Page 1 of 3 Meeting of the CCG Governing Body to be held from 0915–1230hrs on Tuesday, 24 May 2022 In response to the challenges facing the NHS and to reduce the risk of coronavirus transmission, the meeting will be ‘live streamed’ for members of the public (a link for the live streaming will be available on the CCG website). Members of the public are invited to submit questions relating to agenda items either, prior to the meeting, via email to [email protected], or during the live streaming when they will be collated and asked at the appropriate time on the agenda. The minutes of the meeting which will include answers to any questions submitted by the public will be published on the CCG website after the meeting. AGENDA GENERAL BUSINESS 09.15 1. Apologies for Absence Dr Mark Shenton 09.17 2. Declarations of Interest and any hospitality or gifts. Declarations of interest made by members of the Governing Body are listed in the CCG’s Register of Interests which, along with the CCG’s Hospitality and Gifts Register is available on the CCG website. All 09.19 3. Minutes of the previous Ipswich and East Suffolk CCG Governing Body meeting To approve as a correct record the Minutes of the Ipswich and East Suffolk CCG Governing Body meeting held on 22 March 2022. Dr Mark Shenton 09.25 4. Matters arising and review of outstanding actions. To note and endorse how we have responded to the outstanding issues which arose at the last meeting. Dr Mark Shenton 09.30 5. General Update What has been happening in the CCG since the last meeting? To receive a verbal report. Ed Garratt STRATEGY 09.40 6. Patient Story 10.00 7. Patient and Public Involvement and Experience To receive and note a report from the Director of Nursing Lisa Nobes Report No: IESCCG 22-16

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Page 1 of 3
Meeting of the CCG Governing Body
to be held from 0915–1230hrs on Tuesday, 24 May 2022
In response to the challenges facing the NHS and to reduce the risk of coronavirus transmission, the meeting will be ‘live streamed’ for members of the public (a link for the live streaming will be available on the CCG website).
Members of the public are invited to submit questions relating to agenda items either, prior to the meeting, via email to [email protected], or during the live streaming when they will be collated and asked at the appropriate time on the agenda. The minutes of the meeting which will include answers to any questions submitted by the public will be published on the CCG website after the meeting.
AGENDA GENERAL BUSINESS
09.15 1. Apologies for Absence Dr Mark Shenton
09.17 2. Declarations of Interest and any hospitality or gifts. Declarations of interest made by members of the Governing Body are listed in the CCG’s Register of Interests which, along with the CCG’s Hospitality and Gifts Register is available on the CCG website.
All
09.19 3. Minutes of the previous Ipswich and East Suffolk CCG
Governing Body meeting To approve as a correct record the Minutes of the Ipswich and East Suffolk CCG Governing Body meeting held on 22 March 2022.
Dr Mark Shenton
09.25 4. Matters arising and review of outstanding actions.
To note and endorse how we have responded to the outstanding issues which arose at the last meeting.
Dr Mark Shenton
09.30 5. General Update What has been happening in the CCG since the last meeting? To receive a verbal report.
Ed Garratt
STRATEGY
09.40 6. Patient Story
10.00 7. Patient and Public Involvement and Experience To receive and note a report from the Director of Nursing
Lisa Nobes Report No:
IESCCG 22-16
Page 2 of 3
10.10 8. Research Strategy for Suffolk and North East Essex Integrated Care System To receive and approve a report from the Director of Nursing
Lisa Nobes Report No:
IESCCG 22-17
10.20 9. Keyworking Function To receive and approve a report from the Director of Nursing
Lisa Nobes Report No:
IESCCG 22-18
10.30 10. Procurement Update: Summary of Activity 2022 To receive and note a report from the Director of Performance Improvement
Paul Gibara Report No:
IESCCG 22-19 FINANCE, PERFORMANCE AND SCRUTINY
10.40 11. 2022-2023 Plan To receive and approve a report from the Director of Finance
Jane Payling Report No:
IESCCG 22-20
10.55 12. Integrated Performance Report To receive and note a report from Directors.
Directors Report No:
IESCCG 22-21
11.44 13. Governing Body Assurance Framework To review and approve the current Governing Body Assurance Framework
Graham Leaf Report No:
IESCCG 22-22 GOVERNANCE AND CORPORATE BUSINESS
11.55 14. Declaration of Interests To review and note a report from the Director of Corporate Services and System Infrastructure
Amanda Lyes Report No:
IESCCG 22-23
11.50 15. National Staff Survey Results 2021 To review and note a report from the Director of Corporate Services and System Infrastructure
Amanda Lyes Report No:
IESCCG 22-24
12.00 16. Health and Safety To review and note a report from the Director of Corporate Services and System Infrastructure
Amanda Lyes Report No:
IESCCG 22-25
12.15 17. Minutes of Meetings: To receive a report from the Lay Member for Governance seeking the endorsement of minutes and decisions from Ipswich and East Suffolk CCG Sub Committees.
a) Audit Committee
The unconfirmed minutes of a meeting held on 5 April 2022
b) Remuneration and HR Committee The unconfirmed minutes of a meeting held on 5 April 2022.
c) Financial Performance Committee
The minutes of meetings held on 18 January and 15 March 2022
d) Covid-19 Resource Approval Committee
The minutes from a meeting held on 16 March 2022
Graham Leaf Report No:
IESCCG 22-26
Page 3 of 3
e) Ipswich and East Suffolk CCG Primary Care Commissioning Committee The unconfirmed minutes of a meeting held on 26 April 2022
f) Commissioning Governance Committee
Decision from a virtual meeting held on 24 March 2022
g) Ipswich and East Suffolk Alliance The minutes of meetings held on 15 February 2022 and 15 March 2022.
12.10 18 Approval of the Suffolk and North East Essex ICB
Constitution To receive and endorse a decision by the CCGs Collaborative Group
Amanda Lyes Report No:
IESCCG 22-27 (To follow)
12.13 19. Date and Time of future Governing Body meetings.
No further meetings are arranged at present.
12.15 20. Questions from the public – Maximum 15 minutes
Please note questions should relate to the items under discussion and must be a question rather than statement. Where individuals deviate from this requirement they will be asked to stop and will not be invited to take any further part in the meeting.
Exclusion of the Press and Public
The Governing Body is recommended to exclude representatives of the press, and other members of the public, from the meeting having regard to the confidential nature of the business to be transacted, publicity
on which would be prejudicial to the public interest; Section 1(2), Public Bodies (Admission to Meetings) Act 1960.
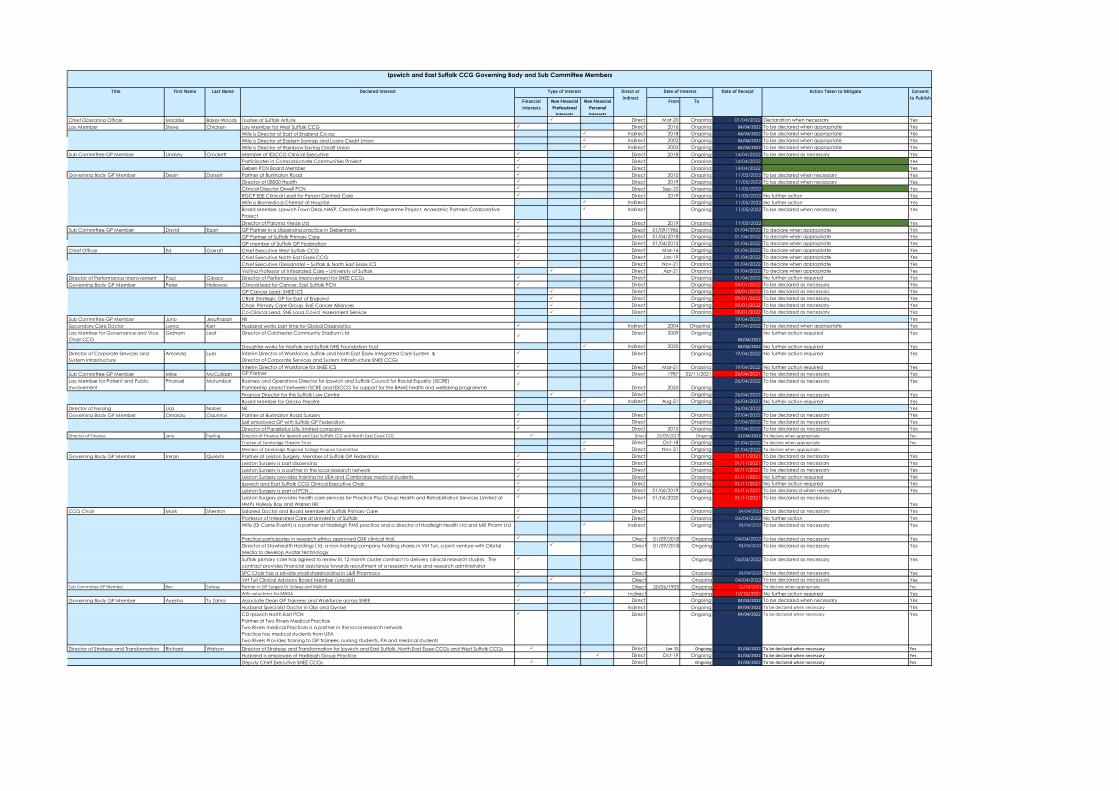
Financial Interests
Non Financial Professional
Interests
Non Financial Personal Interests
From To
Chief Operating Officer Maddie Baker-Woods Trustee of Suffolk ArtLink Direct Mar-20 Ongoing 01/04/2022 Declaration when necessary YesLay Member Steve Chicken Lay Member for West Suffolk CCG Direct 2016 Ongoing 04/04/2022 To be declared when appropriate Yes
Wife is Director of East of England Co-op Indirect 2018 Ongoing 04/04/2022 To be declared when appropriate YesWife is Director of Eastern Savings and Loans Credit Union Indirect 2002 Ongoing 04/04/2022 To be declared when appropriate YesWife is Director of Rainbow Saving Credit Union Indirect 2002 Ongoing 04/04/2022 To be declared when appropriate Yes
Sub Committee GP Member Lindsey Crockett Member of IESCCG Clinical Executive Direct 2018 Ongoing 14/04/2022 To be declared as necessary YesParticipates in Compassionate Communities Project Direct Ongoing 14/04/2022 YesDeben PCN Board Member Direct Ongoing 14/04/2022 Yes
Governing Body GP Member Dean Dorsett Partner at Burlington Road Direct 2010 Ongoing 11/05/2022 To be declared when necessary YesDirector of 08000 Health Direct 2019 Ongoing 11/05/2022 To be declared when necessary YesClinical Director Orwell PCN Direct Sep-22 Ongoing 11/05/2022 YesRGCP E0E Clinical Lead for Person Centred Care Direct 2019 Ongoing 11/05/2022 No further action YesWife is Biomedical Chemist at Hospital Indirect Ongoing 11/05/2022 No further action YesBoard Member, Ipswich Town Deal, NASP, Creative Health Programme Project, Acaedmic Partners Colaborative Project
Indirect Ongoing 11/05/2022 To be declared when necessary Yes
Director of Paloma Vrede Ltd Direct 2019 Ongoing 11/05/2022 YesSub Committee GP Member David Egan GP Partner in a dispensing practice in Debenham Direct 01/09/1986 Ongoing 01/04/2022 To declare when appropriate Yes
GP Partner of Suffolk Primary Care Direct 01/04/2018 Ongoing 01/04/2022 To declare when appropriate YesGP member of Suffolk GP Federation Direct 01/04/2013 Ongoing 01/04/2022 To declare when appropriate Yes
Chief Officer Ed Garratt Chief Executive West Suffolk CCG Direct Mar-16 Ongoing 01/04/2022 To declare when appropriate YesChief Executive North East Essex CCG Direct Jan-19 Ongoing 01/04/2022 To declare when appropriate YesChief Executive (Designate) – Suffolk & North East Essex ICS Direct Nov-21 Ongoing 01/04/2022 To declare when appropriate YesVisiting Professor of Integrated Care – University of Suffolk Direct Apr-21 Ongoing 01/04/2022 To declare when appropriate Yes
Director of Performance Improvement Paul Gibara Director of Performance Improvement for SNEE CCGs Direct Ongoing 01/04/2022 No further action required YesGoverning Body GP Member Peter Holloway Clinical lead for Cancer, East Suffolk PCN Direct Ongoing 09/01/2022 To be declared as necessary Yes
GP Cancer Lead, SNEE ICS Direct Ongoing 09/01/2022 To be declared as necessary YesCRUK Strategic GP for East of England Direct Ongoing 09/01/2022 To be declared as necessary YesChair, Primary Care Group, EoE Cancer Alliances Direct Ongoing 09/01/2022 To be declared as necessary YesCo-Clinical Lead, SNE Long Covid Assessment Service Direct Ongoing 09/01/2022 To be declared as necessary Yes
Sub Committee GP Member Juno Jesuthasan Nil 19/04/2022 YesSecondary Care Doctor Lorna Kerr Husband works part time for Global Diagnostics Indirect 2004 Ongoing 27/04/2022 To be declared when appropriate YesLay Member for Governance and Vice Chair CCG
Graham Leaf Director of Colchester Community Stadium Ltd
Direct 2009 Ongoing04/04/2022
No further action required Yes
Daughter works for Norfolk and Suffolk NHS Foundation Trust Indirect 2020 Ongoing 04/04/2022 No further action required YesDirector of Corporate Services and System Infrastructure
Amanda Lyes Interim Director of Workforce, Suffolk and North East Essex Integrated Care System &Director of Corporate Services and System Infrastructure SNEE CCGs
Direct Ongoing 19/04/2022 No further action required Yes
Interim Director of Workforce for SNEE ICS Direct Mar-21 Ongoing 19/04/2022 No further action required YesSub Committee GP Member Mike McCullagh GP Partner Direct 1987 02/11/2021 26/04/2021 To be declared as necessary YesLay Member for Patient and Public Involvement
Phanuel Mutumburi Business and Operations Director for Ipswich and Suffolk Council for Racial Equality (ISCRE)Partnership project between ISCRE and IESCCG for support for the BAME health and wellbeing programme
Direct 2020 Ongoing
26/04/2022 To be declared as necessary Yes
Finance Director for the Suffolk Law Centre Direct Ongoing 26/04/2022 To be declared as necessary YesBoard Member for Gecko Theatre Indirect Aug-21 Ongoing 26/04/2021 No further action required Yes
Director of Nursing Lisa Nobes Nil 26/04/2022 YesGoverning Body GP Member Omololu Ogunniyi Partner at Burlington Road Surgery Direct Ongoing 27/04/2022 To be declared as necessary Yes
Self employed GP with Suffolk GP Federation Direct Ongoing 27/04/2022 To be declared as necessary YesDirector of Parakletus Life, limited company Direct 2015 Ongoing 27/04/2022 To be declared as necessary Yes
Director of Finance Jane Payling Director of Finance for Ipswich and East Suffolk CCG and North East Essex CCG Direct 25/09/2017 Ongoing 21/04/2022 To declare when appropriate YesTrustee of Cambridge Theatre Trust Direct Oct-18 Ongoing 21/04/2022 To declare when appropriate YesMember of Cambridge Regional College Finance Committee Direct Nov-21 Ongoing 21/04/2022 To declare when appropriate
Governing Body GP Member Imran Qureshi Partner at Leiston Surgery. Member of Suffolk GP Federation Direct Ongoing 01/11/2021 To be declared as necessary YesLeiston Surgery is part dispensing Direct Ongoing 01/11/2021 To be declared as necessary YesLeiston Surgery is a partner in the local research network Direct Ongoing 01/11/2021 To be declared as necessary YesLeiston Surgery provides training for UEA and Cambridge medical students Direct Ongoing 01/11/2021 No further action required YesIpswich and East Suffolk CCG Clinical Executive Chair. Direct Ongoing 01/11/2021 No further action required YesLeiston Surgery is part of PCN. Direct 01/06/2019 Ongoing 01/11/2021 To be declarecd when necessarty YesLeiston Surgery provides health care services for Practice Plus Group Health and Rehabilitation Services Limited at HMPs Hollesly Bay and Warren Hill
Direct 01/06/2020 Ongoing 01/11/2021 To be declared as necessaryYes
CCG Chair Mark Shenton Salaried Doctor and Board Member of Suffolk Primary Care Direct Ongoing 04/04/2022 To be declared as necessary YesProfessor of Integrated Care at University of Suffolk Direct Ongoing 04/04/2022 No further action YesWife (Dr Carrie Everitt) is a partner at Hadleigh PMS practice and a director of Hadleigh Health Ltd and Mill Pharm Ltd Indirect Ongoing 04/04/2022 To be declared as necessary Yes
Practice participates in research ethics approved GSK clinical trial. Direct 01/09/2018 Ongoing 04/04/2022 To be declared as necessary YesDirector of Stowhealth Holdings Ltd, a non-trading company holding shares in Virt Turi, a joint venture with Orbital Media to develop Avatar technology
Direct 01/09/2018 Ongoing 04/04/2022 To be declared as necessary Yes
Suffolk primary care has agreed to renew its 12 month cluster contract to delivery clinical research studies. The contract provides financial assistance towards recruitment of a research nurse and research administrator
Direct Ongoing 04/04/2022 To be declared as necessary Yes
SPC Chair has a private small shareholding in L&R Pharmacy Direct Ongoing 04/04/2022 To be declared as necessary YesVirt Turi Clinical Advisory Board Member (unpaid) Direct Ongoing 04/04/2022 To be declared as necessary Yes
Sub Committee GP Member Ben Solway Partner in GP Surgery Dr Solway and Mallick Direct 20/06/1905 Ongoing 12/10/2021 To declare when appropriate YesWife volunteers for MNDA Indirect Ongoing 12/10/2021 No further action required Yes
Governing Body GP Member Ayesha Tu Zahra Associate Dean GP Trainees and Workforce across SNEE Direct Ongoing 04/04/2022 To be declared when necessary YesHusband Specialist Doctor in Obs and Gynae Indirect Ongoing 04/04/2022 To be declared when necessary YesCD Ipswich North East PCNPartner at Two Rivers Medical PracticeTwo Rivers medical Practices is a partner in the local research networkPractice has medical students from UEATwo Rivers Provides training to GP trainees, nursing students, PA and medical students
Direct Ongoing 04/04/2022 To be declared when necessary Yes
Director of Strategy and Transformation Richard Watson Director of Strategy and Transformation for Ipswich and East Suffolk, North East Essex CCGs and West Suffolk CCGs Direct Jan-15 Ongoing 01/04/2022 To be declared when necessary YesHusband is employee of Hadleigh Group Practice Direct Oct-19 Ongoing 01/04/2022 To be declared when necessary YesDeputy Chief Executive SNEE CCGs Direct Ongoing 01/04/2022 To be declared when necessary Yes
Ipswich and East Suffolk CCG Governing Body and Sub Committee Members
Title First Name Last Name Declared Interest Type of Interest Direct or Indirect
Date of Interest Date of Receipt Action Taken to Mitigate Consent to Publish
Page 1 of 9
Meeting of the Ipswich and East Suffolk CCG Governing Body held on Tuesday 22 March 2022 via
Microsoft Teams and live streamed for members of the public.
PRESENT: Dr Mark Shenton GP Governing Body Member and CCG Chair Maddie Baker-Woods Chief Operating Officer Steve Chicken Lay Member Dr Dean Dorsett GP Governing Body Member Paul Gibara Director of Performance Improvement Dr Peter Holloway GP Governing Body Member Dr Lorna Kerr Secondary Care Doctor Graham Leaf Lay Member: Governance and CCG Vice Chair Amanda Lyes Director of Corporate Services and System Infrastructure Phanuel Mutumburi Lay Member for Patient and Public Involvement Lisa Nobes Director of Nursing Dr Omololu Ogunniyi GP Governing Body Member Jane Payling Director of Finance Dr Imran Qureshi GP Governing Body Member Dr Ayesha Tu Zahra GP Governing Body Member Richard Watson Director of Strategy and Transformation IN ATTENDANCE: Ingrid Kwadzovi Patient Story Simon Morgan Head of Communications Jo Mael Corporate Governance Manager Tonia Wilson Patient Story
22/018 WELCOME AND APOLOGIES FOR ABSENCE
The Chair welcomed everyone to the meeting and apologies for absence were received from; Dr Padmanabhan Badrinath Consultant in Public Health Medicine Ed Garratt, Chief Executive
22/019 DECLARATIONS OF INTEREST AND HOSPITALITY AND GIFTS
Phanuel Mutumburi declared an interest in item 6 on the agenda, (Patient Story), which was a
presentation of the Young Health Ambassadors project co-founded by the NHS Charities and the IESCCG. The Chair expressed thanks to all those working within health and social care during the current challenging times. Covid-19 infections had recently increased significantly and the need to remember hand hygiene in order to reduce the spread of infection was emphasized, together with being tolerate and kind in respect of the request to wear masks within healthcare settings. Two issues previously highlighted at the November 2021 and January 2022 Governing Body’s had been those of capacity in the workforce and deprivation which was driving inequality of health outcomes within the health and care system. There had previously been a plea to see
Page 2 of 9
to address those issues and relieve pressure on finances. Current increased capacity was not funded which was resulting in increased burn out of the workforce which was impacted by abuse to staff. There was a need to carefully consider how the workforce capacity challenge might be met. The current increases to the cost of living would drive deprivation. Publication of a recent Health Foundation Report with regard to general practice was highlighted. The report provided facts on workload, how people accessed services and their preferences in the use of services, together with satisfaction. The report provided a more informed way of developing an opinion of how GP services.
22/020 MINUTES OF THE PREVIOUS MEETING
The minutes of the Ipswich and East Suffolk CCG Governing Body meeting held in public on
25 January 2022 were reviewed and agreed as a correct record.
22/021 MATTERS ARISING AND REVIEW OF OUTSTANDING ACTIONS
There were no matters arising and the action log was complete.
22/022 GENERAL UPDATE
The Deputy Chief Executive reported;
• The Covid-19 vaccination programme was now inviting eligible over 75’s and immuno suppressed over 12’s for their second boosters. There had been an increase in the number of acute beds occupied by patients with Covid-19.
• Draft 2022/23 Plans, setting out how priorities would be met, had been submitted to NHSE.
• Focus continued on elective recovery in order to reduce the numbers of patients that had been waiting for two years and good progress had been made.
• Engagement was currently taking place with patients in respect of the Cardinal Medical Practice.
The management of the supply of vaccine in respect of care home and housebound patients was queried and the Deputy Chief Executive and Director of Nursing agreed to clarify the situation outside of the meeting. The Governing Body noted the update.
22/023 PATIENT STORY
Tonia Wilson and Ingrid Kwadzovi from Volunteering Matters were welcomed to the meeting to
give a presentation on Health Ambassadors. It was highlighted that co-production and talking with young people facilitated good interventions that could deliver true changes for young people. It was explained that it was aimed to create a network of Health Ambassadors to support their communities and enable them to elevate their voices to shape change in Health Care services across Suffolk. There were currently six Health Ambassador programmes from March to July 2022 within primary, secondary and further education. Programmes lasted six weeks, with an additional four weeks to create a Youth Social Action (YSA) project focusing on health within schools or the local community. A Suffolk Youth Conference was to be held in July 2022 to showcase all YSA Ambassador programmes. Work included;
Page 3 of 9
• Exploring the adultification of Black and Minoritized young people within Suffolk Health and Social care students.
• I-Rise Up – Youth Led consultation group tasked with creating visual content and lived experience guidance to support with the development and shaping of our toolkits.
• Suffolk New College intensive three weeks Ambassador Programme – campaign or social action.
• Easter programme – was a three day intensive Health Ambassador Programme (10 young people aged 11-15 years old)
• Six Young people who were Autistic or on the Autistic spectrum would be creating and narrating an immersive audio, visual Art Installation following Autistic Awareness Week
The Lay Member for Public Involvement reported that the work had been part of the Healthy Ambitions Programme and representatives now sat on the Suffolk Safeguarding Partnership. The Governing Body was also shown a video and it was suggested that the CCG might be able to assist with its promotion via its website. Comments included; It was highlighted that the work built confidence amongst young people. The Health and Wellbeing Board had recently looked at adverse childhood experience and its impact and the Ambassador programme was a good grass roots approach. The Director of Strategy and Transformation agreed to discuss offline how young people could participate in current work which included a review of the Childrens and Young People programme. Having queried how it felt to be an Ambassador it was reported that the young people were managed, supported and nurtured in the role. They were encouraged to work with each other and create relationships within their own networks that would enable them to deliver the programme. Although it was queried whether the programme included youth offenders, it was explained that whilst the Health Ambassador Programme did not incorporate them, there were other programmes focussing on youth crime and development of a research base around youth crime. In response to questioning it was explained that whilst there was no specific knowledge of care leavers within the programme there were likely to be some within the school cohorts. It was suggested there might be opportunity to link up with regard to a future project launch with the University College London in respect of social prescribing in children. Dr Dean Dorsett agreed to make contact. The CCG’s Head of Communications offered to showcase the Health Ambassador Programme work within regular System briefings. The Governing Body thanked Tonia and Ingrid for their informative presentation.
22/024 PROCUREMENT UPDATE: SUMMARY OF ACTIVITY 2022
The Governing Body was provided with an update on the procurements completed since the
last procurement update and those currently in progress and planned for 2022. The Chair advised of the following question that had been received by Mr Anthony
Dooley, a member of the public, which it might be more beneficial to respond to now:
Page 4 of 9
Question - in the current financial year how many contracts for health services were given to
private providers, and what was the cost of those contracts? How do those numbers compare
with past financial years?
Response – the Director of Performance Improvement reported that such information was published in respect of each procurement, and whilst unable to share commercially sensitive information was happy to share information on private providers outside of the meeting. As well as private providers procurements also often used community interest companies and the voluntary sector. Key points highlighted from the report included; Pathology Services - the CCG currently commissioned Pathology Services across the Integrated Care System through a contract with North Essex and East Suffolk Pathology Services (NEESPS). The specification and approach to procurement had been agreed by Clinical Executive. The CCGs would be adopting a Commercial Sourcing approach which was scheduled to start in April 2022 subject to approval. Mental Health Assurance - in the summer of 2020 the assurance process for mental health, learning disabilities and autism commenced, concentrating on crisis services. Since then, the assurance of Children, Young people and Families, Community and Learning Disabilities and Autism had started. There had been delays due to covid prioritisation, but the process had continued. Mental Health Procurement - the Mental Health Procurement included the establishment of the Mental Health and Learning Disabilities and Autism Framework, the sourcing of the Daytime Wellbeing Hub and Evening Safe Haven Service and the Suffolk Community Connector Network. Each were subject to a separate evaluation process within a single tender. Documentation was released on the 19 November 2021 and responses were received on the 14 January 2022. Evaluation and moderation of the tenders for the Daytime Wellbeing Hub and Evening Safe Haven Service and the Suffolk Community Connector Network had been undertaken.
Secure Mental Health Transport - an approach to sourcing secure mental health transport had been agreed with colleagues from Norfolk and Suffolk NHS Foundation Trust (NSFT), and the specification was being reviewed internally. A Prior Information Notice was released to the market, and 14 responses had been received from interested providers. The intention was to work with the providers to understand how they believed the framework could work and to get their feedback on the specification and proposed any qualified provider approach. Future Procurements - Level 2B (L2b) neuro-rehabilitation beds was due to go out to procurement imminently. A number of other services were currently under review and the outcome of those reviews might fall into the procurement pipeline depending on the need identified, such as Non-emergency Patient Transport. Procurement Policy continued to develop at pace locally. Supplementary Consultation had been released regarding the new Provider Selection Regime. A review of the consultation would be led by the Procurement Lead, with input from others and the CCG response would be submitted prior to the closing date of 28 March 2022. The Governing Body noted the report.
22/025 2022/23 FINANCIAL PLANNING AND EXTENSION OF TEMPORARY FINANCIAL
ARRANGEMENTS
The report updated the Governing Body on the arrangements for finalising the financial plan for 2022/23 and extension of financial arrangements put into place to support Covid-19.
Page 5 of 9
At its meeting in January 2022 the Governing Body was informed that the timetable for 2022/23 planning had been extended to allow organisations to concentrate on the Covid-19 response over winter. The timetable for the 2022/23 plan was as follows:
• Draft plan –17 March 2022
• Final plan –28 April 2022 The draft plan had now been submitted in line with the above deadline. The timing of the 2022/23 planning deadlines meant that sign-off did not correspond with the schedule of Governing Body meetings. The Governing Body was therefore requested to delegate approval of the various elements of the plans to the following committees
• Financial plan to the Financial Performance Committee
• All other elements of the plan to the Clinical Executive Committee The final plan submissions would be brought back to the Governing Body meetings in May 2022. The NHS commissioning elements for 2022/23 were being constructed as a single plan for the Suffolk and North East Essex Integrated Care Board, from which the relevant CCG elements would be extracted for the months prior to the ICB formation. The expenditure made by the CCGs would be matched with allocation from the full year ICB funding such that the CCG element would be shown as a balanced plan; any surplus or deficit would fall into the combined ICB in the latter part of the year. The report went on to seek approval of a roll-over of the 2021/22 budget for the initial period of
April until such time as the financial plan was finalised (final deadline currently 28 April 2022),
together with continuation of the Covid-19 Resources Approval Committee and previously
agreed changes to delegated authorisation levels.
The Governing Body therefore;
1) Noted the planning timetable for 2022/23 2) Delegated approval of the 2022/23 financial plan and budget to the Financial Performance
Committee, for final sign off by the Governing Body. 3) Delegated approval of the remaining elements of the plan to the Clinical Executive 4) Approved rolling over the 2021/22 budget until such time as the 2022/23 budget had been
developed. 5) Approved the extension of the Covid-19 resource allocation committee and temporary
financial delegation limits until the formal commencement of the ICB.
22/026 INTEGRATED PERFORMANCE REPORT
The Governing Body was in receipt of the Integrated Performance Report. Key points highlighted included;
• The System remained at Level 4 escalation due to Covid-19 numbers increasing.
• Current focus was on key priorities which was reflected in the revised report. Priority areas included elective recovery, cancer and mental health.
• Work was taking place on the use of software which allowed the integration of data within the report and it was hoped that future reports would be more refined.
• Elective Recovery – the System had been directed to maintain urgent elective cases and to reduce 104 week waits, and was on track to hit the trajectory. Mutual aid had carried on

Page 6 of 9
which had resulted in the slight decline of ESNEFT performance due to its support of WSFT. In terms of referral to treatment times, the System was the first in the region to see improvement. The independent sector had been used quite heavily and there was pressure in diagnostics with increased referrals and providers seeking additional capacity.
• Priorities in respect of elective activity included the eradication of 104 week waits and minimisation of 78 week waits. Risks to achievement included Covid-19 and workforce.
• Urgent and Emergency care – Covid-19 rates were increasing although it was thought the current peak would not be reached until 3-4 weeks’ time.
• There had been internal hospital delays in respect of timely discharges and there was increased focus on discharge processes. A level of patient flow had been maintained although if Covid-19 numbers continued to rise there might be a need to consider some cancellation of elective activity.
• The East of England Ambulance Service NHS Trust (EEAST) continued to give cause for concern as response rates were not on target. Initiatives with regard to conveyancing were being explored although workforce was a key issue.
• Cancer – good progress was being made with ESNEFT having treated the highest number of 62 day waiters. Recovery plans were in place for the waiting list.
• Vaccination programme was doing well in programme with over 75’s and immuno suppressed over 12’s being invited for a second booster.
It was felt that the reason EEAST conveyances had reduced might be due to patients going to the hospital under their own steam. The impact of the response rates on the rest of the System and clinicians needed to be addressed. The Governing Body was advised of the intention to establish an Urgent Care Committee as part of the ICB. It was queried whether there was any specific vaccination service for those that might be needle phobic. It was reported that some dedicated clinics had been held and the vaccination bus might prove beneficial for such individuals. There was increased advice and guidance with regard to outpatient referrals although diagnostics were challenging. There had been a lot of work in relation to cancer two week wait referrals and their restoration to pre-pandemic levels although the key standard was due to change away from two week waits to that of 28 day faster diagnosis. Cancer was at 115% of pre-pandemic referrals and the highest in the region for returning and exceeding pre-pandemic levels. ESNEFT was one of the highest in the country for treatment provided. The System was in the process of updating the Cancer Strategy. Expressions of interest had been invited for the roles of ICS Cancer Lead and GP Alliance Cancer Leads. The Governing Body was reminded of the unmet need within other areas of healthcare such as orthopaedics. Clinical Quality
• It would be beneficial to be able to link outcomes to access targets within the IPR.
• Key concerns centred around demand and delays of access to services.
• There were increased Covid-19 numbers within the acutes although individuals were not necessarily unwell with Covid-19. The impact on the workforce had increased.
• ESNEFT – there was concern at the number of children and young people accessing the acute sector for mental health needs and presenting in acute crisis. System work was underway to determine what could be done as a system to support acute services and prevention. ESNEFT had recently lowered its visiting restrictions.
• Norfolk and Suffolk NHS Foundation Trust (NSFT) – focus was on children and young people work with regard to eating disorders and the Emotional Wellbeing hub. There were high numbers accessing services and call response times gave cause for concern. Work was underway to look at frequent users and review the process of referral. The Care Quality Commission report was awaited.
Page 7 of 9
• Ezec – the Care Quality Commission report had been received. There had been an overall ‘requires improvement’ score although the score for ‘safe and caring’ had been good.
• EEAST – C1 response and C3 responses not where they needed to be which had an impact on outcomes. It was suggested that discussion in respect of the perfect day report might identify where support could be provided.
Transformation
• Mental Health – eating disorder service was challenging. Although NSFT had recruited staff and improvement had been seen the situation remained volatile. Dementia prevalence remained poor and only two CCGs had achieved the target. Performance had declined over the last year with current performance being 58.8% v a target of 67%. The CCG was currently working on a community mental health model at present.
• Children and Young People (CYP) – following a recent summit costed improvement proposals had been put together. The Emotional Wellbeing hub demand was reducing and a Barnardos’-CYP parents’ helpline had recently been launched together with a neuro development disorders coordination function and panels.
• Dental – a dental task force had been established which had met twice to look at ways to improve the current position. Focus was on urgent dental access and looked after children.
• There had been acute collaboration work between ESNEFT and WSFT in respect of forming acute provider collaboratives.
• Approval had been obtained to launch an options appraisal for an intelligence function and population health management was moving towards a linked data set.
The Chair advised that linking what the CCG was doing in transformation and wider work through to outcomes would be vital for the ICB. Finance At the end of February 2022, Month 11 the CCG was on track to achieve a break even position by year end after receipt of central allocations for the Hospital Discharge Programme and Elective Recovery Fund. Primary Care
• Primary Care was currently under pressure - improved information was now available with regard to the volume of appointments across the week.
• Staffing remained challenging due to Covid-19 although all practices remained open. Staff were thanked for their hard work.
• The mental health programme of work was a priority which included dementia diagnosis.
• Prescribing – there had been some recovery of the financial position and the CCG was dedicated to making sure prescribing was safe.
• The CCG was due to take on responsibility for dental, pharmacy, and optician work from 2023 and representatives from those sectors had been invited to attend Alliance meetings.
The Governing Body noted the report.
22/027 GOVERNING BODY ASSURANCE FRAMEWORK
The Lay Member for Governance presented the most recent Governing Body Assurance
Framework (GBAF) together with a summary of local risk registers. Amendments and additions to the GBAF were detailed within Section 2 of the report, with key aspects of departmental risk registers being listed in Section 3. The Governing Body noted and approved the GBAF as presented.
Page 8 of 9
22/028 MINUTES OF MEETINGS
Presented by the Lay Member for Governance, consideration was given to minutes and decisions from the following meetings. a) Audit Committee The unconfirmed minutes of a meeting held on 15 February 2022 b) Remuneration and HR Committee The unconfirmed minutes of an meeting held on 15 February 2022. c) Clinical Scrutiny Committee The unconfirmed minutes of a meeting held on 26 October 2021 d) Covid-19 Resource Approval Committee The minutes from a meeting held on 28 January 2022 e) Ipswich and East Suffolk CCG Primary Care Commissioning Committee The unconfirmed minutes of a meeting held on 22 February 2022
f) Commissioning Governance Committee
Decision from a virtual meeting held on 11 November 2021
g) Ipswich and East Suffolk Alliance The confirmed minutes of a meeting held on 18 January 2022
h) CCG Collaborative Group The unconfirmed minutes of a meeting held on 8 February 2022 The Governing Body endorsed the minutes and decisions as presented.
22/029 DATE OF NEXT MEETING
The next meeting was scheduled to take place at 9.15am, Tuesday, 24 May 2022
22/030 QUESTIONS FROM THE PUBLIC
Questions from members of the public were received as follows: Mr Anthony Dooley: Question 1 - Do you agree with the quote attributed to Geoff Barton in the local press recently that 'testing is one of the few tools we (schools) still have to reduce transmission among students and staff, and the government must reverse its decision and continue to provide free tests to people working or studying in educational settings'? Response – testing was a helpful way of understanding the risk of spread and to identify those individuals that were asymptomatic. A decision had been made in terms of how we were to live with Covid-19 but since the reduction in restrictions there had been an uplift in case rates. Question 2 - The DfE response was: ' We are now moving to living with, and managing the virus, while maintaining the population's wall of protection and communicating safer behaviours that the public can follow to manage risk'. This is absurd nonsense, do you agree, yes or no?
Page 9 of 9
Response – as previously mentioned a decision had been taken that we would live with and manage the virus. The importance of maintaining what we can do personally had been emphasized at the start of meeting. The vaccination programme had protected those that were most vulnerable. There was a need for more data and research figures in respect of how serious new variants were and that work was ongoing. Intensive Care Units were not currently overwhelmed which was encouraging and it was about the need for ongoing analysis of casemix and variants. Question 3 - What impact on the tackling health inequalities agenda for the poorest do you anticipate given what is labelled ' the cost of living crisis'? Response – the Chair advised that had been addressed in his preamble to the meeting. Fuel poverty and food poverty were likely to facilitate the making of difficult decisions. Question 4 - In the current financial year how many contracts for health services were given to private providers, and what was the cost of those contracts? How do those numbers compare with past financial years? Response – the question had been responded to as part of procurement item. Question 5 - I applaud your decision not to hold this meeting in public, especially given the removal of legal public health protections, and the inevitable huge rise in infections subsequently, but how is the public meant to understand that GP surgeries rightly insist on patients wearing facemasks but it is optional on public transport and in indoor spaces, such as shops? Response – how society respected those that were vulnerable in settings where they were more likely to be, was highlighted, together with respecting requests to wear masks for the protection of others. Question 6 - Maybe I am jumping the gun but the IPR refers to patient safety. Given the financial statement re workforce (no additional money) what issues concern you, eg maternity? Response – the Director of Nursing reported that whilst there had been an improvement in maternity safety outcomes for women and babies, concerns remained as a system maternity board around the number of pregnant women that were experiencing post partum haemorrhage. Work to address that included improvement of the triage process and to ensure equality of access. Leadership at ESNEFT had been strengthened resulting in improved outcomes. The continuity of carer model was a model that would support reductions in poorer outcomes. ESNEFT was seeking 100% continuity of care by the same time next year. The Chair reported that it was disappointing that the System did not have the financial support to deliver the service and outcomes. Although numbers were important it was also about what we are doing in order that workforce teams were better able to work in an integrated way to look at challenges ahead and the impact of deprivation on co-morbidities.
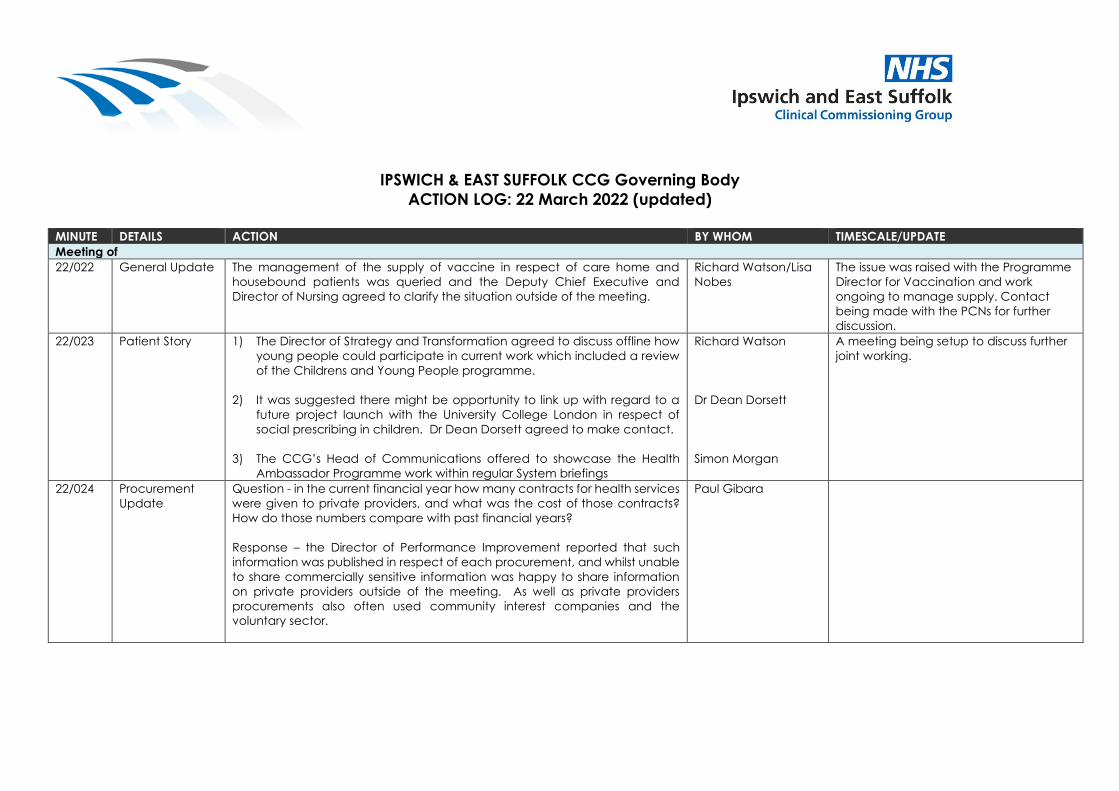
IPSWICH & EAST SUFFOLK CCG Governing Body
ACTION LOG: 22 March 2022 (updated)
MINUTE DETAILS ACTION BY WHOM TIMESCALE/UPDATE
Meeting of
22/022 General Update The management of the supply of vaccine in respect of care home and
housebound patients was queried and the Deputy Chief Executive and
Director of Nursing agreed to clarify the situation outside of the meeting.
Richard Watson/Lisa
Nobes
The issue was raised with the Programme
Director for Vaccination and work
ongoing to manage supply. Contact
being made with the PCNs for further
discussion.
22/023 Patient Story 1) The Director of Strategy and Transformation agreed to discuss offline how
young people could participate in current work which included a review
of the Childrens and Young People programme.
2) It was suggested there might be opportunity to link up with regard to a
future project launch with the University College London in respect of
social prescribing in children. Dr Dean Dorsett agreed to make contact.
3) The CCG’s Head of Communications offered to showcase the Health
Ambassador Programme work within regular System briefings
Richard Watson
Dr Dean Dorsett
Simon Morgan
A meeting being setup to discuss further
joint working.
22/024 Procurement
Update
Question - in the current financial year how many contracts for health services
were given to private providers, and what was the cost of those contracts?
How do those numbers compare with past financial years?
Response – the Director of Performance Improvement reported that such
information was published in respect of each procurement, and whilst unable
to share commercially sensitive information was happy to share information
on private providers outside of the meeting. As well as private providers
procurements also often used community interest companies and the
voluntary sector.
Paul Gibara
Page 1 of 2
GOVERNING BODY
Agenda Item No. 07
Reference No. IESCCG 22-16
Date. 24 May 2022
Title
Patient and Public Involvement and Experience
Lead Director
Lisa Nobes, Director of Nursing
Author(s)
Sophie Martin – Head of Patient and Public Involvement
Purpose
To provide the Governing Body with a broad overview of patient, public involvement and experience.
Applicable CCG Clinical Priorities:
1. To promote self care
2. To ensure high quality local services where possible
3. To improve the health of those most in need
4. To improve health and educational attainment for children and young people
5. To improve access to mental health services
6. To improve outcomes for patients with diabetes to above national averages
7. To improve care for frail elderly individuals
8. To allow patients to die with dignity and compassion and to choose their place of death where appropriate
9. To ensure that the CCG operates within agreed budgets
Action required by Governing Body: To note the report.
Page 2 of 2
1. Background 1.1 This is the fourth quarterly report for year 2021/21. All previous reports have been to
Governing Body for information. 2. Key Issues 2.1 This report shows the Quarter 4 activity of the Patient and Public Involvement and
Experience Team. It records the scope of the activity, number of people involved and impact or outcome achieved.
2.2 The Governing Body is asked to note the activity and impact of coproduction with citizens
across the organisation. 3. Patient and Public Engagement 3.1 The breadth and depth of activity across the organisation and within the Alliances
demonstrates increased collaboration and coproduction with local citizens. 4. Recommendation 4.1 For note.
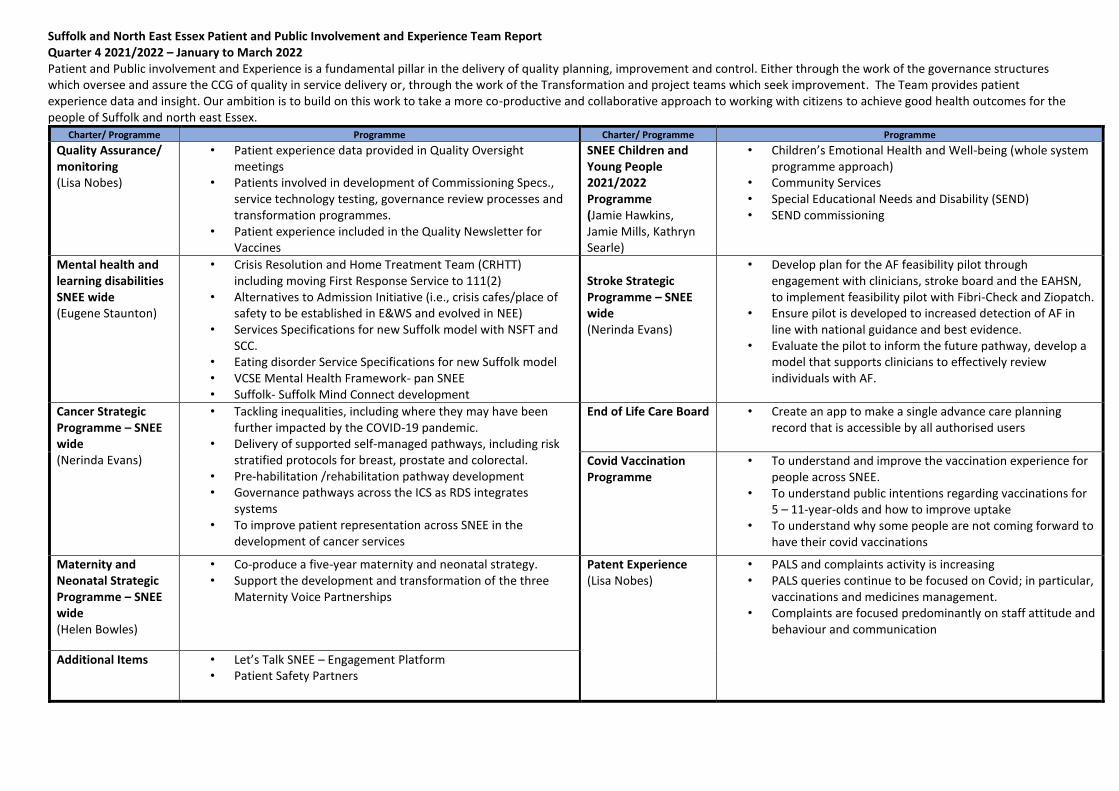
Suffolk and North East Essex Patient and Public Involvement and Experience Team Report Quarter 4 2021/2022 – January to March 2022 Patient and Public involvement and Experience is a fundamental pillar in the delivery of quality planning, improvement and control. Either through the work of the governance structures which oversee and assure the CCG of quality in service delivery or, through the work of the Transformation and project teams which seek improvement. The Team provides patient experience data and insight. Our ambition is to build on this work to take a more co-productive and collaborative approach to working with citizens to achieve good health outcomes for the people of Suffolk and north east Essex.
Charter/ Programme Programme Charter/ Programme Programme
Quality Assurance/ monitoring (Lisa Nobes)
• Patient experience data provided in Quality Oversight meetings
• Patients involved in development of Commissioning Specs., service technology testing, governance review processes and transformation programmes.
• Patient experience included in the Quality Newsletter for Vaccines
SNEE Children and Young People 2021/2022 Programme (Jamie Hawkins, Jamie Mills, Kathryn Searle)
• Children’s Emotional Health and Well-being (whole system programme approach)
• Community Services • Special Educational Needs and Disability (SEND) • SEND commissioning
Mental health and learning disabilities SNEE wide (Eugene Staunton)
• Crisis Resolution and Home Treatment Team (CRHTT) including moving First Response Service to 111(2)
• Alternatives to Admission Initiative (i.e., crisis cafes/place of safety to be established in E&WS and evolved in NEE)
• Services Specifications for new Suffolk model with NSFT and SCC.
• Eating disorder Service Specifications for new Suffolk model • VCSE Mental Health Framework- pan SNEE • Suffolk- Suffolk Mind Connect development
Stroke Strategic Programme – SNEE wide (Nerinda Evans)
• Develop plan for the AF feasibility pilot through engagement with clinicians, stroke board and the EAHSN, to implement feasibility pilot with Fibri-Check and Ziopatch.
• Ensure pilot is developed to increased detection of AF in line with national guidance and best evidence.
• Evaluate the pilot to inform the future pathway, develop a model that supports clinicians to effectively review individuals with AF.
Cancer Strategic Programme – SNEE wide (Nerinda Evans)
• Tackling inequalities, including where they may have been further impacted by the COVID-19 pandemic.
• Delivery of supported self-managed pathways, including risk stratified protocols for breast, prostate and colorectal.
• Pre-habilitation /rehabilitation pathway development • Governance pathways across the ICS as RDS integrates
systems • To improve patient representation across SNEE in the
development of cancer services
End of Life Care Board
• Create an app to make a single advance care planning record that is accessible by all authorised users
Covid Vaccination Programme
• To understand and improve the vaccination experience for people across SNEE.
• To understand public intentions regarding vaccinations for 5 – 11-year-olds and how to improve uptake
• To understand why some people are not coming forward to have their covid vaccinations
Maternity and Neonatal Strategic Programme – SNEE wide (Helen Bowles)
• Co-produce a five-year maternity and neonatal strategy. • Support the development and transformation of the three
Maternity Voice Partnerships
Patent Experience (Lisa Nobes)
• PALS and complaints activity is increasing • PALS queries continue to be focused on Covid; in particular,
vaccinations and medicines management. • Complaints are focused predominantly on staff attitude and
behaviour and communication
Additional Items • Let’s Talk SNEE – Engagement Platform • Patient Safety Partners
Suffolk and North East Essex Patient and Public Involvement and Experience Team Report Quarter 4 2021/2022 – January to March 2022
March 2022 Page 2
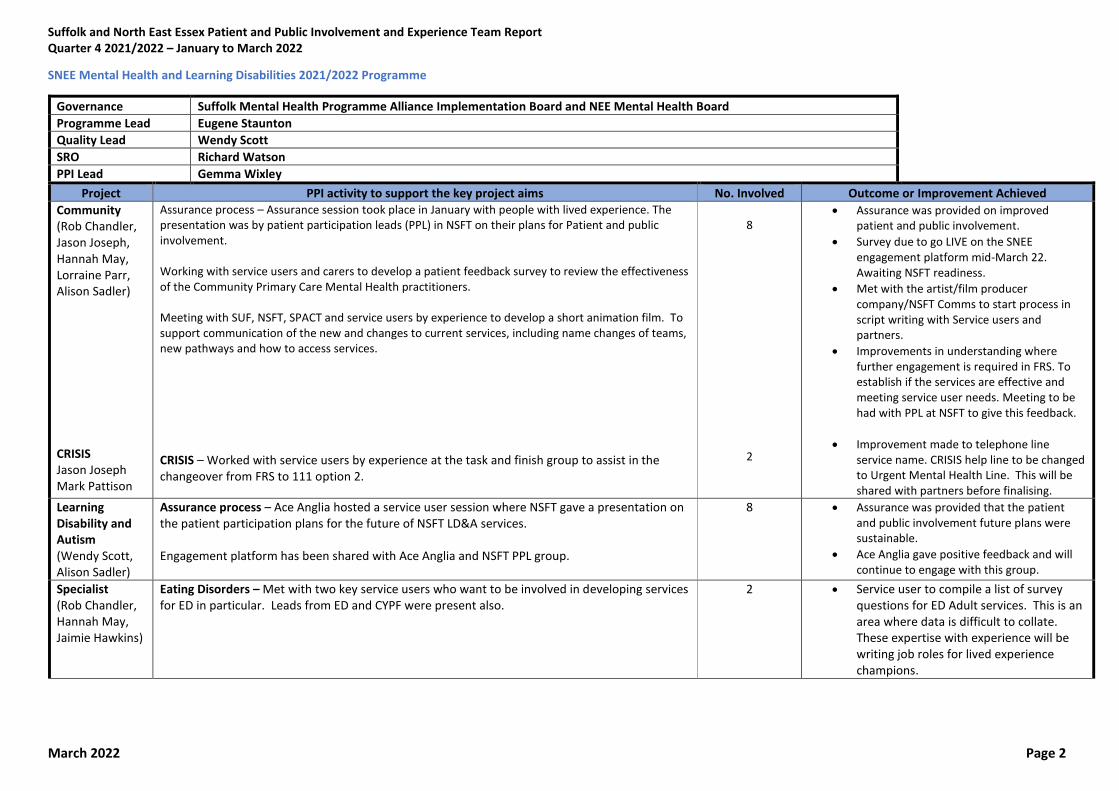
SNEE Mental Health and Learning Disabilities 2021/2022 Programme
Governance Suffolk Mental Health Programme Alliance Implementation Board and NEE Mental Health Board
Programme Lead Eugene Staunton
Quality Lead Wendy Scott
SRO Richard Watson
PPI Lead Gemma Wixley
Project PPI activity to support the key project aims No. Involved Outcome or Improvement Achieved
Community (Rob Chandler, Jason Joseph, Hannah May, Lorraine Parr, Alison Sadler) CRISIS Jason Joseph Mark Pattison
Assurance process – Assurance session took place in January with people with lived experience. The presentation was by patient participation leads (PPL) in NSFT on their plans for Patient and public involvement. Working with service users and carers to develop a patient feedback survey to review the effectiveness of the Community Primary Care Mental Health practitioners. Meeting with SUF, NSFT, SPACT and service users by experience to develop a short animation film. To support communication of the new and changes to current services, including name changes of teams, new pathways and how to access services.
CRISIS – Worked with service users by experience at the task and finish group to assist in the changeover from FRS to 111 option 2.
8
2
• Assurance was provided on improved patient and public involvement.
• Survey due to go LIVE on the SNEE engagement platform mid-March 22. Awaiting NSFT readiness.
• Met with the artist/film producer company/NSFT Comms to start process in script writing with Service users and partners.
• Improvements in understanding where further engagement is required in FRS. To establish if the services are effective and meeting service user needs. Meeting to be had with PPL at NSFT to give this feedback.
• Improvement made to telephone line service name. CRISIS help line to be changed to Urgent Mental Health Line. This will be shared with partners before finalising.
Learning Disability and Autism (Wendy Scott, Alison Sadler)
Assurance process – Ace Anglia hosted a service user session where NSFT gave a presentation on the patient participation plans for the future of NSFT LD&A services. Engagement platform has been shared with Ace Anglia and NSFT PPL group.
8 • Assurance was provided that the patient and public involvement future plans were sustainable.
• Ace Anglia gave positive feedback and will continue to engage with this group.
Specialist (Rob Chandler, Hannah May, Jaimie Hawkins)
Eating Disorders – Met with two key service users who want to be involved in developing services for ED in particular. Leads from ED and CYPF were present also.
2 • Service user to compile a list of survey questions for ED Adult services. This is an area where data is difficult to collate. These expertise with experience will be writing job roles for lived experience champions.
Suffolk and North East Essex Patient and Public Involvement and Experience Team Report Quarter 4 2021/2022 – January to March 2022
March 2022 Page 3
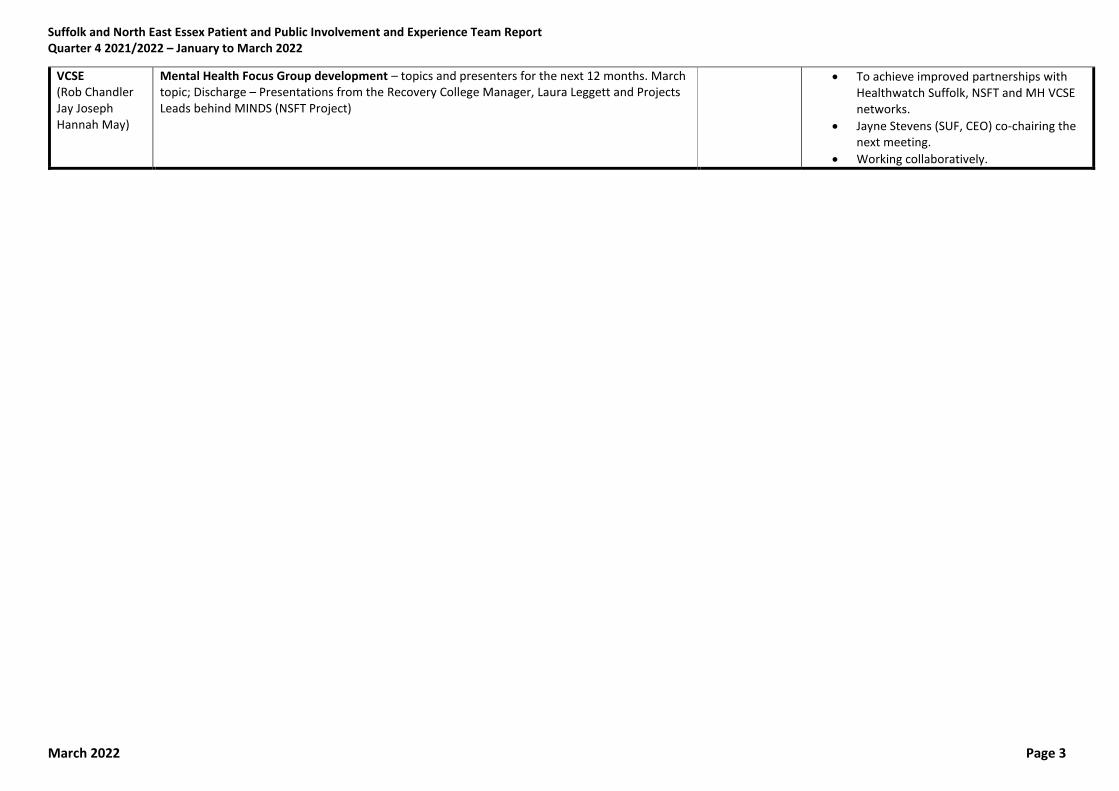
VCSE (Rob Chandler Jay Joseph Hannah May)
Mental Health Focus Group development – topics and presenters for the next 12 months. March topic; Discharge – Presentations from the Recovery College Manager, Laura Leggett and Projects Leads behind MINDS (NSFT Project)
• To achieve improved partnerships with Healthwatch Suffolk, NSFT and MH VCSE networks.
• Jayne Stevens (SUF, CEO) co-chairing the next meeting.
• Working collaboratively.
Suffolk and North East Essex Patient and Public Involvement and Experience Team Report Quarter 4 2021/2022 – January to March 2022
March 2022 Page 4
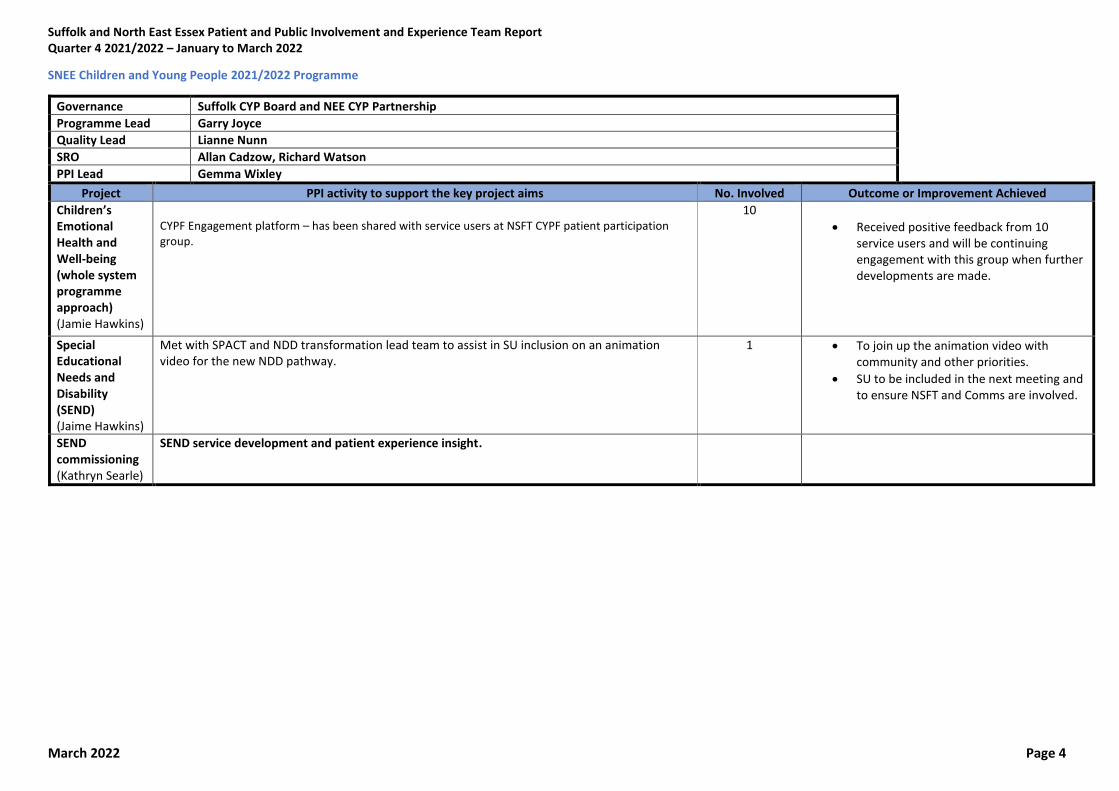
SNEE Children and Young People 2021/2022 Programme
Governance Suffolk CYP Board and NEE CYP Partnership
Programme Lead Garry Joyce
Quality Lead Lianne Nunn
SRO Allan Cadzow, Richard Watson
PPI Lead Gemma Wixley
Project PPI activity to support the key project aims No. Involved Outcome or Improvement Achieved
Children’s Emotional Health and Well-being (whole system programme approach) (Jamie Hawkins)
CYPF Engagement platform – has been shared with service users at NSFT CYPF patient participation group.
10
• Received positive feedback from 10 service users and will be continuing engagement with this group when further developments are made.
Special Educational Needs and Disability (SEND) (Jaime Hawkins)
Met with SPACT and NDD transformation lead team to assist in SU inclusion on an animation video for the new NDD pathway.
1 • To join up the animation video with community and other priorities.
• SU to be included in the next meeting and to ensure NSFT and Comms are involved.
SEND commissioning (Kathryn Searle)
SEND service development and patient experience insight.
Suffolk and North East Essex Patient and Public Involvement and Experience Team Report Quarter 4 2021/2022 – January to March 2022
March 2022 Page 5
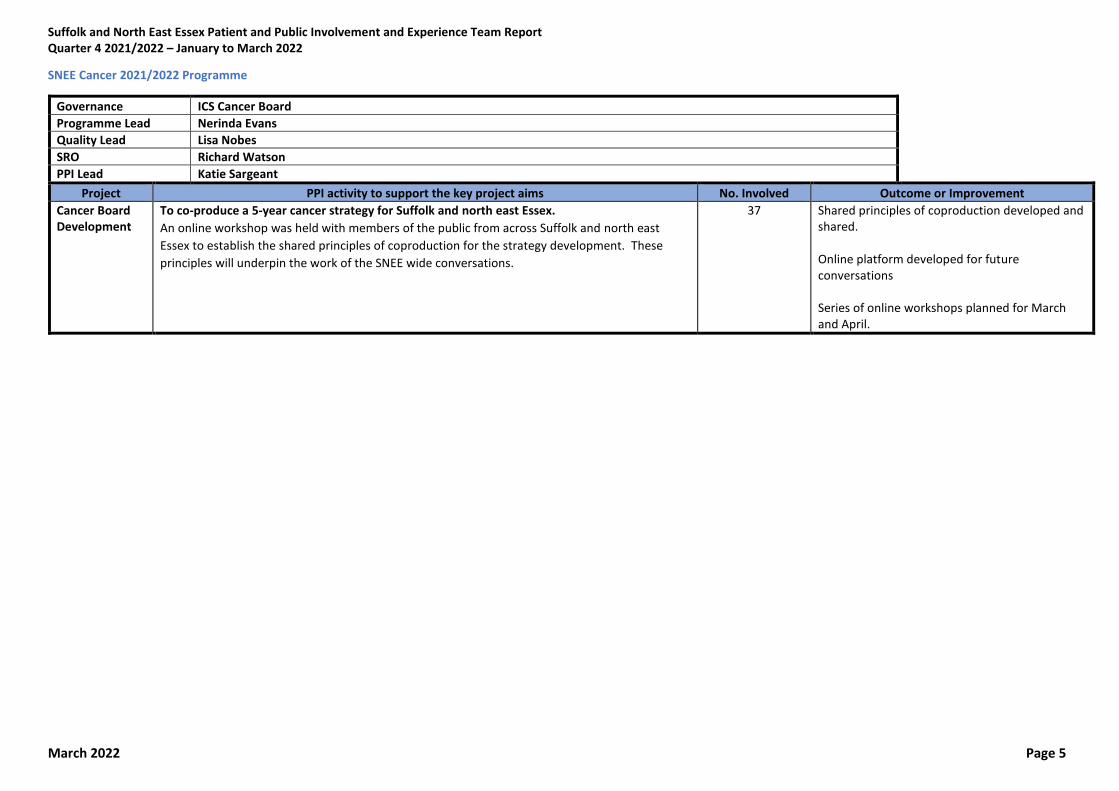
SNEE Cancer 2021/2022 Programme
Governance ICS Cancer Board
Programme Lead Nerinda Evans
Quality Lead Lisa Nobes
SRO Richard Watson
PPI Lead Katie Sargeant
Project PPI activity to support the key project aims No. Involved Outcome or Improvement
Cancer Board Development
To co-produce a 5-year cancer strategy for Suffolk and north east Essex.
An online workshop was held with members of the public from across Suffolk and north east
Essex to establish the shared principles of coproduction for the strategy development. These
principles will underpin the work of the SNEE wide conversations.
37 Shared principles of coproduction developed and shared. Online platform developed for future conversations Series of online workshops planned for March and April.
Suffolk and North East Essex Patient and Public Involvement and Experience Team Report Quarter 4 2021/2022 – January to March 2022
March 2022 Page 6
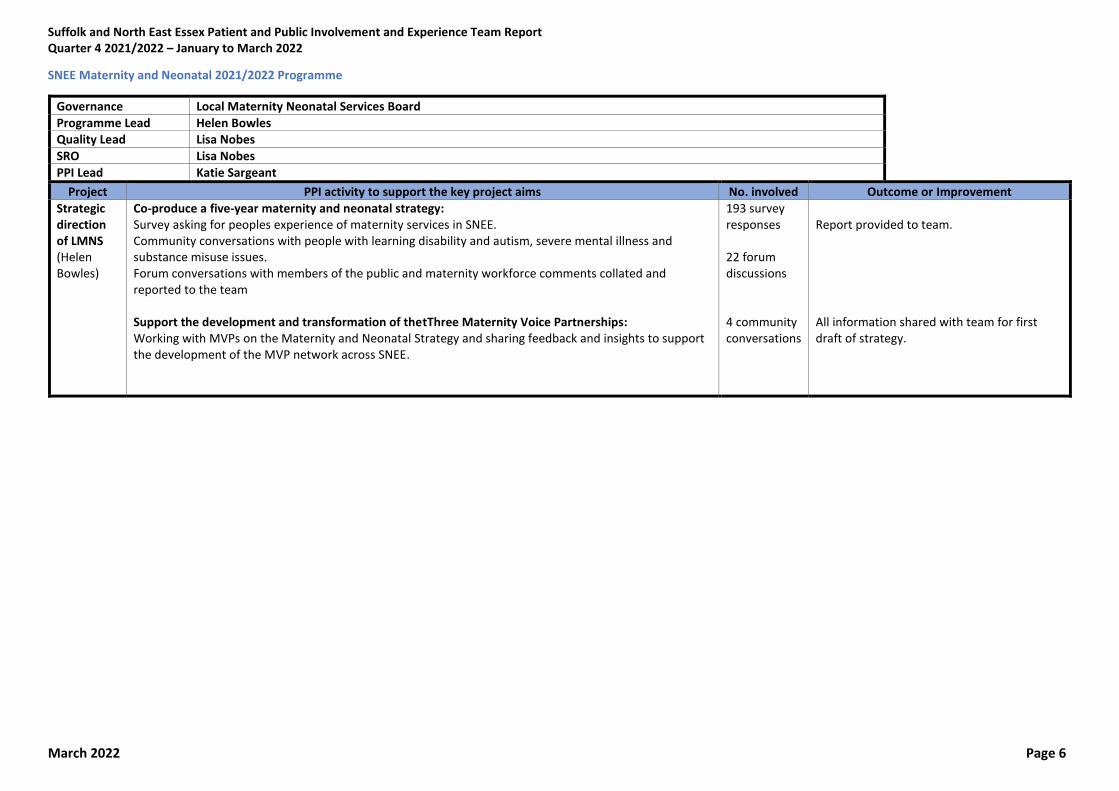
SNEE Maternity and Neonatal 2021/2022 Programme
Governance Local Maternity Neonatal Services Board
Programme Lead Helen Bowles Quality Lead Lisa Nobes
SRO Lisa Nobes
PPI Lead Katie Sargeant
Project PPI activity to support the key project aims No. involved Outcome or Improvement
Strategic direction of LMNS (Helen Bowles)
Co-produce a five-year maternity and neonatal strategy: Survey asking for peoples experience of maternity services in SNEE. Community conversations with people with learning disability and autism, severe mental illness and substance misuse issues. Forum conversations with members of the public and maternity workforce comments collated and reported to the team Support the development and transformation of thetThree Maternity Voice Partnerships: Working with MVPs on the Maternity and Neonatal Strategy and sharing feedback and insights to support the development of the MVP network across SNEE.
193 survey responses 22 forum discussions 4 community conversations
Report provided to team. All information shared with team for first draft of strategy.
Suffolk and North East Essex Patient and Public Involvement and Experience Team Report Quarter 4 2021/2022 – January to March 2022
March 2022 Page 7
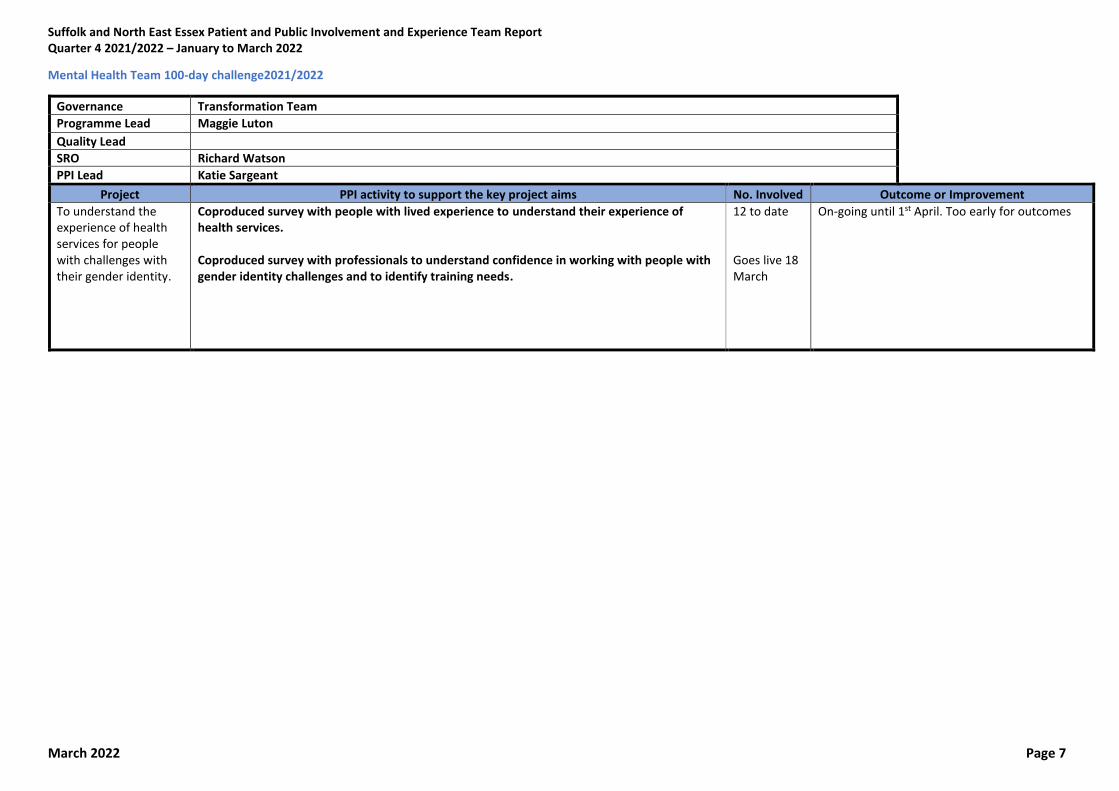
Mental Health Team 100-day challenge2021/2022
Governance Transformation Team
Programme Lead Maggie Luton
Quality Lead
SRO Richard Watson
PPI Lead Katie Sargeant
Project PPI activity to support the key project aims No. Involved Outcome or Improvement
To understand the experience of health services for people with challenges with their gender identity.
Coproduced survey with people with lived experience to understand their experience of health services. Coproduced survey with professionals to understand confidence in working with people with gender identity challenges and to identify training needs.
12 to date Goes live 18 March
On-going until 1st April. Too early for outcomes
Suffolk and North East Essex Patient and Public Involvement and Experience Team Report Quarter 4 2021/2022 – January to March 2022
March 2022 Page 8
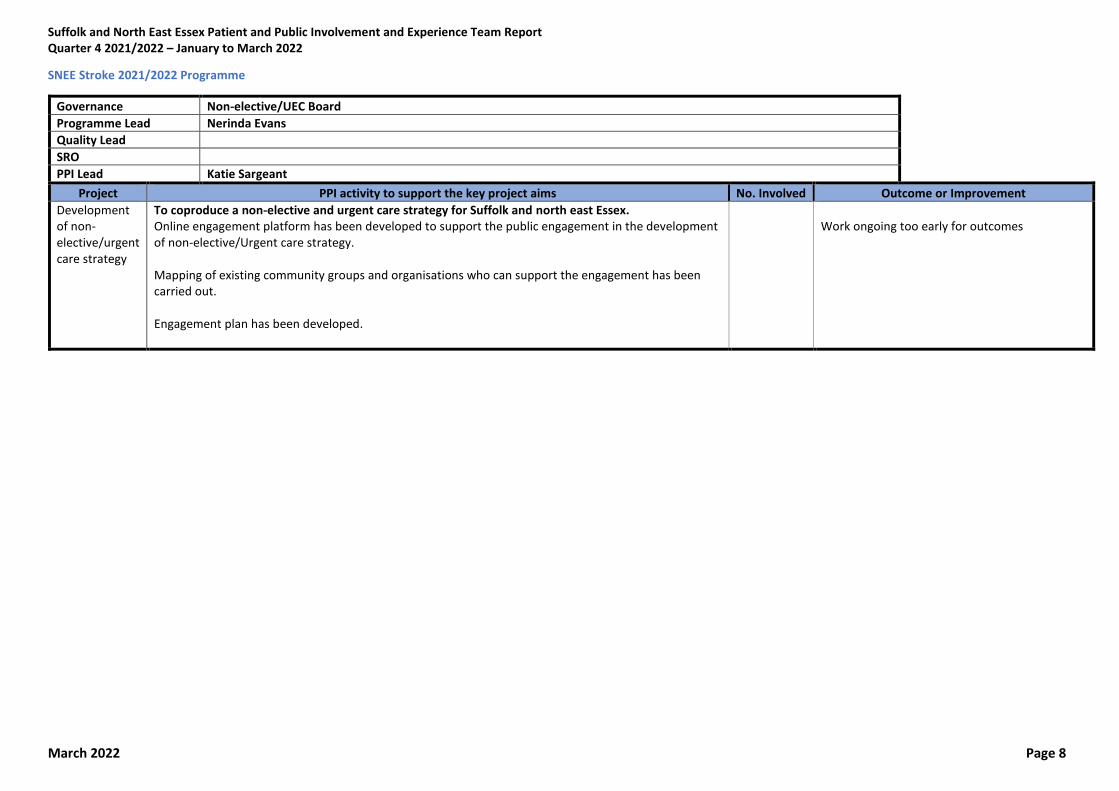
SNEE Stroke 2021/2022 Programme
Governance Non-elective/UEC Board
Programme Lead Nerinda Evans
Quality Lead
SRO
PPI Lead Katie Sargeant
Project PPI activity to support the key project aims No. Involved Outcome or Improvement
Development of non-elective/urgent care strategy
To coproduce a non-elective and urgent care strategy for Suffolk and north east Essex. Online engagement platform has been developed to support the public engagement in the development of non-elective/Urgent care strategy. Mapping of existing community groups and organisations who can support the engagement has been carried out. Engagement plan has been developed.
Work ongoing too early for outcomes
Suffolk and North East Essex Patient and Public Involvement and Experience Team Report Quarter 4 2021/2022 – January to March 2022
March 2022 Page 9
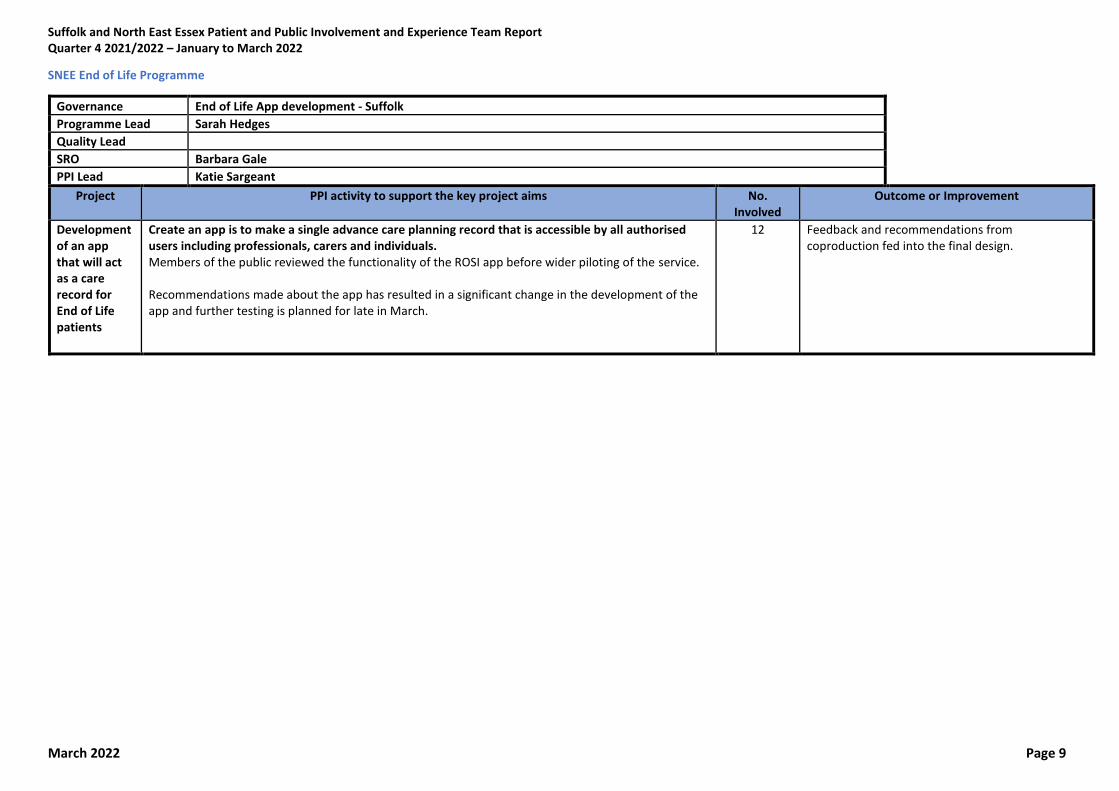
SNEE End of Life Programme
Governance End of Life App development - Suffolk Programme Lead Sarah Hedges Quality Lead
SRO Barbara Gale PPI Lead Katie Sargeant
Project PPI activity to support the key project aims No. Involved
Outcome or Improvement
Development of an app that will act as a care record for End of Life patients
Create an app is to make a single advance care planning record that is accessible by all authorised users including professionals, carers and individuals. Members of the public reviewed the functionality of the ROSI app before wider piloting of the service. Recommendations made about the app has resulted in a significant change in the development of the app and further testing is planned for late in March.
12 Feedback and recommendations from coproduction fed into the final design.
Suffolk and North East Essex Patient and Public Involvement and Experience Team Report Quarter 4 2021/2022 – January to March 2022
March 2022 Page 10
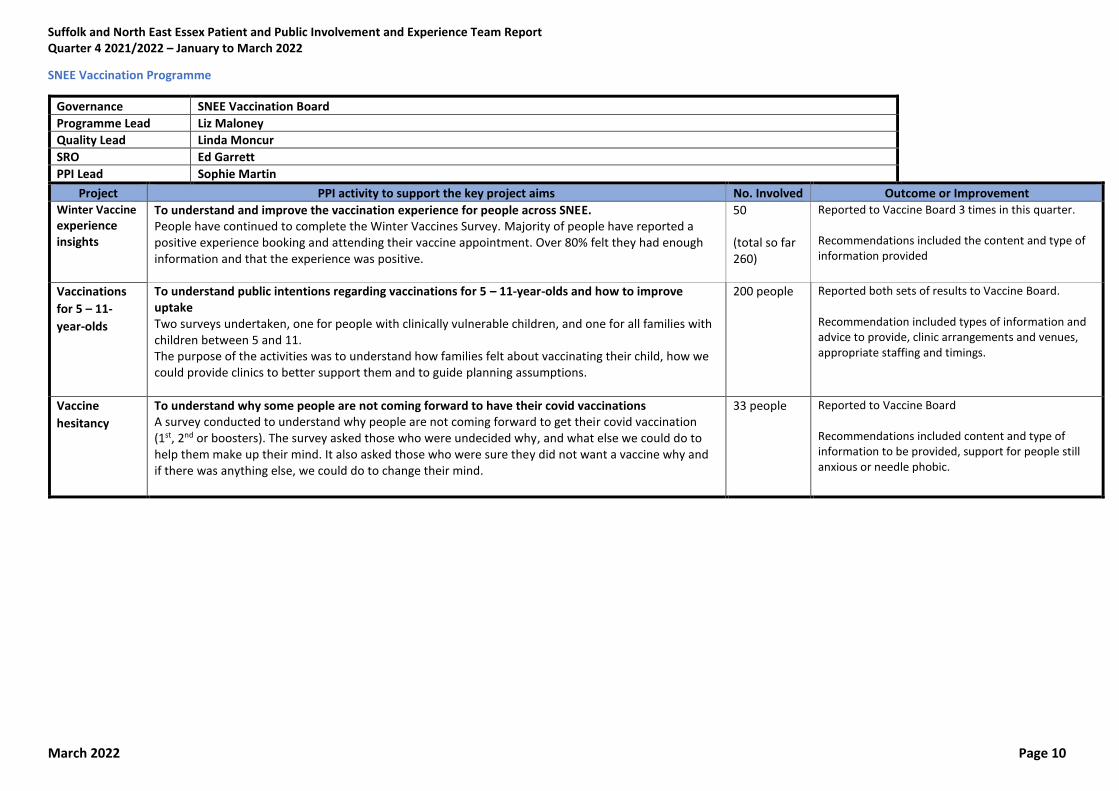
SNEE Vaccination Programme
Governance SNEE Vaccination Board
Programme Lead Liz Maloney
Quality Lead Linda Moncur
SRO Ed Garrett
PPI Lead Sophie Martin
Project PPI activity to support the key project aims No. Involved Outcome or Improvement Winter Vaccine experience insights
To understand and improve the vaccination experience for people across SNEE. People have continued to complete the Winter Vaccines Survey. Majority of people have reported a positive experience booking and attending their vaccine appointment. Over 80% felt they had enough information and that the experience was positive.
50 (total so far 260)
Reported to Vaccine Board 3 times in this quarter. Recommendations included the content and type of information provided
Vaccinations
for 5 – 11-
year-olds
To understand public intentions regarding vaccinations for 5 – 11-year-olds and how to improve uptake Two surveys undertaken, one for people with clinically vulnerable children, and one for all families with children between 5 and 11. The purpose of the activities was to understand how families felt about vaccinating their child, how we could provide clinics to better support them and to guide planning assumptions.
200 people Reported both sets of results to Vaccine Board. Recommendation included types of information and advice to provide, clinic arrangements and venues, appropriate staffing and timings.
Vaccine
hesitancy
To understand why some people are not coming forward to have their covid vaccinations A survey conducted to understand why people are not coming forward to get their covid vaccination (1st, 2nd or boosters). The survey asked those who were undecided why, and what else we could do to help them make up their mind. It also asked those who were sure they did not want a vaccine why and if there was anything else, we could do to change their mind.
33 people Reported to Vaccine Board Recommendations included content and type of information to be provided, support for people still anxious or needle phobic.
Suffolk and North East Essex Patient and Public Involvement and Experience Team Report Quarter 4 2021/2022 – January to March 2022
March 2022 Page 11
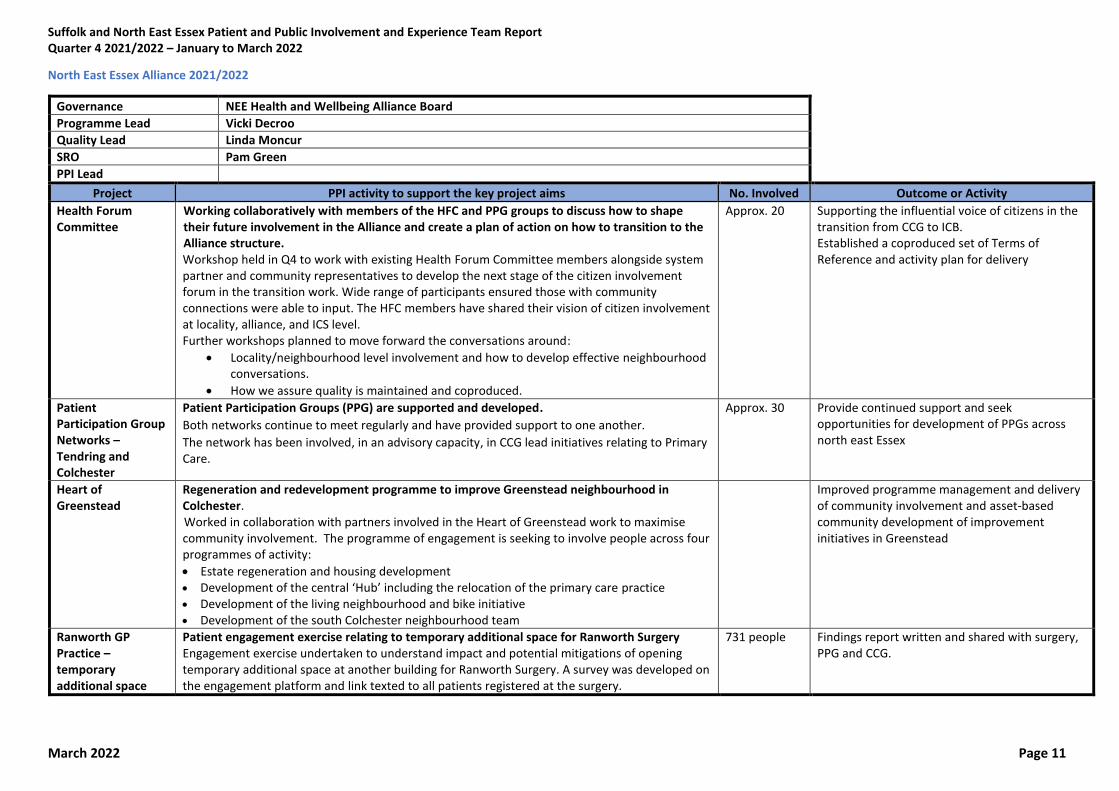
North East Essex Alliance 2021/2022
Governance NEE Health and Wellbeing Alliance Board
Programme Lead Vicki Decroo
Quality Lead Linda Moncur
SRO Pam Green
PPI Lead
Project PPI activity to support the key project aims No. Involved Outcome or Activity Health Forum Committee
Working collaboratively with members of the HFC and PPG groups to discuss how to shape their future involvement in the Alliance and create a plan of action on how to transition to the Alliance structure. Workshop held in Q4 to work with existing Health Forum Committee members alongside system partner and community representatives to develop the next stage of the citizen involvement forum in the transition work. Wide range of participants ensured those with community connections were able to input. The HFC members have shared their vision of citizen involvement at locality, alliance, and ICS level. Further workshops planned to move forward the conversations around:
• Locality/neighbourhood level involvement and how to develop effective neighbourhood conversations.
• How we assure quality is maintained and coproduced.
Approx. 20 Supporting the influential voice of citizens in the transition from CCG to ICB. Established a coproduced set of Terms of Reference and activity plan for delivery
Patient Participation Group Networks – Tendring and Colchester
Patient Participation Groups (PPG) are supported and developed. Both networks continue to meet regularly and have provided support to one another. The network has been involved, in an advisory capacity, in CCG lead initiatives relating to Primary Care.
Approx. 30 Provide continued support and seek opportunities for development of PPGs across north east Essex
Heart of Greenstead
Regeneration and redevelopment programme to improve Greenstead neighbourhood in Colchester. Worked in collaboration with partners involved in the Heart of Greenstead work to maximise community involvement. The programme of engagement is seeking to involve people across four programmes of activity:
• Estate regeneration and housing development
• Development of the central ‘Hub’ including the relocation of the primary care practice • Development of the living neighbourhood and bike initiative • Development of the south Colchester neighbourhood team
Improved programme management and delivery of community involvement and asset-based community development of improvement initiatives in Greenstead
Ranworth GP Practice – temporary additional space
Patient engagement exercise relating to temporary additional space for Ranworth Surgery Engagement exercise undertaken to understand impact and potential mitigations of opening temporary additional space at another building for Ranworth Surgery. A survey was developed on the engagement platform and link texted to all patients registered at the surgery.
731 people Findings report written and shared with surgery, PPG and CCG.
Suffolk and North East Essex Patient and Public Involvement and Experience Team Report Quarter 4 2021/2022 – January to March 2022
March 2022 Page 12
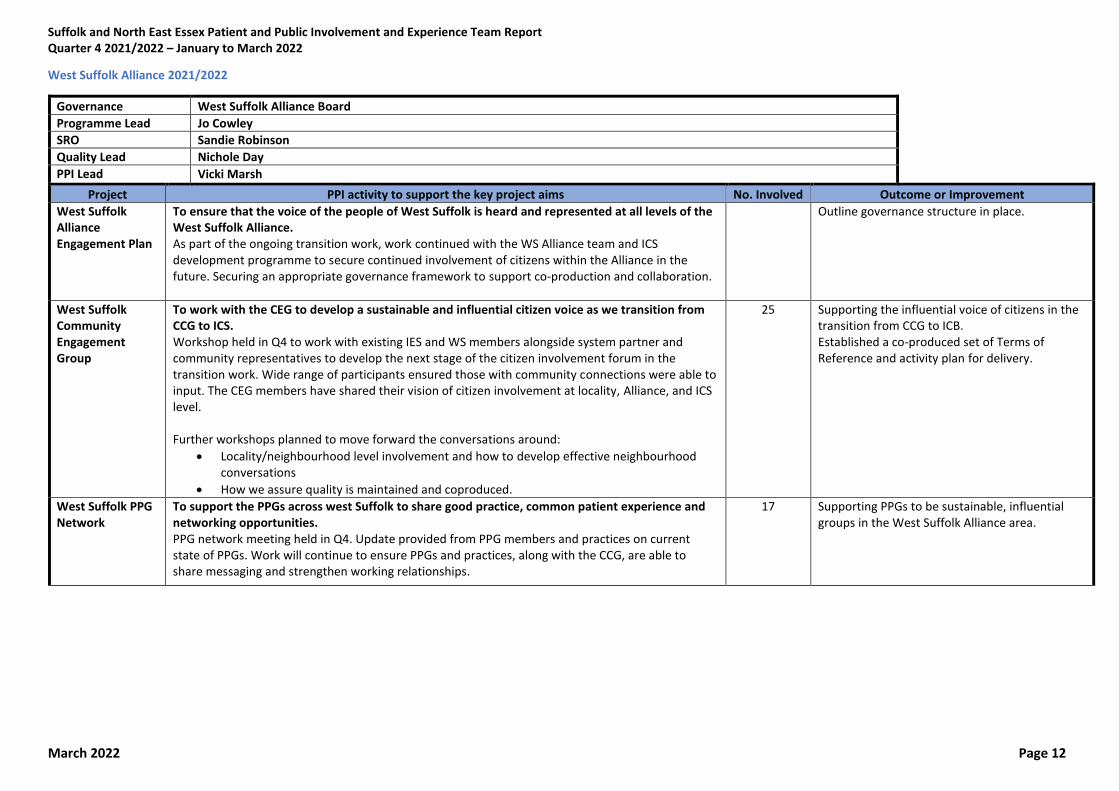
West Suffolk Alliance 2021/2022
Governance West Suffolk Alliance Board
Programme Lead Jo Cowley
SRO Sandie Robinson
Quality Lead Nichole Day
PPI Lead Vicki Marsh
Project PPI activity to support the key project aims No. Involved Outcome or Improvement
West Suffolk Alliance Engagement Plan
To ensure that the voice of the people of West Suffolk is heard and represented at all levels of the West Suffolk Alliance. As part of the ongoing transition work, work continued with the WS Alliance team and ICS development programme to secure continued involvement of citizens within the Alliance in the future. Securing an appropriate governance framework to support co-production and collaboration.
Outline governance structure in place.
West Suffolk Community Engagement Group
To work with the CEG to develop a sustainable and influential citizen voice as we transition from CCG to ICS. Workshop held in Q4 to work with existing IES and WS members alongside system partner and community representatives to develop the next stage of the citizen involvement forum in the transition work. Wide range of participants ensured those with community connections were able to input. The CEG members have shared their vision of citizen involvement at locality, Alliance, and ICS level. Further workshops planned to move forward the conversations around:
• Locality/neighbourhood level involvement and how to develop effective neighbourhood conversations
• How we assure quality is maintained and coproduced.
25 Supporting the influential voice of citizens in the transition from CCG to ICB. Established a co-produced set of Terms of Reference and activity plan for delivery.
West Suffolk PPG Network
To support the PPGs across west Suffolk to share good practice, common patient experience and networking opportunities. PPG network meeting held in Q4. Update provided from PPG members and practices on current state of PPGs. Work will continue to ensure PPGs and practices, along with the CCG, are able to share messaging and strengthen working relationships.
17 Supporting PPGs to be sustainable, influential groups in the West Suffolk Alliance area.
Suffolk and North East Essex Patient and Public Involvement and Experience Team Report Quarter 4 2021/2022 – January to March 2022
March 2022 Page 13
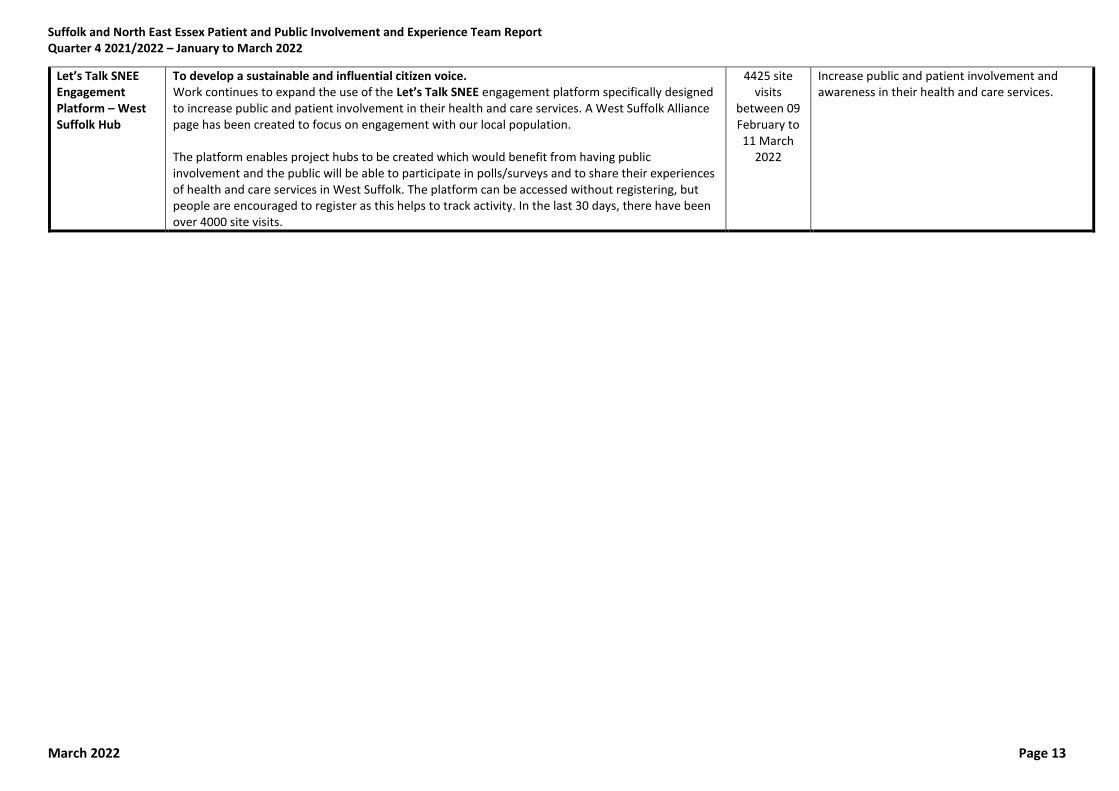
Let’s Talk SNEE Engagement Platform – West Suffolk Hub
To develop a sustainable and influential citizen voice. Work continues to expand the use of the Let’s Talk SNEE engagement platform specifically designed to increase public and patient involvement in their health and care services. A West Suffolk Alliance page has been created to focus on engagement with our local population. The platform enables project hubs to be created which would benefit from having public involvement and the public will be able to participate in polls/surveys and to share their experiences of health and care services in West Suffolk. The platform can be accessed without registering, but people are encouraged to register as this helps to track activity. In the last 30 days, there have been over 4000 site visits.
4425 site visits
between 09 February to 11 March
2022
Increase public and patient involvement and awareness in their health and care services.
Suffolk and North East Essex Patient and Public Involvement and Experience Team Report Quarter 4 2021/2022 – January to March 2022
March 2022 Page 14
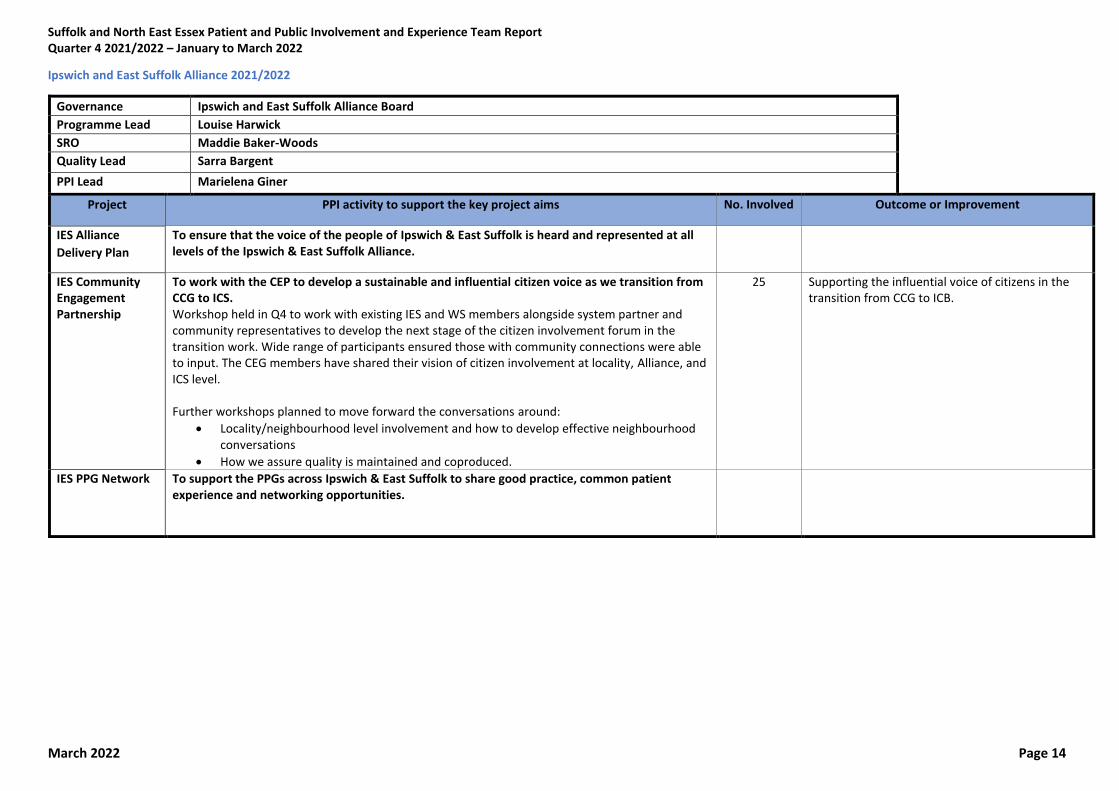
Ipswich and East Suffolk Alliance 2021/2022
Governance Ipswich and East Suffolk Alliance Board
Programme Lead Louise Harwick
SRO Maddie Baker-Woods
Quality Lead Sarra Bargent
PPI Lead Marielena Giner
Project PPI activity to support the key project aims No. Involved Outcome or Improvement
IES Alliance
Delivery Plan
To ensure that the voice of the people of Ipswich & East Suffolk is heard and represented at all levels of the Ipswich & East Suffolk Alliance.
IES Community Engagement Partnership
To work with the CEP to develop a sustainable and influential citizen voice as we transition from CCG to ICS. Workshop held in Q4 to work with existing IES and WS members alongside system partner and community representatives to develop the next stage of the citizen involvement forum in the transition work. Wide range of participants ensured those with community connections were able to input. The CEG members have shared their vision of citizen involvement at locality, Alliance, and ICS level. Further workshops planned to move forward the conversations around:
• Locality/neighbourhood level involvement and how to develop effective neighbourhood conversations
• How we assure quality is maintained and coproduced.
25 Supporting the influential voice of citizens in the transition from CCG to ICB.
IES PPG Network To support the PPGs across Ipswich & East Suffolk to share good practice, common patient experience and networking opportunities.
Suffolk and North East Essex Patient and Public Involvement and Experience Team Report Quarter 4 2021/2022 – January to March 2022
March 2022 Page 15
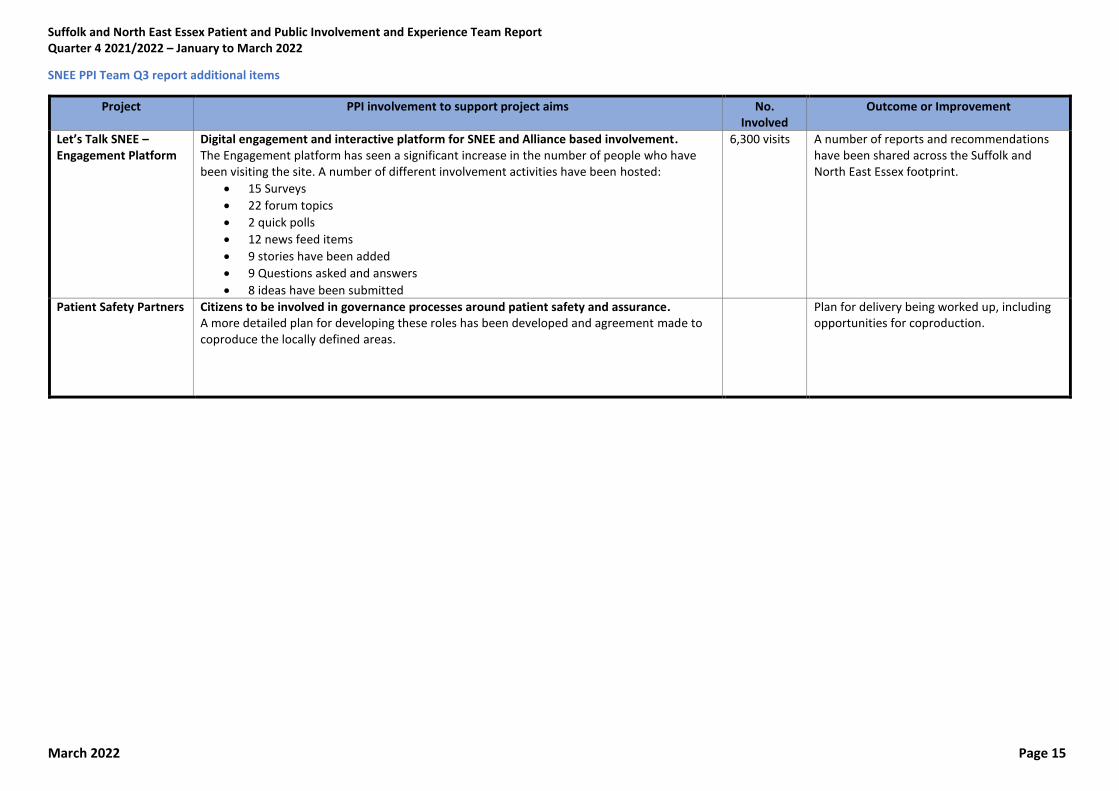
SNEE PPI Team Q3 report additional items
Project PPI involvement to support project aims No. Involved
Outcome or Improvement
Let’s Talk SNEE – Engagement Platform
Digital engagement and interactive platform for SNEE and Alliance based involvement. The Engagement platform has seen a significant increase in the number of people who have been visiting the site. A number of different involvement activities have been hosted:
• 15 Surveys
• 22 forum topics
• 2 quick polls
• 12 news feed items
• 9 stories have been added
• 9 Questions asked and answers
• 8 ideas have been submitted
6,300 visits
A number of reports and recommendations have been shared across the Suffolk and North East Essex footprint.
Patient Safety Partners
Citizens to be involved in governance processes around patient safety and assurance. A more detailed plan for developing these roles has been developed and agreement made to coproduce the locally defined areas.
Plan for delivery being worked up, including opportunities for coproduction.
Suffolk and North East Essex Patient and Public Involvement and Experience Team Report Quarter 4 2021/2022 – January to March 2022
March 2022 Page 16
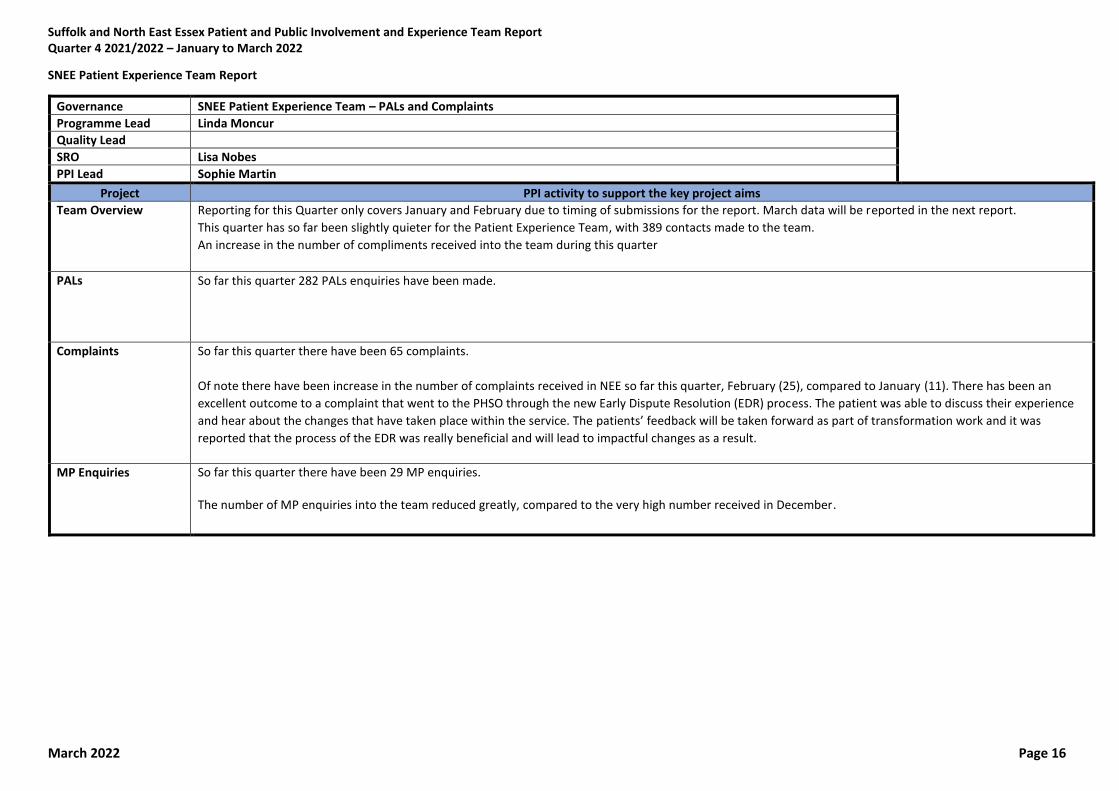
SNEE Patient Experience Team Report
Governance SNEE Patient Experience Team – PALs and Complaints
Programme Lead Linda Moncur
Quality Lead
SRO Lisa Nobes
PPI Lead Sophie Martin
Project PPI activity to support the key project aims
Team Overview Reporting for this Quarter only covers January and February due to timing of submissions for the report. March data will be reported in the next report.
This quarter has so far been slightly quieter for the Patient Experience Team, with 389 contacts made to the team.
An increase in the number of compliments received into the team during this quarter
PALs So far this quarter 282 PALs enquiries have been made.
Complaints So far this quarter there have been 65 complaints.
Of note there have been increase in the number of complaints received in NEE so far this quarter, February (25), compared to January (11). There has been an
excellent outcome to a complaint that went to the PHSO through the new Early Dispute Resolution (EDR) process. The patient was able to discuss their experience
and hear about the changes that have taken place within the service. The patients’ feedback will be taken forward as part of transformation work and it was
reported that the process of the EDR was really beneficial and will lead to impactful changes as a result.
MP Enquiries So far this quarter there have been 29 MP enquiries. The number of MP enquiries into the team reduced greatly, compared to the very high number received in December.
Page 1 of 3
GOVERNING BODY
Agenda Item No. 08
Reference No. IESCCG 22-17
Date. 24 May 2022
Title
Research Strategy for Suffolk and North East Essex Integrated Care System
Lead Director
Lisa Nobes, Director of Nursing
Author(s)
Clare Symms, Head of Research Management, Finance and PPI, Norfolk and Waveney CCG, on behalf of CCGs in Suffolk
Purpose
For approval
Applicable CCG Clinical Priorities:
1. To promote self care
2. To ensure high quality local services where possible x
3. To improve the health of those most in need x
4. To improve health and educational attainment for children and young people
5. To improve access to mental health services
6. To improve outcomes for patients with diabetes to above national averages x
7. To improve care for frail elderly individuals x
8. To allow patients to die with dignity and compassion and to choose their place of death where appropriate
9. To ensure that the CCG operates within agreed budgets
Action required by Governing Body: For approval with a view to the strategy being adopted as we move from CCGs to an ICB. This strategy is being taken to all 3 SNEE CCG Governing Bodies.
Page 2 of 3
1. Background 1.1 Research brings a number of benefits - It is one of the main drivers in providing evidence-
based improved treatment and care, organisations that are research active have better outcomes for their patients and service users, even within services that are not directly involved, it can help with staff recruitment and retention and professional development.
1.2 ICBs will have specific duties to promote research and innovation across their system and
support partners within the system to do the same. 1.3 Two stakeholder workshops were held in December 2021 to look at developing a research
strategy for Suffolk and North East Essex. This was facilitated by the Research Team at NHS Norfolk and Waveney CCG (with whom we have an SLA) and included a wide range of stakeholders across the system to look at the current strengths and weaknesses in the system and what a good research system might look like. Reports from the workshops were sent to all stakeholders and this strategy was developed following.
1.4 Individual partners within the Suffolk and North East Essex ICS have a good track record of
delivering research and collaborating on studies, the strategy aims to build on the good work that already exists.
2. Key Issues 2.1 This research strategy, the first for the Suffolk and North East Essex Integrated Care System
(SNEE ICS), sets out a vision to build a culture of research across that is responsive to those in most need in the communities that it serves, building on what has already been achieved. The strategy outlines 5 key aims: 1. To build a flexible, system-wide approach to research across the Suffolk and North East
Essex ICS
2. To build on our academic partnerships to develop research ideas and achieve research
funding
3. To empower research teams, services, service users and carers to work as partners to
help deliver, develop and support high quality research
4. To embed a culture of research, innovation and use of evidence across the ICS
5. For research to be visible, meaningful and accessible
2.2 The strategy also sets out the key outcomes we expect to see if the strategy is delivered and
how this would be measured. 2.3 The strategy is expected to provide a framework for delivering the research duties of the ICS
and creating a research rich environment that will meet the needs of our population and communities as we move forwards into an ICS.
2.4 Partnership and system wide working, collaboration and co-production are key drivers behind
the aims to build a robust and accessible research system within SNEE. 2.5 Leadership will be a key aspect in delivering of this strategy and achieving the desired
outcomes across the ICS, alongside a mechanism for overseeing research activity at an ICS level either through existing structures or collaborations or through the establishment of a research specific forum.
2.6 Research infrastructure within the ICS is through research teams within NHS Trusts (the
resources and funding for which varies by organisation), and via the NIHR Clinical Research Network (CRN) East of England. The CRN also provide some funding and infrastructure for research in social care and public health.
Page 3 of 3
2.7 A Service Level Agreement for Research support exists between the Suffolk CCGs and
Norfolk and Waveney CCG via the Research Office at Norfolk and Waveney CCG for support within the CCG and within Primary Care, however ownership of the strategy by the SNEE ICS will be critical if the ambitions within the strategy are to be realised.
2.8 It is hoped that through this strategy and collaborative working further research monies will
be attracted into the region through attracting research studies to the region and achieving research grant funding.
2.9 The strategy has been written with a view to being adopted by the CCGs and taken forward
into the ICB. 3. Patient and Public Engagement 3.1 42 attendees (excluding facilitators) took part in two stakeholder workshops to inform the
development of the strategy. A wide range of stakeholders were represented including representatives from Healthwatch and other patient and public involvement representatives, as well as representatives from the Suffolk and North East Essex CCGs, SuNEE Trusts, GP practices, academic partners, National Institute for Health and Care Research (NIHR) Clinical Research Network (CRN) East of England, and Public Health.
3.2 Across the two workshops, stakeholders explored: where we currently were as a system; our
strengths, weaknesses, opportunities, and challenges; what we would like to see in a successful research system; and what steps we might need to take to get there.
3.3 Individuals who expressed interest in helping to draft the strategy following the workshops
have been given the opportunity to review a draft of this strategy and a number of changes have been made as a result.
4. Recommendation 4.1 It is recommended that the CCG adopt the strategy with a view to this being taken forward as
we move from CCGs to an ICB. This strategy is being taken to all 3 SNEE CCG Governing Bodies
1 | P a g e
Research Strategy for Suffolk and North East Essex Integrated Care
System – 2022 - 2027
1 INTRODUCTION
The Suffolk and North East Essex (SNEE) Integrated care system (ICS)1 is one of 42 ICSs
across England, as announced by the Chief Executive of the NHS on April 1, 2021. These
bring together providers and commissioners of NHS services across a geographical area
with local authorities and other local partners to collectively plan health and care services to
meet the needs of their population. ICSs were a key part of the NHS Long Term Plan, and
the Health and Care Bill, which is set to become the Health and Care Act, will put Integrated
Care Systems (ICSs) on a statutory footing from 1st July 2022.
The central aim of each ICSs is to integrate care across different organisations and settings,
joining up hospital and community-based services, physical and mental health, and health
and social care. Research is a core function of health and social care. Thus, development of
a robust research and evidence culture is an essential ingredient to the success of ICSs.
The Suffolk and North East Essex ICS builds on the earlier work of the Suffolk and North
East Essex Sustainability and Transformation Partnership (STP). The full spectrum of
partners engaged in the ICS includes NHS Commissioners, NHS Provider Trusts, Local
government, NHS regulators, primary care – GPs, community pharmacists, optometrists and
dentists, independent sector providers, community and voluntary sector, public, patient and
carer groups, education and research and other sectors including industry, police and
education.
The new Health and Care Bill gives ICSs duties to promote research and innovation, and to
facilitate partners to do the same; the NHS constitution provides a commitment to
“innovation and to the promotion, conduct and use of research to improve the current and
future health and care of the population” and expectation that users of the NHS will be given
opportunities to participate in research relevant to their care. To ensure research that is
aligned with the Suffolk and North East Essex Integrated Care System, this document sets
out our inaugural research strategy over the next 5 years.
2 ACHIEVING OUR AMBITIONS AS AN ICS
Our eight ‘Higher Ambitions’ as an ICS, as set out below, and on our website relate to the
key long standing health and care challenges in our region, and link to the priorities set by
the Health and Wellbeing Boards in Essex and Suffolk in their Joint Health and Wellbeing
Strategies.
• Our Primary Ambition: Reducing Health Inequalities
1 Suffolk & North East Essex Integrated Care System - Suffolk & North East Essex Integrated Care System (sneeics.org.uk)
2 | P a g e
• A healthier life for everyone
• Emotional wellbeing from the start of life
• Zero Suicide
• Earlier diagnosis and treatment for cancer
• An effective treatment pathway for obesity
• The best quality of life as we grow older
• The care and support we need at the end of life
It is the intention that this research strategy will inform the development of a robust
collaborative infrastructure and culture for research across our ICS, enabling the delivery,
development and dissemination of research aligned to these ambitions and the key needs of
our population.
ACADEMIC LINKS Our key academic partners currently include the University of Suffolk (UoS), Anglia Ruskin
University (ARU), University of Essex and University of East Anglia (UEA).
The University of Suffolk (UoS), established in 2016, is the first university in the county, and
fully embraces a culture of research, as demonstrated by its four new research institutes
launched this year; Institute for Social Justice and Crime; Suffolk Sustainability Institute;
Institute of Health and Wellbeing; and the Digital Futures Institute. The Integrated Care
Academy (ICA) at UoS is a unique partnership between SNEE ICS, UoS, Suffolk County
Council and Healthwatch Suffolk; the first in the country to formally bring together the four
pillars of higher education, an integrated care system, local authority, and the voluntary and
community sector. At the ICA co-production is key, with specialised integrated care training
courses offered through its Co-production Hub.
The three priority areas of the ICA purposefully align with SNEE ICS:
• Improving mental health and wellbeing
• Supporting best quality of life as we grow older
• Optimising care and support towards end of life
We have close working relationships through East Suffolk and North Essex NHS Foundation
Trust (ESNEFT) with Anglia Ruskin University (ARU), particularly in relation to AI and the
medical school, and University of Essex. With ARU launching its Wellbeing Research and
Innovation Network in January 2022, with a key goal of improving health and wellbeing
across the Eastern region.
SNEE NHS Trusts and CCGs were also founder partners of the University of East Anglia
(UEA) Health and Social Care Partners (UEAHSCP), which brings together researchers and
academics across health and social care organisations in Norfolk, Suffolk and North East
Essex to conduct collaborative research to address the key health and care challenges for
the region.
Given the infancy of our Integrated Care System, which like the rest of the England, comes
into being on 1st July 2022, this strategy is designed to be flexible to respond to changing
priorities and focus both locally, within SNEE, as well as changes to national strategy and
direction.
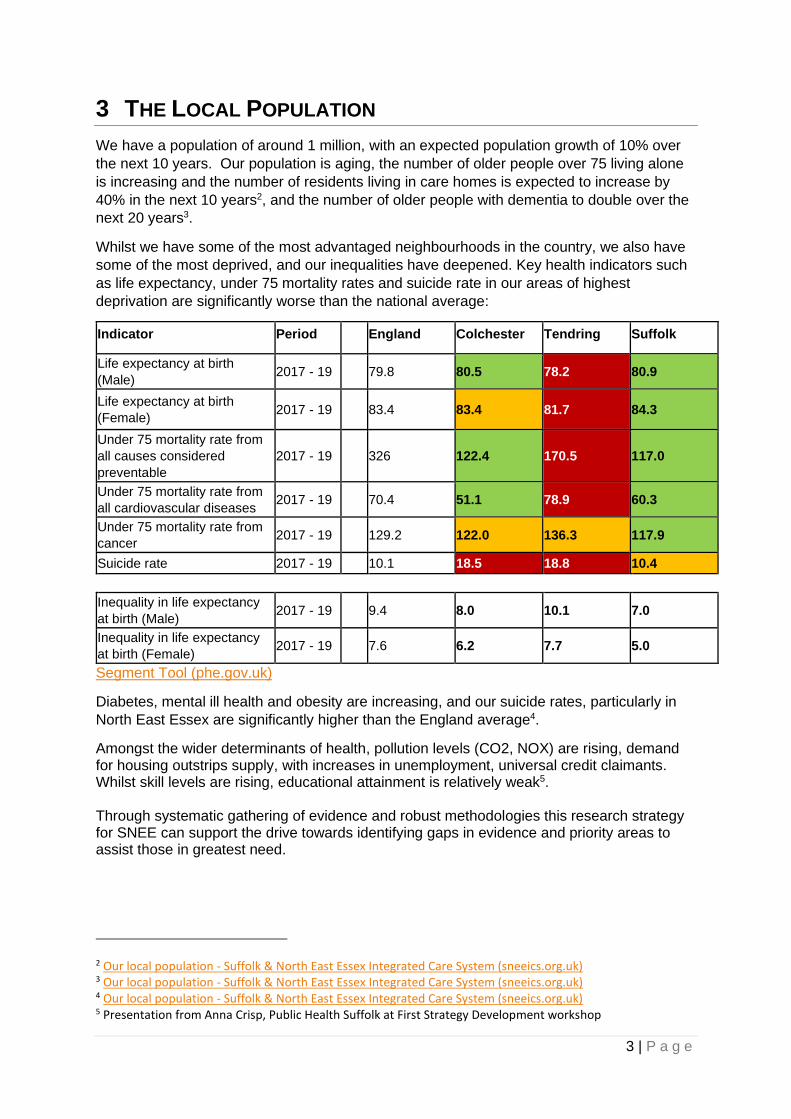
3 | P a g e
3 THE LOCAL POPULATION
We have a population of around 1 million, with an expected population growth of 10% over
the next 10 years. Our population is aging, the number of older people over 75 living alone
is increasing and the number of residents living in care homes is expected to increase by
40% in the next 10 years2, and the number of older people with dementia to double over the
next 20 years3.
Whilst we have some of the most advantaged neighbourhoods in the country, we also have
some of the most deprived, and our inequalities have deepened. Key health indicators such
as life expectancy, under 75 mortality rates and suicide rate in our areas of highest
deprivation are significantly worse than the national average:
Indicator Period England Colchester Tendring Suffolk
Life expectancy at birth
(Male) 2017 - 19 79.8 80.5 78.2 80.9
Life expectancy at birth
(Female) 2017 - 19 83.4 83.4 81.7 84.3
Under 75 mortality rate from
all causes considered
preventable
2017 - 19 326 122.4 170.5 117.0
Under 75 mortality rate from
all cardiovascular diseases 2017 - 19 70.4 51.1 78.9 60.3
Under 75 mortality rate from
cancer 2017 - 19 129.2 122.0 136.3 117.9
Suicide rate 2017 - 19 10.1 18.5 18.8 10.4
Inequality in life expectancy
at birth (Male) 2017 - 19 9.4 8.0 10.1 7.0
Inequality in life expectancy
at birth (Female) 2017 - 19 7.6 6.2 7.7 5.0
Segment Tool (phe.gov.uk)
Diabetes, mental ill health and obesity are increasing, and our suicide rates, particularly in
North East Essex are significantly higher than the England average4.
Amongst the wider determinants of health, pollution levels (CO2, NOX) are rising, demand for housing outstrips supply, with increases in unemployment, universal credit claimants. Whilst skill levels are rising, educational attainment is relatively weak5. Through systematic gathering of evidence and robust methodologies this research strategy for SNEE can support the drive towards identifying gaps in evidence and priority areas to assist those in greatest need.
2 Our local population - Suffolk & North East Essex Integrated Care System (sneeics.org.uk) 3 Our local population - Suffolk & North East Essex Integrated Care System (sneeics.org.uk) 4 Our local population - Suffolk & North East Essex Integrated Care System (sneeics.org.uk) 5 Presentation from Anna Crisp, Public Health Suffolk at First Strategy Development workshop
4 | P a g e
4 WHY IS RESEARCH IMPORTANT?
Research is essential in health and social care. It is one of the main drivers in providing
evidence-based improved treatment and care options for individuals, helping us to find out
which treatments work better and improving our understanding of individuals experience of
care and what is important to them in managing their health. Research can, and must, help
identify gaps in knowledge and change the way that we work. The research undertaken
during the COVID-19 pandemic not only gave us effective treatments and vaccinations, but it
also led to a greater understanding of how COVID-19 spread, and how the pandemic
affected individuals and society as a whole6.
Co-production in research, working in collaboration with service users and those with whom
the research will have the most impact, to develop and deliver research is recognised as
essential to delivering robust and impactful research. Service users, carers and frontline
staff can not only offer a unique perspective on the questions that are most important, but
also on the deliverability of research and engagement of differing populations and
communities. This is essential if we are to make research accessible to our differing
communities.
There is a growing body of evidence7891011 which demonstrates that hospitals that are
research active have better outcomes, and that patients and services not directly involved in
the trials themselves still benefit from being in research-active organisations. Evidence is
also growing that this also applies to other health and care settings.
The Care Quality Commission (CQC) now includes an assessment of opportunities for
service users to join research projects and clinical trials as one of the characteristics of a
‘Well-Led’ organisation, and research offers learning and development opportunities for staff,
and can help with recruitment and retention, helping organisations to flourish.
This research strategy, the first for SNEE, is key to creating a research rich environment to
identify and generate the reforms necessary as we move into a phase of recovery for a
better future.
5 DEVELOPMENT OF THIS STRATEGY AND VISION
The development of this strategy for research has been informed through two system wide
workshops, held in December 2021 with stakeholders able to comment and shape the
resulting strategy (this strategy) that has emerged.
We would like to express our thanks to all those who attended the workshop and helped to
shape the strategy as it now stands.
6 NIHR Evidence - Browse content - Informative and accessible health and care research 7Patients admitted to more research‐active hospitals have more confidence in staff and are better informed about
their condition and medication: Results from a retrospective cross‐sectional study 8 The correlation between National Health Service trusts' clinical trial activity and both mortality rates and care quality commission ratings: a retrospective cross-sectional study 9 Research activity and the association with mortality; 10 High hospital research participation and improved colorectal cancer survival outcomes: a population-based study 11 Does the engagement of clinicians and organisations in research improve healthcare performance: a three-stage review
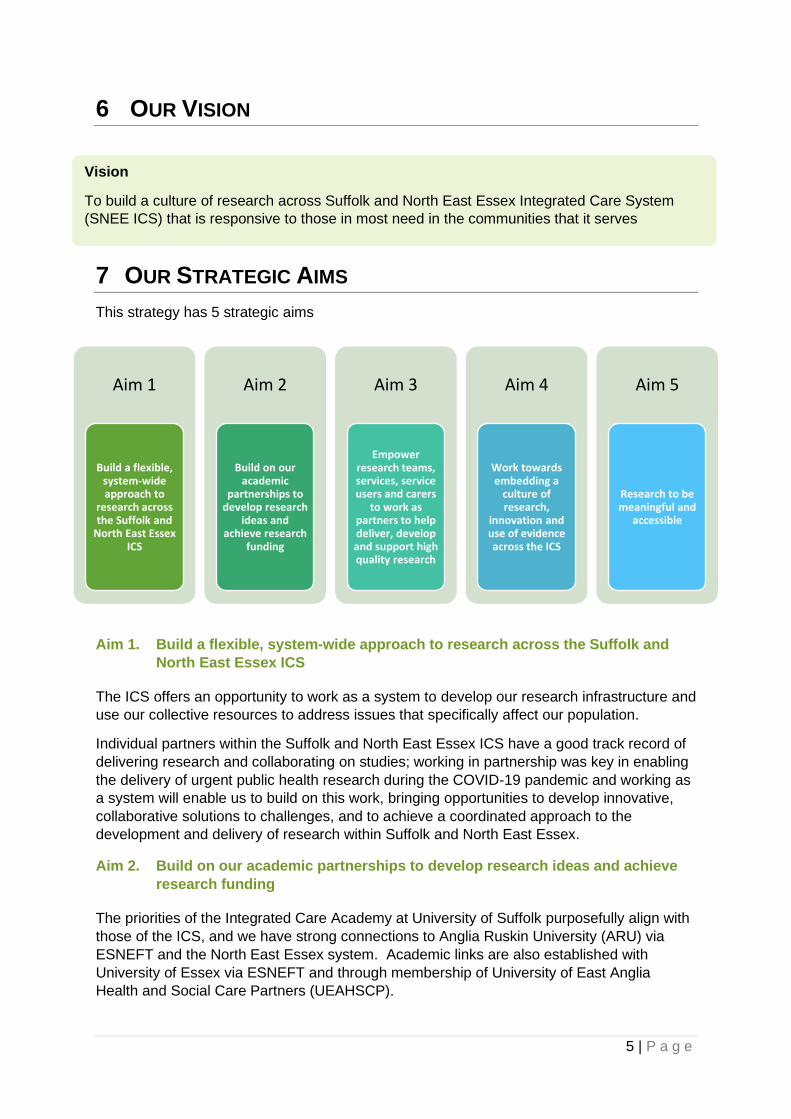
5 | P a g e
6 OUR VISION
7 OUR STRATEGIC AIMS
This strategy has 5 strategic aims
Aim 1. Build a flexible, system-wide approach to research across the Suffolk and
North East Essex ICS
The ICS offers an opportunity to work as a system to develop our research infrastructure and
use our collective resources to address issues that specifically affect our population.
Individual partners within the Suffolk and North East Essex ICS have a good track record of
delivering research and collaborating on studies; working in partnership was key in enabling
the delivery of urgent public health research during the COVID-19 pandemic and working as
a system will enable us to build on this work, bringing opportunities to develop innovative,
collaborative solutions to challenges, and to achieve a coordinated approach to the
development and delivery of research within Suffolk and North East Essex.
Aim 2. Build on our academic partnerships to develop research ideas and achieve
research funding
The priorities of the Integrated Care Academy at University of Suffolk purposefully align with
those of the ICS, and we have strong connections to Anglia Ruskin University (ARU) via
ESNEFT and the North East Essex system. Academic links are also established with
University of Essex via ESNEFT and through membership of University of East Anglia
Health and Social Care Partners (UEAHSCP).
Vision
To build a culture of research across Suffolk and North East Essex Integrated Care System
(SNEE ICS) that is responsive to those in most need in the communities that it serves
Aim 1
Build a flexible, system-wide approach to
research across the Suffolk and
North East Essex ICS
Aim 2
Build on our academic
partnerships to develop research
ideas and achieve research
funding
Aim 3
Empower research teams, services, service users and carers
to work as partners to help deliver, develop and support high quality research
Aim 4
Work towards embedding a
culture of research,
innovation and use of evidence across the ICS
Aim 5
Research to be meaningful and
accessible
6 | P a g e
Building and strengthening these partnerships gives opportunities to identify and develop
ideas at a system wide level and bid for research monies. Bringing together individuals from
across the system to develop truly collaborative projects that are realistic, achievable,
academically sound and meet the needs of our population, to get the best chance of
achieving funding.
Aim 3. Empower research teams, services, service users and carers to work as
partners to help deliver, develop and support high quality research
Involving service users and frontline staff in all aspects of the research pathway helps to
ensure research focuses on what is most important to service users and staff delivering
care; is practical and acceptable to those it is aimed to help; and supports inclusion across
different populations and communities. Co-production is an essential element in addressing
the needs and challenges of the communities the research is designed to serve.
Aim 4. Embedding a culture of research, innovation and use of evidence across the
ICS
As described in section 4, increasing evidence shows that research active organisations
have better outcomes for their patients and services users, providing evidence-based
improved treatment and care options, and offering staff professional developmental
opportunities. Engagement of our services in research also ensures that the findings from
that research are applicable to our population.
Raising awareness and visibility of research, promoting opportunities for staff and service
users and highlighting how staff can get involved, will help to embed research within the
everyday working of the ICS, increasing opportunities for service users and staff to
participate.
Embedding learning from local, national and international research into the commissioning
and delivery of services helps to ensure people receive the most effective services and
provide the best possible outcomes for their health and wellbeing.
Aim 5. Research to be visible, meaningful and accessible
To achieve the best outcomes and engagement, research needs to be accessible to all.
Increasing communication and visibility of research in a format that is accessible and
inclusive will help support the development of a research culture within the ICS, increase
knowledge and engagement of staff and service users and support inclusivity of research.
Consideration is needed around communication of research opportunities, dissemination of
research results and findings, identification of local impact as well as access to, availability
and use of evidence. Much research in health and care is publicly funded, communication
and visibility of research helps demonstrate the benefits of public money invested in
research.
7 | P a g e
8 KEY OUTCOMES
DELIVERY OF THIS STRATEGY IS EXPECTED TO RESULT IN THE FOLLOWING
OUTCOMES.
By 2027 we will have:
1. Built the profile of research within the Suffolk and North East Essex ICS
2. Built a positive reputation for delivery of research within the region
3. Developed locally led collaborative research aligned to local and national priorities
that attracting national funding into the region
4. Established strong networks and partnerships for research across the Suffolk, North
East Essex region – working together across system, place and neighbourhood to
address challenges in research, deliver solutions and champion research
5. Empowered individuals to engage in and champion research
6. Increased dissemination of findings, activities, impact and stories to partners and
service users across our ICS
Measured through:
• An increase in the number and scope of research projects delivered locally
(Outcomes 1,4,5)
• Increased engagement of communities in research, particularly in areas of most need
(Outcomes 1,2,4,5,6)
• Achieving repeat business from external research teams coming back to the SNEE
region to deliver their research (Outcomes 1,2)
• An increase in the number and value of research grants achieving national funding
held by SNEE ICS partners (Outcomes 2,3,4,5).
• An increase in the number of and grant applications developed collaboratively within
SNEE (Outcomes 3,4,5)
• Research champions embedded within ICS partners (Outcome 5)
• An increase in locally led research publications and communications (Outcome 6)
• Research activity featuring more regularly within ICS and partner communications
(Outcome 6)
9 ACKNOWLEDGEMENTS
This strategy was developed following two virtual workshops held in Quarter 3 21/22 which
explored: where we currently were as a system; our strengths, weaknesses, opportunities,
and challenges; what we would like to see in a successful research system; and what steps
we might need to take to get there.
Delegates included: commissioners and practitioners from across the healthcare sector in
Suffolk and North East Essex; representatives from public health, social care, and the public
voice; academic partners and other relevant stakeholders such as the National Institute for
Health and Care Research Clinical Research Network (NIHR CRN) for the Eastern region -
CRN East of England.
8 | P a g e
The workshops were organised and led by the Research Office at NHS Norfolk and
Waveney CCG (Clinical Commissioning Group) with whom Ipswich and East Suffolk CCG
and West Suffolk CCG hold a Service Level Agreement (SLA), with the support of Lisa
Nobes, Director of Nursing, NHS Suffolk and North East Essex CCG and Mark Shenton
Chair/ GP East Suffolk.
10 GLOSSARY
Acronym Title Description
ARU Anglia Ruskin University
CCG Clinical Commissioning Group
CCGs commission most of the hospital and community NHS services in the local areas for which they are responsible. Commissioning involves deciding what services are needed for diverse local populations, and ensuring that they are provided. From 1st July 2022 CCGs will be replaced by Integrated Care Boards (ICB)
CQC Care Quality Commission
CQC is the independent regulator of health and social care in England. They make sure health and social care services provide people with safe, effective, compassionate, high-quality care and encourage care services to improve. https://www.cqc.org.uk/
CRN Clinical Research Network
The NIHR CRN includes 15 local networks who coordinate and support the delivery of research in England. They provide local funding for staff, facilities, equipment and support services to support research within health and social care organisations. Clinical Research Network | NIHR
ESNEFT East Suffolk and North Essex NHS Foundation Trust
ESNEFT provides hospital and community health care services for Colchester, Ipswich and local areas. Formed on 1st July 2018, ESNEFT is the largest NHS organisation in the region.
ICA Integrated Care Academy
The Integrated Care Academy (ICA) at University of Suffolk is a partnership between the University of Suffolk, the Suffolk and North East Essex ICS, Suffolk County Council and Healthwatch Suffolk and others from the voluntary and community sector. It is the leading academic partner for local health and social care services working in mental health, care for older people and end of life care, and for all people and communities who are interested in learning, including service users, their families and carers.
ICB Integrated Care Board
Each ICS will be led by an ICB, the organisation with responsibility for NHS functions and budgets. ICBs will replace CCGs on 1st July 2022 as the organisation responsible for commissioning services
9 | P a g e
ICS Integrated Care System
ICSs are new partnerships between the organisations that meet health and care needs across an area, to coordinate services and to plan in a way that improves population health and reduces inequalities between different groups
NIHR National Institute for Health and Care Research
The NIHR was established in 2006, and is funded by Department of Health and Social Care. Working in partnership with the NHS, universities, local government, other research funders, patients and the public, the NIHR funds, enables and delivers world-leading health and social care research that improves people's health and wellbeing and promotes economic growth. https://www.nihr.ac.uk/
SLA Service Level Agreement
Agreement between partners to deliver a service – in the case of this document – this is an agreement between Suffolk CCGs and the Norfolk and Waveney CCG to deliver research support
SNEE Suffolk and North East Essex
SNEE is the region this strategy applies to and the region covered by the SNEE ICS
STP Sustainability and Transformation Partnership
Sustainability and transformation partnerships (STPs) were introduced in 2016 to bring together local NHS organisations and local authorities to develop proposals to improve health and the quality of care to provide better services for patients in the areas they serve. These have been replaced by ICSs
UEA University of East Anglia
UEAHSCP UEA Health and Social Care Partners
UEA Health and Social Care Partners (UEAHSCP), brings together world-class researchers and academics across health and social care organisations in Norfolk, Suffolk and North East Essex to conduct collaborative research to address the key health challenges in the region
UoS University of Suffolk
Page 1 of 3
GOVERNING BODY
Agenda Item No. 09
Reference No. IESCCG 22-18
Date. 24 May 2022
Title
Keyworking Function
Lead Director
Lisa Nobes, Director of Nursing
Author(s)
Anita Farrant
Purpose
Decision making
Applicable CCG Clinical Priorities:
1. To promote self care
2. To ensure high quality local services where possible ✓
3. To improve the health of those most in need ✓
4. To improve health and educational attainment for children and young people ✓
5. To improve access to mental health services ✓
6. To improve outcomes for patients with diabetes to above national averages
7. To improve care for frail elderly individuals
8. To allow patients to die with dignity and compassion and to choose their place of death where appropriate
9. To ensure that the CCG operates within agreed budgets
Action required by Governing Body: 1. To support the recommendation that the CCG commissions Suffolk County Council (SCC) to
provide the key working Function in Suffolk 2. To sanction a waiver to competitive tendering on the grounds that: there is a clear benefit to be
gained from maintaining continuity with an earlier project.
Page 2 of 3
1. Background 1.1. The Keyworking Function has been developed as a response to the NHS England & NHS
Improvement Long Term Plan (LTP) commitment that by 2023/24, children and young people with a learning disability, autism, or both, with the most complex needs will have a designated Keyworker: implementing the recommendations made by Dame Christine Lenehan. These are our children: a review by Dame Christine Lenehan (publishing.service.gov.uk)
1.2. Aims and Objectives of the Keyworking Function.
cdc.keyworking.guidance.v4.pdf (councilfordisabledchildren.org.uk) 1.2.1. Aim
Initially to provide Keyworking support to vulnerable children and young people (CYP) with a learning disability, autism, or both, to avoid unnecessary admission into mental health or specialist learning disability settings and to keep them and their families safe and well in their community. Support will, in 2023/24, be extended to include those aged up to 25 years.
1.2.2. Objectives
• Identify CYP with a learning disability, autism or both who are at risk of admission to a Tier 4 setting.
• Support these CYP and their families to navigate the system to ensure there is one holistic plan for the family that meets their needs.
• Make a key contribution to the Dynamic Support Register (DSR) which is monitored and overseen by the Ipswich, East and West Suffolk CCG Quality team.
• Review the implementation of Care, Education and Treatment Review (CETR) actions/recommendations
• Hold providers to account when care, education and/or treatment is not being delivered as required.
• Escalate barriers and gaps in services to senior managers and commissioners. 1.3. The key workers will not be delivering care, education, or treatments to CYP or their
families and cannot replace services that are already commissioned. 1.4. The Keyworker Function is funded by NHS England and Suffolk has been allocated
£345,000.00 in 2022/23 and £505,000.00 in 2023/24. Funding beyond 2023/24 has not been confirmed yet, however we are confident that there will be funding to support this project beyond 23/24.
2. Key Issues 2.1. Criteria for an ideal provider to deliver the Keyworking Function are that they:
2.1.1. Can be operational as soon as possible after 01/04/2022, so as to meet the tight time scales dictated by NHSE and meet the KPI’s they have set down.
2.1.2. Have robust information governance processes and information sharing agreements in place to support this function.
2.1.3. Can provide a secure and appropriate data management system on which to record the work of the Keyworking Function. Ideally with access to the Health Information Exchange (HIE).
2.1.4. Can provide a quality service that is trusted by all providers, CYP and their families.
2.1.5. Can recruit to experienced highly motivated staff
Page 3 of 3
3. Patient and Public Engagement
3.1. An engagement event was held in November 2021 with stakeholders, providers, voluntary organisations, the Suffolk Parent Carer Forum and Healthwatch Suffolk. These coproduction partners suggested that a voluntary organisation should provide this service to ensure independence from statutory providers and therefore stimulate trust and engagement from CYP, families and partner organisations.
3.2. This option was pursued at the fortnightly Keyworking Function Steering Group that is made
up of coproduction partners including parents and carers of children with a learning disability and or autism. However, it was found that, at this time, a voluntary organisation could not meet the criteria set above. Therefore, a new option was explored and agreed on as a group.
3.3. An Equality and Quality Impact Screening Tool (Appendix 1) has been completed and
following screening it is considered unnecessary to proceed to a full EQIA.
4. Recommendation 4.1. It is recommended that Suffolk County Council should host the Keyworker Function. This has
been supported at both the Ipswich, East & West Suffolk CCGs Chief Executive Boards because:
4.1.1. SCC are already hosting the CHRIS (Crisis, Help and Risk Intervention
Service) team where there are many synergies to the Keyworking Function, and where Information Governance arrangements already in place could be extended to include the Keyworking Function.
4.1.2. SCC has a record of delivering community health services that are rated “Good” in all categories by the CQC.
4.1.3. SCC has experience and expertise in managing SystmOne which is the preferred data management system for this team.
4.1.4. SCC has experience of delivering independent arm's length services EG. SENDIASS
4.1.5. SCC can offer attractive terms and conditions to potential applicants including an NHS pension to staff already in a current NHS Pension plan.
4.2. It is also recommended that as there is a clear benefit to be gained from maintaining
continuity with an earlier project, i.e., CHRIS, and that the benefit of continuity outweighs any potential financial advantage of going out to tender, that a waver should be granted to going out to competitive tender. Please see Appendix 2 for completed Waver of Competitive Tendering Form.
11. APPENDIX 1
Equality & Quality Impact Assessment (EQIA) Screening Tool
Introduction
This screening tool has been designed to identify proposals that require completion of an EQIA and development of an engagement plan. Proposals that, through this screening, are identified as not having a tangible impact on patients or quality do not require an EQIA or engagement. The screening tool also captures information that tells us about the scale of the proposal and the risk of controversy i.e. reputational impact.
Where an impact on patients is identified through the screening a full EQIA template should be completed.
Scheme Title: Keyworking Function
Scheme Lead: Kathryn Searle /Anita Farrant
Date Screening Completed: 16/02/2022
Projected savings (if any) 2020/21: N/A
Projected savings (if any) 2021/22: N/A
CCG(s) affected: Ipswich East and West Suffolk CCGs
Summary description of the scheme being assessed: The Keyworking Function has been developed as a response to the NHS England & NHS Improvement Long Term Plan (LTP) commitment that by 2023/24, children and young people with a learning disability, autism, or both, with the most complex needs will have a designated Keyworker: implementing the recommendations made by Dame Christine Lenehan. These are our children: a review by Dame Christine Lenehan (publishing.service.gov.uk)
Aim
Initially to provide Keyworking support to vulnerable children and young people (CYP) with a
learning disability, autism, or both, to avoid unnecessary admission into mental health or specialist
learning disability settings and to keep them and their families safe and well in their community.
Support will, in 2023/24, be extended to include those aged up to 25 years.
Objectives
• Identify CYP with a learning disability, autism or both who are at risk of admission to a Tier 4 setting.
• Support these CYP and their families to navigate the system to ensure there is one holistic plan for the family that meets their needs.
• Make a key contribution to the Dynamic Support Register (DSR) which is monitored and overseen by the Ipswich, East and West Suffolk CCG Quality team.
• Review the implementation of Care, Education and Treatment Review (CETR) actions/recommendations
• Hold providers to account when care, education and/or treatment is not being delivered as required.
• Escalate barriers and gaps in services to senior managers and commissioners.
The key workers will not be delivering care, education, or treatments to CYP or their families.
KWF DRAFT Service
Specification Feb 22.docx
SECTION 1: QUESTIONS ON THE IMPACT OF THE CHANGE TO SERVICE USERS
Will the proposal:
• have an impact on who is eligible to access the service e.g. by changing referral criteria and/or
• affect how people access the service e.g. where or when it will be delivered?
Positive Impact Negative Impact No Impact Not Applicable
Comments/rationale:
This is a new service and will only be available to vulnerable children and young people up to the age of 25 with a learning disability and/or autism who are at risk of admission to a Tier 4 inpatient bed. These criteria may be considered by some groups as overly restrictive as there are many vulnerable individuals outside of this definition who would benefit from a Key Worker.
Will the proposal have an impact on patient safety, patient experience or clinical
effectiveness?
Positive Impact Negative Impact No Impact Not Applicable
Comments/rationale:
The expectation is that this team:
• will hold partners to account when they are not delivering the required care, education or treatment required for the CYP to remain safe and well in the community. Thus, reducing the risk of escalation into crisis and admission.
• will identify barriers and gaps to commissioners to support the provision of services that address the unmet needs of this community.
• will advocate for these families, ensuring the wishes, feelings and needs are taken into consideration when planning care, education, and treatment.
• will support CYP and their families to navigate the health and care system to achieve personal goals, enabling them to live more settled lives in the community
Will the proposal have any other impact that will be noticeable to patients or carers?
Positive Impact Negative Impact No Impact Not Applicable
Comments/rationale:
CYP and families should feel listened to.
SECTION 2: QUESTIONS ON THE LIKELY LEVEL OF CONCERN OR CONTROVERSY
Is the proposal likely to result in concern or controversy due to:
• The nature of the service
• The nature of the patients or carers affected
Positive Impact Negative Impact No Impact Not Applicable
Comments/rationale:
The only controversy will be relating to those CYP who do not meet the criteria for this service and any expectation that this team will fill the gaps left by other organisations who are unable to deliver a full service.
Has there been previous concern or controversy around the service resulting in:
• Complaints
• Adverse media coverage
Positive Impact Negative Impact No Impact Not Applicable
Comments/rationale:
This will be a new service. There has however been poor publicity nationally regarding the admission of CYP with LD&A to Tier 4 beds and the poor experience this has provide to them with limited positive outcomes.
Are you aware of any controversy (complaints or adverse media coverage) when this
scheme was introduced elsewhere?
Positive Impact Negative Impact No Impact Not Applicable
Comments/rationale:
No
Has the proposal been risk assessed using the GBAF RAG rating score & if so, is it
considered necessary to add the scheme as a risk to either a departmental Risk Register
or if strategically significant, to the CCGs GBAF (Corporate Register)?
Yes No Not Applicable
Comments/rationale:
Risk review has been carried out and deemed to be low.
Following screening is it considered necessary to complete a full EQIA?
Yes No
Comments/rationale:
Based on this screening tool it is evident that this service is unlikely to have a negative impact on the population of Suffolk and is likely to be well received and have a positive impact on the lives and wellbeing of vulnerable children and young people with a learning disability and/or autism and their families.
However it remains important to be aware that unconscious bias in the way the service is delivered could disadvantage individuals, in particular those with protected characteristics and therefore the service will be collecting data and feedback from CYP and their families to evaluate the impact of the service and ensure that it is providing support and effecting positive change for families.
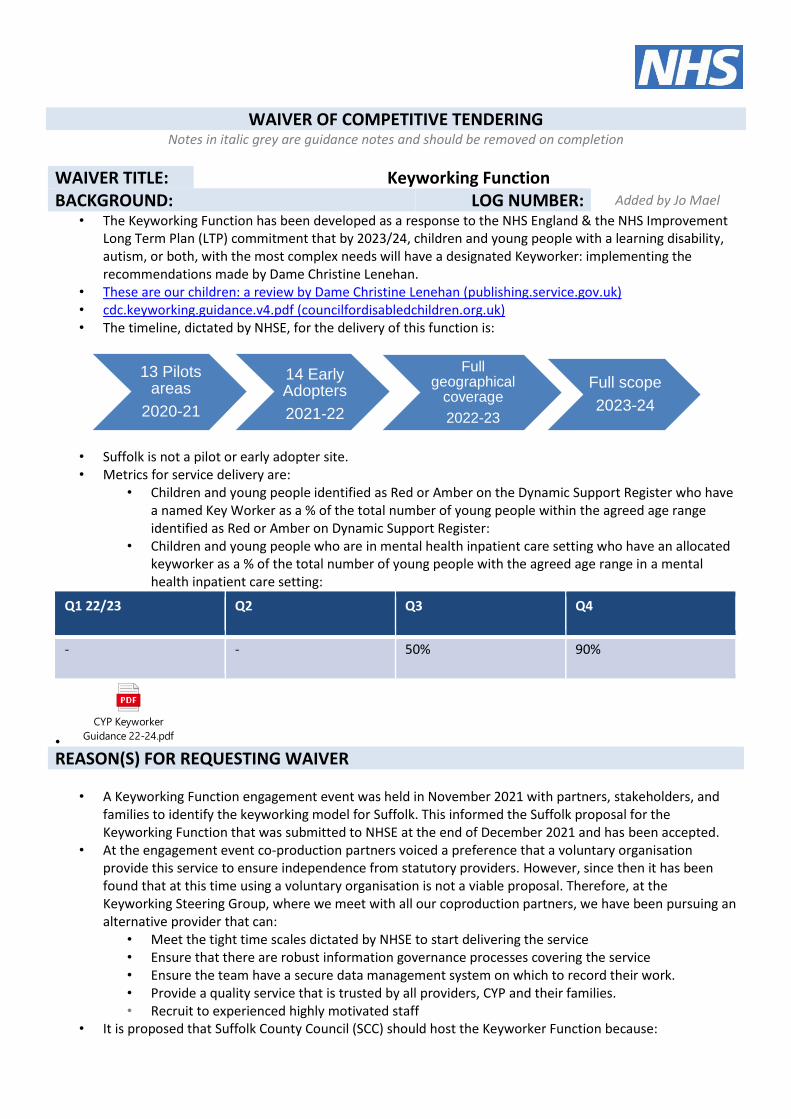
WAIVER OF COMPETITIVE TENDERING Notes in italic grey are guidance notes and should be removed on completion
WAIVER TITLE: Keyworking Function BACKGROUND: LOG NUMBER: Added by Jo Mael
• The Keyworking Function has been developed as a response to the NHS England & the NHS Improvement Long Term Plan (LTP) commitment that by 2023/24, children and young people with a learning disability, autism, or both, with the most complex needs will have a designated Keyworker: implementing the recommendations made by Dame Christine Lenehan.
• These are our children: a review by Dame Christine Lenehan (publishing.service.gov.uk) • cdc.keyworking.guidance.v4.pdf (councilfordisabledchildren.org.uk) • The timeline, dictated by NHSE, for the delivery of this function is:
• Suffolk is not a pilot or early adopter site. • Metrics for service delivery are:
• Children and young people identified as Red or Amber on the Dynamic Support Register who have a named Key Worker as a % of the total number of young people within the agreed age range identified as Red or Amber on Dynamic Support Register:
• Children and young people who are in mental health inpatient care setting who have an allocated keyworker as a % of the total number of young people with the agreed age range in a mental health inpatient care setting:
Q1 22/23 Q2 Q3 Q4
- - 50% 90%
•
CYP Keyworker
Guidance 22-24.pdf REASON(S) FOR REQUESTING WAIVER
• A Keyworking Function engagement event was held in November 2021 with partners, stakeholders, and families to identify the keyworking model for Suffolk. This informed the Suffolk proposal for the Keyworking Function that was submitted to NHSE at the end of December 2021 and has been accepted.
• At the engagement event co-production partners voiced a preference that a voluntary organisation provide this service to ensure independence from statutory providers. However, since then it has been found that at this time using a voluntary organisation is not a viable proposal. Therefore, at the Keyworking Steering Group, where we meet with all our coproduction partners, we have been pursuing an alternative provider that can:
• Meet the tight time scales dictated by NHSE to start delivering the service • Ensure that there are robust information governance processes covering the service • Ensure the team have a secure data management system on which to record their work. • Provide a quality service that is trusted by all providers, CYP and their families. • Recruit to experienced highly motivated staff
• It is proposed that Suffolk County Council (SCC) should host the Keyworker Function because:
13 Pilots areas
2020-21
14 Early Adopters
2021-22
Full geographical
coverage
2022-23
Full scope
2023-24
• SCC are already hosting the CHRIS (Crisis, Help and Risk Intervention Service) team where there are many synergies to the Keyworking Function, and where Information governance arrangements already in place could be extended to include the Keyworking Function.
• SCC has a record of delivering community health services that are rated “Good” in all categories by the CQC.
• SCC has experience and expertise in managing SystmOne which is the preferred data management system for this team.
• SCC has experience of delivering independent arm's length services EG. SENDIASS
Financial Information
RE_ Funding for the
KWF in Suffolk.msg As per the e-mail above the funding comes directly from NHSE. We have been informed that for 2022/23, 50% of funding will be transferred in month 1 and the remaining 50% in month 7. Although funding beyond 23/24 has not been confirmed yet however we are confident that there will be funding to support this project beyond 23/24. Below is the planned budget expenditure for the first 2 years.
2022-23
23-24
Staff FTE Bottom Top FTE Bottom Top
G8 Transforming Care Manager
1 £68,733.00 £84,491.00 1 £68,733.00 £84,491.00
G7 Senior Transforming Care Navigator
1 £53,597.00 £68,733.00 3 £160,791.00 £206,199.00
G5 Transforming Care Navigator
1 £36,071.00 £45,361.00 3 £108,213.00 £136,083.00
G5 Assistant Psychologist
0.5 £18,035.50 £22,680.50 1 £18,035.50 £22,680.50
G4 Administrator 0.5 £14,389.00 £18,035.50 0.5 £14,389.00 £18,035.50
Program Manager 0.6 £36,117.75 £40,197.71 - - -
Total Pay Costs £226943.25 £279,498.71 £370,161.50 £490,169.50
Personal Budgets £10,000.00 £10,000.00 £20,000.00 £20,000.00
Grand total £236,943.25 £289,498.71 £390,161.50 £510,169.50
Budget £345,000.00 £345,000.00 £505,000.00 £505,000.00
To cover travel, training, IT & set up costs.
£108,056.75 £55,501.29 £114,778.50 -£5,169.50
DETAILED FINANCIAL POLICIES 8.5.2 The waiver of this competition requirement is in accordance with the following section of the Detailed Financial Policy.
Formal tendering procedures may be waived in the following circumstances: Please select
a) in very exceptional circumstances where the Accountable Officer decides that formal tendering procedures would not be practicable or the estimated expenditure or income would not warrant formal tendering procedures, and the circumstances are detailed in an appropriate CCG record;
b) where the requirement is covered by an existing contract; c) where Crown Commercial Services agreements are in place; d) where a consortium arrangement is in place and a lead organisation has been appointed to carry
out tendering activity on behalf of the consortium members;
e) where the timescale genuinely precludes competitive tendering but failure to plan the work properly would not be regarded as a justification for a single tender;
f) where specialist expertise is required and is available from only one source; g) when the task is essential to complete the project, and arises as a consequence of a recently
completed assignment and engaging different consultants for the new task would be inappropriate;
h) there is a clear benefit to be gained from maintaining continuity with an earlier project. However in such cases the benefits of such continuity must outweigh any potential financial advantage to be gained by competitive tendering;
✓
i) for the provision of legal advice and services providing that any legal firm or partnership commissioned by the CCG is regulated by the Law Society for England and Wales for the conduct of their business (or by the Bar Council for England and Wales in relation to the obtaining of Counsel’s opinion) and are generally recognised as having sufficient expertise in the area of work for which they are commissioned. The Chief Finance Officer will ensure that any fees paid are reasonable and within commonly accepted rates for the costing of such work;
j) where allowed and provided for in the Capital Investment Manual. The waiving of competitive tendering procedures should not be used to avoid competition or for administrative convenience or to award further work to a consultant originally appointed through a competitive procedure.
INTERNAL REVIEWERS & SUPPORTERS
Waiver Originator: Insert name of individual raising the Waiver and select appropriate counter fraud statement with additional details if required.
Lianne Joyce
I have no interest in the supplier that would constitute a conflict of Interest.
X
I have an interest in the supplier and details are provided below:
Insert details if an interest is declared:
I confirm that the information given on this form is true, complete and accurate. If I supply false information, I am aware the matter may be passed to the CCG’s Local Counter Fraud Specialist or the CCG’s HR Department to consider if criminal or disciplinary action is required.
10/5/2022
Originating Chief Officer:
Lisa Nobes
Contracting supporter:
Helen Abel
Finance supporter:
Jane Payling
SPEND RATIFICATION AND APPROVAL (prior to waiver completion and submission to the Audit Committee)
Date spend and sourcing approach approved by Clinical Executive: (up to £250k total spend)
Insert date if presented to Clinical Executive
Date spend and sourcing approach approved by Governing Body: (if required and / or above £250k total spend)
Insert date if presented to Governing Body
OUTCOME OF RATIFICATION AND APPROVAL
Please insert any comments or requirements as a result of ratification at Clinical Executive or Governing Body which have been taken account of, or should be noted.
Spend Ratification if NOT presented to Clinical Executive or Governing Body
ONLY complete this signature section if the spend has not been ratified by Clinical Executive or Governing Body – NOTE – any spend over £250,000 must be approved by Governing Body prior to commissioning.
Please insert an explanation of where the spend has been signed off, including the board / meeting; the date it was presented and why it has not been through Clinical Executive or Governing Body – i.e. spend is low or Crown Commercial Services Framework has been used.
REVIEWED Insert signature of Chief Officer once reviewed and approved Include this signature for all levels of spend
Insert title
DATE: Insert signature date
If spend is over £38,000 and below £250,000 and has not been presented to Clinical Executive or Governing Body, please complete following signatories:
REVIEWED Insert signature of Chief Finance Officer once approved Include this signature for all spend over £38,000 and below £250,000
Chief Finance Officer
DATE: Insert signature date from Chief Finance Officer
APPROVED: Insert signature of Chief Officer once reviewed and approved Include this signature for all spend over £38,000 and below £250,000
Chief Officer
DATE: Insert signature date from Chief Officer
Following appropriate approval, form to be submitted to the Audit Committee for ratification
DATE OF REPORT TO AUDIT COMMITTEE: Insert date that report was presented to the Audit Committee
EMBEDDED DOCUMENTS:
Please embed any relevant documents in support of this waiver
Page 1 of 5
GOVERNING BODY
Agenda Item No. 10
Reference No. IESCCG 22-19
Date. 24 May 2022
Title Procurement Update: Summary of Activity 2022
Lead Director Paul Gibara, Director of Performance Improvement
Author(s) Jane Garnett, Procurement Lead
Purpose To update the Governing Body on the procurements completed since the last procurement update and those currently in progress and planned for 2022.
Applicable CCG Clinical Priorities:
1. To promote self care
2. To ensure high quality local services where possible
3. To improve the health of those most in need
4. To improve health & educational attainment for children & young people
5. To improve access to mental health services
6. To improve outcomes for patients with diabetes to above national averages
7. To improve care for frail elderly individuals
8. To allow patients to die with dignity & compassion & to choose their placeof death
Action required by Governing Body:
To note the work undertaken and the evolving procurement work programme for 2022.
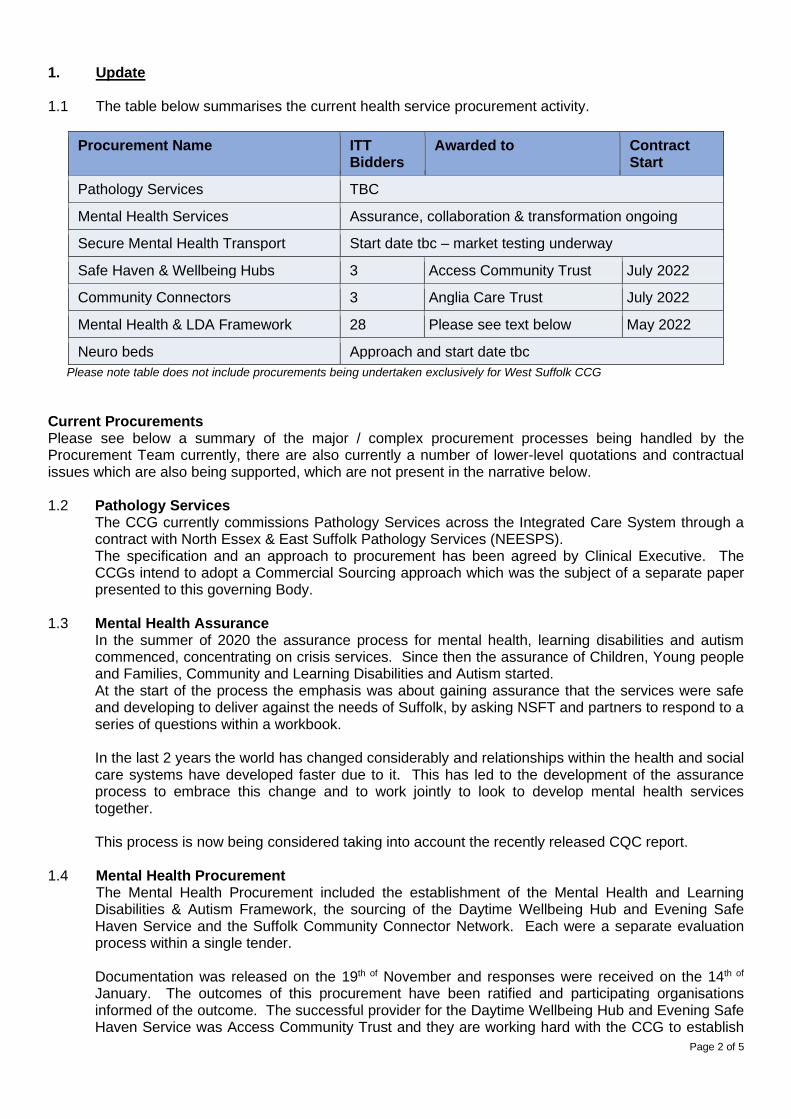
Page 2 of 5
1. Update 1.1 The table below summarises the current health service procurement activity.
Procurement Name ITT Bidders
Awarded to Contract Start
Pathology Services TBC
Mental Health Services Assurance, collaboration & transformation ongoing
Secure Mental Health Transport Start date tbc – market testing underway
Safe Haven & Wellbeing Hubs 3 Access Community Trust July 2022
Community Connectors 3 Anglia Care Trust July 2022
Mental Health & LDA Framework 28 Please see text below May 2022
Neuro beds Approach and start date tbc
Please note table does not include procurements being undertaken exclusively for West Suffolk CCG
Current Procurements Please see below a summary of the major / complex procurement processes being handled by the Procurement Team currently, there are also currently a number of lower-level quotations and contractual issues which are also being supported, which are not present in the narrative below. 1.2 Pathology Services
The CCG currently commissions Pathology Services across the Integrated Care System through a contract with North Essex & East Suffolk Pathology Services (NEESPS). The specification and an approach to procurement has been agreed by Clinical Executive. The CCGs intend to adopt a Commercial Sourcing approach which was the subject of a separate paper presented to this governing Body.
1.3 Mental Health Assurance
In the summer of 2020 the assurance process for mental health, learning disabilities and autism commenced, concentrating on crisis services. Since then the assurance of Children, Young people and Families, Community and Learning Disabilities and Autism started. At the start of the process the emphasis was about gaining assurance that the services were safe and developing to deliver against the needs of Suffolk, by asking NSFT and partners to respond to a series of questions within a workbook. In the last 2 years the world has changed considerably and relationships within the health and social care systems have developed faster due to it. This has led to the development of the assurance process to embrace this change and to work jointly to look to develop mental health services together. This process is now being considered taking into account the recently released CQC report.
1.4 Mental Health Procurement The Mental Health Procurement included the establishment of the Mental Health and Learning Disabilities & Autism Framework, the sourcing of the Daytime Wellbeing Hub and Evening Safe Haven Service and the Suffolk Community Connector Network. Each were a separate evaluation process within a single tender. Documentation was released on the 19th of November and responses were received on the 14th of January. The outcomes of this procurement have been ratified and participating organisations informed of the outcome. The successful provider for the Daytime Wellbeing Hub and Evening Safe Haven Service was Access Community Trust and they are working hard with the CCG to establish
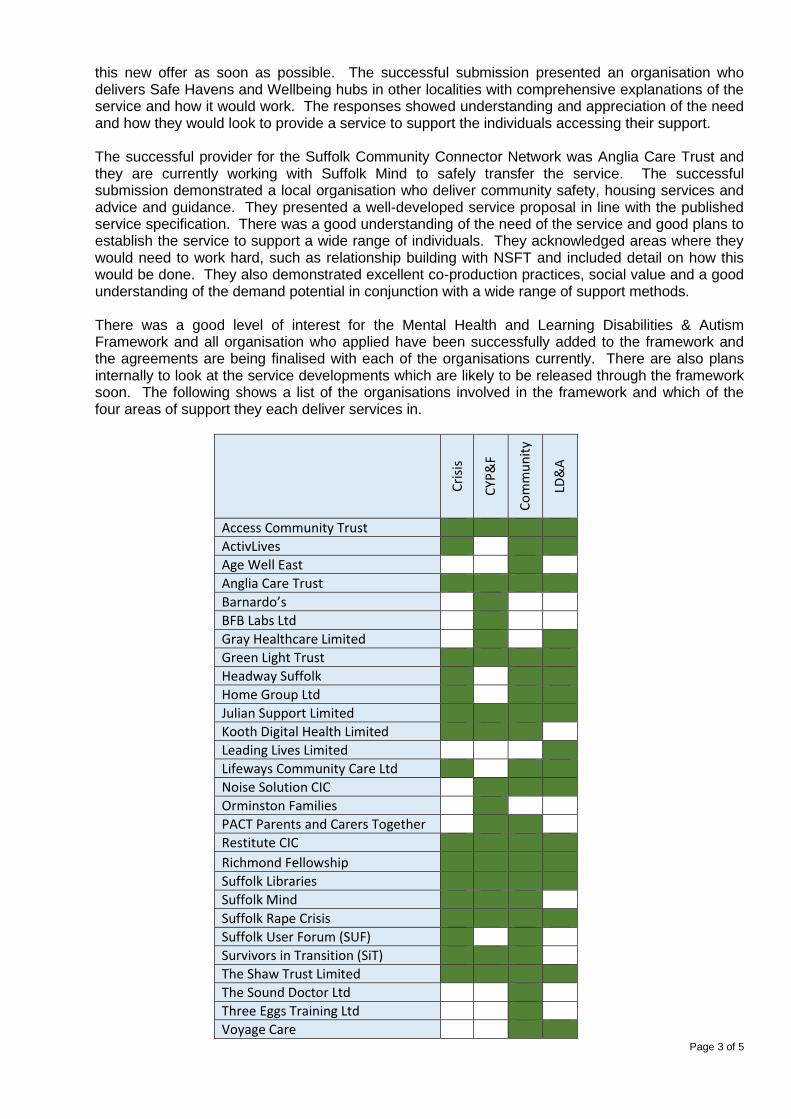
Page 3 of 5
this new offer as soon as possible. The successful submission presented an organisation who delivers Safe Havens and Wellbeing hubs in other localities with comprehensive explanations of the service and how it would work. The responses showed understanding and appreciation of the need and how they would look to provide a service to support the individuals accessing their support.
The successful provider for the Suffolk Community Connector Network was Anglia Care Trust and they are currently working with Suffolk Mind to safely transfer the service. The successful submission demonstrated a local organisation who deliver community safety, housing services and advice and guidance. They presented a well-developed service proposal in line with the published service specification. There was a good understanding of the need of the service and good plans to establish the service to support a wide range of individuals. They acknowledged areas where they would need to work hard, such as relationship building with NSFT and included detail on how this would be done. They also demonstrated excellent co-production practices, social value and a good understanding of the demand potential in conjunction with a wide range of support methods.
There was a good level of interest for the Mental Health and Learning Disabilities & Autism Framework and all organisation who applied have been successfully added to the framework and the agreements are being finalised with each of the organisations currently. There are also plans internally to look at the service developments which are likely to be released through the framework soon. The following shows a list of the organisations involved in the framework and which of the four areas of support they each deliver services in.
Cri
sis
CYP
&F
Co
mm
un
ity
LD&
A
Access Community Trust
ActivLives
Age Well East
Anglia Care Trust
Barnardo’s
BFB Labs Ltd
Gray Healthcare Limited
Green Light Trust
Headway Suffolk
Home Group Ltd
Julian Support Limited
Kooth Digital Health Limited
Leading Lives Limited
Lifeways Community Care Ltd
Noise Solution CIC
Orminston Families
PACT Parents and Carers Together
Restitute CIC
Richmond Fellowship
Suffolk Libraries
Suffolk Mind
Suffolk Rape Crisis
Suffolk User Forum (SUF)
Survivors in Transition (SiT)
The Shaw Trust Limited
The Sound Doctor Ltd
Three Eggs Training Ltd
Voyage Care
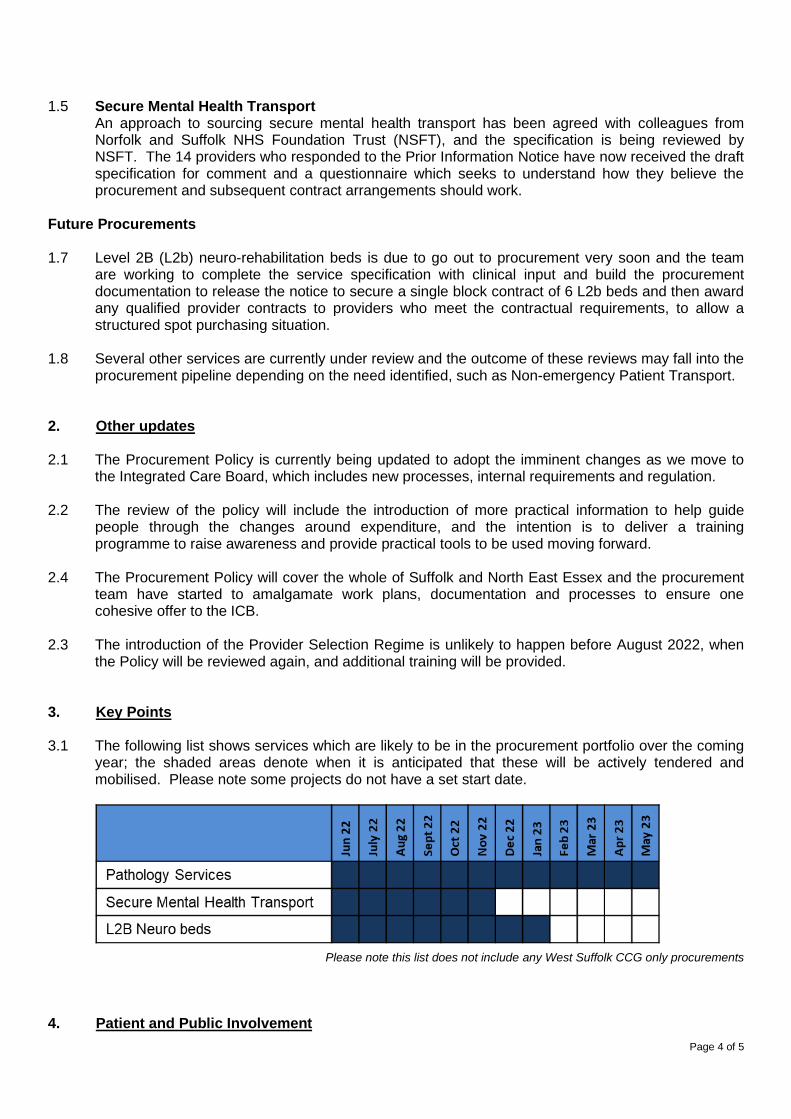
Page 4 of 5
1.5 Secure Mental Health Transport An approach to sourcing secure mental health transport has been agreed with colleagues from
Norfolk and Suffolk NHS Foundation Trust (NSFT), and the specification is being reviewed by NSFT. The 14 providers who responded to the Prior Information Notice have now received the draft specification for comment and a questionnaire which seeks to understand how they believe the procurement and subsequent contract arrangements should work.
Future Procurements 1.7 Level 2B (L2b) neuro-rehabilitation beds is due to go out to procurement very soon and the team
are working to complete the service specification with clinical input and build the procurement documentation to release the notice to secure a single block contract of 6 L2b beds and then award any qualified provider contracts to providers who meet the contractual requirements, to allow a structured spot purchasing situation.
1.8 Several other services are currently under review and the outcome of these reviews may fall into the
procurement pipeline depending on the need identified, such as Non-emergency Patient Transport. 2. Other updates 2.1 The Procurement Policy is currently being updated to adopt the imminent changes as we move to
the Integrated Care Board, which includes new processes, internal requirements and regulation. 2.2 The review of the policy will include the introduction of more practical information to help guide
people through the changes around expenditure, and the intention is to deliver a training programme to raise awareness and provide practical tools to be used moving forward.
2.4 The Procurement Policy will cover the whole of Suffolk and North East Essex and the procurement
team have started to amalgamate work plans, documentation and processes to ensure one cohesive offer to the ICB.
2.3 The introduction of the Provider Selection Regime is unlikely to happen before August 2022, when
the Policy will be reviewed again, and additional training will be provided. 3. Key Points 3.1 The following list shows services which are likely to be in the procurement portfolio over the coming
year; the shaded areas denote when it is anticipated that these will be actively tendered and mobilised. Please note some projects do not have a set start date.
Please note this list does not include any West Suffolk CCG only procurements
4. Patient and Public Involvement
Page 5 of 5
4.1 Patient and Public involvement is sought for all procurements before they commence.
4.2 The Procurement Team retains the commitment to Patient and Public involvement for each process undertaken, and this commitment will continue to be formalised through the reviewed Procurement Policy.
5. Recommendation
5.1 The Governing Body is asked to note the work undertaken and the evolving procurement workprogramme for 2022.
Page 1 of 27
GOVERNING BODY Agenda Item No. 11
Reference No. IESCCG 22-20
Date. 24 May 2022 Title
2022/23 Plan
Lead Director
Jane Payling, Director of Finance
Author(s)
Paul Gibara, Director of Performance Improvement Richard Watson, Deputy Chief Executive and Director of Strategy and Transformation Amanda Lyes, Director of Corporate Services & System Infrastructure
Purpose
To set out, for approval, the 2022/23 plans on activity, workforce and finance and accompanying narrative. To approve the opening budget for 2022/23 for the CCG.
Applicable CCG Clinical Priorities: 1. To promote self care x
2. To ensure high quality local services where possible x
3. To improve the health of those most in need x
4. To improve health & educational attainment for children & young people x
5. To improve access to mental health services x
6. To improve outcomes for patients with diabetes to above national averages x
7. To improve care for frail elderly individuals x
8. To allow patients to die with dignity & compassion & to choose their place of death where appropriate
x
9. To ensure that the CCG operates within agreed budgets x
Action required by the Governing Body: To approve the following plans for 2022/23
• Narrative Plan • Activity and achievement of targets • Workforce • Financial
To approve the opening budget for 2022/23 for the CCG. To delegate sign off for any changes to the finance committee, with reporting back to the Governing Body.
Page 2 of 27
1. Background 1.1 At its meeting in March the Governing Body was provided with an update on the planning
process for 2022/23. The paper noted the timetable for planning required final submissions to be made on 28 April.
1.2 This paper includes the submissions made in April for sign-off • Narrative Plan (appendix A) • Activity & Performance plan (appendix B) • Workforce Plan (appendix C)
1.3 The planning processes have not formally concluded, due in the main to issues regarding financial balance. The paper explains the progress made to date and the expected next steps. The opening budget for the CCG is presented for approval for audit purposes (appendix D).
2. 2022/23 Planning Guidance Summary 2.1 Planning guidance for 2022/23 was issued on 24 December 2021 and updated on 22
February. The detailed guidance document can be accessed via the following link 2022/23 Priorities and Operational Planning.
2.2 The main priority areas highlighted in the document are similar to those issued in 2021-22,
with the introduction to the document explaining:
In 2022/23 we will continue to rise to the challenges of restoring services, meeting the new care demands and reducing the care backlogs that are a direct consequence of the pandemic. While the future pattern of COVID-19 transmission and the resulting demands on the NHS remain uncertain, we know we need to continue to increase our capacity and resilience to deliver safe, high quality services that meet the full range of people’s health and care needs. We will: • accelerate plans to grow the substantive workforce and work differently as we keep our
focus on the health, wellbeing and safety of our staff • use what we have learnt through the pandemic to rapidly and consistently adopt new
models of care that exploit the full potential of digital technologies • work in partnership as systems to make the most effective use of the resources available
to us across acute, community, primary and social care settings, to get above pre-pandemic levels of productivity as the context allows
• use the additional funding government has made available to us to increase our capacity and invest in our buildings and equipment to support staff to deliver safe, effective and efficient care.
2.3 Section 4 of this report introduces the Narrative Plan and sets out the main areas covered. 2.4 The December version of the guidance formally announced the delay in the establishment
of Integrated Care Boards until July, a date which has more recently been confirmed following Royal Assent to the Health and Care Bill. For the purposes of planning, most of the work has been constructed on a Suffolk and North East Essex ICB basis, where the plans differ from this indication has been given in the relevant sections.
3. Process and Timetable 3.1 As discussed at the last meeting, the submission date for the 2022/23 plan was 28 April.
This deadline was achieved by the system.
Page 3 of 27
3.2 At the time of writing the report, we have been made aware by NHSEI that the current financial submissions will not be the final ones, however information on changes which will be required and the timetable for submission have not been confirmed. An update will be provided at the meeting.
4. Suffolk and North East Essex Narrative Plan (Appendx A)
4.1 As part of the 2022/23 Priorities and Operational Planning Guidance submission, a
narrative plan setting out the system approach to achievement was developed. A copy of this document has been included as appendix A, which is a single system level template covering the actions and assumptions that underpin the trajectories within the activity and workforce numerical submission and other critical actions that systems will take to address the priorities set out in the 2022/23 operational planning guidance, including elective recovery.
4.2 The narrative plan sets out priority actions to be taken forward to support delivery of the
planning objectives and by exception, any key areas of concern and emerging risks associated with delivery, including any proposed mitigation to be taken forward. The plan covers the following elements which were requested by NHSE:
• Health Inequalities - Maintain focus on preventing ill-health and tackling health
inequalities. • Invest in our workforce – with more people and new ways of working, and by
strengthening the compassionate and inclusive culture needed to deliver outstanding care. • Maximise elective activity and reduce long waits, taking full advantage of opportunities to
transform the delivery of services. • Complete recovery, to improve performance against cancer waiting times standards. • Diagnostics to outline the priority actions your system will be taking to increase diagnostic
activity to a minimum of 120% of pre-pandemic levels across 2022/23 to support these ambitions and meet local need.
• Urgent and emergency care- keeping patients safe and offering the right care, at the right time, in the right setting. This needs to be supported by creating additional beds, in particular through expansion of virtual ward models, and includes eliminating 12-hour waits in emergency departments (EDs) and minimising ambulance handover delays.
• Transform and build community services capacity to deliver more care at home and improve hospital discharge.
4.3 The Narrative Plan is attached at appendix A. 5. Activity & Performance Plan (Appendix B) 5.1 The planned levels of activity and trajectories for performance for 2022/23 are
shown in appendix B. There is an expectation that activity levels, particularly for elective care, will increase to exceed 2019/20 levels and deliver a sustained reduction in the number of patients waiting more than 18 months for treatment.
5.2 The Narrative Plan (appendix A) provides information on the assumptions made for
delivery of the key targets including elective and cancer waiting times, urgent care delivery and mental health services. It also sets out the actions being taken in each area.
6 Workforce Plan (Appendix C) 6.1 The Narrative Plan contains a section which sets out the context and actions planned for
the workforce in 2022/23. The technical workforce plan (appendix C) shows an increase in establishment of 5% with a more 2% increase in total workforce numbers by 03/23.
Page 4 of 27
6.2 The narrative includes information on the ‘One Workforce’ approach which is being adopted
across the system, included supporting the existing workforce, belonging in health and care, new ways of working and growing for the future.
6.3 Triangulation between the activity, workforce and finance numbers has taken place as part
of the process. 7. Financial Plan and Budget (Appendix D) 7.1 The NHS commissioning elements for 22/23 are being constructed as a single plan for the
Suffolk and North East Essex Integrated Care Board, from which the relevant CCG elements will be extracted for the months prior to the ICB formation. The expenditure made by the CCGs will be matched with allocation from the full year ICB funding such that the CCG element will be shown as a balanced plan; any surplus or deficit will fall into the combined ICB in the latter part of the year.
7.2 Appendix D contains a summary of the system financial plan for 2022/23 as it currently
stands and the corresponding CCG budget for the period April-June 2022. The CCG opening budget, which will be balanced by allocation, has been approved by the finance committee (NEE) and Collaborative Committee (IES & WS).
7.3 Full year plans have been produced for the mental health elements of expenditure as
covered by the Mental Health Investment Standard, these demonstrate that the standard will be achieved in 2022/23.
7.4 Further work is expected on financial plans as recognition of the additional costs associated
with increased inflation and Covid-19 patients during April and May is considered at a national level. This is expected to be concluded during June allowing the ICB budget to be signed off by the relevant ICB committees. The Governing Body as asked to delegate final changes to the CCG budget to the finance committees.
8. Recommendation
The Governing Body is requested to 8.1 Approve the following plans subject to final changes
• Narrative Plan (appendix A) • Activity & Performance plan (appendix B) • Workforce Plan (appendix C) • Opening CCG Budget (appendix D)
8.2 Delegate any final changes to the finance committee.
Appendix A
(instruction sheets summarised)
2022-23 priorities and operational planning
Narrative Submission Template SNEE ICS Version 1.1 28 April 2022
Summary of areas covered
The list below outlines all sections covered in the 2022/23 priorities and operational planning guidance and specifically indicates those which require a narrative response within this submission:
Priorities of 2022-23 priorities and operational planning guidance Narrative Required
Introduction. Health Inequalities - Maintain focus on preventing ill-health and tackling health inequalities. Y
A. Invest in our workforce – with more people and new ways of working, and by strengthening the compassionate and inclusive culture needed to deliver outstanding care. Y
B. Respond to COVID-19 ever more effectively – delivering the NHS COVID-19 vaccination programme and meeting the needs of patients with COVID-19. N
C. Deliver significantly more elective care to tackle the elective backlog, reduce long waits and improve performance against cancer waiting times standards.
C1. Maximise elective activity and reduce long waits, taking full advantage of opportunities to transform the delivery of services
C2. Complete recovery improve performance against cancer waiting times standards. C3. Diagnostics
Y
Y
Y
C4. Deliver improvements in maternity care N
D. Improve the responsiveness of urgent and emergency care (UEC) and build community care capacity – keeping patients safe and offering the right care, at the right time, in the right setting. This needs to be supported by creating the equivalent of 5,000 additional beds, in particular through expansion of virtual ward models, and includes eliminating 12-hour waits in emergency departments (EDs) and minimising ambulance handover delays.
D1. Urgent and emergency care D2. Transform and build community services capacity to deliver more care at home and improve hospital discharge
Y
Y
E. Improve timely access to primary care – expanding capacity and increasing the number of appointments available. N
F. Grow and improve mental health services and services for people with a learning disability and/or autistic people. N
G. Continue to develop our approach to population health management, prevent ill-health and address health inequalities. N
H. Exploit the potential of digital technologies to transform the delivery of care and patient outcomes. N
I. Make the most effective use of our resources. N
J. Establish ICBs and collaborative system working. N
System name: Suffolk and North East Essex ICS
Introduction - Health Inequalities - Maintain focus on preventing ill-health and tackling health inequalities by redoubling efforts on the five priority areas for tackling health inequalities set out in guidance in March 2021. ICSs will take a lead role in tackling health inequalities, building on the Core20PLUS5 approach introduced in 2021/22 to support the reduction of health inequalities experienced by adults, children and young people, at both the national and system level.
Please outline priority actions, assumptions, risks, issues and associated mitigation. Please refer to guidance on the five priority areas and Core20PLUS5 approach to support your response. Actions
Five priority areas Priority 1: Restore NHS services inclusively Health Inequality Improvement funding is supporting the development of comprehensive Equalities and Health Inequalities Impact Assessments (EHIIAs) for all our major programmes. Our first priority area has been elective care recovery, and also, we are developing EHIIAs for maternity, SMI, COPD, cancer and hypertension. These live assessments will inform co-produced action planning to tackle inequalities, and will be live documents, updated as we continue to learn about the impact of the pandemic on groups and communities. The template used includes an action plan with identified mitigations and prioritises these. This approach builds on learning from our Covid19 Vaccination programme. Resources have been shared on our ICS website Covid-19 Vaccine Programme - Suffolk & North East Essex Integrated Care System (sneeics.org.uk) Our Community Ambition programme has invested funding from NHS Charities Together in projects led by grassroots minority ethnic organisations co-producing new solutions to addressing inequalities. Areas include understanding community health needs, culturally competent maternity and mental health services, and healthy lifestyles. Linking these communities to statutory services and strategic forums has enabled these groups’ voices to be heard across our system. A task and finish group, supported by Healthwatch in Suffolk and Essex, will explore improving accessibility to health and care services for people across a wide range of communication needs including language, sensory impairment, and marginalised groups.
Engagement on our ICS maternity and neonatal strategy has been launched. Maternity equality and equity plan submitted to NHSEI and actions are being co-produced with partners and people with lived experience including Black, Asian and minority ethnic organisations. A VCSE Funding Programme has also been launched. A review of work on health equity and equality across mental health programmes was recently submitted to NHSEI. Priority 2: Mitigate against digital exclusion SNEE ICS has a mature digital, data & technology strategy and delivery plan, operating across the whole system. Following rapid adoption of Video Consultation, Remote Care, Virtual Wards, Care Tech, Apps, Channels and Portals in the first wave of Covid we worked with Healthwatch Suffolk & Healthwatch Essex to create the 12 Guiding Principles to address exclusion. This work has allowed assessments of many of our current capabilities. Key findings are: • Digital First not Digital Only – all services are offered as face to face also • Data collected around people and access – usage / utilisation (particularly by pseudonymised people / by characteristics) is
hard to get to, siloed and often incomplete. Would be useful for trend against outcome, and with more timely data we could consider where we were ‘turning the curve’
• Most systems capture people’s communication preferences, but these aren’t shared An Equality & Equity Project / Produce Lifecycle Toolkit has been developed and is being implemented into core practice following approval from the ICS Board in February 2022. Action plans to address gaps found through the assessment are focussed on shared best practice and local adoption. This methodology will be applied to the design and implementation of all new digital channels, capabilities and services for the public, as well as the adoption of best local practice across high use existing digital channels. On CORE20PLUS, Paul Gavin (Deputy Director, National Healthcare Inequalities Improvement Programme for NHS England and NHS Improvement) said: ‘The Suffolk and NE Essex ICS – Healthwatch partnership is demonstrating that successful, co-produced Digital projects that meet the needs of their CORE20PLUS population are achievable. Through establishing a set of agreed guiding principles and designing their development with the input of community groups in a meaningful way, this partnership is a great example for other Integrated Care Systems to consider as they develop their own system initiatives to mitigate against digital exclusion in keeping with NHS England and Improvement’s strategic priorities for talking health inequalities.’ Priority 3: Ensure datasets are complete and timely
The ICS collects and analyses ethnicity data from a range of national datasets covering secondary care, mental health and community services. We are currently starting a programme to extract a range of data from primary care which includes ethnicity data, as part of our PHM programme. We will be able to regularly review the quality and accuracy of ethnicity and other data recording. There is an ICS elective recovery dashboard that also reviews the current waiting list by Age, Gender, Ethnicity and Deprivation. When a national dashboard is available, we will also link in our local datasets. ICS has adopted Outcome Based Accountability across the ICS training in excess of 700 people. We have linked this methodology to our work around Population Health Management. We are now further developing these approaches to inform the way that we can monitor progress at system and place linked to the development of JSNAs/JHWS in both Essex and Suffolk. We have also been part of a comprehensive review of the role of HWBBs in both Suffolk and Essex and how they will align to the ICP. Priority 4: Accelerate preventative programmes that proactively engage those at greatest risk of poor health outcomes We continue to work to identify and tackle inequalities in the Covid-19 vaccination programme. Our dedicated vaccination website is translatable and includes multi-lingual resources, and we have used diverse community-based resources to inform people about vaccination. Mobile units reach into deprived and marginalised communities, taking the opportunity to offer other health prevention services too. Staff and volunteers have guidance on adjustments, and we monitor vaccine uptake by geography and ethnicity, as well as people’s satisfaction with their experience. More detail is available here. Through our Community Ambition programme, the Bangladeshi Women’s Association of Essex is completing a unique health needs assessment of its community. This will be published in June 2022 and shared locally and regionally to help us tackle health inequalities in South Asian communities. SNEE ICS has a well-established Population Health Management Steering Group, which continues to oversee the ongoing development of our PHM Strategy over time as PHM evolves nationally. We recognise the need to work differently, including the tools and intelligence to utilise prevention. SNEE ICS encompasses complementary work in this field from the Suffolk Office for Data Analytics in linking and sharing data on the wider determinants of health, and the equivalent organisation in Essex (ECDA) also now exploring similar approaches enabling us to take PHM forward in its fullest sense. We have historically explored two different approaches to PHM over recent years. This means we have a unique insight into some of the different ways of approaching PHM. We are working towards planning how we harness and exploit the progress made across the ICS in order to meet the national requirements; agreeing and writing a plan by June 2022 which will put in place the systems, skills and data safeguards that will act as a foundation for PHM; and by April 2023 to have longitudinal linked data available covering the entire
ICS, to enable PHM analytics to be used to redesign care pathways and measure outcomes, with a focus on improving access and health equity for underserved communities. The NHS and both County Councils are collaborating to commission a review of the business case for further development of local weight management resources building on thinking from a recent ICS event on this theme For information on CORE20PLUS5 initiatives, please see below. Priority 5: Strengthen leadership and accountability Our SRO Dr Ed Garratt and the wider ICS Partnership Board has oversight of health inequalities, and each of our programmes has responsibility and accountability for tackling health inequalities within its remit. Data from the Public Health Outcomes Framework has been integrated into our ICS strategy for some time. Our ICS Five Year System Strategic Plan includes these measures throughout and they are included in our ICS strategy on our website. HEPP and Health Inequality Improvement funding has been used to develop our Health Equity workshops, which have been delivered to over 200 people in our system, and encouraging and supporting 100 day challenges. Our Anchor Institutions programme is currently developing a dashboard to evaluate progress against our Charter aims, which include recruiting, commissioning and procuring locally that can directly benefit people who live with discrimination and disadvantage, and deprived communities. Our Social Value and Community Microenterprise project, funded by NIHR, is now operational in North East Essex. Our ICS progress on VCSE development has been identified as an area of good practice. Key developments include plans for a VCSE Assembly and Chair, development of a VCSE Resilience Charter, and a VCSE Workforce review. The Secretary of State for Health held a roundtable with local VCSE leaders on 14 February 2022 to hear about this work. System learning is shared on our ICS website including: • Our film competition sharing lived experiences and two events on the theme of ‘How do we help everyone heal?’ • Our ‘Thinking Differently Together’ events explore a wide range of issues through different perspectives; our publications are
here. Written reports of all events, with recommendations, are considered by our ICS Board and associated action plans taken forward e.g. ICS suicide prevention and trauma informed practice training across the ICS.
Those with lived experience who presented within all these events have continued to influence our strategic approaches.
To support the measuring of our impact, we have adopted Outcome Based Approaches across our ICS, training in excess of 700 people. We are now further developing these approaches to inform the way that we can monitor progress at system and place linked to the development of JSNAs/JHWS in both Essex and Suffolk. CORE20PLUS5 Plans are in place for the five target areas, with accountability through the relevant programme boards and ultimately through the ICS Board. The following approaches will be taken to work towards achieving the five targets:
• Maternity: Continuity of carer plans are being finalised to roll out teams in areas where Black, Asian and Mixed ethnic groups and people living in deprived areas are prioritised. Maternity continuity of carer (MCoC) rollout plans have been submitted to NHSE. All provider plan ambitions are to achieve MCoC for 100% of the population by 2024. Initial teams will focus on areas of need/deprivation. Whilst MCoC is mobilised the LMNS has commissioned voluntary sector partners (including AFiUK) to deliver a maternity focussed community ambassador model within our most diverse communities. Commencing in April 2022 the schemes will empower women by educating them about the maternity pathway, helping to understand terminology used, explaining services, and use advocacy to help them access services and ensure they are personalised to their needs. They will also address wider determinants of health such as housing, domestic abuse, and financial hardship; and also educate our teams to be more culturally aware. We will bring the organisations together every three months to share learning and strengthen the networks between our VCSE organisations and maternity/health visiting colleagues. This will support trust between communities and professionals, support system wide roll-out of learning, and help people to access the right help when they need it and to make our services more inclusive to our communities’ needs. April 2022 May 2022 June 2022 Sept 2022 December 22 Feb 2023
VCSE organisations confirm scope and model of delivery. Training provided to community ambassador on pregnancy pathway, services available, key contacts etc. Schemes commence within communities Network meeting and review of initial learning Coproduction event to bring together learning to date and develop sustainable models of support Network meeting and review of initial learning and forward view to 23/24 Celebration event
Alongside voluntary sector partners the LMNS hosts monthly health inequalities meetings which bring together a wide range of VCSE organisations across the ICS footprint.
• SMI: Increasing health checks and supporting access to post-check interventions that have been identified for people with Severe Mental Illness by collaboration with primary and secondary care and VCSE organisations to remove barriers, and with the Covid vaccine programme to combine health checks and vaccination in the same appointment where appropriate.
Through joint working, outcome measures will be developed and monitored to understand and improve life expectancy. Our target is to increase the numbers of people on GP SMI registers receiving a physical health assessment in the last 12 months from 2,572 in Q1 of 2022/23 to 3,448 in Q4, which will enable us to meet the 60% target by Q4.
• COPD: Plan towards population health management approach to identify groups of patients at risk and areas of deprivation. We have begun a data review of the uptake of vaccinations by people with COPD in areas of deprivation, which will be complete by the end of April 2022. Collaboration with primary care and our key partners will identify actions and areas of improvement to address health inequalities in areas of deprivation by the end of May 2022. The plan will be agreed, and monitoring will be in place through the ICS Respiratory dashboard, and a CORE20PLUS5 pilot will be launched by the end of November 2022. Community spirometry service that is being developed will determine early diagnosis for COPD and treatment.
• Cancer: The SNEE cancer programme will explore a population health management approach to increase the uptake of screening opportunities across our communities. We will support earlier identification of Lung Cancer, Targeted Lung Health Checks will be mobilised in our most deprived ward, the pathway will be co-produced to maximise uptake. We will produce outcome data from the last two years to identify and develop plans to support those specialties and communities whose outcomes have been impacted by the pandemic. We are working with the Cancer Alliance data team on outcomes and have held a workshop in March with our Public Health teams to look at cancer survival and population health data. These plans are currently being finalised and will be launched in Q2. We are developing services closer to home, including in our more deprived areas of Clacton, Ipswich East and Forest Heath, which will commence from Q3 onwards. More detail is available in our Cancer Delivery Plan.
• Hypertension: We are working with the Eastern Academic Health and Science Network (EAHSN) to implement the UCLP Proactive care@HOME framework for Blood Pressure. The risk stratification tools will support our PHM approach to case finding and the overall Blood Pressure Optimisation (BPO) programme, and work will also be undertaken with Pharmacies to case find. The ongoing BP@HOME programme supplies free blood pressure devices to patients to help them to self-care. Data from the online CVD Prevent dashboards can be used to identify those patients who are not engaging with CVD related health services. Digital patient information decks provided by Liberate Pro are being developed to support patients identified with hypertension providing information on the condition and how to manage it in a clear and concise manner. The following milestones are planned for 2022: May/June - Gather CORE20 data – 20% most deprived across SNEE May/June - Gather PLUS data – SNEE specific areas such as LD, SMI, digital excluded who may not be part of the CORE20 numbers June - Set up operational group to analyse the data and decide on course of actions including working with the ICS Health Inequality team August/September - Work with community based “African Families” organisation who are commissioned to support Health Inequalities work across SNEE
We have recently been awarded funding to develop CORE20PLUS Community Connectors. We will work in partnership with African Families in the UK to utilise their established Community Ambassador model to recruit and develop volunteers, initially in Colchester and later rolled out across the ICS. We will develop ways in which Connectors can have their voice heard at PCN, Alliance and system levels of the ICS. The project commenced on 1 April 2022; co-production, recruitment and training of Connectors and a coordinator will take place in the coming months with a view to commencing their full roles by September. Development of the ICP from 1 July 2022 will incorporate ways in which Connectors’ voices can be heard as part of its engagement, and we have started to build relationships with the NEE Alliance and local councils so that we can build on existing local champion roles and link our Connectors to their work. We hope to start exploring rolling out the model to other parts of the ICS footprint in Q4 of 2023. Personalised care Literacy and consumable information are key to My Planned Care and PIFU being successful and as part of our Personalised Care and Health Inequalities programmes we are engaging with our patient representatives, community engagement partnerships and VCSE to ensure that we are co-producing plans with our communities and that they have equity in access through tailored, target consumable information and support. Our ICS Personalised Care Strategy’s inequalities, Patient Choice, Shared Decision Making, Social Prescribing and personalised care and support plans workstreams will have a key role in taking forward this work supported by comms, marketing and workforce enablers. Plans are in place as part of the ICS wide Personal care and support plan workstream to identify unmet need with proactive case-finding and collaboration across acute, primary care and VCSE as part personalised care approaches and partnership working. During 22/23 there will be further roll out of personal care and support plans across care pathways and commissioned services and we are embedding this requirement as part of contract and commissioning approaches with our statutory and VCSE providers. Each Alliance has been accelerating personalised approaches to follow-up care in hospitals for patients on Discharge to Assess pathways 0 and 1. The ‘Welcome Home’ Programme, established over winter 2021/22 will further enhance and support the patient pathway process when people are admitted to Ipswich Hospital’s Emergency Assessment Unit (EAU), Surgical Assessment Unit (SAU) and Trauma & Orthopaedics (T&O). The Welcome Home team follows through the journey of the patient in hospital up to and including discharge and onward referral to the community based Connect for Health Social Prescribing service and our multi-cultural social prescribing service. The 7 day a week service model comprises three WTE social prescribing ‘Advice and Support co-ordinators’ managed by Citizens Advice Bureau who provide additional support and capacity to the existing discharge pathway in place by undertaking personalised care and support planning at ward level with the patient, their family, carers and staff during their hospital stay as
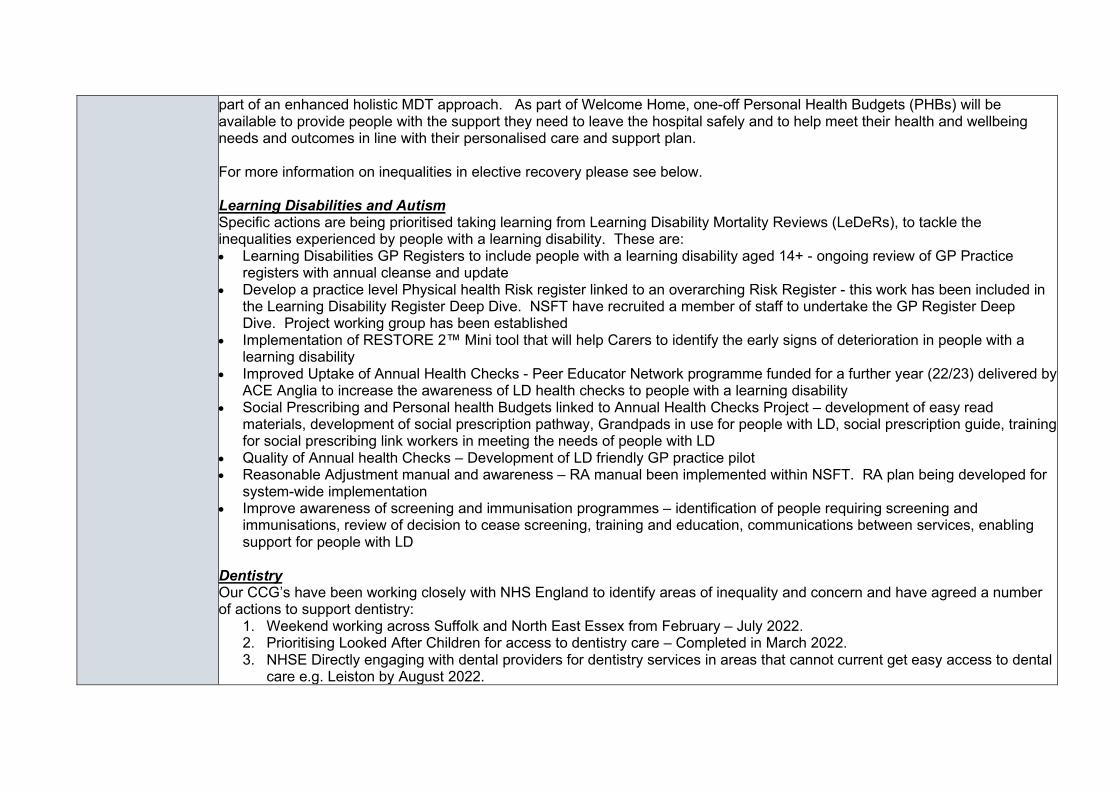
part of an enhanced holistic MDT approach. As part of Welcome Home, one-off Personal Health Budgets (PHBs) will be available to provide people with the support they need to leave the hospital safely and to help meet their health and wellbeing needs and outcomes in line with their personalised care and support plan. For more information on inequalities in elective recovery please see below. Learning Disabilities and Autism Specific actions are being prioritised taking learning from Learning Disability Mortality Reviews (LeDeRs), to tackle the inequalities experienced by people with a learning disability. These are: • Learning Disabilities GP Registers to include people with a learning disability aged 14+ - ongoing review of GP Practice
registers with annual cleanse and update • Develop a practice level Physical health Risk register linked to an overarching Risk Register - this work has been included in
the Learning Disability Register Deep Dive. NSFT have recruited a member of staff to undertake the GP Register Deep Dive. Project working group has been established
• Implementation of RESTORE 2™ Mini tool that will help Carers to identify the early signs of deterioration in people with a learning disability
• Improved Uptake of Annual Health Checks - Peer Educator Network programme funded for a further year (22/23) delivered by ACE Anglia to increase the awareness of LD health checks to people with a learning disability
• Social Prescribing and Personal health Budgets linked to Annual Health Checks Project – development of easy read materials, development of social prescription pathway, Grandpads in use for people with LD, social prescription guide, training for social prescribing link workers in meeting the needs of people with LD
• Quality of Annual health Checks – Development of LD friendly GP practice pilot • Reasonable Adjustment manual and awareness – RA manual been implemented within NSFT. RA plan being developed for
system-wide implementation • Improve awareness of screening and immunisation programmes – identification of people requiring screening and
immunisations, review of decision to cease screening, training and education, communications between services, enabling support for people with LD
Dentistry Our CCG’s have been working closely with NHS England to identify areas of inequality and concern and have agreed a number of actions to support dentistry:
1. Weekend working across Suffolk and North East Essex from February – July 2022. 2. Prioritising Looked After Children for access to dentistry care – Completed in March 2022. 3. NHSE Directly engaging with dental providers for dentistry services in areas that cannot current get easy access to dental
care e.g. Leiston by August 2022.
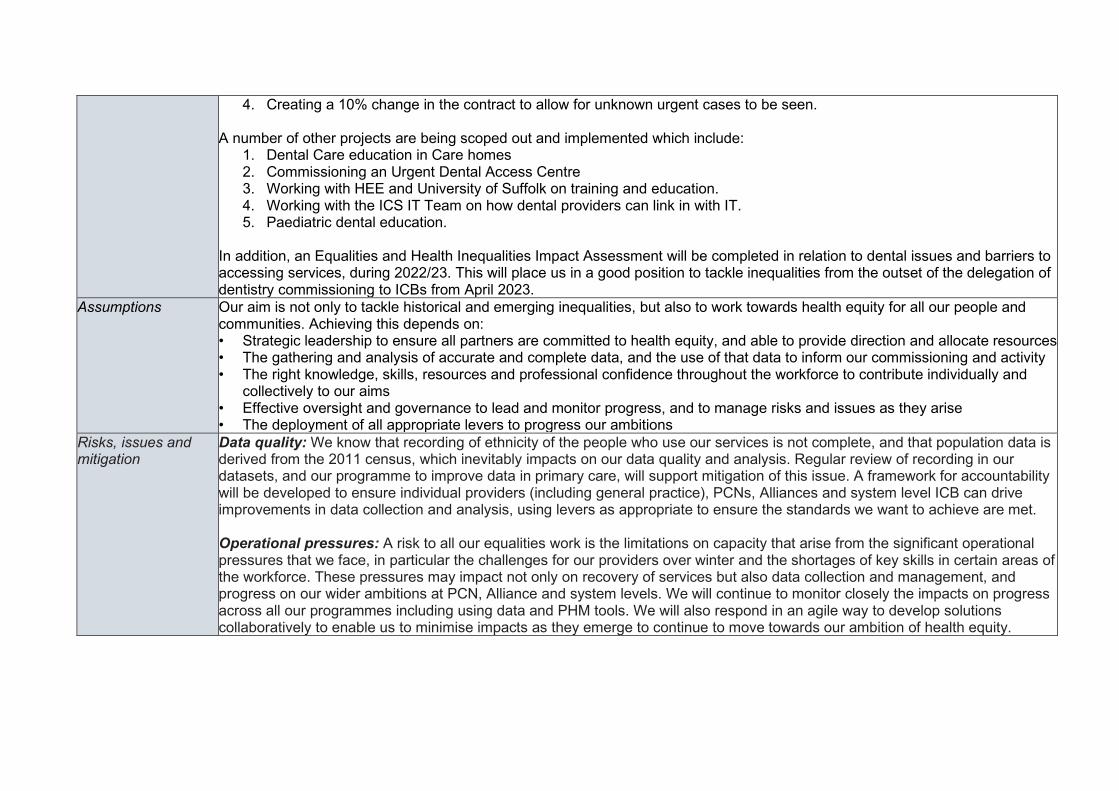
4. Creating a 10% change in the contract to allow for unknown urgent cases to be seen. A number of other projects are being scoped out and implemented which include:
1. Dental Care education in Care homes 2. Commissioning an Urgent Dental Access Centre 3. Working with HEE and University of Suffolk on training and education. 4. Working with the ICS IT Team on how dental providers can link in with IT. 5. Paediatric dental education.
In addition, an Equalities and Health Inequalities Impact Assessment will be completed in relation to dental issues and barriers to accessing services, during 2022/23. This will place us in a good position to tackle inequalities from the outset of the delegation of dentistry commissioning to ICBs from April 2023.
Assumptions Our aim is not only to tackle historical and emerging inequalities, but also to work towards health equity for all our people and communities. Achieving this depends on: • Strategic leadership to ensure all partners are committed to health equity, and able to provide direction and allocate resources • The gathering and analysis of accurate and complete data, and the use of that data to inform our commissioning and activity • The right knowledge, skills, resources and professional confidence throughout the workforce to contribute individually and
collectively to our aims • Effective oversight and governance to lead and monitor progress, and to manage risks and issues as they arise • The deployment of all appropriate levers to progress our ambitions
Risks, issues and mitigation
Data quality: We know that recording of ethnicity of the people who use our services is not complete, and that population data is derived from the 2011 census, which inevitably impacts on our data quality and analysis. Regular review of recording in our datasets, and our programme to improve data in primary care, will support mitigation of this issue. A framework for accountability will be developed to ensure individual providers (including general practice), PCNs, Alliances and system level ICB can drive improvements in data collection and analysis, using levers as appropriate to ensure the standards we want to achieve are met. Operational pressures: A risk to all our equalities work is the limitations on capacity that arise from the significant operational pressures that we face, in particular the challenges for our providers over winter and the shortages of key skills in certain areas of the workforce. These pressures may impact not only on recovery of services but also data collection and management, and progress on our wider ambitions at PCN, Alliance and system levels. We will continue to monitor closely the impacts on progress across all our programmes including using data and PHM tools. We will also respond in an agile way to develop solutions collaboratively to enable us to minimise impacts as they emerge to continue to move towards our ambition of health equity.
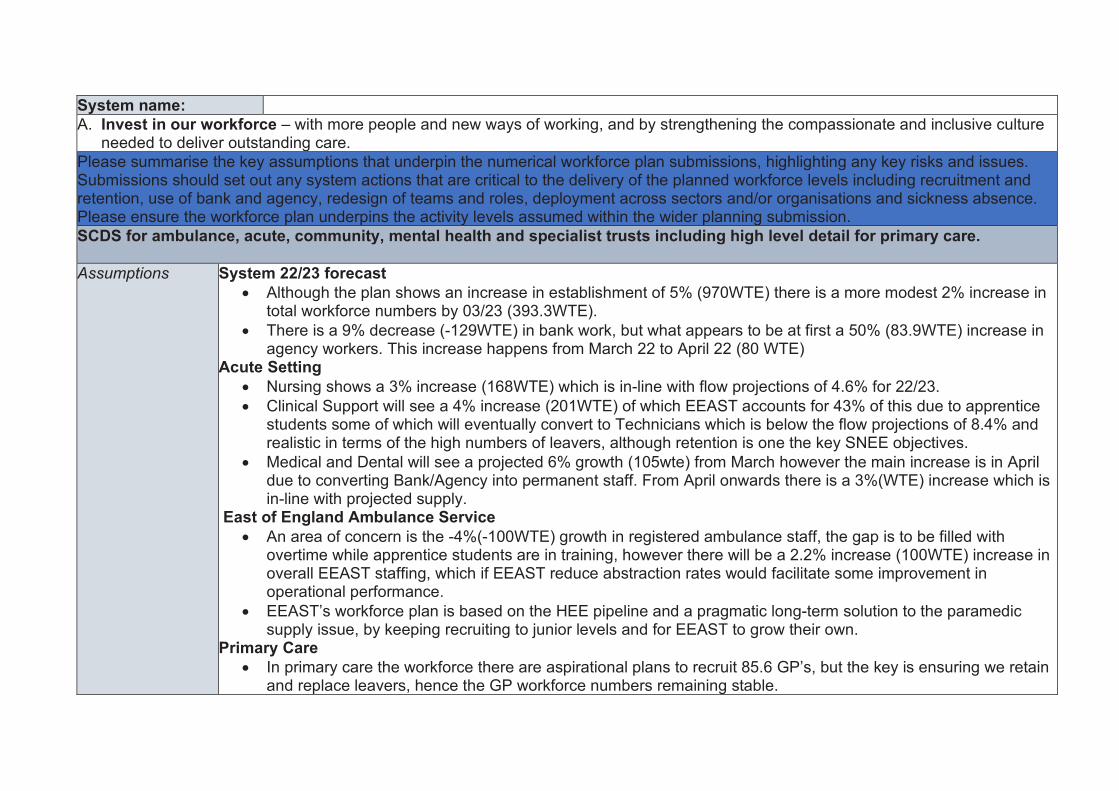
System name: A. Invest in our workforce – with more people and new ways of working, and by strengthening the compassionate and inclusive culture
needed to deliver outstanding care. Please summarise the key assumptions that underpin the numerical workforce plan submissions, highlighting any key risks and issues. Submissions should set out any system actions that are critical to the delivery of the planned workforce levels including recruitment and retention, use of bank and agency, redesign of teams and roles, deployment across sectors and/or organisations and sickness absence. Please ensure the workforce plan underpins the activity levels assumed within the wider planning submission. SCDS for ambulance, acute, community, mental health and specialist trusts including high level detail for primary care. Assumptions System 22/23 forecast
• Although the plan shows an increase in establishment of 5% (970WTE) there is a more modest 2% increase in total workforce numbers by 03/23 (393.3WTE).
• There is a 9% decrease (-129WTE) in bank work, but what appears to be at first a 50% (83.9WTE) increase in agency workers. This increase happens from March 22 to April 22 (80 WTE)
Acute Setting • Nursing shows a 3% increase (168WTE) which is in-line with flow projections of 4.6% for 22/23. • Clinical Support will see a 4% increase (201WTE) of which EEAST accounts for 43% of this due to apprentice
students some of which will eventually convert to Technicians which is below the flow projections of 8.4% and realistic in terms of the high numbers of leavers, although retention is one the key SNEE objectives.
• Medical and Dental will see a projected 6% growth (105wte) from March however the main increase is in April due to converting Bank/Agency into permanent staff. From April onwards there is a 3%(WTE) increase which is in-line with projected supply.
East of England Ambulance Service • An area of concern is the -4%(-100WTE) growth in registered ambulance staff, the gap is to be filled with
overtime while apprentice students are in training, however there will be a 2.2% increase (100WTE) increase in overall EEAST staffing, which if EEAST reduce abstraction rates would facilitate some improvement in operational performance.
• EEAST’s workforce plan is based on the HEE pipeline and a pragmatic long-term solution to the paramedic supply issue, by keeping recruiting to junior levels and for EEAST to grow their own.
Primary Care • In primary care the workforce there are aspirational plans to recruit 85.6 GP’s, but the key is ensuring we retain
and replace leavers, hence the GP workforce numbers remaining stable.
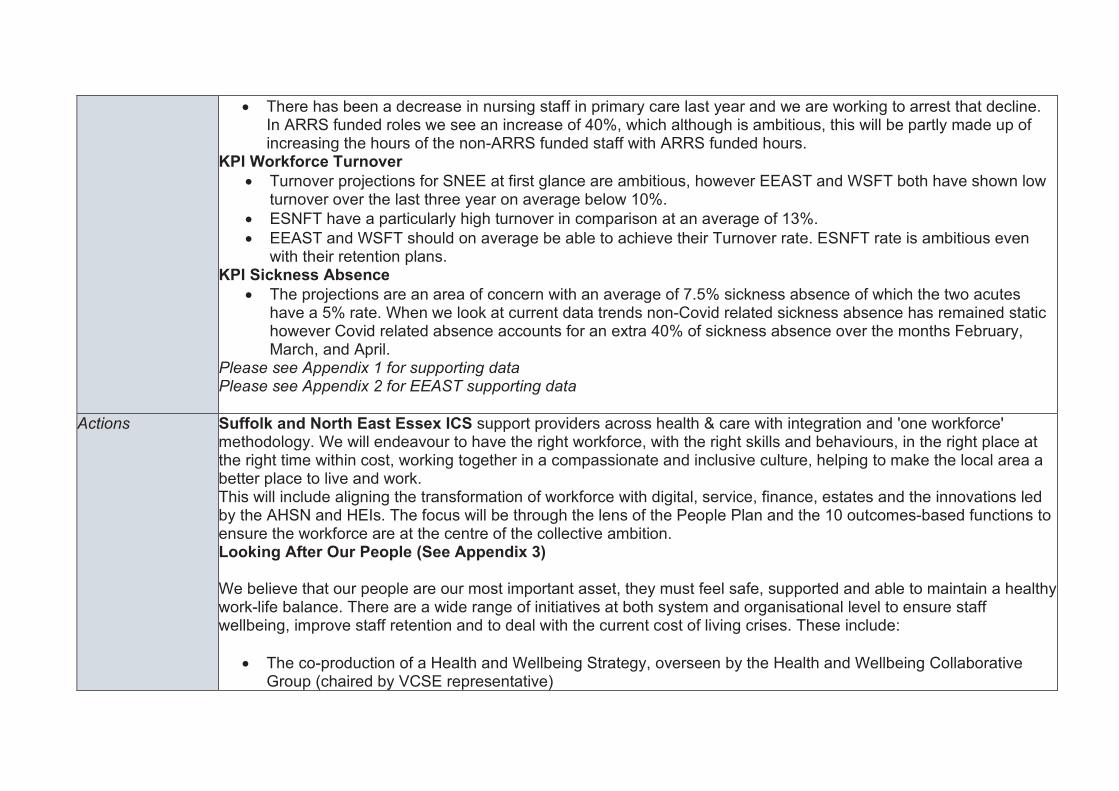
• There has been a decrease in nursing staff in primary care last year and we are working to arrest that decline. In ARRS funded roles we see an increase of 40%, which although is ambitious, this will be partly made up of increasing the hours of the non-ARRS funded staff with ARRS funded hours.
KPI Workforce Turnover • Turnover projections for SNEE at first glance are ambitious, however EEAST and WSFT both have shown low
turnover over the last three year on average below 10%. • ESNFT have a particularly high turnover in comparison at an average of 13%. • EEAST and WSFT should on average be able to achieve their Turnover rate. ESNFT rate is ambitious even
with their retention plans. KPI Sickness Absence
• The projections are an area of concern with an average of 7.5% sickness absence of which the two acutes have a 5% rate. When we look at current data trends non-Covid related sickness absence has remained static however Covid related absence accounts for an extra 40% of sickness absence over the months February, March, and April.
Please see Appendix 1 for supporting data Please see Appendix 2 for EEAST supporting data
Actions Suffolk and North East Essex ICS support providers across health & care with integration and 'one workforce' methodology. We will endeavour to have the right workforce, with the right skills and behaviours, in the right place at the right time within cost, working together in a compassionate and inclusive culture, helping to make the local area a better place to live and work. This will include aligning the transformation of workforce with digital, service, finance, estates and the innovations led by the AHSN and HEIs. The focus will be through the lens of the People Plan and the 10 outcomes-based functions to ensure the workforce are at the centre of the collective ambition. Looking After Our People (See Appendix 3) We believe that our people are our most important asset, they must feel safe, supported and able to maintain a healthy work-life balance. There are a wide range of initiatives at both system and organisational level to ensure staff wellbeing, improve staff retention and to deal with the current cost of living crises. These include:
• The co-production of a Health and Wellbeing Strategy, overseen by the Health and Wellbeing Collaborative Group (chaired by VCSE representative)
• Enhanced Occupational Health including long Covid, Menopause Support and fast-track physiotherapy services as well as procurement of a system-wide OH consultant.
• Enhancing our portfolio of Psychological and Wellbeing Support Services including the launch of My Health My Way and close working with the UoS Institute for Health and Wellbeing.
• Implement a response to the five priorities of the women’s health strategy for staff • To develop a retention plan looking at flexi-working and based on evidence from the learning from the NHS Flex
programme currently being undertaken by ESNEFT • To co-produce and launch the Violence and Aggression Reduction Plan • To continue to work with the ICS Estates colleagues to enhance our system wide Key Worker Housing Project • To support staff with the rising cost of living, by working with Foodbanks for health and social care staff to have
dedicated food bank time slots and finance education and support webinars. Belonging in Health and Care (Appendix 4) It is not enough for any Health and Care system to be non-racist it must be anti-racist. We recognise the need and benefit in championing a racially diverse workforce. Around 5.5% of the SNEE population is minority ethnic, compared to 15% of our workforce. However, at Band 8 and above this drops to just 7%. We know that this is not good enough. We will improve racial equality, diversity, and inclusion so that the system reflects the communities it serves.
• The SNEE ICB have signed Unison’s Anti-Racism Charter and will be encouraging and working with system colleagues to do the same
• An EDI Strategic Lead for workforce has been appointed (jointly with ESNEFT) • An ED&I Strategy will be co-produced in line with the Anti-Racism Charter • Inclusive recruitment training has been rolled out within the ICB during 22/23 • Leadership & Culture Workshop to be organised (Spring’22) – associated strategy/plan to be produced • Expanding Restorative Just and Learning Culture Model (Mersey Care) • Developing a Framework for Clinical and Professional Care Leadership
New Ways of Working and Delivering Care (Appendix 5)
We will continue to positively transform the way in which the community we serve receives it care from a workforce that can meets current and future demands innovatively.
• The Strategic Education Transformation Lead will co-produce a strategic plan with providers including innovations to increase and expand clinical placement capacity and develop a Strategic Education Collaborative Group incl. HEIs to reforming clinical education
• To work in partnership within the SNEE System to develop a “one workforce” integrated plan across health and social care to develop a sustainable workforce that is able to meet the present and future health demands of the Suffolk and North East Essex population.
• The recently established Productivity, Finance and Activity Group will review productivity against workforce and bank/agency spend and then establish productivity interventions in-line with the financial envelope such as better digital rostering, skill mix etc.
• A Dental Working Group (working with HEE Dental Dean) has been established to increase the number of dental staff and practices within the system, which is currently chronically understaffed leading to members of public doing their own dental work. The system is looking at establishing innovative solutions to this.
• The Medical Workforce Collaborative Group (chaired by Associate Post Graduate Dean, HEE) are creating a workforce plan that will focus on a joint approach to International Recruitment, Education Governance, F1 to Consultant career pathway and plans for ‘local’ recruitment
• Working with the Physician Associate Ambassadors to develop a system plan for growing and developing Physician Associates across primary, secondary care and mental health
• The Pharmacy Workforce Collaborative Group (chaired by Chief Pharmacist, ESNEFT) are creating a workforce plan that will focus on cross sector placements, portfolio careers, education support and career development
• The SNEE ICS Reservist Model is being launched in Q1 22/23. The Reservists will work with our system partners (acutes initially) to help services during peak times and emergencies e.g. winter pressures, Covid vaccinations programmes. Year three students will be actively pursued to be part of the programme and then retained when qualified.
• The system is establishing a new roles group to scope and co-ordinate the delivery of several workstreams relating to new roles to avoid duplication across the system (examples include introduction of anaesthetic associates, pathology and cancer.)
Growing for the Future
We believe that the workforce of tomorrow needs to be planned today. We continue to look at attracting local, diverse, and exciting staffing groups to meet the health and social needs of the community we serve.
• The Nursing, Midwifery and AHP Workforce Programme has been established to co-ordinate the delivery of several workstreams relating to the recruitment (including the 50k Nurse Manifesto), retention, and continued professional development of Nurses, Midwives, and Allied Health Professionals across the system footprint. Several pre-existing projects relating to the Clinical Workforce (i.e. Cancer Workforce, CYP Workforce, Pharmacy, Paramedics etc) will feed into these workstreams to avoid duplication across the system.
• The SNEE ICS Health and Care Academy programme will continue to open the eyes of young people to the variety of health and care jobs on offer across the system. The Academies will give young people the opportunity to see what health and care professionals do, to learn some essential life skills, work as a team, solve problems and find out more about what they are interested in.
• The Training Hub – plans to increase student placements, educators, trainers and assessors – working collaboratively on the ARRS to expand workforce
• We will continue to work with system colleagues on the Anchor Programme to show how the local health and care providers can make neighbourhoods healthier, happier and greener. The health and care sector are one of the largest employers in the system, and this programme will enable us to understand better how health and care providers can use their assets and influence to bring about wider positive changes such as local recruitment, apprenticeships, sustainability and helping to address inequality
• Working with providers to increase the numbers of GMTS accessing the scheme • Develop a Leadership and Talent Management Strategy incl. careers coaching service • The implementation of the Medical Applicants Programme which will help young people get the support they
need to apply for Medical School. • Co-ordinate the International Recruitment of workforce across the system • Continue to work with the Integrated Care Academy on Workforce Transformation Training and Development
opportunities and supporting the research and innovation programmes. • We are focusing on an Integrated Care Apprenticeship, which will strengthen the working partnerships between
health and care to support the ‘one workforce’ approach. A system working group is overseeing the progress of this
Risks, issues and mitigation
• Demand on health and care remains high: The back log of activity, continuing pressures on the system and the expectations of both government and public are having an effect on our workforce. This will lead to burnout which will see an increase in sickness absence, turnover and a loss of productivity. To mitigate this we have initiatives as outlined above under “looking after our people”, but our key message is that we are dedicated to ensuring that the system looks at work life balance, creating a flexible working environment that allows staff to truly rest and recuperate.
• The effects of Covid on retention and sickness: Although society and therefore the system needs to “learn to live with Covid” the effects it has had and will continue to have on retention and absence must not be underestimated. Staff can test positive for Covid and be asymptomatic but not test negative for 10 days plus, therefore effecting short term sickness absence, our organisations in the system are looking at how we can address this. There is a great deal of work going into the study of long Covid and its effects, we are currently developing a systemwide approach.
• Turnover: Although turnover has been relatively low in some areas it is seeing a rise within the system at 12.5% (although this is in line with seasonal variations in 2018 & 2019). The areas of concern are that 40% plus of leavers month on month are under the age of 35 and within staff groups in particular care support workers which is at 17.3% turnover and we have 7 FTE less primary care nurses in March 22 compared with the March 21. The system is looking at the work ESNFT has undertaken by recruiting two retention specialists and making the project system wide. The is a co-produced system retention strategy in development and there are also numerous system level projects to look at retention in specific staff groups including CSWs.
• Cost of living impact on the health and care workforce: Inflation is likely to be a minimum of 8% and system cost of living raise is likely to be only 3%, which will lead to retention and sickness absence issues. Although this is a national issue the system has as outlined above looked at what support it can provide to staff. This includes key worker housing, food banks and finance education and support seminars.
• Bank and Agency spend increases: During the planning process it became apparent that in order to mitigate risks and issues such as Bank and Agency spend a Productivity, Finance and Activity Group that can meet to triangulate these issues should be convened. This will allow the system to identify areas of risk and put it place support where necessary.
The actions we propose above will have robust project plans (if not already) including key milestones and mitigations. The People Board will also become more central to the accountability of delivery and therefore holding each other to account
Appendices:
• Clinical Programme • H&WB Programme • Integrated Planning • Demographics • Supporting information for Board Review
System name: Suffolk and North East Essex ICS
C. Deliver significantly more elective care to tackle the elective backlog, reduce long waits and improve performance against cancer waiting times standards.
C1: Maximise elective activity and reduce long waits, taking full advantage of opportunities to transform the delivery of services
Please summarise the key assumptions that underpin the numerical plan submission for elective recovery, highlighting any key risks and issues and mitigation.
Elective Recovery
Activity - National activity plans must deliver in excess of 104% of pre-pandemic value weighted elective activity levels and systems need to agree their (and their constituent providers’) levels of contribution to this ambition, including going further for those that are able to.
Assumptions Our plans demonstrate that we expect to deliver in excess of 104% of pre-pandemic value weighted activity as a system, as individual trusts and in the independent sector. In reaching this assessment we have made the following assumptions:
• The baseline activity is correct and enables a ‘like for like’ comparison with our out-turn
• That mutual aid between trusts and with the independent sector continues, and expands on, the achievements we have realised in 2021/22
• That there is no material withdrawal of independent sector capacity in favour of seeing private patients • That we complete our work in defining a joint access policy and agreeing what a joint PTL across our system means and
that we enact the conclusions of this work • That funding through the revised ERF scheme is sufficient to enable us to put on the additional sessions and capacity
required • That staffing levels are not significantly impacted due to COVID-19, resulting in elective cancellations • That non-elective activity does not impact on elective ward capacity further than outlined below (we are working on further
mitigations against this) • That increased cancer demand does not deplete our resources (beyond our planning assumptions) to deliver 104% • That Reinforced Autoclaved Aerated Concrete (RAAC) plank remedial work at West Suffolk NHS Foundation Trust (WSFT)
will see a reduction in elective activity in January 2023 where we expect the elective ward to be utilised for UEC • That elective activity levels may be impacted by the absence of separate hot and cold elective facilities at WSFT. This will
be addressed in future years, through the development of the Newmarket site, as described in the actions below. • That the visiting surgeon from Cambridge University Hospitals NHS Foundation Trust (CUHFT) remains available to support
East Suffolk and North Essex NHS Foundation Trust (ESNEFT) to clear Oral Maxillo Facial Surgery waiting lists. Actions Modelling methodologies
We have modelled at specialty level what is needed to deliver 104%. We have then discussed with individual specialties what plans they have to increase capacity and assessed the opportunities and risks. Increasing capacity in 2022/23 Building on the approach taken in 2021/22, work will continue with system partners to meet the national thresholds. Mutual aid has been established and inter-trust specialty specific discussions have progressed well in ENT, gynaecology and orthopaedics. Additional capacity has been sourced with the independent sector (orthopaedics, general surgery, urology, gynaecology, ophthalmology diagnostics) and this will continue in 2022/23. Maximising use of existing capacity through weekend working is being progressed. Further work will be taken to explore insourcing opportunities for ophthalmology, urology and general surgery. Capacity options for OMFS are being explored with CUHFT, Norfolk and Norwich University Hospitals NHS Foundation Trust and within Essex. This is to be finalised in March 2022 to ensure no patients are waiting by end of June. Improved productivity: Getting It Right First Time (GIRFT) and High-Volume Low Complexity (HVLC) Actions
Pathway and productivity gains will continue to be taken forward at speciality level within both ESNEFT and WSFT at system level for Eye Care and Musculoskeletal (MSK) pathways. WSFT A high-level review of WSFT’s pathways was undertaken in June 2021 to understand how closely they met the national Get It Right First Time (GIRFT) 29 High Volume Low Capacity (HVLC) procedures. The review of the GIRFT pathways demonstrated that, whilst there is a good degree of compliance, there are opportunities, either at speciality or generic levels, such as advice and guidance (A&G). Recommendations were prioritised at speciality level and form work plans which each speciality is taking forward. The following initiatives are intended to streamline the patient pathway, to enable improved access, shorter lengths of stay and ensuring patients are receiving care in the right place, at the right time. Examples of these initiatives are provided below: ENT:
• Widening the criteria for day case tonsillectomies • Ambulatory care for epistaxis and peri-tonsillar abscess
Eye care: • Looking at expanding community-based pathways for patients • Service review to identify capacity constraints and the potential for new workforce models • Trialling high volume cataract lists and a deep dive into the pathway to identify productivity improvements
MSK: • Engaging with Primary Care/HCP colleagues to redefine pathways • Preparing patients for surgery – patient optimisation • Post -operative care for inpatients • Increase of day case arthroplasty
Urology
• Bladder outflow obstruction – minimally invasive procedure has been launched in DSU • Bladder tumour resection – day case TURBT established • Ureteroscopy/stent management – working to establish a day surgery procedure
ESNEFT Each of the divisional recovery plans are based on three elements:
• Additional capacity • Transformation • Improvements in productivity and efficiency
A detailed evaluation of East Suffolk & North East Essex (ESNEFT) clinical pathways against GIRFT, was undertaken in May 2021. The 29 High Volume Low Complexity (HVLC) procedures were reviewed across all relevant specialties in both Ipswich and Colchester hospitals. The majority of pathways were compliant to best practice, although the review highlighted some variance in practice across the two ESNEFT sites, some of which are being addressed as part of this process. Those specialties requiring improvement were met with, (clinical, operational and nursing leads), and action plans have been created and are being implemented. We are revisiting areas where change has been agreed and implemented, focus areas being reviewed currently for specialties:
– Number of procedures – Follow up appointments – First outpatient appointments – Compliance to best practice
All of the ESNEFT teams are providing continuous updates on their action plans as well as commentary on the additional activity, where services have been impacted by the pandemic. Improved productivity: Digital Aligned to the ‘Delivery plan for tackling the COVID-19 backlog of elective care’ (Feb 2022), digital initiatives are in place and will continue to be developed to support clinical and non-clinical staff in releasing time, for example:
• Implementation of WASP software to speed up referral management time and create a link between Ecare and Advice and Guidance requests
• MMODAL software which improves workflow relating to dictation and transcription. The C2-AI tool has been piloted in Cheshire and Merseyside across three trusts; they have produced a comprehensive toolkit that provides information on how to utilise the C2-Ai system at various stages in the waiting list management process and gives examples of where it has been beneficial for system wide management of waiting lists. ESNEFT began a pilot in February 2022 and this will be reviewed in line with expected benefits of:
• To support HVLC or late notice - the tool will be able to show those patients who fall within a low risk of mortality group and therefore will be more likely to be seen at late notice or within a high-volume low complexity list.
• To be able to give services a comprehensive oversight of their longest waiting patients relating to their risks of mortality, complex co-morbidities and clinical pathways – currently intensive validation is used to manage these patient’s pathways. The tool will allow the patient information to be more accessible and for clinicians to easily review patients who may need to be re-prioritised due to circumstances, i.e. hospital attendances pertaining to their referred condition.
• Assurance around the clinical prioritisation of waiting lists – the algorithm includes the clinical prioritisation assigned to the patient at the time of DTA however once that decision is made the tool will review patients monthly taking into account all available data to ensure the patients deterioration is managed and highlighted if necessary.
• Support operational management and theatre co-ordination – currently patients are reviewed and listed through the administrative and operational staff. The C2Ai tool will allow staff to review patients easier and maintain good oversight.
Improving Productivity: Theatres Theatre Productivity has been reviewed across the system and improvements are planned as described below. Our programme approach:
– Observations in theatres on the day to understand any issues – Planning/Scheduling of theatre lists – Governance and performance framework – Data Quality
Interim Findings: Observations have highlighted various daily and planning issues that disrupt a productive theatre, examples are late list
changes, equipment availability, and getting patients to theatres on time. Theatre capacity planning – renewed look is required in view of current operational pressures, and staff challenges and this
has to be reconciled to the theatre template planning. Theatre governance/framework – there is no formal framework of accountability and forum for clinical leads of theatre &
specialty combined to work together to address cases per list, utilisation, and efficiency to support sustained long-term change.
Data – a renewed focus is required to support improvements to data capture. Clearer understanding of the key elements of data entry which will support accurate representation of utilisation, understanding reasons for cancellations or productivity/efficiency. Further work is needed to assure the accuracy of recording.
Improved Productivity: Outpatients Follow ups - patients that have waited more than 6 months past their agreed “to be seen” follow up appointment. As part of the accelerator programme one of the areas to explore was to contact these patients to ascertain
• Whether an appointment was still required, if so, could this be a virtual appointment rather than face to face or • If “blue card” discharge (PIFU) was an option
As a result of the pilot at ESNEFT in which patients were reviewed by clinical teams, which was deemed successful we have begun to roll out to other specialities and will look to replicate in WSFT.
We will roll out A&G further across the sites to release clinical time further. We will be making changes in speciality use of virtual clinics – During 2021 there were differences across sites and specialities for the use of virtual appointments. We will review this in our work programme for Q1 to assess and review Workforce Our workforce plans detail strategies we are going to employ to improve our recruitment and retention. Initiatives include staff incentives, health and wellbeing support and a reservist model. Better information and support for patients Various initiatives have been established or are being piloted to provide better support to patients and complement the My Planned Care app. These initiatives aim to reduce patient deterioration and optimise health pre-procedure. For example:
• The Waiting Well pilot is a collaboration of WSFT T&O Specialist Care Practitioners with input from Lifelink Suffolk (Social Prescribers), AHPS (Community Physio Team), Forest Health Primary Care Pharmacist and West Suffolk CCG and offers personalised support to patients to reduce the risk of deterioration of their mental and physical health whilst waiting for routine elective surgery. It is expected that the programme will have a positive impact on length of stay and post-operative complications.
• The Surgical School pilot aims to achieve the best possible surgical outcomes by mitigating patient risks thorough preoperative preparation and optimisation. This approach is being trialled in urology and colorectal initially. Outcome measures such as length of stay, post-operative complications and patient satisfaction will be audited through robust data collection. Learning from the pilot project will be shared and acted upon before rolling over the programme to all surgical specialties during autumn 2022. Using apps for patients to be able to access 12-week programmes to “wait well” such as yoga, mindfulness, exercise referred to as CHIP (Complete Health Improvement). This has been piloted in orthopaedics and take up has been good, and there is a plan to rollout across other specialities. A Referral Acknowledgement Letter for patient’s referrals has been initiated, which includes signposting for patients to access helpful tips and hints for them to keep well while waiting. This is an initiative that has also supported primary care and enabled less phone calls to GPs. Continue through 22/23 to monitor this and build on this platform to include other options such as housing, financial support etc.
Medium Term Capacity Developments Medium term, a short form business case has recently been submitted to develop a surgical hub at the Newmarket Community Hospital site. This will comprise 2 laminar-flow operating theatres and a 32-bed inpatient ward together with associated supporting infrastructure. It is assumed that additional activity will be deliverable from Q1 2023/24 as detailed in the business case, subject to approval and consultation timelines.
It is expected that the surgical hub can accommodate an additional 3,300 procedures p.a. which aligns with a requirement for c3,000-3,500 additional procedures per year, in order to make substantial progress to achieve a maximum 18-week wait. ESNEFT are in the process of building an elective orthopaedics centre in Colchester will bring online additional orthopaedic capacity by 2024. In addition, the Trust has applied for other capital schemes which will enable the trust to increase productivity and throughput including additional new laparoscopic theatres at Ipswich. Work is also underway to complete an options appraisal and business case for a community diagnostic hub in West and East Suffolk to support the local community and relieve pressure on the main hospital site for diagnostic testing. We anticipate having additional imaging and endoscopy capacity in these units.
Risks, issues and mitigation
The following are the key risks flagged by our system to the delivery of 104%:
• RAAC plank remedial work at WSFT may impact capacity if deadlines are extended or further work reveals structural findings which requires enhanced or rapid action. Ward work which has commenced and will run through 2022/23, which may impact on ward capacity specifically; an additional decant ward built during 2021 and opened late 2021 for medical Covid capacity, will help to mitigate this risk. RAAC plans will be managed alongside elective delivery plans to pre-empt any likely issues and manage accordingly. Move of the ANC to accommodate RAAC plank remedial work may impact outpatient capacity. Work is underway to develop a virtual consultation pod, which will house a number of specialities and release room capacity for the antenatal service.
• Availability of the independent sector (IS) to support WSFT/ESNEFT, due to capacity, process and workforce issues. Regular meetings and development of standardised processes and SoPs will help to mitigate this risk.
• A general lack of independent sector capacity in and around WSFT and ESNEFT may limit opportunities to outsource. As a system all providers will continue to explore opportunities and will work closely with IS partners.
• Ongoing risk posed by COVID-19 if there continues to be a requirement for patients and staff to self-isolate if positive or sick. This risk can lead to increased cancellations at short notice. We will continue to follow COVID-19 guidance and use a short notice waiting list, to help mitigate this risk.
• Ability to attract staff to specific specialties will impact on capacity to meet waiting list targets. WSFT will work with larger teaching hospitals and explore opportunity to appoint different workforce models such as physician’s assistants, to bridge any foreseen workforce gaps. ESNEFT are proposing to have closer working relationships with HEIs and FE colleges, increasing placement capacity, maximising student/trainee and international recruitment, and widening our participation in apprenticeships. Working differently with New and Advancing roles, training differently (endoscopy and diagnostic capacity, Simulation, multi professional learning), E job planning, e rostering, Leadership development programmes and cultural audits.
• Absence of a ‘cold’ elective site may impact as WSFT is at risk of wards being utilised for non-elective patients. This is in contrast to other sites which have a separate cold site. This will be mitigated through the medium-term development of an elective surgical hub as described above.
• Increase in referrals exceeds capacity to see patients. The intention to further embed PIFU and advice and guidance will help to mitigate this risk by releasing capacity whilst ensuring a personalised approach to patient care.
• Cancer demand remains exceptionally high (up 30% at times) with routine activity being converted to cancer capacity (across all tumour sites) which is increasing the long waiting patients. The implementation of a vague symptoms’ pathway in primary care, as well as the advantage form for referral live being used and ensuring FIT testing is completed prior to referral will mitigate the risk.
• ERF guidance not finalised and it not being financially affordable to deliver this activity within the financial budgets • ‘Red’ rated productivity schemes not being delivered which rely on staffing and establishment increases or slackening of the
national IPC guidance. Eliminate waits of over 104 weeks as a priority by March 2022 and maintain this position through 2022/23 (except where patients choose to wait longer)
Assumptions At the end of March 2022, the system had around 300 patients above 104 weeks. The breaches were in orthopaedics, general surgery, urology and gynaecology (mainly at WSFT due to the significant issues with RAAC planks in main theatres in 2021/22) and OMFS at ESNEFT due to a national capacity shortage.
There are around 125 additional patients across SNEE who will breach 104 weeks if not treated by the end of June 2022. As a system we anticipate we will clear the backlog and additional cases by the end of June 2022 with the exception of 9 OMFS cases at ESNEFT where the national/regional solution has not yet identified sufficient capacity to fully clear the backlog. We have assumed:
• Increased throughput: restoration of elective theatres at WSFT enables increased surgical interventions • mutual aid: ESNEFT will continue to support WSFT and that funding will be adjusted appropriately • independent sector: will continue to be available to support both trusts
That OMFS risk share across the region is recognised and if required patients are transferred to other centres i.e. CUH and NNUH where this surgery is available and waiting times are lower.
Actions Building on the successful approach taken in 2021/22, work will continue with system partners to meet the national threshold. Mutual aid has been established with ESNEFT and inter-trust specialty specific discussions have progressed well in ENT,
gynaecology and orthopaedics. Additional capacity has been sourced with the independent sector and this will continue in 2022/23, with a specific focus on patients waiting over 104 weeks.
Maximising use of existing capacity through weekend working and enhanced theatre productivity are being progressed, and will continue in 2022/23, together with opportunities to undertake increased day surgery aligned to HVLC/GIRFT recommendations and best practice.
Further work will be taken to explore insourcing opportunities for ophthalmology, urology and general surgery.
A continued shift to undertake cases in a day case setting will be pursued (we have not built this into our figures as the plans are not fully worked up yet). An additional theatre at WSFT is scheduled to be available from May 2022.
Ongoing waiting list validation through the use of the DrDoctor app at WSFT and equivalent at ESNEFT.
Clinical prioritisation will remain a feature of our elective strategy.
Through Q1 to reduce the 104 week waits, we are scoping and planning which patients will be transferred over to ESNEFT from WSH through the already agreed clinical pathways and SOPS. We are currently understanding our OMFS capacity options through the regional conversations – a meeting is being set up with CUH and NNUH, as well as options of capacity in Essex. This is to be finalised in March to enable as much clearance as possible during Q1. At the moment we are forecasting 9 breaches at the end of Q1. Use of IS – Discussions with the Nuffield remain ongoing – they are not able to provide regular staffed capacity, however if they do have capacity, they will offer this to us. Plans are in place for use of Ramsay Oaks capacity and this is also being offered to WSFT. We will continue to use the modular Vanguard unit until July 2022.
We will continue to outsource for endoscopy and insourcing for Pain Management (ESNEFT).
Risks, issues and mitigation
The following are the key risks flagged by our system to the delivery of 104 weeks: • RAAC plank remedial work (described above) • Availability of the independent sector (IS) (described above) • A general lack of independent sector capacity (described above) • Ongoing risk posed by COVID-19 (described above) • Ability to attract staff to specific specialties (described above) • Availability of workforce to deliver additional activity and the ability to secure locums as required. • Cancer demand (described above) • Emergency and Covid pressures increase which requires the Elective bed base, which would result in cancellations on the
less urgent patients (which are the longer waiting patients) • The joint access policy is not finalised and rolled out. This will be monitored by the Elective Recovery Board. • OMFS visiting surgeon unable to commit to additional activity required to clear the long waiting patients. • IPC guidance is not changed to enable more activity to return to the baseline of 19/20. • That patients either reject the option to travel to another provider for quicker treatment which will be mitigated by using P6
codes, or, patients choose to wait longer for their care and breach 104 weeks, which will be mitigated as far as possible by applying our access policy.
• That the financial framework does not facilitate the extra activity needed as providers would be making a loss to deliver additional work. We will be seeking to agree an appropriate means of distributing the elective recovery fund to mitigate this.
Reduce waits of over 78 weeks
Assumptions We estimate we will start the financial year within the region of 1,000 patients over 78 weeks. We anticipate significant risks in meeting the requirement in full, specifically in the following specialties:
• Orthopaedics (system wide) • General surgery (system wide) • Gynaecology (system wide) • Urology (WSFT only) • ENT (WSFT only) • Pain Management (ESNEFT only) • OMFS (ESNEFT only – regional issue).
Our key assumptions are: • That Reinforced Autoclaved Aerated Concrete (RAAC) plank remedial work at West Suffolk NHS Foundation Trust (WSFT)
does not impact on elective ward capacity, theatres and other estates areas above our planned levels
• Elective activity levels may be impacted by the absence of separate hot and cold elective facilities at WSFT. This will be addressed in future years, through the development of the Newmarket site, as described in the actions below.
• That work continues with system partners in relation to the provision of mutual aid. • That there is continued access to the independent sector to provide additional capacity. • That staffing levels are not significantly impacted due to COVID-19, resulting in elective cancellations. • That non-elective activity will not impact on elective ward capacity further than outlined • That it is clinically appropriate to dedicate the required level of non-cancer/urgent capacity to those waiting over 78 weeks
(over other priorities) • That a minimal number of patients with no criteria to reside are delayed to enable length of stay (LOS) to reduce and enable
the non-elective activity to be managed within their bed base. Actions We have set out in the action sections above our plans to increase activity and clear backlogs.
The key actions in relation to the risk specialties listed above are as follows:
• Orthopaedics: maximise independent sector throughput; implement key productivity learning from GIRFT and HVLC through our MSK specific programme; where appropriate, use mutual aid to balance out inequalities in our system.
• General Surgery and Gynaecology: the wait times in each trust are broadly similar so our focus will be on internal productivity and securing capacity for at risk sub-specialties such as Urogynaecology and any are with a significant cancer pressure
• Urology: our trusts will be looking at mutual aid opportunities to close the gap in parity between them. Managing cancer capacity against RTT capacity will be a key focus in this specialty.
• Ear, nose and throat: our trusts will be looking at mutual aid opportunities to close the gap in parity between them. • Pain management: our trusts will be looking at mutual aid opportunities to close the gap in parity between them. • OMFS: we will continue to pursue options with NHSE to secure a regional solution to this very specialised area.
More generally:
• we will have the WSFT theatre capacity back in 21/22 which will increase our throughput. This will give significantly more opportunity to clear surgical backlogs
• mutual aid: there are some specialties where we have significant differences in waits. We have been successful in working together (e.g. ophthalmology had a 52 week wait time differential which is now down to 3 weeks and more recently the orthopaedic difference has dropped by 10 weeks) and will seek to expand this into additional areas (specifically urology and pain management).
• Additional capacity: we have extremely strong working relationships with one of our three major independent sector providers and will be seeking to roll out the learning to the other two. We have also been successful in insourcing support.
• Productivity: we have had an extensive MSK programme which will continue into 2022/23 and expand our learning into other areas.
• Validation: We have good engagement in a clinical validation and prioritisation programme, including the conduct of three-monthly reviews for those waiting over 52 weeks from 1 July 2022.
Risks, issues and mitigation
The key risks are the same as described in the 104 week waits section with the addition of: • Insufficient capacity in the pressure specialties (and the sub-specialties within them) identified above where it is clear that
104% activity will be insufficient to meet 78 weeks. We will seek to mitigate by seeking to increase capacity beyond 104% in these areas through the actions above.
Plans will only be signed off if they clearly demonstrate the features set out through a combination of the submitted plan trajectories, narrative submissions and assurance statements as outlined in the elective recovery planning supporting guidance (available on NHS Planning collaboration platform)
Please outline the priority actions that are critical to the delivery of the elective recovery objectives below including any proposed use of multi-year capital funding: [Max 200 words per section]
Maximise cross-system management of demand through prospective, planned arrangements for mutual aid
As set out in the sections above we have a strong track record of delivering mutual aid as demonstrated in ophthalmology, orthopaedics and gynaecology in 2021/22. We have established routes through standard operating protocols that enable us to share staff or transfer patients from organisation to organisation. We have achieved this through strong clinical leadership, cohesive operational working and determination to put patients, not organisations, first. In 2022/23 we will move closer to operating a ‘true’ joint PTL approach whereby we maximise the relative strengths of our organisations including the independent sector. As well as continuing and expanding the existing arrangements we will explore expansion of mutual aid into urology, pain management, dermatology and diagnostics as a minimum. We will proactively engage with patients to facilitate choice and movement across our system to those with the shortest waits at the referral stage and where patients are already on a waiting list. We will ensure constitutional and legal commitments to shared decision making and choice are met. Our joint access policy will underpin delivery of this. [175 words]
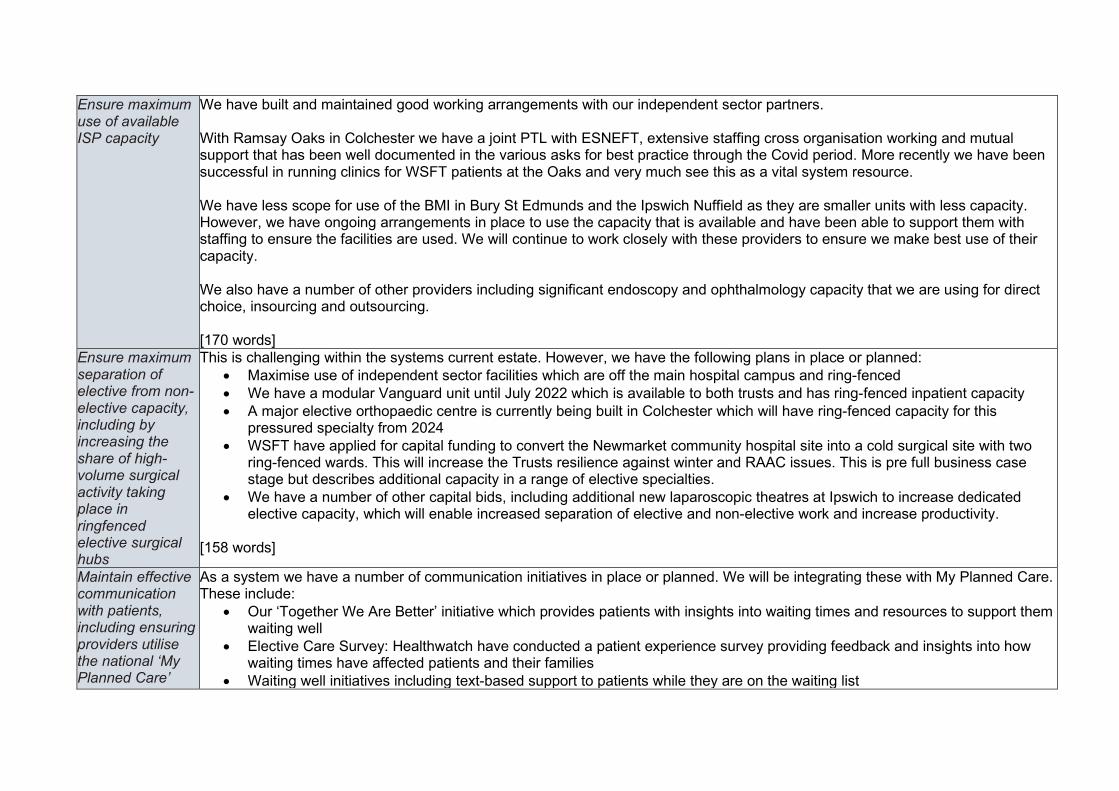
Ensure maximum use of available ISP capacity
We have built and maintained good working arrangements with our independent sector partners. With Ramsay Oaks in Colchester we have a joint PTL with ESNEFT, extensive staffing cross organisation working and mutual support that has been well documented in the various asks for best practice through the Covid period. More recently we have been successful in running clinics for WSFT patients at the Oaks and very much see this as a vital system resource. We have less scope for use of the BMI in Bury St Edmunds and the Ipswich Nuffield as they are smaller units with less capacity. However, we have ongoing arrangements in place to use the capacity that is available and have been able to support them with staffing to ensure the facilities are used. We will continue to work closely with these providers to ensure we make best use of their capacity. We also have a number of other providers including significant endoscopy and ophthalmology capacity that we are using for direct choice, insourcing and outsourcing. [170 words]
Ensure maximum separation of elective from non-elective capacity, including by increasing the share of high-volume surgical activity taking place in ringfenced elective surgical hubs
This is challenging within the systems current estate. However, we have the following plans in place or planned: • Maximise use of independent sector facilities which are off the main hospital campus and ring-fenced • We have a modular Vanguard unit until July 2022 which is available to both trusts and has ring-fenced inpatient capacity • A major elective orthopaedic centre is currently being built in Colchester which will have ring-fenced capacity for this
pressured specialty from 2024 • WSFT have applied for capital funding to convert the Newmarket community hospital site into a cold surgical site with two
ring-fenced wards. This will increase the Trusts resilience against winter and RAAC issues. This is pre full business case stage but describes additional capacity in a range of elective specialties.
• We have a number of other capital bids, including additional new laparoscopic theatres at Ipswich to increase dedicated elective capacity, which will enable increased separation of elective and non-elective work and increase productivity.
[158 words]
Maintain effective communication with patients, including ensuring providers utilise the national ‘My Planned Care’
As a system we have a number of communication initiatives in place or planned. We will be integrating these with My Planned Care. These include:
• Our ‘Together We Are Better’ initiative which provides patients with insights into waiting times and resources to support them waiting well
• Elective Care Survey: Healthwatch have conducted a patient experience survey providing feedback and insights into how waiting times have affected patients and their families
• Waiting well initiatives including text-based support to patients while they are on the waiting list
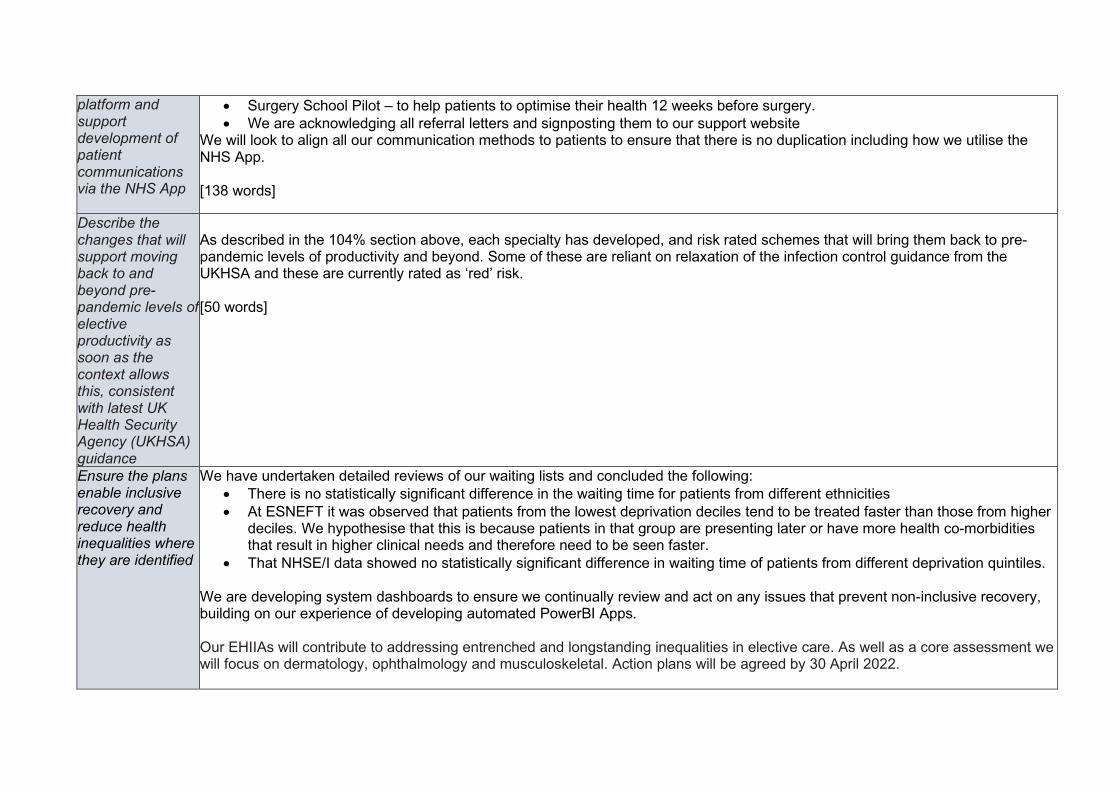
platform and support development of patient communications via the NHS App
• Surgery School Pilot – to help patients to optimise their health 12 weeks before surgery. • We are acknowledging all referral letters and signposting them to our support website
We will look to align all our communication methods to patients to ensure that there is no duplication including how we utilise the NHS App. [138 words]
Describe the changes that will support moving back to and beyond pre-pandemic levels of elective productivity as soon as the context allows this, consistent with latest UK Health Security Agency (UKHSA) guidance
As described in the 104% section above, each specialty has developed, and risk rated schemes that will bring them back to pre-pandemic levels of productivity and beyond. Some of these are reliant on relaxation of the infection control guidance from the UKHSA and these are currently rated as ‘red’ risk. [50 words]
Ensure the plans enable inclusive recovery and reduce health inequalities where they are identified
We have undertaken detailed reviews of our waiting lists and concluded the following: • There is no statistically significant difference in the waiting time for patients from different ethnicities • At ESNEFT it was observed that patients from the lowest deprivation deciles tend to be treated faster than those from higher
deciles. We hypothesise that this is because patients in that group are presenting later or have more health co-morbidities that result in higher clinical needs and therefore need to be seen faster.
• That NHSE/I data showed no statistically significant difference in waiting time of patients from different deprivation quintiles. We are developing system dashboards to ensure we continually review and act on any issues that prevent non-inclusive recovery, building on our experience of developing automated PowerBI Apps. Our EHIIAs will contribute to addressing entrenched and longstanding inequalities in elective care. As well as a core assessment we will focus on dermatology, ophthalmology and musculoskeletal. Action plans will be agreed by 30 April 2022.
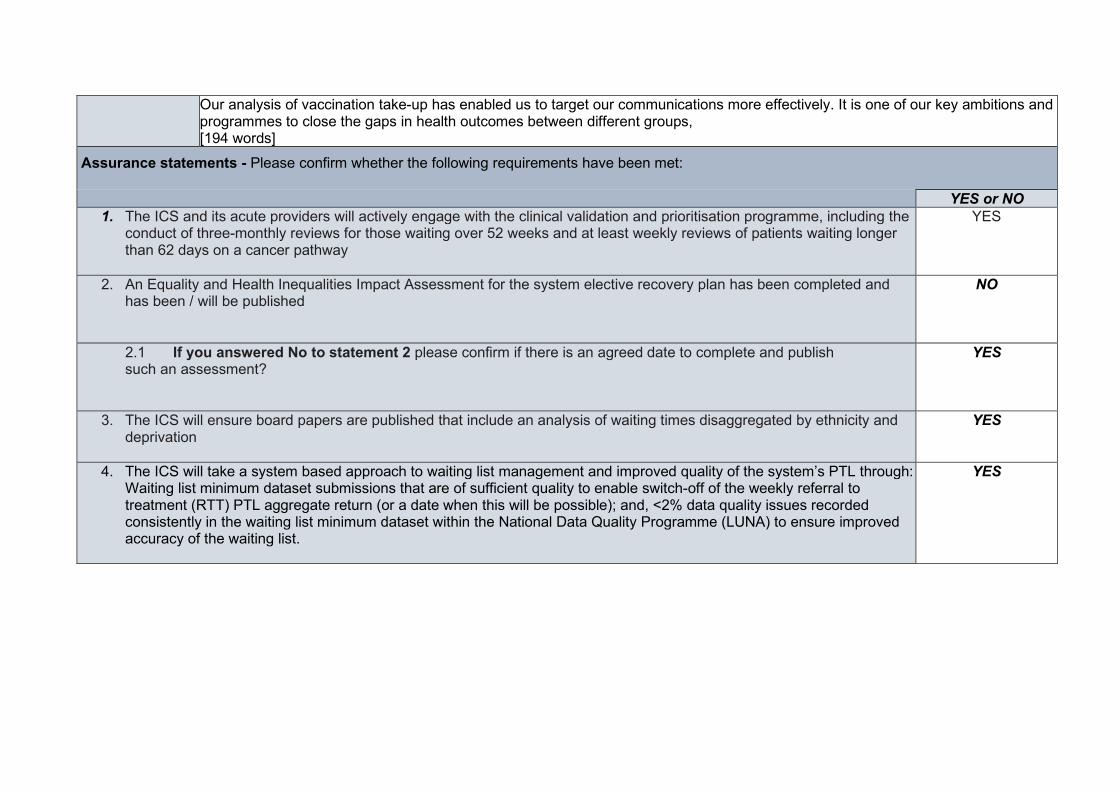
Our analysis of vaccination take-up has enabled us to target our communications more effectively. It is one of our key ambitions and programmes to close the gaps in health outcomes between different groups, [194 words]
Assurance statements - Please confirm whether the following requirements have been met:
YES or NO 1. The ICS and its acute providers will actively engage with the clinical validation and prioritisation programme, including the
conduct of three-monthly reviews for those waiting over 52 weeks and at least weekly reviews of patients waiting longer than 62 days on a cancer pathway
YES
2. An Equality and Health Inequalities Impact Assessment for the system elective recovery plan has been completed and has been / will be published
NO
2.1 If you answered No to statement 2 please confirm if there is an agreed date to complete and publish such an assessment?
YES
3. The ICS will ensure board papers are published that include an analysis of waiting times disaggregated by ethnicity and deprivation
YES
4. The ICS will take a system based approach to waiting list management and improved quality of the system’s PTL through: Waiting list minimum dataset submissions that are of sufficient quality to enable switch-off of the weekly referral to treatment (RTT) PTL aggregate return (or a date when this will be possible); and, <2% data quality issues recorded consistently in the waiting list minimum dataset within the National Data Quality Programme (LUNA) to ensure improved accuracy of the waiting list.
YES
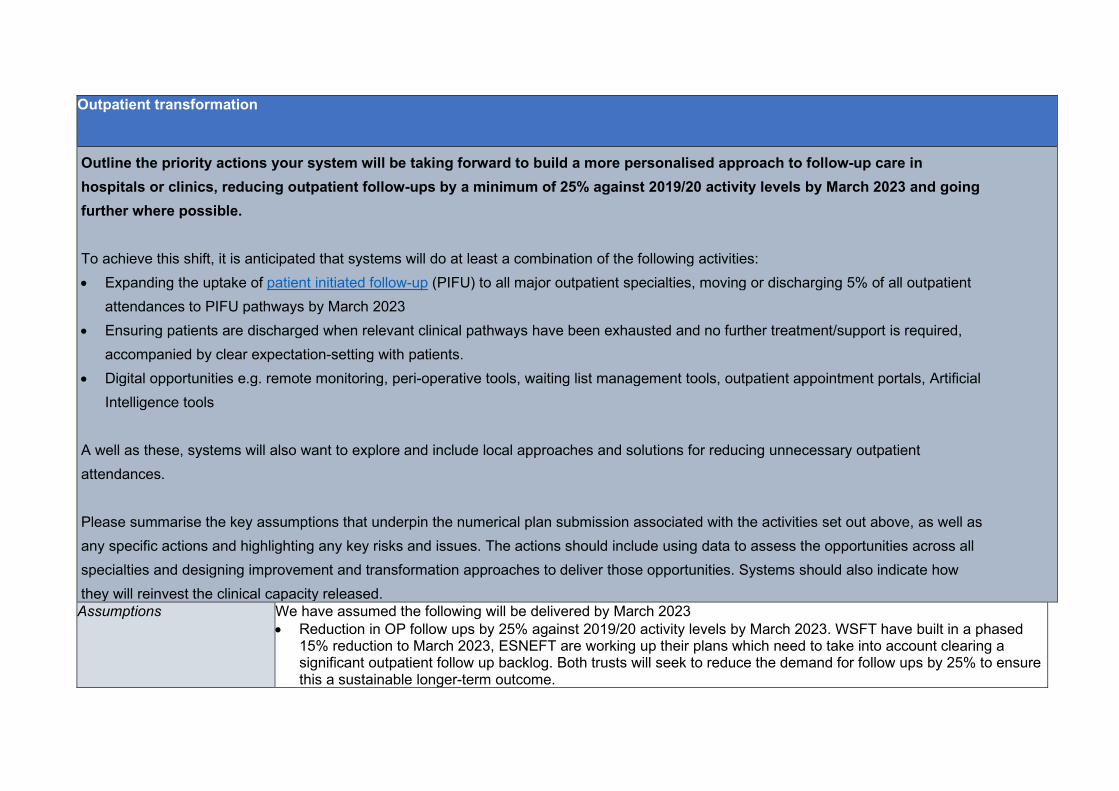
Outpatient transformation Outline the priority actions your system will be taking forward to build a more personalised approach to follow-up care in hospitals or clinics, reducing outpatient follow-ups by a minimum of 25% against 2019/20 activity levels by March 2023 and going further where possible. To achieve this shift, it is anticipated that systems will do at least a combination of the following activities: • Expanding the uptake of patient initiated follow-up (PIFU) to all major outpatient specialties, moving or discharging 5% of all outpatient
attendances to PIFU pathways by March 2023 • Ensuring patients are discharged when relevant clinical pathways have been exhausted and no further treatment/support is required,
accompanied by clear expectation-setting with patients. • Digital opportunities e.g. remote monitoring, peri-operative tools, waiting list management tools, outpatient appointment portals, Artificial
Intelligence tools
A well as these, systems will also want to explore and include local approaches and solutions for reducing unnecessary outpatient attendances. Please summarise the key assumptions that underpin the numerical plan submission associated with the activities set out above, as well as any specific actions and highlighting any key risks and issues. The actions should include using data to assess the opportunities across all specialties and designing improvement and transformation approaches to deliver those opportunities. Systems should also indicate how they will reinvest the clinical capacity released. Assumptions We have assumed the following will be delivered by March 2023
• Reduction in OP follow ups by 25% against 2019/20 activity levels by March 2023. WSFT have built in a phased 15% reduction to March 2023, ESNEFT are working up their plans which need to take into account clearing a significant outpatient follow up backlog. Both trusts will seek to reduce the demand for follow ups by 25% to ensure this a sustainable longer-term outcome.
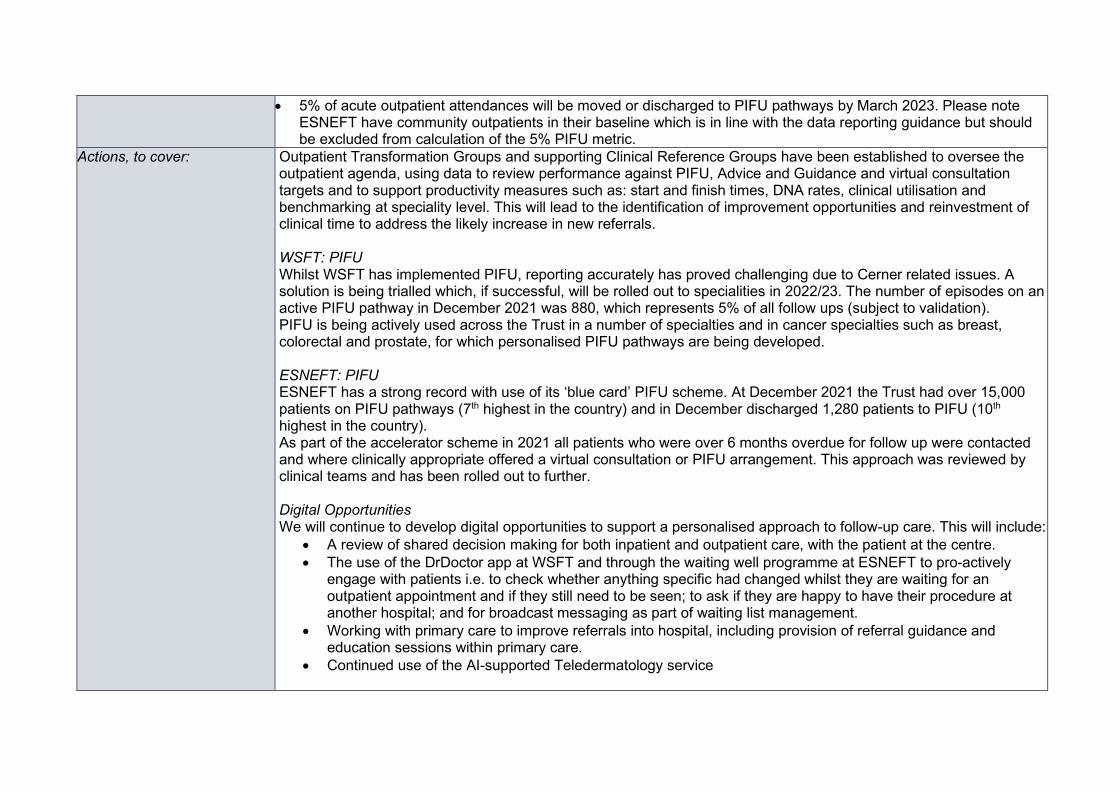
• 5% of acute outpatient attendances will be moved or discharged to PIFU pathways by March 2023. Please note ESNEFT have community outpatients in their baseline which is in line with the data reporting guidance but should be excluded from calculation of the 5% PIFU metric.
Actions, to cover: Outpatient Transformation Groups and supporting Clinical Reference Groups have been established to oversee the outpatient agenda, using data to review performance against PIFU, Advice and Guidance and virtual consultation targets and to support productivity measures such as: start and finish times, DNA rates, clinical utilisation and benchmarking at speciality level. This will lead to the identification of improvement opportunities and reinvestment of clinical time to address the likely increase in new referrals. WSFT: PIFU Whilst WSFT has implemented PIFU, reporting accurately has proved challenging due to Cerner related issues. A solution is being trialled which, if successful, will be rolled out to specialities in 2022/23. The number of episodes on an active PIFU pathway in December 2021 was 880, which represents 5% of all follow ups (subject to validation). PIFU is being actively used across the Trust in a number of specialties and in cancer specialties such as breast, colorectal and prostate, for which personalised PIFU pathways are being developed. ESNEFT: PIFU ESNEFT has a strong record with use of its ‘blue card’ PIFU scheme. At December 2021 the Trust had over 15,000 patients on PIFU pathways (7th highest in the country) and in December discharged 1,280 patients to PIFU (10th highest in the country). As part of the accelerator scheme in 2021 all patients who were over 6 months overdue for follow up were contacted and where clinically appropriate offered a virtual consultation or PIFU arrangement. This approach was reviewed by clinical teams and has been rolled out to further. Digital Opportunities We will continue to develop digital opportunities to support a personalised approach to follow-up care. This will include:
• A review of shared decision making for both inpatient and outpatient care, with the patient at the centre. • The use of the DrDoctor app at WSFT and through the waiting well programme at ESNEFT to pro-actively
engage with patients i.e. to check whether anything specific had changed whilst they are waiting for an outpatient appointment and if they still need to be seen; to ask if they are happy to have their procedure at another hospital; and for broadcast messaging as part of waiting list management.
• Working with primary care to improve referrals into hospital, including provision of referral guidance and education sessions within primary care.
• Continued use of the AI-supported Teledermatology service
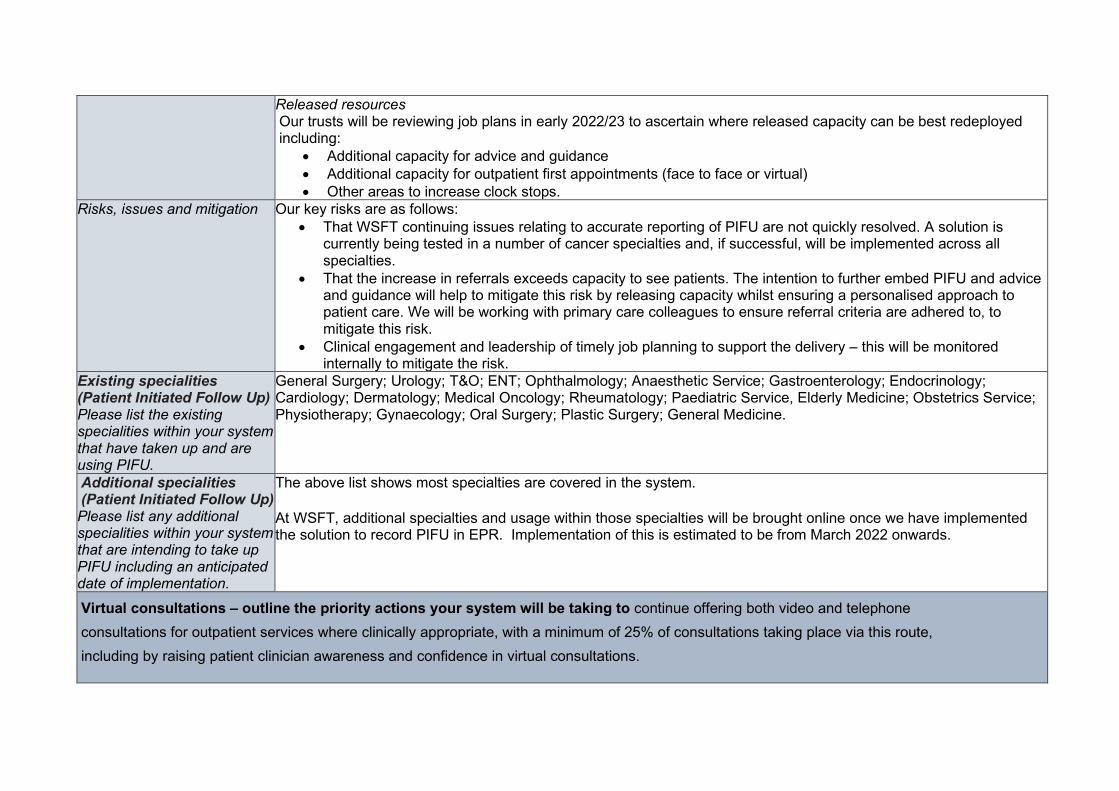
Released resources Our trusts will be reviewing job plans in early 2022/23 to ascertain where released capacity can be best redeployed including:
• Additional capacity for advice and guidance • Additional capacity for outpatient first appointments (face to face or virtual) • Other areas to increase clock stops.
Risks, issues and mitigation Our key risks are as follows: • That WSFT continuing issues relating to accurate reporting of PIFU are not quickly resolved. A solution is
currently being tested in a number of cancer specialties and, if successful, will be implemented across all specialties.
• That the increase in referrals exceeds capacity to see patients. The intention to further embed PIFU and advice and guidance will help to mitigate this risk by releasing capacity whilst ensuring a personalised approach to patient care. We will be working with primary care colleagues to ensure referral criteria are adhered to, to mitigate this risk.
• Clinical engagement and leadership of timely job planning to support the delivery – this will be monitored internally to mitigate the risk.
Existing specialities (Patient Initiated Follow Up) Please list the existing specialities within your system that have taken up and are using PIFU.
General Surgery; Urology; T&O; ENT; Ophthalmology; Anaesthetic Service; Gastroenterology; Endocrinology; Cardiology; Dermatology; Medical Oncology; Rheumatology; Paediatric Service, Elderly Medicine; Obstetrics Service; Physiotherapy; Gynaecology; Oral Surgery; Plastic Surgery; General Medicine.
Additional specialities (Patient Initiated Follow Up) Please list any additional specialities within your system that are intending to take up PIFU including an anticipated date of implementation.
The above list shows most specialties are covered in the system.
At WSFT, additional specialties and usage within those specialties will be brought online once we have implemented the solution to record PIFU in EPR. Implementation of this is estimated to be from March 2022 onwards.
Virtual consultations – outline the priority actions your system will be taking to continue offering both video and telephone consultations for outpatient services where clinically appropriate, with a minimum of 25% of consultations taking place via this route, including by raising patient clinician awareness and confidence in virtual consultations.
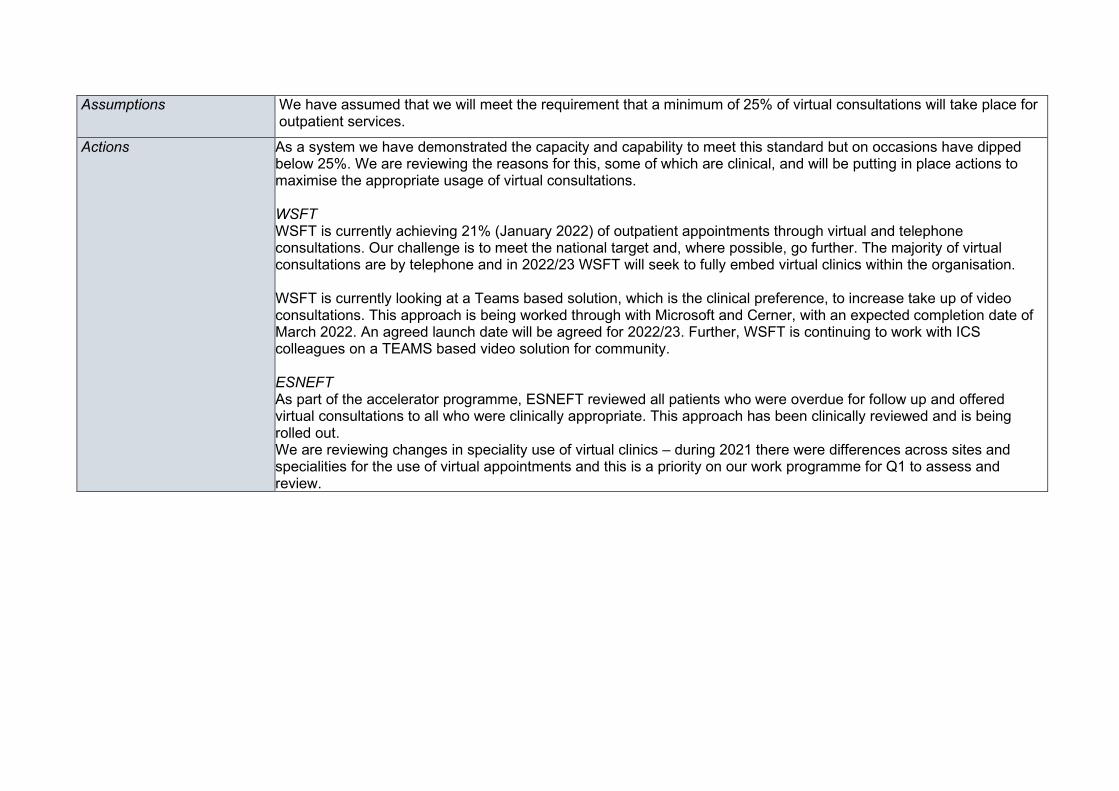
Assumptions We have assumed that we will meet the requirement that a minimum of 25% of virtual consultations will take place for outpatient services.
Actions As a system we have demonstrated the capacity and capability to meet this standard but on occasions have dipped below 25%. We are reviewing the reasons for this, some of which are clinical, and will be putting in place actions to maximise the appropriate usage of virtual consultations. WSFT WSFT is currently achieving 21% (January 2022) of outpatient appointments through virtual and telephone consultations. Our challenge is to meet the national target and, where possible, go further. The majority of virtual consultations are by telephone and in 2022/23 WSFT will seek to fully embed virtual clinics within the organisation. WSFT is currently looking at a Teams based solution, which is the clinical preference, to increase take up of video consultations. This approach is being worked through with Microsoft and Cerner, with an expected completion date of March 2022. An agreed launch date will be agreed for 2022/23. Further, WSFT is continuing to work with ICS colleagues on a TEAMS based video solution for community. ESNEFT As part of the accelerator programme, ESNEFT reviewed all patients who were overdue for follow up and offered virtual consultations to all who were clinically appropriate. This approach has been clinically reviewed and is being rolled out. We are reviewing changes in speciality use of virtual clinics – during 2021 there were differences across sites and specialities for the use of virtual appointments and this is a priority on our work programme for Q1 to assess and review.
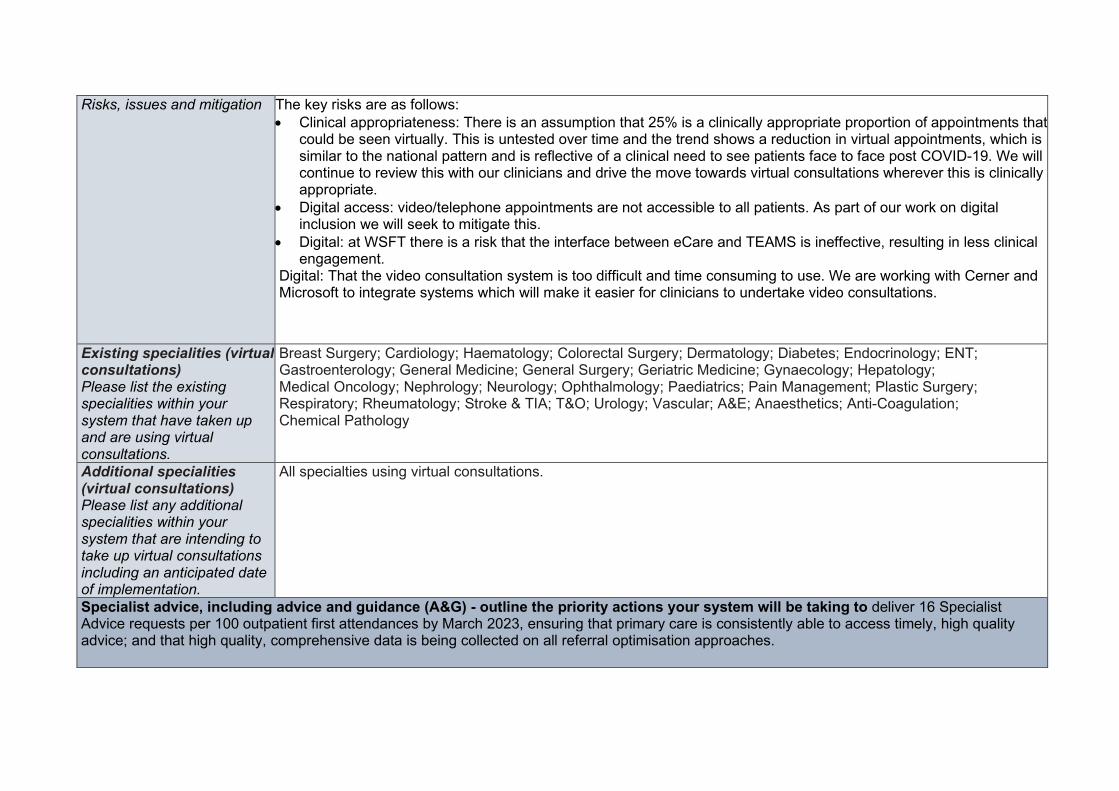
Risks, issues and mitigation The key risks are as follows: • Clinical appropriateness: There is an assumption that 25% is a clinically appropriate proportion of appointments that
could be seen virtually. This is untested over time and the trend shows a reduction in virtual appointments, which is similar to the national pattern and is reflective of a clinical need to see patients face to face post COVID-19. We will continue to review this with our clinicians and drive the move towards virtual consultations wherever this is clinically appropriate.
• Digital access: video/telephone appointments are not accessible to all patients. As part of our work on digital inclusion we will seek to mitigate this.
• Digital: at WSFT there is a risk that the interface between eCare and TEAMS is ineffective, resulting in less clinical engagement.
Digital: That the video consultation system is too difficult and time consuming to use. We are working with Cerner and Microsoft to integrate systems which will make it easier for clinicians to undertake video consultations.
Existing specialities (virtual consultations) Please list the existing specialities within your system that have taken up and are using virtual consultations.
Breast Surgery; Cardiology; Haematology; Colorectal Surgery; Dermatology; Diabetes; Endocrinology; ENT; Gastroenterology; General Medicine; General Surgery; Geriatric Medicine; Gynaecology; Hepatology; Medical Oncology; Nephrology; Neurology; Ophthalmology; Paediatrics; Pain Management; Plastic Surgery; Respiratory; Rheumatology; Stroke & TIA; T&O; Urology; Vascular; A&E; Anaesthetics; Anti-Coagulation; Chemical Pathology
Additional specialities (virtual consultations) Please list any additional specialities within your system that are intending to take up virtual consultations including an anticipated date of implementation.
All specialties using virtual consultations.
Specialist advice, including advice and guidance (A&G) - outline the priority actions your system will be taking to deliver 16 Specialist Advice requests per 100 outpatient first attendances by March 2023, ensuring that primary care is consistently able to access timely, high quality advice; and that high quality, comprehensive data is being collected on all referral optimisation approaches.
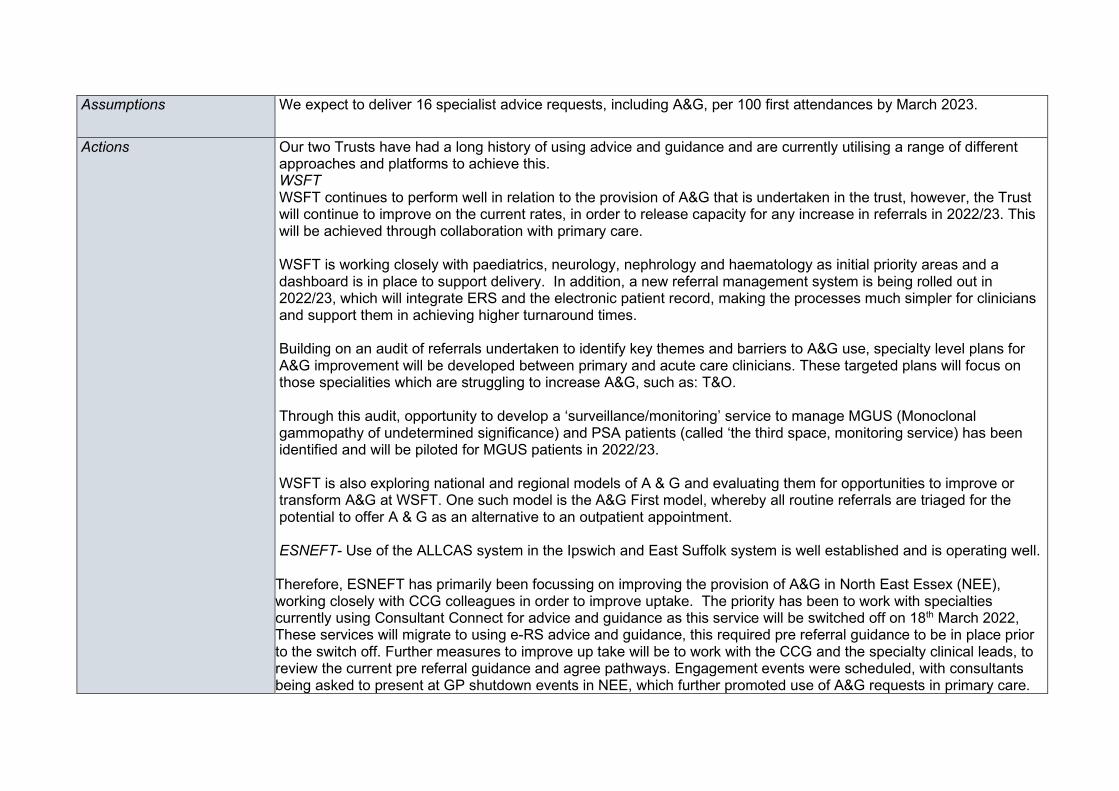
Assumptions We expect to deliver 16 specialist advice requests, including A&G, per 100 first attendances by March 2023.
Actions Our two Trusts have had a long history of using advice and guidance and are currently utilising a range of different approaches and platforms to achieve this. WSFT WSFT continues to perform well in relation to the provision of A&G that is undertaken in the trust, however, the Trust will continue to improve on the current rates, in order to release capacity for any increase in referrals in 2022/23. This will be achieved through collaboration with primary care. WSFT is working closely with paediatrics, neurology, nephrology and haematology as initial priority areas and a dashboard is in place to support delivery. In addition, a new referral management system is being rolled out in 2022/23, which will integrate ERS and the electronic patient record, making the processes much simpler for clinicians and support them in achieving higher turnaround times. Building on an audit of referrals undertaken to identify key themes and barriers to A&G use, specialty level plans for A&G improvement will be developed between primary and acute care clinicians. These targeted plans will focus on those specialities which are struggling to increase A&G, such as: T&O. Through this audit, opportunity to develop a ‘surveillance/monitoring’ service to manage MGUS (Monoclonal gammopathy of undetermined significance) and PSA patients (called ‘the third space, monitoring service) has been identified and will be piloted for MGUS patients in 2022/23. WSFT is also exploring national and regional models of A & G and evaluating them for opportunities to improve or transform A&G at WSFT. One such model is the A&G First model, whereby all routine referrals are triaged for the potential to offer A & G as an alternative to an outpatient appointment. ESNEFT- Use of the ALLCAS system in the Ipswich and East Suffolk system is well established and is operating well. Therefore, ESNEFT has primarily been focussing on improving the provision of A&G in North East Essex (NEE), working closely with CCG colleagues in order to improve uptake. The priority has been to work with specialties currently using Consultant Connect for advice and guidance as this service will be switched off on 18th March 2022, These services will migrate to using e-RS advice and guidance, this required pre referral guidance to be in place prior to the switch off. Further measures to improve up take will be to work with the CCG and the specialty clinical leads, to review the current pre referral guidance and agree pathways. Engagement events were scheduled, with consultants being asked to present at GP shutdown events in NEE, which further promoted use of A&G requests in primary care.
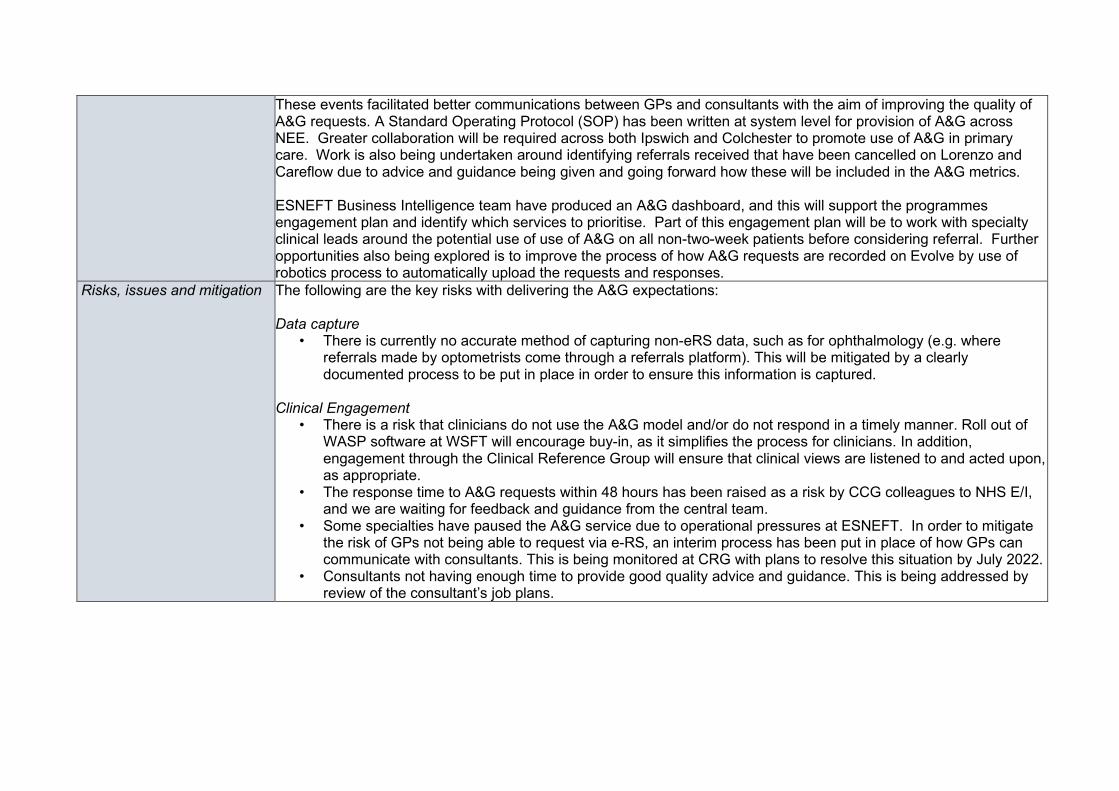
These events facilitated better communications between GPs and consultants with the aim of improving the quality of A&G requests. A Standard Operating Protocol (SOP) has been written at system level for provision of A&G across NEE. Greater collaboration will be required across both Ipswich and Colchester to promote use of A&G in primary care. Work is also being undertaken around identifying referrals received that have been cancelled on Lorenzo and Careflow due to advice and guidance being given and going forward how these will be included in the A&G metrics. ESNEFT Business Intelligence team have produced an A&G dashboard, and this will support the programmes engagement plan and identify which services to prioritise. Part of this engagement plan will be to work with specialty clinical leads around the potential use of use of A&G on all non-two-week patients before considering referral. Further opportunities also being explored is to improve the process of how A&G requests are recorded on Evolve by use of robotics process to automatically upload the requests and responses.
Risks, issues and mitigation The following are the key risks with delivering the A&G expectations: Data capture
• There is currently no accurate method of capturing non-eRS data, such as for ophthalmology (e.g. where referrals made by optometrists come through a referrals platform). This will be mitigated by a clearly documented process to be put in place in order to ensure this information is captured.
Clinical Engagement
• There is a risk that clinicians do not use the A&G model and/or do not respond in a timely manner. Roll out of WASP software at WSFT will encourage buy-in, as it simplifies the process for clinicians. In addition, engagement through the Clinical Reference Group will ensure that clinical views are listened to and acted upon, as appropriate.
• The response time to A&G requests within 48 hours has been raised as a risk by CCG colleagues to NHS E/I, and we are waiting for feedback and guidance from the central team.
• Some specialties have paused the A&G service due to operational pressures at ESNEFT. In order to mitigate the risk of GPs not being able to request via e-RS, an interim process has been put in place of how GPs can communicate with consultants. This is being monitored at CRG with plans to resolve this situation by July 2022.
• Consultants not having enough time to provide good quality advice and guidance. This is being addressed by review of the consultant’s job plans.
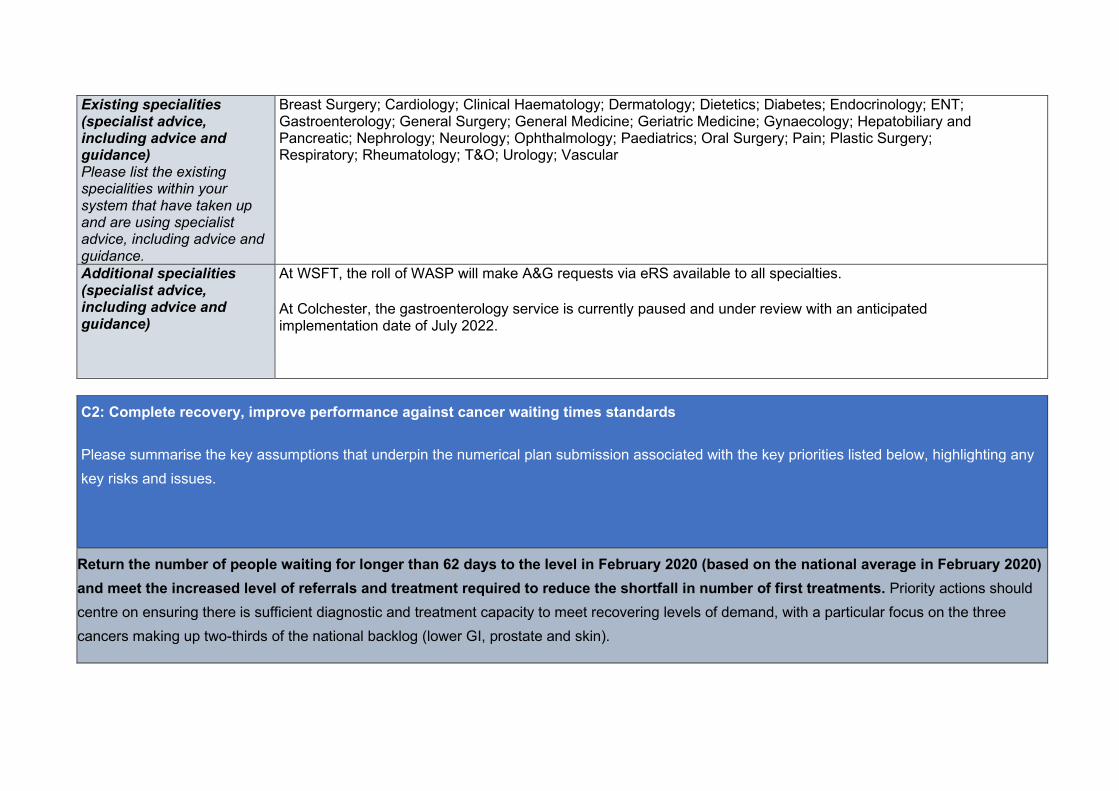
Existing specialities (specialist advice, including advice and guidance) Please list the existing specialities within your system that have taken up and are using specialist advice, including advice and guidance.
Breast Surgery; Cardiology; Clinical Haematology; Dermatology; Dietetics; Diabetes; Endocrinology; ENT; Gastroenterology; General Surgery; General Medicine; Geriatric Medicine; Gynaecology; Hepatobiliary and Pancreatic; Nephrology; Neurology; Ophthalmology; Paediatrics; Oral Surgery; Pain; Plastic Surgery; Respiratory; Rheumatology; T&O; Urology; Vascular
Additional specialities (specialist advice, including advice and guidance)
At WSFT, the roll of WASP will make A&G requests via eRS available to all specialties.
At Colchester, the gastroenterology service is currently paused and under review with an anticipated implementation date of July 2022.
C2: Complete recovery, improve performance against cancer waiting times standards
Please summarise the key assumptions that underpin the numerical plan submission associated with the key priorities listed below, highlighting any key risks and issues.
Return the number of people waiting for longer than 62 days to the level in February 2020 (based on the national average in February 2020) and meet the increased level of referrals and treatment required to reduce the shortfall in number of first treatments. Priority actions should centre on ensuring there is sufficient diagnostic and treatment capacity to meet recovering levels of demand, with a particular focus on the three cancers making up two-thirds of the national backlog (lower GI, prostate and skin).
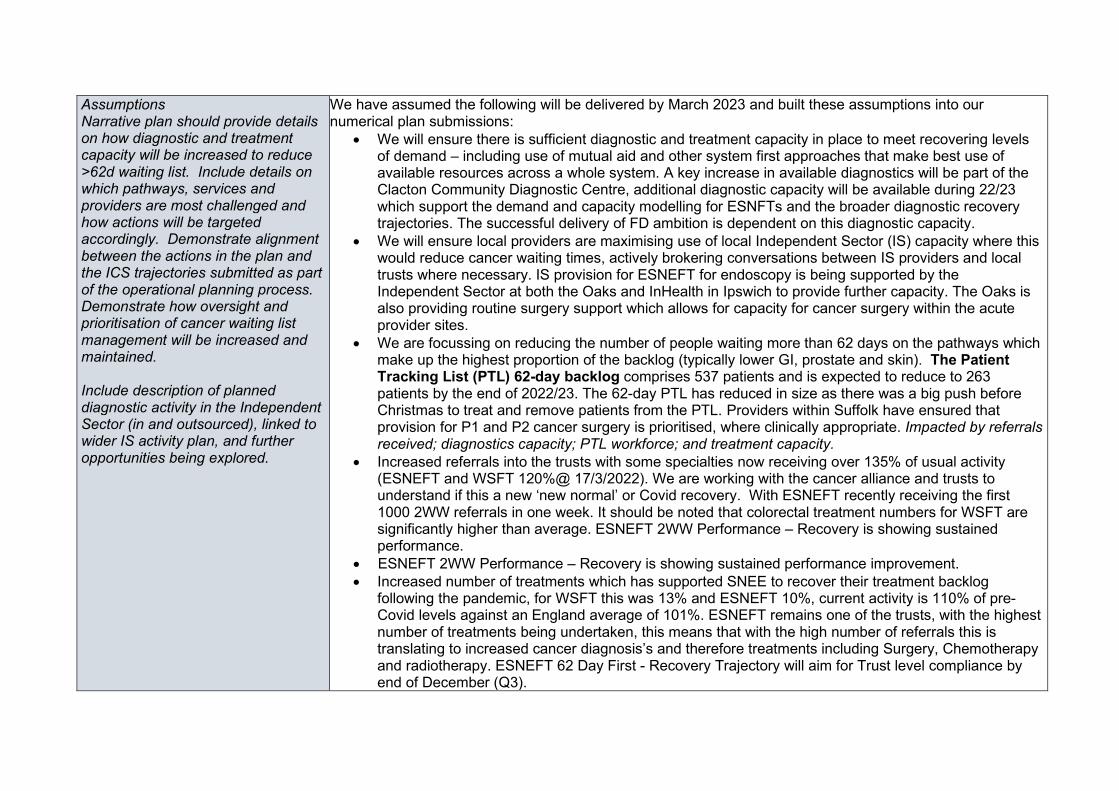
Assumptions Narrative plan should provide details on how diagnostic and treatment capacity will be increased to reduce >62d waiting list. Include details on which pathways, services and providers are most challenged and how actions will be targeted accordingly. Demonstrate alignment between the actions in the plan and the ICS trajectories submitted as part of the operational planning process. Demonstrate how oversight and prioritisation of cancer waiting list management will be increased and maintained. Include description of planned diagnostic activity in the Independent Sector (in and outsourced), linked to wider IS activity plan, and further opportunities being explored.
We have assumed the following will be delivered by March 2023 and built these assumptions into our numerical plan submissions:
• We will ensure there is sufficient diagnostic and treatment capacity in place to meet recovering levels of demand – including use of mutual aid and other system first approaches that make best use of available resources across a whole system. A key increase in available diagnostics will be part of the Clacton Community Diagnostic Centre, additional diagnostic capacity will be available during 22/23 which support the demand and capacity modelling for ESNFTs and the broader diagnostic recovery trajectories. The successful delivery of FD ambition is dependent on this diagnostic capacity.
• We will ensure local providers are maximising use of local Independent Sector (IS) capacity where this would reduce cancer waiting times, actively brokering conversations between IS providers and local trusts where necessary. IS provision for ESNEFT for endoscopy is being supported by the Independent Sector at both the Oaks and InHealth in Ipswich to provide further capacity. The Oaks is also providing routine surgery support which allows for capacity for cancer surgery within the acute provider sites.
• We are focussing on reducing the number of people waiting more than 62 days on the pathways which make up the highest proportion of the backlog (typically lower GI, prostate and skin). The Patient Tracking List (PTL) 62-day backlog comprises 537 patients and is expected to reduce to 263 patients by the end of 2022/23. The 62-day PTL has reduced in size as there was a big push before Christmas to treat and remove patients from the PTL. Providers within Suffolk have ensured that provision for P1 and P2 cancer surgery is prioritised, where clinically appropriate. Impacted by referrals received; diagnostics capacity; PTL workforce; and treatment capacity.
• Increased referrals into the trusts with some specialties now receiving over 135% of usual activity (ESNEFT and WSFT 120%@ 17/3/2022). We are working with the cancer alliance and trusts to understand if this a new ‘new normal’ or Covid recovery. With ESNEFT recently receiving the first 1000 2WW referrals in one week. It should be noted that colorectal treatment numbers for WSFT are significantly higher than average. ESNEFT 2WW Performance – Recovery is showing sustained performance.
• ESNEFT 2WW Performance – Recovery is showing sustained performance improvement. • Increased number of treatments which has supported SNEE to recover their treatment backlog
following the pandemic, for WSFT this was 13% and ESNEFT 10%, current activity is 110% of pre-Covid levels against an England average of 101%. ESNEFT remains one of the trusts, with the highest number of treatments being undertaken, this means that with the high number of referrals this is translating to increased cancer diagnosis’s and therefore treatments including Surgery, Chemotherapy and radiotherapy. ESNEFT 62 Day First - Recovery Trajectory will aim for Trust level compliance by end of December (Q3).
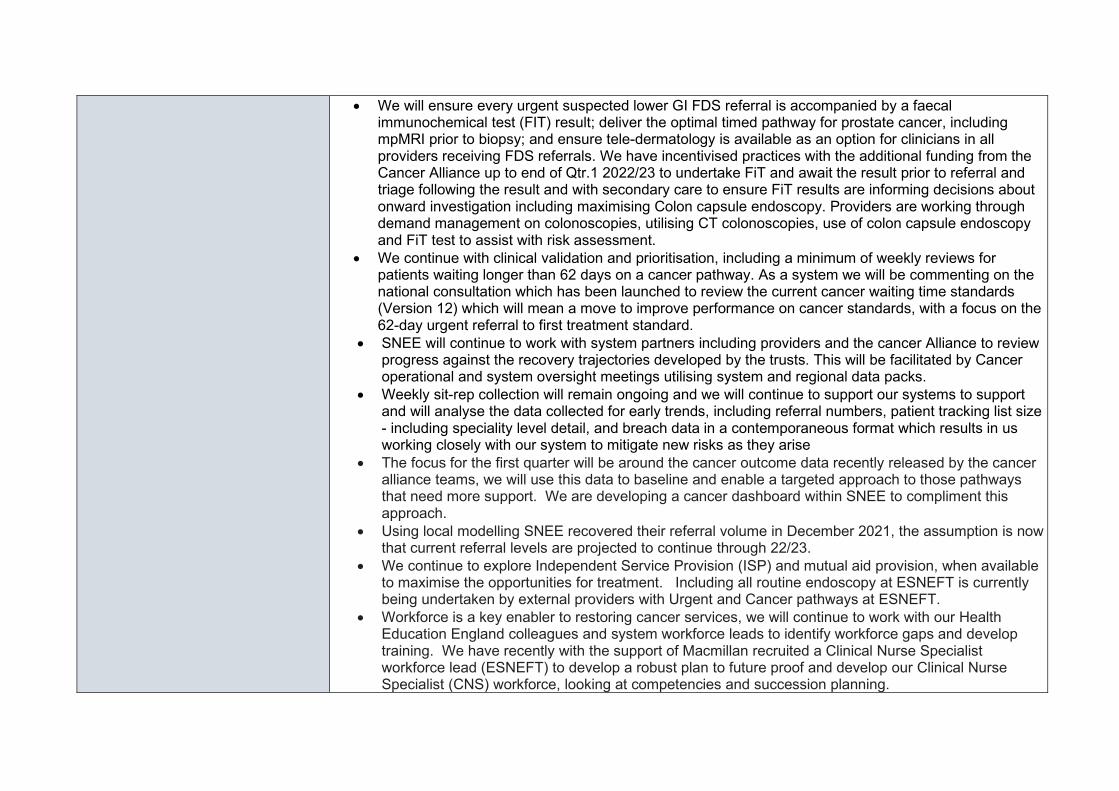
• We will ensure every urgent suspected lower GI FDS referral is accompanied by a faecal immunochemical test (FIT) result; deliver the optimal timed pathway for prostate cancer, including mpMRI prior to biopsy; and ensure tele-dermatology is available as an option for clinicians in all providers receiving FDS referrals. We have incentivised practices with the additional funding from the Cancer Alliance up to end of Qtr.1 2022/23 to undertake FiT and await the result prior to referral and triage following the result and with secondary care to ensure FiT results are informing decisions about onward investigation including maximising Colon capsule endoscopy. Providers are working through demand management on colonoscopies, utilising CT colonoscopies, use of colon capsule endoscopy and FiT test to assist with risk assessment.
• We continue with clinical validation and prioritisation, including a minimum of weekly reviews for patients waiting longer than 62 days on a cancer pathway. As a system we will be commenting on the national consultation which has been launched to review the current cancer waiting time standards (Version 12) which will mean a move to improve performance on cancer standards, with a focus on the 62-day urgent referral to first treatment standard.
• SNEE will continue to work with system partners including providers and the cancer Alliance to review progress against the recovery trajectories developed by the trusts. This will be facilitated by Cancer operational and system oversight meetings utilising system and regional data packs.
• Weekly sit-rep collection will remain ongoing and we will continue to support our systems to support and will analyse the data collected for early trends, including referral numbers, patient tracking list size - including speciality level detail, and breach data in a contemporaneous format which results in us working closely with our system to mitigate new risks as they arise
• The focus for the first quarter will be around the cancer outcome data recently released by the cancer alliance teams, we will use this data to baseline and enable a targeted approach to those pathways that need more support. We are developing a cancer dashboard within SNEE to compliment this approach.
• Using local modelling SNEE recovered their referral volume in December 2021, the assumption is now that current referral levels are projected to continue through 22/23.
• We continue to explore Independent Service Provision (ISP) and mutual aid provision, when available to maximise the opportunities for treatment. Including all routine endoscopy at ESNEFT is currently being undertaken by external providers with Urgent and Cancer pathways at ESNEFT.
• Workforce is a key enabler to restoring cancer services, we will continue to work with our Health Education England colleagues and system workforce leads to identify workforce gaps and develop training. We have recently with the support of Macmillan recruited a Clinical Nurse Specialist workforce lead (ESNEFT) to develop a robust plan to future proof and develop our Clinical Nurse Specialist (CNS) workforce, looking at competencies and succession planning.
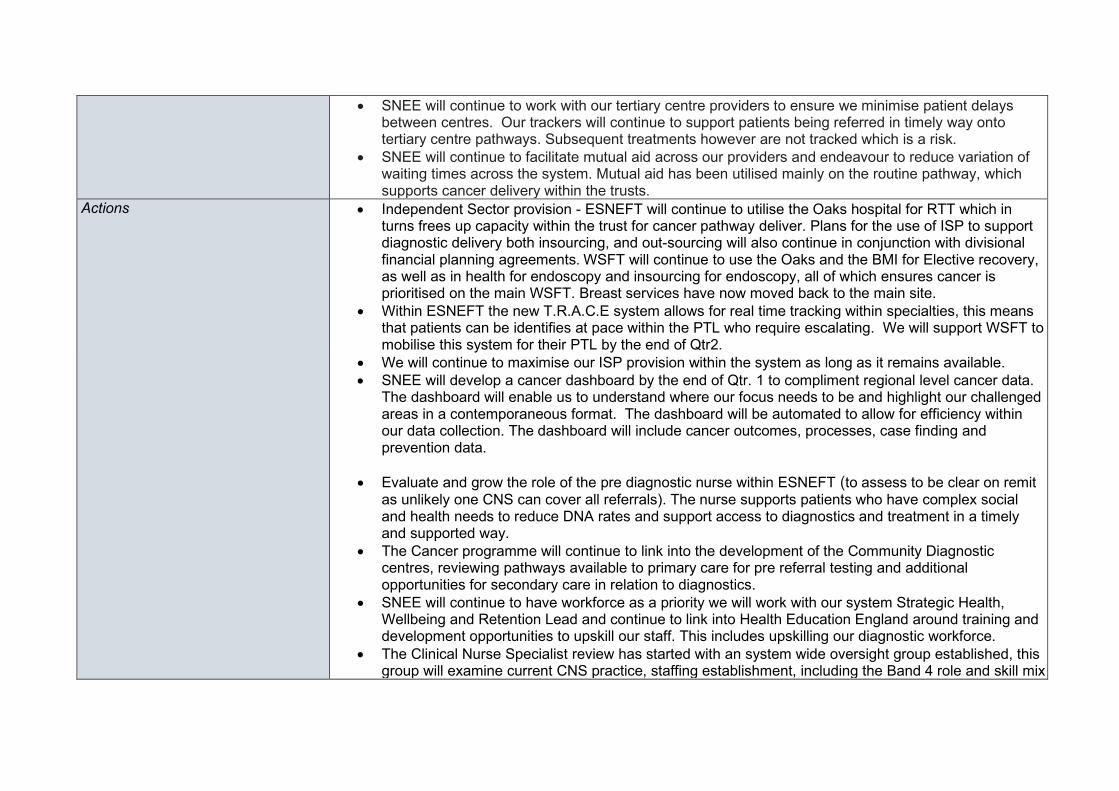
• SNEE will continue to work with our tertiary centre providers to ensure we minimise patient delays between centres. Our trackers will continue to support patients being referred in timely way onto tertiary centre pathways. Subsequent treatments however are not tracked which is a risk.
• SNEE will continue to facilitate mutual aid across our providers and endeavour to reduce variation of waiting times across the system. Mutual aid has been utilised mainly on the routine pathway, which supports cancer delivery within the trusts.
Actions
• Independent Sector provision - ESNEFT will continue to utilise the Oaks hospital for RTT which in turns frees up capacity within the trust for cancer pathway deliver. Plans for the use of ISP to support diagnostic delivery both insourcing, and out-sourcing will also continue in conjunction with divisional financial planning agreements. WSFT will continue to use the Oaks and the BMI for Elective recovery, as well as in health for endoscopy and insourcing for endoscopy, all of which ensures cancer is prioritised on the main WSFT. Breast services have now moved back to the main site.
• Within ESNEFT the new T.R.A.C.E system allows for real time tracking within specialties, this means that patients can be identifies at pace within the PTL who require escalating. We will support WSFT to mobilise this system for their PTL by the end of Qtr2.
• We will continue to maximise our ISP provision within the system as long as it remains available. • SNEE will develop a cancer dashboard by the end of Qtr. 1 to compliment regional level cancer data.
The dashboard will enable us to understand where our focus needs to be and highlight our challenged areas in a contemporaneous format. The dashboard will be automated to allow for efficiency within our data collection. The dashboard will include cancer outcomes, processes, case finding and prevention data.
• Evaluate and grow the role of the pre diagnostic nurse within ESNEFT (to assess to be clear on remit as unlikely one CNS can cover all referrals). The nurse supports patients who have complex social and health needs to reduce DNA rates and support access to diagnostics and treatment in a timely and supported way.
• The Cancer programme will continue to link into the development of the Community Diagnostic centres, reviewing pathways available to primary care for pre referral testing and additional opportunities for secondary care in relation to diagnostics.
• SNEE will continue to have workforce as a priority we will work with our system Strategic Health, Wellbeing and Retention Lead and continue to link into Health Education England around training and development opportunities to upskill our staff. This includes upskilling our diagnostic workforce.
• The Clinical Nurse Specialist review has started with an system wide oversight group established, this group will examine current CNS practice, staffing establishment, including the Band 4 role and skill mix
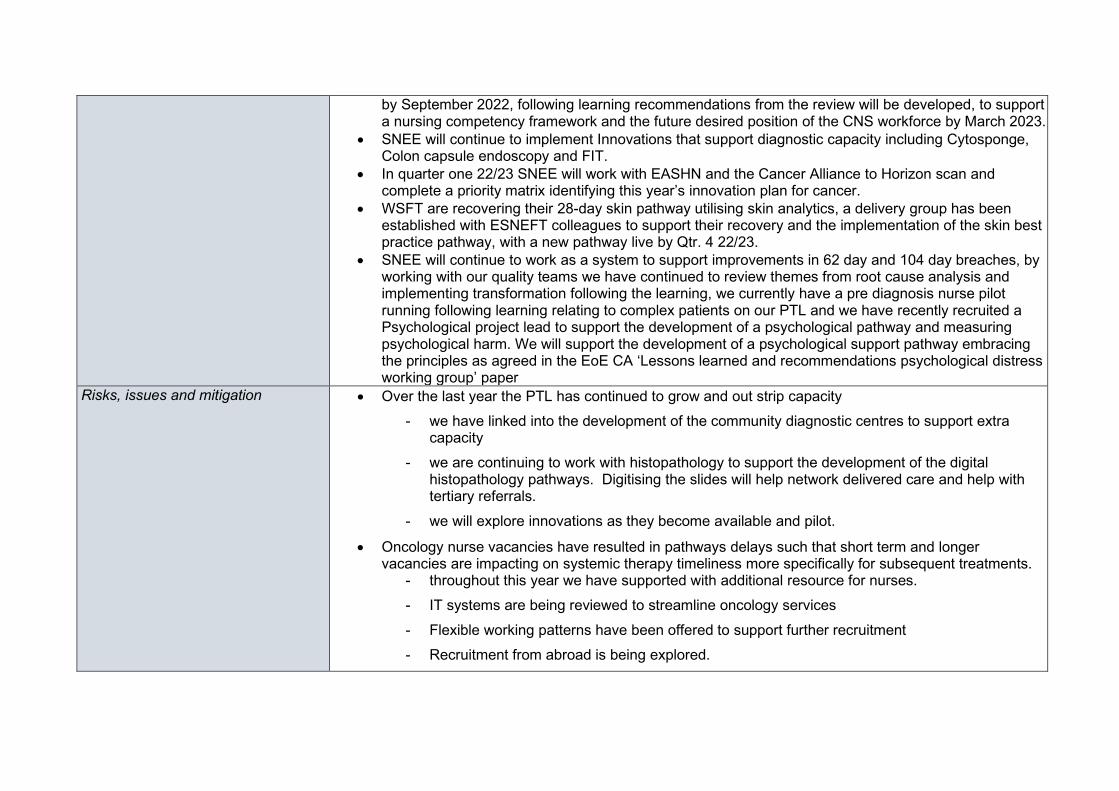
by September 2022, following learning recommendations from the review will be developed, to support a nursing competency framework and the future desired position of the CNS workforce by March 2023.
• SNEE will continue to implement Innovations that support diagnostic capacity including Cytosponge, Colon capsule endoscopy and FIT.
• In quarter one 22/23 SNEE will work with EASHN and the Cancer Alliance to Horizon scan and complete a priority matrix identifying this year’s innovation plan for cancer.
• WSFT are recovering their 28-day skin pathway utilising skin analytics, a delivery group has been established with ESNEFT colleagues to support their recovery and the implementation of the skin best practice pathway, with a new pathway live by Qtr. 4 22/23.
• SNEE will continue to work as a system to support improvements in 62 day and 104 day breaches, by working with our quality teams we have continued to review themes from root cause analysis and implementing transformation following the learning, we currently have a pre diagnosis nurse pilot running following learning relating to complex patients on our PTL and we have recently recruited a Psychological project lead to support the development of a psychological pathway and measuring psychological harm. We will support the development of a psychological support pathway embracing the principles as agreed in the EoE CA ‘Lessons learned and recommendations psychological distress working group’ paper
Risks, issues and mitigation • Over the last year the PTL has continued to grow and out strip capacity - we have linked into the development of the community diagnostic centres to support extra
capacity - we are continuing to work with histopathology to support the development of the digital
histopathology pathways. Digitising the slides will help network delivered care and help with tertiary referrals.
- we will explore innovations as they become available and pilot.
• Oncology nurse vacancies have resulted in pathways delays such that short term and longer vacancies are impacting on systemic therapy timeliness more specifically for subsequent treatments.
- throughout this year we have supported with additional resource for nurses. - IT systems are being reviewed to streamline oncology services - Flexible working patterns have been offered to support further recruitment - Recruitment from abroad is being explored.
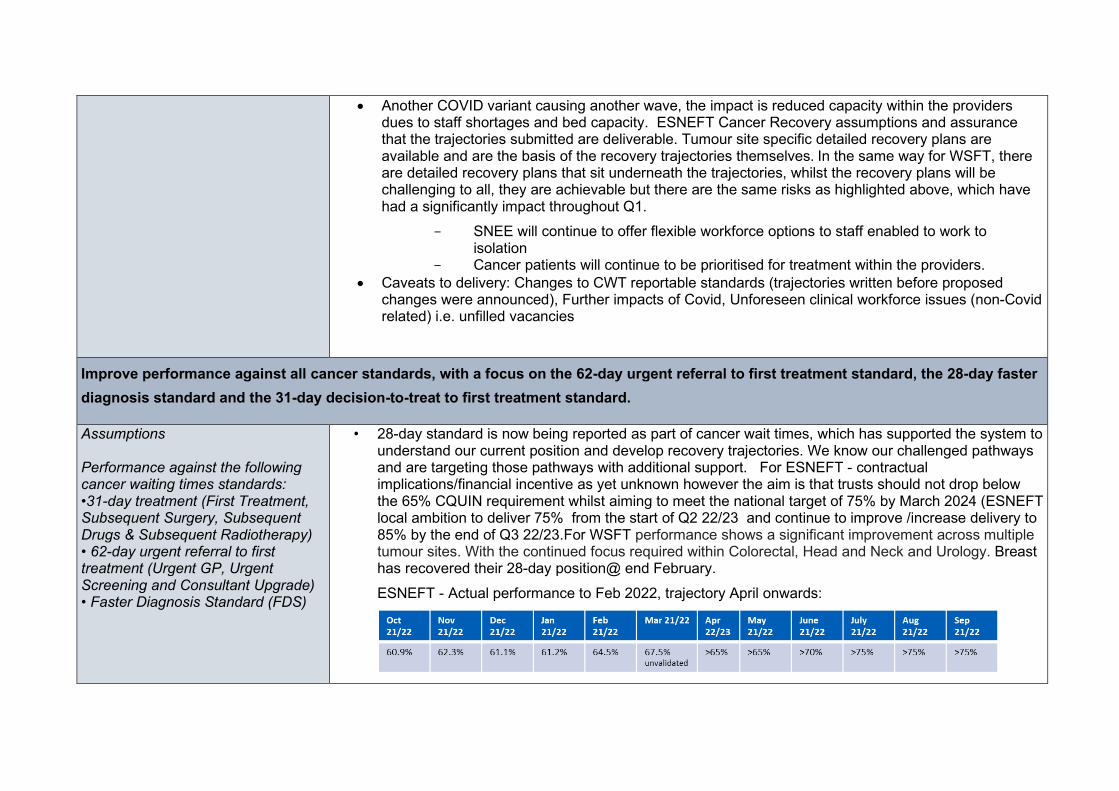
• Another COVID variant causing another wave, the impact is reduced capacity within the providers dues to staff shortages and bed capacity. ESNEFT Cancer Recovery assumptions and assurance that the trajectories submitted are deliverable. Tumour site specific detailed recovery plans are available and are the basis of the recovery trajectories themselves. In the same way for WSFT, there are detailed recovery plans that sit underneath the trajectories, whilst the recovery plans will be challenging to all, they are achievable but there are the same risks as highlighted above, which have had a significantly impact throughout Q1.
SNEE will continue to offer flexible workforce options to staff enabled to work to isolation Cancer patients will continue to be prioritised for treatment within the providers.
• Caveats to delivery: Changes to CWT reportable standards (trajectories written before proposed changes were announced), Further impacts of Covid, Unforeseen clinical workforce issues (non-Covid related) i.e. unfilled vacancies
Improve performance against all cancer standards, with a focus on the 62-day urgent referral to first treatment standard, the 28-day faster diagnosis standard and the 31-day decision-to-treat to first treatment standard.
Assumptions Performance against the following cancer waiting times standards: •31-day treatment (First Treatment, Subsequent Surgery, Subsequent Drugs & Subsequent Radiotherapy) • 62-day urgent referral to first treatment (Urgent GP, Urgent Screening and Consultant Upgrade) • Faster Diagnosis Standard (FDS)
• 28-day standard is now being reported as part of cancer wait times, which has supported the system to understand our current position and develop recovery trajectories. We know our challenged pathways and are targeting those pathways with additional support. For ESNEFT - contractual implications/financial incentive as yet unknown however the aim is that trusts should not drop below the 65% CQUIN requirement whilst aiming to meet the national target of 75% by March 2024 (ESNEFT local ambition to deliver 75% from the start of Q2 22/23 and continue to improve /increase delivery to 85% by the end of Q3 22/23.For WSFT performance shows a significant improvement across multiple tumour sites. With the continued focus required within Colorectal, Head and Neck and Urology. Breast has recovered their 28-day position@ end February. ESNEFT - Actual performance to Feb 2022, trajectory April onwards:
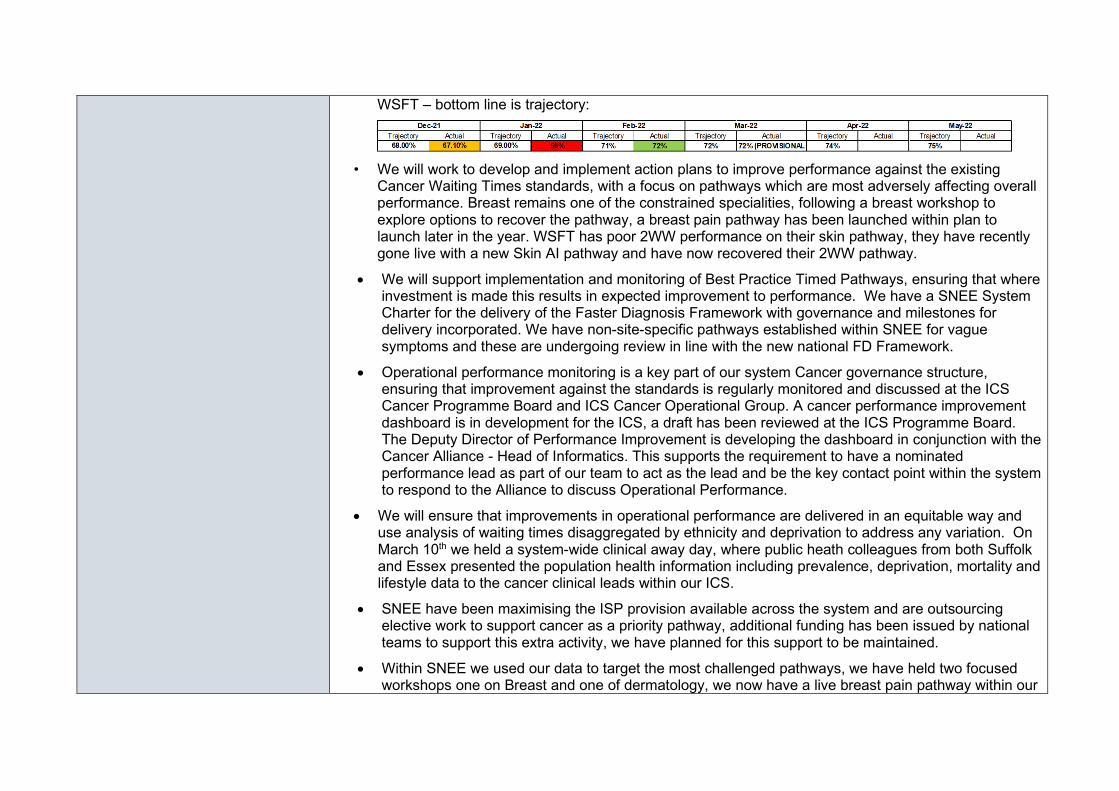
WSFT – bottom line is trajectory:
• We will work to develop and implement action plans to improve performance against the existing
Cancer Waiting Times standards, with a focus on pathways which are most adversely affecting overall performance. Breast remains one of the constrained specialities, following a breast workshop to explore options to recover the pathway, a breast pain pathway has been launched within plan to launch later in the year. WSFT has poor 2WW performance on their skin pathway, they have recently gone live with a new Skin AI pathway and have now recovered their 2WW pathway.
• We will support implementation and monitoring of Best Practice Timed Pathways, ensuring that where investment is made this results in expected improvement to performance. We have a SNEE System Charter for the delivery of the Faster Diagnosis Framework with governance and milestones for delivery incorporated. We have non-site-specific pathways established within SNEE for vague symptoms and these are undergoing review in line with the new national FD Framework.
• Operational performance monitoring is a key part of our system Cancer governance structure, ensuring that improvement against the standards is regularly monitored and discussed at the ICS Cancer Programme Board and ICS Cancer Operational Group. A cancer performance improvement dashboard is in development for the ICS, a draft has been reviewed at the ICS Programme Board. The Deputy Director of Performance Improvement is developing the dashboard in conjunction with the Cancer Alliance - Head of Informatics. This supports the requirement to have a nominated performance lead as part of our team to act as the lead and be the key contact point within the system to respond to the Alliance to discuss Operational Performance.
• We will ensure that improvements in operational performance are delivered in an equitable way and use analysis of waiting times disaggregated by ethnicity and deprivation to address any variation. On March 10th we held a system-wide clinical away day, where public heath colleagues from both Suffolk and Essex presented the population health information including prevalence, deprivation, mortality and lifestyle data to the cancer clinical leads within our ICS.
• SNEE have been maximising the ISP provision available across the system and are outsourcing elective work to support cancer as a priority pathway, additional funding has been issued by national teams to support this extra activity, we have planned for this support to be maintained.
• Within SNEE we used our data to target the most challenged pathways, we have held two focused workshops one on Breast and one of dermatology, we now have a live breast pain pathway within our
system with further transformation planned for this year. Following the dermatology workshop, a delivery group has been established within ESNEFT to embed the best practice skin pathway.
• During the last year SNEE has been successful on opening a community diagnostic centres with additional capacity, the plan continues this year with further centres to be agreed and launched. The cancer programme will remain closely linked to this work to additional capacity within the pathway.
• We know a key enabler to achieving the CWTs is the first few days of the cancer pathway with a completed 2WW referral from primary care, we will work with primary care to support improved referrals and empower further triage, we will do this by, evaluating clinical decision support tools, recruiting an early diagnosis co-ordinator and community cancer nurses with a navigator.
Actions • We will implement a clinical decision tool in primary care to support patients to arrive at secondary care with pre referral tests completed, this will ensure there are minimal delays on first days of the 2WW pathway as patients can be appropriately triaged straight to test or to see a specialist first.
• We will improve the feedback loop to primary care to ensure that primary care is aware of the responsibility to ensure all pre referral guidance is completed and encourage uptake in the Non site-specific pathway alongside site specific pathways.
• Within SNEE we have been innovative around our workforce and have had success on the prostate pathway with Nurse Practitioners now undertaking template biopsies and Colposcopy procedures, we will continue to be a leader in staff development with Gynaecology speciality being the initial focus and developing a nurse led surgical triage pathway.
• In Qtr. 1 we will further develop our Straight to test workforce to remove patients who do not have cancer from the PTL, they will be upskilled to review results and support the specialty and patient to reduce waiting time on the pathway.
• SNEE have developed a robotic surgery pathway in many specialties which substantially increases capacity within the pathway, Gynaecology within ESNEFT are now planning to launch a pathway which will reduce patient risk and increase capacity within the specialty, to support the pathway they will recruit an additional CNS to specialise in ensuring the robotic pathway is maximised.
• Oncology is a key enabler in first treatments and has had some delays this year, we will continue working with our system to support oncology capacity. We will continue to work with our providers to ensure capacity within our system. As part of our workforce review, we will look at recruitment and retention of oncology nurses to ensure a sustained workforce. ESNEFT has implemented a cloud-based integrate radiotherapy system and become ‘paper-light’ enabling resilience through cross-cover potential and remote working’.
• WSFT will improve their reporting time for CTs by implementing a Terarecon system in Qtr. one, this will increase capacity for the current radiology team to report, the specialities impacted will be colorectal for their CtCs and the breast pathway.
• Access to diagnostic is a key constraint within the providers, WSFT will increase their diagnostic capacity within their breast one stop shop in the first quarter which will enable an extra clinic in each session.
Risks, issues and mitigation • Over the last two years there has been huge pressures on our workforce and they have continued to work at an exceptional pace and consistently working extra to keep pace with demand and cover unprecedented levels of sickness due to COVID, our workforce is now fatigued, the risk is they will no longer be able to maintain the work required to deliver the required recovery. SNEE are mitigating this by being innovative with our workforce and upskilling where we can. Encouraging and supporting more flexible working across organisations.
• WSFT surgical capacity has been constrained by RAAC plank work, the theatre element of this is due to be completed in Spring, with RAAC work continuing on the wards and other areas of the hospital, with this cancer services will continue to be prioritised during periods of reduced activity. WSFT are currently utilising mutual aid and ISP provision.
• Over the year SNEE have seen a huge increase in referrals into the 2WW pathways, some specialties have seen as much as 130%, with normal seasonal fluctuations not seen this year. Our providers are now modelling their capacity from these new levels, if further increases are seen the levels would out strip capacity available.
• Diagnostic capacity remains a constraint within our system; - CT at WSFT is currently being supported by an additional scanner which will remain in situ,
subject to appropriate funding. CT at ESNEFT Ipswich site is supported by an additional scanner and Clacton now have a CDC supporting their additional CT
- US capacity at WSFT is a continued challenge which is impacting on 28-day performance for Head and Neck, WSFT are in the process of implementing a one stop service.
- Endoscopy remains constrained across the system; it is currently being supported by ISP and CCE. WSFT have recently reviewed their CTC pathway, which has had a positive impact.
- FiT is now going to be incentivised across primary care to support triaging in the early stages of the pathway.
- Demand and Capacity review being supported by NHSE for colorectal being undertaken in the system,
• Within ESNEFT HDU bed capacity is limited which results in cancelled surgical lists. - Staffing being reviewed to support a more sustainable approach to HDU bed capacity.
Extend coverage of non-specific symptom pathways, with at least 75% population coverage by March 2023.
Assumptions Expected volumes should align with the trajectories submitted against this metric by ICSs as part of the operational planning process. The revised NSS projected referral demand tool will help with this. Narrative plans and milestones should focus on how the Cancer Alliance expects pathway implementation to progress across all relevant providers quarter by quarter, as well as key actions the Cancer Alliance proposes to take to support the embedding of the timed pathways and delivery of key milestones. Where possible, Cancer Alliances should seek out and use 'real' data to populate baseline performance and estimates of performance through the year. Where this is not possible, Cancer Alliances should
• We will deliver referral volumes that reflect at least 75% population coverage for NSS pathways by March 2023. For WSFT for the 28-day standard the unvalidated February performance shows a significant improvement across multiple tumour sites. With the continued focus required within Colorectal, Head and Neck and Urology. We can also see that Breast has recovered their 28-day position. At the end of February, the unvalidated position overall was 70.8% For ESNEFT given the improved overall performance in 2WW standard which once sustained will lead to an improvement in 28FDS performance. This is currently 78.6% @ end February.
• We will ensure NSS services will be sustainably commissioned or in commissioning intentions in 2023/24. We have a dedicated Transformation Lead for FDS delivery with a governance structure to support of a Senior Oversight Group and ICS wide delivery group which are accountable to the ICS Cancer Programme Board. A separate Charter for FDS and work programme have been established to meet the national prescribed best practice pathways for the 7-site specific and NSS pathway. We have completed the NSS referral demand tool with 100% population coverage from 1st April as we already had our primary care practices engaged in referrals to vague symptom services.
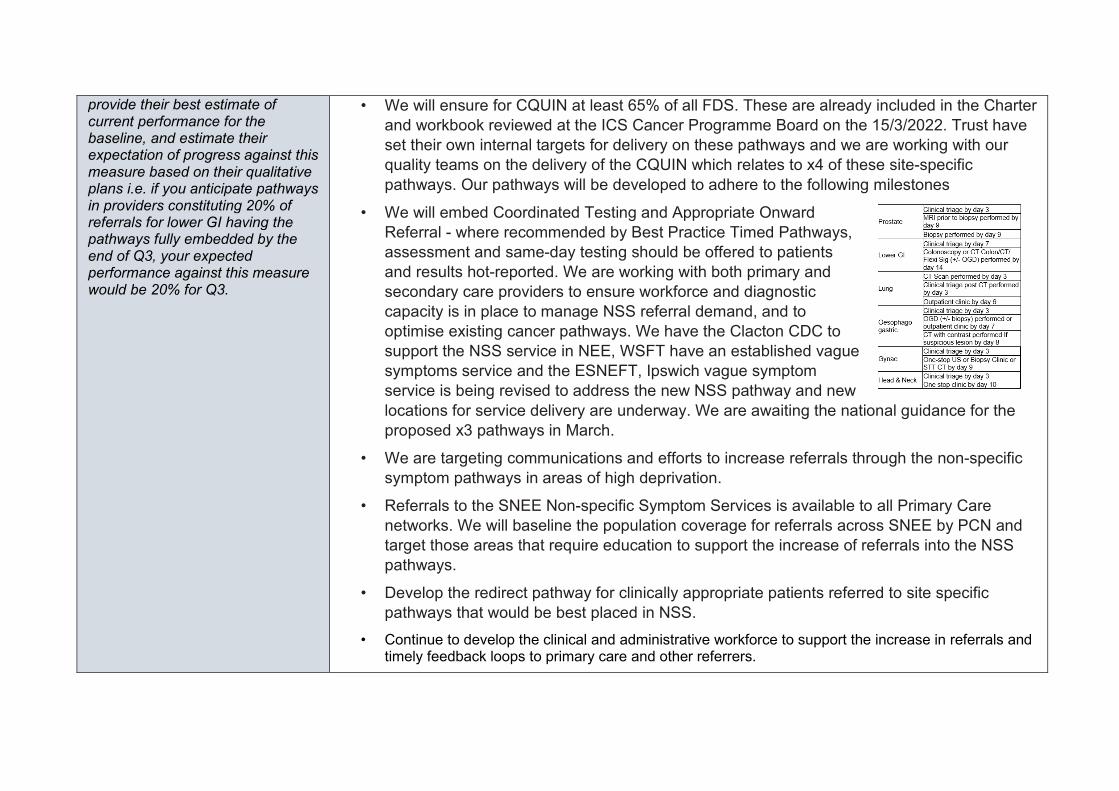
provide their best estimate of current performance for the baseline, and estimate their expectation of progress against this measure based on their qualitative plans i.e. if you anticipate pathways in providers constituting 20% of referrals for lower GI having the pathways fully embedded by the end of Q3, your expected performance against this measure would be 20% for Q3.
• We will ensure for CQUIN at least 65% of all FDS. These are already included in the Charter and workbook reviewed at the ICS Cancer Programme Board on the 15/3/2022. Trust have set their own internal targets for delivery on these pathways and we are working with our quality teams on the delivery of the CQUIN which relates to x4 of these site-specific pathways. Our pathways will be developed to adhere to the following milestones
• We will embed Coordinated Testing and Appropriate Onward Referral - where recommended by Best Practice Timed Pathways, assessment and same-day testing should be offered to patients and results hot-reported. We are working with both primary and secondary care providers to ensure workforce and diagnostic capacity is in place to manage NSS referral demand, and to optimise existing cancer pathways. We have the Clacton CDC to support the NSS service in NEE, WSFT have an established vague symptoms service and the ESNEFT, Ipswich vague symptom service is being revised to address the new NSS pathway and new locations for service delivery are underway. We are awaiting the national guidance for the proposed x3 pathways in March.
• We are targeting communications and efforts to increase referrals through the non-specific symptom pathways in areas of high deprivation.
• Referrals to the SNEE Non-specific Symptom Services is available to all Primary Care networks. We will baseline the population coverage for referrals across SNEE by PCN and target those areas that require education to support the increase of referrals into the NSS pathways.
• Develop the redirect pathway for clinically appropriate patients referred to site specific pathways that would be best placed in NSS.
• Continue to develop the clinical and administrative workforce to support the increase in referrals and timely feedback loops to primary care and other referrers.
• Continue to develop Community Diagnostic Centres (CDC) across SNEE and ensure the NSS is built into this. The CDC at Clacton hospital is operational, resulting in an additional diagnostic capacity within the system which includes CT. Approval for a CDC to be developed on the Newmarket site will commence at end of 22/23, business is in development. A CDC is proposed for IES for 23/24 commencement – venue/location is currently being scoped. As part of the business case development, demand and capacity modelling for cancer referrals are included and colleagues working on FDS are part of the development teams to ensure diagnostics are available to support these pathways. One stop approach for non-site-specific pathways will be part of these new CDCs as spokes with local access.
• Continue to develop and implement innovations that promote earlier identification through screening that will outreach and target existing health inequalities.
Actions • A community (ICE) button has been developed in NEE and IES to facilitate the request for all mandatory first line tests to accompany the NSS referral.
• Implement a communications plan with primary care to advise of any service changes, attend educational sessions and listening events to share experience and practise.
• Monitor and track referral trajectories across PCNs using power BI and pinpoint areas of emerging concern, target communications and educational opportunities. The SNEE Cancer transformation team are working with PCNs to review and improve referral practice: to encourage regular peer review of cancer referrals using templates based on the CRUK NCDA and SEAs; promote the use of clinical decision support tools and use of PCN dashboards they create; use the primary care data pack generated by the EoE CA PCG to identify areas of improvement; and development of electronic referral platforms to ensure completeness of referrals
• Continue the implementation of the Best practice Time Pathways. Ensuring pathways are compliant and developing action plans to support those that require improvement.
• Encourage appropriate access to advice and guidance access across primary and secondary care to promote referring the right patient on the right pathway at the right time.
• Collect high quality patient level data to monitor and improve patient outcomes and experience using the National Minimum data set.
• Analyse and evaluate the SNEE experience of care survey in conjunction with patients, primary and secondary care and third sector stakeholders to drive improvements locally.
Risks, issues and mitigation • Sustaining a workforce with the right skills and experience for the NSS pathway is a key risk in accelerating the referrals to NSS and developing redirect pathways.
- Developing a workforce plan that incorporates timely recruitment, job planning supervision and education will provide an integrated service across primary and secondary care.
• Diagnostic capacity within cancer pathways remain constrained due to demand and diagnostic
workforce. Capital and Revenue funding streams for SNEE are required to develop CDCs and access equipment via the National Procurement Framework in a timely way.
- Strengthen relationships by ensuring early involvement with senior clinicians and diagnostic providers to fully prioritise the demand, capacity and the timeliness required for patients with a suspected cancer.
• Patients presenting to GPs at a late stage. - Actively develop positive patient engagement events. - Deliver targeted early interventions and awareness campaigns. - Incorporate Making Every Contact Count (MECC) to the NSS providing patients with a holistic
assessment that incorporates screening, familial cancer risk and lifestyle support with personalised onward referral and support and affect the working practise and timeliness of patients being reviewed and referred.
Make progress against the ambition in the NHS Long Term Plan to diagnose more people with cancer at an earlier stage, with a particular focus on disadvantaged areas where rates of early diagnosis are lower.
Please outline the priority actions your system and Cancer Alliances will be taking forward that are critical to the delivery of the cancer objectives below: [Max 200 words per section]
Timely presentation and effective primary care pathways (implementation of cancer primary care contract requirements; local awareness campaigns)
Over the last year we have completed cancer champion training with our colleagues in CRUK with our community providers to increase education and awareness in our local communities around the early signs of cancer. We will continue this work over the year by recruiting an Earlier diagnosis and cancer screening transformation lead post in the first quarter of the year. .
SNEE are piloting a community cancer nurse programme, with recruitment planned for June 2022 these nurses with a the support of a cancer co-ordinator will lead on cancer within targeted PCNs, the role of these nurses will be to work with PCNs and their local communities to raise awareness of the early warning signs of cancer and to encourage access. Within PCNs we will ensure complex social and health needs are identified and supported early in the cancer pathway, to maximise clinical outcomes if cancer is diagnosed and subsequent cancer treatment is required. The Social Care role will harmonise with community cancer nurses being developed to ensure that co-morbidity issues are addressed robustly to ensure seamless cancer pathways. Within SNEE we have strong clinical leadership from primary care who continue to work with primary care through GP education to support the implementation of the PCN DES. Supporting PCNs to deliver early diagnosis DES: interrogation of primary care data pack as above; promoting referrals in areas slow to catchup post pandemic (e.g. urology, lung); use of PHM to identify area of lower than expected referral; ensure cancer information is available in multiple languages; and targeted work to increase cancer awareness in underrepresented groups. Co-production is key in developing new services, SNEE are currently developing a patient engagement plan to support improved pathways for cancer patients within primary care. SNEE are part of the GRAIL study, this pilot will run in our system for the next year and support the early identification of cancer patients.
Faster diagnosis (best practice timed pathways and priority pathway improvements including cancer screening) Include information on each provider with teledermatology services in place and the approach to teledermatology being implemented (image taken in primary care, image taken in secondary care, image taken in hub, image taken by patient). Expected activity for each quarter should then be provided as a % of all skin FDS referrals.
• Trusts have set their own internal targets for delivery on these pathways and we are working with our quality teams on the delivery of the CQUIN which relates to x4 of these site-specific pathways. Our pathways will be developed to adhere to the following milestones.
• We will continue to extend the provision of teledermatology services and community spot clinics. We already have well established teledermatology pathways with triage and AI for skin at WSFT which is proving successful for the 28 FDS pathway and consultations reporting that the triage algorithm is very accurate with no clinical assessment changes for onward referral.
• For both trusts SMS reminder systems are in place and being actively utilised. • Targeting communications and efforts to increase referrals to non-specific symptom pathways in areas
of high deprivation. SNEE is working closely with regional diagnostics teams to ensure Community Diagnostic Centres provide required capacity for cancer pathways. Our CDC business case demand and capacity modelling takes into consideration the requirements for increased and faster access to
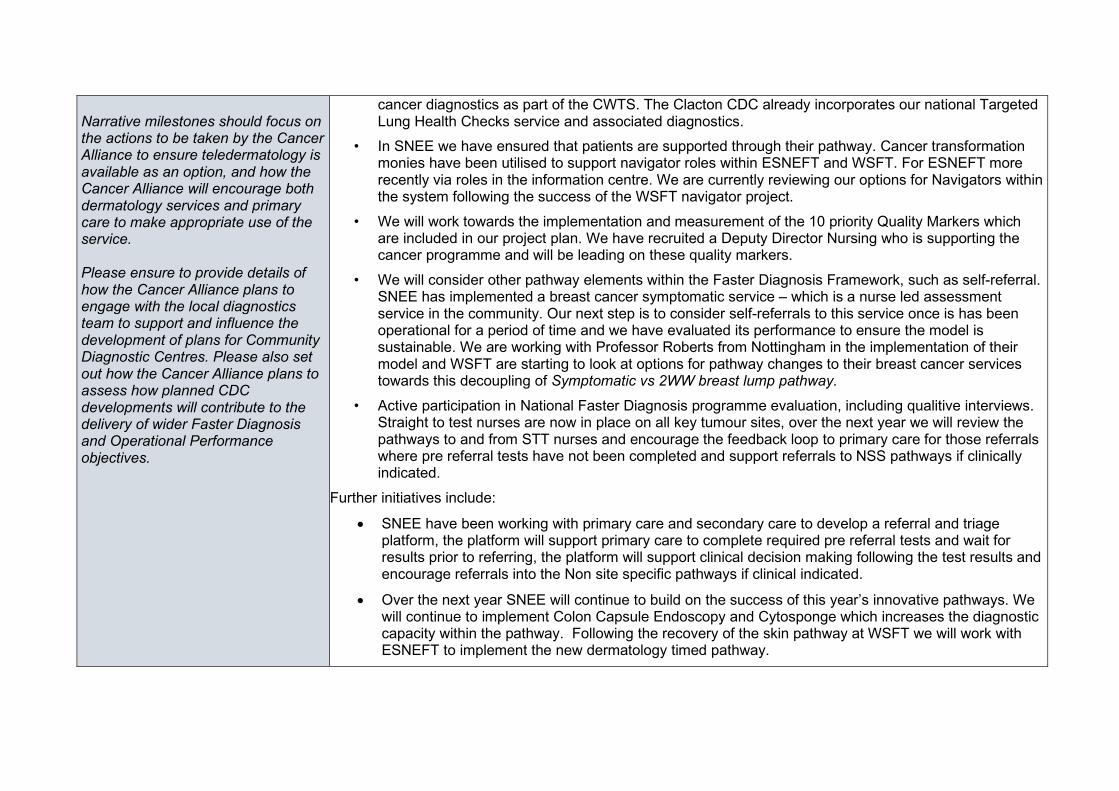
Narrative milestones should focus on the actions to be taken by the Cancer Alliance to ensure teledermatology is available as an option, and how the Cancer Alliance will encourage both dermatology services and primary care to make appropriate use of the service. Please ensure to provide details of how the Cancer Alliance plans to engage with the local diagnostics team to support and influence the development of plans for Community Diagnostic Centres. Please also set out how the Cancer Alliance plans to assess how planned CDC developments will contribute to the delivery of wider Faster Diagnosis and Operational Performance objectives.
cancer diagnostics as part of the CWTS. The Clacton CDC already incorporates our national Targeted Lung Health Checks service and associated diagnostics.
• In SNEE we have ensured that patients are supported through their pathway. Cancer transformation monies have been utilised to support navigator roles within ESNEFT and WSFT. For ESNEFT more recently via roles in the information centre. We are currently reviewing our options for Navigators within the system following the success of the WSFT navigator project.
• We will work towards the implementation and measurement of the 10 priority Quality Markers which are included in our project plan. We have recruited a Deputy Director Nursing who is supporting the cancer programme and will be leading on these quality markers.
• We will consider other pathway elements within the Faster Diagnosis Framework, such as self-referral. SNEE has implemented a breast cancer symptomatic service – which is a nurse led assessment service in the community. Our next step is to consider self-referrals to this service once is has been operational for a period of time and we have evaluated its performance to ensure the model is sustainable. We are working with Professor Roberts from Nottingham in the implementation of their model and WSFT are starting to look at options for pathway changes to their breast cancer services towards this decoupling of Symptomatic vs 2WW breast lump pathway.
• Active participation in National Faster Diagnosis programme evaluation, including qualitive interviews. Straight to test nurses are now in place on all key tumour sites, over the next year we will review the pathways to and from STT nurses and encourage the feedback loop to primary care for those referrals where pre referral tests have not been completed and support referrals to NSS pathways if clinically indicated.
Further initiatives include:
• SNEE have been working with primary care and secondary care to develop a referral and triage platform, the platform will support primary care to complete required pre referral tests and wait for results prior to referring, the platform will support clinical decision making following the test results and encourage referrals into the Non site specific pathways if clinical indicated.
• Over the next year SNEE will continue to build on the success of this year’s innovative pathways. We will continue to implement Colon Capsule Endoscopy and Cytosponge which increases the diagnostic capacity within the pathway. Following the recovery of the skin pathway at WSFT we will work with ESNEFT to implement the new dermatology timed pathway.
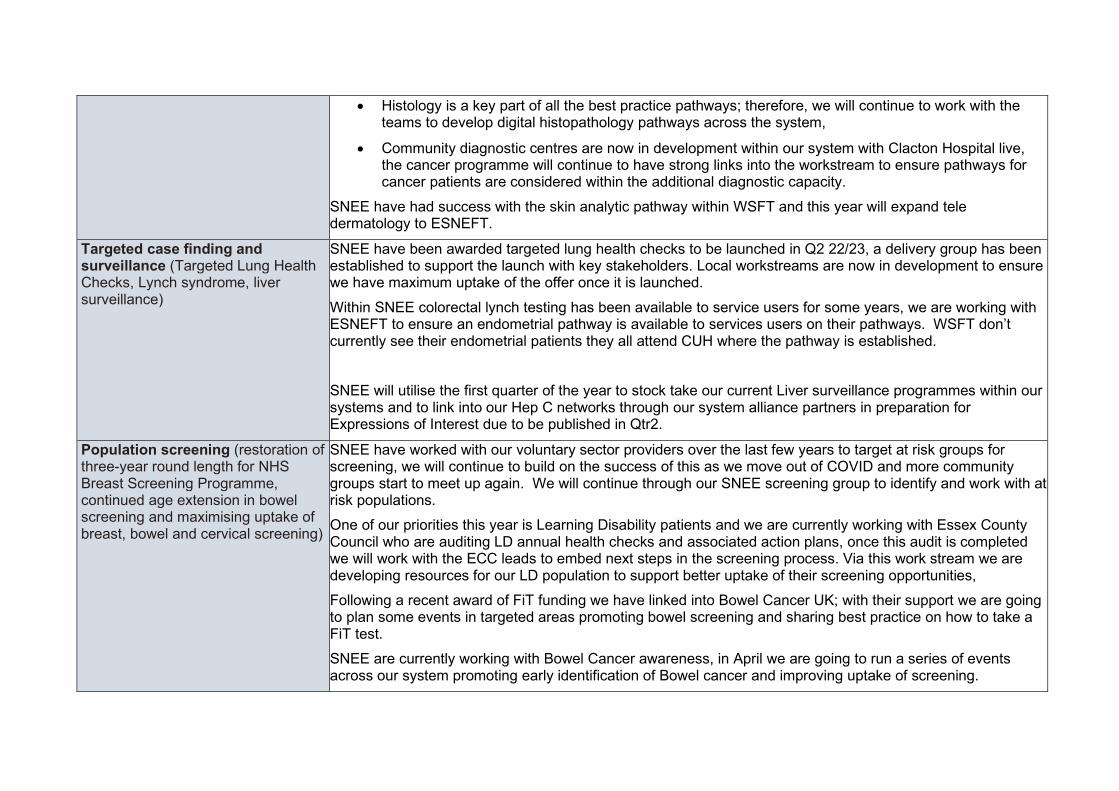
• Histology is a key part of all the best practice pathways; therefore, we will continue to work with the teams to develop digital histopathology pathways across the system,
• Community diagnostic centres are now in development within our system with Clacton Hospital live, the cancer programme will continue to have strong links into the workstream to ensure pathways for cancer patients are considered within the additional diagnostic capacity.
SNEE have had success with the skin analytic pathway within WSFT and this year will expand tele dermatology to ESNEFT.
Targeted case finding and surveillance (Targeted Lung Health Checks, Lynch syndrome, liver surveillance)
SNEE have been awarded targeted lung health checks to be launched in Q2 22/23, a delivery group has been established to support the launch with key stakeholders. Local workstreams are now in development to ensure we have maximum uptake of the offer once it is launched. Within SNEE colorectal lynch testing has been available to service users for some years, we are working with ESNEFT to ensure an endometrial pathway is available to services users on their pathways. WSFT don’t currently see their endometrial patients they all attend CUH where the pathway is established. SNEE will utilise the first quarter of the year to stock take our current Liver surveillance programmes within our systems and to link into our Hep C networks through our system alliance partners in preparation for Expressions of Interest due to be published in Qtr2.
Population screening (restoration of three-year round length for NHS Breast Screening Programme, continued age extension in bowel screening and maximising uptake of breast, bowel and cervical screening)
SNEE have worked with our voluntary sector providers over the last few years to target at risk groups for screening, we will continue to build on the success of this as we move out of COVID and more community groups start to meet up again. We will continue through our SNEE screening group to identify and work with at risk populations. One of our priorities this year is Learning Disability patients and we are currently working with Essex County Council who are auditing LD annual health checks and associated action plans, once this audit is completed we will work with the ECC leads to embed next steps in the screening process. Via this work stream we are developing resources for our LD population to support better uptake of their screening opportunities, Following a recent award of FiT funding we have linked into Bowel Cancer UK; with their support we are going to plan some events in targeted areas promoting bowel screening and sharing best practice on how to take a FiT test. SNEE are currently working with Bowel Cancer awareness, in April we are going to run a series of events across our system promoting early identification of Bowel cancer and improving uptake of screening.
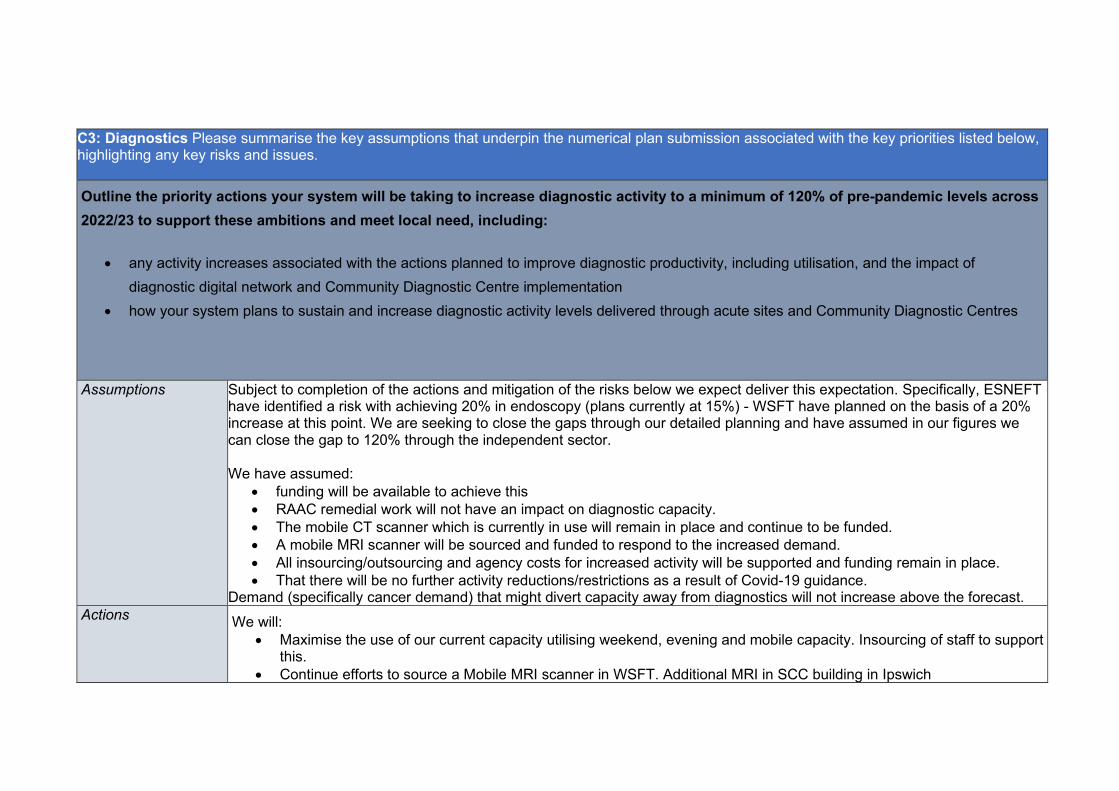
C3: Diagnostics Please summarise the key assumptions that underpin the numerical plan submission associated with the key priorities listed below, highlighting any key risks and issues. Outline the priority actions your system will be taking to increase diagnostic activity to a minimum of 120% of pre-pandemic levels across 2022/23 to support these ambitions and meet local need, including:
• any activity increases associated with the actions planned to improve diagnostic productivity, including utilisation, and the impact of diagnostic digital network and Community Diagnostic Centre implementation
• how your system plans to sustain and increase diagnostic activity levels delivered through acute sites and Community Diagnostic Centres
Assumptions
Subject to completion of the actions and mitigation of the risks below we expect deliver this expectation. Specifically, ESNEFT have identified a risk with achieving 20% in endoscopy (plans currently at 15%) - WSFT have planned on the basis of a 20% increase at this point. We are seeking to close the gaps through our detailed planning and have assumed in our figures we can close the gap to 120% through the independent sector. We have assumed:
• funding will be available to achieve this • RAAC remedial work will not have an impact on diagnostic capacity. • The mobile CT scanner which is currently in use will remain in place and continue to be funded. • A mobile MRI scanner will be sourced and funded to respond to the increased demand. • All insourcing/outsourcing and agency costs for increased activity will be supported and funding remain in place. • That there will be no further activity reductions/restrictions as a result of Covid-19 guidance.
Demand (specifically cancer demand) that might divert capacity away from diagnostics will not increase above the forecast. Actions We will:
• Maximise the use of our current capacity utilising weekend, evening and mobile capacity. Insourcing of staff to support this.
• Continue efforts to source a Mobile MRI scanner in WSFT. Additional MRI in SCC building in Ipswich
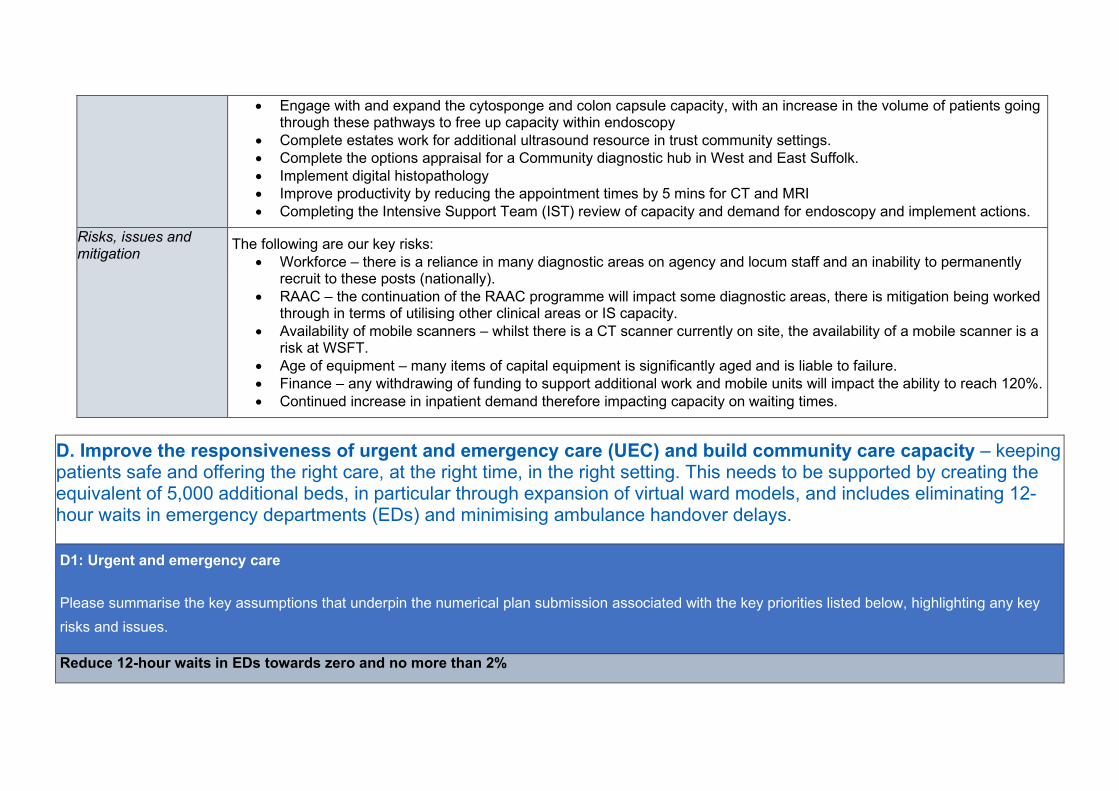
• Engage with and expand the cytosponge and colon capsule capacity, with an increase in the volume of patients going through these pathways to free up capacity within endoscopy
• Complete estates work for additional ultrasound resource in trust community settings. • Complete the options appraisal for a Community diagnostic hub in West and East Suffolk. • Implement digital histopathology • Improve productivity by reducing the appointment times by 5 mins for CT and MRI • Completing the Intensive Support Team (IST) review of capacity and demand for endoscopy and implement actions.
Risks, issues and mitigation
The following are our key risks: • Workforce – there is a reliance in many diagnostic areas on agency and locum staff and an inability to permanently
recruit to these posts (nationally). • RAAC – the continuation of the RAAC programme will impact some diagnostic areas, there is mitigation being worked
through in terms of utilising other clinical areas or IS capacity. • Availability of mobile scanners – whilst there is a CT scanner currently on site, the availability of a mobile scanner is a
risk at WSFT. • Age of equipment – many items of capital equipment is significantly aged and is liable to failure. • Finance – any withdrawing of funding to support additional work and mobile units will impact the ability to reach 120%. • Continued increase in inpatient demand therefore impacting capacity on waiting times.
D. Improve the responsiveness of urgent and emergency care (UEC) and build community care capacity – keeping patients safe and offering the right care, at the right time, in the right setting. This needs to be supported by creating the equivalent of 5,000 additional beds, in particular through expansion of virtual ward models, and includes eliminating 12-hour waits in emergency departments (EDs) and minimising ambulance handover delays.
D1: Urgent and emergency care
Please summarise the key assumptions that underpin the numerical plan submission associated with the key priorities listed below, highlighting any key risks and issues.
Reduce 12-hour waits in EDs towards zero and no more than 2%
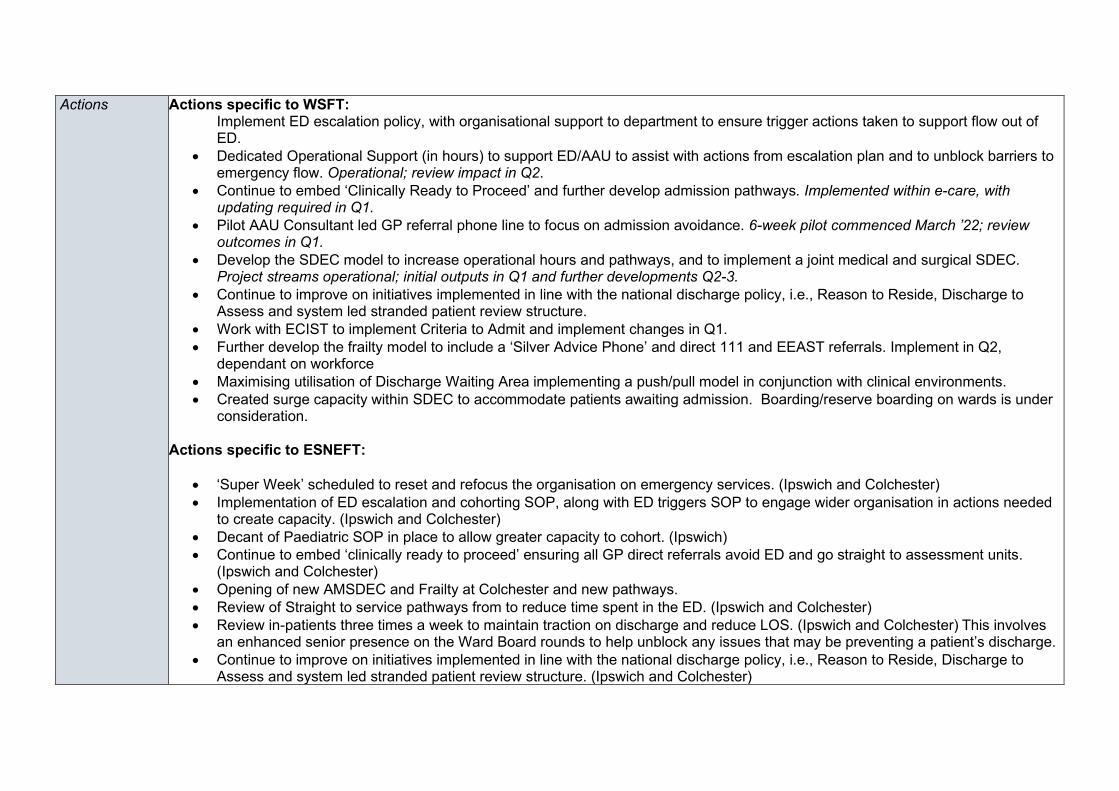
Actions Actions specific to WSFT: Implement ED escalation policy, with organisational support to department to ensure trigger actions taken to support flow out of ED.
• Dedicated Operational Support (in hours) to support ED/AAU to assist with actions from escalation plan and to unblock barriers to emergency flow. Operational; review impact in Q2.
• Continue to embed ‘Clinically Ready to Proceed’ and further develop admission pathways. Implemented within e-care, with updating required in Q1.
• Pilot AAU Consultant led GP referral phone line to focus on admission avoidance. 6-week pilot commenced March ’22; review outcomes in Q1.
• Develop the SDEC model to increase operational hours and pathways, and to implement a joint medical and surgical SDEC. Project streams operational; initial outputs in Q1 and further developments Q2-3.
• Continue to improve on initiatives implemented in line with the national discharge policy, i.e., Reason to Reside, Discharge to Assess and system led stranded patient review structure.
• Work with ECIST to implement Criteria to Admit and implement changes in Q1. • Further develop the frailty model to include a ‘Silver Advice Phone’ and direct 111 and EEAST referrals. Implement in Q2,
dependant on workforce • Maximising utilisation of Discharge Waiting Area implementing a push/pull model in conjunction with clinical environments. • Created surge capacity within SDEC to accommodate patients awaiting admission. Boarding/reserve boarding on wards is under
consideration.
Actions specific to ESNEFT:
• ‘Super Week’ scheduled to reset and refocus the organisation on emergency services. (Ipswich and Colchester) • Implementation of ED escalation and cohorting SOP, along with ED triggers SOP to engage wider organisation in actions needed
to create capacity. (Ipswich and Colchester) • Decant of Paediatric SOP in place to allow greater capacity to cohort. (Ipswich) • Continue to embed ‘clinically ready to proceed’ ensuring all GP direct referrals avoid ED and go straight to assessment units.
(Ipswich and Colchester) • Opening of new AMSDEC and Frailty at Colchester and new pathways. • Review of Straight to service pathways from to reduce time spent in the ED. (Ipswich and Colchester) • Review in-patients three times a week to maintain traction on discharge and reduce LOS. (Ipswich and Colchester) This involves
an enhanced senior presence on the Ward Board rounds to help unblock any issues that may be preventing a patient’s discharge. • Continue to improve on initiatives implemented in line with the national discharge policy, i.e., Reason to Reside, Discharge to
Assess and system led stranded patient review structure. (Ipswich and Colchester)
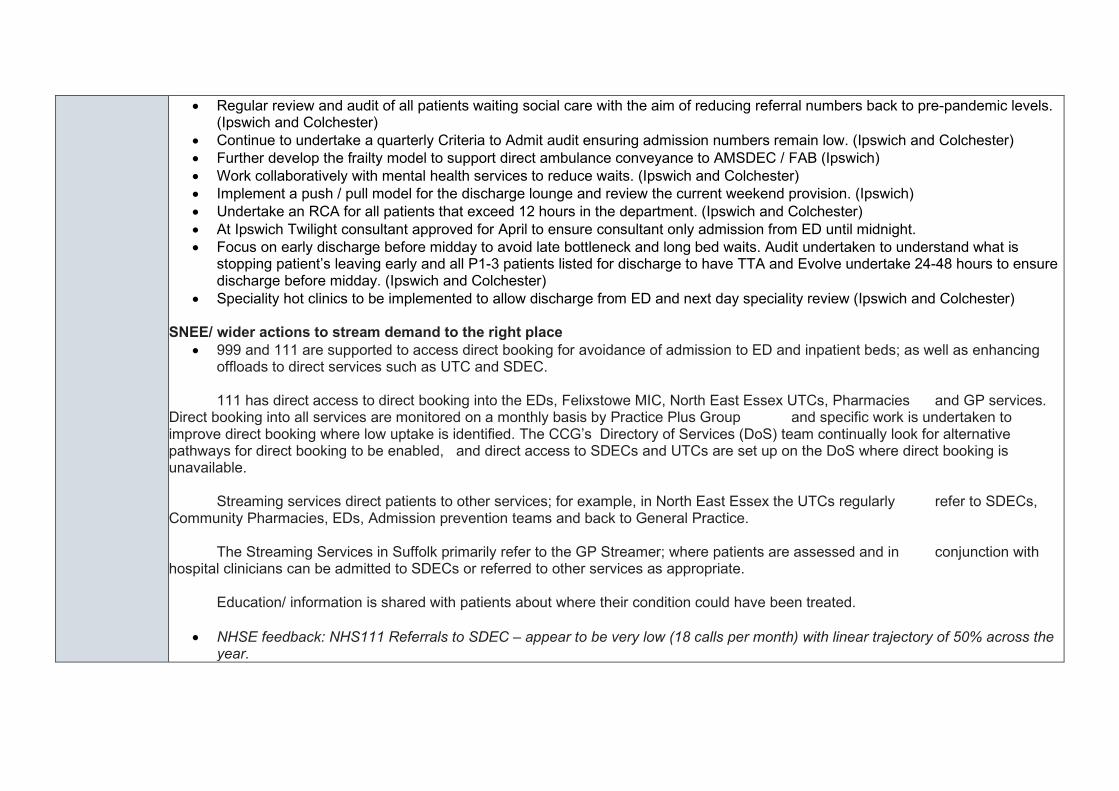
• Regular review and audit of all patients waiting social care with the aim of reducing referral numbers back to pre-pandemic levels. (Ipswich and Colchester)
• Continue to undertake a quarterly Criteria to Admit audit ensuring admission numbers remain low. (Ipswich and Colchester) • Further develop the frailty model to support direct ambulance conveyance to AMSDEC / FAB (Ipswich) • Work collaboratively with mental health services to reduce waits. (Ipswich and Colchester) • Implement a push / pull model for the discharge lounge and review the current weekend provision. (Ipswich) • Undertake an RCA for all patients that exceed 12 hours in the department. (Ipswich and Colchester) • At Ipswich Twilight consultant approved for April to ensure consultant only admission from ED until midnight. • Focus on early discharge before midday to avoid late bottleneck and long bed waits. Audit undertaken to understand what is
stopping patient’s leaving early and all P1-3 patients listed for discharge to have TTA and Evolve undertake 24-48 hours to ensure discharge before midday. (Ipswich and Colchester)
• Speciality hot clinics to be implemented to allow discharge from ED and next day speciality review (Ipswich and Colchester)
SNEE/ wider actions to stream demand to the right place • 999 and 111 are supported to access direct booking for avoidance of admission to ED and inpatient beds; as well as enhancing
offloads to direct services such as UTC and SDEC. 111 has direct access to direct booking into the EDs, Felixstowe MIC, North East Essex UTCs, Pharmacies and GP services. Direct booking into all services are monitored on a monthly basis by Practice Plus Group and specific work is undertaken to improve direct booking where low uptake is identified. The CCG’s Directory of Services (DoS) team continually look for alternative pathways for direct booking to be enabled, and direct access to SDECs and UTCs are set up on the DoS where direct booking is unavailable. Streaming services direct patients to other services; for example, in North East Essex the UTCs regularly refer to SDECs, Community Pharmacies, EDs, Admission prevention teams and back to General Practice. The Streaming Services in Suffolk primarily refer to the GP Streamer; where patients are assessed and in conjunction with hospital clinicians can be admitted to SDECs or referred to other services as appropriate. Education/ information is shared with patients about where their condition could have been treated.
• NHSE feedback: NHS111 Referrals to SDEC – appear to be very low (18 calls per month) with linear trajectory of 50% across the year.
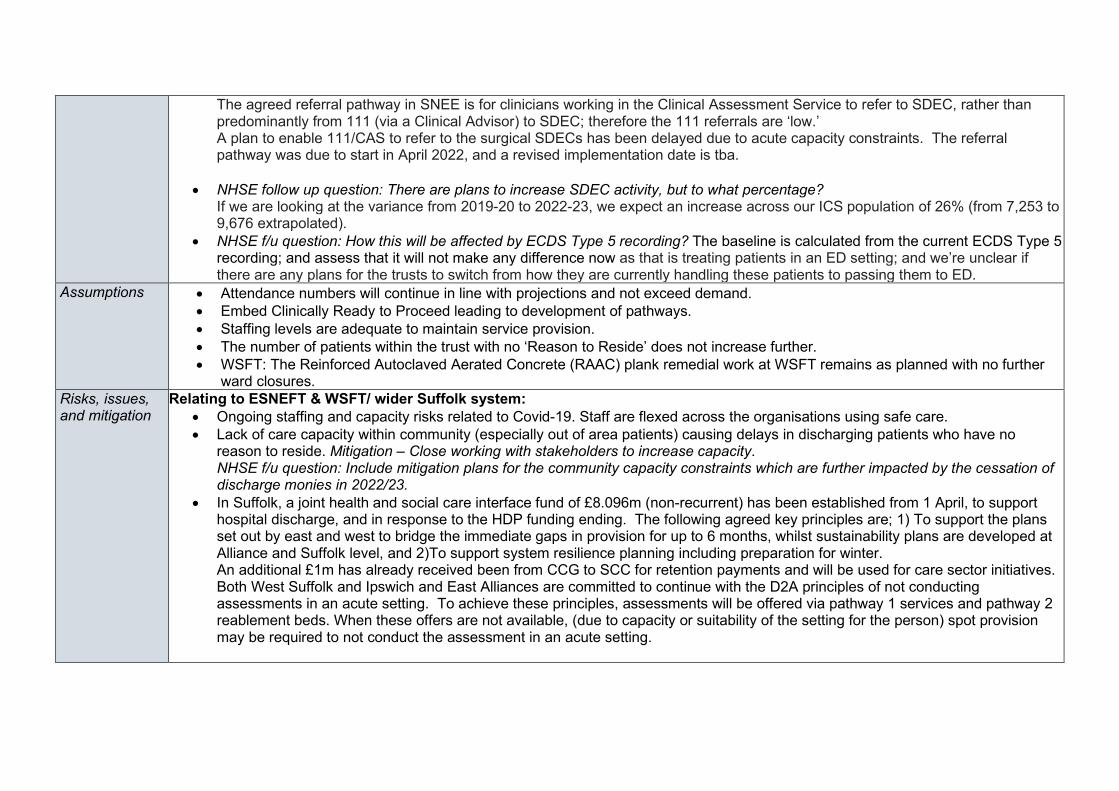
The agreed referral pathway in SNEE is for clinicians working in the Clinical Assessment Service to refer to SDEC, rather than predominantly from 111 (via a Clinical Advisor) to SDEC; therefore the 111 referrals are ‘low.’ A plan to enable 111/CAS to refer to the surgical SDECs has been delayed due to acute capacity constraints. The referral pathway was due to start in April 2022, and a revised implementation date is tba.
• NHSE follow up question: There are plans to increase SDEC activity, but to what percentage? If we are looking at the variance from 2019-20 to 2022-23, we expect an increase across our ICS population of 26% (from 7,253 to 9,676 extrapolated).
• NHSE f/u question: How this will be affected by ECDS Type 5 recording? The baseline is calculated from the current ECDS Type 5 recording; and assess that it will not make any difference now as that is treating patients in an ED setting; and we’re unclear if there are any plans for the trusts to switch from how they are currently handling these patients to passing them to ED.
Assumptions • Attendance numbers will continue in line with projections and not exceed demand. • Embed Clinically Ready to Proceed leading to development of pathways. • Staffing levels are adequate to maintain service provision. • The number of patients within the trust with no ‘Reason to Reside’ does not increase further. • WSFT: The Reinforced Autoclaved Aerated Concrete (RAAC) plank remedial work at WSFT remains as planned with no further
ward closures. Risks, issues, and mitigation
Relating to ESNEFT & WSFT/ wider Suffolk system: • Ongoing staffing and capacity risks related to Covid-19. Staff are flexed across the organisations using safe care. • Lack of care capacity within community (especially out of area patients) causing delays in discharging patients who have no
reason to reside. Mitigation – Close working with stakeholders to increase capacity. NHSE f/u question: Include mitigation plans for the community capacity constraints which are further impacted by the cessation of discharge monies in 2022/23.
• In Suffolk, a joint health and social care interface fund of £8.096m (non-recurrent) has been established from 1 April, to support hospital discharge, and in response to the HDP funding ending. The following agreed key principles are; 1) To support the plans set out by east and west to bridge the immediate gaps in provision for up to 6 months, whilst sustainability plans are developed at Alliance and Suffolk level, and 2)To support system resilience planning including preparation for winter. An additional £1m has already received been from CCG to SCC for retention payments and will be used for care sector initiatives. Both West Suffolk and Ipswich and East Alliances are committed to continue with the D2A principles of not conducting assessments in an acute setting. To achieve these principles, assessments will be offered via pathway 1 services and pathway 2 reablement beds. When these offers are not available, (due to capacity or suitability of the setting for the person) spot provision may be required to not conduct the assessment in an acute setting.
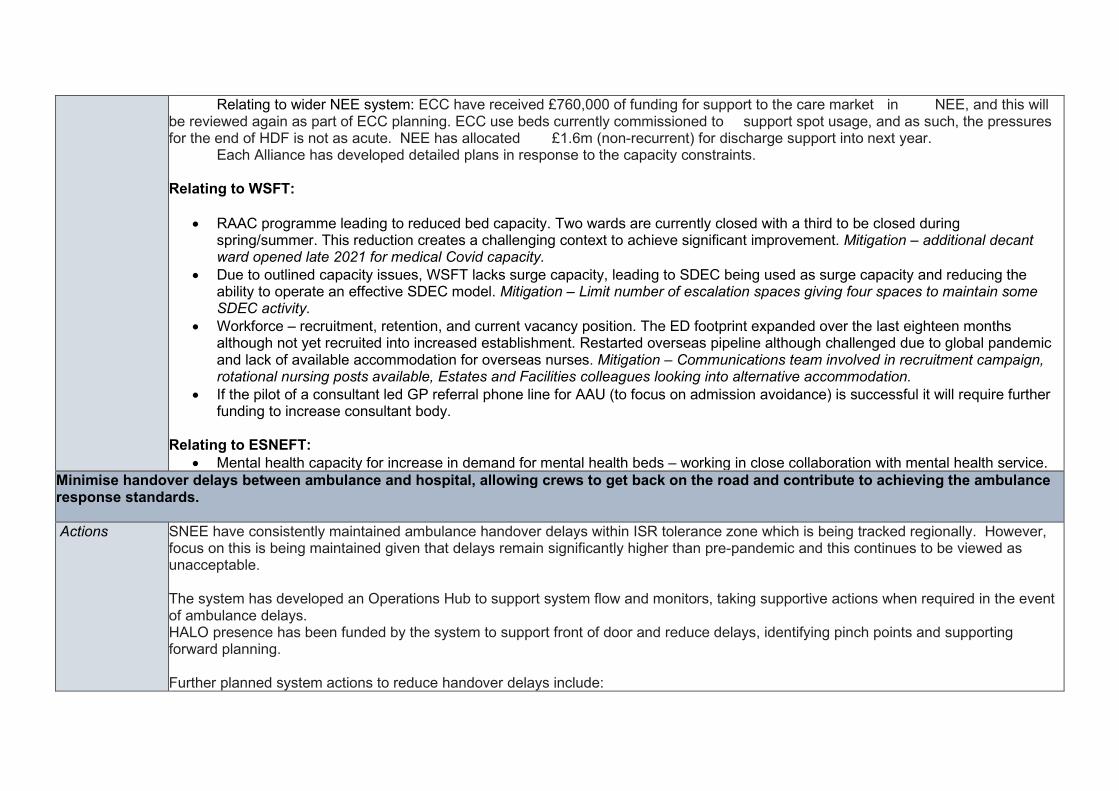
Relating to wider NEE system: ECC have received £760,000 of funding for support to the care market in NEE, and this will be reviewed again as part of ECC planning. ECC use beds currently commissioned to support spot usage, and as such, the pressures for the end of HDF is not as acute. NEE has allocated £1.6m (non-recurrent) for discharge support into next year. Each Alliance has developed detailed plans in response to the capacity constraints. Relating to WSFT:
• RAAC programme leading to reduced bed capacity. Two wards are currently closed with a third to be closed during spring/summer. This reduction creates a challenging context to achieve significant improvement. Mitigation – additional decant ward opened late 2021 for medical Covid capacity.
• Due to outlined capacity issues, WSFT lacks surge capacity, leading to SDEC being used as surge capacity and reducing the ability to operate an effective SDEC model. Mitigation – Limit number of escalation spaces giving four spaces to maintain some SDEC activity.
• Workforce – recruitment, retention, and current vacancy position. The ED footprint expanded over the last eighteen months although not yet recruited into increased establishment. Restarted overseas pipeline although challenged due to global pandemic and lack of available accommodation for overseas nurses. Mitigation – Communications team involved in recruitment campaign, rotational nursing posts available, Estates and Facilities colleagues looking into alternative accommodation.
• If the pilot of a consultant led GP referral phone line for AAU (to focus on admission avoidance) is successful it will require further funding to increase consultant body.
Relating to ESNEFT:
• Mental health capacity for increase in demand for mental health beds – working in close collaboration with mental health service. Minimise handover delays between ambulance and hospital, allowing crews to get back on the road and contribute to achieving the ambulance response standards. Actions SNEE have consistently maintained ambulance handover delays within ISR tolerance zone which is being tracked regionally. However,
focus on this is being maintained given that delays remain significantly higher than pre-pandemic and this continues to be viewed as unacceptable. The system has developed an Operations Hub to support system flow and monitors, taking supportive actions when required in the event of ambulance delays. HALO presence has been funded by the system to support front of door and reduce delays, identifying pinch points and supporting forward planning. Further planned system actions to reduce handover delays include:
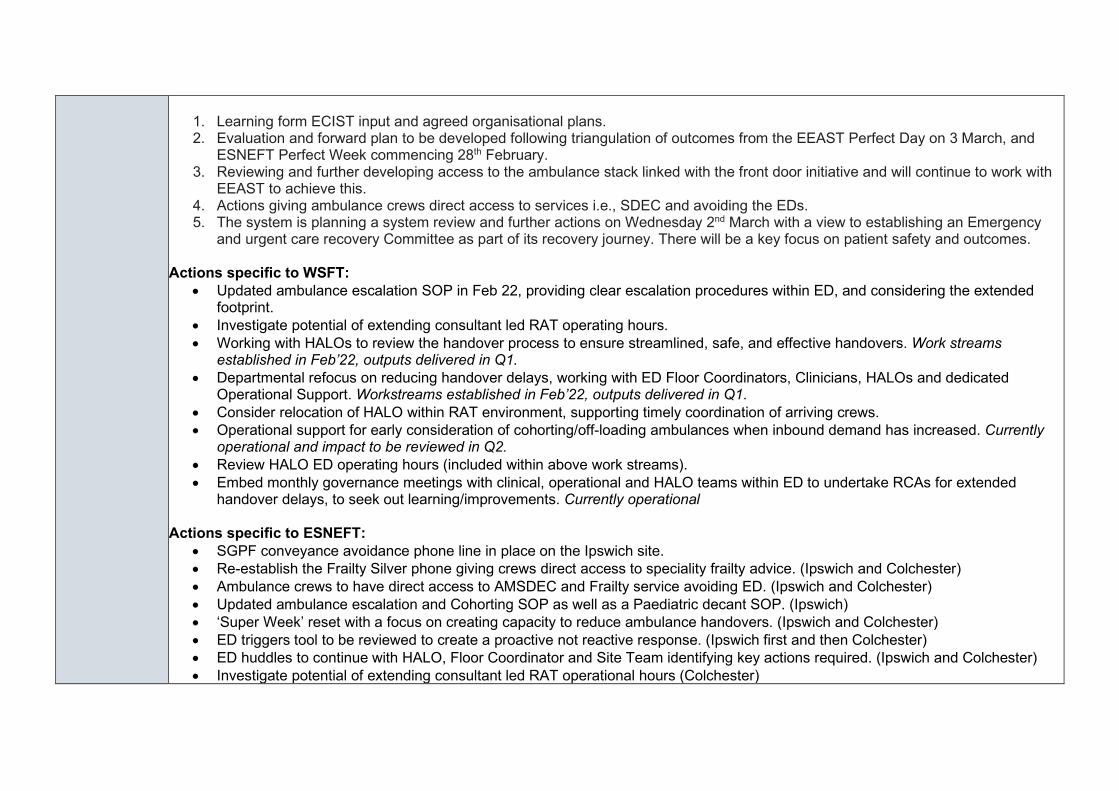
1. Learning form ECIST input and agreed organisational plans. 2. Evaluation and forward plan to be developed following triangulation of outcomes from the EEAST Perfect Day on 3 March, and
ESNEFT Perfect Week commencing 28th February. 3. Reviewing and further developing access to the ambulance stack linked with the front door initiative and will continue to work with
EEAST to achieve this. 4. Actions giving ambulance crews direct access to services i.e., SDEC and avoiding the EDs. 5. The system is planning a system review and further actions on Wednesday 2nd March with a view to establishing an Emergency
and urgent care recovery Committee as part of its recovery journey. There will be a key focus on patient safety and outcomes. Actions specific to WSFT:
• Updated ambulance escalation SOP in Feb 22, providing clear escalation procedures within ED, and considering the extended footprint.
• Investigate potential of extending consultant led RAT operating hours. • Working with HALOs to review the handover process to ensure streamlined, safe, and effective handovers. Work streams
established in Feb’22, outputs delivered in Q1. • Departmental refocus on reducing handover delays, working with ED Floor Coordinators, Clinicians, HALOs and dedicated
Operational Support. Workstreams established in Feb’22, outputs delivered in Q1. • Consider relocation of HALO within RAT environment, supporting timely coordination of arriving crews. • Operational support for early consideration of cohorting/off-loading ambulances when inbound demand has increased. Currently
operational and impact to be reviewed in Q2. • Review HALO ED operating hours (included within above work streams). • Embed monthly governance meetings with clinical, operational and HALO teams within ED to undertake RCAs for extended
handover delays, to seek out learning/improvements. Currently operational Actions specific to ESNEFT:
• SGPF conveyance avoidance phone line in place on the Ipswich site. • Re-establish the Frailty Silver phone giving crews direct access to speciality frailty advice. (Ipswich and Colchester) • Ambulance crews to have direct access to AMSDEC and Frailty service avoiding ED. (Ipswich and Colchester) • Updated ambulance escalation and Cohorting SOP as well as a Paediatric decant SOP. (Ipswich) • ‘Super Week’ reset with a focus on creating capacity to reduce ambulance handovers. (Ipswich and Colchester) • ED triggers tool to be reviewed to create a proactive not reactive response. (Ipswich first and then Colchester) • ED huddles to continue with HALO, Floor Coordinator and Site Team identifying key actions required. (Ipswich and Colchester) • Investigate potential of extending consultant led RAT operational hours (Colchester)
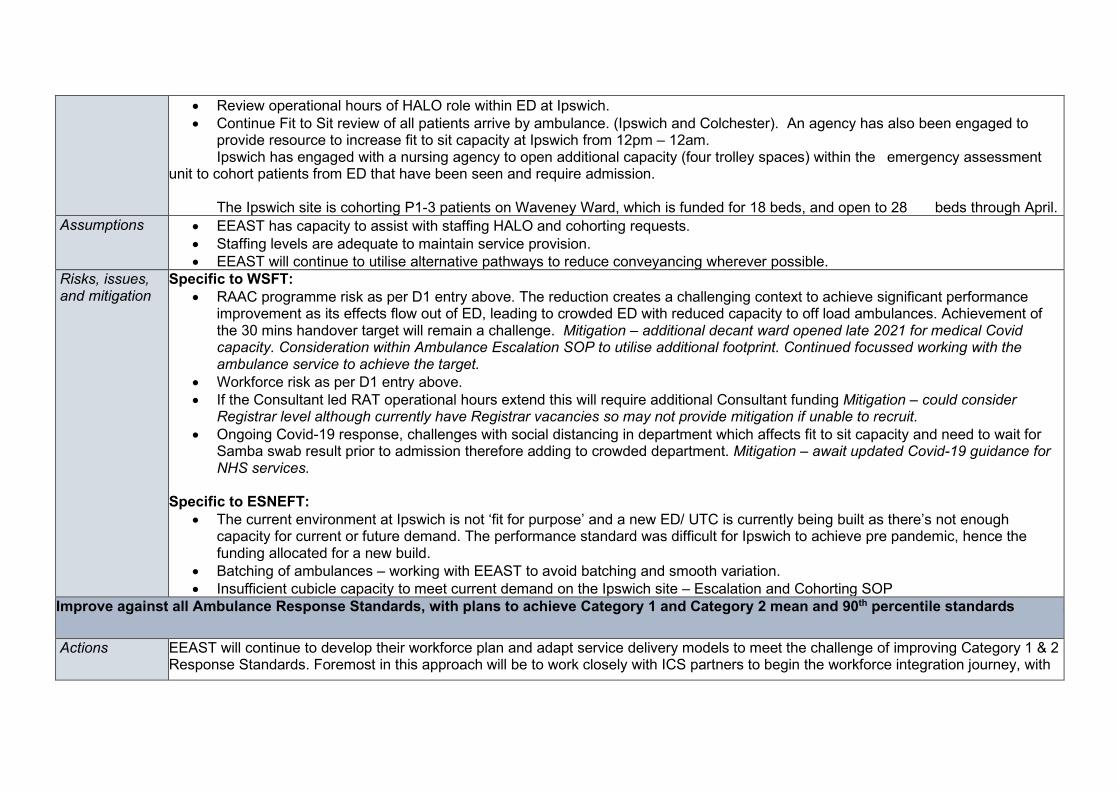
• Review operational hours of HALO role within ED at Ipswich. • Continue Fit to Sit review of all patients arrive by ambulance. (Ipswich and Colchester). An agency has also been engaged to
provide resource to increase fit to sit capacity at Ipswich from 12pm – 12am. Ipswich has engaged with a nursing agency to open additional capacity (four trolley spaces) within the emergency assessment unit to cohort patients from ED that have been seen and require admission. The Ipswich site is cohorting P1-3 patients on Waveney Ward, which is funded for 18 beds, and open to 28 beds through April.
Assumptions • EEAST has capacity to assist with staffing HALO and cohorting requests. • Staffing levels are adequate to maintain service provision. • EEAST will continue to utilise alternative pathways to reduce conveyancing wherever possible.
Risks, issues, and mitigation
Specific to WSFT: • RAAC programme risk as per D1 entry above. The reduction creates a challenging context to achieve significant performance
improvement as its effects flow out of ED, leading to crowded ED with reduced capacity to off load ambulances. Achievement of the 30 mins handover target will remain a challenge. Mitigation – additional decant ward opened late 2021 for medical Covid capacity. Consideration within Ambulance Escalation SOP to utilise additional footprint. Continued focussed working with the ambulance service to achieve the target.
• Workforce risk as per D1 entry above. • If the Consultant led RAT operational hours extend this will require additional Consultant funding Mitigation – could consider
Registrar level although currently have Registrar vacancies so may not provide mitigation if unable to recruit. • Ongoing Covid-19 response, challenges with social distancing in department which affects fit to sit capacity and need to wait for
Samba swab result prior to admission therefore adding to crowded department. Mitigation – await updated Covid-19 guidance for NHS services.
Specific to ESNEFT: • The current environment at Ipswich is not ‘fit for purpose’ and a new ED/ UTC is currently being built as there’s not enough
capacity for current or future demand. The performance standard was difficult for Ipswich to achieve pre pandemic, hence the funding allocated for a new build.
• Batching of ambulances – working with EEAST to avoid batching and smooth variation. • Insufficient cubicle capacity to meet current demand on the Ipswich site – Escalation and Cohorting SOP
Improve against all Ambulance Response Standards, with plans to achieve Category 1 and Category 2 mean and 90th percentile standards
Actions EEAST will continue to develop their workforce plan and adapt service delivery models to meet the challenge of improving Category 1 & 2 Response Standards. Foremost in this approach will be to work closely with ICS partners to begin the workforce integration journey, with
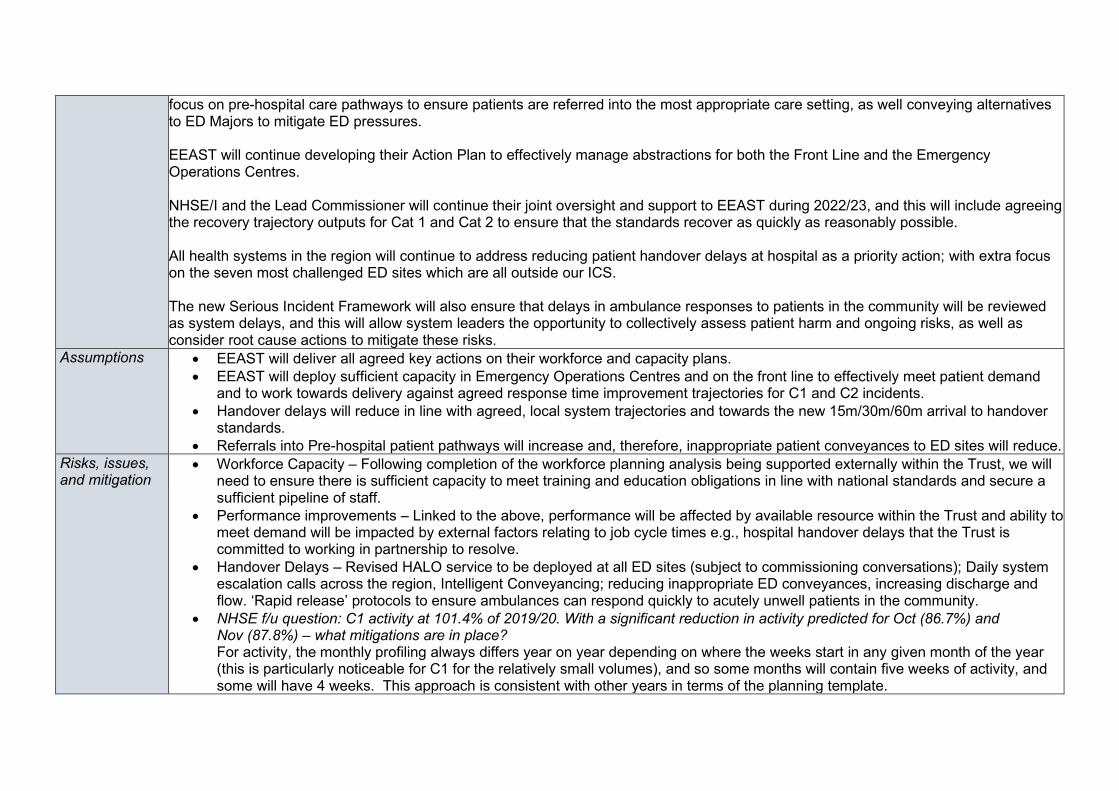
focus on pre-hospital care pathways to ensure patients are referred into the most appropriate care setting, as well conveying alternatives to ED Majors to mitigate ED pressures. EEAST will continue developing their Action Plan to effectively manage abstractions for both the Front Line and the Emergency Operations Centres. NHSE/I and the Lead Commissioner will continue their joint oversight and support to EEAST during 2022/23, and this will include agreeing the recovery trajectory outputs for Cat 1 and Cat 2 to ensure that the standards recover as quickly as reasonably possible. All health systems in the region will continue to address reducing patient handover delays at hospital as a priority action; with extra focus on the seven most challenged ED sites which are all outside our ICS. The new Serious Incident Framework will also ensure that delays in ambulance responses to patients in the community will be reviewed as system delays, and this will allow system leaders the opportunity to collectively assess patient harm and ongoing risks, as well as consider root cause actions to mitigate these risks.
Assumptions • EEAST will deliver all agreed key actions on their workforce and capacity plans. • EEAST will deploy sufficient capacity in Emergency Operations Centres and on the front line to effectively meet patient demand
and to work towards delivery against agreed response time improvement trajectories for C1 and C2 incidents. • Handover delays will reduce in line with agreed, local system trajectories and towards the new 15m/30m/60m arrival to handover
standards. • Referrals into Pre-hospital patient pathways will increase and, therefore, inappropriate patient conveyances to ED sites will reduce.
Risks, issues, and mitigation
• Workforce Capacity – Following completion of the workforce planning analysis being supported externally within the Trust, we will need to ensure there is sufficient capacity to meet training and education obligations in line with national standards and secure a sufficient pipeline of staff.
• Performance improvements – Linked to the above, performance will be affected by available resource within the Trust and ability to meet demand will be impacted by external factors relating to job cycle times e.g., hospital handover delays that the Trust is committed to working in partnership to resolve.
• Handover Delays – Revised HALO service to be deployed at all ED sites (subject to commissioning conversations); Daily system escalation calls across the region, Intelligent Conveyancing; reducing inappropriate ED conveyances, increasing discharge and flow. ‘Rapid release’ protocols to ensure ambulances can respond quickly to acutely unwell patients in the community.
• NHSE f/u question: C1 activity at 101.4% of 2019/20. With a significant reduction in activity predicted for Oct (86.7%) and Nov (87.8%) – what mitigations are in place? For activity, the monthly profiling always differs year on year depending on where the weeks start in any given month of the year (this is particularly noticeable for C1 for the relatively small volumes), and so some months will contain five weeks of activity, and some will have 4 weeks. This approach is consistent with other years in terms of the planning template.
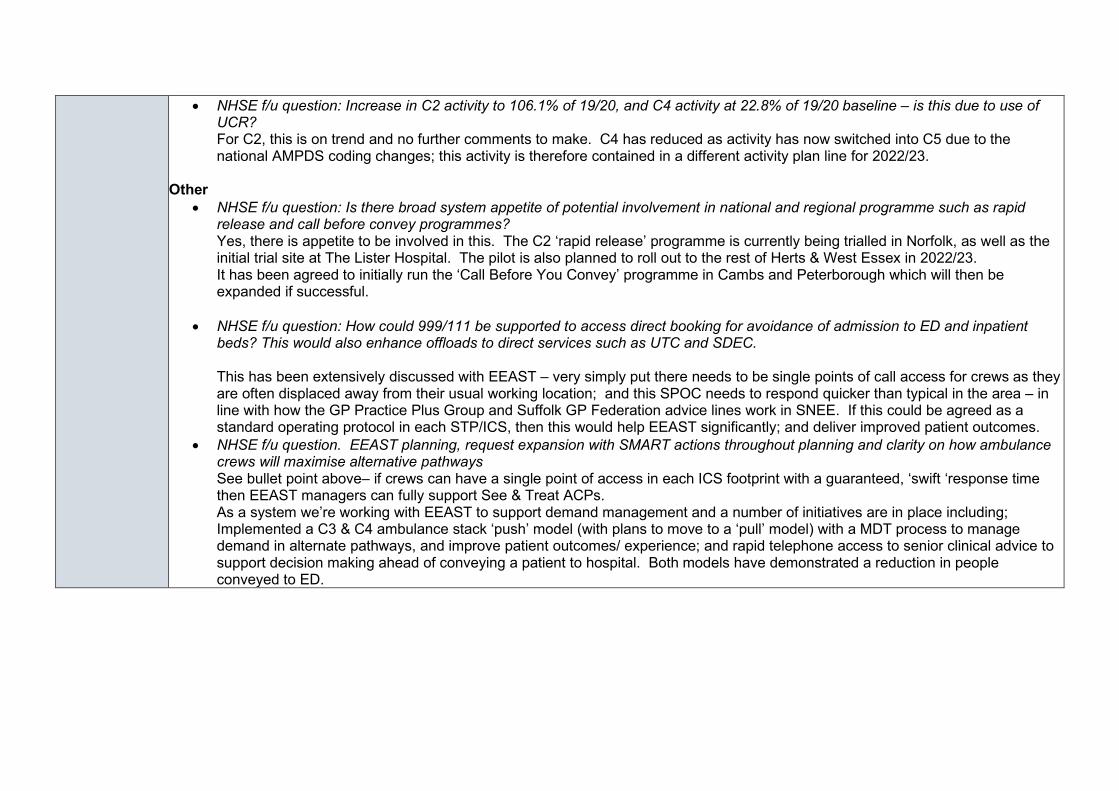
• NHSE f/u question: Increase in C2 activity to 106.1% of 19/20, and C4 activity at 22.8% of 19/20 baseline – is this due to use of UCR? For C2, this is on trend and no further comments to make. C4 has reduced as activity has now switched into C5 due to the national AMPDS coding changes; this activity is therefore contained in a different activity plan line for 2022/23.
Other • NHSE f/u question: Is there broad system appetite of potential involvement in national and regional programme such as rapid
release and call before convey programmes? Yes, there is appetite to be involved in this. The C2 ‘rapid release’ programme is currently being trialled in Norfolk, as well as the initial trial site at The Lister Hospital. The pilot is also planned to roll out to the rest of Herts & West Essex in 2022/23. It has been agreed to initially run the ‘Call Before You Convey’ programme in Cambs and Peterborough which will then be expanded if successful.
• NHSE f/u question: How could 999/111 be supported to access direct booking for avoidance of admission to ED and inpatient beds? This would also enhance offloads to direct services such as UTC and SDEC. This has been extensively discussed with EEAST – very simply put there needs to be single points of call access for crews as they are often displaced away from their usual working location; and this SPOC needs to respond quicker than typical in the area – in line with how the GP Practice Plus Group and Suffolk GP Federation advice lines work in SNEE. If this could be agreed as a standard operating protocol in each STP/ICS, then this would help EEAST significantly; and deliver improved patient outcomes.
• NHSE f/u question. EEAST planning, request expansion with SMART actions throughout planning and clarity on how ambulance crews will maximise alternative pathways See bullet point above– if crews can have a single point of access in each ICS footprint with a guaranteed, ‘swift ‘response time then EEAST managers can fully support See & Treat ACPs. As a system we’re working with EEAST to support demand management and a number of initiatives are in place including; Implemented a C3 & C4 ambulance stack ‘push’ model (with plans to move to a ‘pull’ model) with a MDT process to manage demand in alternate pathways, and improve patient outcomes/ experience; and rapid telephone access to senior clinical advice to support decision making ahead of conveying a patient to hospital. Both models have demonstrated a reduction in people conveyed to ED.
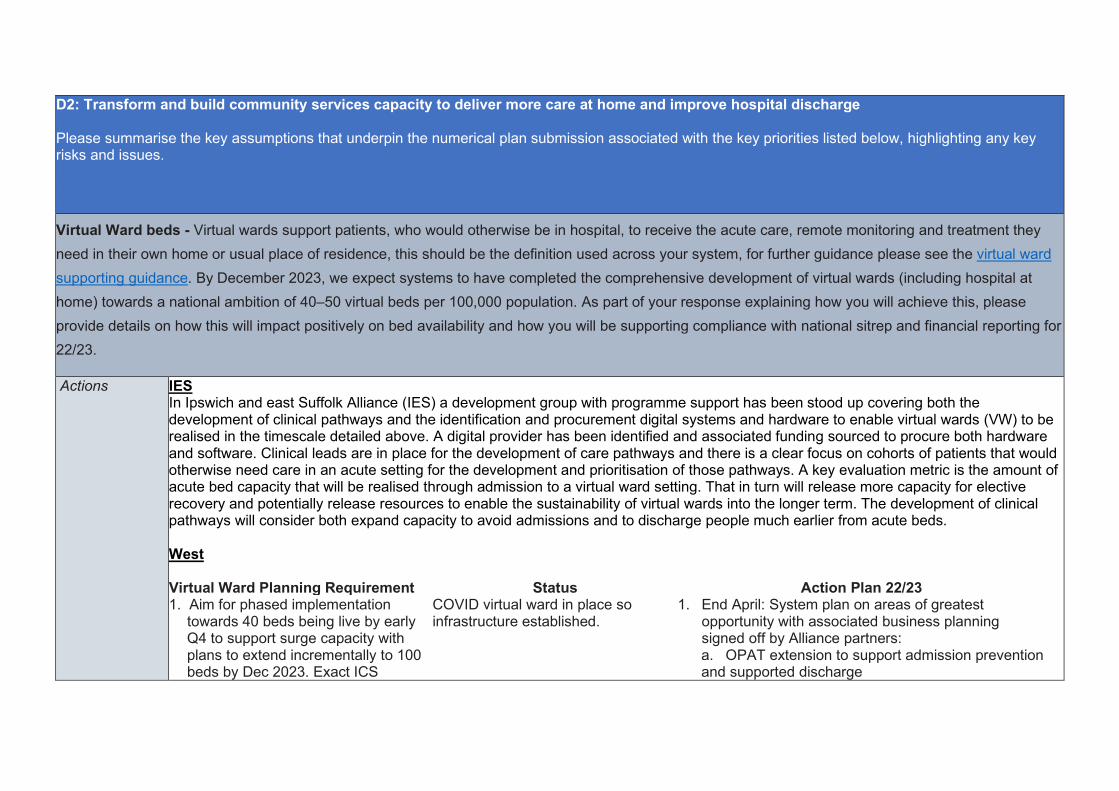
D2: Transform and build community services capacity to deliver more care at home and improve hospital discharge Please summarise the key assumptions that underpin the numerical plan submission associated with the key priorities listed below, highlighting any key risks and issues. Virtual Ward beds - Virtual wards support patients, who would otherwise be in hospital, to receive the acute care, remote monitoring and treatment they need in their own home or usual place of residence, this should be the definition used across your system, for further guidance please see the virtual ward supporting guidance. By December 2023, we expect systems to have completed the comprehensive development of virtual wards (including hospital at home) towards a national ambition of 40–50 virtual beds per 100,000 population. As part of your response explaining how you will achieve this, please provide details on how this will impact positively on bed availability and how you will be supporting compliance with national sitrep and financial reporting for 22/23.
Actions
IES In Ipswich and east Suffolk Alliance (IES) a development group with programme support has been stood up covering both the development of clinical pathways and the identification and procurement digital systems and hardware to enable virtual wards (VW) to be realised in the timescale detailed above. A digital provider has been identified and associated funding sourced to procure both hardware and software. Clinical leads are in place for the development of care pathways and there is a clear focus on cohorts of patients that would otherwise need care in an acute setting for the development and prioritisation of those pathways. A key evaluation metric is the amount of acute bed capacity that will be realised through admission to a virtual ward setting. That in turn will release more capacity for elective recovery and potentially release resources to enable the sustainability of virtual wards into the longer term. The development of clinical pathways will consider both expand capacity to avoid admissions and to discharge people much earlier from acute beds. West Virtual Ward Planning Requirement Status Action Plan 22/23 1. Aim for phased implementation
towards 40 beds being live by early Q4 to support surge capacity with plans to extend incrementally to 100 beds by Dec 2023. Exact ICS
COVID virtual ward in place so infrastructure established.
1. End April: System plan on areas of greatest opportunity with associated business planning signed off by Alliance partners: a. OPAT extension to support admission prevention and supported discharge
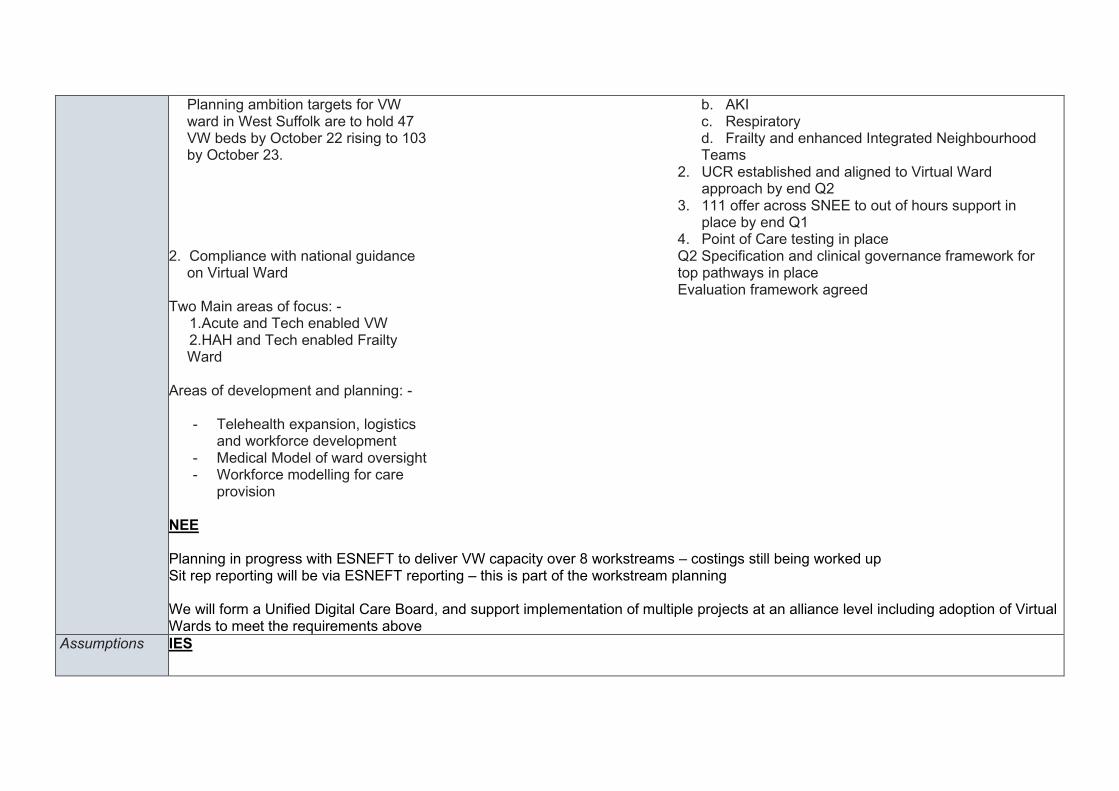
Planning ambition targets for VW ward in West Suffolk are to hold 47 VW beds by October 22 rising to 103 by October 23.
b. AKI c. Respiratory d. Frailty and enhanced Integrated Neighbourhood Teams
2. UCR established and aligned to Virtual Ward approach by end Q2
3. 111 offer across SNEE to out of hours support in place by end Q1
4. Point of Care testing in place 2. Compliance with national guidance
on Virtual Ward Two Main areas of focus: - 1.Acute and Tech enabled VW 2.HAH and Tech enabled Frailty
Ward Areas of development and planning: -
- Telehealth expansion, logistics and workforce development
- Medical Model of ward oversight - Workforce modelling for care
provision
Q2 Specification and clinical governance framework for top pathways in place Evaluation framework agreed
NEE Planning in progress with ESNEFT to deliver VW capacity over 8 workstreams – costings still being worked up Sit rep reporting will be via ESNEFT reporting – this is part of the workstream planning We will form a Unified Digital Care Board, and support implementation of multiple projects at an alliance level including adoption of Virtual Wards to meet the requirements above
Assumptions IES
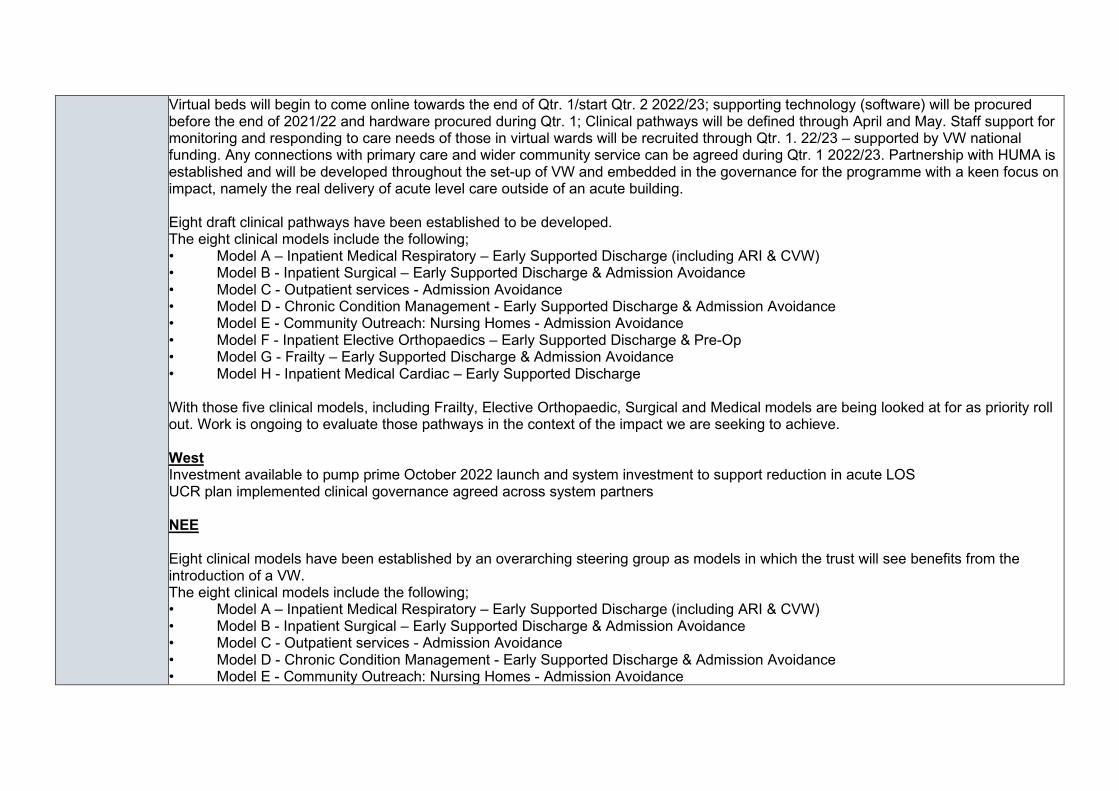
Virtual beds will begin to come online towards the end of Qtr. 1/start Qtr. 2 2022/23; supporting technology (software) will be procured before the end of 2021/22 and hardware procured during Qtr. 1; Clinical pathways will be defined through April and May. Staff support for monitoring and responding to care needs of those in virtual wards will be recruited through Qtr. 1. 22/23 – supported by VW national funding. Any connections with primary care and wider community service can be agreed during Qtr. 1 2022/23. Partnership with HUMA is established and will be developed throughout the set-up of VW and embedded in the governance for the programme with a keen focus on impact, namely the real delivery of acute level care outside of an acute building. Eight draft clinical pathways have been established to be developed. The eight clinical models include the following; • Model A – Inpatient Medical Respiratory – Early Supported Discharge (including ARI & CVW) • Model B - Inpatient Surgical – Early Supported Discharge & Admission Avoidance • Model C - Outpatient services - Admission Avoidance • Model D - Chronic Condition Management - Early Supported Discharge & Admission Avoidance • Model E - Community Outreach: Nursing Homes - Admission Avoidance • Model F - Inpatient Elective Orthopaedics – Early Supported Discharge & Pre-Op • Model G - Frailty – Early Supported Discharge & Admission Avoidance • Model H - Inpatient Medical Cardiac – Early Supported Discharge With those five clinical models, including Frailty, Elective Orthopaedic, Surgical and Medical models are being looked at for as priority roll out. Work is ongoing to evaluate those pathways in the context of the impact we are seeking to achieve. West Investment available to pump prime October 2022 launch and system investment to support reduction in acute LOS UCR plan implemented clinical governance agreed across system partners NEE Eight clinical models have been established by an overarching steering group as models in which the trust will see benefits from the introduction of a VW. The eight clinical models include the following; • Model A – Inpatient Medical Respiratory – Early Supported Discharge (including ARI & CVW) • Model B - Inpatient Surgical – Early Supported Discharge & Admission Avoidance • Model C - Outpatient services - Admission Avoidance • Model D - Chronic Condition Management - Early Supported Discharge & Admission Avoidance • Model E - Community Outreach: Nursing Homes - Admission Avoidance

• Model F - Inpatient Elective Orthopaedics – Early Supported Discharge & Pre-Op • Model G - Frailty – Early Supported Discharge & Admission Avoidance • Model H - Inpatient Medical Cardiac – Early Supported Discharge Five clinical models, including Frailty, Elective Orthopaedic, Surgical and Medical models will be prioritised for FY22/23. The Inpatient Medical Cardiac model will be piloted end of Q1/start of Q2. The following clinical model, to be agreed, will follow at the beginning Q3. The other priority clinical pathways will follow towards the end of financial year. The pilot will enable the trust to test and learn a clinical pathway to provide a proof of concept which subsequent clinical pathways can build on. The clinical model to be lifted as the trailblazer will be the Inpatient Medical Cardiac model. The model will be based around the work that has been successfully embedded and Norfolk & Norwich University Hospital (NNUH). The aim of the model is too safely on-board patients who are awaiting definitive treatment with or without an agreed date to be managed on the VW as appropriate. We have sufficient digital capability & licences exist to enable this (this is part of a wider Unified Digital Care Programme. Application for supporting resources to scale virtual wards will be submitted 11 March – assuming this will be supported, recruitment and programme planning / mobilisation has begun
Risks, issues and mitigation
IES In IES the main risk relates to the ability to recruit staff with sufficient seniority to manage patient risk in virtual wards and to minimise any risks of readmission to acute hospital. Mitigations will include considering support from Physician Associates, ACPs supplemented by support from existing consultant leads to successfully manage risk. West Workforce greatest risk: recruitment plan in development to support new roles Integration of technology solutions across SNEE: SNEE working group on cross cutting themes in development NEE Models still in development with costings still to be reviewed to check they meet the envelop indicated in guidance Risks to not recruiting lead to challenge with mobilising support. Pooled resources at ICS level mitigates this and other associated skills / capacity risks. The risk of widening exclusion will be mitigated by adopting the Equity and Equality approach and through work with Healthwatch and partners
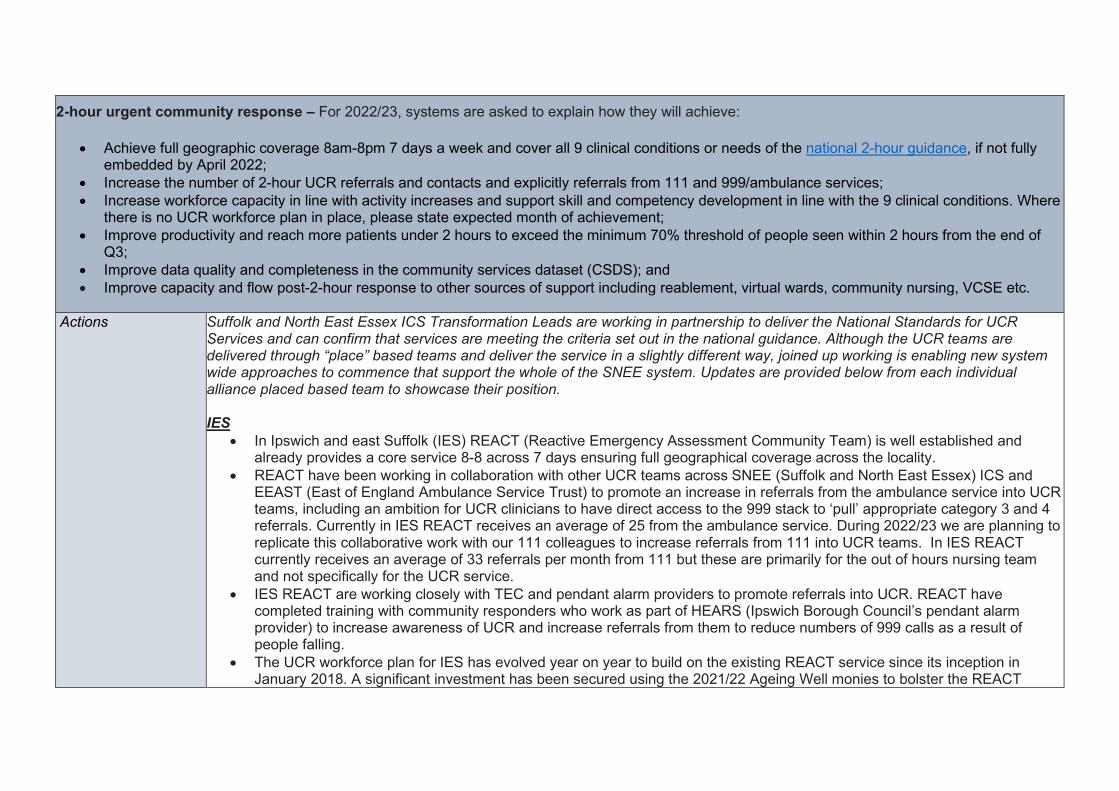
2-hour urgent community response – For 2022/23, systems are asked to explain how they will achieve:
• Achieve full geographic coverage 8am-8pm 7 days a week and cover all 9 clinical conditions or needs of the national 2-hour guidance, if not fully embedded by April 2022;
• Increase the number of 2-hour UCR referrals and contacts and explicitly referrals from 111 and 999/ambulance services; • Increase workforce capacity in line with activity increases and support skill and competency development in line with the 9 clinical conditions. Where
there is no UCR workforce plan in place, please state expected month of achievement; • Improve productivity and reach more patients under 2 hours to exceed the minimum 70% threshold of people seen within 2 hours from the end of
Q3; • Improve data quality and completeness in the community services dataset (CSDS); and • Improve capacity and flow post-2-hour response to other sources of support including reablement, virtual wards, community nursing, VCSE etc.
Actions
Suffolk and North East Essex ICS Transformation Leads are working in partnership to deliver the National Standards for UCR Services and can confirm that services are meeting the criteria set out in the national guidance. Although the UCR teams are delivered through “place” based teams and deliver the service in a slightly different way, joined up working is enabling new system wide approaches to commence that support the whole of the SNEE system. Updates are provided below from each individual alliance placed based team to showcase their position. IES
• In Ipswich and east Suffolk (IES) REACT (Reactive Emergency Assessment Community Team) is well established and already provides a core service 8-8 across 7 days ensuring full geographical coverage across the locality.
• REACT have been working in collaboration with other UCR teams across SNEE (Suffolk and North East Essex) ICS and EEAST (East of England Ambulance Service Trust) to promote an increase in referrals from the ambulance service into UCR teams, including an ambition for UCR clinicians to have direct access to the 999 stack to ‘pull’ appropriate category 3 and 4 referrals. Currently in IES REACT receives an average of 25 from the ambulance service. During 2022/23 we are planning to replicate this collaborative work with our 111 colleagues to increase referrals from 111 into UCR teams. In IES REACT currently receives an average of 33 referrals per month from 111 but these are primarily for the out of hours nursing team and not specifically for the UCR service.
• IES REACT are working closely with TEC and pendant alarm providers to promote referrals into UCR. REACT have completed training with community responders who work as part of HEARS (Ipswich Borough Council’s pendant alarm provider) to increase awareness of UCR and increase referrals from them to reduce numbers of 999 calls as a result of people falling.
• The UCR workforce plan for IES has evolved year on year to build on the existing REACT service since its inception in January 2018. A significant investment has been secured using the 2021/22 Ageing Well monies to bolster the REACT
workforce and ensure the hub and spoke model for UCR is optimised and these posts will be recruited to during 2022/23. There will be a total of 24 WTE posts including nurses, therapists, generic worker & therapy assistant practitioners ensuring a workforce with the competency and skills required for the 9 clinical conditions that present to UCR services: Falls, frailty, reduced function, palliative care, urgent equipment needs, confusion or delirium, urgent catheter care, urgent support for diabetes and carer breakdown. We have also funded additional vehicles (electric cars as art of sustainability plan) to optimise 2-hour response form the three UCR hubs and more community lifting equipment to ensure timely response to non-injured fallers from both UCR and community teams.
• REACT’s current daily admission avoidance target for 21/22 was set at 22 patients referred into the service and this will be stretched to 24 patients per day for 22/23.
• Current indicative data shows REACT historically respond to 68% of crisis referrals within 2 hours. There is a data quality issue that is being resolved to ensure accuracy of CSDS submission. A REACT locality model is in development to optimise numbers of people receiving a 2-hour response. REACT hub and spoke model will see two rural hubs in Woodbridge and Stowmarket mobilised during 2022 which should improve the % to reach 70% or over in line with the national target by the end of Q3 in 2022/23. Advanced plans now moving to implementation for greater flexing of resources between community services to gain more productivity overall.
• From February 2022 the data quality issues with the CSDS submission for SNEE has been addressed. Dedicated data analyst role funded from 2021/22 ageing well monies to work pan-Suffolk to ensure this is maintained and there is data completeness moving forwards.
• REACT’s remit is to provide crisis support for up to 5 days maximum following the initial 2-hour response. Currently the average length of stay (LOS) for a person on the REACT caseload is 2.49 days evidencing good flow out of the service. Delays with transfers of care have historically occurred mainly due to inability to find on-going care. The REACT caseload LOS is regularly monitored, and action plans deployed to address any blockers.
West Suffolk
• Full UCR coverage of 7 day 0800-2000hr provision is in place and established, with an offer of 24/7 to be work through as part of demand and capacity planning by end Q2.
• Source of referral tracked integration with EEAST through pilot at triage in progress. Stretched trajectory to be agreed in Q1 with EEAST and 111 in line with Ageing Well allocation of funding to UCR. Q2 Evaluation of shared triage with EEAST to identify additional workforce and pathways changes relating to high demand 999 calls. Q2 CSDS dashboard in place and DOS review by end Q2
• Workforce mapping in progress and alignment into localities. Trajectory for increase in staffing based on 2021/22 Q4 numbers with a business case for UCR to support service improvement plan approved Q3.
• 70% of 2hr UCR responded within 2 hr by end Q3, with baseline assessment for delivery of response by mid Q1 and improvement trajectory agreed end Q1
• To improve data quality and completeness in CSDS, a digital analyst will be in post to support community compliance with reporting requirements by mid Q1
• To Improve capacity in post urgent community services to support flow and patient outcomes, work is underway to creating capacity in home care market with a review and recovery in progress. WS plan in place by mid Q1
NEE Full geographical coverage is already being delivered across North East Essex, with referrals being accepted between 8am and 8pm 7 days a week for a 2-hour response. The team are able to respond to all 9 clinical conditions in the following ways:
• Direct access to Operation Pendant for non-injured faller pick up - working closely with UCRS in NEE, referrals going both directions to keep patients out of hospital. Work being undertaken to support the service with ECC Adult Social Care Tech services and subsequent referrals through those channels.
• Direct access to Advanced Nurse Practitioners, Community Nursing Teams, the Frailty Unit, and all system admission avoidance partners including Urgent Care Paramedics and Falls vehicles
• Full therapy assessment provided by UCR team in 2-hour response • Working in Partnership with EOL SinglePoint and actively supporting EOL patients with therapy needs • SWAN is the Care / Reablement Provider assigned to the core team who provide ongoing care and support for
the patient, with referrals into core commissioned services • Access to Social Prescribers in the community specifically working with UCR teams to provide non-clinical
community support Increase the number of 2-hour UCR referrals and contacts and explicitly referrals from 111 and 999/ambulance services;
• Work undertaken with EEAST to promote service to all crews with regular review sessions and data sharing on referrals made with EEAST
• Current programme with EEAST to work with UCR teams to take work from the stack which needs further development to continue
• Close working partnership with EEAST Early Intervention Falls and Urgent Paramedic vehicles and referrals being made between services
• 111 – open to DOS and promotion of UCR to clinical leads for referral pathways
Increase workforce capacity in line with activity increases and support skill and competency development in line with the 9 clinical conditions. Where there is no UCR workforce plan in place, please state expected month of achievement;
• Workforce has been developed with ANP offer recently • Additional funding provided for reablement element of the service to provide overflow and meet demand and
capacity issues when referring into Essex County Council
• Current transformation to align other Community Provider and EEAST services to bolster resource in UCR Services
• Currently working in capacity as modelled - model in NEE was always designed to act as a hub and response service, utilising the plethora of admission avoidance services in the system and navigating the referrals into the right service for the right response, whilst responding to those calls appropriate for UCRS directly. The UCRS receive 10 referrals a day on average, however, many more calls through call centre and duty phone line which result in appropriate Admission Avoidance Services being used i.e. Singlepoint EOL, Early Intervention Vehicles, District Nursing etc
• Plans are to integrate the current UCRS with the admission avoidance teams at the front door, OPAT and the urgent response element of community nursing
• The community Nursing element is very much in the planning / funding stage and may need to go out to consultation.
• There will be an additional nurse lead (indicative B7) for the community nurse element of service, with a shared admin across the integrated service and an overarching service lead
• Please see table for full workforce
Core workforce UCRS.docx
Improve productivity and reach more patients under 2 hours to exceed the minimum 70% threshold of people seen within 2 hours from the end of Q3;
• Original productivity in 80+%, but seen a dip in Q3 due to change in reporting frameworks and referrals coming into the team from discharge hub not accurate for a 2-hour response has seen a drop to 61%
Improve data quality and completeness in the community services dataset (CSDS); and
• Data quality is improving, and service is ready to meet CSDS reporting target of March 2022
Improve capacity and flow post-2-hour response to other sources of support including reablement, virtual wards, community nursing, VCSE etc.
• Currently no issues with majority of onward referrals and KPI’s being met, some issues with reablement provision which is a wider issue than North East Essex, being mitigated with regular discussion and system improvement with Newton Europe supporting system flow discussions.
Now receiving CSDS data – next step is to review data to ensure data quality is assured from March 22 Improve response time reporting by March 22 Continue system flow work to enable referrals into reablement in timely fashion
Assumptions ICS wide • Estates will be secured, and capital changes delivered within given timescales and within the providers capital funding
allocation and recurrent budget allocation. • That recruitment is successful and adds capacity in community service delivery rather than moving that capacity about; this is
crucial to picking up extra demand. In the medium/longer term our community integrated neighbourhood teams (INTs) will need to play a greater part in managing crisis demand for their local area.
• Same Day Emergency Care and Virtual Wards aligned and supporting UCR • Ageing Well Funding mapped to delivery of outcomes • Anticipatory Care received from NHSE and model adopted into the ICS • Capacity is within comfort at the moment and no further surges emerge
Risks, issues and mitigation
IES
• 2022/23 Ageing Well funding allocation for SNEE is less than was expected. Majority of investments for UCR in 2021/22 were agreed substantively so considerable proportion of 2022/23 monies is already committed. This leaves minimal amount for further investment into Anticipatory Care (AC) programme. However, this is likely to have minimal impact on UCR performance due to investment already secured. IES system have agreed that remaining ageing well monies for five-year period (e.g., 2023/24) will be focused on AC.
• In IES high vacancy rates across acute and community teams which impact on overall capacity to provide UCR within 2 hours. To mitigate this there are daily capacity meetings to ensure that resources are flexibly deployed to meet areas with most demand.
• Recruitment to new UCR posts (listed above) is challenging and some posts have been recruited to internally which now needs additional recruitment to ensure overall increase in workforce capacity is achieved. Mitigations do relate to the increasing join up in all community services and opportunities thereby in greater flexibility in staff deployment.
• UCR hub and spoke model is dependent upon estates being secured for spoke locations at Woodbridge and Stowmarket.
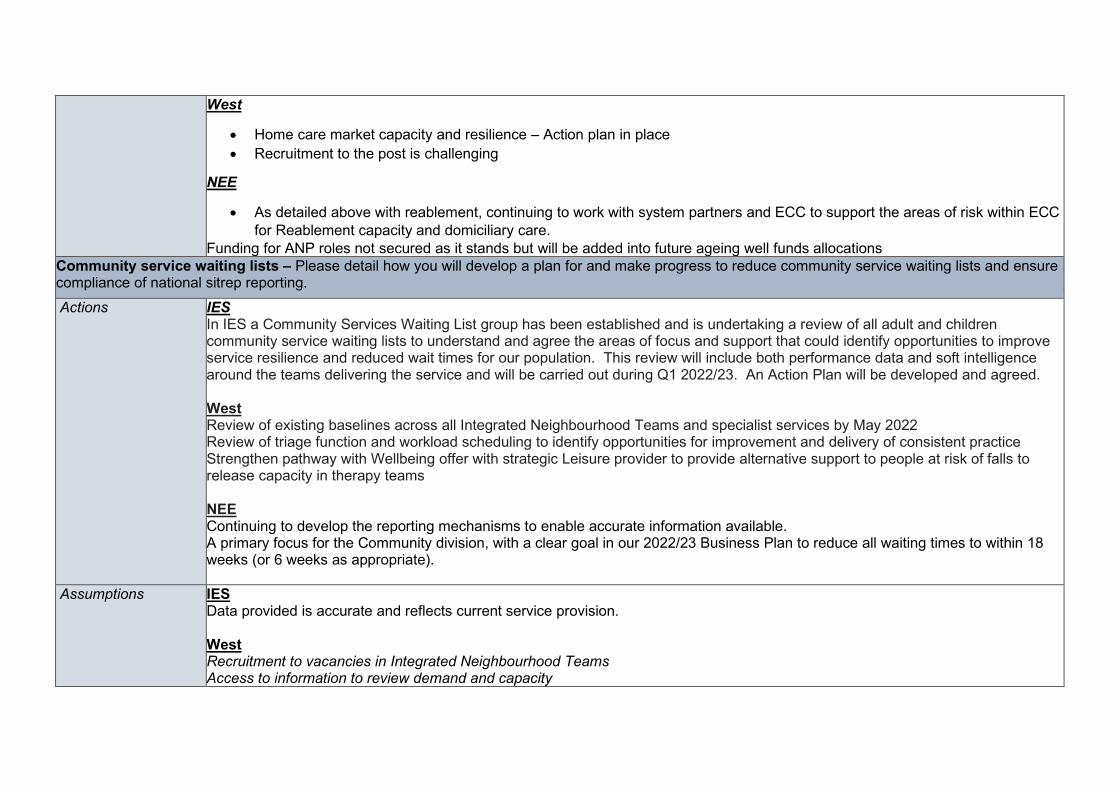
West
• Home care market capacity and resilience – Action plan in place • Recruitment to the post is challenging
NEE
• As detailed above with reablement, continuing to work with system partners and ECC to support the areas of risk within ECC for Reablement capacity and domiciliary care.
Funding for ANP roles not secured as it stands but will be added into future ageing well funds allocations Community service waiting lists – Please detail how you will develop a plan for and make progress to reduce community service waiting lists and ensure compliance of national sitrep reporting. Actions
IES In IES a Community Services Waiting List group has been established and is undertaking a review of all adult and children community service waiting lists to understand and agree the areas of focus and support that could identify opportunities to improve service resilience and reduced wait times for our population. This review will include both performance data and soft intelligence around the teams delivering the service and will be carried out during Q1 2022/23. An Action Plan will be developed and agreed. West Review of existing baselines across all Integrated Neighbourhood Teams and specialist services by May 2022 Review of triage function and workload scheduling to identify opportunities for improvement and delivery of consistent practice Strengthen pathway with Wellbeing offer with strategic Leisure provider to provide alternative support to people at risk of falls to release capacity in therapy teams NEE Continuing to develop the reporting mechanisms to enable accurate information available. A primary focus for the Community division, with a clear goal in our 2022/23 Business Plan to reduce all waiting times to within 18 weeks (or 6 weeks as appropriate).
Assumptions IES Data provided is accurate and reflects current service provision. West Recruitment to vacancies in Integrated Neighbourhood Teams Access to information to review demand and capacity
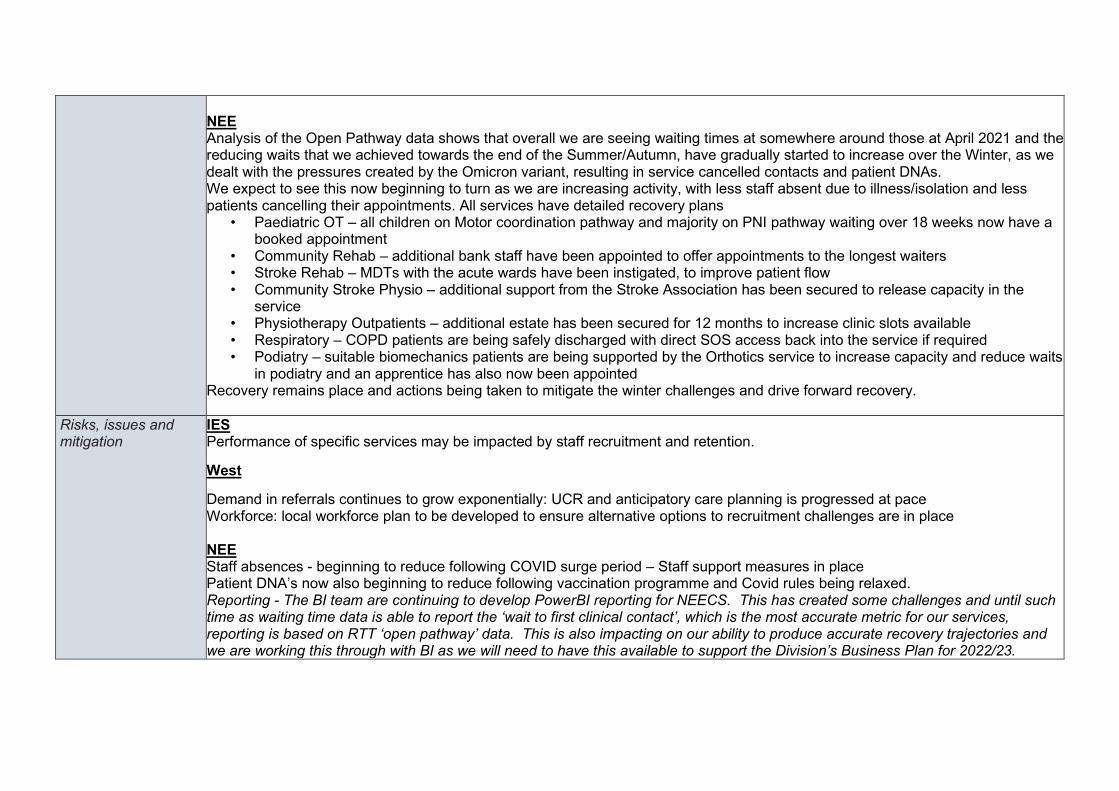
NEE Analysis of the Open Pathway data shows that overall we are seeing waiting times at somewhere around those at April 2021 and the reducing waits that we achieved towards the end of the Summer/Autumn, have gradually started to increase over the Winter, as we dealt with the pressures created by the Omicron variant, resulting in service cancelled contacts and patient DNAs. We expect to see this now beginning to turn as we are increasing activity, with less staff absent due to illness/isolation and less patients cancelling their appointments. All services have detailed recovery plans
• Paediatric OT – all children on Motor coordination pathway and majority on PNI pathway waiting over 18 weeks now have a booked appointment
• Community Rehab – additional bank staff have been appointed to offer appointments to the longest waiters • Stroke Rehab – MDTs with the acute wards have been instigated, to improve patient flow • Community Stroke Physio – additional support from the Stroke Association has been secured to release capacity in the
service • Physiotherapy Outpatients – additional estate has been secured for 12 months to increase clinic slots available • Respiratory – COPD patients are being safely discharged with direct SOS access back into the service if required • Podiatry – suitable biomechanics patients are being supported by the Orthotics service to increase capacity and reduce waits
in podiatry and an apprentice has also now been appointed Recovery remains place and actions being taken to mitigate the winter challenges and drive forward recovery.
Risks, issues and mitigation
IES Performance of specific services may be impacted by staff recruitment and retention.
West
Demand in referrals continues to grow exponentially: UCR and anticipatory care planning is progressed at pace Workforce: local workforce plan to be developed to ensure alternative options to recruitment challenges are in place NEE Staff absences - beginning to reduce following COVID surge period – Staff support measures in place Patient DNA’s now also beginning to reduce following vaccination programme and Covid rules being relaxed. Reporting - The BI team are continuing to develop PowerBI reporting for NEECS. This has created some challenges and until such time as waiting time data is able to report the ‘wait to first clinical contact’, which is the most accurate metric for our services, reporting is based on RTT ‘open pathway’ data. This is also impacting on our ability to produce accurate recovery trajectories and we are working this through with BI as we will need to have this available to support the Division’s Business Plan for 2022/23.
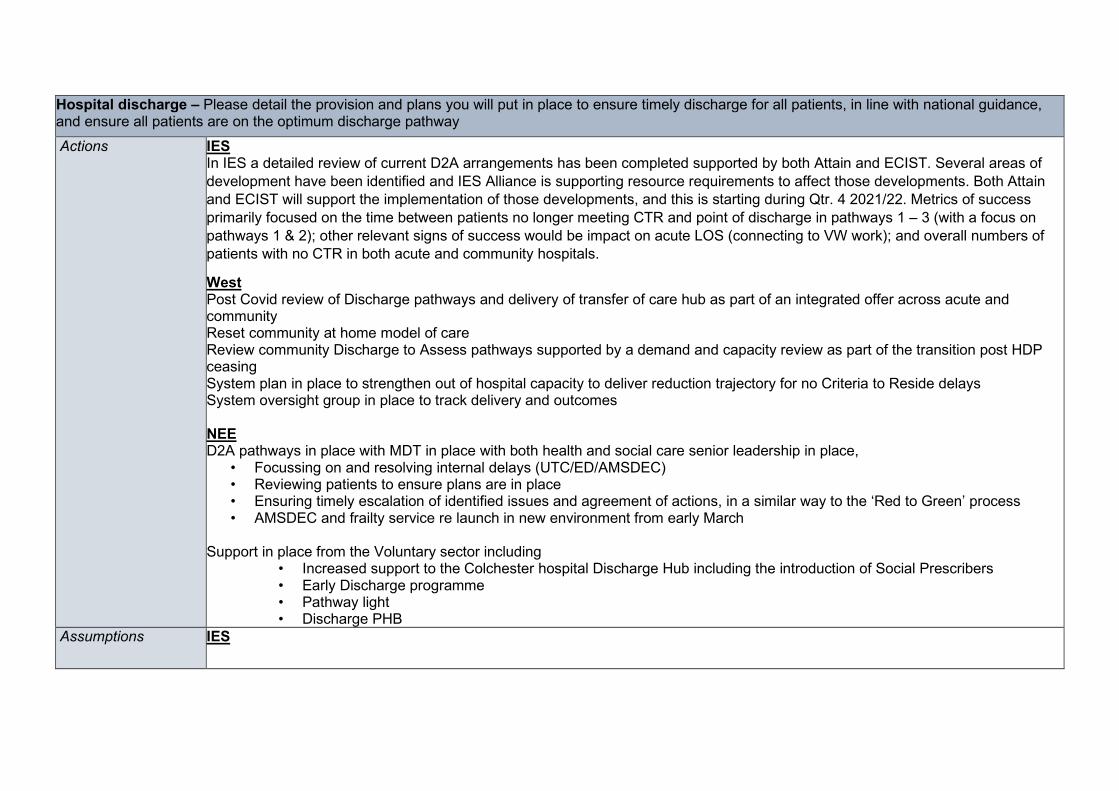
Hospital discharge – Please detail the provision and plans you will put in place to ensure timely discharge for all patients, in line with national guidance, and ensure all patients are on the optimum discharge pathway Actions
IES In IES a detailed review of current D2A arrangements has been completed supported by both Attain and ECIST. Several areas of development have been identified and IES Alliance is supporting resource requirements to affect those developments. Both Attain and ECIST will support the implementation of those developments, and this is starting during Qtr. 4 2021/22. Metrics of success primarily focused on the time between patients no longer meeting CTR and point of discharge in pathways 1 – 3 (with a focus on pathways 1 & 2); other relevant signs of success would be impact on acute LOS (connecting to VW work); and overall numbers of patients with no CTR in both acute and community hospitals.
West Post Covid review of Discharge pathways and delivery of transfer of care hub as part of an integrated offer across acute and community Reset community at home model of care Review community Discharge to Assess pathways supported by a demand and capacity review as part of the transition post HDP ceasing System plan in place to strengthen out of hospital capacity to deliver reduction trajectory for no Criteria to Reside delays System oversight group in place to track delivery and outcomes NEE D2A pathways in place with MDT in place with both health and social care senior leadership in place,
• Focussing on and resolving internal delays (UTC/ED/AMSDEC) • Reviewing patients to ensure plans are in place • Ensuring timely escalation of identified issues and agreement of actions, in a similar way to the ‘Red to Green’ process • AMSDEC and frailty service re launch in new environment from early March
Support in place from the Voluntary sector including
• Increased support to the Colchester hospital Discharge Hub including the introduction of Social Prescribers • Early Discharge programme • Pathway light • Discharge PHB
Assumptions IES
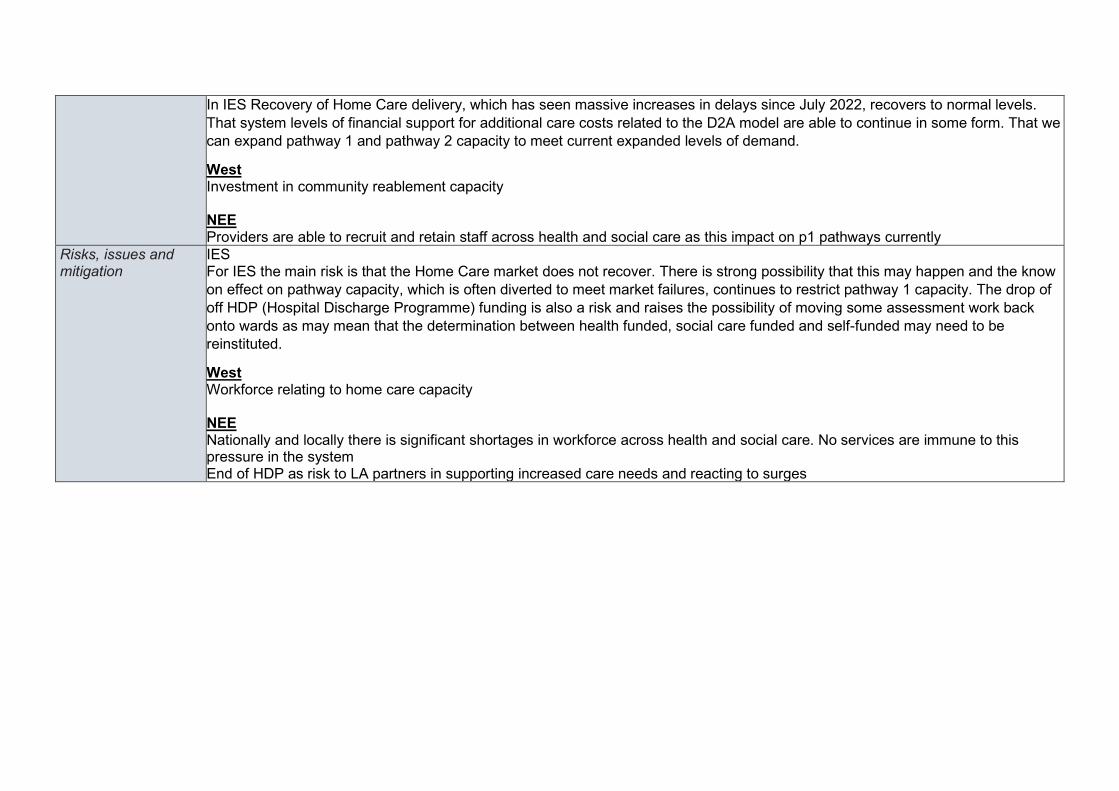
In IES Recovery of Home Care delivery, which has seen massive increases in delays since July 2022, recovers to normal levels. That system levels of financial support for additional care costs related to the D2A model are able to continue in some form. That we can expand pathway 1 and pathway 2 capacity to meet current expanded levels of demand.
West Investment in community reablement capacity NEE Providers are able to recruit and retain staff across health and social care as this impact on p1 pathways currently
Risks, issues and mitigation
IES For IES the main risk is that the Home Care market does not recover. There is strong possibility that this may happen and the know on effect on pathway capacity, which is often diverted to meet market failures, continues to restrict pathway 1 capacity. The drop of off HDP (Hospital Discharge Programme) funding is also a risk and raises the possibility of moving some assessment work back onto wards as may mean that the determination between health funded, social care funded and self-funded may need to be reinstituted.
West Workforce relating to home care capacity NEE Nationally and locally there is significant shortages in workforce across health and social care. No services are immune to this pressure in the system End of HDP as risk to LA partners in supporting increased care needs and reacting to surges
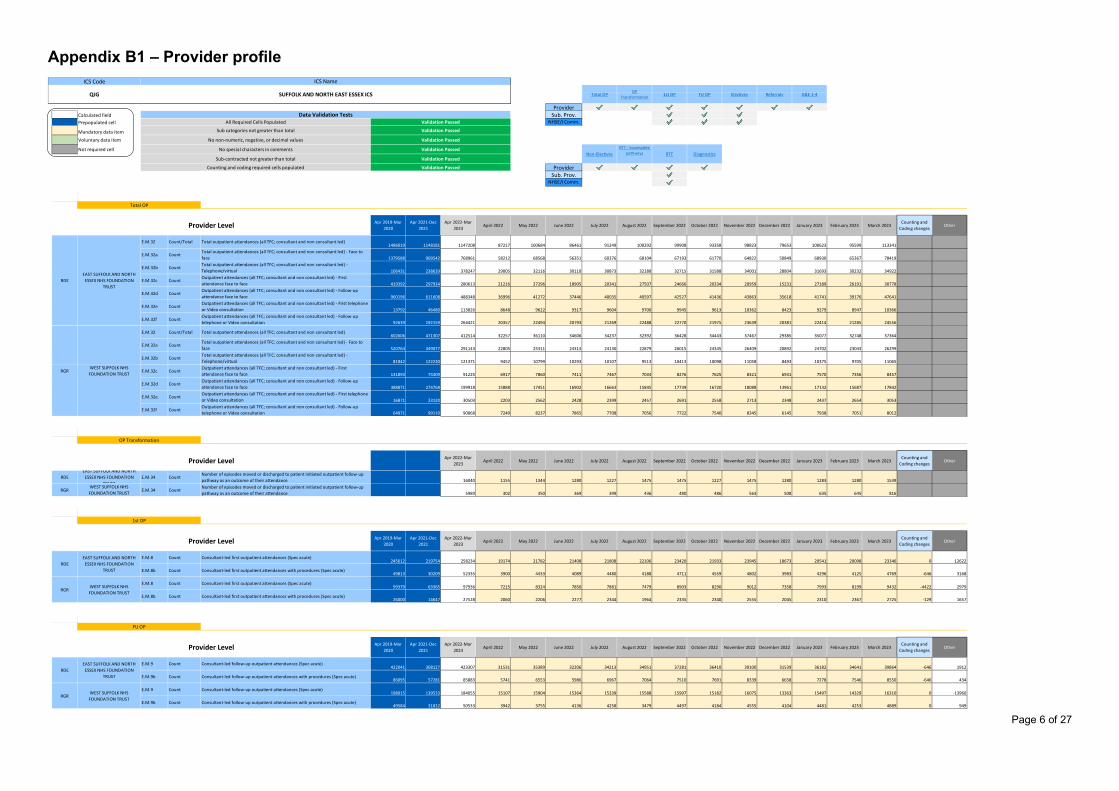
Page 6 of 27
Appendix B1 – Provider profile $H$19 $H$116 $H$135 $H$167 $H$199 $H$270 $H$315
ProviderCalculated field Sub. Prov.Prepopulated cell NHSE/I Comm.
Mandatory data item Activity7 Activity13 Activity12 Activity9Voluntary data item $H$360 $H$431 $H$489 $H$534
Not required cell
ProviderSub. Prov.
NHSE/I Comm.
ActivityCategoryToActivity1
0 1 2 3 4 5
Apr 2019-Mar 2020
Apr 2021-Dec 2021
Apr 2022-Mar 2023
April 2022 May 2022 June 2022 July 2022 August 2022 September 2022 October 2022 November 2022 December 2022 January 2023 February 2023 March 2023Counting and
Coding changesOther
PRE.M.32 Count/Total Total outpatient attendances (all TFC; consultant and non consultant led)
1486019 1148181 1147208 87217 100684 86461 91249 100292 99908 93358 98823 79653 100623 95599 113341
PRE.M.32a Count
Total outpatient attendances (all TFC; consultant and non consultant led) - Face to face 1379588 909542 768961 58212 68568 56351 60376 68104 67193 61770 64822 50849 68930 65367 78419
PRE.M.32b Count
Total outpatient attendances (all TFC; consultant and non consultant led) - Telephone/virtual 106431 238639 378247 29005 32116 30110 30873 32188 32715 31588 34001 28804 31693 30232 34922
PRE.M.32c Count
Outpatient attendances (all TFC; consultant and non consultant led) - First attendance face to face 419392 297934 280613 21216 27296 18905 20341 27507 24666 20334 20959 15231 27189 26191 30778
PRE.M.32d Count
Outpatient attendances (all TFC; consultant and non consultant led) - Follow-up attendance face to face 960196 611608 488348 36996 41272 37446 40035 40597 42527 41436 43863 35618 41741 39176 47641
PRE.M.32e Count
Outpatient attendances (all TFC; consultant and non consultant led) - First telephone or Video consultation 13792 46480 113826 8648 9622 9317 9604 9700 9945 9613 10362 8423 9279 8947 10366
PRE.M.32f Count
Outpatient attendances (all TFC; consultant and non consultant led) - Follow-up telephone or Video consultation 92639 192159 264421 20357 22494 20793 21269 22488 22770 21975 23639 20381 22414 21285 24556
PRE.M.32 Count/Total Total outpatient attendances (all TFC; consultant and non consultant led)
602606 471307 412514 32257 36110 34606 34237 32392 36428 34443 37467 29385 35077 32748 37364
PRE.M.32a Count
Total outpatient attendances (all TFC; consultant and non consultant led) - Face to face 520764 349077 291143 22805 25311 24313 24130 22879 26015 24345 26409 20892 24702 23043 26299
PRE.M.32b Count
Total outpatient attendances (all TFC; consultant and non consultant led) - Telephone/virtual 81842 122230 121371 9452 10799 10293 10107 9513 10413 10098 11058 8493 10375 9705 11065
PRE.M.32c Count
Outpatient attendances (all TFC; consultant and non consultant led) - First attendance face to face 131893 74309 91225 6917 7860 7411 7467 7034 8276 7625 8321 6931 7570 7356 8457
PRE.M.32d Count
Outpatient attendances (all TFC; consultant and non consultant led) - Follow-up attendance face to face 388871 274768 199918 15888 17451 16902 16663 15845 17739 16720 18088 13961 17132 15687 17842
PRE.M.32e Count
Outpatient attendances (all TFC; consultant and non consultant led) - First telephone or Video consultation 16871 23120 30503 2203 2562 2428 2399 2457 2691 2558 2713 2348 2437 2654 3053
PRE.M.32f Count
Outpatient attendances (all TFC; consultant and non consultant led) - Follow-up telephone or Video consultation 64971 99110 90868 7249 8237 7865 7708 7056 7722 7540 8345 6145 7938 7051 8012
ActivityCategoryActivity2
0 1 2 3 4 5 6 7 8 9 10 11
Apr 2022-Mar 2023
April 2022 May 2022 June 2022 July 2022 August 2022 September 2022 October 2022 November 2022 December 2022 January 2023 February 2023 March 2023Counting and
Coding changesOther
PRRDE E.M.34 Count
Number of episodes moved or discharged to patient initiated outpatient follow-up pathway as an outcome of their attendance 16040 1155 1344 1280 1227 1475 1475 1227 1475 1280 1283 1280 1539
PRRGR E.M.34 Count
Number of episodes moved or discharged to patient initiated outpatient follow-up pathway as an outcome of their attendance 5989 302 350 369 399 436 480 486 563 508 635 645 816
ActivityCategoryActivity3
0 1 2 3 4 5 6 7 8 9 10 11
Apr 2019-Mar 2020
Apr 2021-Dec 2021
Apr 2022-Mar 2023
April 2022 May 2022 June 2022 July 2022 August 2022 September 2022 October 2022 November 2022 December 2022 January 2023 February 2023 March 2023Counting and
Coding changesOther
PRE.M.8 Count Consultant-led first outpatient attendances (Spec acute)
245612 219754 258234 19174 21782 21408 21808 22106 23420 21933 23945 18673 20541 20098 23346 0 12622
PRE.M.8b Count Consultant-led first outpatient attendances with procedures (Spec acute)
49813 30209 52335 3900 4433 4089 4480 4188 4711 4559 4802 3983 4296 4125 4769 -646 3168
PRE.M.8 Count Consultant-led first outpatient attendances (Spec acute)
99379 63365 97936 7215 8324 7850 7881 7479 8903 8290 9012 7358 7993 8199 9432 -4422 2979
PRE.M.8b Count Consultant-led first outpatient attendances with procedures (Spec acute)
26000 14647 27528 2060 2206 2277 2344 1964 2335 2340 2555 2045 2310 2367 2725 -129 1657
ActivityCategoryActivity4
0 1 2 3 4 5 6 7 8 9 10 11
Apr 2019-Mar 2020
Apr 2021-Dec 2021
Apr 2022-Mar 2023
April 2022 May 2022 June 2022 July 2022 August 2022 September 2022 October 2022 November 2022 December 2022 January 2023 February 2023 March 2023Counting and
Coding changesOther
PRE.M.9 Count Consultant-led follow-up outpatient attendances (Spec acute)
422041 308127 423307 31531 35389 32206 34213 34951 37281 36410 39100 31539 36182 34641 39864 -646 1912
PRE.M.9b Count Consultant-led follow-up outpatient attendances with procedures (Spec acute)
86095 57281 85883 5741 6553 5986 6967 7064 7510 7691 8339 6658 7278 7546 8550 -646 434
PRE.M.9 Count Consultant-led follow-up outpatient attendances (Spec acute)
198015 139533 184055 15107 15904 15364 15339 15588 15997 15182 16075 13363 15497 14329 16310 0 -13960
PRE.M.9b Count Consultant-led follow-up outpatient attendances with procedures (Spec acute)
49584 31822 50533 3942 3755 4136 4258 3479 4497 4184 4555 4104 4481 4253 4889 0 949
Sub-contracted not greater than total Validation Passed
1st OP
Provider Level
RDEEAST SUFFOLK AND NORTH
ESSEX NHS FOUNDATION TRUST
RGRWEST SUFFOLK NHS
FOUNDATION TRUST
Provider Level
RDEEAST SUFFOLK AND NORTH
ESSEX NHS FOUNDATION TRUST
RGRWEST SUFFOLK NHS
FOUNDATION TRUST
Provider LevelEAST SUFFOLK AND NORTH
ESSEX NHS FOUNDATION TRUST
WEST SUFFOLK NHS FOUNDATION TRUST
OP Transformation
ICS Code ICS Name
Sub categories not greater than total Validation Passed
No non-numeric, negative, or decimal values Validation Passed
QJG SUFFOLK AND NORTH EAST ESSEX ICS
Data Validation TestsAll Required Cells Populated Validation Passed
Total OPOP
Transformation 1st OP FU OP Electives Referrals
Validation PassedNo special characters in comments
A&E 1-4
EAST SUFFOLK AND NORTH ESSEX NHS FOUNDATION
TRUSTRDE
Non-Electives DiagnosticsRTTRTT - Incomplete
pathways
WEST SUFFOLK NHS FOUNDATION TRUST
RGR
Provider Level
Total OP
FU OP
Counting and coding required cells populated Validation Passed
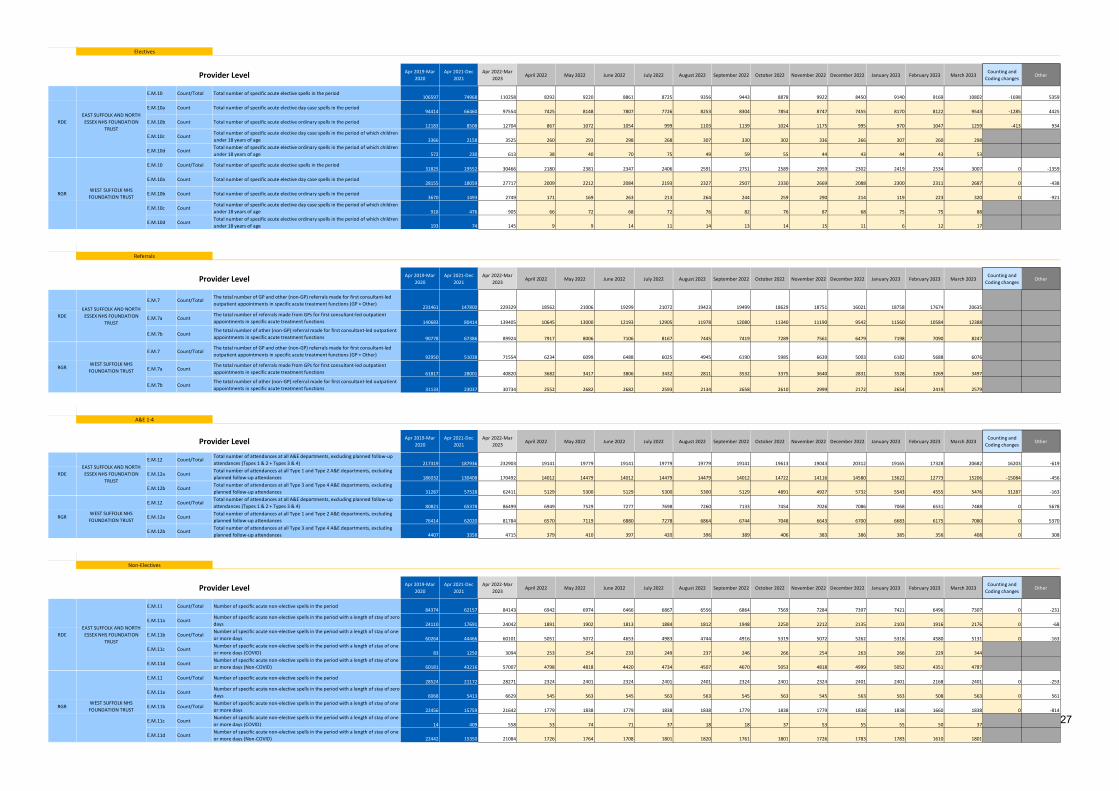
Page 7 of 27
Activity50 1 2 3 4 5 6 7 8 9 10 11
Apr 2019-Mar 2020
Apr 2021-Dec 2021
Apr 2022-Mar 2023
April 2022 May 2022 June 2022 July 2022 August 2022 September 2022 October 2022 November 2022 December 2022 January 2023 February 2023 March 2023Counting and
Coding changesOther
E.M.10 Count/Total Total number of specific acute elective spells in the period106597 74968 110258 8292 9220 8861 8725 9356 9443 8878 9922 8450 9140 9169 10802 -1698 5359
E.M.10a Count Total number of specific acute elective day case spells in the period94414 66460 97554 7425 8148 7807 7726 8253 8304 7854 8747 7455 8170 8122 9543 -1285 4425
E.M.10b Count Total number of specific acute elective ordinary spells in the period12183 8508 12704 867 1072 1054 999 1103 1139 1024 1175 995 970 1047 1259 -413 934
E.M.10c CountTotal number of specific acute elective day case spells in the period of which children under 18 years of age 3366 2158 3525 260 293 298 268 307 330 302 336 266 307 260 298
E.M.10d CountTotal number of specific acute elective ordinary spells in the period of which children under 18 years of age 572 230 613 38 40 70 75 49 59 55 44 43 44 43 53
E.M.10 Count/Total Total number of specific acute elective spells in the period31825 19552 30466 2180 2381 2347 2406 2591 2751 2589 2959 2302 2419 2534 3007 0 -1359
E.M.10a Count Total number of specific acute elective day case spells in the period28155 18059 27717 2009 2212 2084 2193 2327 2507 2330 2669 2088 2300 2311 2687 0 -438
E.M.10b Count Total number of specific acute elective ordinary spells in the period3670 1493 2749 171 169 263 213 264 244 259 290 214 119 223 320 0 -921
E.M.10c CountTotal number of specific acute elective day case spells in the period of which children under 18 years of age 918 476 905 66 72 68 72 76 82 76 87 68 75 75 88
E.M.10d CountTotal number of specific acute elective ordinary spells in the period of which children under 18 years of age 193 74 145 9 9 14 11 14 13 14 15 11 6 12 17
ActivityCategoryActivity8
0 1 2 3 4 5 6 7 8 9 10 11
Apr 2019-Mar 2020
Apr 2021-Dec 2021
Apr 2022-Mar 2023
April 2022 May 2022 June 2022 July 2022 August 2022 September 2022 October 2022 November 2022 December 2022 January 2023 February 2023 March 2023Counting and
Coding changesOther
E.M.7 Count/TotalThe total number of GP and other (non-GP) referrals made for first consultant-led outpatient appointments in specific acute treatment functions (GP + Other)
231461 147800 229329 18562 21006 19299 21072 19423 19499 18629 18751 16021 18758 17674 20635
E.M.7a CountThe total number of referrals made from GPs for first consultant-led outpatient appointments in specific acute treatment functions 140683 80414 139405 10645 13000 12193 12905 11978 12080 11340 11190 9542 11560 10584 12388
E.M.7b CountThe total number of other (non-GP) referral made for first consultant-led outpatient appointments in specific acute treatment functions 90778 67386 89924 7917 8006 7106 8167 7445 7419 7289 7561 6479 7198 7090 8247
E.M.7 Count/TotalThe total number of GP and other (non-GP) referrals made for first consultant-led outpatient appointments in specific acute treatment functions (GP + Other) 92950 51038 71554 6234 6099 6488 6025 4945 6190 5985 6639 5003 6182 5688 6076
E.M.7a CountThe total number of referrals made from GPs for first consultant-led outpatient appointments in specific acute treatment functions 61817 28001 40820 3682 3417 3806 3432 2811 3532 3375 3640 2831 3528 3269 3497
E.M.7b CountThe total number of other (non-GP) referral made for first consultant-led outpatient appointments in specific acute treatment functions 31133 23037 30734 2552 2682 2682 2593 2134 2658 2610 2999 2172 2654 2419 2579
ActivityCategoryActivity6
0 1 2 3 4 5 6 7 8 9 10 11
Apr 2019-Mar 2020
Apr 2021-Dec 2021
Apr 2022-Mar 2023
April 2022 May 2022 June 2022 July 2022 August 2022 September 2022 October 2022 November 2022 December 2022 January 2023 February 2023 March 2023Counting and
Coding changesOther
E.M.12 Count/TotalTotal number of attendances at all A&E departments, excluding planned follow-up attendances (Types 1 & 2 + Types 3 & 4) 217319 187936 232903 19141 19779 19141 19779 19779 19141 19613 19043 20312 19165 17328 20682 16203 -619
E.M.12a CountTotal number of attendances at all Type 1 and Type 2 A&E departments, excluding planned follow-up attendances 186032 130408 170492 14012 14479 14012 14479 14479 14012 14722 14116 14580 13622 12773 15206 -15084 -456
E.M.12b CountTotal number of attendances at all Type 3 and Type 4 A&E departments, excluding planned follow-up attendances 31287 57528 62411 5129 5300 5129 5300 5300 5129 4891 4927 5732 5543 4555 5476 31287 -163
E.M.12 Count/TotalTotal number of attendances at all A&E departments, excluding planned follow-up attendances (Types 1 & 2 + Types 3 & 4) 80821 65378 86499 6949 7529 7277 7698 7260 7133 7454 7026 7086 7068 6531 7488 0 5678
E.M.12a CountTotal number of attendances at all Type 1 and Type 2 A&E departments, excluding planned follow-up attendances 76414 62020 81784 6570 7119 6880 7278 6864 6744 7048 6643 6700 6683 6175 7080 0 5370
E.M.12b CountTotal number of attendances at all Type 3 and Type 4 A&E departments, excluding planned follow-up attendances 4407 3358 4715 379 410 397 420 396 389 406 383 386 385 356 408 0 308
ActivityCategoryActivity7
0 1 2 3 4 5 6 7 8 9 10 11
Apr 2019-Mar 2020
Apr 2021-Dec 2021
Apr 2022-Mar 2023
April 2022 May 2022 June 2022 July 2022 August 2022 September 2022 October 2022 November 2022 December 2022 January 2023 February 2023 March 2023Counting and
Coding changesOther
E.M.11 Count/Total Number of specific acute non-elective spells in the period84374 62157 84143 6942 6974 6466 6867 6556 6864 7569 7284 7397 7421 6496 7307 0 -231
E.M.11a CountNumber of specific acute non-elective spells in the period with a length of stay of zero days 24110 17691 24042 1891 1902 1813 1884 1812 1948 2250 2212 2135 2103 1916 2176 0 -68
E.M.11b Count/TotalNumber of specific acute non-elective spells in the period with a length of stay of one or more days 60264 44466 60101 5051 5072 4653 4983 4744 4916 5319 5072 5262 5318 4580 5131 0 -163
E.M.11c CountNumber of specific acute non-elective spells in the period with a length of stay of one or more days (COVID) 83 1250 3094 253 254 233 249 237 246 266 254 263 266 229 344
E.M.11d CountNumber of specific acute non-elective spells in the period with a length of stay of one or more days (Non-COVID) 60181 43216 57007 4798 4818 4420 4734 4507 4670 5053 4818 4999 5052 4351 4787
E.M.11 Count/Total Number of specific acute non-elective spells in the period28524 21172 28271 2324 2401 2324 2401 2401 2324 2401 2324 2401 2401 2168 2401 0 -253
E.M.11a CountNumber of specific acute non-elective spells in the period with a length of stay of zero days 6068 5413 6629 545 563 545 563 563 545 563 545 563 563 508 563 0 561
E.M.11b Count/TotalNumber of specific acute non-elective spells in the period with a length of stay of one or more days 22456 15759 21642 1779 1838 1779 1838 1838 1779 1838 1779 1838 1838 1660 1838 0 -814
E.M.11c CountNumber of specific acute non-elective spells in the period with a length of stay of one or more days (COVID) 14 409 558 53 74 71 37 18 18 37 53 55 55 50 37
E.M.11d CountNumber of specific acute non-elective spells in the period with a length of stay of one or more days (Non-COVID) 22442 15350 21084 1726 1764 1708 1801 1820 1761 1801 1726 1783 1783 1610 1801
Referrals
Provider Level
WEST SUFFOLK NHS FOUNDATION TRUST
Provider Level
RDEEAST SUFFOLK AND NORTH
ESSEX NHS FOUNDATION TRUST
RGRWEST SUFFOLK NHS
FOUNDATION TRUST
Non-Electives
RGR
RDEEAST SUFFOLK AND NORTH
ESSEX NHS FOUNDATION TRUST
RDEEAST SUFFOLK AND NORTH
ESSEX NHS FOUNDATION TRUST
A&E 1-4
WEST SUFFOLK NHS FOUNDATION TRUST
Provider Level
RGR
EAST SUFFOLK AND NORTH ESSEX NHS FOUNDATION
TRUST
WEST SUFFOLK NHS FOUNDATION TRUST
Provider Level
RGR
RDE
Electives
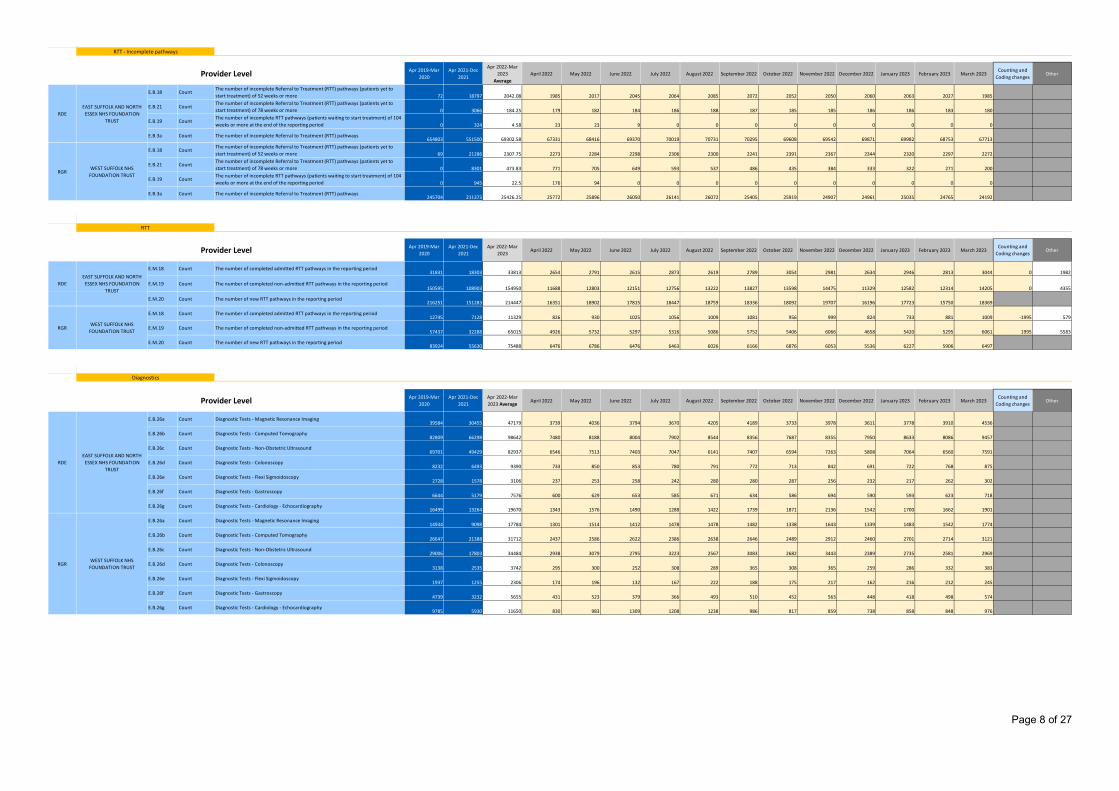
Page 8 of 27
Activity130 1 2 3 4 5 6 7 8 9 10 11
Apr 2019-Mar 2020
Apr 2021-Dec 2021
Apr 2022-Mar 2023
AverageApril 2022 May 2022 June 2022 July 2022 August 2022 September 2022 October 2022 November 2022 December 2022 January 2023 February 2023 March 2023
Counting and Coding changes
Other
E.B.18 CountThe number of incomplete Referral to Treatment (RTT) pathways (patients yet to start treatment) of 52 weeks or more 72 18797 2042.08 1985 2017 2045 2064 2085 2072 2052 2050 2060 2063 2027 1985
E.B.21 CountThe number of incomplete Referral to Treatment (RTT) pathways (patients yet to start treatment) of 78 weeks or more 0 3066 184.25 179 182 184 186 188 187 185 185 186 186 183 180
E.B.19 CountThe number of incomplete RTT pathways (patients waiting to start treatment) of 104 weeks or more at the end of the reporting period 0 324 4.58 23 23 9 0 0 0 0 0 0 0 0 0
E.B.3a Count The number of incomplete Referral to Treatment (RTT) pathways654803 551500 69302.58 67331 68416 69370 70019 70731 70295 69608 69542 69871 69982 68753 67713
E.B.18 CountThe number of incomplete Referral to Treatment (RTT) pathways (patients yet to start treatment) of 52 weeks or more 69 21286 2307.75 2273 2284 2298 2306 2300 2241 2391 2367 2344 2320 2297 2272
E.B.21 CountThe number of incomplete Referral to Treatment (RTT) pathways (patients yet to start treatment) of 78 weeks or more 0 8301 473.83 771 705 649 593 537 486 435 384 333 322 271 200
E.B.19 CountThe number of incomplete RTT pathways (patients waiting to start treatment) of 104 weeks or more at the end of the reporting period 0 945 22.5 176 94 0 0 0 0 0 0 0 0 0 0
E.B.3a Count The number of incomplete Referral to Treatment (RTT) pathways245704 211373 25426.25 25772 25896 26050 26141 26072 25405 25919 24907 24961 25035 24765 24192
ActivityCategoryActivity12
0 1 2 3 4 5 6 7 8 9 10 11
Apr 2019-Mar 2020
Apr 2021-Dec 2021
Apr 2022-Mar 2023
April 2022 May 2022 June 2022 July 2022 August 2022 September 2022 October 2022 November 2022 December 2022 January 2023 February 2023 March 2023Counting and
Coding changesOther
E.M.18 Count The number of completed admitted RTT pathways in the reporting period31831 18303 33813 2654 2791 2615 2873 2619 2789 3054 2981 2634 2946 2813 3044 0 1982
E.M.19 Count The number of completed non-admitted RTT pathways in the reporting period150595 108903 154950 11688 12803 12151 12756 13222 13827 13598 14475 11329 12582 12314 14205 0 4355
E.M.20 Count The number of new RTT pathways in the reporting period216251 151283 214447 16351 18902 17815 18447 18759 18336 18092 19707 16196 17723 15750 18369
E.M.18 Count The number of completed admitted RTT pathways in the reporting period12745 7128 11329 826 930 1025 1056 1009 1081 956 999 824 733 881 1009 -1995 579
E.M.19 Count The number of completed non-admitted RTT pathways in the reporting period57437 32288 65015 4926 5732 5297 5316 5086 5752 5406 6066 4658 5420 5295 6061 1995 5583
E.M.20 Count The number of new RTT pathways in the reporting period83924 55630 75488 6476 6786 6476 6463 6026 6166 6876 6053 5536 6227 5906 6497
ActivityCategoryActivity9
0 1 2 3 4 5 6 7 8 9 10 11
Apr 2019-Mar 2020
Apr 2021-Dec 2021
Apr 2022-Mar 2023 Average
April 2022 May 2022 June 2022 July 2022 August 2022 September 2022 October 2022 November 2022 December 2022 January 2023 February 2023 March 2023Counting and
Coding changesOther
E.B.26a Count Diagnostic Tests - Magnetic Resonance Imaging39584 30455 47179 3739 4036 3794 3670 4205 4189 3733 3978 3611 3778 3910 4536
E.B.26b Count Diagnostic Tests - Computed Tomography82809 66298 98642 7480 8188 8004 7902 8544 8356 7687 8355 7950 8633 8086 9457
E.B.26c Count Diagnostic Tests - Non-Obstetric Ultrasound69701 49429 82937 6546 7513 7403 7047 6141 7407 6594 7263 5808 7064 6560 7591
E.B.26d Count Diagnostic Tests - Colonoscopy8232 6493 9390 733 850 853 780 791 772 713 842 691 722 768 875
E.B.26e Count Diagnostic Tests - Flexi Sigmoidoscopy2728 1578 3106 237 253 258 242 280 280 287 256 232 217 262 302
E.B.26f Count Diagnostic Tests - Gastroscopy6644 5179 7576 600 629 653 585 671 634 586 694 590 593 623 718
E.B.26g Count Diagnostic Tests - Cardiology - Echocardiography16499 13264 19670 1343 1576 1490 1288 1422 1739 1871 2136 1542 1700 1662 1901
E.B.26a Count Diagnostic Tests - Magnetic Resonance Imaging14934 9098 17784 1301 1514 1412 1478 1478 1482 1338 1643 1339 1483 1542 1774
E.B.26b Count Diagnostic Tests - Computed Tomography26647 21388 31712 2437 2586 2622 2386 2638 2646 2489 2912 2460 2701 2714 3121
E.B.26c Count Diagnostic Tests - Non-Obstetric Ultrasound29006 17803 34484 2938 3079 2795 3223 2567 3083 2682 3443 2389 2735 2581 2969
E.B.26d Count Diagnostic Tests - Colonoscopy3138 2535 3742 295 300 252 308 289 365 308 365 259 286 332 383
E.B.26e Count Diagnostic Tests - Flexi Sigmoidoscopy1937 1255 2306 174 196 132 167 222 188 175 217 162 216 212 245
E.B.26f Count Diagnostic Tests - Gastroscopy4739 3232 5655 431 523 379 366 493 510 452 563 448 418 498 574
E.B.26g Count Diagnostic Tests - Cardiology - Echocardiography9785 5930 11650 830 983 1309 1208 1238 986 817 859 738 858 848 976
RDEEAST SUFFOLK AND NORTH
ESSEX NHS FOUNDATION TRUST
RGRWEST SUFFOLK NHS
FOUNDATION TRUST
Diagnostics
Provider Level
RTT - Incomplete pathways
Provider Level
RTT
Provider Level
RDEEAST SUFFOLK AND NORTH
ESSEX NHS FOUNDATION TRUST
RGRWEST SUFFOLK NHS
FOUNDATION TRUST
RDEEAST SUFFOLK AND NORTH
ESSEX NHS FOUNDATION TRUST
RGRWEST SUFFOLK NHS
FOUNDATION TRUST
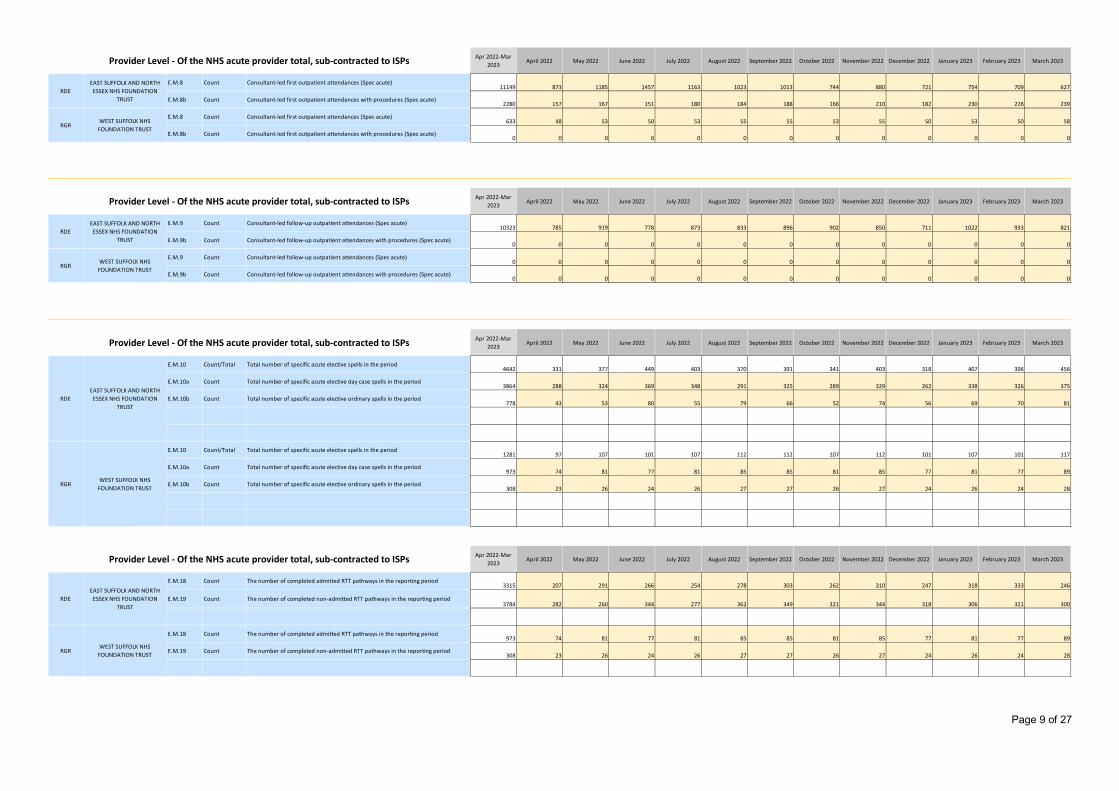
Page 9 of 27
Apr 2022-Mar 2023
April 2022 May 2022 June 2022 July 2022 August 2022 September 2022 October 2022 November 2022 December 2022 January 2023 February 2023 March 2023
E.M.8 Count Consultant-led first outpatient attendances (Spec acute)11149 873 1185 1457 1163 1023 1013 744 880 721 754 709 627
E.M.8b Count Consultant-led first outpatient attendances with procedures (Spec acute)2280 157 167 151 180 184 188 166 210 182 230 226 239
E.M.8 Count Consultant-led first outpatient attendances (Spec acute)633 48 53 50 53 55 55 53 55 50 53 50 58
E.M.8b Count Consultant-led first outpatient attendances with procedures (Spec acute)0 0 0 0 0 0 0 0 0 0 0 0 0
Apr 2022-Mar 2023
April 2022 May 2022 June 2022 July 2022 August 2022 September 2022 October 2022 November 2022 December 2022 January 2023 February 2023 March 2023
E.M.9 Count Consultant-led follow-up outpatient attendances (Spec acute)10323 785 919 778 873 833 896 902 850 711 1022 933 821
E.M.9b Count Consultant-led follow-up outpatient attendances with procedures (Spec acute)0 0 0 0 0 0 0 0 0 0 0 0 0
E.M.9 Count Consultant-led follow-up outpatient attendances (Spec acute)0 0 0 0 0 0 0 0 0 0 0 0 0
E.M.9b Count Consultant-led follow-up outpatient attendances with procedures (Spec acute)0 0 0 0 0 0 0 0 0 0 0 0 0
Apr 2022-Mar 2023
April 2022 May 2022 June 2022 July 2022 August 2022 September 2022 October 2022 November 2022 December 2022 January 2023 February 2023 March 2023
E.M.10 Count/Total Total number of specific acute elective spells in the period4642 331 377 449 403 370 391 341 403 318 407 396 456
E.M.10a Count Total number of specific acute elective day case spells in the period3864 288 324 369 348 291 325 289 329 262 338 326 375
E.M.10b Count Total number of specific acute elective ordinary spells in the period778 43 53 80 55 79 66 52 74 56 69 70 81
E.M.10 Count/Total Total number of specific acute elective spells in the period1281 97 107 101 107 112 112 107 112 101 107 101 117
E.M.10a Count Total number of specific acute elective day case spells in the period973 74 81 77 81 85 85 81 85 77 81 77 89
E.M.10b Count Total number of specific acute elective ordinary spells in the period308 23 26 24 26 27 27 26 27 24 26 24 28
RDE
RGRWEST SUFFOLK NHS
FOUNDATION TRUST
EAST SUFFOLK AND NORTH ESSEX NHS FOUNDATION
TRUST
RGRWEST SUFFOLK NHS
FOUNDATION TRUST
Provider Level - Of the NHS acute provider total, sub-contracted to ISPs
Provider Level - Of the NHS acute provider total, sub-contracted to ISPs
RDEEAST SUFFOLK AND NORTH
ESSEX NHS FOUNDATION TRUST
Provider Level - Of the NHS acute provider total, sub-contracted to ISPs
RDEEAST SUFFOLK AND NORTH
ESSEX NHS FOUNDATION TRUST
RGRWEST SUFFOLK NHS
FOUNDATION TRUST
Apr 2022-Mar 2023
April 2022 May 2022 June 2022 July 2022 August 2022 September 2022 October 2022 November 2022 December 2022 January 2023 February 2023 March 2023
E.M.18 Count The number of completed admitted RTT pathways in the reporting period3315 207 291 266 254 278 303 262 310 247 318 333 246
E.M.19 Count The number of completed non-admitted RTT pathways in the reporting period3784 282 260 344 277 362 349 321 344 318 306 321 300
E.M.18 Count The number of completed admitted RTT pathways in the reporting period973 74 81 77 81 85 85 81 85 77 81 77 89
E.M.19 Count The number of completed non-admitted RTT pathways in the reporting period308 23 26 24 26 27 27 26 27 24 26 24 28
RGRWEST SUFFOLK NHS
FOUNDATION TRUST
Provider Level - Of the NHS acute provider total, sub-contracted to ISPs
RDEEAST SUFFOLK AND NORTH
ESSEX NHS FOUNDATION TRUST
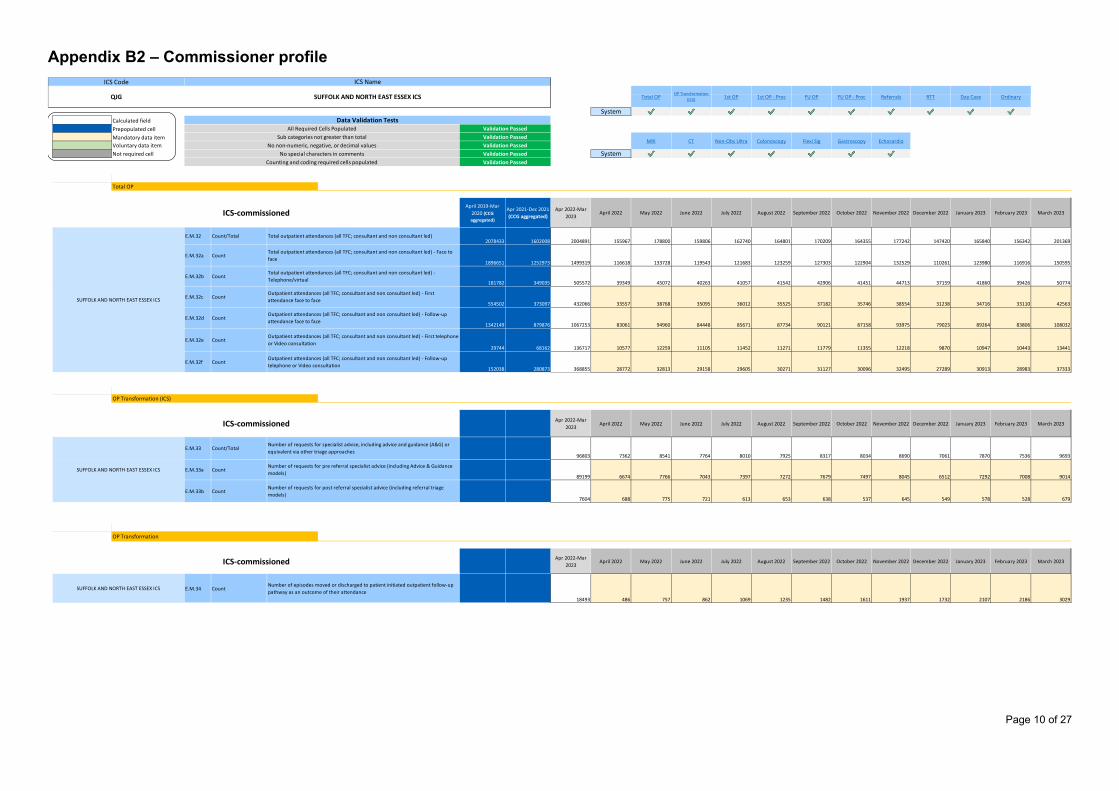
Page 10 of 27
Appendix B2 – Commissioner profile $H$16 $H$29 $H$49 $H$70 $H$82 $H$103 $H$160 $H$169 $H$118 $H$139
SystemCalculated field AlignMeasure7 AlignMeasure8 AlignMeasure9 AlignMeasure10AlignMeasure11AlignMeasure12AlignMeasure13Prepopulated cell $H$177 $H$188 $H$199 $H$210 $H$221 $H$232 $H$243Mandatory data itemVoluntary data itemNot required cell System
ActivityCategoryToActivity1
0 1 2 3 4 5 6 7 8 9 10 5
April 2019-Mar 2020 (CCG aggregated)
Apr 2021-Dec 2021 (CCG aggregated)
Apr 2022-Mar 2023
April 2022 May 2022 June 2022 July 2022 August 2022 September 2022 October 2022 November 2022 December 2022 January 2023 February 2023 March 2023
I QE.M.32 Count/Total
2078433 1602008 2004891 155967 178800 159806 162740 164801 170209 164355 177242 147420 165840 156342 201369
I QE.M.32a Count
1896651 1252973 1499319 116618 133728 119543 121683 123259 127303 122904 132529 110261 123980 116916 150595
I QE.M.32b Count
181782 349035 505572 39349 45072 40263 41057 41542 42906 41451 44713 37159 41860 39426 50774
I QE.M.32c Count
554502 373097 432066 33557 38768 35095 36012 35525 37182 35746 38554 31238 34716 33110 42563
I QE.M.32d Count
1342149 879876 1067253 83061 94960 84448 85671 87734 90121 87158 93975 79023 89264 83806 108032
I QE.M.32e Count
29744 68162 136717 10577 12259 11105 11452 11271 11779 11355 12218 9870 10947 10443 13441
I QE.M.32f Count
152038 280873 368855 28772 32813 29158 29605 30271 31127 30096 32495 27289 30913 28983 37333
ActivityCategoryToActivity11
0 1 2 3 4 5 6 7 8 9 10 5
Apr 2022-Mar 2023
April 2022 May 2022 June 2022 July 2022 August 2022 September 2022 October 2022 November 2022 December 2022 January 2023 February 2023 March 2023
I QE.M.33 Count/Total
96803 7362 8541 7764 8010 7925 8317 8034 8690 7061 7870 7536 9693
I QE.M.33a Count
89199 6674 7766 7043 7397 7272 7679 7497 8045 6512 7292 7008 9014
I QE.M.33b Count
7604 688 775 721 613 653 638 537 645 549 578 528 679
ActivityCategory
Activity20 1 2 3 4 5 6 7 8 9 10 5
Apr 2022-Mar 2023
April 2022 May 2022 June 2022 July 2022 August 2022 September 2022 October 2022 November 2022 December 2022 January 2023 February 2023 March 2023
I Q
E.M.34 Count
18493 486 757 862 1069 1235 1482 1611 1937 1732 2107 2186 3029
Ordinary
Non-Obs Ultra
Counting and coding required cells populated
Outpatient attendances (all TFC; consultant and non consultant led) - Follow-up telephone or Video consultation
OP Transformation (ICS)
ICS-commissioned
SUFFOLK AND NORTH EAST ESSEX ICS
SUFFOLK AND NORTH EAST ESSEX ICS
OP Transformation
ICS-commissioned
Number of requests for post referral specialist advice (including referral triage models)
MRI
Outpatient attendances (all TFC; consultant and non consultant led) - First telephone or Video consultation
No special characters in commentsValidation PassedValidation Passed
Total outpatient attendances (all TFC; consultant and non consultant led)
Number of requests for specialist advice, including advice and guidance (A&G) or equivalent via other triage approaches
Number of requests for pre referral specialist advice (including Advice & Guidance models)
All Required Cells PopulatedSub categories not greater than total
Validation PassedValidation Passed
SUFFOLK AND NORTH EAST ESSEX ICS
Data Validation Tests
No non-numeric, negative, or decimal valuesCT
Number of episodes moved or discharged to patient initiated outpatient follow-up pathway as an outcome of their attendance
ICS Code ICS Name
QJG SUFFOLK AND NORTH EAST ESSEX ICS Total OP 1st OP 1st OP - Proc FU OPOP Transformation
(ICS) FU OP - Proc Referrals RTT Day Case
Echocardio
Total outpatient attendances (all TFC; consultant and non consultant led) - Telephone/virtual
Outpatient attendances (all TFC; consultant and non consultant led) - First attendance face to face
Outpatient attendances (all TFC; consultant and non consultant led) - Follow-up attendance face to face
Total OP
ICS-commissioned
GastroscopyFlexi Sig
Total outpatient attendances (all TFC; consultant and non consultant led) - Face to face
Colonoscopy
Validation Passed
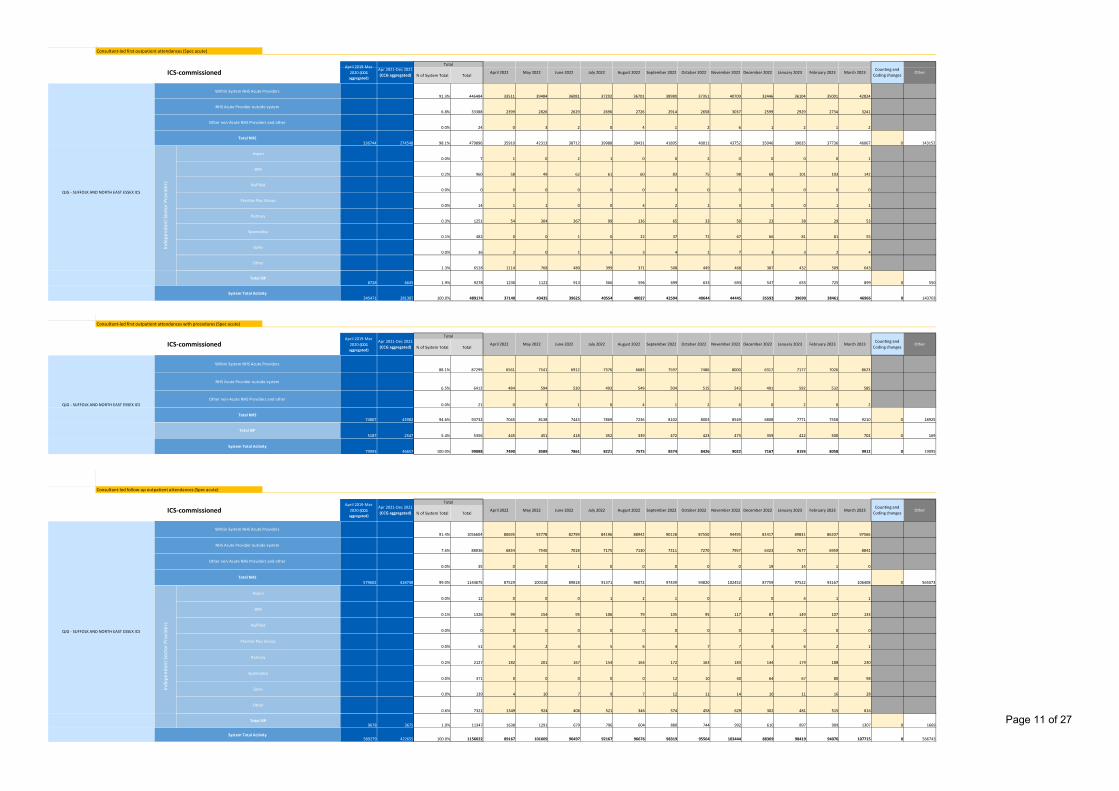
Page 11 of 27
AlignMeasure11095 1096 1097 1098 1099 1100 1101 1102 1103 1104 1105 1106
% of System Total Total
91.3% 446484 33511 39484 36081 37292 36701 38980 37351 40709 32446 36104 35001 42824
6.8% 33388 2399 2826 2629 2696 2726 2914 2658 3037 2599 2929 2734 3241
0.0% 24 0 3 2 0 4 1 2 6 1 2 1 2
336744 274548 98.1% 479896 35910 42313 38712 39988 39431 41895 40011 43752 35046 39035 37736 46067 0 143152
0.0% 7 1 0 2 1 0 0 2 0 0 0 0 1
0.2% 960 58 49 62 61 60 83 75 98 68 101 103 142
0.0% 0 0 0 0 0 0 0 0 0 0 0 0 0
0.0% 14 1 1 0 0 4 2 1 3 0 0 1 1
0.3% 1251 54 304 367 99 136 65 33 50 23 38 29 53
0.1% 482 0 0 1 0 22 37 72 67 66 81 81 55
0.0% 36 2 0 1 6 3 4 1 7 3 3 2 4
1.3% 6528 1114 768 480 399 371 508 449 468 387 432 509 643
8728 6645 1.9% 9278 1230 1122 913 566 596 699 633 693 547 655 725 899 0 550
345471 281387 100.0% 489174 37140 43435 39625 40554 40027 42594 40644 44445 35593 39690 38461 46966 0 143703
E.M.8b MeasureNameAlignMeasure2
1095 1096 1097 1098 1099 1100 1101 1102 1103 1104 1105 1106
% of System Total Total
88.1% 87299 6561 7541 6912 7376 6683 7597 7486 8000 6317 7177 7026 8623
6.5% 6412 484 594 530 493 549 504 515 543 491 592 532 585
0.0% 21 0 3 1 0 4 1 2 6 0 2 0 2
74807 43982 94.6% 93732 7045 8138 7443 7869 7236 8102 8003 8549 6808 7771 7558 9210 0 18925
5187 2547 5.4% 5356 445 451 418 352 339 472 423 473 359 422 500 702 0 169
79993 46657 100.0% 99088 7490 8589 7861 8221 7575 8574 8426 9022 7167 8193 8058 9912 0 19095
E.M.9 MeasureName
AlignMeasure31095 1096 1097 1098 1099 1100 1101 1102 1103 1104 1105 1106
% of System Total Total
91.4% 1056604 80695 92778 82799 84196 88942 90128 87550 94495 81417 89831 86207 97566
7.6% 88036 6834 7540 7018 7175 7130 7311 7270 7957 6323 7677 6959 8842
0.0% 35 0 0 1 0 0 0 0 0 19 14 1 0
579602 418748 99.0% 1144675 87529 100318 89818 91371 96072 97439 94820 102452 87759 97522 93167 106408 0 565073
0.0% 12 0 0 0 1 2 1 0 2 0 4 1 1
0.1% 1326 99 154 95 106 79 105 95 117 87 149 107 133
0.0% 0 0 0 0 0 0 0 0 0 0 0 0 0
0.0% 51 4 2 4 5 6 4 7 7 3 6 2 1
0.2% 2127 182 201 167 154 164 172 163 183 144 179 188 230
0.0% 371 0 0 0 0 0 12 10 40 64 67 80 98
0.0% 139 4 10 7 9 7 12 11 14 10 11 16 28
0.6% 7321 1349 924 406 521 346 574 458 629 302 481 515 816
9678 3675 1.0% 11347 1638 1291 679 796 604 880 744 992 610 897 909 1307 0 1669
589279 422655 100.0% 1156022 89167 101609 90497 92167 96676 98319 95564 103444 88369 98419 94076 107715 0 566743
Total ISP
System Total Activity
Other
Total ISP
System Total Activity
Ramsay
Spamedica
Spire
QJG - SUFFOLK AND NORTH EAST ESSEX ICS
Total ISP
ICS-commissionedApril 2019-Mar
2020 (CCG aggregated)
System Total Activity
Consultant-led follow-up outpatient attendances (Spec acute)
QJG - SUFFOLK AND NORTH EAST ESSEX ICS
Within System NHS Acute Providers
Counting and Coding changes
November 2022 December 2022 January 2023 February 2023 March 2023
Other
Total
October 2022Counting and
Coding changesOther
Counting and Coding changes
Other
Consultant-led first outpatient attendances (Spec acute)
QJG - SUFFOLK AND NORTH EAST ESSEX ICS
Within System NHS Acute Providers
Inde
pend
ent S
ecto
r Pro
vide
rs
Aspen
BMI
Nuffield
Practice Plus Group
Total NHS
Practice Plus Group
Ramsay
Spamedica
Spire
Other
BMI
Nuffield
NHS Acute Provider outside system
Inde
pend
ent S
ecto
r Pro
vide
rs
Consultant-led first outpatient attendances with procedures (Spec acute)
Within System NHS Acute Providers
NHS Acute Provider outside system
Other non-Acute NHS Providers and other
Apr 2021-Dec 2021 (CCG aggregated)
Other non-Acute NHS Providers and other
Total NHS
NHS Acute Provider outside system
Other non-Acute NHS Providers and other
Total NHS
July 2022 August 2022
Aspen
April 2022 May 2022 June 2022 November 2022 December 2022ICS-commissionedApril 2019-Mar
2020 (CCG aggregated)
September 2022 October 2022 January 2023 February 2023 March 2023
September 2022ICS-commissionedApril 2019-Mar
2020 (CCG aggregated)
Apr 2021-Dec 2021 (CCG aggregated)
Total
April 2022 May 2022 June 2022 July 2022 August 2022
Apr 2021-Dec 2021 (CCG aggregated)
Total
April 2022 May 2022 June 2022 July 2022 August 2022 September 2022 October 2022 November 2022 December 2022 January 2023 February 2023 March 2023
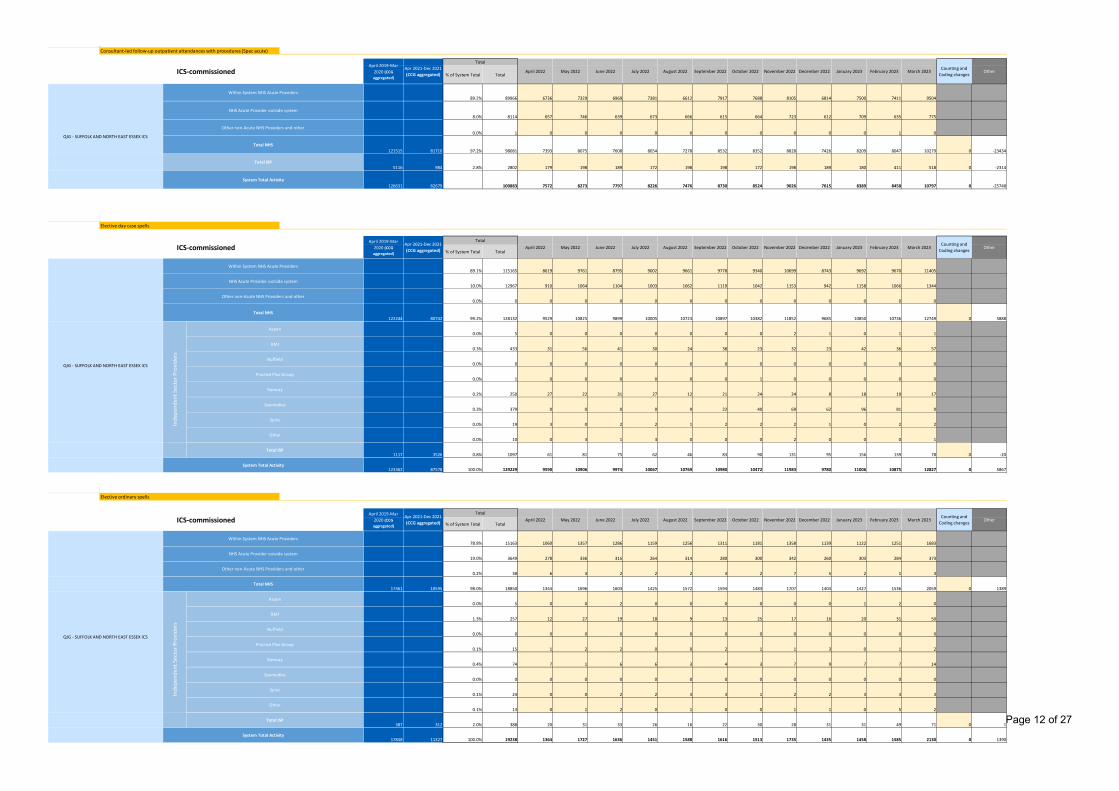
Page 12 of 27
AlignMeasure41095 1096 1097 1098 1099 1100 1101 1102 1103 1104 1105 1106
% of System Total Total
89.2% 89966 6736 7329 6969 7381 6612 7917 7688 8105 6814 7500 7411 9504
8.0% 8114 657 746 639 673 666 615 664 723 612 709 635 775
0.0% 1 0 0 0 0 0 0 0 0 0 0 1 0
121515 81710 97.2% 98081 7393 8075 7608 8054 7278 8532 8352 8828 7426 8209 8047 10279 0 -23434
5116 984 2.8% 2802 179 198 189 172 198 198 172 198 189 180 411 518 0 -2314
126631 82679 100883 7572 8273 7797 8226 7476 8730 8524 9026 7615 8389 8458 10797 0 -25748
E.M.10a MeasureNameAlignMeasure5
1095 1096 1097 1098 1099 1100 1101 1102 1103 1104 1105 1106
% of System Total Total
89.1% 115165 8619 9761 8795 9002 9661 9778 9340 10699 8743 9692 9670 11405
10.0% 12967 910 1064 1104 1003 1062 1119 1042 1153 942 1158 1066 1344
0.0% 0 0 0 0 0 0 0 0 0 0 0 0 0
122244 80742 99.2% 128132 9529 10825 9899 10005 10723 10897 10382 11852 9685 10850 10736 12749 0 5888
0.0% 5 0 0 0 0 0 0 0 2 1 0 1 1
0.3% 433 31 56 41 30 24 38 23 32 23 42 36 57
0.0% 0 0 0 0 0 0 0 0 0 0 0 0 0
0.0% 1 0 0 0 0 0 0 1 0 0 0 0 0
0.2% 250 27 22 31 27 12 21 24 24 8 18 19 17
0.3% 379 0 0 0 0 9 22 40 69 62 96 81 0
0.0% 19 3 0 2 2 1 2 2 2 1 0 2 2
0.0% 10 0 3 1 3 0 0 0 2 0 0 0 1
1117 3526 0.8% 1097 61 81 75 62 46 83 90 131 95 156 139 78 0 -20
123362 87578 100.0% 129229 9590 10906 9974 10067 10769 10980 10472 11983 9780 11006 10875 12827 0 5867
E.M.10b MeasureNameAlignMeasure6
1095 1096 1097 1098 1099 1100 1101 1102 1103 1104 1105 1106
% of System Total Total
78.8% 15163 1060 1357 1286 1159 1256 1311 1181 1358 1139 1122 1251 1683
19.0% 3649 278 336 315 264 314 280 300 342 260 303 284 373
0.2% 38 6 3 2 2 2 3 2 7 5 2 1 3
17461 10595 98.0% 18850 1344 1696 1603 1425 1572 1594 1483 1707 1404 1427 1536 2059 0 1389
0.0% 5 0 0 2 0 0 0 0 0 0 1 2 0
1.3% 257 12 27 19 18 9 13 25 17 16 20 31 50
0.0% 0 0 0 0 0 0 0 0 0 0 0 0 0
0.1% 15 1 2 2 0 0 2 1 1 3 0 1 2
0.4% 74 7 1 6 6 3 4 3 7 9 7 7 14
0.0% 0 0 0 0 0 0 0 0 0 0 0 0 0
0.1% 24 0 0 2 2 3 3 1 2 2 3 3 3
0.1% 13 0 1 2 0 1 0 0 1 1 0 5 2
387 312 2.0% 388 20 31 33 26 16 22 30 28 31 31 49 71 0 1
17848 11327 100.0% 19238 1364 1727 1636 1451 1588 1616 1513 1735 1435 1458 1585 2130 0 1390
April 2019-Mar 2020 (CCG aggregated)
Other non-Acute NHS Providers and other
Consultant-led follow-up outpatient attendances with procedures (Spec acute)
ICS-commissioned July 2022 August 2022 September 2022
Counting and Coding changes
Other
Counting and Coding changes
Other
Counting and Coding changes
Other
October 2022 February 2023 March 2023
October 2022 November 2022
ICS-commissionedApril 2019-Mar
2020 (CCG aggregated)
Other
Total ISP
System Total Activity
ICS-commissionedApril 2019-Mar
2020 (CCG aggregated)
Total
Spire
Other
Total ISP
QJG - SUFFOLK AND NORTH EAST ESSEX ICS
Total NHS
Inde
pend
ent S
ecto
r Pro
vide
rs
Aspen
BMI
Nuffield
Ramsay
Spamedica
Spire
Total
Elective day case spells
System Total Activity
Total NHS
Inde
pend
ent S
ecto
r Pro
vide
rs
Aspen
BMI
Nuffield
Practice Plus Group
Ramsay
Spamedica
Practice Plus Group
Within System NHS Acute Providers
Total ISP
Apr 2021-Dec 2021 (CCG aggregated)
Total
April 2022
Elective ordinary spells
May 2022
NHS Acute Provider outside system
Other non-Acute NHS Providers and other
Within System NHS Acute Providers
NHS Acute Provider outside system
QJG - SUFFOLK AND NORTH EAST ESSEX ICS
Total NHS
System Total Activity
October 2022 November 2022 December 2022 January 2023 February 2023 March 2023
QJG - SUFFOLK AND NORTH EAST ESSEX ICS
Within System NHS Acute Providers
NHS Acute Provider outside system
Other non-Acute NHS Providers and other
Apr 2021-Dec 2021 (CCG aggregated)
April 2022 May 2022 June 2022 July 2022 August 2022 September 2022
August 2022 September 2022Apr 2021-Dec 2021 (CCG aggregated)
April 2022 May 2022 June 2022 July 2022
December 2022 January 2023 February 2023 March 2023
November 2022 December 2022 January 2023
June 2022
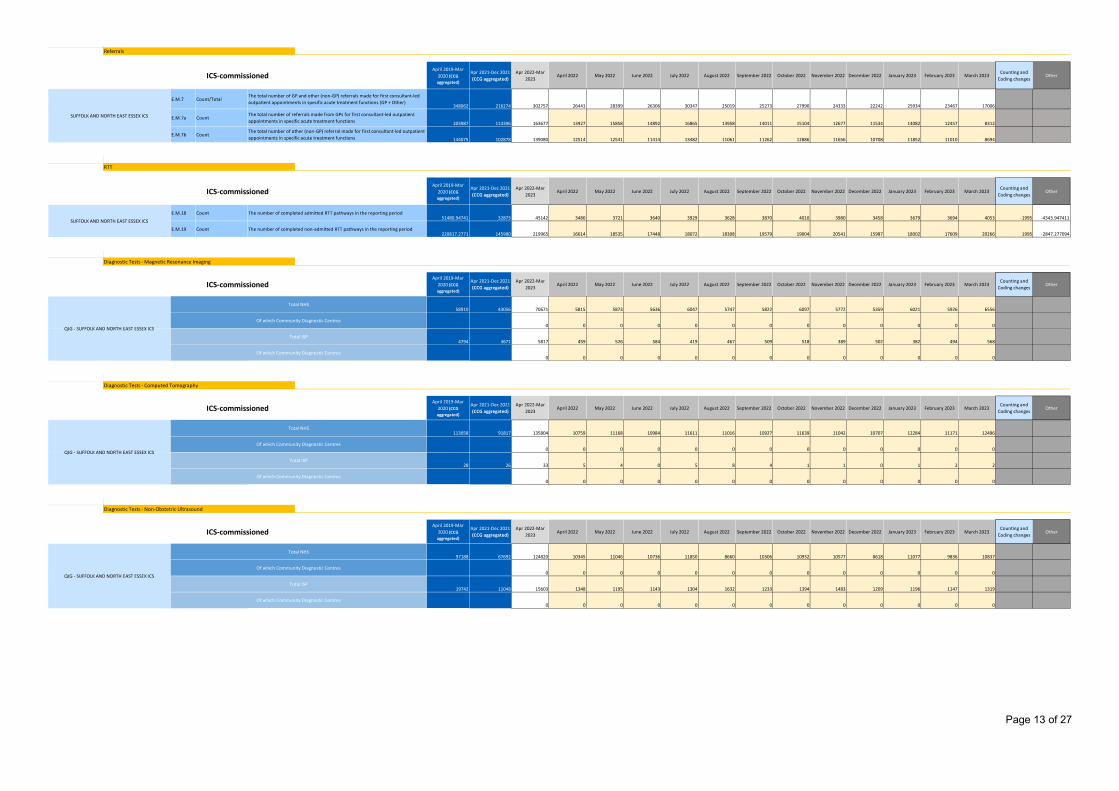
Page 13 of 27
Activity80 1 2 3 4 5 6 7 8 9 10 5
April 2019-Mar 2020 (CCG aggregated)
Apr 2021-Dec 2021 (CCG aggregated)
Apr 2022-Mar 2023
April 2022 May 2022 June 2022 July 2022 August 2022 September 2022 October 2022 November 2022 December 2022 January 2023 February 2023 March 2023Counting and
Coding changesOther
E.M.7 Count/Total348062 216274 302757 26441 28399 26306 30347 25019 25273 27990 24333 22242 25934 23467 17006
E.M.7a Count203987 113396 163677 13927 15858 14892 16865 13958 14011 15104 12677 11534 14082 12457 8312
E.M.7b Count144075 102878 139080 12514 12541 11414 13482 11061 11262 12886 11656 10708 11852 11010 8694
ActivityCategoryActivity12
0 1 2 3 4 5 6 7 8 9 10 5
April 2019-Mar 2020 (CCG aggregated)
Apr 2021-Dec 2021 (CCG aggregated)
Apr 2022-Mar 2023
April 2022 May 2022 June 2022 July 2022 August 2022 September 2022 October 2022 November 2022 December 2022 January 2023 February 2023 March 2023Counting and
Coding changesOther
E.M.18 Count51480.94741 32873 45142 3480 3721 3640 3929 3628 3870 4010 3980 3458 3679 3694 4053 -1995 -4343.947411
E.M.19 Count220817.2771 145980 219965 16614 18535 17448 18072 18308 19579 19004 20541 15987 18002 17609 20266 1995 -2847.277094
E.B.26a MeasureNameAlignMeasure7
1095 1096 1097 1098 1099 1100 1101 1102 1103 1104 1105 1106
58910 43056 70671 5815 5873 5636 6047 5747 5822 6097 5772 5359 6021 5926 6556
0 0 0 0 0 0 0 0 0 0 0 0 0
4794 3671 5817 459 526 584 419 467 509 518 389 502 382 494 568
0 0 0 0 0 0 0 0 0 0 0 0 0
E.B.26b MeasureNameAlignMeasure8
1095 1096 1097 1098 1099 1100 1101 1102 1103 1104 1105 1106
113058 91817 135804 10759 11168 10984 11611 11016 10927 11639 11042 10707 12284 11171 12496
0 0 0 0 0 0 0 0 0 0 0 0 0
28 26 33 5 4 0 5 8 4 1 1 0 1 2 2
0 0 0 0 0 0 0 0 0 0 0 0 0
E.B.26c MeasureNameAlignMeasure9
1095 1096 1097 1098 1099 1100 1101 1102 1103 1104 1105 1106
97188 67692 124820 10345 11046 10736 11850 8660 10306 10932 10577 8618 11077 9836 10837
0 0 0 0 0 0 0 0 0 0 0 0 0
19742 11048 15603 1348 1195 1143 1304 1632 1233 1394 1483 1209 1196 1147 1319
0 0 0 0 0 0 0 0 0 0 0 0 0
Counting and Coding changes
Counting and Coding changes
Other
Counting and Coding changes
Other
February 2023 March 2023
Of which Community Diagnostic Centres
Total NHS
ICS-commissioned
Of which Community Diagnostic Centres
Total ISP
Of which Community Diagnostic Centres
Diagnostic Tests - Computed Tomography
QJG - SUFFOLK AND NORTH EAST ESSEX ICS
Total NHS
Of which Community Diagnostic Centres
Total ISP
Referrals
Apr 2021-Dec 2021 (CCG aggregated)
April 2019-Mar 2020 (CCG aggregated)
Apr 2022-Mar 2023
ICS-commissioned
SUFFOLK AND NORTH EAST ESSEX ICS
The number of completed admitted RTT pathways in the reporting period
The number of completed non-admitted RTT pathways in the reporting period
RTT
QJG - SUFFOLK AND NORTH EAST ESSEX ICS
Diagnostic Tests - Magnetic Resonance Imaging
ICS-commissioned
ICS-commissioned
SUFFOLK AND NORTH EAST ESSEX ICS
The total number of GP and other (non-GP) referrals made for first consultant-led outpatient appointments in specific acute treatment functions (GP + Other)
The total number of referrals made from GPs for first consultant-led outpatient appointments in specific acute treatment functions
The total number of other (non-GP) referral made for first consultant-led outpatient appointments in specific acute treatment functions
August 2022 December 2022 January 2023 OtherSeptember 2022 October 2022
March 2023April 2019-Mar
2020 (CCG aggregated)
Apr 2021-Dec 2021 (CCG aggregated)
Apr 2022-Mar 2023
April 2022 May 2022 June 2022 July 2022 August 2022 September 2022
April 2022 May 2022 June 2022 July 2022 November 2022
ICS-commissionedApril 2019-Mar
2020 (CCG aggregated)
Apr 2021-Dec 2021 (CCG aggregated)
Apr 2022-Mar 2023
April 2022 May 2022 June 2022 July 2022 August 2022
Diagnostic Tests - Non-Obstetric Ultrasound
QJG - SUFFOLK AND NORTH EAST ESSEX ICS
Total NHS
Of which Community Diagnostic Centres
Total ISP
Of which Community Diagnostic Centres
September 2022 October 2022 November 2022 December 2022 January 2023 February 2023 March 2023
October 2022 November 2022 December 2022 January 2023 February 2023
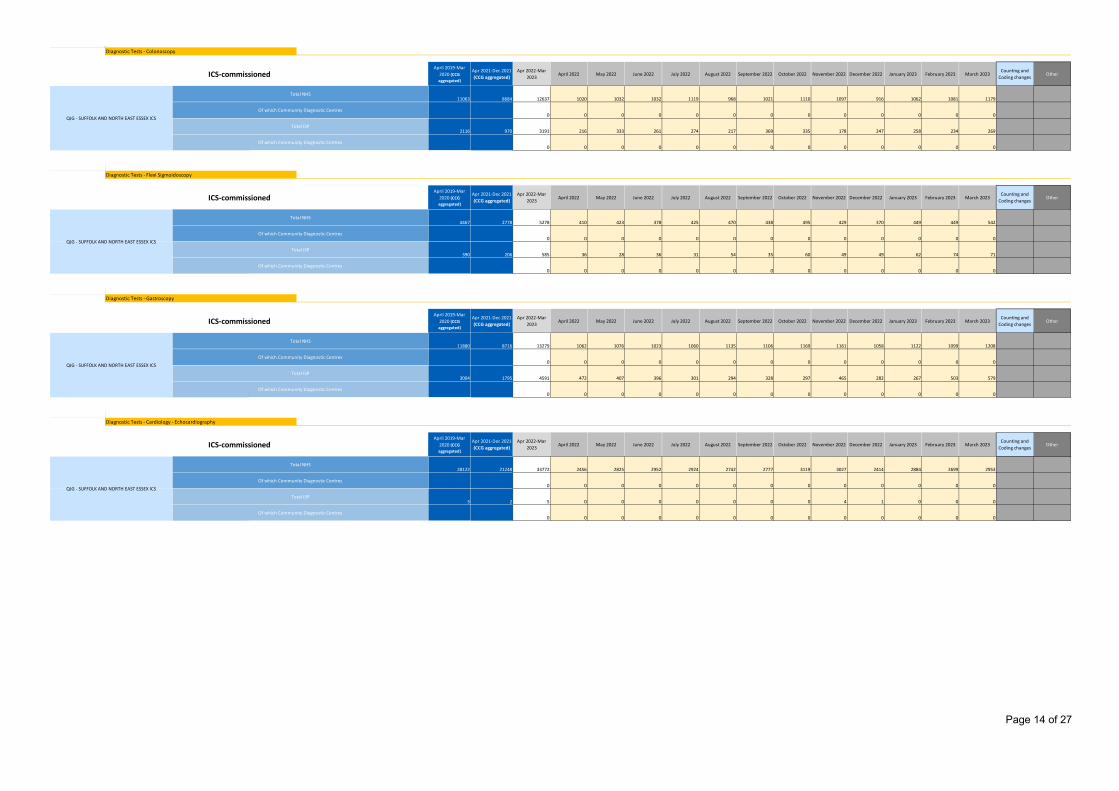
Page 14 of 27
AlignMeasure101095 1096 1097 1098 1099 1100 1101 1102 1103 1104 1105 1106
Q 11063 8684 12637 1020 1032 1032 1119 968 1021 1110 1097 916 1062 1081 1179
Q 0 0 0 0 0 0 0 0 0 0 0 0 0
Q 2116 970 3191 216 333 261 274 217 369 335 178 247 258 234 269
Q 0 0 0 0 0 0 0 0 0 0 0 0 0
E.B.26e MeasureNameAlignMeasure11
1095 1096 1097 1098 1099 1100 1101 1102 1103 1104 1105 1106
Q 4467 2778 5278 410 423 378 425 470 438 495 429 370 449 449 542
Q 0 0 0 0 0 0 0 0 0 0 0 0 0
Q 390 206 585 36 28 36 31 54 35 60 49 49 62 74 71
Q 0 0 0 0 0 0 0 0 0 0 0 0 0
E.B.26f MeasureNameAlignMeasure12
1095 1096 1097 1098 1099 1100 1101 1102 1103 1104 1105 1106
Q 11880 8716 13279 1062 1076 1023 1060 1135 1106 1169 1161 1058 1122 1099 1208
Q 0 0 0 0 0 0 0 0 0 0 0 0 0
Q 3004 1795 4591 472 407 396 301 294 328 297 465 282 267 503 579
Q 0 0 0 0 0 0 0 0 0 0 0 0 0
E.B.26g MeasureNameAlignMeasure13
1095 1096 1097 1098 1099 1100 1101 1102 1103 1104 1105 1106
Q 28122 21248 33772 2456 2825 2952 2924 2742 2777 3119 3027 2414 2884 2699 2953
Q 0 0 0 0 0 0 0 0 0 0 0 0 0
Q 3 2 5 0 0 0 0 0 0 0 4 1 0 0 0
Q 0 0 0 0 0 0 0 0 0 0 0 0 0
Counting and Coding changes
Other
Diagnostic Tests - Gastroscopy
QJG - SUFFOLK AND NORTH EAST ESSEX ICS
Total NHS
Of which Community Diagnostic Centres
Total ISP
Of which Community Diagnostic Centres
QJG - SUFFOLK AND NORTH EAST ESSEX ICS
Of which Community Diagnostic Centres
Of which Community Diagnostic Centres
ICS-commissioned
ICS-commissioned
Diagnostic Tests - Flexi Sigmoidoscopy
Of which Community Diagnostic Centres
QJG - SUFFOLK AND NORTH EAST ESSEX ICS
Total NHS
Of which Community Diagnostic Centres
Total ISP
QJG - SUFFOLK AND NORTH EAST ESSEX ICS
Diagnostic Tests - Colonoscopy
ICS-commissionedApril 2019-Mar
2020 (CCG aggregated)
Apr 2021-Dec 2021 (CCG aggregated)
Diagnostic Tests - Cardiology - Echocardiography
Total NHS
Total ISP
May 2022 July 2022 August 2022 November 2022 December 2022 January 2023June 2022Apr 2022-Mar
2023April 2022 September 2022 October 2022
March 2023
April 2019-Mar 2020 (CCG aggregated)
Apr 2021-Dec 2021 (CCG aggregated)
Apr 2022-Mar 2023
April 2022 May 2022 June 2022 July 2022 August 2022
April 2019-Mar 2020 (CCG aggregated)
Apr 2021-Dec 2021 (CCG aggregated)
Apr 2022-Mar 2023
April 2022 May 2022 June 2022 July 2022 August 2022 December 2022September 2022 October 2022 November 2022Counting and
Coding changesOther
December 2022 January 2023 February 2023 March 2023Counting and
Coding changesSeptember 2022 October 2022 OtherNovember 2022
January 2023 February 2023
Of which Community Diagnostic Centres
Total ISP
Of which Community Diagnostic Centres
Counting and Coding changes
Other
Total NHS
ICS-commissionedApril 2019-Mar
2020 (CCG aggregated)
Apr 2021-Dec 2021 (CCG aggregated)
Apr 2022-Mar 2023
April 2022 May 2022 June 2022 July 2022 August 2022 September 2022 October 2022 November 2022 December 2022 January 2023 February 2023 March 2023
February 2023 March 2023
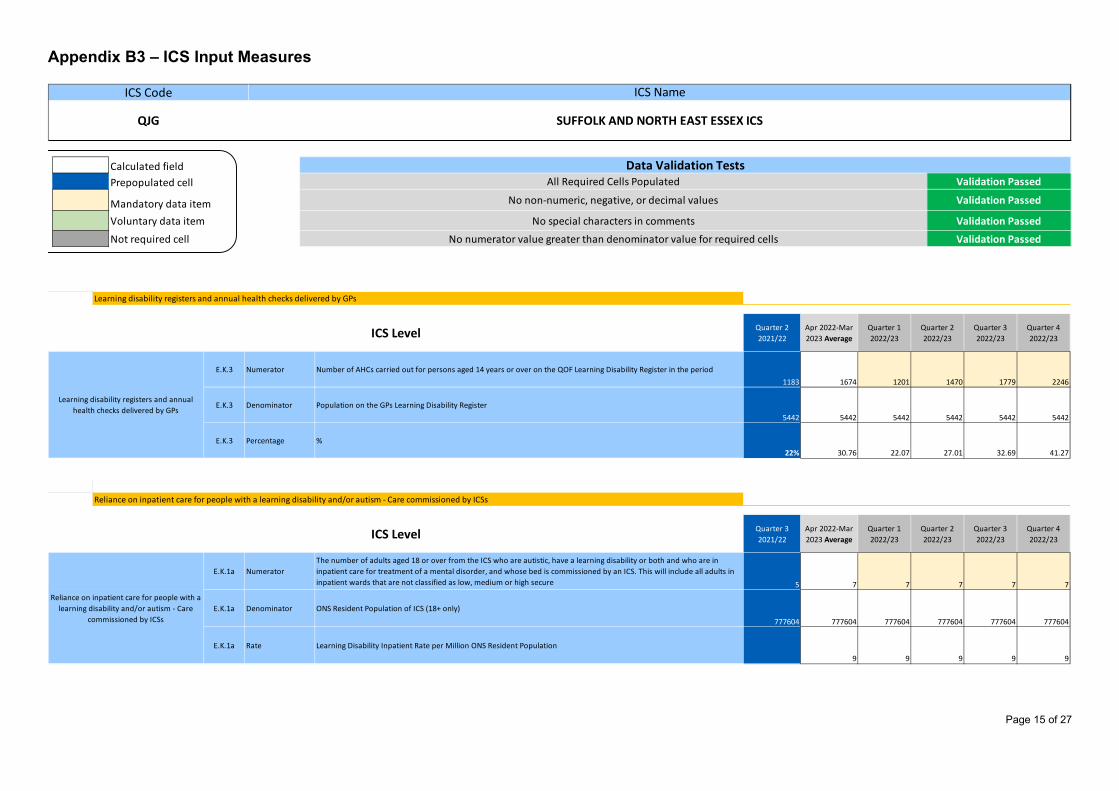
Page 15 of 27
Appendix B3 – ICS Input Measures
Calculated fieldPrepopulated cell
Mandatory data itemVoluntary data item
Not required cell
Validation Passed
Validation Passed
No non-numeric, negative, or decimal values Validation Passed
All Required Cells PopulatedData Validation Tests
ICS Code ICS Name
QJG SUFFOLK AND NORTH EAST ESSEX ICS
No special characters in comments
No numerator value greater than denominator value for required cells Validation Passed
ICSMeasure
PlanningRef 0 1 2 3
Quarter 2 2021/22
Apr 2022-Mar 2023 Average
Quarter 1 2022/23
Quarter 2 2022/23
Quarter 3 2022/23
Quarter 4 2022/23
E.K.3 Numerator Number of AHCs carried out for persons aged 14 years or over on the QOF Learning Disability Register in the period1183 1674 1201 1470 1779 2246
E.K.3 Denominator Population on the GPs Learning Disability Register5442 5442 5442 5442 5442 5442
E.K.3 Percentage %22% 30.76 22.07 27.01 32.69 41.27
MeasureNameICSMeasure
PlanningRef 0 1 2 3
Quarter 3 2021/22
Apr 2022-Mar 2023 Average
Quarter 1 2022/23
Quarter 2 2022/23
Quarter 3 2022/23
Quarter 4 2022/23
E.K.1a NumeratorThe number of adults aged 18 or over from the ICS who are autistic, have a learning disability or both and who are in inpatient care for treatment of a mental disorder, and whose bed is commissioned by an ICS. This will include all adults in inpatient wards that are not classified as low, medium or high secure 5 7 7 7 7 7
E.K.1a Denominator ONS Resident Population of ICS (18+ only)
777604 777604 777604 777604 777604 777604
E.K.1a Rate Learning Disability Inpatient Rate per Million ONS Resident Population 9 9 9 9 9
Reliance on inpatient care for people with a learning disability and/or autism - Care commissioned by ICSs
ICS Level
Reliance on inpatient care for people with a learning disability and/or autism - Care
commissioned by ICSs
Learning disability registers and annual health checks delivered by GPs
ICS Level
Learning disability registers and annual health checks delivered by GPs
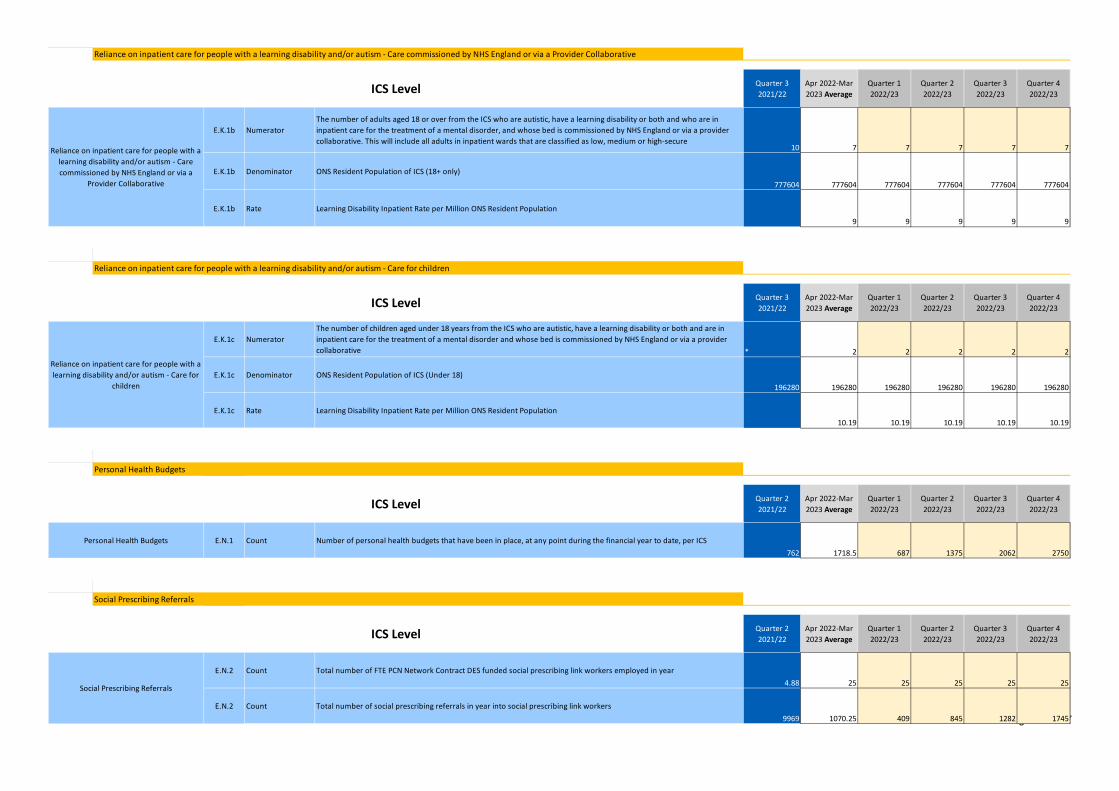
Page 16 of 27
ICSMeasurePlanningRef 0 1 2 3
Quarter 3 2021/22
Apr 2022-Mar 2023 Average
Quarter 1 2022/23
Quarter 2 2022/23
Quarter 3 2022/23
Quarter 4 2022/23
E.K.1b NumeratorThe number of adults aged 18 or over from the ICS who are autistic, have a learning disability or both and who are in inpatient care for the treatment of a mental disorder, and whose bed is commissioned by NHS England or via a provider collaborative. This will include all adults in inpatient wards that are classified as low, medium or high-secure
10 7 7 7 7 7
E.K.1b Denominator ONS Resident Population of ICS (18+ only)
777604 777604 777604 777604 777604 777604
E.K.1b Rate Learning Disability Inpatient Rate per Million ONS Resident Population 9 9 9 9 9
MeasureNameICSMeasure
PlanningRef 0 1 2 3
Quarter 3 2021/22
Apr 2022-Mar 2023 Average
Quarter 1 2022/23
Quarter 2 2022/23
Quarter 3 2022/23
Quarter 4 2022/23
E.K.1c NumeratorThe number of children aged under 18 years from the ICS who are autistic, have a learning disability or both and are in inpatient care for the treatment of a mental disorder and whose bed is commissioned by NHS England or via a provider collaborative * 2 2 2 2 2
E.K.1c Denominator ONS Resident Population of ICS (Under 18)196280 196280 196280 196280 196280 196280
E.K.1c Rate Learning Disability Inpatient Rate per Million ONS Resident Population 10.19 10.19 10.19 10.19 10.19
MeasureNameICSMeasure
PlanningRef 0 1 2 3
Quarter 2 2021/22
Apr 2022-Mar 2023 Average
Quarter 1 2022/23
Quarter 2 2022/23
Quarter 3 2022/23
Quarter 4 2022/23
E.N.1 Count Number of personal health budgets that have been in place, at any point during the financial year to date, per ICS762 1718.5 687 1375 2062 2750
MeasureNameICSMeasure
PlanningRef 0 1 2 3
Quarter 2 2021/22
Apr 2022-Mar 2023 Average
Quarter 1 2022/23
Quarter 2 2022/23
Quarter 3 2022/23
Quarter 4 2022/23
E.N.2 Count Total number of FTE PCN Network Contract DES funded social prescribing link workers employed in year4.88 25 25 25 25 25
E.N.2 Count Total number of social prescribing referrals in year into social prescribing link workers9969 1070.25 409 845 1282 1745
Social Prescribing Referrals
Personal Health Budgets
Social Prescribing Referrals
ICS Level
Personal Health Budgets
ICS Level
Reliance on inpatient care for people with a learning disability and/or autism - Care for
children
ICS Level
ICS Level
Reliance on inpatient care for people with a learning disability and/or autism - Care commissioned by NHS England or via a
Provider Collaborative
Reliance on inpatient care for people with a learning disability and/or autism - Care for children
Reliance on inpatient care for people with a learning disability and/or autism - Care commissioned by NHS England or via a Provider Collaborative
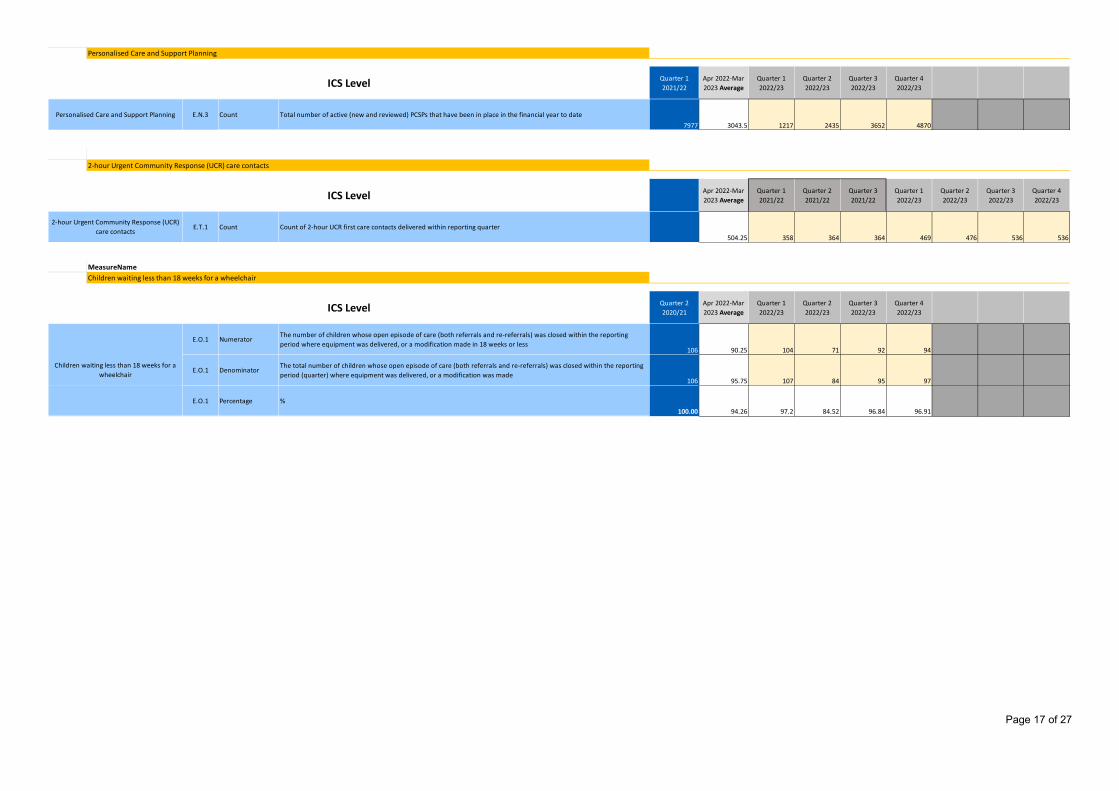
Page 17 of 27
ICSMeasurePlanningRef 0 1 2 3
Quarter 1 2021/22
Apr 2022-Mar 2023 Average
Quarter 1 2022/23
Quarter 2 2022/23
Quarter 3 2022/23
Quarter 4 2022/23
E.N.3 Count Total number of active (new and reviewed) PCSPs that have been in place in the financial year to date7977 3043.5 1217 2435 3652 4870
MeasureNameICSMeasure
PlanningRef 0 1 2 3 4 5 6
Apr 2022-Mar 2023 Average
Quarter 1 2021/22
Quarter 2 2021/22
Quarter 3 2021/22
Quarter 1 2022/23
Quarter 2 2022/23
Quarter 3 2022/23
Quarter 4 2022/23
E.T.1 Count Count of 2-hour UCR first care contacts delivered within reporting quarter504.25 358 364 364 469 476 536 536
MeasureNameICSMeasure
PlanningRef 0 1 2 3
Quarter 2 2020/21
Apr 2022-Mar 2023 Average
Quarter 1 2022/23
Quarter 2 2022/23
Quarter 3 2022/23
Quarter 4 2022/23
E.O.1 NumeratorThe number of children whose open episode of care (both referrals and re-referrals) was closed within the reporting period where equipment was delivered, or a modification made in 18 weeks or less
106 90.25 104 71 92 94
E.O.1 DenominatorThe total number of children whose open episode of care (both referrals and re-referrals) was closed within the reporting period (quarter) where equipment was delivered, or a modification was made
106 95.75 107 84 95 97
E.O.1 Percentage %100.00 94.26 97.2 84.52 96.84 96.91
2-hour Urgent Community Response (UCR) care contacts
Children waiting less than 18 weeks for a wheelchair
ICS Level
Children waiting less than 18 weeks for a wheelchair
Personalised Care and Support Planning
2-hour Urgent Community Response (UCR) care contacts
ICS Level
Personalised Care and Support Planning
ICS Level
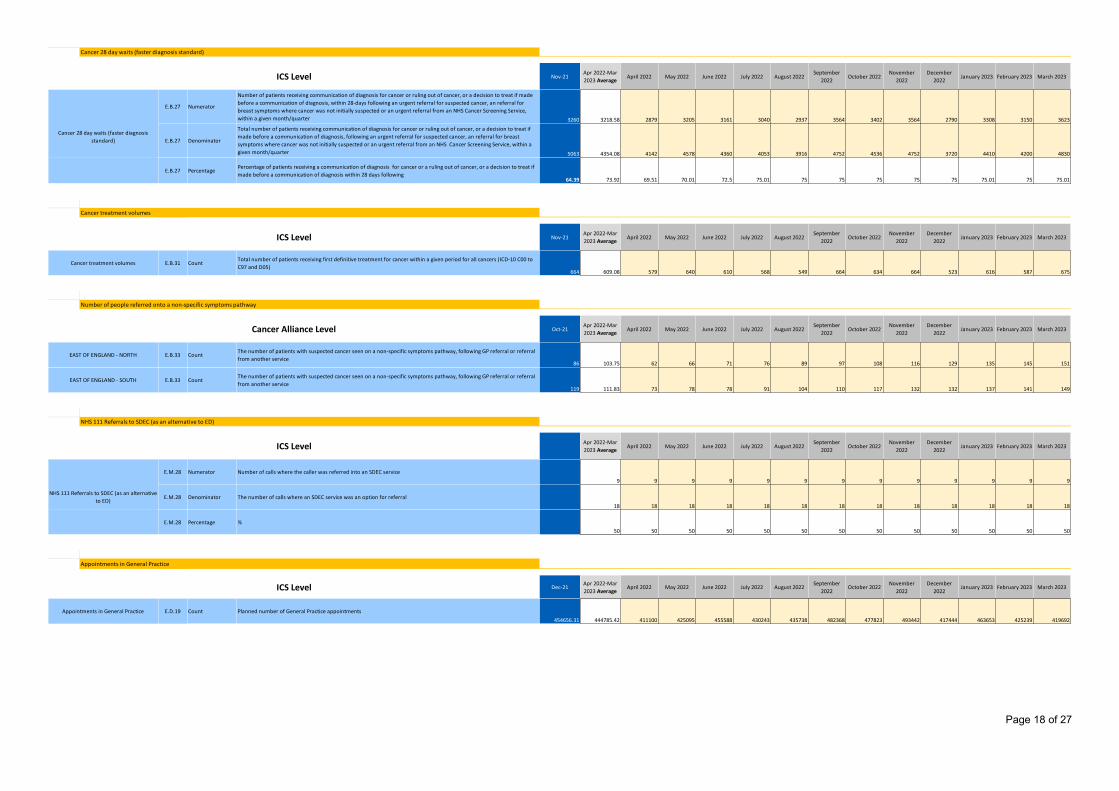
Page 18 of 27
ICSMeasurePlanningRef 0 1 2 3 4 5 6 7 8 9 10 11
Nov-21Apr 2022-Mar 2023 Average
April 2022 May 2022 June 2022 July 2022 August 2022September
2022October 2022
November 2022
December 2022
January 2023 February 2023 March 2023
E.B.27 Numerator
Number of patients receiving communication of diagnosis for cancer or ruling out of cancer, or a decision to treat if made before a communication of diagnosis, within 28-days following an urgent referral for suspected cancer, an referral for breast symptoms where cancer was not initially suspected or an urgent referral from an NHS Cancer Screening Service, within a given month/quarter 3260 3218.58 2879 3205 3161 3040 2937 3564 3402 3564 2790 3308 3150 3623
E.B.27 Denominator
Total number of patients receiving communication of diagnosis for cancer or ruling out of cancer, or a decision to treat if made before a communication of diagnosis, following an urgent referral for suspected cancer, an referral for breast symptoms where cancer was not initially suspected or an urgent referral from an NHS Cancer Screening Service, within a given month/quarter 5063 4354.08 4142 4578 4360 4053 3916 4752 4536 4752 3720 4410 4200 4830
E.B.27 PercentagePercentage of patients receiving a communication of diagnosis for cancer or a ruling out of cancer, or a decision to treat if made before a communication of diagnosis within 28 days following
64.39 73.92 69.51 70.01 72.5 75.01 75 75 75 75 75 75.01 75 75.01
MeasureNameICSMeasure
PlanningRef 0 1 2 3 4 5 6 7 8 9 10 11
Nov-21Apr 2022-Mar 2023 Average
April 2022 May 2022 June 2022 July 2022 August 2022September
2022October 2022
November 2022
December 2022
January 2023 February 2023 March 2023
E.B.31 CountTotal number of patients receiving first definitive treatment for cancer within a given period for all cancers (ICD-10 C00 to C97 and D05)
664 609.08 579 640 610 568 549 664 634 664 523 616 587 675
MeasureNameICSMeasure
PlanningRef 0 1 2 3 4 5 6 7 8 9 10 11
Oct-21Apr 2022-Mar 2023 Average
April 2022 May 2022 June 2022 July 2022 August 2022September
2022October 2022
November 2022
December 2022
January 2023 February 2023 March 2023
E.B.33 CountThe number of patients with suspected cancer seen on a non-specific symptoms pathway, following GP referral or referral from another service
86 103.75 62 66 71 76 89 97 108 116 129 135 145 151
E.B.33 CountThe number of patients with suspected cancer seen on a non-specific symptoms pathway, following GP referral or referral from another service
119 111.83 73 78 78 91 104 110 117 132 132 137 141 149
MeasureNameICSMeasure
PlanningRef 0 1 2 3 4 5
Apr 2022-Mar 2023 Average
April 2022 May 2022 June 2022 July 2022 August 2022September
2022October 2022
November 2022
December 2022
January 2023 February 2023 March 2023
E.M.28 Numerator Number of calls where the caller was referred into an SDEC service9 9 9 9 9 9 9 9 9 9 9 9 9
E.M.28 Denominator The number of calls where an SDEC service was an option for referral18 18 18 18 18 18 18 18 18 18 18 18 18
E.M.28 Percentage %50 50 50 50 50 50 50 50 50 50 50 50 50
MeasureNameICSMeasure
PlanningRef 0 1 2 3 4 5 6 7 8 9 10 11
Dec-21Apr 2022-Mar 2023 Average
April 2022 May 2022 June 2022 July 2022 August 2022September
2022October 2022
November 2022
December 2022
January 2023 February 2023 March 2023
E.D.19 Count Planned number of General Practice appointments454656.31 444785.42 411100 425095 455588 430243 435738 482368 477823 493442 417444 463653 425239 419692
Appointments in General Practice
Appointments in General Practice
ICS Level
Cancer treatment volumes
Cancer 28 day waits (faster diagnosis standard)
Cancer treatment volumes
NHS 111 Referrals to SDEC (as an alternative to ED)
ICS Level
Cancer 28 day waits (faster diagnosis standard)
NHS 111 Referrals to SDEC (as an alternative to ED)
ICS Level
ICS Level
EAST OF ENGLAND - NORTH
EAST OF ENGLAND - SOUTH
Number of people referred onto a non-specific symptoms pathway
Cancer Alliance Level
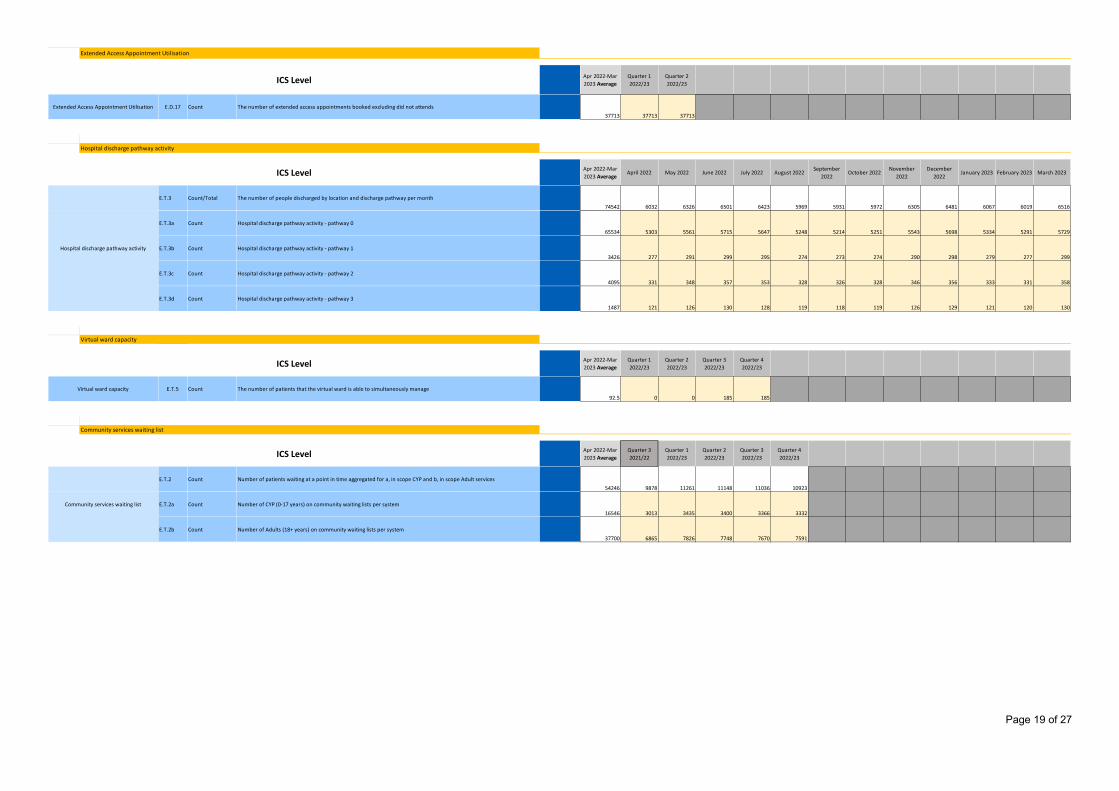
Page 19 of 27
ICSMeasurePlanningRef 0 1
Apr 2022-Mar 2023 Average
Quarter 1 2022/23
Quarter 2 2022/23
E.D.17 Count The number of extended access appointments booked excluding did not attends37713 37713 37713
ActivityCategoryActivity14
0 1 2 3 4 5 6 7 8
Apr 2022-Mar 2023 Average
April 2022 May 2022 June 2022 July 2022 August 2022September
2022October 2022
November 2022
December 2022
January 2023 February 2023 March 2023
E.T.3 Count/Total The number of people discharged by location and discharge pathway per month74542 6032 6326 6501 6423 5969 5931 5972 6305 6481 6067 6019 6516
E.T.3a Count Hospital discharge pathway activity - pathway 065534 5303 5561 5715 5647 5248 5214 5251 5543 5698 5334 5291 5729
E.T.3b Count Hospital discharge pathway activity - pathway 13426 277 291 299 295 274 273 274 290 298 279 277 299
E.T.3c Count Hospital discharge pathway activity - pathway 24095 331 348 357 353 328 326 328 346 356 333 331 358
E.T.3d Count Hospital discharge pathway activity - pathway 31487 121 126 130 128 119 118 119 126 129 121 120 130
MeasureNameICSMeasure
PlanningRef 0 1 2 3
Apr 2022-Mar 2023 Average
Quarter 1 2022/23
Quarter 2 2022/23
Quarter 3 2022/23
Quarter 4 2022/23
E.T.5 Count The number of patients that the virtual ward is able to simultaneously manage92.5 0 0 185 185
ActivityCategoryActivity15
0 1 2 3 4
Apr 2022-Mar 2023 Average
Quarter 3 2021/22
Quarter 1 2022/23
Quarter 2 2022/23
Quarter 3 2022/23
Quarter 4 2022/23
E.T.2 Count Number of patients waiting at a point in time aggregated for a, in scope CYP and b, in scope Adult services54246 9878 11261 11148 11036 10923
E.T.2a Count Number of CYP (0-17 years) on community waiting lists per system16546 3013 3435 3400 3366 3332
E.T.2b Count Number of Adults (18+ years) on community waiting lists per system37700 6865 7826 7748 7670 7591
Community services waiting list
ICS Level
Community services waiting list
Virtual ward capacity
ICS Level
Virtual ward capacity
Hospital discharge pathway activity
Hospital discharge pathway activity
ICS Level
Extended Access Appointment Utilisation
Extended Access Appointment Utilisation
ICS Level
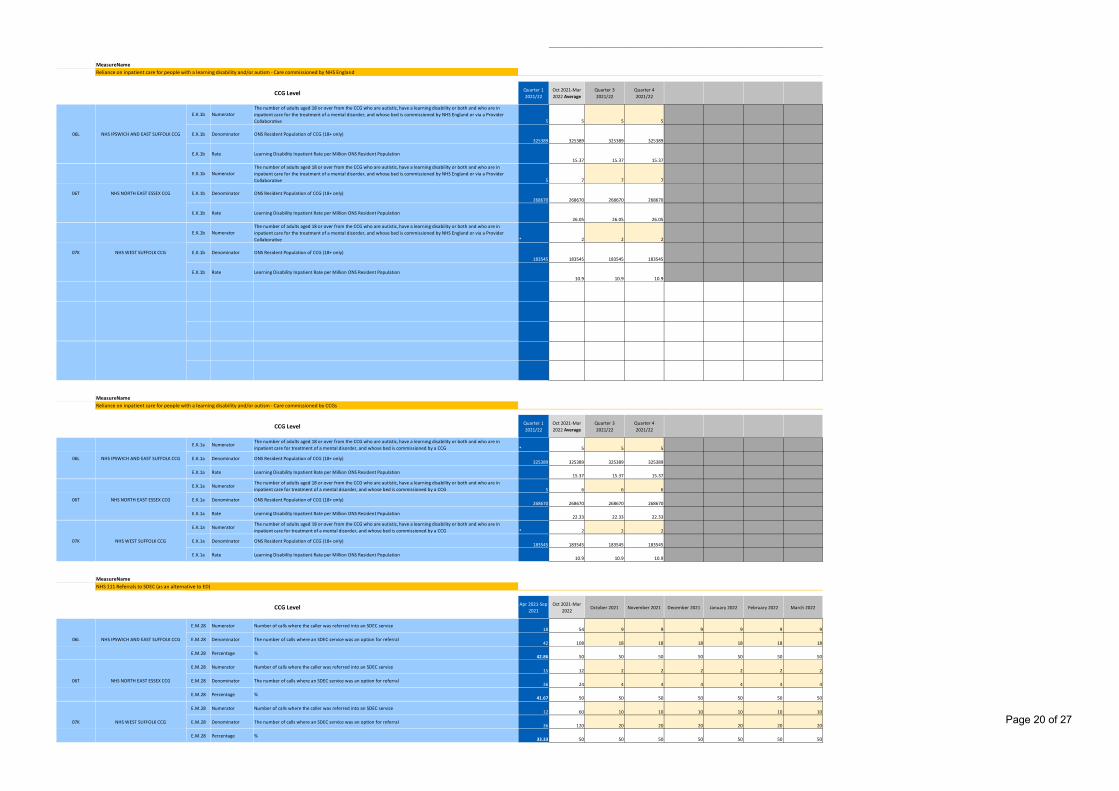
Page 20 of 27
MeasureNameCCGMeasure5
PlanningRef
Quarter 1 2021/22
Oct 2021-Mar 2022 Average
Quarter 3 2021/22
Quarter 4 2021/22
T CC0E.K.1b Numerator
The number of adults aged 18 or over from the CCG who are autistic, have a learning disability or both and who are in inpatient care for the treatment of a mental disorder, and whose bed is commissioned by NHS England or via a Provider Collaborative 5 5 5 5
O CC0E.K.1b Denominator ONS Resident Population of CCG (18+ only)
325389 325389 325389 325389
L CC0E.K.1b Rate Learning Disability Inpatient Rate per Million ONS Resident Population
15.37 15.37 15.37
T CC0E.K.1b Numerator
The number of adults aged 18 or over from the CCG who are autistic, have a learning disability or both and who are in inpatient care for the treatment of a mental disorder, and whose bed is commissioned by NHS England or via a Provider Collaborative 5 7 7 7
O CC0E.K.1b Denominator ONS Resident Population of CCG (18+ only)
268670 268670 268670 268670
L CC0E.K.1b Rate Learning Disability Inpatient Rate per Million ONS Resident Population
26.05 26.05 26.05
T CC0E.K.1b Numerator
The number of adults aged 18 or over from the CCG who are autistic, have a learning disability or both and who are in inpatient care for the treatment of a mental disorder, and whose bed is commissioned by NHS England or via a Provider Collaborative * 2 2 2
O CC0E.K.1b Denominator ONS Resident Population of CCG (18+ only)
183545 183545 183545 183545
L CC0E.K.1b Rate Learning Disability Inpatient Rate per Million ONS Resident Population
10.9 10.9 10.9
CC
CC
CC
CC
CC
MeasureNameCCGMeasure6
PlanningRef
Quarter 1 2021/22
Oct 2021-Mar 2022 Average
Quarter 3 2021/22
Quarter 4 2021/22
T CC0E.K.1a Numerator
The number of adults aged 18 or over from the CCG who are autistic, have a learning disability or both and who are in inpatient care for treatment of a mental disorder, and whose bed is commissioned by a CCG * 5 5 5
O CC0E.K.1a Denominator ONS Resident Population of CCG (18+ only)
325389 325389 325389 325389
L CC0E.K.1a Rate Learning Disability Inpatient Rate per Million ONS Resident Population
15.37 15.37 15.37
T CC0E.K.1a Numerator
The number of adults aged 18 or over from the CCG who are autistic, have a learning disability or both and who are in inpatient care for treatment of a mental disorder, and whose bed is commissioned by a CCG 5 6 6 6
O CC0E.K.1a Denominator ONS Resident Population of CCG (18+ only)
268670 268670 268670 268670
L CC0E.K.1a Rate Learning Disability Inpatient Rate per Million ONS Resident Population
22.33 22.33 22.33
T CC0E.K.1a Numerator
The number of adults aged 18 or over from the CCG who are autistic, have a learning disability or both and who are in inpatient care for treatment of a mental disorder, and whose bed is commissioned by a CCG * 2 2 2
O CC0E.K.1a Denominator ONS Resident Population of CCG (18+ only)
183545 183545 183545 183545
L CC0E.K.1a Rate Learning Disability Inpatient Rate per Million ONS Resident Population
10.9 10.9 10.9
MeasureNameCCGMeasure8
PlanningRef
Apr 2021-Sep 2021
Oct 2021-Mar 2022
October 2021 November 2021 December 2021 January 2022 February 2022 March 2022
N CC0E.M.28 Numerator Number of calls where the caller was referred into an SDEC service
18 54 9 9 9 9 9 9
T CC0E.M.28 Denominator The number of calls where an SDEC service was an option for referral
42 108 18 18 18 18 18 18
%CC0E.M.28 Percentage %
42.86 50 50 50 50 50 50 50
N CC0E.M.28 Numerator Number of calls where the caller was referred into an SDEC service
15 12 2 2 2 2 2 2
T CC0E.M.28 Denominator The number of calls where an SDEC service was an option for referral
36 24 4 4 4 4 4 4
%CC0E.M.28 Percentage %
41.67 50 50 50 50 50 50 50
N CC0E.M.28 Numerator Number of calls where the caller was referred into an SDEC service
12 60 10 10 10 10 10 10
T CC0E.M.28 Denominator The number of calls where an SDEC service was an option for referral
36 120 20 20 20 20 20 20
%CC0E.M.28 Percentage %
33.33 50 50 50 50 50 50 50
06L NHS IPSWICH AND EAST SUFFOLK CCG
06T NHS NORTH EAST ESSEX CCG
07K NHS WEST SUFFOLK CCG
Reliance on inpatient care for people with a learning disability and/or autism - Care commissioned by CCGs
CCG Level
Reliance on inpatient care for people with a learning disability and/or autism - Care commissioned by NHS England
07K NHS WEST SUFFOLK CCG
CCG Level
06L NHS IPSWICH AND EAST SUFFOLK CCG
06T NHS NORTH EAST ESSEX CCG
NHS 111 Referrals to SDEC (as an alternative to ED)
CCG Level
06L NHS IPSWICH AND EAST SUFFOLK CCG
06T NHS NORTH EAST ESSEX CCG
07K NHS WEST SUFFOLK CCG
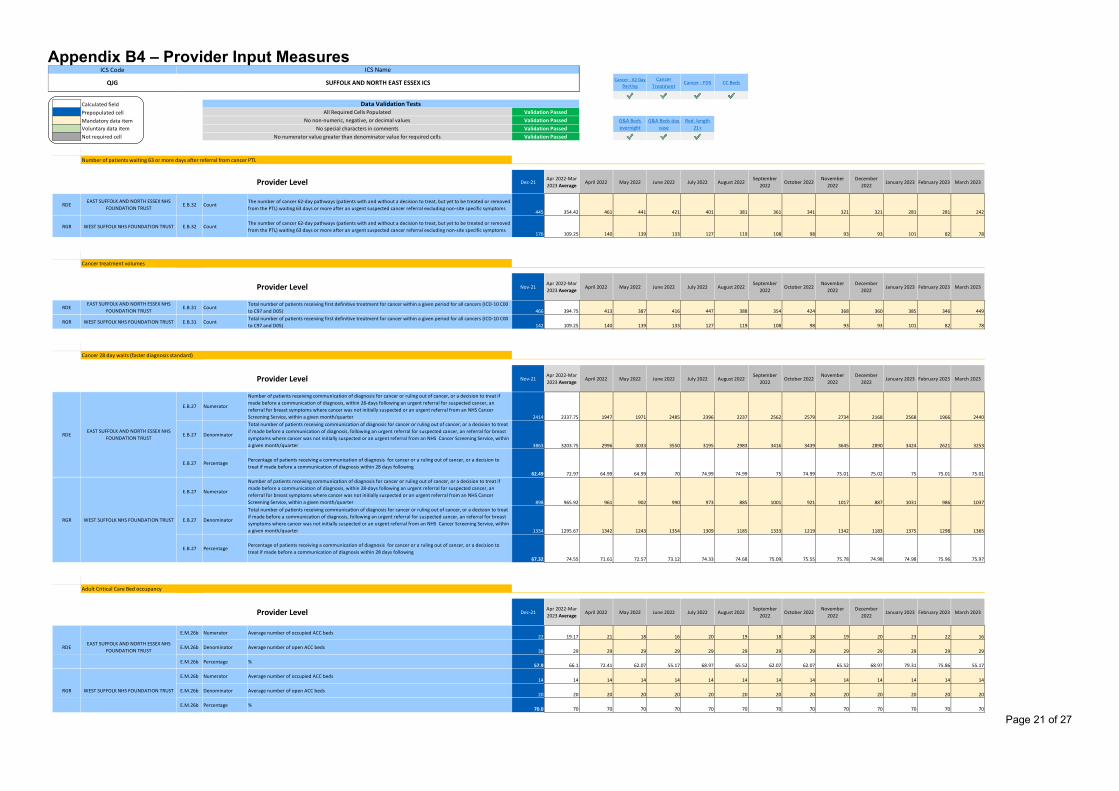
Page 21 of 27
Appendix B4 – Provider Input Measures $H$15 $H$34 $H$53 $H$98
Calculated field ProvMeasure5ProvMeasure6ProvMeasure8Prepopulated cell $H$143 $H$201 $H$233Mandatory data itemVoluntary data itemNot required cell
MeasureNameProvMeasur
PlanningRef
Dec-21Apr 2022-Mar 2023 Average
April 2022 May 2022 June 2022 July 2022 August 2022September
2022October 2022
November 2022
December 2022
January 2023 February 2023 March 2023
PRRDE E.B.32 Count
The number of cancer 62-day pathways (patients with and without a decision to treat, but yet to be treated or removed from the PTL) waiting 63 days or more after an urgent suspected cancer referral excluding non-site specific symptoms
445 354.42 461 441 421 401 381 361 341 321 321 281 281 242
PRRGR E.B.32 Count
The number of cancer 62-day pathways (patients with and without a decision to treat, but yet to be treated or removed from the PTL) waiting 63 days or more after an urgent suspected cancer referral excluding non-site specific symptoms
176 109.25 140 139 133 127 119 108 98 93 93 101 82 78
MeasureNameProvMeasur
PlanningRef
Nov-21Apr 2022-Mar 2023 Average
April 2022 May 2022 June 2022 July 2022 August 2022September
2022October 2022
November 2022
December 2022
January 2023 February 2023 March 2023
PRRDE E.B.31 Count
Total number of patients receiving first definitive treatment for cancer within a given period for all cancers (ICD-10 C00 to C97 and D05) 466 394.75 413 387 416 447 388 354 424 368 360 385 346 449
PRRGR E.B.31 Count
Total number of patients receiving first definitive treatment for cancer within a given period for all cancers (ICD-10 C00 to C97 and D05) 142 109.25 140 139 133 127 119 108 98 93 93 101 82 78
MeasureNameProvMeasur
PlanningRef
Nov-21Apr 2022-Mar 2023 Average
April 2022 May 2022 June 2022 July 2022 August 2022September
2022October 2022
November 2022
December 2022
January 2023 February 2023 March 2023
PR
E.B.27 Numerator
Number of patients receiving communication of diagnosis for cancer or ruling out of cancer, or a decision to treat if made before a communication of diagnosis, within 28-days following an urgent referral for suspected cancer, an referral for breast symptoms where cancer was not initially suspected or an urgent referral from an NHS Cancer Screening Service, within a given month/quarter 2414 2337.75 1947 1971 2485 2396 2237 2562 2579 2734 2168 2568 1966 2440
PR
E.B.27 Denominator
Total number of patients receiving communication of diagnosis for cancer or ruling out of cancer, or a decision to treat if made before a communication of diagnosis, following an urgent referral for suspected cancer, an referral for breast symptoms where cancer was not initially suspected or an urgent referral from an NHS Cancer Screening Service, within a given month/quarter 3863 3203.75 2996 3033 3550 3195 2983 3416 3439 3645 2890 3424 2621 3253
PR
E.B.27 PercentagePercentage of patients receiving a communication of diagnosis for cancer or a ruling out of cancer, or a decision to treat if made before a communication of diagnosis within 28 days following
62.49 72.97 64.99 64.99 70 74.99 74.99 75 74.99 75.01 75.02 75 75.01 75.01
PR
E.B.27 Numerator
Number of patients receiving communication of diagnosis for cancer or ruling out of cancer, or a decision to treat if made before a communication of diagnosis, within 28-days following an urgent referral for suspected cancer, an referral for breast symptoms where cancer was not initially suspected or an urgent referral from an NHS Cancer Screening Service, within a given month/quarter 898 965.92 961 902 990 973 885 1001 921 1017 887 1031 986 1037
PR
E.B.27 Denominator
Total number of patients receiving communication of diagnosis for cancer or ruling out of cancer, or a decision to treat if made before a communication of diagnosis, following an urgent referral for suspected cancer, an referral for breast symptoms where cancer was not initially suspected or an urgent referral from an NHS Cancer Screening Service, within a given month/quarter 1334 1295.67 1342 1243 1354 1309 1185 1333 1219 1342 1183 1375 1298 1365
PR
E.B.27 PercentagePercentage of patients receiving a communication of diagnosis for cancer or a ruling out of cancer, or a decision to treat if made before a communication of diagnosis within 28 days following
67.32 74.55 71.61 72.57 73.12 74.33 74.68 75.09 75.55 75.78 74.98 74.98 75.96 75.97
MeasureNameProvMeasur
PlanningRef
Dec-21Apr 2022-Mar 2023 Average
April 2022 May 2022 June 2022 July 2022 August 2022September
2022October 2022
November 2022
December 2022
January 2023 February 2023 March 2023
PRE.M.26b Numerator Average number of occupied ACC beds
22 19.17 21 18 16 20 19 18 18 19 20 23 22 16
PRE.M.26b Denominator Average number of open ACC beds
38 29 29 29 29 29 29 29 29 29 29 29 29 29
PRE.M.26b Percentage %
57.9 66.1 72.41 62.07 55.17 68.97 65.52 62.07 62.07 65.52 68.97 79.31 75.86 55.17
PRE.M.26b Numerator Average number of occupied ACC beds
14 14 14 14 14 14 14 14 14 14 14 14 14 14
PRE.M.26b Denominator Average number of open ACC beds
20 20 20 20 20 20 20 20 20 20 20 20 20 20
PRE.M.26b Percentage %
70.0 70 70 70 70 70 70 70 70 70 70 70 70 70
Provider Level
Cancer 28 day waits (faster diagnosis standard)
RDEEAST SUFFOLK AND NORTH ESSEX NHS
FOUNDATION TRUST
RGR WEST SUFFOLK NHS FOUNDATION TRUST
Provider Level
EAST SUFFOLK AND NORTH ESSEX NHS FOUNDATION TRUST
WEST SUFFOLK NHS FOUNDATION TRUST
Cancer treatment volumes
Provider Level
EAST SUFFOLK AND NORTH ESSEX NHS FOUNDATION TRUST
Validation PassedNo numerator value greater than denominator value for required cells Validation Passed
WEST SUFFOLK NHS FOUNDATION TRUST
G&A Beds overnight
G&A Beds day case
Red. length 21+
ICS Code ICS Name
QJG SUFFOLK AND NORTH EAST ESSEX ICS
Data Validation Tests
Cancer - 62 Day Backlog
All Required Cells Populated Validation PassedNo non-numeric, negative, or decimal values Validation Passed
Number of patients waiting 63 or more days after referral from cancer PTL
No special characters in comments
Cancer Treatment
Cancer - FDS CC Beds
Adult Critical Care Bed occupancy
Provider Level
RDEEAST SUFFOLK AND NORTH ESSEX NHS
FOUNDATION TRUST
RGR WEST SUFFOLK NHS FOUNDATION TRUST
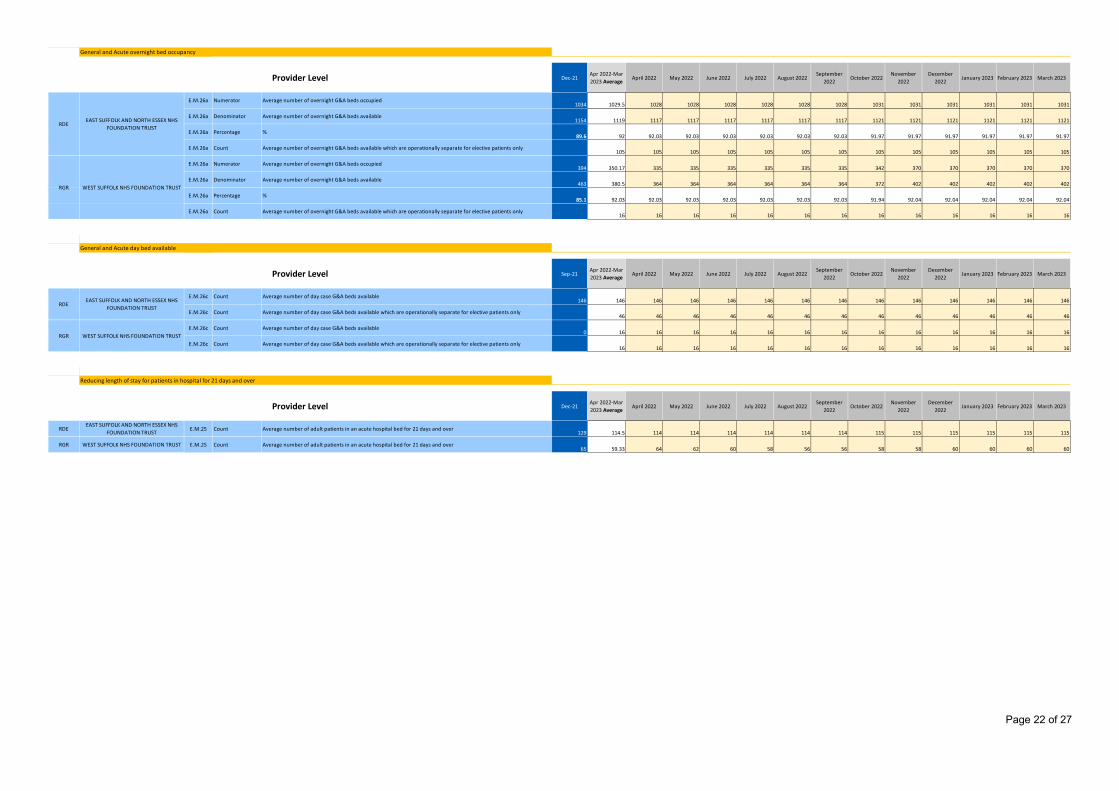
Page 22 of 27
ProvMeasurPlanningRef
Dec-21Apr 2022-Mar 2023 Average
April 2022 May 2022 June 2022 July 2022 August 2022September
2022October 2022
November 2022
December 2022
January 2023 February 2023 March 2023
E.M.26a Numerator Average number of overnight G&A beds occupied1034 1029.5 1028 1028 1028 1028 1028 1028 1031 1031 1031 1031 1031 1031
E.M.26a Denominator Average number of overnight G&A beds available1154 1119 1117 1117 1117 1117 1117 1117 1121 1121 1121 1121 1121 1121
E.M.26a Percentage %89.6 92 92.03 92.03 92.03 92.03 92.03 92.03 91.97 91.97 91.97 91.97 91.97 91.97
E.M.26a Count Average number of overnight G&A beds available which are operationally separate for elective patients only105 105 105 105 105 105 105 105 105 105 105 105 105
E.M.26a Numerator Average number of overnight G&A beds occupied394 350.17 335 335 335 335 335 335 342 370 370 370 370 370
E.M.26a Denominator Average number of overnight G&A beds available463 380.5 364 364 364 364 364 364 372 402 402 402 402 402
E.M.26a Percentage %85.1 92.03 92.03 92.03 92.03 92.03 92.03 92.03 91.94 92.04 92.04 92.04 92.04 92.04
E.M.26a Count Average number of overnight G&A beds available which are operationally separate for elective patients only16 16 16 16 16 16 16 16 16 16 16 16 16
MeasureNameProvMeasur
PlanningRef
Sep-21Apr 2022-Mar 2023 Average
April 2022 May 2022 June 2022 July 2022 August 2022September
2022October 2022
November 2022
December 2022
January 2023 February 2023 March 2023
E.M.26c Count Average number of day case G&A beds available146 146 146 146 146 146 146 146 146 146 146 146 146 146
E.M.26c Count Average number of day case G&A beds available which are operationally separate for elective patients only46 46 46 46 46 46 46 46 46 46 46 46 46
E.M.26c Count Average number of day case G&A beds available0 16 16 16 16 16 16 16 16 16 16 16 16 16
E.M.26c Count Average number of day case G&A beds available which are operationally separate for elective patients only16 16 16 16 16 16 16 16 16 16 16 16 16
MeasureNameProvMeasur
PlanningRef
Dec-21Apr 2022-Mar 2023 Average
April 2022 May 2022 June 2022 July 2022 August 2022September
2022October 2022
November 2022
December 2022
January 2023 February 2023 March 2023
RDE E.M.25 Count Average number of adult patients in an acute hospital bed for 21 days and over129 114.5 114 114 114 114 114 114 115 115 115 115 115 115
RGR E.M.25 Count Average number of adult patients in an acute hospital bed for 21 days and over65 59.33 64 62 60 58 56 56 58 58 60 60 60 60
Provider Level
EAST SUFFOLK AND NORTH ESSEX NHS FOUNDATION TRUST
WEST SUFFOLK NHS FOUNDATION TRUST
Reducing length of stay for patients in hospital for 21 days and over
Provider Level
General and Acute overnight bed occupancy
General and Acute day bed available
Provider Level
RDEEAST SUFFOLK AND NORTH ESSEX NHS
FOUNDATION TRUST
RGR WEST SUFFOLK NHS FOUNDATION TRUST
RDEEAST SUFFOLK AND NORTH ESSEX NHS
FOUNDATION TRUST
RGR WEST SUFFOLK NHS FOUNDATION TRUST
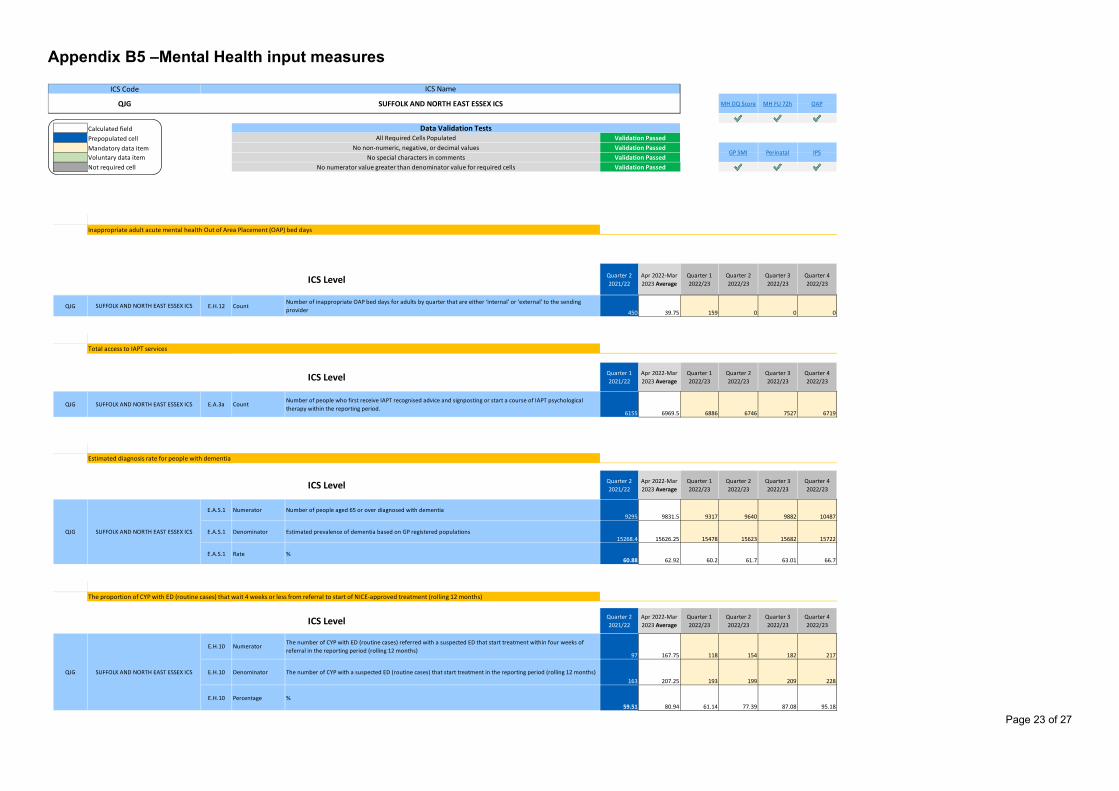
Page 23 of 27
Appendix B5 –Mental Health input measures
$H$17 $H$27 $H$45
Calculated field MeasureMH6MeasureMH7MeasureMH8Prepopulated cell $H$93 $H$100 $H$107Mandatory data itemVoluntary data itemNot required cell
MeasureNameMeasureMH
PlanningRef
PlanningRef
Quarter 2 2021/22
Apr 2022-Mar 2023 Average
Quarter 1 2022/23
Quarter 2 2022/23
Quarter 3 2022/23
Quarter 4 2022/23
I QQJG E.H.12 Count
Number of inappropriate OAP bed days for adults by quarter that are either ‘internal’ or ‘external’ to the sending provider 450 39.75 159 0 0 0
MeasureNameMeasureMH
PlanningRef
Quarter 1 2021/22
Apr 2022-Mar 2023 Average
Quarter 1 2022/23
Quarter 2 2022/23
Quarter 3 2022/23
Quarter 4 2022/23
I QQJG E.A.3a Count
Number of people who first receive IAPT recognised advice and signposting or start a course of IAPT psychological therapy within the reporting period.
6155 6969.5 6886 6746 7527 6719
MeasureNameMeasureMH
PlanningRef
Quarter 2 2021/22
Apr 2022-Mar 2023 Average
Quarter 1 2022/23
Quarter 2 2022/23
Quarter 3 2022/23
Quarter 4 2022/23
I QE.A.S.1 Numerator Number of people aged 65 or over diagnosed with dementia
9295 9831.5 9317 9640 9882 10487
I QE.A.S.1 Denominator Estimated prevalence of dementia based on GP registered populations
15268.4 15626.25 15478 15623 15682 15722
I QE.A.S.1 Rate %
60.88 62.92 60.2 61.7 63.01 66.7
MeasureNameMeasureMH
PlanningRefQuarter 2 2021/22
Apr 2022-Mar 2023 Average
Quarter 1 2022/23
Quarter 2 2022/23
Quarter 3 2022/23
Quarter 4 2022/23
I QE.H.10 Numerator
The number of CYP with ED (routine cases) referred with a suspected ED that start treatment within four weeks of referral in the reporting period (rolling 12 months)
97 167.75 118 154 182 217
I QE.H.10 Denominator The number of CYP with a suspected ED (routine cases) that start treatment in the reporting period (rolling 12 months)
163 207.25 193 199 209 228
I QE.H.10 Percentage %
59.51 80.94 61.14 77.39 87.08 95.18
Perinatal IPSNo special characters in comments Validation Passed
Data Validation TestsAll Required Cells Populated Validation Passed
No non-numeric, negative, or decimal values Validation PassedGP SMI
The proportion of CYP with ED (routine cases) that wait 4 weeks or less from referral to start of NICE-approved treatment (rolling 12 months)
QJG SUFFOLK AND NORTH EAST ESSEX ICS
ICS Level
QJG SUFFOLK AND NORTH EAST ESSEX ICS
ICS Level
ICS Level
Estimated diagnosis rate for people with dementia
Inappropriate adult acute mental health Out of Area Placement (OAP) bed days
SUFFOLK AND NORTH EAST ESSEX ICS
SUFFOLK AND NORTH EAST ESSEX ICS
ICS Level
Total access to IAPT services
No numerator value greater than denominator value for required cells Validation Passed
ICS Code ICS Name
QJG SUFFOLK AND NORTH EAST ESSEX ICS MH DQ Score MH FU 72h OAP
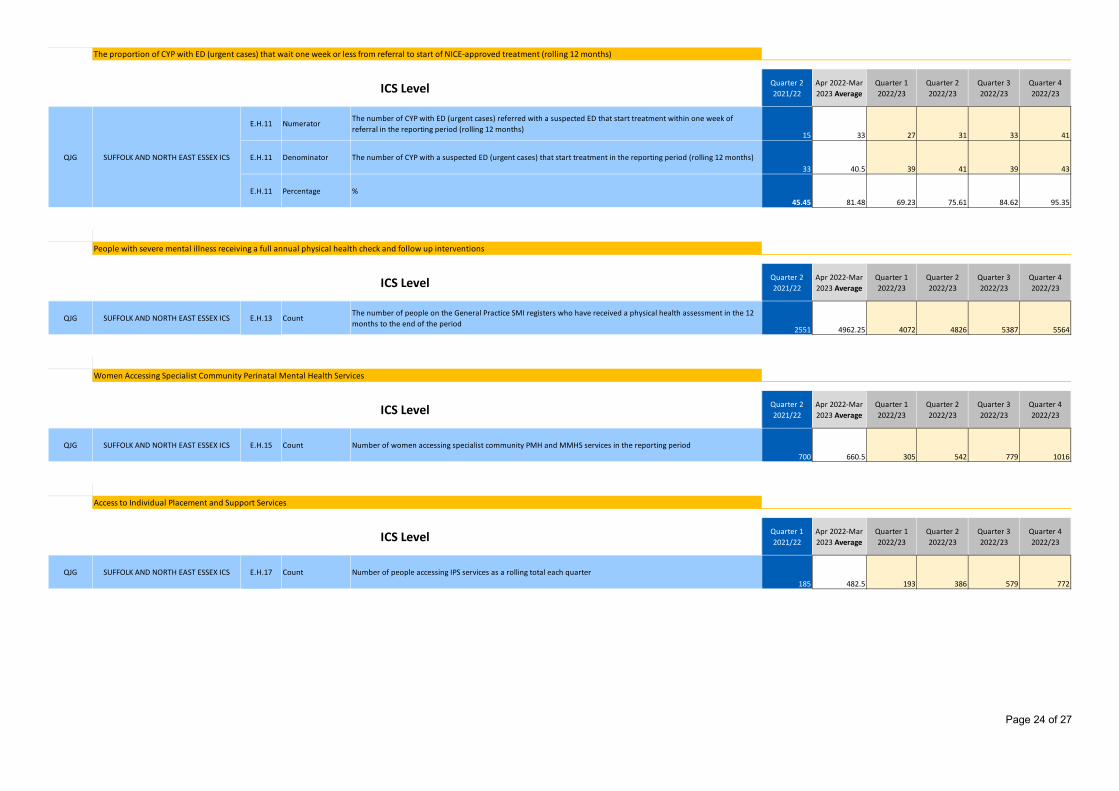
Page 24 of 27
MeasureMHPlanningRef
Quarter 2 2021/22
Apr 2022-Mar 2023 Average
Quarter 1 2022/23
Quarter 2 2022/23
Quarter 3 2022/23
Quarter 4 2022/23
E.H.11 NumeratorThe number of CYP with ED (urgent cases) referred with a suspected ED that start treatment within one week of referral in the reporting period (rolling 12 months)
15 33 27 31 33 41
E.H.11 Denominator The number of CYP with a suspected ED (urgent cases) that start treatment in the reporting period (rolling 12 months)33 40.5 39 41 39 43
E.H.11 Percentage %45.45 81.48 69.23 75.61 84.62 95.35
MeasureNameMeasureMH
PlanningRef
Quarter 2 2021/22
Apr 2022-Mar 2023 Average
Quarter 1 2022/23
Quarter 2 2022/23
Quarter 3 2022/23
Quarter 4 2022/23
QJG E.H.13 CountThe number of people on the General Practice SMI registers who have received a physical health assessment in the 12 months to the end of the period
2551 4962.25 4072 4826 5387 5564
MeasureNameMeasureMH
PlanningRef
Quarter 2 2021/22
Apr 2022-Mar 2023 Average
Quarter 1 2022/23
Quarter 2 2022/23
Quarter 3 2022/23
Quarter 4 2022/23
QJG E.H.15 Count Number of women accessing specialist community PMH and MMHS services in the reporting period700 660.5 305 542 779 1016
MeasureNameMeasureMH
PlanningRef
Quarter 1 2021/22
Apr 2022-Mar 2023 Average
Quarter 1 2022/23
Quarter 2 2022/23
Quarter 3 2022/23
Quarter 4 2022/23
QJG E.H.17 Count Number of people accessing IPS services as a rolling total each quarter185 482.5 193 386 579 772
People with severe mental illness receiving a full annual physical health check and follow up interventions
ICS Level
QJG SUFFOLK AND NORTH EAST ESSEX ICS
Women Accessing Specialist Community Perinatal Mental Health Services
Access to Individual Placement and Support Services
SUFFOLK AND NORTH EAST ESSEX ICS
SUFFOLK AND NORTH EAST ESSEX ICS
ICS Level
ICS Level
The proportion of CYP with ED (urgent cases) that wait one week or less from referral to start of NICE-approved treatment (rolling 12 months)
ICS Level
SUFFOLK AND NORTH EAST ESSEX ICS
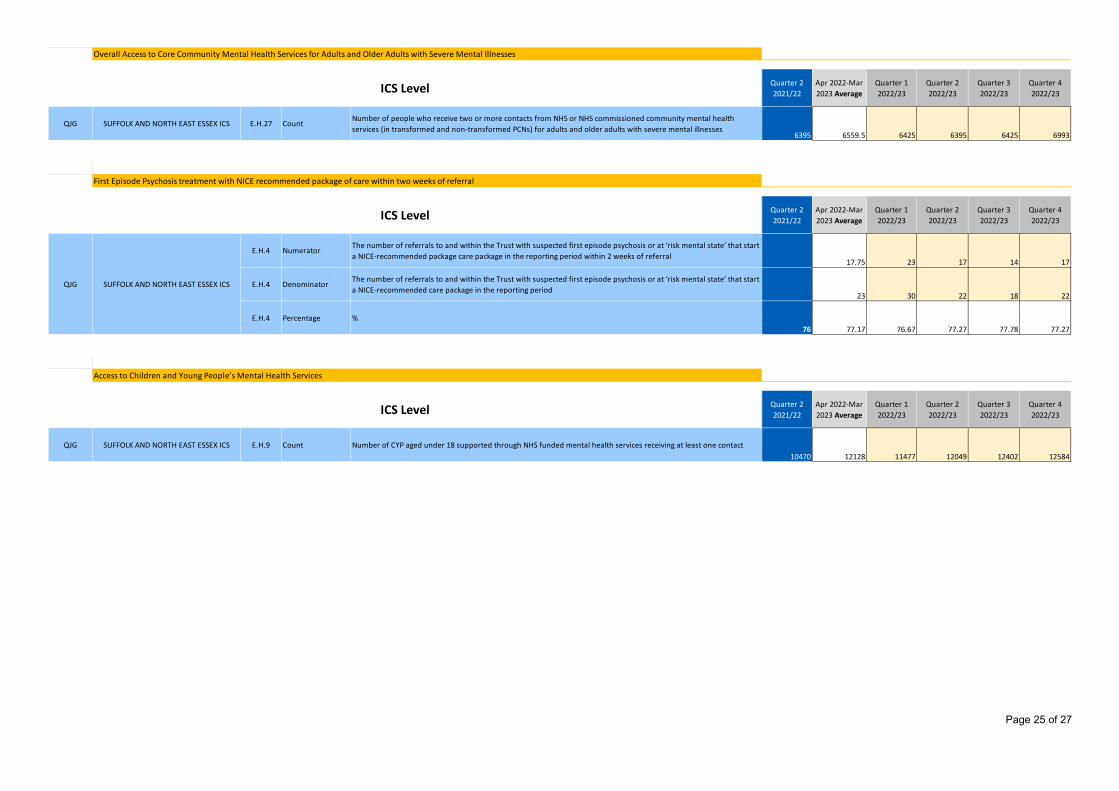
Page 25 of 27
MeasureMHPlanningRef
Quarter 2 2021/22
Apr 2022-Mar 2023 Average
Quarter 1 2022/23
Quarter 2 2022/23
Quarter 3 2022/23
Quarter 4 2022/23
QJG E.H.27 CountNumber of people who receive two or more contacts from NHS or NHS commissioned community mental health services (in transformed and non-transformed PCNs) for adults and older adults with severe mental illnesses
6395 6559.5 6425 6395 6425 6993
MeasureNameMeasureMH
PlanningRef
Quarter 2 2021/22
Apr 2022-Mar 2023 Average
Quarter 1 2022/23
Quarter 2 2022/23
Quarter 3 2022/23
Quarter 4 2022/23
E.H.4 NumeratorThe number of referrals to and within the Trust with suspected first episode psychosis or at ‘risk mental state’ that start a NICE-recommended package care package in the reporting period within 2 weeks of referral
17.75 23 17 14 17
E.H.4 DenominatorThe number of referrals to and within the Trust with suspected first episode psychosis or at ‘risk mental state’ that start a NICE-recommended care package in the reporting period
23 30 22 18 22
E.H.4 Percentage %76 77.17 76.67 77.27 77.78 77.27
MeasureNameMeasureMH
PlanningRef
Quarter 2 2021/22
Apr 2022-Mar 2023 Average
Quarter 1 2022/23
Quarter 2 2022/23
Quarter 3 2022/23
Quarter 4 2022/23
QJG E.H.9 Count Number of CYP aged under 18 supported through NHS funded mental health services receiving at least one contact10470 12128 11477 12049 12402 12584
Overall Access to Core Community Mental Health Services for Adults and Older Adults with Severe Mental Illnesses
ICS Level
SUFFOLK AND NORTH EAST ESSEX ICS
QJG SUFFOLK AND NORTH EAST ESSEX ICS
First Episode Psychosis treatment with NICE recommended package of care within two weeks of referral
ICS Level
SUFFOLK AND NORTH EAST ESSEX ICS
Access to Children and Young People’s Mental Health Services
ICS Level
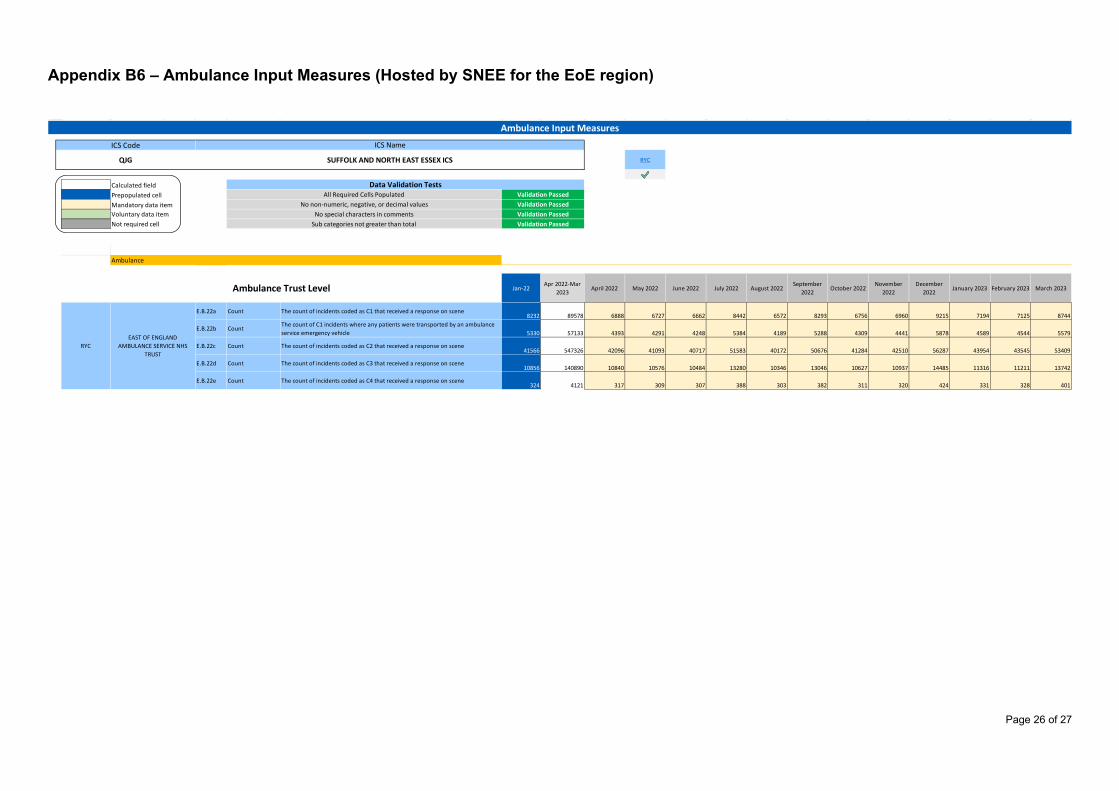
Page 26 of 27
Appendix B6 – Ambulance Input Measures (Hosted by SNEE for the EoE region)
RYC$G$18 #N/A
Calculated fieldPrepopulated cellMandatory data itemVoluntary data itemNot required cell
Ambulance trust PlanningRef 0 1 2 3 4 5
Jan-22Apr 2022-Mar
2023April 2022 May 2022 June 2022 July 2022 August 2022
September 2022
October 2022November
2022December
2022January 2023 February 2023 March 2023
A AARE.B.22a Count The count of incidents coded as C1 that received a response on scene
8232 89578 6888 6727 6662 8442 6572 8293 6756 6960 9215 7194 7125 8744
A AARE.B.22b Count
The count of C1 incidents where any patients were transported by an ambulance service emergency vehicle 5330 57133 4393 4291 4248 5384 4189 5288 4309 4441 5878 4589 4544 5579
A AARE.B.22c Count The count of incidents coded as C2 that received a response on scene
41566 547326 42096 41093 40717 51583 40172 50676 41284 42510 56287 43954 43545 53409
A AARE.B.22d Count The count of incidents coded as C3 that received a response on scene
10856 140890 10840 10576 10484 13280 10346 13046 10627 10937 14485 11316 11211 13742
A AARE.B.22e Count The count of incidents coded as C4 that received a response on scene
324 4121 317 309 307 388 303 382 311 320 424 331 328 401
Ambulance
Ambulance Trust Level
RYCEAST OF ENGLAND
AMBULANCE SERVICE NHS TRUST
No special characters in comments Validation Passed
Ambulance Input Measures
ICS Code ICS Name
QJG SUFFOLK AND NORTH EAST ESSEX ICS RYC
No non-numeric, negative, or decimal values Validation Passed
Data Validation TestsValidation PassedAll Required Cells Populated
Sub categories not greater than total Validation Passed
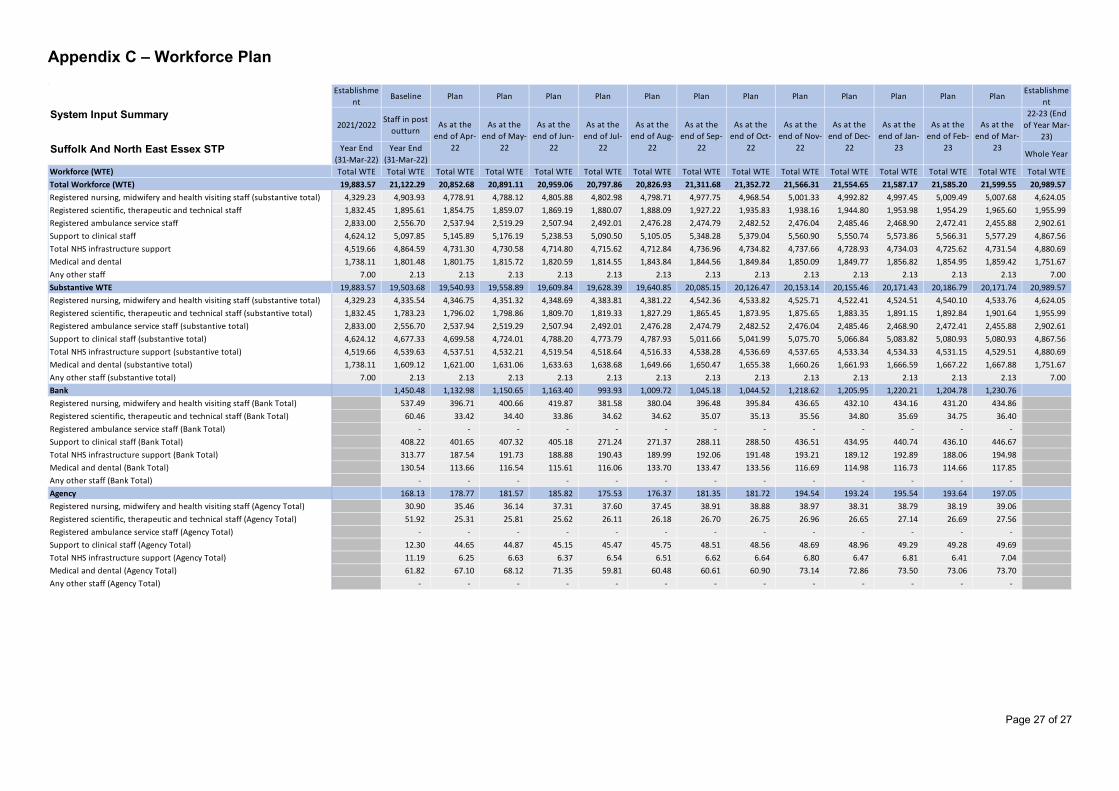
Page 27 of 27
Appendix C – Workforce Plan
Establishment
Baseline Plan Plan Plan Plan Plan Plan Plan Plan Plan Plan Plan PlanEstablishme
ntSystem Input Summary
2021/2022Staff in post
outturn
22-23 (End of Year Mar-
23)Suffolk And North East Essex STP Year End
(31-Mar-22)Year End
(31-Mar-22)Whole Year
Workforce (WTE) Total WTE Total WTE Total WTE Total WTE Total WTE Total WTE Total WTE Total WTE Total WTE Total WTE Total WTE Total WTE Total WTE Total WTE Total WTETotal Workforce (WTE) 19,883.57 21,122.29 20,852.68 20,891.11 20,959.06 20,797.86 20,826.93 21,311.68 21,352.72 21,566.31 21,554.65 21,587.17 21,585.20 21,599.55 20,989.57 Registered nursing, midwifery and health visiting staff (substantive total) 4,329.23 4,903.93 4,778.91 4,788.12 4,805.88 4,802.98 4,798.71 4,977.75 4,968.54 5,001.33 4,992.82 4,997.45 5,009.49 5,007.68 4,624.05 Registered scientific, therapeutic and technical staff 1,832.45 1,895.61 1,854.75 1,859.07 1,869.19 1,880.07 1,888.09 1,927.22 1,935.83 1,938.16 1,944.80 1,953.98 1,954.29 1,965.60 1,955.99 Registered ambulance service staff 2,833.00 2,556.70 2,537.94 2,519.29 2,507.94 2,492.01 2,476.28 2,474.79 2,482.52 2,476.04 2,485.46 2,468.90 2,472.41 2,455.88 2,902.61 Support to clinical staff 4,624.12 5,097.85 5,145.89 5,176.19 5,238.53 5,090.50 5,105.05 5,348.28 5,379.04 5,560.90 5,550.74 5,573.86 5,566.31 5,577.29 4,867.56 Total NHS infrastructure support 4,519.66 4,864.59 4,731.30 4,730.58 4,714.80 4,715.62 4,712.84 4,736.96 4,734.82 4,737.66 4,728.93 4,734.03 4,725.62 4,731.54 4,880.69 Medical and dental 1,738.11 1,801.48 1,801.75 1,815.72 1,820.59 1,814.55 1,843.84 1,844.56 1,849.84 1,850.09 1,849.77 1,856.82 1,854.95 1,859.42 1,751.67 Any other staff 7.00 2.13 2.13 2.13 2.13 2.13 2.13 2.13 2.13 2.13 2.13 2.13 2.13 2.13 7.00 Substantive WTE 19,883.57 19,503.68 19,540.93 19,558.89 19,609.84 19,628.39 19,640.85 20,085.15 20,126.47 20,153.14 20,155.46 20,171.43 20,186.79 20,171.74 20,989.57 Registered nursing, midwifery and health visiting staff (substantive total) 4,329.23 4,335.54 4,346.75 4,351.32 4,348.69 4,383.81 4,381.22 4,542.36 4,533.82 4,525.71 4,522.41 4,524.51 4,540.10 4,533.76 4,624.05 Registered scientific, therapeutic and technical staff (substantive total) 1,832.45 1,783.23 1,796.02 1,798.86 1,809.70 1,819.33 1,827.29 1,865.45 1,873.95 1,875.65 1,883.35 1,891.15 1,892.84 1,901.64 1,955.99 Registered ambulance service staff (substantive total) 2,833.00 2,556.70 2,537.94 2,519.29 2,507.94 2,492.01 2,476.28 2,474.79 2,482.52 2,476.04 2,485.46 2,468.90 2,472.41 2,455.88 2,902.61 Support to clinical staff (substantive total) 4,624.12 4,677.33 4,699.58 4,724.01 4,788.20 4,773.79 4,787.93 5,011.66 5,041.99 5,075.70 5,066.84 5,083.82 5,080.93 5,080.93 4,867.56 Total NHS infrastructure support (substantive total) 4,519.66 4,539.63 4,537.51 4,532.21 4,519.54 4,518.64 4,516.33 4,538.28 4,536.69 4,537.65 4,533.34 4,534.33 4,531.15 4,529.51 4,880.69 Medical and dental (substantive total) 1,738.11 1,609.12 1,621.00 1,631.06 1,633.63 1,638.68 1,649.66 1,650.47 1,655.38 1,660.26 1,661.93 1,666.59 1,667.22 1,667.88 1,751.67 Any other staff (substantive total) 7.00 2.13 2.13 2.13 2.13 2.13 2.13 2.13 2.13 2.13 2.13 2.13 2.13 2.13 7.00 Bank 1,450.48 1,132.98 1,150.65 1,163.40 993.93 1,009.72 1,045.18 1,044.52 1,218.62 1,205.95 1,220.21 1,204.78 1,230.76 Registered nursing, midwifery and health visiting staff (Bank Total) 537.49 396.71 400.66 419.87 381.58 380.04 396.48 395.84 436.65 432.10 434.16 431.20 434.86 Registered scientific, therapeutic and technical staff (Bank Total) 60.46 33.42 34.40 33.86 34.62 34.62 35.07 35.13 35.56 34.80 35.69 34.75 36.40 Registered ambulance service staff (Bank Total) - - - - - - - - - - - - - Support to clinical staff (Bank Total) 408.22 401.65 407.32 405.18 271.24 271.37 288.11 288.50 436.51 434.95 440.74 436.10 446.67 Total NHS infrastructure support (Bank Total) 313.77 187.54 191.73 188.88 190.43 189.99 192.06 191.48 193.21 189.12 192.89 188.06 194.98 Medical and dental (Bank Total) 130.54 113.66 116.54 115.61 116.06 133.70 133.47 133.56 116.69 114.98 116.73 114.66 117.85 Any other staff (Bank Total) - - - - - - - - - - - - - Agency 168.13 178.77 181.57 185.82 175.53 176.37 181.35 181.72 194.54 193.24 195.54 193.64 197.05 Registered nursing, midwifery and health visiting staff (Agency Total) 30.90 35.46 36.14 37.31 37.60 37.45 38.91 38.88 38.97 38.31 38.79 38.19 39.06 Registered scientific, therapeutic and technical staff (Agency Total) 51.92 25.31 25.81 25.62 26.11 26.18 26.70 26.75 26.96 26.65 27.14 26.69 27.56 Registered ambulance service staff (Agency Total) - - - - - - - - - - - - - Support to clinical staff (Agency Total) 12.30 44.65 44.87 45.15 45.47 45.75 48.51 48.56 48.69 48.96 49.29 49.28 49.69 Total NHS infrastructure support (Agency Total) 11.19 6.25 6.63 6.37 6.54 6.51 6.62 6.64 6.80 6.47 6.81 6.41 7.04 Medical and dental (Agency Total) 61.82 67.10 68.12 71.35 59.81 60.48 60.61 60.90 73.14 72.86 73.50 73.06 73.70 Any other staff (Agency Total) - - - - - - - - - - - - -
As at the end of Oct-
22
As at the end of Nov-
22
As at the end of Dec-
22
As at the end of Jan-
23
As at the end of Feb-
23
As at the end of Mar-
23
As at the end of Apr-
22
As at the end of May-
22
As at the end of Jun-
22
As at the end of Jul-
22
As at the end of Aug-
22
As at the end of Sep-
22
Financial Plan & Budgets 2022-23 Governing Body May 2022
1
Appendix D
Updated Guidance from NHSEI£
2
• NHSE/I have formally acknowledged the 2022/23 guidance sets out levels of inflation and COVID-19 which are significantly below current levels.
• For the submission on 28 April they required plans to reflect the reality of current cost pressures – specifically price inflation and the current COVID-19 wave.
• Items which were allowed for the submission as ‘acceptable drivers of deficit’ agreed by EoE NHSE/I included:• Price inflation at current (rather than prospective) levels.• Existing high rates until the end of April, tailing off during May to a ‘low-level’ of COVID-19 for the rest of the year.
• Items to be included were ‘unmitigated risks’: • Any estimate of further non-pay inflation (in expectation of further increases in CPI/energy costs for example);• The impact of COVID-19, greater than low-level, extending beyond May 22: either the current wave or any possible
future wave.
• It is anticipated that NHSE/I will issue further allocations to systems to support (not fully mitigate) inflationary costs and there will be another planning submission in mid June.
Background£
3
• ICB and its partner trusts must ensure both capital and revenue resources do not exceed the limit set by NHSEI.• ICBs have a duty to at least break even individually and collectively with partner Trusts.• CCG expenditure will be matched with allocation such that the CCGs will break even; any surplus or deficit for
the year will fall into the combined ICB in the latter part of the year.
• Rollover of system envelopes from (H2) 2021/22 adjusted to remove back pay and provider income support.• Convergence adjustment applied to all systems to move towards underlying funding. Value for SNEE is -0.45%
which is the second lowest in the region.• Growth included to reflect 1.7% net tariff increase and other price/activity increases. • Covid funding reduced by 57%.• Hospital Discharge Programme (HDP) no longer available.• Elective Recovery Fund (ERF) indicative value £32m but dependent on delivery of 104% of 19/20 levels.• Delegated Primary Care Allocation increased by 6.6% to reflect national contractual commitments.• ICB Running Cost Allowance uplifted only for impact of employer NI increases due to Health & Social Care levy.
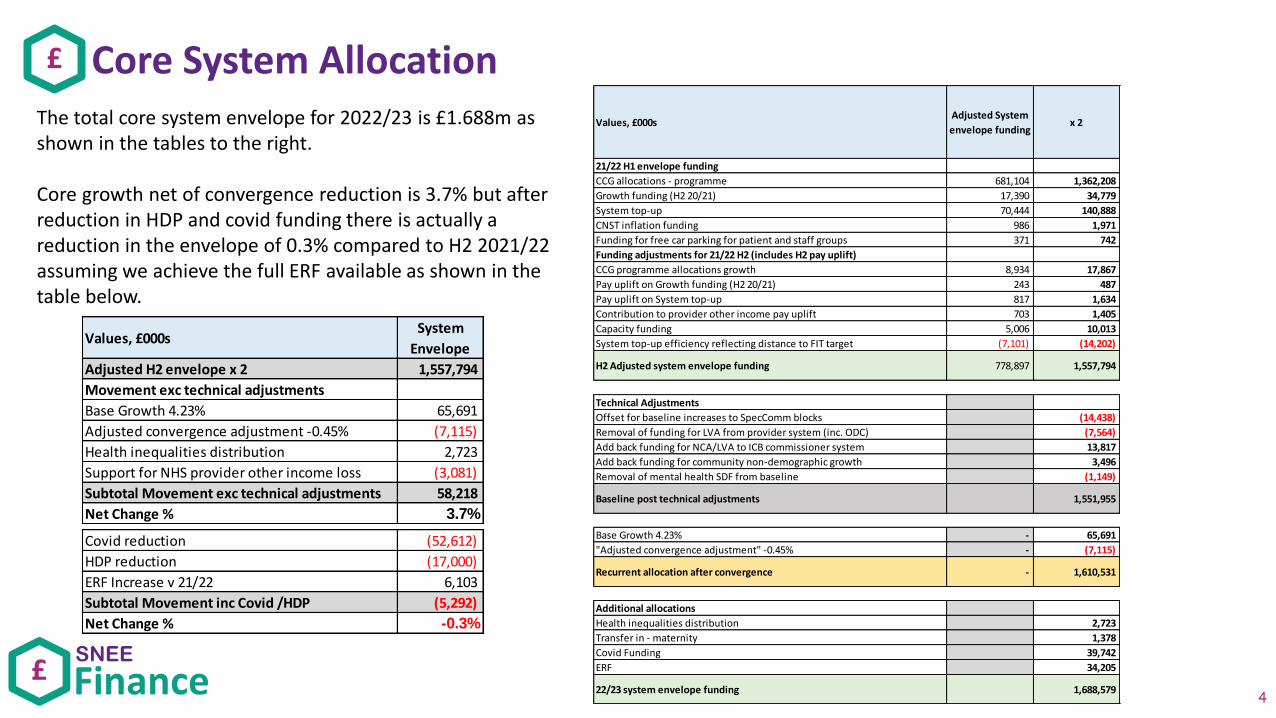
Core System Allocation£
4
Values, £000sAdjusted System
envelope fundingx 2
21/22 H1 envelope funding
CCG allocations - programme 681,104 1,362,208
Growth funding (H2 20/21) 17,390 34,779
System top-up 70,444 140,888
CNST inflation funding 986 1,971
Funding for free car parking for patient and staff groups 371 742
Funding adjustments for 21/22 H2 (includes H2 pay uplift)
CCG programme allocations growth 8,934 17,867
Pay uplift on Growth funding (H2 20/21) 243 487
Pay uplift on System top-up 817 1,634
Contribution to provider other income pay uplift 703 1,405
Capacity funding 5,006 10,013
System top-up efficiency reflecting distance to FIT target (7,101) (14,202)
H2 Adjusted system envelope funding 778,897 1,557,794
Technical Adjustments
Offset for baseline increases to SpecComm blocks (14,438)
Removal of funding for LVA from provider system (inc. ODC) (7,564)
Add back funding for NCA/LVA to ICB commissioner system 13,817
Add back funding for community non-demographic growth 3,496
Removal of mental health SDF from baseline (1,149)
Baseline post technical adjustments 1,551,955
Base Growth 4.23% - 65,691
"Adjusted convergence adjustment" -0.45% - (7,115)
Recurrent allocation after convergence - 1,610,531
Additional allocations
Health inequalities distribution 2,723
Transfer in - maternity 1,378
Covid Funding 39,742
ERF 34,205
22/23 system envelope funding 1,688,579
The total core system envelope for 2022/23 is £1.688m as shown in the tables to the right.
Core growth net of convergence reduction is 3.7% but after reduction in HDP and covid funding there is actually a reduction in the envelope of 0.3% compared to H2 2021/22 assuming we achieve the full ERF available as shown in the table below.
Values, £000sSystem
Envelope
Adjusted H2 envelope x 2 1,557,794
Movement exc technical adjustments
Base Growth 4.23% 65,691
Adjusted convergence adjustment -0.45% (7,115)
Health inequalities distribution 2,723
Support for NHS provider other income loss (3,081)
Subtotal Movement exc technical adjustments 58,218
Net Change % 3.7%
Covid reduction (52,612)
HDP reduction (17,000)
ERF Increase v 21/22 6,103
Subtotal Movement inc Covid /HDP (5,292)
Net Change % -0.3%
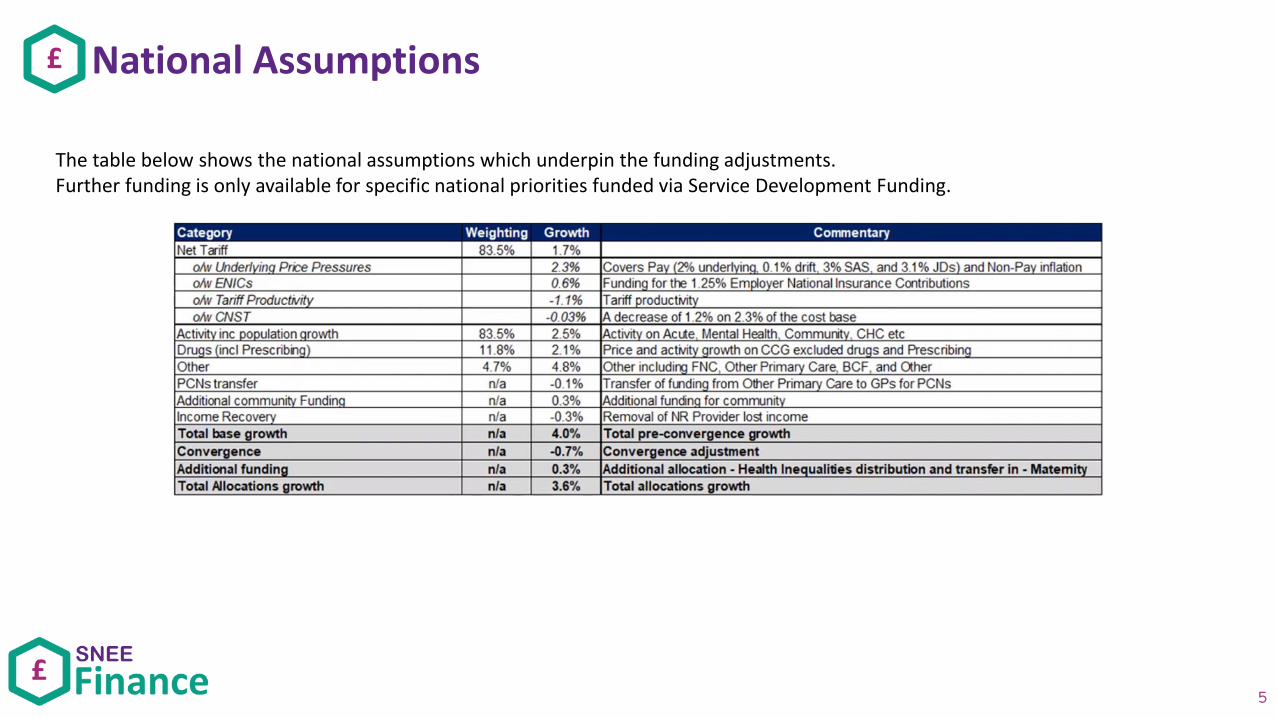
National Assumptions£
5
The table below shows the national assumptions which underpin the funding adjustments.Further funding is only available for specific national priorities funded via Service Development Funding.
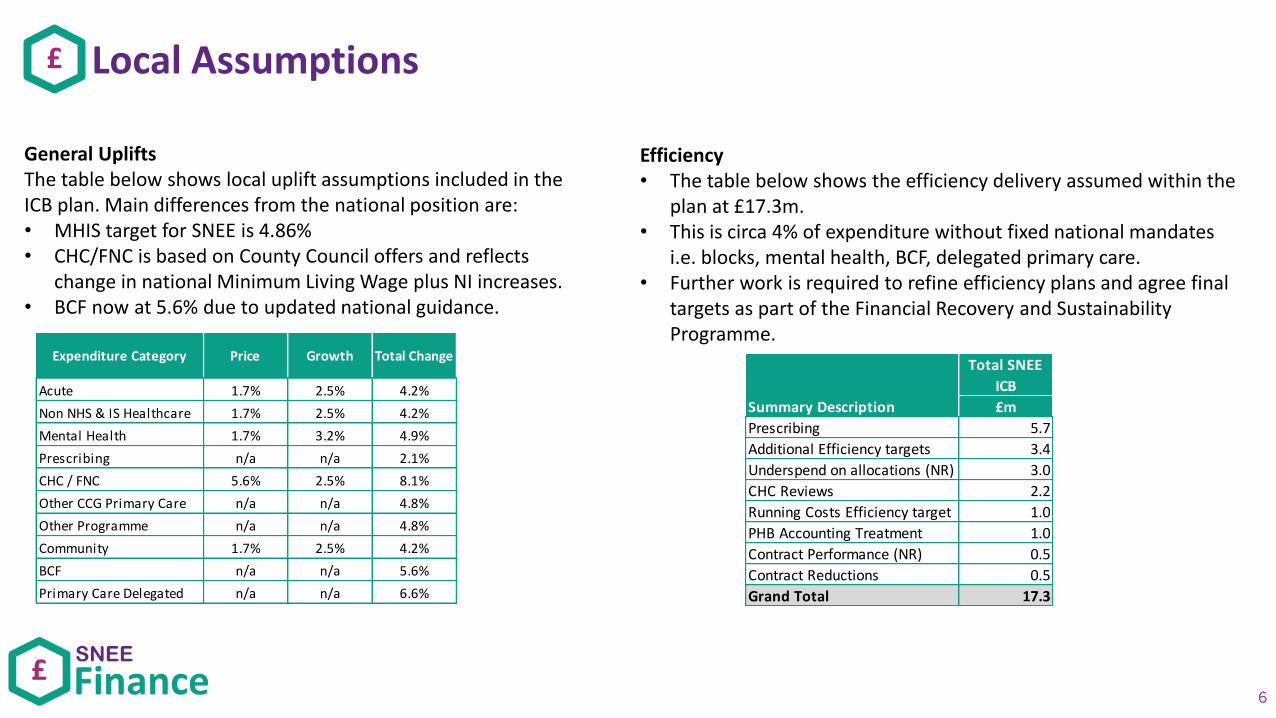
Local Assumptions£
6
General UpliftsThe table below shows local uplift assumptions included in the ICB plan. Main differences from the national position are:• MHIS target for SNEE is 4.86%• CHC/FNC is based on County Council offers and reflects
change in national Minimum Living Wage plus NI increases.• BCF now at 5.6% due to updated national guidance.
Efficiency• The table below shows the efficiency delivery assumed within the
plan at £17.3m. • This is circa 4% of expenditure without fixed national mandates
i.e. blocks, mental health, BCF, delegated primary care.• Further work is required to refine efficiency plans and agree final
targets as part of the Financial Recovery and Sustainability Programme.
Expenditure Category Price Growth Total Change
Acute 1.7% 2.5% 4.2%
Non NHS & IS Healthcare 1.7% 2.5% 4.2%
Mental Health 1.7% 3.2% 4.9%
Prescribing n/a n/a 2.1%
CHC / FNC 5.6% 2.5% 8.1%
Other CCG Primary Care n/a n/a 4.8%
Other Programme n/a n/a 4.8%
Community 1.7% 2.5% 4.2%
BCF n/a n/a 5.6%
Primary Care Delegated n/a n/a 6.6%
Total SNEE
ICB
£m
Prescribing 5.7
Additional Efficiency targets 3.4
Underspend on allocations (NR) 3.0
CHC Reviews 2.2
Running Costs Efficiency target 1.0
PHB Accounting Treatment 1.0
Contract Performance (NR) 0.5
Contract Reductions 0.5
Grand Total 17.3
Summary Description
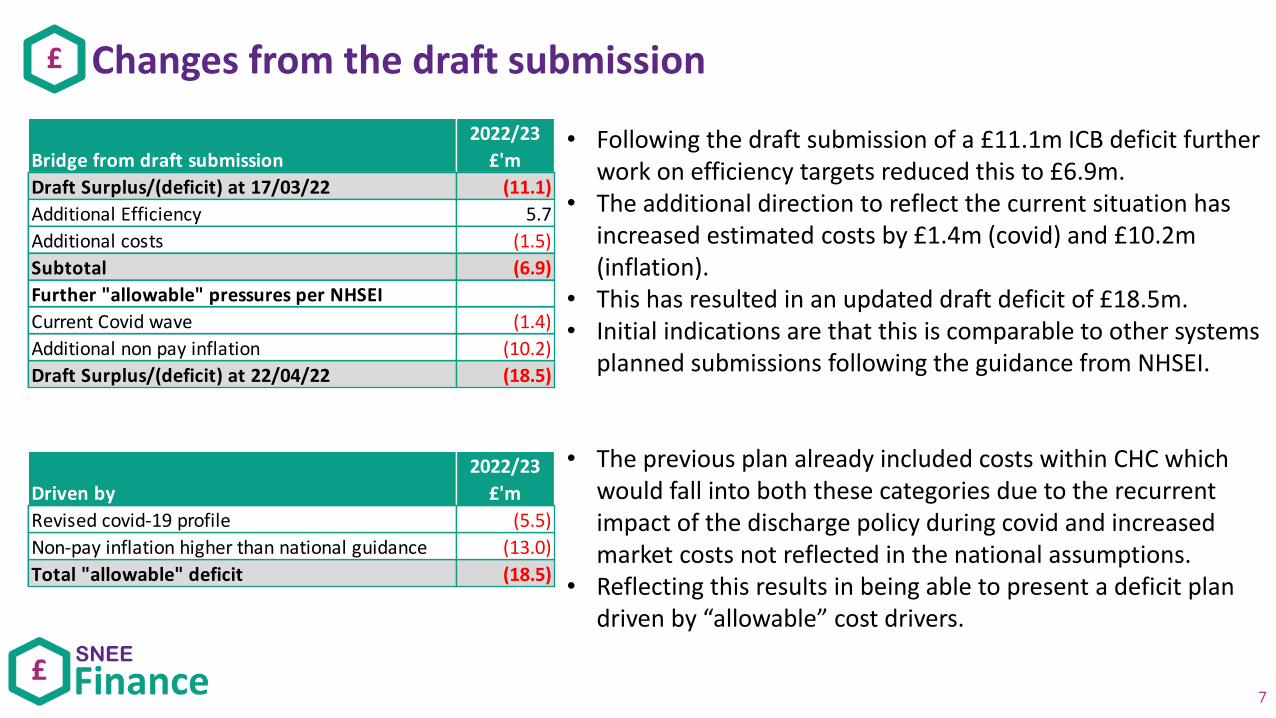
Changes from the draft submission£
7
• Following the draft submission of a £11.1m ICB deficit further work on efficiency targets reduced this to £6.9m.
• The additional direction to reflect the current situation has increased estimated costs by £1.4m (covid) and £10.2m (inflation).
• This has resulted in an updated draft deficit of £18.5m.• Initial indications are that this is comparable to other systems
planned submissions following the guidance from NHSEI.
• The previous plan already included costs within CHC which would fall into both these categories due to the recurrent impact of the discharge policy during covid and increased market costs not reflected in the national assumptions.
• Reflecting this results in being able to present a deficit plan driven by “allowable” cost drivers.
Bridge from draft submission
2022/23
£'m
Draft Surplus/(deficit) at 17/03/22 (11.1)
Additional Efficiency 5.7
Additional costs (1.5)
Subtotal (6.9)
Further "allowable" pressures per NHSEI
Current Covid wave (1.4)
Additional non pay inflation (10.2)
Draft Surplus/(deficit) at 22/04/22 (18.5)
Driven by
2022/23
£'m
Revised covid-19 profile (5.5)
Non-pay inflation higher than national guidance (13.0)
Total "allowable" deficit (18.5)
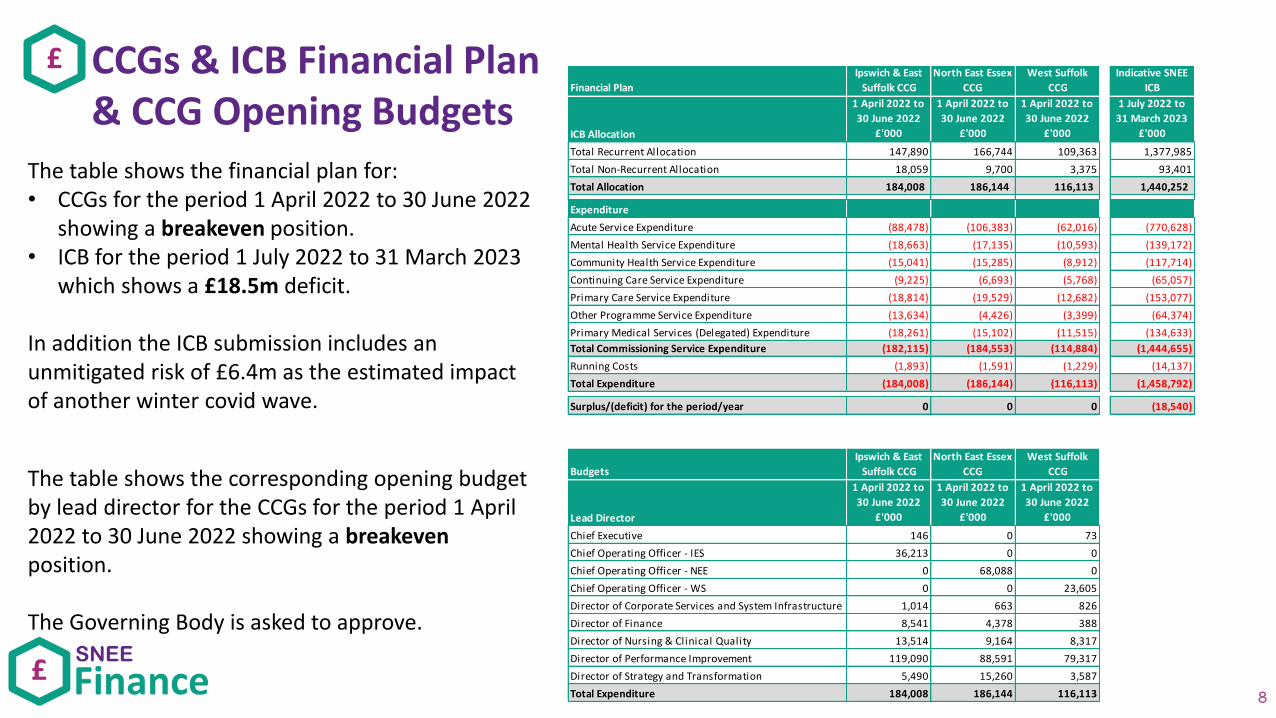
CCGs & ICB Financial Plan& CCG Opening Budgets
£
8
The table shows the financial plan for:• CCGs for the period 1 April 2022 to 30 June 2022
showing a breakeven position.• ICB for the period 1 July 2022 to 31 March 2023
which shows a £18.5m deficit.
In addition the ICB submission includes an unmitigated risk of £6.4m as the estimated impact of another winter covid wave.
Financial Plan
Ipswich & East
Suffolk CCG
North East Essex
CCG
West Suffolk
CCG
Indicative SNEE
ICB
ICB Allocation
1 April 2022 to
30 June 2022
£'000
1 April 2022 to
30 June 2022
£'000
1 April 2022 to
30 June 2022
£'000
1 July 2022 to
31 March 2023
£'000
Total Recurrent Allocation 147,890 166,744 109,363 1,377,985
Total Non-Recurrent Allocation 18,059 9,700 3,375 93,401
Total Allocation 184,008 186,144 116,113 1,440,252
Expenditure
Acute Service Expenditure (88,478) (106,383) (62,016) (770,628)
Mental Health Service Expenditure (18,663) (17,135) (10,593) (139,172)
Community Health Service Expenditure (15,041) (15,285) (8,912) (117,714)
Continuing Care Service Expenditure (9,225) (6,693) (5,768) (65,057)
Primary Care Service Expenditure (18,814) (19,529) (12,682) (153,077)
Other Programme Service Expenditure (13,634) (4,426) (3,399) (64,374)
Primary Medical Services (Delegated) Expenditure (18,261) (15,102) (11,515) (134,633)
Total Commissioning Service Expenditure (182,115) (184,553) (114,884) (1,444,655)
Running Costs (1,893) (1,591) (1,229) (14,137)
Total Expenditure (184,008) (186,144) (116,113) (1,458,792)
Surplus/(deficit) for the period/year 0 0 0 (18,540)
Budgets
Ipswich & East
Suffolk CCG
North East Essex
CCG
West Suffolk
CCG
Lead Director
1 April 2022 to
30 June 2022
£'000
1 April 2022 to
30 June 2022
£'000
1 April 2022 to
30 June 2022
£'000
Chief Executive 146 0 73
Chief Operating Officer - IES 36,213 0 0
Chief Operating Officer - NEE 0 68,088 0
Chief Operating Officer - WS 0 0 23,605
Director of Corporate Services and System Infrastructure 1,014 663 826
Director of Finance 8,541 4,378 388
Director of Nursing & Clinical Quality 13,514 9,164 8,317
Director of Performance Improvement 119,090 88,591 79,317
Director of Strategy and Transformation 5,490 15,260 3,587
Total Expenditure 184,008 186,144 116,113
The table shows the corresponding opening budget by lead director for the CCGs for the period 1 April 2022 to 30 June 2022 showing a breakevenposition.
The Governing Body is asked to approve.
GOVERNING BODY
Agenda Item No. 12
Reference No. IESCCG 22-21
Date. 24 May 2022
Title
Integrated Performance Report
Lead Director
Joint Leadership Team
Author(s)
Joint Leadership Team
Purpose
To present the up to date Integrated Performance report.
Applicable CCG Clinical Priorities:
1. To promote self-care
2. To ensure high quality local services where possible
3. To improve the health of those most in need
4. To improve health and educational attainment for children and young people
5. To improve access to mental health services
6. To improve outcomes for patients with diabetes to above national averages
7. To improve care for frail elderly individuals
8. To allow patients to die with dignity and compassion and to choose their place of death where appropriate
9. To ensure that the CCG operates within agreed budgets
Action required by Governing Body: To note the report.
1
IESCCG Performance Pack May 2022
*** Please note all slides in this pack show data for March M12 unless otherwise stated ***
2
Contents (Ctrl + Click on Heading to follow the link)
• Elective Care, RTT & Diagnostics
• Urgent Emergency Care
• Cancer
• COVID Vaccination
• CYP & Mental Health
• Quality
• Transformation
• CCG Finance

Elective Care RTT & Diagnostics
Elective Care (March 2022)ContextMarch was a productive month in our hospitals and independent sector partners. Significant activity was undertaken and our longest waiter numbers reduced. WSFT had access to additional theatres and were able to increase the numbers of patients treated in this month.
System workingESNEFT supported WSFT by providing support in the form of enabling orthopaedic and gynaecology patients to transfer and receive their care earlier.
Independent SectorOur independent sector partners have continued to support our elective recovery by providing additional capacity to the system.
Waiting timesAs detailed on the following pages overall waiting times were relatively stable, but the number of patients waiting longer than 2 years for treatment fell. In April, we have seen further reductions in the very long waiters and aim to have eliminated all 2 year waiters by July 2022.
With the exception of CT waits at ESNEFT diagnostic waiting times were either stable or grew in March and we are seeking to source additional capacity to address this issue.
Outpatient TransformationBoth Trusts continue to focus on the following initiatives:• Advice and Guidance is being made more available to GPs and
patients who wish to discuss care with a consultant and may not need to come to hospital for an appointment
• Patient Initiated Follow Ups (PIFU): where clinically appropriate, patients are being offered the opportunity to have a patient initiated follow up such that they only need come back into the hospital if they are worried or are experiencing symptoms that have been discussed with the team on discharge from the hospital
• Virtual consultations: where clinically appropriate, patients are being offered telephone or video consultations as an alternative to them having to attend the hospital.
Other transformationOur trusts are focussing on the following initiatives to increase productivity:• Theatre productivity: reviews are taking place to understand the
potential for increasing theatre throughput• High Volume, Low Complexity (HVLC) pathways: reviews of routine
elective pathways are ongoing to identify and realise greater efficiencies
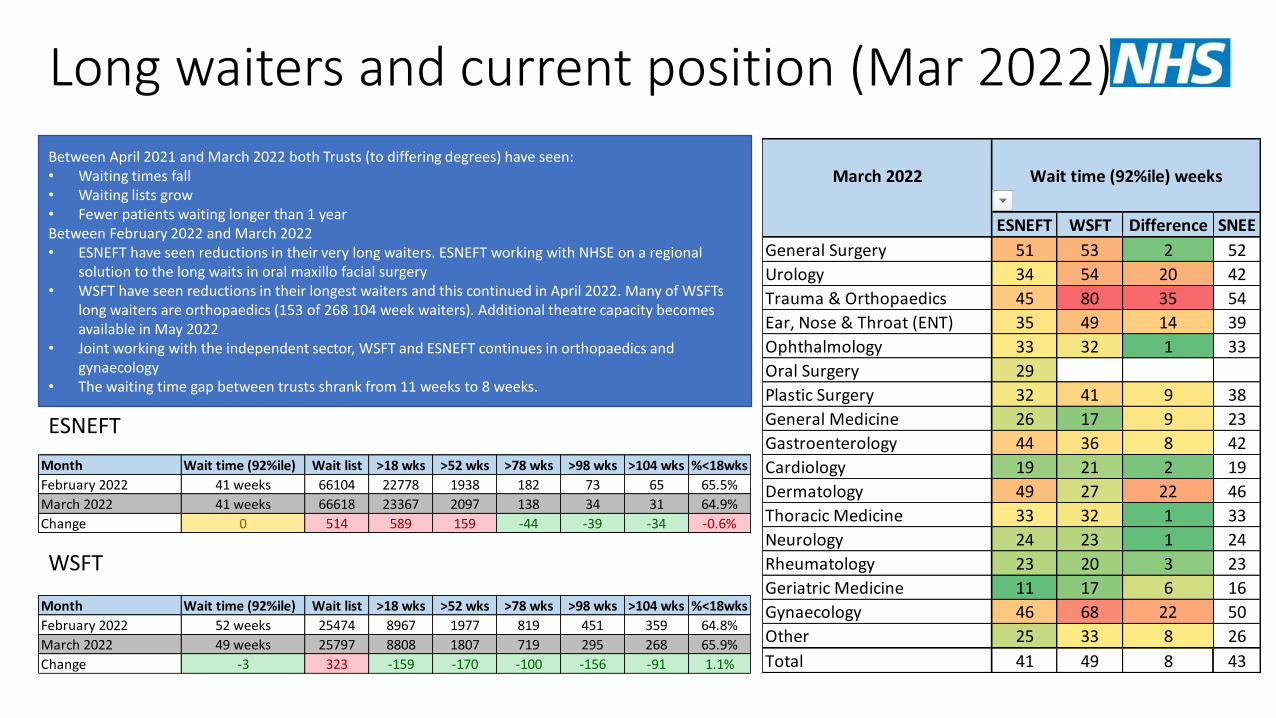
Long waiters and current position (Mar 2022)
ESNEFT
WSFT
Between April 2021 and March 2022 both Trusts (to differing degrees) have seen:• Waiting times fall• Waiting lists grow• Fewer patients waiting longer than 1 yearBetween February 2022 and March 2022• ESNEFT have seen reductions in their very long waiters. ESNEFT working with NHSE on a regional
solution to the long waits in oral maxillo facial surgery• WSFT have seen reductions in their longest waiters and this continued in April 2022. Many of WSFTs
long waiters are orthopaedics (153 of 268 104 week waiters). Additional theatre capacity becomes available in May 2022
• Joint working with the independent sector, WSFT and ESNEFT continues in orthopaedics and gynaecology
• The waiting time gap between trusts shrank from 11 weeks to 8 weeks.
Month Wait time (92%ile) Wait list >18 wks >52 wks >78 wks >98 wks >104 wks %<18wks
February 2022 41 weeks 66104 22778 1938 182 73 65 65.5%
March 2022 41 weeks 66618 23367 2097 138 34 31 64.9%
Change 0 514 589 159 -44 -39 -34 -0.6%
Month Wait time (92%ile) Wait list >18 wks >52 wks >78 wks >98 wks >104 wks %<18wks
February 2022 52 weeks 25474 8967 1977 819 451 359 64.8%
March 2022 49 weeks 25797 8808 1807 719 295 268 65.9%
Change -3 323 -159 -170 -100 -156 -91 1.1%
March 2022
ESNEFT WSFT Difference SNEE
General Surgery 51 53 2 52
Urology 34 54 20 42
Trauma & Orthopaedics 45 80 35 54
Ear, Nose & Throat (ENT) 35 49 14 39
Ophthalmology 33 32 1 33
Oral Surgery 29
Plastic Surgery 32 41 9 38
General Medicine 26 17 9 23
Gastroenterology 44 36 8 42
Cardiology 19 21 2 19
Dermatology 49 27 22 46
Thoracic Medicine 33 32 1 33
Neurology 24 23 1 24
Rheumatology 23 20 3 23
Geriatric Medicine 11 17 6 16
Gynaecology 46 68 22 50
Other 25 33 8 26
Total 41 49 8 43
Wait time (92%ile) weeks
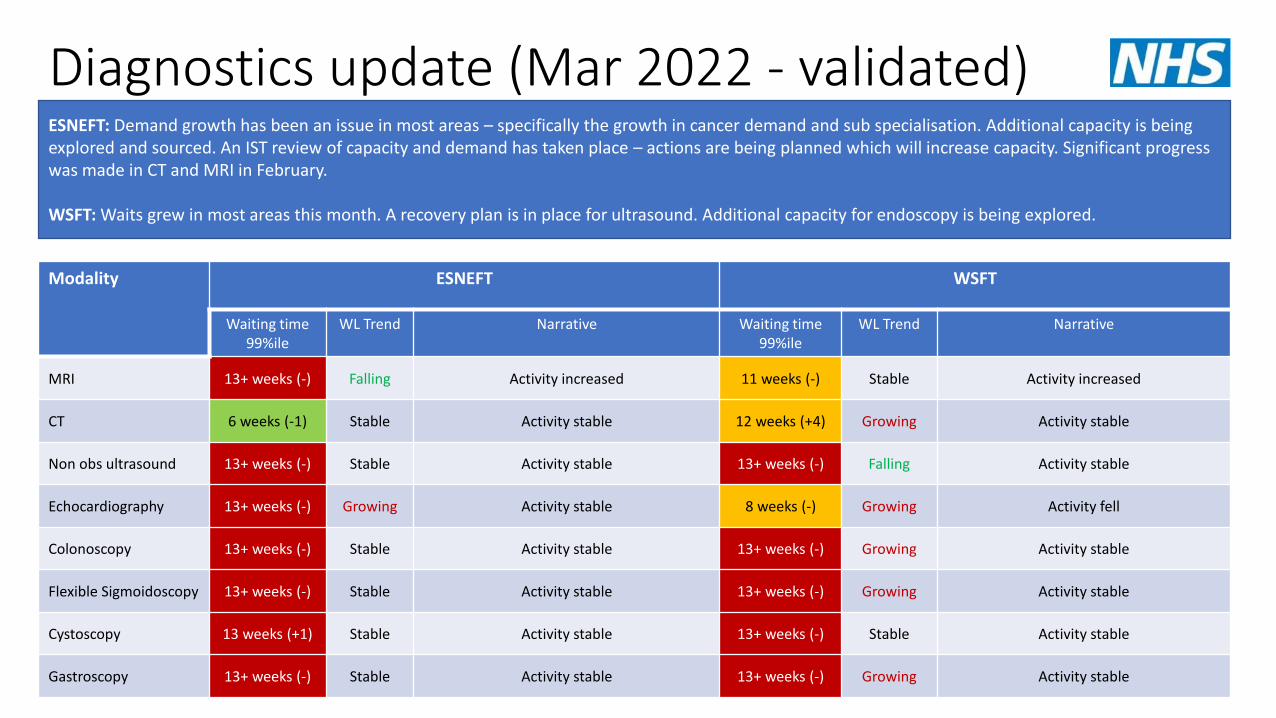
Diagnostics update (Mar 2022 - validated)ESNEFT: Demand growth has been an issue in most areas – specifically the growth in cancer demand and sub specialisation. Additional capacity is being explored and sourced. An IST review of capacity and demand has taken place – actions are being planned which will increase capacity. Significant progress was made in CT and MRI in February.
WSFT: Waits grew in most areas this month. A recovery plan is in place for ultrasound. Additional capacity for endoscopy is being explored.
Modality ESNEFT WSFT
Waiting time99%ile
WL Trend Narrative Waiting time99%ile
WL Trend Narrative
MRI 13+ weeks (-) Falling Activity increased 11 weeks (-) Stable Activity increased
CT 6 weeks (-1) Stable Activity stable 12 weeks (+4) Growing Activity stable
Non obs ultrasound 13+ weeks (-) Stable Activity stable 13+ weeks (-) Falling Activity stable
Echocardiography 13+ weeks (-) Growing Activity stable 8 weeks (-) Growing Activity fell
Colonoscopy 13+ weeks (-) Stable Activity stable 13+ weeks (-) Growing Activity stable
Flexible Sigmoidoscopy 13+ weeks (-) Stable Activity stable 13+ weeks (-) Growing Activity stable
Cystoscopy 13 weeks (+1) Stable Activity stable 13+ weeks (-) Stable Activity stable
Gastroscopy 13+ weeks (-) Stable Activity stable 13+ weeks (-) Growing Activity stable

Urgent Emergency Care
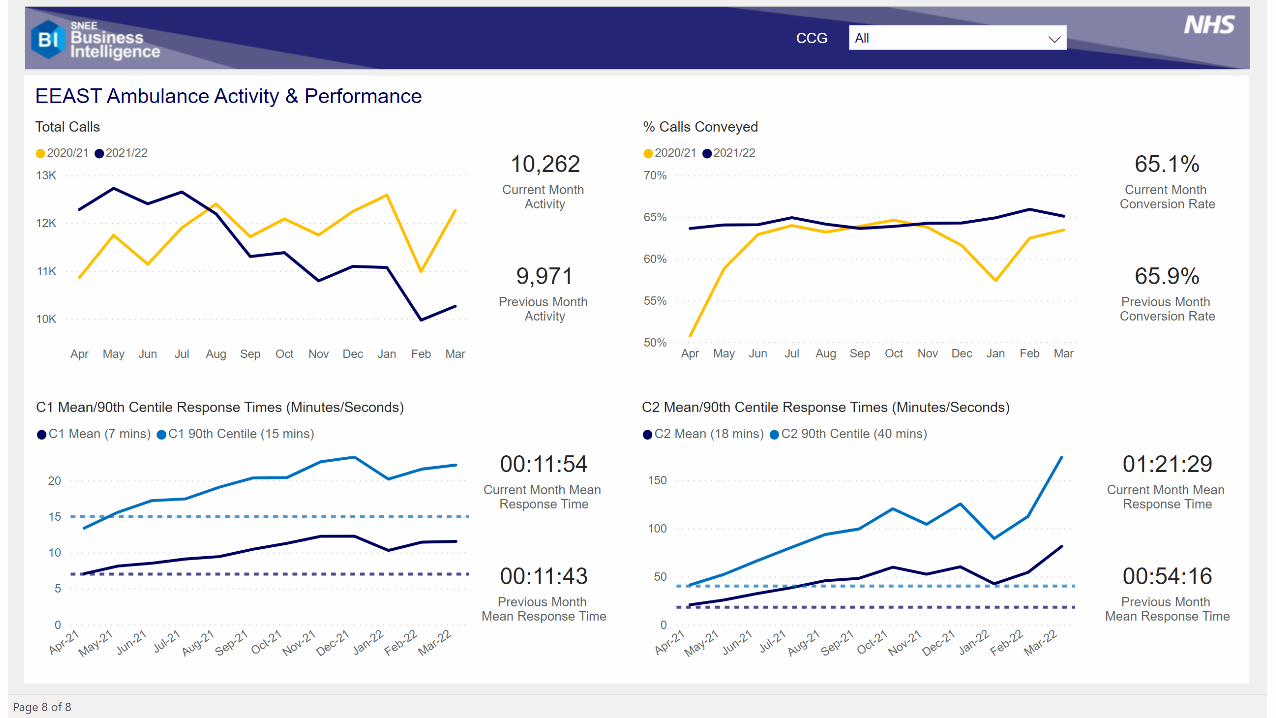
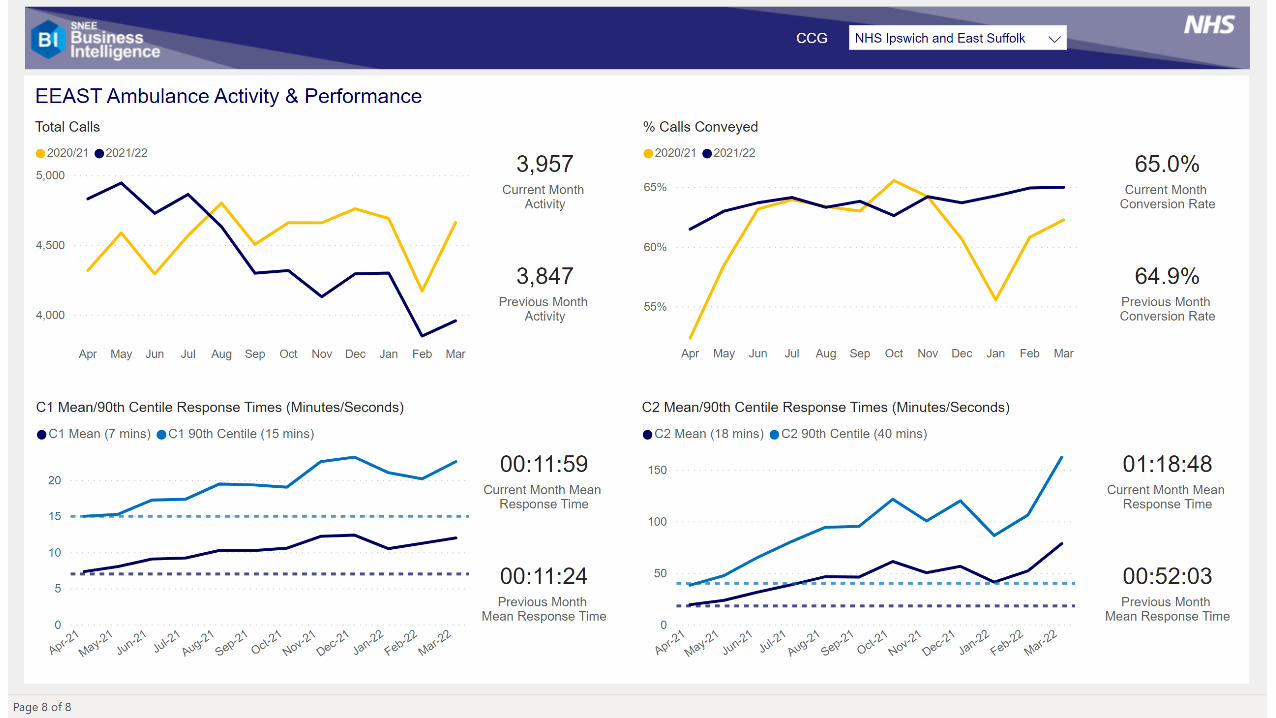
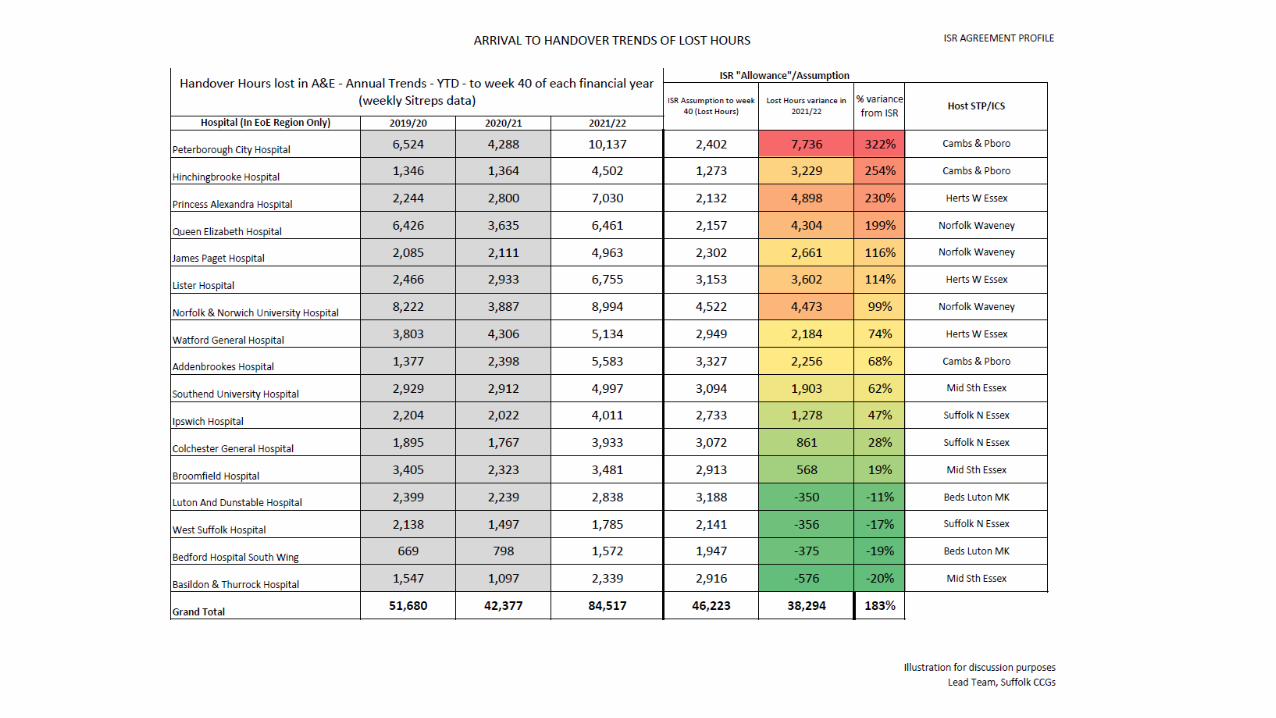
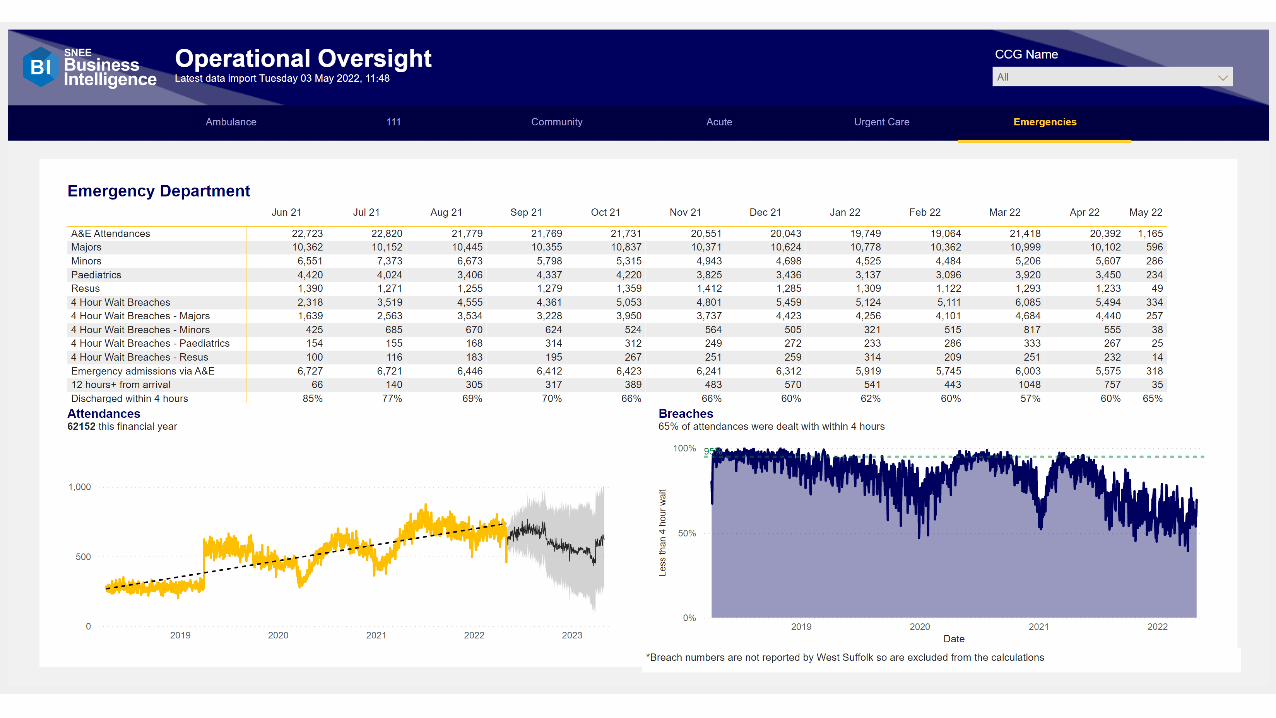
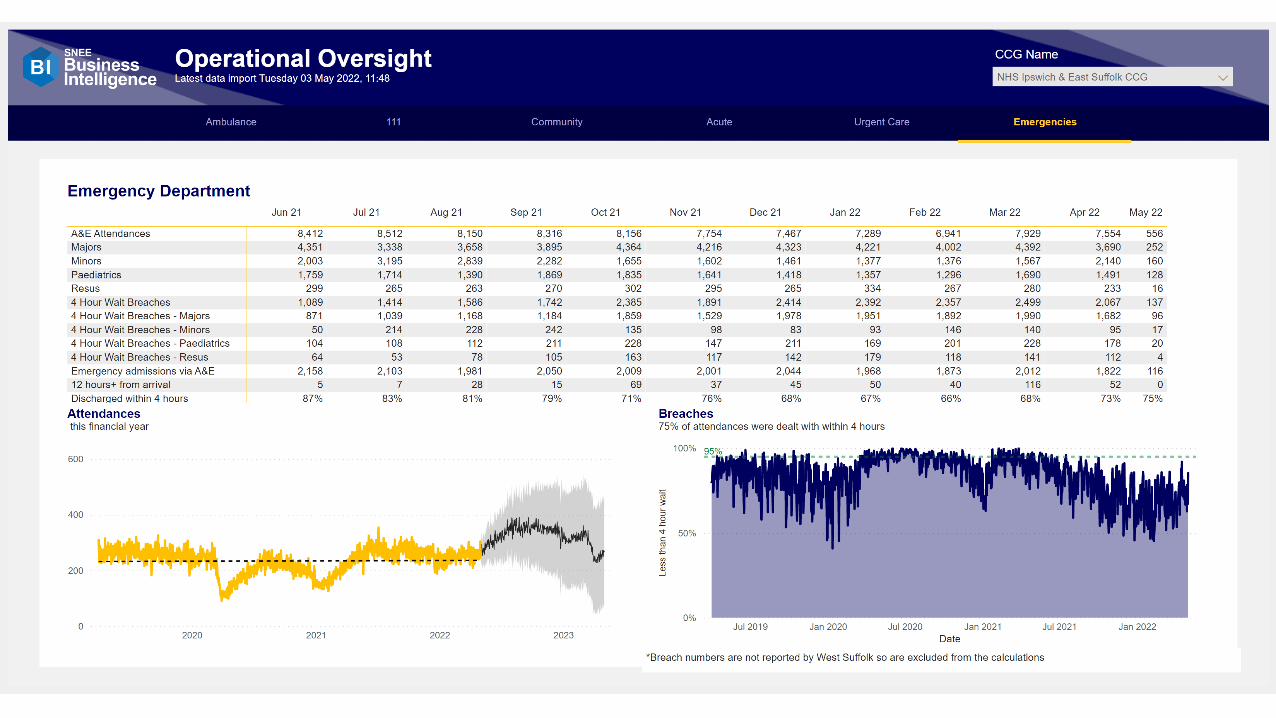
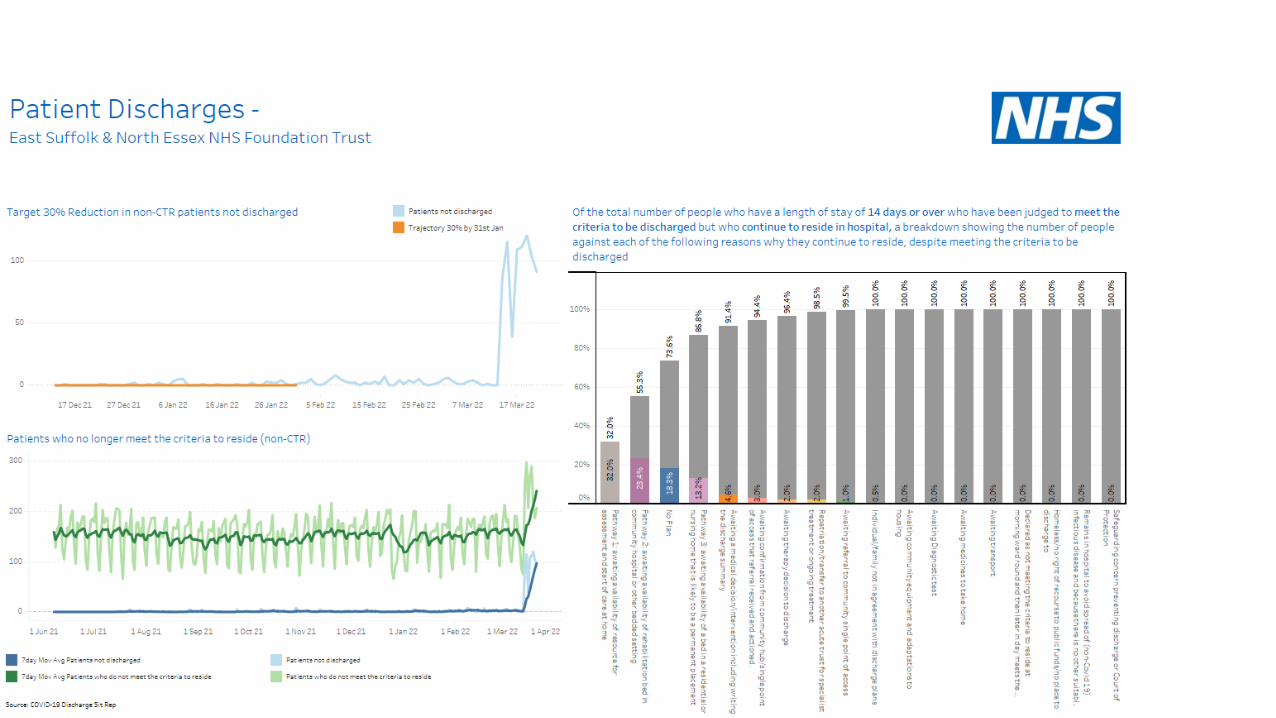
Urgent and emergency care summary
• The National Incident Level remains at Level 4 and the SNEE Command, Control and Coordination structures continue to support 0800-1800 seven days a week.
• Our Operating Pressure Escalation Level (OPEL) reduced to OPEL 3 on the 8th April and this has further reduced to OPEL 2 on the 28th April (we are one of a handful of systems nationally at this stable level). EEAST remain at REAP level 4, although we have seen more frequent de-escalation of Surge levels during the end of April/ beginning of May.
• Workforce absence has improved across all providers with the Acute sites now showing 27.8% of sickness Covid related which is reduced from 44.8% mid April.
• Covid patients occupying hospital beds has also reduced to 158 patients as of 4/5/22. Overall occupancy in hospitals remains high (>95%).
• ED 4 hour performance at ESNEFT has continued to be below national standards, but generally one of the highest in the EoE region. We have seen a slight improvement over April. WSFT average journey time for April was 278 minutes.
• Discharges have continued to be challenging, partly because of care availability (impacted by workforce and holidays – both of which are improving) and differences in national guidance on Covid for health and care. This is also now improving with teams supporting to improve understanding and confidence across the care sector. Pathway 2 (Carehome) patients with no criteria to reside remain high in Ipswich & east.
Overall, the system continues to be challenged due to high demand at ED, impacts of bank holidays on flow and recovery activities. The focus for the system remains on flow, reducing occupancy and planning for the Jubilee weekend.
▪ EEAST activity reduced on 20/21 levels, achieving required patient facing staff hours on day to day basis remains the focus and issue.
▪ Performance in March showing stable or worsening response times. Expected this will show small improvements in April however still not achieving national standards.
▪ Additional support and process now formalised for c3/c4 ambulance stacked patients to transfer to IUC CAS. Also conveyance reduction support lines (paramedic on scene to GP access) remain in place.
▪ Handover delays, West Suffolk remain below allowance planned into EEAST models for handover performance. Colchester and Ipswich are above allowance however benchmark well against other hospital sites. HALO continuation has been agreed for Ipswich and West Suffolk and NEE going through final governance sign off. HALO will now become part of ESNEFT core contract moving forwards.
Urgent and emergency care summary
• As a system we’re working with EEAST to support demand management and a number of initiatives are now in place including; Implemented a C3 & C4 ambulance stack ‘push’ model (with plans to move to an electronic solution directly transferring cases to the IUC for validation being advanced with NHS England); and rapid telephone access to senior clinical advice to support decision making ahead of conveying a patient to hospital. Both models have demonstrated a reduction in the number of people conveyed to ED.
• The IUC Service have implemented additional training for advisors to look to reduce Cat 2 ambulance, this has broadly been very successful with a 8% drop in C2 ambulances, however this has resulted in more C3 ambulance so ambulances sent remains the same. The implementation of DoS Validation has also resulted in a 2% drop in ED outcomes to around 7% of triaged calls, both of these initiatives have been extremely positive for helping reduce demand on the Urgent and Emergency Care Services.

Cancer
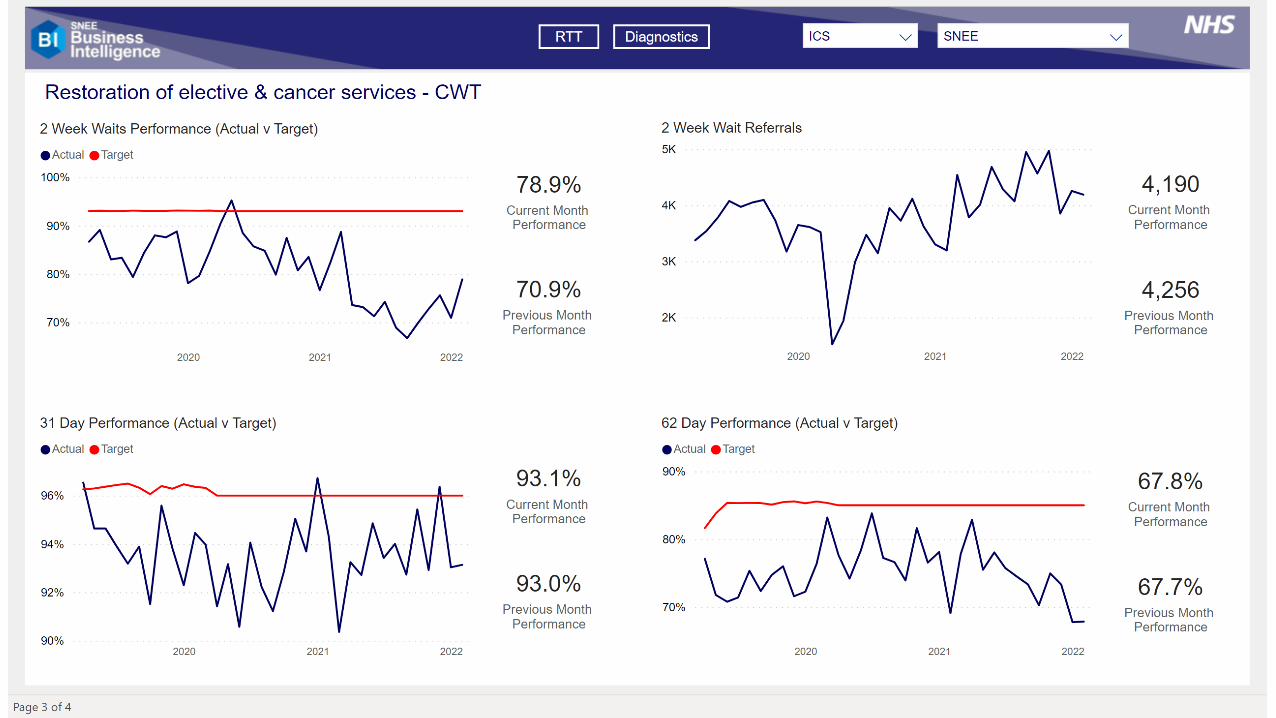
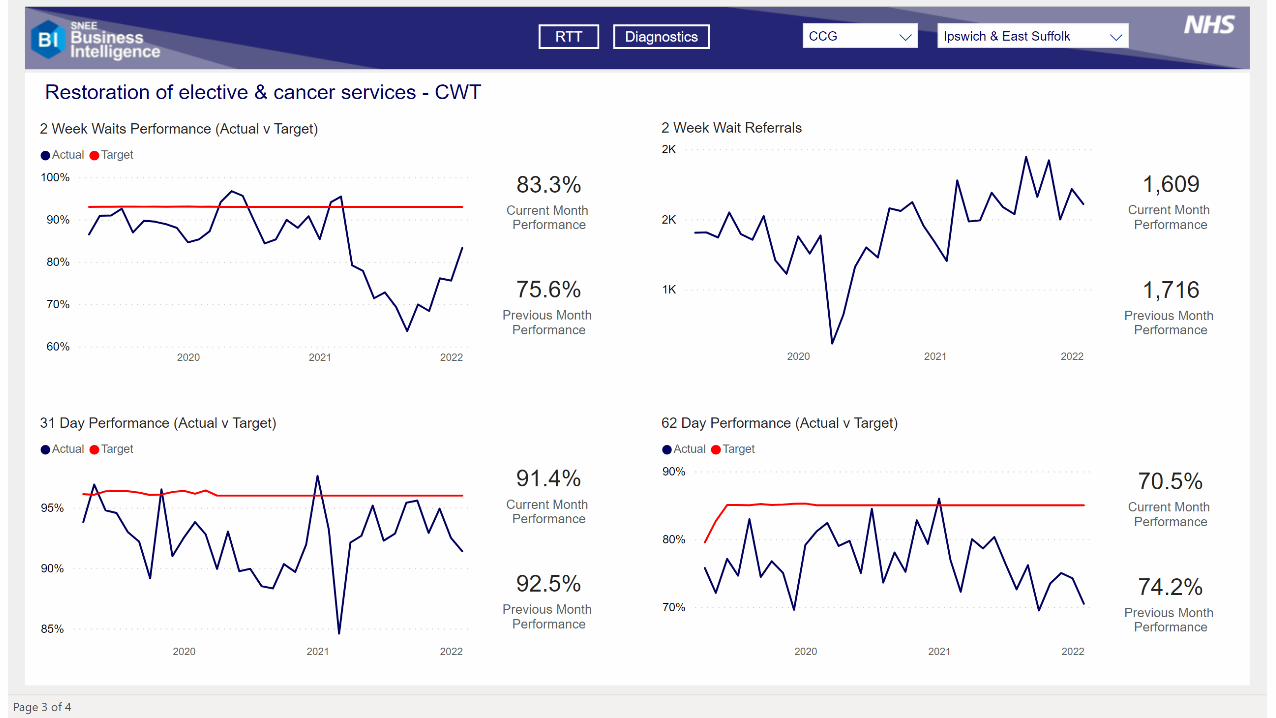
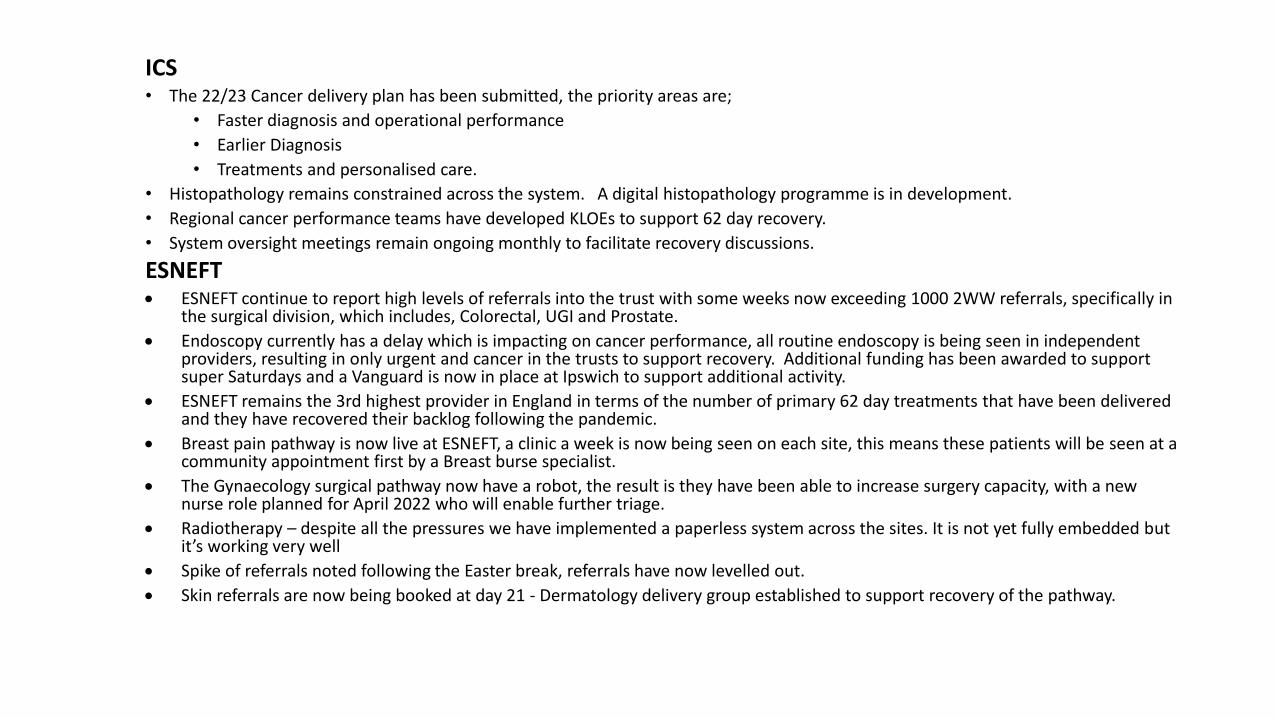
ICS • The 22/23 Cancer delivery plan has been submitted, the priority areas are;
• Faster diagnosis and operational performance
• Earlier Diagnosis
• Treatments and personalised care.
• Histopathology remains constrained across the system. A digital histopathology programme is in development.
• Regional cancer performance teams have developed KLOEs to support 62 day recovery.
• System oversight meetings remain ongoing monthly to facilitate recovery discussions.
ESNEFT• ESNEFT continue to report high levels of referrals into the trust with some weeks now exceeding 1000 2WW referrals, specifically in
the surgical division, which includes, Colorectal, UGI and Prostate.
• Endoscopy currently has a delay which is impacting on cancer performance, all routine endoscopy is being seen in independent providers, resulting in only urgent and cancer in the trusts to support recovery. Additional funding has been awarded to support super Saturdays and a Vanguard is now in place at Ipswich to support additional activity.
• ESNEFT remains the 3rd highest provider in England in terms of the number of primary 62 day treatments that have been delivered and they have recovered their backlog following the pandemic.
• Breast pain pathway is now live at ESNEFT, a clinic a week is now being seen on each site, this means these patients will be seen at a community appointment first by a Breast burse specialist.
• The Gynaecology surgical pathway now have a robot, the result is they have been able to increase surgery capacity, with a newnurse role planned for April 2022 who will enable further triage.
• Radiotherapy – despite all the pressures we have implemented a paperless system across the sites. It is not yet fully embedded but it’s working very well
• Spike of referrals noted following the Easter break, referrals have now levelled out.
• Skin referrals are now being booked at day 21 - Dermatology delivery group established to support recovery of the pathway.
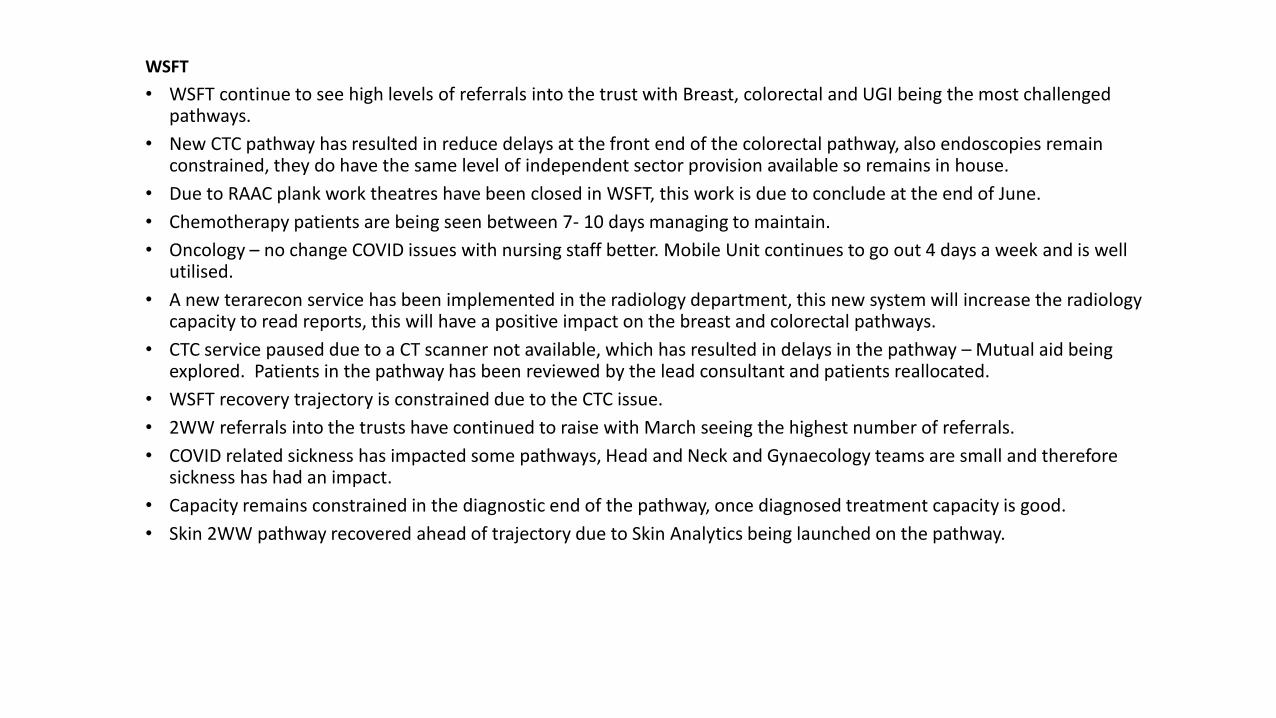
WSFT
• WSFT continue to see high levels of referrals into the trust with Breast, colorectal and UGI being the most challenged pathways.
• New CTC pathway has resulted in reduce delays at the front end of the colorectal pathway, also endoscopies remain constrained, they do have the same level of independent sector provision available so remains in house.
• Due to RAAC plank work theatres have been closed in WSFT, this work is due to conclude at the end of June.
• Chemotherapy patients are being seen between 7- 10 days managing to maintain.
• Oncology – no change COVID issues with nursing staff better. Mobile Unit continues to go out 4 days a week and is well utilised.
• A new terarecon service has been implemented in the radiology department, this new system will increase the radiology capacity to read reports, this will have a positive impact on the breast and colorectal pathways.
• CTC service paused due to a CT scanner not available, which has resulted in delays in the pathway – Mutual aid being explored. Patients in the pathway has been reviewed by the lead consultant and patients reallocated.
• WSFT recovery trajectory is constrained due to the CTC issue.
• 2WW referrals into the trusts have continued to raise with March seeing the highest number of referrals.
• COVID related sickness has impacted some pathways, Head and Neck and Gynaecology teams are small and therefore sickness has had an impact.
• Capacity remains constrained in the diagnostic end of the pathway, once diagnosed treatment capacity is good.
• Skin 2WW pathway recovered ahead of trajectory due to Skin Analytics being launched on the pathway.
Covid Vaccination
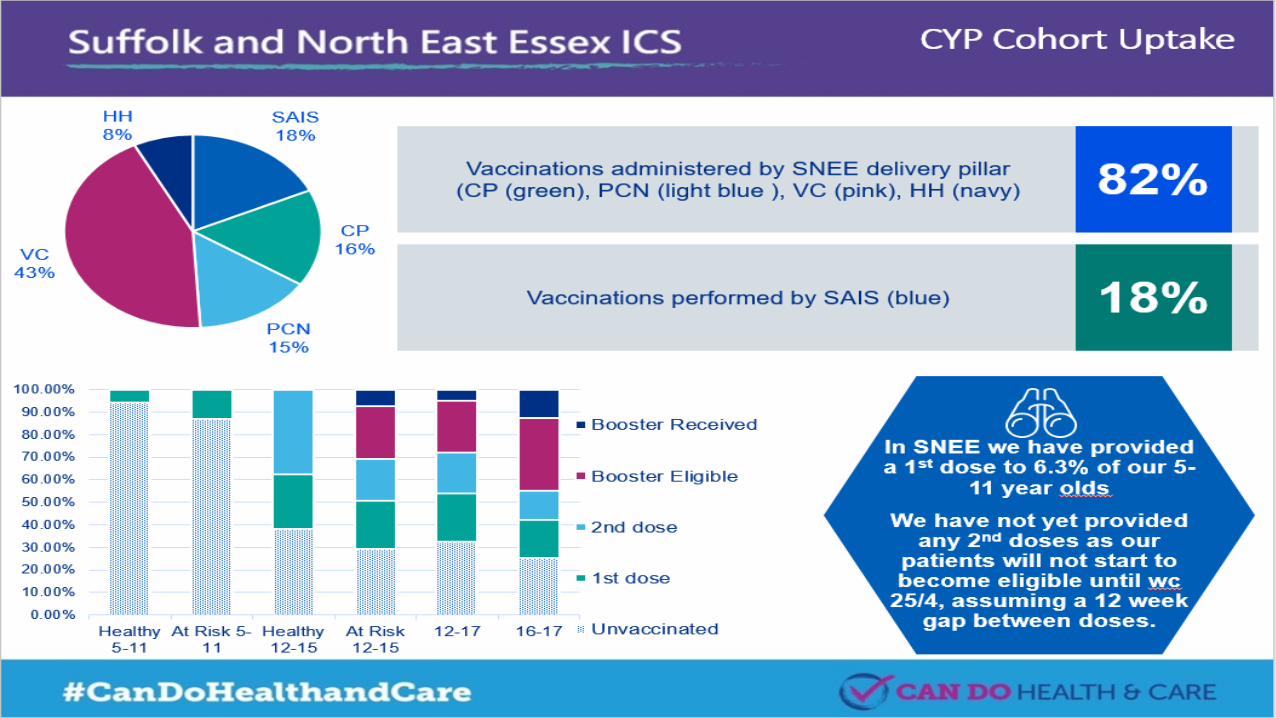
Children and Young People/Mental
Health
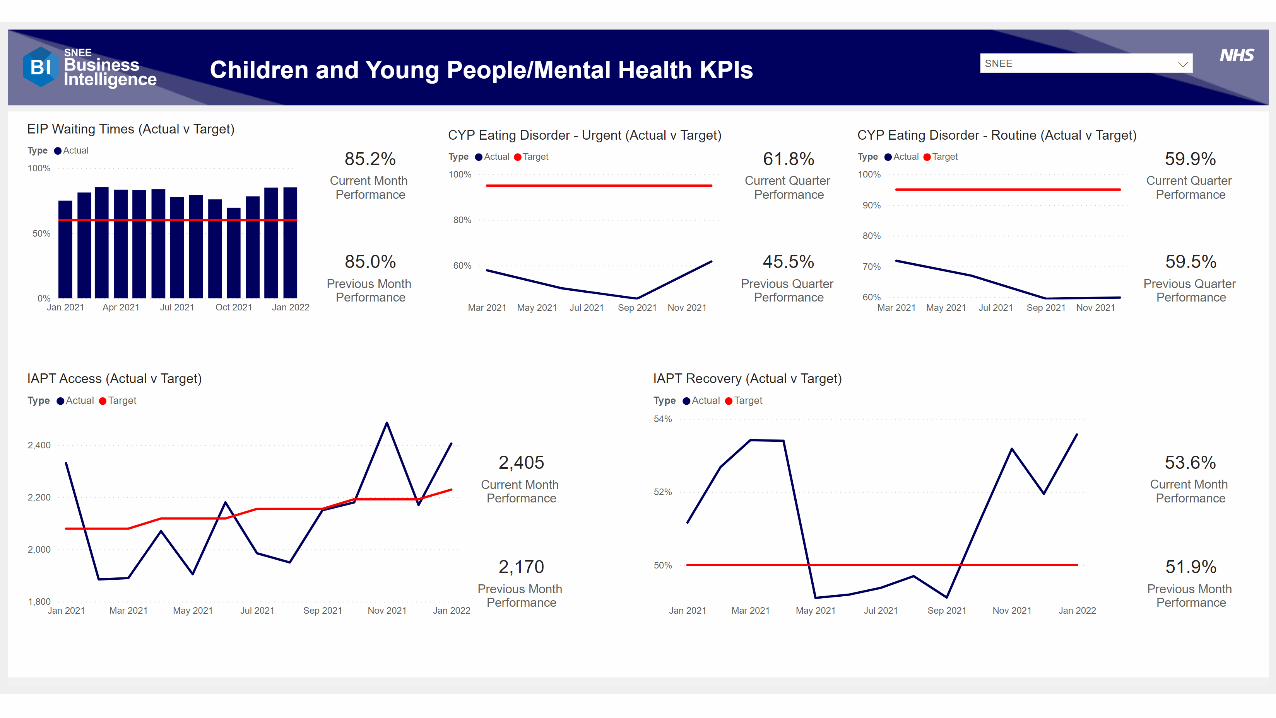
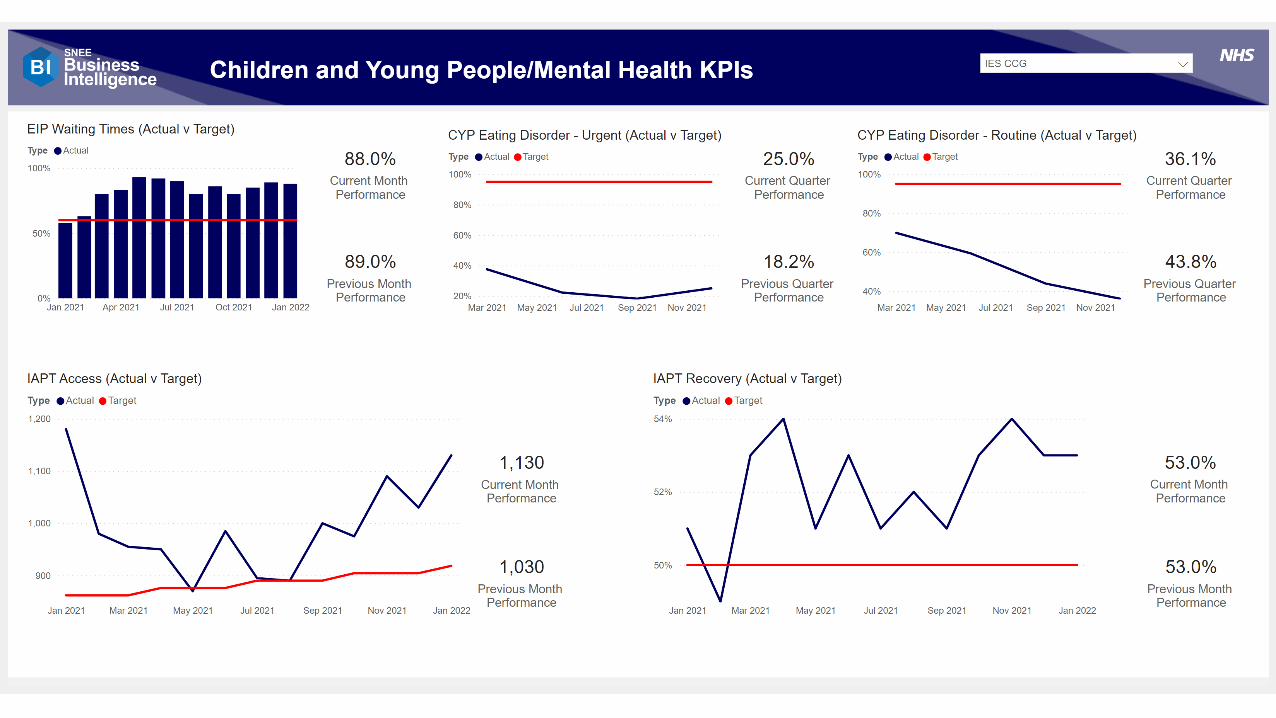
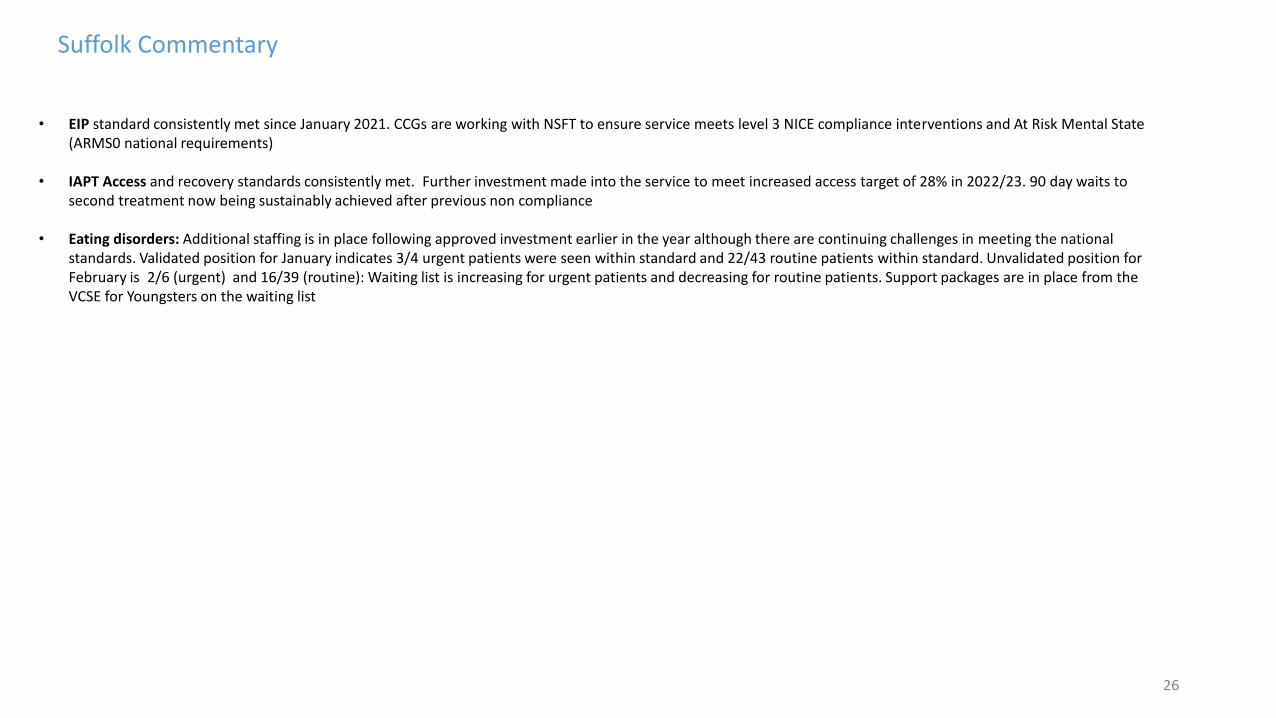
26
Suffolk Commentary
• EIP standard consistently met since January 2021. CCGs are working with NSFT to ensure service meets level 3 NICE compliance interventions and At Risk Mental State (ARMS0 national requirements)
• IAPT Access and recovery standards consistently met. Further investment made into the service to meet increased access target of 28% in 2022/23. 90 day waits to second treatment now being sustainably achieved after previous non compliance
• Eating disorders: Additional staffing is in place following approved investment earlier in the year although there are continuing challenges in meeting the national standards. Validated position for January indicates 3/4 urgent patients were seen within standard and 22/43 routine patients within standard. Unvalidated position for February is 2/6 (urgent) and 16/39 (routine): Waiting list is increasing for urgent patients and decreasing for routine patients. Support packages are in place from the VCSE for Youngsters on the waiting list

Quality Assurance Updates
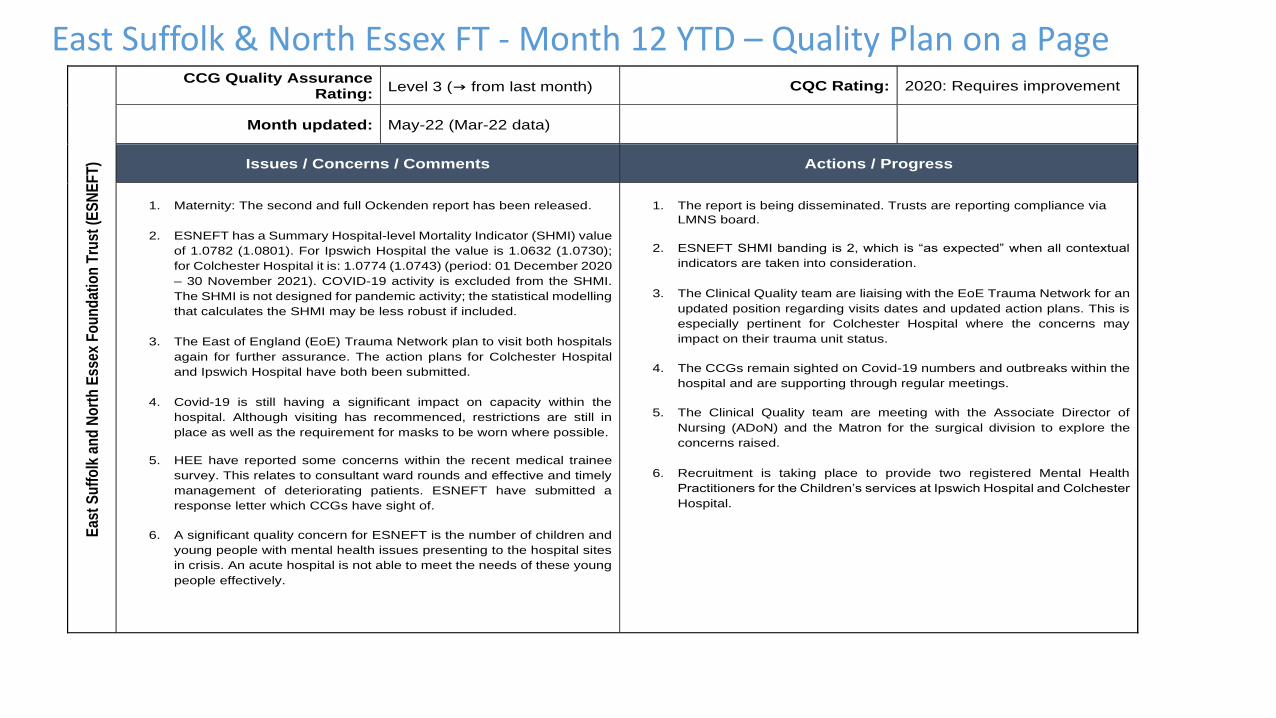
East Suffolk & North Essex FT - Month 12 YTD – Quality Plan on a Page
Eas
t S
uff
olk
an
d N
ort
h E
ssex
Fo
un
dat
ion
Tru
st (
ES
NE
FT
) CCG Quality Assurance
Rating: Level 3 (→ from last month) CQC Rating: 2020: Requires improvement
Month updated: May-22 (Mar-22 data)
Issues / Concerns / Comments Actions / Progress
1. Maternity: The second and full Ockenden report has been released.
2. ESNEFT has a Summary Hospital-level Mortality Indicator (SHMI) value
of 1.0782 (1.0801). For Ipswich Hospital the value is 1.0632 (1.0730);
for Colchester Hospital it is: 1.0774 (1.0743) (period: 01 December 2020
– 30 November 2021). COVID-19 activity is excluded from the SHMI.
The SHMI is not designed for pandemic activity; the statistical modelling
that calculates the SHMI may be less robust if included.
3. The East of England (EoE) Trauma Network plan to visit both hospitals
again for further assurance. The action plans for Colchester Hospital
and Ipswich Hospital have both been submitted.
4. Covid-19 is still having a significant impact on capacity within the
hospital. Although visiting has recommenced, restrictions are still in
place as well as the requirement for masks to be worn where possible.
5. HEE have reported some concerns within the recent medical trainee
survey. This relates to consultant ward rounds and effective and timely
management of deteriorating patients. ESNEFT have submitted a
response letter which CCGs have sight of.
6. A significant quality concern for ESNEFT is the number of children and
young people with mental health issues presenting to the hospital sites
in crisis. An acute hospital is not able to meet the needs of these young
people effectively.
1. The report is being disseminated. Trusts are reporting compliance via
LMNS board.
2. ESNEFT SHMI banding is 2, which is “as expected” when all contextual
indicators are taken into consideration.
3. The Clinical Quality team are liaising with the EoE Trauma Network for an
updated position regarding visits dates and updated action plans. This is
especially pertinent for Colchester Hospital where the concerns may
impact on their trauma unit status.
4. The CCGs remain sighted on Covid-19 numbers and outbreaks within the
hospital and are supporting through regular meetings.
5. The Clinical Quality team are meeting with the Associate Director of
Nursing (ADoN) and the Matron for the surgical division to explore the
concerns raised.
6. Recruitment is taking place to provide two registered Mental Health
Practitioners for the Children’s services at Ipswich Hospital and Colchester
Hospital.
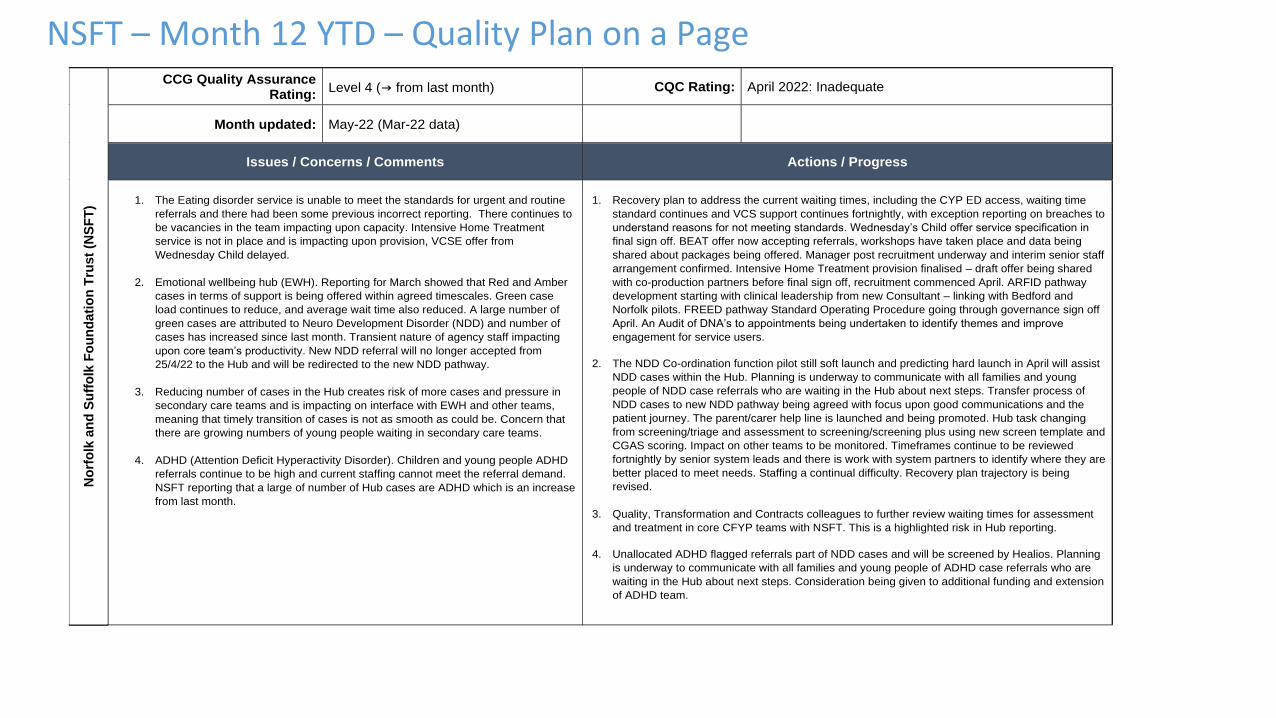
NSFT – Month 12 YTD – Quality Plan on a Page
No
rfo
lk a
nd
Su
ffo
lk F
ou
nd
ati
on
Tru
st
(NS
FT
)
CCG Quality Assurance
Rating: Level 4 (→ from last month) CQC Rating: April 2022: Inadequate
Month updated: May-22 (Mar-22 data)
Issues / Concerns / Comments Actions / Progress
1. The Eating disorder service is unable to meet the standards for urgent and routine
referrals and there had been some previous incorrect reporting. There continues to
be vacancies in the team impacting upon capacity. Intensive Home Treatment
service is not in place and is impacting upon provision, VCSE offer from
Wednesday Child delayed.
2. Emotional wellbeing hub (EWH). Reporting for March showed that Red and Amber
cases in terms of support is being offered within agreed timescales. Green case
load continues to reduce, and average wait time also reduced. A large number of
green cases are attributed to Neuro Development Disorder (NDD) and number of
cases has increased since last month. Transient nature of agency staff impacting
upon core team’s productivity. New NDD referral will no longer accepted from
25/4/22 to the Hub and will be redirected to the new NDD pathway.
3. Reducing number of cases in the Hub creates risk of more cases and pressure in
secondary care teams and is impacting on interface with EWH and other teams,
meaning that timely transition of cases is not as smooth as could be. Concern that
there are growing numbers of young people waiting in secondary care teams.
4. ADHD (Attention Deficit Hyperactivity Disorder). Children and young people ADHD
referrals continue to be high and current staffing cannot meet the referral demand.
NSFT reporting that a large of number of Hub cases are ADHD which is an increase
from last month.
1. Recovery plan to address the current waiting times, including the CYP ED access, waiting time
standard continues and VCS support continues fortnightly, with exception reporting on breaches to
understand reasons for not meeting standards. Wednesday’s Child offer service specification in
final sign off. BEAT offer now accepting referrals, workshops have taken place and data being
shared about packages being offered. Manager post recruitment underway and interim senior staff
arrangement confirmed. Intensive Home Treatment provision finalised – draft offer being shared
with co-production partners before final sign off, recruitment commenced April. ARFID pathway
development starting with clinical leadership from new Consultant – linking with Bedford and
Norfolk pilots. FREED pathway Standard Operating Procedure going through governance sign off
April. An Audit of DNA’s to appointments being undertaken to identify themes and improve
engagement for service users.
2. The NDD Co-ordination function pilot still soft launch and predicting hard launch in April will assist
NDD cases within the Hub. Planning is underway to communicate with all families and young
people of NDD case referrals who are waiting in the Hub about next steps. Transfer process of
NDD cases to new NDD pathway being agreed with focus upon good communications and the
patient journey. The parent/carer help line is launched and being promoted. Hub task changing
from screening/triage and assessment to screening/screening plus using new screen template and
CGAS scoring. Impact on other teams to be monitored. Timeframes continue to be reviewed
fortnightly by senior system leads and there is work with system partners to identify where they are
better placed to meet needs. Staffing a continual difficulty. Recovery plan trajectory is being
revised.
3. Quality, Transformation and Contracts colleagues to further review waiting times for assessment
and treatment in core CFYP teams with NSFT. This is a highlighted risk in Hub reporting.
4. Unallocated ADHD flagged referrals part of NDD cases and will be screened by Healios. Planning
is underway to communicate with all families and young people of ADHD case referrals who are
waiting in the Hub about next steps. Consideration being given to additional funding and extension
of ADHD team.
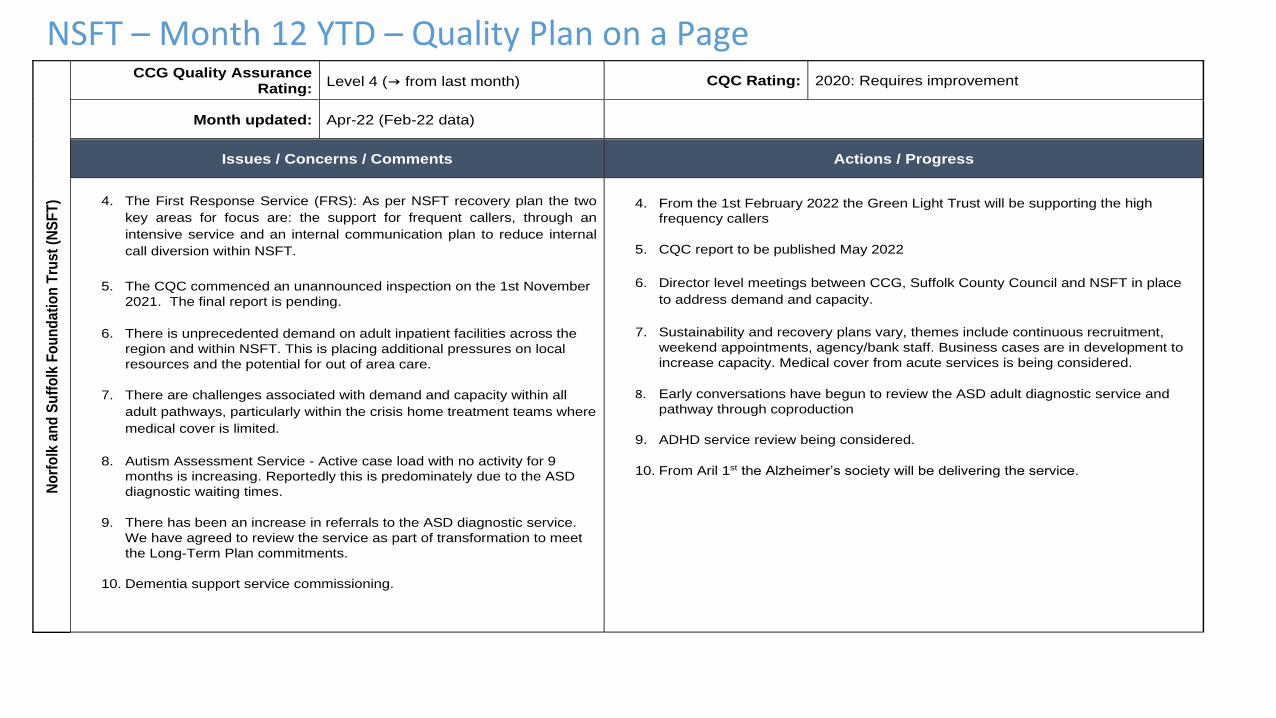
NSFT – Month 12 YTD – Quality Plan on a PageN
orf
olk
an
d S
uff
olk
Fo
un
da
tio
n T
rust
(NS
FT
)
CCG Quality Assurance
Rating: Level 4 (→ from last month) CQC Rating: 2020: Requires improvement
Month updated: Apr-22 (Feb-22 data)
Issues / Concerns / Comments Actions / Progress
4. The First Response Service (FRS): As per NSFT recovery plan the two
key areas for focus are: the support for frequent callers, through an
intensive service and an internal communication plan to reduce internal
call diversion within NSFT.
5. The CQC commenced an unannounced inspection on the 1st November
2021. The final report is pending.
6. There is unprecedented demand on adult inpatient facilities across the
region and within NSFT. This is placing additional pressures on local
resources and the potential for out of area care.
7. There are challenges associated with demand and capacity within all
adult pathways, particularly within the crisis home treatment teams where
medical cover is limited.
8. Autism Assessment Service - Active case load with no activity for 9
months is increasing. Reportedly this is predominately due to the ASD
diagnostic waiting times.
9. There has been an increase in referrals to the ASD diagnostic service.
We have agreed to review the service as part of transformation to meet
the Long-Term Plan commitments.
10. Dementia support service commissioning.
4. From the 1st February 2022 the Green Light Trust will be supporting the high
frequency callers
5. CQC report to be published May 2022
6. Director level meetings between CCG, Suffolk County Council and NSFT in place
to address demand and capacity.
7. Sustainability and recovery plans vary, themes include continuous recruitment,
weekend appointments, agency/bank staff. Business cases are in development to
increase capacity. Medical cover from acute services is being considered.
8. Early conversations have begun to review the ASD adult diagnostic service and
pathway through coproduction
9. ADHD service review being considered.
10. From Aril 1st the Alzheimer’s society will be delivering the service.
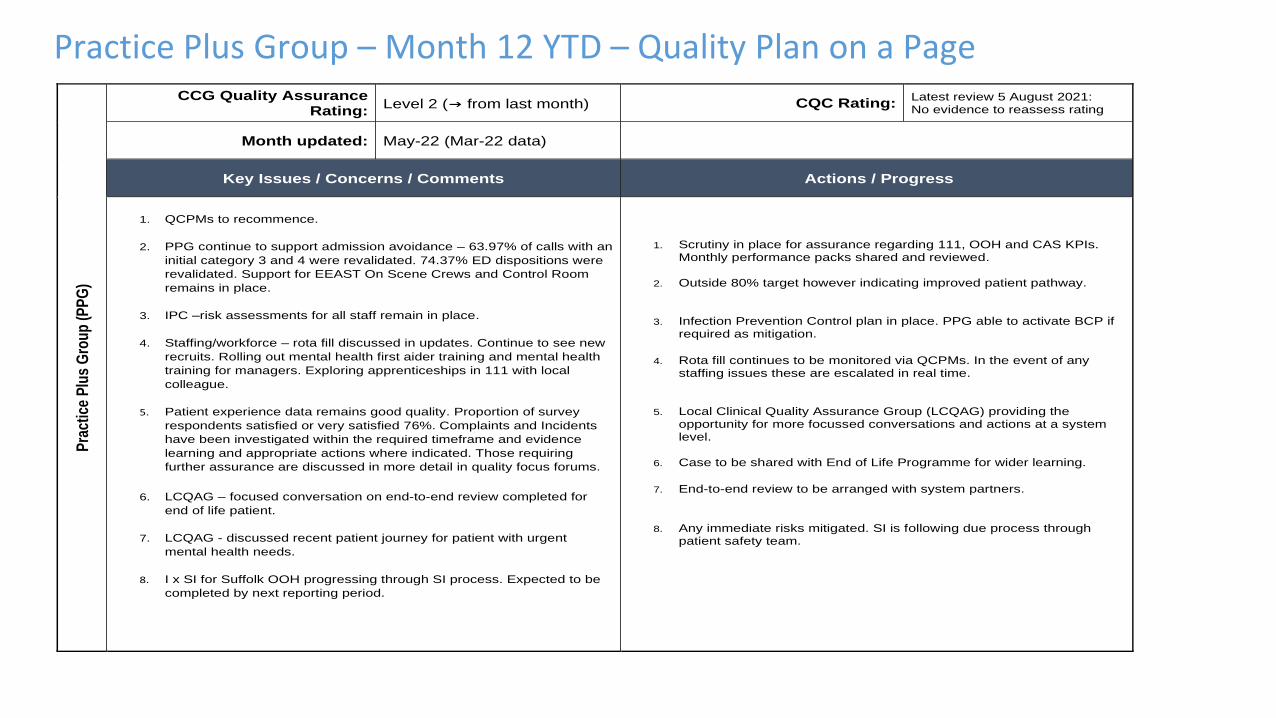
Practice Plus Group – Month 12 YTD – Quality Plan on a PageP
ract
ice
Plu
s G
rou
p (
PP
G)
CCG Quality Assurance Rating:
Level 2 (→ from last month) CQC Rating: Latest review 5 August 2021: No evidence to reassess rating
Month updated: May-22 (Mar-22 data)
Key Issues / Concerns / Comments Actions / Progress
1. QCPMs to recommence.
2. PPG continue to support admission avoidance – 63.97% of calls with an
initial category 3 and 4 were revalidated. 74.37% ED dispositions were
revalidated. Support for EEAST On Scene Crews and Control Room
remains in place.
3. IPC –risk assessments for all staff remain in place.
4. Staffing/workforce – rota fill discussed in updates. Continue to see new
recruits. Rolling out mental health first aider training and mental health
training for managers. Exploring apprenticeships in 111 with local
colleague.
5. Patient experience data remains good quality. Proportion of survey
respondents satisfied or very satisfied 76%. Complaints and Incidents
have been investigated within the required timeframe and evidence
learning and appropriate actions where indicated. Those requiring
further assurance are discussed in more detail in quality focus forums.
6. LCQAG – focused conversation on end-to-end review completed for
end of life patient.
7. LCQAG - discussed recent patient journey for patient with urgent
mental health needs.
8. I x SI for Suffolk OOH progressing through SI process. Expected to be
completed by next reporting period.
1. Scrutiny in place for assurance regarding 111, OOH and CAS KPIs. Monthly performance packs shared and reviewed.
2. Outside 80% target however indicating improved patient pathway.
3. Infection Prevention Control plan in place. PPG able to activate BCP if required as mitigation.
4. Rota fill continues to be monitored via QCPMs. In the event of any staffing issues these are escalated in real time.
5. Local Clinical Quality Assurance Group (LCQAG) providing the opportunity for more focussed conversations and actions at a system level.
6. Case to be shared with End of Life Programme for wider learning.
7. End-to-end review to be arranged with system partners.
8. Any immediate risks mitigated. SI is following due process through
patient safety team.
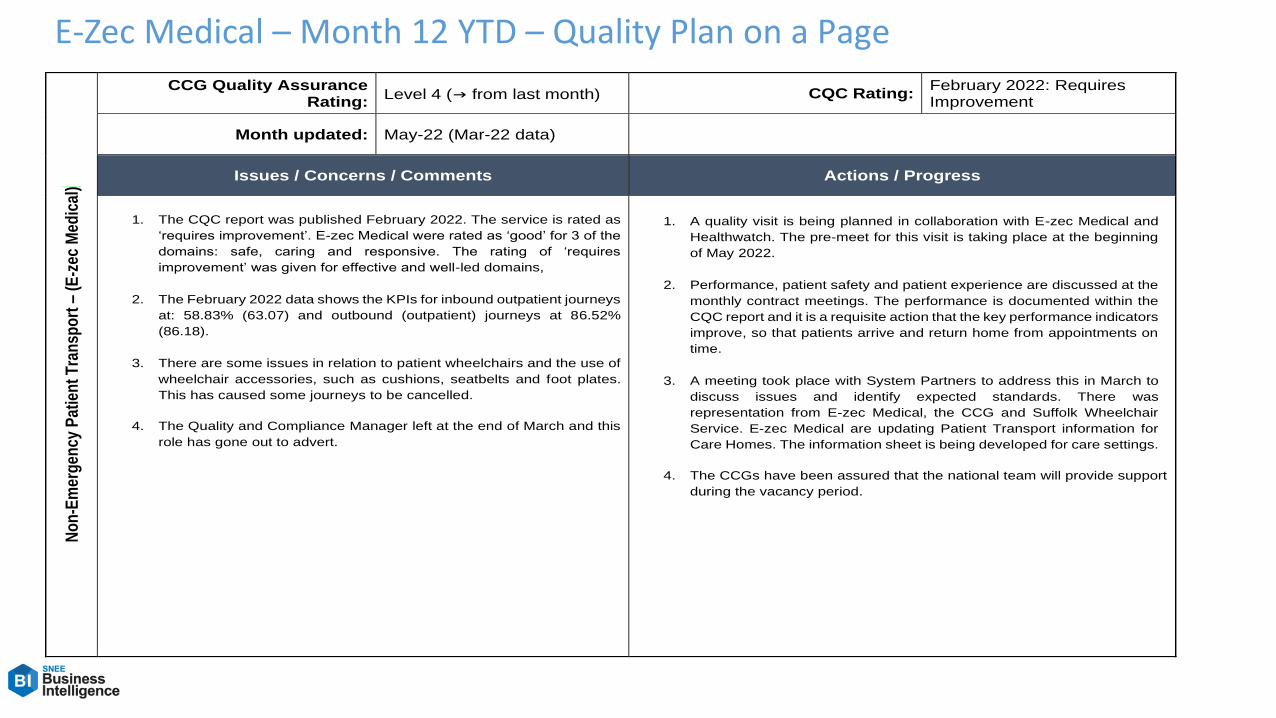
E-Zec Medical – Month 12 YTD – Quality Plan on a PageN
on
-Em
erg
ency
Pat
ien
t T
ran
spo
rt –
(E
-zec
Med
ical
) CCG Quality Assurance
Rating: Level 4 (→ from last month) CQC Rating:
February 2022: Requires Improvement
Month updated: May-22 (Mar-22 data)
Issues / Concerns / Comments Actions / Progress
1. The CQC report was published February 2022. The service is rated as
‘requires improvement’. E-zec Medical were rated as ‘good’ for 3 of the
domains: safe, caring and responsive. The rating of ‘requires
improvement’ was given for effective and well-led domains,
2. The February 2022 data shows the KPIs for inbound outpatient journeys
at: 58.83% (63.07) and outbound (outpatient) journeys at 86.52%
(86.18).
3. There are some issues in relation to patient wheelchairs and the use of
wheelchair accessories, such as cushions, seatbelts and foot plates.
This has caused some journeys to be cancelled.
4. The Quality and Compliance Manager left at the end of March and this
role has gone out to advert.
1. A quality visit is being planned in collaboration with E-zec Medical and
Healthwatch. The pre-meet for this visit is taking place at the beginning
of May 2022.
2. Performance, patient safety and patient experience are discussed at the
monthly contract meetings. The performance is documented within the
CQC report and it is a requisite action that the key performance indicators
improve, so that patients arrive and return home from appointments on
time.
3. A meeting took place with System Partners to address this in March to
discuss issues and identify expected standards. There was
representation from E-zec Medical, the CCG and Suffolk Wheelchair
Service. E-zec Medical are updating Patient Transport information for
Care Homes. The information sheet is being developed for care settings.
4. The CCGs have been assured that the national team will provide support
during the vacancy period.
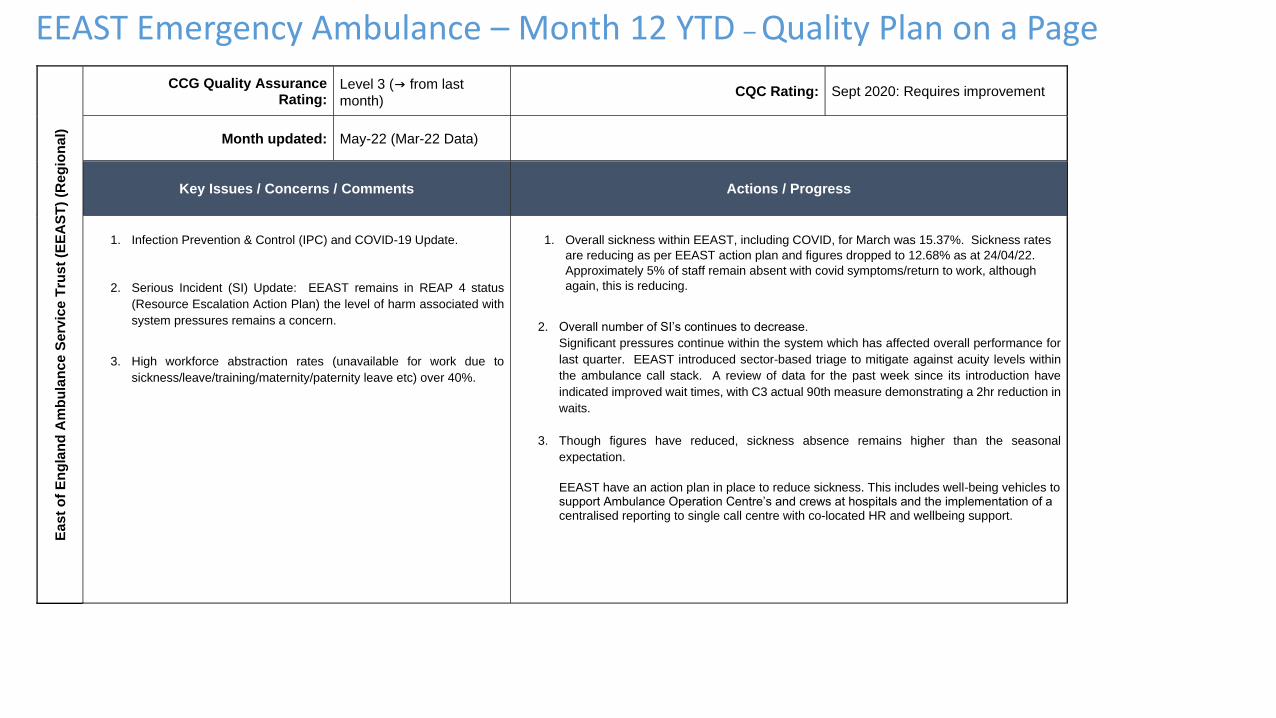
EEAST Emergency Ambulance – Month 12 YTD – Quality Plan on a PageE
as
t o
f E
ng
lan
d A
mb
ula
nc
e S
erv
ice
Tru
st
(EE
AS
T)
(Re
gio
na
l)
CCG Quality Assurance Rating:
Level 3 (→ from last
month) CQC Rating: Sept 2020: Requires improvement
Month updated: May-22 (Mar-22 Data)
Key Issues / Concerns / Comments Actions / Progress
1. Infection Prevention & Control (IPC) and COVID-19 Update.
2. Serious Incident (SI) Update: EEAST remains in REAP 4 status
(Resource Escalation Action Plan) the level of harm associated with
system pressures remains a concern.
3. High workforce abstraction rates (unavailable for work due to
sickness/leave/training/maternity/paternity leave etc) over 40%.
1. Overall sickness within EEAST, including COVID, for March was 15.37%. Sickness rates
are reducing as per EEAST action plan and figures dropped to 12.68% as at 24/04/22.
Approximately 5% of staff remain absent with covid symptoms/return to work, although
again, this is reducing.
2. Overall number of SI’s continues to decrease.
Significant pressures continue within the system which has affected overall performance for
last quarter. EEAST introduced sector-based triage to mitigate against acuity levels within
the ambulance call stack. A review of data for the past week since its introduction have
indicated improved wait times, with C3 actual 90th measure demonstrating a 2hr reduction in
waits.
3. Though figures have reduced, sickness absence remains higher than the seasonal
expectation.
EEAST have an action plan in place to reduce sickness. This includes well-being vehicles to support Ambulance Operation Centre’s and crews at hospitals and the implementation of a centralised reporting to single call centre with co-located HR and wellbeing support.
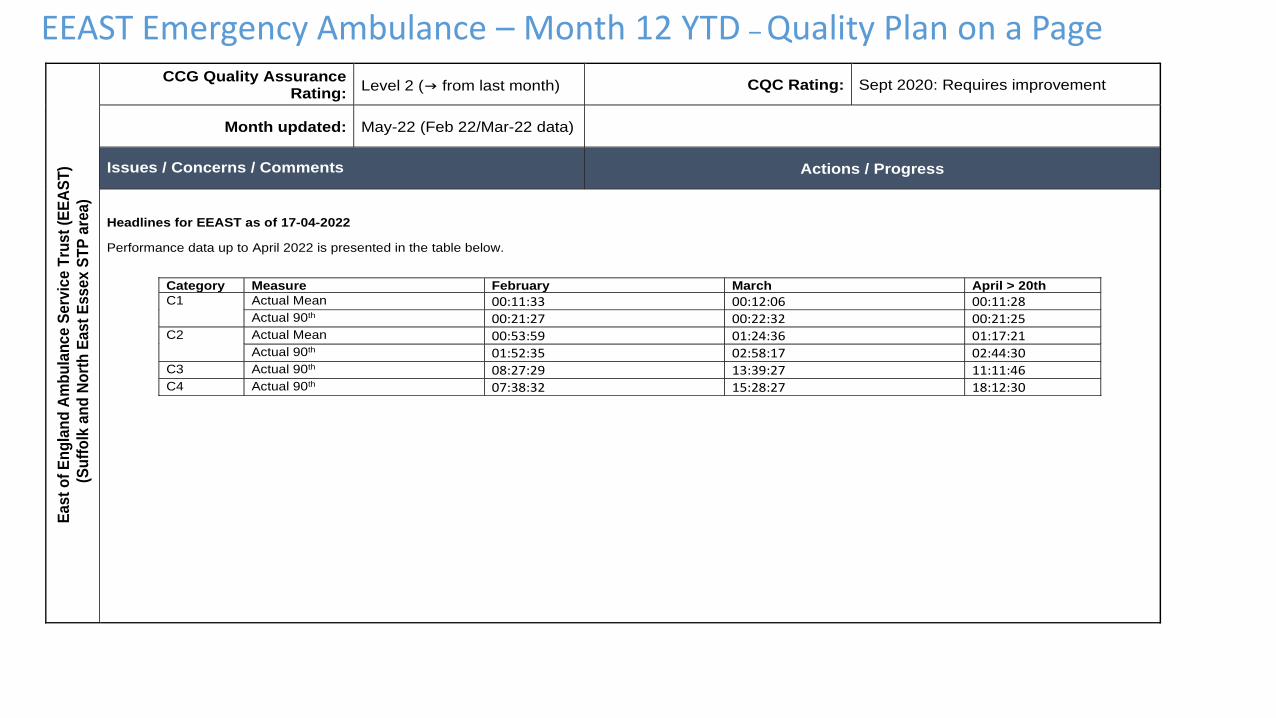
EEAST Emergency Ambulance – Month 12 YTD – Quality Plan on a Page
E
as
t o
f E
ng
lan
d A
mb
ula
nc
e S
erv
ice
Tru
st
(EE
AS
T)
(S
uff
olk
an
d N
ort
h E
as
t E
ss
ex S
TP
are
a)
CCG Quality Assurance Rating:
Level 2 (→ from last month) CQC Rating: Sept 2020: Requires improvement
Month updated: May-22 (Feb 22/Mar-22 data)
Issues / Concerns / Comments Actions / Progress
Headlines for EEAST as of 17-04-2022
Performance data up to April 2022 is presented in the table below.
Category Measure February March April > 20th
C1 Actual Mean 00:11:33 00:12:06 00:11:28
Actual 90th 00:21:27 00:22:32 00:21:25
C2 Actual Mean 00:53:59 01:24:36 01:17:21
Actual 90th 01:52:35 02:58:17 02:44:30
C3 Actual 90th 08:27:29 13:39:27 11:11:46
C4 Actual 90th 07:38:32 15:28:27 18:12:30
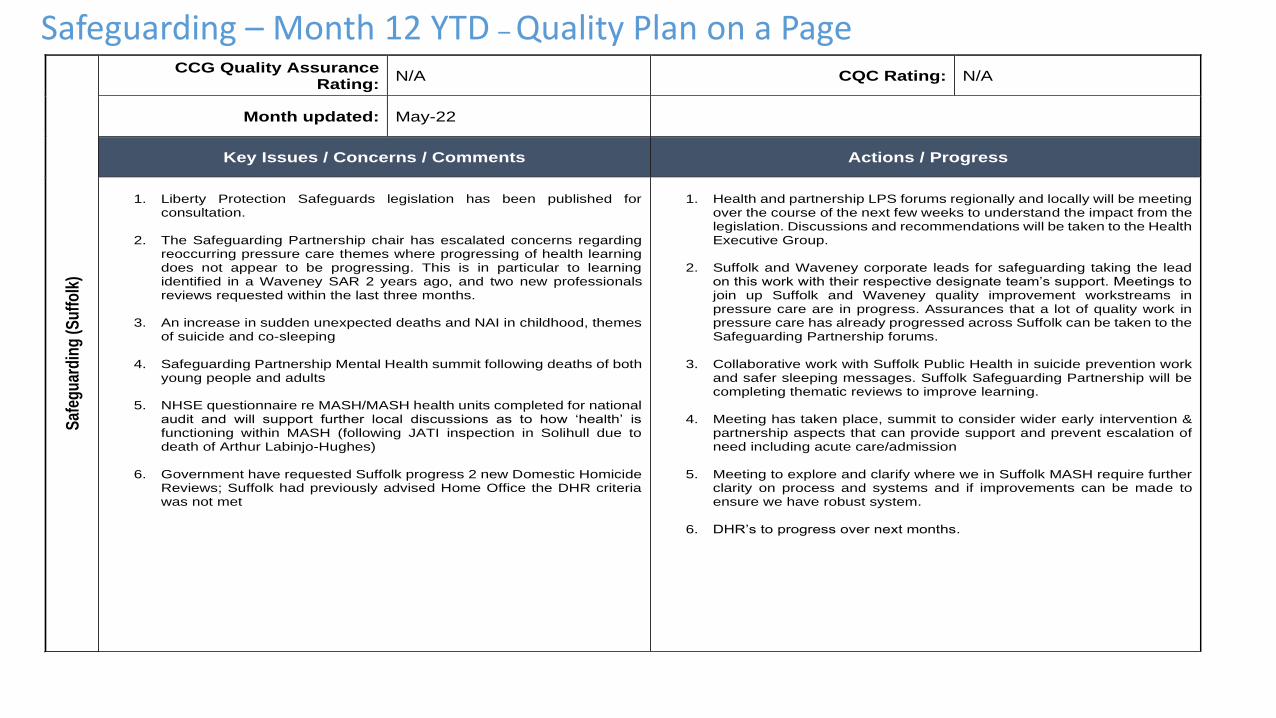
Safeguarding – Month 12 YTD – Quality Plan on a PageS
afeg
uar
din
g (
Su
ffo
lk)
CCG Quality Assurance Rating:
N/A CQC Rating: N/A
Month updated: May-22
Key Issues / Concerns / Comments Actions / Progress
1. Liberty Protection Safeguards legislation has been published for
consultation.
2. The Safeguarding Partnership chair has escalated concerns regarding reoccurring pressure care themes where progressing of health learning does not appear to be progressing. This is in particular to learning identified in a Waveney SAR 2 years ago, and two new professionals reviews requested within the last three months.
3. An increase in sudden unexpected deaths and NAI in childhood, themes
of suicide and co-sleeping
4. Safeguarding Partnership Mental Health summit following deaths of both young people and adults
5. NHSE questionnaire re MASH/MASH health units completed for national
audit and will support further local discussions as to how ‘health’ is functioning within MASH (following JATI inspection in Solihull due to death of Arthur Labinjo-Hughes)
6. Government have requested Suffolk progress 2 new Domestic Homicide
Reviews; Suffolk had previously advised Home Office the DHR criteria was not met
1. Health and partnership LPS forums regionally and locally will be meeting
over the course of the next few weeks to understand the impact from the legislation. Discussions and recommendations will be taken to the Health Executive Group.
2. Suffolk and Waveney corporate leads for safeguarding taking the lead
on this work with their respective designate team’s support. Meetings to join up Suffolk and Waveney quality improvement workstreams in pressure care are in progress. Assurances that a lot of quality work in pressure care has already progressed across Suffolk can be taken to the Safeguarding Partnership forums.
3. Collaborative work with Suffolk Public Health in suicide prevention work
and safer sleeping messages. Suffolk Safeguarding Partnership will be completing thematic reviews to improve learning.
4. Meeting has taken place, summit to consider wider early intervention &
partnership aspects that can provide support and prevent escalation of need including acute care/admission
5. Meeting to explore and clarify where we in Suffolk MASH require further
clarity on process and systems and if improvements can be made to ensure we have robust system.
6. DHR’s to progress over next months.
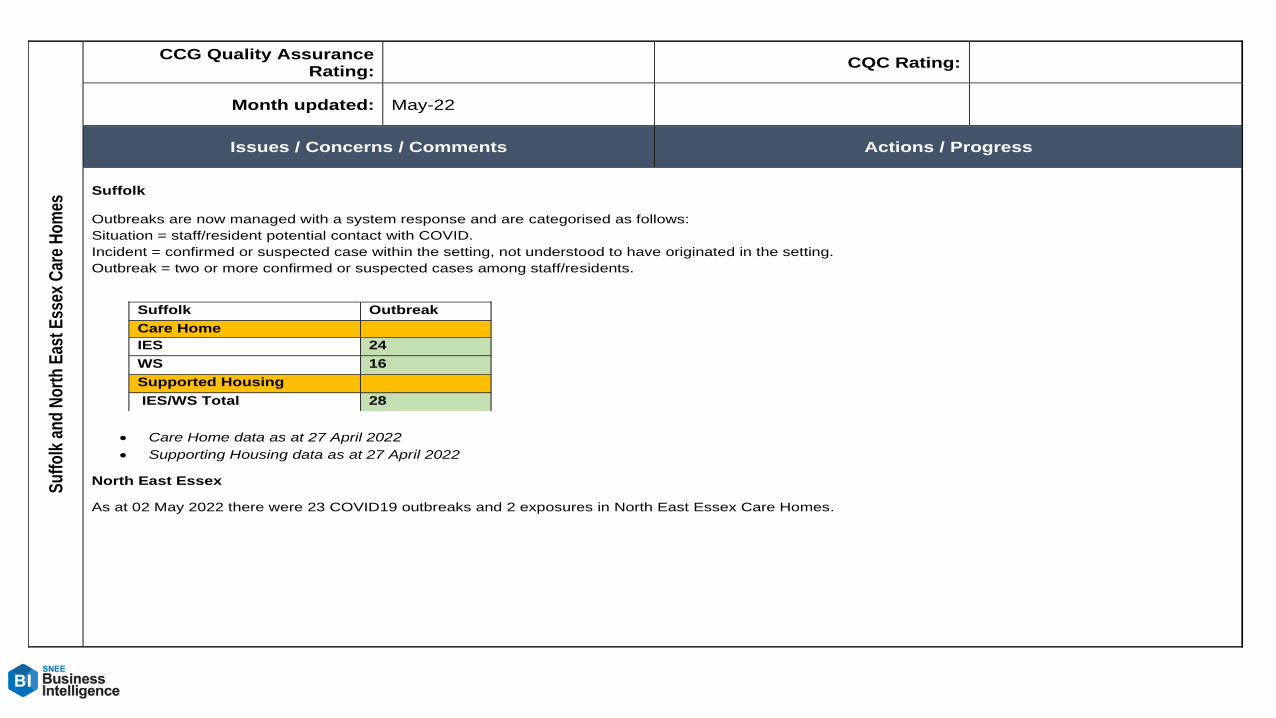
Su
ffo
lk a
nd
No
rth
Eas
t E
ssex
Car
e H
om
es
CCG Quality Assurance Rating:
CQC Rating:
Month updated: May-22
Issues / Concerns / Comments Actions / Progress
Suffolk Outbreaks are now managed with a system response and are categorised as follows:
Situation = staff/resident potential contact with COVID.
Incident = confirmed or suspected case within the setting, not understood to have originated in the setting.
Outbreak = two or more confirmed or suspected cases among staff/residents.
• Care Home data as at 27 April 2022
• Supporting Housing data as at 27 April 2022
North East Essex
As at 02 May 2022 there were 23 COVID19 outbreaks and 2 exposures in North East Essex Care Homes.
Suffolk Outbreak
Care Home
IES 24
WS 16
Supported Housing
IES/WS Total 28
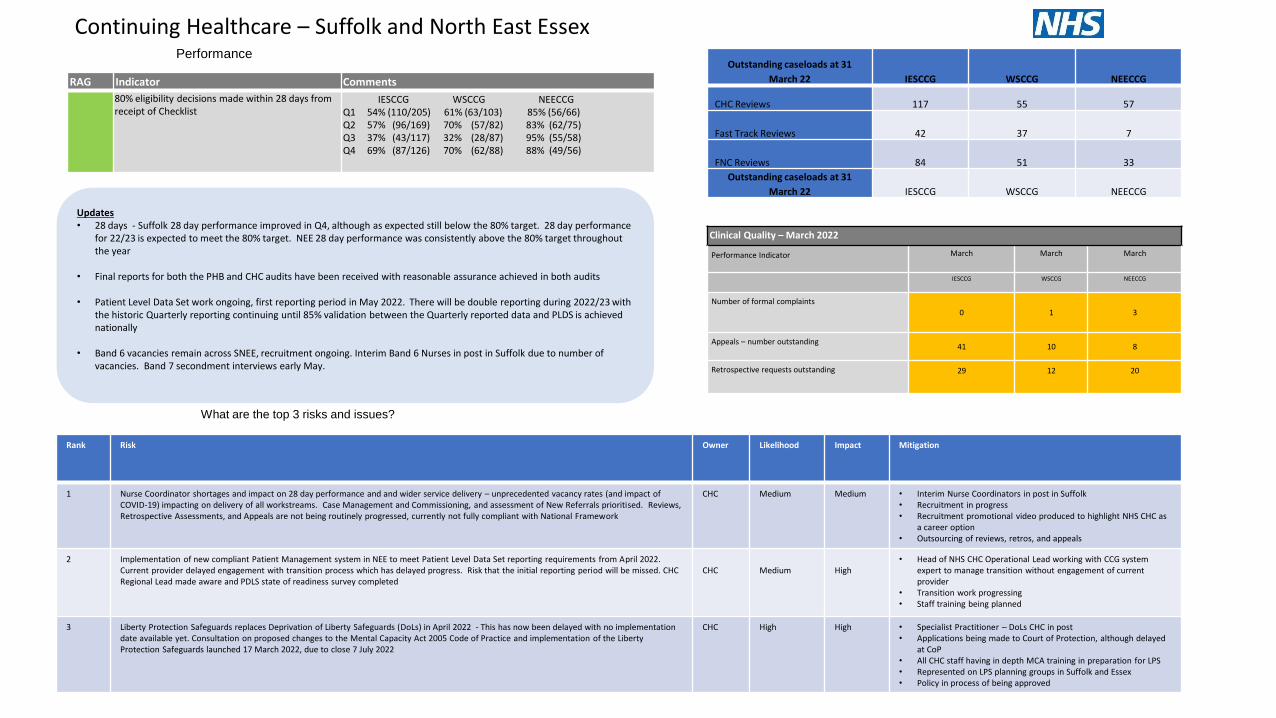
What are the top 3 risks and issues?
Continuing Healthcare – Suffolk and North East EssexPerformance
Outstanding caseloads at 31
March 22 IESCCG WSCCG NEECCG
CHC Reviews 117 55 57
Fast Track Reviews 42 37 7
FNC Reviews 84 51 33
Outstanding caseloads at 31
March 22 IESCCG WSCCG NEECCG
Updates• 28 days - Suffolk 28 day performance improved in Q4, although as expected still below the 80% target. 28 day performance
for 22/23 is expected to meet the 80% target. NEE 28 day performance was consistently above the 80% target throughout the year
• Final reports for both the PHB and CHC audits have been received with reasonable assurance achieved in both audits
• Patient Level Data Set work ongoing, first reporting period in May 2022. There will be double reporting during 2022/23 with the historic Quarterly reporting continuing until 85% validation between the Quarterly reported data and PLDS is achieved nationally
• Band 6 vacancies remain across SNEE, recruitment ongoing. Interim Band 6 Nurses in post in Suffolk due to number of vacancies. Band 7 secondment interviews early May.
Clinical Quality – March 2022
Performance Indicator March March March
IESCCG WSCCG NEECCG
Number of formal complaints
0 1 3
Appeals – number outstanding41 10 8
Retrospective requests outstanding 29 12 20
Rank Risk Owner Likelihood Impact Mitigation
1 Nurse Coordinator shortages and impact on 28 day performance and and wider service delivery – unprecedented vacancy rates (and impact of COVID-19) impacting on delivery of all workstreams. Case Management and Commissioning, and assessment of New Referrals prioritised. Reviews, Retrospective Assessments, and Appeals are not being routinely progressed, currently not fully compliant with National Framework
CHC Medium Medium • Interim Nurse Coordinators in post in Suffolk• Recruitment in progress• Recruitment promotional video produced to highlight NHS CHC as
a career option• Outsourcing of reviews, retros, and appeals
2 Implementation of new compliant Patient Management system in NEE to meet Patient Level Data Set reporting requirements from April 2022. Current provider delayed engagement with transition process which has delayed progress. Risk that the initial reporting period will be missed. CHC Regional Lead made aware and PDLS state of readiness survey completed
CHC Medium High• Head of NHS CHC Operational Lead working with CCG system
expert to manage transition without engagement of current provider
• Transition work progressing• Staff training being planned
3 Liberty Protection Safeguards replaces Deprivation of Liberty Safeguards (DoLs) in April 2022 - This has now been delayed with no implementation date available yet. Consultation on proposed changes to the Mental Capacity Act 2005 Code of Practice and implementation of the Liberty Protection Safeguards launched 17 March 2022, due to close 7 July 2022
CHC High High • Specialist Practitioner – DoLs CHC in post• Applications being made to Court of Protection, although delayed
at CoP• All CHC staff having in depth MCA training in preparation for LPS• Represented on LPS planning groups in Suffolk and Essex• Policy in process of being approved
RAG Indicator Comments
80% eligibility decisions made within 28 days from receipt of Checklist
IESCCG WSCCG NEECCGQ1 54% (110/205) 61% (63/103) 85% (56/66)Q2 57% (96/169) 70% (57/82) 83% (62/75) Q3 37% (43/117) 32% (28/87) 95% (55/58)Q4 69% (87/126) 70% (62/88) 88% (49/56)
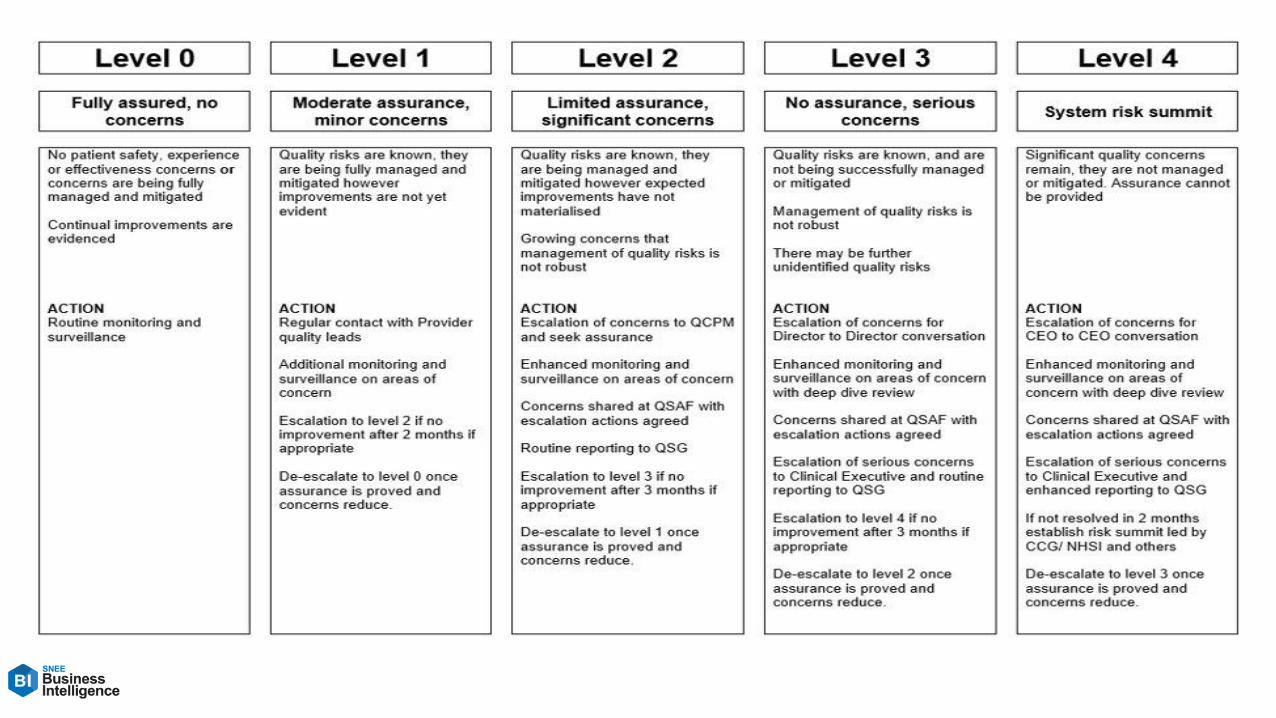

Transformation Programmes 21-22
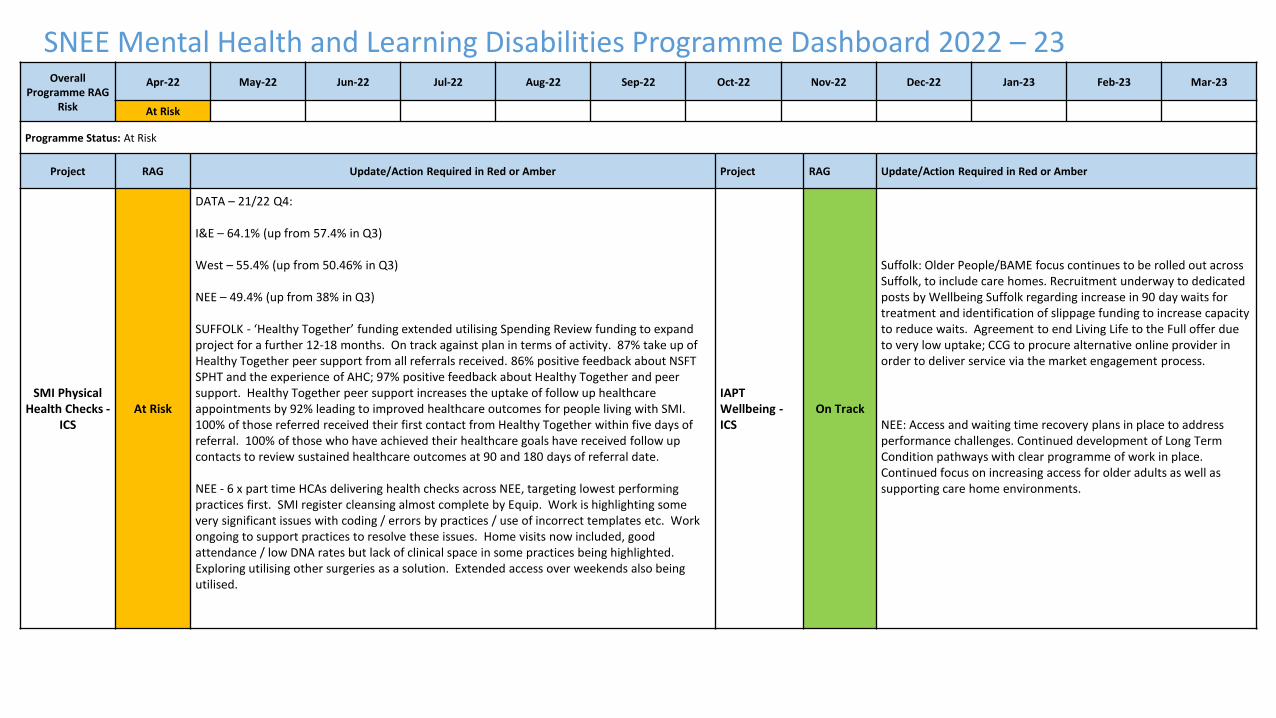
SNEE Mental Health and Learning Disabilities Programme Dashboard 2022 – 23Overall
Programme RAG Risk
Apr-22 May-22 Jun-22 Jul-22 Aug-22 Sep-22 Oct-22 Nov-22 Dec-22 Jan-23 Feb-23 Mar-23
At Risk
Programme Status: At Risk
Project RAG Update/Action Required in Red or Amber Project RAG Update/Action Required in Red or Amber
SMI Physical Health Checks -
ICSAt Risk
DATA – 21/22 Q4:
I&E – 64.1% (up from 57.4% in Q3)
West – 55.4% (up from 50.46% in Q3)
NEE – 49.4% (up from 38% in Q3)
SUFFOLK - ‘Healthy Together’ funding extended utilising Spending Review funding to expand project for a further 12-18 months. On track against plan in terms of activity. 87% take up of Healthy Together peer support from all referrals received. 86% positive feedback about NSFT SPHT and the experience of AHC; 97% positive feedback about Healthy Together and peer support. Healthy Together peer support increases the uptake of follow up healthcare appointments by 92% leading to improved healthcare outcomes for people living with SMI. 100% of those referred received their first contact from Healthy Together within five days of referral. 100% of those who have achieved their healthcare goals have received follow up contacts to review sustained healthcare outcomes at 90 and 180 days of referral date.
NEE - 6 x part time HCAs delivering health checks across NEE, targeting lowest performing practices first. SMI register cleansing almost complete by Equip. Work is highlighting some very significant issues with coding / errors by practices / use of incorrect templates etc. Work ongoing to support practices to resolve these issues. Home visits now included, good attendance / low DNA rates but lack of clinical space in some practices being highlighted. Exploring utilising other surgeries as a solution. Extended access over weekends also being utilised.
IAPT Wellbeing -ICS
On Track
Suffolk: Older People/BAME focus continues to be rolled out across Suffolk, to include care homes. Recruitment underway to dedicated posts by Wellbeing Suffolk regarding increase in 90 day waits for treatment and identification of slippage funding to increase capacity to reduce waits. Agreement to end Living Life to the Full offer due to very low uptake; CCG to procure alternative online provider in order to deliver service via the market engagement process.
NEE: Access and waiting time recovery plans in place to address performance challenges. Continued development of Long Term Condition pathways with clear programme of work in place. Continued focus on increasing access for older adults as well as supporting care home environments.
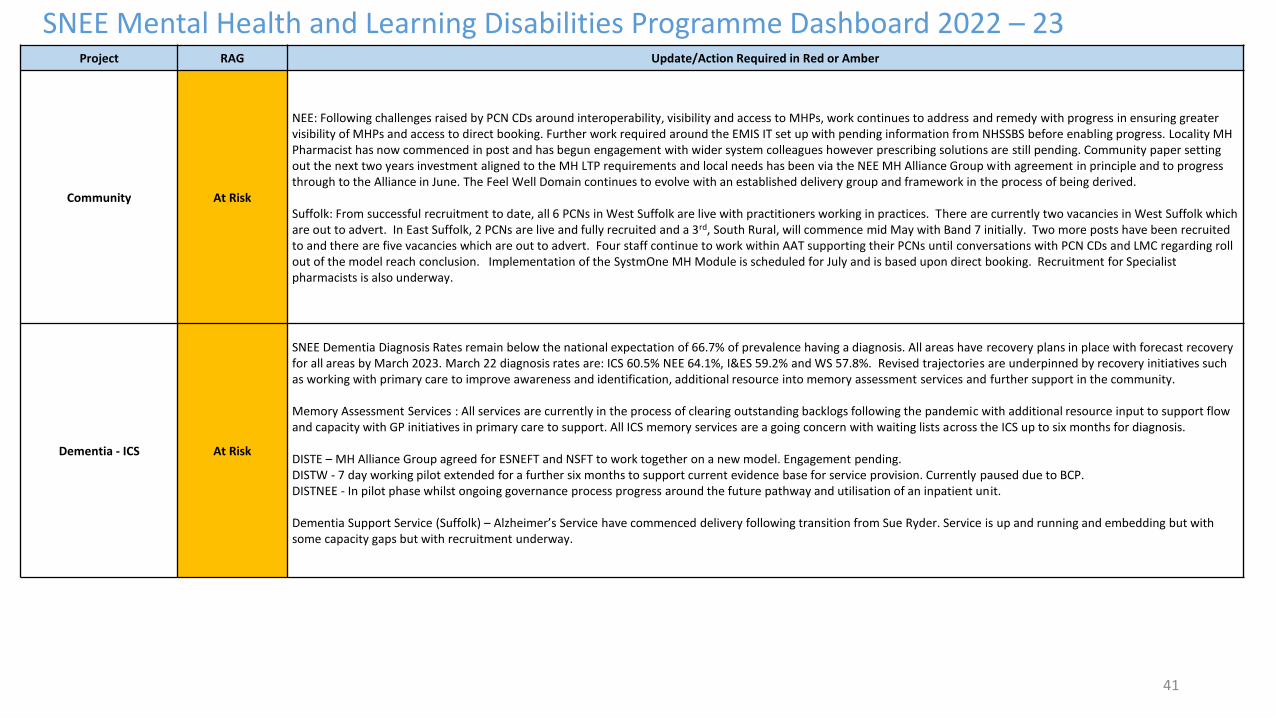
41
SNEE Mental Health and Learning Disabilities Programme Dashboard 2022 – 23Project RAG Update/Action Required in Red or Amber
Community At Risk
NEE: Following challenges raised by PCN CDs around interoperability, visibility and access to MHPs, work continues to address and remedy with progress in ensuring greater visibility of MHPs and access to direct booking. Further work required around the EMIS IT set up with pending information from NHSSBS before enabling progress. Locality MH Pharmacist has now commenced in post and has begun engagement with wider system colleagues however prescribing solutions are still pending. Community paper setting out the next two years investment aligned to the MH LTP requirements and local needs has been via the NEE MH Alliance Group with agreement in principle and to progress through to the Alliance in June. The Feel Well Domain continues to evolve with an established delivery group and framework in the process of being derived.
Suffolk: From successful recruitment to date, all 6 PCNs in West Suffolk are live with practitioners working in practices. There are currently two vacancies in West Suffolk which are out to advert. In East Suffolk, 2 PCNs are live and fully recruited and a 3rd, South Rural, will commence mid May with Band 7 initially. Two more posts have been recruited to and there are five vacancies which are out to advert. Four staff continue to work within AAT supporting their PCNs until conversations with PCN CDs and LMC regarding roll out of the model reach conclusion. Implementation of the SystmOne MH Module is scheduled for July and is based upon direct booking. Recruitment for Specialist pharmacists is also underway.
Dementia - ICS At Risk
SNEE Dementia Diagnosis Rates remain below the national expectation of 66.7% of prevalence having a diagnosis. All areas have recovery plans in place with forecast recovery for all areas by March 2023. March 22 diagnosis rates are: ICS 60.5% NEE 64.1%, I&ES 59.2% and WS 57.8%. Revised trajectories are underpinned by recovery initiatives such as working with primary care to improve awareness and identification, additional resource into memory assessment services and further support in the community.
Memory Assessment Services : All services are currently in the process of clearing outstanding backlogs following the pandemic with additional resource input to support flow and capacity with GP initiatives in primary care to support. All ICS memory services are a going concern with waiting lists across the ICS up to six months for diagnosis.
DISTE – MH Alliance Group agreed for ESNEFT and NSFT to work together on a new model. Engagement pending. DISTW - 7 day working pilot extended for a further six months to support current evidence base for service provision. Currently paused due to BCP.DISTNEE - In pilot phase whilst ongoing governance process progress around the future pathway and utilisation of an inpatient unit.
Dementia Support Service (Suffolk) – Alzheimer’s Service have commenced delivery following transition from Sue Ryder. Service is up and running and embedding but with some capacity gaps but with recruitment underway.
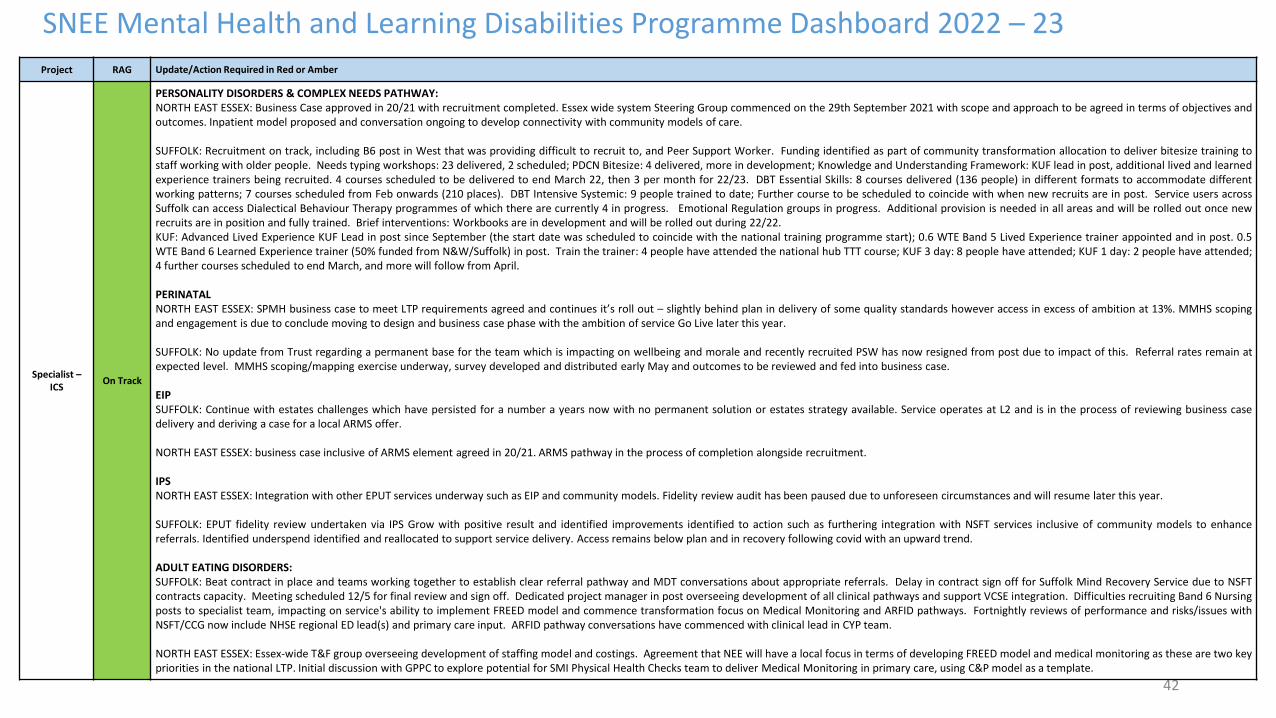
42
SNEE Mental Health and Learning Disabilities Programme Dashboard 2022 – 23
Project RAG Update/Action Required in Red or Amber
Specialist –ICS
On Track
PERSONALITY DISORDERS & COMPLEX NEEDS PATHWAY:NORTH EAST ESSEX: Business Case approved in 20/21 with recruitment completed. Essex wide system Steering Group commenced on the 29th September 2021 with scope and approach to be agreed in terms of objectives andoutcomes. Inpatient model proposed and conversation ongoing to develop connectivity with community models of care.
SUFFOLK: Recruitment on track, including B6 post in West that was providing difficult to recruit to, and Peer Support Worker. Funding identified as part of community transformation allocation to deliver bitesize training tostaff working with older people. Needs typing workshops: 23 delivered, 2 scheduled; PDCN Bitesize: 4 delivered, more in development; Knowledge and Understanding Framework: KUF lead in post, additional lived and learnedexperience trainers being recruited. 4 courses scheduled to be delivered to end March 22, then 3 per month for 22/23. DBT Essential Skills: 8 courses delivered (136 people) in different formats to accommodate differentworking patterns; 7 courses scheduled from Feb onwards (210 places). DBT Intensive Systemic: 9 people trained to date; Further course to be scheduled to coincide with when new recruits are in post. Service users acrossSuffolk can access Dialectical Behaviour Therapy programmes of which there are currently 4 in progress. Emotional Regulation groups in progress. Additional provision is needed in all areas and will be rolled out once newrecruits are in position and fully trained. Brief interventions: Workbooks are in development and will be rolled out during 22/22.KUF: Advanced Lived Experience KUF Lead in post since September (the start date was scheduled to coincide with the national training programme start); 0.6 WTE Band 5 Lived Experience trainer appointed and in post. 0.5WTE Band 6 Learned Experience trainer (50% funded from N&W/Suffolk) in post. Train the trainer: 4 people have attended the national hub TTT course; KUF 3 day: 8 people have attended; KUF 1 day: 2 people have attended;4 further courses scheduled to end March, and more will follow from April.
PERINATALNORTH EAST ESSEX: SPMH business case to meet LTP requirements agreed and continues it’s roll out – slightly behind plan in delivery of some quality standards however access in excess of ambition at 13%. MMHS scopingand engagement is due to conclude moving to design and business case phase with the ambition of service Go Live later this year.
SUFFOLK: No update from Trust regarding a permanent base for the team which is impacting on wellbeing and morale and recently recruited PSW has now resigned from post due to impact of this. Referral rates remain atexpected level. MMHS scoping/mapping exercise underway, survey developed and distributed early May and outcomes to be reviewed and fed into business case.
EIPSUFFOLK: Continue with estates challenges which have persisted for a number a years now with no permanent solution or estates strategy available. Service operates at L2 and is in the process of reviewing business casedelivery and deriving a case for a local ARMS offer.
NORTH EAST ESSEX: business case inclusive of ARMS element agreed in 20/21. ARMS pathway in the process of completion alongside recruitment.
IPSNORTH EAST ESSEX: Integration with other EPUT services underway such as EIP and community models. Fidelity review audit has been paused due to unforeseen circumstances and will resume later this year.
SUFFOLK: EPUT fidelity review undertaken via IPS Grow with positive result and identified improvements identified to action such as furthering integration with NSFT services inclusive of community models to enhancereferrals. Identified underspend identified and reallocated to support service delivery. Access remains below plan and in recovery following covid with an upward trend.
ADULT EATING DISORDERS:SUFFOLK: Beat contract in place and teams working together to establish clear referral pathway and MDT conversations about appropriate referrals. Delay in contract sign off for Suffolk Mind Recovery Service due to NSFTcontracts capacity. Meeting scheduled 12/5 for final review and sign off. Dedicated project manager in post overseeing development of all clinical pathways and support VCSE integration. Difficulties recruiting Band 6 Nursingposts to specialist team, impacting on service's ability to implement FREED model and commence transformation focus on Medical Monitoring and ARFID pathways. Fortnightly reviews of performance and risks/issues withNSFT/CCG now include NHSE regional ED lead(s) and primary care input. ARFID pathway conversations have commenced with clinical lead in CYP team.
NORTH EAST ESSEX: Essex-wide T&F group overseeing development of staffing model and costings. Agreement that NEE will have a local focus in terms of developing FREED model and medical monitoring as these are two keypriorities in the national LTP. Initial discussion with GPPC to explore potential for SMI Physical Health Checks team to deliver Medical Monitoring in primary care, using C&P model as a template.
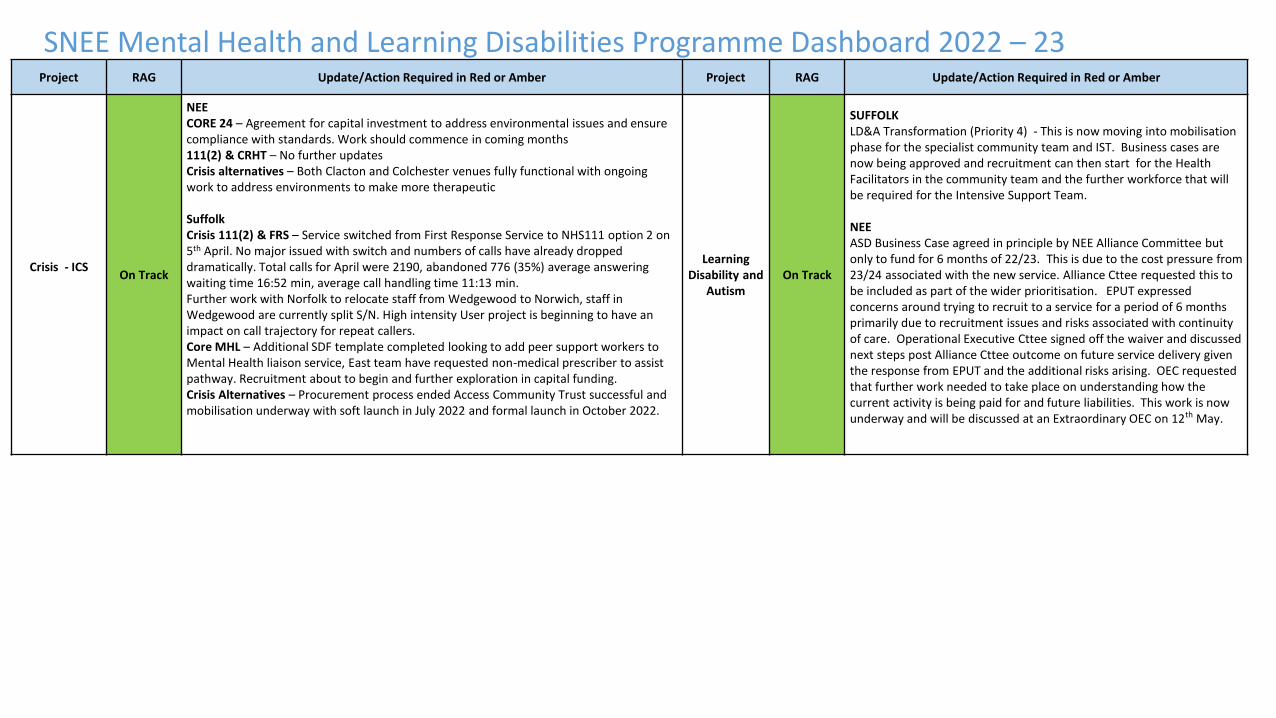
SNEE Mental Health and Learning Disabilities Programme Dashboard 2022 – 23Project RAG Update/Action Required in Red or Amber Project RAG Update/Action Required in Red or Amber
Crisis - ICSOn Track
NEECORE 24 – Agreement for capital investment to address environmental issues and ensure compliance with standards. Work should commence in coming months111(2) & CRHT – No further updates Crisis alternatives – Both Clacton and Colchester venues fully functional with ongoing work to address environments to make more therapeutic
Suffolk Crisis 111(2) & FRS – Service switched from First Response Service to NHS111 option 2 on 5th April. No major issued with switch and numbers of calls have already dropped dramatically. Total calls for April were 2190, abandoned 776 (35%) average answering waiting time 16:52 min, average call handling time 11:13 min.Further work with Norfolk to relocate staff from Wedgewood to Norwich, staff in Wedgewood are currently split S/N. High intensity User project is beginning to have an impact on call trajectory for repeat callers.Core MHL – Additional SDF template completed looking to add peer support workers to Mental Health liaison service, East team have requested non-medical prescriber to assist pathway. Recruitment about to begin and further exploration in capital funding.Crisis Alternatives – Procurement process ended Access Community Trust successful and mobilisation underway with soft launch in July 2022 and formal launch in October 2022.
Learning Disability and
AutismOn Track
SUFFOLKLD&A Transformation (Priority 4) - This is now moving into mobilisation phase for the specialist community team and IST. Business cases are now being approved and recruitment can then start for the Health Facilitators in the community team and the further workforce that will be required for the Intensive Support Team.
NEEASD Business Case agreed in principle by NEE Alliance Committee but only to fund for 6 months of 22/23. This is due to the cost pressure from 23/24 associated with the new service. Alliance Cttee requested this to be included as part of the wider prioritisation. EPUT expressed concerns around trying to recruit to a service for a period of 6 months primarily due to recruitment issues and risks associated with continuity of care. Operational Executive Cttee signed off the waiver and discussed next steps post Alliance Cttee outcome on future service delivery given the response from EPUT and the additional risks arising. OEC requested that further work needed to take place on understanding how the current activity is being paid for and future liabilities. This work is now underway and will be discussed at an Extraordinary OEC on 12th May.
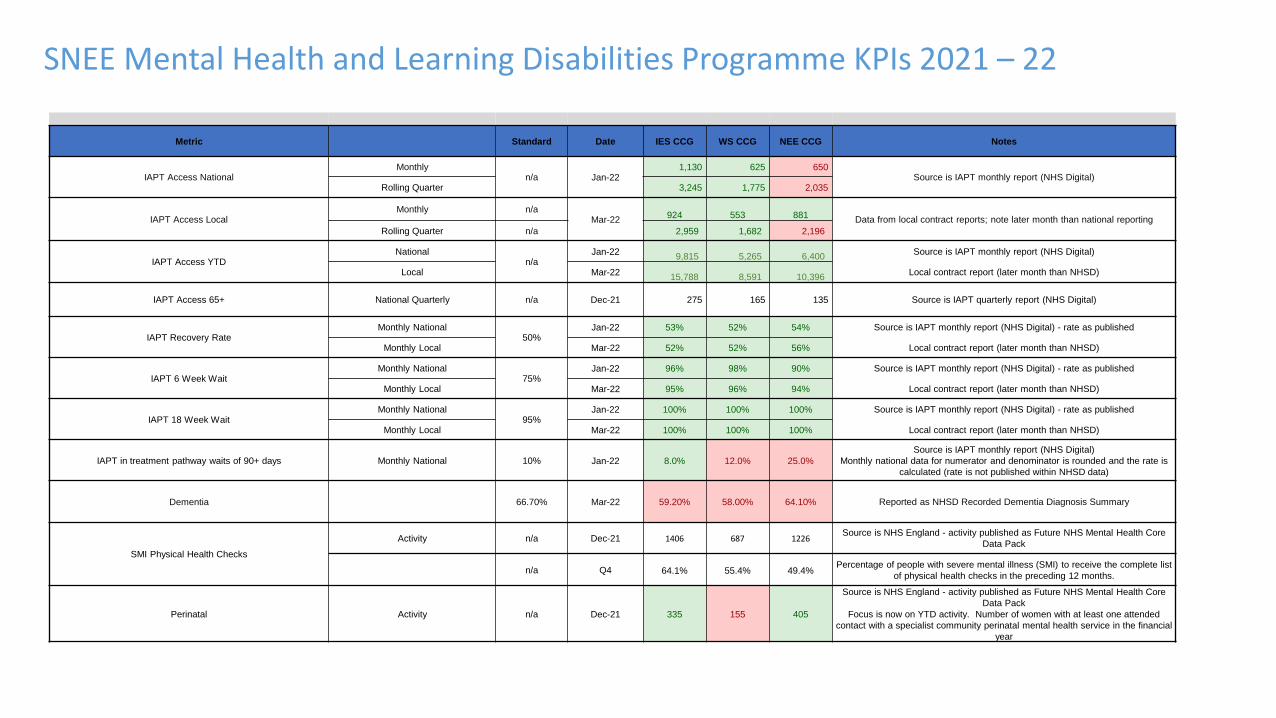
SNEE Mental Health and Learning Disabilities Programme KPIs 2021 – 22
Metric Standard Date IES CCG WS CCG NEE CCG Notes
IAPT Access NationalMonthly
n/a Jan-221,130 625 650
Source is IAPT monthly report (NHS Digital)Rolling Quarter 3,245 1,775 2,035
IAPT Access LocalMonthly n/a
Mar-22924 553 881
Data from local contract reports; note later month than national reporting
Rolling Quarter n/a 2,959 1,682 2,196
IAPT Access YTDNational
n/aJan-22
9,815 5,265 6,400 Source is IAPT monthly report (NHS Digital)
Local Mar-2215,788 8,591 10,396
Local contract report (later month than NHSD)
IAPT Access 65+ National Quarterly n/a Dec-21 275 165 135 Source is IAPT quarterly report (NHS Digital)
IAPT Recovery RateMonthly National
50%Jan-22 53% 52% 54% Source is IAPT monthly report (NHS Digital) - rate as published
Monthly Local Mar-22 52% 52% 56% Local contract report (later month than NHSD)
IAPT 6 Week WaitMonthly National
75%Jan-22 96% 98% 90% Source is IAPT monthly report (NHS Digital) - rate as published
Monthly Local Mar-22 95% 96% 94% Local contract report (later month than NHSD)
IAPT 18 Week WaitMonthly National
95%Jan-22 100% 100% 100% Source is IAPT monthly report (NHS Digital) - rate as published
Monthly Local Mar-22 100% 100% 100% Local contract report (later month than NHSD)
IAPT in treatment pathway waits of 90+ days Monthly National 10% Jan-22 8.0% 12.0% 25.0%
Source is IAPT monthly report (NHS Digital)
Monthly national data for numerator and denominator is rounded and the rate is
calculated (rate is not published within NHSD data)
Dementia 66.70% Mar-22 59.20% 58.00% 64.10% Reported as NHSD Recorded Dementia Diagnosis Summary
SMI Physical Health Checks
Activity n/a Dec-21 1406 687 1226Source is NHS England - activity published as Future NHS Mental Health Core
Data Pack
n/a Q4 64.1% 55.4% 49.4%Percentage of people with severe mental illness (SMI) to receive the complete list
of physical health checks in the preceding 12 months.
Perinatal Activity n/a Dec-21 335 155 405
Source is NHS England - activity published as Future NHS Mental Health Core
Data Pack
Focus is now on YTD activity. Number of women with at least one attended
contact with a specialist community perinatal mental health service in the financial
year
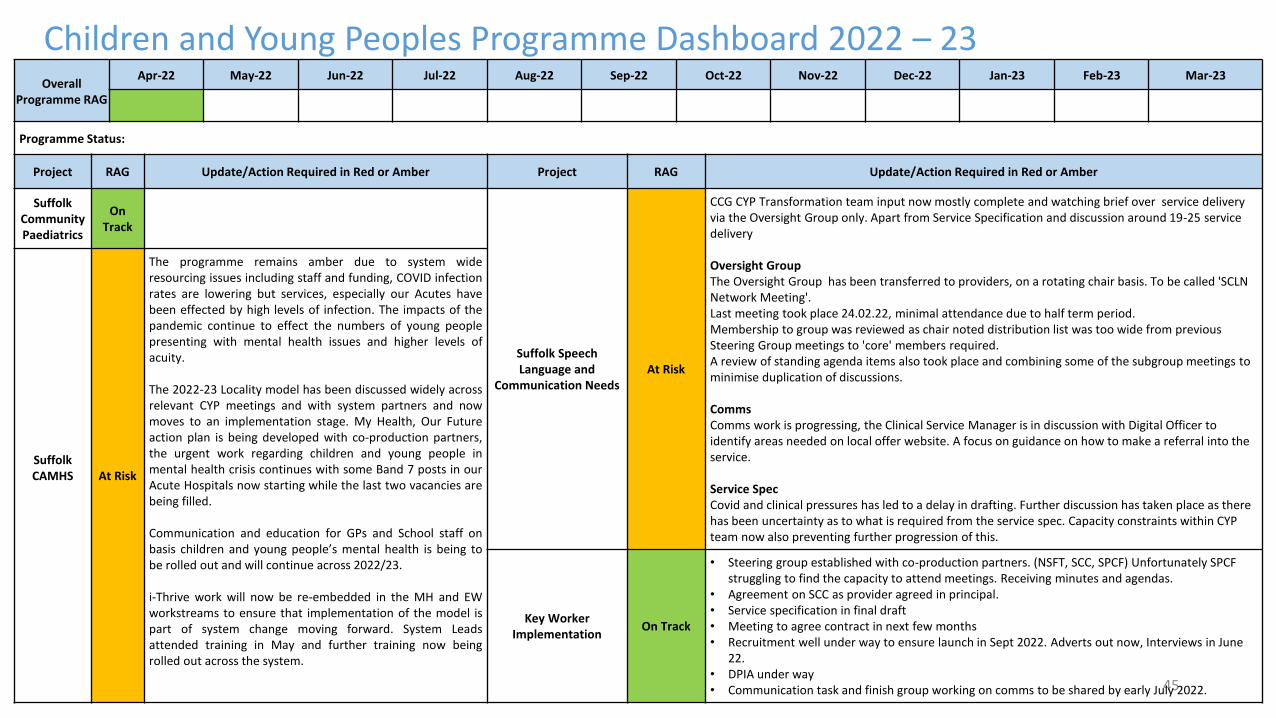
45
Children and Young Peoples Programme Dashboard 2022 – 23Overall
Programme RAG
Apr-22 May-22 Jun-22 Jul-22 Aug-22 Sep-22 Oct-22 Nov-22 Dec-22 Jan-23 Feb-23 Mar-23
Programme Status:
Project RAG Update/Action Required in Red or Amber Project RAG Update/Action Required in Red or Amber
Suffolk Community Paediatrics
OnTrack
Suffolk Speech Language and
Communication NeedsAt Risk
CCG CYP Transformation team input now mostly complete and watching brief over service delivery via the Oversight Group only. Apart from Service Specification and discussion around 19-25 service delivery
Oversight GroupThe Oversight Group has been transferred to providers, on a rotating chair basis. To be called 'SCLN Network Meeting'.Last meeting took place 24.02.22, minimal attendance due to half term period. Membership to group was reviewed as chair noted distribution list was too wide from previous Steering Group meetings to 'core' members required. A review of standing agenda items also took place and combining some of the subgroup meetings to minimise duplication of discussions.
CommsComms work is progressing, the Clinical Service Manager is in discussion with Digital Officer to identify areas needed on local offer website. A focus on guidance on how to make a referral into the service.
Service SpecCovid and clinical pressures has led to a delay in drafting. Further discussion has taken place as there has been uncertainty as to what is required from the service spec. Capacity constraints within CYP team now also preventing further progression of this.
Suffolk CAMHS At Risk
The programme remains amber due to system wideresourcing issues including staff and funding, COVID infectionrates are lowering but services, especially our Acutes havebeen effected by high levels of infection. The impacts of thepandemic continue to effect the numbers of young peoplepresenting with mental health issues and higher levels ofacuity.
The 2022-23 Locality model has been discussed widely acrossrelevant CYP meetings and with system partners and nowmoves to an implementation stage. My Health, Our Futureaction plan is being developed with co-production partners,the urgent work regarding children and young people inmental health crisis continues with some Band 7 posts in ourAcute Hospitals now starting while the last two vacancies arebeing filled.
Communication and education for GPs and School staff onbasis children and young people’s mental health is being tobe rolled out and will continue across 2022/23.
i-Thrive work will now be re-embedded in the MH and EWworkstreams to ensure that implementation of the model ispart of system change moving forward. System Leadsattended training in May and further training now beingrolled out across the system.
Key Worker Implementation
On Track
• Steering group established with co-production partners. (NSFT, SCC, SPCF) Unfortunately SPCF struggling to find the capacity to attend meetings. Receiving minutes and agendas.
• Agreement on SCC as provider agreed in principal. • Service specification in final draft• Meeting to agree contract in next few months• Recruitment well under way to ensure launch in Sept 2022. Adverts out now, Interviews in June
22.• DPIA under way• Communication task and finish group working on comms to be shared by early July 2022.
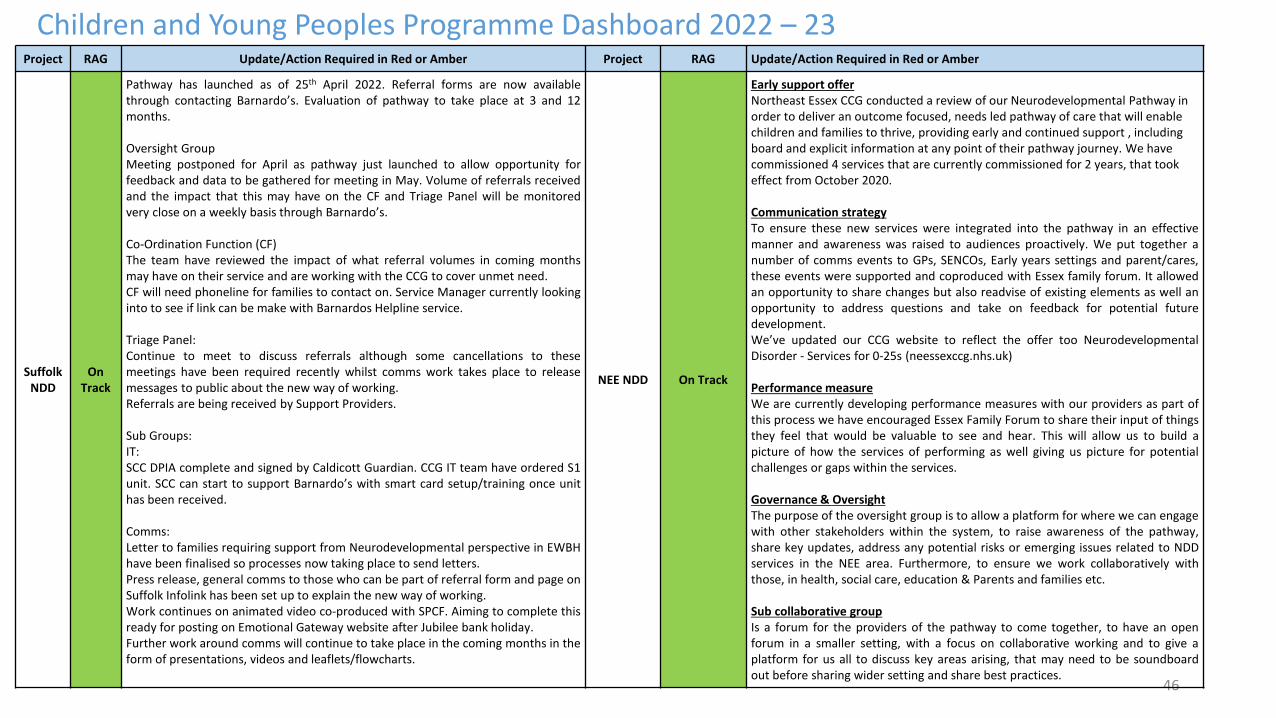
46
Children and Young Peoples Programme Dashboard 2022 – 23Project RAG Update/Action Required in Red or Amber Project RAG Update/Action Required in Red or Amber
Suffolk NDD
On Track
Pathway has launched as of 25th April 2022. Referral forms are now availablethrough contacting Barnardo’s. Evaluation of pathway to take place at 3 and 12months.
Oversight GroupMeeting postponed for April as pathway just launched to allow opportunity forfeedback and data to be gathered for meeting in May. Volume of referrals receivedand the impact that this may have on the CF and Triage Panel will be monitoredvery close on a weekly basis through Barnardo’s.
Co-Ordination Function (CF)The team have reviewed the impact of what referral volumes in coming monthsmay have on their service and are working with the CCG to cover unmet need.CF will need phoneline for families to contact on. Service Manager currently lookinginto to see if link can be make with Barnardos Helpline service.
Triage Panel:Continue to meet to discuss referrals although some cancellations to thesemeetings have been required recently whilst comms work takes place to releasemessages to public about the new way of working.Referrals are being received by Support Providers.
Sub Groups:IT:SCC DPIA complete and signed by Caldicott Guardian. CCG IT team have ordered S1unit. SCC can start to support Barnardo’s with smart card setup/training once unithas been received.
Comms:Letter to families requiring support from Neurodevelopmental perspective in EWBHhave been finalised so processes now taking place to send letters.Press release, general comms to those who can be part of referral form and page onSuffolk Infolink has been set up to explain the new way of working.Work continues on animated video co-produced with SPCF. Aiming to complete thisready for posting on Emotional Gateway website after Jubilee bank holiday.Further work around comms will continue to take place in the coming months in theform of presentations, videos and leaflets/flowcharts.
NEE NDD On Track
Early support offer Northeast Essex CCG conducted a review of our Neurodevelopmental Pathway in order to deliver an outcome focused, needs led pathway of care that will enable children and families to thrive, providing early and continued support , including board and explicit information at any point of their pathway journey. We have commissioned 4 services that are currently commissioned for 2 years, that took effect from October 2020.
Communication strategyTo ensure these new services were integrated into the pathway in an effectivemanner and awareness was raised to audiences proactively. We put together anumber of comms events to GPs, SENCOs, Early years settings and parent/cares,these events were supported and coproduced with Essex family forum. It allowedan opportunity to share changes but also readvise of existing elements as well anopportunity to address questions and take on feedback for potential futuredevelopment.We’ve updated our CCG website to reflect the offer too NeurodevelopmentalDisorder - Services for 0-25s (neessexccg.nhs.uk)
Performance measureWe are currently developing performance measures with our providers as part ofthis process we have encouraged Essex Family Forum to share their input of thingsthey feel that would be valuable to see and hear. This will allow us to build apicture of how the services of performing as well giving us picture for potentialchallenges or gaps within the services.
Governance & OversightThe purpose of the oversight group is to allow a platform for where we can engagewith other stakeholders within the system, to raise awareness of the pathway,share key updates, address any potential risks or emerging issues related to NDDservices in the NEE area. Furthermore, to ensure we work collaboratively withthose, in health, social care, education & Parents and families etc.
Sub collaborative groupIs a forum for the providers of the pathway to come together, to have an openforum in a smaller setting, with a focus on collaborative working and to give aplatform for us all to discuss key areas arising, that may need to be soundboardout before sharing wider setting and share best practices.
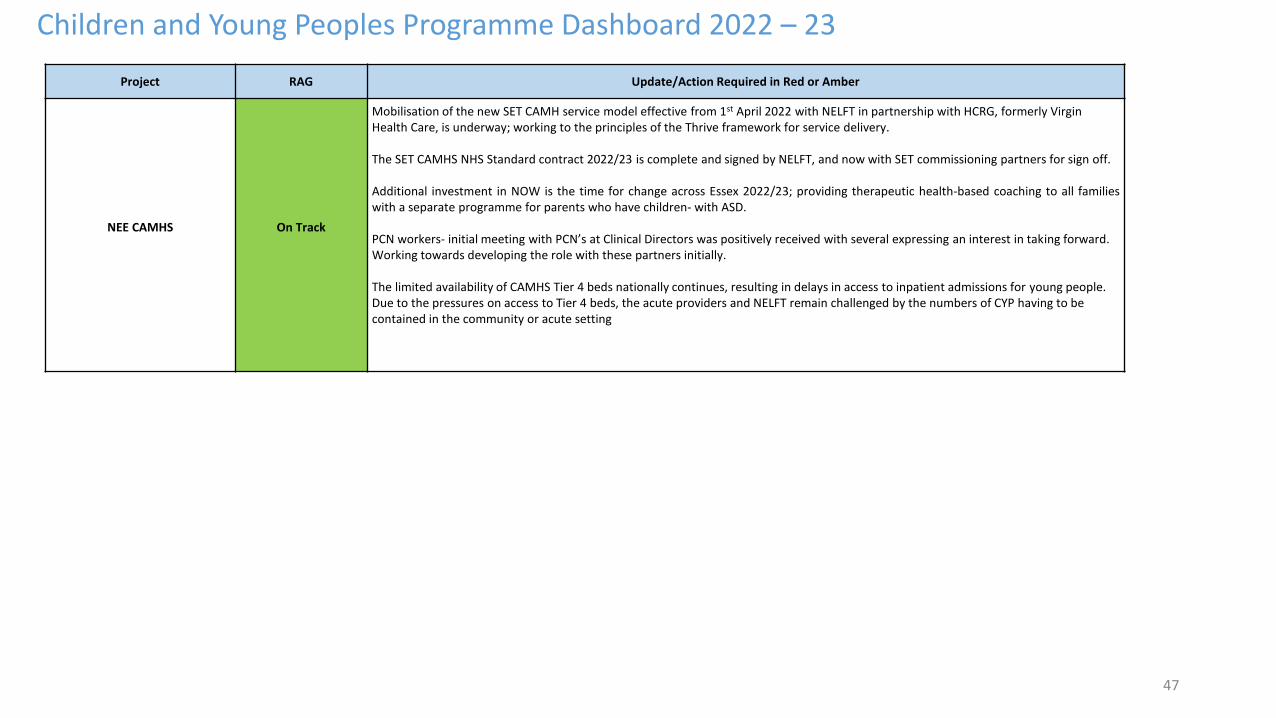
Project RAG Update/Action Required in Red or Amber
NEE CAMHS On Track
Mobilisation of the new SET CAMH service model effective from 1st April 2022 with NELFT in partnership with HCRG, formerly Virgin Health Care, is underway; working to the principles of the Thrive framework for service delivery.
The SET CAMHS NHS Standard contract 2022/23 is complete and signed by NELFT, and now with SET commissioning partners for sign off.
Additional investment in NOW is the time for change across Essex 2022/23; providing therapeutic health-based coaching to all familieswith a separate programme for parents who have children- with ASD.
PCN workers- initial meeting with PCN’s at Clinical Directors was positively received with several expressing an interest in taking forward. Working towards developing the role with these partners initially.
The limited availability of CAMHS Tier 4 beds nationally continues, resulting in delays in access to inpatient admissions for young people. Due to the pressures on access to Tier 4 beds, the acute providers and NELFT remain challenged by the numbers of CYP having to becontained in the community or acute setting
47
Children and Young Peoples Programme Dashboard 2022 – 23
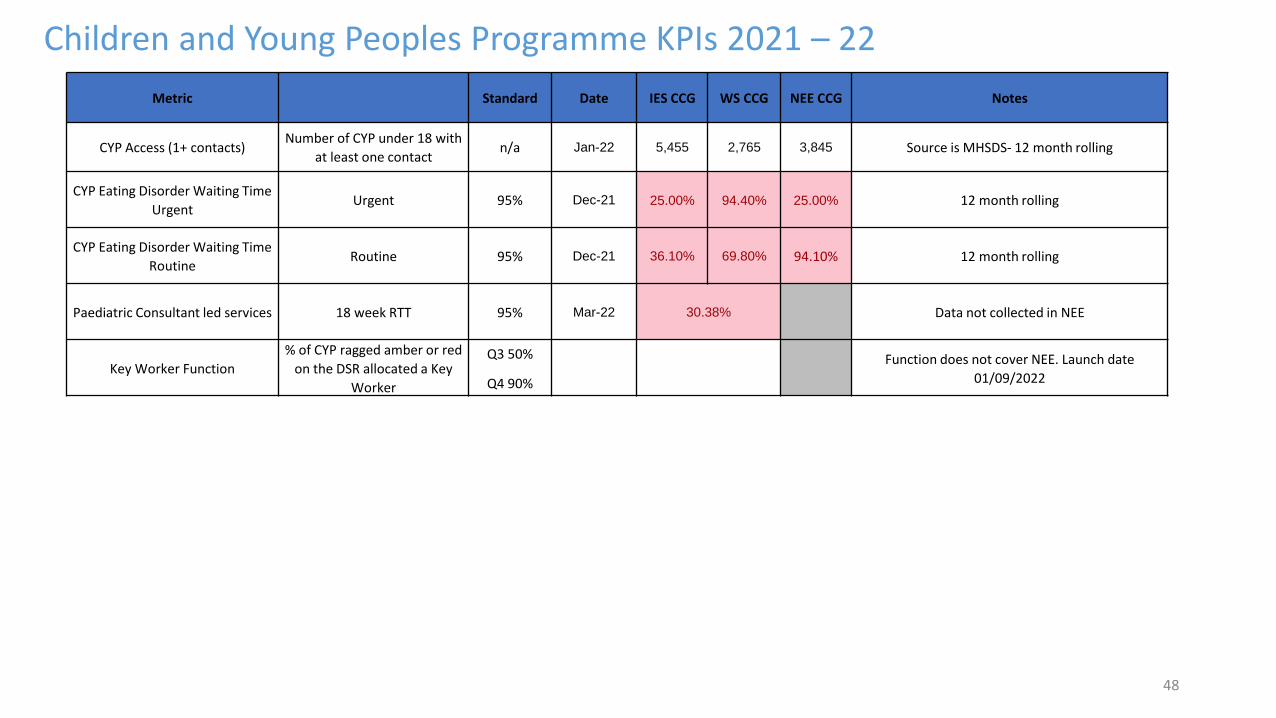
48
Children and Young Peoples Programme KPIs 2021 – 22
Metric Standard Date IES CCG WS CCG NEE CCG Notes
CYP Access (1+ contacts)Number of CYP under 18 with
at least one contactn/a Jan-22 5,455 2,765 3,845 Source is MHSDS- 12 month rolling
CYP Eating Disorder Waiting Time
UrgentUrgent 95% Dec-21 25.00% 94.40% 25.00% 12 month rolling
CYP Eating Disorder Waiting Time
RoutineRoutine 95% Dec-21 36.10% 69.80% 94.10% 12 month rolling
Paediatric Consultant led services 18 week RTT 95% Mar-22 30.38% Data not collected in NEE
Key Worker Function
% of CYP ragged amber or red
on the DSR allocated a Key
Worker
Q3 50%
Q4 90%
Function does not cover NEE. Launch date
01/09/2022
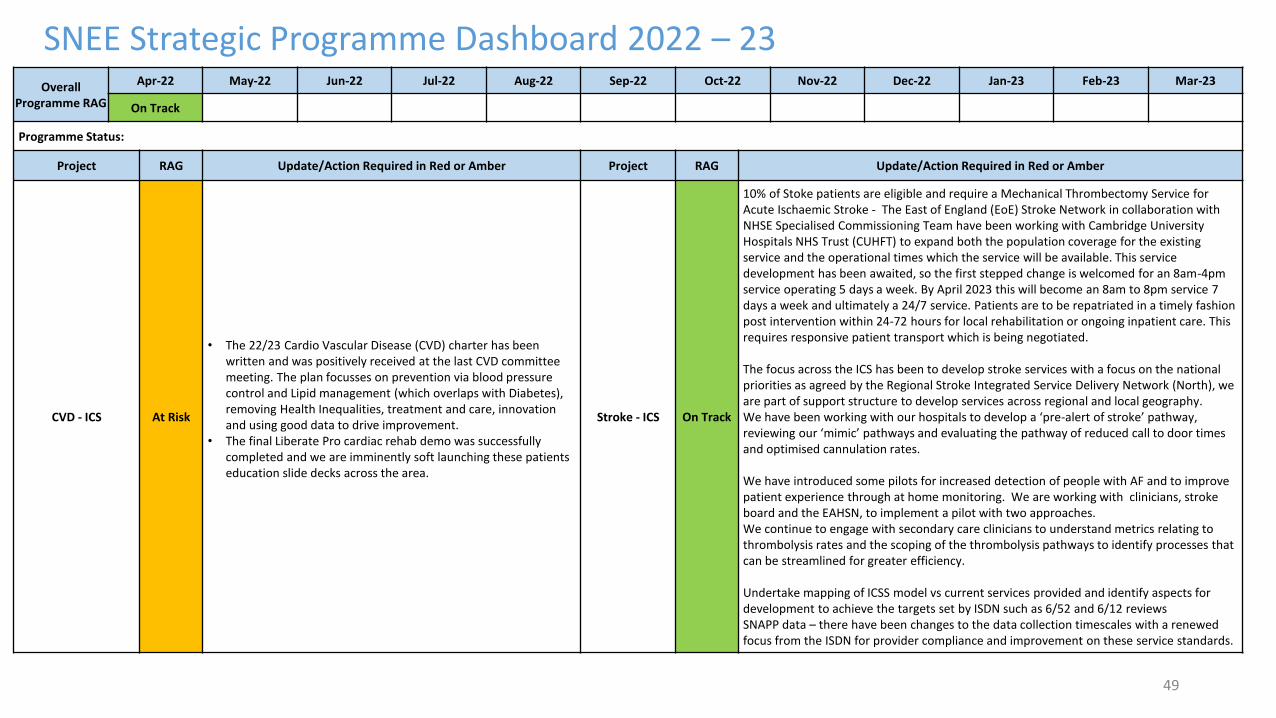
49
SNEE Strategic Programme Dashboard 2022 – 23Overall
Programme RAG
Apr-22 May-22 Jun-22 Jul-22 Aug-22 Sep-22 Oct-22 Nov-22 Dec-22 Jan-23 Feb-23 Mar-23
On Track
Programme Status:
Project RAG Update/Action Required in Red or Amber Project RAG Update/Action Required in Red or Amber
CVD - ICS At Risk
• The 22/23 Cardio Vascular Disease (CVD) charter has been written and was positively received at the last CVD committee meeting. The plan focusses on prevention via blood pressure control and Lipid management (which overlaps with Diabetes), removing Health Inequalities, treatment and care, innovation and using good data to drive improvement.
• The final Liberate Pro cardiac rehab demo was successfully completed and we are imminently soft launching these patients education slide decks across the area.
Stroke - ICS On Track
10% of Stoke patients are eligible and require a Mechanical Thrombectomy Service for Acute Ischaemic Stroke - The East of England (EoE) Stroke Network in collaboration with NHSE Specialised Commissioning Team have been working with Cambridge University Hospitals NHS Trust (CUHFT) to expand both the population coverage for the existing service and the operational times which the service will be available. This service development has been awaited, so the first stepped change is welcomed for an 8am-4pm service operating 5 days a week. By April 2023 this will become an 8am to 8pm service 7 days a week and ultimately a 24/7 service. Patients are to be repatriated in a timely fashion post intervention within 24-72 hours for local rehabilitation or ongoing inpatient care. This requires responsive patient transport which is being negotiated.
The focus across the ICS has been to develop stroke services with a focus on the national priorities as agreed by the Regional Stroke Integrated Service Delivery Network (North), we are part of support structure to develop services across regional and local geography. We have been working with our hospitals to develop a ‘pre-alert of stroke’ pathway, reviewing our ‘mimic’ pathways and evaluating the pathway of reduced call to door times and optimised cannulation rates.
We have introduced some pilots for increased detection of people with AF and to improve patient experience through at home monitoring. We are working with clinicians, stroke board and the EAHSN, to implement a pilot with two approaches.We continue to engage with secondary care clinicians to understand metrics relating to thrombolysis rates and the scoping of the thrombolysis pathways to identify processes that can be streamlined for greater efficiency.
Undertake mapping of ICSS model vs current services provided and identify aspects for development to achieve the targets set by ISDN such as 6/52 and 6/12 reviews SNAPP data – there have been changes to the data collection timescales with a renewed focus from the ISDN for provider compliance and improvement on these service standards.
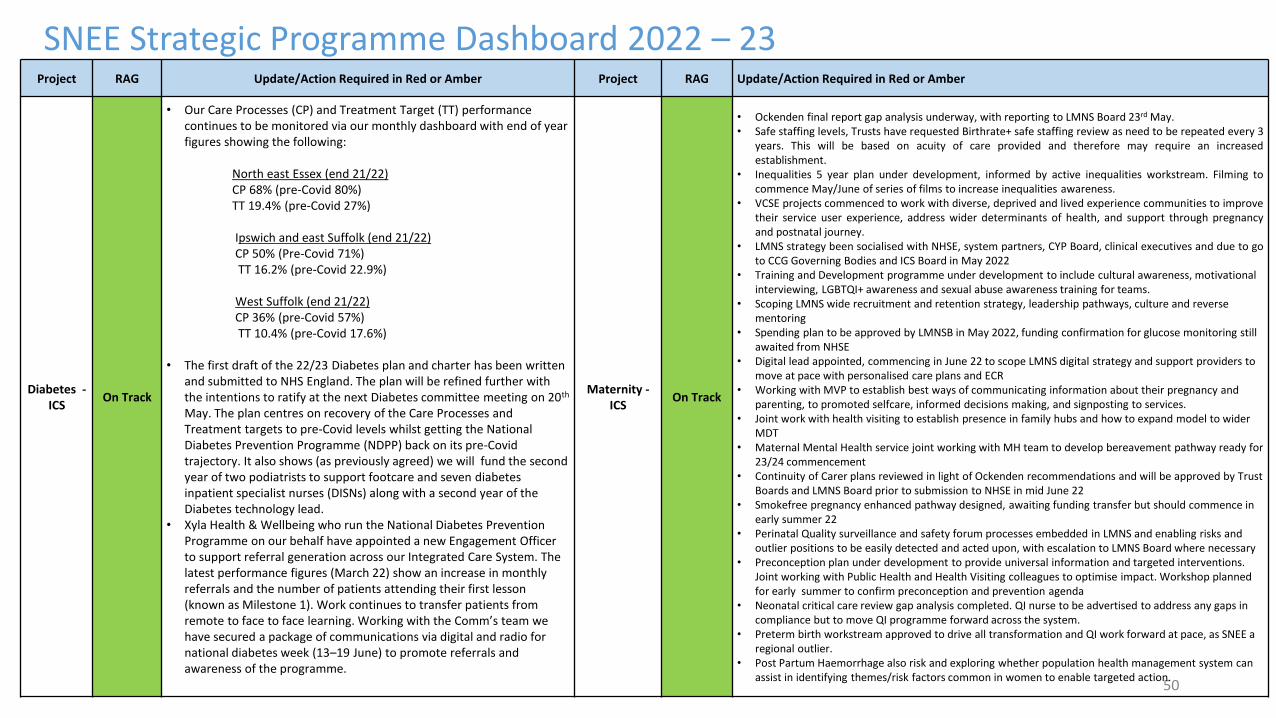
50
SNEE Strategic Programme Dashboard 2022 – 23Project RAG Update/Action Required in Red or Amber Project RAG Update/Action Required in Red or Amber
Diabetes -ICS
On Track
• Our Care Processes (CP) and Treatment Target (TT) performance continues to be monitored via our monthly dashboard with end of year figures showing the following:
North east Essex (end 21/22)CP 68% (pre-Covid 80%) TT 19.4% (pre-Covid 27%)
Ipswich and east Suffolk (end 21/22)CP 50% (Pre-Covid 71%)TT 16.2% (pre-Covid 22.9%)
West Suffolk (end 21/22)CP 36% (pre-Covid 57%)TT 10.4% (pre-Covid 17.6%)
• The first draft of the 22/23 Diabetes plan and charter has been written and submitted to NHS England. The plan will be refined further with the intentions to ratify at the next Diabetes committee meeting on 20th
May. The plan centres on recovery of the Care Processes and Treatment targets to pre-Covid levels whilst getting the National Diabetes Prevention Programme (NDPP) back on its pre-Covid trajectory. It also shows (as previously agreed) we will fund the second year of two podiatrists to support footcare and seven diabetes inpatient specialist nurses (DISNs) along with a second year of the Diabetes technology lead.
• Xyla Health & Wellbeing who run the National Diabetes Prevention Programme on our behalf have appointed a new Engagement Officer to support referral generation across our Integrated Care System. The latest performance figures (March 22) show an increase in monthly referrals and the number of patients attending their first lesson (known as Milestone 1). Work continues to transfer patients from remote to face to face learning. Working with the Comm’s team we have secured a package of communications via digital and radio for national diabetes week (13–19 June) to promote referrals and awareness of the programme.
Maternity -ICS
On Track
• Ockenden final report gap analysis underway, with reporting to LMNS Board 23rd May.• Safe staffing levels, Trusts have requested Birthrate+ safe staffing review as need to be repeated every 3
years. This will be based on acuity of care provided and therefore may require an increasedestablishment.
• Inequalities 5 year plan under development, informed by active inequalities workstream. Filming tocommence May/June of series of films to increase inequalities awareness.
• VCSE projects commenced to work with diverse, deprived and lived experience communities to improvetheir service user experience, address wider determinants of health, and support through pregnancyand postnatal journey.
• LMNS strategy been socialised with NHSE, system partners, CYP Board, clinical executives and due to goto CCG Governing Bodies and ICS Board in May 2022
• Training and Development programme under development to include cultural awareness, motivational interviewing, LGBTQI+ awareness and sexual abuse awareness training for teams.
• Scoping LMNS wide recruitment and retention strategy, leadership pathways, culture and reverse mentoring
• Spending plan to be approved by LMNSB in May 2022, funding confirmation for glucose monitoring still awaited from NHSE
• Digital lead appointed, commencing in June 22 to scope LMNS digital strategy and support providers to move at pace with personalised care plans and ECR
• Working with MVP to establish best ways of communicating information about their pregnancy and parenting, to promoted selfcare, informed decisions making, and signposting to services.
• Joint work with health visiting to establish presence in family hubs and how to expand model to wider MDT
• Maternal Mental Health service joint working with MH team to develop bereavement pathway ready for 23/24 commencement
• Continuity of Carer plans reviewed in light of Ockenden recommendations and will be approved by Trust Boards and LMNS Board prior to submission to NHSE in mid June 22
• Smokefree pregnancy enhanced pathway designed, awaiting funding transfer but should commence in early summer 22
• Perinatal Quality surveillance and safety forum processes embedded in LMNS and enabling risks and outlier positions to be easily detected and acted upon, with escalation to LMNS Board where necessary
• Preconception plan under development to provide universal information and targeted interventions. Joint working with Public Health and Health Visiting colleagues to optimise impact. Workshop planned for early summer to confirm preconception and prevention agenda
• Neonatal critical care review gap analysis completed. QI nurse to be advertised to address any gaps in compliance but to move QI programme forward across the system.
• Preterm birth workstream approved to drive all transformation and QI work forward at pace, as SNEE a regional outlier.
• Post Partum Haemorrhage also risk and exploring whether population health management system can assist in identifying themes/risk factors common in women to enable targeted action.
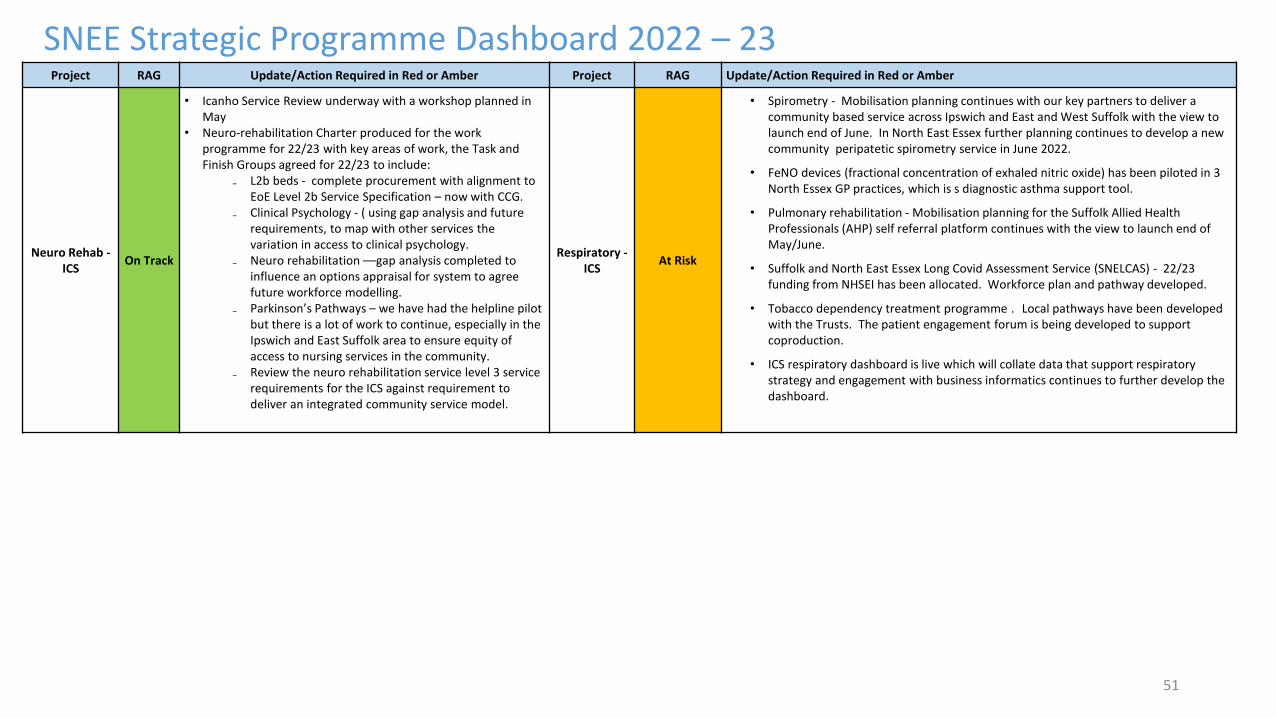
51
SNEE Strategic Programme Dashboard 2022 – 23Project RAG Update/Action Required in Red or Amber Project RAG Update/Action Required in Red or Amber
Neuro Rehab -ICS
On Track
• Icanho Service Review underway with a workshop planned in May
• Neuro-rehabilitation Charter produced for the work programme for 22/23 with key areas of work, the Task and Finish Groups agreed for 22/23 to include:
₋ L2b beds - complete procurement with alignment to EoE Level 2b Service Specification – now with CCG.
₋ Clinical Psychology - ( using gap analysis and future requirements, to map with other services the variation in access to clinical psychology.
₋ Neuro rehabilitation ––gap analysis completed to influence an options appraisal for system to agree future workforce modelling.
₋ Parkinson’s Pathways – we have had the helpline pilot but there is a lot of work to continue, especially in the Ipswich and East Suffolk area to ensure equity of access to nursing services in the community.
₋ Review the neuro rehabilitation service level 3 service requirements for the ICS against requirement to deliver an integrated community service model.
Respiratory -ICS
At Risk
• Spirometry - Mobilisation planning continues with our key partners to deliver a community based service across Ipswich and East and West Suffolk with the view to launch end of June. In North East Essex further planning continues to develop a new community peripatetic spirometry service in June 2022.
• FeNO devices (fractional concentration of exhaled nitric oxide) has been piloted in 3 North Essex GP practices, which is s diagnostic asthma support tool.
• Pulmonary rehabilitation - Mobilisation planning for the Suffolk Allied Health Professionals (AHP) self referral platform continues with the view to launch end of May/June.
• Suffolk and North East Essex Long Covid Assessment Service (SNELCAS) - 22/23 funding from NHSEI has been allocated. Workforce plan and pathway developed.
• Tobacco dependency treatment programme . Local pathways have been developed with the Trusts. The patient engagement forum is being developed to support coproduction.
• ICS respiratory dashboard is live which will collate data that support respiratory strategy and engagement with business informatics continues to further develop the dashboard.
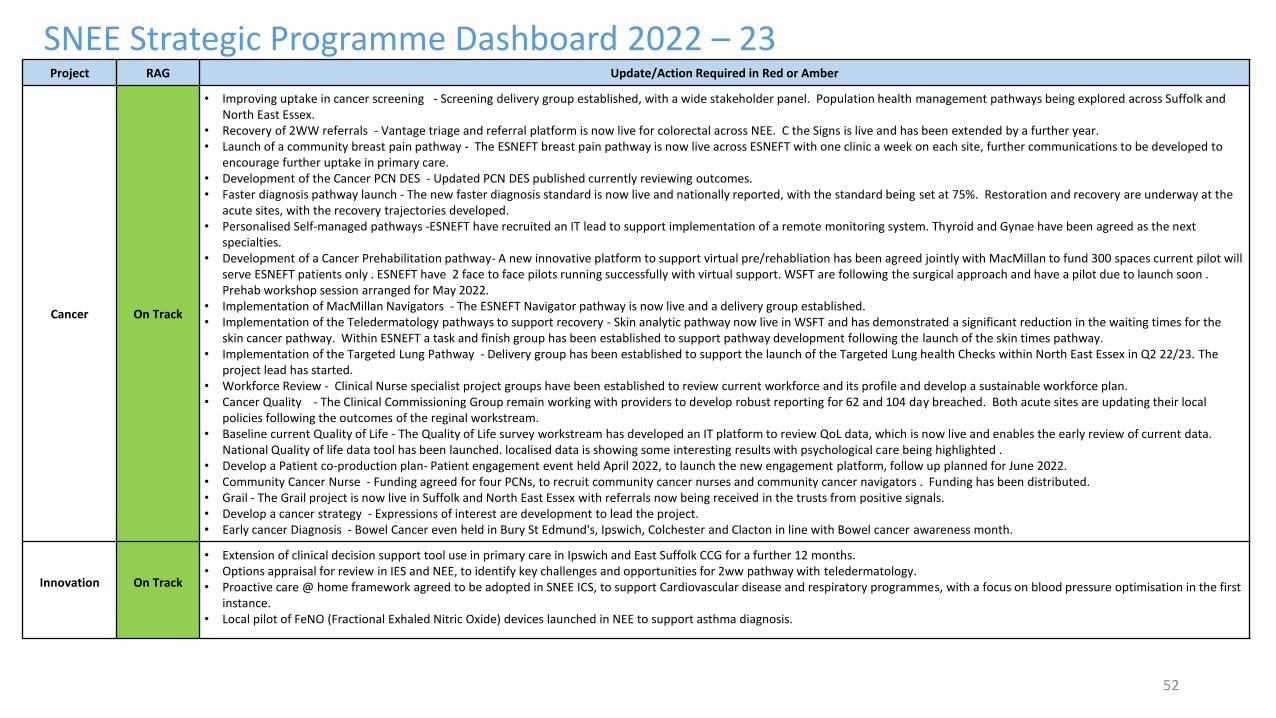
52
SNEE Strategic Programme Dashboard 2022 – 23Project RAG Update/Action Required in Red or Amber
Cancer On Track
• Improving uptake in cancer screening - Screening delivery group established, with a wide stakeholder panel. Population health management pathways being explored across Suffolk and North East Essex.
• Recovery of 2WW referrals - Vantage triage and referral platform is now live for colorectal across NEE. C the Signs is live and has been extended by a further year. • Launch of a community breast pain pathway - The ESNEFT breast pain pathway is now live across ESNEFT with one clinic a week on each site, further communications to be developed to
encourage further uptake in primary care. • Development of the Cancer PCN DES - Updated PCN DES published currently reviewing outcomes. • Faster diagnosis pathway launch - The new faster diagnosis standard is now live and nationally reported, with the standard being set at 75%. Restoration and recovery are underway at the
acute sites, with the recovery trajectories developed. • Personalised Self-managed pathways -ESNEFT have recruited an IT lead to support implementation of a remote monitoring system. Thyroid and Gynae have been agreed as the next
specialties. • Development of a Cancer Prehabilitation pathway- A new innovative platform to support virtual pre/rehabliation has been agreed jointly with MacMillan to fund 300 spaces current pilot will
serve ESNEFT patients only . ESNEFT have 2 face to face pilots running successfully with virtual support. WSFT are following the surgical approach and have a pilot due to launch soon . Prehab workshop session arranged for May 2022.
• Implementation of MacMillan Navigators - The ESNEFT Navigator pathway is now live and a delivery group established. • Implementation of the Teledermatology pathways to support recovery - Skin analytic pathway now live in WSFT and has demonstrated a significant reduction in the waiting times for the
skin cancer pathway. Within ESNEFT a task and finish group has been established to support pathway development following the launch of the skin times pathway. • Implementation of the Targeted Lung Pathway - Delivery group has been established to support the launch of the Targeted Lung health Checks within North East Essex in Q2 22/23. The
project lead has started. • Workforce Review - Clinical Nurse specialist project groups have been established to review current workforce and its profile and develop a sustainable workforce plan. • Cancer Quality - The Clinical Commissioning Group remain working with providers to develop robust reporting for 62 and 104 day breached. Both acute sites are updating their local
policies following the outcomes of the reginal workstream. • Baseline current Quality of Life - The Quality of Life survey workstream has developed an IT platform to review QoL data, which is now live and enables the early review of current data.
National Quality of life data tool has been launched. localised data is showing some interesting results with psychological care being highlighted .• Develop a Patient co-production plan- Patient engagement event held April 2022, to launch the new engagement platform, follow up planned for June 2022.• Community Cancer Nurse - Funding agreed for four PCNs, to recruit community cancer nurses and community cancer navigators . Funding has been distributed. • Grail - The Grail project is now live in Suffolk and North East Essex with referrals now being received in the trusts from positive signals. • Develop a cancer strategy - Expressions of interest are development to lead the project. • Early cancer Diagnosis - Bowel Cancer even held in Bury St Edmund's, Ipswich, Colchester and Clacton in line with Bowel cancer awareness month.
Innovation On Track
• Extension of clinical decision support tool use in primary care in Ipswich and East Suffolk CCG for a further 12 months.• Options appraisal for review in IES and NEE, to identify key challenges and opportunities for 2ww pathway with teledermatology.• Proactive care @ home framework agreed to be adopted in SNEE ICS, to support Cardiovascular disease and respiratory programmes, with a focus on blood pressure optimisation in the first
instance.• Local pilot of FeNO (Fractional Exhaled Nitric Oxide) devices launched in NEE to support asthma diagnosis.
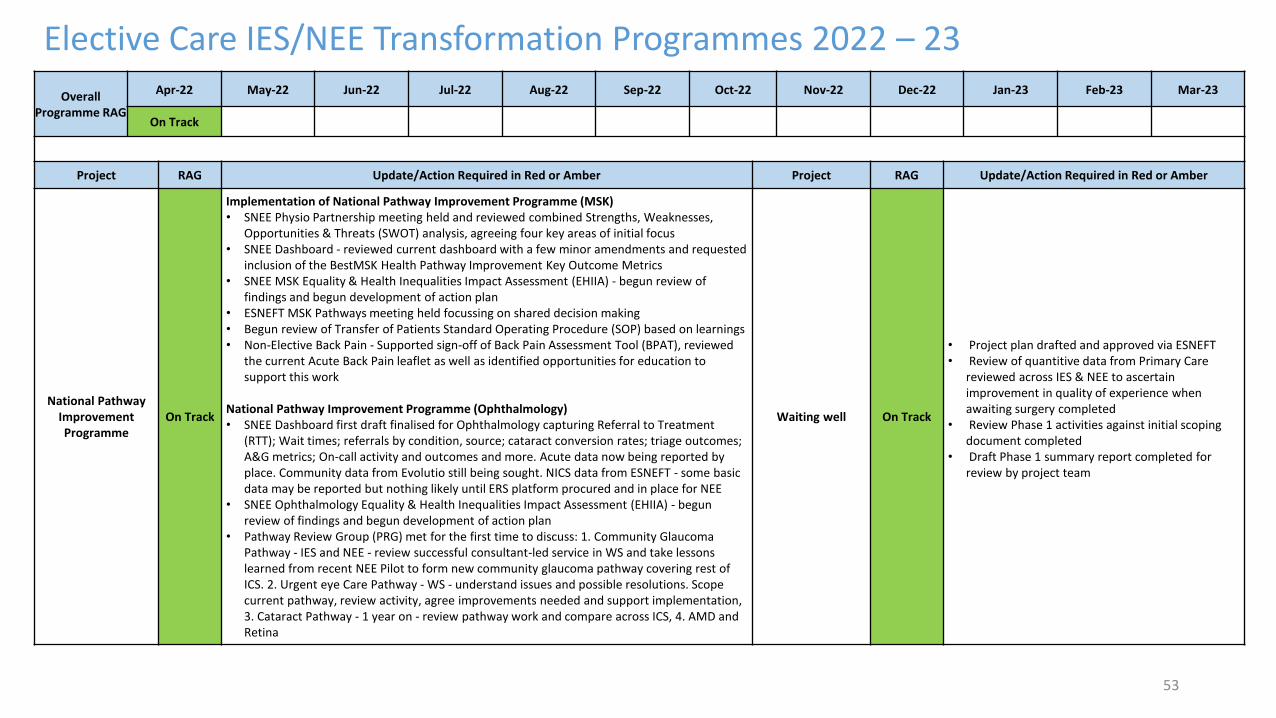
53
Elective Care IES/NEE Transformation Programmes 2022 – 23
Overall Programme RAG
Apr-22 May-22 Jun-22 Jul-22 Aug-22 Sep-22 Oct-22 Nov-22 Dec-22 Jan-23 Feb-23 Mar-23
On Track
Project RAG Update/Action Required in Red or Amber Project RAG Update/Action Required in Red or Amber
National Pathway Improvement Programme
On Track
Implementation of National Pathway Improvement Programme (MSK)• SNEE Physio Partnership meeting held and reviewed combined Strengths, Weaknesses,
Opportunities & Threats (SWOT) analysis, agreeing four key areas of initial focus• SNEE Dashboard - reviewed current dashboard with a few minor amendments and requested
inclusion of the BestMSK Health Pathway Improvement Key Outcome Metrics• SNEE MSK Equality & Health Inequalities Impact Assessment (EHIIA) - begun review of
findings and begun development of action plan• ESNEFT MSK Pathways meeting held focussing on shared decision making• Begun review of Transfer of Patients Standard Operating Procedure (SOP) based on learnings• Non-Elective Back Pain - Supported sign-off of Back Pain Assessment Tool (BPAT), reviewed
the current Acute Back Pain leaflet as well as identified opportunities for education to support this work
National Pathway Improvement Programme (Ophthalmology)• SNEE Dashboard first draft finalised for Ophthalmology capturing Referral to Treatment
(RTT); Wait times; referrals by condition, source; cataract conversion rates; triage outcomes; A&G metrics; On-call activity and outcomes and more. Acute data now being reported by place. Community data from Evolutio still being sought. NICS data from ESNEFT - some basic data may be reported but nothing likely until ERS platform procured and in place for NEE
• SNEE Ophthalmology Equality & Health Inequalities Impact Assessment (EHIIA) - begun review of findings and begun development of action plan
• Pathway Review Group (PRG) met for the first time to discuss: 1. Community Glaucoma Pathway - IES and NEE - review successful consultant-led service in WS and take lessons learned from recent NEE Pilot to form new community glaucoma pathway covering rest of ICS. 2. Urgent eye Care Pathway - WS - understand issues and possible resolutions. Scope current pathway, review activity, agree improvements needed and support implementation, 3. Cataract Pathway - 1 year on - review pathway work and compare across ICS, 4. AMD and Retina
Waiting well On Track
• Project plan drafted and approved via ESNEFT• Review of quantitive data from Primary Care
reviewed across IES & NEE to ascertain improvement in quality of experience when awaiting surgery completed
• Review Phase 1 activities against initial scoping document completed
• Draft Phase 1 summary report completed for review by project team
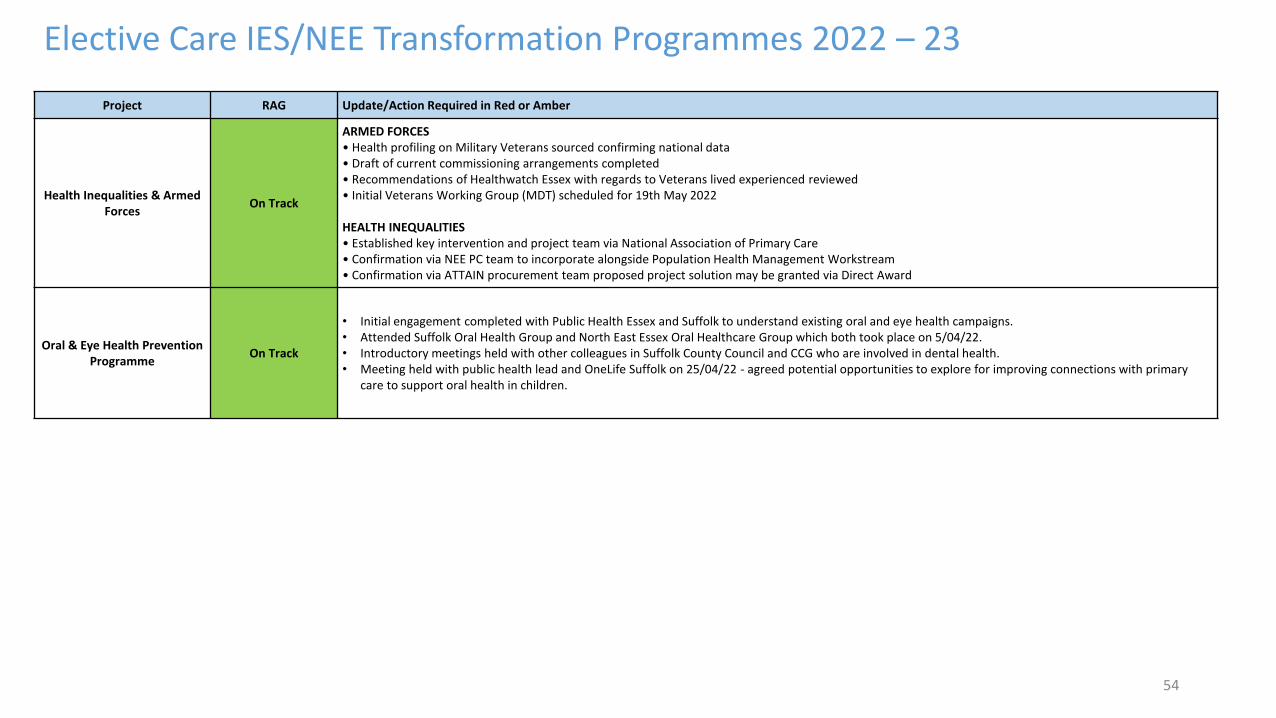
54
Elective Care IES/NEE Transformation Programmes 2022 – 23
Project RAG Update/Action Required in Red or Amber
Health Inequalities & Armed Forces
On Track
ARMED FORCES • Health profiling on Military Veterans sourced confirming national data • Draft of current commissioning arrangements completed• Recommendations of Healthwatch Essex with regards to Veterans lived experienced reviewed• Initial Veterans Working Group (MDT) scheduled for 19th May 2022
HEALTH INEQUALITIES• Established key intervention and project team via National Association of Primary Care• Confirmation via NEE PC team to incorporate alongside Population Health Management Workstream• Confirmation via ATTAIN procurement team proposed project solution may be granted via Direct Award
Oral & Eye Health Prevention Programme
On Track
• Initial engagement completed with Public Health Essex and Suffolk to understand existing oral and eye health campaigns. • Attended Suffolk Oral Health Group and North East Essex Oral Healthcare Group which both took place on 5/04/22.• Introductory meetings held with other colleagues in Suffolk County Council and CCG who are involved in dental health. • Meeting held with public health lead and OneLife Suffolk on 25/04/22 - agreed potential opportunities to explore for improving connections with primary
care to support oral health in children.
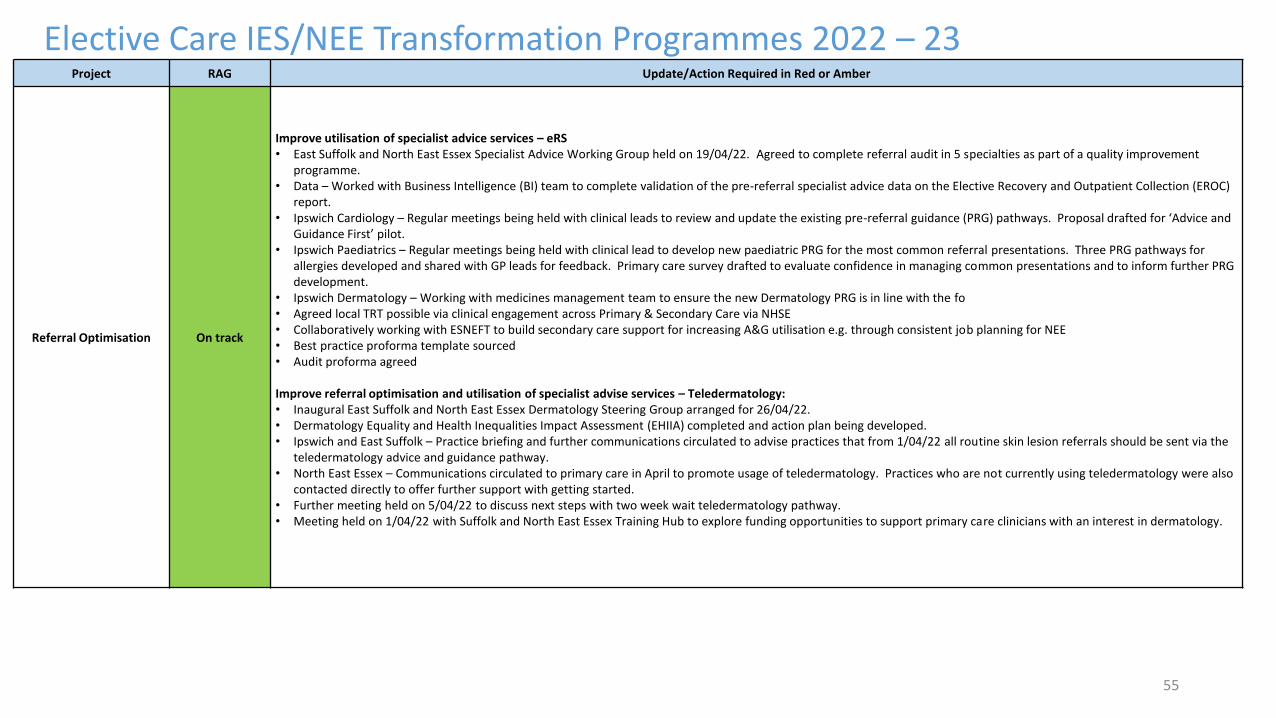
55
Elective Care IES/NEE Transformation Programmes 2022 – 23Project RAG Update/Action Required in Red or Amber
Referral Optimisation On track
Improve utilisation of specialist advice services – eRS• East Suffolk and North East Essex Specialist Advice Working Group held on 19/04/22. Agreed to complete referral audit in 5 specialties as part of a quality improvement
programme. • Data – Worked with Business Intelligence (BI) team to complete validation of the pre-referral specialist advice data on the Elective Recovery and Outpatient Collection (EROC)
report. • Ipswich Cardiology – Regular meetings being held with clinical leads to review and update the existing pre-referral guidance (PRG) pathways. Proposal drafted for ‘Advice and
Guidance First’ pilot. • Ipswich Paediatrics – Regular meetings being held with clinical lead to develop new paediatric PRG for the most common referral presentations. Three PRG pathways for
allergies developed and shared with GP leads for feedback. Primary care survey drafted to evaluate confidence in managing common presentations and to inform further PRG development.
• Ipswich Dermatology – Working with medicines management team to ensure the new Dermatology PRG is in line with the fo• Agreed local TRT possible via clinical engagement across Primary & Secondary Care via NHSE• Collaboratively working with ESNEFT to build secondary care support for increasing A&G utilisation e.g. through consistent job planning for NEE• Best practice proforma template sourced • Audit proforma agreed
Improve referral optimisation and utilisation of specialist advise services – Teledermatology:• Inaugural East Suffolk and North East Essex Dermatology Steering Group arranged for 26/04/22. • Dermatology Equality and Health Inequalities Impact Assessment (EHIIA) completed and action plan being developed. • Ipswich and East Suffolk – Practice briefing and further communications circulated to advise practices that from 1/04/22 all routine skin lesion referrals should be sent via the
teledermatology advice and guidance pathway. • North East Essex – Communications circulated to primary care in April to promote usage of teledermatology. Practices who are not currently using teledermatology were also
contacted directly to offer further support with getting started. • Further meeting held on 5/04/22 to discuss next steps with two week wait teledermatology pathway. • Meeting held on 1/04/22 with Suffolk and North East Essex Training Hub to explore funding opportunities to support primary care clinicians with an interest in dermatology.
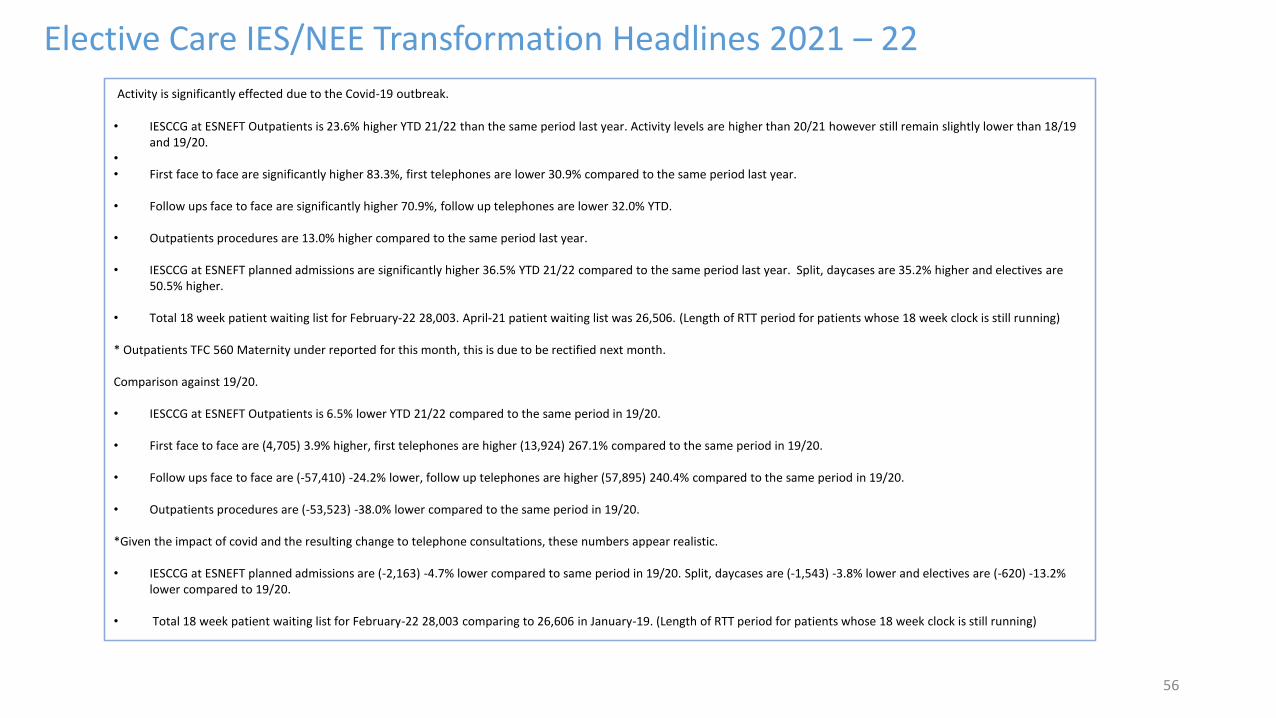
56
Elective Care IES/NEE Transformation Headlines 2021 – 22
Activity is significantly effected due to the Covid-19 outbreak.
• IESCCG at ESNEFT Outpatients is 23.6% higher YTD 21/22 than the same period last year. Activity levels are higher than 20/21 however still remain slightly lower than 18/19 and 19/20.
•
• First face to face are significantly higher 83.3%, first telephones are lower 30.9% compared to the same period last year.
• Follow ups face to face are significantly higher 70.9%, follow up telephones are lower 32.0% YTD.
• Outpatients procedures are 13.0% higher compared to the same period last year.
• IESCCG at ESNEFT planned admissions are significantly higher 36.5% YTD 21/22 compared to the same period last year. Split, daycases are 35.2% higher and electives are 50.5% higher.
• Total 18 week patient waiting list for February-22 28,003. April-21 patient waiting list was 26,506. (Length of RTT period for patients whose 18 week clock is still running)
* Outpatients TFC 560 Maternity under reported for this month, this is due to be rectified next month.
Comparison against 19/20.
• IESCCG at ESNEFT Outpatients is 6.5% lower YTD 21/22 compared to the same period in 19/20.
• First face to face are (4,705) 3.9% higher, first telephones are higher (13,924) 267.1% compared to the same period in 19/20.
• Follow ups face to face are (-57,410) -24.2% lower, follow up telephones are higher (57,895) 240.4% compared to the same period in 19/20.
• Outpatients procedures are (-53,523) -38.0% lower compared to the same period in 19/20.
*Given the impact of covid and the resulting change to telephone consultations, these numbers appear realistic.
• IESCCG at ESNEFT planned admissions are (-2,163) -4.7% lower compared to same period in 19/20. Split, daycases are (-1,543) -3.8% lower and electives are (-620) -13.2% lower compared to 19/20.
• Total 18 week patient waiting list for February-22 28,003 comparing to 26,606 in January-19. (Length of RTT period for patients whose 18 week clock is still running)
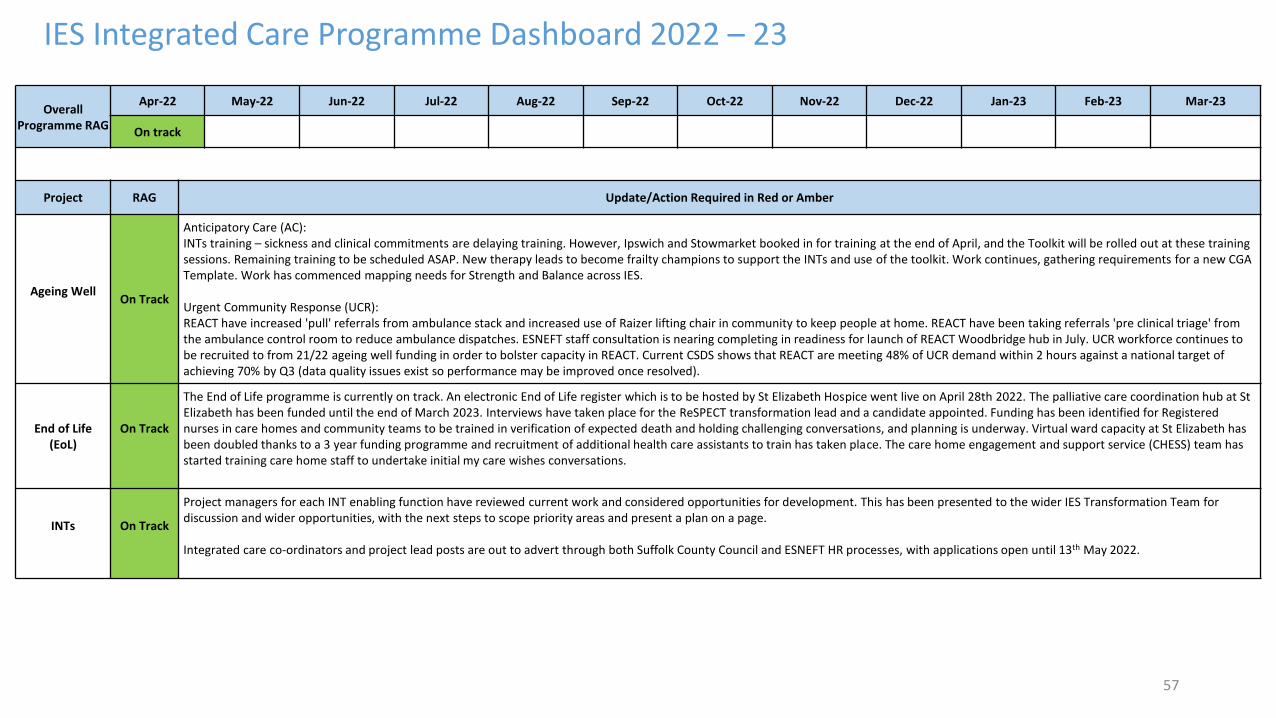
57
IES Integrated Care Programme Dashboard 2022 – 23
Overall Programme RAG
Apr-22 May-22 Jun-22 Jul-22 Aug-22 Sep-22 Oct-22 Nov-22 Dec-22 Jan-23 Feb-23 Mar-23
On track
Project RAG Update/Action Required in Red or Amber
Ageing WellOn Track
Anticipatory Care (AC):INTs training – sickness and clinical commitments are delaying training. However, Ipswich and Stowmarket booked in for training at the end of April, and the Toolkit will be rolled out at these training sessions. Remaining training to be scheduled ASAP. New therapy leads to become frailty champions to support the INTs and use of the toolkit. Work continues, gathering requirements for a new CGA Template. Work has commenced mapping needs for Strength and Balance across IES.
Urgent Community Response (UCR):REACT have increased 'pull' referrals from ambulance stack and increased use of Raizer lifting chair in community to keep people at home. REACT have been taking referrals 'pre clinical triage' from the ambulance control room to reduce ambulance dispatches. ESNEFT staff consultation is nearing completing in readiness for launch of REACT Woodbridge hub in July. UCR workforce continues to be recruited to from 21/22 ageing well funding in order to bolster capacity in REACT. Current CSDS shows that REACT are meeting 48% of UCR demand within 2 hours against a national target of achieving 70% by Q3 (data quality issues exist so performance may be improved once resolved).
End of Life(EoL)
On Track
The End of Life programme is currently on track. An electronic End of Life register which is to be hosted by St Elizabeth Hospice went live on April 28th 2022. The palliative care coordination hub at St Elizabeth has been funded until the end of March 2023. Interviews have taken place for the ReSPECT transformation lead and a candidate appointed. Funding has been identified for Registered nurses in care homes and community teams to be trained in verification of expected death and holding challenging conversations, and planning is underway. Virtual ward capacity at St Elizabeth has been doubled thanks to a 3 year funding programme and recruitment of additional health care assistants to train has taken place. The care home engagement and support service (CHESS) team has started training care home staff to undertake initial my care wishes conversations.
INTs On Track
Project managers for each INT enabling function have reviewed current work and considered opportunities for development. This has been presented to the wider IES Transformation Team for discussion and wider opportunities, with the next steps to scope priority areas and present a plan on a page.
Integrated care co-ordinators and project lead posts are out to advert through both Suffolk County Council and ESNEFT HR processes, with applications open until 13th May 2022.
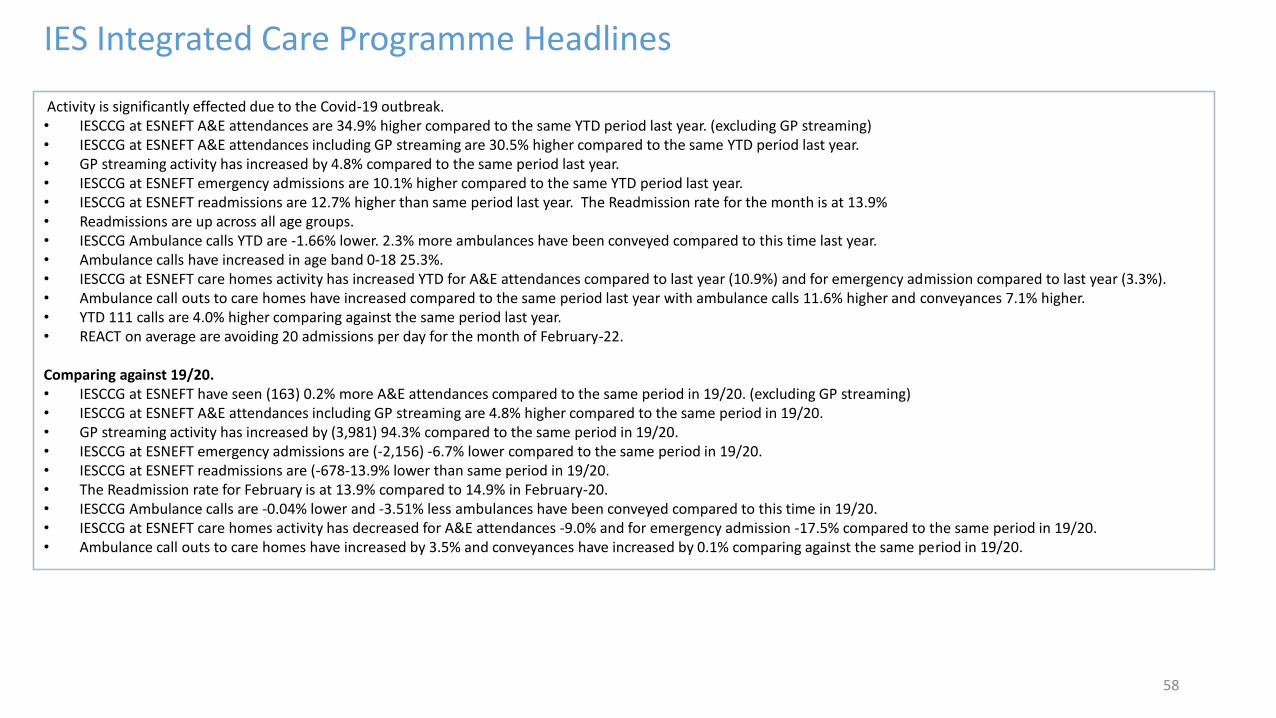
58
IES Integrated Care Programme Headlines
Activity is significantly effected due to the Covid-19 outbreak.• IESCCG at ESNEFT A&E attendances are 34.9% higher compared to the same YTD period last year. (excluding GP streaming)• IESCCG at ESNEFT A&E attendances including GP streaming are 30.5% higher compared to the same YTD period last year.• GP streaming activity has increased by 4.8% compared to the same period last year.• IESCCG at ESNEFT emergency admissions are 10.1% higher compared to the same YTD period last year.• IESCCG at ESNEFT readmissions are 12.7% higher than same period last year. The Readmission rate for the month is at 13.9%• Readmissions are up across all age groups.• IESCCG Ambulance calls YTD are -1.66% lower. 2.3% more ambulances have been conveyed compared to this time last year. • Ambulance calls have increased in age band 0-18 25.3%.• IESCCG at ESNEFT care homes activity has increased YTD for A&E attendances compared to last year (10.9%) and for emergency admission compared to last year (3.3%). • Ambulance call outs to care homes have increased compared to the same period last year with ambulance calls 11.6% higher and conveyances 7.1% higher. • YTD 111 calls are 4.0% higher comparing against the same period last year. • REACT on average are avoiding 20 admissions per day for the month of February-22.
Comparing against 19/20.• IESCCG at ESNEFT have seen (163) 0.2% more A&E attendances compared to the same period in 19/20. (excluding GP streaming)• IESCCG at ESNEFT A&E attendances including GP streaming are 4.8% higher compared to the same period in 19/20.• GP streaming activity has increased by (3,981) 94.3% compared to the same period in 19/20.• IESCCG at ESNEFT emergency admissions are (-2,156) -6.7% lower compared to the same period in 19/20.• IESCCG at ESNEFT readmissions are (-678-13.9% lower than same period in 19/20. • The Readmission rate for February is at 13.9% compared to 14.9% in February-20.• IESCCG Ambulance calls are -0.04% lower and -3.51% less ambulances have been conveyed compared to this time in 19/20. • IESCCG at ESNEFT care homes activity has decreased for A&E attendances -9.0% and for emergency admission -17.5% compared to the same period in 19/20.• Ambulance call outs to care homes have increased by 3.5% and conveyances have increased by 0.1% comparing against the same period in 19/20.
Financial Position Updates 21-22
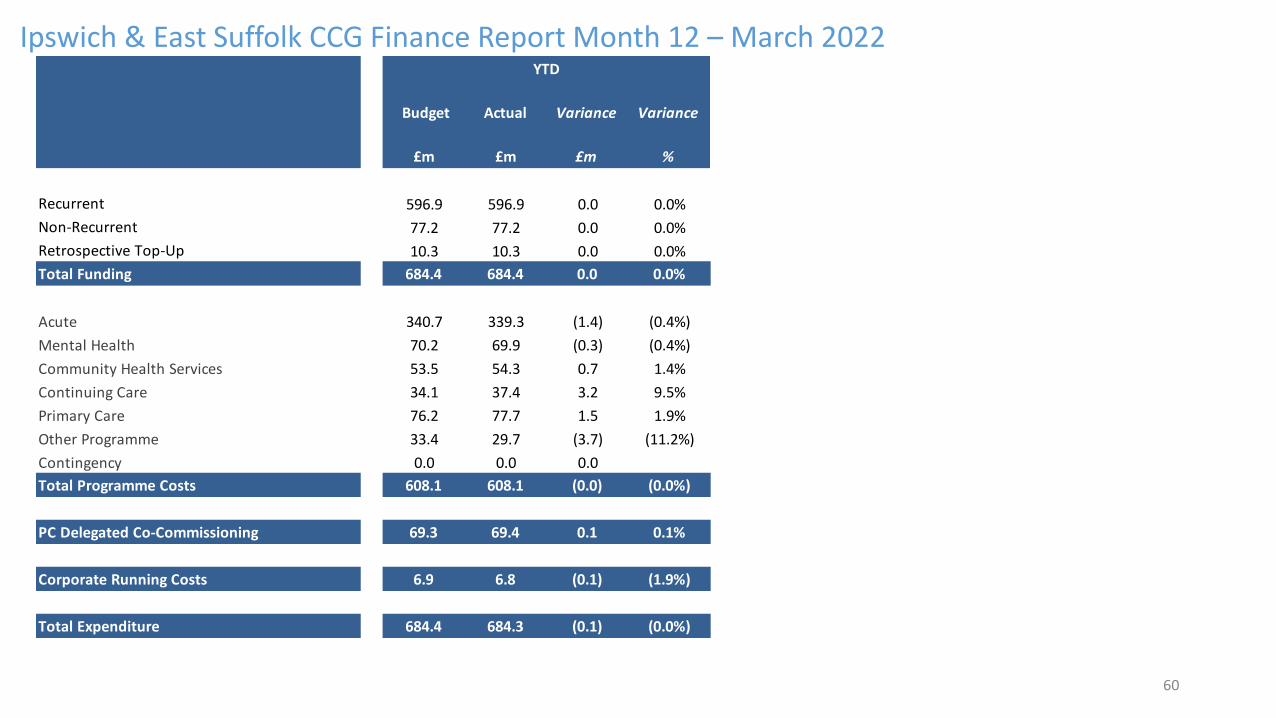
60
Ipswich & East Suffolk CCG Finance Report Month 12 – March 2022
Budget Actual Variance Variance
£m £m £m %
Recurrent 596.9 596.9 0.0 0.0%
Non-Recurrent 77.2 77.2 0.0 0.0%
Retrospective Top-Up 10.3 10.3 0.0 0.0%
Total Funding 684.4 684.4 0.0 0.0%
Acute 340.7 339.3 (1.4) (0.4%)
Mental Health 70.2 69.9 (0.3) (0.4%)
Community Health Services 53.5 54.3 0.7 1.4%
Continuing Care 34.1 37.4 3.2 9.5%
Primary Care 76.2 77.7 1.5 1.9%
Other Programme 33.4 29.7 (3.7) (11.2%)
Contingency 0.0 0.0 0.0
Total Programme Costs 608.1 608.1 (0.0) (0.0%)
PC Delegated Co-Commissioning 69.3 69.4 0.1 0.1%
Corporate Running Costs 6.9 6.8 (0.1) (1.9%)
Total Expenditure 684.4 684.3 (0.1) (0.0%)
YTD
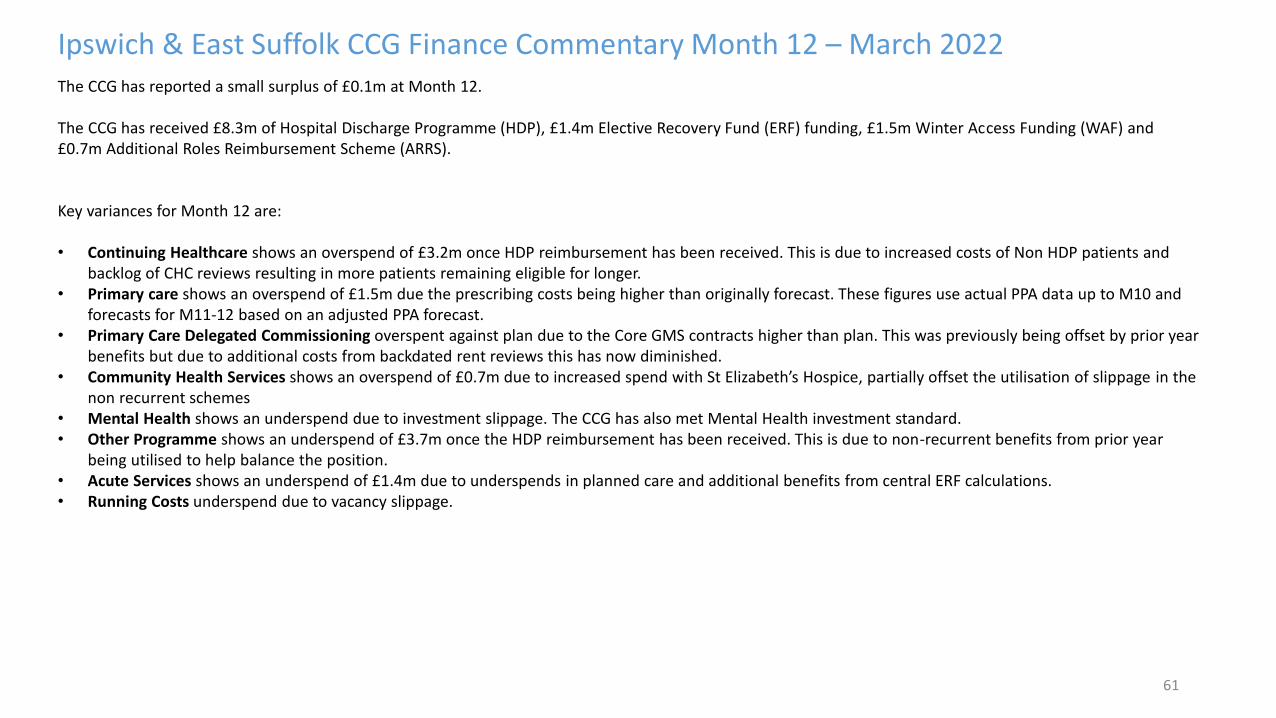
61
Ipswich & East Suffolk CCG Finance Commentary Month 12 – March 2022The CCG has reported a small surplus of £0.1m at Month 12.
The CCG has received £8.3m of Hospital Discharge Programme (HDP), £1.4m Elective Recovery Fund (ERF) funding, £1.5m Winter Access Funding (WAF) and £0.7m Additional Roles Reimbursement Scheme (ARRS).
Key variances for Month 12 are:
• Continuing Healthcare shows an overspend of £3.2m once HDP reimbursement has been received. This is due to increased costs of Non HDP patients and backlog of CHC reviews resulting in more patients remaining eligible for longer.
• Primary care shows an overspend of £1.5m due the prescribing costs being higher than originally forecast. These figures use actual PPA data up to M10 and forecasts for M11-12 based on an adjusted PPA forecast.
• Primary Care Delegated Commissioning overspent against plan due to the Core GMS contracts higher than plan. This was previously being offset by prior year benefits but due to additional costs from backdated rent reviews this has now diminished.
• Community Health Services shows an overspend of £0.7m due to increased spend with St Elizabeth’s Hospice, partially offset the utilisation of slippage in the non recurrent schemes
• Mental Health shows an underspend due to investment slippage. The CCG has also met Mental Health investment standard.• Other Programme shows an underspend of £3.7m once the HDP reimbursement has been received. This is due to non-recurrent benefits from prior year
being utilised to help balance the position.• Acute Services shows an underspend of £1.4m due to underspends in planned care and additional benefits from central ERF calculations.• Running Costs underspend due to vacancy slippage.
Page 1 of 4
GOVERNING BODY
Agenda Item No. 13
Reference No. IESCCG 22-22
Date. 24 May 2022
Title
Governing Body Assurance Framework and Directors Risk Registers
Lead Director
Amanda Lyes, Director of Corporate Services and System Infrastructure
Author(s)
Tony Buckle, Risk Manager
Purpose
To provide the committee with the updated CCG Governing Body Assurance Framework (GBAF) document for May 2022
Applicable CCG Clinical Priorities:
1. To promote self care
2. To ensure high quality local services where possible ✓
3. To improve the health of those most in need ✓
4. To improve health & educational attainment for children & young people ✓
5. To improve access to mental health services ✓
6. To improve outcomes for patients with diabetes to above national averages ✓
7. To improve care for frail elderly individuals ✓
8. To allow patients to die with dignity & compassion & to choose their place of death where appropriate
9. To ensure that the CCG operates within agreed budgets
Action required by the Governing Body: The Governing Body is requested to review and approve the updated Ipswich & East Suffolk CCG GBAF for May 2022.
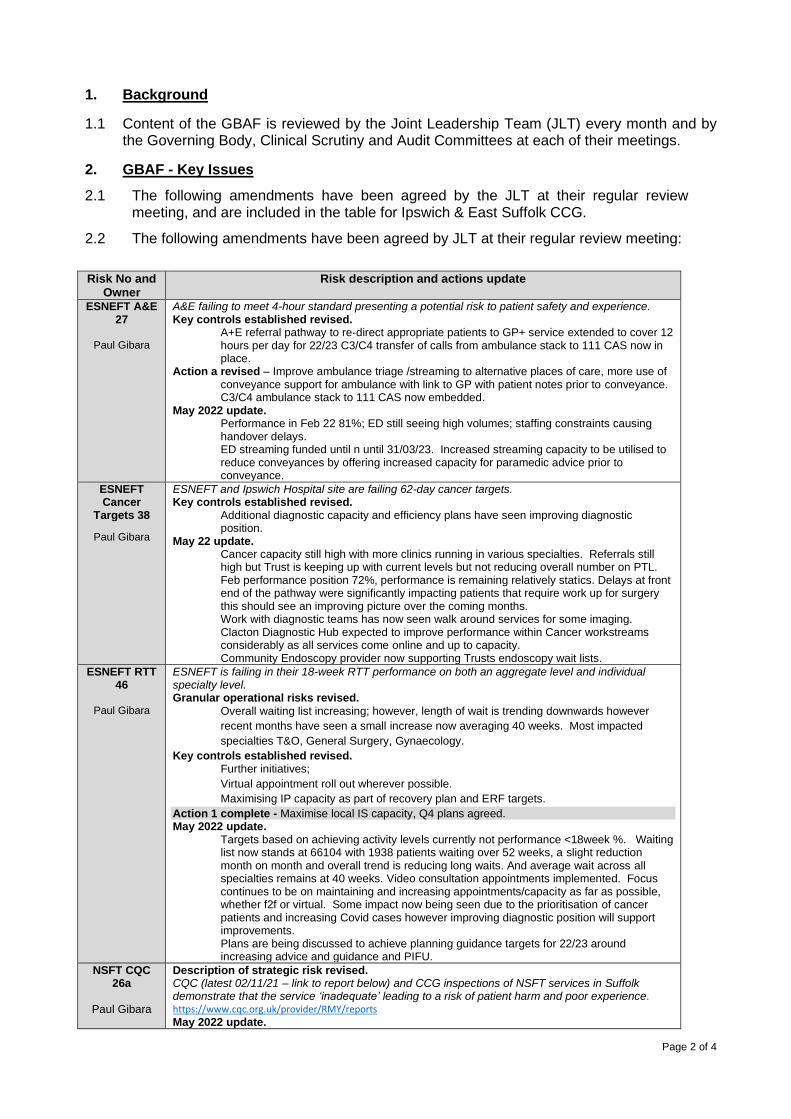
Page 2 of 4
1. Background
1.1 Content of the GBAF is reviewed by the Joint Leadership Team (JLT) every month and by the Governing Body, Clinical Scrutiny and Audit Committees at each of their meetings.
2. GBAF - Key Issues
2.1 The following amendments have been agreed by the JLT at their regular review meeting, and are included in the table for Ipswich & East Suffolk CCG.
2.2 The following amendments have been agreed by JLT at their regular review meeting:
Risk No and Owner
Risk description and actions update
ESNEFT A&E 27
Paul Gibara
A&E failing to meet 4-hour standard presenting a potential risk to patient safety and experience. Key controls established revised. A+E referral pathway to re-direct appropriate patients to GP+ service extended to cover 12 hours per day for 22/23 C3/C4 transfer of calls from ambulance stack to 111 CAS now in place. Action a revised – Improve ambulance triage /streaming to alternative places of care, more use of conveyance support for ambulance with link to GP with patient notes prior to conveyance. C3/C4 ambulance stack to 111 CAS now embedded. May 2022 update. Performance in Feb 22 81%; ED still seeing high volumes; staffing constraints causing handover delays. ED streaming funded until n until 31/03/23. Increased streaming capacity to be utilised to reduce conveyances by offering increased capacity for paramedic advice prior to conveyance.
ESNEFT Cancer
Targets 38
Paul Gibara
ESNEFT and Ipswich Hospital site are failing 62-day cancer targets. Key controls established revised.
Additional diagnostic capacity and efficiency plans have seen improving diagnostic position.
May 22 update. Cancer capacity still high with more clinics running in various specialties. Referrals still high but Trust is keeping up with current levels but not reducing overall number on PTL. Feb performance position 72%, performance is remaining relatively statics. Delays at front end of the pathway were significantly impacting patients that require work up for surgery this should see an improving picture over the coming months. Work with diagnostic teams has now seen walk around services for some imaging. Clacton Diagnostic Hub expected to improve performance within Cancer workstreams considerably as all services come online and up to capacity. Community Endoscopy provider now supporting Trusts endoscopy wait lists.
ESNEFT RTT 46
Paul Gibara
ESNEFT is failing in their 18-week RTT performance on both an aggregate level and individual specialty level. Granular operational risks revised. Overall waiting list increasing; however, length of wait is trending downwards however
recent months have seen a small increase now averaging 40 weeks. Most impacted
specialties T&O, General Surgery, Gynaecology.
Key controls established revised. Further initiatives;
Virtual appointment roll out wherever possible.
Maximising IP capacity as part of recovery plan and ERF targets.
Action 1 complete - Maximise local IS capacity, Q4 plans agreed. May 2022 update. Targets based on achieving activity levels currently not performance <18week %. Waiting list now stands at 66104 with 1938 patients waiting over 52 weeks, a slight reduction month on month and overall trend is reducing long waits. And average wait across all specialties remains at 40 weeks. Video consultation appointments implemented. Focus continues to be on maintaining and increasing appointments/capacity as far as possible, whether f2f or virtual. Some impact now being seen due to the prioritisation of cancer patients and increasing Covid cases however improving diagnostic position will support improvements. Plans are being discussed to achieve planning guidance targets for 22/23 around increasing advice and guidance and PIFU.
NSFT CQC 26a
Paul Gibara
Description of strategic risk revised. CQC (latest 02/11/21 – link to report below) and CCG inspections of NSFT services in Suffolk demonstrate that the service ‘inadequate’ leading to a risk of patient harm and poor experience. https://www.cqc.org.uk/provider/RMY/reports
May 2022 update.
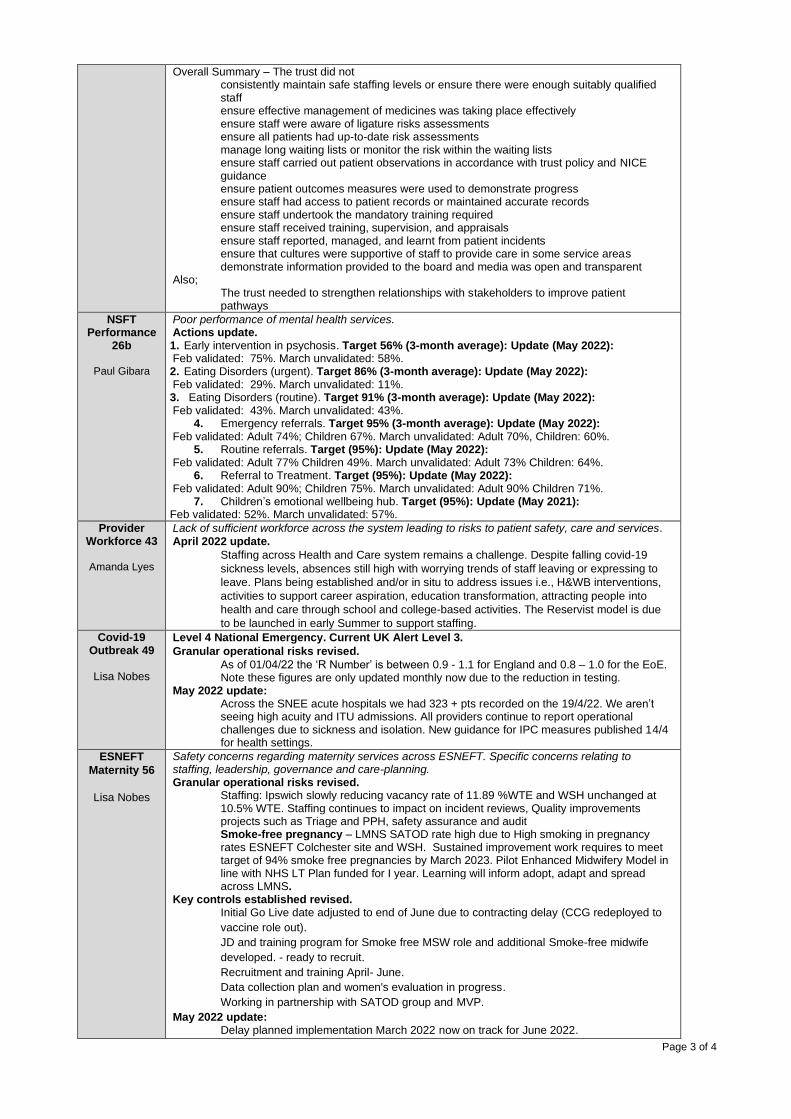
Page 3 of 4
Overall Summary – The trust did not consistently maintain safe staffing levels or ensure there were enough suitably qualified staff ensure effective management of medicines was taking place effectively ensure staff were aware of ligature risks assessments ensure all patients had up-to-date risk assessments manage long waiting lists or monitor the risk within the waiting lists ensure staff carried out patient observations in accordance with trust policy and NICE guidance ensure patient outcomes measures were used to demonstrate progress ensure staff had access to patient records or maintained accurate records ensure staff undertook the mandatory training required ensure staff received training, supervision, and appraisals ensure staff reported, managed, and learnt from patient incidents ensure that cultures were supportive of staff to provide care in some service areas demonstrate information provided to the board and media was open and transparent Also; The trust needed to strengthen relationships with stakeholders to improve patient pathways
NSFT Performance
26b
Paul Gibara
Poor performance of mental health services. Actions update. 1. Early intervention in psychosis. Target 56% (3-month average): Update (May 2022): Feb validated: 75%. March unvalidated: 58%. 2. Eating Disorders (urgent). Target 86% (3-month average): Update (May 2022): Feb validated: 29%. March unvalidated: 11%. 3. Eating Disorders (routine). Target 91% (3-month average): Update (May 2022): Feb validated: 43%. March unvalidated: 43%.
4. Emergency referrals. Target 95% (3-month average): Update (May 2022): Feb validated: Adult 74%; Children 67%. March unvalidated: Adult 70%, Children: 60%.
5. Routine referrals. Target (95%): Update (May 2022): Feb validated: Adult 77% Children 49%. March unvalidated: Adult 73% Children: 64%.
6. Referral to Treatment. Target (95%): Update (May 2022): Feb validated: Adult 90%; Children 75%. March unvalidated: Adult 90% Children 71%.
7. Children’s emotional wellbeing hub. Target (95%): Update (May 2021): Feb validated: 52%. March unvalidated: 57%.
Provider Workforce 43
Amanda Lyes
Lack of sufficient workforce across the system leading to risks to patient safety, care and services. April 2022 update.
Staffing across Health and Care system remains a challenge. Despite falling covid-19
sickness levels, absences still high with worrying trends of staff leaving or expressing to
leave. Plans being established and/or in situ to address issues i.e., H&WB interventions,
activities to support career aspiration, education transformation, attracting people into
health and care through school and college-based activities. The Reservist model is due
to be launched in early Summer to support staffing.
Covid-19 Outbreak 49
Lisa Nobes
Level 4 National Emergency. Current UK Alert Level 3.
Granular operational risks revised.
As of 01/04/22 the ‘R Number’ is between 0.9 - 1.1 for England and 0.8 – 1.0 for the EoE. Note these figures are only updated monthly now due to the reduction in testing. May 2022 update: Across the SNEE acute hospitals we had 323 + pts recorded on the 19/4/22. We aren’t seeing high acuity and ITU admissions. All providers continue to report operational challenges due to sickness and isolation. New guidance for IPC measures published 14/4 for health settings.
ESNEFT
Maternity 56
Lisa Nobes
Safety concerns regarding maternity services across ESNEFT. Specific concerns relating to staffing, leadership, governance and care-planning. Granular operational risks revised. Staffing: Ipswich slowly reducing vacancy rate of 11.89 %WTE and WSH unchanged at 10.5% WTE. Staffing continues to impact on incident reviews, Quality improvements projects such as Triage and PPH, safety assurance and audit Smoke-free pregnancy – LMNS SATOD rate high due to High smoking in pregnancy rates ESNEFT Colchester site and WSH. Sustained improvement work requires to meet target of 94% smoke free pregnancies by March 2023. Pilot Enhanced Midwifery Model in line with NHS LT Plan funded for I year. Learning will inform adopt, adapt and spread across LMNS. Key controls established revised. Initial Go Live date adjusted to end of June due to contracting delay (CCG redeployed to
vaccine role out).
JD and training program for Smoke free MSW role and additional Smoke-free midwife
developed. - ready to recruit.
Recruitment and training April- June.
Data collection plan and women's evaluation in progress.
Working in partnership with SATOD group and MVP.
May 2022 update: Delay planned implementation March 2022 now on track for June 2022.
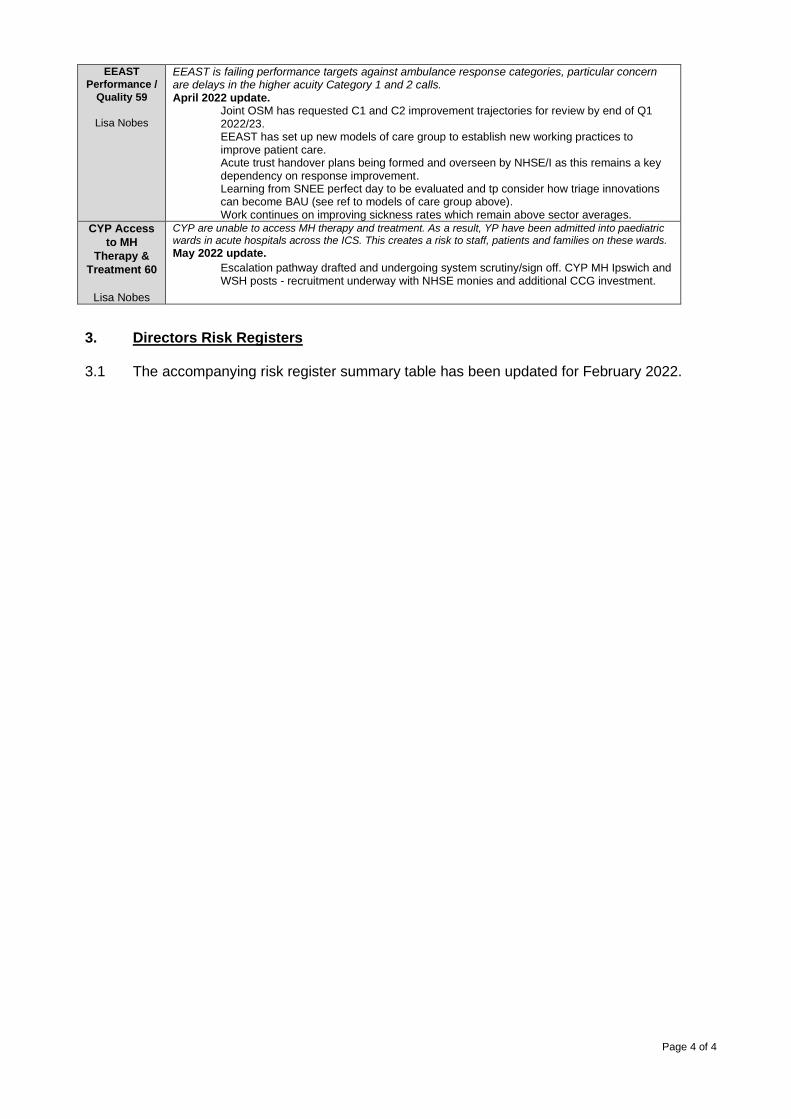
Page 4 of 4
EEAST
Performance /
Quality 59
Lisa Nobes
EEAST is failing performance targets against ambulance response categories, particular concern are delays in the higher acuity Category 1 and 2 calls. April 2022 update. Joint OSM has requested C1 and C2 improvement trajectories for review by end of Q1 2022/23. EEAST has set up new models of care group to establish new working practices to improve patient care. Acute trust handover plans being formed and overseen by NHSE/I as this remains a key dependency on response improvement. Learning from SNEE perfect day to be evaluated and tp consider how triage innovations can become BAU (see ref to models of care group above). Work continues on improving sickness rates which remain above sector averages.
CYP Access
to MH
Therapy &
Treatment 60
Lisa Nobes
CYP are unable to access MH therapy and treatment. As a result, YP have been admitted into paediatric wards in acute hospitals across the ICS. This creates a risk to staff, patients and families on these wards.
May 2022 update.
Escalation pathway drafted and undergoing system scrutiny/sign off. CYP MH Ipswich and WSH posts - recruitment underway with NHSE monies and additional CCG investment.
3. Directors Risk Registers 3.1 The accompanying risk register summary table has been updated for February 2022.
Governing Body Assurance Framework
2022 - 2023
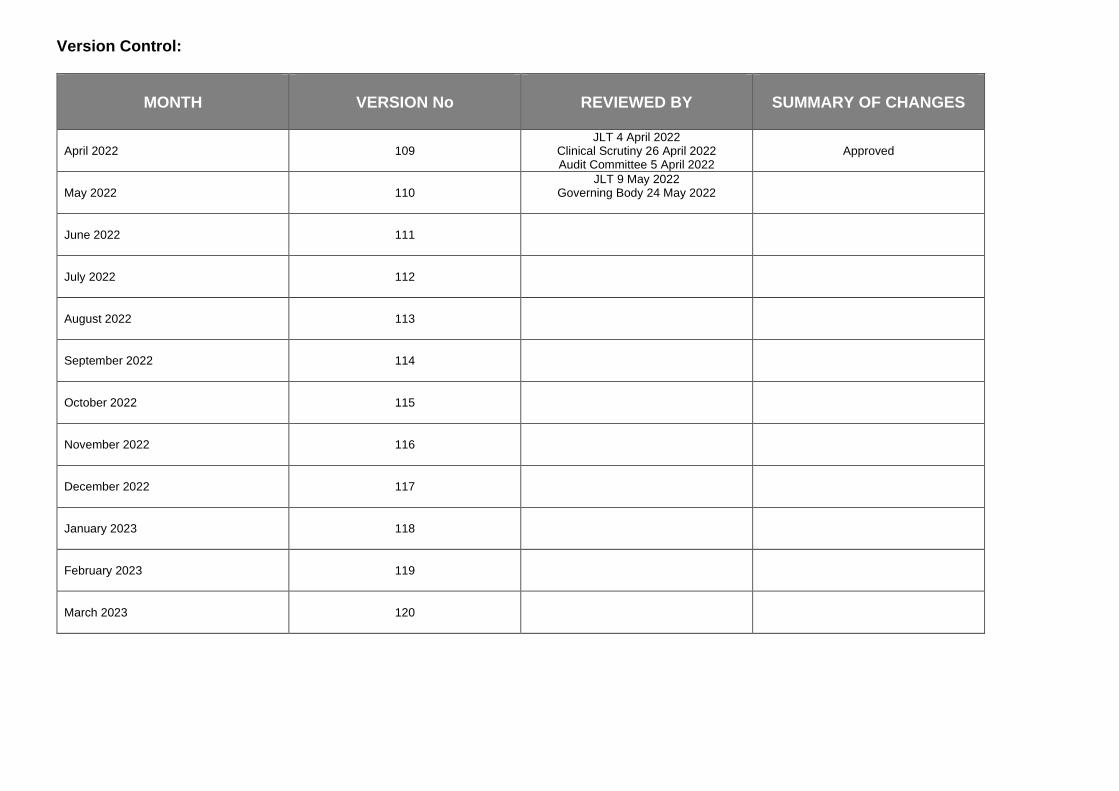
Version Control:
MONTH
VERSION No
REVIEWED BY
SUMMARY OF CHANGES
April 2022
109
JLT 4 April 2022 Clinical Scrutiny 26 April 2022 Audit Committee 5 April 2022
Approved
May 2022
110
JLT 9 May 2022 Governing Body 24 May 2022
June 2022
111
July 2022
112
August 2022
113
September 2022
114
October 2022
115
November 2022
116
December 2022
117
January 2023
118
February 2023
119
March 2023
120
Governing Body Assurance Framework
Overview
The Governing Body Assurance Framework (GBAF hereafter) provides the NHS Ipswich and East Suffolk Clinical Commissioning Group (CCG) with a simple but comprehensive method for the effective and focused management of risk. Through the GBAF the CCG Governing Body gains assurance that risks are being appropriately managed throughout the organisation. The GBAF identifies which of the organisation’s strategic objectives may be at risk because of inadequacies in the operation of controls, or where the CCG has insufficient assurance. At the same time, it encompasses the control of risk, provides structured assurances about where risks are being managed and ensures that objectives are being delivered. This allows the Governing Body to determine how to make the most efficient use of resources and address the issues identified to improve the quality and safety of care. The GBAF also brings together all the evidence required to support the Annual Governance Statement. The GBAF should be a working document and will be updated regularly by the Joint Leadership Team, monitored by the Audit Committee, Clinical Scrutiny and reported to the Governing Body at each of its meetings. The GBAF is linked to the Directorate Risk Register’s, the content of which is also provided for review by the Joint Leadership Team. A flow chart setting out how risks are identified and managed is set out overleaf. In order to ensure consistency in the risk assessment process, the likelihood and consequences of all risks on the Risk Register are assessed against the former National Patient Safety Agency (NPSA) 5X5 risk matrix and those scoring 15 and above and are of strategic concern migrate to the GBAF and thereby inform the Governing Body agenda. Once added to the GBAF, a risk should remain in place until its RAG rating has been mitigated to a score of 1-6 when it is considered manageable and therefore no longer a strategic concern. The 5X5 risk matrix and subsequent red, amber, green (RAG) score identify the level at which identified risks will be managed within the organisation. It also assigns priorities for remedial action and determines whether risks are to be accepted based on the colour bandings and risk ratings. In terms of evaluation of effectiveness, the RAG rating system is also used to present how well the agreed controls are operating.
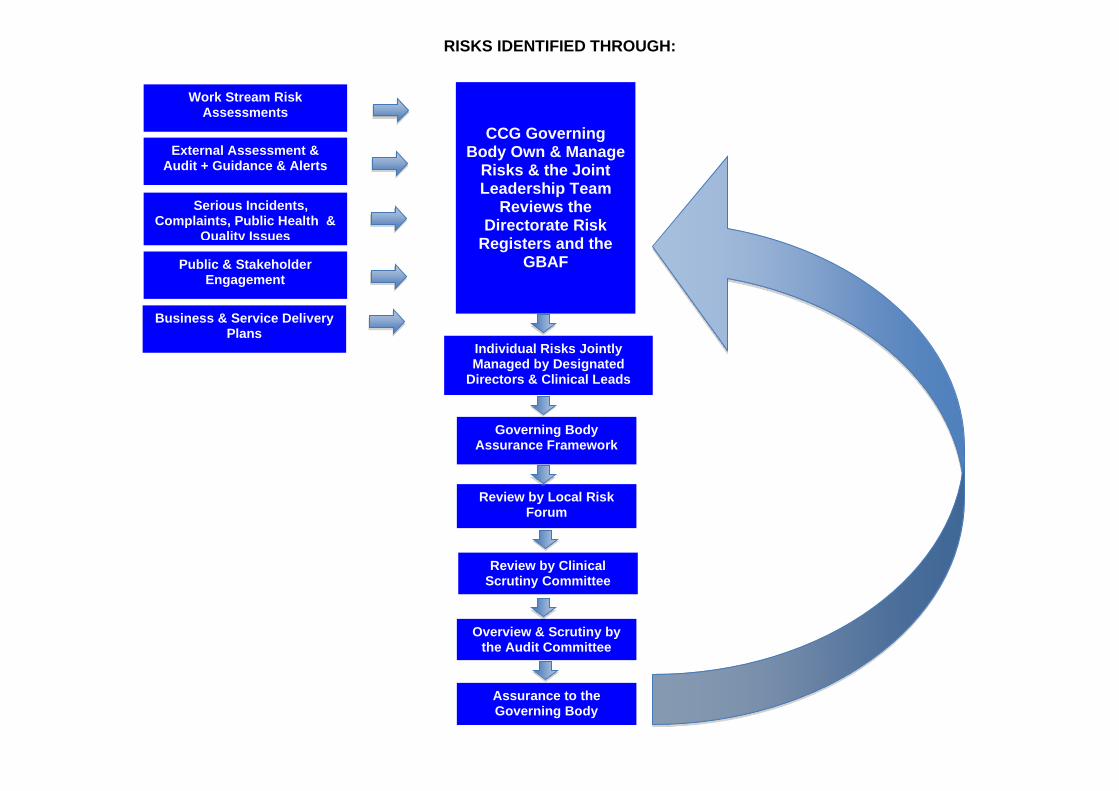
RISKS IDENTIFIED THROUGH:
External Assessment & Audit + Guidance & Alerts
Serious Incidents, Complaints, Public Health &
Quality Issues
Public & Stakeholder Engagement
Business & Service Delivery Plans
CCG Governing Body Own & Manage
Risks & the Joint Leadership Team
Reviews the Directorate Risk
Registers and the GBAF
Governing Body Assurance Framework
Overview & Scrutiny by the Audit Committee
Assurance to the Governing Body
Individual Risks Jointly Managed by Designated
Directors & Clinical Leads
Work Stream Risk Assessments
Review by Local Risk Forum
Review by Clinical Scrutiny Committee
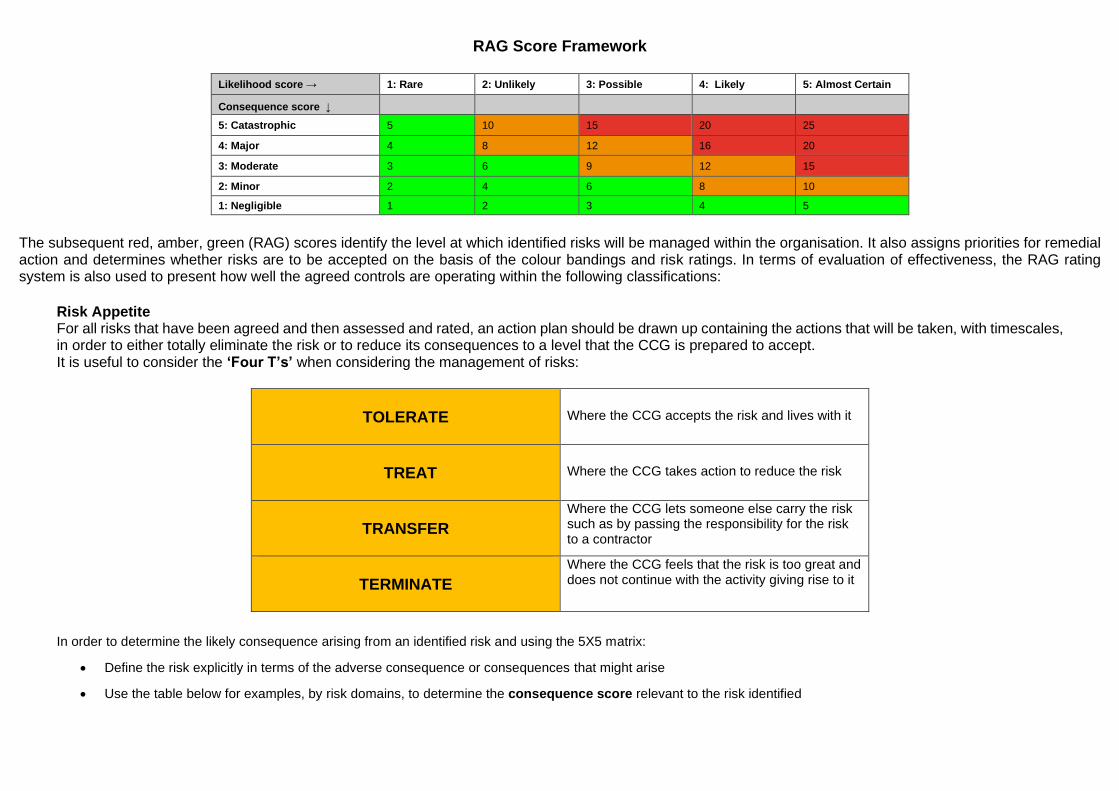
RAG Score Framework
Likelihood score → 1: Rare 2: Unlikely 3: Possible 4: Likely 5: Almost Certain
Consequence score ↓
5: Catastrophic 5 10 15 20 25
4: Major 4 8 12 16 20
3: Moderate 3 6 9 12 15
2: Minor 2 4 6 8 10
1: Negligible 1 2 3 4 5
The subsequent red, amber, green (RAG) scores identify the level at which identified risks will be managed within the organisation. It also assigns priorities for remedial action and determines whether risks are to be accepted on the basis of the colour bandings and risk ratings. In terms of evaluation of effectiveness, the RAG rating system is also used to present how well the agreed controls are operating within the following classifications:
Risk Appetite For all risks that have been agreed and then assessed and rated, an action plan should be drawn up containing the actions that will be taken, with timescales, in order to either totally eliminate the risk or to reduce its consequences to a level that the CCG is prepared to accept. It is useful to consider the ‘Four T’s’ when considering the management of risks:
TOLERATE
Where the CCG accepts the risk and lives with it
TREAT
Where the CCG takes action to reduce the risk
TRANSFER
Where the CCG lets someone else carry the risk such as by passing the responsibility for the risk to a contractor
TERMINATE
Where the CCG feels that the risk is too great and does not continue with the activity giving rise to it
In order to determine the likely consequence arising from an identified risk and using the 5X5 matrix:
• Define the risk explicitly in terms of the adverse consequence or consequences that might arise
• Use the table below for examples, by risk domains, to determine the consequence score relevant to the risk identified
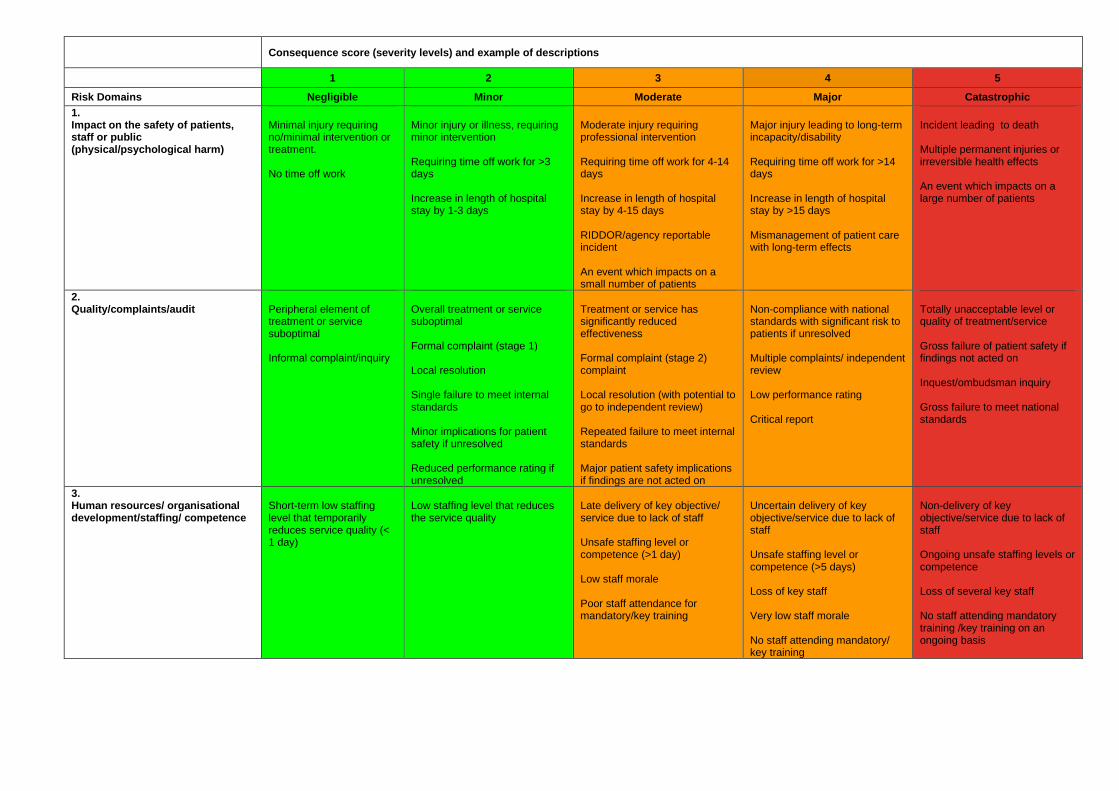
Consequence score (severity levels) and example of descriptions
1 2 3 4 5
Risk Domains Negligible Minor Moderate Major Catastrophic
1. Impact on the safety of patients, staff or public (physical/psychological harm)
Minimal injury requiring no/minimal intervention or treatment. No time off work
Minor injury or illness, requiring minor intervention Requiring time off work for >3 days Increase in length of hospital stay by 1-3 days
Moderate injury requiring professional intervention Requiring time off work for 4-14 days Increase in length of hospital stay by 4-15 days RIDDOR/agency reportable incident An event which impacts on a small number of patients
Major injury leading to long-term incapacity/disability Requiring time off work for >14 days Increase in length of hospital stay by >15 days Mismanagement of patient care with long-term effects
Incident leading to death Multiple permanent injuries or irreversible health effects An event which impacts on a large number of patients
2. Quality/complaints/audit
Peripheral element of treatment or service suboptimal Informal complaint/inquiry
Overall treatment or service suboptimal Formal complaint (stage 1) Local resolution Single failure to meet internal standards Minor implications for patient safety if unresolved Reduced performance rating if unresolved
Treatment or service has significantly reduced effectiveness Formal complaint (stage 2) complaint Local resolution (with potential to go to independent review) Repeated failure to meet internal standards Major patient safety implications if findings are not acted on
Non-compliance with national standards with significant risk to patients if unresolved Multiple complaints/ independent review Low performance rating Critical report
Totally unacceptable level or quality of treatment/service Gross failure of patient safety if findings not acted on Inquest/ombudsman inquiry Gross failure to meet national standards
3. Human resources/ organisational development/staffing/ competence
Short-term low staffing level that temporarily reduces service quality (< 1 day)
Low staffing level that reduces the service quality
Late delivery of key objective/ service due to lack of staff Unsafe staffing level or competence (>1 day) Low staff morale Poor staff attendance for mandatory/key training
Uncertain delivery of key objective/service due to lack of staff Unsafe staffing level or competence (>5 days) Loss of key staff Very low staff morale No staff attending mandatory/ key training
Non-delivery of key objective/service due to lack of staff Ongoing unsafe staffing levels or competence Loss of several key staff No staff attending mandatory training /key training on an ongoing basis

4. Statutory duty/ inspections
No or minimal impact or breech of guidance/ statutory duty
Breech of statutory legislation Reduced performance rating if unresolved
Single breech in statutory duty Challenging external recommendations/ improvement notice
Enforcement action Multiple breeches in statutory duty Improvement notices Low performance rating Critical report
Multiple breeches in statutory duty Prosecution Complete systems change required Zero performance rating Severely critical report
5. Adverse publicity/ reputation
Rumours
Potential for public concern
Local media coverage – short-term reduction in public confidence Elements of public expectation not being met
Local media coverage – long-term reduction in public confidence
National media coverage with <3 days service well below reasonable public expectation
National media coverage with >3 days service well below reasonable public expectation. MP concerned (questions in the House) Total loss of public confidence
6. Business objectives/ projects
Insignificant cost increase/ schedule slippage
<5 per cent over project budget Schedule slippage
5–10 per cent over project budget Schedule slippage
Non-compliance with national 10–25 per cent over project budget Schedule slippage Key objectives not met
Incident leading >25 per cent over project budget Schedule slippage Key objectives not met
7. Finance including claims
Small loss Risk of claim remote
Loss of 0.1–0.25 per cent of budget Claim less than £10,000
Loss of 0.25–0.5 per cent of budget Claim(s) between £10,000 and £100,000
Uncertain delivery of key objective/Loss of 0.5–1.0 per cent of budget Claim(s) between £100,000 and £1 million Purchasers failing to pay on time
Non-delivery of key objective/ Loss of >1 per cent of budget Failure to meet specification/ slippage Loss of contract / payment by results Claim(s) >£1 million
8. Service/business interruption
Loss/interruption of >1 hour
Loss/interruption of >8 hours
Loss/interruption of >1 day
Loss/interruption of >1 week
Permanent loss of service or facility
9. Environmental impact
Minimal or no impact on the environment
Minor impact on environment
Moderate impact on environment
Major impact on environment
Catastrophic impact on environment
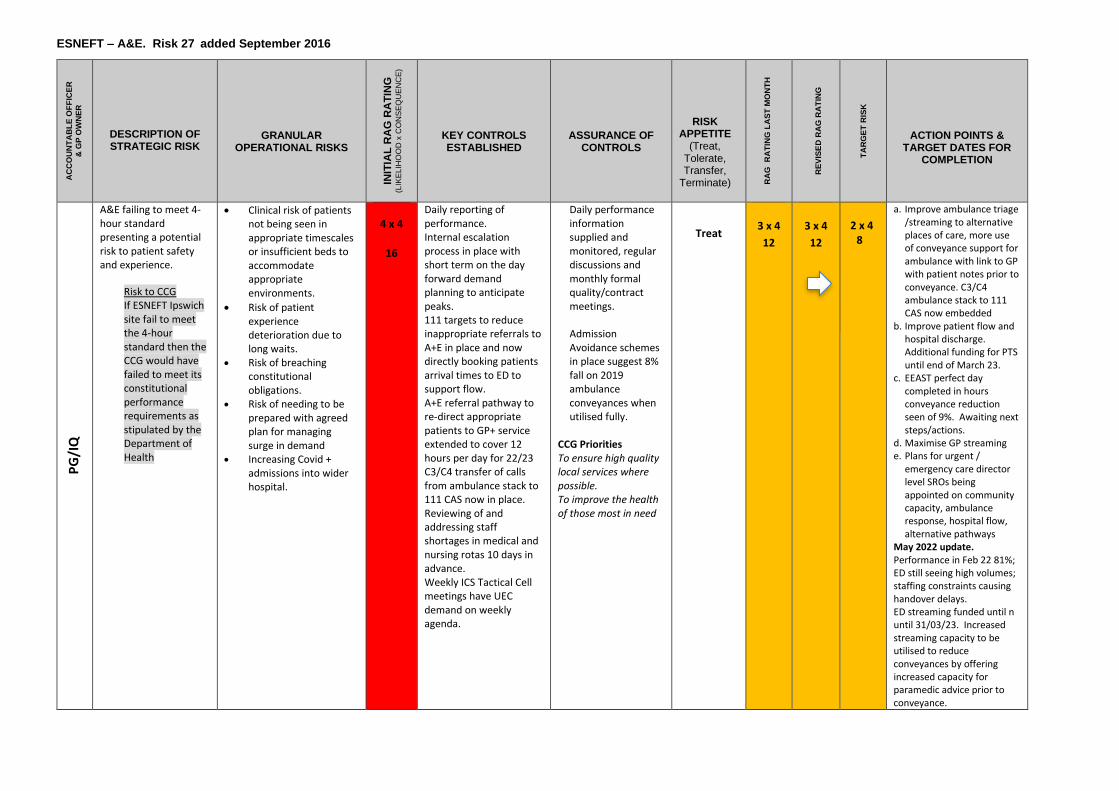
ESNEFT – A&E. Risk 27 added September 2016
AC
CO
UN
TA
BL
E O
FF
ICE
R
& G
P O
WN
ER
DESCRIPTION OF STRATEGIC RISK
GRANULAR OPERATIONAL RISKS
INIT
IAL
RA
G R
AT
ING
(L
IKE
LIH
OO
D x
CO
NS
EQ
UE
NC
E)
KEY CONTROLS ESTABLISHED
ASSURANCE OF CONTROLS
RISK APPETITE
(Treat, Tolerate, Transfer,
Terminate)
RA
G
RA
TIN
G L
AS
T M
ON
TH
R
EV
ISE
D R
AG
RA
TIN
G
TA
RG
ET
RIS
K
ACTION POINTS & TARGET DATES FOR
COMPLETION
PG
/IQ
A&E failing to meet 4-hour standard presenting a potential risk to patient safety and experience.
Risk to CCG If ESNEFT Ipswich site fail to meet the 4-hour standard then the CCG would have failed to meet its constitutional performance requirements as stipulated by the Department of Health
• Clinical risk of patients not being seen in appropriate timescales or insufficient beds to accommodate appropriate environments.
• Risk of patient experience deterioration due to long waits.
• Risk of breaching constitutional obligations.
• Risk of needing to be prepared with agreed plan for managing surge in demand
• Increasing Covid + admissions into wider hospital.
4 x 4
16
Daily reporting of performance. Internal escalation process in place with short term on the day forward demand planning to anticipate peaks. 111 targets to reduce inappropriate referrals to A+E in place and now directly booking patients arrival times to ED to support flow. A+E referral pathway to re-direct appropriate patients to GP+ service extended to cover 12 hours per day for 22/23 C3/C4 transfer of calls from ambulance stack to 111 CAS now in place. Reviewing of and addressing staff shortages in medical and nursing rotas 10 days in advance. Weekly ICS Tactical Cell meetings have UEC demand on weekly agenda.
Daily performance information supplied and monitored, regular discussions and monthly formal quality/contract meetings.
Admission Avoidance schemes in place suggest 8% fall on 2019 ambulance conveyances when utilised fully.
CCG Priorities To ensure high quality local services where possible. To improve the health of those most in need
Treat
3 x 4
12
3 x 4
12
2 x 4 8
a. Improve ambulance triage /streaming to alternative places of care, more use of conveyance support for ambulance with link to GP with patient notes prior to conveyance. C3/C4 ambulance stack to 111 CAS now embedded
b. Improve patient flow and hospital discharge. Additional funding for PTS until end of March 23.
c. EEAST perfect day completed in hours conveyance reduction seen of 9%. Awaiting next steps/actions.
d. Maximise GP streaming e. Plans for urgent /
emergency care director level SROs being appointed on community capacity, ambulance response, hospital flow, alternative pathways
May 2022 update. Performance in Feb 22 81%; ED still seeing high volumes; staffing constraints causing handover delays. ED streaming funded until n until 31/03/23. Increased streaming capacity to be utilised to reduce conveyances by offering increased capacity for paramedic advice prior to conveyance.
a
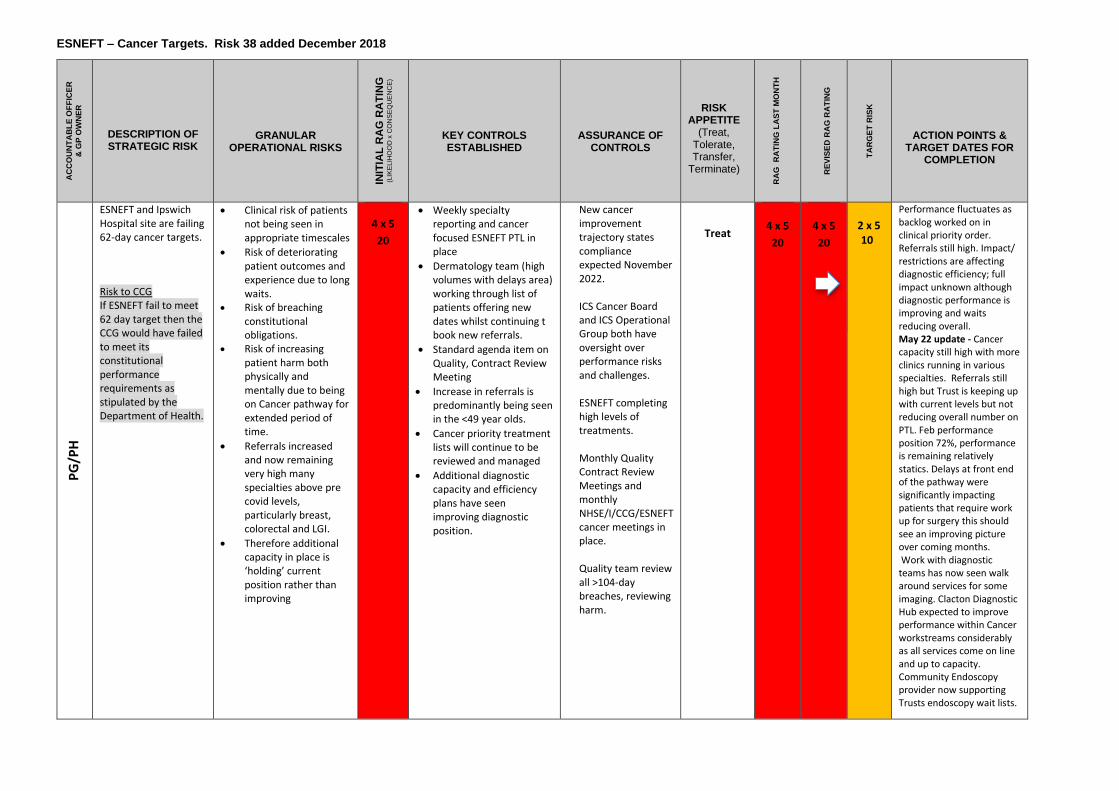
ESNEFT – Cancer Targets. Risk 38 added December 2018
AC
CO
UN
TA
BL
E O
FF
ICE
R
& G
P O
WN
ER
DESCRIPTION OF STRATEGIC RISK
GRANULAR OPERATIONAL RISKS
INIT
IAL
RA
G R
AT
ING
(L
IKE
LIH
OO
D x
CO
NS
EQ
UE
NC
E)
KEY CONTROLS ESTABLISHED
ASSURANCE OF CONTROLS
RISK
APPETITE (Treat,
Tolerate, Transfer,
Terminate)
RA
G
RA
TIN
G L
AS
T M
ON
TH
R
EV
ISE
D R
AG
RA
TIN
G
TA
RG
ET
RIS
K
ACTION POINTS & TARGET DATES FOR
COMPLETION
PG
/PH
ESNEFT and Ipswich Hospital site are failing 62-day cancer targets.
Risk to CCG If ESNEFT fail to meet 62 day target then the CCG would have failed to meet its constitutional performance requirements as stipulated by the Department of Health.
• Clinical risk of patients not being seen in appropriate timescales
• Risk of deteriorating patient outcomes and experience due to long waits.
• Risk of breaching constitutional obligations.
• Risk of increasing patient harm both physically and mentally due to being on Cancer pathway for extended period of time.
• Referrals increased and now remaining very high many specialties above pre covid levels, particularly breast, colorectal and LGI.
• Therefore additional capacity in place is ‘holding’ current position rather than improving
4 x 5
20
• Weekly specialty reporting and cancer focused ESNEFT PTL in place
• Dermatology team (high volumes with delays area) working through list of patients offering new dates whilst continuing t book new referrals.
• Standard agenda item on Quality, Contract Review Meeting
• Increase in referrals is predominantly being seen in the <49 year olds.
• Cancer priority treatment lists will continue to be reviewed and managed
• Additional diagnostic capacity and efficiency plans have seen improving diagnostic position.
New cancer improvement trajectory states compliance expected November 2022. ICS Cancer Board and ICS Operational Group both have oversight over performance risks and challenges. ESNEFT completing high levels of treatments.
Monthly Quality Contract Review Meetings and monthly NHSE/I/CCG/ESNEFT cancer meetings in place. Quality team review all >104-day breaches, reviewing harm.
Treat
4 x 5
20
4 x 5
20
2 x 5 10
Performance fluctuates as backlog worked on in clinical priority order. Referrals still high. Impact/ restrictions are affecting diagnostic efficiency; full impact unknown although diagnostic performance is improving and waits reducing overall. May 22 update - Cancer capacity still high with more clinics running in various specialties. Referrals still high but Trust is keeping up with current levels but not reducing overall number on PTL. Feb performance position 72%, performance is remaining relatively statics. Delays at front end of the pathway were significantly impacting patients that require work up for surgery this should see an improving picture over coming months. Work with diagnostic teams has now seen walk around services for some imaging. Clacton Diagnostic Hub expected to improve performance within Cancer workstreams considerably as all services come on line and up to capacity. Community Endoscopy provider now supporting Trusts endoscopy wait lists.
a
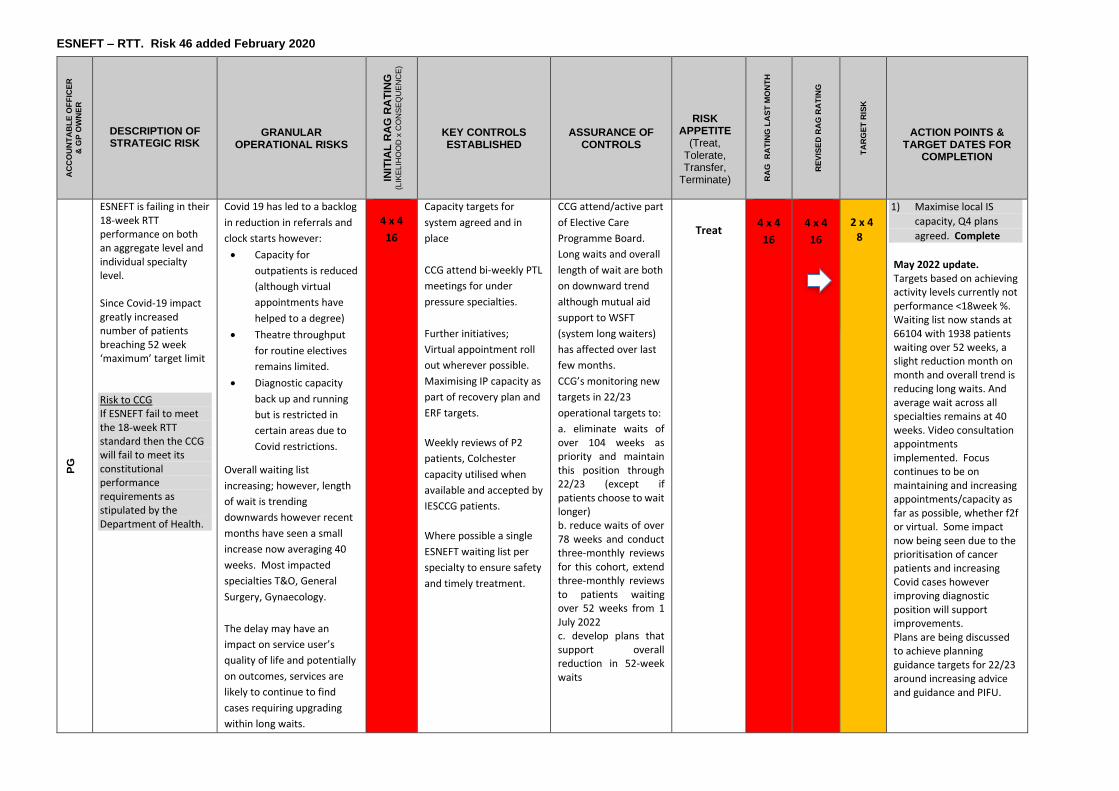
ESNEFT – RTT. Risk 46 added February 2020
AC
CO
UN
TA
BL
E O
FF
ICE
R
& G
P O
WN
ER
DESCRIPTION OF STRATEGIC RISK
GRANULAR OPERATIONAL RISKS
INIT
IAL
RA
G R
AT
ING
(L
IKE
LIH
OO
D x
CO
NS
EQ
UE
NC
E)
KEY CONTROLS ESTABLISHED
ASSURANCE OF CONTROLS
RISK APPETITE
(Treat, Tolerate, Transfer,
Terminate)
RA
G
RA
TIN
G L
AS
T M
ON
TH
R
EV
ISE
D R
AG
RA
TIN
G
TA
RG
ET
RIS
K
ACTION POINTS & TARGET DATES FOR
COMPLETION
PG
ESNEFT is failing in their 18-week RTT performance on both an aggregate level and individual specialty level. Since Covid-19 impact greatly increased number of patients breaching 52 week ‘maximum’ target limit Risk to CCG If ESNEFT fail to meet the 18-week RTT standard then the CCG will fail to meet its constitutional performance requirements as stipulated by the Department of Health.
Covid 19 has led to a backlog
in reduction in referrals and
clock starts however:
• Capacity for
outpatients is reduced
(although virtual
appointments have
helped to a degree)
• Theatre throughput
for routine electives
remains limited.
• Diagnostic capacity
back up and running
but is restricted in
certain areas due to
Covid restrictions.
Overall waiting list
increasing; however, length
of wait is trending
downwards however recent
months have seen a small
increase now averaging 40
weeks. Most impacted
specialties T&O, General
Surgery, Gynaecology.
The delay may have an
impact on service user’s
quality of life and potentially
on outcomes, services are
likely to continue to find
cases requiring upgrading
within long waits.
4 x 4
16
Capacity targets for
system agreed and in
place
CCG attend bi-weekly PTL
meetings for under
pressure specialties.
Further initiatives;
Virtual appointment roll
out wherever possible.
Maximising IP capacity as
part of recovery plan and
ERF targets.
Weekly reviews of P2
patients, Colchester
capacity utilised when
available and accepted by
IESCCG patients.
Where possible a single
ESNEFT waiting list per
specialty to ensure safety
and timely treatment.
CCG attend/active part
of Elective Care
Programme Board.
Long waits and overall
length of wait are both
on downward trend
although mutual aid
support to WSFT
(system long waiters)
has affected over last
few months.
CCG’s monitoring new
targets in 22/23
operational targets to:
a. eliminate waits of over 104 weeks as priority and maintain this position through 22/23 (except if patients choose to wait longer) b. reduce waits of over 78 weeks and conduct three-monthly reviews for this cohort, extend three-monthly reviews to patients waiting over 52 weeks from 1 July 2022 c. develop plans that support overall reduction in 52-week waits
Treat
4 x 4
16
4 x 4
16
2 x 4 8
1) Maximise local IS
capacity, Q4 plans
agreed. Complete
May 2022 update. Targets based on achieving activity levels currently not performance <18week %. Waiting list now stands at 66104 with 1938 patients waiting over 52 weeks, a slight reduction month on month and overall trend is reducing long waits. And average wait across all specialties remains at 40 weeks. Video consultation appointments implemented. Focus continues to be on maintaining and increasing appointments/capacity as far as possible, whether f2f or virtual. Some impact now being seen due to the prioritisation of cancer patients and increasing Covid cases however improving diagnostic position will support improvements. Plans are being discussed to achieve planning guidance targets for 22/23 around increasing advice and guidance and PIFU.
a
NSFT – CQC inspection. Risk 26a added July 2015 (Renumbered January 2016)
AC
CO
UN
TA
BL
E
OF
FIC
ER
& G
P O
WN
ER
DESCRIPTION OF STRATEGIC RISK
GRANULAR OPERATIONAL RISKS
INIT
IAL
RA
G
RA
TIN
G
(LIK
EL
IHO
OD
x
CO
NS
EQ
UE
NC
E)
KEY CONTROLS ESTABLISHED
ASSURANCE OF CONTROLS
RISK APPETITE
(Treat, Tolerate, Transfer,
Terminate)
RA
G R
AT
ING
LA
ST
MO
NT
H
RE
VIS
ED
RA
G
RA
TIN
G
TA
RG
ET
RIS
K
ACTION POINTS & TARGET DATES FOR
COMPLETION
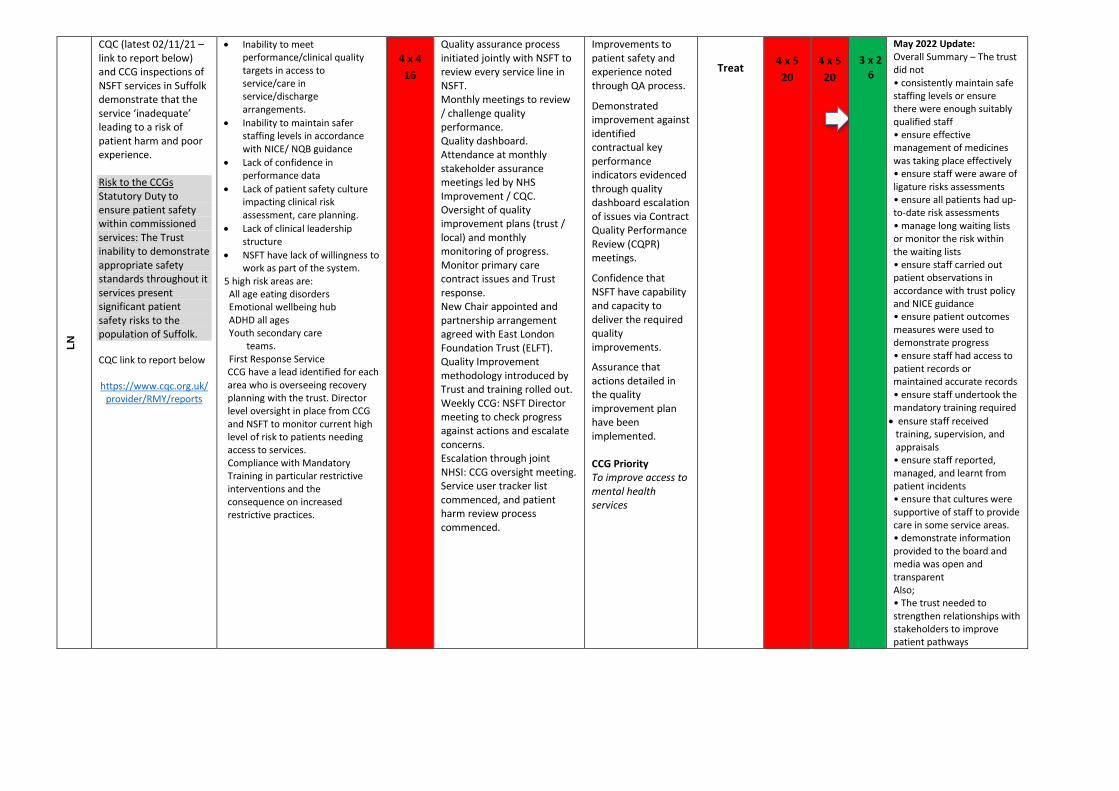
LN
CQC (latest 02/11/21 – link to report below) and CCG inspections of NSFT services in Suffolk demonstrate that the service ‘inadequate’ leading to a risk of patient harm and poor experience. Risk to the CCGs Statutory Duty to ensure patient safety within commissioned services: The Trust inability to demonstrate appropriate safety standards throughout it services present significant patient safety risks to the population of Suffolk. CQC link to report below https://www.cqc.org.uk/
provider/RMY/reports
• Inability to meet performance/clinical quality targets in access to service/care in service/discharge arrangements.
• Inability to maintain safer staffing levels in accordance with NICE/ NQB guidance
• Lack of confidence in performance data
• Lack of patient safety culture impacting clinical risk assessment, care planning.
• Lack of clinical leadership structure
• NSFT have lack of willingness to work as part of the system.
5 high risk areas are: All age eating disorders
Emotional wellbeing hub
ADHD all ages Youth secondary care teams. First Response Service
CCG have a lead identified for each area who is overseeing recovery planning with the trust. Director level oversight in place from CCG and NSFT to monitor current high level of risk to patients needing access to services. Compliance with Mandatory Training in particular restrictive interventions and the consequence on increased restrictive practices.
4 x 4
16
Quality assurance process initiated jointly with NSFT to review every service line in NSFT. Monthly meetings to review / challenge quality performance. Quality dashboard. Attendance at monthly stakeholder assurance meetings led by NHS Improvement / CQC. Oversight of quality improvement plans (trust / local) and monthly monitoring of progress. Monitor primary care contract issues and Trust response. New Chair appointed and partnership arrangement agreed with East London Foundation Trust (ELFT). Quality Improvement methodology introduced by Trust and training rolled out. Weekly CCG: NSFT Director meeting to check progress against actions and escalate concerns. Escalation through joint NHSI: CCG oversight meeting. Service user tracker list commenced, and patient harm review process commenced.
Improvements to patient safety and experience noted through QA process.
Demonstrated improvement against identified contractual key performance indicators evidenced through quality dashboard escalation of issues via Contract Quality Performance Review (CQPR) meetings.
Confidence that NSFT have capability and capacity to deliver the required quality improvements.
Assurance that actions detailed in the quality improvement plan have been implemented. CCG Priority To improve access to mental health services
Treat
4 x 5
20
4 x 5
20
3 x 2 6
May 2022 Update: Overall Summary – The trust did not • consistently maintain safe staffing levels or ensure there were enough suitably qualified staff • ensure effective management of medicines was taking place effectively • ensure staff were aware of ligature risks assessments • ensure all patients had up-to-date risk assessments • manage long waiting lists or monitor the risk within the waiting lists • ensure staff carried out patient observations in accordance with trust policy and NICE guidance • ensure patient outcomes measures were used to demonstrate progress • ensure staff had access to patient records or maintained accurate records • ensure staff undertook the mandatory training required
• ensure staff received training, supervision, and appraisals • ensure staff reported, managed, and learnt from patient incidents • ensure that cultures were supportive of staff to provide care in some service areas. • demonstrate information provided to the board and media was open and transparent Also; • The trust needed to strengthen relationships with stakeholders to improve patient pathways
a
NSFT – Performance. Risk 26b added January 2016
AC
CO
UN
TA
BL
E O
FF
ICE
R
& G
P O
WN
ER
DESCRIPTION OF STRATEGIC RISK
GRANULAR OPERATIONAL RISKS
INIT
IAL
RA
G R
AT
ING
(L
IKE
LIH
OO
D x
CO
NS
EQ
UE
NC
E)
KEY CONTROLS ESTABLISHED
ASSURANCE OF CONTROLS
RISK APPETITE
(Treat, Tolerate, Transfer,
Terminate)
RA
G
RA
TIN
G L
AS
T M
ON
TH
R
EV
ISE
D R
AG
RA
TIN
G
TA
RG
ET
RIS
K
ACTION POINTS & TARGET DATES FOR
COMPLETION
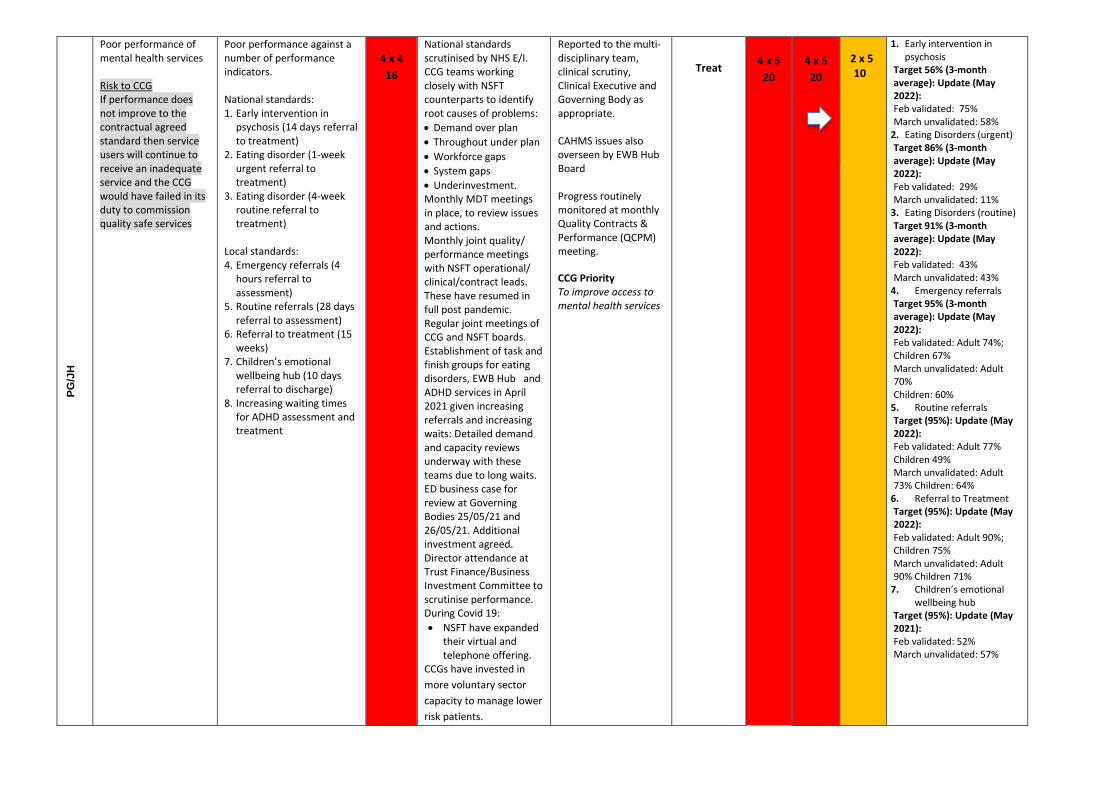
PG
/JH
Poor performance of mental health services Risk to CCG If performance does not improve to the contractual agreed standard then service users will continue to receive an inadequate service and the CCG would have failed in its duty to commission quality safe services
Poor performance against a number of performance indicators. National standards: 1. Early intervention in
psychosis (14 days referral to treatment)
2. Eating disorder (1-week urgent referral to treatment)
3. Eating disorder (4-week routine referral to treatment)
Local standards: 4. Emergency referrals (4
hours referral to assessment)
5. Routine referrals (28 days referral to assessment)
6. Referral to treatment (15 weeks)
7. Children’s emotional wellbeing hub (10 days referral to discharge)
8. Increasing waiting times for ADHD assessment and treatment
4 x 4
16
National standards scrutinised by NHS E/I. CCG teams working closely with NSFT counterparts to identify root causes of problems:
• Demand over plan
• Throughout under plan
• Workforce gaps
• System gaps
• Underinvestment. Monthly MDT meetings in place, to review issues and actions. Monthly joint quality/ performance meetings with NSFT operational/ clinical/contract leads. These have resumed in full post pandemic. Regular joint meetings of CCG and NSFT boards. Establishment of task and finish groups for eating disorders, EWB Hub and ADHD services in April 2021 given increasing referrals and increasing waits: Detailed demand and capacity reviews underway with these teams due to long waits. ED business case for review at Governing Bodies 25/05/21 and 26/05/21. Additional investment agreed. Director attendance at Trust Finance/Business Investment Committee to scrutinise performance. During Covid 19:
• NSFT have expanded their virtual and telephone offering.
CCGs have invested in
more voluntary sector
capacity to manage lower
risk patients.
Reported to the multi-disciplinary team, clinical scrutiny, Clinical Executive and Governing Body as appropriate. CAHMS issues also overseen by EWB Hub Board Progress routinely monitored at monthly Quality Contracts & Performance (QCPM) meeting. CCG Priority To improve access to mental health services
Treat
4 x 5
20
4 x 5
20
2 x 5 10
1. Early intervention in psychosis
Target 56% (3-month average): Update (May 2022): Feb validated: 75% March unvalidated: 58%
2. Eating Disorders (urgent) Target 86% (3-month average): Update (May 2022): Feb validated: 29% March unvalidated: 11%
3. Eating Disorders (routine) Target 91% (3-month average): Update (May 2022): Feb validated: 43% March unvalidated: 43%
4. Emergency referrals Target 95% (3-month average): Update (May 2022): Feb validated: Adult 74%; Children 67% March unvalidated: Adult 70% Children: 60%
5. Routine referrals Target (95%): Update (May 2022): Feb validated: Adult 77% Children 49% March unvalidated: Adult 73% Children: 64%
6. Referral to Treatment Target (95%): Update (May 2022): Feb validated: Adult 90%; Children 75% March unvalidated: Adult 90% Children 71%
7. Children’s emotional wellbeing hub
Target (95%): Update (May 2021): Feb validated: 52% March unvalidated: 57%
a
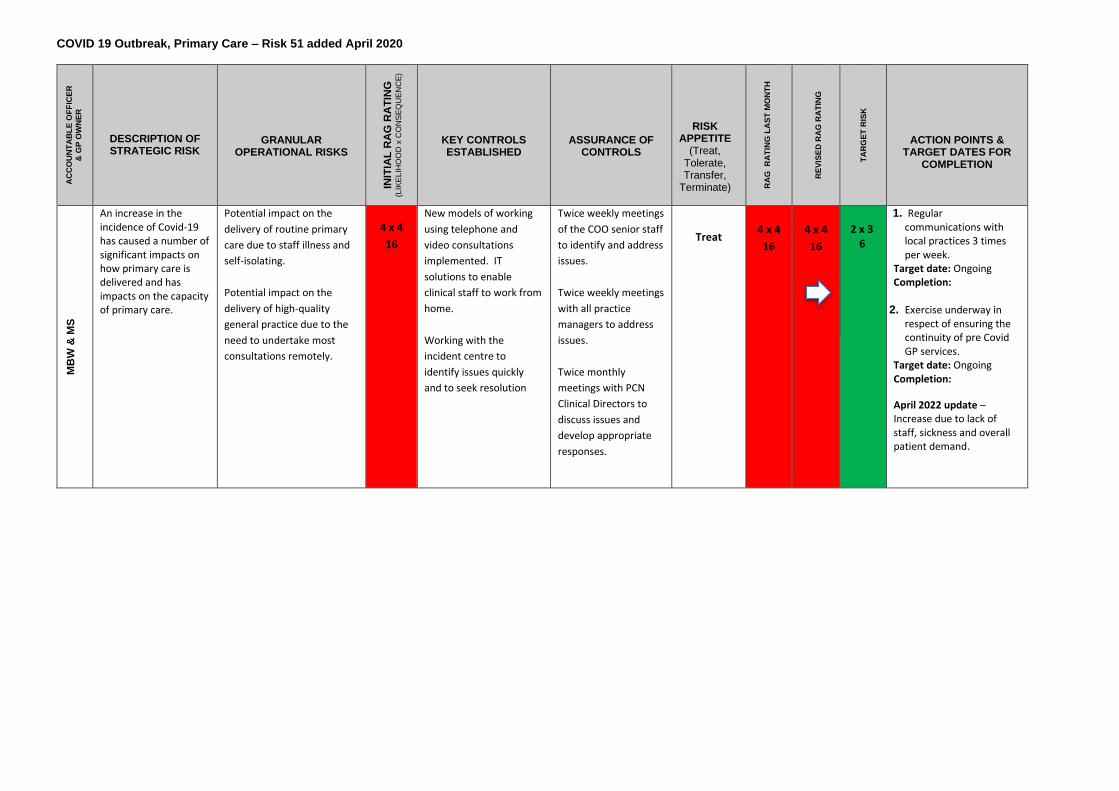
COVID 19 Outbreak, Primary Care – Risk 51 added April 2020
AC
CO
UN
TA
BL
E O
FF
ICE
R
& G
P O
WN
ER
DESCRIPTION OF STRATEGIC RISK
GRANULAR OPERATIONAL RISKS
INIT
IAL
RA
G R
AT
ING
(L
IKE
LIH
OO
D x
CO
NS
EQ
UE
NC
E)
KEY CONTROLS ESTABLISHED
ASSURANCE OF CONTROLS
RISK APPETITE
(Treat, Tolerate, Transfer,
Terminate)
RA
G
RA
TIN
G L
AS
T M
ON
TH
R
EV
ISE
D R
AG
RA
TIN
G
TA
RG
ET
RIS
K
ACTION POINTS & TARGET DATES FOR
COMPLETION
MB
W &
MS
An increase in the incidence of Covid-19 has caused a number of significant impacts on how primary care is delivered and has impacts on the capacity of primary care.
Potential impact on the
delivery of routine primary
care due to staff illness and
self-isolating.
Potential impact on the
delivery of high-quality
general practice due to the
need to undertake most
consultations remotely.
4 x 4
16
New models of working
using telephone and
video consultations
implemented. IT
solutions to enable
clinical staff to work from
home.
Working with the
incident centre to
identify issues quickly
and to seek resolution
Twice weekly meetings
of the COO senior staff
to identify and address
issues.
Twice weekly meetings
with all practice
managers to address
issues.
Twice monthly
meetings with PCN
Clinical Directors to
discuss issues and
develop appropriate
responses.
Treat
4 x 4
16
4 x 4
16
2 x 3 6
1. Regular communications with local practices 3 times per week.
Target date: Ongoing Completion:
2. Exercise underway in respect of ensuring the continuity of pre Covid GP services.
Target date: Ongoing Completion:
April 2022 update – Increase due to lack of staff, sickness and overall patient demand.
Cyber Security. Risk 36 added September 2018
AC
CO
UN
TA
BL
E O
FF
ICE
R
& G
P O
WN
ER
DESCRIPTION OF STRATEGIC RISK
GRANULAR OPERATIONAL RISKS
INIT
IAL
RA
G R
AT
ING
(L
IKE
LIH
OO
D x
CO
NS
EQ
UE
NC
E)
KEY CONTROLS ESTABLISHED
ASSURANCE OF CONTROLS
RISK APPETITE
(Treat, Tolerate, Transfer,
Terminate)
RA
G
RA
TIN
G L
AS
T M
ON
TH
R
EV
ISE
D R
AG
RA
TIN
G
TA
RG
ET
RIS
K
ACTION POINTS & TARGET DATES FOR
COMPLETION
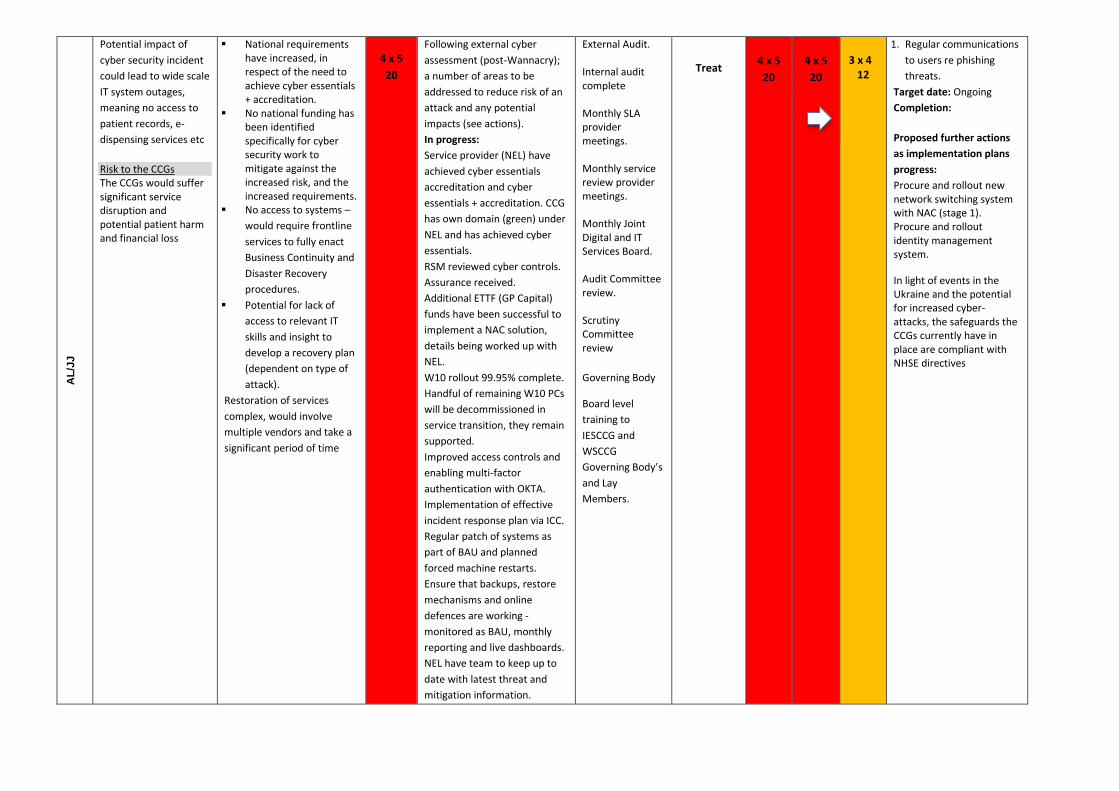
AL
/JJ
Potential impact of
cyber security incident
could lead to wide scale
IT system outages,
meaning no access to
patient records, e-
dispensing services etc
Risk to the CCGs The CCGs would suffer significant service disruption and potential patient harm and financial loss
▪ National requirements have increased, in respect of the need to achieve cyber essentials + accreditation.
▪ No national funding has been identified specifically for cyber security work to mitigate against the increased risk, and the increased requirements.
▪ No access to systems –
would require frontline
services to fully enact
Business Continuity and
Disaster Recovery
procedures.
▪ Potential for lack of
access to relevant IT
skills and insight to
develop a recovery plan
(dependent on type of
attack).
Restoration of services
complex, would involve
multiple vendors and take a
significant period of time
4 x 5
20
Following external cyber
assessment (post-Wannacry);
a number of areas to be
addressed to reduce risk of an
attack and any potential
impacts (see actions).
In progress:
Service provider (NEL) have
achieved cyber essentials
accreditation and cyber
essentials + accreditation. CCG
has own domain (green) under
NEL and has achieved cyber
essentials.
RSM reviewed cyber controls.
Assurance received.
Additional ETTF (GP Capital)
funds have been successful to
implement a NAC solution,
details being worked up with
NEL.
W10 rollout 99.95% complete.
Handful of remaining W10 PCs
will be decommissioned in
service transition, they remain
supported.
Improved access controls and
enabling multi-factor
authentication with OKTA.
Implementation of effective
incident response plan via ICC.
Regular patch of systems as
part of BAU and planned
forced machine restarts.
Ensure that backups, restore
mechanisms and online
defences are working -
monitored as BAU, monthly
reporting and live dashboards.
NEL have team to keep up to
date with latest threat and
mitigation information.
External Audit. Internal audit complete Monthly SLA provider meetings. Monthly service review provider meetings. Monthly Joint Digital and IT Services Board. Audit Committee review. Scrutiny Committee review
Governing Body
Board level
training to
IESCCG and
WSCCG
Governing Body’s
and Lay
Members.
Treat
4 x 5
20
4 x 5
20
3 x 4
12
1. Regular communications
to users re phishing
threats.
Target date: Ongoing
Completion:
Proposed further actions
as implementation plans
progress:
Procure and rollout new network switching system with NAC (stage 1). Procure and rollout identity management system.
In light of events in the Ukraine and the potential for increased cyber-attacks, the safeguards the CCGs currently have in place are compliant with NHSE directives
a
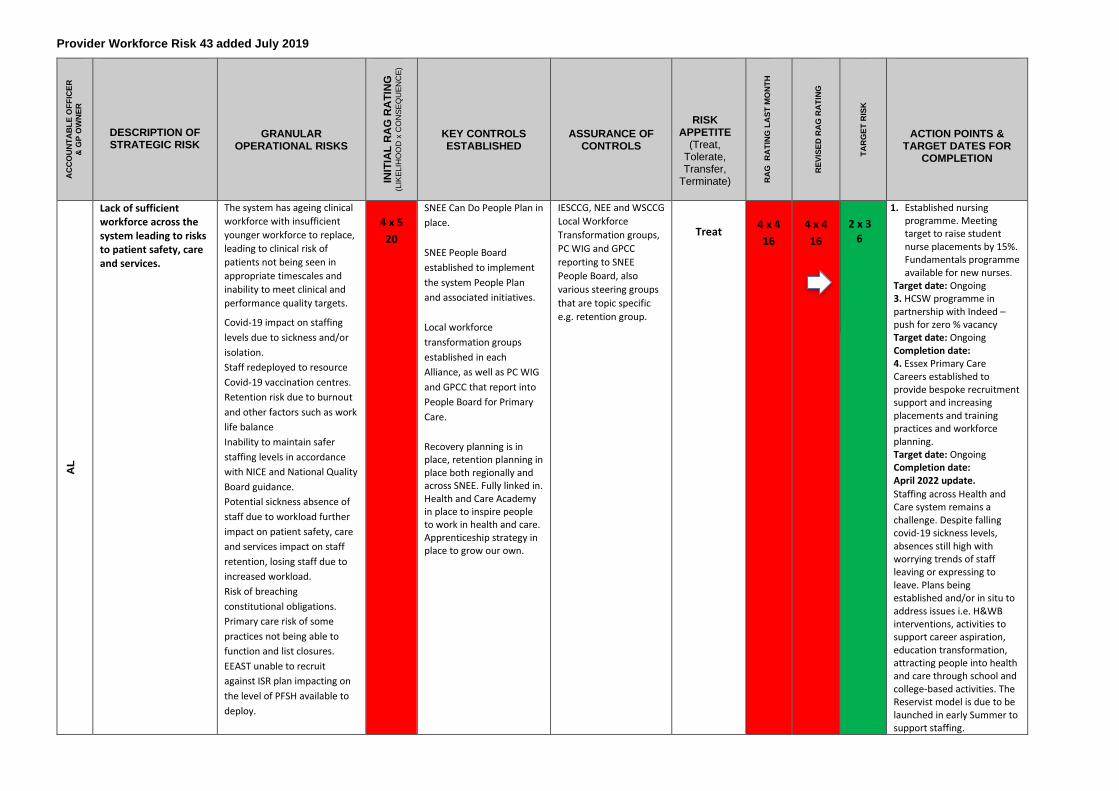
Provider Workforce Risk 43 added July 2019
AC
CO
UN
TA
BL
E O
FF
ICE
R
& G
P O
WN
ER
DESCRIPTION OF STRATEGIC RISK
GRANULAR OPERATIONAL RISKS
INIT
IAL
RA
G R
AT
ING
(L
IKE
LIH
OO
D x
CO
NS
EQ
UE
NC
E)
KEY CONTROLS ESTABLISHED
ASSURANCE OF CONTROLS
RISK APPETITE
(Treat, Tolerate, Transfer,
Terminate)
RA
G
RA
TIN
G L
AS
T M
ON
TH
R
EV
ISE
D R
AG
RA
TIN
G
TA
RG
ET
RIS
K
ACTION POINTS & TARGET DATES FOR
COMPLETION
AL
Lack of sufficient workforce across the system leading to risks to patient safety, care and services.
The system has ageing clinical
workforce with insufficient
younger workforce to replace,
leading to clinical risk of
patients not being seen in
appropriate timescales and
inability to meet clinical and
performance quality targets. Covid-19 impact on staffing
levels due to sickness and/or
isolation. Staff redeployed to resource
Covid-19 vaccination centres. Retention risk due to burnout
and other factors such as work
life balance
Inability to maintain safer
staffing levels in accordance
with NICE and National Quality
Board guidance. Potential sickness absence of
staff due to workload further
impact on patient safety, care
and services impact on staff
retention, losing staff due to
increased workload.
Risk of breaching
constitutional obligations. Primary care risk of some
practices not being able to
function and list closures. EEAST unable to recruit
against ISR plan impacting on
the level of PFSH available to
deploy.
4 x 5
20
SNEE Can Do People Plan in
place.
SNEE People Board
established to implement
the system People Plan
and associated initiatives.
Local workforce
transformation groups
established in each
Alliance, as well as PC WIG
and GPCC that report into
People Board for Primary
Care.
Recovery planning is in place, retention planning in place both regionally and across SNEE. Fully linked in. Health and Care Academy in place to inspire people to work in health and care. Apprenticeship strategy in place to grow our own.
IESCCG, NEE and WSCCG
Local Workforce
Transformation groups,
PC WIG and GPCC
reporting to SNEE
People Board, also
various steering groups
that are topic specific
e.g. retention group.
Treat
4 x 4
16
4 x 4
16
2 x 3 6
1. Established nursing programme. Meeting target to raise student nurse placements by 15%. Fundamentals programme available for new nurses.
Target date: Ongoing 3. HCSW programme in partnership with Indeed – push for zero % vacancy Target date: Ongoing Completion date: 4. Essex Primary Care Careers established to provide bespoke recruitment support and increasing placements and training practices and workforce planning. Target date: Ongoing Completion date: April 2022 update.
Staffing across Health and Care system remains a challenge. Despite falling covid-19 sickness levels, absences still high with worrying trends of staff leaving or expressing to leave. Plans being established and/or in situ to address issues i.e. H&WB interventions, activities to support career aspiration, education transformation, attracting people into health and care through school and college-based activities. The Reservist model is due to be launched in early Summer to support staffing.
a
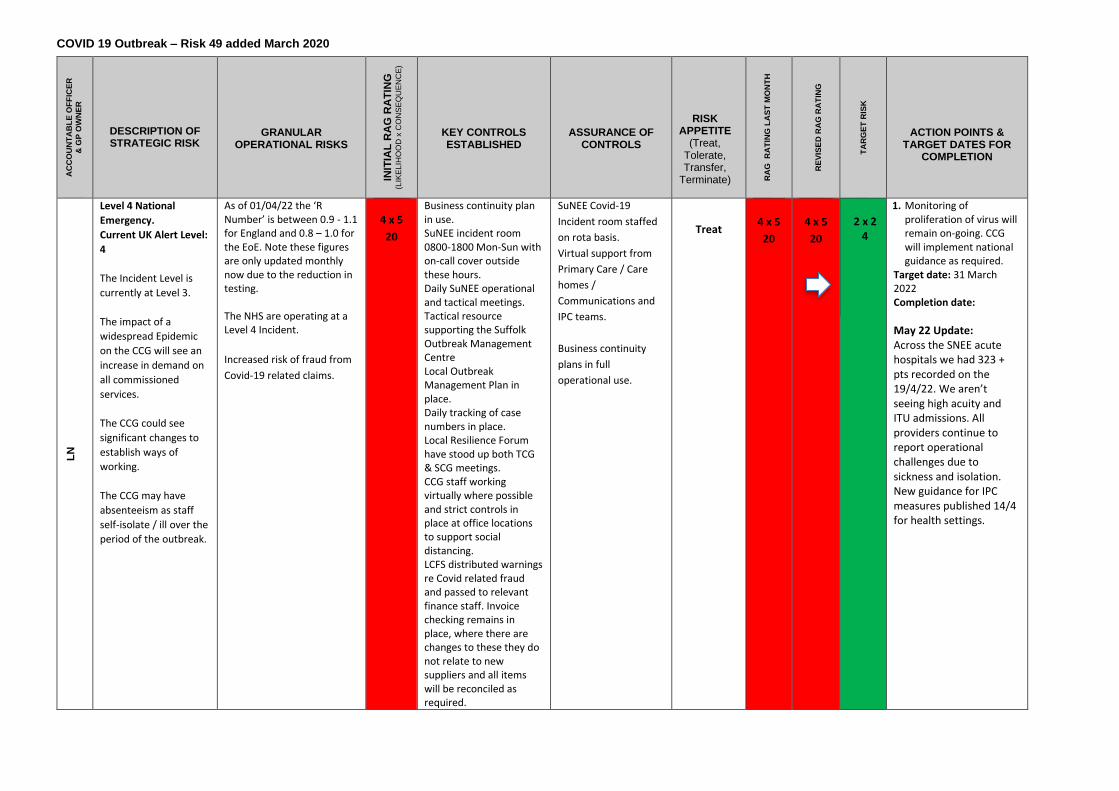
COVID 19 Outbreak – Risk 49 added March 2020
AC
CO
UN
TA
BL
E O
FF
ICE
R
& G
P O
WN
ER
DESCRIPTION OF STRATEGIC RISK
GRANULAR OPERATIONAL RISKS
INIT
IAL
RA
G R
AT
ING
(L
IKE
LIH
OO
D x
CO
NS
EQ
UE
NC
E)
KEY CONTROLS ESTABLISHED
ASSURANCE OF CONTROLS
RISK APPETITE
(Treat, Tolerate, Transfer,
Terminate)
RA
G
RA
TIN
G L
AS
T M
ON
TH
R
EV
ISE
D R
AG
RA
TIN
G
TA
RG
ET
RIS
K
ACTION POINTS & TARGET DATES FOR
COMPLETION
LN
Level 4 National
Emergency.
Current UK Alert Level:
4
The Incident Level is
currently at Level 3.
The impact of a
widespread Epidemic
on the CCG will see an
increase in demand on
all commissioned
services.
The CCG could see
significant changes to
establish ways of
working.
The CCG may have
absenteeism as staff
self-isolate / ill over the
period of the outbreak.
As of 01/04/22 the ‘R Number’ is between 0.9 - 1.1 for England and 0.8 – 1.0 for the EoE. Note these figures are only updated monthly now due to the reduction in testing. The NHS are operating at a Level 4 Incident.
Increased risk of fraud from
Covid-19 related claims.
4 x 5
20
Business continuity plan in use. SuNEE incident room 0800-1800 Mon-Sun with on-call cover outside these hours. Daily SuNEE operational and tactical meetings. Tactical resource supporting the Suffolk Outbreak Management Centre Local Outbreak Management Plan in place. Daily tracking of case numbers in place. Local Resilience Forum have stood up both TCG & SCG meetings. CCG staff working virtually where possible and strict controls in place at office locations to support social distancing. LCFS distributed warnings re Covid related fraud and passed to relevant finance staff. Invoice checking remains in place, where there are changes to these they do not relate to new suppliers and all items will be reconciled as required.
SuNEE Covid-19
Incident room staffed
on rota basis.
Virtual support from
Primary Care / Care
homes /
Communications and
IPC teams.
Business continuity
plans in full
operational use.
Treat
4 x 5
20
4 x 5
20
2 x 2 4
1. Monitoring of proliferation of virus will remain on-going. CCG will implement national guidance as required.
Target date: 31 March 2022 Completion date:
May 22 Update: Across the SNEE acute hospitals we had 323 + pts recorded on the 19/4/22. We aren’t seeing high acuity and ITU admissions. All providers continue to report operational challenges due to sickness and isolation. New guidance for IPC measures published 14/4 for health settings.
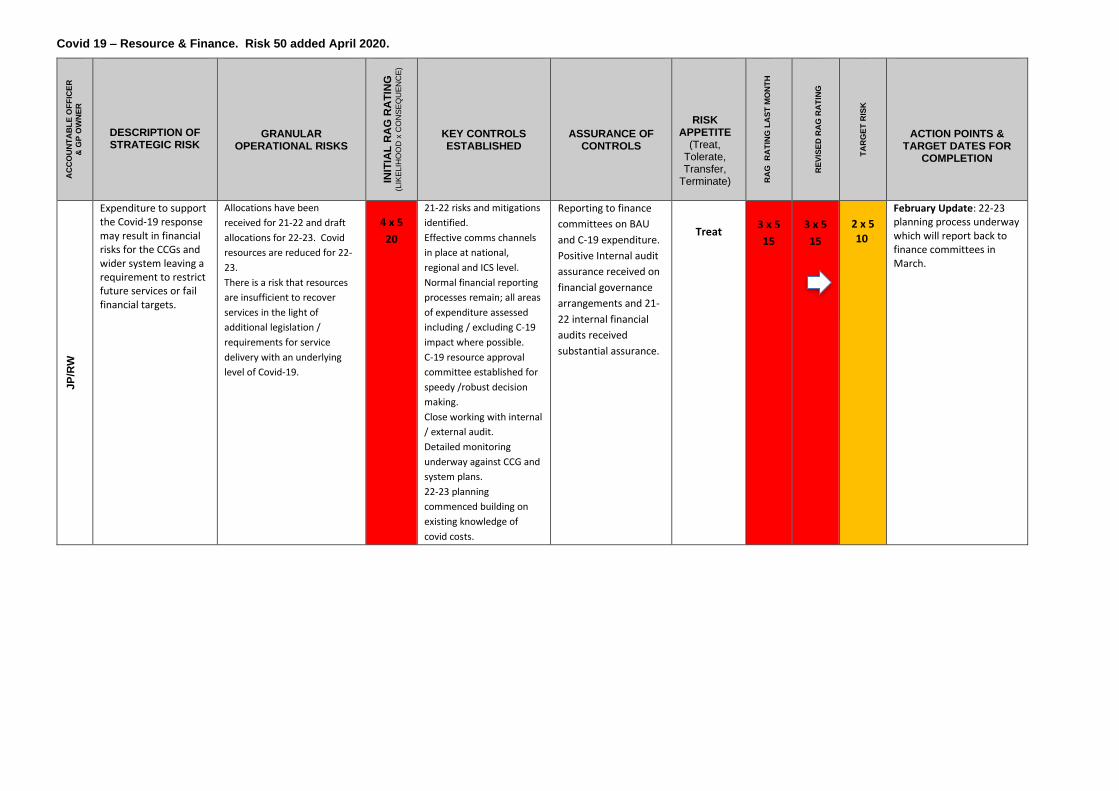
Covid 19 – Resource & Finance. Risk 50 added April 2020.
AC
CO
UN
TA
BL
E O
FF
ICE
R
& G
P O
WN
ER
DESCRIPTION OF STRATEGIC RISK
GRANULAR OPERATIONAL RISKS
INIT
IAL
RA
G R
AT
ING
(L
IKE
LIH
OO
D x
CO
NS
EQ
UE
NC
E)
KEY CONTROLS ESTABLISHED
ASSURANCE OF CONTROLS
RISK APPETITE
(Treat, Tolerate, Transfer,
Terminate)
RA
G
RA
TIN
G L
AS
T M
ON
TH
R
EV
ISE
D R
AG
RA
TIN
G
TA
RG
ET
RIS
K
ACTION POINTS & TARGET DATES FOR
COMPLETION
JP
/RW
Expenditure to support the Covid-19 response may result in financial risks for the CCGs and wider system leaving a requirement to restrict future services or fail financial targets.
Allocations have been
received for 21-22 and draft
allocations for 22-23. Covid
resources are reduced for 22-
23.
There is a risk that resources
are insufficient to recover
services in the light of
additional legislation /
requirements for service
delivery with an underlying
level of Covid-19.
4 x 5
20
21-22 risks and mitigations
identified.
Effective comms channels
in place at national,
regional and ICS level.
Normal financial reporting
processes remain; all areas
of expenditure assessed
including / excluding C-19
impact where possible.
C-19 resource approval
committee established for
speedy /robust decision
making.
Close working with internal
/ external audit.
Detailed monitoring
underway against CCG and
system plans.
22-23 planning
commenced building on
existing knowledge of
covid costs.
Reporting to finance
committees on BAU
and C-19 expenditure.
Positive Internal audit
assurance received on
financial governance
arrangements and 21-
22 internal financial
audits received
substantial assurance.
Treat
3 x 5
15
3 x 5
15
2 x 5 10
February Update: 22-23 planning process underway which will report back to finance committees in March.
a
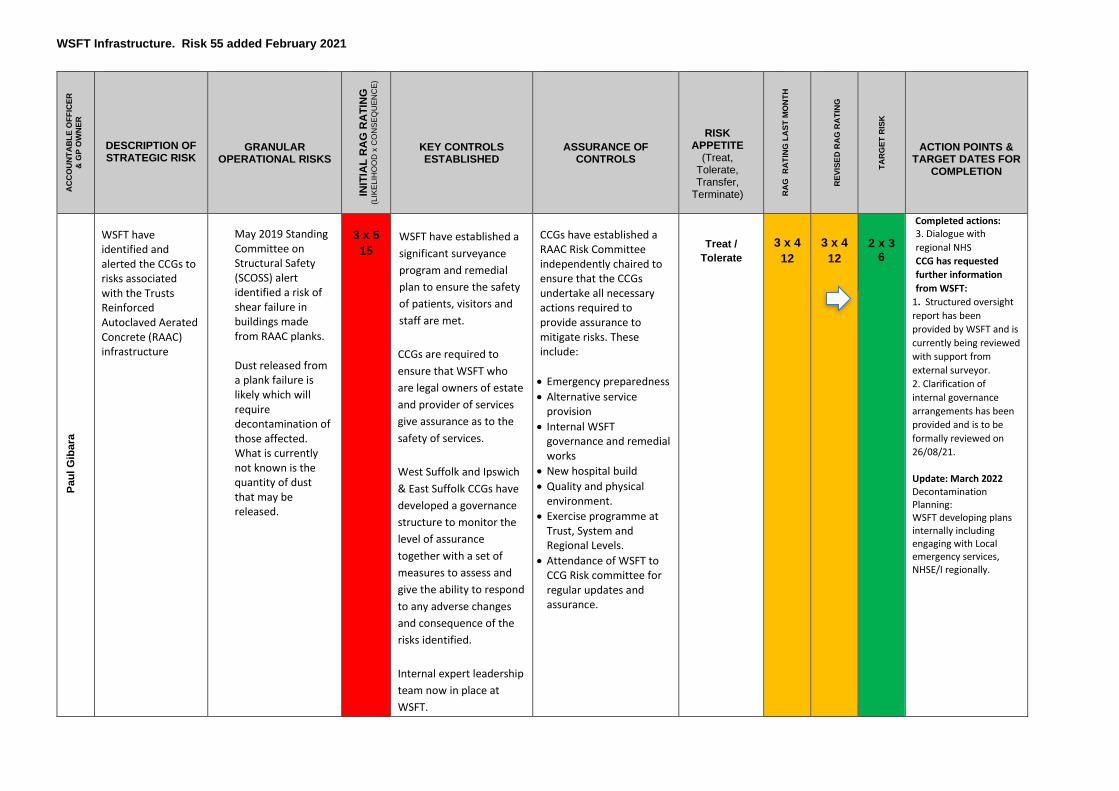
WSFT Infrastructure. Risk 55 added February 2021
AC
CO
UN
TA
BL
E O
FF
ICE
R
& G
P O
WN
ER
DESCRIPTION OF STRATEGIC RISK
GRANULAR OPERATIONAL RISKS
INIT
IAL
RA
G R
AT
ING
(L
IKE
LIH
OO
D x
CO
NS
EQ
UE
NC
E)
KEY CONTROLS ESTABLISHED
ASSURANCE OF CONTROLS
RISK APPETITE
(Treat, Tolerate, Transfer,
Terminate)
RA
G
RA
TIN
G L
AS
T M
ON
TH
R
EV
ISE
D R
AG
RA
TIN
G
TA
RG
ET
RIS
K
ACTION POINTS & TARGET DATES FOR
COMPLETION
Pau
l G
iba
ra
WSFT have identified and alerted the CCGs to risks associated with the Trusts Reinforced Autoclaved Aerated Concrete (RAAC) infrastructure
May 2019 Standing Committee on Structural Safety (SCOSS) alert identified a risk of shear failure in buildings made from RAAC planks. Dust released from a plank failure is likely which will require decontamination of those affected. What is currently not known is the quantity of dust that may be released.
3 x 5
15
WSFT have established a
significant surveyance
program and remedial
plan to ensure the safety
of patients, visitors and
staff are met.
CCGs are required to
ensure that WSFT who
are legal owners of estate
and provider of services
give assurance as to the
safety of services.
West Suffolk and Ipswich
& East Suffolk CCGs have
developed a governance
structure to monitor the
level of assurance
together with a set of
measures to assess and
give the ability to respond
to any adverse changes
and consequence of the
risks identified.
Internal expert leadership
team now in place at
WSFT.
CCGs have established a RAAC Risk Committee independently chaired to ensure that the CCGs undertake all necessary actions required to provide assurance to mitigate risks. These include:
• Emergency preparedness
• Alternative service provision
• Internal WSFT governance and remedial works
• New hospital build
• Quality and physical environment.
• Exercise programme at Trust, System and Regional Levels.
• Attendance of WSFT to CCG Risk committee for regular updates and assurance.
Treat /
Tolerate
3 x 4
12
3 x 4
12
2 x 3 6
Completed actions: 3. Dialogue with
regional NHS
CCG has requested
further information
from WSFT:
1. Structured oversight
report has been
provided by WSFT and is
currently being reviewed
with support from
external surveyor.
2. Clarification of
internal governance
arrangements has been
provided and is to be
formally reviewed on
26/08/21.
Update: March 2022 Decontamination Planning: WSFT developing plans internally including engaging with Local emergency services, NHSE/I regionally.
a
System has developed initial plans which will be reviewed via a tabletop exercise on 19/08/21. CCGs have worked with
Region to ensure
regional/local plans are
aligned
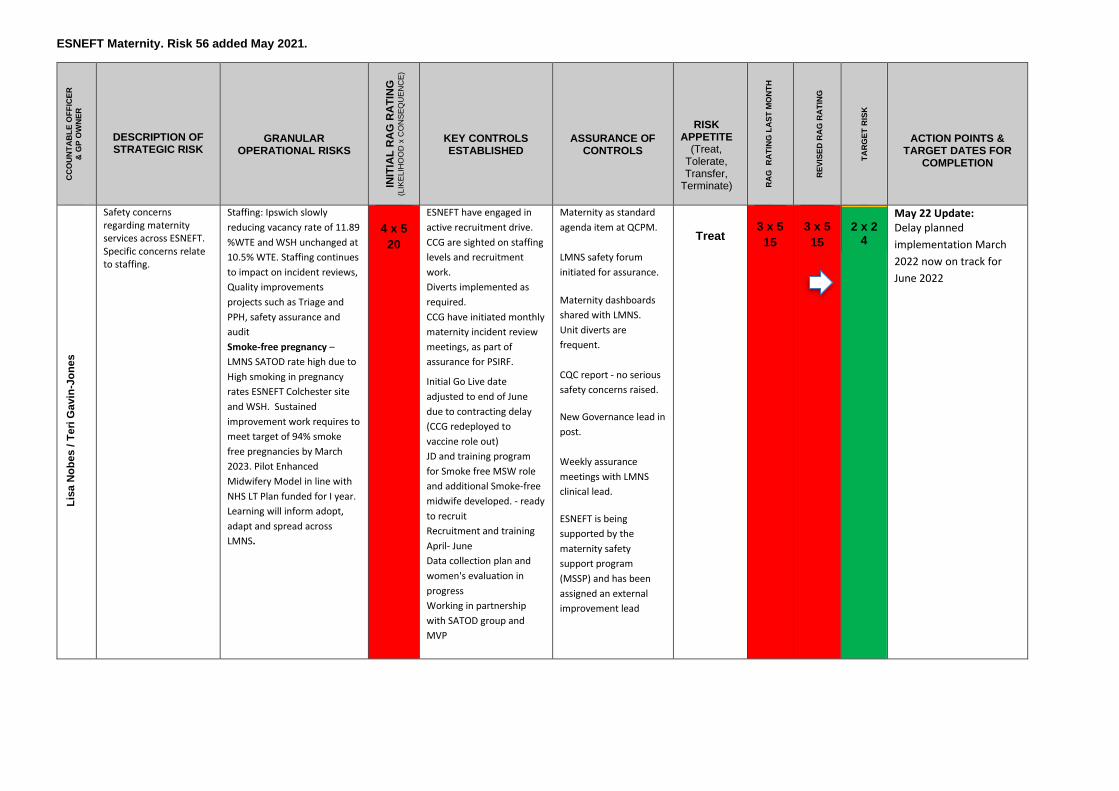
ESNEFT Maternity. Risk 56 added May 2021.
CC
OU
NT
AB
LE
OF
FIC
ER
& G
P O
WN
ER
DESCRIPTION OF STRATEGIC RISK
GRANULAR OPERATIONAL RISKS
INIT
IAL
RA
G R
AT
ING
(L
IKE
LIH
OO
D x
CO
NS
EQ
UE
NC
E)
KEY CONTROLS ESTABLISHED
ASSURANCE OF CONTROLS
RISK APPETITE
(Treat, Tolerate, Transfer,
Terminate)
RA
G
RA
TIN
G L
AS
T M
ON
TH
R
EV
ISE
D R
AG
RA
TIN
G
TA
RG
ET
RIS
K
ACTION POINTS & TARGET DATES FOR
COMPLETION
Lis
a N
ob
es / T
eri
Gavin
-Jo
ne
s
Safety concerns regarding maternity services across ESNEFT. Specific concerns relate to staffing.
Staffing: Ipswich slowly
reducing vacancy rate of 11.89
%WTE and WSH unchanged at
10.5% WTE. Staffing continues
to impact on incident reviews,
Quality improvements
projects such as Triage and
PPH, safety assurance and
audit
Smoke-free pregnancy –
LMNS SATOD rate high due to
High smoking in pregnancy
rates ESNEFT Colchester site
and WSH. Sustained
improvement work requires to
meet target of 94% smoke
free pregnancies by March
2023. Pilot Enhanced
Midwifery Model in line with
NHS LT Plan funded for I year.
Learning will inform adopt,
adapt and spread across
LMNS.
4 x 5
20
ESNEFT have engaged in
active recruitment drive.
CCG are sighted on staffing
levels and recruitment
work.
Diverts implemented as
required.
CCG have initiated monthly
maternity incident review
meetings, as part of
assurance for PSIRF.
Initial Go Live date
adjusted to end of June
due to contracting delay
(CCG redeployed to
vaccine role out)
JD and training program
for Smoke free MSW role
and additional Smoke-free
midwife developed. - ready
to recruit
Recruitment and training
April- June
Data collection plan and
women's evaluation in
progress
Working in partnership
with SATOD group and
MVP
Maternity as standard
agenda item at QCPM.
LMNS safety forum
initiated for assurance.
Maternity dashboards
shared with LMNS.
Unit diverts are
frequent.
CQC report - no serious
safety concerns raised.
New Governance lead in
post.
Weekly assurance
meetings with LMNS
clinical lead.
ESNEFT is being
supported by the
maternity safety
support program
(MSSP) and has been
assigned an external
improvement lead
Treat
3 x 5
15
3 x 5
15
2 x 2 4
May 22 Update: Delay planned
implementation March
2022 now on track for
June 2022
a
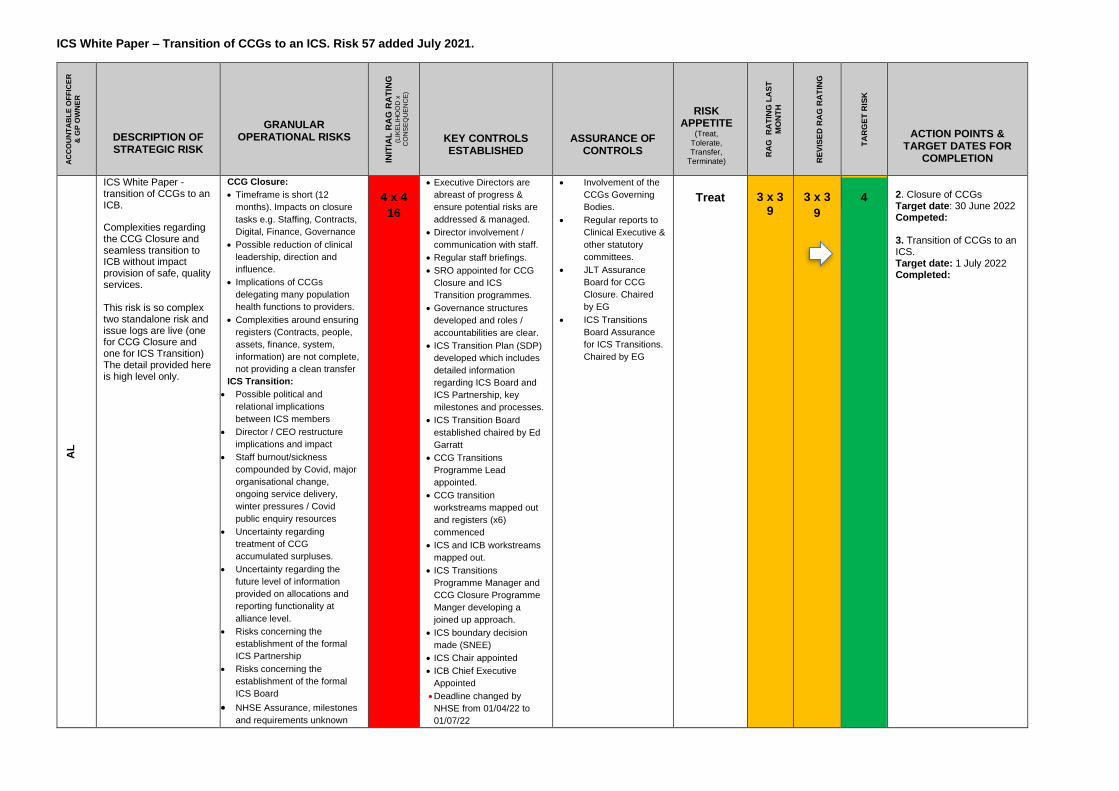
ICS White Paper – Transition of CCGs to an ICS. Risk 57 added July 2021.
AC
CO
UN
TA
BL
E O
FF
ICE
R
& G
P O
WN
ER
DESCRIPTION OF STRATEGIC RISK
GRANULAR OPERATIONAL RISKS
INIT
IAL
RA
G R
AT
ING
(L
IKE
LIH
OO
D x
C
ON
SE
QU
EN
CE
)
KEY CONTROLS ESTABLISHED
ASSURANCE OF CONTROLS
RISK
APPETITE (Treat,
Tolerate, Transfer,
Terminate)
RA
G
RA
TIN
G L
AS
T
MO
NT
H
R
EV
ISE
D R
AG
RA
TIN
G
TA
RG
ET
RIS
K
ACTION POINTS & TARGET DATES FOR
COMPLETION
AL
ICS White Paper - transition of CCGs to an ICB.
Complexities regarding the CCG Closure and seamless transition to ICB without impact provision of safe, quality services. This risk is so complex two standalone risk and issue logs are live (one for CCG Closure and one for ICS Transition) The detail provided here is high level only.
CCG Closure:
• Timeframe is short (12
months). Impacts on closure
tasks e.g. Staffing, Contracts,
Digital, Finance, Governance
• Possible reduction of clinical
leadership, direction and
influence.
• Implications of CCGs
delegating many population
health functions to providers.
• Complexities around ensuring
registers (Contracts, people,
assets, finance, system,
information) are not complete,
not providing a clean transfer
ICS Transition:
• Possible political and
relational implications
between ICS members
• Director / CEO restructure
implications and impact
• Staff burnout/sickness
compounded by Covid, major
organisational change,
ongoing service delivery,
winter pressures / Covid
public enquiry resources
• Uncertainty regarding
treatment of CCG
accumulated surpluses.
• Uncertainty regarding the
future level of information
provided on allocations and
reporting functionality at
alliance level.
• Risks concerning the
establishment of the formal
ICS Partnership
• Risks concerning the
establishment of the formal
ICS Board
• NHSE Assurance, milestones
and requirements unknown
4 x 4
16
• Executive Directors are
abreast of progress &
ensure potential risks are
addressed & managed.
• Director involvement /
communication with staff.
• Regular staff briefings.
• SRO appointed for CCG
Closure and ICS
Transition programmes.
• Governance structures
developed and roles /
accountabilities are clear.
• ICS Transition Plan (SDP)
developed which includes
detailed information
regarding ICS Board and
ICS Partnership, key
milestones and processes.
• ICS Transition Board
established chaired by Ed
Garratt
• CCG Transitions
Programme Lead
appointed.
• CCG transition
workstreams mapped out
and registers (x6)
commenced
• ICS and ICB workstreams
mapped out.
• ICS Transitions
Programme Manager and
CCG Closure Programme
Manger developing a
joined up approach.
• ICS boundary decision
made (SNEE)
• ICS Chair appointed
• ICB Chief Executive
Appointed
• Deadline changed by
NHSE from 01/04/22 to
01/07/22
• Involvement of the
CCGs Governing
Bodies.
• Regular reports to
Clinical Executive &
other statutory
committees.
• JLT Assurance
Board for CCG
Closure. Chaired
by EG
• ICS Transitions
Board Assurance
for ICS Transitions.
Chaired by EG
Treat
3 x 3
9
3 x 3
9
4
2. Closure of CCGs Target date: 30 June 2022 Competed: 3. Transition of CCGs to an ICS. Target date: 1 July 2022 Completed:
a
System Resilience. Risk 58 added August 2021.
AC
CO
UN
TA
BL
E O
FF
ICE
R
& G
P O
WN
ER
DESCRIPTION OF STRATEGIC RISK
GRANULAR OPERATIONAL RISKS
INIT
IAL
RA
G R
AT
ING
(L
IKE
LIH
OO
D x
CO
NS
EQ
UE
NC
E)
KEY CONTROLS ESTABLISHED
ASSURANCE OF CONTROLS
RISK APPETITE
(Treat, Tolerate, Transfer,
Terminate)
RA
G R
AT
ING
LA
ST
MO
NT
H
R
EV
ISE
D R
AG
RA
TIN
G
TA
RG
ET
RIS
K
ACTION POINTS & TARGET DATES FOR
COMPLETION
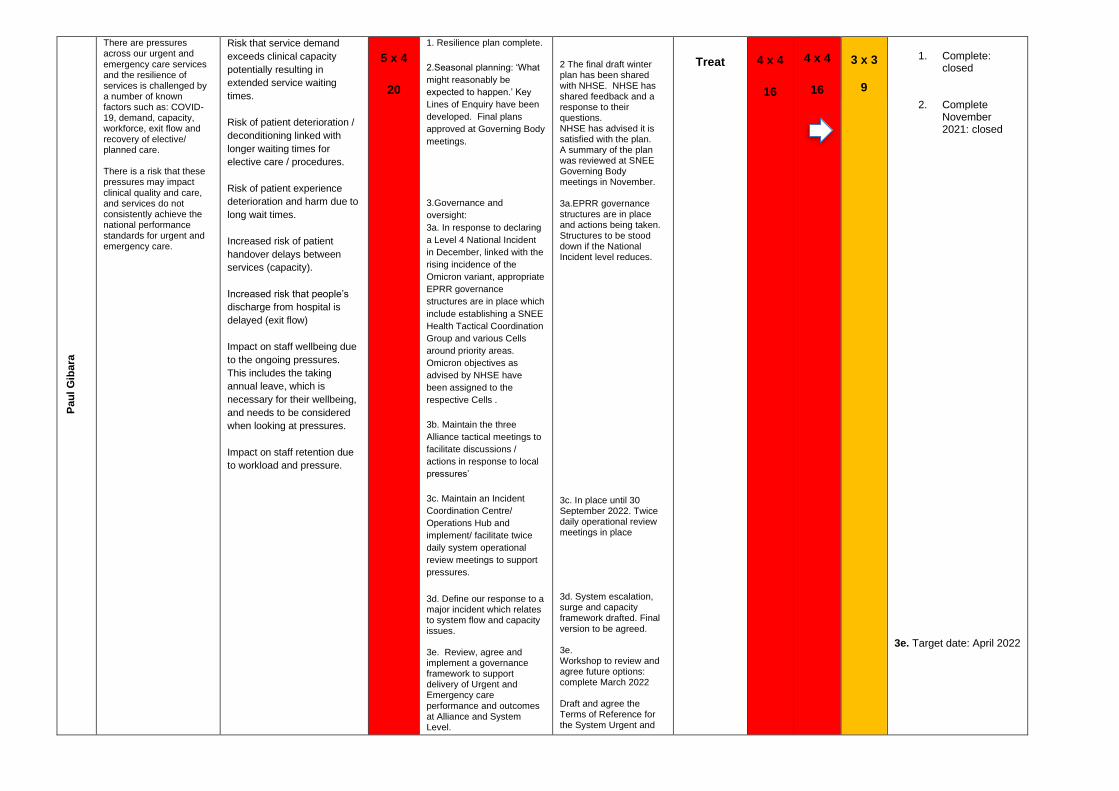
Pau
l G
iba
ra
There are pressures across our urgent and emergency care services and the resilience of services is challenged by a number of known factors such as: COVID-19, demand, capacity, workforce, exit flow and recovery of elective/ planned care. There is a risk that these pressures may impact clinical quality and care, and services do not consistently achieve the national performance standards for urgent and emergency care.
Risk that service demand
exceeds clinical capacity
potentially resulting in
extended service waiting
times.
Risk of patient deterioration /
deconditioning linked with
longer waiting times for
elective care / procedures.
Risk of patient experience
deterioration and harm due to
long wait times.
Increased risk of patient
handover delays between
services (capacity).
Increased risk that people’s
discharge from hospital is
delayed (exit flow)
Impact on staff wellbeing due
to the ongoing pressures.
This includes the taking
annual leave, which is
necessary for their wellbeing,
and needs to be considered
when looking at pressures.
Impact on staff retention due
to workload and pressure.
5 x 4
20
1. Resilience plan complete.
2.Seasonal planning: ‘What
might reasonably be
expected to happen.’ Key
Lines of Enquiry have been
developed. Final plans
approved at Governing Body
meetings.
3.Governance and
oversight:
3a. In response to declaring
a Level 4 National Incident
in December, linked with the
rising incidence of the
Omicron variant, appropriate
EPRR governance
structures are in place which
include establishing a SNEE
Health Tactical Coordination
Group and various Cells
around priority areas.
Omicron objectives as
advised by NHSE have
been assigned to the
respective Cells .
3b. Maintain the three
Alliance tactical meetings to
facilitate discussions /
actions in response to local
pressures’
3c. Maintain an Incident
Coordination Centre/
Operations Hub and
implement/ facilitate twice
daily system operational
review meetings to support
pressures.
3d. Define our response to a major incident which relates to system flow and capacity issues. 3e. Review, agree and implement a governance framework to support delivery of Urgent and Emergency care performance and outcomes at Alliance and System Level.
2 The final draft winter plan has been shared with NHSE. NHSE has shared feedback and a response to their questions. NHSE has advised it is satisfied with the plan. A summary of the plan was reviewed at SNEE Governing Body meetings in November. 3a.EPRR governance structures are in place and actions being taken. Structures to be stood down if the National Incident level reduces.
3c. In place until 30 September 2022. Twice daily operational review meetings in place 3d. System escalation, surge and capacity framework drafted. Final version to be agreed. 3e. Workshop to review and agree future options: complete March 2022 Draft and agree the Terms of Reference for the System Urgent and
Treat
4 x 4
16
4 x 4
16
3 x 3
9
1. Complete:
closed
2. Complete November 2021: closed
3e. Target date: April 2022
a
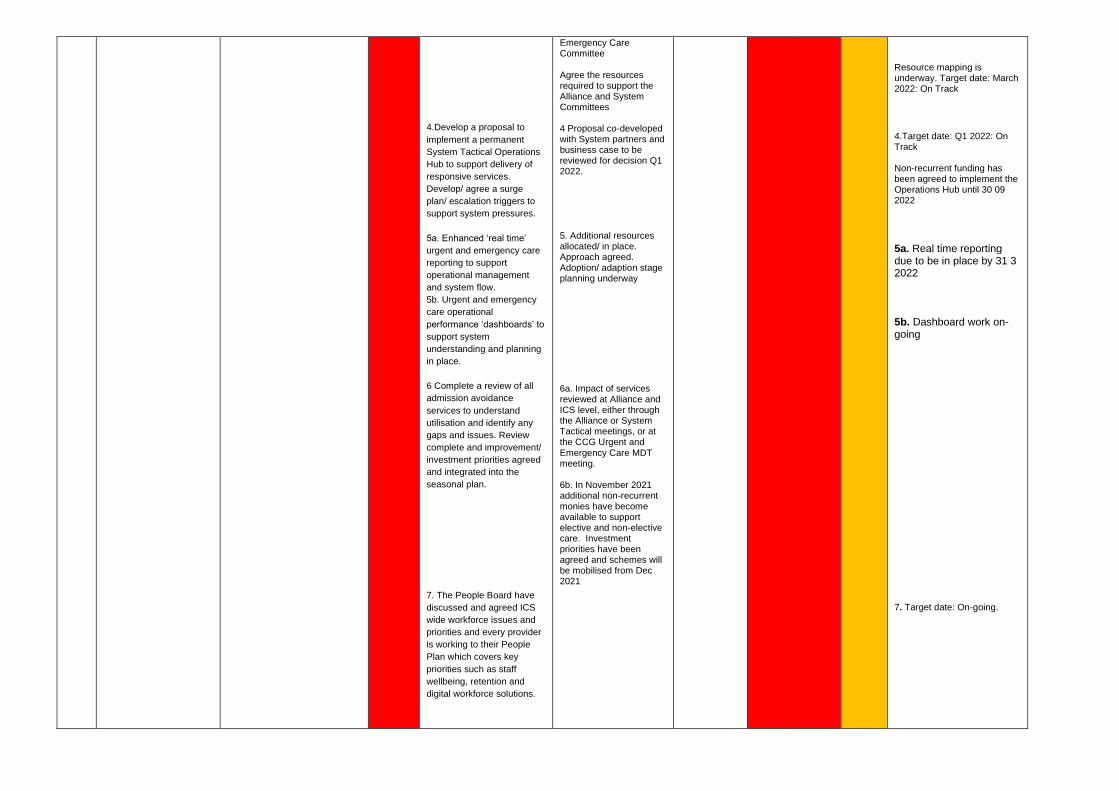
4.Develop a proposal to
implement a permanent
System Tactical Operations
Hub to support delivery of
responsive services.
Develop/ agree a surge
plan/ escalation triggers to
support system pressures.
5a. Enhanced ‘real time’
urgent and emergency care
reporting to support
operational management
and system flow.
5b. Urgent and emergency
care operational
performance ‘dashboards’ to
support system
understanding and planning
in place.
6 Complete a review of all
admission avoidance
services to understand
utilisation and identify any
gaps and issues. Review
complete and improvement/
investment priorities agreed
and integrated into the
seasonal plan.
7. The People Board have
discussed and agreed ICS
wide workforce issues and
priorities and every provider
is working to their People
Plan which covers key
priorities such as staff
wellbeing, retention and
digital workforce solutions.
Emergency Care Committee Agree the resources required to support the Alliance and System Committees 4 Proposal co-developed with System partners and business case to be reviewed for decision Q1 2022. 5. Additional resources allocated/ in place. Approach agreed. Adoption/ adaption stage planning underway
6a. Impact of services reviewed at Alliance and ICS level, either through the Alliance or System Tactical meetings, or at the CCG Urgent and Emergency Care MDT meeting. 6b. In November 2021 additional non-recurrent monies have become available to support elective and non-elective care. Investment priorities have been agreed and schemes will be mobilised from Dec 2021
Resource mapping is underway. Target date: March 2022: On Track
4.Target date: Q1 2022: On Track Non-recurrent funding has been agreed to implement the Operations Hub until 30 09 2022
5a. Real time reporting due to be in place by 31 3 2022 5b. Dashboard work on-going
7. Target date: On-going.
EEAST – Performance/Quality. Risk 59. December 2021.
AC
CO
UN
TA
BL
E O
FF
ICE
R
& G
P O
WN
ER
DESCRIPTION OF STRATEGIC
RISK
GRANULAR OPERATIONAL RISKS
INIT
IAL
RA
G R
AT
ING
(L
IKE
LIH
OO
D x
CO
NS
EQ
UE
NC
E)
KEY CONTROLS ESTABLISHED
ASSURANCE OF CONTROLS
RISK
APPETITE (Treat,
Tolerate, Transfer,
Terminate)
RA
G
RA
TIN
G L
AS
T M
ON
TH
R
EV
ISE
D R
AG
RA
TIN
G
TA
RG
ET
RIS
K
ACTION POINTS & TARGET DATES FOR
COMPLETION
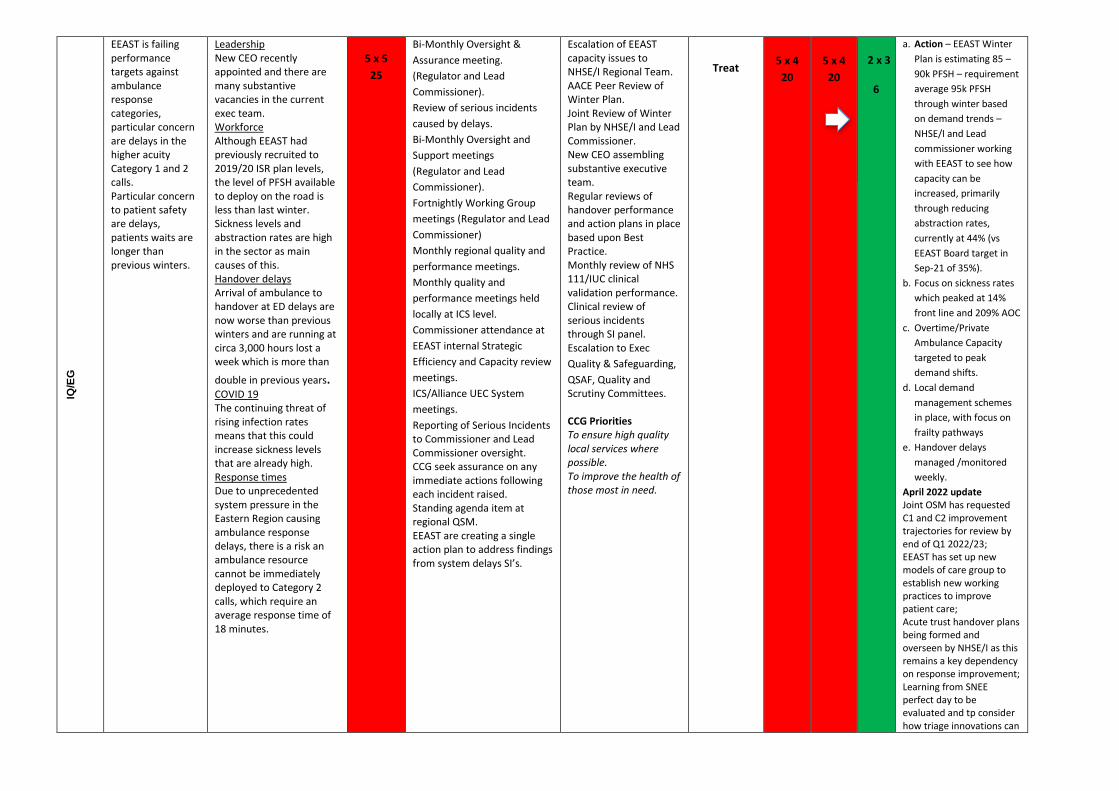
IQ/E
G
EEAST is failing performance targets against ambulance response categories, particular concern are delays in the higher acuity Category 1 and 2 calls. Particular concern to patient safety are delays, patients waits are longer than previous winters.
Leadership New CEO recently appointed and there are many substantive vacancies in the current exec team. Workforce Although EEAST had previously recruited to 2019/20 ISR plan levels, the level of PFSH available to deploy on the road is less than last winter. Sickness levels and abstraction rates are high in the sector as main causes of this. Handover delays Arrival of ambulance to handover at ED delays are now worse than previous winters and are running at circa 3,000 hours lost a week which is more than
double in previous years. COVID 19 The continuing threat of rising infection rates means that this could increase sickness levels that are already high. Response times Due to unprecedented system pressure in the Eastern Region causing ambulance response delays, there is a risk an ambulance resource cannot be immediately deployed to Category 2 calls, which require an average response time of 18 minutes.
5 x 5
25
Bi-Monthly Oversight &
Assurance meeting.
(Regulator and Lead
Commissioner).
Review of serious incidents
caused by delays.
Bi-Monthly Oversight and
Support meetings
(Regulator and Lead
Commissioner).
Fortnightly Working Group
meetings (Regulator and Lead
Commissioner)
Monthly regional quality and
performance meetings.
Monthly quality and
performance meetings held
locally at ICS level.
Commissioner attendance at
EEAST internal Strategic
Efficiency and Capacity review
meetings.
ICS/Alliance UEC System
meetings.
Reporting of Serious Incidents to Commissioner and Lead Commissioner oversight. CCG seek assurance on any immediate actions following each incident raised. Standing agenda item at regional QSM. EEAST are creating a single action plan to address findings from system delays SI’s.
Escalation of EEAST capacity issues to NHSE/I Regional Team. AACE Peer Review of Winter Plan. Joint Review of Winter Plan by NHSE/I and Lead Commissioner. New CEO assembling substantive executive team. Regular reviews of handover performance and action plans in place based upon Best Practice. Monthly review of NHS 111/IUC clinical validation performance. Clinical review of serious incidents through SI panel. Escalation to Exec
Quality & Safeguarding,
QSAF, Quality and Scrutiny Committees. CCG Priorities To ensure high quality local services where possible. To improve the health of those most in need.
Treat
5 x 4
20
5 x 4
20
2 x 3
6
a. Action – EEAST Winter
Plan is estimating 85 –
90k PFSH – requirement
average 95k PFSH
through winter based
on demand trends –
NHSE/I and Lead
commissioner working
with EEAST to see how
capacity can be
increased, primarily
through reducing
abstraction rates,
currently at 44% (vs
EEAST Board target in
Sep-21 of 35%).
b. Focus on sickness rates
which peaked at 14%
front line and 209% AOC
c. Overtime/Private
Ambulance Capacity
targeted to peak
demand shifts.
d. Local demand
management schemes
in place, with focus on
frailty pathways
e. Handover delays
managed /monitored
weekly.
April 2022 update Joint OSM has requested C1 and C2 improvement trajectories for review by end of Q1 2022/23; EEAST has set up new models of care group to establish new working practices to improve patient care; Acute trust handover plans being formed and overseen by NHSE/I as this remains a key dependency on response improvement; Learning from SNEE perfect day to be evaluated and tp consider how triage innovations can
a
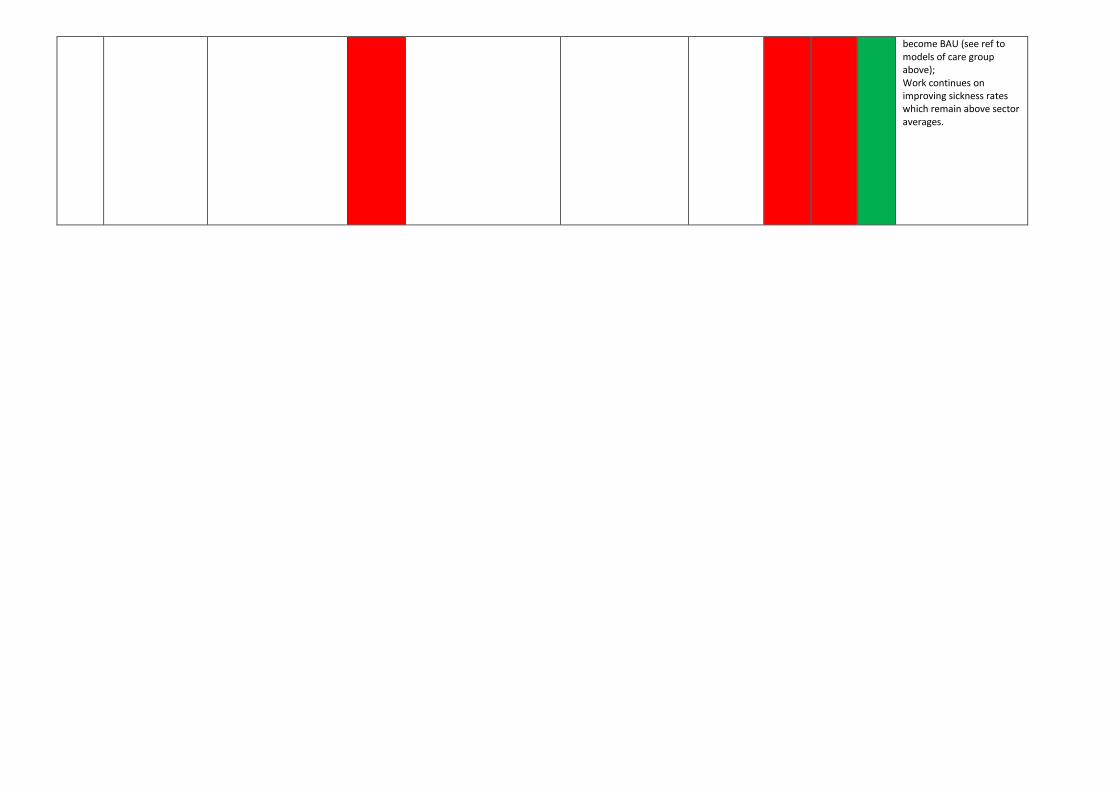
become BAU (see ref to models of care group above); Work continues on improving sickness rates which remain above sector averages.
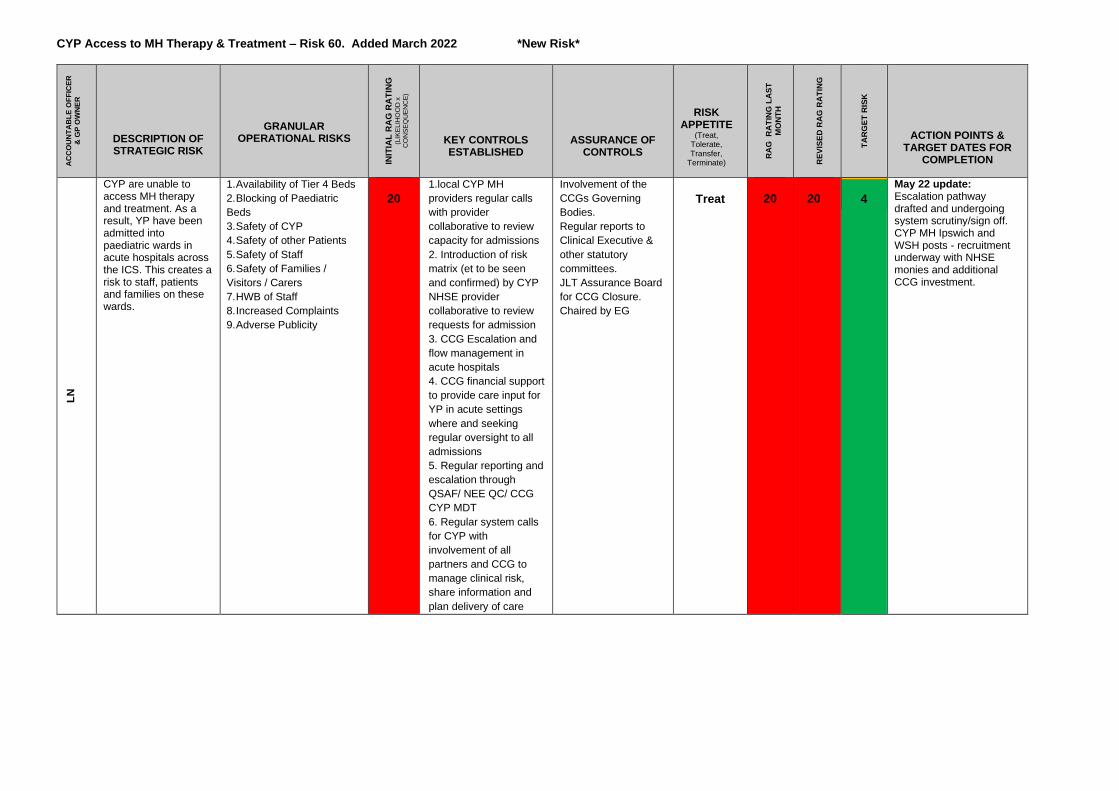
CYP Access to MH Therapy & Treatment – Risk 60. Added March 2022 *New Risk*
AC
CO
UN
TA
BL
E O
FF
ICE
R
& G
P O
WN
ER
DESCRIPTION OF STRATEGIC RISK
GRANULAR OPERATIONAL RISKS
INIT
IAL
RA
G R
AT
ING
(L
IKE
LIH
OO
D x
C
ON
SE
QU
EN
CE
)
KEY CONTROLS ESTABLISHED
ASSURANCE OF CONTROLS
RISK
APPETITE (Treat,
Tolerate, Transfer,
Terminate)
RA
G
RA
TIN
G L
AS
T
MO
NT
H
R
EV
ISE
D R
AG
RA
TIN
G
TA
RG
ET
RIS
K
ACTION POINTS & TARGET DATES FOR
COMPLETION
LN
CYP are unable to access MH therapy and treatment. As a result, YP have been admitted into paediatric wards in acute hospitals across the ICS. This creates a risk to staff, patients and families on these wards.
1. Availability of Tier 4 Beds
2. Blocking of Paediatric
Beds
3. Safety of CYP
4. Safety of other Patients
5. Safety of Staff
6. Safety of Families /
Visitors / Carers
7. HWB of Staff
8. Increased Complaints
9. Adverse Publicity
20
1.local CYP MH
providers regular calls
with provider
collaborative to review
capacity for admissions
2. Introduction of risk
matrix (et to be seen
and confirmed) by CYP
NHSE provider
collaborative to review
requests for admission
3. CCG Escalation and
flow management in
acute hospitals
4. CCG financial support
to provide care input for
YP in acute settings
where and seeking
regular oversight to all
admissions
5. Regular reporting and
escalation through
QSAF/ NEE QC/ CCG
CYP MDT
6. Regular system calls
for CYP with
involvement of all
partners and CCG to
manage clinical risk,
share information and
plan delivery of care
Involvement of the
CCGs Governing
Bodies.
Regular reports to
Clinical Executive &
other statutory
committees.
JLT Assurance Board
for CCG Closure.
Chaired by EG
Treat
20
20
4
May 22 update: Escalation pathway drafted and undergoing system scrutiny/sign off. CYP MH Ipswich and WSH posts - recruitment underway with NHSE monies and additional CCG investment.
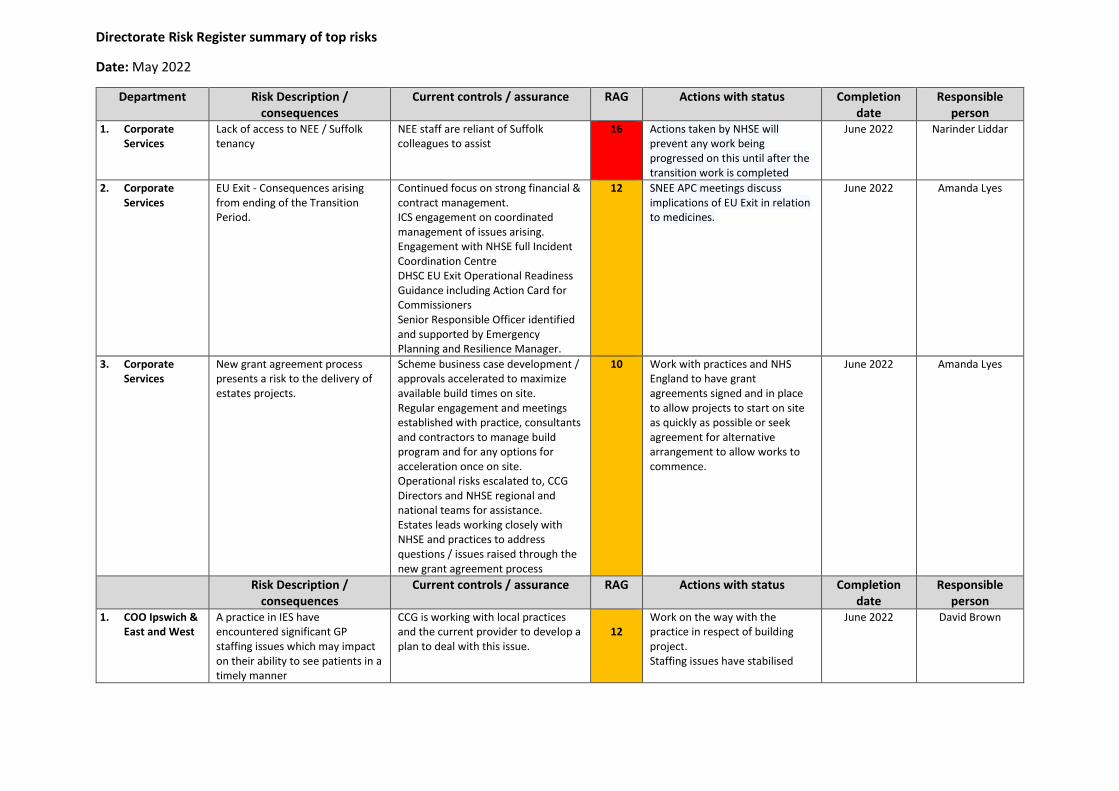
Directorate Risk Register summary of top risks
Date: May 2022
Department Risk Description / consequences
Current controls / assurance RAG Actions with status Completion date
Responsible person
1. Corporate Services
Lack of access to NEE / Suffolk tenancy
NEE staff are reliant of Suffolk colleagues to assist
16 Actions taken by NHSE will prevent any work being progressed on this until after the transition work is completed
June 2022 Narinder Liddar
2. Corporate Services
EU Exit - Consequences arising from ending of the Transition Period.
Continued focus on strong financial & contract management. ICS engagement on coordinated management of issues arising. Engagement with NHSE full Incident Coordination Centre DHSC EU Exit Operational Readiness Guidance including Action Card for Commissioners Senior Responsible Officer identified and supported by Emergency Planning and Resilience Manager.
12 SNEE APC meetings discuss implications of EU Exit in relation to medicines.
June 2022 Amanda Lyes
3. Corporate Services
New grant agreement process presents a risk to the delivery of estates projects.
Scheme business case development / approvals accelerated to maximize available build times on site. Regular engagement and meetings established with practice, consultants and contractors to manage build program and for any options for acceleration once on site. Operational risks escalated to, CCG Directors and NHSE regional and national teams for assistance. Estates leads working closely with NHSE and practices to address questions / issues raised through the new grant agreement process
10 Work with practices and NHS England to have grant agreements signed and in place to allow projects to start on site as quickly as possible or seek agreement for alternative arrangement to allow works to commence.
June 2022 Amanda Lyes
Risk Description / consequences
Current controls / assurance RAG Actions with status Completion date
Responsible person
1. COO Ipswich & East and West
A practice in IES have encountered significant GP staffing issues which may impact on their ability to see patients in a timely manner
CCG is working with local practices and the current provider to develop a plan to deal with this issue.
12
Work on the way with the practice in respect of building project. Staffing issues have stabilised
June 2022 David Brown
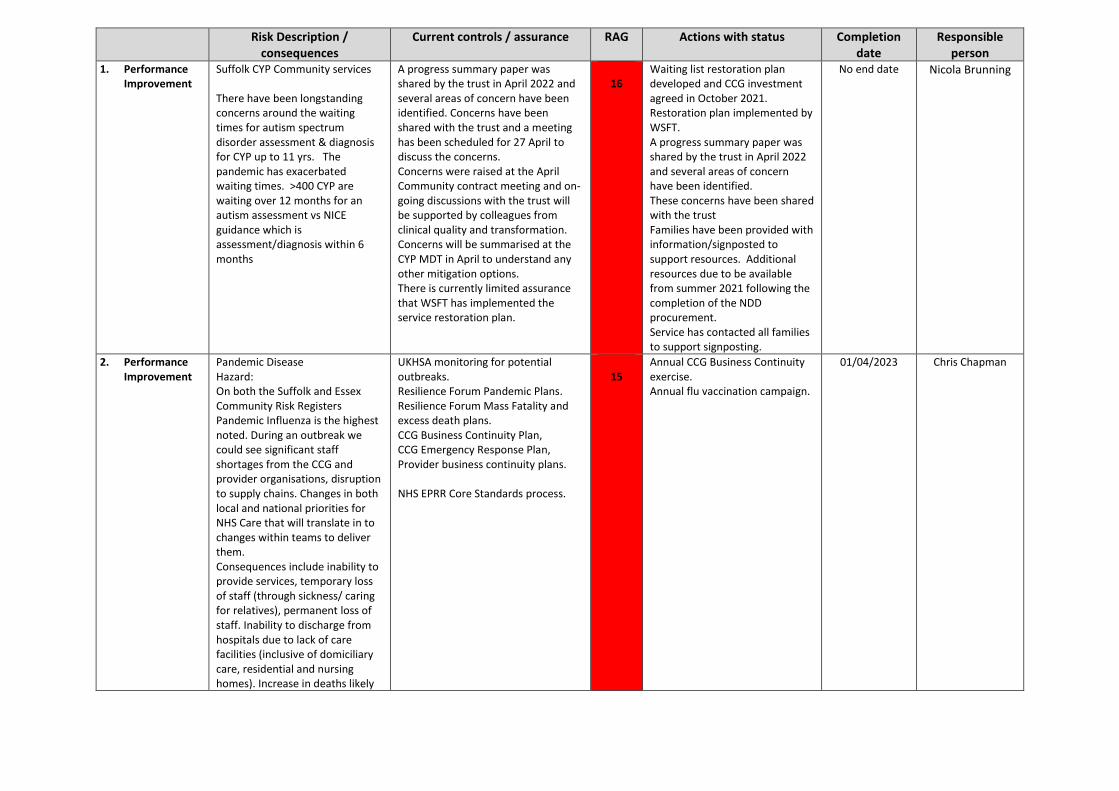
Risk Description / consequences
Current controls / assurance RAG Actions with status Completion date
Responsible person
1. Performance Improvement
Suffolk CYP Community services There have been longstanding concerns around the waiting times for autism spectrum disorder assessment & diagnosis for CYP up to 11 yrs. The pandemic has exacerbated waiting times. >400 CYP are waiting over 12 months for an autism assessment vs NICE guidance which is assessment/diagnosis within 6 months
A progress summary paper was shared by the trust in April 2022 and several areas of concern have been identified. Concerns have been shared with the trust and a meeting has been scheduled for 27 April to discuss the concerns. Concerns were raised at the April Community contract meeting and on-going discussions with the trust will be supported by colleagues from clinical quality and transformation. Concerns will be summarised at the CYP MDT in April to understand any other mitigation options. There is currently limited assurance that WSFT has implemented the service restoration plan.
16
Waiting list restoration plan developed and CCG investment agreed in October 2021. Restoration plan implemented by WSFT. A progress summary paper was shared by the trust in April 2022 and several areas of concern have been identified. These concerns have been shared with the trust Families have been provided with information/signposted to support resources. Additional resources due to be available from summer 2021 following the completion of the NDD procurement. Service has contacted all families to support signposting.
No end date Nicola Brunning
2. Performance Improvement
Pandemic Disease Hazard: On both the Suffolk and Essex Community Risk Registers Pandemic Influenza is the highest noted. During an outbreak we could see significant staff shortages from the CCG and provider organisations, disruption to supply chains. Changes in both local and national priorities for NHS Care that will translate in to changes within teams to deliver them. Consequences include inability to provide services, temporary loss of staff (through sickness/ caring for relatives), permanent loss of staff. Inability to discharge from hospitals due to lack of care facilities (inclusive of domiciliary care, residential and nursing homes). Increase in deaths likely
UKHSA monitoring for potential outbreaks. Resilience Forum Pandemic Plans. Resilience Forum Mass Fatality and excess death plans. CCG Business Continuity Plan, CCG Emergency Response Plan, Provider business continuity plans. NHS EPRR Core Standards process.
15
Annual CCG Business Continuity exercise. Annual flu vaccination campaign.
01/04/2023 Chris Chapman
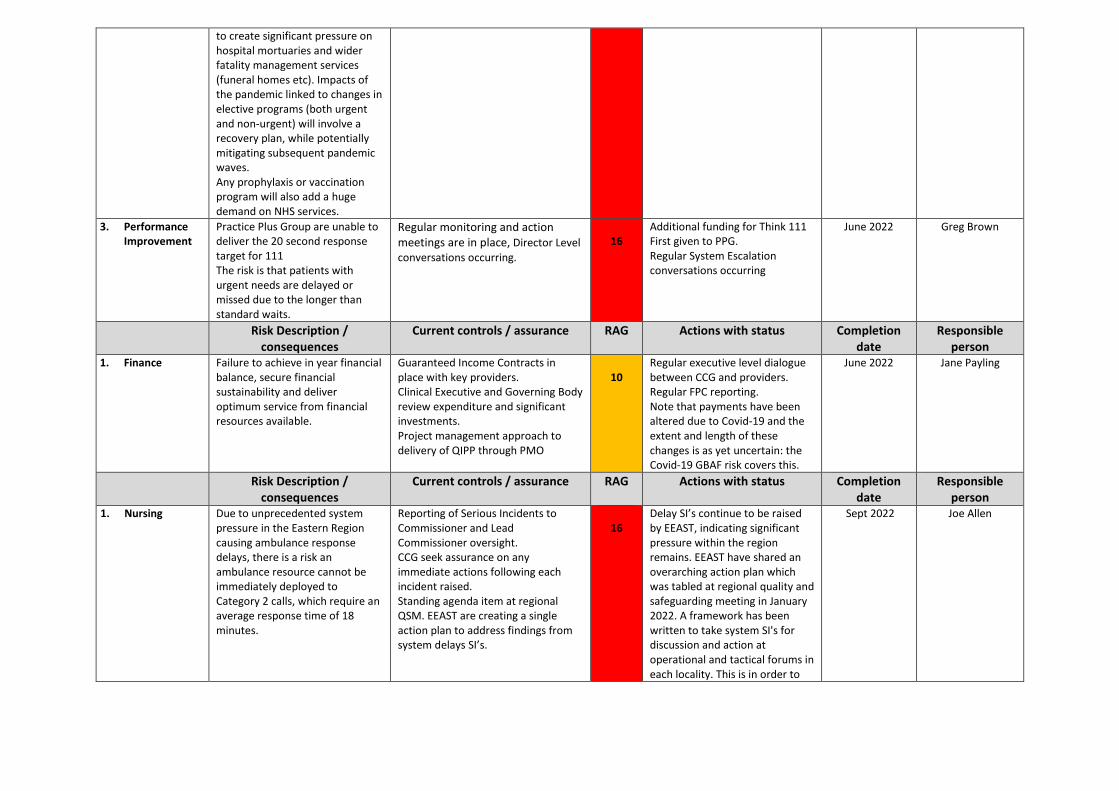
to create significant pressure on hospital mortuaries and wider fatality management services (funeral homes etc). Impacts of the pandemic linked to changes in elective programs (both urgent and non-urgent) will involve a recovery plan, while potentially mitigating subsequent pandemic waves. Any prophylaxis or vaccination program will also add a huge demand on NHS services.
3. Performance Improvement
Practice Plus Group are unable to deliver the 20 second response target for 111 The risk is that patients with urgent needs are delayed or missed due to the longer than standard waits.
Regular monitoring and action meetings are in place, Director Level conversations occurring.
16
Additional funding for Think 111 First given to PPG. Regular System Escalation conversations occurring
June 2022 Greg Brown
Risk Description / consequences
Current controls / assurance RAG Actions with status Completion date
Responsible person
1. Finance Failure to achieve in year financial balance, secure financial sustainability and deliver optimum service from financial resources available.
Guaranteed Income Contracts in place with key providers. Clinical Executive and Governing Body review expenditure and significant investments. Project management approach to delivery of QIPP through PMO
10
Regular executive level dialogue between CCG and providers. Regular FPC reporting. Note that payments have been altered due to Covid-19 and the extent and length of these changes is as yet uncertain: the Covid-19 GBAF risk covers this.
June 2022 Jane Payling
Risk Description / consequences
Current controls / assurance RAG Actions with status Completion date
Responsible person
1. Nursing Due to unprecedented system pressure in the Eastern Region causing ambulance response delays, there is a risk an ambulance resource cannot be immediately deployed to Category 2 calls, which require an average response time of 18 minutes.
Reporting of Serious Incidents to Commissioner and Lead Commissioner oversight. CCG seek assurance on any immediate actions following each incident raised. Standing agenda item at regional QSM. EEAST are creating a single action plan to address findings from system delays SI’s.
16
Delay SI’s continue to be raised by EEAST, indicating significant pressure within the region remains. EEAST have shared an overarching action plan which was tabled at regional quality and safeguarding meeting in January 2022. A framework has been written to take system SI's for discussion and action at operational and tactical forums in each locality. This is in order to
Sept 2022 Joe Allen
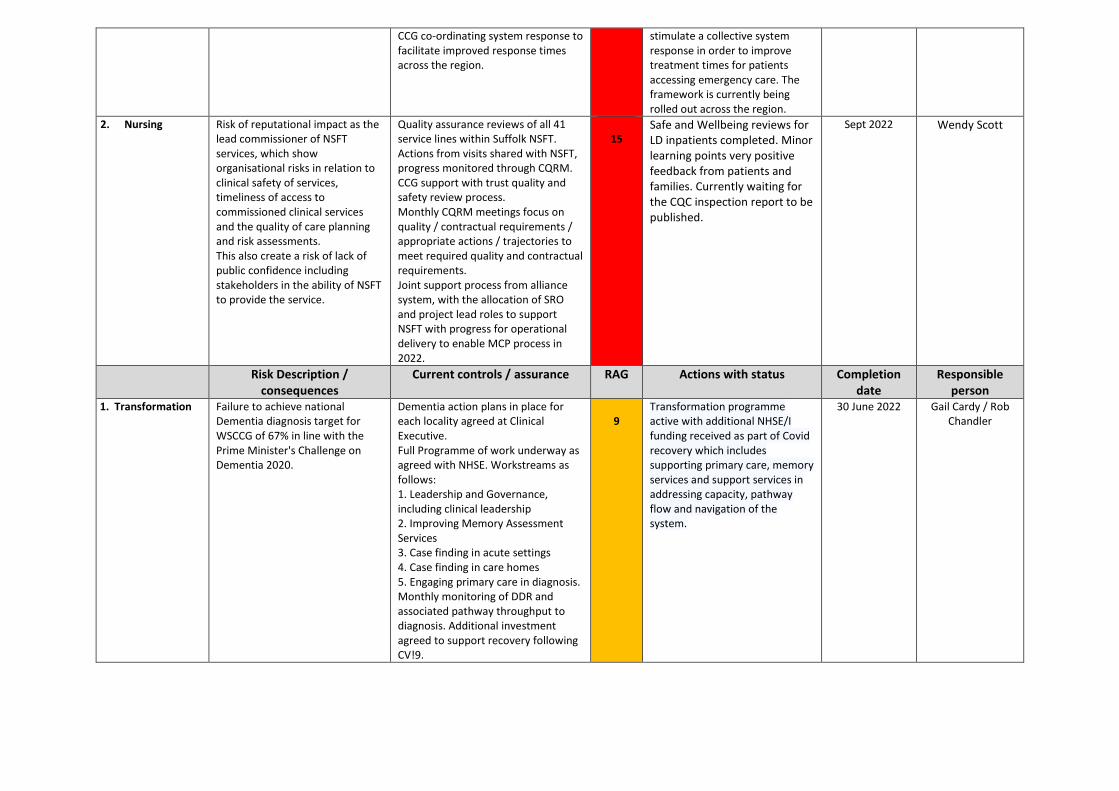
CCG co-ordinating system response to facilitate improved response times across the region.
stimulate a collective system response in order to improve treatment times for patients accessing emergency care. The framework is currently being rolled out across the region.
2. Nursing Risk of reputational impact as the lead commissioner of NSFT services, which show organisational risks in relation to clinical safety of services, timeliness of access to commissioned clinical services and the quality of care planning and risk assessments. This also create a risk of lack of public confidence including stakeholders in the ability of NSFT to provide the service.
Quality assurance reviews of all 41 service lines within Suffolk NSFT. Actions from visits shared with NSFT, progress monitored through CQRM. CCG support with trust quality and safety review process. Monthly CQRM meetings focus on quality / contractual requirements / appropriate actions / trajectories to meet required quality and contractual requirements. Joint support process from alliance system, with the allocation of SRO and project lead roles to support NSFT with progress for operational delivery to enable MCP process in 2022.
15
Safe and Wellbeing reviews for LD inpatients completed. Minor learning points very positive feedback from patients and families. Currently waiting for the CQC inspection report to be published.
Sept 2022 Wendy Scott
Risk Description / consequences
Current controls / assurance RAG Actions with status Completion date
Responsible person
1. Transformation Failure to achieve national Dementia diagnosis target for WSCCG of 67% in line with the Prime Minister's Challenge on Dementia 2020.
Dementia action plans in place for each locality agreed at Clinical Executive. Full Programme of work underway as agreed with NHSE. Workstreams as follows: 1. Leadership and Governance, including clinical leadership 2. Improving Memory Assessment Services 3. Case finding in acute settings 4. Case finding in care homes 5. Engaging primary care in diagnosis. Monthly monitoring of DDR and associated pathway throughput to diagnosis. Additional investment agreed to support recovery following CV!9.
9
Transformation programme active with additional NHSE/I funding received as part of Covid recovery which includes supporting primary care, memory services and support services in addressing capacity, pathway flow and navigation of the system.
30 June 2022
Gail Cardy / Rob Chandler
Page 1 of 2
GOVERNING BODY
Agenda Item No. 14
Reference No. IESCCG 22-23
Date. 24 May 2022
Title Declaration of Interests
Lead Director Amanda Lyes, Chief Corporate Services Officer
Author(s) Colin Boakes, Independent Governance Advisor
Purpose The report provides a public record of relevant and material interests declared by members of the Ipswich and East Suffolk CCG Governing Body, its sub-committees, decision making staff and member practices.
Applicable CCG Clinical Priorities: 1. To promote self-care
2. To ensure high quality local services where possible
3. To improve the health of those most in need
4. To improve health & educational attainment for children & young people
5. To improve access to mental health services
6. To improve outcomes for patients with diabetes to above nationalaverages
7. To improve care for frail elderly individuals
8. To allow patients to die with dignity & compassion & to choose theirplace of death where appropriate.
9. To ensure that the CCG operates within agreed budgets
Action required by Governing Body:
The Governing Body is asked to review the current register and consider whether any action in relation to non-responders might be required.
Page 2 of 2
1. Background 1.1 Clinical commissioning groups (CCGs) manage conflicts of interest as part of their day-
to-day activities. Effective handling of conflicts of interest is crucial to give confidence to patients, tax payers, healthcare providers and Parliament that CCG commissioning decisions are robust, fair and transparent and offer value for money. It is essential in order to protect healthcare professionals and maintain public trust in the NHS. Failure to manage conflicts of interest could lead to legal challenge and even criminal action in the event of fraud, bribery and corruption.
1.2 Conflicts of interest are inevitable in commissioning. It is how we manage them that
matters. Section 14O of the National Health Service Act 2006 (as amended by the Health and Social Care Act 2012) (“the Act”) sets out the minimum requirements of what both NHS England and CCGs must do in terms of managing conflicts of interest.
1.3 As a minimum, CCGs must have robust systems in place to identify and manage
conflicts of interest. This should involve creating an environment in which CCG staff, Governing Body and sub-committee members, and member practices feel able, encouraged and obliged to be open, honest and upfront about actual or potential conflicts. Transparency in this regard is expected to lead to effective identification and management of conflicts. The effect should be to make everyone aware of what to do if they suspect a conflict and ensure decision-making is efficient, transparent and fair.
1.4 CCGs are required to have systems in place to satisfy themselves that their registers of
interest are accurate and up-to-date. 2. Key Points 2.1 As regards declarations and registers of interest, guidance requires that all CCG
Officers, Governing Body members, GPs, all staff, including students, agency and seconded staff, together with practice staff with involvement in CCG business complete declarations. However, only those staff classed as ‘decision makers’ will be included in the register published on the CCG’s web site.
2.2 Declarations are sought by the CCG on a six-monthly basis – in October by submission
of a signed declaration and in April by exception should there have been changes. The decision makers declarations constitute the register published on the CCG’s website. The current register is attached to the report at Appendix 1. (Dates highlighted in ‘Red’ denote where there has been no response to the request for declarations in April 2022)
2.3 In view of the Covid19 pandemic, we have managed the collection of declarations of
interest slightly differently. For example, we have accepted e-mailed copies of declarations with electronic signatures. Similarly, where there has been no change to an individual’s declaration or where there is a nil return, these have been signed off by the Corporate Governance Manager on my behalf.
3. Recommendation 3.1 The Governing Body is asked to review the current register and consider whether any
action in relation to non-responders might be required.
Interests of:
Governing Body and Sub-Committee MembersAll Decision Making CCG Staff
Member Practices
Register of Interests
April 2022
Ipswich and East Suffolk CCG
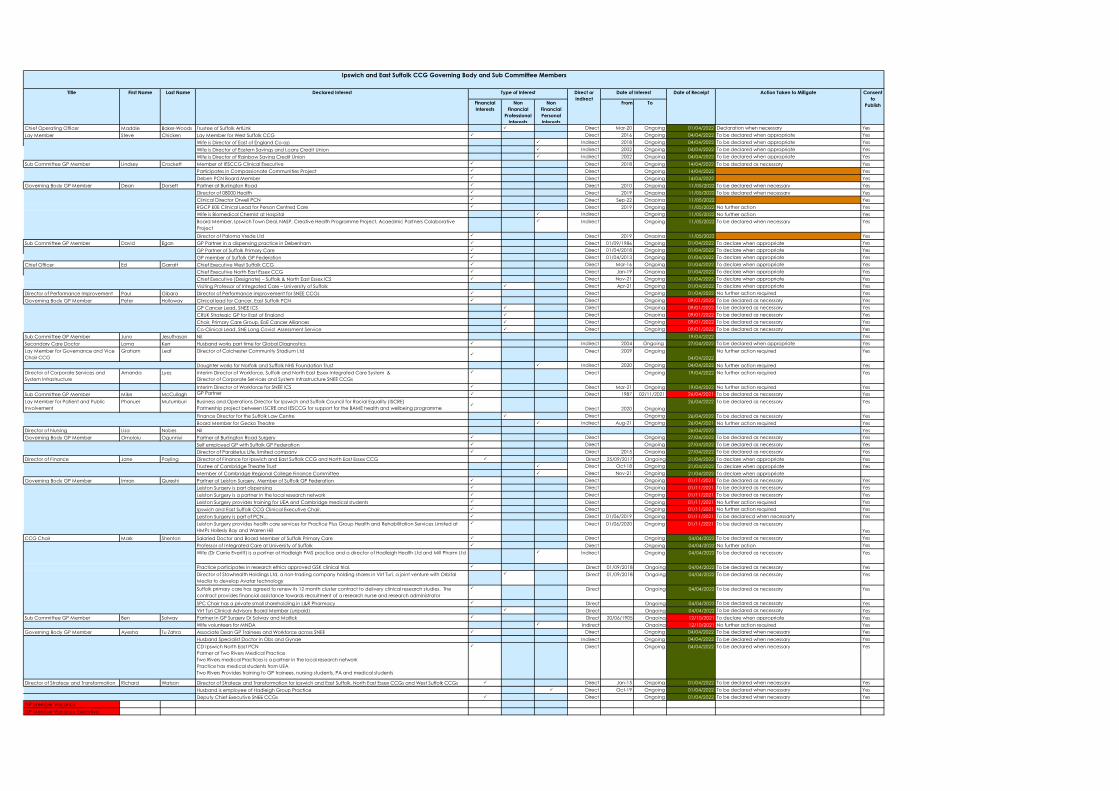
Financial Interests
Non Financial
Professional Interests
Non Financial Personal Interests
From To
Chief Operating Officer Maddie Baker-Woods Trustee of Suffolk ArtLink Direct Mar-20 Ongoing 01/04/2022 Declaration when necessary YesLay Member Steve Chicken Lay Member for West Suffolk CCG Direct 2016 Ongoing 04/04/2022 To be declared when appropriate Yes
Wife is Director of East of England Co-op Indirect 2018 Ongoing 04/04/2022 To be declared when appropriate YesWife is Director of Eastern Savings and Loans Credit Union Indirect 2002 Ongoing 04/04/2022 To be declared when appropriate YesWife is Director of Rainbow Saving Credit Union Indirect 2002 Ongoing 04/04/2022 To be declared when appropriate Yes
Sub Committee GP Member Lindsey Crockett Member of IESCCG Clinical Executive Direct 2018 Ongoing 14/04/2022 To be declared as necessary YesParticipates in Compassionate Communities Project Direct Ongoing 14/04/2022 YesDeben PCN Board Member Direct Ongoing 14/04/2022 Yes
Governing Body GP Member Dean Dorsett Partner at Burlington Road Direct 2010 Ongoing 11/05/2022 To be declared when necessary YesDirector of 08000 Health Direct 2019 Ongoing 11/05/2022 To be declared when necessary YesClinical Director Orwell PCN Direct Sep-22 Ongoing 11/05/2022 YesRGCP E0E Clinical Lead for Person Centred Care Direct 2019 Ongoing 11/05/2022 No further action YesWife is Biomedical Chemist at Hospital Indirect Ongoing 11/05/2022 No further action YesBoard Member, Ipswich Town Deal, NASP, Creative Health Programme Project, Acaedmic Partners Colaborative Project
Indirect Ongoing 11/05/2022 To be declared when necessary Yes
Director of Paloma Vrede Ltd Direct 2019 Ongoing 11/05/2022 YesSub Committee GP Member David Egan GP Partner in a dispensing practice in Debenham Direct 01/09/1986 Ongoing 01/04/2022 To declare when appropriate Yes
GP Partner of Suffolk Primary Care Direct 01/04/2018 Ongoing 01/04/2022 To declare when appropriate YesGP member of Suffolk GP Federation Direct 01/04/2013 Ongoing 01/04/2022 To declare when appropriate Yes
Chief Officer Ed Garratt Chief Executive West Suffolk CCG Direct Mar-16 Ongoing 01/04/2022 To declare when appropriate YesChief Executive North East Essex CCG Direct Jan-19 Ongoing 01/04/2022 To declare when appropriate YesChief Executive (Designate) – Suffolk & North East Essex ICS Direct Nov-21 Ongoing 01/04/2022 To declare when appropriate YesVisiting Professor of Integrated Care – University of Suffolk Direct Apr-21 Ongoing 01/04/2022 To declare when appropriate Yes
Director of Performance Improvement Paul Gibara Director of Performance Improvement for SNEE CCGs Direct Ongoing 01/04/2022 No further action required YesGoverning Body GP Member Peter Holloway Clinical lead for Cancer, East Suffolk PCN Direct Ongoing 09/01/2022 To be declared as necessary Yes
GP Cancer Lead, SNEE ICS Direct Ongoing 09/01/2022 To be declared as necessary YesCRUK Strategic GP for East of England Direct Ongoing 09/01/2022 To be declared as necessary YesChair, Primary Care Group, EoE Cancer Alliances Direct Ongoing 09/01/2022 To be declared as necessary YesCo-Clinical Lead, SNE Long Covid Assessment Service Direct Ongoing 09/01/2022 To be declared as necessary Yes
Sub Committee GP Member Juno Jesuthasan Nil 19/04/2022 YesSecondary Care Doctor Lorna Kerr Husband works part time for Global Diagnostics Indirect 2004 Ongoing 27/04/2022 To be declared when appropriate YesLay Member for Governance and Vice Chair CCG
Graham Leaf Director of Colchester Community Stadium Ltd
Direct 2009 Ongoing04/04/2022
No further action required Yes
Daughter works for Norfolk and Suffolk NHS Foundation Trust Indirect 2020 Ongoing 04/04/2022 No further action required YesDirector of Corporate Services and System Infrastructure
Amanda Lyes Interim Director of Workforce, Suffolk and North East Essex Integrated Care System &Director of Corporate Services and System Infrastructure SNEE CCGs
Direct Ongoing 19/04/2022 No further action required Yes
Interim Director of Workforce for SNEE ICS Direct Mar-21 Ongoing 19/04/2022 No further action required YesSub Committee GP Member Mike McCullagh GP Partner Direct 1987 02/11/2021 26/04/2021 To be declared as necessary YesLay Member for Patient and Public Involvement
Phanuel Mutumburi Business and Operations Director for Ipswich and Suffolk Council for Racial Equality (ISCRE)Partnership project between ISCRE and IESCCG for support for the BAME health and wellbeing programme
Direct 2020 Ongoing
26/04/2022 To be declared as necessary Yes
Finance Director for the Suffolk Law Centre Direct Ongoing 26/04/2022 To be declared as necessary YesBoard Member for Gecko Theatre Indirect Aug-21 Ongoing 26/04/2021 No further action required Yes
Director of Nursing Lisa Nobes Nil 26/04/2022 YesGoverning Body GP Member Omololu Ogunniyi Partner at Burlington Road Surgery Direct Ongoing 27/04/2022 To be declared as necessary Yes
Self employed GP with Suffolk GP Federation Direct Ongoing 27/04/2022 To be declared as necessary YesDirector of Parakletus Life, limited company Direct 2015 Ongoing 27/04/2022 To be declared as necessary Yes
Director of Finance Jane Payling Director of Finance for Ipswich and East Suffolk CCG and North East Essex CCG Direct 25/09/2017 Ongoing 21/04/2022 To declare when appropriate YesTrustee of Cambridge Theatre Trust Direct Oct-18 Ongoing 21/04/2022 To declare when appropriate YesMember of Cambridge Regional College Finance Committee Direct Nov-21 Ongoing 21/04/2022 To declare when appropriate
Governing Body GP Member Imran Qureshi Partner at Leiston Surgery. Member of Suffolk GP Federation Direct Ongoing 01/11/2021 To be declared as necessary YesLeiston Surgery is part dispensing Direct Ongoing 01/11/2021 To be declared as necessary YesLeiston Surgery is a partner in the local research network Direct Ongoing 01/11/2021 To be declared as necessary YesLeiston Surgery provides training for UEA and Cambridge medical students Direct Ongoing 01/11/2021 No further action required YesIpswich and East Suffolk CCG Clinical Executive Chair. Direct Ongoing 01/11/2021 No further action required YesLeiston Surgery is part of PCN. Direct 01/06/2019 Ongoing 01/11/2021 To be declarecd when necessarty YesLeiston Surgery provides health care services for Practice Plus Group Health and Rehabilitation Services Limited at HMPs Hollesly Bay and Warren Hill
Direct 01/06/2020 Ongoing 01/11/2021 To be declared as necessaryYes
CCG Chair Mark Shenton Salaried Doctor and Board Member of Suffolk Primary Care Direct Ongoing 04/04/2022 To be declared as necessary YesProfessor of Integrated Care at University of Suffolk Direct Ongoing 04/04/2022 No further action YesWife (Dr Carrie Everitt) is a partner at Hadleigh PMS practice and a director of Hadleigh Health Ltd and Mill Pharm Ltd Indirect Ongoing 04/04/2022 To be declared as necessary Yes
Practice participates in research ethics approved GSK clinical trial. Direct 01/09/2018 Ongoing 04/04/2022 To be declared as necessary YesDirector of Stowhealth Holdings Ltd, a non-trading company holding shares in Virt Turi, a joint venture with Orbital Media to develop Avatar technology
Direct 01/09/2018 Ongoing 04/04/2022 To be declared as necessary Yes
Suffolk primary care has agreed to renew its 12 month cluster contract to delivery clinical research studies. The contract provides financial assistance towards recruitment of a research nurse and research administrator
Direct Ongoing 04/04/2022 To be declared as necessary Yes
SPC Chair has a private small shareholding in L&R Pharmacy Direct Ongoing 04/04/2022 To be declared as necessary YesVirt Turi Clinical Advisory Board Member (unpaid) Direct Ongoing 04/04/2022 To be declared as necessary Yes
Sub Committee GP Member Ben Solway Partner in GP Surgery Dr Solway and Mallick Direct 20/06/1905 Ongoing 12/10/2021 To declare when appropriate YesWife volunteers for MNDA Indirect Ongoing 12/10/2021 No further action required Yes
Governing Body GP Member Ayesha Tu Zahra Associate Dean GP Trainees and Workforce across SNEE Direct Ongoing 04/04/2022 To be declared when necessary YesHusband Specialist Doctor in Obs and Gynae Indirect Ongoing 04/04/2022 To be declared when necessary YesCD Ipswich North East PCNPartner at Two Rivers Medical PracticeTwo Rivers medical Practices is a partner in the local research networkPractice has medical students from UEATwo Rivers Provides training to GP trainees, nursing students, PA and medical students
Direct Ongoing 04/04/2022 To be declared when necessary Yes
Director of Strategy and Transformation Richard Watson Director of Strategy and Transformation for Ipswich and East Suffolk, North East Essex CCGs and West Suffolk CCGs Direct Jan-15 Ongoing 01/04/2022 To be declared when necessary YesHusband is employee of Hadleigh Group Practice Direct Oct-19 Ongoing 01/04/2022 To be declared when necessary YesDeputy Chief Executive SNEE CCGs Direct Ongoing 01/04/2022 To be declared when necessary Yes
GP Member VacancyGP Member Vacancy Executive
Ipswich and East Suffolk CCG Governing Body and Sub Committee Members
Direct or Indirect
Date of Interest Date of Receipt Action Taken to Mitigate Consent to
Publish
Declared Interest Type of InterestTitle First Name Last Name
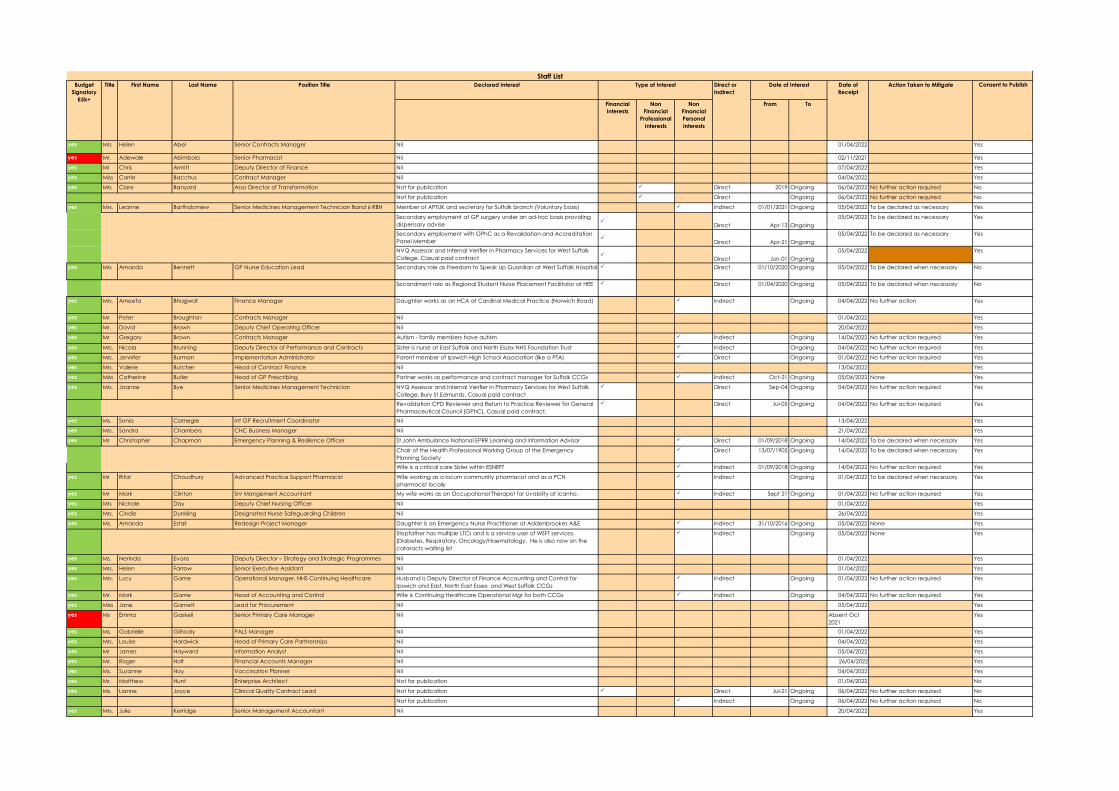
Declared Interest
Financial Interests
Non Financial
Professional Interests
Non Financial Personal Interests
From To
yes Mrs Helen Abel Senior Contracts Manager Nil 01/04/2022 Yes
yes Mr. Adewale Abimbola Senior Pharmacist Nil 02/11/2021 Yes
yes Mr Chris Armitt Deputy Director of Finance Nil 07/04/2022 Yes
yes Miss Carrie Bacchus Contract Manager Nil 04/04/2022 Yes
yes Mrs Clare Banyard Asso Director of Transformation Not for publication Direct 2019 Ongoing 06/04/2022 No further action required No
Not for publication Direct Ongoing 06/04/2022 No further action required No
yes Mrs. Leanne Bartholomew Senior Medicines Management Technician Band 6 RBH Member of APTUK and secretary for Suffolk branch (Voluntary basis) Indirect 01/01/2021 Ongoing 05/04/2022 To be declared as necessary Yes
Secondary employment at GP surgery under an ad-hoc basis providing dispensary advise
Direct Apr-13 Ongoing05/04/2022 To be declared as necessary Yes
Secondary employment with GPhC as a Revalidation and Accreditation Panel Member
Direct Apr-21 Ongoing05/04/2022 To be declared as necessary Yes
NVQ Assessor and Internal Verifier in Pharmacy Services for West Suffolk College. Casual paid contract
Direct Jun-01 Ongoing05/04/2022 Yes
yes Mrs Amanda Bennett GP Nurse Education Lead Secondary role as Freedom to Speak Up Guardian at West Suffolk Hospital Direct 01/10/2020 Ongoing 05/04/2022 To be declared when necessary No
Secondment role as Regional Student Nurse Placement Facilitator at HEE Direct 01/04/2020 Ongoing 05/04/2022 To be declared when necessary No
yes Mrs. Ameeta Bhagwat Finance Manager Daughter works as an HCA at Cardinal Medical Practice (Norwich Road) Indirect Ongoing 04/04/2022 No further action Yes
yes Mr Peter Broughton Contracts Manager Nil 01/04/2022 Yes
yes Mr. David Brown Deputy Chief Operating Officer Nil 20/04/2022 Yes
yes Mr Gregory Brown Contracts Manager Autism - family members have autism Indirect Ongoing 14/04/2022 No further action required Yes
yes Mrs. Nicola Brunning Deputy Director of Performance and Contracts Sister is nurse at East Suffolk and North Essex NHS Foundation Trust Indirect Ongoing 04/04/2022 No further action required Yes
yes Mrs. Jennifer Burman Implementation Administrator Parent member of Ipswich High School Association (like a PTA) Direct Ongoing 01/04/2022 No further action required Yes
yes Mrs. Valerie Butcher Head of Contract Finance Nil 13/04/2022 Yes
yes Miss Catherine Butler Head of GP Prescribing Partner works as performance and contract manager for Suffolk CCGs Indirect Oct-21 Ongoing 05/04/2022 None Yes
yes Mrs. Joanne Bye Senior Medicines Management Technician NVQ Assessor and Internal Verifier in Pharmacy Services for West Suffolk College, Bury St Edmunds. Casual paid contract
Direct Sep-04 Ongoing 04/04/2022 No further action required Yes
Revalidation CPD Reviewer and Return to Practice Reviewer for General Pharmaceutical Council (GPhC). Casual paid contract.
Direct Jul-05 Ongoing 04/04/2022 No further action required Yes
yes Ms. Sonia Carnegie Int GP Recruitment Coordinator Nil 13/04/2022 Yes
yes Mrs. Sandra Chambers CHC Business Manager Nil 21/04/2022 Yes
yes Mr Christopher Chapman Emergency Planning & Resilience Officer St John Ambulance National EPRR Learning and Information Advisor Direct 01/09/2018 Ongoing 14/04/2022 To be declared when necessary Yes
Chair of the Health Professional Working Group of the Emergency Planning Society
Direct 13/07/1905 Ongoing 14/04/2022 To be declared when necessary Yes
Wife is a critical care Sister within ESNEFT Indirect 01/09/2018 Ongoing 14/04/2022 No further action required Yes
yes Mr Rifat Choudhury Advanced Practice Support Pharmacist Wife working as a locum community pharmacist and as a PCN pharmacist locally
Indirect Ongoing 01/04/2022 To be declared when necessary Yes
yes Mr Mark Clinton Snr Mangement Accountant My wife works as an Occupational Therapist for Livability at Icanho. Indirect Sept 21 Ongoing 01/04/2022 No further action required Yes
yes Mrs Nichole Day Deputy Chief Nursing Officer Nil 01/04/2022 Yes
yes Mrs. Cindie Dunkling Designated Nurse Safeguarding Children Nil 26/04/2022 Yes
yes Ms. Amanda Estall Redesign Project Manager Daughter is an Emergency Nurse Practitioner at Addenbrookes A&E Indirect 31/10/2016 Ongoing 05/04/2022 None Yes
Stepfather has multiple LTCs and is a service user of WSFT services. (Diabetes, Respiratory, Oncology/Haematology. He is also now on the cataracts waiting list
Indirect Ongoing 05/04/2022 None Yes
yes Ms. Nerinda Evans Deputy Director – Strategy and Strategic Programmes Nil 01/04/2022 Yes
yes Mrs. Helen Farrow Senior Executive Assistant Nil 01/04/2022 Yes
yes Mrs. Lucy Game Operational Manager, NHS Continuing Healthcare Husband is Deputy Director of Finance Accounting and Control for Ipswich and East, North East Essex and West Suffolk CCGs
Indirect Ongoing 01/04/2022 No further action required Yes
yes Mr. Mark Game Head of Accounting and Control Wife is Continuing Healthcare Operational Mgr for both CCGs Indirect Ongoing 04/04/2022 No further action required Yes
yes Miss Jane Garnett Lead for Procurement Nil 05/04/2022 Yes
yes Ms Emma Gaskell Senior Primary Care Manager Nil Absent Oct 2021
Yes
yes Ms. Gabrielle Gilhooly PALS Manager Nil 01/04/2022 Yes
yes Mrs. Louise Hardwick Head of Primary Care Partnerships Nil 04/04/2022 Yes
yes Mr James Hayward Information Analyst Nil 05/04/2022 Yes
yes Mr. Roger Holt Financial Accounts Manager Nil 26/04/2022 Yes
yes Ms. Suzanne Hoy Vaccination Planner Nil 04/04/2022 Yes
yes Mr. Matthew Hunt Enterprise Architect Not for publication 01/04/2022 No
yes Ms. Lianne Joyce Clinical Quality Contract Lead Not for publication Direct Jul-21 Ongoing 06/04/2022 No further action required No
Not for publication Indirect Ongoing 06/04/2022 No further action required No
yes Mrs. Julie Kerridge Senior Management Accountant Nil 20/04/2022 Yes
Direct or Indirect
Staff ListBudget
Signatory £5k+
Consent to PublishDate of Receipt
Action Taken to MitigateTitle First Name Last Name Type of Interest Date of InterestPosition Title
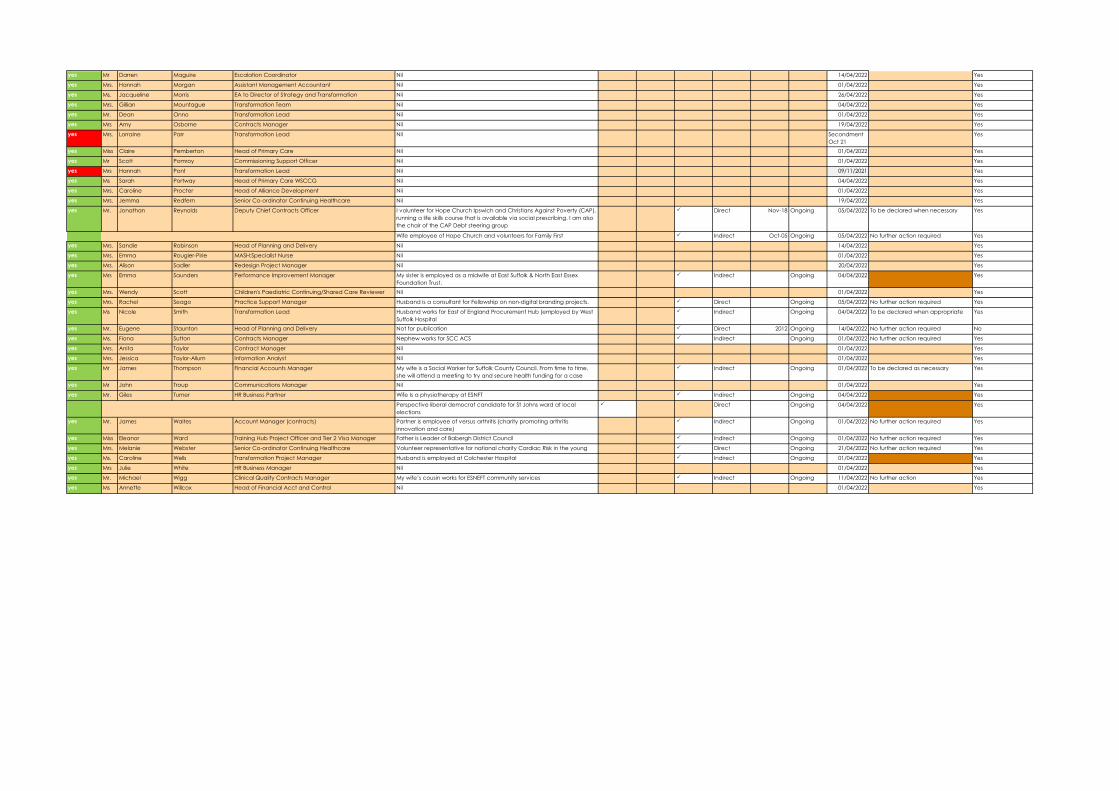
yes Mr Darren Maguire Escalation Coordinator Nil 14/04/2022 Yes
yes Mrs. Hannah Morgan Assistant Management Accountant Nil 01/04/2022 Yes
yes Ms. Jacqueline Morris EA to Director of Strategy and Transformation Nil 26/04/2022 Yes
yes Mrs. Gillian Mountague Transformation Team Nil 04/04/2022 Yes
yes Mr. Dean Onno Transformation Lead Nil 01/04/2022 Yes
yes Mrs Amy Osborne Contracts Manager Nil 19/04/2022 Yes
yes Mrs. Lorraine Parr Transformation Lead Nil Secondment Oct 21
Yes
yes Miss Claire Pemberton Head of Primary Care Nil 01/04/2022 Yes
yes Mr Scott Pomroy Commissioning Support Officer Nil 01/04/2022 Yes
yes Mrs Hannah Pont Transformation Lead Nil 09/11/2021 Yes
yes Ms Sarah Portway Head of Primary Care WSCCG Nil 04/04/2022 Yes
yes Mrs. Caroline Procter Head of Alliance Development Nil 01/04/2022 Yes
yes Mrs. Jemma Redfern Senior Co-ordinator Continuing Healthcare Nil 19/04/2022 Yes
yes Mr. Jonathan Reynolds Deputy Chief Contracts Officer I volunteer for Hope Church Ipswich and Christians Against Poverty (CAP), running a life skills course that is available via social prescribing. I am also the chair of the CAP Debt steering group
Direct Nov-18 Ongoing 05/04/2022 To be declared when necessary Yes
Wife employee of Hope Church and volunteers for Family First Indirect Oct-05 Ongoing 05/04/2022 No further action required Yes
yes Mrs. Sandie Robinson Head of Planning and Delivery Nil 14/04/2022 Yes
yes Mrs. Emma Rougier-Pirie MASH:Specialist Nurse Nil 01/04/2022 Yes
yes Mrs. Alison Sadler Redesign Project Manager Nil 20/04/2022 Yes
yes Mrs Emma Saunders Performance Improvement Manager My sister is employed as a midwife at East Suffolk & North East Essex Foundation Trust.
Indirect Ongoing 04/04/2022 Yes
yes Mrs. Wendy Scott Children's Paediatric Continuing/Shared Care Reviewer Nil 01/04/2022 Yes
yes Mrs. Rachel Seago Practice Support Manager Husband is a consultant for Fellowship on non-digital branding projects. Direct Ongoing 05/04/2022 No further action required Yes
yes Ms Nicole Smith Transformation Lead Husband works for East of England Procurement Hub (employed by West Suffolk Hospital
Indirect Ongoing 04/04/2022 To be declared when appropriate Yes
yes Mr. Eugene Staunton Head of Planning and Delivery Not for publication Direct 2012 Ongoing 14/04/2022 No further action required No
yes Ms. Fiona Sutton Contracts Manager Nephew works for SCC ACS Indirect Ongoing 01/04/2022 No further action required Yes
yes Mrs. Anita Taylor Contract Manager Nil 01/04/2022 Yes
yes Mrs. Jessica Taylor-Allum Information Analyst Nil 01/04/2022 Yes
yes Mr James Thompson Financial Accounts Manager My wife is a Social Worker for Suffolk County Council. From time to time, she will attend a meeting to try and secure health funding for a case
Indirect Ongoing 01/04/2022 To be declared as necessary Yes
yes Mr John Troup Communications Manager Nil 01/04/2022 Yes
yes Mr. Giles Turner HR Business Partner Wife Is a physiotherapy at ESNFT Indirect Ongoing 04/04/2022 Yes
Perspective liberal democrat candidate for St Johns ward at local elections
Direct Ongoing 04/04/2022 Yes
yes Mr. James Waites Account Manager (contracts) Partner is employee of versus arthritis (charity promoting arthritis innovation and care)
Indirect Ongoing 01/04/2022 No further action required Yes
yes Miss Eleanor Ward Training Hub Project Officer and Tier 2 Visa Manager Father is Leader of Babergh District Council Indirect Ongoing 01/04/2022 No further action required Yes
yes Mrs. Melanie Webster Senior Co-ordinator Continuing Healthcare Volunteer representative for national charity Cardiac Risk in the young Direct Ongoing 21/04/2022 No further action required Yes
yes Ms. Caroline Wells Transformation Project Manager Husband is employed at Colchester Hospital Indirect Ongoing 01/04/2022 Yes
yes Mrs Julie White HR Business Manager Nil 01/04/2022 Yes
yes Mr. Michael Wigg Clinical Quality Contracts Manager My wife’s cousin works for ESNEFT community services Indirect Ongoing 11/04/2022 No further action Yes
yes Ms Annette Willcox Head of Financial Acct and Control Nil 01/04/2022 Yes
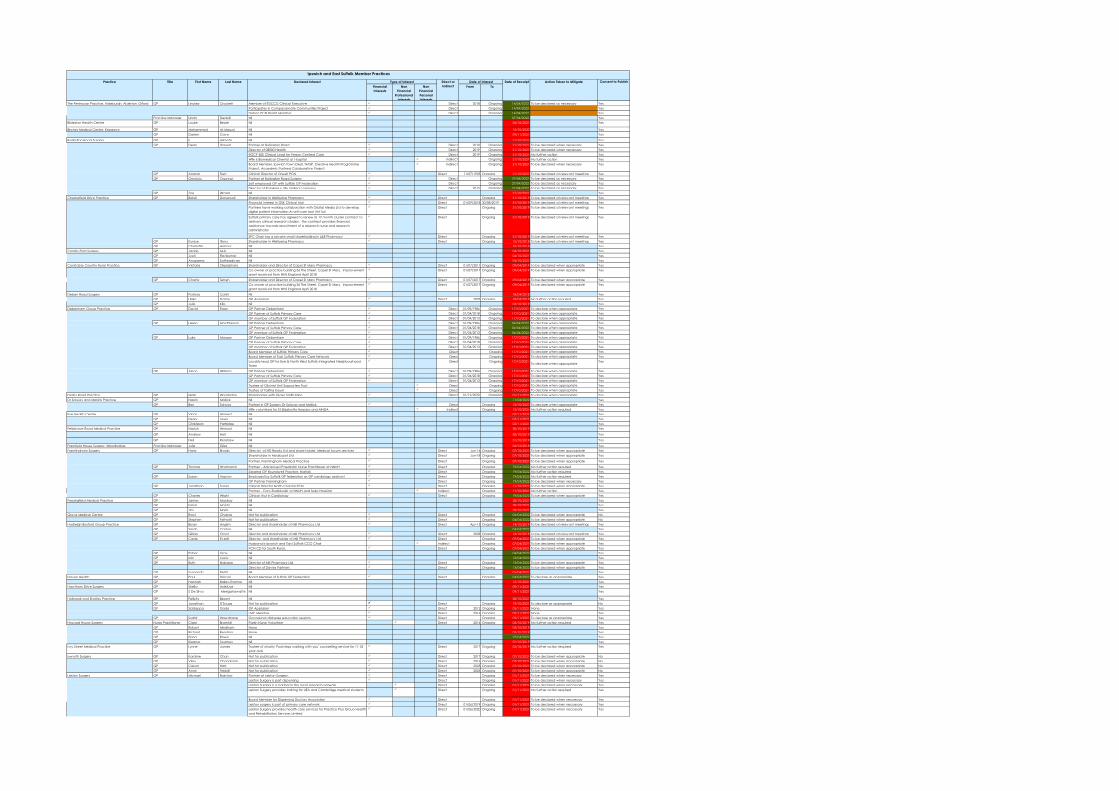
Financial Interests
Non Financial
Professional Interests
Non Financial Personal Interests
From To
The Peninsular Practice, Aldeburgh, Alderton, Orford GP Lindsey Crockett Member of IESCCG Clinical Executive Direct 2018 Ongoing 14/04/2022 To be declared as necessary YesParticipates in Compassionate Communities Project Direct Ongoing 14/04/2022 YesDeben PCN Board Member Direct Ongoing 14/04/2022 Yes
Practice Manager Linda Deabill Nil 07/04/2022 YesBildeston Health Centre GP Louise Beale Nil 06/10/2021 Yes
Birches Medical Centre, Kesgrave GP Mohammed Al-Masud Nil 12/10/2020 YesGP Darren Cave Nil 09/11/2021 Yes
Burlington Road Surgery GP E Alimeta Nil 21/10/2021 YesGP Dean Dorsett Partner at Burlington Road Direct 2010 Ongoing 21/10/2021 To be declared when necessary Yes
Director of 08000 Health Direct 2019 Ongoing 21/10/2021 To be declared when necessary YesRGCP E0E Clinical Lead for Person Centred Care Direct 2019 Ongoing 21/10/2021 No further action YesWife is Biomedical Chemist at Hospital Indirect Ongoing 21/10/2021 No further action YesBoard Member, Ipswich Town Deal, NASP, Creative Health Programme Project, Acaedmic Partners Colaborative Project
Indirect Ongoing 21/10/2021 To be declared when necessary Yes
GP Alastair Flett Clinical Director of Orwell PCN Direct 11/07/1905 Ongoing 21/10/2021 To be declared at relevant meetings YesGP Omololu Ogunniyi Partner at Burlington Road Surgery Direct Ongoing 27/04/2022 To be declared as necessary Yes
Self employed GP with Suffolk GP Federation Direct Ongoing 27/04/2022 To be declared as necessary YesDirector of Parakletus Life, limited company Direct 2015 Ongoing 27/04/2022 To be declared as necessary Yes
GP Zoe Wragg Nil 21/10/2021 YesChesterfield Drive Practice GP Balaji Donepudi Shareholder in Wellbeing Pharmacy Direct Ongoing 31/10/2019 To be declared at relevant meetings Yes
Financial interest in GSK Clinical trial Direct 01/09/2018 30/08/2019 31/10/2019 To be declared at relevant meetings YesPartners have working collaboration with Orbital Media Ltd to develop digital patient information AI self care tool Virt Turi
Direct Ongoing 31/10/2019 To be declared at relevant meetings Yes
Suffolk primary care has agreed to renew its 12 month cluster contract to delivery clinical research studies. The contract provides financial assistance towards recruitment of a research nurse and research administrator
Direct Ongoing 31/10/2019 To be declared at relevant meetings Yes
SPC Chair has a private small shareholding in L&R Pharmacy Direct Ongoing 31/10/2019 To be declared at relevant meetings YesGP Eunice Ifionu Shareholder in Wellbeing Pharmacy Direct Ongoing 15/10/2018 To be declared at relevant meetings YesGP Charlotte Armour Nil 10/10/2018 Yes
Combs Ford Surgery GP Jackie Muir Nil 04/10/2021 YesGP Jyoti Ravikumar Nil 04/10/2021 YesGP Anupama Satheadivan Nil 04/10/2021 Yes
Constable Country Rural Practice GP Victoria Okpiabhele Shareholder and Director of Capel St Mary Pharmacy Direct 01/07/2017 Ongoing 09/04/2019 To be declared when appropriate YesCo-owner of practice building 36 The Street, Capel St Mary. Improvement grant received from NHS England April 2018
Direct 01/07/2017 Ongoing 09/04/2019 To be declared when appropriate Yes
GP Charity Tetteh Shareholder and Director of Capel St Mary Pharmacy Direct 01/07/2017 Ongoing 09/04/2019 To be declared when appropriate YesCo-owner of practice building 36 The Street, Capel St Mary. Improvement grant received from NHS England April 2018
Direct 01/07/2017 Ongoing 09/04/2019 To be declared when appropriate Yes
Deben Road Surgery GP Patricia Cahill Nil 18/04/2018 YesGP Ulrike Datan GP Appraiser Direct 2005 Ongoing 18/04/2018 No further action required YesGP Julie Kite Nil 03/10/2019 Yes
Debenham Group Practice GP David Egan GP Partner Debenham Direct 01/09/1986 Ongoing 17/10/2021 To declare when appropriate YesGP Partner of Suffolk Primary Care Direct 01/04/2018 Ongoing 17/10/2021 To declare when appropriate YesGP member of Suffolk GP Federation Direct 01/04/2013 Ongoing 17/10/2021 To declare when appropriate Yes
GP Helen MacPherson GP Partner Debenham Direct 01/09/1986 Ongoing 04/04/2022 To declare when appropriate YesGP Partner of Suffolk Primary Care Direct 01/04/2018 Ongoing 04/04/2022 To declare when appropriate YesGP member of Suffolk GP Federation Direct 01/04/2013 Ongoing 04/04/2022 To declare when appropriate Yes
GP Luke Morgan GP Partner Debenham Direct 01/09/1986 Ongoing 17/10/2021 To declare when appropriate YesGP Partner of Suffolk Primary Care Direct 01/04/2018 Ongoing 17/10/2021 To declare when appropriate YesGP member of Suffolk GP Federation Direct 01/04/2013 Ongoing 17/10/2021 To declare when appropriate YesBoard Member of Suffolk Primary Care Direct Ongoing 17/10/2021 To declare when appropriate YesBoard Member of East Suffolk Primary Care Network Direct Ongoing 17/10/2021 To declare when appropriate YesLocality lead GP for Eye & North West Suffolk Integrated Neiqhbourhood Team
Direct Ongoing 17/10/2021To declare when appropriate
Yes
GP Alison Williams GP Partner Debenham Direct 01/09/1986 Ongoing 17/10/2021 To declare when appropriate YesGP Partner of Suffolk Primary Care Direct 01/04/2018 Ongoing 17/10/2021 To declare when appropriate YesGP member of Suffolk GP Federation Direct 01/04/2013 Ongoing 17/10/2021 To declare when appropriate YesTrustee of Gilchrist Unit Supporters Trust Direct Ongoing 17/10/2021 To declare when appropriate YesTrustee of Talitha Koum Direct Ongoing 17/10/2021 To declare when appropriate Yes
Derby Road Practice GP Mark Woolterton Shareholder with Glaxo Smith Kline Direct 01/12/2020 Ongoing 01/11/2021 To declare when appropriate YesDr Solway and Mallick Practice GP Nasrin Mallick Nil 11/04/2022 Yes
GP Ben Solway Partner in GP Surgery Dr Solway and Mallick Direct Ongoing 12/10/2021 To declare when appropriate YesWife volunteers for St Elizabeths Hospice and MNDA Indirect Ongoing 12/10/2021 No further action required Yes
Eye Health Centre GP Viqar Ahmed Nil 02/11/2021 YesGP Henry Lewis Nil 02/11/2021 YesGP Christiaan Partridge Nil 02/11/2021 Yes
Felixstowe Road Medical Practice GP Naziuh Ahmad Nil 30/10/2019 Yes
GP Andrew Hall Nil 30/10/2019 Yes
GP Neil Renshaw Nil 31/10/2019 Yes
Framfield House Surgery, Woodbridge Practice Manager Julie Giles Nil 06/12/2018 YesFramlingham Surgery GP Harry Brooks Director of HD Brooks Ltd and share holder. Medical locum services Direct Jun-16 Ongoing 07/10/2021 To be declared when appropriate Yes
Shareholder in Medicspot Ltd Direct Jun-18 Ongoing 07/10/2021 To be declared when appropriate Yes
Partner, Framlingham Medical Practice Direct Ongoing 07/10/2021 To be declared when appropriate Yes
GP Thomas Hindmarch Partner – Advanced Paediatric Nurse Practitioner at NNUH Direct Ongoing 19/04/2022 No further action required YesSalaried GP Roundwell Practice, Norfolk Direct Ongoing 19/04/2022 No further action required Yes
GP Susan Hopton Employed by Suffolk GP federation as GP cardiology assistant Direct Ongoing 19/04/2022 No further action required YesGP Partner Framlingham Direct Ongoing 19/04/2022 To be declared when necessary Yes
GP Jonathan Turner Clinical Director North Coastal PCN Direct Ongoing 11/10/2021 To be declared when appropriate YesPartner - Cons Radiologist at NNUH and Spire Hospital Indirect Ongoing 11/10/2021 No further action Yes
GP Charles Wright Clinical Asst in Cardiology Direct Ongoing 19/04/2022 To be declared when appropriate YesFressingfield Medical Practice GP James Mackay Nil 28/10/2021 Yes
GP Faisal Manto Nil 28/10/2021 YesGP Jim Morris Nil 28/10/2021 Yes
Grove Medical Centre GP Ravji Chabra Not for publication Direct Ongoing 04/04/2022 To be declared when appropriate NoGP Stephen Feltwell Not for publication Direct Ongoing 04/04/2022 To be declared when appropriate No
Hadleigh Boxford Group Practice GP Bryan Anglim Director and shareholder of Mill Pharmacy Ltd Direct Apr-15 Ongoing 14/10/2019 To be declared at relevant meetings YesGP Sarah Caston Nil 04/04/2022 YesGP Gillian Croot Director and shareholder of Mill Pharmacy Ltd Direct 2009 Ongoing 16/10/2019 To be declared at relevant meetings YesGP Carrie Everitt Director and shareholder of Mill Pharmacy Ltd Direct Ongoing 07/04/2021 To be declared when appropriate Yes
Husband is Ipswich and East Suffolk CCG Chair Indirect Ongoing 07/04/2021 To be declared when appropriate YesPCN CD for South Rural, Direct Ongoing 07/04/2021 To be declared when appropriate Yes
GP Esther Gray Nil 04/04/2022 YesGP Iain Lyons Nil 13/04/2022 YesGP Ruth Nabarro Director of Mill Pharmacy Ltd Direct Ongoing 13/04/2022 To be declared when appropriate Yes
Director of Davies Partners Direct Ongoing 13/04/2022 To be declared when appropriate YesGP Susannah Pettit Nil 01/04/2021 Yes
Haven Health GP Paul Driscoll Board Member of Suffolk GP Federation Direct Ongoing 04/04/2022 To declare as appropriate YesGP Hannah Bailey-Thomas Nil 15/10/2021 Yes
Hawthorn Drive Surgery GP Sheila Adefuye Nil 09/11/2021 YesGP S De Silva Meegahawatte Nil 09/11/2021 Yes
Holbrook and Shotley Practice GP Feliicity Bezant Nil 28/10/2021 YesGP Jonathan D'Souza Not for publication Direct Ongoing 19/10/2021 To declare as appropriate NoGP Siddappa Gada GP Appraiser Direct 2012 Ongoing 03/11/2021 None Yes
LMC Member Direct 2016 Ongoing 03/11/2021 None YesGP Sudhir Wawdhane Occasional diabetes education sessions Direct Ongoing 03/11/2021 To declare as appropriate Yes
Howard House Surgery Nurse Practitioner Clare Bramhill Parish Nurse Volunteer Direct 2016 Ongoing 02/10/2019 No further action required YesGP Robert Mindham None 03/10/2019 YesGP Richard Reading None 03/10/2019 YesGP Fiona Rowe Nil 27/04/2022 YesGP Eleanor Twomey Nil 07/10/2019 Yes
Ivry Street Medical Practice GP Lynne James Trustee of charity 'Footsteps walking with you' counselling service for 11-25 year olds
Direct 2017 Ongoing 02/10/2019 No further action required Yes
Ixworth Surgery GP Karoline Chan Not for publication Direct 2017 Ongoing 07/10/2021 To be declared when appropriate NoGP Vijay Chandraraj Not for publication Direct 2016 Ongoing 07/10/2021 To be declared when appropriate NoGP Calum Hart Not for publication Direct 2005 Ongoing 07/10/2021 To be declared when appropriate NoGP Anne Tebbitt Not for publication Direct 2005 Ongoing 07/10/2021 To be declared when appropriate No
Leiston Surgery GP Michael Bairstow Partner at Leiston Surgery. Direct Ongoing 01/11/2021 To be declared when necessary YesLeiston Surgery is part dispensing Direct Ongoing 01/11/2021 To be declared when necessary YesLeiston Surgery is a partner in the local research network Direct Ongoing 01/11/2021 To be declared when neccesary YesLeiston Surgery provides training for UEA and Cambridge medical students Direct Ongoing 01/11/2021 No further action required Yes
Board Member for Dispensing Doctors Association Direct Ongoing 01/11/2021 To be declared when neccesary YesLeiston surgery is part of primary care network Direct 01/06/2019 Ongoing 01/11/2021 To be declared when neccesary YesLeiston Surgery provides health care services for Practice Plus Grouo Health and Rehabilitation Services Limited
Direct 01/06/2020 Ongoing 01/11/2021 To be declared when neccesary Yes
Ipswich and East Suffolk Member Practices
Practice First Name Last Name Declared Interest Type of Interest Direct or Indirect
Date of Interest Date of Receipt Action Taken to Mitigate Consent to PublishTitle
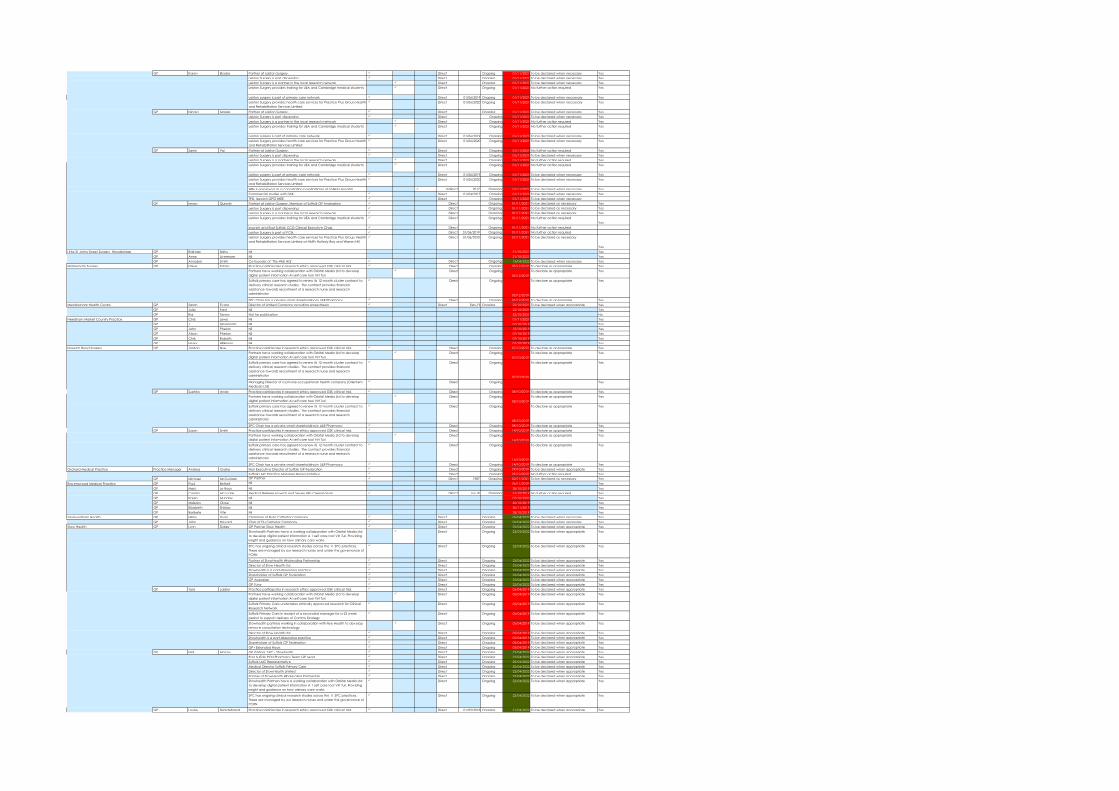
GP Karen Blades Partner at Leiston Surgery. Direct Ongoing 01/11/2021 To be declared when necessary YesLeiston Surgery is part dispensing Direct Ongoing 01/11/2021 To be declared when necessary YesLeiston Surgery is a partner in the local research network Direct Ongoing 01/11/2021 To be declared when necessary YesLeiston Surgery provides training for UEA and Cambridge medical students Direct Ongoing 01/11/2021 No further action required Yes
Leiston surgery is part of primary care network Direct 01/06/2019 Ongoing 01/11/2021 To be declared when neccesary YesLeiston Surgery provides health care services for Practice Plus Grouo Health and Rehabilitation Services Limited
Direct 01/06/2020 Ongoing 01/11/2021 To be declared when neccesary Yes
GP Nicola Maggs Partner at Leiston Surgery. Direct Ongoing 01/11/2021 To be declared when necessary YesLeiston Surgery is part dispensing Direct Ongoing 01/11/2021 To be declared when necessary YesLeiston Surgery is a partner in the local research network Direct Ongoing 01/11/2021 No further action required YesLeiston Surgery provides training for UEA and Cambridge medical students Direct Ongoing 01/11/2021 No further action required Yes
Leiston surgery is part of primary care network Direct 01/06/2019 Ongoing 01/11/2021 To be declared when necessary YesLeiston Surgery provides health care services for Practice Plus Grouo Health and Rehabilitation Services Limited
Direct 01/06/2020 Ongoing 01/11/2021 To be declared when necessary Yes
GP Samir Pai Partner at Leiston Surgery. Direct Ongoing 01/11/2021 No further action required YesLeiston Surgery is part dispensing Direct Ongoing 01/11/2021 To be declared when necessary YesLeiston Surgery is a partner in the local research network Direct Ongoing 01/11/2021 No further action required YesLeiston Surgery provides training for UEA and Cambridge medical students Direct Ongoing 01/11/2021 No further action required Yes
Leiston surgery is part of primary care network Direct 01/06/2019 Ongoing 01/11/2021 To be declared when necessary YesLeiston Surgery provides health care services for Practice Plus Grouo Health and Rehabilitation Services Limited
Direct 01/06/2020 Ongoing 01/11/2021 To be declared when necessary Yes
Wife is employed as a consultation paediatrician at ESNEFT Hosoital. Indirect 2017 Ongoing 01/11/2021 To be declared when necessary YesCommercial studies with GSK. Direct 01/04/2017 Ongoing 01/11/2021 To be declared when necessary YesTPD, lpswich GPST {HEE Direct Ongoing 01/11/2021 To be declared when necessary
GP Imran Qureshi Partner at Leiston Surgery. Member of Suffolk GP Federation Direct Ongoing 01/11/2021 To be declared as necessary YesLeiston Surgery is part dispensing Direct Ongoing 01/11/2021 To be declared as necessary YesLeiston Surgery is a partner in the local research network Direct Ongoing 01/11/2021 To be declared as necessary YesLeiston Surgery provides training for UEA and Cambridge medical students Direct Ongoing 01/11/2021 No further action required
YesIpswich and East Suffolk CCG Clinical Executive Chair. Direct Ongoing 01/11/2021 No further action requiredLeiston Surgery is part of PCN. Direct 01/06/2019 Ongoing 01/11/2021 No further action requiredLeiston Surgery provides health care services for Practice Plus Group Health and Rehabilitation Services Limited at HMPs Hollesly Bay and Warren Hill
Direct 01/06/2020 Ongoing 01/11/2021 To be declared as necessary
YesLittle St Johns Street Surgery, Woodbridge GP Rajinder Sidhu Nil 21/10/2021 Yes
GP Anne Livermore Nil 21/10/2021 YesGP Annabel Smith Co-founder of ‘The Well HQ’ Direct Ongoing 13/04/2022 To be declared when necessary Yes
Martlesham Surgery GP Oliver Tobias Practice participates in research ethics approved GSK clinical trial. Direct Ongoing 05/12/2019 To declare as appropriate YesPartners have working collaboration with Orbital Media Ltd to develop digital patient information AI self care tool Virt Turi
Direct Ongoing05/12/2019
To declare as appropriate Yes
Suffolk primary care has agreed to renew its 12 month cluster contract to delivery clinical research studies. The contract provides financial assistance towards recruitment of a research nurse and research administrator
Direct Ongoing
05/12/2019
To declare as appropriate Yes
SPC Chair has a private small shareholding in L&R Pharmacy Direct Ongoing 05/12/2019 To declare as appropriate YesMendlesham Health Centre GP Sarah Evans Director of Limited Company providing Anaesthesia Direct Feb-19 Ongoing 22/10/2021 To be declared when appropriate Yes
GP Julia Ford Nil 22/10/2021 YesGP Raj Tanna Not for publication 22/10/2021 No
Needham Market Country Practice GP Chris Lewis Nil 01/11/2021 YesGP J Messenger Nil 07/10/2019 YesGP John Phelan Nil 15/10/2019 YesGP Alison Phelan Nil 07/10/2019 YesGP Chris Roberts Nil 07/10/2019 YesGP Henry Wilkinson Nil 07/10/2019 Yes
Norwich Road Surgery GP Jordan Nye Practice participates in research ethics approved GSK clinical trial. Direct Ongoing 07/10/2019 To declare as appropriate YesPartners have working collaboration with Orbital Media Ltd to develop digital patient information AI self care tool Virt Turi
Direct Ongoing07/10/2019
To declare as appropriate Yes
Suffolk primary care has agreed to renew its 12 month cluster contract to delivery clinical research studies. The contract provides financial assistance towards recruitment of a research nurse and research administrator
Direct Ongoing
07/10/2019
To declare as appropriate Yes
Managing Director of a private occupational health company (Orientem Medicals Ltd)
Direct Ongoing Yes
GP Suehita Ande Practice participates in research ethics approved GSK clinical trial. Direct Ongoing 08/10/2019 To declare as appropriate YesPartners have working collaboration with Orbital Media Ltd to develop digital patient information AI self care tool Virt Turi
Direct Ongoing08/10/2019
To declare as appropriate Yes
Suffolk primary care has agreed to renew its 12 month cluster contract to delivery clinical research studies. The contract provides financial assistance towards recruitment of a research nurse and research administrator
Direct Ongoing
08/10/2019
To declare as appropriate Yes
SPC Chair has a private small shareholding in L&R Pharmacy Direct Ongoing 08/10/2019 To declare as appropriate YesGP Susan Smith Practice participates in research ethics approved GSK clinical trial. Direct Ongoing 14/10/2019 To declare as appropriate Yes
Partners have working collaboration with Orbital Media Ltd to develop digital patient information AI self care tool Virt Turi
Direct Ongoing14/10/2019
To declare as appropriate Yes
Suffolk primary care has agreed to renew its 12 month cluster contract to delivery clinical research studies. The contract provides financial assistance towards recruitment of a research nurse and research administrator
Direct Ongoing
14/10/2019
To declare as appropriate Yes
SPC Chair has a private small shareholding in L&R Pharmacy Direct Ongoing 14/10/2019 To declare as appropriate YesOrchard Medical Practice Practice Manager Andrea Clarke Non Executive Director of Suffolk GP Federation Direct Ongoing 29/10/2019 To be declared when appropriate Yes
Suffolk LMC Practice Manager Representative Direct Ongoing 29/10/2019 No further action required YesGP Michael McCullagh GP Partner Direct 1987 Ongoing 02/11/2021 To be declared as necessary Yes
Ravenswood Medical Practice GP Paul Bethell Nil 26/11/2019 YesGP Marc Le Roux Nil 28/10/2019 YesGP Camila McLuckie Medical Referee Ipswich and Seven Hills Crematorium Direct Jul-19 Ongoing 31/10/2019 No further action required YesGP Karen Munday Nil 07/10/2020 YesGP Mojisola Olose Nil 25/10/2019 YesGP Elizabeth Shirlaw Nil 20/11/2019 YesGP Baribefe Vite Nil 28/10/2019 Yes
Saxmundham Health GP Hilary Dunn Chairman of Flute Catheter Company Direct Ongoing 06/04/2022 To be declared when necessary YesGP John Havard Char of Flu Catheter Company Direct Ongoing 06/04/2022 To be declared when necessary Yes
Stow Health GP Lynn Dailey GP Partner Stow Health Direct Ongoing 22/04/2022 To be declared when appropriate YesStowhealth Partners have a working collaboration with Orbital Media Ltd to develop digital patient information A 1 self care tool Virt Turi. Providing insight and guidance on how orimary care works
Direct Ongoing 22/04/2022 To be declared when appropriate Yes
SPC has ongoing clinical research studies across the 11 SPC practices. These are managed by our research nurses and under the governance of PCRN
Direct Ongoing 22/04/2022 To be declared when appropriate Yes
Partner of StowHealth Wholesaling Partnership Direct Ongoing 22/04/2022 To be declared when appropriate YesDirector of Stow Health Ltd Direct Ongoing 22/04/2022 To be declared when appropriate YesStowhealth is a part-dispensing practice Direct Ongoing 22/04/2022 To be declared when appropriate YesShareholder of Suffolk GP Federation Direct Ongoing 22/04/2022 To be declared when appropriate YesGP Appraiser Direct Ongoing 22/04/2022 To be declared when appropriate YesGP Tutor Direct Ongoing 22/04/2022 To be declared when appropriate Yes
GP Tara Laidler Practice participates in research ethics approved GSK clinical trial. Direct Ongoing 05/04/2019 To be declared when appropriate YesPartners have working collaboration with Orbital Media Ltd to develop digital patient information AI self care tool Virt Turi
Direct Ongoing 05/04/2019 To be declared when appropriate Yes
Suffolk Primary Care undertakes ethically approved research for Clinical Research Network
Direct Ongoing 05/04/2019 To be declared when appropriate Yes
Suffolk Primary Care in receipt of a seconded manager for a 23 week period to support delivery of Comms Strategy
Direct Ongoing 05/04/2019 To be declared when appropriate Yes
Stowhealth partners working in collaboration with Nye Health to develop remove consultation technology
Direct Ongoing 05/04/2019 To be declared when appropriate Yes
Director of Stow Health Ltd Direct Ongoing 05/04/2019 To be declared when appropriate YesStowhealth is a part-dispensing practice Direct Ongoing 05/04/2019 To be declared when appropriate YesShareholder of Suffolk GP Federation Direct Ongoing 05/04/2019 To be declared when appropriate YesGP+ Extended Hours Direct Ongoing 05/04/2019 To be declared when appropriate Yes
GP Neil Macey GP Partner, SPC - Stowheath Direct Ongoing 22/04/2022 To be declared when appropriate YesEast Suffolk PCN Pharmacy Team GP Lead Direct Ongoing 22/04/2022 To be declared when appropriate YesSuffolk LMC Representative Direct Ongoing 22/04/2022 To be declared when appropriate YesMedical Director Suffolk Primary Care Direct Ongoing 22/04/2022 To be declared when appropriate YesDirector of StowHealth Limited Direct Ongoing 22/04/2022 To be declared when appropriate YesPartner of StowHealth Wholesaling Partnership Direct Ongoing 22/04/2022 To be declared when appropriate YesStowhealth Partners have a working collaboration with Orbital Media Ltd to develop digital patient information A 1 self care tool Virt Turi. Providing insight and guidance on how orimary care works
Direct Ongoing 22/04/2022 To be declared when appropriate Yes
SPC has ongoing clinical research studies across the 11 SPC practices. These are managed by our research nurses and under the governance of PCRN
Direct Ongoing 22/04/2022 To be declared when appropriate Yes
GP Louise Skioldebrand Practice participates in research ethics approved GSK clinical trial. Direct 01/09/2018 Ongoing 21/04/2022 To be declared when appropriate Yes
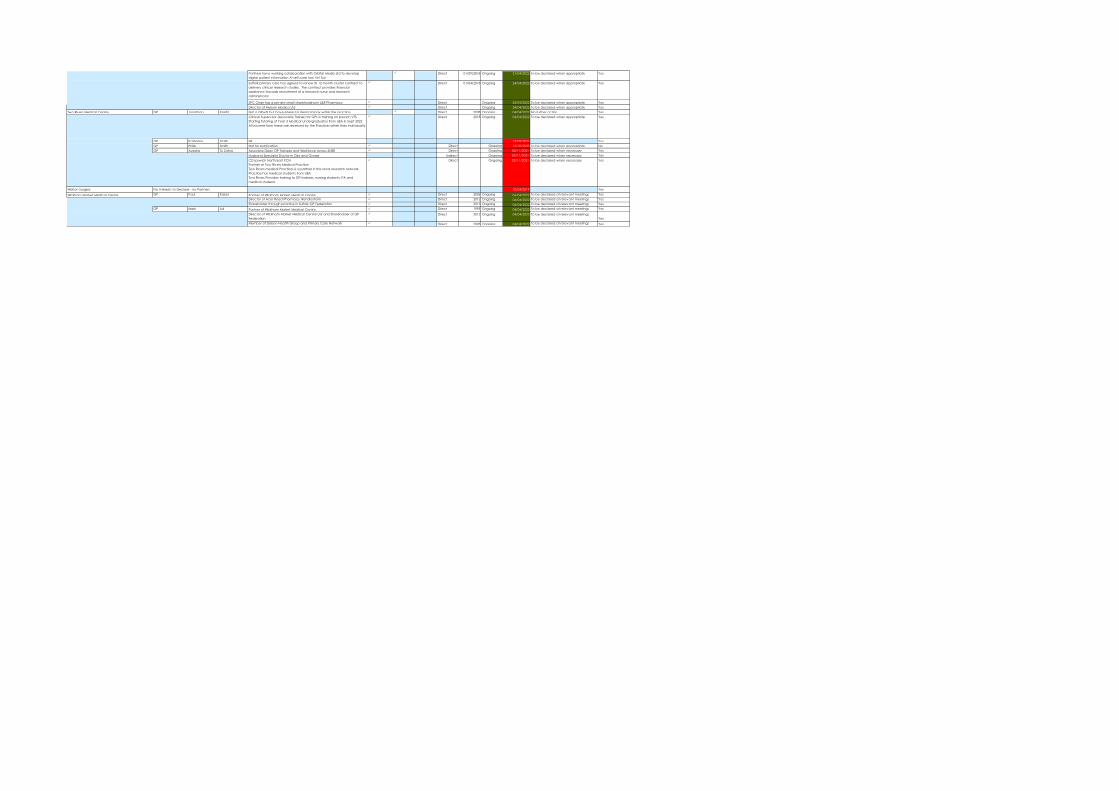
Partners have working collaboration with Orbital Media Ltd to develop digital patient information AI self care tool Virt Turi
Direct 01/09/2018 Ongoing 21/04/2022 To be declared when appropriate Yes
Suffolk primary care has agreed to renew its 12 month cluster contract to delivery clinical research studies. The contract provides financial assistance towards recruitment of a research nurse and research administrator
Direct 01/04/2018 Ongoing 24/04/2022 To be declared when appropriate Yes
SPC Chair has a private small shareholding in L&R Pharmacy Direct Ongoing 24/04/2022 To be declared when appropriate YesDirector of Mysium Medica Ltd Direct Ongoing 24/04/2022 To be declared when appropriate Yes
Two Rivers Medical Centre GP Jonathan Knight Not a GPwSI but have interest in dermatology within the practice Direct 2008 Ongoing 04/04/2022 No further action YesClinical Supervisor (Associate Trainer) for GPs in training on Ipswich VTSStarting Tutoring of Year 3 Medical Undergraduates from UEA in Sept 2022All income from these are received by the Practice rather than individually
Direct 2018 Ongoing 04/04/2022 To be declared when appropriate Yes
GP Katherine Smith Nil 13/05/2021 YesGP Philip Smith Not for publication Direct Ongoing 12/10/2020 To be declared when appropriate NoGP Ayesha Tu Zahra Associate Dean GP Trainees and Workforce across SNEE Direct Ongoing 02/11/2021 To be declared when necessary Yes
Husband Specialist Doctor in Obs and Gynae Indirect Ongoing 02/11/2021 To be declared when necessary YesCD Ipswich North East PCNPartner at Two Rivers Medical PracticeTwo Rivers medical Practices is a partner in the local research networkPractice has medical students from UEATwo Rivers Provides training to GP trainees, nursing students, PA and medical students
Direct Ongoing 02/11/2021 To be declared when necessary Yes
Walton Surgery 10/04/2019 Yes
Wickham Market Medical Centre GP Paul Kaiser Partner of Wickham Market Medical Centre, Direct 2006 Ongoing 06/04/2022 To be declared at relevant meetings YesDirector of Acer Road Pharmacy, Rendlesham Direct 2012 Ongoing 06/04/2022 To be declared at relevant meetings YesShareholder through practice in Suffolk GP Federation Direct 2013 Ongoing 06/04/2022 To be declared at relevant meetings Yes
GP Mark Lal Partner of Wickham Market Medical Centre, Direct 1995 Ongoing 04/04/2022 To be declared at relevant meetings YesDirector of Wickham Market Medical Centre Ltd and Shareholder of GP Federation
Direct 2012 Ongoing 04/04/2022 To be declared at relevant meetingsYes
Member of Deben Health Group and Primary Care Network Direct 2003 Ongoing 04/04/2022 To be declared at relevant meetings Yes
No Interests to Declare - no Partners
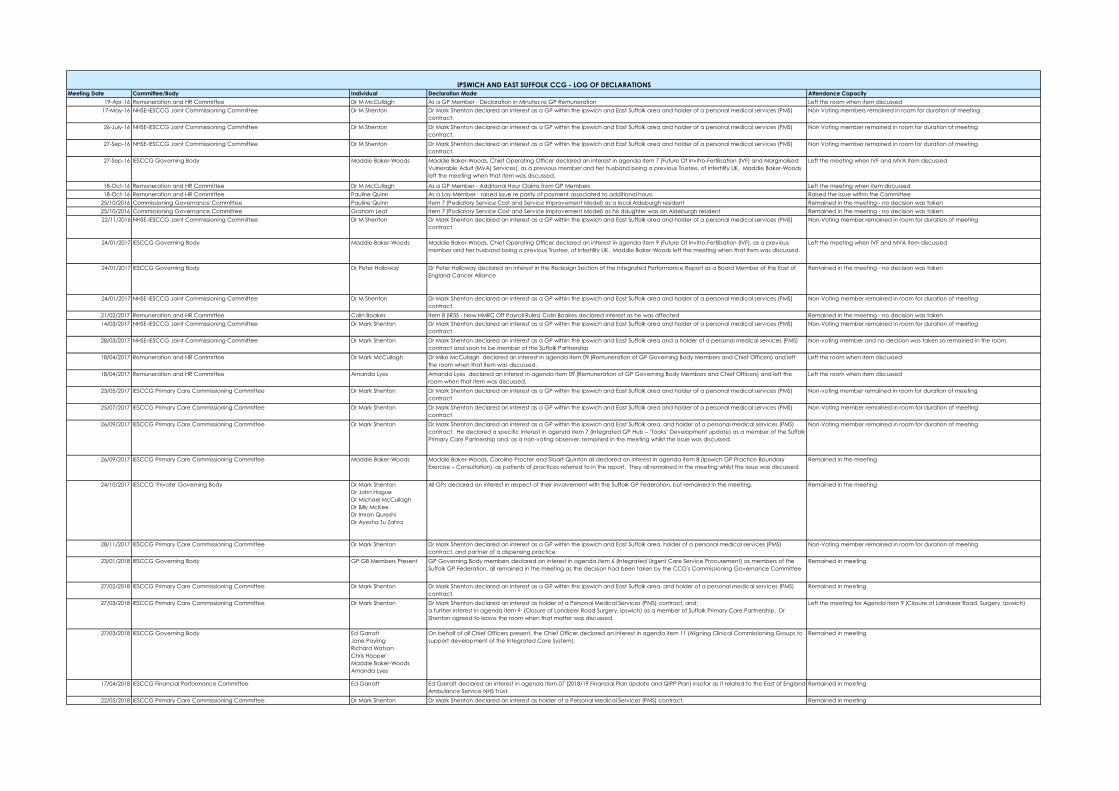
Meeting Date Committee/Body Individual Declaration Made Attendance Capacity19-Apr-16 Remuneration and HR Committee Dr M McCullagh As a GP Member - Declaration in Minutes re GP Remuneration Left the room when item discussed
17-May-16 NHSE-IESCCG Joint Commissioning Committee Dr M Shenton Dr Mark Shenton declared an interest as a GP within the Ipswich and East Suffolk area and holder of a personal medical services (PMS) contract.
Non Voting members remained in room for duration of meeting
26-July-16 NHSE-IESCCG Joint Commissioning Committee Dr M Shenton Dr Mark Shenton declared an interest as a GP within the Ipswich and East Suffolk area and holder of a personal medical services (PMS) contract.
Non Voting member remained in room for duration of meeting
27-Sep-16 NHSE-IESCCG Joint Commissioning Committee Dr M Shenton Dr Mark Shenton declared an interest as a GP within the Ipswich and East Suffolk area and holder of a personal medical services (PMS) contract.
Non Voting member remained in room for duration of meeting
27-Sep-16 IESCCG Governing Body Maddie Baker-Woods Maddie Baker-Woods, Chief Operating Officer declared an interest in agenda item 7 (Future Of Invitro-Fertilisation (IVF) and Marginalised Vulnerable Adult (MVA) Services), as a previous member and her husband being a previous Trustee, of Infertility UK. Maddie Baker-Woods left the meeting when that item was discussed.
Left the meeting when IVF and MVA item discussed
18-Oct-16 Remuneration and HR Committee Dr M McCullagh As a GP Member - Additonal Hour Claims from GP Members Left the meeting when item discussed18-Oct-16 Remuneration and HR Committee Pauline Quinn As a Lay Member - raised issue re parity of payment associated to additional hours Raised the issue within the Committee
25/10/2016 Commissioning Governance Committee Pauline Quinn Item 7 (Podiatory Service Cost and Service Improvement Model) as a local Aldeburgh resident Remained in the meeting - no decision was taken25/10/2016 Commissioning Governance Committee Graham Leaf Item 7 (Podiatory Service Cost and Service Improvement Model) as his daughter was an Aldeburgh resident Remained in the meeting - no decision was taken22/11/2016 NHSE-IESCCG Joint Commissioning Committee Dr M Shenton Dr Mark Shenton declared an interest as a GP within the Ipswich and East Suffolk area and holder of a personal medical services (PMS)
contract. Non-Voting member remained in room for duration of meeting
24/01/2017 IESCCG Governing Body Maddie Baker-Woods Maddie Baker-Woods, Chief Operating Officer declared an interest in agenda item 9 (Future Of Invitro-Fertilisation (IVF), as a previous member and her husband being a previous Trustee, of Infertility UK. Maddie Baker-Woods left the meeting when that item was discussed.
Left the meeting when IVF and MVA item discussed
24/01/2017 IESCCG Governing Body Dr Peter Holloway Dr Peter Holloway declared an interest in the Redesign Section of the Integrated Performance Report as a Board Member of the East of England Cancer Alliance
Remained in the meeting - no decision was taken
24/01/2017 NHSE-IESCCG Joint Commissioning Committee Dr M Shenton Dr Mark Shenton declared an interest as a GP within the Ipswich and East Suffolk area and holder of a personal medical services (PMS) contract.
Non-Voting member remained in room for duration of meeting
21/02/2017 Remuneration and HR Committee Colin Boakes Item 8 (IR35 - New HMRC Off Payroll Rules) Colin Boakes declared interest as he was affected Remained in the meeting - no decision was taken14/03/2017 NHSE-IESCCG Joint Commissioning Committee Dr Mark Shenton Dr Mark Shenton declared an interest as a GP within the Ipswich and East Suffolk area and holder of a personal medical services (PMS)
contract.Non-Voting member remained in room for duration of meeting
28/03/2017 NHSE-IESCCG Joint Commissioning Committee Dr Mark Shenton Dr Mark Shenton declared an interest as a GP within the Ipswich and East Suffolk area and a holder of a personal medical services (PMS) contract and soon to be member of the Suffolk Partnership
Non-voting member and no decision was taken so remained in the room.
18/04/2017 Remuneration and HR Committee Dr Mark McCullagh Dr Mike McCullagh declared an interest in agenda item 09 (Remuneration of GP Governing Body Members and Chief Officers) and left the room when that item was discussed.
Left the room when item discussed
18/04/2017 Remuneration and HR Committee Amanda Lyes Amanda Lyes declared an interest in agenda item 09 (Remuneration of GP Governing Body Members and Chief Officers) and left the room when that item was discussed.
Left the room when item discussed
23/05/2017 IESCCG Primary Care Commissioning Committee Dr Mark Shenton Dr Mark Shenton declared an interest as a GP within the Ipswich and East Suffolk area and holder of a personal medical services (PMS) contract
Non-voting member remained in room for duration of meeting
25/07/2017 IESCCG Primary Care Commissioning Committee Dr Mark Shenton Dr Mark Shenton declared an interest as a GP within the Ipswich and East Suffolk area and holder of a personal medical services (PMS) contract
Non-Voting member remained in room for duration of meeting
26/09/2017 IESCCG Primary Care Commissioning Committee Dr Mark Shenton Dr Mark Shenton declared an interest as a GP within the Ipswich and East Suffolk area, and holder of a personal medical services (PMS) contract. He declared a specific interest in agenda item 7 (Integrated GP Hub – ‘Tooks’ Development update) as a member of the Suffolk Primary Care Partnership and, as a non-voting observer, remained in the meeting whilst the issue was discussed.
Non-Voting member remained in room for duration of meeting
26/09/2017 IESCCG Primary Care Commissioning Committee Maddie Baker-Woods Maddie Baker-Woods, Caroline Procter and Stuart Quinton all declared an interest in agenda item 8 (Ipswich GP Practice Boundary Exercise – Consultation), as patients of practices referred to in the report. They all remained in the meeting whilst the issue was discussed.
Remained in the meeting
24/10/2017 IESCCG 'Private' Governing Body Dr Mark ShentonDr John HagueDr Michael McCullaghDr Billy McKeeDr Imran QureshiDr Ayesha Tu Zahra
All GPs declared an interest in respect of their involvement with the Suffolk GP Federation, but remained in the meeting. Remained in the meeting
28/11/2017 IESCCG Primary Care Commissioning Committee Dr Mark Shenton Dr Mark Shenton declared an interest as a GP within the Ipswich and East Suffolk area, holder of a personal medical services (PMS) contract, and partner of a dispensing practice
Non-Voting member remained in room for duration of meeting
23/01/2018 IESCCG Governing Body GP GB Members Present GP Governing Body members declared an interest in agenda item 6 (Integrated Urgent Care Service Procurement) as members of the Suffolk GP Federation, all remained in the meeting as the decision had been taken by the CCG's Commissioning Governance Committee
Remained in meeting
27/02/2018 IESCCG Primary Care Commissioning Committee Dr Mark Shenton Dr Mark Shenton declared an interest as a GP within the Ipswich and East Suffolk area, and holder of a personal medical services (PMS) contract.
Remained in meeting
27/03/2018 IESCCG Primary Care Commissioning Committee Dr Mark Shenton Dr Mark Shenton declared an interest as holder of a Personal Medical Services (PMS) contract, and;a further interest in agenda item 9 (Closure of Landseer Road Surgery, Ipswich) as a member of Suffolk Primary Care Partnership. Dr Shenton agreed to leave the room when that matter was discussed.
Left the meeting for Agenda item 9 (Closure of Landseer Road, Surgery, Ipswich)
27/03/2018 IESCCG Governing Body Ed GarrattJane PaylingRichard WatsonChris HooperMaddie Baker-WoodsAmanda Lyes
On behalf of all Chief Officers present, the Chief Officer declared an interest in agenda item 11 (Aligning Clinical Commissioning Groups to support development of the Integrated Care System).
Remained in meeting
17/04/2018 IESCCG Financial Performance Committee Ed Garratt Ed Garratt declared an interest in agenda item 07 (2018/19 Financial Plan Update and QIPP Plan) insofar as it related to the East of England Ambulance Service NHS Trust.
Remained in meeting
22/05/2018 IESCCG Primary Care Commissioning Committee Dr Mark Shenton Dr Mark Shenton declared an interest as holder of a Personal Medical Services (PMS) contract. Remained in meeting
IPSWICH AND EAST SUFFOLK CCG - LOG OF DECLARATIONS
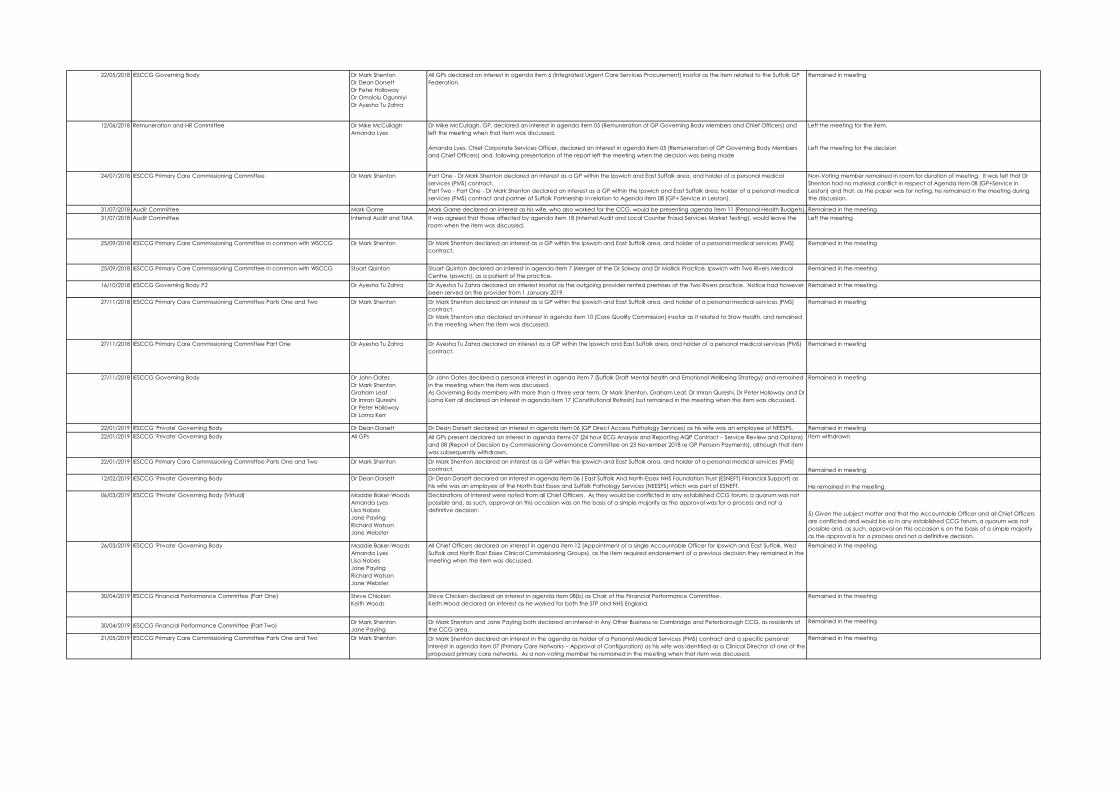
22/05/2018 IESCCG Governing Body Dr Mark ShentonDr Dean DorsettDr Peter HollowayDr Omololu OgunniyiDr Ayesha Tu Zahra
All GPs declared an interest in agenda item 6 (Integrated Urgent Care Services Procurement) insofar as the item related to the Suffolk GP Federation.
Remained in meeting
12/06/2018 Remuneration and HR Committee Dr Mike McCullaghAmanda Lyes
Dr Mike McCullagh, GP, declared an interest in agenda item 05 (Remuneration of GP Governing Body Members and Chief Officers) and left the meeting when that item was discussed.
Amanda Lyes, Chief Corporate Services Officer, declared an interest in agenda item 05 (Remuneration of GP Governing Body Members and Chief Officers) and, following presentation of the report left the meeting when the decision was being made
Left the meeting for the item.
Left the meeting for the decision
24/07/2018 IESCCG Primary Care Commissioning Committee Dr Mark Shenton Part One - Dr Mark Shenton declared an interest as a GP within the Ipswich and East Suffolk area, and holder of a personal medical services (PMS) contract.Part Two - Part One - Dr Mark Shenton declared an interest as a GP within the Ipswich and East Suffolk area, holder of a personal medical services (PMS) contract and partner of Suffolk Partnership in relation to Agenda item 08 (GP+ Service in Leiston).
Non-Voting member remained in room for duration of meeting. It was felt that Dr Shenton had no material conflict in respect of Agenda item 08 (GP+Service in Leiston) and that, as the paper was for noting, he remained in the meeting during the discussion.
31/07/2018 Audit Committee Mark Game Mark Game declared an interest as his wife, who also worked for the CCG, would be presenting agenda item 11 (Personal Health Budgets). Remained in the meeting31/07/2018 Audit Committee Internal Audit and TIAA It was agreed that those affected by agenda item 18 (Internal Audit and Local Counter Fraud Services Market Testing), would leave the
room when the item was discussed.Left the meeting
25/09/2018 IESCCG Primary Care Commissioning Committee in common with WSCCG Dr Mark Shenton Dr Mark Shenton declared an interest as a GP within the Ipswich and East Suffolk area, and holder of a personal medical services (PMS) contract.
Remained in the meeting
25/09/2018 IESCCG Primary Care Commissioning Committee in common with WSCCG Stuart Quinton Stuart Quinton declared an interest in agenda item 7 (Merger of the Dr Solway and Dr Mallick Practice, Ipswich with Two Rivers Medical Centre, Ipswich), as a patient of the practice.
Remained in the meeting
16/10/2018 IESCCG Governing Body P2 Dr Ayesha Tu Zahra Dr Ayesha Tu Zahra declared an interest insofar as the outgoing provider rented premises at the Two Rivers practice. Notice had however been served on the provider from 1 January 2019.
Remained in the meeting
27/11/2018 IESCCG Primary Care Commissioning Committee Parts One and Two Dr Mark Shenton Dr Mark Shenton declared an interest as a GP within the Ipswich and East Suffolk area, and holder of a personal medical services (PMS) contract.Dr Mark Shenton also declared an interest in agenda item 10 (Care Quality Commission) insofar as it related to Stow Health, and remained in the meeting when the item was discussed.
Remained in meeting
27/11/2018 IESCCG Primary Care Commissioning Committee Part One Dr Ayesha Tu Zahra Dr Ayesha Tu Zahra declared an interest as a GP within the Ipswich and East Suffolk area, and holder of a personal medical services (PMS) contract.
Remained in meeting
27/11/2018 IESCCG Governing Body Dr John OatesDr Mark ShentonGraham LeafDr Imran QureshiDr Peter HollowayDr Lorna Kerr
Dr John Oates declared a personal interest in agenda item 7 (Suffolk Draft Mental health and Emotional Wellbeing Strategy) and remained in the meeting when the item was discussed.As Governing Body members with more than a three year term, Dr Mark Shenton, Graham Leaf, Dr Imran Qureshi, Dr Peter Holloway and Dr Lorna Kerr all declared an interest in agenda item 17 (Constitutional Refresh) but remained in the meeting when the item was discussed.
Remained in meeting
22/01/2019 IESCCG 'Private' Governing Body Dr Dean Dorsett Dr Dean Dorsett declared an interest in agenda item 06 (GP Direct Access Pathology Services) as his wife was an employee of NEESPS. Remained in meeting22/01/2019 IESCCG 'Private' Governing Body All GPs All GPs present declared an interest in agenda items 07 (24 hour ECG Analysis and Reporting AQP Contract – Service Review and Options)
and 08 (Report of Decision by Commissioning Governance Committee on 23 November 2018 re GP Pension Payments), although that item was subsequently withdrawn.
Item withdrawn
22/01/2019 IESCCG Primary Care Commissioning Committee Parts One and Two Dr Mark Shenton Dr Mark Shenton declared an interest as a GP within the Ipswich and East Suffolk area, and holder of a personal medical services (PMS) contract. Remained in meeting
12/02/2019 IESCCG 'Private' Governing Body Dr Dean Dorsett Dr Dean Dorsett declared an interest in agenda item 06 ( East Suffolk And North Essex NHS Foundation Trust (ESNEFT) Financial Support) as his wife was an employee of the North East Essex and Suffolk Pathology Services (NEESPS) which was part of ESNEFT. He remained in the meeting.
06/03/2019 IESCCG 'Private' Governing Body (Virtual) Maddie Baker-WoodsAmanda LyesLisa NobesJane PaylingRichard WatsonJane Webster
Declarations of interest were noted from all Chief Officers. As they would be conflicted in any established CCG forum, a quorum was not possible and, as such, approval on this occasion was on the basis of a simple majority as the approval was for a process and not a definitive decision. 5) Given the subject matter and that the Accountable Officer and all Chief Officers
are conflicted and would be so in any established CCG forum, a quorum was not possible and, as such, approval on this occasion is on the basis of a simple majority as the approval is for a process and not a definitive decision.
26/03/2019 IESCCG 'Private' Governing Body Maddie Baker-WoodsAmanda LyesLisa NobesJane PaylingRichard WatsonJane Webster
All Chief Officers declared an interest in agenda item 12 (Appointment of a single Accountable Officer for Ipswich and East Suffolk, West Suffolk and North East Essex Clinical Commissioning Groups), as the item required endorsement of a previous decision they remained in the meeting when the item was discussed.
Remained in the meeting
30/04/2019 IESCCG Financial Performance Committee (Part One) Steve ChickenKeith Woods
Steve Chicken declared an interest in agenda item 08(b) as Chair of the Financial Performance Committee.Keith Wood declared an interest as he worked for both the STP and NHS England.
Remained in the meeting
30/04/2019 IESCCG Financial Performance Committee (Part Two) Dr Mark ShentonJane Payling
Dr Mark Shenton and Jane Payling both declared an interest in Any Other Business re Cambridge and Peterborough CCG, as residents of the CCG area.
Remained in the meeting
21/05/2019 IESCCG Primary Care Commissioning Committee Parts One and Two Dr Mark Shenton Dr Mark Shenton declared an interest in the agenda as holder of a Personal Medical Services (PMS) contract and a specific personal interest in agenda item 07 (Primary Care Networks – Approval of Configuration) as his wife was identified as a Clinical Director of one of the proposed primary care networks. As a non-voting member he remained in the meeting when that item was discussed.
Remained in the meeting
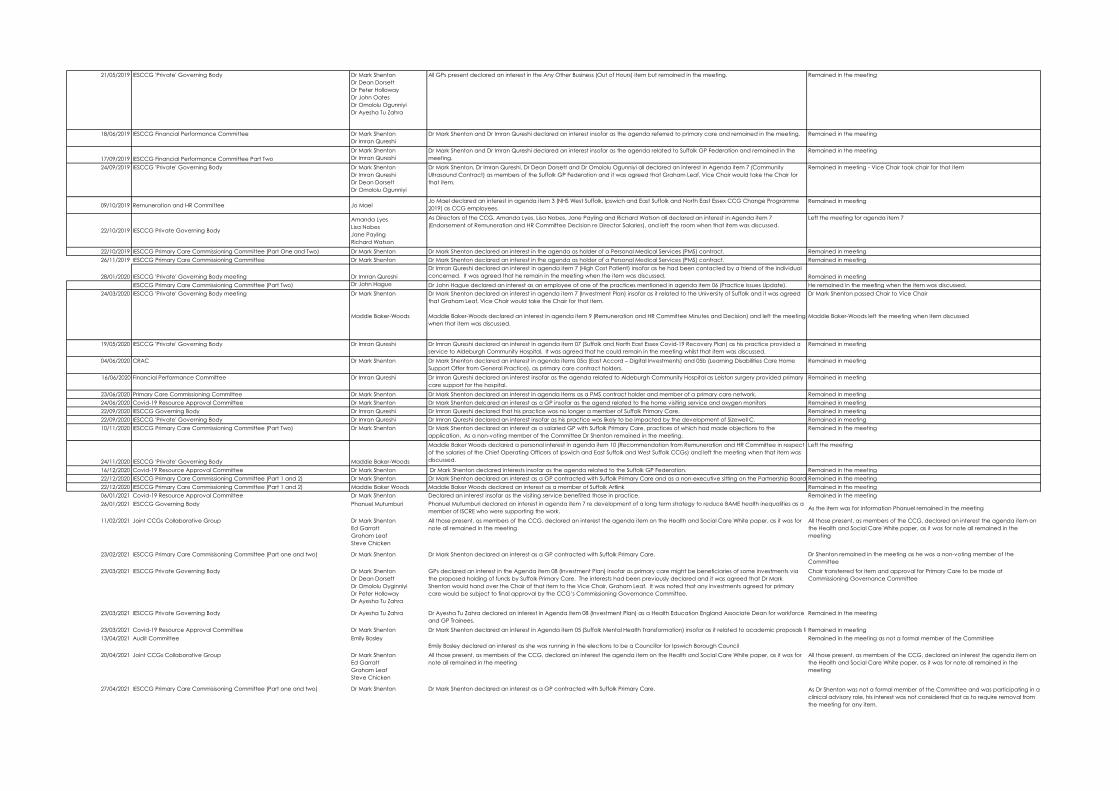
21/05/2019 IESCCG 'Private' Governing Body Dr Mark ShentonDr Dean DorsettDr Peter HollowayDr John OatesDr Omololu OgunniyiDr Ayesha Tu Zahra
All GPs present declared an interest in the Any Other Business (Out of Hours) item but remained in the meeting. Remained in the meeting
18/06/2019 IESCCG Financial Performance Committee Dr Mark ShentonDr Imran Qureshi
Dr Mark Shenton and Dr Imran Qureshi declared an interest insofar as the agenda referred to primary care and remained in the meeting. Remained in the meeting
17/09/2019 IESCCG Financial Performance Committee Part TwoDr Mark ShentonDr Imran Qureshi
Dr Mark Shenton and Dr Imran Qureshi declared an interest insofar as the agenda related to Suffolk GP Federation and remained in the meeting.
Remained in the meeting
24/09/2019 IESCCG 'Private' Governing Body Dr Mark ShentonDr Imran QureshiDr Dean DorsettDr Omololu Ogunniyi
Dr Mark Shenton, Dr Imran Qureshi, Dr Dean Dorsett and Dr Omololu Ogunniyi all declared an interest in Agenda item 7 (Community Ultrasound Contract) as members of the Suffolk GP Federation and it was agreed that Graham Leaf, Vice Chair would take the Chair for that item.
Remained in meeting - Vice Chair took chair for that item
09/10/2019 Remuneration and HR Committee Jo MaelJo Mael declared an interest in agenda item 3 (NHS West Suffolk, Ipswich and East Suffolk and North East Essex CCG Change Programme 2019) as CCG employees.
Remained in meeting
22/10/2019 IESCCG Private Governing Body
Amanda LyesLisa NobesJane PaylingRichard Watson
As Directors of the CCG, Amanda Lyes, Lisa Nobes, Jane Payling and Richard Watson all declared an interest in Agenda item 7 (Endorsement of Remuneration and HR Committee Decision re Director Salaries), and left the room when that item was discussed.
Left the meeting for agenda item 7
22/10/2019 IESCCG Primary Care Commissioning Committee (Part One and Two) Dr Mark Shenton Dr Mark Shenton declared an interest in the agenda as holder of a Personal Medical Services (PMS) contract. Remained in meeting26/11/2019 IESCCG Primary Care Commissioning Committee Dr Mark Shenton Dr Mark Shenton declared an interest in the agenda as holder of a Personal Medical Services (PMS) contract. Remained in meeting
28/01/2020 IESCCG 'Private' Governing Body meeting Dr Imrran QureshiDr Imran Qureshi declared an interest in agenda item 7 (High Cost Patient) insofar as he had been contacted by a friend of the individual concerned. It was agreed that he remain in the meeting when the item was discussed. Remained in meeting
IESCCG Primary Care Commissioning Committee (Part Two) Dr John Hague Dr John Hague declared an interest as an employee of one of the practices mentioned in agenda item 06 (Practice Issues Update). He remained in the meeting when the item was discussed.24/03/2020 IESCCG 'Private' Governing Body meeting Dr Mark Shenton
Maddie Baker-Woods
Dr Mark Shenton declared an interest in agenda item 7 (Investment Plan) insofar as it related to the University of Suffolk and it was agreed that Graham Leaf, Vice Chair would take the Chair for that item.
Maddie Baker-Woods declared an interest in agenda item 9 (Remuneration and HR Committee Minutes and Decision) and left the meeting when that item was discussed.
Dr Mark Shenton passed Chair to Vice Chair
Maddie Baker-Woods left the meeting when item discussed
19/05/2020 IESCCG 'Private' Governing Body Dr Imran Qureshi Dr Imran Qureshi declared an interest in agenda item 07 (Suffolk and North East Essex Covid-19 Recovery Plan) as his practice provided a service to Aldeburgh Community Hospital. It was agreed that he could remain in the meeting whilst that item was discussed.
Remained in meeting
04/06/2020 CRAC Dr Mark Shenton Dr Mark Shenton declared an interest in agenda items 05a (East Accord – Digital Investments) and 05b (Learning Disabilities Care Home Support Offer from General Practice), as primary care contract holders.
Remained in meeting
16/06/2020 Financial Performance Committee Dr Imran Qureshi Dr Imran Qureshi declared an interest insofar as the agenda related to Aldeburgh Community Hospital as Leiston surgery provided primary care support for the hospital.
Remained in meeting
23/06/2020 Primary Care Commissioning Committee Dr Mark Shenton Dr Mark Shenton declared an interest in agenda items as a PMS contract holder and member of a primary care network. Remained in meeting24/06/2020 Covid-19 Resource Approval Committee Dr Mark Shenton Dr Mark Shenton delcared an interest as a GP insofar as the agend related to the home visiting service and oxygen monitors Remained in meeting22/09/2020 IESCCG Governing Body Dr Imran Qureshi Dr Imran Qureshi declared that his practice was no longer a member of Suffolk Primary Care. Remained in meeting22/09/2020 IESCCG 'Private' Governing Body Dr Imran Qureshi Dr Imran Qureshi declared an interest insofar as his practice was likely to be impacted by the development of Sizewell C. Remained in meeting10/11/2020 IESCCG Primary Care Commissioning Committee (Part Two) Dr Mark Shenton Dr Mark Shenton declared an interest as a salaried GP with Suffolk Primary Care, practices of which had made objections to the
application. As a non-voting member of the Committee Dr Shenton remained in the meeting.Remained in the meeting
24/11/2020 IESCCG 'Private' Governing Body Maddie Baker-Woods
Maddie Baker Woods declared a personal interest in agenda item 10 (Recommendation from Remuneration and HR Committee in respect of the salaries of the Chief Operating Officers of Ipswich and East Suffolk and West Suffolk CCGs) and left the meeting when that item was discussed.
Left the meeting
16/12/2020 Covid-19 Resource Approval Committee Dr Mark Shenton Dr Mark Shenton declared interests insofar as the agenda related to the Suffolk GP Federation. Remained in the meeting22/12/2020 IESCCG Primary Care Commissioning Committee (Part 1 and 2) Dr Mark Shenton Dr Mark Shenton declared an interest as a GP contracted with Suffolk Primary Care and as a non-executive sitting on the Partnership Board Remained in the meeting22/12/2020 IESCCG Primary Care Commissioning Committee (Part 1 and 2) Maddie Baker Woods Maddie Baker Woods declared an interest as a member of Suffolk Artlink Remained in the meeting06/01/2021 Covid-19 Resource Approval Committee Dr Mark Shenton Declared an interest insofar as the visiting service benefited those in practice. Remained in the meeting26/01/2021 IESCCG Governing Body Phanuel Mutumburi Phanuel Mutumburi declared an interest in agenda item 7 re development of a long term strategy to reduce BAME health inequalities as a
member of ISCRE who were supporting the work. As the item was for information Phanuel remained in the meeting
11/02/2021 Joint CCGs Collaborative Group Dr Mark ShentonEd GarrattGraham LeafSteve Chicken
All those present, as members of the CCG, declared an interest the agenda item on the Health and Social Care White paper, as it was for note all remained in the meeting
All those present, as members of the CCG, declared an interest the agenda item on the Health and Social Care White paper, as it was for note all remained in the meeting
23/02/2021 IESCCG Primary Care Commisisoning Committee (Part one and two) Dr Mark Shenton Dr Mark Shenton declared an interest as a GP contracted with Suffolk Primary Care. Dr Shenton remained in the meeting as he was a non-voting member of the Committee
23/03/2021 IESCCG Private Governing Body Dr Mark ShentonDr Dean DorsettDr Omololu OyginniyiDr Peter HollowayDr Ayesha Tu Zahra
GPs declared an interest in the Agenda item 08 (Investment Plan) insofar as primary care might be beneficiaries of some investments via the proposed holding of funds by Suffolk Primary Care. The interests had been previously declared and it was agreed that Dr Mark Shenton would hand over the Chair of that item to the Vice Chair, Graham Leaf. It was noted that any investments agreed for primary care would be subject to final approval by the CCG’s Commissioning Governance Committee.
Chair transferred for item and approval for Primary Care to be made at Commissioning Governance Committee
23/03/2021 IESCCG Private Governing Body Dr Ayesha Tu Zahra Dr Ayesha Tu Zahra declared an interest in Agenda item 08 (Investment Plan) as a Health Education England Associate Dean for workforce and GP Trainees.
Remained in the meeting
23/03/2021 Covid-19 Resource Approval Committee Dr Mark Shenton Dr Mark Shenton declared an interest in Agenda item 05 (Suffolk Mental Health Transformation) insofar as it related to academic proposals fr Remained in meeting13/04/2021 Audit Committee Emily Bosley
Emily Bosley declared an interest as she was running in the elections to be a Councillor for Ipswich Borough CouncilRemained in the meeting as not a formal member of the Committee
20/04/2021 Joint CCGs Collaborative Group Dr Mark ShentonEd GarrattGraham LeafSteve Chicken
All those present, as members of the CCG, declared an interest the agenda item on the Health and Social Care White paper, as it was for note all remained in the meeting
All those present, as members of the CCG, declared an interest the agenda item on the Health and Social Care White paper, as it was for note all remained in the meeting
27/04/2021 IESCCG Primary Care Commisisoning Committee (Part one and two) Dr Mark Shenton Dr Mark Shenton declared an interest as a GP contracted with Suffolk Primary Care. As Dr Shenton was not a formal member of the Committee and was participating in a clinical advisory role, his interest was not considered that as to require removal from the meeting for any item.
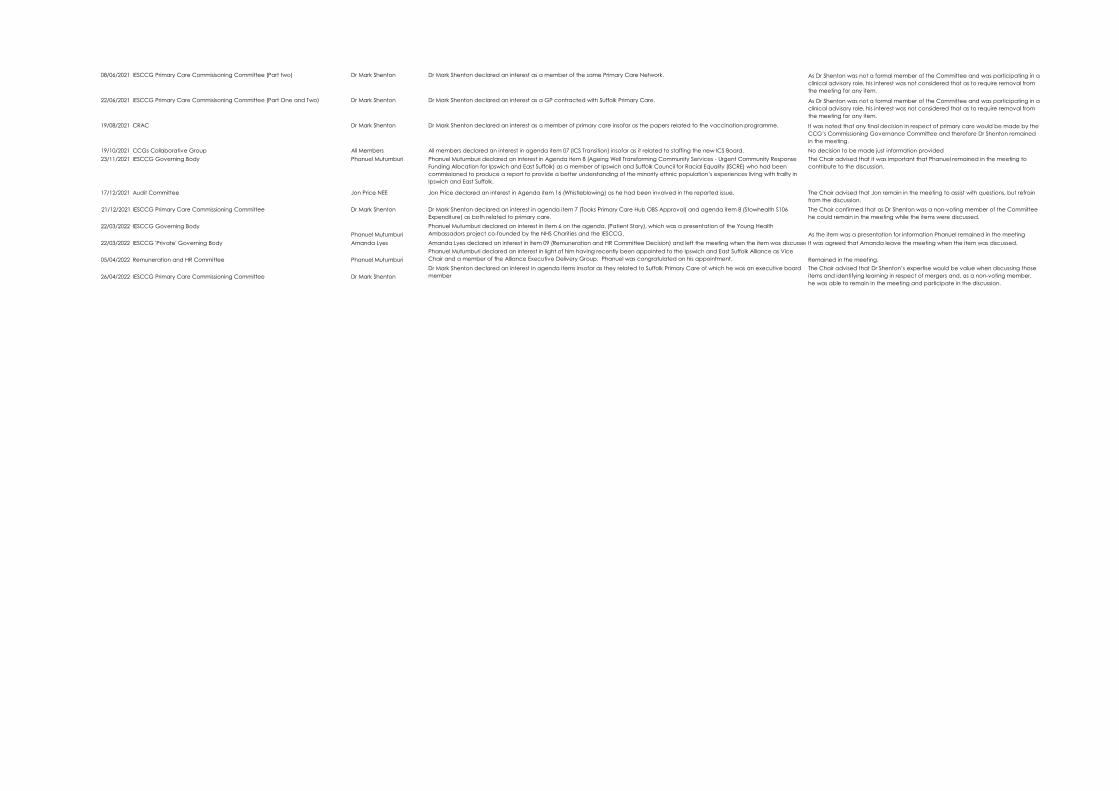
08/06/2021 IESCCG Primary Care Commisisoning Committee (Part two) Dr Mark Shenton Dr Mark Shenton declared an interest as a member of the same Primary Care Network. As Dr Shenton was not a formal member of the Committee and was participating in a clinical advisory role, his interest was not considered that as to require removal from the meeting for any item.
22/06/2021 IESCCG Primary Care Commisisoning Committee (Part One and Two) Dr Mark Shenton Dr Mark Shenton declared an interest as a GP contracted with Suffolk Primary Care. As Dr Shenton was not a formal member of the Committee and was participating in a clinical advisory role, his interest was not considered that as to require removal from the meeting for any item.
19/08/2021 CRAC Dr Mark Shenton Dr Mark Shenton declared an interest as a member of primary care insofar as the papers related to the vaccination programme. It was noted that any final decision in respect of primary care would be made by the CCG’s Commissioning Governance Committee and therefore Dr Shenton remained in the meeting.
19/10/2021 CCGs Collaborative Group All Members All members declared an interest in agenda item 07 (ICS Transition) insofar as it related to staffing the new ICS Board. No decision to be made just information provided23/11/2021 IESCCG Governing Body Phanuel Mutumburi Phanuel Mutumburi declared an interest in Agenda item 8 (Ageing Well Transforming Community Services - Urgent Community Response
Funding Allocation for Ipswich and East Suffolk) as a member of Ipswich and Suffolk Council for Racial Equality (ISCRE) who had been commissioned to produce a report to provide a better understanding of the minority ethnic population’s experiences living with frailty in Ipswich and East Suffolk.
The Chair advised that it was important that Phanuel remained in the meeting to contribute to the discussion.
17/12/2021 Audit Committee Jon Price NEE Jon Price declared an interest in Agenda item 16 (Whistleblowing) as he had been involved in the reported issue. The Chair advised that Jon remain in the meeting to assist with questions, but refrain from the discussion.
21/12/2021 IESCCG Primary Care Commissioning Committee Dr Mark Shenton Dr Mark Shenton declared an interest in agenda item 7 (Tooks Primary Care Hub OBS Approval) and agenda item 8 (Stowhealth S106 Expenditure) as both related to primary care.
The Chair confirmed that as Dr Shenton was a non-voting member of the Committee he could remain in the meeting while the items were discussed.
22/03/2022 IESCCG Governing BodyPhanuel Mutumburi
Phanuel Mutumburi declared an interest in item 6 on the agenda, (Patient Story), which was a presentation of the Young Health Ambassadors project co-founded by the NHS Charities and the IESCCG. As the item was a presentation for information Phanuel remained in the meeting
22/03/2022 IESCCG 'Private' Governing Body Amanda Lyes Amanda Lyes declared an interest in item 09 (Remuneration and HR Committee Decision) and left the meeting when the item was discussedIt was agreed that Amanda leave the meeting when the item was discussed.
05/04/2022 Remuneration and HR Committee Phanuel MutumburiPhanuel Mutumburi declared an interest in light of him having recently been appointed to the Ipswich and East Suffolk Alliance as Vice Chair and a member of the Alliance Executive Delivery Group. Phanuel was congratulated on his appointment. Remained in the meeting.
26/04/2022 IESCCG Primary Care Commissioning Committee Dr Mark ShentonDr Mark Shenton declared an interest in agenda items insofar as they related to Suffolk Primary Care of which he was an executive board member
The Chair advised that Dr Shenton’s expertise would be value when discussing those items and identifying learning in respect of mergers and, as a non-voting member, he was able to remain in the meeting and participate in the discussion.
Page 1 of 5
GOVERNING BODY
Agenda Item No. 15
Reference No. IESCCG 22-24
Date. 24 May 2022
Title
National Staff Survey Results 2021
Lead Director
Amanda Lyes, Interim Director of Workforce, Suffolk and North East Essex Integrated Care System & Director of Corporate Services and System Infrastructure
Author(s)
Ben Askew, Head of People and Culture
Purpose
For Information
Applicable CCG Clinical Priorities:
1. To promote self care
2. To ensure high quality local services where possible *
3. To improve the health of those most in need
4. To improve health and educational attainment for children and young people
5. To improve access to mental health services
6. To improve outcomes for patients with diabetes to above national averages
7. To improve care for frail elderly individuals
8. To allow patients to die with dignity and compassion and to choose their place of death where appropriate
9. To ensure that the CCG operates within agreed budgets
Action required by Governing Body: For information only.
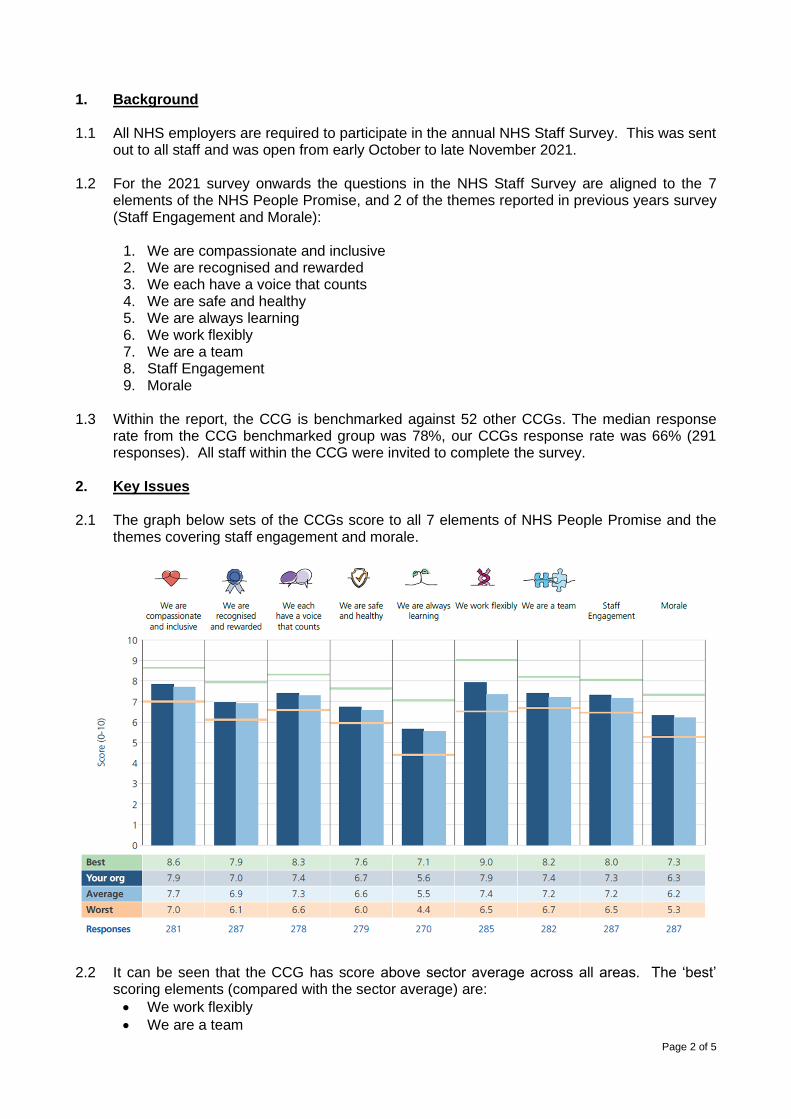
Page 2 of 5
1. Background 1.1 All NHS employers are required to participate in the annual NHS Staff Survey. This was sent
out to all staff and was open from early October to late November 2021. 1.2 For the 2021 survey onwards the questions in the NHS Staff Survey are aligned to the 7
elements of the NHS People Promise, and 2 of the themes reported in previous years survey (Staff Engagement and Morale):
1. We are compassionate and inclusive 2. We are recognised and rewarded 3. We each have a voice that counts 4. We are safe and healthy 5. We are always learning 6. We work flexibly 7. We are a team 8. Staff Engagement 9. Morale
1.3 Within the report, the CCG is benchmarked against 52 other CCGs. The median response
rate from the CCG benchmarked group was 78%, our CCGs response rate was 66% (291 responses). All staff within the CCG were invited to complete the survey.
2. Key Issues 2.1 The graph below sets of the CCGs score to all 7 elements of NHS People Promise and the
themes covering staff engagement and morale.
2.2 It can be seen that the CCG has score above sector average across all areas. The ‘best’
scoring elements (compared with the sector average) are:
• We work flexibly
• We are a team
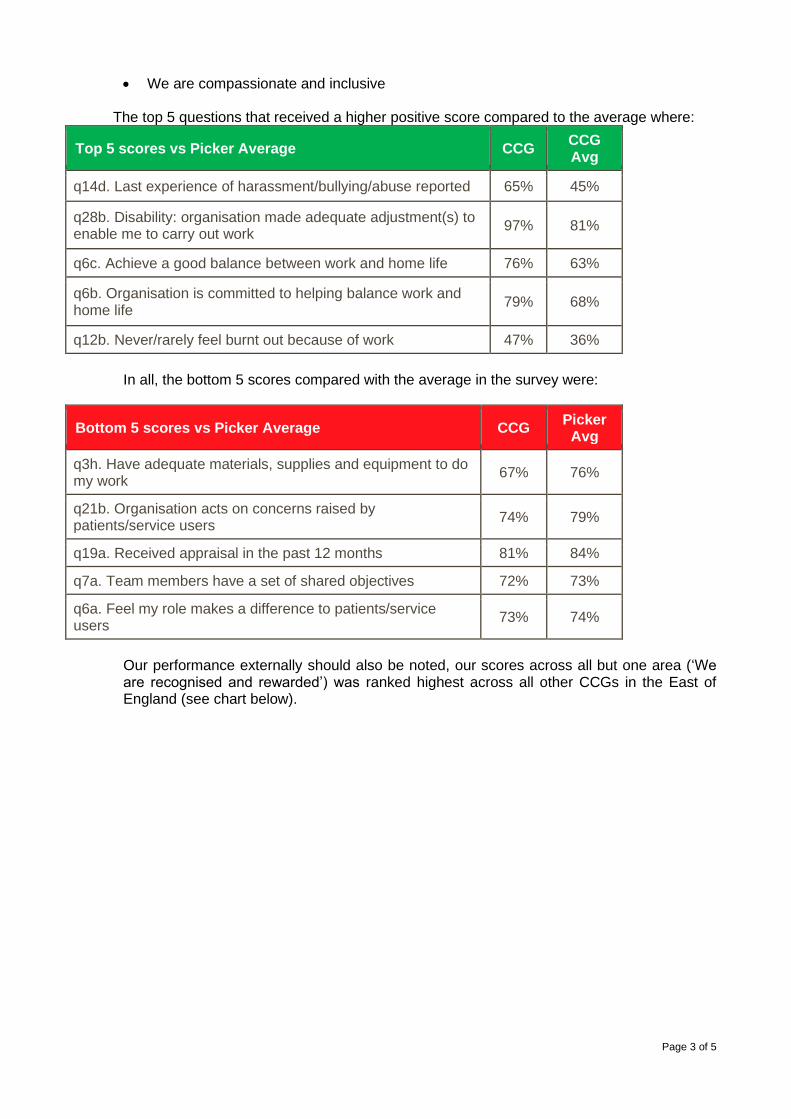
Page 3 of 5
• We are compassionate and inclusive
The top 5 questions that received a higher positive score compared to the average where:
Top 5 scores vs Picker Average CCG CCG Avg
q14d. Last experience of harassment/bullying/abuse reported 65% 45%
q28b. Disability: organisation made adequate adjustment(s) to enable me to carry out work
97% 81%
q6c. Achieve a good balance between work and home life 76% 63%
q6b. Organisation is committed to helping balance work and home life
79% 68%
q12b. Never/rarely feel burnt out because of work 47% 36%
In all, the bottom 5 scores compared with the average in the survey were:
Bottom 5 scores vs Picker Average CCG Picker
Avg
q3h. Have adequate materials, supplies and equipment to do my work
67% 76%
q21b. Organisation acts on concerns raised by patients/service users
74% 79%
q19a. Received appraisal in the past 12 months 81% 84%
q7a. Team members have a set of shared objectives 72% 73%
q6a. Feel my role makes a difference to patients/service users
73% 74%
Our performance externally should also be noted, our scores across all but one area (‘We are recognised and rewarded’) was ranked highest across all other CCGs in the East of England (see chart below).
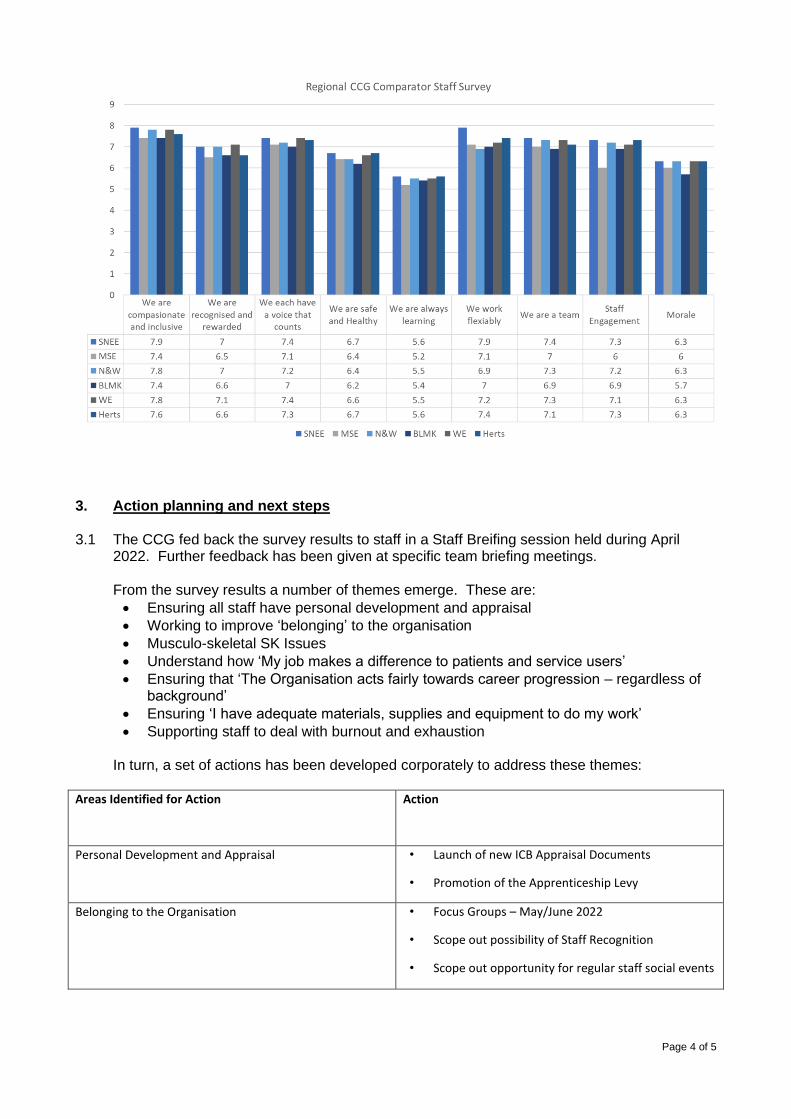
Page 4 of 5
3. Action planning and next steps
3.1 The CCG fed back the survey results to staff in a Staff Breifing session held during April
2022. Further feedback has been given at specific team briefing meetings. From the survey results a number of themes emerge. These are:
• Ensuring all staff have personal development and appraisal
• Working to improve ‘belonging’ to the organisation
• Musculo-skeletal SK Issues
• Understand how ‘My job makes a difference to patients and service users’
• Ensuring that ‘The Organisation acts fairly towards career progression – regardless of background’
• Ensuring ‘I have adequate materials, supplies and equipment to do my work’
• Supporting staff to deal with burnout and exhaustion In turn, a set of actions has been developed corporately to address these themes:
Areas Identified for Action Action
Personal Development and Appraisal • Launch of new ICB Appraisal Documents
• Promotion of the Apprenticeship Levy
Belonging to the Organisation • Focus Groups – May/June 2022
• Scope out possibility of Staff Recognition
• Scope out opportunity for regular staff social events
Page 5 of 5
MSK Issues • ‘Your Back Matters Campaign’
• Promote Physio referral and advice
• Initiatives around equipment set up and use of
equipment
• Exercise initiatives through the Health and
Wellbeing Ambassadors
‘My job makes a difference to patients and service users’ • Better use of intranet to promote patient care
• Discuss at induction (7 steps to patient care)
‘The Organisation acts fairly towards career progression –
regardless of background’
• EDI training
• Staff Networks
• Inclusive recruitment
• Anti-Racism Charter
4. Patient and Public Engagement
4.1 Adverse trends in workforce performance have quality implications for our patients and service users. There is an evidence base1 that improving staff experience and engagement is directly correlated to improved experience and outcomes for patients and service users.
5. Recommendation
5.1 This report is presented for information.
1 Work of Professor Michael West
Page 1 of 2
GOVERNING BODY
Agenda Item No. 16
Reference No. IESCCG 22-25
Date. 24 May 2022
Title
Health and Safety Committee
Lead Director
Amanda Lyes, Director of Corporate Services and System Infrastructure
Author(s)
Tony Buckle, Risk Manager
Purpose
To update the Governing Body on current health and safety issues
Applicable CCG Clinical Priorities:
1. To promote self care
2. To ensure high quality local services where possible
3. To improve the health of those most in need
4. To improve health & educational attainment for children & young people
5. To improve access to mental health services
6. To improve outcomes for patients with diabetes to above national averages
7. To improve care for frail elderly individuals
8. To allow patients to die with dignity & compassion & to choose their place of death where appropriate.
9. To ensure that the CCG operates within agreed budgets
Action required by Governing Body: To note the report.
Page 2 of 2
1. Purpose
To advise the Governing Body of work currently being undertaken in relation to Health & Safety.
2. Background
The Health and Safety Committee, chaired by the Director of Corporate Services and System Infrastructure, continues to meet twice per year. The committee review the H&S annual plan at these meetings to ensure that the CCGs remain compliant with current H&S legislation.
3. Key Points
The last meeting of the committee was on 28 April 2022. Issues reviewed included the following items.
• TB gave an update on the status of the Building User Group meetings. These are continuing and TB agreed to provide an update for the next meeting regarding the frequency and any actions following the ending of Covid restrictions.
• TB went through the updated (2022 – 2023) version of the annual plan. The annual plan will be revised to reflect the closure of the CCGs and the move to an ICB from 1 July 2022.
• There have been no health and safety related incidents since the last meeting.
• The Risk Manager presented the latest HR report which included sickness absence report, the following were highlighted. - Absence due to mental health reasons shows a slight reduction year on year. - The slide for January 2022 shows an increase in respiratory/chest and
colds/coughs/flu absences which may be linked to Covid-19 cases. Following a deep dive, chest/respiratory average duration of sickness has increased from 5 to 8 days year on year.
• This was the last meeting of the Suffolk and North East Essex Health and Safety Committee. All duties and responsibilities will be transferred to the SNEE ICB upon its inception on 1 July 2022.
Page 1 of 47
GOVERNING BODY
Agenda Item No. 17
Reference No. IESCCG 22-26
Date. 24 May 2022
Title Minutes of Meetings
Lead Director Amanda Lyes, Director of Corporate Services and System Infrastructure
Author(s) Jo Mael, Corporate Governance Manager
Purpose Minutes of Meetings:
To receive a report from the Lay Member for Governance seeking the endorsement of minutes and decisions from the following Ipswich and East Suffolk CCG Sub Committees.
a) Audit CommitteeThe unconfirmed minutes of a meeting held on 5 April 2022
b) Remuneration and HR CommitteeThe unconfirmed minutes of a meeting held on 5 April 2022.
c) Financial Performance CommitteeThe minutes of meetings held on 18 January and 15 March 2022
d) Covid-19 Resource Approval CommitteeThe minutes from a meeting held on 16 March 2022
e) Ipswich and East Suffolk CCG Primary Care CommissioningCommitteeThe unconfirmed minutes of a meeting held on 26 April 2022
f) Commissioning Governance CommitteeDecision from a virtual meeting held on 24 March 2022
g) Ipswich and East Suffolk AllianceThe minutes of meetings held on 15 February 2022 and 15 March2022.
Applicable CCG Clinical Priorities:
1. To promote self-care
2. To ensure high quality local services where possible
3. To improve the health of those most in need
Page 2 of 47
4. To improve health & educational attainment for children and young people
5. To improve access to mental health services
6. To improve outcomes for patients with diabetes to above national averages
7. To improve care for frail elderly individuals
8. To allow patients to die with dignity and compassion and to choose their place of death where appropriate.
9. To ensure that the CCG operates within agreed budgets
Action required by Governing Body: To endorse the minutes and decisions as attached to the report whilst noting that ‘unconfirmed’ minutes remain subject to change by the relevant Committee/Group.
Page 3 of 47
Minutes of a Meeting of the Ipswich and East Suffolk Clinical Commissioning Group
Audit Committee held on 5 April 2022
(The meeting was held ‘in common’ with the Audit Committees of North East Essex CCG and West Suffolk CCG)
PRESENT Graham Leaf - Lay Member for Governance (Chair) Phanuel Mutumburi - Lay Member for Patient and Public Involvement IN ATTENDANCE Emily Bosley - Governance Accountant Tony Buckle - Risk Manager (Item 22/028 only) Christopher Chapman - Emergency Preparedness, Resilience, Response Manager Gerald Chanduru - BDO, External Audit Geoff Dobson - Lay Member for Governance, West Suffolk CCG Mark Game - Deputy Director of Finance Satinder Jas - BDO, External Audit Mark Kidd - RSM UK, Local Counter Fraud Specialist Jo Mael - Corporate Governance Manager Dr Mike McCullagh - GP Clinical Executive Member, Ipswich and East Suffolk CCG Jane Payling - Director of Finance Jon Price - Lay Member, North East Essex CCG Emma Seabrook - Corporate Governance Officer Liz Wright - RSM UK, Internal Audit 22/019 WELCOME AND APOLOGIES FOR ABSENCE
The Chair welcomed everyone to the meeting and apologies for absence were received from; Lisa Blake - BDO, External Auditors Colin Boakes - Governance Advisor, Suffolk CCGs Steve Chicken - Lay Member Amanda Lyes - Director of Corporate Services and System Infrastructure
22/020 DECLARATIONS OF INTEREST AND HOSPITALITY AND GIFTS
No declarations of interest were received.
22/021 MINUTES OF PREVIOUS MEETING
The minutes of an Audit Committee meeting held on 15 February 2022 were
approved as a correct record. 22/022 MATTERS ARISING AND REVIEW OF ACTION LOG
There were no matters arising and the action log was reviewed and updated.
Page 4 of 47
22/023 AUDIT SECTOR UPDATE REPORT
The Committee received the Auditor Sector Update report from the External
Auditors. The Committee noted the update.
22/024 EXTERNAL AUDIT PROGRESS REPORT
The Committee was in receipt of the External Audit Progress report, with key
points highlighted being;
• Planning work had been completed across the three CCGs and there was nothing significant to note or raise.
• The Auditors were confident that they had everything in hand to enable the deadline to be met and intended to meet with the Finance Team and be on site more often during the audit.
The need to ensure that there was nothing outstanding at the 10 June 2022 was emphasized. There was an aim to provide the external audit opinion prior to the deadline, although there might be minor items outstanding for resolution prior to sign off. The Committee noted the report.
22/025 DRAFT HEAD OF INTERNAL AUDIT OPINION 2021-22
The Committee was in receipt of the draft Head of Internal Audit Opinion for
2021/22 which was as follows; The organisation had an adequate and effective framework for risk management, governance and internal control. However, our work had identified further enhancements to the framework of risk management, governance and internal control to ensure that it remained adequate and effective. The opinion was a positive opinion and not expected to change unless there were issues identified by external audit. Although the opinion had been presented in draft it was suggested it be used as the basis for the annual governance statement within the annual report. Having queried whether there had been more issues as a result of the pandemic, it was reported that any impact had mainly been seen in operational areas such as continuing healthcare and personal health budgets where staff had been redeployed. New controls in respect of ICB checklists had been introduced. The Committee noted the report.
22/026 INTERNAL AUDIT PROGRESS REPORT
The Committee was in receipt of the current internal audit progress report together
with the following internal audit reports; a) Safeguarding Children – Substantial Assurance b) Personal Health Budgets – Reasonable Assurance c) Continuing Healthcare – Reasonable Assurance d) Conflict of Interest – Reasonable Assurance
Page 5 of 47
e) Patient and Public Involvement – Reasonable Assurance Conflicts of Interest was expected to become more complex within the ICS. Comments included; Having noted that there was reference to some NEECCG provider performance board meeting minutes not having been provided, the Governance Accountant agreed to investigate. Reference to patient and public involvement staff not having access to shared drives was highlighted and it was explained that the issue was ongoing and due to the use of differing systems across CCGs. With regard to actions, it was reported that they were agreed with teams and followed up on a regular basis. Also attached to the report was information on key outcomes from the pandemic with regard to the need for remote working resilience and business continuity. There had, to date, been no confirmation with regard to internal audit requirements for the new organisation and therefore it was proposed that Quarter 1 would consist of the carrying out of mandatory checklists or audits from the Centre as well as top up testing. Quarter 2 work would be dependent on mandatory requirements. It was anticipated that there would be a flexible and pragmatic approach to the use of internal audit time going forward. The Committee noted and accepted the reports.
22/027 LOCAL COUNTER FRAUD PROGRESS REPORT
The Committee was in receipt of the Local Counter Fraud Work Plan and
Progress Report, key points highlighted included;
• The Counter Fraud Functional Standard return was due by 31 May 2022. Audit Committee Chairs would be approached to complete sign off mid May 2022.
• There was a need to adhere to the 12 functional standards set out within the plan.
• Training – there was some flexibility with key areas being the ICB senior leadership team and continuing healthcare team, together with a local exercise regarding recruitment and key employment checks. There was also a blank exercise set aside for use when the ICB commenced.
The differing allocated resource days between CCGs of 12.5 for Suffolk CCGs and 25 for North East Essex CCG was queried. It was explained they were determined as part of the tender process but could be utilised across the CCGs. With regard to investigations, there had been two West Suffolk referrals, one in relation to continuing healthcare payments and the other due to over charges on the CCGs credit card by a supplier. The Committee approved the workplan and noted the report.
22/028 TIMETABLE FOR PRODUCTION OF ANNUAL REPORT AND ACCOUNTS
The report sought to update the Committee on the production timetable and
governance processes in relation to the year-end accounts and annual report.
Page 6 of 47
As in previous years we propose to hold an informal Audit Committee to review the accounts prior to their submission to the auditors and NHS England in draft. The timetable in Section 2 of the report had been designed to give the Governing Body the chance to review the accounts and the annual reports in their draft state, make any comments or recommended changes and allow time for those to be actioned. There was then a second opportunity for the Audit Committee to review, prior to the formally recommending the accounts and annual reports for signature. The Governing Bodies might then approve the accounts virtually, prior to the audit reports being signed and submission to NHS England. Having noted that there were formal dates for the Governing Body to sign off the accounts and a certain time that signatures were valid, the possible need for an additional Audit Committee was highlighted. It was thought that assuming there were no audit changes required after signature an additional meeting would not be required but should perhaps be in the diary in case it was needed. The Director of Finance agreed to liaise with the Corporate Governance Manager regarding a possible date. Members were reminded that an informal meeting was planned on 25 April 2022 and that details of timings etc would be forthcoming. The Committee noted the report.
22/029 GOVERNING BODY ASSURANCE FRAMEWORK (GBAF) AND RISK
REGISTERS
The Committee was in receipt of the latest Governing Body Assurance Framework (GBAF) and risk registers in order to satisfy itself that appropriate risk management processes were in place. There was one new risk across all three CCGs with regard to Children and Young People and access to mental health services. Having noted that there were two risks on the NEECCG register that had a risk rating the same as the target risk rating, the Risk Manager agreed to investigate and report back to the NEECCG Lay Member for Governance outside of the meeting. The Committee noted the GBAF as presented and was assured of the robustness of risk management processes.
22/030 GOVERNANCE LOGS
Waivers
The Committee received the following waivers of competitive tendering.
127 Survivors in Transition
128 Evolution Recruitment Solutions
129 Green Light Trust
130 Community Discovery
131 NHS Suffolk and North East Essex Intranet
Page 7 of 47
development
132 Procurement of 220 laptops by WAF
133 Ideal (Digital Healthcare Specialists)
134 Barnardo’s Link ‘Families Together’
135 UK Babies – Antenatal Education Classes
And Support Online
136 Suffolk User Forum – Serious Mental Illness
(SMI) Support
Hospitality and Gifts Register . The Committee received the current hospitality and gifts register for review.
The Committee noted the waivers of competitive tendering and hospitality and gifts register as presented and congratulated Emily Bosley on her award
22/031 ICB POLICIES OVERVIEW REPORT
The ICB being formed in July would need various policies to comply with regulations/statute to be prepared and ready for adoption on the first day of the ICB’s operation. A variety of those policies had been prepared and had been reviewed and approved by the Committee in the past. One additional policy in the form of the Emergency Preparedness, Resilience Response (EPRR) policy was provided for review today, as well as an overview of the remaining policies still expected. Additionally, an update on the SFIs and Scheme of Reservation and Delegation was provided. Policies and items for review were detailed in Section 3 of the report.
Points highlighted included;
The EPRR policy would change and adapt going forward.
Having queried whether, as stated in the Standing Financial Instructions, the role of the Audit Committee was to ensure effective systems were in place, or rather to seek assurance that effective systems were in place, the Director of Finance agreed to revise and also ensure that the name of the Committee was consistent throughout.
It was also queried how potential conflicts of interest associated to the Remuneration and HR Committee might be handled within the ICB and set out within the SoRD. The Director of Finance agreed to investigate.
It was noted that the documents would require formal sign off by the ICB at a later date.
The Committee;
1) Approved, subject to minor amendment as discussed, the Suffolk and NorthEast Essex ICB Standing Financial Instructions
2) Approved, subject to minor amendment as discussed, the Suffolk and NorthEast Essex ICB Schedule of Matters Reserved to the ICB and Scheme ofDelegation (SoRD)
3) Approved the principles of working as set out within the attached Suffolk
Page 8 of 47
and North East Essex ICB Emergency Preparedness, Resilience, Response and Business Continuity Policy.
22/032 ANY OTHER BUSINESS AND REFLECTION
No items of other business were received.
22/033 DATE OF NEXT MEETING
An ‘Extraordinary’ meeting was scheduled to take place on 10 June 2022.
Page 9 of 47
Minutes of a meeting of the Ipswich and East Suffolk Clinical Commissioning Group Remuneration and Human Resources Committee Meeting held on Tuesday, 5 April
2022
PRESENT: Graham Leaf Lay Member for Governance (Chair) Steve Chicken Lay Member (Part) Dr Mike McCullagh GP Member Phanuel Mutumburi Lay Member for Patient and Public Involvement
IN ATTENDANCE: Ben Askew Head of Workforce Geoff Dobson Lay Member, West Suffolk CCG Susannah Howard ICS Programme Director, SNEE ICS (Item 22/023 only) Amanda Lyes Director of Corporate Services and System Infrastructure Jo Mael Corporate Governance Manager Giles Turner Head of Workforce Jerry Wedge Lay Member, North East Essex CCG
22/018 WELCOME AND APOLOGIES FOR ABSENCE
The Chair welcomed everyone to the meeting and no apologies for absence were received.
22/019 DECLARATIONS OF INTEREST
Phanuel Mutumburi declared an interest in light of him having recently been appointed to the role of Ipswich and East Suffolk Alliance Vice Chair and a member of the Alliance Executive Delivery Group. Phanuel was congratulated on his appointment.
Members were reminded of the need to declare any hospitality or gifts via completion of the relevant documentation.
22/020 MINUTES OF THE PREVIOUS MEETING
The minutes of the Remuneration and Human Resources Committee meeting held on 15 February 2022 were approved as a correct record.
22/021 MATTERS ARISING AND REVIEW OF THE ACTION LOG
There were no matters arising and the action log was reviewed and updated.
22/022 ANNUAL REVIEW OF TERMS OF REFERENCE
The Committee was in receipt of its terms of reference for annual review.
Part One
Page 10 of 47
The Committee approved its terms of reference as presented.
(The Chair agreed that the CCG Closure and ICS Transition item would be taken next)
22/023 CCG CLOSURE AND ICS TRANSITION UPDATE
Susannah Howard, ICS Programme Director was welcomed to the meeting and proceeded to provide a presentation on progress in respect of transition to the ICS. Key points of the presentation included;
• The SNEE ICS had been one of the first to be established and had apopulation of just over one million which was small compared to otherSystems.
• The ICS had moved on place based working at an early stage and madegood progress to put it in a good place for transition in line with the newlegislation.
• The ICS was working towards a higher ambition with focus on healthequality.
• The presentation provided detail on the Health and Social Care Billtogether with ICS Design Framework principles.
• The presentation included a transition timeline to the ICS being establishedfrom 1 July 2022 and detailed how it was expected ICSs’ should beorganised.
• Detail was provided on the components of the Integrated Care System andthe transition programme.
• A functions and decisions map had been included.
• It was explained that the ICB was an NHS body that had brought otherpartners around the table and the ICP consisted of a range of partnersacross the System.
• Key issues were population accountability and performance accountabilitytogether with Health and Wellbeing.
Comments included;
Having noted that a key element was partnership across the System, it was queried how that might be achieved to ensure partners felt equal and able to contribute to discussions, together with the feasibility of including other wider partners. Whilst the integration programme had been led by the NHS previously the intention was to move to a statutory mechanism of joint partners. Support would be provided to ensure partners were able to be at the table which included resilience work with the voluntary and community sectors. Work was underway to ensure a health and wellbeing focus on wider determinates with Health and Social Care as partners but not always dominating the agenda.
The Committee noted the report.
(Steve Chicken left the meeting)
22/024 WORKFORCE REPORT
The Committee was in receipt of the combined workforce report for Suffolk and North East Essex CCGs. Key points highlighted included;
• Staff Headcount and FTE had increased slowly for three months and wasnow remaining stable.
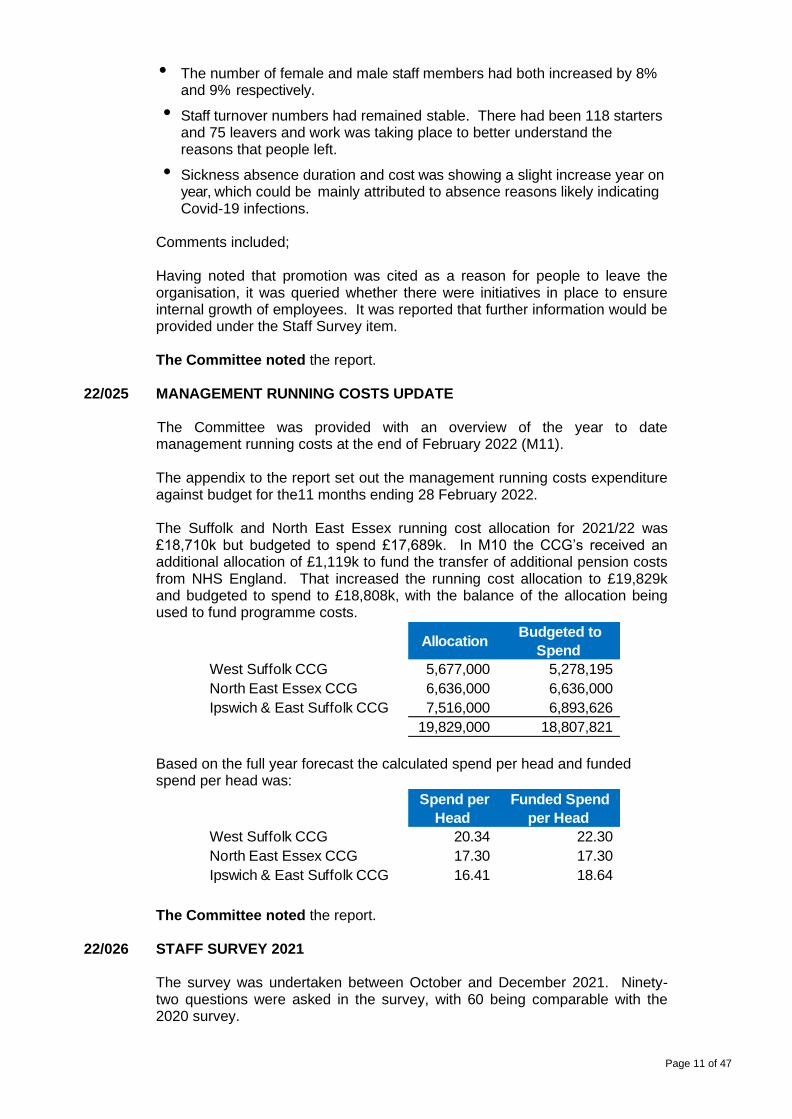
Page 11 of 47
Allocation Budgeted to
Spend
West Suffolk CCG 5,677,000 5,278,195
North East Essex CCG 6,636,000 6,636,000
Ipswich & East Suffolk CCG 7,516,000 6,893,626
19,829,000 18,807,821
Spend per
Head
Funded Spend
per Head
West Suffolk CCG 20.34 22.30
North East Essex CCG 17.30 17.30
Ipswich & East Suffolk CCG 16.41 18.64
• The number of female and male staff members had both increased by 8% and 9% respectively.
• Staff turnover numbers had remained stable. There had been 118 starters and 75 leavers and work was taking place to better understand the reasons that people left.
• Sickness absence duration and cost was showing a slight increase year on year, which could be mainly attributed to absence reasons likely indicating Covid-19 infections.
Comments included; Having noted that promotion was cited as a reason for people to leave the organisation, it was queried whether there were initiatives in place to ensure internal growth of employees. It was reported that further information would be provided under the Staff Survey item. The Committee noted the report.
22/025 MANAGEMENT RUNNING COSTS UPDATE
The Committee was provided with an overview of the year to date
management running costs at the end of February 2022 (M11). The appendix to the report set out the management running costs expenditure against budget for the11 months ending 28 February 2022.
The Suffolk and North East Essex running cost allocation for 2021/22 was £18,710k but budgeted to spend £17,689k. In M10 the CCG’s received an additional allocation of £1,119k to fund the transfer of additional pension costs from NHS England. That increased the running cost allocation to £19,829k and budgeted to spend to £18,808k, with the balance of the allocation being used to fund programme costs.
Based on the full year forecast the calculated spend per head and funded spend per head was: The Committee noted the report.
22/026 STAFF SURVEY 2021
The survey was undertaken between October and December 2021. Ninety-
two questions were asked in the survey, with 60 being comparable with the 2020 survey.
Page 12 of 47
From 2021, NHS England results of the NHS Staff Survey questions were now grouped into seven People Promise elements and against two of the themes reported in previous years results (Staff Engagement and Morale). The CCGs were now reporting as one organisation, whereas the 2020 results were reported as North East Essex and Suffolk. The report went on to detail feedback from the survey and identified actions, with key points highlighted including; The results of the survey had been good compared to other areas which was a result of the organisation having attempted to listen to staff in order to make improvements. Key actions going forward included;
• An aim to be top, not only within the Region but within the Country.
• A need to address the lack of equipment issue which would involve understanding what that meant for different people.
• Attempt to make appraisals more meaningful, by reviewing the documentation and exploring use of the apprenticeship levy.
• Focus Groups – during May/June it was intended that there would be events for teams to get together to discuss work. A series of ICB wide groups were also to take place looking at subjects such as reward and recognition and future ways of working.
• The pursuance of initiatives such as ‘your back matters’
• Work to attempt to identify the impact of people’s roles on patients and service users. Ensure, via induction that staff understood the 7 steps to patient care.
• Facilitate network groups such as the BAME group, and LGBT+ network.
• Flexible working – ensure there was equality in respect of flexible working. The results were welcomed, especially as they had been achieved during difficult and challenging times. It was highlighted that flexible working could create disconnect amongst the workforce and recognised that a hybrid way of working was more beneficial. Induction difficulties were noted in respect of ensuring new colleagues were able to get to know others and know how systems and processes worked. The need to ensure that those with disability received the same focus as other groups was highlighted and it was reported that a Disability Group had just been established. The Committee noted the report.
22/027 POLICIES FOR APPROVAL
No policies were received for approval. 22/028 JOINT STAFF PARTNERSHIP COMMITTEE
The report provided an update on items discussed at a meeting of the Joint
Staff Partnership Committee held on 24 March 2022. The Director of Corporate Services and System Infrastructure reported that the CCGs had recently become the first to sign up to Unison’s Anti-Racism Charter. The Committee noted the report.
Page 13 of 47
22/029 GENDER PAY GAP (SUFFOLK ONLY)
Under the Equality Act 2010 (Gender Pay Gap Information) Regulations 2017,
all employers with 250 or more staff were required to report, on an annual basis, their gender pay gap. The report:
• Provided information on the requirements.
• Set out the gender pay gap and provided some analysis.
• Proposed next steps. Of the 339 people employed by the CCG, as at 31 March 2021, the gender profile within the CCG was 25% male (84 people) and 75% female (255). The CCG was required to submit and publish its Gender Pay Gap by 31 March 2022. It was proposed that our data was published with some brief supporting narrative to confirm:
• That we paid staff in line with nationally agreed NHS pay structures and terms and conditions of employment.
• Some of the factors influencing our data.
• Our compliance with policies and systems to safeguard equal pay, for example, job evaluation and starting salary criteria.
• Our commitment to recruiting and retaining a diverse workforce and paying staff fairly, regardless of gender, in line with contractual requirements.
Having queried how the pay gap had been reduced since 2018, it was explained that had been largely due to attracting increased numbers of female GPs onto the Governing Bodies and changes within the Joint Leadership Team. The Committee noted the report.
22/030 ANY OTHER BUSINESS
No items of other business were received. 22/031
DATE AND TIME OF NEXT MEETING
It was agreed that attempt be made to convene a meeting in June 2022.
Page 14 of 47
Minutes of a Meeting of the Ipswich and East Suffolk CCG
Financial Performance Committee held on Tuesday, 18 January 2022
PRESENT: Steve Chicken Lay Member (Chair) Ed Garratt Chief Executive Dr Mike McCullagh GP Member Jane Payling Director of Finance Dr Imran Qureshi GP Member Dr Mark Shenton CCG Chair IN ATTENDANCE: Chris Armitt Deputy Director of Finance Julie Kerridge Senior Management Accountant Jo Mael Corporate Governance Manager
22/001 WELCOME AND APOLOGIES FOR ABSENCE
No apologies for absence were received. 22/002 DECLARATIONS OF INTEREST HOSPITALITY AND GIFTS
No declarations were received. 22/003 MINUTES OF PREVIOUS MEETING
The minutes of the meeting held on 2 November 2021 were agreed as a correct record. 22/004 MATTERS ARISING AND REVIEW OF ACTION LOG
There were no matters arising and the action log was reviewed and updated.
21/037 - Community Contract discussion – the Director of Finance reported that following discussion with ESNEFT it had been suggested that joint work commence in respect of the Emergency Department (ED). Whilst it was queried whether there was potential for savings within ED, the Committee agreed commencement of work in that area in the first instance.
22/005 CCG FINANCES MONTH 9
The Committee was in receipt of a report that provided detailed information in respect of Month
9 finances. Points highlighted included;
• The CCG had reported a balanced position for Month 9 as per the H2 planning submission.
• In line with the H2 plan, the CCG had required £4.2m of non recurrent benefits in order to offset overspends; £1.8m of prior year, £0.8m of unutilised covid funding, £1.3m unutilised non recurrent funding and £0.3m CHC provision release.
• The CCG had received £3.7m of Hospital Discharge Programme (HDP) and £1.2m Elective
Page 15 of 47
Recovery Fund (ERF) funding. It anticipated further reimbursements of: HDP £1.3m and ERF £0.1m YTD.
• The forecast was in line with the H2 plan once retrospective top-ups have been received. Key variances for Month 9 are:
• Continuing Healthcare showed an overspend of £2.0m once HDP reimbursement had been received. That was due to increased costs of Non HDP patients and backlog of CHC reviews resulting in more patients remaining eligible for longer. In H2 the CHC budgets were reset and current H2 YTD spend was in line with plan. The YTD spend also included a provision release of £0.3m.
• Primary care showed an overspend due the prescribing costs being higher than originally forecast. Those figures used actual PPA data up to M07 and forecasts for M08-09 based on PPA forecast.
• Mental Health showed an overspend due to the forecast shared care with Suffolk County Council being higher than anticipated. Mental Investment slippage had not been factored into the position and the CCG was still forecasting to meet the Mental Health investment standard.
• Primary Care Delegated Commissioning overspent against plan due to the Core GMS contracts higher than plan. That was previously being offset by prior year benefits but due to additional costs from backdated rent reviews that had now diminished.
• Other Programme showed an underspend of £0.9m once the HDP reimbursement had been received. That was due to non-recurrent benefits from prior year being utilised to help balance the position.
• Community Health Services showed an underspend of £1.2m due the utilisation of slippage in the non recurrent schemes
• Acute Services showed a YTD underspend once ERF and HDP had been reimbursed. That was due to underspends in planned care and additional benefits from central ERF calculations.
• Running Costs underspend due to vacancy slippage. The Committee was informed that, as could be seen from detailed information within the report, there was approximately £33.8m additional monies available for the second half of the year through funding streams such as the accelerator and elective discharge funding. However, due to workforce issues and the current Covid-19 response it was challenging to deliver schemes as intended. Comments included; It was questioned whether planning was for a 15 or 12 month year due to the delay associated to transition to the ICB. In response, it was explained that as the CCG was to remain in place until July, or possibly October 2022 there would be a normal full financial year in 21/22 followed by 22/23 being split into two parts. It was anticipated that the first three months of 2022/23 would be a CCG budget with the remainder being ICB. Having queried whether budgets would take the form of those prior to the pandemic or those during the pandemic, it was reported that the current regime would continue with a step move towards normal pre-pandemic budgets. There was indication that CCG allocations for the first three months of 2022/23, whatever the level of spend, would be adjusted in order to breakeven with the balance of the full year allocations being transferred into the new ICB. It was questioned how primary care delegated budgets would be managed and whether they would be managed by the ICB or the Alliances. The Committee was informed that, as much of the budget was fixed, it was likely the majority of costs would be reviewed across the ICB with Alliances reviewing those areas that were variable. Discussion would be required in order to clarify sign off arrangements. There was concern that such discussion had not already taken
Page 16 of 47
place in order to achieve some certainty going forward. With regard to Norfolk and Suffolk NHS Foundation Trust (NSFT) there was concern as to how to ensure future value for money and quality of services. The Committee was informed that NSFT was currently carrying out work to review its baseline and cost of services in order to obtain clarity with regard to the contract. It was recognised that, although the CCGs were commissioners, the debate was likely to be wider as Regulators had previously held a view. It was felt that further information might be required in order to better understand the pressures on the prescribing budget like in light of the uncertainty and changes over the last few years. It was reported that the prescribing team had carried out work in October 2021 to ascertain the current CCG position, but since then had been redeployed to assist the vaccination programme. The Committee requested that the prescribing team be asked to consider some analysis of current pressures and realistic plans for 2022/23 for presentation to the Committee in March 2022. The Director of Finance reported that the Finance Team had been working on a Month 9 set of accounts which could be circulated to members if required. The Committee approved the report.
22/006 ICS FINANCES MONTH 8
Key points highlighted included;
• Balanced financial positions had been reported by all organisations within SNEE with the exception of the East of England Ambulance Service.
• Risks to the delivery of NHS plans included, an increased requirement to deliver efficiency targets, the impact on capacity of RAAC plank replacement at West Suffolk NHS Foundation Trust (WSFT), a redesign of the Elective Recovery Fund scheme which would make it difficult to access recovery funding, the rapidly rising prevalence and impact of Covid 19 and the uncertainty of the extent of influenza and other respiratory disease in winter.
• In light of the rapid rise of the Omicron variant, and its likely impact in January and February 2022, NHSEI had committed to offset any reasonable approved additional revenue expenditure on elective capacity, winter capacity, cancer waits and the vaccination programme.
Comments included; Having highlighted gaps within the mental health information, the Committee was advised that work was taking place with EPUT to ensure consistency across the System and to address the situation for future reports. System working by ESNEFT and the East of England Ambulance NHS Service Trust (EEAST) was recognised and welcomed. Having noted that EEAST was a significant outlier, it was queried whether that was due to agency costs. It was explained that whilst the CCGs were lead commissioner much of the work associated to EEAST was being carried out at regional level in order to get finances back on track. That work included benchmarking and efficiency programmes. The Trust currently had an extremely high level of vacancies due to sickness and vacancies caused by a shortage of staffing. The Trust benchmarked in the middle nationally in respect of absences and similar pressures were replicated in other trusts. The Chief Executive agreed to invite Tom Burton , who is seconded to the Trust to assist with Strategic Planning to the next meeting. When commencing the joint working on the Emergency Department, it was suggested there was a need to consider ambulance handover delays. The Director of Finance agreed to take
Page 17 of 47
the matter forward in those discussions. The Committee noted the report.
22/007 COVID-19 RESOURCES APPROVAL COMMITTEE UPDATE
The Covid-19 Resources Approval Committee was initially set up to cover the period April to
July, that had now been extended to the end of March 2022 to assist decision through the Winter period and support the vaccination programme. The report set out the approvals made from the last detailed report (which was up to 13 October 2021). As requested, approvals had been broken down in terms of approximate value per CCG. It was noted that those values had in some cases been apportioned using usual CCG splits and therefore might not match the final values. From 1 October 2020 the NHS had moved away from central reimbursements to local allocations for Covid and growth, with continuation of central reimbursement for the hospital discharge programme (HDP) and vaccination costs. Additional national funding had been received in 2021/22 for Integrated Urgent Care which had also been approved through the Committee. The Chair advised that oversight of Covid-19 spend should remain with the Committee going forward. The Director of Finance reported that there was currently approval for the Covid-19 Resource Approval Committee to remain in place until the end of March 2022 although that might require extension in light of the transition delay. The Committee noted the approvals made by CRAC on behalf of the Governing Body.
22/008 FINANCIAL PLANNING 2022/23 UPDATE
Key points highlighted with the report included;
• The financial planning process had been delayed, reflecting current covid response and delay to the implementation of Integrated Care Boards.
• Limited information had been released to date with further information expected by mid January 2022.
• Systems were required to submit a single overall plan for the full year with a draft required in March and final plans in April 2022.
• Trusts were required to also submit an organisation level plan.
• Each ICB and its partner trusts must ensure in each financial year that both capital and revenue resources did not exceed the limit set by NHSEI.
• ICBs would have a duty to at least break even individually and collectively with partner Trusts.
• Revenue allocations were to be published for 2022/23 only, draft allocations received but not finalised
• Capital allocations were to be published for three years.
• There was a new fair shares formula at ICS level which included previous Provider Sustainability Funding and replaced CCG pace of change and Trust financial improvement trajectories (FIT).
• Rollover of core system envelopes from months 7 to 12 (H2) 2021/22 adjusted to remove back pay and provider income support.
• Convergence adjustment applied to all systems to move towards underlying national funding. Value was dependent on distance from fair shares and for SNEE was -0.45% which was the second lowest in the region.
• Growth included to reflect 1.7% net tariff increase and other price/activity increases.
• Covid funding reduced by 57%.
• Hospital Discharge Programme (HDP) no longer available.
• Elective Recovery Fund (ERF) still available but significantly changed and further guidance
Page 18 of 47
awaited.
• Core growth net of convergence reduction was 3.7% but after reduction in HDP and covid funding there was actually a reduction in the total expenditure envelope of 0.7% compared to H2 2021/22.
• Delegated Primary Care Allocation increased by 6.6% net of -0.1% convergence reduction to reflect national contractual commitments.
• ICB Running Cost Allowance uplifted only for impact of employer NI increases due to Health & Social Care levy.
The Committee was informed that there used to be non contracted activity where providers invoiced commissioners and during the pandemic that funding went through System top-ups to providers. It was likely that there would now be a step back towards fixed low value activity payments. Comments included; It was reported that capacity funding was an area for future work together with growth and Covid-19 allocations. Work was taking place by planning leads across the System and it was anticipated that an update of progress could be provided in March 2022. The funding regime was a combination of new and old, with overall resources moving back to the System having a fair share. Where funding sat between the CCGs and Trusts, Trust had seen the benefit during the pandemic. It was likely to challenging for CCGs going forward. Having recognised that the CCG was close to its funding target, the position of neighbouring CCGs such as Cambridge and Peterborough was queried and the Director of Finance agreed to make such figures available to the Chief Executive outside of the meeting. There was an expectation that final allocations would be issued soon and then work could commence to timetable draft plans in March, and final submission in April 2022. Overall resources would be tighter and there was a shift between the financial powerbase of Trusts and CCGs. There were also pressures associated to the end of the hospital discharge programme and efficiencies expected in order to bring the System to a breakeven position. The Committee noted the report.
22/009 ANY OTHER BUSINESS AND REFLECTION
The Chair queried how extension of the CCG’s life might reflect on the workload of the Finance
Team. The Committee was informed that whilst previously the Team had anticipated closedown on 31 March and had been working to that date, it was now anticipated that the CCGs would roll forward to July 2022. Such a rollover was likely to require the need for part year accounts which it was preferable to do in October rather than July should the transition be delayed further. Whilst there had been a lot of discussion, there had not been much clarification to date. There was concern in respect of capacity of the team but a temporary member of staff had been extended and as much forward work as possible was being carried out. The Chief Executive reported that recruitment for the ICB Finance Director continued with interviews scheduled for 19 January 2022.
22/010 DATE OF NEXT MEETING
The next meeting was scheduled to take place on 15 March 2022.

Page 19 of 47
Page 20 of 47
Minutes of a Meeting of the Ipswich and East Suffolk CCG
Financial Performance Committee held on Tuesday, 15 March 2022
PRESENT: Steve Chicken Lay Member (Chair) Ed Garratt Chief Executive Dr Mike McCullagh GP Member Jane Payling Director of Finance Dr Imran Qureshi GP Member Dr Mark Shenton CCG Chair IN ATTENDANCE: Chris Armitt Deputy Director of Finance Tom Burton Strategic Planning Director, East of England Ambulance NHS Trust (Item 22-017 only) Julie Kerridge Senior Management Accountant Jo Mael Corporate Governance Manager
22/011 WELCOME AND APOLOGIES FOR ABSENCE
No apologies for absence were received. 22/012 DECLARATIONS OF INTEREST HOSPITALITY AND GIFTS
No declarations were received. 22/013 MINUTES OF PREVIOUS MEETING
The minutes of the meeting held on 18 January 2022 were agreed as a correct record. 22/014 MATTERS ARISING AND REVIEW OF ACTION LOG
There were no matters arising and the action log was reviewed and updated. 22/015 CCG FINANCES MONTH 11
The Committee was in receipt of a report that provided detailed information in respect of Month
11 finances. Points highlighted included;
• The CCG had reported a balanced position for Month 11 as per the H2 planning submission.
• The CCG had received £5.3m of Hospital Discharge Programme (HDP) and £1.2m Elective Recovery Fund (ERF) funding. It anticipated further reimbursements of: HDP £1.6m YTD.
• The forecast was in line with the H2 plan once retrospective top-ups had been received. Key variances for Month 11 were:
Page 21 of 47
Continuing Healthcare showed an overspend of £2.5m once HDP reimbursement had been received. That was due to increased costs of Non HDP patients and backlog of CHC reviews resulting in more patients remaining eligible for longer.
Primary Care showed an overspend due to prescribing costs being higher than originally forecast. Those figures used actual PPA data up to M09 and forecasts for M10-11 based on the PPA forecast adjusted to mitigate some of the risk relating to category M reductions not being achieved.
Primary Care Delegated Commissioning was overspent against plan due to the primary care contract spend being higher than plan. That was previously being offset by prior year benefits but, due to additional costs from backdated rent reviews, that had now diminished.
Mental Health showed an underspend due to the forecast shared care with Suffolk County Council being lower than anticipated and prior year benefits. Mental Investment slippage had not been factored into the position and the CCG was still forecasting to meet the Mental Health Investment standard.
Other Programme showed an underspend of £0.8m once the HDP reimbursement had been received. That was due to non-recurrent benefits from prior year being utilised.
Community Health Services showed an underspend of £0.5m due the utilisation of slippage in the non-recurrent schemes.
Acute Services showed a year-to-date underspend once ERF and HDP had been reimbursed. That was due to underspends in planned care and additional benefits from central ERF calculations.
Running Costs underspend due to vacancy slippage. Comments included; As the last Committee minutes had stated a mental health overspend, the current reported underspend was queried. The Committee was advised that the change had been due to the impact of shared care updates. It was explained that the variation in acute spend across the Alliances was a result of differing top ups across the CCGs. Having queried whether continuing healthcare assessment standards were being managed and whether there had been a reduction in the number of people going into care homes, it was reported that 28-day reviews were on track with general reviews being behind and outsourcing of that work being explored. Overall package numbers remained steady and no decrease had been seen although the average package cost had increased significantly with there being more complex patients. It was queried whether, in light of the Guaranteed Income Contract, the planned care underspend was a virtual underspend or actual cost to the System. It was explained that the planned care underspend was in respect of the independent sector and providers other than ESNEFT. The Director of Finance reported that, at its meeting in March 2022, the Governing Body was to receive reports including a summary of winter additional capacity schemes. Having suggested how support might be provided to the domiciliary care market going forward, it was agreed that a report be presented to a future meeting. It was suggested that the hospital might wish to consider support for the hospital discharge programme following the demise of the CCGs.
Page 22 of 47
The Committee approved the report.
22/016 ICS FINANCES MONTH 10
Key points highlighted included;
• NHS organisations were on schedule to deliver a net break-even position for the SNEE
system. There are offsetting variances at EEAST and ESNEFT. • The current reported position and forecast of both County Councils showed a small surplus
on the elements of budget included in this report, which predominantly relate to social care. • The NHS system capital position was in line with Regional expectations. The forecast
positions of all organisations required a significant increase in spending in the latter stages of the year, but all were providing assurance that it would be achieved. The forecast overspend at the two acute providers related to resources yet to be allocated (accelerator funding), or a request to increase expenditure (ESNEFT) to balance an expected Regional underspend.
• Risks to the delivery of NHS plans were reducing for 21/22. The availability of staff was in some cases an impediment to being able to use resources that were available, creating a natural mitigation to financial pressures.
Comments included; Although the Guaranteed Income Contract with ESNEFT was a fixed amount to the Trust, it had also received a significant amount of additional funding to support extra capacity for elective and emergency services. The forecast underspend was lower than additional monies it had received. The Trust had retained a financial discipline in order to maintain momentum with regard to delivering financial sustainability in the longer term. It was questioned whether commissioning expenditure breakdown by alliance had been affected by Covid-19 costs as, if not, it would seem to be a good benchmarking tool. In response it was reported that the commissioning expenditure had been distorted by Covid-19 and top up funding and that both ESNEFT and EEAST extra monies had flowed through NEE CCG. It was also queried how the position of the East of England Ambulance Services NHS Trust (EEAST) was managed within the overall System control total. The CCGs had been hosting EEAST within the SNEE system control total for three years and, when taking on the hosting of EEAST, had agreed with region that EEAST could be counted within the system on a neutral basis, with any EEAST variances effectively being reported below the line. The ICB would have statutory accountability for financial balance within the System and the implication of having EEAST reporting within the ICB on that position was currently not fully understood. The Director of Finance agreed to include notes within the Month 12 ICS report that would address and remove larger items of expenditure which are distorting the underlying commissioning expenditure for comparative purposes. The Committee noted the report.
22/017 EAST OF ENGLAND AMBULANCE SERVICE NHS TRUST (EEAST) Tom Burton, Strategic Planning Director for EEAST was welcomed to the meeting and
proceeded to give a short presentation on EEAST with key points highlighted including:
• A review of the year which advised that work had been driven by activity, demand had increased significantly, the Trust had been subject to regulatory impacts and structural changes.
• Key priority areas were strengthening the executive, review of operational plans, tackling employee relations, engagement and communication, and a review of governance and culture.
• The presentation provided detailed information on operational performance, the impact of Covid-19, and handover delays.
Page 23 of 47
• An overview of priorities included information on sickness absence, the instigation of a call handling recruitment plan and performance.
• SNEE data – volumes had reduced although handover delay performance had declined. The Trust had been challenged in recent weeks due to Covid-19.
• The financial plan for next year was showing a deficit which was likely to challenging at a System level.
Comments included; The opportunity to share learning from the ‘Perfect Day’ exercise was queried. This included the need for increased access to shared records at a System level in order to facilitate improved decision making. It was recognised that further work on C1 and C2 response was required, and the Committee was informed that specific concerns, once highlighted, could be investigated. The Chief Executive agreed to ask the Director of Performance Improvement to take the issue of pursuing shared learning via the tactical group. Concern was raised that when GPs might have worrying situations at their surgeries, the control room seemed to downgraded the response as a clinician was already present. The quality of clinical supervision for call handlers was questioned, together with the quality of referral from the 111 service. The Committee was reassured that there was no process for the downgrade of calls, supervision had increased for call handlers and there was clinical presence within the call room. There was improved liaison with the 111 service although working in partnership remained challenging. Having queried financial risk, it was reported that 2021/22 outturn is currently reporting a deficit. There had been resourcing issues which had seen increased overtime and additional resource. The Trust was currently trying to understand the driver of inflationary costs and the impact of increased fuel costs. The feasibility of an electric fleet was queried, and the Committee informed that the first electric rapid response vehicles would be introduced this year although full sized electric ambulances were a way off at present. The Committee noted the presentation.
22/018 COVID-19 RESOURCES APPROVAL COMMITTEE UPDATE
The Covid-19 Resources Approval Committee had been extended to the end of March 2022 to
assist decision making through the Winter period and support the vaccination programme. The report set out the approvals made since the last detailed report (which was up to 21 December 2021). From 1 October 2020 the NHS had moved away from central reimbursements to local allocations for Covid-19 and growth, with continuation of central reimbursement for the hospital discharge programme (HDP) and vaccination costs. Additional national funding had been received in 2021/22 for Integrated Urgent Care which had also been approved through the committee. The Committee noted the approvals made by CRAC on behalf of the Governing Body.
22/019 FINANCIAL PLANNING 2022/23 UPDATE
Key points highlighted with the report included;
• ICB and its partner trusts must ensure both capital and revenue resources did not exceed
Page 24 of 47
the limit set by NHSEI. • ICBs had a duty to at least break even individually and collectively with partner Trusts. • CCG expenditure would be matched with allocation such that the CCGs would break even;
any surplus or deficit for the year would fall into the combined ICB in the latter part of the year.
• Rollover of system envelopes from (H2) 2021/22 had been adjusted to remove back pay and provider income support.
• Convergence adjustment applied to all systems to move towards fair share of national funding. Value for SNEE was -0.45% which was the second lowest in the region.
• Growth included to reflect 1.7% net tariff increase and other price/activity increases. • Covid funding reduced by 57%. • Hospital Discharge Programme (HDP) ceases on 1 April 2022. • Elective Recovery Fund (ERF) details only just received causing uncertainty. • Delegated Primary Care Allocation increased by 6.6% to reflect national contractual
commitments. • ICB Running Cost Allowance uplifted only for impact of employer NI increases due to
Health and Social Care levy, cost associated with pay awards for 21/22 and 22/23 is not funded.
The report went on to detail the System draft financial position, cost pressures and risks and next steps which included;
• The draft submission was due on 17 March 2022 with the final submission on 28 April 2022.
• Due to the timing of meetings, and the remaining financial gap, the Governing Body would be asked to delegate responsibility to the finance committees for sign off of the ICB financial plan.
• The system would need to find solutions to the remaining local gap.
• Solutions used in other systems would be considered for application in SNEE.
• The Directors of Finance meeting on 15 March 2022 would be used to collate and quantify solutions.
• Resources were being reassigned to support the initiation of internal financial recovery within the ICB.
Comments included; The forecast running costs for the ICB compared to the cost of running the three CCGs was queried. The Committee was informed that whilst overall the SNEE System had low running costs compared to other areas, the future running costs of the ICB were currently more than the CCGs. In response to questioning it was confirmed that plans had not taken into account previous support provided to other Systems. The Director of Finance advised that things had moved on since circulation of the report. EEEAST was reporting a £12m deficit which was currently treated as a separate issue. There was a £11m gap across the rest of the system, which is sitting in the CCGs/ICB. A week ago NHSEI had been seeking to close the gap, but was now advising that the underlying position should be identified in the draft plan. Whilst there might be opportunity to argue for historic drawdown, that would only be a temporary solution. A key issue going forward was ensuring the utilisation of ring-fenced monies. The need to think cohesively going forward was emphasized. The challenges for 2022/23 and 2023/24 were recognised and clinical input in transformation would be key. There was concern that the use of ring-fenced funds might be reliant on the good will of primary care and it was queried whether the hospital recognised the need to invest in community services and the hospital discharge programme.
Page 25 of 47
Ipswich & East Suffolk Clinical Commissioning Group
West Suffolk Clinical Commissioning Group North East Essex Clinical Commissioning Group
Minutes of the CCG Covid-19 Resource Approval Committee meeting held on 16 March 2022
PRESENT Dr Hasan Chowhan Chair, North East Essex CCG (Chair) Dr Christopher Browning Chair, West Suffolk CCG Dr Mark Shenton Chair, Ipswich and East Suffolk CCG Jane Payling Director of Finance Richard Watson Director of Strategy and Transformation IN ATTENDANCE Jo Mael Corporate Governance Manager
Minute
22/009 Welcome and apologies The Chair welcomed everyone to the meeting. Apologies for absence were received from; Ed Garratt, Chief Executive Amanda Lyes, Director of Corporate Services and System Infrastructure
22/010 Declarations of Interest, Hospitality and Gifts
No declarations of interest were received.
22/011 Minutes of the previous meeting
The minutes of the previous meeting held on 28 January 2022 were approved as a correct record.
22/012 Matters Arising and Review of Action Log
Although the existence of centrally held contingency funds was queried, the Committee was informed that current advice was that all funds had been allocated. The Committee noted the report.
22/020 ANY OTHER BUSINESS AND REFLECTION
No items of other business were received 22/021 DATE OF NEXT MEETING
The next meeting was scheduled to take place on 14 June 2022.
Page 26 of 47
There were no matters arising and the action log was reviewed and updated. 22/013 Requests for Covid-19 related investment
Continuing Healthcare Outsourcing Extension The report sought to gain approval to use £370k of Covid-19 funding to extend the remit of the current contract between Carehome Selection Limited t/a CHS Healthcare Clinical Services (CHS) and NHS West Suffolk Clinical Commissioning Group/NHS Ipswich and East Suffolk Clinical Commissioning Group to complete outstanding NHS Continuing Healthcare reviews resulting from the impact of Covid-19 and unprecedented Nurse Coordinator vacancy rates. The Committee approved the use of £370k of Covid-19 funds in order to support the recovery of the NHS CHC service. ICS Demand and Capacity Model post Covid-19 The report sought agreement to provide £250k non recurrent funding to support the development of an ICS demand and capacity model to take account of the impact of Covid-19 on our health and care services. The principal objective of the project was to quantify demand for health and care services across the SNEE Integrated Care System over the next 5-10 (TBC) years and deliver insights on capacity gaps that would need to be addressed through changes to the way we planned and delivered care. The immediate, priority deliverables were detailed in paragraph 1.4 of the report. The Committee was informed that it was intended that a Memorandum of Understanding agreement would be established with Suffolk County Council who would host the funding which was for utilisation by the end of 2022/23. Monies available had now been increased to £450k which included the £250k being sought by the report supplemented by an additional contribution from system partners. Whilst there was concern was to whether the scheme needed to be so acute focussed as there could be a risk that a capacity model, based on acute demand, would be developed, it was explained that the additional funding should allow for everything to be considered. Having queried the potential data source, it was explained that funding had been sought in the first instance prior to taking the work forward. The end outcome was anticipated to be development of a demand and capacity model over the next 5-10 years. The model should assist with the required ICS refresh, ICB clinical strategy and also help inform the Alliance delivery plan. There was likely to be some overlap with population health work. The Committee approved the provision of £450k non recurrent funding to support the development of an ICS demand and capacity model as described within the report. Covid-19 Vaccination Costs The Covid-19 vaccination scheme was a rapidly changing landscape, with requirements for the delivery of the programme continuing to evolve. The reimbursement methods and the scope of reimbursement had become clearer as the year had progressed, although there remained some uncertainty as we move into 2022-23. In order to meet NHS England requirements some costs were being incurred locally and would need retrospective reimbursement. In the meetings up to and including the 19 August 2021, the Committee had approved
Page 27 of 47
£1,072,920 of expenses which were expected to be picked up by the CCGs in respect of the vaccination programme. The report set out the additional expenditure made since 19 August 2021. The Committee was being asked to review and approve Covid-19 vaccination costs totalling £7,076.77 (to be paid directly to PCNs by NHSE) and £99,941 (covered by an allocation from NHSE specifically for that purpose), as well as £92,065 (reclaimed from NHSE). Where those related to payments to primary care the payments would be authorised by the Commissioning Governance Committee It was highlighted that work was underway to identify the likely costs for 22/23 for which some central funding would be made available. The Committee approved the vaccination costs as outlined within the report. Month 9 to 11 (December 2021 to February 2022) Covid-19 expenditure returns The report sought to approve all expenditure included in the month 9 (December 2021) to month 11 (February 2022) Covid-19 expenditure returns. The Hospital Discharge Programme was due to cease on 1 April 2022 and work was underway with County Councils to seek to mitigate the impact. The Committee noted the total expenditure returns submitted by the CCGs for months 9 to 11 and approved the month 9 to 11 elements of previously approved expenditure areas included in the returns as detailed in sections 2.5 and 2.6 of the report.
21/014 Forward Planner
There was nothing on the Forward Planner. 21/015 Date of Next Meeting
Meetings are arranged on an as and when required.
Page 28 of 47
Meeting of the Ipswich and East Suffolk CCG Primary Care Commissioning Committee held
on Tuesday 26 April 2022, via Microsoft Teams
Members of the public were invited to email questions prior to the meeting.
PRESENT: Phanuel Mutumburi Lay Member for Patient and Public Involvement (Chair) Maddie Baker-Woods Chief Operating Officer Dr Lorna Kerr Secondary Care Doctor Jane Payling Director of Finance Simon Jones Suffolk Local Medical Committee Kerry Overton Healthwatch Dr Mark Shenton CCG Chair
IN ATTENDANCE: Sarra Bargent Ipswich and East Suffolk Alliance Quality Lead David Brown Deputy Chief Operating Officer Jo Mael Corporate Governance Manager Julie Purnell Executive Assistant, Chief Operating Office Stuart Quinton Primary Care Commissioning Manager Claire Pemberton Head of Primary Care, Ipswich and East Suffolk CCG Daniel Turner Senior Estates Development Manager
22/11 APOLOGIES FOR ABSENCE
Apologies for absence were noted from: Steve Chicken , Lay Member Ed Garratt, Chief Executive Paul Gibara, Director of Performance Improvement Kathleen Hedges, Contracting Support Manager (Suffolk and North East Essex STP) Cllr Rebecca Hopfensperger, Suffolk County Council Amanda Lyes, Director of Corporate Services and System Infrastructure Laura Traill, Contracting Manager (Suffolk and North East Essex STP)
22/12 DECLARATIONS OF INTEREST AND HOSPITALITY AND GIFTS
No declarations of interest were received.
22/13 MINUTES OF THE PREVIOUS MEETING
The minutes of meetings of the Ipswich and East Suffolk CCG Primary Care Commissioning Committee held on 21 December 2021 and 22 February 2022 were approved as correct records.
22/14 MATTERS ARISING AND REVIEW OF OUTSTANDING ACTIONS
Page 29 of 47
There were no matters arising and the action log was reviewed and updated.
22/15 GENERAL UPDATE
The Chief Operating Officer reported;
• Julie Purnell was welcomed to the meeting as the new Executive Assistant for the Chief Operating Officer.
• It was anticipated that the Integrated Care System would be established on 1 July 2022 and as it moved forward it was envisaged that there would be a dedicated Primary Care Group within the three Alliance areas. The Ipswich and East Group would report to the Alliance Committee and meet as appropriate with colleagues from West Suffolk and North East Essex.
• Suffolk Primary Care had shared a picture of primary care demand which included the numbers of calls received and face to face consultations carried out. There were consistent patterns within the information with Mondays being the busiest day.
• Despite increased sickness levels due to Covid-19, practices had continued to sustain urgent on the day services and no practices had been shut as a result of the sickness. All practice staff were thanked for the contribution and patients thanked for their understanding and patience.
• The CCG was now close to the year end in respect to special services that it provided and was able to report that Serious Mental Illness health checks and Learning Disability health checks were now meeting or exceeding targets.
• Sarra Bargent was welcomed to the meeting as the new Ipswich and East Suffolk Alliance Quality Lead.
It was queried whether Monday being the busiest day for primary care was a result of the weekend or behavioural and whether there was any influence that could be brought to bear. It was explained that the way patients chose to contact practices had not changed much despite the offer of a demand led service and Monday being the busiest day had been the same prior to the pandemic. The Committee noted the update.
22/16 PRIMARY CARE CONTRACTS AND PERFORMANCE REPORT
The report provided an overview of primary care performance and updated on primary care
activity where relevant. Detailed information was provided on the following areas:
• Prescribing and Medicines Management
• Learning Disabilities and Serious Mental Illness Health Checks
• Dementia Diagnosis Rates
• Flu Vaccination
• Childhood Immunisation 2020/21
• Primary Care Network Development
• PMS (Personal Medical Services) Development Framework
• Local Enhanced Services
• CQRS (Calculating Quality Reporting Service) Local Key points highlighted included:
• The prescribing budget at month 10 was slightly overspent although antibiotic prescribing performance was better than national targets.
• Learning Disability health checks at quarter three were ahead of the same point in 2021 and 64/1% of Serious Mental Illness health checks had been completed which was the highest achievement to date.
• Flu vaccination coverage was above previous years.
• Primary Care Network (PCNs) development – guidance had been published at the end of
Page 30 of 47
March 2022 for 2022/23. GP contract changes would be identified under a separate agenda item. One key change was related to enhanced access. At present practices were responsible for extended hours and the CCG commissioned a separate GP+ service from Suffolk GP Federation. From October the PCN would be responsible for providing enhanced access outside core hours.
• Personal Medical Services (PMS) Development Framework – a refreshed draft for 2022/23 had been issued to the Local Medical Committee for review and a response was awaited.
• Local Enhanced Services – in the main they had been rolled forward from last year to next year and were currently with the Local Medical Committee prior to them going through the CCG governance process and being issued to practices.
• CQRS (Calculating Quality Reporting Service) Local - used by practices to monitor Quality Outcome Framework and Direct Enhanced Services it enabled the CCG to process local enhanced services online.
Comments included: Clarification on child immunisation data was sought and the Primary Care Commissioning Manager agreed to investigate and report back to the Secondary Care Doctor outside of the meeting. Having queried the number of Learning Disability health checks carried out, it was explained that final numbers reported indicated that the 75% national standard would be met. There was now focus on continuous improvement. In light of the recent pandemic and recognising that pregnant women were major suffers of flu, it was questioned what might be done to facilitate midwifery participation in immunisation programmes. It was suggested that vaccination programmes should form a strand of the midwifery strategy and be included within general midwifery training. The Chief Operating Officer agreed to explore with relevant staff how it might be incorporated within the strategy development. Much of the Primary Care Network development framework where population health management methods could assist clinical directors with teams and integrated neighbourhood teams to manage work seemed to be working well by aligning clinical directors with integrated neighbourhood team management and analysts to work with linked datasets to deliver significant change. It was highlighted that investment would be needed to influence change. The cause of low Serious Mental Illness health check performance at Ixworth and Solway and Mallick practices was queried. It was explained that the exact cause could not be pinpointed although the CCG continued to liaise with those practices and provide support. The Committee noted the update.
22/17 PRIMARY CARE DELEGATED COMMISSIONING – FINANCE REPORT
The report provided an overview of the Month 12 Primary Care Delegated Commissioning
Budget. At the end of Month 12, the Primary Care Delegated Budget was £903k overspent. That was mainly due to expected increase in Quality Outcome Framework achievement offset by a reduction in dispensing/ prescribing professional fees.
The allocation received for Primary Care Delegated Commissioning was lower than the budget required. The shortfall was funded from the CCG programme as detailed in the table within the report. If that was not the case the overspend on Primary Care Delegated Commissioning would be £2.6m. Other Primary Care showed an overspend of £59k at the end of Month 12.
Page 31 of 47
Comments included; Having queried the budgeting process, it was explained that during the years when there had not been a delegated budget, NHSE had supported contracts with practices signing PMS or GMS contracts. After delegated commissioning NHSE had made a choice to only reimburse GMS contracts ignoring PMS contract holders and that change was reflected in the allocated budget. The system was mandated to manage the gap. The CCG had chosen to support PMS contracts despite not being funded for them with them being supplemented from the programme budget. 2022/23 – in light of the move towards the Integrated Care System, budgets for 2022/23 had been allocated based on the ICS and the finance team was currently working through plans for 2022/23 which for commissioning had come in on the larger footprint. Challenges remained as there were significant amounts of PMS contracts which would need to continue to be supplemented from the primary care overall budget overall moving forward. Discussions with regard to financial recovery and efficiencies for next year were taking place. It was suggested that thought be given to whether support provided over the last few years could be recurrent and space left within the budget to offset that. There was a risk that the deficit remained at the discretion of future commissioning decisions and therefore over the heads of practices and PCNs. The need for any future Committee to monitor the situation closely going forward was emphasized. The Committee noted the update.
22/18 GENERAL PRACTICE CONTRACT CHANGES 2022-23
NHS England and Improvement’s National team had produced the document General Practice
Contract Arrangements in 2022-23, attached as Appendix 1 to the report, which provided an overview of the contractual changes for 2022-23. Key points from the document were highlighted in paragraph 2.1 of the report. Key points included:
• The largest change was associated to extended access arrangements as mentioned earlier.
• There was support for the management of PCNs and Clinical Directors -15 PCN roles were to be funded 100%.
• There was an increase in the scope and number of service specifications.
• The Impact and Investment Fund was a scheme that rewarded PCNs if they achieved targets and milestones.
The need for increased liaison between secondary and primary care was highlighted. There was an issue of budget allocation not meeting the spend, then squeezing the ability to provide recurrent funding in estate. Less available estate per patient resulted in less workforce space needed to manage the demand and less capacity to train the new workforce. There was a need to ensure available funding entered the system. A key priority for the Integrated Care System would be to develop a prioritisation mechanism with regard to primary care estate. The Committee noted the report and contract changes.
22/19 CARE QUALITY COMMISSION (CQC)
The purpose of the report was to inform the Committee about the outcomes of Care Quality
Commission (CQC) inspections of Ipswich and East Suffolk GP practices and the actions which were proposed to address issues, share good practice and enable continuous
Page 32 of 47
improvement. The Committee was invited to review the report and advise on any areas for action. Although the CQC had put formal reviews on hold whilst the practices dealt with Covid-19, reviews had now restarted and they had been in contact with Saxmundham. A visit to Cardinal had been planned on the 22 April 2022 and there was no update as yet. The CQC had concentrated on practices that were at high or very high risk during Covid-19 by calling each practice and asking them a number of questions as part of the Emergency Support Framework (ESF). Whilst Ipswich and East Suffolk did not have any practices in that category the CCG had contacted practices to ask the questions to ensure they felt supported with positive results. The Committee noted the update.
22/20 PRIMARY CARE DELEGATION AGREEMENT AND FUTURE PRIMARY CARE
GOVERNANCE ARRANGEMENTS
The report provided an overview of: Part 1 - the proposed Primary Care Delegation Agreement for the Suffolk and North East Essex Integrated Care Board from 1 July 2022 and Part 2 - the proposed governance arrangements for primary care decisions from 1 July 2022. Subject to the passage of the Health and Care Bill through Parliament and the granting of Royal Assent, Integrated Care Boards (ICBs) would be established on 1 July 2022; and NHS England (NHSE), via a Delegation Agreement would delegate the exercise of the following delegated functions to ICBs: o Primary medical services o Primary dental services and Prescribed Dental Services o Primary ophthalmic services o Pharmaceutical services and local pharmaceutical services
It was proposed that primary medical services would be delegated to the Suffolk and North East Essex (SNEE) ICB from 1 July 2022 and the other services from 1 July 2023 (with closer working between NHSE and the ICB during the twelve months leading up to that date)
The ICB would be required to perform the Delegated Functions in such a manner as to ensure NHSE’s compliance with NHSE’s statutory duties in respect of the Delegated Functions, having regard to NHSE’s accountability to the Secretary of State and Parliament. The report went onto to detail the delegation agreement, points for consideration and feedback. There were a lot more functions than currently and it was proposed that NHSE staff would transfer into ICBs. It was unclear as to what the overall resource would be and whether there would be trade off in respect of the resources received and the amount of additional functions needing to be carried out. With regard to governance arrangements, neither the Health and Care Bill nor the aforementioned Delegation Agreement mandated ICBs to establish a Primary Care Commissioning Committee (PCCC) to discharge primary care functions. However, ICBs might wish to retain their PCCC while considering how to integrate Primary Care with wider responsibilities. The following parameters though, were stated within the agreement:
• ICBs might delegate the discharge of its primary care functions to another relevant body or to joint committees of ICBs but not to providers nor to joint ICB / provider committees (although providers might be members of a delegated committee at ‘place’ level
• Other delegations or joint committees were permitted subject to approval by NHSE
• The further delegation of a function from a body which had delegated functions from the
Page 33 of 47
ICB (‘triple delegation’) was prohibited.
ICBs must develop an operational scheme of delegation defining those individuals or groups of individuals, including committees, who might discharge aspects of the delegated functions. The arrangements made must be effective, safe, efficient and economic. SNEE ICS was proposing that the three Alliances (Ipswich and East Suffolk, West Suffolk and North East Essex) exercise the delegated primary care functions as sub-committees of the ICB; but via their own separate primary care commissioning committee or group reporting into the Alliance Terms of reference for those future primary care commissioning committees / groups were currently being drafted by the CCGs’ independent governance advisor. The Committee was advised of the following questions posed within the report which Members were asked to consider and provide comment on; ➢ Is a primary care commissioning committee / group the most effective mechanism for
discharging primary care functions from 1st July 2022 onwards? If yes, why? ➢ If you consider the answer to the above is ‘no’, what other mechanism would you propose? ➢ Would a hybrid model be a better option i.e. the primary care commissioning committee /
group making some decisions; and another body or individual ICB officers making other decisions? If so, what type of decisions sit best with each body / individual?
➢ Who should be members of the primary care commissioning committee / group; and which members should constitute the quorate for making decisions?
➢ Should meetings be, by default, in public (with only sensitive items being discussed in private)?
➢ How often should the committee / group meet; and should the three committees across the Alliances ever meet in common?
Comments included; It was felt important to have focus on needs, performance and funding for primary care via a dedicated primary care group. As a delegated function of the Alliance Committee it was important that matters were brought to committee for support. The group should include current colleagues and be strengthened by relationships with districts and boroughs. The need to work with colleagues in West Suffolk and North East Essex was recognised but there was also a need to be flexible in that approach. The need for such a committee was seen as important for the local system, to build on what was already in place. It was likely that terms of reference would need amending when dentists, opticians and pharmacists became formally delegated. It was highlighted that it would be tough for the NHS to take on extra responsibility when it had not had adequate resource to date and there was a need to ensure it was properly resourced going forward. The importance of a primary care presence to provide expertise was recognised and it was suggested that thought be given as to how that might be facilitated in future. Whilst noting comments made, the Primary Care Commissioning Manager reminded Members that any further comments could be fed back to him outside of the meeting. The Committee noted the report.
22/21 DATE OF NEXT MEETING
The next meeting was scheduled to take place on Tuesday, 28 June 2022

Page 34 of 47
22/22 QUESTIONS FROM THE PUBLIC
No questions were received.
Page 35 of 47
Decisions from a virtual meeting of the Ipswich and East Suffolk CCG Commissioning Governance Committee held on 24 March 2022
DECISION RECORD
Commissioning Governance Committee Members:
Graham Leaf, Lay Member for Governance
Steve Chicken, Lay Member Dr Lorna Kerr, Secondary Care Doctor Phanuel Mutumburi, Lay Member for Patient and Public Involvement Jane Payling, Director of Finance Declarations of Interest
No declarations of interest were received.
2 GP Streaming – additional hours to support Covid-19 response and
Winter To receive and approve a report from the Director of Performance Improvement
Paul Gibara Report No:
IESCCG/CGC 22-01
3 Covid Vaccination Programme costs – PCN sites
To receive and approve a report from the Director of Finance Jane Payling
Report No: IESCCG/CGC 22-02
4 Additional Funding for Refugee Health Care
To receive and approve a report from the Chief Operating Officer Maddie Baker-Woods
Report No: IESCCG/CGC 22-03
Decision
GP Streaming – additional hours to support Covid-19 response and Winter The Committee approved the IES element of payments (up to £61,200) to Suffolk GP Federation for provision of additional GP Streaming as set out in the report. Covid Vaccination Programme costs – PCN sites The Committee approved Covid-19 vaccination costs of £34,870 for IESCCG as set out in the report and recommended by the Covid-19 Resource Allocation Committee.

Page 36 of 47
Additional Funding for Refugee Health Care The Committee approved the payment of up to £35,00 to Derby Road Practice for the support of refugees. And recommended that the extension of the health outreach service is given consideration across SNEE.
Page 37 of 47
Ipswich and East Suffolk Alliance Committee
Minutes of meeting held on 15 February 2022, 1030-1230 Via Teams365
Present: Kirsten Alderson, Suffolk Family Carers (KA) Sarra Bargent, IESCCG (SB) Dr Ruth Bushaway, Suffolk GP Federation (RB) Dr Shane Gordon, ESNEFT (SG) Chair Paul Little, SCC/ESNEFT (PL) -left at 1200 Judi Newman, St Elizabeth Hospice (JN) Dr Mark Shenton, IESCCG (MS) Kathy Nixon, Babergh and Mid Suffolk District Councils (KN) Lisa Nobes, IESCCG (LN) – joined at 1103 Jane Payling, IESCCG (JP) Dr Imran Qureshi, IESCCG (IQ) Martin Seymour, SCC – Public Health (MSe) Maddie Baker- Woods, IESCCG (MBW) Apologies: Georgia Chimbani, SCC (GC) Kathryn Ellis, NSFT (KE) Ed Garratt, IESCCG (EG) Neill Moloney, ESNEFT (NM) Lianne Nunn, IESCCG/SCC (LNu) David Pannell, Suffolk GP Federation (DP) Stuart Richardson, NSFT (SR) Dr Angela Tillett, ESNEFT (AT) Richard Watson, IESCCG (RW) Andy Yacoub, Healthwatch (AY) In attendance: Clare Banyard, IESCCG (CB) Paul Duell (PD) Liz Hallworth, IESCCG (LH) (to minute meeting) Louise Hardwick, IESCCG (LHa) Karen Lough, ESNEFT (KL) Alastair Mitchell-Baker, Tridant (AM-B) (Functions and Accountability item) Caroline Procter, IESCCG (CP) Wendy Scott, IESCCG (WS) (LD&A Update)
1 Welcome, introductions and apologies Action
SG welcomed all to the meeting. Apologies were noted. No declarations of interest were received.
2. Update Action Log & Minutes
The minutes from the meeting held on 18.01.22 were agreed as a correct record. The action log was reviewed and updated.
3. Briefing and discussion re The Government’s proposals for health and care integration, ‘Joining up care for people, places and populations’, published 09.02.22
MBW presented the paper. It was highlighted that the briefing was provided to ensure that all Alliance Committee members had a common understanding of the headlines within the White Paper and the associated timelines. A constructive discussion was held around the implications of the proposals for IES Alliance. All members agreed that integration of the workforce, together with shared learning and training will be vital for successful delivery of our plans. It was also felt that some of the digital goals are very ambitious and that the model of
Page 38 of 47
governance proposed is not entirely clear. The Committee agreed that a formal response on behalf of the IES Alliance to the questions raised at the end of the White Paper should be submitted. MBW agreed to action this on behalf of the Committee.
4. ICS/Alliance Transition – Focus on Functions and Accountabilities of the Committee
AM-B was welcomed to the meeting and with MBW, took the Committee through the presentation. It was highlighted that the purpose of the paper was to ensure that everyone is comfortable with the emerging list of functions; understood what the currently described accountabilities of this committee are; and sets out the specific functions of the ICB and the delegation of those accountabilities to the Alliances. A concern was raised that an opportunity may being missed to make the ICB truly integrated rather than just an NHS system. As such there may be a disconnection between what we want to do conceptually and what in reality we will be able to do, as all the functions relate to health and are not about system integrated delivery. It was felt that there needs to be some flexibility and to look at this as a commitment to an ambition with a timeline trajectory of making it a truly integrated system. It was agreed that all members share the ambition of the ICS system becoming truly integrated and that the context of the previously discussed White Paper can help us with this. Whilst a timeline would be helpful, it was stressed that the functions that are currently being formally delegated are still only NHS ones. We will need to take on these functions and do them well but have the ambition, with an agreed timeline, on how we move to the next stage. As such, we will be able to move from aligned projects to those that are collectively delivered with pooled budgets if it is appropriate to do so. JP confirmed that the financial limits are still ‘draft’ and cannot be finalised or approved until the ICB has been formed. It was felt that the financial limits seem to be very low given the amount of money in the system. It was agreed that the limits might appear low but we are trying across the ICB to bring three systems together that currently work in different ways. This is about agreeing a budget and what will be devolved to the Alliance Committee and is about individual transactions for the Alliance to handle and make appropriate decisions rather than the total budget. It was queried whether this will be permissive enough for the approach we want to take, especially in terms of the financial limits being proposed. It was suggested that we start with this and then feedback what these are stopping us from doing. We will need to have an ICB which commits to reviewing this with their Alliances - either after the first 6 months or 12 months – to establish whether the limits are stifling work or are sufficient to allow Alliances to get on and do the work that is needed. However, all other system members will also need to show the desire to work in an integrated way and put in appropriate finances. It was agreed that the system working slide does not clearly identify all areas and members of the ICS (in particular SCC and District and Boroughs) and that it would be beneficial for this diagram to be enhanced. It was felt that this would be helpful as the District and Boroughs are on a trajectory for more integration and want to have conversations about joint commissioning and what this will mean in the future, along with joint points at senior and middle management. It was reported that the next steps relate to the ICB and Alliance Schemes of Delegation and Reservation which are in the process of being pulled together. Another draft of these and further functions will be available next month. It is the aim that by the start of April, we are all clear and in agreement. However, there is still the opportunity to look at alternative suggestions before moving to approval in
Page 39 of 47
the new financial year. The Committee agreed that it was clear on the proposed Alliance functions but that there remains further work to be undertaken about what functions and governance is required to enable true integration with other partners. It was agreed that the system diagram would be reviewed and revised. In addition, Committee members would submit any further suggestions/alternatives for consideration to MBW, AMB or CP.
5. Development of the Strategy and Operational Plans using Outcome Based Accountability (OBA) methodology
MS and CP provided a comprehensive overview of the paper. The Committee was asked to consider whether they were still supportive of Outcome Based Accountability methodology being the system of choice for the Alliance. The Committee agreed with the use of this approach for all the good reasons that had been outlined within the paper and presentation. However, it was felt that it will work better if the rest of the ICS and our partners adopt the same sort of approach. As such, there needs to be a commitment to this effect from teams across the system. However, it was felt that there is a lack of understanding as to what this means to individuals on the ground and support will be needed to clearly demonstrate the benefits for our workforce and local population. It was suggested that it would be helpful for a Committee member to take on the responsibility of making this happen across the transformation work we are trying to undertake in order to provide the appropriate assurance at both the EDG and Alliance Committee levels. MS and CP confirmed that they would continue to work on the next steps and welcomed the offers from those willing to be involved either as a champion or with the overall OBA methodology.
6. Learning Disability and Autism (LD&A) Update
WS was welcomed to the meeting and provided the Committee with a verbal update on the progress to date. The main points highlighted included:
• The Peer Educators from ACE are continuing in their role and are supporting the uptake of annual health checks both virtually and face to face. They have also extended their remit, as it is recognised that a number of people live in supported residential schemes and there is a need to educate through that workforce.
• The original funding finishes at the end of the financial year but a further year will continue to be funded through slippage.
• It is recognised that data is very driven in terms of numbers but we need to know the experience of those people having an annual health check. This will be sought from questionnaires so that learning can be taken forward to establish what can be done collectively to make the necessary improvements.
• Membership of the Suffolk LD Partnership Board has been recently reviewed. In the new governance arrangements, this Board will be feed into the three Alliances.
• Whilst there has been a strategy refresh, it is more about a commitment of how we can work better to ensure people have the right support of a good quality, in the right place, at the right time.
A constructive discussion was held. It was agreed that there is a need to ensure true coproduction and to work with individuals with LD&A in all our plans. This current peer group has provided us with a role model and we need to start incorporating it into other programmes of work that we have. It was felt that the Learning Disability strategy is a really good exemplar of an OBA
Page 40 of 47
approach and that the health check approach is really about personalisation from a health care perspective. Whilst there have been some successes with learning disability being threaded through the mental health transformation and the work during the vaccination programme, we need to consider how it is threaded through everything that we do and make it the norm for us all, for example when looking at the Urgent Treatment Centre design. It was agreed that there is a need for a robust and true Equality Impact Assessment process, whereby those that are using the service truly assess the impact of the design. LN confirmed that she would like to undertake a piece of work across the ICS which would properly look at the impacts on all groups for the work we do. It was agreed that those with LD&A are a group of people who suffer great inequalities but there are also others. When looking at dashboards and outcomes we need to focus on specific groups of people who are at the greatest risk of inequality. As such, as we develop it, its needs to be part of our performance framework. WS thanked the Committee for the feedback provided and confirmed that she would like to attend a future meeting to report on progress and next steps.
7. Priority Focus Deep Dive – Integrating Pharmacy within IES Alliance
PD was welcomed to the meeting and presented a comprehensive overview in respect of the integration of pharmacy within IES and the wider ICS. The Committee was asked to consider the rationale for, and to endorse the current ICS programme of work to integrate pharmacy into the system and achieve medicines optimisation. In addition, the Committee was asked to discuss what more is required at Alliance level to secure an integrated approach. A constructive discussion ensued. The key points highlighted included:
• All agreed that the presentation was informative and helpful.
• The previously discussed joined up and integrated health and social care White Paper was highlighted. It was felt that whilst the Regional perspective is to look at integration of community pharmacy with PCNs, locally the bigger opportunity may be with the INTs, as these would provide a much broader group of health and care professionals integrating with pharmacy. It was highlighted that there is some funding within the pharmacy contract to enable a lead pharmacist in each PCN footprint and this model can be utilised initially and then expanded into the INTs.
• The challenge around the use of a single care record was acknowledged. If this could be resolved, better communication channels would be available with all parties being able to see the same records which would allow pharmacy to play its part in supporting primary care and hospitals. It was agreed that digital alignment will be a key enabler to make pharmacy more integrated. There is currently a pilot underway utilising SystmOne and the ability for the pilot sites to be able to read, write and use task functions of SystmOne rather than to just have access to the summary care record.
• It was also acknowledged that communications are not as joined up as they need to be and this is a key element that needs to be looked at and worked on.
• The simple logistical benefit of pharmacy working directly primary care practices would ensure good relationships are built and maintained. The main aim is to improve patient journeys and we need to consider how we can join up to help patients get the best messages in a joined up and integrated way.
Page 41 of 47
• It was agreed that pharmacy can bring more to the table in terms of support for self care and prevention. However, it was acknowledged that those with limited health literacy can find it very difficult to self care and we need to put ways in place to assist with this.
• It was acknowledged that there is a responsibility and opportunity for primary care to include pharmacy when considering infrastructure particularly in respect to digital and estate.
• The need to ensure links are established and maintained with hospital pharmacy in respect of integration was highlighted. It was confirmed that the hospital Chief Pharmacists are involved and those conversations are taking place. It was however, highlighted that it is currently a rather centric group having these conversations, and as such there is a need to broaden it wider rather than just pharmacists. This would enable system ownership and ultimately help create a pharmacy that works for everyone.
The Committee thanked PD for his attendance and agreed that further discussions would be continued.
8. Any Other Business
JN reported that The Lancet Commission on the Value of Death has been published and the link to this would be shared (see below). It was felt that this is very much aligned with what we are trying to achieve through our Compassionate Communities and would be discussed at the next End of Life Committee meeting. (Lancet Commission on the Value of Death - The Lancet.
Date of Next meeting
Tuesday 15 March 2022
CLOSE
Page 42 of 47
Ipswich and East Suffolk Alliance Committee Minutes of meeting held on 15 March 2022, 1030-1230
Via Teams365 Present: Kirsten Alderson, Suffolk Family Carers (KA) -left at 1200 Sarra Bargent, IESCCG (SB) Dr Ruth Bushaway, Suffolk GP Federation (RB) Dr Shane Gordon, ESNEFT (SG) Paul Little, SCC/ESNEFT (PL) -left at 1200 Judi Newman, St Elizabeth Hospice (JN) David Pannell, Suffolk GP Federation (DP) Prof Mark Shenton, IESCCG (MS) Chair Kathy Nixon, Babergh and Mid Suffolk District Councils (KN) Dr Imran Qureshi, IESCCG (IQ) Martin Seymour, SCC – Public Health (MSe) Richard Watson, IESCCG (RW) -joined at 1100 Maddie Baker- Woods, IESCCG (MBW) Andy Yacoub, Healthwatch (AY) Apologies: Georgia Chimbani, SCC (GC) Kathryn Ellis, NSFT (KE) Ed Garratt, IESCCG (EG) Neill Moloney, ESNEFT (NM) Lisa Nobes, IESCCG (LN) – joined at 1103 Lianne Nunn, IESCCG/SCC (LNu) Jane Payling, IESCCG (JP) Stuart Richardson, NSFT (SR) Dr Angela Tillett, ESNEFT (AT) In attendance: Clare Banyard, IESCCG (CB) Liz Hallworth, IESCCG (LH) (to minute meeting) Justin Jupp, Ipswich Borough Council (JJ) Peter McElduff, Local Optical Council (PMc) Caroline Procter, IESCCG (CP)
1 Welcome, introductions and apologies Action
MS welcomed all to the meeting. Apologies were noted. No declarations of interest were received.
2. Update Action Log & Minutes
The minutes from the meeting held on 15.02.22 were agreed as a correct record. The action log was reviewed and updated.
3. IES Strategic Priorities Update
MBW presented the paper, which provided an update on the current status and progress in respect of the 12 priorities for action that the Committee had agreed in January 2022; namely:
1. Progress Outcomes Based Accountability Framework for forward strategy and delivery plans
2. Continue Evergreen 1st, 2nd and Booster vaccines, particularly in communities with lower take-up
3. Accelerate locally based admission prevention enabled by expanded Integrated Neighbourhood Teams (INTs) with devolved Reactive Emergency Assessment Community Team (REACT) support and Connect with District, Borough and voluntary sector partners to meet urgent two-hour community response target
4. Restore pace of elective recovery and long-term condition management with particular focus on addressing inequalities
Page 43 of 47
5. Deliver community mental health model within Primary Care Networks (PCNs)/INTs
6. Initiate induction and prepare for shadow commissioning of wider primary care services (optoms, dental and pharmacy)
7. Accelerate recruitment and training programmes within care, primary and community based services, specifically including carers, nurses and GPs
8. Expand social prescribing in response to demand and re-procure 9. Scope methodology to develop holistic health and care plan for the town of
Ipswich (NB this does not infer any changes to INT geographies) 10. Scope response to Anchor Institution and voluntary sector strategies
It was highlighted that Action 10 will be a priority for April and that a presentation in respect to Action 9 will come to the Committee in May. During the ensuing discussion the following points were raised:
• It was agreed that this had been a helpful and informative narrative in respect of the agreed priorities. Data as it emerges will be critical in guiding the future actions on our priorities.
• A concern was raised that in respect of the delivery of the community mental health model in PCNs/INTs, we do not as yet have a clear vision on how this interacts with neighbourhood and delivery. It was agreed that it might be a useful focus for the next Committee meeting to look at how integration is progressing alongside the next steps for mental health.
• It was reported that as part of the community mental health programme we are looking to try and see how we get this moving by running a One Team Programme with participants taking a practical approach as to how it will work. Defining the vision will be important but learning how it all works together will be important too.
• It was agreed that in an ideal world we would have INT based plans and overlay these with that of the alliance as well. Whilst we must not lose the work we have started, it has to be acknowledged that the COVID pandemic delayed the empowerment of the INTs and PCNs. This must, however, be part of next year’s focus.
• In respect of recruitment and training, it was felt that there is a need to think about the wider care sector and recruitment and retention.
• It was suggested that Paul Leppard in ESNEFT’s Finance Team might be a useful contact in respect of the Anchor Institution action. ESNEFT has prepared a response to the Anchor Institutions internally and there may be other organisations who have also taken steps in this regard. MS reported that the ICS Chairs Group had received a presentation on the way ESNEFT has gone about this. It was felt to be very impressive and we should consider using the approach and learning from this. It was highlighted that Population Health Management (PHM) and an Outcomes Based Accountability (OBA) approach to much of this work will be vital so that we know what we want to measure, and what change we want to see as a consequence of working differently at place level. The Clacton Community Diagnostic Hub was highlighted as a good example of how needs based data has been utilised effectively. It was agreed that this will be a really important part of the work we do in Ipswich which must be data driven.
• A concern was raised that full awareness in respect of Connect for Health and social prescribing opportunities, especially in relation to the Hospice and ED is missing. Having full sight on these to maximise the benefit would be helpful, especially in respect of the new Urgent Treatment Centre development which provides ESNEFT and the Alliance partners to build on these.
• It was reiterated that the INTs are a community service team working in our neighbourhoods, with PCNs and the voluntary care services,
Page 44 of 47
especially the Hospice, alongside our specialist teams be they acute, mental health based or from the voluntary care services. We need to recognise that we are a neighbourhood and that we are all participating and delivering health and care in that neighbourhood. As such we need to ensure relationships continue to bridge and not divide us. It was agreed that this was a helpful reminder and we need to fill any gaps and make the necessary connections which are all ‘doable’.
• It was highlighted that work has been continuing with primary care to get the Electronic Palliative Care Co-ordination System - shared record (EPaCCS) ‘live’ and this should be reflected in the appropriate sections of the report going forwards.
• It was reported that a further One Team Programme is in the process of being planned and members were asked to highlight this to their teams.
The Committee noted the update and it was agreed that MBW would contact individual members as appropriate outside of the meeting.
4. IES Alliance Quality Committee
SB presented the paper and highlighted that this was the first iteration and socialisation of thoughts and processes as to what the IES Alliance Quality Committee could look like. The paper provided details on the background of how this been brought together using guidance from the National Quality Board, including the six key principles for delivering quality care in systems, alongside the governance and responsibilities articulated in respect of ‘Place’. The purpose of the IES Quality Committee will be to provide a forum at which IES place-based partners from across health, social care, voluntary sector, public health and wider can routinely share insight and intelligence into local quality matters, identify opportunities for improvement and concerns/risks to quality, and develop place-based responses to support ongoing quality improvement for the local population. The proposed specific duties were outlined in detail within the paper. The Committee was asked to review the proposed ‘purpose’ and ‘duties’; agree for this to be socialised wider; and to commit to the co-development of, and participation in, the Alliance Quality Committee going forwards. It was highlighted that the name of this group will need to be changed from ‘Committee’ with a new name being agreed and utilised going forwards. A constructive discussion ensued with the following points being made:
• It was highlighted that a vital part of quality assurance and outcome improvement is to look forward, not just backwards at what has already happened. This is important to demonstrate learning of what we need to do differently in the future.
• A query was raised around wider clinical engagement within the Committee, and for consultants and GPs to be part of this to ensure breadth of assurance and appropriateness. It was confirmed that once the principles of the committee have been agreed, conversations would be started to ensure that we have the right people around the table. However, we also need to understand how output from this committee feeds into other forums so it is imperative that we get the governance correct from the outset.
• It was highlighted that there is also a need to ensure the patient voice is part of the committee. It was reiterated that we will be looking for representation from all Alliance partners, not just health, and that the voluntary care sector and patient voices will be needed; it is about holistic quality.
• It was acknowledged that each organisation will continue to have their own
Page 45 of 47
statutory committees etc to examine quality.
• It was acknowledged that the Quality Committee will have to connect with the ICS/ICB governance and as a consequence its purpose in respect of assurance on statutory and national priorities will dictate some of the priorities for the Alliance Committee. However, we need to ensure that duplication of activity is avoided.
• The use of the wording “Co-production with people using services, the public and staff” was widely welcomed. It was highlighted that the use of ‘people’ rather than ‘patients’ is important language as quality of care is more than just about health. It was suggested that this language should be more obvious across the paper as a whole as it still feels very health centric. It was agreed that this was helpful feedback and that whilst a lot of the slide information had been taken from the National Quality Board, it is not the finished article and adaptions will be incorporated taking on the feedback received.
• It was highlighted that Healthwatch Suffolk has a Co-production team who would be willing and able to provide any appropriate training to eventual members of the Quality Committee through a workshop to help set the standard to ensure that any co-production work going forwards remains authentic. This offer would be welcomed.
• It was noted that the CQC was included within the ‘Business as Usual’ section of the National Quality Board’s guidance. It was felt that their strategy is not business as usual and that it would be timely for us to challenge ourselves as a whole system, as this is what the CQC will be looking at going forwards.
• A query was raised as to whether we need to look at how we manage the continuous quality improvement process outside of the Committee and whether this provides us with an opportunity to put in train something that helps peer review. We need to assure ourselves outside of the Providers’ individual quality committees that we are getting what we are hoping for, and we need to consider how we proactively take that quality improvement process forward in a systematic rather than reactive way within the system.
• It was highlighted that we also need to consider staff in the system, and not just people, patients and customers; for example as a result of ambulance delays, clinicians are having to work in different ways which is increasing their risk. It will be important that the Quality Committee is able to pick up on such issues to ensure that they are looking at learning from outside the room as well.
In conclusion, it was agreed that a number of actions and offers of help have been put forward, in particular around co-production. Consideration must be given to how this committee will be broader than health, it is not just patients but all people using and delivering the services. It was agreed that we must continue to work in a proactive way to bring better outcomes for everyone.
5. Optometry
PMc from the Local Optical Committee (LOC) was welcomed to the meeting and gave a very enlightening and informative presentation about the challenges, opportunities, and possible solutions in respect of eye care provision locally and nationally. A constructive discussion ensued, the key points of which included:
• It was acknowledged that a local Optom who is engaged with a primary care practice makes a real difference to the care that can be given to patients. It was highlighted that Evolutio does have a telephone support line that patients and local Opticians can use to get early support if it is required (patients are typically seen in the clinic in Ipswich). It was agreed that it would be helpful for the LOC to liaise more with the Local Medical
Page 46 of 47
Committee (LMC) to keep them informed as to what is available and to make the GPs job easier. (NB the telephone number will be shared so that it can circulated more widely).
• It was highlighted that if it was possible for everyone to use SystmOne as a joined up clinical record, we could easily share the transfer of concerns.
• It was reported that Healthwatch’s feedback from the public during the pandemic suggested that optometry services were resourceful and consistent in their delivery of the services that were possible and that this had been really appreciated.
• A query was raised around the care of Looked After Children and Young People. The offer of the Healthwatch Community Team, to help the LOC understand what services are needed where, was made. This was accepted by PMc who felt that further integration of what is currently on offer would be very much welcomed.
• A concern was raised that Alliance members may need to do more to highlight the need to look after your eyes – not just to their employees but also to other professionals and personally. PMc agreed that the LOC would welcome the opportunity to do anything that promotes the importance of regular eye examinations.
• It was reported that there is a SNEE Eye Care Clinical Programme Board of which PMc and the LOC are key members. As part of this, ESNEFT has led a local programme of work in respect of demand and capacity which members may be interested in reading; the outcome from this being six key recommendations. It noted that there is a need for an increased role of the optom community to meet the expected increase in demand, particularly in view of our aging population over the next four to six years. We need to understand what more can be done by reviewing our existing community pathways, not just in respect of cataracts but also retinal disorders. It is recognised that the national tariffs and national contract are an inhibitor, but we need to find a way round this looking at what can we do differently to take account of some of the challenges. It was highlighted that the group is establishing close working relationships from clinical and professional levels across the area. RW would be happy to bring back more details if required.
• A query was raised as to whether there are any proactive or specific pieces of work in respect of children, dementia or frail patients ie is there more that we can do within care homes or own homes. There is also a need to consider what more can we do within the prevention space and how we address inequality as we will undoubtedly see more problems arising in communities where we have deprivation and inequality. How can we work together to try and ensure we get better coverage not only of services but information about what is available. PMc outlined some of the work that is already undertaken in respect of children services (highlighting that children’s eye exams are free but recognising that children in deprived areas may not have access), work with the elderly and vulnerable particularly in care homes and in relation to falls. However, it was acknowledged that much more can be done going forwards.
• It was reported that as part of the Community Diagnostic Hub in Clacton phase 2 planning, they are looking to implement an ophthalmology bus to serve people who need specialist eye care and consideration should possible be given as to whether a similar model would be applicable in our locality.
• The use of technology was highlighted and in particular the Femtosecond Laser that ESNEFT has invested in at Ipswich Hospital which will help with cataract productivity. It was suggested that ESNEFT could potentially look at how we get investment in the right way to join up optometry services and secondary services better possibly by making revenue investment into the services.
Page 47 of 47
• A prevention approach was welcomed and the query raised as to whether a Public Health approach had been taken. MSe offered to speak off-line with PMc to review potential future health promotion campaigns.
The Committee thanked PMc for his attendance and for providing such an informative presentation which generated a constructive discussion with plenty of connections and offers of assistance being made. A method to capture all the outputs from these connections will be considered to ensure we are fully aware of what has happened and what more is needed to support the importance of optometry as part of primary care.
6. District and Borough Partnership working within our Alliance
KN and JJ took the Committee through the considerable and varied programmes of work within Babergh and Mid Suffolk Council and Ipswich Borough Council localities. Due to a prior commitment, the East Suffolk Council representative had been unable to attend but an update had been provided within the presentation. It was highlighted that there is a lot of similarity to how the three local authorities are working to tackle the wider determinants of health The Committee agreed that the updates clearly showed the breadth and depth of programmes that are taking place together with the shared learning opportunities that are available as a consequence. It was reported that the Public Health team are looking internally at their structure. The proposed structure will give more commitment to place with consultant leads within each of the District and Boroughs. The aim is to ensure that better relationships are in place and for more opportunities to work together. MBW thanked KN, JJ, NR for their update and particularly LHa who is a great facilitator of relationships and partnership working. It was highlighted that the Alliance, with the Districts and Boroughs, has a shared vision focused on the wider determinates of health which will also be authority and community specific within each of the localities. We now have organic relationships, with delivery focused in terms of our strategy and the different services and sites. Investment, both joint and aligned has been critical, as have the appointment of joint roles. However, we need to prepare for the next stage when we move into an ICB and it is very important that we evolve today’s narrative and share what we have done with wider system colleagues across the ICS. Informed data will be imperative, using what is available from the Suffolk Office of Data and Analytics (SODA), Population Health Management and Outcomes Based Assessment. We will also need to consider the next stages of our governance and shared leadership, together with the future investment that will be required. The Committee agreed that the updates had shown just how much has been achieved and provides a great deal of optimism going forwards.
8. Any Other Business
MBW on behalf of the Committee thanked LH for her administration of the Alliance Committee meetings prior to her retirement at the end of the month.
Date of Next meeting
Tuesday 19 April 2022
CLOSE
Related Documents











