MEDICAL CLASSIFICATION CODE VS. CLINICAL TERMINOLOGY CODE Dr SB Bhattacharyya MBBS, MBA. FCGP Member, National EHR Standardisation Committee, Moh&FW, GoI Member, Health Informatics Sectional Committee (MHD-17), BIS Hony. State Secretary (2015), IMA Haryana President (2010 – 2011), IAMI

Medical classification coding vs clinical terminology coding
Jan 14, 2017
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
MEDICAL CLASSIFICATION CODE VS. CLINICAL TERMINOLOGY CODE
Dr SB Bhattacharyya
MBBS, MBA. FCGP
Member, National EHR Standardisation Committee, Moh&FW, GoI
Member, Health Informatics Sectional Committee (MHD-17), BIS
Hony. State Secretary (2015), IMA Haryana
President (2010 – 2011), IAMI

RECORDS – WHY KEEP THEM?
• For reuse
• As a source of historical data & information
• Information exchange among providers
• To anticipate future health problems
• As a record standard preventive measures
• To identify deviations from the expected
• As basis for clinical research – trials and observational
• As legal evidence
2
Dr SB Bhattacharyya©

WHY CODE?
• Computers hold information as sequences of binary bits and work by matching strings all of which need precisely coded data
• Codes are needed and used by computers, not humans
• These are a sequence of symbols, usually digits or letters, which designate an object or concept for identification or selection purposes and is just an alternative name for something, an identifier, designed for computer processing
• All free-text data needs to be redacted during anonymisation/de-identification process, not the coded ones
Dr SB Bhattacharyya©
3
CLASSIFICATION & TERMINOLOGY: APPLES AND ORANGES OR CHALK
AND CHEESE?
4
Dr SB Bhattacharyya© : Images as sourced from Internet
CLASSIFICATION & TERMINOLOGY SYSTEMS
Classification Systems
• Semasiological or meaning-based approach to building the code system
• Starting point is the word (term)
• Studying a term, the lexicographer ponders on its many meanings or the different concepts it reflects, i.e. the term’s point-of-view
Terminology Systems
• Onomasiological or concept-based approach to building the code system
• Starting point is the concept
• Studying a term, the terminologist ponders on the various terms that could best reflect a particular concept, i.e., the conceptual point-of-view
5
Dr SB Bhattacharyya©
POINTS OF DIFFERENCE
Classification Systems
• Codes specific data items, e.g.,
• Diseases & diagnosis (ICD, ICD-O, DRG, etc.)
• Lab reports (LOINC)
• Procedures/services – for billing (CPT)
• Pharma products (RxNorm, ATC)
• Combination of codes required to query several items simultaneously
Terminology Systems
• Codes the entire domain, e.g. SNOMED CT covers terms from abscess to zygote
• Ability to function as a common reference code system that maps to others
• Using compositional grammar complex concepts can be coded and queried
6
Dr SB Bhattacharyya©
APPLICATION AREAS
Classification Systems
• Statistical analysis
• Administrative
• Performance
• Activity Based Analysis
• Epidemiological studies
• Billing & Accounting
• Reporting
Terminology Systems
• Semantic interoperability
• Detailed analysis including those that classification can do
• Predictive analytics
• Personalised medicine
• Robust support for clinical trials and observational research
7
Dr SB Bhattacharyya©
EXAMPLES OF MEDICAL CLASSIFICATION CODE SYSTEMS – ICD
• ICD-10 Version : 2016
• I Certain infectious and parasitic diseases
• II Neoplasms
• III Diseases of the blood and blood-forming organs and certain disorders involving the immune mechanism
• IV Endocrine, nutritional and metabolic diseases
• V Mental and behavioural disorders
• VI Diseases of the nervous system
• VII Diseases of the eye and adnexa
• Certain infectious and parasitic diseases
• A00-A09 Intestinal infectious diseases • A00 Cholera
• A00.0 Cholera due to Vibrio cholerae 01, biovar cholerae
• A00.1 Cholera due to Vibrio cholerae 01, biovar eltor
• A00.9 Cholera, unspecified
• A01 Typhoid and paratyphoid fevers
• A02 Other salmonella infections
• A03 Shigellosis
• A04 Other bacterial intestinal infections
Dr SB Bhattacharyya© : Codes as sourced from the Internet
8
EXAMPLES OF CLINICAL TERMINOLOGY CODE – SNOMED CT
• Infectious disease (disorder)
• Infectious disease
• Disease due to infection
• Infective disorder
• Disorder due to infection
• Infection
• Term fully defined as ...
• | is a | = disease
• (has a) pathological process = infectious process
• Infectious disease
• Acute infectious disease
• Bacterial infectious disease
• Chronic infectious disease
• Congenital infectious disease
• Disease caused by parasite
• Dust-borne infectious disease
• Fomite transmitted infectious disease
• Ill-defined infectious disease
Dr SB Bhattacharyya©
9
CONCEPTS
• Concepts are a clinical idea with a unique identifier that is machine-processable pseudo-random number.
• The Concepts (thought or idea) themselves are in people's heads, while the corresponding codes are its unique identifiers and is a unique numeric code representing a “unit of meaning” like “pain in right leg”
Dr SB Bhattacharyya©
10
CONCEPTS
• Based on the principle of ‘one code per meaning, one meaning per code’
• Unique concept identifiers are actually strings of machine-processable digits with lengths ranging from 6 to 18, although most commonly 8 or 9 digits
Dr SB Bhattacharyya©
11

CONCEPTS
Each clinical idea is called a concept
that has a concept ID (e.g. 195967001 | asthma |)
which is a pseudo-random number
Allows multiple names for the same clinical idea in many
languages (e.g. English, Spanish, Danish)
dialects of the same language (e.g. US English, UK English)
12
Dr SB Bhattacharyya©
MULTIPLE DESCRIPTIONS FOR EACH CONCEPT
• Some descriptions are what clinicians prefer to use while communicating, e.g. Myocardial Infarction
• Some descriptions are other names that can be used for the same thing, but are not the preferable term e.g. cardiac infarction, infarction of heart, heart attack
• SNOMED CT includes all these synonyms as distinct terms that are all related to the same concept
• Thus, anyone subsequently studying it would understand what clinical idea the author of the record had when making the entry
13
Dr SB Bhattacharyya©

14
Image courtesy IHTSDO

CODINGClassification & Terminology
15Dr SB Bhattacharyya©
SEVERE BURN BETWEEN 4TH & 5TH
LEFT TOE
ICD-10
• One cannot implicitly code
• One cannot explicitly code
• Nearest code:T25.3 – burn of 3° ankle and foot
• T31.0 to T31.9 – indicating %-age of burn (<10% to >90%)
SNOMED CT
• One cannot implicitly code
• One can explicitly code as follows284196006|Burn of skin|: 246112005|Severity|= 24484000|severe, 363698007|Finding Site|= (113185004|Structure of skin between fourth and fifth toes|:272741003|Laterality|= 7771000|left)
16
Dr SB Bhattacharyya©
LAPAROSCOPIC EMERGENCY APPENDECTOMY
ICD - 9 - CM (Year 2001 – WHO – International Classification of Diseases – Ninth Revision – Clinical Modification)
17
Diagnosis Acute Appendicitis 541
with perforation 540.0
with peritoneal abscess 540.1
Dr SB Bhattacharyya© : As sourced from the Internet
LAPAROSCOPIC EMERGENCY APPENDECTOMY
International Statistical Classification of Diseases and Related Health Problems 10th Revision (ICD-10)-WHO Version for 2016
Chapter XI : Diseases of the digestive system (K00-K93)
Diseases of appendix (K35-K38)
18
Dr SB Bhattacharyya© : As sourced from the Internet
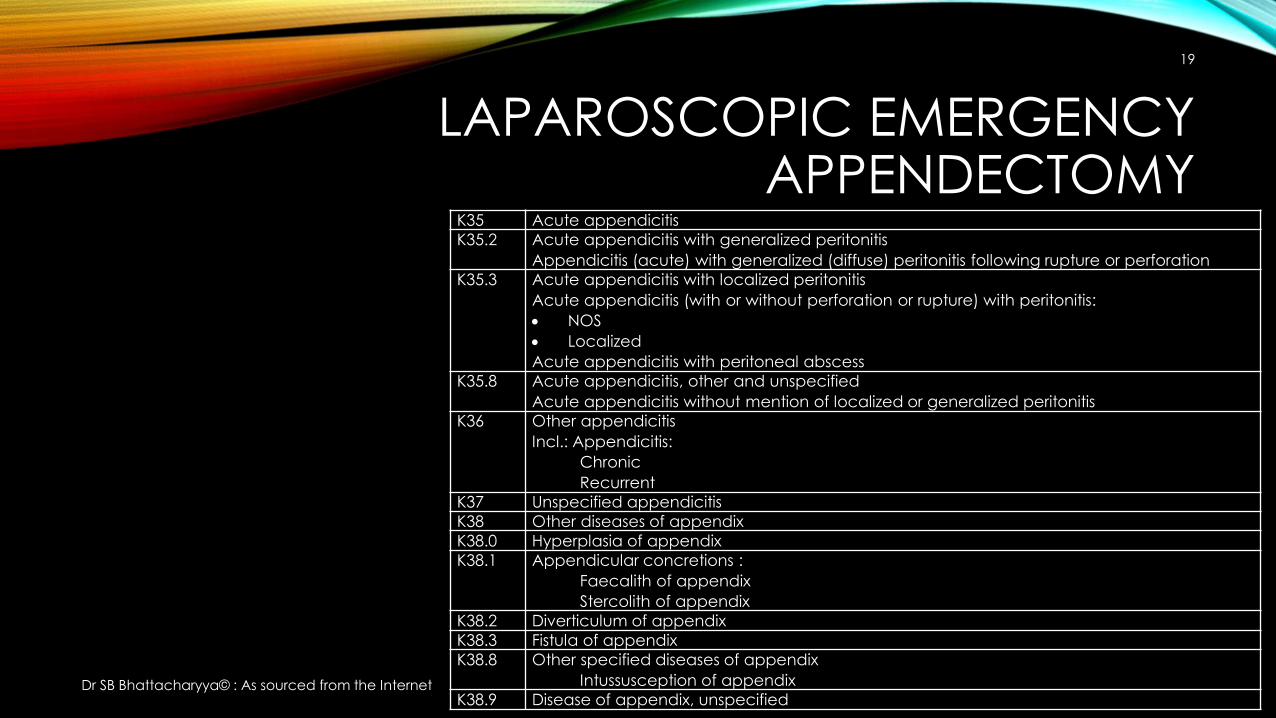
LAPAROSCOPIC EMERGENCY APPENDECTOMY
K35 Acute appendicitis
K35.2 Acute appendicitis with generalized peritonitis
Appendicitis (acute) with generalized (diffuse) peritonitis following rupture or perforation
K35.3 Acute appendicitis with localized peritonitis
Acute appendicitis (with or without perforation or rupture) with peritonitis:
NOS
Localized
Acute appendicitis with peritoneal abscess
K35.8 Acute appendicitis, other and unspecified
Acute appendicitis without mention of localized or generalized peritonitis
K36 Other appendicitis
Incl.: Appendicitis:
Chronic
Recurrent
K37 Unspecified appendicitis
K38 Other diseases of appendix
K38.0 Hyperplasia of appendix
K38.1 Appendicular concretions :
Faecalith of appendix
Stercolith of appendix
K38.2 Diverticulum of appendix
K38.3 Fistula of appendix
K38.8 Other specified diseases of appendix
Intussusception of appendix
K38.9 Disease of appendix, unspecified
19
Dr SB Bhattacharyya© : As sourced from the Internet
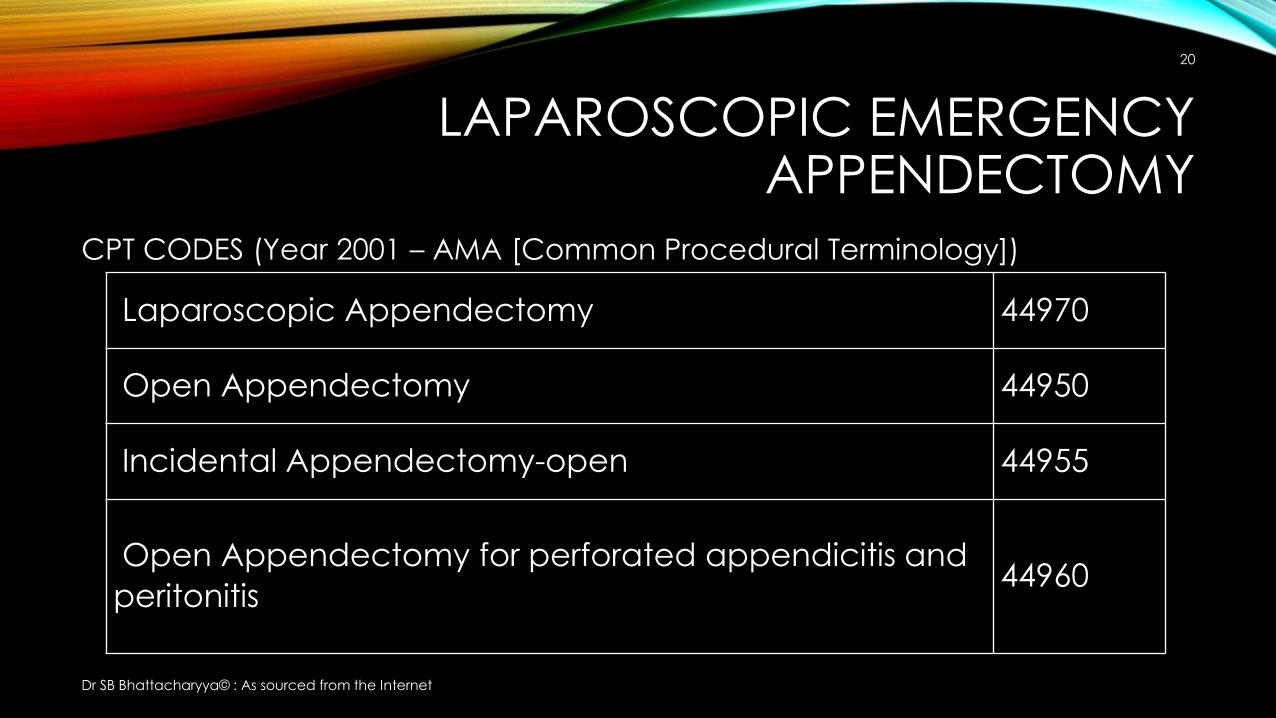
LAPAROSCOPIC EMERGENCY APPENDECTOMY
CPT CODES (Year 2001 – AMA [Common Procedural Terminology])
20
Laparoscopic Appendectomy 44970
Open Appendectomy 44950
Incidental Appendectomy-open 44955
Open Appendectomy for perforated appendicitis and
peritonitis44960
Dr SB Bhattacharyya© : As sourced from the Internet
LAPAROSCOPIC EMERGENCY APPENDECTOMY
• Cannot write procedure as “laparoscopic emergency appendectomy” as such, which surgeons would normally prefer
• Procedure performed has to be entered using ICD-10 : K35.8 (Acute appendicitis without mention of localized or generalized peritonitis) –since no information about anything other than appendicitis is available – best guesstimate
• Procedure performed has to be entered using CPT : 44970 (Laparoscopic Appendectomy)
• Need TWO (2) separate entries – one for procedure name and another for billing purposes
• The fact that it was an emergency needs to be implicitly derived
21
Dr SB Bhattacharyya©
LAPAROSCOPIC EMERGENCY APPENDICECTOMY
• Difficult as the term “appendicectomy” is not available in either ICD or CPT code systems
• Needs to be implicitly understood that “appendicectomy” and “appendectomy” are synonyms
• Users need to be taught how to code correctly, not-so-easy to automate the coding activity
22
Dr SB Bhattacharyya©
LAPAROSCOPIC EMERGENCY APPENDECTOMY
SNOMED CT (US-English) :
174041007 | laparoscopic emergency appendectomy |
23
Dr SB Bhattacharyya© : Sourced using CliniClue™
LAPAROSCOPIC EMERGENCY APPENDICECTOMY
SNOMED CT (GB-English):
174041007 | laparoscopic emergency appendicectomy |
24
Dr SB Bhattacharyya© : Sourced using CliniClue™
WHAT THE SURGEON RECORDS…
Procedure: (any one of the following)
laparoscopic emergency appendicectomylaparoscopic emergency appendectomyendoscopic emergency appendectomy endoscopic emergency appendicectomy
25
Dr SB Bhattacharyya© : Sourced using CliniClue™
WHAT THE GP SEES (ON REVIEW)…
Procedure performed: laparoscopic emergency appendicectomy
26
Dr SB Bhattacharyya©

HOW IT CAN HELP THE INSURANCE SECTOR?
Within medical records…
• More accurate terms for services rendered
• Consistent terms for diagnosis / procedure performed
• Robust support for fraud analysis and detection, even in real-time
27
Dr SB Bhattacharyya©

INTRODUCTION TO SNOMED CT BY DR SB BHATTACHARYYA AVAILABLE
AT• http://www.amazon.com/Introduction-SNOMED-CT-S-B-
Bhattacharyya/dp/9812878939/ref=sr_1_1?ie=UTF8&qid=1453269681&sr=8-1&keywords=introduction+to+snomed+ct – hardcopy only
• http://www.amazon.in/Introduction-SNOMED-CT-2016-Bhattacharyya/dp/9812878939/ref=sr_1_1?ie=UTF8&qid=1453269722&sr=8-1&keywords=introduction+to+snomed+ct – hardcopy only
• http://www.springer.com/gp/book/9789812878939 – ebook and hardcopy
• http://link.springer.com/book/10.1007/978-981-287-895-3 – chapter-wise online access only
Dr SB Bhattacharyya©
28

Related Documents











