Meditation and Somatic Arousal Reduction A Review of the Experimental Evidence David S. Holmes University of Kansas ABSTRACT: The conceptual and methodological is- sues associated with research on the effects of med- itation are reviewed. A summary of the research in which the somatic arousal of meditating subjects was compared to the somatic arousal of resting subjects did not reveal any consistent differences between med- itating and resting subjects on measures of heart rate, electrodermal activity, respiration rate, systolic blood pressure, diastolic blood pressure, skin temperature, oxygen consumption, EMG activity, blood flow, or various biochemicalfactors. Similarly, a review of the research on the effects of meditation in controlling arousal in threatening situations did not reveal any consistent differences between meditating and non- meditating (no-treatment, antimeditation, or relax- ation) subjects. The implications of these findings for research and practice are discussed. Over the past 15 years there has been widespread interest in the practice of meditation, with the most publicized and popular technique being transcenden- tal meditation (TM; Maharishi, 1963). It appears that many persons use meditation to reduce physiological and subjective arousal, and because of its purported effects on arousal, meditation is used to treat nu- merous disorders that stem from or involve hyper- arousal. For example, meditation has been used to treat a variety of psychiatric disorders (Bloomfield, Cain, Jaffee, & Kory, 1975; Glueck & Stroebel, 1975), hypertension (Benson, Rosner, & Marzetta, 1973; Benson & Wallace, 1972; Blackwell et al., 1975; Mi- chaels, Huber, & McCann, 1976; Simon, Oparil, & Kimball, 1977), asthma (Wilson, Honsberger, Chiu, & Novey, 1975), inflammation of the gums (Klemons, 1977), drug abuse (Benson & Wallace, 1972; Sham', Lavely, & Jaffe, 1974), alcohol abuse (Shafii, Lavely, &Jafte, 1975), insomnia (Miskiman, 1977a, 1977b), and stuttering (Mclntyre, Silverman, & Trotter, 1974). Furthermore, meditation has been suggested as an alternative to progressive muscle relaxation training (Boudreau, 1972). In view of the pervasive interest in the use of meditation to reduce arousal, it seemed important to carefully review the empirical research on the effects of meditation on somatic arousal, and therefore the present review was prepared. 1 This review is divided into four sections. In the first section, conceptual and methodological issues and problems will be discussed, thus providing a per- spective within which to evaluate the research. The second section will be focused on the question of whether subjects who meditate show lower somatic arousal while they are meditating than other subjects show while they are simply resting. The third section will be focused on the question of whether subjects who meditate show less somatic response to threat. In the fourth section overall conclusions will be drawn. Conceptual and Methodological Considerations Types of Investigations Case study. The research on meditation can be di- vided into three distinct groups. The first group con- tains case studies of the effects of meditation. Those accounts provide a rich source of hypotheses con- cerning the effects of meditation, but because they lack controls they cannot be used as empirical tests of the effects of meditation, and consequently they will not be considered here. Requests for reprints should be sent to David S. Holmes, Depart- ment of Psychology, University of Kansas, Fraser Hall, Lawrence, Kansas 66045. 1 It should be recognized that not all forms of meditation are designed to reduce arousal. Indeed, some types of meditation— such as Maulavi, the dancing practice of the "whirling dervishes"— involve considerable bodily activity and serve to increase arousal. The present review focuses on more passive forms of meditation that are designed to reduce arousal. For a discussion of the types of meditation, see Naranjo and Ornstein (1971). The influence of meditation on arousal has been examined in a number of previous reviews (Akishige, 1968; Davidson, 1976; Oellhorn & Kiely, 1972; Kanellakos & Lukas, 1974; Rigby, 1977; Schuman, 1980; Shapiro, 1980; Woolfolk, 1975). Unfortunately, the conclusions drawn in previous reviews generally cannot be accepted because the authors were selective in the investigations they cited; disregarded methodological problems in drawing con- clusions from investigations; and/or indiscriminantly mixed results of case studies, uncontrolled investigations, and appropriately con- trolled experiments in drawing their conclusions. This manuscript focuses on the somatic responses associated with meditation, but is not intended to deny the wide variety of potentially important subjective experiences that have been at- January 1984 • American Psychologist Copyright 1984 by the American Psychological Association, Inc. Vol. 39, No. 1, !-10

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Meditation and Somatic Arousal ReductionA Review of the Experimental Evidence
David S. Holmes University of Kansas
ABSTRACT: The conceptual and methodological is-sues associated with research on the effects of med-itation are reviewed. A summary of the research inwhich the somatic arousal of meditating subjects wascompared to the somatic arousal of resting subjectsdid not reveal any consistent differences between med-itating and resting subjects on measures of heart rate,electrodermal activity, respiration rate, systolic bloodpressure, diastolic blood pressure, skin temperature,oxygen consumption, EMG activity, blood flow, orvarious biochemical factors. Similarly, a review of theresearch on the effects of meditation in controllingarousal in threatening situations did not reveal anyconsistent differences between meditating and non-meditating (no-treatment, antimeditation, or relax-ation) subjects. The implications of these findings forresearch and practice are discussed.
Over the past 15 years there has been widespreadinterest in the practice of meditation, with the mostpublicized and popular technique being transcenden-tal meditation (TM; Maharishi, 1963). It appears thatmany persons use meditation to reduce physiologicaland subjective arousal, and because of its purportedeffects on arousal, meditation is used to treat nu-merous disorders that stem from or involve hyper-arousal. For example, meditation has been used totreat a variety of psychiatric disorders (Bloomfield,Cain, Jaffee, & Kory, 1975; Glueck & Stroebel, 1975),hypertension (Benson, Rosner, & Marzetta, 1973;Benson & Wallace, 1972; Blackwell et al., 1975; Mi-chaels, Huber, & McCann, 1976; Simon, Oparil, &Kimball, 1977), asthma (Wilson, Honsberger, Chiu,& Novey, 1975), inflammation of the gums (Klemons,1977), drug abuse (Benson & Wallace, 1972; Sham',Lavely, & Jaffe, 1974), alcohol abuse (Shafii, Lavely,&Jafte, 1975), insomnia (Miskiman, 1977a, 1977b),and stuttering (Mclntyre, Silverman, & Trotter, 1974).Furthermore, meditation has been suggested as analternative to progressive muscle relaxation training(Boudreau, 1972). In view of the pervasive interestin the use of meditation to reduce arousal, it seemedimportant to carefully review the empirical researchon the effects of meditation on somatic arousal, andtherefore the present review was prepared.1
This review is divided into four sections. In thefirst section, conceptual and methodological issuesand problems will be discussed, thus providing a per-spective within which to evaluate the research. Thesecond section will be focused on the question ofwhether subjects who meditate show lower somaticarousal while they are meditating than other subjectsshow while they are simply resting. The third sectionwill be focused on the question of whether subjectswho meditate show less somatic response to threat.In the fourth section overall conclusions will be drawn.
Conceptual and MethodologicalConsiderations
Types of Investigations
Case study. The research on meditation can be di-vided into three distinct groups. The first group con-tains case studies of the effects of meditation. Thoseaccounts provide a rich source of hypotheses con-cerning the effects of meditation, but because theylack controls they cannot be used as empirical testsof the effects of meditation, and consequently theywill not be considered here.
Requests for reprints should be sent to David S. Holmes, Depart-ment of Psychology, University of Kansas, Fraser Hall, Lawrence,Kansas 66045.
1 It should be recognized that not all forms of meditation aredesigned to reduce arousal. Indeed, some types of meditation—such as Maulavi, the dancing practice of the "whirling dervishes"—involve considerable bodily activity and serve to increase arousal.The present review focuses on more passive forms of meditationthat are designed to reduce arousal. For a discussion of the typesof meditation, see Naranjo and Ornstein (1971).
The influence of meditation on arousal has been examinedin a number of previous reviews (Akishige, 1968; Davidson, 1976;Oellhorn & Kiely, 1972; Kanellakos & Lukas, 1974; Rigby, 1977;Schuman, 1980; Shapiro, 1980; Woolfolk, 1975). Unfortunately,the conclusions drawn in previous reviews generally cannot beaccepted because the authors were selective in the investigationsthey cited; disregarded methodological problems in drawing con-clusions from investigations; and/or indiscriminantly mixed resultsof case studies, uncontrolled investigations, and appropriately con-trolled experiments in drawing their conclusions.
This manuscript focuses on the somatic responses associatedwith meditation, but is not intended to deny the wide variety ofpotentially important subjective experiences that have been at-
January 1984 • American PsychologistCopyright 1984 by the American Psychological Association, Inc.Vol. 39, No. 1, !-10

Own-control. The second group contains in-vestigations in which the own-control research designis employed (e.g., Bakker, 1977; Beary & Benson,1974; Benson, Steinart, Greenwood, Klemchuk, &Peterson, 1975; Herbert, 1977;Janby, 1977;McCuaig,1974; Wallace, 1970; Wallace & Benson, 1972; Wal-lace, Benson, & Wilson, 1971; West, 1977; Younger,Adriance, & Berger, 1975). In this type of investi-gation, subjects are first asked to simply sit quietlywithout meditating, then they are asked to meditate,and finally they usually are asked again to simply sitquietly. The pre- and postmeditation periods are usedas "control" periods, and the levels of arousal evi-denced during those periods are compared to thelevel of arousal evidenced during the meditation pe-riod.
The results obtained with the own-control designhave indicated consistently that subjects had lowerarousal while meditating than they did before or aftermeditating, and those results have been generally ac-cepted as evidence for the effectiveness of meditationfor reducing arousal. It is important to recognize,however, that those investigations suffer from a seriouslimitation because they do not indicate whether med-itation is more effective than other arousal-reducingstrategies such as simply resting. Indeed, subjects whosit quietly and then rest may show the same decreasein arousal as subjects who sit quietly and then med-itate. Because it is generally assumed that meditationresults in different effects than does simply resting,and because those proposed differences have a varietyof important theoretical and practical implications,it is essential to directly compare the effects of med-itation to the effects of resting. Therefore, this reviewwill not rely on data from investigations that employedthe own-control approach.2
Experimental control. The third group containsinvestigations in which the experimental-control ap-proach was used. With that approach, a group ofsubjects trained in meditation are asked to meditate,whereas another group of subjects not trained inmeditation are asked to rest. Then the arousal levelsof meditating subjects are compared to the arousallevels of resting subjects. This is generally the most
tributed to meditation. Space limitations do not permit a consid-eration of all of the responses associated with meditation, and thesomatic responses were selected for study because of their relevancefor the treatment of the disorders noted previously. Readers in-terested in the research concerning the influence of meditation onsubjective or cognitive responses should consult other reviews (e.g.,Shapiro, 1980; Smith, 1975).
2 It might be noted that to overcome some of the limitationsof the typical own-control procedure, a multiple-activity own-controlprocedure could be used in which, for example, subjects sat quietly,meditated, sat quietly, rested, sat quietly, rested, and sat quietly.Unfortunately, this procedure has not been used to study meditation,although an own-control with different activities on different dayshas been used (see the discussion of the research of Pagano, Rose,Stivers, & Warrenburg, 1976, in the next section).
effective approach to studying the effects of medi-tation, and my review focuses on the results of ex-periments in which this approach was used.
Before concluding this overview of approaches,I should note that some investigators have used acombination of the own-control design and the ex-perimental-control design. In one case, the subjectsparticipated in a sit/meditation/sit sequence on somedays and in a sit/rest/sit sequence on other days, thusmaking it possible to compare meditation and restingwithin the same subjects (Pagano, Rose, Stivers, &Warrenburg, 1976). Unfortunately, if this approachdid not yield differences between the meditation andrest days, it could be argued that on the rest days themeditatiors "slipped into" their meditative state. Inanother group of investigations, subjects' arousal levelswere assessed while resting before they had beentaught to meditate, and then three to four monthslater after the subjects had been taught to meditatetheir arousal levels were assessed while meditating(Jevning, Wilson, Smith, & Morton, 1978; Jevning,Pirkle, & Wilson, 1977; Jevning, Wilson, & Davidson,1978; Jevning, Wilson, & VanderLaan, 1978). Withthat approach, however, the meditation versus restcomparison is confounded with factors such as time,history, laboratory experience, and so on, thus makingthe conclusions drawn from the data subject to al-ternative interpretations.
Methodological Issues
Although the experimental-control design is generallythe best approach for studying the effects of medi-tation, many of the investigations in which that ap-proach was used suffer from one or more potentiallyserious methodological problems, and some brief at-tention should be given to those problems before re-viewing the data.
Amount of training/experience with meditation.One potential problem revolves around the natureand amount of training and experience the meditatingsubjects had with meditation. Obviously, if the sub-jects in the meditation condition were not adequatelytrained or experienced with the technique, the com-parison with the nonmeditating subjects would bemeaningless. It has been asserted that almost anyonecan learn the TM technique in only a few trainingsessions (Maharishi, 1963), but a number of inves-tigations have revealed differences between novicesand advanced meditators (cf. Jevning et al., 1977;Jevning, Wilson, & Davidson, 1978; Jevning, Wilson,Smith, & Morton, 1978; Jevning, Wilson, &VanderLann, 1978; Lang, Dehob, Meurer, & Kauf-man, 1979). Certainly, if subjects with limited trainingor experience served in an experiment that did notreveal differences between meditating and restingsubjects, the lack of a difference might be attributedto an ineffective manipulation of the independent
January 1984 • American Psychologist

variable (i.e., meditation). With regard to the training/experience issue, it might be noted that in some in-vestigations the meditators had as little as two orthree weeks of experience (cf. Boswell & Murray,1979; Parker, Gilbert, & Thoreson, 1978), whereasin others the subjects had between three and five yearsof experience or were qualified as teachers of TM (cf.Holmes, Solomon, Cappo, & Greenberg, 1983; Jevn-ing et al., 1977; Jevning, Wilson, & Davidson, 1978;Jevning, Wilson, Smith, & Morton, 1978; Jevning,Wilson, & VanderLann, 1978).
Subject selection. It is, of course, desirable torandomly assign subjects to conditions, but if subjectsare randomly assigned it may be practically impossibleto conduct and maintain the experimental manipu-lation (learning and practicing meditation) over thenumber of weeks, months, or years that may be nec-essary to assure that the meditators receive sufficienttraining and experience. Consequently, in the inves-tigations that involved prolonged training or expe-riencej subjects were not randomly assigned to con-ditions. Instead, persons who earlier had voluntarilyelected to become meditators and who had main-tained the practice for some time were compared (a)to a matched group of nonmeditators, (b) to a ran-domly selected group of nonmeditators, or (c) to agroup of nonmeditators who had recently elected tolearn meditation but who had not yet learned orpracticed the technique. Those procedures may in-troduce problems, because persons who elect to learnto meditate and who continue the practice for manyyears may differ in some ways from persons who donot elect to learn to meditate or who do not continuewith meditation once it is learned.
Analyses of data. The major statistical problemencountered in this body of research revolves aroundthe failure of investigators to control for the influenceof initial differences in arousal between meditatingand nonmeditating subjects (i.e., the law of initialvalues; Lacey, 1956; Wilder, 1962). Initial differencesbetween meditating and nonmeditating subjects caninfluence subsequent scores directly (e.g., in the ab-sence of any change, subjects with lower initial arousalmay appear to have decreased their arousal at sub-sequent times relative to subjects with higher initialarousal) and can inhibit the degree to which subjectscan change their levels of arousal (e.g., ceiling andfloor effects). The effects of initial differences are par-ticularly pronounced with physiological measures, andit has been demonstrated that even nonreliable initialdifferences can create or obscure subsequent reliabledifferences (Kinsman & Staudenmayer, 1978). Simpledifference scores are insufficient for controlling forthe effects of initial differences, and therefore eithercovariance or residualization procedures must beemployed (Benjamin, 1967; Cronbach & Furby,1970). Unfortunately, these controls have been used
only rarely. In the absence of those corrections, at aminimum it would be necessary to conduct a con-ditions (meditating subjects vs. resting subjects) bytrials (premeditation/prerest period vs. meditation/rest period) analysis of variance in which a conditionsby trials interaction is predicted (e.g., greater reductionin arousal across trials for meditating than for restingsubjects). Regrettably, in most cases the investigatorssimply compared the meditating and resting subjectsduring the meditation/rest period.
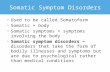
Somatic Arousal During MeditationHaving identified the types of investigations that havebeen conducted and the various potential method-ological problems, in this section I will examinewhether subjects who are meditating evidence lowerlevels of arousal than subjects who are resting. Table1 contains a summary of the experimental findingsconcerning heart rate, electrodermal activity, respi-ration rate, blood pressure, EMG activity, skin tem-perature, oxygen consumption, and blood flow. Thefindings concerning biochemical factors could not beefficiently summarized in tabular form because somany substances have been examined, and thereforea summary of the experimental findings concerningbiochemical factors is presented in a subsequentparagraph. The information in Table 1 and the para-graph on biochemical factors make it possible to ex-amine the effects of meditation on any one responseacross experiments and to examine the effects ofmeditation across responses within any one experi-ment.3
Heart Rate
In none of the 16 experiments in which heart ratewas monitored did the meditating subjects evidencereliably greater decreases in heart rate than did theresting subjects. On the other hand, in four of theexperiments the meditating subjects actually evi-denced greater increases in heart rate than did theresting subjects (Elson, Huari, & Cunis, 1977; Gole-man & Schwartz, 1976; Michaels, Parra, McCann,& Vander, 1979; Travis, Kondo, & Knott, 1976).4
Electrodermal Activity
Of the 13 experiments in which electrodermal activitywas measured, only one provided reliable evidence
3 Research that was only reported in an abstract was not con-sidered in this review because such reports rarely contain sufficientinformation to enable an adequate evaluation of the proceduresand results. Research concerning EEG responses was not consideredin this review because adequate ways of quantifying and comparingEEG activity in different groups were not available or used.
4 Heart rate was considered in one other experiment involvingmeditating and resting subjects, but the measurement of heart ratedid not occur until after the meditation/rest period and thus thedata do not reflect directly on the meditation (Corey, 1977).
January 1984 • American Psychologist
Table 1Experiments Measuring Somatic Arousal and Whether Meditating Subjects Experienced LowerArousal Than Resting Subjects
ExperimentHeartrate Electodermal Respiration
Bloodpressure EMG Other
Bahrke & Morgan (1978) No
Boswell & Murray (1979) No NoCauthen & Prymak
(1977) No NoCurtis & Wessberg
(1975/1976) No NoDhanaraj & Singh (1977) No
No
NoNo
O2, noTemperature, no
Temperature, no
O2, yesRespiratory tidal volume, yes
Elsonet al. (1977)Goleman & Schwartz
(1976)Holmes et al. (1983)Jevning, Wilson, Smith, &
Morton (1978)Lintel (1980)Malec & Sipprelle (1977)Michaels et al. (1979)Morse et al. (1977)Orme-Johnson (1 973)Parker et al. (1978)Raskin et al. (1980)Routt (1 977)Travis et al. (1976)Walrath & Hamilton
(1975)Zuroff & Schwarz(1978)
No8
No"No
NoNo8
No
No
NoNoa
NoNo
Yesb Yes Temperature, no
NoNo No" No
Blood flow, yesNoNo Yes
NoNo No No YesNoNo Yes
NoNo No Blood flow, no
No Heart-rate variability, no
No No
' Reliably higher arousal observed In meditating than resting subjects.3 Meditating subjects were Initially more aroused, and hence their greater decrease in arousal may have been due to regression to the mean.
that meditating subjects achieved greater decreasesin arousal than did resting subjects. Caution must beexercised in accepting the results of that investigation,however, because the meditating subjects began withconsiderably higher arousal than did the resting sub-jects (/[20] = 1.48, p = .15; test computed by thepresent author based on data in the original report;Elson et al., 1977, Table 1). Indeed, at the end of themeditation/rest period, the meditating subjectsshowed only slightly lower arousal than the restingsubjects (Elson et al., 1977, Figure 2), and the declinein arousal evidenced by meditating subjects can prob-ably be attributed to regression to the mean.
In considering the findings concerning electro-dermal measures, some attention should be given tothe often-cited work of Orme-Johnson (1973). Theresults of his investigation indicated that experiencedmeditators showed reliably fewer spontaneous GSRresponses while meditating than nonmeditators didwhile resting, and thus it was concluded that medi-tation served to reduce arousal. It is important to
recognize, however, that the meditators also showedreliably fewer spontaneous GSR responses than didthe nonmeditators when the two groups of subjectswere simply asked to sit quietly (i.e., during a periodin which the meditators were not meditating). In fact,the difference between the groups during the sittingperiod was almost identical to the difference betweenthe groups during the meditation/rest period, thusclearly indicating that the meditation did not serveto reduce arousal from the initial level. Of course, itcould be argued that the long-term practice of med-itation had served to reduce the chronic levels ofarousal of meditators, but the other research reviewedin Table 1 has not supported that possibility (i.e., theother research has not generally revealed differencesbetween experienced meditators and nonmeditatorsin resting levels of arousal). Therefore, it is most likelythat the effects noted in this investigation were dueto subject-selection factors. In any event, this inves-tigation did not provide evidence that the act of med-itating reduced subjects' phasic levels of arousal, al-
January 1984 • American Psychologist

though it did highlight the importance of controllingfor initial levels of arousal (see earlier discussion).5
Respiration Rate
The eight comparisons of the changes in respirationrates associated with meditation and rest revealedonly one case in which the meditating subjects evi-denced a reliably greater decrease in respiration ratethan did resting subjects (Elson et al., 1977). Inter-estingly, there was also one experiment in which med-itating subjects showed reliably higher respiration ratesthan resting subjects did (Holmes et al., 1983).
Blood Pressure
Only one of four experiments in which blood pressurewas measured indicated that decreases in blood pres-sure were greater with meditation than with rest (Par-ker et al., 1978). It might be noted, however, that theone set of positive findings was based on 10 alcoholicsubjects who had only been exposed to meditationfor three weeks (the amount of time spent meditatingin that period is not clear from the report). Becauseother investigations with larger samples of more ex-perienced meditators did not reveal changes in bloodpressure, one must question both the replicabilityand the generalizability of the one set of positive find-ings.
EMG Activity
EMG activity was assessed in four experiments, butonly two of those provided evidence that meditatingsubjects experienced less muscle tension than didresting subjects.
Other Variables
None of the three experiments that measured skintemperature revealed reliable differences betweenmeditating and resting subjects. In only one of thetwo investigations of blood flow did the meditatingsubjects evidence a reduced blood flow relative toresting subjects. In only one of two experiments deal-ing with oxygen consumption did meditating subjectsevidence reliably lower levels than resting subjects.6
Finally, in one comparison for each variable, medi-tating subjects were found to have reduced respiratory
5 One other experiment reported that meditating subjects ev-idenced lower arousal as measured by skin resistance than didcontrol subjects (Laurie, 1977). In that experiment, however, thecontrol subjects were told to "meditate" (rather than to rest), butthey had not had any experience with meditation and were notinstructed in how to meditate. Under those circumstances, com-plying with the instructions might have been difficult or anxiety-provoking for the control subjects, and thus the arousal of thosesubjects may not have declined as much as if they had been askedto simply rest.
6 Oxygen consumption was also measured in one other ex-periment, but in that case the control subjects listened to classicalmusic rather than simply resting and it is likely that the musicinfluenced respiration (Fenwick et al., 1977).
tidal volume but not different heart-rate variabilitythan resting subjects.
Biochemical Factors
Of the 29 comparisons that were made regarding 27substances in 6 experiments, only 4 reliable differencesbetween meditating and resting subjects were found.Specifically, no reliable differences were found inplasma renin or aldosterone (Michaels et al., 1979);VMA, urine adrenaline, urine noradrenaline orplasma adrenaline (Lang et al., 1979); growth hor-mone (Jevning, Wilson, & VanderLaan, 1978); tes-tosterone (Jevning, Wilson, & Davidson, 1978); nor-epinephrine or epinephrine (Michaels et al., 1976);plasma lactate (Michaels et al., 1976, 1979); threo-nine, serine, asparagine, glutamic, glutamine, glycine,alanine, citrulline, valine, isoleucine, leucine, or ty-rosine (Jevning et al., 1977). Some comments shouldbe made concerning the four reliable differences thatwere found. First, one investigation yielded a differ-ence in plasma cortisol (Jevning, Wilson, & Davidson,1978), but another did not (Michaels et al., 1979).Second, levels of plasma prolactin were found to differbetween meditating and resting subjects, but the dif-ference did not appear until the rest period after themeditation period (Jevning, Wilson, & VanderLaan,1978). Third, meditators were found to have higherlevels of plasma noradrenaline (Lang et al., 1979).Fourth, meditating subjects were found to have higherlevels of phenylalanine than resting subjects, a findingwhich reflects high arousal in meditators and a findingthe authors described as "unexpected" (Jevning etal., 1977). Overall then, these findings do not provideevidence that meditation reduces arousal as measuredby various biochemical factors.
Comments and Conclusions
A number of comments should be made concerningthe results of the experiments in which the levels ofarousal of meditating subjects were compared to thelevels of arousal of resting subjects. First, from Table1 and the accompanying discussion, it is clear thatacross experiments there is not a measure of arousalon which the meditating subjects were consistentlyfound to have reliably lower arousal than resting sub-jects. Indeed, the most consistent finding was thatthere were not reliable differences between meditatingand resting subjects. Furthermore, there appear to beabout as many instances in which the meditating sub-jects showed reliably higher arousal as there are in-stances in which they showed reliably lower arousalthan their resting counterparts.
Second, it is clear that within any one experimentthere is no consistent evidence across measures thatmeditating subjects have reliably lower arousal thanresting subjects. In fact, of the 21 experiments thatinvolved more than one measure of arousal, only 2
January 1984 • American Psychologist
experiments revealed reliably lower arousal of med-itating subjects on more than one of the measuresconsidered (Dhanaraj & Singh, 1977; Elson et al.,1977), and in the latter of those two experiments themeditating subjects evidenced reliably higher arousalon one of the other measures.
Third, it is very important to recognize that theresults of one well-done experiment can outweigh theresults of numerous less-well-done experiments, andthus in addition to simply counting findings, thequality of the research must be considered. With thepresent set of experiments, considering those withmore or fewer problems does not change the pat-terning of results. Furthermore, as noted in the pre-ceeding paragraph, not one experiment providedconsistent evidence that meditating subjects were lessaroused than resting subjects, and thus the possibilitythat there is one good experiment confirming theutility of meditation for reducing arousal is precluded.Indeed, there does not even appear to be one badexperiment offering consistent evidence that medi-tating reduces arousal more than resting.
Fourth, in this review I have only been able todraw conclusions from published research, and giventhe differential difficulty associated with publishingconfirming results versus null results, the incidenceof null results summarized here is probably an un-derestimate of those which have actually been found.
Fifth, although in the majority of experimentsthe meditating subjects used the TM technique, ex-periments in which other techniques were used didnot yield appreciably different results (Bahrke &Morgan, 1978; Elson et al., 1977). Although it is pos-sible that other meditation techniques might be moreeffective for reducing somatic arousal than thosewhich were reviewed here, at the present time thereare no data to support that speculation.
Sixth and finally, although the investigations inwhich the experimental-control procedure was useddid not provide evidence for the arousal-reducingfunction of meditation, the investigations in whichthe own-control procedure was used did provide suchevidence (see earlier citations). As noted earlier, how-ever, the own-control procedure does not permit theappropriate comparison. Regarding this difference inconclusions, it might be noted that in one investigationthe data were analyzed both ways, thus providing adirect comparison of the two approaches (Holmes etal., 1983). The own-control comparison indicated thatmeditation reduced arousal from the premeditationlevel, but the experimental-control comparison in-dicated that meditation did not reduce arousal morethan did resting. The sharp difference in findings il-lustrates the importance of the methodological issue;the distinction between the types of research shouldbe kept in mind when evaluating the research findingsand the conclusions of authors.
Overall then, it appears that there is no measurewhich across experiments reflects lower arousal inmeditating than in resting subjects and that there isno experiment which across measures reflects lowerarousal in meditating than in resting subjects. In viewof those results I must conclude that at the presenttime there is no evidence that meditation is moreeffective for reducing somatic arousal than is simplyresting.
Meditation and Control of SomaticArousal in Threatening SituationsIn this section, attention will be focused on the ques-tion of whether subjects who practice meditation arebetter able to control their arousal in threatening sit-uations than are subjects who do not practice med-itation. There are three reasons why it is importantto answer that question. First, it is practically im-portant. One of the reasons why meditation is oftenused as a psychotherapeutic technique is that it iswidely believed that meditation will facilitate the con-trol of arousal in threatening situations.
Second, an examination of the ability of med-itators and nonmeditators to control arousal inthreatening situations might reflect on differences inthe processes involved in meditating and resting.Consider the following: In the previous section it wasfound that meditating and resting subjects evidencedcomparable reductions in arousal, but it is possiblethat the meditating and resting subjects achieved theircomparable reductions through different processes.Specifically, in resting subjects the arousal reductionsmay have been due to adaptation, whereas in med-itating subjects the reductions may have been due toadaptation or to something the meditating subjectslearned as a consequence of their meditation. It isunlikely that the adaptation that the resting subjectsexperienced would be of any value in a subsequentthreatening situation, but it is possible that if themeditating subjects learned something as a conse-quence of the meditation they might be able to applythat knowledge in a subsequent threatening situation.Differences in arousal levels between meditators andnonmeditators under stress might then influence in-terpretation of the results that were reviewed in theprevious section.
Third, if there are differences in the ability tocontrol arousal between meditators and nonmedi-tators, the differences may be more apparent inthreatening situations because the opportunity for dif-ferences in arousal are greater in threatening situationsthan they are in nonthreatening situations. For prac-tical, theoretical, and methodological reasons, then,the ability to control arousal in threatening situationsprovides an excellent test of the effects of meditation.
Surprisingly, despite the importance of experi-ments on the effect of meditation on arousal in
January 1984 • American Psychologist

threatening situations, there are only four such ex-periments. Because these experiments are more com-plex than those in the previous section and becauseit is important to consider the types of threats thatwere used, in this section I will consider each exper-iment individually.
Review of the ResearchThe first experiment in this series provided a test ofthe effects of meditation in a threatening "real-life"situation that was personally relevant for the subjects(Kirsch & Henry, 1979). Thirty-eight speech-anxioussubjects were each asked to give a speech and theirheart rates were assessed immediately before thespeeches were given. For three weeks following thespeeches, the subjects participated in one of four con-ditions: (a) systematic desensitization in which thesubjects used progressive muscle relaxation training;(b) systematic desensitization in which meditationreplaced the muscle relaxation training; (c) medita-tion; or (d) no-treatment. Following the treatmentperiod, each subject was asked to give a second speechand again heart rates were assessed. Comparisons ofsubjects' speech-related heart rates before and afterthe treatments revealed that only the subjects in thedesensitization-with-relaxation-training conditionevidenced a reliable decrease in heart rate. Meditationdid not result in a decrease in heart rate. (It shouldalso be noted, however, that comparisons among thegroups indicated that the change observed in the de-sensitization-with-relaxation-training conditions wasnot reliably greater than the changes observed in theother conditions.) These findings did not provide anyevidence for the utility of meditation for controllingarousal in threatening situations.
In the second experiment in this series, each of80 subjects was randomly assigned to one of fourconditions: (1) a TM-like mantra meditation condi-tion, (2) an antimeditation (placebo) condition inwhich the subjects walked actively and concentratedon problems, (3) a progressive muscle relaxationtraining condition, and (4) a no-treatment condition(Boswell & Murray, 1979). The treatments were prac-ticed for 15 minutes twice a day for 2 weeks. In thestressful situation which followed the training period,the subjects were required to take a college-level IQtest and a digits backwards test, and the subjects werelead to believe that they had performed poorly onboth tests. To assess stress, data on spontaneous GSR,skin conductance, and heart rate were collected duringthe stressful situation. Comparisons of the subjectsin the four conditions on those measures failed toreveal any reliable differences, and again meditationwas left without any support for its hypothesizedstress-reducing function.
The third and most recent experiment in whichthe stress-reducing function of meditation was tested
involved a comparison of the effects of (a) TM, (b)behavior therapy consisting of progressive muscle re-laxation training and cognitive restructuring, (c) self-relaxation training, and (d) no treatment (Puente &Beiman, 1980). The treatments were conducted overa four-week period. In the stress-testing sessions thatoccured before and after the treatment/no-treatmentperiod, the subjects were shown slides of medical/surgical stimuli that in a pilot study had been foundto elicit physiological and subjective stress responses.While the subjects watched the slides, their heart rateswere recorded. Only the subjects in the behavior ther-apy and the self-relaxation conditions evidenced re-liable reductions in heart rate responses from pre- toposttreatment measurements. The results suggest that,contrary to what is usually assumed, training in med-itation may be less effective for controlling arousalin threatening situations than is training in behaviortherapy or relaxation therapy, and not more effectivethan no treatment.
The fourth and final investigation to be consid-ered is somewhat different from the others in thatalthough it was designed as an experiment, it was notanalyzed as such (Goleman & Schwartz, 1976). Thirtyexperienced meditators were randomly assigned toeither a meditation condition or to a nonmeditationcondition, and 30 nonmeditators were also randomlyassigned to the meditation and nonmeditation con-ditions. Apparently subjects were randomly assignedto the conditions so that the responses of subjects inthe meditation condition could be compared to theresponses of subjects in the nonmeditation condition,but those comparisons were not reported. Instead,responses of experienced meditators were comparedto the responses of nonmeditators regardless of theconditions in which the meditators and nonmeditatorshad served. Obviously, although the investigation wasdesigned as an experiment and gives the initial ap-pearance of an experiment, it was in fact a correla-tional study with the potential problems attendantthereto. Despite this problem, the results of this in-vestigation deserve attention because they are fre-quently cited as evidence for the stress-reducing effectsof meditation.
In this investigation, the responses of meditatorsand nonmeditators were compared while the subjectswatched a stressful film. The film portrayed threeindustrial accidents: "the fingers of a worker are lac-erated, a finger of another is cut off, and an innocentbystander is killed by a wooden plank driven throughhis midsection as a result of carelessness" (Goleman& Schwartz, 1976, p. 458).
Contrary to what might be expected, first it wasfound that during the minute prior to each accident(i.e., when the subjects were anticipating what wasgoing to happen), the meditators showed reliablygreater increases in skin conductance response fre-
January 1984 • American Psychologist
quencies than did the nonmeditators. The authorsacknowledged that generally such a finding would beinterpreted as evidence that meditators showed agreater stress response in the face of threat than didnonmeditators, but the authors chose to interpret thefindings as evidence for a "defensive reaction" (e.g.,vigilance) on the part of the meditators that mightfacilitate adaptive coping reactions. That is certainlyan interesting speculation, but as the other findingswill indicate, it is without support in this investigation.
The second finding was that immediately aftereach accident the meditators showed a reliably greaterdecline in skin conductance response frequencies thandid the nonmeditators, but it is important to recognizethat those declines simply brought the meditatorsdown from their high level of arousal to the level ofarousal of the nonmeditators. That is, the greaterdecline evidenced by the meditators did not result ina lower level of arousal. The authors pointed out thatthe greater postaccident decline in arousal by med-itators may have been due to simple regression fromtheir initially higher levels, but the authors arguedthat was not the case and suggested instead that thedecline was due to a more rapid habituation on thepart of the meditators. No evidence was offered forthat interpretation, however. Furthermore, even if thedeclines were due to faster habituation, the faster ha-bituation did not in any way improve the position ofthe meditators relative to the nonmeditators becausethe habituations did not take the meditators to a lowerlevel of arousal than the nonmeditators had achieved.
The third finding of this investigation involvedheart rate. Although data concerning heart rate werecollected, they were incompletely and inconsistentlyreported, thus making it difficult to draw conclusionsconcerning the reliability of the differences in heartrate between the meditators and nonmeditators. In-spection of the figure presented by the authors (Gole-man & Schwartz, 1976, p. 462, Figure 3) indicates,however, that throughout the stressful film the med-itators had higher heart rates than did the nonmedita-tors.
In summary, this investigation provided no ev-idence that experienced meditators can achieve ormaintain lower levels of arousal in threatening situ-ations than nonmeditators. In fact, the reverse seemsto have been the case.
Summary and Conclusion
In the four experiments described in the proceedingsection, subjects in meditation conditions were com-pared to subjects in no-treatment conditions fourtimes; they were compared to subjects in an anti-meditation condition once; and they were comparedto subjects in conditions involving some sort of re-laxation training five times. Heart rate was used asthe dependent variable four times, and electrodermal
measures (skin conductance response frequencies,skin conductance) were used in three investigations.That combination of conditions and variables yielded17 basic paired comparisons between subjects whomeditated and subjects in other conditions who didnot meditate. The results were very consistent: notone of the comparisons yielded evidence that med-itation was effective for reducing arousal in threat-ening situations. That is, in none of the comparisonsdid the subjects who had meditated show lower so-matic arousal when in a threatening situation thandid subjects in other conditions who did not meditate.On the other hand, in four comparisons it was foundthat the subjects who meditated evidenced greatersomatic arousal in the threatening situations than didthe subjects in the other conditions who did not med-itate (higher skin conductance response frequency andhigher heart rate than nonmeditators, Goleman &Schwartz, 1976; higher heart rates than subjects givenbehavior therapy or self-relaxation training, Puente& Beiman, 1980). These findings provide no evidencewhatsoever that meditation facilitates the control ofarousal in threatening situations. It is possible, ofcourse, that with different types of threat and/or dif-ferent measures of somatic arousal, future researchwill document the often-hypothesized effects of med-itation on arousal.
Overall Conclusions and ImplicationsThis review of the published experimental researchon the influence of meditation on somatic arousaldid not reveal any evidence that meditating subjectsattained lower levels of somatic arousal than did rest-ing subjects. Furthermore, the review did not revealany evidence that subjects who had meditated hadless somatic response to stressful situations than didsubjects who had not meditated. These conclusionsare in sharp contrast to the widely held beliefs aboutthe effects of meditation.
The conclusions generated by this review of theexperimental research have implications for the per-sonal and professional use of meditation as an antidotefor high somatic arousal. Clearly, such use is not jus-tified by the existing research data. This is not to saythat the practice of meditation might not have othereffects, but any such effects could not be due to theusually assumed effect of meditation on somaticarousal. Obviously, that restriction limits the rangeof potential effects of meditation.
The review also illustrated the need for carefulattention to methodological issues and problems whenconsidering research in this area. Indeed, the originalconclusion that meditation resulted in a unique re-duction of somatic arousal was undoubtedly basedon the uncritical acceptance of conclusions from own-control comparisons rather than from experimentaltests involving appropriate control conditions.
January 1984 • American Psychologist

The practice of meditation has a long history, itis now well established in Western society, and itsalleged effects have a good deal of face validity andare widely accepted. In view of those factors, it isimportant that we recognize that within the existingresearch there is no evidence that meditation is moreeffective for reducing somatic arousal than is simpleresting.
REFERENCES
Akishige, Y, (Ed.). (1968). Psychological studies on Zen (KyushuPsychological Studies, No. 5). Fukuoka, Japan: Kyushu Uni-versity.
Bahrke, M. S., & Morgan, W. P. (1978). Anxiety reduction followingexercise and meditation. Cognitive Therapy and Research, 2,323-333.
Bakker, R. (1977). Decreased respiratory rate during the transcen-dental meditation technique: A replication. In D. Orme-Johnson& J. Farrow (Eds.), Scientific research on the transcendental med-itation program (Vol. 1, pp. 140-141). Los Angeles: MaharishiEuropean Research University Press.
Beary, J. F., & Benson, H. (1974). A simple psychophysiologictechnique which elicits the hypometabolic changes on the relax-ation response. Psychosomatic Medicine, 36, 115-120.
Benjamin, L. (1967). Facts and artifacts in using analysis of co-variance to "undo" the law of initial values. Psychophysiology,4, 187-206.
Benson, H., Rosner, B. A., & Marzetta, B. R. (1973). Decreasedblood pressure in hypertensive subjects who practiced meditation.Journal of Clinical Investigation, 52, 8a-lla.
Benson, A. H., Steinart, R. F, Greenwood, M. M., Klemchuk,H. M., & Peterson, N. H. (1975). Continuous measurement ofO2 consumption^ and CO2 elimination during a wakeful hypo-metabolic state. Journal of Human Stress, 1, 37-44.
Benson, H., & Wallace, R. K. (1972). Decreased drug abuse withtranscendental meditation: A study of 1,862 subjects. In C. Zar-afonetis (Ed.), Drug abuse: Proceedings of the International Con-ference (pp. 239-252). Philadelphia: Lea & Febiger.
Blackwell, B., Hanenson, I. B., Bloomfield, S. S., Magenheim,H. G., Nidich, S. I., &Gartside, P. (1975). Effects of transcendentalmeditation on blood pressure: A controlled pilet experiment.Psychosomatic Medicine, 37, 86.
Bloomfield, H. H., Cain, M. P., Jaffee, D. T., & Kory, R. B. (1975).T.M.: Discovering inner energy and overcoming stress. New \brk:Dell.
Boswell, P. C., & Murray, E. J, (1979). Effects of meditation onpsychological and physiological measures of anxiety. Journal ofConsulting and Clinical Psychology, 47, 606-607.
Boudreau, L. (1972). Transcendental meditation and yoga as re-ciprocal inhibitors. Journal of Behavior Therapy and ExperimentalPsychiatry, 3, 97-98.
Cauthen, N. R., & Prymak, C. A. (1977). Meditation versus re-laxation: An examination of the physiological effects of relaxationtraining and different levels of experience with transcendentalmeditation. Journal of Consulting and Clinical Psychology, 45,496-497.
Corey, P. W. (1977). Airway conductance and oxygen consumptionchanges associated with practice of the transcendental meditationtechnique. In D. Orme-Johnson & J. Farrow (Eds.), Scientificresearch on the transcendental meditation program (Vol. 1, pp.94-107). Los Angeles: Maharishi European Research UniversityPress.
Cronbach, L., & Furby, L. (1970). How we should*measure change—Or should we? Psychological Bulletin, 74, 68-80.
Curtis, W. D., & Wessberg, H. W. (1975/1976). A comparison ofheart rate, respiration, and galvanic skin response among med-
itators, relaxers, and controls. Journal of Altered States of Con-sciousness, 2, 319-324.
Davidson, J. M. (1976). The physiology of meditation and mysticalstates of consciousness. Perspectives in Biology and Medicine,19, 345-379.
Dhanaraj, V. H., & Singh, M. (1977). Reduction in metabolic rateduring the practice of the transcendental meditation technique.In D. Orme-Johnson & J. Farrow (Eds.), Scientific research onthe transcendental meditation program (Vol. 1, pp. 137-139).Los Angeles: Maharishi European Research University Press.
Elson, B. D., Hauri, P., & Cunis, D. (1977). Physiological changesin yoga meditation. Psychophysiology, 14, 52-57.
Fenwick, P. B., Donaldson, S., Gillis, L., Bushman, J., Fenton,G. W., Perry, I., Tilsley, C., & Serafmowicz, H. (1977). Metabolicand EEG changes during transcendental meditation: An expla-nation. Biological Psychology, 5, 101-118.
Gellhorn, E., & Kiely, W. F. (1972). Mystical states of consciousness:Neurophysiological and clinical aspects. Journal of Nervous andMental Disease, 154, 399-405.
Glueck, B., & Stroebel, C. (1975). Biofeedback and meditation inthe treatment of psychiatric illnesses. Comprehensive Psychiatry,7(5,303-321.
Goleman, D. J., & Schwartz, G. E. (1976). Meditation as an in-tervention in stress reactivity. Journal of Consulting and ClinicalPsychology, 44, 456-466.
Herbert, J. R. (1977). Periodic suspension of respiration duringthe transcendental meditation technique. In D. Orme-Johnson& J. Farrow (Eds.), Scientific research on the transcendental med-itation Program (Vol. 1, pp. 134-135). Los Angeles: MaharishiEuropean Research University Press.
Holmes, D. S., Solomon, S., Cappo, B. M., & Greenberg, J. L.(1983). Effects of transcendental meditation versus resting onphysiological and subjective arousal. Journal of Personality andSocial Psychology, 44, 1244-1252.
Janby, J. (1977). Immediate effects of the transcendental meditationtechnique: Increased skin resistance during first meditation afterinstruction. In D. Orme-Johnson & J. Farrow (Eds.), Scientificresearch on the transcendental meditation program (Vol. 1, pp.213-215). Los Angeles: Maharishi European Research UniversityPress.
Jevning, R., Pirkle, H. C., & Wilson, A. F. (1977). Behavioralalteration of plasma phenylalanine concentration. Physiology andBehavior, 19, 611-614.
Jevning, R., Wilson, A. F., & Davidson, J. M. (1978). Adrenocorticalactivity during meditation. Hormones and Behavior, 10, 54-60.
Jevning, R., Wilson, A. F., Smith, W. R., & Morton, M. E. (1978).Redistribution of blood flow in acute hypometabolic behavior.American Journal of Physiology, 235, R89-R92.
Jevning, R., Wilson, A. F., & VanderLann, E. F. (1978). Plasmaprolactin and growth hormone during meditation. PsychosomaticMedicine, 40, 329-333.
Kanellakos, D., & Lukas, J. (1974). The psychobiology of tran-scendental meditation. Menlo Park, CA: Benjamin.
Kinsman, R. A., & Staudenmayer, H. (1978). Baseline levels inmuscle relaxation training. Biofeedback and Self-Regulation, 3,97-104.
Kirsch, I., & Henry, D. (1979). Self-desensitization and meditationin the reduction of public speaking anxiety. Journal of Consultingand Clinical Psychology, 47, 536-541.
Klemons, I. M. (1977). Changes in inflammation in persons prac-ticing the transcendental meditation technique. In D. Orme-Johnson & J. Farrow (Eds.), Scientific research on the transcen-dental meditation program (Vol. 1, pp. 287-291). Los Angeles:Maharishi European Research University Press.
Lacey, J. (1956). The evaluation of autonomic responses: Towarda general solution. Annals of New York Academy of Sciences, 67,123-164.
Lang, R., Dehob, K., Meurer, K., & Kaufman, W. (1979). Sym-pathetic activity and transcendental meditation. Journal of NeuralTransmission, 44, 117-135.
January 1984 • American Psychologist

Laurie, G. (1977). An investigation into the changes in skin resis-tance during the transcendental meditation technique. In D.Orme-Johnson & J. Farrow (Eds.), Scientific research on thetranscendental meditation program (Vol. 1, pp. 216-223). LosAngeles: Maharishi European Research University Press.
Lintel, A. G. (1980). Physiological anxiety responses in transcen-dental meditators and nonmeditators. Perceptual and Motor Skills,50, 295-300.
Maharishi Mahesh Yogi. (1963). The science of being and art ofliving. London: Unwin.
Malec, J., & Sipprelle, C. (1977). Physiological and subjective effectsof Zen meditation and demand characteristics. Journal of Con-sulting and Clinical Psychology, 44, 339-340.
McCuaig, L. (1974). Salivary electrolytes, protein, and pH duringtranscendental meditation. Experimentia, 30, 988-989.
Mclntyre, M. E., Silverman, F. H., & Trotter, W. D. (1974). Tran-scendental meditation and stuttering: A preliminary report. Per-ceptual and Motor Skills, 39, 294.
Michaels, R. R., Huber, M. J., & McCann, D. S. (1976). Evaluationof transcendental meditation as a method of reducing stress.Science, 192, 1242-1244.
Michaels, R. R., Parra, J., McCann, D. S., & Vander, A. J. (1979).Renin, cortisol, and aldosterone during transcendental meditation.Psychosomatic Medicine, 41, 50-54.
Miskiman, D. E. (I977a). The treatment of insomnia by the tran-scendental meditation program. In D. Orme-Johnson & J. Farrow(Eds.), Scientific research on the transcendental meditation pro-gram (Vol. 1, pp. 296-298). Los Angeles: Maharishi EuropeanResearch University Press.
Miskiman, D. E. (1977b). Long-term effects of the transcendentalmeditation program in the treatment of insomnia. In D. Orme-Johnson & J. Farrow (Eds.), Scientific research on the transcen-dental meditation program (Vol. 1, pp. 299-300). Los Angeles:Maharishi European Research University Press.
Morse, D. R., Martin, J. S., Furst, M. L., & Dubin, L. L. (1977).A physiological and subjective evaluation of meditation, hypnosis,and relaxation. Psychosomatic Medicine, 39, 304-324.
Naranjo, C., & Ornstein, R. E. (1971). On the psychology of med-itation, New \brk: Viking Press.
Orme-Johnson, D. W. (1973). Autonomic stability and transcen-dental meditation. Psychosomatic Medicine, 35, 341-349.
Pagano, R. R., Rose, R. M., Stivers, R. M., & Warrenburg, S.(1976). Sleep during transcendental meditation. Science, 191,308-309.
Parker, J. C., Gilbert, G. S., & Thoreson, R. W. (1978). Reductionof autonomic arousal in alcoholics: A comparison of relaxationand meditation techniques. Journal of Consulting and ClinicalPsychology, 46, 879-886.
Puente, A. E., &Beiman, I. (1980). The effects of behavior therapy,self-relaxation, and transcendental meditation on cardiovascularstress response. Journal of Clinical Psychology, 36, 291-295.
Raskin, M., Bali, L. R., &Peeke, H. V. (1980). Muscle biofeedbackand transcendental meditation. Archives of General Psychiatry,37, 93-97.
Rigby, B. P. (1977). Higher states of consciousness through thetranscendental meditation programme: A literature review. Jour-nal of Chronic Diseases and Therapeutics Research, 1, 35-55.
Routt, T. J. (1977). Low normal heart and respiration rates inindividuals practicing the transcendental meditation technique.In D. Orme-Johnson & J. Farrow (Eds.), Scientific research onthe transcendental meditation program (Vol. 1, pp. 256-260).Los Angeles: Maharishi European Research University Press.
Schuman, M. (1980). The psychophysiological model of meditationand altered states of consciousness: A critical review. In J. M.Davidson & R. J. Davidson (Eds.), The psychobiology of con-sciousness (pp. 333-378). New York: Plenum Press.
Shafii, M., Lavely, R. A., & Jaffe, R. D. (1974). Meditation andmarijuana. American Journal of Psychiatry, 131, 60-63.
Shafii, M., Lavely, R. A., & Jaffe, R. D. (1975). Meditation andthe prevention of alcohol abuse. American Journal of Psychiatry,132, 924-945.
Shapiro, D. (1980). Meditation. Chicago: Aldine.Simon, D. B., Oparil, S., & Kimball, C. P. (1977). The transcendental
meditation program and essential hypertension. In D. Orme-Johnson & J. Farrow (Eds.), Scientific research on the transcen-dental meditation program (Vol. 1, pp. 268-269). Los Angeles:Mararishi European Research University Press.
Smith, J. C. (1975). Meditation as psychotherapy: A review of theliterature. Psychological Bulletin, 82, 558-564.
Travis, X, Rondo, C., & Knott, J. (1976). Heart rate, muscle tension,and alpha production of transcendental meditation and relaxationcontrols. Biofeedback and Self Regulation, 1, 387-394.
Wallace, R. K. (1970). Physiological effects of transcendental med-itation. Science, 167, 1751-1754.
Wallace, R. K., & Benson, H. (1972). The physiology of meditation.Scientific American, 226, 84-90.
Wallace, R. K., Benson, H., & Wilson, A. F. (1971). A wakefulhypometabolic physiologic state. American Journal of Physiology,221, 795-799.
Walrath, L. C., & Hamilton, D. W. (1975). Autonomic correlatesof meditation and hypnosis. American Journal of Clinical Hyp-nosis, 17, 190-197.
West, M. A. (1977). Changes in skin resistances in subjects resting,reading, listening to music, or practicing the transcendental med-itation technique. In D. Orme-Johnson & J. Farrow (Eds.), Sci-entific research on the transcendental meditation Program (Vol.1, pp. 224-229). Los Angeles: Mararishi European ResearchUniversity Press.
Wilder, J. (1962). Basimetric approach (law of initial values) tobiological rhythms. Annals of New York Academy of Sciences,98, 1211-1220.
Wilson, A. F., Honsterger, R., Chiu, J. T, & Novey, H. S. (1975).Transcendental meditation and asthma. Respiration, 32, 74-80.
Woolfolk, R. L. (1975). Psychophysiological correlates of meditation.Archives of General Psychiatry, 32, 1326-1333.
Younger, J., Adriance, W, & Berger, R. J. (1975). Sleep duringtranscendental meditation. Perceptual and Motor Skills, 40, 953-954.
Zuroff, D. C., & Schwarz, J. C. (1978). Effects of transcendentalmeditation and muscle relaxation on trait anxiety, maladjustment,locus of control, and drug use. Journal of Consulting and ClinicalPsychology, 46, 264-271.
10 January 1984 • American Psychologist
Related Documents