Amanda Paton Parkerville Children and Youth Care Mental Health and Complex Trauma

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Amanda Paton
Parkerville Children and Youth Care
Mental Health and Complex
Trauma

Providing specialist therapeutic services to children, young people and their families who have been effected
by trauma and abuse.

Client Background
• Complex family histories ▫ Intergenerational abuse
• Multiple abuse experiences • Chronic rather than acute episodes • Multiple perpetrators • System abuse
▫ Placement breakdowns
• Early onset abuse • Disrupted attachment

Complex Trauma
• Exposure to multiple or prolonged traumatic events • Impacts development • Simultaneous or sequential occurrence of child
maltreatment ▫ psychological maltreatment ▫ neglect ▫ physical abuse ▫ sexual abuse ▫ domestic violence
• Chronic, begins in early childhood, and occurs within primary care giving relationship

Symptoms • Physiological hyper-arousal • Emotional numbing • Hyperactivity • Dysphoria • Dissociation • Distractibility and attention problems • Impulsivity • Increased startle response • Social avoidance • Poor school achievement • Sleep problems • Aggressive play/ interactions with peers • General regressed/ delayed development

PTSD
• Children exposed to trauma have higher rates than general population – 15-90%
• Ackerman ▫ 34% met criteria ▫ Over 50% of children exp SA and PA met criteria ▫ Majority met diagnostic criteria for three or more Axis
I diagnoses in addition to PTSD
• The younger a child the more likely they are to develop trauma-related symptoms
• % of children developing PTSD following a traumatic event is sign. higher than % of adults

Common Misdiagnosis
• Hyperactivity, Impulsivity and inattention – ADHD
• Cognitive profile with low verbal and average performance – Learning Disability
• Poor emotional expression and response to emotional cues – Autism Spectrum Disorder
• Behavioural problems – ODD, CD
Mental Health
• One’s ability to enjoy life, and create a balance
• Psychological resilience
• Expression of emotions
• Adaptation
• Well being
• Cope with ‘normal’ stresses of life
• Aware of ones own abilities

Poor Mental Health
• Axis I: Clinical Syndromes
▫ e.g. Depression, Schizophrenia, Anxiety
• Axis II: Developmental Disorders and Personality Disorders
▫ DD – e.g. Autism PDD and others first evident in childhood
▫ PD – e.g. Paranoid, Antisocial, and Borderline Personality Disorders.
Complex Trauma
Child and carer factors
General Poor MH and risk
Diagnosis & misdiagnosis
Symptoms
Child
Physical
Medical
Trauma Experience
Social;
Cognitive
Education
Emotional
Behavioural
11

Our assessments
are about
putting the
pieces of the
puzzle together
and working out
how the child’s
behaviours fit
with their
experience of
their world
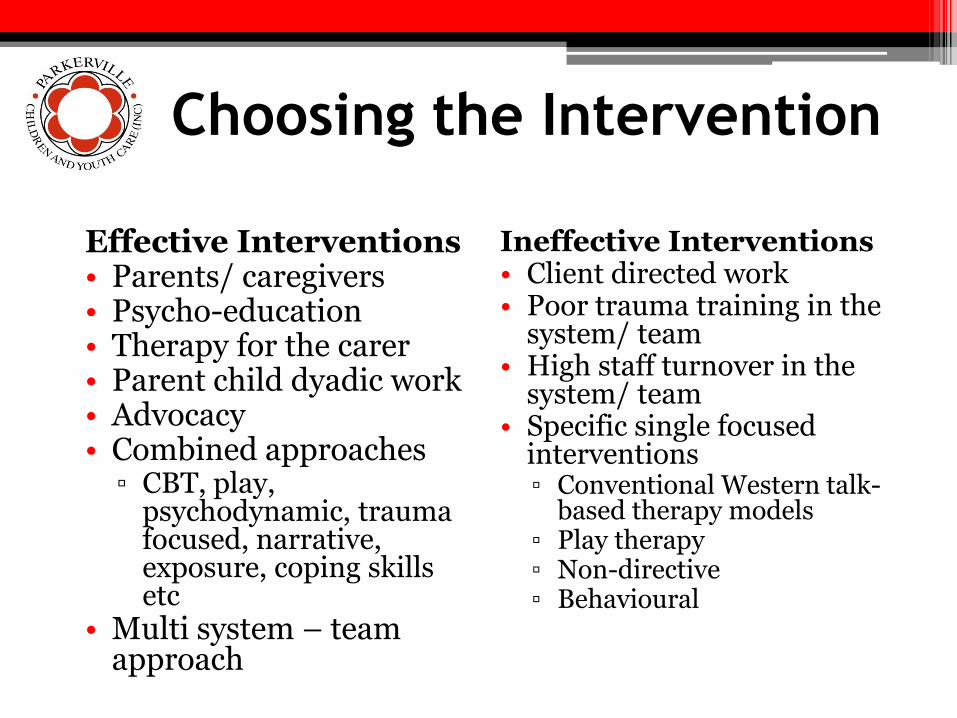
Choosing the Intervention
Ineffective Interventions • Client directed work • Poor trauma training in the
system/ team • High staff turnover in the
system/ team • Specific single focused
interventions ▫ Conventional Western talk-
based therapy models ▫ Play therapy ▫ Non-directive ▫ Behavioural
Effective Interventions • Parents/ caregivers • Psycho-education • Therapy for the carer • Parent child dyadic work • Advocacy • Combined approaches
▫ CBT, play, psychodynamic, trauma focused, narrative, exposure, coping skills etc
• Multi system – team approach

Brain Region Age of greatest
developmental activity
Age of functional
maturity
Key functions
Neocortex Childhood Adult Reasoning
Problem solving
Abstraction
Spatial reasoning
Limbic Early Childhood Puberty Memory
Attachment
Affect regulation
Primary Sensory Integration
Diencephalon Infancy Childhood Motor Control
Balance
Brainstem In utero Infancy Core physiological state regulation
e.g. Heart rate, temperature,
breathing, blood pressure and
sucking reflex
Adapted from ‘Shifting Developmental Activity across Brain Regions; Bruce Perry 2007
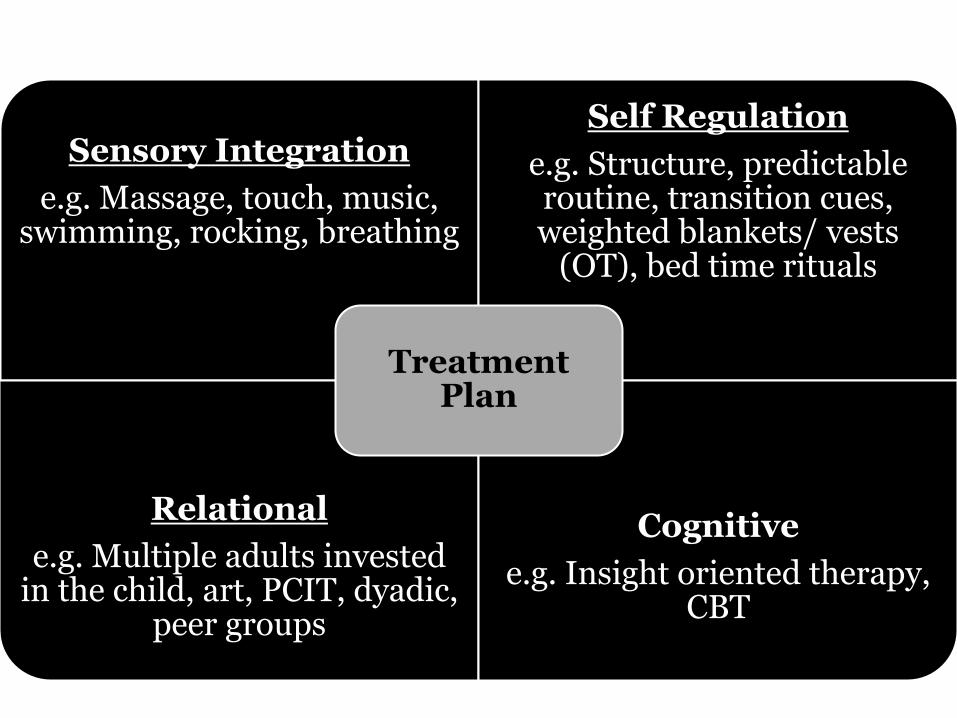
Sensory Integration
e.g. Massage, touch, music, swimming, rocking, breathing
Self Regulation
e.g. Structure, predictable routine, transition cues, weighted blankets/ vests
(OT), bed time rituals
Relational
e.g. Multiple adults invested in the child, art, PCIT, dyadic,
peer groups
Cognitive
e.g. Insight oriented therapy, CBT
Treatment Plan

Laura
• Hx neglect, DV, SA
• Multiple perp
• Chronic abuse
• Parental care of siblings
• No food in house, frequent carer absence, hyper vigilant
• Poor school attendance, poor supervision
• Apprehended at 6 years
• Failed reunification attempts
• Multiple placements
• Poor family contact
• Long term placement
▫ Further SA and carer rejection
• Sibling group separated
• Long term placement – one on one care

Presentation
• Nightmares • Frequent flashbacks • Highly dis-regulated • General affect regulation difficulties • Dysphoria • Visual hallucinations • Self harm, suicidal ideation and attempt • Paranoia • Violence towards carer • Poor attention, diff at school • Peer difficulties • Fluctuating developmental presentation • Poor memory

• Diagnosis
▫ Complex PTSD, GAD, Dep, Disorganised Attachment
• Multiple hospital admissions
• Psychiatric treatment
• Medications
▫ Mood stabilisers
▫ Tranquilisers
▫ Respiratory depressant
▫ Anti depressants
▫ Anti anxiety

1
Sensory Integration
Controlled timed breathing, gentle massage by carer, touch/ hugs, rocking, nails and hair, music
Self Regulation
Highly structured and predictable environment, all changes heavily
planned in advance, verbal prompts and reminders for change/
transition, highly routine bedtime, swings, emotional prompts/ cues
Relational
Psych for six yrs, carer 4 yrs, respite 2 years, CM, 4 years, dyadic
sessions with carer, parallel play with carer, peer interactions – one on one and small groups, siblings
facilitated contact
Cognitive
CBT, trauma narrative, exposure, life story
Laura

Intervention/ Progress
• Therapy responsive to child and carer needs • Care Team approach across agencies and disciplines • Trauma informed practice • Planned co-ordinated response • Long term placement for 4 years • Emotional growth – hampered by puberty and family
factors (uncontrollable in treatment) • Dev insight into hx and current fx • Dev ability to co regulate and in certain times, self
regulate • Returned to extended family • Maintained relationship with long term carer • Avoided the ‘system’
Some helpful References
• Haddad & Garralda. 1992 • Perry, Pollard, Blakley, Baker, & Vigilante. 1995 • Perry, Pollard, Baker, Sturges, Vigilante, & Blakley.
1995; Perry. 1994; Perry. 2000 • Kaufman. 1991; Ornitz & Pynoos. 1989; Perry. 2000 • Ackerman, Newton, McPHerson, Jones, & Dykman.
1998 • Pfefferbaum. 1997 • Joseph Spinazzola, Ph.D., Julian Ford, Ph.D., Bessel
van der Kolk, M.D., Margaret Blaustein, Ph.D., Melissa Brymer, Psy.D., Laura Gardner, BsPH, Susan Silva, Ph.D., Stephanie Smith, Ph.D.
Related Documents











