Dear Provider, As the health care industry continues to evolve, we as a system are preparing ourselves to act as industry leaders in the shift from fee for service to value-based payment models. It’s inevitable, but if we’re proactive and prepare appropriately, it’s a shift that will support our ministry of delivering high quality, Franciscan health care to our patients. Focusing on value-based payment models will require us to take on and manage a greater amount of risk. We will no longer be reimbursed based on the procedures performed, but rather on our ability to better manage population health—we will be rewarded for keeping our patients at their highest level of personal wellness. For this reason, our recently completed yearly Governance Retreat revolved around the theme of risk. The Governance Retreat, which was hosted in Green Bay on Sept. 23, invited the Boards of Directors from Prevea Health and all HSHS Wisconsin Hospitals, our Executive Leadership Teams and also Leadership from Springfield to join in discussions on how we as a system can proactively manage risk to ensure our continued success in an ever-changing marketplace. The day included a panel discussion on population health, one with brokers, and one with patients; a presentation by Dr. Kavita Patel that discussed navigating politics and policy; break-out sessions on leveraging our own health plan, Prevea360, for long-term success; and a motivational keynote presentation by SEAL Team Six leader, Rob O’Neil. Overall, the day helped us examine the change-causing forces in our industry, what risk we will need to take on, our current assets, and it sparked an ongoing dialogue around the changes we will need to make to realize the opportunities that are before us. We learned to take the emotion out of the decision making process, to never quit and that complacency could be a downfall, and most importantly, our day ended with the voice of our patients reminding us to treat the whole family. Now that they’ve begun, I’m excited about the momentum of these conversations and look forward to involving more members of our medical staff and our colleagues as we prepare for tomorrow. Together, we can ensure that health, healing and hope will be provided in Northeast Wisconsin well into the future. medical staff E-News Therese Pandl, RN, MSN, MBA, FACHE President and Chief Executive Officer HSHS Division – Eastern Wisconsin HSHS St. Vincent Hospital Green Bay, Wisconsin www.stvincenthospital.org HSHS St. Mary’s Hospital Medical Center Green Bay, Wisconsin www.stmgb.org HSHS St. Nicholas Hospital Sheboygan, Wisconsin www.stnicholashospital.org HSHS St. Clare Memorial Hospital Oconto Falls, Wisconsin www.stclarememorial.org October 2016 St.Vincent St. Mary’s St. Nicholas St. Clare HSHS All members of the medical staff are invited to contribute to the e-Newsletter. Send your information to Ken Johnson, MD, Chief Physician Executive at [email protected]. The e-Newsletter is distributed at the beginning of even- numbered months. medical staff and allied health professional update Respect, Care, Competence, Joy

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Dear Provider, As the health care industry continues to evolve, we as a system are preparing ourselves to act as industry leaders in the shift from fee for service to value-based payment models. It’s inevitable, but if we’re proactive and prepare appropriately, it’s a shift that will support our ministry of delivering high quality, Franciscan health care to our patients.
Focusing on value-based payment models will require us to take on and manage a greater amount of risk. We will no longer be reimbursed based on the procedures performed, but rather on our ability to better manage population health—we will be rewarded for keeping our patients at their highest level of personal wellness. For this reason, our recently completed yearly Governance Retreat revolved around the theme of risk.
The Governance Retreat, which was hosted in Green Bay on Sept. 23, invited the Boards of Directors from Prevea Health and all HSHS Wisconsin Hospitals, our Executive Leadership Teams and also Leadership from Springfield to join in discussions on how we as a system can proactively manage risk to ensure our continued success in an ever-changing marketplace. The day included a panel discussion on population health, one with brokers, and one with patients; a presentation by Dr. Kavita Patel that discussed navigating politics and policy; break-out sessions on leveraging our own health plan, Prevea360, for long-term success; and a motivational keynote presentation by SEAL Team Six leader, Rob O’Neil.
Overall, the day helped us examine the change-causing forces in our industry, what risk we will need to take on, our current assets, and it sparked an ongoing dialogue around the changes we will need to make to realize the opportunities that are before us. We learned to take the emotion out of the decision making process, to never quit and that complacency could be a downfall, and most importantly, our day ended with the voice of our patients reminding us to treat the whole family.
Now that they’ve begun, I’m excited about the momentum of these conversations and look forward to involving more members of our medical staff and our colleagues as we prepare for tomorrow. Together, we can ensure that health, healing and hope will be provided in Northeast Wisconsin well into the future.
medical staff
E-News
Therese Pandl, RN, MSN, MBA, FACHEPresident and Chief Executive Officer HSHS Division – Eastern Wisconsin
Ascend Design Inc. ©2012 Designer: Jef f rey P. Hojnacki
Pr in t Version:Pantone® Black C (Process)
Pr in t Version:Pantone® 877C Si lver (Metal l ic )
St. Vincents HospitalIconic Element (#9.C -Final)
Graphic Guidelines for Print
HSHS St. Vincent HospitalGreen Bay, Wisconsin
www.stvincenthospital.org
HSHS St. Mary’s Hospital Medical Center
Green Bay, Wisconsinwww.stmgb.org
HSHS St. Nicholas HospitalSheboygan, Wisconsin
www.stnicholashospital.org
HSHS St. Clare Memorial HospitalOconto Falls, Wisconsin
www.stclarememorial.org
October 2016 St. VincentSt. Mary’sSt. NicholasSt. Clare
HSHS
All members of the
medical staff are invited
to contribute to the
e-Newsletter. Send your
information to Ken
Johnson, MD, Chief
Physician Executive at
The e-Newsletter is
distributed at the
beginning of even-
numbered months.
medical staff and allied health professional update
Respect, Care, Competence, Joy

2E-
New
s –
Oct
obe
r 20
16
Flu Vaccination Required by October 31All Medical Staff and Allied Health Professionals with privileges at the following hospitals will be required to receive a flu vaccine, which is the most effective way we can help stem the spread of this preventable, and in some cases deadly, disease.
If you have privileges at the following hospital(s) you are required to comply with the Medical Staff/Allied Health Professional policy for Health Screening Requirements MS-024.
• HSHS St. Vincent Hospital
• HSHS St. Mary’s Hospital Medical Center
• HSHS St. Nicholas Hospital
• HSHS St. Clare Memorial Hospital
• Libertas Treatment Center
Free flu vaccination clinics are now available at all four Eastern Wisconsin Division (EWD) hospitals and are scheduled to conclude by end of October. You may also receive the flu vaccine on the hospitals’ clinical floors from the designated flu vaccinators.
If you receive the flu vaccine at your clinic or other facility, please forward a copy of the documentation showing you received the flu vaccine to Medical Staff Services at any one of the four EWD hospitals or email [email protected] or fax to Denise Benning at 920-451-7480.
Because we recognize there will be a small number of individuals with a medical or religious reason that prevents them from receiving the vaccine, we will offer a declination process. Those who decline the vaccine are required to complete a declination form available from any EWD Medical Staff Services Department. If you decline, you will also be required to wear a mask while at any of the hospitals when flu activity is reported per the Medical Staff/Allied Health Professionals Policy for Health Screening Requirements MS-024.
Colleagues who are credentialed need to provide proof that you have received your flu vaccine. If you received your flu vaccine from an EWD hospital, just go into PeopleSoft Self Service, print a copy, and forward it to Medical Staff Services.
Medical Staff and Allied Health Professionals who fail to get vaccinated or participate in the declination process by October 31, 2016 will no longer be able to provide patient care in the hospital until the declination form has been received. This is part of your Medical Staff appointment and Allied Health Professional authorization.
Thank you in advance for
your cooperation and for
continued dedication to
protecting the health and
well-being of our patients
and one another.
Day, Date Time Location
Wed., Oct. 12 10:00 a.m.-12:30 p.m. Heritage C
Mon., Oct. 17 7:30-9:30 a.m. Heritage C
Thurs., Oct. 20 9:00-10:30 a.m. Allouez plaza (On-site colleagues only)
Fri., Oct. 21 1:00-3:00 p.m. Cancer Center 1-2
Mon., Oct. 24 1:30-4:00 p.m. Cancer Center 1-2
Tues., Oct. 25 10:00 a.m.-Noon People Services
HSHS St. Vincent Hospital Flu Clinics
Day, Date Time Location
Wed., Oct. 19 7:30-9:30 a.m. Colleague Health Office
Day, Date Time Location
Wed., Oct. 12 2:00-4:00 p.m. Café Conference Room
Fri., Oct. 14 7:00-9:00 a.m. People Services
Tues., Oct. 18 2:00-4:00 p.m. Café Conference Room
Fri., Oct. 21 10:00 a.m.-Noon People Services
Mon., Oct. 24 12:30-3:00 p.m. Café Conference Room
Wed., Oct. 26 9:00-11:30 a.m. People Services
Day, Date Time Location
Tues., Oct. 18 10:00 a.m.-1:00 p.m. Colleague Health
Thurs., Oct. 20 1:00-3:00 p.m. Administrative Wing
Tues., Oct. 25 10:00 a.m.-3:00 p.m. Colleague Health
DAILY 3:00-9:00 a.m. Emergency Department
HSHS St. Mary’s Hospital Medical Center Flu Clinics
HSHS St. Nicholas Hospital Flu Clinics
HSHS St. Clare Memorial Hospital Flu Clinics

3E-N
ews – O
ctober 2016
CPI OpportunitiesWe have a few Continuous Performance Improvement (CPI) initiatives we are focusing on to improve patient experience.
(1) Patient experience results indicate that our patients that are admitted through the ED at HSHS St. Vincent and HSHS St. Mary’s Hospitals are significantly less satisfied than other patients so we will be doing a deeper dive into the process and issues that may cause this result.
(2) Another program that has been successful in other organizations to improve workflow and patient experience is a departure/discharge lounge. HSHS St. Mary’s and HSHS St. Nicholas Med Surg along with HSHS St. Vincent surgical floors collected data last month to determine how many patients would have qualified to go to a lounge environment. This data and literature review will help determine what is needed in CPI.
(3) New staffing models will be developed in the HSHS St. Vincent rehab and EWD Emergency Departments with the goal of having the right person doing the right job at the right time.
We are very interested in having providers engaged in these process improvements. If you have an interest or a recommendation for who should be involved, please contact Paula Hafeman, CNO or Mary Martin, CNO.
HSHS Medication Prescription Pad Security and New “Not for Medication” Prescription PadEffective Wednesday September 7, HSHS EWD Medication Prescription Blanks (pads) will be stored in a locked location to reduce the risk of diversion. Should you need a Medication Prescription Blank you will need to obtain one through the patient’s nurse.
We realize that providers have been using these pads to write for DME prescriptions and short notes/release from work. To assist with meeting this need, a “Not for Medication” prescription has been developed. This “Not for Medication” pad does not have the necessary tamper resistant features and therefore cannot be used for medication / controlled substance prescriptions. These “Not for Medication” pads will be readily available on nursing units.
Name _______________________________________Address _______________________Date __________
_________________________________________ MD
Not for Medication
Patient label
EWD_ADMIN000087-4 8/16
After Hours Outpatient Imaging Services at HSHS St. NicholasTo meet your need for advanced imaging services, HSHS St. Nicholas Hospital is offering urgent, unscheduled outpatient CT services until 8:00 p.m. Monday through Friday.
To provide a safe patient care experience, we ask for a few items:
• Please enter the order in Epic or Epic Carelink. If you are not an Epic user, please fax the order to 920-459-5183.
• Call the HSHS St. Nicholas Nursing Supervisor at 920-377-1216 to inform them of your request and to provide medical history.
• Please direct your patient to the Emergency Department entrance lobby for hospital registration. Your patient will not be seen by an ED physician.
• Once the CT scan is completed, the patient will relax in the ED lobby while the radiologys reviews the imaging study. The patient will wait in the ED lobby for your communication. The radiologist will dictate the report, which will be availabe to you thorugh Epic or faxed to your office if you are not an Epic user. Critcal findings will be reported directly to you using the phone number you provide on the order.
• As the patient’s medical provider, you will need to communicate the findings to your patient. At your direction, the patient will be sent home, back to your office for additional care, or admitted to the hospital.
HSHS St. Nicholas Hospital Imaging Services maintains a vigilant view of imaging needs. As additional imaging services are identified, safe, efficient and convenient, services will be made available to your patients.
If you have questions or concerns, please contact Chris Handrow, Manager, Imaging Services, at 920-459-4756.

4E-
New
s –
Oct
obe
r 20
16
HIM UPDATES
HIM Hours RestructureTo improve the customer service experience (assisting at the nurses stations) and manage time and resources appropriately, Health Information Management (HIM) is making adjustments to its schedule at the HSHS St. Vincent site.
New Hours of Operation for HIM:
HSHS St. Vincent and HSHS St. Mary’s Hospitals 0600 – 2230
HSHS St. Nicholas Hospital* 0700 – 2030
HSHS St. Clare Memorial Hospital* 0700 – 1630
*HSHS St. Nicholas and HSHS St. Clare are supported until 2230 through the HIM call center.
From 2230 – 0600, Nursing Supervisors will complete emergent requests.
If you have questions, concerns or feedback, please contact:
Sheila Bertrand, RHIT HIM Manager (920) 884-5641 (ext. 54641)
Trista Mersberger, HSHS St. Mary’s HIM Facilitator (920) 272-3242 (ext. 63242)
Michelle Martinez, HSHS St. Nicholas HIM Facilitator (920) 459-4691 (ext. 54691)
Clinical Documentation Improvement – A Quality InitiativeClinical documentation captures the quality and extent of care that was provided.
Thorough clinical documentation improves communication among Medical Staff, increases recognition of comorbid conditions that are responsive to treatment, validates the care that was provided, and shows compliance with quality and safety guidelines.
Our hospitals provide care to very ill patients; proper documentation supports the care we provide. Your documentation determines the severity of illness and risk of mortality scores for patients. These scores are derived from specific codeable diagnoses. The more specific and complete the diagnoses, the less need for clarification through queries.
An example of a frequently queried diagnosis for our facility is hyponatremia. Medical diagnoses should be utilized to describe electrolyte imbalances and other abnormal lab values. Documenting “sodium is 129” or “low sodium” cannot be coded to hyponatremia. Documenting “hyponatremia” as a diagnosis allows the Coder to properly assign the code.
Our HSHS Clinical Documentation Specialist team is here to provide support to bridge the gap between documentation and coding. For further assistance, please contact us at 884-5929.
Thank you for your
patience and feedback
as we make this
implementation a success.

5E-N
ews – O
ctober 2016
HIM UPDATES
Updates to HSHS Record Destruction PolicyAfter review of regulatory requirements and requests for records older than 10 years, HSHS has updated the Records Retention and Disposal Policy to allow destruction of paper records 10 years after the date of service. This includes records maintained on micro-fiche, micro-film or CD’s.
The policy reads: “Paper Medical Records maintained by the HSHS entities may be destroyed Ten (10) years after the date of service, or in the case of a minor, Three (3) years after the patient would have reached the age of eighteen (18), whichever period is longer. For purpose of this policy Microfilmed records or records stored on CD’s shall be considered Paper Medical Records.”
Within EWD, we will begin the review and confidential destruction of Paper Records in the next few months.
Documentation RequirementsRecently there has been some confusion related to documentation requirements. As a reminder, per CMS guidelines and hospital policy, please be aware of the following:
Timing:
• H&P’s can be accepted only if the original documentation was completed within 30 days or less of the admission date to the hospital or procedure date. This is not a new requirement; however, recently we are seeing H&P’s submitted that are more than thirty days old (30 days, not a month). An addendum added to a document that is more than 30 days old is not acceptable. An interval H&P is always required if the original H&P is not written on the day of admission or on the day of the surgery/procedure; however, the original H&P must still be documented within 30 days of the visit.
Elements:
• Elements for H&P’s, operative notes and discharge summaries have been defined per CMS requirements and physician input. The surveyors are scrutinizing documentation for all required elements. As a result, deficiencies may be posted in your InBasket asking that you document elements that may be missing from the original report.
• The COS colleagues are available to assist in setting up or updating templates so that all required documentation is captured.
Please contact Jodi Kaftan, HIM Director, at 920-498-4575 or Michelle Martinez, SNS HIM Facilitator, at 920-459-4691 with questions.
Please call
Health Information
Management with
any questions
(920-433-8172).
HIM – Here to HelpOver the past several months, the Compass consultants performed mock surveys at our EWD locations. HIM has reviewed their reports and would like to take this opportunity to provide you with the following reminders in regards to documentation.
1. Blanks: A simple no, none, negative or N/A will suffice where applicable. Blanks are regarded as incomplete documentation.
2. Informed Consent: Must be documented in the medical record or by signing, dating and timing the ‘Performing Provider Statement of Informed Consent’ on the Informed Consent for Medical and/or Surgical Treatment form.
3. Brief Op Note: Should be on the chart immediately after surgery.
4. Verbal Orders: To be used only when it is not feasible to write or electronically enter.
5. Signatures: Must be legible or print name after/under signature.

6E-
New
s –
Oct
obe
r 20
16
SEPSIS UPDATESThe Inpatient Admission Sepsis Order Set [518] has been updated and two NEW Sepsis Addendum order sets have been put into production: IP Adult Severe Sepsis/Septic Shock Addendum [1006] and IP Adult Sepsis Non-ICU Addendum [30400116]. The order sets include a link to the Sepsis Treatment Algorithm and the Algorithm is posted in departments for your reference.
If a patient has two or more SIRS and a suspected infection and evidence of organ dysfunction the patient’s care will be evaluated to assess compliance with the following 7 components:
1. Lactic Acid Level within 3 hours
2. Blood Cultures within 3 hours
3. Broad Spectrum Antibiotics within 3 hours
4. Repeat Lactic Acid within 6 hours if initial result is ≥ 2
If the patient is in Septic Shock – has persistent hypotension and/or the Lactic Acid is > 4 administer:
5. 30 ml/kg of NS or LR within 3 hours
6. Pressors if no response to fluid bolus
7. Within 6 hours the provider completes a focused examination which must include a Capillary Refill Evaluation.
The Sepsis measure is an “all or none” measure and crosses all hospital settings. Studies have shown that adherence to these 7 measures decrease mortality in septic patients. http://www.survivingsepsis.org/Resources/Pages/Literature.aspx
Fluid ResuscitationUpdated guidelines on Sepsis were published effective July 1, 2016. The most significant change is regarding fluid resuscitation. A fluid bolus of 30ml/kg of either lactated ringers or 0.9% normal saline is required for “initial” hypotension in addition to being required for “persistent” hypotension. So for a patient who presents to ED or deteriorates as an inpatient with:
1) Documented infection and
2) 2 or more SIRS criteria and
3) evidence of organ dysfunction with associated hypotension is to receive the full 30 ml/kg bolus, even if the hypotension resolves with less volume. Fluids from IV antibiotics and KVO lines are not considered part of the bolus.
Example – Patient presents with Severe Sepsis:1. Infection: Pneumonia2. SIRS: Pulse 110, WBC’s 21,0003. Organ Dysfunction: Lactic acid 2.8
and BP is 86/50 – 30 ml/kg fluid bolus is the required treatment. Patient stated or actual weight is 120 kg:
120kg X 30ml = 3,600 ml bolus required
If the Lactic Acid is ≥ 4 the patient is considered to be in Septic Shock and the fluid bolus is also required even without hypotension. If hypotension persists after fluid resuscitation, it is appropriate to proceed to vasopressors.
The Sepsis Algorithm posted on units and available in Epic has been updated to include fluid resuscitation for Severe Sepsis. All sepsis orders sets are under revision to clarify this change.
Sepsis Treatment AlgorithmSepsis = Suspected Bacterial Infection + 2 or more SIRS Criteria
a. HR > 90 b. Temp < 36C (96.8F) or > 38.3C (100.9F)
c. RR > 20 d. WBC > 12,000 or < 4,000 or > 10% bands
ACTION: USE THE SEPSIS OR INFECTION ED ORDER SET!Note: Antibiotic choices listed on p. 2
ORDER CMP, LACTIC ACID, Blood Cultures x2, Start Broad-Spectrum Antibiotics
Physician Directed Fluids (0.9% normal saline or LR)(Consider UA, Urine culture, Influenza, CXR)
Severe Sepsis = Sepsis + Organ Failure Organ Failure = evidence by ANY ONE of the following:
• Systolic blood pressure (SBP) < 90, or Mean arterial pressure < 65, or A decrease in SBP by > 40 mmHg points from the last previously recorded SBP considered normal for that patient
• Creatinine > 2.0, or urine output < 0.5 mL/kg/hour for 2 hours• Bilirubin > 2 mg/dL (34.2 mmol/L)• Platelet count < 100,000• INR > 1.5 or aPTT > 60 sec• Lactate > 2 mmol/L (18.0 mg/dL)• Acute Respiratory Failure evidenced by a new need for
invasive or noninvasive mechanical ventilation
ACTION:ORDER Repeat lactic acid
(Will already be ordered if used the order set)
Monitor BP A) If hypotensive - Give 30 mL/kg of LR or NS within
3 hours, repeat lactate and complete reassessment note after 30 mL/kg
B) If BP remains low after fluid resuscitation with total of 30 ml/kg
BROAD SPECTRUM ANTIBIOTIC SELECTIONS MUST BE INITIATED WITHIN 3 HOURS
ORANTIBIOTIC MONOTHERAPY OPTIONS – CHOOSE ONEDoripenem Ceftriaxone Amp/Sulb GatifloxacinImipenem/cilastatin Cefotaxime Pip/Tazo LevofloxacinErtapenem Ceftazidime Tic/Clav MoxifloxacinMeropenem Cefepime Ceftaroline/
fosamil
Hyperlinked to:HSHS ED Sepsis/Pneumonia Evaluation and Treatment (882)HSHS IP Adult Sepsis or Infection Admission (518)HSHS IP Adult Severe Sepsis/Shock Addendum (1006)HSHS IP Adult Sepsis or Infection Non-ICU Addendum (30400116)
Source: HSHS Sepsis TeamApproved by: HSHS Sepsis Team
Combination Antibiotic Therapy Table (MUST CHOOSE TWO – one from each column)
Column A Column BAminoglycoside Cephalosporin
(1st or 2nd Generation) IVOR Clindamycin IV OR
Aztreonam Daptomycin OROR Glycopeptide OR
Ciprofloxacin IV Linezolid ORMacrolide IV OR
Penicillin IV
All patients with the diagnosis of SEPSIS should have focused exam documented prior to departing the ED and if InPt within 6 hours of identification of Septic Shock to evaluate adequacy of resuscitation and risk of decompensation. Sepsis reassessment MUST include ALL elements of the FOCUSED EXAM including:
❏ Vital Signs, AND ❏ Cardiopulmonary Exam, AND ❏ Capillary Refill Evaluation, AND❏ Peripheral Pulse Evaluation, AND ❏ Skin Examination
Septic ShockIf Initial Lactic Acid is > or EQUAL TO 4
ACTION:Give 30 mL/kg of LR or NS within 3 hours, repeat lactate
and complete reassessment note after 30 mL/kg
Septic ShockIf Lactic Acid is > or EQUAL TO 4
OR SBP is less than 90 OR decrease in SBP by greater than 40
OR MAP less than 65 mmHg after total of 30 mL/Kg fluid bolus
ACTION:Start Pressors (levophed preferred)
if persistent hypotension
EWD_QUAL000003-2 9/16
EWD_QUAL000003 11x14 Sepsis.indd 1 9/22/16 1:39 PM

7E-N
ews – O
ctober 2016
Comprehensive Women’s Services Added to St. Gianna ClinicSt. Gianna Clinic, the Division’s Catholic-based medical clinic, now offers comprehensive women’s care services and treatments, including Creighton Model FertilityCare System and Natural Procreative Technology, or NaProTECHNOLOGY.
Women’s care services are provided by Dr. Melissa Weidert, an OB/GYN specializing in general obstetrics and gynecology for women of all ages, reproductive health and infertility, natural family planning, high-risk pregnancy care and minimally- invasive and robotic-assisted surgeries. Dr. Weidert utilizes the Creighton Model FertilityCare
System to diagnose a variety of gynecological and reproductive health concerns including infertility, PMS, menstrual cramps, ovarian cysts, polycystic ovarian disease, repetitive miscarriages, postpartum depression and hormonal abnormalities.
The Creighton Model FertilityCare System uses a natural approach to diagnosing these health concerns, by having the patient and physician monitor certain biomarkers to track various hormonal events during the patient’s menstrual cycle. Once a diagnosis is made, Dr. Weidert may then apply medical or surgical NaProTECHNOLOGY techniques to correct the problem. Dr. Weidert is one of 20 physicians in the country to be medically and surgically fellowship trained in NaProTECHNOLOGY from the Pope Paul VI Institute for the Study of Human Reproduction in Omaha, Neb. She completed medical school at the University of Wisconsin School of Medicine and Public Health and residency at Sisters of Charity Hospital in Buffalo, N.Y.
DocHalo UpdateBy Ted Collson, MD, Chief Medical Information Officer
On August 29 the HSHS-sponsored mobile application of DocHalo went live for Prevea providers as well as the majority of our EWD-privileged providers. The following week, the desktop-based application of DocHalo went live for specific HSHS ancillary and support staff. While you have access to the mobile version on your personal phone AND the desktop version of DocHalo on any HSHS or Prevea computer, support and ancillary staff only have access to the desktop version.
As of the morning of September 14, 87% of those offered the use of DocHalo had elected to register and use it (1,948 out of 2,230). While those numbers are very encouraging, the DocHalo project team (headed by Ryan Lewis and Adam Nichol of HSHS) would like to see that number climb even higher. I support this ideal as the more individuals that elect to use DocHalo, the more functional the application will become.
As a reminder, DocHalo is a secure messaging platform that allows you to communicate with other providers as well as support staff in a HIPAA-compliant and secure manner through a simplified application. Through the mobile version of DocHalo, you can send and receive text, image, and file messages to communicate in real-time with colleagues while ensuring you are complying with current regulations and protecting your patients’ Protected Health Information (PHI). HSHS is treating all communications via the Doc Halo application similar to telephone communication with the exception that no orders will be allowed via DocHalo. All messages will be archived and retrievable for 30 days.
If you haven’t loaded the application yet, please take a few moments to download DocHalo and give it a try. It should serve to enhance your workflows and efficiency in caring for your patients while continuing to keep their important medical health information private and secure.
If you have any questions regarding this, please do not hesitate to contact me.
Important information regarding patient labels:In Epic, when a patient name exceeds 25 characters, the 25th character is replaced with a # sign on the patient labels that are printed out of Epic. The entire patient name displays in Epic but since there is a limited amount of room on the patient labels, the 25th character displays as a # indicating that there are additional characters that are not able to display on the patient labels.
Important information regard ing pat ient l abels : In Epic, when a patient name exceeds 25 characters, the 25th character is replaced with a # sign on the patient labels that are printed out of Epic. The entire patient name displays in Epic but since there is a limited amount of room on the patient labels, the 25th character displays as a # indicating that there are additional characters that are not able to display on the patient labels.
Xxxxxxxxxxxx
8E-
New
s –
Oct
obe
r 20
16
New DME Supply Ordering ProcessDue to recent CMS changes, specific patient details need to be documented BEFORE specific Durable Medical Equipment (DME) Supplies will be covered/dispensed by the payer. This is a significant change as previously this required documentation could be completed AFTER the DME was dispensed and it would still be covered/dispensed by the payer. This is no longer the case. Our patients and providers have been put into a very difficult situation where if very specific/detailed information is not provided prior to the DME being dispensed, the patient will likely be denied distribution of the equipment they need, or they may be left with the entire bill.
In an effort to assist both patients and the practitioners who care for them, we have placed some specific questions within the DME order set to address the majority of these requirements at the time of ordering. The answers that you provide to these embedded questions within the order set will be a part of the
patient’s medical record and, as such, should help to satisfy the requirements for distribution. This order set is available in both the discharge navigator under new orders (order sets and Pathways) as well as the normal clinical smartset area. Please see Standard Workflow for the more information and a screen shot of the IP section.
This workflow is available on the Physician learning dashboard and should be reviewed there. It is now available in production to start using. Please be reminded that the DME smartset/order set is the ONLY place the orders will print/fax properly. Please remind providers to use the orders set.
Currently, CMS has mandated specific parameters be answered when it comes to the ordering of wheelchairs, in-home hospital beds, home oxygen, vacuum-assisted closure devices, bi-pap, c-pap and nebulizers. We believe that in time, there will be other DMEs that will be added to this list by CMS.
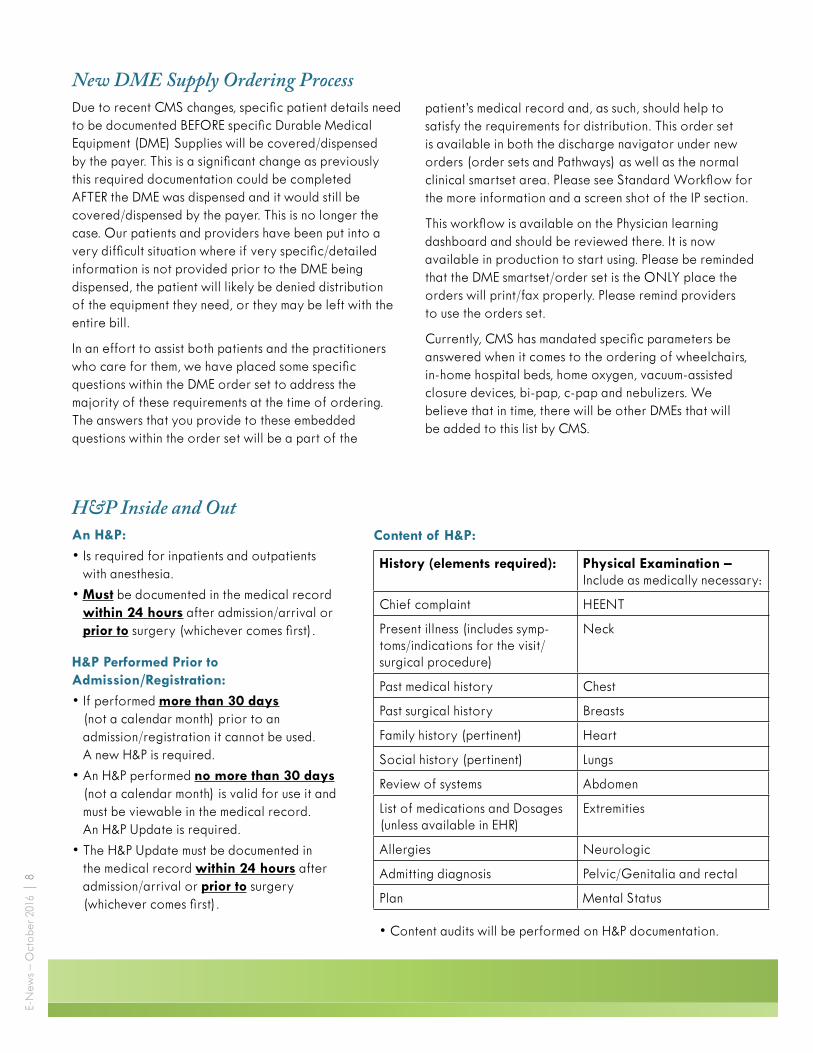
H&P Inside and OutAn H&P:
• Is required for inpatients and outpatients with anesthesia.
• Must be documented in the medical record within 24 hours after admission/arrival or prior to surgery (whichever comes first).
H&P Performed Prior to Admission/Registration:
• If performed more than 30 days (not a calendar month) prior to an admission/registration it cannot be used. A new H&P is required.
• An H&P performed no more than 30 days (not a calendar month) is valid for use it and must be viewable in the medical record. An H&P Update is required.
• The H&P Update must be documented in the medical record within 24 hours after admission/arrival or prior to surgery (whichever comes first).
History (elements required): Physical Examination – Include as medically necessary:
Chief complaint HEENT
Present illness (includes symp-toms/indications for the visit/surgical procedure)
Neck
Past medical history Chest
Past surgical history Breasts
Family history (pertinent) Heart
Social history (pertinent) Lungs
Review of systems Abdomen
List of medications and Dosages (unless available in EHR)
Extremities
Allergies Neurologic
Admitting diagnosis Pelvic/Genitalia and rectal
Plan Mental Status
• Content audits will be performed on H&P documentation.
Content of H&P:

9E-N
ews – O
ctober 2016
Enhanced Special Contact Isolation Signage
Evidence-Based Medicine (EBM) Order Set Standardization Program UpdateThe goal of the HSHS Evidence-Based Medicine (EBM) Order Set Standardization Program has been to provide clinical decision support, using the tool of Order Sets, to improve the quality, safety, and efficiency of patient care. Over the last decade, as our Local Systems have implemented Meditech, approximately 400 HSHS standard EBM order sets have been deployed.
To assist in creating, maintaining, and providing additional educational information for each order set, HSHS subscribed to Zynx Health in 2007. This web-based, software application provided us with more than 950 pre-configured order set templates our System-wide order set committee could modify to fit HSHS’ needs, as well as peer-reviewed, literature-linked, references embedded in those order sets for additional “evidence.”
Earlier this year, HSHS switched from Zynx Health to UpToDate for providing embedded evidence links in our EBM order sets. More than 8,000 Zynx links built into Meditech order sets were updated with UpToDate’s information. As EBM order sets are updated in the Epic library for Project UnITy, UpToDate’s evidence-based, physician-authored, clinical decision tools will be added.
HSHS’ subscription to UpToDate includes access to more than 10,000 topics in more than 22 specialties. All topics are updated and become available after a rigorous peer-review process. By implementing EBM order sets and now updating the evidence presented with them, ITS Performance Improvement is providing another method of point-of-care, clinical-decision support for our clinicians. This approach helps to keep HSHS in compliance with the Centers for Medicare and Medicaid Services’ (CMS) Center for Clinical Standards and Quality and the Joint Commission’s expectation that “order sets are consistent with nationally recognized and evidenced-based guidelines.”
For any questions regarding EBM, UpToDate, or Performance Improvement, please contact Chris Cinciripini, ITS Performance Improvement and Evidence-Based Medicine Informaticist.
EWD Isolation Cart StandardizationWe now have standardized Isolation Cart for HSHS St. Clare, HSHS St. Vincent, HSHS St. Mary’s and HSHS St. Nicholas with:
• Standard placement outside patient room, standard placement of PPE in each cart
• EWD Special Contact Isolation signage enhanced to assist patient families, visitors and colleagues.
Contact Infection Preventionist at each hospital for any questions.
EWD Isolation Cart Standardization • Standardized Isolation Cart for St. Clare, St. Vincent, St. Mary’s and St. Nicholas • Standard placement outside patient room, standard placement of PPE in each cart • EWD Special Contact Isolation signage enhanced to assist patient families, visitors and
colleagues.
Standard Isolation Cart Enhanced Special Contact Isolation Signage
Props for appropriate donning and doffing of PPE, assisting families and visitors Contact Infection Preventionist at each hospital for any questions.
EWD Isolation Cart Standardization • Standardized Isolation Cart for St. Clare, St. Vincent, St. Mary’s and St. Nicholas • Standard placement outside patient room, standard placement of PPE in each cart • EWD Special Contact Isolation signage enhanced to assist patient families, visitors and
colleagues.
Standard Isolation Cart Enhanced Special Contact Isolation Signage
Props for appropriate donning and doffing of PPE, assisting families and visitors Contact Infection Preventionist at each hospital for any questions.
EWD Isolation Cart Standardization • Standardized Isolation Cart for St. Clare, St. Vincent, St. Mary’s and St. Nicholas • Standard placement outside patient room, standard placement of PPE in each cart • EWD Special Contact Isolation signage enhanced to assist patient families, visitors and
colleagues.
Standard Isolation Cart Enhanced Special Contact Isolation Signage
Props for appropriate donning and doffing of PPE, assisting families and visitors Contact Infection Preventionist at each hospital for any questions.
Standard Isolation Cart

10E-
New
s –
Oct
obe
r 20
16
Diabetic Educator ServicesServices are available at HSHS St. Vincent and HSHS St. Mary’s Hospitals Monday through Friday by one of 2 RN’s (Mary Georgia, RN CDE and Amanda Griffin, RN). They are available from approximately 9 a.m. until 3 p.m. and flex their schedule to accommodate the needs of patients and patients families. To reach a diabetic educator: put in consult, vocera “diabetic educator” or phone extension 45770.
The educators serve as a resource for all team members within their scope of practice to assist with coordination of diabetic needs, focusing on teaching, patient safety, and survival skills. Our goal is to meet the needs of the patients so they can be successful in controlling blood glucose and preventing additional hospitalizations.
We address issues from admission to discharge planning. Some examples are:
• Insulin pump patients – Assisting nurses and physicians who have less experience with the pump and may need assistance in navigating the insulin pump or plan of care associated with the pump. Evaluating a patient’s knowledge and safety with pump use. Assisting physicians going into surgery where the pump was left in place – a desired standard of practice – and an insulin drip was also utilized to allow the patient to have good blood glucose control through the surgery and post-op.
• Hyper/Hypoglycemia – In collaboration with the provider, we can assist the patient to determine the best plan of care based on resources available to them, insurance benefits and their willingness to manage blood glucose.
• Supply procurement – There are no set supplies for any one insurance vendor. We can escribe a prescription to a pharmacy to check coverage so the patient has co-payment information before discharge. Plan of care and direction is discussed. We understand affordability
of insulin and supplies in discussing co-pay with the patient prior to discharge so there is no surprise at the pharmacy preventing the patient from purchasing insulin and supplies. This assists the patient to be successful in managing their blood glucose.
Recently we assisted a patient admitted for complications due to poor blood glucose control to find out that he was not taking insulin as prescribed. The insulin was costing him about $950 every three months and we saved him about $800 quarterly, making his insulin affordable.
• Patients admitted under a specialty provider can consult a diabetic educator to evaluate diabetic needs. Services of hospitalists are not always required.
Reasons to consult a diabetic educator:
• No fee for inpatient services.
• Pump patients can be evaluated for smooth transition from home to hospital as well as knowledge needs.
• Assess patient and the possible barriers (knowledge, supplies/finances, insurance coverage) that do not allow the patient to be successful in managing their diabetes at home.
• Collaborate with provider on best strategies to assist the patient with the goal of blood glucose control.
Proposed EPIC enhancements:
• Consults- auto consult to procure prescriptions for over the counter diabetic supplies and insulin pens that will be prescribed once insurance coverage established.
• Auto consults for admissions of insulin pump patients.
Patients diagnosed with diabetes who have controlled blood glucose, and the supplies and resources they need to continue controlling blood glucose at home do not always need a consult for diabetic education.
Enhanced Cell Phone Coverage Comes to HSHS St. NicholasHSHS St. Nicholas Hospital has deployed a cellular carrier neutral DAS (distributed antenna system) to enhance cell phone coverage in the hospital, 1621 Taylor, and 2920 Superior Avenue locations. This has been a much desired improvement to cellular access in our facility and will be a satisfier for colleagues, providers, patients, and visitors.
The DAS will support AT&T, Verizon Wireless, Sprint PCS, Cellcom and US Cellular mobile devices for voice, data and 4G services. The system has been designed for -85dB across the space (3 bars of coverage) for 95% of the hospital building space. We cannot place antennas in the elevators or stairwells, so coverage enhancement is incidental in these spaces.
If you have one of the carriers listed and continue to experience issues, please contact the HelpDesk at 48000. When you call, it is important that you share what carrier you have and a detailed location of where you are having issues.

11E-N
ews – O
ctober 2016
The Secret of Life is…By Cathy Mileski, RN, CHPN, Unity Nursing Practice Facilitator
Providing hospice care for the past five years, I have been witness to the most beautiful acts of love and kindness. They have taught me the following secrets of life:
Choose Joy. Find joy in the every day. Every day brings new opportunities to find the joy in your life. Take five minutes to reflect and be grateful for all of the beauty that we are a part of.
Be hopeful. Hope NEVER dies it only changes, we hope for different things. Whether it be a short term or a long term goal we choose what our story is. Even if our time is limited, we can set goals and achieve them.
Be prepared. Talk to your loved ones about what you want for end-of-life care. You never know when your end-of-life care decisions will be needed. Complete a Durable Power of Attorney for Health care and let them know your wishes. Being prepared makes things easier in a difficult time.
Say what you need to say. Tell your loved ones that you love and appreciate them as often as possible. These tender words are never wasted. They create everlasting feelings and memories. You can never hear I love you too often.
Be present. In today’s busy world we are all too often racing through our lives getting to the next thing. We forget to enjoy what we are doing at this moment. Slow down and be present in what you are doing. We are forgetting to make memories because we are too busy with technology. Memories are important, they will bring joy when you may need it the most.
Look for the helpers. Mr. Rogers said, “When I was a boy and I would see scary things in the news, my mother would say to me, look for the helpers. You will always find people who are helping.” I would add, be one of the helpers. Doing something positive makes life richer. You never know how your actions will affect others.
Laugh. Really laugh…it is good for your soul. Besides, funny things happen every day. Make it a point to belly laugh every day. It reduces pain and lightens your spirit.
Love. Love is all you need. The Beatles are correct on that point! When people are looking back on their lives, you know what they think about? Love, the people and things that they love.
There are many secrets of life and many have their own variation. The important thing is to not take life for granted. Pay attention, be present and choose joy!
Teachable Momentsby Leah Hamby, RN, Unity Hospice
Being at the bedside while a loved one dies can be distressing for family members. Most people have never witnessed a death before. Uncertainty, sadness and perhaps conflicting emotions, can diminish one’s ability to process such an experience.
What nurses bring to the bedside is experience, understanding, knowledge and comfort. In addition to the management of symptoms like anxiety, dyspnea and pain; a nurse can help the family anticipate what may happen and be better prepared. Mottling and apnea are two examples of symptoms that hospice nurses can help families understand. Nurses provide the reassurance that while these symptoms may cause concern, they are a normal part of the dying process and their loved one is not suffering.
In my role as a hospice nurse I have been at the bedside for many deaths. One of my cherished memories was being able to help a patient and their family recognize their perception of death, work through their fears and gain acceptance. This process sometimes gets overlooked, but is so important. It is beautiful and inspiring to observe the patient and family’s growth.
As I was working to manage severe dyspnea in an unresponsive patient, I taught the family about the work of breathing and how to watch for discomfort in their loved one. I taught them about accessory muscle use and what things they could do to help their loved one. I reassured them that medication would help and they allowed me to initiate this. This teaching not only gave them better understanding, but also a greater sense of control and the feeling they were doing something for the person they loved.
With all of this I still saw fear in their faces. They were afraid, not only of losing a family member, but of death itself. When the patient was breathing comfortably, I reinforced the teaching and reminded them hospice was only a phone call away, if they had any concerns at all. I assured them we would see them tomorrow.
When I arrived to the home the next day, the interventions had been effective and with some minor medication changes, the patient was breathing easily. I spent some time talking with the family, reinforced previous teaching and left the patient in the care of his family. The next day I received a call that the patient had passed away. I arrived to the door and could hear laughter coming from inside. As I entered the home, the peace and joy were palpable. There were tears on faces yes, but everyone was smiling. Some were singing! A daughter told me how afraid she had been to die but she wasn’t afraid anymore. The family felt joy and saw the beauty in the death they had witnessed. The family told me he passed away at the exact moment the sun was setting through the living room window and his favorite hymn was being sung by his children.
UNITY UPDATES

Ascend Design Inc. ©2012 Designer: Jef f rey P. Hojnacki
Pr in t Version:Pantone® Black C (Process)
Pr in t Version:Pantone® 877C Si lver (Metal l ic )
St. Vincents HospitalIconic Element (#9.C -Final)
Graphic Guidelines for Print
medical staff
E-Newslet us know!
Your opinion counts. And your suggestions are appreciated. If
you have ideas on how to improve our services, outcomes or our
interface with you or your patients, I encourage you to share that input
with any hospital leader. If you would like to meet to discuss any
suggestions please contact Paula Hunsader, Director, Medical Staff Services, at 920-433-8508, who will be happy to facilitate a designated
meeting time with the appropriate hospital leaders.
Therese Pandl, RN, MSN, MBA, FACHE, President & Chief Executive Officer, HSHS Division – Eastern Wisconsin
920-884-5801 ~ [email protected]
Gail Ostrander, RN, MS, MBA, FACHE Chief Performance Improvement Officer
HSHS Division – Eastern Wisconsin 920-498-4154 ~ [email protected]
Rose Turba, MD, HSHS St. Vincent Medical Staff President
920-272-1611 ~ [email protected]
Todd Fergus, MD, HSHS St. Mary’s Hospital Medical Center
Medical Staff President 920-272-1050 ~ [email protected]
Larry Connors, HSHS St. Mary’s/HSHS St. Vincent Hospital, Chief Operating Officer
920-498-4601 ~ [email protected]
Ken Johnson, MD, Chief Physician Executive, HSHS St. Vincent and HSHS
St. Mary’s Hospital 920-433-8351 ~ [email protected]
Ken Hujet, MD, Board Member, HSHS St. Vincent and HSHS St. Mary’s Hospital
920-498-4200 ~ [email protected]
Andrew J. Bagnall, FACHE, President and Chief Executive Officer, HSHS St. Nicholas Hospital
920-459-4705 ~ [email protected]
Nicholas Barnes, MD, President, Medical Staff, HSHS St. Nicholas Hospital
920-452-6000 ~ [email protected]
S. Mark Bettag, MD, Board Member, HSHS St. Nicholas Hospital
920-452-3594 ~ [email protected]
Christopher L. Larson, MD, Board Member, HSHS St. Nicholas Hospital
920-452-5400 ~ [email protected]
William L. Trager, MD, Board Member, HSHS St. Nicholas Hospital
920-458-3331 ~ [email protected]
Keith Elkins, MD, Medical Staff President, HSHS St. Clare Memorial Hospital
920-846-8187 ~ [email protected]
New Location for Prevea Endocrinology, Diabetes and Nutrition CentersPrevea Endocrinology, Diabetes and Nutrition Centers will be consolidating their three existing locations to the Prevea St. Mary’s Health Center on the 2R floor.
There will be a phased approach of transitioning the services to HSHS St. Mary’s resulting in separate dates in which patients will start being seen at HSHS St. Mary’s. They are:
Monday, October 17 Prevea East DePere patients
Monday, Octpber 24 Prevea Ashwaubenon patients
Monday November 7 Prevea Allouez patients
The appointment line of (920) 272-1010 will remain unchanged.
Cardiology SymposiumJoin us Saturday, October 15, 2016 at Lambeau Field for the 4th Annual Cardiology Symposium
$75 for physicians $25 for non-physicians
For more information, and to register online visit www.prevea.com/Heart2016
Email Brad [email protected] if you have any questions
Cardiology Symposium
Join us Saturday, October 15, 2016 at Lambeau Field for the 4th Annual Cardiology Symposium $75 for physicians ● $25 for non-physicians For more information, see attached PDF To register online visit www.prevea.com/Heart2016 Email Brad [email protected] if you have any questions
On August 11, colleagues, board members and donors came together to bless the new memorial garden in front of the hospital. The garden was donated by KC and Georgia Stock in memory of Patricia Drews.
Related Documents








![MAG MODEL MEDICAL STAFF BYLAWS - Leadership in Web viewNCMS MODEL MEDICAL STAFF BYLAWS. Annotated ©2012 Legal Counsel for the Medical Staff PLLC. ... [Medical Staff Manager/Coordinator]](https://static.cupdf.com/doc/110x72/5a78edb27f8b9a68148ca2ae/mag-model-medical-staff-bylaws-leadership-in-web-viewncms-model-medical.jpg)


