P.O. Box 1039 Appleton, WI 54912-1039 Starting Your Mail Order and Specialty Prescription Service S9701_2022_UCA_NEW_MAIL_V01_C Dear University of California Retiree, Navitus MedicareRx (PDP) would like to inform you of some changes to your Medicare prescription drug coverage effective 1/1/2022. This will affect you if you get your medications through mail order or if you take specialty medications. Starting 1/1/2022, your mail order prescriptions will be available through your recommended pharmacy, Costco Mail Order. Also, Lumicera Specialty Pharmacy will be your recommended specialty pharmacies. The Select UC Pharmacies are still available in your network. On the following pages you will learn how to fill medications at your preferred mail order pharmacy or specialty pharmacy and ways to contact them. It is important to provide your new Navitus MedicareRx ID Card information to your pharmacies. Please refer to the following pages for help. Please note: • Medicare guidelines require that members initiate any prescription mail order or specialty prescription refill transfers. If you take prescription medications, you can help ensure a smooth transition to your new plan by having an adequate supply of your medication on hand prior to December 31, 2021. Important: Please dispose of your old card(s) as these will no longer be active as of 1/1/2022. If you try to fill a prescription using your old prescription ID card, the pharmacy may say that your prescription coverage has ended. Before filling a new prescription and/or refilling a current prescription, please provide your new Navitus MedicareRx ID card information to your pharmacy to avoid any delay. If you are not sure where to start, please call Navitus MedicareRx Customer Care at 1-866-270-3877 (TTY 711). Someone is always there to take your call every day except on Thanksgiving and Christmas Day.

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

P.O. Box 1039
Appleton, WI 54912-1039
Starting Your Mail Order and Specialty Prescription Service
S9701_2022_UCA_NEW_MAIL_V01_C
Dear University of California Retiree, Navitus MedicareRx (PDP) would like to inform you of some changes to your Medicare prescription drug coverage effective 1/1/2022. This will affect you if you get your medications through mail order or if you take specialty medications. Starting 1/1/2022, your mail order prescriptions will be available through your recommended pharmacy, Costco Mail Order. Also, Lumicera Specialty Pharmacy will be your recommended specialty pharmacies. The Select UC Pharmacies are still available in your network. On the following pages you will learn how to fill medications at your preferred mail order pharmacy or specialty pharmacy and ways to contact them. It is important to provide your new Navitus MedicareRx ID Card information to your pharmacies. Please refer to the following pages for help. Please note:
• Medicare guidelines require that members initiate any prescription mail order or specialty prescription refill transfers.
If you take prescription medications, you can help ensure a smooth transition to your new plan by having an adequate supply of your medication on hand prior to December 31, 2021. Important: Please dispose of your old card(s) as these will no longer be active as of 1/1/2022. If you try to fill a prescription using your old prescription ID card, the pharmacy may say that your prescription coverage has ended. Before filling a new prescription and/or refilling a current prescription, please provide your new Navitus MedicareRx ID card information to your pharmacy to avoid any delay. If you are not sure where to start, please call Navitus MedicareRx Customer Care at 1-866-270-3877 (TTY 711). Someone is always there to take your call every day except on Thanksgiving and Christmas Day.

Costco Mail Order Pharmacy
You can use any network mail order pharmacy you want; however, Costco Mail Order Pharmacy is the recommended mail order pharmacy and serves members nationwide. You do not need to be a member of Costco warehouse/club stores to utilize Costco mail order services. Both Costco mail order and retail locations are unable to fill Medicare Part B products - for example, diabetic testing strips. Costco can refer you to an affiliated provider that can fill these supplies or you can locate a participating retail pharmacy that can process Part B products. How do I register with Costco mail order? You will receive a new Navitus MedicareRx ID card in the mail from Navitus MedicareRx with updated prescription information. Since your Medicare Part D prescription drug benefits will be through Navitus MedicareRx as of 1/1/2022, please call and register your Costco patient profile information (Rx Member ID, BIN, PCN, and RxGroup). You can do so by calling Costco at 1-800-607-6861, or by going to www.pharmacy.costco.com. Registering with Costco.com allows you to manage your prescriptions online. How do I start a new prescription? You can mail original prescriptions to Costco Mail Order Pharmacy to start this service. It is important to allow at least 14 days before you will need your medications. Please include the following information with your prescriptions (no form required). Costco may need to contact you for additional information.
• Your Name Please send to: • Date of Birth Costco Mail Order Pharmacy • Phone Number 215 Deininger Circle • Shipping Address Corona, CA 92880
What if I already use Costco Mail Order Pharmacy? Will my mail order prescriptions automatically transfer? If you currently have a prescription on file with Costco, you can call Costco at 1-800-607-6861 to determine if a new prescription is necessary on or after 1/1/2022. You will need to provide Costco with your new Navitus MedicareRx ID card information. How can my physician reach Costco Mail Order Pharmacy or provide my prescriptions? You can also ask your provider to send the prescriptions directly to Costco Pharmacy. New prescriptions or order clarifications can be provided to Costco by your prescriber, using one of the following ways:
• Fax: 1-888-545-4615 • Call Costco’s Physician Line: 1-800-607-6861, option #3 • E-Prescribe: NCPDP# Corona: #5633753
S9701_2022_UCA_NEW_MAIL_V01_C
Costco calls you when new prescriptions are received and within 14 days of the date your prescriptions are eligible for refill. You may view your prescription order status and tracking information by logging onto www.pharmacy.costco.com. For questions about home delivery, call Costco at 1-800-607-6861. Their pharmacy agents are available Monday–Friday from 5:00 a.m. to 7:00 p.m. PST, and Saturday from 9:30 a.m. to 2:00 p.m. PST.
Lumicera Specialty Pharmacy
What should I do if I take a medication considered a specialty medication? You can use any specialty pharmacy you want; however, Lumicera Specialty Pharmacy is the recommended pharmacy for specialty medications. These medications usually:
• Have a high manufacturer cost. • Are hard to get locally. • Treat rare and complicated conditions. Examples of conditions include Rheumatoid
Arthritis, Hepatitis C, and Cancer. Note: If you decide to stay with your current specialty pharmacy and it is contracted with the pharmacy network, please call them and provide your new Navitus MedicareRx ID card information by 1/1/2022. The Select UC Pharmacies are still available in your network. Will my prescriptions automatically transfer to this new program? Lumicera will assist you with the transfer of your specialty prescription. If you are already on a specialty medication, you can call Lumicera’s Customer Care at 1-855-847-3553 (TTY 711), Monday through Thursday 6:00 a.m. to 5:00 p.m. and Friday from 6:00 a.m. to 4:00 p.m. PST, to set up an account and provide your new Navitus MedicareRx ID card information. It is important to call at least 14 days before you need your specialty mediation refill. Your prescriber can call Lumicera at 1-855-847-3554, or they can fax a prescription to 1-855-847-3558. What if I am not sure where to start or have questions about benefits or copays? You can get the answers you need by calling Navitus MedicareRx Customer Care at 1-866-270-3877 (TTY 711) 24 hours a day, 7 days a week, except on Thanksgiving and Christmas Day. Calls to these numbers are free. You can also visit our website at https://Memberportal.navitus.com for more information. Sincerely, The University of California and Navitus MedicareRx (PDP)
S9701_2022_UCA_FORM_Comp_V01.8_C This formulary was updated on 10/28/2021
Navitus MedicareRx (PDP) NAVITUS MEDICARERX (PDP) 2022 FORMULARY LIST OF COVERED DRUGS UNIVERSITY OF CALIFORNIA
PLEASE READ: THIS DOCUMENT CONTAINS INFORMATION ABOUT THE DRUGS WE COVER IN THIS PLAN
HPMS Approved Formulary File Submission ID 00022105, Version Number 8
This formulary was updated on 10/28/2021. For more recent information or other questions, please contact Navitus MedicareRx Customer Care at 1-866-270-3877 (for TTY users, please call 711), available 24 hours a day, 7 days a week (except on Thanksgiving and Christmas Day) or visit the member portal at https://memberportal.navitus.com.

1
When this formulary refers to “we,” “us”, “our”, “plan” or “our plan”, it means Navitus MedicareRx Prescription Drug Plan (PDP).
This document includes a list of the drugs (formulary) for our plan which is current as of 10/28/2021. For an updated formulary, please contact us. Our contact information, along with the date we last updated the formulary, appears on the front and back cover pages.
You must generally use network pharmacies to use your prescription drug benefit. Benefits, formulary, pharmacy network, and/or copayments/coinsurance may change on January 1, 2023, and from time to time during the year.
What is the Navitus MedicareRx (PDP) Formulary? A formulary is a list of covered drugs selected by Navitus MedicareRx in consultation with a team of health care providers, which represents the prescription therapies believed to be a necessary part of a quality treatment program. Navitus MedicareRx will generally cover the drugs listed in our formulary as long as the drug is medically necessary, the prescription is filled at a Navitus MedicareRx network pharmacy, and other plan rules are followed. For more information on how to fill your prescriptions, please review your Evidence of Coverage.
Can the Formulary (drug list) change? Most changes in drug coverage happen on January 1, but we may add or remove drugs on the Formulary during the year, move them to different cost-sharing tiers, or add new restrictions. We must follow the Medicare rules in making these changes.
Changes that can affect you this year: In the below cases, you will be affected by coverage changes during the year:
• New generic drugs. We may immediately remove a brand name drug on our Formulary if weare replacing it with a new generic drug that will appear on the same or lower cost sharing tierand with the same or fewer restrictions. Also, when adding the new generic drug, we maydecide to keep the brand name drug on our Formulary, but immediately move it to a differentcost-sharing tier or add new restrictions. If you are currently taking that brand name drug, wemay not tell you in advance before we make that change, but we will later provide you withinformation about the specific change(s) we have made.
o If we make such a change, you or your prescriber can ask us to make an exception andcontinue to cover the brand name drug for you. The notice we provide you will alsoinclude information on how to request an exception, and you can find information inthe section below titled “How do I request an exception to the Navitus MedicareRxFormulary?”

2
• Drugs removed from the market. If the Food and Drug Administration (FDA) deems a drugon our formulary to be unsafe or the drug’s manufacturer removes the drug from the market,we will immediately remove the drug from our formulary and provide notice to members whotake the drug.
• Other changes. We may make other changes that affect members currently taking a drug. Forinstance, we may add a generic drug that is not new to market to replace a brand name drugcurrently on the formulary; or add new restrictions to the brand name drug or move it to adifferent cost sharing tier or both. Or we may make changes based on new clinical guidelines.If we remove drugs from our formulary, add prior authorization, quantity limits and/or steptherapy restrictions on a drug or move a drug to a higher cost-sharing tier, we must notifyaffected members of the change at least 30 days before the change becomes effective, or atthe time the member requests a refill of the drug, at which time the member will receive a30-day supply of the drug.
o If we make these other changes, you or your prescriber can ask us to make anexception and continue to cover the brand name drug for you. The notice we provideyou will also include information on how to request an exception, and you can also findinformation in the section below entitled “How do I request an exception to the NavitusMedicareRx Formulary?”
Changes that will not affect you if you are currently taking the drug. Generally, if you are taking a drug on our 2022 formulary that was covered at the beginning of the year, we will not discontinue or reduce coverage of the drug during the 2022 coverage year except as described above. This means these drugs will remain available at the same cost sharing and with no new restrictions for those members taking them for the remainder of the coverage year. You will not get direct notice this year about changes that do not affect you. However, on January 1 of the next year, such changes would affect you, and it is important to check the Formulary for the new benefit year for any changes to drugs.
The enclosed formulary is current as of 10/28/2021. The formulary is updated each month and is available on the Member Portal at https://memberportal.navitus.com. We update our online formulary on a regularly scheduled basis to include any changes that have occurred after the last update. When changes to the formulary occur during the year, we post the formulary on our Member Portal including those changes. In the event of CMS-approved non-maintenance changes to the formulary throughout the plan year, Navitus MedicareRx will notify you. To get updated information about the drugs covered by Navitus MedicareRx please contact us. Our contact information appears on the front and back cover pages.
How do I use the Formulary? There are two ways to find your drug within the formulary:

3
Medical Condition The formulary begins on page 9. The drugs in this formulary are grouped into categories depending on the type of medical conditions that they are used to treat. For example, drugs used to treat a heart condition are listed under the category, “Cardiovascular Agents”. If you know what your drug is used for, look for the category name in the list that begins on page 9. Then look under the category name for your drug.
Alphabetical Listing If you are not sure what category to look under, you should look for your drug in the Index that begins on page 113. The Index provides an alphabetical list of all of the drugs included in this document. Both brand name drugs and generic drugs are listed in the Index. Look in the Index and find your drug. Next to your drug, you will see the page number where you can find coverage information. Turn to the page listed in the Index and find the name of your drug in the first column of the list.
What are generic drugs? Navitus MedicareRx covers both brand name drugs and generic drugs. A generic drug is approved by the FDA as having the same active ingredient as the brand name drug. Generally, generic drugs cost less than brand name drugs.
Are there any restrictions on my coverage? Some covered drugs may have additional requirements or limits on coverage. These requirements and limits may include:
• Prior Authorization: Navitus MedicareRx requires you or your physician to get priorauthorization for certain drugs. This means that you will need to get approval from NavitusMedicareRx before you fill your prescriptions. If you do not get approval, Navitus MedicareRxmay not cover the drug.
• Quantity Limits: For certain drugs, Navitus MedicareRx limits the amount of the drug thatNavitus MedicareRx will cover. For example, Navitus MedicareRx provides 18 tablets perprescription for Imitrex. This may be in addition to a standard one-month or three-monthsupply.
• Step Therapy: In some cases, Navitus MedicareRx requires you to first try certain drugs totreat your medical condition before we will cover another drug for that condition. Forexample, if Drug A and Drug B both treat your medical condition, Navitus MedicareRx maynot cover Drug B unless you try Drug A first. If Drug A does not work for you, NavitusMedicareRx will then cover Drug B.
4
You can find out if your drug has any additional requirements or limits by looking in the formulary that begins on page 9. You can also get more information about the restrictions applied to specific covered drugs by visiting the Member Portal. We have posted online documents that explain our prior authorization and step therapy restrictions. You may also ask us to send you a copy. Our contact information, along with the date we last updated the formulary, appears on the front and back cover pages. You can ask Navitus MedicareRx to make an exception to these restrictions or limits or for a list of other, similar drugs that may treat your health condition. See the section, “How do I request an exception to the Navitus MedicareRx formulary?” for information about how to request an exception.
Cost Sharing – Brand vs. Generic Drugs The Formulary indicates what you will pay for your drug. A generic drug is the same as a brand-name drug in dosage, safety and strength. If you and/or your prescriber specifies that a brand name drug must be dispensed and there is a lower tier generic equivalent available on the formulary, you must pay the applicable brand copay plus the difference between the cost of the brand-name drug and the generic equivalent. With prior authorization, exceptions for medical necessity can be made and you will pay the Tier 3 (non-preferred) copay. This Dispense as Written (DAW) cost-sharing penalty will not exceed the cost of the medication.
What are over-the-counter (OTC) drugs? OTC drugs are non-prescription drugs that are not normally covered by a Medicare Prescription Drug Plan. Navitus MedicareRx pays for certain OTC drugs. The covered OTC drugs are listed on your Formulary. Navitus MedicareRx will provide these OTC drugs at no cost to you. The cost to Navitus MedicareRx of these OTC drugs will not count toward your total Part D drug costs (that is, the cost of the OTC drugs does not count for the coverage gap). Your plan also covers certain prescribed Cough and Cold, or Vitamin and Mineral medications. The Formulary indicates what tier applies to these drugs.
What if my drug is not on the Formulary? If your drug is not included in this formulary (list of covered drugs), you should first contact Customer Care and ask if your drug is covered. If you learn that Navitus MedicareRx does not cover your drug, you have two options:
• You can ask Customer Care for a list of similar drugs that are covered by Navitus MedicareRx. When you receive the list, show it to your doctor and ask him or her to prescribe a similar drug that is covered by Navitus MedicareRx.

5
• You can ask Navitus MedicareRx to make an exception and cover your drug. See below for information about how to request an exception.
How do I request an exception to the Navitus MedicareRx (PDP) Formulary? You can ask Navitus MedicareRx to make an exception to our coverage rules. There are several types of exceptions that you can ask us to make.
• You can ask us to cover a drug even if it is not on our formulary. If approved, this drug will be covered at a pre-determined cost-sharing level, and you would not be able to ask us to provide the drug at a lower cost-sharing level.
• You can ask us to cover a formulary drug at lower cost-sharing level, unless the drug is on the specialty tier. If approved, this would lower the amount you must pay for your drug.
• You can ask us to waive coverage restrictions or limits on your drug. For example, for certain drugs, Navitus MedicareRx limits the amount of the drug that we will cover. If your drug has a quantity limit, you can ask us to waive the limit and cover a greater amount.
Generally, Navitus MedicareRx will only approve your request for an exception if the alternative drugs included on the plan’s formulary, the lower cost-sharing drug, or additional utilization restrictions would not be as effective in treating your condition and/or would cause you to have adverse medical effects. You should contact us to ask us for an initial coverage decision for a formulary, tier, or utilization restriction exception. When you request a formulary, tier, or utilization restriction exception you should submit a statement from your prescriber or physician supporting your request. Generally, we must make our decision within 72 hours of getting your prescriber’s supporting statement. You can request an expedited (fast) exception if you or your doctor believe that your health could be seriously harmed by waiting up to 72 hours for a decision. If your request to expedite is granted, we must give you a decision no later than 24 hours after we get a supporting statement from your doctor or other prescriber.
What do I do before I can talk to my doctor about changing my drugs or requesting an exception? As a new or continuing member in our plan you may be taking drugs that are not on our formulary. Or, you may be taking a drug that is on our formulary but your ability to get it is limited. For example, you may need a prior authorization from us before you can fill your prescription. You should talk to your doctor to decide if you should switch to an appropriate drug that we cover or request a formulary exception so that we will cover the drug you take. While you talk to your doctor to
6
determine the right course of action for you, we may cover your drug in certain cases during the first 90 days you are a member of our plan. For each of your drugs that is not on our formulary or if your ability to get your drugs is limited, we will cover a temporary 30-day supply. If your prescription is written for fewer days, we’ll allow refills to provide up to a maximum 30-day supply of medication. After your first 30-day supply, we will not pay for these drugs, even if you have been a member of the plan less than 90 days. If you are a resident of a long-term care facility and you need a drug that is not on our formulary or if your ability to get your drugs is limited, but you are past the first 90 days of membership in our plan, we will cover a 31-day emergency supply of that drug while you pursue a formulary exception.
Level of Care Changes Navitus MedicareRx’s level of care transition process accounts for unplanned changes for members. In some instances, these changes may result in the prescribed drug regimen(s) not being available on our formulary. These instances usually occur when a member moves from one treatment setting to another. This could include members who:
• Enter long-term care (LTC) facilities with a discharge list of medications from the hospital with very short-term planning taken into account (e.g., less than 8 hours).
• Are discharged from a hospital to a home with very short-term planning taken into account. • End their skilled nursing facility Medicare Part A stay (where payments include all pharmacy
charges) and who need to go back to their Part D plan formulary. • Give up hospice status to revert to standard Medicare Part A and Part B benefits. • End an LTC facility stay and return to their home. • Are discharged from psychiatric hospitals with drug regimens that are highly tailored to them.
These changes often result in members and/or prescribers using Navitus’ exceptions and/or appeals processes. For these types of changes, we will make coverage determinations and re-determinations as quickly as the member’s health requires. Navitus MedicareRx ensures proper medication continuance for members upon discharge from an LTC facility or other facilities to ensure an effective transition of care. This may include:
• A refill upon entrance to, or discharge from, an LTC facility. The current standard of care promotes caregivers receiving outpatient Part D prescriptions before discharge from a Part A stay. Members, through no fault of their own, may not have access to the balance of their prescription.
• Navitus MedicareRx allows the member to access a refill upon entrance to, or discharge from, an LTC facility.

7
To process these transition refills, the pharmacy may need to call Navitus MedicareRx Customer Care (phone numbers are on the back cover of this booklet). Navitus MedicareRx Customer Care can help the pharmacy process an override.
For more information For more detailed information about your Navitus MedicareRx prescription drug coverage, please review your Evidence of Coverage and other plan materials.
If you have questions about Navitus MedicareRx, please contact us. Our contact information, along with the date we last updated the formulary, appears on the front and back cover pages. If you have general questions about Medicare prescription drug coverage, please call Medicare at 1-800-MEDICARE (1-800-633-4227) 24 hours a day/7 days a week. TTY users should call 1-877-486-2048. Or, visit www.medicare.gov.
Navitus MedicareRx (PDP) Formulary The formulary below provides coverage information about the drugs covered by Navitus MedicareRx.
If you have trouble finding your drug in the list, turn to the Index that begins on page 113.
The first column of the chart lists the drug name.
• Brand name drugs are capitalized (e.g., LIPITOR)• Generic drugs are listed in lower-case italics (e.g., atorvastatin).
The second column of the chart lists the Drug Tier. You can reference the Summary of Benefits booklet or Chapter 4 (Section 5.2) in the Evidence of Coverage booklet to learn what your copay or coinsurance will be.
• Tier 1: Preferred generics and certain lower cost brand products• Tier 2: Preferred brand products and some high cost non-preferred generics• Tier 3: Non-preferred products (could include some high cost non-preferred generics)• Tier 4: Specialty products
And • Tier $0: Select Generics (not all dosages of these drugs are covered at the Select Generics cost
share); certain over-the-counter drugs.
The third column of the chart lists information in the Requirements/Limits column which tells you if Navitus MedicareRx has any special requirements for coverage of your drug.
• Limited Distribution (LD): This prescription may be available only at certain pharmacies. Formore information consult your Pharmacy Directory or call Customer Care.

8
• Non-Extended Day Supply (NDS): You may be able to receive greater than a 1-month supply of most of the drugs on your Formulary. Drugs noted with “NDS” are limited to a 1-month supply for both Retail and Mail Order.
• Prior Authorization (PA): The Plan requires you or your physician to get prior authorization for certain drugs. This means that you will need to get approval from The Plan before you fill your prescriptions. If you don’t get approval, Navitus MedicareRx may not cover the drug.
• Prior Authorization Restriction for Part B vs Part D Determination (PA_BvD): This drug may be eligible for payment under Medicare Part B or Part D. You (or your physician) are required to get prior authorization from Navitus MedicareRx to determine that this drug is covered under Medicare Part D before you fill your prescription for this drug. Without prior approval, Navitus MedicareRx may not cover this drug.
• Prior Authorization Restriction for New Starts Only (PA_NSO): If this drug is new to you, you (or your physician) are required to get prior authorization from Navitus MedicareRx before you fill your prescription for this drug. Without prior approval, Navitus MedicareRx may not cover this drug.
• Step Therapy (ST): In some cases, Navitus MedicareRx requires you to first try certain drugs to treat your medical condition before we will cover another drug for that condition. For example, if Drug A and Drug B both treat your medical condition, Navitus MedicareRx may not cover Drug B unless you try Drug A first. If Drug A does not work for you, Navitus MedicareRx will then cover Drug B.
• Step Therapy for New Starts Only (ST_NSO): If this drug is new to you, you are required to first try certain drugs to treat your medical condition before we will cover another drug for that condition.
• Quantity Limits (QL): For certain drugs, Navitus MedicareRx limits the amount of the drug that Navitus MedicareRx will cover. This could include a: per fill, daily, monthly, or yearly limitation.
• Rx Cents (RXC): This medication is offered at half the stated tier copay when your prescriber writes a prescription for half-tab daily. For example, if you take one 20mg tablet per day that is listed on the Formulary as a Tier 1 drug, the prescriber might write the prescription for half of a 40mg tab per day. Then you would pay $2.50 per month instead of $5 per month. For more information or to acquire a tablet splitter, contact Customer Care.
The * symbol after the Tier indicates these prescription drugs are not normally covered in a Medicare Prescription Drug Plan. The amount you pay when you fill a prescription for this drug does not count towards your total drug costs (that is, the amount you pay does not help you qualify for catastrophic coverage). In addition, if you are receiving extra help to pay for your prescriptions, you will not get any extra help to pay for these drugs.
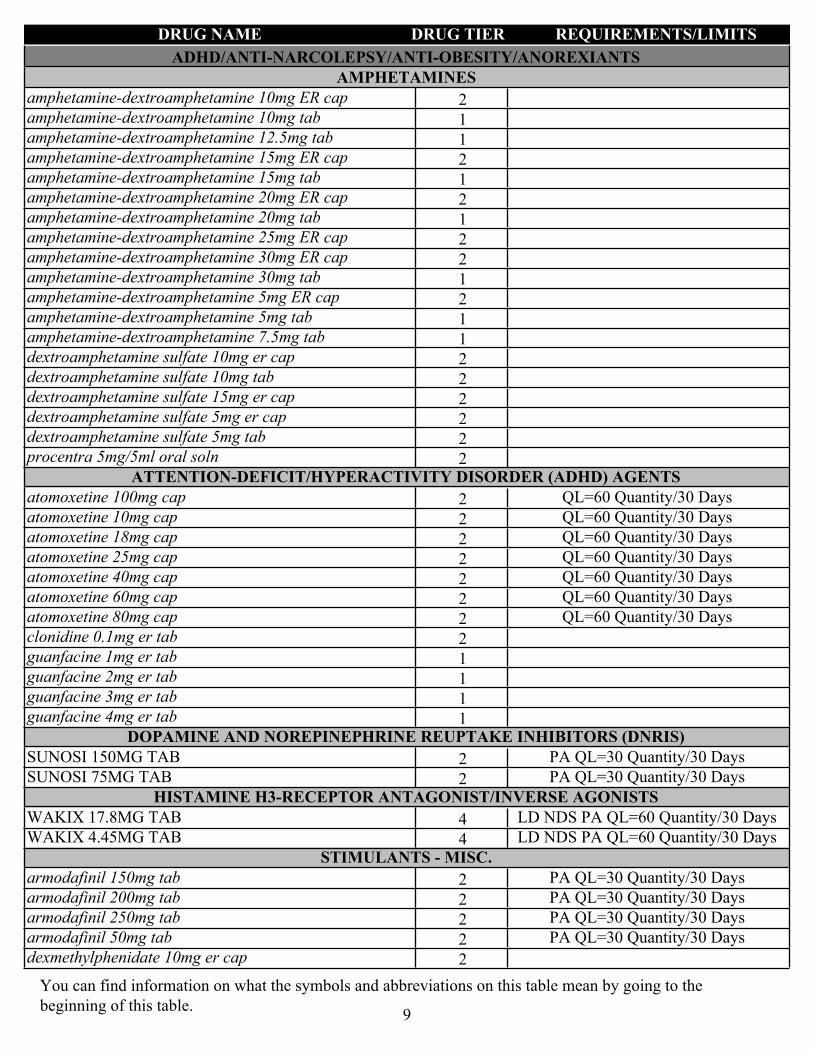
DRUG NAME DRUG TIER REQUIREMENTS/LIMITS
ADHD/ANTI-NARCOLEPSY/ANTI-OBESITY/ANOREXIANTSAMPHETAMINES
2amphetamine-dextroamphetamine 10mg ER cap
1amphetamine-dextroamphetamine 10mg tab
1amphetamine-dextroamphetamine 12.5mg tab
2amphetamine-dextroamphetamine 15mg ER cap
1amphetamine-dextroamphetamine 15mg tab
2amphetamine-dextroamphetamine 20mg ER cap
1amphetamine-dextroamphetamine 20mg tab
2amphetamine-dextroamphetamine 25mg ER cap
2amphetamine-dextroamphetamine 30mg ER cap
1amphetamine-dextroamphetamine 30mg tab
2amphetamine-dextroamphetamine 5mg ER cap
1amphetamine-dextroamphetamine 5mg tab
1amphetamine-dextroamphetamine 7.5mg tab
2dextroamphetamine sulfate 10mg er cap
2dextroamphetamine sulfate 10mg tab
2dextroamphetamine sulfate 15mg er cap
2dextroamphetamine sulfate 5mg er cap
2dextroamphetamine sulfate 5mg tab
2procentra 5mg/5ml oral solnATTENTION-DEFICIT/HYPERACTIVITY DISORDER (ADHD) AGENTS
2atomoxetine 100mg cap QL=60 Quantity/30 Days
2atomoxetine 10mg cap QL=60 Quantity/30 Days
2atomoxetine 18mg cap QL=60 Quantity/30 Days
2atomoxetine 25mg cap QL=60 Quantity/30 Days
2atomoxetine 40mg cap QL=60 Quantity/30 Days
2atomoxetine 60mg cap QL=60 Quantity/30 Days
2atomoxetine 80mg cap QL=60 Quantity/30 Days
2clonidine 0.1mg er tab
1guanfacine 1mg er tab
1guanfacine 2mg er tab
1guanfacine 3mg er tab
1guanfacine 4mg er tabDOPAMINE AND NOREPINEPHRINE REUPTAKE INHIBITORS (DNRIS)
2SUNOSI 150MG TAB PA QL=30 Quantity/30 Days
2SUNOSI 75MG TAB PA QL=30 Quantity/30 DaysHISTAMINE H3-RECEPTOR ANTAGONIST/INVERSE AGONISTS
4WAKIX 17.8MG TAB LD NDS PA QL=60 Quantity/30 Days
4WAKIX 4.45MG TAB LD NDS PA QL=60 Quantity/30 DaysSTIMULANTS - MISC.
2armodafinil 150mg tab PA QL=30 Quantity/30 Days
2armodafinil 200mg tab PA QL=30 Quantity/30 Days
2armodafinil 250mg tab PA QL=30 Quantity/30 Days
2armodafinil 50mg tab PA QL=30 Quantity/30 Days
2dexmethylphenidate 10mg er cap
You can find information on what the symbols and abbreviations on this table mean by going to the beginning of this table.
9

DRUG NAME DRUG TIER REQUIREMENTS/LIMITS
1dexmethylphenidate 10mg tab
2dexmethylphenidate 15mg er cap
1dexmethylphenidate 2.5mg tab
2dexmethylphenidate 20mg er cap
2dexmethylphenidate 25mg er cap
2dexmethylphenidate 30mg er cap
2dexmethylphenidate 35mg er cap
2dexmethylphenidate 40mg er cap
2dexmethylphenidate 5mg er cap
1dexmethylphenidate 5mg tab
2methylphenidate 10mg chew tab
2methylphenidate 10mg cr cap
2methylphenidate 10mg er tab
2methylphenidate 10mg la cap
1methylphenidate 10mg tab
2METHYLPHENIDATE 18MG ER TAB
2methylphenidate 18mg er tab
2methylphenidate 1mg/ml oral soln
2methylphenidate 2.5mg chew tab
2methylphenidate 20mg cr cap
2methylphenidate 20mg er tab
2methylphenidate 20mg la cap
1methylphenidate 20mg tab
1methylphenidate 27mg sr tab
2methylphenidate 2mg/ml oral soln
2methylphenidate 30mg cr cap
2methylphenidate 30mg la cap
1methylphenidate 36mg sr tab
2methylphenidate 40mg cr cap
2methylphenidate 40mg la cap
2methylphenidate 50mg cr cap
1methylphenidate 54mg sr tab
2methylphenidate 5mg chew tab
1methylphenidate 5mg tab
2methylphenidate 60mg cr cap
1methylphenidate 60mg la cap
2methylphenidate ER osmotic 27mg tab
2methylphenidate ER osmotic 36mg tab
2methylphenidate ER osmotic 54mg tab
2modafinil 100mg tab PA QL=60 Quantity/30 Days
2modafinil 200mg tab PA QL=60 Quantity/30 Days
AMEBICIDESAMEBICIDES
3SOLOSEC 2GM GRANULES PA
AMINOGLYCOSIDESAMINOGLYCOSIDES
You can find information on what the symbols and abbreviations on this table mean by going to the beginning of this table.
10

DRUG NAME DRUG TIER REQUIREMENTS/LIMITS
2amikacin 250mg/ml inj
2amikacin sulfate 1gm/4ml inj
4ARIKAYCE 590MG/8.4ML INH SUSP LD NDS PA QL=252 Quantity/30 Days
2GENTAMICIN 0.8MG/ML INJ
2gentamicin 1.2mg/ml inj
2GENTAMICIN 1.6MG/ML INJ
2GENTAMICIN 1MG/ML INJ
2gentamicin 40mg/ml inj
1neomycin sulfate 500mg tab
3paromomycin 250mg cap
3STREPTOMYCIN 1000MG INJ
2tobramycin 1.2gm inj
2tobramycin 1.2gm/30ml inj
2TOBRAMYCIN 10MG/ML INJ
2TOBRAMYCIN 2GM/50ML INJ
2tobramycin 40mg/ml inj
4TOBRAMYCIN 60MG/ML INH SOLN NDS PA QL=300 Quantity/30 Days
4tobramycin 60mg/ml inh soln PA QL=300 Quantity/30 Days
ANALGESICS - ANTI-INFLAMMATORYANTIRHEUMATIC - ENZYME INHIBITORS
4OLUMIANT 1MG TAB NDS PA QL=30 Quantity/30 Days
4OLUMIANT 2MG TAB NDS PA QL=30 Quantity/30 Days
4RINVOQ 15MG ER TAB NDS PA QL=30 Quantity/30 Days
4XELJANZ 10MG TAB NDS PA QL=60 Quantity/30 Days
4XELJANZ 1MG/ML ORAL SOLN NDS PA QL=300 Quantity/30 Days
4XELJANZ 5MG TAB NDS PA QL=60 Quantity/30 Days
4XELJANZ XR 11MG TAB NDS PA QL=30 Quantity/30 Days
4XELJANZ XR 22MG TAB NDS PA QL=30 Quantity/30 DaysANTI-TNF-ALPHA - MONOCLONAL ANTIBODIES
4HUMIRA 10MG/0.1ML SYRINGE NDS PA QL=2 Quantity/28 Days
4HUMIRA 10MG/0.2ML SYRINGE NDS PA QL=2 Quantity/28 Days
4HUMIRA 20MG/0.2ML SYRINGE NDS PA QL=2 Quantity/28 Days
4HUMIRA 20MG/0.4ML SYRINGE NDS PA QL=2 Quantity/28 Days
4HUMIRA 40MG/0.4ML AUTO-INJECTOR NDS PA QL=6 Quantity/28 Days
4HUMIRA 40MG/0.4ML SYRINGE NDS PA QL=6 Quantity/28 Days
4HUMIRA 40MG/0.8ML AUTO-INJECTOR NDS PA QL=6 Quantity/28 Days
4HUMIRA 40MG/0.8ML SYRINGE NDS PA QL=6 Quantity/28 Days
4HUMIRA 80MG/0.8ML AUTO-INJECTOR NDS PA QL=2 Quantity/28 Days
4HUMIRA PEDIATRIC CROHN'S STARTER PACK (3) 80MG/0.8ML SYRINGE
NDS PA QL=3 Quantity/180 Days
4HUMIRA PEDIATRIC CROHN'S STARTER PACK SYRINGE (2) 40MG/0.4ML, 80MG/0.8ML
NDS PA QL=2 Quantity/180 Days
4HUMIRA PEN - CROHN'S STARTER PACK 40MG/0.8ML INJ
PA QL=6 Quantity/180 Days
4HUMIRA PEN - PEDIATRIC UC STARTER PACK 80MG/0.8ML INJ
PA QL=4 Quantity/180 Days
You can find information on what the symbols and abbreviations on this table mean by going to the beginning of this table.
11
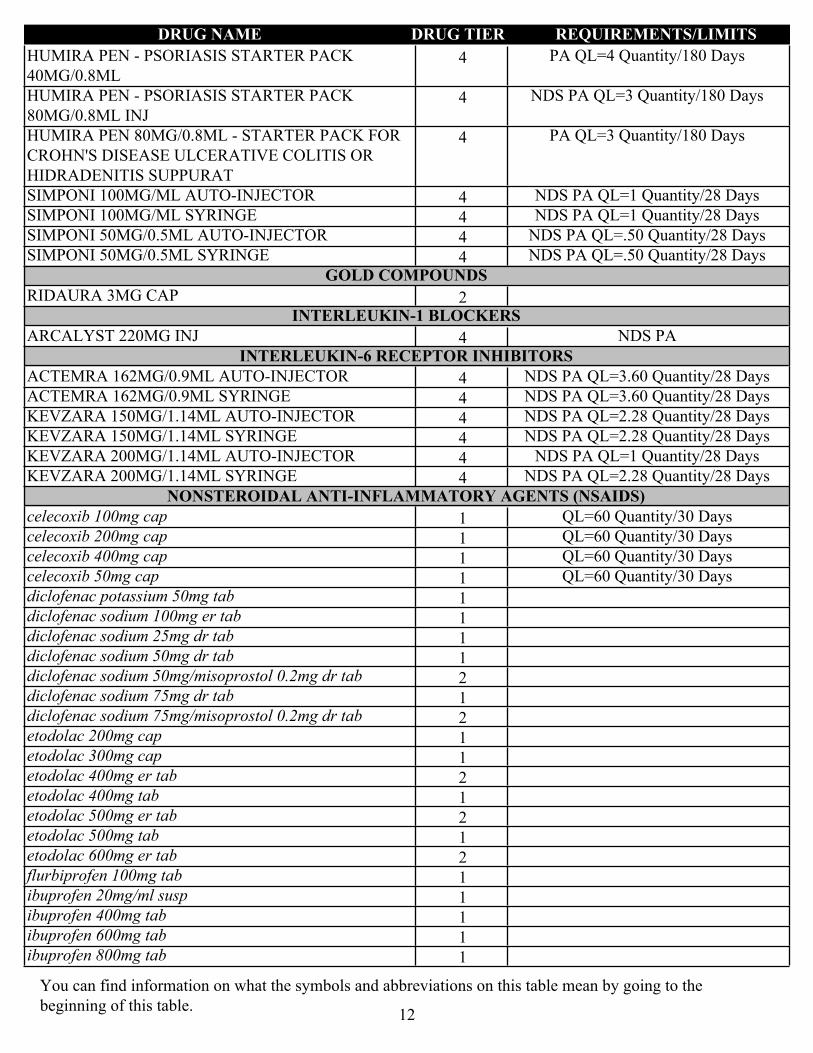
DRUG NAME DRUG TIER REQUIREMENTS/LIMITS
4HUMIRA PEN - PSORIASIS STARTER PACK 40MG/0.8ML
PA QL=4 Quantity/180 Days
4HUMIRA PEN - PSORIASIS STARTER PACK 80MG/0.8ML INJ
NDS PA QL=3 Quantity/180 Days
4HUMIRA PEN 80MG/0.8ML - STARTER PACK FOR CROHN'S DISEASE ULCERATIVE COLITIS OR HIDRADENITIS SUPPURAT
PA QL=3 Quantity/180 Days
4SIMPONI 100MG/ML AUTO-INJECTOR NDS PA QL=1 Quantity/28 Days
4SIMPONI 100MG/ML SYRINGE NDS PA QL=1 Quantity/28 Days
4SIMPONI 50MG/0.5ML AUTO-INJECTOR NDS PA QL=.50 Quantity/28 Days
4SIMPONI 50MG/0.5ML SYRINGE NDS PA QL=.50 Quantity/28 DaysGOLD COMPOUNDS
2RIDAURA 3MG CAPINTERLEUKIN-1 BLOCKERS
4ARCALYST 220MG INJ NDS PAINTERLEUKIN-6 RECEPTOR INHIBITORS
4ACTEMRA 162MG/0.9ML AUTO-INJECTOR NDS PA QL=3.60 Quantity/28 Days
4ACTEMRA 162MG/0.9ML SYRINGE NDS PA QL=3.60 Quantity/28 Days
4KEVZARA 150MG/1.14ML AUTO-INJECTOR NDS PA QL=2.28 Quantity/28 Days
4KEVZARA 150MG/1.14ML SYRINGE NDS PA QL=2.28 Quantity/28 Days
4KEVZARA 200MG/1.14ML AUTO-INJECTOR NDS PA QL=1 Quantity/28 Days
4KEVZARA 200MG/1.14ML SYRINGE NDS PA QL=2.28 Quantity/28 DaysNONSTEROIDAL ANTI-INFLAMMATORY AGENTS (NSAIDS)
1celecoxib 100mg cap QL=60 Quantity/30 Days
1celecoxib 200mg cap QL=60 Quantity/30 Days
1celecoxib 400mg cap QL=60 Quantity/30 Days
1celecoxib 50mg cap QL=60 Quantity/30 Days
1diclofenac potassium 50mg tab
1diclofenac sodium 100mg er tab
1diclofenac sodium 25mg dr tab
1diclofenac sodium 50mg dr tab
2diclofenac sodium 50mg/misoprostol 0.2mg dr tab
1diclofenac sodium 75mg dr tab
2diclofenac sodium 75mg/misoprostol 0.2mg dr tab
1etodolac 200mg cap
1etodolac 300mg cap
2etodolac 400mg er tab
1etodolac 400mg tab
2etodolac 500mg er tab
1etodolac 500mg tab
2etodolac 600mg er tab
1flurbiprofen 100mg tab
1ibuprofen 20mg/ml susp
1ibuprofen 400mg tab
1ibuprofen 600mg tab
1ibuprofen 800mg tab
You can find information on what the symbols and abbreviations on this table mean by going to the beginning of this table.
12
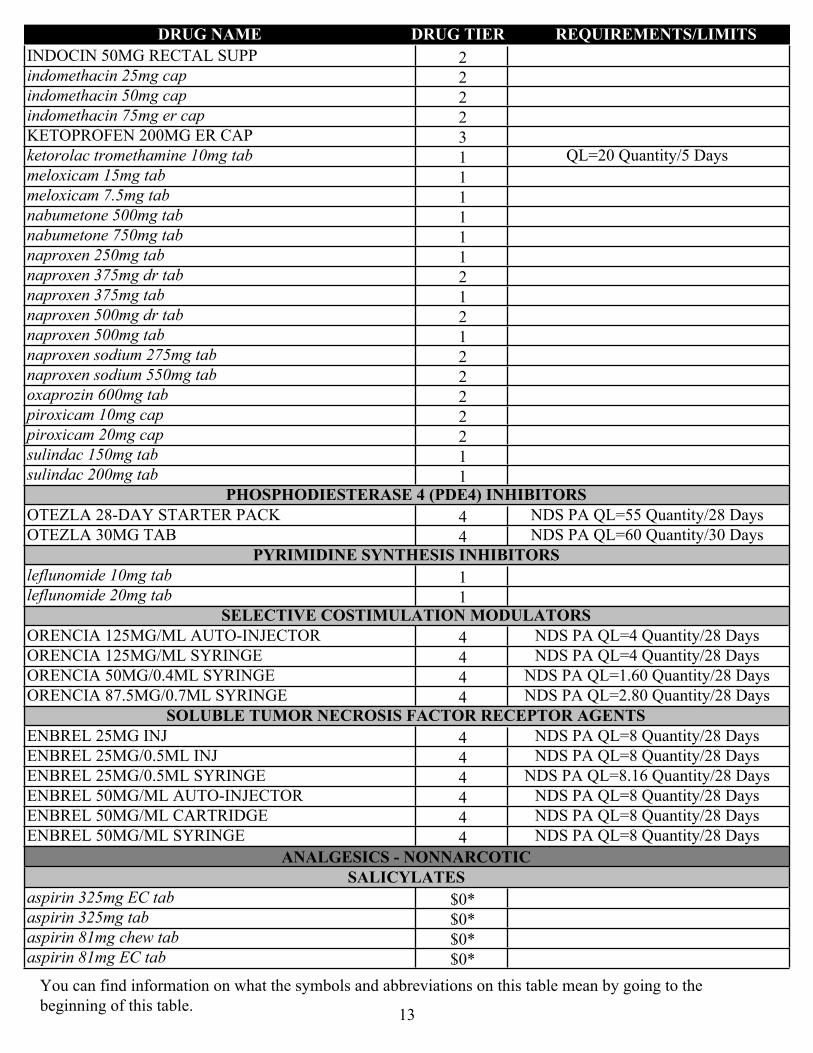
DRUG NAME DRUG TIER REQUIREMENTS/LIMITS
2INDOCIN 50MG RECTAL SUPP
2indomethacin 25mg cap
2indomethacin 50mg cap
2indomethacin 75mg er cap
3KETOPROFEN 200MG ER CAP
1ketorolac tromethamine 10mg tab QL=20 Quantity/5 Days
1meloxicam 15mg tab
1meloxicam 7.5mg tab
1nabumetone 500mg tab
1nabumetone 750mg tab
1naproxen 250mg tab
2naproxen 375mg dr tab
1naproxen 375mg tab
2naproxen 500mg dr tab
1naproxen 500mg tab
2naproxen sodium 275mg tab
2naproxen sodium 550mg tab
2oxaprozin 600mg tab
2piroxicam 10mg cap
2piroxicam 20mg cap
1sulindac 150mg tab
1sulindac 200mg tabPHOSPHODIESTERASE 4 (PDE4) INHIBITORS
4OTEZLA 28-DAY STARTER PACK NDS PA QL=55 Quantity/28 Days
4OTEZLA 30MG TAB NDS PA QL=60 Quantity/30 DaysPYRIMIDINE SYNTHESIS INHIBITORS
1leflunomide 10mg tab
1leflunomide 20mg tabSELECTIVE COSTIMULATION MODULATORS
4ORENCIA 125MG/ML AUTO-INJECTOR NDS PA QL=4 Quantity/28 Days
4ORENCIA 125MG/ML SYRINGE NDS PA QL=4 Quantity/28 Days
4ORENCIA 50MG/0.4ML SYRINGE NDS PA QL=1.60 Quantity/28 Days
4ORENCIA 87.5MG/0.7ML SYRINGE NDS PA QL=2.80 Quantity/28 DaysSOLUBLE TUMOR NECROSIS FACTOR RECEPTOR AGENTS
4ENBREL 25MG INJ NDS PA QL=8 Quantity/28 Days
4ENBREL 25MG/0.5ML INJ NDS PA QL=8 Quantity/28 Days
4ENBREL 25MG/0.5ML SYRINGE NDS PA QL=8.16 Quantity/28 Days
4ENBREL 50MG/ML AUTO-INJECTOR NDS PA QL=8 Quantity/28 Days
4ENBREL 50MG/ML CARTRIDGE NDS PA QL=8 Quantity/28 Days
4ENBREL 50MG/ML SYRINGE NDS PA QL=8 Quantity/28 Days
ANALGESICS - NONNARCOTICSALICYLATES
$0*aspirin 325mg EC tab
$0*aspirin 325mg tab
$0*aspirin 81mg chew tab
$0*aspirin 81mg EC tab
You can find information on what the symbols and abbreviations on this table mean by going to the beginning of this table.
13
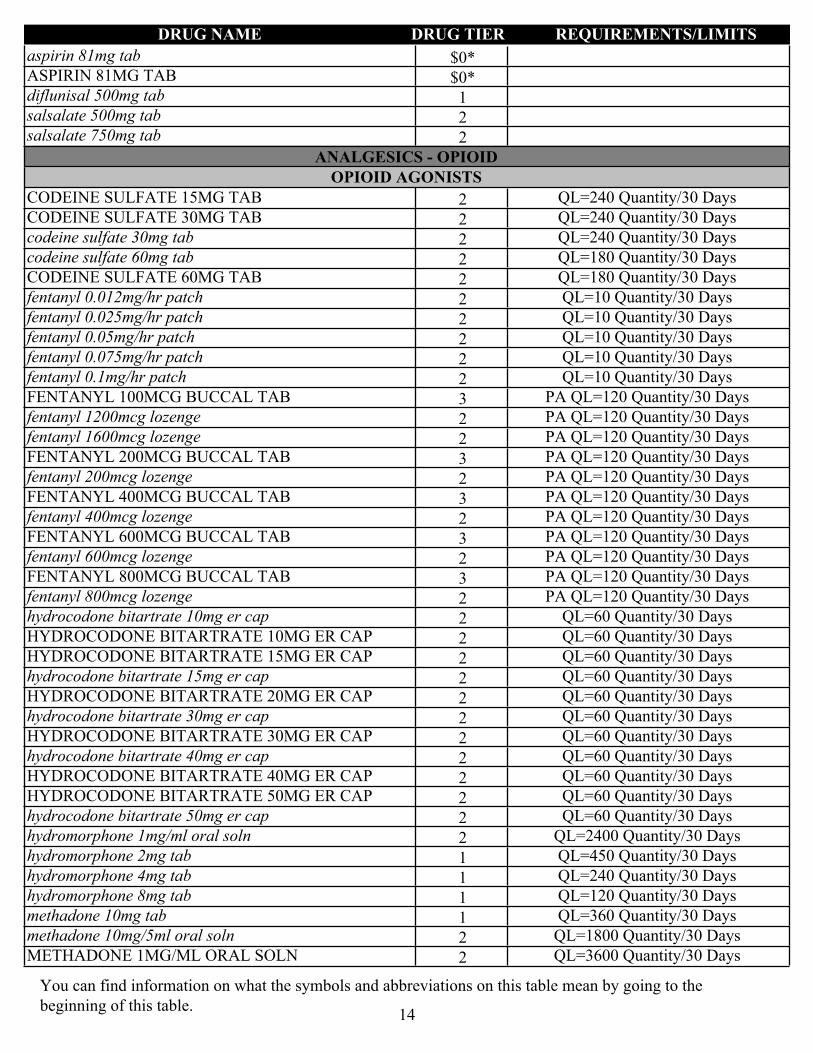
DRUG NAME DRUG TIER REQUIREMENTS/LIMITS
$0*aspirin 81mg tab
$0*ASPIRIN 81MG TAB
1diflunisal 500mg tab
2salsalate 500mg tab
2salsalate 750mg tab
ANALGESICS - OPIOIDOPIOID AGONISTS
2CODEINE SULFATE 15MG TAB QL=240 Quantity/30 Days
2CODEINE SULFATE 30MG TAB QL=240 Quantity/30 Days
2codeine sulfate 30mg tab QL=240 Quantity/30 Days
2codeine sulfate 60mg tab QL=180 Quantity/30 Days
2CODEINE SULFATE 60MG TAB QL=180 Quantity/30 Days
2fentanyl 0.012mg/hr patch QL=10 Quantity/30 Days
2fentanyl 0.025mg/hr patch QL=10 Quantity/30 Days
2fentanyl 0.05mg/hr patch QL=10 Quantity/30 Days
2fentanyl 0.075mg/hr patch QL=10 Quantity/30 Days
2fentanyl 0.1mg/hr patch QL=10 Quantity/30 Days
3FENTANYL 100MCG BUCCAL TAB PA QL=120 Quantity/30 Days
2fentanyl 1200mcg lozenge PA QL=120 Quantity/30 Days
2fentanyl 1600mcg lozenge PA QL=120 Quantity/30 Days
3FENTANYL 200MCG BUCCAL TAB PA QL=120 Quantity/30 Days
2fentanyl 200mcg lozenge PA QL=120 Quantity/30 Days
3FENTANYL 400MCG BUCCAL TAB PA QL=120 Quantity/30 Days
2fentanyl 400mcg lozenge PA QL=120 Quantity/30 Days
3FENTANYL 600MCG BUCCAL TAB PA QL=120 Quantity/30 Days
2fentanyl 600mcg lozenge PA QL=120 Quantity/30 Days
3FENTANYL 800MCG BUCCAL TAB PA QL=120 Quantity/30 Days
2fentanyl 800mcg lozenge PA QL=120 Quantity/30 Days
2hydrocodone bitartrate 10mg er cap QL=60 Quantity/30 Days
2HYDROCODONE BITARTRATE 10MG ER CAP QL=60 Quantity/30 Days
2HYDROCODONE BITARTRATE 15MG ER CAP QL=60 Quantity/30 Days
2hydrocodone bitartrate 15mg er cap QL=60 Quantity/30 Days
2HYDROCODONE BITARTRATE 20MG ER CAP QL=60 Quantity/30 Days
2hydrocodone bitartrate 30mg er cap QL=60 Quantity/30 Days
2HYDROCODONE BITARTRATE 30MG ER CAP QL=60 Quantity/30 Days
2hydrocodone bitartrate 40mg er cap QL=60 Quantity/30 Days
2HYDROCODONE BITARTRATE 40MG ER CAP QL=60 Quantity/30 Days
2HYDROCODONE BITARTRATE 50MG ER CAP QL=60 Quantity/30 Days
2hydrocodone bitartrate 50mg er cap QL=60 Quantity/30 Days
2hydromorphone 1mg/ml oral soln QL=2400 Quantity/30 Days
1hydromorphone 2mg tab QL=450 Quantity/30 Days
1hydromorphone 4mg tab QL=240 Quantity/30 Days
1hydromorphone 8mg tab QL=120 Quantity/30 Days
1methadone 10mg tab QL=360 Quantity/30 Days
2methadone 10mg/5ml oral soln QL=1800 Quantity/30 Days
2METHADONE 1MG/ML ORAL SOLN QL=3600 Quantity/30 Days
You can find information on what the symbols and abbreviations on this table mean by going to the beginning of this table.
14
DRUG NAME DRUG TIER REQUIREMENTS/LIMITS
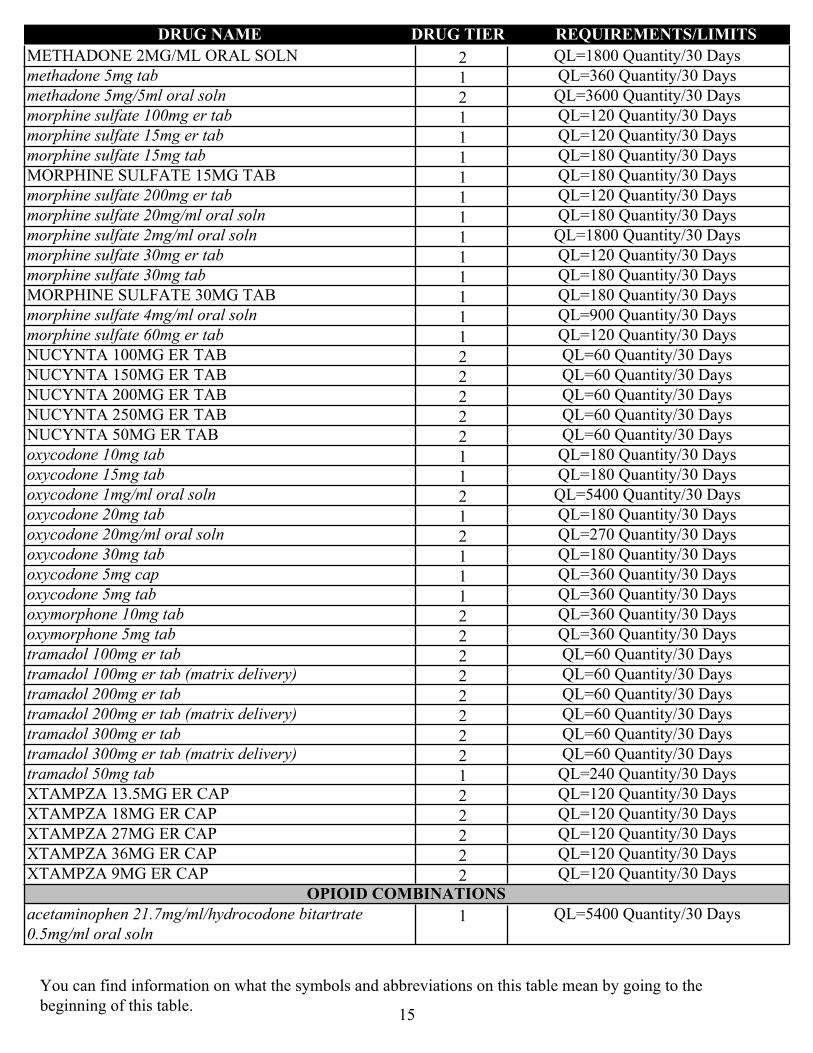
2METHADONE 2MG/ML ORAL SOLN QL=1800 Quantity/30 Days
1methadone 5mg tab QL=360 Quantity/30 Days
2methadone 5mg/5ml oral soln QL=3600 Quantity/30 Days
1morphine sulfate 100mg er tab QL=120 Quantity/30 Days
1morphine sulfate 15mg er tab QL=120 Quantity/30 Days
1morphine sulfate 15mg tab QL=180 Quantity/30 Days
1MORPHINE SULFATE 15MG TAB QL=180 Quantity/30 Days
1morphine sulfate 200mg er tab QL=120 Quantity/30 Days
1morphine sulfate 20mg/ml oral soln QL=180 Quantity/30 Days
1morphine sulfate 2mg/ml oral soln QL=1800 Quantity/30 Days
1morphine sulfate 30mg er tab QL=120 Quantity/30 Days
1morphine sulfate 30mg tab QL=180 Quantity/30 Days
1MORPHINE SULFATE 30MG TAB QL=180 Quantity/30 Days
1morphine sulfate 4mg/ml oral soln QL=900 Quantity/30 Days
1morphine sulfate 60mg er tab QL=120 Quantity/30 Days
2NUCYNTA 100MG ER TAB QL=60 Quantity/30 Days
2NUCYNTA 150MG ER TAB QL=60 Quantity/30 Days
2NUCYNTA 200MG ER TAB QL=60 Quantity/30 Days
2NUCYNTA 250MG ER TAB QL=60 Quantity/30 Days
2NUCYNTA 50MG ER TAB QL=60 Quantity/30 Days
1oxycodone 10mg tab QL=180 Quantity/30 Days
1oxycodone 15mg tab QL=180 Quantity/30 Days
2oxycodone 1mg/ml oral soln QL=5400 Quantity/30 Days
1oxycodone 20mg tab QL=180 Quantity/30 Days
2oxycodone 20mg/ml oral soln QL=270 Quantity/30 Days
1oxycodone 30mg tab QL=180 Quantity/30 Days
1oxycodone 5mg cap QL=360 Quantity/30 Days
1oxycodone 5mg tab QL=360 Quantity/30 Days
2oxymorphone 10mg tab QL=360 Quantity/30 Days
2oxymorphone 5mg tab QL=360 Quantity/30 Days
2tramadol 100mg er tab QL=60 Quantity/30 Days
2tramadol 100mg er tab (matrix delivery) QL=60 Quantity/30 Days
2tramadol 200mg er tab QL=60 Quantity/30 Days
2tramadol 200mg er tab (matrix delivery) QL=60 Quantity/30 Days
2tramadol 300mg er tab QL=60 Quantity/30 Days
2tramadol 300mg er tab (matrix delivery) QL=60 Quantity/30 Days
1tramadol 50mg tab QL=240 Quantity/30 Days
2XTAMPZA 13.5MG ER CAP QL=120 Quantity/30 Days
2XTAMPZA 18MG ER CAP QL=120 Quantity/30 Days
2XTAMPZA 27MG ER CAP QL=120 Quantity/30 Days
2XTAMPZA 36MG ER CAP QL=120 Quantity/30 Days
2XTAMPZA 9MG ER CAP QL=120 Quantity/30 DaysOPIOID COMBINATIONS
1acetaminophen 21.7mg/ml/hydrocodone bitartrate 0.5mg/ml oral soln
QL=5400 Quantity/30 Days
You can find information on what the symbols and abbreviations on this table mean by going to the beginning of this table.
15
DRUG NAME DRUG TIER REQUIREMENTS/LIMITS
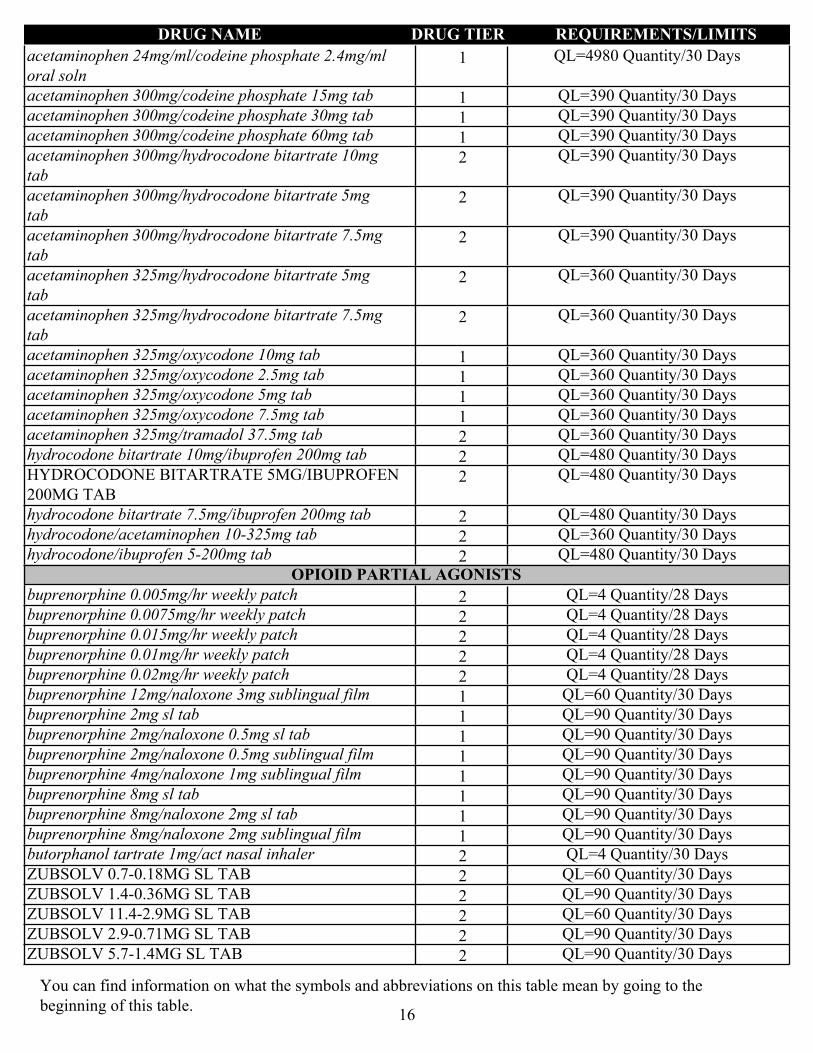
1acetaminophen 24mg/ml/codeine phosphate 2.4mg/ml oral soln
QL=4980 Quantity/30 Days
1acetaminophen 300mg/codeine phosphate 15mg tab QL=390 Quantity/30 Days
1acetaminophen 300mg/codeine phosphate 30mg tab QL=390 Quantity/30 Days
1acetaminophen 300mg/codeine phosphate 60mg tab QL=390 Quantity/30 Days
2acetaminophen 300mg/hydrocodone bitartrate 10mg tab
QL=390 Quantity/30 Days
2acetaminophen 300mg/hydrocodone bitartrate 5mg tab
QL=390 Quantity/30 Days
2acetaminophen 300mg/hydrocodone bitartrate 7.5mg tab
QL=390 Quantity/30 Days
2acetaminophen 325mg/hydrocodone bitartrate 5mg tab
QL=360 Quantity/30 Days
2acetaminophen 325mg/hydrocodone bitartrate 7.5mg tab
QL=360 Quantity/30 Days
1acetaminophen 325mg/oxycodone 10mg tab QL=360 Quantity/30 Days
1acetaminophen 325mg/oxycodone 2.5mg tab QL=360 Quantity/30 Days
1acetaminophen 325mg/oxycodone 5mg tab QL=360 Quantity/30 Days
1acetaminophen 325mg/oxycodone 7.5mg tab QL=360 Quantity/30 Days
2acetaminophen 325mg/tramadol 37.5mg tab QL=360 Quantity/30 Days
2hydrocodone bitartrate 10mg/ibuprofen 200mg tab QL=480 Quantity/30 Days
2HYDROCODONE BITARTRATE 5MG/IBUPROFEN 200MG TAB
QL=480 Quantity/30 Days
2hydrocodone bitartrate 7.5mg/ibuprofen 200mg tab QL=480 Quantity/30 Days
2hydrocodone/acetaminophen 10-325mg tab QL=360 Quantity/30 Days
2hydrocodone/ibuprofen 5-200mg tab QL=480 Quantity/30 DaysOPIOID PARTIAL AGONISTS
2buprenorphine 0.005mg/hr weekly patch QL=4 Quantity/28 Days
2buprenorphine 0.0075mg/hr weekly patch QL=4 Quantity/28 Days
2buprenorphine 0.015mg/hr weekly patch QL=4 Quantity/28 Days
2buprenorphine 0.01mg/hr weekly patch QL=4 Quantity/28 Days
2buprenorphine 0.02mg/hr weekly patch QL=4 Quantity/28 Days
1buprenorphine 12mg/naloxone 3mg sublingual film QL=60 Quantity/30 Days
1buprenorphine 2mg sl tab QL=90 Quantity/30 Days
1buprenorphine 2mg/naloxone 0.5mg sl tab QL=90 Quantity/30 Days
1buprenorphine 2mg/naloxone 0.5mg sublingual film QL=90 Quantity/30 Days
1buprenorphine 4mg/naloxone 1mg sublingual film QL=90 Quantity/30 Days
1buprenorphine 8mg sl tab QL=90 Quantity/30 Days
1buprenorphine 8mg/naloxone 2mg sl tab QL=90 Quantity/30 Days
1buprenorphine 8mg/naloxone 2mg sublingual film QL=90 Quantity/30 Days
2butorphanol tartrate 1mg/act nasal inhaler QL=4 Quantity/30 Days
2ZUBSOLV 0.7-0.18MG SL TAB QL=60 Quantity/30 Days
2ZUBSOLV 1.4-0.36MG SL TAB QL=90 Quantity/30 Days
2ZUBSOLV 11.4-2.9MG SL TAB QL=60 Quantity/30 Days
2ZUBSOLV 2.9-0.71MG SL TAB QL=90 Quantity/30 Days
2ZUBSOLV 5.7-1.4MG SL TAB QL=90 Quantity/30 Days
You can find information on what the symbols and abbreviations on this table mean by going to the beginning of this table.
16

DRUG NAME DRUG TIER REQUIREMENTS/LIMITS
2ZUBSOLV 8.6-2.1MG SL TAB QL=60 Quantity/30 Days
ANDROGENS-ANABOLICANABOLIC STEROIDS
1oxandrolone 10mg tab PA QL=60 Quantity/30 Days
1oxandrolone 2.5mg tab PA QL=120 Quantity/30 DaysANDROGENS
2ANDRODERM 2MG/24HR PATCH PA QL=60 Quantity/30 Days
2ANDRODERM 4MG/24HR PATCH PA QL=30 Quantity/30 Days
2danazol 100mg cap
2danazol 200mg cap
2danazol 50mg cap
3METHITEST 10MG TAB PA
3METHYLTESTOSTERONE 10MG CAP PA
3testosterone 1% (12.5mg) gel pump bottle PA QL=4 Quantity/30 Days
3TESTOSTERONE 1% (12.5MG/ACT) GEL PUMP PA QL=4 Quantity/30 Days
2testosterone 1% (25mg) gel packet PA QL=120 Quantity/30 Days
2TESTOSTERONE 1% (50MG) GEL PACKET PA QL=60 Quantity/30 Days
2testosterone 1.62% (1.25gm) gel packet PA QL=60 Quantity/30 Days
2testosterone 1.62% (2.5gm) gel packet PA QL=60 Quantity/30 Days
2testosterone 20.25mg/act gel pump PA QL=2 Quantity/30 Days
2testosterone 30mg/act topical soln PA QL=2 Quantity/30 Days
1testosterone cypionate 100mg/ml inj
1testosterone cypionate 200mg/ml inj
2TESTOSTERONE ENANTHATE 200MG/ML INJ
2testosterone gel 1% (50mg) packet PA QL=60 Quantity/30 Days
ANORECTAL AGENTSINTRARECTAL STEROIDS
2hydrocortisone 1.67mg/ml enema
3UCERIS 2MG/ACT RECTAL FOAM PARECTAL COMBINATIONS
3*ANALPRAM-HC CREAM
2hydrocortisone/pramoxine 1-1% rectal cream
1*hydrocortisone/pramoxine 2.5-1% rectal cream
2*lidocaine/hydrocortisone creamRECTAL STEROIDS
3*ANUSOL-HC SUPP
1hydrocortisone 1% cream (RX Only) QL=240 Quantity/30 Days
2*hydrocortisone supp
1procto-med 2.5% cream
1procto-pak 1% rectal creamVASODILATING AGENTS
3RECTIV 0.4% RECTAL OINTMENT QL=30 Quantity/30 Days
ANTHELMINTICSANTHELMINTICS
2albendazole 200mg tab
2BENZNIDAZOLE 100MG TAB PA
You can find information on what the symbols and abbreviations on this table mean by going to the beginning of this table.
17

DRUG NAME DRUG TIER REQUIREMENTS/LIMITS
2BENZNIDAZOLE 12.5MG TAB PA
2ivermectin 3mg tab
2praziquantel 600mg tab
ANTIANGINAL AGENTSANTIANGINALS-OTHER
2ranolazine 1000mg er tab
2ranolazine 500mg er tabNITRATES
1isosorbide dinitrate 10mg tab
1isosorbide dinitrate 20mg tab
1isosorbide dinitrate 30mg tab
2isosorbide dinitrate 40mg tab
1isosorbide dinitrate 5mg tab
1isosorbide mononitrate 10mg tab
1isosorbide mononitrate 120mg er tab
1isosorbide mononitrate 20mg tab
1isosorbide mononitrate 30mg er tab
1isosorbide mononitrate 60mg er tab
2NITRO-BID 2% OINTMENT
3NITRO-DUR 0.3MG/HR PATCH
3NITRO-DUR 0.8MG/HR PATCH
1nitroglycerin 0.1mg/hr patch
1nitroglycerin 0.2mg/hr patch
1nitroglycerin 0.3mg sl tab
1nitroglycerin 0.4mg sl tab
2nitroglycerin 0.4mg/act spray
1nitroglycerin 0.4mg/hr patch
1nitroglycerin 0.6mg sl tab
1nitroglycerin 0.6mg/hr patch
1*NITROGLYCERIN CAP
ANTIANXIETY AGENTSANTIANXIETY AGENTS - MISC.
1buspirone 10mg tab
1buspirone 15mg tab
1buspirone 30mg tab
1buspirone 5mg tab
1buspirone 7.5mg tab
1hydroxyzine 10mg tab
1hydroxyzine 25mg tab
1hydroxyzine 2mg/ml oral soln
1hydroxyzine 50mg tab
2HYDROXYZINE PAMOATE 100MG CAP
1hydroxyzine pamoate 25mg cap
1hydroxyzine pamoate 50mg capBENZODIAZEPINES
1alprazolam 0.25mg tab QL=120 Quantity/30 Days
You can find information on what the symbols and abbreviations on this table mean by going to the beginning of this table.
18
DRUG NAME DRUG TIER REQUIREMENTS/LIMITS
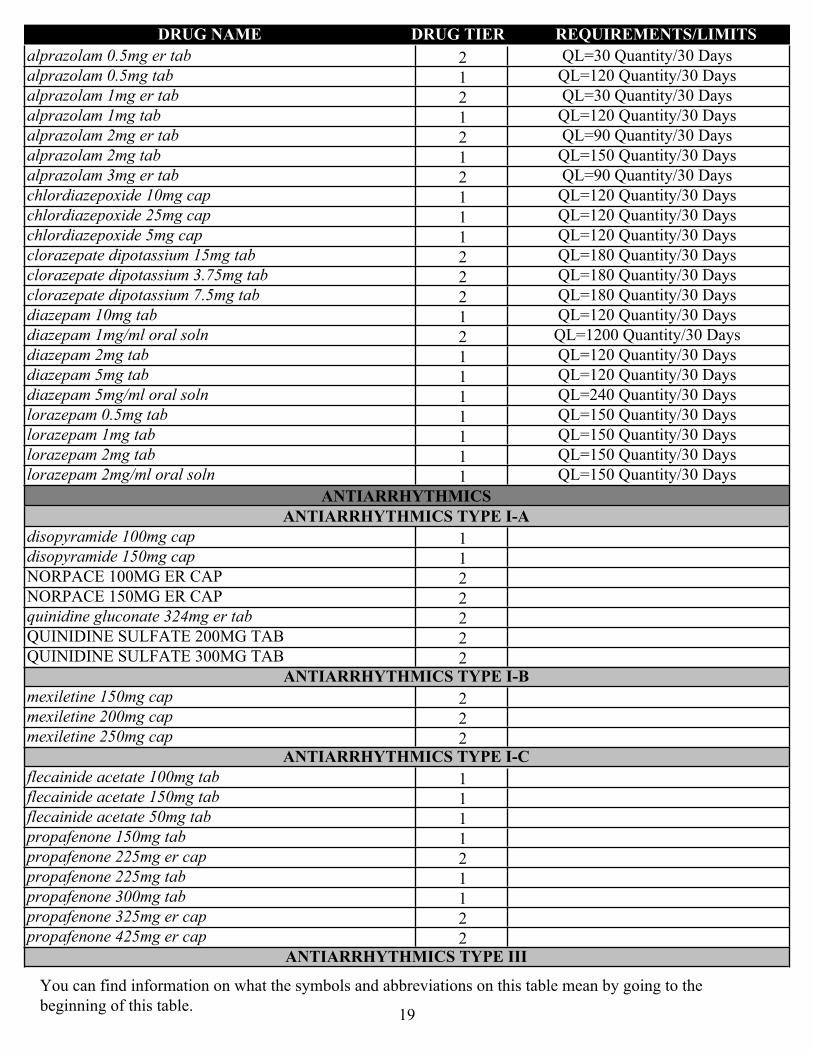
2alprazolam 0.5mg er tab QL=30 Quantity/30 Days
1alprazolam 0.5mg tab QL=120 Quantity/30 Days
2alprazolam 1mg er tab QL=30 Quantity/30 Days
1alprazolam 1mg tab QL=120 Quantity/30 Days
2alprazolam 2mg er tab QL=90 Quantity/30 Days
1alprazolam 2mg tab QL=150 Quantity/30 Days
2alprazolam 3mg er tab QL=90 Quantity/30 Days
1chlordiazepoxide 10mg cap QL=120 Quantity/30 Days
1chlordiazepoxide 25mg cap QL=120 Quantity/30 Days
1chlordiazepoxide 5mg cap QL=120 Quantity/30 Days
2clorazepate dipotassium 15mg tab QL=180 Quantity/30 Days
2clorazepate dipotassium 3.75mg tab QL=180 Quantity/30 Days
2clorazepate dipotassium 7.5mg tab QL=180 Quantity/30 Days
1diazepam 10mg tab QL=120 Quantity/30 Days
2diazepam 1mg/ml oral soln QL=1200 Quantity/30 Days
1diazepam 2mg tab QL=120 Quantity/30 Days
1diazepam 5mg tab QL=120 Quantity/30 Days
1diazepam 5mg/ml oral soln QL=240 Quantity/30 Days
1lorazepam 0.5mg tab QL=150 Quantity/30 Days
1lorazepam 1mg tab QL=150 Quantity/30 Days
1lorazepam 2mg tab QL=150 Quantity/30 Days
1lorazepam 2mg/ml oral soln QL=150 Quantity/30 Days
ANTIARRHYTHMICSANTIARRHYTHMICS TYPE I-A
1disopyramide 100mg cap
1disopyramide 150mg cap
2NORPACE 100MG ER CAP
2NORPACE 150MG ER CAP
2quinidine gluconate 324mg er tab
2QUINIDINE SULFATE 200MG TAB
2QUINIDINE SULFATE 300MG TABANTIARRHYTHMICS TYPE I-B
2mexiletine 150mg cap
2mexiletine 200mg cap
2mexiletine 250mg capANTIARRHYTHMICS TYPE I-C
1flecainide acetate 100mg tab
1flecainide acetate 150mg tab
1flecainide acetate 50mg tab
1propafenone 150mg tab
2propafenone 225mg er cap
1propafenone 225mg tab
1propafenone 300mg tab
2propafenone 325mg er cap
2propafenone 425mg er capANTIARRHYTHMICS TYPE III
You can find information on what the symbols and abbreviations on this table mean by going to the beginning of this table.
19
DRUG NAME DRUG TIER REQUIREMENTS/LIMITS
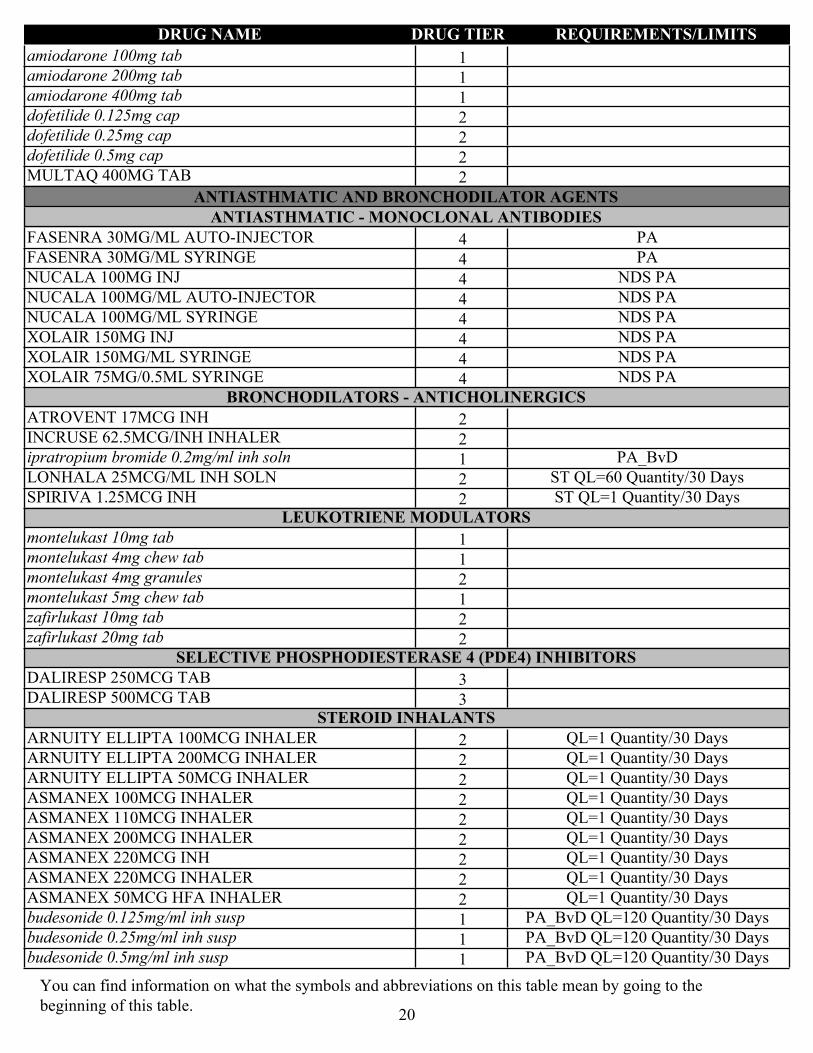
1amiodarone 100mg tab
1amiodarone 200mg tab
1amiodarone 400mg tab
2dofetilide 0.125mg cap
2dofetilide 0.25mg cap
2dofetilide 0.5mg cap
2MULTAQ 400MG TAB
ANTIASTHMATIC AND BRONCHODILATOR AGENTSANTIASTHMATIC - MONOCLONAL ANTIBODIES
4FASENRA 30MG/ML AUTO-INJECTOR PA
4FASENRA 30MG/ML SYRINGE PA
4NUCALA 100MG INJ NDS PA
4NUCALA 100MG/ML AUTO-INJECTOR NDS PA
4NUCALA 100MG/ML SYRINGE NDS PA
4XOLAIR 150MG INJ NDS PA
4XOLAIR 150MG/ML SYRINGE NDS PA
4XOLAIR 75MG/0.5ML SYRINGE NDS PABRONCHODILATORS - ANTICHOLINERGICS
2ATROVENT 17MCG INH
2INCRUSE 62.5MCG/INH INHALER
1ipratropium bromide 0.2mg/ml inh soln PA_BvD
2LONHALA 25MCG/ML INH SOLN ST QL=60 Quantity/30 Days
2SPIRIVA 1.25MCG INH ST QL=1 Quantity/30 DaysLEUKOTRIENE MODULATORS
1montelukast 10mg tab
1montelukast 4mg chew tab
2montelukast 4mg granules
1montelukast 5mg chew tab
2zafirlukast 10mg tab
2zafirlukast 20mg tabSELECTIVE PHOSPHODIESTERASE 4 (PDE4) INHIBITORS
3DALIRESP 250MCG TAB
3DALIRESP 500MCG TABSTEROID INHALANTS
2ARNUITY ELLIPTA 100MCG INHALER QL=1 Quantity/30 Days
2ARNUITY ELLIPTA 200MCG INHALER QL=1 Quantity/30 Days
2ARNUITY ELLIPTA 50MCG INHALER QL=1 Quantity/30 Days
2ASMANEX 100MCG INHALER QL=1 Quantity/30 Days
2ASMANEX 110MCG INHALER QL=1 Quantity/30 Days
2ASMANEX 200MCG INHALER QL=1 Quantity/30 Days
2ASMANEX 220MCG INH QL=1 Quantity/30 Days
2ASMANEX 220MCG INHALER QL=1 Quantity/30 Days
2ASMANEX 50MCG HFA INHALER QL=1 Quantity/30 Days
1budesonide 0.125mg/ml inh susp PA_BvD QL=120 Quantity/30 Days
1budesonide 0.25mg/ml inh susp PA_BvD QL=120 Quantity/30 Days
1budesonide 0.5mg/ml inh susp PA_BvD QL=120 Quantity/30 Days
You can find information on what the symbols and abbreviations on this table mean by going to the beginning of this table.
20

DRUG NAME DRUG TIER REQUIREMENTS/LIMITS
2FLOVENT 100MCG DISKUS QL=1 Quantity/30 Days
2FLOVENT 110MCG HFA INH QL=2 Quantity/30 Days
2FLOVENT 220MCG HFA INH QL=2 Quantity/30 Days
2FLOVENT 250MCG DISKUS QL=1 Quantity/30 Days
2FLOVENT 44MCG HFA INH QL=2 Quantity/30 Days
2FLOVENT 50MCG DISKUS QL=1 Quantity/30 DaysSYMPATHOMIMETICS
2ADVAIR 100-50MCG DISKUS QL=1 Quantity/30 Days
2ADVAIR 115-21MCG HFA INHALER QL=1 Quantity/30 Days
2ADVAIR 230-21MCG HFA INHALER QL=1 Quantity/30 Days
2ADVAIR 250-50MCG DISKUS QL=1 Quantity/30 Days
2ADVAIR 45-21MCG/ACT HFA INHALER QL=1 Quantity/30 Days
2ADVAIR 500-50MCG DISKUS QL=1 Quantity/30 Days
1albuterol 0.21mg/ml inh soln PA_BvD
1albuterol 0.417mg/ml inh soln PA_BvD
1albuterol 0.4mg/ml oral soln
2albuterol 0.83mg/ml inh soln PA_BvD
1albuterol 2mg tab
1albuterol 4mg tab
2albuterol 5mg/ml inh soln PA_BvD
1albuterol HFA inhaler (6.7gm) QL=2 Quantity/30 Days
1albuterol HFA inhaler (8.5gm) QL=2 Quantity/30 Days
2ANORO ELLIPTA 62.5-25MCG INHALER QL=1 Quantity/30 Days
2arformoterol tartrate 15mcg/2ml neb soln PA_BvD QL=120 Quantity/30 Days
2BREO ELLIPTA 100-25MCG INHALER QL=1 Quantity/30 Days
2BREO ELLIPTA 200-25MCG INHALER QL=1 Quantity/30 Days
2BREZTRI AEROSPHERE 160-9-4.8MCG/ACT INH QL=1 Quantity/30 Days
2COMBIVENT 20-100MCG/ACT INH
2DULERA 100-5MCG INHALER QL=1 Quantity/30 Days
2DULERA 200-5MCG INHALER QL=1 Quantity/30 Days
2DULERA 50-5MCG INHALER QL=1 Quantity/30 Days
1fluticasone propionate/salmeterol 100-50mcg/act dry powder inhaler, wixela 100-50mcg inhaler
QL=1 Quantity/30 Days
1fluticasone propionate/salmeterol 250-50mcg/act dry powder inhaler, wixela 250-50mcg inhaler
QL=1 Quantity/30 Days
1fluticasone propionate/salmeterol 500-50mcg/act dry powder inhaler, wixela 500-50mcg inhaler
QL=1 Quantity/30 Days
2formoterol fumarate 20mcg/2ml neb soln PA_BvD QL=120 Quantity/30 Days
1ipratropium/albuterol 0.5-2.5mg/3ml inh soln PA_BvD
2levalbuterol 0.103mg/ml inh soln PA_BvD
2levalbuterol 0.21mg/ml inh soln PA_BvD
2levalbuterol 0.417mg/ml inh soln PA_BvD
2levalbuterol 2.5mg/ml inh soln PA_BvD
2SEREVENT 50MCG/DOSE INH
2STIOLTO 2.5-2.5MCG/ACT INH QL=1 Quantity/30 Days
2SYMBICORT 160-4.5MCG/ACT INHALER QL=1 Quantity/30 Days
You can find information on what the symbols and abbreviations on this table mean by going to the beginning of this table.
21

DRUG NAME DRUG TIER REQUIREMENTS/LIMITS
2SYMBICORT 80-4.5MCG/ACT INHALER QL=1 Quantity/30 Days
1terbutaline sulfate 2.5mg tab
1terbutaline sulfate 5mg tab
2TRELEGY ELLIPTA 100- 62.5-25MCG INHALER QL=1 Quantity/30 Days
2TRELEGY ELLIPTA 200-62.5-25MCG INHALER QL=1 Quantity/30 Days
2VENTOLIN 108MCG INH (18GM) QL=2 Quantity/30 Days
2VENTOLIN 108MCG INH (8GM) QL=5 Quantity/30 Days
3XOPENEX 45MCG INH, LEVALBUTEROL 45MCG INHALER
ST QL=2 Quantity/30 Days
XANTHINES
3THEO-24 100MG ER CAP
3THEO-24 200MG ER CAP
3THEO-24 300MG ER CAP
3THEO-24 400MG ER CAP
2THEOPHYLLINE 300MG ER TAB
1theophylline 400mg er tab
2THEOPHYLLINE 450MG ER TAB
1theophylline 5.33mg/ml oral soln
1theophylline 600mg er tab
ANTICOAGULANTSCOUMARIN ANTICOAGULANTS
1warfarin sodium 10mg tab
1warfarin sodium 1mg tab
1warfarin sodium 2.5mg tab
1warfarin sodium 2mg tab
1warfarin sodium 3mg tab
1warfarin sodium 4mg tab
1warfarin sodium 5mg tab
1warfarin sodium 6mg tab
1warfarin sodium 7.5mg tabDIRECT FACTOR XA INHIBITORS
2ELIQUIS 2.5MG TAB
2ELIQUIS 5MG TAB
2ELIQUIS 5MG TAB 30-DAY STARTER PACK
2XARELTO 10MG TAB
2XARELTO 15MG TAB
2XARELTO 2.5MG TAB
2XARELTO 20MG TAB
2XARELTO KIT PACKHEPARINS AND HEPARINOID-LIKE AGENTS
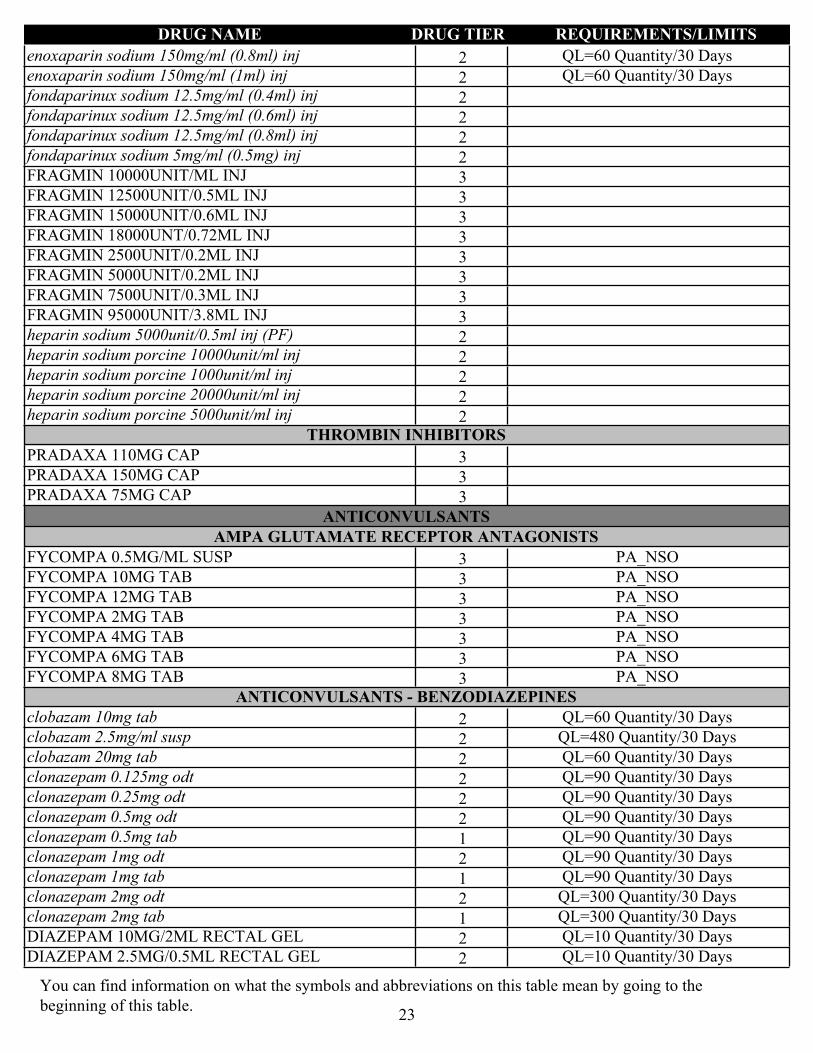
2enoxaparin 300mg/3ml inj QL=30 Quantity/30 Days
2enoxaparin sodium 100mg/ml (0.3ml) inj QL=60 Quantity/30 Days
2enoxaparin sodium 100mg/ml (0.4ml) inj QL=60 Quantity/30 Days
2enoxaparin sodium 100mg/ml (0.6ml) inj QL=60 Quantity/30 Days
2enoxaparin sodium 100mg/ml (0.8ml) inj QL=60 Quantity/30 Days
2enoxaparin sodium 100mg/ml (1ml) inj QL=60 Quantity/30 Days
You can find information on what the symbols and abbreviations on this table mean by going to the beginning of this table.
22
DRUG NAME DRUG TIER REQUIREMENTS/LIMITS
2enoxaparin sodium 150mg/ml (0.8ml) inj QL=60 Quantity/30 Days
2enoxaparin sodium 150mg/ml (1ml) inj QL=60 Quantity/30 Days
2fondaparinux sodium 12.5mg/ml (0.4ml) inj
2fondaparinux sodium 12.5mg/ml (0.6ml) inj
2fondaparinux sodium 12.5mg/ml (0.8ml) inj
2fondaparinux sodium 5mg/ml (0.5mg) inj
3FRAGMIN 10000UNIT/ML INJ
3FRAGMIN 12500UNIT/0.5ML INJ
3FRAGMIN 15000UNIT/0.6ML INJ
3FRAGMIN 18000UNT/0.72ML INJ
3FRAGMIN 2500UNIT/0.2ML INJ
3FRAGMIN 5000UNIT/0.2ML INJ
3FRAGMIN 7500UNIT/0.3ML INJ
3FRAGMIN 95000UNIT/3.8ML INJ
2heparin sodium 5000unit/0.5ml inj (PF)
2heparin sodium porcine 10000unit/ml inj
2heparin sodium porcine 1000unit/ml inj
2heparin sodium porcine 20000unit/ml inj
2heparin sodium porcine 5000unit/ml injTHROMBIN INHIBITORS
3PRADAXA 110MG CAP
3PRADAXA 150MG CAP
3PRADAXA 75MG CAP
ANTICONVULSANTSAMPA GLUTAMATE RECEPTOR ANTAGONISTS
3FYCOMPA 0.5MG/ML SUSP PA_NSO
3FYCOMPA 10MG TAB PA_NSO
3FYCOMPA 12MG TAB PA_NSO
3FYCOMPA 2MG TAB PA_NSO
3FYCOMPA 4MG TAB PA_NSO
3FYCOMPA 6MG TAB PA_NSO
3FYCOMPA 8MG TAB PA_NSOANTICONVULSANTS - BENZODIAZEPINES
2clobazam 10mg tab QL=60 Quantity/30 Days
2clobazam 2.5mg/ml susp QL=480 Quantity/30 Days
2clobazam 20mg tab QL=60 Quantity/30 Days
2clonazepam 0.125mg odt QL=90 Quantity/30 Days
2clonazepam 0.25mg odt QL=90 Quantity/30 Days
2clonazepam 0.5mg odt QL=90 Quantity/30 Days
1clonazepam 0.5mg tab QL=90 Quantity/30 Days
2clonazepam 1mg odt QL=90 Quantity/30 Days
1clonazepam 1mg tab QL=90 Quantity/30 Days
2clonazepam 2mg odt QL=300 Quantity/30 Days
1clonazepam 2mg tab QL=300 Quantity/30 Days
2DIAZEPAM 10MG/2ML RECTAL GEL QL=10 Quantity/30 Days
2DIAZEPAM 2.5MG/0.5ML RECTAL GEL QL=10 Quantity/30 Days
You can find information on what the symbols and abbreviations on this table mean by going to the beginning of this table.
23
DRUG NAME DRUG TIER REQUIREMENTS/LIMITS
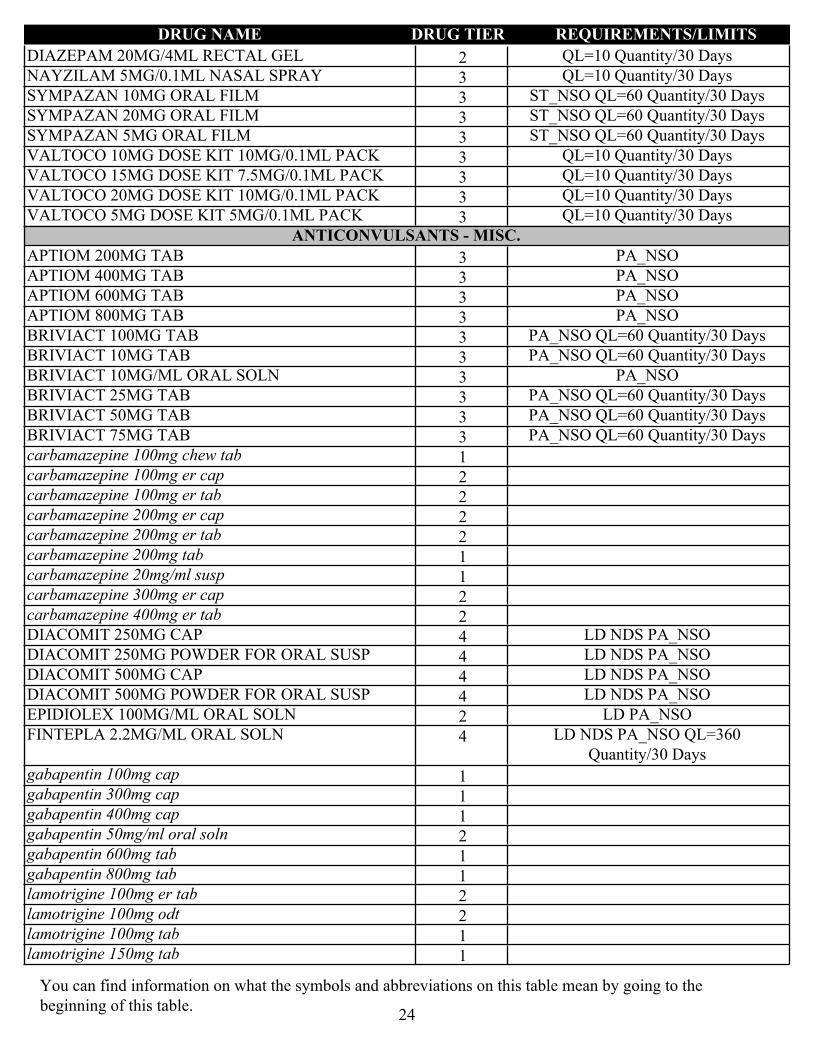
2DIAZEPAM 20MG/4ML RECTAL GEL QL=10 Quantity/30 Days
3NAYZILAM 5MG/0.1ML NASAL SPRAY QL=10 Quantity/30 Days
3SYMPAZAN 10MG ORAL FILM ST_NSO QL=60 Quantity/30 Days
3SYMPAZAN 20MG ORAL FILM ST_NSO QL=60 Quantity/30 Days
3SYMPAZAN 5MG ORAL FILM ST_NSO QL=60 Quantity/30 Days
3VALTOCO 10MG DOSE KIT 10MG/0.1ML PACK QL=10 Quantity/30 Days
3VALTOCO 15MG DOSE KIT 7.5MG/0.1ML PACK QL=10 Quantity/30 Days
3VALTOCO 20MG DOSE KIT 10MG/0.1ML PACK QL=10 Quantity/30 Days
3VALTOCO 5MG DOSE KIT 5MG/0.1ML PACK QL=10 Quantity/30 DaysANTICONVULSANTS - MISC.
3APTIOM 200MG TAB PA_NSO
3APTIOM 400MG TAB PA_NSO
3APTIOM 600MG TAB PA_NSO
3APTIOM 800MG TAB PA_NSO
3BRIVIACT 100MG TAB PA_NSO QL=60 Quantity/30 Days
3BRIVIACT 10MG TAB PA_NSO QL=60 Quantity/30 Days
3BRIVIACT 10MG/ML ORAL SOLN PA_NSO
3BRIVIACT 25MG TAB PA_NSO QL=60 Quantity/30 Days
3BRIVIACT 50MG TAB PA_NSO QL=60 Quantity/30 Days
3BRIVIACT 75MG TAB PA_NSO QL=60 Quantity/30 Days
1carbamazepine 100mg chew tab
2carbamazepine 100mg er cap
2carbamazepine 100mg er tab
2carbamazepine 200mg er cap
2carbamazepine 200mg er tab
1carbamazepine 200mg tab
1carbamazepine 20mg/ml susp
2carbamazepine 300mg er cap
2carbamazepine 400mg er tab
4DIACOMIT 250MG CAP LD NDS PA_NSO
4DIACOMIT 250MG POWDER FOR ORAL SUSP LD NDS PA_NSO
4DIACOMIT 500MG CAP LD NDS PA_NSO
4DIACOMIT 500MG POWDER FOR ORAL SUSP LD NDS PA_NSO
2EPIDIOLEX 100MG/ML ORAL SOLN LD PA_NSO
4FINTEPLA 2.2MG/ML ORAL SOLN LD NDS PA_NSO QL=360 Quantity/30 Days
1gabapentin 100mg cap
1gabapentin 300mg cap
1gabapentin 400mg cap
2gabapentin 50mg/ml oral soln
1gabapentin 600mg tab
1gabapentin 800mg tab
2lamotrigine 100mg er tab
2lamotrigine 100mg odt
1lamotrigine 100mg tab
1lamotrigine 150mg tab
You can find information on what the symbols and abbreviations on this table mean by going to the beginning of this table.
24

DRUG NAME DRUG TIER REQUIREMENTS/LIMITS
2lamotrigine 200mg er tab
2lamotrigine 200mg odt
1lamotrigine 200mg tab
2lamotrigine 250mg er tab
1lamotrigine 25mg chew tab
2lamotrigine 25mg er tab
2lamotrigine 25mg odt
1lamotrigine 25mg tab
2lamotrigine 300mg er tab
2lamotrigine 50mg er tab
2lamotrigine 50mg odt
1lamotrigine 5mg chew tab
1levetiracetam 1000mg tab
1levetiracetam 100mg/ml oral soln
1levetiracetam 250mg tab
1levetiracetam 500mg er tab
1levetiracetam 500mg tab
1levetiracetam 750mg er tab
1levetiracetam 750mg tab
1oxcarbazepine 150mg tab
1oxcarbazepine 300mg tab
1oxcarbazepine 600mg tab
1oxcarbazepine 60mg/ml susp
1pregabalin 100mg cap
1pregabalin 150mg cap
1pregabalin 200mg cap
2pregabalin 20mg/ml oral soln
1pregabalin 225mg cap
1pregabalin 25mg cap
1pregabalin 300mg cap
1pregabalin 50mg cap
1pregabalin 75mg cap
1primidone 250mg tab
1primidone 50mg tab
2rufinamide 200mg tab PA_NSO
2rufinamide 40mg/ml susp PA_NSO
3SPRITAM 1000MG TAB FOR ORAL SUSP PA_NSO
3SPRITAM 250MG TAB FOR ORAL SUSP PA_NSO
3SPRITAM 500MG TAB FOR ORAL SUSP PA_NSO
3SPRITAM 750MG TAB FOR ORAL SUSP PA_NSO
1topiramate 100mg tab
1topiramate 15mg cap
1topiramate 200mg tab
1topiramate 25mg cap
1topiramate 25mg tab
1topiramate 50mg tab
You can find information on what the symbols and abbreviations on this table mean by going to the beginning of this table.
25
DRUG NAME DRUG TIER REQUIREMENTS/LIMITS
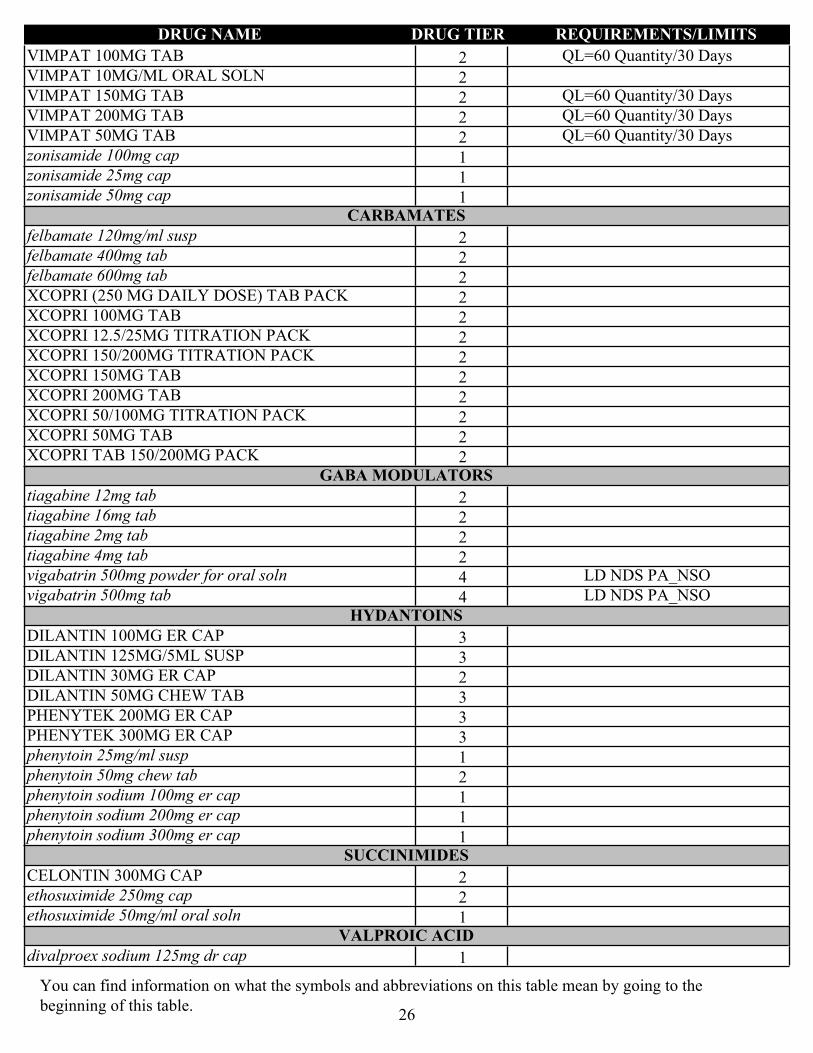
2VIMPAT 100MG TAB QL=60 Quantity/30 Days
2VIMPAT 10MG/ML ORAL SOLN
2VIMPAT 150MG TAB QL=60 Quantity/30 Days
2VIMPAT 200MG TAB QL=60 Quantity/30 Days
2VIMPAT 50MG TAB QL=60 Quantity/30 Days
1zonisamide 100mg cap
1zonisamide 25mg cap
1zonisamide 50mg capCARBAMATES
2felbamate 120mg/ml susp
2felbamate 400mg tab
2felbamate 600mg tab
2XCOPRI (250 MG DAILY DOSE) TAB PACK
2XCOPRI 100MG TAB
2XCOPRI 12.5/25MG TITRATION PACK
2XCOPRI 150/200MG TITRATION PACK
2XCOPRI 150MG TAB
2XCOPRI 200MG TAB
2XCOPRI 50/100MG TITRATION PACK
2XCOPRI 50MG TAB
2XCOPRI TAB 150/200MG PACKGABA MODULATORS
2tiagabine 12mg tab
2tiagabine 16mg tab
2tiagabine 2mg tab
2tiagabine 4mg tab
4vigabatrin 500mg powder for oral soln LD NDS PA_NSO
4vigabatrin 500mg tab LD NDS PA_NSOHYDANTOINS
3DILANTIN 100MG ER CAP
3DILANTIN 125MG/5ML SUSP
2DILANTIN 30MG ER CAP
3DILANTIN 50MG CHEW TAB
3PHENYTEK 200MG ER CAP
3PHENYTEK 300MG ER CAP
1phenytoin 25mg/ml susp
2phenytoin 50mg chew tab
1phenytoin sodium 100mg er cap
1phenytoin sodium 200mg er cap
1phenytoin sodium 300mg er capSUCCINIMIDES
2CELONTIN 300MG CAP
2ethosuximide 250mg cap
1ethosuximide 50mg/ml oral solnVALPROIC ACID
1divalproex sodium 125mg dr cap
You can find information on what the symbols and abbreviations on this table mean by going to the beginning of this table.
26
DRUG NAME DRUG TIER REQUIREMENTS/LIMITS
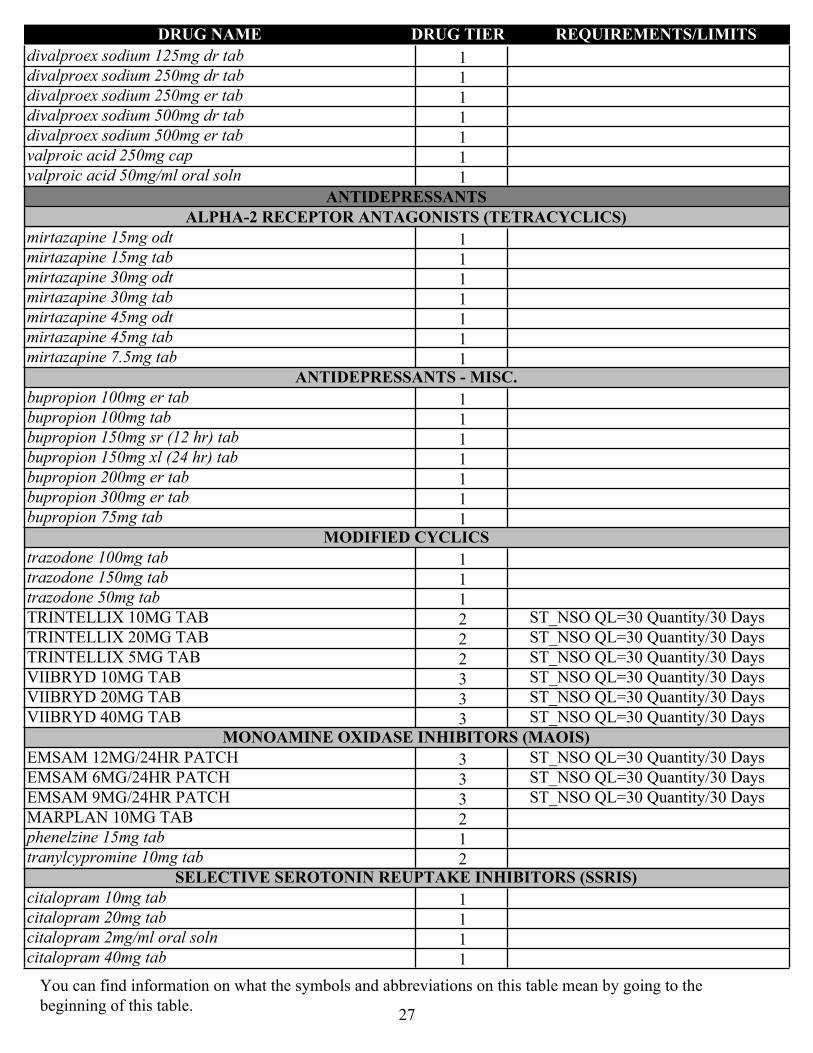
1divalproex sodium 125mg dr tab
1divalproex sodium 250mg dr tab
1divalproex sodium 250mg er tab
1divalproex sodium 500mg dr tab
1divalproex sodium 500mg er tab
1valproic acid 250mg cap
1valproic acid 50mg/ml oral soln
ANTIDEPRESSANTSALPHA-2 RECEPTOR ANTAGONISTS (TETRACYCLICS)
1mirtazapine 15mg odt
1mirtazapine 15mg tab
1mirtazapine 30mg odt
1mirtazapine 30mg tab
1mirtazapine 45mg odt
1mirtazapine 45mg tab
1mirtazapine 7.5mg tabANTIDEPRESSANTS - MISC.
1bupropion 100mg er tab
1bupropion 100mg tab
1bupropion 150mg sr (12 hr) tab
1bupropion 150mg xl (24 hr) tab
1bupropion 200mg er tab
1bupropion 300mg er tab
1bupropion 75mg tabMODIFIED CYCLICS
1trazodone 100mg tab
1trazodone 150mg tab
1trazodone 50mg tab
2TRINTELLIX 10MG TAB ST_NSO QL=30 Quantity/30 Days
2TRINTELLIX 20MG TAB ST_NSO QL=30 Quantity/30 Days
2TRINTELLIX 5MG TAB ST_NSO QL=30 Quantity/30 Days
3VIIBRYD 10MG TAB ST_NSO QL=30 Quantity/30 Days
3VIIBRYD 20MG TAB ST_NSO QL=30 Quantity/30 Days
3VIIBRYD 40MG TAB ST_NSO QL=30 Quantity/30 DaysMONOAMINE OXIDASE INHIBITORS (MAOIS)
3EMSAM 12MG/24HR PATCH ST_NSO QL=30 Quantity/30 Days
3EMSAM 6MG/24HR PATCH ST_NSO QL=30 Quantity/30 Days
3EMSAM 9MG/24HR PATCH ST_NSO QL=30 Quantity/30 Days
2MARPLAN 10MG TAB
1phenelzine 15mg tab
2tranylcypromine 10mg tabSELECTIVE SEROTONIN REUPTAKE INHIBITORS (SSRIS)
1citalopram 10mg tab
1citalopram 20mg tab
1citalopram 2mg/ml oral soln
1citalopram 40mg tab
You can find information on what the symbols and abbreviations on this table mean by going to the beginning of this table.
27

DRUG NAME DRUG TIER REQUIREMENTS/LIMITS
1escitalopram 10mg tab
2escitalopram 1mg/ml oral soln
1escitalopram 20mg tab
1escitalopram 5mg tab
1fluoxetine 10mg cap
1fluoxetine 20mg cap
1fluoxetine 40mg cap
1fluoxetine 4mg/ml oral soln
1fluvoxamine maleate 100mg tab
1fluvoxamine maleate 25mg tab
1fluvoxamine maleate 50mg tab
1paroxetine 10mg tab
3paroxetine 10mg/5ml susp
2paroxetine 12.5mg er tab
1paroxetine 20mg tab
2paroxetine 25mg er tab
1paroxetine 30mg tab
2paroxetine 37.5mg er tab
1paroxetine 40mg tab
3PAXIL 10MG/5ML SUSP
1sertraline 100mg tab
1sertraline 20mg/ml oral soln
1sertraline 25mg tab
1sertraline 50mg tabSEROTONIN MODULATORS
3NEFAZODONE 100MG TAB
3NEFAZODONE 150MG TAB
3NEFAZODONE 200MG TAB
1NEFAZODONE 250MG TAB
1NEFAZODONE 50MG TAB
3VIIBRYD 10/20MG STARTER PACK ST_NSO QL=30 Quantity/30 DaysSEROTONIN-NOREPINEPHRINE REUPTAKE INHIBITORS (SNRIS)
2desvenlafaxine succinate 100mg er tab
2desvenlafaxine succinate 25mg er tab
2desvenlafaxine succinate 50mg er tab
3DRIZALMA 20MG DR CAP ST_NSO QL=60 Quantity/30 Days
3DRIZALMA 30MG DR CAP ST_NSO QL=60 Quantity/30 Days
3DRIZALMA 40MG DR CAP ST_NSO QL=60 Quantity/30 Days
3DRIZALMA 60MG DR CAP ST_NSO QL=60 Quantity/30 Days
1duloxetine 20mg dr cap
1duloxetine 30mg dr cap
1duloxetine 60mg dr cap
3FETZIMA 120MG ER CAP ST_NSO QL=30 Quantity/30 Days
3FETZIMA 20MG ER CAP ST_NSO QL=30 Quantity/30 Days
3FETZIMA 40MG ER CAP ST_NSO QL=30 Quantity/30 Days
3FETZIMA 80MG ER CAP ST_NSO QL=30 Quantity/30 Days
You can find information on what the symbols and abbreviations on this table mean by going to the beginning of this table.
28

DRUG NAME DRUG TIER REQUIREMENTS/LIMITS
3FETZIMA PACK ST_NSO QL=30 Quantity/30 Days
1venlafaxine 100mg tab
1venlafaxine 150mg er cap
1venlafaxine 25mg tab
1venlafaxine 37.5mg er cap
1venlafaxine 37.5mg tab
1venlafaxine 50mg tab
1venlafaxine 75mg er cap
1venlafaxine 75mg tabTRICYCLIC AGENTS
1amitriptyline 100mg tab
1amitriptyline 10mg tab
1amitriptyline 150mg tab
1amitriptyline 25mg tab
1amitriptyline 50mg tab
1amitriptyline 75mg tab
2AMOXAPINE 100MG TAB
2AMOXAPINE 150MG TAB
2AMOXAPINE 25MG TAB
2AMOXAPINE 50MG TAB
2clomipramine 25mg cap
2clomipramine 50mg cap
2clomipramine 75mg cap
2desipramine 100mg tab
2desipramine 10mg tab
2desipramine 150mg tab
2desipramine 25mg tab
2desipramine 50mg tab
2desipramine 75mg tab
1doxepin 100mg cap
1doxepin 10mg cap
1doxepin 10mg/ml oral soln
1doxepin 150mg cap
1doxepin 25mg cap
1doxepin 50mg cap
1doxepin 75mg cap
1imipramine 10mg tab
1imipramine 25mg tab
1imipramine 50mg tab
1nortriptyline 10mg cap
1nortriptyline 25mg cap
2NORTRIPTYLINE 2MG/ML ORAL SOLN
1nortriptyline 50mg cap
1nortriptyline 75mg cap
2protriptyline 10mg tab
2protriptyline 5mg tab
You can find information on what the symbols and abbreviations on this table mean by going to the beginning of this table.
29

DRUG NAME DRUG TIER REQUIREMENTS/LIMITS
2trimipramine 100mg cap
2trimipramine 25mg cap
2trimipramine 50mg cap
ANTIDIABETICSALPHA-GLUCOSIDASE INHIBITORS
1acarbose 100mg tab
1acarbose 25mg tab
1acarbose 50mg tab
2miglitol 100mg tab
2miglitol 25mg tab
2miglitol 50mg tabANTIDIABETIC COMBINATIONS
$0glipizide 2.5mg/metformin 250mg tab
$0glipizide 2.5mg/metformin 500mg tab
$0glipizide 5mg/metformin 500mg tab
1glyburide 1.25mg/metformin 250mg tab
1glyburide 2.5mg/metformin 500mg tab
1glyburide 5mg/metformin 500mg tab
2GLYXAMBI 10-5MG TAB QL=30 Quantity/30 Days
2GLYXAMBI 25-5MG TAB QL=30 Quantity/30 Days
2JANUMET 1000-100MG ER TAB QL=30 Quantity/30 Days
2JANUMET 1000-50MG ER TAB QL=60 Quantity/30 Days
2JANUMET 1000-50MG TAB QL=60 Quantity/30 Days
2JANUMET 500-50MG ER TAB QL=60 Quantity/30 Days
2JANUMET 500-50MG TAB QL=60 Quantity/30 Days
2JENTADUETO 2.5-1000MG ER TAB QL=30 Quantity/30 Days
2JENTADUETO 2.5-1000MG TAB QL=60 Quantity/30 Days
2JENTADUETO 2.5-500MG TAB QL=60 Quantity/30 Days
2JENTADUETO 2.5-850MG TAB QL=60 Quantity/30 Days
2JENTADUETO 5-1000MG ER TAB QL=30 Quantity/30 Days
2SOLIQUA PEN INJ PA QL=1 Quantity/25 Days
2SYNJARDY 10-1000MG ER TAB QL=30 Quantity/30 Days
2SYNJARDY 12.5-1000MG ER TAB QL=60 Quantity/30 Days
2SYNJARDY 12.5-1000MG TAB QL=60 Quantity/30 Days
2SYNJARDY 12.5-500MG TAB QL=60 Quantity/30 Days
2SYNJARDY 25-1000MG ER TAB QL=30 Quantity/30 Days
2SYNJARDY 5-1000MG ER TAB QL=60 Quantity/30 Days
2SYNJARDY 5-1000MG TAB QL=60 Quantity/30 Days
2SYNJARDY 5-500MG TAB QL=60 Quantity/30 Days
2TRIJARDY 10-5-1000MG ER TAB QL=30 Quantity/30 Days
2TRIJARDY 12.5-2.5-1000MG ER TAB QL=60 Quantity/30 Days
2TRIJARDY 25-5-1000MG ER TAB QL=30 Quantity/30 Days
2TRIJARDY 5-2.5-1000MG ER TAB QL=60 Quantity/30 Days
2XIGDUO 10-1000MG ER TAB QL=30 Quantity/30 Days
2XIGDUO 10-500MG ER TAB QL=30 Quantity/30 Days
2XIGDUO 2.5-1000MG ER TAB QL=60 Quantity/30 Days
You can find information on what the symbols and abbreviations on this table mean by going to the beginning of this table.
30

DRUG NAME DRUG TIER REQUIREMENTS/LIMITS
2XIGDUO 5-1000MG ER TAB QL=60 Quantity/30 Days
2XIGDUO 5-500MG ER TAB QL=30 Quantity/30 Days
2XULTOPHY 100UNIT-3.6MG/ML PEN INJ PA QL=15 Quantity/30 DaysBIGUANIDES
$0metformin 1000mg tab
2metformin 100mg/ml soln
$0metformin 500mg er tab
$0metformin 500mg tab
$0metformin 750mg er tab
$0metformin 850mg tabDIABETIC OTHER
2BAQSIMI 3MG/DOSE NASAL POWDER QL=2 Quantity/7 Days
2diazoxide 50mg/ml susp
2GLUCAGEN 1MG INJ QL=2 Quantity/7 Days
2glucagon (rdna) 1mg inj kit QL=2 Quantity/7 Days
2GLUCAGON 1MG KIT QL=2 Quantity/7 Days
2GVOKE 0.5MG/0.1ML AUTO-INJECTOR QL=2 Quantity/7 Days
2GVOKE 0.5MG/0.1ML SYRINGE QL=2 Quantity/7 Days
2GVOKE 1MG/0.2ML AUTO-INJECTOR QL=2 Quantity/7 Days
2GVOKE 1MG/0.2ML SYRINGE QL=2 Quantity/7 Days
4KORLYM 300MG TAB LD NDS PADIPEPTIDYL PEPTIDASE-4 (DPP-4) INHIBITORS
2JANUVIA 100MG TAB RXC QL=30 Quantity/30 Days
2JANUVIA 25MG TAB RXC QL=30 Quantity/30 Days
2JANUVIA 50MG TAB RXC QL=30 Quantity/30 Days
2TRADJENTA 5MG TAB QL=30 Quantity/30 DaysDOPAMINE RECEPTOR AGONISTS - ANTIDIABETIC
3CYCLOSET 0.8MG TABINCRETIN MIMETIC AGENTS (GLP-1 RECEPTOR AGONISTS)
2BYDUREON 2MG PEN INJ QL=4 Quantity/28 Days
2BYDUREON 2MG/0.85ML AUTO-INJECTOR QL=4 Quantity/28 Days
2OZEMPIC 2MG/1.5ML PEN INJ QL=1 Quantity/28 Days
2OZEMPIC 2MG/1.5ML PEN INJ (1MG DOSE) QL=2 Quantity/28 Days
2OZEMPIC 4MG/3ML PEN INJ QL=1 Quantity/28 Days
2RYBELSUS 14MG TAB QL=30 Quantity/30 Days
2RYBELSUS 3MG TAB QL=30 Quantity/30 Days
2RYBELSUS 7MG TAB QL=30 Quantity/30 Days
2TRULICITY 0.75MG/0.5ML AUTO-INJECTOR QL=4 Quantity/28 Days
2TRULICITY 1.5MG/0.5ML AUTO-INJECTOR QL=4 Quantity/28 Days
2TRULICITY 3MG/0.5ML AUTO-INJECTOR QL=4 Quantity/28 Days
2TRULICITY 4.5MG/0.5ML AUTO-INJECTOR QL=4 Quantity/28 Days
2VICTOZA 18MG/3ML PEN INJ QL=9 Quantity/30 DaysINSULIN
2FIASP 100UNIT/ML CARTRIDGE
2FIASP 100UNIT/ML INJ PA_BvD
2FIASP 100UNIT/ML PEN INJ
You can find information on what the symbols and abbreviations on this table mean by going to the beginning of this table.
31

DRUG NAME DRUG TIER REQUIREMENTS/LIMITS
2HUMULIN R 500UNIT/ML INJ PA_BvD
2HUMULIN R 500UNIT/ML PEN INJ
2LANTUS 100UNIT/ML INJ
2LANTUS SOLOSTAR 100UNIT/ML INJ
2LEVEMIR 100UNIT/ML INJ
2LEVEMIR 100UNIT/ML PEN INJ
2NOVOLIN MIX (70/30) 100UNIT/ML INJ
2NOVOLIN MIX (70/30) FLEXPEN 100UNIT/ML
2NOVOLIN N 100UNIT/ML INJ
2NOVOLIN N 100UNIT/ML PEN INJ
2NOVOLIN R 100UNIT/ML INJ
2NOVOLIN R FLEXPEN RELION
2NOVOLOG 100UNIT/ML CARTRIDGE, INSULIN ASPART HUMAN 100UNIT/ML CARTRIDGE
2NOVOLOG 100UNIT/ML INJ, INSULIN ASPART HUMAN 100UNIT/ML INJ
PA_BvD
2NOVOLOG 100UNIT/ML PEN INJ, INSULIN ASPART HUMAN 100UNIT/ML PEN INJ
2NOVOLOG MIX (70/30) 100UNIT/ML INJ, INSULIN ASPART MIX 70UNIT-30UNIT/ML INJ
2NOVOLOG MIX 70-30UNIT/ML PEN INJ, INSULIN ASPART MIX 70UNIT-30UNIT/ML PEN INJ
2TOUJEO 300UNIT/ML PEN INJ
2TOUJEO MAX 300UNIT/ML PEN INJ (3ML)
2TRESIBA 100UNIT/ML INJ
2TRESIBA 100UNIT/ML PEN INJ
2TRESIBA 200UNIT/ML PEN INJINSULIN SENSITIZING AGENTS
1pioglitazone 15mg tab
1pioglitazone 30mg tab
1pioglitazone 45mg tabMEGLITINIDE ANALOGUES
1nateglinide 120mg tab
1nateglinide 60mg tab
1repaglinide 0.5mg tab
1repaglinide 1mg tab
1repaglinide 2mg tabSODIUM-GLUCOSE CO-TRANSPORTER 2 (SGLT2) INHIBITORS
2FARXIGA 10MG TAB QL=30 Quantity/30 Days
2FARXIGA 5MG TAB QL=30 Quantity/30 Days
2JARDIANCE 10MG TAB QL=30 Quantity/30 Days
2JARDIANCE 25MG TAB QL=30 Quantity/30 DaysSULFONYLUREAS
$0glimepiride 1mg tab
$0glimepiride 2mg tab
$0glimepiride 4mg tab
You can find information on what the symbols and abbreviations on this table mean by going to the beginning of this table.
32
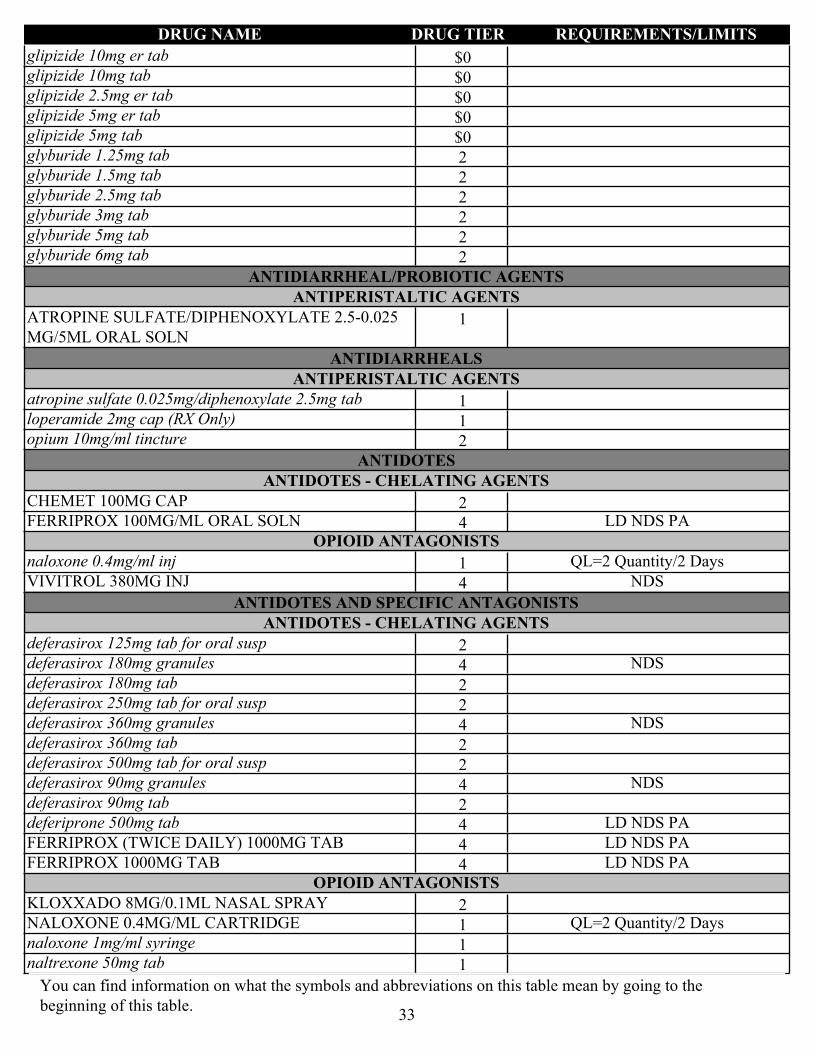
DRUG NAME DRUG TIER REQUIREMENTS/LIMITS
$0glipizide 10mg er tab
$0glipizide 10mg tab
$0glipizide 2.5mg er tab
$0glipizide 5mg er tab
$0glipizide 5mg tab
2glyburide 1.25mg tab
2glyburide 1.5mg tab
2glyburide 2.5mg tab
2glyburide 3mg tab
2glyburide 5mg tab
2glyburide 6mg tab
ANTIDIARRHEAL/PROBIOTIC AGENTSANTIPERISTALTIC AGENTS
1ATROPINE SULFATE/DIPHENOXYLATE 2.5-0.025 MG/5ML ORAL SOLN
ANTIDIARRHEALSANTIPERISTALTIC AGENTS
1atropine sulfate 0.025mg/diphenoxylate 2.5mg tab
1loperamide 2mg cap (RX Only)
2opium 10mg/ml tincture
ANTIDOTESANTIDOTES - CHELATING AGENTS
2CHEMET 100MG CAP
4FERRIPROX 100MG/ML ORAL SOLN LD NDS PAOPIOID ANTAGONISTS
1naloxone 0.4mg/ml inj QL=2 Quantity/2 Days
4VIVITROL 380MG INJ NDS
ANTIDOTES AND SPECIFIC ANTAGONISTSANTIDOTES - CHELATING AGENTS
2deferasirox 125mg tab for oral susp
4deferasirox 180mg granules NDS
2deferasirox 180mg tab
2deferasirox 250mg tab for oral susp
4deferasirox 360mg granules NDS
2deferasirox 360mg tab
2deferasirox 500mg tab for oral susp
4deferasirox 90mg granules NDS
2deferasirox 90mg tab
4deferiprone 500mg tab LD NDS PA
4FERRIPROX (TWICE DAILY) 1000MG TAB LD NDS PA
4FERRIPROX 1000MG TAB LD NDS PAOPIOID ANTAGONISTS
2KLOXXADO 8MG/0.1ML NASAL SPRAY
1NALOXONE 0.4MG/ML CARTRIDGE QL=2 Quantity/2 Days
1naloxone 1mg/ml syringe
1naltrexone 50mg tab
You can find information on what the symbols and abbreviations on this table mean by going to the beginning of this table.
33

DRUG NAME DRUG TIER REQUIREMENTS/LIMITS
1NARCAN 4MG/0.1ML NASAL SPRAY
ANTIEMETICS5-HT3 RECEPTOR ANTAGONISTS
1granisetron 1mg tab PA_BvD QL=60 Quantity/30 Days
1ondansetron 0.8mg/ml oral soln PA_BvD
1ONDANSETRON 24MG TAB PA_BvD
1ondansetron 4mg odt PA_BvD
1ondansetron 4mg tab PA_BvD
1ondansetron 8mg odt PA_BvD
1ondansetron 8mg tab PA_BvD
3SANCUSO 3.1MG/24HR PATCH QL=2 Quantity/14 DaysANTIEMETICS - ANTICHOLINERGIC
1meclizine 12.5mg tab
1meclizine 25mg tab (RX Only)
2scopolamine 0.0139mg/hr patch
1trimethobenzamide 300mg capANTIEMETICS - MISCELLANEOUS
2doxylamine succinate 10mg/pyridoxine 10mg dr tab QL=120 Quantity/30 Days
2dronabinol 10mg cap PA QL=60 Quantity/30 Days
2dronabinol 2.5mg cap PA QL=60 Quantity/30 Days
2dronabinol 5mg cap PA QL=60 Quantity/30 DaysSUBSTANCE P/NEUROKININ 1 (NK1) RECEPTOR ANTAGONISTS
2aprepitant 125mg cap PA_BvD QL=3 Quantity/2 Days
2aprepitant 125mg/aprepitant 80mg pack PA_BvD QL=6 Quantity/4 Days
2aprepitant 40mg cap PA_BvD QL=3 Quantity/2 Days
2aprepitant 80mg cap PA_BvD QL=6 Quantity/4 Days
3VARUBI 90MG TAB PA_BvD QL=4 Quantity/28 Days
ANTIFUNGALSANTIFUNGAL - GLUCAN SYNTHESIS INHIBITORS (ECHINOCANDINS)
4caspofungin acetate 50mg inj NDS
4CASPOFUNGIN ACETATE 50MG INJ NDS
2CASPOFUNGIN ACETATE 70MG INJ
2caspofungin acetate 70mg inj
2ERAXIS 100MG INJ
2ERAXIS 50MG INJ
2micafungin sodium 100mg inj
2micafungin sodium 50mg injANTIFUNGALS
3ABELCET 5MG/ML INJ PA_BvD
3AMBISOME 50MG INJ PA_BvD
3AMPHOTERICIN B 50MG INJ PA_BvD
2flucytosine 250mg cap
2flucytosine 500mg cap
2griseofulvin 125mg tab
2griseofulvin 250mg tab
2griseofulvin 25mg/ml susp
You can find information on what the symbols and abbreviations on this table mean by going to the beginning of this table.
34
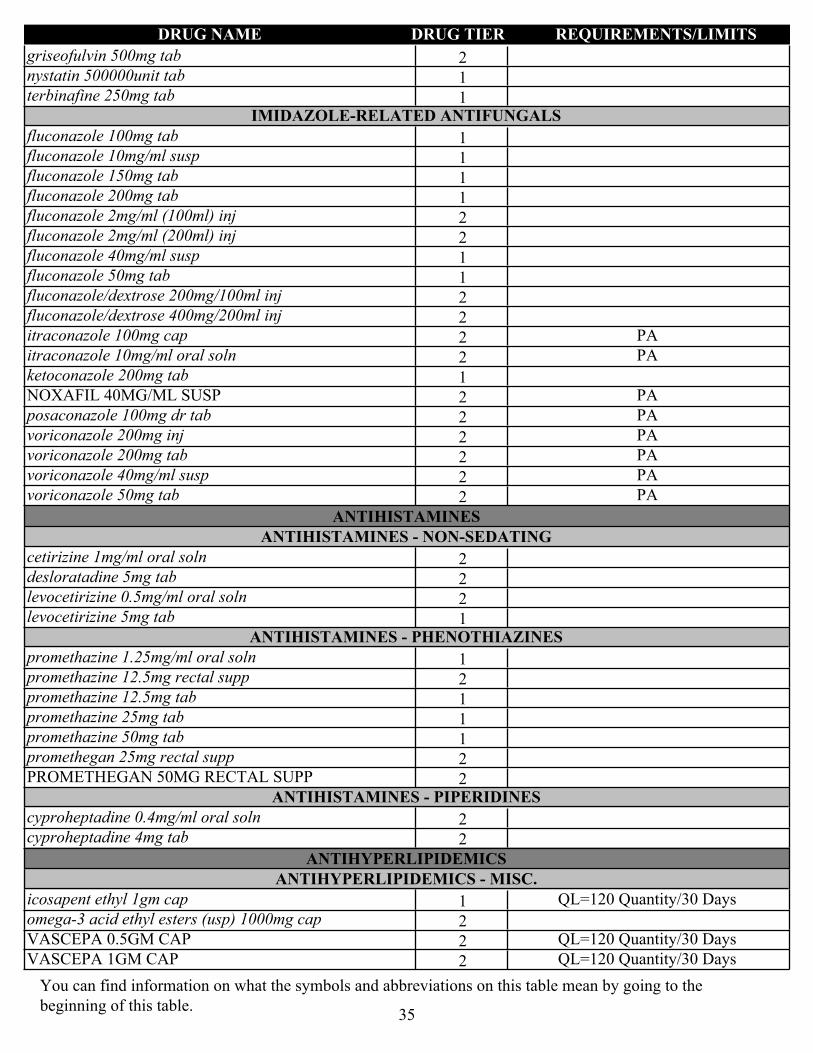
DRUG NAME DRUG TIER REQUIREMENTS/LIMITS
2griseofulvin 500mg tab
1nystatin 500000unit tab
1terbinafine 250mg tabIMIDAZOLE-RELATED ANTIFUNGALS
1fluconazole 100mg tab
1fluconazole 10mg/ml susp
1fluconazole 150mg tab
1fluconazole 200mg tab
2fluconazole 2mg/ml (100ml) inj
2fluconazole 2mg/ml (200ml) inj
1fluconazole 40mg/ml susp
1fluconazole 50mg tab
2fluconazole/dextrose 200mg/100ml inj
2fluconazole/dextrose 400mg/200ml inj
2itraconazole 100mg cap PA
2itraconazole 10mg/ml oral soln PA
1ketoconazole 200mg tab
2NOXAFIL 40MG/ML SUSP PA
2posaconazole 100mg dr tab PA
2voriconazole 200mg inj PA
2voriconazole 200mg tab PA
2voriconazole 40mg/ml susp PA
2voriconazole 50mg tab PA
ANTIHISTAMINESANTIHISTAMINES - NON-SEDATING
2cetirizine 1mg/ml oral soln
2desloratadine 5mg tab
2levocetirizine 0.5mg/ml oral soln
1levocetirizine 5mg tabANTIHISTAMINES - PHENOTHIAZINES
1promethazine 1.25mg/ml oral soln
2promethazine 12.5mg rectal supp
1promethazine 12.5mg tab
1promethazine 25mg tab
1promethazine 50mg tab
2promethegan 25mg rectal supp
2PROMETHEGAN 50MG RECTAL SUPPANTIHISTAMINES - PIPERIDINES
2cyproheptadine 0.4mg/ml oral soln
2cyproheptadine 4mg tab
ANTIHYPERLIPIDEMICSANTIHYPERLIPIDEMICS - MISC.
1icosapent ethyl 1gm cap QL=120 Quantity/30 Days
2omega-3 acid ethyl esters (usp) 1000mg cap
2VASCEPA 0.5GM CAP QL=120 Quantity/30 Days
2VASCEPA 1GM CAP QL=120 Quantity/30 Days
You can find information on what the symbols and abbreviations on this table mean by going to the beginning of this table.
35

DRUG NAME DRUG TIER REQUIREMENTS/LIMITS
BILE ACID SEQUESTRANTS
2cholestyramine 4gm bulk powder
2cholestyramine resin 4gm sf powder for oral susp
2cholestyramine resin 4gm sf powder for oral susp (sugar free)
2colesevelam 3750mg powder for oral susp
2colesevelam 625mg tab
1colestipol 1000mg tab
2colestipol 5000mg granules for oral susp
2colestipol 5gm granule
2prevalite 4gm powder for oral suspFIBRIC ACID DERIVATIVES
3ANTARA 30MG CAP
3ANTARA 90MG CAP
1fenofibrate 134mg cap
1fenofibrate 145mg tab
3FENOFIBRATE 150MG CAP
1fenofibrate 160mg tab
1fenofibrate 200mg cap
1fenofibrate 48mg tab
3FENOFIBRATE 50MG CAP
1fenofibrate 54mg tab
1fenofibrate 67mg cap
2fenofibric acid 135mg dr cap
2fenofibric acid 45mg dr cap
1gemfibrozil 600mg tabHMG COA REDUCTASE INHIBITORS
$0atorvastatin 10mg tab
$0atorvastatin 20mg tab
$0atorvastatin 40mg tab
$0atorvastatin 80mg tab
2fluvastatin 20mg cap
2fluvastatin 40mg cap
2fluvastatin 80mg er tab
3LIVALO 1MG TAB ST
3LIVALO 2MG TAB ST
3LIVALO 4MG TAB ST
$0lovastatin 10mg tab
$0lovastatin 20mg tab
$0lovastatin 40mg tab
$0pravastatin sodium 10mg tab
$0pravastatin sodium 20mg tab
$0pravastatin sodium 40mg tab
$0pravastatin sodium 80mg tab
$0rosuvastatin calcium 10mg tab
$0rosuvastatin calcium 20mg tab
You can find information on what the symbols and abbreviations on this table mean by going to the beginning of this table.
36
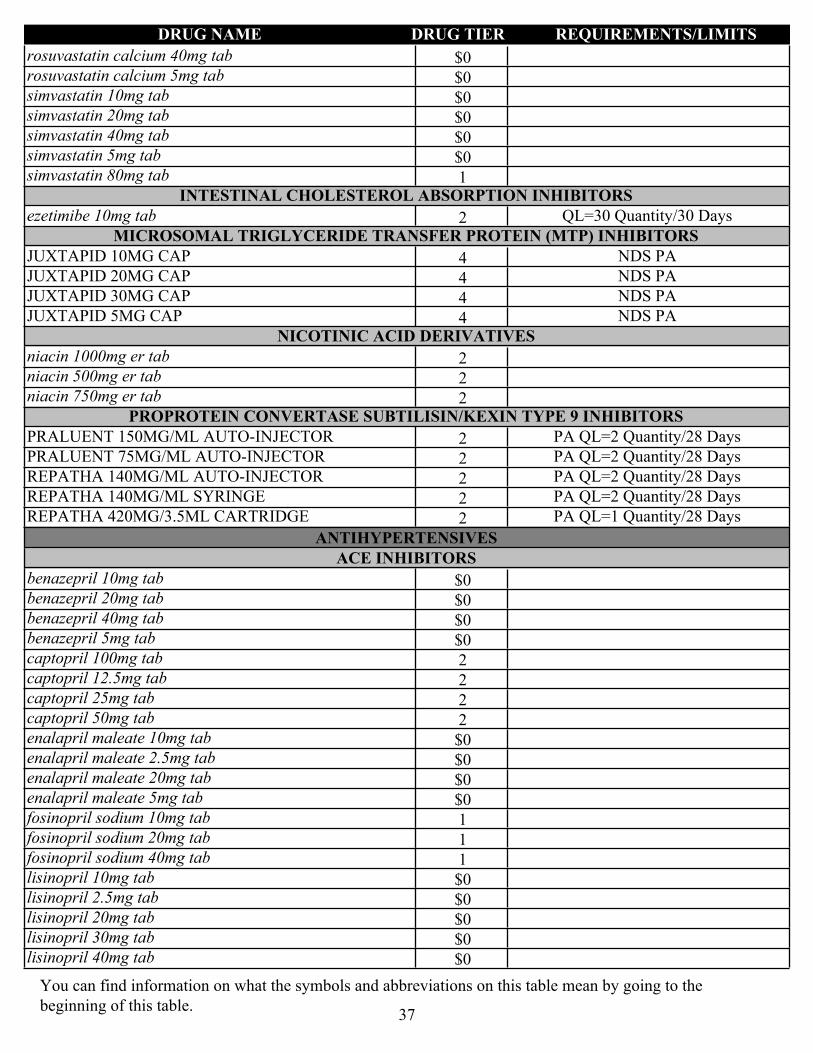
DRUG NAME DRUG TIER REQUIREMENTS/LIMITS
$0rosuvastatin calcium 40mg tab
$0rosuvastatin calcium 5mg tab
$0simvastatin 10mg tab
$0simvastatin 20mg tab
$0simvastatin 40mg tab
$0simvastatin 5mg tab
1simvastatin 80mg tabINTESTINAL CHOLESTEROL ABSORPTION INHIBITORS
2ezetimibe 10mg tab QL=30 Quantity/30 DaysMICROSOMAL TRIGLYCERIDE TRANSFER PROTEIN (MTP) INHIBITORS
4JUXTAPID 10MG CAP NDS PA
4JUXTAPID 20MG CAP NDS PA
4JUXTAPID 30MG CAP NDS PA
4JUXTAPID 5MG CAP NDS PANICOTINIC ACID DERIVATIVES
2niacin 1000mg er tab
2niacin 500mg er tab
2niacin 750mg er tabPROPROTEIN CONVERTASE SUBTILISIN/KEXIN TYPE 9 INHIBITORS
2PRALUENT 150MG/ML AUTO-INJECTOR PA QL=2 Quantity/28 Days
2PRALUENT 75MG/ML AUTO-INJECTOR PA QL=2 Quantity/28 Days
2REPATHA 140MG/ML AUTO-INJECTOR PA QL=2 Quantity/28 Days
2REPATHA 140MG/ML SYRINGE PA QL=2 Quantity/28 Days
2REPATHA 420MG/3.5ML CARTRIDGE PA QL=1 Quantity/28 Days
ANTIHYPERTENSIVESACE INHIBITORS
$0benazepril 10mg tab
$0benazepril 20mg tab
$0benazepril 40mg tab
$0benazepril 5mg tab
2captopril 100mg tab
2captopril 12.5mg tab
2captopril 25mg tab
2captopril 50mg tab
$0enalapril maleate 10mg tab
$0enalapril maleate 2.5mg tab
$0enalapril maleate 20mg tab
$0enalapril maleate 5mg tab
1fosinopril sodium 10mg tab
1fosinopril sodium 20mg tab
1fosinopril sodium 40mg tab
$0lisinopril 10mg tab
$0lisinopril 2.5mg tab
$0lisinopril 20mg tab
$0lisinopril 30mg tab
$0lisinopril 40mg tab
You can find information on what the symbols and abbreviations on this table mean by going to the beginning of this table.
37
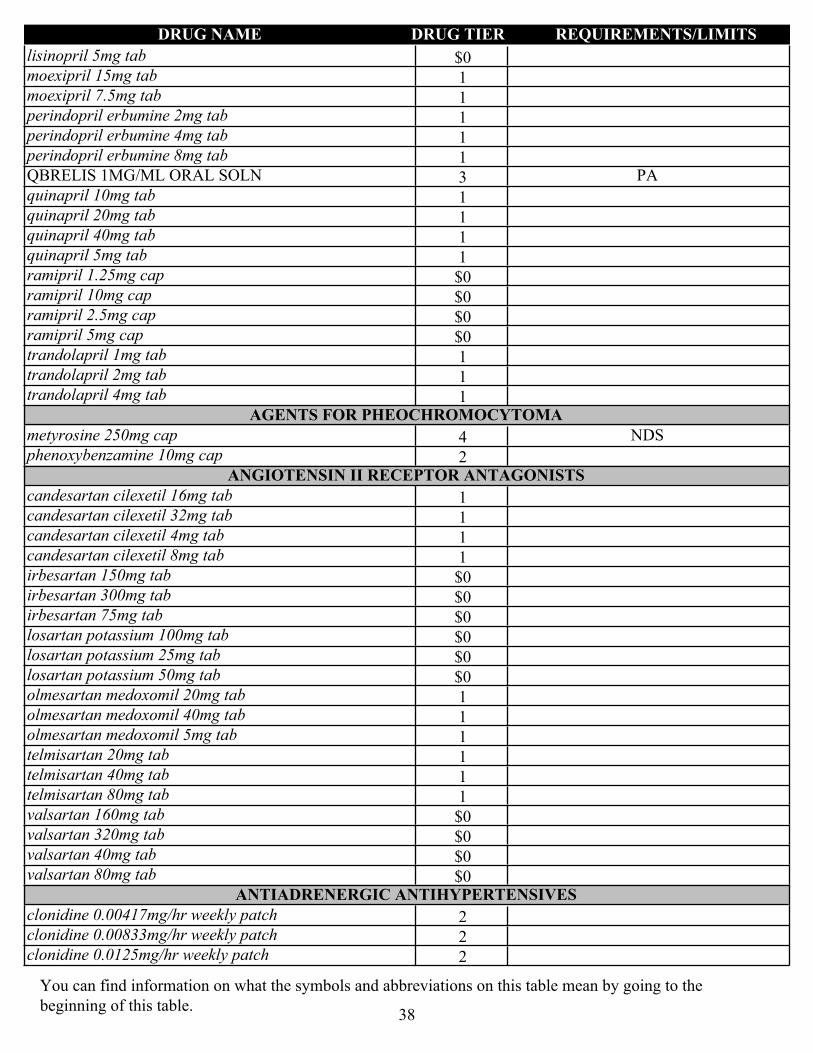
DRUG NAME DRUG TIER REQUIREMENTS/LIMITS
$0lisinopril 5mg tab
1moexipril 15mg tab
1moexipril 7.5mg tab
1perindopril erbumine 2mg tab
1perindopril erbumine 4mg tab
1perindopril erbumine 8mg tab
3QBRELIS 1MG/ML ORAL SOLN PA
1quinapril 10mg tab
1quinapril 20mg tab
1quinapril 40mg tab
1quinapril 5mg tab
$0ramipril 1.25mg cap
$0ramipril 10mg cap
$0ramipril 2.5mg cap
$0ramipril 5mg cap
1trandolapril 1mg tab
1trandolapril 2mg tab
1trandolapril 4mg tabAGENTS FOR PHEOCHROMOCYTOMA
4metyrosine 250mg cap NDS
2phenoxybenzamine 10mg capANGIOTENSIN II RECEPTOR ANTAGONISTS
1candesartan cilexetil 16mg tab
1candesartan cilexetil 32mg tab
1candesartan cilexetil 4mg tab
1candesartan cilexetil 8mg tab
$0irbesartan 150mg tab
$0irbesartan 300mg tab
$0irbesartan 75mg tab
$0losartan potassium 100mg tab
$0losartan potassium 25mg tab
$0losartan potassium 50mg tab
1olmesartan medoxomil 20mg tab
1olmesartan medoxomil 40mg tab
1olmesartan medoxomil 5mg tab
1telmisartan 20mg tab
1telmisartan 40mg tab
1telmisartan 80mg tab
$0valsartan 160mg tab
$0valsartan 320mg tab
$0valsartan 40mg tab
$0valsartan 80mg tabANTIADRENERGIC ANTIHYPERTENSIVES
2clonidine 0.00417mg/hr weekly patch
2clonidine 0.00833mg/hr weekly patch
2clonidine 0.0125mg/hr weekly patch
You can find information on what the symbols and abbreviations on this table mean by going to the beginning of this table.
38
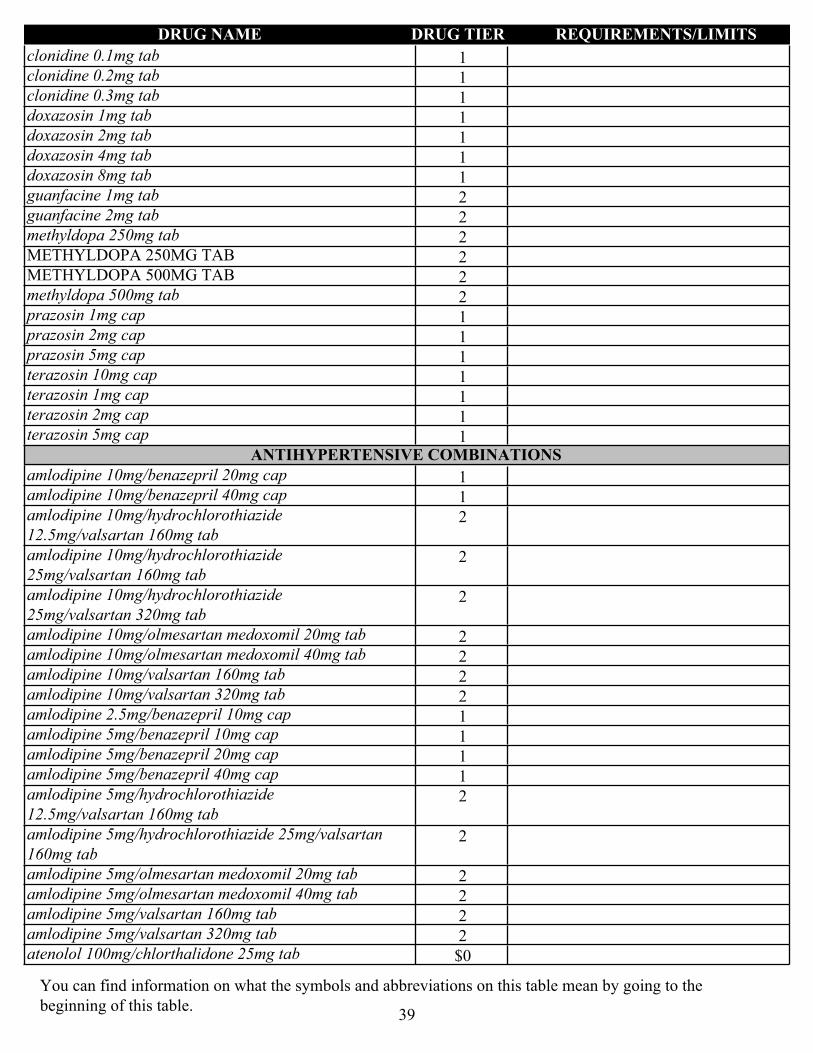
DRUG NAME DRUG TIER REQUIREMENTS/LIMITS
1clonidine 0.1mg tab
1clonidine 0.2mg tab
1clonidine 0.3mg tab
1doxazosin 1mg tab
1doxazosin 2mg tab
1doxazosin 4mg tab
1doxazosin 8mg tab
2guanfacine 1mg tab
2guanfacine 2mg tab
2methyldopa 250mg tab
2METHYLDOPA 250MG TAB
2METHYLDOPA 500MG TAB
2methyldopa 500mg tab
1prazosin 1mg cap
1prazosin 2mg cap
1prazosin 5mg cap
1terazosin 10mg cap
1terazosin 1mg cap
1terazosin 2mg cap
1terazosin 5mg capANTIHYPERTENSIVE COMBINATIONS
1amlodipine 10mg/benazepril 20mg cap
1amlodipine 10mg/benazepril 40mg cap
2amlodipine 10mg/hydrochlorothiazide 12.5mg/valsartan 160mg tab
2amlodipine 10mg/hydrochlorothiazide 25mg/valsartan 160mg tab
2amlodipine 10mg/hydrochlorothiazide 25mg/valsartan 320mg tab
2amlodipine 10mg/olmesartan medoxomil 20mg tab
2amlodipine 10mg/olmesartan medoxomil 40mg tab
2amlodipine 10mg/valsartan 160mg tab
2amlodipine 10mg/valsartan 320mg tab
1amlodipine 2.5mg/benazepril 10mg cap
1amlodipine 5mg/benazepril 10mg cap
1amlodipine 5mg/benazepril 20mg cap
1amlodipine 5mg/benazepril 40mg cap
2amlodipine 5mg/hydrochlorothiazide 12.5mg/valsartan 160mg tab
2amlodipine 5mg/hydrochlorothiazide 25mg/valsartan 160mg tab
2amlodipine 5mg/olmesartan medoxomil 20mg tab
2amlodipine 5mg/olmesartan medoxomil 40mg tab
2amlodipine 5mg/valsartan 160mg tab
2amlodipine 5mg/valsartan 320mg tab
$0atenolol 100mg/chlorthalidone 25mg tab
You can find information on what the symbols and abbreviations on this table mean by going to the beginning of this table.
39
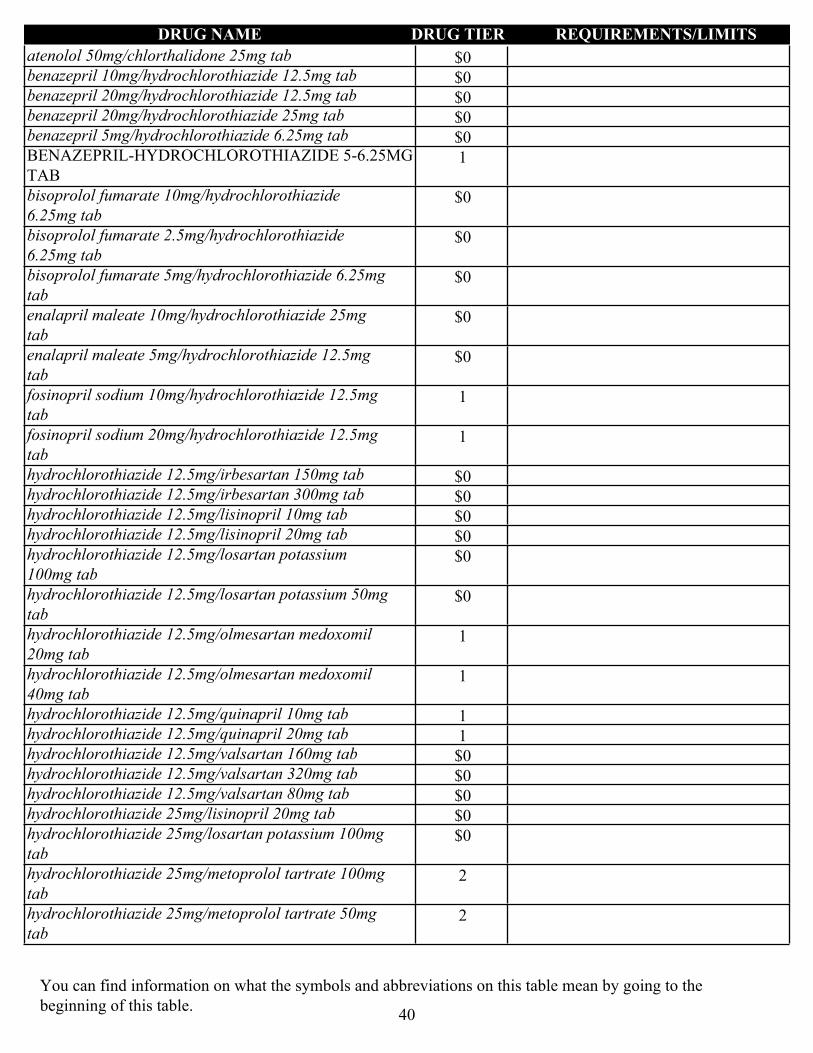
DRUG NAME DRUG TIER REQUIREMENTS/LIMITS
$0atenolol 50mg/chlorthalidone 25mg tab
$0benazepril 10mg/hydrochlorothiazide 12.5mg tab
$0benazepril 20mg/hydrochlorothiazide 12.5mg tab
$0benazepril 20mg/hydrochlorothiazide 25mg tab
$0benazepril 5mg/hydrochlorothiazide 6.25mg tab
1BENAZEPRIL-HYDROCHLOROTHIAZIDE 5-6.25MG TAB
$0bisoprolol fumarate 10mg/hydrochlorothiazide 6.25mg tab
$0bisoprolol fumarate 2.5mg/hydrochlorothiazide 6.25mg tab
$0bisoprolol fumarate 5mg/hydrochlorothiazide 6.25mg tab
$0enalapril maleate 10mg/hydrochlorothiazide 25mg tab
$0enalapril maleate 5mg/hydrochlorothiazide 12.5mg tab
1fosinopril sodium 10mg/hydrochlorothiazide 12.5mg tab
1fosinopril sodium 20mg/hydrochlorothiazide 12.5mg tab
$0hydrochlorothiazide 12.5mg/irbesartan 150mg tab
$0hydrochlorothiazide 12.5mg/irbesartan 300mg tab
$0hydrochlorothiazide 12.5mg/lisinopril 10mg tab
$0hydrochlorothiazide 12.5mg/lisinopril 20mg tab
$0hydrochlorothiazide 12.5mg/losartan potassium 100mg tab
$0hydrochlorothiazide 12.5mg/losartan potassium 50mg tab
1hydrochlorothiazide 12.5mg/olmesartan medoxomil 20mg tab
1hydrochlorothiazide 12.5mg/olmesartan medoxomil 40mg tab
1hydrochlorothiazide 12.5mg/quinapril 10mg tab
1hydrochlorothiazide 12.5mg/quinapril 20mg tab
$0hydrochlorothiazide 12.5mg/valsartan 160mg tab
$0hydrochlorothiazide 12.5mg/valsartan 320mg tab
$0hydrochlorothiazide 12.5mg/valsartan 80mg tab
$0hydrochlorothiazide 25mg/lisinopril 20mg tab
$0hydrochlorothiazide 25mg/losartan potassium 100mg tab
2hydrochlorothiazide 25mg/metoprolol tartrate 100mg tab
2hydrochlorothiazide 25mg/metoprolol tartrate 50mg tab
You can find information on what the symbols and abbreviations on this table mean by going to the beginning of this table.
40
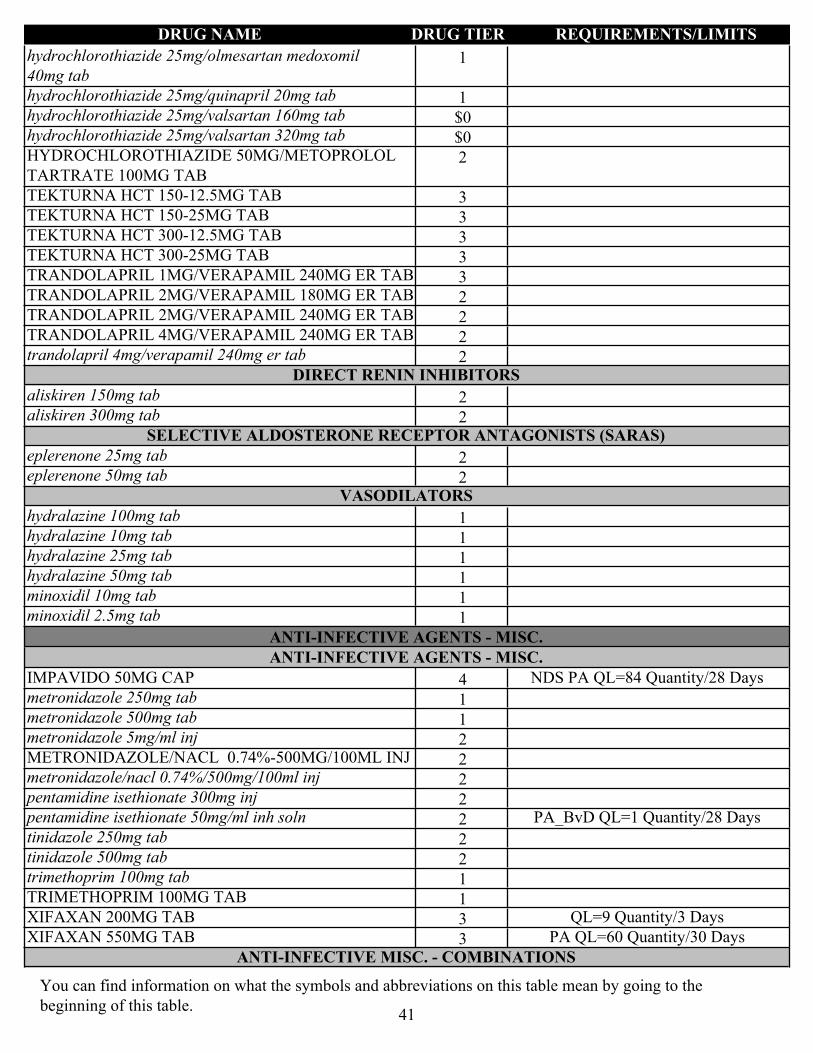
DRUG NAME DRUG TIER REQUIREMENTS/LIMITS
1hydrochlorothiazide 25mg/olmesartan medoxomil 40mg tab
1hydrochlorothiazide 25mg/quinapril 20mg tab
$0hydrochlorothiazide 25mg/valsartan 160mg tab
$0hydrochlorothiazide 25mg/valsartan 320mg tab
2HYDROCHLOROTHIAZIDE 50MG/METOPROLOL TARTRATE 100MG TAB
3TEKTURNA HCT 150-12.5MG TAB
3TEKTURNA HCT 150-25MG TAB
3TEKTURNA HCT 300-12.5MG TAB
3TEKTURNA HCT 300-25MG TAB
3TRANDOLAPRIL 1MG/VERAPAMIL 240MG ER TAB
2TRANDOLAPRIL 2MG/VERAPAMIL 180MG ER TAB
2TRANDOLAPRIL 2MG/VERAPAMIL 240MG ER TAB
2TRANDOLAPRIL 4MG/VERAPAMIL 240MG ER TAB
2trandolapril 4mg/verapamil 240mg er tabDIRECT RENIN INHIBITORS
2aliskiren 150mg tab
2aliskiren 300mg tabSELECTIVE ALDOSTERONE RECEPTOR ANTAGONISTS (SARAS)
2eplerenone 25mg tab
2eplerenone 50mg tabVASODILATORS
1hydralazine 100mg tab
1hydralazine 10mg tab
1hydralazine 25mg tab
1hydralazine 50mg tab
1minoxidil 10mg tab
1minoxidil 2.5mg tab
ANTI-INFECTIVE AGENTS - MISC.ANTI-INFECTIVE AGENTS - MISC.
4IMPAVIDO 50MG CAP NDS PA QL=84 Quantity/28 Days
1metronidazole 250mg tab
1metronidazole 500mg tab
2metronidazole 5mg/ml inj
2METRONIDAZOLE/NACL 0.74%-500MG/100ML INJ
2metronidazole/nacl 0.74%/500mg/100ml inj
2pentamidine isethionate 300mg inj
2pentamidine isethionate 50mg/ml inh soln PA_BvD QL=1 Quantity/28 Days
2tinidazole 250mg tab
2tinidazole 500mg tab
1trimethoprim 100mg tab
1TRIMETHOPRIM 100MG TAB
3XIFAXAN 200MG TAB QL=9 Quantity/3 Days
3XIFAXAN 550MG TAB PA QL=60 Quantity/30 DaysANTI-INFECTIVE MISC. - COMBINATIONS
You can find information on what the symbols and abbreviations on this table mean by going to the beginning of this table.
41
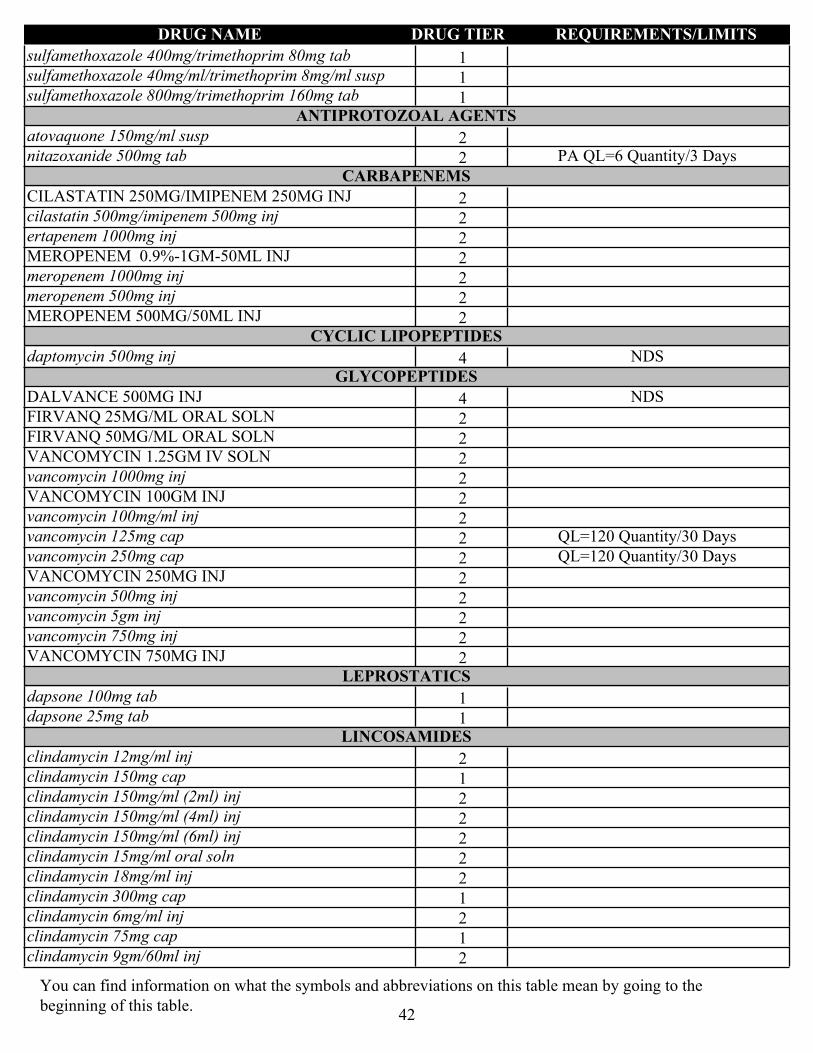
DRUG NAME DRUG TIER REQUIREMENTS/LIMITS
1sulfamethoxazole 400mg/trimethoprim 80mg tab
1sulfamethoxazole 40mg/ml/trimethoprim 8mg/ml susp
1sulfamethoxazole 800mg/trimethoprim 160mg tabANTIPROTOZOAL AGENTS
2atovaquone 150mg/ml susp
2nitazoxanide 500mg tab PA QL=6 Quantity/3 DaysCARBAPENEMS
2CILASTATIN 250MG/IMIPENEM 250MG INJ
2cilastatin 500mg/imipenem 500mg inj
2ertapenem 1000mg inj
2MEROPENEM 0.9%-1GM-50ML INJ
2meropenem 1000mg inj
2meropenem 500mg inj
2MEROPENEM 500MG/50ML INJCYCLIC LIPOPEPTIDES
4daptomycin 500mg inj NDSGLYCOPEPTIDES
4DALVANCE 500MG INJ NDS
2FIRVANQ 25MG/ML ORAL SOLN
2FIRVANQ 50MG/ML ORAL SOLN
2VANCOMYCIN 1.25GM IV SOLN
2vancomycin 1000mg inj
2VANCOMYCIN 100GM INJ
2vancomycin 100mg/ml inj
2vancomycin 125mg cap QL=120 Quantity/30 Days
2vancomycin 250mg cap QL=120 Quantity/30 Days
2VANCOMYCIN 250MG INJ
2vancomycin 500mg inj
2vancomycin 5gm inj
2vancomycin 750mg inj
2VANCOMYCIN 750MG INJLEPROSTATICS
1dapsone 100mg tab
1dapsone 25mg tabLINCOSAMIDES
2clindamycin 12mg/ml inj
1clindamycin 150mg cap
2clindamycin 150mg/ml (2ml) inj
2clindamycin 150mg/ml (4ml) inj
2clindamycin 150mg/ml (6ml) inj
2clindamycin 15mg/ml oral soln
2clindamycin 18mg/ml inj
1clindamycin 300mg cap
2clindamycin 6mg/ml inj
1clindamycin 75mg cap
2clindamycin 9gm/60ml inj
You can find information on what the symbols and abbreviations on this table mean by going to the beginning of this table.
42
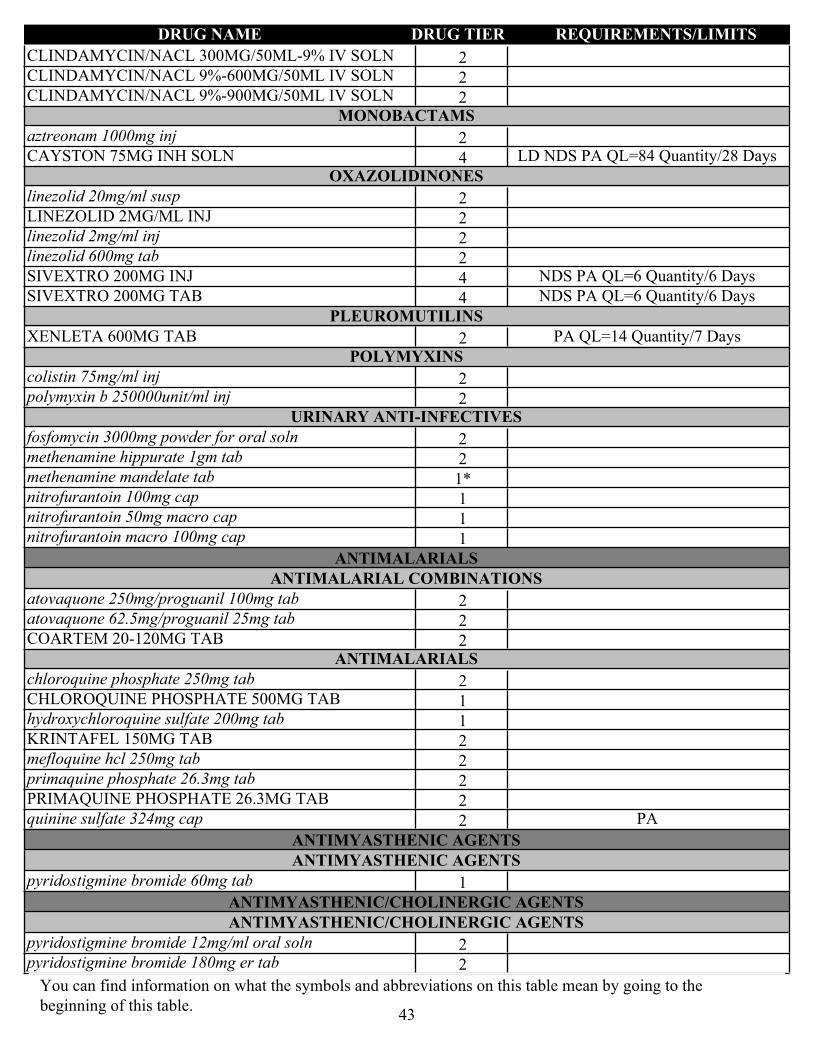
DRUG NAME DRUG TIER REQUIREMENTS/LIMITS
2CLINDAMYCIN/NACL 300MG/50ML-9% IV SOLN
2CLINDAMYCIN/NACL 9%-600MG/50ML IV SOLN
2CLINDAMYCIN/NACL 9%-900MG/50ML IV SOLNMONOBACTAMS
2aztreonam 1000mg inj
4CAYSTON 75MG INH SOLN LD NDS PA QL=84 Quantity/28 DaysOXAZOLIDINONES
2linezolid 20mg/ml susp
2LINEZOLID 2MG/ML INJ
2linezolid 2mg/ml inj
2linezolid 600mg tab
4SIVEXTRO 200MG INJ NDS PA QL=6 Quantity/6 Days
4SIVEXTRO 200MG TAB NDS PA QL=6 Quantity/6 DaysPLEUROMUTILINS
2XENLETA 600MG TAB PA QL=14 Quantity/7 DaysPOLYMYXINS
2colistin 75mg/ml inj
2polymyxin b 250000unit/ml injURINARY ANTI-INFECTIVES
2fosfomycin 3000mg powder for oral soln
2methenamine hippurate 1gm tab
1*methenamine mandelate tab
1nitrofurantoin 100mg cap
1nitrofurantoin 50mg macro cap
1nitrofurantoin macro 100mg cap
ANTIMALARIALSANTIMALARIAL COMBINATIONS
2atovaquone 250mg/proguanil 100mg tab
2atovaquone 62.5mg/proguanil 25mg tab
2COARTEM 20-120MG TABANTIMALARIALS
2chloroquine phosphate 250mg tab
1CHLOROQUINE PHOSPHATE 500MG TAB
1hydroxychloroquine sulfate 200mg tab
2KRINTAFEL 150MG TAB
2mefloquine hcl 250mg tab
2primaquine phosphate 26.3mg tab
2PRIMAQUINE PHOSPHATE 26.3MG TAB
2quinine sulfate 324mg cap PA
ANTIMYASTHENIC AGENTSANTIMYASTHENIC AGENTS
1pyridostigmine bromide 60mg tab
ANTIMYASTHENIC/CHOLINERGIC AGENTSANTIMYASTHENIC/CHOLINERGIC AGENTS
2pyridostigmine bromide 12mg/ml oral soln
2pyridostigmine bromide 180mg er tab
You can find information on what the symbols and abbreviations on this table mean by going to the beginning of this table.
43
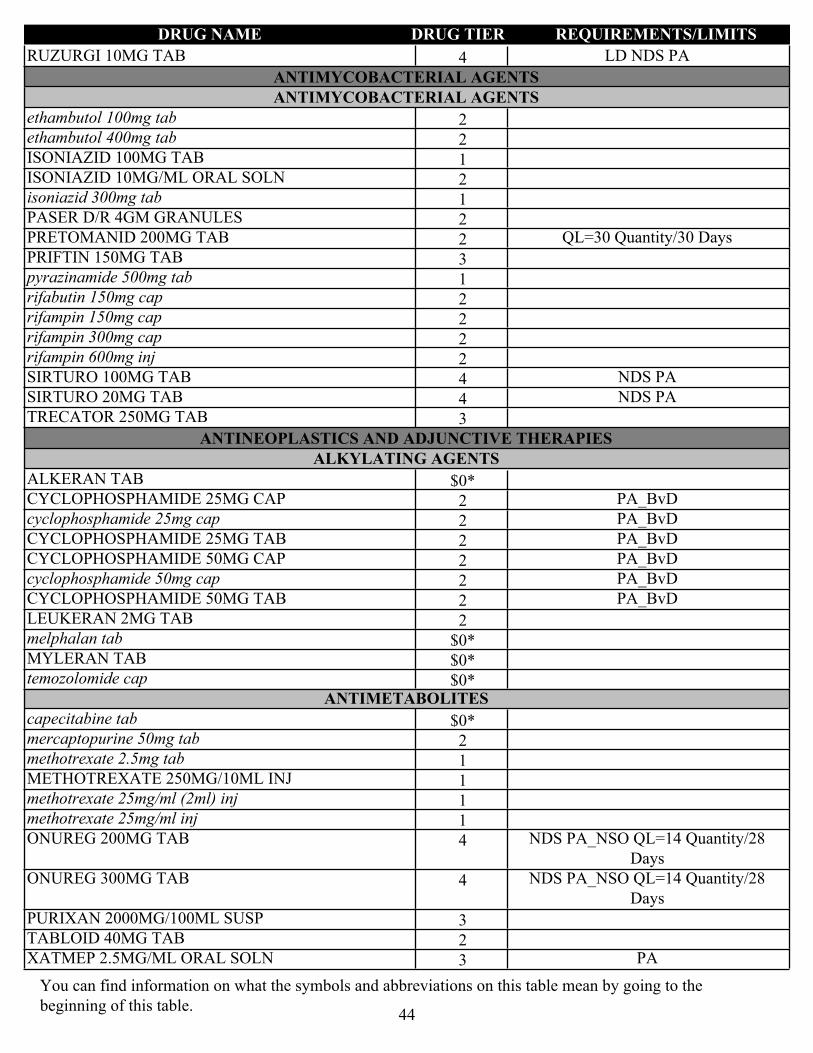
DRUG NAME DRUG TIER REQUIREMENTS/LIMITS
4RUZURGI 10MG TAB LD NDS PA
ANTIMYCOBACTERIAL AGENTSANTIMYCOBACTERIAL AGENTS
2ethambutol 100mg tab
2ethambutol 400mg tab
1ISONIAZID 100MG TAB
2ISONIAZID 10MG/ML ORAL SOLN
1isoniazid 300mg tab
2PASER D/R 4GM GRANULES
2PRETOMANID 200MG TAB QL=30 Quantity/30 Days
3PRIFTIN 150MG TAB
1pyrazinamide 500mg tab
2rifabutin 150mg cap
2rifampin 150mg cap
2rifampin 300mg cap
2rifampin 600mg inj
4SIRTURO 100MG TAB NDS PA
4SIRTURO 20MG TAB NDS PA
3TRECATOR 250MG TAB
ANTINEOPLASTICS AND ADJUNCTIVE THERAPIESALKYLATING AGENTS
$0*ALKERAN TAB
2CYCLOPHOSPHAMIDE 25MG CAP PA_BvD
2cyclophosphamide 25mg cap PA_BvD
2CYCLOPHOSPHAMIDE 25MG TAB PA_BvD
2CYCLOPHOSPHAMIDE 50MG CAP PA_BvD
2cyclophosphamide 50mg cap PA_BvD
2CYCLOPHOSPHAMIDE 50MG TAB PA_BvD
2LEUKERAN 2MG TAB
$0*melphalan tab
$0*MYLERAN TAB
$0*temozolomide capANTIMETABOLITES
$0*capecitabine tab
2mercaptopurine 50mg tab
1methotrexate 2.5mg tab
1METHOTREXATE 250MG/10ML INJ
1methotrexate 25mg/ml (2ml) inj
1methotrexate 25mg/ml inj
4ONUREG 200MG TAB NDS PA_NSO QL=14 Quantity/28 Days
4ONUREG 300MG TAB NDS PA_NSO QL=14 Quantity/28 Days
3PURIXAN 2000MG/100ML SUSP
2TABLOID 40MG TAB
3XATMEP 2.5MG/ML ORAL SOLN PA
You can find information on what the symbols and abbreviations on this table mean by going to the beginning of this table.
44

DRUG NAME DRUG TIER REQUIREMENTS/LIMITS
ANTINEOPLASTIC - ANGIOGENESIS INHIBITORS
4INLYTA 1MG TAB NDS PA_NSO
4INLYTA 5MG TAB NDS PA_NSO
4LENVIMA CAP THERAPY PACK (10MG) LD NDS PA_NSO QL=30 Quantity/30 Days
4LENVIMA CAP THERAPY PACK (12MG) LD NDS PA_NSO QL=90 Quantity/30 Days
4LENVIMA CAP THERAPY PACK (14MG) LD NDS PA_NSO QL=60 Quantity/30 Days
4LENVIMA CAP THERAPY PACK (18MG) LD NDS PA_NSO QL=90 Quantity/30 Days
4LENVIMA CAP THERAPY PACK (20MG) LD NDS PA_NSO QL=60 Quantity/30 Days
4LENVIMA CAP THERAPY PACK (24MG) LD NDS PA_NSO QL=90 Quantity/30 Days
4LENVIMA CAP THERAPY PACK (4MG) LD NDS PA_NSO QL=30 Quantity/30 Days
4LENVIMA CAP THERAPY PACK (8MG) LD NDS PA_NSO QL=60 Quantity/30 Days
ANTINEOPLASTIC - ANTI-HER2 AGENTS
4TUKYSA 150MG TAB LD NDS PA_NSO QL=120 Quantity/30 Days
4TUKYSA 50MG TAB LD NDS PA_NSO QL=120 Quantity/30 Days
ANTINEOPLASTIC - BCL-2 INHIBITORS
4VENCLEXTA 100MG TAB LD NDS PA_NSO
2VENCLEXTA 10MG TAB LD PA_NSO
2VENCLEXTA 50MG TAB LD PA_NSO
4VENCLEXTA STARTING PACK LD NDS PA_NSOANTINEOPLASTIC - EGFR INHIBITORS
2erlotinib 100mg tab PA_NSO
2erlotinib 150mg tab PA_NSO
2erlotinib 25mg tab PA_NSO
4GILOTRIF 20MG TAB LD NDS PA_NSO QL=30 Quantity/30 Days
4GILOTRIF 30MG TAB LD NDS PA_NSO QL=30 Quantity/30 Days
4GILOTRIF 40MG TAB LD NDS PA_NSO QL=30 Quantity/30 Days
4IRESSA 250MG TAB LD NDS PA_NSO
4TAGRISSO 40MG TAB LD NDS PA_NSO
4TAGRISSO 80MG TAB LD NDS PA_NSO
4VIZIMPRO 15MG TAB NDS PA_NSO QL=30 Quantity/30 Days
4VIZIMPRO 30MG TAB NDS PA_NSO QL=30 Quantity/30 Days
You can find information on what the symbols and abbreviations on this table mean by going to the beginning of this table.
45

DRUG NAME DRUG TIER REQUIREMENTS/LIMITS
4VIZIMPRO 45MG TAB NDS PA_NSO QL=30 Quantity/30 Days
ANTINEOPLASTIC - HEDGEHOG PATHWAY INHIBITORS
4DAURISMO 100MG TAB NDS PA_NSO
4DAURISMO 25MG TAB NDS PA_NSO
4ERIVEDGE 150MG CAP NDS PA_NSO
4ODOMZO 200MG CAP NDS PA_NSOANTINEOPLASTIC - HORMONAL AGENTS
$0anastrozole 1mg tab
1bicalutamide 50mg tab
3ELIGARD 22.5MG INJ QL=1 Quantity/84 Days
3ELIGARD 30MG INJ QL=1 Quantity/112 Days
3ELIGARD 45MG INJ QL=1 Quantity/168 Days
3ELIGARD 7.5MG INJ QL=1 Quantity/28 Days
2EMCYT 140MG CAP
$0exemestane 25mg tab
2flutamide 125mg cap
1letrozole 2.5mg tab
2leuprolide acetate 5mg/ml inj
4LUPRON 11.25MG INJ QL=1 Quantity/84 Days
4LUPRON 22.5MG INJ QL=1 Quantity/84 Days
4LUPRON 3.75MG INJ QL=1 Quantity/28 Days
4LUPRON 30MG INJ QL=1 Quantity/112 Days
4LUPRON 45MG INJ QL=1 Quantity/168 Days
4LUPRON 7.5MG INJ QL=1 Quantity/28 Days
2LYSODREN 500MG TAB LD
1megestrol acetate 20mg tab PA_NSO
1megestrol acetate 40mg tab PA_NSO
1megestrol acetate 40mg/ml susp PA
$0tamoxifen 10mg tab
$0tamoxifen 20mg tab
4TRELSTAR 11.25MG INJ QL=1 Quantity/84 Days
4TRELSTAR 22.5MG INJ QL=1 Quantity/168 Days
4TRELSTAR 3.75MG INJ QL=1 Quantity/28 DaysANTINEOPLASTIC - HORMONAL AND RELATED AGENTS
1abiraterone acetate 250mg tab QL=120 Quantity/30 Days
4ERLEADA 60MG TAB NDS PA_NSO QL=120 Quantity/30 Days
2FIRMAGON 120MG INJ PA_NSO
2FIRMAGON 80MG INJ PA_NSO
2FLUTAMIDE 125MG CAP
4nilutamide 150mg tab NDS
4NUBEQA 300MG TAB NDS PA_NSO QL=120 Quantity/30 Days
4ORGOVYX 120MG TAB LD NDS PA_NSO QL=30 Quantity/28 Days
You can find information on what the symbols and abbreviations on this table mean by going to the beginning of this table.
46
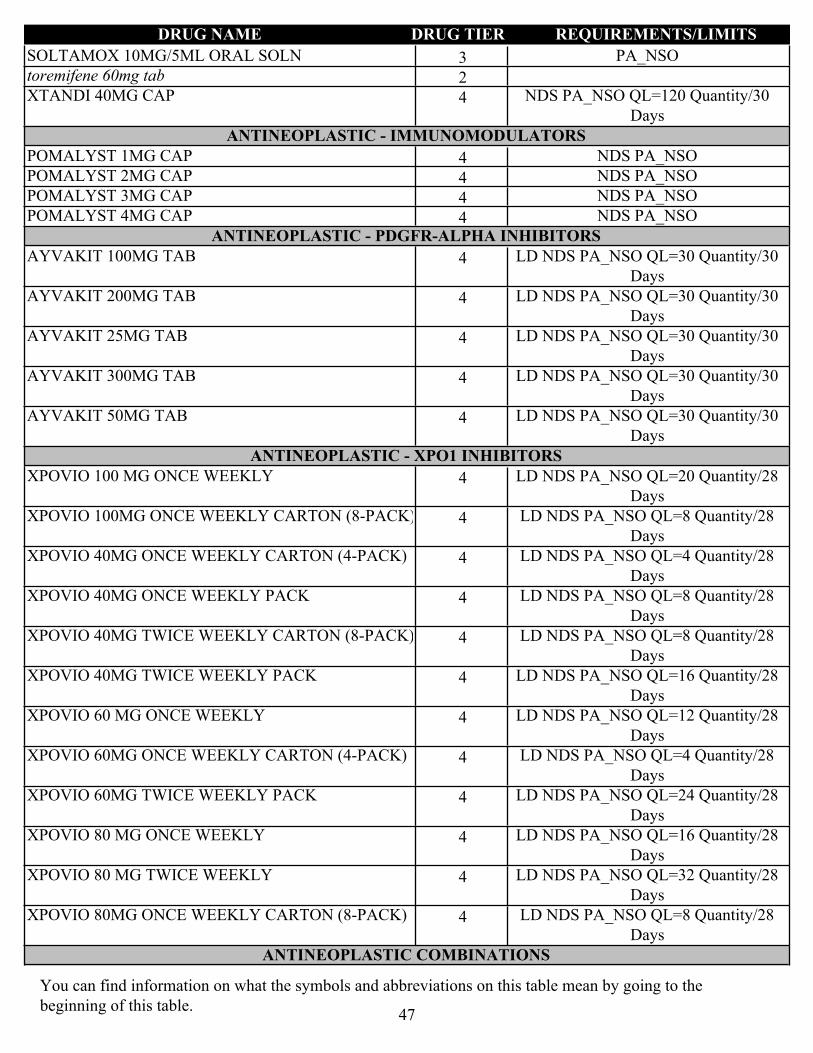
DRUG NAME DRUG TIER REQUIREMENTS/LIMITS
3SOLTAMOX 10MG/5ML ORAL SOLN PA_NSO
2toremifene 60mg tab
4XTANDI 40MG CAP NDS PA_NSO QL=120 Quantity/30 Days
ANTINEOPLASTIC - IMMUNOMODULATORS
4POMALYST 1MG CAP NDS PA_NSO
4POMALYST 2MG CAP NDS PA_NSO
4POMALYST 3MG CAP NDS PA_NSO
4POMALYST 4MG CAP NDS PA_NSOANTINEOPLASTIC - PDGFR-ALPHA INHIBITORS
4AYVAKIT 100MG TAB LD NDS PA_NSO QL=30 Quantity/30 Days
4AYVAKIT 200MG TAB LD NDS PA_NSO QL=30 Quantity/30 Days
4AYVAKIT 25MG TAB LD NDS PA_NSO QL=30 Quantity/30 Days
4AYVAKIT 300MG TAB LD NDS PA_NSO QL=30 Quantity/30 Days
4AYVAKIT 50MG TAB LD NDS PA_NSO QL=30 Quantity/30 Days
ANTINEOPLASTIC - XPO1 INHIBITORS
4XPOVIO 100 MG ONCE WEEKLY LD NDS PA_NSO QL=20 Quantity/28 Days
4XPOVIO 100MG ONCE WEEKLY CARTON (8-PACK) LD NDS PA_NSO QL=8 Quantity/28 Days
4XPOVIO 40MG ONCE WEEKLY CARTON (4-PACK) LD NDS PA_NSO QL=4 Quantity/28 Days
4XPOVIO 40MG ONCE WEEKLY PACK LD NDS PA_NSO QL=8 Quantity/28 Days
4XPOVIO 40MG TWICE WEEKLY CARTON (8-PACK) LD NDS PA_NSO QL=8 Quantity/28 Days
4XPOVIO 40MG TWICE WEEKLY PACK LD NDS PA_NSO QL=16 Quantity/28 Days
4XPOVIO 60 MG ONCE WEEKLY LD NDS PA_NSO QL=12 Quantity/28 Days
4XPOVIO 60MG ONCE WEEKLY CARTON (4-PACK) LD NDS PA_NSO QL=4 Quantity/28 Days
4XPOVIO 60MG TWICE WEEKLY PACK LD NDS PA_NSO QL=24 Quantity/28 Days
4XPOVIO 80 MG ONCE WEEKLY LD NDS PA_NSO QL=16 Quantity/28 Days
4XPOVIO 80 MG TWICE WEEKLY LD NDS PA_NSO QL=32 Quantity/28 Days
4XPOVIO 80MG ONCE WEEKLY CARTON (8-PACK) LD NDS PA_NSO QL=8 Quantity/28 Days
ANTINEOPLASTIC COMBINATIONS
You can find information on what the symbols and abbreviations on this table mean by going to the beginning of this table.
47
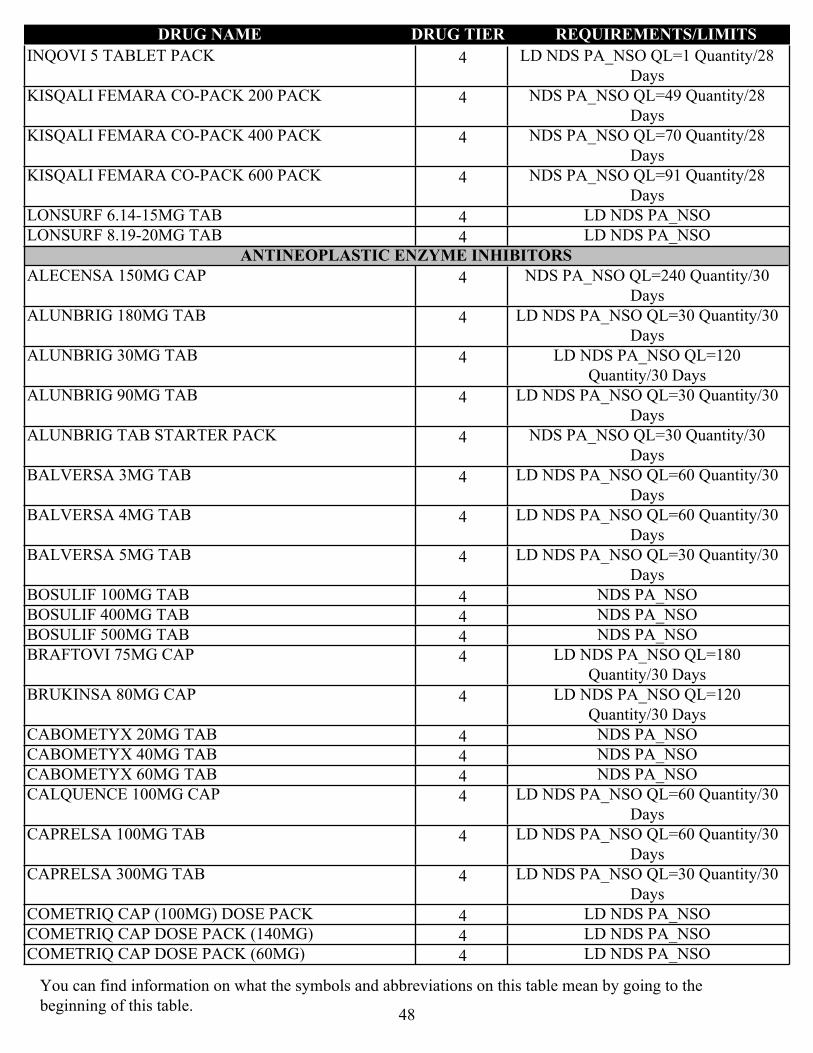
DRUG NAME DRUG TIER REQUIREMENTS/LIMITS
4INQOVI 5 TABLET PACK LD NDS PA_NSO QL=1 Quantity/28 Days
4KISQALI FEMARA CO-PACK 200 PACK NDS PA_NSO QL=49 Quantity/28 Days
4KISQALI FEMARA CO-PACK 400 PACK NDS PA_NSO QL=70 Quantity/28 Days
4KISQALI FEMARA CO-PACK 600 PACK NDS PA_NSO QL=91 Quantity/28 Days
4LONSURF 6.14-15MG TAB LD NDS PA_NSO
4LONSURF 8.19-20MG TAB LD NDS PA_NSOANTINEOPLASTIC ENZYME INHIBITORS
4ALECENSA 150MG CAP NDS PA_NSO QL=240 Quantity/30 Days
4ALUNBRIG 180MG TAB LD NDS PA_NSO QL=30 Quantity/30 Days
4ALUNBRIG 30MG TAB LD NDS PA_NSO QL=120 Quantity/30 Days
4ALUNBRIG 90MG TAB LD NDS PA_NSO QL=30 Quantity/30 Days
4ALUNBRIG TAB STARTER PACK NDS PA_NSO QL=30 Quantity/30 Days
4BALVERSA 3MG TAB LD NDS PA_NSO QL=60 Quantity/30 Days
4BALVERSA 4MG TAB LD NDS PA_NSO QL=60 Quantity/30 Days
4BALVERSA 5MG TAB LD NDS PA_NSO QL=30 Quantity/30 Days
4BOSULIF 100MG TAB NDS PA_NSO
4BOSULIF 400MG TAB NDS PA_NSO
4BOSULIF 500MG TAB NDS PA_NSO
4BRAFTOVI 75MG CAP LD NDS PA_NSO QL=180 Quantity/30 Days
4BRUKINSA 80MG CAP LD NDS PA_NSO QL=120 Quantity/30 Days
4CABOMETYX 20MG TAB NDS PA_NSO
4CABOMETYX 40MG TAB NDS PA_NSO
4CABOMETYX 60MG TAB NDS PA_NSO
4CALQUENCE 100MG CAP LD NDS PA_NSO QL=60 Quantity/30 Days
4CAPRELSA 100MG TAB LD NDS PA_NSO QL=60 Quantity/30 Days
4CAPRELSA 300MG TAB LD NDS PA_NSO QL=30 Quantity/30 Days
4COMETRIQ CAP (100MG) DOSE PACK LD NDS PA_NSO
4COMETRIQ CAP DOSE PACK (140MG) LD NDS PA_NSO
4COMETRIQ CAP DOSE PACK (60MG) LD NDS PA_NSO
You can find information on what the symbols and abbreviations on this table mean by going to the beginning of this table.
48
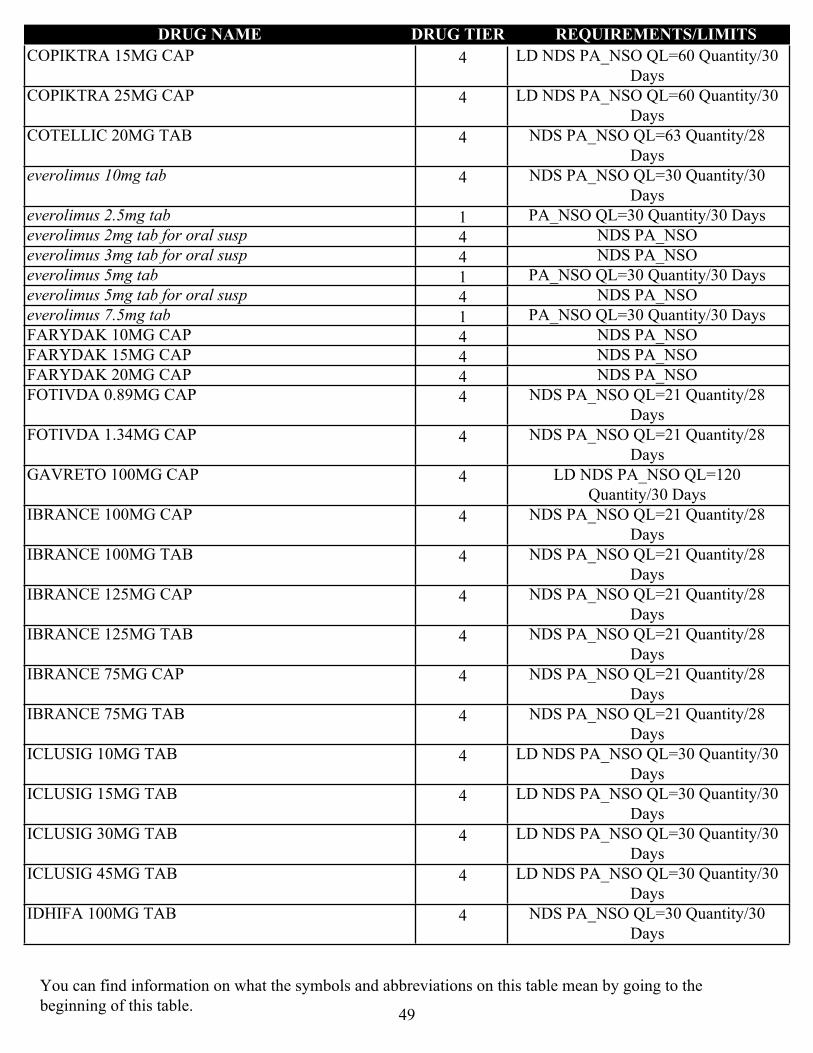
DRUG NAME DRUG TIER REQUIREMENTS/LIMITS
4COPIKTRA 15MG CAP LD NDS PA_NSO QL=60 Quantity/30 Days
4COPIKTRA 25MG CAP LD NDS PA_NSO QL=60 Quantity/30 Days
4COTELLIC 20MG TAB NDS PA_NSO QL=63 Quantity/28 Days
4everolimus 10mg tab NDS PA_NSO QL=30 Quantity/30 Days
1everolimus 2.5mg tab PA_NSO QL=30 Quantity/30 Days
4everolimus 2mg tab for oral susp NDS PA_NSO
4everolimus 3mg tab for oral susp NDS PA_NSO
1everolimus 5mg tab PA_NSO QL=30 Quantity/30 Days
4everolimus 5mg tab for oral susp NDS PA_NSO
1everolimus 7.5mg tab PA_NSO QL=30 Quantity/30 Days
4FARYDAK 10MG CAP NDS PA_NSO
4FARYDAK 15MG CAP NDS PA_NSO
4FARYDAK 20MG CAP NDS PA_NSO
4FOTIVDA 0.89MG CAP NDS PA_NSO QL=21 Quantity/28 Days
4FOTIVDA 1.34MG CAP NDS PA_NSO QL=21 Quantity/28 Days
4GAVRETO 100MG CAP LD NDS PA_NSO QL=120 Quantity/30 Days
4IBRANCE 100MG CAP NDS PA_NSO QL=21 Quantity/28 Days
4IBRANCE 100MG TAB NDS PA_NSO QL=21 Quantity/28 Days
4IBRANCE 125MG CAP NDS PA_NSO QL=21 Quantity/28 Days
4IBRANCE 125MG TAB NDS PA_NSO QL=21 Quantity/28 Days
4IBRANCE 75MG CAP NDS PA_NSO QL=21 Quantity/28 Days
4IBRANCE 75MG TAB NDS PA_NSO QL=21 Quantity/28 Days
4ICLUSIG 10MG TAB LD NDS PA_NSO QL=30 Quantity/30 Days
4ICLUSIG 15MG TAB LD NDS PA_NSO QL=30 Quantity/30 Days
4ICLUSIG 30MG TAB LD NDS PA_NSO QL=30 Quantity/30 Days
4ICLUSIG 45MG TAB LD NDS PA_NSO QL=30 Quantity/30 Days
4IDHIFA 100MG TAB NDS PA_NSO QL=30 Quantity/30 Days
You can find information on what the symbols and abbreviations on this table mean by going to the beginning of this table.
49

DRUG NAME DRUG TIER REQUIREMENTS/LIMITS
4IDHIFA 50MG TAB NDS PA_NSO QL=30 Quantity/30 Days
1imatinib 100mg tab
1imatinib 400mg tab
4IMBRUVICA 140MG CAP LD NDS PA_NSO QL=90 Quantity/30 Days
4IMBRUVICA 140MG TAB LD NDS PA_NSO QL=30 Quantity/30 Days
4IMBRUVICA 280MG TAB LD NDS PA_NSO QL=30 Quantity/30 Days
4IMBRUVICA 420MG TAB LD NDS PA_NSO QL=30 Quantity/30 Days
4IMBRUVICA 560MG TAB LD NDS PA_NSO QL=30 Quantity/30 Days
4IMBRUVICA 70MG CAP LD NDS PA_NSO QL=30 Quantity/30 Days
4INREBIC 100MG CAP NDS PA_NSO QL=120 Quantity/30 Days
4JAKAFI 10MG TAB NDS PA_NSO QL=60 Quantity/30 Days
4JAKAFI 15MG TAB NDS PA_NSO QL=60 Quantity/30 Days
4JAKAFI 20MG TAB NDS PA_NSO QL=60 Quantity/30 Days
4JAKAFI 25MG TAB NDS PA_NSO QL=60 Quantity/30 Days
4JAKAFI 5MG TAB NDS PA_NSO QL=60 Quantity/30 Days
4KISQALI 200MG DAILY DOSE PACK NDS PA_NSO QL=21 Quantity/28 Days
4KISQALI 400MG DAILY DOSE PACK NDS PA_NSO QL=42 Quantity/28 Days
4KISQALI 600MG DAILY DOSE PACK NDS PA_NSO QL=63 Quantity/28 Days
4KOSELUGO 10MG CAP LD NDS PA_NSO QL=120 Quantity/30 Days
4KOSELUGO 25MG CAP LD NDS PA_NSO QL=120 Quantity/30 Days
4lapatinib ditosylate 250mg tab NDS PA_NSO
4LORBRENA 100MG TAB NDS PA_NSO QL=30 Quantity/30 Days
4LORBRENA 25MG TAB NDS PA_NSO QL=90 Quantity/30 Days
4LUMAKRAS 120MG TAB NDS PA_NSO QL=240 Quantity/30 Days
You can find information on what the symbols and abbreviations on this table mean by going to the beginning of this table.
50
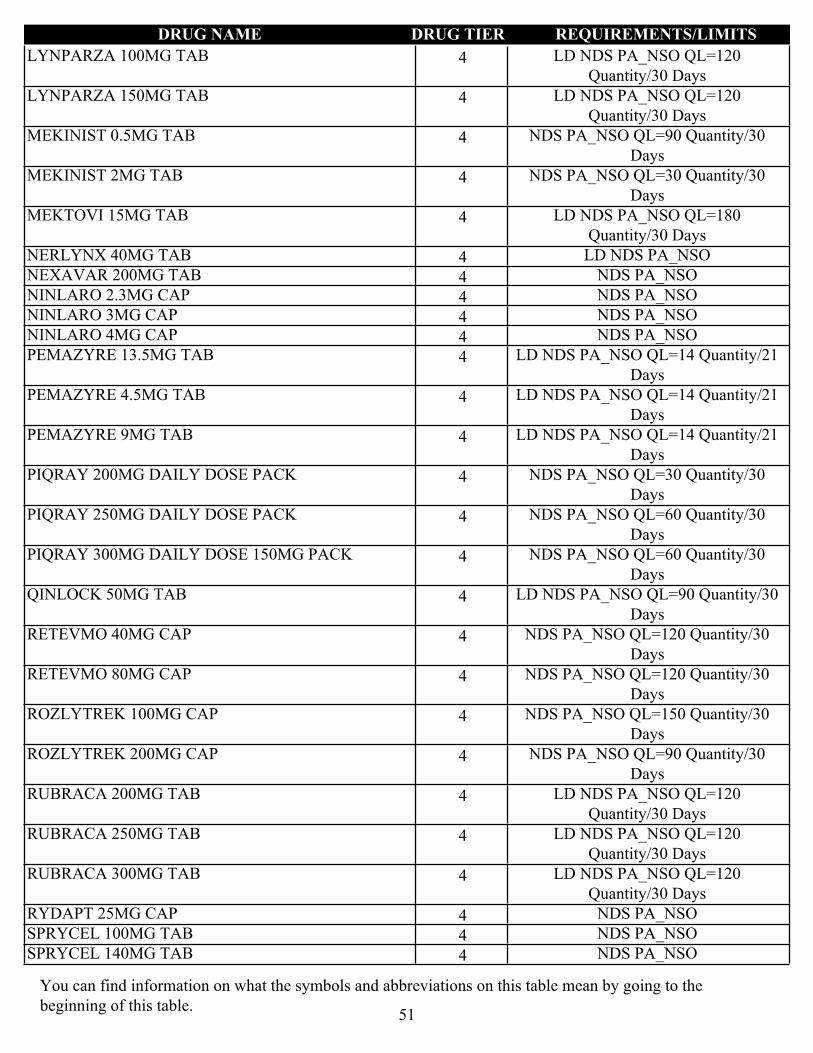
DRUG NAME DRUG TIER REQUIREMENTS/LIMITS
4LYNPARZA 100MG TAB LD NDS PA_NSO QL=120 Quantity/30 Days
4LYNPARZA 150MG TAB LD NDS PA_NSO QL=120 Quantity/30 Days
4MEKINIST 0.5MG TAB NDS PA_NSO QL=90 Quantity/30 Days
4MEKINIST 2MG TAB NDS PA_NSO QL=30 Quantity/30 Days
4MEKTOVI 15MG TAB LD NDS PA_NSO QL=180 Quantity/30 Days
4NERLYNX 40MG TAB LD NDS PA_NSO
4NEXAVAR 200MG TAB NDS PA_NSO
4NINLARO 2.3MG CAP NDS PA_NSO
4NINLARO 3MG CAP NDS PA_NSO
4NINLARO 4MG CAP NDS PA_NSO
4PEMAZYRE 13.5MG TAB LD NDS PA_NSO QL=14 Quantity/21 Days
4PEMAZYRE 4.5MG TAB LD NDS PA_NSO QL=14 Quantity/21 Days
4PEMAZYRE 9MG TAB LD NDS PA_NSO QL=14 Quantity/21 Days
4PIQRAY 200MG DAILY DOSE PACK NDS PA_NSO QL=30 Quantity/30 Days
4PIQRAY 250MG DAILY DOSE PACK NDS PA_NSO QL=60 Quantity/30 Days
4PIQRAY 300MG DAILY DOSE 150MG PACK NDS PA_NSO QL=60 Quantity/30 Days
4QINLOCK 50MG TAB LD NDS PA_NSO QL=90 Quantity/30 Days
4RETEVMO 40MG CAP NDS PA_NSO QL=120 Quantity/30 Days
4RETEVMO 80MG CAP NDS PA_NSO QL=120 Quantity/30 Days
4ROZLYTREK 100MG CAP NDS PA_NSO QL=150 Quantity/30 Days
4ROZLYTREK 200MG CAP NDS PA_NSO QL=90 Quantity/30 Days
4RUBRACA 200MG TAB LD NDS PA_NSO QL=120 Quantity/30 Days
4RUBRACA 250MG TAB LD NDS PA_NSO QL=120 Quantity/30 Days
4RUBRACA 300MG TAB LD NDS PA_NSO QL=120 Quantity/30 Days
4RYDAPT 25MG CAP NDS PA_NSO
4SPRYCEL 100MG TAB NDS PA_NSO
4SPRYCEL 140MG TAB NDS PA_NSO
You can find information on what the symbols and abbreviations on this table mean by going to the beginning of this table.
51
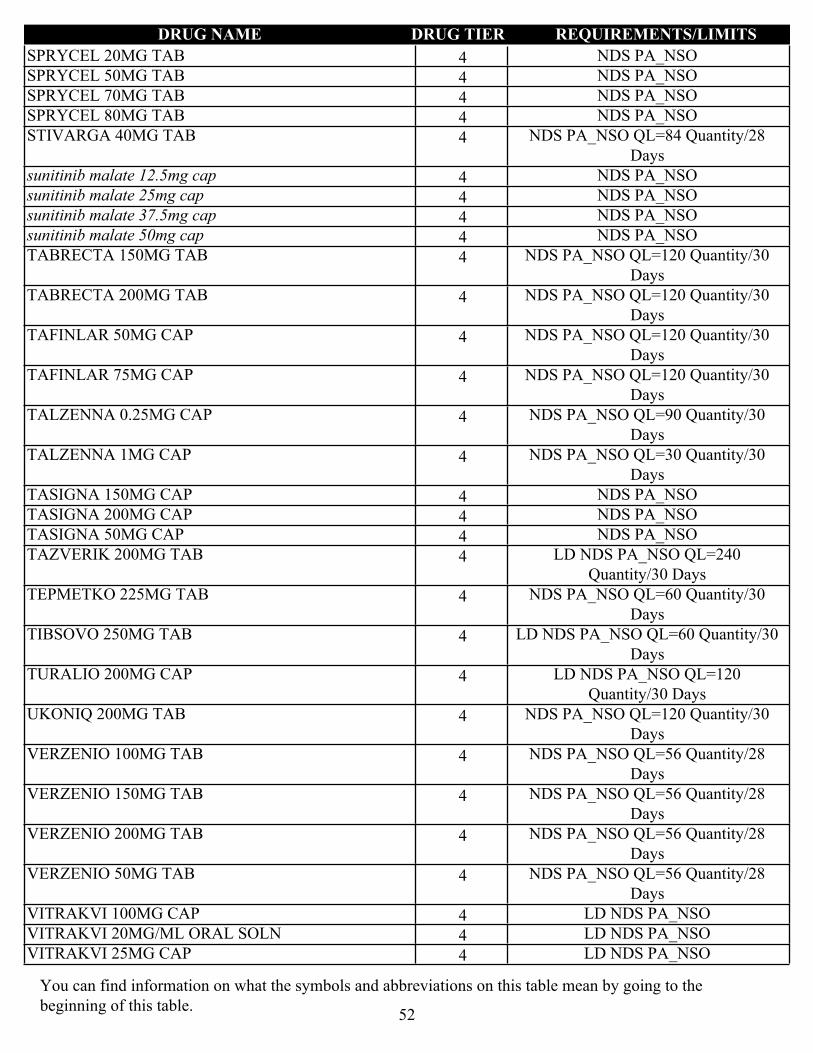
DRUG NAME DRUG TIER REQUIREMENTS/LIMITS
4SPRYCEL 20MG TAB NDS PA_NSO
4SPRYCEL 50MG TAB NDS PA_NSO
4SPRYCEL 70MG TAB NDS PA_NSO
4SPRYCEL 80MG TAB NDS PA_NSO
4STIVARGA 40MG TAB NDS PA_NSO QL=84 Quantity/28 Days
4sunitinib malate 12.5mg cap NDS PA_NSO
4sunitinib malate 25mg cap NDS PA_NSO
4sunitinib malate 37.5mg cap NDS PA_NSO
4sunitinib malate 50mg cap NDS PA_NSO
4TABRECTA 150MG TAB NDS PA_NSO QL=120 Quantity/30 Days
4TABRECTA 200MG TAB NDS PA_NSO QL=120 Quantity/30 Days
4TAFINLAR 50MG CAP NDS PA_NSO QL=120 Quantity/30 Days
4TAFINLAR 75MG CAP NDS PA_NSO QL=120 Quantity/30 Days
4TALZENNA 0.25MG CAP NDS PA_NSO QL=90 Quantity/30 Days
4TALZENNA 1MG CAP NDS PA_NSO QL=30 Quantity/30 Days
4TASIGNA 150MG CAP NDS PA_NSO
4TASIGNA 200MG CAP NDS PA_NSO
4TASIGNA 50MG CAP NDS PA_NSO
4TAZVERIK 200MG TAB LD NDS PA_NSO QL=240 Quantity/30 Days
4TEPMETKO 225MG TAB NDS PA_NSO QL=60 Quantity/30 Days
4TIBSOVO 250MG TAB LD NDS PA_NSO QL=60 Quantity/30 Days
4TURALIO 200MG CAP LD NDS PA_NSO QL=120 Quantity/30 Days
4UKONIQ 200MG TAB NDS PA_NSO QL=120 Quantity/30 Days
4VERZENIO 100MG TAB NDS PA_NSO QL=56 Quantity/28 Days
4VERZENIO 150MG TAB NDS PA_NSO QL=56 Quantity/28 Days
4VERZENIO 200MG TAB NDS PA_NSO QL=56 Quantity/28 Days
4VERZENIO 50MG TAB NDS PA_NSO QL=56 Quantity/28 Days
4VITRAKVI 100MG CAP LD NDS PA_NSO
4VITRAKVI 20MG/ML ORAL SOLN LD NDS PA_NSO
4VITRAKVI 25MG CAP LD NDS PA_NSO
You can find information on what the symbols and abbreviations on this table mean by going to the beginning of this table.
52

DRUG NAME DRUG TIER REQUIREMENTS/LIMITS
4VOTRIENT 200MG TAB NDS PA_NSO
4XALKORI 200MG CAP NDS PA_NSO QL=60 Quantity/30 Days
4XALKORI 250MG CAP NDS PA_NSO QL=60 Quantity/30 Days
4XOSPATA 40MG TAB LD NDS PA_NSO
4ZEJULA 100MG CAP LD NDS PA_NSO QL=90 Quantity/30 Days
4ZELBORAF 240MG TAB NDS PA_NSO QL=240 Quantity/30 Days
4ZOLINZA 100MG CAP NDS PA_NSO
4ZYDELIG 100MG TAB LD NDS PA_NSO QL=60 Quantity/30 Days
4ZYDELIG 150MG TAB LD NDS PA_NSO QL=60 Quantity/30 Days
4ZYKADIA 150MG TAB NDS PA_NSO QL=90 Quantity/30 Days
ANTINEOPLASTICS MISC.
4ACTIMMUNE 2000000UNIT/0.5ML INJ LD NDS PA_NSO
2bexarotene 75mg cap PA_NSO
1hydroxyurea 500mg cap
2INTRON A 10MU INJ
2INTRON A 10MU/ML INJ
4INTRON A 18MU INJ NDS
4INTRON A 50MU INJ NDS
2INTRON A 6000000UNIT/ML INJ
4MATULANE 50MG CAP NDS
4SYNRIBO 3.5MG INJ NDS PA_NSO
1tretinoin 10mg capCHEMOTHERAPY RESCUE/ANTIDOTE AGENTS
2leucovorin 10mg tab
2leucovorin 15mg tab
1leucovorin 25mg tab
1leucovorin 5mg tab
2MESNEX 400MG TAB
ANTIPARKINSON AGENTSANTIPARKINSON ADJUVANTS
2carbidopa 25mg tabANTIPARKINSON ANTICHOLINERGICS
1benztropine mesylate 0.5mg tab
1benztropine mesylate 1mg tab
1benztropine mesylate 2mg tab
1trihexyphenidyl 2mg tab
1trihexyphenidyl 5mg tabANTIPARKINSON COMT INHIBITORS
2entacapone 200mg tab
You can find information on what the symbols and abbreviations on this table mean by going to the beginning of this table.
53

DRUG NAME DRUG TIER REQUIREMENTS/LIMITS
2tolcapone 100mg tabANTIPARKINSON DOPAMINERGICS
1amantadine 100mg cap
2amantadine 100mg tab
1amantadine 10mg/ml oral soln
2bromocriptine 2.5mg tab
2bromocriptine 5mg cap
1carbidopa 10mg/levodopa 100mg tab
2CARBIDOPA 12.5MG/ENTACAPONE 200MG/LEVODOPA 50MG TAB
2CARBIDOPA 25MG/ENTACAPONE 200MG/LEVODOPA 100MG TAB, STALEVO 25-200-100MG TAB
1carbidopa 25mg/levodopa 100mg er tab
1carbidopa 25mg/levodopa 100mg tab
1carbidopa 25mg/levodopa 250mg tab
2CARBIDOPA 31.25MG/ENTACAPONE 200MG/LEVODOPA 125MG TAB, STALEVO 31.25-200-125MG TAB
2CARBIDOPA 37.5MG/ENTACAPONE 200MG/LEVODOPA 150MG TAB
1carbidopa 50mg/levodopa 200mg er tab
2CARBIDOPA/LEVODOPA/ENTACAPONE 50-200-200MG TAB
2CARBIDOPA/LEVODOPA/ENTACAPONE18.75-75-200MG TAB, STALEVO 12.5-200-50MG TAB
3NEUPRO 1MG/24HR PATCH
3NEUPRO 2MG/24HR PATCH
3NEUPRO 3MG/24HR PATCH
3NEUPRO 4MG/24HR PATCH
3NEUPRO 6MG/24HR PATCH
3NEUPRO 8MG/24HR PATCH
1pramipexole 0.125mg tab
1pramipexole 0.25mg tab
2pramipexole 0.375mg er tab
1pramipexole 0.5mg tab
2pramipexole 0.75mg er tab
1pramipexole 0.75mg tab
2pramipexole 1.5mg er tab
1pramipexole 1.5mg tab
1pramipexole 1mg tab
2pramipexole 2.25mg er tab
2pramipexole 3.75mg er tab
2pramipexole 3mg er tab
2pramipexole 4.5mg er tab
1ropinirole 0.25mg tab
You can find information on what the symbols and abbreviations on this table mean by going to the beginning of this table.
54
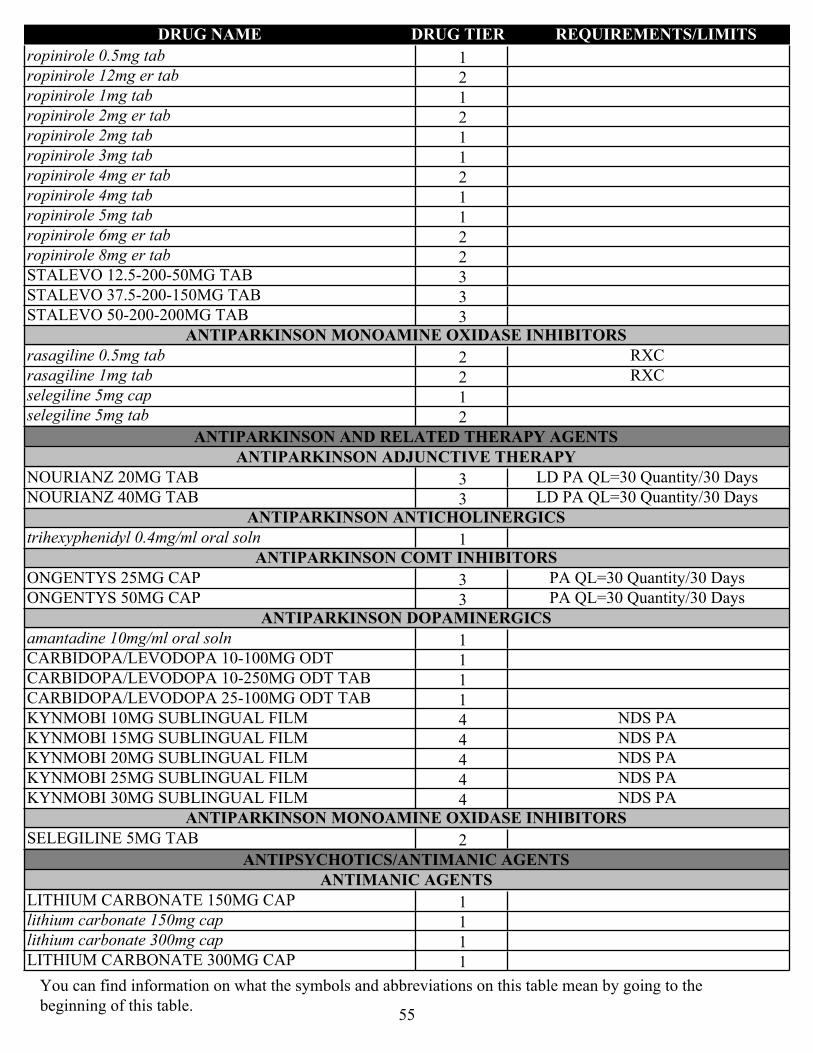
DRUG NAME DRUG TIER REQUIREMENTS/LIMITS
1ropinirole 0.5mg tab
2ropinirole 12mg er tab
1ropinirole 1mg tab
2ropinirole 2mg er tab
1ropinirole 2mg tab
1ropinirole 3mg tab
2ropinirole 4mg er tab
1ropinirole 4mg tab
1ropinirole 5mg tab
2ropinirole 6mg er tab
2ropinirole 8mg er tab
3STALEVO 12.5-200-50MG TAB
3STALEVO 37.5-200-150MG TAB
3STALEVO 50-200-200MG TABANTIPARKINSON MONOAMINE OXIDASE INHIBITORS
2rasagiline 0.5mg tab RXC
2rasagiline 1mg tab RXC
1selegiline 5mg cap
2selegiline 5mg tab
ANTIPARKINSON AND RELATED THERAPY AGENTSANTIPARKINSON ADJUNCTIVE THERAPY
3NOURIANZ 20MG TAB LD PA QL=30 Quantity/30 Days
3NOURIANZ 40MG TAB LD PA QL=30 Quantity/30 DaysANTIPARKINSON ANTICHOLINERGICS
1trihexyphenidyl 0.4mg/ml oral solnANTIPARKINSON COMT INHIBITORS
3ONGENTYS 25MG CAP PA QL=30 Quantity/30 Days
3ONGENTYS 50MG CAP PA QL=30 Quantity/30 DaysANTIPARKINSON DOPAMINERGICS
1amantadine 10mg/ml oral soln
1CARBIDOPA/LEVODOPA 10-100MG ODT
1CARBIDOPA/LEVODOPA 10-250MG ODT TAB
1CARBIDOPA/LEVODOPA 25-100MG ODT TAB
4KYNMOBI 10MG SUBLINGUAL FILM NDS PA
4KYNMOBI 15MG SUBLINGUAL FILM NDS PA
4KYNMOBI 20MG SUBLINGUAL FILM NDS PA
4KYNMOBI 25MG SUBLINGUAL FILM NDS PA
4KYNMOBI 30MG SUBLINGUAL FILM NDS PAANTIPARKINSON MONOAMINE OXIDASE INHIBITORS
2SELEGILINE 5MG TAB
ANTIPSYCHOTICS/ANTIMANIC AGENTSANTIMANIC AGENTS
1LITHIUM CARBONATE 150MG CAP
1lithium carbonate 150mg cap
1lithium carbonate 300mg cap
1LITHIUM CARBONATE 300MG CAP
You can find information on what the symbols and abbreviations on this table mean by going to the beginning of this table.
55
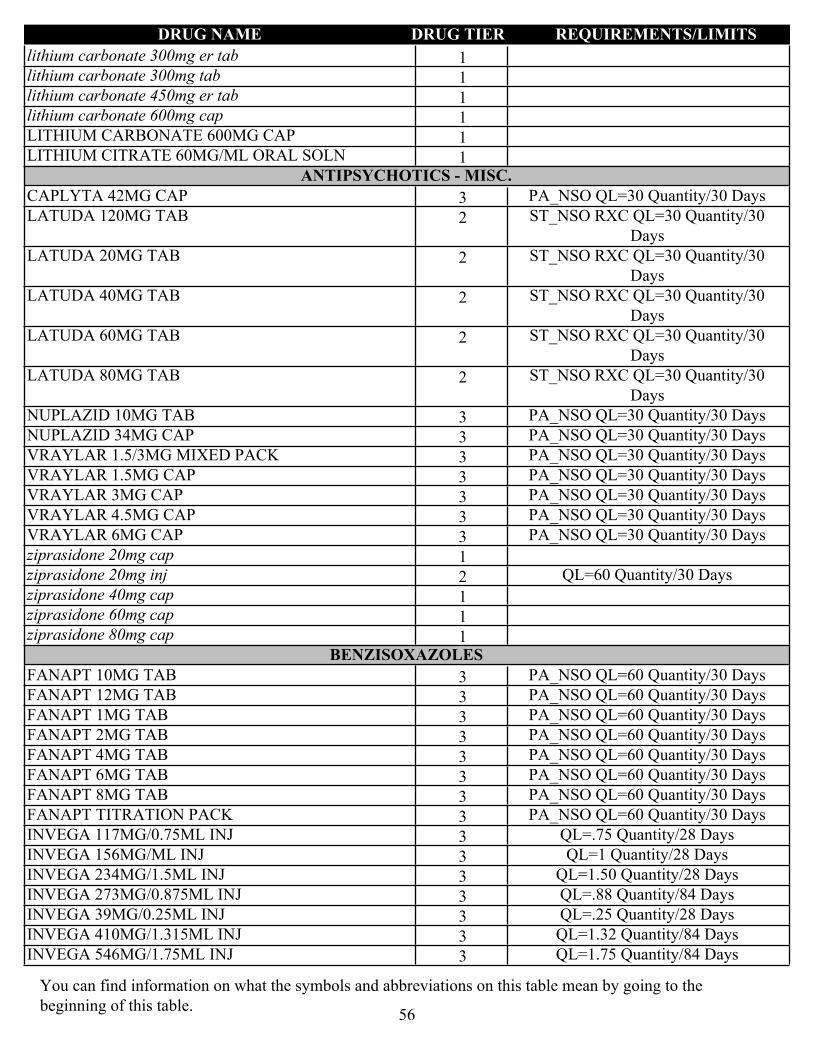
DRUG NAME DRUG TIER REQUIREMENTS/LIMITS
1lithium carbonate 300mg er tab
1lithium carbonate 300mg tab
1lithium carbonate 450mg er tab
1lithium carbonate 600mg cap
1LITHIUM CARBONATE 600MG CAP
1LITHIUM CITRATE 60MG/ML ORAL SOLNANTIPSYCHOTICS - MISC.
3CAPLYTA 42MG CAP PA_NSO QL=30 Quantity/30 Days
2LATUDA 120MG TAB ST_NSO RXC QL=30 Quantity/30 Days
2LATUDA 20MG TAB ST_NSO RXC QL=30 Quantity/30 Days
2LATUDA 40MG TAB ST_NSO RXC QL=30 Quantity/30 Days
2LATUDA 60MG TAB ST_NSO RXC QL=30 Quantity/30 Days
2LATUDA 80MG TAB ST_NSO RXC QL=30 Quantity/30 Days
3NUPLAZID 10MG TAB PA_NSO QL=30 Quantity/30 Days
3NUPLAZID 34MG CAP PA_NSO QL=30 Quantity/30 Days
3VRAYLAR 1.5/3MG MIXED PACK PA_NSO QL=30 Quantity/30 Days
3VRAYLAR 1.5MG CAP PA_NSO QL=30 Quantity/30 Days
3VRAYLAR 3MG CAP PA_NSO QL=30 Quantity/30 Days
3VRAYLAR 4.5MG CAP PA_NSO QL=30 Quantity/30 Days
3VRAYLAR 6MG CAP PA_NSO QL=30 Quantity/30 Days
1ziprasidone 20mg cap
2ziprasidone 20mg inj QL=60 Quantity/30 Days
1ziprasidone 40mg cap
1ziprasidone 60mg cap
1ziprasidone 80mg capBENZISOXAZOLES
3FANAPT 10MG TAB PA_NSO QL=60 Quantity/30 Days
3FANAPT 12MG TAB PA_NSO QL=60 Quantity/30 Days
3FANAPT 1MG TAB PA_NSO QL=60 Quantity/30 Days
3FANAPT 2MG TAB PA_NSO QL=60 Quantity/30 Days
3FANAPT 4MG TAB PA_NSO QL=60 Quantity/30 Days
3FANAPT 6MG TAB PA_NSO QL=60 Quantity/30 Days
3FANAPT 8MG TAB PA_NSO QL=60 Quantity/30 Days
3FANAPT TITRATION PACK PA_NSO QL=60 Quantity/30 Days
3INVEGA 117MG/0.75ML INJ QL=.75 Quantity/28 Days
3INVEGA 156MG/ML INJ QL=1 Quantity/28 Days
3INVEGA 234MG/1.5ML INJ QL=1.50 Quantity/28 Days
3INVEGA 273MG/0.875ML INJ QL=.88 Quantity/84 Days
3INVEGA 39MG/0.25ML INJ QL=.25 Quantity/28 Days
3INVEGA 410MG/1.315ML INJ QL=1.32 Quantity/84 Days
3INVEGA 546MG/1.75ML INJ QL=1.75 Quantity/84 Days
You can find information on what the symbols and abbreviations on this table mean by going to the beginning of this table.
56

DRUG NAME DRUG TIER REQUIREMENTS/LIMITS
3INVEGA 78MG/0.5ML INJ QL=.50 Quantity/28 Days
3INVEGA 819MG/2.625ML INJ QL=2.63 Quantity/84 Days
2paliperidone 1.5mg er tab QL=30 Quantity/30 Days
2paliperidone 3mg er tab QL=30 Quantity/30 Days
2paliperidone 6mg er tab QL=60 Quantity/30 Days
2paliperidone 9mg er tab QL=30 Quantity/30 Days
4PERSERIS 120MG INJ NDS QL=1 Quantity/28 Days
4PERSERIS 90MG INJ NDS QL=1 Quantity/28 Days
3RISPERDAL 12.5MG INJ QL=2 Quantity/28 Days
3RISPERDAL 25MG INJ QL=2 Quantity/28 Days
3RISPERDAL 37.5MG INJ QL=2 Quantity/28 Days
3RISPERDAL 50MG INJ QL=2 Quantity/28 Days
2RISPERIDONE 0.25MG ODT
1risperidone 0.25mg tab
2risperidone 0.5mg odt
1risperidone 0.5mg tab
2risperidone 1mg odt
1risperidone 1mg tab
1risperidone 1mg/ml oral soln
2risperidone 2mg odt
1risperidone 2mg tab
2risperidone 3mg odt
1risperidone 3mg tab
2risperidone 4mg odt
1risperidone 4mg tabBUTYROPHENONES
1haloperidol 0.5mg tab
1haloperidol 10mg tab
1haloperidol 1mg tab
1haloperidol 20mg tab
1haloperidol 2mg tab
1haloperidol 2mg/ml oral soln
1haloperidol 5mg tab
2haloperidol 5mg/ml inj
2haloperidol decanoate 100mg/ml inj
2haloperidol decanoate 50mg/ml injDIBENZAPINES
2asenapine 10mg sl tab PA_NSO QL=60 Quantity/30 Days
2asenapine 2.5mg sl tab PA_NSO QL=60 Quantity/30 Days
2asenapine 5mg sl tab PA_NSO QL=60 Quantity/30 Days
2clozapine 100mg odt
2clozapine 100mg tab
2CLOZAPINE 12.5MG ODT
3CLOZAPINE 150MG ODT
3CLOZAPINE 200MG ODT
2clozapine 200mg tab
You can find information on what the symbols and abbreviations on this table mean by going to the beginning of this table.
57
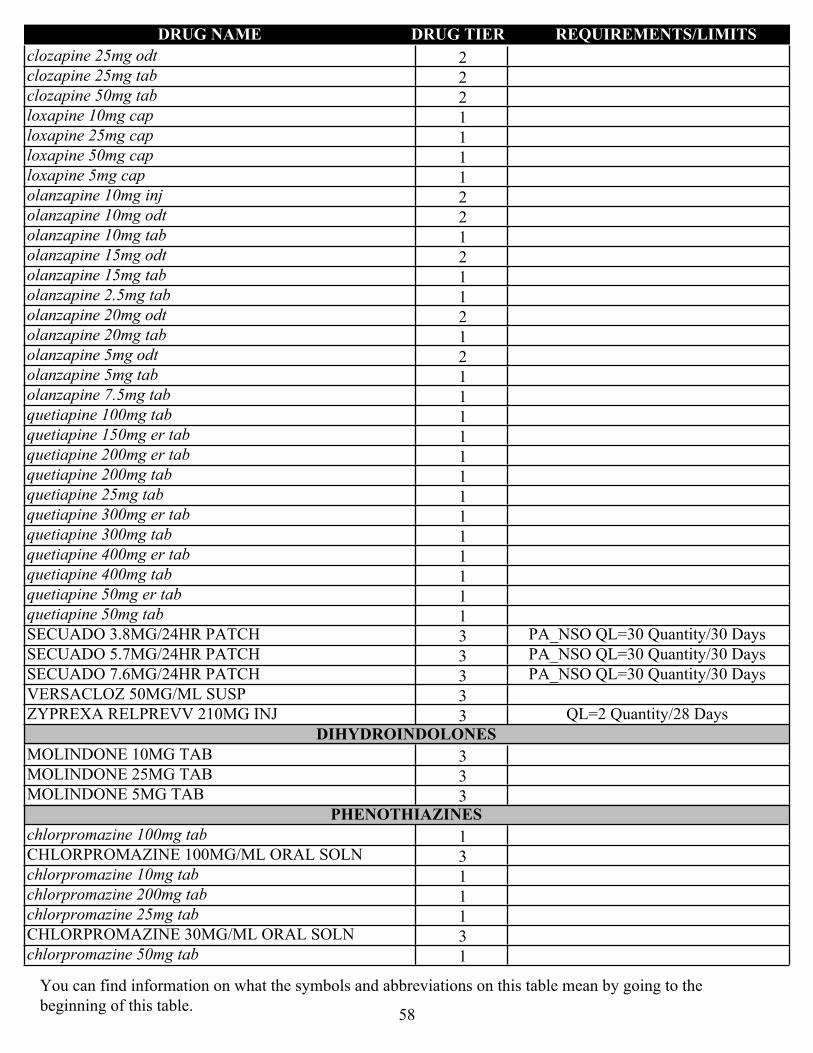
DRUG NAME DRUG TIER REQUIREMENTS/LIMITS
2clozapine 25mg odt
2clozapine 25mg tab
2clozapine 50mg tab
1loxapine 10mg cap
1loxapine 25mg cap
1loxapine 50mg cap
1loxapine 5mg cap
2olanzapine 10mg inj
2olanzapine 10mg odt
1olanzapine 10mg tab
2olanzapine 15mg odt
1olanzapine 15mg tab
1olanzapine 2.5mg tab
2olanzapine 20mg odt
1olanzapine 20mg tab
2olanzapine 5mg odt
1olanzapine 5mg tab
1olanzapine 7.5mg tab
1quetiapine 100mg tab
1quetiapine 150mg er tab
1quetiapine 200mg er tab
1quetiapine 200mg tab
1quetiapine 25mg tab
1quetiapine 300mg er tab
1quetiapine 300mg tab
1quetiapine 400mg er tab
1quetiapine 400mg tab
1quetiapine 50mg er tab
1quetiapine 50mg tab
3SECUADO 3.8MG/24HR PATCH PA_NSO QL=30 Quantity/30 Days
3SECUADO 5.7MG/24HR PATCH PA_NSO QL=30 Quantity/30 Days
3SECUADO 7.6MG/24HR PATCH PA_NSO QL=30 Quantity/30 Days
3VERSACLOZ 50MG/ML SUSP
3ZYPREXA RELPREVV 210MG INJ QL=2 Quantity/28 DaysDIHYDROINDOLONES
3MOLINDONE 10MG TAB
3MOLINDONE 25MG TAB
3MOLINDONE 5MG TABPHENOTHIAZINES
1chlorpromazine 100mg tab
3CHLORPROMAZINE 100MG/ML ORAL SOLN
1chlorpromazine 10mg tab
1chlorpromazine 200mg tab
1chlorpromazine 25mg tab
3CHLORPROMAZINE 30MG/ML ORAL SOLN
1chlorpromazine 50mg tab
You can find information on what the symbols and abbreviations on this table mean by going to the beginning of this table.
58

DRUG NAME DRUG TIER REQUIREMENTS/LIMITS
2FLUPHENAZINE 0.5MG/ML ORAL SOLN
2fluphenazine 10mg tab
2fluphenazine 1mg tab
2fluphenazine 2.5mg tab
2FLUPHENAZINE 2.5MG/ML INJ
2fluphenazine 5mg tab
2FLUPHENAZINE 5MG/ML ORAL SOLN
2fluphenazine decanoate 25mg/ml inj
1perphenazine 16mg tab
1perphenazine 2mg tab
1perphenazine 4mg tab
1perphenazine 8mg tab
1prochlorperazine 10mg tab
1prochlorperazine 25mg rectal supp
1prochlorperazine 5mg tab
1thioridazine 100mg tab
1thioridazine 10mg tab
1thioridazine 25mg tab
1thioridazine 50mg tab
1trifluoperazine 10mg tab
1trifluoperazine 1mg tab
1trifluoperazine 2mg tab
1trifluoperazine 5mg tabQUINOLINONE DERIVATIVES
4ABILIFY 300MG INJ NDS QL=1 Quantity/28 Days
4ABILIFY 300MG SYRINGE NDS QL=1 Quantity/28 Days
4ABILIFY 400MG INJ NDS QL=1 Quantity/28 Days
4ABILIFY 400MG SYRINGE NDS QL=1 Quantity/28 Days
2aripiprazole 10mg odt QL=60 Quantity/30 Days
1aripiprazole 10mg tab
2aripiprazole 15mg odt QL=60 Quantity/30 Days
1aripiprazole 15mg tab
2aripiprazole 1mg/ml oral soln
1aripiprazole 20mg tab
1aripiprazole 2mg tab
1aripiprazole 30mg tab
1aripiprazole 5mg tab
4ARISTADA 1064MG/3.9ML INJ QL=3.90 Quantity/56 Days
4ARISTADA 441MG/1.6ML INJ NDS QL=1.60 Quantity/28 Days
4ARISTADA 662MG/2.4ML INJ NDS QL=2.40 Quantity/28 Days
4ARISTADA 675MG/2.4ML INJ NDS QL=2.40 Quantity/42 Days
4ARISTADA 882MG/3.2ML INJ QL=3.20 Quantity/28 Days
3REXULTI 0.25MG TAB PA_NSO QL=30 Quantity/30 Days
3REXULTI 0.5MG TAB PA_NSO QL=30 Quantity/30 Days
3REXULTI 1MG TAB PA_NSO QL=30 Quantity/30 Days
3REXULTI 2MG TAB PA_NSO QL=30 Quantity/30 Days
You can find information on what the symbols and abbreviations on this table mean by going to the beginning of this table.
59
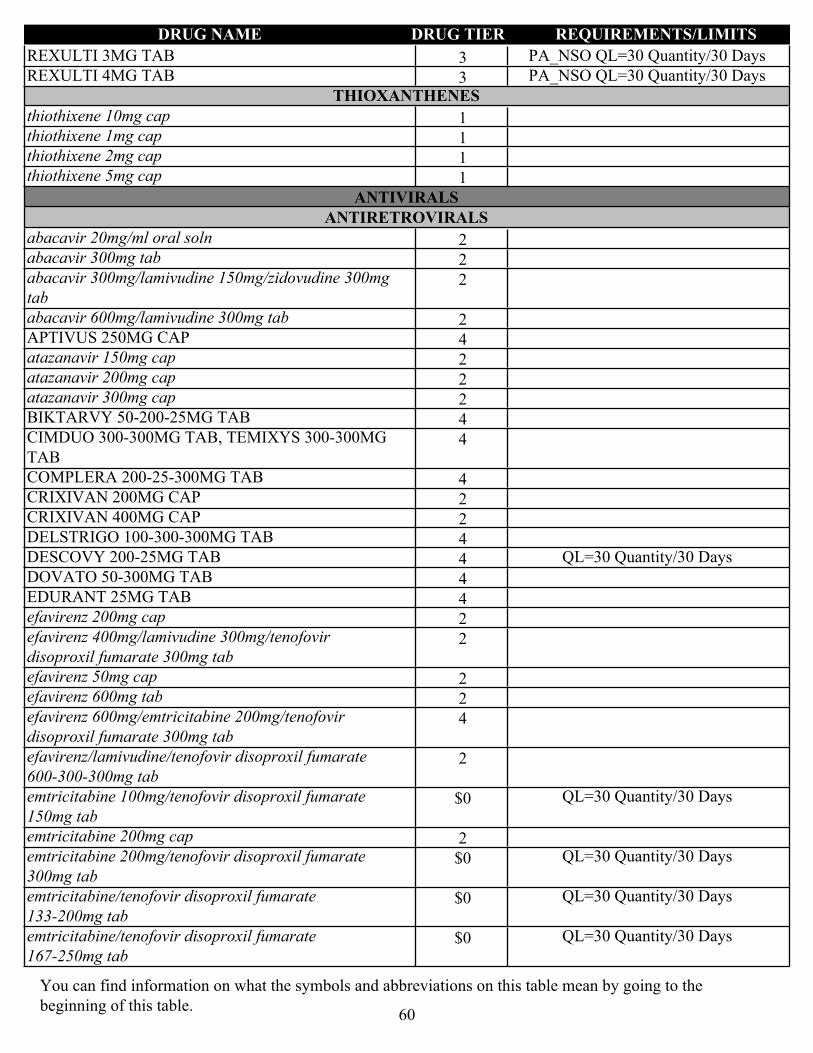
DRUG NAME DRUG TIER REQUIREMENTS/LIMITS
3REXULTI 3MG TAB PA_NSO QL=30 Quantity/30 Days
3REXULTI 4MG TAB PA_NSO QL=30 Quantity/30 DaysTHIOXANTHENES
1thiothixene 10mg cap
1thiothixene 1mg cap
1thiothixene 2mg cap
1thiothixene 5mg cap
ANTIVIRALSANTIRETROVIRALS
2abacavir 20mg/ml oral soln
2abacavir 300mg tab
2abacavir 300mg/lamivudine 150mg/zidovudine 300mg tab
2abacavir 600mg/lamivudine 300mg tab
4APTIVUS 250MG CAP
2atazanavir 150mg cap
2atazanavir 200mg cap
2atazanavir 300mg cap
4BIKTARVY 50-200-25MG TAB
4CIMDUO 300-300MG TAB, TEMIXYS 300-300MG TAB
4COMPLERA 200-25-300MG TAB
2CRIXIVAN 200MG CAP
2CRIXIVAN 400MG CAP
4DELSTRIGO 100-300-300MG TAB
4DESCOVY 200-25MG TAB QL=30 Quantity/30 Days
4DOVATO 50-300MG TAB
4EDURANT 25MG TAB
2efavirenz 200mg cap
2efavirenz 400mg/lamivudine 300mg/tenofovir disoproxil fumarate 300mg tab
2efavirenz 50mg cap
2efavirenz 600mg tab
4efavirenz 600mg/emtricitabine 200mg/tenofovir disoproxil fumarate 300mg tab
2efavirenz/lamivudine/tenofovir disoproxil fumarate 600-300-300mg tab
$0emtricitabine 100mg/tenofovir disoproxil fumarate 150mg tab
QL=30 Quantity/30 Days
2emtricitabine 200mg cap
$0emtricitabine 200mg/tenofovir disoproxil fumarate 300mg tab
QL=30 Quantity/30 Days
$0emtricitabine/tenofovir disoproxil fumarate 133-200mg tab
QL=30 Quantity/30 Days
$0emtricitabine/tenofovir disoproxil fumarate 167-250mg tab
QL=30 Quantity/30 Days
You can find information on what the symbols and abbreviations on this table mean by going to the beginning of this table.
60

DRUG NAME DRUG TIER REQUIREMENTS/LIMITS
2EMTRIVA 10MG/ML ORAL SOLN
2etravirine 100mg tab
2etravirine 200mg tab
4EVOTAZ 300-150MG TAB
4fosamprenavir 700mg tab
4FUZEON 90MG INJ
4GENVOYA 150-150-200-10MG TAB
3INTELENCE 25MG TAB
4INVIRASE 500MG TAB
2ISENTRESS 100MG CHEW TAB
2ISENTRESS 100MG GRANULES FOR ORAL SUSP
2ISENTRESS 25MG CHEW TAB
2ISENTRESS 400MG TAB
2ISENTRESS 600MG TAB
4JULUCA 50-25MG TAB
2lamivudine 10mg/ml oral soln
2lamivudine 150mg tab
2lamivudine 150mg/zidovudine 300mg tab
2lamivudine 300mg tab
2LEXIVA 50MG/ML SUSP
2lopinavir 80mg/ml/ritonavir 20mg/ml oral solution
2lopinavir/ritonavir 100-25mg tab
2lopinavir/ritonavir 200-50mg tab
2NEVIRAPINE 100MG ER TAB
2NEVIRAPINE 10MG/ML SUSP
1nevirapine 200mg tab
2nevirapine 400mg er tab
2NORVIR 100MG ORAL POWDER
2NORVIR 80MG/ML ORAL SOLN
4ODEFSEY 200-25-25MG TAB
4PIFELTRO 100MG TAB
4PREZCOBIX 150-800MG TAB
2PREZISTA 100MG/ML SUSP
2PREZISTA 150MG TAB
4PREZISTA 600MG TAB
2PREZISTA 75MG TAB
4PREZISTA 800MG TAB
4REYATAZ 50MG ORAL POWDER
2ritonavir 100mg tab
4RUKOBIA 600MG ER TAB
4SELZENTRY 150MG TAB
4SELZENTRY 20MG/ML ORAL SOLN
2SELZENTRY 25MG TAB
4SELZENTRY 300MG TAB
4SELZENTRY 75MG TAB
4STRIBILD 150-150-200-300MG TAB
You can find information on what the symbols and abbreviations on this table mean by going to the beginning of this table.
61
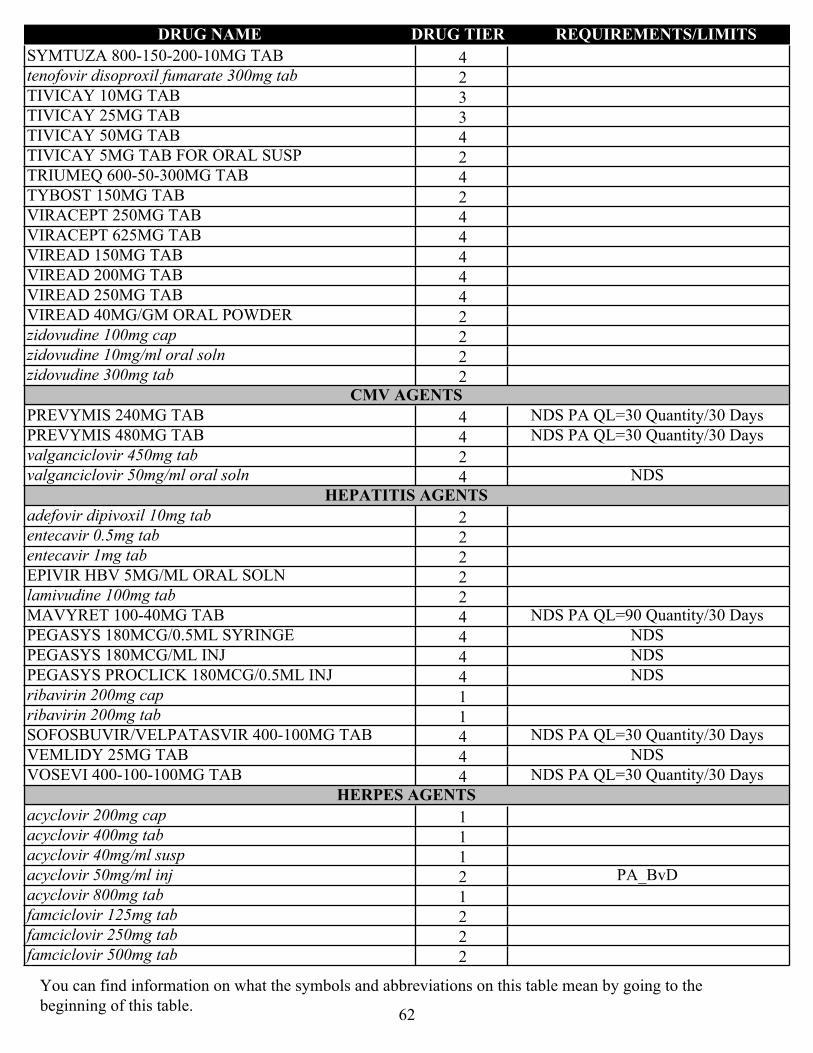
DRUG NAME DRUG TIER REQUIREMENTS/LIMITS
4SYMTUZA 800-150-200-10MG TAB
2tenofovir disoproxil fumarate 300mg tab
3TIVICAY 10MG TAB
3TIVICAY 25MG TAB
4TIVICAY 50MG TAB
2TIVICAY 5MG TAB FOR ORAL SUSP
4TRIUMEQ 600-50-300MG TAB
2TYBOST 150MG TAB
4VIRACEPT 250MG TAB
4VIRACEPT 625MG TAB
4VIREAD 150MG TAB
4VIREAD 200MG TAB
4VIREAD 250MG TAB
2VIREAD 40MG/GM ORAL POWDER
2zidovudine 100mg cap
2zidovudine 10mg/ml oral soln
2zidovudine 300mg tabCMV AGENTS
4PREVYMIS 240MG TAB NDS PA QL=30 Quantity/30 Days
4PREVYMIS 480MG TAB NDS PA QL=30 Quantity/30 Days
2valganciclovir 450mg tab
4valganciclovir 50mg/ml oral soln NDSHEPATITIS AGENTS
2adefovir dipivoxil 10mg tab
2entecavir 0.5mg tab
2entecavir 1mg tab
2EPIVIR HBV 5MG/ML ORAL SOLN
2lamivudine 100mg tab
4MAVYRET 100-40MG TAB NDS PA QL=90 Quantity/30 Days
4PEGASYS 180MCG/0.5ML SYRINGE NDS
4PEGASYS 180MCG/ML INJ NDS
4PEGASYS PROCLICK 180MCG/0.5ML INJ NDS
1ribavirin 200mg cap
1ribavirin 200mg tab
4SOFOSBUVIR/VELPATASVIR 400-100MG TAB NDS PA QL=30 Quantity/30 Days
4VEMLIDY 25MG TAB NDS
4VOSEVI 400-100-100MG TAB NDS PA QL=30 Quantity/30 DaysHERPES AGENTS
1acyclovir 200mg cap
1acyclovir 400mg tab
1acyclovir 40mg/ml susp
2acyclovir 50mg/ml inj PA_BvD
1acyclovir 800mg tab
2famciclovir 125mg tab
2famciclovir 250mg tab
2famciclovir 500mg tab
You can find information on what the symbols and abbreviations on this table mean by going to the beginning of this table.
62
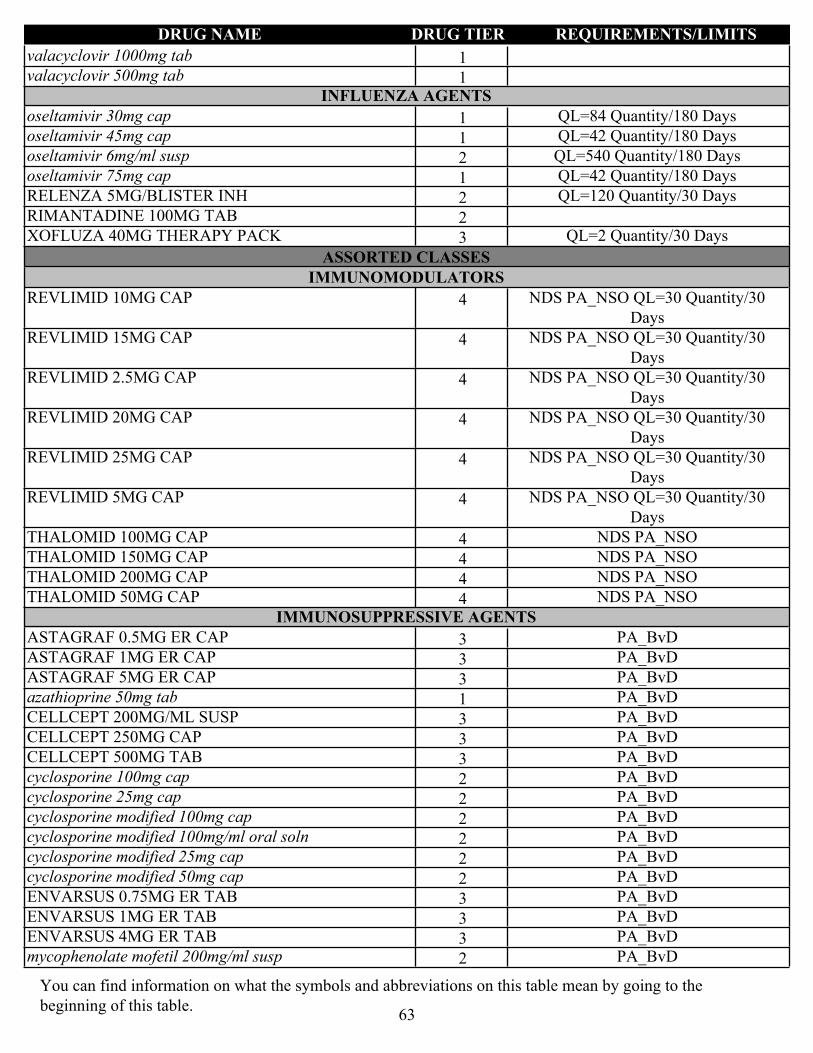
DRUG NAME DRUG TIER REQUIREMENTS/LIMITS
1valacyclovir 1000mg tab
1valacyclovir 500mg tabINFLUENZA AGENTS
1oseltamivir 30mg cap QL=84 Quantity/180 Days
1oseltamivir 45mg cap QL=42 Quantity/180 Days
2oseltamivir 6mg/ml susp QL=540 Quantity/180 Days
1oseltamivir 75mg cap QL=42 Quantity/180 Days
2RELENZA 5MG/BLISTER INH QL=120 Quantity/30 Days
2RIMANTADINE 100MG TAB
3XOFLUZA 40MG THERAPY PACK QL=2 Quantity/30 Days
ASSORTED CLASSESIMMUNOMODULATORS
4REVLIMID 10MG CAP NDS PA_NSO QL=30 Quantity/30 Days
4REVLIMID 15MG CAP NDS PA_NSO QL=30 Quantity/30 Days
4REVLIMID 2.5MG CAP NDS PA_NSO QL=30 Quantity/30 Days
4REVLIMID 20MG CAP NDS PA_NSO QL=30 Quantity/30 Days
4REVLIMID 25MG CAP NDS PA_NSO QL=30 Quantity/30 Days
4REVLIMID 5MG CAP NDS PA_NSO QL=30 Quantity/30 Days
4THALOMID 100MG CAP NDS PA_NSO
4THALOMID 150MG CAP NDS PA_NSO
4THALOMID 200MG CAP NDS PA_NSO
4THALOMID 50MG CAP NDS PA_NSOIMMUNOSUPPRESSIVE AGENTS
3ASTAGRAF 0.5MG ER CAP PA_BvD
3ASTAGRAF 1MG ER CAP PA_BvD
3ASTAGRAF 5MG ER CAP PA_BvD
1azathioprine 50mg tab PA_BvD
3CELLCEPT 200MG/ML SUSP PA_BvD
3CELLCEPT 250MG CAP PA_BvD
3CELLCEPT 500MG TAB PA_BvD
2cyclosporine 100mg cap PA_BvD
2cyclosporine 25mg cap PA_BvD
2cyclosporine modified 100mg cap PA_BvD
2cyclosporine modified 100mg/ml oral soln PA_BvD
2cyclosporine modified 25mg cap PA_BvD
2cyclosporine modified 50mg cap PA_BvD
3ENVARSUS 0.75MG ER TAB PA_BvD
3ENVARSUS 1MG ER TAB PA_BvD
3ENVARSUS 4MG ER TAB PA_BvD
2mycophenolate mofetil 200mg/ml susp PA_BvD
You can find information on what the symbols and abbreviations on this table mean by going to the beginning of this table.
63
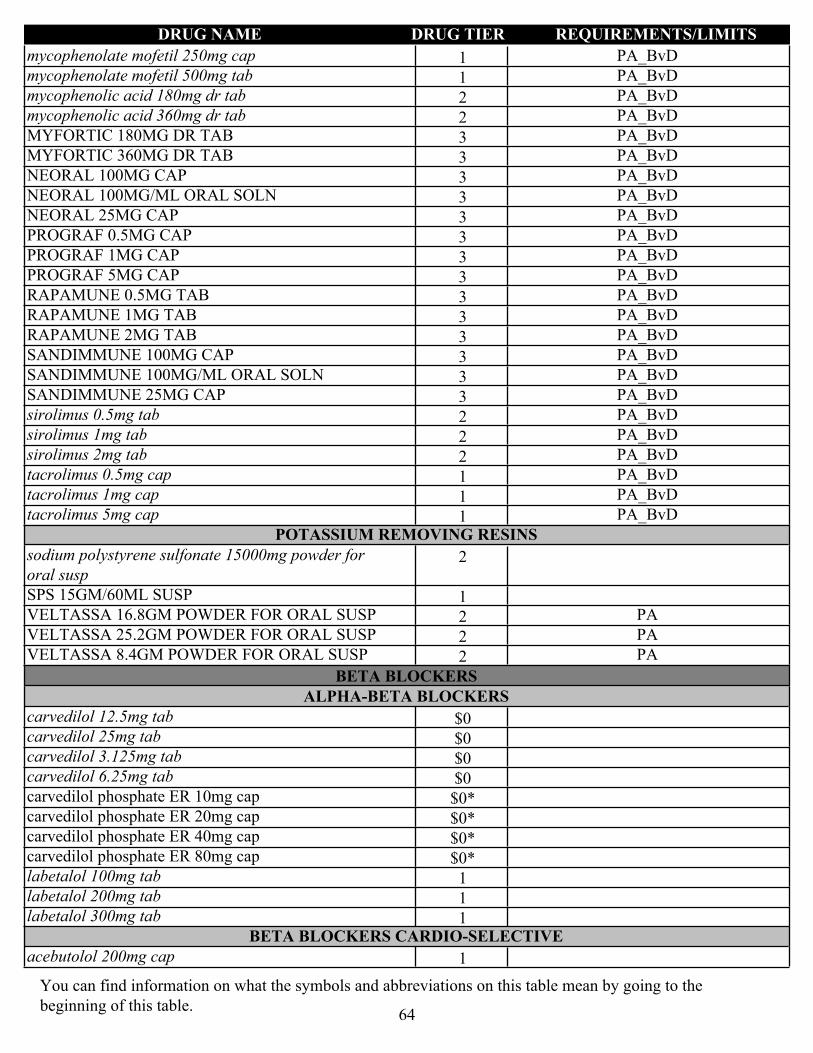
DRUG NAME DRUG TIER REQUIREMENTS/LIMITS
1mycophenolate mofetil 250mg cap PA_BvD
1mycophenolate mofetil 500mg tab PA_BvD
2mycophenolic acid 180mg dr tab PA_BvD
2mycophenolic acid 360mg dr tab PA_BvD
3MYFORTIC 180MG DR TAB PA_BvD
3MYFORTIC 360MG DR TAB PA_BvD
3NEORAL 100MG CAP PA_BvD
3NEORAL 100MG/ML ORAL SOLN PA_BvD
3NEORAL 25MG CAP PA_BvD
3PROGRAF 0.5MG CAP PA_BvD
3PROGRAF 1MG CAP PA_BvD
3PROGRAF 5MG CAP PA_BvD
3RAPAMUNE 0.5MG TAB PA_BvD
3RAPAMUNE 1MG TAB PA_BvD
3RAPAMUNE 2MG TAB PA_BvD
3SANDIMMUNE 100MG CAP PA_BvD
3SANDIMMUNE 100MG/ML ORAL SOLN PA_BvD
3SANDIMMUNE 25MG CAP PA_BvD
2sirolimus 0.5mg tab PA_BvD
2sirolimus 1mg tab PA_BvD
2sirolimus 2mg tab PA_BvD
1tacrolimus 0.5mg cap PA_BvD
1tacrolimus 1mg cap PA_BvD
1tacrolimus 5mg cap PA_BvDPOTASSIUM REMOVING RESINS
2sodium polystyrene sulfonate 15000mg powder for oral susp
1SPS 15GM/60ML SUSP
2VELTASSA 16.8GM POWDER FOR ORAL SUSP PA
2VELTASSA 25.2GM POWDER FOR ORAL SUSP PA
2VELTASSA 8.4GM POWDER FOR ORAL SUSP PA
BETA BLOCKERSALPHA-BETA BLOCKERS
$0carvedilol 12.5mg tab
$0carvedilol 25mg tab
$0carvedilol 3.125mg tab
$0carvedilol 6.25mg tab
$0*carvedilol phosphate ER 10mg cap
$0*carvedilol phosphate ER 20mg cap
$0*carvedilol phosphate ER 40mg cap
$0*carvedilol phosphate ER 80mg cap
1labetalol 100mg tab
1labetalol 200mg tab
1labetalol 300mg tabBETA BLOCKERS CARDIO-SELECTIVE
1acebutolol 200mg cap
You can find information on what the symbols and abbreviations on this table mean by going to the beginning of this table.
64
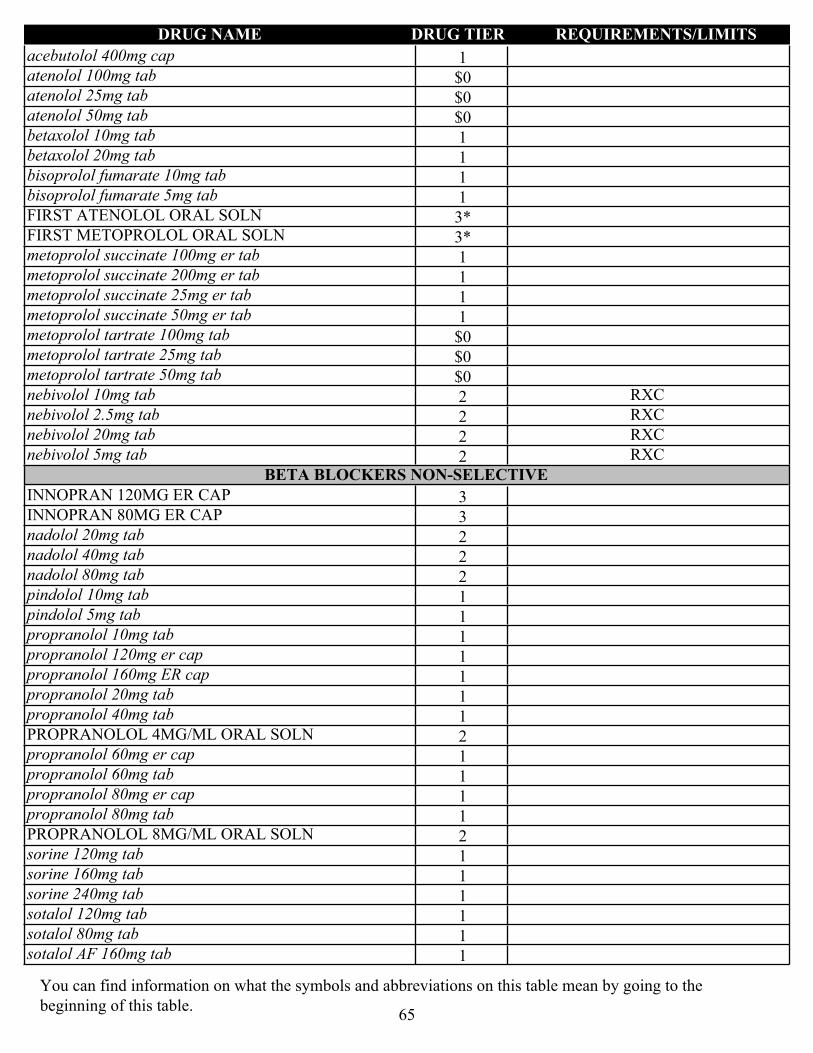
DRUG NAME DRUG TIER REQUIREMENTS/LIMITS
1acebutolol 400mg cap
$0atenolol 100mg tab
$0atenolol 25mg tab
$0atenolol 50mg tab
1betaxolol 10mg tab
1betaxolol 20mg tab
1bisoprolol fumarate 10mg tab
1bisoprolol fumarate 5mg tab
3*FIRST ATENOLOL ORAL SOLN
3*FIRST METOPROLOL ORAL SOLN
1metoprolol succinate 100mg er tab
1metoprolol succinate 200mg er tab
1metoprolol succinate 25mg er tab
1metoprolol succinate 50mg er tab
$0metoprolol tartrate 100mg tab
$0metoprolol tartrate 25mg tab
$0metoprolol tartrate 50mg tab
2nebivolol 10mg tab RXC
2nebivolol 2.5mg tab RXC
2nebivolol 20mg tab RXC
2nebivolol 5mg tab RXCBETA BLOCKERS NON-SELECTIVE
3INNOPRAN 120MG ER CAP
3INNOPRAN 80MG ER CAP
2nadolol 20mg tab
2nadolol 40mg tab
2nadolol 80mg tab
1pindolol 10mg tab
1pindolol 5mg tab
1propranolol 10mg tab
1propranolol 120mg er cap
1propranolol 160mg ER cap
1propranolol 20mg tab
1propranolol 40mg tab
2PROPRANOLOL 4MG/ML ORAL SOLN
1propranolol 60mg er cap
1propranolol 60mg tab
1propranolol 80mg er cap
1propranolol 80mg tab
2PROPRANOLOL 8MG/ML ORAL SOLN
1sorine 120mg tab
1sorine 160mg tab
1sorine 240mg tab
1sotalol 120mg tab
1sotalol 80mg tab
1sotalol AF 160mg tab
You can find information on what the symbols and abbreviations on this table mean by going to the beginning of this table.
65

DRUG NAME DRUG TIER REQUIREMENTS/LIMITS
1sotalol AF 80mg tab
1timolol 10mg tab
1timolol 20mg tab
1timolol 5mg tab
CALCIUM CHANNEL BLOCKERSCALCIUM CHANNEL BLOCKERS
1amlodipine 10mg tab
1amlodipine 2.5mg tab
1amlodipine 5mg tab
3CARDIZEM 120MG ER TAB
1cartia 180mg er cap
1cartia 240mg er cap
1cartia 300mg er cap
1dilt 120mg er cap
1dilt 180mg er cap
1dilt 240mg er cap
1diltiazem 120mg er (12 hr) cap
1diltiazem 120mg er (24 hr) cap
1diltiazem 120mg tab
2diltiazem 180mg er tab
2diltiazem 300mg er tab
1diltiazem 30mg tab
1diltiazem 360mg cd cap
2diltiazem 360mg er tab
1diltiazem 420mg er cap
1diltiazem 60mg er cap
1diltiazem 60mg tab
1diltiazem 90mg er cap
1diltiazem 90mg tab
1felodipine 10mg er tab
1felodipine 2.5mg er tab
1felodipine 5mg er tab
1isradipine 2.5mg cap
1isradipine 5mg cap
2matzim 240mg er tab
2matzim 420mg er tab
1nicardipine 20mg cap
1nicardipine 30mg cap
2nifedipine 10mg cap
2nifedipine 20mg cap
1nifedipine 30mg er tab
1nifedipine 30mg osmotic er tab
1nifedipine 60mg er tab
1nifedipine 60mg osmotic er tab
1nifedipine 90mg er tab
1nifedipine 90mg osmotic er tab
You can find information on what the symbols and abbreviations on this table mean by going to the beginning of this table.
66

DRUG NAME DRUG TIER REQUIREMENTS/LIMITS
2nimodipine 30mg cap
2nisoldipine 17mg er tab
2NISOLDIPINE 20MG ER TAB
2NISOLDIPINE 25.5MG ER TAB
2NISOLDIPINE 30MG ER TAB
2nisoldipine 34mg er tab
2NISOLDIPINE 40MG ER TAB
2nisoldipine 8.5mg er tab
1taztia 120mg er cap
1taztia 180mg er cap
1taztia 240mg er cap
1taztia 300mg er cap
1taztia 360mg er cap
2VERAPAMIL 100MG ER CAP
2verapamil 120mg er cap
1verapamil 120mg er tab
1verapamil 120mg tab
2verapamil 180mg er cap
1verapamil 180mg er tab
2VERAPAMIL 200MG ER CAP
2verapamil 240mg er cap
1verapamil 240mg er tab
2VERAPAMIL 300MG ER CAP
2VERAPAMIL 360MG ER CAP
1verapamil 40mg tab
1verapamil 80mg tab
3VERELAN 100MG ER CAP
3VERELAN 200MG ER CAP
3VERELAN 300MG ER CAP
3VERELAN 360MG ER CAP
CARDIOTONICSCARDIAC GLYCOSIDES
1digox 125mcg tab
1digoxin 0.05mg/ml oral soln
1DIGOXIN 0.05 MG/ML ORAL SOLN
1digoxin 0.25mg tab
1DIGOXIN ORAL 0.05MG/ML SOLN
3LANOXIN 125MCG TAB
3LANOXIN 250MCG TAB
CARDIOVASCULAR AGENTS - MISC.CARDIOVASCULAR AGENTS MISC. - COMBINATIONS
2amlodipine 10mg/atorvastatin 10mg tab
2amlodipine 10mg/atorvastatin 20mg tab
2amlodipine 10mg/atorvastatin 40mg tab
2amlodipine 10mg/atorvastatin 80mg tab
2amlodipine 2.5mg/atorvastatin 10mg tab
You can find information on what the symbols and abbreviations on this table mean by going to the beginning of this table.
67
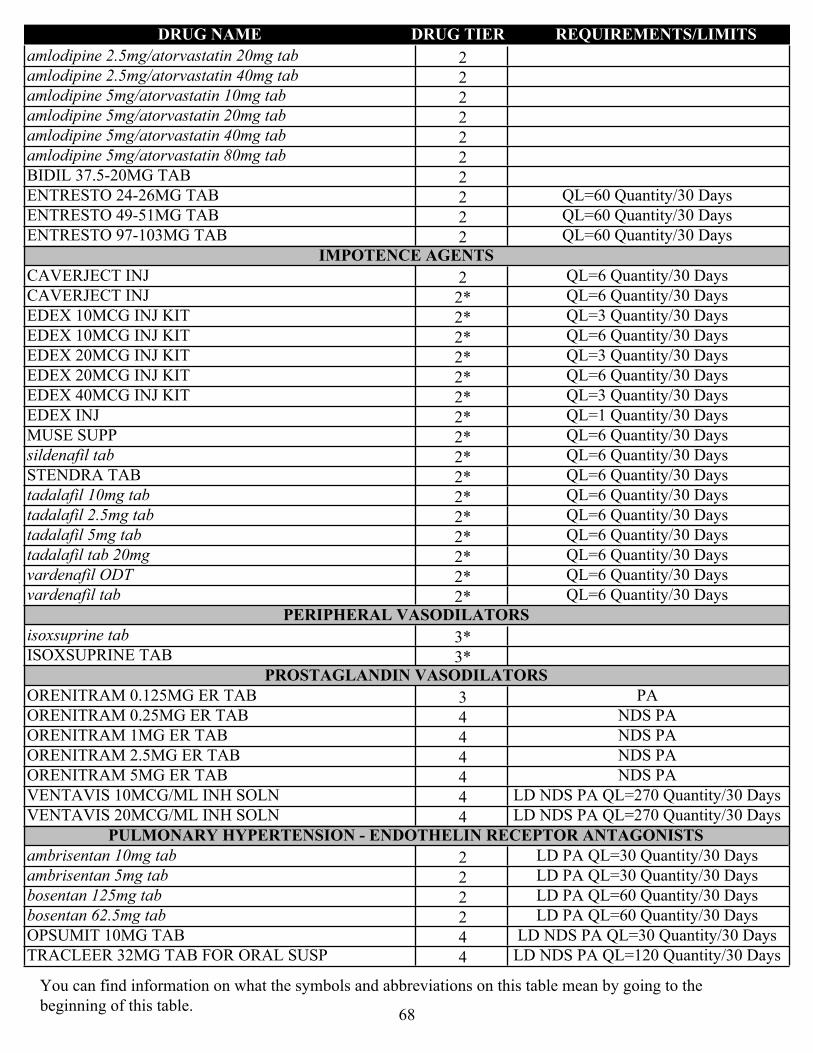
DRUG NAME DRUG TIER REQUIREMENTS/LIMITS
2amlodipine 2.5mg/atorvastatin 20mg tab
2amlodipine 2.5mg/atorvastatin 40mg tab
2amlodipine 5mg/atorvastatin 10mg tab
2amlodipine 5mg/atorvastatin 20mg tab
2amlodipine 5mg/atorvastatin 40mg tab
2amlodipine 5mg/atorvastatin 80mg tab
2BIDIL 37.5-20MG TAB
2ENTRESTO 24-26MG TAB QL=60 Quantity/30 Days
2ENTRESTO 49-51MG TAB QL=60 Quantity/30 Days
2ENTRESTO 97-103MG TAB QL=60 Quantity/30 DaysIMPOTENCE AGENTS
2CAVERJECT INJ QL=6 Quantity/30 Days
2*CAVERJECT INJ QL=6 Quantity/30 Days
2*EDEX 10MCG INJ KIT QL=3 Quantity/30 Days
2*EDEX 10MCG INJ KIT QL=6 Quantity/30 Days
2*EDEX 20MCG INJ KIT QL=3 Quantity/30 Days
2*EDEX 20MCG INJ KIT QL=6 Quantity/30 Days
2*EDEX 40MCG INJ KIT QL=3 Quantity/30 Days
2*EDEX INJ QL=1 Quantity/30 Days
2*MUSE SUPP QL=6 Quantity/30 Days
2*sildenafil tab QL=6 Quantity/30 Days
2*STENDRA TAB QL=6 Quantity/30 Days
2*tadalafil 10mg tab QL=6 Quantity/30 Days
2*tadalafil 2.5mg tab QL=6 Quantity/30 Days
2*tadalafil 5mg tab QL=6 Quantity/30 Days
2*tadalafil tab 20mg QL=6 Quantity/30 Days
2*vardenafil ODT QL=6 Quantity/30 Days
2*vardenafil tab QL=6 Quantity/30 DaysPERIPHERAL VASODILATORS
3*isoxsuprine tab
3*ISOXSUPRINE TABPROSTAGLANDIN VASODILATORS
3ORENITRAM 0.125MG ER TAB PA
4ORENITRAM 0.25MG ER TAB NDS PA
4ORENITRAM 1MG ER TAB NDS PA
4ORENITRAM 2.5MG ER TAB NDS PA
4ORENITRAM 5MG ER TAB NDS PA
4VENTAVIS 10MCG/ML INH SOLN LD NDS PA QL=270 Quantity/30 Days
4VENTAVIS 20MCG/ML INH SOLN LD NDS PA QL=270 Quantity/30 DaysPULMONARY HYPERTENSION - ENDOTHELIN RECEPTOR ANTAGONISTS
2ambrisentan 10mg tab LD PA QL=30 Quantity/30 Days
2ambrisentan 5mg tab LD PA QL=30 Quantity/30 Days
2bosentan 125mg tab LD PA QL=60 Quantity/30 Days
2bosentan 62.5mg tab LD PA QL=60 Quantity/30 Days
4OPSUMIT 10MG TAB LD NDS PA QL=30 Quantity/30 Days
4TRACLEER 32MG TAB FOR ORAL SUSP LD NDS PA QL=120 Quantity/30 Days
You can find information on what the symbols and abbreviations on this table mean by going to the beginning of this table.
68

DRUG NAME DRUG TIER REQUIREMENTS/LIMITS
PULMONARY HYPERTENSION - PHOSPHODIESTERASE INHIBITORS
1sildenafil 20mg tab PA
1tadalafil 20mg tab (PAH) PAPULMONARY HYPERTENSION - PROSTACYCLIN RECEPTOR AGONIST
4UPTRAVI 1000MCG TAB LD NDS PA
4UPTRAVI 1200MCG TAB LD NDS PA
4UPTRAVI 1400MCG TAB LD NDS PA
4UPTRAVI 1600MCG TAB LD NDS PA
4UPTRAVI 200MCG TAB LD NDS PA
4UPTRAVI 400MCG TAB LD NDS PA
4UPTRAVI 600MCG TAB LD NDS PA
4UPTRAVI 800MCG TAB LD NDS PA
4UPTRAVI TITRATION PACK LD NDS PA QL=200 Quantity/28 DaysPULMONARY HYPERTENSION - SOL GUANYLATE CYCLASE STIMULATOR
4ADEMPAS 0.5MG TAB LD NDS PA
4ADEMPAS 1.5MG TAB LD NDS PA
4ADEMPAS 1MG TAB LD NDS PA
4ADEMPAS 2.5MG TAB LD NDS PA
4ADEMPAS 2MG TAB LD NDS PASINUS NODE INHIBITORS
3CORLANOR 5MG TAB PA
3CORLANOR 5MG/5ML ORAL SOLN PA
3CORLANOR 7.5MG TAB PATRANSTHYRETIN STABILIZERS
4VYNDAMAX 61MG CAP NDS PA QL=30 Quantity/30 Days
4VYNDAQEL 20MG CAP NDS PA QL=120 Quantity/30 DaysVASOACTIVE SOLUBLE GUANYLATE CYCLASE STIMULATOR (SGC)
2VERICIGUAT 10MG TAB PA QL=30 Quantity/30 Days
2VERICIGUAT 2.5MG TAB PA QL=30 Quantity/30 Days
2VERICIGUAT 5MG TAB PA QL=30 Quantity/30 Days
CEPHALOSPORINSCEPHALOSPORIN COMBINATIONS
4AVYCAZ 500-2000MG INJ NDS
4ZERBAXA 1000-500MG INJ NDSCEPHALOSPORINS - 1ST GENERATION
1cefadroxil 100mg/ml susp
1cefadroxil 1gm tab
1CEFADROXIL 1GM TAB
1cefadroxil 500mg cap
1cefadroxil 50mg/ml susp
2cefazolin 1000mg inj
2CEFAZOLIN 100GM INJ
2CEFAZOLIN 1GM INJ
2cefazolin 200mg/ml inj
2CEFAZOLIN 20GM INJ
2CEFAZOLIN 300GM INJ
You can find information on what the symbols and abbreviations on this table mean by going to the beginning of this table.
69

DRUG NAME DRUG TIER REQUIREMENTS/LIMITS
2cefazolin 500mg inj
2CEFAZOLIN/DEXTROSE 1GM-4% IV SOLN
2CEFAZOLIN/DEXTROSE 1GM/50ML-4% IV SOLN
1cephalexin 250mg cap
1cephalexin 25mg/ml susp
1cephalexin 500mg cap
1cephalexin 50mg/ml suspCEPHALOSPORINS - 2ND GENERATION
2cefaclor 250mg cap
2CEFACLOR 250MG CAP
3CEFACLOR 25MG/ML SUSP
2cefaclor 500mg cap
2CEFACLOR 500MG CAP
3CEFACLOR 500MG ER TAB
3CEFACLOR 50MG/ML SUSP
3CEFACLOR 75MG/ML SUSP
2cefotetan 1000mg inj
2cefotetan 2000mg inj
2CEFOTETAN/DEXTROSE 1GM/3.58% INJ
2CEFOTETAN/DEXTROSE 2GM-2.08% INJ
2cefoxitin 1000mg inj
2cefoxitin 2000mg inj
2cefoxitin 200mg/ml inj
2CEFOXITIN/DEXTROSE 1GM-4% INJ
2CEFOXITIN/DEXTROSE 2GM/2.2% INJ
1cefprozil 250mg tab
1cefprozil 25mg/ml susp
1cefprozil 500mg tab
1cefprozil 50mg/ml susp
2cefuroxime 1500mg inj
1cefuroxime 250mg tab
1cefuroxime 500mg tab
2cefuroxime 750mg inj
2cefuroxime 95mg/ml injCEPHALOSPORINS - 3RD GENERATION
1cefdinir 25mg/ml susp
1cefdinir 300mg cap
1cefdinir 50mg/ml susp
2cefixime 20mg/ml susp
2cefixime 400mg cap
2cefixime 40mg/ml susp
2cefpodoxime 100mg tab
2cefpodoxime 10mg/ml susp
2cefpodoxime 200mg tab
2cefpodoxime 20mg/ml susp
2ceftazidime 1000mg inj
You can find information on what the symbols and abbreviations on this table mean by going to the beginning of this table.
70

DRUG NAME DRUG TIER REQUIREMENTS/LIMITS
2ceftazidime 200mg/ml inj
2CEFTAZIDIME/D5W 1GM/50ML INJ
2CEFTAZIDIME/DEXTROSE 2GM/50ML/5% INJ
2ceftriaxone 1000mg inj
2ceftriaxone 100mg/ml inj
2ceftriaxone 2000mg inj
2ceftriaxone 250mg inj
2ceftriaxone 500mg inj
2CEFTRIAXONE SODIUM 100GM INJ
2ceftriaxone sodium 1gm inj
2ceftriaxone sodium 2gm inj
2CEFTRIAXONE/DEXTROSE 1GM-3.74% IV SOLN
2CEFTRIAXONE/DEXTROSE 20MG/ML INJ
2CEFTRIAXONE/DEXTROSE 2GM-2.22% IV SOLN
2CEFTRIAXONE/DEXTROSE 40MG/ML INJ
3SUPRAX 100MG CHEW TAB
3SUPRAX 200MG CHEW TAB
3SUPRAX 500MG/5ML SUSP
2TAZICEF 1GM INJ
2tazicef 2gm inj
2TAZICEF 6GM INJCEPHALOSPORINS - 4TH GENERATION
2cefepime 1000mg inj
2CEFEPIME 1GM/50ML IV SOLN
2cefepime 2000mg inj
2CEFEPIME 2GM/100ML IV SOLN
2CEFEPIME/DEXTROSE 1GM/50ML-5% INJ
2CEFEPIME/DEXTROSE 2GM/50ML-5% INJCEPHALOSPORINS - 5TH GENERATION
4TEFLARO 400MG INJ NDS
4TEFLARO 600MG INJ NDS
CONTRACEPTIVESCOMBINATION CONTRACEPTIVES - ORAL
$0altavera 28 day pack
$0apri 28 day pack
$0aranelle 28 pack
$0ashlyna 91 day pack
$0briellyn 28 day pack
$0camreselo 91 day pack
$0caziant 28 day pack
$0cyclafem 7/7/7 28 day pack
$0desogestrel/ethinyl estradiol pack
$0dolishale 28 day pack
$0estarylla 28 day pack
$0ethinyl estradiol 0.02mg/inert ingredients 1mg/levonorgestrel 0.1mg pack
You can find information on what the symbols and abbreviations on this table mean by going to the beginning of this table.
71

DRUG NAME DRUG TIER REQUIREMENTS/LIMITS
$0ethinyl estradiol 0.035mg/ethynodiol 1mg 28 day pack
$0ethinyl estradiol 0.035mg/inert/norgestimate 0.18mg/0.215mg/0.25mg pack
$0ethinyl estradiol 0.03mg/inert ingredients 1mg/levonorgestrel 0.15mg pack
$0ethinyl estradiol 0.05mg/ethynodiol 1mg/inert ingredients 1mg 28 day pack
$0ethinyl estradiol/levonorgestrel 91 day pack
$0jasmiel 28 day pack
2junel fe 1.5/30 28 day pack
2larin 1.5/30 pack
2larin 1/20 pack
$0layolis fe 28 pack
3LO LOESTRIN FE 28 DAY PACK
$0low-ogestrel 28 day pack
2melodetta 24 fe chewable 28 day pack
2microgestin fe 1/20 28 day pack
3NATAZIA 28 DAY PACK
$0nortrel 0.5/35 28 day pack
$0ocella 28 day pack
$0pirmella 1/35 28 day pack
2tarina 24 fe 1/20 28 day pack
$0tri-legest 28 day pack
$0tri-lo-sprintec 28 day pack
$0trivora 28 day pack
2tydemy 28 day pack
$0wymzya fe 28 day packCOMBINATION CONTRACEPTIVES - TRANSDERMAL
$0xulane 150-35mcg/24hr patchCOMBINATION CONTRACEPTIVES - VAGINAL
$0eluryng 0.120-0.015mg/24hr vaginal systemCOPPER CONTRACEPTIVES - IUD
$0*PARAGARD IUDEMERGENCY CONTRACEPTIVES
$0*levonorgestrel tab
$0*PLAN B TAB PROGESTIN CONTRACEPTIVES - IMPLANTS
$0*IMPLANON IMPLANT, NEXPLANON IMPLANTPROGESTIN CONTRACEPTIVES - INJECTABLE
$0medroxyprogesterone acetate 150mg/ml inj
$0medroxyprogesterone acetate 150mg/ml syringePROGESTIN CONTRACEPTIVES - IUD
$0*MIRENA IUDPROGESTIN CONTRACEPTIVES - ORAL
$0norethindrone 0.35mg pack
3SLYND 4MG PACK
You can find information on what the symbols and abbreviations on this table mean by going to the beginning of this table.
72
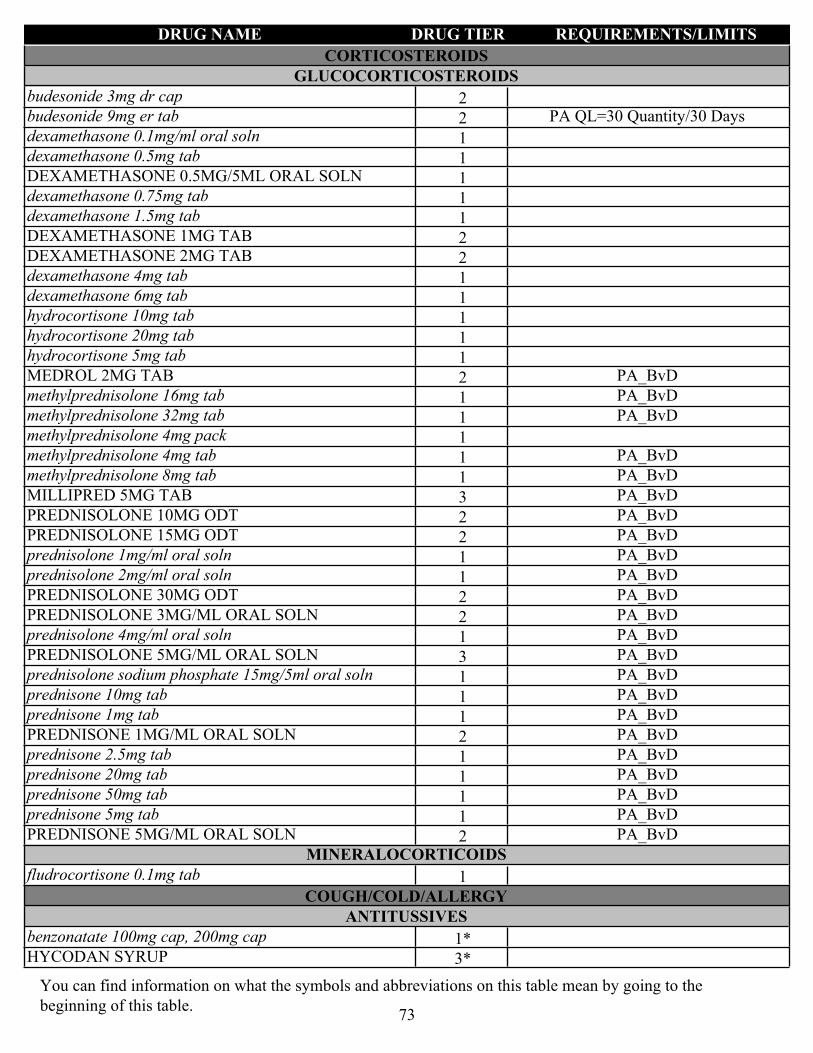
DRUG NAME DRUG TIER REQUIREMENTS/LIMITS
CORTICOSTEROIDSGLUCOCORTICOSTEROIDS
2budesonide 3mg dr cap
2budesonide 9mg er tab PA QL=30 Quantity/30 Days
1dexamethasone 0.1mg/ml oral soln
1dexamethasone 0.5mg tab
1DEXAMETHASONE 0.5MG/5ML ORAL SOLN
1dexamethasone 0.75mg tab
1dexamethasone 1.5mg tab
2DEXAMETHASONE 1MG TAB
2DEXAMETHASONE 2MG TAB
1dexamethasone 4mg tab
1dexamethasone 6mg tab
1hydrocortisone 10mg tab
1hydrocortisone 20mg tab
1hydrocortisone 5mg tab
2MEDROL 2MG TAB PA_BvD
1methylprednisolone 16mg tab PA_BvD
1methylprednisolone 32mg tab PA_BvD
1methylprednisolone 4mg pack
1methylprednisolone 4mg tab PA_BvD
1methylprednisolone 8mg tab PA_BvD
3MILLIPRED 5MG TAB PA_BvD
2PREDNISOLONE 10MG ODT PA_BvD
2PREDNISOLONE 15MG ODT PA_BvD
1prednisolone 1mg/ml oral soln PA_BvD
1prednisolone 2mg/ml oral soln PA_BvD
2PREDNISOLONE 30MG ODT PA_BvD
2PREDNISOLONE 3MG/ML ORAL SOLN PA_BvD
1prednisolone 4mg/ml oral soln PA_BvD
3PREDNISOLONE 5MG/ML ORAL SOLN PA_BvD
1prednisolone sodium phosphate 15mg/5ml oral soln PA_BvD
1prednisone 10mg tab PA_BvD
1prednisone 1mg tab PA_BvD
2PREDNISONE 1MG/ML ORAL SOLN PA_BvD
1prednisone 2.5mg tab PA_BvD
1prednisone 20mg tab PA_BvD
1prednisone 50mg tab PA_BvD
1prednisone 5mg tab PA_BvD
2PREDNISONE 5MG/ML ORAL SOLN PA_BvDMINERALOCORTICOIDS
1fludrocortisone 0.1mg tab
COUGH/COLD/ALLERGYANTITUSSIVES
1*benzonatate 100mg cap, 200mg cap
3*HYCODAN SYRUP
You can find information on what the symbols and abbreviations on this table mean by going to the beginning of this table.
73
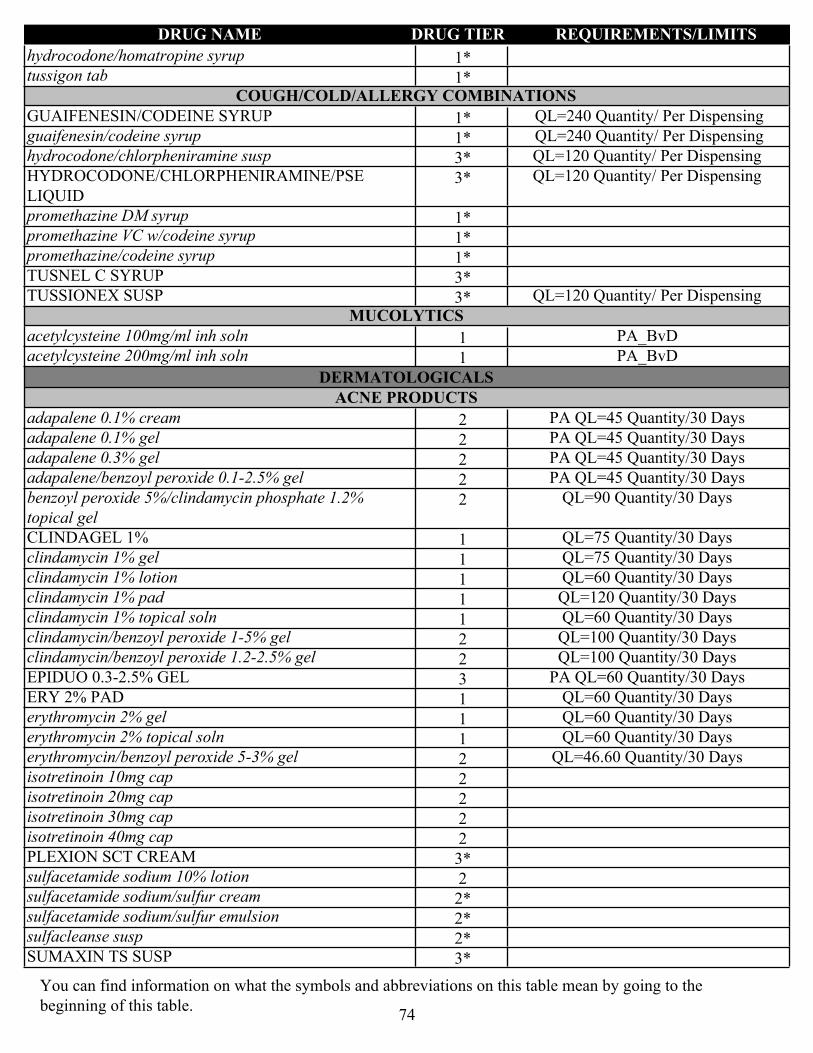
DRUG NAME DRUG TIER REQUIREMENTS/LIMITS
1*hydrocodone/homatropine syrup
1*tussigon tabCOUGH/COLD/ALLERGY COMBINATIONS
1*GUAIFENESIN/CODEINE SYRUP QL=240 Quantity/ Per Dispensing
1*guaifenesin/codeine syrup QL=240 Quantity/ Per Dispensing
3*hydrocodone/chlorpheniramine susp QL=120 Quantity/ Per Dispensing
3*HYDROCODONE/CHLORPHENIRAMINE/PSE LIQUID
QL=120 Quantity/ Per Dispensing
1*promethazine DM syrup
1*promethazine VC w/codeine syrup
1*promethazine/codeine syrup
3*TUSNEL C SYRUP
3*TUSSIONEX SUSP QL=120 Quantity/ Per DispensingMUCOLYTICS
1acetylcysteine 100mg/ml inh soln PA_BvD
1acetylcysteine 200mg/ml inh soln PA_BvD
DERMATOLOGICALSACNE PRODUCTS
2adapalene 0.1% cream PA QL=45 Quantity/30 Days
2adapalene 0.1% gel PA QL=45 Quantity/30 Days
2adapalene 0.3% gel PA QL=45 Quantity/30 Days
2adapalene/benzoyl peroxide 0.1-2.5% gel PA QL=45 Quantity/30 Days
2benzoyl peroxide 5%/clindamycin phosphate 1.2% topical gel
QL=90 Quantity/30 Days
1CLINDAGEL 1% QL=75 Quantity/30 Days
1clindamycin 1% gel QL=75 Quantity/30 Days
1clindamycin 1% lotion QL=60 Quantity/30 Days
1clindamycin 1% pad QL=120 Quantity/30 Days
1clindamycin 1% topical soln QL=60 Quantity/30 Days
2clindamycin/benzoyl peroxide 1-5% gel QL=100 Quantity/30 Days
2clindamycin/benzoyl peroxide 1.2-2.5% gel QL=100 Quantity/30 Days
3EPIDUO 0.3-2.5% GEL PA QL=60 Quantity/30 Days
1ERY 2% PAD QL=60 Quantity/30 Days
1erythromycin 2% gel QL=60 Quantity/30 Days
1erythromycin 2% topical soln QL=60 Quantity/30 Days
2erythromycin/benzoyl peroxide 5-3% gel QL=46.60 Quantity/30 Days
2isotretinoin 10mg cap
2isotretinoin 20mg cap
2isotretinoin 30mg cap
2isotretinoin 40mg cap
3*PLEXION SCT CREAM
2sulfacetamide sodium 10% lotion
2*sulfacetamide sodium/sulfur cream
2*sulfacetamide sodium/sulfur emulsion
2*sulfacleanse susp
3*SUMAXIN TS SUSP
You can find information on what the symbols and abbreviations on this table mean by going to the beginning of this table.
74
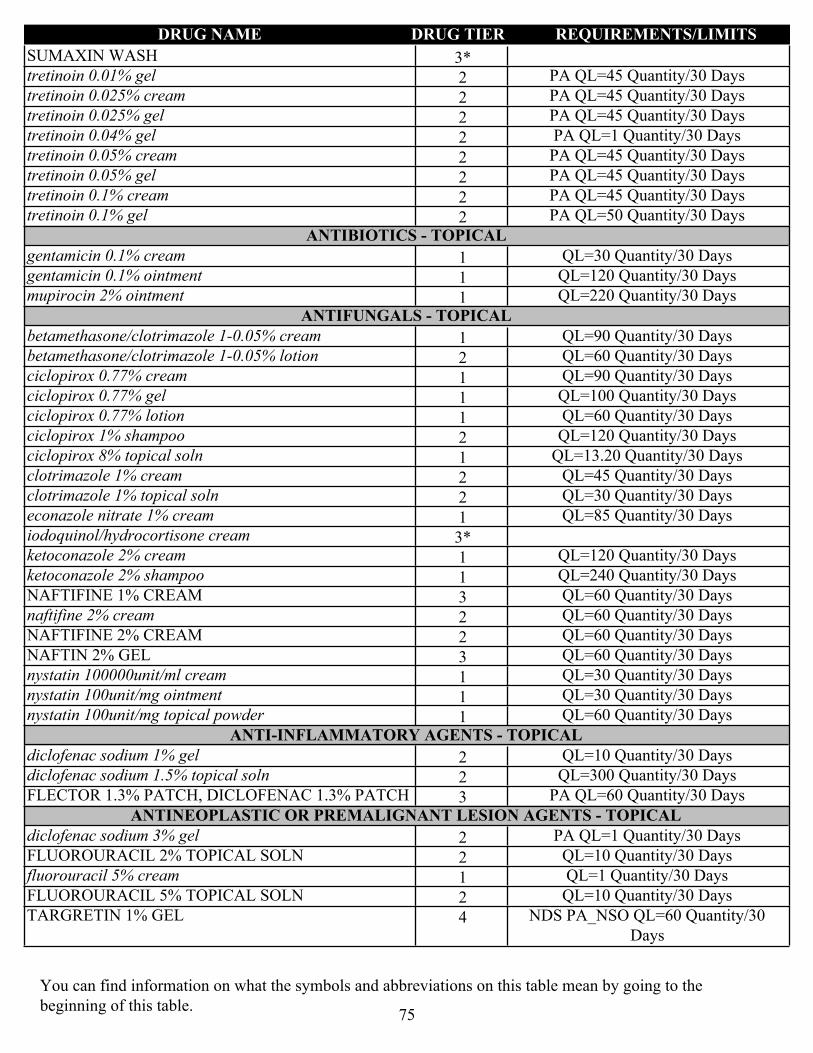
DRUG NAME DRUG TIER REQUIREMENTS/LIMITS
3*SUMAXIN WASH
2tretinoin 0.01% gel PA QL=45 Quantity/30 Days
2tretinoin 0.025% cream PA QL=45 Quantity/30 Days
2tretinoin 0.025% gel PA QL=45 Quantity/30 Days
2tretinoin 0.04% gel PA QL=1 Quantity/30 Days
2tretinoin 0.05% cream PA QL=45 Quantity/30 Days
2tretinoin 0.05% gel PA QL=45 Quantity/30 Days
2tretinoin 0.1% cream PA QL=45 Quantity/30 Days
2tretinoin 0.1% gel PA QL=50 Quantity/30 DaysANTIBIOTICS - TOPICAL
1gentamicin 0.1% cream QL=30 Quantity/30 Days
1gentamicin 0.1% ointment QL=120 Quantity/30 Days
1mupirocin 2% ointment QL=220 Quantity/30 DaysANTIFUNGALS - TOPICAL
1betamethasone/clotrimazole 1-0.05% cream QL=90 Quantity/30 Days
2betamethasone/clotrimazole 1-0.05% lotion QL=60 Quantity/30 Days
1ciclopirox 0.77% cream QL=90 Quantity/30 Days
1ciclopirox 0.77% gel QL=100 Quantity/30 Days
1ciclopirox 0.77% lotion QL=60 Quantity/30 Days
2ciclopirox 1% shampoo QL=120 Quantity/30 Days
1ciclopirox 8% topical soln QL=13.20 Quantity/30 Days
2clotrimazole 1% cream QL=45 Quantity/30 Days
2clotrimazole 1% topical soln QL=30 Quantity/30 Days
1econazole nitrate 1% cream QL=85 Quantity/30 Days
3*iodoquinol/hydrocortisone cream
1ketoconazole 2% cream QL=120 Quantity/30 Days
1ketoconazole 2% shampoo QL=240 Quantity/30 Days
3NAFTIFINE 1% CREAM QL=60 Quantity/30 Days
2naftifine 2% cream QL=60 Quantity/30 Days
2NAFTIFINE 2% CREAM QL=60 Quantity/30 Days
3NAFTIN 2% GEL QL=60 Quantity/30 Days
1nystatin 100000unit/ml cream QL=30 Quantity/30 Days
1nystatin 100unit/mg ointment QL=30 Quantity/30 Days
1nystatin 100unit/mg topical powder QL=60 Quantity/30 DaysANTI-INFLAMMATORY AGENTS - TOPICAL
2diclofenac sodium 1% gel QL=10 Quantity/30 Days
2diclofenac sodium 1.5% topical soln QL=300 Quantity/30 Days
3FLECTOR 1.3% PATCH, DICLOFENAC 1.3% PATCH PA QL=60 Quantity/30 DaysANTINEOPLASTIC OR PREMALIGNANT LESION AGENTS - TOPICAL
2diclofenac sodium 3% gel PA QL=1 Quantity/30 Days
2FLUOROURACIL 2% TOPICAL SOLN QL=10 Quantity/30 Days
1fluorouracil 5% cream QL=1 Quantity/30 Days
2FLUOROURACIL 5% TOPICAL SOLN QL=10 Quantity/30 Days
4TARGRETIN 1% GEL NDS PA_NSO QL=60 Quantity/30 Days
You can find information on what the symbols and abbreviations on this table mean by going to the beginning of this table.
75

DRUG NAME DRUG TIER REQUIREMENTS/LIMITS
4VALCHLOR 0.016% GEL LD NDS PA_NSO QL=240 Quantity/30 Days
ANTIPSORIATICS
2acitretin 10mg cap
2acitretin 17.5mg cap
2acitretin 25mg cap
2calcipotriene 0.005% cream PA QL=120 Quantity/30 Days
2calcipotriene 0.005% ointment PA QL=120 Quantity/30 Days
2calcipotriene 0.005% topical soln PA QL=120 Quantity/30 Days
2METHOXSALEN 10MG CAP
4SKYRIZI 150MG DOSE PACK (75MG/0.83ML) PA QL=7 Quantity/365 Days
4SKYRIZI 150MG/ML AUTO-INJECTOR PA QL=7 Quantity/365 Days
4SKYRIZI 150MG/ML SYRINGE PA QL=7 Quantity/365 Days
4STELARA 45MG/0.5ML INJ PA QL=.50 Quantity/28 Days
4STELARA 45MG/0.5ML SYRINGE PA QL=.50 Quantity/28 Days
4STELARA 90MG/ML SYRINGE PA QL=1 Quantity/28 Days
4TALTZ 80MG/ML AUTO-INJECTOR NDS PA QL=3 Quantity/28 Days
4TALTZ 80MG/ML SYRINGE NDS PA QL=3 Quantity/28 Days
2tazarotene 0.1% cream PA QL=60 Quantity/30 Days
3TAZORAC 0.05% CREAM PA QL=60 Quantity/30 Days
4TREMFYA 100MG/ML AUTO-INJECTOR NDS PA QL=2 Quantity/28 Days
4TREMFYA 100MG/ML SYRINGE NDS PA QL=2 Quantity/28 DaysANTISEBORRHEIC PRODUCTS
3*OVACE CREAM
3*OVACE PLUS SHAMPOO
3*OVACE PLUS WASH
3*OVACE WASH
3*seb-prev cream
2*selenium sulfide 2.25% shampoo
1selenium sulfide 2.5% shampoo
3*sulfacetamide sodium gel
3*sulfacetamide sodium shampoo
2*sulfacetamide sodium washANTIVIRALS - TOPICAL
2acyclovir 5% cream QL=5 Quantity/7 Days
2acyclovir 5% ointment QL=30 Quantity/30 DaysBURN PRODUCTS
1ssd 1% cream
2SULFAMYLON 85MG/GM CREAMCORTICOSTEROIDS - TOPICAL
1ala-cort 2.5% cream QL=454 Quantity/30 Days
2alclometasone dipropionate 0.05% cream QL=120 Quantity/30 Days
2alclometasone dipropionate 0.05% ointment QL=120 Quantity/30 Days
1betamethasone 0.05% aug cream QL=100 Quantity/30 Days
1betamethasone 0.05% aug lotion QL=120 Quantity/30 Days
1betamethasone 0.05% aug ointment QL=100 Quantity/30 Days
You can find information on what the symbols and abbreviations on this table mean by going to the beginning of this table.
76
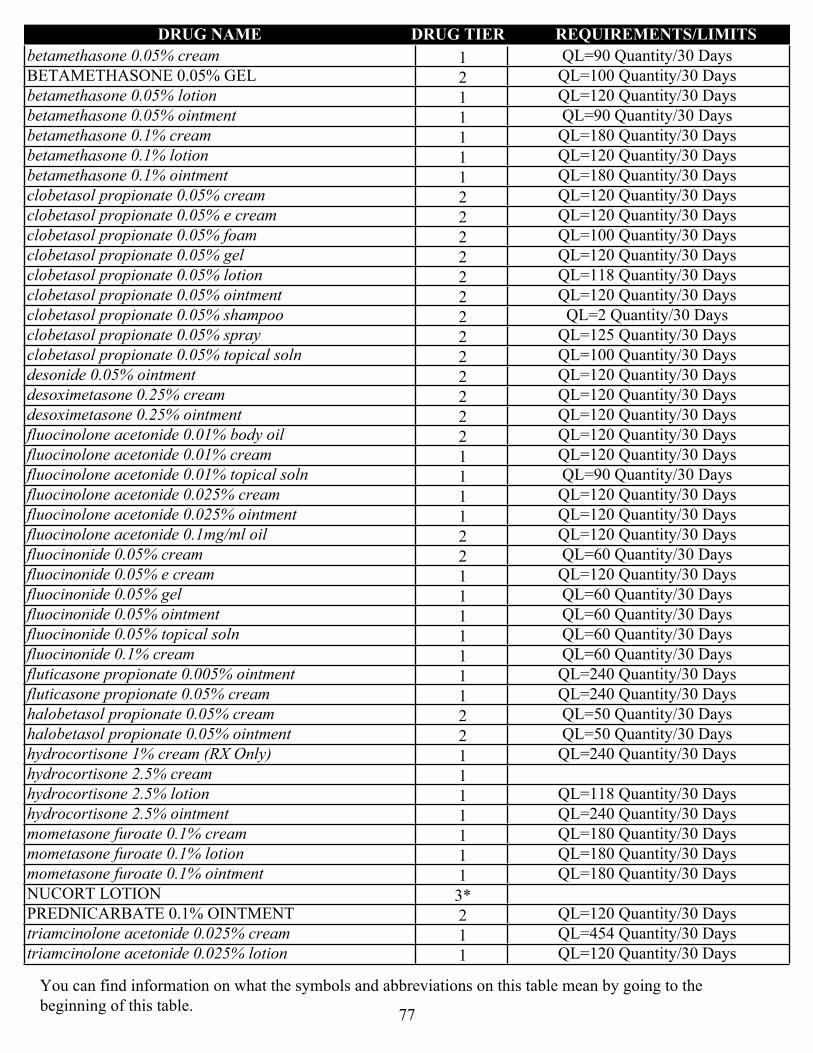
DRUG NAME DRUG TIER REQUIREMENTS/LIMITS
1betamethasone 0.05% cream QL=90 Quantity/30 Days
2BETAMETHASONE 0.05% GEL QL=100 Quantity/30 Days
1betamethasone 0.05% lotion QL=120 Quantity/30 Days
1betamethasone 0.05% ointment QL=90 Quantity/30 Days
1betamethasone 0.1% cream QL=180 Quantity/30 Days
1betamethasone 0.1% lotion QL=120 Quantity/30 Days
1betamethasone 0.1% ointment QL=180 Quantity/30 Days
2clobetasol propionate 0.05% cream QL=120 Quantity/30 Days
2clobetasol propionate 0.05% e cream QL=120 Quantity/30 Days
2clobetasol propionate 0.05% foam QL=100 Quantity/30 Days
2clobetasol propionate 0.05% gel QL=120 Quantity/30 Days
2clobetasol propionate 0.05% lotion QL=118 Quantity/30 Days
2clobetasol propionate 0.05% ointment QL=120 Quantity/30 Days
2clobetasol propionate 0.05% shampoo QL=2 Quantity/30 Days
2clobetasol propionate 0.05% spray QL=125 Quantity/30 Days
2clobetasol propionate 0.05% topical soln QL=100 Quantity/30 Days
2desonide 0.05% ointment QL=120 Quantity/30 Days
2desoximetasone 0.25% cream QL=120 Quantity/30 Days
2desoximetasone 0.25% ointment QL=120 Quantity/30 Days
2fluocinolone acetonide 0.01% body oil QL=120 Quantity/30 Days
1fluocinolone acetonide 0.01% cream QL=120 Quantity/30 Days
1fluocinolone acetonide 0.01% topical soln QL=90 Quantity/30 Days
1fluocinolone acetonide 0.025% cream QL=120 Quantity/30 Days
1fluocinolone acetonide 0.025% ointment QL=120 Quantity/30 Days
2fluocinolone acetonide 0.1mg/ml oil QL=120 Quantity/30 Days
2fluocinonide 0.05% cream QL=60 Quantity/30 Days
1fluocinonide 0.05% e cream QL=120 Quantity/30 Days
1fluocinonide 0.05% gel QL=60 Quantity/30 Days
1fluocinonide 0.05% ointment QL=60 Quantity/30 Days
1fluocinonide 0.05% topical soln QL=60 Quantity/30 Days
1fluocinonide 0.1% cream QL=60 Quantity/30 Days
1fluticasone propionate 0.005% ointment QL=240 Quantity/30 Days
1fluticasone propionate 0.05% cream QL=240 Quantity/30 Days
2halobetasol propionate 0.05% cream QL=50 Quantity/30 Days
2halobetasol propionate 0.05% ointment QL=50 Quantity/30 Days
1hydrocortisone 1% cream (RX Only) QL=240 Quantity/30 Days
1hydrocortisone 2.5% cream
1hydrocortisone 2.5% lotion QL=118 Quantity/30 Days
1hydrocortisone 2.5% ointment QL=240 Quantity/30 Days
1mometasone furoate 0.1% cream QL=180 Quantity/30 Days
1mometasone furoate 0.1% lotion QL=180 Quantity/30 Days
1mometasone furoate 0.1% ointment QL=180 Quantity/30 Days
3*NUCORT LOTION
2PREDNICARBATE 0.1% OINTMENT QL=120 Quantity/30 Days
1triamcinolone acetonide 0.025% cream QL=454 Quantity/30 Days
1triamcinolone acetonide 0.025% lotion QL=120 Quantity/30 Days
You can find information on what the symbols and abbreviations on this table mean by going to the beginning of this table.
77
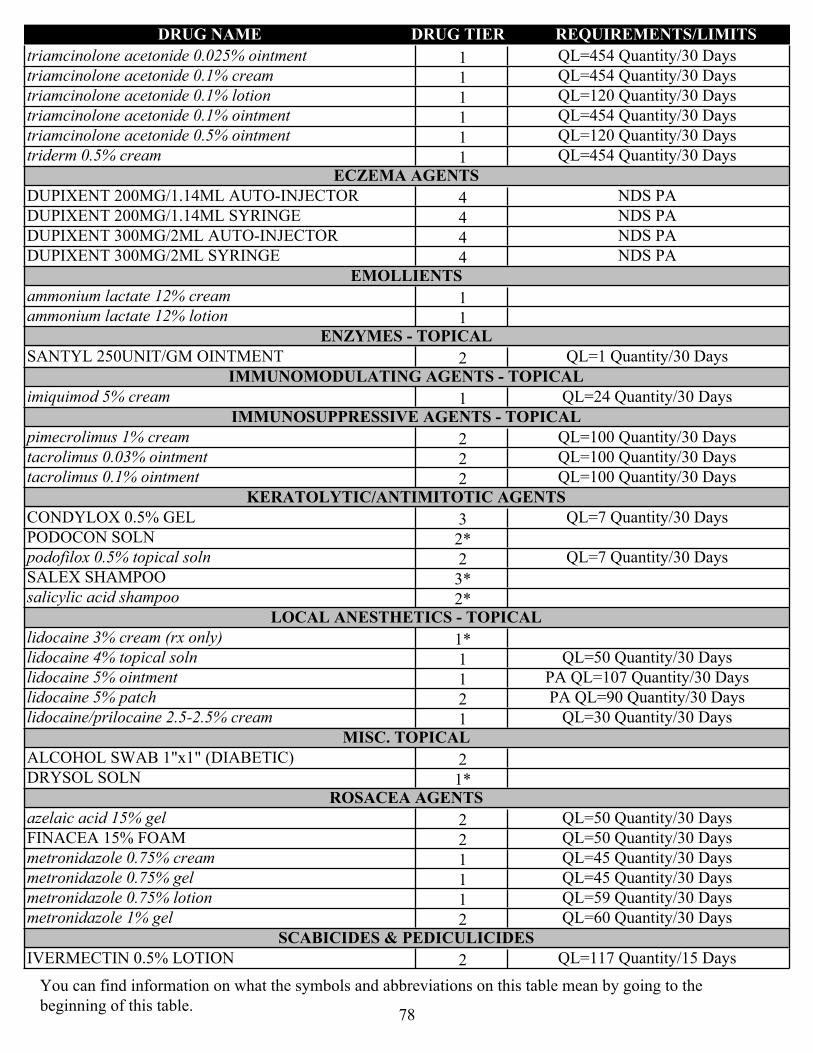
DRUG NAME DRUG TIER REQUIREMENTS/LIMITS
1triamcinolone acetonide 0.025% ointment QL=454 Quantity/30 Days
1triamcinolone acetonide 0.1% cream QL=454 Quantity/30 Days
1triamcinolone acetonide 0.1% lotion QL=120 Quantity/30 Days
1triamcinolone acetonide 0.1% ointment QL=454 Quantity/30 Days
1triamcinolone acetonide 0.5% ointment QL=120 Quantity/30 Days
1triderm 0.5% cream QL=454 Quantity/30 DaysECZEMA AGENTS
4DUPIXENT 200MG/1.14ML AUTO-INJECTOR NDS PA
4DUPIXENT 200MG/1.14ML SYRINGE NDS PA
4DUPIXENT 300MG/2ML AUTO-INJECTOR NDS PA
4DUPIXENT 300MG/2ML SYRINGE NDS PAEMOLLIENTS
1ammonium lactate 12% cream
1ammonium lactate 12% lotionENZYMES - TOPICAL
2SANTYL 250UNIT/GM OINTMENT QL=1 Quantity/30 DaysIMMUNOMODULATING AGENTS - TOPICAL
1imiquimod 5% cream QL=24 Quantity/30 DaysIMMUNOSUPPRESSIVE AGENTS - TOPICAL
2pimecrolimus 1% cream QL=100 Quantity/30 Days
2tacrolimus 0.03% ointment QL=100 Quantity/30 Days
2tacrolimus 0.1% ointment QL=100 Quantity/30 DaysKERATOLYTIC/ANTIMITOTIC AGENTS
3CONDYLOX 0.5% GEL QL=7 Quantity/30 Days
2*PODOCON SOLN
2podofilox 0.5% topical soln QL=7 Quantity/30 Days
3*SALEX SHAMPOO
2*salicylic acid shampooLOCAL ANESTHETICS - TOPICAL
1*lidocaine 3% cream (rx only)
1lidocaine 4% topical soln QL=50 Quantity/30 Days
1lidocaine 5% ointment PA QL=107 Quantity/30 Days
2lidocaine 5% patch PA QL=90 Quantity/30 Days
1lidocaine/prilocaine 2.5-2.5% cream QL=30 Quantity/30 DaysMISC. TOPICAL
2ALCOHOL SWAB 1"x1" (DIABETIC)
1*DRYSOL SOLNROSACEA AGENTS
2azelaic acid 15% gel QL=50 Quantity/30 Days
2FINACEA 15% FOAM QL=50 Quantity/30 Days
1metronidazole 0.75% cream QL=45 Quantity/30 Days
1metronidazole 0.75% gel QL=45 Quantity/30 Days
1metronidazole 0.75% lotion QL=59 Quantity/30 Days
2metronidazole 1% gel QL=60 Quantity/30 DaysSCABICIDES & PEDICULICIDES
2IVERMECTIN 0.5% LOTION QL=117 Quantity/15 Days
You can find information on what the symbols and abbreviations on this table mean by going to the beginning of this table.
78
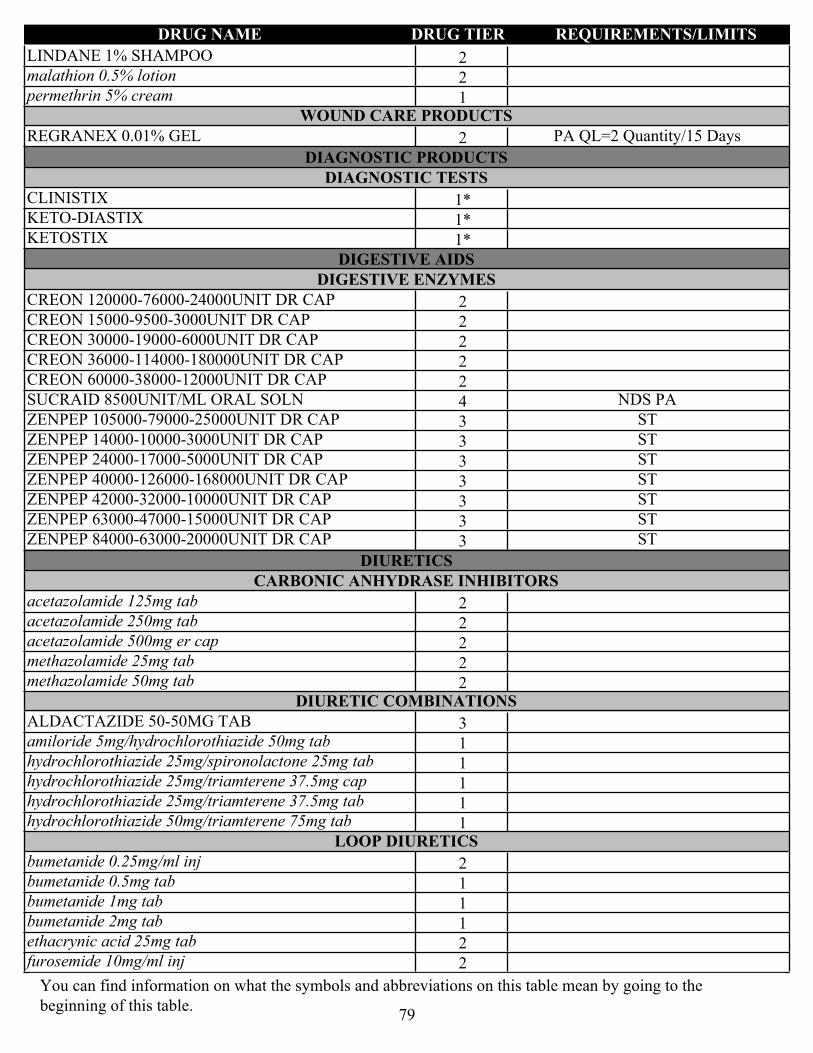
DRUG NAME DRUG TIER REQUIREMENTS/LIMITS
2LINDANE 1% SHAMPOO
2malathion 0.5% lotion
1permethrin 5% creamWOUND CARE PRODUCTS
2REGRANEX 0.01% GEL PA QL=2 Quantity/15 Days
DIAGNOSTIC PRODUCTSDIAGNOSTIC TESTS
1*CLINISTIX
1*KETO-DIASTIX
1*KETOSTIX
DIGESTIVE AIDSDIGESTIVE ENZYMES
2CREON 120000-76000-24000UNIT DR CAP
2CREON 15000-9500-3000UNIT DR CAP
2CREON 30000-19000-6000UNIT DR CAP
2CREON 36000-114000-180000UNIT DR CAP
2CREON 60000-38000-12000UNIT DR CAP
4SUCRAID 8500UNIT/ML ORAL SOLN NDS PA
3ZENPEP 105000-79000-25000UNIT DR CAP ST
3ZENPEP 14000-10000-3000UNIT DR CAP ST
3ZENPEP 24000-17000-5000UNIT DR CAP ST
3ZENPEP 40000-126000-168000UNIT DR CAP ST
3ZENPEP 42000-32000-10000UNIT DR CAP ST
3ZENPEP 63000-47000-15000UNIT DR CAP ST
3ZENPEP 84000-63000-20000UNIT DR CAP ST
DIURETICSCARBONIC ANHYDRASE INHIBITORS
2acetazolamide 125mg tab
2acetazolamide 250mg tab
2acetazolamide 500mg er cap
2methazolamide 25mg tab
2methazolamide 50mg tabDIURETIC COMBINATIONS
3ALDACTAZIDE 50-50MG TAB
1amiloride 5mg/hydrochlorothiazide 50mg tab
1hydrochlorothiazide 25mg/spironolactone 25mg tab
1hydrochlorothiazide 25mg/triamterene 37.5mg cap
1hydrochlorothiazide 25mg/triamterene 37.5mg tab
1hydrochlorothiazide 50mg/triamterene 75mg tabLOOP DIURETICS
2bumetanide 0.25mg/ml inj
1bumetanide 0.5mg tab
1bumetanide 1mg tab
1bumetanide 2mg tab
2ethacrynic acid 25mg tab
2furosemide 10mg/ml inj
You can find information on what the symbols and abbreviations on this table mean by going to the beginning of this table.
79

DRUG NAME DRUG TIER REQUIREMENTS/LIMITS
1furosemide 10mg/ml oral soln
$0furosemide 20mg tab
$0furosemide 40mg tab
$0furosemide 80mg tab
2FUROSEMIDE 8MG/ML ORAL SOLN
1torsemide 100mg tab
1torsemide 10mg tab
1torsemide 20mg tab
1torsemide 5mg tabPOTASSIUM SPARING DIURETICS
1amiloride 5mg tab
1spironolactone 100mg tab
1spironolactone 25mg tab
1spironolactone 50mg tab
2triamterene 100mg cap
2triamterene 50mg capTHIAZIDES AND THIAZIDE-LIKE DIURETICS
$0chlorthalidone 25mg tab
$0chlorthalidone 50mg tab
2DIURIL 250MG/5ML SUSP
$0hydrochlorothiazide 12.5mg cap
$0hydrochlorothiazide 12.5mg tab
$0hydrochlorothiazide 25mg tab
$0hydrochlorothiazide 50mg tab
1indapamide 1.25mg tab
1indapamide 2.5mg tab
1metolazone 10mg tab
1metolazone 2.5mg tab
1metolazone 5mg tab
ENDOCRINE AND METABOLIC AGENTS - MISC.ADRENAL STEROID INHIBITORS
4ISTURISA 10MG TAB LD NDS PA QL=180 Quantity/30 Days
4ISTURISA 1MG TAB LD NDS PA QL=240 Quantity/30 Days
4ISTURISA 5MG TAB LD NDS PA QL=60 Quantity/30 DaysBONE DENSITY REGULATORS
$0alendronate 10mg tab
$0alendronate 35mg tab
$0alendronate 70mg tab
3alendronate 70mg/75ml oral soln
4FORTEO 600MCG/2.4ML PEN INJ NDS QL=1 Quantity/28 Days
1ibandronate 150mg tab QL=1 Quantity/30 Days
4NATPARA 100MCG CARTRIDGE LD NDS PA
4NATPARA 25MCG CARTRIDGE LD NDS PA
4NATPARA 50MCG CARTRIDGE LD NDS PA
4NATPARA 75MCG CARTRIDGE LD NDS PA
3PROLIA 60MG/ML SYRINGE PA QL=1 Quantity/168 Days
You can find information on what the symbols and abbreviations on this table mean by going to the beginning of this table.
80

DRUG NAME DRUG TIER REQUIREMENTS/LIMITS
2risedronate sodium 150mg tab
2risedronate sodium 30mg tab
2risedronate sodium 35mg tab
2risedronate sodium 5mg tab
2salmon calcitonin 200unit/act nasal spray
4TYMLOS 3120MCG/1.56ML PEN INJ NDS QL=1.56 Quantity/30 Days
4XGEVA 120MG/1.7ML INJ NDS PA QL=1 Quantity/28 DaysGNRH/LHRH ANTAGONISTS
2ORILISSA 150MG TAB PA QL=30 Quantity/30 Days
2ORILISSA 200MG TAB PA QL=60 Quantity/30 DaysGROWTH HORMONE RECEPTOR ANTAGONISTS
4SOMAVERT 10MG INJ LD NDS PA
4SOMAVERT 15MG INJ LD NDS PA
4SOMAVERT 20MG INJ LD NDS PA
4SOMAVERT 25MG INJ LD NDS PA
4SOMAVERT 30MG INJ LD NDS PAGROWTH HORMONES
4GENOTROPIN 0.2MG INJ NDS PA
4GENOTROPIN 0.4MG INJ NDS PA
4GENOTROPIN 0.6MG INJ NDS PA
4GENOTROPIN 0.8MG INJ NDS PA
4GENOTROPIN 1.2MG INJ NDS PA
4GENOTROPIN 1.4MG INJ NDS PA
4GENOTROPIN 1.6MG INJ NDS PA
4GENOTROPIN 1.8MG INJ NDS PA
4GENOTROPIN 12MG CARTRIDGE NDS PA
4GENOTROPIN 1MG INJ NDS PA
4GENOTROPIN 2MG INJ NDS PA
4GENOTROPIN 5MG CARTRIDGE NDS PAHORMONE RECEPTOR MODULATORS
3OSPHENA 60MG TAB PA
$0raloxifene 60mg tabINSULIN-LIKE GROWTH FACTORS (SOMATOMEDINS)
4INCRELEX 40MG/4ML INJ NDS PALHRH/GNRH AGONIST ANALOG PITUITARY SUPPRESSANTS
4LUPANETA 3-MONTH PACK PA QL=1 Quantity/84 Days
4LUPANETA PACK 1-MONTH PACK NDS PA QL=1 Quantity/28 Days
4LUPRON 11.25MG INJ PED KIT (3 MONTH) QL=1 Quantity/84 Days
4LUPRON 7.5MG INJ PED KIT (1 MONTH) QL=1 Quantity/28 Days
4SYNAREL 2MG/ML NASAL INHALER NDS PAMETABOLIC MODIFIERS
1calcitriol 0.00025mg cap
1calcitriol 0.0005mg cap
1calcitriol 0.001mg/ml oral soln
3CARBAGLU 200MG TAB FOR ORAL SUSP PA
2cinacalcet 30mg tab
You can find information on what the symbols and abbreviations on this table mean by going to the beginning of this table.
81
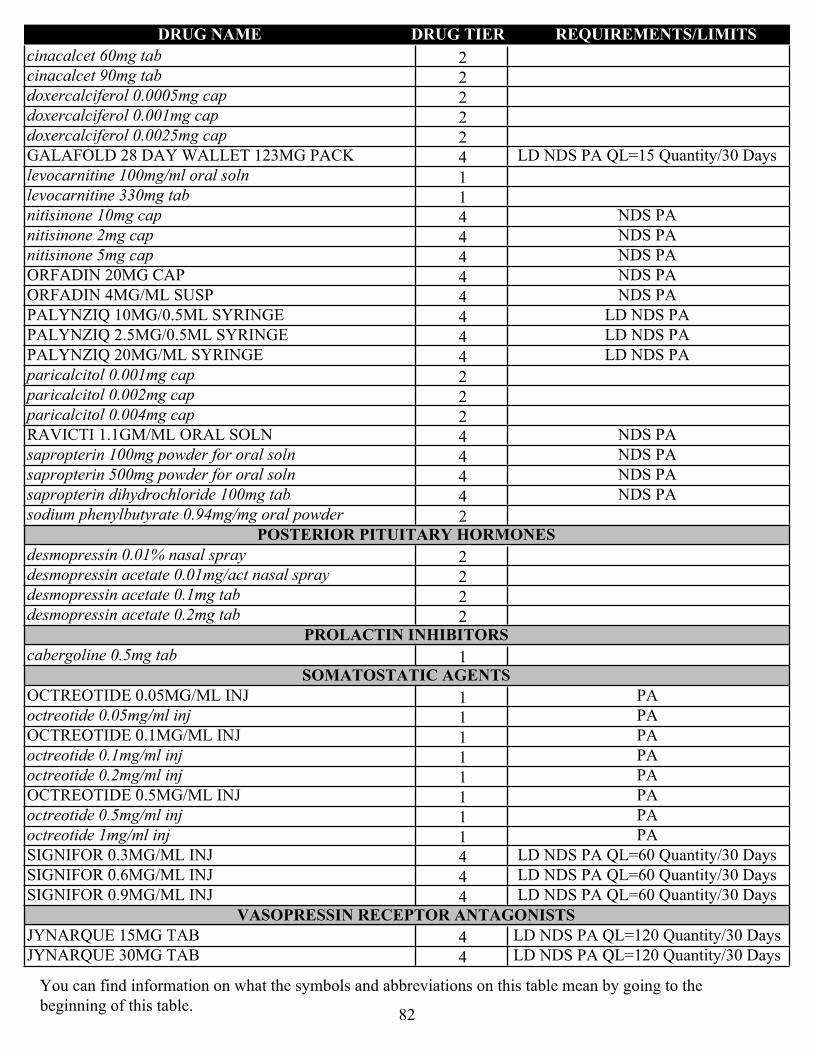
DRUG NAME DRUG TIER REQUIREMENTS/LIMITS
2cinacalcet 60mg tab
2cinacalcet 90mg tab
2doxercalciferol 0.0005mg cap
2doxercalciferol 0.001mg cap
2doxercalciferol 0.0025mg cap
4GALAFOLD 28 DAY WALLET 123MG PACK LD NDS PA QL=15 Quantity/30 Days
1levocarnitine 100mg/ml oral soln
1levocarnitine 330mg tab
4nitisinone 10mg cap NDS PA
4nitisinone 2mg cap NDS PA
4nitisinone 5mg cap NDS PA
4ORFADIN 20MG CAP NDS PA
4ORFADIN 4MG/ML SUSP NDS PA
4PALYNZIQ 10MG/0.5ML SYRINGE LD NDS PA
4PALYNZIQ 2.5MG/0.5ML SYRINGE LD NDS PA
4PALYNZIQ 20MG/ML SYRINGE LD NDS PA
2paricalcitol 0.001mg cap
2paricalcitol 0.002mg cap
2paricalcitol 0.004mg cap
4RAVICTI 1.1GM/ML ORAL SOLN NDS PA
4sapropterin 100mg powder for oral soln NDS PA
4sapropterin 500mg powder for oral soln NDS PA
4sapropterin dihydrochloride 100mg tab NDS PA
2sodium phenylbutyrate 0.94mg/mg oral powderPOSTERIOR PITUITARY HORMONES
2desmopressin 0.01% nasal spray
2desmopressin acetate 0.01mg/act nasal spray
2desmopressin acetate 0.1mg tab
2desmopressin acetate 0.2mg tabPROLACTIN INHIBITORS
1cabergoline 0.5mg tabSOMATOSTATIC AGENTS
1OCTREOTIDE 0.05MG/ML INJ PA
1octreotide 0.05mg/ml inj PA
1OCTREOTIDE 0.1MG/ML INJ PA
1octreotide 0.1mg/ml inj PA
1octreotide 0.2mg/ml inj PA
1OCTREOTIDE 0.5MG/ML INJ PA
1octreotide 0.5mg/ml inj PA
1octreotide 1mg/ml inj PA
4SIGNIFOR 0.3MG/ML INJ LD NDS PA QL=60 Quantity/30 Days
4SIGNIFOR 0.6MG/ML INJ LD NDS PA QL=60 Quantity/30 Days
4SIGNIFOR 0.9MG/ML INJ LD NDS PA QL=60 Quantity/30 DaysVASOPRESSIN RECEPTOR ANTAGONISTS
4JYNARQUE 15MG TAB LD NDS PA QL=120 Quantity/30 Days
4JYNARQUE 30MG TAB LD NDS PA QL=120 Quantity/30 Days
You can find information on what the symbols and abbreviations on this table mean by going to the beginning of this table.
82

DRUG NAME DRUG TIER REQUIREMENTS/LIMITS
4JYNARQUE 45/15 THERAPY PACK LD NDS PA QL=60 Quantity/30 Days
4JYNARQUE 60/30 THERAPY PACK LD NDS PA QL=60 Quantity/30 Days
4JYNARQUE 90/30 THERAPY PACK LD NDS PA QL=60 Quantity/30 Days
4JYNARQUE TAB 15/15 CARTON 15MG PACK LD NDS PA QL=60 Quantity/30 Days
4JYNARQUE TAB 30/15MG THERAPY PACK LD NDS PA QL=60 Quantity/30 Days
ESTROGENSESTROGEN COMBINATIONS
2amabelz 0.5/0.1mg 28 day pack
3ANGELIQ 0.25/0.5MG 28 DAY PACK
3ANGELIQ 0.5/1MG 28 DAY PACK
3CLIMARA PRO 0.00188-0.000625MG/HR PATCH
3COMBIPATCH 0.00208-0.00583MG/HR PATCH
3COMBIPATCH 0.00208-0.0104MG/HR PATCH
1*esterified estrogens/methyltestosterone tab
2ethinyl estradiol 0.005mg/norethindrone acetate 1mg pack
2fyavolv 0.0025-0.5mg tab
2mimvey pack
2ORIAHNN 28 DAY KIT PACK PA QL=56 Quantity/28 Days
3PREFEST 30 DAY PACK
2PREMPHASE 28 DAY PACK
2PREMPRO 0.3/1.5MG 28 DAY PACK
2PREMPRO 0.45/1.5 28 DAY PACK
2PREMPRO 0.625/2.5MG 28 DAY PACK
2PREMPRO 0.625/5MG 28 DAY PACKESTROGENS
3DELESTROGEN 10MG/ML INJ
3DEPO-ESTRADIOL 5MG/ML INJ
1estradiol 0.00104mg/hr weekly patch
1estradiol 0.00156mg/hr weekly patch
1estradiol 0.00208mg/hr weekly patch
1estradiol 0.0025mg/hr weekly patch
1estradiol 0.00312mg/hr weekly patch
1estradiol 0.00417mg/hr weekly patch
2estradiol 0.025mg twice weekly patch
2estradiol 0.0375mg/24hr twice weekly patch
2estradiol 0.05mg/24hr twice weekly patch
2estradiol 0.075mg/24hr twice weekly patch
2estradiol 0.1mg/24hr twice weekly patch
1estradiol 0.5mg tab
1estradiol 1mg tab
1estradiol 2mg tab
2estradiol valerate 20mg/ml inj
2estradiol valerate 40mg/ml inj
3EVAMIST 1.53MG/SPRAY SPRAY
3MENEST 0.3MG TAB
You can find information on what the symbols and abbreviations on this table mean by going to the beginning of this table.
83
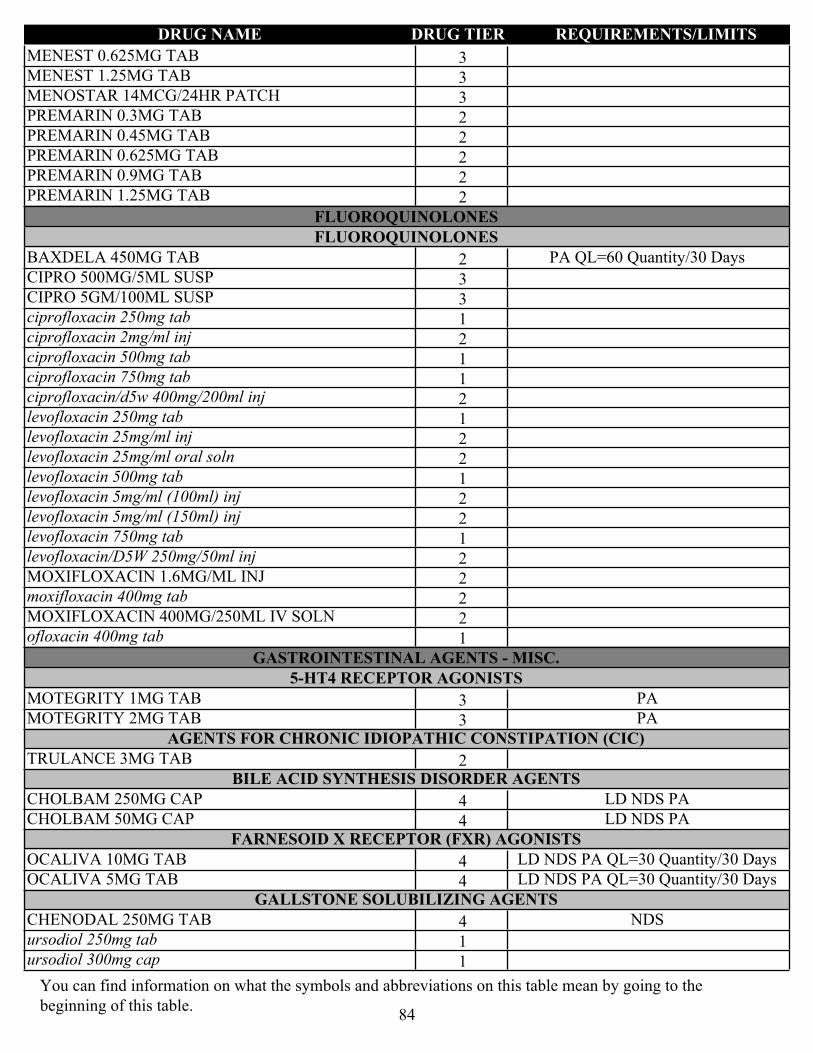
DRUG NAME DRUG TIER REQUIREMENTS/LIMITS
3MENEST 0.625MG TAB
3MENEST 1.25MG TAB
3MENOSTAR 14MCG/24HR PATCH
2PREMARIN 0.3MG TAB
2PREMARIN 0.45MG TAB
2PREMARIN 0.625MG TAB
2PREMARIN 0.9MG TAB
2PREMARIN 1.25MG TAB
FLUOROQUINOLONESFLUOROQUINOLONES
2BAXDELA 450MG TAB PA QL=60 Quantity/30 Days
3CIPRO 500MG/5ML SUSP
3CIPRO 5GM/100ML SUSP
1ciprofloxacin 250mg tab
2ciprofloxacin 2mg/ml inj
1ciprofloxacin 500mg tab
1ciprofloxacin 750mg tab
2ciprofloxacin/d5w 400mg/200ml inj
1levofloxacin 250mg tab
2levofloxacin 25mg/ml inj
2levofloxacin 25mg/ml oral soln
1levofloxacin 500mg tab
2levofloxacin 5mg/ml (100ml) inj
2levofloxacin 5mg/ml (150ml) inj
1levofloxacin 750mg tab
2levofloxacin/D5W 250mg/50ml inj
2MOXIFLOXACIN 1.6MG/ML INJ
2moxifloxacin 400mg tab
2MOXIFLOXACIN 400MG/250ML IV SOLN
1ofloxacin 400mg tab
GASTROINTESTINAL AGENTS - MISC.5-HT4 RECEPTOR AGONISTS
3MOTEGRITY 1MG TAB PA
3MOTEGRITY 2MG TAB PAAGENTS FOR CHRONIC IDIOPATHIC CONSTIPATION (CIC)
2TRULANCE 3MG TABBILE ACID SYNTHESIS DISORDER AGENTS
4CHOLBAM 250MG CAP LD NDS PA
4CHOLBAM 50MG CAP LD NDS PAFARNESOID X RECEPTOR (FXR) AGONISTS
4OCALIVA 10MG TAB LD NDS PA QL=30 Quantity/30 Days
4OCALIVA 5MG TAB LD NDS PA QL=30 Quantity/30 DaysGALLSTONE SOLUBILIZING AGENTS
4CHENODAL 250MG TAB NDS
1ursodiol 250mg tab
1ursodiol 300mg cap
You can find information on what the symbols and abbreviations on this table mean by going to the beginning of this table.
84
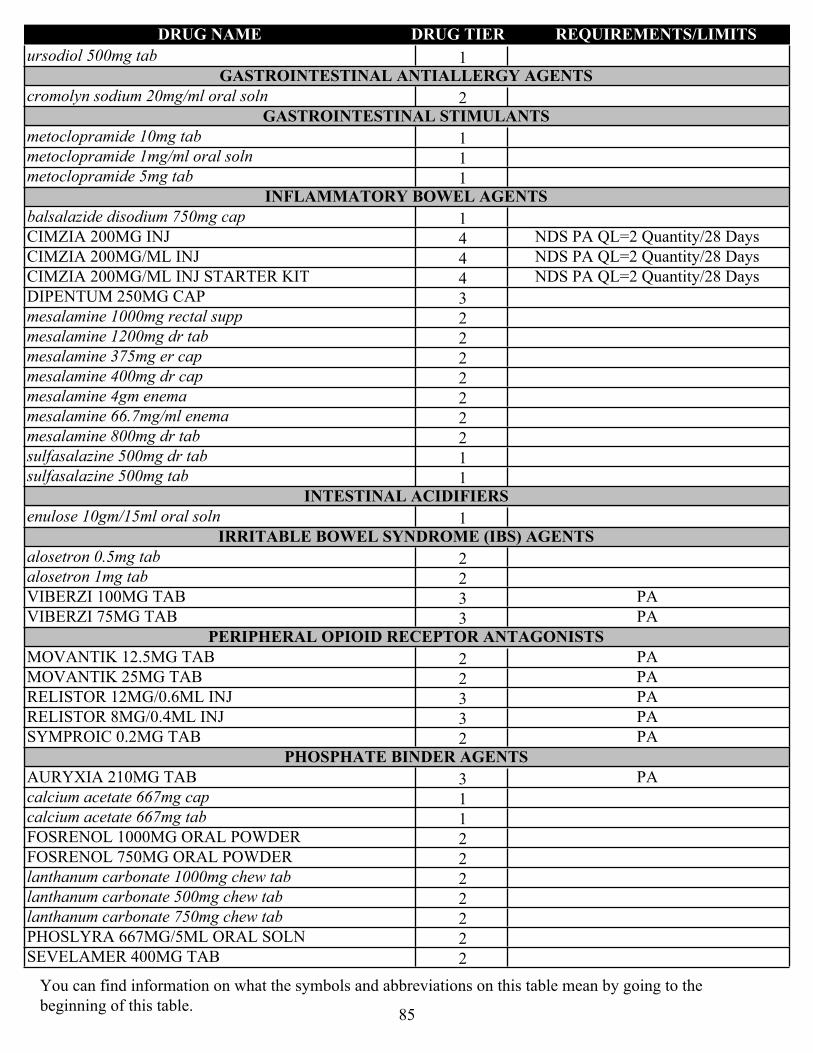
DRUG NAME DRUG TIER REQUIREMENTS/LIMITS
1ursodiol 500mg tabGASTROINTESTINAL ANTIALLERGY AGENTS
2cromolyn sodium 20mg/ml oral solnGASTROINTESTINAL STIMULANTS
1metoclopramide 10mg tab
1metoclopramide 1mg/ml oral soln
1metoclopramide 5mg tabINFLAMMATORY BOWEL AGENTS
1balsalazide disodium 750mg cap
4CIMZIA 200MG INJ NDS PA QL=2 Quantity/28 Days
4CIMZIA 200MG/ML INJ NDS PA QL=2 Quantity/28 Days
4CIMZIA 200MG/ML INJ STARTER KIT NDS PA QL=2 Quantity/28 Days
3DIPENTUM 250MG CAP
2mesalamine 1000mg rectal supp
2mesalamine 1200mg dr tab
2mesalamine 375mg er cap
2mesalamine 400mg dr cap
2mesalamine 4gm enema
2mesalamine 66.7mg/ml enema
2mesalamine 800mg dr tab
1sulfasalazine 500mg dr tab
1sulfasalazine 500mg tabINTESTINAL ACIDIFIERS
1enulose 10gm/15ml oral solnIRRITABLE BOWEL SYNDROME (IBS) AGENTS
2alosetron 0.5mg tab
2alosetron 1mg tab
3VIBERZI 100MG TAB PA
3VIBERZI 75MG TAB PAPERIPHERAL OPIOID RECEPTOR ANTAGONISTS
2MOVANTIK 12.5MG TAB PA
2MOVANTIK 25MG TAB PA
3RELISTOR 12MG/0.6ML INJ PA
3RELISTOR 8MG/0.4ML INJ PA
2SYMPROIC 0.2MG TAB PAPHOSPHATE BINDER AGENTS
3AURYXIA 210MG TAB PA
1calcium acetate 667mg cap
1calcium acetate 667mg tab
2FOSRENOL 1000MG ORAL POWDER
2FOSRENOL 750MG ORAL POWDER
2lanthanum carbonate 1000mg chew tab
2lanthanum carbonate 500mg chew tab
2lanthanum carbonate 750mg chew tab
2PHOSLYRA 667MG/5ML ORAL SOLN
2SEVELAMER 400MG TAB
You can find information on what the symbols and abbreviations on this table mean by going to the beginning of this table.
85
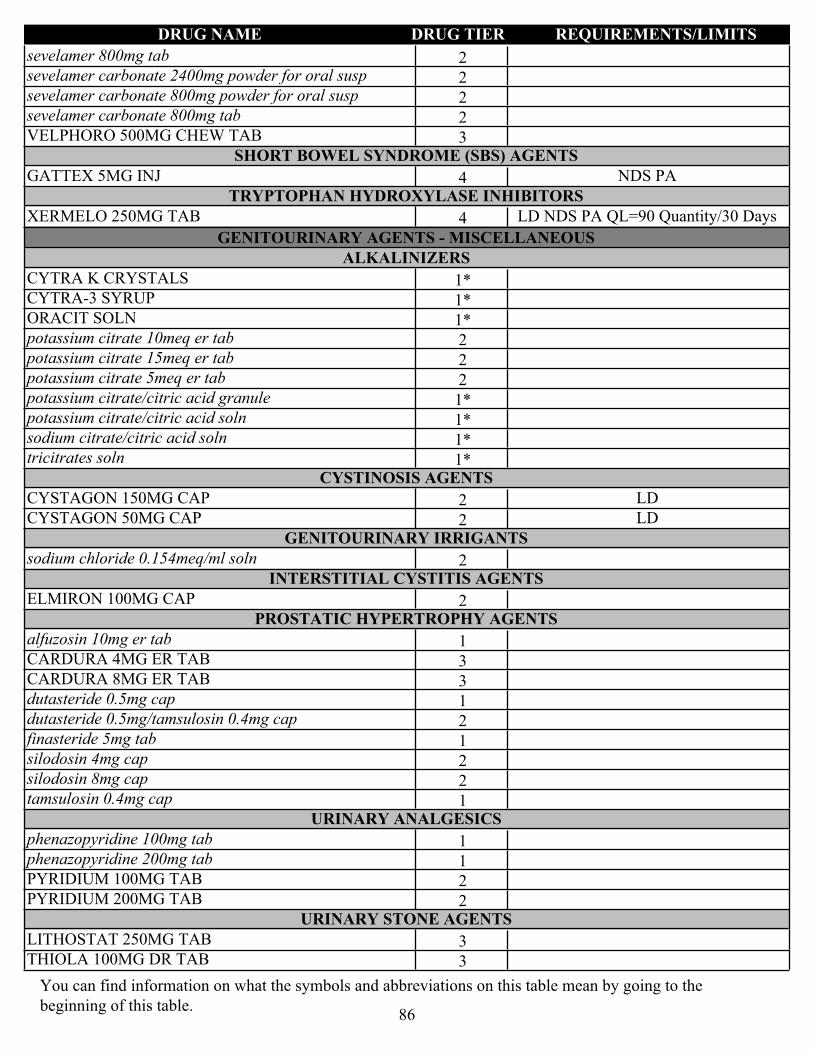
DRUG NAME DRUG TIER REQUIREMENTS/LIMITS
2sevelamer 800mg tab
2sevelamer carbonate 2400mg powder for oral susp
2sevelamer carbonate 800mg powder for oral susp
2sevelamer carbonate 800mg tab
3VELPHORO 500MG CHEW TABSHORT BOWEL SYNDROME (SBS) AGENTS
4GATTEX 5MG INJ NDS PATRYPTOPHAN HYDROXYLASE INHIBITORS
4XERMELO 250MG TAB LD NDS PA QL=90 Quantity/30 Days
GENITOURINARY AGENTS - MISCELLANEOUSALKALINIZERS
1*CYTRA K CRYSTALS
1*CYTRA-3 SYRUP
1*ORACIT SOLN
2potassium citrate 10meq er tab
2potassium citrate 15meq er tab
2potassium citrate 5meq er tab
1*potassium citrate/citric acid granule
1*potassium citrate/citric acid soln
1*sodium citrate/citric acid soln
1*tricitrates solnCYSTINOSIS AGENTS
2CYSTAGON 150MG CAP LD
2CYSTAGON 50MG CAP LDGENITOURINARY IRRIGANTS
2sodium chloride 0.154meq/ml solnINTERSTITIAL CYSTITIS AGENTS
2ELMIRON 100MG CAPPROSTATIC HYPERTROPHY AGENTS
1alfuzosin 10mg er tab
3CARDURA 4MG ER TAB
3CARDURA 8MG ER TAB
1dutasteride 0.5mg cap
2dutasteride 0.5mg/tamsulosin 0.4mg cap
1finasteride 5mg tab
2silodosin 4mg cap
2silodosin 8mg cap
1tamsulosin 0.4mg capURINARY ANALGESICS
1phenazopyridine 100mg tab
1phenazopyridine 200mg tab
2PYRIDIUM 100MG TAB
2PYRIDIUM 200MG TABURINARY STONE AGENTS
3LITHOSTAT 250MG TAB
3THIOLA 100MG DR TAB
You can find information on what the symbols and abbreviations on this table mean by going to the beginning of this table.
86

DRUG NAME DRUG TIER REQUIREMENTS/LIMITS
3THIOLA 300MG DR TAB
2tiopronin 100mg tab
GOUT AGENTSGOUT AGENT COMBINATIONS
1colchicine 0.5mg/probenecid 500mg tabGOUT AGENTS
1allopurinol 100mg tab
1allopurinol 300mg tab
2colchicine 0.6mg tab
2febuxostat 40mg tab ST RXC
2febuxostat 80mg tab ST RXCURICOSURICS
1probenecid 500mg tab
HEMATOLOGICAL AGENTS - MISC.BRADYKININ B2 RECEPTOR ANTAGONISTS
4icatibant 10mg/ml inj NDS PACOMPLEMENT INHIBITORS
4BERINERT 500UNIT INJ LD NDS PA
4CINRYZE 500UNIT INJ LD NDS PA
4HAEGARDA 2000UNIT INJ LD NDS PA
4HAEGARDA 3000UNIT INJ LD NDS PA
4RUCONEST 2100UNIT INJ LD NDS PAHEMATAOLOGIC - TYROSINE KINASE INHIBITORS
4TAVALISSE 100MG TAB LD NDS PA QL=60 Quantity/30 Days
4TAVALISSE 150MG TAB LD NDS PA QL=60 Quantity/30 DaysHEMATORHEOLOGIC AGENTS
1pentoxifylline 400mg er tabPLASMA KALLIKREIN INHIBITORS
4TAKHZYRO 300MG/2ML INJ LD NDS PA QL=2 Quantity/28 DaysPLATELET AGGREGATION INHIBITORS
1anagrelide 0.5mg cap
1anagrelide 1mg cap
2aspirin 25mg/dipyridamole 200mg er cap
3BRILINTA 60MG TAB
3BRILINTA 90MG TAB
4CABLIVI 11MG INJ LD NDS PA QL=30 Quantity/30 Days
1cilostazol 100mg tab
1cilostazol 50mg tab
1clopidogrel 75mg tab
2dipyridamole 25mg tab
2dipyridamole 50mg tab
2dipyridamole 75mg tab
1prasugrel 10mg tab
1prasugrel 5mg tab
3ZONTIVITY 2.08MG TAB PA
HEMATOPOIETIC AGENTS
You can find information on what the symbols and abbreviations on this table mean by going to the beginning of this table.
87
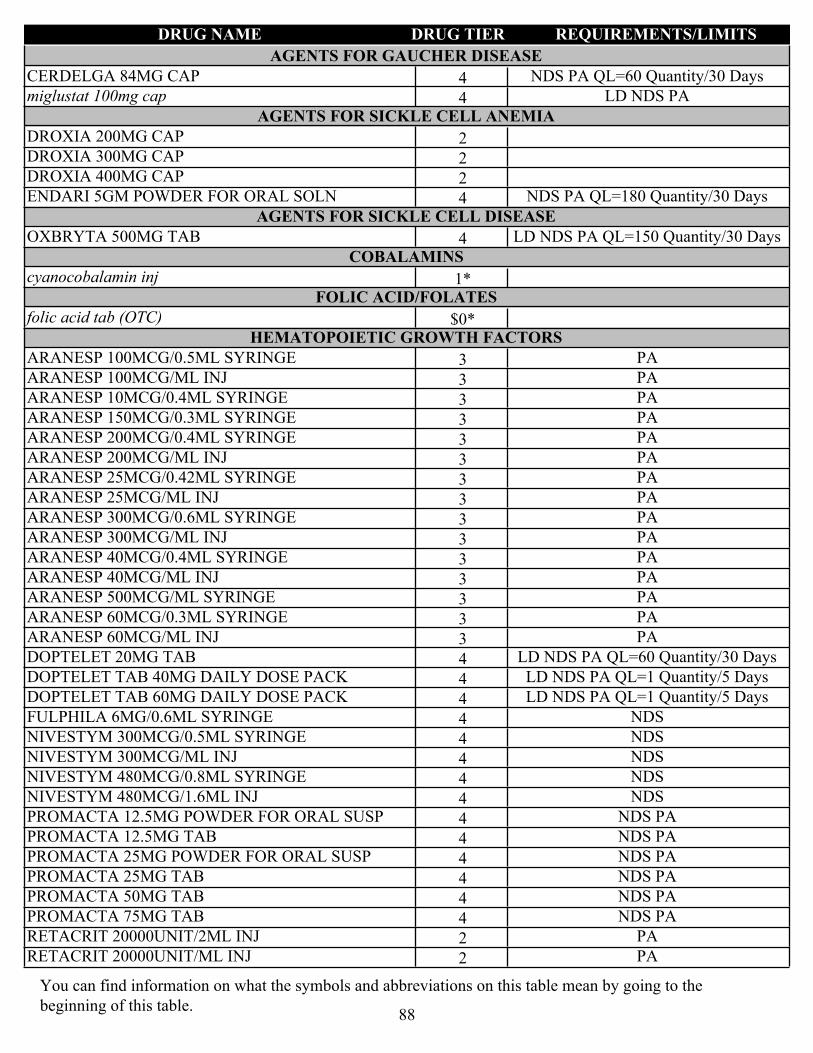
DRUG NAME DRUG TIER REQUIREMENTS/LIMITS
AGENTS FOR GAUCHER DISEASE
4CERDELGA 84MG CAP NDS PA QL=60 Quantity/30 Days
4miglustat 100mg cap LD NDS PAAGENTS FOR SICKLE CELL ANEMIA
2DROXIA 200MG CAP
2DROXIA 300MG CAP
2DROXIA 400MG CAP
4ENDARI 5GM POWDER FOR ORAL SOLN NDS PA QL=180 Quantity/30 DaysAGENTS FOR SICKLE CELL DISEASE
4OXBRYTA 500MG TAB LD NDS PA QL=150 Quantity/30 DaysCOBALAMINS
1*cyanocobalamin injFOLIC ACID/FOLATES
$0*folic acid tab (OTC) HEMATOPOIETIC GROWTH FACTORS
3ARANESP 100MCG/0.5ML SYRINGE PA
3ARANESP 100MCG/ML INJ PA
3ARANESP 10MCG/0.4ML SYRINGE PA
3ARANESP 150MCG/0.3ML SYRINGE PA
3ARANESP 200MCG/0.4ML SYRINGE PA
3ARANESP 200MCG/ML INJ PA
3ARANESP 25MCG/0.42ML SYRINGE PA
3ARANESP 25MCG/ML INJ PA
3ARANESP 300MCG/0.6ML SYRINGE PA
3ARANESP 300MCG/ML INJ PA
3ARANESP 40MCG/0.4ML SYRINGE PA
3ARANESP 40MCG/ML INJ PA
3ARANESP 500MCG/ML SYRINGE PA
3ARANESP 60MCG/0.3ML SYRINGE PA
3ARANESP 60MCG/ML INJ PA
4DOPTELET 20MG TAB LD NDS PA QL=60 Quantity/30 Days
4DOPTELET TAB 40MG DAILY DOSE PACK LD NDS PA QL=1 Quantity/5 Days
4DOPTELET TAB 60MG DAILY DOSE PACK LD NDS PA QL=1 Quantity/5 Days
4FULPHILA 6MG/0.6ML SYRINGE NDS
4NIVESTYM 300MCG/0.5ML SYRINGE NDS
4NIVESTYM 300MCG/ML INJ NDS
4NIVESTYM 480MCG/0.8ML SYRINGE NDS
4NIVESTYM 480MCG/1.6ML INJ NDS
4PROMACTA 12.5MG POWDER FOR ORAL SUSP NDS PA
4PROMACTA 12.5MG TAB NDS PA
4PROMACTA 25MG POWDER FOR ORAL SUSP NDS PA
4PROMACTA 25MG TAB NDS PA
4PROMACTA 50MG TAB NDS PA
4PROMACTA 75MG TAB NDS PA
2RETACRIT 20000UNIT/2ML INJ PA
2RETACRIT 20000UNIT/ML INJ PA
You can find information on what the symbols and abbreviations on this table mean by going to the beginning of this table.
88
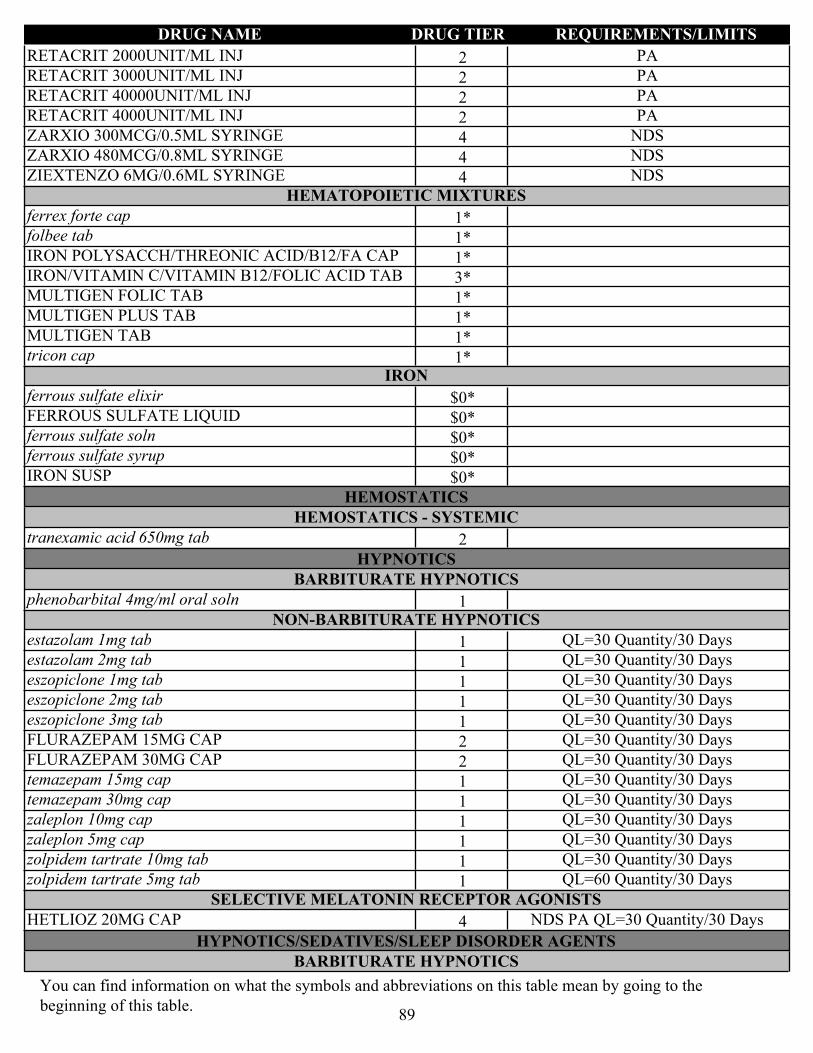
DRUG NAME DRUG TIER REQUIREMENTS/LIMITS
2RETACRIT 2000UNIT/ML INJ PA
2RETACRIT 3000UNIT/ML INJ PA
2RETACRIT 40000UNIT/ML INJ PA
2RETACRIT 4000UNIT/ML INJ PA
4ZARXIO 300MCG/0.5ML SYRINGE NDS
4ZARXIO 480MCG/0.8ML SYRINGE NDS
4ZIEXTENZO 6MG/0.6ML SYRINGE NDSHEMATOPOIETIC MIXTURES
1*ferrex forte cap
1*folbee tab
1*IRON POLYSACCH/THREONIC ACID/B12/FA CAP
3*IRON/VITAMIN C/VITAMIN B12/FOLIC ACID TAB
1*MULTIGEN FOLIC TAB
1*MULTIGEN PLUS TAB
1*MULTIGEN TAB
1*tricon capIRON
$0*ferrous sulfate elixir
$0*FERROUS SULFATE LIQUID
$0*ferrous sulfate soln
$0*ferrous sulfate syrup
$0*IRON SUSP
HEMOSTATICSHEMOSTATICS - SYSTEMIC
2tranexamic acid 650mg tab
HYPNOTICSBARBITURATE HYPNOTICS
1phenobarbital 4mg/ml oral solnNON-BARBITURATE HYPNOTICS
1estazolam 1mg tab QL=30 Quantity/30 Days
1estazolam 2mg tab QL=30 Quantity/30 Days
1eszopiclone 1mg tab QL=30 Quantity/30 Days
1eszopiclone 2mg tab QL=30 Quantity/30 Days
1eszopiclone 3mg tab QL=30 Quantity/30 Days
2FLURAZEPAM 15MG CAP QL=30 Quantity/30 Days
2FLURAZEPAM 30MG CAP QL=30 Quantity/30 Days
1temazepam 15mg cap QL=30 Quantity/30 Days
1temazepam 30mg cap QL=30 Quantity/30 Days
1zaleplon 10mg cap QL=30 Quantity/30 Days
1zaleplon 5mg cap QL=30 Quantity/30 Days
1zolpidem tartrate 10mg tab QL=30 Quantity/30 Days
1zolpidem tartrate 5mg tab QL=60 Quantity/30 DaysSELECTIVE MELATONIN RECEPTOR AGONISTS
4HETLIOZ 20MG CAP NDS PA QL=30 Quantity/30 Days
HYPNOTICS/SEDATIVES/SLEEP DISORDER AGENTSBARBITURATE HYPNOTICS
You can find information on what the symbols and abbreviations on this table mean by going to the beginning of this table.
89
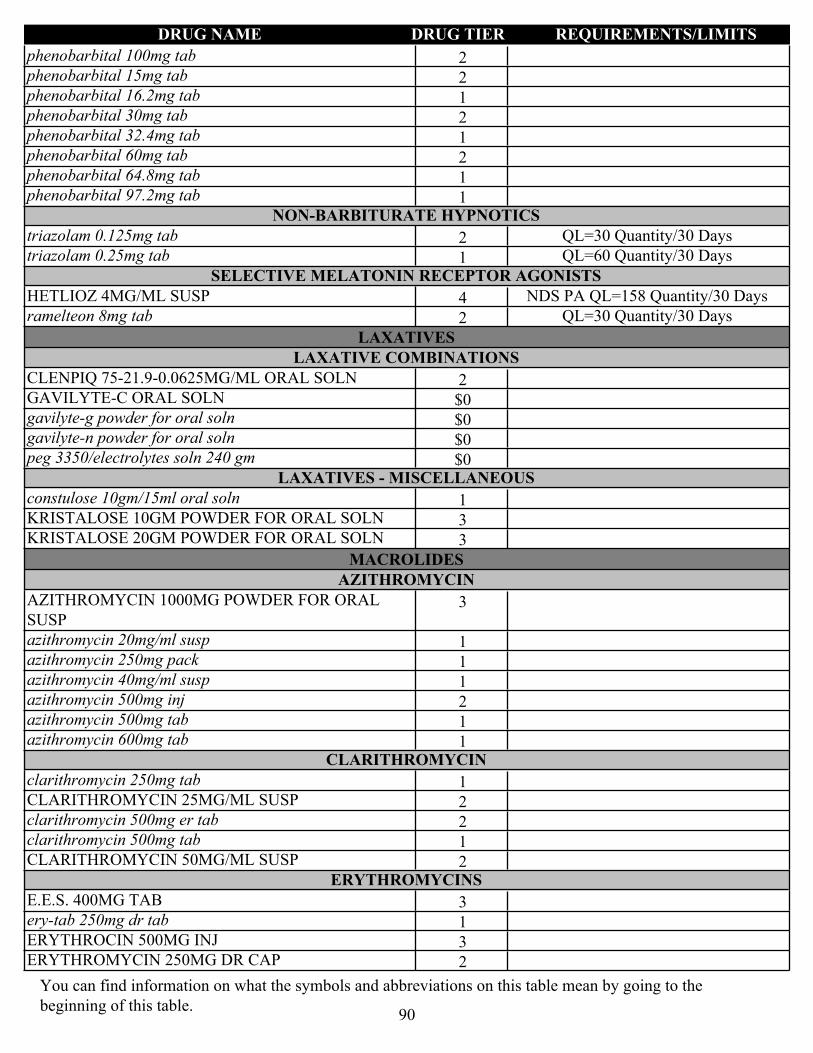
DRUG NAME DRUG TIER REQUIREMENTS/LIMITS
2phenobarbital 100mg tab
2phenobarbital 15mg tab
1phenobarbital 16.2mg tab
2phenobarbital 30mg tab
1phenobarbital 32.4mg tab
2phenobarbital 60mg tab
1phenobarbital 64.8mg tab
1phenobarbital 97.2mg tabNON-BARBITURATE HYPNOTICS
2triazolam 0.125mg tab QL=30 Quantity/30 Days
1triazolam 0.25mg tab QL=60 Quantity/30 DaysSELECTIVE MELATONIN RECEPTOR AGONISTS
4HETLIOZ 4MG/ML SUSP NDS PA QL=158 Quantity/30 Days
2ramelteon 8mg tab QL=30 Quantity/30 Days
LAXATIVESLAXATIVE COMBINATIONS
2CLENPIQ 75-21.9-0.0625MG/ML ORAL SOLN
$0GAVILYTE-C ORAL SOLN
$0gavilyte-g powder for oral soln
$0gavilyte-n powder for oral soln
$0peg 3350/electrolytes soln 240 gmLAXATIVES - MISCELLANEOUS
1constulose 10gm/15ml oral soln
3KRISTALOSE 10GM POWDER FOR ORAL SOLN
3KRISTALOSE 20GM POWDER FOR ORAL SOLN
MACROLIDESAZITHROMYCIN
3AZITHROMYCIN 1000MG POWDER FOR ORAL SUSP
1azithromycin 20mg/ml susp
1azithromycin 250mg pack
1azithromycin 40mg/ml susp
2azithromycin 500mg inj
1azithromycin 500mg tab
1azithromycin 600mg tabCLARITHROMYCIN
1clarithromycin 250mg tab
2CLARITHROMYCIN 25MG/ML SUSP
2clarithromycin 500mg er tab
1clarithromycin 500mg tab
2CLARITHROMYCIN 50MG/ML SUSPERYTHROMYCINS
3E.E.S. 400MG TAB
1ery-tab 250mg dr tab
3ERYTHROCIN 500MG INJ
2ERYTHROMYCIN 250MG DR CAP
You can find information on what the symbols and abbreviations on this table mean by going to the beginning of this table.
90
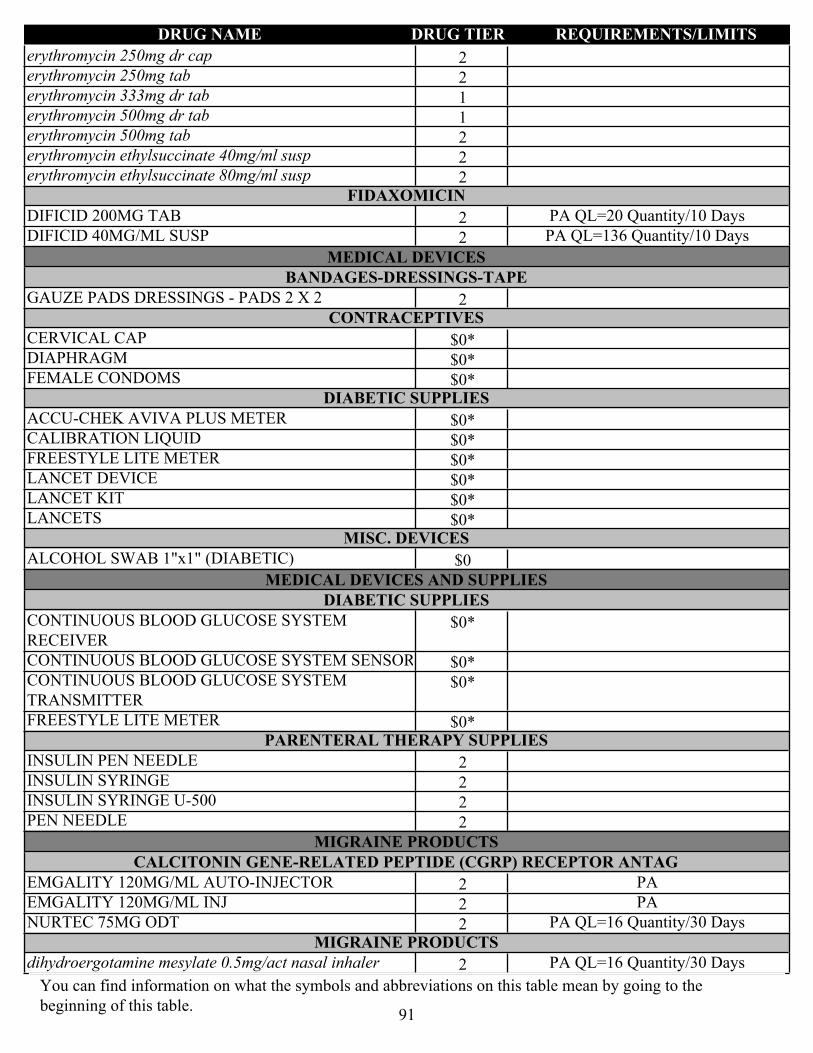
DRUG NAME DRUG TIER REQUIREMENTS/LIMITS
2erythromycin 250mg dr cap
2erythromycin 250mg tab
1erythromycin 333mg dr tab
1erythromycin 500mg dr tab
2erythromycin 500mg tab
2erythromycin ethylsuccinate 40mg/ml susp
2erythromycin ethylsuccinate 80mg/ml suspFIDAXOMICIN
2DIFICID 200MG TAB PA QL=20 Quantity/10 Days
2DIFICID 40MG/ML SUSP PA QL=136 Quantity/10 Days
MEDICAL DEVICESBANDAGES-DRESSINGS-TAPE
2GAUZE PADS DRESSINGS - PADS 2 X 2 CONTRACEPTIVES
$0*CERVICAL CAP
$0*DIAPHRAGM
$0*FEMALE CONDOMS DIABETIC SUPPLIES
$0*ACCU-CHEK AVIVA PLUS METER
$0*CALIBRATION LIQUID
$0*FREESTYLE LITE METER
$0*LANCET DEVICE
$0*LANCET KIT
$0*LANCETS MISC. DEVICES
$0ALCOHOL SWAB 1"x1" (DIABETIC)
MEDICAL DEVICES AND SUPPLIESDIABETIC SUPPLIES
$0*CONTINUOUS BLOOD GLUCOSE SYSTEM RECEIVER
$0*CONTINUOUS BLOOD GLUCOSE SYSTEM SENSOR
$0*CONTINUOUS BLOOD GLUCOSE SYSTEM TRANSMITTER
$0*FREESTYLE LITE METER PARENTERAL THERAPY SUPPLIES
2INSULIN PEN NEEDLE
2INSULIN SYRINGE
2INSULIN SYRINGE U-500
2PEN NEEDLE
MIGRAINE PRODUCTSCALCITONIN GENE-RELATED PEPTIDE (CGRP) RECEPTOR ANTAG
2EMGALITY 120MG/ML AUTO-INJECTOR PA
2EMGALITY 120MG/ML INJ PA
2NURTEC 75MG ODT PA QL=16 Quantity/30 DaysMIGRAINE PRODUCTS
2dihydroergotamine mesylate 0.5mg/act nasal inhaler PA QL=16 Quantity/30 Days
You can find information on what the symbols and abbreviations on this table mean by going to the beginning of this table.
91

DRUG NAME DRUG TIER REQUIREMENTS/LIMITS
MIGRAINE PRODUCTS - MONOCLONAL ANTIBODIES
2AIMOVIG 140MG/ML AUTO-INJECTOR PA
2AIMOVIG 70MG/ML AUTO-INJECTOR PA
2EMGALITY 100MG/ML INJ PA
2UBRELVY 100MG TAB PA QL=16 Quantity/30 Days
2UBRELVY 50MG TAB PA QL=16 Quantity/30 DaysSEROTONIN AGONISTS
2eletriptan 20mg tab QL=18 Quantity/30 Days
2eletriptan 40mg tab QL=18 Quantity/30 Days
2naratriptan 1mg tab QL=18 Quantity/30 Days
2naratriptan 2.5mg tab QL=18 Quantity/30 Days
2REYVOW 100MG TAB PA QL=8 Quantity/30 Days
2REYVOW 50MG TAB PA QL=8 Quantity/30 Days
1rizatriptan 10mg odt QL=36 Quantity/60 Days
1rizatriptan 10mg tab QL=36 Quantity/60 Days
1rizatriptan 5mg odt QL=36 Quantity/60 Days
1rizatriptan 5mg tab QL=36 Quantity/60 Days
1sumatriptan 100mg tab QL=18 Quantity/30 Days
2sumatriptan 12mg/ml auto-injector QL=10 Quantity/30 Days
2sumatriptan 12mg/ml inj QL=10 Quantity/30 Days
2sumatriptan 20mg/act nasal spray QL=12 Quantity/30 Days
1sumatriptan 25mg tab QL=18 Quantity/30 Days
1sumatriptan 50mg tab QL=18 Quantity/30 Days
2sumatriptan 5mg/act nasal spray QL=12 Quantity/30 Days
2sumatriptan 6mg/0.5ml refill inj QL=10 Quantity/30 Days
2sumatriptan 8mg/ml cartridge QL=10 Quantity/30 Days
2zolmitriptan 2.5mg odt QL=18 Quantity/30 Days
2zolmitriptan 2.5mg tab QL=18 Quantity/30 Days
2zolmitriptan 5mg odt QL=18 Quantity/30 Days
2zolmitriptan 5mg tab QL=18 Quantity/30 Days
3ZOMIG 2.5MG NASAL SPRAY QL=16 Quantity/30 Days
3ZOMIG 5MG NASAL SPRAY QL=12 Quantity/30 Days
MINERALS & ELECTROLYTESELECTROLYTE MIXTURES
2d2.5w/nacl 0.45% inj
2d5w/nacl 5%-0.33% inj
2DEXTROSE 10% W/ SODIUM CHLORIDE 0.2% PA_BvD
2DEXTROSE 10% W/ SODIUM CHLORIDE 0.45% PA_BvD
2DEXTROSE/SODIUM CHLORIDE 5-0.225% INJ
2dextrose/sodium chloride 5%-0.225% inj
2GLUCOSE 25MG/ML/SODIUM CHLORIDE 0.0769 MEQ/ML INJ
2glucose 50 mg/ml/potassium chloride 0.04meq/ml/sodium chloride 4.5mg/ml inj
2glucose 50mg/ml/potassium chloride 0.01 meq/ml/sodium chloride 0.0769 meq/ml inj
You can find information on what the symbols and abbreviations on this table mean by going to the beginning of this table.
92
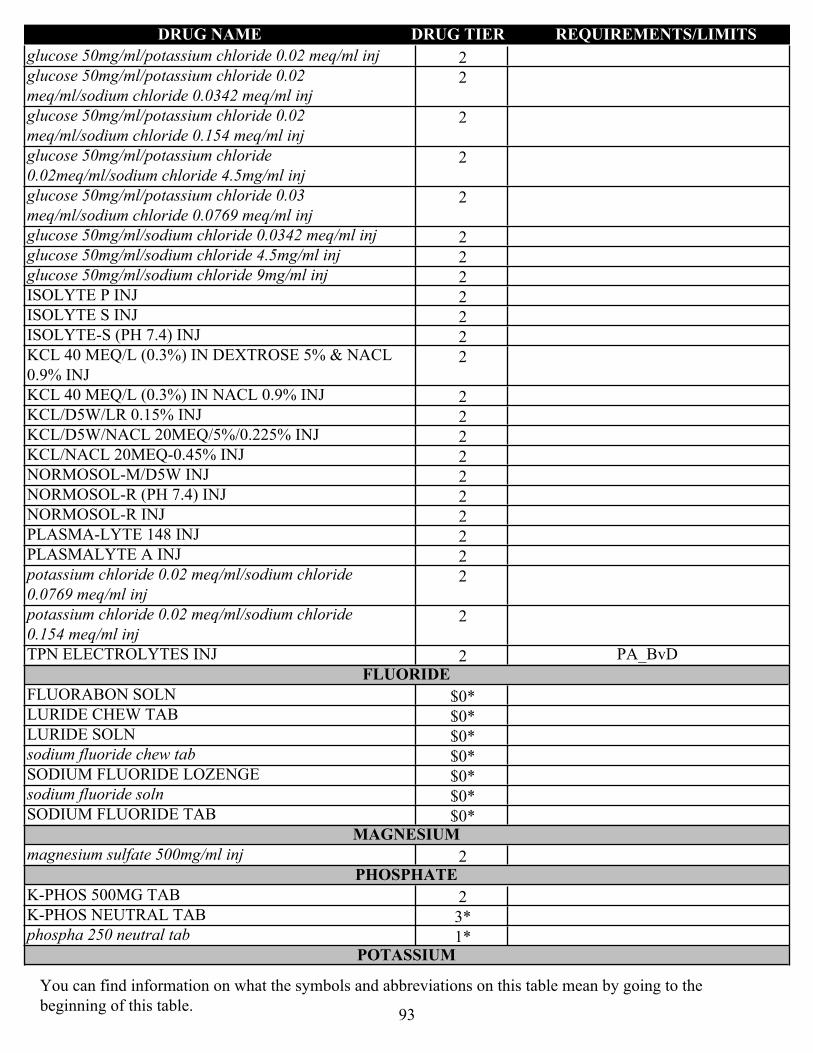
DRUG NAME DRUG TIER REQUIREMENTS/LIMITS
2glucose 50mg/ml/potassium chloride 0.02 meq/ml inj
2glucose 50mg/ml/potassium chloride 0.02 meq/ml/sodium chloride 0.0342 meq/ml inj
2glucose 50mg/ml/potassium chloride 0.02 meq/ml/sodium chloride 0.154 meq/ml inj
2glucose 50mg/ml/potassium chloride 0.02meq/ml/sodium chloride 4.5mg/ml inj
2glucose 50mg/ml/potassium chloride 0.03 meq/ml/sodium chloride 0.0769 meq/ml inj
2glucose 50mg/ml/sodium chloride 0.0342 meq/ml inj
2glucose 50mg/ml/sodium chloride 4.5mg/ml inj
2glucose 50mg/ml/sodium chloride 9mg/ml inj
2ISOLYTE P INJ
2ISOLYTE S INJ
2ISOLYTE-S (PH 7.4) INJ
2KCL 40 MEQ/L (0.3%) IN DEXTROSE 5% & NACL 0.9% INJ
2KCL 40 MEQ/L (0.3%) IN NACL 0.9% INJ
2KCL/D5W/LR 0.15% INJ
2KCL/D5W/NACL 20MEQ/5%/0.225% INJ
2KCL/NACL 20MEQ-0.45% INJ
2NORMOSOL-M/D5W INJ
2NORMOSOL-R (PH 7.4) INJ
2NORMOSOL-R INJ
2PLASMA-LYTE 148 INJ
2PLASMALYTE A INJ
2potassium chloride 0.02 meq/ml/sodium chloride 0.0769 meq/ml inj
2potassium chloride 0.02 meq/ml/sodium chloride 0.154 meq/ml inj
2TPN ELECTROLYTES INJ PA_BvDFLUORIDE
$0*FLUORABON SOLN
$0*LURIDE CHEW TAB
$0*LURIDE SOLN
$0*sodium fluoride chew tab
$0*SODIUM FLUORIDE LOZENGE
$0*sodium fluoride soln
$0*SODIUM FLUORIDE TABMAGNESIUM
2magnesium sulfate 500mg/ml injPHOSPHATE
2K-PHOS 500MG TAB
3*K-PHOS NEUTRAL TAB
1*phospha 250 neutral tabPOTASSIUM
You can find information on what the symbols and abbreviations on this table mean by going to the beginning of this table.
93
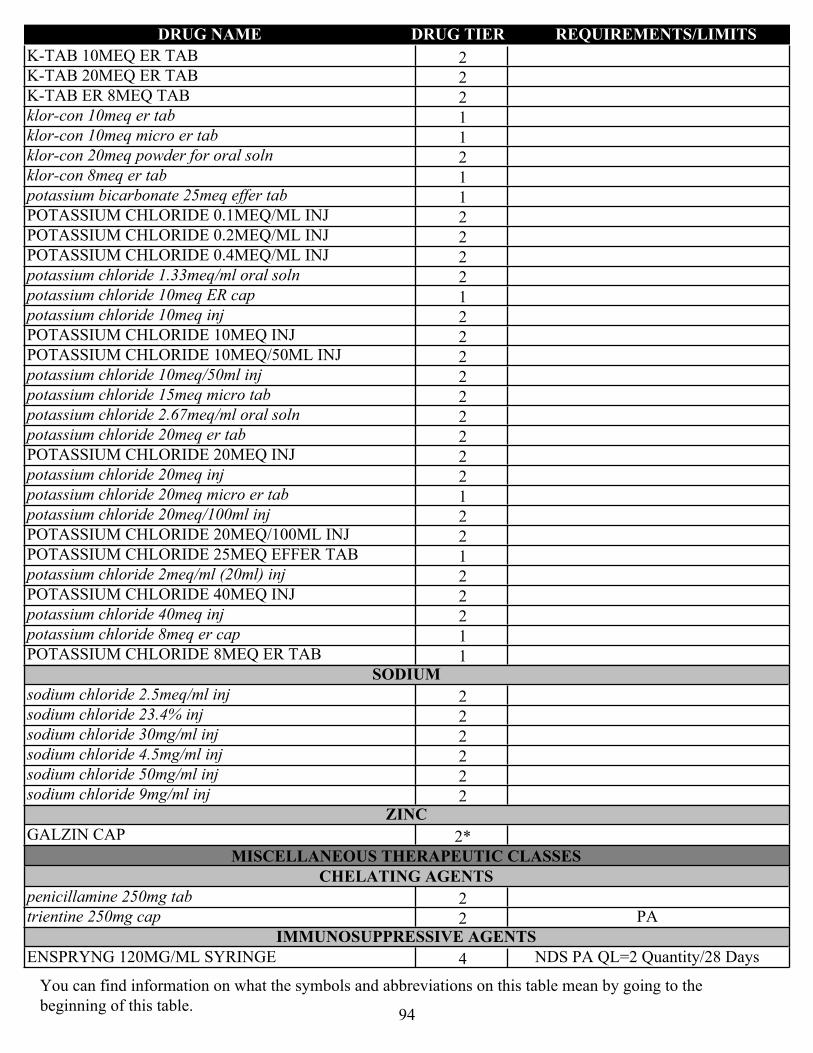
DRUG NAME DRUG TIER REQUIREMENTS/LIMITS
2K-TAB 10MEQ ER TAB
2K-TAB 20MEQ ER TAB
2K-TAB ER 8MEQ TAB
1klor-con 10meq er tab
1klor-con 10meq micro er tab
2klor-con 20meq powder for oral soln
1klor-con 8meq er tab
1potassium bicarbonate 25meq effer tab
2POTASSIUM CHLORIDE 0.1MEQ/ML INJ
2POTASSIUM CHLORIDE 0.2MEQ/ML INJ
2POTASSIUM CHLORIDE 0.4MEQ/ML INJ
2potassium chloride 1.33meq/ml oral soln
1potassium chloride 10meq ER cap
2potassium chloride 10meq inj
2POTASSIUM CHLORIDE 10MEQ INJ
2POTASSIUM CHLORIDE 10MEQ/50ML INJ
2potassium chloride 10meq/50ml inj
2potassium chloride 15meq micro tab
2potassium chloride 2.67meq/ml oral soln
2potassium chloride 20meq er tab
2POTASSIUM CHLORIDE 20MEQ INJ
2potassium chloride 20meq inj
1potassium chloride 20meq micro er tab
2potassium chloride 20meq/100ml inj
2POTASSIUM CHLORIDE 20MEQ/100ML INJ
1POTASSIUM CHLORIDE 25MEQ EFFER TAB
2potassium chloride 2meq/ml (20ml) inj
2POTASSIUM CHLORIDE 40MEQ INJ
2potassium chloride 40meq inj
1potassium chloride 8meq er cap
1POTASSIUM CHLORIDE 8MEQ ER TABSODIUM
2sodium chloride 2.5meq/ml inj
2sodium chloride 23.4% inj
2sodium chloride 30mg/ml inj
2sodium chloride 4.5mg/ml inj
2sodium chloride 50mg/ml inj
2sodium chloride 9mg/ml injZINC
2*GALZIN CAP
MISCELLANEOUS THERAPEUTIC CLASSESCHELATING AGENTS
2penicillamine 250mg tab
2trientine 250mg cap PAIMMUNOSUPPRESSIVE AGENTS
4ENSPRYNG 120MG/ML SYRINGE NDS PA QL=2 Quantity/28 Days
You can find information on what the symbols and abbreviations on this table mean by going to the beginning of this table.
94

DRUG NAME DRUG TIER REQUIREMENTS/LIMITS
2everolimus 0.25mg tab PA_BvD
2everolimus 0.5mg tab PA_BvD
2everolimus 0.75mg tab PA_BvD
4LUPKYNIS 7.9MG CAP LD NDS PA QL=180 Quantity/30 Days
3PROGRAF 0.2MG GRANULES FOR ORAL SUSP PA_BvD
3PROGRAF 1MG GRANULES FOR ORAL SUSP PA_BvD
3RAPAMUNE 1MG/ML ORAL SOLN PA_BvD
2sirolimus 1mg/ml oral soln PA_BvD
3ZORTRESS 1MG TAB PA_BvDPOTASSIUM REMOVING AGENTS
2LOKELMA 10GM POWDER FOR ORAL SUSP PA
2LOKELMA 5GM POWDER FOR ORAL SUSP PASYSTEMIC LUPUS ERYTHEMATOSUS AGENTS
4BENLYSTA 200MG/ML AUTO-INJECTOR NDS PA QL=4 Quantity/28 Days
4BENLYSTA 200MG/ML SYRINGE NDS PA QL=4 Quantity/28 Days
MOUTH/THROAT/DENTAL AGENTSANESTHETICS TOPICAL ORAL
3*FIRST MOUTHWASH BLM SUSP
1lidocaine 2% topical soln
1LIDOCAINE 4% ORAL SOLN QL=50 Quantity/30 DaysANTI-INFECTIVES - THROAT
1clotrimazole 10mg lozenge
1nystatin 100000unit/ml susp
3ORAVIG 50MG BUCCAL TABANTISEPTICS - MOUTH/THROAT
1chlorhexidine gluconate 0.12% mouthwashDENTAL PRODUCTS
2*PREVIDENT 5000 BOOSTER PASTE
2*PREVIDENT 5000 DRY MOUTH GEL
2*PREVIDENT 5000 PASTE
1*PREVIDENT 5000 PASTE
$0*PREVIDENT 5000 PLUS CREAM
2*PREVIDENT RINSE
$0*sodium fluoride cream
1*sodium fluoride gel
1*sodium fluoride paste
1*sodium fluoride rinse
1*sodium fluoride/potassium nitrate pasteSTEROIDS - MOUTH/THROAT
1triamcinolone acetonide 0.1% oral pasteTHROAT PRODUCTS - MISC.
2cevimeline 30mg cap
1pilocarpine 5mg tab
1pilocarpine 7.5mg tab
MULTIVITAMINSB-COMPLEX W/ FOLIC ACID
You can find information on what the symbols and abbreviations on this table mean by going to the beginning of this table.
95
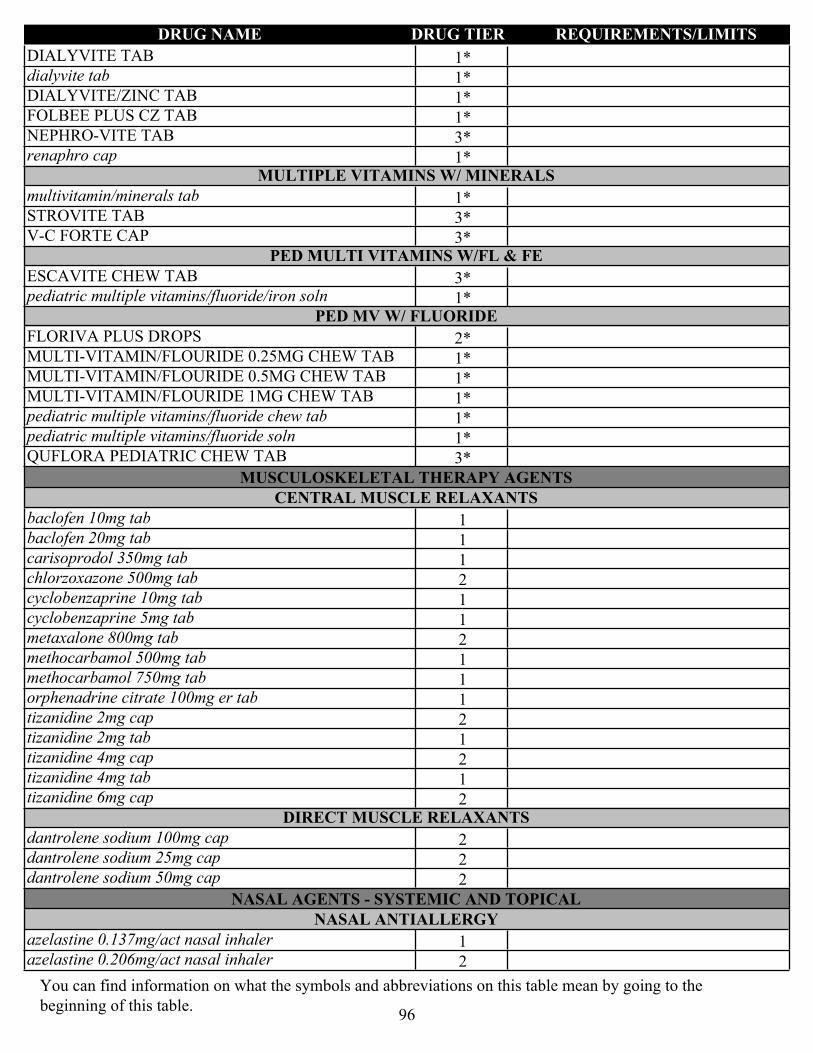
DRUG NAME DRUG TIER REQUIREMENTS/LIMITS
1*DIALYVITE TAB
1*dialyvite tab
1*DIALYVITE/ZINC TAB
1*FOLBEE PLUS CZ TAB
3*NEPHRO-VITE TAB
1*renaphro capMULTIPLE VITAMINS W/ MINERALS
1*multivitamin/minerals tab
3*STROVITE TAB
3*V-C FORTE CAPPED MULTI VITAMINS W/FL & FE
3*ESCAVITE CHEW TAB
1*pediatric multiple vitamins/fluoride/iron solnPED MV W/ FLUORIDE
2*FLORIVA PLUS DROPS
1*MULTI-VITAMIN/FLOURIDE 0.25MG CHEW TAB
1*MULTI-VITAMIN/FLOURIDE 0.5MG CHEW TAB
1*MULTI-VITAMIN/FLOURIDE 1MG CHEW TAB
1*pediatric multiple vitamins/fluoride chew tab
1*pediatric multiple vitamins/fluoride soln
3*QUFLORA PEDIATRIC CHEW TAB
MUSCULOSKELETAL THERAPY AGENTSCENTRAL MUSCLE RELAXANTS
1baclofen 10mg tab
1baclofen 20mg tab
1carisoprodol 350mg tab
2chlorzoxazone 500mg tab
1cyclobenzaprine 10mg tab
1cyclobenzaprine 5mg tab
2metaxalone 800mg tab
1methocarbamol 500mg tab
1methocarbamol 750mg tab
1orphenadrine citrate 100mg er tab
2tizanidine 2mg cap
1tizanidine 2mg tab
2tizanidine 4mg cap
1tizanidine 4mg tab
2tizanidine 6mg capDIRECT MUSCLE RELAXANTS
2dantrolene sodium 100mg cap
2dantrolene sodium 25mg cap
2dantrolene sodium 50mg cap
NASAL AGENTS - SYSTEMIC AND TOPICALNASAL ANTIALLERGY
1azelastine 0.137mg/act nasal inhaler
2azelastine 0.206mg/act nasal inhaler
You can find information on what the symbols and abbreviations on this table mean by going to the beginning of this table.
96

DRUG NAME DRUG TIER REQUIREMENTS/LIMITS
2olopatadine 0.665mg/act nasal inhalerNASAL ANTICHOLINERGICS
1ipratropium 0.03% nasal spray
1ipratropium 0.06% nasal sprayNASAL STEROIDS
3FLUNISOLIDE 0.025MG/ACT NASAL INHALER QL=1 Quantity/30 Days
1fluticasone propionate 0.05mg/act nasal inhaler QL=2 Quantity/30 Days
NEUROMUSCULAR AGENTSALS AGENTS
2riluzole 50mg tabSPINAL MUSCULAR ATROPHY AGENTS (SMA)
4EVRYSDI 0.75MG/ML ORAL SOLN LD NDS PA QL=200 Quantity/30 Days
NUTRIENTSCARBOHYDRATES
2glucose 100mg/ml inj PA_BvD
2glucose 50mg/ml injLIPIDS
3INTRALIPID 30GM/100ML INJ PA_BvD
2NUTRILIPID 20GM/100ML INJ PA_BvDPROTEINS
3AMINOSYN-PF 7% INJ PA_BvD
2CLINIMIX 4.25/10 INJ PA_BvD
2CLINIMIX 4.25/5 INJ PA_BvD
2CLINIMIX 5/15 INJ PA_BvD
2CLINIMIX 5/20 INJ PA_BvD
2CLINIMIX E 2.75/5 INJ PA_BvD
2CLINIMIX E 4.25/10 INJ PA_BvD
2CLINIMIX E 4.25/5 INJ PA_BvD
2CLINIMIX E 5/15 INJ PA_BvD
2CLINIMIX E 5/20 INJ PA_BvD
2clinisol 15% inj PA_BvD
3FREAMINE HBC 6.9% INJ PA_BvD
2HEPATAMINE 8% INJ PA_BvD
3PROCALAMINE 3% INJ PA_BvD
3PROSOL 20% INJ PA_BvD
3TRAVASOL 10% INJ PA_BvD
OPHTHALMIC AGENTSBETA-BLOCKERS - OPHTHALMIC
1betaxolol 0.5% ophth soln
3BETIMOL 0.25% OPHTH SOLN
2BETIMOL 0.5% OPHTH SOLN
3BETOPTIC S 0.25% OPHTH SUSP
1CARTEOLOL 1% OPHTH SOLN
2COMBIGAN 2-5MG/ML OPHTH SOLN
1dorzolamide/timolol 22.3-6.8mg/ml ophth soln
You can find information on what the symbols and abbreviations on this table mean by going to the beginning of this table.
97

DRUG NAME DRUG TIER REQUIREMENTS/LIMITS
2dorzolamide/timolol 22.3-6.8mg/ml ophth soln (preservative-free)
1LEVOBUNOLOL 0.5% OPHTH SOLN
2timolol 0.25% ophth gel
1timolol 0.25% ophth soln
2timolol 0.5% (pf) ophth soln
2timolol 0.5% ophth gel
1timolol 0.5% ophth soln
2timolol 5mg/ml ophth 24hr ophth soln
3TIMOPTIC 0.25% OPHTH SOLN (PRESERVATIVE-FREE)
CYCLOPLEGIC MYDRIATICS
2ATROPINE SULFATE 1% OPHTH SOLN
1*homatropine ophth soln
2*HOMATROPINE OPHTH SOLNMIOTICS
1pilocarpine 1% ophth soln
1pilocarpine 2% ophth soln
1pilocarpine 4% ophth solnOPHTHALMIC ADRENERGIC AGENTS
3ALPHAGAN 0.1% OPHTH SOLN
2apraclonidine 0.5% ophth soln
2brimonidine tartrate 0.15% ophth soln
1brimonidine tartrate 0.2% ophth soln
3IOPIDINE 1% OPHTH SOLN
2SIMBRINZA 0.2-1% OPHTH SUSPOPHTHALMIC ANTI-INFECTIVES
2AZASITE 1% OPHTH SOLN
2BACITRACIN 0.5UNIT/MG OPHTH OINTMENT
1bacitracin 0.5unit/mg/polymyxin b 10unit/mg ophth ointment
QL=7 Quantity/7 Days
3CILOXAN 0.3% OPHTH OINTMENT QL=7 Quantity/7 Days
1ciprofloxacin 0.3% ophth soln QL=60 Quantity/30 Days
1erythromycin 0.5% ophth ointment QL=7 Quantity/7 Days
2gatifloxacin 0.5% ophth soln QL=2 Quantity/7 Days
2GENTAK 0.3% OPHTH OINTMENT QL=7 Quantity/7 Days
1gentamicin 0.3% ophth soln QL=10 Quantity/7 Days
1GRAMICIDIN 0.025MG/ML/NEOMYCIN 1.75MG/ML/POLYMYXIN B 10000UNIT/ML OPHTH SOLN
QL=1 Quantity/7 Days
1levofloxacin 0.5% ophth soln QL=12 Quantity/30 Days
1moxifloxacin 0.5% ophth soln QL=2 Quantity/7 Days
1moxifloxacin 0.5% ophth soln QL=6 Quantity/7 Days
2NATACYN 5% OPHTH SUSP QL=1 Quantity/7 Days
1neomycin/bacitracin/polymyxin ophth ointment 5(3.5)mg-400unit-10000unit
QL=7 Quantity/7 Days
You can find information on what the symbols and abbreviations on this table mean by going to the beginning of this table.
98

DRUG NAME DRUG TIER REQUIREMENTS/LIMITS
1ofloxacin 0.3% ophth soln QL=60 Quantity/30 Days
1polymyxin b 10000unit/ml/trimethoprim 1mg/ml ophth soln
QL=1 Quantity/7 Days
2SULFACETAMIDE SODIUM 10% OPHTH OINTMENT QL=7 Quantity/7 Days
1sulfacetamide sodium 10% ophth soln QL=15 Quantity/7 Days
1tobramycin 0.3% ophth soln QL=12 Quantity/30 Days
3TOBREX 0.3% OPHTH OINTMENT QL=7 Quantity/7 Days
2TRIFLURIDINE 1% OPHTH SOLN QL=2 Quantity/7 Days
2ZIRGAN 0.15% OPHTH GEL QL=10 Quantity/7 DaysOPHTHALMIC IMMUNOMODULATORS
2RESTASIS 0.05% OPHTH SUSPOPHTHALMIC KINASE INHIBITORS
2RHOPRESSA 0.02% OPHTH SOLN QL=2 Quantity/30 Days
2ROCKLATAN 0.05-0.2MG/ML OPHTH SOLN QL=2 Quantity/30 DaysOPHTHALMIC LOCAL ANESTHETICS
1proparacaine 0.5% ophth solnOPHTHALMIC NERVE GROWTH FACTORS
4OXERVATE 0.002% OPHTH SOLN LD NDS PA QL=112 Quantity/365 Days
OPHTHALMIC STEROIDS
2ALREX 0.2% OPHTH SUSP
3BLEPHAMIDE 0.2-10% OPHTH OINTMENT
3BLEPHAMIDE 0.2-10% OPHTH SUSP
2DEXAMETHASONE PHOSPHATE 0.1% OPHTH SOLN
1dexamethasone/neomycin/polymyxin b 0.1% ophth ointment
1dexamethasone/neomycin/polymyxin b 0.1% ophth susp
1dexamethasone/tobramycin 0.3-0.1% ophth susp
2difluprednate 0.05% ophth emulsion
3FLAREX 0.1% OPHTH SUSP
1fluorometholone 0.1% ophth susp
3FML 0.1% OPHTH OINTMENT
3FML FORTE LIQUIFILM 0.25% OPHTH SUSP
2LOTEMAX 0.5% OPHTH OINTMENT
2loteprednol etabonate 0.5% ophth gel
2loteprednol etabonate 0.5% ophth susp
2MAXIDEX 0.1% OPHTH SUSP
1NEOMYCIN-POLYMYXIN-HC OPHTH SUSP
1neomycin/polymyxin/bacitracin/hydrocortisone 1% ophth ointment
3PRED FORTE 1% OPHTH SUSP
2PRED MILD 0.12% OPHTH SUSP
3PRED-G 0.3-0.6% OPHTH OINTMENT
2PRED-G 0.3-1% OPHTH SUSP
You can find information on what the symbols and abbreviations on this table mean by going to the beginning of this table.
99

DRUG NAME DRUG TIER REQUIREMENTS/LIMITS
2PREDNISOLONE 1% OPHTH SOLN
2PREDNISOLONE ACETATE 1% OPHTH SUSP
1PREDNISOLONE SODIUM PHOSPHATE 2.5MG/ML/SULFACETAMIDE SODIUM 100MG/ML OPHTH SOLN
3TOBRADEX 0.05-0.3% OPHTH SUSP
2TOBRADEX 0.1-0.3% OPHTH OINTMENT
2ZYLET 0.5-0.3% OPHTH SUSPOPHTHALMICS - MISC.
3ACUVAIL 0.45% OPHTH SOLN QL=60 Quantity/365 Days
2ALOCRIL 2% OPHTH SOLN
2ALOMIDE 0.1% OPHTH SOLN
1azelastine 0.05% ophth soln
2bepotastine besilate 1.5% ophth soln
2brinzolamide 1% ophth susp
1bromfenac 0.09% ophth soln QL=6.80 Quantity/365 Days
1cromolyn sodium 4% ophth soln
4CYSTADROPS 0.37% OPHTH SOLN LD NDS PA QL=4 Quantity/28 Days
4CYSTARAN 0.44% OPHTH SOLN LD NDS PA QL=60 Quantity/28 Days
1diclofenac sodium 0.1% ophth soln QL=20 Quantity/365 Days
1dorzolamide 2% ophth soln
2epinastine 0.05% ophth soln
2FLURBIPROFEN SODIUM 0.03% OPHTH SOLN
2ILEVRO 0.3% OPHTH SUSP QL=12 Quantity/365 Days
1ketorolac tromethamine 0.4% ophth soln QL=20 Quantity/365 Days
1ketorolac tromethamine 0.5% ophth soln
3LASTACAFT 0.25% OPHTH SOLN
2NEVANAC 0.1% OPHTH SUSP QL=12 Quantity/365 Days
1olopatadine 0.1% ophth soln
1olopatadine 0.2% ophth soln
3PROLENSA 0.07% OPHTH SOLN QL=12 Quantity/365 DaysPROSTAGLANDINS - OPHTHALMIC
2bimatoprost 0.03% ophth soln QL=5 Quantity/30 Days
1latanoprost 0.005% ophth soln QL=5 Quantity/30 Days
2LUMIGAN 0.01% OPHTH SOLN QL=5 Quantity/30 Days
2travoprost 0.004% ophth soln QL=5 Quantity/30 Days
3ZIOPTAN 0.015MG/ML OPHTH SOLN ST QL=30 Quantity/30 Days
OTIC AGENTSOTIC AGENTS - MISCELLANEOUS
1acetic acid 2% otic solnOTIC ANTI-INFECTIVES
2CIPROFLOXACIN 0.2% OTIC SOLN
1ofloxacin 0.3% otic solnOTIC COMBINATIONS
3CIPRO HC 0.2-1% OTIC SUSP
2ciprofloxacin/dexamethasone 0.3-0.1% otic susp
You can find information on what the symbols and abbreviations on this table mean by going to the beginning of this table.
100

DRUG NAME DRUG TIER REQUIREMENTS/LIMITS
1hydrocortisone 10mg/ml/neomycin 3.5mg/ml/polymyxin b 10000unit/ml otic soln
1hydrocortisone 10mg/ml/neomycin 3.5mg/ml/polymyxin b 10000unit/ml otic susp
OTIC STEROIDS
1acetic acid/hydrocortisone 1-2% otic soln
2fluocinolone acetonide 0.01% otic soln
PASSIVE IMMUNIZING AGENTSIMMUNE SERUMS
4BIVIGAM 5GM/50ML INJ NDS PA
4FLEBOGAMMA 0.5GM/10ML INJ NDS PA
4GAMMAGARD 10GM INJ NDS PA
4GAMMAGARD 10GM/100ML INJ NDS PA
4GAMMAGARD 2.5GM/25ML INJ NDS PA
4GAMMAGARD 20GM/200ML INJ NDS PA
4GAMMAGARD 30GM/300ML INJ NDS PA
4GAMMAGARD 5GM INJ NDS PA
4GAMMAGARD 5GM/50ML INJ NDS PA
4GAMMAKED 1GM/10ML INJ NDS PA
4GAMMAPLEX 10GM/100ML INJ NDS PA
4GAMMAPLEX 10GM/200ML INJ NDS PA
4GAMMAPLEX 20GM/400ML INJ NDS PA
4GAMUNEX-C 40GM/400ML INJ NDS PA
4OCTAGAM 1GM/20ML INJ NDS PA
4OCTAGAM 2.5GM/50ML INJ NDS PA
4OCTAGAM 25GM/500ML INJ NDS PA
4OCTAGAM 2GM/20ML INJ NDS PA
4OCTAGAM 30GM/300ML INJ NDS PA
4OCTAGAM 5GM/100ML INJ NDS PA
4PRIVIGEN 20GM/200ML INJ NDS PA
4PRIVIGEN 40GM/400ML INJ NDS PA
PASSIVE IMMUNIZING AND TREATMENT AGENTSIMMUNE SERUMS
4PANZYGA 10GM/100ML INJ NDS PA
4PANZYGA 1GM/10ML INJ NDS PA
4PANZYGA 2.5GM/25ML INJ NDS PA
4PANZYGA 20GM/200ML INJ NDS PA
4PANZYGA 30GM/300ML INJ NDS PA
4PANZYGA 5GM/50ML INJ NDS PA
4VARIZIG 125UNIT/1.2ML INJ NDS
PENICILLINSAMINOPENICILLINS
1AMOXICILLIN 125MG CHEW TAB
1amoxicillin 250mg cap
2AMOXICILLIN 250MG CHEW TAB
1amoxicillin 25mg/ml susp
You can find information on what the symbols and abbreviations on this table mean by going to the beginning of this table.
101

DRUG NAME DRUG TIER REQUIREMENTS/LIMITS
1amoxicillin 40mg/ml susp
1amoxicillin 500mg cap
1amoxicillin 500mg tab
1amoxicillin 50mg/ml susp
1amoxicillin 80mg/ml susp
1amoxicillin 875mg tab
2ampicillin 1000mg inj
2ampicillin 100mg/ml inj
2AMPICILLIN 125MG INJ
2ampicillin 250mg inj
2ampicillin 2gm inj
2AMPICILLIN 2GM INJ
1AMPICILLIN 500MG CAP
2ampicillin 500mg inj
2AMPICILLIN SODIUM 1GM INJNATURAL PENICILLINS
2BICILLIN L-A 1200000UNIT/2ML INJ
2BICILLIN L-A 2400000UNIT/4ML INJ
2BICILLIN L-A 600000UNIT/ML INJ
2penicillin g potassium 1000000unit/ml inj
2PENICILLIN G POTASSIUM 40000UNIT/ML INJ
2PENICILLIN G POTASSIUM 60000UNIT/ML INJ
2PENICILLIN G PROCAINE 600000UNIT/ML INJ
2PENICILLIN G SODIUM 100000UNIT/ML INJ
2penicillin gk 5000000unit inj
1penicillin v potassium 250mg tab
1PENICILLIN V POTASSIUM 25MG/ML ORAL SOLN
1penicillin v potassium 500mg tab
1PENICILLIN V POTASSIUM 50MG/ML ORAL SOLNPENICILLIN COMBINATIONS
3AMOXICILLIN 1000MG/CLAVULANATE 62.5MG ER TAB
1amoxicillin 120mg/ml/clavulanate 8.58mg/ml susp
2AMOXICILLIN 200MG/CLAVULANATE 28.5MG CHEW TAB
1amoxicillin 250mg/clavulanate 125mg tab
2AMOXICILLIN 400MG/CLAVULANATE 57MG CHEW TAB
1amoxicillin 40mg/ml/clavulanate 5.7mg/ml susp
1amoxicillin 500mg/clavulanate 125mg tab
1amoxicillin 50mg/ml/clavulanate 12.5mg/ml susp
1amoxicillin 80mg/ml/clavulanate 11.4mg/ml susp
1amoxicillin 875mg/clavulanate 125mg tab
3amoxicillin/k clavulanate 1000-62.5mg er tab
2ampicillin 1000mg/sulbactam 500mg inj
2ampicillin 100mg/ml/sulbactam 50mg/ml inj
You can find information on what the symbols and abbreviations on this table mean by going to the beginning of this table.
102
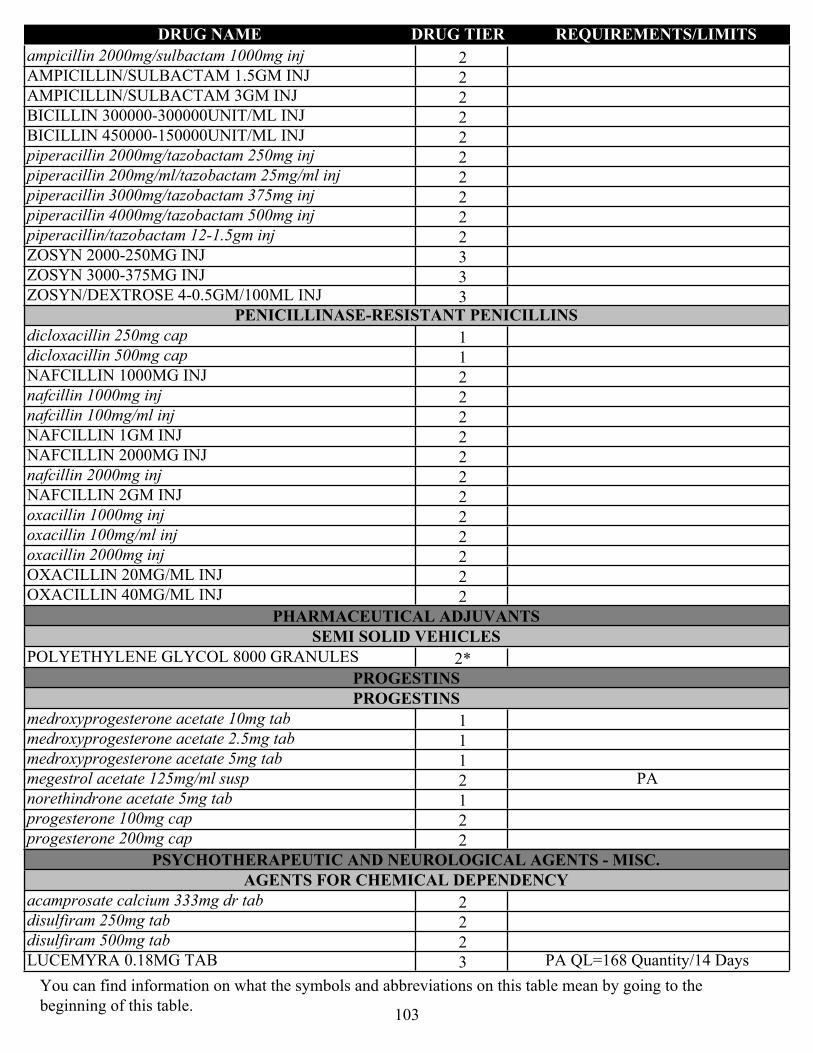
DRUG NAME DRUG TIER REQUIREMENTS/LIMITS
2ampicillin 2000mg/sulbactam 1000mg inj
2AMPICILLIN/SULBACTAM 1.5GM INJ
2AMPICILLIN/SULBACTAM 3GM INJ
2BICILLIN 300000-300000UNIT/ML INJ
2BICILLIN 450000-150000UNIT/ML INJ
2piperacillin 2000mg/tazobactam 250mg inj
2piperacillin 200mg/ml/tazobactam 25mg/ml inj
2piperacillin 3000mg/tazobactam 375mg inj
2piperacillin 4000mg/tazobactam 500mg inj
2piperacillin/tazobactam 12-1.5gm inj
3ZOSYN 2000-250MG INJ
3ZOSYN 3000-375MG INJ
3ZOSYN/DEXTROSE 4-0.5GM/100ML INJPENICILLINASE-RESISTANT PENICILLINS
1dicloxacillin 250mg cap
1dicloxacillin 500mg cap
2NAFCILLIN 1000MG INJ
2nafcillin 1000mg inj
2nafcillin 100mg/ml inj
2NAFCILLIN 1GM INJ
2NAFCILLIN 2000MG INJ
2nafcillin 2000mg inj
2NAFCILLIN 2GM INJ
2oxacillin 1000mg inj
2oxacillin 100mg/ml inj
2oxacillin 2000mg inj
2OXACILLIN 20MG/ML INJ
2OXACILLIN 40MG/ML INJ
PHARMACEUTICAL ADJUVANTSSEMI SOLID VEHICLES
2*POLYETHYLENE GLYCOL 8000 GRANULES
PROGESTINSPROGESTINS
1medroxyprogesterone acetate 10mg tab
1medroxyprogesterone acetate 2.5mg tab
1medroxyprogesterone acetate 5mg tab
2megestrol acetate 125mg/ml susp PA
1norethindrone acetate 5mg tab
2progesterone 100mg cap
2progesterone 200mg cap
PSYCHOTHERAPEUTIC AND NEUROLOGICAL AGENTS - MISC.AGENTS FOR CHEMICAL DEPENDENCY
2acamprosate calcium 333mg dr tab
2disulfiram 250mg tab
2disulfiram 500mg tab
3LUCEMYRA 0.18MG TAB PA QL=168 Quantity/14 Days
You can find information on what the symbols and abbreviations on this table mean by going to the beginning of this table.
103

DRUG NAME DRUG TIER REQUIREMENTS/LIMITS
ANTI-CATAPLECTIC AGENTS
4XYREM 500MG/ML ORAL SOLN LD NDS PA QL=540 Quantity/30 DaysANTIDEMENTIA AGENTS
1donepezil 10mg odt QL=30 Quantity/30 Days
1donepezil 10mg tab
2donepezil 23mg tab QL=30 Quantity/30 Days
1donepezil 5mg odt QL=30 Quantity/30 Days
1donepezil 5mg tab
1galantamine 12mg tab
1galantamine 4mg tab
1galantamine 8mg tab
2galantamine hydrobromide 16mg er cap
2galantamine hydrobromide 24mg er cap
3GALANTAMINE HYDROBROMIDE 4MG/ML ORAL SOLN
2galantamine hydrobromide 8mg er cap
1memantine 10mg tab
1memantine 10mg/memantine 5mg pack
2memantine 14mg er cap
2memantine 21mg er cap
2memantine 28mg er cap
2memantine 2mg/ml oral soln
1memantine 5mg tab
2memantine 7mg er cap
2rivastigmine 0.192mg/hr patch
2rivastigmine 0.396mg/hr patch
2rivastigmine 0.554mg/hr patch
1rivastigmine 1.5mg cap
1rivastigmine 3mg cap
1rivastigmine 4.5mg cap
1rivastigmine 6mg capFIBROMYALGIA AGENTS
2SAVELLA 100MG TAB QL=60 Quantity/30 Days
2SAVELLA 12.5MG TAB QL=60 Quantity/30 Days
2SAVELLA 25MG TAB QL=60 Quantity/30 Days
2SAVELLA 4-WEEK TITRATION PACK
2SAVELLA 50MG TAB QL=60 Quantity/30 DaysMOVEMENT DISORDER DRUG THERAPY
4AUSTEDO 12MG TAB NDS PA
4AUSTEDO 6MG TAB NDS PA
4AUSTEDO 9MG TAB NDS PA
4INGREZZA 40MG CAP LD NDS PA
4INGREZZA 60MG CAP LD NDS PA
4INGREZZA 80MG CAP LD NDS PA
2tetrabenazine 12.5mg tab PA
2tetrabenazine 25mg tab PA
You can find information on what the symbols and abbreviations on this table mean by going to the beginning of this table.
104
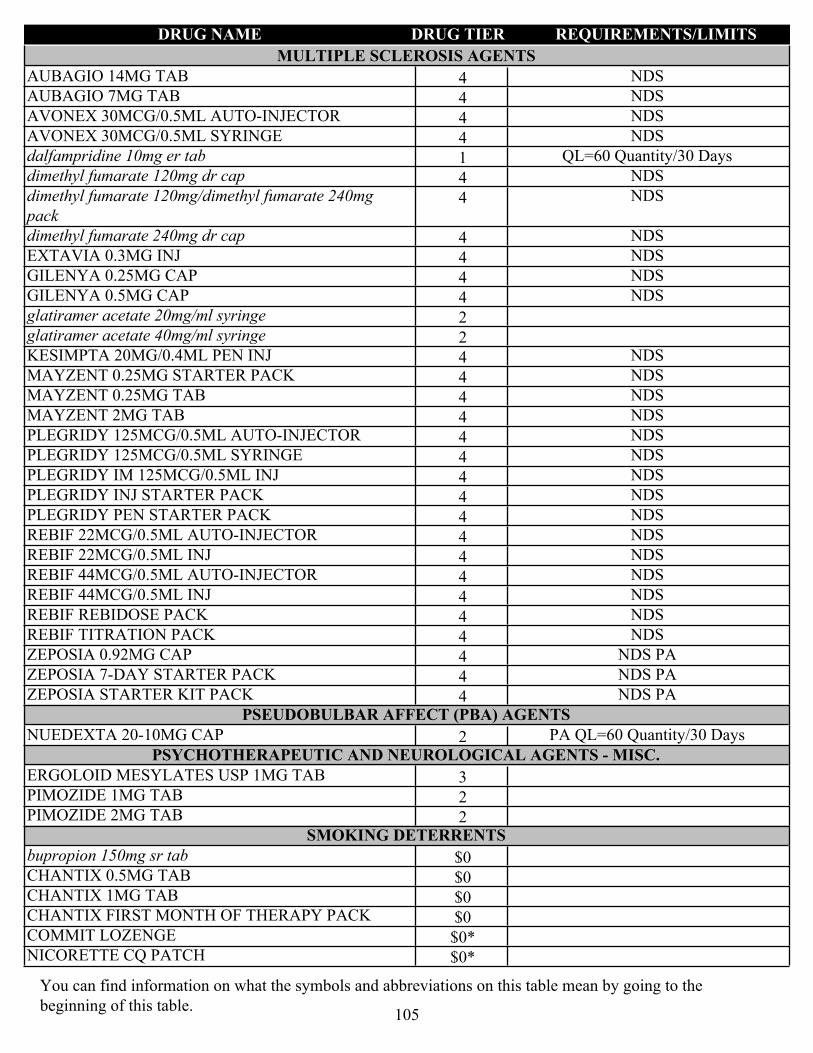
DRUG NAME DRUG TIER REQUIREMENTS/LIMITS
MULTIPLE SCLEROSIS AGENTS
4AUBAGIO 14MG TAB NDS
4AUBAGIO 7MG TAB NDS
4AVONEX 30MCG/0.5ML AUTO-INJECTOR NDS
4AVONEX 30MCG/0.5ML SYRINGE NDS
1dalfampridine 10mg er tab QL=60 Quantity/30 Days
4dimethyl fumarate 120mg dr cap NDS
4dimethyl fumarate 120mg/dimethyl fumarate 240mg pack
NDS
4dimethyl fumarate 240mg dr cap NDS
4EXTAVIA 0.3MG INJ NDS
4GILENYA 0.25MG CAP NDS
4GILENYA 0.5MG CAP NDS
2glatiramer acetate 20mg/ml syringe
2glatiramer acetate 40mg/ml syringe
4KESIMPTA 20MG/0.4ML PEN INJ NDS
4MAYZENT 0.25MG STARTER PACK NDS
4MAYZENT 0.25MG TAB NDS
4MAYZENT 2MG TAB NDS
4PLEGRIDY 125MCG/0.5ML AUTO-INJECTOR NDS
4PLEGRIDY 125MCG/0.5ML SYRINGE NDS
4PLEGRIDY IM 125MCG/0.5ML INJ NDS
4PLEGRIDY INJ STARTER PACK NDS
4PLEGRIDY PEN STARTER PACK NDS
4REBIF 22MCG/0.5ML AUTO-INJECTOR NDS
4REBIF 22MCG/0.5ML INJ NDS
4REBIF 44MCG/0.5ML AUTO-INJECTOR NDS
4REBIF 44MCG/0.5ML INJ NDS
4REBIF REBIDOSE PACK NDS
4REBIF TITRATION PACK NDS
4ZEPOSIA 0.92MG CAP NDS PA
4ZEPOSIA 7-DAY STARTER PACK NDS PA
4ZEPOSIA STARTER KIT PACK NDS PAPSEUDOBULBAR AFFECT (PBA) AGENTS
2NUEDEXTA 20-10MG CAP PA QL=60 Quantity/30 DaysPSYCHOTHERAPEUTIC AND NEUROLOGICAL AGENTS - MISC.
3ERGOLOID MESYLATES USP 1MG TAB
2PIMOZIDE 1MG TAB
2PIMOZIDE 2MG TABSMOKING DETERRENTS
$0bupropion 150mg sr tab
$0CHANTIX 0.5MG TAB
$0CHANTIX 1MG TAB
$0CHANTIX FIRST MONTH OF THERAPY PACK
$0*COMMIT LOZENGE
$0*NICORETTE CQ PATCH
You can find information on what the symbols and abbreviations on this table mean by going to the beginning of this table.
105

DRUG NAME DRUG TIER REQUIREMENTS/LIMITS
$0*NICORETTE GUM
$0*nicotine gum
$0*nicotine lozenge
$0*nicotine patch
$0*NICOTINE PATCH KIT
$0NICOTROL 10MG INH SOLN
$0NICOTROL 10MG/ML NASAL INHALERTRANSTHYRETIN AMYLOIDOSIS AGENTS
4TEGSEDI 284MG/1.5ML INJ LD NDS PA QL=4 Quantity/28 Days
RESPIRATORY AGENTS - MISC.ALPHA-PROTEINASE INHIBITOR (HUMAN)
4ARALAST NP 500MG INJ NDS PA
4GLASSIA 1000MG/50ML INJ NDS PA
4PROLASTIN-C 1000MG INJ NDS PA
4ZEMAIRA 1000MG INJ NDS PACYSTIC FIBROSIS AGENTS
4KALYDECO 150MG TAB LD NDS PA QL=60 Quantity/30 Days
4KALYDECO 25MG GRANULES LD NDS PA QL=60 Quantity/30 Days
4KALYDECO 50MG GRANULES LD NDS PA QL=60 Quantity/30 Days
4KALYDECO 75MG GRANULES LD NDS PA QL=60 Quantity/30 Days
4ORKAMBI 125-100MG GRANULES LD NDS PA QL=60 Quantity/30 Days
4ORKAMBI 125-100MG TAB LD NDS PA QL=120 Quantity/30 Days
4ORKAMBI 125-200MG TAB LD NDS PA QL=120 Quantity/30 Days
4ORKAMBI 188-150MG GRANULES LD NDS PA QL=60 Quantity/30 Days
4PULMOZYME 1MG/ML INH SOLN NDS PA_BvD QL=150 Quantity/30 Days
4SYMDEKO 50-75MG/75MG PACK LD NDS PA QL=60 Quantity/30 Days
4SYMDEKO TAB 4-WEEK PACK LD NDS PA QL=60 Quantity/30 Days
4TRIKAFTA 100-50-75MG/150MG PACK LD NDS PA QL=90 Quantity/30 Days
4TRIKAFTA 50-37.5-25MG/75MG TAB PACK LD NDS PA QL=84 Quantity/28 DaysPULMONARY FIBROSIS AGENTS
4ESBRIET 267MG CAP NDS PA
4ESBRIET 267MG TAB NDS PA
4ESBRIET 801MG TAB NDS PA
4OFEV 100MG CAP LD NDS PA
4OFEV 150MG CAP LD NDS PA
SULFONAMIDESSULFONAMIDES
2SULFADIAZINE 500MG TAB
TETRACYCLINESAMINOMETHYLCYCLINES
4NUZYRA 150MG TAB LD NDS PA QL=30 Quantity/14 DaysGLYCYLCYCLINES
4TIGECYCLINE 50MG INJ NDS
4tigecycline 50mg inj NDSTETRACYCLINES
You can find information on what the symbols and abbreviations on this table mean by going to the beginning of this table.
106
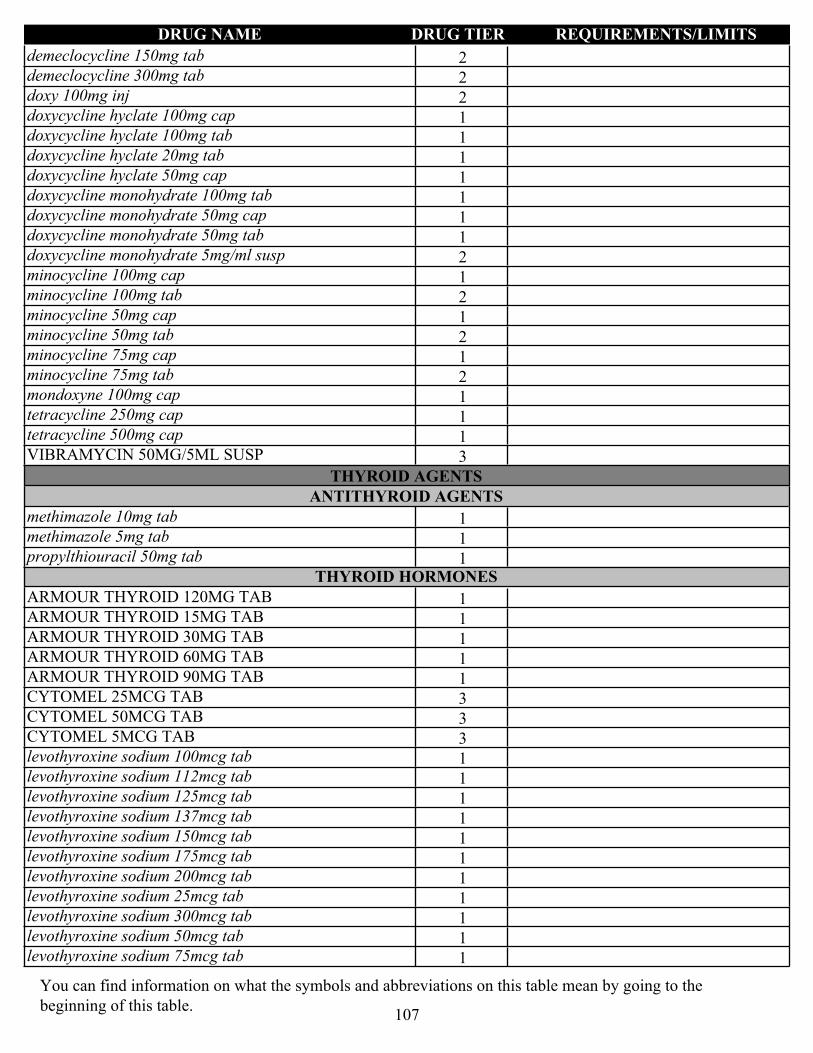
DRUG NAME DRUG TIER REQUIREMENTS/LIMITS
2demeclocycline 150mg tab
2demeclocycline 300mg tab
2doxy 100mg inj
1doxycycline hyclate 100mg cap
1doxycycline hyclate 100mg tab
1doxycycline hyclate 20mg tab
1doxycycline hyclate 50mg cap
1doxycycline monohydrate 100mg tab
1doxycycline monohydrate 50mg cap
1doxycycline monohydrate 50mg tab
2doxycycline monohydrate 5mg/ml susp
1minocycline 100mg cap
2minocycline 100mg tab
1minocycline 50mg cap
2minocycline 50mg tab
1minocycline 75mg cap
2minocycline 75mg tab
1mondoxyne 100mg cap
1tetracycline 250mg cap
1tetracycline 500mg cap
3VIBRAMYCIN 50MG/5ML SUSP
THYROID AGENTSANTITHYROID AGENTS
1methimazole 10mg tab
1methimazole 5mg tab
1propylthiouracil 50mg tabTHYROID HORMONES
1ARMOUR THYROID 120MG TAB
1ARMOUR THYROID 15MG TAB
1ARMOUR THYROID 30MG TAB
1ARMOUR THYROID 60MG TAB
1ARMOUR THYROID 90MG TAB
3CYTOMEL 25MCG TAB
3CYTOMEL 50MCG TAB
3CYTOMEL 5MCG TAB
1levothyroxine sodium 100mcg tab
1levothyroxine sodium 112mcg tab
1levothyroxine sodium 125mcg tab
1levothyroxine sodium 137mcg tab
1levothyroxine sodium 150mcg tab
1levothyroxine sodium 175mcg tab
1levothyroxine sodium 200mcg tab
1levothyroxine sodium 25mcg tab
1levothyroxine sodium 300mcg tab
1levothyroxine sodium 50mcg tab
1levothyroxine sodium 75mcg tab
You can find information on what the symbols and abbreviations on this table mean by going to the beginning of this table.
107

DRUG NAME DRUG TIER REQUIREMENTS/LIMITS
1levothyroxine sodium 88mcg tab
1liothyronine sodium 0.005mg tab
1liothyronine sodium 0.025mg tab
1liothyronine sodium 0.05mg tab
3SYNTHROID 100MCG TAB
3SYNTHROID 112MCG TAB
3SYNTHROID 125MCG TAB
3SYNTHROID 137MCG TAB
3SYNTHROID 150MCG TAB
3SYNTHROID 175MCG TAB
3SYNTHROID 200MCG TAB
3SYNTHROID 25MCG TAB
3SYNTHROID 300MCG TAB
3SYNTHROID 50MCG TAB
3SYNTHROID 75MCG TAB
3SYNTHROID 88MCG TAB
TOXOIDSTOXOID COMBINATIONS
$0ADACEL INJ
$0BOOSTRIX INJ
$0DAPTACEL INJ
$0DIPHTHERIA/TETANUS TOXOID INJ PA_BvD
$0INFANRIX INJ
$0KINRIX INJ
$0KINRIX PF INJ
$0PEDIARIX INJ
$0PENTACEL INJ
$0TDVAX 4-4UNIT/ML INJ PA_BvD
$0TENIVAC 4-10UNIT/ML INJ PA_BvD
ULCER DRUGSANTISPASMODICS
3*ANASPAZ TAB
2*BELLADONNA ALKALOID/OPIUM SUPP
3CUVPOSA 1MG/5ML ORAL SOLN
1dicyclomine 10mg cap
1dicyclomine 20mg tab
2dicyclomine 2mg/ml oral soln
2glycopyrrolate 1mg tab
2glycopyrrolate 2mg tab
1*hyoscyamine sulfate CR tab
1*hyoscyamine sulfate elixir
1*hyoscyamine sulfate ODT
1*hyoscyamine sulfate SL tab
1*hyoscyamine sulfate tab
3*LEVBID TAB
3*LEVSIN SL TAB
You can find information on what the symbols and abbreviations on this table mean by going to the beginning of this table.
108
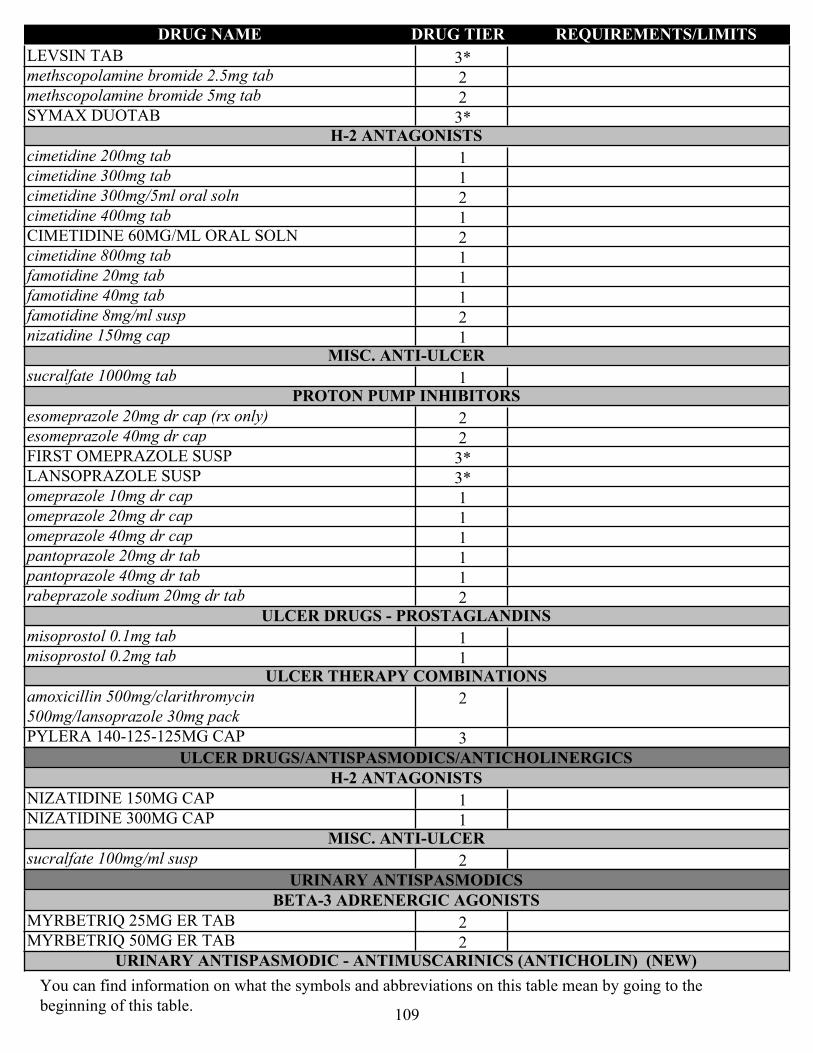
DRUG NAME DRUG TIER REQUIREMENTS/LIMITS
3*LEVSIN TAB
2methscopolamine bromide 2.5mg tab
2methscopolamine bromide 5mg tab
3*SYMAX DUOTABH-2 ANTAGONISTS
1cimetidine 200mg tab
1cimetidine 300mg tab
2cimetidine 300mg/5ml oral soln
1cimetidine 400mg tab
2CIMETIDINE 60MG/ML ORAL SOLN
1cimetidine 800mg tab
1famotidine 20mg tab
1famotidine 40mg tab
2famotidine 8mg/ml susp
1nizatidine 150mg capMISC. ANTI-ULCER
1sucralfate 1000mg tabPROTON PUMP INHIBITORS
2esomeprazole 20mg dr cap (rx only)
2esomeprazole 40mg dr cap
3*FIRST OMEPRAZOLE SUSP
3*LANSOPRAZOLE SUSP
1omeprazole 10mg dr cap
1omeprazole 20mg dr cap
1omeprazole 40mg dr cap
1pantoprazole 20mg dr tab
1pantoprazole 40mg dr tab
2rabeprazole sodium 20mg dr tabULCER DRUGS - PROSTAGLANDINS
1misoprostol 0.1mg tab
1misoprostol 0.2mg tabULCER THERAPY COMBINATIONS
2amoxicillin 500mg/clarithromycin 500mg/lansoprazole 30mg pack
3PYLERA 140-125-125MG CAP
ULCER DRUGS/ANTISPASMODICS/ANTICHOLINERGICSH-2 ANTAGONISTS
1NIZATIDINE 150MG CAP
1NIZATIDINE 300MG CAPMISC. ANTI-ULCER
2sucralfate 100mg/ml susp
URINARY ANTISPASMODICSBETA-3 ADRENERGIC AGONISTS
2MYRBETRIQ 25MG ER TAB
2MYRBETRIQ 50MG ER TABURINARY ANTISPASMODIC - ANTIMUSCARINICS (ANTICHOLIN) (NEW)
You can find information on what the symbols and abbreviations on this table mean by going to the beginning of this table.
109

DRUG NAME DRUG TIER REQUIREMENTS/LIMITS
1oxybutynin chloride 10mg er tab
1oxybutynin chloride 15mg er tab
1oxybutynin chloride 1mg/ml oral soln
1oxybutynin chloride 5mg er tab
1oxybutynin chloride 5mg tab
1tolterodine tartrate 1mg tab
1tolterodine tartrate 2mg tab
1trospium chloride 20mg tab
2trospium chloride 60mg er capURINARY ANTISPASMODIC - ANTIMUSCARINICS (ANTICHOLINERGIC)
2darifenacin 15mg er tab
2darifenacin 7.5mg er tab
1solifenacin succinate 10mg tab
1solifenacin succinate 5mg tab
2tolterodine tartrate 2mg er cap
2tolterodine tartrate 4mg er capURINARY ANTISPASMODICS - CHOLINERGIC AGONISTS (NEW)
1bethanechol chloride 10mg tab
1bethanechol chloride 25mg tab
1bethanechol chloride 50mg tab
1bethanechol chloride 5mg tabURINARY ANTISPASMODICS - DIRECT MUSCLE RELAXANTS
2flavoxate 100mg tab
VACCINESBACTERIAL VACCINES
$0ACTHIB INJ
$0BCG LIVE TICE STRAIN 50MG INJ
$0BEXSERO SYRINGE
$0HIBERIX 10MCG INJ
$0MENACTRA INJ
$0MENQUADFI INJ
$0MENVEO INJ
$0PEDVAXHIB 7.5MCG/0.5ML INJ
$0TRUMENBA INJ
$0TYPHIM VI 25MCG/0.5ML INJ
$0*VIVOTIF BERNA CAP QL=4 Quantity/ Per DispensingVIRAL VACCINES
$0ENGERIX-B 10MCG/0.5ML INJ PA_BvD
$0ENGERIX-B 20MCG/ML INJ PA_BvD
$0GARDASIL 9 INJ
$0GARDASIL 9 SYRINGE
$0HAVRIX 1440ELU/ML INJ
$0HAVRIX 720ELU/0.5ML INJ
$0IMOVAX 2.5UNIT/ML INJ PA_BvD
$0IPOL INJ
$0IXIARO 0.012MG/ML INJ
You can find information on what the symbols and abbreviations on this table mean by going to the beginning of this table.
110

DRUG NAME DRUG TIER REQUIREMENTS/LIMITS
$0M-M-R II INJ
$0PROQUAD INJ
$0RABAVERT 2.5UNIT/ML INJ PA_BvD
$0RECOMBIVAX 10MCG/ML INJ PA_BvD
$0RECOMBIVAX 40MCG/ML INJ PA_BvD
$0RECOMBIVAX 5MCG/0.5ML INJ PA_BvD
$0ROTARIX SUSP
$0ROTATEQ SUSP
$0SHINGRIX 50MCG/0.5ML INJ QL=2 Quantity/365 Days
$0TWINRIX 720UNIT INJ
$0VAQTA 25UNIT/0.5ML INJ
$0VAQTA 50UNIT/ML INJ
$0VARIVAX 1350PFU/0.5ML INJ
$0YF-VAX 4000UNIT/ML INJ
VAGINAL PRODUCTSMISCELLANEOUS VAGINAL PRODUCTS
3*FEM PH GELSPERMICIDES
$0*CONTRACEPTIVE FILM
$0*CONTRACEPTIVE FOAM
$0*CONTRACEPTIVE GEL
$0*CONTRACEPTIVE SPONGE
$0*CONTRACEPTIVE SUPP VAGINAL ANTI-INFECTIVES
3CLEOCIN 100MG VAGINAL INSERT
1clindamycin 2% vaginal cream
3CLINDESSE 2% VAGINAL CREAM
1metronidazole 0.75% vaginal gel
3MICONAZOLE NITRATE 200MG VAGINAL INSERT
1terconazole 0.4% vaginal cream
2terconazole 0.8% vaginal cream
2TERCONAZOLE 0.8% VAGINAL CREAM
1terconazole 80mg vaginal insertVAGINAL ESTROGENS
2estradiol 0.01% vaginal cream
2estradiol 0.01mg vaginal insert
3ESTRING 2MG VAGINAL SYSTEM ST
3FEMRING 0.05MG/24HR VAGINAL SYSTEM ST
3FEMRING 0.1MG/24HR VAGINAL SYSTEM ST
2PREMARIN 0.625MG/GM VAGINAL CREAMVAGINAL PROGESTINS
2CRINONE 4% VAGINAL GEL PA
2CRINONE 8% VAGINAL GEL PA
VASOPRESSORSANAPHYLAXIS THERAPY AGENTS
2epinephrine 0.15mg/0.3ml auto-injector (2 pack) QL=2 Quantity/15 Days
You can find information on what the symbols and abbreviations on this table mean by going to the beginning of this table.
111

DRUG NAME DRUG TIER REQUIREMENTS/LIMITS
2epinephrine 0.3mg/0.3ml auto-injector (2 pack) QL=2 Quantity/15 Days
2SYMJEPI 0.15MG/0.3ML SYRINGE QL=2 Quantity/15 Days
2SYMJEPI 0.3MG/0.3ML SYRINGE QL=2 Quantity/15 DaysNEUROGENIC ORTHOSTATIC HYPOTENSION (NOH) - AGENTS
2droxidopa 100mg cap PA
2droxidopa 200mg cap PA
2droxidopa 300mg cap PAVASOPRESSORS
1midodrine 10mg tab
1midodrine 2.5mg tab
1midodrine 5mg tab
VITAMINSOIL SOLUBLE VITAMINS
3*DRISDOL CAP
1*vitamin D 50000unit capWATER SOLUBLE VITAMINS
3*POTABA CAP
You can find information on what the symbols and abbreviations on this table mean by going to the beginning of this table.
112

ALPHABETICAL LISTING OF DRUGS
A
abacavir 20mg/ml oral soln
60
abacavir 300mg tab 60 abacavir 300mg/lamivudine 150mg/zidovudine 300mg tab
60
abacavir 600mg/lamivudine 300mg tab
60
ABELCET 5MG/ML INJ 34 ABILIFY 300MG INJ 59 ABILIFY 300MG SYRINGE
59
ABILIFY 400MG INJ 59 ABILIFY 400MG SYRINGE
59
abiraterone acetate 250mg tab
46
acamprosate calcium 333mg dr tab
103
acarbose 100mg tab 30 acarbose 25mg tab 30 acarbose 50mg tab 30 ACCU-CHEK AVIVA PLUS METER
91
acebutolol 200mg cap 64 acebutolol 400mg cap 65 acetaminophen 21.7mg/ml/hydrocodone bitartrate 0.5mg/ml oral soln
15
acetaminophen 24mg/ml/codeine phosphate 2.4mg/ml oral soln
16
acetaminophen 300mg/codeine phosphate 15mg tab
16
acetaminophen 300mg/codeine phosphate 30mg tab
16
acetaminophen 300mg/codeine phosphate 60mg tab
16
acetaminophen 300mg/hydrocodone bitartrate 10mg tab
16
acetaminophen 300mg/hydrocodone bitartrate 5mg tab
16
acetaminophen 300mg/hydrocodone bitartrate 7.5mg tab
16
acetaminophen 325mg/hydrocodone bitartrate 5mg tab
16
acetaminophen 325mg/hydrocodone bitartrate 7.5mg tab
16
acetaminophen 325mg/oxycodone 10mg tab
16
acetaminophen 325mg/oxycodone 2.5mg tab
16
acetaminophen 325mg/oxycodone 5mg tab
16
acetaminophen 325mg/oxycodone 7.5mg tab
16
acetaminophen 325mg/tramadol 37.5mg tab
16
acetazolamide 125mg tab 79 acetazolamide 250mg tab 79 acetazolamide 500mg er cap
79
acetic acid 2% otic soln 100 acetic acid/hydrocortisone 1-2% otic soln
101
acetylcysteine 100mg/ml inh soln
74
acetylcysteine 200mg/ml inh soln
74
acitretin 10mg cap 76 acitretin 17.5mg cap 76 acitretin 25mg cap 76 ACTEMRA 162MG/0.9ML AUTO-INJECTOR
12
ACTEMRA 162MG/0.9ML SYRINGE
12
ACTHIB INJ 110 ACTIMMUNE 2000000UNIT/0.5ML INJ
53
ACUVAIL 0.45% OPHTH SOLN
100
acyclovir 200mg cap 62 acyclovir 400mg tab 62 acyclovir 40mg/ml susp 62 acyclovir 5% cream 76 acyclovir 5% ointment 76 acyclovir 50mg/ml inj 62 acyclovir 800mg tab 62 ADACEL INJ 108 adapalene 0.1% cream 74 adapalene 0.1% gel 74 adapalene 0.3% gel 74 adapalene/benzoyl peroxide 0.1-2.5% gel
74
adefovir dipivoxil 10mg tab
62
ADEMPAS 0.5MG TAB 69 ADEMPAS 1.5MG TAB 69 ADEMPAS 1MG TAB 69 ADEMPAS 2.5MG TAB 69 ADEMPAS 2MG TAB 69 ADVAIR 100-50MCG DISKUS
21
ADVAIR 115-21MCG HFA INHALER
21
ADVAIR 230-21MCG HFA INHALER
21
ADVAIR 250-50MCG DISKUS
21
You can find information on what the symbols and abbreviations on this table mean by going to the beginning of this table.
113

ALPHABETICAL LISTING OF DRUGS
ADVAIR 45-21MCG/ACT HFA INHALER
21
ADVAIR 500-50MCG DISKUS
21
AIMOVIG 140MG/ML AUTO-INJECTOR
92
AIMOVIG 70MG/ML AUTO-INJECTOR
92
ala-cort 2.5% cream 76 albendazole 200mg tab 17 albuterol 0.21mg/ml inh soln
21
albuterol 0.417mg/ml inh soln
21
albuterol 0.4mg/ml oral soln
21
albuterol 0.83mg/ml inh soln
21
albuterol 2mg tab 21 albuterol 4mg tab 21 albuterol 5mg/ml inh soln 21 albuterol HFA inhaler (6.7gm)
21
albuterol HFA inhaler (8.5gm)
21
alclometasone dipropionate 0.05% cream
76
alclometasone dipropionate 0.05% ointment
76
ALCOHOL SWAB 1"x1" (DIABETIC)
78
ALCOHOL SWAB 1"x1" (DIABETIC)
78
ALDACTAZIDE 50-50MG TAB
79
ALECENSA 150MG CAP 48 alendronate 10mg tab 80 alendronate 35mg tab 80 alendronate 70mg tab 80 alendronate 70mg/75ml oral soln
80
alfuzosin 10mg er tab 86 aliskiren 150mg tab 41
aliskiren 300mg tab 41 ALKERAN TAB 44 allopurinol 100mg tab 87 allopurinol 300mg tab 87 ALOCRIL 2% OPHTH SOLN
100
ALOMIDE 0.1% OPHTH SOLN
100
alosetron 0.5mg tab 85 alosetron 1mg tab 85 ALPHAGAN 0.1% OPHTH SOLN
98
alprazolam 0.25mg tab 18 alprazolam 0.5mg er tab 19 alprazolam 0.5mg tab 19 alprazolam 1mg er tab 19 alprazolam 1mg tab 19 alprazolam 2mg er tab 19 alprazolam 2mg tab 19 alprazolam 3mg er tab 19 ALREX 0.2% OPHTH SUSP
99
altavera 28 day pack 71 ALUNBRIG 180MG TAB 48 ALUNBRIG 30MG TAB 48 ALUNBRIG 90MG TAB 48 ALUNBRIG TAB STARTER PACK
48
amabelz 0.5/0.1mg 28 day pack
83
amantadine 100mg cap 54 amantadine 100mg tab 54 amantadine 10mg/ml oral soln
54
amantadine 10mg/ml oral soln
54
AMBISOME 50MG INJ 34 ambrisentan 10mg tab 68 ambrisentan 5mg tab 68 amikacin 250mg/ml inj 11 amikacin sulfate 1gm/4ml inj
11
amiloride 5mg tab 80
amiloride 5mg/hydrochlorothiazide 50mg tab
79
AMINOSYN-PF 7% INJ 97 amiodarone 100mg tab 20 amiodarone 200mg tab 20 amiodarone 400mg tab 20 amitriptyline 100mg tab 29 amitriptyline 10mg tab 29 amitriptyline 150mg tab 29 amitriptyline 25mg tab 29 amitriptyline 50mg tab 29 amitriptyline 75mg tab 29 amlodipine 10mg tab 66 amlodipine 10mg/atorvastatin 10mg tab
67
amlodipine 10mg/atorvastatin 20mg tab
67
amlodipine 10mg/atorvastatin 40mg tab
67
amlodipine 10mg/atorvastatin 80mg tab
67
amlodipine 10mg/benazepril 20mg cap
39
amlodipine 10mg/benazepril 40mg cap
39
amlodipine 10mg/hydrochlorothiazide 12.5mg/valsartan 160mg tab
39
amlodipine 10mg/hydrochlorothiazide 25mg/valsartan 160mg tab
39
amlodipine 10mg/hydrochlorothiazide 25mg/valsartan 320mg tab
39
You can find information on what the symbols and abbreviations on this table mean by going to the beginning of this table.
114

ALPHABETICAL LISTING OF DRUGS
amlodipine 10mg/olmesartan medoxomil 20mg tab
39
amlodipine 10mg/olmesartan medoxomil 40mg tab
39
amlodipine 10mg/valsartan 160mg tab
39
amlodipine 10mg/valsartan 320mg tab
39
amlodipine 2.5mg tab 66 amlodipine 2.5mg/atorvastatin 10mg tab
67
amlodipine 2.5mg/atorvastatin 20mg tab
68
amlodipine 2.5mg/atorvastatin 40mg tab
68
amlodipine 2.5mg/benazepril 10mg cap
39
amlodipine 5mg tab 66 amlodipine 5mg/atorvastatin 10mg tab
68
amlodipine 5mg/atorvastatin 20mg tab
68
amlodipine 5mg/atorvastatin 40mg tab
68
amlodipine 5mg/atorvastatin 80mg tab
68
amlodipine 5mg/benazepril 10mg cap
39
amlodipine 5mg/benazepril 20mg cap
39
amlodipine 5mg/benazepril 40mg cap
39
amlodipine 5mg/hydrochlorothiazide 12.5mg/valsartan 160mg tab
39
amlodipine 5mg/hydrochlorothiazide 25mg/valsartan 160mg tab
39
amlodipine 5mg/olmesartan medoxomil 20mg tab
39
amlodipine 5mg/olmesartan medoxomil 40mg tab
39
amlodipine 5mg/valsartan 160mg tab
39
amlodipine 5mg/valsartan 320mg tab
39
ammonium lactate 12% cream
78
ammonium lactate 12% lotion
78
AMOXAPINE 100MG TAB
29
AMOXAPINE 150MG TAB
29
AMOXAPINE 25MG TAB 29 AMOXAPINE 50MG TAB 29 AMOXICILLIN 1000MG/CLAVULANATE 62.5MG ER TAB
102
amoxicillin 120mg/ml/clavulanate 8.58mg/ml susp
102
AMOXICILLIN 125MG CHEW TAB
101
AMOXICILLIN 200MG/CLAVULANATE 28.5MG CHEW TAB
102
amoxicillin 250mg cap 101 AMOXICILLIN 250MG CHEW TAB
101
amoxicillin 250mg/clavulanate 125mg tab
102
amoxicillin 25mg/ml susp 101 AMOXICILLIN 400MG/CLAVULANATE 57MG CHEW TAB
102
amoxicillin 40mg/ml susp 102 amoxicillin 40mg/ml/clavulanate 5.7mg/ml susp
102
amoxicillin 500mg cap 102 amoxicillin 500mg tab 102 amoxicillin 500mg/clarithromycin 500mg/lansoprazole 30mg pack
109
amoxicillin 500mg/clavulanate 125mg tab
102
amoxicillin 50mg/ml susp 102 amoxicillin 50mg/ml/clavulanate 12.5mg/ml susp
102
amoxicillin 80mg/ml susp 102 amoxicillin 80mg/ml/clavulanate 11.4mg/ml susp
102
amoxicillin 875mg tab 102 amoxicillin 875mg/clavulanate 125mg tab
102
amoxicillin/k clavulanate 1000-62.5mg er tab
102
amphetamine-dextroamphetamine 10mg ER cap
9
amphetamine-dextroamphetamine 10mg tab
9
amphetamine-dextroamphetamine 12.5mg tab
9
amphetamine-dextroamphetamine 15mg ER cap
9
amphetamine-dextroamphetamine 15mg tab
9
amphetamine-dextroamphetamine 20mg ER cap
9
amphetamine-dextroamphetamine 20mg tab
9
You can find information on what the symbols and abbreviations on this table mean by going to the beginning of this table.
115

ALPHABETICAL LISTING OF DRUGS
amphetamine-dextroamphetamine 25mg ER cap
9
amphetamine-dextroamphetamine 30mg ER cap
9
amphetamine-dextroamphetamine 30mg tab
9
amphetamine-dextroamphetamine 5mg ER cap
9
amphetamine-dextroamphetamine 5mg tab
9
amphetamine-dextroamphetamine 7.5mg tab
9
AMPHOTERICIN B 50MG INJ
34
ampicillin 1000mg inj 102 ampicillin 1000mg/sulbactam 500mg inj
102
ampicillin 100mg/ml inj 102 ampicillin 100mg/ml/sulbactam 50mg/ml inj
102
AMPICILLIN 125MG INJ 102 ampicillin 2000mg/sulbactam 1000mg inj
103
ampicillin 250mg inj 102 ampicillin 2gm inj 102 AMPICILLIN 2GM INJ 102 AMPICILLIN 500MG CAP
102
ampicillin 500mg inj 102 AMPICILLIN SODIUM 1GM INJ
102
AMPICILLIN/SULBACTAM 1.5GM INJ
103
AMPICILLIN/SULBACTAM 3GM INJ
103
anagrelide 0.5mg cap 87 anagrelide 1mg cap 87 ANALPRAM-HC CREAM 17 ANASPAZ TAB 108 anastrozole 1mg tab 46 ANDRODERM 2MG/24HR PATCH
17
ANDRODERM 4MG/24HR PATCH
17
ANGELIQ 0.25/0.5MG 28 DAY PACK
83
ANGELIQ 0.5/1MG 28 DAY PACK
83
ANORO ELLIPTA 62.5-25MCG INHALER
21
ANTARA 30MG CAP 36 ANTARA 90MG CAP 36 ANUSOL-HC SUPP 17 apraclonidine 0.5% ophth soln
98
aprepitant 125mg cap 34 aprepitant 125mg/aprepitant 80mg pack
34
aprepitant 40mg cap 34 aprepitant 80mg cap 34 apri 28 day pack 71 APTIOM 200MG TAB 24 APTIOM 400MG TAB 24 APTIOM 600MG TAB 24 APTIOM 800MG TAB 24 APTIVUS 250MG CAP 60 ARALAST NP 500MG INJ 106 aranelle 28 pack 71 ARANESP 100MCG/0.5ML SYRINGE
88
ARANESP 100MCG/ML INJ
88
ARANESP 10MCG/0.4ML SYRINGE
88
ARANESP 150MCG/0.3ML SYRINGE
88
ARANESP 200MCG/0.4ML SYRINGE
88
ARANESP 200MCG/ML INJ
88
ARANESP 25MCG/0.42ML SYRINGE
88
ARANESP 25MCG/ML INJ
88
ARANESP 300MCG/0.6ML SYRINGE
88
ARANESP 300MCG/ML INJ
88
ARANESP 40MCG/0.4ML SYRINGE
88
ARANESP 40MCG/ML INJ
88
ARANESP 500MCG/ML SYRINGE
88
ARANESP 60MCG/0.3ML SYRINGE
88
ARANESP 60MCG/ML INJ
88
ARCALYST 220MG INJ 12 arformoterol tartrate 15mcg/2ml neb soln
21
ARIKAYCE 590MG/8.4ML INH SUSP
11
aripiprazole 10mg odt 59 aripiprazole 10mg tab 59 aripiprazole 15mg odt 59 aripiprazole 15mg tab 59 aripiprazole 1mg/ml oral soln
59
aripiprazole 20mg tab 59 aripiprazole 2mg tab 59 aripiprazole 30mg tab 59 aripiprazole 5mg tab 59 ARISTADA 1064MG/3.9ML INJ
59
ARISTADA 441MG/1.6ML INJ
59
ARISTADA 662MG/2.4ML INJ
59
ARISTADA 675MG/2.4ML INJ
59
ARISTADA 882MG/3.2ML INJ
59
armodafinil 150mg tab 9 armodafinil 200mg tab 9 armodafinil 250mg tab 9
You can find information on what the symbols and abbreviations on this table mean by going to the beginning of this table.
116

ALPHABETICAL LISTING OF DRUGS
armodafinil 50mg tab 9 ARMOUR THYROID 120MG TAB
107
ARMOUR THYROID 15MG TAB
107
ARMOUR THYROID 30MG TAB
107
ARMOUR THYROID 60MG TAB
107
ARMOUR THYROID 90MG TAB
107
ARNUITY ELLIPTA 100MCG INHALER
20
ARNUITY ELLIPTA 200MCG INHALER
20
ARNUITY ELLIPTA 50MCG INHALER
20
asenapine 10mg sl tab 57 asenapine 2.5mg sl tab 57 asenapine 5mg sl tab 57 ashlyna 91 day pack 71 ASMANEX 100MCG INHALER
20
ASMANEX 110MCG INHALER
20
ASMANEX 200MCG INHALER
20
ASMANEX 220MCG INH 20 ASMANEX 220MCG INHALER
20
ASMANEX 50MCG HFA INHALER
20
aspirin 25mg/dipyridamole 200mg er cap
87
aspirin 325mg EC tab 13 aspirin 325mg tab 13 aspirin 81mg chew tab 13 aspirin 81mg EC tab 13 aspirin 81mg tab 14 ASPIRIN 81MG TAB 14 ASTAGRAF 0.5MG ER CAP
63
ASTAGRAF 1MG ER CAP 63 ASTAGRAF 5MG ER CAP 63
atazanavir 150mg cap 60 atazanavir 200mg cap 60 atazanavir 300mg cap 60 atenolol 100mg tab 65 atenolol 100mg/chlorthalidone 25mg tab
39
atenolol 25mg tab 65 atenolol 50mg tab 65 atenolol 50mg/chlorthalidone 25mg tab
40
atomoxetine 100mg cap 9 atomoxetine 10mg cap 9 atomoxetine 18mg cap 9 atomoxetine 25mg cap 9 atomoxetine 40mg cap 9 atomoxetine 60mg cap 9 atomoxetine 80mg cap 9 atorvastatin 10mg tab 36 atorvastatin 20mg tab 36 atorvastatin 40mg tab 36 atorvastatin 80mg tab 36 atovaquone 150mg/ml susp
42
atovaquone 250mg/proguanil 100mg tab
43
atovaquone 62.5mg/proguanil 25mg tab
43
atropine sulfate 0.025mg/diphenoxylate 2.5mg tab
33
ATROPINE SULFATE 1% OPHTH SOLN
98
ATROPINE SULFATE/DIPHENOXYLATE 2.5-0.025 MG/5ML ORAL SOLN
33
ATROVENT 17MCG INH 20 AUBAGIO 14MG TAB 105 AUBAGIO 7MG TAB 105 AURYXIA 210MG TAB 85 AUSTEDO 12MG TAB 104
AUSTEDO 6MG TAB 104 AUSTEDO 9MG TAB 104 AVONEX 30MCG/0.5ML AUTO-INJECTOR
105
AVONEX 30MCG/0.5ML SYRINGE
105
AVYCAZ 500-2000MG INJ
69
AYVAKIT 100MG TAB 47 AYVAKIT 200MG TAB 47 AYVAKIT 25MG TAB 47 AYVAKIT 300MG TAB 47 AYVAKIT 50MG TAB 47 AZASITE 1% OPHTH SOLN
98
azathioprine 50mg tab 63 azelaic acid 15% gel 78 azelastine 0.05% ophth soln
100
azelastine 0.137mg/act nasal inhaler
96
azelastine 0.206mg/act nasal inhaler
96
AZITHROMYCIN 1000MG POWDER FOR ORAL SUSP
90
azithromycin 20mg/ml susp
90
azithromycin 250mg pack 90 azithromycin 40mg/ml susp
90
azithromycin 500mg inj 90 azithromycin 500mg tab 90 azithromycin 600mg tab 90 aztreonam 1000mg inj 43
B
BACITRACIN 0.5UNIT/MG OPHTH OINTMENT
98
bacitracin 0.5unit/mg/polymyxin b 10unit/mg ophth ointment
98
baclofen 10mg tab 96 baclofen 20mg tab 96
You can find information on what the symbols and abbreviations on this table mean by going to the beginning of this table.
117

ALPHABETICAL LISTING OF DRUGS
balsalazide disodium 750mg cap
85
BALVERSA 3MG TAB 48 BALVERSA 4MG TAB 48 BALVERSA 5MG TAB 48 BAQSIMI 3MG/DOSE NASAL POWDER
31
BAXDELA 450MG TAB 84 BCG LIVE TICE STRAIN 50MG INJ
110
BELLADONNA ALKALOID/OPIUM SUPP
108
benazepril 10mg tab 37 benazepril 10mg/hydrochlorothiazide 12.5mg tab
40
benazepril 20mg tab 37 benazepril 20mg/hydrochlorothiazide 12.5mg tab
40
benazepril 20mg/hydrochlorothiazide 25mg tab
40
benazepril 40mg tab 37 benazepril 5mg tab 37 benazepril 5mg/hydrochlorothiazide 6.25mg tab
40
BENAZEPRIL-HYDROCHLOROTHIAZIDE 5-6.25MG TAB
40
BENLYSTA 200MG/ML AUTO-INJECTOR
95
BENLYSTA 200MG/ML SYRINGE
95
BENZNIDAZOLE 100MG TAB
17
BENZNIDAZOLE 12.5MG TAB
18
benzonatate 100mg cap, 200mg cap
73
benzoyl peroxide 5%/clindamycin phosphate 1.2% topical gel
74
benztropine mesylate 0.5mg tab
53
benztropine mesylate 1mg tab
53
benztropine mesylate 2mg tab
53
bepotastine besilate 1.5% ophth soln
100
BERINERT 500UNIT INJ 87 betamethasone 0.05% aug cream
76
betamethasone 0.05% aug lotion
76
betamethasone 0.05% aug ointment
76
betamethasone 0.05% cream
77
BETAMETHASONE 0.05% GEL
77
betamethasone 0.05% lotion
77
betamethasone 0.05% ointment
77
betamethasone 0.1% cream
77
betamethasone 0.1% lotion
77
betamethasone 0.1% ointment
77
betamethasone/clotrimazole 1-0.05% cream
75
betamethasone/clotrimazole 1-0.05% lotion
75
betaxolol 0.5% ophth soln
97
betaxolol 10mg tab 65 betaxolol 20mg tab 65 bethanechol chloride 10mg tab
110
bethanechol chloride 25mg tab
110
bethanechol chloride 50mg tab
110
bethanechol chloride 5mg tab
110
BETIMOL 0.25% OPHTH SOLN
97
BETIMOL 0.5% OPHTH SOLN
97
BETOPTIC S 0.25% OPHTH SUSP
97
bexarotene 75mg cap 53 BEXSERO SYRINGE 110 bicalutamide 50mg tab 46 BICILLIN 300000-300000UNIT/ML INJ
103
BICILLIN 450000-150000UNIT/ML INJ
103
BICILLIN L-A 1200000UNIT/2ML INJ
102
BICILLIN L-A 2400000UNIT/4ML INJ
102
BICILLIN L-A 600000UNIT/ML INJ
102
BIDIL 37.5-20MG TAB 68 BIKTARVY 50-200-25MG TAB
60
bimatoprost 0.03% ophth soln
100
bisoprolol fumarate 10mg tab
65
bisoprolol fumarate 10mg/hydrochlorothiazide 6.25mg tab
40
bisoprolol fumarate 2.5mg/hydrochlorothiazide 6.25mg tab
40
bisoprolol fumarate 5mg tab
65
bisoprolol fumarate 5mg/hydrochlorothiazide 6.25mg tab
40
BIVIGAM 5GM/50ML INJ
101
You can find information on what the symbols and abbreviations on this table mean by going to the beginning of this table.
118
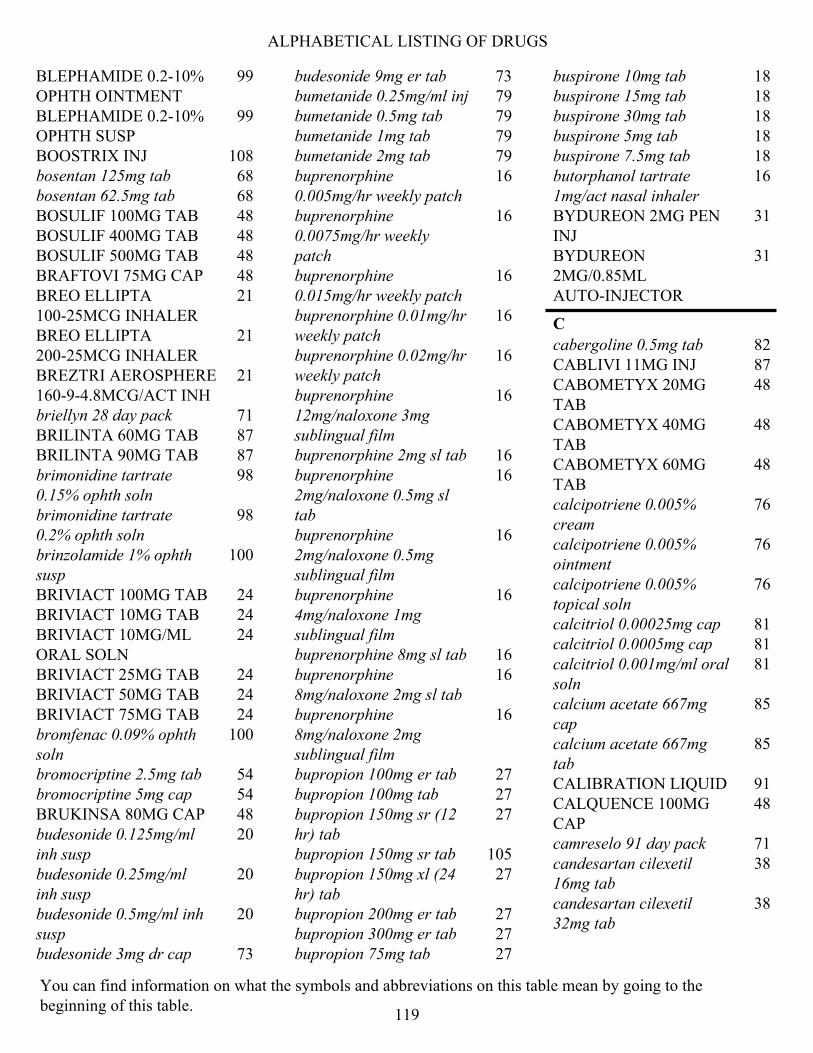
ALPHABETICAL LISTING OF DRUGS
BLEPHAMIDE 0.2-10% OPHTH OINTMENT
99
BLEPHAMIDE 0.2-10% OPHTH SUSP
99
BOOSTRIX INJ 108 bosentan 125mg tab 68 bosentan 62.5mg tab 68 BOSULIF 100MG TAB 48 BOSULIF 400MG TAB 48 BOSULIF 500MG TAB 48 BRAFTOVI 75MG CAP 48 BREO ELLIPTA 100-25MCG INHALER
21
BREO ELLIPTA 200-25MCG INHALER
21
BREZTRI AEROSPHERE 160-9-4.8MCG/ACT INH
21
briellyn 28 day pack 71 BRILINTA 60MG TAB 87 BRILINTA 90MG TAB 87 brimonidine tartrate 0.15% ophth soln
98
brimonidine tartrate 0.2% ophth soln
98
brinzolamide 1% ophth susp
100
BRIVIACT 100MG TAB 24 BRIVIACT 10MG TAB 24 BRIVIACT 10MG/ML ORAL SOLN
24
BRIVIACT 25MG TAB 24 BRIVIACT 50MG TAB 24 BRIVIACT 75MG TAB 24 bromfenac 0.09% ophth soln
100
bromocriptine 2.5mg tab 54 bromocriptine 5mg cap 54 BRUKINSA 80MG CAP 48 budesonide 0.125mg/ml inh susp
20
budesonide 0.25mg/ml inh susp
20
budesonide 0.5mg/ml inh susp
20
budesonide 3mg dr cap 73
budesonide 9mg er tab 73 bumetanide 0.25mg/ml inj 79 bumetanide 0.5mg tab 79 bumetanide 1mg tab 79 bumetanide 2mg tab 79 buprenorphine 0.005mg/hr weekly patch
16
buprenorphine 0.0075mg/hr weekly patch
16
buprenorphine 0.015mg/hr weekly patch
16
buprenorphine 0.01mg/hr weekly patch
16
buprenorphine 0.02mg/hr weekly patch
16
buprenorphine 12mg/naloxone 3mg sublingual film
16
buprenorphine 2mg sl tab 16 buprenorphine 2mg/naloxone 0.5mg sl tab
16
buprenorphine 2mg/naloxone 0.5mg sublingual film
16
buprenorphine 4mg/naloxone 1mg sublingual film
16
buprenorphine 8mg sl tab 16 buprenorphine 8mg/naloxone 2mg sl tab
16
buprenorphine 8mg/naloxone 2mg sublingual film
16
bupropion 100mg er tab 27 bupropion 100mg tab 27 bupropion 150mg sr (12 hr) tab
27
bupropion 150mg sr tab 105 bupropion 150mg xl (24 hr) tab
27
bupropion 200mg er tab 27 bupropion 300mg er tab 27 bupropion 75mg tab 27
buspirone 10mg tab 18 buspirone 15mg tab 18 buspirone 30mg tab 18 buspirone 5mg tab 18 buspirone 7.5mg tab 18 butorphanol tartrate 1mg/act nasal inhaler
16
BYDUREON 2MG PEN INJ
31
BYDUREON 2MG/0.85ML AUTO-INJECTOR
31
C
cabergoline 0.5mg tab 82 CABLIVI 11MG INJ 87 CABOMETYX 20MG TAB
48
CABOMETYX 40MG TAB
48
CABOMETYX 60MG TAB
48
calcipotriene 0.005% cream
76
calcipotriene 0.005% ointment
76
calcipotriene 0.005% topical soln
76
calcitriol 0.00025mg cap 81 calcitriol 0.0005mg cap 81 calcitriol 0.001mg/ml oral soln
81
calcium acetate 667mg cap
85
calcium acetate 667mg tab
85
CALIBRATION LIQUID 91 CALQUENCE 100MG CAP
48
camreselo 91 day pack 71 candesartan cilexetil 16mg tab
38
candesartan cilexetil 32mg tab
38
You can find information on what the symbols and abbreviations on this table mean by going to the beginning of this table.
119

ALPHABETICAL LISTING OF DRUGS
candesartan cilexetil 4mg tab
38
candesartan cilexetil 8mg tab
38
capecitabine tab 44 CAPLYTA 42MG CAP 56 CAPRELSA 100MG TAB 48 CAPRELSA 300MG TAB 48 captopril 100mg tab 37 captopril 12.5mg tab 37 captopril 25mg tab 37 captopril 50mg tab 37 CARBAGLU 200MG TAB FOR ORAL SUSP
81
carbamazepine 100mg chew tab
24
carbamazepine 100mg er cap
24
carbamazepine 100mg er tab
24
carbamazepine 200mg er cap
24
carbamazepine 200mg er tab
24
carbamazepine 200mg tab
24
carbamazepine 20mg/ml susp
24
carbamazepine 300mg er cap
24
carbamazepine 400mg er tab
24
carbidopa 10mg/levodopa 100mg tab
54
CARBIDOPA 12.5MG/ENTACAPONE 200MG/LEVODOPA 50MG TAB
54
carbidopa 25mg tab 53 CARBIDOPA 25MG/ENTACAPONE 200MG/LEVODOPA 100MG TAB, STALEVO 25-200-100MG TAB
54
carbidopa 25mg/levodopa 100mg er tab
54
carbidopa 25mg/levodopa 100mg tab
54
carbidopa 25mg/levodopa 250mg tab
54
CARBIDOPA 31.25MG/ENTACAPONE 200MG/LEVODOPA 125MG TAB, STALEVO 31.25-200-125MG TAB
54
CARBIDOPA 37.5MG/ENTACAPONE 200MG/LEVODOPA 150MG TAB
54
carbidopa 50mg/levodopa 200mg er tab
54
CARBIDOPA/LEVODOPA 10-100MG ODT
55
CARBIDOPA/LEVODOPA 10-250MG ODT TAB
55
CARBIDOPA/LEVODOPA 25-100MG ODT TAB
55
CARBIDOPA/LEVODOPA/ENTACAPONE 50-200-200MG TAB
54
CARBIDOPA/LEVODOPA/ENTACAPONE18.75-75-200MG TAB, STALEVO 12.5-200-50MG TAB
54
CARDIZEM 120MG ER TAB
66
CARDURA 4MG ER TAB 86 CARDURA 8MG ER TAB 86 carisoprodol 350mg tab 96 CARTEOLOL 1% OPHTH SOLN
97
cartia 180mg er cap 66 cartia 240mg er cap 66 cartia 300mg er cap 66 carvedilol 12.5mg tab 64
carvedilol 25mg tab 64 carvedilol 3.125mg tab 64 carvedilol 6.25mg tab 64 carvedilol phosphate ER 10mg cap
64
carvedilol phosphate ER 20mg cap
64
carvedilol phosphate ER 40mg cap
64
carvedilol phosphate ER 80mg cap
64
caspofungin acetate 50mg inj
34
CASPOFUNGIN ACETATE 50MG INJ
34
CASPOFUNGIN ACETATE 70MG INJ
34
caspofungin acetate 70mg inj
34
CAVERJECT INJ 68 CAVERJECT INJ 68 CAYSTON 75MG INH SOLN
43
caziant 28 day pack 71 cefaclor 250mg cap 70 CEFACLOR 250MG CAP 70 CEFACLOR 25MG/ML SUSP
70
cefaclor 500mg cap 70 CEFACLOR 500MG CAP 70 CEFACLOR 500MG ER TAB
70
CEFACLOR 50MG/ML SUSP
70
CEFACLOR 75MG/ML SUSP
70
cefadroxil 100mg/ml susp 69 cefadroxil 1gm tab 69 CEFADROXIL 1GM TAB 69 cefadroxil 500mg cap 69 cefadroxil 50mg/ml susp 69 cefazolin 1000mg inj 69 CEFAZOLIN 100GM INJ 69 CEFAZOLIN 1GM INJ 69 cefazolin 200mg/ml inj 69
You can find information on what the symbols and abbreviations on this table mean by going to the beginning of this table.
120

ALPHABETICAL LISTING OF DRUGS
CEFAZOLIN 20GM INJ 69 CEFAZOLIN 300GM INJ 69 cefazolin 500mg inj 70 CEFAZOLIN/DEXTROSE 1GM/50ML-4% IV SOLN
70
CEFAZOLIN/DEXTROSE 1GM-4% IV SOLN
70
cefdinir 25mg/ml susp 70 cefdinir 300mg cap 70 cefdinir 50mg/ml susp 70 cefepime 1000mg inj 71 CEFEPIME 1GM/50ML IV SOLN
71
cefepime 2000mg inj 71 CEFEPIME 2GM/100ML IV SOLN
71
CEFEPIME/DEXTROSE 1GM/50ML-5% INJ
71
CEFEPIME/DEXTROSE 2GM/50ML-5% INJ
71
cefixime 20mg/ml susp 70 cefixime 400mg cap 70 cefixime 40mg/ml susp 70 cefotetan 1000mg inj 70 cefotetan 2000mg inj 70 CEFOTETAN/DEXTROSE 1GM/3.58% INJ
70
CEFOTETAN/DEXTROSE 2GM-2.08% INJ
70
cefoxitin 1000mg inj 70 cefoxitin 2000mg inj 70 cefoxitin 200mg/ml inj 70 CEFOXITIN/DEXTROSE 1GM-4% INJ
70
CEFOXITIN/DEXTROSE 2GM/2.2% INJ
70
cefpodoxime 100mg tab 70 cefpodoxime 10mg/ml susp
70
cefpodoxime 200mg tab 70 cefpodoxime 20mg/ml susp
70
cefprozil 250mg tab 70 cefprozil 25mg/ml susp 70 cefprozil 500mg tab 70
cefprozil 50mg/ml susp 70 ceftazidime 1000mg inj 70 ceftazidime 200mg/ml inj 71 CEFTAZIDIME/D5W 1GM/50ML INJ
71
CEFTAZIDIME/DEXTROSE 2GM/50ML/5% INJ
71
ceftriaxone 1000mg inj 71 ceftriaxone 100mg/ml inj 71 ceftriaxone 2000mg inj 71 ceftriaxone 250mg inj 71 ceftriaxone 500mg inj 71 CEFTRIAXONE SODIUM 100GM INJ
71
ceftriaxone sodium 1gm inj
71
ceftriaxone sodium 2gm inj
71
CEFTRIAXONE/DEXTROSE 1GM-3.74% IV SOLN
71
CEFTRIAXONE/DEXTROSE 20MG/ML INJ
71
CEFTRIAXONE/DEXTROSE 2GM-2.22% IV SOLN
71
CEFTRIAXONE/DEXTROSE 40MG/ML INJ
71
cefuroxime 1500mg inj 70 cefuroxime 250mg tab 70 cefuroxime 500mg tab 70 cefuroxime 750mg inj 70 cefuroxime 95mg/ml inj 70 celecoxib 100mg cap 12 celecoxib 200mg cap 12 celecoxib 400mg cap 12 celecoxib 50mg cap 12 CELLCEPT 200MG/ML SUSP
63
CELLCEPT 250MG CAP 63 CELLCEPT 500MG TAB 63 CELONTIN 300MG CAP 26 cephalexin 250mg cap 70 cephalexin 25mg/ml susp 70 cephalexin 500mg cap 70 cephalexin 50mg/ml susp 70 CERDELGA 84MG CAP 88
CERVICAL CAP 91 cetirizine 1mg/ml oral soln
35
cevimeline 30mg cap 95 CHANTIX 0.5MG TAB 105 CHANTIX 1MG TAB 105 CHANTIX FIRST MONTH OF THERAPY PACK
105
CHEMET 100MG CAP 33 CHENODAL 250MG TAB 84 chlordiazepoxide 10mg cap
19
chlordiazepoxide 25mg cap
19
chlordiazepoxide 5mg cap
19
chlorhexidine gluconate 0.12% mouthwash
95
chloroquine phosphate 250mg tab
43
CHLOROQUINE PHOSPHATE 500MG TAB
43
chlorpromazine 100mg tab
58
CHLORPROMAZINE 100MG/ML ORAL SOLN
58
chlorpromazine 10mg tab 58 chlorpromazine 200mg tab
58
chlorpromazine 25mg tab 58 CHLORPROMAZINE 30MG/ML ORAL SOLN
58
chlorpromazine 50mg tab 58 chlorthalidone 25mg tab 80 chlorthalidone 50mg tab 80 chlorzoxazone 500mg tab 96 CHOLBAM 250MG CAP 84 CHOLBAM 50MG CAP 84 cholestyramine 4gm bulk powder
36
cholestyramine resin 4gm sf powder for oral susp
36
You can find information on what the symbols and abbreviations on this table mean by going to the beginning of this table.
121
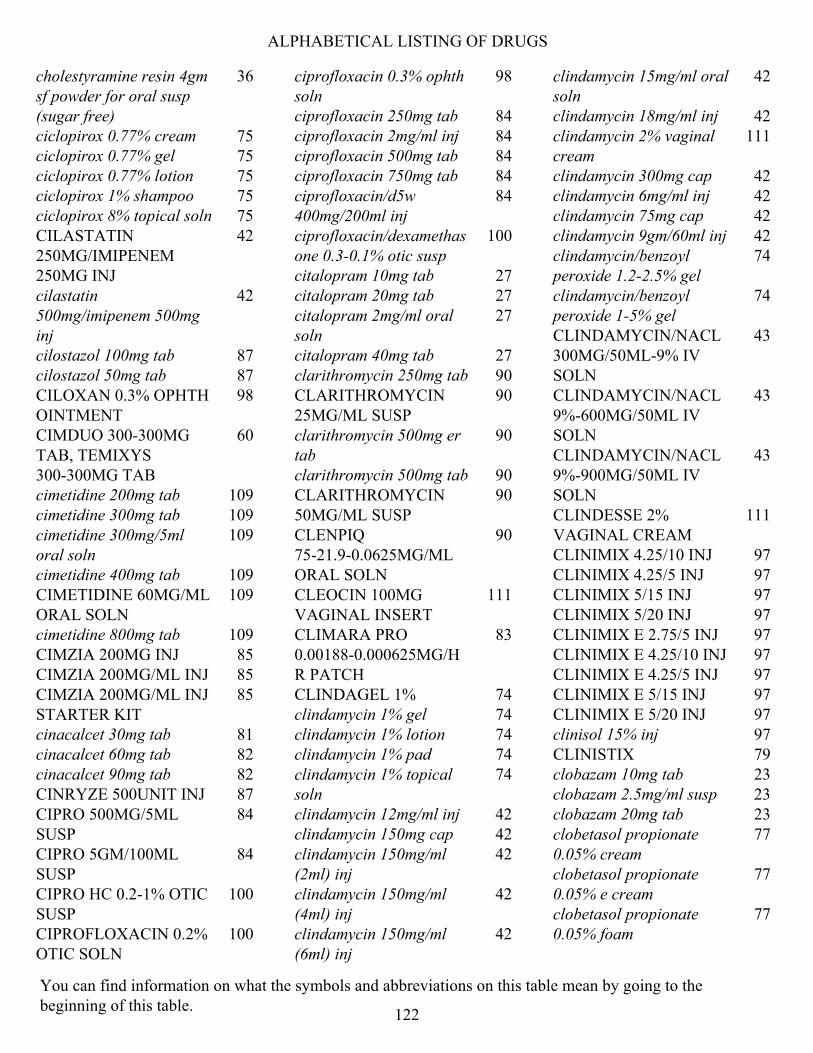
ALPHABETICAL LISTING OF DRUGS
cholestyramine resin 4gm sf powder for oral susp (sugar free)
36
ciclopirox 0.77% cream 75 ciclopirox 0.77% gel 75 ciclopirox 0.77% lotion 75 ciclopirox 1% shampoo 75 ciclopirox 8% topical soln 75 CILASTATIN 250MG/IMIPENEM 250MG INJ
42
cilastatin 500mg/imipenem 500mg inj
42
cilostazol 100mg tab 87 cilostazol 50mg tab 87 CILOXAN 0.3% OPHTH OINTMENT
98
CIMDUO 300-300MG TAB, TEMIXYS 300-300MG TAB
60
cimetidine 200mg tab 109 cimetidine 300mg tab 109 cimetidine 300mg/5ml oral soln
109
cimetidine 400mg tab 109 CIMETIDINE 60MG/ML ORAL SOLN
109
cimetidine 800mg tab 109 CIMZIA 200MG INJ 85 CIMZIA 200MG/ML INJ 85 CIMZIA 200MG/ML INJ STARTER KIT
85
cinacalcet 30mg tab 81 cinacalcet 60mg tab 82 cinacalcet 90mg tab 82 CINRYZE 500UNIT INJ 87 CIPRO 500MG/5ML SUSP
84
CIPRO 5GM/100ML SUSP
84
CIPRO HC 0.2-1% OTIC SUSP
100
CIPROFLOXACIN 0.2% OTIC SOLN
100
ciprofloxacin 0.3% ophth soln
98
ciprofloxacin 250mg tab 84 ciprofloxacin 2mg/ml inj 84 ciprofloxacin 500mg tab 84 ciprofloxacin 750mg tab 84 ciprofloxacin/d5w 400mg/200ml inj
84
ciprofloxacin/dexamethasone 0.3-0.1% otic susp
100
citalopram 10mg tab 27 citalopram 20mg tab 27 citalopram 2mg/ml oral soln
27
citalopram 40mg tab 27 clarithromycin 250mg tab 90 CLARITHROMYCIN 25MG/ML SUSP
90
clarithromycin 500mg er tab
90
clarithromycin 500mg tab 90 CLARITHROMYCIN 50MG/ML SUSP
90
CLENPIQ 75-21.9-0.0625MG/ML ORAL SOLN
90
CLEOCIN 100MG VAGINAL INSERT
111
CLIMARA PRO 0.00188-0.000625MG/HR PATCH
83
CLINDAGEL 1% 74 clindamycin 1% gel 74 clindamycin 1% lotion 74 clindamycin 1% pad 74 clindamycin 1% topical soln
74
clindamycin 12mg/ml inj 42 clindamycin 150mg cap 42 clindamycin 150mg/ml (2ml) inj
42
clindamycin 150mg/ml (4ml) inj
42
clindamycin 150mg/ml (6ml) inj
42
clindamycin 15mg/ml oral soln
42
clindamycin 18mg/ml inj 42 clindamycin 2% vaginal cream
111
clindamycin 300mg cap 42 clindamycin 6mg/ml inj 42 clindamycin 75mg cap 42 clindamycin 9gm/60ml inj 42 clindamycin/benzoyl peroxide 1.2-2.5% gel
74
clindamycin/benzoyl peroxide 1-5% gel
74
CLINDAMYCIN/NACL 300MG/50ML-9% IV SOLN
43
CLINDAMYCIN/NACL 9%-600MG/50ML IV SOLN
43
CLINDAMYCIN/NACL 9%-900MG/50ML IV SOLN
43
CLINDESSE 2% VAGINAL CREAM
111
CLINIMIX 4.25/10 INJ 97 CLINIMIX 4.25/5 INJ 97 CLINIMIX 5/15 INJ 97 CLINIMIX 5/20 INJ 97 CLINIMIX E 2.75/5 INJ 97 CLINIMIX E 4.25/10 INJ 97 CLINIMIX E 4.25/5 INJ 97 CLINIMIX E 5/15 INJ 97 CLINIMIX E 5/20 INJ 97 clinisol 15% inj 97 CLINISTIX 79 clobazam 10mg tab 23 clobazam 2.5mg/ml susp 23 clobazam 20mg tab 23 clobetasol propionate 0.05% cream
77
clobetasol propionate 0.05% e cream
77
clobetasol propionate 0.05% foam
77
You can find information on what the symbols and abbreviations on this table mean by going to the beginning of this table.
122
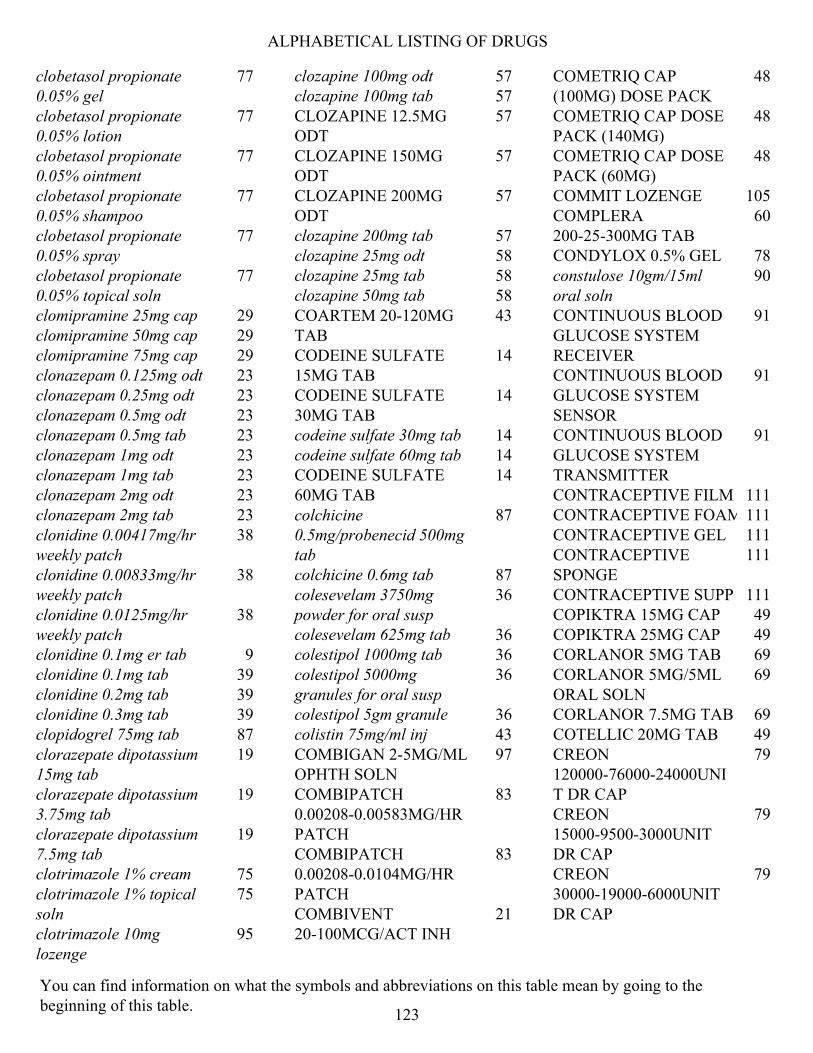
ALPHABETICAL LISTING OF DRUGS
clobetasol propionate 0.05% gel
77
clobetasol propionate 0.05% lotion
77
clobetasol propionate 0.05% ointment
77
clobetasol propionate 0.05% shampoo
77
clobetasol propionate 0.05% spray
77
clobetasol propionate 0.05% topical soln
77
clomipramine 25mg cap 29 clomipramine 50mg cap 29 clomipramine 75mg cap 29 clonazepam 0.125mg odt 23 clonazepam 0.25mg odt 23 clonazepam 0.5mg odt 23 clonazepam 0.5mg tab 23 clonazepam 1mg odt 23 clonazepam 1mg tab 23 clonazepam 2mg odt 23 clonazepam 2mg tab 23 clonidine 0.00417mg/hr weekly patch
38
clonidine 0.00833mg/hr weekly patch
38
clonidine 0.0125mg/hr weekly patch
38
clonidine 0.1mg er tab 9 clonidine 0.1mg tab 39 clonidine 0.2mg tab 39 clonidine 0.3mg tab 39 clopidogrel 75mg tab 87 clorazepate dipotassium 15mg tab
19
clorazepate dipotassium 3.75mg tab
19
clorazepate dipotassium 7.5mg tab
19
clotrimazole 1% cream 75 clotrimazole 1% topical soln
75
clotrimazole 10mg lozenge
95
clozapine 100mg odt 57 clozapine 100mg tab 57 CLOZAPINE 12.5MG ODT
57
CLOZAPINE 150MG ODT
57
CLOZAPINE 200MG ODT
57
clozapine 200mg tab 57 clozapine 25mg odt 58 clozapine 25mg tab 58 clozapine 50mg tab 58 COARTEM 20-120MG TAB
43
CODEINE SULFATE 15MG TAB
14
CODEINE SULFATE 30MG TAB
14
codeine sulfate 30mg tab 14 codeine sulfate 60mg tab 14 CODEINE SULFATE 60MG TAB
14
colchicine 0.5mg/probenecid 500mg tab
87
colchicine 0.6mg tab 87 colesevelam 3750mg powder for oral susp
36
colesevelam 625mg tab 36 colestipol 1000mg tab 36 colestipol 5000mg granules for oral susp
36
colestipol 5gm granule 36 colistin 75mg/ml inj 43 COMBIGAN 2-5MG/ML OPHTH SOLN
97
COMBIPATCH 0.00208-0.00583MG/HR PATCH
83
COMBIPATCH 0.00208-0.0104MG/HR PATCH
83
COMBIVENT 20-100MCG/ACT INH
21
COMETRIQ CAP (100MG) DOSE PACK
48
COMETRIQ CAP DOSE PACK (140MG)
48
COMETRIQ CAP DOSE PACK (60MG)
48
COMMIT LOZENGE 105 COMPLERA 200-25-300MG TAB
60
CONDYLOX 0.5% GEL 78 constulose 10gm/15ml oral soln
90
CONTINUOUS BLOOD GLUCOSE SYSTEM RECEIVER
91
CONTINUOUS BLOOD GLUCOSE SYSTEM SENSOR
91
CONTINUOUS BLOOD GLUCOSE SYSTEM TRANSMITTER
91
CONTRACEPTIVE FILM 111 CONTRACEPTIVE FOAM 111 CONTRACEPTIVE GEL 111 CONTRACEPTIVE SPONGE
111
CONTRACEPTIVE SUPP 111 COPIKTRA 15MG CAP 49 COPIKTRA 25MG CAP 49 CORLANOR 5MG TAB 69 CORLANOR 5MG/5ML ORAL SOLN
69
CORLANOR 7.5MG TAB 69 COTELLIC 20MG TAB 49 CREON 120000-76000-24000UNIT DR CAP
79
CREON 15000-9500-3000UNIT DR CAP
79
CREON 30000-19000-6000UNIT DR CAP
79
You can find information on what the symbols and abbreviations on this table mean by going to the beginning of this table.
123
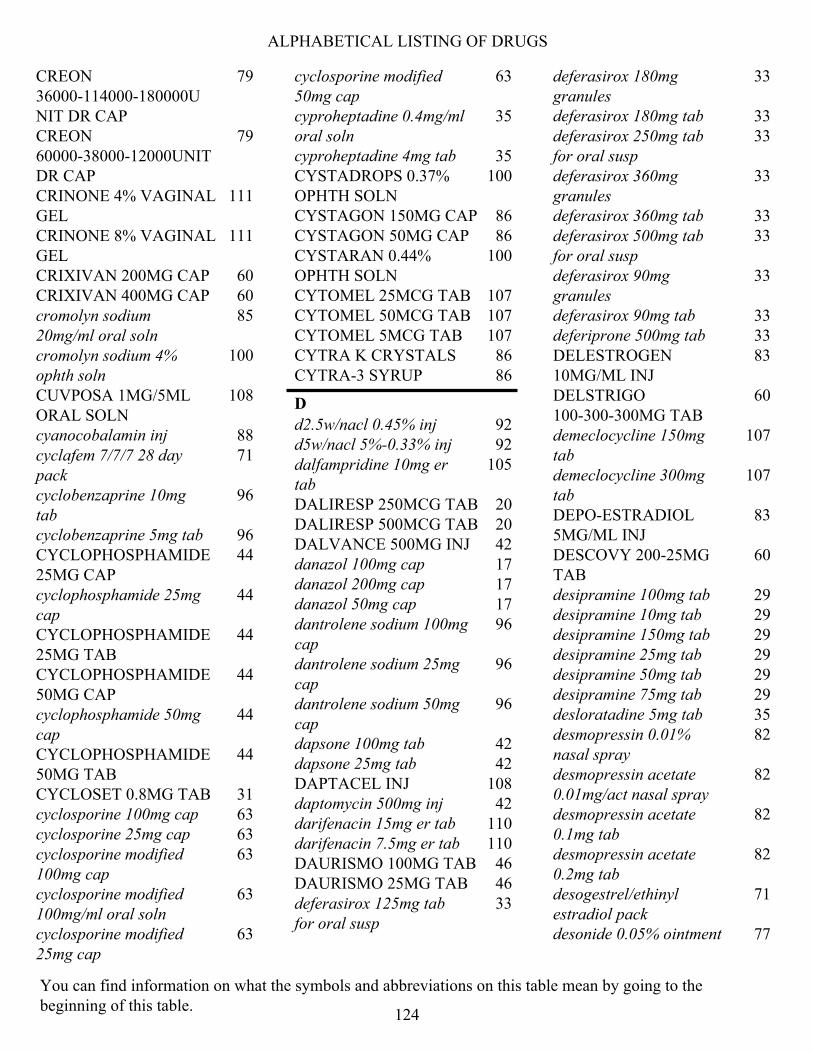
ALPHABETICAL LISTING OF DRUGS
CREON 36000-114000-180000UNIT DR CAP
79
CREON 60000-38000-12000UNIT DR CAP
79
CRINONE 4% VAGINAL GEL
111
CRINONE 8% VAGINAL GEL
111
CRIXIVAN 200MG CAP 60 CRIXIVAN 400MG CAP 60 cromolyn sodium 20mg/ml oral soln
85
cromolyn sodium 4% ophth soln
100
CUVPOSA 1MG/5ML ORAL SOLN
108
cyanocobalamin inj 88 cyclafem 7/7/7 28 day pack
71
cyclobenzaprine 10mg tab
96
cyclobenzaprine 5mg tab 96 CYCLOPHOSPHAMIDE 25MG CAP
44
cyclophosphamide 25mg cap
44
CYCLOPHOSPHAMIDE 25MG TAB
44
CYCLOPHOSPHAMIDE 50MG CAP
44
cyclophosphamide 50mg cap
44
CYCLOPHOSPHAMIDE 50MG TAB
44
CYCLOSET 0.8MG TAB 31 cyclosporine 100mg cap 63 cyclosporine 25mg cap 63 cyclosporine modified 100mg cap
63
cyclosporine modified 100mg/ml oral soln
63
cyclosporine modified 25mg cap
63
cyclosporine modified 50mg cap
63
cyproheptadine 0.4mg/ml oral soln
35
cyproheptadine 4mg tab 35 CYSTADROPS 0.37% OPHTH SOLN
100
CYSTAGON 150MG CAP 86 CYSTAGON 50MG CAP 86 CYSTARAN 0.44% OPHTH SOLN
100
CYTOMEL 25MCG TAB 107 CYTOMEL 50MCG TAB 107 CYTOMEL 5MCG TAB 107 CYTRA K CRYSTALS 86 CYTRA-3 SYRUP 86
D
d2.5w/nacl 0.45% inj 92 d5w/nacl 5%-0.33% inj 92 dalfampridine 10mg er tab
105
DALIRESP 250MCG TAB 20 DALIRESP 500MCG TAB 20 DALVANCE 500MG INJ 42 danazol 100mg cap 17 danazol 200mg cap 17 danazol 50mg cap 17 dantrolene sodium 100mg cap
96
dantrolene sodium 25mg cap
96
dantrolene sodium 50mg cap
96
dapsone 100mg tab 42 dapsone 25mg tab 42 DAPTACEL INJ 108 daptomycin 500mg inj 42 darifenacin 15mg er tab 110 darifenacin 7.5mg er tab 110 DAURISMO 100MG TAB 46 DAURISMO 25MG TAB 46 deferasirox 125mg tab for oral susp
33
deferasirox 180mg granules
33
deferasirox 180mg tab 33 deferasirox 250mg tab for oral susp
33
deferasirox 360mg granules
33
deferasirox 360mg tab 33 deferasirox 500mg tab for oral susp
33
deferasirox 90mg granules
33
deferasirox 90mg tab 33 deferiprone 500mg tab 33 DELESTROGEN 10MG/ML INJ
83
DELSTRIGO 100-300-300MG TAB
60
demeclocycline 150mg tab
107
demeclocycline 300mg tab
107
DEPO-ESTRADIOL 5MG/ML INJ
83
DESCOVY 200-25MG TAB
60
desipramine 100mg tab 29 desipramine 10mg tab 29 desipramine 150mg tab 29 desipramine 25mg tab 29 desipramine 50mg tab 29 desipramine 75mg tab 29 desloratadine 5mg tab 35 desmopressin 0.01% nasal spray
82
desmopressin acetate 0.01mg/act nasal spray
82
desmopressin acetate 0.1mg tab
82
desmopressin acetate 0.2mg tab
82
desogestrel/ethinyl estradiol pack
71
desonide 0.05% ointment 77
You can find information on what the symbols and abbreviations on this table mean by going to the beginning of this table.
124
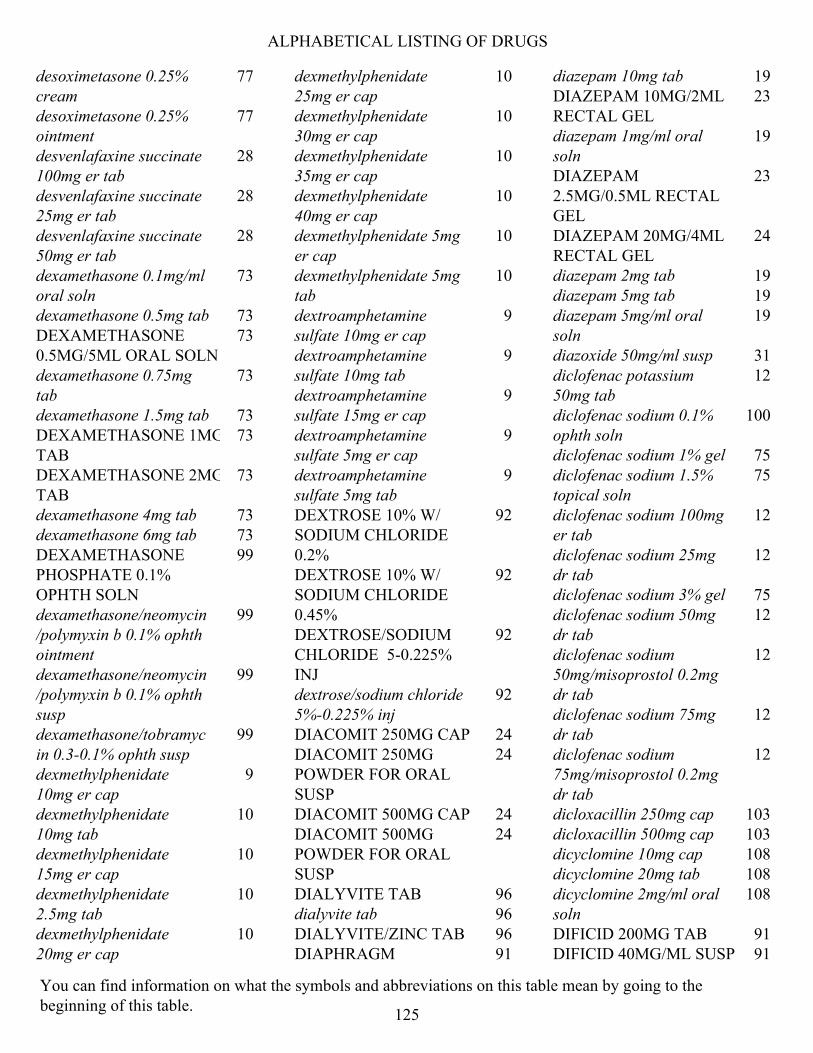
ALPHABETICAL LISTING OF DRUGS
desoximetasone 0.25% cream
77
desoximetasone 0.25% ointment
77
desvenlafaxine succinate 100mg er tab
28
desvenlafaxine succinate 25mg er tab
28
desvenlafaxine succinate 50mg er tab
28
dexamethasone 0.1mg/ml oral soln
73
dexamethasone 0.5mg tab 73 DEXAMETHASONE 0.5MG/5ML ORAL SOLN
73
dexamethasone 0.75mg tab
73
dexamethasone 1.5mg tab 73 DEXAMETHASONE 1MG TAB
73
DEXAMETHASONE 2MG TAB
73
dexamethasone 4mg tab 73 dexamethasone 6mg tab 73 DEXAMETHASONE PHOSPHATE 0.1% OPHTH SOLN
99
dexamethasone/neomycin/polymyxin b 0.1% ophth ointment
99
dexamethasone/neomycin/polymyxin b 0.1% ophth susp
99
dexamethasone/tobramycin 0.3-0.1% ophth susp
99
dexmethylphenidate 10mg er cap
9
dexmethylphenidate 10mg tab
10
dexmethylphenidate 15mg er cap
10
dexmethylphenidate 2.5mg tab
10
dexmethylphenidate 20mg er cap
10
dexmethylphenidate 25mg er cap
10
dexmethylphenidate 30mg er cap
10
dexmethylphenidate 35mg er cap
10
dexmethylphenidate 40mg er cap
10
dexmethylphenidate 5mg er cap
10
dexmethylphenidate 5mg tab
10
dextroamphetamine sulfate 10mg er cap
9
dextroamphetamine sulfate 10mg tab
9
dextroamphetamine sulfate 15mg er cap
9
dextroamphetamine sulfate 5mg er cap
9
dextroamphetamine sulfate 5mg tab
9
DEXTROSE 10% W/ SODIUM CHLORIDE 0.2%
92
DEXTROSE 10% W/ SODIUM CHLORIDE 0.45%
92
DEXTROSE/SODIUM CHLORIDE 5-0.225% INJ
92
dextrose/sodium chloride 5%-0.225% inj
92
DIACOMIT 250MG CAP 24 DIACOMIT 250MG POWDER FOR ORAL SUSP
24
DIACOMIT 500MG CAP 24 DIACOMIT 500MG POWDER FOR ORAL SUSP
24
DIALYVITE TAB 96 dialyvite tab 96 DIALYVITE/ZINC TAB 96 DIAPHRAGM 91
diazepam 10mg tab 19 DIAZEPAM 10MG/2ML RECTAL GEL
23
diazepam 1mg/ml oral soln
19
DIAZEPAM 2.5MG/0.5ML RECTAL GEL
23
DIAZEPAM 20MG/4ML RECTAL GEL
24
diazepam 2mg tab 19 diazepam 5mg tab 19 diazepam 5mg/ml oral soln
19
diazoxide 50mg/ml susp 31 diclofenac potassium 50mg tab
12
diclofenac sodium 0.1% ophth soln
100
diclofenac sodium 1% gel 75 diclofenac sodium 1.5% topical soln
75
diclofenac sodium 100mg er tab
12
diclofenac sodium 25mg dr tab
12
diclofenac sodium 3% gel 75 diclofenac sodium 50mg dr tab
12
diclofenac sodium 50mg/misoprostol 0.2mg dr tab
12
diclofenac sodium 75mg dr tab
12
diclofenac sodium 75mg/misoprostol 0.2mg dr tab
12
dicloxacillin 250mg cap 103 dicloxacillin 500mg cap 103 dicyclomine 10mg cap 108 dicyclomine 20mg tab 108 dicyclomine 2mg/ml oral soln
108
DIFICID 200MG TAB 91 DIFICID 40MG/ML SUSP 91
You can find information on what the symbols and abbreviations on this table mean by going to the beginning of this table.
125
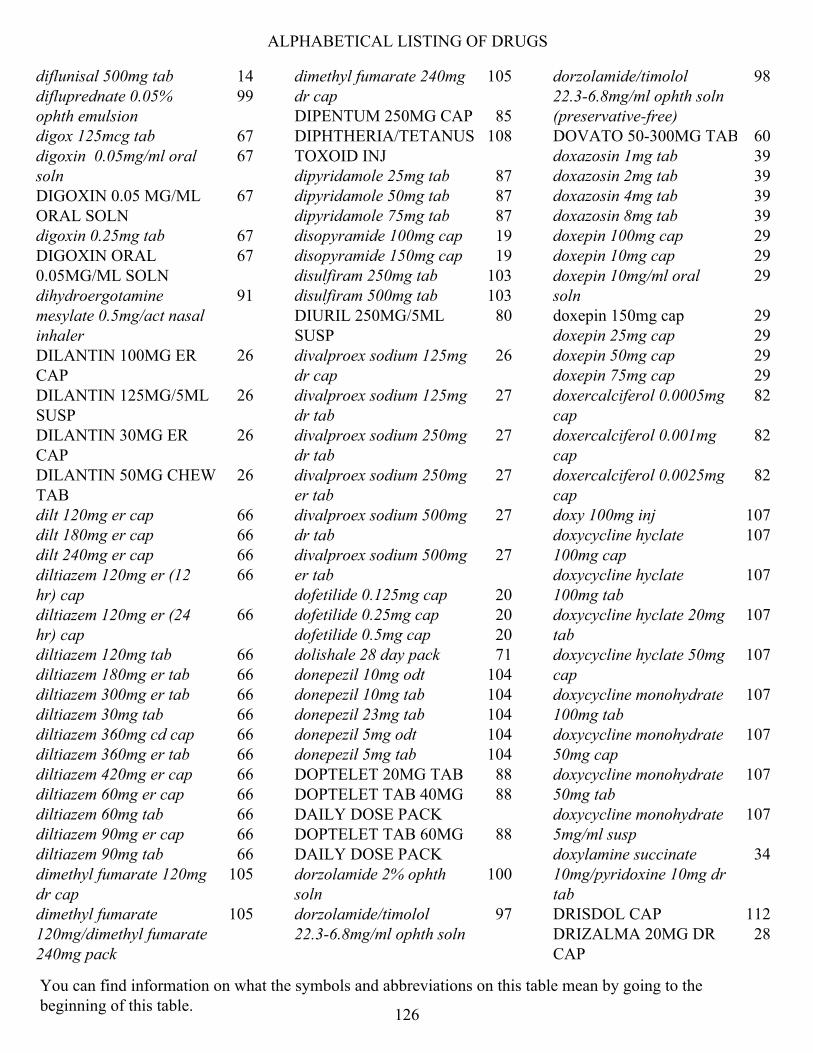
ALPHABETICAL LISTING OF DRUGS
diflunisal 500mg tab 14 difluprednate 0.05% ophth emulsion
99
digox 125mcg tab 67 digoxin 0.05mg/ml oral soln
67
DIGOXIN 0.05 MG/ML ORAL SOLN
67
digoxin 0.25mg tab 67 DIGOXIN ORAL 0.05MG/ML SOLN
67
dihydroergotamine mesylate 0.5mg/act nasal inhaler
91
DILANTIN 100MG ER CAP
26
DILANTIN 125MG/5ML SUSP
26
DILANTIN 30MG ER CAP
26
DILANTIN 50MG CHEW TAB
26
dilt 120mg er cap 66 dilt 180mg er cap 66 dilt 240mg er cap 66 diltiazem 120mg er (12 hr) cap
66
diltiazem 120mg er (24 hr) cap
66
diltiazem 120mg tab 66 diltiazem 180mg er tab 66 diltiazem 300mg er tab 66 diltiazem 30mg tab 66 diltiazem 360mg cd cap 66 diltiazem 360mg er tab 66 diltiazem 420mg er cap 66 diltiazem 60mg er cap 66 diltiazem 60mg tab 66 diltiazem 90mg er cap 66 diltiazem 90mg tab 66 dimethyl fumarate 120mg dr cap
105
dimethyl fumarate 120mg/dimethyl fumarate 240mg pack
105
dimethyl fumarate 240mg dr cap
105
DIPENTUM 250MG CAP 85 DIPHTHERIA/TETANUS TOXOID INJ
108
dipyridamole 25mg tab 87 dipyridamole 50mg tab 87 dipyridamole 75mg tab 87 disopyramide 100mg cap 19 disopyramide 150mg cap 19 disulfiram 250mg tab 103 disulfiram 500mg tab 103 DIURIL 250MG/5ML SUSP
80
divalproex sodium 125mg dr cap
26
divalproex sodium 125mg dr tab
27
divalproex sodium 250mg dr tab
27
divalproex sodium 250mg er tab
27
divalproex sodium 500mg dr tab
27
divalproex sodium 500mg er tab
27
dofetilide 0.125mg cap 20 dofetilide 0.25mg cap 20 dofetilide 0.5mg cap 20 dolishale 28 day pack 71 donepezil 10mg odt 104 donepezil 10mg tab 104 donepezil 23mg tab 104 donepezil 5mg odt 104 donepezil 5mg tab 104 DOPTELET 20MG TAB 88 DOPTELET TAB 40MG DAILY DOSE PACK
88
DOPTELET TAB 60MG DAILY DOSE PACK
88
dorzolamide 2% ophth soln
100
dorzolamide/timolol 22.3-6.8mg/ml ophth soln
97
dorzolamide/timolol 22.3-6.8mg/ml ophth soln (preservative-free)
98
DOVATO 50-300MG TAB 60 doxazosin 1mg tab 39 doxazosin 2mg tab 39 doxazosin 4mg tab 39 doxazosin 8mg tab 39 doxepin 100mg cap 29 doxepin 10mg cap 29 doxepin 10mg/ml oral soln
29
doxepin 150mg cap 29 doxepin 25mg cap 29 doxepin 50mg cap 29 doxepin 75mg cap 29 doxercalciferol 0.0005mg cap
82
doxercalciferol 0.001mg cap
82
doxercalciferol 0.0025mg cap
82
doxy 100mg inj 107 doxycycline hyclate 100mg cap
107
doxycycline hyclate 100mg tab
107
doxycycline hyclate 20mg tab
107
doxycycline hyclate 50mg cap
107
doxycycline monohydrate 100mg tab
107
doxycycline monohydrate 50mg cap
107
doxycycline monohydrate 50mg tab
107
doxycycline monohydrate 5mg/ml susp
107
doxylamine succinate 10mg/pyridoxine 10mg dr tab
34
DRISDOL CAP 112 DRIZALMA 20MG DR CAP
28
You can find information on what the symbols and abbreviations on this table mean by going to the beginning of this table.
126

ALPHABETICAL LISTING OF DRUGS
DRIZALMA 30MG DR CAP
28
DRIZALMA 40MG DR CAP
28
DRIZALMA 60MG DR CAP
28
dronabinol 10mg cap 34 dronabinol 2.5mg cap 34 dronabinol 5mg cap 34 DROXIA 200MG CAP 88 DROXIA 300MG CAP 88 DROXIA 400MG CAP 88 droxidopa 100mg cap 112 droxidopa 200mg cap 112 droxidopa 300mg cap 112 DRYSOL SOLN 78 DULERA 100-5MCG INHALER
21
DULERA 200-5MCG INHALER
21
DULERA 50-5MCG INHALER
21
duloxetine 20mg dr cap 28 duloxetine 30mg dr cap 28 duloxetine 60mg dr cap 28 DUPIXENT 200MG/1.14ML AUTO-INJECTOR
78
DUPIXENT 200MG/1.14ML SYRINGE
78
DUPIXENT 300MG/2ML AUTO-INJECTOR
78
DUPIXENT 300MG/2ML SYRINGE
78
dutasteride 0.5mg cap 86 dutasteride 0.5mg/tamsulosin 0.4mg cap
86
E
E.E.S. 400MG TAB 90 econazole nitrate 1% cream
75
EDEX 10MCG INJ KIT 68
EDEX 10MCG INJ KIT 68 EDEX 20MCG INJ KIT 68 EDEX 20MCG INJ KIT 68 EDEX 40MCG INJ KIT 68 EDEX INJ 68 EDURANT 25MG TAB 60 efavirenz 200mg cap 60 efavirenz 400mg/lamivudine 300mg/tenofovir disoproxil fumarate 300mg tab
60
efavirenz 50mg cap 60 efavirenz 600mg tab 60 efavirenz 600mg/emtricitabine 200mg/tenofovir disoproxil fumarate 300mg tab
60
efavirenz/lamivudine/tenofovir disoproxil fumarate 600-300-300mg tab
60
eletriptan 20mg tab 92 eletriptan 40mg tab 92 ELIGARD 22.5MG INJ 46 ELIGARD 30MG INJ 46 ELIGARD 45MG INJ 46 ELIGARD 7.5MG INJ 46 ELIQUIS 2.5MG TAB 22 ELIQUIS 5MG TAB 22 ELIQUIS 5MG TAB 30-DAY STARTER PACK
22
ELMIRON 100MG CAP 86 eluryng 0.120-0.015mg/24hr vaginal system
72
EMCYT 140MG CAP 46 EMGALITY 100MG/ML INJ
92
EMGALITY 120MG/ML AUTO-INJECTOR
91
EMGALITY 120MG/ML INJ
91
EMSAM 12MG/24HR PATCH
27
EMSAM 6MG/24HR PATCH
27
EMSAM 9MG/24HR PATCH
27
emtricitabine 100mg/tenofovir disoproxil fumarate 150mg tab
60
emtricitabine 200mg cap 60 emtricitabine 200mg/tenofovir disoproxil fumarate 300mg tab
60
emtricitabine/tenofovir disoproxil fumarate 133-200mg tab
60
emtricitabine/tenofovir disoproxil fumarate 167-250mg tab
60
EMTRIVA 10MG/ML ORAL SOLN
61
enalapril maleate 10mg tab
37
enalapril maleate 10mg/hydrochlorothiazide 25mg tab
40
enalapril maleate 2.5mg tab
37
enalapril maleate 20mg tab
37
enalapril maleate 5mg tab
37
enalapril maleate 5mg/hydrochlorothiazide 12.5mg tab
40
ENBREL 25MG INJ 13 ENBREL 25MG/0.5ML INJ
13
ENBREL 25MG/0.5ML SYRINGE
13
ENBREL 50MG/ML AUTO-INJECTOR
13
You can find information on what the symbols and abbreviations on this table mean by going to the beginning of this table.
127
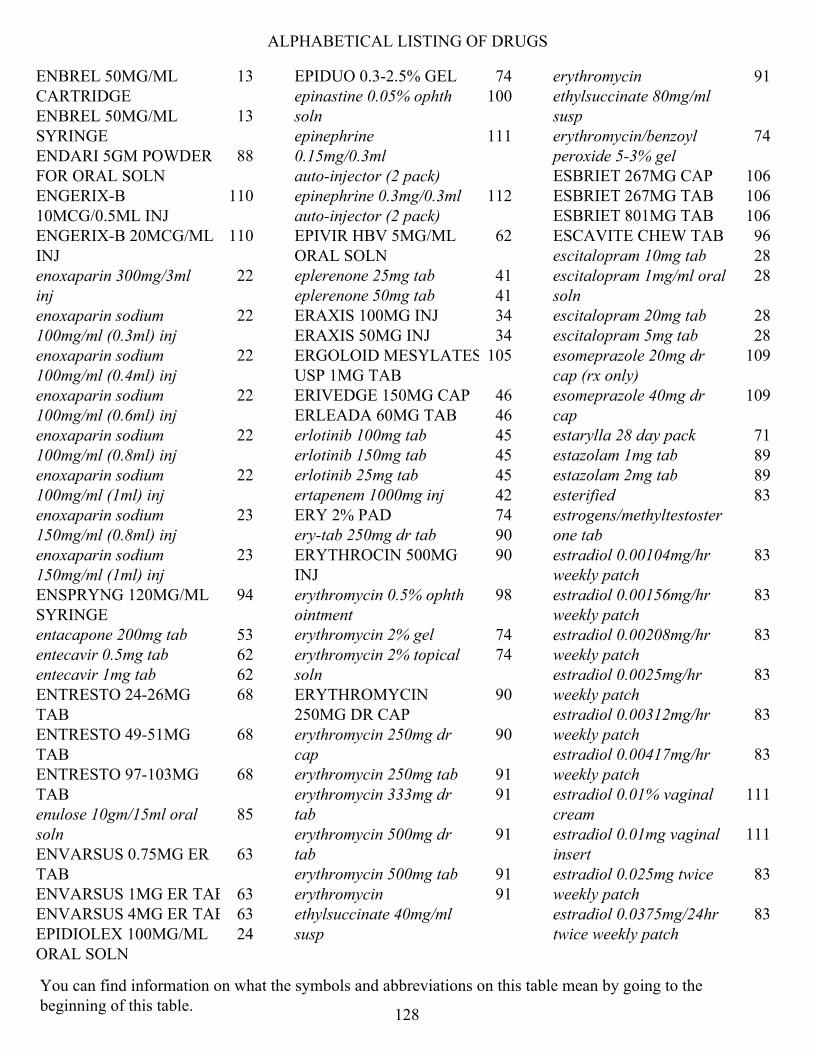
ALPHABETICAL LISTING OF DRUGS
ENBREL 50MG/ML CARTRIDGE
13
ENBREL 50MG/ML SYRINGE
13
ENDARI 5GM POWDER FOR ORAL SOLN
88
ENGERIX-B 10MCG/0.5ML INJ
110
ENGERIX-B 20MCG/ML INJ
110
enoxaparin 300mg/3ml inj
22
enoxaparin sodium 100mg/ml (0.3ml) inj
22
enoxaparin sodium 100mg/ml (0.4ml) inj
22
enoxaparin sodium 100mg/ml (0.6ml) inj
22
enoxaparin sodium 100mg/ml (0.8ml) inj
22
enoxaparin sodium 100mg/ml (1ml) inj
22
enoxaparin sodium 150mg/ml (0.8ml) inj
23
enoxaparin sodium 150mg/ml (1ml) inj
23
ENSPRYNG 120MG/ML SYRINGE
94
entacapone 200mg tab 53 entecavir 0.5mg tab 62 entecavir 1mg tab 62 ENTRESTO 24-26MG TAB
68
ENTRESTO 49-51MG TAB
68
ENTRESTO 97-103MG TAB
68
enulose 10gm/15ml oral soln
85
ENVARSUS 0.75MG ER TAB
63
ENVARSUS 1MG ER TAB 63 ENVARSUS 4MG ER TAB 63 EPIDIOLEX 100MG/ML ORAL SOLN
24
EPIDUO 0.3-2.5% GEL 74 epinastine 0.05% ophth soln
100
epinephrine 0.15mg/0.3ml auto-injector (2 pack)
111
epinephrine 0.3mg/0.3ml auto-injector (2 pack)
112
EPIVIR HBV 5MG/ML ORAL SOLN
62
eplerenone 25mg tab 41 eplerenone 50mg tab 41 ERAXIS 100MG INJ 34 ERAXIS 50MG INJ 34 ERGOLOID MESYLATES USP 1MG TAB
105
ERIVEDGE 150MG CAP 46 ERLEADA 60MG TAB 46 erlotinib 100mg tab 45 erlotinib 150mg tab 45 erlotinib 25mg tab 45 ertapenem 1000mg inj 42 ERY 2% PAD 74 ery-tab 250mg dr tab 90 ERYTHROCIN 500MG INJ
90
erythromycin 0.5% ophth ointment
98
erythromycin 2% gel 74 erythromycin 2% topical soln
74
ERYTHROMYCIN 250MG DR CAP
90
erythromycin 250mg dr cap
90
erythromycin 250mg tab 91 erythromycin 333mg dr tab
91
erythromycin 500mg dr tab
91
erythromycin 500mg tab 91 erythromycin ethylsuccinate 40mg/ml susp
91
erythromycin ethylsuccinate 80mg/ml susp
91
erythromycin/benzoyl peroxide 5-3% gel
74
ESBRIET 267MG CAP 106 ESBRIET 267MG TAB 106 ESBRIET 801MG TAB 106 ESCAVITE CHEW TAB 96 escitalopram 10mg tab 28 escitalopram 1mg/ml oral soln
28
escitalopram 20mg tab 28 escitalopram 5mg tab 28 esomeprazole 20mg dr cap (rx only)
109
esomeprazole 40mg dr cap
109
estarylla 28 day pack 71 estazolam 1mg tab 89 estazolam 2mg tab 89 esterified estrogens/methyltestosterone tab
83
estradiol 0.00104mg/hr weekly patch
83
estradiol 0.00156mg/hr weekly patch
83
estradiol 0.00208mg/hr weekly patch
83
estradiol 0.0025mg/hr weekly patch
83
estradiol 0.00312mg/hr weekly patch
83
estradiol 0.00417mg/hr weekly patch
83
estradiol 0.01% vaginal cream
111
estradiol 0.01mg vaginal insert
111
estradiol 0.025mg twice weekly patch
83
estradiol 0.0375mg/24hr twice weekly patch
83
You can find information on what the symbols and abbreviations on this table mean by going to the beginning of this table.
128
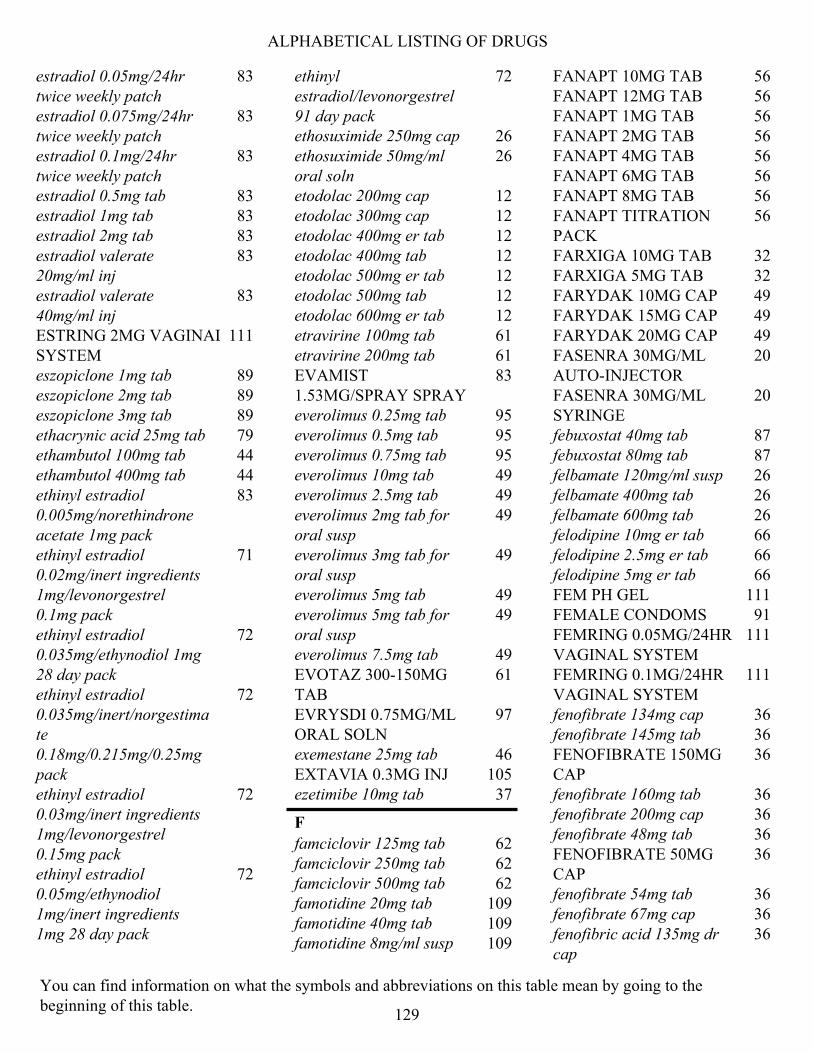
ALPHABETICAL LISTING OF DRUGS
estradiol 0.05mg/24hr twice weekly patch
83
estradiol 0.075mg/24hr twice weekly patch
83
estradiol 0.1mg/24hr twice weekly patch
83
estradiol 0.5mg tab 83 estradiol 1mg tab 83 estradiol 2mg tab 83 estradiol valerate 20mg/ml inj
83
estradiol valerate 40mg/ml inj
83
ESTRING 2MG VAGINAL SYSTEM
111
eszopiclone 1mg tab 89 eszopiclone 2mg tab 89 eszopiclone 3mg tab 89 ethacrynic acid 25mg tab 79 ethambutol 100mg tab 44 ethambutol 400mg tab 44 ethinyl estradiol 0.005mg/norethindrone acetate 1mg pack
83
ethinyl estradiol 0.02mg/inert ingredients 1mg/levonorgestrel 0.1mg pack
71
ethinyl estradiol 0.035mg/ethynodiol 1mg 28 day pack
72
ethinyl estradiol 0.035mg/inert/norgestimate 0.18mg/0.215mg/0.25mg pack
72
ethinyl estradiol 0.03mg/inert ingredients 1mg/levonorgestrel 0.15mg pack
72
ethinyl estradiol 0.05mg/ethynodiol 1mg/inert ingredients 1mg 28 day pack
72
ethinyl estradiol/levonorgestrel 91 day pack
72
ethosuximide 250mg cap 26 ethosuximide 50mg/ml oral soln
26
etodolac 200mg cap 12 etodolac 300mg cap 12 etodolac 400mg er tab 12 etodolac 400mg tab 12 etodolac 500mg er tab 12 etodolac 500mg tab 12 etodolac 600mg er tab 12 etravirine 100mg tab 61 etravirine 200mg tab 61 EVAMIST 1.53MG/SPRAY SPRAY
83
everolimus 0.25mg tab 95 everolimus 0.5mg tab 95 everolimus 0.75mg tab 95 everolimus 10mg tab 49 everolimus 2.5mg tab 49 everolimus 2mg tab for oral susp
49
everolimus 3mg tab for oral susp
49
everolimus 5mg tab 49 everolimus 5mg tab for oral susp
49
everolimus 7.5mg tab 49 EVOTAZ 300-150MG TAB
61
EVRYSDI 0.75MG/ML ORAL SOLN
97
exemestane 25mg tab 46 EXTAVIA 0.3MG INJ 105 ezetimibe 10mg tab 37
F
famciclovir 125mg tab 62 famciclovir 250mg tab 62 famciclovir 500mg tab 62 famotidine 20mg tab 109 famotidine 40mg tab 109 famotidine 8mg/ml susp 109
FANAPT 10MG TAB 56 FANAPT 12MG TAB 56 FANAPT 1MG TAB 56 FANAPT 2MG TAB 56 FANAPT 4MG TAB 56 FANAPT 6MG TAB 56 FANAPT 8MG TAB 56 FANAPT TITRATION PACK
56
FARXIGA 10MG TAB 32 FARXIGA 5MG TAB 32 FARYDAK 10MG CAP 49 FARYDAK 15MG CAP 49 FARYDAK 20MG CAP 49 FASENRA 30MG/ML AUTO-INJECTOR
20
FASENRA 30MG/ML SYRINGE
20
febuxostat 40mg tab 87 febuxostat 80mg tab 87 felbamate 120mg/ml susp 26 felbamate 400mg tab 26 felbamate 600mg tab 26 felodipine 10mg er tab 66 felodipine 2.5mg er tab 66 felodipine 5mg er tab 66 FEM PH GEL 111 FEMALE CONDOMS 91 FEMRING 0.05MG/24HR VAGINAL SYSTEM
111
FEMRING 0.1MG/24HR VAGINAL SYSTEM
111
fenofibrate 134mg cap 36 fenofibrate 145mg tab 36 FENOFIBRATE 150MG CAP
36
fenofibrate 160mg tab 36 fenofibrate 200mg cap 36 fenofibrate 48mg tab 36 FENOFIBRATE 50MG CAP
36
fenofibrate 54mg tab 36 fenofibrate 67mg cap 36 fenofibric acid 135mg dr cap
36
You can find information on what the symbols and abbreviations on this table mean by going to the beginning of this table.
129
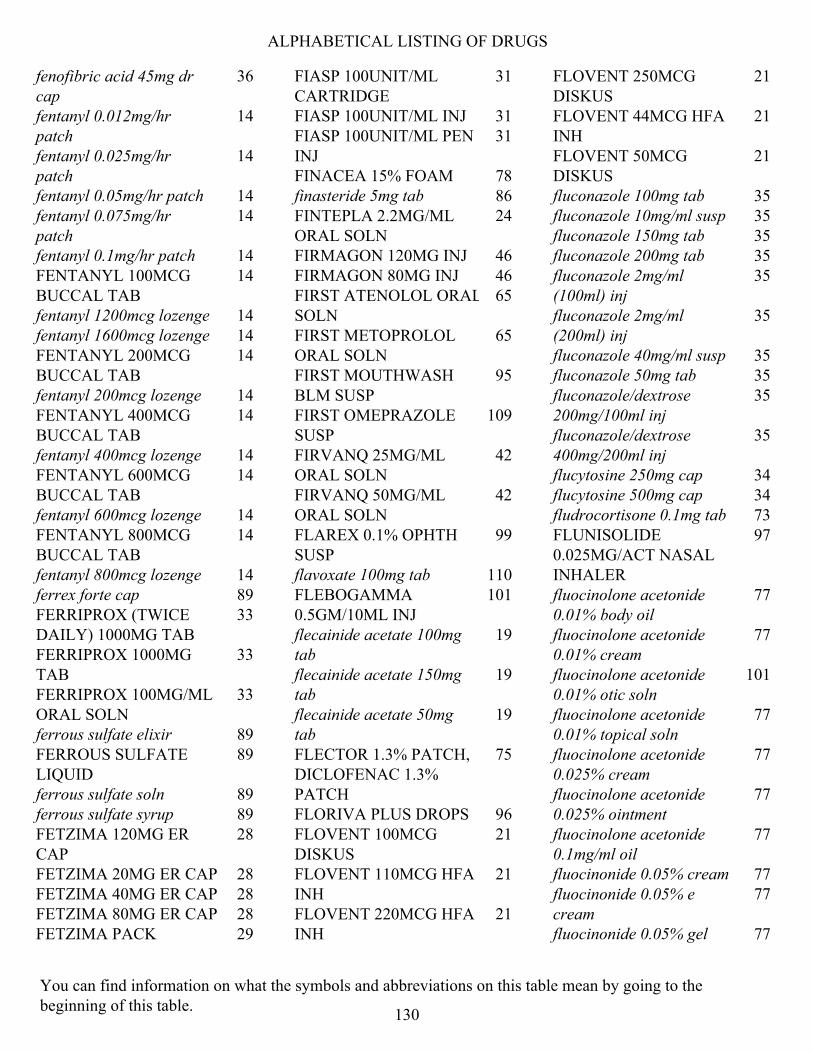
ALPHABETICAL LISTING OF DRUGS
fenofibric acid 45mg dr cap
36
fentanyl 0.012mg/hr patch
14
fentanyl 0.025mg/hr patch
14
fentanyl 0.05mg/hr patch 14 fentanyl 0.075mg/hr patch
14
fentanyl 0.1mg/hr patch 14 FENTANYL 100MCG BUCCAL TAB
14
fentanyl 1200mcg lozenge 14 fentanyl 1600mcg lozenge 14 FENTANYL 200MCG BUCCAL TAB
14
fentanyl 200mcg lozenge 14 FENTANYL 400MCG BUCCAL TAB
14
fentanyl 400mcg lozenge 14 FENTANYL 600MCG BUCCAL TAB
14
fentanyl 600mcg lozenge 14 FENTANYL 800MCG BUCCAL TAB
14
fentanyl 800mcg lozenge 14 ferrex forte cap 89 FERRIPROX (TWICE DAILY) 1000MG TAB
33
FERRIPROX 1000MG TAB
33
FERRIPROX 100MG/ML ORAL SOLN
33
ferrous sulfate elixir 89 FERROUS SULFATE LIQUID
89
ferrous sulfate soln 89 ferrous sulfate syrup 89 FETZIMA 120MG ER CAP
28
FETZIMA 20MG ER CAP 28 FETZIMA 40MG ER CAP 28 FETZIMA 80MG ER CAP 28 FETZIMA PACK 29
FIASP 100UNIT/ML CARTRIDGE
31
FIASP 100UNIT/ML INJ 31 FIASP 100UNIT/ML PEN INJ
31
FINACEA 15% FOAM 78 finasteride 5mg tab 86 FINTEPLA 2.2MG/ML ORAL SOLN
24
FIRMAGON 120MG INJ 46 FIRMAGON 80MG INJ 46 FIRST ATENOLOL ORAL SOLN
65
FIRST METOPROLOL ORAL SOLN
65
FIRST MOUTHWASH BLM SUSP
95
FIRST OMEPRAZOLE SUSP
109
FIRVANQ 25MG/ML ORAL SOLN
42
FIRVANQ 50MG/ML ORAL SOLN
42
FLAREX 0.1% OPHTH SUSP
99
flavoxate 100mg tab 110 FLEBOGAMMA 0.5GM/10ML INJ
101
flecainide acetate 100mg tab
19
flecainide acetate 150mg tab
19
flecainide acetate 50mg tab
19
FLECTOR 1.3% PATCH, DICLOFENAC 1.3% PATCH
75
FLORIVA PLUS DROPS 96 FLOVENT 100MCG DISKUS
21
FLOVENT 110MCG HFA INH
21
FLOVENT 220MCG HFA INH
21
FLOVENT 250MCG DISKUS
21
FLOVENT 44MCG HFA INH
21
FLOVENT 50MCG DISKUS
21
fluconazole 100mg tab 35 fluconazole 10mg/ml susp 35 fluconazole 150mg tab 35 fluconazole 200mg tab 35 fluconazole 2mg/ml (100ml) inj
35
fluconazole 2mg/ml (200ml) inj
35
fluconazole 40mg/ml susp 35 fluconazole 50mg tab 35 fluconazole/dextrose 200mg/100ml inj
35
fluconazole/dextrose 400mg/200ml inj
35
flucytosine 250mg cap 34 flucytosine 500mg cap 34 fludrocortisone 0.1mg tab 73 FLUNISOLIDE 0.025MG/ACT NASAL INHALER
97
fluocinolone acetonide 0.01% body oil
77
fluocinolone acetonide 0.01% cream
77
fluocinolone acetonide 0.01% otic soln
101
fluocinolone acetonide 0.01% topical soln
77
fluocinolone acetonide 0.025% cream
77
fluocinolone acetonide 0.025% ointment
77
fluocinolone acetonide 0.1mg/ml oil
77
fluocinonide 0.05% cream 77 fluocinonide 0.05% e cream
77
fluocinonide 0.05% gel 77
You can find information on what the symbols and abbreviations on this table mean by going to the beginning of this table.
130

ALPHABETICAL LISTING OF DRUGS
fluocinonide 0.05% ointment
77
fluocinonide 0.05% topical soln
77
fluocinonide 0.1% cream 77 FLUORABON SOLN 93 fluorometholone 0.1% ophth susp
99
FLUOROURACIL 2% TOPICAL SOLN
75
fluorouracil 5% cream 75 FLUOROURACIL 5% TOPICAL SOLN
75
fluoxetine 10mg cap 28 fluoxetine 20mg cap 28 fluoxetine 40mg cap 28 fluoxetine 4mg/ml oral soln
28
FLUPHENAZINE 0.5MG/ML ORAL SOLN
59
fluphenazine 10mg tab 59 fluphenazine 1mg tab 59 fluphenazine 2.5mg tab 59 FLUPHENAZINE 2.5MG/ML INJ
59
fluphenazine 5mg tab 59 FLUPHENAZINE 5MG/ML ORAL SOLN
59
fluphenazine decanoate 25mg/ml inj
59
FLURAZEPAM 15MG CAP
89
FLURAZEPAM 30MG CAP
89
flurbiprofen 100mg tab 12 FLURBIPROFEN SODIUM 0.03% OPHTH SOLN
100
flutamide 125mg cap 46 FLUTAMIDE 125MG CAP
46
fluticasone propionate 0.005% ointment
77
fluticasone propionate 0.05% cream
77
fluticasone propionate 0.05mg/act nasal inhaler
97
fluticasone propionate/salmeterol 100-50mcg/act dry powder inhaler, wixela 100-50mcg inhaler
21
fluticasone propionate/salmeterol 250-50mcg/act dry powder inhaler, wixela 250-50mcg inhaler
21
fluticasone propionate/salmeterol 500-50mcg/act dry powder inhaler, wixela 500-50mcg inhaler
21
fluvastatin 20mg cap 36 fluvastatin 40mg cap 36 fluvastatin 80mg er tab 36 fluvoxamine maleate 100mg tab
28
fluvoxamine maleate 25mg tab
28
fluvoxamine maleate 50mg tab
28
FML 0.1% OPHTH OINTMENT
99
FML FORTE LIQUIFILM 0.25% OPHTH SUSP
99
FOLBEE PLUS CZ TAB 96 folbee tab 89 folic acid tab (OTC) 88 fondaparinux sodium 12.5mg/ml (0.4ml) inj
23
fondaparinux sodium 12.5mg/ml (0.6ml) inj
23
fondaparinux sodium 12.5mg/ml (0.8ml) inj
23
fondaparinux sodium 5mg/ml (0.5mg) inj
23
formoterol fumarate 20mcg/2ml neb soln
21
FORTEO 600MCG/2.4ML PEN INJ
80
fosamprenavir 700mg tab 61 fosfomycin 3000mg powder for oral soln
43
fosinopril sodium 10mg tab
37
fosinopril sodium 10mg/hydrochlorothiazide 12.5mg tab
40
fosinopril sodium 20mg tab
37
fosinopril sodium 20mg/hydrochlorothiazide 12.5mg tab
40
fosinopril sodium 40mg tab
37
FOSRENOL 1000MG ORAL POWDER
85
FOSRENOL 750MG ORAL POWDER
85
FOTIVDA 0.89MG CAP 49 FOTIVDA 1.34MG CAP 49 FRAGMIN 10000UNIT/ML INJ
23
FRAGMIN 12500UNIT/0.5ML INJ
23
FRAGMIN 15000UNIT/0.6ML INJ
23
FRAGMIN 18000UNT/0.72ML INJ
23
FRAGMIN 2500UNIT/0.2ML INJ
23
FRAGMIN 5000UNIT/0.2ML INJ
23
FRAGMIN 7500UNIT/0.3ML INJ
23
FRAGMIN 95000UNIT/3.8ML INJ
23
FREAMINE HBC 6.9% INJ
97
FREESTYLE LITE METER
91
FREESTYLE LITE METER
91
FULPHILA 6MG/0.6ML SYRINGE
88
You can find information on what the symbols and abbreviations on this table mean by going to the beginning of this table.
131
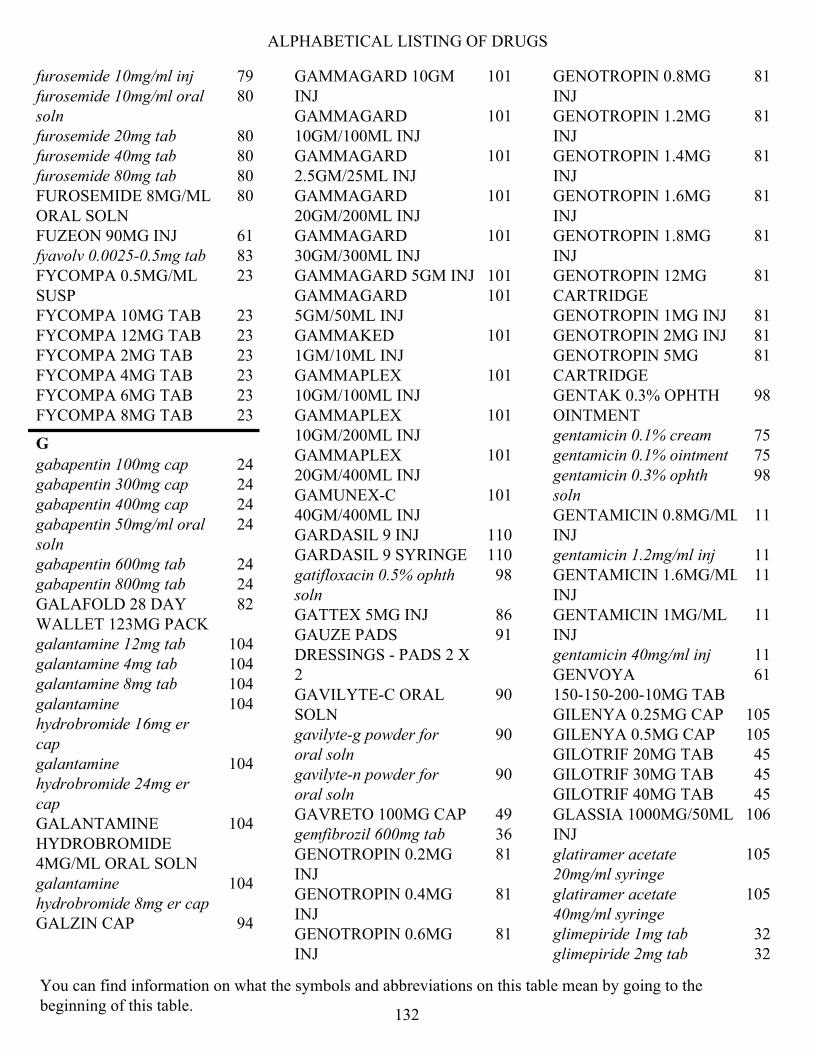
ALPHABETICAL LISTING OF DRUGS
furosemide 10mg/ml inj 79 furosemide 10mg/ml oral soln
80
furosemide 20mg tab 80 furosemide 40mg tab 80 furosemide 80mg tab 80 FUROSEMIDE 8MG/ML ORAL SOLN
80
FUZEON 90MG INJ 61 fyavolv 0.0025-0.5mg tab 83 FYCOMPA 0.5MG/ML SUSP
23
FYCOMPA 10MG TAB 23 FYCOMPA 12MG TAB 23 FYCOMPA 2MG TAB 23 FYCOMPA 4MG TAB 23 FYCOMPA 6MG TAB 23 FYCOMPA 8MG TAB 23
G
gabapentin 100mg cap 24 gabapentin 300mg cap 24 gabapentin 400mg cap 24 gabapentin 50mg/ml oral soln
24
gabapentin 600mg tab 24 gabapentin 800mg tab 24 GALAFOLD 28 DAY WALLET 123MG PACK
82
galantamine 12mg tab 104 galantamine 4mg tab 104 galantamine 8mg tab 104 galantamine hydrobromide 16mg er cap
104
galantamine hydrobromide 24mg er cap
104
GALANTAMINE HYDROBROMIDE 4MG/ML ORAL SOLN
104
galantamine hydrobromide 8mg er cap
104
GALZIN CAP 94
GAMMAGARD 10GM INJ
101
GAMMAGARD 10GM/100ML INJ
101
GAMMAGARD 2.5GM/25ML INJ
101
GAMMAGARD 20GM/200ML INJ
101
GAMMAGARD 30GM/300ML INJ
101
GAMMAGARD 5GM INJ 101 GAMMAGARD 5GM/50ML INJ
101
GAMMAKED 1GM/10ML INJ
101
GAMMAPLEX 10GM/100ML INJ
101
GAMMAPLEX 10GM/200ML INJ
101
GAMMAPLEX 20GM/400ML INJ
101
GAMUNEX-C 40GM/400ML INJ
101
GARDASIL 9 INJ 110 GARDASIL 9 SYRINGE 110 gatifloxacin 0.5% ophth soln
98
GATTEX 5MG INJ 86 GAUZE PADS DRESSINGS - PADS 2 X 2
91
GAVILYTE-C ORAL SOLN
90
gavilyte-g powder for oral soln
90
gavilyte-n powder for oral soln
90
GAVRETO 100MG CAP 49 gemfibrozil 600mg tab 36 GENOTROPIN 0.2MG INJ
81
GENOTROPIN 0.4MG INJ
81
GENOTROPIN 0.6MG INJ
81
GENOTROPIN 0.8MG INJ
81
GENOTROPIN 1.2MG INJ
81
GENOTROPIN 1.4MG INJ
81
GENOTROPIN 1.6MG INJ
81
GENOTROPIN 1.8MG INJ
81
GENOTROPIN 12MG CARTRIDGE
81
GENOTROPIN 1MG INJ 81 GENOTROPIN 2MG INJ 81 GENOTROPIN 5MG CARTRIDGE
81
GENTAK 0.3% OPHTH OINTMENT
98
gentamicin 0.1% cream 75 gentamicin 0.1% ointment 75 gentamicin 0.3% ophth soln
98
GENTAMICIN 0.8MG/ML INJ
11
gentamicin 1.2mg/ml inj 11 GENTAMICIN 1.6MG/ML INJ
11
GENTAMICIN 1MG/ML INJ
11
gentamicin 40mg/ml inj 11 GENVOYA 150-150-200-10MG TAB
61
GILENYA 0.25MG CAP 105 GILENYA 0.5MG CAP 105 GILOTRIF 20MG TAB 45 GILOTRIF 30MG TAB 45 GILOTRIF 40MG TAB 45 GLASSIA 1000MG/50ML INJ
106
glatiramer acetate 20mg/ml syringe
105
glatiramer acetate 40mg/ml syringe
105
glimepiride 1mg tab 32 glimepiride 2mg tab 32
You can find information on what the symbols and abbreviations on this table mean by going to the beginning of this table.
132
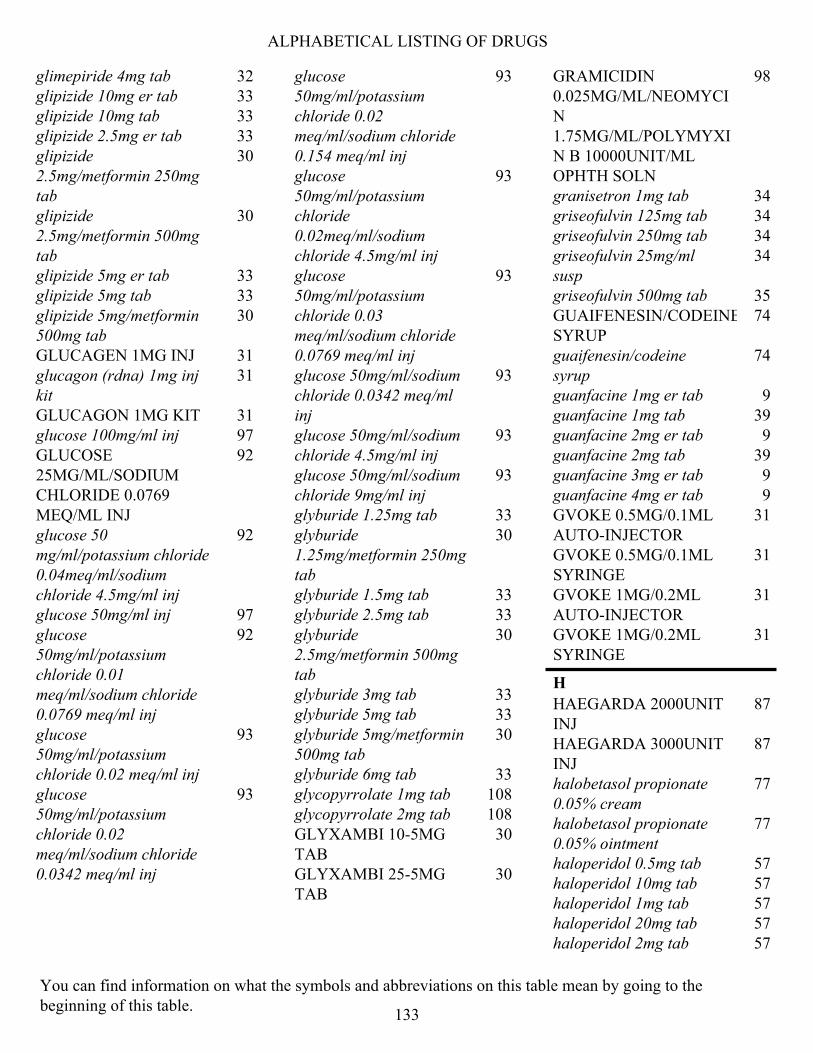
ALPHABETICAL LISTING OF DRUGS
glimepiride 4mg tab 32 glipizide 10mg er tab 33 glipizide 10mg tab 33 glipizide 2.5mg er tab 33 glipizide 2.5mg/metformin 250mg tab
30
glipizide 2.5mg/metformin 500mg tab
30
glipizide 5mg er tab 33 glipizide 5mg tab 33 glipizide 5mg/metformin 500mg tab
30
GLUCAGEN 1MG INJ 31 glucagon (rdna) 1mg inj kit
31
GLUCAGON 1MG KIT 31 glucose 100mg/ml inj 97 GLUCOSE 25MG/ML/SODIUM CHLORIDE 0.0769 MEQ/ML INJ
92
glucose 50 mg/ml/potassium chloride 0.04meq/ml/sodium chloride 4.5mg/ml inj
92
glucose 50mg/ml inj 97 glucose 50mg/ml/potassium chloride 0.01 meq/ml/sodium chloride 0.0769 meq/ml inj
92
glucose 50mg/ml/potassium chloride 0.02 meq/ml inj
93
glucose 50mg/ml/potassium chloride 0.02 meq/ml/sodium chloride 0.0342 meq/ml inj
93
glucose 50mg/ml/potassium chloride 0.02 meq/ml/sodium chloride 0.154 meq/ml inj
93
glucose 50mg/ml/potassium chloride 0.02meq/ml/sodium chloride 4.5mg/ml inj
93
glucose 50mg/ml/potassium chloride 0.03 meq/ml/sodium chloride 0.0769 meq/ml inj
93
glucose 50mg/ml/sodium chloride 0.0342 meq/ml inj
93
glucose 50mg/ml/sodium chloride 4.5mg/ml inj
93
glucose 50mg/ml/sodium chloride 9mg/ml inj
93
glyburide 1.25mg tab 33 glyburide 1.25mg/metformin 250mg tab
30
glyburide 1.5mg tab 33 glyburide 2.5mg tab 33 glyburide 2.5mg/metformin 500mg tab
30
glyburide 3mg tab 33 glyburide 5mg tab 33 glyburide 5mg/metformin 500mg tab
30
glyburide 6mg tab 33 glycopyrrolate 1mg tab 108 glycopyrrolate 2mg tab 108 GLYXAMBI 10-5MG TAB
30
GLYXAMBI 25-5MG TAB
30
GRAMICIDIN 0.025MG/ML/NEOMYCIN 1.75MG/ML/POLYMYXIN B 10000UNIT/ML OPHTH SOLN
98
granisetron 1mg tab 34 griseofulvin 125mg tab 34 griseofulvin 250mg tab 34 griseofulvin 25mg/ml susp
34
griseofulvin 500mg tab 35 GUAIFENESIN/CODEINE SYRUP
74
guaifenesin/codeine syrup
74
guanfacine 1mg er tab 9 guanfacine 1mg tab 39 guanfacine 2mg er tab 9 guanfacine 2mg tab 39 guanfacine 3mg er tab 9 guanfacine 4mg er tab 9 GVOKE 0.5MG/0.1ML AUTO-INJECTOR
31
GVOKE 0.5MG/0.1ML SYRINGE
31
GVOKE 1MG/0.2ML AUTO-INJECTOR
31
GVOKE 1MG/0.2ML SYRINGE
31
H
HAEGARDA 2000UNIT INJ
87
HAEGARDA 3000UNIT INJ
87
halobetasol propionate 0.05% cream
77
halobetasol propionate 0.05% ointment
77
haloperidol 0.5mg tab 57 haloperidol 10mg tab 57 haloperidol 1mg tab 57 haloperidol 20mg tab 57 haloperidol 2mg tab 57
You can find information on what the symbols and abbreviations on this table mean by going to the beginning of this table.
133

ALPHABETICAL LISTING OF DRUGS
haloperidol 2mg/ml oral soln
57
haloperidol 5mg tab 57 haloperidol 5mg/ml inj 57 haloperidol decanoate 100mg/ml inj
57
haloperidol decanoate 50mg/ml inj
57
HAVRIX 1440ELU/ML INJ
110
HAVRIX 720ELU/0.5ML INJ
110
heparin sodium 5000unit/0.5ml inj (PF)
23
heparin sodium porcine 10000unit/ml inj
23
heparin sodium porcine 1000unit/ml inj
23
heparin sodium porcine 20000unit/ml inj
23
heparin sodium porcine 5000unit/ml inj
23
HEPATAMINE 8% INJ 97 HETLIOZ 20MG CAP 89 HETLIOZ 4MG/ML SUSP 90 HIBERIX 10MCG INJ 110 homatropine ophth soln 98 HOMATROPINE OPHTH SOLN
98
HUMIRA 10MG/0.1ML SYRINGE
11
HUMIRA 10MG/0.2ML SYRINGE
11
HUMIRA 20MG/0.2ML SYRINGE
11
HUMIRA 20MG/0.4ML SYRINGE
11
HUMIRA 40MG/0.4ML AUTO-INJECTOR
11
HUMIRA 40MG/0.4ML SYRINGE
11
HUMIRA 40MG/0.8ML AUTO-INJECTOR
11
HUMIRA 40MG/0.8ML SYRINGE
11
HUMIRA 80MG/0.8ML AUTO-INJECTOR
11
HUMIRA PEDIATRIC CROHN'S STARTER PACK (3) 80MG/0.8ML SYRINGE
11
HUMIRA PEDIATRIC CROHN'S STARTER PACK SYRINGE (2) 40MG/0.4ML, 80MG/0.8ML
11
HUMIRA PEN - CROHN'S STARTER PACK 40MG/0.8ML INJ
11
HUMIRA PEN - PEDIATRIC UC STARTER PACK 80MG/0.8ML INJ
11
HUMIRA PEN - PSORIASIS STARTER PACK 40MG/0.8ML
12
HUMIRA PEN - PSORIASIS STARTER PACK 80MG/0.8ML INJ
12
HUMIRA PEN 80MG/0.8ML - STARTER PACK FOR CROHN'S DISEASE ULCERATIVE COLITIS OR HIDRADENITIS SUPPURAT
12
HUMULIN R 500UNIT/ML INJ
32
HUMULIN R 500UNIT/ML PEN INJ
32
HYCODAN SYRUP 73 hydralazine 100mg tab 41 hydralazine 10mg tab 41 hydralazine 25mg tab 41 hydralazine 50mg tab 41 hydrochlorothiazide 12.5mg cap
80
hydrochlorothiazide 12.5mg tab
80
hydrochlorothiazide 12.5mg/irbesartan 150mg tab
40
hydrochlorothiazide 12.5mg/irbesartan 300mg tab
40
hydrochlorothiazide 12.5mg/lisinopril 10mg tab
40
hydrochlorothiazide 12.5mg/lisinopril 20mg tab
40
hydrochlorothiazide 12.5mg/losartan potassium 100mg tab
40
hydrochlorothiazide 12.5mg/losartan potassium 50mg tab
40
hydrochlorothiazide 12.5mg/olmesartan medoxomil 20mg tab
40
hydrochlorothiazide 12.5mg/olmesartan medoxomil 40mg tab
40
hydrochlorothiazide 12.5mg/quinapril 10mg tab
40
hydrochlorothiazide 12.5mg/quinapril 20mg tab
40
hydrochlorothiazide 12.5mg/valsartan 160mg tab
40
hydrochlorothiazide 12.5mg/valsartan 320mg tab
40
hydrochlorothiazide 12.5mg/valsartan 80mg tab
40
hydrochlorothiazide 25mg tab
80
hydrochlorothiazide 25mg/lisinopril 20mg tab
40
You can find information on what the symbols and abbreviations on this table mean by going to the beginning of this table.
134
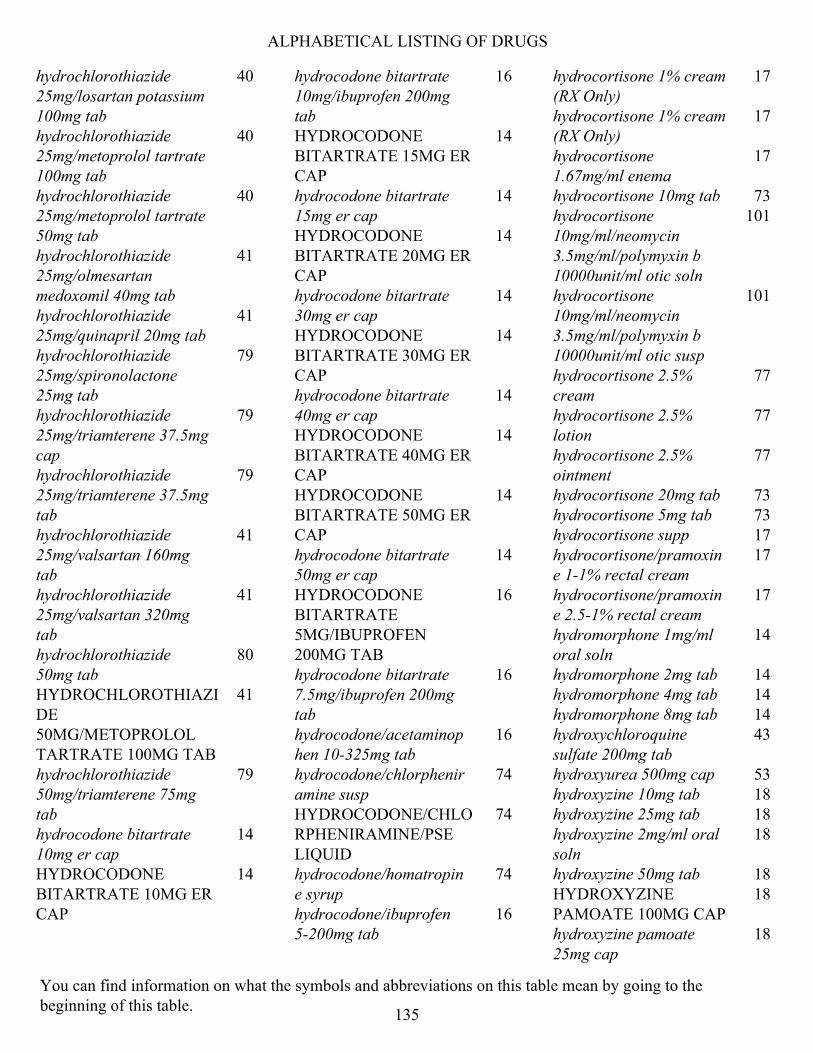
ALPHABETICAL LISTING OF DRUGS
hydrochlorothiazide 25mg/losartan potassium 100mg tab
40
hydrochlorothiazide 25mg/metoprolol tartrate 100mg tab
40
hydrochlorothiazide 25mg/metoprolol tartrate 50mg tab
40
hydrochlorothiazide 25mg/olmesartan medoxomil 40mg tab
41
hydrochlorothiazide 25mg/quinapril 20mg tab
41
hydrochlorothiazide 25mg/spironolactone 25mg tab
79
hydrochlorothiazide 25mg/triamterene 37.5mg cap
79
hydrochlorothiazide 25mg/triamterene 37.5mg tab
79
hydrochlorothiazide 25mg/valsartan 160mg tab
41
hydrochlorothiazide 25mg/valsartan 320mg tab
41
hydrochlorothiazide 50mg tab
80
HYDROCHLOROTHIAZIDE 50MG/METOPROLOL TARTRATE 100MG TAB
41
hydrochlorothiazide 50mg/triamterene 75mg tab
79
hydrocodone bitartrate 10mg er cap
14
HYDROCODONE BITARTRATE 10MG ER CAP
14
hydrocodone bitartrate 10mg/ibuprofen 200mg tab
16
HYDROCODONE BITARTRATE 15MG ER CAP
14
hydrocodone bitartrate 15mg er cap
14
HYDROCODONE BITARTRATE 20MG ER CAP
14
hydrocodone bitartrate 30mg er cap
14
HYDROCODONE BITARTRATE 30MG ER CAP
14
hydrocodone bitartrate 40mg er cap
14
HYDROCODONE BITARTRATE 40MG ER CAP
14
HYDROCODONE BITARTRATE 50MG ER CAP
14
hydrocodone bitartrate 50mg er cap
14
HYDROCODONE BITARTRATE 5MG/IBUPROFEN 200MG TAB
16
hydrocodone bitartrate 7.5mg/ibuprofen 200mg tab
16
hydrocodone/acetaminophen 10-325mg tab
16
hydrocodone/chlorpheniramine susp
74
HYDROCODONE/CHLORPHENIRAMINE/PSE LIQUID
74
hydrocodone/homatropine syrup
74
hydrocodone/ibuprofen 5-200mg tab
16
hydrocortisone 1% cream (RX Only)
17
hydrocortisone 1% cream (RX Only)
17
hydrocortisone 1.67mg/ml enema
17
hydrocortisone 10mg tab 73 hydrocortisone 10mg/ml/neomycin 3.5mg/ml/polymyxin b 10000unit/ml otic soln
101
hydrocortisone 10mg/ml/neomycin 3.5mg/ml/polymyxin b 10000unit/ml otic susp
101
hydrocortisone 2.5% cream
77
hydrocortisone 2.5% lotion
77
hydrocortisone 2.5% ointment
77
hydrocortisone 20mg tab 73 hydrocortisone 5mg tab 73 hydrocortisone supp 17 hydrocortisone/pramoxine 1-1% rectal cream
17
hydrocortisone/pramoxine 2.5-1% rectal cream
17
hydromorphone 1mg/ml oral soln
14
hydromorphone 2mg tab 14 hydromorphone 4mg tab 14 hydromorphone 8mg tab 14 hydroxychloroquine sulfate 200mg tab
43
hydroxyurea 500mg cap 53 hydroxyzine 10mg tab 18 hydroxyzine 25mg tab 18 hydroxyzine 2mg/ml oral soln
18
hydroxyzine 50mg tab 18 HYDROXYZINE PAMOATE 100MG CAP
18
hydroxyzine pamoate 25mg cap
18
You can find information on what the symbols and abbreviations on this table mean by going to the beginning of this table.
135

ALPHABETICAL LISTING OF DRUGS
hydroxyzine pamoate 50mg cap
18
hyoscyamine sulfate CR tab
108
hyoscyamine sulfate elixir 108 hyoscyamine sulfate ODT 108 hyoscyamine sulfate SL tab
108
hyoscyamine sulfate tab 108
I
ibandronate 150mg tab 80 IBRANCE 100MG CAP 49 IBRANCE 100MG TAB 49 IBRANCE 125MG CAP 49 IBRANCE 125MG TAB 49 IBRANCE 75MG CAP 49 IBRANCE 75MG TAB 49 ibuprofen 20mg/ml susp 12 ibuprofen 400mg tab 12 ibuprofen 600mg tab 12 ibuprofen 800mg tab 12 icatibant 10mg/ml inj 87 ICLUSIG 10MG TAB 49 ICLUSIG 15MG TAB 49 ICLUSIG 30MG TAB 49 ICLUSIG 45MG TAB 49 icosapent ethyl 1gm cap 35 IDHIFA 100MG TAB 49 IDHIFA 50MG TAB 50 ILEVRO 0.3% OPHTH SUSP
100
imatinib 100mg tab 50 imatinib 400mg tab 50 IMBRUVICA 140MG CAP
50
IMBRUVICA 140MG TAB 50 IMBRUVICA 280MG TAB 50 IMBRUVICA 420MG TAB 50 IMBRUVICA 560MG TAB 50 IMBRUVICA 70MG CAP 50 imipramine 10mg tab 29 imipramine 25mg tab 29 imipramine 50mg tab 29 imiquimod 5% cream 78
IMOVAX 2.5UNIT/ML INJ
110
IMPAVIDO 50MG CAP 41 IMPLANON IMPLANT, NEXPLANON IMPLANT
72
INCRELEX 40MG/4ML INJ
81
INCRUSE 62.5MCG/INH INHALER
20
indapamide 1.25mg tab 80 indapamide 2.5mg tab 80 INDOCIN 50MG RECTAL SUPP
13
indomethacin 25mg cap 13 indomethacin 50mg cap 13 indomethacin 75mg er cap
13
INFANRIX INJ 108 INGREZZA 40MG CAP 104 INGREZZA 60MG CAP 104 INGREZZA 80MG CAP 104 INLYTA 1MG TAB 45 INLYTA 5MG TAB 45 INNOPRAN 120MG ER CAP
65
INNOPRAN 80MG ER CAP
65
INQOVI 5 TABLET PACK 48 INREBIC 100MG CAP 50 INSULIN PEN NEEDLE 91 INSULIN SYRINGE 91 INSULIN SYRINGE U-500
91
INTELENCE 25MG TAB 61 INTRALIPID 30GM/100ML INJ
97
INTRON A 10MU INJ 53 INTRON A 10MU/ML INJ 53 INTRON A 18MU INJ 53 INTRON A 50MU INJ 53 INTRON A 6000000UNIT/ML INJ
53
INVEGA 117MG/0.75ML INJ
56
INVEGA 156MG/ML INJ 56
INVEGA 234MG/1.5ML INJ
56
INVEGA 273MG/0.875ML INJ
56
INVEGA 39MG/0.25ML INJ
56
INVEGA 410MG/1.315ML INJ
56
INVEGA 546MG/1.75ML INJ
56
INVEGA 78MG/0.5ML INJ
57
INVEGA 819MG/2.625ML INJ
57
INVIRASE 500MG TAB 61 iodoquinol/hydrocortisone cream
75
IOPIDINE 1% OPHTH SOLN
98
IPOL INJ 110 ipratropium 0.03% nasal spray
97
ipratropium 0.06% nasal spray
97
ipratropium bromide 0.2mg/ml inh soln
20
ipratropium/albuterol 0.5-2.5mg/3ml inh soln
21
irbesartan 150mg tab 38 irbesartan 300mg tab 38 irbesartan 75mg tab 38 IRESSA 250MG TAB 45 IRON POLYSACCH/THREONIC ACID/B12/FA CAP
89
IRON SUSP 89 IRON/VITAMIN C/VITAMIN B12/FOLIC ACID TAB
89
ISENTRESS 100MG CHEW TAB
61
ISENTRESS 100MG GRANULES FOR ORAL SUSP
61
You can find information on what the symbols and abbreviations on this table mean by going to the beginning of this table.
136

ALPHABETICAL LISTING OF DRUGS
ISENTRESS 25MG CHEW TAB
61
ISENTRESS 400MG TAB 61 ISENTRESS 600MG TAB 61 ISOLYTE P INJ 93 ISOLYTE S INJ 93 ISOLYTE-S (PH 7.4) INJ 93 ISONIAZID 100MG TAB 44 ISONIAZID 10MG/ML ORAL SOLN
44
isoniazid 300mg tab 44 isosorbide dinitrate 10mg tab
18
isosorbide dinitrate 20mg tab
18
isosorbide dinitrate 30mg tab
18
isosorbide dinitrate 40mg tab
18
isosorbide dinitrate 5mg tab
18
isosorbide mononitrate 10mg tab
18
isosorbide mononitrate 120mg er tab
18
isosorbide mononitrate 20mg tab
18
isosorbide mononitrate 30mg er tab
18
isosorbide mononitrate 60mg er tab
18
isotretinoin 10mg cap 74 isotretinoin 20mg cap 74 isotretinoin 30mg cap 74 isotretinoin 40mg cap 74 isoxsuprine tab 68 ISOXSUPRINE TAB 68 isradipine 2.5mg cap 66 isradipine 5mg cap 66 ISTURISA 10MG TAB 80 ISTURISA 1MG TAB 80 ISTURISA 5MG TAB 80 itraconazole 100mg cap 35 itraconazole 10mg/ml oral soln
35
IVERMECTIN 0.5% LOTION
78
ivermectin 3mg tab 18 IXIARO 0.012MG/ML INJ 110
J
JAKAFI 10MG TAB 50 JAKAFI 15MG TAB 50 JAKAFI 20MG TAB 50 JAKAFI 25MG TAB 50 JAKAFI 5MG TAB 50 JANUMET 1000-100MG ER TAB
30
JANUMET 1000-50MG ER TAB
30
JANUMET 1000-50MG TAB
30
JANUMET 500-50MG ER TAB
30
JANUMET 500-50MG TAB
30
JANUVIA 100MG TAB 31 JANUVIA 25MG TAB 31 JANUVIA 50MG TAB 31 JARDIANCE 10MG TAB 32 JARDIANCE 25MG TAB 32 jasmiel 28 day pack 72 JENTADUETO 2.5-1000MG ER TAB
30
JENTADUETO 2.5-1000MG TAB
30
JENTADUETO 2.5-500MG TAB
30
JENTADUETO 2.5-850MG TAB
30
JENTADUETO 5-1000MG ER TAB
30
JULUCA 50-25MG TAB 61 junel fe 1.5/30 28 day pack
72
JUXTAPID 10MG CAP 37 JUXTAPID 20MG CAP 37 JUXTAPID 30MG CAP 37 JUXTAPID 5MG CAP 37 JYNARQUE 15MG TAB 82
JYNARQUE 30MG TAB 82 JYNARQUE 45/15 THERAPY PACK
83
JYNARQUE 60/30 THERAPY PACK
83
JYNARQUE 90/30 THERAPY PACK
83
JYNARQUE TAB 15/15 CARTON 15MG PACK
83
JYNARQUE TAB 30/15MG THERAPY PACK
83
K
KALYDECO 150MG TAB 106 KALYDECO 25MG GRANULES
106
KALYDECO 50MG GRANULES
106
KALYDECO 75MG GRANULES
106
KCL 40 MEQ/L (0.3%) IN DEXTROSE 5% & NACL 0.9% INJ
93
KCL 40 MEQ/L (0.3%) IN NACL 0.9% INJ
93
KCL/D5W/LR 0.15% INJ 93 KCL/D5W/NACL 20MEQ/5%/0.225% INJ
93
KCL/NACL 20MEQ-0.45% INJ
93
KESIMPTA 20MG/0.4ML PEN INJ
105
ketoconazole 2% cream 75 ketoconazole 2% shampoo
75
ketoconazole 200mg tab 35 KETO-DIASTIX 79 KETOPROFEN 200MG ER CAP
13
ketorolac tromethamine 0.4% ophth soln
100
ketorolac tromethamine 0.5% ophth soln
100
You can find information on what the symbols and abbreviations on this table mean by going to the beginning of this table.
137
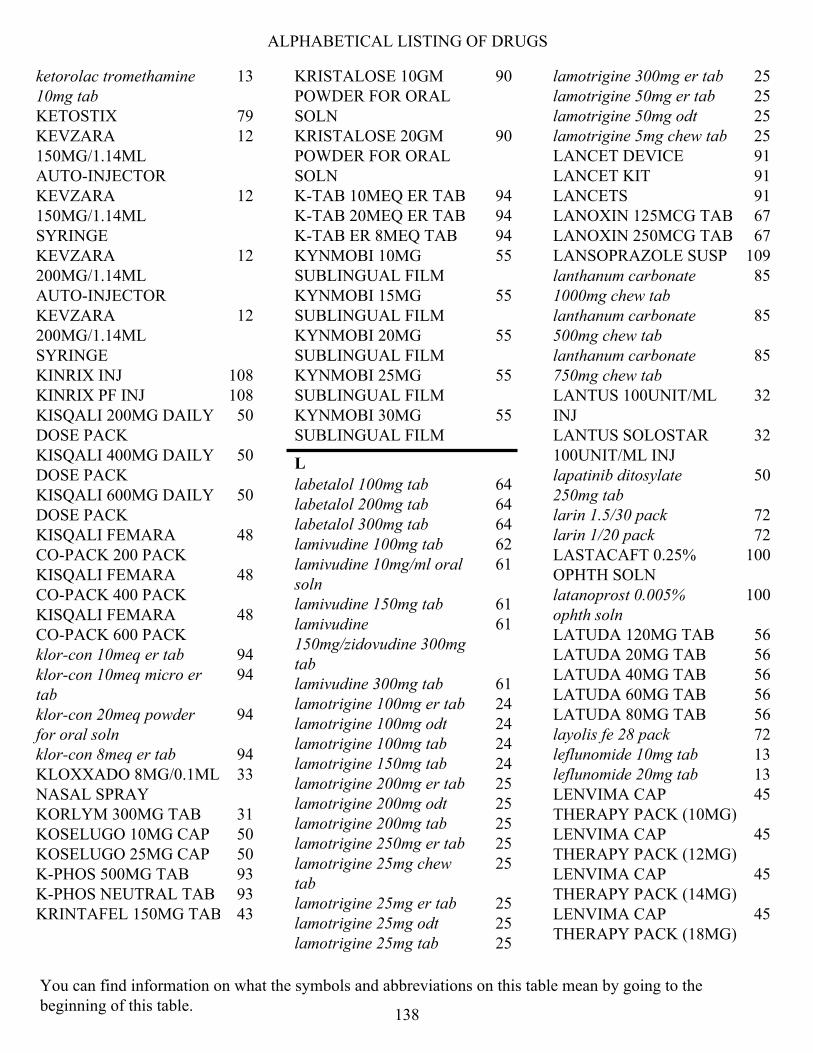
ALPHABETICAL LISTING OF DRUGS
ketorolac tromethamine 10mg tab
13
KETOSTIX 79 KEVZARA 150MG/1.14ML AUTO-INJECTOR
12
KEVZARA 150MG/1.14ML SYRINGE
12
KEVZARA 200MG/1.14ML AUTO-INJECTOR
12
KEVZARA 200MG/1.14ML SYRINGE
12
KINRIX INJ 108 KINRIX PF INJ 108 KISQALI 200MG DAILY DOSE PACK
50
KISQALI 400MG DAILY DOSE PACK
50
KISQALI 600MG DAILY DOSE PACK
50
KISQALI FEMARA CO-PACK 200 PACK
48
KISQALI FEMARA CO-PACK 400 PACK
48
KISQALI FEMARA CO-PACK 600 PACK
48
klor-con 10meq er tab 94 klor-con 10meq micro er tab
94
klor-con 20meq powder for oral soln
94
klor-con 8meq er tab 94 KLOXXADO 8MG/0.1ML NASAL SPRAY
33
KORLYM 300MG TAB 31 KOSELUGO 10MG CAP 50 KOSELUGO 25MG CAP 50 K-PHOS 500MG TAB 93 K-PHOS NEUTRAL TAB 93 KRINTAFEL 150MG TAB 43
KRISTALOSE 10GM POWDER FOR ORAL SOLN
90
KRISTALOSE 20GM POWDER FOR ORAL SOLN
90
K-TAB 10MEQ ER TAB 94 K-TAB 20MEQ ER TAB 94 K-TAB ER 8MEQ TAB 94 KYNMOBI 10MG SUBLINGUAL FILM
55
KYNMOBI 15MG SUBLINGUAL FILM
55
KYNMOBI 20MG SUBLINGUAL FILM
55
KYNMOBI 25MG SUBLINGUAL FILM
55
KYNMOBI 30MG SUBLINGUAL FILM
55
L
labetalol 100mg tab 64 labetalol 200mg tab 64 labetalol 300mg tab 64 lamivudine 100mg tab 62 lamivudine 10mg/ml oral soln
61
lamivudine 150mg tab 61 lamivudine 150mg/zidovudine 300mg tab
61
lamivudine 300mg tab 61 lamotrigine 100mg er tab 24 lamotrigine 100mg odt 24 lamotrigine 100mg tab 24 lamotrigine 150mg tab 24 lamotrigine 200mg er tab 25 lamotrigine 200mg odt 25 lamotrigine 200mg tab 25 lamotrigine 250mg er tab 25 lamotrigine 25mg chew tab
25
lamotrigine 25mg er tab 25 lamotrigine 25mg odt 25 lamotrigine 25mg tab 25
lamotrigine 300mg er tab 25 lamotrigine 50mg er tab 25 lamotrigine 50mg odt 25 lamotrigine 5mg chew tab 25 LANCET DEVICE 91 LANCET KIT 91 LANCETS 91 LANOXIN 125MCG TAB 67 LANOXIN 250MCG TAB 67 LANSOPRAZOLE SUSP 109 lanthanum carbonate 1000mg chew tab
85
lanthanum carbonate 500mg chew tab
85
lanthanum carbonate 750mg chew tab
85
LANTUS 100UNIT/ML INJ
32
LANTUS SOLOSTAR 100UNIT/ML INJ
32
lapatinib ditosylate 250mg tab
50
larin 1.5/30 pack 72 larin 1/20 pack 72 LASTACAFT 0.25% OPHTH SOLN
100
latanoprost 0.005% ophth soln
100
LATUDA 120MG TAB 56 LATUDA 20MG TAB 56 LATUDA 40MG TAB 56 LATUDA 60MG TAB 56 LATUDA 80MG TAB 56 layolis fe 28 pack 72 leflunomide 10mg tab 13 leflunomide 20mg tab 13 LENVIMA CAP THERAPY PACK (10MG)
45
LENVIMA CAP THERAPY PACK (12MG)
45
LENVIMA CAP THERAPY PACK (14MG)
45
LENVIMA CAP THERAPY PACK (18MG)
45
You can find information on what the symbols and abbreviations on this table mean by going to the beginning of this table.
138
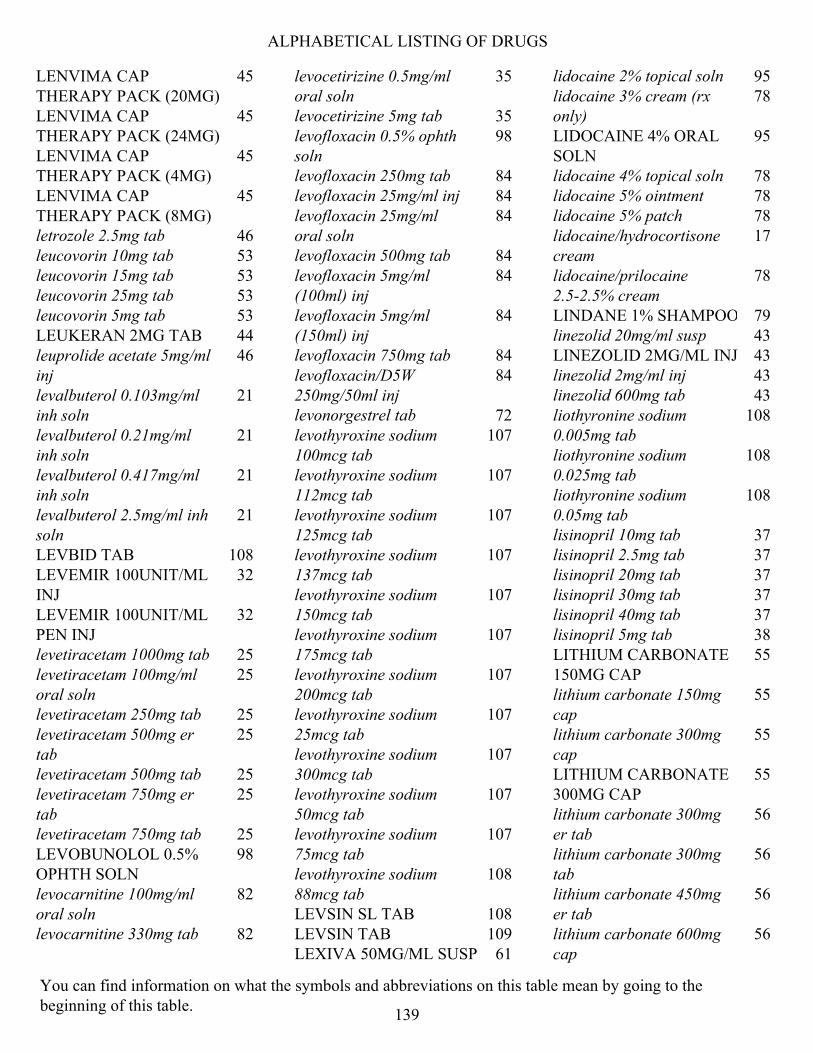
ALPHABETICAL LISTING OF DRUGS
LENVIMA CAP THERAPY PACK (20MG)
45
LENVIMA CAP THERAPY PACK (24MG)
45
LENVIMA CAP THERAPY PACK (4MG)
45
LENVIMA CAP THERAPY PACK (8MG)
45
letrozole 2.5mg tab 46 leucovorin 10mg tab 53 leucovorin 15mg tab 53 leucovorin 25mg tab 53 leucovorin 5mg tab 53 LEUKERAN 2MG TAB 44 leuprolide acetate 5mg/ml inj
46
levalbuterol 0.103mg/ml inh soln
21
levalbuterol 0.21mg/ml inh soln
21
levalbuterol 0.417mg/ml inh soln
21
levalbuterol 2.5mg/ml inh soln
21
LEVBID TAB 108 LEVEMIR 100UNIT/ML INJ
32
LEVEMIR 100UNIT/ML PEN INJ
32
levetiracetam 1000mg tab 25 levetiracetam 100mg/ml oral soln
25
levetiracetam 250mg tab 25 levetiracetam 500mg er tab
25
levetiracetam 500mg tab 25 levetiracetam 750mg er tab
25
levetiracetam 750mg tab 25 LEVOBUNOLOL 0.5% OPHTH SOLN
98
levocarnitine 100mg/ml oral soln
82
levocarnitine 330mg tab 82
levocetirizine 0.5mg/ml oral soln
35
levocetirizine 5mg tab 35 levofloxacin 0.5% ophth soln
98
levofloxacin 250mg tab 84 levofloxacin 25mg/ml inj 84 levofloxacin 25mg/ml oral soln
84
levofloxacin 500mg tab 84 levofloxacin 5mg/ml (100ml) inj
84
levofloxacin 5mg/ml (150ml) inj
84
levofloxacin 750mg tab 84 levofloxacin/D5W 250mg/50ml inj
84
levonorgestrel tab 72 levothyroxine sodium 100mcg tab
107
levothyroxine sodium 112mcg tab
107
levothyroxine sodium 125mcg tab
107
levothyroxine sodium 137mcg tab
107
levothyroxine sodium 150mcg tab
107
levothyroxine sodium 175mcg tab
107
levothyroxine sodium 200mcg tab
107
levothyroxine sodium 25mcg tab
107
levothyroxine sodium 300mcg tab
107
levothyroxine sodium 50mcg tab
107
levothyroxine sodium 75mcg tab
107
levothyroxine sodium 88mcg tab
108
LEVSIN SL TAB 108 LEVSIN TAB 109 LEXIVA 50MG/ML SUSP 61
lidocaine 2% topical soln 95 lidocaine 3% cream (rx only)
78
LIDOCAINE 4% ORAL SOLN
95
lidocaine 4% topical soln 78 lidocaine 5% ointment 78 lidocaine 5% patch 78 lidocaine/hydrocortisone cream
17
lidocaine/prilocaine 2.5-2.5% cream
78
LINDANE 1% SHAMPOO 79 linezolid 20mg/ml susp 43 LINEZOLID 2MG/ML INJ 43 linezolid 2mg/ml inj 43 linezolid 600mg tab 43 liothyronine sodium 0.005mg tab
108
liothyronine sodium 0.025mg tab
108
liothyronine sodium 0.05mg tab
108
lisinopril 10mg tab 37 lisinopril 2.5mg tab 37 lisinopril 20mg tab 37 lisinopril 30mg tab 37 lisinopril 40mg tab 37 lisinopril 5mg tab 38 LITHIUM CARBONATE 150MG CAP
55
lithium carbonate 150mg cap
55
lithium carbonate 300mg cap
55
LITHIUM CARBONATE 300MG CAP
55
lithium carbonate 300mg er tab
56
lithium carbonate 300mg tab
56
lithium carbonate 450mg er tab
56
lithium carbonate 600mg cap
56
You can find information on what the symbols and abbreviations on this table mean by going to the beginning of this table.
139

ALPHABETICAL LISTING OF DRUGS
LITHIUM CARBONATE 600MG CAP
56
LITHIUM CITRATE 60MG/ML ORAL SOLN
56
LITHOSTAT 250MG TAB 86 LIVALO 1MG TAB 36 LIVALO 2MG TAB 36 LIVALO 4MG TAB 36 LO LOESTRIN FE 28 DAY PACK
72
LOKELMA 10GM POWDER FOR ORAL SUSP
95
LOKELMA 5GM POWDER FOR ORAL SUSP
95
LONHALA 25MCG/ML INH SOLN
20
LONSURF 6.14-15MG TAB
48
LONSURF 8.19-20MG TAB
48
loperamide 2mg cap (RX Only)
33
lopinavir 80mg/ml/ritonavir 20mg/ml oral solution
61
lopinavir/ritonavir 100-25mg tab
61
lopinavir/ritonavir 200-50mg tab
61
lorazepam 0.5mg tab 19 lorazepam 1mg tab 19 lorazepam 2mg tab 19 lorazepam 2mg/ml oral soln
19
LORBRENA 100MG TAB 50 LORBRENA 25MG TAB 50 losartan potassium 100mg tab
38
losartan potassium 25mg tab
38
losartan potassium 50mg tab
38
LOTEMAX 0.5% OPHTH OINTMENT
99
loteprednol etabonate 0.5% ophth gel
99
loteprednol etabonate 0.5% ophth susp
99
lovastatin 10mg tab 36 lovastatin 20mg tab 36 lovastatin 40mg tab 36 low-ogestrel 28 day pack 72 loxapine 10mg cap 58 loxapine 25mg cap 58 loxapine 50mg cap 58 loxapine 5mg cap 58 LUCEMYRA 0.18MG TAB
103
LUMAKRAS 120MG TAB 50 LUMIGAN 0.01% OPHTH SOLN
100
LUPANETA 3-MONTH PACK
81
LUPANETA PACK 1-MONTH PACK
81
LUPKYNIS 7.9MG CAP 95 LUPRON 11.25MG INJ 46 LUPRON 11.25MG INJ PED KIT (3 MONTH)
81
LUPRON 22.5MG INJ 46 LUPRON 3.75MG INJ 46 LUPRON 30MG INJ 46 LUPRON 45MG INJ 46 LUPRON 7.5MG INJ 46 LUPRON 7.5MG INJ PED KIT (1 MONTH)
81
LURIDE CHEW TAB 93 LURIDE SOLN 93 LYNPARZA 100MG TAB 51 LYNPARZA 150MG TAB 51 LYSODREN 500MG TAB 46
M
magnesium sulfate 500mg/ml inj
93
malathion 0.5% lotion 79 MARPLAN 10MG TAB 27
MATULANE 50MG CAP 53 matzim 240mg er tab 66 matzim 420mg er tab 66 MAVYRET 100-40MG TAB
62
MAXIDEX 0.1% OPHTH SUSP
99
MAYZENT 0.25MG STARTER PACK
105
MAYZENT 0.25MG TAB 105 MAYZENT 2MG TAB 105 meclizine 12.5mg tab 34 meclizine 25mg tab (RX Only)
34
MEDROL 2MG TAB 73 medroxyprogesterone acetate 10mg tab
103
medroxyprogesterone acetate 150mg/ml inj
72
medroxyprogesterone acetate 150mg/ml syringe
72
medroxyprogesterone acetate 2.5mg tab
103
medroxyprogesterone acetate 5mg tab
103
mefloquine hcl 250mg tab 43 megestrol acetate 125mg/ml susp
103
megestrol acetate 20mg tab
46
megestrol acetate 40mg tab
46
megestrol acetate 40mg/ml susp
46
MEKINIST 0.5MG TAB 51 MEKINIST 2MG TAB 51 MEKTOVI 15MG TAB 51 melodetta 24 fe chewable 28 day pack
72
meloxicam 15mg tab 13 meloxicam 7.5mg tab 13 melphalan tab 44 memantine 10mg tab 104
You can find information on what the symbols and abbreviations on this table mean by going to the beginning of this table.
140
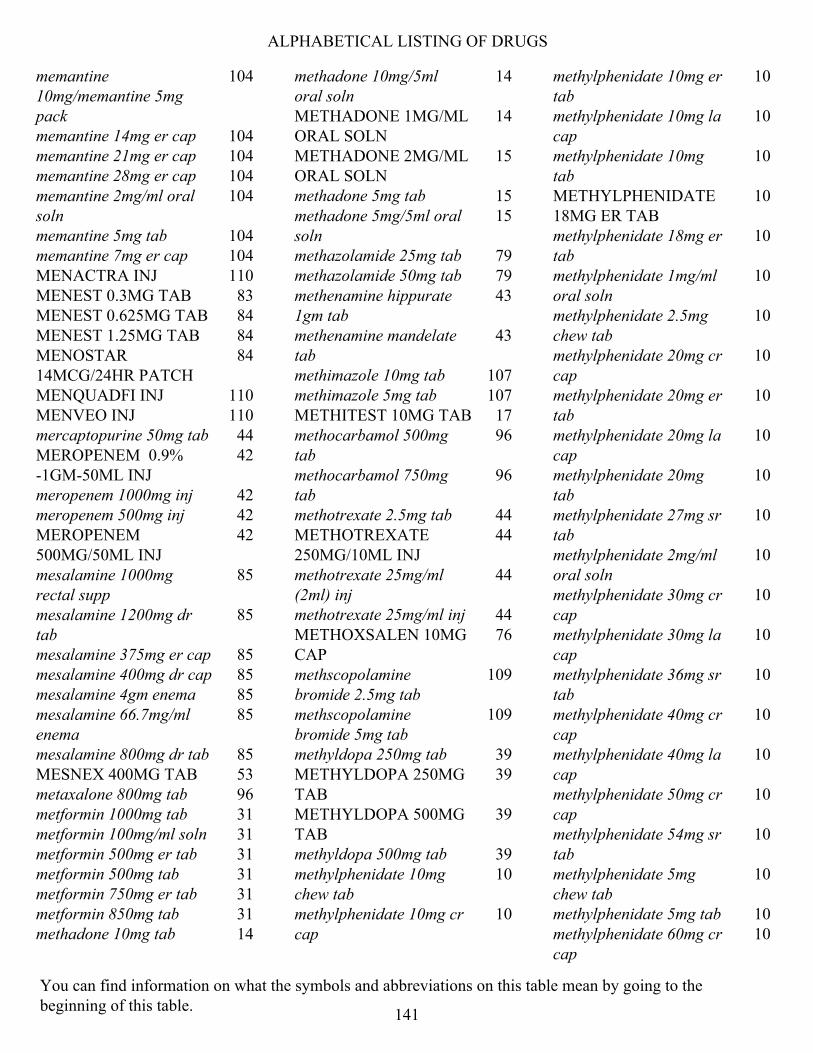
ALPHABETICAL LISTING OF DRUGS
memantine 10mg/memantine 5mg pack
104
memantine 14mg er cap 104 memantine 21mg er cap 104 memantine 28mg er cap 104 memantine 2mg/ml oral soln
104
memantine 5mg tab 104 memantine 7mg er cap 104 MENACTRA INJ 110 MENEST 0.3MG TAB 83 MENEST 0.625MG TAB 84 MENEST 1.25MG TAB 84 MENOSTAR 14MCG/24HR PATCH
84
MENQUADFI INJ 110 MENVEO INJ 110 mercaptopurine 50mg tab 44 MEROPENEM 0.9%-1GM-50ML INJ
42
meropenem 1000mg inj 42 meropenem 500mg inj 42 MEROPENEM 500MG/50ML INJ
42
mesalamine 1000mg rectal supp
85
mesalamine 1200mg dr tab
85
mesalamine 375mg er cap 85 mesalamine 400mg dr cap 85 mesalamine 4gm enema 85 mesalamine 66.7mg/ml enema
85
mesalamine 800mg dr tab 85 MESNEX 400MG TAB 53 metaxalone 800mg tab 96 metformin 1000mg tab 31 metformin 100mg/ml soln 31 metformin 500mg er tab 31 metformin 500mg tab 31 metformin 750mg er tab 31 metformin 850mg tab 31 methadone 10mg tab 14
methadone 10mg/5ml oral soln
14
METHADONE 1MG/ML ORAL SOLN
14
METHADONE 2MG/ML ORAL SOLN
15
methadone 5mg tab 15 methadone 5mg/5ml oral soln
15
methazolamide 25mg tab 79 methazolamide 50mg tab 79 methenamine hippurate 1gm tab
43
methenamine mandelate tab
43
methimazole 10mg tab 107 methimazole 5mg tab 107 METHITEST 10MG TAB 17 methocarbamol 500mg tab
96
methocarbamol 750mg tab
96
methotrexate 2.5mg tab 44 METHOTREXATE 250MG/10ML INJ
44
methotrexate 25mg/ml (2ml) inj
44
methotrexate 25mg/ml inj 44 METHOXSALEN 10MG CAP
76
methscopolamine bromide 2.5mg tab
109
methscopolamine bromide 5mg tab
109
methyldopa 250mg tab 39 METHYLDOPA 250MG TAB
39
METHYLDOPA 500MG TAB
39
methyldopa 500mg tab 39 methylphenidate 10mg chew tab
10
methylphenidate 10mg cr cap
10
methylphenidate 10mg er tab
10
methylphenidate 10mg la cap
10
methylphenidate 10mg tab
10
METHYLPHENIDATE 18MG ER TAB
10
methylphenidate 18mg er tab
10
methylphenidate 1mg/ml oral soln
10
methylphenidate 2.5mg chew tab
10
methylphenidate 20mg cr cap
10
methylphenidate 20mg er tab
10
methylphenidate 20mg la cap
10
methylphenidate 20mg tab
10
methylphenidate 27mg sr tab
10
methylphenidate 2mg/ml oral soln
10
methylphenidate 30mg cr cap
10
methylphenidate 30mg la cap
10
methylphenidate 36mg sr tab
10
methylphenidate 40mg cr cap
10
methylphenidate 40mg la cap
10
methylphenidate 50mg cr cap
10
methylphenidate 54mg sr tab
10
methylphenidate 5mg chew tab
10
methylphenidate 5mg tab 10 methylphenidate 60mg cr cap
10
You can find information on what the symbols and abbreviations on this table mean by going to the beginning of this table.
141

ALPHABETICAL LISTING OF DRUGS
methylphenidate 60mg la cap
10
methylphenidate ER osmotic 27mg tab
10
methylphenidate ER osmotic 36mg tab
10
methylphenidate ER osmotic 54mg tab
10
methylprednisolone 16mg tab
73
methylprednisolone 32mg tab
73
methylprednisolone 4mg pack
73
methylprednisolone 4mg tab
73
methylprednisolone 8mg tab
73
METHYLTESTOSTERONE 10MG CAP
17
metoclopramide 10mg tab 85 metoclopramide 1mg/ml oral soln
85
metoclopramide 5mg tab 85 metolazone 10mg tab 80 metolazone 2.5mg tab 80 metolazone 5mg tab 80 metoprolol succinate 100mg er tab
65
metoprolol succinate 200mg er tab
65
metoprolol succinate 25mg er tab
65
metoprolol succinate 50mg er tab
65
metoprolol tartrate 100mg tab
65
metoprolol tartrate 25mg tab
65
metoprolol tartrate 50mg tab
65
metronidazole 0.75% cream
78
metronidazole 0.75% gel 78
metronidazole 0.75% lotion
78
metronidazole 0.75% vaginal gel
111
metronidazole 1% gel 78 metronidazole 250mg tab 41 metronidazole 500mg tab 41 metronidazole 5mg/ml inj 41 METRONIDAZOLE/NACL 0.74%-500MG/100ML INJ
41
metronidazole/nacl 0.74%/500mg/100ml inj
41
metyrosine 250mg cap 38 mexiletine 150mg cap 19 mexiletine 200mg cap 19 mexiletine 250mg cap 19 micafungin sodium 100mg inj
34
micafungin sodium 50mg inj
34
MICONAZOLE NITRATE 200MG VAGINAL INSERT
111
microgestin fe 1/20 28 day pack
72
midodrine 10mg tab 112 midodrine 2.5mg tab 112 midodrine 5mg tab 112 miglitol 100mg tab 30 miglitol 25mg tab 30 miglitol 50mg tab 30 miglustat 100mg cap 88 MILLIPRED 5MG TAB 73 mimvey pack 83 minocycline 100mg cap 107 minocycline 100mg tab 107 minocycline 50mg cap 107 minocycline 50mg tab 107 minocycline 75mg cap 107 minocycline 75mg tab 107 minoxidil 10mg tab 41 minoxidil 2.5mg tab 41 MIRENA IUD 72 mirtazapine 15mg odt 27
mirtazapine 15mg tab 27 mirtazapine 30mg odt 27 mirtazapine 30mg tab 27 mirtazapine 45mg odt 27 mirtazapine 45mg tab 27 mirtazapine 7.5mg tab 27 misoprostol 0.1mg tab 109 misoprostol 0.2mg tab 109 M-M-R II INJ 111 modafinil 100mg tab 10 modafinil 200mg tab 10 moexipril 15mg tab 38 moexipril 7.5mg tab 38 MOLINDONE 10MG TAB 58 MOLINDONE 25MG TAB 58 MOLINDONE 5MG TAB 58 mometasone furoate 0.1% cream
77
mometasone furoate 0.1% lotion
77
mometasone furoate 0.1% ointment
77
mondoxyne 100mg cap 107 montelukast 10mg tab 20 montelukast 4mg chew tab
20
montelukast 4mg granules
20
montelukast 5mg chew tab
20
morphine sulfate 100mg er tab
15
morphine sulfate 15mg er tab
15
morphine sulfate 15mg tab
15
MORPHINE SULFATE 15MG TAB
15
morphine sulfate 200mg er tab
15
morphine sulfate 20mg/ml oral soln
15
morphine sulfate 2mg/ml oral soln
15
You can find information on what the symbols and abbreviations on this table mean by going to the beginning of this table.
142

ALPHABETICAL LISTING OF DRUGS
morphine sulfate 30mg er tab
15
morphine sulfate 30mg tab
15
MORPHINE SULFATE 30MG TAB
15
morphine sulfate 4mg/ml oral soln
15
morphine sulfate 60mg er tab
15
MOTEGRITY 1MG TAB 84 MOTEGRITY 2MG TAB 84 MOVANTIK 12.5MG TAB 85 MOVANTIK 25MG TAB 85 moxifloxacin 0.5% ophth soln
98
moxifloxacin 0.5% ophth soln
98
MOXIFLOXACIN 1.6MG/ML INJ
84
moxifloxacin 400mg tab 84 MOXIFLOXACIN 400MG/250ML IV SOLN
84
MULTAQ 400MG TAB 20 MULTIGEN FOLIC TAB 89 MULTIGEN PLUS TAB 89 MULTIGEN TAB 89 MULTI-VITAMIN/FLOURIDE 0.25MG CHEW TAB
96
MULTI-VITAMIN/FLOURIDE 0.5MG CHEW TAB
96
MULTI-VITAMIN/FLOURIDE 1MG CHEW TAB
96
multivitamin/minerals tab 96 mupirocin 2% ointment 75 MUSE SUPP 68 mycophenolate mofetil 200mg/ml susp
63
mycophenolate mofetil 250mg cap
64
mycophenolate mofetil 500mg tab
64
mycophenolic acid 180mg dr tab
64
mycophenolic acid 360mg dr tab
64
MYFORTIC 180MG DR TAB
64
MYFORTIC 360MG DR TAB
64
MYLERAN TAB 44 MYRBETRIQ 25MG ER TAB
109
MYRBETRIQ 50MG ER TAB
109
N
nabumetone 500mg tab 13 nabumetone 750mg tab 13 nadolol 20mg tab 65 nadolol 40mg tab 65 nadolol 80mg tab 65 NAFCILLIN 1000MG INJ 103 nafcillin 1000mg inj 103 nafcillin 100mg/ml inj 103 NAFCILLIN 1GM INJ 103 NAFCILLIN 2000MG INJ 103 nafcillin 2000mg inj 103 NAFCILLIN 2GM INJ 103 NAFTIFINE 1% CREAM 75 naftifine 2% cream 75 NAFTIFINE 2% CREAM 75 NAFTIN 2% GEL 75 NALOXONE 0.4MG/ML CARTRIDGE
33
naloxone 0.4mg/ml inj 33 naloxone 1mg/ml syringe 33 naltrexone 50mg tab 33 naproxen 250mg tab 13 naproxen 375mg dr tab 13 naproxen 375mg tab 13 naproxen 500mg dr tab 13 naproxen 500mg tab 13 naproxen sodium 275mg tab
13
naproxen sodium 550mg tab
13
naratriptan 1mg tab 92 naratriptan 2.5mg tab 92
NARCAN 4MG/0.1ML NASAL SPRAY
34
NATACYN 5% OPHTH SUSP
98
NATAZIA 28 DAY PACK 72 nateglinide 120mg tab 32 nateglinide 60mg tab 32 NATPARA 100MCG CARTRIDGE
80
NATPARA 25MCG CARTRIDGE
80
NATPARA 50MCG CARTRIDGE
80
NATPARA 75MCG CARTRIDGE
80
NAYZILAM 5MG/0.1ML NASAL SPRAY
24
nebivolol 10mg tab 65 nebivolol 2.5mg tab 65 nebivolol 20mg tab 65 nebivolol 5mg tab 65 NEFAZODONE 100MG TAB
28
NEFAZODONE 150MG TAB
28
NEFAZODONE 200MG TAB
28
NEFAZODONE 250MG TAB
28
NEFAZODONE 50MG TAB
28
neomycin sulfate 500mg tab
11
neomycin/bacitracin/polymyxin ophth ointment 5(3.5)mg-400unit-10000unit
98
neomycin/polymyxin/bacitracin/hydrocortisone 1% ophth ointment
99
NEOMYCIN-POLYMYXIN-HC OPHTH SUSP
99
NEORAL 100MG CAP 64 NEORAL 100MG/ML ORAL SOLN
64
You can find information on what the symbols and abbreviations on this table mean by going to the beginning of this table.
143

ALPHABETICAL LISTING OF DRUGS
NEORAL 25MG CAP 64 NEPHRO-VITE TAB 96 NERLYNX 40MG TAB 51 NEUPRO 1MG/24HR PATCH
54
NEUPRO 2MG/24HR PATCH
54
NEUPRO 3MG/24HR PATCH
54
NEUPRO 4MG/24HR PATCH
54
NEUPRO 6MG/24HR PATCH
54
NEUPRO 8MG/24HR PATCH
54
NEVANAC 0.1% OPHTH SUSP
100
NEVIRAPINE 100MG ER TAB
61
NEVIRAPINE 10MG/ML SUSP
61
nevirapine 200mg tab 61 nevirapine 400mg er tab 61 NEXAVAR 200MG TAB 51 niacin 1000mg er tab 37 niacin 500mg er tab 37 niacin 750mg er tab 37 nicardipine 20mg cap 66 nicardipine 30mg cap 66 NICORETTE CQ PATCH 105 NICORETTE GUM 106 nicotine gum 106 nicotine lozenge 106 nicotine patch 106 NICOTINE PATCH KIT 106 NICOTROL 10MG INH SOLN
106
NICOTROL 10MG/ML NASAL INHALER
106
nifedipine 10mg cap 66 nifedipine 20mg cap 66 nifedipine 30mg er tab 66 nifedipine 30mg osmotic er tab
66
nifedipine 60mg er tab 66
nifedipine 60mg osmotic er tab
66
nifedipine 90mg er tab 66 nifedipine 90mg osmotic er tab
66
nilutamide 150mg tab 46 nimodipine 30mg cap 67 NINLARO 2.3MG CAP 51 NINLARO 3MG CAP 51 NINLARO 4MG CAP 51 nisoldipine 17mg er tab 67 NISOLDIPINE 20MG ER TAB
67
NISOLDIPINE 25.5MG ER TAB
67
NISOLDIPINE 30MG ER TAB
67
nisoldipine 34mg er tab 67 NISOLDIPINE 40MG ER TAB
67
nisoldipine 8.5mg er tab 67 nitazoxanide 500mg tab 42 nitisinone 10mg cap 82 nitisinone 2mg cap 82 nitisinone 5mg cap 82 NITRO-BID 2% OINTMENT
18
NITRO-DUR 0.3MG/HR PATCH
18
NITRO-DUR 0.8MG/HR PATCH
18
nitrofurantoin 100mg cap 43 nitrofurantoin 50mg macro cap
43
nitrofurantoin macro 100mg cap
43
nitroglycerin 0.1mg/hr patch
18
nitroglycerin 0.2mg/hr patch
18
nitroglycerin 0.3mg sl tab 18 nitroglycerin 0.4mg sl tab 18 nitroglycerin 0.4mg/act spray
18
nitroglycerin 0.4mg/hr patch
18
nitroglycerin 0.6mg sl tab 18 nitroglycerin 0.6mg/hr patch
18
NITROGLYCERIN CAP 18 NIVESTYM 300MCG/0.5ML SYRINGE
88
NIVESTYM 300MCG/ML INJ
88
NIVESTYM 480MCG/0.8ML SYRINGE
88
NIVESTYM 480MCG/1.6ML INJ
88
nizatidine 150mg cap 109 NIZATIDINE 150MG CAP 109 NIZATIDINE 300MG CAP 109 norethindrone 0.35mg pack
72
norethindrone acetate 5mg tab
103
NORMOSOL-M/D5W INJ 93 NORMOSOL-R (PH 7.4) INJ
93
NORMOSOL-R INJ 93 NORPACE 100MG ER CAP
19
NORPACE 150MG ER CAP
19
nortrel 0.5/35 28 day pack
72
nortriptyline 10mg cap 29 nortriptyline 25mg cap 29 NORTRIPTYLINE 2MG/ML ORAL SOLN
29
nortriptyline 50mg cap 29 nortriptyline 75mg cap 29 NORVIR 100MG ORAL POWDER
61
NORVIR 80MG/ML ORAL SOLN
61
NOURIANZ 20MG TAB 55 NOURIANZ 40MG TAB 55
You can find information on what the symbols and abbreviations on this table mean by going to the beginning of this table.
144

ALPHABETICAL LISTING OF DRUGS
NOVOLIN MIX (70/30) 100UNIT/ML INJ
32
NOVOLIN MIX (70/30) FLEXPEN 100UNIT/ML
32
NOVOLIN N 100UNIT/ML INJ
32
NOVOLIN N 100UNIT/ML PEN INJ
32
NOVOLIN R 100UNIT/ML INJ
32
NOVOLIN R FLEXPEN RELION
32
NOVOLOG 100UNIT/ML CARTRIDGE, INSULIN ASPART HUMAN 100UNIT/ML CARTRIDGE
32
NOVOLOG 100UNIT/ML INJ, INSULIN ASPART HUMAN 100UNIT/ML INJ
32
NOVOLOG 100UNIT/ML PEN INJ, INSULIN ASPART HUMAN 100UNIT/ML PEN INJ
32
NOVOLOG MIX (70/30) 100UNIT/ML INJ, INSULIN ASPART MIX 70UNIT-30UNIT/ML INJ
32
NOVOLOG MIX 70-30UNIT/ML PEN INJ, INSULIN ASPART MIX 70UNIT-30UNIT/ML PEN INJ
32
NOXAFIL 40MG/ML SUSP
35
NUBEQA 300MG TAB 46 NUCALA 100MG INJ 20 NUCALA 100MG/ML AUTO-INJECTOR
20
NUCALA 100MG/ML SYRINGE
20
NUCORT LOTION 77 NUCYNTA 100MG ER TAB
15
NUCYNTA 150MG ER TAB
15
NUCYNTA 200MG ER TAB
15
NUCYNTA 250MG ER TAB
15
NUCYNTA 50MG ER TAB
15
NUEDEXTA 20-10MG CAP
105
NUPLAZID 10MG TAB 56 NUPLAZID 34MG CAP 56 NURTEC 75MG ODT 91 NUTRILIPID 20GM/100ML INJ
97
NUZYRA 150MG TAB 106 nystatin 100000unit/ml cream
75
nystatin 100000unit/ml susp
95
nystatin 100unit/mg ointment
75
nystatin 100unit/mg topical powder
75
nystatin 500000unit tab 35
O
OCALIVA 10MG TAB 84 OCALIVA 5MG TAB 84 ocella 28 day pack 72 OCTAGAM 1GM/20ML INJ
101
OCTAGAM 2.5GM/50ML INJ
101
OCTAGAM 25GM/500ML INJ
101
OCTAGAM 2GM/20ML INJ
101
OCTAGAM 30GM/300ML INJ
101
OCTAGAM 5GM/100ML INJ
101
OCTREOTIDE 0.05MG/ML INJ
82
octreotide 0.05mg/ml inj 82
OCTREOTIDE 0.1MG/ML INJ
82
octreotide 0.1mg/ml inj 82 octreotide 0.2mg/ml inj 82 OCTREOTIDE 0.5MG/ML INJ
82
octreotide 0.5mg/ml inj 82 octreotide 1mg/ml inj 82 ODEFSEY 200-25-25MG TAB
61
ODOMZO 200MG CAP 46 OFEV 100MG CAP 106 OFEV 150MG CAP 106 ofloxacin 0.3% ophth soln 99 ofloxacin 0.3% otic soln 100 ofloxacin 400mg tab 84 olanzapine 10mg inj 58 olanzapine 10mg odt 58 olanzapine 10mg tab 58 olanzapine 15mg odt 58 olanzapine 15mg tab 58 olanzapine 2.5mg tab 58 olanzapine 20mg odt 58 olanzapine 20mg tab 58 olanzapine 5mg odt 58 olanzapine 5mg tab 58 olanzapine 7.5mg tab 58 olmesartan medoxomil 20mg tab
38
olmesartan medoxomil 40mg tab
38
olmesartan medoxomil 5mg tab
38
olopatadine 0.1% ophth soln
100
olopatadine 0.2% ophth soln
100
olopatadine 0.665mg/act nasal inhaler
97
OLUMIANT 1MG TAB 11 OLUMIANT 2MG TAB 11 omega-3 acid ethyl esters (usp) 1000mg cap
35
omeprazole 10mg dr cap 109 omeprazole 20mg dr cap 109
You can find information on what the symbols and abbreviations on this table mean by going to the beginning of this table.
145

ALPHABETICAL LISTING OF DRUGS
omeprazole 40mg dr cap 109 ondansetron 0.8mg/ml oral soln
34
ONDANSETRON 24MG TAB
34
ondansetron 4mg odt 34 ondansetron 4mg tab 34 ondansetron 8mg odt 34 ondansetron 8mg tab 34 ONGENTYS 25MG CAP 55 ONGENTYS 50MG CAP 55 ONUREG 200MG TAB 44 ONUREG 300MG TAB 44 opium 10mg/ml tincture 33 OPSUMIT 10MG TAB 68 ORACIT SOLN 86 ORAVIG 50MG BUCCAL TAB
95
ORENCIA 125MG/ML AUTO-INJECTOR
13
ORENCIA 125MG/ML SYRINGE
13
ORENCIA 50MG/0.4ML SYRINGE
13
ORENCIA 87.5MG/0.7ML SYRINGE
13
ORENITRAM 0.125MG ER TAB
68
ORENITRAM 0.25MG ER TAB
68
ORENITRAM 1MG ER TAB
68
ORENITRAM 2.5MG ER TAB
68
ORENITRAM 5MG ER TAB
68
ORFADIN 20MG CAP 82 ORFADIN 4MG/ML SUSP
82
ORGOVYX 120MG TAB 46 ORIAHNN 28 DAY KIT PACK
83
ORILISSA 150MG TAB 81 ORILISSA 200MG TAB 81
ORKAMBI 125-100MG GRANULES
106
ORKAMBI 125-100MG TAB
106
ORKAMBI 125-200MG TAB
106
ORKAMBI 188-150MG GRANULES
106
orphenadrine citrate 100mg er tab
96
oseltamivir 30mg cap 63 oseltamivir 45mg cap 63 oseltamivir 6mg/ml susp 63 oseltamivir 75mg cap 63 OSPHENA 60MG TAB 81 OTEZLA 28-DAY STARTER PACK
13
OTEZLA 30MG TAB 13 OVACE CREAM 76 OVACE PLUS SHAMPOO 76 OVACE PLUS WASH 76 OVACE WASH 76 oxacillin 1000mg inj 103 oxacillin 100mg/ml inj 103 oxacillin 2000mg inj 103 OXACILLIN 20MG/ML INJ
103
OXACILLIN 40MG/ML INJ
103
oxandrolone 10mg tab 17 oxandrolone 2.5mg tab 17 oxaprozin 600mg tab 13 OXBRYTA 500MG TAB 88 oxcarbazepine 150mg tab 25 oxcarbazepine 300mg tab 25 oxcarbazepine 600mg tab 25 oxcarbazepine 60mg/ml susp
25
OXERVATE 0.002% OPHTH SOLN
99
oxybutynin chloride 10mg er tab
110
oxybutynin chloride 15mg er tab
110
oxybutynin chloride 1mg/ml oral soln
110
oxybutynin chloride 5mg er tab
110
oxybutynin chloride 5mg tab
110
oxycodone 10mg tab 15 oxycodone 15mg tab 15 oxycodone 1mg/ml oral soln
15
oxycodone 20mg tab 15 oxycodone 20mg/ml oral soln
15
oxycodone 30mg tab 15 oxycodone 5mg cap 15 oxycodone 5mg tab 15 oxymorphone 10mg tab 15 oxymorphone 5mg tab 15 OZEMPIC 2MG/1.5ML PEN INJ
31
OZEMPIC 2MG/1.5ML PEN INJ (1MG DOSE)
31
OZEMPIC 4MG/3ML PEN INJ
31
P
paliperidone 1.5mg er tab 57 paliperidone 3mg er tab 57 paliperidone 6mg er tab 57 paliperidone 9mg er tab 57 PALYNZIQ 10MG/0.5ML SYRINGE
82
PALYNZIQ 2.5MG/0.5ML SYRINGE
82
PALYNZIQ 20MG/ML SYRINGE
82
pantoprazole 20mg dr tab 109 pantoprazole 40mg dr tab 109 PANZYGA 10GM/100ML INJ
101
PANZYGA 1GM/10ML INJ
101
PANZYGA 2.5GM/25ML INJ
101
You can find information on what the symbols and abbreviations on this table mean by going to the beginning of this table.
146
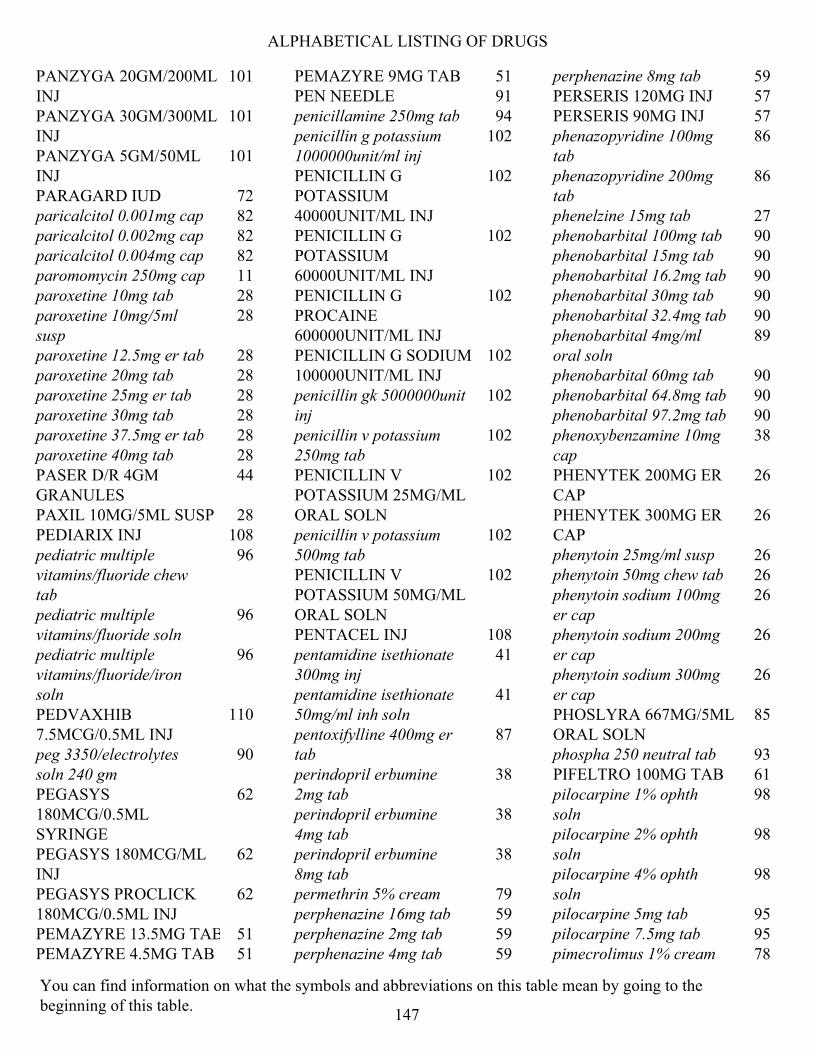
ALPHABETICAL LISTING OF DRUGS
PANZYGA 20GM/200ML INJ
101
PANZYGA 30GM/300ML INJ
101
PANZYGA 5GM/50ML INJ
101
PARAGARD IUD 72 paricalcitol 0.001mg cap 82 paricalcitol 0.002mg cap 82 paricalcitol 0.004mg cap 82 paromomycin 250mg cap 11 paroxetine 10mg tab 28 paroxetine 10mg/5ml susp
28
paroxetine 12.5mg er tab 28 paroxetine 20mg tab 28 paroxetine 25mg er tab 28 paroxetine 30mg tab 28 paroxetine 37.5mg er tab 28 paroxetine 40mg tab 28 PASER D/R 4GM GRANULES
44
PAXIL 10MG/5ML SUSP 28 PEDIARIX INJ 108 pediatric multiple vitamins/fluoride chew tab
96
pediatric multiple vitamins/fluoride soln
96
pediatric multiple vitamins/fluoride/iron soln
96
PEDVAXHIB 7.5MCG/0.5ML INJ
110
peg 3350/electrolytes soln 240 gm
90
PEGASYS 180MCG/0.5ML SYRINGE
62
PEGASYS 180MCG/ML INJ
62
PEGASYS PROCLICK 180MCG/0.5ML INJ
62
PEMAZYRE 13.5MG TAB 51 PEMAZYRE 4.5MG TAB 51
PEMAZYRE 9MG TAB 51 PEN NEEDLE 91 penicillamine 250mg tab 94 penicillin g potassium 1000000unit/ml inj
102
PENICILLIN G POTASSIUM 40000UNIT/ML INJ
102
PENICILLIN G POTASSIUM 60000UNIT/ML INJ
102
PENICILLIN G PROCAINE 600000UNIT/ML INJ
102
PENICILLIN G SODIUM 100000UNIT/ML INJ
102
penicillin gk 5000000unit inj
102
penicillin v potassium 250mg tab
102
PENICILLIN V POTASSIUM 25MG/ML ORAL SOLN
102
penicillin v potassium 500mg tab
102
PENICILLIN V POTASSIUM 50MG/ML ORAL SOLN
102
PENTACEL INJ 108 pentamidine isethionate 300mg inj
41
pentamidine isethionate 50mg/ml inh soln
41
pentoxifylline 400mg er tab
87
perindopril erbumine 2mg tab
38
perindopril erbumine 4mg tab
38
perindopril erbumine 8mg tab
38
permethrin 5% cream 79 perphenazine 16mg tab 59 perphenazine 2mg tab 59 perphenazine 4mg tab 59
perphenazine 8mg tab 59 PERSERIS 120MG INJ 57 PERSERIS 90MG INJ 57 phenazopyridine 100mg tab
86
phenazopyridine 200mg tab
86
phenelzine 15mg tab 27 phenobarbital 100mg tab 90 phenobarbital 15mg tab 90 phenobarbital 16.2mg tab 90 phenobarbital 30mg tab 90 phenobarbital 32.4mg tab 90 phenobarbital 4mg/ml oral soln
89
phenobarbital 60mg tab 90 phenobarbital 64.8mg tab 90 phenobarbital 97.2mg tab 90 phenoxybenzamine 10mg cap
38
PHENYTEK 200MG ER CAP
26
PHENYTEK 300MG ER CAP
26
phenytoin 25mg/ml susp 26 phenytoin 50mg chew tab 26 phenytoin sodium 100mg er cap
26
phenytoin sodium 200mg er cap
26
phenytoin sodium 300mg er cap
26
PHOSLYRA 667MG/5ML ORAL SOLN
85
phospha 250 neutral tab 93 PIFELTRO 100MG TAB 61 pilocarpine 1% ophth soln
98
pilocarpine 2% ophth soln
98
pilocarpine 4% ophth soln
98
pilocarpine 5mg tab 95 pilocarpine 7.5mg tab 95 pimecrolimus 1% cream 78
You can find information on what the symbols and abbreviations on this table mean by going to the beginning of this table.
147
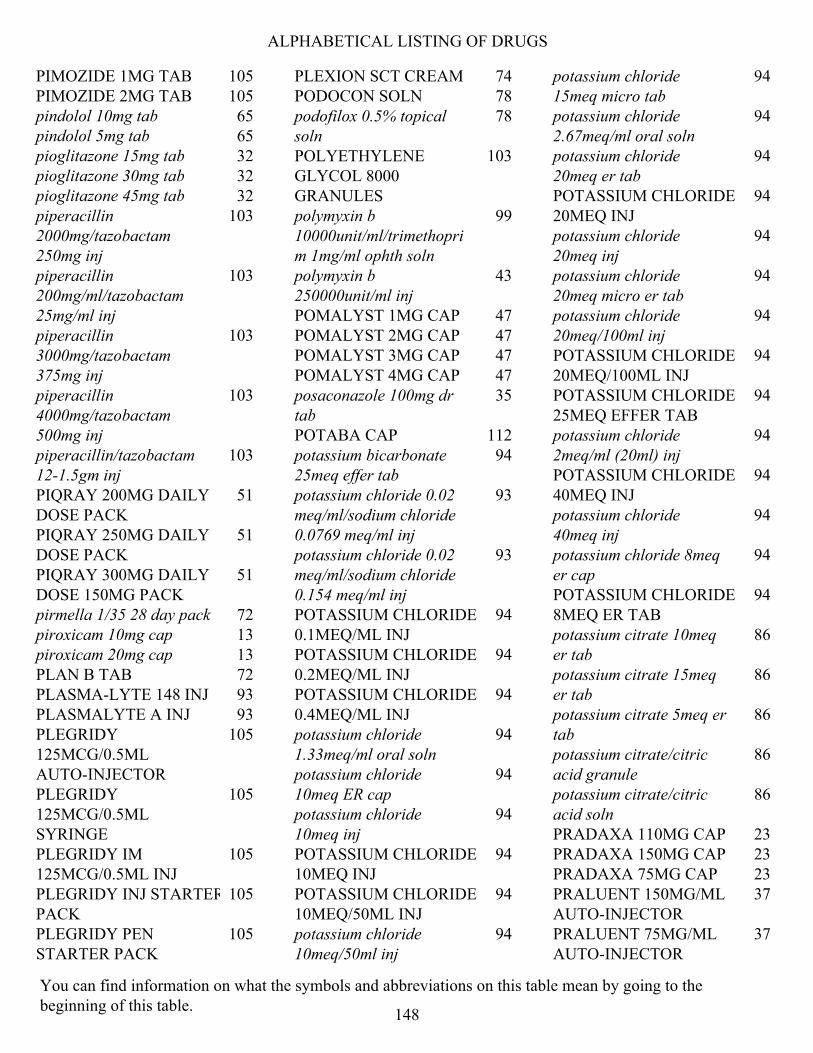
ALPHABETICAL LISTING OF DRUGS
PIMOZIDE 1MG TAB 105 PIMOZIDE 2MG TAB 105 pindolol 10mg tab 65 pindolol 5mg tab 65 pioglitazone 15mg tab 32 pioglitazone 30mg tab 32 pioglitazone 45mg tab 32 piperacillin 2000mg/tazobactam 250mg inj
103
piperacillin 200mg/ml/tazobactam 25mg/ml inj
103
piperacillin 3000mg/tazobactam 375mg inj
103
piperacillin 4000mg/tazobactam 500mg inj
103
piperacillin/tazobactam 12-1.5gm inj
103
PIQRAY 200MG DAILY DOSE PACK
51
PIQRAY 250MG DAILY DOSE PACK
51
PIQRAY 300MG DAILY DOSE 150MG PACK
51
pirmella 1/35 28 day pack 72 piroxicam 10mg cap 13 piroxicam 20mg cap 13 PLAN B TAB 72 PLASMA-LYTE 148 INJ 93 PLASMALYTE A INJ 93 PLEGRIDY 125MCG/0.5ML AUTO-INJECTOR
105
PLEGRIDY 125MCG/0.5ML SYRINGE
105
PLEGRIDY IM 125MCG/0.5ML INJ
105
PLEGRIDY INJ STARTER PACK
105
PLEGRIDY PEN STARTER PACK
105
PLEXION SCT CREAM 74 PODOCON SOLN 78 podofilox 0.5% topical soln
78
POLYETHYLENE GLYCOL 8000 GRANULES
103
polymyxin b 10000unit/ml/trimethoprim 1mg/ml ophth soln
99
polymyxin b 250000unit/ml inj
43
POMALYST 1MG CAP 47 POMALYST 2MG CAP 47 POMALYST 3MG CAP 47 POMALYST 4MG CAP 47 posaconazole 100mg dr tab
35
POTABA CAP 112 potassium bicarbonate 25meq effer tab
94
potassium chloride 0.02 meq/ml/sodium chloride 0.0769 meq/ml inj
93
potassium chloride 0.02 meq/ml/sodium chloride 0.154 meq/ml inj
93
POTASSIUM CHLORIDE 0.1MEQ/ML INJ
94
POTASSIUM CHLORIDE 0.2MEQ/ML INJ
94
POTASSIUM CHLORIDE 0.4MEQ/ML INJ
94
potassium chloride 1.33meq/ml oral soln
94
potassium chloride 10meq ER cap
94
potassium chloride 10meq inj
94
POTASSIUM CHLORIDE 10MEQ INJ
94
POTASSIUM CHLORIDE 10MEQ/50ML INJ
94
potassium chloride 10meq/50ml inj
94
potassium chloride 15meq micro tab
94
potassium chloride 2.67meq/ml oral soln
94
potassium chloride 20meq er tab
94
POTASSIUM CHLORIDE 20MEQ INJ
94
potassium chloride 20meq inj
94
potassium chloride 20meq micro er tab
94
potassium chloride 20meq/100ml inj
94
POTASSIUM CHLORIDE 20MEQ/100ML INJ
94
POTASSIUM CHLORIDE 25MEQ EFFER TAB
94
potassium chloride 2meq/ml (20ml) inj
94
POTASSIUM CHLORIDE 40MEQ INJ
94
potassium chloride 40meq inj
94
potassium chloride 8meq er cap
94
POTASSIUM CHLORIDE 8MEQ ER TAB
94
potassium citrate 10meq er tab
86
potassium citrate 15meq er tab
86
potassium citrate 5meq er tab
86
potassium citrate/citric acid granule
86
potassium citrate/citric acid soln
86
PRADAXA 110MG CAP 23 PRADAXA 150MG CAP 23 PRADAXA 75MG CAP 23 PRALUENT 150MG/ML AUTO-INJECTOR
37
PRALUENT 75MG/ML AUTO-INJECTOR
37
You can find information on what the symbols and abbreviations on this table mean by going to the beginning of this table.
148

ALPHABETICAL LISTING OF DRUGS
pramipexole 0.125mg tab 54 pramipexole 0.25mg tab 54 pramipexole 0.375mg er tab
54
pramipexole 0.5mg tab 54 pramipexole 0.75mg er tab
54
pramipexole 0.75mg tab 54 pramipexole 1.5mg er tab 54 pramipexole 1.5mg tab 54 pramipexole 1mg tab 54 pramipexole 2.25mg er tab
54
pramipexole 3.75mg er tab
54
pramipexole 3mg er tab 54 pramipexole 4.5mg er tab 54 prasugrel 10mg tab 87 prasugrel 5mg tab 87 pravastatin sodium 10mg tab
36
pravastatin sodium 20mg tab
36
pravastatin sodium 40mg tab
36
pravastatin sodium 80mg tab
36
praziquantel 600mg tab 18 prazosin 1mg cap 39 prazosin 2mg cap 39 prazosin 5mg cap 39 PRED FORTE 1% OPHTH SUSP
99
PRED MILD 0.12% OPHTH SUSP
99
PRED-G 0.3-0.6% OPHTH OINTMENT
99
PRED-G 0.3-1% OPHTH SUSP
99
PREDNICARBATE 0.1% OINTMENT
77
PREDNISOLONE 1% OPHTH SOLN
100
PREDNISOLONE 10MG ODT
73
PREDNISOLONE 15MG ODT
73
prednisolone 1mg/ml oral soln
73
prednisolone 2mg/ml oral soln
73
PREDNISOLONE 30MG ODT
73
PREDNISOLONE 3MG/ML ORAL SOLN
73
prednisolone 4mg/ml oral soln
73
PREDNISOLONE 5MG/ML ORAL SOLN
73
PREDNISOLONE ACETATE 1% OPHTH SUSP
100
prednisolone sodium phosphate 15mg/5ml oral soln
73
PREDNISOLONE SODIUM PHOSPHATE 2.5MG/ML/SULFACETAMIDE SODIUM 100MG/ML OPHTH SOLN
100
prednisone 10mg tab 73 prednisone 1mg tab 73 PREDNISONE 1MG/ML ORAL SOLN
73
prednisone 2.5mg tab 73 prednisone 20mg tab 73 prednisone 50mg tab 73 prednisone 5mg tab 73 PREDNISONE 5MG/ML ORAL SOLN
73
PREFEST 30 DAY PACK 83 pregabalin 100mg cap 25 pregabalin 150mg cap 25 pregabalin 200mg cap 25 pregabalin 20mg/ml oral soln
25
pregabalin 225mg cap 25 pregabalin 25mg cap 25 pregabalin 300mg cap 25
pregabalin 50mg cap 25 pregabalin 75mg cap 25 PREMARIN 0.3MG TAB 84 PREMARIN 0.45MG TAB 84 PREMARIN 0.625MG TAB
84
PREMARIN 0.625MG/GM VAGINAL CREAM
111
PREMARIN 0.9MG TAB 84 PREMARIN 1.25MG TAB 84 PREMPHASE 28 DAY PACK
83
PREMPRO 0.3/1.5MG 28 DAY PACK
83
PREMPRO 0.45/1.5 28 DAY PACK
83
PREMPRO 0.625/2.5MG 28 DAY PACK
83
PREMPRO 0.625/5MG 28 DAY PACK
83
PRETOMANID 200MG TAB
44
prevalite 4gm powder for oral susp
36
PREVIDENT 5000 BOOSTER PASTE
95
PREVIDENT 5000 DRY MOUTH GEL
95
PREVIDENT 5000 PASTE 95 PREVIDENT 5000 PASTE 95 PREVIDENT 5000 PLUS CREAM
95
PREVIDENT RINSE 95 PREVYMIS 240MG TAB 62 PREVYMIS 480MG TAB 62 PREZCOBIX 150-800MG TAB
61
PREZISTA 100MG/ML SUSP
61
PREZISTA 150MG TAB 61 PREZISTA 600MG TAB 61 PREZISTA 75MG TAB 61 PREZISTA 800MG TAB 61 PRIFTIN 150MG TAB 44
You can find information on what the symbols and abbreviations on this table mean by going to the beginning of this table.
149

ALPHABETICAL LISTING OF DRUGS
primaquine phosphate 26.3mg tab
43
PRIMAQUINE PHOSPHATE 26.3MG TAB
43
primidone 250mg tab 25 primidone 50mg tab 25 PRIVIGEN 20GM/200ML INJ
101
PRIVIGEN 40GM/400ML INJ
101
probenecid 500mg tab 87 PROCALAMINE 3% INJ 97 procentra 5mg/5ml oral soln
9
prochlorperazine 10mg tab
59
prochlorperazine 25mg rectal supp
59
prochlorperazine 5mg tab 59 procto-med 2.5% cream 17 procto-pak 1% rectal cream
17
progesterone 100mg cap 103 progesterone 200mg cap 103 PROGRAF 0.2MG GRANULES FOR ORAL SUSP
95
PROGRAF 0.5MG CAP 64 PROGRAF 1MG CAP 64 PROGRAF 1MG GRANULES FOR ORAL SUSP
95
PROGRAF 5MG CAP 64 PROLASTIN-C 1000MG INJ
106
PROLENSA 0.07% OPHTH SOLN
100
PROLIA 60MG/ML SYRINGE
80
PROMACTA 12.5MG POWDER FOR ORAL SUSP
88
PROMACTA 12.5MG TAB
88
PROMACTA 25MG POWDER FOR ORAL SUSP
88
PROMACTA 25MG TAB 88 PROMACTA 50MG TAB 88 PROMACTA 75MG TAB 88 promethazine 1.25mg/ml oral soln
35
promethazine 12.5mg rectal supp
35
promethazine 12.5mg tab 35 promethazine 25mg tab 35 promethazine 50mg tab 35 promethazine DM syrup 74 promethazine VC w/codeine syrup
74
promethazine/codeine syrup
74
promethegan 25mg rectal supp
35
PROMETHEGAN 50MG RECTAL SUPP
35
propafenone 150mg tab 19 propafenone 225mg er cap
19
propafenone 225mg tab 19 propafenone 300mg tab 19 propafenone 325mg er cap
19
propafenone 425mg er cap
19
proparacaine 0.5% ophth soln
99
propranolol 10mg tab 65 propranolol 120mg er cap
65
propranolol 160mg ER cap
65
propranolol 20mg tab 65 propranolol 40mg tab 65 PROPRANOLOL 4MG/ML ORAL SOLN
65
propranolol 60mg er cap 65 propranolol 60mg tab 65 propranolol 80mg er cap 65
propranolol 80mg tab 65 PROPRANOLOL 8MG/ML ORAL SOLN
65
propylthiouracil 50mg tab
107
PROQUAD INJ 111 PROSOL 20% INJ 97 protriptyline 10mg tab 29 protriptyline 5mg tab 29 PULMOZYME 1MG/ML INH SOLN
106
PURIXAN 2000MG/100ML SUSP
44
PYLERA 140-125-125MG CAP
109
pyrazinamide 500mg tab 44 PYRIDIUM 100MG TAB 86 PYRIDIUM 200MG TAB 86 pyridostigmine bromide 12mg/ml oral soln
43
pyridostigmine bromide 180mg er tab
43
pyridostigmine bromide 60mg tab
43
Q
QBRELIS 1MG/ML ORAL SOLN
38
QINLOCK 50MG TAB 51 quetiapine 100mg tab 58 quetiapine 150mg er tab 58 quetiapine 200mg er tab 58 quetiapine 200mg tab 58 quetiapine 25mg tab 58 quetiapine 300mg er tab 58 quetiapine 300mg tab 58 quetiapine 400mg er tab 58 quetiapine 400mg tab 58 quetiapine 50mg er tab 58 quetiapine 50mg tab 58 QUFLORA PEDIATRIC CHEW TAB
96
quinapril 10mg tab 38 quinapril 20mg tab 38 quinapril 40mg tab 38
You can find information on what the symbols and abbreviations on this table mean by going to the beginning of this table.
150
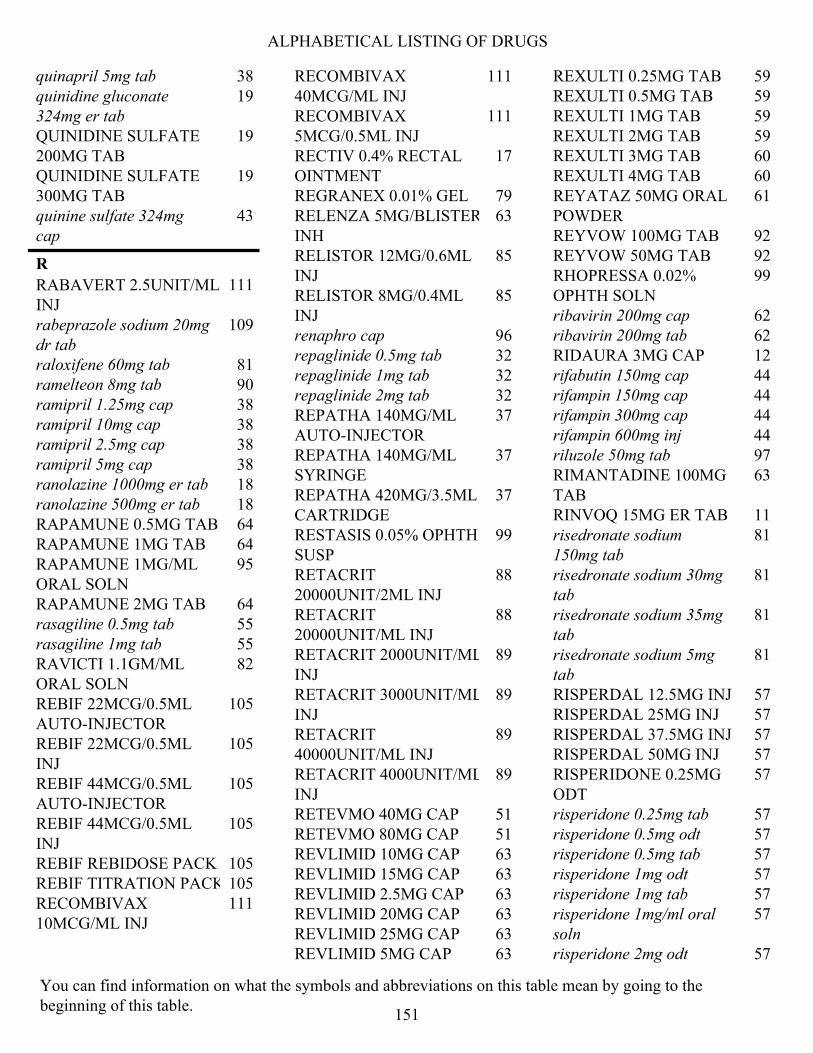
ALPHABETICAL LISTING OF DRUGS
quinapril 5mg tab 38 quinidine gluconate 324mg er tab
19
QUINIDINE SULFATE 200MG TAB
19
QUINIDINE SULFATE 300MG TAB
19
quinine sulfate 324mg cap
43
R
RABAVERT 2.5UNIT/ML INJ
111
rabeprazole sodium 20mg dr tab
109
raloxifene 60mg tab 81 ramelteon 8mg tab 90 ramipril 1.25mg cap 38 ramipril 10mg cap 38 ramipril 2.5mg cap 38 ramipril 5mg cap 38 ranolazine 1000mg er tab 18 ranolazine 500mg er tab 18 RAPAMUNE 0.5MG TAB 64 RAPAMUNE 1MG TAB 64 RAPAMUNE 1MG/ML ORAL SOLN
95
RAPAMUNE 2MG TAB 64 rasagiline 0.5mg tab 55 rasagiline 1mg tab 55 RAVICTI 1.1GM/ML ORAL SOLN
82
REBIF 22MCG/0.5ML AUTO-INJECTOR
105
REBIF 22MCG/0.5ML INJ
105
REBIF 44MCG/0.5ML AUTO-INJECTOR
105
REBIF 44MCG/0.5ML INJ
105
REBIF REBIDOSE PACK 105 REBIF TITRATION PACK 105 RECOMBIVAX 10MCG/ML INJ
111
RECOMBIVAX 40MCG/ML INJ
111
RECOMBIVAX 5MCG/0.5ML INJ
111
RECTIV 0.4% RECTAL OINTMENT
17
REGRANEX 0.01% GEL 79 RELENZA 5MG/BLISTER INH
63
RELISTOR 12MG/0.6ML INJ
85
RELISTOR 8MG/0.4ML INJ
85
renaphro cap 96 repaglinide 0.5mg tab 32 repaglinide 1mg tab 32 repaglinide 2mg tab 32 REPATHA 140MG/ML AUTO-INJECTOR
37
REPATHA 140MG/ML SYRINGE
37
REPATHA 420MG/3.5ML CARTRIDGE
37
RESTASIS 0.05% OPHTH SUSP
99
RETACRIT 20000UNIT/2ML INJ
88
RETACRIT 20000UNIT/ML INJ
88
RETACRIT 2000UNIT/ML INJ
89
RETACRIT 3000UNIT/ML INJ
89
RETACRIT 40000UNIT/ML INJ
89
RETACRIT 4000UNIT/ML INJ
89
RETEVMO 40MG CAP 51 RETEVMO 80MG CAP 51 REVLIMID 10MG CAP 63 REVLIMID 15MG CAP 63 REVLIMID 2.5MG CAP 63 REVLIMID 20MG CAP 63 REVLIMID 25MG CAP 63 REVLIMID 5MG CAP 63
REXULTI 0.25MG TAB 59 REXULTI 0.5MG TAB 59 REXULTI 1MG TAB 59 REXULTI 2MG TAB 59 REXULTI 3MG TAB 60 REXULTI 4MG TAB 60 REYATAZ 50MG ORAL POWDER
61
REYVOW 100MG TAB 92 REYVOW 50MG TAB 92 RHOPRESSA 0.02% OPHTH SOLN
99
ribavirin 200mg cap 62 ribavirin 200mg tab 62 RIDAURA 3MG CAP 12 rifabutin 150mg cap 44 rifampin 150mg cap 44 rifampin 300mg cap 44 rifampin 600mg inj 44 riluzole 50mg tab 97 RIMANTADINE 100MG TAB
63
RINVOQ 15MG ER TAB 11 risedronate sodium 150mg tab
81
risedronate sodium 30mg tab
81
risedronate sodium 35mg tab
81
risedronate sodium 5mg tab
81
RISPERDAL 12.5MG INJ 57 RISPERDAL 25MG INJ 57 RISPERDAL 37.5MG INJ 57 RISPERDAL 50MG INJ 57 RISPERIDONE 0.25MG ODT
57
risperidone 0.25mg tab 57 risperidone 0.5mg odt 57 risperidone 0.5mg tab 57 risperidone 1mg odt 57 risperidone 1mg tab 57 risperidone 1mg/ml oral soln
57
risperidone 2mg odt 57
You can find information on what the symbols and abbreviations on this table mean by going to the beginning of this table.
151

ALPHABETICAL LISTING OF DRUGS
risperidone 2mg tab 57 risperidone 3mg odt 57 risperidone 3mg tab 57 risperidone 4mg odt 57 risperidone 4mg tab 57 ritonavir 100mg tab 61 rivastigmine 0.192mg/hr patch
104
rivastigmine 0.396mg/hr patch
104
rivastigmine 0.554mg/hr patch
104
rivastigmine 1.5mg cap 104 rivastigmine 3mg cap 104 rivastigmine 4.5mg cap 104 rivastigmine 6mg cap 104 rizatriptan 10mg odt 92 rizatriptan 10mg tab 92 rizatriptan 5mg odt 92 rizatriptan 5mg tab 92 ROCKLATAN 0.05-0.2MG/ML OPHTH SOLN
99
ropinirole 0.25mg tab 54 ropinirole 0.5mg tab 55 ropinirole 12mg er tab 55 ropinirole 1mg tab 55 ropinirole 2mg er tab 55 ropinirole 2mg tab 55 ropinirole 3mg tab 55 ropinirole 4mg er tab 55 ropinirole 4mg tab 55 ropinirole 5mg tab 55 ropinirole 6mg er tab 55 ropinirole 8mg er tab 55 rosuvastatin calcium 10mg tab
36
rosuvastatin calcium 20mg tab
36
rosuvastatin calcium 40mg tab
37
rosuvastatin calcium 5mg tab
37
ROTARIX SUSP 111 ROTATEQ SUSP 111
ROZLYTREK 100MG CAP
51
ROZLYTREK 200MG CAP
51
RUBRACA 200MG TAB 51 RUBRACA 250MG TAB 51 RUBRACA 300MG TAB 51 RUCONEST 2100UNIT INJ
87
rufinamide 200mg tab 25 rufinamide 40mg/ml susp 25 RUKOBIA 600MG ER TAB
61
RUZURGI 10MG TAB 44 RYBELSUS 14MG TAB 31 RYBELSUS 3MG TAB 31 RYBELSUS 7MG TAB 31 RYDAPT 25MG CAP 51
S
SALEX SHAMPOO 78 salicylic acid shampoo 78 salmon calcitonin 200unit/act nasal spray
81
salsalate 500mg tab 14 salsalate 750mg tab 14 SANCUSO 3.1MG/24HR PATCH
34
SANDIMMUNE 100MG CAP
64
SANDIMMUNE 100MG/ML ORAL SOLN
64
SANDIMMUNE 25MG CAP
64
SANTYL 250UNIT/GM OINTMENT
78
sapropterin 100mg powder for oral soln
82
sapropterin 500mg powder for oral soln
82
sapropterin dihydrochloride 100mg tab
82
SAVELLA 100MG TAB 104 SAVELLA 12.5MG TAB 104
SAVELLA 25MG TAB 104 SAVELLA 4-WEEK TITRATION PACK
104
SAVELLA 50MG TAB 104 scopolamine 0.0139mg/hr patch
34
seb-prev cream 76 SECUADO 3.8MG/24HR PATCH
58
SECUADO 5.7MG/24HR PATCH
58
SECUADO 7.6MG/24HR PATCH
58
selegiline 5mg cap 55 selegiline 5mg tab 55 SELEGILINE 5MG TAB 55 selenium sulfide 2.25% shampoo
76
selenium sulfide 2.5% shampoo
76
SELZENTRY 150MG TAB 61 SELZENTRY 20MG/ML ORAL SOLN
61
SELZENTRY 25MG TAB 61 SELZENTRY 300MG TAB 61 SELZENTRY 75MG TAB 61 SEREVENT 50MCG/DOSE INH
21
sertraline 100mg tab 28 sertraline 20mg/ml oral soln
28
sertraline 25mg tab 28 sertraline 50mg tab 28 SEVELAMER 400MG TAB
85
sevelamer 800mg tab 86 sevelamer carbonate 2400mg powder for oral susp
86
sevelamer carbonate 800mg powder for oral susp
86
sevelamer carbonate 800mg tab
86
You can find information on what the symbols and abbreviations on this table mean by going to the beginning of this table.
152
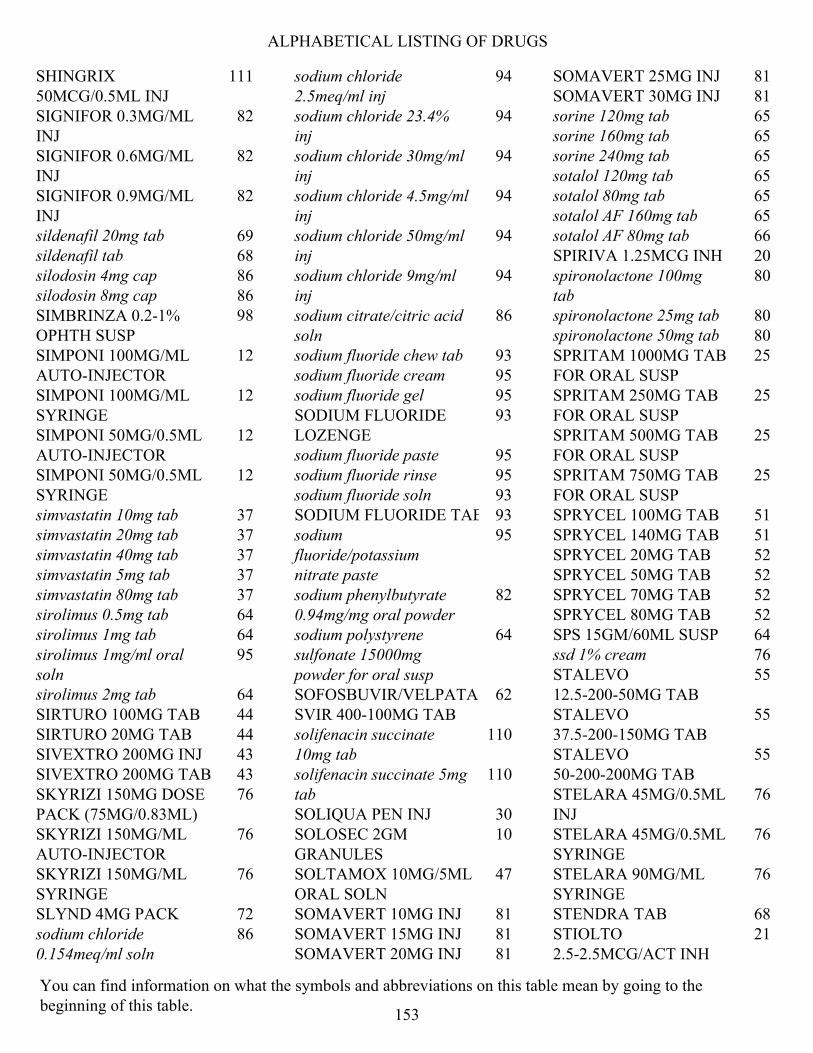
ALPHABETICAL LISTING OF DRUGS
SHINGRIX 50MCG/0.5ML INJ
111
SIGNIFOR 0.3MG/ML INJ
82
SIGNIFOR 0.6MG/ML INJ
82
SIGNIFOR 0.9MG/ML INJ
82
sildenafil 20mg tab 69 sildenafil tab 68 silodosin 4mg cap 86 silodosin 8mg cap 86 SIMBRINZA 0.2-1% OPHTH SUSP
98
SIMPONI 100MG/ML AUTO-INJECTOR
12
SIMPONI 100MG/ML SYRINGE
12
SIMPONI 50MG/0.5ML AUTO-INJECTOR
12
SIMPONI 50MG/0.5ML SYRINGE
12
simvastatin 10mg tab 37 simvastatin 20mg tab 37 simvastatin 40mg tab 37 simvastatin 5mg tab 37 simvastatin 80mg tab 37 sirolimus 0.5mg tab 64 sirolimus 1mg tab 64 sirolimus 1mg/ml oral soln
95
sirolimus 2mg tab 64 SIRTURO 100MG TAB 44 SIRTURO 20MG TAB 44 SIVEXTRO 200MG INJ 43 SIVEXTRO 200MG TAB 43 SKYRIZI 150MG DOSE PACK (75MG/0.83ML)
76
SKYRIZI 150MG/ML AUTO-INJECTOR
76
SKYRIZI 150MG/ML SYRINGE
76
SLYND 4MG PACK 72 sodium chloride 0.154meq/ml soln
86
sodium chloride 2.5meq/ml inj
94
sodium chloride 23.4% inj
94
sodium chloride 30mg/ml inj
94
sodium chloride 4.5mg/ml inj
94
sodium chloride 50mg/ml inj
94
sodium chloride 9mg/ml inj
94
sodium citrate/citric acid soln
86
sodium fluoride chew tab 93 sodium fluoride cream 95 sodium fluoride gel 95 SODIUM FLUORIDE LOZENGE
93
sodium fluoride paste 95 sodium fluoride rinse 95 sodium fluoride soln 93 SODIUM FLUORIDE TAB 93 sodium fluoride/potassium nitrate paste
95
sodium phenylbutyrate 0.94mg/mg oral powder
82
sodium polystyrene sulfonate 15000mg powder for oral susp
64
SOFOSBUVIR/VELPATASVIR 400-100MG TAB
62
solifenacin succinate 10mg tab
110
solifenacin succinate 5mg tab
110
SOLIQUA PEN INJ 30 SOLOSEC 2GM GRANULES
10
SOLTAMOX 10MG/5ML ORAL SOLN
47
SOMAVERT 10MG INJ 81 SOMAVERT 15MG INJ 81 SOMAVERT 20MG INJ 81
SOMAVERT 25MG INJ 81 SOMAVERT 30MG INJ 81 sorine 120mg tab 65 sorine 160mg tab 65 sorine 240mg tab 65 sotalol 120mg tab 65 sotalol 80mg tab 65 sotalol AF 160mg tab 65 sotalol AF 80mg tab 66 SPIRIVA 1.25MCG INH 20 spironolactone 100mg tab
80
spironolactone 25mg tab 80 spironolactone 50mg tab 80 SPRITAM 1000MG TAB FOR ORAL SUSP
25
SPRITAM 250MG TAB FOR ORAL SUSP
25
SPRITAM 500MG TAB FOR ORAL SUSP
25
SPRITAM 750MG TAB FOR ORAL SUSP
25
SPRYCEL 100MG TAB 51 SPRYCEL 140MG TAB 51 SPRYCEL 20MG TAB 52 SPRYCEL 50MG TAB 52 SPRYCEL 70MG TAB 52 SPRYCEL 80MG TAB 52 SPS 15GM/60ML SUSP 64 ssd 1% cream 76 STALEVO 12.5-200-50MG TAB
55
STALEVO 37.5-200-150MG TAB
55
STALEVO 50-200-200MG TAB
55
STELARA 45MG/0.5ML INJ
76
STELARA 45MG/0.5ML SYRINGE
76
STELARA 90MG/ML SYRINGE
76
STENDRA TAB 68 STIOLTO 2.5-2.5MCG/ACT INH
21
You can find information on what the symbols and abbreviations on this table mean by going to the beginning of this table.
153

ALPHABETICAL LISTING OF DRUGS
STIVARGA 40MG TAB 52 STREPTOMYCIN 1000MG INJ
11
STRIBILD 150-150-200-300MG TAB
61
STROVITE TAB 96 SUCRAID 8500UNIT/ML ORAL SOLN
79
sucralfate 1000mg tab 109 sucralfate 100mg/ml susp 109 sulfacetamide sodium 10% lotion
74
SULFACETAMIDE SODIUM 10% OPHTH OINTMENT
99
sulfacetamide sodium 10% ophth soln
99
sulfacetamide sodium gel 76 sulfacetamide sodium shampoo
76
sulfacetamide sodium wash
76
sulfacetamide sodium/sulfur cream
74
sulfacetamide sodium/sulfur emulsion
74
sulfacleanse susp 74 SULFADIAZINE 500MG TAB
106
sulfamethoxazole 400mg/trimethoprim 80mg tab
42
sulfamethoxazole 40mg/ml/trimethoprim 8mg/ml susp
42
sulfamethoxazole 800mg/trimethoprim 160mg tab
42
SULFAMYLON 85MG/GM CREAM
76
sulfasalazine 500mg dr tab
85
sulfasalazine 500mg tab 85 sulindac 150mg tab 13
sulindac 200mg tab 13 sumatriptan 100mg tab 92 sumatriptan 12mg/ml auto-injector
92
sumatriptan 12mg/ml inj 92 sumatriptan 20mg/act nasal spray
92
sumatriptan 25mg tab 92 sumatriptan 50mg tab 92 sumatriptan 5mg/act nasal spray
92
sumatriptan 6mg/0.5ml refill inj
92
sumatriptan 8mg/ml cartridge
92
SUMAXIN TS SUSP 74 SUMAXIN WASH 75 sunitinib malate 12.5mg cap
52
sunitinib malate 25mg cap
52
sunitinib malate 37.5mg cap
52
sunitinib malate 50mg cap
52
SUNOSI 150MG TAB 9 SUNOSI 75MG TAB 9 SUPRAX 100MG CHEW TAB
71
SUPRAX 200MG CHEW TAB
71
SUPRAX 500MG/5ML SUSP
71
SYMAX DUOTAB 109 SYMBICORT 160-4.5MCG/ACT INHALER
21
SYMBICORT 80-4.5MCG/ACT INHALER
22
SYMDEKO 50-75MG/75MG PACK
106
SYMDEKO TAB 4-WEEK PACK
106
SYMJEPI 0.15MG/0.3ML SYRINGE
112
SYMJEPI 0.3MG/0.3ML SYRINGE
112
SYMPAZAN 10MG ORAL FILM
24
SYMPAZAN 20MG ORAL FILM
24
SYMPAZAN 5MG ORAL FILM
24
SYMPROIC 0.2MG TAB 85 SYMTUZA 800-150-200-10MG TAB
62
SYNAREL 2MG/ML NASAL INHALER
81
SYNJARDY 10-1000MG ER TAB
30
SYNJARDY 12.5-1000MG ER TAB
30
SYNJARDY 12.5-1000MG TAB
30
SYNJARDY 12.5-500MG TAB
30
SYNJARDY 25-1000MG ER TAB
30
SYNJARDY 5-1000MG ER TAB
30
SYNJARDY 5-1000MG TAB
30
SYNJARDY 5-500MG TAB
30
SYNRIBO 3.5MG INJ 53 SYNTHROID 100MCG TAB
108
SYNTHROID 112MCG TAB
108
SYNTHROID 125MCG TAB
108
SYNTHROID 137MCG TAB
108
SYNTHROID 150MCG TAB
108
SYNTHROID 175MCG TAB
108
You can find information on what the symbols and abbreviations on this table mean by going to the beginning of this table.
154

ALPHABETICAL LISTING OF DRUGS
SYNTHROID 200MCG TAB
108
SYNTHROID 25MCG TAB
108
SYNTHROID 300MCG TAB
108
SYNTHROID 50MCG TAB
108
SYNTHROID 75MCG TAB
108
SYNTHROID 88MCG TAB
108
T
TABLOID 40MG TAB 44 TABRECTA 150MG TAB 52 TABRECTA 200MG TAB 52 tacrolimus 0.03% ointment
78
tacrolimus 0.1% ointment 78 tacrolimus 0.5mg cap 64 tacrolimus 1mg cap 64 tacrolimus 5mg cap 64 tadalafil 10mg tab 68 tadalafil 2.5mg tab 68 tadalafil 20mg tab (PAH) 69 tadalafil 5mg tab 68 tadalafil tab 20mg 68 TAFINLAR 50MG CAP 52 TAFINLAR 75MG CAP 52 TAGRISSO 40MG TAB 45 TAGRISSO 80MG TAB 45 TAKHZYRO 300MG/2ML INJ
87
TALTZ 80MG/ML AUTO-INJECTOR
76
TALTZ 80MG/ML SYRINGE
76
TALZENNA 0.25MG CAP 52 TALZENNA 1MG CAP 52 tamoxifen 10mg tab 46 tamoxifen 20mg tab 46 tamsulosin 0.4mg cap 86 TARGRETIN 1% GEL 75
tarina 24 fe 1/20 28 day pack
72
TASIGNA 150MG CAP 52 TASIGNA 200MG CAP 52 TASIGNA 50MG CAP 52 TAVALISSE 100MG TAB 87 TAVALISSE 150MG TAB 87 tazarotene 0.1% cream 76 TAZICEF 1GM INJ 71 tazicef 2gm inj 71 TAZICEF 6GM INJ 71 TAZORAC 0.05% CREAM
76
taztia 120mg er cap 67 taztia 180mg er cap 67 taztia 240mg er cap 67 taztia 300mg er cap 67 taztia 360mg er cap 67 TAZVERIK 200MG TAB 52 TDVAX 4-4UNIT/ML INJ 108 TEFLARO 400MG INJ 71 TEFLARO 600MG INJ 71 TEGSEDI 284MG/1.5ML INJ
106
TEKTURNA HCT 150-12.5MG TAB
41
TEKTURNA HCT 150-25MG TAB
41
TEKTURNA HCT 300-12.5MG TAB
41
TEKTURNA HCT 300-25MG TAB
41
telmisartan 20mg tab 38 telmisartan 40mg tab 38 telmisartan 80mg tab 38 temazepam 15mg cap 89 temazepam 30mg cap 89 temozolomide cap 44 TENIVAC 4-10UNIT/ML INJ
108
tenofovir disoproxil fumarate 300mg tab
62
TEPMETKO 225MG TAB 52 terazosin 10mg cap 39 terazosin 1mg cap 39
terazosin 2mg cap 39 terazosin 5mg cap 39 terbinafine 250mg tab 35 terbutaline sulfate 2.5mg tab
22
terbutaline sulfate 5mg tab
22
terconazole 0.4% vaginal cream
111
terconazole 0.8% vaginal cream
111
TERCONAZOLE 0.8% VAGINAL CREAM
111
terconazole 80mg vaginal insert
111
testosterone 1% (12.5mg) gel pump bottle
17
TESTOSTERONE 1% (12.5MG/ACT) GEL PUMP
17
testosterone 1% (25mg) gel packet
17
TESTOSTERONE 1% (50MG) GEL PACKET
17
testosterone 1.62% (1.25gm) gel packet
17
testosterone 1.62% (2.5gm) gel packet
17
testosterone 20.25mg/act gel pump
17
testosterone 30mg/act topical soln
17
testosterone cypionate 100mg/ml inj
17
testosterone cypionate 200mg/ml inj
17
TESTOSTERONE ENANTHATE 200MG/ML INJ
17
testosterone gel 1% (50mg) packet
17
tetrabenazine 12.5mg tab 104 tetrabenazine 25mg tab 104 tetracycline 250mg cap 107 tetracycline 500mg cap 107
You can find information on what the symbols and abbreviations on this table mean by going to the beginning of this table.
155
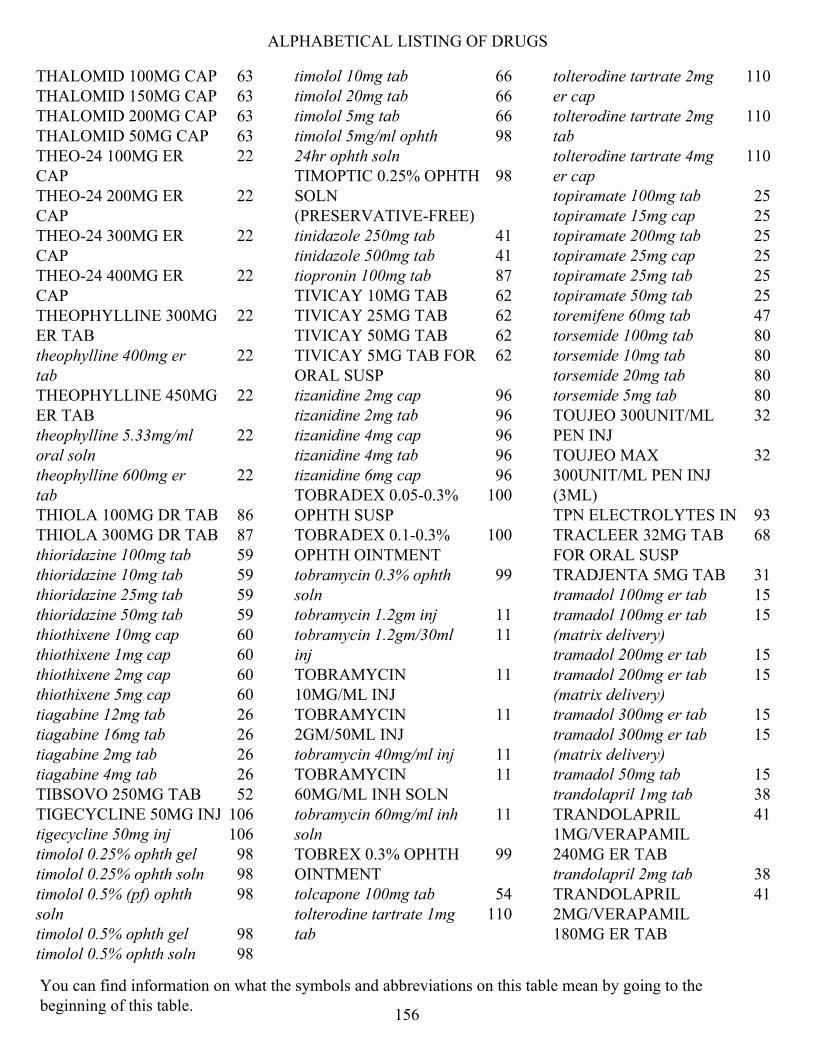
ALPHABETICAL LISTING OF DRUGS
THALOMID 100MG CAP 63 THALOMID 150MG CAP 63 THALOMID 200MG CAP 63 THALOMID 50MG CAP 63 THEO-24 100MG ER CAP
22
THEO-24 200MG ER CAP
22
THEO-24 300MG ER CAP
22
THEO-24 400MG ER CAP
22
THEOPHYLLINE 300MG ER TAB
22
theophylline 400mg er tab
22
THEOPHYLLINE 450MG ER TAB
22
theophylline 5.33mg/ml oral soln
22
theophylline 600mg er tab
22
THIOLA 100MG DR TAB 86 THIOLA 300MG DR TAB 87 thioridazine 100mg tab 59 thioridazine 10mg tab 59 thioridazine 25mg tab 59 thioridazine 50mg tab 59 thiothixene 10mg cap 60 thiothixene 1mg cap 60 thiothixene 2mg cap 60 thiothixene 5mg cap 60 tiagabine 12mg tab 26 tiagabine 16mg tab 26 tiagabine 2mg tab 26 tiagabine 4mg tab 26 TIBSOVO 250MG TAB 52 TIGECYCLINE 50MG INJ 106 tigecycline 50mg inj 106 timolol 0.25% ophth gel 98 timolol 0.25% ophth soln 98 timolol 0.5% (pf) ophth soln
98
timolol 0.5% ophth gel 98 timolol 0.5% ophth soln 98
timolol 10mg tab 66 timolol 20mg tab 66 timolol 5mg tab 66 timolol 5mg/ml ophth 24hr ophth soln
98
TIMOPTIC 0.25% OPHTH SOLN (PRESERVATIVE-FREE)
98
tinidazole 250mg tab 41 tinidazole 500mg tab 41 tiopronin 100mg tab 87 TIVICAY 10MG TAB 62 TIVICAY 25MG TAB 62 TIVICAY 50MG TAB 62 TIVICAY 5MG TAB FOR ORAL SUSP
62
tizanidine 2mg cap 96 tizanidine 2mg tab 96 tizanidine 4mg cap 96 tizanidine 4mg tab 96 tizanidine 6mg cap 96 TOBRADEX 0.05-0.3% OPHTH SUSP
100
TOBRADEX 0.1-0.3% OPHTH OINTMENT
100
tobramycin 0.3% ophth soln
99
tobramycin 1.2gm inj 11 tobramycin 1.2gm/30ml inj
11
TOBRAMYCIN 10MG/ML INJ
11
TOBRAMYCIN 2GM/50ML INJ
11
tobramycin 40mg/ml inj 11 TOBRAMYCIN 60MG/ML INH SOLN
11
tobramycin 60mg/ml inh soln
11
TOBREX 0.3% OPHTH OINTMENT
99
tolcapone 100mg tab 54 tolterodine tartrate 1mg tab
110
tolterodine tartrate 2mg er cap
110
tolterodine tartrate 2mg tab
110
tolterodine tartrate 4mg er cap
110
topiramate 100mg tab 25 topiramate 15mg cap 25 topiramate 200mg tab 25 topiramate 25mg cap 25 topiramate 25mg tab 25 topiramate 50mg tab 25 toremifene 60mg tab 47 torsemide 100mg tab 80 torsemide 10mg tab 80 torsemide 20mg tab 80 torsemide 5mg tab 80 TOUJEO 300UNIT/ML PEN INJ
32
TOUJEO MAX 300UNIT/ML PEN INJ (3ML)
32
TPN ELECTROLYTES INJ 93 TRACLEER 32MG TAB FOR ORAL SUSP
68
TRADJENTA 5MG TAB 31 tramadol 100mg er tab 15 tramadol 100mg er tab (matrix delivery)
15
tramadol 200mg er tab 15 tramadol 200mg er tab (matrix delivery)
15
tramadol 300mg er tab 15 tramadol 300mg er tab (matrix delivery)
15
tramadol 50mg tab 15 trandolapril 1mg tab 38 TRANDOLAPRIL 1MG/VERAPAMIL 240MG ER TAB
41
trandolapril 2mg tab 38 TRANDOLAPRIL 2MG/VERAPAMIL 180MG ER TAB
41
You can find information on what the symbols and abbreviations on this table mean by going to the beginning of this table.
156

ALPHABETICAL LISTING OF DRUGS
TRANDOLAPRIL 2MG/VERAPAMIL 240MG ER TAB
41
trandolapril 4mg tab 38 TRANDOLAPRIL 4MG/VERAPAMIL 240MG ER TAB
41
trandolapril 4mg/verapamil 240mg er tab
41
tranexamic acid 650mg tab
89
tranylcypromine 10mg tab
27
TRAVASOL 10% INJ 97 travoprost 0.004% ophth soln
100
trazodone 100mg tab 27 trazodone 150mg tab 27 trazodone 50mg tab 27 TRECATOR 250MG TAB 44 TRELEGY ELLIPTA 100- 62.5-25MCG INHALER
22
TRELEGY ELLIPTA 200-62.5-25MCG INHALER
22
TRELSTAR 11.25MG INJ 46 TRELSTAR 22.5MG INJ 46 TRELSTAR 3.75MG INJ 46 TREMFYA 100MG/ML AUTO-INJECTOR
76
TREMFYA 100MG/ML SYRINGE
76
TRESIBA 100UNIT/ML INJ
32
TRESIBA 100UNIT/ML PEN INJ
32
TRESIBA 200UNIT/ML PEN INJ
32
tretinoin 0.01% gel 75 tretinoin 0.025% cream 75 tretinoin 0.025% gel 75 tretinoin 0.04% gel 75 tretinoin 0.05% cream 75 tretinoin 0.05% gel 75
tretinoin 0.1% cream 75 tretinoin 0.1% gel 75 tretinoin 10mg cap 53 triamcinolone acetonide 0.025% cream
77
triamcinolone acetonide 0.025% lotion
77
triamcinolone acetonide 0.025% ointment
78
triamcinolone acetonide 0.1% cream
78
triamcinolone acetonide 0.1% lotion
78
triamcinolone acetonide 0.1% ointment
78
triamcinolone acetonide 0.1% oral paste
95
triamcinolone acetonide 0.5% ointment
78
triamterene 100mg cap 80 triamterene 50mg cap 80 triazolam 0.125mg tab 90 triazolam 0.25mg tab 90 tricitrates soln 86 tricon cap 89 triderm 0.5% cream 78 trientine 250mg cap 94 trifluoperazine 10mg tab 59 trifluoperazine 1mg tab 59 trifluoperazine 2mg tab 59 trifluoperazine 5mg tab 59 TRIFLURIDINE 1% OPHTH SOLN
99
trihexyphenidyl 0.4mg/ml oral soln
55
trihexyphenidyl 2mg tab 53 trihexyphenidyl 5mg tab 53 TRIJARDY 10-5-1000MG ER TAB
30
TRIJARDY 12.5-2.5-1000MG ER TAB
30
TRIJARDY 25-5-1000MG ER TAB
30
TRIJARDY 5-2.5-1000MG ER TAB
30
TRIKAFTA 100-50-75MG/150MG PACK
106
TRIKAFTA 50-37.5-25MG/75MG TAB PACK
106
tri-legest 28 day pack 72 tri-lo-sprintec 28 day pack
72
trimethobenzamide 300mg cap
34
trimethoprim 100mg tab 41 TRIMETHOPRIM 100MG TAB
41
trimipramine 100mg cap 30 trimipramine 25mg cap 30 trimipramine 50mg cap 30 TRINTELLIX 10MG TAB 27 TRINTELLIX 20MG TAB 27 TRINTELLIX 5MG TAB 27 TRIUMEQ 600-50-300MG TAB
62
trivora 28 day pack 72 trospium chloride 20mg tab
110
trospium chloride 60mg er cap
110
TRULANCE 3MG TAB 84 TRULICITY 0.75MG/0.5ML AUTO-INJECTOR
31
TRULICITY 1.5MG/0.5ML AUTO-INJECTOR
31
TRULICITY 3MG/0.5ML AUTO-INJECTOR
31
TRULICITY 4.5MG/0.5ML AUTO-INJECTOR
31
TRUMENBA INJ 110 TUKYSA 150MG TAB 45 TUKYSA 50MG TAB 45 TURALIO 200MG CAP 52
You can find information on what the symbols and abbreviations on this table mean by going to the beginning of this table.
157

ALPHABETICAL LISTING OF DRUGS
TUSNEL C SYRUP 74 tussigon tab 74 TUSSIONEX SUSP 74 TWINRIX 720UNIT INJ 111 TYBOST 150MG TAB 62 tydemy 28 day pack 72 TYMLOS 3120MCG/1.56ML PEN INJ
81
TYPHIM VI 25MCG/0.5ML INJ
110
U
UBRELVY 100MG TAB 92 UBRELVY 50MG TAB 92 UCERIS 2MG/ACT RECTAL FOAM
17
UKONIQ 200MG TAB 52 UPTRAVI 1000MCG TAB 69 UPTRAVI 1200MCG TAB 69 UPTRAVI 1400MCG TAB 69 UPTRAVI 1600MCG TAB 69 UPTRAVI 200MCG TAB 69 UPTRAVI 400MCG TAB 69 UPTRAVI 600MCG TAB 69 UPTRAVI 800MCG TAB 69 UPTRAVI TITRATION PACK
69
ursodiol 250mg tab 84 ursodiol 300mg cap 84 ursodiol 500mg tab 85
V
valacyclovir 1000mg tab 63 valacyclovir 500mg tab 63 VALCHLOR 0.016% GEL 76 valganciclovir 450mg tab 62 valganciclovir 50mg/ml oral soln
62
valproic acid 250mg cap 27 valproic acid 50mg/ml oral soln
27
valsartan 160mg tab 38 valsartan 320mg tab 38 valsartan 40mg tab 38 valsartan 80mg tab 38
VALTOCO 10MG DOSE KIT 10MG/0.1ML PACK
24
VALTOCO 15MG DOSE KIT 7.5MG/0.1ML PACK
24
VALTOCO 20MG DOSE KIT 10MG/0.1ML PACK
24
VALTOCO 5MG DOSE KIT 5MG/0.1ML PACK
24
VANCOMYCIN 1.25GM IV SOLN
42
vancomycin 1000mg inj 42 VANCOMYCIN 100GM INJ
42
vancomycin 100mg/ml inj 42 vancomycin 125mg cap 42 vancomycin 250mg cap 42 VANCOMYCIN 250MG INJ
42
vancomycin 500mg inj 42 vancomycin 5gm inj 42 vancomycin 750mg inj 42 VANCOMYCIN 750MG INJ
42
VAQTA 25UNIT/0.5ML INJ
111
VAQTA 50UNIT/ML INJ 111 vardenafil ODT 68 vardenafil tab 68 VARIVAX 1350PFU/0.5ML INJ
111
VARIZIG 125UNIT/1.2ML INJ
101
VARUBI 90MG TAB 34 VASCEPA 0.5GM CAP 35 VASCEPA 1GM CAP 35 V-C FORTE CAP 96 VELPHORO 500MG CHEW TAB
86
VELTASSA 16.8GM POWDER FOR ORAL SUSP
64
VELTASSA 25.2GM POWDER FOR ORAL SUSP
64
VELTASSA 8.4GM POWDER FOR ORAL SUSP
64
VEMLIDY 25MG TAB 62 VENCLEXTA 100MG TAB
45
VENCLEXTA 10MG TAB 45 VENCLEXTA 50MG TAB 45 VENCLEXTA STARTING PACK
45
venlafaxine 100mg tab 29 venlafaxine 150mg er cap 29 venlafaxine 25mg tab 29 venlafaxine 37.5mg er cap
29
venlafaxine 37.5mg tab 29 venlafaxine 50mg tab 29 venlafaxine 75mg er cap 29 venlafaxine 75mg tab 29 VENTAVIS 10MCG/ML INH SOLN
68
VENTAVIS 20MCG/ML INH SOLN
68
VENTOLIN 108MCG INH (18GM)
22
VENTOLIN 108MCG INH (8GM)
22
VERAPAMIL 100MG ER CAP
67
verapamil 120mg er cap 67 verapamil 120mg er tab 67 verapamil 120mg tab 67 verapamil 180mg er cap 67 verapamil 180mg er tab 67 VERAPAMIL 200MG ER CAP
67
verapamil 240mg er cap 67 verapamil 240mg er tab 67 VERAPAMIL 300MG ER CAP
67
VERAPAMIL 360MG ER CAP
67
verapamil 40mg tab 67 verapamil 80mg tab 67
You can find information on what the symbols and abbreviations on this table mean by going to the beginning of this table.
158

ALPHABETICAL LISTING OF DRUGS
VERELAN 100MG ER CAP
67
VERELAN 200MG ER CAP
67
VERELAN 300MG ER CAP
67
VERELAN 360MG ER CAP
67
VERICIGUAT 10MG TAB 69 VERICIGUAT 2.5MG TAB 69 VERICIGUAT 5MG TAB 69 VERSACLOZ 50MG/ML SUSP
58
VERZENIO 100MG TAB 52 VERZENIO 150MG TAB 52 VERZENIO 200MG TAB 52 VERZENIO 50MG TAB 52 VIBERZI 100MG TAB 85 VIBERZI 75MG TAB 85 VIBRAMYCIN 50MG/5ML SUSP
107
VICTOZA 18MG/3ML PEN INJ
31
vigabatrin 500mg powder for oral soln
26
vigabatrin 500mg tab 26 VIIBRYD 10/20MG STARTER PACK
28
VIIBRYD 10MG TAB 27 VIIBRYD 20MG TAB 27 VIIBRYD 40MG TAB 27 VIMPAT 100MG TAB 26 VIMPAT 10MG/ML ORAL SOLN
26
VIMPAT 150MG TAB 26 VIMPAT 200MG TAB 26 VIMPAT 50MG TAB 26 VIRACEPT 250MG TAB 62 VIRACEPT 625MG TAB 62 VIREAD 150MG TAB 62 VIREAD 200MG TAB 62 VIREAD 250MG TAB 62 VIREAD 40MG/GM ORAL POWDER
62
vitamin D 50000unit cap 112
VITRAKVI 100MG CAP 52 VITRAKVI 20MG/ML ORAL SOLN
52
VITRAKVI 25MG CAP 52 VIVITROL 380MG INJ 33 VIVOTIF BERNA CAP 110 VIZIMPRO 15MG TAB 45 VIZIMPRO 30MG TAB 45 VIZIMPRO 45MG TAB 46 voriconazole 200mg inj 35 voriconazole 200mg tab 35 voriconazole 40mg/ml susp
35
voriconazole 50mg tab 35 VOSEVI 400-100-100MG TAB
62
VOTRIENT 200MG TAB 53 VRAYLAR 1.5/3MG MIXED PACK
56
VRAYLAR 1.5MG CAP 56 VRAYLAR 3MG CAP 56 VRAYLAR 4.5MG CAP 56 VRAYLAR 6MG CAP 56 VYNDAMAX 61MG CAP 69 VYNDAQEL 20MG CAP 69
W
WAKIX 17.8MG TAB 9 WAKIX 4.45MG TAB 9 warfarin sodium 10mg tab
22
warfarin sodium 1mg tab 22 warfarin sodium 2.5mg tab
22
warfarin sodium 2mg tab 22 warfarin sodium 3mg tab 22 warfarin sodium 4mg tab 22 warfarin sodium 5mg tab 22 warfarin sodium 6mg tab 22 warfarin sodium 7.5mg tab
22
wymzya fe 28 day pack 72
X
XALKORI 200MG CAP 53 XALKORI 250MG CAP 53
XARELTO 10MG TAB 22 XARELTO 15MG TAB 22 XARELTO 2.5MG TAB 22 XARELTO 20MG TAB 22 XARELTO KIT PACK 22 XATMEP 2.5MG/ML ORAL SOLN
44
XCOPRI (250 MG DAILY DOSE) TAB PACK
26
XCOPRI 100MG TAB 26 XCOPRI 12.5/25MG TITRATION PACK
26
XCOPRI 150/200MG TITRATION PACK
26
XCOPRI 150MG TAB 26 XCOPRI 200MG TAB 26 XCOPRI 50/100MG TITRATION PACK
26
XCOPRI 50MG TAB 26 XCOPRI TAB 150/200MG PACK
26
XELJANZ 10MG TAB 11 XELJANZ 1MG/ML ORAL SOLN
11
XELJANZ 5MG TAB 11 XELJANZ XR 11MG TAB 11 XELJANZ XR 22MG TAB 11 XENLETA 600MG TAB 43 XERMELO 250MG TAB 86 XGEVA 120MG/1.7ML INJ
81
XIFAXAN 200MG TAB 41 XIFAXAN 550MG TAB 41 XIGDUO 10-1000MG ER TAB
30
XIGDUO 10-500MG ER TAB
30
XIGDUO 2.5-1000MG ER TAB
30
XIGDUO 5-1000MG ER TAB
31
XIGDUO 5-500MG ER TAB
31
XOFLUZA 40MG THERAPY PACK
63
You can find information on what the symbols and abbreviations on this table mean by going to the beginning of this table.
159

ALPHABETICAL LISTING OF DRUGS
XOLAIR 150MG INJ 20 XOLAIR 150MG/ML SYRINGE
20
XOLAIR 75MG/0.5ML SYRINGE
20
XOPENEX 45MCG INH, LEVALBUTEROL 45MCG INHALER
22
XOSPATA 40MG TAB 53 XPOVIO 100 MG ONCE WEEKLY
47
XPOVIO 100MG ONCE WEEKLY CARTON (8-PACK)
47
XPOVIO 40MG ONCE WEEKLY CARTON (4-PACK)
47
XPOVIO 40MG ONCE WEEKLY PACK
47
XPOVIO 40MG TWICE WEEKLY CARTON (8-PACK)
47
XPOVIO 40MG TWICE WEEKLY PACK
47
XPOVIO 60 MG ONCE WEEKLY
47
XPOVIO 60MG ONCE WEEKLY CARTON (4-PACK)
47
XPOVIO 60MG TWICE WEEKLY PACK
47
XPOVIO 80 MG ONCE WEEKLY
47
XPOVIO 80 MG TWICE WEEKLY
47
XPOVIO 80MG ONCE WEEKLY CARTON (8-PACK)
47
XTAMPZA 13.5MG ER CAP
15
XTAMPZA 18MG ER CAP
15
XTAMPZA 27MG ER CAP
15
XTAMPZA 36MG ER CAP
15
XTAMPZA 9MG ER CAP 15 XTANDI 40MG CAP 47 xulane 150-35mcg/24hr patch
72
XULTOPHY 100UNIT-3.6MG/ML PEN INJ
31
XYREM 500MG/ML ORAL SOLN
104
Y
YF-VAX 4000UNIT/ML INJ
111
Z
zafirlukast 10mg tab 20 zafirlukast 20mg tab 20 zaleplon 10mg cap 89 zaleplon 5mg cap 89 ZARXIO 300MCG/0.5ML SYRINGE
89
ZARXIO 480MCG/0.8ML SYRINGE
89
ZEJULA 100MG CAP 53 ZELBORAF 240MG TAB 53 ZEMAIRA 1000MG INJ 106 ZENPEP 105000-79000-25000UNIT DR CAP
79
ZENPEP 14000-10000-3000UNIT DR CAP
79
ZENPEP 24000-17000-5000UNIT DR CAP
79
ZENPEP 40000-126000-168000UNIT DR CAP
79
ZENPEP 42000-32000-10000UNIT DR CAP
79
ZENPEP 63000-47000-15000UNIT DR CAP
79
ZENPEP 84000-63000-20000UNIT DR CAP
79
ZEPOSIA 0.92MG CAP 105 ZEPOSIA 7-DAY STARTER PACK
105
ZEPOSIA STARTER KIT PACK
105
ZERBAXA 1000-500MG INJ
69
zidovudine 100mg cap 62 zidovudine 10mg/ml oral soln
62
zidovudine 300mg tab 62 ZIEXTENZO 6MG/0.6ML SYRINGE
89
ZIOPTAN 0.015MG/ML OPHTH SOLN
100
ziprasidone 20mg cap 56 ziprasidone 20mg inj 56 ziprasidone 40mg cap 56 ziprasidone 60mg cap 56 ziprasidone 80mg cap 56 ZIRGAN 0.15% OPHTH GEL
99
ZOLINZA 100MG CAP 53 zolmitriptan 2.5mg odt 92 zolmitriptan 2.5mg tab 92 zolmitriptan 5mg odt 92 zolmitriptan 5mg tab 92 zolpidem tartrate 10mg tab
89
zolpidem tartrate 5mg tab 89 ZOMIG 2.5MG NASAL SPRAY
92
ZOMIG 5MG NASAL SPRAY
92
zonisamide 100mg cap 26 zonisamide 25mg cap 26 zonisamide 50mg cap 26 ZONTIVITY 2.08MG TAB 87 ZORTRESS 1MG TAB 95 ZOSYN 2000-250MG INJ 103 ZOSYN 3000-375MG INJ 103
You can find information on what the symbols and abbreviations on this table mean by going to the beginning of this table.
160

ALPHABETICAL LISTING OF DRUGS
ZOSYN/DEXTROSE 4-0.5GM/100ML INJ
103
ZUBSOLV 0.7-0.18MG SL TAB
16
ZUBSOLV 1.4-0.36MG SL TAB
16
ZUBSOLV 11.4-2.9MG SL TAB
16
ZUBSOLV 2.9-0.71MG SL TAB
16
ZUBSOLV 5.7-1.4MG SL TAB
16
ZUBSOLV 8.6-2.1MG SL TAB
17
ZYDELIG 100MG TAB 53 ZYDELIG 150MG TAB 53 ZYKADIA 150MG TAB 53 ZYLET 0.5-0.3% OPHTH SUSP
100
ZYPREXA RELPREVV 210MG INJ
58
You can find information on what the symbols and abbreviations on this table mean by going to the beginning of this table.
161
S9701_2022_UCA_FORM_Comp_V01.8_C
This formulary was updated on 10/28/2021. For more recent information or other questions, please contact Navitus MedicareRx Customer Care at 1-866-270-3877 (TTY users should call 711), available 24 hours a day, 7 days a week (except on Thanksgiving and Christmas Day) or visit the member portal at https://memberportal.navitus.com.
Pharmacies can reach Navitus Customer Care 24 hours a day, 7 days a week.
This formulary was updated on 10/28/2021

NAVITUS MEDICARERX (PDP) JANUARY 1 – DECEMBER 31, 2022 EVIDENCE OF COVERAGE UNIVERSITY OF CALIFORNIA High Option Supplement to Medicare and Medicare PPO
Your Medicare Prescription Drug Coverage as a Member of Navitus MedicareRx Prescription Drug Plan (PDP) This booklet gives you the details about your Medicare prescription drug coverage from January 1 – December 31, 2022. It explains how to get coverage for the prescription drugs you need. This is an important legal document. Please keep it in a safe place.
This plan, Navitus MedicareRx (PDP), offered by Dean Health Insurance, Inc., is a Federally-Qualified Medicare Contracting Prescription Drug Plan.
(When this Evidence of Coverage says “we,” “us,” or “our,” “plan,” or “our plan,” it means Navitus MedicareRx.)
The University of California has implemented an Employer Group Waiver Plan (EGWP) for Medicare-eligible retirees. This plan is administered by Navitus Health Solutions. This means that Medicare-eligible retirees and/or dependents are enrolled in a Group Medicare Part D Plan. Your employer group plan also includes supplemental coverage that wraps around the benefits provided by this plan. Please contact our Customer Care number at 1-866-270-3877 for additional information. (TTY/TDD users should call 711.) Hours are 24 hours a day, 7 days a week, except on Thanksgiving and Christmas Day. Calls to these numbers are free.
Customer Care has free language interpreter services available for non-English speakers if needed. This booklet is also available in different formats, including braille and large print. Please call Customer Care if you need plan information in another format.
For plan premium or enrollment questions, please contact the UC Retirement Administration Service Center (RASC) at (800) 888-8267 (in U.S.) or (510) 987-0200 (from outside the U.S.). Representatives are available Monday through Friday, 8:30 a.m. to 4:30 p.m. (Pacific).
Benefits, premium, deductible, and/or copayments/coinsurance may change on January 1, 2023.
The formulary, pharmacy network, and/or provider network may change at any time. You will receive notice when necessary.
S9701_2022_UCA_EOC_V01_C
2022 Evidence of Coverage for Navitus MedicareRx (PDP) 1 Table of Contents
2022 Evidence of Coverage
Table of Contents
This list of chapters and page numbers is your starting point. For more help in finding information you need, go to the first page of a chapter. You will find a detailed list of topics at the beginning of each chapter.
Chapter 1. Getting started as a member ...................................................................... 4 Explains what it means to be in a Medicare prescription drug plan and how to use this booklet. Tells about materials we will send you, your plan premium, the Part D late enrollment penalty, your plan membership card, and keeping your membership record up to date.
Chapter 2. Important phone numbers and resources.............................................. 21 Tells you how to get in touch with our plan (Navitus MedicareRx) and with other organizations including Medicare, the State Health Insurance Assistance Program (SHIP), the Quality Improvement Organization, Social Security, Medicaid (the state health insurance program for people with low incomes), programs that help people pay for their prescription drugs, and the Railroad Retirement Board.
Chapter 3. Using the plan’s coverage for your Part D prescription drugs .......... 36 Explains rules you need to follow when you get your Part D drugs. Tells how to use the plan’s List of Covered Drugs (Formulary) to find out which drugs are covered. Tells which kinds of drugs are not covered. Explains several kinds of restrictions that apply to coverage for certain drugs. Explains where to get your prescriptions filled. Tells about the plan’s programs for drug safety and managing medications.
Chapter 4. What you pay for your Part D prescription drugs ................................. 62 Tells about the four stages of drug coverage (Deductible Stage, Initial Coverage Stage, Coverage Gap Stage, Catastrophic Coverage Stage) and how these stages affect what you pay for your drugs. Explains the four cost-sharing tiers for your Part D drugs and tells what you must pay for a drug in each cost-sharing tier.
Chapter 5. Asking us to pay our share of the costs for covered drugs ............... 86 Explains when and how to send a bill to us when you want to ask us to pay you back for our share of the cost for your covered drugs.

2022 Evidence of Coverage for Navitus MedicareRx (PDP) 2 Table of Contents
Chapter 6. Your rights and responsibilities............................................................... 93 Explains the rights and responsibilities you have as a member of our plan. Tells what you can do if you think your rights are not being respected.
Chapter 7. What to do if you have a problem or complaint (coverage decisions, appeals, complaints) ......................................... 103 Tells you step-by-step what to do if you are having problems or concerns as a member of our plan.
• Explains how to ask for coverage decisions and make appeals if you are having trouble getting the prescription drugs you think are covered by our plan. This includes asking us to make exceptions to the rules and/or extra restrictions on your coverage.
• Explains how to make complaints about quality of care, waiting times, customer care, and other concerns.
Chapter 8. Ending your membership in the plan .................................................... 129 Explains when and how you can end your membership in the plan. Explains situations in which our plan is required to end your membership.
Chapter 9. Legal notices ............................................................................................. 140 Includes notices about governing law and about non-discrimination.
Chapter 10. Definitions of important words ............................................................... 143 Explains key terms used in this booklet.
Exhibit A - Listing of State Health Insurance Assistance Programs (SHIPs)…....149
Exhibit B - Listing of Quality Improvement Organizations (QIOs)…………………156
Exhibit C - Listing of State Medical Assistance Offices (Medicaid)……………….157
Exhibit D - Listing of State Pharmaceutical Assistance Programs (SPAPs)…….162
Exhibit E - Listing of State AIDS Drug Assistance Programs (ADAPs) ………….164
CHAPTER 1 Getting started as a member
2022 Evidence of Coverage for Navitus MedicareRx (PDP) 4 Chapter 1. Getting started as a member
Chapter 1. Getting started as a member
SECTION 1 Introduction.............................................................................................. 6
Section 1.1 You are enrolled in Navitus MedicareRx, which is a Medicare Prescription Drug Plan (PDP) ......................................................................6
Section 1.2 What is the Evidence of Coverage booklet about? ........................................6
Section 1.3 Legal information about the Evidence of Coverage.......................................6
SECTION 2 What makes you eligible to be a plan member?................................ 7
Section 2.1 Your eligibility requirements .......................................................................7
Section 2.2 What are Medicare Part A and Medicare Part B? ..........................................7
Section 2.3 Here is the plan service area for Navitus MedicareRx ...................................8
Section 2.4 U.S. Citizen or Lawful Presence ..................................................................8
SECTION 3 What other materials will you get from us? ....................................... 8
Section 3.1 Your plan membership card – Use it to get all covered prescription drugs .....8
Section 3.2 The Pharmacy Directory: Your guide to pharmacies in our network .............9
Section 3.3 The plan’s List of Covered Drugs (Formulary)........................................... 10
Section 3.4 The Part D Explanation of Benefits (the “Part D EOB”): Reports with a summary of payments made for your Part D prescription drugs .................. 10
SECTION 4 Your monthly premium for Navitus MedicareRx (PDP) .................. 10
Section 4.1 How much is your plan premium? ............................................................. 10
SECTION 5 Do you have to pay the Part D “late enrollment penalty”? ............ 12
Section 5.1 What is the Part D “late enrollment penalty”? ............................................ 12
Section 5.2 How much is the Part D late enrollment penalty? ....................................... 12
Section 5.3 In some situations, you can enroll late and not have to pay the penalty........ 13
Section 5.4 What can you do if you disagree about your Part D late enrollment penalty? .................................................................................................... 14
SECTION 6 Do you have to pay an extra Part D amount because of your income? .................................................................................................. 14
Section 6.1 Who pays an extra Part D amount because of income? ............................... 14
Section 6.2 How much is the extra Part D amount? ...................................................... 15
Section 6.3 What can you do if you disagree about paying an extra Part D amount? ...... 15
Section 6.4 What happens if you do not pay the extra Part D amount? .......................... 15

2022 Evidence of Coverage for Navitus MedicareRx (PDP) 5 Chapter 1. Getting started as a member
SECTION 7 More information about your monthly premium ............................. 15
Section 7.1 Many members are required to pay other Medicare premiums .................... 15
Section 7.2 There are several ways you can pay your plan premium ............................. 16
Section 7.3 Can we change your monthly plan premium during the year? ..................... 16
SECTION 8 Please keep your plan membership record up to date .................. 17
Section 8.1 How to help make sure that we have accurate information about you .......... 17
SECTION 9 We protect the privacy of your personal health information ........ 18
Section 9.1 We make sure that your health information is protected.............................. 18
SECTION 10 How other insurance works with our plan ........................................ 18
Section 10.1 Which plan pays first when you have other insurance? ............................... 18
2022 Evidence of Coverage for Navitus MedicareRx (PDP) 6 Chapter 1. Getting started as a member
SECTION 1 Introduction
Section 1.1 You are enrolled in Navitus MedicareRx, which is a Medicare Prescription Drug Plan (PDP)
You are covered by Original Medicare for your health care coverage, and you have chosen to get your Medicare prescription drug coverage through our plan, Navitus MedicareRx.
There are different types of Medicare plans. Navitus MedicareRx is a Medicare prescription drug plan (PDP). Like all Medicare plans, this Medicare prescription drug plan is approved by Medicare and run by a private company. In addition, your retiree drug coverage includes non-Medicare supplemental drug coverage provided by your Navitus MedicareRx benefits.
Section 1.2 What is the Evidence of Coverage booklet about?
This Evidence of Coverage booklet explains how to get your Medicare prescription drug coverage through our plan. This booklet explains your rights and responsibilities, what is covered, and what you pay as a member of the plan.
The word “coverage” or “covered drugs” refers to the prescription drug coverage available to you as a member of Navitus MedicareRx.
It’s important for you to learn what your plan’s rules are and what coverage is available to you. We encourage you to set aside some time to look through this Evidence of Coverage booklet.
If you are confused or concerned or just have a question, please contact our plan’s Customer Care (phone numbers are printed on the back cover of this booklet).
Section 1.3 Legal information about the Evidence of Coverage
It’s part of our contract with you
This Evidence of Coverage is part of our contract with you about how Navitus MedicareRx covers your care. Other parts of this contract include your enrollment form, the List of Covered Drugs (Formulary), and any notices you receive from us about changes to your coverage or conditions that affect your coverage. These notices are sometimes called “riders” or “amendments.”
The contract is in effect for months in which you are enrolled in Navitus MedicareRx between January 1, 2022 and December 31, 2022.
Each calendar year, Medicare allows us to make changes to the plans that we offer. This means we can change the costs and benefits of Navitus MedicareRx after December 31, 2022. We can

2022 Evidence of Coverage for Navitus MedicareRx (PDP) 7 Chapter 1. Getting started as a member
also choose to stop offering the plan, or to offer it in a different service area, after December 31, 2022.
Medicare must approve our plan each year
Medicare (the Centers for Medicare & Medicaid Services) must approve Navitus MedicareRx each year. You can continue to get Medicare coverage as a member of our plan as long as we choose to continue to offer the plan and Medicare renews its approval of the plan.
SECTION 2 What makes you eligible to be a plan member?
Section 2.1 Your eligibility requirements
You are eligible for membership in our plan as long as:
• You have Medicare Part A and Medicare Part B (Section 2.2 tells you about Medicare Part A and Medicare Part B)
• -- and -- you are a United States citizen or are lawfully present in the United States
• -- and -- you live in our geographic service area (Section 2.3 below describes our service area)
• -- and -- you are eligible for coverage under your group sponsored health plan retiree benefits.
Section 2.2 What are Medicare Part A and Medicare Part B?
As discussed in Section 1.1 above, you have chosen to get your prescription drug coverage (sometimes called Medicare Part D) through our plan. Our plan has contracted with Medicare to provide you with most of these Medicare benefits. We describe the drug coverage you receive under your Medicare Part D coverage in Chapter 3.
When you first signed up for Medicare, you received information about what services are covered under Medicare Part A and Medicare Part B. Remember:
• Medicare Part A generally helps cover services provided by hospitals (for inpatient services, skilled nursing facilities, or home health agencies).
• Medicare Part B is for most other medical services (such as physician’s services, home infusion therapy, and other outpatient services) and certain items (such as durable medical equipment (DME) and supplies).
2022 Evidence of Coverage for Navitus MedicareRx (PDP) 8 Chapter 1. Getting started as a member
Section 2.3 Here is the plan service area for Navitus MedicareRx
Although Medicare is a Federal program, Navitus MedicareRx is available only to individuals who live in our plan service area. To remain a member of our plan, you must continue to reside in the plan service area. The service area is described as all 50 states and Puerto Rico. The service area excludes most U.S. Territories, such as the U.S. Virgin Islands, Guam, American Samoa, and the Northern Mariana Islands.
If you move outside of our service area, you cannot remain a member of our plan. If you plan to move out of the service area, please contact the UC Retirement Administration Service Center (RASC) at (800) 888-8267 (in U.S.) or (510) 987-0200 (from outside the U.S.). Representatives are available Monday through Friday, 8:30 a.m. to 4:30 p.m. (Pacific).
It is also important that you call Social Security if you move or change your mailing address. You can find phone numbers and contact information for Social Security in Chapter 2, Section 5.
Section 2.4 U.S. Citizen or Lawful Presence
A member of a Medicare health plan must be a U.S. citizen or lawfully present in the United States. Medicare (the Centers for Medicare & Medicaid Services) will notify Navitus MedicareRx if you are not eligible to remain a member on this basis. Navitus MedicareRx must disenroll you if you do not meet this requirement.
SECTION 3 What other materials will you get from us?
Section 3.1 Your plan membership card – Use it to get all covered prescription drugs
While you are a member of our plan, you must use your membership card for our plan for prescription drugs you get at network pharmacies. You should also show the pharmacy your Medicaid card, if applicable. Here’s a sample membership card to show you what yours will look like:
2022 Evidence of Coverage for Navitus MedicareRx (PDP) 9 Chapter 1. Getting started as a member
Please carry your membership card with you at all times and remember to show your card when you get covered drugs. If your plan membership card is damaged, lost, or stolen, call Customer Care right away and we will send you a new card. (Phone numbers for Customer Care are printed on the back cover of this booklet.)
You may need to use your red, white, and blue Medicare card to get covered medical care and services under Original Medicare.
Section 3.2 The Pharmacy Directory: Your guide to pharmacies in our network
What are “network pharmacies”?
Network pharmacies are all of the pharmacies that have agreed to fill covered prescriptions for our plan members.
Why do you need to know about network pharmacies?
You can use the pharmacy search tool to find the network pharmacy you want to use. You can find a pharmacy search tool on our Member Portal at https://memberportal.navitus.com. There are changes to our network of pharmacies for next year. Also, an updated Pharmacy Directory is located on our Member Portal at https://memberportal.navitus.com. You may also call Customer Care for updated pharmacy information or to ask us to mail you a Pharmacy Directory. Please review your pharmacies to see which pharmacies are in our network.
If you don’t have the Pharmacy Directory, you can get a copy from Customer Care (phone numbers are printed on the back cover of this booklet). At any time, you can call Customer Care to get up-to-date information about changes in the pharmacy network. You can also find a pharmacy search tool on our Member Portal at https://memberportal.navitus.com.

2022 Evidence of Coverage for Navitus MedicareRx (PDP) 10 Chapter 1. Getting started as a member
Section 3.3 The plan’s List of Covered Drugs (Formulary)
The plan has a List of Covered Drugs (Formulary). It tells which Part D prescription drugs are covered by Navitus MedicareRx. The drugs on this list are selected by the plan with the help of a team of doctors and pharmacists. The list must meet requirements set by Medicare. Medicare has approved the Navitus MedicareRx Formulary.
The Formulary also explains if there are any rules that restrict coverage for your drugs.
A copy of the Formulary is located on our Member Portal at https://memberportal.navitus.com. If one of your drugs is not listed in the Formulary, you should visit our Member Portal or contact Customer Care to find out if we cover it. To get the most complete and current information about which drugs are covered, you can visit the plan’s Member Portal (https://memberportal.navitus.com) or call Customer Care (phone numbers are printed on the back cover of this booklet).
Section 3.4 The Part D Explanation of Benefits (the “Part D EOB”): Reports with a summary of payments made for your Part D prescription drugs
When you use your Part D prescription drug benefits, we will send you a summary report to help you understand and keep track of payments for your Part D prescription drugs. This summary report is called the Part D Explanation of Benefits (or the “Part D EOB”).
A Part D Explanation of Benefits explains the total amount you, or others on your behalf, have spent on your Part D prescription drugs and the total amount your retiree drug coverage has paid for each of your Part D prescription drugs during each month the Part D benefit is used. The Part D EOB is not a bill. The Part D EOB provides more information about the drugs you take, such as increases in price and other drugs with lower cost sharing that may be available. You should consult with your prescriber about these lower cost options. Chapter 4 (What you pay for your Part D prescription drugs) gives more information about the Part D Explanation of Benefits and how it can help you keep track of your drug coverage.
The Part D Explanation of Benefits is also available upon request. To get a copy, please contact Customer Care (phone numbers are printed on the back cover of this booklet).
SECTION 4 Your monthly premium for Navitus MedicareRx (PDP)
Section 4.1 How much is your plan premium?
As a member of our plan, you pay a monthly plan premium. In addition, you must continue to pay your Medicare Part B premium (unless your Part B premium is paid for you by Medicaid or another third party).
2022 Evidence of Coverage for Navitus MedicareRx (PDP) 11 Chapter 1. Getting started as a member
Your coverage is provided through a contract with your current employer or former employer. Please contact the UC Retirement Administration Service Center (RASC) at (800) 888-8267 (in U.S.) or (510) 987-0200 (from outside the U.S.) for information about your plan premium amounts. Representatives are available Monday through Friday, 8:30 a.m. to 4:30 p.m. (Pacific).
In some situations, your plan premium could be less There are programs to help people with limited resources pay for their drugs. These include “Extra Help” and State Pharmaceutical Assistance Programs. The “Extra Help” program helps people with limited resources pay for their drugs. Chapter 2, Section 7 tells more about these programs. If you qualify, enrolling in the program might lower your monthly plan premium.
If you are already enrolled and getting help from one of these programs, the information about premiums in this Evidence of Coverage may not apply to you. We have included a separate insert, called the “Evidence of Coverage Rider for People Who Get Extra Help Paying for Prescription Drugs” (also known as the “Low Income Subsidy Rider” or the “LIS Rider”), which explains your drug coverage. If you didn’t receive this insert and it applies to you, please call Customer Care and ask for the “LIS Rider.” (Phone numbers for Customer Care are printed on the back cover of this booklet.) In most cases, because you’re enrolled in a group sponsored plan, we’ll credit the amount of “Extra Help” received to your group’s bill on your behalf. If your group plan pays 100% of the premium for your retiree coverage, then the group sponsor plan is entitled to keep these funds. However, if you contribute to the premium, your group must apply the subsidy toward the amount you contribute to this plan.
In some situations, your plan premium could be more In some situations, you may owe additional money because of your income or when you enrolled in Part D. Some members are required to pay a Part D late enrollment penalty because they did not join a Medicare drug plan when they first became eligible or because they had a continuous period of 63 days or more when they didn’t have “creditable” prescription drug coverage. (“Creditable” means the drug coverage is expected to pay, on average, at least as much as Medicare’s standard prescription drug coverage. If applicable to you, Navitus MedicareRx will bill you directly each month.
• If you are required to pay the Part D late enrollment penalty, the cost of the late enrollment penalty depends on how long you went without Part D or other creditable prescription drug coverage. Chapter 1, Section 5 explains the Part D late enrollment penalty.
If you have a Part D late enrollment penalty and do not pay it, you could be disenrolled from your plan. Some members may be required to pay an extra charge, known as the Part D Income Related Monthly Adjustment Amount, also known as IRMAA, because, 2 years ago, they had a modified adjusted gross income, above a certain amount, on their IRS tax return. Members subject to an IRMAA will have to pay the standard premium amount and this extra charge, which will be added to their premium. Chapter 1, Section 6 explains the IRMAA in further detail.

2022 Evidence of Coverage for Navitus MedicareRx (PDP) 12 Chapter 1. Getting started as a member
SECTION 5 Do you have to pay the Part D “late enrollment penalty”?
Section 5.1 What is the Part D “late enrollment penalty”?
Note: If you receive “Extra Help” from Medicare to pay for your prescription drugs, you will not pay a late enrollment penalty.
You may owe a Part D late enrollment penalty if you did not enroll in a plan offering Medicare Part D drug coverage when you first became eligible for this drug coverage, or if there is a period of 63 days or more in a row when you did not have Part D or other creditable prescription drug coverage. (“Creditable prescription drug coverage” is coverage that meets Medicare’s minimum standards since it is expected to pay, on average, at least as much as Medicare’s standard prescription drug coverage.) The cost of the late enrollment penalty depends on how long you went without Part D or other creditable prescription drug coverage. You will have to pay this penalty for as long as you have Part D coverage.
When you first enroll in Navitus MedicareRx, we will let you know the amount of the penalty. Navitus MedicareRx will directly bill you for any applicable late enrollment penalties. If you do not pay your Part D late enrollment penalty, you could be disenrolled from the plan.
Section 5.2 How much is the Part D late enrollment penalty?
Medicare determines the amount of the penalty. Here is how it works:
• First count the number of full months that you delayed enrolling in a Medicare drug plan after you were eligible to enroll. Or count the number of full months in which you did not have creditable prescription drug coverage, if the break in coverage was 63 days or more. The penalty is 1% for every month that you didn’t have creditable coverage. For example, if you go 14 months without coverage, the penalty will be 14%.
• Then Medicare determines the amount of the average monthly premium for Medicare drug plans in the nation from the previous year. For 2022, the average premium amount is $33.37.
• To calculate your monthly penalty, you multiply the penalty percentage and the average monthly premium and then round it to the nearest 10 cents. In the example here, it would be 14% times $33.37, which equals $4.67. This rounds to $4.70. This amount would be added to the monthly premium for someone with a Part D late enrollment penalty.
There are three important things to note about this monthly Part D late enrollment penalty:
2022 Evidence of Coverage for Navitus MedicareRx (PDP) 13 Chapter 1. Getting started as a member
• First, the penalty may change each year, because the average monthly premium can change each year. If the national average premium (as determined by Medicare) increases, your penalty will increase.
• Second, you will continue to pay a penalty every month for as long as you are enrolled in a plan that has Medicare Part D drug benefits, even if you change plans.
• Third, if you are under 65 and currently receiving Medicare benefits, the Part D late enrollment penalty will reset when you turn 65. After age 65, your Part D late enrollment penalty will be based only on the months that you don’t have coverage after your initial enrollment period for aging into Medicare.
Section 5.3 In some situations, you can enroll late and not have to pay the penalty
Even if you have delayed enrolling in a plan offering Medicare Part D coverage when you were first eligible, sometimes you do not have to pay the Part D late enrollment penalty.
You will not have to pay a penalty for late enrollment if you are in any of these situations:
• If you already have prescription drug coverage that is expected to pay, on average, at least as much as Medicare’s standard prescription drug coverage. Medicare calls this “creditable drug coverage.” Please note:
o Creditable coverage could include drug coverage from a group sponsor, TRICARE, or the Department of Veterans Affairs. Your insurer or your human resources department will tell you each year if your drug coverage is creditable coverage. This information may be sent to you in a letter or included in a newsletter from the plan. Keep this information, because you may need it if you join a Medicare drug plan later. Please note: If you receive a “certificate of creditable coverage” when
your health coverage ends, it may not mean your prescription drug coverage was creditable. The notice must state that you had “creditable” prescription drug coverage that expected to pay as much as Medicare’s standard prescription drug plan pays.
o The following are not creditable prescription drug coverage: prescription drug discount cards, free clinics, and drug discount websites.
o For additional information about creditable coverage, please look in your Medicare & You 2022 handbook or call Medicare at 1-800-MEDICARE (1-800-633-4227). TTY/TDD users call 1-877-486-2048. You can call these numbers for free, 24 hours a day, 7 days a week.
• If you were without creditable coverage, but you were without it for less than 63 days in a row.
• If you are receiving “Extra Help” from Medicare.

2022 Evidence of Coverage for Navitus MedicareRx (PDP) 14 Chapter 1. Getting started as a member
Section 5.4 What can you do if you disagree about your Part D late enrollment penalty?
If you disagree about your Part D late enrollment penalty, you or your representative can ask for a review of the decision about your late enrollment penalty. Generally, you must request this review within 60 days from the date on the first letter you receive stating you have to pay a late enrollment penalty. If you were paying a penalty before joining our plan, you may not have another chance to request a review of that late enrollment penalty. Call Customer Care to find out more about how to do this (phone numbers are printed on the back cover of this booklet).
Important: Do not stop paying your Part D late enrollment penalty while you’re waiting for a review of the decision about your late enrollment penalty. If you do, you could be disenrolled for failure to pay your plan premiums.
SECTION 6 Do you have to pay an extra Part D amount because of your income?
Section 6.1 Who pays an extra Part D amount because of income?
If your modified adjusted gross income as reported on your IRS tax return from 2 years ago is above a certain amount, you’ll pay the standard premium amount and an Income Related Monthly Adjustment Amount, also known as IRMAA. IRMAA is an extra charge added to your premium.
Part D-IRMAA is assessed to all Medicare beneficiaries with Part D coverage whose incomes exceed the federal government established threshold amounts. Failure by a Medicare beneficiary to pay the Part D-IRMAA will result in involuntary disenrollment from their Part D plan and, thus, the loss of retiree drug and/or health coverage through their group sponsor.
Please carefully review all communications you receive from Medicare. As a Part D group sponsor, your group sponsor will not be billing or collecting the Part D-IRMAA; however, as a group sponsor we must be prepared to effectuate accurate disenrollments in situations where individuals fail to pay the income-related adjustment.
If you have to pay an extra amount, Social Security, not your Medicare plan, will send you a letter telling you what that extra amount will be and how to pay it. The extra amount will be withheld from your Social Security, Railroad Retirement Board, or Office of Personnel Management benefit check, no matter how you usually pay your plan premium, unless your monthly benefit isn’t enough to cover the extra amount owed. If your benefit check isn’t enough to cover the extra amount, you will get a bill from Medicare. You must pay the extra amount to the government. It cannot be paid with your monthly plan premium.

2022 Evidence of Coverage for Navitus MedicareRx (PDP) 15 Chapter 1. Getting started as a member
Section 6.2 How much is the extra Part D amount?
If your modified adjusted gross income (MAGI) as reported on your IRS tax return is above a certain amount, you will pay an extra amount in addition to your monthly plan premium. For more information on the extra amount you may have to pay based on your income, visit www.medicare.gov/part-d/costs/premiums/drug-plan-premiums.html.
Section 6.3 What can you do if you disagree about paying an extra Part D amount?
If you disagree about paying an extra amount because of your income, you can ask Social Security to review the decision. To find out more about how to do this, contact Social Security at 1-800-772-1213 (TTY/TDD 1-800-325-0778).
Section 6.4 What happens if you do not pay the extra Part D amount?
The extra amount is paid directly to the government (not your Medicare plan) for your Medicare Part D coverage. If you are required by law to pay the extra amount and you do not pay it, you will be disenrolled from retiree drug and/or health coverage through the group sponsor.
SECTION 7 More information about your monthly premium
Section 7.1 Many members are required to pay other Medicare premiums
In addition to paying the monthly plan premium, many members are required to pay other Medicare premiums. Some plan members (those who aren’t eligible for premium-free Part A) pay a premium for Medicare Part A. Most plan members pay a premium for Medicare Part B. You must continue to pay your Medicare premiums for you to remain a member of your plan.
If your modified adjusted gross income as reported on your IRS tax return from 2 years ago is above a certain amount, you’ll pay the standard premium amount and an Income Related Monthly Adjustment Amount, also known as IRMAA. IRMAA is an extra charge added to your premium.
• If you are required to pay the extra amount and you do not pay it, you will be disenrolled from your plan and lose prescription drug coverage.
• If you have to pay an extra amount, Social Security, not your Medicare plan, will send you a letter telling you what that extra amount will be.
• For more information about Part D premiums based on income, go to Chapter 1, Section 6 of this booklet. You can also visit www.medicare.gov on the Web or call 1-800-MEDICARE (1-800-633-4227), 24 hours a day, 7 days a week. TTY/TDD users should
2022 Evidence of Coverage for Navitus MedicareRx (PDP) 16 Chapter 1. Getting started as a member
call 1-877-486-2048. Or you may call Social Security at 1-800-772-1213. TTY/TDD users should call 1-800-325-0778.
Your copy of the Medicare & You 2022 handbook gives information about the Medicare premiums in the section called “2022 Medicare Costs.” This explains how the Medicare Part B and Part D premiums differ for people with different incomes. Everyone with Medicare receives a copy of the Medicare & You 2022 handbook each year in the fall. Those new to Medicare receive it within a month after first signing up. You can also download a copy of the Medicare & You 2022 handbook from the Medicare website (www.medicare.gov). Or, you can order a printed copy by phone at 1-800-MEDICARE (1-800-633-4227), 24 hours a day, 7 days a week. TTY/TDD users call 1-877-486-2048.
Section 7.2 There are several ways you can pay your plan premium Please contact the UC Retirement Administration Service Center (RASC) at (800) 888-8267 (in U.S.) or (510) 987-0200 (from outside the U.S.). Representatives are available Monday through Friday, 8:30 a.m. to 4:30 p.m. (Pacific) to find out what your plan premium is and how you are required to pay for it. Your benefits administrator can discuss different payment options with you. If you think we have wrongfully ended your enrollment in the Part D plan, you have a right to ask us to reconsider this decision by making a complaint. Chapter 7, Section 7 of this booklet tells how to make a complaint. If you had an emergency circumstance that was out of your control and it caused you to not be able to pay your plan premium within the grace period, you can ask us to reconsider this decision by calling the RASC. TTY/TDD users should call 711. You must make your request no later than 60 days after the date your membership ends.
Section 7.3 Can we change your monthly plan premium during the year?
Medicare Part D Coverage: No. Generally, your plan premium won’t change during the benefit year. You will be notified, in advance, if there will be any changes for the next benefit year in your plan premiums or in the amounts you will have to pay when you get your prescriptions covered.
However, in some cases the part of the premium that you have to pay can change during the year. This happens if you become eligible for the “Extra Help” program or if you lose your eligibility for the “Extra Help” program during the year. If you qualify for “Extra Help” with their prescription drug costs, the “Extra Help” program will pay part of the member’s monthly plan premium. If Medicare pays only a portion of this premium, we will bill you for the amount Medicare doesn’t cover. A member who loses their eligibility during the year, will need to start paying their full monthly premium. You can find out more about the “Extra Help” program in Chapter 2, Section 7.
If you lose Extra Help, you may be subject to the late enrollment penalty if you go 63 days or more in a row without Part D or other creditable prescription drug coverage.

2022 Evidence of Coverage for Navitus MedicareRx (PDP) 17 Chapter 1. Getting started as a member
SECTION 8 Please keep your plan membership record up to date
Section 8.1 How to help make sure that we have accurate information about you
Your membership record has information including your address and telephone number. It shows your specific plan coverage.
The pharmacists in your plan’s network need to have correct information about you. These network providers use your membership record to know what drugs are covered and the cost sharing amounts for you. Because of this, it is very important that you help us keep your information up to date.
Let us and RASC know about these changes:
• Changes to your name, your address, or your phone number
• Changes in any other medical or drug insurance coverage you have (such as from a group sponsor, your spouse’s employer, workers’ compensation, or Medicaid)
• If you have any liability claims, such as claims from an automobile accident
• If you have been admitted to a nursing home
• If your designated responsible party (such as a caregiver) changes/
If any of this information changes, please let us know by calling Customer Care (phone numbers are printed on the back cover of this booklet). Please remember to also notify the RASC so they will have your most up-to-date contact information on file.
It is also important to contact Social Security if you move or change your mailing address. You can find phone numbers and contact information for Social Security in Chapter 2, Section 5.
Read over the information we send you about any other insurance coverage you have
Medicare requires that we collect information from you about any medical or drug insurance coverage that you have in addition to this retiree drug coverage. That’s because we must coordinate any other coverage you have with your benefits under our plan. (For more information about how our coverage works when you have other insurance, see Section 10 in this chapter.)
Once each year, we will send you a letter that lists any other medical or drug insurance coverage that we know about. Please read over this information carefully. If it is correct, you don’t need to do anything. If the information is incorrect, or if you have other coverage that is not listed, please call Customer Care (phone numbers are printed on the back cover of this booklet).

2022 Evidence of Coverage for Navitus MedicareRx (PDP) 18 Chapter 1. Getting started as a member
SECTION 9 We protect the privacy of your personal health information
Section 9.1 We make sure that your health information is protected
Federal and state laws protect the privacy of your medical records and personal health information. We protect your personal health information as required by these laws.
For more information about how we protect your personal health information, please go to Chapter 6, Section 1.3 of this booklet.
SECTION 10 How other insurance works with our plan
Section 10.1 Which plan pays first when you have other insurance?
When you have other insurance (like employer group health coverage), there are rules set by Medicare that decide whether our plan or your other insurance pays first. The insurance that pays first is called the “primary payer” and pays up to the limits of its coverage. The one that pays second, called the “secondary payer,” only pays if there are costs left uncovered by the primary coverage. The secondary payer may not pay all of the uncovered costs. Your retiree drug coverage includes basic coverage provided by Group Part D benefits and additional coverage provided by your Navitus MedicareRx supplemental benefits.
These rules apply for employer or union group health plan coverage:
• If you have retiree coverage, Medicare pays first.
• If your group health plan coverage is based on your or a family member’s current employment, who pays first depends on your age, the number of people employed by your employer, and whether you have Medicare based on age, disability, or End-Stage Renal Disease (ESRD):
o If you’re under 65 and disabled and you or your family member is still working, your group health plan pays first if the employer has 100 or more employees or at least one employer in a multiple employer plan that has more than 100 employees.
o If you’re over 65 and you or your spouse/domestic partner is still working, your group health plan pays first if the employer has 20 or more employees or at least one employer in a multiple employer plan that has more than 20 employees.
• If you have Medicare because of ESRD, your group sponsored health plan will pay first for the first 30 months after you become eligible for Medicare.
These types of coverage usually pay first for services related to each type:

2022 Evidence of Coverage for Navitus MedicareRx (PDP) 19 Chapter 1. Getting started as a member
• No-fault insurance (including automobile insurance)
• Liability (including automobile insurance)
• Black lung benefits
• Workers’ compensation
Medicaid and TRICARE never pay first for Medicare-covered services. They only pay after Medicare, group sponsored health plans, and/or Medigap have paid.
If you have other insurance, tell your doctor, hospital, and pharmacy. If you have questions about who pays first, or you need to update your other insurance information, call Customer Care (phone numbers are printed on the back cover of this booklet). You may need to give your plan member ID number to your other insurers (once you have confirmed their identity) so your bills are paid correctly and on time.

CHAPTER 2 Important phone numbers and
resources

2022 Evidence of Coverage for Navitus MedicareRx (PDP) 21 Chapter 2. Important phone numbers and resources
Chapter 2. Important phone numbers and resources
SECTION 1 Navitus MedicareRx (PDP) contacts (how to contact us, including how to reach Customer Care at the plan) ............................. 22
SECTION 2 Medicare (how to get help and information directly from the Federal Medicare program) .................................................................... 27
SECTION 3 State Health Insurance Assistance Program (free help, information, and answers to your questions about Medicare) ............. 28
SECTION 4 Quality Improvement Organization (paid by Medicare to check on the quality of care for people with Medicare) ........................ 29
SECTION 5 Social Security ...................................................................................... 29
SECTION 6 Medicaid (a joint Federal and state program that helps with medical costs for some people with limited income and resources) ................................................................................................ 30
SECTION 7 Information about programs to help people pay for their prescription drugs ................................................................................ 31
SECTION 8 How to contact the Railroad Retirement Board ............................... 34
SECTION 9 Do you have “group insurance” or other health insurance from another employer? ...................................................................... 34
2022 Evidence of Coverage for Navitus MedicareRx (PDP) 22 Chapter 2. Important phone numbers and resources
SECTION 1 Navitus MedicareRx (PDP) contacts (how to contact us, including how to reach Customer Care at the plan)
How to contact our plan’s Customer Care
For assistance with claims, billing, or member card questions, please call or write to Navitus MedicareRx Customer Care. We will be happy to help you.
Method Customer Care – Contact Information
CALL 1-866-270-3877 Calls to this number are free. We are available 24 hours a day, 7 days a week, except on Thanksgiving and Christmas Day. Pharmacies can also reach Navitus Customer Care 24 hours a day, 7 days a week. Customer Care also has free language interpreter services available for non-English speakers.
TTY/TDD 711 This number requires special telephone equipment and is only for people who have difficulties with hearing or speaking. Calls to this number are free. Members can reach Navitus Customer Care 24 hours a day, 7 days a week, except on Thanksgiving and Christmas Day.
WRITE Navitus MedicareRx (PDP) Customer Care P.O. Box 1039 Appleton, WI 54912-1039
WEBSITE https://memberportal.navitus.com

2022 Evidence of Coverage for Navitus MedicareRx (PDP) 23 Chapter 2. Important phone numbers and resources
How to contact us when you are asking for a coverage decision about your Part D prescription drugs
A coverage decision is a decision we make about your benefits and coverage or about the amount we will pay for your prescription drugs covered under the Part D benefit included in your plan. For more information on asking for coverage decisions about your Part D prescription drugs, see Chapter 7 (What to do if you have a problem or complaint (coverage decisions, appeals, complaints)).
You may call us if you have questions about our coverage decision process your request against both your Group Part D and Navitus MedicareRx coverage.
Method Coverage Decisions for Part D Prescription Drugs – Contact Information
CALL 1-866-270-3877 Calls to this number are free. We are available 24 hours a day, 7 days a week, except on Thanksgiving and Christmas Day. Pharmacies can also reach Navitus Customer Care 24 hours a day, 7 days a week. Customer Care also has free language interpreter services available for non-English speakers.
TTY/TDD 711 This number requires special telephone equipment and is only for people who have difficulties with hearing or speaking. Calls to this number are free. Members can reach Navitus Customer Care 24 hours a day, 7 days a week, except on Thanksgiving and Christmas Day.
FAX 1-855-668-8552
WRITE Navitus MedicareRx (PDP) Prior Authorization P.O. Box 1039 Appleton, WI 54912-1039
WEBSITE https://memberportal.navitus.com
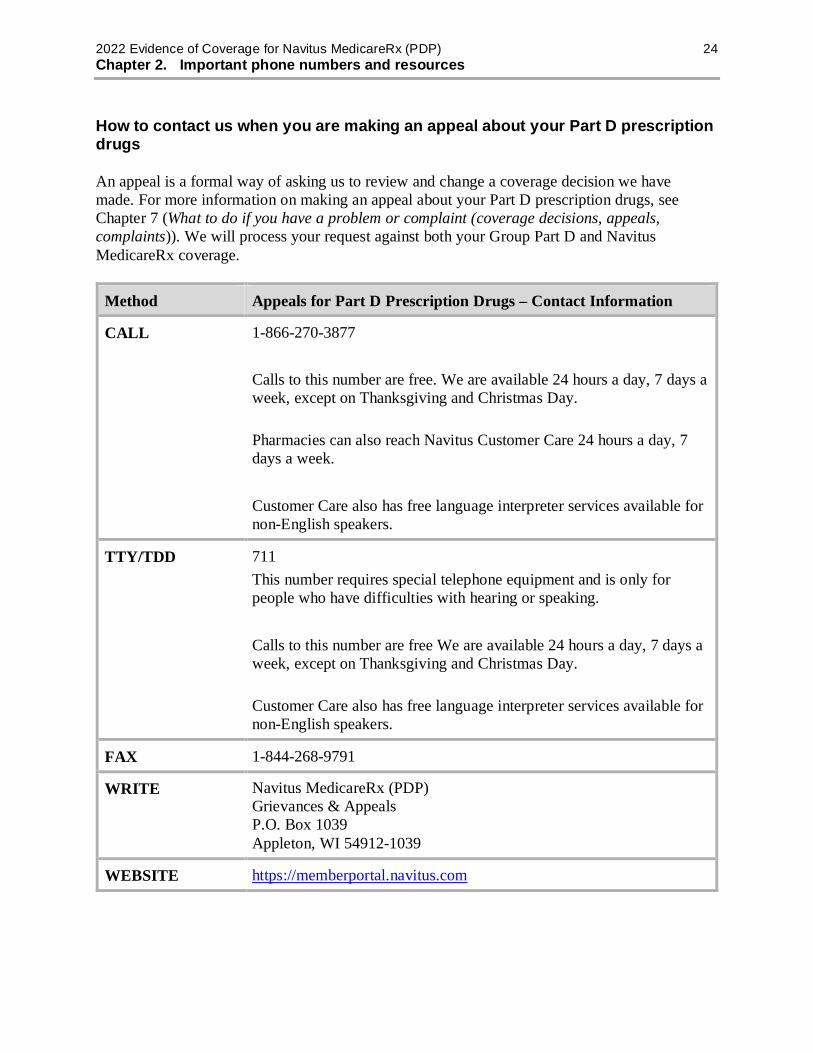
2022 Evidence of Coverage for Navitus MedicareRx (PDP) 24 Chapter 2. Important phone numbers and resources
How to contact us when you are making an appeal about your Part D prescription drugs
An appeal is a formal way of asking us to review and change a coverage decision we have made. For more information on making an appeal about your Part D prescription drugs, see Chapter 7 (What to do if you have a problem or complaint (coverage decisions, appeals, complaints)). We will process your request against both your Group Part D and Navitus MedicareRx coverage.
Method Appeals for Part D Prescription Drugs – Contact Information
CALL 1-866-270-3877 Calls to this number are free. We are available 24 hours a day, 7 days a week, except on Thanksgiving and Christmas Day. Pharmacies can also reach Navitus Customer Care 24 hours a day, 7 days a week. Customer Care also has free language interpreter services available for non-English speakers.
TTY/TDD 711 This number requires special telephone equipment and is only for people who have difficulties with hearing or speaking. Calls to this number are free We are available 24 hours a day, 7 days a week, except on Thanksgiving and Christmas Day. Customer Care also has free language interpreter services available for non-English speakers.
FAX 1-844-268-9791
WRITE Navitus MedicareRx (PDP) Grievances & Appeals P.O. Box 1039 Appleton, WI 54912-1039
WEBSITE https://memberportal.navitus.com

2022 Evidence of Coverage for Navitus MedicareRx (PDP) 25 Chapter 2. Important phone numbers and resources
How to contact us when you are making a complaint about your Part D prescription drugs
You can make a complaint about us or one of our network pharmacies, including a complaint about the quality of your care. This type of complaint does not involve coverage or payment disputes. (If your problem is about the plan’s coverage or payment, you should look at the section above about making an appeal.) For more information on making a complaint about your Part D prescription drugs, see Chapter 7 (What to do if you have a problem or complaint (coverage decisions, appeals, complaints)).
Method Complaints about Part D prescription drugs – Contact Information
CALL 1-866-270-3877 Calls to this number are free. We are available 24 hours a day, 7 days a week, except on Thanksgiving and Christmas Day. Pharmacies can also reach Navitus Customer Care 24 hours a day, 7 days a week. Customer Care also has free language interpreter services available for non-English speakers.
TTY/TDD 711 This number requires special telephone equipment and is only for people who have difficulties with hearing or speaking. Calls to this number are free. Members can reach Navitus Customer Care 24 hours a day, 7 days a week, except on Thanksgiving and Christmas Day.
FAX 1-844-268-9791
WRITE Navitus MedicareRx (PDP) Grievances & Appeals P.O. Box 1039 Appleton, WI 54912-1039
MEDICARE WEBSITE
You can submit a complaint about Navitus MedicareRx directly to Medicare. To submit an online complaint to Medicare go to www.medicare.gov/MedicareComplaintForm/home.aspx.
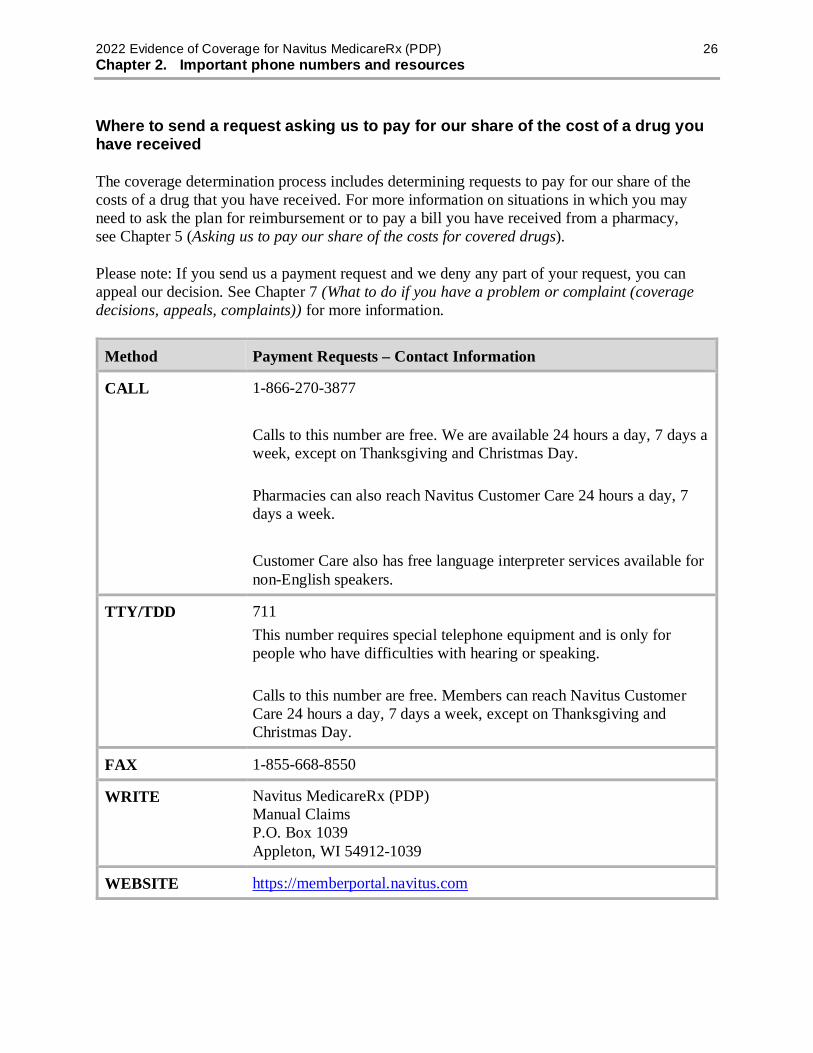
2022 Evidence of Coverage for Navitus MedicareRx (PDP) 26 Chapter 2. Important phone numbers and resources
Where to send a request asking us to pay for our share of the cost of a drug you have received
The coverage determination process includes determining requests to pay for our share of the costs of a drug that you have received. For more information on situations in which you may need to ask the plan for reimbursement or to pay a bill you have received from a pharmacy, see Chapter 5 (Asking us to pay our share of the costs for covered drugs).
Please note: If you send us a payment request and we deny any part of your request, you can appeal our decision. See Chapter 7 (What to do if you have a problem or complaint (coverage decisions, appeals, complaints)) for more information.
Method Payment Requests – Contact Information
CALL 1-866-270-3877 Calls to this number are free. We are available 24 hours a day, 7 days a week, except on Thanksgiving and Christmas Day. Pharmacies can also reach Navitus Customer Care 24 hours a day, 7 days a week. Customer Care also has free language interpreter services available for non-English speakers.
TTY/TDD 711 This number requires special telephone equipment and is only for people who have difficulties with hearing or speaking. Calls to this number are free. Members can reach Navitus Customer Care 24 hours a day, 7 days a week, except on Thanksgiving and Christmas Day.
FAX 1-855-668-8550
WRITE Navitus MedicareRx (PDP) Manual Claims P.O. Box 1039 Appleton, WI 54912-1039
WEBSITE https://memberportal.navitus.com

2022 Evidence of Coverage for Navitus MedicareRx (PDP) 27 Chapter 2. Important phone numbers and resources
SECTION 2 Medicare (how to get help and information directly from the Federal Medicare program)
Medicare is the Federal health insurance program for people 65 years of age or older, some people under age 65 with disabilities, and people with End-Stage Renal Disease (permanent kidney failure requiring dialysis or a kidney transplant).
The Federal agency in charge of Medicare is the Centers for Medicare & Medicaid Services (sometimes called “CMS”). This agency contracts with Medicare Prescription Drug Plans, including us.
Method Medicare – Contact Information
CALL 1-800-MEDICARE, or 1-800-633-4227 Calls to this number are free. 24 hours a day, 7 days a week.
TTY/TDD 1-877-486-2048 This number requires special telephone equipment and is only for people who have difficulties with hearing or speaking. Calls to this number are free.
WEBSITE www.medicare.gov This is the official government website for Medicare. It gives you up-to-date information about Medicare and current Medicare issues. It also has information about hospitals, nursing homes, physicians, home health agencies, and dialysis facilities. It includes booklets you can print directly from your computer. You can also find Medicare contacts in your state. The Medicare website also has detailed information about your Medicare eligibility and enrollment options with the following tools:
• Medicare Eligibility Tool: Provides Medicare eligibility status information.
• Medicare Plan Finder: Provides personalized information about available Medicare prescription drug plans, Medicare health plans, and Medigap (Medicare Supplement Insurance) policies in your area. These tools provide an estimate of what your out-of-pocket costs might be in different Medicare plans.
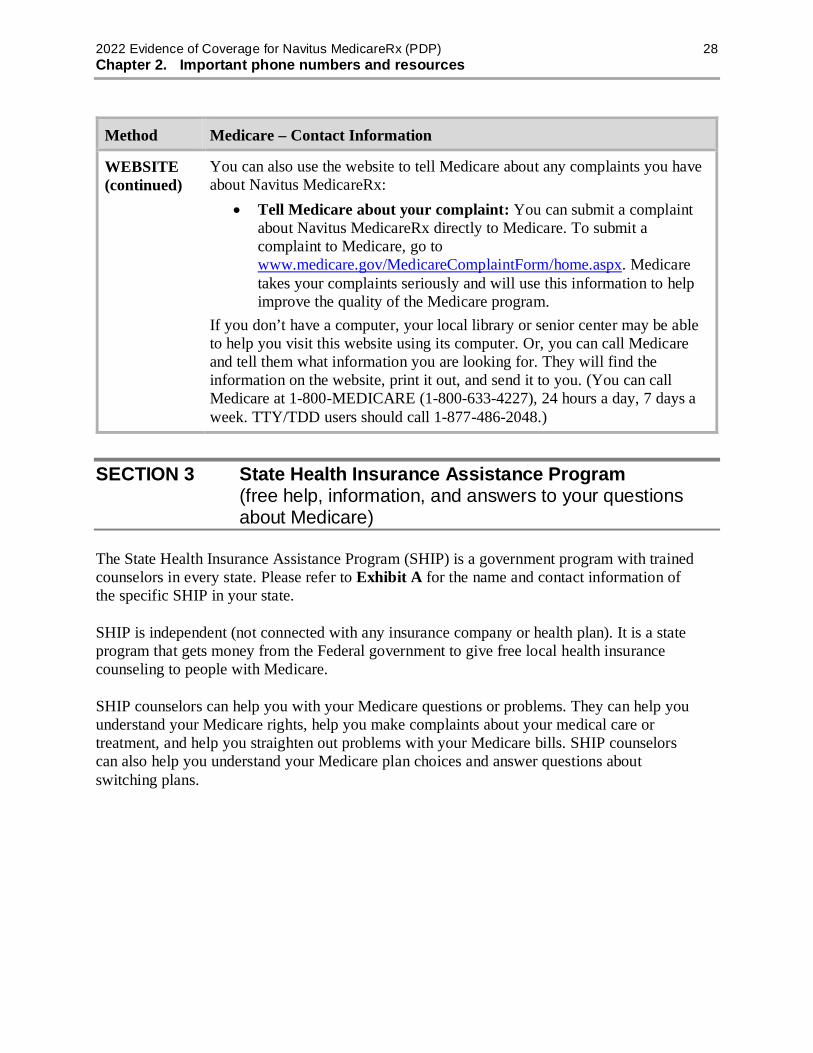
2022 Evidence of Coverage for Navitus MedicareRx (PDP) 28 Chapter 2. Important phone numbers and resources
Method Medicare – Contact Information
WEBSITE (continued)
You can also use the website to tell Medicare about any complaints you have about Navitus MedicareRx:
• Tell Medicare about your complaint: You can submit a complaint about Navitus MedicareRx directly to Medicare. To submit a complaint to Medicare, go to www.medicare.gov/MedicareComplaintForm/home.aspx. Medicare takes your complaints seriously and will use this information to help improve the quality of the Medicare program.
If you don’t have a computer, your local library or senior center may be able to help you visit this website using its computer. Or, you can call Medicare and tell them what information you are looking for. They will find the information on the website, print it out, and send it to you. (You can call Medicare at 1-800-MEDICARE (1-800-633-4227), 24 hours a day, 7 days a week. TTY/TDD users should call 1-877-486-2048.)
SECTION 3 State Health Insurance Assistance Program (free help, information, and answers to your questions about Medicare)
The State Health Insurance Assistance Program (SHIP) is a government program with trained counselors in every state. Please refer to Exhibit A for the name and contact information of the specific SHIP in your state.
SHIP is independent (not connected with any insurance company or health plan). It is a state program that gets money from the Federal government to give free local health insurance counseling to people with Medicare.
SHIP counselors can help you with your Medicare questions or problems. They can help you understand your Medicare rights, help you make complaints about your medical care or treatment, and help you straighten out problems with your Medicare bills. SHIP counselors can also help you understand your Medicare plan choices and answer questions about switching plans.

2022 Evidence of Coverage for Navitus MedicareRx (PDP) 29 Chapter 2. Important phone numbers and resources
METHOD TO ACCESS SHIP and OTHER RESOURCES:
Visit www.medicare.gov Click on “Forms, Help, and Resources” on far right of menu on top In the drop down click on “Phone Numbers & Websites” You now have several options
o Option #1: You can have a live chat o Option #2: You can click on any of the “TOPICS” in the menu
on bottom o Option #3: You can select your STATE from the dropdown
menu and click GO. This will take you to a page with phone numbers and resources specific to your state.
SECTION 4 Quality Improvement Organization (paid by Medicare to check on the quality of care for people with Medicare)
There is a designated Quality Improvement Organization (QIO) for serving Medicare beneficiaries in each state. Please refer to Exhibit B for the name and contact information of the specific Quality Improvement Organization in your area.
The QIO has a group of doctors and other health care professionals who are paid by the Federal government. This organization is paid by Medicare to check on and help improve the quality of care for people with Medicare. The QIO is an independent organization. It is not connected with our plan.
You should contact the QIO if you have a complaint about the quality of care you have received. For example, you can contact the QIO if you were given the wrong medication or if you were given medications that interact in a negative way.
SECTION 5 Social Security
Social Security is responsible for determining eligibility and handling enrollment for Medicare. U.S. citizens and lawful permanent residents who are 65 or older, or who have a disability or End-Stage Renal Disease and meet certain conditions, are eligible for Medicare. If you are already getting Social Security checks, enrollment into Medicare is automatic. If you are not getting Social Security checks, you have to enroll in Medicare. To apply for Medicare, you can call Social Security or visit your local Social Security office.
Social Security is also responsible for determining who has to pay an extra amount for their Part D drug coverage because they have a higher income. If you got a letter from Social Security telling you that you have to pay the extra amount and have questions about the
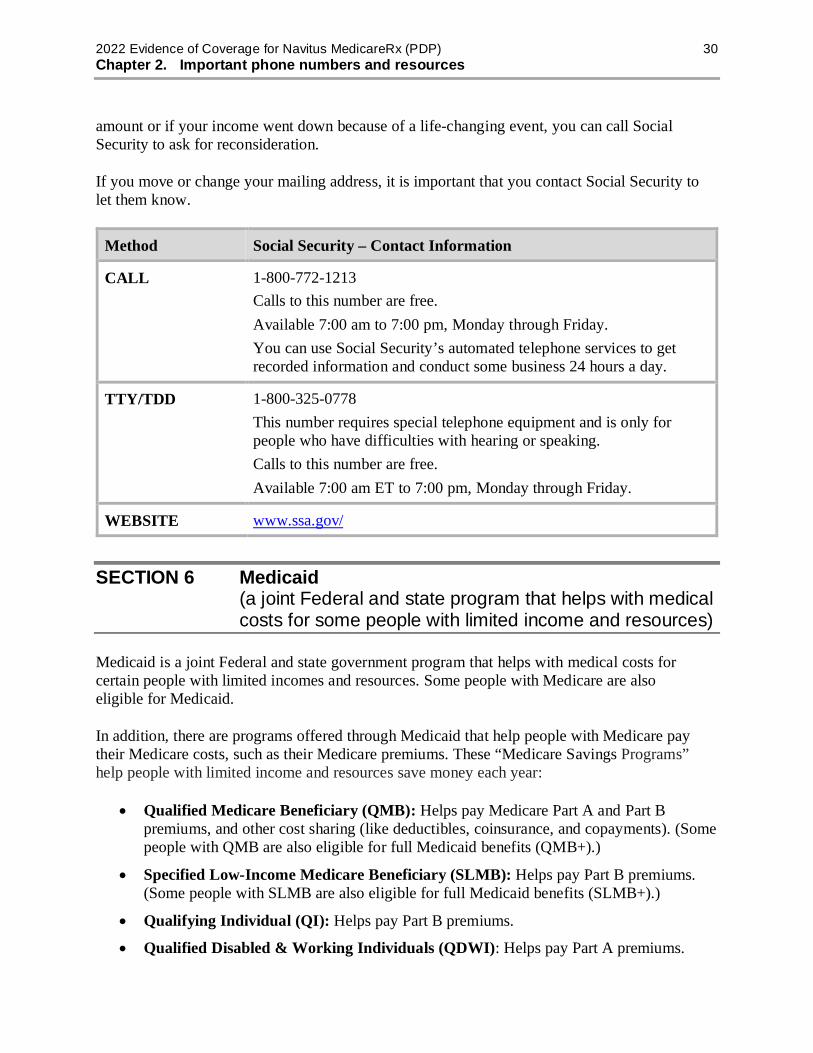
2022 Evidence of Coverage for Navitus MedicareRx (PDP) 30 Chapter 2. Important phone numbers and resources
amount or if your income went down because of a life-changing event, you can call Social Security to ask for reconsideration.
If you move or change your mailing address, it is important that you contact Social Security to let them know.
Method Social Security – Contact Information
CALL 1-800-772-1213 Calls to this number are free. Available 7:00 am to 7:00 pm, Monday through Friday. You can use Social Security’s automated telephone services to get recorded information and conduct some business 24 hours a day.
TTY/TDD 1-800-325-0778 This number requires special telephone equipment and is only for people who have difficulties with hearing or speaking. Calls to this number are free. Available 7:00 am ET to 7:00 pm, Monday through Friday.
WEBSITE www.ssa.gov/
SECTION 6 Medicaid (a joint Federal and state program that helps with medical costs for some people with limited income and resources)
Medicaid is a joint Federal and state government program that helps with medical costs for certain people with limited incomes and resources. Some people with Medicare are also eligible for Medicaid.
In addition, there are programs offered through Medicaid that help people with Medicare pay their Medicare costs, such as their Medicare premiums. These “Medicare Savings Programs” help people with limited income and resources save money each year:
• Qualified Medicare Beneficiary (QMB): Helps pay Medicare Part A and Part B premiums, and other cost sharing (like deductibles, coinsurance, and copayments). (Some people with QMB are also eligible for full Medicaid benefits (QMB+).)
• Specified Low-Income Medicare Beneficiary (SLMB): Helps pay Part B premiums. (Some people with SLMB are also eligible for full Medicaid benefits (SLMB+).)
• Qualifying Individual (QI): Helps pay Part B premiums.
• Qualified Disabled & Working Individuals (QDWI): Helps pay Part A premiums.
2022 Evidence of Coverage for Navitus MedicareRx (PDP) 31 Chapter 2. Important phone numbers and resources
To find out more about Medicaid and its programs, please refer to Exhibit C for the name and contact information of your state specific Medicaid program.
SECTION 7 Information about programs to help people pay for their prescription drugs
Medicare’s “Extra Help” Program
Medicare provides “Extra Help” to pay prescription drug costs for people who have limited income and resources. Resources include your savings and stocks, but not your home or car. If you qualify, you get help paying for any Medicare drug plan’s monthly premium, and prescription copayments or coinsurance. This “Extra Help” also counts toward your out-of-pocket costs.
Some people automatically qualify for “Extra Help” and don’t need to apply. Medicare mails a letter to people who automatically qualify for “Extra Help.”
You may be able to get “Extra Help” to pay for your prescription drug premiums and costs. To see if you qualify for getting “Extra Help,” call:
• 1-800-MEDICARE (1-800-633-4227). TTY/TDD users should call 1-877-486-2048, 24 hours a day, 7 days a week;
• The Social Security Office at 1-800-772-1213, between 7 am to 7 pm, Monday through Friday. TTY/TDD users should call 1-800-325-0778 (applications); or
• Your State Medicaid Office (applications). (See Section 6 of this chapter for contact information.)
If you believe you have qualified for “Extra Help” and you believe that you are paying an incorrect cost-sharing amount when you get your prescription at a pharmacy, our plan has established a process that allows you to either request assistance in obtaining evidence of your proper copayment level, or, if you already have the evidence, to provide this evidence to us.
• If you do not have evidence of “Extra Help”, notify the pharmacy when you pick up your prescription. The pharmacy will contact us and we will work with Medicare to get this evidence for you.
• When we receive the evidence showing your copayment level, we will update our system so that you can pay the correct copayment when you get your next prescription at the pharmacy. If you overpay your copayment, we will reimburse you.
• When we receive the evidence showing your copayment level, we will update our system so that you can pay the correct copayment when you get your next prescription at the pharmacy. If you overpay your copayment, we will reimburse you. We will forward a check to you in the amount of your overpayment. Please contact Customer Care if you have questions (phone numbers are printed on the back cover of this booklet).
2022 Evidence of Coverage for Navitus MedicareRx (PDP) 32 Chapter 2. Important phone numbers and resources
There are programs in Puerto Rico to help people with limited income and resources pay their Medicare costs. Programs vary in these areas. Call your local Medical Assistance (Medicaid) office to find out more about their rules (phone numbers are in Section 6 of this chapter). Or call 1-800-MEDICARE (1-800-633-4227) 24 hours a day, 7 days a week and say “Medicaid” for more information. TTY/TDD users should call 1-877-486-2048. You can also visit www.medicare.gov for more information.
Medicare Coverage Gap Discount Program
The plan continues to cover your drugs at your regular cost-sharing amount through the Gap Coverage Stage.
The Medicare Coverage Gap Discount Program provides manufacturer discounts on brand name drugs to Part D members who have reached the coverage gap and are not receiving “Extra Help.” For brand name drugs, the 70% discount provided by manufacturers excludes any dispensing fee for costs in the gap. Members pay 25% of the negotiated price which includes a portion of the dispensing fee for brand name drugs.
If you reach the coverage gap, we will automatically apply the discount when your pharmacy bills you for your prescription and your Part D Explanation of Benefits (EOB) will show any discount provided. It will also reflect the coverage provided by your Navitus MedicareRx supplemental coverage after the discount is applied. Both the amount you pay and the amount discounted by the manufacturer count toward your out-of-pocket costs as if you had paid them and move you through the coverage gap. The amount paid by the plan (5%) does not count toward your out-of-pocket costs.
You also receive some coverage for generic drugs. For generic drugs, the amount paid by the plan (75%) does not count toward your out-of-pocket costs. Only the amount you pay counts and moves you through the coverage gap. Also, the dispensing fee is included as part of the cost of the drug.
The Medicare Coverage Gap Discount Program is available nationwide. Because Navitus MedicareRx offers additional gap coverage during the Coverage Gap Stage. Please go to Chapter 4, Section 6 for more information about your coverage during the Coverage Gap Stage.
If you have any questions about the availability of discounts for the drugs you are taking or about the Medicare Coverage Gap Discount Program in general, please contact Customer Care (phone numbers are printed on the back cover of this booklet).
What if you have coverage from a State Pharmaceutical Assistance Program (SPAP)?
If you are enrolled in a State Pharmaceutical Assistance Program (SPAP), or any other program that provides coverage for Part D drugs (other than “Extra Help”), you still get the 70% discount on covered brand name drugs. Also, the plan pays 5% of the costs of brand drugs in the coverage gap. The 70% discount and the 5% paid by the plan are both applied to the price of the drug before any SPAP or other coverage.

2022 Evidence of Coverage for Navitus MedicareRx (PDP) 33 Chapter 2. Important phone numbers and resources
What if you have coverage from an AIDS Drug Assistance Program (ADAP)? What is the AIDS Drug Assistance Program (ADAP)?
The AIDS Drug Assistance Program (ADAP) helps ADAP-eligible individuals living with HIV/AIDS have access to life-saving HIV medications. Medicare Part D prescription drugs that are also covered by ADAP qualify for prescription cost-sharing assistance. Note: To be eligible for the ADAP operating in your State, individuals must meet certain criteria, including proof of State residence and HIV status, low income as defined by the State, and uninsured/under-insured status.
If you are currently enrolled in an ADAP, it can continue to provide you with Medicare Part D prescription cost-sharing assistance for drugs on the ADAP formulary. In order to be sure you continue receiving this assistance, please notify your local ADAP enrollment worker of any changes in your Medicare Part D plan name or policy number.
For information on eligibility criteria, covered drugs, or how to enroll in the program, refer to Exhibit E for the name and contact information of your state specific ADAP.
What if you get “Extra Help” from Medicare to help pay your prescription drug costs? Can you get the discounts?
No. If you get “Extra Help,” you already get coverage for your prescription drug costs during the coverage gap.
What if you don’t get a discount, and you think you should have?
If you think that you have reached the coverage gap and did not get a discount when you paid for your brand name drug, you should review your next Part D Explanation of Benefits (Part D EOB) notice. If the discount doesn’t appear on your Part D Explanation of Benefits, you should contact us to make sure that your prescription records are correct and up-to-date. If we don’t agree that you are owed a discount, you can appeal. You can get help filing an appeal from your State Health Insurance Assistance Program (SHIP) (refer to Exhibit A for the name and contact information of the specific SHIP in your state) or by calling 1-800-MEDICARE (1-800-633-4227), 24 hours a day, 7 days a week. TTY/TDD users should call 1-877-486-2048.
State Pharmaceutical Assistance Programs Many states have State Pharmaceutical Assistance Programs that help some people pay for prescription drugs based on financial need, age, medical condition, or disabilities. Each state has different rules to provide drug coverage to its members.
To find out more about a State Pharmaceutical Assistance Program (SPAP), please refer to Exhibit D for the name and contact information of your state specific SPAP.

2022 Evidence of Coverage for Navitus MedicareRx (PDP) 34 Chapter 2. Important phone numbers and resources
SECTION 8 How to contact the Railroad Retirement Board
The Railroad Retirement Board is an independent Federal agency that administers comprehensive benefit programs for the nation’s railroad workers and their families. If you have questions regarding your benefits from the Railroad Retirement Board, contact the agency.
If you receive your Medicare through the Railroad Retirement Board, it is important that you let them know if you move or change your mailing address.
Method Railroad Retirement Board – Contact Information
CALL 1-877-772-5772 Calls to this number are free. If you press “0,” you may speak with an RRB representative from 9:00 am to 3:30 pm, Monday, Tuesday, Thursday, and Friday, and from 9:00 am to 12:00 pm on Wednesday. If you press “1”, you may access the automated RRB HelpLine and recorded information 24 hours a day, including weekends and holidays.
TTY/TDD 1-312-751-4701 This number requires special telephone equipment and is only for people who have difficulties with hearing or speaking. Calls to this number are not free.
WEBSITE rrb.gov/
SECTION 9 Do you have “group insurance” or other health insurance from another employer?
If you (or your spouse) get benefits from your (or your spouse’s) employer or retiree group as part of this plan, you may call the RASC or Customer Care if you have any questions. You can ask about your (or your spouse’s) employer or retiree health benefits, premiums, or the enrollment period. (Phone numbers for Customer Care are printed on the back cover of this booklet.) You may also call 1-800-MEDICARE (1-800-633-4227; TTY/TDD: 1-877-486-2048) with questions related to your Medicare coverage under this plan.
If you have other prescription drug coverage through your (or your spouse’s) employer or retiree group, please contact that group’s benefits administrator. That benefits administrator can help you determine how your current prescription drug coverage will work with our plan.

CHAPTER 3 Using the plan’s coverage for your
Part D prescription drugs

2022 Evidence of Coverage for Navitus MedicareRx (PDP) 36 Chapter 3. Using the plan’s coverage for your Part D prescription drugs
Chapter 3. Using the plan’s coverage for your Part D prescription drugs
SECTION 1 Introduction............................................................................................ 38
Section 1.1 This chapter describes your coverage for Part D drugs ............................... 38
Section 1.2 Basic rules for the plan’s Part D drug coverage .......................................... 38
SECTION 2 Fill your prescription at a network pharmacy or through the plan’s mail-order service ..................................................................... 39
Section 2.1 To have your prescription covered, use a network pharmacy ...................... 39
Section 2.2 Finding network pharmacies ...................................................................... 39
Section 2.3 Using the plan’s mail-order services .......................................................... 40
Section 2.4 How can you get a long-term supply of drugs? ........................................... 42
Section 2.5 When can you use a pharmacy that is not in the plan’s network? ................ 43
SECTION 3 Your drugs need to be on the plan’s “Formulary” .......................... 44
Section 3.1 The “Formulary” tells which Part D drugs are covered ............................... 44
Section 3.2 There are four “cost-sharing tiers” for drugs on the Formulary ................... 44
Section 3.3 How can you find out if a specific drug is on the Formulary? ..................... 45
SECTION 4 There are restrictions on coverage for some drugs ....................... 45
Section 4.1 Why do some drugs have restrictions? ....................................................... 45
Section 4.2 What kinds of restrictions? ........................................................................ 46
Section 4.3 Do any of these restrictions apply to your drugs? ....................................... 47
SECTION 5 What if one of your drugs is not covered in the way you’d like it to be covered? ............................................................................ 48
Section 5.1 There are things you can do if your drug is not covered in the way you’d like it to be covered ................................................................................... 48
Section 5.2 What can you do if your drug is not on the Formulary or if the drug is restricted in some way? ............................................................................. 48
Section 5.3 What can you do if your drug is in a cost-sharing tier you think is too high? ......................................................................................................... 50
SECTION 6 What if your coverage changes for one of your drugs? ................ 51
Section 6.1 The Formulary can change during the year ................................................. 51
Section 6.2 What happens if coverage changes for a drug you are taking?..................... 51
SECTION 7 What types of drugs are not covered by the plan? ......................... 53
Section 7.1 Types of drugs we do not cover ................................................................. 53
2022 Evidence of Coverage for Navitus MedicareRx (PDP) 37 Chapter 3. Using the plan’s coverage for your Part D prescription drugs
SECTION 8 Show your plan membership card when you fill a prescription ............................................................................................ 55
Section 8.1 Show your membership card...................................................................... 55
Section 8.2 What if you don’t have your membership card with you? ........................... 55
SECTION 9 Part D drug coverage in special situations ...................................... 55
Section 9.1 What if you’re in a hospital or a skilled nursing facility for a stay that is covered by Original Medicare? .................................................................. 55
Section 9.2 What if you’re a resident in a long-term care (LTC) facility? ...................... 56
Section 9.3 What if you are taking drugs covered by Original Medicare? ...................... 56
Section 9.4 What if you have a Medigap (Medicare Supplement Insurance) policy with prescription drug coverage? ............................................................... 57
Section 9.5 What if you’re also getting drug coverage from an employer or retiree group plan? ............................................................................................... 57
Section 9.6 What if you are in Medicare-certified Hospice?.......................................... 58
SECTION 10 Programs on drug safety and managing medications ................... 58
Section 10.1 Programs to help members use drugs safely ............................................... 58
Section 10.2 Drug Management Program (DMP) to help members safely use their opioid medications .................................................................................... 59
Section 10.3 Medication Therapy Management (MTM) program to help members manage their medications .......................................................................... 59
2022 Evidence of Coverage for Navitus MedicareRx (PDP) 38 Chapter 3. Using the plan’s coverage for your Part D prescription drugs
Did you know there are programs to help people pay for their drugs?
There are programs to help people with limited resources pay for their drugs. These include “Extra Help” and State Pharmaceutical Assistance Programs. For more information, see Chapter 2, Section 7.
Are you currently getting help to pay for your drugs?
If you are in a program that helps pay for your drugs, some information in this Evidence of Coverage about the costs for Part D prescription drugs may not apply to you. If you qualify, we have included a separate insert, called the “Evidence of Coverage Rider for People Who Get Extra Help Paying for Prescription Drugs” (also known as the “Low Income Subsidy Rider” or the “LIS Rider”), which explains your drug coverage. If you don’t have this insert and it is applicable to you, please call Customer Care and ask for the “LIS Rider.” (Phone numbers for Customer Care are printed on the back cover of this booklet.)
SECTION 1 Introduction
Section 1.1 This chapter describes your coverage for Part D drugs
This chapter explains rules for using your coverage for Part D drugs. The next chapter tells what you pay for Part D drugs (Chapter 4, What you pay for your Part D prescription drugs).
In addition to your coverage for Part D drugs through your plan, Original Medicare (Medicare Part A and Part B) also covers some drugs:
• Medicare Part A covers drugs you are given during Medicare-covered stays in the hospital or in a skilled nursing facility.
• Medicare Part B also provides benefits for some drugs. Part B drugs include certain chemotherapy drugs, certain drug injections you are given during an office visit, drugs you are given at a dialysis facility, and certain drugs you receive via medical equipment such as nebulizers.
The two examples of drugs described above are covered by Original Medicare. (To find out more about this coverage, see your Medicare & You 2022 handbook.) Your Part D prescription drugs are covered under our plan.
Section 1.2 Basic rules for the plan’s Part D drug coverage
The plan will generally cover your drugs as long as you follow these basic rules:
• You must have a provider (a doctor, dentist, or other prescriber) write your prescription.

2022 Evidence of Coverage for Navitus MedicareRx (PDP) 39 Chapter 3. Using the plan’s coverage for your Part D prescription drugs
• Your prescriber must either accept Medicare or file documentation with CMS showing that they are qualified to write prescriptions, or your Part D claim will be denied. You should ask your prescribers the next time you call or visit if they meet this condition. If not, please be aware it takes time for your prescriber to submit the necessary paperwork to be processed.
• You generally must use a network pharmacy to fill your prescription. (See Section 2, Fill your prescriptions at a network pharmacy or through your plan’s mail-order service.)
• Your drug must be on the plan’s List of Covered Drugs (Formulary). (See Section 3, Your drugs need to be on the plan’s “Formulary”.)
• Your drug must be used for a medically accepted indication. A “medically accepted indication” is a use of the drug that is either approved by the Food and Drug Administration or supported by certain reference books. (See Section 3 for more information about a medically accepted indication.)
SECTION 2 Fill your prescription at a network pharmacy or through the plan’s mail-order service
Section 2.1 To have your prescription covered, use a network pharmacy
In most cases, your prescriptions are covered only if they are filled at your plan’s network pharmacies. (See Section 2.5 for information about when we would cover prescriptions filled at out-of-network pharmacies.)
A network pharmacy is a pharmacy that has a contract with us to provide your covered prescription drugs. The term “covered drugs” means all of the Part D prescription drugs that are covered on the plan’s Formulary.
Section 2.2 Finding network pharmacies
How do you find a network pharmacy in your area?
To find a network pharmacy, you can look in your Pharmacy Directory, visit our Member Portal (https://memberportal.navitus.com), or call Customer Care (phone numbers are printed on the back cover of this booklet). You can also find a pharmacy search tool on our Member Portal.
You may go to any of our network pharmacies. If you switch from one network pharmacy to another, and you need a refill of a drug you have been taking, you can ask either to have a new prescription written by a prescriber or to have your prescription transferred to your new network pharmacy.

2022 Evidence of Coverage for Navitus MedicareRx (PDP) 40 Chapter 3. Using the plan’s coverage for your Part D prescription drugs
What if the pharmacy you have been using leaves the network?
If the pharmacy you have been using leaves your plan’s network, you will have to find a new pharmacy that is in the network. To find another network pharmacy in your area, you can get help from Customer Care (phone numbers are printed on the back cover of this booklet) or use the Pharmacy Directory. You can find information on our Member Portal at https://memberportal.navitus.com. You can also find a pharmacy search tool on our Member Portal.
What if you need a specialized pharmacy?
Sometimes prescriptions must be filled at a specialized pharmacy. Specialized pharmacies include:
• Pharmacies that supply drugs for home infusion therapy.
• Pharmacies that supply drugs for residents of a long-term care (LTC) facility. Usually, a long-term care facility (such as a nursing home) has its own pharmacy. If you are in an LTC facility, we must ensure that you are able to routinely receive your Part D benefits through our network of LTC pharmacies, which is typically the pharmacy that the LTC facility uses. If you have any difficulty accessing your Part D benefits in an LTC facility, please contact Customer Care.
• Pharmacies that serve the Indian Health Service / Tribal / Urban Indian Health Program (not available in Puerto Rico). Except in emergencies, only Native Americans or Alaska Natives have access to these pharmacies in our network.
• Pharmacies that dispense drugs that are restricted by the FDA to certain locations or that require special handling, pharmacy coordination, or education on their use. (Note: This scenario should happen rarely.)
To locate a specialized pharmacy, look in your Pharmacy Directory or call Customer Care (phone numbers are printed on the back cover of this booklet). You can find information on our Member Portal at https://memberportal.navitus.com. You can also find a pharmacy search tool on our Member Portal.
Section 2.3 Using the plan’s mail-order services
You can use the plan’s network mail-order services. Generally, the drugs provided through mail order are drugs that you take on a regular basis, for a chronic or long-term medical condition.
Our plan’s mail-order service allows you to order up to a 90-day supply for most drugs. Specialty drugs are only available for up to a 30-day supply.
To get order forms and information about filling your prescriptions by mail call Customer Care (phone numbers are on the back cover of this booklet).
2022 Evidence of Coverage for Navitus MedicareRx (PDP) 41 Chapter 3. Using the plan’s coverage for your Part D prescription drugs
You may use any contracted pharmacy you like, currently the recommended mail order pharmacy is Costco Mail Order Pharmacy. Note: Costco Mail Order is not to be confused with Costco Warehouse/Club Stores. You do not need to be a member of Costco Warehouse/Club Stores to utilize Costco Mail Order Pharmacy services.
Costco Mail Order can be reached at 1-800-607-6861. Costco representatives are available Monday through Friday, 5am to 7pm PST and Saturdays 9:30am to 2pm PST. Refill orders can be placed and tracked 24 hours a day, 7 days a week. Your physician can send new prescriptions in by calling (1-800-607-6861) or by fax at 1-888-545-4615.
Usually a mail-order pharmacy order will get to you in no more than 14 days.
New prescriptions the pharmacy receives directly from your doctor’s office. After the pharmacy receives a prescription from a health care provider, it will contact you to see if you want the medication filled immediately or at a later time. This will give you an opportunity to make sure that the pharmacy is delivering the correct drug (including strength, amount, and form) and, if needed, allow you to stop or delay the order before you are billed and it is shipped. It is important that you respond each time you are contacted by the pharmacy, to let them know what to do with the new prescription and to prevent any delays in shipping.
Refills on mail-order prescriptions. For refills, please contact your pharmacy 14 days before you think the drugs you have on hand will run out to make sure your next order is shipped to you in time.
Note: Both Costco mail order and retail locations are unable to fill Medicare Part B products, for example, Diabetic Testing Strips. Costco can either refer you to an affiliated provider that can fill these supplies, or you can locate a participating retail pharmacy that can process Part B products.
What should I do if I need my mail order prescription urgently from Costco?
Usually Costco Mail Order will get to you within 14 days. If the medication does not arrive in that timeframe, you should contact Costco to report that you did not receive your prescription. Costco will verify how many days of medication you have left.
If you have 5 days or less of medication left, you should contact your doctor to ask for a two-week supply to be called into your local pharmacy.
If you have more than 6 days remaining, Costco will continue to process your order. Costco can expedite shipping your order at an additional cost to you. The overnight shipping happens after the usual processing time of 24 to 96 hours.
In an emergency circumstance where Costco failed to comply with their protocol, they will expedite the patient medication at Costco’s cost. If Costco provided unrealistic expectations to
2022 Evidence of Coverage for Navitus MedicareRx (PDP) 42 Chapter 3. Using the plan’s coverage for your Part D prescription drugs
you which results in you not getting your medication in time, Costco will investigate and immediately resolve the situation to prevent gaps in therapy.
So the pharmacy can reach you to confirm your order before shipping, please make sure to let the pharmacy know the best ways to contact you. Communication preferences can be updated by contacting our recommended mail order partner, Costco Mail Order Pharmacy.
Section 2.4 How can you get a long-term supply of drugs?
When you get a long-term supply of drugs, your cost sharing may be lower. Your plan offers two ways to get a long-term supply (also called an “extended supply”) of “maintenance” drugs on your plan’s Formulary. (Maintenance drugs are drugs that you take on a regular basis, for a chronic or long-term medical condition.) You may order this supply through mail order (see Section 2.3) or you may go to a retail pharmacy.
1. Some retail pharmacies in our network allow you to get a long-term supply of maintenance drugs. Some of these retail pharmacies agree to accept the mail-order cost-sharing amount for a long-term supply of maintenance drugs. Other retail pharmacies may not agree to accept the mail-order cost-sharing amounts for a long-term supply of maintenance drugs. In this case you may be responsible for the difference in price. Your Pharmacy Directory tells you which pharmacies in our network can give you a long-term supply of maintenance drugs. You can find a pharmacy search tool on our Member Portal at https://memberportal.navitus.com. You can also call Customer Care for more information (phone numbers are printed on the back cover of this booklet).
2. Select Retail pharmacies in our network allow you to get a long-term supply of drugs for a reduced copayment. For these Select Retail pharmacies, you will only be charged twice your 1-month retail copayment for a 90-day supply. You can take advantage of this benefit by visiting one of the participating Select Retail pharmacies which include the UC Medical Center retail pharmacies, Costco, CVS, Vons/Safeway, Walmart or Walgreens.
3. You can use the plan’s network mail-order services. Our plan’s mail-order service allows you to order up to a 90-day supply. See Section 2.3 for more information about using our mail-order services.
You may be able to receive greater than a 1-month supply for most of the drugs on your formulary. Drugs noted with “NDS” (Non-extended Day Supply) on the list are limited to a 1-month supply for retail, mail-order and specialty pharmacies.
2022 Evidence of Coverage for Navitus MedicareRx (PDP) 43 Chapter 3. Using the plan’s coverage for your Part D prescription drugs
Section 2.5 When can you use a pharmacy that is not in the plan’s network?
Your prescription may be covered in certain situations
Generally, we cover drugs filled at an out-of-network pharmacy only when you are not able to use a network pharmacy. If you cannot use a network pharmacy, here are the circumstances when we would cover prescriptions filled at an out-of-network pharmacy:
• If you are unable to get a covered drug in a timely manner within your area because there are no network pharmacies within a reasonable driving distance that provides 24-hour services.
• If you are trying to fill a covered drug that is not regularly stocked at an eligible network retail pharmacy or mail order pharmacy. (These drugs include orphan drugs or other specialty pharmaceuticals.)
• Please note that out-of-network prescriptions are limited to reimbursement for a single refill of up to a 30-day supply. If you are planning an extended stay in an area without a network pharmacy, please call Customer Care for assistance in signing up for mail order service.
• If you are filling prescriptions at an out-of-network pharmacy related to a medical emergency.
• Additionally, the pharmacy is not located outside the United States or its territories.
In these situations, please check first with Customer Care to see if there is a network pharmacy nearby. (Phone numbers for Customer Care are printed on the back cover of this booklet.) You may be required to pay the difference between what you pay for the drug at the out-of-network pharmacy and the cost that we would cover at an in-network pharmacy.
How do you ask for reimbursement from your plan?
If you must use an out-of-network pharmacy, you will generally have to pay the full cost (rather than your normal share of the cost) at the time you fill your prescription. You can ask us to reimburse you for our share of the cost. (Chapter 5, Section 2.1 explains how to ask your plan to pay you back.)
After all benefits are provided under your retiree drug coverage, in addition to paying your copayments/coinsurances, you will be required to pay the difference between what we would pay for a prescription filled at an in-network pharmacy and what the out-of-network pharmacy charged for your prescriptions.
2022 Evidence of Coverage for Navitus MedicareRx (PDP) 44 Chapter 3. Using the plan’s coverage for your Part D prescription drugs
SECTION 3 Your drugs need to be on the plan’s “Formulary”
Section 3.1 The “Formulary” tells which Part D drugs are covered
The plan has a “List of Covered Drugs (Formulary)”.
The drugs on this list are selected by your plan with the help of a team of doctors and pharmacists. The list must meet requirements set by Medicare. Medicare has approved the plan’s Formulary.
The drugs on the Formulary are only those covered under Medicare Part D (earlier in this chapter, Section 1.1 explains about Part D drugs).
We will generally cover a drug on your plan’s Formulary as long as you follow the other coverage rules explained in this chapter and the use of the drug is a medically accepted indication. A “medically accepted indication” is a use of the drug that is either:
• Approved by the Food and Drug Administration. (That is, the Food and Drug Administration has approved the drug for the diagnosis or condition for which it is being prescribed.)
• -- or -- Supported by certain references, such as the American Hospital Formulary Service Drug Information and the DRUGDEX Information System.
The Formulary includes both brand name and generic drugs
A generic drug is a prescription drug that has the same active ingredients as the brand name drug. Generally, it works just as well as the brand name drug and usually costs less. There are generic drug substitutes available for many brand name drugs.
What is not on the Formulary?
Your plan does not cover all prescription drugs.
• In some cases, the law does not allow any Medicare plan to cover certain types of drugs (for more about this, see Section 7.1 in this chapter).
• In other cases, we have decided not to include a particular drug on our Formulary.
Section 3.2 There are four “cost-sharing tiers” for drugs on the Formulary
Every drug on your plan’s Formulary is in one of four cost-sharing tiers. In general, the higher the cost-sharing tier, the higher your cost for the drug.
To find out which cost-sharing tier your drug is in, look it up in the Formulary.

2022 Evidence of Coverage for Navitus MedicareRx (PDP) 45 Chapter 3. Using the plan’s coverage for your Part D prescription drugs
The amount you pay for drugs in each cost-sharing tier is shown in Chapter 4 (What you pay for your Part D prescription drugs).
• Tier $0: Select generics (not all dosages of these drugs are covered at the Select Generics cost share)
• Tier 1: Preferred generics and certain lower cost brand products
• Tier 2: Preferred brand products and some high cost non-preferred generics
• Tier 3: Non-preferred products (could include some high cost non-preferred generics)
• Tier 4: Specialty products
Section 3.3 How can you find out if a specific drug is on the Formulary?
You have two ways to find out:
1. Check the most recent Formulary provided electronically on the Navitus MedicareRx Member Portal (https://memberportal.navitus.com). (Please note: If one of your drugs is not listed in the Formulary, you should visit our Member Portal or contact Customer Care to find out if we cover it.) The Formulary on the Member Portal is always the most current.
2. Call Customer Care to find out if a particular drug is on the plan’s Formulary or to ask for a copy of the list. (Phone numbers for Customer Care are printed on the back cover of this booklet.)
SECTION 4 There are restrictions on coverage for some drugs
Section 4.1 Why do some drugs have restrictions?
For certain prescription drugs, special rules restrict how and when your plan covers them. A team of doctors and pharmacists developed these rules to help our members use drugs in the most effective ways. These special rules also help control overall drug costs, which keeps your drug coverage more affordable.
In general, our rules encourage you to get a drug that works for your medical condition and is safe and effective. Whenever a safe, lower-cost drug will work just as well medically as a higher-cost drug, your plan’s rules are designed to encourage you and your prescriber to use that lower-cost option. We also need to comply with Medicare’s rules and regulations for drug coverage and cost sharing.
If there is a restriction for your drug, it usually means that you or your prescriber will have to take extra steps in order for us to cover the drug. If you want us to waive the restriction for you, you will need to use the coverage decision process and ask us to make an exception. We
2022 Evidence of Coverage for Navitus MedicareRx (PDP) 46 Chapter 3. Using the plan’s coverage for your Part D prescription drugs
may or may not agree to waive the restriction for you. (See Chapter 7, Section 5.2 for information about asking for exceptions.)
Please note that sometimes a drug may appear more than once in our Formulary. This is because different restrictions or cost sharing may apply based on factors such as the strength, amount, or form of the drug prescribed by your health care provider (for instance, 10 mg versus 100 mg; one per day versus two per day; tablet versus liquid).
Section 4.2 What kinds of restrictions?
Our plan uses different types of restrictions to help our members use drugs in the most effective ways. The sections below tell you more about the types of restrictions we use for certain drugs.
Restricting brand name drugs when a generic version is available
Generally, a “generic” drug works the same as a brand name drug and usually costs less. In most cases, when a generic version of a brand name drug is available, our network pharmacies will provide you the generic version. We usually will not cover the brand name drug when a generic version is available.
The Formulary indicates what you will pay for your drug. A generic drug is the same as a brand-name drug in dosage, safety and strength. When a generic drug is available and you or your prescriber choose the brand-name drug, you must pay the applicable brand copay plus the difference between the cost of the brand-name drug and the generic equivalent. With a prior authorization request, an exception for medical necessity may be made and you will pay the Tier 3 (non-preferred) applicable copay.
Note: The difference between the cost of the brand drug and the generic (DAW penalty) does not accumulate toward the UC High Option Supplement to Medicare Annual Prescription Maximum Out-of-Pocket.
This Dispense as Written (DAW) cost-sharing penalty will not exceed the cost of the medication.
Coverage for out-of-country drugs
Outpatient prescription drugs are not covered by Medicare Part D plans when they are filled by pharmacies outside of the United States.
Your UC plan provides coverage for outpatient prescription drugs when all of the following apply:
• You remain a permanent resident of the United States while you are out of country, • The drug is approved by the Food and Drug Administration (FDA), and • The drug would be a covered drug by your plan if the drug was filled by a pharmacy
located within the United States.

2022 Evidence of Coverage for Navitus MedicareRx (PDP) 47 Chapter 3. Using the plan’s coverage for your Part D prescription drugs
When you receive coverage for outpatient prescription drugs filled at a pharmacy outside the United States, you will need to pay the full cost of the drug and request that we reimburse you for our share. Your share of a covered outpatient drug will be your coinsurance or copayment amount. Please see “How to ask us to pay you back” in Chapter 5, Section 2, for detailed instructions.
Getting plan approval in advance
For certain drugs, you or your prescriber need to get approval from us before we will agree to cover the drug for you. This is called “prior authorization.” Sometimes the requirement for getting approval in advance helps guide appropriate use of certain drugs. If you do not get this approval, your drug might not be covered by the plan.
Trying a different drug first
This requirement encourages you to try less costly but usually just as effective drugs before your plan covers another drug. For example, if Drug A and Drug B treat the same medical condition, your plan may require you to try Drug A first. If Drug A does not work for you, your plan will then cover Drug B. This requirement to try a different drug first is called “step therapy.”
Quantity limits
For certain drugs, we limit the amount of the drug that you can have by limiting how much of a drug you can get each time you fill your prescription. For example, if it is normally considered safe to take only one pill per day for a certain drug, we may limit coverage for your prescription to no more than one pill per day.
Section 4.3 Do any of these restrictions apply to your drugs?
The plan’s Formulary includes information about the restrictions described above. To find out if any of these restrictions apply to a drug you take or want to take, check the Formulary. For the most up-to-date information, call Customer Care (phone numbers are printed on the back cover of this booklet) or check our Member Portal (https://memberportal.navitus.com).
If there is a restriction for your drug, it usually means that you or your prescriber will have to take extra steps in order for us to cover the drug. If there is a restriction on the drug you want to take, you should contact Customer Care to learn what you or your prescriber would need to do to get coverage for the drug. If you want us to waive the restriction for you, you will need to use the coverage decision process and ask us to make an exception. We may or may not agree to waive the restriction for you. (See Chapter 7, Section 5.2 for information about asking for exceptions.)

2022 Evidence of Coverage for Navitus MedicareRx (PDP) 48 Chapter 3. Using the plan’s coverage for your Part D prescription drugs
SECTION 5 What if one of your drugs is not covered in the way you’d like it to be covered?
Section 5.1 There are things you can do if your drug is not covered in the way you’d like it to be covered
We hope that your drug coverage will work well for you. But it’s possible that there could be a prescription drug you are currently taking, or one that you and your prescriber think you should be taking that is not on our formulary or is on our formulary with restrictions. For example:
• The drug might not be covered at all. Or maybe a generic version of the drug is covered but the brand name version you want to take is not covered.
• The drug is covered, but there are extra rules or restrictions on coverage for that drug. As explained in Section 4, some of the drugs covered by your plan have extra rules to restrict their use. For example, you might be required to try a different drug first, to see if it will work, before the drug you want to take will be covered for you. Or there might be limits on what amount of the drug (number of pills, etc.) is covered during a particular time period. In some cases, you may want us to waive the restriction for you.
• The drug is covered, but it is in a cost-sharing tier that makes your cost sharing more expensive than you think it should be. Your plan puts each covered drug into one of four different cost-sharing tiers. How much you pay for your prescription depends in part on which cost-sharing tier your drug is in.
There are things you can do if your drug is not covered in the way that you’d like it to be covered. Your options depend on what type of problem you have:
• If your drug is not on the Formulary or if your drug is restricted, go to Section 5.2 to learn what you can do.
• If your drug is in a cost-sharing tier that makes your cost more expensive than you think it should be, go to Section 5.3 to learn what you can do.
Section 5.2 What can you do if your drug is not on the Formulary or if the drug is restricted in some way?
If your drug is not on the Formulary or is restricted, here are things you can do:
• You may be able to get a temporary supply of the drug (only members in certain situations can get a temporary supply). This will give you and your prescriber time to change to another drug or to file a request to have the drug covered.
• You can change to another drug.
• You can request an exception and ask your plan to cover the drug or remove restrictions from the drug.
2022 Evidence of Coverage for Navitus MedicareRx (PDP) 49 Chapter 3. Using the plan’s coverage for your Part D prescription drugs
You may be able to get a temporary supply
Under certain circumstances, your plan must offer a temporary supply of a drug to you when your drug is not on the Formulary or when it is restricted in some way. Doing this gives you time to talk with your prescriber about the change in coverage and figure out what to do.
To be eligible for a temporary supply, you must meet the two requirements below:
1. The change to your drug coverage must be one of the following types of changes:
• The drug you have been taking is no longer on your plan’s Formulary.
• -- or -- The drug you have been taking is now restricted in some way (Section 4 in this chapter explains restrictions).
2. You must be in one of the situations described below:
• For those members who are new or who were in the plan last year: We will cover a temporary supply of your drug during the first 90 days of your membership in the plan if you were new and during the first 90 days of the calendar year if you were in the plan last year. This temporary supply will be for a maximum of a 30-day supply. If your prescription is written for fewer days, we will allow multiple fills to provide up to a maximum of a 30-day supply of medication. The prescription must be filled at a network pharmacy. (Please note that the long-term care pharmacy may provide the drug in smaller amounts at a time to prevent waste.)
• For those members who have been in the plan for more than 90 days and reside in a long-term care (LTC) facility and need a supply right away: We will cover one 31-day supply of a particular drug, or less if your prescription is written for fewer days. This is in addition to the above temporary supply situation.
Level of Care Changes
We will provide a one-time 31-day transition supply per drug, which will cover a temporary supply if you have a change in your medications due to a level-of-care change. A level of care change may include:
• Entering or leaving a LTC facility • Being discharged from a hospital to a home • Ending a Medicare Part A skilled nursing facility stay • Giving up hospice status and reverting back to standard Medicare benefits • Ending an LTC facility stay and return home
To ask for a temporary supply, call Customer Care (phone numbers are printed on the back cover of this booklet).
2022 Evidence of Coverage for Navitus MedicareRx (PDP) 50 Chapter 3. Using the plan’s coverage for your Part D prescription drugs
During the time when you are getting a temporary supply of a drug, you should talk with your prescriber to decide what to do when your temporary supply runs out. You can either switch to a different drug covered by your plan or ask your plan to make an exception for you and cover your current drug. The sections below tell you more about these options.
You can change to another drug
Start by talking with your prescriber. Perhaps there is a different drug covered by your plan that might work just as well for you. You can call Customer Care to ask for a list of covered drugs that treat the same medical condition. This list can help your prescriber find a covered drug that might work for you. (Phone numbers for Customer Care are printed on the back cover of this booklet.)
You can ask for an exception
You and your prescriber can ask us to make an exception for you and cover the drug in the way you would like it to be covered. If your prescriber says that you have medical reasons that justify asking us for an exception, your prescriber can help you request an exception to the rule. For example, you can ask us to cover a drug even though it is not on your plan’s Formulary. Or you can ask us to make an exception and cover the drug without restrictions.
If you are a current member and a drug you are taking will be removed from the formulary or restricted in some way for next year, we will allow you to request a formulary exception in advance for next year. We will explain any change in the coverage for your drug for next year. You can ask for an exception before next year, and we will give you an answer within 72 hours after we receive your request (or your prescriber’s supporting statement). If we approve your request, we will authorize the coverage before the change takes effect.
If you and your prescriber want to ask for an exception, Chapter 7, Section 5.4 tells what to do. It explains the procedures and deadlines that have been set by Medicare to make sure your request is handled promptly and fairly.
Section 5.3 What can you do if your drug is in a cost-sharing tier you think is too high?
If your drug is in a cost-sharing tier you think is too high, here are things you can do:
You can change to another drug
If your drug is in a cost-sharing tier you think is too high, start by talking with your prescriber. Perhaps there is a different drug in a lower cost-sharing tier that might work just as well for you. You can call Customer Care to ask for a list of covered drugs that treat the same medical condition. This list can help your prescriber find a covered drug that might work for you. (Phone numbers for Customer Care are printed on the back cover of this booklet.)
2022 Evidence of Coverage for Navitus MedicareRx (PDP) 51 Chapter 3. Using the plan’s coverage for your Part D prescription drugs
You can ask for an exception
You and your prescriber can ask us to make an exception in the cost-sharing tier for the drug so that you pay less for it. If your prescriber says that you have medical reasons that justify asking us for an exception, your prescriber can help you request an exception to the rule.
If you and your prescriber want to ask for an exception, Chapter 7, Section 5.4 tells what to do. It explains the procedures and deadlines that have been set by Medicare to make sure your request is handled promptly and fairly.
Drugs of our Tier 4 (Specialty products) are not eligible for this type of exception. We do not lower the cost-sharing amount for drugs in this tier.
SECTION 6 What if your coverage changes for one of your drugs?
Section 6.1 The Formulary can change during the year
Most of the changes in drug coverage happen at the beginning of each year (January 1). However, during the year, your plan might make changes to the Formulary. For example, the plan might:
• Add or remove drugs from the Formulary. New drugs become available, including new generic drugs. Perhaps the government has given approval to a new use for an existing drug. Sometimes, a drug gets recalled and we decide not to cover it. Or we might remove a drug from the list because it has been found to be ineffective.
• Move a drug to a higher or lower cost-sharing tier.
• Add or remove a restriction on coverage for a drug (for more information about restrictions to coverage, see Section 4 in this chapter).
• Replace a brand name drug with a generic drug.
We must follow Medicare requirements before we change your plan’s Formulary.
Section 6.2 What happens if coverage changes for a drug you are taking?
Information on changes to drug coverage
When changes to the Formulary occur during the year, we post information on our Member Portal about those changes. We will update our online Formulary on a regularly scheduled basis to include any changes that have occurred after the last update. Below we point out the times that you would get direct notice if changes are made to a drug that you are then taking. You can also call Customer Care for more information (phone numbers are printed on the back cover of this booklet).
2022 Evidence of Coverage for Navitus MedicareRx (PDP) 52 Chapter 3. Using the plan’s coverage for your Part D prescription drugs
Do changes to your drug coverage affect you right away?
Changes that can affect you this year: In the below cases, you will be affected by the coverage changes during the current year:
Advance General Notice that Navitus MedicareRx may immediately substitute new generic drugs:
• A new generic drug replaces a brand name drug on the Formulary (or we change the cost-sharing tier or add new restrictions to the brand name drug or both)
o We may immediately remove a brand name drug on our Formulary if we are replacing it with a newly approved generic version of the same drug that will appear on the same or lower cost-sharing tier and with the same or fewer restrictions. Also, when adding the new generic drug, we may decide to keep the brand name drug on our Formulary, but immediately move it to a higher cost-sharing tier or add new restrictions or both.
o We may not tell you in advance before we make that change—even if you are currently taking the brand name drug,
o You or your prescriber can ask us to make an exception and continue to cover the brand name drug for you. For information on how to ask for an exception, see Chapter 7 (What to do if you have a problem or complaint (coverage decisions, appeals, complaints)).
o If you are taking the brand name drug at the time we make the change, we will provide you with information about the specific change(s) we made. This will also include information on the steps you may take to request an exception to cover the brand name drug. You may not get this notice before we make the change.
• Unsafe drugs and other drugs on the Formulary that are withdrawn from the market
o Once in a while, a drug may be suddenly withdrawn because it has been found to be unsafe or removed from the market for another reason. If this happens, we will immediately remove the drug from the Formulary. If you are taking that drug, we will let you know of this change right away.
o Your prescriber will also know about this change, and can work with you to find another drug for your condition.
• Other changes to drugs on the Formulary o We may make other changes once the year has started that affect drugs you are
taking. For instance, we might add a generic drug that is not new to the market to replace a brand name drug or change the cost-sharing tier or add new restrictions to the brand name drug or both. We also might make changes based on FDA boxed warnings or new clinical guidelines recognized by Medicare. We must give

2022 Evidence of Coverage for Navitus MedicareRx (PDP) 53 Chapter 3. Using the plan’s coverage for your Part D prescription drugs
you at least 30 days’ advance notice of the change or give you notice of the change and a 30-day refill of the drug you are taking at a network pharmacy.
o After you receive notice of the change, you should be working with your prescriber to switch to a different drug that we cover.
o Or you or your prescriber can ask us to make an exception and continue to cover the drug for you. For information on how to ask for an exception, see Chapter 7 (What to do if you have a problem or complaint (coverage decisions, appeals, complaints)).
Changes to drugs on the Formulary that will not affect people currently taking the drug: For changes to the Formulary that are not described above, if you are currently taking the drug, the following types of changes will not affect you until January 1 of the next year if you stay in your plan:
• If we move your drug into a higher cost-sharing tier.
• If we put a new restriction on your use of the drug.
• If we remove your drug from the Formulary.
If any of these changes happen for a drug you are taking (but not because of a market withdrawal, a generic drug replacing a brand name drug, a Part D status change or other change noted in the sections above), then the change won’t affect your use or what you pay as your share of the cost until January 1 of the next year. Until that date, you probably won’t see any increase in your payments or any added restriction to your use of the drug. You will not get direct notice this year about changes that do not affect you. However, on January 1 of the next year, the changes will affect you, and it is important to check the Formulary in the new benefit year for any changes to drugs.
SECTION 7 What types of drugs are not covered by the plan?
Section 7.1 Types of drugs we do not cover
This section tells you what kinds of prescription drugs are “excluded.” This means Medicare does not pay for these drugs.
If you get drugs that are excluded and not on the formulary, you must pay for them yourself. We won’t pay for the drugs that are listed in this section (except for certain excluded drugs covered under our supplemental drug coverage). In some cases, excluded drugs may be covered under your medical plan. The only exception: If the requested drug is found upon appeal to be a drug that is not excluded under Part D and we should have paid for or covered it because of your specific situation. (For information about appealing a decision we have made to not cover a drug, go to Chapter 7, Section 5.5 in this booklet.)

2022 Evidence of Coverage for Navitus MedicareRx (PDP) 54 Chapter 3. Using the plan’s coverage for your Part D prescription drugs
Here are a few general rules about drugs that Medicare drug plans will not cover under Part D:
• Our plan’s Part D drug coverage cannot cover a drug that would be covered under Medicare Part A or Part B.
• Our plan cannot cover a drug purchased outside the United States and its territories.
• Our plan usually cannot cover off-label use. “Off-label use” is any use of the drug other than those indicated on a drug’s label as approved by the Food and Drug Administration.
o Generally, coverage for “off-label use” is allowed only when the use is supported by certain references, such as the American Hospital Formulary Service Drug Information and the DRUGDEX Information System. If the use is not supported by any of these references, then our plan cannot cover its “off-label use.”
• Your plan does cover drugs listed on your Formulary, including when these drugs are ingredients in a compound drug.
Also, by law, these categories of drugs are not covered by Medicare drug plans unless your plan covers them as “Extra Covered Drugs”. Please see the “Extra Covered Drugs” section of the benefits chart located in Chapter 4 to find out which of the drugs listed below are covered under your group sponsored plan.
• Non-prescription drugs (also called over-the-counter drugs)
• Drugs when used to promote fertility
• Drugs when used for the relief of cough or cold symptoms
• Drugs when used for cosmetic purposes or to promote hair growth
• Prescription vitamins and mineral products, except prenatal vitamins and fluoride preparations
• Drugs when used for the treatment of sexual or erectile dysfunction
• Drugs when used for treatment of anorexia, weight loss, or weight gain, unless used to treat HIV or cancer wasting
• Outpatient drugs for which the manufacturer seeks to require that associated tests or monitoring services be purchased exclusively from the manufacturer as a condition of sale
We offer additional coverage of some prescription drugs not normally covered in a Medicare prescription drug plan (supplemental drug coverage). These drugs can be found on the Formulary. The amount you pay when you fill a prescription for these drugs does not count toward qualifying you for the Catastrophic Coverage Stage. (The Catastrophic Coverage Stage is described in Chapter 4, Section 7 of this booklet.)
In addition, if you are receiving “Extra Help” from Medicare to pay for your prescriptions, the “Extra Help” program will not pay for the drugs not normally covered. (Please refer to the plan’s Formulary or call Customer Care for more information. Phone numbers for Customer Care are printed on the back cover of this booklet.) However, if you have drug coverage through
2022 Evidence of Coverage for Navitus MedicareRx (PDP) 55 Chapter 3. Using the plan’s coverage for your Part D prescription drugs
Medicaid, your state Medicaid program may cover some prescription drugs not normally covered in a Medicare drug plan. Please contact your state Medicaid program to determine what drug coverage may be available to you. (You can find phone numbers and contact information for Medicaid in Chapter 2, Section 6.)
SECTION 8 Show your plan membership card when you fill a prescription
Section 8.1 Show your membership card
To fill your prescription, show your plan membership card at the network pharmacy you choose. When you show your plan membership card, the network pharmacy will automatically bill your plan for our share of your covered prescription drug cost. You will need to pay the pharmacy your share of the cost when you pick up your prescription.
Section 8.2 What if you don’t have your membership card with you?
If you don’t have your plan membership card with you when you fill your prescription, ask the pharmacy to contact Customer Care to get the necessary information (phone numbers are printed on the back cover of this booklet).
If the pharmacy is not able to get the necessary information, you may have to pay the full cost of the prescription when you pick it up. (You can then ask us to reimburse you for our share. See Chapter 5, Section 2.1 for information about how to ask the plan for reimbursement.)
SECTION 9 Part D drug coverage in special situations
Section 9.1 What if you’re in a hospital or a skilled nursing facility for a stay that is covered by Original Medicare?
If you are admitted to a hospital for a stay covered by Original Medicare, Medicare Part A will generally cover the cost of your prescription drugs during your stay. Once you leave the hospital, our plan will cover your drugs as long as the drugs meet all of our rules for coverage. See the previous parts of this chapter that tell about the rules for getting drug coverage.
If you are admitted to a skilled nursing facility for a stay covered by Original Medicare, Medicare Part A will generally cover your prescription drugs during all or part of your stay. If you are still in the skilled nursing facility, and Part A is no longer covering your drugs, our plan will cover your drugs as long as the drugs meet all of our rules for coverage. See the previous parts of this chapter that tell about the rules for getting drug coverage.
Please Note: When you enter, live in, or leave a skilled nursing facility, you are entitled to a Special Enrollment Period. During this time period, you can switch plans or change your
2022 Evidence of Coverage for Navitus MedicareRx (PDP) 56 Chapter 3. Using the plan’s coverage for your Part D prescription drugs
coverage. (Chapter 8, Ending your membership in the plan, tells when you can leave our plan and join a different Medicare plan.)
Section 9.2 What if you’re a resident in a long-term care (LTC) facility?
Usually, a long-term care facility (LTC) (such as a nursing home) has its own pharmacy, or a pharmacy that supplies drugs for all of its residents. If you are a resident of a long-term care facility, you may get your prescription drugs through the facility’s pharmacy as long as it is part of our network.
Check your Pharmacy Directory to find out if your LTC facility’s pharmacy is part of our network. There is also a pharmacy search tool on our Member Portal at https://memberportal.navitus.com. If the LTC pharmacy isn’t in our network, or if you need more information, please contact Customer Care (phone numbers are printed on the back cover of this booklet).
What if you’re a resident in a long-term care (LTC) facility and become a new member of the plan?
If you need a drug that is not on our Formulary or is restricted in some way, the plan will cover a temporary supply of your drug during the first 90 days of your membership. The total supply will be for a maximum of a 31-day supply, or less if your prescription is written for fewer days. (Please note that the long-term care pharmacy may provide the drug in smaller amounts at a time to prevent waste.) If you have been a member of the plan for more than 90 days and need a drug that is not on our Formulary or if the plan has any restriction on the drug’s coverage, we will cover one 31-day supply, or less if your prescription is written for fewer days.
During the time when you are getting a temporary supply of a drug, you should talk with your prescriber to decide what to do when your temporary supply runs out. Perhaps there is a different drug covered by the plan that might work just as well for you. Or you and your prescriber can ask the plan to make an exception for you and cover the drug in the way you would like it to be covered. If you and your prescriber want to ask for an exception, Chapter 7, Section 5.4 tells what to do.
Section 9.3 What if you are taking drugs covered by Original Medicare?
Your enrollment in Navitus MedicareRx doesn’t affect your coverage for drugs covered under Medicare Part A or Part B. If you meet Medicare’s coverage requirements, your drug will still be covered under Medicare Part A or Part B, even though you are enrolled in this plan. In addition, if your drug would be covered by Medicare Part A or Part B, our plan can’t cover it, even if you choose not to enroll in Part A or Part B.
Some drugs may be covered under Medicare Part B in some situations and through Navitus MedicareRx in other situations. But drugs are never covered by both Part B and our plan at the
2022 Evidence of Coverage for Navitus MedicareRx (PDP) 57 Chapter 3. Using the plan’s coverage for your Part D prescription drugs
same time. In general, your pharmacist or prescriber will determine whether to bill Medicare Part B or Navitus MedicareRx for the drug.
Section 9.4 What if you have a Medigap (Medicare Supplement Insurance) policy with prescription drug coverage?
If you currently have a Medigap policy that includes coverage for prescription drugs, you must contact your Medigap issuer and tell them you have enrolled in our plan. If you decide to keep your current Medigap policy, your Medigap issuer will remove the prescription drug coverage portion of your Medigap policy and lower your premium.
Each year your Medigap insurance company should send you a notice that tells if your prescription drug coverage is “creditable,” and the choices you have for drug coverage. (If the coverage from the Medigap policy is “creditable,” it means that it is expected to pay, on average, at least as much as Medicare’s standard prescription drug coverage.) The notice will also explain how much your premium would be lowered if you remove the prescription drug coverage portion of your Medigap policy. If you didn’t get this notice, or if you can’t find it, contact your Medigap insurance company and ask for another copy.
Section 9.5 What if you’re also getting drug coverage from an employer or retiree group plan?
Do you currently have other prescription drug coverage through your (or your spouse’s) employer or retiree group? If so, please contact that group’s sponsor. They can help you determine how your current prescription drug coverage will work with our plan.
In general, if you are currently employed, the prescription drug coverage you get from us will be secondary to your employer or retiree group coverage. That means your group coverage would pay first.
Special note about ‘creditable coverage’:
Each year your employer or retiree group should provide you a notice that tells if your prescription drug coverage for the next calendar year is “creditable” and the choices you have for drug coverage.
If the coverage from the group plan is “creditable,” it means that the plan has drug coverage that is expected to pay, on average, at least as much as Medicare’s standard prescription drug coverage.
Keep these notices about creditable coverage, because you may need them later. If you enroll in a Medicare plan that includes Part D drug coverage, you may need these notices to show that you have maintained creditable coverage. If you didn’t get a notice about creditable coverage from your employer or retiree group plan, you can get a copy from the employer or retiree group’s benefits administrator or the employer.

2022 Evidence of Coverage for Navitus MedicareRx (PDP) 58 Chapter 3. Using the plan’s coverage for your Part D prescription drugs
Section 9.6 What if you are in Medicare-certified Hospice?
Drugs are never covered by both hospice and our plan at the same time. If you are enrolled in Medicare hospice and require an anti-nausea, laxative, pain medication, or anti-anxiety drug that is not covered by your hospice because it is unrelated to your terminal illness and related conditions, our plan must receive notification from either the prescriber or your hospice provider that the drug is unrelated before our plan can cover the drug. To prevent delays in receiving any unrelated drugs that should be covered by our plan, you can ask your hospice provider or prescriber to make sure we have the notification that the drug is unrelated before you ask a pharmacy to fill your prescription.
In the event you either revoke your hospice election or are discharged from hospice, our plan should cover all your drugs. To prevent any delays at a pharmacy when your Medicare hospice benefit ends, you should bring documentation to the pharmacy to verify your revocation or discharge. See the previous parts of this section that tell about the rules for getting drug coverage under Part D. Chapter 4 (What you pay for your Part D prescription drugs) gives more information about drug coverage and what you pay.
SECTION 10 Programs on drug safety and managing medications
Section 10.1 Programs to help members use drugs safely
We conduct drug use reviews for our members to help make sure that they are getting safe and appropriate care. These reviews are especially important for members who have more than one prescriber who prescribes their drugs.
We do a review each time you fill a prescription. We also review our records on a regular basis. During these reviews, we look for potential problems such as:
• Possible medication errors
• Drugs that may not be necessary because you are taking another drug to treat the same medical condition
• Drugs that may not be safe or appropriate because of your age or gender
• Certain combinations of drugs that could harm you if taken at the same time
• Prescriptions written for drugs that have ingredients you are allergic to
• Possible errors in the amount (dosage) of a drug you are taking
• Unsafe amounts of opioid pain medications
If we see a possible problem in your use of medications, we will work with your prescriber to correct the problem.

2022 Evidence of Coverage for Navitus MedicareRx (PDP) 59 Chapter 3. Using the plan’s coverage for your Part D prescription drugs
Section 10.2 Drug Management Program (DMP) to help members safely use their opioid medications
We have a program that can help make sure our members safely use their prescription opioid medications, and other medications that are frequently abused. This program is called a Drug Management Program (DMP). If you use opioid medications that you get from several doctors or pharmacies, or if you had a recent opioid overdose, we may talk to your doctors to make sure your use of opioid medications is appropriate and medically necessary. Working with your doctors, if we decide your use of prescription opioid or benzodiazepine medications is not safe, we may limit how you can get those medications. The limitations may be:
• Requiring you to get all your prescriptions for opioid or benzodiazepine medications from a certain pharmacy(ies)
• Requiring you to get all your prescriptions for opioid or benzodiazepine medications from a certain doctor(s)
• Limiting the amount of opioid or benzodiazepine medications we will cover for you
If we think that one or more of these limitations should apply to you, we will send you a letter in advance. The letter will have information explaining the limitations we think should apply to you. You will also have an opportunity to tell us which doctors or pharmacies you prefer to use, and about any other information you think is important for us to know. After you have had the opportunity to respond, if we decide to limit your coverage for these medications, we will send you another letter confirming the limitation. If you think we made a mistake or you disagree with our determination that you are at-risk for prescription drug misuse or with the limitation, you and your prescriber have the right to ask us for an appeal. If you choose to appeal, we will review your case and give you a decision. If we continue to deny any part of your request related to the limitations that apply to your access to medications, we will automatically send your case to an independent reviewer outside of our plan for review and resolution. See Chapter 7 for information about how to ask for an appeal.
The DMP may not apply to you if you have certain medical conditions, such as cancer or sickle cell disease, you are receiving hospice, palliative, or end-of-life care, or live in a long-term care facility.
Section 10.3 Medication Therapy Management (MTM) program to help members manage their medications
We have a program that can help our members with complex health needs.
This program is voluntary and free to members. A team of pharmacists and doctors developed the program for us. This program can help make sure that our members get the most benefit from the drugs they take. Our program is called a Medication Therapy Management (MTM) program.
Some members who take medications for different medical conditions and have high drug costs, or are in a Drug Management Program (DMP) to help members use their opioids safely, may be able to get services through an MTM program. A pharmacist or other health professional will

2022 Evidence of Coverage for Navitus MedicareRx (PDP) 60 Chapter 3. Using the plan’s coverage for your Part D prescription drugs
give you a comprehensive review of all your medications. You can talk about how best to take your medications, your costs, and any problems or questions you have about your prescription and over-the-counter medications. You’ll get a written summary of this discussion. The summary has a medication action plan that recommends what you can do to make the best use of your medications, with space for you to take notes or write down any follow-up questions. You’ll also get a personal medication list that will include all the medications you’re taking and why you take them. In addition, members in the MTM program will receive information on the safe disposal of prescription medications that are controlled substances.
It’s a good idea to have your medication review before your yearly “Wellness” visit, so you can talk to your doctor about your action plan and medication list. Bring your action plan and medication list with you to your visit or anytime you talk with your doctors, pharmacists, and other health care prescribers. Also, keep your medication list with you (for example, with your ID) in case you go to the hospital or emergency room.
If we have a program that fits your needs, we will automatically enroll you in the program and send you information. If you decide not to participate, please notify us and we will withdraw you from the program. If you have any questions about these programs, please contact Customer Care (phone numbers are printed on the back cover of this booklet).
If you have specific questions about this program, please contact the Medication Therapy Management (MTM) program team. You can call us at 1-833-837-4304, Monday through Thursday 9 am to 6 pm Central Standard Time and on Friday 9 am to 4 pm Central Standard Time. TTY/TDD users should call 711.
CHAPTER 4 What you pay for your Part D
prescription drugs

2022 Evidence of Coverage for Navitus MedicareRx (PDP) 62 Chapter 4. What you pay for your Part D prescription drugs
Chapter 4. What you pay for your Part D prescription drugs
SECTION 1 Introduction............................................................................................ 64
Section 1.1 Use this chapter together with other materials that explain your drug coverage ................................................................................................... 64
Section 1.2 Types of out-of-pocket costs you may pay for covered drugs ...................... 65
SECTION 2 What you pay for a drug depends on which “drug payment stage” you are in when you get the drug.......................................... 65
Section 2.1 What are the drug payment stages for Navitus MedicareRx (PDP) members?.................................................................................................. 65
SECTION 3 We send you reports that explain payments for your drugs and which payment stage you are in ................................................. 66
Section 3.1 We send you a monthly summary called the “Part D Explanation of Benefits” (the “Part D EOB”) .................................................................... 66
Section 3.2 Help us keep our information about your drug payments up to date ............ 67
SECTION 4 There is no deductible for Navitus MedicareRx .............................. 68
Section 4.1 You do not pay a deductible for your Part D drugs. .................................... 68
SECTION 5 During the Initial Coverage Stage, the plan pays its share of your drug costs and you pay your share.......................................... 68
Section 5.1 What you pay for a drug depends on the drug and where you fill your prescription ............................................................................................... 68
Section 5.2 A table that shows your costs for a one-month supply of a drug .................. 69
Section 5.3 If your doctor prescribes less than a full month’s supply, you may not have to pay the cost of the entire month’s supply........................................ 73
Section 5.4 A table that shows your costs for a long-term (up to a 90-day) supply of a drug .......................................................................................................... 73
Section 5.5 You stay in the Initial Coverage Stage until total drug costs for the year reach $4,430.............................................................................................. 77
SECTION 6 During the Coverage Gap Stage, the plan provides some drug coverage........................................................................................ 77
Section 6.1 You stay in the Coverage Gap Stage until your out-of-pocket costs reach $7,050 ....................................................................................................... 77
Section 6.2 How Medicare calculates your out-of-pocket costs for prescription drugs ... 78

2022 Evidence of Coverage for Navitus MedicareRx (PDP) 63 Chapter 4. What you pay for your Part D prescription drugs
SECTION 7 During the Catastrophic Coverage Stage, the plan pays most of the cost for your drugs.......................................................... 80
Section 7.1 Once you are in the Catastrophic Coverage Stage, you will stay in this stage for the rest of the year ....................................................................... 80
SECTION 8 What you pay for vaccinations covered by Part D depends on how and where you get them ........................................................ 83
Section 8.1 Our plan may have separate coverage for the Part D vaccine medication itself and for the cost of giving you the vaccine .......................................... 83
Section 8.2 You may want to call us at Customer Care before you get a vaccination ..... 84
2022 Evidence of Coverage for Navitus MedicareRx (PDP) 64 Chapter 4. What you pay for your Part D prescription drugs
Did you know there are programs to help people pay for their drugs?
There are programs to help people with limited resources pay for their drugs. These include “Extra Help” and State Pharmaceutical Assistance Programs. For more information, see Chapter 2, Section 7.
Are you currently getting help to pay for your drugs?
If you are in a program that helps pay for your drugs, some information in this Evidence of Coverage about the costs for Part D prescription drugs may not apply to you. We will provide a separate insert, called the “Evidence of Coverage Rider for People Who Get Extra Help Paying for Prescription Drugs” (also known as the “Low Income Subsidy Rider” or the “LIS Rider”), which tells you about your drug coverage. If you are eligible and don’t have this insert, please call Customer Care and ask for the “LIS Rider.” (Phone numbers for Customer Care are printed on the back cover of this booklet.)
SECTION 1 Introduction
Section 1.1 Use this chapter together with other materials that explain your drug coverage
This chapter focuses on what you pay for your Part D prescription drugs. To keep things simple, we use “drug” in this chapter to mean a Part D prescription drug. As explained in Chapter 3, not all drugs are Part D drugs – some drugs are covered under Medicare Part A or Part B and other drugs are excluded from Medicare coverage by law. Some excluded drugs may be covered by our plan because of your supplemental (wrap) drug coverage, and will be included on our Formulary.
To understand the payment information, we give you in this chapter, you need to know the basics of what drugs are covered, where to fill your prescriptions, and what rules to follow when you get your covered drugs. Here are materials that explain these basics:
• The plan’s List of Covered Drugs (Formulary). o This Formulary tells which drugs are covered for you. o It also tells which of the four “cost-sharing tiers” the drug is in and whether there
are any restrictions on your coverage for the drug.
o If you need a copy of the Formulary, call Customer Care (phone numbers are printed on the back cover of this booklet). You can also find the Formulary on our Member Portal at https://memberportal.navitus.com. The Formulary on the Member Portal is always the most current.
• Chapter 3 of this booklet. Chapter 3 gives the details about your prescription drug coverage, including rules you need to follow when you get your covered drugs. Chapter 3 also tells which types of prescription drugs are not covered by our plan.
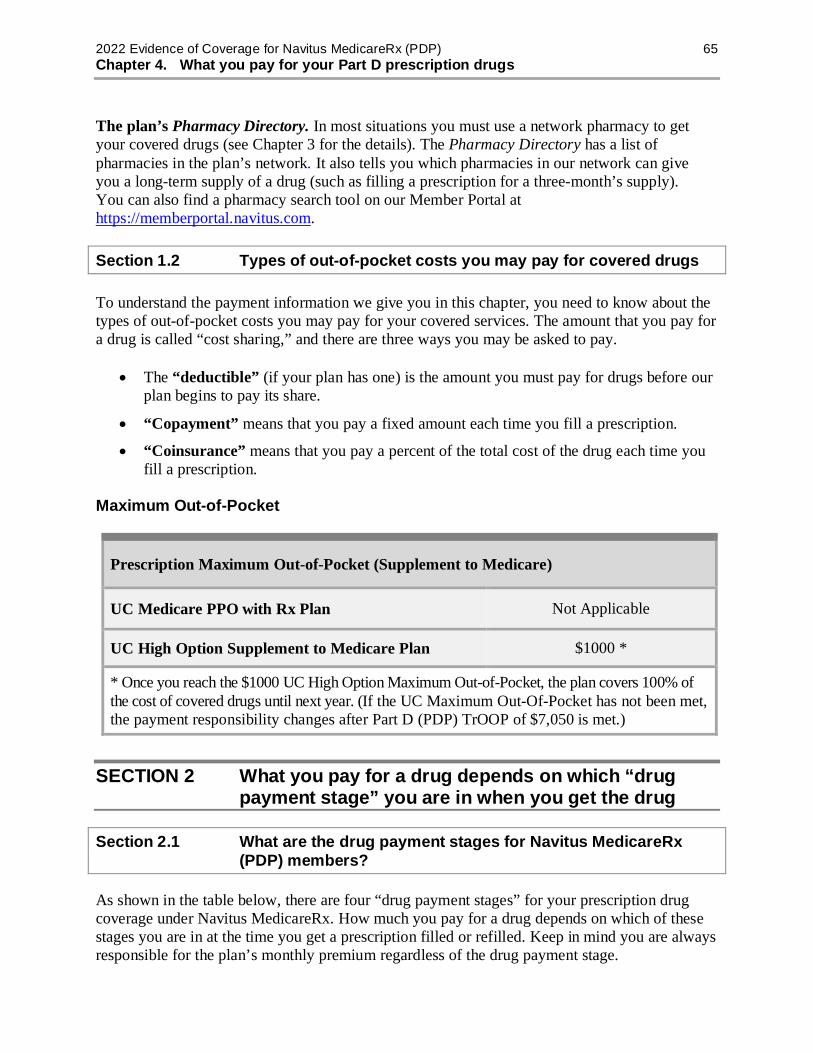
2022 Evidence of Coverage for Navitus MedicareRx (PDP) 65 Chapter 4. What you pay for your Part D prescription drugs
The plan’s Pharmacy Directory. In most situations you must use a network pharmacy to get your covered drugs (see Chapter 3 for the details). The Pharmacy Directory has a list of pharmacies in the plan’s network. It also tells you which pharmacies in our network can give you a long-term supply of a drug (such as filling a prescription for a three-month’s supply). You can also find a pharmacy search tool on our Member Portal at https://memberportal.navitus.com.
Section 1.2 Types of out-of-pocket costs you may pay for covered drugs
To understand the payment information we give you in this chapter, you need to know about the types of out-of-pocket costs you may pay for your covered services. The amount that you pay for a drug is called “cost sharing,” and there are three ways you may be asked to pay.
• The “deductible” (if your plan has one) is the amount you must pay for drugs before our plan begins to pay its share.
• “Copayment” means that you pay a fixed amount each time you fill a prescription.
• “Coinsurance” means that you pay a percent of the total cost of the drug each time you fill a prescription.
Maximum Out-of-Pocket
Prescription Maximum Out-of-Pocket (Supplement to Medicare)
UC Medicare PPO with Rx Plan Not Applicable
UC High Option Supplement to Medicare Plan $1000 *
* Once you reach the $1000 UC High Option Maximum Out-of-Pocket, the plan covers 100% of the cost of covered drugs until next year. (If the UC Maximum Out-Of-Pocket has not been met, the payment responsibility changes after Part D (PDP) TrOOP of $7,050 is met.)
SECTION 2 What you pay for a drug depends on which “drug payment stage” you are in when you get the drug
Section 2.1 What are the drug payment stages for Navitus MedicareRx (PDP) members?
As shown in the table below, there are four “drug payment stages” for your prescription drug coverage under Navitus MedicareRx. How much you pay for a drug depends on which of these stages you are in at the time you get a prescription filled or refilled. Keep in mind you are always responsible for the plan’s monthly premium regardless of the drug payment stage.
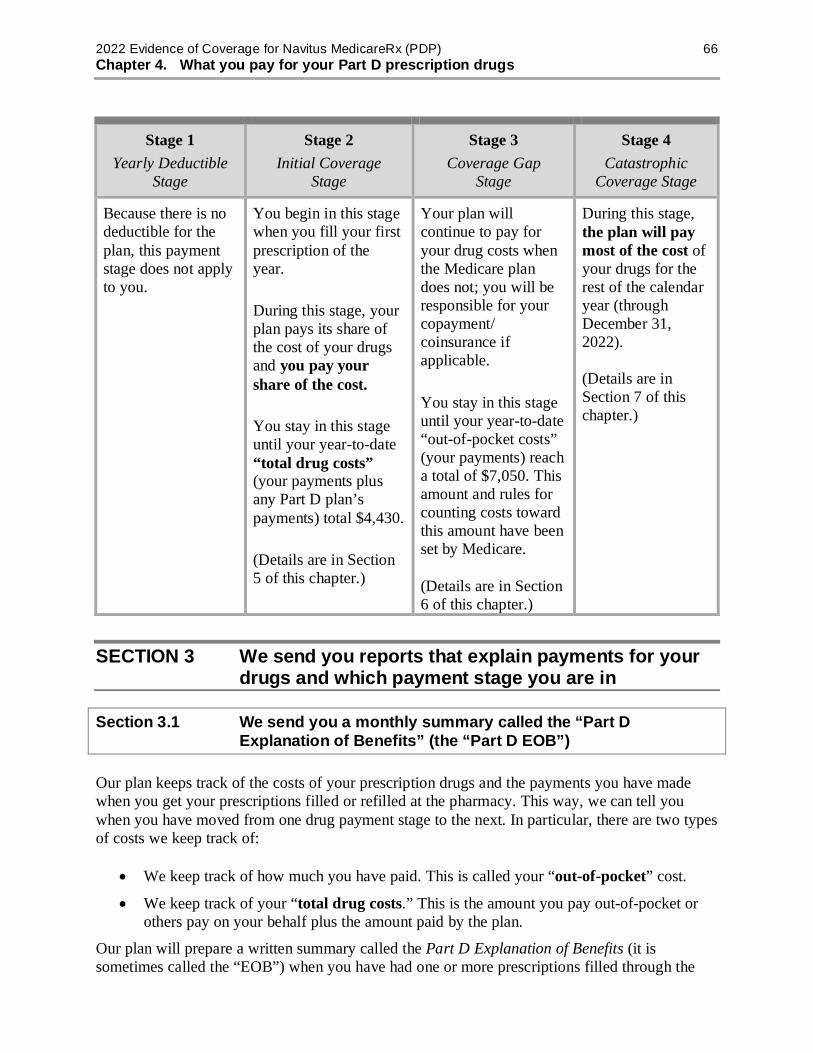
2022 Evidence of Coverage for Navitus MedicareRx (PDP) 66 Chapter 4. What you pay for your Part D prescription drugs
Stage 1 Yearly Deductible
Stage
Stage 2 Initial Coverage
Stage
Stage 3 Coverage Gap
Stage
Stage 4 Catastrophic
Coverage Stage
Because there is no deductible for the plan, this payment stage does not apply to you.
You begin in this stage when you fill your first prescription of the year. During this stage, your plan pays its share of the cost of your drugs and you pay your share of the cost. You stay in this stage until your year-to-date “total drug costs” (your payments plus any Part D plan’s payments) total $4,430. (Details are in Section 5 of this chapter.)
Your plan will continue to pay for your drug costs when the Medicare plan does not; you will be responsible for your copayment/ coinsurance if applicable. You stay in this stage until your year-to-date “out-of-pocket costs” (your payments) reach a total of $7,050. This amount and rules for counting costs toward this amount have been set by Medicare. (Details are in Section 6 of this chapter.)
During this stage, the plan will pay most of the cost of your drugs for the rest of the calendar year (through December 31, 2022). (Details are in Section 7 of this chapter.)
SECTION 3 We send you reports that explain payments for your drugs and which payment stage you are in
Section 3.1 We send you a monthly summary called the “Part D Explanation of Benefits” (the “Part D EOB”)
Our plan keeps track of the costs of your prescription drugs and the payments you have made when you get your prescriptions filled or refilled at the pharmacy. This way, we can tell you when you have moved from one drug payment stage to the next. In particular, there are two types of costs we keep track of:
• We keep track of how much you have paid. This is called your “out-of-pocket” cost.
• We keep track of your “total drug costs.” This is the amount you pay out-of-pocket or others pay on your behalf plus the amount paid by the plan.
Our plan will prepare a written summary called the Part D Explanation of Benefits (it is sometimes called the “EOB”) when you have had one or more prescriptions filled through the

2022 Evidence of Coverage for Navitus MedicareRx (PDP) 67 Chapter 4. What you pay for your Part D prescription drugs
plan during the previous month. The Part D EOB provides more information about the drugs you take, such as increases in price and other drugs with lower cost sharing that may be available. You should consult with your prescriber about these lower cost options. The Part D EOB includes:
• Information for that month. This report gives the payment details about the prescriptions you have filled during the previous month. It shows the total drugs costs, what your plan paid, and what you and others on your behalf paid.
• Totals for the year since January 1. This is called “year-to-date” information. It shows you the total drug costs and total payments for your drugs since the year began.
• Drug price information. This information will display the total drug price, and any percentage change from the first fill for each prescription claim of the same quantity.
• Available lower cost alternative prescriptions. This will include information about other drugs with lower cost sharing for each prescription claim that may be available.
Section 3.2 Help us keep our information about your drug payments up to date
To keep track of your drug costs and the payments you make for drugs, we use records we get from pharmacies. Here is how you can help us keep your information correct and up to date:
• Show your membership ID card when you get a prescription filled. To make sure we know about the prescriptions you are filling and what you are paying, show your plan membership card every time you get a prescription filled.
• Make sure we have the information we need. There are times you may pay for prescription drugs when we will not automatically get the information we need to keep track of your out-of-pocket costs. To help us keep track of your out-of-pocket costs, you may give us copies of receipts for drugs that you have purchased. (If you are billed for a covered drug, you can ask our plan to pay our share of the cost. For instructions on how to do this, go to Chapter 5, Section 2 of this booklet.) Here are some types of situations when you may want to give us copies of your drug receipts to be sure we have a complete record of what you have spent for your drugs:
o When you purchase a covered drug at a network pharmacy at a special price or using a discount card that is not part of our plan’s benefit.
o When you made a copayment for drugs that are provided under a drug manufacturer patient assistance program.
o Any time you have purchased covered drugs at out-of-network pharmacies or other times you have paid the full price for a covered drug under special circumstances.
• Send us information about the payments others have made for you. Payments made by certain other individuals and organizations also count toward your out-of-pocket costs and help qualify you for catastrophic coverage. For example, payments made by a State Pharmaceutical Assistance Program, an AIDS drug assistance program (ADAP), the

2022 Evidence of Coverage for Navitus MedicareRx (PDP) 68 Chapter 4. What you pay for your Part D prescription drugs
Indian Health Service, and most charities count toward your out-of-pocket costs. You should keep a record of these payments and send them to us so we can track your costs.
• Check the written report we send you. When you receive the Part D Explanation of Benefits (an EOB) in the mail, please look it over to be sure the information is complete and correct. If you think something is missing from the report, or you have any questions, please call us at Customer Care (phone numbers are printed on the back cover of this booklet). Be sure to keep these reports. They are an important record of your drug expenses.
SECTION 4 There is no deductible for Navitus MedicareRx
Section 4.1 You do not pay a deductible for your Part D drugs.
There is no deductible for Navitus MedicareRx. You begin in the Initial Coverage Stage when you fill your first prescription of the year. See Section 5 for information about your coverage in the Initial Coverage Stage.
SECTION 5 During the Initial Coverage Stage, the plan pays its share of your drug costs and you pay your share
Section 5.1 What you pay for a drug depends on the drug and where you fill your prescription
During the Initial Coverage Stage, the plan pays its share of the cost of your covered prescription drugs, and you pay your share (your copayment or coinsurance amount). Your share of the cost will vary depending on the drug and where you fill your prescription.
The plan has four Cost-Sharing Tiers To find out which cost-sharing tier your drug is in, please check our plan’s Formulary. Every drug on the plan’s Formulary is in one of four cost-sharing tiers. In general, the higher the cost-sharing tier number, the higher your cost for the drug:
• Tier $0 includes select generics
• Tier 1 includes preferred generics and certain lower cost brand products
• Tier 2 includes preferred brand products and some high cost non-preferred generics
• Tier 3 includes non-preferred products (could include some high cost non-preferred generics)
• Tier 4 includes specialty products
2022 Evidence of Coverage for Navitus MedicareRx (PDP) 69 Chapter 4. What you pay for your Part D prescription drugs
Your pharmacy choices
How much you pay for a drug depends on whether you get the drug from:
• A retail pharmacy that is in our plan’s network
• A pharmacy that is not in the plan’s network
• The plan’s mail-order pharmacy
• The plan’s specialty pharmacy
For more information about these pharmacy choices and filling your prescriptions, see Chapter 3 in this booklet and the plan’s Pharmacy Directory.
Section 5.2 A table that shows your costs for a one-month supply of a drug
During the Initial Coverage Stage, your share of the cost of a covered drug will be either a copayment or coinsurance.
• “Copayment” means that you pay a fixed amount each time you fill a prescription.
• “Coinsurance” means that you pay a percent of the total cost of the drug each time you fill a prescription.
As shown in the table below, the amount of the copayment or coinsurance depends on which tier your drug is in. Please note:
• If your covered drug costs less than the copayment amount listed in the chart, you will pay that lower price for the drug. You pay either the full price of the drug or the copayment amount, whichever is lower.
• We cover prescriptions filled at out-of-network pharmacies in only limited situations. Please see Chapter 3, Section 2.5 for information about when we will cover a prescription filled at an out-of-network pharmacy.
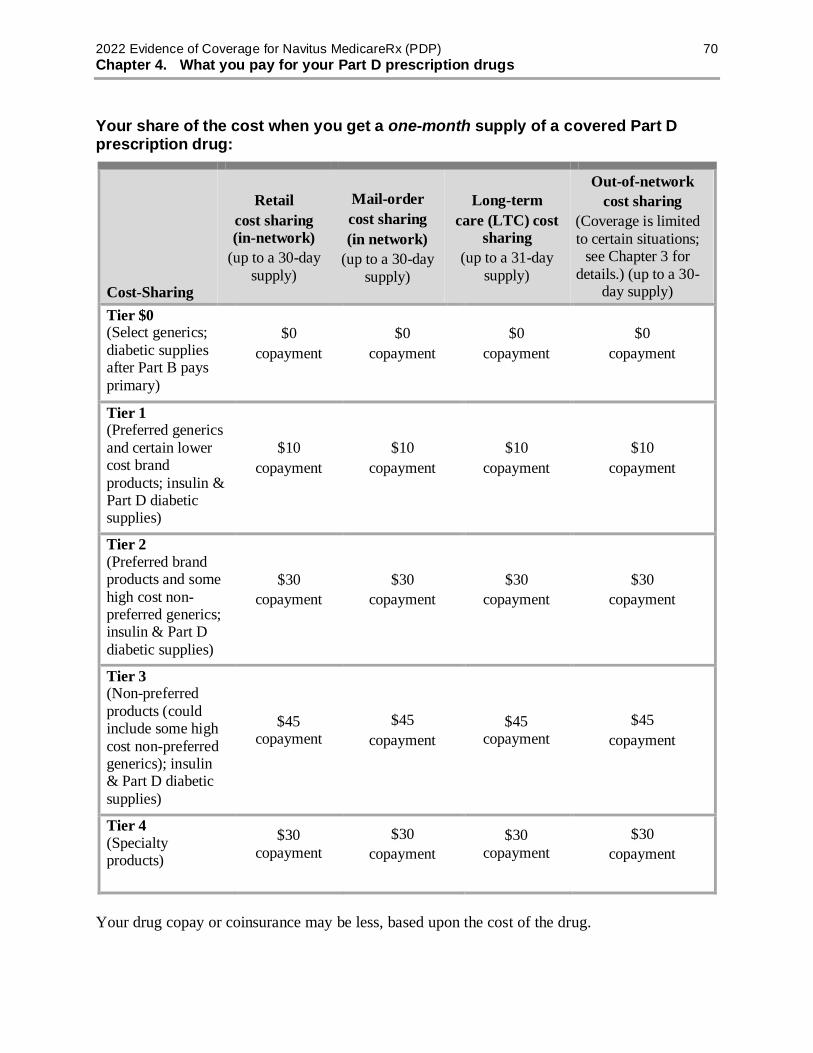
2022 Evidence of Coverage for Navitus MedicareRx (PDP) 70 Chapter 4. What you pay for your Part D prescription drugs
Your share of the cost when you get a one-month supply of a covered Part D prescription drug:
Cost-Sharing
Retail cost sharing (in-network)
(up to a 30-day supply)
Mail-order cost sharing (in network)
(up to a 30-day supply)
Long-term care (LTC) cost
sharing (up to a 31-day
supply)
Out-of-network cost sharing
(Coverage is limited to certain situations;
see Chapter 3 for details.) (up to a 30-
day supply) Tier $0 (Select generics; diabetic supplies after Part B pays primary)
$0 copayment
$0 copayment
$0 copayment
$0 copayment
Tier 1 (Preferred generics and certain lower cost brand products; insulin & Part D diabetic supplies)
$10 copayment
$10 copayment
$10 copayment
$10 copayment
Tier 2 (Preferred brand products and some high cost non-preferred generics; insulin & Part D diabetic supplies)
$30 copayment
$30 copayment
$30 copayment
$30 copayment
Tier 3 (Non-preferred products (could include some high cost non-preferred generics); insulin & Part D diabetic supplies)
$45 copayment
$45 copayment
$45 copayment
$45 copayment
Tier 4 (Specialty products)
$30 copayment
$30 copayment
$30 copayment
$30 copayment
Your drug copay or coinsurance may be less, based upon the cost of the drug.
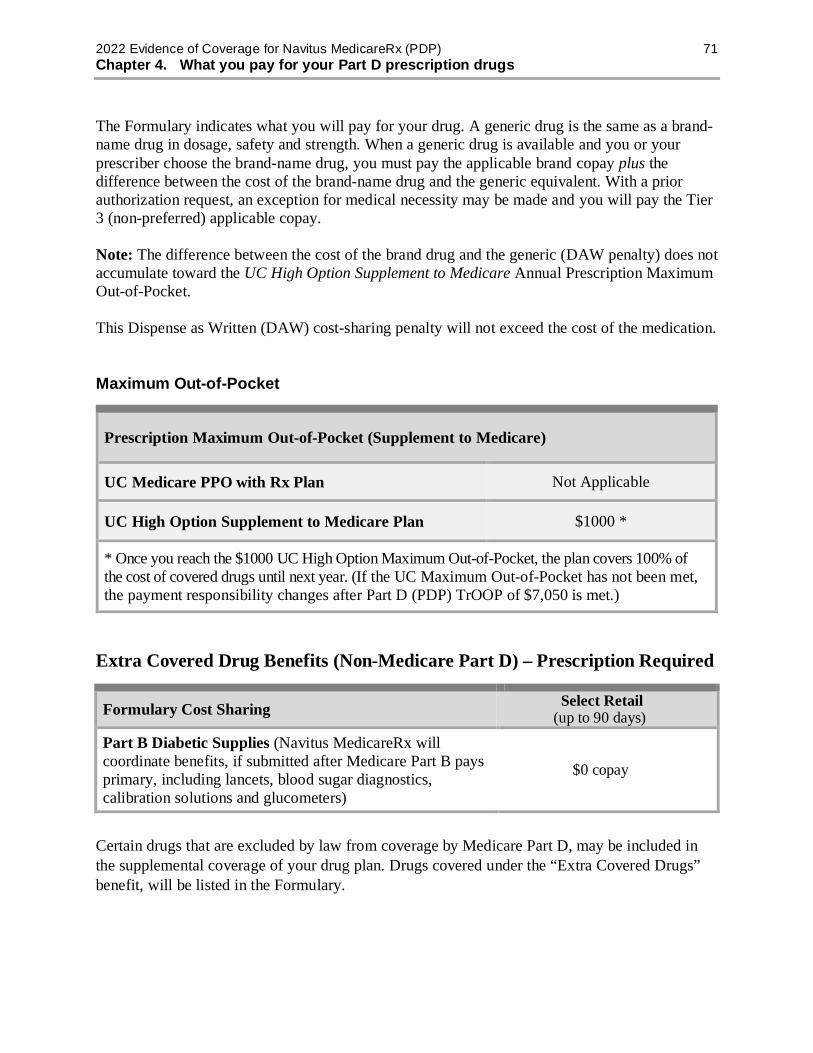
2022 Evidence of Coverage for Navitus MedicareRx (PDP) 71 Chapter 4. What you pay for your Part D prescription drugs
The Formulary indicates what you will pay for your drug. A generic drug is the same as a brand-name drug in dosage, safety and strength. When a generic drug is available and you or your prescriber choose the brand-name drug, you must pay the applicable brand copay plus the difference between the cost of the brand-name drug and the generic equivalent. With a prior authorization request, an exception for medical necessity may be made and you will pay the Tier 3 (non-preferred) applicable copay. Note: The difference between the cost of the brand drug and the generic (DAW penalty) does not accumulate toward the UC High Option Supplement to Medicare Annual Prescription Maximum Out-of-Pocket.
This Dispense as Written (DAW) cost-sharing penalty will not exceed the cost of the medication.
Maximum Out-of-Pocket
Prescription Maximum Out-of-Pocket (Supplement to Medicare)
UC Medicare PPO with Rx Plan Not Applicable
UC High Option Supplement to Medicare Plan $1000 *
* Once you reach the $1000 UC High Option Maximum Out-of-Pocket, the plan covers 100% of the cost of covered drugs until next year. (If the UC Maximum Out-of-Pocket has not been met, the payment responsibility changes after Part D (PDP) TrOOP of $7,050 is met.)
Extra Covered Drug Benefits (Non-Medicare Part D) – Prescription Required
Formulary Cost Sharing Select Retail (up to 90 days)
Part B Diabetic Supplies (Navitus MedicareRx will coordinate benefits, if submitted after Medicare Part B pays primary, including lancets, blood sugar diagnostics, calibration solutions and glucometers)
$0 copay
Certain drugs that are excluded by law from coverage by Medicare Part D, may be included in the supplemental coverage of your drug plan. Drugs covered under the “Extra Covered Drugs” benefit, will be listed in the Formulary.

2022 Evidence of Coverage for Navitus MedicareRx (PDP) 72 Chapter 4. What you pay for your Part D prescription drugs
Extra covered drug benefits (non-Medicare Part D) – prescription required
Extra Covered Drugs Cost Sharing
Retail & Mail Order
(up to 30 days)
Retail (31-60 days)
Retail (61-90 days)
Mail Order (31-90 days)
Tier 1 non-Medicare covered drugs
$10 copay $20 copay $30 copay $20 copay
Tier 2 non-Medicare covered drugs
$30 copay $60 copay $90 copay $60 copay
Tier 3 non-Medicare covered drugs
$45 copay $90 copay $135 copay $90 copay
Note: These Extra Covered Drugs do not count towards the Medicare TrOOP ($7,050) expenses and they do not qualify for lower catastrophic copays.
Member cost share per tier values in the above table, for:
• Cough and Cold Prescriptions • Erectile Disfunction (ED) – with quantity limit (QL) • Vitamins and Minerals Prescriptions
Coverage for Out of Country Drugs: Outpatient prescription drugs are not covered by Medicare Part D plans when they are filled by pharmacies outside of the United States. Your UC plan provides coverage for outpatient prescription drugs when all of the following apply:
You remain a permanent resident of the United States while you are out of country, and The drug is approved by the Food and Drug Administration (FDA), and The drug would be a covered drug by your plan if the drug was filled by a pharmacy
located within the United States. When you receive coverage for outpatient prescription drugs filled at a pharmacy outside the United States, you will need to pay the full cost of the drug and request that we reimburse you for our share. Your share of a covered outpatient drug will be your coinsurance or copayment amount. Please see “How to ask us to pay you back” for detailed instructions, which can be found in the Evidence of Coverage, Chapter 5, Section 2.
2022 Evidence of Coverage for Navitus MedicareRx (PDP) 73 Chapter 4. What you pay for your Part D prescription drugs
Section 5.3 If your doctor prescribes less than a full month’s supply, you may not have to pay the cost of the entire month’s supply
Typically, the amount you pay for a prescription drug covers a full month’s supply of a covered drug. However, your doctor can prescribe less than a month’s supply of drugs. There may be times when you want to ask your doctor about prescribing less than a month’s supply of a drug (for example, when you are trying a medication for the first time that is known to have serious side effects). If your doctor prescribes less than a full month’s supply, you may not have to pay for the full month’s supply for certain drugs.
The amount you pay when you get less than a full month’s supply will depend on whether you are responsible for paying coinsurance (a percentage of the total cost) or a copayment (a flat dollar amount).
• If you are responsible for coinsurance, you pay a percentage of the total cost of the drug. You pay the same percentage regardless of whether the prescription is for a full month’s supply or for fewer days. However, because the entire drug cost will be lower if you get less than a full month’s supply, the amount you pay will be less.
Section 5.4 A table that shows your costs for a long-term (up to a 90-day) supply of a drug
For some drugs, you can get a long-term supply (also called an “extended supply”) when you fill your prescription. A long-term supply is up to a 90-day supply. (For details on where and how to get a long-term supply of a drug, see Chapter 3, Section 2.4.)
The table below shows what you pay when you get a long-term (up to a 90-day) supply of a drug.
• Please note: If your covered drug costs less than the copayment amount listed in the chart, you will pay that lower price for the drug. You pay either the full price of the drug or the copayment amount, whichever is lower.
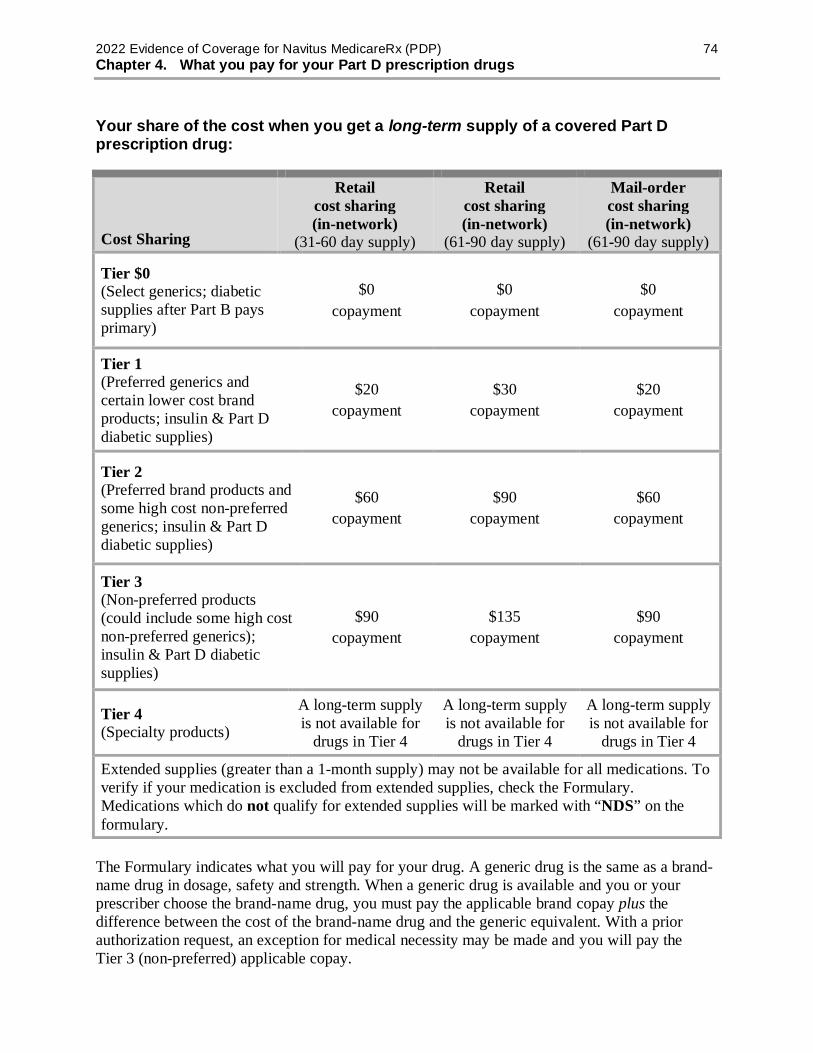
2022 Evidence of Coverage for Navitus MedicareRx (PDP) 74 Chapter 4. What you pay for your Part D prescription drugs
Your share of the cost when you get a long-term supply of a covered Part D prescription drug:
Cost Sharing
Retail cost sharing (in-network)
(31-60 day supply)
Retail cost sharing (in-network)
(61-90 day supply)
Mail-order cost sharing (in-network)
(61-90 day supply)
Tier $0 (Select generics; diabetic supplies after Part B pays primary)
$0 copayment
$0 copayment
$0 copayment
Tier 1 (Preferred generics and certain lower cost brand products; insulin & Part D diabetic supplies)
$20 copayment
$30 copayment
$20 copayment
Tier 2 (Preferred brand products and some high cost non-preferred generics; insulin & Part D diabetic supplies)
$60 copayment
$90 copayment
$60 copayment
Tier 3 (Non-preferred products (could include some high cost non-preferred generics); insulin & Part D diabetic supplies)
$90 copayment
$135 copayment
$90 copayment
Tier 4 (Specialty products)
A long-term supply is not available for
drugs in Tier 4
A long-term supply is not available for
drugs in Tier 4
A long-term supply is not available for
drugs in Tier 4
Extended supplies (greater than a 1-month supply) may not be available for all medications. To verify if your medication is excluded from extended supplies, check the Formulary. Medications which do not qualify for extended supplies will be marked with “NDS” on the formulary.
The Formulary indicates what you will pay for your drug. A generic drug is the same as a brand-name drug in dosage, safety and strength. When a generic drug is available and you or your prescriber choose the brand-name drug, you must pay the applicable brand copay plus the difference between the cost of the brand-name drug and the generic equivalent. With a prior authorization request, an exception for medical necessity may be made and you will pay the Tier 3 (non-preferred) applicable copay.
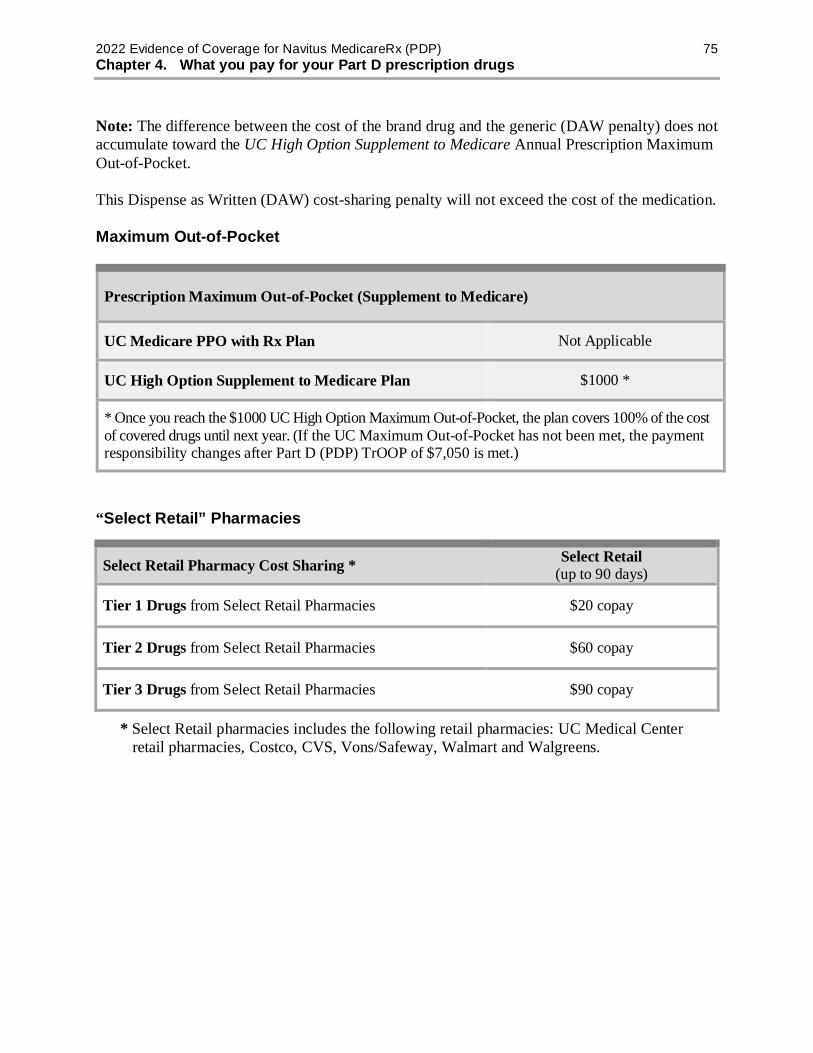
2022 Evidence of Coverage for Navitus MedicareRx (PDP) 75 Chapter 4. What you pay for your Part D prescription drugs
Note: The difference between the cost of the brand drug and the generic (DAW penalty) does not accumulate toward the UC High Option Supplement to Medicare Annual Prescription Maximum Out-of-Pocket.
This Dispense as Written (DAW) cost-sharing penalty will not exceed the cost of the medication.
Maximum Out-of-Pocket
Prescription Maximum Out-of-Pocket (Supplement to Medicare)
UC Medicare PPO with Rx Plan Not Applicable
UC High Option Supplement to Medicare Plan $1000 *
* Once you reach the $1000 UC High Option Maximum Out-of-Pocket, the plan covers 100% of the cost of covered drugs until next year. (If the UC Maximum Out-of-Pocket has not been met, the payment responsibility changes after Part D (PDP) TrOOP of $7,050 is met.)
“Select Retail” Pharmacies
Select Retail Pharmacy Cost Sharing * Select Retail (up to 90 days)
Tier 1 Drugs from Select Retail Pharmacies $20 copay
Tier 2 Drugs from Select Retail Pharmacies $60 copay
Tier 3 Drugs from Select Retail Pharmacies $90 copay
* Select Retail pharmacies includes the following retail pharmacies: UC Medical Center retail pharmacies, Costco, CVS, Vons/Safeway, Walmart and Walgreens.

2022 Evidence of Coverage for Navitus MedicareRx (PDP) 76 Chapter 4. What you pay for your Part D prescription drugs
Extra Covered Drug Benefits (Non-Medicare Part D) – Prescription Required
Formulary Cost Sharing Select Retail (up to 90 days)
Part B Diabetic Supplies (Navitus MedicareRx will coordinate benefits, if submitted after Medicare Part B pays primary, including lancets, blood sugar diagnostics, calibration solutions and glucometers)
$0 copay
Certain drugs that are excluded by law from coverage by Medicare Part D, may be included in the supplemental coverage of your drug plan. Drugs covered under the “Extra Covered Drugs” benefit, will be listed in the Formulary.
Extra Covered Drugs Cost Sharing
Retail & Mail Order
(up to 30 days)
Retail (31-60 days)
Retail (61-90 days)
Mail Order (31-90 days)
Tier 1 non-Medicare covered drugs
$10 copay $20 copay $30 copay $20 copay
Tier 2 non-Medicare covered drugs
$30 copay $60 copay $90 copay $60 copay
Tier 3 non-Medicare covered drugs
$45 copay $90 copay $135 copay $90 copay
Note: These Extra Covered Drugs do not count towards the Medicare TrOOP ($7,050) expenses and they do not qualify for lower catastrophic copays.
Member cost share per tier values in the above table, for:
• Cough and Cold Prescriptions • Erectile Disfunction (ED) – with quantity limit (QL) • Vitamins and Minerals Prescriptions
Coverage for Out of Country Drugs: Outpatient prescription drugs are not covered by Medicare Part D plans when they are filled by pharmacies outside of the United States. Your UC plan provides coverage for outpatient prescription drugs when all of the following apply:
You remain a permanent resident of the United States while you are out of country, and The drug is approved by the Food and Drug Administration (FDA), and The drug would be a covered drug by your plan if the drug was filled by a pharmacy
located within the United States.
2022 Evidence of Coverage for Navitus MedicareRx (PDP) 77 Chapter 4. What you pay for your Part D prescription drugs
When you receive coverage for outpatient prescription drugs filled at a pharmacy outside the United States, you will need to pay the full cost of the drug and request that we reimburse you for our share. Your share of a covered outpatient drug will be your coinsurance or copayment amount. Please see “How to ask us to pay you back” for detailed instructions, which can be found in the Evidence of Coverage, Chapter 5, Section 2.
Section 5.5 You stay in the Initial Coverage Stage until total drug costs for the year reach $4,430
You stay in the Initial Coverage Stage until the total amount for the prescription drugs you have filled and refilled reaches the $4,430 limit for the Initial Coverage Stage.
Your total drug cost is based on adding together what you have paid and what any Part D plan has paid:
• What you have paid for all the covered drugs you have gotten since you started with your first drug purchase of the year. (See Section 6.2 for more information about how Medicare calculates your out-of-pocket costs.) This includes:
o The total you paid as your share of the cost for your drugs during the Initial Coverage Stage.
• What the plan has paid as its share of the cost for your drugs during the Initial Coverage Stage. (If you were enrolled in a different Part D plan at any time during 2022, the amount that plan paid during the Initial Coverage Stage also counts toward your total drug costs.)
We offer additional coverage on some prescription drugs that are not normally covered in a Medicare Prescription Drug Plan. Payments made for these drugs will not count toward your initial coverage limit or total out-of-pocket costs.
The Explanation of Benefits (EOB) that we send to you will help you keep track of how much you and the plan, as well as any third parties, have spent on your behalf during the year. Many people do not reach the $4,430 limit in a year.
We will let you know if you reach this $4,430 amount. If you do reach this amount, you will leave the Initial Coverage Stage and move on to the Coverage Gap Stage.
SECTION 6 During the Coverage Gap Stage, the plan provides some drug coverage
Section 6.1 You stay in the Coverage Gap Stage until your out-of-pocket costs reach $7,050
When you are in the Coverage Gap Stage, the Medicare Coverage Gap Discount Program provides manufacturer discounts on brand name drugs. Your plan will continue to pay for your

2022 Evidence of Coverage for Navitus MedicareRx (PDP) 78 Chapter 4. What you pay for your Part D prescription drugs
drug costs at the Initial Coverage Stage copayments, when the Medicare plan does not; you will be responsible for your formulary copayment as applicable.
Medicare has rules about what counts and what does not count as your out-of-pocket costs. When you reach an out-of-pocket limit of $7,050, you leave the Coverage Gap Stage and move on to the Catastrophic Coverage Stage.
Section 6.2 How Medicare calculates your out-of-pocket costs for prescription drugs
Here are Medicare’s rules that we must follow when we keep track of your out-of-pocket (TrOOP) costs for your drugs.
These payments are included in your out-of-pocket costs
When you add up your out-of-pocket costs, you can include the payments listed below (as long as they are for Part D covered drugs and you followed the rules for drug coverage that are explained in Chapter 3 of this booklet):
• The amount you pay for drugs when you are in any of the following drug payment stages:
o The Initial Coverage Stage o The Coverage Gap Stage
• Any payments you made during this calendar year as a member of a different Medicare prescription drug plan before you joined our plan.
It matters who pays:
• If you make these payments yourself, they are included in your out-of-pocket costs.
• These payments are also included if they are made on your behalf by certain other individuals or organizations. This includes payments for your drugs made by a friend or relative, by most charities, by AIDS drug assistance programs, by a State Pharmaceutical Assistance Program that is qualified by Medicare, or by the Indian Health Service. Payments made by Medicare’s “Extra Help” Program are also included.
• Some of the payments made by the Medicare Coverage Gap Discount Program are included. The amount the manufacturer pays for your brand name drugs is included. But the amount the plan pays for your generic drugs is not included.

2022 Evidence of Coverage for Navitus MedicareRx (PDP) 79 Chapter 4. What you pay for your Part D prescription drugs
Moving on to the Catastrophic Coverage Stage:
When the amount you (or those paying on your behalf) have paid for covered drugs reaches $7,050 in out-of-pocket costs within the calendar year, you will move from the Coverage Gap Stage to the Catastrophic Coverage Stage.
These payments are not included in your out-of-pocket costs
When you add up your out-of-pocket costs, you are not allowed to include any of these types of payments for prescription drugs:
• The amount you pay for your monthly premium.
• Drugs you buy outside the United States and Puerto Rico.
• Drugs that are not covered by our plan.
• Drugs you get at an out-of-network pharmacy that do not meet the plan’s requirements for out-of-network coverage.
• Non-Part D drugs, including prescription drugs covered by Part A or Part B and other drugs excluded from coverage by Medicare.
• Prescription drugs covered by Part A or Part B. • Payments you make toward drugs covered under our additional coverage but not
normally covered in a Medicare Prescription Drug Plan (for example, the “Extra Covered Drugs” benefit).
• Payments you make toward prescription drugs not normally covered in a Medicare Prescription Drug Plan.
• Payments made by the plan for your brand or generic drugs while in the Coverage Gap. • Payments for your drugs that are made by group health plans including employer health
plans. • Payments for your drugs that are made by certain insurance plans and government-funded
health programs such as TRICARE and Veterans Affairs. • Payments for your drugs made by a third-party with a legal obligation to pay for
prescription costs (for example, Workers’ Compensation). Reminder: If any other organization such as the ones listed above pays part or all of your out-of-pocket costs for drugs, you are required to tell our plan. Call Customer Care to let us know (phone numbers are printed on the back cover of this booklet).
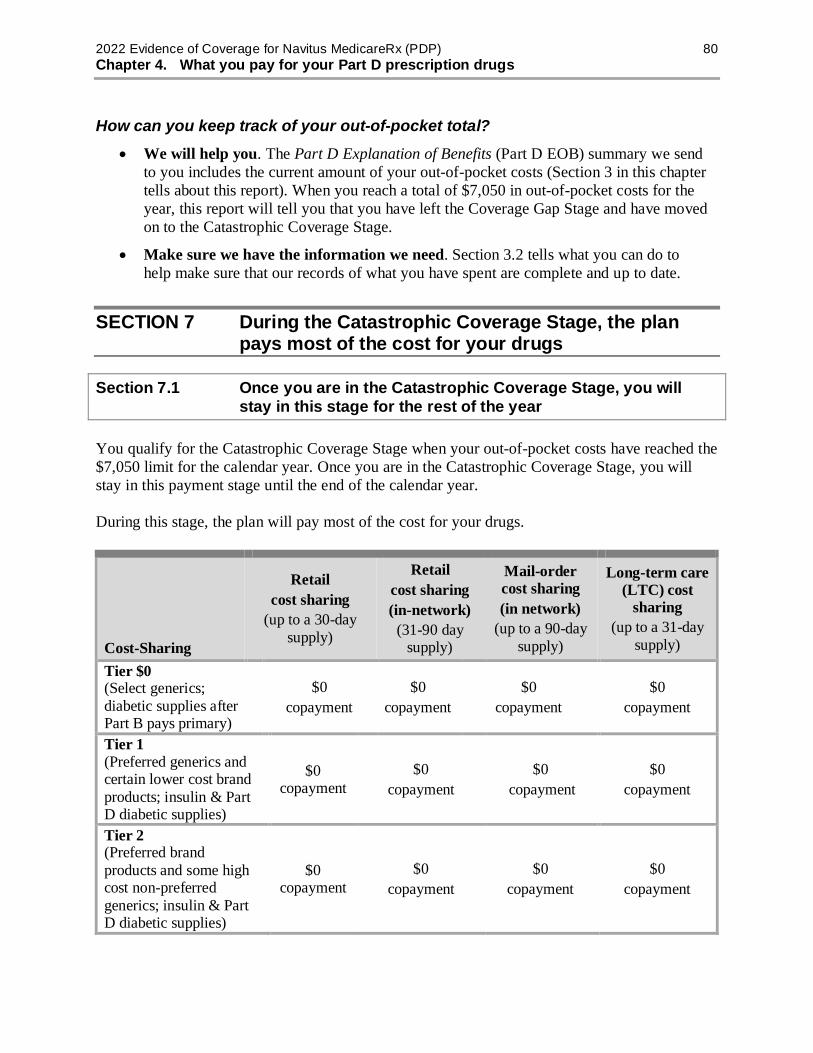
2022 Evidence of Coverage for Navitus MedicareRx (PDP) 80 Chapter 4. What you pay for your Part D prescription drugs
How can you keep track of your out-of-pocket total? • We will help you. The Part D Explanation of Benefits (Part D EOB) summary we send
to you includes the current amount of your out-of-pocket costs (Section 3 in this chapter tells about this report). When you reach a total of $7,050 in out-of-pocket costs for the year, this report will tell you that you have left the Coverage Gap Stage and have moved on to the Catastrophic Coverage Stage.
• Make sure we have the information we need. Section 3.2 tells what you can do to help make sure that our records of what you have spent are complete and up to date.
SECTION 7 During the Catastrophic Coverage Stage, the plan pays most of the cost for your drugs
Section 7.1 Once you are in the Catastrophic Coverage Stage, you will stay in this stage for the rest of the year
You qualify for the Catastrophic Coverage Stage when your out-of-pocket costs have reached the $7,050 limit for the calendar year. Once you are in the Catastrophic Coverage Stage, you will stay in this payment stage until the end of the calendar year.
During this stage, the plan will pay most of the cost for your drugs.
Cost-Sharing
Retail cost sharing
(up to a 30-day supply)
Retail cost sharing (in-network)
(31-90 day supply)
Mail-order cost sharing (in network)
(up to a 90-day supply)
Long-term care (LTC) cost
sharing (up to a 31-day
supply)
Tier $0 (Select generics; diabetic supplies after Part B pays primary)
$0 copayment
$0 copayment
$0 copayment
$0 copayment
Tier 1 (Preferred generics and certain lower cost brand products; insulin & Part D diabetic supplies)
$0 copayment
$0 copayment
$0 copayment
$0 copayment
Tier 2 (Preferred brand products and some high cost non-preferred generics; insulin & Part D diabetic supplies)
$0 copayment
$0 copayment
$0 copayment
$0 copayment
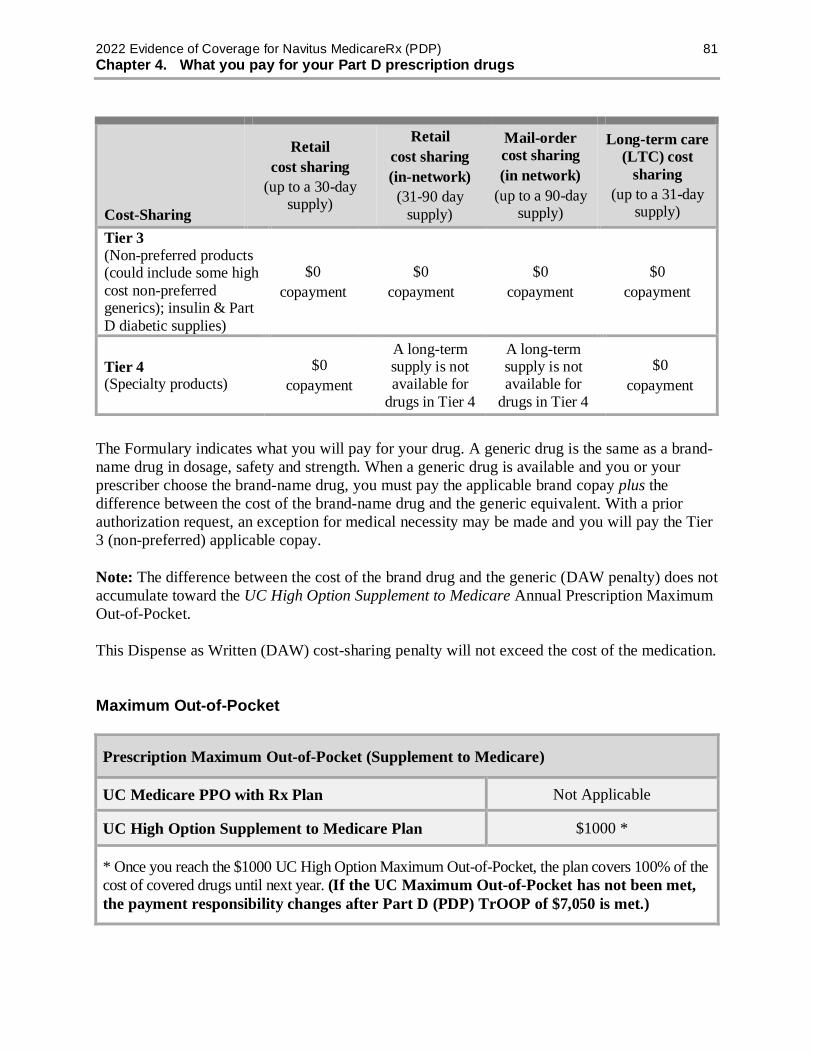
2022 Evidence of Coverage for Navitus MedicareRx (PDP) 81 Chapter 4. What you pay for your Part D prescription drugs
Cost-Sharing
Retail cost sharing
(up to a 30-day supply)
Retail cost sharing (in-network)
(31-90 day supply)
Mail-order cost sharing (in network)
(up to a 90-day supply)
Long-term care (LTC) cost
sharing (up to a 31-day
supply)
Tier 3 (Non-preferred products (could include some high cost non-preferred generics); insulin & Part D diabetic supplies)
$0 copayment
$0 copayment
$0 copayment
$0 copayment
Tier 4 (Specialty products)
$0 copayment
A long-term supply is not available for
drugs in Tier 4
A long-term supply is not available for
drugs in Tier 4
$0 copayment
The Formulary indicates what you will pay for your drug. A generic drug is the same as a brand-name drug in dosage, safety and strength. When a generic drug is available and you or your prescriber choose the brand-name drug, you must pay the applicable brand copay plus the difference between the cost of the brand-name drug and the generic equivalent. With a prior authorization request, an exception for medical necessity may be made and you will pay the Tier 3 (non-preferred) applicable copay. Note: The difference between the cost of the brand drug and the generic (DAW penalty) does not accumulate toward the UC High Option Supplement to Medicare Annual Prescription Maximum Out-of-Pocket.
This Dispense as Written (DAW) cost-sharing penalty will not exceed the cost of the medication.
Maximum Out-of-Pocket
Prescription Maximum Out-of-Pocket (Supplement to Medicare)
UC Medicare PPO with Rx Plan Not Applicable
UC High Option Supplement to Medicare Plan $1000 *
* Once you reach the $1000 UC High Option Maximum Out-of-Pocket, the plan covers 100% of the cost of covered drugs until next year. (If the UC Maximum Out-of-Pocket has not been met, the payment responsibility changes after Part D (PDP) TrOOP of $7,050 is met.)

2022 Evidence of Coverage for Navitus MedicareRx (PDP) 82 Chapter 4. What you pay for your Part D prescription drugs
For UC High Option Supplement to Medicare – once members reach the $1000 UC Maximum Out-of-Pocket, the plan covers 100% of the cost of covered drugs until next year.
• Out-of-pocket costs for Extra Covered Drugs apply toward the $1,000 out-of-pocket maximum, but not the Medicare TrOOP of $7,050.
• Members qualifying for the Coverage Gap Discount could reach Medicare TrOOP before the $1,000 out-of-pocket maximum because out-of-pocket expenses covered by the Coverage Gap Discount apply only toward the Medicare TrOOP, but not the UC out-of-pocket maximum. If this happens, members will continue to pay a copayment for Extra Covered Drugs until reaching the $1,000 out-of-pocket maximum. After that, the plan will pay 100% for all covered drugs (including Extra Covered Drugs).
For PPO Plan Members – members continue to pay the cost of Extra Covered Drugs, even after the CMS TrOOP is met.
Extra Covered Drug Benefits (Non-Medicare Part D) – Prescription Required Certain drugs that are excluded by law from coverage by Medicare Part D, may be included in the supplemental coverage of your drug plan. Drugs covered under the “Extra Covered Drugs” benefit, will be listed in the Formulary.
Extra Covered Drugs Cost Sharing
Retail & Mail Order
(up to 30 days)
Retail (31-60 days)
Retail (61-90 days)
Mail Order (31-90 days)
Tier 1 non-Medicare covered drugs
$10 copay $20 copay $30 copay $20 copay
Tier 2 non-Medicare covered drugs
$30 copay $60 copay $90 copay $60 copay
Tier 3 non-Medicare covered drugs
$45 copay $90 copay $135 copay $90 copay
Note: These Extra Covered Drugs do not count towards the Medicare TrOOP ($7,050) expenses and they do not qualify for lower catastrophic copays. Member cost share per tier values in the above table, for:
• Cough and Cold Prescriptions • Erectile Disfunction (ED) – with quantity limit (QL) • Vitamins and Minerals Prescriptions
2022 Evidence of Coverage for Navitus MedicareRx (PDP) 83 Chapter 4. What you pay for your Part D prescription drugs
SECTION 8 What you pay for vaccinations covered by Part D depends on how and where you get them
Section 8.1 Our plan may have separate coverage for the Part D vaccine medication itself and for the cost of giving you the vaccine
Our plan provides coverage of a number of Part D vaccines. There are two parts to our coverage of vaccinations:
• The first part of coverage is the cost of the vaccine medication itself. The vaccine is a prescription medication.
• The second part of coverage is for the cost of giving you the vaccine. (This is sometimes called the “administration” of the vaccine.)
What do you pay for a Part D vaccination?
What you pay for a Part D vaccination depends on three things: 1. The type of vaccine (what you are being vaccinated for).
o Some vaccines are considered Part D drugs. You can find these vaccines listed in the plan’s List of Covered Drugs (Formulary).
o Other vaccines are considered medical benefits. They are covered under Original Medicare.
2. Where you get the vaccine medication. 3. Who gives you the vaccine.
What you pay at the time you get the Part D vaccination can vary depending on the circumstances. For example:
• Sometimes when you get your vaccine, you will have to pay the entire cost for both the vaccine medication and for getting the vaccine. You can ask our plan to pay you back for our share of the cost.
• Other times, when you get the vaccine medication or the vaccine, you will pay only your share of the cost.
To show how this works, here are three common ways you might get a Part D vaccine.
Situation 1: You buy the Part D vaccine at the pharmacy and you get your vaccine at the network pharmacy. (Whether you have this choice depends on where you live. Some states do not allow pharmacies to administer a vaccination.)
• You will have to pay the pharmacy the amount of your coinsurance or copayment for the vaccine and the cost of giving you the vaccine.
• Our plan will pay the remainder of the costs.

2022 Evidence of Coverage for Navitus MedicareRx (PDP) 84 Chapter 4. What you pay for your Part D prescription drugs
Situation 2: You get the Part D vaccination at your doctor’s office.
• When you get the vaccination, you will pay for the entire cost of the vaccine and its administration.
• You can then ask our plan to pay our share of the cost by using the procedures that are described in Chapter 5 of this booklet (Asking us to pay our share of the costs for covered drugs).
• You will be reimbursed the amount you paid, less your normal coinsurance or copayment for the vaccine (including administration) and less any difference between the amount the doctor charges and what we normally pay, up to the plan limits. (If you get “Extra Help”, we will reimburse you for this difference.)
Situation 3: You buy the Part D vaccine at your pharmacy, and then take it to your doctor’s office where they give you the vaccine.
• You will have to pay the pharmacy the amount of your coinsurance or copayment for the vaccine itself.
• When your doctor gives you the vaccine, you will pay the entire cost for this service. You can then ask our plan to pay our share of the cost by using the procedures described in Chapter 5 of this booklet.
• You will be reimbursed the amount charged by the doctor for administering the vaccine, less any difference between the amount the doctor charges and what we normally pay, up to the plan limits. (If you get “Extra Help”, we will reimburse you for this difference.)
Section 8.2 You may want to call us at Customer Care before you get a vaccination
The rules for coverage of vaccinations are complicated. We are here to help. We recommend that you call us first at Customer Care whenever you are planning to get a vaccination. (Phone numbers for Customer Care are printed on the back cover of this booklet.)
• We can tell you about how your vaccination is covered by our plan and explain your share of the cost.
• We can tell you how to keep your own cost down by using providers and pharmacies in the network.
• If you are not able to use a network provider or pharmacy, we can tell you what you need to do to get payment from us for our share of the cost.

CHAPTER 5 Asking us to pay our share of the
costs for covered drugs
2022 Evidence of Coverage for Navitus MedicareRx (PDP) 86 Chapter 5. Asking us to pay our share of the costs for covered drugs
Chapter 5. Asking us to pay our share of the costs for covered drugs
SECTION 1 Situations in which you should ask us to pay our share of the cost of your covered drugs .......................................................... 87
Section 1.1 If you pay our plan’s share of the cost of your covered drugs, you can ask us for payment .......................................................................................... 87
SECTION 2 How to ask us to pay you back........................................................... 88
Section 2.1 How and where to send us your request for payment .................................. 88
SECTION 3 We will consider your request for payment and say yes or no ............................................................................................................. 89
Section 3.1 We check to see whether we should cover the drug and how much we owe ........................................................................................................... 89
Section 3.2 If we tell you that we will not pay for all or part of the drug, you can make an appeal .......................................................................................... 89
SECTION 4 Other situations in which you should save your receipts and send copies to us .......................................................................... 90
Section 4.1 In some cases, you should send copies of your receipts to us to help us track your out-of-pocket drug costs ............................................................ 90
2022 Evidence of Coverage for Navitus MedicareRx (PDP) 87 Chapter 5. Asking us to pay our share of the costs for covered drugs
SECTION 1 Situations in which you should ask us to pay our share of the cost of your covered drugs
Section 1.1 If you pay our plan’s share of the cost of your covered drugs, you can ask us for payment
Sometimes when you get a prescription drug, you may need to pay the full cost right away. Other times, you may find that you have paid more than you expected under the coverage rules of the plan. In either case, you can ask our plan to pay you back (paying you back is often called “reimbursing” you). Please note that depending on the coverage rules for your specific drug, there may be a difference in the amount you are reimbursed and the total amount you paid.
Here are examples of situations in which you may need to ask our plan to pay you back. All of these examples are types of coverage decisions (for more information about coverage decisions, go to Chapter 7 of this booklet).
1. When you use an out-of-network pharmacy to get a prescription filled If you go to an out-of-network pharmacy and try to use your membership card to fill a prescription, the pharmacy may not be able to submit the claim directly to us. When that happens, you will have to pay the full cost of your prescription. (We cover prescriptions filled at out-of-network pharmacies only in a few special situations. Please go to Chapter 3, Section 2.5 to learn more.)
Save your receipt and send a copy to us when you ask us to pay you back for our share of the cost.
2. When you pay the full cost for a prescription because you don’t have your plan membership card with you If you do not have your plan membership card with you, you can ask the pharmacy to call the plan or look up your enrollment information. However, if the pharmacy cannot get the enrollment information they need right away, you may need to pay the full cost of the prescription yourself. Save your receipt and send a copy to us when you ask us to pay you back for our share of the cost.
3. When you pay the full cost for a prescription in other situations You may pay the full cost of the prescription because you find that the drug is not covered for some reason.
• For example, the drug may not be on the plan’s List of Covered Drugs (Formulary); or it could have a requirement or restriction that you didn’t know about or don’t think should apply to you. If you decide to get the drug immediately, you may need to pay the full cost for it.
2022 Evidence of Coverage for Navitus MedicareRx (PDP) 88 Chapter 5. Asking us to pay our share of the costs for covered drugs
• Save your receipt and send a copy to us when you ask us to pay you back. In some situations, we may need to get more information from your doctor in order to pay you back for our share of the cost.
4. If you are retroactively enrolled in our plan Sometimes a person’s enrollment in the plan is retroactive. (Retroactive means that the first day of their enrollment has already passed. The enrollment date may even have occurred last year.) If you were retroactively enrolled in our plan and you paid out-of-pocket for any of your drugs after your enrollment date, you can ask us to pay you back for our share of the costs. You will need to submit paperwork for us to handle the reimbursement. Please call Customer Care for additional information about how to ask us to pay you back and deadlines for making your request. (Phone numbers for Customer Care are printed on the back cover of this booklet.)
All of the examples above are types of coverage decisions. This means that if we deny your request for payment, you can appeal our decision. Chapter 7 of this booklet (What to do if you have a problem or complaint (coverage decisions, appeals, complaints)) has information about how to make an appeal.
SECTION 2 How to ask us to pay you back
Section 2.1 How and where to send us your request for payment
Send us your request for payment, along with your receipt documenting the payment you have made. It’s a good idea to make a copy of your receipts for your records.
To make sure you are giving us all the information we need to make a decision, you can fill out our claim form to make your request for payment.
• You don’t have to use the form, but it will help us process the information faster.
• Either download a copy of the form from our Member Portal (https://memberportal.navitus.com) or call Customer Care and ask for the form. (Phone numbers for Customer Care are printed on the back cover of this booklet.)
Mail your request for payment together with any bills and paid receipts to us at this address:
Navitus MedicareRx Manual Claims P.O. Box 1039 Appleton, WI 54912-1039

2022 Evidence of Coverage for Navitus MedicareRx (PDP) 89 Chapter 5. Asking us to pay our share of the costs for covered drugs
You must submit your claim to us within 36 months of the date you received the service, item, or drug.
Contact Customer Care if you have any questions (phone numbers are printed on the back cover of this booklet). If you don’t know what you should have paid, we can help. You can also call if you want to give us more information about a request for payment you have already sent to us.
SECTION 3 We will consider your request for payment and say yes or no
Section 3.1 We check to see whether we should cover the drug and how much we owe
When we receive your request for payment, we will let you know if we need any additional information from you. Otherwise, we will consider your request and make a coverage decision.
• If we decide that the drug is covered and you followed all the rules for getting the drug, we will pay for our share of the cost. We will mail your reimbursement of our share of the cost to you. (Chapter 3 explains the rules you need to follow for getting your Part D prescription drugs covered.) We will send payment within 30 days after your request was received.
• If we decide that the drug is not covered, or you did not follow all the rules, we will not pay for our share of the cost. Instead, we will send you a letter that explains the reasons why we are not sending the payment you have requested and your rights to appeal that decision.
Section 3.2 If we tell you that we will not pay for all or part of the drug, you can make an appeal
If you think we have made a mistake in turning down your request for payment or you don’t agree with the amount we are paying, you can make an appeal. If you make an appeal, it means you are asking us to change the decision we made when we turned down your request for payment.
For the details on how to make this appeal, go to Chapter 7 of this booklet (What to do if you have a problem or complaint (coverage decisions, appeals, complaints)). The appeals process is a formal process with detailed procedures and important deadlines. If making an appeal is new to you, you will find it helpful to start by reading Section 4 of Chapter 7. Section 4 is an introductory section that explains the process for coverage decisions and appeals and gives definitions of terms such as “appeal.” Then after you have read Section 4, you can go to Section 5.5 in Chapter 7 for a step-by-step explanation of how to file an appeal.
2022 Evidence of Coverage for Navitus MedicareRx (PDP) 90 Chapter 5. Asking us to pay our share of the costs for covered drugs
SECTION 4 Other situations in which you should save your receipts and send copies to us
Section 4.1 In some cases, you should send copies of your receipts to us to help us track your out-of-pocket drug costs
There are some situations when you should let us know about payments you have made for your drugs. In these cases, you are not asking us for payment. Instead, you are telling us about your payments so that we can calculate your out-of-pocket costs correctly. This may help you to qualify for the Catastrophic Coverage Stage more quickly.
Here are two situations when you should send us copies of receipts to let us know about payments you have made for your drugs:
1. When you buy the drug for a price that is lower than our price Sometimes you can buy your drug at a network pharmacy for a price that is lower than our price.
• For example, a pharmacy might offer a special price on the drug. Or you may have a discount card that is outside our benefit that offers a lower price.
• Unless special conditions apply, you must use a network pharmacy in these situations and your drug must be on our Formulary.
• Save your receipt and send a copy to us so that we can have your out-of-pocket expenses count toward qualifying you for the Catastrophic Coverage Stage.
• Please note: We may not pay for any share of these drug costs. But sending a copy of the receipt allows us to calculate your out-of-pocket costs correctly and may help you qualify for the Catastrophic Coverage Stage more quickly.
2. When you get a drug through a patient assistance program offered by a drug manufacturer Some members are enrolled in a patient assistance program offered by a drug manufacturer that is outside your Part D plan benefits. If you get any drugs through a program offered by a drug manufacturer, you may pay a copayment to the patient assistance program.
• Save your receipt and send a copy to us so that we can have your out-of-pocket expenses count toward qualifying you for the Catastrophic Coverage Stage.
• Please note: Because you are getting your drug through the patient assistance program and not through your Part D plan’s benefits, will not pay for any share of these drug costs. But sending a copy of the receipt allows us to calculate your out-of-pocket costs correctly and may help you qualify for the Catastrophic Coverage Stage more quickly.
2022 Evidence of Coverage for Navitus MedicareRx (PDP) 91 Chapter 5. Asking us to pay our share of the costs for covered drugs
Since you are not asking for payment in the two cases described above, these situations are not considered coverage decisions. Therefore, you cannot make an appeal if you disagree with our decision.
CHAPTER 6 Your rights and responsibilities
2022 Evidence of Coverage for Navitus MedicareRx (PDP) 93 Chapter 6. Your rights and responsibilities
Chapter 6. Your rights and responsibilities
SECTION 1 Our plan must honor your rights as a member of the plan ........... 94
Section 1.1 We must provide information in a way that works for you (in languages other than English, in braille, in large print, or other alternate formats, etc.)........................................................................................................... 94
Section 1.2 We must ensure that you get timely access to your covered drugs ............... 94
Section 1.3 We must protect the privacy of your personal health information ................ 94
Section 1.4 We must give you information about the plan, its network of pharmacies, and your covered drugs.............................................................................. 95
Section 1.5 We must support your right to make decisions about your care ................... 97
Section 1.6 You have the right to make complaints and to ask us to reconsider decisions we have made ............................................................................ 98
Section 1.7 What can you do if you believe you are being treated unfairly or your rights are not being respected? ................................................................... 98
Section 1.8 How to get more information about your rights .......................................... 99
SECTION 2 You have some responsibilities as a member of the plan ............. 99
Section 2.1 What are your responsibilities? .................................................................. 99

2022 Evidence of Coverage for Navitus MedicareRx (PDP) 94 Chapter 6. Your rights and responsibilities
SECTION 1 Our plan must honor your rights as a member of the plan
Section 1.1 We must provide information in a way that works for you (in languages other than English, in braille, in large print, or other alternate formats, etc.)
To get information from us in a way that works for you, please call Customer Care (phone numbers are printed on the back cover of this booklet).
Our plan has people and free interpreter services available to answer questions from disabled and non-English speaking members. We can also give you information in braille, in large print, or other alternate formats at no cost if you need it. We are required to give you information about the plan’s benefits in a format that is accessible and appropriate for you. To get information from us in a way that works for you, please call Customer Care (phone numbers are printed on the back cover of this booklet).
If you have any trouble getting information from our plan in a format that is accessible and appropriate for you, please call to file a grievance with Navitus MedicareRx Customer Care (phone numbers are printed on the back cover of this booklet). You may also file a complaint with Medicare by calling 1-800-MEDICARE (1-800-633-4227) or directly with the Office for Civil Rights. Contact information is included in this Evidence of Coverage or with this mailing, or you may contact Navitus MedicareRx Customer Care for additional information (phone numbers are printed on the back cover of this booklet).
Section 1.2 We must ensure that you get timely access to your covered drugs
As a member of our plan, you have the right to get your prescriptions filled or refilled at any of our network pharmacies without long delays. If you think that you are not getting your Part D drugs within a reasonable amount of time, Chapter 7, Section 7 of this booklet tells what you can do. (If we have denied coverage for your prescription drugs and you don’t agree with our decision, Chapter 7, Section 4 tells what you can do.)
Section 1.3 We must protect the privacy of your personal health information
Federal and state laws protect the privacy of your medical records and personal health information. We protect your personal health information as required by these laws.
• Your “personal health information” includes the personal information you gave us when you enrolled in this plan as well as your medical records and other medical and health information.
2022 Evidence of Coverage for Navitus MedicareRx (PDP) 95 Chapter 6. Your rights and responsibilities
• The laws that protect your privacy give you rights related to getting information and controlling how your health information is used. We give you a written notice, called a “Notice of Privacy Practice,” that tells about these rights and explains how we protect the privacy of your health information.
How do we protect the privacy of your health information? • We make sure that unauthorized people don’t see or change your records.
• In most situations, if we give your health information to anyone who isn’t providing your care or paying for your care, we are required to get written permission from you first. Written permission can be given by you or by someone you have given legal power to make decisions for you.
• There are certain exceptions that do not require us to get your written permission first. These exceptions are allowed or required by law.
o For example, we are required to release health information to government agencies that are checking on quality of care.
o Because you are a member of our plan through Medicare, we are required to give Medicare your health information including information about your Part D prescription drugs. If Medicare releases your information for research or other uses, this will be done according to Federal statutes and regulations.
You can see the information in your records and know how it has been shared with others
You have the right to look at your medical records held at the plan, and to get a copy of your records. We are allowed to charge you a fee for making copies. You also have the right to ask us to make additions or corrections to your medical records. If you ask us to do this, we will work with your healthcare provider to decide whether the changes should be made.
You have the right to know how your health information has been shared with others for any purposes that are not routine.
If you have questions or concerns about the privacy of your personal health information, please call Customer Care (phone numbers are printed on the back cover of this booklet).
Section 1.4 We must give you information about the plan, its network of pharmacies, and your covered drugs
As a member of Navitus MedicareRx, you have the right to get several kinds of information from us. (As explained above in Section 1.1, you have the right to get information from us in a way that works for you. This includes getting the information in languages other than English and in large print or other alternate formats.)
2022 Evidence of Coverage for Navitus MedicareRx (PDP) 96 Chapter 6. Your rights and responsibilities
If you want any of the following kinds of information, please call Customer Care (phone numbers are printed on the back cover of this booklet):
• Information about our plan. This includes, for example, information about your plan’s financial condition, the number of appeals made by members and the plan’s Star Ratings, including how it has been rated by plan members and how it compares to other Medicare prescription drug plans.
• Information about our network pharmacies. o For example, you have the right to get information from us about the pharmacies
in our network. o For a list of the pharmacies in the plan’s network, see the Pharmacy Directory. o For more detailed information about our pharmacies, you can call Customer Care
(phone numbers are printed on the back cover of this booklet) or visit our Member Portal at https://memberportal.navitus.com. There is also a pharmacy search tool on our Member Portal at https://memberportal.navitus.com.
• Information about your coverage and the rules you must follow when using your coverage.
o To get the details on your Part D prescription drug coverage, see Chapters 3 and 4 of this booklet plus the plan’s List of Covered Drugs (Formulary). These chapters, together with the List of Covered Drugs (Formulary), tell you what drugs are covered and explain the rules you must follow and the restrictions to your coverage for certain drugs.
o If you have questions about the rules or restrictions, please call Customer Care (phone numbers are printed on the back cover of this booklet).
• Information about why something is not covered and what you can do about it. o If a Part D drug is not covered for you, or if your coverage is restricted in some
way, you can ask us for a written explanation. You have the right to this explanation even if you received the drug from an out-of-network pharmacy.
o If you are not happy or if you disagree with a decision we make about what Part D drug is covered for you, you have the right to ask us to change the decision. You can ask us to change the decision by making an appeal. For details on what to do if something is not covered for you in the way you think it should be covered, see Chapter 7 of this booklet. It gives you the details about how to make an appeal if you want us to change our decision. (Chapter 7 also tells about how to make a complaint about quality of care, waiting times, and other concerns.)
o If you want to ask our plan to pay our share of the cost for a Part D prescription drug, see Chapter 5 of this booklet.

2022 Evidence of Coverage for Navitus MedicareRx (PDP) 97 Chapter 6. Your rights and responsibilities
Section 1.5 We must support your right to make decisions about your care
You have the right to give instructions about what is to be done if you are not able to make medical decisions for yourself
Sometimes people become unable to make health care decisions for themselves due to accidents or serious illness. You have the right to say what you want to happen if you are in this situation. This means that, if you want to, you can:
• Fill out a written form to give someone the legal authority to make medical decisions for you if you ever become unable to make decisions for yourself.
• Give your doctors written instructions about how you want them to handle your medical care if you become unable to make decisions for yourself.
The legal documents that you can use to give your directions in advance in these situations are called “advance directives.” There are different types of advance directives and different names for them. Documents called “living will” and “power of attorney for health care” are examples of advance directives.
If you want to use an “advance directive” to give your instructions, here is what to do:
• Get the form. If you want to have an advance directive, you can get a form from your lawyer, from a social worker, or from some office supply stores. You can sometimes get advance directive forms from organizations that give people information about Medicare.
• Fill it out and sign it. Regardless of where you get this form, keep in mind that it is a legal document. You should consider having a lawyer help you prepare it.
• Give copies to appropriate people. You should give a copy of the form to your doctor and to the person you name on the form as the one to make decisions for you if you can’t. You may want to give copies to close friends or family members as well. Be sure to keep a copy at home.
If you know ahead of time that you are going to be hospitalized, and you have signed an advance directive, take a copy with you to the hospital.
• If you are admitted to the hospital, they will ask you whether you have signed an advance directive form and whether you have it with you.
• If you have not signed an advance directive form, the hospital has forms available and will ask if you want to sign one.
Remember, it is your choice whether you want to fill out an advance directive (including whether you want to sign one if you are in the hospital). According to law, no one can deny you care or discriminate against you based on whether or not you have signed an advance directive.

2022 Evidence of Coverage for Navitus MedicareRx (PDP) 98 Chapter 6. Your rights and responsibilities
What if your instructions are not followed?
If you have signed an advance directive, and you believe that a doctor or hospital did not follow the instructions in it, you may file a complaint with the state agency. For contact information on the State Medical Assistance Office in your state, please refer to Exhibit C or call Customer Care (phone numbers are printed on the back cover of this booklet).
Section 1.6 You have the right to make complaints and to ask us to reconsider decisions we have made
If you have any problems or concerns about your covered services or care, Chapter 7 of this booklet tells what you can do. It gives the details about how to deal with all types of problems and complaints. What you need to do to follow up on a problem or concern depends on the situation. You might need to ask our plan to make a coverage decision for you, make an appeal to us to change a coverage decision, or make a complaint. Whatever you do – ask for a coverage decision, make an appeal, or make a complaint – we are required to treat you fairly.
You have the right to get a summary of information about the appeals and complaints that other members have filed against our plan in the past. To get this information, please call Customer Care (phone numbers are printed on the back cover of this booklet).
Section 1.7 What can you do if you believe you are being treated unfairly or your rights are not being respected?
If it is about discrimination, call the Office for Civil Rights
If you believe you have been treated unfairly or your rights have not been respected due to your race, disability, religion, sex, health, ethnicity, creed (beliefs), age, or national origin, you should call the Department of Health and Human Services’ Office for Civil Rights at 1-800-368-1019 or TTY/TDD 1-800-537-7697, or call your local Office for Civil Rights.
Is it about something else?
If you believe you have been treated unfairly or your rights have not been respected, and it’s not about discrimination, you can get help dealing with the problem you are having:
• You can call Customer Care (phone numbers are printed on the back cover of this booklet).
• You can call the State Health Insurance Assistance Program. For details about this organization and how to contact it, go to Chapter 2, Section 3.
• Or, you can call Medicare at 1-800-MEDICARE (1-800-633-4227), 24 hours a day, 7 days a week. TTY/TDD users should call 1-877-486-2048.
2022 Evidence of Coverage for Navitus MedicareRx (PDP) 99 Chapter 6. Your rights and responsibilities
Section 1.8 How to get more information about your rights
There are several places where you can get more information about your rights:
• You can call Customer Care (phone numbers are printed on the back cover of this booklet).
• You can call the State Health Insurance Assistance Program. For details about this organization and how to contact it, go to Chapter 2, Section 3.
• You can contact Medicare. o You can visit the Medicare website to read or download the publication
“Medicare Rights & Protections.” (The publication is available at: www.medicare.gov/Pubs/pdf/11534-Medicare-Rights-and-Protections.pdf.)
o Or, you can call 1-800-MEDICARE (1-800-633-4227), 24 hours a day, 7 days a week. TTY/TDD users should call 1-877-486-2048.
SECTION 2 You have some responsibilities as a member of the plan
Section 2.1 What are your responsibilities?
Things you need to do as a member of the plan are listed below. If you have any questions, please call Customer Care (phone numbers are printed on the back cover of this booklet). We’re here to help.
• Get familiar with your covered drugs and the rules you must follow to get these covered drugs. Use this Evidence of Coverage booklet to learn what is covered for you and the rules you need to follow to get your covered drugs.
o Chapters 3 and 4 give the details about your coverage for Part D prescription drugs.
• If you have any other prescription drug coverage in addition to our plan, you are required to tell us. Please call Customer Care to let us know (phone numbers are printed on the back cover of this booklet).
o We are required to follow rules set by Medicare to make sure that you are using all of your coverage in combination when you get your covered drugs from our plan. This is called “coordination of benefits” because it involves coordinating the drug benefits you get from our plan with any other drug benefits available to you. We’ll help you coordinate your benefits. (For more information about coordination of benefits, go to Chapter 1, Section 10.)
• Tell your doctor and pharmacist that you are enrolled in our plan. Show your plan membership card whenever you get your Part D prescription drugs.
2022 Evidence of Coverage for Navitus MedicareRx (PDP) 100 Chapter 6. Your rights and responsibilities
• Help your doctors and other prescribers help you, by giving them information, asking questions, and following through on your care.
o To help your doctors and other health providers give you the best care, learn as much as you are able to about your health problems and give them the information they need about you and your health. Follow the treatment plans and instructions that you and your doctors agree upon.
o Make sure your doctors know all of the drugs you are taking, including over-the-counter drugs, vitamins, and supplements.
o If you have any questions, be sure to ask. Your doctors and other health care providers are supposed to explain things in a way you can understand. If you ask a question and you don’t understand the answer you are given, ask again.
• Pay what you owe. As a plan member, you are responsible for these payments: o Your plan premiums must be paid to continue being a member of our plan. o For most of your drugs covered by the plan, you must pay your share of the cost
when you get the drug. This will be a copayment (a fixed amount) or coinsurance (a percentage of the total cost). Chapter 4 tells what you must pay for your Part D prescription drugs.
o If you get any drugs that are not covered by our plan or by other insurance you may have, you must pay the full cost. If you disagree with our decision to deny coverage for a drug, you can
make an appeal. Please see Chapter 7 of this booklet for information about how to make an appeal.
o If you are required to pay a late enrollment penalty, you must pay the penalty to remain a member of the plan.
o If you are required to pay the extra amount for Part D because of your yearly income, you must pay the extra amount directly to the government to remain a member of the plan.
Tell us if you move. If you are going to move, it’s important to tell us right away. Please remember to also notify UC Retirement Administration Service Center (RASC) at (800) 888-8267 (in U.S.) or (510) 987-0200 (from outside the U.S.), so they will have your most up-to-date contact information on file. Representatives are available Monday through Friday, 8:30 a.m. to 4:30 p.m. (Pacific). We need to keep your membership record up to date and know how to contact you.
o If you move outside of the United States or Puerto Rico, you cannot remain a member of our plan. (Chapter 1 tells about our service area.) We can help you figure out whether you are moving outside our service area.
o If you move within our service area, we still need to know so we can keep your membership record up to date and know how to contact you.
2022 Evidence of Coverage for Navitus MedicareRx (PDP) 101 Chapter 6. Your rights and responsibilities
o If you move, it is also important to tell Social Security (or the Railroad Retirement Board). You can find phone numbers and contact information for these organizations in Chapter 2.
• Call Customer Care for help if you have questions or concerns. We also welcome any suggestions you may have for improving our plan.
o Phone numbers and calling hours for Customer Care are printed on the back cover of this booklet.
o For more information on how to reach us, including our mailing address, please see Chapter 2.
CHAPTER 7 What to do if you have a problem or
complaint (coverage decisions, appeals, complaints)
2022 Evidence of Coverage for Navitus MedicareRx (PDP) 103 Chapter 7. What to do if you have a problem or complaint
(coverage decisions, appeals, complaints)
Chapter 7. What to do if you have a problem or complaint (coverage decisions, appeals, complaints)
SECTION 1 Introduction.......................................................................................... 105
Section 1.1 What to do if you have a problem or concern ........................................... 105
Section 1.2 What about the legal terms? ..................................................................... 105
SECTION 2 You can get help from government organizations that are not connected with us ........................................................................ 106
Section 2.1 Where to get more information and personalized assistance ...................... 106
SECTION 3 To deal with your problem, which process should you use? ..... 106
Section 3.1 Should you use the process for coverage decisions and appeals? Or should you use the process for making complaints? .................................. 106
COVERAGE DECISIONS AND APPEALS .................................................................... 107
SECTION 4 A guide to the basics of coverage decisions and appeals .......... 107
Section 4.1 Asking for coverage decisions and making appeals: the big picture .......... 107
Section 4.2 How to get help when you are asking for a coverage decision or making an appeal ................................................................................................. 108
SECTION 5 Your Part D prescription drugs: How to ask for a coverage decision or make an appeal .............................................................. 109
Section 5.1 This section tells you what to do if you have problems getting a Part D drug or you want us to pay you back for a Part D drug ............................. 109
Section 5.2 What is an exception? .............................................................................. 111
Section 5.3 Important things to know about asking for exceptions .............................. 113
Section 5.4 Step-by-step: How to ask for a coverage decision, including an exception 113
Section 5.5 Step-by-step: How to make a Level 1 Appeal (how to ask for a review of a coverage decision made by our plan) ..................................................... 117
Section 5.6 Step-by-step: How to make a Level 2 Appeal ........................................... 120
SECTION 6 Taking your appeal to Level 3 and beyond .................................... 122
Section 6.1 Appeal Levels 3, 4 and 5 for Part D Drug Requests .................................. 122
MAKING COMPLAINTS................................................................................................... 123
SECTION 7 How to make a complaint about quality of care, waiting times, customer service, or other concerns .................................. 123
Section 7.1 What kinds of problems are handled by the complaint process? ................ 123

2022 Evidence of Coverage for Navitus MedicareRx (PDP) 104 Chapter 7. What to do if you have a problem or complaint
(coverage decisions, appeals, complaints)
Section 7.2 The formal name for “making a complaint” is “filing a grievance” ........... 125
Section 7.3 Step-by-step: Making a complaint............................................................ 125
Section 7.4 You can also make complaints about quality of care to the Quality Improvement Organization ...................................................................... 126
Section 7.5 You can also tell Medicare about your complaint ..................................... 127
2022 Evidence of Coverage for Navitus MedicareRx (PDP) 105 Chapter 7. What to do if you have a problem or complaint
(coverage decisions, appeals, complaints)
SECTION 1 Introduction
Section 1.1 What to do if you have a problem or concern
Please call us first
Your health and satisfaction are important to us. When you have a problem or concern, we hope you’ll try an informal approach first. Please call Navitus MedicareRx Customer Care, our phone numbers are printed on the back cover of this booklet. We will work with you on a mutually satisfactory solution to your concern. We pledge to honor your rights, to take your problems and concerns seriously, and to treat you with respect.
This chapter explains two types of processes for handling problems and concerns:
• For some types of problems, you need to use the process for coverage decisions and appeals.
• For other types of problems, you need to use the process for making complaints.
Both of these processes have been approved by Medicare. To ensure fairness and prompt handling of your problems, each process has a set of rules, procedures, and deadlines that must be followed by us and by you.
Which one do you use? That depends on the type of problem you are having. The guide in Section 3 will help you identify the right process to use.
Section 1.2 What about the legal terms?
There are technical legal terms for some of the rules, procedures, and types of deadlines explained in this chapter. Many of these terms are unfamiliar to most people and can be hard to understand.
To keep things simple, this chapter explains the legal rules and procedures using simpler words in place of certain legal terms. For example, this chapter generally says “making a complaint” rather than “filing a grievance,” “coverage decision” rather than “coverage determination” or “at-risk determination,” and “Independent Review Organization” instead of “Independent Review Entity.” It also uses abbreviations as little as possible.
However, it can be helpful – and sometimes quite important – for you to know the correct legal terms for the situation you are in. Knowing which terms to use will help you communicate more clearly and accurately when you are dealing with your problem and get the right help or information for your situation. To help you know which terms to use, we include legal terms when we give the details for handling specific types of situations.

2022 Evidence of Coverage for Navitus MedicareRx (PDP) 106 Chapter 7. What to do if you have a problem or complaint
(coverage decisions, appeals, complaints)
SECTION 2 You can get help from government organizations that are not connected with us
Section 2.1 Where to get more information and personalized assistance
Sometimes it can be confusing to start or follow through the process for dealing with a problem. This can be especially true if you do not feel well or have limited energy. Other times, you may not have the knowledge you need to take the next step.
Get help from an independent government organization
We are always available to help you. But in some situations you may also want help or guidance from someone who is not connected with us. You can always contact your State Health Insurance Assistance Program (SHIP). This government program has trained counselors in every state. The program is not connected with us or with any insurance company or health plan. The counselors at this program can help you understand which process you should use to handle a problem you are having. They can also answer your questions, give you more information, and offer guidance on what to do.
The services of SHIP counselors are free You will find contact information for the SHIP program in your state in Exhibit A (located in the back of this booklet).
You can also get help and information from Medicare
For more information and help in handling a problem, you can also contact Medicare. Here are two ways to get information directly from Medicare:
• You can call 1-800-MEDICARE (1-800-633-4227), 24 hours a day, 7 days a week. TTY/TDD users should call 1-877-486-2048.
• You can visit the Medicare website (www.medicare.gov).
SECTION 3 To deal with your problem, which process should you use?
Section 3.1 Should you use the process for coverage decisions and appeals? Or should you use the process for making complaints?
If you have a problem or concern, you only need to read the parts of this chapter that apply to your situation. The guide that follows will help.

2022 Evidence of Coverage for Navitus MedicareRx (PDP) 107 Chapter 7. What to do if you have a problem or complaint
(coverage decisions, appeals, complaints)
To figure out which part of this chapter will help with your specific problem or concern, START HERE
Is your problem or concern about your benefits or coverage?
(This includes problems about whether particular medical care or prescription drugs are covered or not, the way in which they are covered, and problems related to payment for medical care or prescription drugs.)
Yes. My problem is about benefits or coverage.
Go on to the next section of this chapter, Section 4, “A guide to the basics of coverage decisions and appeals.”
No. My problem is not about benefits or coverage.
Skip ahead to Section 7 at the end of this chapter: “How to make a complaint about quality of care, waiting times, customer service or other concerns.”
COVERAGE DECISIONS AND APPEALS
SECTION 4 A guide to the basics of coverage decisions and appeals
Section 4.1 Asking for coverage decisions and making appeals: the big picture
The process for coverage decisions and appeals deals with problems related to your benefits and coverage for prescription drugs, including problems related to payment. This is the process you use for issues such as whether a drug is covered or not and the way in which the drug is covered.
Asking for coverage decisions
A coverage decision is a decision we make about your benefits and coverage or about the amount we will pay for your prescription drugs.
We are making a coverage decision for you whenever we decide what is covered for you and how much we pay. In some cases, we might decide a drug is not covered or is no longer covered by Medicare for you. If you disagree with this coverage decision, you can make an appeal.

2022 Evidence of Coverage for Navitus MedicareRx (PDP) 108 Chapter 7. What to do if you have a problem or complaint
(coverage decisions, appeals, complaints)
Making an appeal
If we make a coverage decision and you are not satisfied with this decision, you can “appeal” the decision. An appeal is a formal way of asking us to review and change a coverage decision we have made.
When you appeal a decision for the first time, this is called a Level 1 Appeal. In this appeal, we review the coverage decision we made to check to see if we were following all of the rules properly. Your appeal is handled by different reviewers than those who made the original unfavorable decision. When we have completed the review, we give you our decision. Under certain circumstances, which we discuss later, you can request an expedited or “fast coverage decision” or fast appeal of a coverage decision. In limited circumstances a request for a coverage decision will be dismissed, which means we won’t review the request. Examples of when a request will be dismissed include if the request is incomplete, if someone makes the request on your behalf but isn’t legally authorized to do so or if you ask for your request to be withdrawn. If we dismiss a request for a coverage decision, we will send a notice explaining why the request was dismissed and how to ask for a review of the dismissal.
If we say no to all or part of your Level 1 Appeal, you can ask for a Level 2 Appeal. The Level 2 Appeal is conducted by an Independent Review Organization that is not connected to us. If you are not satisfied with the decision at the Level 2 Appeal, you may be able to continue through additional levels of appeal.
Section 4.2 How to get help when you are asking for a coverage decision or making an appeal
Would you like some help? Here are resources you may wish to use if you decide to ask for any kind of coverage decision or appeal a decision:
• You can call us at Customer Care (phone numbers are printed on the back cover of this booklet).
• You can get free help from your State Health Insurance Assistance Program (SHIP) (see Section 2 of this chapter).
• Your doctor or other prescriber can make a request for you. For Part D prescription drugs, your doctor or other prescriber can request a coverage decision or a Level 1 or Level 2 Appeal on your behalf. To request any appeal after Level 2, your doctor or other prescriber must be appointed as your representative.
• You can ask someone to act on your behalf. If you want to, you can name another person to act for you as your “representative” to ask for a coverage decision or make an appeal.
o There may be someone who is already legally authorized to act as your representative under State law.

2022 Evidence of Coverage for Navitus MedicareRx (PDP) 109 Chapter 7. What to do if you have a problem or complaint
(coverage decisions, appeals, complaints)
o If you want a friend, relative, your doctor or other prescriber, or other person to be your representative, call Customer Care (phone numbers are printed on the back cover of this booklet) and ask for the “Appointment of Representative” form. (The form is also available on Medicare’s website at www.cms.gov/Medicare/CMS-Forms/CMS-Forms/downloads/cms1696.pdf or on our Member Portal at https://memberportal.navitus.com.) The form gives that person permission to act on your behalf. It must be signed by you and by the person who you would like to act on your behalf. You must give us a copy of the signed form.
• You also have the right to hire a lawyer to act for you. You may contact your own lawyer, or get the name of a lawyer from your local bar association or other referral service. There are also groups that will give you free legal services if you qualify. However, you are not required to hire a lawyer to ask for any kind of coverage decision or appeal a decision.
SECTION 5 Your Part D prescription drugs: How to ask for a coverage decision or make an appeal
Have you read Section 4 of this chapter (A guide to “the basics” of coverage decisions and appeals)? If not, you may want to read it before you start this section.
Section 5.1 This section tells you what to do if you have problems getting a Part D drug or you want us to pay you back for a Part D drug
Your benefits as a member of our plan include coverage for many prescription drugs. Please refer to our plan’s List of Covered Drugs (Formulary). To be covered, the drug must be used for a medically accepted indication. (A “medically accepted indication” is a use of the drug that is either approved by the Food and Drug Administration or supported by certain reference books. See Chapter 3, Section 3 for more information about a medically accepted indication.)
• This section is about your Part D drugs only. To keep things simple, we generally say “drug” in the rest of this section, instead of repeating “covered outpatient prescription drug” or “Part D drug” every time.
• For details about what we mean by Part D drugs, the List of Covered Drugs (Formulary), rules and restrictions on coverage, and cost information, see Chapter 3 (Using our plan’s coverage for your Part D prescription drugs) and Chapter 4 (What you pay for your Part D prescription drugs).

2022 Evidence of Coverage for Navitus MedicareRx (PDP) 110 Chapter 7. What to do if you have a problem or complaint
(coverage decisions, appeals, complaints)
Part D coverage decisions and appeals
As discussed in Section 4 of this chapter, a coverage decision is a decision we make about your benefits and coverage or about the amount we will pay for your drugs.
Legal Terms
An initial coverage decision about your Part D drugs is called a “coverage determination.”
Here are examples of coverage decisions you ask us to make about your Part D drugs:
• You ask us to make an exception, including: o Asking us to cover a Part D drug that is not on the plan’s List of Covered Drugs
(Formulary) o Asking us to waive a restriction on the plan’s coverage for a drug (such as limits
on the amount of the drug you can get) o Asking to pay a lower cost-sharing amount for a covered drug on a higher cost-
sharing tier
• You ask us whether a drug is covered for you and whether you satisfy any applicable coverage rules. (For example, when your drug is on the plan’s List of Covered Drugs (Formulary) but we require you to get approval from us before we will cover it for you.)
o Please note: If your pharmacy tells you that your prescription cannot be filled as written, the pharmacy will give you a written notice explaining how to contact us to ask for a coverage decision.
• You ask us to pay for a prescription drug you already bought. This is a request for a coverage decision about payment.
If you disagree with a coverage decision we have made, you can appeal our decision.
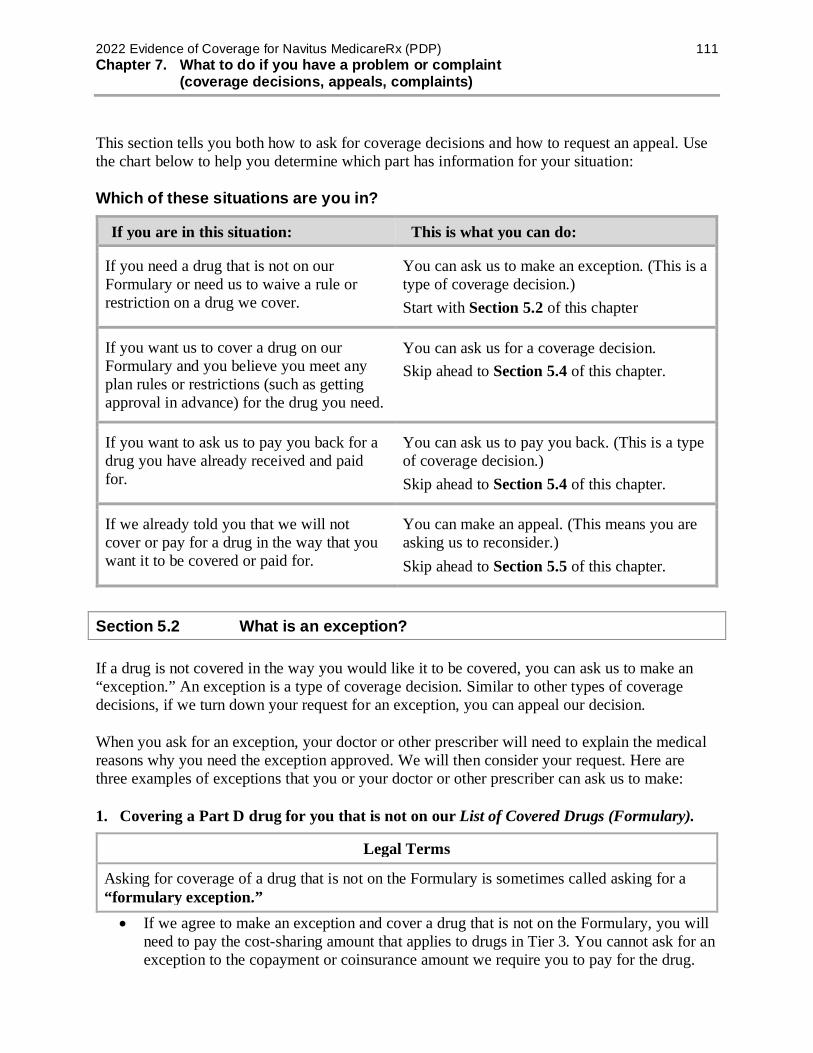
2022 Evidence of Coverage for Navitus MedicareRx (PDP) 111 Chapter 7. What to do if you have a problem or complaint
(coverage decisions, appeals, complaints)
This section tells you both how to ask for coverage decisions and how to request an appeal. Use the chart below to help you determine which part has information for your situation:
Which of these situations are you in?
If you are in this situation: This is what you can do:
If you need a drug that is not on our Formulary or need us to waive a rule or restriction on a drug we cover.
You can ask us to make an exception. (This is a type of coverage decision.) Start with Section 5.2 of this chapter
If you want us to cover a drug on our Formulary and you believe you meet any plan rules or restrictions (such as getting approval in advance) for the drug you need.
You can ask us for a coverage decision. Skip ahead to Section 5.4 of this chapter.
If you want to ask us to pay you back for a drug you have already received and paid for.
You can ask us to pay you back. (This is a type of coverage decision.) Skip ahead to Section 5.4 of this chapter.
If we already told you that we will not cover or pay for a drug in the way that you want it to be covered or paid for.
You can make an appeal. (This means you are asking us to reconsider.) Skip ahead to Section 5.5 of this chapter.
Section 5.2 What is an exception?
If a drug is not covered in the way you would like it to be covered, you can ask us to make an “exception.” An exception is a type of coverage decision. Similar to other types of coverage decisions, if we turn down your request for an exception, you can appeal our decision.
When you ask for an exception, your doctor or other prescriber will need to explain the medical reasons why you need the exception approved. We will then consider your request. Here are three examples of exceptions that you or your doctor or other prescriber can ask us to make:
1. Covering a Part D drug for you that is not on our List of Covered Drugs (Formulary).
Legal Terms
Asking for coverage of a drug that is not on the Formulary is sometimes called asking for a “formulary exception.” • If we agree to make an exception and cover a drug that is not on the Formulary, you will
need to pay the cost-sharing amount that applies to drugs in Tier 3. You cannot ask for an exception to the copayment or coinsurance amount we require you to pay for the drug.
2022 Evidence of Coverage for Navitus MedicareRx (PDP) 112 Chapter 7. What to do if you have a problem or complaint
(coverage decisions, appeals, complaints)
2. Removing a restriction on our coverage for a covered drug. There are extra rules or restrictions that apply to certain drugs on our List of Covered Drugs (Formulary) (for more information, go to Chapter 3).
Legal Terms
Asking for removal of a restriction on coverage for a drug is sometimes called asking for a “formulary exception.”
• The extra rules and restrictions on coverage for certain drugs include: o Being required to use the generic version of a drug instead of the brand name
drug. o Getting plan approval in advance before we will agree to cover the drug for you.
(This is sometimes called “prior authorization.”) o Being required to try a different drug first before we will agree to cover the drug
you are asking for. (This is sometimes called “step therapy.”) o Quantity limits. For some drugs, there are restrictions on the amount of the drug
you can have.
• If we agree to make an exception and waive a restriction for you, you can ask for an exception to the copayment or coinsurance amount we require you to pay for the drug.
3. Changing coverage of a drug to a lower cost-sharing tier. Every drug on our Formulary is in one of four cost-sharing tiers. In general, the lower the cost-sharing tier number, the less you will pay as your share of the cost of the drug.
Legal Terms
Asking to pay a lower price for a covered non-preferred drug is sometimes called asking for a “tiering exception.”
• If our Formulary contains alternative drug(s) for treating your medical condition that are in a lower cost-sharing tier than your drug, you can ask us to cover your drug at the cost-sharing amount that applies to the alternative drug(s). This would lower your share of the cost for the drug.
o If the drug you’re taking is a biological product you can ask us to cover your drug at the cost-sharing amount that applies to the lowest tier that contains biological product alternatives for treating your condition.
o If the drug you’re taking is a brand name drug you can ask us to cover your drug at the cost-sharing amount that applies to the lowest tier that contains brand name alternatives for treating your condition.

2022 Evidence of Coverage for Navitus MedicareRx (PDP) 113 Chapter 7. What to do if you have a problem or complaint
(coverage decisions, appeals, complaints)
o If the drug you’re taking is a generic drug you can ask us to cover your drug at the cost-sharing amount that applies to the lowest tier that contains either brand or generic alternatives for treating your condition.
• You cannot ask us to change the cost-sharing tier for any drug in Tier 4 (Specialty products).
• If we approve your request for a tiering exception and there is more than one lower cost-sharing tier with alternative drugs you can’t take, you will usually pay the lowest amount. Please contact Customer Care with any questions (phone numbers are printed on the back cover of this booklet).
Section 5.3 Important things to know about asking for exceptions
Your doctor must tell us the medical reasons Your doctor or other prescriber must give us a statement that explains the medical reasons for requesting an exception. For a faster decision, include this medical information from your doctor or other prescriber when you ask for the exception.
Typically, our Formulary includes more than one drug for treating a particular condition. These different possibilities are called “alternative” drugs. If an alternative drug would be just as effective as the drug you are requesting and would not cause more side effects or other health problems, we will generally not approve your request for an exception. If you ask us for a tiering exception, we will generally not approve your request for an exception unless all the alternative drugs in the lower cost-sharing tier(s) won’t work as well for you or are likely to cause an adverse reaction or other harm.
We can say yes or no to your request
• If we approve your request for an exception, our approval usually is valid until the end of the calendar year. This is true as long as your doctor continues to prescribe the drug for you and that drug continues to be safe and effective for treating your condition.
• If we say no to your request for an exception, you can ask for a review of our decision by making an appeal. Section 5.5 tells you how to make an appeal if we say no.
The next section tells you how to ask for a coverage decision, including an exception.
Section 5.4 Step-by-step: How to ask for a coverage decision, including an exception
Step 1: You ask us to make a coverage decision about the drug(s) or payment you need. If your health requires a quick response, you must ask us to make a
2022 Evidence of Coverage for Navitus MedicareRx (PDP) 114 Chapter 7. What to do if you have a problem or complaint
(coverage decisions, appeals, complaints)
“fast coverage decision.” You cannot ask for a fast coverage decision if you are asking us to pay you back for a drug you already bought.
What to do
• Request the type of coverage decision you want. Start by calling, writing, or faxing us to make your request. You, your representative, or your doctor (or other prescriber) can do this. You can also access the coverage decision process through our Member Portal. For the details, go to Chapter 2, Section 1 and look for the section called How to contact us when you are asking for a coverage decision about your Part D prescription drugs. Or if you are asking us to pay you back for a drug, go to the section called Where to send a request asking us to pay for our share of the cost of a drug you have received.
• You or your doctor or someone else who is acting on your behalf can ask for a coverage decision. Section 4 of this chapter tells how you can give written permission to someone else to act as your representative. You can also have a lawyer act on your behalf.
• If you want to ask us to pay you back for a drug, start by reading Chapter 5 of this booklet: Asking us to pay our share of the costs for covered drugs. Chapter 5 describes the situations in which you may need to ask for reimbursement. It also tells how to send us the paperwork that asks us to pay you back for our share of the cost of a drug you have paid for.
• If you are requesting an exception, provide the “supporting statement.” Your doctor or other prescriber must give us the medical reasons for the drug exception you are requesting. (We call this the “supporting statement.”) Your doctor or other prescriber can fax or mail the statement to us. Or your doctor or other prescriber can tell us on the phone and follow up by faxing or mailing a written statement if necessary. See Sections 5.2 and 5.3 for more information about exception requests.
• We must accept any written request, including a request submitted on the CMS Model Coverage Determination Request Form, which is available on our Member Portal.
• For electronic submission, you can go to our website (https://memberportal.navitus.com) to sign into your Member Portal and complete the Request for Coverage Determination form. Note that if attachments need to be submitted, please fax or mail the form and supporting documentation.
If your health requires it, ask us to give you a “fast coverage decision”
Legal Terms
A “fast coverage decision” is called an “expedited coverage determination.”
• When we give you our decision, we will use the “standard” deadlines unless we have agreed to use the “fast” deadlines. A standard coverage decision means we will give you
2022 Evidence of Coverage for Navitus MedicareRx (PDP) 115 Chapter 7. What to do if you have a problem or complaint
(coverage decisions, appeals, complaints)
an answer within 72 hours after we receive your doctor’s statement. A fast coverage decision means we will answer within 24 hours after we receive your doctor’s statement.
• To get a fast coverage decision, you must meet two requirements: o You can get a fast coverage decision only if you are asking for a drug you have
not yet received. (You cannot ask for a fast coverage decision if you are asking us to pay you back for a drug you have already bought.)
o You can get a fast coverage decision only if using the standard deadlines could cause serious harm to your health or hurt your ability to function.
• If your doctor or other prescriber tells us that your health requires a “fast coverage decision,” we will automatically agree to give you a fast coverage decision.
• If you ask for a fast coverage decision on your own (without your doctor’s or other prescriber’s support), we will decide whether your health requires that we give you a fast coverage decision.
o If we decide that your medical condition does not meet the requirements for a fast coverage decision, we will send you a letter that says so (and we will use the standard deadlines instead).
o This letter will tell you that if your doctor or other prescriber asks for the fast coverage decision, we will automatically give a fast coverage decision.
o The letter will also tell how you can file a complaint about our decision to give you a standard coverage decision instead of the fast coverage decision you requested. It tells how to file a “fast” complaint, which means you would get our answer to your complaint within 24 hours of receiving the complaint. (The process for making a complaint is different from the process for coverage decisions and appeals. For more information about the process for making complaints, see Section 7 of this chapter.)
Step 2: We consider your request and we give you our answer.
Deadlines for a “fast” coverage decision
• If we are using the fast deadlines, we must give you our answer within 24 hours. o Generally, this means within 24 hours after we receive your request. If you are
requesting an exception, we will give you our answer within 24 hours after we receive your doctor’s statement supporting your request. We will give you our answer sooner if your health requires us to.
o If we do not meet this deadline, we are required to send your request on to Level 2 of the appeals process, where it will be reviewed by an Independent Review Organization. Later in this section, we talk about this review organization and explain what happens at Appeal Level 2.

2022 Evidence of Coverage for Navitus MedicareRx (PDP) 116 Chapter 7. What to do if you have a problem or complaint
(coverage decisions, appeals, complaints)
• If our answer is yes to part or all of what you requested, we must provide the coverage we have agreed to provide within 24 hours after we receive your request or doctor’s statement supporting your request.
• If our answer is no to part or all of what you requested, we will send you a written statement that explains why we said no. We will also tell you how you can appeal.
Deadlines for a “standard” coverage decision about a drug you have not yet received
• If we are using the standard deadlines, we must give you our answer within 72 hours. o Generally, this means within 72 hours after we receive your request. If you are
requesting an exception, we will give you our answer within 72 hours after we receive your doctor’s statement supporting your request. We will give you our answer sooner if your health requires us to.
o If we do not meet this deadline, we are required to send your request on to Level 2 of the appeals process, where it will be reviewed by an Independent Review Organization. Later in this section, we talk about this review organization and explain what happens at Appeal Level 2.
• If our answer is yes to part or all of what you requested – o If we approve your request for coverage, we must provide the coverage we have
agreed to provide within 72 hours after we receive your request or doctor’s statement supporting your request.
• If our answer is no to part or all of what you requested, we will send you a written statement that explains why we said no. We will also tell you how you can appeal.
Deadlines for a “standard” coverage decision about payment for a drug you have already bought
• We must give you our answer within 14 calendar days after we receive your request. o If we do not meet this deadline, we are required to send your request on to Level 2
of the appeals process, where it will be reviewed by an Independent Review Organization. Later in this section, we talk about this review organization and explain what happens at Appeal Level 2.
• If our answer is yes to part or all of what you requested, we are also required to make payment to you within 14 calendar days after we receive your request.
• If our answer is no to part or all of what you requested, we will send you a written statement that explains why we said no. We will also tell you how you can appeal.
Step 3: If we say no to your coverage request, you decide if you want to make an appeal.
• If we say no, you have the right to request an appeal. Requesting an appeal means asking us to reconsider – and possibly change – the decision we made.
2022 Evidence of Coverage for Navitus MedicareRx (PDP) 117 Chapter 7. What to do if you have a problem or complaint
(coverage decisions, appeals, complaints)
Section 5.5 Step-by-step: How to make a Level 1 Appeal (how to ask for a review of a coverage decision made by our plan)
Legal Terms
An appeal to the plan about a Part D drug coverage decision is called a plan “redetermination.”
Step 1: You contact us and make your Level 1 Appeal. If your health requires a quick response, you must ask for a “fast appeal.”
What to do
• To start your appeal, you (or your representative or your doctor or other prescriber) must contact us.
o For details on how to reach us by phone, fax, or mail, or on our Member Portal, for any purpose related to your appeal, go to Chapter 2, Section 1, and look for the section called How to contact us when you are making an appeal about your Part D prescription drugs.
• If you are asking for a standard appeal, make your appeal by submitting a written request. You may also ask for an appeal by calling us at the phone number shown in Chapter 2, Section 1 (How to contact us when you are making an appeal about your Part D prescription drugs).
• If you are asking for a fast appeal, you may make your appeal in writing or you may call us at the phone number shown in Chapter 2, Section 1 (How to contact us when you are making an appeal about your Part D prescription drugs).
• We must accept any written request, including a request submitted on the CMS Model Coverage Determination Request Form, which is available on our Member Portal.
• For electronic submission, you can go to our Member Portal (https://memberportal.navitus.com) to sign into your Member Portal and complete the Request for Redetermination of Medicare Prescription Drug Denial form. Note that if attachments need to be submitted, please fax or mail the form and supporting documentation.
• You must make your appeal request within 60 calendar days from the date on the written notice we sent to tell you our answer to your request for a coverage decision. If you miss this deadline and have a good reason for missing it, we may give you more time to make your appeal. Examples of good cause for missing the deadline may include if you had a serious illness that prevented you from contacting us or if we provided you with incorrect or incomplete information about the deadline for requesting an appeal.

2022 Evidence of Coverage for Navitus MedicareRx (PDP) 118 Chapter 7. What to do if you have a problem or complaint
(coverage decisions, appeals, complaints)
• You can ask for a copy of the information in your appeal and add more information.
o You have the right to ask us for a copy of the information regarding your appeal. o If you wish, you and your doctor or other prescriber may give us additional
information to support your appeal.
If your health requires it, ask for a “fast appeal”
Legal Terms
A “fast appeal” is also called an “expedited redetermination.”
• If you are appealing a decision we made about a drug you have not yet received, you and your doctor or other prescriber will need to decide if you need a “fast appeal.”
• The requirements for getting a “fast appeal” are the same as those for getting a “fast coverage decision” in Section 5.4 of this chapter.
Step 2: We consider your appeal and we give you our answer.
• When we are reviewing your appeal, we take another careful look at all of the information about your coverage request. We check to see if we were following all the rules when we said no to your request. We may contact you or your doctor or other prescriber to get more information.
Deadlines for a “fast appeal”
• If we are using the fast deadlines, we must give you our answer within 72 hours after we receive your appeal. We will give you our answer sooner if your health requires it.
o If we do not give you an answer within 72 hours, we are required to send your request on to Level 2 of the appeals process, where it will be reviewed by an Independent Review Organization. (Later in this section, we talk about this review organization and explain what happens at Level 2 of the appeals process.)
• If our answer is yes to part or all of what you requested, we must provide the coverage we have agreed to provide within 72 hours after we receive your appeal.
• If our answer is no to part or all of what you requested, we will send you a written statement that explains why we said no and how you can appeal our decision.
Deadlines for a “standard” appeal
• If we are using the standard deadlines, we must give you our answer within 7 calendar days after we receive your appeal for a drug you have not received yet. We will give you our decision sooner if you have not received the drug yet and your health condition requires us to do so. If you believe your health requires it, you should ask for “fast” appeal.

2022 Evidence of Coverage for Navitus MedicareRx (PDP) 119 Chapter 7. What to do if you have a problem or complaint
(coverage decisions, appeals, complaints)
o If we do not give you a decision within 7 calendar days, we are required to send your request on to Level 2 of the appeals process, where it will be reviewed by an Independent Review Organization. Later in this section, we talk about this review organization and explain what happens at Level 2 of the appeals process.
• If our answer is yes to part or all of what you requested – o If we approve a request for coverage, we must provide the coverage we have
agreed to provide as quickly as your health requires, but no later than 7 calendar days after we receive your appeal.
o If we approve a request to pay you back for a drug you already bought, we are required to send payment to you within 30 calendar days after we receive your appeal request.
• If our answer is no to part or all of what you requested, we will send you a written statement that explains why we said no and how you can appeal our decision.
• If you are requesting that we pay you back for a drug you have already bought, we must give you our answer within 14 calendar days after we receive your request.
o If we do not give you a decision within 14 calendar days, we are required to send your request on to Level 2 of the appeals process, where it will be reviewed by an Independent Review Organization. Later in this section, we talk about this review organization and explain what happens at Appeal Level 2.
• If our answer is yes to part or all of what you requested, we are also required to make payment to you within 30 calendar days after we receive your request.
• If our answer is no to part or all of what you requested, we will send you a written statement that explains why we said no. We will also tell you how you can appeal our decision.
Step 3: If we say no to your appeal, you decide if you want to continue with the appeals process and make another appeal.
• If we say no to your appeal, you then choose whether to accept this decision or continue by making another appeal.
• If you decide to make another appeal, it means your appeal is going on to Level 2 of the appeals process (see below).
2022 Evidence of Coverage for Navitus MedicareRx (PDP) 120 Chapter 7. What to do if you have a problem or complaint
(coverage decisions, appeals, complaints)
Section 5.6 Step-by-step: How to make a Level 2 Appeal
If we say no to your appeal, you then choose whether to accept this decision or continue by making another appeal. If you decide to go on to a Level 2 Appeal, the Independent Review Organization reviews the decision we made when we said no to your first appeal. This organization decides whether the decision we made should be changed.
Legal Terms
The formal name for the “Independent Review Organization” is the “Independent Review Entity.” It is sometimes called the “IRE.”
Step 1: To make a Level 2 Appeal, you (or your representative or your doctor or other prescriber) must contact the Independent Review Organization and ask for a review of your case.
• If we say no to your Level 1 Appeal, the written notice we send you will include instructions on how to make a Level 2 Appeal with the Independent Review Organization. These instructions will tell who can make this Level 2 Appeal, what deadlines you must follow, and how to reach the review organization.
• When you make an appeal to the Independent Review Organization, we will send the information we have about your appeal to this organization. This information is called your “case file.” You have the right to ask us for a copy of your case file.
• You have a right to give the Independent Review Organization additional information to support your appeal.
Step 2: The Independent Review Organization does a review of your appeal and gives you an answer.
• The Independent Review Organization is an independent organization that is hired by Medicare. This organization is not connected with us and it is not a government agency. This organization is a company chosen by Medicare to review our decisions about your Part D benefits with us.
• Reviewers at the Independent Review Organization will take a careful look at all of the information related to your appeal. The organization will tell you its decision in writing and explain the reasons for it.
Deadlines for “fast appeal” at Level 2
• If your health requires it, ask the Independent Review Organization for a “fast appeal.”
• If the review organization agrees to give you a “fast appeal,” the review organization must give you an answer to your Level 2 Appeal within 72 hours after it receives your appeal request.

2022 Evidence of Coverage for Navitus MedicareRx (PDP) 121 Chapter 7. What to do if you have a problem or complaint
(coverage decisions, appeals, complaints)
• If the Independent Review Organization says yes to part or all of what you requested, we must provide the drug coverage that was approved by the review organization within 24 hours after we receive the decision from the review organization.
Deadlines for “standard appeal” at Level 2
• If you have a standard appeal at Level 2, the review organization must give you an answer to your Level 2 Appeal within 7 calendar days after it receives your appeal if it is for a drug you have not received yet. If you are requesting that we pay you back for a drug you have already bought, the review organization must give you an answer to your level 2 appeal within 14 calendar days after it receives your request.
• If the Independent Review Organization says yes to part or all of what you requested
• If the Independent Review Organization approves a request for coverage, we must provide the drug coverage that was approved by the review organization within 72 hours after we receive the decision from the review organization.
• If the Independent Review Organization approves a request to pay you back for a drug you already bought, we are required to send payment to you within 30 calendar days after we receive the decision from the review organization.
What if the review organization says no to your appeal?
If this organization says no to your appeal, it means the organization agrees with our decision not to approve your request. (This is called “upholding the decision.” It is also called “turning down your appeal.”)
If the Independent Review Organization “upholds the decision” you have the right to a Level 3 Appeal. However, to make another appeal at Level 3, the dollar value of the drug coverage you are requesting must meet a minimum amount. If the dollar value of the drug coverage you are requesting is too low, you cannot make another appeal and the decision at Level 2 is final. The notice you get from the Independent Review Organization will tell you the dollar value that must be in dispute to continue with the appeals process.
Step 3: If the dollar value of the coverage you are requesting meets the requirement, you choose whether you want to take your appeal further.
• There are three additional levels in the appeals process after Level 2 (for a total of five levels of appeal).
• If your Level 2 Appeal is turned down and you meet the requirements to continue with the appeals process, you must decide whether you want to go on to Level 3 and make a third appeal. If you decide to make a third appeal, the details on how to do this are in the written notice you got after your second appeal.
• The Level 3 Appeal is handled by an Administrative Law Judge or attorney adjudicator. Section 6 in this chapter tells more about Levels 3, 4, and 5 of the appeals process.
2022 Evidence of Coverage for Navitus MedicareRx (PDP) 122 Chapter 7. What to do if you have a problem or complaint
(coverage decisions, appeals, complaints)
SECTION 6 Taking your appeal to Level 3 and beyond
Section 6.1 Appeal Levels 3, 4 and 5 for Part D Drug Requests
This section may be appropriate for you if you have made a Level 1 Appeal and a Level 2 Appeal, and both of your appeals have been turned down.
If the value of the drug you have appealed meets a certain dollar amount, you may be able to go on to additional levels of appeal. If the dollar amount is less, you cannot appeal any further. The written response you receive to your Level 2 Appeal will explain who to contact and what to do to ask for a Level 3 Appeal.
For most situations that involve appeals, the last three levels of appeal work in much the same way. Here is who handles the review of your appeal at each of these levels.
Level 3 Appeal A judge (called an Administrative Law Judge) or an attorney adjudicator who works for the Federal government will review your appeal and give you an answer.
• If the answer is yes, the appeals process is over. What you asked for in the appeal has been approved. We must authorize or provide the drug coverage that was approved by the Administrative Law Judge or attorney adjudicator within 72 hours (24 hours for expedited appeals) or make payment no later than 30 calendar days after we receive the decision.
• If the Administrative Law Judge or attorney adjudicator says no to your appeal, the appeals process may or may not be over.
o If you decide to accept this decision that turns down your appeal, the appeals process is over.
o If you do not want to accept the decision, you can continue to the next level of the review process. If the Administrative Law Judge or attorney adjudicator says no to your appeal, the notice you get will tell you what to do next if you choose to continue with your appeal.
Level 4 Appeal The Medicare Appeals Council (Council) will review your appeal and give you an answer. The Council is part of the Federal government.
• If the answer is yes, the appeals process is over. What you asked for in the appeal has
been approved. We must authorize or provide the drug coverage that was approved by the Council within 72 hours (24 hours for expedited appeals) or make payment no later than 30 calendar days after we receive the decision.

2022 Evidence of Coverage for Navitus MedicareRx (PDP) 123 Chapter 7. What to do if you have a problem or complaint
(coverage decisions, appeals, complaints)
• If the answer is no, the appeals process may or may not be over. o If you decide to accept this decision that turns down your appeal, the appeals
process is over. o If you do not want to accept the decision, you might be able to continue to the
next level of the review process. If the Council says no to your appeal or denies your request to review the appeal, the notice you get will tell you whether the rules allow you to go on to a Level 5 Appeal. If the rules allow you to go on, the written notice will also tell you who to contact and what to do next if you choose to continue with your appeal.
Level 5 Appeal A judge at the Federal District Court will review your appeal.
• This is the last step of the appeals process.
MAKING COMPLAINTS
SECTION 7 How to make a complaint about quality of care, waiting times, customer service, or other concerns
If your problem is about decisions related to benefits, coverage, or payment, then this section is not for you. Instead, you need to use the process for coverage decisions and appeals. Go to Section 4 of this chapter.
Section 7.1 What kinds of problems are handled by the complaint process?
This section explains how to use the process for making complaints. The complaint process is used for certain types of problems only. This includes problems related to quality of care, waiting times, and the customer service you receive. Here are examples of the kinds of problems handled by the complaint process.
If you have any of these kinds of problems, you can “make a complaint”
Complaint Example
Quality of your medical care
• Are you unhappy with the quality of the care you have received?
Respecting your privacy
• Do you believe that someone did not respect your right to privacy or shared information about you that you feel should be confidential?
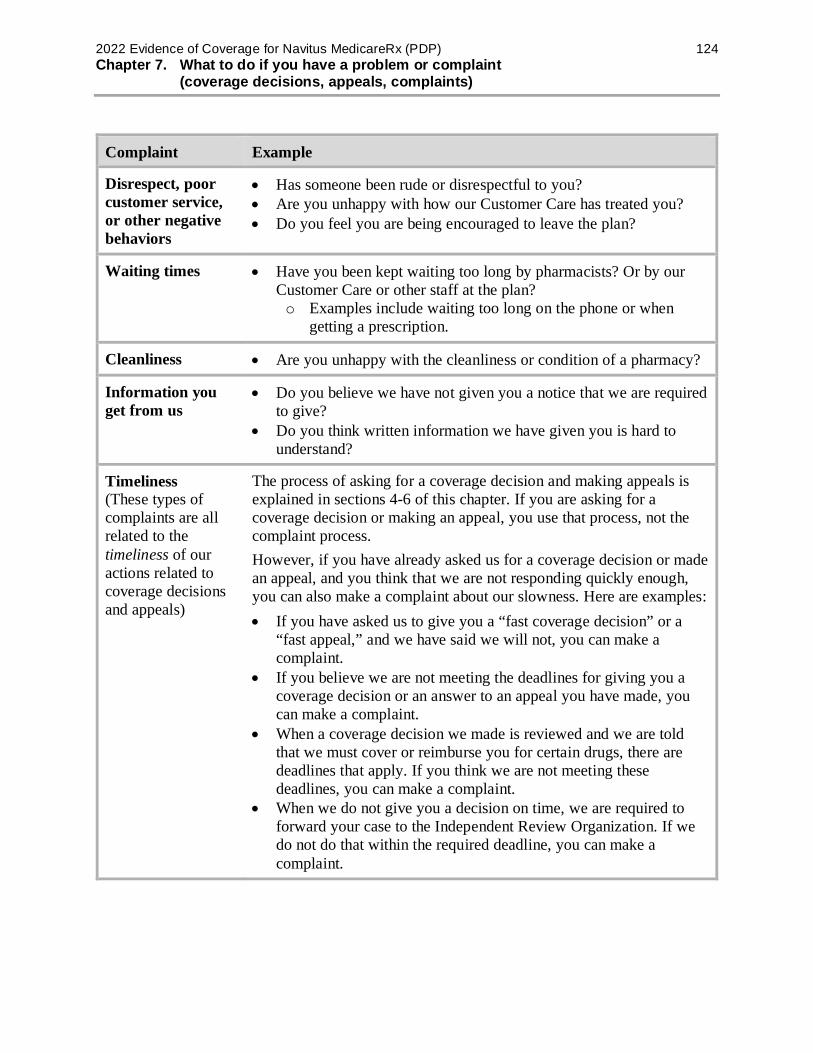
2022 Evidence of Coverage for Navitus MedicareRx (PDP) 124 Chapter 7. What to do if you have a problem or complaint
(coverage decisions, appeals, complaints)
Complaint Example
Disrespect, poor customer service, or other negative behaviors
• Has someone been rude or disrespectful to you? • Are you unhappy with how our Customer Care has treated you? • Do you feel you are being encouraged to leave the plan?
Waiting times • Have you been kept waiting too long by pharmacists? Or by our Customer Care or other staff at the plan? o Examples include waiting too long on the phone or when
getting a prescription.
Cleanliness • Are you unhappy with the cleanliness or condition of a pharmacy?
Information you get from us
• Do you believe we have not given you a notice that we are required to give?
• Do you think written information we have given you is hard to understand?
Timeliness (These types of complaints are all related to the timeliness of our actions related to coverage decisions and appeals)
The process of asking for a coverage decision and making appeals is explained in sections 4-6 of this chapter. If you are asking for a coverage decision or making an appeal, you use that process, not the complaint process. However, if you have already asked us for a coverage decision or made an appeal, and you think that we are not responding quickly enough, you can also make a complaint about our slowness. Here are examples: • If you have asked us to give you a “fast coverage decision” or a
“fast appeal,” and we have said we will not, you can make a complaint.
• If you believe we are not meeting the deadlines for giving you a coverage decision or an answer to an appeal you have made, you can make a complaint.
• When a coverage decision we made is reviewed and we are told that we must cover or reimburse you for certain drugs, there are deadlines that apply. If you think we are not meeting these deadlines, you can make a complaint.
• When we do not give you a decision on time, we are required to forward your case to the Independent Review Organization. If we do not do that within the required deadline, you can make a complaint.

2022 Evidence of Coverage for Navitus MedicareRx (PDP) 125 Chapter 7. What to do if you have a problem or complaint
(coverage decisions, appeals, complaints)
Section 7.2 The formal name for “making a complaint” is “filing a grievance”
Legal Terms
• What this section calls a “complaint” is also called a “grievance.”
• Another term for “making a complaint” is “filing a grievance.” Another way to say “using the process for complaints” is “using the process for filing a grievance.”
Section 7.3 Step-by-step: Making a complaint
Step 1: Contact us promptly – either by phone or in writing.
• Usually, calling Customer Care is the first step. If there is anything else you need to do, Customer Care will let you know. Please contact our Customer Care number at 1-866-270-3877. TTY users should call 711. Navitus MedicareRx Customer Care are available 24 hours a day, 7 days a week, except on Thanksgiving and Christmas Day.
• If you do not wish to call (or you called and were not satisfied), you can put your complaint in writing and send it to us. If you put your complaint in writing, we will respond to your complaint in writing.
• When a complaint is received in any department of Navitus Health Solutions, it is immediately forwarded to the Navitus MedicareRx Grievance and Appeals Department. All information related to the complaint is collected. You will be advised of the decision no later than 30 calendar days after the date the oral or written complaint is received. Navitus MedicareRx may extend the 30-calendar day timeframe by up to an additional 14 calendar days. Extensions may be given if you request the extension, or if the Grievance and Appeals Department justifies a need for more information. We must inform you of the status of the grievance within 30 days of receipt of the complaint.
o You may file for a faster response time when sending an expedited complaint. This request may be filed either verbally or in writing. The same procedures apply for documentation as with standard complaints. However, the Grievance and Appeals Department must notify the member of the decision within 24 hours of receipt of the complaint. The decision is usually presented verbally to the member. Navitus MedicareRx then sends written notice of the decision within three (3) calendar days of the oral notification.
• Whether you call or write, you should contact Customer Care right away (phone numbers are printed on the back cover of this booklet). The complaint must be made within 60 calendar days after you had the problem you want to complain about.
2022 Evidence of Coverage for Navitus MedicareRx (PDP) 126 Chapter 7. What to do if you have a problem or complaint
(coverage decisions, appeals, complaints)
• If you are making a complaint because we denied your request for a “fast coverage decision” or a “fast appeal,” we will automatically give you a “fast” complaint. If you have a “fast” complaint, it means we will give you an answer within 24 hours.
Legal Terms
What this section calls a “fast complaint” is also called an “expedited grievance.”
Step 2: We look into your complaint and give you our answer.
• If possible, we will answer you right away. If you call us with a complaint, we may be able to give you an answer on the same phone call. If your health condition requires us to answer quickly, we will do that.
• Most complaints are answered within 30 calendar days. If we need more information and the delay is in your best interest or if you ask for more time, we can take up to 14 more calendar days (44 calendar days total) to answer your complaint. If we decide to take extra days, we will tell you in writing.
• If we do not agree with some or all of your complaint or don’t take responsibility for the problem you are complaining about, we will let you know. Our response will include our reasons for this answer. We must respond whether we agree with the complaint or not.
Section 7.4 You can also make complaints about quality of care to the Quality Improvement Organization
You can make your complaint about the quality of care you received by using the step-by-step process outlined above.
When your complaint is about quality of care, you also have two extra options:
• You can make your complaint to the Quality Improvement Organization. If you prefer, you can make your complaint about the quality of care you received directly to this organization (without making the complaint to us).
o The Quality Improvement Organization is a group of practicing doctors and other health care experts paid by the Federal government to check and improve the care given to Medicare patients.
o You will find the name, address, and phone number of the Quality Improvement Organization for your state in Exhibit B (located in the back of this booklet). If you make a complaint to this organization, we will work with them to resolve your complaint.
• Or you can make your complaint to both at the same time. If you wish, you can make your complaint about quality of care to us and also to the Quality Improvement Organization.

2022 Evidence of Coverage for Navitus MedicareRx (PDP) 127 Chapter 7. What to do if you have a problem or complaint
(coverage decisions, appeals, complaints)
Section 7.5 You can also tell Medicare about your complaint
You can submit a complaint about Navitus MedicareRx directly to Medicare. To submit a complaint to Medicare, go to www.medicare.gov/MedicareComplaintForm/home.aspx. Medicare takes your complaints seriously and will use this information to help improve the quality of the Medicare program.
If you have any other feedback or concerns, or if you feel the plan is not addressing your issue, please call 1-800-MEDICARE (1-800-633-4227). TTY/TDD users can call 1-877-486-2048.

CHAPTER 8 Ending your membership in the plan
2022 Evidence of Coverage for Navitus MedicareRx (PDP) 129 Chapter 8. Ending your membership in the plan
Chapter 8. Ending your membership in the plan
SECTION 1 Introduction.......................................................................................... 130
Section 1.1 This chapter focuses on ending your membership in our plan ................... 130
SECTION 2 When can you end your membership in our plan? ....................... 130
Section 2.1 You can end your membership during the Annual Enrollment Period ....... 130
Section 2.2 In certain situations, you can end your membership during a Special Enrollment Period ................................................................................... 132
Section 2.3 Where can you get more information about when you can end your membership? ........................................................................................... 133
SECTION 3 How do you end your membership in our plan? ........................... 134
Section 3.1 Usually, you end your membership by enrolling in another plan ............... 134
SECTION 4 Until your membership ends, you must keep getting your drugs through our plan ...................................................................... 136
Section 4.1 Until your membership ends, you are still a member of our plan ............... 136
SECTION 5 Navitus MedicareRx must end your membership in the plan in certain situations ............................................................................ 136
Section 5.1 When must we end your membership in the plan? .................................... 136
Section 5.2 We cannot ask you to leave our plan for any reason related to your health 137
Section 5.3 You have the right to make a complaint if we end your membership in our plan ................................................................................................... 138
2022 Evidence of Coverage for Navitus MedicareRx (PDP) 130 Chapter 8. Ending your membership in the plan
SECTION 1 Introduction
Section 1.1 This chapter focuses on ending your membership in our plan
Ending your membership in Navitus MedicareRx may be voluntary (your own choice) or involuntary (not your own choice):
• You might leave our plan because you have decided that you want to leave. o There are only certain times during the year, or certain situations, when you may
voluntarily end your membership in the plan. Section 2 tells you when you can end your membership in the plan.
o The process for voluntarily ending your membership varies depending on what type of new coverage you are choosing. Section 3 tells you how to end your membership in each situation.
• There are also limited situations where you do not choose to leave, but we are required to end your membership. Section 5 tells you about situations when we must end your membership.
If you are leaving our plan, you must continue to get your Part D prescription drugs through our plan until your membership ends.
SECTION 2 When can you end your membership in our plan?
You may end your membership in our plan anytime during the year. Ending your group sponsored Medicare Part D plan may impact your eligibility for other coverage sponsored by your group. You may not be able to re-enroll in your plan in the future. If you end your group Medicare Part D coverage, your Navitus MedicareRx coverage will end on the same date. Before ending your group sponsored Medicare Part D coverage, please contact your group sponsor.
Note: If you disenroll from Medicare prescription drug coverage and go without creditable prescription drug coverage for 63 days or more in a row, you may need to pay a late penalty if you join a Medicare drug plan later. “Creditable” coverage means the coverage is expected to pay, on average, at least as much as Medicare’s standard prescription drug coverage. See Chapter 1, Section 5 for more information about the late enrollment penalty.
Section 2.1 You can end your membership during the Annual Enrollment Period
You can end your membership and enroll in a different plan during the Annual Enrollment Period (also known as the “Annual Open Enrollment Period”). This is the time when you should review your health and drug coverage and make a decision about your coverage for the upcoming year.

2022 Evidence of Coverage for Navitus MedicareRx (PDP) 131 Chapter 8. Ending your membership in the plan
• When is the Medicare Annual Enrollment Period? This happens for Medicare from October 15 to December 7. The University of California’s Open Enrollment Period is from October 28 through November 18, 2021.
• What type of plan can you switch to during the Medicare Annual Enrollment Period? You can choose to keep your current coverage or make changes to your coverage for the upcoming year. If you decide to change to a new plan, you can choose any of the following types of plans:
o Another Medicare prescription drug plan. o Original Medicare without a separate Medicare prescription drug plan.
If you receive “Extra Help” from Medicare to pay for your prescription drugs: If you do not enroll in a separate Medicare prescription drug plan, Medicare may enroll you in a drug plan, unless you have opted out of automatic enrollment.
o – or – A Medicare health plan. A Medicare health plan is a plan offered by a private company that contracts with Medicare to provide all of the Medicare Part A (Hospital) and Part B (Medical) benefits. Some Medicare health plans also include Part D prescription drug coverage. Note: Ending your group sponsored Medicare Part D plan may impact your eligibility for other coverage sponsored by your group, or mean that you will not be able to re-enroll in your plan in the future. Before ending your group sponsored Medicare Part D coverage, please contact your group sponsor. If you end your group Medicare Part D coverage, your Navitus MedicareRx coverage will end on the same date.
• If you enroll in most Medicare health plans, you will be disenrolled from Navitus MedicareRx when your new plan’s coverage begins. However, if you choose a Private Fee-for-Service plan without Part D drug coverage, a Medicare Medical Savings Account plan, or a Medicare Cost Plan, you can enroll in that new plan, however enrollment in the new plan will not end your membership in our plan. Your group benefits administrator can best explain your options, the implications of leaving this plan (such as if there would be loss of medical or dental benefits) and the process to follow to disenroll. If you do not want to keep our plan, you can choose to enroll in another Medicare prescription drug plan or drop Medicare prescription drug coverage.
Note: If you disenroll from Medicare prescription drug coverage and go without creditable prescription drug coverage for 63 or more days in a row, you may have to pay a late enrollment penalty if you join a Medicare drug plan later. (“Creditable” coverage means the coverage is expected to pay, on average, at least as much as Medicare’s standard prescription drug coverage.) See Chapter 1, Section 5 for more information about the late enrollment penalty.
• When will your membership end? Your membership will end when your new plan’s coverage begins on January 1.

2022 Evidence of Coverage for Navitus MedicareRx (PDP) 132 Chapter 8. Ending your membership in the plan
Section 2.2 In certain situations, you can end your membership during a Special Enrollment Period
In certain situations, members of Navitus MedicareRx may be eligible to end their membership at other times of the year. This is known as a Special Enrollment Period.
• Who is eligible for a Special Enrollment Period? If any of the following situations apply to you, you may be eligible to end your membership during a Special Enrollment Period. These are just examples, for the full list you can contact the plan, call Medicare, or visit the Medicare website (www.medicare.gov):
o If you have moved out of your plan’s service area. o If you have Medicaid. o If you are eligible for “Extra Help” with paying for your Medicare prescriptions. o If we violate our contract with you. o If you are getting care in an institution, such as a nursing home or long-term care
(LTC) hospital. o If you enroll in the Program of All-inclusive Care for the Elderly (PACE). PACE
is not available in all states. If you would like to know if PACE is available in your state, please contact Customer Care (phone numbers are printed on the back cover of this booklet).
o Note: If you are in a drug management program, you may not be able to change plans. Chapter 3, Section 10 tells you more about drug management programs.
• When are Special Enrollment Periods? The enrollment periods vary depending on your situation.
• What can you do? To find out if you are eligible for a Special Enrollment Period, please call Medicare at 1-800-MEDICARE (1-800-633-4227), 24 hours a day, 7 days a week. TTY/TDD users call 1-877-486-2048. If you are eligible to end your membership because of a special situation, you can choose to change both your Medicare health coverage and prescription drug coverage. This means you can choose any of the following types of plans:
o Another Medicare prescription drug plan. o Original Medicare without a separate Medicare prescription drug plan.
If you receive “Extra Help” from Medicare to pay for your prescription drugs: If you switch to Original Medicare and do not enroll in a separate Medicare prescription drug plan, Medicare may enroll you in a drug plan, unless you have opted out of automatic enrollment.
o – or – A Medicare health plan. A Medicare health plan is a plan offered by a private company that contracts with Medicare to provide all of the Medicare Part A (Hospital) and Part B (Medical) benefits. Some Medicare health plans also include Part D prescription drug coverage.
2022 Evidence of Coverage for Navitus MedicareRx (PDP) 133 Chapter 8. Ending your membership in the plan
Note: Ending your group sponsored Medicare Part D plan may impact your eligibility for other coverage sponsored by your group, or mean that you will not be able to re-enroll in your plan in the future. Before ending your group sponsored Medicare Part D coverage, please contact your group sponsor. If you end your group Medicare Part D coverage, your Navitus MedicareRx coverage will end on the same date. If you enroll in most Medicare health plans, you will automatically be
disenrolled from Navitus MedicareRx when your new plan’s coverage begins. However, if you choose a Private Fee-for-Service plan without Part D drug coverage, a Medicare Medical Savings Account plan, or a Medicare Cost Plan, you can enroll in that new plan, however enrollment in the new plan will not end your membership in our plan. Contact your group benefits administrator for information about disenrolling from this plan. Your group benefits administrator can best explain your options, the implications of leaving this plan (such as if there would be loss of medical or dental benefits) and the process to follow to disenroll. If you do not want to keep our plan, you can choose to enroll in another Medicare prescription drug plan or to drop Medicare prescription drug coverage.
Note: If you disenroll from Medicare prescription drug coverage and go without creditable prescription drug coverage for a continuous period of 63 days or more, you may have to pay a Part D late enrollment penalty if you join a Medicare drug plan later. (“Creditable” coverage means the coverage is expected to pay, on average, at least as much as Medicare’s standard prescription drug coverage.) See Chapter 1, Section 5 for more information about the late enrollment penalty.
• When will your membership end? Your membership will usually end on the first day of the month after we receive your request to change your plan.
Section 2.3 Where can you get more information about when you can end your membership?
If you have any questions or would like more information on when you can end your membership:
• You can call Customer Care (phone numbers are printed on the back cover of this booklet).
• You can find the information in the Medicare & You 2022 handbook. o Everyone with Medicare receives a copy of the Medicare & You 2022 handbook
each fall. Those new to Medicare receive it within a month after first signing up. o You can also download a copy from the Medicare website (www.medicare.gov).
Or, you can order a printed copy by calling Medicare at the number below.
• You can contact Medicare at 1-800-MEDICARE (1-800-633-4227), 24 hours a day, 7 days a week. TTY/TDD users should call 1-877-486-2048.

2022 Evidence of Coverage for Navitus MedicareRx (PDP) 134 Chapter 8. Ending your membership in the plan
SECTION 3 How do you end your membership in our plan?
Section 3.1 Usually, you end your membership by enrolling in another plan
If you are considering ending your Part D membership with Navitus MedicareRx, please first contact RASC at (800) 888-8267 (in U.S.) or (510) 987-0200 (from outside the U.S.), to talk about how this may affect your UC Medicare Supplement PPO plan coverage.
Usually, to end your membership in our plan, you simply enroll in another Medicare plan during one of the enrollment periods (see Section 2 in this chapter for information about the enrollment periods). However, there are two situations in which you will need to end your membership in a different way:
• If you want to switch from our plan to Original Medicare without a Medicare prescription drug plan, you must ask to be disenrolled from our plan.
• If you join a Private Fee-for-Service plan without prescription drug coverage, a Medicare Medical Savings Account Plan, or a Medicare Cost Plan, you can enroll in that new plan, however your enrollment in that new plan will not end your membership in our plan. Contact your group benefits administrator for information about disenrolling from this plan. Your group benefits administrator can best explain your options, the implications of leaving this plan (such as loss of medical or dental benefits) and the process to follow to disenroll. If you do not want to keep our plan, you can choose to enroll in another Medicare prescription drug plan or ask to be disenrolled from our plan.
If you are in one of these two situations and want to leave our plan, there are two ways you can ask to be disenrolled:
• You can make a request in writing to us. Contact Customer Care if you need more information on how to do this (phone numbers are printed on the back cover of this booklet).
• --or--You can contact Medicare at 1-800-MEDICARE (1-800-633-4227), 24 hours a day, 7 days a week. TTY/TDD users should call 1-877-486-2048.
Ending your group sponsored Medicare Part D plan may impact your eligibility for other coverage sponsored by your group, or mean that you will not be able to re-enroll in your plan in the future. Before ending your group sponsored Medicare Part D coverage, please contact your group sponsor. If you end your group Medicare Part D coverage, your Navitus MedicareRx coverage will end on the same date.
Note: If you disenroll from Medicare prescription drug coverage and go without creditable prescription drug coverage for 63 days or more in a row, you may have to pay a Part D late enrollment penalty if you join a Medicare drug plan later. (“Creditable” coverage means the

2022 Evidence of Coverage for Navitus MedicareRx (PDP) 135 Chapter 8. Ending your membership in the plan
coverage is expected to pay, on average, at least as much as Medicare’s standard prescription drug coverage.) See Chapter 1, Section 5 for more information about the late enrollment penalty.
The table below explains how you should end your membership in our plan.
If you would like to switch from our plan to: This is what you should do:
• Another Medicare prescription drug plan.
• Enroll in the new Medicare prescription drug plan between October 15 and December 7. You will automatically be disenrolled from Navitus MedicareRx when your new plan’s coverage begins.
• A Medicare health plan. • Enroll in the Medicare health plan by December 7. With most Medicare health plans, you will automatically be disenrolled from Navitus MedicareRx when your new plan’s coverage begins. However, if you choose a Private Fee-For-Service plan without Part D drug coverage, a Medicare Medical Savings Account plan, or a Medicare Cost Plan, you can enroll in that new plan, however enrollment in the new plan will not end your membership in our plan. Contact your group benefits administrator for information about dis-enrolling from this plan. Your group benefits administrator can best explain your options, the implications of leaving this plan (such as if there would be loss of medical or dental benefits) and the process to follow to dis-enroll. If you want to leave our plan, you must either enroll in another Medicare prescription drug plan or ask to be disenrolled. To ask to be disenrolled, you must send us a written request (contact Customer Care (phone numbers are printed on the back cover of this booklet) if you need more information on how to do this) or contact Medicare at 1-800-MEDICARE (1-800-633-4227), 24 hours a day, 7 days a week (TTY/TDD users should call 1-877-486-2048).
2022 Evidence of Coverage for Navitus MedicareRx (PDP) 136 Chapter 8. Ending your membership in the plan
If you would like to switch from our plan to: This is what you should do:
• Original Medicare without a separate Medicare prescription drug plan.
Note: If you disenroll from a Medicare prescription drug plan and go without creditable prescription drug coverage for 63 days or more in a row, you may have to pay a late enrollment penalty if you join a Medicare drug plan later. See Chapter 1, Section 5 for more information about the late enrollment penalty.
• Send us a written request to disenroll. Contact Customer Care if you need more information on how to do this (phone numbers are printed on the back cover of this booklet).
• You can also contact Medicare at 1-800-MEDICARE (1-800-633-4227), 24 hours a day, 7 days a week, and ask to be disenrolled. TTY/TDD users should call 1-877-486-2048.
• – or – Contact your group benefits administrator.
SECTION 4 Until your membership ends, you must keep getting your drugs through our plan
Section 4.1 Until your membership ends, you are still a member of our plan
If you leave Navitus MedicareRx, it may take time before your membership ends and your new Medicare coverage goes into effect. (See Section 2 for information on when your new coverage begins.) During this time, you must continue to get your prescription drugs through our plan.
• You should continue to use our network pharmacies to get your prescriptions filled until your membership in our plan ends. Usually, your prescription drugs are only covered if they are filled at a network pharmacy including through our mail-order pharmacy services.
SECTION 5 Navitus MedicareRx must end your membership in the plan in certain situations
Section 5.1 When must we end your membership in the plan?
Navitus MedicareRx must end your membership in the plan if any of the following happen:
• If you no longer have Medicare Part A and Medicare Part B.
• If you move out of our service area.

2022 Evidence of Coverage for Navitus MedicareRx (PDP) 137 Chapter 8. Ending your membership in the plan
• If you are away from our service area for more than 12 months. o If you move or take a long trip, you need to call Customer Care to find out if the
place you are moving or traveling to is in our plan’s area. (Phone numbers for Customer Care are printed on the back cover of this booklet.)
• If you become incarcerated (go to prison).
• If you are not a United States citizen or lawfully present in the United States.
• If you lie about or withhold information about other insurance you have that provides prescription drug coverage.
• If you intentionally give us incorrect information when you are enrolling in our plan and that information affects your eligibility for our plan. (We cannot make you leave our plan for this reason unless we get permission from Medicare first.)
• If you continuously behave in a way that is disruptive and makes it difficult for us to provide care for you and other members of our plan. (We cannot make you leave our plan for this reason unless we get permission from Medicare first.)
• If you let someone else use your membership card to get prescription drugs. (We cannot make you leave our plan for this reason unless we get permission from Medicare first.)
o If we end your membership because of this reason, Medicare may have your case investigated by the Inspector General.
• If plan premiums are not paid. o We must notify you in writing that you have 3 months to pay the plan premium
before we end your membership. • If you are required to pay the extra Part D amount because of your income and you do not
pay it, Medicare will disenroll you from our plan and you will lose prescription drug coverage.
Where can you get more information?
If you have questions or would like more information on when we can end your membership:
• You can call Customer Care for more information (phone numbers are printed on the back cover of this booklet).
Section 5.2 We cannot ask you to leave our plan for any reason related to your health
Navitus MedicareRx is not allowed to ask you to leave our plan for any reason related to your health.

2022 Evidence of Coverage for Navitus MedicareRx (PDP) 138 Chapter 8. Ending your membership in the plan
What should you do if this happens?
If you feel that you are being asked to leave our plan because of a health-related reason, you should call Medicare at 1-800-MEDICARE (1-800-633-4227). TTY/TDD users should call 1-877-486-2048. You may call 24 hours a day, 7 days a week.
Section 5.3 You have the right to make a complaint if we end your membership in our plan
If we end your membership in our plan, we must tell you our reasons in writing for ending your membership. We must also explain how you file a grievance or can make a complaint about our decision to end your membership. You can also look in Chapter 7, Section 7 for information about how to make a complaint.

CHAPTER 9 Legal notices
2022 Evidence of Coverage for Navitus MedicareRx (PDP) 140 Chapter 9. Legal notices
Chapter 9. Legal notices
SECTION 1 Notice about governing law .............................................................. 141
SECTION 2 Notice about non-discrimination ...................................................... 141
SECTION 3 Notice about Medicare Secondary Payer subrogation rights ..... 141
2022 Evidence of Coverage for Navitus MedicareRx (PDP) 141 Chapter 9. Legal notices
SECTION 1 Notice about governing law
Many laws apply to this Evidence of Coverage and some additional provisions may apply because they are required by law. This may affect your rights and responsibilities even if the laws are not included or explained in this document. The principal law that applies to this document is Title XVIII of the Social Security Act and the regulations created under the Social Security Act by the Centers for Medicare & Medicaid Services, or CMS. In addition, other Federal laws may apply and, under certain circumstances, the laws of the state you live in.
SECTION 2 Notice about non-discrimination
Our plan must obey laws that protect you from discrimination or unfair treatment. We don’t discriminate based on race, ethnicity, national origin, color, religion, sex, gender, age, mental or physical disability, health status, claims experience, medical history, genetic information, evidence of insurability, or geographic location within the service area. All organizations that provide Medicare prescription drug plans, like our plan, must obey Federal laws against discrimination, including Title VI of the Civil Rights Act of 1964, the Rehabilitation Act of 1973, the Age Discrimination Act of 1975, the Americans with Disabilities Act, Section 1557 of the Affordable Care Act, all other laws that apply to organizations that get Federal funding, and any other laws and rules that apply for any other reason.
If you want more information or have concerns about discrimination or unfair treatment, please call the Department of Health and Human Services’ Office for Civil Rights at 1-800-368-1019 (TTY/TDD 1-800-537-7697) or your local Office for Civil Rights.
If you have a disability and need help with access to care, please call us at Customer Care (phone numbers are printed on the back cover of this booklet). If you have a complaint, such as a problem with wheelchair access, Customer Care can help.
SECTION 3 Notice about Medicare Secondary Payer subrogation rights
We have the right and responsibility to collect for covered Medicare prescription drugs for which Medicare is not the primary payer. According to CMS regulations at 42 CFR sections 422.108 and 423.462, Navitus MedicareRx (PDP), as a Medicare prescription drug plan sponsor, will exercise the same rights of recovery that the Secretary exercises under CMS regulations in subparts B through D of part 411 of 42 CFR and the rules established in this section supersede any State laws.

CHAPTER 10 Definitions of important words

2022 Evidence of Coverage for Navitus MedicareRx (PDP) 143 Chapter 10. Definitions of important words
Chapter 10. Definitions of important words
Appeal – An appeal is something you do if you disagree with our decision to deny a request for coverage of prescription drugs or payment for drugs you already received. For example, you may ask for an appeal if we don’t pay for a drug you think you should be able to receive. Chapter 7 explains appeals, including the process involved in making an appeal.
Annual Enrollment Period (Original Medicare) – A set time each fall when members can change their health or drug plans or switch to Original Medicare. The Medicare Annual Enrollment Period is from October 15 until December 7.
Brand Name Drug – A prescription drug that is manufactured and sold by the pharmaceutical company that originally researched and developed the drug. Brand name drugs have the same active-ingredient formula as the generic version of the drug. However, generic drugs are manufactured and sold by other drug manufacturers and are generally not available until after the patent on the brand name drug has expired.
Catastrophic Coverage Stage – The stage in the Part D Drug Benefit where you pay a low copayment or coinsurance for your drugs after you or other qualified parties on your behalf have spent $7,050 in covered drugs during the covered year.
Centers for Medicare & Medicaid Services (CMS) – The Federal agency that administers Medicare. Chapter 2 explains how to contact CMS.
Coinsurance – An amount you may be required to pay as your share of the cost for prescription drugs (after you pay any deductibles, if applicable). Coinsurance is usually a percentage (for example, 20%).
Complaint – The formal name for “making a complaint” is “filing a grievance.” The complaint process is used for certain types of problems only. This includes problems related to quality of care, waiting times, and the customer service you receive. See also “Grievance,” in this list of definitions.
Copayment (or “copay”) – An amount you may be required to pay as your share of the cost for a prescription drug. A copayment is a set amount, rather than a percentage. For example, you might pay $10 or $20 for a prescription drug.
Cost Sharing – Cost sharing refers to amounts that a member has to pay when drugs are received. (This is in addition to the plan’s monthly premium.) Cost sharing includes any combination of the following three types of payments: (1) any deductible amount a plan may impose before drugs are covered; (2) any fixed “copayment” amount that a plan requires when a specific drug is received; or (3) any “coinsurance” amount, a percentage of the total amount paid for a drug, that a plan requires when a specific drug is received.
Cost-Sharing Tier – Every drug on the list of covered drugs is in one of four cost-sharing tiers. In general, the higher the cost-sharing tier, the higher your cost for the drug.
2022 Evidence of Coverage for Navitus MedicareRx (PDP) 144 Chapter 10. Definitions of important words
Coverage Determination – A decision about whether a drug prescribed for you is covered by the plan and the amount, if any, you are required to pay for the prescription. In general, if you bring your prescription to a pharmacy and the pharmacy tells you the prescription isn’t covered under your plan, that isn’t a coverage determination. You need to call or write to your plan to ask for a formal decision about the coverage. Coverage determinations are called “coverage decisions” in this booklet. Chapter 7 explains how to ask us for a coverage decision.
Covered Drugs – The term we use to mean all of the prescription drugs covered by our plan.
Creditable Prescription Drug Coverage – Prescription drug coverage (for example, from an employer or union) that is expected to pay, on average, at least as much as Medicare’s standard prescription drug coverage. People who have this kind of coverage when they become eligible for Medicare can generally keep that coverage without paying a penalty, if they decide to enroll in Medicare prescription drug coverage later.
Customer Care – A department within our plan responsible for answering your questions about your membership, benefits, grievances, and appeals. See Chapter 2 for information about how to contact Customer Care.
Deductible – The amount you must pay for prescriptions before our plan begins to pay (if applicable).
Disenroll or Disenrollment – The process of ending your membership in our plan. Disenrollment may be voluntary (your own choice) or involuntary (not your own choice).
Dispensing Fee – A fee charged each time a covered drug is dispensed to pay for the cost of filling a prescription. The dispensing fee covers costs such as the pharmacist’s time to prepare and package the prescription.
Emergency – A medical emergency is when you, or any other prudent layperson with an average knowledge of health and medicine, believe that you have medical symptoms that require immediate medical attention to prevent loss of life, loss of a limb, or loss of function of a limb. The medical symptoms may be an illness, injury, severe pain, or a medical condition that is quickly getting worse.
Evidence of Coverage (EOC) and Disclosure Information – This document along with any other attachments, riders, or other optional coverage selected, which explains your coverage, what we must do, your rights, and what you have to do as a member of our plan.
Exception – A type of coverage decision that, if approved, allows you to get a drug that is not on your plan sponsor’s formulary (a formulary exception), or get a non-preferred drug at a lower cost-sharing level (a tiering exception). You may also request an exception if your plan sponsor requires you to try another drug before receiving the drug you are requesting, or the plan limits the quantity or dosage of the drug you are requesting (a formulary exception).
2022 Evidence of Coverage for Navitus MedicareRx (PDP) 145 Chapter 10. Definitions of important words
Extra Covered Drugs – Certain drugs that are excluded by law from coverage by Medicare Part D, may be included in the supplemental coverage of your drug plan. Drugs covered under the “Extra Covered Drugs” benefit, will be listed in the Formulary.
Extra Help – A Medicare program to help people with limited income and resources pay Medicare prescription drug program costs, such as premiums, deductibles, and coinsurance.
Formulary – A list of covered drugs provided by your plan.
Generic Drug – A prescription drug that is approved by the Food and Drug Administration (FDA) as having the same active ingredient(s) as the brand name drug. Generally, a “generic” drug works the same as a brand name drug and usually costs less.
Grievance – A type of complaint you make about us or one of our network pharmacies, including a complaint concerning the quality of your care. This type of complaint does not involve coverage or payment disputes.
Income Related Monthly Adjustment Amount (IRMAA) – If your modified adjusted gross income as reported on your IRS tax return from 2 years ago is above a certain amount, you’ll pay the standard premium amount and an Income Related Monthly Adjustment Amount, also known as IRMAA. IRMAA is an extra charge added to your premium. Less than 5% of people with Medicare are affected, so most people will not pay a higher premium.
Initial Coverage Limit – The maximum limit of coverage under the Initial Coverage Stage.
Initial Coverage Stage – This is the stage before your total drug costs including amounts you have paid and what your plan has paid on your behalf for the year have reached $4,430.
Initial Enrollment Period – When you are first eligible for Medicare, the period of time when you can sign up for Medicare Part A and Part B. For example, if you’re eligible for Medicare when you turn 65, your Initial Enrollment Period is the 7-month period that begins 3 months before the month you turn 65, includes the month you turn 65, and ends 3 months after the month you turn 65.
List of Covered Drugs (Formulary) – A list of prescription drugs covered by the plan. The drugs on this list are selected by the plan with the help of doctors and pharmacists. The list includes both brand name and generic drugs.
Low Income Subsidy (LIS) – See “Extra Help.”
Medicaid (or Medical Assistance) – A joint Federal and state program that helps with medical costs for some people with low incomes and limited resources. Medicaid programs vary from state to state, but most health care costs are covered if you qualify for both Medicare and Medicaid. See Chapter 2, Section 6 for information about how to contact Medicaid in your state.
2022 Evidence of Coverage for Navitus MedicareRx (PDP) 146 Chapter 10. Definitions of important words
Medically Accepted Indication – A use of a drug that is either approved by the Food and Drug Administration or supported by certain reference books. See Chapter 3, Section 3 for more information about a medically accepted indication.
Medicare – The Federal health insurance program for people 65 years of age or older, some people under age 65 with certain disabilities, and people with End-Stage Renal Disease (generally those with permanent kidney failure who need dialysis or a kidney transplant). People with Medicare can get their Medicare health coverage through Original Medicare, a Medicare Cost Plan, a PACE plan, or a Medicare Advantage Plan.
Medicare Advantage (MA) Plan – Sometimes called Medicare Part C. A plan offered by a private company that contracts with Medicare to provide you with all your Medicare Part A and Part B benefits. A Medicare Advantage Plan can be an HMO, PPO, a Private Fee-for-Service (PFFS) plan, or a Medicare Medical Savings Account (MSA) plan. If you are enrolled in a Medicare Advantage Plan, Medicare services are covered through the plan, and are not paid for under Original Medicare. In most cases, Medicare Advantage Plans also offer Medicare Part D (prescription drug coverage). These plans are called Medicare Advantage Plans with Prescription Drug Coverage. Everyone who has Medicare Part A and Part B is eligible to join any Medicare Advantage health plan that is offered in their area.
Medicare Cost Plan – A Medicare Cost Plan is a plan operated by a Health Maintenance Organization (HMO) or Competitive Medical Plan (CMP) in accordance with a cost-reimbursed contract under section 1876(h) of the Act.
Medicare Coverage Gap Discount Program – A program that provides discounts on most covered Part D brand name drugs to Part D members who have reached the Coverage Gap Stage and who are not already receiving “Extra Help.” Discounts are based on agreements between the Federal government and certain drug manufacturers. For this reason, most, but not all, brand name drugs are discounted.
Medicare-Covered Services – Services covered by Medicare Part A and Part B.
Medicare Health Plan – A Medicare health plan is offered by a private company that contracts with Medicare to provide Part A and Part B benefits to people with Medicare who enroll in the plan. This term includes all Medicare Advantage Plans, Medicare Cost Plans, Demonstration/Pilot Programs, and Programs of All-inclusive Care for the Elderly (PACE).
Medicare Prescription Drug Coverage (Medicare Part D) – Insurance to help pay for outpatient prescription drugs, vaccines, biologicals, and some supplies not covered by Medicare Part A or Part B.
“Medigap” (Medicare Supplement Insurance) Policy – Medicare supplement insurance sold by private insurance companies to fill “gaps” in Original Medicare. Medigap policies only work with Original Medicare. (A Medicare Advantage Plan is not a Medigap policy.)
2022 Evidence of Coverage for Navitus MedicareRx (PDP) 147 Chapter 10. Definitions of important words
Member (Member of our Plan, or “Plan Member”) – A person with Medicare who is eligible to get covered services, who has enrolled in our plan and whose enrollment has been confirmed by the Centers for Medicare & Medicaid Services (CMS).
Network Pharmacy – A network pharmacy is a pharmacy where members of our plan can get their prescription drug benefits. We call them “network pharmacies” because they contract with our plan. In most cases, your prescriptions are covered only if they are filled at one of our network pharmacies.
Original Medicare (“Traditional Medicare” or “Fee-for-service” Medicare) – Original Medicare is offered by the government, and not a private health plan like Medicare Advantage Plans and prescription drug plans. Under Original Medicare, Medicare services are covered by paying doctors, hospitals, and other health care providers payment amounts established by Congress. You can see any doctor, hospital, or other health care provider that accepts Medicare. You must pay the deductible. Medicare pays its share of the Medicare-approved amount, and you pay your share. Original Medicare has two parts: Part A (Hospital Insurance) and Part B (Medical Insurance) and is available everywhere in the United States.
Out-of-Network Pharmacy – A pharmacy that doesn’t have a contract with our plan to coordinate or provide covered drugs to members of our plan. As explained in this Evidence of Coverage, most drugs you get from out-of-network pharmacies are not covered by our plan unless certain conditions apply.
Out-of-Pocket Costs – See the definition for “cost sharing” above. A member’s cost-sharing requirement to pay for a portion of drugs received is also referred to as the member’s “out-of-pocket” cost requirement.
PACE Plan – A PACE (Program of All-Inclusive Care for the Elderly) plan combines medical, social, and long-term care (LTC) services for frail people to help people stay independent and living in their community (instead of moving to a nursing home) as long as possible, while getting the high-quality care they need. People enrolled in PACE plans receive both their Medicare and Medicaid benefits through the plan. PACE is not available in all states. If you would like to know if PACE is available in your state, please contact Customer Care (phone numbers are printed on the back cover of this booklet).
Part C – see “Medicare Advantage (MA) Plan.”
Part D – The voluntary Medicare Prescription Drug Benefit Program. (For ease of reference, we will refer to the prescription drug benefit program as Part D.)
Part D Drugs – Drugs that can be covered under Part D. We may or may not offer all Part D drugs. (See your formulary for a specific list of covered drugs.) Certain categories of drugs were specifically excluded by Congress from being covered as Part D drugs.
Part D Late Enrollment Penalty – An amount added to your monthly premium for Medicare drug coverage if you go without creditable coverage (coverage that is expected to pay, on average, at least as much as standard Medicare prescription drug coverage) for a continuous

2022 Evidence of Coverage for Navitus MedicareRx (PDP) 148 Chapter 10. Definitions of important words
period of 63 days or more after you are first eligible to join a Part D plan. You pay this higher amount as long as you have a Medicare drug plan. There are some exceptions. For example, if you receive “Extra Help” from Medicare to pay your prescription drug plan costs, the late enrollment penalty rules do not apply to you. If you receive “Extra Help,” you do not pay a late enrollment penalty.
Premium – The periodic payment to Medicare, an insurance company, or a health care plan for health or prescription drug coverage.
Prior Authorization – Approval in advance to get certain drugs that may or may not be on our formulary. Some drugs are covered only if your doctor or other network prescriber gets “prior authorization” from us. Covered drugs that need prior authorization are marked in the formulary.
Quality Improvement Organization (QIO) – A group of practicing doctors and other health care experts paid by the Federal government to check and improve the care given to Medicare patients. See Chapter 2, Section 4 for information about how to contact the QIO for your state.
Quantity Limits – A management tool that is designed to limit the use of selected drugs for quality, safety, or utilization reasons. Limits may be on the amount of the drug that we cover per prescription or for a defined period of time.
Select Generics - A specific list of generic drugs that have been on the market long enough to have a proven track record for effectiveness and value. Your plan has reduced copayments for “Select Generics”.
Service Area – A geographic area where a prescription drug plan accepts members if it limits membership based on where people live. The plan may disenroll you if you permanently move out of the plan’s service area.
Specialty Drugs - The Centers for Medicare & Medicaid Services (CMS) defines specialty drugs as any drug that costs $830 or more per unit.
Special Enrollment Period – A set time when members can change their health or drug plans or return to Original Medicare. Situations in which you may be eligible for a Special Enrollment Period include: if you are getting “Extra Help” with your prescription drug costs, if you move into a nursing home, or if we violate our contract with you.
Step Therapy – A utilization tool that requires you to first try another drug to treat your medical condition before we will cover the drug your physician may have initially prescribed.
Supplemental Security Income (SSI) – A monthly benefit paid by Social Security to people with limited income and resources who are disabled, blind, or age 65 and older. SSI benefits are not the same as Social Security benefits.

2022 Evidence of Coverage for Navitus MedicareRx (PDP) 149 Exhibit A – Listing of State Health Assistance Programs (SHIPs)
Exhibit A - Listing of State Health Insurance Assistance Programs (SHIPs) SHIP is a state program that gets money from the Federal government to give free local health insurance counseling to people with Medicare. TTY numbers require special telephone equipment and are only for people who have difficulties with hearing or speaking. If there is no TTY number indicated, you may try 711.
State Agency Name/Address Contact Information Alabama State Health Insurance Assistance
Program (SHIP) 201 Monroe St, Ste 350 Montgomery AL 36104
Toll Free: 1-800-243-5463 Local: 1-334-242-5743
Fax: 1-334-242-5594
Website: http://www.alabamaageline.gov/ Alaska Alaska Medicare Information
Office (SHIP) 550 W. 8th Ave Anchorage AK 99501
Toll Free (within AK): 1-800-478-6065 Local (in Anchorage): 1-907-269-3680
Outside AK: Call Anchorage TTY: 1-800-770-8973
Website: http://www.medicare.alaska.gov Arizona State Health Insurance Assistance
Program (SHIP) 1789 W. Jefferson St #950A Phoenix AZ 85007
Toll Free: 1-800-432-4040 (leave message)
Local: 1-602-542-4446
Website: https://des.az.gov/services/older-adults/medicare-assistance Arkansas Senior Health Insurance Information
Program (SHIP) 1200 W. 3rd St Little Rock AR 72201-1904
Toll Free: 1-800-224-6330 Local: 1-501-371-2782 TTY: 1-501-371-2782
Website: https://insurance.arkansas.gov/pages/consumer-services/senior-health/ California California Health Insurance
Counseling and Advocacy Program (HICAP) 1300 National Dr, Ste 200 Sacramento CA 95834
Toll Free (within CA): 1-800-434-0222 Toll Free (outside CA): 1-800-677-1116
TTY: 1-800-735-2929
Website: https://www.aging.ca.gov/hicap/ Colorado State Health Insurance Assistance
Program 1560 Broadway, Ste 850 Denver CO 80202
Toll Free: 1-888-696-7213 Local: 1-303-894-7855 TTY: 1-303-894-7880
Spanish: 1-866-665-9668 Website: https://www.colorado.gov/dora/senior-healthcare-medicare
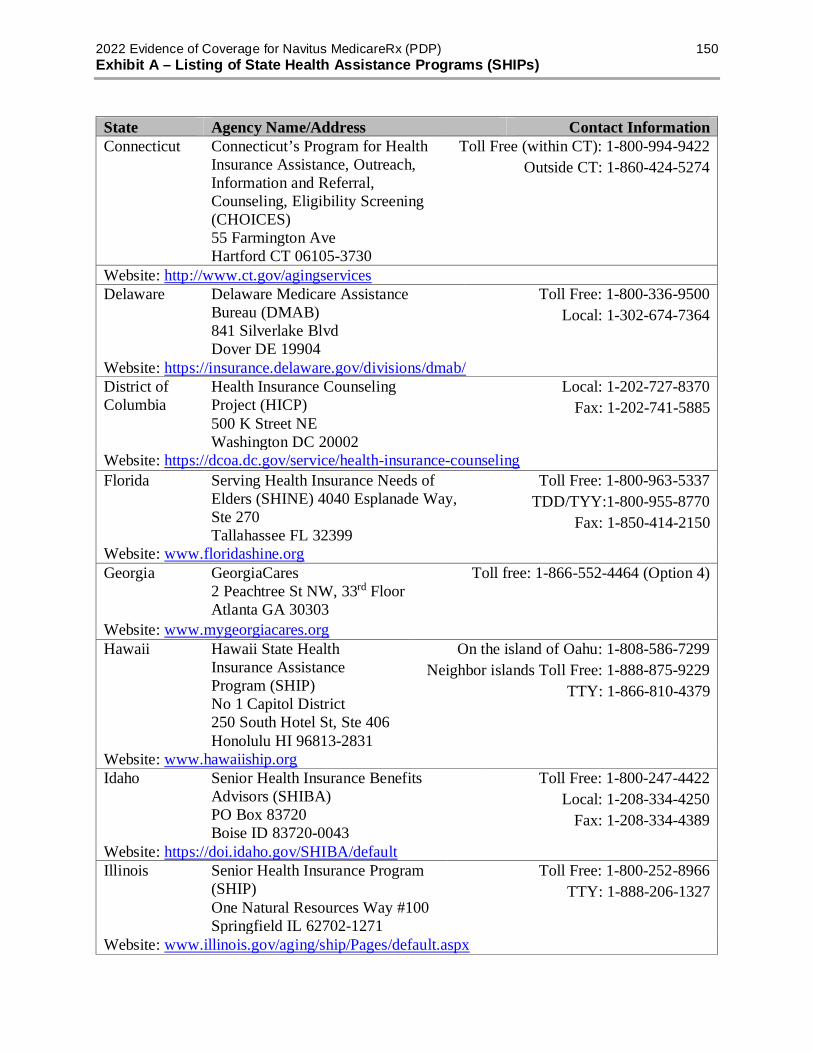
2022 Evidence of Coverage for Navitus MedicareRx (PDP) 150 Exhibit A – Listing of State Health Assistance Programs (SHIPs)
State Agency Name/Address Contact Information Connecticut Connecticut’s Program for Health
Insurance Assistance, Outreach, Information and Referral, Counseling, Eligibility Screening (CHOICES) 55 Farmington Ave Hartford CT 06105-3730
Toll Free (within CT): 1-800-994-9422 Outside CT: 1-860-424-5274
Website: http://www.ct.gov/agingservices Delaware Delaware Medicare Assistance
Bureau (DMAB) 841 Silverlake Blvd Dover DE 19904
Toll Free: 1-800-336-9500 Local: 1-302-674-7364
Website: https://insurance.delaware.gov/divisions/dmab/ District of Columbia
Health Insurance Counseling Project (HICP) 500 K Street NE Washington DC 20002
Local: 1-202-727-8370 Fax: 1-202-741-5885
Website: https://dcoa.dc.gov/service/health-insurance-counseling Florida Serving Health Insurance Needs of
Elders (SHINE) 4040 Esplanade Way, Ste 270 Tallahassee FL 32399
Toll Free: 1-800-963-5337 TDD/TYY:1-800-955-8770
Fax: 1-850-414-2150
Website: www.floridashine.org Georgia GeorgiaCares
2 Peachtree St NW, 33rd Floor Atlanta GA 30303
Toll free: 1-866-552-4464 (Option 4)
Website: www.mygeorgiacares.org Hawaii Hawaii State Health
Insurance Assistance Program (SHIP) No 1 Capitol District 250 South Hotel St, Ste 406 Honolulu HI 96813-2831
On the island of Oahu: 1-808-586-7299 Neighbor islands Toll Free: 1-888-875-9229
TTY: 1-866-810-4379
Website: www.hawaiiship.org Idaho Senior Health Insurance Benefits
Advisors (SHIBA) PO Box 83720 Boise ID 83720-0043
Toll Free: 1-800-247-4422 Local: 1-208-334-4250
Fax: 1-208-334-4389
Website: https://doi.idaho.gov/SHIBA/default Illinois Senior Health Insurance Program
(SHIP) One Natural Resources Way #100 Springfield IL 62702-1271
Toll Free: 1-800-252-8966 TTY: 1-888-206-1327
Website: www.illinois.gov/aging/ship/Pages/default.aspx

2022 Evidence of Coverage for Navitus MedicareRx (PDP) 151 Exhibit A – Listing of State Health Assistance Programs (SHIPs)
State Agency Name/Address Contact Information Indiana State Health Insurance Assistance
Program (SHIP) 311 W. Washington St, Ste 300 Indianapolis IN 46204-2787
Toll Free: 1-800-452-4800 TDD/TYY: 1-866-846-0139
Website: www.in.gov/idoi/2495.htm Iowa Senior Health Insurance Information
Program (SHIIP) 601 Locust St, 4th Floor Des Moines IA 50309-3738
Toll Free: 1-800-351-4664 TTY: 1-800-735-2942
Website: https://shiip.iowa.gov/ Kansas Senior Health Insurance
Counseling for Kansas (SHICK) 503 S. Kansas Ste 612 Topeka KS 66603
Toll Free: 1-800-860-5260 TTY: 1-800-766-3777 Fax: 1-785-296-0256
Website: https://www.kdads.ks.gov/commissions/commission-on-aging/medicare-programs/shick Kentucky State Health Insurance
Assistance Program (SHIP) 275 E. Main St 3E-E Frankfort KY 40621
Toll Free: 1-877-293-7447 (Option #2) Local (DAIL): 1-502-564-6930
(Ask for a SHIP counselor) TTY: 1-888-642-1137
Website: https://chfs.ky.gov/agencies/dail/Pages/ship.aspx Louisiana Senior Health Insurance
Information Program (SHIIP) 1702 N 3rd Baton Rouge LA 70802
Toll Free: 1-800-259-5300 Local: 1-225-342-5301
Website: www.ldi.la.gov/consumers/senior-health-shiip Maine Office of Aging and Disability
Services 41 Anthony Ave Augusta ME 04333
Toll Free: 1-800-262-2232
Website: http://www.maine.gov/dhhs/oads/community-support/ship.html Maryland Senior Health Insurance
Assistance Program (SHIP) 301 W. Preston St, Ste 1007 Baltimore MD 21201
Toll Free: 1-800-243-3425 Local: 1-410-767-1100
Website: http://www.aging.maryland.gov/Pages/StateHealthInsuranceProgram.aspx Massachusetts Serving Health Insurance Needs
of Elders (SHINE) 1 Ashburton Pl, 5th Floor Boston MA 02108
Toll Free: 1-800-243-4636 TTY: 1-877-610-0241
Website: https://www.mass.gov/health-insurance-counseling
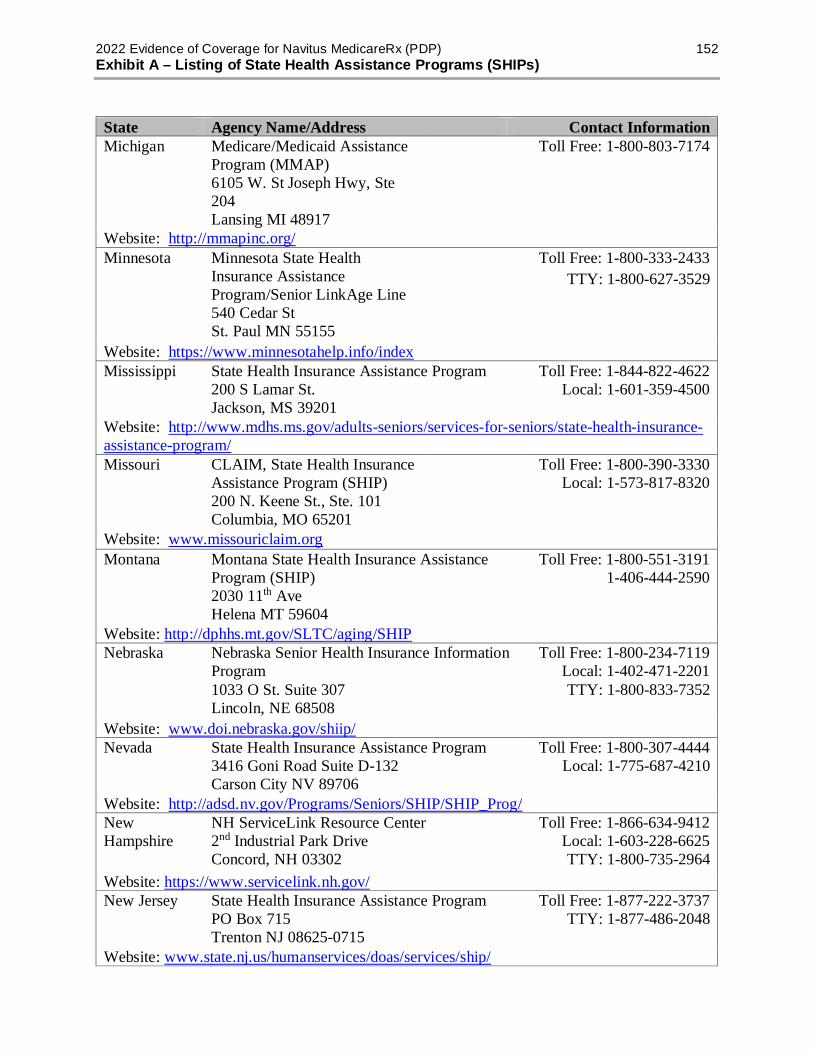
2022 Evidence of Coverage for Navitus MedicareRx (PDP) 152 Exhibit A – Listing of State Health Assistance Programs (SHIPs)
State Agency Name/Address Contact Information Michigan Medicare/Medicaid Assistance
Program (MMAP) 6105 W. St Joseph Hwy, Ste 204 Lansing MI 48917
Toll Free: 1-800-803-7174
Website: http://mmapinc.org/ Minnesota Minnesota State Health
Insurance Assistance Program/Senior LinkAge Line 540 Cedar St St. Paul MN 55155
Toll Free: 1-800-333-2433 TTY: 1-800-627-3529
Website: https://www.minnesotahelp.info/index Mississippi State Health Insurance Assistance Program
200 S Lamar St. Jackson, MS 39201
Toll Free: 1-844-822-4622 Local: 1-601-359-4500
Website: http://www.mdhs.ms.gov/adults-seniors/services-for-seniors/state-health-insurance-assistance-program/ Missouri CLAIM, State Health Insurance
Assistance Program (SHIP) 200 N. Keene St., Ste. 101 Columbia, MO 65201
Toll Free: 1-800-390-3330 Local: 1-573-817-8320
Website: www.missouriclaim.org Montana Montana State Health Insurance Assistance
Program (SHIP) 2030 11th Ave Helena MT 59604
Toll Free: 1-800-551-3191 1-406-444-2590
Website: http://dphhs.mt.gov/SLTC/aging/SHIP Nebraska Nebraska Senior Health Insurance Information
Program 1033 O St. Suite 307 Lincoln, NE 68508
Toll Free: 1-800-234-7119 Local: 1-402-471-2201 TTY: 1-800-833-7352
Website: www.doi.nebraska.gov/shiip/ Nevada State Health Insurance Assistance Program
3416 Goni Road Suite D-132 Carson City NV 89706
Toll Free: 1-800-307-4444 Local: 1-775-687-4210
Website: http://adsd.nv.gov/Programs/Seniors/SHIP/SHIP_Prog/ New Hampshire
NH ServiceLink Resource Center 2nd Industrial Park Drive Concord, NH 03302
Toll Free: 1-866-634-9412 Local: 1-603-228-6625 TTY: 1-800-735-2964
Website: https://www.servicelink.nh.gov/ New Jersey State Health Insurance Assistance Program
PO Box 715 Trenton NJ 08625-0715
Toll Free: 1-877-222-3737 TTY: 1-877-486-2048
Website: www.state.nj.us/humanservices/doas/services/ship/
http://www.mdhs.ms.gov/adults-seniors/services-for-seniors/state-health-insurance-assistance-program

2022 Evidence of Coverage for Navitus MedicareRx (PDP) 153 Exhibit A – Listing of State Health Assistance Programs (SHIPs)
State Agency Name/Address Contact Information New Mexico New Mexico ADRC
2550 Cerrillos Rd Santa Fe NM 87505
Toll Free: 1-800-432-2080 Local: 1-505-476-4799 TTY: 1-505-476-4937
Website: http://www.nmaging.state.nm.us/ New York Health Insurance Information Counseling and
Assistance Program (HIICAP) 2 Empire State Plaza 4th Floor Albany NY 12223
Toll Free: 1-800-701-0501 Local: 1-800-342-9871
Website: www.aging.ny.gov/HealthBenefits/Index.cfm North Carolina
Seniors’ Health Insurance Information Program 325 N Salisbury St Raleigh, NC 27603
Toll Free: 1-855-408-1212 Local: 1-919-807-6900 TTY: 1-800-735-2962
Website: www.ncdoi.com/SHIIP/Default.aspx North Dakota State Health Insurance Counseling Program
600 E Boulevard Ave Bismarck, ND 58505
Toll Free: 1-888-575-6611 Local: 1-701-328-2440 TTY: 1-800-366-6888
Website: www.nd.gov/ndins/shic Ohio Ohio Senior Health Insurance Information
Program 50 W. Town St 3rd Floor, Ste 300 Columbus OH 43215
Toll Free:1-800-686-1578 Local: 1-614-644-2658 TTY: 1-614-644-3745
Website: http://www.insurance.ohio.gov/Pages/default.aspx Oklahoma Medicare Assistance Program
5 Corporate Plaza 3625 NW 56th St, Ste 100 Oklahoma City, OK 73112
Toll Free: 1-800-763-2828 Local: 1-405-521-2828
Website: www.ok.gov/oid/Consumers/Information_for_Seniors/SHIP.html Oregon Senior Health Insurance Benefits Assistance
(SHIBA) 350 Winter St NE Salem OR 97309-2555
Toll Free: 1-800-722-4134 TTY: 1-800-735-2900
Website: https://healthcare.oregon.gov/shiba/pages/index.aspx Pennsylvania APPRISE Pennsylvania State Health
Assistance Program 600 S Wycombe Ave, Yeadon, PA 19050
Toll Free: 1-800-783-7067 Local: 1-484-494-3769
Website: http://www.aging.pa.gov/aging-services/insurance/Pages/default.aspx Puerto Rico State Health Insurance Assistance Program
San Juan PR 00907 Toll Free: 1-877-725-4300
TTY: 1-787-919-7291 Website: http://www.oppea.pr.gov/

2022 Evidence of Coverage for Navitus MedicareRx (PDP) 154 Exhibit A – Listing of State Health Assistance Programs (SHIPs)
State Agency Name/Address Contact Information Rhode Island Senior Health Insurance Program
57 Howard Ave Louis Pasteur Bldg. 2nd Floor Cranston RI 02920
Toll Free: 1-888-884-8721 Local: 1-401-462-0510 TTY: 1-401-462-0740
Website: www.dea.ri.gov/insurance/ South Carolina
State Health Insurance Assistance Program (SHIP) 1301 Gervais St, Ste 350 Columbus SC 29201
Toll Free: 1-800-868-9095 Local: 1-803-734-9900
Website: https://aging.sc.gov/programs-and-initiatives South Dakota Senior Health Information & Insurance
Education (SHIINE) 2300 W 46th St Sioux Falls SD 57105
Toll Free: 1-800-536-8197 Local: 1-605-333-3314
Website: www.shiine.net
Tennessee State Health Insurance Assistance Program 502 Deaderick St, 9th Floor Nashville TN, 37243-0860
Toll Free: 1-877-801-0044 Local: 1-615-741-2056 TTY: 1-615-532-3893
Website: http://tnmedicarehelp.com/ Texas Health Information Counseling and Advocacy
Program (HICAP) 701 W. 51st St Austin TX 78751
Toll Free: 1-800-252-9240 TTY: 1-800-735-2989
Website: https://hhs.texas.gov/services/health/medicare Utah Senior Health Insurance Information Program
195 N. 1950 W Salt Lake City UT 84116
Toll Free: 1-800-541-7735 Local: 1-801-538-4171
Website: https://daas.utah.gov/seniors/ Vermont State Health Insurance Assistance Program
476 Main St Ste #3 Winooski VT 05404
Toll Free: 1-800-642-5119 Local: 1-802-578-7094
Website: https://www.vermont4a.org/ Virginia Virginia Insurance Counseling and Assistance
Program (VICAP) 1610 Forest Ave, Ste 100 Henrico VA 23229
Toll Free: 1-800-552-3402 Local: 1-804-662-9333
Website: www.vda.virginia.gov/vicap.asp Washington Statewide Health Insurance Benefits Advisors
(SHIBA) PO Box 40255 Olympia WA 98504-0255
Toll Free: 1-800-562-6900 TDD: 1-360-586-0241
Website: www.insurance.wa.gov/about-oic/what-we-do/advocate-for-consumers/shiba/
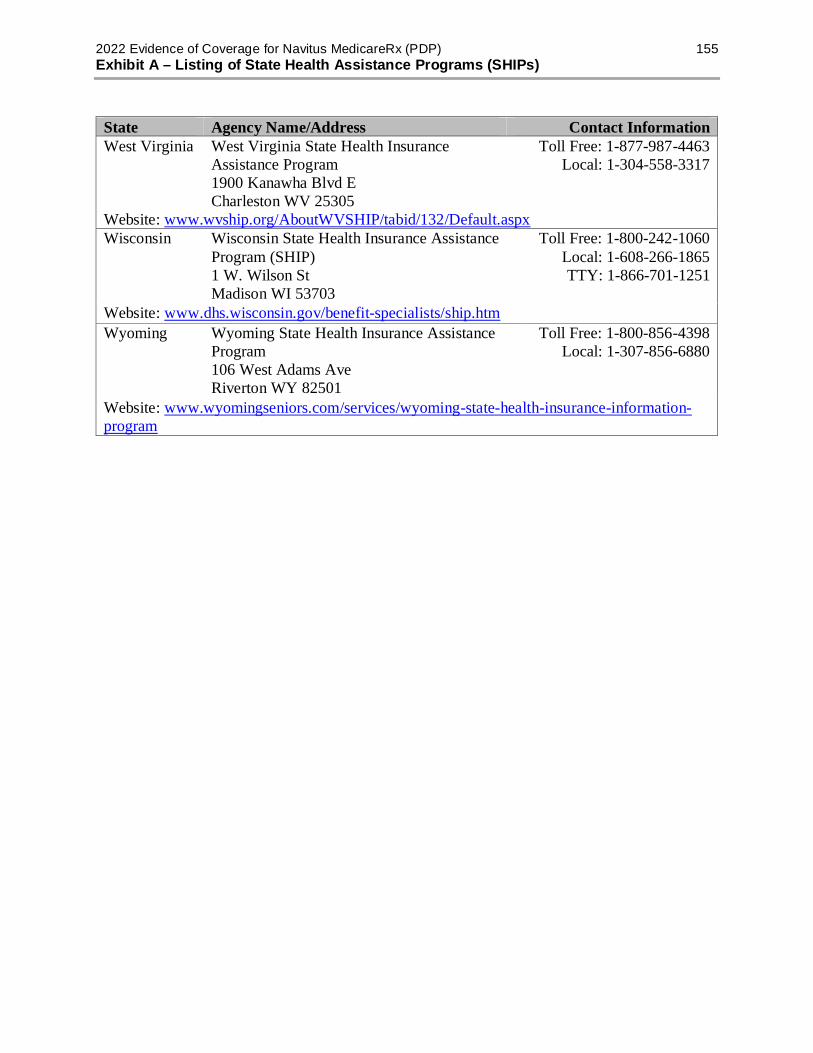
2022 Evidence of Coverage for Navitus MedicareRx (PDP) 155 Exhibit A – Listing of State Health Assistance Programs (SHIPs)
State Agency Name/Address Contact Information West Virginia West Virginia State Health Insurance
Assistance Program 1900 Kanawha Blvd E Charleston WV 25305
Toll Free: 1-877-987-4463 Local: 1-304-558-3317
Website: www.wvship.org/AboutWVSHIP/tabid/132/Default.aspx Wisconsin Wisconsin State Health Insurance Assistance
Program (SHIP) 1 W. Wilson St Madison WI 53703
Toll Free: 1-800-242-1060 Local: 1-608-266-1865 TTY: 1-866-701-1251
Website: www.dhs.wisconsin.gov/benefit-specialists/ship.htm Wyoming Wyoming State Health Insurance Assistance
Program 106 West Adams Ave Riverton WY 82501
Toll Free: 1-800-856-4398 Local: 1-307-856-6880
Website: www.wyomingseniors.com/services/wyoming-state-health-insurance-information-program
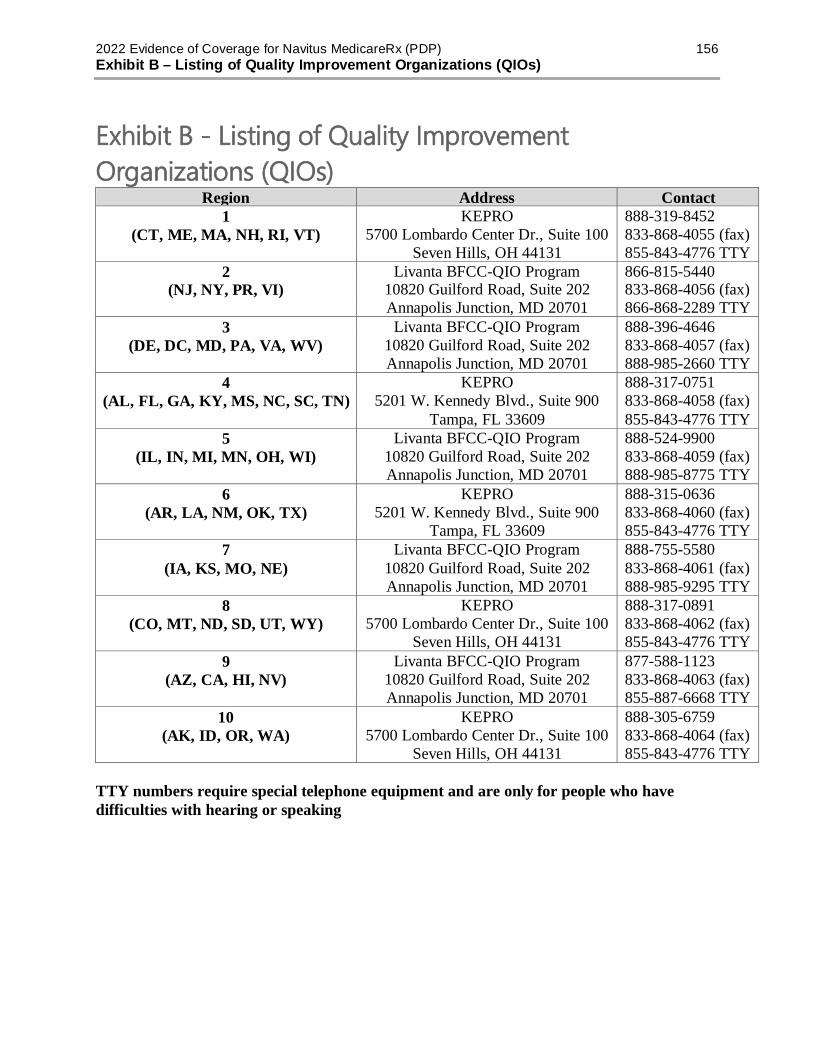
2022 Evidence of Coverage for Navitus MedicareRx (PDP) 156 Exhibit B – Listing of Quality Improvement Organizations (QIOs)
Exhibit B - Listing of Quality Improvement Organizations (QIOs)
Region Address Contact 1 KEPRO 888-319-8452
(CT, ME, MA, NH, RI, VT) 5700 Lombardo Center Dr., Suite 100 833-868-4055 (fax) Seven Hills, OH 44131 855-843-4776 TTY 2 Livanta BFCC-QIO Program 866-815-5440
(NJ, NY, PR, VI) 10820 Guilford Road, Suite 202 833-868-4056 (fax) Annapolis Junction, MD 20701 866-868-2289 TTY 3 Livanta BFCC-QIO Program 888-396-4646
(DE, DC, MD, PA, VA, WV) 10820 Guilford Road, Suite 202 833-868-4057 (fax) Annapolis Junction, MD 20701 888-985-2660 TTY 4 KEPRO 888-317-0751
(AL, FL, GA, KY, MS, NC, SC, TN) 5201 W. Kennedy Blvd., Suite 900 833-868-4058 (fax) Tampa, FL 33609 855-843-4776 TTY 5 Livanta BFCC-QIO Program 888-524-9900
(IL, IN, MI, MN, OH, WI) 10820 Guilford Road, Suite 202 833-868-4059 (fax) Annapolis Junction, MD 20701 888-985-8775 TTY 6 KEPRO 888-315-0636
(AR, LA, NM, OK, TX) 5201 W. Kennedy Blvd., Suite 900 833-868-4060 (fax) Tampa, FL 33609 855-843-4776 TTY 7 Livanta BFCC-QIO Program 888-755-5580
(IA, KS, MO, NE) 10820 Guilford Road, Suite 202 833-868-4061 (fax) Annapolis Junction, MD 20701 888-985-9295 TTY 8 KEPRO 888-317-0891
(CO, MT, ND, SD, UT, WY) 5700 Lombardo Center Dr., Suite 100 833-868-4062 (fax) Seven Hills, OH 44131 855-843-4776 TTY 9 Livanta BFCC-QIO Program 877-588-1123
(AZ, CA, HI, NV) 10820 Guilford Road, Suite 202 833-868-4063 (fax) Annapolis Junction, MD 20701 855-887-6668 TTY
10 KEPRO 888-305-6759 (AK, ID, OR, WA) 5700 Lombardo Center Dr., Suite 100 833-868-4064 (fax)
Seven Hills, OH 44131 855-843-4776 TTY TTY numbers require special telephone equipment and are only for people who have difficulties with hearing or speaking

2022 Evidence of Coverage for Navitus MedicareRx (PDP) 157 Exhibit C – Listing of State Medical Assistance Offices (Medicaid)
Exhibit C - Listing of State Medical Assistance Offices (Medicaid) STATE PROGRAM
NAME ADDRESS PHONE NUMBERS/WEBSITES
Alabama Medicaid Agency of Alabama
501 Dexter Ave PO Box 5624 Montgomery AL 36103-5624
1-800-362-1504 www.medicaid.alabama.gov
Alaska
Alaska Department of Health and Social Services
350 Main St Rm 304 PO Box 110640 Juneau AK 99811-0640
1-800-780-9972 http://dhss.alaska.gov
Arizona
Arizona Health Care Cost Containment System (AHCCCS)
801 E. Jefferson St Phoenix AZ 85034
1-855-432-7587 www.azahcccs.gov
Arkansas Arkansas Medicaid
PO Box 1437 Slot S401 Little Rock AR 72203-1437
1-800-482-8988 1-800-285-1131 x26789 (TDD) * https://medicaid.mmis.arkansas.gov
California Medi-Cal PO Box 997417
MS 4607 Sacramento CA 95899-7417
1-800-541-5555 1-916-636-1980 (outside California) www.dhca.ca.gov
Colorado Health First Colorado
1570 Grant St Denver CO 80203-1818
1-800-221-3943 TTY: 711 www.colorado.gov/hcpf
Connecticut Husky Health 55 Farmington Ave Hartford CT 06105-3730
1-877-284-8759 1-866-492-5276 (TDD/TTY) * http://www.ct.gov/hh/
Delaware Diamond State Health
1901 N. Dupont Hwy New Castle DE 19720
1-866-843-7212 1-302-571-4900 http://www.dhss.delaware.gov/dss/medicaid.html
District of Columbia
DC Medicaid 441 4th St NW 900S Washington DC 20001
1-202-727-5355 www.dc-medicaid.com
Florida Statewide Medicaid Managed Care
2727 Mahan Dr Mail Stop #8 Tallahassee FL 32308
1-877-254-1055 1-866-467-4970 (TDD) * www.fdhc.state.fl.us/Medicaid
Georgia Georgia Medicaid
2 Peachtree St NW Atlanta GA 30303
1-866-211-0950 https://dch.georgia.gov/medicaid

2022 Evidence of Coverage for Navitus MedicareRx (PDP) 158 Exhibit C – Listing of State Medical Assistance Offices (Medicaid)
STATE PROGRAM NAME ADDRESS PHONE NUMBERS/WEBSITES
Hawaii Hawaii QUEST
801 Dillingham Blvd 3rd Floor Honolulu HI 96817
Oahu: 1-808-524-3370 TTY/TDD: 1-808-692-7182* Neighbor Islands: 1-800-316-8005 TTY/TDD 1-800-603-1201 * https://medquest.hawaii.gov
Idaho Idaho Medicaid
1720 N Westgate Dr Boise ID 83704
1-877-456-1233 1-208-334-6801 (TTY) * http://www.medicaid.idaho.gov/
Illinois HFS Medical Benefits
201 S. Grand Ave E. 2nd Springfield IL 62704-0001
1-800-843-6154 1-800-447-6404 (TTY) * http://www.illinois.gov/hfs/
Indiana Hoosier Healthwise
PO Box 1810 Marion IN 46952
1-800-457-4584 https://fssabenefits.in.gov
Iowa IA Health Link 1305 E Walnut St Des Moines IA 50319
1-800-338-8366 1-800-735-2942 (TTY) * http://dhs.iowa.gov/iahealthlink
Kansas KanCare 900 SW Jackson St Ste 900N Topeka KS 66612
1-800-792-4884 www.kancare.ks.gov
Kentucky Kentucky Medicaid
275 E Main St 6W-A Frankfurt KY 40602
1-855-306-8959 https://chfs.ky.gov/
Louisiana Healthy Louisiana
PO Box 629 Baton Rouge LA 70821-0629
1-888-342-6207 1-855-526-3346 (TTY) * www.bayouhealth.com
Maine MaineCare 114 Corn Shop Ln Farmington ME 04938
1-855-797-4357 TTY: 711 * https://www.maine.gov/DHHS/oms
Maryland Maryland Medicaid
201 W Preston St Baltimore MD 21201
1-877-463-3464 1-410-767-6500 mmcp.dhmh.maryland.gov
Massachusetts MassHealth PO Box 290794 Charleston MA 02129
1-800-841-2900 1-800-497-4648 (TTY) * www.mass.gov/masshealth
Michigan Michigan Medicaid Program
333 S Grand Ave PO Box 30195 Lansing MI 48909
1-800-642-3195 1-800-649-3777 (TTY) * www.michigan.gov/medicaid
Minnesota MinnesotaCare PO Box 64838 St Paul MN 55164
1-800-657-3672 http://mn.gov/dhs
Mississippi Mississippi Medicaid
550 High St Ste 1000 Jackson MS 39201-1399
1-800-421-2408 www.medicaid.ms.gov
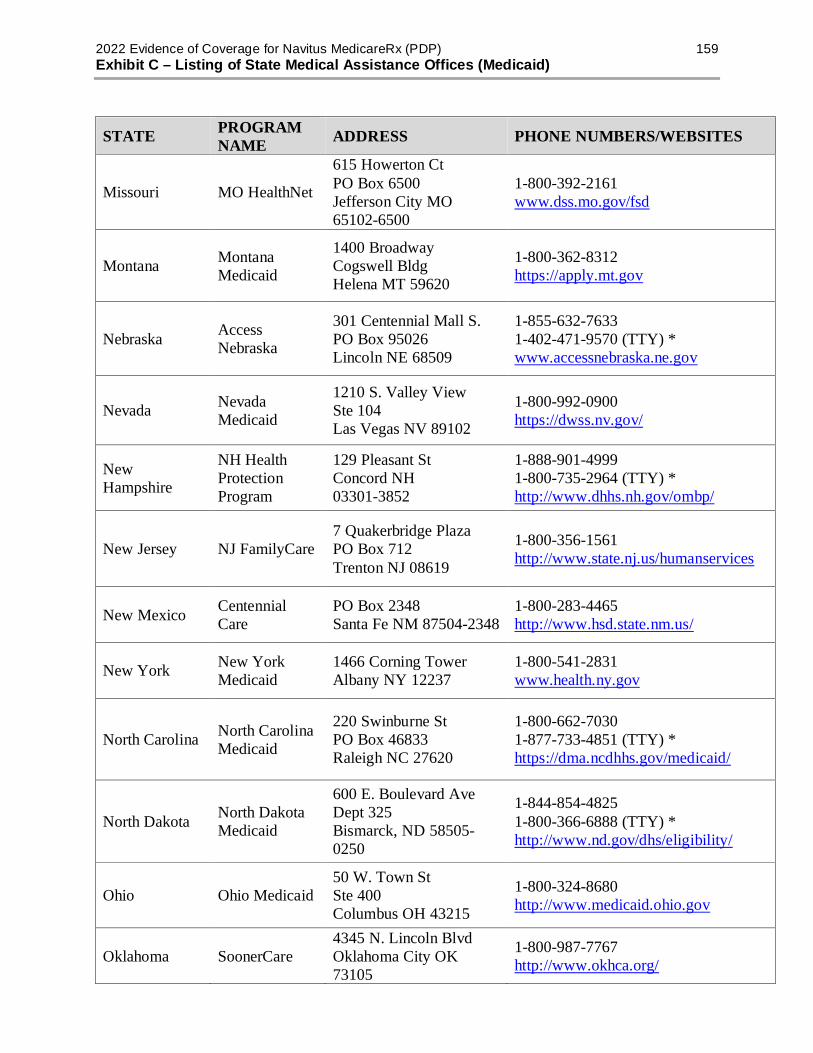
2022 Evidence of Coverage for Navitus MedicareRx (PDP) 159 Exhibit C – Listing of State Medical Assistance Offices (Medicaid)
STATE PROGRAM NAME ADDRESS PHONE NUMBERS/WEBSITES
Missouri MO HealthNet
615 Howerton Ct PO Box 6500 Jefferson City MO 65102-6500
1-800-392-2161 www.dss.mo.gov/fsd
Montana Montana Medicaid
1400 Broadway Cogswell Bldg Helena MT 59620
1-800-362-8312 https://apply.mt.gov
Nebraska Access Nebraska
301 Centennial Mall S. PO Box 95026 Lincoln NE 68509
1-855-632-7633 1-402-471-9570 (TTY) * www.accessnebraska.ne.gov
Nevada Nevada Medicaid
1210 S. Valley View Ste 104 Las Vegas NV 89102
1-800-992-0900 https://dwss.nv.gov/
New Hampshire
NH Health Protection Program
129 Pleasant St Concord NH 03301-3852
1-888-901-4999 1-800-735-2964 (TTY) * http://www.dhhs.nh.gov/ombp/
New Jersey NJ FamilyCare 7 Quakerbridge Plaza PO Box 712 Trenton NJ 08619
1-800-356-1561 http://www.state.nj.us/humanservices
New Mexico Centennial Care
PO Box 2348 Santa Fe NM 87504-2348
1-800-283-4465 http://www.hsd.state.nm.us/
New York New York Medicaid
1466 Corning Tower Albany NY 12237
1-800-541-2831 www.health.ny.gov
North Carolina North Carolina Medicaid
220 Swinburne St PO Box 46833 Raleigh NC 27620
1-800-662-7030 1-877-733-4851 (TTY) * https://dma.ncdhhs.gov/medicaid/
North Dakota North Dakota Medicaid
600 E. Boulevard Ave Dept 325 Bismarck, ND 58505-0250
1-844-854-4825 1-800-366-6888 (TTY) * http://www.nd.gov/dhs/eligibility/
Ohio Ohio Medicaid 50 W. Town St Ste 400 Columbus OH 43215
1-800-324-8680 http://www.medicaid.ohio.gov
Oklahoma SoonerCare 4345 N. Lincoln Blvd Oklahoma City OK 73105
1-800-987-7767 http://www.okhca.org/

2022 Evidence of Coverage for Navitus MedicareRx (PDP) 160 Exhibit C – Listing of State Medical Assistance Offices (Medicaid)
STATE PROGRAM NAME ADDRESS PHONE NUMBERS/WEBSITES
Oregon Oregon Health Plan
500 Summer St NE Salem OR 97301
1-800-699-9075 http://healthcare.oregon.gov/
Pennsylvania Pennsylvania Medicaid
625 Forester St Rm 515 PO Box 2675 Harrisburg PA 17105
1-800-692-7462 1-717-705-7103 (TTY) * http://www.dhs.pa.gov/citizens/healthcaremedicalassistance/
Puerto Rico Puerto Rico Medicaid
PO Box 70184 San Juan PR 00936
1-787-765-6000 www.medicaid.pr.gov
Rhode Island Rhody Health Options
57 Howard Ave Cranston RI 02920
1-800-984-8989 1-401-462-0740 (TTY) * http://www.eohhs.ri.gov/
South Carolina Healthy Connections
PO Box 100101 Columbia SC 29202
1-888-549-0820 www.scdhhs.gov
South Dakota South Dakota Medicaid
700 Governors Dr Pierre SD 57501
1-800-226-1033 http://dss.sd.gov/medicaid/
Tennessee TennCare 310 Great Circle Rd Nashville TN 37243
1-800-342-3145 1-877-779-3103 (TTY) * www.tn.gov/tenncare/
Texas Texas Medicaid
4900 N. Lamar Blvd Austin TX 78751
1-800-252-8263 1-512-424-6597 (TTY) * www.yourtexasbenefits.com
Utah Utah Medicaid 288 N. 1460 West PO Box 143106 Salt Lake City UT 84114
1-800-662-9651 https://medicaid.utah.gov/
Vermont Vermont Medicaid
103 S. Main St Waterbury VT 05671-0204
1-800-250-8427 http://dcf.vermont.gov/benefits/MABD
Virginia Virginia Medicaid
600 E. Broad St Ste 1300 Richmond VA 23219
1-804-786-7933 1-800-343-0634 (TTY) * http://www.dmas.virginia.gov/
Washington Washington Apple Health
PO Box 45502 Olympia WA 98504-5502
1-800-562-3022 1-360-586-0226 (TTY) * http://www.hca.wa.gov/Medicaid
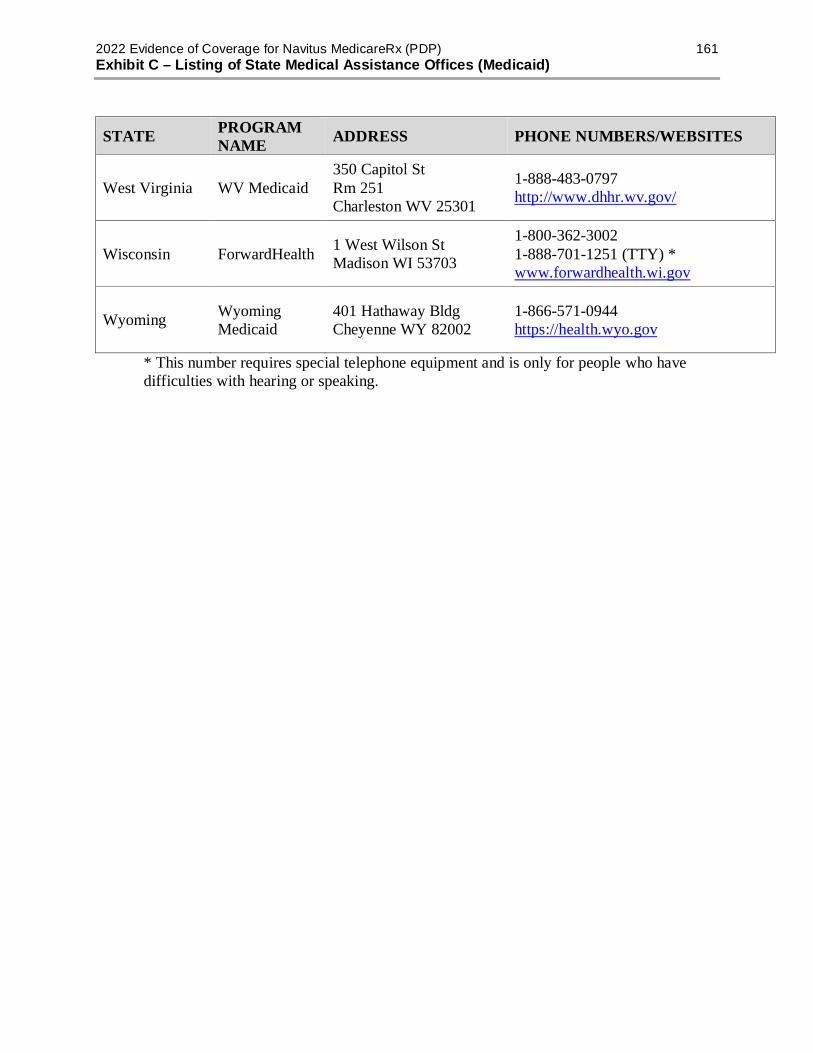
2022 Evidence of Coverage for Navitus MedicareRx (PDP) 161 Exhibit C – Listing of State Medical Assistance Offices (Medicaid)
STATE PROGRAM NAME ADDRESS PHONE NUMBERS/WEBSITES
West Virginia WV Medicaid 350 Capitol St Rm 251 Charleston WV 25301
1-888-483-0797 http://www.dhhr.wv.gov/
Wisconsin ForwardHealth 1 West Wilson St Madison WI 53703
1-800-362-3002 1-888-701-1251 (TTY) * www.forwardhealth.wi.gov
Wyoming Wyoming Medicaid
401 Hathaway Bldg Cheyenne WY 82002
1-866-571-0944 https://health.wyo.gov
*.This number requires special telephone equipment and is only for people who have difficulties with hearing or speaking.

2021 Evidence of Coverage for Navitus MedicareRx (PDP) 162 Exhibit D – Listing of State Pharmaceutal Assistance Programs (SPAPs)
Exhibit D - Listing of State Pharmaceutical Assistance Programs (SPAPs) STATE AGENCY ADDRESS PHONE NUMBERS
Colorado Colorado Bridging the Gap
Colorado Department of Public Health and Environment 4300 Cherry Creek Drive South Denver, CO 80246
1-303-692-2716
1-303-692-2783
https://www.colorado.gov
Connecticut
Connecticut Pharmaceutical Assistance Contract to the Elderly and the Disabled Program (ConnPACE)
PO Box 5011 Harford CT 06102
1-860-269-2029 (Hartford/Farmington and
out-of-state) 1-800-423-5026
(in-state only)
https://portal.ct.gov/dors
Delaware Delaware Prescription Assistance Program
PO Box 950 New Castle DE 19720 1-800-996-9969 Ext:2
https://www.dhss.delaware.gov/dhss/dmma/dpap.html
Idaho IdaGAP PO Box 83720 Boise ID 83720
1-208-334-5612
http://healthandwelfare.idaho.gov/Health/FamilyPlanningSTDHIV/HIVCareandTreatment
Indiana HoosierRx 402 W. Washington St Room W374, MS07 Indianapolis IN 46204
1-866-267-4679
https://www.payingforseniorcare.com/pharmaceutical-assistance/in-hoosierrx.html
Massachusetts Massachusetts Prescription Advantage
PO Box 15153 Worcester MA 01615 1-800-243-4636 Ext: 2
TTY (877) 610-0241 https://www.mass.gov/prescription-drug-assistance
Maryland Maryland SPAP c/o Pool Administrators 628 Hebron Ave Ste 502 Glastonbury CT 06033
1-800-551-5995 TTY/TDD 1-800-877-
5156 http://marylandspdap.com/
Maine MaineCare Services 242 State St Augusta ME 04333 1-866-796-2463
https://www.maine.gov/dhhs/oads/community-support/medicare-assistance.html
Missouri Missouri Rx Plan PO Box 6500 Jefferson City MO 65102
1-800-375-1406
https://www.payingforseniorcare.com/pharmaceutical-assistance/mo-missouri-rx-plan.html

2021 Evidence of Coverage for Navitus MedicareRx (PDP) 163 Exhibit D – Listing of State Pharmaceutal Assistance Programs (SPAPs)
STATE AGENCY ADDRESS PHONE NUMBERS
Montana Montana Big Sky Rx Program
PO Box 202915 Helena MT 59620
1-866-369-1233
https://dphhs.mt.gov/MontanaHealthcarePrograms/BigSky
North Carolina North Carolina SPAP 1902 Mail Service Center
Raleigh NC 27699 1-877-466-2232
https://epi.dph.ncdhhs.gov/cd/hiv/hmap.html
New Jersey NJ Senior Gold Prescription Discount Program
PO Box 715 Trenton NJ 08625
1-800-792-9745
https://www.state.nj.us/humanservices/doas/services/seniorgold/
Nevada Nevada Senior Rx 3416 Goni Road Ste D-132 Carson City NV 89706
1-866-303-6323 Option 2 702-486-4307
http://adsd.nv.gov/Programs/Seniors/SeniorRx/SrRxProg/
New York New York EPIC PO Box 15018 Albany NY 12212
1-800-332-3742
https://www.health.ny.gov/health_care/epic/
Pennsylvania PACE PO Box 8806 Harrisburg PA 17105 1-800-225-7223
https://www.aging.pa.gov/aging-services/prescriptions/Pages/default.aspx
Rhode Island RIPAE 74 West Rd Cranston RI 02920 1-401-462-3000
https://www.payingforseniorcare.com/pharmaceutical-assistance/ri-ripae.html
Texas Texas KHC PO Box 149347 Austin TX 78714 1-800-222-3986
https://hhs.texas.gov/services/health/kidney-health-care
Virginia Virginia SPAP 109 Governor St Richmond VA 23219 1-855-362-0658
http://www.vdh.virginia.gov/disease-prevention/virginia-aids-drug-assistance-program-adap/
Vermont VPharm 312 Hurricane Ln Ste 201 Williston VT 05495
1-800-250-8427
https://www.payingforseniorcare.com/pharmaceutical-assistance/vt-vpharm-vhap-vscript.html
Washington Washington State Health Insurance Pool
PO Box 1090 Great Bend KS 67530 1-800-877-5187
https://www.wship.org/Default.asp
Wisconsin SeniorCare PO Box 6710 Madison WI 53716 1-800-657-2038
https://www.dhs.wisconsin.gov/seniorcare/index.htm

2022 Evidence of Coverage for Navitus MedicareRx (PDP) 164 Exhibit E – Listing of State AIDS Drug Assistance Programs (ADAPs)
Exhibit E - Listing of State AIDS Drug Assistance Programs (ADAPs) STATE AGENCY ADDRESS PHONE
NUMBERS Alabama
http://www.adph.org/aids/index.asp
Alabama ADAP 201 Monroe St Ste 1400 Montgomery AL 36104
1-866-574-9964
Alaska Alaska ADAP 3601 C Street Ste 540 Anchorage AK 99503
1-907-269-8058
http://www.adph.org/aids/index.asp Arizona Arizona ADAP 150 N. 18th
Ave, Ste 110 Phoenix AZ 85007
1-800-334-1540
http://www.azdhs.gov/phs/hiv/adap/ Arkansas Arkansas ADAP 4815 W.
Markham Little Rock AR 72205
1-800-232-4636
http://www.healthy.arkansas.gov/programsServices/infectiousDisease/ California California ADAP 1616 Capitol
Ave Ste 616 Sacramento CA 95814
1-888-311-7632
http://www.cdph.ca.gov/programs/aids/Pages/toaADAPIndiv.aspx Colorado Colorado ADAP 4300 Cherry
Creek Dr South Denver CO 80246
1-303-692-2716
https://www.colorado.gov/pacific/cdphe/colorado-aids-drug-assistance-program-adap Connecticut Connecticut
ADAP 25 Sigourney St Hartford CT 06106
1-800-233-2503
http://www.ct.gov/dss/lib/dss/PDFs/CADAPapp03.pdf Delaware Delaware ADAP 540 DuPoint
Hwy Dover DE 19901
1-302-739-3032
http://www.dhss.delaware.gov/dph/dpc/hivtreatment.html
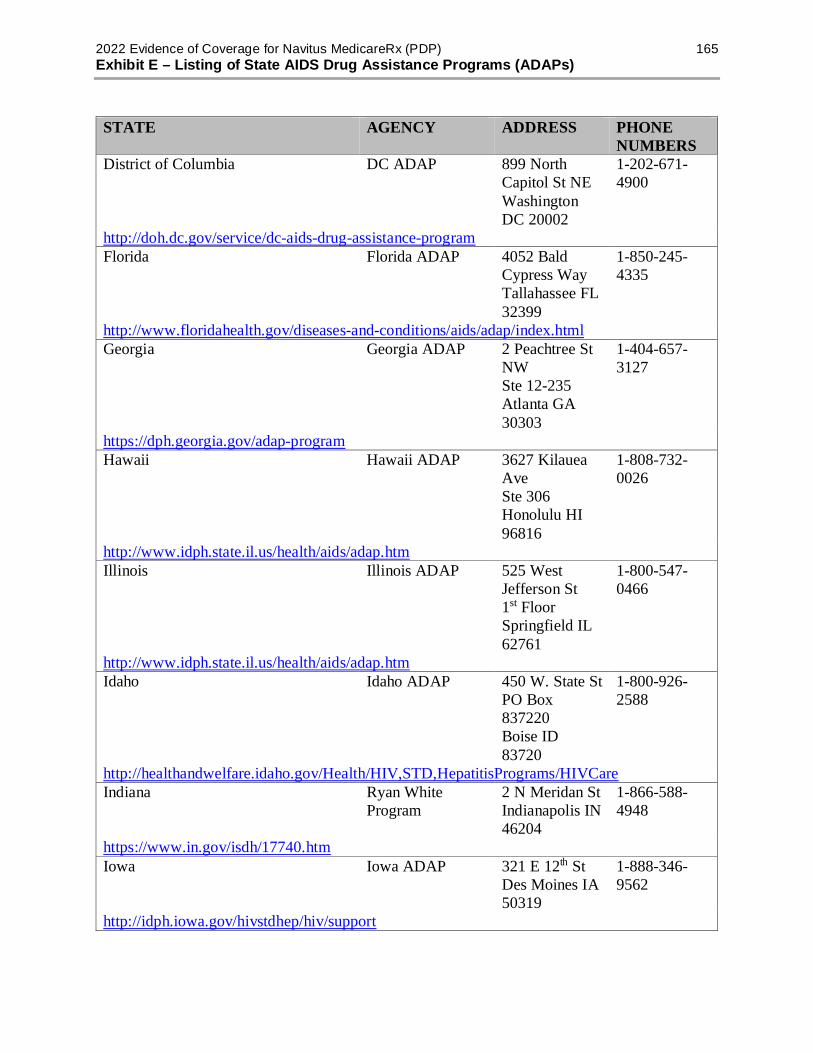
2022 Evidence of Coverage for Navitus MedicareRx (PDP) 165 Exhibit E – Listing of State AIDS Drug Assistance Programs (ADAPs)
STATE AGENCY ADDRESS PHONE NUMBERS
District of Columbia DC ADAP 899 North Capitol St NE Washington DC 20002
1-202-671-4900
http://doh.dc.gov/service/dc-aids-drug-assistance-program Florida Florida ADAP 4052 Bald
Cypress Way Tallahassee FL 32399
1-850-245-4335
http://www.floridahealth.gov/diseases-and-conditions/aids/adap/index.html Georgia Georgia ADAP 2 Peachtree St
NW Ste 12-235 Atlanta GA 30303
1-404-657-3127
https://dph.georgia.gov/adap-program Hawaii Hawaii ADAP 3627 Kilauea
Ave Ste 306 Honolulu HI 96816
1-808-732-0026
http://www.idph.state.il.us/health/aids/adap.htm Illinois Illinois ADAP 525 West
Jefferson St 1st Floor Springfield IL 62761
1-800-547-0466
http://www.idph.state.il.us/health/aids/adap.htm Idaho Idaho ADAP 450 W. State St
PO Box 837220 Boise ID 83720
1-800-926-2588
http://healthandwelfare.idaho.gov/Health/HIV,STD,HepatitisPrograms/HIVCare Indiana Ryan White
Program 2 N Meridan St Indianapolis IN 46204
1-866-588-4948
https://www.in.gov/isdh/17740.htm Iowa Iowa ADAP 321 E 12th St
Des Moines IA 50319
1-888-346-9562
http://idph.iowa.gov/hivstdhep/hiv/support

2022 Evidence of Coverage for Navitus MedicareRx (PDP) 166 Exhibit E – Listing of State AIDS Drug Assistance Programs (ADAPs)
STATE AGENCY ADDRESS PHONE NUMBERS
Kansas Kansas ADAP 1000 SW Jackson Ste 210 Topeka KS 66612
1-785-296-8701
http://www.kdheks.gov/sti_hiv/ryan_white_care.htm Kentucky Kentucky ADAP 275 E. Main St
1E-B Frankfort KY 40621
1-800-420-7431
http://chfs.ky.gov/dph/epi/hivaids/services.htm Louisiana Louisiana Health
Access Program 1450 Poydras St Ste 2136 New Orleans LA 70112
1-504-568-7474
http://new.dhh.louisiana.gov/index.cfm/page/1118 Maine Maine ADAP 221 State St
Augusta ME 04333
1-800-851-8437
http://www.maine.gov/dhhs/mecdc/infectious-disease/hiv-std/contacts/adap.shtml Maryland Maryland ADAP 201 W. Preston
St Baltimore MD 21201
1-800-205-6308
http://phpa.dhmh.maryland.gov/OIDPCS/CHCS/pages/madap.aspx Massachusetts Community
Research Initiative of New England/HDAP
38 Chauncy St Ste 500 Boston MA 02111
1-800-228-2714
http://crine.org/hdap/contact-us/ Michigan MiDAP 109 Michigan
Ave 9th Floor Lansing MI 48913
1-888-826-6565
http://www.michigan.gov/mdhhs/0,5885,7-339-71550_2955_2982---,00.html Minnesota MN ADAP PO Box 64972
St Paul MN 55164
1-800-657-3761
1-800-627-3529 (TTY) *
https://mn.gov/dhs/people-we-serve/adults/health-care/hiv-aids/
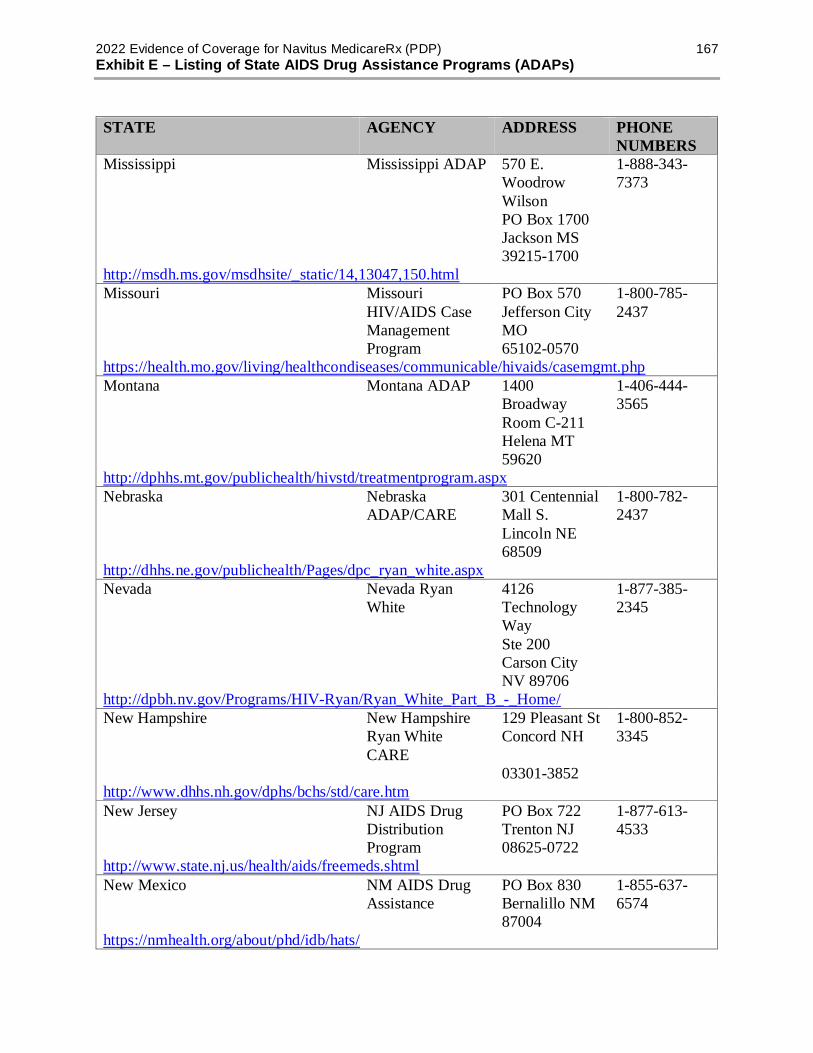
2022 Evidence of Coverage for Navitus MedicareRx (PDP) 167 Exhibit E – Listing of State AIDS Drug Assistance Programs (ADAPs)
STATE AGENCY ADDRESS PHONE NUMBERS
Mississippi Mississippi ADAP 570 E. Woodrow Wilson PO Box 1700 Jackson MS 39215-1700
1-888-343-7373
http://msdh.ms.gov/msdhsite/_static/14,13047,150.html Missouri Missouri
HIV/AIDS Case Management Program
PO Box 570 Jefferson City MO 65102-0570
1-800-785-2437
https://health.mo.gov/living/healthcondiseases/communicable/hivaids/casemgmt.php Montana Montana ADAP 1400
Broadway Room C-211 Helena MT 59620
1-406-444-3565
http://dphhs.mt.gov/publichealth/hivstd/treatmentprogram.aspx Nebraska Nebraska
ADAP/CARE 301 Centennial Mall S. Lincoln NE 68509
1-800-782-2437
http://dhhs.ne.gov/publichealth/Pages/dpc_ryan_white.aspx Nevada Nevada Ryan
White 4126 Technology Way Ste 200 Carson City NV 89706
1-877-385-2345
http://dpbh.nv.gov/Programs/HIV-Ryan/Ryan_White_Part_B_-_Home/ New Hampshire New Hampshire
Ryan White CARE
129 Pleasant St Concord NH
03301-3852
1-800-852-3345
http://www.dhhs.nh.gov/dphs/bchs/std/care.htm New Jersey NJ AIDS Drug
Distribution Program
PO Box 722 Trenton NJ 08625-0722
1-877-613-4533
http://www.state.nj.us/health/aids/freemeds.shtml New Mexico NM AIDS Drug
Assistance PO Box 830 Bernalillo NM 87004
1-855-637-6574
https://nmhealth.org/about/phd/idb/hats/

2022 Evidence of Coverage for Navitus MedicareRx (PDP) 168 Exhibit E – Listing of State AIDS Drug Assistance Programs (ADAPs)
STATE AGENCY ADDRESS PHONE NUMBERS
New York HIV Uninsured CARE
PO Box 2052 Albany NY 12220-0052
1-800-542-2437
1-518-459-0121 (TTY) *
http://www.health.ny.gov/diseases/aids/general/resources/adap/ North Carolina NC ADAP 1902 Mail
Service Center Raleigh NC 27699
1-877-466-2232
http://epi.publichealth.nc.gov/cd/hiv/adap.html North Dakota Ryan White
HIV/AIDS Program
2635 E. Main Ave Bismarck ND 58506
1-800-472-2180
https://www.ndhealth.gov/HIV/HIV%20Care/ADAP/ADAP.htm Ohio Ohio HIV Drug
Assistance Program
246 N. High St Columbus OH 43215
1-800-777-4775
https://www.odh.ohio.gov/odhprograms/hastpac/hivcare/OHDAP/drgasst1.aspx Oklahoma Oklahoma ADAP 1000 NE Tenth
Rm 614 Oklahoma City OK 73117
1-800-884-1572
https://www.ok.gov/health2/documents/HIV-HDAPbrochure14.pdf Oregon CAREassist PO Box 14450
Portland OR 97293
1-800-805-2313
https://www.oregon.gov/oha/ph/DiseasesConditions/HIVSTDViralHepatitis/HIVCareTreatment/CAREAssist Pennsylvania Special
Pharmaceutical Benefits Program
PO Box 8808 Harrisburg PA 17105-8808
1-800-922-9384
https://www.health.pa.gov/topics/programs/HIV/Pages/Special-Pharmaceutical-Benefits.aspx Puerto Rico Ryan White
Program PO Box 70184 San Juan PR 00936-8184
1-787-765-2929
http://www.salud.gov.pr/Servicios-al-Ciudadano/Pages/default.aspx Rhode Island Ryan White
Program 74 West Rd Ste 60 Cranston RI 02920
1-401-462-3294
http://www.eohhs.ri.gov/Portals/0/Uploads/Documents/ADAPEnrollmentForm.pdf

2022 Evidence of Coverage for Navitus MedicareRx (PDP) 169 Exhibit E – Listing of State AIDS Drug Assistance Programs (ADAPs)
STATE AGENCY ADDRESS PHONE NUMBERS
South Carolina SC ADAP PO Box 101106 Columbia SC 29211
1-800-856-9954
http://www.scdhec.gov/Health/DiseasesandConditions/InfectiousDiseases/HIVandSTDs/ South Dakota Ryan White
Program 615 E. 4th St Pierre SD 57501
1-800-592-1861
http://doh.sd.gov/diseases/infectious/ryanwhite/ Tennessee Ryan White
Program 425 5th Ave N. 3rd Fl Nashville TN 37243
1-800- 525-2437
http://www.tn.gov/health/topic/STD-ryanwhite
Texas Texas HIV Medication Program
PO Box 149347 MC 1873 Austin TX 78714
1-800-255-1090
https://www.dshs.texas.gov/hivstd/meds/document.shtm Utah Utah ADAP PO Box
142104 Salt Lake City UT 84114-2104
1-801-538-6197
http://health.utah.gov/epi/treatment/ Vermont VT Medication
Assistance Program
108 Cherry St Burlington VT 05402
1-802-863-7245
http://healthvermont.gov/prevent/aids/aids_index.aspx Virginia Virginia ADAP VA Dept of
Health 109 Governor St 1st Floor Richmond VA 23219
1-855-362-0658
http://166.67.66.226/epidemiology/DiseasePrevention/Programs/ADAP/ Washington Early Intervention
Program PO Box 47841 Olympia WA 98504-7841
1-877-376-9316
http://www.doh.wa.gov/portals/1/documents/pubs/430-025-EIPBrochure.pdf
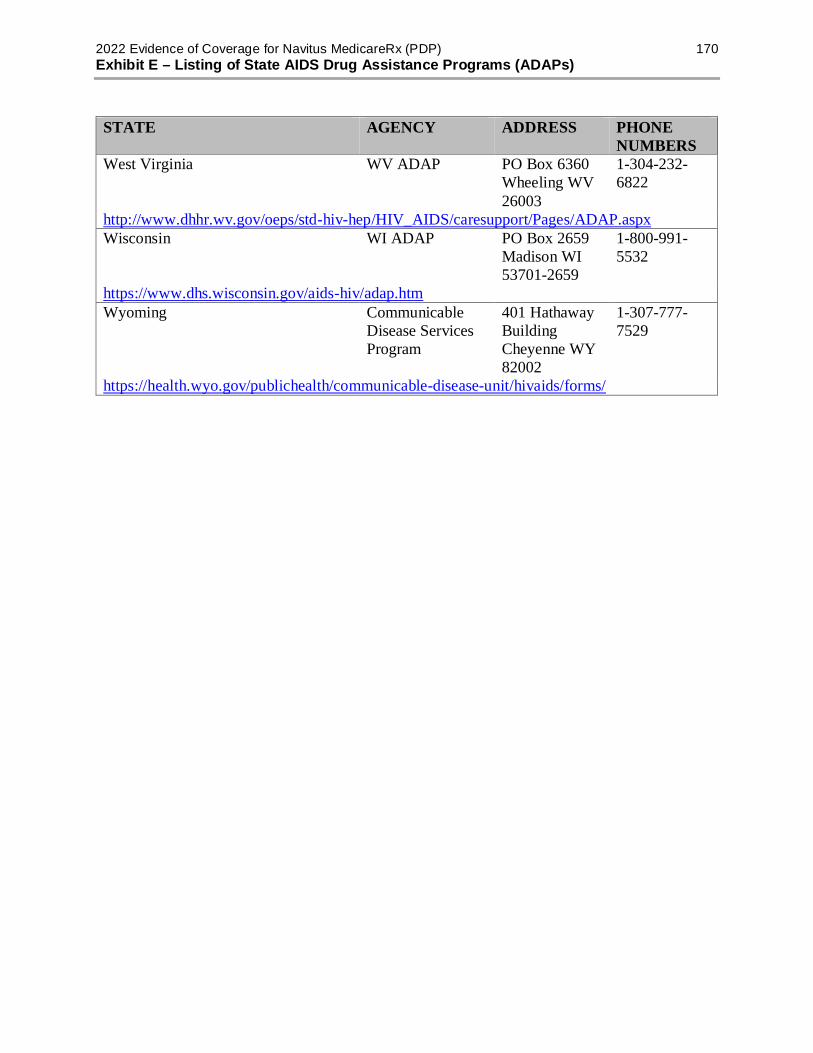
2022 Evidence of Coverage for Navitus MedicareRx (PDP) 170 Exhibit E – Listing of State AIDS Drug Assistance Programs (ADAPs)
STATE AGENCY ADDRESS PHONE NUMBERS
West Virginia WV ADAP PO Box 6360 Wheeling WV 26003
1-304-232-6822
http://www.dhhr.wv.gov/oeps/std-hiv-hep/HIV_AIDS/caresupport/Pages/ADAP.aspx Wisconsin WI ADAP PO Box 2659
Madison WI 53701-2659
1-800-991-5532
https://www.dhs.wisconsin.gov/aids-hiv/adap.htm Wyoming Communicable
Disease Services Program
401 Hathaway Building Cheyenne WY 82002
1-307-777-7529
https://health.wyo.gov/publichealth/communicable-disease-unit/hivaids/forms/

Navitus MedicareRx (PDP) Customer Care
Method Customer Care – Contact Information
CALL 1-866-270-3877 Calls to this number are free. We are available 24 hours a day, 7 days a week except on Thanksgiving and Christmas Day. Pharmacies can also reach Customer Care 24 hours a day, 7 days a week. Customer Care also has free language interpreter services available for non-English speakers.
TTY/TDD 711 This number requires special telephone equipment and is only for people who have difficulties with hearing or speaking. Calls to this number are free. We are available 24 hours a day, 7 days a week except on Thanksgiving and Christmas Day. Customer Care also has free language interpreter services available for non-English speakers.
WRITE Navitus MedicareRx (PDP) Customer Care P.O. Box 1039 Appleton, WI 54912-1039
WEBSITE https://memberportal.navitus.com
SHIP (State Health Insurance Assistance Program) is a state program that gets money from the Federal government to give free local health insurance counseling to people with Medicare. Refer to Exhibit A in this Evidence of Coverage.
PRA Disclosure Statement According to the Paperwork Reduction Act of 1995, no persons are required to respond to a collection of information unless it displays a valid OMB control number. The valid OMB control number for this information collection is 0938-1051. If you have comments or suggestions for improving this form, please write to: CMS, 7500 Security Boulevard, Attn: PRA Reports Clearance Officer, Mail Stop C4-26-05, Baltimore, Maryland 21244-1850.
S9701_2022_UCA_EOC_V01_C
S9701_2022_UCA_VACC_V01_C
Your Vaccine Coverage
Navitus MedicareRx (PDP) is committed to your health. Your prescription benefit covers
Medicare Part D vaccinations to prevent illness. Navitus covers the following common vaccines,
which are available at a $0 cost to you at a participating pharmacy. It is always recommended to
check with your prescriber to see which vaccinations are right for you.
• Shingles
• Hepatitis A and Hepatitis B (for members at low risk)
• Travel vaccines (including typhoid, yellow fever, Rabies, Japanese Encephalitis, and
Polio)
• Tetanus (for preventative use)
• Meningitis
Please note that some common vaccines are covered by your Medicare Part B benefit. These
include influenza (flu), pneumonia, COVID-19, tetanus (for injury or exposure) and hepatitis
B (for members at medium or high risk of hepatitis). Please contact your Medicare Part B
plan for more information.
How to Receive Your Part D Vaccinations
We recommend scheduling your Part D vaccinations at an in-network pharmacy. These
pharmacies can bill directly to Navitus MedicareRx for a quick, easy, no-cost appointment.
Part D vaccinations may also be covered by Medicare at your provider’s office. However, you
may have to pay additional out-of-pocket costs. You can ask us to reimburse you for our share of
the cost. To do this, submit vaccination records along with payment receipts to Navitus
MedicareRx.
Questions?
If you have questions, please call Navitus MedicareRx Customer Care. We can be reached toll-
free at 1-866-270-3877. For the hearing impaired, please call TTY at 711. Members can reach
Navitus MedicareRx Customer Care 24 hours a day, 7 days a week, except on Thanksgiving and
Christmas Day.
Our online portal can help you find an in-network pharmacy and manage your pharmacy benefit.
You can find the Member Portal at https://memberportal.navitus.com to get started.
Related Documents











