Medical Education Series © 2005 National Abortion Federation E A R L Y O P T I O N S A PROVIDER’S GUIDE TO MEDICAL ABORTION

Medical Education Series © 2005 National Abortion Federation E A R L Y O P T I O N S A PROVIDER’S GUIDE TO MEDICAL ABORTION.
Dec 17, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Medical Education Series© 2005 National Abortion Federation
E A R L Y O P T I O N
SA PROVIDER’S GUIDE TO MEDICAL ABORTION

E A R L Y O P T I O N
SA PROVIDER’S GUIDE TO MEDICAL ABORTION
MEDICAL ABORTIONMEDICAL ABORTIONREGIMENSREGIMENS
Objectives
• Review the mechanism of action and pharmacology of medical abortion agents
• Describe and compare safety and efficacy data for mifepristone/misoprostol regimens
• Describe safety and efficacy data for alternative medical abortion regimens, including methotrexate/misoprostol and misoprostol alone
• Discuss clinical and practical issues relating to medical abortion

Overview
• Mifepristone/misoprostol: mechanism of action
• Mifepristone/misoprostol regimens
• Clinical issues
• Alternatives– methotrexate/misoprostol– misoprostol alone
Medical Abortion Agents
• Antiprogestin: mifepristone
• Antimetabolite: methotrexate
• Prostaglandin analogue: misoprostol
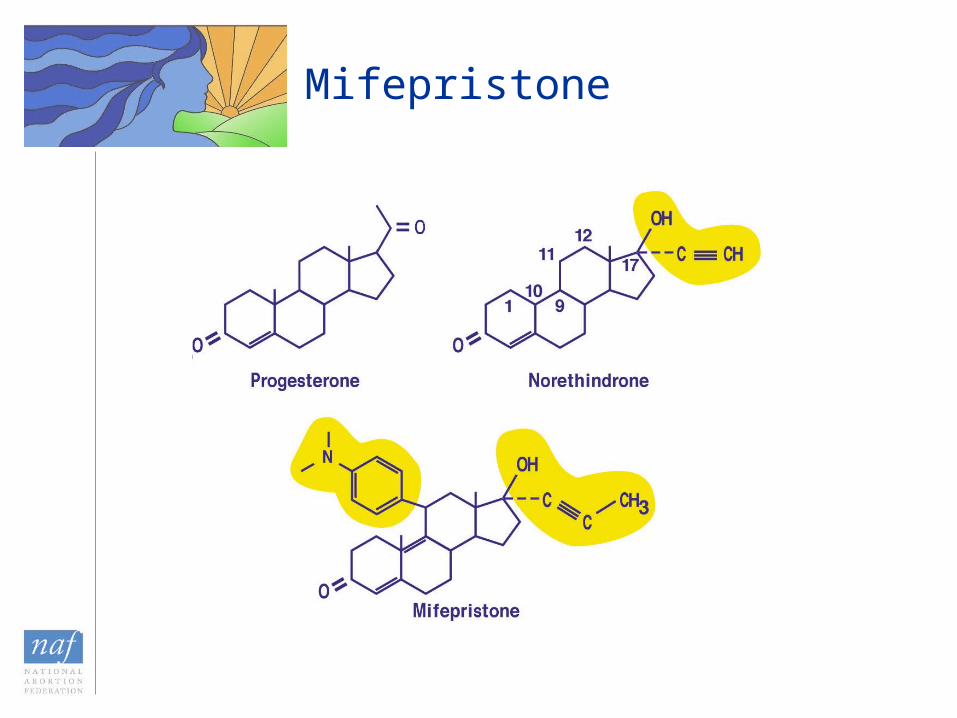
Mifepristone

Mechanism of Action: Mifepristone
• Derivative of norethindrone
• Side chains added at the 11-C and 17-C positions
• Binds to progesterone receptor with high affinity; does not activate receptor

Mechanism of Action: Misoprostol
• PGE1 analogue
• Absorbed from oral, vaginal, buccal, sublingual, or rectal routes
• Inexpensive
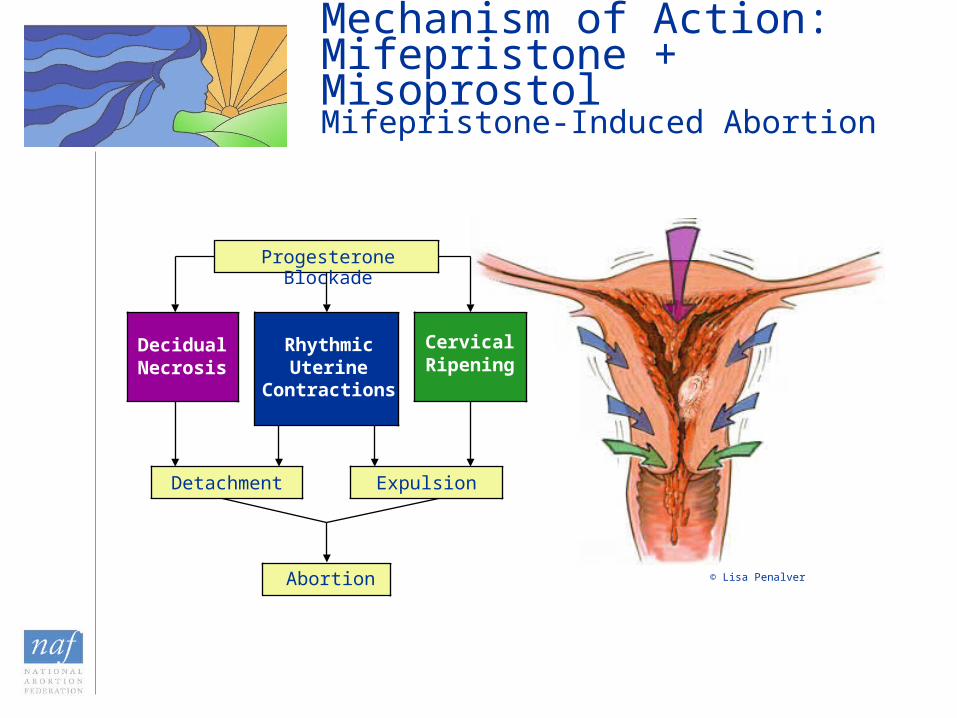
RhythmicUterine
Contractions
Progesterone Blockade
DecidualNecrosis
CervicalRipening
Detachment Expulsion
Abortion
Mechanism of Action: Mifepristone + MisoprostolMifepristone-Induced Abortion
© Lisa Penalver
Overview
• Mifepristone/misoprostol: mechanism of action
• Mifepristone/misoprostol regimens
• Clinical issues
• Alternatives– methotrexate/misoprostol– misoprostol alone

FDA-Approved & Evidence-Based Alternative Regimens
49 days LMPGestational limit
Approximately Day 14Timing of initial follow-up examination
48 hrs later (Day 3)When misoprostol taken
At homeAt office or clinicWhere misoprostol taken
800 µg PV400 µg PO Misoprostol dosage
200 mg (one 200-mg tablet)
600 mg (three 200-mg tablets)
Mifepristone dosage
Evidence- Based Alternatives
FDA-Approved Regimen
6-72 hrs later < 56 days
6-48 hrs later < 63 days
From Day 4-14
Up to 63 days LMP
ONLY in studies using 800µg VAGINAL miso

FDA-Approved Regimen*
• Day 1– Mifepristone 600 mg PO (three 200-mg tablets)– Rh immune globulin, if indicated
• Day 3– Misoprostol 400 µg orally– Provided in the office
• Day 14 (approximately)– Follow-up– Ultrasound, if necessary– Vacuum aspiration, if necessary
*For pregnancies up to 49 days’ gestation
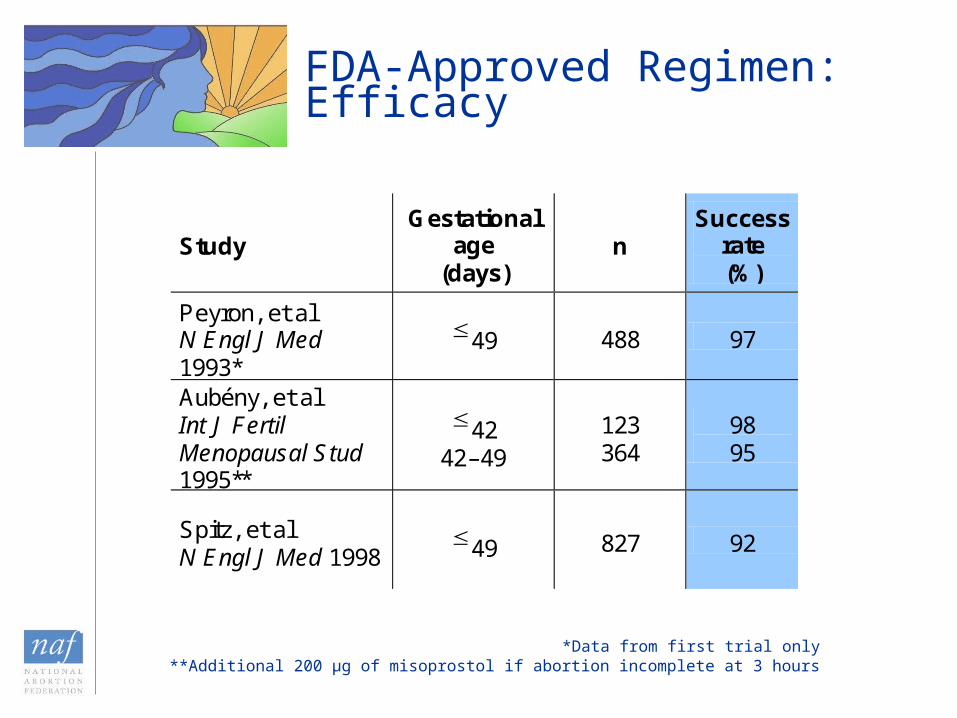
FDA-Approved Regimen: Efficacy
*Data from first trial only**Additional 200 µg of misoprostol if abortion incomplete at 3 hours
Study Gestational
age (days)
n Success
rate (%)
Peyron, et al N Engl J Med 1993*
49 488 97
Aubény, et al Int J Fertil Menopausal Stud 1995**
42 42–49
123 364
98 95
Spitz, et al N Engl J Med 1998
49 827 92

Evidence-Based Alternative Regimens
• Mifepristone dose• Vaginal misoprostol • Home use of misoprostol• Gestational age limits• Timing of vaginal misoprostol administration• Timing of follow-up evaluation

Mifepristone Pharmacology
• Peak serum levels in 2 hours
• Same pharmacokinetics for all doses 100 mg or greater
• Total serum concentration same during first 72 hours for 200-mg and 600-mg dosing
• Same peak concentration with 100-, 400-, 600-, and 800-mg doses
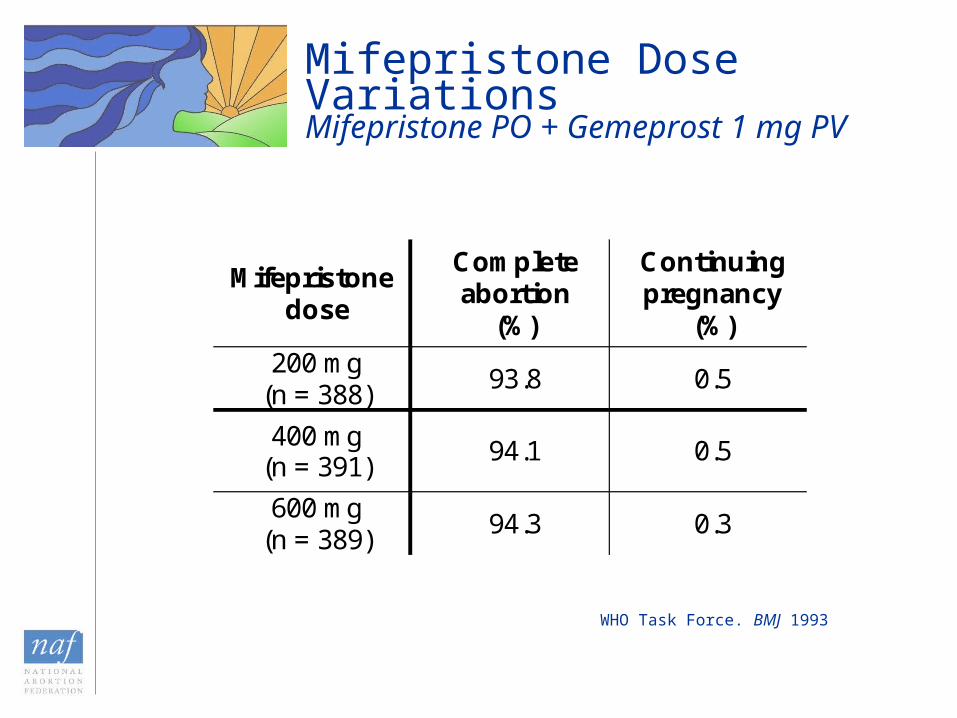
Mifepristone dose
Complete abortion
(%)
Continuing pregnancy
(%) 200 mg
(n = 388) 93.8 0.5
400 mg (n = 391)
94.1 0.5
600 mg (n = 389)
94.3 0.3
WHO Task Force. BMJ 1993
Mifepristone Dose VariationsMifepristone PO + Gemeprost 1 mg PV
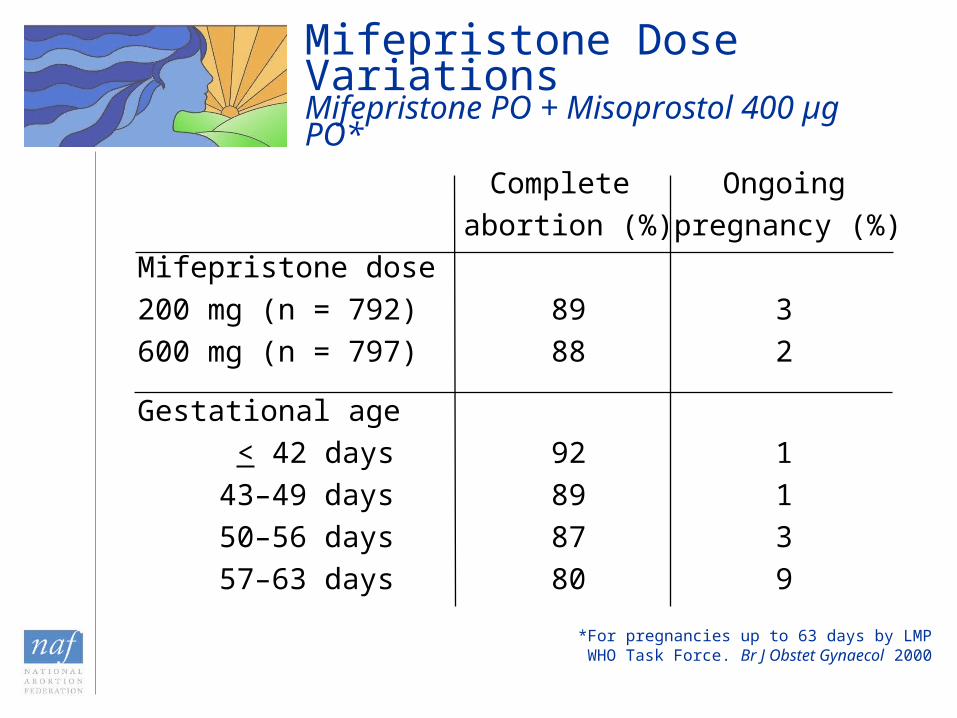
Mifepristone Dose VariationsMifepristone PO + Misoprostol 400 µg PO*
Complete Ongoing
abortion (%) pregnancy (%)
Mifepristone dose
200 mg (n = 792) 89 3
600 mg (n = 797) 88 2
Gestational age
< 42 days 92 1
43–49 days 89 1
50–56 days 87 3
57–63 days 80 9
*For pregnancies up to 63 days by LMPWHO Task Force. Br J Obstet Gynaecol 2000

Zieman, et al. Obstet Gynecol 1997
Vaginal vs. Oral Misoprostol

Success
(%)*
Abortion in 4 hours
(%)**
Continued pregnancy
(%)***
Missed abortion
(%)
Incomplete abortion
(%)
Oral misoprostol 800 µg (n = 130)
87 78 7 3 3
Vaginal misoprostol 800 µg (n = 133)
95 93 1 1 4
El-Refaey, et al. N Engl J Med 1995
*P = 0.03** P < 0.001*** P = 0.01
Vaginal vs. Oral Misoprostol 63 Days’ Gestation

Schaff, et al. Contraception 2001
*P = 0.001** P = 0.001
Vaginal vs. Oral Misoprostol 63 Days’ Gestation
Success (%)*
Complete abortion @ 1
week (%)**
Continued pregnancy
(%)
Oral misoprostol 400 µg + 400 µg 2 hrs later(n = 548)
95 90 1.1
Vaginal misoprostol800 µg (n = 596)
99 97 0

Misoprostol Routes of Administration
• Vaginal vs. oral misoprostol associated with:– Higher efficacy rates– Lower rate of GI side effects– More rapid expulsion– Lower rate of continuing pregnancy
• Sublingual misoprostol• Buccal misoprostol
Kahn, et al. Contraception 2000Tang, et al. Hum Reprod 2003Shannon, et al. 2003

Mifepristone (various doses) PO + Misoprostol 800 µg PV
StudyMifepristone
doseGestational
ageSuccess
(%)
Ongoingpregnancy
(%)
El-RefaeyContraception 1994
600 mg 63 days(n = 100)
100 0
Schaff, et alJ Fam Pract 1997
600 mg 56 days(n = 166)
98 0
Ashok, et alHum Reprod 1998 200 mg
49 days(n = 928)
50–63 days(n = 1,072)
99
97
0.2
0.8
Schaff, et alContraception 1999
200 mg
49 days(n = 660)
50–56 days(n = 273)
97
96
0.3
1.1
Schaff, et alContraception 2000
200 mg
49 days(n = 578)
50–56 days(n = 251)
57–63 days(n = 308)
98
97
96
0.2
0.4
1.0

Acceptable responses (%)
Prior surgical abortion (n = 449)
No prior surgical abortion (n = 471)
Procedure
Home use of misoprostol
Bleeding
Side effects
Waiting
Pain
Would choose procedure again
Would recommend procedure
93
90
89
86
85
75
85
84
95
92
90
85
86
73
89
86
Schaff, et al. Contraception 1999
Home Use of Misoprostol: AcceptabilitySurvey Results
Gestational Age and Outcomes
• FDA approved regimen– Oral misoprostol– High efficacy through 49 days’ gestation– Efficacy decreases with increasing gestational
age
• Evidence-based alternative regimens with vaginal misoprostol– Sustained high efficacy through 63 days’
gestation

Timing of Vaginal Misoprostol Administration
• In regimens of 200 mg mifepristone + 800 µg vaginal misoprostol
• Administer misoprostol:– 6-72 hours after mifepristone < 56 days– 6-48 hours after mifepristone < 63 days
• Sustained high efficacy
Timing of Vaginal Misoprostol Administration
• Randomized trial of 2,295 women through 56 days’ gestation– Mifepristone 200 mg– Misoprostol 800 µg PV 1, 2, or 3 days after
mifepristone• Efficacy by interval
– 1-day: 98% (95% CI 97%99%)– 2-day: 98% (95% CI 97%99%)– 3-day: 96% (95% CI 95%97%)
• Acceptability of waiting time: significantly greater with 1-day vs. 2-day or 3-day interval
Schaff, et al. JAMA 2000

Timing of Vaginal Misoprostol Administration
• Randomized trial of 1,080 women through 63 days’ gestation– Mifepristone 200 mg– Misoprostol 800 µg PV 6-8 hours or 23-25 hours
after mifepristone• Efficacy by interval
– 6-8 hours: 96%(95% CI 93.7%97.3%)– 23-25 hours: 98% (95% CI 96.6%99.1%)
• Significantly higher rates of side effects after mifepristone and significantly higher rates of nausea & vomiting after misoprostol in 23-25 hour group.
Creinin, et al. Obstet Gynecol 2004
Timing of Follow-up Evaluation
• FDA regimen: Follow-up about 14 days after mifepristone
• Data support acceptable earlier follow-up when:– Regimens involve vaginal misoprostol– Transvaginal ultrasonography is used for dating
and evaluation after treatment
• Follow-up may be performed as early as 1 day after vaginal misoprostol
• Abortion complete at 1-week evaluation in > 95% of women
Schaff, et al. Contraception 1999Schaff, et al. Contraception 2000Schaff, et al. JAMA 2000

Evidence-Based Alternative Regimens
• 200-mg dose of mifepristone• Vaginal administration of misoprostol
– Lower incidence of side effects compared to oral misoprostol
– More rapid expulsion compared to oral misoprostol– Increases efficacy of medical abortion for gestations
up to 63 days– Decreases continuing pregnancy rate
• Home use of misoprostol• Flexibility in timing of vaginal misoprostol use• Flexibility in initial follow-up evaluation

Overview
• Mifepristone/misoprostol: mechanism of action
• Mifepristone/misoprostol regimens
• Clinical issues
• Alternatives– methotrexate/misoprostol– misoprostol alone
Sample Protocol
First visit*• Counseling (including Medication Guide & Patient
Agreement)• Lab work• Medical history & gestational dating (ultrasound if
needed)• Mifepristone (Serial number recorded in patient chart)• Rh immune globulin, if indicated • Misoprostol tablets or prescription dispensed for later use• Medication and/or prescriptions given as needed for
cramping• Emergency contact information given• Discuss post-abortion contraception, STDs, & EC as
appropriate*In states with required waiting periods between a first visit and the abortion, these may be divided between two visits.

Sample Protocol (con’t)
Misoprostol administration• 6-72 hours after mifepristone• Most often used at home
First follow-up visit • Approximately 4-14 days after mifepristone• Ultrasound, if necessary• Vacuum aspiration, if necessary

Contraindications
• Allergy to mifepristone, misoprostol, or other prostaglandin analogues
• Concurrent long-term systemic corticosteroid use
• Chronic adrenal failure
• Hemorrhagic disorder or concurrent anticoagulant therapy
• Intrauterine device in situ
• Possible ectopic pregnancy
• Inherited porphyria
Special Considerations
• Chronic medical conditions– Cardiovascular disease– Hypertension– Hepatic disease– Renal disease– Pulmonary disorders– IDDM– Severe anemia– Heavy smoking
• Breast-feeding• Women over 35 years
who smoke > 10 cigarettes daily
Teratogenicity
• Mifepristone: data do not indicate teratogenicity
• Methotrexate– High-dose therapy is teratogenic– Low-dose therapy with unknown risk
• Misoprostol: associated with birth defects
Ultrasound
• Standard in US medical abortion trials
• Usage varies in inter national studies
• Should be available for specific indications
• Useful, but not mandatory in the FDA labeling
Assessing When Ultrasound is Needed: Study Results1
• Gestational age & abortion outcome assessed based on history & physical exam, and compared with TVU results
• Gestational age– TVU rated as “not indicated” for 60% of women at <42
days, 66% at 43-49 days, and 46% >50 days.– 1.4% clinically assessed <63 days but >63 days by TVU– 9.1% clinically assessed >63 days but <63 days by TVU
• Abortion outcome– Confident in clinical assessment for 59.5% of women– 1.3% (7/522) were assessed with clinical confidence to
have a complete abortion, but did not by TVU– Clinicians assessed ultrasound was desired or indicated in
71% (17/24) of women who did not have a complete abortion
1Fielding et al, Contraception 2002

Medical Abortion: Acceptability
• Generally well-accepted by providers and patients
• Patient attitudes towards mifepristone/misoprostol– “Satisfactory” or “very satisfactory”: 88%–97%– % of eligible women choosing mifepristone
varies– More than half of eligible women choose
mifepristone in France, Scotland & Sweden– Patients dislike multiple-visit requirements
Winikoff, et al. Int Fam Plann Perspect 1997Winikoff, et al. Arch Fam Med 1998Ngoc, et al. Int Fam Plann Perspect 1999Jones, et al. Perspect Sexual Reprod Health 2002
Overview
• Mifepristone/misoprostol: mechanism of action
• Mifepristone/misoprostol regimens
• Clinical issues
• Alternatives– methotrexate/misoprostol– misoprostol alone
Alternatives: MethotrexateMechanism of Action
• Over 40 years of use in cancer chemotherapy
• Antimetabolite– Blocks dihydrofolate reductase– Primary effect is to impede DNA synthesis
• Affects cytotrophoblast cells—impairs implantation
Medical Abortion with Methotrexate/ Misoprostol: Contraindications
• Anemia (Hgb < 10 g/dL)
• Known coagulopathy
• Active renal or liver disease
• Uncontrolled seizure disorder
• Acute inflammatory bowel disease
• Intrauterine device in situ
• Intolerance of methotrexate or misoprostol
Methotrexate/Misoprostol Regimens*
• Methotrexate: 50 mg/m2 IM or 50 mg PO• Misoprostol: 800 µg PV 3–7 days later• Efficacy decreases after 49 days’ gestation• Rh immune globulin to Rh negative patients
before misoprostol• Initial follow-up ~1 week after methotrexate• Subsequent care based on results of
physical exam, ultrasonography
*For pregnancies up to 49 days’ gestation
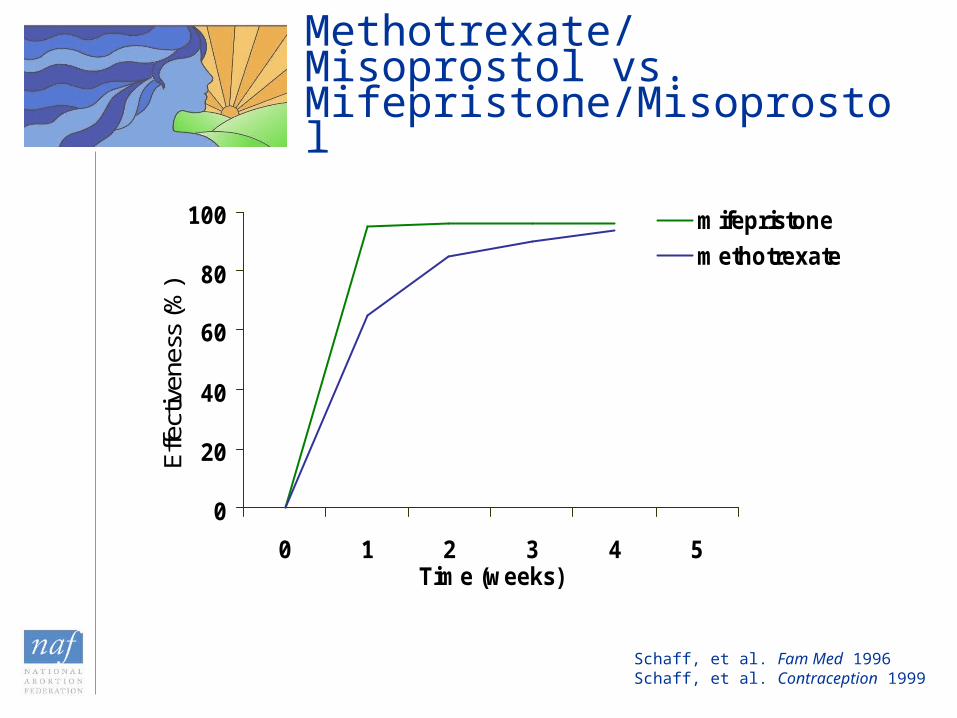
Methotrexate/Misoprostol vs. Mifepristone/Misoprostol
Schaff, et al. Fam Med 1996Schaff, et al. Contraception 1999
0
20
40
60
80
100
0 1 2 3 4 5Time (weeks)
Effe
ctiv
enes
s (%
)
mifepristone
methotrexate

Clinical Trial Results: Mifepristone vs. Methotrexate
83.2% **88%Acceptability
0.4%0%Ongoing pregnancy
96.0%
74.5% *20.3% *
96.1%
90.5%3.9%
Overall Success
By day 8 After day 8
Methotrexate/misoprostol
Mifepristone/misoprostol
* p<.001
** p=.031
Wiebe, et al. Obstet Gynecol 2002

Study Rx n Gestational
age Success rate (%)
Creinin, et al JAMA 1994
800 µg PV x 1 if needed
30 56 days 47
Carbonell, et al Contraception 1997
800 µg PV* every 48h x 3 if needed**
141 70 days 94
Carbonell, et al Eur J Contraception Reprod Health Care 1997
800 µg PV* every 48h x 3 if needed** 175 63 days 92
Carbonell, et al Contraception 1999
800 µg PV* every 24h x 3 if needed**
720 35–63 days 89
Jain, et al Am J Obstet Gynecol 1999
800 µg PV*, then a second dose in 24 hours if needed
63
25
49 days
50–56 days
88
89
Misoprostol as a Single Agent
*Moistened**Plus additional 400–1,200 µg after expulsion was confirmed

Misoprostol-Alone Regimen*
• 2 doses 800 µg vaginal misoprostol
• 24 hours apart
• Up to 9 weeks LMP
• Moistening tablets may increase success
*Consensus Statement, 2003
Conclusion
• Various mifepristone/misoprostol regimens have 95-99% efficacy rates
• Evidence-based regimens
– 200 mg mifepristone
– Vaginal misoprostol 800 µg
– Gestations < 63 days with vaginal misoprostol
– Home use of misoprostol
– Flexibility in timing of vaginal misoprostol use
– Flexibility in initial follow-up evaluation
• Methotrexate/misoprostol and misoprostol-alone regimens are safe & effective alternatives
E A R L Y O P T I O N
SA PROVIDER’S GUIDE TO MEDICAL ABORTIONThis educational program does not define a standard of care, nor does it dictate an
exclusive course of management. It contains recognized methods and techniques of medical care that represent currently appropriate clinical practice. Variations in patient needs and available resources may justify alternative approaches. Laws governing abortion, informed consent, and medical malpractice vary among states. These materials are strictly for informational purposes, and do not constitute legal advice or representation. These materials are not intended as a substitute for the advice of a health care provider. Neither NAF nor its agents are responsible for adverse clinical outcomes that might occur where they are not expressly and directly involved in the role of primary caregiver.
This educational program is protected by copyright. Any unauthorized duplication, reproduction, or alteration of the presentations or any part of the presentations contained therein is strictly prohibited. This educational program is intended for the use of the original recipient and his/her agents and cannot be sold, distributed, transmitted or transferred in any form without prior written authorization by the National Abortion Federation.
© 2005 National Abortion Federation
Related Documents











