Medical Debaters: Brooks Cash, MD Lin Chang, MD Moderator: Philip Schoenfeld, MD William D. Chey, MD Mark Pimentel, MD This activity is supported by an educational grant from Salix Pharmaceuticals, Inc. Jointly sponsored by the Gi Health Foundation and Purdue University College of Pharmacy. This event is neither sponsored by nor endorsed by the American College of Gastroenterology. Accredited by: Sponsored by: 1

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Medical Debaters:
Brooks Cash, MDLin Chang, MD
Moderator:
Philip Schoenfeld, MD William D. Chey, MDMark Pimentel, MD
This activity is supported by an educational grant from Salix Pharmaceuticals, Inc. Jointly sponsored by the Gi Health Foundation and Purdue University College of Pharmacy.
This event is neither sponsored by nor endorsed by the American College of Gastroenterology.
Accredited by: Sponsored by:
1
Breaking News: ACG 2012Philip Schoenfeld, MD

Mesalamine granules 1500 mg once daily for 12 weeks provides adequate relief of IBS symptoms in IBS with diarrhea: Results
from a Phase 2 trial
Aron J et al. Program no. 7
Design
• Background: Mesalamine granules are approved for ulcerative colitis
• Study design– Randomized, double-blind, placebo-controlled, multicenter study– 148 patients with IBS-D (Rome III criteria)– Placebo (n=50) vs Mesalamine granules 750 mg qd (n=47) vs
mesalamine granules 1500 mg once daily (n=51)
• Endpoint: Monthly responders for both abdominal pain and stool consistency during the 3-month treatment period
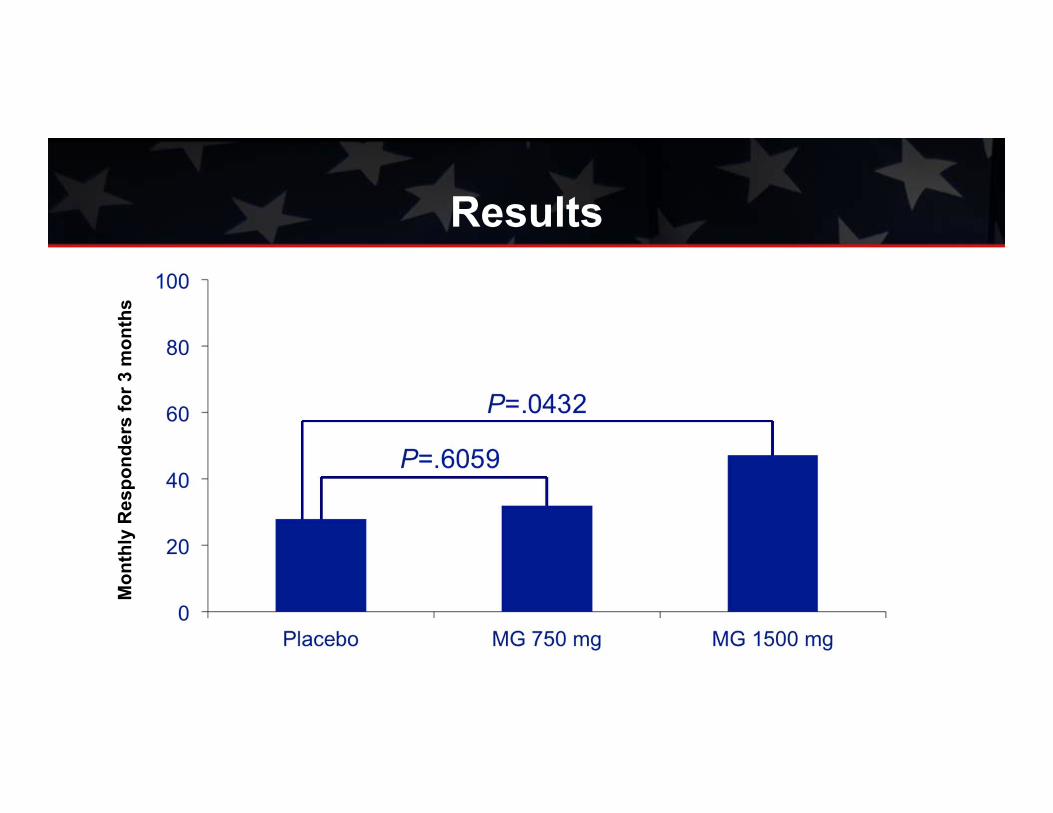
Results
Mon
thly
Res
pond
ers
for 3
mon
ths

Fecal incontinence in US adults from 2005-10: Epidemiology and Risk Factors
Ditah I et al. Program no. P445

Design• Purpose: Estimate prevalence of FI and identify risk factors
• Study design: Population-based survey of US residents. Data obtained annually (2005-2010) from NHANES Fecal Incontinence Severity Index
• Participants: Men and women aged ≥20 years (N=52,195)
Results• Prevalence of fecal incontinence in 2009-2010 survey: 9.01%
• FI occurred at least weekly in 1.13% of participants
• Prevalence similar in women (9.13%) and men (7.36%)
• Among individuals ≥70 years old: Prevalence = 17.46%
• Other independent risk factors: diabetes and level of education

Effects of linaclotide on abdominal and bowel symptoms over the first 7 days of
treatment in patients with IBS with constipation
Chang L et al. Program no. P1559
Design• Purpose: Assess changes from baseline in abdominal discomfort and bowel
symptoms in IBS-C patients during first 7 days of linaclotide
• Methods: IBS-C patients (Rome II) randomized to linaclotide 290 µg or placebo– Data from first 7 days of treatment analyzed for daily percent change from
baseline in abdominal symptoms and stool consistency– Percentages of patients having ≥1 spontaneous bowel movement (SBM)
and complete SBM (CSBM) on each of the first 7 days of treatment and mean number of SBMs and CSBMs calculated

Results• Significantly more linaclotide patients had an SBM (50% vs 6%) and CSBM
(20% vs 6%) on day one
• Linaclotide statistically significantly improved abdominal bloating and fullness on day one, pain and discomfort by day two, and cramping by day three
• Weekly SBM (6.6 vs 3.5) and weekly CSBM (2.4 vs 0.9) were significantly higher in linaclotide patients vs placebo. (P<.001)
• Diarrhea incidence during the first seven days of treatment was 10% (n=80) and 0.4% (n=3) for linaclotide and placebo patients, respectively

Medical Debaters:
Brooks Cash, MDLin Chang, MD
Moderator:
Philip Schoenfeld, MD William D. Chey, MDMark Pimentel, MD
This activity is supported by an educational grant from Salix Pharmaceuticals, Inc. Jointly sponsored by the Gi Health Foundation and Purdue University College of Pharmacy.
This event is neither sponsored by nor endorsed by the American College of Gastroenterology.
Accredited by: Sponsored by:
12

Faculty Introductions

History• 52-year-old senior account executive for oil exploration company
• Got “food poisoning” during trip to Central America one year ago
• For the last 11 months, has been seeing a primary care physician for intermittent diarrhea with abdominal pain and severe urgency
• When questioned carefully, indicates that she experiences occasional episodes of FI (≥2 times monthly)
– She feels urgency but can’t always make it to the bathroom in time – Notes that she has never discussed this with her primary care physician.

History• She also experiences occasional urinary incontinence when
coughing, laughing, or sneezing
• She has dramatically curtailed her travel schedule because of her fecal incontinence, but she does not feel this is something she can discuss or admit to her supervisor
• Has taken Imodium, which decreases diarrhea and reduces fecal incontinence but results in severe bloating and cramping

History• She has 2 children, both delivered vaginally, the last
being 12 years ago• No history of diabetes, rheumatologic disease, anorectal
surgeries• Current medications
– Taking fiber supplements
Physical Exam and Diagnostic Evaluations
• Physical exam– Some skin irritation in perianal region– Anal sphincter tone at rest is slightly decreased– Mild augmentation of anal sphincter tone during squeeze command– No anatomic sphincter defects were noted
• Anorectal manometry– Slightly decreased anal sphincter tone at rest – An adequate anal sphincter squeeze pressure could not be sustained– Rectal compliance decreased– Sensory thresholds normal
Physical Exam and Diagnostic Evaluations
• Anal endosonography– Some mild scarring of the EAS (external anal sphincter)
• Colonoscopy – Normal; random biopsies are normal
• Capsule endoscopy– Normal
• Laboratory evaluations– Normal TFTs, CBC, ESR, CRP, LFTs
CBC=complete blood count; CRP=C-reactive protein; ESR=erythrocyte sedimentation rate; LFT=liver function tests; TFT=thyroid function test.

Fecal Incontinence:Diagnosis

Types of Fecal Incontinence• Passive incontinence1,2
– Unaware of stool or gas passage; associated with diseased or disrupted IAS
• Urge incontinence1,2
– Release of feces despite awareness and attempted retention; 88% associated with EAS dysfunction
• Fecal seepage1,2
– Presence of small amount of fecal material on undergarments; thought to be due to impaired rectal sensation
1. Rao SS et al. Am J Gastroenterol. 2004;99:1585-1604; 2. Rao SS et al. 2004;126:S14-S22.
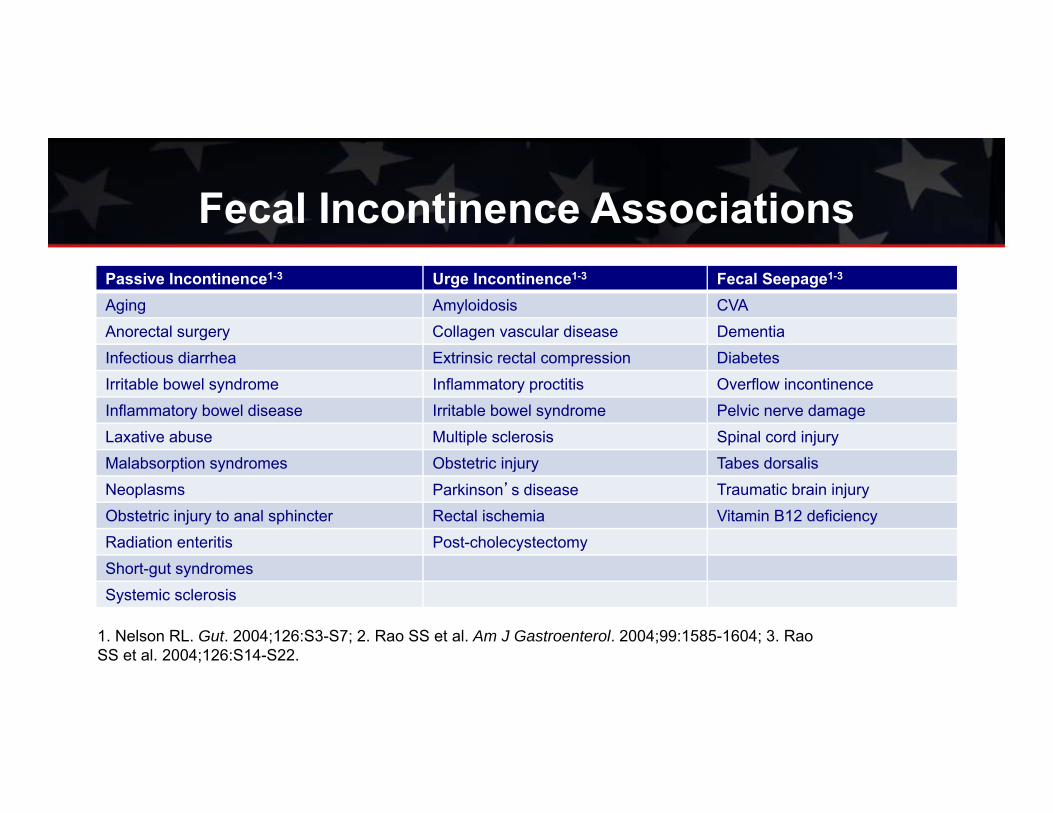
Fecal Incontinence AssociationsPassive Incontinence1-3 Urge Incontinence1-3 Fecal Seepage1-3
Aging Amyloidosis CVAAnorectal surgery Collagen vascular disease DementiaInfectious diarrhea Extrinsic rectal compression DiabetesIrritable bowel syndrome Inflammatory proctitis Overflow incontinenceInflammatory bowel disease Irritable bowel syndrome Pelvic nerve damageLaxative abuse Multiple sclerosis Spinal cord injuryMalabsorption syndromes Obstetric injury Tabes dorsalisNeoplasms Parkinson’s disease Traumatic brain injuryObstetric injury to anal sphincter Rectal ischemia Vitamin B12 deficiencyRadiation enteritis Post-cholecystectomyShort-gut syndromesSystemic sclerosis
1. Nelson RL. Gut. 2004;126:S3-S7; 2. Rao SS et al. Am J Gastroenterol. 2004;99:1585-1604; 3. RaoSS et al. 2004;126:S14-S22.

Diagnostic Evaluation• History:1,2 Duration, nature, impact on quality of life, obstetric history, other
medical conditions, urinary incontinence• Physical exam1,2 Digital rectal exam• Diagnostic examinations1,2
– Anorectal manometry– Rectal sensory and compliance testing– Anal endosonography– Anal or pelvic MRI (static or dynamic)– Defecography– Anal sphincter EMG*– Motor-evoked potentials
*Pudendal nerve latency testing no longer recommended1. Rao SS et al. Am J Gastroenterol. 2004;99:1585-1604; 2. Rao SS et al. 2004;126:S14-S22.

PuborectalisPuborectalisInternal anal
sphincter
Internal anal
sphincter
Symphysispubis
Symphysispubis
External anal sphincter (EAS)
External anal sphincter (EAS)
Digital Exam for Continence
Adapted from: Rome Foundation FunctionalGI Disorders. Specialty Modules.

PuborectalisPuborectalis
Symphysispubis
Symphysispubis
External anal sphincter (EAS)
External anal sphincter (EAS)
Digital Exam for Continence
Adapted from: Rome Foundation FunctionalGI Disorders. Specialty Modules.
Internal anal
sphincter
Internal anal
sphincter

Yield of Diagnostic TestingPhysiologic Test Clinical Utility Evidence
Strengths Weaknesses
Anorectal manometry
Quantifies sphincter pressures, sensation, rectal compliance and recto-anal
reflexes
Not standardized Good
Endoanal U/S Assesses IAS and EAS thickness, integrity Subjective interpretation Good
MRIEvaluate global pelvic floor
anatomy, sphincter morphology, motion
Expensive, not standardized, availability Fair
Needle EMG Distinguishes between neuropathy and myopathy Invasive, painful Fair
Surface EMG Provides information on normal or weak tone Inaccurate, artifacts Fair
Adapted from: Rao SSC. Clin Gastroenterol Hepatol. 2010;8:910-919.

Debate 1Every patient with FI needs an extensive diagnostic
evaluation, including anal ultrasound
VS

Treatment Options:Fecal Incontinence

Behavioral Techniques for Fecal Incontinence• Stop, don’t run: Avoid rushing to the toilet
– Increases abdominal wall contraction which increases chance of FI
– Reduces focus on pelvic floor– Stop and perform Kegel exercise and proceed to toilet
• Clean, squeeze, reclean– After BM, clean anus, perform 2-3 Kegel exercises, then re-clean– If stool present, may have avoided FI
• Delay bowel movement after biofeedback therapy– Start with brief periods, then increase; improves confidence
• Wean off laxatives and antidiarrheals
Heyman S et al. Dis Colon Rectum. 2009;52:1730-1737.
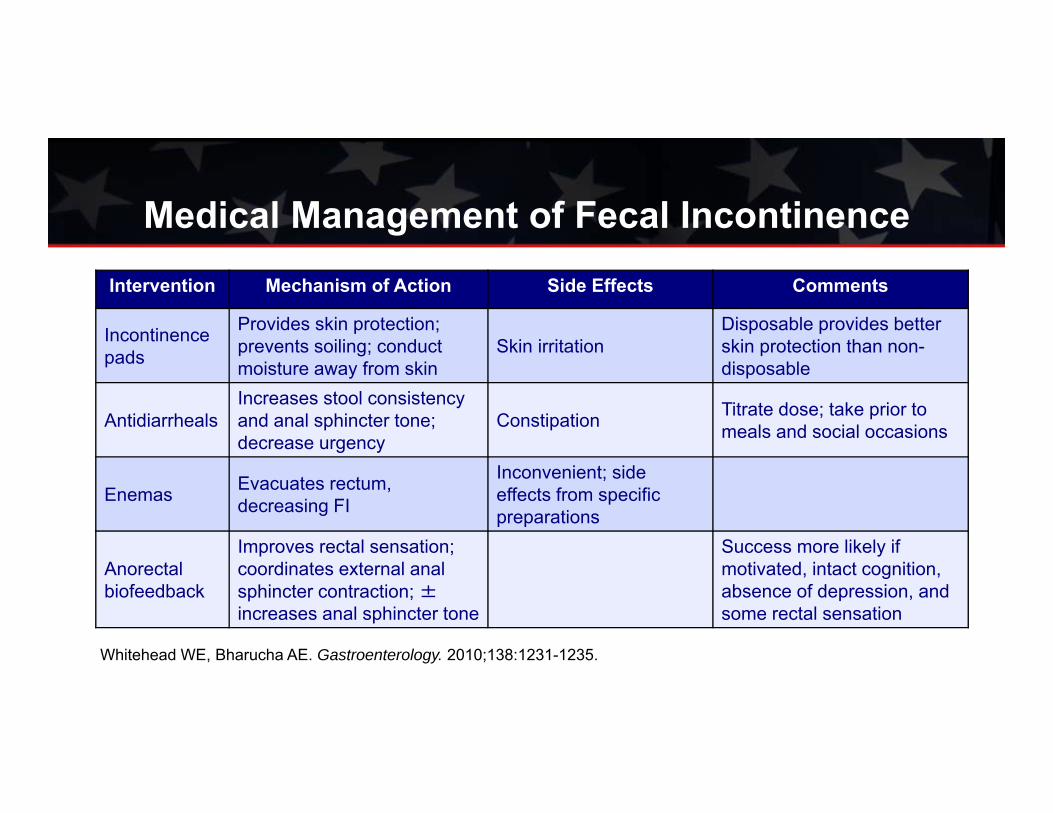
Medical Management of Fecal IncontinenceIntervention Mechanism of Action Side Effects Comments
Incontinence pads
Provides skin protection; prevents soiling; conduct moisture away from skin
Skin irritationDisposable provides better skin protection than non-disposable
AntidiarrhealsIncreases stool consistency and anal sphincter tone; decrease urgency
Constipation Titrate dose; take prior to meals and social occasions
Enemas Evacuates rectum, decreasing FI
Inconvenient; side effects from specific preparations
Anorectal biofeedback
Improves rectal sensation; coordinates external anal sphincter contraction; ±increases anal sphincter tone
Success more likely if motivated, intact cognition, absence of depression, and some rectal sensation
Whitehead WE, Bharucha AE. Gastroenterology. 2010;138:1231-1235.

Pharmacologic Treatment of Fecal Incontinence
• Antidiarrheal agents– Loperamide, diphenoxylate
• Anticholinergics
• Tricyclic agents
• Alosetron for refractory diarrhea
• Cholestyramine for post-cholecystectomy diarrhea
Rao SS et al. Am J Gastroenterol. 2004;99:1585-1604.

T31
Biofeedback for Fecal Incontinence:Training Methods
Squeeze in response to reflex inhibition of IAS
during rectal filling
Improving rectal sensation
Strengthtraining
Coordination

*P=.01FISI=Fecal Incontinence Severity IndexHeyman S et al. Dis Colon Rectum. 2009;52:1730-1737.
Biofeedback + Pelvic Floor Exercises (PFE) vs Pelvic Floor Exercise in FI

Surgical Management of Fecal IncontinenceIntervention Mechanism of
ActionSide Effects Comments
Sphincteroplasty for sphincter defects
Restores sphincterintegrity
Wound infection; delayed recurrent FI
Beneficial effects decrease over time; indicated for IAS defects without denervation
Sacral nerve stimulation
Increases stool consistency and anal sphincter tone; decrease urgency
Infection; lead fracture or migration Relatively safe
Artificial sphincterGracilis transposition
Restores anal barrier
Device erosion, failure, infection
High morbidity; seldom used
Colostomy Reserve for most severe
Whitehead WE, Bharucha AE. Gastroenterology. 2010;138:1231-1235.Glasgow SC, Lowry A. Dis Colon Rectum 2012;55:482-490

New Treatment Options for Fecal
Incontinence
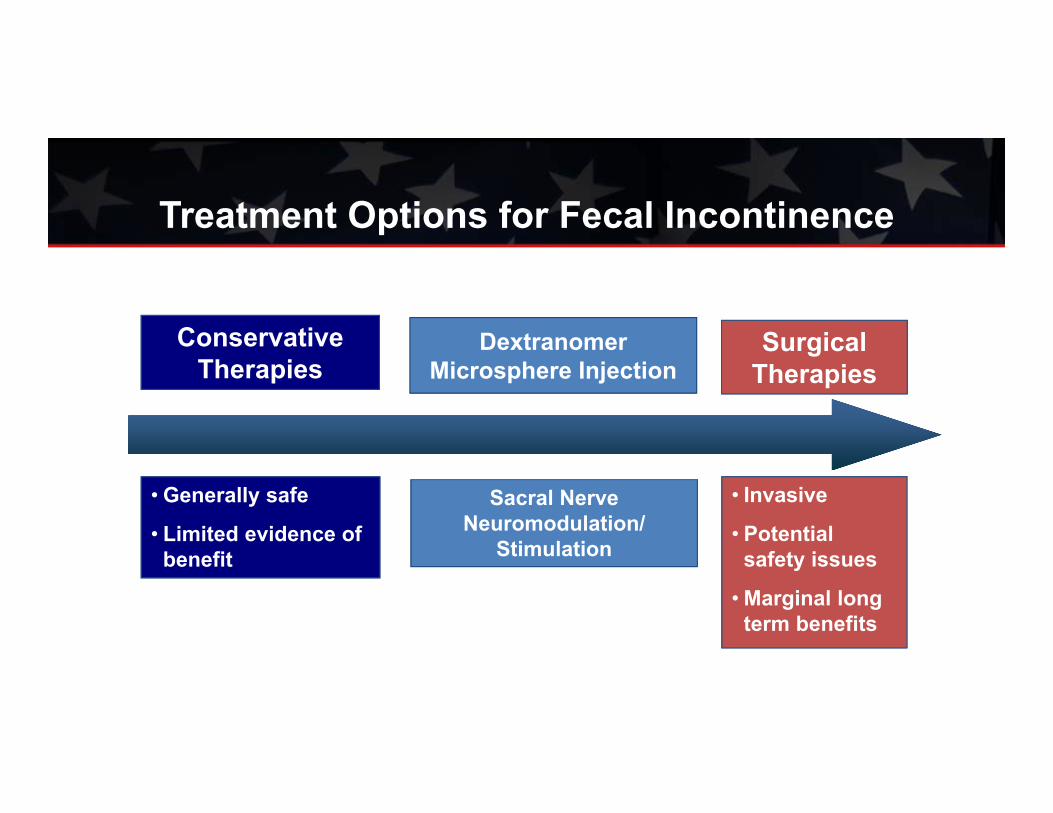
Conservative Therapies
Surgical Therapies
DextranomerMicrosphere Injection
• Generally safe
• Limited evidence of benefit
Sacral Nerve Neuromodulation/
Stimulation
• Invasive
• Potential safety issues
• Marginal long term benefits
Treatment Options for Fecal Incontinence

Injectable Gel Treatment for FI• Biocompatible, injectable gel consisting of dextranomer
microspheres in stabilized hyaluronic acid• FDA approved for the treatment of fecal incontinence in patients
aged ≥18 years who have failed conservative therapy• Administration
– Done in physician office or hospital out-patient department– Four injections through an anoscope– Injected into submucosal layer of the anal canal– No anesthesia required
Solesta [package insert]. Oceana Therapeutics, Edison NJ, 2012.

Significantly higher responder rates in injection group at 6 months (Responder50)*
53.2%n=136
30.7%n=70
0
20
40
60
80
Injection Sham
Median # incontinence episodes during
2 weeks in the active treatment group
decreased from 15.0(IQR 9.6–27.5) at baseline
to 6.2 (2.0–15.5) at12 months (P<.0001)
*Responder50 = ≥50% reduction in incontinence episodes as compared with baseline.Graf W et al. Lancet. 2011; 377: 997–1003.
P=.004
Dextranomer Microspheres Injection Pivotal Trial: Primary Endpoint Data
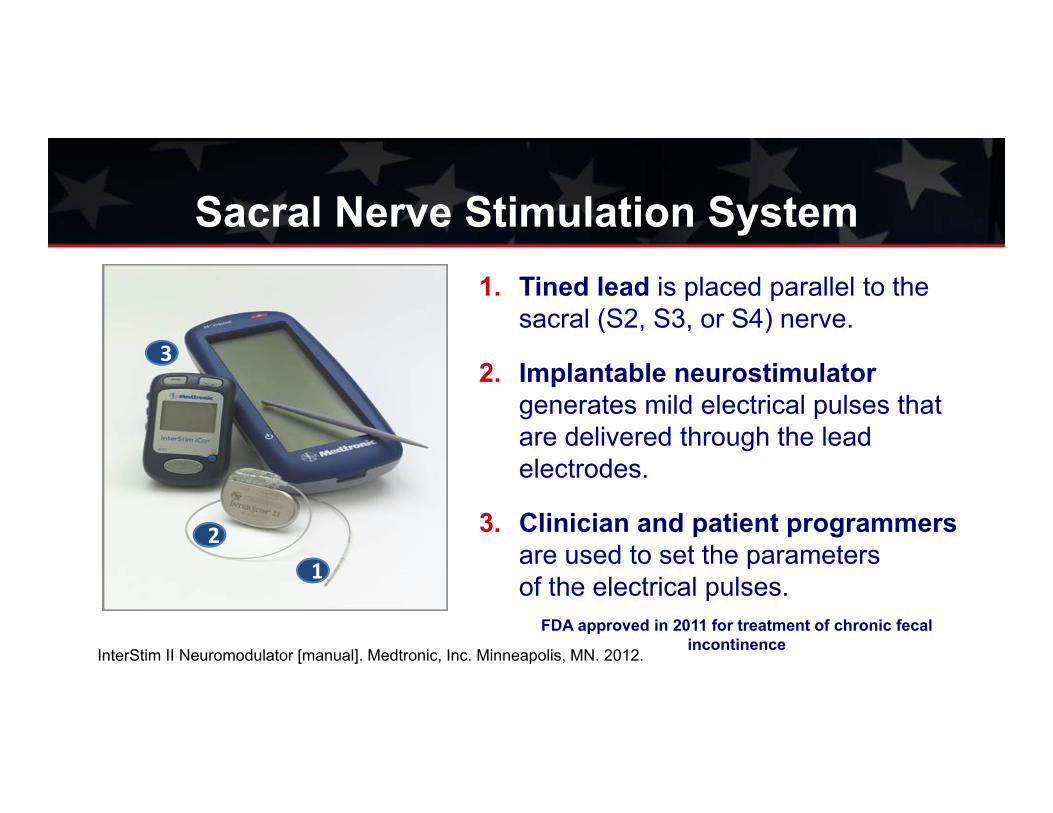
Sacral Nerve Stimulation System1. Tined lead is placed parallel to the
sacral (S2, S3, or S4) nerve.
2. Implantable neurostimulator generates mild electrical pulses that are delivered through the lead electrodes.
3. Clinician and patient programmersare used to set the parameters of the electrical pulses.1
2
3
FDA approved in 2011 for treatment of chronic fecal incontinence
InterStim II Neuromodulator [manual]. Medtronic, Inc. Minneapolis, MN. 2012.

Sacral Nerve Stimulation Bowel Control Study
41%36%
Wexner SD, Coller JA et al. Ann Surg. 2010;251:441-449.

Sacral Nerve Stimulation Bowel Control Study
Most common adverse events (≥5%) reported during the implant phase:1
Adverse Event Frequency (%)Implant site pain 25.8%
Paresthesia 12.5%
Implant site infection 10.8%
Change in sensation of stimulation 8.3%
Urinary incontinence 6.7%
Diarrhea 5.0%
InterStim II Neuromodulator [clinical summary insert]. Medtronic, Inc. Minneapolis, MN. 2012Wexner SD, Coller JA et al. Ann Surg. 2010;251:441-449.
26 SAEs, 13 (10.8%) experienced implant site infection. 5 infections treated with medication, 7 infections (5.8%) required surgical intervention (5 (4%) device explants & 2 (1.6%) device replacements

Debate 2Conventional vs Newer Therapies for FI
VS

How Does the Presence of FI Affect the Diagnosis/Pretest Probability of IBS-D

Rome III Criteria for IBS
Recurrent abdominal pain or discomfort at least 3 days/month in the last 3 months associated with 2 or
more of the following:
Improvement with defecation
Onset associated with a change in
frequency of stool
Onset associated with a change in
form of stool
*Criteria fulfilled for the last 3 months with symptom onset at least 6 months prior to diagnosis
Longstreth GF et al. Gastroenterology. 2006;130:1480-1491.
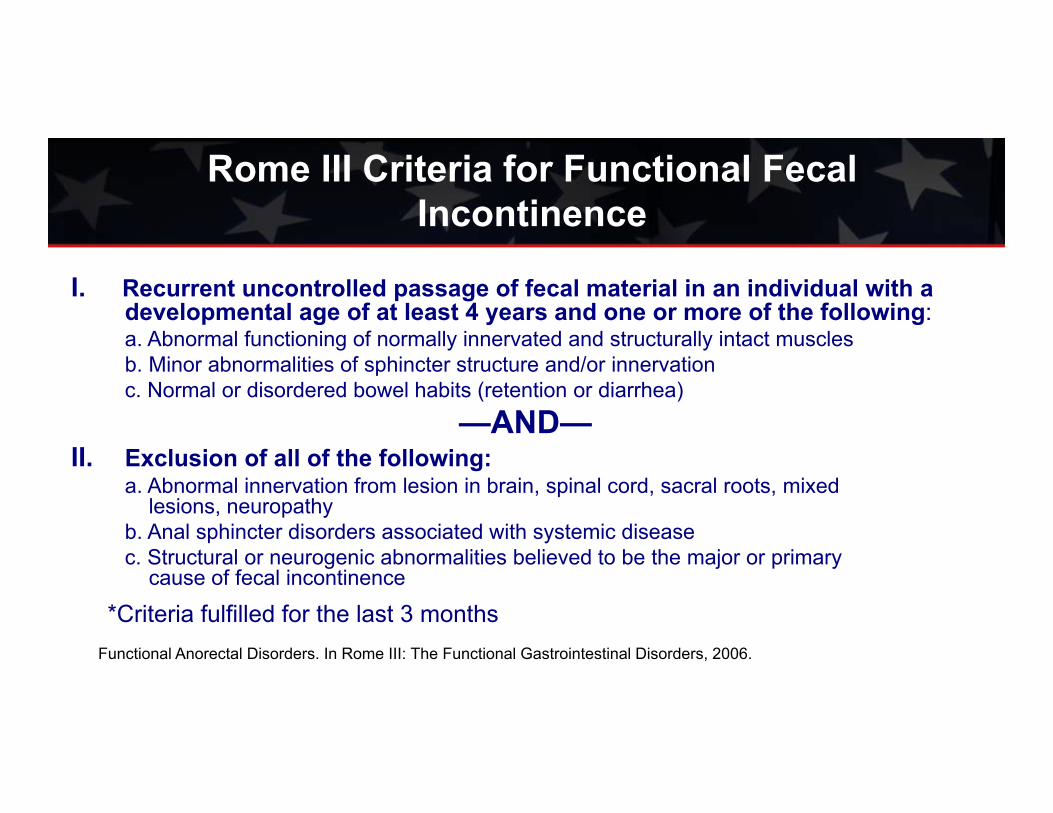
Rome III Criteria for Functional Fecal Incontinence
I. Recurrent uncontrolled passage of fecal material in an individual with a developmental age of at least 4 years and one or more of the following:a. Abnormal functioning of normally innervated and structurally intact musclesb. Minor abnormalities of sphincter structure and/or innervationc. Normal or disordered bowel habits (retention or diarrhea)
—AND—II. Exclusion of all of the following:
a. Abnormal innervation from lesion in brain, spinal cord, sacral roots, mixed lesions, neuropathy
b. Anal sphincter disorders associated with systemic diseasec. Structural or neurogenic abnormalities believed to be the major or primary
cause of fecal incontinence
*Criteria fulfilled for the last 3 monthsFunctional Anorectal Disorders. In Rome III: The Functional Gastrointestinal Disorders, 2006.
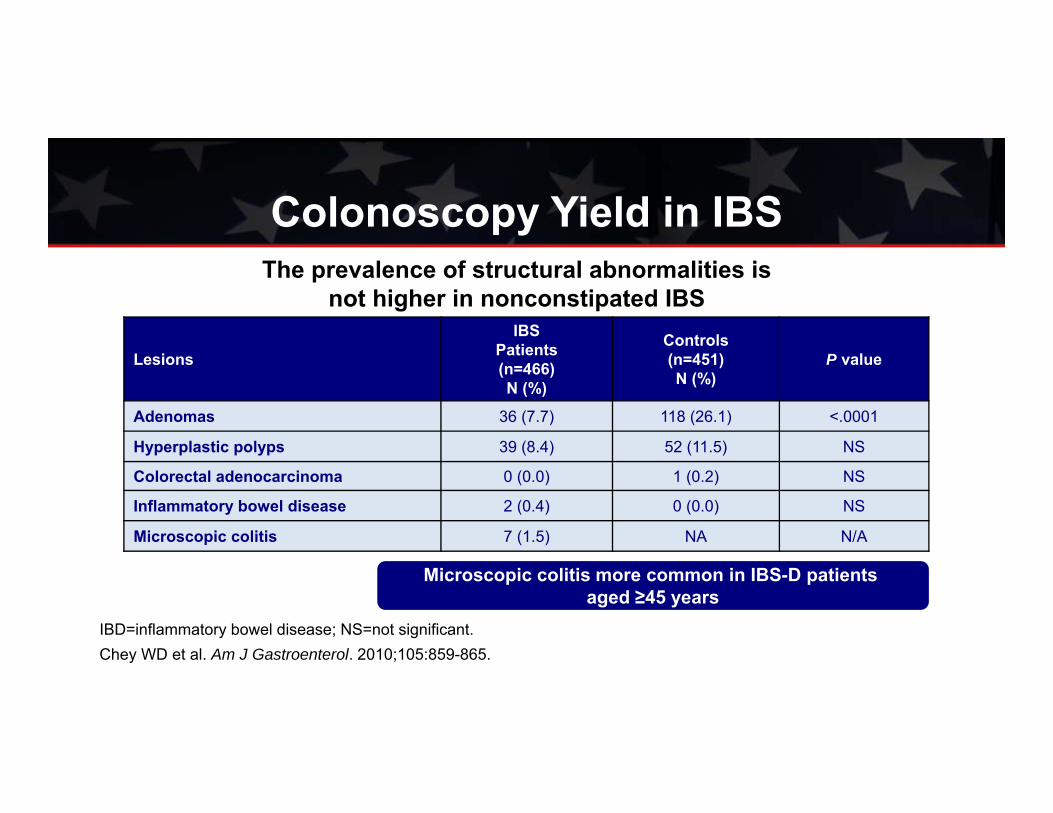
Colonoscopy Yield in IBS
Lesions
IBSPatients(n=466) N (%)
Controls(n=451) N (%)
P value
Adenomas 36 (7.7) 118 (26.1) <.0001
Hyperplastic polyps 39 (8.4) 52 (11.5) NS
Colorectal adenocarcinoma 0 (0.0) 1 (0.2) NS
Inflammatory bowel disease 2 (0.4) 0 (0.0) NS
Microscopic colitis 7 (1.5) NA N/A
Microscopic colitis more common in IBS-D patients aged ≥45 years
IBD=inflammatory bowel disease; NS=not significant.Chey WD et al. Am J Gastroenterol. 2010;105:859-865.
The prevalence of structural abnormalities is not higher in nonconstipated IBS
Linkage Between Fecal Incontinence and IBS/FGID
• Common associations (urinary incontinence, somatic disorders)• Diarrhea and rectal urgency are both risk factors for fecal
incontinence– Loperamide can increase the IAS tone– Diphenoxylate can improve diarrhea/incontinence
• Constipation associated with fecal incontinence– Regularized defecation patterns (laxatives, bulking agents, digital
maneuvers, biofeedback) can decrease fecal incontinence associated with constipation
Longstreth GF et al. Gastroenterology. 2006;130:1480-1491.

Fecal Incontinence and IBS • Presence of fecal incontinence should prompt diagnostic
evaluations– DRE, lower GI endoscopy, ARM, endoanal U/S
• Normal results of diagnostic testing increase the likelihood of IBS as an etiology of fecal incontinence
• Concomitant improvement in symptoms of IBS and fecal incontinence suggest linkage

Post-infectious IBS

Normal
Acute Gastroenteritis
Complete Recovery
~Genetic susceptibility~Abnormal host response~Toxin intensity
POST-INFECTIOUS IBSFunctional GI Diseases?
90% 10%
Risk Factors for PI-IBS• Female1
• Increased diarrhea during acute infection1
• Younger patient with acute diarrhea1
• Absence of vomiting2
• Psychology3,4
PI-IBS=post-infectious IBS1. Neal KR et al. Gut. 202;3:410-413; 2. Neal KR et al. BMJ. 1997;314:779-782; 3. Gwee KA et al. Gut. 1999;44:400-406; 4. Dunlop SP et al. Gastroenterology. 2003;125:1651-1659.

Risk for PI-IBS Increases 7-fold After Infectious Gastroenteritis*
9.8% IBS in cases vs 1.2% IBS in controls
2.8 (1.0-7.5)
8.7 (3.3-22.6)
10.7 (2.5-45.6)
10.1 (0.6-181.4)
6.6 (2.0-22.3)
2.7 (0.2-30.2)
9.9 (3.2-30.0)
11.3 (6.3-20.1)
7.3 (4.8-11.1)
0.1 0.5 1 10 50
Protective Effect Increased Risk OR (95% Cl) Study (year/bacteria)
Ji (2005/Shigella)
Mearin (2005/Salmonella)
Wang (2004/Unspecified)
Okhuysen (2004/Unspecified)
Cumberland (2003/Unspecified)
llnyckyj (2003/Unspecified)
Parry (2003/Bacterial NOS)
Rodriguez (1999/Bacterial NOS)
Pooled estimate
*Systematic review of 8 studies involving 588,061 subjects; follow-up ranged from 3 to 12 months.Halvorsen HA et al. Am J Gastroenterol. 2006;101:1894-1899.
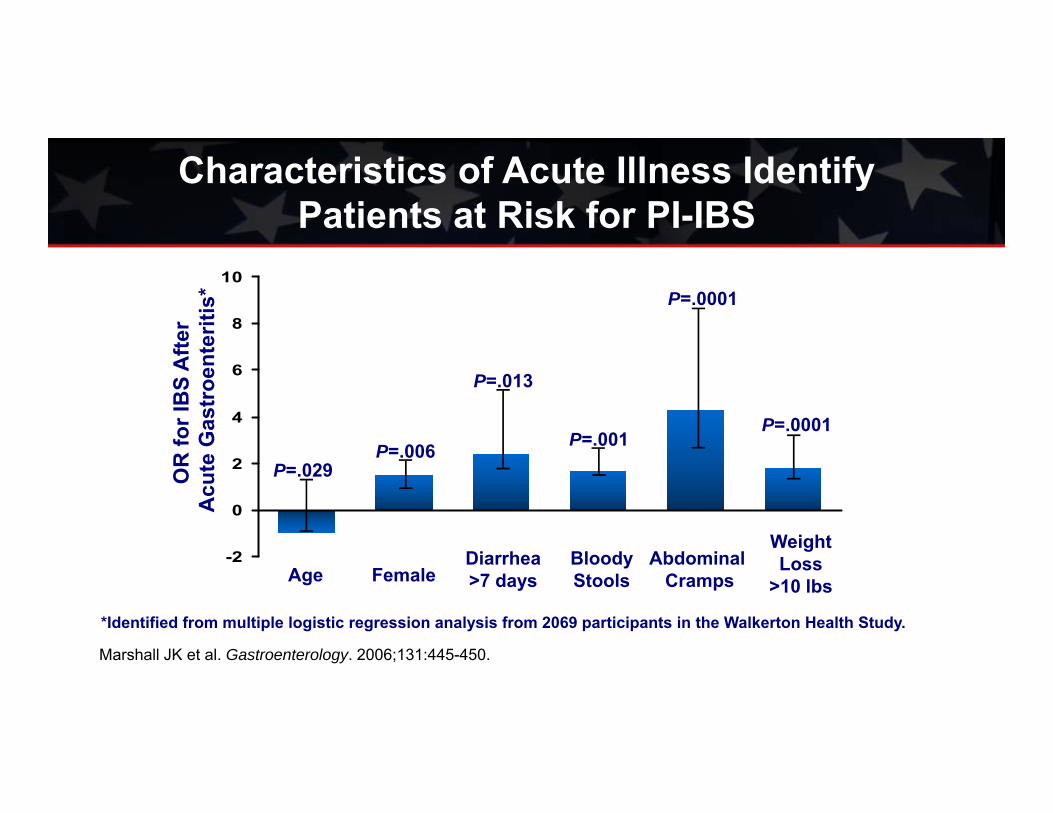
Characteristics of Acute Illness Identify Patients at Risk for PI-IBS
-2
0
2
4
6
8
10
Age FemaleDiarrhea>7 days
BloodyStools
Abdominal Cramps
Weight Loss
>10 lbs
OR
for I
BS
Afte
r A
cute
Gas
troe
nter
itis*
P=.029P=.006
P=.013
P=.001
P=.0001
P=.0001
Marshall JK et al. Gastroenterology. 2006;131:445-450.
*Identified from multiple logistic regression analysis from 2069 participants in the Walkerton Health Study.
Debate 3Does the presence of PI-IBS change approach
to management?
VS

Lifestyle Modifications
for IBS?

n=38 n=37
• 102 IBS patients by Rome II
• 12-week intervention
• 20-60” moderate to vigorous activity 3-5 times/week
• Durable results up to 3 years reported
IBS Severity Scoring System, IBS Score
Johannesson E et al. Am J Gastroenterol. 2011;106:915-922;Johannesson E et al. Abstract presented at DDW 2012.
500
400
300
200
100
0
Control group Physical activity group
P=.001Start Weeks
Impact of Physical Activity on IBS

Food allergy or intolerance
Up to two-thirds of IBS patients associate
symptoms with eating a meal
Gastrocolonicresponse
Psychological Factors
Microbiome/ Fermentation
Gas Handling
1. Simren M et al. Clin Gastroenterol Hepatol. 2007;5:201-218; 2. Eswaran S et al. Gastroenterol Clin North Am. 2011;1:141-162.
Food and IBS Symptoms

Potential Dietary Interventions for IBS
• Gluten-free diet• Empiric food elimination diets • Reduced lactose diet • Low carbohydrate diet• Low FODMAP diet
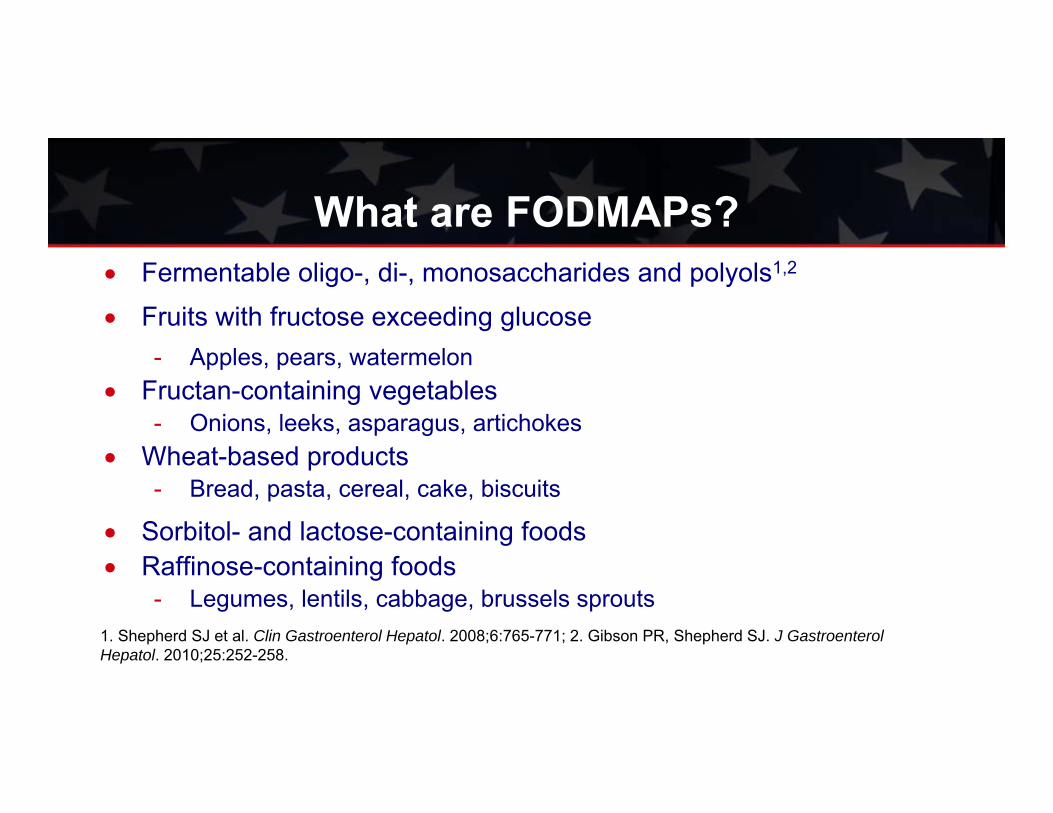
What are FODMAPs?
1. Shepherd SJ et al. Clin Gastroenterol Hepatol. 2008;6:765-771; 2. Gibson PR, Shepherd SJ. J GastroenterolHepatol. 2010;25:252-258.
Fermentable oligo-, di-, monosaccharides and polyols1,2
Fruits with fructose exceeding glucose- Apples, pears, watermelon
Fructan-containing vegetables- Onions, leeks, asparagus, artichokes
Wheat-based products- Bread, pasta, cereal, cake, biscuits
Sorbitol- and lactose-containing foods Raffinose-containing foods
- Legumes, lentils, cabbage, brussels sprouts

0102030405060708090
Symptoms
Prop
ortio
n of
pat
ient
s (%
)
ControlIntervention
*
*
Staudacher HM et al. J Nutr. 2012;142:1510-1515.
* **P<.05
Daily Symptom Scores on Low-FODMAP vs Control Diet

Pharmacologic Options for
Managing IBS-D?
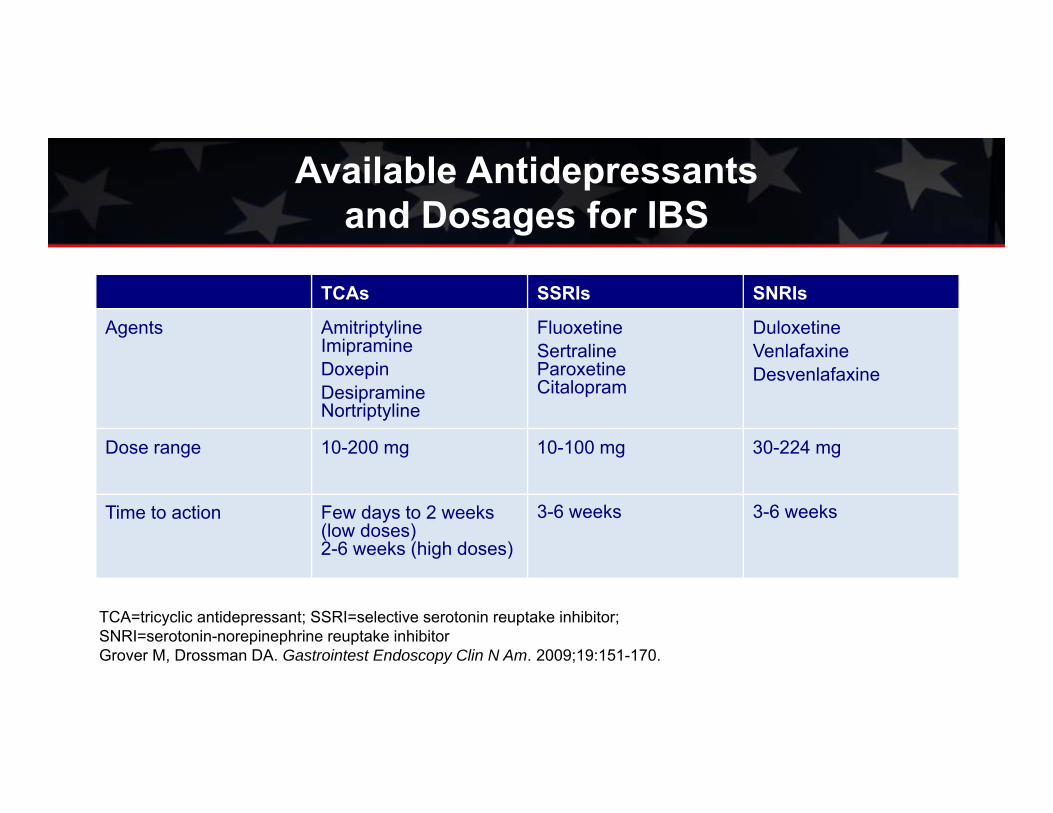
TCAs SSRIs SNRIs
Agents Amitriptyline Imipramine DoxepinDesipramineNortriptyline
Fluoxetine Sertraline Paroxetine Citalopram
DuloxetineVenlafaxineDesvenlafaxine
Dose range 10-200 mg 10-100 mg 30-224 mg
Time to action Few days to 2 weeks (low doses)2-6 weeks (high doses)
3-6 weeks 3-6 weeks
TCA=tricyclic antidepressant; SSRI=selective serotonin reuptake inhibitor; SNRI=serotonin-norepinephrine reuptake inhibitorGrover M, Drossman DA. Gastrointest Endoscopy Clin N Am. 2009;19:151-170.
Available Antidepressants and Dosages for IBS

Study (Drug, Dose) Treatment n/N Control n/N RR (Random) 95% CI
Heefner (desipramine 150 once daily) 10/22 12/22
Myren (trimipramine 50 once daily) 5/30 10/31
Nigam (amitriptyline 12.5 once daily) 14/21 21/21
Boerner (doxepin 50 once daily) 16/42 19/41
Bergmann (trimipramine 50 once daily) 5/19 14/16
Vij (doxepin 75 once daily) 14/25 20/25
Drossman (desipramine 50-150 once daily) 60/115 36/57
Talley (imipramine 50 once daily) 0/18 5/16
Vahedi (amitriptyline 10 once daily) 8/27 16/27
Subtotal (95% CI) 319 256
RR=0.68(95% CI=0.56-0.83)
NNT=4
0.1 0.2 0.5 1 2 5 10 Favors Treatment Favors Control
*Significant heterogeneity among studies may limit conclusions.Study duration ranged from 4 weeks to 3 months.Ford AC et al. Gut. 2009;58:367-378.
Efficacy of TCAs in RelievingGlobal IBS Symptoms*

Study ID OR (95% Cl) % Weight
Sharara et al 3.70 (0.92, 14.89) 3.06
Pimentel et al 4.83 (1.44, 16.18) 3.99
Lembo et al 1.39 (0.93, 2.07) 26.01
TARGET 1 1.52 (1.09, 2.11) 33.20
TARGET 2 1.44 (1.04, 2.00) 33.73
Overall 1.57 (1.22, 2.01) 100.00
Menees SB et al. Am J Gastroenterol. 2012;107:28-35.
Efficacy of Rifaximin for Adequate Relief of IBS Symptoms

Efficacy OutcomeProportion of Patients with a
Response Odds Ratio (95% CI)P Value for Treatment
EffectPlacebo Rifaximin
no./total no.
Secondary end points
Daily abdominal pain
Target 1 132/314 159/309 1.48 0.02
Target 2 138/320 165/315 1.46 0.02
Combined 270/634 324/624 1.46 <0.001
Daily stool consistency
Target 1 212/314 244/309 1.80 0.002
Target 2 206/320 233/315 1.57 0.01
Combined 418/634 477/624 1.64 <0.001
Analyses of Primary, Key Secondary, and Other Secondary End Points
Pimentel M, et al. N Engl J Med 2011;364:22.
0.50 1.00 1.50 2.00 2.50 3.00
Placebo Better Rifaximin Better

RTX=retreatmentPimentel M et al. Dig Dis Sci. 2011;56:2067-2072.
Retreatment With Rifaximin After Return of IBS Symptoms
0
10
20
30
40
50
60
70
80
90
100
1st RTX 2nd RTX 3rd RTX 4th RTX 5th RTX 0
2
4
6
8
10
12
1st RTX 2nd RTX 3rd RTX 4th RTX 5th RTX Perc
ent o
f sub
ject
s w
ho re
spon
ded
Med
ian
num
ber o
f mon
ths
befo
re re
laps
e
54/65
38/40 17/18
6/73/4
N=63Range:
0.5- 45 mo
N=46Range: 1-45 mo N=21
Range:2-37 mo
N=6Range:1-18 mo
N=4Range:2-24 mo

Alosetron Camilleri (1999) Bardhan (2000) Camilleri (2000) Camilleri (2001) Lembo (2001) Chey (2004) Chang (2005) Krause (2007)Subtotal (95% Cl) Total events: 1576 (treatment), 1,127 (control) Test for heterogenerity: x2 = 46.22, df = 7 (P<0.00001, l2 = 84.9% Test for overall effect: Z = 3.45 (P = 0.0006)
179/290166/345191/324182/309144/532167/351268/534279/529
3,214
54/8057/117
229/323235/317156/269197/36377/128122/176
1,173
8.297.289.949.978.419.169.639.6271.29
0.91 [0.77, 1.09]0.99 [0.80, 1.23]0.83 [0.74, 0.93]0.79 [0.71, 0.89]0.47 [0.39, 0.55]0.88 [0.76, 1.01]0.83 [0.67, 0.86]0.76 [0.69, 0.90]
71.29 [0.69, 0.90]
Studyor sub-category
Treatmentn/N
Controln/N
RR (random)95% Cl
RR (random)95% Cl
Weight%
Ford AC et al. Am J Gastroenterol. 2009;104:1831-1843.
Efficacy of Alosetron (5-HT3 Antagonist) in IBS:A Meta-Analysis of RCTs

• Only for women with severe diarrhea-predominant IBS who have– Chronic IBS symptoms (6 months) – No evidence of anatomic or biochemical abnormalities of the GI tract – Failed to respond to conventional therapy
• IBS is severe if it includes diarrhea and 1 of the following:– Frequent, severe abdominal pain / discomfort– Frequent bowel urgency or fecal incontinence– Disability or restriction of daily activities due to IBS
Harris LA, Chang L.. Women’s Health. 2007;3:15-27.
Indications for Restricted Use of Alosetron

IBS Therapies:Safety
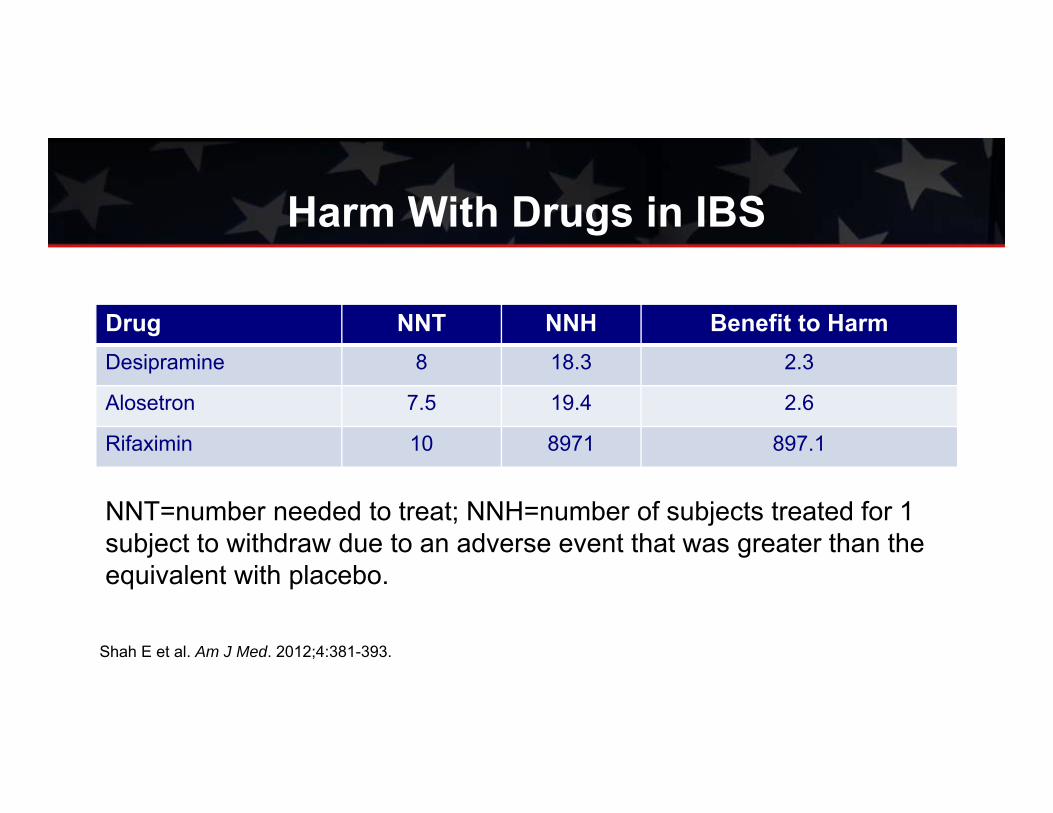
Harm With Drugs in IBS
Drug NNT NNH Benefit to HarmDesipramine 8 18.3 2.3
Alosetron 7.5 19.4 2.6
Rifaximin 10 8971 897.1
NNT=number needed to treat; NNH=number of subjects treated for 1 subject to withdraw due to an adverse event that was greater than the equivalent with placebo.
Shah E et al. Am J Med. 2012;4:381-393.

Harm With Drugs in IBS
Drug Excess of Placebo OnlyDesipramine Dry mouth, flushing, constipation, insomnia,
decreased appetite, palpitationsAlosetron Constipation, abdominal pain/discomfort
Rifaximin Bad taste in mouth
Shah E et al. Am J Med. 2012;4:381-393.

Functional Net Value
‐25‐20‐15‐10‐505
10152025
Benefit over placebo
GI side effect in excessof placebo
+12.5%
-16.0% -17.0%
+13.0% +10.0%
Desipramine Alosetron RifaximinNet value: -3.5% -4% +10%
Shah E et al. Abstract presented at Digestive Disease Week 2012.

This activity is supported by an educational grant from Salix Pharmaceuticals, Inc. Jointly sponsored by the Gi Health Foundation and Purdue University College of Pharmacy.
This event is neither sponsored by nor endorsed by the American College of Gastroenterology.
Accredited by: Sponsored by:
Faculty:
Brooks Cash, MDLin Chang, MD
Moderator:
Philip Schoenfeld, MD William Chey, MD
Mark Pimentel, MD
72
Related Documents











