: Knownasthmatics with an acute exacerbation shouldhave pulse oximetry and either PEF or FEV1measurement. All 3 measures help establishthe severity of an exacerbation and documenttreatment response. PEF values are inter-preted in light of the patient’s personal best,which may vary widely among patients whoare equally well controlled. A 15 to 20% reduc-tion from this baseline indicates a significantexacerbation. When baseline values are notknown, the percent predicted value gives ageneral idea of airflow limitation but not theindividual patient’s degree of worsening.
Chest x-ray is not necessary for most ex-acerbations but should be obtained in patientswith symptoms suggestive of pneumonia orpneumothorax.
ABG measurements should be obtained inpatients with marked respiratory distress orsigns and symptoms of impending respira-tory failure.
PrognosisAsthma resolves in most children with the
disease, but for as many as one in four, wheez-ing persists into adulthood or relapse occursin later years. Female sex, smoking, earlierage of onset, sensitization to household dustmites, and airway hyperresponsiveness arerisk factors for persistence and relapse.
About 5000 deaths/yr are attributable toasthma in the US, most of which are prevent-able with treatment. Thus, the prognosis isgood with adequate access and adherence to
treatment. Risk factors for death include in-creasing requirements for oral corticoste-roids before hospitalization, previous hospi-talization for acute exacerbations, and lowerpeak flows at presentation. Several studiesshow that use of inhaled corticosteroids de-creases hospital admission and mortalityrates.
Over time, the airways in some asthmaticpatients undergo permanent structuralchanges (remodeling) that prevent return tonormal lung functioning. Early aggressiveuse of anti-inflammatory drugs may help pre-vent this remodeling.
TreatmentTreatment of asthma—both chronic dis-
ease and acute exacerbations—involves con-trol of triggering factors, drug treatment tai-lored to severity of disease, monitoring ofresponse to treatment and disease progres-sion, and patient education to maximize self-management of disease. Objectives are toprevent exacerbations and chronic symp-toms, including nocturnal awakenings; min-imize the need for emergency departmentvisits or hospitalizations; maintain baseline(normal) pulmonary function and activitylevels; and avoid adverse treatment effects.
Control of triggering factors: Trigger-ing factors may in some patients be controlledwith use of synthetic fiber pillows and imper-meable mattress covers and frequent washingof bedsheets, pillowcases, and blankets in hotwater. Upholstered furniture, soft toys, car-pets, and pets should be removed (dust mites,animal dander), and dehumidifiers should beused in basements and in other poorly aerated,damp rooms (molds). Steam treatment ofhomes diminishes dust mite allergens. Thefact that control of triggering factors is moredifficult in urban environments does not di-minish the importance of these measures;elimination of cockroach exposure by way ofhouse cleaning and extermination is espe-cially important. High-efficiency particulateair (HEPA) vacuums and filters may relievesymptoms, but their effects on pulmonaryfunction and on the need for drugs are un-proven. Sulfite-sensitive patients should avoidred wine. Nonallergenic triggers, such as cig-arette smoke, strong odors, irritant fumes, coldtemperatures, high humidity, and exercise,should also be avoided or controlled when pos-sible. Patients with aspirin-induced asthmacan use acetaminophen, choline magnesiumsalicylate, or cyclooxygenase (COX)-2 inhibi-
045_062PUL Page 386 Tuesday, November 8, 2005 10:54 AM

48 ASTHMA 387
tors in place of NSAIDs. Asthma is a relativecontraindication to the use of nonselectiveβ-blockers, including topical formulations,but cardioselective drugs (eg metoprolol,atenolol) probably have no adverse effects.
Drug therapy: Major drug classes com-monly used in the treatment of chronicasthma and asthma exacerbations includebronchodilators (β-agonists, anticholinergics),corticosteroids, mast cell stabilizers, leuko-triene modifiers, and methylxanthines (seeTABLE 48–2). Drugs in these classes areinhaled or taken orally; inhaled drugs comein aerosolized and powdered forms. Use ofaerosolized forms with a spacer or holdingchamber facilitates deposition of the drug inthe airways rather than the pharynx; patientsshould be advised to wash and dry their spac-ers after each use to prevent bacterial contam-ination. In addition, use of aerosolized formsrequires coordination between actuation ofthe inhaler (drug delivery) and inhalation;powdered forms reduce the need for coordi-nation, because drug is delivered only whenthe patient inhales. In addition, powderedforms reduce the release of fluorocarbon pro-pellants into the environment.
b-Agonists (β-adrenergics) relax bron-chial smooth muscle, decrease mast cell de-granulation and histamine release, inhibitmicrovascular leakage into the airways, andincrease mucociliary clearance. β-Agonistscome in short- and long-acting preparations(see TABLE 48–2). Short-acting β-agonists(eg, albuterol) inhaled 2 to 8 puffs as neededare the drug of choice for relieving acutebronchoconstriction and preventing exer-cise-induced bronchoconstriction. They takeeffect within minutes and are active for up to6 to 8 h, depending on the drug. Long-actingdrugs, inhaled at bedtime or bid and active forup to 12 h, are used for moderate and severeasthma as well as for mild asthma that causesnocturnal awakening. Long-acting β-ago-nists also interact synergistically with in-haled corticosteroids and permit lower dos-ing of corticosteroids. Oral β-agonists havemore systemic effects and generally shouldbe avoided. Tachycardia and tremor are themost common acute adverse effects of in-haled β-agonists and are dose-related. Hy-pokalemia occurs uncommonly and to only amild extent. The safety of regular long-termuse of β-agonists is controversial; regular,possibly excessive use is associated with in-creased mortality, but it is unclear whether
this is an adverse effect or if regular use re-flects suboptimal treatment of the diseasewith other drugs. Daily use of β-agonists, in-creased dosing or diminishing effects, or useof one or more canisters a month suggests in-adequate control of disease and the need tobegin or intensify other therapies. Use oflevalbuterol (a solution containing the R-iso-mer of albuterol) theoretically minimizesadverse effects, but its long-term efficacy andsafety is unproven.
Anticholinergics relax bronchial smoothmuscle through competitive inhibition ofmuscarinic (M3) cholinergic receptors. Ipra-tropium has minimal effect when used alonefor asthma but may have an additive effectwhen combined with short-acting β-agonists.Adverse effects include pupillary dilation,blurred vision, and dry mouth. Tiotropium isa 24-h inhaled anticholinergic that has notbeen adequately evaluated for asthma use.
Corticosteroids inhibit airway inflamma-tion, reverse β-receptor down-regulation,block leukotriene synthesis, and inhibit cyto-kine production and adhesion protein activa-tion. They block the late response (but not theearly response) to inhaled allergens. Routes ofadministration include oral, IV, and inhaled. Inacute asthma exacerbation, early use of sys-temic corticosteroids often aborts the exacer-bation, decreases the need for hospitalization,prevents relapse, and speeds recovery. Oral andIV routes are equally effective. Inhaled corti-costeroids have no role in acute exacerbationbut are indicated for long-term suppression,control, and reversal of inflammation andsymptoms. They substantially reduce the needfor maintenance oral corticosteroid therapyand are considered disease-modifying drugsbecause they slow or halt the deterioration ofpulmonary function characteristic of untreatedasthma. Adverse local effects of inhaled corti-costeroids include dysphonia and oral candi-diasis, which can be prevented or minimized byhaving the patient use a spacer and/or garglewith water after corticosteroid inhalation. Sys-temic effects are all dose-related, can occurwith oral or inhaled forms, and occur mainlywith inhaled doses > 800 µg/day. They includesuppression of the adrenal-pituitary axis, os-teoporosis, cataracts, skin atrophy, hyperpha-gia, and easy bruisability. Whether inhaledcorticosteroids suppress growth in children iscontroversial: Most children reach their pre-dicted adult height. Quiescent TB may be reac-tivated by systemic corticosteroid use.
Text continues on page 392.
045_062PUL Page 387 Tuesday, November 8, 2005 10:54 AM

388 SECTION 5 PULMONARY DISORDERS
TABLE 48–2. DRUG TREATMENT OF CHRONIC ASTHMA
DRUG FORM
DOSAGECOMMENTSChild Adult
Short-acting β-agonistsAlbuterol MDI: 90 µg/
puff
DPI: 200 µg/capsule
Nebulized solution: 2.5 and 5 mg/mL 0.63 and 1.25 mg/3 mL
2 puffs tid to qid and 5 min before exercise prn
1 capsule q 4–6 h and before exer-cise
0.05 mg/kg (minimum 1.25 mg, maximum 2.5 mg) in 3 mL saline q 4–6 h
2 puffs tid to qid and 5 min before exercise prn
1–2 capsules q 4–6 h and before exer-cise
1.25–5 mg in 3 mL saline q 4–8 h
Used mainly as res-cue drug; not rec-ommended for maintenance treat-ment. Regular use indicates diminish-ing asthma control and need for addi-tional drug. Dou-ble MDI/DPI dose for mild and nebu-lized dose for severe exacerba-tions. MDI/DPI as effective as nebu-lized therapy if patient can coordi-nate inhalation maneuver using spacer/holding chamber. Nebulized albuterol can be mixed with other nebulizer solutions
Bitolterol MDI: 370 µg/puff
Nebulized solution:2 mg/mL (0.2%)
Not estab-lished
0.5–3.5 mg Cannot mix with other nebulizer solutions
(0.25–1 mL)in 2–3 mL saline q 4–8 h
Leval-buterol
Nebulized solution: 0.31, 0.63, and 1.25 mg/3 mL
0.025 mg/kg (minimum 0.63 mg, maximum 1.25 mg) q 4–8 h
0.63–2.5 mg q 4–8 h
R-isomer of albuterol. 0.63 mg is equivalent to 1.25 mg racemic albuterol. May have fewer adverse effects
Pirbuterol MDI: 200 µg/puff
Same as albuterol
Long-acting β-agonistsFormot-
erolDPI: 12 µg/
capsule1 capsule q
12 h1 capsule q
12 hMay be used for
acute symptom relief in an exacer-bation. Efficacy and safety unstudied in children < 5 yr. Capsules for single use; patients should be educated to avoid swallowing
045_062PUL Page 388 Tuesday, November 8, 2005 10:54 AM
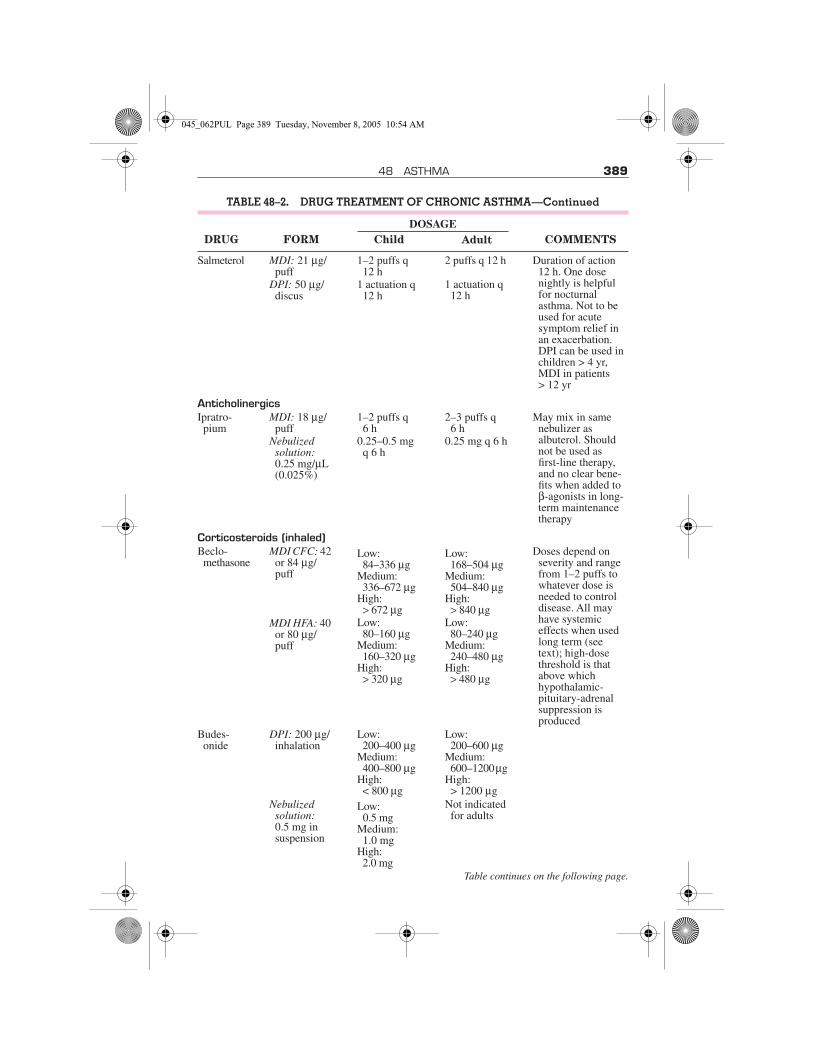
48 ASTHMA 389
Salmeterol MDI: 21 µg/puff
DPI: 50 µg/discus
1–2 puffs q 12 h
1 actuation q 12 h
2 puffs q 12 h
1 actuation q 12 h
Duration of action 12 h. One dose nightly is helpful for nocturnal asthma. Not to be used for acute symptom relief in an exacerbation. DPI can be used in children > 4 yr, MDI in patients> 12 yr
AnticholinergicsIpratro-
piumMDI: 18 µg/
puff Nebulized
solution: 0.25 mg/µL (0.025%)
1–2 puffs q6 h
0.25–0.5 mg q 6 h
2–3 puffs q6 h
0.25 mg q 6 h
May mix in same nebulizer as albuterol. Should not be used as first-line therapy, and no clear bene-fits when added to β-agonists in long-term maintenance therapy
Corticosteroids (inhaled)Beclo-
methasoneMDI CFC: 42
or 84 µg/puff
MDI HFA: 40 or 80 µg/puff
Low: 84–336 µg
Medium: 336–672 µg
High: > 672 µg
Low: 80–160 µg
Medium: 160–320 µg
High: > 320 µg
Low: 168–504 µg
Medium: 504–840 µg
High: > 840 µg
Low: 80–240 µg
Medium: 240–480 µg
High: > 480 µg
Doses depend on severity and range from 1–2 puffs to whatever dose is needed to control disease. All may have systemic effects when used long term (see text); high-dose threshold is that above which hypothalamic-pituitary-adrenal suppression is produced
Budes-onide
DPI: 200 µg/inhalation
Low: 200–400 µg
Medium: 400–800 µg
High: < 800 µg
Low: 200–600 µg
Medium: 600–1200 µg
High: > 1200 µg
Nebulized solution: 0.5 mg in suspension
Low: 0.5 mg
Medium: 1.0 mg
High: 2.0 mg
Not indicated for adults
Table continues on the following page.
TABLE 48–2. DRUG TREATMENT OF CHRONIC ASTHMA—Continued
DRUG FORM
DOSAGECOMMENTSChild Adult
045_062PUL Page 389 Tuesday, November 8, 2005 10:54 AM

390 SECTION 5 PULMONARY DISORDERS
Flunisolide MDI: 250 µg/puff
Low: 500–750 µg
Medium: 750–1250 µg
High: > 1250 µg
Low: 500–1000 µg
Medium: 1000–2000 µg
High: > 2000 µg
Fluticasone MDI: 44, 100, or 220 µg/puff
Low: 88–176 µg
Medium: 176–440 µg
High: > 440 µg
Low: 88–264 µg
Medium: 264–660 µg
High: < 660 µg
DPI: 50, 100, or 250 µg/inhalation
Low: 100–200 µg
Medium: 200–400 µg
High: > 400 µg
Low: 100–300 µg
Medium: 300–600 µg
High: > 600 µg
Triamci-nolone
MDI: 100 µg/puff
Low: 400–800 µg
Medium: 800–1200 µg
High:> 1200 µg
Low: 400–1000 µg
Medium:1000–1200 µg
High: > 2000 µg
Systemic corticosteroidsMethyl-
pred-nisolone
Tablets: 2, 4, 8, 32 mg
Mainte-nance: 0.25–2 mg/kg/day
Short-course burst: 1–2 mg/kg/day, max 60 mg/day for 3 to 10 days
Mainte-nance: 7.5–60 mg/day
Short-course burst: 40–60 mg/day as single or 2 divided doses for 3–10 days
Maintenance doses should be given in a single dose in the morning or every other day as needed for control. Some evidence suggests clinical effective-ness increases with no increase in adre-nal suppression when dose given at 3 PM. Short-course burst doses are effective for estab-lishing control when initiating therapy or during a period of gradual deterioration. The burst should be continued until the patient achieves 80% PEF personal best or symptoms resolve; may require longer than 3–10 days of therapy
Predniso-lone
Pred-nisone
Tablets: 5 mgSolution: 5 or
15 mg/5 mLTablets: 1,
2.5, 5, 10, 20, 50 mg
Solution:5 mg/mL,5 mg/5mL
TABLE 48–2. DRUG TREATMENT OF CHRONIC ASTHMA—Continued
DRUG FORM
DOSAGECOMMENTSChild Adult
045_062PUL Page 390 Tuesday, November 8, 2005 10:54 AM
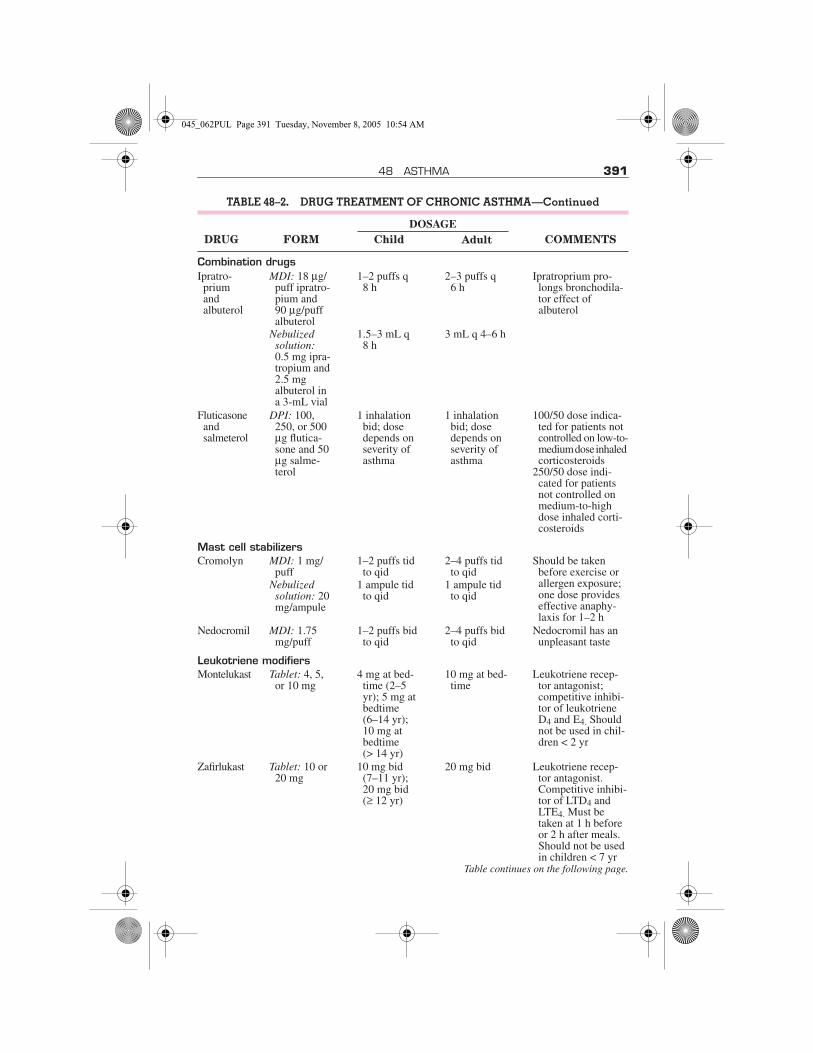
48 ASTHMA 391
Combination drugsIpratro-
prium and albuterol
MDI: 18 µg/puff ipratro-pium and90 µg/puff albuterol
1–2 puffs q8 h
2–3 puffs q6 h
Ipratroprium pro-longs bronchodila-tor effect of albuterol
Nebulized solution:0.5 mg ipra-tropium and 2.5 mg albuterol in a 3-mL vial
1.5–3 mL q8 h
3 mL q 4–6 h
Fluticasone and salmeterol
DPI: 100, 250, or 500 µg flutica-sone and 50 µg salme-terol
1 inhalation bid; dose depends on severity of asthma
1 inhalation bid; dose depends on severity of asthma
100/50 dose indica-ted for patients not controlled on low-to-medium dose inhaled corticosteroids
250/50 dose indi-cated for patients not controlled on medium-to-high dose inhaled corti-costeroids
Mast cell stabilizersCromolyn MDI: 1 mg/
puff Nebulized
solution: 20 mg/ampule
1–2 puffs tid to qid
1 ampule tid to qid
2–4 puffs tid to qid
1 ampule tid to qid
Should be taken before exercise or allergen exposure; one dose provides effective anaphy-laxis for 1–2 h
Nedocromil MDI: 1.75 mg/puff
1–2 puffs bid to qid
2–4 puffs bid to qid
Nedocromil has an unpleasant taste
Leukotriene modifiersMontelukast Tablet: 4, 5,
or 10 mg4 mg at bed-
time (2–5 yr); 5 mg at bedtime (6–14 yr);10 mg at bedtime(> 14 yr)
10 mg at bed-time
Leukotriene recep-tor antagonist; competitive inhibi-tor of leukotriene D4 and E4. Should not be used in chil-dren < 2 yr
Zafirlukast Tablet: 10 or 20 mg
10 mg bid(7–11 yr);20 mg bid (≥ 12 yr)
20 mg bid Leukotriene recep-tor antagonist. Competitive inhibi-tor of LTD4 and LTE4. Must be taken at 1 h before or 2 h after meals. Should not be used in children < 7 yr
Table continues on the following page.
TABLE 48–2. DRUG TREATMENT OF CHRONIC ASTHMA—Continued
DRUG FORM
DOSAGECOMMENTSChild Adult
045_062PUL Page 391 Tuesday, November 8, 2005 10:54 AM

392 SECTION 5 PULMONARY DISORDERS
Mast cell stabilizers inhibit histamine re-lease from mast cells, reduce airway hyper-responsiveness, and block the early and lateresponses to allergens. They are given by in-halation prophylactically to patients with ex-ercise- and allergen-induced asthma; they areineffective once symptoms have occurred.They are the safest of all antiasthmatic drugsbut the least effective.
Leukotriene modifiers are taken orallyand can be used for long-term control and pre-vention of symptoms in patients with mild
persistent to severe persistent asthma. Themain adverse effect is liver enzyme elevation;extremely rarely, patients develop a clinical syn-drome resembling Churg-Strauss syndrome.
Methylxanthines relax bronchial smoothmuscle (probably by nonselectively inhibitingphosphodiesterase) and may improve myocar-dial and diaphragmatic contractility throughunknown mechanisms. Methylxanthines ap-pear to inhibit intracellular release of Ca, de-crease microvascular leakage into the airwaymucosa, and inhibit the late response to aller-
Zileuton Tablet: 300 or 600 mg
600 mg qid(> 12 yr)
600 mg qid 5-Lipoxygenase inhibitor. Dosing may limit adher-ence. May cause liver enzyme eleva-tions and inhibit metabolism of drugs processed by CYP3A4, including theophylline. Should not be used in children < 12 yr
MethylxanthinesTheophyl-
lineTablet: 100,
200, 300, 400, or600 mg
Initial dose 10 mg/kg/day up to 300 mg, then adjust dose to achieve serum con-centration of 5–15 µg/mL at steady state
Maximum usually 800 mg/day
Initial dose 10 mg/kg/day, then adjust dose to achieve serum con-centration of 5–15 µg/mL at steady state
Maximum(< 1 yr): 0.2 (age in wk) + 5 = mg/kg/day
Maximum (≥ 1 yr): 16 mg/kg/day
Wide interpatient variability in meta-bolic clearance, drug interactions, potential for adverse effects mandate routine serum level moni-toring. Availability of safer alterna-tives has led to declining use of this drug
MDI = metered dose inhaler; DPI = dry-powder inhaler; CFC = chlorofluorocarbon; HFA =hydrofluroalkane; PEF = peak expiratory flow.
Adapted from NAEPP Expert Panel Report, Guidelines for the Diagnosis and Management ofAsthma.
TABLE 48–2. DRUG TREATMENT OF CHRONIC ASTHMA—Continued
DRUG FORM
DOSAGECOMMENTSChild Adult
045_062PUL Page 392 Tuesday, November 8, 2005 10:54 AM

48 ASTHMA 393
gens. They decrease the infiltration of eosino-phils into bronchial mucosa and of T lympho-cytes into epithelium. Methylxanthines areused for long-term control as an adjunct to β-agonists; extended-release theophylline helpsmanage nocturnal asthma. The drug is fallinginto disuse because of its many adverse effectsand interactions compared with other drugs.Adverse effects include headache, vomiting,cardiac arrhythmias, and seizures. Methylxan-thines have a narrow therapeutic index; multi-ple drugs (any metabolized by the cytochromeP450 pathway, eg, macrolide antibiotics) andconditions (eg, fever, liver disease, heart fail-ure) alter methylxanthine metabolism andelimination. Serum theophylline levels shouldbe monitored periodically and maintained be-tween 5 and 15 µg/mL (28 and 83 µmol/L).
Other drugs are used uncommonly in spe-cific circumstances. Immunotherapy may beindicated when symptoms are triggered by al-lergy, as suggested by history and confirmedby allergy testing. Immunotherapy is moresuccessful in children than adults. If symp-toms are not significantly relieved by 24 mo,then therapy is stopped. If symptoms are re-lieved, therapy should continue for ≥ 3 yr, al-though the optimum duration is unknown.Corticosteroid-sparing drugs are occasionallyprescribed to reduce dependence on high-doseoral corticosteroids. All carry significant tox-icities. Low-dose methotrexate (5 to 15 mg/wk) can lead to modest improvements in FEV1and modest decreases (3.3 mg/day) in dailyoral corticosteroid use. Gold and cyclosporineare also modestly effective, but toxicity andneed for monitoring limit their use. Omali-zumab is an anti-IgE antibody developed foruse in severely allergic asthmatic patients withelevated IgE levels. It decreases oral cortico-steroid requirements and relieves symptoms.Dose is determined by a dosing chart based onthe patient’s weight and IgE levels; the drug isadministered sc every 2 wk. Other therapiesfor management of chronic asthma includenebulized lidocaine, nebulized heparin, col-chicine, and high-dose IV immune globulin.Limited evidence supports the use of thesetherapies, and their benefits are unproven, sonone can yet be recommended for clinical use.
Monitoring response to treatment: Peakexpiratory flow (PEF) testing, a measure ofairflow and airway obstruction, helps estab-lish the severity of an asthma exacerbation bydocumenting response to treatments andmonitoring trends in disease severity in real-world settings through patient-kept diaries.
Home PEF monitoring is especially usefulfor charting disease progression and re-sponses to treatment in patients with moder-ate to severe persistent asthma. When asthmais quiescent, one PEF measurement in themorning suffices. If the patient’s PEF falls be-low 80% of his personal best, then twice-a-day monitoring to assess circadian variationis useful. Circadian variation of > 20% indi-cates airway instability and the need to re-evaluate the therapeutic regimen.
Patient education: The importance ofpatient education cannot be overemphasized.Patients do better the more they know aboutasthma—what triggers an attack, what drugto use when, proper inhaler technique, how touse a spacer with a metered-dose inhaler(MDI), and the importance of early use of cor-ticosteroids in exacerbations. Every patientshould have a written action plan for day-to-day management, especially for manage-ment of acute attacks, that is based on the pa-tient’s best personal peak flow rather than onpredicted normal value. Such a plan leads tomuch better asthma control, largely attribut-able to improved adherence to therapies.
Treatment of acute exacerbation: Thegoal of asthma exacerbation treatment is torelieve symptoms and return patients to theirpersonal best PEF. Patients should be in-structed to self-administer inhaled albuterolor a similar short-acting β-agonist for anacute exacerbation and measure PEF if pos-sible. Patients who feel better after 2 to 4 puffsfrom an MDI administered up to 3 times upto 20 min apart and who have a PEF > 80%of baseline can manage the acute exacerba-tion at home. Patients who do not respond,have severe symptoms, or have a PEF < 80%should follow a treatment management pro-gram outlined by the physician or should goto the emergency department for drug inter-vention (see TABLE 48–3 for specific dosinginformation).
Inhaled bronchodilators (β-agonists andanticholinergics) are the mainstay of asthmatreatment in the emergency department. Inadults and older children, albuterol given byan MDI and spacer is as effective as that givenby nebulizer. Nebulized treatment is pre-ferred for younger children because of diffi-culties coordinating MDIs and spacers; re-cent evidence suggests that bronchodilatorresponse improves when the nebulizer ispowered with helium-O2 (heliox) rather thanwith O2. Subcutaneous epinephrine 1:1000solution or terbutaline is an alternative for
045_062PUL Page 393 Tuesday, November 8, 2005 10:54 AM
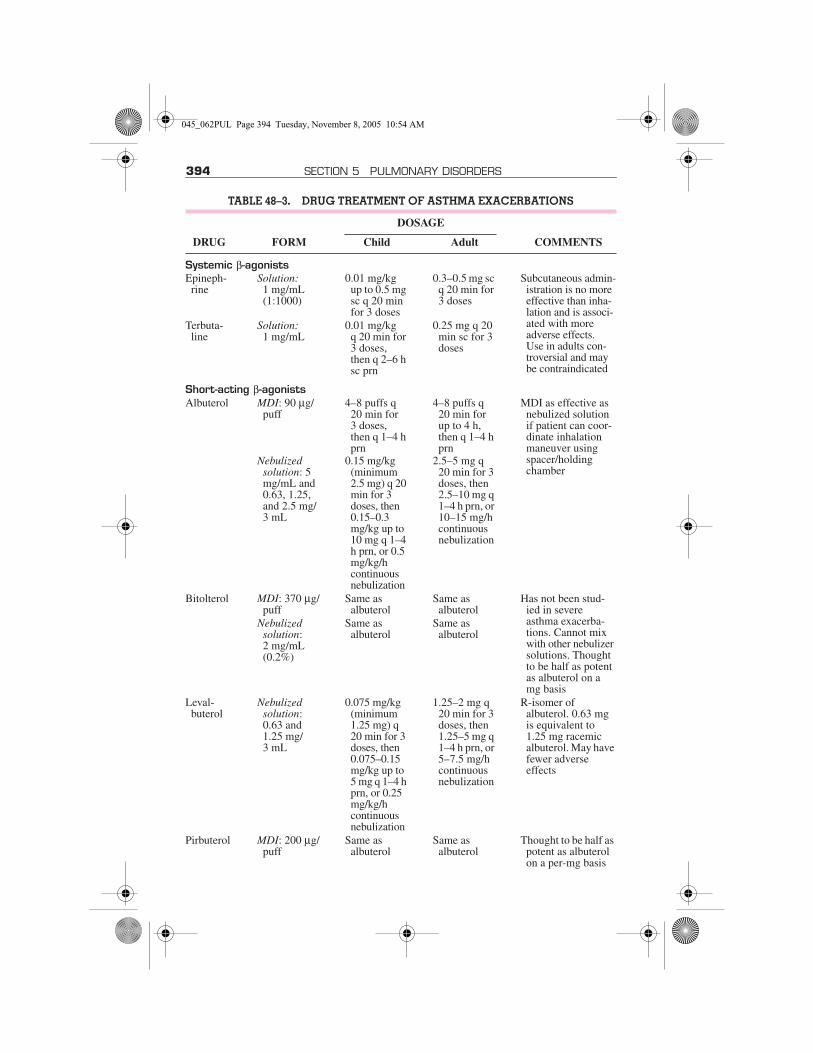
394 SECTION 5 PULMONARY DISORDERS
TABLE 48–3. DRUG TREATMENT OF ASTHMA EXACERBATIONS
DRUG FORM
DOSAGE
COMMENTSChild Adult
Systemic β-agonistsEpineph-
rineSolution:
1 mg/mL (1:1000)
0.01 mg/kg up to 0.5 mg sc q 20 min for 3 doses
0.3–0.5 mg sc q 20 min for 3 doses
Subcutaneous admin-istration is no more effective than inha-lation and is associ-ated with more adverse effects.Use in adults con-troversial and may be contraindicated
Terbuta-line
Solution:1 mg/mL
0.01 mg/kgq 20 min for 3 doses, then q 2–6 h sc prn
0.25 mg q 20 min sc for 3 doses
Short-acting β-agonistsAlbuterol MDI: 90 µg/
puff
Nebulized solution: 5 mg/mL and 0.63, 1.25, and 2.5 mg/3 mL
4–8 puffs q 20 min for3 doses, then q 1–4 h prn
0.15 mg/kg (minimum 2.5 mg) q 20 min for 3 doses, then 0.15–0.3 mg/kg up to 10 mg q 1–4 h prn, or 0.5 mg/kg/h continuous nebulization
4–8 puffs q 20 min for up to 4 h, then q 1–4 h prn
2.5–5 mg q 20 min for 3 doses, then 2.5–10 mg q 1–4 h prn, or 10–15 mg/h continuous nebulization
MDI as effective as nebulized solution if patient can coor-dinate inhalation maneuver using spacer/holding chamber
Bitolterol MDI: 370 µg/puff
Nebulized solution:2 mg/mL (0.2%)
Same as albuterol
Same as albuterol
Same as albuterol
Same as albuterol
Has not been stud-ied in severe asthma exacerba-tions. Cannot mix with other nebulizer solutions. Thought to be half as potent as albuterol on a mg basis
Leval-buterol
Nebulized solution: 0.63 and 1.25 mg/3 mL
0.075 mg/kg (minimum 1.25 mg) q 20 min for 3 doses, then 0.075–0.15 mg/kg up to 5 mg q 1–4 h prn, or 0.25 mg/kg/h continuous nebulization
1.25–2 mg q 20 min for 3 doses, then 1.25–5 mg q 1–4 h prn, or 5–7.5 mg/h continuous nebulization
R-isomer of albuterol. 0.63 mg is equivalent to1.25 mg racemic albuterol. May have fewer adverse effects
Pirbuterol MDI: 200 µg/puff
Same as albuterol
Same as albuterol
Thought to be half as potent as albuterol on a per-mg basis
045_062PUL Page 394 Tuesday, November 8, 2005 10:54 AM

48 ASTHMA 395
AnticholinergicsIpratro-
priumMDI: 18 µg/
puff 4–8 puffs prn 4–8 puffs prn Should be added to
β-agonists and not used as first-line therapy. May be mixed in same neb-ulizer as albuterol. Dose delivered from MDI is low and has not been studied in exacerbations
Nebulized solution: 0.25 mg/mL (0.025%)
0.25 mg q 20 min for 3 doses, then q 2–4 h prn
0.5 mg q 30 min for 3 doses, then q 2–4 h prn
Combination drugsIpratro-
prium and albuterol
MDI: 18 µg/puff ipratro-prium and90 µg/puff albuterol
4–8 puffs prn 4–8 puffs prn Ipratroprium pro-longs bronchodila-tor effect of albuterol
Nebulized solution:0.5 mg ipra-troprium and 2.5 mg albuterol in a 3 mL vial
1.5 mL q 20 min for 3 doses, thenq 2–4 h
3 mL q 30 m for 3 doses, then q 2–4 h prn
Systemic corticosteroidsMethyl-
pred-nisolone
Predniso-lone
Tablets: 2, 4, 8, 32 mg
Tablets: 5 mg Solution: 5 or
15 mg/5 mLTablets: 1,
2.5, 5, 10, 20, 50 mg
Solution: 5 mg/mL, 5 mg/5mL
Inpatient:1 mg/kg q 6 h for 48 h, then 0.5–1.0 mg/kg bid (maxi-mum, 60 mg/day) until PEF = 70% of pre-dicted or personal best
Outpatient burst: 0.5–1.0 mg/kg bid, maxi-mum 60 mg/day for 3–10 days
Inpatient:40–60 mg q 6 h or q 8 h for 48 h, then 60–80 mg/day until PEF reaches 70% of pre-dicted or personal best
Outpatient burst: 40 to 60 mg in single or 2 divided doses for 3–10 days
No advantage to IV over oral administra-tion if GI function is normal. No advan-tage to higher doses in severe exacerba-tions. Usual regi-men is to continue frequent multiple daily dose until the patient achieves an FEV1 or PEF of 50% of predicted or personal best and then lower the dose to bid, usually within 48 h. Therapy following a hospital-ization or ED visit may last 3–10 days. No need to taper does if patients are also given inhaled corticosteroids
Predni-sone
MDI = metered dose inhaler; PEF = peak expiratory flow; ED = emergency department.Adapted from NAEPP Expert Panel Report, Guidelines for the Diagnosis and Management of Asthma.
TABLE 48–3. DRUG TREATMENT OF ASTHMA EXACERBATIONS—Continued
DRUG FORM
DOSAGE
COMMENTSChild Adult
045_062PUL Page 395 Tuesday, November 8, 2005 10:54 AM

396 SECTION 5 PULMONARY DISORDERS
children. Terbutaline may be preferable toepinephrine because of its lesser cardiovas-cular effect and longer duration of action, butit is no longer produced in large quantities andis expensive. Subcutaneous administrationof β-agonists is theoretically problematic foradults because of adverse cardiostimulatoryeffects. However, clinically demonstrable illeffects are few, and subcutaneous adminis-tration may benefit patients unresponsive tomaximal inhaled therapy or those unable toreceive effective nebulized treatment (eg,those who cough excessively, have poor ven-tilation, or are uncooperative). Nebulizedipratropium can be co-administered withnebulized albuterol for patients who do notrespond optimally to albuterol alone; someevidence favors simultaneous high-doseβ-agonist and ipratropium as first-line treat-ment, but no data favor continuous β-agonistnebulization over intermittent administra-tion. Theophylline has very little role in treat-ment.
Systemic corticosteroids (prednisone,prednisolone, methylprednisolone) shouldbe given for all but the mildest acute exacer-bation; they are unnecessary for patientswhose PEF normalizes after 1 or 2 broncho-dilator doses. IV and oral routes of adminis-tration are equally effective. IV methylpred-nisolone can be given if an IV line is alreadyin place and can be switched to oral dosingwhenever necessary or convenient. Taperingusually starts after 7 to 10 days and should last2 to 3 wk.
Antibiotics are indicated only when his-tory, examination, or chest x-ray suggestsunderlying bacterial infection; most infec-tions underlying asthma exacerbations areviral in origin, but mycoplasma and chlamy-dia have been demonstrated in recent studypopulations.
O2 is indicated when patients with asthmaexacerbation have an O2sat < 90% as mea-sured by pulse oximetry or ABG measure-ments; O2 should be given by nasal cannulaor face mask at a flow rate or concentrationsufficient to correct hypoxemia.
Reassurance is the best approach whenanxiety is the cause of asthma exacerbation.Anxiolytics and morphine are relatively con-traindicated because they are associated withincreased mortality and the need for mechan-ical ventilation.
Hospitalization generally is required if pa-tients have not returned to their baselinewithin 4 h. Criteria for hospitalization vary,
but definite indications are failure to improve,worsening fatigue, relapse after repeatedβ-agonist therapy, and significant decrease inPaO2 (< 50 mm Hg) or increase in PaCO2(> 40 mm Hg), indicating progression to res-piratory failure.
Patients who continue to deteriorate de-spite aggressive treatment are candidates fornoninvasive positive pressure ventilation or,for severely affected patients and those fail-ing to respond, endotracheal intubation andmechanical ventilation (see p. 544). Patientsrequiring intubation may benefit from seda-tion, but paralytics should be avoided be-cause of possible interactions with cortico-steroids that can cause prolonged neuromus-cular weakness.
Generally, volume-cycled ventilation inassist-control mode is used because it pro-vides constant alveolar ventilation whenairway resistance is high and changing. Theventilator should be set to a rate of 8 to 14breaths/min with a rapid inspiratory flowrate (> 60 to 80 L/min) to prolong exhala-tion and to minimize auto-PEEP (positiveend-expiratory pressure).
Initial tidal volumes can be set to 10 to12 mL/kg. High peak airway pressures cangenerally be ignored, because they resultfrom high airway resistance and inspiratoryflow rates and do not reflect the degree of lungdistention produced by alveolar pressure.However, if plateau pressures exceed 30 to 35cm H2O, then tidal volume should be reducedto between 5 and 7 mL/kg to limit the risk ofpneumothorax. An exception is when de-creased compliance of the chest wall (eg, obe-sity) or abdomen (eg, ascites) may substan-tially contribute to the elevated pressures.When reduced tidal volumes are necessary, amoderate degree of hypercapnia is accept-able, but if arterial pH falls below 7.10, a slowsodium bicarbonate infusion is indicated tomaintain pH between 7.20 and 7.25. Onceairflow obstruction is relieved and PaCO2 andarterial pH normalize, patients can usually bequickly weaned from the ventilator.
Other therapies are reported effective forasthma exacerbation, but none have beenthoroughly studied. Heliox is used to de-crease the work of breathing and improveventilation through a decrease in turbulentflow attributable to helium, a gas less densethan O2. Despite the theoretical benefits ofheliox, studies have reported conflicting re-sults concerning its efficacy; lack of readyavailability also limits its use. Magnesium
045_062PUL Page 396 Tuesday, November 8, 2005 10:54 AM
48 ASTHMA 397
sulfate relaxes smooth muscle, but efficacy inmanagement of asthma exacerbation in theemergency department is controversial. Gen-eral anesthesia in patients with status asth-maticus causes bronchodilation by an un-clear mechanism, perhaps by a direct relaxanteffect on airway smooth muscle or attenua-tion of cholinergic tone.
Treatment of chronic asthma: Appro-priate drug use keeps most chronic asthmat-ics out of the emergency department and hos-pital. Many drugs are available, and selectionand sequence of drugs are based on asthmaseverity (see TABLE 48–2). “Step-down”therapy—a reduction in drug dose to the min-imal amount needed for control of symp-toms—is indicated for all asthma severities.
Patients with mild intermittent asthma donot need drugs daily. A short-acting β-ago-nist (eg, 2 inhalations of albuterol as a rescuedrug) is sufficient for acute symptoms; usefor more than 2 times/wk, use of ≥ 2 canistersa year, or decreasing response to the drugmay indicate the need for long-term controltherapy. Regardless of the severity of theasthma, the frequent need for a rescue β-agonist indicates that the asthma is not well-controlled.
Patients with mild persistent asthma(adults and children) should receive anti-inflammatory therapy. Low-dose inhaledcorticosteroids are the treatment of choice,but some patients may be controlled withmast cell stabilizers, leukotriene modifiers,or extended-release theophylline. A short-acting rescue β-agonist (eg, albuterol, 2 to 4puffs) is indicated as rescue therapy forbreakthrough symptoms. Patients who re-quire rescue therapy daily require medium-dose inhaled corticosteroids or combinationtherapy (see below).
Patients with moderate persistent asthmashould be treated with inhaled corticoste-roids in a dose adjusted to response combinedwith a long-acting inhaled β-agonist (salme-terol, 2 puffs bid). A long-acting inhaled β-agonist alone is insufficient treatment but incombined therapy allows for a lower inhaledcorticosteroid dosage and is more effectivefor nocturnal symptoms. Alternatives to thisapproach include inhaled corticosteroidsalone in medium dose range or substitution ofleukotriene receptor antagonists or ex-tended-release theophylline for long-actingβ-agonists in combination with low-to-me-dium-dose inhaled corticosteroids. In pa-tients with GERD and moderate persistent
asthma, anti-reflux treatment may reduce thefrequency and dose of drugs needed forsymptom control. In patients with allergicrhinitis and moderate persistent asthma, na-sal corticosteroids may reduce the frequencyof asthma exacerbations requiring emer-gency department visits.
Patients with severe persistent asthma are aminority who require several drugs in highdoses. Options include a combination high-dose inhaled corticosteroid combined withlong-acting β-agonist (salmeterol) or a com-bination of an inhaled corticosteroid, long-act-ing β-agonist, and leukotriene modifier. Short-acting inhaled β-agonists are indicated in bothcases for rescue of breakthrough symptoms.Systemic corticosteroids are indicated for pa-tients inadequately managed on these regi-mens; alternate-day dosing helps minimizeadverse effects associated with a daily dosing.
Exercise-induced asthma: Exercise-induced asthma can generally be preventedby inhalation of a short-acting β-agonist ormast cell stabilizers before starting the exer-cise. If β-agonists are not effective or if exer-cise-induced asthma is frequent or severe, inmost cases the patient has more severeasthma than is recognized and requires long-term therapy aimed at control.
Aspirin-sensitive asthma: The primarytreatment for aspirin-sensitive asthma isavoidance of NSAIDs. Cyclooxygenase-2(COX-2) inhibitors do not appear to be trig-gers. Leukotriene modifiers can blunt the re-sponse to NSAIDs. Alternatively, inpatientdesensitization has been successful in smallseries of patients.
Future therapies: Multiple therapies arebeing developed to target specific compo-nents of the inflammatory cascade. Therapiesdirected at IL-4 and IL-13 are under investi-gation.
Special PopulationsInfants, children, and adolescents:
Asthma is difficult to diagnose in infants,thus underrecognition and undertreatmentare common. Empiric trials of inhaledbronchodilators and anti-inflammatorydrugs may be helpful for both. Drugs may begiven by nebulizer or MDI with a holdingchamber with or without a face mask. In-fants and children < 5 yr requiring treatmentmore than 2 times/wk should be given dailyanti-inflammatory therapy with inhaled corti-costeroids (preferred), leukotriene receptorantagonists, or cromolyn.
045_062PUL Page 397 Tuesday, November 8, 2005 10:54 AM

398 SECTION 5 PULMONARY DISORDERS
Children > 5 yr and adolescents withasthma can be treated similar to adults butshould be encouraged to maintain physicalactivities, exercise, and sports. Predictednorms for pulmonary function tests in ado-lescents are closer to childhood (not adult)standards. Adolescents and mature youngerchildren should participate in developingtheir own asthma management plans and es-tablishing their own goals for therapy to im-prove compliance. The action plan should beunderstood by teachers and school nurses toensure reliable and prompt access to rescuedrugs. Cromolyn and nedocromil are oftentried in this group but are not as beneficial asinhaled corticosteroids; long-acting drugsprevent the embarrassment of having to takedrugs at school.
Pregnant women: About 1⁄3 of femaleasthmatics who become pregnant noticerelief of symptoms; 1⁄3 notice worsening (attimes to a severe degree); and 1⁄3 notice nochange. GERD may be an important con-tributor to symptomatic disease in preg-nancy. Asthma control during pregnancy iscrucial (see p. 2168), because poorly con-trolled maternal disease can result in in-creased prenatal mortality, premature de-livery, and low birth weight. Asthma drugshave not been shown to have adverse fetaleffects, but no large well-controlled studieshave been conducted to truly documentsafety for the developing fetus.
ALLERGIC BRONCHOPULMONARY
ASPERGILLOSISAllergic bronchopulmonary aspergillosis is ahypersensitivity reaction to Aspergillusfumigatus that occurs almost exclusively inpatients with asthma or, less commonly, cysticfibrosis. Immune responses to Aspergillusantigens cause airway obstruction and, ifuntreated, bronchiectasis and pulmonaryfibrosis. Symptoms and signs are those ofasthma with the addition of productive coughand, occasionally, fever and anorexia. Diag-nosis is suspected based on history and imag-ing tests and confirmed by Aspergillus skintesting and measurement of IgE levels, circu-lating precipitins, and A. fumigatus–specificantibodies. Treatment is with corticoste-roids and, in patients with refractory disease,itraconazole.
Etiology and PathophysiologyAllergic bronchopulmonary aspergillosis
(ABPA) develops when airways of patientswith asthma or cystic fibrosis become colo-nized with Aspergillus fumigatus (a ubiqui-tous fungus in the soil). For unclear reasons,colonization in these patients prompts vigor-ous antibody (IgE and IgG) and cell-medi-ated immune responses (type I, III, and IVhypersensitivity reactions) to Aspergillus an-tigens, leading to frequent, recurrent asthmaexacerbations. Over time, the immune reac-tions, combined with direct toxic effects ofthe fungus, lead to airway damage with dila-tation and, ultimately, bronchiectasis and fi-brosis. The disease is characterized histolog-ically by mucoid impaction of airways, eosin-ophilic pneumonia, infiltration of alveolarsepta with plasma and mononuclear cells,and an increase in the number of bronchiolarmucous glands and goblet cells. Rarely, otherfungi, such as Penicillium, Candida, Curvu-laria, Helminthosporium, and/or Drechsleraspp, cause an identical syndrome called aller-gic bronchopulmonary mycosis in the ab-sence of underlying asthma or cystic fibrosis.
Aspergillus is present intraluminally but isnot invasive. Thus, allergic bronchopulmo-nary aspergillosis must be distinguishedfrom invasive aspergillosis, which occurs ex-clusively in immunocompromised patients;from aspergillomas, which are collections ofAspergillus in patients with established cav-itary lesions or cystic airspaces; and from therare Aspergillus pneumonia, which occurs inpatients who take low doses of prednisonelong term (eg, those with COPD).
Symptoms and SignsSymptoms are those of asthma or pulmo-
nary cystic fibrosis exacerbation, with the ad-dition of cough productive of dirty-green orbrown plugs and, occasionally, hemoptysis.Fever, headache, and anorexia are commonsystemic symptoms in severe disease. Signsare those of airway obstruction, specifically,wheezing and prolonged expiration, which areindistinguishable from asthma exacerbation.
DiagnosisThe diagnosis is suspected in asthmatic pa-
tients with any combination of recurrentasthma exacerbations, migratory or nonre-solving infiltrates on chest x-ray (often due toatelectasis from mucoid plugging and bron-chial obstruction), evidence of bronchiecta-
045_062PUL Page 398 Tuesday, November 8, 2005 10:54 AM
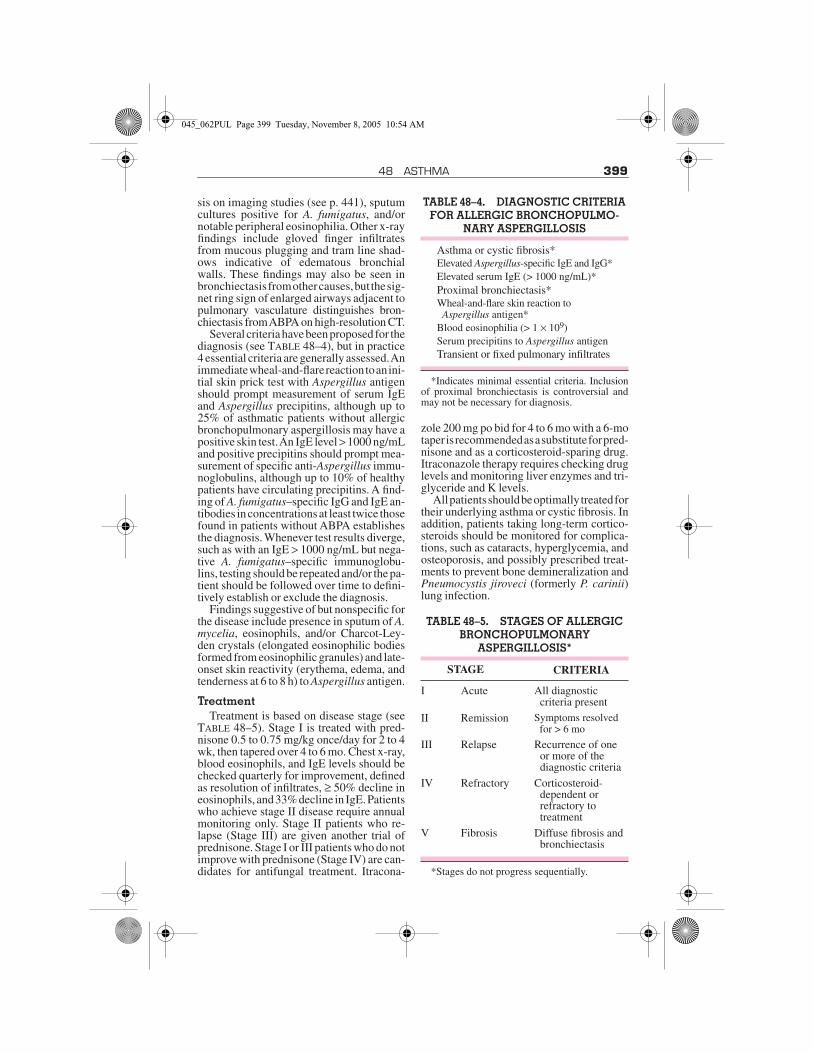
48 ASTHMA 399
sis on imaging studies (see p. 441), sputumcultures positive for A. fumigatus, and/ornotable peripheral eosinophilia. Other x-rayfindings include gloved finger infiltratesfrom mucous plugging and tram line shad-ows indicative of edematous bronchialwalls. These findings may also be seen inbronchiectasis from other causes, but the sig-net ring sign of enlarged airways adjacent topulmonary vasculature distinguishes bron-chiectasis from ABPA on high-resolution CT.
Several criteria have been proposed for thediagnosis (see TABLE 48–4), but in practice4 essential criteria are generally assessed. Animmediate wheal-and-flare reaction to an ini-tial skin prick test with Aspergillus antigenshould prompt measurement of serum IgEand Aspergillus precipitins, although up to25% of asthmatic patients without allergicbronchopulmonary aspergillosis may have apositive skin test. An IgE level > 1000 ng/mLand positive precipitins should prompt mea-surement of specific anti-Aspergillus immu-noglobulins, although up to 10% of healthypatients have circulating precipitins. A find-ing of A. fumigatus–specific IgG and IgE an-tibodies in concentrations at least twice thosefound in patients without ABPA establishesthe diagnosis. Whenever test results diverge,such as with an IgE > 1000 ng/mL but nega-tive A. fumigatus–specific immunoglobu-lins, testing should be repeated and/or the pa-tient should be followed over time to defini-tively establish or exclude the diagnosis.
Findings suggestive of but nonspecific forthe disease include presence in sputum of A.mycelia, eosinophils, and/or Charcot-Ley-den crystals (elongated eosinophilic bodiesformed from eosinophilic granules) and late-onset skin reactivity (erythema, edema, andtenderness at 6 to 8 h) to Aspergillus antigen.
TreatmentTreatment is based on disease stage (see
TABLE 48–5). Stage I is treated with pred-nisone 0.5 to 0.75 mg/kg once/day for 2 to 4wk, then tapered over 4 to 6 mo. Chest x-ray,blood eosinophils, and IgE levels should bechecked quarterly for improvement, definedas resolution of infiltrates, ≥ 50% decline ineosinophils, and 33% decline in IgE. Patientswho achieve stage II disease require annualmonitoring only. Stage II patients who re-lapse (Stage III) are given another trial ofprednisone. Stage I or III patients who do notimprove with prednisone (Stage IV) are can-didates for antifungal treatment. Itracona-
zole 200 mg po bid for 4 to 6 mo with a 6-motaper is recommended as a substitute for pred-nisone and as a corticosteroid-sparing drug.Itraconazole therapy requires checking druglevels and monitoring liver enzymes and tri-glyceride and K levels.
All patients should be optimally treated fortheir underlying asthma or cystic fibrosis. Inaddition, patients taking long-term cortico-steroids should be monitored for complica-tions, such as cataracts, hyperglycemia, andosteoporosis, and possibly prescribed treat-ments to prevent bone demineralization andPneumocystis jiroveci (formerly P. carinii)lung infection.
TABLE 48–4. DIAGNOSTIC CRITERIA FOR ALLERGIC BRONCHOPULMO-
NARY ASPERGILLOSIS
Asthma or cystic fibrosis*Elevated Aspergillus-specific IgE and IgG*Elevated serum IgE (> 1000 ng/mL)*Proximal bronchiectasis*Wheal-and-flare skin reaction to Aspergillus antigen*
Blood eosinophilia (> 1 × 109)Serum precipitins to Aspergillus antigenTransient or fixed pulmonary infiltrates
*Indicates minimal essential criteria. Inclusionof proximal bronchiectasis is controversial andmay not be necessary for diagnosis.
TABLE 48–5. STAGES OF ALLERGIC BRONCHOPULMONARY
ASPERGILLOSIS*
STAGE CRITERIA
I Acute All diagnosticcriteria present
II Remission Symptoms resolved for > 6 mo
III Relapse Recurrence of one or more of the diagnostic criteria
IV Refractory Corticosteroid-dependent or refractory totreatment
V Fibrosis Diffuse fibrosis andbronchiectasis
*Stages do not progress sequentially.
045_062PUL Page 399 Tuesday, November 8, 2005 10:54 AM

400
49CHRONIC OBSTRUCTIVE PULMONARY DISEASE
Chronic obstructive pulmonary disease is par-tially reversible airflow obstruction causedby an abnormal inflammatory response totoxins, often cigarette smoke. α1-Antitrypsindeficiency and a variety of occupational expo-sures are less common causes in nonsmokers.Symptoms are productive cough and dyspneathat develop over years; common signsinclude decreased breath sounds and wheez-ing. Severe cases may be complicated byweight loss, pneumothorax, right heart fail-ure, and respiratory failure. Diagnosis isbased on history, physical examination, chestx-ray, and pulmonary function tests. Treat-ment is with bronchodilators, corticosteroids,and, when necessary, O2. About 50% ofpatients die within 10 yr of initial diagnosis.
Chronic obstructive pulmonary disease(COPD) comprises chronic obstructive bron-chitis and emphysema. Many patients havefeatures of both.
Chronic obstructive bronchitis ischronic bronchitis with airflow obstruction.Chronic bronchitis (also called chronic mu-cous hypersecretion syndrome) is definedas productive cough for at least 3 mo in 2 suc-cessive years. Chronic bronchitis becomeschronic obstructive bronchitis if spirometricevidence of airflow obstruction develops.Chronic asthmatic bronchitis is a similar,overlapping condition characterized bychronic productive cough, wheezing, andpartially reversible airflow obstruction insmokers with a history of asthma. In somecases, the distinction between chronic ob-structive bronchitis and asthmatic bronchitisis unclear.
Emphysema is destruction of lung paren-chyma leading to loss of elastic recoil and lossof alveolar septa and radial airway traction,which increases the tendency for airway col-lapse. Lung hyperinflation, airflow limita-tion, and air trapping follow. Airspaces en-large and may eventually develop bullae.
EpidemiologyIn 2000, an estimated 24 million people in
the US had COPD, of whom only 10 millionwere diagnosed. In the same year, COPD wasthe 4th leading cause of death, resulting in119,054 deaths—compared with 52,193deaths in 1980. From 1980 to 2000, the COPDmortality rate increased 64% (from 40.7 to66.9/100,000).
Prevalence, incidence, and mortality ratesincrease with age. Prevalence is higher inmales, but total mortality is similar in bothsexes. Incidence and mortality are generallyhigher in whites, blue-collar workers, andpeople with fewer years of formal education,probably because these groups have a higherprevalence of smoking. COPD seems to ag-gregate in families independent of α1-anti-trypsin (α1-antiprotease inhibitor) deficiency(see p. 410).
COPD is increasing worldwide because ofthe increase in smoking in nonindustrializedcountries, the reduction in mortality due toinfectious diseases, and the widespread useof biomass fuels. It caused an estimated2.74 million deaths worldwide in 2000 and isprojected to become 1 of the top 5 causes ofdisease burden globally by the year 2020.
Etiology and PathophysiologyCigarette smoking is the primary risk fac-
tor in most countries, although only about15% of smokers develop clinically apparentCOPD; an exposure history of 40 or morepack-years is especially predictive. Smokefrom burning biomass fuels for indoor cook-ing and heating is an important contributingfactor in underdeveloped countries. Smokerswith preexisting airway reactivity (definedby increased sensitivity to inhaled methacho-line), even in the absence of clinical asthma,are at greater risk of developing COPD thanare those without. Low body weight, child-hood respiratory diseases, passive cigarettesmoke exposure, air pollution, and occupa-tional dust (eg, mineral or cotton dust) orchemical (eg, cadmium) exposure contributeto the risk of COPD but are of minor impor-tance compared with cigarette smoking.
Genetic factors also contribute. The best-defined genetic disorder is α1-antitrypsin de-ficiency (see p. 410), which is a significantcause of emphysema in nonsmokers and in-fluences susceptibility to disease in smokers.Polymorphisms in microsomal epoxide
045_062PUL Page 400 Tuesday, November 8, 2005 10:54 AM

49 CHRONIC OBSTRUCTIVE PULMONARY DISEASE 401
hydrolase, vitamin D–binding protein, IL-1β,and IL-1 receptor antagonist genes are all as-sociated with rapid decline in forced expi-ratory volume in 1 sec (FEV1) in selectedpopulations.
In genetically susceptible people, inhala-tional exposures trigger an inflammatory re-sponse in airways and alveoli that leads to dis-ease. The process is thought to be mediatedby an increase in protease activity and a de-crease in antiprotease activity (see p. 410).Lung proteases, such as neutrophil elastase,matrix metalloproteinases, and cathepsins,break down elastin and connective tissue inthe normal process of tissue repair. Their ac-tivity is balanced by antiproteases, such asα1-antitrypsin, airway epithelium–derivedsecretory leukoproteinase inhibitor, elafin,and matrix metalloproteinase tissue inhibi-tor. In people with COPD, activated neutro-phils and other inflammatory cells releaseproteases as part of the inflammatory pro-cess; protease activity exceeds antiproteaseactivity, and tissue destruction and mucus hy-persecretion result. Neutrophil and macro-phage activation also leads to accumulationof free radicals, superoxide anions, and hy-drogen peroxide, which inhibit antiproteasesand cause bronchoconstriction, mucosaledema, and mucous hypersecretion. Neutro-phil-induced oxidative damage, release ofprofibrotic neuropeptides (eg, bombesin),and reduced levels of vascular endothelialgrowth factor may also play a role, as doesinfection.
Bacteria, especially Haemophilus influen-zae, colonize the normally sterile lower air-ways of about 30% of patients with activeCOPD. In more severely affected patients(eg, those with previous hospitalizations),Pseudomonas aeruginosa is common. Someexperts postulate that smoking and airflowobstruction lead to impaired mucus clearancein lower airways, which predisposes to infec-tion. The repeated bouts of infection lead toincreased inflammatory burden that hastensdisease progression. There is no evidence,however, that long-term use of antibioticsslows the progression of COPD in susceptiblesmokers.
The cardinal pathophysiologic feature ofCOPD is airflow limitation caused by emphy-sema and/or airflow obstruction caused bymucus hypersecretion, mucus plugging, and/or bronchospasm. Increased airway resis-tance increases the work of respiration, as
does lung hyperinflation. Increased work ofbreathing may lead to alveolar hypoventila-tion with hypoxia and hypercapnia, althoughhypoxia is also caused by ventilation/perfu-sion (V/Q) mismatch. Some patients with ad-vanced disease develop chronic hypoxemiaand hypercapnia. Chronic hypoxemia in-creases pulmonary vascular tone which, ifdiffuse, causes pulmonary hypertension andcor pulmonale. O2 administration may thenworsen hypercapnia in some patients by de-creasing hypoxic ventilatory drive, leading toalveolar hypoventilation.
Histologic changes include peribronchiolarinflammatory infiltrates, bronchial smoothmuscle hypertrophy, and airspace distortiondue to loss of alveolar attachments and alveolarseptal destruction. Enlarged alveolar spacessometimes consolidate into bullae, defined asairspaces ≥ 1 cm in diameter. Bullae may beentirely empty or have strands of lung tissuetraversing them in areas of locally severe em-physema; they occasionally occupy the en-tire hemithorax.
Symptoms and SignsCOPD takes years to develop and progress.
Productive cough usually is the initial sign inpatients in their 40s and 50s who have smoked≥ 20 cigarettes/day for > 20 yr. Dyspnea thatis progressive, persistent, exertional, orworse during respiratory infection eventu-ally appears by the time patients reach theirlate 50s. Symptoms usually progress quicklyin patients who continue to smoke and whohave higher lifetime tobacco exposure.Morning headache develops in more ad-vanced disease and signals nocturnal hyper-capnia or hypoxemia.
Acute exacerbations occur sporadicallyduring the course of COPD and are heraldedby increased symptom severity. The specificcause of any exacerbation is almost alwaysimpossible to determine, but exacerbationsare often attributed to viral URIs or acute bac-terial bronchitis. As COPD progresses, acuteexacerbations tend to become more frequent,averaging about 3 episodes/yr. Those whosuffer acute exacerbations are much morelikely to have recurrent exacerbations.
Signs include wheezing, lung hyperinfla-tion manifest as decreased heart and lungsounds, and increased anteroposterior diam-eter of the thorax (barrel chest). Patients withadvanced emphysema lose weight and expe-rience muscle wasting because of immobility;
045_062PUL Page 401 Tuesday, November 8, 2005 10:54 AM
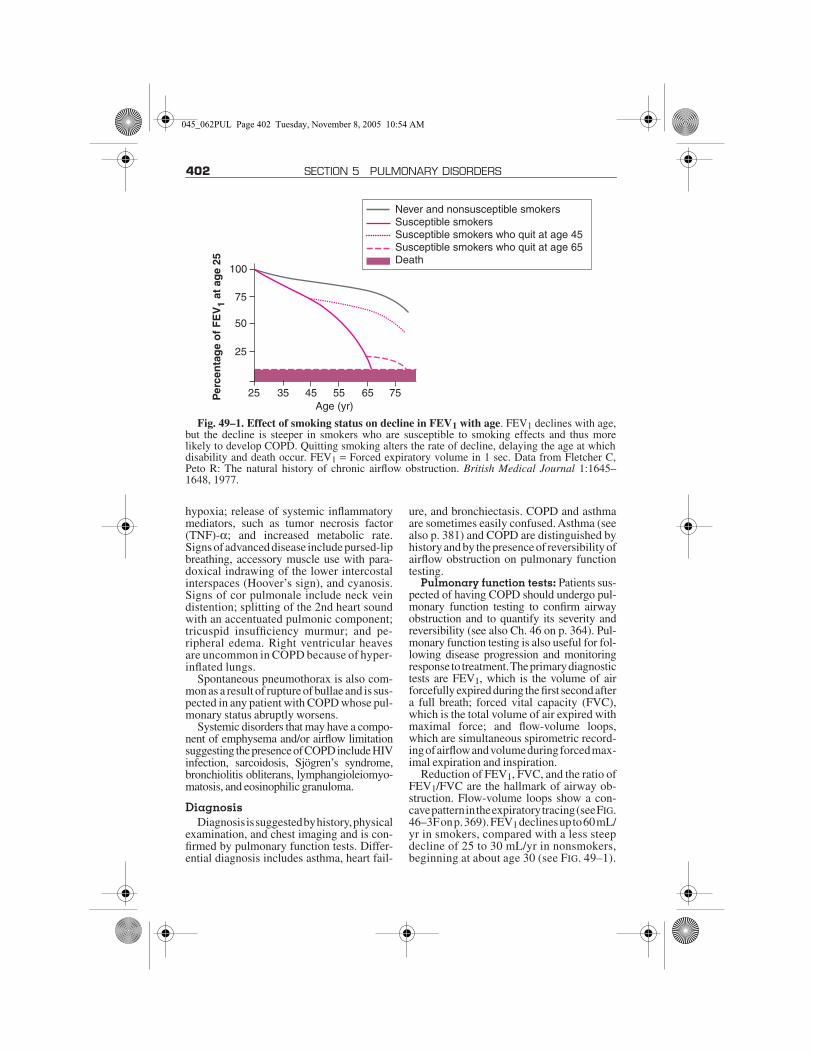
402 SECTION 5 PULMONARY DISORDERS
hypoxia; release of systemic inflammatorymediators, such as tumor necrosis factor(TNF)-α; and increased metabolic rate.Signs of advanced disease include pursed-lipbreathing, accessory muscle use with para-doxical indrawing of the lower intercostalinterspaces (Hoover’s sign), and cyanosis.Signs of cor pulmonale include neck veindistention; splitting of the 2nd heart soundwith an accentuated pulmonic component;tricuspid insufficiency murmur; and pe-ripheral edema. Right ventricular heavesare uncommon in COPD because of hyper-inflated lungs.
Spontaneous pneumothorax is also com-mon as a result of rupture of bullae and is sus-pected in any patient with COPD whose pul-monary status abruptly worsens.
Systemic disorders that may have a compo-nent of emphysema and/or airflow limitationsuggesting the presence of COPD include HIVinfection, sarcoidosis, Sjögren’s syndrome,bronchiolitis obliterans, lymphangioleiomyo-matosis, and eosinophilic granuloma.
DiagnosisDiagnosis is suggested by history, physical
examination, and chest imaging and is con-firmed by pulmonary function tests. Differ-ential diagnosis includes asthma, heart fail-
ure, and bronchiectasis. COPD and asthmaare sometimes easily confused. Asthma (seealso p. 381) and COPD are distinguished byhistory and by the presence of reversibility ofairflow obstruction on pulmonary functiontesting.
Pulmonary function tests: Patients sus-pected of having COPD should undergo pul-monary function testing to confirm airwayobstruction and to quantify its severity andreversibility (see also Ch. 46 on p. 364). Pul-monary function testing is also useful for fol-lowing disease progression and monitoringresponse to treatment. The primary diagnostictests are FEV1, which is the volume of airforcefully expired during the first second aftera full breath; forced vital capacity (FVC),which is the total volume of air expired withmaximal force; and flow-volume loops,which are simultaneous spirometric record-ing of airflow and volume during forced max-imal expiration and inspiration.
Reduction of FEV1, FVC, and the ratio ofFEV1/FVC are the hallmark of airway ob-struction. Flow-volume loops show a con-cave pattern in the expiratory tracing (see FIG.46–3F on p. 369). FEV1 declines up to 60 mL/yr in smokers, compared with a less steepdecline of 25 to 30 mL/yr in nonsmokers,beginning at about age 30 (see FIG. 49–1).
Fig. 49–1. Effect of smoking status on decline in FEV1 with age. FEV1 declines with age,but the decline is steeper in smokers who are susceptible to smoking effects and thus morelikely to develop COPD. Quitting smoking alters the rate of decline, delaying the age at whichdisability and death occur. FEV1 = Forced expiratory volume in 1 sec. Data from Fletcher C,Peto R: The natural history of chronic airflow obstruction. British Medical Journal 1:1645–1648, 1977.
100
75
50
25
25 35 45 55 65 75Age (yr)
Never and nonsusceptible smokersSusceptible smokersSusceptible smokers who quit at age 45Susceptible smokers who quit at age 65Death
Per
cen
tag
e o
f F
EV
1 at
ag
e 25
045_062PUL Page 402 Tuesday, November 8, 2005 10:54 AM

49 CHRONIC OBSTRUCTIVE PULMONARY DISEASE 403
In middle-aged smokers who already have alow FEV1, the decline occurs at a more rapidrate. When the FEV1 falls below about 1 L,patients develop dyspnea with activities ofdaily living; when the FEV1 falls below about0.8 L, they are at risk of hypoxemia, hyper-
capnia, and cor pulmonale. FEV1 and FVCare easily measured with office spirometryand define severity of disease (see TABLE 49–1)because they correlate with symptoms andmortality. Normal reference values are deter-mined by patient age, sex, and height.
TABLE 49–1. SEVERITY AND TREATMENT OF COPD
STAGE CHARACTERISTICSRECOMMENDED
TREATMENTADDITIONAL TREATMENT
All Avoidance of risk factors
Influenza vaccination
0: At risk Chronic symptoms (cough, sputum)
Exposure to risk factors Normal spirometry
I: Mild COPD
FEV1/FVC < 70% FEV1 ≥ 80% predicted
Short-acting bronchodi-lator when needed
With or without symp-toms
II: Moder-ate COPD
IIAFEV1/FVC < 70% 50% ≤ FEV1 < 80%
predicted
Regular treatment with one or more bronchodilators
RehabilitationWith or without symp-toms
IIBFEV1/FVC < 70% 30% ≤ FEV1 > 50%
predicted With or without symptoms
Regular treatment with one or more bronchodilators
Rehabilitation
Inhaled corticoste-roids for recur-rent exacerba-tions
III: Severe COPD
FEV1/FVC < 70% FEV1 < 30% predicted or presence of respiratory failure or right heart failure
Regular treatment with one or more bronchodilators
Inhaled corticosteroids for recurrent exacerbations
Treatment of complications
Rehabilitation Long-term oxygen ther-apy if respiratory failure
Consider surgical treatments
FEV1 = Forced expiratory volume in 1 sec; FVC = forced vital capacity.Modified from Pauwels RA, Buist AS, Calverley PM, Jenkins CR, Hurd SS. Global strategy for the
diagnosis, management, and prevention of chronic obstructive pulmonary disease. NHLBI/WHOGlobal Initiative for Chronic Obstructive Lung Disease (GOLD) Workshop summary. AmericanJournal of Respiratory and Critical Care Medicine 163:1256–1276, 2001.
045_062PUL Page 403 Tuesday, November 8, 2005 10:54 AM

404 SECTION 5 PULMONARY DISORDERS
Additional pulmonary function testing isnecessary only in specific circumstances,such as before lung volume reduction surgery(see p. 408). Other test abnormalities may in-clude an increased total lung capacity, func-tional residual capacity, and residual volume,which can help distinguish COPD from re-strictive pulmonary disease, in which thesemeasures are diminished; decreased vital ca-pacity; and decreased single-breath diffusingcapacity for carbon monoxide (DLCO). De-creased DLCO is nonspecific and is reduced inother disorders that affect the pulmonary vas-cular bed, such as interstitial lung disease, butcan help distinguish COPD from asthma, inwhich DLCO is normal or elevated.
Imaging tests: The chest x-ray has char-acteristic, though not diagnostic, findings.Changes with emphysema include lung hy-perinflation manifested as a flat diaphragm,narrow heart, rapid tapering of hilar vessels(anteroposterior view), and widening of theretrosternal airspace. The flattening of the di-aphragm due to hyperinflation causes an in-crease in the angle formed by the sternumand anterior diaphragm on a lateral film fromthe normal value of 45° to > 90°. Bullae—radiolucencies > 1 cm surrounded by arcuatehairline shadows—reflect locally severe dis-ease. Emphysematous changes predomi-nantly in the lung bases indicate α1-anti-trypsin deficiency (see p. 410). The lungs maylook normal or have increased lucency sec-ondary to loss of parenchyma. The chest x-raysof patients with chronic obstructive bron-chitis may be normal or may demonstratea bi-basilar increase in bronchovascularmarkings.
Prominent hila may suggest large centralpulmonary arteries seen with pulmonary hy-pertension. Right ventricular enlargementseen in cor pulmonale may be masked by lunghyperinflation or may manifest as encroach-ment of the heart shadow on the retrosternalspace or by widening of the transverse car-diac shadow in comparison with previouschest x-rays.
CT scans may clarify abnormalities seenon chest x-ray suggestive of coexisting orcomplicating diseases, such as pneumonia,pneumoconiosis, or lung cancer. CT helpsassess the extent and distribution of emphy-sema, estimated either by visual scoring orwith analysis of the distribution of lung den-sity. These parameters may be useful inpreparation for lung volume reductionsurgery.
Adjunctive tests: α1-Antitrypsin levelsshould be measured in patients < 50 yr withsymptomatic COPD and in nonsmokers ofany age with COPD to detect α1-antitrypsindeficiency (see p. 410). Other indications ofα1-antitrypsin deficiency include a familyhistory of premature COPD or infantile liverdisease, lower-lobe distribution of emphy-sema, and COPD associated with antineutro-phil cytoplasmic antibody (ANCA)-positivevasculitis. Low levels of α1-antitrypsinshould be confirmed by phenotyping.
The ECG, often performed to exclude car-diac causes of dyspnea, typically demon-strates diffusely low QRS voltage with a ver-tical heart axis caused by lung hyperinflationand increased P-wave voltage or rightwardshifts of the P-wave vector caused by rightatrial enlargement in patients with ad-vanced emphysema. Findings of right ven-tricular hypertrophy include an R or R′ waveas tall as or taller than the S wave in lead V1;an R wave smaller than the S wave in lead V6;and/or right-axis deviation > 110° withoutright bundle branch block. Multifocal atrialtachycardia, an arrhythmia that can accom-pany COPD, manifests as a tachyarrhythmiawith polymorphic P waves and variable PRintervals.
Echocardiography is occasionally usefulfor assessing right ventricular function andpulmonary hypertension, although it istechnically difficult in COPD patients. It ismost often indicated when coexistent leftventricular or valvular heart disease is sus-pected.
CBC is of little diagnostic value in the eval-uation of COPD but may show erythro-cythemia (Hct > 48%) as a reflection ofchronic hypoxemia.
Evaluation of exacerbations: Patientswith acute exacerbations who display in-creased work of breathing, somnolence, andlow O2 saturations on oximetry should un-dergo ABG sampling to quantify hypoxemiaand hypercapnia. Hypercapnia may existwith hypoxemia. In such patients, the hypox-emia often provides more respiratory stimu-lation than hypercapnia (which is the norm),and O2 therapy may worsen hypercapnia byattenuating hypoxic ventilatory drive andworsening hypoventilation.
Findings of partial pressure of arterial O2(PaO2) < 50 mm Hg or partial pressure of ar-terial CO2 (PaCO2) > 50 mm Hg in the settingof respiratory acidemia define acute respira-tory failure (see p. 544). However, some
045_062PUL Page 404 Tuesday, November 8, 2005 10:54 AM

49 CHRONIC OBSTRUCTIVE PULMONARY DISEASE 405
patients with chronic COPD survive at suchlevels for prolonged periods.
A chest x-ray is often obtained to check forpneumonia or pneumothorax. Rarely, infil-trates in patients receiving chronic systemiccorticosteroids may represent Aspergilluspneumonia.
Yellow or green sputum is a reliable indi-cator of sputum neutrophils and suggestsbacterial colonization or infection. Gramstain usually shows neutrophils with a mix-ture of organisms, often gram-positive diplo-cocci (Streptococcus pneumoniae) and/orgram-negative rods (H. influenzae). Otheroropharyngeal commensal flora, such asMoraxella (Branhamella) catarrhalis, occa-sionally cause exacerbations. In hospitalizedpatients, Gram stains and cultures may dem-onstrate resistant gram-negative organisms(eg, Pseudomonas) or, rarely, gram-positiveinfection with Staphylococcus.
PrognosisSeverity of airway obstruction predicts
survival in patients with COPD. The mortal-ity rate in patients with an FEV1 ≥ 50% of pre-dicted is slightly greater than that of the gen-eral population. If the FEV1 is 0.75 to 1.25 L,5-yr survival is about 40 to 60%; if < 0.75 L,about 30 to 40%. Cardiac disease, low bodyweight, resting tachycardia, hypercapnia,and hypoxemia decrease survival, whereas asignificant response to bronchodilators is as-sociated with improved survival. Risk factorsfor death in patients with acute exacerbationrequiring hospitalization include older age,higher PaCO2, and use of maintenance oralcorticosteroids.
Mortality in COPD often results from in-tercurrent illnesses rather than from progres-sion of the underlying disease in those whohave stopped smoking. Death is generallycaused by acute respiratory failure, pneumo-nia, lung cancer, cardiac disease, or pulmo-nary embolism.
Treatment of Stable COPDTreatment of cor pulmonale, a common
complication of long-standing, severe COPD,is discussed on p. 664.
Treatment of chronic stable COPD aims toprevent exacerbations and provide long-termimprovement in lung and physical functionthrough drug and O2 therapy, smoking ces-sation, exercise, enhancement of nutrition,and pulmonary rehabilitation. Surgical treat-ment of COPD is indicated for selected pa-
tients. COPD management involves treat-ment of both chronic stable disease and ofexacerbations.
Drug therapy: Recommended drug ther-apy is summarized in TABLE 49–1. Bron-chodilators are the mainstay of COPD man-agement; drugs include inhaled β-agonistsand anticholinergics. Any patient with symp-tomatic COPD should be taking 1 or both ofthese classes of drugs, which are equally ef-fective. For initial therapy, the choice be-tween short-acting β-agonists, long-actingβ-agonists, anticholinergics (which have agreater bronchodilating effect), or combina-tion β-agonist and anticholinergic therapy isoften a matter of tailoring cost and conve-nience to the patient's preferences and symp-toms. There is no evidence that regular bron-chodilator use slows deterioration of pulmo-nary function, but the drugs acutely relievesymptoms and increase pulmonary functionand exercise capacity.
In treatment of chronic stable disease, ad-ministration by metered-dose inhaler ordry-powder inhaler is preferred over nebu-lized home treatment; home nebulizers areprone to contamination from incompletecleaning and drying. Patients should betaught to exhale to functional residual ca-pacity, inhale the aerosol slowly to total lungcapacity, and hold the inhalation for 3 to 4 secbefore exhaling. Spacers help ensure opti-mal delivery of drug to the distal airways andreduce the importance of coordinating acti-vation of the inhaler with inhalation. Somespacers alert the patient if they are inhalingtoo rapidly.
β-Agonists relax bronchial smooth mus-cle and increase mucociliary clearance. Al-buterol aerosol, 2 puffs (100 µg/puff) inhaledfrom a metered-dose inhaler 4 to 6 times/dayprn, is usually the drug of choice because oflow cost; regular dosing offers no advantagesover as-needed use and causes more adverseeffects. Long-acting β-agonists are prefera-ble for patients with nocturnal symptoms orfor those who find frequent dosing inconve-nient; options include salmeterol powder, 1puff (50 µg) inhaled bid; or formoterol pow-der (12 µg) inhaled bid. The dry-powder for-mulations may be more effective for patientswho have trouble coordinating use of a me-tered-dose inhaler. Patients should be taughtthe difference between short- and long-act-ing drugs, because long-acting drugs that areused as needed or more than twice/day in-crease the risk of cardiac arrhythmias. Ad-
045_062PUL Page 405 Tuesday, November 8, 2005 10:54 AM

406 SECTION 5 PULMONARY DISORDERS
verse effects commonly result from use ofany β-agonist and include tremor, anxiety, ta-chycardia, and mild hypokalemia.
Anticholinergics relax bronchial smoothmuscle through competitive inhibition ofmuscarinic receptors (M1, M2, and M3). Ip-ratropium is most commonly used because oflow cost and availability; dose is 2 to 4 puffsq 4 to 6 h. Ipratropium has a slower onset ofaction (within 30 min; peak effect in 1 to 2 h),so a β2-agonist is often prescribed with it ina single combination inhaler or as a separateas-needed rescue drug. Tiotropium, a long-acting quaternary anticholinergic, is M1 andM3 selective and may therefore have an ad-vantage over ipratropium, because M2 recep-tor blockade (as occurs with ipratropium)may limit bronchodilation. Dose is 18 µgonce/day. Tiotropium is not available world-wide, however, and additional studies areneeded before its precise role can be clarified.Adverse effects of all anticholinergics arepupillary dilation, blurred vision, and drymouth.
Inhaled corticosteroids inhibit airway in-flammation, reverse β-receptor down-regu-lation, and inhibit leukotriene and cytokineproduction. They do not alter the course ofpulmonary function decline in COPD pa-tients who continue to smoke, but they doimprove short-term pulmonary function insome patients, are additive to the effect ofbronchodilators, and may diminish the fre-quency of COPD exacerbations. Dose de-pends on the drug; examples include flutica-sone 500 to 1000 µg/day and beclometha-sone 400 to 2000 µg/day. The long-termrisks of inhaled corticosteroids in older pop-ulations are not proven but probably includeosteoporosis and cataract formation. Long-term users therefore should undergo peri-odic ophthalmologic and bone densitometryscreening and should possibly receive sup-plemental calcium, vitamin D, and a bispho-sphonate as indicated.
Combinations of a long-acting β-agonist(eg, salmeterol) and an inhaled corticosteroid(eg, fluticasone) are more effective than ei-ther drug alone in the treatment of chronic sta-ble disease.
Oral or systemic corticosteroids can beused to treat chronic stable COPD but seemto benefit only 10 to 20% of patients, andlong-term risks may exceed benefits. Formalcomparisons between oral and inhaled corti-costeroids have not been performed. Oraldosing should start at 30 mg prednisone once/
day, and response to treatment should bemonitored by spirometry. If the FEV1improves ≥ 20%, then the dose should be ta-pered at a rate of a 5-mg equivalent of pred-nisone per week to the lowest amount thatmaintains the improvement. If exacerbationoccurs during tapering, inhaled corticoste-roids may be helpful, but a resumption ofhigher dosing is likely to provide more rapidsymptom relief and improvement in FEV1.By contrast, if initial FEV1 improvement is< 20%, then corticosteroids should be taperedrapidly and stopped. Alternate-day dosing isan option if it reduces adverse effects whilesustaining daily improvement.
Theophylline plays a small role in the treat-ment of chronic stable COPD and of acuteCOPD exacerbations now that safer, moreeffective drugs are available. Theophyllinedecreases smooth muscle spasm, enhancesmucociliary clearance, improves right ven-tricular function, and decreases pulmonaryvascular resistance and arterial pressure. Itsmode of action is poorly understood but ap-pears to differ from that of β2-agonists and an-ticholinergics. Its role in improving diaphrag-matic function and dyspnea during exerciseis controversial. Low-dose theophylline (300to 400 mg/day) has anti-inflammatory prop-erties and may enhance the effects of inhaledcorticosteroids.
Theophylline can be used for patients whohave not adequately responded to inhaledagents and who have shown symptomaticbenefit from a trial of the drug. Serum levelsneed not be monitored unless the patient doesnot respond to the drug, develops symptomsof toxicity, or is questionably adherent;slowly absorbed oral theophylline prepara-tions, which require less frequent dosing, en-hance compliance. Toxicity is common andincludes sleeplessness and GI upset, even atlow blood levels. More serious adverse ef-fects, such as supraventricular and ventricu-lar arrhythmias and seizures, tend to occur atblood levels > 20 mg/L. Hepatic metabolismof theophylline varies greatly and is influencedby genetic factors, age, cigarette smoking,hepatic dysfunction, and some drugs, such asmacrolide and fluoroquinolone antibioticsand nonsedating histamine2 blockers.
Phosphodiesterase-4 antagonists and anti-oxidants are under investigation for anti-inflammatory effects in the treatment ofCOPD.
Oxygen therapy: Long-term O2 therapyprolongs life in COPD patients whose PaO2
045_062PUL Page 406 Tuesday, November 8, 2005 10:54 AM

49 CHRONIC OBSTRUCTIVE PULMONARY DISEASE 407
is chronically < 55 mm Hg. Continual 24-h useis more effective than a 12-h nocturnal regi-men. O2 therapy brings Hct toward normallevels; moderately improves neuropsycho-logic factors, possibly by facilitating sleep;and ameliorates pulmonary hemodynamicabnormalities. O2 therapy also increases ex-ercise tolerance in many patients.
A sleep study should be considered for pa-tients with advanced COPD who do not meetthe criteria for long-term O2 therapy (see TA-BLE 49–2) but whose clinical assessment sug-gests pulmonary hypertension in the absenceof daytime hypoxemia. Nocturnal O2 may beprescribed if a sleep study shows episodic de-saturation to ≤ 88%. Such treatment preventsprogression of pulmonary hypertension, butits effects on survival are unknown.
O2 is administered by nasal cannula at aflow rate sufficient to achieve a PaO2 > 60 mmHg (SaO2 > 90%), usually ≤ 3 L/min at rest.O2 is supplied by electrically driven O2 con-centrators, liquid O2 systems, or cylinders ofcompressed gas. Concentrators, which limitmobility but are the least expensive, are pref-erable for patients who spend most of theirtime at home. Such patients require small O2tanks for backup in case of an electrical fail-ure and for portable use.
A liquid system is preferable for patientswho spend much time out of their homes. Por-table canisters of liquid O2 are easier to carryand have more capacity than portable cylin-ders of compressed gas. Large compressed-air cylinders are the most expensive way ofproviding O2 and should be used only if noother source is available. All patients must betaught the dangers of smoking during O2 use.
Various devices can conserve the amountof O2 used by the patient, either by using a res-ervoir system or by permitting O2 flow onlyduring inspiration. These devices correct hy-poxemia as effectively as do continuous flowsystems.
Some patients need supplemental O2 dur-ing air travel, because flight cabin pressure incommercial airliners is low. Eucapnic COPDpatients with a sea level PaO2 > 68 mm Hggenerally have an in-flight PaO2 > 50 mm Hgand do not require supplemental O2. AllCOPD patients with hypercapnia, significantanemia (Hct < 30), or coexisting heart or cere-brovascular disease should use supplementalO2 during long flights and should notify theairline when making their reservation. Pa-tients are not permitted to transport or usetheir own O2. The airline provides its own O2
system, and most require a minimum noticeof 24 h, a physician's statement of necessity,and an O2 prescription before the flight.Patients should bring their own nasal cannu-las, because some airlines provide only facemasks. Arrangements for O2 equipment inthe destination city, if required, should bemade in advance so that the supplier can meetthe traveler at the airport.
Smoking cessation: Smoking cessation(see p. 2733) is both extremely difficult andextremely important; it slows but does not al-together halt the progression of airway in-flammation (see FIG. 49–1). Simultaneoususe of multiple strategies is most effective:establishment of a quit date, behavior modi-fication techniques, group sessions, nicotinereplacement therapy (by gum, transdermalpatch, inhaler, lozenge, or nasal spray), bu-propion, and physician encouragement. Quitrates are about 30% at 1 yr even with bupro-pion combined with nicotine replacement,the most effective intervention.
Vaccinations: All patients with COPDshould be given annual influenza vaccina-tions. If a patient is unable to receive an in-fluenza vaccination or if the prevailing in-fluenza strain is not included in the annualvaccine formulation, prophylactic treatment(amantadine, rimantadine, oseltamivir, orzanamivir) is appropriate during community
TABLE 49–2. INDICATIONS FOR LONG-TERM O2 THERAPY IN COPD
PaO2 ≤ 55 mm Hg or SaO2 ≤ 88%* in patients receiving optimal medical regimen for at least 30 days†
PaO2 = 55 to 59 mm Hg or SaO2 ≤ 89%* for patients with cor pulmonale or erythrocyto-sis (Hct > 55%)
Can be considered for PaO2 ≥ 60 mm Hg or SaO2 ≥ 90%* for patients whose room-air PaO2 is ≤ 55 mm Hg or SaO2 ≤ 88% during exercise or sleep
PaO2 = partial pressure of arterial O2; SaO2 =arterial O2 saturation.
*Arterial O2 levels measured at rest during airbreathing.
†Patients who are recovering from an acuterespiratory illness and who meet the listed crite-ria should be given O2 and rechecked on roomair in 30 days.
045_062PUL Page 407 Tuesday, November 8, 2005 10:54 AM

408 SECTION 5 PULMONARY DISORDERS
influenza outbreaks. Pneumococcal polysac-charide vaccine, although of unproven effi-cacy in COPD, has minimal adverse effectsand should probably also be administered.
Physical activity: Skeletal muscle de-conditioning resulting from inactivity or pro-longed hospitalization for respiratory failurecan be ameliorated with a program of gradedexercise. Specific training of respiratory mus-cles is less helpful than general aerobic con-ditioning. A typical training program beginswith slow walking on a treadmill or unloadedcycling on an ergometer for a few minutes.Duration and exercise load is progressivelyincreased over 4 to 6 wk until the patient canexercise for 20 to 30 min nonstop with man-ageable dyspnea. Patients with very severeCOPD can usually achieve an exercise regi-men of walking for 30 min at 1 to 2 mph. Main-tenance exercise should be performed 3 to 4times/wk to maintain fitness levels. O2 satu-ration is monitored and supplemental O2 pro-vided as needed. Upper extremity resistancetraining is helpful in performing daily taskssuch as bathing, dressing, and housecleaning.COPD patients should be taught ways to con-serve energy during activities of daily livingand pace their activities. Difficulties in sexualfunction should be discussed and advice givenon using energy-conserving techniques forsexual gratification.
Nutrition: COPD patients are at risk ofweight loss and nutritional deficiencies be-cause of a 15 to 25% increase in resting energyexpenditure from breathing; a larger post-prandial increase in metabolism and heat pro-duction (ie, the thermal effect of feeding), per-haps because a distended stomach interfereswith descent of the already flattened dia-phragm and increases the work of breathing;a higher energy cost of daily activities; re-duced caloric intake relative to need; and thecatabolic effect of inflammatory cytokinessuch as TNF-α. Generalized muscle strengthand efficiency of O2 use are impaired. Patientswith poorer nutritional status have a worseprognosis, so it is prudent to recommend abalanced diet with adequate caloric intake inconjunction with exercise to prevent or re-verse malnutrition and muscle atrophy. How-ever, excessive weight gain should beavoided, and obese patients should strive toachieve more normal body mass index. Stud-ies of nutritional supplementation alone havenot resulted in improvement in pulmonaryfunction or exercise capacity. The roles ofanabolic steroids (eg, megace, oxandrolone),
growth hormone supplementation, and TNFantagonists in reversing malnutrition andimproving functional status and prognosis inCOPD are not well defined.
Pulmonary rehabilitation: Pulmonaryrehabilitation programs serve as adjuncts todrug treatment to improve physical function;many hospitals and health care organizationsoffer formal multidisciplinary rehabilitationprograms. Pulmonary rehabilitation in-cludes exercise, education, and behavioralintervention. Treatment should be individu-alized; patients and family members aretaught about COPD and medical treatments,and the patient is encouraged to take as muchresponsibility for personal care as possible. Acarefully integrated rehabilitation programhelps patients with severe COPD accommo-date to physiologic limitations while provid-ing realistic expectations for improvement.
The benefits of rehabilitation are greaterindependence and improved quality of lifeand exercise capacity. Modest increases areseen in lower extremity strength, endurance,and maximum O2 consumption. Pulmonaryrehabilitation typically does not improve pul-monary function or increase longevity, how-ever. Patients with severe disease require aminimum of 3 mo of rehabilitation to ben-efit and should continue with maintenanceprograms.
Specialized programs are available forpatients who remain ventilator-bound afteracute respiratory failure. Some patients canbe liberated from the ventilator entirely,whereas others can remain off the ventilatorduring the day. For patients with adequatehome support, training of family memberscan permit some patients to be sent home withventilators.
Surgery: Surgical options for treatmentof severe COPD include lung volume reduc-tion and transplantation.
Lung volume reduction by resection ofnonfunctioning emphysematous areas im-proves exercise tolerance and 2-yr mortalityin patients with severe, predominantly upper-lung emphysema who have low baseline ex-ercise capacity after pulmonary rehabilita-tion. Other patients may experience symp-tom relief and improved exercise capacityafter surgery, but mortality has been shown tobe the same or increased compared with thatfor drug therapy. Long-term effects of theprocedure are unknown. Improvement is lessthan that with lung transplantation. Themechanism of improvement is believed to be
045_062PUL Page 408 Tuesday, November 8, 2005 10:54 AM

49 CHRONIC OBSTRUCTIVE PULMONARY DISEASE 409
enhanced lung recoil and improved dia-phragmatic function and V/Q relationships.Operative mortality is about 5%. The bestcandidates for lung volume reduction arethose with an FEV1 20 to 40% of predicted,a DLCO > 20% of predicted, significantly im-paired exercise capacity, heterogeneous pul-monary disease on CT with an upper-lobepredominance, PaCO2 < 50 mm Hg, and ab-sence of severe pulmonary hypertension andcoronary artery disease.
Rarely, patients have extremely large bul-lae that compress the functional lung. Thesepatients can be helped by surgical resectionof these bullae, with resulting relief of symp-toms and improved pulmonary function. Ingeneral, resection is most beneficial for pa-tients with bullae affecting > 1⁄3 of a hemi-thorax and an FEV1 about 1⁄2 the predicted nor-mal value. Improved pulmonary function isrelated to the amount of normal or minimallydiseased lung tissue that was compressed bythe resected bullae. Serial chest x-rays andCT are the most useful procedures for deter-mining whether a patient's functional statusis due to compression of viable lung by bullaeor to generalized emphysema. A markedlyreduced DLCO (< 40% predicted) indicateswidespread emphysema and suggests a poor-er outcome from surgical resection.
Since 1989, single-lung transplantationhas largely replaced double-lung transplan-tation in COPD patients. Candidates fortransplantation are patients < 60 yr with anFEV1 < 25% predicted or with severe pulmo-nary hypertension. The goal of lung trans-plantation is to improve quality of life, be-cause survival time is rarely increased. The5-yr survival after transplantation for emphy-sema is 45 to 60%. Lifelong immunosuppres-sion is required, with the attendant risk of op-portunistic infections.
Treatment of Acute COPD Exacerbation
The immediate objectives are to ensure ad-equate oxygenation, reverse airway obstruc-tion, and treat underlying causes.
The cause is usually unknown, althoughsome acute exacerbations result from bacte-rial or viral infections. Smoking, irritative in-halational exposure, and high levels of airpollution also contribute. Mild exacerbationsoften can be treated on an outpatient basis inpatients with adequate home support. Elderlyfrail patients and patients with comorbidities,
a history of respiratory failure, or acutechanges in ABG measurements are admittedto the hospital for observation and treatment.Patients with life-threatening exacerbationsmanifested by uncorrected hypoxemia, acuterespiratory acidosis, new arrhythmias, or de-teriorating respiratory function despite hos-pital treatment and those who require seda-tion for management should be admitted tothe ICU and their respiratory status moni-tored frequently.
Oxygen: Most patients require O2 sup-plementation, even those who do not need itchronically. O2 administration may worsenhypercapnia by attenuating hypoxic respira-tory drive. After 30 days, room-air PaO2should be reassessed to determine if the pa-tient still requires supplemental O2.
Ventilatory assistance: Noninvasivepositive-pressure ventilation (eg, pressuresupport or bi-level positive airway pressureventilation by face mask [see p. 547]) is an al-ternative to full mechanical ventilation. Non-invasive ventilation appears to decrease theneed for intubation, reduce hospital stay, andreduce mortality in patients with severe ex-acerbations (defined as a pH < 7.30 in hemo-dynamically stable patients not at immediaterisk of respiratory arrest). Noninvasive ven-tilation appears to have no effect in patientswith less severe exacerbation. However, itmay be indicated for patients in this groupwhose ABGs worsen despite initial drug ther-apy or who appear to be imminent candidatesfor full mechanical ventilation but who do notrequire intubation for control of the airway orsedation for agitation. Deterioration on non-invasive ventilation should prompt conver-sion to invasive mechanical ventilation.
Deteriorating ABG levels and mental sta-tus and progressive respiratory fatigue areindications for endotracheal intubation andmechanical ventilation. Ventilator settings,management strategies, and complicationsare discussed in Ch. 65 on p. 544. Risk factorsfor ventilatory dependence include an FEV1< 0.5 L, stable ABGs with a PaO2 < 50 mm Hgand/or PaCO2 > 60 mm Hg, severe exerciselimitation, and poor nutritional status. There-fore, a discussion of the patient's wishes re-garding intubation and mechanical ventila-tion should be initiated and documented (seep. 2768).
If a patient requires prolonged intubation(eg, > 2 wk), a tracheostomy is indicated to fa-cilitate comfort, communication, and eating.With a good multidisciplinary rehabilitation
045_062PUL Page 409 Tuesday, November 8, 2005 10:54 AM

410 SECTION 5 PULMONARY DISORDERS
program, including nutritional and psycho-logic support (see p. 378), many patients re-quiring prolonged mechanical ventilationcan be successfully weaned and can return totheir former level of function.
Drug therapy: β-agonists, anticholiner-gics, and/or corticosteroids should be startedconcurrently with O2 therapy (regardless ofhow O2 is administered) with the aim of re-versing airway obstruction.
β-agonists are the cornerstone of drugtherapy for acute exacerbations. The mostwidely used drug is albuterol, 2.5 mg by neb-ulizer or 2 to 4 inhalations (100 µg/puff) bymetered-dose inhaler q 2 to 6 h. Inhalationusing a metered-dose inhaler produces rapidbronchodilation; there are no data indicatingthat nebulizers are more effective than me-tered-dose inhalers.
Ipratropium, the most commonly used an-ticholinergic, is proven effective in acuteCOPD exacerbation and should be given con-currently or alternating with β-agonists usinga metered-dose inhaler. Dosage is 0.25 to 0.5mg by nebulizer or 2 to 4 inhalations (21 µg/puff) by metered-dose inhaler q 4 to 6 h. Ip-ratropium generally provides bronchodilat-ing effect similar to β-agonists. The role ofthe longer-acting anticholinergic tiotropiumin treating acute exacerbations has not beendefined.
Corticosteroids should be begun immedi-ately for all but mild exacerbations. Optionsinclude prednisone, 60 mg once/day po ta-pered over 7 to 14 days, and methylpredniso-lone, 60 mg once/day IV tapered over 7 to14 days. These drugs are equivalent in theiracute effects; inhaled corticosteroids have norole in the treatment of acute exacerbation.
Methylxanthines, once considered essen-tial to treatment of acute COPD exacerbation,are no longer used. Toxicities exceededbenefit.
Antibiotics are recommended for exacer-bations in patients with purulent sputum.Some physicians give antibiotics empiricallyfor change in sputum color or for nonspecificchest x-ray abnormalities. Routine culturesand Gram stains are not necessary beforetreatment unless an unusual or resistant or-ganism is suspected. Trimethoprim-sul-famethoxazole 160 mg/800 mg bid, amox-icillin 250 to 500 mg tid, tetracycline 250 mgqid, and doxycycline 50 to 100 bid given for7 to 14 days are all effective and inexpensivefirst-line drugs. The choice of drug should bedictated by local patterns of bacterial sensitiv-
ity and patient history. In most cases, treat-ment should be initiated with oral drugs if tol-erated. If the patient is seriously ill or if clinicalevidence suggests that the infectious organ-isms are resistant, more expensive second-line drugs can be used. These drugs includeamoxicillin-clavulanate 250 to 500 mg tid;fluoroquinolones, such as ciprofloxacin, levo-floxacin, or gatifloxacin; 2nd-generationcephalosporins, such as cefuroxime or cefa-clor; and extended-spectrum macrolides,such as azithromycin, clarithromycin, ortelithromycin. These drugs are effectiveagainst β-lactamase–producing strains of H.influenzae and M. catarrhalis but have notbeen shown to be more effective than first-linedrugs for most patients. Patients can be taughtto recognize a change in sputum from normalto purulent as a sign of impending exacerba-tion and to start a 10- to 14-day course of an-tibiotic therapy. Long-term antibiotic prophy-laxis is recommended only for patients withunderlying structural changes in the lung,such as bronchiectasis or infected bullae.
a1-ANTITRYPSIN DEFICIENCY
a1-Antitrypsin deficiency is congenital lackof a primary lung antiprotease—a1-anti-trypsin—leading to increased protease tis-sue destruction and emphysema in adults.Hepatic accumulation of abnormal a1-anti-trypsin can cause liver disease in both chil-dren and adults. Serum a1-antitrypsin level< 11 mmol/L (80 mg/dL) confirms the diag-nosis. Treatment is smoking cessation, bron-chodilators, early treatment of infection, and,in selected cases, a1-antitrypsin replace-ment. Severe liver disease may require trans-plantation. Prognosis is related mainly todegree of lung impairment.
α1-Antitrypsin is a neutrophil elastaseinhibitor (an antiprotease), the major func-tion of which is to protect the lungs fromprotease-mediated tissue destruction. Mostα1-antitrypsin is synthesized by liver cellsand monocytes and passively diffuses throughthe circulation into the lungs; some is sec-ondarily produced by alveolar macrophagesand epithelial cells. The protein conforma-tion (and, hence, functionality) and quantityof circulating α1-antitrypsin is determinedby codominant expression of parental al-leles; > 90 different alleles have been identi-
045_062PUL Page 410 Tuesday, November 8, 2005 10:54 AM

49 CHRONIC OBSTRUCTIVE PULMONARY DISEASE 411
fied and described by protease inhibitor (PI*)phenotype.
Inheritance of some variant alleles causesa change in conformation of the α1-anti-trypsin molecule, leading to polymerizationand retention within hepatocytes. The hepaticaccumulation of aberrant α1-antitrypsin mol-ecules causes neonatal cholestatic jaundicein 10 to 20% of patients; the remainder areprobably able to degrade the abnormal protein,although the exact protective mechanism isunclear. About 20% of cases of neonatal he-patic involvement result in development ofcirrhosis in childhood. About 10% withoutchildhood liver disease develop cirrhosis asadults. Liver involvement increases the riskof liver cancer.
In the lung, α1-antitrypsin deficiency in-creases neutrophil elastase activity, which fa-cilitates tissue destruction leading to emphy-sema (especially in smokers, because ciga-rette smoke also increases protease activity).α1-Antitrypsin deficiency is estimated to ac-count for 1 to 2% of all cases of COPD.
Other disorders possibly associated withα1-antitrypsin variants include panniculitis,life-threatening hemorrhage (through a mu-tation that converts α1-antitrypsin from aneutrophil elastase to a coagulation factor in-hibitor), aneurysms, ulcerative colitis, andglomerular disease.
Epidemiology and ClassificationMore than 95% of people with severe α1-
antitrypsin deficiency and emphysema arehomozygous for the Z allele (PI*ZZ) andhave α1-antitrypsin levels of about 30 to 40mg/dL (5 to 6 µmol/L). Prevalence in the nor-mal population is 1/1500 to 5000. Most arewhites of Northern European descent; the Zallele is rare in Asians and blacks. Thoughemphysema is common in PI*ZZ patients,many nonsmoking homozygotes do not de-velop emphysema; those who do typicallyhave a family history of COPD. PI*ZZ smok-ers have a lower life expectancy than PI*ZZnonsmokers, who have a lower life expect-ancy than PI*MM nonsmokers and smok-ers. Nonsmoking PI*MZ heterozygotes maybe at increased risk of developing a morerapid fall in FEV1 over time than do normalsubjects.
Other rare phenotypes include PI*SZ andtwo types with nonexpressing alleles, PI*Z-null and PI*null-null (see TABLE 49–3). Thenull phenotype leads to undetectable serumlevels of α1-antitrypsin. Normal serum levels
of malfunctioning α1-antitrypsin may beseen with rare mutations.
Symptoms and SignsInfants with hepatic involvement present
with cholestatic jaundice and hepatomagalyduring the first week of life; jaundice usuallyresolves by 2 to 4 mo of age. Cirrhosis maydevelop in childhood or adulthood (symp-toms and signs of cirrhosis and hepatocellu-lar carcinoma are discussed elsewhere in THEMANUAL).
α1-Antitrypsin deficiency most com-monly causes early emphysema; symptomsand signs are those of COPD (see p. 401).Lung involvement occurs earlier in smokersthan in nonsmokers but in both cases is rarebefore age 25. Severity of pulmonary dis-ease varies greatly; pulmonary function iswell preserved in some PI*ZZ smokers andcan be severely impaired in some PI*ZZnonsmokers. PI*ZZ people identified inpopulation surveys (ie, those without symp-toms or pulmonary disease) tend to have bet-ter pulmonary function, whether they smokeor not, than do index people (those identifiedbecause they have pulmonary disease). As agroup, nonindex people with severe α1-an-titrypsin deficiency who have never smokedhave a normal life expectancy and only mod-erate impairment of pulmonary function.Airflow obstruction occurs more frequentlyin men and in people with asthma, recurrentrespiratory infections, occupational dust
TABLE 49–3. EXPRESSION OF PHENOTYPE IN α1-ANTITRYPSIN
DEFICIENCY
PHENO-TYPE
α1-ANTI-TRYPSIN SERUM LEVEL
RISK OF EMPHY-
SEMA
PI*ZZ 2.5–7 µmol/L High
PI*MZ 17–33 µmol/L Minimallyincreased
PI*SZ 8–16 µmol/L Slightly increased
PI*SS 15–33 µmol/L Minimallyincreased
PI*null-null 0 HighPI*Z-null 0–5 µmol/L HighPI*MM 20–48 µmol/L Normal
045_062PUL Page 411 Tuesday, November 8, 2005 10:54 AM

412 SECTION 5 PULMONARY DISORDERS
exposure, and a family history of pulmonarydisease. The most common cause of death inα1-antitrypsin deficiency is emphysema,followed by cirrhosis, often with hepaticcarcinoma.
Panniculitis, an inflammatory disease ofsubcutaneous soft tissue, manifests as indu-rated, tender, discolored plaques or nodules,typically on the lower abdomen, buttocks,and thighs (see p. 976).
Diagnosisα1-Antitrypsin deficiency is suspected in
smokers who develop emphysema beforeage 45; in nonsmokers without occupationalexposures who develop emphysema at anyage; in patients with predominately lowerlung emphysema (as shown on chest x-ray);in patients with a family history of emphy-sema or unexplained cirrhosis; in patientswith panniculitis; in newborns with jaundiceor liver enzyme elevations; and in any patientwith unexplained liver disease. Diagnosis isconfirmed by serum α1-antitrypsin levels< 80 mg/dL (< 11 µmol/L).
TreatmentTreatment of pulmonary disease is with
purified human α1-antitrypsin (60 mg/kg IVover 45 to 60 min given once weekly, or 250mg/kg over 4 to 6 h given once monthly[pooled only]), which can maintain the serumα1-antitrypsin level above a target protectivelevel of 80 mg/dL (35% of normal). Because
emphysema produces permanent structuralchange, therapy cannot improve damagedlung structure or function but is given to haltprogression. Treatment is extremely expen-sive and is therefore reserved for nonsmokingpatients with mild to moderately abnormalpulmonary function and serum α1-anti-trypsin < 80 mg/dL (< 11 µmol/L). It is not in-dicated for patients who have severe diseaseor for patients with normal or heterozygousphenotypes.
Smoking cessation, use of bronchodila-tors, and early treatment of respiratory infec-tions are particularly important for α1-anti-trypsin–deficient patients with emphysema.Experimental treatments, such as phenylbu-tyric acid that can reverse the misfolding ofthe abnormal α1-antitrypsin proteins in thehepatocytes, thereby stimulating protein re-lease, are being investigated. For severely im-paired people < 60 yr, lung transplantationshould be considered. Lung volume reduc-tion in treating the emphysema of α1-anti-trypsin deficiency is controversial. Genetherapy is under study.
Treatment of liver disease is supportive.Enzyme replacement does not help becausethe disease is caused by abnormal processingrather than by enzyme deficiency. Livertransplantation may be used for patients withliver failure.
Treatment of panniculitis is not well de-fined. Corticosteroids, antimalarials, and tet-racyclines have been used.
50PULMONARY EMBOLISM
Pulmonary embolism is the occlusion of oneor more pulmonary arteries by thrombi thatoriginate elsewhere, typically in the largeveins of the lower extremities or pelvis. Riskfactors are conditions that impair venousreturn and that cause endothelial injury ordysfunction, especially in patients with anunderlying hypercoagulable state. Symp-toms include dyspnea, pleuritic chest pain,cough, and, in severe cases, syncope or car-diorespiratory arrest. Signs are nonspecific
and may include tachypnea, tachycardia,hypotension, and loud pulmonic componentof the 2nd heart sound. Diagnosis is based ona ventilation/perfusion scan, a CT angio-gram, or a pulmonary arteriogram. Treat-ment is with anticoagulants, thrombolytics,and, occasionally, surgery to remove the clot.
Pulmonary embolism (PE) affects an esti-mated 650,000 people and causes up to200,000 deaths/yr, accounting for an esti-mated 15% of all hospital deaths/yr. The in-cidence of PE in children is about 5/10,000admissions.
Etiology and PathophysiologyNearly all PEs arise from thrombi in the
lower extremity or pelvic veins (deep venous
045_062PUL Page 412 Tuesday, November 8, 2005 10:54 AM

50 PULMONARY EMBOLISM 413
thrombosis [DVT]—see p. 754). Thrombi ineither system may be occult. Thromboembolican also originate in upper extremity veins orin right cardiac chambers. Risk factors forDVT and PE are similar in children and adultsand include conditions that impair venous re-turn or that cause endothelial injury or dys-function particularly in patients with an un-derlying baseline hypercoagulable state (seeTABLE 50–1). Bed rest and confinementwithout walking, even for a few hours, arecommon precipitators.
Once DVT develops, the clot may dislodgeand travel through the venous system andright heart to lodge in the pulmonary arteries,where it partially or completely occludes oneor more vessels. The consequences dependon the size and number of emboli, the pulmo-nary reaction, and the ability of the body's in-trinsic thrombolytic system to dissolve theclot.
Small emboli may have no acute physio-logic effects; many begin to lyse immediatelyand resolve within hours or days. Larger em-boli can cause a reflex increase in ventilation(tachypnea); hypoxemia from ventilation/perfusion (V/Q) mismatch and shunting;atelectasis from alveolar hypocapnia and ab-normalities in surfactant; and an increase inpulmonary vascular resistance caused by me-chanical obstruction and vasoconstriction.Endogenous lysis reduces most emboli, eventhose of moderate size, without treatment,and physiologic alterations decrease overhours or days. Some emboli resist lysis andmay organize and persist. Occasionally,chronic residual obstruction leads to pulmo-nary hypertension (chronic thromboembolicpulmonary hypertension) that may developover years and result in chronic right heartfailure. When large emboli occlude major ar-teries, or when many small emboli occlude> 50% of the distal arterial system, right ven-tricular pressure increases, causing acuteright ventricular failure, failure with shock(massive PE), or sudden death in severecases. The risk of death depends on the degreeand rate of rise of right-sided pressures and onthe patient’s underlying cardiopulmonarystatus; higher pressures more commonly oc-cur in patients with preexisting cardiopulmo-nary disease. Healthy patients may survive aPE that occludes > 50% of the pulmonary vas-cular bed.
Pulmonary infarction occurs in < 10% ofpatients diagnosed with PE. This low rate hasbeen attributed to the dual blood supply to the
lung (ie, bronchial and pulmonary). Infarc-tion is typically characterized by a radio-graphic infiltrate, chest pain, fever, and,occasionally, hemoptysis.
Nonthrombotic PE: PE from a variety ofnonthrombotic sources causes clinical syn-dromes that differ from thrombotic PE.
TABLE 50–1. RISK FACTORS FOR DEEP VENOUS THROMBOSIS AND
PULMONARY EMBOLISM
Age > 60 yrAtrial fibrillationCigarette smoking (including passive
smoke)Estrogen receptor modulators (raloxifene,
tamoxifen)Extremity traumaHeart failure*Hypercoagulability disorders*
Antiphospholipid antibodysyndrome
Antithrombin III deficiencyFactor V Leiden mutation
(activated protein C resistance)Heparin-induced thrombocy-
topenia and thrombosisHereditary fibrinolytic defectsHyperhomocystinemiaIncrease in factor VIIIIncrease in factor XIIncrease in von Willebrand’s
factorParoxysmal nocturnal
hemoglobinuriaProtein C deficiencyProtein S deficiencyProthrombin G-A gene variantTissue factor pathway inhibitor
Immobilization*Indwelling venous cathetersMalignancy*Myeloproliferative disease
(hyperviscosity)Nephrotic syndromeObesityOral contraceptives/estrogen
replacementPregnancy and postpartum*Prior venous thromboembolismSickle cell anemiaSurgery within past 3 mo*
*One of the most common risk factors.
045_062PUL Page 413 Tuesday, November 8, 2005 10:54 AM

414 SECTION 5 PULMONARY DISORDERS
Air embolism is caused by introduction oflarge amounts of air into systemic veins or intothe right heart, which then move to the pulmo-nary arterial system. Causes include surgery,blunt or barometric trauma (such as from me-chanical ventilation), defective or uncappedvenous catheters, and rapid decompressionafter underwater diving. Microbubble forma-tion in the pulmonary circulation may causeendothelial damage, hypoxemia, and diffuseinfiltrates. In large volume air embolism, pul-monary outflow tract obstruction may occur,which can be rapidly fatal.
Fat embolism is caused by introductionof fat or bone marrow particles into the sys-temic venous system and then to pulmonaryarteries. Causes include long bone frac-tures, orthopedic procedures, microvascu-lar occlusion or necrosis of bone marrow inpatients with sickle cell crisis, and, rarely,toxic modification of native or parenteralserum lipids. Fat embolism causes a pulmo-nary syndrome similar to the acute respira-tory distress syndrome, with severe hypox-emia of rapid onset often accompanied byneurologic changes and a petechial rash.
Amniotic fluid embolism is a rare syndromecaused by introduction of amniotic fluid into thematernal venous and then pulmonary arterialsystem associated with labor (see p. 2205).The syndrome can occasionally occur duringprepartum uterine manipulations. Patients canhave cardiac and respiratory distress due to ana-phylaxis, vasoconstriction causing acute severepulmonary hypertension, and direct pulmonarymicrovascular toxicity.
Septic embolism occurs when infectedmaterial embolizes to the lung. Causes in-clude drug use, right-sided infective en-docarditis, and septic thrombophlebitis. Sep-tic embolism causes symptoms and signs ofpneumonia or sepsis and is initially associ-ated with nodular opacities on the chest x-ray,which may progress to peripheral infiltratesand may cavitate.
Foreign body embolism is caused by intro-duction of particulate matter into the pulmo-nary arterial system, usually by IV injectionof inorganic substances such as talc by heroinusers or elemental mercury by patients withmental disorders.
Tumor embolism is a rare complication ofmalignancy (usually adenocarcinomas) inwhich neoplastic cells from an organ enter thesystemic venous and pulmonary arterial sys-tem, where they lodge, proliferate, and ob-struct flow. Patients typically present with
symptoms of dyspnea and pleuritic chest painand signs of cor pulmonale that develop overweeks to months. Diagnosis, which is sug-gested by micronodules or diffuse pulmonaryinfiltrates, can be confirmed by biopsy or oc-casionally by cytologic aspiration and histo-logic study of pulmonary capillary blood.
Systemic gas embolism is a rare syndromethat occurs when barotrauma during mechan-ical ventilation with high airway pressureleads to air dissection from lung parenchymain the pulmonary venous and then systemicarterial system. Gas emboli cause CNSchanges (including stroke), cardiac injury,and shoulder or anterior chest livedo reticu-laris. Diagnosis is based on exclusion of othervascular processes in the setting of recog-nized barotrauma.
Symptoms and SignsMost PEs are small, physiologically insig-
nificant, and asymptomatic. Even when pre-sent, symptoms are nonspecific and vary infrequency and intensity, depending on the ex-tent of pulmonary vascular occlusion and pre-existing cardiopulmonary function.
Larger emboli cause acute dyspnea andpleuritic chest pain and, less commonly,cough and/or hemoptysis. Massive PE pre-sents with hypotension, tachycardia, syn-cope, or cardiac arrest.
The most common signs of PE are tachy-cardia and tachypnea. Less commonly, pa-tients have hypotension, a loud 2nd heartsound (S2) due to a loud pulmonic component(P2), and/or crackles or wheezing. In the pres-ence of right ventricular failure, distendedinternal jugular veins and a right ventricularheave may be evident, and right ventriculargallop (3rd and 4th heart sounds [S3 and S4]),with or without tricuspid regurgitation, may beaudible. Fever can occur; DVT and PE are of-ten overlooked causes of fever.
Chronic thromboembolic pulmonary hy-pertension causes symptoms and signs ofright heart failure, including exertional dys-pnea, easy fatigue, and peripheral edema thatdevelops over months to years.
DiagnosisDiagnosis is challenging, because symp-
toms and signs are nonspecific and diagnostictests are either imperfect or invasive. Diag-nosis starts by including PE in the differentialdiagnosis of a large number of conditionswith similar symptoms, including cardiacischemia, heart failure, COPD exacerbation,
045_062PUL Page 414 Tuesday, November 8, 2005 10:54 AM

50 PULMONARY EMBOLISM 415
pneumothorax, pneumonia, sepsis, acutechest syndrome (in sickle cell patients), andacute anxiety with hyperventilation. Initialevaluation should include pulse oximetry,ECG, and chest x-ray. The chest x-ray usuallyis nonspecific but may show atelectasis, focalinfiltrates, an elevated hemidiaphragm, and/or a pleural effusion. The classic findings offocal loss of vascular markings (Wester-mark's sign), a peripheral wedge-shaped den-sity (Hampton's hump), or enlargement of theright descending pulmonary artery (Palla'ssign) are suggestive but very insensitive.
Pulse oximetry provides a quick way to as-sess oxygenation; hypoxemia is one sign ofPE, and other significant disorders must beinvestigated.
ECG most often shows tachycardia and var-ious ST-T wave abnormalities, which are notspecific for PE (see FIG. 50–1). An S1Q3T3 ora new right bundle branch block may indicatethe effect of abrupt rise in right ventricularpressure on right ventricular conduction; theseare specific but insensitive, occurring in onlyabout 5% of patients. Right axis deviation(R > S in V1) and P-pulmonale may be present.T-wave inversion in leads V1 to V4 also occurs.
Clinical probability of PE can be assessedby combining ECG and chest x-ray findingswith those from the history and physical ex-amination (see TABLE 50–2). Patients witha low clinical probability of PE may needno or only minimal additional testing. Pa-tients with an intermediate clinical probabil-ity need additional testing. Patients with ahigh probability may be candidates for im-mediate treatment pending confirmationwith additional testing.
Noninvasive testing: Noninvasive test-ing typically can be obtained more quicklyand carries less morbidity than invasive test-ing. Tests most useful for diagnosing or ex-cluding PE are D-dimer testing, V/Q scan-ning, duplex ultrasonography, helical CTscanning, and echocardiography.
There is no universally accepted algorithmfor the best choice and sequence of tests, butone common approach is to screen with theD-dimer, obtain lower extremity ultrasonogra-phy when the D-dimer is positive, and progressto CT or V/Q if the duplex is negative. Patientswith moderate to high probability of diseasebased on clinical criteria who have low or in-termediate probability V/Q scans usually re-quire pulmonary arteriography or helical CTto make or exclude the diagnosis. A positivelower extremity ultrasound establishes the
need for anticoagulation and obviates the needfor further diagnostic testing. A negative ultra-sound study does not negate the need for ad-ditional studies. Positive D-dimers, ECG,ABG measurements, chest x-ray, and echo-cardiograms are adjunctive tests that lack suf-ficient specificity to be diagnostic alone.
D-dimer is a by-product of intrinsic fibrin-olysis; thus elevated levels suggest recentpresence of a thrombus. The test is extremelysensitive; > 90% of patients with DVT/PEhave elevated levels. However, a positive re-sult is not specific for venous thrombus be-cause many patients without DVT/PE alsohave elevated levels. In contrast, a low D-dimer has a negative predictive value of> 90%, making it useful for excluding DVT/PE, especially when initial estimates of like-lihood of disease are < 50%. Documentedcases of PE have occurred in the context ofnegative D-dimers using older enzyme-linkedimmunosorbent assays, but newer highlyspecific and rapid assays make a negative D-dimer sufficiently reliable for excluding thediagnosis of PE in routine practice.
V/Q scans detect areas of lung that are ven-tilated but not perfused, as occurs in PE; resultsare reported as low, intermediate, or high prob-ability of PE based on patterns of V/Q mis-match. A completely normal scan essentiallyexcludes PE with nearly 100% accuracy, but alow-probability scan still carries a 15% likeli-hood of PE. Perfusion deficits may occur inmany other lung conditions, including pleuraleffusion, chest mass, pulmonary hypertension,pneumonia, and COPD.
Duplex ultrasonography is a safe, nonin-vasive, portable technique for detectinglower extremity (primarily femoral vein)thrombi. A clot can be detected in up to 3ways: by visualizing the lining of the vein, bydemonstrating incompressibility of the vein,and by demonstrating reduced flow by Dop-pler. The test has a sensitivity of > 90% and aspecificity of > 95% for thrombus. It cannotreliably detect a clot in calf or iliac veins. Ab-sence of thrombi in the femoral veins does notexclude the possibility of thrombus fromother sources, but patients with negative du-plex test results have > 95% event-free sur-vival, because thrombi from other sources areso much less common. Ultrasonography hasbeen incorporated into many diagnostic al-gorithms, because an ultrasound positive forfemoral vein thrombosis indicates the needfor anticoagulation, which may make furthertesting for PE or other thrombi unnecessary.
045_062PUL Page 415 Tuesday, November 8, 2005 10:54 AM

416
Fig
. 50–
1. E
CG
in p
ulm
onar
y em
bolis
m. E
CG
sho
ws
sinu
s rh
ythm
at a
rat
e of
75
beat
s/m
in; S
wav
e in
lead
I w
ith Q
-wav
e, T
-wav
e in
vers
ion,
and
ST-s
egm
ent e
leva
tion
in le
ad I
II (
S1Q
3T3)
; and
QR
S ri
ght a
xis
devi
atio
n w
ith R
-wav
e am
plitu
de g
reat
er th
an S
-wav
e am
plitu
de in
lead
V1.
The
re a
repe
aked
P w
aves
in le
ad I
I.
045_062PUL Page 416 Tuesday, November 8, 2005 10:54 AM

50 PULMONARY EMBOLISM 417
Contrast helical (spiral) CT scanning is an al-ternative to V/Q scanning and pulmonary arte-riography in many settings because it is fast,available, and noninvasive and gives more in-formation about other lung pathology. How-ever, the patient must be able to hold his breath
for several seconds. The sensitivity of CT ishighest for PE in lobar and segmental vesselsand lowest for emboli in smaller subsegmentalvessels (about 30% of all PEs) and thus is lesssensitive than perfusion scans (60% vs > 99%).It is also less specific than pulmonary arterio-
TABLE 50–2. CLINICAL PREDICTION RULE FOR DIAGNOSING PULMONARY EMBOLISM
I. Establish clinical probability— add risks to determine probability
CLINICAL RISK POINTS
Clinical signs and symptoms of DVT (objective leg swelling, pain with palpation) 3PE as or more likely than alternative diagnosis 3Heart rate > 100 beats/min 1.5Immobilization ≥ 3 days 1.5Surgery in previous 4 wk 1.5Previous DVT or PE 1.5Hemoptysis 1Malignancy (including those stopping cancer treatment within 6 mo) 1
High probability: > 6Moderate probability: 2–6Low probability: < 2
II. Use pretest probability to determine testing
DVT = Deep venous thrombosis; PE = pulmonary embolism; V/Q = ventilation/perfusion.
Low PretestProbability
Moderate PretestProbability
High PretestProbability
D-dimer
D-dimer Duplex ultrasonography* (if negative, → CT), CT**, or V/Q scan
Not sick Sick Not sick Sick
Negative Positive
Negative Positive
Negative Positive
Negative Positive
Negative Positive
Negative PositiveQuit CT, duplex
ultrasonography,or V/Q scan
Quit CT, duplexultrasonography,
or V/Q scan
Full evaluationfor other diagnoses
Full evaluationfor other diagnoses
CT, V/Q scan,or duplex
ultrasonography
Heparinize
Treat
Treat
Considerangiographyor V/Q scan
Considerangiographyor V/Q scan
Discontinueheparin; treat for other
diagnoses
Treat forother
diagnoses*Quickest in most places.** Quickest in some places.
045_062PUL Page 417 Tuesday, November 8, 2005 10:54 AM

418 SECTION 5 PULMONARY DISORDERS
grams (90% vs > 95%), because visual artifactscan result from incomplete mixing of contrast.A positive scan may be diagnostic of PE, but anegative scan does not necessarily exclude sub-segmental disease, though the clinical signifi-cance of emboli in smaller subsegmental ves-sels remains to be determined. New scannerswith higher resolution are likely to improve thediagnostic accuracy, thereby replacing perfu-sion scans and arteriograms.
Echocardiography as a diagnostic test for PEis controversial. Its sensitivity is > 80% for de-tecting right ventricular dysfunction (eg, dila-tion and hypokinesis, which occur where pul-monary artery pressure exceeds 40 mm Hg).This is a useful measure of hemodynamic sever-ity in acute PE, but right ventricular dysfunctionis present in multiple conditions, includingCOPD, heart failure, and sleep apnea and istherefore a nonspecific finding. Estimation ofpulmonary artery systolic pressure using Dop-pler flow signals gives additional useful infor-mation about the severity of acute PE. Absenceof right ventricular dysfunction or pulmonaryhypertension makes the diagnosis of a large PEunlikely but does not exclude the diagnosis.
Cardiac marker testing is evolving as a use-ful means of stratifying mortality risk in pa-tients with acute PE. Elevated troponin levelscan signify right ventricular strain. Elevatedbrain natriuretic peptide (BNP) and pro-BNPlevels are not helpful, but low levels appear tosignify good prognosis. The clinical role ofthese tests remains to be determined, becausethey are not specific either for right ventricu-lar strain or pulmonary embolism.
ABG and exhaled PCO2 measurement al-lows for estimation of physiologic dead space(ie, the fraction of ventilated lung that is notperfused). When dead space is < 15% and D-dimer is low, the negative predictive value foracute PE is 98%.
Invasive tests: Pulmonary angiographyis indicated when the pretest probability ofPE is moderate or high and noninvasive testsare inconclusive; when the need to make orexclude the diagnosis is urgent, such as in anacutely ill patient; and when anticoagulationis contraindicated.
Pulmonary arteriography is still the mostaccurate test for diagnosing PE, but it is neededmuch less often because of the sensitivity of ul-trasonography and helical CT. An arteriogramwith intraluminal filling defects or abrupt cut-off of flow is positive. Findings suggestive butnot diagnostic of PE include partial occlusionof pulmonary arterial branches with increased
proximal and decreased distal caliber,oligemic zones, and persistence of dye in theproximal artery during the late (venous) phaseof the arteriogram. In lung segments with ob-structed arteries, venous filling with contrastmedium is delayed or absent.
PrognosisAn estimated 10% of patients with PE die
within 1 h. Of those who survive the 1st hour,only about 30% are diagnosed and receivetreatment; > 95% of these patients survive.Thus, most mortality from PE occurs in patientswho are never diagnosed, and the best prospectsfor reducing mortality lie in improving diagno-sis, not in improving treatment. Patients withchronic thromboembolic disease represent atiny fraction of patients with PE who survive.Anticoagulant therapy reduces the rate of re-currence of PE to about 5% in all patients.
TreatmentInitial treatment of PE is O2 for hypoxemia
and IV 0.9% saline and vasopressors forhypotension. All patients with strongly sus-pected or confirmed PE should be hospital-ized and, ideally, should also be continuallymonitored for life-threatening cardiovascu-lar complications in the first 24 to 48 h. Sub-sequent treatment involves anticoagulationand sometimes clot elimination.
Clot elimination: Clot dissolution or re-moval should be considered for hypotensivepatients. It may also be indicated for patientswith clinical, ECG, and/or echocardiographicevidence of right ventricular overload or fail-ure, but data supporting this indication are notdefinitive. Clot dissolution is achieved usingembolectomy or IV thrombolytic therapy.
Embolectomy is reserved for patients withPE who are on the verge of cardiac or respiratoryarrest (persistent systolic BP ≤ 90 mm Hg afterfluid therapy and O2 or if pressor therapy isrequired). Suction or fragmentation of theembolus through a pulmonary artery catheterminimizes the morbidity of surgical embolec-tomy but with undocumented advantages in ef-ficacy. Surgical embolectomy appears to im-prove survival in patients with massive PE butis not widely available and is associated withsubstantial mortality. The decision to proceedwith embolectomy and the choice of techniquedepends on local resources and expertise.
Thrombolytic therapy with tissue plasmino-gen activator (tPA), streptokinase, or urokinaseoffers a noninvasive way to rapidly restore pul-monary blood flow but is controversial, because
045_062PUL Page 418 Tuesday, November 8, 2005 10:54 AM

50 PULMONARY EMBOLISM 419
long-term benefits do not clearly outweigh therisk of hemorrhage. Thrombolytics speed theresolution of radiographic abnormalities andhemodynamic function (heart rate and rightventricular function) and prevent cardiopulmo-nary deterioration in patients with submassivePE but have not been shown to improve survival.Thrombolytics are recommended by some fornormotensive PE patients with echocardio-graphic evidence of proximal pulmonary artery(large) embolism or of right ventricular dys-function due to PE or preexisting disease. Othersreserve thrombolytic therapy for patients withmassive PE (hypotension, hypoxemia, or ob-struction of 2 or more lobar arteries). Absolutecontraindications to thrombolytics include priorhemorrhagic stroke; active bleeding from anysource; intracranial trauma or surgery within2 mo; recent femoral or large arterial puncture;GI bleeding, including guaiac-positive stools(< 6 mo); and CPR. Relative contraindicationsinclude recent surgery (≤ 10 days), hemorrhagicdiathesis (as in hepatic insufficiency), preg-nancy, and severe hypertension (systolic BP> 180 or diastolic BP > 110 mm Hg).
Options for thrombolysis include strep-tokinase, urokinase, and alteplase (recombi-nant tPA). No agent is proven superior. Stan-dard IV regimens are streptokinase 250,000units over 30 min followed by continuous in-fusion of 100,000 units/h for 24 h; urokinase4400 units/kg over 10 min followed by 4400units/kg/h for 12 h; or alteplase 100 mg con-tinuous infusion over 2 h followed by an ad-ditional 40 mg over another 4 h (10 mg/h) ifclinical presentation and repeat pulmonaryangiogram suggests failure of clot lysis andinitial dosing does not cause bleeding. Strep-tokinase is now rarely used because it is as-sociated with allergic and pyrogenic reac-tions and requires constant infusion.
An initial loading dose of heparin should begiven concurrently, but the activated PTTshould be allowed to fall to 1.5 to 2.5 times thebaseline value before beginning continuous in-fusion. Direct delivery of thrombolytics to theclot via a pulmonary artery catheter is occa-sionally used for patients with massive PE orfor those with relative contraindications to sys-temic thrombolytics, but this approach doesnot prevent systemic thrombolysis. Bleeding,if it occurs, can be reversed with cryoprecipi-tate or fresh frozen plasma and compression ofvascular access sites.
Anticoagulation: Because venous throm-boses rarely embolize completely, anticoagu-lation is required acutely to prevent residual
clots from extending and embolizing. Patientsin whom anticoagulants are contraindicated orthose who have thromboemboli despite thera-peutic anticoagulation should have placementof a percutaneous inferior vena cava filter.
Heparin, either unfractionated or low molwt, is the mainstay of treatment of acute DVTand PE and should be given immediately on di-agnosis or sooner if clinical suspicion is high;inadequate anticoagulation in the first 24 h islinked to increased risk of recurrent PE for upto 3 mo. Heparin accelerates the action of anti-thrombin III, an inhibitor of coagulation fac-tors; unfractionated heparin also has antithrom-bin III–mediated anti-inflammatory properties,which may facilitate clot organization and re-duce thrombophlebitis. Unfractionated hep-arin should be given as a bolus and infusionby protocol (see TABLE 50–3) to achieve anactivated PTT 1.5 to 2.5 times that of normalcontrol. Subcutaneous low mol wt heparin(LMWH) is as efficacious as unfractionated he-parin and may cause less thrombocytopenia.Because of its long half-life, it is useful in out-
TABLE 50–3. WEIGHT-BASEDNOMOGRAM FOR HEPARIN
1. Heparin bolus 80 units/kg, followed by2. Heparin infusion 18 units/kg/h*3. Check PTT 6 h after bolus4. Adjust heparin as needed:
PTT(sec)
Infusion RateChange (mL/h)*
< 35 Repeat 80 units/kg bolus, increase rate by 4 units/kg/h
35−45 Repeat 80 units/kg bolus, increase rate by 2 units/kg/h
46−70 No change71−90 Reduce rate by
2 units/kg/h> 90 Hold infusion for 1 h,
reduce rate by3 units/kg/h
5. Check PTT 6 h after dosage change; when two consecutive PTTs are therapeutic, check q 24 h.
*Heparin concentration = 40 units/mL, usu-ally as 20,000 units/500 mL.
Adapted from Raschke RA et al. Annals ofInternal Medicine 119:874–881, 1993.
045_062PUL Page 419 Tuesday, November 8, 2005 10:54 AM

420 SECTION 5 PULMONARY DISORDERS
patient treatment of DVT and to facilitate earlierdischarge of patients who have not achievedtherapeutic anticoagulation with warfarin.
All heparins can cause bleeding, throm-bocytopenia, urticaria, and, rarely, thrombosisor anaphylaxis. Long-term heparin adminis-tration may cause hypokalemia, liver enzymeelevations, and osteoporosis. Patients shouldbe screened for bleeding with serial CBCs andtests for occult blood in stool. Bleeding causedby overheparinization can be stopped with amaximum of 50 mg of protamine per 5000units unfractionated heparin (or 1 mg in 20 mLnormal saline infused over 10 to 20 min forLMWH, though the precise dose is undefinedbecause protamine only partially neutralizesLMWH inactivation of factor Xa). Treatmentwith heparin or LMWH is continued until fullanticoagulation has been achieved with oralwarfarin. The use of LMWH in long-term an-ticoagulation after acute PE has not been stud-ied but will likely be limited by cost and easeof administration compared with oral warfarin.
Warfarin is the oral drug of choice for long-term anticoagulation in all patients exceptpregnant women and patients with new orworsening venous thromboembolism duringwarfarin treatment. Five to 10 mg po once/day should be started within 48 h of onset ofeffective heparinization or, in the rare patientwith protein C deficiency, only after thera-peutic anticoagulation is achieved. The ther-apeutic goal is usually an INR of 2 to 3.
Physicians prescribing warfarin should bewary of multiple drug interactions, includinginteractions with nonprescription medicinalherbs. Patients with transient risk factors forDVT or PE (eg, fracture or surgery) can stop thedrug after 3 to 6 mo. Patients with nontransientrisk factors (eg, hypercoagulability), no knownrisk factors, or recurrent DVT or PE should takewarfarin for at least 6 mo and possibly for lifeunless complications of therapy intervene. Inlow-risk patients, low-intensity warfarin (tomaintain INR at 1.5 to 2.0) may be safe and ef-fective for at least 2 to 4 yr, but this regimen re-quires further proof of safety before it can beroutinely recommended. Bleeding is the mostcommon complication of warfarin treatment;patients > 65 and those with comorbidities (es-pecially diabetes, recent MI, Hct < 30%, cre-atinine > 1.5 mg/dL) and a history of stroke orGI bleeding appear to be at greatest risk. Bleed-ing can be reversed with 2.5 to 10 mg of vitaminK sc or po and, in an emergency, with fresh fro-zen plasma. Vitamin K may cause flushing, lo-cal pain, and, rarely, anaphylaxis.
Inferior vena cava filter (IVCF) placementis reserved for patients with contraindica-tions to anticoagulation and thrombolysis,with recurrent emboli on adequate anticoag-ulation, or after pulmonary embolectomy.Several kinds of filters are available, differingin size and retrievability. The filter is placedvia catheterization of the internal jugular orfemoral veins; optimum location is just be-low the entry of the renal veins. Filters reduceacute and subacute thrombotic complica-tions but are associated with longer termcomplications; for example, venous collateralscan develop and provide a pathway by whichPE can still occur around the filter. Patientswith recurrent DVT or chronic risks for DVTmay therefore still require anticoagulation;the filters provide some protection until con-traindications to anticoagulation subside orresolve. Despite widespread use of filters,efficacy in preventing PE is unstudied andunproven.
PreventionPrevention of PE means prevention of
DVT; the need depends on the patient's risks.Bed-bound patients and those undergoingsurgical, especially orthopedic, proceduresespecially benefit, and most of these patientscan be identified before a thrombus forms(see TABLE 50–4). Preventive drugs includelow-dose unfractionated heparin (LDUH),LMWH, warfarin, newer anticoagulants, com-pression devices, and stockings.
Choice of drug or device depends on dura-tion of treatment, contraindications, relativecosts, and ease of use.
LDUH is given in doses of 5000 units sc 2 hpreoperatively and q 8 to 12 h thereafter for 7 to10 days or until the patient is fully ambulatory.Immobilized patients not undergoing surgeryshould receive 5000 units sc q 12 h indefinitelyor until reversal of risk.
LMWH dosing depends on the drug;enoxaparin 30 mg sc q 12 h, dalteparin 2500units once/day, and tinzaparin 3500 unitsonce/day are 3 of many equally effectiveLMWHs that are as efficacious as LDUH forpreventing DVT and PE.
Warfarin is usually effective and safe at adose of 2 to 5 mg once/day or at a dose ad-justed to maintain an INR of 1.5 to 2.
Newer anticoagulants, including hirudin,a subcutaneous direct thrombin inhibitor;ximelagatran (melagatran), an oral directthrombin inhibitor; and danaparoid andfondaparinux, which are selective factor Xa
045_062PUL Page 420 Tuesday, November 8, 2005 10:54 AM
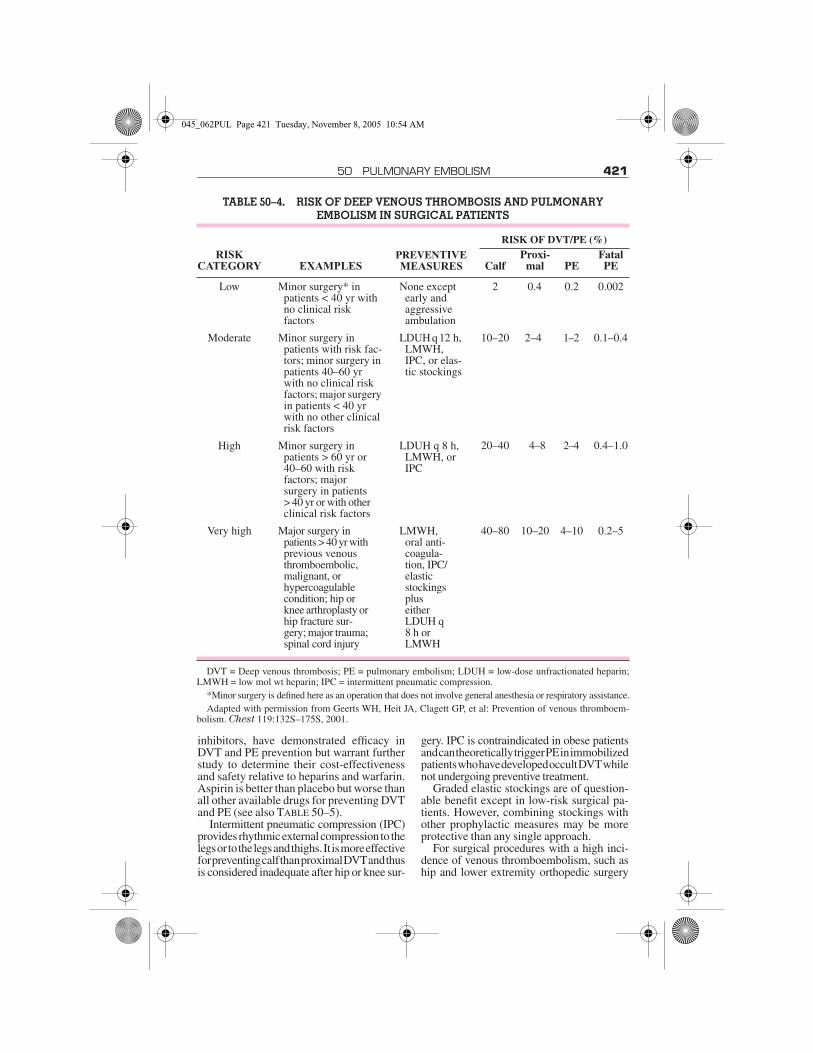
50 PULMONARY EMBOLISM 421
inhibitors, have demonstrated efficacy inDVT and PE prevention but warrant furtherstudy to determine their cost-effectivenessand safety relative to heparins and warfarin.Aspirin is better than placebo but worse thanall other available drugs for preventing DVTand PE (see also TABLE 50–5).
Intermittent pneumatic compression (IPC)provides rhythmic external compression to thelegs or to the legs and thighs. It is more effectivefor preventing calf than proximal DVT and thusis considered inadequate after hip or knee sur-
gery. IPC is contraindicated in obese patientsand can theoretically trigger PE in immobilizedpatients who have developed occult DVT whilenot undergoing preventive treatment.
Graded elastic stockings are of question-able benefit except in low-risk surgical pa-tients. However, combining stockings withother prophylactic measures may be moreprotective than any single approach.
For surgical procedures with a high inci-dence of venous thromboembolism, such aship and lower extremity orthopedic surgery
TABLE 50–4. RISK OF DEEP VENOUS THROMBOSIS AND PULMONARY EMBOLISM IN SURGICAL PATIENTS
RISKCATEGORY EXAMPLES
PREVENTIVE MEASURES
RISK OF DVT/PE (%)
CalfProxi-
mal PEFatal PE
Low Minor surgery* in patients < 40 yr with no clinical riskfactors
None except early and aggressive ambulation
2 0.4 0.2 0.002
Moderate Minor surgery in patients with risk fac-tors; minor surgery in patients 40–60 yr with no clinical risk factors; major surgery in patients < 40 yr with no other clinical risk factors
LDUH q 12 h, LMWH, IPC, or elas-tic stockings
10–20 2–4 1–2 0.1–0.4
High Minor surgery in patients > 60 yr or 40–60 with riskfactors; majorsurgery in patients > 40 yr or with other clinical risk factors
LDUH q 8 h, LMWH, or IPC
20–40 4–8 2–4 0.4–1.0
Very high Major surgery in patients > 40 yr with previous venous thromboembolic, malignant, or hypercoagulable condition; hip or knee arthroplasty or hip fracture sur-gery; major trauma; spinal cord injury
LMWH, oral anti-coagula-tion, IPC/elastic stockings plus either LDUH q 8 h or LMWH
40–80 10–20 4–10 0.2–5
DVT = Deep venous thrombosis; PE = pulmonary embolism; LDUH = low-dose unfractionated heparin;LMWH = low mol wt heparin; IPC = intermittent pneumatic compression.
*Minor surgery is defined here as an operation that does not involve general anesthesia or respiratory assistance.Adapted with permission from Geerts WH, Heit JA, Clagett GP, et al: Prevention of venous thromboem-
bolism. Chest 119:132S–175S, 2001.
045_062PUL Page 421 Tuesday, November 8, 2005 10:54 AM

422 SECTION 5 PULMONARY DISORDERS
(see TABLE 50–4), both LDUH and aspirin areinadequate; LMWH or adjusted-dose war-farin is recommended. For total knee replace-ment, risk reductions provided by LMWH andIPC are comparable, and the combinationshould be considered for patients with con-comitant clinical risks. The regimens for or-thopedic surgery may be initiated preopera-tively and should be continued for at least 7days postoperatively. In selected patients atvery high risk of both venous thromboembo-lism and bleeding, placement of an IVCF is aprophylactic option.
A high incidence of venous thromboembo-lism is also associated with elective neurosur-gery, acute spinal cord injury, and multipletrauma. Although physical methods (IPC,elastic stockings) have been used in neurosur-gical patients because of concern about intra-cranial bleeding, LMWH appears to be an ac-ceptable alternative. The combination of IPC
and LMWH may be more effective than eitheralone in high-risk patients. Limited data sup-port the combination of IPC, elastic stockings,and LMWH in spinal cord injury or in multipletrauma. For very high risk patients, an IVCFmay be considered.
The most common nonsurgical conditionsin which DVT prophylaxis is indicated areacute MI and ischemic stroke. For MI pa-tients, LDUH is effective; IPC, elastic stock-ings, or both may be used when anticoagu-lants are contraindicated. For stroke patients,LDUH or LMWH can be used; IPC, elasticstockings, or both may be beneficial.
Recommendations for some other nonsur-gical conditions include LDUH for patientswith heart failure; adjusted-dose warfarin(INR 1.3 to 1.9) for patients with metastaticbreast cancer; and warfarin 1 mg/day for can-cer patients with an indwelling centralvenous catheter.
TABLE 50–5. ANTICOAGULATION OPTIONS IN THROMBOEMBOLIC DISEASE
CATEGORY DOSE COMMENTS CATEGORY DOSE COMMENTS
Heparins Tinzaparin 175 units/kg sc dailyUnfractionated
heparinSee TABLE 50–3 Vitamin K inhibitor
Low mol wt Warfarin 5 mg daily initially, then titrate to desired INR
Ardeparin 50 units/kg sc q 12 h
Not for IM or IV use—not indicated for PE
Certoparin 3000 units sc daily Thrombin inhibitors
Hirudin 0.75 mg/kg sc q 12 hDalteparin 2500 units
IV bolus200 units/kg sc daily
Lepirudin 1.25 mg/kg sc q 12 hDanaparoid 2000 unit IV
bolus, then 750 units sc q 12 h
Heparinoid; monitor using antifactor Xa assay
Argatroban 2 µg/kg/min IV infusion (for HIT) or 350 µg/kg IV bolus, then 25 µg/kg/min (for PCI)
Enoxaparin 1 mg/kg sc q 12 h or 1.5 mg/kg sc daily
Nadroparin 200 units/kg sc q 12 h
Parnaparin 3200 to 4250 units sc daily
Prophylaxis dose
Ximelagatran (melagatran)
24 µg po q 12 h
Factor Xa inhibitorReviparin 1750 units
sc dailyProphylaxis dose
Fonda-parinux
2.5 mg sc daily
PE = pulmonary embolism; HIT = heparin-induced thrombocytopenia; PCI = percutaneous coronaryintervention.
045_062PUL Page 422 Tuesday, November 8, 2005 10:54 AM

423
51ACUTE BRONCHITISAcute bronchitis is inflammation of theupper airways, commonly following a URI.The cause is usually a viral infection thoughit is sometimes a bacterial infection; thepathogen is rarely identified. The most com-mon symptom is cough with or without feverand/or sputum production. In patients withCOPD, hemoptysis, burning chest pain, andhypoxemia may also occur. Diagnosis isclinical. Treatment is supportive; antibioticsare necessary only for patients with chroniclung disease. Prognosis is excellent in patientswithout lung disease, but in patients withCOPD, acute respiratory failure mayresult.
Acute bronchitis is frequently a compo-nent of a URI caused by rhinovirus, para-influenza, influenza A or B, respiratory syn-cytial virus, coronavirus, or other viral in-fection. Less common causes may be My-coplasma pneumoniae, Bordetella pertussis,and Chlamydia pneumoniae. Patients at riskinclude those who smoke and those withCOPD and other diseases that impair bron-chial clearance mechanisms, such as cystic fi-brosis or conditions leading to bronchiectasis(see p. 439).
Symptoms, Signs, and DiagnosisSymptoms are a nonproductive or mini-
mally productive cough accompanied or pre-ceded by URI symptoms. Subjective dyspnearesults from chest pain with breathing, not
hypoxia, except in those with underlyinglung disease. Signs are often absent but mayinclude scattered rhonchi and wheezing.Sputum may be clear, purulent, or, occasion-ally, bloody. Sputum characteristics do notcorrespond with a particular etiology (ie, vi-ral vs bacterial).
Diagnosis is based on clinical presenta-tion. Chest x-ray is only necessary if fever,dyspnea, or other symptoms and signs sug-gest pneumonia. Sputum gram stain and cul-ture have no role.
Treatment and PrognosisAcute bronchitis in otherwise healthy sub-
jects is a major reason that antibiotics areoverused. Nearly all patients require onlysymptomatic treatment, such as acetamin-ophen and hydration. Antitussives shouldonly be used to facilitate sleep (see p. 356).Patients with wheezing may benefit from aninhaled β-agonist (eg, albuterol) or an anti-cholinergic (eg, ipratropium) for ≤ 7 days.Oral antibiotics (eg, 7 days of amoxicillin500 mg tid, doxycycline 100 mg bid, or tri-methoprim-sulfamethoxazole 160/800 mgbid) are presumed to be beneficial for patientswith COPD (see p. 400) or other serious pul-monary disease who have at least 2 of the fol-lowing: increased cough, increased dyspnea,increase in sputum purulence.
Cough resolves within 2 wk in 75% of pa-tients. Patients with persistent cough shouldundergo a chest x-ray and be evaluated forpertussis (whooping cough) and noninfec-tious etiologies, such as postnasal drip, aller-gic rhinitis, and cough-variant asthma. Somepatients benefit from inhaled corticosteroidsfor a few days if cough persists because of air-way irritation.
52PNEUMONIA(See also Neonatal Pneumonia on p. 2332.)
Pneumonia is acute inflammation of thelungs caused by infection. Initial diagnosis isusually based on chest x-ray. Causes, symp-toms, treatment, preventive measures, andprognosis differ depending on whether the
infection is bacterial, viral, fungal, or para-sitic; whether it is acquired in the commu-nity, hospital, or nursing home; and whetherit develops in a patient who is immunocom-petent or immunocompromised.
An estimated 2 to 3 million people in theUS develop pneumonia each year, of whomabout 45,000 die. Pneumonia is the most
045_062PUL Page 423 Tuesday, November 8, 2005 10:54 AM

424 SECTION 5 PULMONARY DISORDERS
common fatal hospital-acquired infectionand the most common overall cause of deathin developing countries.
Bacteria are the most common cause ofpneumonia in adults > 30 yr, Streptococcuspneumoniae infection being the most com-mon pathogen across all age groups, settings,and geographic regions. However, pathogensof every sort, from viruses to parasites, causepneumonia.
The airways and lungs are constantly ex-posed to pathogens in the external environ-ment; the upper airways and oropharynx inparticular are colonized with so-called nor-mal flora rendered harmless by host defenses.Infection develops when pathogens over-come multiple host defenses.
Upper airway defenses include salivaryIgA, proteases, and lysozymes; growth in-hibitors produced by normal flora; and fi-bronectin, which coats the mucosae and in-hibits adherence. Nonspecific lower airwaydefenses include cough, mucociliary clear-ance, and airway angulation preventing in-fection in airspaces. Specific lower airwaydefenses include a variety of pathogen-specific immune mechanisms, includingIgA and IgG opsonization, anti-inflamma-tory effects of surfactant, phagocytosis by al-veolar macrophages, and T-cell–mediatedimmune responses. These mechanisms pro-tect most people against infection. But nu-merous conditions alter normal flora (eg,systemic illness, malnutrition, hospital ornursing home exposure, antibiotic expo-sure), increase virulence (eg, antibiotic ex-posure), or impair these defenses (eg, ciga-rette smoking, nasogastric or endotrachealintubation). Pathogens that then reach air-spaces by inhalation, contiguous or hema-togenous spread, or aspiration can multiplyand cause pneumonia.
Specific pathogens causing pneumoniacannot be found in > 1⁄2 of patients, even withextensive diagnostic investigation. But be-cause pathogens and outcomes tend to besimilar by setting and host risk factors, cate-gorization of pneumonias as community-acquired, hospital-acquired (including ven-tilator-acquired and postoperative), nursinghome–acquired, and those that occur in theimmunocompromised host allows treatmentto be established empirically.
The term interstitial pneumonia refers toa variety of unrelated conditions of un-known cause characterized by inflammationand fibrosis of the pulmonary interstitium.
These conditions bear little resemblance toinfectious pneumonia and are discussed inCh. 55 on p. 443.
COMMUNITY-ACQUIRED PNEUMONIA
Community-acquired pneumonia developsin people with limited or no contact withmedical institutions or settings. The mostcommonly identified pathogens are Strepto-coccus pneumoniae, Haemophilus influen-zae, and atypical organisms (ie, Chlamydiapneumoniae, Mycoplasma pneumoniae,Legionella sp). Symptoms and signs arefever, cough, dyspnea, tachypnea, andtachycardia. Diagnosis is based on clinicalpresentation and chest x-ray. Treatment iswith empirically chosen antibiotics. Prog-nosis is excellent for relatively young and/or healthy patients, but many pneumonias,especially when caused by S. pneumoniaeand influenza virus, are fatal in older, sickerpatients.
EtiologyMany organisms cause community-ac-
quired pneumonia, including bacteria, viruses,and fungi. Pathogens vary by patient age andother factors (see TABLES 52–1 and 52–2), butthe relative importance of each as a cause ofcommunity-acquired pneumonia is uncertain,because most patients do not undergo thor-ough testing, and because even with testing,specific agents are identified in < 50% of cases.
S. pneumoniae, H. influenzae, C. pneumo-niae, and M. pneumoniae are the most com-mon bacterial causes. Chlamydia and myco-plasma are clinically indistinguishable fromother causes. Common viral agents includerespiratory syncytial virus (RSV), adenovi-rus, influenza, metapneumovirus, and para-influenza virus in children and influenza inthe elderly. Bacterial superinfection canmake distinguishing viral from bacterialinfection difficult.
C. pneumoniae accounts for 5 to 10% ofcommunity-acquired pneumonia and is the 2ndmost common cause of lung infections inhealthy people aged 5 to 35 yr. C. pneumoniaeis commonly responsible for outbreaks of res-piratory infection within families, in collegedormitories, and in military training camps. Itcauses a relatively benign form of pneumoniathat infrequently requires hospitalization.
045_062PUL Page 424 Tuesday, November 8, 2005 10:54 AM

52 PNEUMONIA 425
Chlamydia psittaci pneumonia (psittacosis)occurs in patients who own birds.
A host of other organisms cause lung infec-tion in immunocompetent patients, althoughthe term community-acquired pneumonia isusually reserved for the more common bacte-rial and viral etiologies.
Q fever, tularemia, anthrax, and plague areuncommon bacterial syndromes in whichpneumonia may be a prominent feature; thelatter three should raise the suspicion of bio-terrorism.
Adenovirus, Epstein-Barr virus, and cox-sackievirus are common viruses that rarelycause pneumonia. Varicella virus and hanta-virus cause lung infection as part of adultchickenpox and hantavirus pulmonary syn-drome; a novel coronavirus causes severeacute respiratory syndrome (SARS—seep.1600).
The most common fungal pathogens areHistoplasma capsulatum (histoplasmosis)and Coccidioides immitis (coccidioidomy-cosis). Less common fungi include Blasto-myces dermatitidis (blastomycosis) andParacoccidioides braziliensis (paracoccid-ioidomycosis).
Parasites causing lung infection in devel-oped countries include Plasmodium sp (ma-laria), Toxocara canis or catis (visceral larvamigrans), Dirofilaria immitis (dirofilariasis),and Paragonimus westermani (paragonimi-asis). (For a discussion of pulmonary TB orof specific microorganisms, see p. 1508.)
Symptoms and SignsSymptoms include malaise, cough, dysp-
nea, and chest pain. Cough typically is pro-ductive in older children and adults and dry
TABLE 52–1. COMMUNITY-ACQUIRED PNEUMONIA IN CHILDREN
AGE ORGANISMS TREATMENT
Birth to 3 wk Group B streptococci, Listeria monocytogenes, gram-negative bacilli, cytomegalovirus
Ampicillin (or nafcillin)and
Gentamicin (or cefotaxime)*
3 wk to 3 mo Streptococcus pneumoniae, viral infection (RSV, parain-fluenza, metapneumovirus), Bordetella pertussis, Staphylo-coccus aureus, Chlamydia tra-chomatis (transnatal exposure)
Outpatient: Erythromycin 10 mg/kg IV q 6 h for 10−14 days
Inpatient non-ICU: Cefuroxime 50 mg/kg IV q 8−12 hInpatient ICU: Cefotaxime 66 mg/kg IV tid
and Cloxacillin 50 mg/kg IV q 6 h
4 mo to 4 yr S. pneumoniae, viral infection (RSV, parainfluenza, influ-enza, adenovirus, rhinovirus, metapneumovirus), Myco-plasma pneumoniae (in older children), group A streptococci
Outpatient:Erythromycin 10 mg/kg po qid
Inpatient: Erythromycin 10 mg/kg po qid and
Cefuroxime 50 mg/kg IV q 8 h
5 to 15 yr S. pneumoniae, M. pneumoniae, Chlamydia pneumoniae
Outpatient: Clarithromycin 500 mg po bid Inpatient: Ceftriaxone 50 mg/kg once/day IV (maximum 2 g) and
Azithromycin 10 mg/kg once/day (maximum 500 mg)
RSV = respiratory syncytial virus.*For doses and discussion of neonatal pneumonia, see p. 2332.Data from McIntosh K: Community-acquired pneumonia in children. The New England Jour-
nal of Medicine 346:429–437, 2002.
045_062PUL Page 425 Tuesday, November 8, 2005 10:54 AM

426 SECTION 5 PULMONARY DISORDERS
TABLE 52–2. COMMUNITY-ACQUIRED PNEUMONIA IN ADULTS
GROUP LIKELY ORGANISMS EMPIRIC TREATMENT
I. Outpatients—No modify-ing factors present*
Streptococcus pneumoniae, Mycoplasma pneumoniae, Chlamydia pneumoniae, Hae-mophilus influenzae, respira-tory viruses, miscellaneous (Legionella sp, Mycobacterium tuberculosis, endemic fungi)
Macrolide (azithromycin 500 mg po once, then 250 mg once/day; clarithromycin 250 to 500 mg po bid); or extended-release clarithromycin 1 g once/dayor
Doxycycline 100 mg po bid (if allergic to macrolide)
II. Outpatients—Modifying factors present
S. pneumoniae, including drug-resistant forms; M. pneumo-niae; C. pneumoniae; mixed infection (bacteria + atypical pathogen or virus); H. influen-zae; enteric gram negatives; res-piratory viruses; miscellaneous (Moraxella catarrhalis, Legionella sp, anaerobes [aspi-ration], M. tuberculosis, endemic fungi)
β-lactam (cefpodoxime 200 mg po q 12 h; cefuroxime 500 mg po q 12 h; amoxicillin 1 g q 8 h; amoxicillin/clavulanate 875/125 mg q 12 h) plus
Macrolide or doxycycline (if allergic to macrolide) po or
Antipneumococcal fluoroqui-nolone† po
IIIA. Inpatient—Not in ICU, no modifying factors
S. pneumoniae, H. influenzae; M. pneumoniae; C. pneumoniae; mixed infection (bacteria + atypical pathogen or virus); res-piratory viruses; Legionella sp, miscellaneous (M. tuberculosis, endemic fungi, Pneumocystis jiroveci (formerly P. carinii)
Azithromycin 500 mg IV q 24 h,or
Doxycycline 100 mg po bidplus
β-lactam (see Group II forchoices) if macrolide allergic or intolerantor
Antipneumococcal fluoroqui-nolone† IV
IIIB. Inpatient—Not in ICU, modify-ing factors
S. pneumoniae, including drug-resistant forms; H. influenzae; M. pneumoniae; C. pneumo-niae; mixed infection (bacteria + atypical pathogen or virus); enteric gram-negatives; anaer-obes (aspiration); respiratory viruses; Legionella sp, miscella-neous (M. tuberculosis, endemic fungi, P. jiroveci)
β-lactam‡ IV (cefotaxime 1 to 2 g IV q 8 to 12 h; ceftriaxone 1 g IV q 24 h)plus
Macrolide (erythromycin 4−5 mg/kg po qid, azithromycin 500 mg IV or po q 24 h, or clarithromycin 250 to 500 mg po bid, or extended-release clarithromycin 1 g once/day), or doxycycline 100 mg po bidor
Antipneumococcal fluoroqui-nolone† IV
IVA. ICU patient—no Pseudomo-nas risk factors
S. pneumoniae, including drug-resistant forms, Legionella sp, H. influenzae, enteric gram-neg-atives, S. aureus, M. pneumo-niae, respiratory viruses, mis-cellaneous (C. pneumoniae, M. tuberculosis, endemic fungi)
β-lactam IV (cefotaxime 1 to 2 g IV q 8 to 12 h; ceftriaxone 1 g IV q 24 h) plus either
Antipneumococcal fluoroqui-nolone† IVor
Azithromycin 500 mg IV q 24 h
045_062PUL Page 426 Tuesday, November 8, 2005 10:54 AM

52 PNEUMONIA 427
in infants, young children, and the elderly.Dyspnea usually is mild and exertional and israrely present at rest. Chest pain is pleuriticand is adjacent to the infected area. Pneumo-nia may manifest as upper abdominal painwhen lower lobe infection irritates the dia-phragm. Symptoms become variable at theextremes of age; infection in infants maymanifest as nonspecific irritability and rest-lessness; in the elderly, as confusion and ob-tundation.
Signs include fever, tachypnea, tachycar-dia, crackles, bronchial breath sounds, ego-phony, and dullness to percussion. Signs ofpleural effusion may also be present (see p.493). Nasal flaring, use of accessory muscles,and cyanosis are common in infants.
Symptoms and signs were previouslythought to differ by type of pathogen, but pre-sentations overlap considerably. In addition,no single symptom or sign is sensitive or spe-cific enough to predict the organism. Symp-
toms are even similar for noninfective lungdiseases such as pulmonary embolism, pul-monary malignancy, and other inflammatorylung diseases.
DiagnosisDiagnosis is suspected on the basis of
clinical presentation and is confirmed bychest x-ray (see TABLE 52–3). The most se-rious condition misdiagnosed as pneumoniais pulmonary embolism, which may be morelikely in patients with minimal sputum pro-duction, no accompanying URI or systemicsymptoms, and risk factors for thromboem-bolism (see TABLE 50–1 on p. 413).
Chest x-ray almost always demonstratessome degree of infiltrate; rarely, an infiltrateis absent in the first 24 to 48 h of illness. Ingeneral, no specific findings distinguish onetype of infection from another, though mul-tilobar infiltrates suggest S. pneumoniaeor Legionella pneumophila infection, and
IVB. ICU patient—Pseudomo-nas risk factors present
Same as previous plus Pseudomonas sp
Antipseudomonal β-lactam§ or if β-lactam allergic or intolerant, aztreonam 1 to 2 g q 8 h, an aminoglycosideplus
Ciprofloxacin 400 mg IV q 12 hor
Antipseudomonal β-lactam§plus an aminoglycoside plus azithromycin or a nonpseu-domonal fluoroquinolone*
*Modifying factors:Increased risk of drug-resistant pneumococcus: Age > 65, alcoholism, β-lactam antibiotic within
3 mo, exposure to child in day care center, immunosuppression (including corticosteroid use; HIVinfection considered separately), multiple coexisting illnesses.
Increased risk of enteric gram-negatives: Antibiotic use within 3 mo, cardiopulmonary disease(including COPD and heart failure), multiple coexisting illnesses, nursing home residence.
Increased risk of Pseudomonas aeruginosa: Broad spectrum antibiotics > 7 days in past month, cor-ticosteroid use, malnutrition, structural pulmonary disease.† Antipneumococcal fluoroquinolones = levofloxacin 500 to 750 mg po or IV q 24 h, trovafloxacin
200 mg po or IV once/day (300 mg initial loading dose for hospital-acquired pneumonia), gemifloxa-cin 320 mg po once/day.
‡ Antipseudomonal fluoroquinolones = levofloxacin 500 mg po or IV q 24 h, gatifloxacin 400 mgpo or IV q 24 h.
§ Antipseudomonal β-lactams = cefepime 1 to 2 g IV q 12 h, imipenem 500 mg IV q 6 h, meropenem500 mg to 1 g IV q 8 h, piperacillin/ tazobactam 3.375 g IV q 4 h.
Data from Niederman MS, Mandell LA, Anzueto A, et al: Guidelines for the management of adultswith community-acquired pneumonia: Diagnosis, assessment of severity, antimicrobial therapy, andprevention. American Journal of Respiratory and Critical Care Medicine 163:1730–1754, 2001.
TABLE 52–2. COMMUNITY-ACQUIRED PNEUMONIA IN ADULTS—Continued
GROUP LIKELY ORGANISMS EMPIRIC TREATMENT
045_062PUL Page 427 Tuesday, November 8, 2005 10:54 AM

428 SECTION 5 PULMONARY DISORDERS
interstitial pneumonia suggests viral ormycoplasma etiology.
Hospitalized patients (see p. 430) shouldundergo WBC count and electrolytes, BUN,and creatinine testing to classify risk and hy-dration status. Two sets of blood cultures areoften obtained to detect pneumococcal bac-teremia and sepsis, because about 12% of allpatients hospitalized with pneumonia havebacteremia; S. pneumoniae accounts for 2⁄3of these cases. Whether the results of bloodcultures actually alter therapy commonlyenough to warrant the expense is under study.Pulse oximetry or ABG should also be per-formed.
Attempts to identify a pathogen are notroutinely indicated; exceptions may be madefor critically ill patients, patients in whom adrug-resistant or unusual organism is sus-pected (eg, TB), and patients who are dete-riorating or not responding to treatmentwithin 72 h. Sputum Gram stain and cultureare controversial, because specimens oftenare contaminated and because overall diag-nostic yield is low. Samples can be obtainednoninvasively by simple expectoration or af-ter hypertonic saline nebulization for thoseunable to produce sputum. Alternatively, pa-tients can undergo bronchoscopy or endo-tracheal suctioning, either of which can beeasily performed through an endotrachealtube in mechanically ventilated patients.
Testing should include mycobacterial andfungal stains and cultures in deterioratingpatients and in those unresponsive to broad-spectrum antibiotics.
Additional tests are indicated in some cir-cumstances. Patients at risk of Legionellapneumonia (eg, patients who smoke, havechronic pulmonary disease, are > 40, receivechemotherapy, or take immunosuppressantsfor organ transplantation) should undergourinary Legionella antigen testing, whichstays positive long after treatment is initiatedbut detects only L. pneumophila serogroup 1(70% of cases). A 4-fold rise in antibody titersto ≥ 1:128 (or a single convalescent serum of≥ 1:256) is also considered diagnostic. Thesetests are specific (95 to 100%) but are not verysensitive (40 to 60%); thus, a positive test in-dicates infection, but a negative test does notexclude it.
Infants and young children with possibleRSV infection should undergo rapid antigentesting of nasal or throat swabs. No other testsfor viral pneumonias exist; viral culture andserologic tests are rarely clinically warranted.
PCR testing for mycoplasma and chlamy-dia species, although not widely available,holds promise as a highly sensitive and spe-cific rapid diagnostic test and is likely to playa greater role as PCR technologies are refined.
A test for SARS-associated coronavirusexists, but its role in clinical practice is un-known, and its application is limited outsideof known outbreaks (see p. 1600). In rare sit-uations, anthrax should be considered (seep. 1449).
PrognosisCandidates for outpatient treatment usu-
ally improve over 24 to 72 h. Hospitalized pa-tients may improve or deteriorate dependingon comorbidities. Aspiration is a major riskfactor for death, as is older age, number andtype of comorbidities, and certain infectiousagents. Death may be caused by pneumoniaitself, progression to sepsis syndrome affect-ing other organs, or exacerbation of underly-ing comorbidities.
Pneumococcal infection still accounts forabout 66% of all fatal cases of community-acquired pneumonia in which an etiologicagent is known. The overall mortality rate inhospitalized patients is about 12%. Poorprognostic factors include age < 1 or > 60 yr;involvement of more than one lobe; periph-eral WBC count < 5000/µL; comorbidities(heart failure, alcoholism, hepatic and renal
TABLE 52–3. PROBABILITY OF PNEUMONIA GIVEN CHEST
X-RAY INFILTRATE
Assign 1 point each for:� Temperature > 37.8°C� Heart rate > 100 beats/min� Crackles on auscultation� Decreased breath sounds� Absence of asthma
SCORE
LIKELI-HOOD RATIO
PROBABILITY OF PNEUMONIA*
0–1 0.3 ≤ 1%2–3 — 3–10%4–5 8.2 25–50%
*Based on baseline prevalence (pretest proba-bility) of 5%.
Data from Heckerling PS, Tape TG, WigtonRS, et al: Clinical prediction rule for pulmonaryinfiltrates. Annals of Internal Medicine 113:664–670, 1990.
045_062PUL Page 428 Tuesday, November 8, 2005 10:54 AM

52 PNEUMONIA 429
insufficiency), immunosuppression (agam-maglobulinemia, anatomic or functionalasplenia), infection with serotypes 3 and 8;and hematogenous spread with either posi-tive blood cultures or extrapulmonary com-plications (arthritis, meningitis, or endocardi-tis). Infants and children are at special risk ofpneumococcal otitis media, bacteremia, andmeningitis.
Mortality in Legionella infection is 10 to20% among community-acquired cases andis higher among immunosuppressed or hos-pitalized patients. Patients who respond do soslowly, and x-ray abnormalities usually per-sist for ≥ 1 mo. Most patients require hospi-talization, many require ventilator support,and 10 to 20% die despite appropriate antibi-otic therapy.
Prognosis in mycoplasma pneumonia isexcellent; nearly all patients recover. Chla-mydial pneumoniae responds slower to treat-ment than mycoplasma and tends to recur iftherapy is stopped prematurely. Young adultsusually do well, but the elderly have a mor-tality rate of 5 to 10%.
TreatmentA prediction rule may be used to identify
those patients who can be safely treated asoutpatients and those who require hospital-ization because of high risk of complications(see TABLE 52–4). The rule should supple-ment, not replace, clinical judgment, becausemany unrepresented factors, such as likeli-hood of adherence, ability to care for self, andwishes to avoid hospitalization, should alsoinfluence triage decisions. ICU admission isrequired for patients who need mechanicalventilation and for those with hypotension(systolic BP < 90 mm Hg). Other criteria forICU admission include respiratory rate > 30/min, PaO2/inspired O2 (FIO2) < 250, multilo-bar pneumonia, diastolic BP < 60 mm Hg,confusion, and BUN > 19.6 mg/dL. Appro-priate treatment involves starting antibioticsas soon as possible, preferably ≤ 8 h after pre-sentation. Supportive care includes fluids,antipyretics, analgesics, and O2 for patientswith hypoxemia.
Because organisms are difficult to iden-tify, antibiotics are selected based on likelypathogens and severity of illness. Consen-sus guidelines have been developed by manyprofessional organizations; one widely usedset is detailed in TABLE 52–2. Guidelinesshould be adapted to local susceptibility pat-
terns, drug formularies, and individual pa-tient circumstances. Importantly, none pro-vide recommendations for treatment of viralpneumonia.
TABLE 52–4. RISK STRATIFICATION FOR COMMUNITY-ACQUIRED
PNEUMONIA
FACTOR POINTS
AgeMenWomen
Age (yr)Age (yr) −10
Nursing home resident 10
Coexisting illnessMalignancy 30Liver disease 20Heart failure 10Cerebrovascular disease 10Renal disease 10
Physical examinationAltered mental status 20Respiratory rate ≥ 30 20Systolic BP < 90 mm Hg 20Temperature ≥ 40° or < 35°C 15Heart rate ≥ 125 beats/min 10
Test resultsArterial pH < 7.35 30BUN ≥ 30 mg/dL (11 mmol/L)
20
Na <130 mmol/L 20Glucose ≥ 250 mg/dL (14 mmol/L)
10
Hematocrit < 30% 10PaO2 < 60 mm Hg or O2sat < 90%*
10
Pleural effusion 10
POINTS MORTALITY RECOMMENDATION
≤ 70 <1% Outpatient treatment†
71−90 <5% Outpatient treatment†
91−130 5−15% Admit>130 >15% Admit
*Many consider hypoxemia an absolute indi-cation for admission.
†Consider acute care admission, subacute careadmission, observation period, home IV antibi-otics, or home nursing visits for patients who arefrail, isolated, or living in unstable environments.
Adapted from Pneumonia: New predictionmodel proves promising (AHCPR Publication No.97-R031).
045_062PUL Page 429 Tuesday, November 8, 2005 10:54 AM
430 SECTION 5 PULMONARY DISORDERS
Ribavirin and RSV Ig have been used aloneand in combination for RSV bronchiolitis inchildren, but their effectiveness is controver-sial, and neither is standard practice. Ribavi-rin is not used in adults with RSV infection.Amantadine or rimantadine 200 mg po once/day started within 48 h of symptom onset re-duces the duration and severity of symptomsin patients who develop presumed influenzaA infection as part of an outbreak, but efficacyfor preventing adverse outcomes of influenzapneumonia is unknown. Zanamivir (10 mginhaled bid) and oseltamivir (75 mg po bid)are similarly effective in reducing the dura-tion of symptoms caused by influenza A or Bif started within 48 h of symptom onset,though zanamivir may be contraindicated inpatients with asthma. Acyclovir 5 to 10 mg/kg IV q 8 h for adults or 250 to 500 mg/m2
body surface area IV q 8 h for children is ad-vocated for varicella lung infections. Somepatients with viral pneumonia, especiallythose with influenza, develop superimposedbacterial infections and require antibioticsdirected against S. pneumoniae, H. influen-zae, and Staphylococcus aureus.
With empiric treatment, 90% of patientswith bacterial pneumonia improve, mani-fested by decreased cough and dyspnea, de-fervescence, relief of chest pain, and declinein WBC count. Failure to improve shouldtrigger suspicion of an unusual organism, an-tibiotic resistance with inadequate coverage,co-infection or superinfection with a 2nd in-fectious agent, an obstructive endobronchiallesion, immunosuppression, metastatic fo-cus of infection with reseeding (in the case ofpneumococcal infection), or nonadherenceto treatment (in the case of outpatients). Ifnone of these can be proven, treatment failureis likely due to inadequate host defenses.
Most viral pneumonias resolve withoutspecific treatment.
Follow-up x-rays should be obtained 6 wkafter treatment in patients > 35; persistence ofan infiltrate at ≤ 6 wk raises suspicions of anunderlying, possibly malignant endobron-chial lesion or of TB.
PreventionSome forms of community-acquired
pneumonia are preventable with pneumo-coccal conjugate vaccine (for patients < 2 yr),H. influenzae B (HIB) vaccine (for patients< 2 yr), and influenza vaccine (for patients> 65 yr)—see p. 1399 and FIG. 266–3 on
p. 2235. Pneumococcus, HIB, and influenzavaccines are also recommended for high-riskpatients. High-risk patients not vaccinatedagainst influenza may be given amantadine,rimantadine, or oseltamivir during influenzaepidemics.
HOSPITAL-ACQUIRED PNEUMONIA
Hospital-acquired pneumonia develops atleast 48 h after hospitalization. The mostcommon pathogens are gram-negative bacilliand Staphylococcus aureus; drug-resistantorganisms are an important concern. Symp-toms and signs are the same as those for com-munity-acquired pneumonia, but in ventilatedpatients, pneumonia may also manifest asworsening oxygenation and increased tra-cheal secretions. Diagnosis is suspected onthe basis of clinical presentation and chestx-ray and is confirmed by blood culture orbronchoscopic sampling of the lower respi-ratory tract. Treatment is with antibiotics.Overall prognosis is poor, due in part tocomorbidities.
Hospital-acquired pneumonia includesventilator-associated pneumonia, postopera-tive pneumonia, and pneumonia that devel-ops in unventilated but otherwise moderatelyor critically ill hospitalized inpatients.
EtiologyThe most common cause is microaspira-
tion of bacteria that colonize the oropharynxand upper airways in seriously ill patients.
Risk factors: Endotracheal intubation withmechanical ventilation poses the greatestoverall risk; ventilator-associated pneumoniaconstitutes > 85% of all cases, with pneu-monia occurring in 17 to 23% of ventilatedpatients. Endotracheal intubation breachesairway defenses, impairs cough and muco-ciliary clearance, and facilitates microaspi-ration of bacteria-laden secretions that poolabove the inflated endotracheal tube cuff. Inaddition, bacteria form a biofilm on andwithin the endotracheal tube that protectsthem from antibiotics and host defenses.
In nonintubated patients, risk factors in-clude previous antibiotic treatment, highgastric pH (from stress ulcer prophylaxistherapy), and coexisting cardiac, pulmonary,hepatic, and renal insufficiency. Major risk
045_062PUL Page 430 Tuesday, November 8, 2005 10:54 AM

52 PNEUMONIA 431
factors for postoperative pneumonia are age> 70, abdominal or thoracic surgery, and de-pendent functional status.
Pathogens: Pathogens and antibiotic re-sistance patterns vary significantly amonginstitutions and can vary within institutionsover short periods (eg, month to month). Ingeneral, the most important pathogen isPseudomonas aeruginosa, which is espe-cially common in pneumonias acquired in in-tensive care settings and in patients with cys-tic fibrosis, neutropenia, advanced AIDS, andbronchiectasis. Other important pathogensinclude enteric gram-negative bacteria (En-terobacter sp, Klebsiella pneumoniae, Es-cherichia coli, Serratia marcescens, Proteussp, Acinetobacter sp) and both methicillin-sensitive and methicillin-resistant Staphylo-coccus aureus.
S. aureus, pneumococcus, and Haemophi-lus influenzae are most commonly implicatedwhen pneumonia develops within 4 to 7 daysof hospitalization, whereas enteric gram-negative organisms become more commonwith increasing duration of intubation.
Prior antibiotic treatment greatly increasesthe likelihood of polymicrobial infection;resistant organisms, particularly methicillin-resistant S. aureus; and Pseudomonas infec-tion. Infection with a resistant organismmarkedly worsens mortality and morbidity.
High-dose corticosteroids increase the riskof Legionella and Pseudomonas infections.
Symptoms, Signs, and DiagnosisSymptoms and signs in nonintubated pa-
tients are generally the same as those for com-munity-acquired pneumonia (see p. 425).Pneumonia in critically ill, mechanically ven-tilated patients more typically causes fever andincreased respiratory and/or heart rate orchanges in respiratory parameters, such as anincrease in purulent secretions or worseninghypoxemia. Noninfectious causes of pulmo-nary deterioration, such as acute respiratorydistress syndrome (ARDS), pneumothorax,and pulmonary edema, must be excluded.
Diagnosis is imperfect. In practice, hospi-tal-acquired pneumonia is often suspected onthe basis of the appearance of a new infiltrateon a chest x-ray that is taken for evaluation ofnew symptoms or signs or of leucocytosis.However, no symptom, sign, or x-ray findingis sensitive or specific for the diagnosis, be-cause all can be caused by atelectasis, pulmo-nary embolism, or pulmonary edema andmay be part of the clinical findings in ARDS.
Gram stain and culture of endotracheal as-pirates are controversial, because specimensare likely to be contaminated with bacteriathat are colonizers as well as pathogens, anda positive culture may or may not indicate in-fection. Bronchoscopic sampling of lower air-way secretions for quantitative culture seemsto yield more reliable specimens, but the effectof this approach on outcomes is controversial.Measurement of inflammatory mediators inbronchoalveolar lavage fluid may play a futurerole in diagnosis; eg, a concentration of solu-ble triggering receptor expressed on myeloidcells (a protein expressed and shed byimmune cells during infection) > 5 pg/mLmay help distinguish bacterial and fungalpneumonia from noninfectious causes ofclinical and radiographic changes in venti-lated patients. However, this approach re-quires further investigation, and the onlyfinding that reliably identifies both pneumo-nia and the responsible organism is a blood orpleural fluid culture that is positive for a res-piratory pathogen.
PrognosisThe mortality associated with hospital-ac-
quired pneumonia due to gram-negative in-fection is about 25 to 50% despite the avail-ability of effective antibiotics. Whether deathis due to underlying illness or to the pneumo-nia itself is uncertain. Women may be atgreater risk of death. The mortality rate asso-ciated with S. aureus pneumonia is 10 to40%, in part due to the serious conditionswith which it is associated (eg, need for a ven-tilator, advanced age, cancer chemotherapy,chronic pulmonary disease).
TreatmentA few patients may have a pneumonia risk
score (see TABLE 52–5) low enough to suggestthat alternative diagnoses should be sought.Otherwise, treatment is with antibiotics thatare chosen empirically based on local sensi-tivity patterns, specific patient risk factors, andthe conditions noted in TABLE 52–2.
Indiscriminate use of antibiotics is a majorcontributor to development of antimicrobialresistance. Therefore, treatment may beginwith initial use of broad-spectrum drugs,which are replaced by the most specific drugavailable for the pathogens identified by cul-ture. Alternative strategies for limiting resis-tance that has not proven effective include stop-ping antibiotics after 72 h in patients whosepulmonary infection scores (see TABLE 52–5)
045_062PUL Page 431 Tuesday, November 8, 2005 10:54 AM

432 SECTION 5 PULMONARY DISORDERS
improve to < 6 and regularly rotating empir-ically chosen antibiotics (eg, q 3 to 6 mo).
Initial antibiotics: Multiple regimensexist, but all should include antibiotics thatcover both resistant gram-negative and gram-
positive organisms. Options include a carba-penem (imipenem-cilastatin 500 mg IV q 6 hor meropenem 1 to 2 g IV q 8 h), monobactam(aztreonam 1 to 2 g IV q 8 h), or anti-pseudomonal β-lactam (ticarcillin 3 g IV withor without clavulanic acid q 4 h, piperacillin3 g IV with or without tazobactam q 4 to 6 h,ceftazidime 2 g IV q 8 h, or cefepime 1 to 2 gq 12 h), given alone or combined with anaminoglycoside (gentamicin or tobramycin1.7 mg/kg IV q 8 h or 5 to 6 mg/kg once/dayor amikacin 5 mg/kg q 8 h) and/or vancomycin1 g q 12 h. Linezolid may be used for some pul-monary infections involving methicillin-re-sistant S. aureus, especially in patients whocannot take vancomycin. Daptomycin shouldnot be used for pulmonary infections.
PreventionNoninvasive ventilation using continuous
positive airway pressure (CPAP) or bi-levelpositive airway pressure (BiPAP) prevents thebreach in airway defense that occurs with en-dotracheal intubation and eliminates the needfor intubation in some patients. Semi-upright orupright positioning reduces risk of aspirationand pneumonia compared with recumbent po-sitioning.
Continuous aspiration of subglottic secre-tions using a specially designed endotrachealtube attached to a suction device seems to re-duce the risk of aspiration.
Selective decontamination of the oropharynx(using topical gentamicin, colistin, and vanco-mycin cream) or of the entire GI tract (usingpolymyxin, an aminoglycoside or quinolone,and either nystatin or amphotericin) also seemsto be effective, although it may increase the riskof colonization with resistant organisms.
Surveillance cultures and routinely chang-ing ventilator circuits or endotracheal tubeshave not been shown to decrease ventilator-associated pneumonia.
NURSING HOME–ACQUIRED PNEUMONIA
Common nursing home–acquired pneumoniapathogens are usually gram-negative bacilli,Staphylococcus aureus, Streptococcuspneumoniae, Haemophilus influenzae,anaerobes, and influenza. Symptoms andsigns are similar to those of pneumonia inother settings, except many elderly patientshave less prominent changes in vital signs.Diagnosis is based on clinical presentation
TABLE 52–5. HOSPITAL-ACQUIRED PNEUMONIA RISK INDEX
FACTOR POINTS
Temperature (°C)≥ 36.5 and ≤ 38.4 0≥ 38.5 and ≤ 38.9 1≥ 39 and ≤ 36 2
Blood leukocytes, µL≥ 4,000 and ≤ 11, 000 0< 4,000 or > 11,000 1Band forms ≥ 50% 1
Tracheal secretionsNone 0Nonpurulent 1Purulent 2
Oxygenation: PaO2/FIO2, mm Hg> 240 or ARDS 0≤ 240 and no ARDS 2
Pulmonary radiographyNo infiltrate 0Diffuse (or patchy)
infiltrate1
Localized infiltrate 2
Progression of infiltrate*None 0Progression
(heart failure and ARDS excluded)
2
Growth of pathogenic bacteria on tracheal aspirate culture*
No, rare, or light growth 0Moderate or heavy
growth1
Same bacteria as on Gram stain
1
PaO2/FIO2 = ratio of arterial O2 pressure to frac-tion of inspired O2; ARDS = acute respiratorydistress syndrome.
*Criteria applicable 72 h after initial diagnosis.Score > 6 suggests hospital-acquired pneumonia.Score < 6 suggests alternative process.Adapted from Singh N, Rogers P, Atwood CW,
et al: Short-course empiric antibiotic therapy forpatients with pulmonary infiltrates in the inten-sive care unit. American Journal of Respira-tory and Critical Care Medicine 162:505–511, 2000.
045_062PUL Page 432 Tuesday, November 8, 2005 10:54 AM

52 PNEUMONIA 433
and chest x-ray, which are often not availablein nursing homes immediately. Treatment iswith antibiotics provided in the nursing homefor less severe illness and in the hospital formore severe infection. Mortality is moderatelyhigh but may be due in part to comorbidities.
Nursing home–acquired pneumonia fallsbetween community- and hospital-acquiredpneumonia in etiology and management.S. pneumoniae and gram-negative bacillimay be roughly equally responsible for mostinfections, though there is debate overwhether gram-negative bacilli are pathogensor merely colonizers. H. influenzae and Mo-raxella catarrhalis are next most common;Chlamydia, Mycoplasma, and Legionellaspp are rarely identified. Risk factors arethose common among debilitated nursinghome residents, such as poor functional sta-tus; impaired mood, mental status, and swal-lowing; and presence of a tracheostomy tube.
Symptoms, Signs, and DiagnosisSymptoms often resemble those of commu-
nity- or hospital-acquired pneumonia but maybe more subtle; cough and altered mental sta-tus are common, as are nonspecific symptomsof anorexia, weakness, restlessness and agita-tion, falling, and incontinence. Subjectivedyspnea occurs but is less common. Signs in-clude diminished or absent responsiveness,fever, tachycardia, tachypnea, wheezes orcrackles, and stentorous, wet breathing.
Diagnosis is based on clinical presentationand chest x-ray. X-rays are often difficult toobtain in nursing home patients, so it may benecessary to transfer them to a hospital atleast for initial evaluation. In some cases,treatment may be started without x-ray confir-mation. Nursing home residents may initiallylack a radiographic infiltrate, presumably be-cause of the dehydration that commonly ac-companies febrile pneumonia in the elderlyand/or a blunted immune response, althoughthe phenomenon is not proven to occur. Be-cause detection of physical changes may bedelayed in a nursing home setting and be-cause residents are at greater risk of compli-cations, evaluation for hypoxemia with pulseoximetry and for decreased intravascular vol-ume with serum BUN and creatinine shouldalso be performed.
PrognosisMortality rate for patients requiring admis-
sion for treatment is 13 to 41%, whereas that
TABLE 52–6. NURSING HOME−ACQUIRED PNEUMONIA RISK INDEX
VARIABLEAND VALUE
POINTSASSIGNED
Serum urea nitrogen (mg/dL)*≤ 16 016.1–27 127.1–38 238.1–49 349.1–60 460.1–71 5> 71 6
WBC count (103/µL)≤ 14 014.1–24 1>24 2
Absolute lymphocyte count> 800/µL (0.8 × 109/L) 0≤ 800/µL (0.8 × 109/L) 1
Pulse (beats/min)≤ 72 073–102 1> 132 3
SexFemale 0Male 1
Body mass index (kg/m2)> 31 025.1–31 119.1–25 213.1–19 3≤ 13 4
Activities of daily living†0 01–2 13–4 2
Mood deterioration over last 90 daysNo 0Yes 2
*To convert to mmol/L, multiply by 0.357; toconvert a value in mmol/L to mg/dL, multiply by 6.
†Based on grooming, using the toilet, locomo-tion, and eating. Each is assigned a zero if theresident is independent, requires supervision, orrequires limited assistance or 1 if the residentrequires extensive assistance or is totally depen-dent. The 4 scores are summed to derive a scoreof zero to 4 and assigned points as shown.
Score Mortality1–4 Low (2–3%)5–6 Relatively low (6–7%)7–8 Moderate (15–16%)9–10 High (34–36%)
11–17 Very high (60–62%)
045_062PUL Page 433 Tuesday, November 8, 2005 10:54 AM

434 SECTION 5 PULMONARY DISORDERS
for patients treated in the nursing home is 7 to19%. Mortality rate exceeds 30% in patientswith more than 2 of the following findings:respiratory rate > 30 breaths/min, heart rate> 125 beats/min, acute mental status change,and history of dementia. An alternative pre-dictive index incorporates laboratory data(see TABLE52–6). Physicians should followall medical directives, because pneumoniais often a terminal event in debilitated nurs-ing home patients.
TreatmentFew data are available to guide decisions
about where treatment should take place, butin general, patients should be hospitalized ifthey have 2 or more unstable vital signs andif the nursing home cannot administer acutecare. Some nursing home residents are notcandidates for hospital transfer. One dose ofantibiotics to cover S. pneumoniae, H. in-fluenzae, common gram-negative bacilli, andS. aureus should be given before transfer; acommon regimen is an oral antipneumococ-cal quinolone (eg, levofloxacin 750 mg once/day, moxifloxacin 400 mg once/day, or gemi-floxacin 400 mg once/day).
PNEUMONIA IN THE IMMU-NOCOMPROMISED HOST
Pneumonia in the immunocompromisedhost is often caused by unusual pathogens.Symptoms and signs depend on the patho-gen. Diagnosis is based on blood culturesand bronchoscopic sampling of respiratorysecretions, sometimes with quantitative cul-tures. Treatment depends on the host defectand pathogen.
The potential pathogens in patients withcompromised defenses are legion. Likelypathogens based on the type of defect in host de-fenses are listed in TABLE 52–7. However, res-piratory symptoms and changes on chest x-raysin immunocompromised hosts may be due toa variety of processes other than infection,such as pulmonary hemorrhage, pulmonaryedema, radiation injury, pulmonary toxicitydue to cytotoxic drugs, and tumor infiltrates.
Symptoms, Signs, and DiagnosisSymptoms and signs may be the same
as those found with community-acquiredpneumonia or hospital-acquired pneumo-nia in immunocompetent patients, though
immunocompromised patients may have nofever or respiratory signs and are less likelyto have purulent sputum if they are neutro-penic. In some patients, the only sign is fever.
An immunocompromised patient withrespiratory symptoms, signs, or fever shouldundergo chest x-ray. If an infiltrate is present,diagnostic studies should include sputumGram stain and culture and blood cultures.Optimally, firm diagnosis is made with in-duced sputum and/or bronchoscopy, espe-cially in patients with chronic pneumonia,atypical presentation, severe defects in im-mune function, and failure to respond tobroad-spectrum antibiotics.
Likely pathogens can often be predicted onthe basis of symptoms, x-ray changes, and thetype of immunodeficiency. In patients withacute symptoms, likely diagnoses are bacte-rial infection, hemorrhage, pulmonaryedema, a leukocyte agglutinin reaction, andpulmonary emboli. A subacute or chronicpresentation is more suggestive of a fungalor mycobacterial infection, an opportunis-tic viral infection, Pneumocystis jiroveci(formerly P. carinii) pneumonia, tumor, a cy-totoxic drug reaction, or radiation injury.
X-rays showing localized consolidationusually indicate an infection involving bac-teria, mycobacteria, fungi, or Nocardia sp. Adiffuse interstitial pattern is more likely torepresent a viral infection, P. jiroveci pneu-monia, drug or radiation injury, or pulmonaryedema. Diffuse nodular lesions suggestmycobacteria, Nocardia sp, fungi, or tumor.Cavitary disease suggests mycobacteria,Nocardia sp, fungi, or bacteria.
In organ or marrow transplantation recip-ients with bilateral interstitial pneumonia,the usual cause is cytomegalovirus, or thedisease is idiopathic. A pleural-based con-solidation is usually aspergillosis. In AIDSpatients, bilateral pneumonia is usuallyP. jiroveci pneumonia. About 30% of patientswith HIV infection have P. jiroveci pneumo-nia as the initial AIDS-defining diagnosis,and > 80% of AIDS patients have this infec-tion at some time if prophylaxis is not given(see p. 1640). Patients with HIV infection be-come vulnerable to P. jiroveci pneumoniawhen the CD4+ helper cell count is < 200/µL.
TreatmentIn neutropenic patients, empiric treatment
depends on the host defect, x-ray, and severityof illness. Generally, broad-spectrum drugsare needed to cover gram-negative bacilli,
045_062PUL Page 434 Tuesday, November 8, 2005 10:54 AM

52 PNEUMONIA 435
Staphylococcus aureus, and anaerobes, as forhospital-acquired pneumonia (see p. 431).
PNEUMOCYSTIS JIROVECI PNEUMONIAP. jiroveci (formerly P. carinii) is a commoncause of pneumonia in immunosuppressedpatients, especially in those infected withHIV. Symptoms include fever, dyspnea, and
cough. Diagnosis requires demonstration ofthe organism in a sputum specimen. Treat-ment is with antibiotics, usually trimethoprim-sulfamethoxazole or pentamidine, and corti-costeroids for patients with PaO2 < 70 mmHg. Prognosis is generally good with timelytreatment.
P. jiroveci is a ubiquitous organism trans-mitted by aerosol route and causes no disease
TABLE 52–7. PNEUMONIA IN THE IMMUNOCOMPROMISED HOST
HOST DEFECT
DISORDERS OR THERAPY
ASSOCIATED WITH DEFECT* LIKELY PATHOGENS
Defective polymorphonuclear neutrophils
Neutropenia Acute leukemia, aplastic anemia, cancer chemo-therapy
Gram-negative bacteria, Staphylo-coccus aureus, Aspergillus sp, Candida sp
Defective chemotaxis Diabetes mellitus S. aureus, gram-negative aerobesDefective intracellular killing
Chronic granulomatous disease
S. aureus
Defective alternative pathway
Sickle cell disease Streptococcus pneumoniae, Haemophilus influenzae
C5 deficiency Congenital disorder S. pneumoniae, S. aureus, gram-negative bacteria
Cell-mediatedimmunodeficiency
(T-cell deficiency/dysfunction)
Hodgkin lymphoma, cancer chemotherapy, corticosteroid therapy
Mycobacteria, viruses (herpes sim-plex, cytomegalovirus), Strongy-loides sp, opportunistic fungi (Aspergillus, Mucor, Crypto-coccus spp), Nocardia sp, Toxo-plasma sp
AIDS Pneumocystis jiroveci (formerly P. carinii), Toxoplasma sp, cytomegalovirus, herpes simplex virus, opportunistic fungi (Aspergillus, Mucor, Crypto-coccus spp), mycobacteria
Humoralimmunodeficiency
(B-cell deficiency/dysfunction)
Multiple myeloma, agammaglobulinemia
S. pneumoniae, H. influenzae, Neisseria meningitidis
Selective deficiency: IgA, IgG, IgM
S. pneumoniae, H. influenzae
Hypogammaglobuline-mia
P. jiroveci, cytomegalovirus, S. pneumoniae, H. influenzae
*Examples.
045_062PUL Page 435 Tuesday, November 8, 2005 10:54 AM
436 SECTION 5 PULMONARY DISORDERS
in immunocompetent patients. Patientswith HIV infection and CD4+ counts < 200/µL, organ transplant recipients, those whohave hematologic malignancies, and pa-tients taking corticosteroids are at risk ofdeveloping P. jiroveci pneumonia. Most havefever, dyspnea, and a dry, nonproductivecough that evolves subacutely over severalweeks (HIV infection) or acutely over sev-eral days (other causes of compromisedcell-mediated immunity). The chest x-raycharacteristically shows diffuse, bilateralperihilar infiltrates, but 20 to 30% of patientshave normal x-rays. ABGs show hypoxemia,with an increase in the alveolar-arterial O2gradient, and pulmonary function tests showaltered diffusing capacity (although this israrely done as a diagnostic test). Diagnosisrequires histopathologic demonstration ofthe organism with methenamine silver,Giemsa, Wright-Giemsa, modified Grocott,Weigert-Gram, or monoclonal antibodystain. Sputum specimens are usually ob-tained by induced sputum or bronchoscopy.Sensitivity ranges from 30 to 80% for in-duced sputum and is > 95% for bronchoscopywith bronchoalveolar lavage.
Treatment is with trimethoprim-sulfa-methoxazole (TMP-SMX) 4 to 5 mg/kg IV orpo tid for 14 to 21 days. Treatment can bestarted before diagnosis is confirmed becauseP. jiroveci cysts persist in the lungs for weeks.Adverse effects more common in patientswith AIDS include skin rash, neutropenia,hepatitis, and fever. Alternative regimens arepentamidine 4 mg/kg IV once/day, atova-quone 750 mg po bid, TMP-SMX 5 mg/kg poqid with dapsone 100 mg po once/day, or clin-damycin 300 to 900 mg IV q 6 to 8 h with pri-maquine base 15 to 30 mg/day po, also for21 days. The major limitation of pentamidineis the high frequency of toxic adverse effects,including renal failure, hypotension, and hy-poglycemia. Adjunctive therapy with corti-costeroids is advocated for those with a PaO2< 70 mm Hg. The suggested regimen is pred-nisone 40 mg bid (or its equivalent) for thefirst 5 days, 40 mg/day for the next 5 days (asa single dose or as 20 mg bid), and then 20 mgonce/day for the duration of treatment.
HIV-infected patients who have had P.jiroveci pneumonia or who have a CD4+ count< 200/µL should receive prophylaxis with TMP-SMX 80/400 mg once/day; if this treatment isnot tolerated, dapsone 100 mg po once/day oraerosolized pentamidine 300 mg once/monthcan be used. These prophylactic regimens are
also probably indicated for non-HIV-infectedpatients at risk of P. jiroveci pneumonia.
Overall mortality for P. jiroveci pneumoniain hospitalized patients is 15 to 20%. Risk fac-tors for death may include previous history ofP. jiroveci pneumonia, older age, and, in HIV-infected patients, CD4+ cell count < 50/µL.
ASPIRATION PNEUMONITIS AND PNEUMONIA
Aspiration pneumonitis and pneumonia arecaused by inhaling toxic substances, usuallygastric contents into the lungs. The resultmay be undetectable or chemical pneu-monitis, bacterial pneumonia, or airwayobstruction. Symptoms include cough anddyspnea. Diagnosis is based on clinical pre-sentation and x-ray. Treatment and progno-sis differ by aspirated substance.
Aspiration can cause lung inflammation(chemical pneumonitis), infection (bacterialpneumonia or abscess), or airway obstruc-tion. Drowning is discussed on p. 2617; air-way obstruction, on p. 524. Most episodes ofaspiration cause minor symptoms or pneu-monitis rather than infection or obstruction.
Risks for aspiration include impaired cog-nition, impaired swallowing, vomiting, GIand respiratory devices and procedures (eg,nasogastric or endotracheal tube), and gas-troesophageal reflux disease.
Chemical pneumonitis: Multiple sub-stances are either directly toxic to the lung orstimulate an inflammatory response when as-pirated; gastric acid is the prototype, but othersinclude petroleum products (such as petro-leum jelly) and laxative oils (such as mineral,castor, and paraffin oil), all of which cause li-poid pneumonia. Aspirated gasoline and ker-osene also cause a chemical pneumonitis.
Gastric contents produce damage mainlyfrom gastric acid, although food and other in-gested material (eg, activated charcoal as intreatment of overdose) are injurious in quan-tity. Gastric acid causes a chemical burn of theairways and lung leading to rapid broncho-constriction, atelectasis, edema, and alveolarhemorrhage. Symptoms include acute dysp-nea with cough, sometimes productive ofpink frothy sputum; tachypnea; tachycardia;fever; diffuse crackles; and wheezing. Chestx-ray shows diffuse infiltrates frequently butnot exclusively in dependent segments, whilepulse-oximetry and ABGs demonstrate
045_062PUL Page 436 Tuesday, November 8, 2005 10:54 AM

53 LUNG ABSCESS 437
hypoxemia. Treatment is supportive, ofteninvolving mechanical ventilation. Antibio-tics often are given to patients with witnessedor known gastric aspiration. The syndromemay resolve spontaneously, usually within afew days; may progress to acute respiratorydistress syndrome; and/or may be compli-cated by bacterial superinfection.
Aspiration of oils or petroleum jelly causesexogenous lipoid pneumonia, which is char-acterized histologically by chronic granulo-matous inflammation with fibrosis. It is oftenasymptomatic and is detected incidentally onchest x-ray or may present with low-gradefever, gradual weight loss, and crackles. Chestx-ray findings vary; consolidation, cavita-tion, interstitial or nodular infiltrates, pleuraleffusion, and other changes may be slowlyprogressive. Treatment is avoidance of thetoxic substance.
Aspiration pneumonia: Healthy peoplecommonly aspirate small amounts of oralsecretions, but normal defense mechanismsusually clear the inoculum without sequelae.Aspiration of larger amounts, or aspiration ina patient with impaired pulmonary defenses,often causes pneumonia and/or abscess (seealso Ch. 53, below).
Symptoms and signs of pneumonia and ab-scess are similar and include chronic low-grade dyspnea, fever, weight loss, and coughproductive of putrid, foul-tasting sputum. Pa-tients may have signs of poor oral hygiene.
Chest x-ray shows an infiltrate, frequentlybut not exclusively, in the dependent lungsegments, ie, the superior segment of a lowerlobe or the posterior segment of an upperlobe. Anaerobes often can be cultured fromsputum, but it is unclear whether they are pri-mary infecting organisms to which treat-ment should be directed or whether they aresimply one of several organisms causinginfection.
Treatment is with clindamycin 450 to 900mg IV q 8 h followed by 300 mg po qid oncefever and clinical symptoms subside. Peni-cillin (either penicillin G 1 to 2 million unitsq 4 to 6 h or amoxicillin 0.5 to 1 g po tid) pluseither metronidazole 500 mg po tid, amox-icillin-clavulanate 875/125 mg po tid, orimipenem is an acceptable alternative to clin-damycin. Duration of treatment is usually 1to 2 wk unless the pneumonia is complicatedby lung abscess formation, in which casetreatment may be required for 6 wk, and upto 3 mo. Empyema is another common com-plication.
Airway obstruction: Airway obstructionby fluid (eg, near-drowning) or solid food hasa range of consequences, from atelectasis tohypoxemia and death. Diagnosis is obviousfrom history; treatment is suction aspiration(fluid) or bronchoscopic removal of food ifpossible. Corticosteroids are sometimes usedwhen food cannot be completely retrieved,but efficacy is unproven.
53LUNG ABSCESS
Lung abscess is a necrotizing infection char-acterized by localized pus. It is almostalways caused by aspiration of oral secre-tions by patients who have impaired con-sciousness. Symptoms are persistent cough,fever, sweats, and weight loss. Diagnosisis based on history, physical examination,and chest x-ray. Treatment usually is withclindamycin or combination β-lactam /β -lactamase inhibitors.
Etiology and PathophysiologyMost lung abscesses develop after aspira-
tion of oral secretions by patients with gingi-
vitis or poor oral hygiene who are uncon-scious or obtunded from alcohol, illicit drugs,anesthesia, sedatives, or opioids. Older pa-tients and those unable to handle their oral se-cretions, often because of neurologic disease,are also at risk. Lung abscess less commonlycomplicates necrotizing pneumonia that maydevelop from hematogenous seeding of thelungs due to septic embolism from IV druguse or suppurative thromboembolism. Incontrast to aspiration, these conditions typi-cally cause multiple rather than isolated lungabscesses.
The most common pathogens are anaero-bic bacteria, but about 1⁄2 of all cases involveboth anaerobic and aerobic organisms (seeTABLE 53–1). The most common aerobicpathogens are streptococci. Immunocom-promised patients with lung abscess are more
045_062PUL Page 437 Tuesday, November 8, 2005 10:54 AM

438 SECTION 5 PULMONARY DISORDERS
likely to have infection with Nocardia, my-cobacteria, or fungi. People from developingcountries are at risk of abscess due to Myco-
bacterium tuberculosis, amebic infection(Entamoeba histolytica), paragonimiasis, orBurkholderia pseudomallei.
Introduction of these pathogens into thelungs first causes inflammation, which leads totissue necrosis and then abscess formation.Most commonly, the abscess ruptures into abronchus, and its contents are expectorated,leaving an air- and fluid-filled cavity. In about 1⁄3of cases, direct or indirect extension (via bron-chopleural fistula) into the pleural cavity resultsin empyema. Cavitary pulmonary lesions arenot always abscesses (see TABLE 53–1).
Symptoms and SignsSymptoms of abscess due to anaerobic bac-
teria or mixed anaerobic/aerobic bacteria areusually chronic (eg, over weeks or months) andinclude productive cough, fever, sweats, andweight loss. Severe prostration may occur.Sputum may be purulent or blood-streakedand classically smells or tastes foul. Symp-toms of abscess due to aerobic bacteria developmore acutely and resemble bacterial pneumo-nia. Abscesses due to organisms other thananaerobes (eg, Mycobacteria, Nocardia) lackputrid respiratory secretions, may be morelikely to occur in nondependent lung regions,and do not respond to standard antibiotics.
Signs of lung abscess, when present, arenonspecific and resemble those of pneumo-nia: decreased breath sounds indicating con-solidation or effusion, temperature ≥ 39.4°C, crackles over the affected area, egophony,and dullness to percussion in the presence ofeffusion. Patients typically have signs ofperiodontal disease and a history of a prob-lem or condition causing impaired con-sciousness.
DiagnosisLung abscess is suspected based on his-
tory, physical examination, and chest x-ray.In anaerobic infection due to aspiration, chestx-ray classically shows consolidation, with asingle cavity containing an air-fluid level inportions of the lung that are dependent whenthe patient is recumbent (eg, posterior seg-ment upper lobe or superior segment lowerlobe). This pattern helps distinguish anaero-bic abscess from other causes of cavitary pul-monary disease, such as diffuse or embolicpulmonary disease, which may cause multi-ple cavitations, or TB, which involves the api-ces. CT scan is not routinely needed but maybe useful when the x-ray suggests a cavitatinglesion or when an underlying pulmonary
TABLE 53–1. CAUSES OF CAVITARY LUNG LESIONS
Lung abscessAnaerobic bacteria
Gram-negative bacilliFusobacterium spPrevotella spBacteroides sp
Gram-positive cocciPeptostreptococcus sp
Gram-positive bacilliClostridium spActinomyces sp
Aerobic bacteriaGram-positive cocci
Streptococcus milleri and otherstreptococciStaphylococcus aureus
Gram-negative bacilliKlebsiella pneumoniaePseudomonas aeruginosaBurkholderia pseudomallei
Gram-positive bacilliNocardia
MycobacteriaMycobacterium tuberculosisMycobacterium avium-cellulareMycobacterium kansasii
FungiHistoplasmosisAspergillosisCoccidioidomycosisBlastomycosisCryptococcal infectionMucormycosisSporotrichosisPneumocystis jiroveci (formerly P. carinii)
infectionParasites
ParagonimiasisEchinococcal infectionAmebic infection
BronchiectasisNoninfectious causes
Lung cancerBullae with air-fluid levelPulmonary sequestrationPulmonary embolismWegener’s granulomatosisNodular silicosis nodule with central necrosis
045_062PUL Page 438 Tuesday, November 8, 2005 10:54 AM

54 BRONCHIECTASIS 439
mass obstructing the drainage of a lung seg-ment is suspected. Anaerobic bacteria arerarely identifiable on culture because uncon-taminated specimens are difficult to obtainand because most laboratories do not cultureanaerobes well or often. If sputum is putrid,then anaerobic infection is assumed to be thecause. Bronchoscopy is sometimes indicatedto exclude malignancy.
When anaerobic infection is less likely,then aerobic, fungal, or mycobacterial infec-tion is suspected, and attempts are made toidentify a pathogen. Cultures of sputum,bronchoscopic aspirates, or both are helpful.
TreatmentTreatment is with antibiotics. Clindamy-
cin 600 mg IV q 6 to 8 h is usually the drugof choice given its excellent anaerobic andstreptococcal coverage. The primary alterna-tive is a combination β-lactam/β-lactamaseinhibitor (eg, ampicillin/sulbactam 1 to 2 g IVq 6 h, ticarcillin/clavulanate 3 to 6 g IV q 6 h,piperacillin/tazobactam 3 g IV q 6 h). Met-ronidazole 500 mg q 8 h may be used but mustbe combined with penicillin 2 million units q6 h IV. Less seriously ill patients may be givenoral antibiotics such as clindamycin 300 mgpo q 6 h or amoxicillin/clavulanate 875/125mg po q 12 h. IV regimens can be convertedto oral ones when the patient defervesces.
Optimal duration of treatment is un-known, but common practice is to treat for3 to 6 wk unless the chest x-ray shows com-plete resolution sooner. In general, the largerthe abscess, the longer it will take to resolveon x-ray. Larger abscesses, therefore, typi-cally require several weeks or months oftreatment.
Most authorities do not recommendchest physical therapy and postural drain-age because they may cause spillage of in-fection into other bronchi with extension ofthe infection or acute obstruction. If the pa-tient is weak or paralyzed or has respiratoryfailure, tracheostomy and suctioning maybe necessary. Rarely, bronchoscopic aspi-ration helps facilitate drainage. An accom-panying empyema must be drained; fluidprovides a good source for anaerobic cul-ture. Percutaneous or surgical drainage oflung abscesses is necessary in the roughly10% of patients in whom lesions do not re-spond to antibiotics. Resistance to antibi-otic treatment is most common with largecavities and with infections that compli-cate obstructions.
When surgery is necessary, lobectomy isthe most common procedure; segmental re-section may suffice for small lesions. Pneu-monectomy may be necessary for multipleabscesses or for pulmonary gangrene unre-sponsive to drug therapy.
54BRONCHIECTASIS
Bronchiectasis is dilation and destruction oflarger bronchi caused by chronic infectionand inflammation. Common causes are cys-tic fibrosis, immune defects, and infections,though some cases appear to be idiopathic.Symptoms are chronic cough and purulentsputum expectoration; some patients mayalso have fever and dyspnea. Diagnosis isbased on history and imaging, usuallyinvolving high-resolution CT, though stan-dard chest x-rays may be diagnostic. Treat-ment and prevention of acute exacerbationsare with antibiotics, drainage of secretions,and management of complications, such assuperinfection and hemoptysis. Treatment
of underlying causes is important wheneverpossible.
Etiology and PathophysiologyDiffuse bronchiectasis develops in pa-
tients with genetic, immune, or anatomic de-fects that affect the airways. Cystic fibrosis isthe most common cause; ciliary dyskinesiaand severe α1-antitrypsin deficiency are lesscommon genetic causes. Hypogammaglob-ulinemia and immune deficiencies may alsocause diffuse disease, as may rare abnormal-ities in airway structure (eg, tracheobron-chomegaly [Mounier-Kuhn syndrome],cartilage deficiency [Williams-Campbellsyndrome]). Diffuse bronchiectasis is anuncommon complication of more commonconditions, such as RA, Sjögren’s syndrome,and allergic bronchopulmonary aspergillo-sis, probably via multiple mechanisms.
045_062PUL Page 439 Tuesday, November 8, 2005 10:54 AM
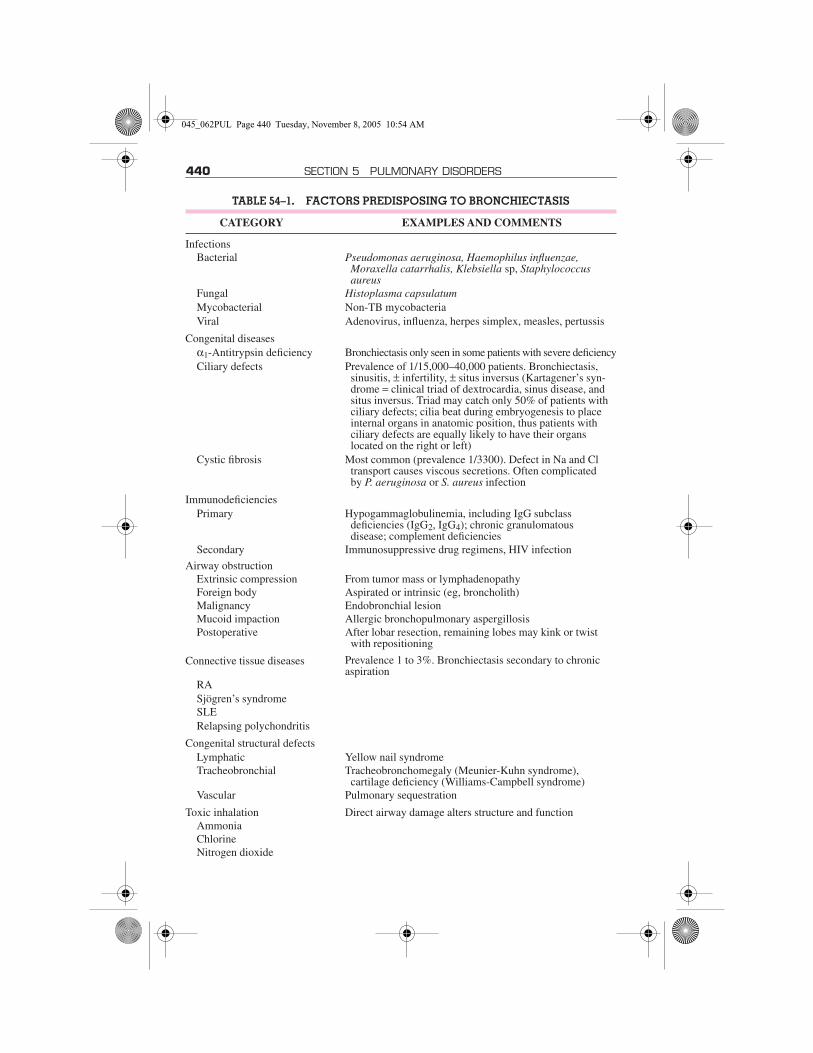
440 SECTION 5 PULMONARY DISORDERS
TABLE 54–1. FACTORS PREDISPOSING TO BRONCHIECTASIS
CATEGORY EXAMPLES AND COMMENTS
InfectionsBacterial Pseudomonas aeruginosa, Haemophilus influenzae,
Moraxella catarrhalis, Klebsiella sp, Staphylococcus aureus
Fungal Histoplasma capsulatumMycobacterial Non-TB mycobacteriaViral Adenovirus, influenza, herpes simplex, measles, pertussis
Congenital diseasesα1-Antitrypsin deficiency Bronchiectasis only seen in some patients with severe deficiencyCiliary defects Prevalence of 1/15,000–40,000 patients. Bronchiectasis,
sinusitis, ± infertility, ± situs inversus (Kartagener’s syn-drome = clinical triad of dextrocardia, sinus disease, and situs inversus. Triad may catch only 50% of patients with ciliary defects; cilia beat during embryogenesis to place internal organs in anatomic position, thus patients withciliary defects are equally likely to have their organslocated on the right or left)
Cystic fibrosis Most common (prevalence 1/3300). Defect in Na and Cl transport causes viscous secretions. Often complicatedby P. aeruginosa or S. aureus infection
ImmunodeficienciesPrimary Hypogammaglobulinemia, including IgG subclass
deficiencies (IgG2, IgG4); chronic granulomatousdisease; complement deficiencies
Secondary Immunosuppressive drug regimens, HIV infection
Airway obstructionExtrinsic compression From tumor mass or lymphadenopathyForeign body Aspirated or intrinsic (eg, broncholith)Malignancy Endobronchial lesionMucoid impaction Allergic bronchopulmonary aspergillosisPostoperative After lobar resection, remaining lobes may kink or twist
with repositioning
Connective tissue diseases Prevalence 1 to 3%. Bronchiectasis secondary to chronic aspiration
RASjögren’s syndromeSLERelapsing polychondritis
Congenital structural defectsLymphatic Yellow nail syndromeTracheobronchial Tracheobronchomegaly (Meunier-Kuhn syndrome),
cartilage deficiency (Williams-Campbell syndrome)Vascular Pulmonary sequestration
Toxic inhalation Direct airway damage alters structure and functionAmmoniaChlorineNitrogen dioxide
045_062PUL Page 440 Tuesday, November 8, 2005 10:54 AM

54 BRONCHIECTASIS 441
Focal bronchiectasis develops from un-treated pneumonia or obstruction (eg, fromforeign bodies and tumors, extrinsic com-pression, or shifts in anatomy after lobar re-section). Other disorders are listed in TABLE54–1; some cases have no readily apparentcause.
All of these conditions impair airway clear-ance mechanisms and host defenses, confer-ring an inability to clear secretions and predis-posing to infection and chronic inflammation.As a result of frequent infection, most com-monly with Haemophilus influenzae (35%),Pseudomonas aeruginosa (31%), Moraxellacatarrhalis (20%), Staphylococcus aureus(14%), and Streptococcus pneumoniae (13%),airways become inspissated with viscousmucous containing inflammatory mediatorsand pathogens and slowly become dilated,scarred, and distorted. Histologically, bron-chial walls are thickened by edema, inflamma-tion, and neovascularization. Destruction ofsurrounding interstitium and alveoli causesfibrosis, emphysema, or both.
Mycobacteria other than TB can causebronchiectasis as well as colonize the lungsof patients with bronchiectasis from othercauses.
Symptoms and SignsThe primary symptom of bronchiectasis is
chronic cough that may produce large vol-umes of thick, tenacious, purulent sputum.Dyspnea and wheezing are common. He-moptysis, which can be massive, is due toneovascularization of the airways from thebronchial (as opposed to pulmonary) arter-ies. Low-grade fever occurs with acute exac-erbations of disease, during which the extentof cough and the volume and purulence ofsputum production increase. Chronic bron-chitis (see p. 400) may mimic bronchiectasisclinically, but bronchiectasis is distinguishedby more voluminous production of purulent
sputum on a daily basis and typical CT scanabnormalities.
Halitosis and abnormal breath sounds, in-cluding crackles, rhonchi, and wheezing, aretypical signs of disease. Finger clubbing mayalso be present.
Symptoms characteristically begin insidi-ously and recur increasingly, worseninggradually over years. In advanced cases, hy-poxemia, pulmonary hypertension, and rightheart failure can occur.
Superinfection with multidrug-resistantorganisms including mycobacteria otherthan TB should be considered a possible un-derlying cause of symptoms in patients withrecurrent exacerbations or worsening air-flow limitation on pulmonary functiontests.
DiagnosisDiagnosis is based on a history, physical
examination, and radiologic testing, begin-ning with a chest x-ray. X-ray findings sug-gestive of bronchiectasis include scattered ir-regular opacities caused by mucous plugs,honeycombing, and rings and “tram lines”caused by thickened, dilated airways facinginto or perpendicular to the x-ray beam, re-spectively. Radiographic patterns may differby underlying disease: Bronchiectasis due tocystic fibrosis develops predominantly in up-per lobes, whereas that due to other causes ismore diffuse or predominates in the lowerlobes. High-resolution CT is the test of choicefor defining the extent of bronchiectasis. Thetest is nearly 100% sensitive and specific. CTtypically shows bronchial varicosities andcysts (sometimes appearing as grapelikeclusters), scattered mucous plugs, and air-ways that are dilated > 1.5 times the diameterof nearby blood vessels. Dilated medium-sized bronchi may extend almost to the pleu-rae. Atelectasis, consolidation, and de-creased vascularity are nonspecific findings.
MiscellaneousInflammatory bowel
diseaseUsually chronic ulcerative colitis; bowel resection may
exacerbate pulmonary diseaseTransplantation May be secondary to frequent infection from immunosup-
pression
Data from Barker, AF: Bronchiectasis. The New England Journal of Medicine 346:1383–1393, 2002.
TABLE 54–1. FACTORS PREDISPOSING TO BRONCHIECTASIS—Continued
CATEGORY EXAMPLES AND COMMENTS
045_062PUL Page 441 Tuesday, November 8, 2005 10:54 AM

442 SECTION 5 PULMONARY DISORDERS
A differential diagnosis of dilated airways in-cludes bronchitis and “traction bronchiecta-sis” that occurs when pulmonary fibrosispulls airways open.
Pulmonary function tests should be ob-tained for purposes of documenting baselinefunction and for following the progression ofdisease over time. Bronchiectasis is associ-ated with airflow limitation (reduced forcedexpiratory volume in 1 sec [FEV1], forcedvital capacity [FVC], and FEV1/FVC); theFEV1 can improve in response to β-agonistbronchodilators. Lung volume measurementsand diffusing capacity for carbon monoxide(DLCO) may be decreased.
Tests to help diagnose an underlying causeinclude sputum evaluation, including stain-ing and cultures for bacterial, mycobacterial(Mycobacterium avium complex and Myco-bacterium tuberculosis), and fungal (As-pergillus) infection. Mycobacterial superin-fection is diagnosed by repeatedly culturingmycobacteria other than TB in high colonycounts and by finding granulomas on biopsywith concurrent radiologic evidence of dis-ease. Additional tests may include sweatchloride testing to diagnose cystic fibrosis,which should be performed even in older pa-tients; rheumatoid factor and other serologictests to look for connective tissue disease; im-munoglobulins including IgG subclasses todocument some immunodeficiencies; As-pergillus precipitins, IgE, and eosinophilia torule out allergic bronchopulmonary as-pergillosis; and α1-antitrypsin levels to doc-ument α1-antitrypsin deficiency. When theclinical presentation suggests ciliary dyski-nesia (by concurrent sinus disease and mid-dle and lower lobe bronchiectasis with orwithout infertility), a nasal or bronchial epi-thelial biopsy should be obtained and exam-ined by transmission electron microscopy forabnormal ciliary structure. A less invasive al-ternative is examination of sperm motility.The diagnosis of ciliary dyskinesia should bemade cautiously by an experienced physiciantrained in specialized techniques, becausenonspecific structural defects can be presentin up to 10% of cilia in healthy patients andin those with pulmonary disease; infectioncan cause transient dyskinesia; and ciliary ul-trastructure may be normal in patients withprimary ciliary dyskinesia syndromes char-acterized by abnormal ciliary function.
Bronchoscopy is indicated when an ana-tomic or an obstructing object or lesion issuspected.
Prognosis and PreventionOverall, prognosis is thought to be good,
with about 80% of patients having no furtherdeterioration of lung function on the basis ofbronchiectasis alone. However, cystic fibro-sis patients have a median survival of 32 yr,and most patients continue to have intermit-tent acute exacerbations.
Prevention of bronchiectasis requirestimely recognition and treatment of underly-ing causes. Unfortunately, most patients seekmedical attention because the disease is al-ready established.
TreatmentTreatment involves preventing exacerba-
tions, treating underlying causes, aggres-sively managing acute exacerbations, andcontrolling complications.
There is no consensus on the best approachto prevent or limit acute exacerbations. Optionsinclude daily prophylactic oral antibiotics (eg,ciprofloxacin 500 mg bid) and, in patients withcystic fibrosis who are colonized with P.aeruginosa, inhaled tobramycin (300 mg bidevery other month). In patients with diffusebronchiectasis due to other causes, aerosolizedgentamicin (40 mg bid) may also be effective.
As with all chronic pulmonary disease, an-nual vaccination against influenza and againstpneumococcus is recommended.
Various techniques can facilitate clearanceof secretions, including postural drainage andchest percussion, positive expiratory pressuredevices, intrapulmonary percussive ventila-tors, pneumatic vests, and autogenic drainage(a breathing technique thought to help move se-cretions from peripheral to central airways). Amucolytic (rhDNase) has been shown to haveclinical utility in patients with cystic fibrosis.Patients should be introduced to these tech-niques by a respiratory therapist and should usewhichever technique is most effective; no evi-dence favors one technique over another.
Additional treatment depends on the un-derlying cause. For cystic fibrosis, see p. 2308.Allergic bronchopulmonary aspergillosis istreated with corticosteroids and possibly withazole antifungals (see p. 398). Patients withimmunoglobulin deficiencies should receivereplacement therapy. Those with α1-anti-trypsin deficiency should receive replace-ment therapy.
Treatment of acute exacerbations is withantibiotics that will cover H. influenzae, P.aeruginosa, M. catarrhalis, S. aureus, and S.pneumoniae (eg, ciprofloxacin 500 mg po bid
045_062PUL Page 442 Tuesday, November 8, 2005 10:54 AM

55 INTERSTITIAL LUNG DISEASES 443
or levofloxacin 500 mg po once/day for 7 to14 days). Azithromycin 500 mg 3 times/wkhas demonstrated efficacy in cystic fibrosisbronchiectasis, but it is unclear whether mac-rolides are useful in other forms of the disorder.Antibiotic treatment should be accompaniedby increased efforts to facilitate clearance ofsputum from the airway.
Control of acute complications includestreating mycobacterial superinfection andhemorrhage.
An empirical multidrug regimen for M.avium complex may include clarithromycin500 mg po bid or azithromycin 250 mg once/
day; rifampin 600 mg po once/day or rifab-utin 300 mg po once/day; and ethambutol25 mg/kg po once/day for 2 mo followed by15 mg/kg once/day. All drugs should be takenon a continuous maintenance basis untilsputum cultures are negative for 12 mo. Sur-gical resection is rarely necessary but shouldbe considered when antibiotic treatment isinadequate and the disease is sufficientlylocalized.
Massive hemorrhage is generally treatedwith bronchial artery embolization alongwith antibiotic treatment for an acute exacer-bation.
55INTERSTITIAL LUNG DISEASES(Diffuse Interstitial Lung Diseases)
Interstitial lung diseases are characterizedby alveolar septal thickening, fibroblast pro-liferation, collagen deposition, and, if theprocess remains unchecked, pulmonary fi-brosis. Numerous conditions and agents, in-cluding most connective tissue diseases andoccupational lung exposures, and manydrugs cause similar interstitial changes (seeCh. 57 on p. 469 and TABLE 55–1). But in upto 30% of patients, no clear cause can befound; the term idiopathic interstitial pneu-monia refers to these patients. Other idio-pathic interstitial diseases differ in histology,clinical features, and presentation and thusare considered unique diseases; these includeeosinophilic pulmonary diseases, hypersen-sitivity pneumonitis, pulmonary Langerhans’cell granulomatosis, lymphangioleiomyoma-tosis, pulmonary alveolar proteinosis, andsarcoidosis.
IDIOPATHIC INTERSTITIAL PNEUMONIAS
Idiopathic interstitial pneumonias are inter-stitial lung diseases of unknown etiologythat share similar clinical features. Classi-fied into 6 histologic subtypes, all are char-acterized by varying degrees of inflammation
and fibrosis and all cause dyspnea and typicalradiographic abnormalities. Diagnosis isbased on history, physical examination,imaging, pulmonary function tests, and lungbiopsy. Treatment varies by subtype but typ-ically involves corticosteroids, cytotoxicdrugs, or both; treatment is frequently inef-fective. Prognosis varies by subtype andranges from excellent to nearly always fatal.
The 6 histologic subtypes of idiopathic in-terstitial pneumonia (IIP) in decreasing orderof frequency are usual interstitial pneumonia(UIP), known clinically as idiopathic pulmo-nary fibrosis; nonspecific interstitial pneu-monia; bronchiolitis obliterans organizingpneumonia; respiratory bronchiolitis-asso-ciated interstitial lung disease (ILD); desqua-mative interstitial pneumonia; and acute in-terstitial pneumonia. Lymphoid interstitialpneumonia, although still considered a sub-type of IIP, is now thought to be part of thelymphoproliferative disease spectrum ratherthan primary ILD (see p. 459). These sub-types are characterized by varying degrees ofinterstitial inflammation and fibrosis, and allcause dyspnea; diffuse, usually reticularopacities on chest x-ray; and inflammationand/or fibrosis on biopsy. The subtypes areimportant to distinguish, however, becausethey have different clinical features and re-sponses to treatment (see TABLE 55–2).
DiagnosisKnown causes of ILD must be excluded.
Chest x-ray is always obtained as well as pul-monary function tests (see p. 364) and high-resolution CT (HRCT), which distinguishes
045_062PUL Page 443 Tuesday, November 8, 2005 10:54 AM

444 SECTION 5 PULMONARY DISORDERS
airspace from interstitial disease, providesbetter assessment of the extent and distribu-tion of disease, and is more likely to detectunderlying or coexisting disease (eg, occultmediastinal adenopathy, carcinoma, em-physema). HRCT is best performed with thepatient prone to reduce dependent lungatelectasis.
Lung biopsy is usually needed to confirmthe diagnosis except when HRCT demon-strates a diagnostic pattern. Bronchoscopictransbronchial biopsy can rule out ILD by de-tecting other diseases but does not yieldenough tissue to diagnose ILD. Biopsy ofmultiple sites with an open or video-assistedthoracoscopic surgery (VATS) procedure isrequired.
Bronchoalveolar lavage helps narrow thedifferential diagnosis in selected patients andcan provide information about disease progres-sion and response to therapy. The usefulness ofthis procedure in the initial clinical assessmentand follow-up of most patients with these dis-eases has not been established, however.
IDIOPATHIC PULMONARY FIBROSIS(Cryptogenic Fibrosing Alveolitis)
Idiopathic pulmonary fibrosis, the most com-mon form of IIP, causes progressive pulmo-nary fibrosis predominantly in male smokers.Symptoms and signs develop over months toyears and include exertional dyspnea, cough,and fine (Velcro) crackles. Diagnosis is basedon history, physical examination, chest x-ray,and pulmonary function tests and is con-firmed with HRCT, lung biopsy, or both if nec-essary. No specific treatment has proveneffective, but corticosteroids, cyclophospha-mide, azathioprine, or a combination areoften given. Most patients deteriorate evenwith treatment; median survival is < 3 yr fromdiagnosis.
Etiology and PathophysiologyIdiopathic pulmonary fibrosis (IPF), iden-
tified histologically as UIP, accounts for 50%of cases of IIP. IPF affects men and women intheir 50s and 60s in a ratio of 2 :1. Current orformer cigarette smoking is most stronglyassociated with the disease. There is somegenetic predisposition; familial clusteringoccurs in up to 3% of cases.
Although IPF is called a pneumonia, in-flammation seems to play a relatively minorrole. Environmental, genetic, or other un-
TABLE 55–1. CAUSES OF INTERSTITIAL LUNG DISEASE*
CAUSEDIFFERENTIAL
DIAGNOSIS
Circulatory disorders
Pulmonary edemaPulmonary veno-
occlusive disease
Connective tissuedisease
Ankylosing spondylitis Behçet’s syndromeDermatomyositisGoodpasture’s syndrome Mixed connective tissue diseasePolymyositisRASjögren’s syndromeSLE
Environ-mentalpulmonary disease
Inorganic:* Aluminum oxide fibrosis, asbestosis, baritosis, berylliosis, coal worker’s lung, metal polisher’s lung/hard metal fibrosis, sidero-sis, silicosis, stannosis, talc pneumoconiosis
Organic:* Bagassosis, bird fancier’s lung, coffee worker’s lung, farmer’s lung, humidifier’s lung, hot tub lung, malt worker’s lung, maple bark stripper’s lung, mushroom worker’s lung, tea grower’s lung
Infections AspergillosisHistoplasmosisParasitic infectionTBViral infection
Vasculitis Churg-Strauss syndrome Giant cell arteritisWegener’s granulomatosis
Miscel-laneousdiseases
Alveolar proteinosis AmyloidosisChronic aspirationEosinophilic granuloma Eosinophilic pneumonia Gaucher’s diseaseLipoid pneumoniaLymphangioleiomyomatosisMicrolithiasisNeurofibromatosisNiemann-Pick disease Pulmonary lymphoma SarcoidosisTuberous sclerosis
*For drug causes, see TABLE 55–3.
045_062PUL Page 444 Tuesday, November 8, 2005 10:54 AM

55 INTERSTITIAL LUNG DISEASES 445
known factors are thought to initially triggeralveolar epithelial cell injury, but self-perpet-uating and aberrant interstitial fibroblast andmesenchymal cell proliferation (with col-lagen deposition and fibrosis) are thought toaccount for development of clinical disease.The key histologic findings are subpleural fi-brosis with sites of fibroblast proliferation (fi-broblast foci) and dense scarring, alternatingwith areas of normal lung tissue (heteroge-neity). Scattered interstitial inflammationoccurs with lymphocyte, plasma cell, andhistiocyte infiltration. Cystic dilatation of pe-ripheral alveoli (honeycombing) is found inall patients and increases with advanced dis-ease. A similar histologic pattern uncommonlyoccurs in cases of ILD of known etiology (seeTABLE 55–1); the term UIP is reserved for id-iopathic lesions not associated with knownconditions.
Symptoms and SignsSymptoms and signs typically develop
over 6 mo to several years and include dysp-nea on exertion and nonproductive cough.Constitutional symptoms, such as low-gradefever and myalgias, are uncommon. The clas-sic sign of IPF is fine, dry, bibasilar inspira-tory crackles (Velcro crackles). Clubbing ispresent in about 50% of cases. The remainderof the examination is normal until disease isadvanced; in advanced disease, signs of pul-monary hypertension and right ventricularsystolic dysfunction may develop.
DiagnosisDiagnosis is based on history, imaging
tests, pulmonary function tests, and biopsy.IPF is commonly overlooked at first becauseof clinical similarities to other diseases, suchas bronchitis, asthma, and heart failure.
Chest x-ray typically shows diffuse retic-ular opacities in the lower and peripheral lungzones. Small cystic lesions (honeycombing)and dilated airways due to traction bron-chiectasis are additional findings.
Pulmonary function tests typically reveala restrictive pattern (see Ch. 46 on p. 364).Diffusing capacity for carbon monoxide(DLCO) is also reduced. ABGs show hypox-emia, which is often exaggerated or elicitedby exercise and low arterial CO2 levels.
HRCT shows diffuse, patchy, subpleural,reticular opacities with irregularly thickenedinterlobular septa and intralobular lines; sub-pleural honeycombing; and traction bron-chiectasis. Ground-glass opacities affecting
> 30% of the lung suggest an alternative di-agnosis.
Laboratory testing plays little role in diag-nosis. Elevated ESR, C-reactive protein, andhypergammaglobulinemia are common. An-tinuclear antibody or rheumatoid factor is el-evated in up to 30% of patients and, depend-ing on the titer, may not imply underlyingconnective tissue disease.
PrognosisMost patients have moderate to advanced
clinical disease at the time of diagnosis anddeteriorate despite treatment. Normal PaO2 atpresentation and fewer fibroblastic foci on bi-opsy improve the prognosis. Prognosis isworse with advanced age, poor pulmonaryfunction at presentation, and severe dyspnea.Median survival is < 3 yr from time of diag-nosis. An increase in the frequency of hospi-talization for unexpected respiratory infec-tion and insufficiency indicates the approachof the patient’s end of life and should promptdiscussions about advance care planning (seep. 2768). Lung cancer occurs more frequentlyin patients with IPF, but cause of death is usu-ally respiration failure, respiratory infection,or heart failure with ischemia and arrhythmia.
TreatmentNo specific treatment has proven effective.
Supportive therapy consists of O2 for hypox-emia and antibiotics for pneumonias. End-stage disease may qualify selected patientsfor lung transplantation. Corticosteroids andcytotoxic drugs (cyclophosphamide, azathi-oprine) have traditionally been given to IPFpatients empirically in an attempt to halt theprogression of inflammation, but limited datasupport their efficacy. Nevertheless, it is com-mon practice to attempt treatment with pred-nisone (0.5 to 1.0 mg/kg po once/day for 3 mo,tapered to 0.25 mg/kg once/day over the next3 to 6 mo) combined with cyclophosphamideor azathioprine (1 to 2 mg/kg po once/day).Every 3 mo for 1 yr, clinical, radiographic,and physiologic responses are assessed, anddrug doses are increased or decreased ac-cordingly. Therapy is stopped if there is noobjective response.
Pirfenidone, an antifibrotic agent, may sta-bilize pulmonary function and reduce exac-erbations. Antifibrotics that inhibit collagensynthesis (relaxin), profibrotic growth fac-tors (suramin), and endothelin-1 (an angio-tensin receptor blocker) have only been dem-onstrated effective in vitro.
045_062PUL Page 445 Tuesday, November 8, 2005 10:54 AM

446
TABL
E 55
–2.
KEY
FEA
TUR
ES O
F ID
IOPA
THIC
INTE
RST
ITIA
L PN
EUM
ON
IAS
KE
Y F
EA
TU
RE
IPF
/CFA
NSI
PD
IPR
BIL
DA
IPC
OP
LIP
*
Age
at o
nset
(yr
)>
6040
–60
40–5
040
–50
Any
age
40–5
0A
ny a
ge
M:F
rat
ioM
ale
pred
omi-
nanc
eE
qual
Mal
e pr
edom
i-na
nce
Slig
ht m
ale
pre-
dom
inan
ceE
qual
Equ
alFe
mal
e pr
edom
i-na
nce
Prod
rom
eC
hron
ic(>
12
mo)
Suba
cute
to
chro
nic
(mon
ths
to
year
s)
Suba
cute
(w
eeks
to
mon
ths)
Suba
cute
(w
eeks
to
mon
ths)
Abr
upt (
1–
2 w
k)Su
bacu
te(<
3 m
o)C
hron
ic(>
12
mo)
His
tory
of
ciga
rette
smok
ing
> 6
0%>
40%
> 9
0%>
90%
Unk
now
n<
50%
Unk
now
n
Che
st x
-ray
findi
ngs
Bas
al-p
redo
mi-
nant
ret
icul
ar
abno
rmal
ity
with
vol
ume
loss
Gro
und-
glas
s an
d re
ticul
ar
opac
ity
Gro
und-
glas
s op
acity
Bro
nchi
al w
all
thic
keni
ng;
grou
nd-g
lass
op
acity
Prog
ress
ive
dif-
fuse
gro
und-
glas
s de
nsity
/co
nsol
idat
ion
Patc
hy b
ilate
ral
cons
olid
atio
nR
etic
ular
opac
ities
,no
dule
s
Hig
h-re
solu
tion
CT
find
ings
Peri
pher
al, s
ub-
pleu
ral,
basa
l; re
ticul
ar;
hone
ycom
b-in
g; tr
actio
n br
onch
iect
a-si
s/br
onch
i-ol
ecta
sis;
ar
chite
ctur
al
dist
ortio
n;
foca
l gro
und
glas
s
Peri
pher
al, s
ub-
pleu
ral,
basa
l, sy
mm
etri
c;
grou
nd-g
lass
at
tenu
atio
n;
irre
gula
r lin
es; c
onso
l-id
atio
n
Low
er z
one,
pe
riph
eral
pr
edom
i-na
nce
in
mos
t; gr
ound
-gla
ss
atte
nuat
ion;
re
ticul
ar li
nes
Dif
fuse
pat
tern
; br
onch
ial
wal
l thi
cken
-in
g; c
entr
i-lo
bula
r no
dule
s;
patc
hy
grou
nd-g
lass
op
acity
Dif
fuse
con
soli-
datio
n an
d gr
ound
-gla
ss
opac
ity, o
ften
w
ith lo
bula
r sp
arin
g; tr
ac-
tion
bron
chi-
ecta
sis
late
r
Subp
leur
al/p
eri-
bron
chia
l; pa
tchy
con
-so
lidat
ion
and/
or n
od-
ules
Dif
fuse
pat
tern
. C
entr
ilobu
lar
nod-
ules
; gro
und-
glas
s at
tenu
a-tio
n; s
epta
l and
bron
chov
ascu
-la
r th
icke
ning
; th
in-w
alle
d cy
sts
045_062PUL Page 446 Tuesday, November 8, 2005 10:54 AM
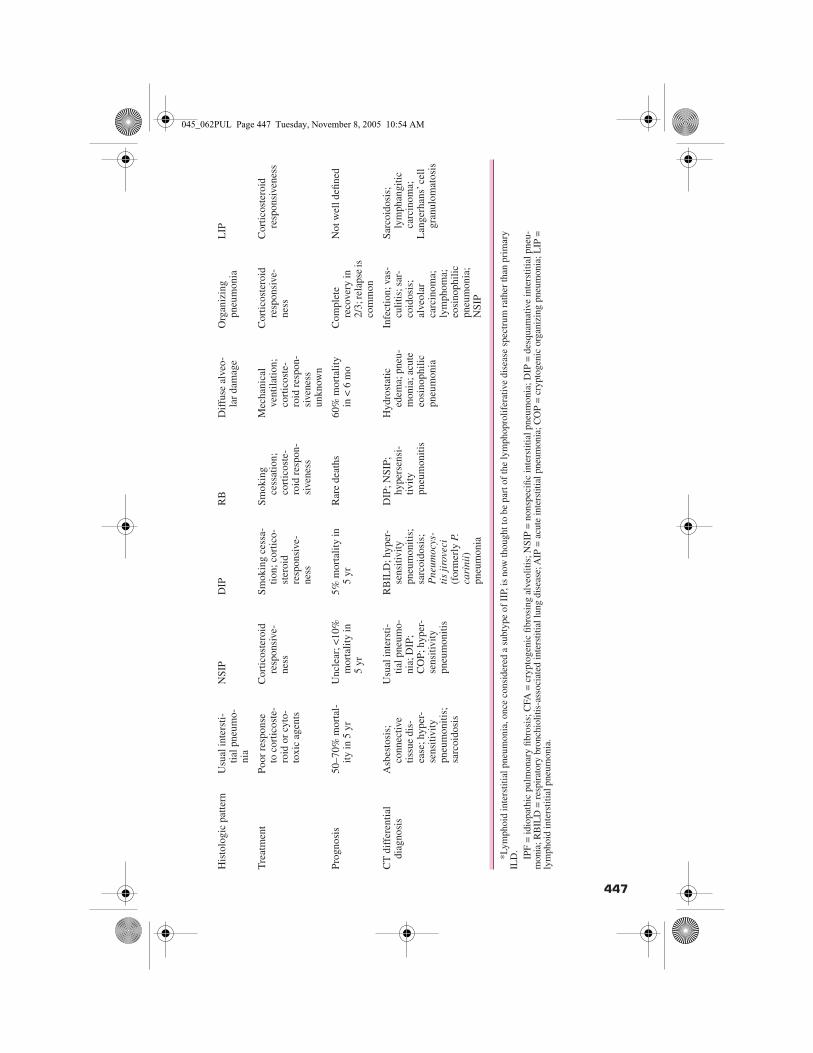
447
His
tolo
gic
patte
rnU
sual
inte
rsti-
tial p
neum
o-ni
a
NSI
PD
IPR
BD
iffu
se a
lveo
-la
r da
mag
eO
rgan
izin
g pn
eum
onia
LIP
Tre
atm
ent
Poor
res
pons
e to
cor
ticos
te-
roid
or
cyto
-to
xic
agen
ts
Cor
ticos
tero
id
resp
onsi
ve-
ness
Smok
ing
cess
a-tio
n; c
ortic
o-st
eroi
d re
spon
sive
-ne
ss
Smok
ing
cess
atio
n;
cort
icos
te-
roid
res
pon-
sive
ness
Mec
hani
cal
vent
ilatio
n;
cort
icos
te-
roid
res
pon-
sive
ness
un
know
n
Cor
ticos
tero
id
resp
onsi
ve-
ness
Cor
ticos
tero
id
resp
onsi
vene
ss
Prog
nosi
s50
–70%
mor
tal-
ity in
5 y
rU
ncle
ar; <
10%
m
orta
lity
in
5 yr
5% m
orta
lity
in
5 yr
Rar
e de
aths
60%
mor
talit
y in
< 6
mo
Com
plet
e re
cove
ry in
2/
3; re
laps
e is
co
mm
on
Not
wel
l defi
ned
CT
dif
fere
ntia
l di
agno
sis
Asb
esto
sis;
conn
ectiv
etis
sue
dis-
ease
; hyp
er-
sens
itivi
ty
pneu
mon
itis;
sa
rcoi
dosi
s
Usu
al in
ters
ti-tia
l pne
umo-
nia;
DIP
; C
OP;
hyp
er-
sens
itivi
ty
pneu
mon
itis
RB
ILD
; hyp
er-
sens
itivi
ty
pneu
mon
itis;
sa
rcoi
dosi
s;
Pne
umoc
ys-
tis
jiro
veci
(f
orm
erly
P.
cari
nii)
pneu
mon
ia
DIP
; NSI
P;
hype
rsen
si-
tivity
pneu
mon
itis
Hyd
rost
atic
ed
ema;
pne
u-m
onia
; acu
te
eosi
noph
ilic
pneu
mon
ia
Infe
ctio
n; v
as-
culit
is; s
ar-
coid
osis
; al
veol
ar
carc
inom
a;
lym
phom
a;
eosi
noph
ilic
pneu
mon
ia;
NSI
P
Sarc
oido
sis;
lym
phan
gitic
ca
rcin
oma;
L
ange
rhan
s’ c
ell
gran
ulom
atos
is
*Lym
phoi
d in
ters
titia
l pne
umon
ia, o
nce
cons
ider
ed a
sub
type
of
IIP,
is n
ow th
ough
t to
be p
art o
f th
e ly
mph
opro
lifer
ativ
e di
seas
e sp
ectr
um r
athe
r th
an p
rim
ary
ILD
.IP
F =
idio
path
ic p
ulm
onar
y fib
rosi
s; C
FA =
cry
ptog
enic
fibr
osin
g al
veol
itis;
NSI
P =
non
spec
ific
inte
rstit
ial p
neum
onia
; DIP
= d
esqu
amat
ive
inte
rstit
ial p
neu-
mon
ia; R
BIL
D =
res
pira
tory
bro
nchi
oliti
s-as
soci
ated
inte
rstit
ial l
ung
dise
ase;
AIP
= a
cute
inte
rstit
ial p
neum
onia
; CO
P =
cryp
toge
nic
orga
nizi
ng p
neum
onia
; LIP
=ly
mph
oid
inte
rstit
ial p
neum
onia
.
TABL
E 55
–2.
KEY
FEA
TUR
ES O
F ID
IOPA
THIC
INTE
RST
ITIA
L PN
EUM
ON
IAS
045_062PUL Page 447 Tuesday, November 8, 2005 10:54 AM

448 SECTION 5 PULMONARY DISORDERS
Interferon-γ-1b has shown promise whencombined with prednisone in a small groupof patients, but a larger double-blind multi-national randomized trial found no effect onprogression-free survival time, pulmonaryfunction, or quality of life.
Lung transplantation is successful for oth-erwise healthy IPF patients < 55 yr with end-stage pulmonary disease (< 40% of all IPFpatients).
DESQUAMATIVE INTERSTITIAL PNEUMONIADesquamative interstitial pneumonia ischronic lung inflammation characterizedby mononuclear cell infiltration of the air-spaces.
Over 90% of patients with desquamativeinterstitial pneumonia are smokers, whotend to develop the disease in their 30s or 40s.The disease tends to affect the lung paren-chyma uniformly. The alveolar walls arelined with plump cuboidal pneumocytes;there is moderate infiltration of the alveolarseptum by lymphocytes, plasma cells, and,occasionally, eosinophils, and alveolar sep-tal fibrosis is mild at worst. The most strikingfeature is the presence of numerous pig-mented macrophages within distal airspaces,mistaken as desquamated pneumocytes whenthe disease was first described. Honeycomb-ing is rare. Similar but much less extensivefindings are seen in respiratory bronchiolitis-associated ILD (RBILD), leading to thesuggestion that desquamative interstitialpneumonia and RBILD are different mani-festations of the same disease caused bycigarette smoking.
The symptoms, signs, pulmonary functiontest findings, and approach to diagnosis areotherwise the same as for idiopathic pulmo-nary fibrosis (IPF).
Chest x-ray abnormalities are less severethan in IPF; findings may be normal in up to20% of cases. HRCT shows patchy, subpleu-ral ground-glass opacities, usually withoutreticular opacities.
Treatment with smoking cessation results inclinical improvement in an estimated 75% ofpatients; those who do not improve may re-spond to corticosteroid or cytotoxic drugs.Prognosis is good, with about 70% survivalat 10 yr.
RESPIRATORY BRONCHIOLITIS-ASSOCIATED INTERSTITIAL LUNG DISEASERespiratory bronchiolitis-associated ILD is asyndrome of small airway inflammation andinterstitial lung disease occurring in smokers.
Most smokers develop a subclinicalbronchiolitis characterized by mild or mod-erate inflammation of the small airways.The few patients who develop more severeinflammation with clinically significant in-terstitial disease are said to have respiratorybronchiolitis-associated ILD (RBILD). Male-to-female ratio is 2:1. RBILD is character-ized histologically by submucosal inflam-mation of the membranous and respiratorybronchioles manifested by the presence oftan-brown pigmented macrophages (result-ing from increased iron content, as is seenin smokers), mucus stasis, and metaplasticcuboidal epithelium in bronchioles and al-veoli. Alveolar septal scarring always occurs.These findings, however, occur in some hy-persensitivity reactions, occupational lungexposures (usually due to mineral dusts),viral infections, and drug reactions. RBILDalso resembles desquamative interstitialpneumonia histologically, but in RBILD in-flammation is patchier and less extensive.The similarity of the 2 conditions has led tothe suggestion that they are different man-ifestations of the same disease caused bycigarette smoking.
Symptoms of cough and breathlessnesswith exertion resemble those of other ILDs,especially IPF, but are milder. Crackles on ex-amination are the only physical finding.
Diagnosis is based on history, imagingtests, pulmonary function tests, and biopsy.Chest x-ray findings include diffuse, fine re-ticular or nodular opacities; bronchial wallthickening; prominent peribronchovascularinterstitium; small regular and irregular opac-ities; and small peripheral ring shadows.HRCT scanning often shows hazy ground-glass opacities. A mixed obstructive-restrictivepattern is common on pulmonary functiontests, although results may be normal or showan isolated increase in residual volume. ABGmeasurements show mild hypoxemia. Rou-tine laboratory tests are not helpful.
Treatment of RBILD is smoking cessa-tion; evidence of efficacy of corticosteroids isanecdotal. The natural clinical course of the
045_062PUL Page 448 Tuesday, November 8, 2005 10:54 AM

55 INTERSTITIAL LUNG DISEASES 449
disease is unknown, but prognosis is goodwith smoking cessation.
ACUTE INTERSTITIAL PNEUMONIA(Accelerated Interstitial Pneumonia; Hamman-Rich Syndrome)
Acute interstitial pneumonia is an idiopathicversion of the acute respiratory distress syn-drome (ARDS—see p. 556).
Acute interstitial pneumonia (AIP) affectsapparently healthy men and women usually> 40 yr equally.
AIP is defined histologically by organiz-ing diffuse alveolar damage, a nonspecificpattern seen in other causes of lung injury un-related to IIP. The hallmark of organizing dif-fuse alveolar damage is diffuse, marked al-veolar septal edema with inflammatory cellinfiltration; fibroblast proliferation; occa-sional hyaline membranes; and thickening.Septa are lined with atypical, hyperplastictype II pneumocytes, and airspaces are col-lapsed. Thrombi develop in small arteries butare nonspecific.
Symptoms are abrupt onset of fever,cough, and shortness of breath and last 7 to14 days, quickly progressing in most patientsto respiratory failure.
Diagnosis is based on history, imagingtests, pulmonary function tests, and biopsy.Chest x-ray findings are similar to those inARDS and show diffuse bilateral airspaceopacification. HRCT scan shows bilateralpatchy symmetric areas of ground-glass at-tenuation and sometimes bilateral areas ofairspace consolidation in a predominantlysubpleural distribution. Mild honeycomb-ing, usually affecting < 10% of the lung, maybe seen. Routine laboratory tests are nonspe-cific and generally not helpful.
Diagnosis is confirmed by biopsy showingdiffuse alveolar damage in the absence ofknown causes of ARDS and diffuse alveolardamage (eg, sepsis, drugs, toxins, radiation,and viral infection). The disease must also bedistinguished from diffuse alveolar hemor-rhage syndrome, acute eosinophilic pneumo-nia, and idiopathic bronchiolitis obliteransorganizing pneumonia.
Treatment is supportive and usually re-quires mechanical ventilation. Corticoste-roid therapy is generally used, but efficacyhas not been established.
Mortality is > 60%; most patients diewithin 6 mo of presentation, and death is usu-ally due to respiratory failure. In patients whosurvive the initial acute episode, recovery ofpulmonary function is complete, althoughthe disease may recur.
BRONCHIOLITIS OBLITERANS ORGANIZING PNEUMONIA(Cryptogenic Organizing Pneumonia)
Bronchiolitis obliterans organizing pneumo-nia is an idiopathic condition in which gran-ulation tissue obstructs bronchioles andalveolar ducts with chronic inflammation andorganizing pneumonia in adjacent alveoli.
Idiopathic bronchiolitis obliterans orga-nizing pneumonia (BOOP) affects men andwomen equally, usually in their 40s or 50s.Cigarette smoking does not appear to be a riskfactor.
About 1⁄2 the patients recall having a com-munity-acquired pneumonia-like syndrome(ie, a nonresolving flu-like illness character-ized by cough, fever, malaise, fatigue, andweight loss). Progressive cough and exer-tional dyspnea are what usually prompt thepatient to seek medical attention. Examina-tion demonstrates inspiratory crackles.
Diagnosis is based on history, physical ex-amination, imaging tests, pulmonary func-tion tests, and biopsy. Chest x-ray showsbilateral, diffuse, peripherally distributed al-veolar opacities with normal lung volumes; aperipheral distribution similar to that seen inchronic eosinophilic pneumonia may occur.Rarely, alveolar opacities are unilateral. Re-current and migratory pulmonary opacitiesare common. Rarely, irregular linear or nod-ular interstitial opacities or honeycombingare seen at presentation. HRCT scans of thelung show patchy airspace consolidation,ground-glass opacities, small nodular opac-ities, and bronchial wall thickening and dila-tation. The patchy opacities are more com-mon in the periphery of the lung, often in thelower lung zone. CT scans may show muchmore extensive disease than is expected fromreview of the chest x-ray.
Pulmonary function tests usually show arestrictive defect, although an obstructive de-fect ([FEV1/FVC] < 70%) is found in 21% ofpatients, and pulmonary function is occa-sionally normal.
045_062PUL Page 449 Tuesday, November 8, 2005 10:54 AM
450 SECTION 5 PULMONARY DISORDERS
Routine laboratory tests are nonspecific.Leukocytosis without an increase in eosino-phils occurs in about 1⁄2 of patients. The initialESR often is elevated. Rest and exercise hy-poxemia is common.
Lung biopsy shows excessive prolifera-tion of granulation tissue within small airwaysand alveolar ducts, with chronic inflamma-tion in the surrounding alveoli. Foci of or-ganizing pneumonia (ie, a BOOP pattern) arenonspecific and can occur secondary to otherpathologic processes, including infections,Wegener’s granulomatosis, lymphoma, hy-persensitivity pneumonitis, and eosinophilicpneumonia.
Treatment is similar to that for idiopathicpulmonary fibrosis. Clinical recovery occursin 2⁄3 of treated patients, often within 2 wk.Relapses occur in up to 50% of patients, butthese patients are responsive to additionalcourses of corticosteroids.
NONSPECIFIC INTERSTITIAL PNEUMONIANonspecific interstitial pneumonia refers toa histologic appearance in ILD that does notconform to the other more specific histo-logic patterns.
Nonspecific interstitial pneumonia ap-pears to be a discrete entity. Its incidence andprevalence are unknown, but it appears to bethe 2nd most common form of IIP (14 to 36%of reported cases). Most cases occur in pa-tients who have connective-tissue disease,drug-induced ILD, or chronic hypersensitiv-ity pneumonitis as an underlying feature.Some cases have no identified etiology andare not associated with another disease.
Clinical presentation is similar to that ofIPF. Most patients are between 40 and 60 yr.Cough and dyspnea are present for months toyears.
Chest x-ray primarily demonstrates lower-zone reticular opacities. Bilateral patchyopacities can also be seen. HRCT scan find-ings include bilateral patchy ground-glassattenuation, bilateral areas of consolidation,irregular lines, and bronchial dilatation.Ground-glass attenuation is the predominantfinding in most cases and is the sole abnor-mality in about 1⁄3 of cases.
The main histologic feature of nonspecificinterstitial pneumonia is homogenous inflam-mation and fibrosis, as opposed to the heter-ogeneity in usual interstitial pneumonia.
The changes are temporally uniform, but theprocess may be patchy, with intervening ar-eas of unaffected lung. Honeycomb areas arerare.
Most patients have a good prognosis aftertreatment with corticosteroids. Relapse mayoccur. The disease progresses in a few pa-tients, who die 5 to 10 yr after diagnosis. Theestimated 10-yr mortality is < 15 to 20%.
DRUG-INDUCED PULMONARY DISEASE
Drug-induced pulmonary disease is not asingle disorder, but rather, a common clinicalproblem in which a patient without previouspulmonary disease develops respiratorysymptoms, chest x-ray changes, deteriora-tion of pulmonary function, and/or histo-logic changes while receiving drug therapy.Over 150 drugs or categories of drugs havebeen reported to cause pulmonary disease;the mechanism is rarely known, but manydrugs are thought to provoke a hypersensi-tivity response.
Depending on the drug, drug-induced syn-dromes can resemble interstitial fibrosis,bronchiolitis obliterans organizing pneumo-nia, asthma, noncardiogenic pulmonaryedema, pleural effusions, pulmonary eosino-philia, pulmonary hemorrhage, or veno-occlusive disease (see TABLE 55–3), with cor-responding chest x-ray, CT, and pulmonaryfunction test findings.
Diagnosis is based on observation of re-sponses to withdrawal from and, if practical,reintroduction to the suspected drug.
Treatment is drug discontinuation. Ascreening pulmonary function test is com-monly obtained in patients about to begin oralready taking drugs with pulmonary toxici-ties, but the benefits of screening for predic-tion or early detection of toxicity is unproven.
EOSINOPHILIC PULMONARY DISEASES
Eosinophilic pulmonary diseases are agroup of diseases characterized by the accu-mulation of eosinophils in alveolar spaces,the interstitium, or both. Peripheral bloodeosinophilia is also common. Known causesof eosinophilic pulmonary disease includeinfections (especially helminthic infections),
045_062PUL Page 450 Tuesday, November 8, 2005 10:54 AM

55 INTERSTITIAL LUNG DISEASES 451
drug-induced pneumonitis (eg, antibiotics,phenytoin, L-tryptophan), inhaled toxins(eg, cocaine), systemic diseases (eg, Churg-Strauss), and allergic bronchopulmonary as-pergillosis, but often the cause is unknown.
Diagnosis is based on demonstration ofopacities on chest x-ray and identification ofeosinophilia (> 450/µL) in peripheral blood,bronchoalveolar lavage fluid, or lung biopsy
tissue. Pulmonary opacities on chest x-ray as-sociated with blood eosinophilia are some-times called the PIE (pulmonary infiltrateswith eosinophilia) syndrome.
Eosinophils are primarily tissue-dwellingand are several hundred–fold more abundantin tissues than in blood. Consequently, bloodeosinophil numbers do not necessarily indi-cate the extent of eosinophilic involvement in
TABLE 55–3. DRUGS CAUSING SPECIFIC CLINICAL PRESENTATIONSOF PULMONARY TOXICITY
CONDITION DRUG OR AGENT
Asthma Aspirin, β-blockers (timolol), cocaine, dipyridamole, hydrocortisone, IL-2, methylphenidate, nitrofurantoin, protamine, sulfasalazine, vinca alkaloids (with mitomycin)
Bronchiolitis obliterans organizing pneumonia
Amiodarone, bleomycin, cocaine, cyclophosphamide, methotrexate, minocycline, mitomycin-C, penicil-lamine, sulfasalazine, tetracycline
Hypersensitivitypneumonitis
Azathioprine plus 6-mercaptopurine, busulfan, fluoxe-tine, radiation
Interstitial pneumonia or fibrosis
Amphotericin B, bleomycin, busulfan, carbamazepine, chlorambucil, cocaine, cyclophosphamide, diphenyl-hydantoin, flecainide, heroin, melphalan, methadone, methotrexate, methylphenidate, methysergide, mineral oil, nitrofurantoin, nitrosoureas, procarbazine, silicone, tocainide, vinca alkaloids (with mitomycin)
Noncardiac pulmonary edema
Beta mimetics (terbutaline, ritodrine), chlordiazepoxide, cocaine, cytarabine, ethiodized oil, gemcitabine, her-oin, hydrochlorothiazide, methadone, mitomycin-C, phenothiazines, protamine, sulfasalazine, tocolytic agents, tricyclics, tumor necrosis factor, vinca alkaloids (with mitomycin)
Parenchymal hemorrhage Anticoagulants, azathioprine plus 6-mercaptopurine, cocaine, mineral oil, nitrofurantoin, radiation
Pleural effusion Amiodarone, anticoagulants, bleomycin, bromocriptine, busulfan, granulocyte-macrophage colony-stimulating factor, IL-2, methotrexate, methysergide, mitomycin-C, nitrofurantoin, para-aminosalicylic acid, procarbazine, radiation, tocolytic agents
Pulmonary infiltrate with eosinophilia
Amiodarone, amphotericin B, bleomycin, carba-mazepine, diphenylhydantoin, ethambutol, etoposide, granulocyte-macrophage colony-stimulating factor, isoniazid, methotrexate, minocycline, mitomycin-C, nitrofurantoin, para-aminosalicylic acid, procarbazine, radiation, sulfasalazine, sulfonamides, tetracycline,trazodone
Pulmonary vasculardisease
Appetite suppressants (dexfenfluramine, fenfluramine, phentermine), busulfan, cocaine, heroin, methadone, methylphenidate, nitrosoureas, radiation
045_062PUL Page 451 Tuesday, November 8, 2005 10:54 AM

452 SECTION 5 PULMONARY DISORDERS
affected tissues. Eosinophils are most numer-ous in tissues with a mucosal epithelial inter-face with the environment, such as the respi-ratory, GI, and lower GU tracts. Eosinophilsare not found in the lungs of healthy people,so their presence in tissue or bronchoalveolarlavage (> 5% of differential count) identifiesa pathologic process. Pulmonary eosino-philia may occur in the absence of peripheraleosinophilia.
Eosinophils are exquisitely sensitive tocorticosteroids and completely disappearfrom the bloodstream within a few hours afteradministration of corticosteroids. This rapiddisappearance from the blood may obscurethe diagnosis in patients who receive corti-costeroids before the diagnostic assessmentis instituted.
The 2 primary eosinophilic pulmonarydiseases of unknown etiology are chronic andacute eosinophilic pneumonia. Hypereosin-ophilia syndrome, a systemic disease affect-ing multiple organs, is discussed on p. 1095.
CHRONIC EOSINOPHILIC PNEUMONIAChronic eosinophilic pneumonia is an abnor-mal, chronic accumulation of eosinophils inthe lung.
Prevalence and incidence of chronic eosin-ophilic pneumonia (CEP) are unknown. Eti-ology is suspected to be an allergic diathesis.Most patients are nonsmokers.
Symptoms, Signs, and DiagnosisPatients often present with fulminant ill-
ness characterized by cough, fever, progres-sive breathlessness, weight loss, wheezing,and night sweats. Asthma accompanies orprecedes the illness in > 50% of cases.
Diagnosis requires exclusion of infectiouscauses and is based on clinical presentation,blood tests, and chest x-ray. Peripheral bloodeosinophilia, a very high ESR, iron defi-ciency anemia, and thrombocytosis are allfrequently found. Chest x-ray findings of bi-lateral peripheral or pleural-based opacities(present in about 60% of cases), most com-monly in the middle and upper lung zones, isdescribed as the “photographic negative” ofpulmonary edema and is virtually pathogno-monic (although seen in < 25% of patients).A similar pattern is identified on CT in virtu-ally all cases. Bronchoalveolar lavage eosin-ophilia > 40% is suggestive of CEP; serial
bronchoalveolar lavage examinations mayhelp document the course of disease. Biopsydemonstrates interstitial and alveolar eosino-phils and histiocytes, including multinucle-ated giant cells, and bronchiolitis obliteransorganizing pneumonia. Fibrosis is minimal.
TreatmentPatients with CEP are uniformly responsive
to IV or oral corticosteroids; failure to respondindicates another diagnosis. Initial treatmentis prednisone 40 to 60 mg once/day. Clinicalimprovement is often striking and rapid, oftenoccurring within 48 h. Complete resolution ofsymptoms and x-ray abnormalities occurswithin 14 days in most patients and by 1 mo inalmost all. Symptoms and plain chest x-raysare both reliable and efficient guides to ther-apy. Although CT scanning is more sensitivefor the detection of radiographic abnormali-ties, there is no benefit gained by repeating it.Peripheral eosinophil counts, ESR, and IgElevels can also be used to follow the clinicalcourse during treatment. However, not all pa-tients have abnormal laboratory test results.
Symptomatic or radiographic relapse oc-curs in 50 to 80% of cases either after cessa-tion of therapy or, less commonly, with taper-ing of the corticosteroid dose. Relapse canoccur months to years after the initial present-ing episode. Thus, corticosteroid therapy isoccasionally continued indefinitely. Inhaledcorticosteroids (eg, fluticasone or beclo-methasone 500 to 750 µg bid) appear to beeffective, especially in reducing the main-tenance dose of oral corticosteroid.
CEP occasionally leads to physiologicallyimportant, irreversible fibrosis, althoughdeath is extremely unusual. Relapse does notappear to indicate treatment failure, a worseprognosis, or greater morbidity. Patients con-tinue to respond to corticosteroids similar tothose before relapse. Fixed airflow obstruc-tion can occur in some patients who recover,but the abnormalities are usually of border-line clinical significance.
ACUTE EOSINOPHILIC PNEUMONIAAcute eosinophilic pneumonia is character-ized by rapid eosinophilic infiltration of thelung interstitium.
Incidence and prevalence of acute eosino-philic pneumonia (AEP) are unknown. AEPcan occur at any age but most often affects pa-tients between 20 and 40 yr, with a male-to-
045_062PUL Page 452 Tuesday, November 8, 2005 10:54 AM

55 INTERSTITIAL LUNG DISEASES 453
female ratio of 21:1. The cause is unknown,but AEP may be an acute hypersensitivity re-action to an unidentified inhaled antigen in anotherwise healthy person. Cigarette or othersmoke exposure may be involved.
Symptoms and SignsAEP causes an acute febrile illness of short
duration (usually < 7 days). Symptoms arenonproductive cough, dyspnea, malaise, myal-gias, night sweats, and pleuritic chest pain. Signsinclude tachypnea, fever (often > 38.5°C), andbibasilar inspiratory crackles and, occasion-ally, rhonchi on forced exhalation. AEP fre-quently presents as acute respiratory failurerequiring mechanical ventilation. Rarely, hy-perdynamic shock can occur.
DiagnosisThe diagnosis is based on clinical presen-
tation and findings from routine testing and isconfirmed by bronchoscopy. AEP is a diag-nosis of exclusion and requires the absence ofknown causes of eosinophilic pneumoniaand of respiratory failure. The CBC in mostpatients demonstrates markedly elevatedeosinophil counts. ESR and IgE levels arehigh but are nonspecific.
The chest x-ray initially may show onlysubtle reticular or ground-glass opacities, of-ten with Kerley B lines. Isolated alveolar(about 25% of cases) or reticular (about 25%of cases) opacities may also be seen on pre-sentation. The pattern is unlike that seen inchronic eosinophilic pneumonia, in which theopacities are localized to the lung periphery.Small pleural effusions occur in 2⁄3 of pa-tients and are frequently bilateral. High-resolution CT is always abnormal with bilat-eral, random, patchy ground-glass or reticularopacities. Pleural fluid examination showsmarked eosinophilia with high pH. Pulmo-nary function tests often demonstrate a restric-tive process with reduced diffusing capacityfor carbon monoxide (DLCO).
Bronchoscopy should be performed for la-vage and, occasionally, biopsy. Bronchoal-veolar lavage fluid often shows a high numberand percentage (> 25%) of eosinophils. Themost common histopathologic features onbiopsy include eosinophilic infiltration withacute and organizing diffuse alveolar damage,but few cases have undergone lung biopsy.
Treatment and PrognosisSome patients improve spontaneously.
Most are treated with prednisone 40 to 60 mg
po once/day. In the setting of respiratory fail-ure, methylprednisolone 60 to 125 mg q 6 his preferred. The prognosis is excellent; re-sponse to corticosteroids and complete re-covery without recurrence is almost univer-sal. Pleural effusions resolve more slowlythan parenchymal opacities.
LÖFFLER’S SYNDROMELöffler’s syndrome is characterized by ab-
sent or mild respiratory symptoms, fleetingmigratory pulmonary opacities, and periph-eral blood eosinophilia. Parasitic infections,especially Ascaris lumbricoides, may be thecause, but an identifiable etiologic agent isnot found in up to 1⁄3 of patients. The diseaseusually resolves within 1 mo.
HYPERSENSITIVITY PNEUMONITIS
(Extrinsic Allergic Alveolitis)
Hypersensitivity pneumonitis is a syndromeof cough, dyspnea, and fatigue caused bysensitization and subsequent hypersensitiv-ity to environmental (frequently occupa-tional) antigens. Acute, subacute, andchronic forms exist; all are characterized byacute interstitial inflammation and develop-ment of granulomas and fibrosis with long-term exposure. Diagnosis is based on a com-bination of history, physical examination,imaging tests, bronchoalveolar lavage, andbiopsy. Short-term treatment is with corti-costeroids; long-term treatment is antigenavoidance.
Etiology and PathophysiologyOver 300 antigens have been identified as
triggers for hypersensitivity pneumonitis, al-though 8 account for about 75% of cases. An-tigens are commonly categorized by type andoccupation (see TABLE 55–4); farmer’s lung,caused by inhalation of hay dust containingthermophilic actinomycetes, is the proto-type. Substantial overlap exists between hy-persensitivity pneumonitis and chronic bron-chitis in farmers, in whom chronic bronchitisis far more common, occurs independent ofsmoking status, is linked to thermophilic ac-tinomycete exposure, and leads to findingssimilar to those of hypersensitivity pneu-monitis on diagnostic testing.
045_062PUL Page 453 Tuesday, November 8, 2005 10:54 AM

454 SECTION 5 PULMONARY DISORDERS
TABLE 55–4. EXAMPLES OF HYPERSENSITIVITY PNEUMONITIS
ASSOCI-ATION DISEASE ANTIGEN SOURCE
Farming Farmer’s lung Thermophilic actino-mycetes; fungi, espe-cially Aspergillus sp
Vegetable compost (moldy grain, hay, silage)
Tobacco grower’s lung
Aspergillus sp, Scopu-lariopsis brevicaulis
Tobacco plants
Mushroom worker’s lung
Thermophilic actino-mycetes, Hypsizigus marumoreus
Mushroom compost
Potato riddler’s lung Thermophilic actino-mycetes, Aspergillus sp
Moldy hay around pota-toes
Cheese washer’s lung
Penicillium casei, Aspergillus clavatus
Moldy cheese
Bagassosis Thermophilic actino-mycetes
Moldy bagasse (sugar cane)
Compost lung Aspergillus sp CompostWine grower’s lung Botrytis cincrea Moldy grapesCoffee worker’s lung Coffee bean dust Coffee beans
Water Sewer worker’s lung Cephalosporium sp Contaminated basement (sewage)
Tap water lung Unknown Contaminated tap waterHumidifier lung Aureobasidium sp, Can-
dida albicans, thermo-philic actinomycetes
Contaminated water in humidification or air-conditioning systems
Hot tub lung Cladosporium sp, Mycobacterium avium complex
Contaminated mist and mold on ceilings and around tub
Sauna taker’s lung Aureobasidium sp Contaminated sauna water
Birds Bird fancier’s lung Parakeet, pigeon, chicken, turkey, and duck proteins
Avian droppings or feathers
Animals Sausage worker’s lung
Penicillium nalgiovense Dry sausage mold
Pituitary snuff taker’s lung
Animal proteins Heterologous (bovine, porcine) pituitary snuff
Furrier’s lung Animal fur dust Animal peltsLaboratory worker’s hypersensitivity pneumonitis
Rodent proteins Male rat urine and fur
Fish food lung Unknown Fish foodFish meal worker’s lung
Fish meal dust Fish meal dust
Mummy handler’s lung
Unknown Cloth mummy wrap-pings
Grains Miller’s lung Sitophilus granarius (wheat weevil)
Infested wheat flour
Malt worker’s lung Aspergillus sp Moldy barley
045_062PUL Page 454 Tuesday, November 8, 2005 10:54 AM

55 INTERSTITIAL LUNG DISEASES 455
The disease seems to represent a type IVhypersensitivity reaction, in which repeatedexposure to antigen in genetically suscepti-ble people leads to acute neutrophilic andmononuclear alveolitis, followed by intersti-tial lymphocytic infiltration and granuloma-tous reaction. Fibrosis with bronchiolarobliteration occurs with continued exposure.
Circulating precipitins (antibodies sensi-tized to antigen) seem not to have a primaryetiologic role, and clinical history of allergy(such as asthma and seasonal allergies) is nota predisposing factor. Cigarette smokingseems to delay or prevent development, per-haps through down-regulation of the lung’simmune response to inhaled antigens. How-ever, smoking may exacerbate the diseaseonce established.
Hypersensitivity pneumonitis must be dis-tinguished from disorders that are clinicallysimilar but that have different pathophysiol-ogies. Organic dust toxic syndrome (pulmo-nary mycotoxicosis, grain fever), for exam-ple, is a syndrome consisting of fever, chills,myalgias, and dyspnea that does not requireprior sensitization and is thought to be causedby inhalation of toxins produced by fungi or
other contaminants of organic dust. Silofiller’s disease may lead to respiratory failure,acute respiratory distress syndrome (ARDS),and bronchiolitis obliterans or bronchitis butis caused by inhalation of toxic nitrogen ox-ides produced by freshly fermented corn oralfalfa silage. Occupational asthma causesdyspnea in people previously sensitized to aninhaled antigen, but features such as airflowobstruction, airway eosinophilia, and differ-ences in triggering antigens distinguish itfrom hypersensitivity pneumonitis (seep. 476).
Symptoms and SignsSymptoms and signs tend to depend on
whether onset is acute, subacute, or chronic.Only a small proportion of exposed peopledevelop symptoms and in most cases only af-ter weeks to months of exposure and sensiti-zation.
Acute disease occurs in previously sensi-tized people with acute high-level antigen ex-posure and manifests as fever, chills, cough,chest tightness, and dyspnea 4 to 8 h after ex-posure. Anorexia, nausea, and vomiting mayalso be present. Physical examination shows
Milling and con-struction
Woodworker’s lung Wood dust, Alternaria sp, Baccilus subtilis
Oak, cedar, pine, spruce, and mahogany dusts
Wood trimmer’s disease
Rhizopus, Mucor spp Contaminated wood trimmings
Wood pulp worker’s disease
Penicillium sp Oak and maple tree pulp
Sequoiosis Aureobasidium, Graph-ium spp
Redwood sawdust
Thatched-roof worker’s disease
Sacchoromonospora viridis
Dried grass and leaves
Industry Detergent worker’s lung
Bacillus subtilis Bacillus subtilus enzymes in detergent
Chemical worker’s lung
Isocyanates Polyurethane foam, varnishes, lacquer
Vineyard sprayer’s lung
Copper sulfate Copper sulfate use
Textiles Byssinosis (brown lung)
Mill dust Cotton, flax, and hemp dust
Lycoperdonosis Puffball spores Folk medicine
TABLE 55–4. EXAMPLES OF HYPERSENSITIVITY PNEUMONITIS—Continued
ASSOCI-ATION DISEASE ANTIGEN SOURCE
045_062PUL Page 455 Tuesday, November 8, 2005 10:54 AM

456 SECTION 5 PULMONARY DISORDERS
tachypnea, diffuse fine-to-medium inspira-tory rales, and, in almost all cases, absence ofwheezing.
Chronic disease occurs in people withchronic low-level antigen exposure (such asowners of birds) and manifests as onset overmonths to years of exertional dyspnea, pro-ductive cough, fatigue, and weight loss.There are few physical findings; clubbing un-commonly occurs and fever is absent. In ad-
vanced cases, pulmonary fibrosis producessigns and symptoms of right heart failure, res-piratory failure, or both.
Subacute disease falls between the acuteand chronic forms and manifests either ascough, dyspnea, fatigue, and anorexia thatdevelops over days to weeks or as acute su-perimposed on chronic symptoms.
DiagnosisDiagnosis is based on a combination of his-
tory, physical examination, imaging tests,pulmonary function tests, bronchoalveolarlavage, and biopsy (see TABLE 55–5). Thedifferential diagnosis is broad and includesenvironmental pulmonary diseases (see Ch.57 on p. 469), sarcoidosis, bronchiolitis oblit-erans, connective tissue–associated pulmo-nary disease, and other ILDs.
Clues in the history include atypical pneu-monias recurring at roughly regular inter-vals; symptom onset after moving to a newjob or home; a hot tub, a sauna, a swimmingpool, or other sources of standing water orwater damage in the home or regular expo-sure to them elsewhere; having birds as pets;and exacerbation and relief of symptoms inand away from specific settings, respectively.
Examination often is not useful in makingthe diagnosis, although abnormal lung soundsand clubbing may be present.
Imaging tests typically are obtained forpatients with the above history, signs, andsymptoms. Chest x-ray is neither sensitivenor specific for detecting disease and is fre-quently normal in patients with acute andsubacute forms. It may demonstrate reticularor nodular opacities, usually when symptomsare present. Chest x-rays of patients withchronic disease are more likely to show retic-ular or nodular opacities in the upper lobeswith reduced lung volumes and honeycomb-ing, similar to that of idiopathic pulmonaryfibrosis. Abnormalities are far more com-monly detected by high-resolution CT(HRCT), and HRCT is considered standardfor evaluating parenchymal changes in hy-persensitivity pneumonitis. The most typicalHRCT finding is the presence of profusepoorly defined centrilobular micronodules.These micronodules may be found in patientswith acute, subacute, or chronic disease and,in the correct clinical context, strongly sug-gest hypersensitivity pneumonitis. Occa-sionally, ground-glass attenuation is the pre-dominant or only finding. It is usually diffusebut sometimes spares the periphery of the
TABLE 55–5. DIAGNOSTIC CRITERIA FOR HYPERSENSITIVITY PNEUMONITIS
DIAGNOSTIC CATEGORY CRITERIA
Definite HP 1, 2, and 3 1, 2, and 4a 1, 2a, 3, and 5 2, 3, and 5
Probable HP 1, 2a, and 3Subclinical HP 1 and 3aSensitized 1 only
Criteria1. Known exposure to antigen
a. History of exposureb. Confirmation of presence of
antigen in environment by investigation
c. Presence of elevated, specific IgG serum precipitins
2. Clinical, chest x-ray, and pulmonary function test findings
a. Characteristic symptoms and signs (especially after antigen exposure)
b. Characteristic chest x-ray or high-resolution CT findings
c. Abnormal pulmonary function test results
3. Lymphocytosis on bronchoalveolar lavagea. CD4+/CD8+ ratio < 1b. Positive response to lymphocyte
transformation testing
4. Recurrence of clinical and pulmonary function test findings with antigen challenge testing
a. Environmental exposureb. Controlled exposure to antigen
extract
5. Histologya. Noncaseating granulomasb. Mononuclear cell infiltrate
HP = Hypersensitivity pneumonitis.
045_062PUL Page 456 Tuesday, November 8, 2005 10:54 AM
55 INTERSTITIAL LUNG DISEASES 457
secondary lobule. Focal areas of hyperlu-cency, similar to those seen in obliterativebronchiolitis, may be a prominent feature insome patients (eg, mosaic attenuation withair trapping on expiratory HRCT). In chronichypersensitivity pneumonitis, there are signsof lung fibrosis (eg, lobar volume loss, linear/reticular opacities, or honeycombing). Somenonsmoking patients with chronic hypersen-sitivity pneumonitis have findings of upperlobe emphysema. Mediastinal lymphadenop-athy is uncommon, thereby distinguishing hy-persensitivity pneumonitis from sarcoidosis.
Pulmonary function tests should be ob-tained as part of the standard evaluation ofsuspected cases of hypersensitivity pneu-monitis. The disease can produce obstruc-tive, restrictive, or a mixed pattern of airwaychanges. Advanced disease most commonlyproduces a restrictive defect (decreased lungvolumes), a decreased diffusing capacity forcarbon monoxide (DLCO), and hypoxemia.Airway obstruction is unusual in acute dis-ease but may develop in chronic disease.
Bronchoalveolar lavage is rarely specificfor the diagnosis but is often a component ofthe diagnostic assessment for chronic respi-ratory symptoms and pulmonary function ab-normalities. A lymphocytosis in lavage fluid(> 60%) with CD4+/CD8+ ratio < 1.0 is char-acteristic of disease; by contrast, lymphocy-tosis with CD4+ predominance (ratio > 1.0)is more characteristic of sarcoidosis. Otherfindings may include mast cells > 1% (afteracute exposure) and increased neutrophilsand eosinophils.
Lung biopsy is indicated when noninva-sive testing is inconclusive. Transbronchialbiopsy performed through a bronchoscope issufficient as long as multiple specimens aretaken from areas of active disease and multi-ple sequential sections of tissue are examinedhistologically. Findings vary but includelymphocytic alveolitis, noncaseating granu-lomas, and granulomatosis. Interstitial fibro-sis may be seen but is usually mild in the ab-sence of advanced radiographic changes.
Additional testing is indicated when addi-tional support for the diagnosis is required orto detect other causes of ILD. Circulating pre-cipitins (specific precipitating antibodies tothe suspected antigen) are suggestive but areneither sensitive nor specific and thus are nothelpful. Identification of a specific precipi-tating antigen may require detailed aerobio-logic and/or microbiologic assessment of theworkplace by industrial hygiene specialists
but usually are guided by known sources ofinciting antigens (eg, Bacillus subtilis in de-tergent factories). Skin tests are not helpful,and eosinophilia is absent. Tests helpful in de-tecting other diseases include serologies andcultures (for psittacosis and other pneumo-nias) and autoantibodies (for collagen-vas-cular disease). Elevated eosinophils may sug-gest chronic eosinophilic pneumonias, andhilar and paratracheal lymph node enlarge-ment is more characteristic of sarcoidosis.
Prognosis, Treatment, and Prevention
Pathologic changes are completely revers-ible if detected early and if antigen exposure iseliminated. Acute disease is self-limiting withantigen avoidance; symptoms usually lessenwithin hours. Chronic disease has a more com-plicated prognosis: once fibrosis has been es-tablished, patients usually have irreversiblepathophysiology, although these changes of-ten stabilize if the patient is no longer exposedto the offending environment.
Treatment of acute or subacute hypersen-sitivity pneumonitis is with corticosteroids,usually prednisone 60 mg once/day for 1 to2 wk, then tapered over the next 2 to 4 wk to20 mg once/day, followed by weekly decre-ments of 2.5 mg until the drug is stopped. Thisregimen relieves initial symptoms but doesnot appear to alter long-term outcome.
The most important long-term treatment isavoidance of exposure to antigens. A com-plete change of environment is rarely realis-tic, especially for farmers and other workers,in which case dust control measures (such aswetting down compost before disturbing it)or using air filters or protective masks may beeffective. Fungicides may be used to preventthe growth of antigenic microorganisms (eg,in hay or on sugar cane), but the long-termsafety of this approach is unproven. Exten-sive cleaning of wet ventilation systems, re-moval of moist carpets, and maintenance oflow humidity are also effective in some set-tings. Patients must be told, however, thatthese measures may be inadequate in thepresence of continued exposure.
LYMPHANGIOLEIOMYO-MATOSIS
Lymphangioleiomyomatosis is nonmalig-nant growth of smooth muscle cells through-out the lung, pulmonary blood vessels,
045_062PUL Page 457 Tuesday, November 8, 2005 10:54 AM

458 SECTION 5 PULMONARY DISORDERS
lymphatics, and pleurae. It is rare and occursexclusively in young women. The cause isunknown. Symptoms are dyspnea, cough,chest pain, and hemoptysis; spontaneouspneumothorax is common. Diagnosis is sus-pected on the basis of symptoms and chestx-ray and is confirmed by high-resolutionCT. Prognosis is uncertain, but the diseaseis slowly progressive and over years oftenleads to respiratory failure and death. Pri-mary treatment is lung transplantation.
Epidemiology, Etiology, and Pathophysiology
Lymphangioleiomyomatosis (LAM) is adisease exclusive to women, affecting mostbetween 20 and 40 yr. Whites are at greatestrisk. LAM affects < 1 in 1 million people. Itis characterized by nonmalignant prolifera-tion of atypical smooth muscle cells through-out the chest, including lung parenchyma,vasculature, lymphatics, and pleurae, lead-ing to distortion of lung architecture, cysticemphysema, and progressive deterioration oflung function. It is included in the currentchapter because patients with LAM are oc-casionally misdiagnosed as having ILD.
The cause of LAM is unknown. The tempt-ing hypothesis that female sex hormones playa role in pathogenesis remains unproven. Thedisease usually arises spontaneously, butLAM bears many similarities to the pulmo-nary findings of tuberous sclerosis (TS—seep. 2379); LAM occurs in some patients withTS and is thought by some to be a forme frusteof TS. Mutations in the tuberous sclerosiscomplex-2 gene (TSC-2) have been de-scribed in LAM cells and angiomyolipomas.These observations suggest 1 of 2 possibili-ties: (1) somatic mosaicism for TSC-2 muta-tions within the lungs and kidneys results infoci of disease superimposed against a back-ground of normal cells within these tissues(although multiple discrete sites of diseasemight be expected) or (2) LAM representsdissemination of angiomyolipoma tissue tothe lung in a fashion analogous to the syn-drome of benign metastasizing leiomyoma.
Symptoms and SignsInitial symptoms are dyspnea and, less
commonly, cough, chest pain, and hemopty-sis. There are few signs of disease, but somewomen have crackles and rhonchi. Many pa-tients present with spontaneous pneumotho-rax. They may also present with manifesta-tions of lymphatic obstruction, including
chylothorax, chylous ascites, and chyluria.Symptoms are thought to worsen duringpregnancy and possibly during air travel; airtravel is especially contraindicated in womenwith new or worsening respiratory symp-toms; history of a pneumothorax or hemop-tysis; or evidence of extensive subpleuralbullous or cystic changes on high-resolutionCT (HRCT) scans. Renal angiomyolipomas(hamartomas made of smooth muscle, bloodvessels, and adipose) occur in up to 50% ofpatients and, although usually asymptomatic,can cause bleeding, which usually presents ashematuria or flank pain if they grow large.
DiagnosisDiagnosis is suspected in young women
with dyspnea, interstitial changes with nor-mal or increased lung volumes on chest x-ray,spontaneous pneumothorax, and/or chylouseffusion. Diagnosis is confirmed by biopsy,but HRCT is performed in all patients sus-pected of having the disease. Findings ofmultiple, small, diffusely distributed cystsare generally pathognomonic for LAM.
Biopsy is indicated only when HRCT find-ings are nondiagnostic. Findings of an abnor-mal proliferation of smooth muscle cells(LAM cells) associated with cystic changeson histologic examination confirm disease.
Pulmonary function tests support the diag-nosis and are especially useful for monitor-ing. Typical findings are of an obstructive ormixed obstructive/restrictive pattern. Thelungs are usually hyperinflated with an in-crease in the total lung capacity (TLC) andthoracic gas volume. Gas trapping (an in-crease in residual volume [RV] and RV/TLCratio) is commonly present. The PaO2 and dif-fusing capacity for carbon monoxide (DLCO)are commonly reduced. Diminished exerciseperformance is found in most patients.
Prognosis and TreatmentPrognosis is unclear because the disease is
so rare and because the clinical course of pa-tients with LAM is variable. In general, thedisease is slowly progressive, leading even-tually to respiratory failure and death, but thetime to death varies widely among reports.Women should be advised that progressionmay accelerate during pregnancy. Mediansurvival is likely > 8 yr from diagnosis.
Standard treatment is lung transplantation,but disease can recur in grafted lungs. Alterna-tive treatments, such as hormonal manipula-tion with progestins, tamoxifen, and oophorec-
045_062PUL Page 458 Tuesday, November 8, 2005 10:54 AM

55 INTERSTITIAL LUNG DISEASES 459
tomy, are largely ineffective. Pneumothora-ces may be difficult to manage because theyare often recurrent, bilateral, and less respon-sive to standard measures. Recurrent pneu-mothorax requires pleural abrasion, talc orchemical pleurodesis, or pleurectomy. Pa-tients can receive psychologic support fromthe LAM Foundation in the US.
LYMPHOID INTERSTITIAL PNEUMONIA
(Lymphocytic Interstitial Pneumonitis)
Lymphoid interstitial pneumonia is lympho-cytic infiltration of the alveolar interstitiumand air spaces. The cause is unknown. It mostoften occurs in children with HIV infectionand in people of any age with autoimmune dis-ease. Symptoms and signs are cough, pro-gressive dyspnea, and crackles. Diagnosis isbased on history, physical examination, imag-ing tests, pulmonary function tests, and lungbiopsy. Treatment is with corticosteroids,cytotoxic drugs, or both, although efficacy isunknown. Five-year survival is 50 to 66%.
Lymphoid interstitial pneumonia (LIP) isa rare disease characterized by infiltration ofalveoli and alveolar septa with small lympho-cytes and varying numbers of plasma cells.Noncaseating granulomas may be presentbut are usually rare and inconspicuous.
LIP is the most common cause of pulmo-nary disease after Pneumocystis infectionin HIV-positive children and is an AIDS-defining illness in up to 1⁄2 of HIV-positivechildren. LIP affects < 1% of adults with orwithout HIV infection. Females are affectedmore commonly.
The cause is postulated to be an autoimmunedisease or a nonspecific response to infectionwith Epstein-Barr virus, HIV, or other viruses.Evidence of an autoimmune etiology includesits frequent association with Sjögren’s syn-drome (25% of cases) and other diseases (eg,SLE, RA, Hashimoto’s disease—14% ofcases). Evidence of an indirect viral etiologyincludes frequent association with immunode-ficient states (HIV/AIDS, combined variableimmunodeficiency, agammaglobulinemia—14% of cases) and findings of Epstein-Barr vi-rus DNA and HIV RNA in lung tissue of LIPpatients. According to this theory, LIP is an ex-treme manifestation of the normal ability oflymphoid tissue in the lung to respond to in-haled and circulating antigen.
Symptoms and SignsIn adults, LIP causes symptoms of progres-
sive dyspnea and cough. These manifestationsprogress over months or, in some cases, yearsand appear at a mean age of 54. Weight loss,fever, arthralgias, and night sweats occur butare less common.
In children, LIP causes bronchospasm,cough, and/or respiratory distress and failureto thrive, usually at age 2 or 3 yr.
Examination may reveal crackles. Findingssuch as hepatosplenomegaly, arthritis, andlymphadenopathy are uncommon and suggestan accompanying or alternative diagnosis.
DiagnosisDiagnosis is based on history, physical
examination, imaging tests, and pulmonaryfunction tests and is confirmed by lung biopsy.
Chest x-ray shows bibasilar linear reticu-lar or nodular opacities, a nonspecific findingthat is seen in a number of pulmonary infec-tions. Alveolar opacities, honeycombing, orboth may be present in more advanced dis-ease. High-resolution CT of the chest helpsestablish the extent of disease, define the hilaranatomy, and identify pleural involvement.Characteristic findings are centrilobular andsubpleural nodules, thickened bronchovas-cular bundles, ground-glass opacities, and,rarely, diffuse cystic structures.
Pulmonary function tests show restrictivedefects with reduced lung volumes and dif-fusing capacity for carbon monoxide (DLCO)and preserved airflow. Marked hypoxemiamay occur. Bronchoalveolar lavage shouldbe performed to rule out infection and may re-veal an increased number of lymphocytes.
About 80% of patients have a serumprotein abnormality, most commonly a poly-clonal gammopathy and, especially in chil-dren, hypogammaglobulinemia, the signifi-cance of which is unknown. These elementsare sufficient to confirm the diagnosis in HIV-positive children. In adults, diagnosis re-quires demonstration of expansion of thealveolar septae with lymphocytic and otherimmune cell (plasma cell, immunoblastic,and histiocytic) infiltrates. Germinal centersand multinucleated giant cells with non-caseating granulomas are also seen. Infil-trates appear occasionally along bronchi andvessels but most commonly along alveolarsepta. Immunohistochemical staining andflow cytometry must be performed on the tis-sue to distinguish LIP from primary lympho-mas; in LIP, the infiltrate is polyclonal (both
045_062PUL Page 459 Tuesday, November 8, 2005 10:54 AM

460 SECTION 5 PULMONARY DISORDERS
T and B cells), whereas other lymphomas pro-duce monoclonal infiltrates.
Prognosis and TreatmentThe natural history and prognosis of LIP
are poorly understood. Good prognosis maybe linked to severity of radiographic abnor-malities, which may indicate a more vigorousimmune response. Spontaneous resolution,resolution after treatment with corticoste-roids or other immunosuppressive drugs, pro-gression to lymphoma, or development ofpulmonary fibrosis with respiratory insuffi-ciency may ensue. Five-year survival is 50 to66%. Common causes of death are infection,development of malignant lymphoma (5%),and progressive fibrosis.
Treatment is with corticosteroids, cyto-toxic drugs, or both, but, as with many othercauses of ILD, the efficacy of this approachis unknown.
PULMONARY ALVEOLAR PROTEINOSIS
Pulmonary alveolar proteinosis is accumula-tion of surfactant in alveoli. Etiology is almostalways unknown. Symptoms are dyspnea,fatigue, and malaise. Diagnosis is based onbronchoalveolar lavage, although character-istic x-ray and laboratory test abnormalitiesoccur. Treatment is with whole lung lavage.Prognosis is generally good with treatment.
Etiology and PathophysiologyPulmonary alveolar proteinosis is most
often idiopathic and occurs in otherwisehealthy men and women between 30 and50 yr. Rare secondary forms occur in patientswith acute silicosis, Pneumocystis jiroveci(formerly P. carinii) infection, hematologicmalignancies, or immunosuppression and inthose with significant inhalation exposures toaluminum, titanium, cement, and cellulosedusts. Rare congenital forms causing neona-tal respiratory failure also exist. It is unclearwhether idiopathic and secondary casesshare a common pathophysiology. Impairedalveolar macrophage processing of surfac-tant due to abnormal granulocyte-macro-phage colony-stimulating factor (GM-CSF)signaling is thought to contribute to the dis-order, perhaps due to reduced or absent func-tion of the common β chain of the GM-CSF/IL-13/IL-5 receptor on mononuclear cells
(seen in some children but not in adults withthe disorder). Anti–GM-CSF antibodies havealso been found in most patients. Toxic lunginjury is suspected but not proven in second-ary inhalation causes.
Alveoli are filled with acellular PAS-positive lipoproteinacious surfactant. Alve-olar and interstitial cells remain normal. Pos-terobasal lung segments are mostly affected.The pleura and mediastinum are unaffected.
Symptoms, Signs, and DiagnosisMost patients present with progressive ex-
ertional dyspnea and weight loss, fatigue,malaise, or low-grade fever. Cough, occa-sionally producing chunky or gummy spu-tum, occurs but is less common. Clubbingand cyanosis are uncommon. Inspiratorycrackles are rare because alveoli are fluid-filled; when crackles are present, they sug-gest infection.
Pulmonary alveolar proteinosis is usuallyfirst suspected when a chest x-ray is taken fornonspecific respiratory symptoms. The x-rayshows bilateral mid- and lower-lung fieldopacities in a butterfly distribution with nor-mal hila.
Diagnosis requires bronchoalveolar lav-age, with or without transbronchial biopsy.Lavage fluid is milky or opaque, stains PAS-positive, and is characterized by scatteredsurfactant-engorged macrophages, an in-crease in T lymphocytes, and high levels ofsurfactant apoprotein-A. Thoracoscopic oropen lung biopsy is performed when bron-choscopy is contraindicated or when speci-mens from lavage fluid are nondiagnostic.Tests typically ordered before treatment be-gins include high-resolution CT (HRCT),pulmonary function tests, ABGs, and labora-tory tests.
HRCT shows ground-glass opacification,thickened intralobular structures, and inter-lobular septa in typical polygonal shapes(crazy-paving). This finding is not specific,however, as it may also be seen in patientswith lipoid pneumonia, bronchoalveolar cellcarcinoma, and Pneumocystis jiroveci pneu-monia.
Pulmonary function tests show reductionin diffusing capacity for carbon monoxide(DLCO) that is disproportionate to the de-creases in vital capacity, residual volume,functional residual capacity, and total lungcapacity.
Laboratory abnormalities include polycy-themia, hypergammaglobulinemia, increased
045_062PUL Page 460 Tuesday, November 8, 2005 10:54 AM

55 INTERSTITIAL LUNG DISEASES 461
serum LDH levels, and increased serum sur-factant proteins A and D: All are suggestivebut nondiagnostic. ABGs may show hypox-emia with mild to moderate exercise or at restif disease is more severe.
PrognosisWithout treatment, pulmonary alveolar
proteinosis remits spontaneously in up to10% of patients. A single whole lung lavageis curative in up to 40%; other patients requirelavage every 6 to 12 mo for many years. Five-year survival is about 80%; the most commoncause of death is respiratory failure, typicallyoccurring within the 1st yr after diagnosis.Secondary pulmonary infections with bacte-rial (Mycobacteria, Nocardia) and other or-ganisms (Aspergillus, Cryptococcus, andother opportunistic fungi) occasionally de-velop because of impaired macrophage func-tion; these infections require treatment.
TreatmentTreatment is unnecessary for patients
without symptoms or for those with only mildsymptoms. Whole lung lavage is performedin patients with troubling dyspnea using gen-eral anesthesia and a double-lumen endotra-cheal tube. One lung is lavaged up to 15 timeswith 1 to 2 L saline while the other lung is ven-tilated. The process is then reversed. Lungtransplantation is not performed because thedisorder recurs in the grafted lung.
Systemic corticosteroids play no role inmanagement and may increase the risk ofsecondary infection. The role of GM-CSF(IV or sc) in management remains to be de-termined. An open-label study showed clinicalimprovement in 57% of the patients studied.
PULMONARY LANGERHANS’ CELL GRANULOMATOSIS
(Eosinophilic Granuloma, Pulmonary Granulomatosis X, Histiocytosis X)
Pulmonary Langerhans’ cell granulomato-sis (histiocytosis) is proliferation of mono-clonal Langerhans’ cells in lung interstitiumand airspaces. Etiology is unknown, but cig-arette smoking plays a primary role. Symp-toms are dyspnea, cough, fatigue, and/orpleuritic chest pain. Diagnosis is based onhistory with imaging tests or bronchoalveo-lar lavage and biopsy. Treatment is smoking
cessation. Corticosteroids are given inmany cases, but efficacy is unknown. Lungtransplantation is curative when combinedwith smoking cessation. Prognosis is goodoverall, although patients are at increasedrisk of malignancy.
Pulmonary Langerhans’ cell granuloma-tosis (PLCG) is a disease in which mono-clonal CD1a-positive Langerhans’ cells (atype of histiocyte) infiltrate the bronchiolesand alveolar interstitium, accompanied bylymphocytes, plasma cells, neutrophils, andeosinophils. PLCG is one manifestation ofLangerhans’ cell histiocytosis (see p. 1096),which can affect organs in isolation (most no-tably the lungs, skin, bones, pituitary, andlymph nodes) or simultaneously. PLCG oc-curs in isolation ≥ 85% of the time.
The etiology of PLCG is unknown, but thedisease occurs almost exclusively in whites20 to 40 yr who smoke. Men and women areaffected equally. Women develop disease later,but any differences in disease presentation bysex may represent differences in smokingbehavior. Pathophysiology may involve re-cruitment and proliferation of Langerhans’cells in response to cytokines and growth fac-tors secreted by alveolar macrophages in re-sponse to cigarette smoke.
Symptoms and SignsTypical symptoms and signs of PLCG are
dyspnea, nonproductive cough, fatigue, and/or pleuritic chest pain, and 10 to 25% of pa-tients have sudden, spontaneous pneumo-thorax (see p. 496). About 15% of patientsare asymptomatic, with disease noted inci-dentally on a chest x-ray taken for anotherreason. Bone pain from bone cysts (18%),skin rash (13%), and polyuria from diabetesinsipidus (5%) are the most common mani-festations of extrapulmonary involvementand occur in up to 15% of patients, rarely be-ing the presenting symptoms of PLCG. Thereare few signs of PLCG; the physical exami-nation results are usually normal.
DiagnosisPLCG is suspected based on history, phys-
ical examination, and chest x-ray and is con-firmed by high-resolution CT (HRCT) andbronchoscopy with biopsy and bronchoalve-olar lavage.
Chest x-ray classically demonstrates bilat-erally symmetric nodular opacities in themiddle and upper lung fields with cystic
045_062PUL Page 461 Tuesday, November 8, 2005 10:54 AM

462 SECTION 5 PULMONARY DISORDERS
changes and normal or increased lung vol-umes. The lung bases are often spared. Ap-pearance may mimic COPD or lymphangi-oleiomyomatosis (see p. 457). Confirmationon HRCT of middle and upper lobe cysts (of-ten with bizarre shapes) and/or nodules withinterstitial thickening is considered diagnos-tic of PLCG. Pulmonary function test find-ings are normal, restrictive, obstructive, ormixed depending on when the test is per-formed during the course of the disease. Mostcommonly, the diffusing capacity for carbonmonoxide (DLCO) is reduced and exercise isimpaired.
Bronchoscopy and biopsy are indicatedwhen imaging and pulmonary function testsare inconclusive. Finding > 5% of CD1a cellsin bronchoalveolar lavage fluid is highly sug-gestive of the disease. Biopsy shows prolif-eration of Langerhans’ cells with occasionalclustering of eosinophils (the origin of theoutdated term eosinophilic granuloma) in themidst of cellular and fibrotic nodules thatmay take on a stellate configuration. Immu-nohistochemical staining is positive for CD1a,S-100 protein, and HLA-DR antigens.
TreatmentThe main treatment is smoking cessation,
which leads to symptom resolution in up to1⁄3 of patients. As with other ILDs, empiricuse of corticosteroids and cytotoxic drugs iscommon practice even though their effective-ness is unproven. Lung transplantation is anoption for otherwise healthy patients with ac-celerating respiratory insufficiency, but thedisease may recur in the transplanted lung ifthe patient continues or resumes smoking.
Spontaneous resolution of symptoms oc-curs in some patients with minimally symp-tomatic disease; 5-yr survival is about 75%,and median survival is 12 yr. However, somepatients develop slowly progressive disease,for which the clinical markers include con-tinued smoking, age extremes, multiorganinvolvement, persistent constitutional symp-toms, numerous cysts on chest x-ray, reducedDLCO, low FEV1/FVC (< 66%), high residualvolume (RV)/total lung capacity (TLC) ratio(> 33%), and need for prolonged corticoste-roids. Cause of death is respiratory insuffi-ciency or malignancy. Lung cancer risk is in-creased because of cigarette smoking.
56SARCOIDOSIS
Sarcoidosis is characterized by noncaseat-ing granulomas in one or more organs andtissues; etiology is unknown. The lungs andlymphatic system are most often affected,but sarcoidosis may affect any organ. Pul-monary symptoms range from none (lim-ited disease) to exertional dyspnea and,rarely, respiratory or other organ failure(advanced disease). Diagnosis usually isfirst suspected because of pulmonaryinvolvement and is confirmed by chest x-ray, biopsy, and exclusion of other causesof granulomatous inflammation. First-linetreatment is corticosteroids. Prognosis isexcellent for limited disease but poor formore advanced disease.
Sarcoidosis primarily affects people aged20 to 40 but occasionally affects children andolder adults. Worldwide, prevalence is greatestin black Americans and northern Europeans,
especially Scandinavians. Disease presenta-tion varies widely by racial and ethnic back-ground, with black Americans and PuertoRicans demonstrating more frequent ex-trathoracic manifestations. Sarcoidosis isslightly more prevalent in women. Incidenceincreases in winter and early spring, for un-known reasons.
Etiology and PathophysiologySarcoidosis is thought to be due to an in-
flammatory response to an environmentalexposure in a genetically susceptible person.Although uncertain, proposed triggers in-clude viral, bacterial, and mycobacterial in-fections and inhalation of inorganic (eg, alu-minum, zirconium, talc) or organic (eg, pinetree pollen, clay) agents. The unknown anti-gen triggers a cell-mediated immune re-sponse characterized by the accumulation ofT lymphocytes and macrophages, release ofcytokines and chemokines, and organizationof responding cells into granulomas. Clustersof disease in families and communities sug-gest a genetic predisposition, shared expo-
045_062PUL Page 462 Tuesday, November 8, 2005 10:54 AM

56 SARCOIDOSIS 463
sures, or, less likely, person-to-person trans-mission.
The result of the inflammatory process isformation of noncaseating granulomas, thehallmark of sarcoidosis. Granulomas are col-lections of mononuclear cells and macro-phages that are differentiated into epithelioidand multinucleated giant cells, surroundedby lymphocytes, plasma cells, mast cells, fi-broblasts, and collagen. Granulomas occurmost commonly in the lung and lymph nodesbut can involve many other sites, includingthe liver, spleen, eyes (see p. 914), sinuses,skin, bones, joints, skeletal muscle, kidney,reproductive organs, heart, salivary glands,and nervous system. The granulomas in thelung are distributed along lymphatics, withmost found in peribronchiolar, subpleural,and perilobular regions.
Symptoms and SignsSymptoms and signs depend on the site and
degree of involvement and vary over time,ranging from spontaneous remission tochronic indolent illness. Therefore, frequentreassessment for new symptoms in differentorgans is needed. Most cases are probablyasymptomatic and thus go undetected. Pulmo-nary disease occurs in > 90% of adult patients.
Symptoms and signs may include dysp-nea, cough, chest discomfort, and crackles onexamination. Fatigue, malaise, weakness,anorexia, weight loss, and low-grade feverare also common; sarcoidosis is an unusualcause of fever of unknown origin. Nontenderlymphadenopathy is often the only sign. Sys-temic involvement causes various symptoms(see TABLE 56–1), which vary by race, sex,and age. Blacks are more likely than whitesto have involvement of the eye, liver, bonemarrow, peripheral lymph nodes, and skinother than erythema nodosum. Women aremore likely to have erythema nodosum andeye or nervous system involvement. Men andolder patients are more likely to be hypercal-cemic.
In children < 4 yr, arthritis, rash, and uvei-tis are the most common presentations. Sar-coidosis may be confused with juvenile RAin this age group.
DiagnosisSarcoidosis is most often suspected when
hilar adenopathy is incidentally detected onchest x-ray. These changes are the most com-mon abnormality, and x-ray appearance isroughly predictive of the likelihood of spon-
taneous remission (see TABLE 56–2) in pa-tients with pulmonary involvement. There-fore, a chest x-ray should be the first test if ithas not already been obtained in patients sus-pected of having sarcoidosis.
Because pulmonary involvement is so fre-quent, a normal chest x-ray generally ex-cludes the diagnosis. In cases in which thedisease is highly suspected despite a normalchest x-ray, high-resolution chest CT is moresensitive for detecting hilar and mediastinallymphadenopathy; CT findings in more ad-vanced stages (II to IV) include thickening ofthe bronchovascular bundles and bronchialwalls; beading of the interlobular septa;ground-glass opacification; parenchymalnodules, cysts, or cavities; and/or tractionbronchiectasis.
When imaging suggests sarcoidosis, thediagnosis is confirmed by demonstration ofnoncaseating granulomas on biopsy and ex-clusion of alternative causes of granuloma-tous disease (see TABLE 56–3). The diagnos-tic evaluation, therefore, requires selection ofa biopsy site; exclusion of other causes ofgranulomatous disease; and assessment ofthe severity and extent of disease to determineif therapy is indicated.
Sites for biopsy may be obvious fromphysical examination and initial assessment:peripheral lymph nodes, skin lesions, andconjunctivae are all easily accessible. How-ever, bronchoscopic transbronchial biopsy isthe diagnostic procedure of choice in patientswith intrathoracic involvement, because thesensitivity is as high as 90% in experiencedhands. Video-assisted thoracoscopy can pro-vide access to lung tissue when bronchoscopictransbronchial biopsy is nondiagnostic. Me-diastinoscopy is sometimes performed whenhilar or mediastinal lymphadenopathy existsin the absence of pulmonary infiltrates, espe-cially if lymphoma is in the differential diag-nosis. However, even in patients with onlymediastinal adenopathy on x-ray or CT,transbronchial biopsies are often diagnostic.Open lung biopsy provides another way toobtain tissue but requires general anesthesiaand is now rarely necessary. Clinical and x-rayfindings may be accurate enough for diagno-sis in stage I disease or in stage II diseasewhen biopsy is not possible.
Exclusion of other diagnoses is critical, es-pecially when symptoms and x-ray signs areminimal, because many other diseases andprocesses can cause granulomatous inflam-mation (see TABLE 56–3). Biopsy tissue
045_062PUL Page 463 Tuesday, November 8, 2005 10:54 AM

464 SECTION 5 PULMONARY DISORDERS
TABLE 56–1. SYSTEMIC INVOLVEMENT IN SARCOIDOSIS
SYSTEMESTIMATED FREQUENCY COMMENTS
PleuropulmonaryPulmonary > 90% Granulomas form in alveolar septa, bronchiolar, and
bronchial walls, causing diffuse pulmonary disease; pulmonary arteries and veins are also involved
Often asymptomatic. Spontaneously resolves in many patients but can cause progressive pulmonary dysfunc-tion leading to limitations in physical function, respiratory failure, and death in a few
Pleural Rare Produces lymphocytic exudative effusions, usually bilateral
Lymphatic 90% Hilar or mediastinal involvement incidentally detected by chest x-ray in most patients. Others display non-tender peripheral or cervical lymphadenopathy
GI Hepatic 40–75% Usually asymptomatic; manifests as mild elevations in
liver function test results, hypolucencies on CT scans with radiopaque dye
Rarely causes clinically significant cholestasis, cirrhosisUnclear distinction between sarcoidosis and granulo-matous hepatitis when sarcoidosis affects liver only
Splenic 10% Usually asymptomatic, manifests with left upper quadrant pain, thrombocytopenia, incidental finding on x-ray or CT
Other Rare Rare reports of gastric granulomas, rare intestinal involvement; mesenteric lymphadenopathy may cause abdominal pain
Ocular 25% Uveitis most common, causing blurred vision, photo-phobia, and tearing. Can cause blindness, but sponta-neously resolves in most
Conjunctivitis, iridocyclitis, chorioretinitis, dacryocys-titis, lacrimal gland infiltration causing dry eyes, optic neuritis, glaucoma, and cataracts also reported
Ocular involvement more common in black Americans and Japanese
Annual or biannual screening indicated for earlydisease detection
MusculoskeletalMuscle 50–80% Asymptomatic disease with or without enzyme
elevations in most; sometimes insidious or acute myopathy with muscle weakness
Joint 25–50% Ankle, knee, wrist, elbow arthritis most common; may cause chronic arthritis with Jaccoud’s deformities or dactylitis
Löfgren’s syndrome is triad of acute polyarthritis, erythema nodosum, and hilar adenopathy. Has distinct features; more common in Scandinavian and Irish women, often responsive to NSAIDs, and often self-limited; low rate of relapse
Bone 5% Osteolytic or cystic lesions; osteopenia
045_062PUL Page 464 Tuesday, November 8, 2005 10:54 AM
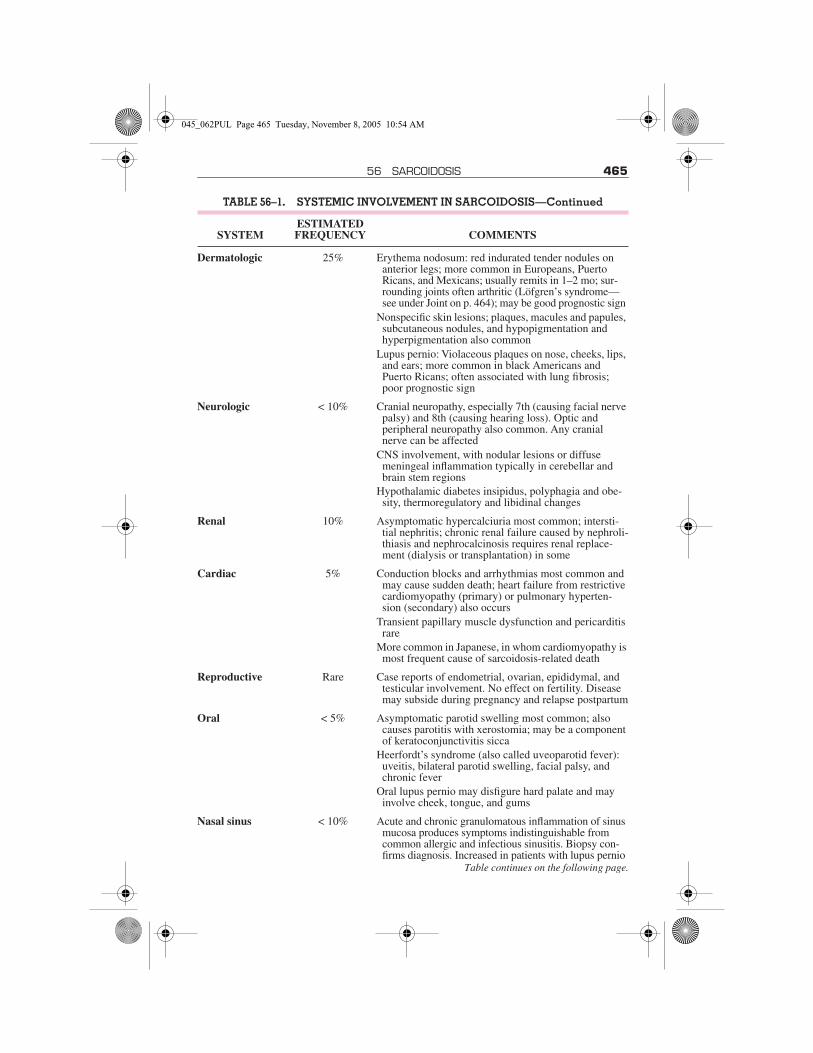
56 SARCOIDOSIS 465
Dermatologic 25% Erythema nodosum: red indurated tender nodules on anterior legs; more common in Europeans, Puerto Ricans, and Mexicans; usually remits in 1–2 mo; sur-rounding joints often arthritic (Löfgren’s syndrome—see under Joint on p. 464); may be good prognostic sign
Nonspecific skin lesions; plaques, macules and papules, subcutaneous nodules, and hypopigmentation and hyperpigmentation also common
Lupus pernio: Violaceous plaques on nose, cheeks, lips, and ears; more common in black Americans and Puerto Ricans; often associated with lung fibrosis; poor prognostic sign
Neurologic < 10% Cranial neuropathy, especially 7th (causing facial nerve palsy) and 8th (causing hearing loss). Optic and peripheral neuropathy also common. Any cranial nerve can be affected
CNS involvement, with nodular lesions or diffuse meningeal inflammation typically in cerebellar and brain stem regions
Hypothalamic diabetes insipidus, polyphagia and obe-sity, thermoregulatory and libidinal changes
Renal 10% Asymptomatic hypercalciuria most common; intersti-tial nephritis; chronic renal failure caused by nephroli-thiasis and nephrocalcinosis requires renal replace-ment (dialysis or transplantation) in some
Cardiac 5% Conduction blocks and arrhythmias most common and may cause sudden death; heart failure from restrictive cardiomyopathy (primary) or pulmonary hyperten-sion (secondary) also occurs
Transient papillary muscle dysfunction and pericarditis rare
More common in Japanese, in whom cardiomyopathy is most frequent cause of sarcoidosis-related death
Reproductive Rare Case reports of endometrial, ovarian, epididymal, and testicular involvement. No effect on fertility. Disease may subside during pregnancy and relapse postpartum
Oral < 5% Asymptomatic parotid swelling most common; also causes parotitis with xerostomia; may be a component of keratoconjunctivitis sicca
Heerfordt’s syndrome (also called uveoparotid fever): uveitis, bilateral parotid swelling, facial palsy, and chronic fever
Oral lupus pernio may disfigure hard palate and may involve cheek, tongue, and gums
Nasal sinus < 10% Acute and chronic granulomatous inflammation of sinus mucosa produces symptoms indistinguishable from common allergic and infectious sinusitis. Biopsy con-firms diagnosis. Increased in patients with lupus pernio
Table continues on the following page.
TABLE 56–1. SYSTEMIC INVOLVEMENT IN SARCOIDOSIS—Continued
SYSTEMESTIMATED FREQUENCY COMMENTS
045_062PUL Page 465 Tuesday, November 8, 2005 10:54 AM

466 SECTION 5 PULMONARY DISORDERS
should be cultured for fungi and mycobacte-ria. Exposure history to occupational (sili-cates, beryllium), environmental (moldy hay,birds, and other antigenic triggers of hyper-sensitivity pneumonitis), and infectious (TB,coccidioidomycosis, histoplasmosis) anti-gens should be explored. PPD skin testingshould be performed early in the assessmentalong with anergy controls.
Pulmonary function tests and exercisepulse-oximetry assess disease severity. Pul-monary function test results are often normalin early stages but demonstrate restrictionand reduced diffusing capacity for carbonmonoxide (DLCO) in advanced disease. Air-flow obstruction also occurs and may suggestinvolvement of the bronchial mucosae. Pulseoximetry is often normal when measured atrest but may show effort desaturation withmore extensive lung involvement. ABG anal-ysis at rest and during exercise is more sen-sitive than pulse oximetry.
Recommended screening tests for extra-pulmonary disease include ECG, slit-lampophthalmologic examination, and routinerenal and liver function testing. Echocardio-graphy, neuroimaging, lumbar puncture,bone films or MRI, and electromyographymay be appropriate when symptoms suggestcardiac, neurologic, or rheumatologic dis-ease. Abdominal CT with radiopaque dye isnot routinely recommended but can provideevidence of hepatic or splenic involvementwith enlargement and hyperlucent lesions.
Laboratory testing plays an adjunctive rolein establishing the diagnosis and extent of organ
involvement. CBC, electrolytes (includingcalcium), BUN, creatinine, and liver func-tion tests generally provide useful informa-tion in screening for extrathoracic involve-ment. CBC may show anemia, eosinophilia,or leukopenia. Serum Ca may be elevatedbecause of production of vitamin D analogsby activated macrophages. BUN, creati-nine, and liver function tests may be elevatedin renal and hepatic sarcoidosis. Total pro-tein may be elevated because of hypergam-maglobulinemia. Elevated ESR is nonspe-cific. Measurement of Ca in a urine specimencollected over 24 h is recommended to ex-clude hypercalciuria, even in patients withnormal serum Ca levels. Elevated serum ACElevels also suggest sarcoidosis but are non-specific and may be low in patients takingACE inhibitors or elevated in patients with avariety of other conditions (eg, hyperthyroid-ism, Gaucher’s disease, silicosis, mycobac-terial disease, hypersensitivity pneumoni-tis). ACE levels may be useful for followingdisease activity and therapeutic response inpatients with confirmed sarcoidosis. In-creased ACE levels in CSF may be useful fordiagnosing CNS sarcoidosis.
Other adjunctive tests include bronchoal-veolar lavage and gallium scanning. The find-ings on bronchoalveolar lavage vary con-siderably, but lymphocytosis (lymphocytes> 10%) and/or a CD4+/CD8+ ratio of > 3.5 inthe lavage fluid cell differential suggests thediagnosis in the proper clinical context. Ab-sence of these findings does not excludesarcoidosis, however.
Endocrine Rare Hypothalamic and pituitary stalk infiltration may cause panhypopituitarism; may cause thyroid infiltration without dysfunction; secondary hypoparathyroidism from hypercalcemia
Psychiatric 10% Depression common, uncertain if a primary manifesta-tion of sarcoidosis or a response to prolonged course of disease and frequent recurrences
Hematologic < 5–30% Lymphopenia; anemia of chronic disease; anemia due to granulomatous infiltration of bone marrow some-times producing pancytopenia; splenic sequestration producing thrombocytopenia; leukopenia
TABLE 56–1. SYSTEMIC INVOLVEMENT IN SARCOIDOSIS—Continued
SYSTEMESTIMATED FREQUENCY COMMENTS
045_062PUL Page 466 Tuesday, November 8, 2005 10:54 AM

56 SARCOIDOSIS 467
Whole-body gallium scanning may pro-vide useful supportive evidence in the absenceof tissue confirmation. Symmetrical in-creased uptake in mediastinal and hilar nodes(lambda sign) and in lacrimal, parotid, and sal-ivary glands (panda sign) are patterns highlysuggestive of sarcoidosis. A negative result inpatients taking prednisone is unreliable.
PrognosisAlthough spontaneous improvement is
common, the severity and manifestations ofdisease are highly variable, and many pa-tients require courses of corticosteroids sometime during the course of their disease. Thus,serial monitoring for evidence of relapse isimperative. About 90% of patients who havespontaneous remission do so within the first2 yr after diagnosis; < 10% of these patientshave relapses after 2 yr. Those patients whodo not experience remission within 2 yr arelikely to have chronic disease.
Sarcoidosis is thought to be chronic in upto 30% of patients, and 10 to 20% experiencepermanent sequelae. The disease is fatal in1 to 5% of patients. Pulmonary fibrosis withrespiratory failure is the most common causeof death worldwide, followed by pulmonaryhemorrhage from aspergilloma. In Japan,however, infiltrative cardiomyopathy caus-ing heart failure and arrhythmias is the mostcommon cause of death.
Prognosis is worse for patients with extra-pulmonary sarcoidosis and for blacks. Recov-ery occurs in 89% of whites and 76% of blackswith no extrathoracic disease and in 70% ofwhites and 46% of blacks with extrathoracicdisease. The presence of erythema nodosumand acute arthritis are good prognostic signs.Uveitis, lupus pernio, chronic hypercalce-mia, neurosarcoidosis, nephrocalcinosis,myocardial disease, and extensive pulmo-nary involvement are all poor prognosticsigns. However, little difference is demon-strable in long-term outcome between treatedand untreated patients, and relapse is com-mon when treatment ends.
TreatmentBecause sarcoidosis often spontaneously
resolves, asymptomatic patients and thosewith mild symptoms do not require treat-ment, although they should be monitored forsigns of deterioration. These patients can befollowed with serial x-rays, pulmonary func-tion tests (including diffusing capacity), and
markers of extrathoracic involvement (eg,routine renal and liver function testing). Pa-tients who require treatment regardless ofstage include those with worsening symp-toms; limitation of activity; markedly abnor-mal or deteriorating lung function; worri-some x-ray changes (cavitation, fibrosis,conglomerate masses, signs of pulmonaryhypertension); heart, nervous system, or eyeinvolvement; renal or hepatic insufficiency orfailure; or disfiguring skin and joint disease.
Treatment is with corticosteroids. A stan-dard protocol is prednisone 0.3 to 1mg/kg poonce/day depending on symptoms and severity
TABLE 56–2. STAGING SARCOIDOSIS
STAGE DEFINITION
INCIDENCE OF SPONTA-
NEOUS REMISSION
0 Normal chest x-ray
Usually remits; no correla-tion with prognosis
I Bilateral hilar, paratracheal, and mediasti-nal lympha-denopathy without paren-chymal infil-trates
60–80%
II Bilateral hilar/mediastinal adenopathy with intersti-tial infiltrates (usually upper lung fields)
50–65%
III Diffuse intersti-tial infiltrates without hilar adenopathy
< 30%
IV Diffuse fibrosis, often associ-ated with fibrotic-appearing conglomerate masses, trac-tion bron-chiectasis, traction cysts
0%
045_062PUL Page 467 Tuesday, November 8, 2005 10:54 AM

468 SECTION 5 PULMONARY DISORDERS
of findings. Alternate-day regimens are alsoused (eg, prednisone 40 to 60 mg po onceevery other day). It is rare to exceed 40 mg/day;however, higher doses may be needed to re-duce complications in patients with ocular,myocardial, or neurologic disease. Responseusually occurs within 2 to 4 wk, so symptomsand results of chest x-ray and pulmonary func-tion tests may be reassessed between 4 and 12wk. Chronic, insidious cases may respondmore slowly. The drug is tapered to a mainte-nance dose (eg, prednisone ≤ 10 mg everyother day if possible) after evidence of re-sponse and is continued for a minimum of12 mo if improvement occurs. The optimalduration of treatment is unknown. Prematuretaper can result in relapse. The drug is slowlystopped if response is absent or equivocal.Corticosteroids can ultimately be stopped inmost patients, but because relapse occurs upto 50% of the time, monitoring should be re-peated, usually every 3 to 6 mo. Corticosteroidtreatment should be resumed for recurrence ofsymptoms and signs, including dyspnea, ar-thralgia, fever, hepatic insufficiency, cardiacarrhythmia, CNS involvement, hypercalce-mia, ocular disease uncontrolled by localdrugs, and disfiguring skin lesions.
Data on use of inhaled corticosteroids forpulmonary sarcoidosis are not definitive, butsome evidence suggests that this route of ad-ministration can relieve cough in patientswith endobronchial involvement. Topicalcorticosteroids may be useful in some casesof dermatologic and ocular disease.
About 10% of patients requiring therapyare unresponsive to tolerable doses of a cor-ticosteroid and should be given a 6-mo trialof methotrexate starting at 2.5 mg po once/wkand increasing in increments of 2.5 mg/wk toa total of 10 to 15 mg/wk as tolerated to keepWBC > 3000/µL. Initially, methotrexate andcorticosteroids are both given; over 8 wk, thecorticosteroid dose can be tapered and, inmany cases, stopped. The maximal responseto methotrexate, however, may take 6 to 12mo. In such cases, prednisone must be ta-pered more slowly. Serial blood counts andliver enzyme tests should be performed every1 to 2 wk initially and then every 4 to 6 wkonce a stable dose is achieved. Folic acid(1 mg po once/day) is recommended for pa-tients treated with methotrexate.
Other drugs reported to be effective insmall numbers of patients who are cortico-steroid-resistant or who experience compli-cating adverse effects include azathioprine,
TABLE 56–3. DIFFERENTIAL DIAG-NOSIS OF SARCOIDOSIS
InfectiousMycobacterial
TBAtypical mycobacteria
FungalAspergillosisBlastomycosisCoccidioidomycosisCryptococcal infectionHistoplasmosis
OtherBrucellosisCat-scratch disease (lymph nodes only)Mycoplasmal infectionPneumocystis jiroveci (formerly P. carinii)
infectionSyphilis
RheumatologicJuvenile RAKikuchi’s lymphadenitis (lymph nodes only)
Necrotizing sarcoid granulomatosisRASjögren’s syndromeWegener’s granulomatosis
Hematologic malignancyHodgkin lymphomaNon-Hodgkin lymphomaSplenic lymphoma
HypersensitivityOccupational metals
AluminumBerylliosisTitaniumZirconium
Organic antigens producing hypersensitivity pneumonitis
ActinomycetesAtypical mycobacterial antigensFungiMushroom sporesOther bioaerosols
Inorganic antigens producing hypersensitivity pneumonitis
IsocyanatesPyrethrins
Drug reaction
OtherInflammatory bowel diseaseForeign body aspiration or inoculationGranulomatous hepatitisGranulomatous lesion of unknown significance
Lymphoid interstitial pneumonia
045_062PUL Page 468 Tuesday, November 8, 2005 10:54 AM
57 ENVIRONMENTAL PULMONARY DISEASES 469
cyclophosphamide, chlorambucil, chloro-quine or hydroxychloroquine, thalidomide,pentoxifylline, and infliximab.
Hydroxychloroquine 200 mg po bid to tidcan be as effective as corticosteroids for treat-ment of disfiguring skin sarcoidosis and intreatment of hypercalciuria. Although immu-nosuppressants are often more effective in
refractory cases, relapse is common aftercessation.
No available drugs have consistently pre-vented pulmonary fibrosis.
Lung transplantation is an option for pa-tients with end-stage pulmonary involve-ment, although disease may recur in thetransplanted organ.
57ENVIRONMENTAL PULMONARY DISEASES
Environmental pulmonary diseases resultfrom inhalation of dusts, allergens, chemicals,gases, and environmental pollutants. Thelungs are continually exposed to the externalenvironment and are susceptible to a host ofenvironmental diseases. Pathologic processescan involve any part of the lung, including theairways (eg, occupational asthma, reactiveairways dysfunction syndrome, toxic inhala-tions), interstitium (eg, pneumoconioses, hy-persensitivity pneumonitis), and pleurae (eg,asbestos-related diseases).
Prevention of occupational and environ-mental respiratory disease centers on reduc-ing exposure (primary prevention). This in-cludes administrative controls (eg, limitingthe number of people placed in hazardousconditions), engineering controls (eg, enclo-sures, ventilation systems, safe clean-up pro-cedures), product substitution (eg, usingsafer, less toxic materials), and use of respi-ratory protection devices.
Many clinicians erroneously assume that apatient who has used a respirator or respira-tory protection device (dust mask or gasmask) has been well protected. While respi-rators do afford a degree of protection, espe-cially in situations in which fresh air is pro-vided by tank or air hose, the benefit is limitedand idiosyncratic. When recommending useof a respirator, clinicians should considerseveral factors. Workers with cardiovasculardisease may be unable to perform jobs that re-quire strenuous work, especially if they must
wear a self-contained breathing apparatus(tank). Respirators that are tight-fitting andthat require the wearer to draw air through fil-ter cartridges can increase the work of breath-ing, especially troublesome for patients withasthma, COPD, or interstitial lung disorders.
Medical surveillance is a form of second-ary prevention. Workers can be offered med-ical tests that identify disease at early stateswhen medical treatment might help reducelong-term consequences.
AIR POLLUTION–RELATED ILLNESS
The major components of air pollution indeveloped countries are nitrogen dioxide(from combustion of fossil fuels), ozone(from the effect of sunlight on nitrogen diox-ide and hydrocarbons), and suspended solidor liquid particles. Burning of biomass fuel isan additional important source of particulatematter indoors in developing countries. Pas-sive smoking can be considered as related.
The effect of air pollution on lung diseasecan be substantial at high pollution levels,which can trigger asthma and COPD exacer-bations. People living in areas with high traf-fic, especially when stagnant air is created bythermal inversions, are at particular risk. Ofthe so-called criteria air pollutants (oxides ofnitrogen, oxides of sulfur, ozone, carbonmonoxide, lead, and particulates), only COand lead do not affect airways hyperreactiv-ity. Long-term exposure may increase respi-ratory infections and symptoms in the gen-eral population, especially children.
Ozone, which is the major component ofsmog, is a strong respiratory irritant and ox-idant. Levels tend to be highest in the sum-mer, late morning, and early afternoon.Short-term exposures can produce dyspnea,
045_062PUL Page 469 Tuesday, November 8, 2005 10:54 AM

470 SECTION 5 PULMONARY DISORDERS
chest pain, and airways reactivity. Childrenwho participate in outdoor sports during highozone pollution days are more likely to de-velop asthma. Long-term exposure to ozoneproduces a small, permanent decrease in lungfunction.
Oxides of sulfur, resulting from combustionof fossil fuels that are high in sulfur content,can create acid aerosols with high solubility,resulting in upper airway deposition. Sulfuroxides can induce airways inflammation, pos-sibly increasing the risk for chronic bronchitisas well as inducing bronchoconstriction.
Particulate air pollution is a complex mix-ture, derived from fossil fuel combustion (es-pecially diesel). The particles can have bothlocal and systemic inflammatory effects, sug-gesting an explanation for their impact onboth respiratory and cardiovascular health.Ultrafine particles (< 2.5 µm) produce agreater inflammatory response per mass thando larger particles. Data to date suggest thatparticulate air pollution increases death ratesfrom all causes, especially cardiovascularand respiratory illness.
ASBESTOS-RELATED DISORDERS
Asbestos-related disorders are caused byinhalation of asbestos fibers. The disordersinclude asbestosis; lung carcinoma; nonma-lignant pleural plaque formation and thicken-ing; benign pleural effusions; and malignantmesothelioma. Asbestosis and mesotheliomaboth cause progressive dyspnea. Diagnosisis based on history and chest x-ray or CT and,in the case of malignancy, tissue biopsy.Treatment is supportive, except for malig-nancies, which may require surgery and/orchemotherapy.
Asbestos is a naturally occurring silicatewhose heat-resistant and structural proper-ties made it useful for inclusion in construc-tion and shipbuilding materials, automobilebrakes, and some textiles. Chrysotile (a ser-pentine fiber), crocidolite, and amosite (am-phibole, or straight, fibers) are the 3 maintypes of asbestos that cause disease. Asbestoscan affect the lung and/or the pleura.
PULMONARY DISEASEPulmonary disease can be nonmalignant
or malignant.
Asbestosis: Asbestosis, a form of inter-stitial pulmonary fibrosis, is much more com-mon than malignant disease. Shipbuilders,textile and construction workers, home re-modelers, workers who do asbestos abate-ment, and miners exposed to asbestos fibersare among the many categories of workers atrisk of the disease. Secondhand exposuremay occur among family members of ex-posed workers and among those who liveclose to mines. Pathophysiology is similarto that of other pneumoconioses—alveolarmacrophages attempting to engulf inhaled fi-bers release cytokines and growth factors thatstimulate inflammation, collagen deposition,and ultimately fibrosis—except that asbestosfibers themselves may also be directly toxicto lung tissue. Risk of disease is generally re-lated to duration and intensity of exposure andtype, length, and thickness of inhaled fibers.
Asbestosis is initially asymptomatic butcan cause progressive dyspnea, nonproduc-tive cough, and fatigue; the disease progressesin > 10% of patients after cessation of expo-sure. Advanced asbestosis may cause club-bing, dry bibasilar crackles, and, in severecases, symptoms and signs of right ventricu-lar failure (cor pulmonale).
Diagnosis is based on history of exposureand chest x-ray or chest CT. Chest x-rayshows linear reticular or nodular opacitiessignifying fibrosis, usually in the peripherallower lobes, often accompanied by pleuralchanges (see p. 471). Honeycombing signi-fies more advanced disease, which may in-volve the mid lung fields. As with silicosis, se-verity is graded on the International LaborOrganization scale based on size, shape, loca-tion, and profusion of opacities. In contrast tosilicosis, asbestosis produces reticular opaci-ties with a lower lobe predominance. Hilar andmediastinal adenopathy are uncharacteristicand suggest a different diagnosis. Chest x-rayis insensitive; high-resolution chest CT(HRCT) is useful when asbestosis is a likelydiagnosis. HRCT is also superior to the chestx-ray in identifying the pleural abnormali-ties. Pulmonary function tests, which mayshow reduced lung volumes and DLco, arenonspecific but help characterize changes inlung function over time after the diagnosis ismade. Bronchoalveolar lavage or lung bi-opsy is indicated only when noninvasivemeasures fail to provide conclusive diagno-sis; demonstration of asbestos fibers indi-cates asbestosis in people with pulmonary fi-brosis, although such fibers can occasionally
045_062PUL Page 470 Tuesday, November 8, 2005 10:54 AM

57 ENVIRONMENTAL PULMONARY DISEASES 471
be found in lungs of exposed people withoutdisease.
No specific treatment exists. Early detec-tion of hypoxemia and right ventricular fail-ure leads to use of supplemental O2 andtreatment of heart failure. Pulmonary reha-bilitation can be helpful for patients withimpairment. Preventive measures includeeliminating exposure, asbestos abatement innonoccupational settings, smoking cessa-tion, and pneumococcal and influenza vacci-nation. Smoking cessation is particularly im-portant in light of the multiplicative risk oflung cancer in those who have both tobaccosmoke and asbestos exposures. Prognosisvaries; many patients do well with no ormild symptoms, whereas some develop pro-gressive dyspnea and a few develop respira-tory failure, right ventricular failure, andmalignancy.
Lung carcinoma (nonsmall cell) developsin patients with asbestosis at 8 to 10 timesthe rate of those without asbestosis and is es-pecially common in workers exposed to am-phibole fibers, although all forms of inhaledasbestos have been associated with an ele-vated cancer risk. Asbestos and smokinghave a synergistic effect on lung cancer risk(see p. 503).
PLEURAL DISEASEPleural disease, a hallmark of asbestos
exposure, includes formation of pleuralplaques, calcification, thickening, adhe-sions, effusion, and mesothelioma. Pleuraldisease produces effusion and malignancybut few symptoms. All pleural changes arediagnosed by chest x-ray or HRCT, thoughchest CT is more sensitive than chest x-ray fordetecting pleural disorders. Treatment israrely needed except in the case of malignantmesothelioma.
Discrete plaques, which occur in up to 60%of workers exposed to asbestos, typically af-fect the bilateral parietal pleurae between the5th and 9th ribs and adjacent to the dia-phragm. Plaque calcification is common andcan lead to misdiagnosis of severe pulmonarydisease when radiographically superim-posed on lung fields. HRCT can distinguishpleural from parenchymal disease in thissetting.
Diffuse thickening affects visceral as wellas parietal pleurae. It may be an extension ofpulmonary fibrosis from parenchyma to thepleurae or a nonspecific reaction to pleural
effusion. With or without calcification, pleu-ral thickening can cause a restrictive defect.Rounded atelectasis is a manifestation ofpleural thickening in which invagination ofpleura into the parenchyma can entrap lungtissue, causing atelectasis. On chest x-ray andCT, it typically appears as a curvilinear cica-tricial mass, often in the lower lung zones,and can be confused radiographically with apulmonary malignancy.
Pleural effusions occur but are less com-mon than the other pleural changes they ac-company. Effusions are exudative, oftenhemorrhagic, and typically resolve sponta-neously (see p. 490).
Pleural mesothelioma: Pleural meso-thelioma is the only known pleural malig-nancy and is caused by asbestos exposure innearly all cases. Asbestos workers have up toa 10% lifetime risk of developing the disease,with an average latency of 30 yr. Risk is in-dependent of smoking. Mesothelioma canspread locally or metastasize to the pericar-dium, diaphragm, peritoneum, and, rarely,the tunica vaginalis of the testis. Patients mostoften present with dyspnea and nonpleuriticchest pain. Constitutional symptoms are un-common at time of clinical presentation.Invasion of the chest wall and other adjacentstructures may cause severe pain, hoarseness,dysphagia, Horner’s syndrome, brachialplexopathy, or ascites. Extrathoracic spreadoccurs in up to 80% of patients, most com-monly including the hilar and mediastinallymph nodes, liver, adrenals, and kidneys.
The pleural form of mesothelioma, whichrepresents more than 90% of all cases, pre-sents on x-ray as diffuse unilateral or bilateralpleural thickening that appears to encase thelungs, usually producing blunting of thecostophrenic angles. Pleural effusions arepresent in 95% of cases and are typically uni-lateral, massive effusions. Diagnosis is basedon pleural fluid cytology or pleural biopsyand, if these are nondiagnostic, biopsy byvideo-assisted thorascopic surgery (VATS)or thoracotomy. Staging is done with chestCT, mediastinoscopy, and MRI. Sensitivityand specificity of MRI and CT are compara-ble, although MRI is helpful in determiningtumor extension into the spine or spinal cord.PET may have better sensitivity and specific-ity for distinguishing benign from malignantpleural thickening. Bronchoscopy rules outcoexisting endobronchial malignancies. In-creased hyaluronidase levels in pleural fluidare suggestive but not diagnostic of disease.
045_062PUL Page 471 Tuesday, November 8, 2005 10:54 AM

472 SECTION 5 PULMONARY DISORDERS
Soluble mesothelin-related proteins releasedinto the serum by mesothelial cells are beingstudied as possible tumor markers for diseasedetection and monitoring.
Mesothelioma remains an incurable can-cer. Surgery to remove the pleura; ipsilaterallung, phrenic nerve, and hemidiaphragm;and pericardium combined with chemother-apy or radiation therapy may be considered,although it does not substantially changeprognosis or survival time, and long-termsurvival is uncommon. Moreover, completesurgical resection is not feasible in most pa-tients. Combination pemetrexed (an anti-folate antimetabolite) and cisplatin showspromise but warrants further study.
The major focus of supportive care is onrelief of pain and dyspnea. Given the diffusenature of the disease, radiation therapy is usu-ally unsuitable except as a tool for treating lo-calized pain and for needle-tract metastasesbut should be avoided for treatment of nerveroot pain. To help reduce dyspnea caused bypleural effusions, pleurodesis or pleurec-tomy can be used. Adequate analgesia is dif-ficult but important to achieve, usually re-quiring opioids, with both transcutaneousand indwelling epidural catheters being usedin pain management. Chemotherapy usingcisplatin with gemcitabine has relieved symp-toms in most cases and has demonstratedtumor shrinkage in 1⁄2 of patients studied.Multimodality therapies are advocated by someauthorities. Intrapleural injection of granulo-cyte-macrophage colony-stimulating factoror interferon-γ ; IV ranpirnase (a ribonucle-ase); and gene therapies are under study.
No treatment has been shown to substan-tially prolong survival. Survival from time ofdiagnosis averages 8 to 15 mo depending onthe location and cell type. A small number ofpatients, usually younger patients with shorterduration of symptoms, have a more favorableprognosis, sometimes surviving for severalyears after diagnosis.
BERYLLIUM DISEASE(Berylliosis)
Acute beryllium disease (ABD) and chronicberyllium disease (CBD) are caused by inha-lation of dust or fumes from beryllium com-pounds and products. ABD is now rare;CBD is characterized by formation of gran-ulomas throughout the body, especially thelungs, intrathoracic lymph nodes, and skin.
CBD causes progressive dyspnea, cough,and fatigue. Diagnosis is by history, beryl-lium lymphocyte proliferation test, andbiopsy. Treatment is with corticosteroids.
Etiology and PathophysiologyBeryllium exposure is a common but under-
recognized cause of illness in many industries,including beryllium mining and extraction,alloy production, metal alloy machining, elec-tronics, telecommunications, nuclear weap-ons, defense, aircraft, automotive, aerospace,and computers and electronics recycling.
ABD is a chemical pneumonitis causingdiffuse parenchymal inflammatory infil-trates and nonspecific intra-alveolar edema.Other tissues (eg, skin and conjunctivae) maybe affected. ABD is now rare because most in-dustries have reduced exposure levels, butcases were common between 1940 and 1970,and many progressed from ABD to CBD.
CBD remains a common illness in indus-tries that use beryllium and beryllium alloy.It differs from most pneumoconioses in thatit is a cell-mediated hypersensitivity disease.Beryllium is presented to CD4+ T lympho-cytes by antigen-presenting cells, principallyin the context of HLA-DP molecules. T cellsin the blood, lung, or other organs, in turn,recognize the beryllium, proliferate, andform T-cell clones. These clones then releaseproinflammatory cytokines, such as tumornecrosis factor-α, IL-2, and interferon-γ.These amplify the immune response, result-ing in formation of mononuclear cell infil-trates and noncaseating granulomas in targetorgans where beryllium has deposited. Onaverage, 2 to 6% of beryllium-exposed peo-ple develop beryllium sensitization (definedby positive blood lymphocyte proliferation toberyllium salts in vitro), with most progress-ing to disease. Certain high-risk populations,such as beryllium metal and alloy machinists,have CBD prevalence > 17%. Workers withbystander exposures, such as secretaries andsecurity guards, also develop sensitizationand disease but at lower rates. The typicalpathologic consequence is a diffuse pulmo-nary, hilar, and mediastinal lymph node gran-ulomatous reaction histologically indistin-guishable from sarcoidosis. Early granulomaformation with mononuclear and giant cellscan also occur. Many lymphocytes are foundwhen cells are washed from the lungs (bron-choalveolar lavage [BAL]) during bron-choscopy. These T cells proliferate when ex-posed to beryllium in vitro, much as the blood
045_062PUL Page 472 Tuesday, November 8, 2005 10:54 AM

57 ENVIRONMENTAL PULMONARY DISEASES 473
cells do (beryllium lymphocyte proliferationtest [BeLPT]).
Symptoms, Signs, and DiagnosisPatients with CBD often have dyspnea,
cough, weight loss, and a highly variablechest x-ray pattern, usually showing diffuseinterstitial consolidation. Patients complainof insidious and progressive exertional dysp-nea, cough, chest pain, weight loss, nightsweats, and fatigue. Symptoms may developwithin months of 1st exposure or > 40 yr afterexposure has ceased. Some people remainasymptomatic. The chest x-ray may be normalor show diffuse infiltrates that can be nodular,reticular, or have a hazy ground-glass appear-ance, often with hilar adenopathy resemblingthe pattern seen in sarcoidosis. A miliary pat-tern also occurs. High-resolution chest x-rayis more sensitive than x-ray, although cases ofbiopsy-proven disease occur even in peoplewith normal imaging tests.
Diagnosis depends on a history of expo-sure, the appropriate clinical manifestations,and an abnormal blood and/or BAL BeLPT.BAL BeLPT is highly sensitive and specific,helping to distinguish CBD from sarcoidosisand other forms of diffuse pulmonary disease.
PrognosisABD can be fatal, but prognosis is usually
excellent if patients do not progress to CBD.CBD often results in progressive loss of res-piratory function. Early abnormalities in-clude air flow obstruction and decreased ox-ygenation on ABG at rest and during exercisetesting. Decreased diffusing capacity for car-bon monoxide (DLCO) and restriction appearlater. Pulmonary hypertension and right heartfailure develop in about 10% of cases, withdeath from cor pulmonale. Beryllium sensi-tization progresses to CBD at a rate of about8%/yr after initial detection through work-place medical surveillance programs. Subcu-taneous granulomatous nodules caused byinoculation with beryllium splinters or dustusually persist until excised.
TreatmentSome CBD patients never require treat-
ment because of the relatively slow rate ofdisease progression. Treatment is with corti-costeroids, which result in symptomatic im-provement and better oxygenation. Treat-ment is generally started only in those patientswith significant symptoms and evidence of ab-normal gas exchange or evidence of an accel-
erated decline in lung function or oxygen-ation. In symptomatic patients with abnormalpulmonary function, prednisone 40 to 60 mgpo once/day or every other day is given for 3to 6 mo, after which measures of pulmonaryphysiology and gas exchange are repeated todocument a response to therapy. The dose isthen gradually tapered to the lowest that main-tains symptomatic and objective improve-ment (usually about 10 to 15 mg once/day orevery other day). Lifelong treatment withcorticosteroids is usually required. There isanecdotal evidence that the addition of meth-otrexate (10 to 25 mg po once/wk) has a cor-ticosteroid-sparing effect in CBD, similar tothat observed in sarcoidosis.
In ABD, the lungs often become edema-tous and hemorrhagic. Mechanical ventila-tion is necessary in severely affected patients.
Unlike many cases of sarcoidosis, sponta-neous remission of CBD is rare. In patientswith end-stage CBD, lung transplantationcan be lifesaving. Other supportive measures,such as supplemental O2 therapy, pulmonaryrehabilitation, and drugs for treatment ofright heart failure, are used as needed.
PreventionIndustrial dust suppression is the basis for
preventing beryllium exposure. Exposuresmust be reduced to levels that are as low as rea-sonably achievable—preferably more than10-fold below current OSHA standards—toreduce the risk of sensitization and CBD.Medical surveillance, using the blood BeLPTand chest x-ray, is recommended for all ex-posed workers, including those with direct orindirect contact. The disease (both acute andchronic) must be promptly recognized and af-fected workers removed from further beryl-lium exposure.
BUILDING-RELATED ILLNESSES
Building-related illnesses (BRIs) are a het-erogeneous group of disorders whose etiol-ogy is linked to the environment of modernairtight buildings. Such buildings are charac-terized by sealed windows and dependenceon heating, ventilation, and air conditioningsystems for circulation of air. Most cases oc-cur in nonindustrial office buildings but canoccur in apartment buildings, single familydwellings, schools, museums, and libraries.
BRIs can be specific or nonspecific.
045_062PUL Page 473 Tuesday, November 8, 2005 10:54 AM

474 SECTION 5 PULMONARY DISORDERS
Specific BRIs: Specific BRIs are those forwhich a link between building-related expo-sure and illness is proven. Examples includeLegionella infection (see p. 1464), occupa-tional asthma (see p. 476), hypersensitivitypneumonitis (see p. 453), and inhalationalfever.
Inhalational fever is a febrile reactioncaused by exposures to organic aerosols ordusts. Names used to describe this type ofBRI include humidifier fever, grain fever,swine confinement fever, and mycotoxicosis.Metal fumes and polymer fumes can also pro-duce febrile illness. The term organic dusttoxic syndrome (ODTS) has been used to en-compass the reaction to any organic dust, al-though the term toxic pneumonitis has alsoentered common parlance.
In nonindustrial building settings, the BRIcalled humidifier fever occurs as a conse-quence of humidifiers or other types of ven-tilation units serving as a reservoir for thegrowth of microbes (bacteria, fungi) and as amethod of aerosolizing these contaminants.The disorder usually manifests as low-gradefever, malaise, cough, and dyspnea. Improve-ment with removal from exposure (eg, week-end away from the office building) is often oneof the 1st indications of etiology. The condi-tion has an acute onset and is self-limiting(usually 2 to 3 days). Physical signs may beabsent or subtle. Clusters of cases are com-mon. Unlike immunologically mediatedconditions, such as hypersensitivity pneu-monitis and building-related asthma, inhala-tional fevers do not require a period of sensi-tization. Disease can occur on 1st exposure.Acute episodes do not generally requiretreatment apart from removal from the con-taminated environment and antipyretics. Ifsymptoms persist, further investigation maybe required to rule out infection, hypersensi-tivity pneumonitis, or other conditions. Bio-logic sampling (to detect airborne microbialsin the work environment) can be costly andtime consuming but is necessary in somecases to document the source of contami-nated air. Inhalational fevers of all types areusually prevented by good maintenance ofventilation systems.
Nonspecific BRIs: Nonspecific BRIs arethose for which a link between building-related exposure and illness are more difficultto prove. The term sick building syndromehas been used to refer to illnesses that occurin clusters within a building for which thesymptoms are often nonspecific, including
itchy, irritated, dry or watery eyes; rhinorrheaor nasal congestion; throat soreness or tight-ness; dry itchy skin or unexplained skinrashes; and headache, lethargy, and difficultyconcentrating.
Some building-related factors appear toaccount for symptoms in some instances;these include higher building temperature,higher humidity, and poor ventilation, typi-cally with a failure to incorporate sufficientfresh air from outdoors. But patient factors,including female sex, history of atopy, in-creased attention to body sensations, worryabout the meaning of symptoms, anxiety, de-pression, and occasionally mass hysteria, alsoseem to underlie experience of symptoms.
BYSSINOSISByssinosis is a form of reactive airway dis-ease characterized by bronchoconstrictionin cotton, flax, and hemp workers. The eti-ologic agent is unknown. Symptoms arechest tightness and dyspnea that worsen onthe 1st day of the work week and subside asthe week progresses. Diagnosis is based onhistory and pulmonary function tests. Treat-ment includes avoidance of exposure anduse of asthma drugs.
Byssinosis occurs almost entirely in work-ers who contact unprocessed, raw cotton, es-pecially those exposed to open bales or whowork in cotton spinning or in the card room.Byssinosis can occur after acute exposure butusually occurs in workers with a history ofchronic exposure. Evidence suggests thatsome agent in the cotton bract leads to bron-choconstriction. Although bacterial endo-toxin is a likely cause, the absence of similarsymptoms in other settings in which workersare exposed to endotoxin leaves some uncer-tainty. Prolonged exposure to cotton dust wasonce thought to cause emphysema, a theorynot disproved. Chronic bronchitis symptomsare common among those exposed to cottondust.
Symptoms and SignsSymptoms are chest tightness and dyspnea
that lessen with repeated exposure. Symp-toms develop on the 1st day of work after aweekend or vacation and diminish or disap-pear by the end of the week. With repeated ex-posure over a period of years, chest tightnesstends to return and persist through midweek
045_062PUL Page 474 Tuesday, November 8, 2005 10:54 AM

57 ENVIRONMENTAL PULMONARY DISEASES 475
and occasionally to the end of the week or aslong as the person continues to work. Thistypical temporal pattern distinguishes byssi-nosis from asthma.
Signs of acute exposure are tachypnea andwheezing. Patients with more chronic expo-sure may have crackles.
Diagnosis and TreatmentDiagnosis is based on history and pulmo-
nary function tests that show typical airflowobstruction and a reduction in ventilatory ca-pacity, especially if measured at the start andend of a 1st work shift. Hyperresponsivenessto methacholine is also often observed. Sur-veillance measures, including symptom re-porting and spirometry in textile workers, canaid in early detection.
Treatment includes avoidance or reduc-tion of exposure and use of asthma drugs.
COAL WORKERS’ PNEUMOCONIOSIS
(Anthracosis; Black Lung Disease;Coal Miner’s Pneumoconiosis)
Coal workers’ pneumoconiosis (CWP) iscaused by inhalation of coal dust. Deposi-tion of dust produces dust-laden macro-phages around bronchioles (coal macules),occasionally causing focal bronchiolaremphysema. CWP usually causes no symp-toms but can progress to progressive mas-sive fibrosis with impaired lung function.Diagnosis is based on history and chestx-ray. Treatment is generally supportive.
Etiology and PathophysiologyCWP is caused by chronic inhalation of
dust from high-carbon coal (anthracite andbituminous), typically over ≥ 20 yr. Inhala-tion of silica contained in coal may also con-tribute to clinical disease. Alveolar macro-phages engulf the dust, release cytokines thatstimulate inflammation, and collect in lunginterstitium around bronchioles and alveoli(coal macules). Coal nodules develop as col-lagen accumulates, and focal emphysema de-velops as bronchiole walls weaken and dilate.Fibrosis can occur but is usually limited to ar-eas adjacent to coal macules. Distortion of lungarchitecture, airflow obstruction, and func-tional impairment are usually mild but can behighly destructive in a subset of patients.
Two forms are described: simple, with in-dividual coal macules, and complicated, withcoalescence of macules and progressive mas-sive fibrosis (PMF). Patients with simpleCWP develop PMF at a rate of about 1 to 2%.In this condition, nodules coalesce to formblack, rubbery parenchymal masses usuallyin the upper posterior fields. The masses mayencroach on and destroy vascular supply andairways or may cavitate. PMF can developand progress even after exposure to coal dusthas ceased. Despite the similarity of coal-induced PMF and conglomerate silicosis, thedevelopment of PMF in coal workers is un-related to silica content of the coal.
An association between CWP and featuresof RA is well-described. It is unclear whetherCWP predisposes miners to developing RA,whether RA takes on a unique form in pa-tients with CWP, or whether RA alters theresponse of miners to coal dust. Multiplerounded nodules in the lung appearing overa relatively short time (Caplan’s syndrome)represent an immunopathologic responserelated to rheumatoid diathesis. Histologi-cally, they resemble rheumatoid nodules buthave a peripheral region of more acute in-flammation. Patients with CWP are at aslightly increased risk of developing activeTB and non-TB mycobacterial infections.The same principles of TB surveillance andtreatment apply to CWP as for silicosis.Weak associations have been reported be-tween CWP and progressive systemic scle-rosis and stomach cancer.
Symptoms and SignsCWP does not usually cause symptoms.
Most chronic pulmonary symptoms in coalminers are caused by other conditions, suchas industrial bronchitis from coal dust or co-incident emphysema from smoking. Coughcan be chronic and problematic in patientseven after they leave the workplace, even inthose who do not smoke.
PMF causes progressive dyspnea. Blacksputum (melanoptysis) is rare and is causedby rupture of PMF lesions into the airways.PMF often progresses to pulmonary hyper-tension with right ventricular and respiratoryfailure.
DiagnosisDiagnosis depends on a history of expo-
sure and chest x-ray or thoracic CT appear-ance of diffuse, small rounded opacities or nod-ules (CWP) or of at least one opacity > 10 mm
045_062PUL Page 475 Tuesday, November 8, 2005 10:54 AM

476 SECTION 5 PULMONARY DISORDERS
against a background of CWP (PMF). Thespecificity of the chest x-ray for PMF is low,because up to 1⁄3 of lesions identified as beingPMF turn out to be malignancies, scars, orother lesions. Chest CT is also more sensitivethan chest x-ray for detecting coalescing nod-ules, early PMF, and cavitation. Pulmonaryfunction tests are nondiagnostic but are use-ful for characterizing lung function in pa-tients in whom obstructive, restrictive, ormixed defects may develop. Because abnor-malities of gas exchange are observed insome patients with extensive simple CWPand in those with complicated CWP, baselineand periodic measures of diffusing capacityfor carbon monoxide (DLCO) and ABG at restand during exercise are recommended.
Treatment and PreventionTreatment is rarely necessary in simple
CWP, although smoking cessation and TBsurveillance are recommended. Patients withpulmonary hypertension and/or hypoxemiaare given supplemental O2 therapy. Pulmo-nary rehabilitation can help the more severelyaffected workers perform activities of dailyliving. Preventive measures include elimi-nating exposure, smoking cessation, andpneumococcal and influenza vaccination.Workers with CWP, especially those withPMF, should be restricted from further expo-sure, especially to high concentrations ofdust. TB is treated in accordance with currentrecommendations (see p. 1511).
CWP can be prevented by suppressing coaldust at the coal face. Despite long-standingregulations, exposures continue to occur inthe mining trade. Respiratory masks provideonly limited protection.
OCCUPATIONAL ASTHMAOccupational asthma is reversible airwayobstruction that develops after months toyears of sensitization to an allergen encoun-tered in the workplace. Symptoms are dysp-nea, wheezing, cough, and, occasionally,upper respiratory allergic symptoms. Diag-nosis is based on occupational history,including assessment of job activities, aller-gens in the work environment, and a tempo-ral association between work and symptoms.Allergen skin testing and provocative inha-lational challenge may be used in special-ized centers but are usually unnecessary.
Treatment involves removing the personfrom the environment and using asthmadrugs as needed (see also p. 387).
Occupational asthma is development ofasthma in a worker who has no previous his-tory of asthma; symptoms typically developover months to years from sensitization to anallergen encountered in the workplace. Oncesensitized, the worker invariably responds tomuch lower concentrations of the allergenthan that which initiated the response. Occu-pational asthma differs from occupationallyaggravated asthma, which is an exacerbationor worsening of asthma in workers with pre-viously existing clinical or subclinical dis-ease as a result of single or repeated work-place exposures to pulmonary irritants suchas dusts and fumes. Occupationally aggra-vated asthma, which is more common thanoccupational asthma, generally subsideswith reduction of exposure and appropriateasthma treatment. It has a better prognosisand does not require the same level of clinicalinvestigation of specific triggering allergens.
Several other airway diseases caused byinhalational workplace exposures can be dis-tinguished from occupational and occupa-tionally aggravated asthma.
In reactive airways dysfunction syndrome(RADS), which is nonallergenic, people withno history of asthma develop persistent, re-versible airway obstruction after acute over-exposure to irritant dust, fume, or gas. Airwayinflammation persists even after removal ofthe acute irritant, and the syndrome is indis-tinguishable from asthma.
In reactive upper airways syndrome, up-per airway (ie, nasal, pharyngeal) mucosalsymptoms develop after acute or repeated ex-posure to airways irritants.
In irritant-associated vocal cord dysfunc-tion, which mimics asthma, abnormal appo-sition and closure of the vocal cords, espe-cially during inspiration, occurs after acuteirritant inhalation.
In industrial bronchitis (irritant-inducedchronic bronchitis), bronchial inflammationcauses cough after acute or chronic inhala-tional exposures to irritants.
In bronchiolitis obliterans, bronchiolardamage occurs after acute inhalational expo-sure to gases (eg, anhydrous ammonia). The2 major forms are proliferative and constric-tive. The constrictive form is more commonand may or may not be associated with otherforms of diffuse lung injury.
045_062PUL Page 476 Tuesday, November 8, 2005 10:54 AM

57 ENVIRONMENTAL PULMONARY DISEASES 477
EtiologyOccupational asthma is caused by both im-
mune- and non–immune-mediated mecha-nisms. Immune mechanisms involve IgE-and non–IgE-mediated hypersensitivity toworkplace allergens. Hundreds of occupa-tional allergens exist, ranging from low molwt chemicals to large proteins. Examples in-clude grain dust, proteolytic enzymes used indetergent manufacturing, red cedar wood,isocyanates, formalin (rarely), antibiotics(eg, ampicillin, spiramycin), epoxy resins,and tea.
Non–immune-mediated inflammatorymechanisms, responsible for occupationalairways disease, cause direct irritation of therespiratory epithelium and upper airway mu-cosae.
Symptoms and SignsSymptoms include shortness of breath,
chest tightness, wheezing, and cough, oftenwith upper respiratory symptoms such assneezing, rhinorrhea, and tearing. Upper air-way and conjunctival symptoms may pre-cede the typical asthmatic symptoms bymonths or years. Symptoms may developduring work hours after specific dust or vaporexposure but often do not become apparentuntil several hours after leaving work,thereby making the association with occupa-tional exposure less obvious. Nocturnalwheezing may be the only symptom. Often,the symptoms disappear on weekends or dur-ing vacations, although with ongoing expo-sure temporal exacerbations and relief be-come less apparent.
DiagnosisDiagnosis depends on recognizing the link
between workplace allergens and clinicalasthma. Diagnosis is suspected on the basisof an occupational history of allergen expo-sures. A materials safety data sheet can beused to list potential allergens and confirmwhen immunologic tests (eg, skin prick, pud-dle, or patch testing), through use of sus-pected antigens, demonstrate that a causativeagent in the workplace is affecting a person.An increase in bronchial hyperresponsive-ness after exposure to the suspected antigenis also helpful in making the diagnosis.
In difficult cases, a carefully controlledinhalation challenge test performed in thelaboratory confirms the cause of the airwayobstruction. Such procedures should be re-served for clinical centers experienced in in-
halation challenge testing and capable ofmonitoring the sometimes severe reactionsthat can occur. Pulmonary function tests orpeak expiratory flow measurements thatshow decreasing airflow during work are fur-ther evidence that occupational exposure iscausative. Methacholine challenge tests canbe used to establish the degree of airway hy-perreactivity. Sensitivity to methacholinemay decrease after exposure to the occupa-tional allergen has ceased.
Differentiation from idiopathic asthma isgenerally based on the pattern of symptoms,demonstration that allergens are present inthe workplace, and the relationship betweenexposure to allergens and symptoms andphysiologic worsening.
Treatment and PreventionTreatment is the same as for idiopathic
asthma, including inhaled bronchodilatorsand corticosteroids (see p. 387).
Dust suppression is essential. However,elimination of all instances of sensitizationand clinical disease may not be possible.Once sensitized, patients with occupationalasthma may react to extremely low levels ofairborne allergen. Those who return to envi-ronments in which the allergen persists gen-erally have a poorer prognosis, with more res-piratory symptoms, more abnormal lungphysiology, a greater need for drugs, andmore frequent and severe exacerbations.Whenever possible, a symptomatic personshould be removed from a setting known toproduce symptoms. If exposure continues,symptoms tend to persist. Occupationalasthma can sometimes be cured if it is diag-nosed early and exposure ceases.
SILICOSISSilicosis is caused by inhalation of crystal-line-free silica dust and is characterized bynodular pulmonary fibrosis. Chronic silico-sis initially causes no symptoms or only milddyspnea but over years can advance toinvolve most of the lung and cause dyspnea,hypoxemia, pulmonary hypertension, andrespiratory impairment. Diagnosis is basedon history and chest x-ray. No effectivetreatment exists except supportive careand, for severe cases, lung transplantation.
EtiologySilicosis, the oldest known occupational
pulmonary disease, is caused by inhalation of
045_062PUL Page 477 Tuesday, November 8, 2005 10:54 AM

478 SECTION 5 PULMONARY DISORDERS
tiny particles of silicon in the form of crystal-line “free” silica (usually quartz) or, less com-monly, by inhalation of silicates, mineralscontaining silicon dioxide bound to other el-ements, such as talc. Workers at greatest riskare those who move or blast rock and sand(miners, quarry workers, stonecutters) orwho use silica-containing rock or sand abra-sives (sand blasters; glass makers; foundry,gemstone, and ceramic workers; potters).Coal miners are at risk of mixed silicosis andcoal workers’ pneumoconiosis (see p. 475).
Chronic silicosis is the most common formand generally develops only after exposureover decades. Accelerated silicosis (rare) andacute silicosis may develop after more in-tense exposures over several years or months.Silica is also a cause of lung cancer.
Factors that influence the likelihood ofprogression to silicosis include duration andintensity of exposure, the form of silicon (ex-posure to crystalline form poses greater riskthan bound form), surface characteristics(exposure to uncoated form poses greater riskthan coated form), and rapidity of inhalationafter the dust is fractured and becomes air-borne (exposure immediately after fracturingposes greater risk than delayed exposure).The current limit for free silica in the indus-trial atmosphere is 100 µg/m3, an 8-h time-weighted average based on the percentage ofsilica in the dust.
PathophysiologyAlveolar macrophages engulf inhaled free
silica particles and enter lymphatics and in-terstitial tissue. The macrophages cause re-lease of cytokines (tumor necrosis factor-α,IL-1), growth factors (tumor growth factor-β), and oxidants, stimulating parenchymalinflammation, collagen synthesis, and, ulti-mately, fibrosis.
When the macrophages die, they releasethe silica into interstitial tissue around thesmall bronchioles, causing formation of thepathognomonic silicotic nodule. These nod-ules initially contain macrophages, lympho-cytes, mast cells, fibroblasts with disorga-nized patches of collagen, and scatteredbirefringent particles that are best seen by po-larized light microscopy. As they mature, thenodule centers become a dense ball of fibroticscar with a classic onion-skin appearance,surrounded by an outer layer of inflammatorycells. In low-intensity or short-term expo-sures, these nodules remain discrete andcause no compromise of lung function (sim-
ple chronic silicosis). But, with higher-inten-sity or more prolonged exposures (compli-cated chronic silicosis), these nodules coa-lesce and cause progressive fibrosis andreduction of lung volumes (TLC, VC) on pul-monary function tests, or they coalesce, some-times forming large conglomerate masses(also called progressive massive fibrosis).
In acute silicosis, which is caused by in-tense silica dust exposure over short periods,alveolar spaces fill with a PAS-positive stain-ing proteinaceous material similar to thatfound in pulmonary alveolar proteinosis (si-licoproteinosis—see p. 460). Mononuclearcells infiltrate alveolar septa. The occupa-tional history of acute exposure is needed todistinguish silicoproteinosis from the idio-pathic variety.
Symptoms, Signs, and Complications
Chronic silicosis patients are often asymp-tomatic but many eventually develop dysp-nea on exertion that progresses to dyspnea atrest. Productive cough, when present, may bedue to silicosis, coexisting chronic occupa-tional (industrial) bronchitis, or smoking.Breath sounds diminish as the disease ad-vances, and pulmonary consolidation, pul-monary hypertension, and respiratory failurewith or without right ventricular failure maydevelop in advanced disease.
Accelerated silicosis patients experiencethe same symptoms as those with chronicsilicosis but over a shorter period. Similarpathologic lesions and radiographic abnor-malities often develop over months to years.
Acute silicosis patients experience rapidprogression of dyspnea, weight loss, and fa-tigue, with diffuse bilateral crackles. Respi-ratory failure often develops within 2 yr.
Conglomerate (complicated) silicosis, theadvanced form of chronic or accelerated dis-ease characterized by widespread masses offibrosis, typically occurs in the upper lungzones. It causes severe, chronic respiratorysymptoms.
All patients with silicosis are at increasedrisk of pulmonary TB or nontubercular my-cobacterial disease, possibly from impairedmacrophage function and an increased risk ofactivation of latent infection. Other compli-cations include spontaneous pneumothorax,broncholithiasis, and tracheobronchial ob-struction. Emphysema is a common findingin areas immediately peripheral to conglom-erate nodules and in areas of progressive mas-
045_062PUL Page 478 Tuesday, November 8, 2005 10:54 AM

57 ENVIRONMENTAL PULMONARY DISEASES 479
sive fibrosis. Silica exposure and silicosis arerisk factors for lung cancer.
DiagnosisDiagnosis is based on x-ray findings in
conjunction with exposure history. Biopsyplays a confirmatory role when x-ray findingsare unclear. Adjunctive tests are performed todistinguish silicosis from other diseases.
Chronic silicosis is recognized by multiple1- to 3-mm rounded opacities or nodules onchest x-ray or CT, usually in upper lung fields.CT is more sensitive than x-ray, especiallywhen spiral and high-resolution algorithmsare used. Severity is graded on a standardizedscale developed by the International LaborOrganization, in which specially trainedreaders examine the chest x-ray for size andshape of opacities; concentration of opacities(profusion); and pleural changes. An equiv-alent scale does not exist for CT appearance.Calcified hilar and mediastinal lymph nodesare common and occasionally take on an egg-shell appearance. Pleural thickening is un-common unless a severe parenchymal dis-ease abuts the pleura. Rarely, calcified pleuralthickening is seen in patients with little pa-renchymal involvement. Bullae commonlyform around the conglomerate masses. Tra-cheal deviation may occur when the massesbecome large and cause volume loss. Truecavities may indicate TB. Numerous diseasesresemble chronic silicosis on x-ray, includingwelders’ siderosis, hemosiderosis, sarcoido-sis, chronic beryllium disease, hypersensitiv-ity pneumonitis, coal workers’ pneumoconi-osis, miliary TB, fungal pulmonary diseases,and metastatic malignancy. Eggshell calcifi-cations in hilar and mediastinal lymph nodesmay help distinguish silicosis from other pul-monary diseases but are not a pathognomonicfinding and are not commonly present.
Accelerated silicosis looks like chronicsilicosis on x-ray but develops more rapidly.
Acute silicosis is recognized by rapid pro-gression of symptoms and by diffuse alveolarbibasilar opacities on x-ray because of thefilling of the alveoli with fluid. On CT, areasof ground-glass density consisting of reticu-lar infiltration and areas of patchy increasedattenuation and inhomogeneity occur. Themultiple rounded opacities of chronic andaccelerated silicosis are not characteristic ofacute silicosis.
Conglomerate silicosis is recognizable byconfluent opacities > 10 mm in diameteragainst a background of chronic silicosis.
Adjunctive tests: Chest CT may be usedto distinguish asbestosis from silicosis, al-though this differentiation can usually bemade on the basis of chest x-ray and exposurehistory. CT is better at detecting the transitionfrom simple to conglomerate silicosis.
Tuberculin skin testing, sputum cultureand cytology, CT scan, PET scan, and bron-choscopy all may assist in distinguishing sil-icosis from disseminated TB or malignancy.
Pulmonary function tests (PFTs) and mea-sures of gas exchange (diffusing capacity forcarbon monoxide [DLCO], ABG) are not di-agnostic but help monitor disease. Earlychronic silicosis may manifest with reducedlung volumes that are at the lower end of thepredicted range and with normal functionalresidual capacity and residual volume. PFTsin conglomerate silicosis reveal decreasedlung volumes, DLCO, and airway obstruction.ABGs show hypoxemia usually without CO2retention. Measurements of gas exchangeduring exercise, using pulse oximetry orpreferably indwelling arterial catheter, is oneof the most sensitive measures of pulmonaryimpairment.
Antinuclear antibodies and elevated rheu-matoid factor are detectable in some patientsand are suggestive but not diagnostic of co-existing connective tissue disease. There is anexcess risk of progressive systemic sclerosis(scleroderma) in patients with silicosis, andsome patients with silicosis develop RA as-sociated with 3- to 5-mm pulmonary rheuma-toid nodules on chest x-ray or CT.
TreatmentWhole lung lavage may be useful in some
cases of acute silicosis. Whole lung lavagecan reduce the total mineral dust load in thelungs of patients with chronic silicosis. Caseseries have shown short-term reduction insymptoms after lavage, but controlled trialshave not been performed. Anecdotal evi-dence supports the use of oral corticosteroidsin acute and accelerated silicosis. Lung trans-plantation is a last-resort therapy.
Patients with obstruction may be treatedempirically with bronchodilators and inhaledcorticosteroids. Patients should be monitoredand treated for hypoxemia to forestall pulmo-nary hypertension. Pulmonary rehabilitationmay help patients perform activities of dailyliving. Workers who develop silicosis shouldbe removed from further exposure. Other pre-ventive measures include smoking cessationand pneumococcal and influenza vaccination.
045_062PUL Page 479 Tuesday, November 8, 2005 10:54 AM

480 SECTION 5 PULMONARY DISORDERS
PreventionThe most effective preventive interven-
tions occur at an industrial rather than clinicallevel and include dust suppression, processisolation, ventilation, and use of non–silica–containing abrasives. Respiratory masksprovide imperfect protection and, althoughhelpful, are not an adequate solution. Surveil-lance of exposed workers with respiratoryquestionnaires, spirometry, and chest x-raysis recommended. Frequency of surveillancedepends to some degree on the expected in-tensity of the exposure. Physicians must bealert to the risk of TB and nontuberculous my-cobacterial infections in silica-exposed pa-tients, especially miners. People exposed tosilica but without silicosis have 3 times therisk of developing TB compared with thenonexposed general population. Miners withsilicosis have a > 20-fold risk of TB and non-TB mycobacterial infection compared withthe general population and are more likely todevelop both pulmonary and extrapulmonarymanifestations. Patients exposed to silica witha positive tuberculin test and negative spu-tum TB cultures should be given isoniazidchemoprophylaxis in keeping with guide-lines for other tuberculin reactors. Recom-mendations for treatment are the same as forother patients with TB. Relapse is more com-mon in patients with silicotuberculosis, some-times necessitating longer courses than areusually recommended.
TOXIC INHALATION INJURYThe effect of inhaling toxic gases depends
on the extent and duration of exposure and onthe specific irritant. Toxic exposures predom-inantly affect the airways, causing tracheitis,bronchitis, and bronchiolitis.
ACUTE EXPOSUREAcute exposure to high concentrations of
toxic gas over a short time is characteristic ofindustrial accidents resulting from a faultyvalve or pump in a gas tank or during gastransport. Many people may be exposed andaffected. Chlorine, phosgene, sulfur dioxide,hydrogen chloride or sulfide, nitrogen diox-ide, ozone, and ammonia are among the mostimportant irritant gases.
Respiratory damage is related to the size ofinhaled particles and the solubility of the gas.More water-soluble gases (eg, chlorine, am-
monia, sulfur dioxide, hydrogen chloride)immediately cause mucous membrane irrita-tion, which may alert the victims to the needto escape the exposure. Permanent damage tothe upper respiratory tract, distal airways,and lung parenchyma occurs only if the vic-tim’s escape from the gas source is impeded.Less soluble gases (eg, nitrogen dioxide,phosgene, ozone) do not produce early warn-ing signs and are more likely to cause severebronchiolitis, with or without pulmonaryedema. In nitrogen dioxide intoxication (asoccurs in silo fillers and welders), a lag of upto 12 h may occur before symptoms of pul-monary edema develop.
Symptoms, Signs, and DiagnosisSoluble irritant gases cause severe burning
and other manifestations of irritation of theeyes, nose, throat, trachea, and major bron-chi. Marked cough, hemoptysis, wheezing,retching, and dyspnea are common. Severityis generally dose-related. Nonsoluble gasescause fewer immediate symptoms but canpresent with dyspnea or cough.
Diagnosis is usually obvious from the his-tory; management does not differ by specificinhaled agent but rather by symptoms. Theupper airway may be obstructed by edema,secretions, and/or laryngospasm. Chest x-rayfindings of patchy or confluent alveolar con-solidation usually indicates pulmonary edema.Evidence of any of these indicates a need forprophylactic endotracheal intubation.
PrognosisMost people recover fully. Bacterial infec-
tions, which are common, are the most seri-ous complication. A few develop acute respi-ratory distress syndrome (ARDS), usuallywithin 24 h. Bronchiolitis obliterans pro-gressing to respiratory failure can develop 10to 14 days after acute exposure to ammonia,nitrogen oxides, sulfur dioxide, and mercury.This pattern of injury is associated with air-flow obstruction mixed with restriction and isseen on CT as a pattern of bronchiolar thick-ening and a patchy mosaic of hyperinflation.Bronchiolitis obliterans with organizedpneumonia can ensue when granulation tis-sue accumulates in the terminal airways andalveolar ducts during the body’s reparativeprocess. ARDS without or with late pulmo-nary fibrosis may develop in a minority ofcases.
Occasionally, heavy exposures lead to re-versible airway obstruction (reactive airways
045_062PUL Page 480 Tuesday, November 8, 2005 10:54 AM

58 PULMONARY HYPERTENSION 481
dysfunction syndrome) persistent for ≥ 1 yr,resolving slowly in some cases. Smokersmay be more susceptible to persistent toxin-related lung injury. Injuries to the lower air-ways can obstruct airflow long-term, espe-cially after exposures to ammonia, ozone,chlorine, and gas mixtures.
TreatmentImmediate management includes removal
from exposure, observation, and supportivecare. If possible, the victim should be movedinto fresh air and given supplemental O2.Treatment is directed toward maintainingsufficient gas exchange by ensuring adequateoxygenation and alveolar ventilation. Severeairflow obstruction is managed with inhaledracemic epinephrine, endotracheal intuba-tion or tracheostomy, and mechanical venti-lation, if necessary. Bronchodilators and O2therapy may suffice in less severe cases. Theefficacy of corticosteroid therapy (eg, pred-nisone 45 to 60 mg once/day for 1 to 2 wk)is difficult to prove but is frequently usedempirically.
After the acute phase has been managed,physicians must remain alert to the develop-ment of reactive airways dysfunction syn-drome, bronchiolitis obliterans with or without
organized pneumonia, pulmonary fibrosis,and delayed-onset ARDS. Because of the riskof ARDS, any patient with acute upper airwayinjury after inhalation of toxic aerosols orgases should be observed for 24 h.
PreventionCare in handling gases and chemicals is the
most important preventive measure. Theavailability of adequate respiratory protec-tion (eg, gas masks with self-contained airsupply) is also very important if accidentalexposure occurs; rescuers without protectivegear who rush in to extricate a victim oftensuccumb themselves or develop acute andchronic airways disease.
CHRONIC EXPOSURELow-level continuous or intermittent ex-
posure to irritant gases or chemical vaporsmay lead to chronic bronchitis, although therole of such exposure is especially difficult tosubstantiate in smokers.
Chronic inhalational exposure to someagents (eg, bis[chloromethyl]ether or certainmetals) causes lung and other cancers (eg, liverangiosarcomas after vinyl chloride monomerexposure, mesothelioma with asbestos).
58PULMONARY HYPERTENSION
Pulmonary hypertension is increased pres-sure in the pulmonary circulation. It hasmany secondary causes; when the cause isunknown it is called primary pulmonaryhypertension (PPH). In PPH, pulmonary ves-sels become constricted, hypertrophied,and fibrosed. Pulmonary hypertension leadsto right ventricular overload and failure.Symptoms are fatigue, exertional dyspnea,and, occasionally, chest discomfort and syn-cope. Diagnosis is by measuring pulmonaryartery pressure. Treatment is with vasodila-tors and, in selected advanced cases, lungtransplantation. Prognosis is poor overall ifa treatable secondary cause is not found.
Epidemiology, Etiology, and Pathophysiology
Pulmonary hypertension is defined as amean pulmonary arterial pressure ≥ 25 mmHg at rest or ≥ 35 mm Hg during exercise.Many conditions and drugs cause pulmo-nary hypertension (see TABLE 58–1). PPH ispulmonary hypertension in the absence ofsuch causes. However, the end result can besimilar. PPH is rare, affecting 1 or 2 per mil-lion people.
PPH affects women about twice as often asmen. The mean age at diagnosis is 35 yr. Thedisease can be familial or sporadic; sporadiccases are about 10 times more common. Mostfamilial cases have mutations in the gene forthe bone morphogenetic protein receptortype 2 (BMPR2), part of the transforminggrowth factor (TGF)-β family of receptors.About 20% of sporadic cases also haveBMPR2 mutations. Many people with PPH
045_062PUL Page 481 Tuesday, November 8, 2005 10:54 AM

482 SECTION 5 PULMONARY DISORDERS
have increased levels of angiopoietin-1;angiopoietin-1 appears to down-regulateBMPR1A, a sister receptor to BMPR2, and
may stimulate serotonin production and en-dothelial smooth muscle proliferation. Otherpossible contributing factors include abnor-malities in serotonin transport and previousinfection with human herpesvirus 8.
PPH is characterized by variable vasocon-striction, smooth muscle hypertrophy, andvascular wall remodeling. Vasoconstrictionis thought to be due in part to enhanced activ-ity of thromboxane and endothelin-1 (bothvasoconstrictors) and reduced activity ofprostacyclin and nitric oxide (both vasodila-tors). The increased pulmonary vascularpressure that results from vascular obstruc-tion further injures the endothelium. Injuryactivates coagulation at the intimal surface,which may worsen the hypertension. Throm-botic coagulopathy from increased plasmin-ogen activator inhibitor type 1 and fibrin-opeptide A and decreased tissue plasminogenactivator activity may also contribute. Focalcoagulation at the endothelial surface shouldnot be confused with chronic thromboembolicpulmonary hypertension, which is pulmo-nary hypertension caused by organized pul-monary emboli.
In most patients, PPH eventually leads toright ventricular hypertrophy followed bydilatation and right ventricular failure.
Symptoms and SignsProgressive exertional dyspnea and easy
fatigability occur in almost all cases. Atypicalchest discomfort and exertional lightheaded-ness or presyncope may accompany dyspnea.These symptoms are due primarily to insuf-ficient cardiac output. Raynaud’s phenome-non occurs in about 10% of PPH patients. Ofthis 10%, 99% are women. Hemoptysis israre but may be fatal; hoarseness due to re-current laryngeal nerve compression by anenlarged pulmonary artery (Ortner’s syn-drome) also occurs rarely.
In advanced disease, signs may include rightventricular heave, widely split second heartsound (S2), accentuated pulmonic componentof S2 (P2), pulmonary ejection click, rightventricular third heart sound (S3), and jugularvein distention. Liver congestion and periph-eral edema are common late manifestations.
DiagnosisThe diagnosis of PPH is suspected in patients
with significant exertional dyspnea who areotherwise relatively healthy and have no his-tory or signs of other diseases known to causepulmonary hypertension (see TABLE 58–1).
TABLE 58–1. CAUSES OF SECOND-ARY PULMONARY HYPERTENSION
PulmonaryChronic high altitude exposureChronic thromboembolic diseaseCongenital pulmonary arterio-
venous shuntsCOPDHypoventilation syndromesInterstitial lung disease/pulmonary
fibrosisObstructive sleep apneaPulmonary capillary hemangioma-
tosis (rare)
CardiacCongenital heart diseaseHigh-output heart failureLeft ventricular diastolic
dysfunction (multiple causes)Left-to-right shunt with
Eisenmenger’s complexPatent ductus arteriosus
Connective tissue diseasesMixed connective tissue diseaseRAScleroderma and CREST (calcino-
sis cutis, Raynaud’s phenome-non, esophageal dysmotility, sclerodactyly, telangiectasias) syndrome
SLEVasculitis
Portal hypertension/liver failure
Infectious diseaseHIVParasitic disease (schistosomiasis,
filariasis, helminthiasis)
Drugs and toxinsAmphetaminesAnorexigens (fenfluramine,
dexfenfluramine)CocaineL-tryptophan (contaminated)Toxic rapeseed oil ingestion
HematologicPolycythemia veraSickle cell anemia
Persistent pulmonary hypertension of the newborn
045_062PUL Page 482 Tuesday, November 8, 2005 10:54 AM

58 PULMONARY HYPERTENSION 483
Patients initially undergo chest x-ray,spirometry, and ECG to identify more com-mon causes of dyspnea, followed by Dopplerechocardiography to assess right ventricularand pulmonary artery pressures as well as todetect structural heart disease causing sec-ondary pulmonary hypertension.
The most common x-ray result in PPH isenlarged hilar vessels that rapidly prune intothe periphery. Spirometry and lung volumesmay be normal or show mild restriction, butdiffusing capacity for carbon monoxide(DLCO) is usually reduced. Common ECGfindings include right axis deviation, R > S inV1, S1Q3T3, and peaked P waves.
Additional tests are obtained as indicated todiagnose secondary causes not apparent clin-ically. These include ventilation-perfusionscanning to detect thromboembolic disease;pulmonary function tests to identify obstruc-tive or restrictive lung disease; and serum se-rologic tests to gather evidence for or againstrheumatologic disease. Chronic thromboem-bolic pulmonary hypertension is suggested byCT or lung scan and is diagnosed by arterio-graphy. Other tests, such as HIV testing, liverfunction tests, and polysomnography, are per-formed in the appropriate clinical context.
When initial evaluation reveals no condi-tions associated with secondary pulmonaryhypertension, pulmonary artery catheter-ization is necessary to measure right atrialand ventricular, pulmonary artery, and pul-monary capillary wedge pressures and car-diac output. Right-sided O2 saturationshould be measured to exclude atrial septaldefect. Mean pulmonary arterial pressure> 25 mm Hg in the absence of an underlyingcause defines PPH. However, most patientswith PPH present with significantly higherpressure (eg, 60 mm Hg). Vasodilating drugs(eg, inhaled nitric oxide, IV epoprostenol,adenosine) are often administered duringthe procedure; decrease in right-sided pres-sures in response to these drugs helps in theselection of drugs for treatment. Biopsy,once widely performed, is neither needednor recommended because of high morbid-ity and mortality.
Once PPH is diagnosed, the patient's fam-ily history is reviewed to detect possible ge-netic transmission, which is suggested bypremature deaths in otherwise healthy mem-bers of the extended family. In familial PPH,genetic counseling is needed to advise familymembers of the risk of disease (about 20%)and to advocate serial screening with echocar-
diograms. Testing for mutations in the BMPR2gene in familial PPH may play a future role.
PrognosisUntreated patients have a median survival
of 2.5 yr. Cause of death is usually suddendeath in the context of right ventricular fail-ure. Five-year survival for epoprostenol-treated patients is 54%, whereas that for theminority of patients who respond to Ca chan-nel blockers is > 90%. Signs predictive ofpoor survival include low cardiac output,higher pulmonary artery and right atrial pres-sures, lack of response to vasodilators, heartfailure, hypoxemia, and reduced overall phys-ical functioning.
TreatmentSecondary pulmonary hypertension:
Treatment of secondary pulmonary hyper-tension involves management of the under-lying disorder. Patients with severe pulmo-nary hypertension secondary to chronicthromboembolic disease should undergopulmonary thromboendarterectomy. Undercardiopulmonary bypass, organized endo-thelialized thrombus is dissected along thepulmonary trunk in a procedure more com-plex than acute surgical embolectomy. Thisprocedure cures pulmonary hypertension ina substantial percentage of patients and re-stores cardiopulmonary function; operativemortality is < 10% in experienced centers.
Primary pulmonary hypertension:Treatment of PPH is rapidly evolving. OralCa channel blockers sustain reduction in pul-monary artery pressure or pulmonary vascu-lar resistance in about 10 to 15% of patientsand are the first drugs used. No differences inefficacy exist by Ca channel blocker type,though most specialists avoid verapamil be-cause of its negative inotropic effects. Re-sponse to Ca channel blockers is a favorableprognostic sign, and patients who respondshould continue this treatment. Those who donot respond are given other drugs.
IV epoprostenol, a prostacyclin analog,improves function and lengthens survivaleven in patients who are unresponsive to a va-sodilator during catheterization. Disadvan-tages are the need for continuous central cath-eter infusion and significant adverse effects,including flushing, diarrhea, and bacteremiadue to the indwelling central catheter. Inhaled(iloprost), oral (beraprost), and subcutaneous(treprostinil) prostacyclin analogs are understudy as alternatives.
045_062PUL Page 483 Tuesday, November 8, 2005 10:54 AM

484 SECTION 5 PULMONARY DISORDERS
Bosentan, an oral endothelin-receptor an-tagonist, is also useful in some patients, gen-erally those with milder disease who are notvasodilator-responsive. Oral sildenafil and L-arginine are also under study.
Lung transplantation offers the only hopeof cure but has high morbidity due to theproblems of rejection and infection and a60% 5-yr survival rate related to bronchiolitisobliterans. Lung transplantation is reservedfor patients with New York Heart Associationclass IV disease (defined as dyspnea associ-ated with minimal activity, leading to bed tochair limitations) who have not been helpedby prostacyclin analogs.
Many patients require adjunctive thera-pies to treat heart failure, including diuretics,and should receive warfarin to prevent throm-boembolism.
PORTOPULMONARY HYPERTENSION
Portopulmonary hypertension is severe pul-monary hypertension with portal hyperten-sion in patients without other secondarycauses.
Pulmonary hypertension occurs in pa-tients with a variety of conditions leading toportal hypertension with or without cirrhosis.Portopulmonary hypertension occurs lesscommonly than the hepatopulmonary syn-drome in patients with chronic liver disease(3.5 to 12%).
Presenting symptoms are dyspnea and fa-tigue. Chest pain and hemoptysis can also oc-cur. Patients have physical findings and ECGabnormalities consistent with pulmonary hy-pertension and may develop evidence of corpulmonale (elevated jugular venous pulse,edema). Tricuspid regurgitation is common.The diagnosis is suspected by echocardiog-raphy and confirmed by right heart catheter-ization. Treatment is that of primary pulmo-nary hypertension except for avoidance ofhepatotoxic drugs. Some patients have ben-efitted from vasodilator therapy. The under-lying liver disease is a major determinantof outcome. Portopulmonary hypertensionis a relative contraindication to liver trans-plantation because of increased morbidityand mortality. Some patients with mildpulmonary hypertension regress aftertransplantation.
HEPATOPULMONARY SYNDROME
Hepatopulmonary syndrome is hypoxemiacaused by vasodilation in patients with portalhypertension; dyspnea and hypoxemia areworse in the upright position.
The hepatopulmonary syndrome resultsfrom the formation of microscopic intrapul-monary arteriovenous dilatations in patientswith chronic liver disease. The mechanism isunknown but is thought to be due to increasedhepatic production or decreased hepaticclearance of vasodilators, possibly involvingnitric oxide. The vascular dilatations causeoverperfusion relative to ventilation, leadingto hypoxemia. Because the lesions frequentlyare more numerous at the lung bases, thehepatopulmonary syndrome causes platyp-nea (dyspnea) and orthodeoxia (hypoxemia)in the seated or upright position that subsidewith recumbency. Most patients also have stig-mata of chronic liver disease, such as spider an-giomas. About 20% of patients, however,present with pulmonary symptoms alone.
The hepatopulmonary syndrome is sus-pected in any patient with known liver diseasewho reports dyspnea (particularly platyp-nea). Patients with clinically significantsymptoms should undergo pulse oximetry. Ifthe syndrome is advanced, ABGs should bemeasured on air and on 100% O2 to determineshunt fraction.
A useful diagnostic test is contrast echocar-diography. IV microbubbles from agitated sa-line that are normally obstructed by pulmo-nary capillaries rapidly transit the lung andappear in the left atrium within 7 beats. Sim-ilarly, IV technetium-99m–labeled albuminmay transit the lungs and appear in the kidneyand brain. Pulmonary angiography may re-veal diffusely fine or blotchy vascular config-uration. Angiography is generally not neededunless thromboembolism is suspected.
The main treatment is supplemental O2 forsymptoms. Other therapies, such as soma-tostatin to inhibit vasodilation, are of modestbenefit in only some patients. Coil emboliza-tion is virtually impossible because of thenumber and size of the lesions. Inhaled nitricoxide synthesis inhibitors may be a futuretreatment option. Hepatopulmonary syn-drome may regress after liver transplantationor if the underlying liver disease subsides.Prognosis is poor without treatment (survival< 2 yr).
045_062PUL Page 484 Tuesday, November 8, 2005 10:54 AM

485
59DIFFUSE ALVEOLAR HEMORRHAGE AND PULMONARY-RENAL SYNDROMES
DIFFUSE ALVEOLARHEMORRHAGE SYNDROME
Diffuse alveolar hemorrhage syndrome is per-sistent or recurrent pulmonary hemorrhage.
Diffuse alveolar hemorrhage syndrome isan independent diagnostic entity because itsuggests a differential diagnosis and a spe-cific sequence of tests and treatments. Thedifferential diagnosis is broad and includesautoimmune diseases, including systemicvasculitides and Goodpasture’s syndrome;antiphospholipid antibody syndrome; pul-monary infections; toxic exposures; drug re-actions; bone marrow and solid organ trans-plantation; cardiac disorders such as mitralstenosis; coagulation disorders caused bydiseases or anticoagulant drugs; isolatedpauci-immune pulmonary capillaritis; andidiopathic pulmonary hemosiderosis.
Isolated pauci-immune pulmonary capil-laritis is a small-vessel vasculitis limited tothe lung; its only manifestation is alveolarhemorrhage affecting people aged 18 to 35 yr.
Idiopathic pulmonary hemosiderosis isdiffuse alveolar hemorrhage syndrome withno detectable underlying disease. It occursmainly in children < 10 yr and is thought to bedue to a defect in the alveolar capillary endo-thelium, possibly from autoimmune injury.
Some of these diseases can also cause glom-erulonephritis, in which case the patient is saidto have pulmonary-renal syndrome (see p. 486).
Symptoms, Signs, and DiagnosisSymptoms and signs of milder diffuse al-
veolar hemorrhage syndrome are dyspnea,
cough, and fever; however, many patientspresent with acute respiratory failure. He-moptysis is common but may be absent in upto 1⁄3 of patients. Children with idiopathicpulmonary hemosiderosis may have failureto thrive. There are no specific physical ex-amination findings.
Diagnosis is often suggested by chest x-rayfindings of diffuse bilateral alveolar infil-trates. Urinalysis is indicated to excludeglomerulonephritis and pulmonary-renal syn-drome. Others tests include CBC, coagula-tion studies, platelet counts, and serologictests (antinuclear antibody, anti-dsDNA, anti-glomerular basement membrane [anti-GBM]antibodies, antineutrophil cytoplasmic anti-bodies [ANCA], antiphospholipid antibody)to look for underlying causes; p-ANCA titersare elevated in some cases of isolated pauci-immune pulmonary capillaritis. Diagnosis ofidiopathic pulmonary hemosiderosis involvesdemonstration of iron-deficiency anemia andhemosiderin-laden macrophages on broncho-alveolar lavage or lung biopsy in the absenceof evidence of small-vessel vasculitis (pulmo-nary capillaritis) or of other diagnoses.
Other tests depend on clinical context.Pulmonary function tests may be performedto document lung function; increased diffus-ing capacity for carbon monoxide (DLCO)due to increased uptake of carbon monoxideby intra-alveolar Hb is consistent with hem-orrhage. Echocardiography may be indi-cated to exclude mitral stenosis. Broncho-alveolar lavage typically returns lavagefluid that remains hemorrhagic even aftersequential sampling. Lung biopsy is fre-quently needed when an underlying causeremains unclear.
Prognosis and TreatmentRecurrent diffuse alveolar hemorrhage
syndrome causes pulmonary hemosiderosisand fibrosis, both of which develop when fer-ritin aggregates within alveoli and exertstoxic effects. COPD occurs in some patientswith recurrent diffuse alveolar hemorrhagesecondary to microscopic polyarteritis.
Treatment involves correcting the cause.Corticosteroids and possibly cyclophos-phamide are used to treat vasculitides, con-nective tissue diseases, and Goodpasture’ssyndrome. Corticosteroids are also used totreat idiopathic pulmonary hemosiderosis;immunosuppressants are added for nonre-sponders.
045_062PUL Page 485 Tuesday, November 8, 2005 10:54 AM

486 SECTION 5 PULMONARY DISORDERS
PULMONARY-RENAL SYNDROME
Pulmonary-renal syndrome (PRS) is dif-fuse alveolar hemorrhage and glomerulone-phritis occurring simultaneously. PRS isalways a manifestation of underlying au-toimmune disease but is gaining recognitionas a diagnostic entity because it suggests adifferential diagnosis and a specific sequenceof tests and treatments. Goodpasture’s syn-drome is the prototype cause, but PRS canalso be caused by SLE, Wegener’s granulo-matosis, microscopic polyangiitis, and, lesscommonly, by other vasculitides and connec-tive tissue disease (see TABLE 59–1). Thenumber of cases of PRS caused by these latterdiseases is probably greater than those causedby Goodpasture’s syndrome, but patients withthose diseases more commonly present inother ways; only a few present with PRS.
PRS is less commonly a manifestation ofIgA-mediated disease, such as IgA nephrop-athy and Henoch-Schönlein purpura, and ofimmune complex–mediated renal disease,such as essential mixed cryoglobulinemia.Rarely, rapidly progressive glomerulone-
phritis alone can cause PRS through a mech-anism of renal failure, volume overload, andpulmonary edema with hemoptysis.
PRS is suspected in patients with hemoptysisnot obviously attributable to other causes (suchas pneumonia, carcinoma, or bronchiectasis),particularly when hemoptysis is accompaniedby diffuse parenchymal infiltrates. Initial test-ing includes urinalysis for evidence of hema-turia, serum creatinine for renal function as-sessment, and CBC for evidence of anemia.Pulmonary function tests are not diagnostic, butthe finding of an increased diffusing capacityfor carbon monoxide (DLCO) suggests pulmo-nary hemorrhage and is due to the increased up-take of carbon monoxide by intra-alveolar Hb.
Serum antibody testing may help distinguishsome causes. Antiglomerular basement mem-brane (anti-GBM) antibodies are pathogno-monic for Goodpasture’s syndrome, althoughthey also occur in patients with Alport’s syn-drome after kidney transplantation. Antibodiesto double-stranded DNA and reduced serumcomplements are typical of SLE. Antineutro-phil cytoplasmic antibodies (ANCA) directedagainst proteinase-3 (PR3-ANCA or cyto-plasmic ANCA [c-ANCA]) are present inWegener’s granulomatosis. Antineutrophil cy-toplasmic antibodies directed against myelo-peroxidase (MPO-ANCA, or perinuclear ANCA[p-ANCA]) suggest microscopic polyangiitis.
GOODPASTURE’S SYNDROME (Anti-GBM Antibody Disease)
Goodpasture’s syndrome is an autoimmunesyndrome of alveolar hemorrhage and glom-erulonephritis caused by circulating anti-GBM antibodies. Goodpasture’s syndromemost often develops in genetically susceptiblepeople who smoke cigarettes, but hydrocar-bon exposure and viral respiratory infectionsare additional possible triggers. Symptomsare dyspnea, cough, fatigue, hemoptysis,and/or hematuria. Goodpasture’s syndromeis suspected in patients with hemoptysis orhematuria and is confirmed by the presence ofanti-GBM antibodies in the blood. Treatmentincludes plasmapheresis, corticosteroids, andimmunosuppressants, such as cyclophospha-mide. Prognosis is good when treatment isbegun before onset of respiratory or renalfailure.
Goodpasture’s syndrome is the combina-tion of glomerulonephritis with alveolarhemorrhage in the presence of anti-GBM an-
TABLE 59–1. DIFFERENTIAL DIAGNOSIS OF PULMONARY-
RENAL SYNDROME
Connective tissue diseasePolymyositis or dermatomyositisProgressive systemic sclerosis RASLE
Goodpasture’s syndrome
Renal diseaseIdiopathic immune complex
glomerulonephritisIgA nephropathyRapidly progressive glomerulo-
nephritis with heart failure
Systemic vasculitisBehçet’s syndromeChurg-Strauss syndrome CryoglobulinemiaHenoch-Schönlein purpura Microscopic polyarteritisWegener’s granulomatosis
OtherDrugs (penicillamine)Heart failure
045_062PUL Page 486 Tuesday, November 8, 2005 10:54 AM

59 ALVEOLAR HEMORRHAGE AND PULMONARY-RENAL SYNDROMES 487
tibodies. Goodpasture’s syndrome most of-ten manifests as diffuse alveolar hemorrhageand glomerulonephritis together but can oc-casionally cause glomerulonephritis (10 to20%) or pulmonary disease (10%) alone.Men are affected more often than women.
Anti-GBM antibodies are directed againstthe noncollagenous (NC-1) domain of the α3chain of type IV collagen, which is found inhighest concentration in the basement mem-branes of renal and pulmonary capillaries. En-vironmental exposures—cigarette smoking,viral URI, and hydrocarbon solvent inhalationmost commonly and pneumonia less com-monly—expose alveolar capillary antigens tocirculating antibody in genetically susceptiblepeople, most notably those with HLA-DRw15,-DR4, and -DRB1 alleles. Circulating anti-GBM antibodies bind to basement membranes,fix complement, and trigger a cell-mediated in-flammatory response, causing glomerulone-phritis and/or pulmonary capillaritis.
Symptoms and SignsHemoptysis is the most prominent symp-
tom; however, hemoptysis may be absent inthe presence of hemorrhage, and the patientmay present with only chest x-ray infiltratesor infiltrates and respiratory distress and/orfailure. Dyspnea, cough, fatigue, fever, andweight loss are common. Up to 40% of pa-tients have gross hematuria, although pulmo-nary hemorrhage may precede renal manifes-tations by weeks to years.
Signs vary over time and range from clearlungs on auscultation to crackles and rhonchi.Some patients have peripheral edema andpallor from anemia.
DiagnosisIf initial testing supports the diagnosis of
PRS, additional tests are required. Diagnosis ofGoodpasture’s syndrome requires demonstra-tion of serum anti-GBM antibodies by indirectimmunofluorescence testing or, when avail-able, direct enzyme-linked immunosorbent as-say (ELISA) testing with recombinant or hu-man NC-1 α3. Other serologic tests are ob-tained, such as an antinuclear antibody (ANA)to detect SLE and antistreptolysin-O titer to de-tect poststreptococcal glomerulonephritis,which may be associated with many of thecauses of PRS. ANCA testing is positive (in pe-ripheral pattern) in 25% of Goodpasture’scases. In the presence of glomerulonephritis(hematuria, proteinuria, red cell casts on urinal-ysis, and/or renal insufficiency), renal biopsy
may be indicated. A rapidly progressive focalsegmental necrotizing glomerulonephritiswith crescent formation is found on biopsy inGoodpasture’s syndrome and all other causesof PRS. Immunofluorescence staining of renalor lung tissue classically demonstrates linearIgG deposition along the glomerular or alveo-lar capillaries. This also occurs in the diabetickidney and in fibrillary glomerulonephritis, arare disorder causing PRS, but GBM binding ofantibodies in these disorders is nonspecific.
Pulmonary function tests and bronchoalve-olar lavage are not diagnostic of Goodpasture’ssyndrome but can be used to help confirm dif-fuse alveolar hemorrhage in patients withglomerulonephritis and pulmonary infiltratesbut without hemoptysis. Lavage fluid that re-mains hemorrhagic after sequential samplingestablishes diffuse alveolar hemorrhage, espe-cially in the context of falling Hct.
Prognosis and TreatmentGoodpasture’s syndrome is often rapidly
progressive and can be fatal if prompt recog-nition and treatment are delayed; prognosis isgood when treatment is begun before onset ofrespiratory or renal failure.
Immediate survival in the face of pulmo-nary hemorrhage and respiratory failure islinked to airway control; endotracheal intu-bation and mechanical ventilation are recom-mended for patients with borderline ABGsand impending respiratory failure.
Treatment is daily or every-other-day plas-mapheresis for 2 to 3 wk using 4-L exchangesto remove anti-GBM antibodies, combinedwith an IV corticosteroid (usually methylpred-nisolone 1 g over 20 min every other day for3 doses followed by 1 mg/kg prednisone once/day) and cyclophosphamide (2 mg/kg once/day) for 6 to 12 mo to prevent formation of newantibodies. Therapy can be tapered when pul-monary and renal function stop improving.Long-term morbidity is related to the degree ofrenal impairment at presentation; patients re-quiring dialysis at presentation and those with> 50% crescents on biopsy have < 2-yr survivaland often require dialysis unless kidney trans-plantation is performed. Hemoptysis may be agood prognostic sign because it leads to earlierdetection of disease; the minority of patientswho are ANCA-positive respond better totreatment. Relapse occurs in a small numberand is linked to continued tobacco use and res-piratory infection. In patients with end-stagerenal disease who receive kidney transplanta-tion, disease can recur in the graft.
045_062PUL Page 487 Tuesday, November 8, 2005 10:54 AM

488
60MEDIASTINAL AND PLEURAL DISORDERS
Mediastinal and pleural disorders includemasses, mediastinitis, pleural effusion, pleu-ral fibrosis and calcification, pneumomedi-astinum, pneumothorax, and viral pleuritis.
MEDIASTINAL MASSESMediastinal masses are caused by a varietyof cysts and tumors; likely causes differ bypatient age and by whether the mass occursin the anterior, middle, or posterior mediasti-num. The masses may be asymptomatic (inadults) or cause obstructive respiratorysymptoms (in children). Testing involves CTscan with biopsy and adjunctive tests asneeded. Treatment differs by cause.
Classification and EtiologyMediastinal masses are divided into those
that occur in the anterior, middle, and poste-rior mediastinum. Each compartment hascharacteristic lesions (see FIG. 60–1). The an-terior mediastinum extends from the sternumto the pericardium and brachiocephalic ves-sels posteriorly. The middle mediastinum liesbetween the anterior and posterior mediasti-num. The posterior mediastinum is boundedby the pericardium and trachea anteriorly andthe vertebral column posteriorly.
The most common mediastinal masses inchildren are neurogenic tumors and cysts. Inadults, neurogenic tumors and thymoma arethe most common anterior lesions; lympho-mas (both Hodgkin and non-Hodgkin) occurmost frequently between ages 20 and 40 in theanterior mediastinum.
Symptoms and SignsSymptoms and signs of mediastinal
masses depend on location. Many are asymp-tomatic. In general, malignant lesions aremuch more likely to produce symptoms thanare benign lesions. The most common symp-toms are chest pain and weight loss. In chil-
dren, mediastinal masses are more likely tocause tracheobronchial compression andstridor or symptoms of recurrent bronchitisor pneumonia. Large anterior mediastinalmasses may cause dyspnea on lying supine.Lesions in the middle mediastinum maycompress blood vessels or airways, produc-ing the superior vena cava syndrome or air-way obstruction. Lesions in the posterior me-diastinum may encroach on the esophagus,producing dysphagia or odynophagia.
DiagnosisMediastinal masses are most often inci-
dentally discovered on chest x-ray or otherimaging tests during an examination for chestsymptoms. Additional diagnostic testing,usually imaging and biopsy, is indicated todetermine etiology.
CT scanning with IV contrast is the mostvaluable imaging technique. With thoracicCT, normal variants and benign tumors, suchas fat- and fluid-filled cysts, can be distin-guished from other processes. A definitive di-agnosis can be obtained for many mediastinalmasses with needle aspiration or needle bi-opsy. Fine-needle aspiration techniques usu-ally suffice for carcinomatous lesions, but acutting-needle biopsy should be performedwhenever lymphoma, thymoma, or a neuralmass is suspected (see TABLE 60–1). If TB isa concern, a PPD is performed. If ectopic thy-roid is considered, thyroid-stimulating hor-mone is measured.
TreatmentTreatment depends on etiology. Some be-
nign lesions, such as pericardial cysts, can beobserved. Most malignant tumors should beremoved surgically, but some, such as lym-phomas, are best treated with chemotherapy.Granulomatous disease should be treatedwith the appropriate antimicrobial drug.
MEDIASTINITISMediastinitis is acute inflammation of themediastinum.
The two most common causes of medias-tinitis are esophageal perforation and mediansternotomy.
Esophageal perforation may complicateesophagoscopy or insertion of a Sengstaken-Blakemore or Minnesota tube (for esophageal
045_062PUL Page 488 Tuesday, November 8, 2005 10:54 AM

60 MEDIASTINAL AND PLEURAL DISORDERS 489
variceal bleeding). It may occur with vomiting(Boerhaave’s syndrome). Patients with esoph-ageal perforation are generally acutely ill, withsevere chest pain and dyspnea due to medias-tinal infection and inflammation. Diagnosisusually is obvious from clinical presentationbut is confirmed by chest x-ray or CT showingair in the mediastinum. Treatment is withparenteral antibiotics selected to cover oraland GI flora, eg, clindamycin 450 mg IV q 6 hplus ceftriaxone 2 g once/day, for at least 2 wk.Many patients require emergency explorationof the mediastinum with primary repair of theesophageal tear and drainage of the pleuralspace and mediastinum.
Median sternotomy is complicated by me-diastinitis in about 1% of cases. These patientsmost commonly present with wound drainageor sepsis. Diagnosis is based on finding in-fected fluid from a needle aspiration throughthe sternum. Treatment consists of immediatesurgical drainage, debridement, and parenteralbroad-spectrum antibiotics. Mortality ap-proaches 50% in some series.
Chronic fibrosing mediastinitis usually isdue to TB or histoplasmosis but can be dueto sarcoidosis, silicosis, or other fungal dis-
eases. Patients develop an intense fibroticprocess that leads to compression of medi-astinal structures that can lead to the supe-rior vena cava syndrome, tracheal stenosis,or obstruction of the pulmonary arteries orveins.
Diagnosis is based on demonstration ofenlarged mediastinal lymph nodes by chestx-ray or CT scan. If the cause is TB, anti-TBtherapy is indicated. Otherwise, no knowntreatment is beneficial, but some physicianshave begun inserting vascular stents in an at-tempt to limit compression of selected cen-tral vessels.
PLEURAL EFFUSIONPleural effusions are accumulations of fluidwithin the pleural space. They have multiplecauses and usually are classified as transu-dates or exudates. Detection is by physicalexamination and chest x-ray; thoracentesisand pleural fluid analysis are often requiredto determine cause. Asymptomatic transu-dates require no treatment. Symptomatictransudates and almost all exudates require
Fig. 60–1. Common diagnostic possibilities of mediastinal masses by compartment.
Posterior mediastinumAneurysmBronchogenic tumorEnteric cystEsophageal diverticulaEsophageal tumorMeningoceleMeningomyeloceleNeurogenic tumor
Anterior mediastinumAneurysmAngiomatous tumorEsophageal tumorGoiterLipomaLymphomaMorgagni herniaParathyroid tumorPericardial cystTeratomaThymomaThyroid tumor
Middle mediastinumBronchogenic cystBronchogenic tumorLymph node hyperplasiaLymphomaPleuropericardial cystVascular masses
Esophagus
Aorta
Diaphragm
Heart inpericardium
Trachea
045_062PUL Page 489 Tuesday, November 8, 2005 10:54 AM

490 SECTION 5 PULMONARY DISORDERS
thoracentesis, chest tube drainage, pleu-rodesis, and/or pleurectomy.
Normally, 10 to 20 mL of pleural fluidsimilar in composition to plasma but lowerin protein (< 1.5 g/dL) is spread thinly overvisceral and parietal pleurae, facilitatingmovement between the lung and chest wall.The fluid enters the pleural space from sys-temic capillaries in the parietal pleurae andexits via parietal pleural stomas and lym-phatics. Pleural fluid accumulates when toomuch fluid enters or too little exits the pleu-ral space.
Classification and EtiologyPleural effusions have numerous causes
(see TABLE 60–2) and usually are categorizedas transudates or exudates based on labora-tory characteristics of the fluid (see TABLE60–3). A transudate can usually be treatedwithout extensive evaluation, whereas thecause of an exudate requires investigation.Bilateral effusions usually share the samecharacteristics.
Transudative effusions are caused bysome combination of increased hydrostatic
pressure and decreased oncotic pressurein the pulmonary or systemic circulation.Heart failure is the most common cause,followed by cirrhosis with ascites and hy-poalbuminemia, usually from the nephroticsyndrome.
Exudative effusions are caused by localprocesses leading to increased capillary per-meability resulting in exudation of fluid,protein, cells, and other serum constituents.Causes are numerous, the most commonbeing pneumonia, malignancy, pulmonaryembolism, viral infection, and TB. Yellownail syndrome is a rare disorder causingchronic exudative pleural effusions, lymph-edema, and dystrophic yellow nails, allthought to be the result of impaired lymphaticdrainage.
Chylous effusion (chylothorax) is amilky white effusion high in triglyceridescaused by traumatic or neoplastic (most of-ten lymphomatous) damage to the thoracicduct.
Chyliform (cholesterol or pseudochy-lous) effusions resemble chylous effusionsbut are low in triglycerides and high in cho-lesterol. Chyliform effusions are thought tobe due to release of cholesterol from lysed
TABLE 60–1. DIFFERENTIAL DIAGNOSIS OF MEDIASTINAL MASSES
POPU-LATION ANTERIOR MIDDLE POSTERIOR
Adults Anterior aortic aneurysm
Azygous vein Descending aortic aneurysmBronchogenic cyst Neurogenic tumors
Ectopic thyroid Ectopic thyroid Paraspinal infectionLymphoma Esophageal abnormalityMorgani hernia Hiatus herniaPericardial cyst LymphadenopathyTeratoma VaricesThymoma Vascular aneurysm
Children Ectopic thyroid Bronchogenic cyst MeningomyeloceleLymphoma Cardiac tumor Neuroenteric anomaliesSarcoma Cystic hygroma Neurogenic tumorsTeratoma Esophageal duplicationThymus
CystHistiocytosisHistoplasmosisNormalThymoma
HemangiomaLymphadenopathyLymphomaPericardial cystVascular anomalies
045_062PUL Page 490 Tuesday, November 8, 2005 10:54 AM
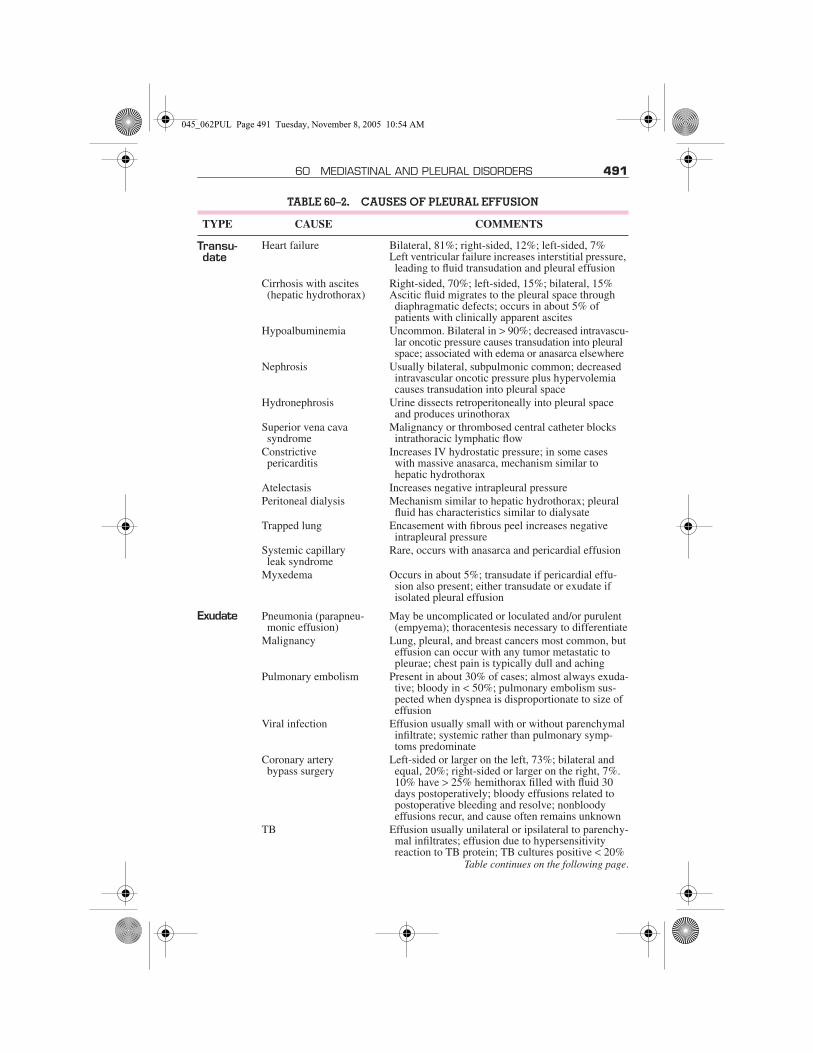
60 MEDIASTINAL AND PLEURAL DISORDERS 491
TABLE 60–2. CAUSES OF PLEURAL EFFUSION
TYPE CAUSE COMMENTS
Transu-date
Heart failure Bilateral, 81%; right-sided, 12%; left-sided, 7% Left ventricular failure increases interstitial pressure, leading to fluid transudation and pleural effusion
Cirrhosis with ascites (hepatic hydrothorax)
Right-sided, 70%; left-sided, 15%; bilateral, 15% Ascitic fluid migrates to the pleural space through diaphragmatic defects; occurs in about 5% of patients with clinically apparent ascites
Hypoalbuminemia Uncommon. Bilateral in > 90%; decreased intravascu-lar oncotic pressure causes transudation into pleural space; associated with edema or anasarca elsewhere
Nephrosis Usually bilateral, subpulmonic common; decreased intravascular oncotic pressure plus hypervolemia causes transudation into pleural space
Hydronephrosis Urine dissects retroperitoneally into pleural space and produces urinothorax
Superior vena cava syndrome
Malignancy or thrombosed central catheter blocks intrathoracic lymphatic flow
Constrictive pericarditis
Increases IV hydrostatic pressure; in some cases with massive anasarca, mechanism similar to hepatic hydrothorax
Atelectasis Increases negative intrapleural pressurePeritoneal dialysis Mechanism similar to hepatic hydrothorax; pleural
fluid has characteristics similar to dialysateTrapped lung Encasement with fibrous peel increases negative
intrapleural pressureSystemic capillary leak syndrome
Rare, occurs with anasarca and pericardial effusion
Myxedema Occurs in about 5%; transudate if pericardial effu-sion also present; either transudate or exudate if isolated pleural effusion
Exudate Pneumonia (parapneu-monic effusion)
May be uncomplicated or loculated and/or purulent (empyema); thoracentesis necessary to differentiate
Malignancy Lung, pleural, and breast cancers most common, but effusion can occur with any tumor metastatic to pleurae; chest pain is typically dull and aching
Pulmonary embolism Present in about 30% of cases; almost always exuda-tive; bloody in < 50%; pulmonary embolism sus-pected when dyspnea is disproportionate to size of effusion
Viral infection Effusion usually small with or without parenchymal infiltrate; systemic rather than pulmonary symp-toms predominate
Coronary artery bypass surgery
Left-sided or larger on the left, 73%; bilateral and equal, 20%; right-sided or larger on the right, 7%. 10% have > 25% hemithorax filled with fluid 30 days postoperatively; bloody effusions related to postoperative bleeding and resolve; nonbloody effusions recur, and cause often remains unknown
TB Effusion usually unilateral or ipsilateral to parenchy-mal infiltrates; effusion due to hypersensitivity reaction to TB protein; TB cultures positive < 20%
Table continues on the following page.
045_062PUL Page 491 Tuesday, November 8, 2005 10:54 AM

492 SECTION 5 PULMONARY DISORDERS
Sarcoidosis Effusion in 1–2%; patients have extensive parenchy-mal sarcoid and often extrathoracic sarcoid; pleural fluid is predominantly lymphocytic
Uremia Effusion in about 3%; > 50% have chest symptoms, most commonly fever (50%), chest pain (30%), cough (35%), and dyspnea (20%); diagnosis of exclusion
Infradiaphragmatic abscess
Causes “sympathetic” subpulmonic effusion; neutro-phils predominant in pleural fluid, but pH and glu-cose normal
HIV infection Effusion multifactorial: parapneumonic, TB, pulmo-nary Kaposi’s sarcoma, Pneumocystis jiroveci (for-merly called P. carinii) pneumonia, and other opportunistic infections
Rheumatoid disease Patient is typically an elderly man with rheumatoid nodules and deforming arthritis; must differentiate from parapneumonic effusion
Lupus erythematosus May be first manifestation of SLE; common with drug-induced SLE; diagnosis established by sero-logic tests of blood, not of pleural fluid
Drugs Many drugs, most notably bromocriptine, dantrolene nitrofurantoin, IL-2 (for treatment of renal cell can-cer and melanoma), and methysergide. Also seen with drug-induced lupus
Ovarian hyperstimula-tion syndrome
Complicates ovulation induction with human chori-onic gonadotropin (hCG) and occasionally clomi-phene; effusion develops 7–14 days after hCG injection; 52% right-sided, 27% bilateral
Pancreatitis Acute: Present in about 50%; bilateral, 77%; left-sided, 16%; right-sided, 8%. Due to transdiaphrag-matic transfer of the exudative inflammatory fluid and diaphragmatic inflammation
Chronic: Due to sinus tract from pancreatic pseudocyst through diaphragm into pleural space, chest symptoms rather than abdominal symptoms dominant, patients look like they have cancer
Esophageal rupture Patients extremely sick, medical emergency, morbid-ity and mortality due to infection of the mediasti-num and pleural space
Benign asbestos pleu-ral effusion
Occurs > 30 yr after initial exposure; frequently asymptomatic, tends to come and go, must rule out mesothelioma
Ovarian tumor (Meige’s disease)
Mechanism similar to hepatic hydrothorax; not all patients with ovarian mass, ascites, and pleural effusion are inoperable; diagnosis requires disappearance of ascites and effusion postoperatively
Yellow nail syndrome Triad of pleural effusion, lymphedema, and yellow nails; elements may appear decades apart; pleural fluid has relatively high protein but low LDH; effu-sion tends to recur, and there is no pleuritic chest pain
TABLE 60–2. CAUSES OF PLEURAL EFFUSION—Continued
TYPE CAUSE COMMENTS
045_062PUL Page 492 Tuesday, November 8, 2005 10:54 AM

60 MEDIASTINAL AND PLEURAL DISORDERS 493
RBCs and neutrophils in long-standing effu-sions when absorption is blocked by thethickened pleura.
Hemothorax is bloody fluid (pleural fluidhematocrit > 50% peripheral hematocrit) inthe pleural space due to trauma or, rarely, asa result of coagulopathy or after rupture of amajor blood vessel, such as the aorta or pul-monary artery.
Empyema is pus in the pleural space. Itcan occur as a complication of pneumonia,thoracotomy, abscesses (lung, hepatic, orsubdiaphragmatic), or penetrating trauma.Empyema necessitans is soft-tissue exten-sion of empyema leading to chest wall infec-tion and external drainage.
Trapped lung is lung encased by a fibrouspeel caused by empyema or tumor. Becausethe lung cannot expand, the pleural pressurebecomes more negative than normal, increas-ing transudation of fluid from parietal pleuralcapillaries. The fluid characteristically isborderline between a transudate and an exu-date, ie, the biochemical values are within15% of the cutoff levels for Light’s criteria(see TABLE 60–3).
Iatrogenic effusions can be caused by mi-gration or misplacement of a feeding tube orcentral venous catheter, leading to infusion oftube feedings or IV solution into the pleuralspace.
Effusions with no obvious cause are of-ten due to occult pulmonary emboli, TB, ormalignancy. Etiology is unknown for about15% of effusions even after extensive study;many of these effusions are thought to be dueto viral infection.
Symptoms and SignsSome pleural effusions are asymptomatic
and are discovered incidentally on physicalexamination or chest x-ray. Many causedyspnea, pleuritic chest pain, or both. Pleu-ritic chest pain, a vague discomfort or sharppain that worsens on inspiration, indicates in-flammation of the parietal pleura. Pain isusually felt over the inflamed site, but the pos-terior and peripheral portions of the dia-phragmatic pleura are supplied by the lower6 intercostal nerves, and irritation there maycause pain in the lower chest wall or abdomen
TABLE 60–3. CRITERIA FOR IDENTIFYING EXUDATIVE PLEURAL EFFUSIONS
TEST EXUDATE SENSITIVITY SPECIFICITY
Light’s criteria (1 or more of the following 3)
98 83
Fluid LDH* ≥ 2/3 ULN for serum LDH
82 89
Pleural fluid: serum total protein ratio
≥ 0.5 86 84
Pleural fluid: serum LDH ratio
≥ 0.6 90 82
Fluid total protein ≥ 3 g/dL 90 90
Fluid cholesterol ≥ 60 mg/dL≥ 43 mg/dL
5475
9280
Pleural fluid: Serum cholesterol ratio
≥ 0.3 89 81
Serum–pleural fluidprotein†
≤ 3.1 g/dL 87 92
ULN = upper limit of normal.*Correction for increase in LDH from RBC lysis = measured LDH − 0.0012 × RBC count/µL.†Preferred test for patients prescribed diuretics after development of effusion if Light’s exudative
criteria are met.Data from Light RW: Pleural effusion. New England Journal of Medicine 346:1971–1977, 2002.
045_062PUL Page 493 Tuesday, November 8, 2005 10:54 AM

494 SECTION 5 PULMONARY DISORDERS
that may simulate intra-abdominal disease.Irritation of the central portion of the dia-phragmatic pleura, innervated by the phrenicnerves, causes pain referred to the neck andshoulder.
Physical examination reveals absent tac-tile fremitus, dullness to percussion, and de-creased breath sounds on the side of the effu-sion. These findings can also be produced bypleural thickening. With large-volume effu-sions, respiration is usually rapid and shallow.A pleural friction rub, although infrequent, isthe classic physical sign. The friction rub var-ies from a few intermittent sounds that maysimulate crackles to a fully developed harshgrating, creaking, or leathery sound synchro-nous with respiration, heard on inspirationand expiration. Friction sounds adjacent tothe heart (pleuropericardial rub) may varywith the heartbeat and may be confusedwith the friction rub of pericarditis. Pericar-dial rub is best heard over the left border ofthe sternum in the 3rd and 4th intercostalspaces, is characteristically a to-and-frosound synchronous with the heartbeat, andis not influenced significantly by respira-tion. Sensitivity and specificity of the phys-ical examination for detecting effusion areprobably low.
DiagnosisDiagnostic tests are indicated to document
the presence of pleural fluid and to determineits cause.
Chest x-ray is the first test performed toconfirm the presence of pleural fluid. The lat-eral upright chest x-ray should be examinedwhen a pleural effusion is suspected. In an up-right film, 75 mL of fluid blunts the posteriorcostophrenic angle. Larger pleural effusionsopacify portions of the hemithorax; effusions> 4 L may cause complete opacification andeven mediastinal shift.
Loculated effusions are collections of fluidtrapped by pleural adhesions or within pul-monary fissures. Lateral decubitus x-rays,chest CT, or ultrasound should be performedif it is unclear whether an x-ray density rep-resents fluid or whether suspected fluid is loc-ulated or free-flowing; these tests are moresensitive than upright films and can detectfluid volumes < 10 mL. Loculated effusions,particularly those in the horizontal or obliquefissure, can be confused with a solid pulmo-nary mass (pseudotumor). They may change
shape and size with changes in the patient’sposition and amount of pleural fluid.
CT scan is not routinely indicated but isvaluable for evaluating the underlying lungparenchyma for infiltrates or masses whenthe lung is obscured by the effusion and fordistinguishing loculated fluid from solidmass.
Thoracentesis (see p. 378) should be per-formed on almost all patients who have pleu-ral fluid that is ≥10 mm in thickness on lat-eral decubitus x-ray or ultrasound that is newor of uncertain etiology. Despite commonpractice, chest x-ray need not be repeatedafter thoracentesis unless the patient devel-ops symptoms suggestive of pneumothorax(dyspnea or chest pain) or unless air mayhave entered the pleural space during theprocedure. Thoracentesis and subsequentpleural fluid analysis (see below) often arenot necessary for pleural effusions that arechronic, have a known cause, and cause nosymptoms.
Ultrasonography is helpful for identifyingpleural fluid collections for thoracentesiswhen blind thoracentesis is unsuccessful.
Pleural fluid analysis is performed to diag-nose the cause of pleural effusion. Analysisbegins with visual inspection, which can dis-tinguish bloody and chylous (or chyliform)from other effusions; can identify purulenteffusions strongly suggestive of empyema;and can identify viscous fluid, which is char-acteristic of some mesotheliomas. Fluidshould always be sent for total protein, LDH,cell count and cell differential, Gram stain,and aerobic and anaerobic bacterial cultures.Other tests (glucose, cytology, TB fluidmarkers [adenosine deaminase or interfe-ron-γ], amylase, mycobacterial, and fungalstains and cultures) are used in appropriateclinical settings.
Fluid chemistries help distinguish transu-dates from exudates; multiple criteria exist,not one of which perfectly discriminates be-tween the two. When Light’s criteria are used(see TABLE 60–3), the serum LDH and totalprotein for comparison with pleural fluidshould be obtained as close as possible to thetime of thoracentesis. Light’s criteria cor-rectly identify almost all exudates but misi-dentify about 20% of transudates as exudates.If transudative effusion is suspected (eg, due toheart failure or cirrhosis) and none of the bio-chemical measurements are > 15% above thecutoff levels for Light’s criteria, then the dif-
045_062PUL Page 494 Tuesday, November 8, 2005 10:54 AM

60 MEDIASTINAL AND PLEURAL DISORDERS 495
ference between the serum and the pleuralfluid protein is measured. If the difference is> 3.1 g/dL, then the patient probably has atransudative effusion.
If the diagnosis remains unclear after pleu-ral fluid analysis, a spiral CT scan is indicatedto look for pulmonary emboli, pulmonary in-filtrates, or mediastinal lesions. Findings ofpulmonary emboli indicate the need for long-term anticoagulation; parenchymal infil-trates, the need for bronchoscopy; and medi-astinal lesions, the need for transthoracicneedle aspiration or mediastinoscopy. How-ever, spiral CT requires a patient to hold hisbreath for ≥ 24 sec, and not all patients cancomply. If spiral CT is unrevealing, observa-tion is the best course unless the patient hasa history of malignancy, weight loss, persis-tent fever, or other findings suggestive of ma-lignancy or TB, in which case thoracoscopymay be indicated. Needle biopsy of thepleura can be performed when thoracoscopyis unavailable. When thoracoscopy is unre-vealing, an open thoracotomy must some-times be performed. Most patients with exu-dative effusions should have a PPD placedwith controls.
TreatmentThe underlying cause is treated; the effu-
sion itself generally does not require treat-ment if it is asymptomatic, because many re-sorb spontaneously, especially those due touncomplicated pneumonias, pulmonary em-bolism, and surgery. Pleuritic pain can usu-ally be managed with oral analgesics, thougha short course of oral opioids is sometimesnecessary.
Thoracentesis is sufficient treatment formany symptomatic effusions and can be re-peated for effusions that reaccumulate. Re-moval of > 1.5 L of pleural fluid at a timeshould be avoided, because it can lead to pul-monary edema due to rapid re-expansion ofalveoli previously compressed by fluid.
Effusions that are chronic, recurrent, andcausing symptoms can be treated with pleu-rodesis or with an indwelling catheter (seep. 498). Effusions caused by pneumonia andmalignancy may require additional specificmeasures.
Parapneumonic effusion: In the pres-ence of adverse prognostic factors (pH < 7.20,glucose < 60 mg/dL, positive Gram stain orculture, loculations), the effusion should be
completely drained via thoracentesis or tubethoracostomy. If complete drainage is impos-sible, fibrinolytics (urokinase 100,000 unitsin 100 mL saline solution) should be admin-istered intrapleurally. If this is ineffective,thoracoscopy should be performed to lyse ad-hesions and facilitate drainage. If thoracos-copy is unsuccessful, thoracotomy with surgi-cal decortication (eg, removal of scar, clot, orfibrous membrane surrounding the lung)should be performed.
Malignant pleural effusion: If dysp-nea caused by malignant pleural effusion isrelieved by thoracentesis but fluid reaccumu-lates (with dyspnea) more than once, chronicdrainage or pleurodesis is indicated; asymp-tomatic effusions and those unresponsiveto thoracentesis do not require additionalprocedures.
Indwelling catheter drainage is the preferredapproach for ambulatory patients, becausethe catheter can be inserted on an outpatientbasis and the pleural fluid drained intermit-tently into vacuum bottles. Shunting of pleu-ral fluid to the peritoneum (pleuroperitonealshunt) is useful for patients with malignanteffusion who fail pleurodesis or who havetrapped lung.
Pleurodesis is created by instilling a scle-rosing agent into the pleural space to fuse thevisceral and parietal pleura and eliminate thespace. The most effective and commonlyused sclerosing agents are talc, doxycycline,and bleomycin delivered via chest tube orthoracoscopy. Pleurodesis is contraindicatedif the mediastinum has shifted toward the sideof the effusion or if the lung does not expandafter a chest tube is inserted.
PLEURAL FIBROSIS AND CALCIFICATION
Pleural fibrosis and calcification are usuallybenign sequelae of pleural inflammation orasbestos exposure.
Pleural fibrosis and calcification can be ei-ther postinflammatory or asbestos related.
Postinflammatory: Pleural inflamma-tion commonly causes acute pleural thick-ening. In most cases, the thickening resolvesalmost completely. Some patients are leftwith minor degrees of pleural thickening,
045_062PUL Page 495 Tuesday, November 8, 2005 10:54 AM

496 SECTION 5 PULMONARY DISORDERS
which usually produces no symptoms or im-pairment of lung function. Occasionally, thelung becomes encased with a thick, fibrouspleural peel that limits expansion, pulls themediastinum toward the side of disease, andimpairs pulmonary function. Chest x-rayshows asymmetry of the lungs with thick-ened pleura (trapped lung). Differentiatinglocalized pleural thickening from loculatedpleural fluid may be difficult on x-ray, but theentire pleural surface may be seen on a CTscan.
Pleural fibrosis after inflammation can, onoccasion, calcify. Calcification produces adense image on the chest x-ray and almost al-ways involves the visceral pleura. Postin-flammatory calcifications are invariablyunilateral.
Asbestos related: Exposure to asbestoscan lead to focal, plaquelike pleural fibrosis,at times with calcification, occurring ≥ 20 yrafter the initial exposure. Any pleural or peri-cardial surface can be affected, but asbestos-related pleural plaques are usually in thelower 2⁄3 of the thorax and are bilateral. Cal-cification most often affects the parietal dia-phragmatic pleura and may be the only evi-dence of exposure. Dense pleural fibrosis canalso follow asbestos exposure.
PNEUMOMEDIASTINUMPneumomediastinum is air in mediastinalinterstices.
The three main causes of pneumomedi-astinum are alveolar rupture with dissectionof air into the mediastinum, esophageal per-foration, and esophageal or bowel rupturewith dissection of air from the neck or the ab-domen into the mediastinum. The primarysymptom is substernal chest pain which can,on occasion, be severe. Physical examinationshows subcutaneous emphysema, usually inthe suprasternal notch, along with a crunch-ing or clicking noise synchronous with theheartbeat which is best heard over the heartwhen the patient is in the left lateral decubitusposition (Hamman’s sign). The diagnosis isconfirmed by chest x-ray, which shows air inthe mediastinum. Treatment usually is notnecessary, although tension pneumomedi-astinum with compression of mediastinalstructures (rare) can be relieved with needleaspiration, leaving the needle open to the
atmosphere as is done with tension pneu-mothorax.
PNEUMOTHORAXPneumothorax is air in the pleural spacecausing partial or complete lung collapse.Pneumothorax can occur spontaneously orfrom underlying pulmonary disease, trauma,or medical procedures. Diagnosis is basedon physical examination and chest x-ray.Most pneumothoraces require transcatheteraspiration or tube thoracostomy.
Intrapleural pressure is normally negative(less than atmospheric pressure) because ofinward lung and outward chest wall recoil. Inpneumothorax, air enters the pleural spacefrom outside the chest or from the lung itselfvia mediastinal tissue planes or direct pleuralperforation. Intrapleural pressure rises, andlung volume decreases.
Classification and EtiologyPrimary spontaneous pneumothorax
occurs in patients without underlying pulmo-nary disease, typically in tall, thin young menin their teens and 20s. It is thought to be dueto spontaneous rupture of subpleural apicalblebs or bullae that result from smoking orthat are inherited. It generally occurs at rest,although some cases occur with activitiesinvolving reaching or stretching. Primaryspontaneous pneumothorax also occurs dur-ing diving and high-altitude flying because ofunequally transmitted pressure changes inthe lung.
Secondary spontaneous pneumotho-rax occurs in patients with underlying pul-monary disease. It most often results fromrupture of a bleb or bulla in patients with se-vere COPD (forced expiratory volume in1 sec [FEV1] < 1 L), HIV-related Pneumocys-tis jiroveci (formerly called P. carinii) infec-tion, cystic fibrosis, or any underlying pul-monary parenchymal disease (see TABLE60–4). Secondary spontaneous pneumotho-rax is typically more serious than primaryspontaneous pneumothorax because it occursin older patients who have less pulmonaryand cardiac reserve. Catamenial pneumotho-rax is a rare form of secondary spontaneouspneumothorax that occurs within 48 h of theonset of menstruation in premenopausalwomen and sometimes in postmenopausal
045_062PUL Page 496 Tuesday, November 8, 2005 10:54 AM

60 MEDIASTINAL AND PLEURAL DISORDERS 497
women taking estrogen. The cause is in-trathoracic endometriosis, possibly frommigration of peritoneal endometrial tissuethrough diaphragmatic defects or emboliza-tion through pelvic veins. With menstrua-tion, a hole develops in the pleura as the en-dometrial tissue is shed.
Traumatic pneumothorax is a commoncomplication of blunt and penetrating chestinjuries.
Tension pneumothorax is a pneumotho-rax causing progressive rise in intrapleuralpressure to levels that become positivethroughout the respiratory cycle and collapsethe lung, shift the mediastinum, and impairvenous return to the heart. Air continues to getinto the pleural space but cannot exit. Withoutproper treatment, the impaired venous returncan cause systemic hypotension and respira-tory and cardiac arrest within minutes. Ten-sion pneumothorax most commonly occursin patients receiving positive-pressure me-chanical ventilation (particularly during re-suscitation). It is rarely a complication oftraumatic pneumothorax, when a chestwound acts as a one-way valve that traps in-creasing volumes of air in the pleural spacewith inspiration.
Iatrogenic pneumothorax is caused bymedical interventions, including transtho-racic needle aspiration, thoracentesis, centralvenous catheter placement, mechanical ven-tilation, and cardiopulmonary resuscitation.
Symptoms and SignsNontraumatic pneumothoraces are some-
times asymptomatic. Symptoms includedyspnea, pleuritic chest pain, and anxiety.Dyspnea may be sudden or gradual in onsetdepending on the rate of development andsize of the pneumothorax. Pain can simulatecardiac ischemia, musculoskeletal injury(when referred to the shoulder), or an intra-abdominal process (when referred to theabdomen).
Physical findings classically consist of ab-sent tactile fremitus, hyperresonance to per-cussion, and decreased breath sounds on theside with the pneumothorax. If the pneu-mothorax is large, the side with the pneu-mothorax may be enlarged with the tracheavisibly shifted to the opposite side.
DiagnosisDiagnosis is made with upright inspiratory
chest x-ray. Radiolucent air and the absence
of lung markings juxtaposed between ashrunken lobe or lung and the parietal pleuraare diagnostic of pneumothorax. Trachealdeviation and mediastinal shift occur withlarge pneumothoraces.
The size of a pneumothorax is defined asthe percentage of the hemithorax that is va-cant. This is determined by taking 1 minus theratio of the cubes of the width of the lung andhemithorax. For example, if the width of thehemithorax is 10 cm and the width of the lungis 5 cm, the ratio is 53/103 = 0.125. Thus thesize of the pneumothorax is 1 minus 0.125, or87.5%. If adhesions are present between thelung and the chest wall, the lung will not col-lapse symmetrically, the pneumothorax mayappear atypical or loculated, and the calcula-tion will not hold.
Small pneumothoraces are sometimesoverlooked on chest x-ray. Conditions thatmimic pneumothorax radiographically in-clude emphysematous bullae, skin folds, and
TABLE 60–4. CAUSES OF SPONTANE-OUS PNEUMOTHORAX
PrimarySubpleural blebs attributed to smoking
SecondaryMore common
AsthmaCOPDCystic fibrosisNecrotizing pneumoniaPneumocystic jiroveci (formerly P. carinii) infection
TBLess common
PulmonaryIdiopathic pulmonary fibrosisLangerhans’ cell granulomatosisLung cancerLymphangioleiomyomatosisSarcoidosisConnective-tissue diseaseAnkylosing spondylitisEhlers-Danlos syndromeMarfan’s syndromePolymyositis/dermatomyositisRASarcomaScleroderma
OtherThoracic endometriosisTuberous sclerosis
045_062PUL Page 497 Tuesday, November 8, 2005 10:54 AM

498 SECTION 5 PULMONARY DISORDERS
overlap of stomach or bowel markings onlung fields.
TreatmentPatients should receive supplemental O2
until the chest x-ray is available; O2 acceler-ates pleural reabsorption of air. Treatmentthen depends on the type, size, and effects ofpneumothorax. Primary spontaneous pneu-mothorax that is < 20% and that does notcause respiratory or cardiac symptoms can besafely observed without treatment if follow-up chest x-rays obtained at about 6 and 48 hshow no progression. Larger or symptomaticprimary spontaneous pneumothoraces shouldbe evacuated by catheter drainage.
Catheter drainage is accomplished by in-sertion of a small-bore IV or pigtail catheterinto the chest in the 2nd intercostal space atthe mid-clavicular line. The catheter is at-tached to a three-way stopcock and syringe.Air is withdrawn from the pleural spacethrough the stopcock into the syringe and ex-pelled into the room. The process is repeateduntil the lung re-expands or until 4 L of air areremoved. If the lung expands, the catheter canbe removed or kept in place attached to a one-way Heimlich valve (thus permitting ambu-lation). If the lung does not expand, a chesttube should be inserted; in either approach,patients are usually hospitalized for observa-tion. Primary spontaneous pneumothoracescan also be managed initially with a chesttube attached to a water seal without or withsuction. Patients with primary spontaneouspneumothoraces should also undergo smok-ing cessation counseling, because smoking isa primary risk.
Secondary and traumatic pneumothoracesare generally treated with tube thoracostomy(see p. 380), although hospitalization and ob-servation may not be needed for some pa-tients with a small pneumothorax. Symptom-atic patients with iatrogenic pneumothoracesare best managed initially with aspiration.
Tension pneumothorax is a medical emer-gency. It should be treated immediately by in-serting a 14- or 16-gauge needle with catheterthrough the chest wall in the 2nd intercostalspace at the mid-clavicular line. The sound ofhigh-pressure air escaping confirms diagno-sis. The catheter can be left open to air or at-tached to a Heimlich valve. Emergency de-compression must be followed immediatelyby tube thoracostomy, after which the cathe-ter is removed.
ComplicationsThe three main problems encountered when
treating pneumothorax are air leaks, failure ofthe lung to expand, and re-expansion pulmo-nary edema.
Air leaks are usually due to the primarydefect—ie, continued leakage of air from thelung into the pleural space—but can be due toair leaking around the chest tube insertion siteif the site is not properly sutured and sealed. Airleaks are more common in secondary than inprimary spontaneous pneumothorax. Mostresolve spontaneously in < 1 wk.
Failure of the lung to re-expand is usuallydue to a persistent air leak, an endobronchialobstruction, a trapped lung, or a malposi-tioned chest tube. If an air leak or an incom-pletely expanded lung persists beyond 1 wk,the patient should be evaluated for thoracos-copy or thoracotomy.
Re-expansion pulmonary edema occurswhen the lung is rapidly expanded, as occurswhen a chest tube is connected to negativepressure after having been collapsed for > 2days. Treatment is supportive with O2, di-uretics, and cardiopulmonary support asneeded.
PreventionRecurrence approaches 50% in the 3 yr af-
ter initial spontaneous pneumothorax; thebest preventive procedure is a video-assistedthoracic surgery (VATS) procedure in whichblebs are stapled and a pleurodesis is createdwith pleural abrasion, parietal pleurectomy,or talc insufflation; in some medical centersthoracotomy is still used. These proceduresare recommended when catheter drainagefails with spontaneous pneumothorax, whenthere is a recurrent pneumothorax, or in pa-tients with secondary spontaneous pneu-mothorax. Recurrence after these proce-dures is < 5%. Patients who cannot undergothoracoscopy may undergo chemical pleu-rodesis through a chest tube (see p. 495), aprocedure that, though much less invasive,reduces the recurrence rate to only about25%.
VIRAL PLEURITISViral pleuritis is a viral infection of thepleurae.
Viral pleuritis is most commonly causedby infection with coxsackie B virus. Occa-
045_062PUL Page 498 Tuesday, November 8, 2005 10:54 AM

61 SLEEP APNEA 499
sionally, echovirus causes a rare conditionknown as epidemic or Bornholm’s pleuro-dynia, manifesting as pleuritis, fever, andchest muscle spasms; the condition occurs inthe late summer and affects adolescents and
young adults. The primary symptom is pleu-ritic pain; pleural friction rub may be a sign(see p. 494). Diagnosis is made clinically, andtreatment is symptomatic, with oral NSAIDsor a short course of oral opioids if needed.
61SLEEP APNEA
Breathing disorders that occur duringsleep include obstructive sleep apnea and cen-tral sleep apnea. Less severe forms includesnoring and upper airway resistance syn-drome. The term sleep-disordered breathingis used to encompass all such disorders. (Seealso Ch. 215 on p. 1834.)
OBSTRUCTIVE SLEEP APNEAObstructive sleep apnea comprises epi-sodes of partial and/or complete closure ofthe upper airway during sleep leading tobreathing cessation, defined as > 10 sec.Symptoms include restlessness, snoring,recurrent awakening, morning headache,and excessive daytime sleepiness. Diagno-sis is based on sleep history, physical exam-ination, and polysomnography. Treatmentis with nasal continuous positive airwaypressure, oral appliances, and, in refractorycases, surgery. Prognosis is good with treat-ment, but most cases are undiagnosed anduntreated, resulting in hypertension, heartfailure, and injury and death from motorvehicle and other accidents resulting fromhypersomnolence.
In at-risk patients, sleep destabilizes theupper airway, causing partial or complete ob-struction of the nasopharynx, oropharynx, orboth. When breathing is diminished but notabsent, the condition is called obstructivesleep hypopnea.
The prevalence of obstructive sleep apnea(OSA) in developed countries is 2 to 4%; thecondition is underrecognized and often un-
diagnosed even in symptomatic patients.OSA is up to 4 times more common in men,perhaps because it is underdiagnosed inwomen, because women may be more reluc-tant to report symptoms of snoring, or be-cause of gender bias in referral.
EtiologyAnatomic risk factors include obesity
(body mass index > 30); an oropharynx“crowded” by a short or retracted mandibleand prominent tongue, tonsils, lateral pha-ryngeal walls, or lateral parapharyngeal fatpads; a rounded head; and a shirt collar size> 18 inches. Other identified risk factors in-clude postmenopausal status and alcohol orsedative use. Family history of sleep apnea ispresent in 25 to 40% of cases, perhaps reflec-tive of intrinsic ventilatory drive or pharyn-geal structure; the likelihood of the diseaseincreases progressively as more family mem-bers have it. OSA is also often found in asso-ciation with chronic disease, such as hyper-tension, stroke, diabetes, gastroesophagealreflux disease, nocturnal angina, heart fail-ure, and hypothyroidism.
Because obesity is a common risk factorfor both OSA and the obesity-hypoventila-tion syndrome (see p. 57), the two conditionsmay coexist.
Airway obstruction causes paroxysms ofinspiratory effort, reductions in gas ex-change, disruption of normal sleep architec-ture, and partial or complete arousals fromsleep. Hypoxia and/or hypercapnia and sleepfragmentation interact to produce character-istic symptoms and signs.
OSA is an extreme form of sleep-relatedupper airway resistance. Less severe formsdo not produce O2 desaturation and includeprimary snoring; pharyngeal airflow resis-tance causing noisy inspiration but withoutsleep arousals; and the upper airway resistancesyndrome, which is more severe pharyngeal
045_062PUL Page 499 Tuesday, November 8, 2005 10:54 AM

500 SECTION 5 PULMONARY DISORDERS
airflow resistance causing snoring and tran-sient sleep arousals. People with upper airwayresistance syndrome are typically youngerand less obese than those with OSA and com-plain of daytime sleepiness more than dothose with primary snoring. But the symp-toms, diagnostic evaluation, and treatment ofsnoring and upper airway resistance syn-drome are otherwise the same as for OSA.
Symptoms and SignsSymptoms include loud disruptive snor-
ing, which is reported by 80 to 85% of OSApatients. However, most people who snore donot have OSA, and few need extensive eval-uation. Other symptoms include choking,gasping, or snorting during sleep, restlesssleep, and difficulty staying asleep (seeTABLE 61–1). Most patients are unaware ofsymptoms during sleep but are informed bybed partners or roommates. Daytime symp-toms include fatigue, hypersomnolence, andimpaired concentration. The frequency ofsleep complaints and degree of daytimesleepiness roughly correlate with the numberand length of nocturnal arousals. Hyperten-sion and diabetes are twice as commonamong people who snore, even after age andobesity are accounted for. OSA can be asso-ciated with cardiac arrhythmias (eg, brady-cardia, asystole) and heart failure.
DiagnosisThe diagnosis is suspected in patients with
identifiable risk factors and/or symptoms.
The patient and sleeping partner should be in-terviewed. The differential diagnosis of ex-cessive daytime sleepiness is broad (see p.1839) and includes reduced quantity orquality of sleep due to poor sleep hygiene;narcolepsy; sedation or mental status changesfrom drugs; chronic diseases, including car-diovascular, respiratory, or metabolic distur-bances and accompanying therapies (eg, di-uretics, insulin); depression; alcohol or drugabuse; and other primary sleep disorders (eg,periodic limb movement disorder, restlesslegs syndrome). A sleep history should betaken in all older patients; in patients withsymptoms of daytime fatigue, sleepiness,and lack of energy; in overweight or obese pa-tients; and in patients with chronic medicalconditions such as hypertension (which maybe caused by OSA), heart failure (which maycause and be caused by OSA), and stroke.Most patients who report only snoring, with-out other symptoms or cardiovascular risk,however, do not need an extensive evaluationfor OSA.
The physical examination should includeevaluation for nasal obstruction, tonsillar hy-pertrophy, signs of poor control of hyperten-sion, and measurement of neck size.
The diagnosis is confirmed with polysom-nography (see p. 1837), which comprisescontinuous measures of breathing effort byplethysmography; airflow at the nose andmouth by flow sensors; O2 saturation byoximetry; sleep architecture by EEG (forsleep stages), chin electromyography (forhypotonia), and electro-oculograms for rapideye movements. Also, the patient is observedby video. ECG is useful for determiningwhether arrhythmias occur with apneic epi-sodes. Other variables evaluated include limbmuscle activity (to assess nonrespiratorycauses of sleep arousal, such as restless legssyndrome and periodic limb movements dis-order) and body position (apnea may occuronly in the supine position).
Some facilities use portable monitors thatmeasure only heart rate, pulse oximetry, andnasal airflow to diagnose OSA. Althoughsome studies show excellent correlation be-tween these monitors and polysomnography,controversy over their routine use persists,because coexisting sleep disorders (eg, rest-less legs syndrome) may go unrecognized.
The common summary measure used todescribe respiratory disturbances duringsleep is the apnea-hypopnea index (AHI)—the total number of episodes of apnea and hy-
TABLE 61–1. DEFINITION OF OBSTRUCTIVE SLEEP APNEA
Excessive daytime sleepiness unex-plained by other factors and ≥ 2 ofthe following:
� Loud disruptive snoring� Nocturnal choking/gasping/
snorting� Recurrent nocturnal awakening� Unrefreshing sleep� Daytime fatigue� Impaired concentration
andSleep monitoring documenting > 5 episodes of hypopnea and apnea per hour
045_062PUL Page 500 Tuesday, November 8, 2005 10:54 AM
61 SLEEP APNEA 501
popnea during sleep divided by the hours ofsleep time. AHI values can be computed fordifferent sleep stages. The respiratory distur-bance index (RDI) is a similar measure,which refers to the number of times per hourthat blood O2 saturation falls > 3%. With anEEG, an arousal index (AI) can be computed,which is the number of arousals per hour ofsleep. The AI may be correlated with AHI orRDI, but about 20% of apneas and desatura-tion episodes are not accompanied by arous-als, or other causes of arousals are present. AnAHI > 5 is required for the diagnosis of OSA;values > 15 and > 30 indicate moderate andsevere levels of sleep apnea, respectively.Snoring confers a 7-fold increase in the like-lihood of having AHI > 5. The AI and RDIcorrelate only moderately with a patient’ssymptoms.
Adjunctive testing may include upper air-way imaging, thyroid-stimulating hormone,and other tests as appropriate to assesschronic medical conditions associated withOSA.
PrognosisPrognosis is excellent with proper treat-
ment. However, untreated OSA, which is com-mon because it is so frequently undiagnosed,can have long-term sequelae, including poorlycontrolled hypertension and heart failure. Theadverse effects of hypersomnolence, such asloss of employment and sexual dysfunction,can affect families considerably.
Perhaps most importantly, excessive day-time sleepiness is a major risk factor for seriousinjury and death from accidents, especiallymotor vehicle accidents. Sleepy patientsshould therefore be warned of the risk of op-erating a motor vehicle or engaging in activ-ities during which sleep attacks would behazardous. In addition, perioperative cardiacarrest has been attributed to OSA, probablydue to the effects of anesthesia on the condi-tion after removal of a mechanical airway. Pa-tients should therefore inform an anesthesi-ologist of the diagnosis before undergoingsurgery and should expect to receive contin-uous positive airway pressure (CPAP) duringhospitalization.
TreatmentInitial treatment addresses underlying risk
factors. Modifiable risk factors include obe-sity, alcohol and sedative use, and poor con-trol of chronic disease. Weight loss is an im-portant component of OSA treatment but is
extremely difficult for most people, espe-cially those fatigued or sleepy.
Surgical correction of upper airway ob-struction caused by enlarged tonsils and nasalpolyps should be considered; surgery for mac-roglossia or micrognathia is also an option.
The aim of treatment specific to OSA is toreduce episodes of hypoxia and sleep frag-mentation; treatment is tailored to the patientand to the degree of impairment. Cure is de-fined as a resolution of symptoms with AHIreduction below a threshold, usually 10/h.Moderate and severe levels of sleepiness arepredictors of treatment success.
CPAP: Nasal CPAP is the treatment ofchoice for most patients with subjectivesleepiness; it is of questionable benefit for pa-tients who deny sleepiness. CPAP improvesupper airway patency by application of pos-itive pressure to the collapsible upper airway.Effective pressures typically range from 3 to15 cm H2O. Disease severity does not corre-late with pressure requirements. If clinicalimprovement is not apparent, pressure can betitrated by repeat polysomnography. Regard-less of AHI, CPAP can also reduce neurocog-nitive impairments and blood pressure. IfCPAP is withdrawn, symptoms recur overseveral days, though short interruptions oftherapy for acute medical conditions are usu-ally well tolerated. Duration of therapy is in-definite.
Failures of nasal CPAP commonly occurbecause of limited patient adherence. Ad-verse effects include sore throat, which can bealleviated in some cases with the use of warmhumidified air, and discomfort resulting froma poorly fitting mask.
CPAP can be augmented with inspiratoryassistance (bi-level positive airway pressure)for patients with obesity-hypoventilationsyndrome (see p. 57).
Oral appliances: Oral appliances aredesigned to advance the mandible or, at thevery least, prevent mandible retrusion withsleep. Some are also designed to pull thetongue forward. Use of these appliances totreat both snoring and OSA is gainingacceptance. Comparisons of appliances toCPAP are limited, and specific indicationsand cost-effectiveness have not beenestablished.
Surgery: Surgery is reserved for patientsrefractory to noninvasive therapies. Uvulo-palatopharyngoplasty (UPPP) is the mostcommon procedure. It involves a submucosalresection of tissue from the tonsillar pillars to
045_062PUL Page 501 Tuesday, November 8, 2005 10:54 AM
502 SECTION 5 PULMONARY DISORDERS
the arytenoepiglottic folds, including resec-tion of the adenoids, to enlarge the upper air-way. Equivalence with CPAP was demon-strated in one study using CPAP as a bridgeto surgery, but the two interventions have notbeen directly compared. Patients who aremorbidly obese or who have anatomic nar-rowing of the airway may not realize successwith UPPP. Moreover, recognition of sleepapnea after UPPP is obscured because snor-ing is absent. These silent obstructions maybe as severe as apneic episodes before surgi-cal intervention.
Adjunctive surgical procedures includemidline glossectomy and mandibulomaxil-lary advancement. The latter is often offered asa 2nd-stage procedure if UPPP is not curative.Studies of this 2-stage approach across centersin unselected patients are not available.
Tracheostomy is the most effective thera-peutic maneuver for obstructive apnea but isa procedure of last resort. It bypasses the siteof obstruction during sleep. It is indicated forpatients who are most severely affected byOSA and/or obstructive sleep hypopnea (eg,those with cor pulmonale). It may take ≥ 1 yrbefore the stoma is healed.
Laser-assisted uvuloplasty has been pro-moted as a treatment for loud snoring alongwith radiofrequency tissue ablation. It pro-vides 2- to 6-mo reductions of 70 to 80% insnoring loudness; however, efficacy declinesafter 1 yr. Sleep apnea syndrome should beconsidered in these evaluations so as not todelay more appropriate treatment.
Adjunctive treatments: Adjunctive treat-ments are commonly used but have no provenrole as first-line treatment.
O2 may provoke respiratory acidosis andmorning headache in some patients, and itis impossible to predict who will respondfavorably.
A number of drugs have been used as ven-tilatory drive stimulants (eg, tricyclic antide-pressants, theophylline) but cannot be rou-tinely advocated because of limited efficacyand/or a low therapeutic index.
Nasal dilatory devices and throat sprayssold OTC for snoring have no proven benefits.
Patient education and support: An in-formed patient and family are better able tocope with a treatment strategy, including tra-cheostomy in patients refractory to othertreatment. Patient support groups are effec-tive in providing information and in support-ing timely and effective treatment.
CENTRAL SLEEP APNEACentral sleep apnea is a heterogenousgroup of conditions characterized bychanges in ventilatory drive or decreasedability to breathe without airway obstruc-tion; most of these conditions cause asymp-tomatic changes in breathing pattern duringsleep.
Patients with central sleep apnea (CSA) fallinto two categories. One group presents withhypercapnia with decreased ventilatory driveor a decreased ability to breathe. Causes in-clude central lesions, such as brain stem infarc-tions, encephalitis, and Arnold-Chiari malfor-mation; neuromuscular diseases, such as mus-cular dystrophy, amyotrophic lateral sclerosis,and postpolio syndrome; and chest wall abnor-malities, notably, kyphoscoliosis. The othergroup presents with eucapnia or hypocapniawith increased ventilatory drive but sleep-induced apnea and periodic breathing. Cheyne-Stokes breathing is a discrete pattern of thisform of CSA thought to be caused by delays incerebral circulation that, in turn, cause a lag inrecognition by respiratory centers of acidosis/hypoxia (causing hyperpnea) and of alkalosis/hypocapnia (causing apnea). Causes includeheart failure, high altitude, pain, and anxiety.
Congenital central hypoventilation (On-dine’s curse) is a rare disorder of idiopathicCSA in newborns and may be associated withHirschsprung’s disease. It may be related toan inborn error in neurogenesis.
CSA is mostly asymptomatic and is de-tected by caretakers or bed partners who no-tice long respiratory pauses, shallow breaths,or restless sleep. Patients with hypercapnicforms may experience daytime somnolence,lethargy, and morning headache.
Diagnosis is suspected on the basis of his-tory and confirmed by polysomnography.Testing may not be necessary, however, ifCSA causes no symptoms or is clearly relatedto an identifiable disorder. Additional testingmay involve brain or brain stem imaging toevaluate central causes.
Primary treatment is correction of underlyingconditions and avoidance of sedatives. Second-ary treatment is provision of supplemental O2or, in patients with hypercapnic CSA, noninva-sive continuous or bi-level positive airway pres-sure. Acetazolamide is effective in CSA causedby high altitude. Phrenic nerve pacing is an op-tion for children > 2 yr with congenital CSA.
045_062PUL Page 502 Tuesday, November 8, 2005 10:54 AM

503
62TUMORS OF THE LUNGS
Lung tumors may be malignant or be-nign, primary or metastatic (see TABLE 62–1).Lung carcinoma, also called bronchogeniccarcinoma or lung cancer, is the most com-mon nondermatologic cancer and the mostcommon lung tumor.
LUNG CARCINOMALung carcinoma is a malignant lung tumorusually categorized as small cell or non–small cell. Cigarette smoking is the majorrisk factor for most types. Symptomsinclude cough, chest discomfort, and, lesscommonly, hemoptysis, but many patientsare asymptomatic and some present withmetastatic disease. Diagnosis is suspectedby chest x-ray or CT scan and confirmed bybiopsy. Treatment is with surgery, chemo-therapy, and/or radiation therapy. Despiteadvances in treatment, the prognosis ispoor, and attention is focused on earlydetection and prevention.
Epidemiology, Pathophysiology, and Classification
An estimated 171,900 new cases of lungcarcinoma are diagnosed each year in the US,and the disease causes 157,200 deaths annu-ally. The incidence is rising in women and ap-pears to be leveling off in men. Black men areat especially high risk.
Cigarette smoking, including passive (sec-ondhand) smoking, is the most importantcause. Risk differs by age and smoking inten-sity and duration; risk after smoking cessa-tion declines but probably never returns tobaseline. Exposure to radon, a breakdownproduct of naturally occurring radium anduranium, is the most important environmen-tal risk factor in nonsmokers. Occupationalexposure to radon (in uranium miners); as-bestos (in construction and demolition work-ers, pipefitters, shipbuilders, and automotivemechanics); silica (in miners and sandblast-ers); arsenic (in workers in copper smelting,pesticide manufacturing, and wood-treat-ment plants); chromates (in stainless steel and
pigment manufacturing plants); nickel (inbattery and stainless steel manufacturingplants); chloromethyl ethers; beryllium; andcoke oven emissions (in steel workers)accounts for a small number of cases per year(see Ch. 57 on p. 469). The risk of cancer isgreater with combined exposure to occupa-tional toxins and cigarette smoking than witheither one alone. COPD and pulmonary fibro-sis may increase susceptibility; β-carotenesupplementation may increase susceptibility
TABLE 62–1. CLASSIFICATION OF PRIMARY LUNG TUMORS
MalignantCarcinoma
Small cellOat cellIntermediate cellCombined
Non–small cellAdenocarcinoma
AcinarBronchioloalveolarPapillarySolid
AdenosquamousLarge cell
Clear cellGiant cell
Squamous cellSpindle cell
OtherBronchial gland carcinoma
Adenoid cysticMucoepidermoid
CarcinoidLymphoma
Primary pulmonary HodgkinPrimary pulmonary
non-Hodgkin
BenignLaryngotracheobronchial
AdenomaHamartomaMyoblastomaPapilloma
ParenchymalFibromaHamartomaLeiomyomaLipomaNeurofibroma/schwannomaSclerosing hemangioma
045_062PUL Page 503 Tuesday, November 8, 2005 10:54 AM
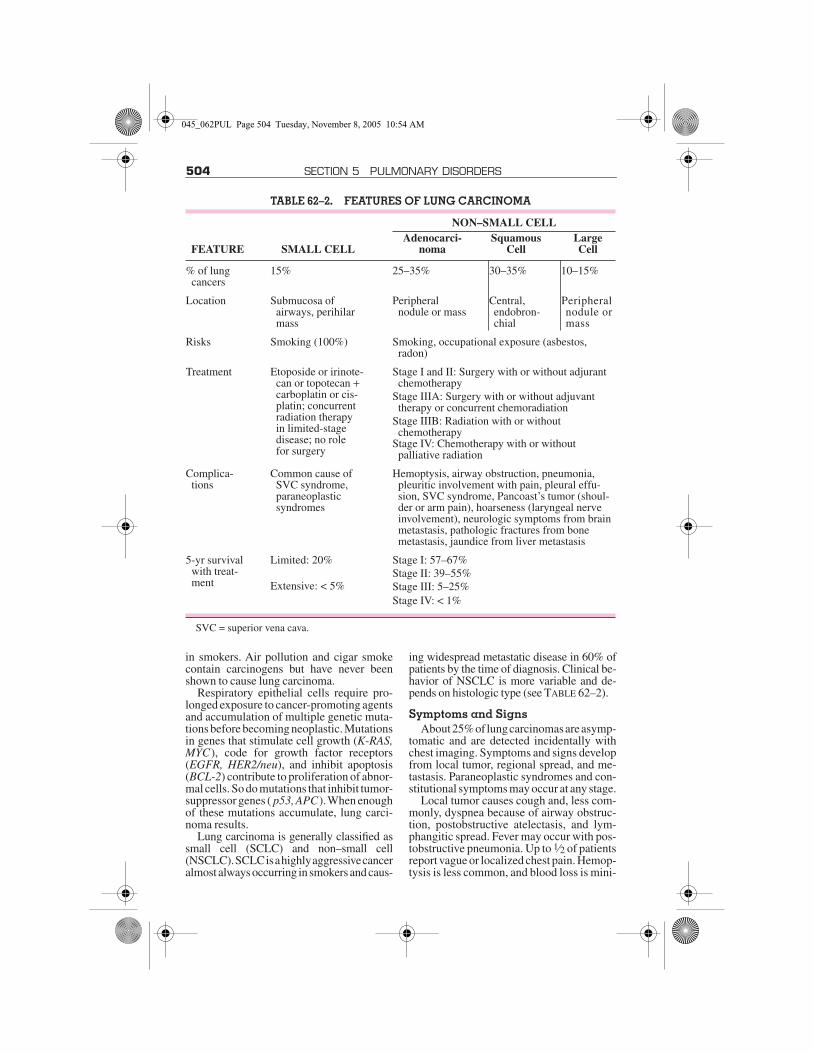
504 SECTION 5 PULMONARY DISORDERS
in smokers. Air pollution and cigar smokecontain carcinogens but have never beenshown to cause lung carcinoma.
Respiratory epithelial cells require pro-longed exposure to cancer-promoting agentsand accumulation of multiple genetic muta-tions before becoming neoplastic. Mutationsin genes that stimulate cell growth (K-RAS,MYC), code for growth factor receptors(EGFR, HER2/neu), and inhibit apoptosis(BCL-2) contribute to proliferation of abnor-mal cells. So do mutations that inhibit tumor-suppressor genes ( p53, APC). When enoughof these mutations accumulate, lung carci-noma results.
Lung carcinoma is generally classified assmall cell (SCLC) and non–small cell(NSCLC). SCLC is a highly aggressive canceralmost always occurring in smokers and caus-
ing widespread metastatic disease in 60% ofpatients by the time of diagnosis. Clinical be-havior of NSCLC is more variable and de-pends on histologic type (see TABLE 62–2).
Symptoms and SignsAbout 25% of lung carcinomas are asymp-
tomatic and are detected incidentally withchest imaging. Symptoms and signs developfrom local tumor, regional spread, and me-tastasis. Paraneoplastic syndromes and con-stitutional symptoms may occur at any stage.
Local tumor causes cough and, less com-monly, dyspnea because of airway obstruc-tion, postobstructive atelectasis, and lym-phangitic spread. Fever may occur with pos-tobstructive pneumonia. Up to 1⁄2 of patientsreport vague or localized chest pain. Hemop-tysis is less common, and blood loss is mini-
TABLE 62–2. FEATURES OF LUNG CARCINOMA
FEATURE SMALL CELL
NON–SMALL CELLAdenocarci-
nomaSquamous
CellLarge Cell
% of lung cancers
15% 25–35% 30–35% 10–15%
Location Submucosa ofairways, perihilar mass
Peripheralnodule or mass
Central, endobron-chial
Peripheral nodule or mass
Risks Smoking (100%) Smoking, occupational exposure (asbestos, radon)
Treatment Etoposide or irinote-can or topotecan + carboplatin or cis-platin; concurrent radiation therapyin limited-stagedisease; no rolefor surgery
Stage I and II: Surgery with or without adjurant chemotherapy
Stage IIIA: Surgery with or without adjuvant therapy or concurrent chemoradiation
Stage IIIB: Radiation with or withoutchemotherapy
Stage IV: Chemotherapy with or withoutpalliative radiation
Complica-tions
Common cause of SVC syndrome, paraneoplasticsyndromes
Hemoptysis, airway obstruction, pneumonia, pleuritic involvement with pain, pleural effu-sion, SVC syndrome, Pancoast’s tumor (shoul-der or arm pain), hoarseness (laryngeal nerve involvement), neurologic symptoms from brain metastasis, pathologic fractures from bone metastasis, jaundice from liver metastasis
5-yr survival with treat-ment
Limited: 20% Stage I: 57–67% Stage II: 39–55%
Extensive: < 5% Stage III: 5–25%Stage IV: < 1%
SVC = superior vena cava.
045_062PUL Page 504 Tuesday, November 8, 2005 10:54 AM

62 TUMORS OF THE LUNGS 505
mal, except in rare instances when tumorerodes a major artery, causing massive hem-orrhage and death by asphyxiation.
Regional spread may cause pleuritic chestpain or dyspnea from pleural effusion,hoarseness due to tumor encroachment on therecurrent laryngeal nerve, and dyspnea andhypoxia from diaphragmatic paralysis due toinvolvement of the phrenic nerve.
Compression or invasion of the superiorvena cava (SVC syndrome) can produceheadache or a sensation of head fullness, fa-cial or upper extremity swelling, and supinebreathlessness and flushing (plethora). Signsof SVC syndrome are facial and upper ex-tremity edema, dilated neck and subcutane-ous veins over the face and upper trunk, andfacial and truncal plethora. SVC syndrome ismore common in patients with SCLC.
Apical tumors, usually NSCLC, can invadethe brachial plexus, pleura, or ribs, causingshoulder and upper extremity pain and weak-ness or atrophy of the ipsilateral hand (Pan-coast's tumor). Horner's syndrome (ptosis,miosis, enophthalmos, and anhidrosis) resultswhen the paravertebral sympathetic chain orcervical stellate ganglion is involved. Spread oftumor to pericardium may be asymptomatic orlead to constrictive pericarditis or cardiactamponade (see p. 732). Rarely, esophagealcompression causes dysphagia.
Metastases always eventually causesymptoms that vary by location. Metastasesto the liver cause GI symptoms and ultimatelyhepatic insufficiency. Metastases to the braincause behavioral changes, confusion, apha-sia, seizures, paresis or paralysis, nausea andvomiting, and, ultimately, coma and death.Bone metastases cause severe pain andpathologic fractures. Lung carcinoma com-monly metastasizes to the adrenal glands butrarely leads to adrenal insufficiency.
Paraneoplastic syndromes are not causedby cancer directly (see p. 1150). Commonparaneoplastic syndromes in patients withlung carcinoma include hypercalcemia(caused by tumor production of parathyroidhormone-related protein), syndrome of inap-propriate antidiuretic hormone secretion(SIADH), finger clubbing with or without hy-pertrophic osteoarthropathy, hypercoagula-bility with migratory superficial throm-bophlebitis (Trousseau’s syndrome), myas-thenia (Eaton-Lambert syndrome), and avariety of neurologic syndromes, includingneuropathies, encephalopathies, encephalit-ides, myelopathies, and cerebellar disease.
Mechanisms for neuromuscular syndromesinvolve tumor expression of autoantigenswith production of autoantibodies, but thecause of most others is unknown.
Constitutional symptoms most commonlyinclude weight loss and fatigue and are some-times the first indication of underlying ma-lignancy.
DiagnosisChest x-ray is the initial test. It may show
clearly defined abnormalities, such as a singlemass or multifocal masses or a solitary pulmo-nary nodule (see p. 361), or more subtlechanges, such as an enlarged hilum, widenedmediastinum, tracheobronchial narrowing,atelectasis, nonresolving parenchymal infil-trate, cavitary lesion, or unexplained pleuralthickening or effusion. These findings are sug-gestive but not diagnostic of lung carcinomaand require follow-up with high-resolutionCT (HRCT) and cytopathologic confirmation.
CT demonstrates many characteristic pat-terns and appearances that may confirm thediagnosis. CT also can guide needle biopsy ofaccessible lesions and is useful for staging.
The method used to obtain cells or tissue forconfirmation depends on the accessibility of tis-sue and the location of suspect lesions. Sputumor pleural fluid cytology is the least invasivemethod. In patients with productive cough,sputum specimens obtained on awakeningmay contain high concentrations of malignantcells, but yield for this method is about 50%overall. Pleural fluid is another convenientsource of cells, but effusions accompany ≤ 1⁄3of all lung carcinomas; nevertheless, a malig-nant effusion immediately stages a cancer as atleast stage IIIB (see TABLE 62–3) and is a poorprognostic sign. In general, false-negative cy-tology readings can be minimized by obtainingas large a volume of sputum or fluid as possibleearly in the day and sending the sample to thepathology laboratory immediately to mini-mize delays in processing, which lead to cellbreakdown. Percutaneous biopsy is the nextleast invasive procedure. It is more useful formetastatic sites (supraclavicular or otherperipheral lymph nodes, pleura, liver, andadrenals) than for lung lesions because of a20 to 25% risk of pneumothorax and the riskof false-negative results unlikely to change theperceived need for treatment.
Bronchoscopy is the procedure most oftenused for diagnosing lung carcinoma. In the-ory, the procedure of choice for obtaining tis-sue is the one that is least invasive. In practice,
045_062PUL Page 505 Tuesday, November 8, 2005 10:54 AM
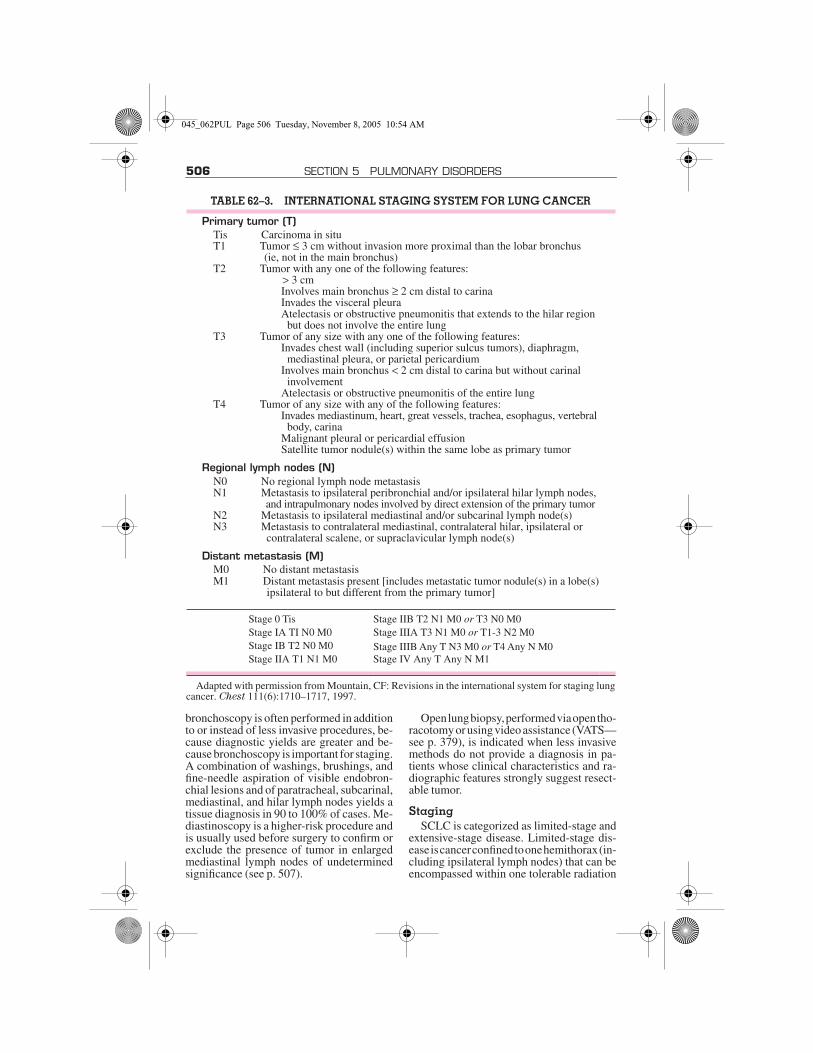
506 SECTION 5 PULMONARY DISORDERS
bronchoscopy is often performed in additionto or instead of less invasive procedures, be-cause diagnostic yields are greater and be-cause bronchoscopy is important for staging.A combination of washings, brushings, andfine-needle aspiration of visible endobron-chial lesions and of paratracheal, subcarinal,mediastinal, and hilar lymph nodes yields atissue diagnosis in 90 to 100% of cases. Me-diastinoscopy is a higher-risk procedure andis usually used before surgery to confirm orexclude the presence of tumor in enlargedmediastinal lymph nodes of undeterminedsignificance (see p. 507).
Open lung biopsy, performed via open tho-racotomy or using video assistance (VATS—see p. 379), is indicated when less invasivemethods do not provide a diagnosis in pa-tients whose clinical characteristics and ra-diographic features strongly suggest resect-able tumor.
StagingSCLC is categorized as limited-stage and
extensive-stage disease. Limited-stage dis-ease is cancer confined to one hemithorax (in-cluding ipsilateral lymph nodes) that can beencompassed within one tolerable radiation
TABLE 62–3. INTERNATIONAL STAGING SYSTEM FOR LUNG CANCER
Primary tumor (T)Tis Carcinoma in situT1 Tumor ≤ 3 cm without invasion more proximal than the lobar bronchus
(ie, not in the main bronchus)T2 Tumor with any one of the following features:
> 3 cmInvolves main bronchus ≥ 2 cm distal to carinaInvades the visceral pleuraAtelectasis or obstructive pneumonitis that extends to the hilar region
but does not involve the entire lungT3 Tumor of any size with any one of the following features:
Invades chest wall (including superior sulcus tumors), diaphragm, mediastinal pleura, or parietal pericardium
Involves main bronchus < 2 cm distal to carina but without carinal involvement
Atelectasis or obstructive pneumonitis of the entire lungT4 Tumor of any size with any of the following features:
Invades mediastinum, heart, great vessels, trachea, esophagus, vertebralbody, carina
Malignant pleural or pericardial effusionSatellite tumor nodule(s) within the same lobe as primary tumor
Regional lymph nodes (N)N0 No regional lymph node metastasisN1 Metastasis to ipsilateral peribronchial and/or ipsilateral hilar lymph nodes,
and intrapulmonary nodes involved by direct extension of the primary tumorN2 Metastasis to ipsilateral mediastinal and/or subcarinal lymph node(s)N3 Metastasis to contralateral mediastinal, contralateral hilar, ipsilateral or
contralateral scalene, or supraclavicular lymph node(s)
Distant metastasis (M)M0 No distant metastasisM1 Distant metastasis present [includes metastatic tumor nodule(s) in a lobe(s)
ipsilateral to but different from the primary tumor]
Stage 0 Tis Stage IIB T2 N1 M0 or T3 N0 M0Stage IA TI N0 M0 Stage IIIA T3 N1 M0 or T1-3 N2 M0Stage IB T2 N0 M0 Stage IIIB Any T N3 M0 or T4 Any N M0Stage IIA T1 N1 M0 Stage IV Any T Any N M1
Adapted with permission from Mountain, CF: Revisions in the international system for staging lungcancer. Chest 111(6):1710–1717, 1997.
045_062PUL Page 506 Tuesday, November 8, 2005 10:54 AM

62 TUMORS OF THE LUNGS 507
therapy port, excluding the presence of pleu-ral or pericardial effusion. Extensive-stagedisease is cancer outside a single hemithoraxand presence of malignant pleural or pericar-dial effusion. About 1⁄3 of patients with SCLChave limited-stage disease; the remainder of-ten have extensive distant metastases.
NSCLC staging involves determining tu-mor size, tumor and lymph node location, andthe presence or absence of distant metastases(see TABLES 62–2 and 62–3).
Thin-section CT from the neck to upper ab-domen (to detect cervical and supraclavicularand hepatic and adrenal metastases) is the firststaging test for both SCLC and NSCLC. How-ever, CT often cannot distinguish postinflam-matory from malignant intrathoracic lymphnode enlargement or benign from malignanthepatic or adrenal lesions (distinctions that de-termine stage). Thus, other tests are usuallyperformed when CT abnormalities are presentin these areas. PET scanning is an accurate,noninvasive test used to identify malignantmediastinal lymph nodes and other distant me-tastases (metabolic staging). Integrated PET-CT, in which PET and CT images are combinedinto a single image by scanners in a single gan-try, is more accurate for NSCLC staging thanCT or PET alone or than visual correlation ofthe two tests. The use of PET and PET-CT islimited by cost and availability. When a PETscan is unavailable, bronchoscopy and, lesscommonly, mediastinoscopy or video-as-sisted thoracoscopy can be used to biopsyquestionable mediastinal lymph nodes. With-out PET scanning, suspect hepatic or adrenallesions must be evaluated by needle biopsy.
MRI of the chest is slightly more accuratethan high-chest HRCT for staging apicaltumors and cancers close to the diaphragm.
Patients with headache or neurologic ab-normalities should undergo head CT or MRIand evaluation for SVC syndrome. Patientswith bone pain or elevated serum Ca or alka-line phosphatase should undergo a radionu-clide bone scan. These imaging tests are not in-dicated in the absence of suspicious symp-toms, signs, or laboratory test abnormalities.Other blood tests, such as CBC, serum albu-min, and creatinine, play no role in staging butprovide important prognostic informationabout the patient’s ability to tolerate treatment.
PrognosisPrognosis is poor, even with newer treat-
ments. On average, untreated patients withadvanced NSCLC survive 6 mo, whereas
5-yr survival for treated patients is about 9 mo.Patients with extensive-stage SCLC do espe-cially poorly, with a 5-yr survival rate < 1%.The median survival time for limited-stagedisease is 20 mo, with a 5-yr survival rate of20%. In many patients with SCLC, chemo-therapy prolongs life and improves quality oflife enough to warrant its use. The 5-yr sur-vival rate of patients with NSCLC varies bystage, from 60 to 70% for patients with stageI to virtually 0% for those with stage IV dis-ease; recent evidence suggests improved sur-vival in early-stage disease with a platinum-based chemotherapy regimen. Given the dis-appointing results in late-stage disease,efforts at reducing mortality have increas-ingly focused on early detection and activeinterventions to prevent disease.
A screening chest x-ray in high-risk pa-tients detects lung carcinomas at early stagesbut does not decrease mortality. A screeningCT is more sensitive for detecting tumors, butmore false-positive readings increase thenumber of unnecessary invasive diagnosticprocedures needed to verify CT findings. Suchprocedures are costly and risk complications.A strategy of yearly CT screening of smokerswith follow-up PET scan or HRCT to evaluateindeterminate lesions is being studied. So far,this strategy does not seem to lessen mortalityand cannot be recommended as routine prac-tice. The future of screening may lie in a com-bination of molecular analysis for geneticmarkers (such as K-RAS, p53, EGFR), sputumcytometry, and detection of cancer-relatedvolatile organic compounds (eg, alkane, ben-zene) in exhaled breath.
TreatmentTreatment generally involves assessment
of eligibility for surgery followed by choice ofsurgery, chemotherapy, and/or radiation as ap-propriate, depending on tumor type and stage.Many nontumor-related factors affect eligi-bility. Poor cardiopulmonary reserve; malnu-trition; frailty or poor physical performancestatus; comorbidities, including cytopenias;and psychiatric or cognitive illness all may leadto a decision for palliative over curative treat-ment or for no treatment at all, even though curemight technically be possible.
Surgery is performed only on patients whowill have adequate pulmonary reserve once alobe or lung is resected. Patients with preop-erative forced expiratory volume in 1 sec(FEV1) > 2 L generally tolerate pneumonec-tomy. Those with FEV1 < 2 L should undergo
045_062PUL Page 507 Tuesday, November 8, 2005 10:54 AM

508 SECTION 5 PULMONARY DISORDERS
a quantitative radionuclide perfusion scan todetermine the proportion of function the pa-tient can expect to lose from resection. Post-operative FEV1 can be predicted by multiply-ing percent perfusion of the nonresected lungby the preoperative FEV1. A predicted FEV1> 800 mL or > 40% of the predicted normalFEV1 suggests adequate postoperative lungfunction, though studies of lung volume re-duction surgery in COPD patients suggestthat patients with FEV1 < 800 mL can tolerateresection if the cancer is located in poorlyfunctional bullous (generally apical) lung re-gions. Patients undergoing resection at hos-pitals that perform more resections havefewer complications and are more likely tosurvive than those who undergo surgery atlow-volume hospitals.
Multiple chemotherapy regimens exist fortreatment of lung carcinoma; no one regimenis proven superior. Choice of regimen, there-fore, often depends on local practice, con-traindications, and toxicities. Treatment op-tions for disease that recurs after treatmentvary by location and include repeat chemo-therapy for local recurrence, radiation ther-apy for metastases, and brachytherapy for en-dobronchial disease when additional exter-nal radiation cannot be tolerated.
Radiation treatment carries the risk of ra-diation pneumonitis when large areas of lungare exposed to high doses of radiation overtime. Radiation pneumonitis can occur up to3 mo after treatment. Cough, dyspnea, low-grade fever, or pleuritic chest pain may signalthe condition, as may rales or pleural frictionrub. Chest x-rays may be nonspecific; CTsmay show nonspecific infiltration withoutdiscrete mass. The diagnosis is often one ofexclusion. Radiation pneumonitis is treatedwith 60 mg prednisone for 2 to 4 wk followedby a gradual taper.
Because many patients with lung carci-noma die, the need for end-of-life careshould be anticipated. Symptoms of breath-lessness, pain, anxiety, nausea, and anorexiaare especially common and can be treatedwith parenteral morphine; oral, transdermal,or parenteral opioids; and antiemetics (seep. 2764).
SCLC: SCLC of any stage is typically ini-tially responsive to treatment, but responsesare usually short-lived. Surgery generallyplays no role in treatment of SCLC, althoughit may be curative in the rare patient who hasa small focal tumor without spread (such asa solitary pulmonary nodule).
In limited-stage disease, a combination ofetoposide and a platinum compound (eithercisplatin or carboplatin) in 4 to 6 cycles isthought to be most effective, although combi-nations with other drugs—including vinca al-kaloids (vinblastine, vincristine, vinorelbine),alkylating drugs (cyclophosphamide, ifosfa-mide), doxorubicin, taxanes (docetaxel, pacli-taxel), and gemcitabine—are also commonlyused. Radiation further improves response; thevery definition of limited-stage disease as dis-ease confined to a hemithorax is based on thesignificant improvement in survival observedwith radiation. The use of cranial radiation toprevent brain metastases is advocated by someexperts; micrometastases are common inSCLC, and chemotherapy does not cross theblood-brain barrier.
In extensive-stage disease, treatment is thesame as with limited-stage disease but withoutconcurrent radiation. Replacing etoposidewith topoisomerase inhibitors (irinotecan ortopotecan) may improve survival. These drugsalone or in combination with other drugs arealso commonly used in refractory disease andin cancer of either stage that has recurred. Ra-diation is often used as palliative treatment formetastases to bone or brain.
In general, recurrent SCLC carries a poorprognosis, although patients who maintain agood performance status should be offered aclinical trial.
NSCLC: Treatment of NSCLC dependson the stage. For stage I and II disease, thestandard is surgical resection with eitherlobectomy or pneumonectomy combinedwith mediastinal lymph node sampling orcomplete dissection. Lesser resections, in-cluding segmentectomy and wedge resec-tion, are considered for patients with poorpulmonary reserve. Surgery is curative inabout 55 to 75% of patients with stage I andin 35 to 55% of patients with stage II disease.Adjuvant chemotherapy is probably helpfulin early-stage disease (stages Ib and II). An in-crease in 5-yr overall survival (69% vs 54%)and disease-free survival (61% vs 49%) oc-curs with cisplatin plus vinorelbine. Becausethe improvement is small, the decision foradjuvant chemotherapy should be made onan individual basis. The role of neoadjuvantchemotherapy in early-stage NSCLC is un-der investigation.
Stage III disease is one or more locally ad-vanced tumors with regional nodal involve-ment but no distant metastases. For stage IIIAtumors with occult mediastinal nodal me-
045_062PUL Page 508 Tuesday, November 8, 2005 10:54 AM
62 TUMORS OF THE LUNGS 509
tastases discovered at the time of surgery, re-section results in 20 to 25% 5-yr survival. Ra-diation therapy with or without concurrentchemotherapy is considered standard for un-resectable clinically staged IIIA disease, butsurvival is poor (median survival, 10 to 14mo). Recent trials suggest slightly better re-sults with preoperative chemotherapy plusradiation followed by surgery and subse-quent chemotherapy. This remains an area ofinvestigation.
Stage IIIB patients with contralateral me-diastinal nodal disease, supraclavicularnodal disease, or malignant pleural effusionsare offered radiation or chemotherapy orboth. The addition of radiation-sensitizingchemotherapeutic drugs, such as cisplatin,paclitaxel, vincristine, and cyclophospha-mide, improves survival slightly. Patientswith locally advanced tumors invading theheart, great vessels, mediastinum, or spineusually receive radiation. In select cases(T4N0M0 tumors), surgical resection witheither neoadjuvant or adjuvant chemoradia-tion may be feasible. The 5-yr survival rate fortreated stage IIIB patients is 5%.
In stage IV disease, palliation of symptomsis the goal. Chemotherapy and radiation maybe used to reduce tumor burden, treat symp-toms, and improve quality of life. However,median survival is only 9 mo; < 25% ofpatients survive 1 yr. Surgical palliative pro-cedures may be required and may includethoracentesis and pleurodesis of recurrenteffusions, placement of indwelling pleuraldrainage catheters, bronchoscopic fulgura-tion of tumors involving the trachea andmainstem bronchi, placement of stents to pre-vent airway occlusion, and, in some cases,spinal stabilization for impending spinal cordcompression.
Several novel biologic agents specificallytarget lung tumors. Gefitinib, an epidermalgrowth factor receptor (EGFR) tyrosine kinaseinhibitor, may be used in patients who have notresponded to platinum and docetaxel therapy.Other biologic agents under investigation in-clude other EGFR inhibitors, antisense oligo-nucleotides to EGFR mRNA (messengerRNA), and farnesyl transferase inhibitors.
It is important to distinguish between re-current NSCLC, an independent 2nd primarytumor, locally recurrent NSCLC, and distantmetastatic NSCLC. The treatment of an in-dependent 2nd primary tumor and locally re-current NSCLC follows the same guidelinesas for primary tumor stages I to III. If surgery
was used initially, radiation therapy is themain modality. If recurrence manifests as dis-tant metastases, patients are treated as stageIV with a focus on palliation.
Complications: Initial treatment of ma-lignant pleural effusion is with thoracentesis.Asymptomatic effusions require no treat-ment; symptomatic effusions that recur de-spite multiple thoracenteses are drainedthrough a chest tube. Infusion of talc (or occa-sionally, tetracycline or bleomycin) into thepleural space (a procedure called pleurodesis)scars the pleura, eliminates the pleural space,and is effective in > 90% of cases (see p. 495).
Treatment of SVC syndrome is the same astreatment of lung carcinoma: with chemo-therapy (SCLC), radiation therapy (NSCLC),or both (NSCLC). Corticosteroids are com-monly used but are of unproven benefit.Treatment of apical tumors is with surgerywith or without preoperative radiation or withradiation with or without adjuvant chemo-therapy. Treatment of paraneoplastic syn-dromes varies by syndrome (see p. 1150).
PreventionNo active interventions are proven effec-
tive except for smoking cessation. Remedia-tion of high radon levels in private residencesremoves known cancer-promoting radiation,but a reduction in lung cancer incidence is un-proven. Increasing dietary intake of fruits andvegetables high in retinoids and β-caroteneappears to have no effect on lung carcinomaincidence. Vitamin supplementation is eitherunproven (vitamin E) or harmful (β-caro-tene) in smokers. Preliminary evidence hint-ing that NSAIDs and vitamin E supplemen-tation may protect former smokers from lungcarcinoma requires confirmation. New mo-lecular approaches targeting cell signalingand cell cycle pathways and tumor-associ-ated antigens are under investigation.
AIRWAY TUMORSAirway tumors can arise from primary tra-cheobronchial tumors, adjacent primarytumors with airway invasion, or metastaticdisease to the airway.
Primary tracheal tumors are rare (0.1/100,000 people). They are often malignantand found at a locally advanced stage. Themost common malignant tracheal tumors in-clude adenoid cystic carcinoma, squamous
045_062PUL Page 509 Tuesday, November 8, 2005 10:54 AM

510 SECTION 5 PULMONARY DISORDERS
cell carcinoma, carcinoid, and mucoepider-moid carcinomas. The most common benignairway tumor is a squamous papilloma, al-though pleomorphic adenomas and granularcell and benign cartilaginous tumors alsooccur.
Symptoms, Signs, and DiagnosisPatients often present with dyspnea, cough,
wheezing, hemoptysis, and stridor. Hemop-tysis occurs with squamous cell carcinomaand can lead to earlier diagnosis, whereaswheezing or stridor occurs more often withthe adenoid cystic variant. Dysphagia andhoarseness can also be present initially andusually indicate advanced disease.
Symptoms of airway narrowing can heraldlife-threatening airway obstruction and re-quire immediate hospitalization and evalua-tion with bronchoscopy. Bronchoscopy canboth stabilize the airways and obtain speci-mens for diagnosis. If a malignancy is found,more extensive testing for metastases is done.
Prognosis and TreatmentPrognosis depends on the histology. Squa-
mous cell carcinomas tend to metastasize toregional lymph nodes and directly invade me-diastinal structures, leading to high local andregional recurrence rates. Even with definitivesurgical resection, the 5-yr survival is 20 to40%. Adenoid cystic carcinomas are typicallyindolent but tend to metastasize to the lungsand to spread perineurally, leading to high re-currence rates after resection. However, thesepatients have a higher 5-yr survival of 60 to75% because of the slow rate of growth.
Primary airway tumors should be treateddefinitively with surgical resection if possi-ble. Tracheal, laryngotracheal, or carinal re-sections are the most common procedures.Up to 50% of the length of the trachea can besafely resected with primary re-anastomosis.If a lung or thyroid cancer invades the airway,surgery is sometimes still feasible if assess-ment indicates sufficient tissue available forairway reconstruction. Adjuvant radiation isrecommended if adequate surgical marginscannot be obtained.
Most primary airway tumors are not resec-table because of metastasis, locally advancedstage, or patient comorbidities. In cases of en-doluminal tumors, a therapeutic bronchos-copy can mechanically core-out the tumor.Other techniques to eliminate obstruction in-clude laser vaporization, photodynamic ther-apy, cryotherapy, and endobronchial brachy-
therapy. Tumors that compress the tracheaare treated with airway stenting, radiother-apy, or both.
BRONCHIAL CARCINOIDBronchial carcinoids are rare, slow-growingneuroendocrine tumors arising from bron-chial mucosa that affect patients in their 40sto 60s.
Half of patients are asymptomatic, and 1⁄2present with symptoms of airway obstruc-tion, including dyspnea, wheezing, andcough, which often leads to a misdiagnosis ofasthma. Recurrent pneumonia, hemoptysis,and chest pain are also common. Paraneo-plastic syndromes, including Cushing’s syn-drome due to ectopic ACTH, acromegaly dueto ectopic growth hormone–releasing factor,and Zollinger-Ellison due to ectopic gastrinproduction, are more common than carcinoidsyndrome (see p. 1313), which occurs in < 3%of patients with the tumor. A left-sided heartmurmur (mitral stenosis or regurgitation) oc-curs rarely due to serotonin-induced valvulardamage (as opposed to the right-sided valvu-lar lesions of GI carcinoid).
Diagnosis is based on bronchoscopic bi-opsy, but evaluation often initially involveschest CT, which reveals tumor calcificationsin up to 1⁄3 of patients. Indium-111–labeledoctreotide scans are useful for determiningregional and metastatic spread. Increased uri-nary serotonin and 5-hydroxyindoleaceticacid levels support the diagnosis but are notcommonly present.
Treatment is with surgical removal with orwithout adjuvant chemotherapy. Prognosisdepends on tumor type. Five-year survival fortypical (well-differentiated) carcinoids is >90%; for atypical tumors, 50 to 70%.
CHEST WALL TUMORSPrimary chest wall tumors consist of 5%
of all thoracic tumors and 1 to 2% of all pri-mary tumors. Almost 1⁄2 are benign, the mostcommon of which are osteochondroma,chondroma, and fibrous dysplasia. A widerange of malignant chest wall tumors exist.Over 1⁄2 are metastases from distant organs ordirect invasions from adjacent structures(breast, lung, pleura, mediastinum). Themost common malignant primary tumors
045_062PUL Page 510 Tuesday, November 8, 2005 10:54 AM
62 TUMORS OF THE LUNGS 511
arising from the chest wall are sarcomas;about 45% originate from soft tissue and 55%from cartilaginous or bony tissue. Chondro-sarcomas are the most common primary bonechest wall sarcoma and arise in the anteriortract of ribs and less commonly from the ster-num, scapula, or clavicle. Other bony tumorsinclude osteosarcoma and small-cell malig-nant tumors (Ewing’s sarcoma, Askin’s tu-mor). The most common soft-tissue primarymalignant tumors are fibrosarcomas (des-moids, neurofibrosarcomas) and malignantfibrous histiocytomas. Other primary tumorsinclude chondroblastomas, osteoblastomas,melanomas, lymphomas, rhabdomyosarco-mas, lymphangiosarcomas, multiple my-eloma, and plasmacytomas.
Symptoms, Signs, and DiagnosisSoft-tissue chest wall tumors often present
as a localized mass without other symptoms;some patients have fever. Patients usually donot experience pain until the tumor is moreadvanced. In contrast, primary cartilaginousand bone tumors are often painful.
Patients with chest wall tumors requirechest x-ray, CT, and sometimes an MRI todetermine the original site and extent of thetumor and whether it is a primary chest wall
tumor or a metastasis. Biopsy confirms thediagnosis.
Prognosis and TreatmentPrognosis varies by cell type and stage;
firm conclusions are limited by the low inci-dence of any given tumor. Sarcomas havebeen the most well studied, and primary chestwall sarcomas have a reported 5-yr survivalof 16.7%. Survival is better with early-stagedisease.
Most chest wall tumors are treated withsurgical resection and reconstruction as theprimary modality. Reconstruction often uti-lizes a combination of myocutaneous flapsand prosthetic materials. The presence of amalignant pleural effusion is a contraindica-tion for surgical resection. Also, in cases ofmultiple myeloma or isolated plasmacy-toma, chemotherapy and radiation should bethe primary therapy. Small-cell malignant tu-mors such as Ewing’s sarcoma and Askin’stumor should be treated with a multimodalityapproach combining chemotherapy, radia-tion, and surgery. In cases of chest wall me-tastasis from distant tumors, a palliativechest wall resection is recommended onlywhen nonsurgical options do not alleviatesymptoms.
045_062PUL Page 511 Tuesday, November 8, 2005 10:54 AM
Related Documents











