MEDIATORS IN DEVELOPMENTAL CASCADES 1 Mediating Factors in Within-Person Developmental Cascades of Externalising, Internalising and ADHD Symptoms in Childhood Lydia Gabriela Speyer a , Ingrid Obsuth b , Denis Ribeaud d , Manuel Eisner c,d , Michelle Luciano a , Bonnie Auyeung a,e , and Aja Louise Murray a,c Affiliations: a Department of Psychology, University of Edinburgh, Edinburgh, United Kingdom; b Clinical Psychology Department, University of Edinburgh, Edinburgh, United Kingdom; c Violence Research Centre, Institute of Criminology, University of Cambridge, Cambridge, United Kingdom; d Jacobs Center for Productive Youth Development, University of Zurich, Zurich, Switzerland; and e Autism Research Centre, Department of Psychiatry, University of Cambridge, Cambridge, United Kingdom; Address correspondence to: Lydia Gabriela Speyer, Department of Psychology, University of Edinburgh, 7 George Square, Edinburgh, EH8 9JZ, United Kingdom, [[email protected], 00436506914172]. Conflicts of Interest: The authors have no conflicts of interest relevant to this article to disclose. Acknowledgements: The authors are grateful to the children, parents and teachers who provided data for the z-proso study and the research assistants involved in its collection.

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
MEDIATORS IN DEVELOPMENTAL CASCADES1
Mediating Factors in Within-Person Developmental Cascades of
Externalising, Internalising and ADHD Symptoms in Childhood
Lydia Gabriela Speyera, Ingrid Obsuthb, Denis Ribeaudd, Manuel Eisnerc,d, Michelle
Lucianoa, Bonnie Auyeunga,e, and Aja Louise Murraya,c
Affiliations: aDepartment of Psychology, University of Edinburgh, Edinburgh, United
Kingdom; bClinical Psychology Department, University of Edinburgh, Edinburgh, United
Kingdom; cViolence Research Centre, Institute of Criminology, University of Cambridge,
Cambridge, United Kingdom; dJacobs Center for Productive Youth Development,
University of Zurich, Zurich, Switzerland; and eAutism Research Centre, Department ofPsychiatry, University of Cambridge, Cambridge, United Kingdom;
Address correspondence to: Lydia Gabriela Speyer, Department of Psychology, University
of Edinburgh, 7 George Square, Edinburgh, EH8 9JZ, United Kingdom, [[email protected],
00436506914172].
Conflicts of Interest: The authors have no conflicts of interest relevant to this article to disclose.
Acknowledgements: The authors are grateful to the children, parents and teachers who
provided data for the z-proso study and the research assistants involved in its collection.
MEDIATORS IN DEVELOPMENTAL CASCADES2
Abstract
Previous studies have offered evidence for peer problems and academic achievement as
mediators in developmental cascades from externalising to internalising problems, and from
ADHD symptoms to internalising problems and externalising problems. However, these
mediators have not been found to fully account for these cascades indicating that there may
be additional mediators involved. This study investigated the role of parental involvement
alongside academic achievement and peer problems in mediating within-person
developmental cascades from externalising to internalising problems and from ADHD
symptoms to internalising and externalising problems using autoregressive latent trajectory
models with structured residuals. Models were fit for parent- and teacher-reports on
children’s psychosocial development as measured by the Social Behaviour Questionnaire
(SBQ) collected over ages 7, 9, and 11 in an ethnically diverse Swiss longitudinal cohort
study (zproso; N=1387, 51% male). Results indicated that none of the considered factors
acted as significant mediators in longitudinal relations between ADHD, internalising and
externalising problems; hence, a full picture of the mediating mechanisms in developmental
cascades remains to be identified.
Keywords: Developmental cascades; Internalising; Externalising; ADHD Symptoms; z-
proso;

MEDIATORS IN DEVELOPMENTAL CASCADES3
According to the World Health Organisation (WHO, 2018) up to 20% of children and
adolescents globally suffer from a mental health problem and about 50% of all mental health
conditions have their onset by age 14. The leading mental health concerns among young
people in this age group are Attention deficit hyperactivity disorder (ADHD), behaviour (or
externalising) problems, anxiety and depression (or internalising problems) (e.g. Ghandour et
al., 2019). Importantly, these mental health conditions commonly co-occur (e.g. Reale et al.,
2017). Available longitudinal studies suggest that the negative consequences of experiencing
a number of childhood mental health problems are more serious than experiencing a single
condition (e.g. Biederman, 2004). Comorbidity also significantly impacts the prognosis,
treatment, and outcomes of therapeutic interventions with young people (Sibley et al., 2011).
For these reasons it is crucial to understand the processes through which different childhood
mental health problems are linked over time. To add to this understanding, in this study we
examined the roles of academic achievement, peer problems and parental involvement as
potential mechanisms of longitudinal links between ADHD, internalising and externalising
problems.
One theory that seeks to explain the high externalising-internalising longitudinal
comorbidity within the framework of developmental cascade models is the dual failure model
(Capaldi, 1992). Developmental cascade models hypothesise that links between mental health
domains are the result of problems in one domain causally affecting the other domain,
potentially through a number of linking mechanisms (Masten & Cicchetti, 2010). According
to the dual failure model, externalising problems lead to the development of internalising
problems through unidirectional cascades from externalising problems to educational
underachievement (academic failure) and social difficulties such as peer problems (social
failure) which in turn increase the risk for developing internalising problems such as anxiety
or depression (Capaldi, 1992).
MEDIATORS IN DEVELOPMENTAL CASCADES4
While the focus on linking factors between developmental cascades from
externalising to internalising problems has been mainly on peer relationships and academic
achievement with a number of studies finding support for the dual failure model (e.g. van
Lier et al., 2012), these factors have not been found to fully explain externalising-
internalising cascades (e.g. Evans & Fite, 2019; Poirier et al., 2019). Given the complexity of
the development of mental health problems, it is highly likely that other factors play a
mediating role in these cascades. To date, few studies have investigated the role of parenting
behaviours as a potential mechanism for linking externalising-internalising cascades, even
though Capaldi’s (1992) paper originally hypothesised dual failure model explicitly included
parental relationships in the social domain. Considering that there is substantial evidence
highlighting the role of parenting behaviours for children’s socio-emotional development (for
a review see McKee, Colletti, Rakow, Jones, & Forehand, 2008) as well as the role of
externalising problems in eliciting worse parenting through a coercive cycle of negative
parent-child interaction (Patterson, 2002), parenting behaviours are a strong candidate for
linking the developmental relations of externalising and internalising problems.
One of the few studies that included a parental factor in a developmental cascade
model found that maternal dissatisfaction with their child was a significant mediator in a
developmental cascade from externalising problems at age 5 to internalising problems at age
12 (Wertz et al., 2015). A parental factor that could be particularly relevant in mediating
developmental cascades is parental involvement. A large body of research has highlighted
that parental involvement is not only associated with externalising problems but is also an
important factor in the development of internalising problems (Aboobaker, Jangam, Sagar,
Amaresha, & Jose, 2019; Hawes, Dadds, Frost, & Russell, 2013; Kirkhaug, Drugli, Klöckner,
& Mørch, 2013; Wang & Sheikh-Khalil, 2014). For instance, using the Alabama Parenting
Questionnaire which measures six domains of parenting behaviour, Aboobaker et al. (2019)
MEDIATORS IN DEVELOPMENTAL CASCADES5
found that, out of all measured parenting domains, parental involvement was the only
parenting domain associated with emotional problems in a sample of 10 to 18 year olds.
Further research is needed to examine the role of parental involvement in the links between
externalizing and internalizing problems.
Internalising and externalising problems also commonly co-occur with ADHD, with
up to 50% of children suffering from ADHD symptoms also suffering from co-occurring
internalising and externalising problems (Gnanavel, Sharma, Kaushal, & Hussain, 2019). One
explanation of these comorbidities has been offered by Beauchaine and McNulty (2013)
through the ontogenic process model of externalising psychopathology which hypothesises
that early-onset ADHD symptoms lead to later externalising problems as a result of
longitudinal transaction between contextual risk factors and individual vulnerabilities (e.g.
genetic factors). The theory implies that ADHD symptoms might set up individuals for a
developmental trajectory characterised by increasingly escalating externalising behavioural
problems through coercive parent-child interactions (Theule, Wiener, Tannock, & Jenkins,
2013), poorer peer relationships (Diamantopoulou, Henricsson, & Rydell, 2005; Murray,
Zych, Ribeaud, & Eisner, 2020) and academic underachievement (Barry, Lyman, & Klinger,
2002). While some studies have found evidence for developmental cascades from ADHD
symptoms to externalising problems (e.g. Obsuth, Murray, Di Folco, Ribeaud, & Eisner,
2020), few studies to date have investigated potential linking factors in these relations (e.g.
Sevincok, Ozbay, Ozbek, Tunagur, & Aksu, 2020), hence, further research is needed.
Longitudinal investigations of the relations between ADHD and internalising
problems have also found support for developmental cascades from ADHD symptoms to
internalising problems with some also finding support for cascades in the opposite direction
(Murray, Caye, et al., 2020). Since ADHD has been found to be associated with similar risk
MEDIATORS IN DEVELOPMENTAL CASCADES6
factors as externalising problems, a number of studies have also applied the dual failure
model to ADHD-internalising cascades, finding support for mediating effects of both peer
problems and academic attainment (Powell et al., 2020; Roy, Hartman, Veenstra, &
Oldehinkel, 2015). While the focal linking factors have also been peer relationships and
academic achievement, there has also been some evidence for parental relationships as a link
between ADHD symptoms and depression (Humphreys et al., 2013).
One limitation common to most studies on developmental cascades relates to their
statistical operationalisation. The most frequently used method to investigate developmental
cascades and potential mediating factors is the cross-lagged panel model (CLPM), which
examines the relations between variables over time after adjusting inter-individual stability in
those same variables. However, the CLPM does not separate between-person differences
from within-person relations, which means that its parameters represent a mixture of within-
and between-person effects that provide ambiguous results (Berry & Willoughby, 2017).
Considering that developmental cascades refer to within-person processes, more appropriate
methods are needed to confirm that the established relations between externalising problems
as well as ADHD symptoms and internalising problems still hold when appropriately
accounting for between-person differences. One modelling technique well-suited to overcome
this limitation of the CLPM, is the autoregressive latent trajectory model with structured
residuals (ALT-SR) (Curran, Howard, Bainter, Lane, & McGinley, 2014). ALT-SRs combine
the CLPM with a parallel process latent growth curve model that accounts for between-
person effects through allowing growth intercepts of different variables to covary. Thus, they
are well suited to disaggregate within- from between-person effects. Relatively few studies
have applied ALT-SRs to the study of developmental cascades (Murray, Eisner, & Ribeaud,
2020; Oh et al., 2020), and even fewer to the study of potential mediators (Murray et al.,
2021). The only study on linking factors using an ALT-SR so far has not provided strong
MEDIATORS IN DEVELOPMENTAL CASCADES7
evidence for the dual failure model. Using data from the same cohort as the current study,
Murray et. al (2021) investigated the mediating role of peer- and teacher-relationships in
developmental cascades between self-reported internalising problems and aggression during
adolescence. Murray et al. did not identify any significant mediation effects nor did they find
support for developmental cascades between aggression and internalizing problems.
However, they only investigated these relations during a specific developmental period, that
is adolescence (ages 11, 13 and 15) and did not consider the role of parental involvement or
academic achievement as well as ADHD symptoms in these relations. Since previous
research has shown that the within-person developmental relations between internalising and
externalising problems unfold differently in childhood compared to adolescence (Murray,
Eisner, et al., 2020), it is highly important to also investigate mediators in the dual-failure
model during childhood.
In the current study, we aimed to extend the dual failure model by investigating
whether within-person developmental cascades from externalising problems to internalising
problems as well as cascades from ADHD symptoms to internalising and externalising
problems during childhood (median-ages 7, 9 and 11) were mediated by parental
involvement, peer problems (as indicated by negative social roles in the classroom) and
academic achievement. To overcome one of the main limitations of previous research—the
conflation of within- and between-person effects—we used an autoregressive latent trajectory
model with structured residuals which gives insights into the within-person dynamics of the
studied developmental relations. Since previous research has highlighted the need for multi-
informant approaches to the studies of children’s psychosocial development (De Los Reyes,
2013) we further built two ALT-SRs, one using parent-reported data on internalising,
externalising and ADHD symptoms and one using teacher-reported data to evaluate the
stability of our results across informants. This was deemed to be particularly important since
MEDIATORS IN DEVELOPMENTAL CASCADES8
previous research using the ADHD data used in the current study already highlighted that
agreement on children’s ADHD symptom trajectories was only low to moderate across
parents and teachers (Murray, Booth, Ribeaud, & Eisner, 2018; Murray, Ribeaud, Eisner,
Murray, & McKenzie, 2019).
Methods
Participants
The participants of this study included 1387 (51% male) children who were part of the
Zurich Project on Social Development from Childhood to Adulthood (z-proso), a Swiss
longitudinal cohort study. Z-proso has been following the lives of 1675 children from 2004
when the children entered school at age 7 up until today with data collection still ongoing. To
date, there have been ten waves of data collection at ages 7, 8, 9, 10, 11, 12, 13, 15, 17 and
20. Participants attended one of 56 schools in Zurich that were chosen based on a stratified
random sampling procedure that included the school’s size and location as stratification
variables to ensure representativeness in terms of area-based deprivation. While the official
language of the canton of Zurich is German, Zurich is a very culturally diverse city, thus, in
order to recruit and retain as many of the non-German speaking participants as possible,
contact letters and parent interviews were translated into an additional nine languages.
Further details on assessment procedures, recruitment, retention, and attrition can be found in
the literature (M. Eisner & Ribeaud, 2005, 2007; N. L. Eisner, Murray, Eisner, & Ribeaud,
2019). Further details on the z-proso study can be found on the study website:
https://www.jacobscenter.uzh.ch/en/research/zproso/aboutus.html. This study uses data from
waves at median-ages 7, 9 and 11 since at these ages data on internalising, externalising and
ADHD symptoms as well as on peer problems, academic achievement and parental
involvement were available.
MEDIATORS IN DEVELOPMENTAL CASCADES9
Measures
Psychosocial Development
Internalising problems, externalising problems and ADHD symptoms were measured
using the Social Behaviour Questionnaire (SBQ; Tremblay et al., 1991) which assesses
children’s psychosocial development across five domains: aggression, non-aggressive
externalizing problems, anxiety/depression, ADHD symptoms and prosocial behaviour. At
median-ages 7, 9 and 11, teachers completed a German paper-and-pencil version of the SBQ
while parents completed a computer-assisted personal interview. Most of the interviews were
conducted in German, but parents with other native-languages were able to complete the
interview in an additional nine languages (M. Eisner & Ribeaud, 2007). Items in the paper-
and-pencil version of the SBQ were presented in the same order to all teachers, whereas the
computer assisted interview presented items in a randomised order. Self-reported SBQs were
also available, but those were not used in the current study as they were collected in the form
of an adapted computer-based multimedia version of the SBQ with children answering ‘yes’
or ‘no’ to a series of questions relating to their psycho-social development. Internalising
problems were measured using four items on depression and three items on anxiety. All items
were rated on a 5-point Likert scale from Never to Very Often and subsequently averaged to
create a composite score (parent-report: Cronbach’s αage 7 = 0.71; αage 9 = 0.76; αage 11 = 0.79;
teacher-report: Cronbach’s αage 7 = 0.89; αage 9 = 0.91; αage 11 = 0.91). Higher scores indicate
more mental health problems. Composite scores for externalising problems were created by
averaging item scores of four items related to non-aggressive conduct problems, two items
measuring symptoms of oppositional defiant disorder, five items on physical aggression,
three items on proactive aggression and 3 items on reactive aggression, thus, reflecting the
multi-dimensional nature of externalising problems (parent-report: Cronbach’s αage 7 = 0.81;
αage 9 = 0.82; αage 11 = 0.84; teacher-report: Cronbach’s αage 7 = 0.94; αage 9 = 0.94; αage 11 = 0.94).
MEDIATORS IN DEVELOPMENTAL CASCADES10
The ADHD symptom composite score was derived from four items on inattention and four
items on hyperactivity/impulsivity (parent-report: Cronbach’s αage 7 = 0.79; αage 9 = 0.84; αage 11
= 0.85; teacher-report: Cronbach’s αage 7 = 0.94; αage 9 = 0.95; αage 11 = 0.95). Psychometric
analyses of the SBQ in the current sample have found support for developmental invariance,
factorial and criterion validity and have shown that the SBQ is a reliable measure of
moderately low to very high levels of psychopathology in the general population (Murray,
Eisner, Obsuth, & Ribeaud, 2017; Murray, Eisner, & Ribeaud, 2019).
Mediating Factors
Academic achievement was measured using a composite score of arithmetic skills and
reading and verbal language performance scores which were provided by teachers who
compared the child’s abilities in both domains to an average student on a five-point Likert
scale from ‘worse’ to ‘better than average’. These scores were averaged to create a composite
score with higher scores indicating better academic performance (Cronbach’s αage 7 = 0.79;
αage 9 = 0.80; αage 11 = 0.83).
Peer problems were based on a measure of children’s social roles in the classroom.
Teachers were asked to rate the child’s role on four items relating to popularity, bullying
victimisation, rejection and domination on a 5-point Likert scale from ‘very untrue’ to ‘very
true’. Negative social roles, such as being a bully or a bullying victim, have previously been
identified to be associated with internalising as well as externalising problems (Kelly et al.,
2015). In addition, children with multiple negative social roles (e.g., being a bully and a
bullying victim) have been found to have more internalising and externalising problems than
children with just one negative role (being a bully or a bullying victim) (Kelly et al., 2015).
Before averaging all items to create a composite score, the item on popularity was reverse
coded in order to be consistent with the other items. Higher scores indicate that a child has
MEDIATORS IN DEVELOPMENTAL CASCADES11
more negative social roles in the classroom, thus more peer problems (Cronbach’s αage 7 =
0.67; αage 9 = 0.73; αage 11 = 0.69).
Parental involvement was measured using the Alabama Parenting Questionnaire
(APQ) which measures parenting behaviours in six domains: parental involvement, positive
parenting, poor monitoring, inconsistent discipline, corporal punishment, and other discipline
(Shelton, Frick, & Wootton, 1996). Since past research has offered evidence that parental
involvement may be involved in both the development of internalising and externalising
problems (Aboobaker et al., 2019; Hawes et al., 2013; Kirkhaug et al., 2013; Wang &
Sheikh-Khalil, 2014), we here focus on the parental involvement subscale as a potential
mediator in our models. The involvement subscale includes ten items that parents rated on a
5-point Likert scale ranging from ‘never’ to ‘always’. Scores on all items were averaged to
create a composite score (Cronbach’s αage 7 = 0.63; αage 9 = 0.67; αage 11 = 0.72) with higher
scores being indicative of more parental involvement.
Statistical Analysis
Autoregressive Latent Trajectory Models with Structured Residuals (ALT-SR) were
fitted separately for parent- and teacher-reported data on children’s psychosocial
development to investigate the effects of academic achievement, peer problems and parental
involvement on developmental cascades from externalising problems and ADHD symptoms
to internalising problems. We decided on running separate models for each informant since
teacher- and parent-reports on children’s psychosocial functioning tend to show limited
convergence with cross-informant reports correlating at a low-to-moderate magnitude (De
Los Reyes et al., 2015). Additionally, combining an ALT-SR with a latent variable model
would have likely resulted in estimation difficulties. ALT-SRs combine cross-lagged panel
models with latent growth curve models to optimally account for between-person effects. The
MEDIATORS IN DEVELOPMENTAL CASCADES12
latent growth curve part of the model included random intercepts that are allowed to co-vary
and fixed slopes. Slope factor loadings were fixed proportional to the time intervals between
measurement occasions. Gender was further regressed onto each intercept factor to adjust for
gender differences. The autoregressive and cross lagged effects are defined between the
variables’ residuals, reflecting deviations from the person-specific means and growth curves
at certain time points and, thus, offering insights into within-person dynamics. The cross-
lagged part of the model included all first-order autoregressive and cross-lagged effects as
well as within-time residual covariances. In addition, mediation effects were estimated for
cascades from externalising problems to internalising problems via peer problems, parental
involvement and academic achievement as well as for ADHD symptoms to internalising and
externalising problems via the same potential mediators. Second-order cross-lagged effects
between externalising at time 1 and internalising problems at time 3 as well as between
ADHD symptoms at time 1 and internalising and externalising at time 3 were further
included to allow for testing of longitudinal mediation. To assess statistical significance of
estimated indirect effects, standard errors were computed using the delta method. However,
since the delta method incorrectly assumes a symmetric sampling distribution of indirect
effects (MacKinnon, Warsi, & Dwyer, 1995), we also computed bootstrapped 95%
confidence intervals using standard maximum likelihood estimation.
Models were fit in Mplus 8.5 (Muthén & Muthén, 2018) using a robust maximum
likelihood estimator (MLR) which uses full information maximum likelihood (FIML) to
handle missing data (Enders, 2001). Model fit was judged to be acceptable based on the
following criteria: Tucker Lewis Index (TLI) >.90, Comparative Fit Index (CFI) >.90 and
Root Mean Squared Error of Approximation (RMSEA) <.05 (Kline, 2005). Mplus code and
full model results are provided on the Open Science Framework: https://osf.io/d7wfb/?
view_only=1e61e55ade1f4a53b18c6f376991ffbf.
MEDIATORS IN DEVELOPMENTAL CASCADES13
Results
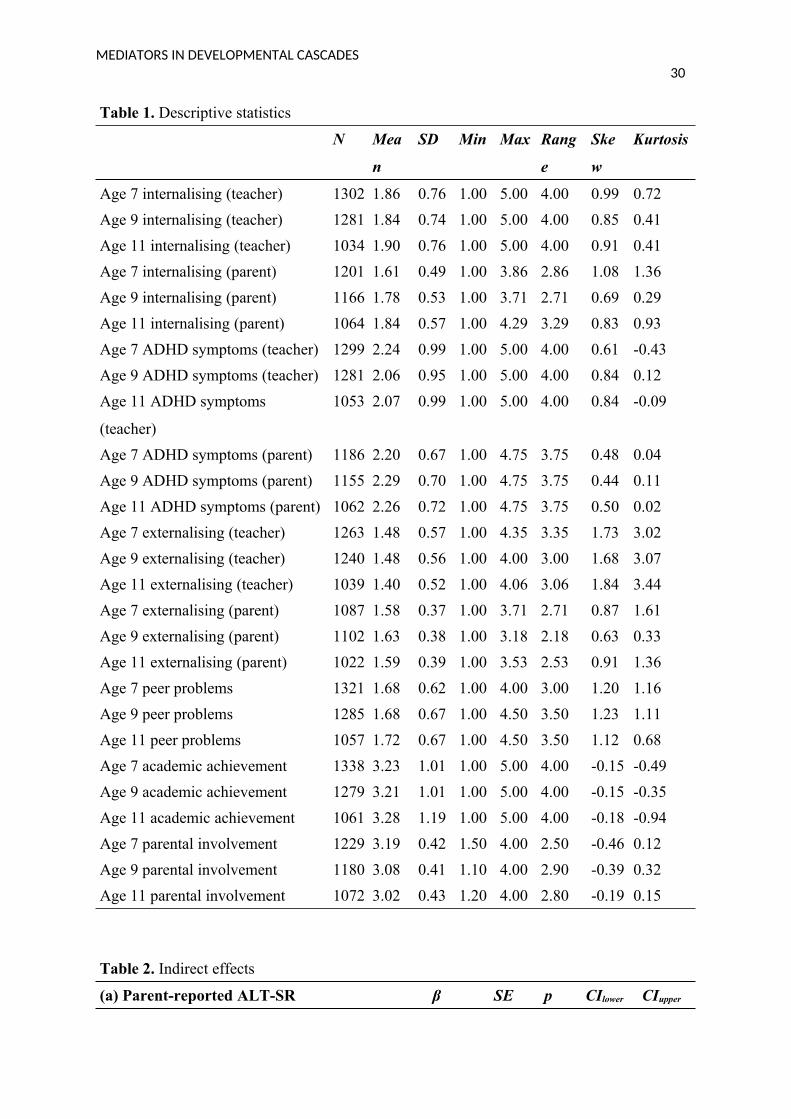
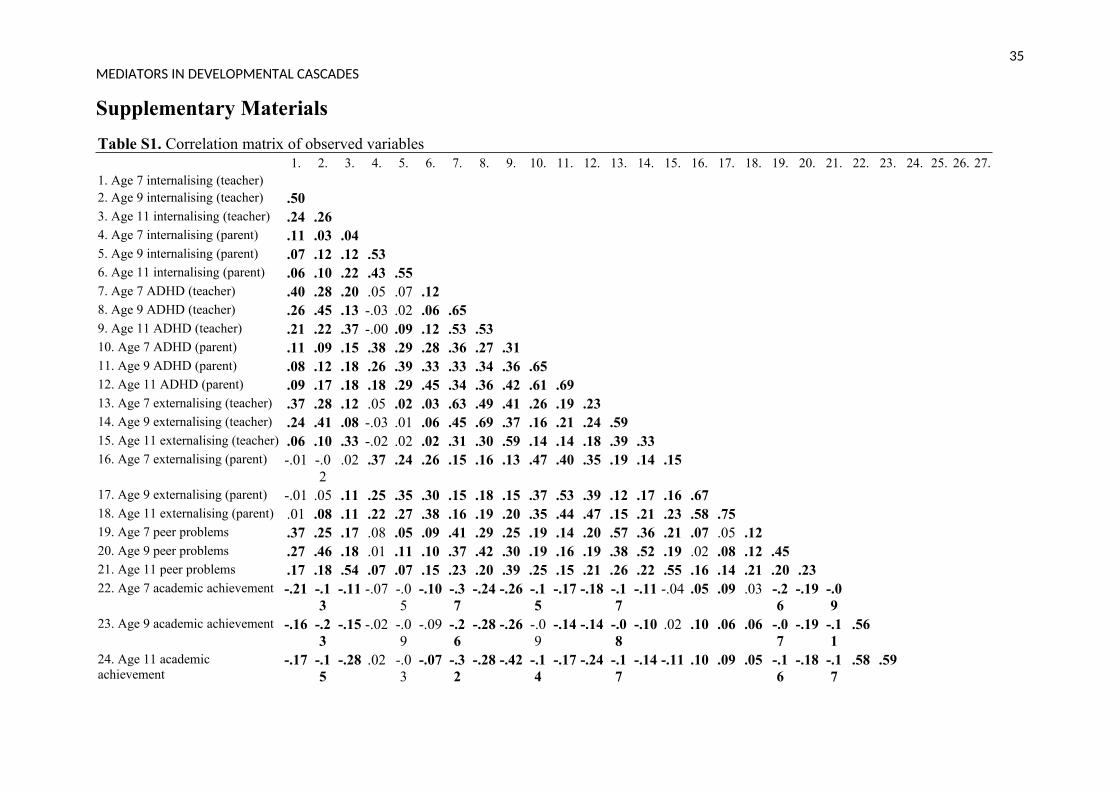
Descriptive statistics are provided in Table 1. For a correlation matrix of all observed
variables, see the online supplementary Table S1. Correlations between parent- and teacher-
reported variables on psychosocial development were relatively small, ranging from .11
to .22 for internalising problems, from .19 to .23 for externalising problems and from .36
to .42 for ADHD symptoms. Model fit indices for the ALT-SR using parent reported data
showed good fit with RMSEA = .038, CFI = .992 and TLI = .954. For a summary of
significant standardised autoregressive and cross-lagged parameters see Figure 1 and for full
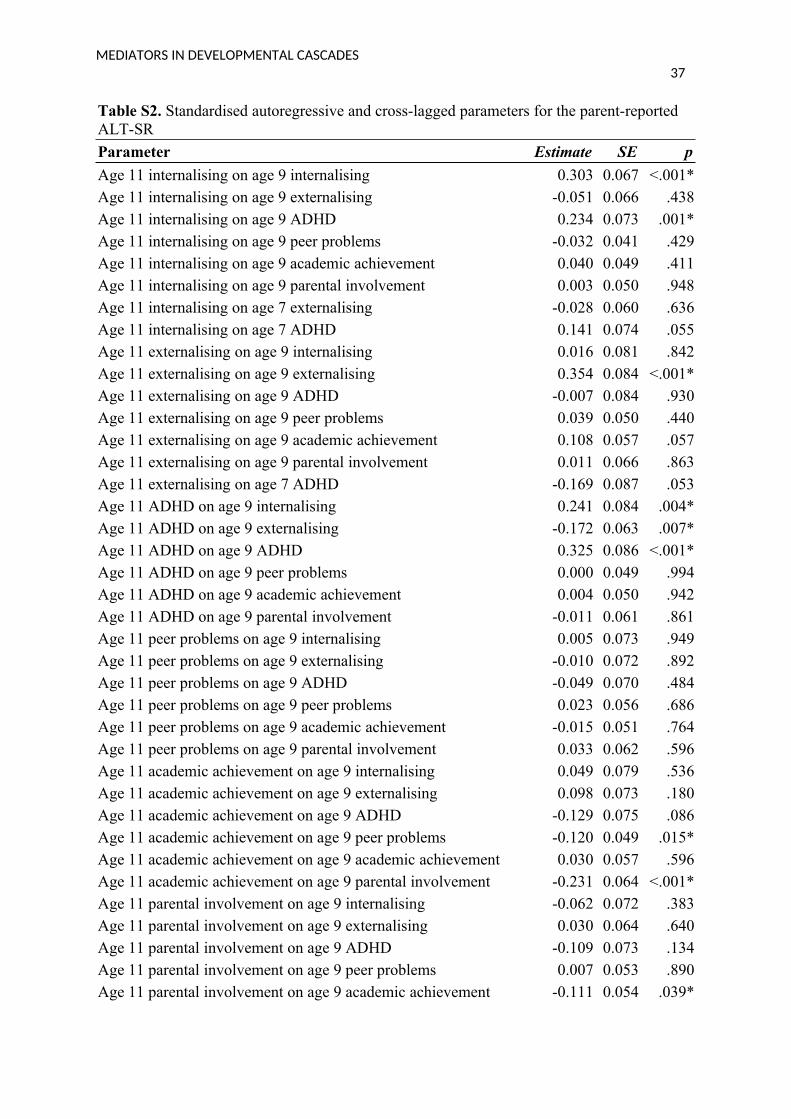
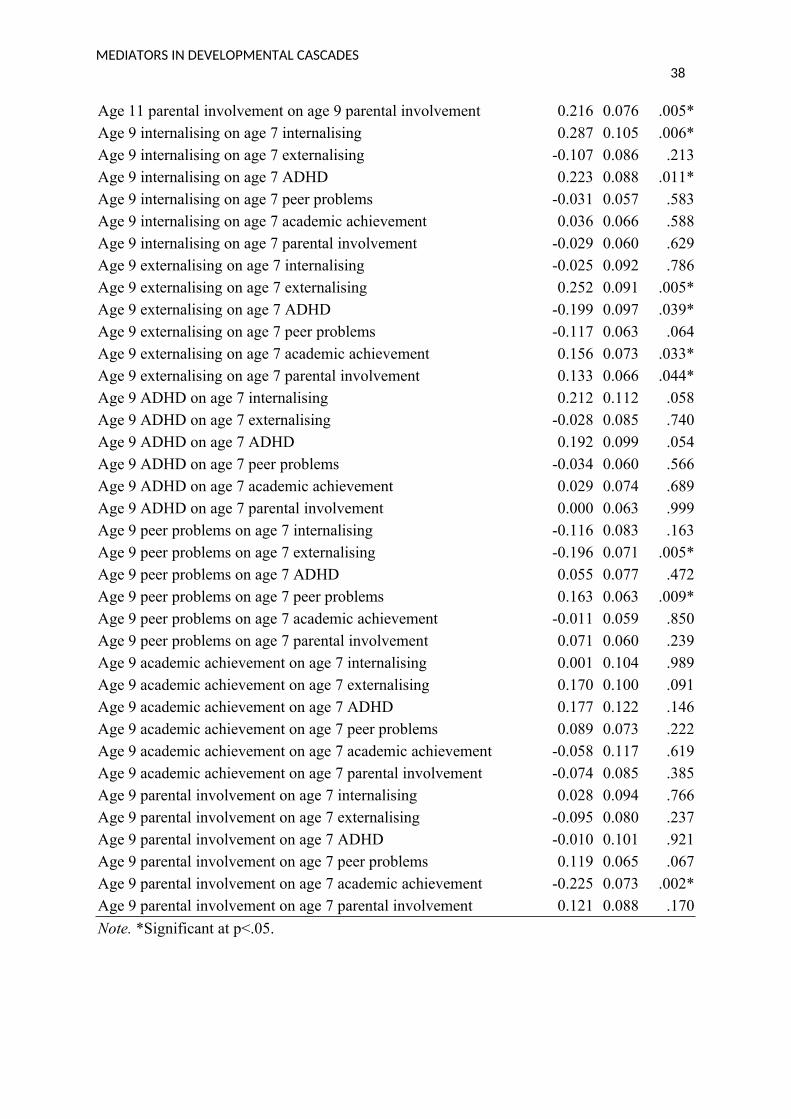
results see the online supplementary Table S2.
[TABLE ONE HERE]
[FIGURE ONE HERE]
While internalising and externalising problems were stable across both lags, ADHD
symptoms only showed evidence for homotypic continuity across the second lag. In terms of
cross-lagged effects, ADHD symptoms at age 7 and at age 9 were found to be predictive of
internalising problems at age 9 and age 11 respectively. Age 9 internalising was also
predictive of age 11 ADHD, thus showing evidence for a reciprocal relation between ADHD
and internalising difficulties during late childhood. The model further identified a significant
cascade from ADHD symptoms at age 7 to externalising problems at age 9 and from age 9
externalising to age 11 ADHD. Results did not indicate any statistically significant cascades
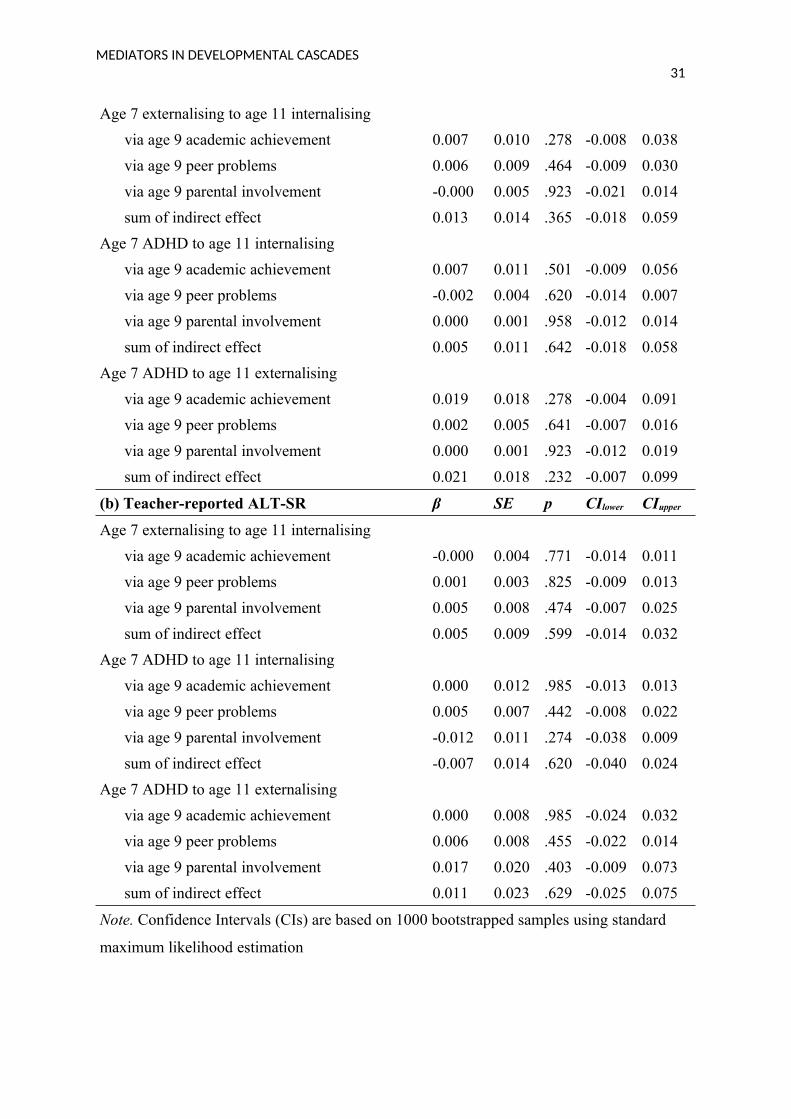
from externalising to internalising problems. Analyses of indirect effects indicated that
neither cascades from externalising to internalising problem nor cascades from ADHD
symptoms to internalising or externalising problems were significantly mediated by peer
problems, academic achievement or parental involvement, see Table 2 (a). Their combined
mediating effect was also not statistically significant which was further confirmed using
MEDIATORS IN DEVELOPMENTAL CASCADES14
bootstrapped confidence intervals (see: https://osf.io/d7wfb/?
view_only=1e61e55ade1f4a53b18c6f376991ffbf). In fact, none of the considered mediating
factors shared any statistically significant longitudinal relations with internalising problems.
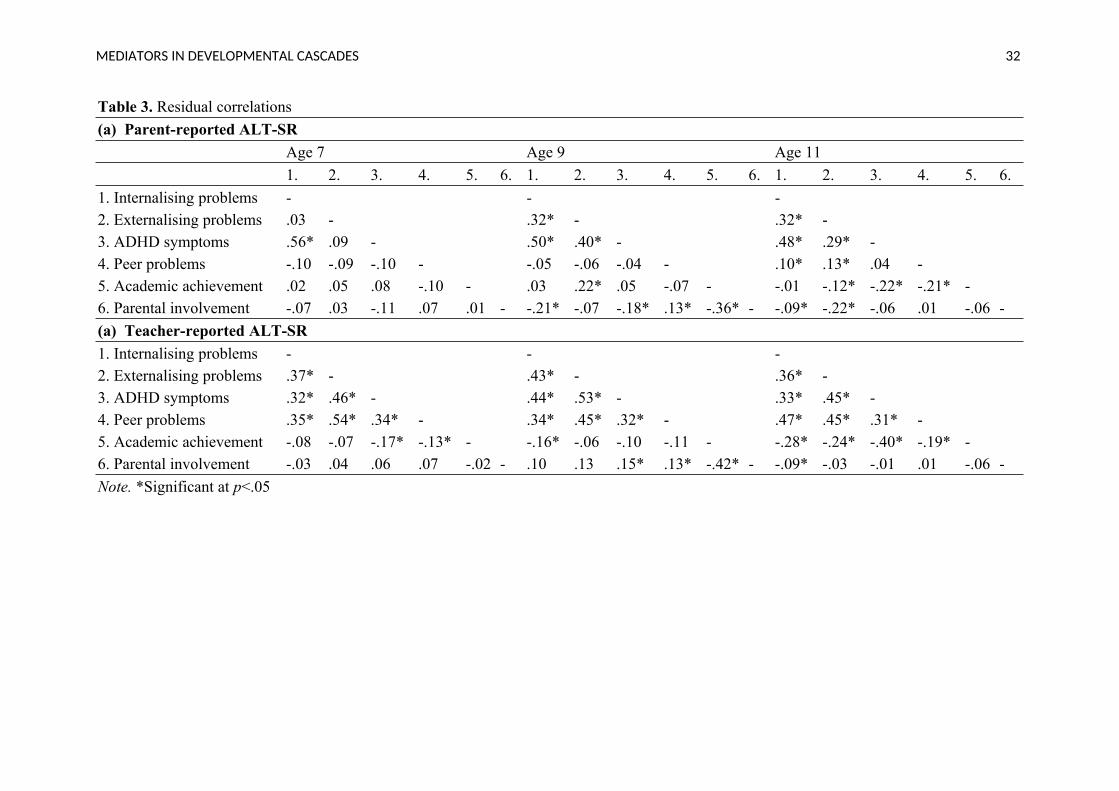
However, all considered mediating factors did share at least some concurrent relations with
the considered domains of psychosocial functioning. See Table 3 (a) for residual correlations.
[TABLE TWO HERE]
[TABLE THREE HERE]
The teacher-reported ALT-SR also showed good fit (RMSEA = .050, CFI = .987, TLI
= .927). Significant standardised autoregressive and cross-lagged parameters visualised in
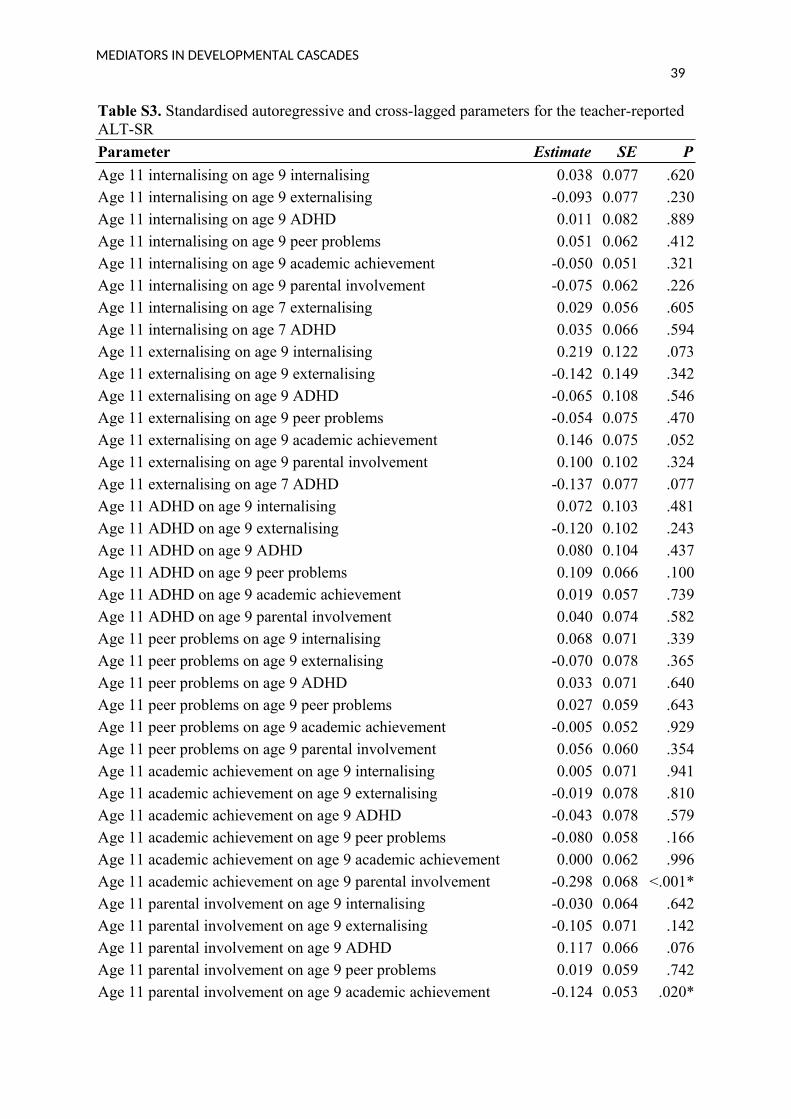
Figure 2 and presented in full in the online supplementary Table S3. In contrast to the parent-
reported model, internalising problems, externalising problems and ADHD symptoms all
showed homotypic continuity over the first lag but not over the second. The model also did
not identify any significant developmental cascades involving psychosocial difficulties. In
line with the parent-reported model, neither externalising-internalising cascades nor ADHD-
internalising or ADHD-externalising cascades were significantly mediated by peer problems,
academic achievement or parental involvement. Their combined mediating effect was also
not statistically significant based on bootstrapped confidence intervals, see Table 2 (b). For
full results see: https://osf.io/d7wfb/?view_only=1e61e55ade1f4a53b18c6f376991ffbf).
Residual correlations are summarised in Table 3 (b).
We also conducted additional exploratory analyses using a standard cross-lagged
panel model in order to provide insights into why our results may have differed from
previous studies. The full model results for both parent-and teacher-reported models can be
found here: https://osf.io/d7wfb/?view_only=1e61e55ade1f4a53b18c6f376991ffbf, The
results of the parent-reported CLPM model suggested that a cascade from ADHD symptoms
MEDIATORS IN DEVELOPMENTAL CASCADES15
at age 7 to externalising problems at age 11 was significantly mediated by peer problems at
age 9. The teacher-reported model identified additional developmental cascades from
externalising problems at age 9 to internalising problems at age 11 and found support for
mediating effects of peer problems and academic achievement in cascades from ADHD to
internalising problems. These differences in results highlight the need for appropriately
disaggregating within- from between-person effects.
[FIGURE TWO HERE]
Discussion
The aim of the current study was to evaluate whether developmental cascades from
externalising to internalising problems and from ADHD symptoms to internalising and
externalising problems were mediated by parental involvement, peer problems and academic
underachievement when appropriately disaggregating within- from between-person effects.
Results indicated that none of these factors acted as significant mediators, thus, calling the
dual failure model into question (Capaldi, 1992). Additionally, we found only limited support
for developmental cascades between the studied domains of psychosocial functioning. While
the parent-reported ALT-SR suggested that there were developmental cascades from ADHD
symptoms to internalising problems across all studied time intervals as well as a
developmental cascade from internalising problems at age 9 to ADHD symptoms at age 11,
these patterns were not found in the model using teacher-reported data on internalising,
externalising and ADHD symptoms. Similarly, the only significant ADHD-externalising
developmental cascade identified from age 7 to age 9 in the parent-reported model was also
not significant in the teacher-reported model. However, concurrent relations of the different
domains of psychosocial functioning and the hypothesised mediating factors did show a
MEDIATORS IN DEVELOPMENTAL CASCADES16
number of significant associations in both teacher- and parent-reported models, suggesting
that these factors may play a role in the risk for mental health problems.
While many previous studies have found evidence for the dual failure model (e.g. van
Lier et al., 2012), this is not the first study to report null-findings. For example, Poirier et al.
(2019) found no evidence for a mediating effect of academic skills on developmental
cascades from conduct problems to depressive symptoms. Similarly, in their study of 912 1st,
2nd and 3rd graders, Evans and Fite (2019) found only limited and mixed support for the dual
failure model in linking aggressive behaviour to depressive symptoms over time. These
authors concluded that the pathways via peer rejection and academic performance may be
observed in younger children but not in children at later elementary school age. The only
other study to date investigating mediating factors in externalising-internalising cascades also
using an ALT-SR which appropriately accounts for between-person effects (Curran et al.,
2014) also found no evidence for peer relationships or teacher relationships to mediate
developmental cascades from aggression to internalising problems (Murray et al., 2021).
Using data from the same cohort as the current study, but with a focus on adolescence (ages
11, 13, and 15), Murray et al. also did not identify any significant developmental cascades
from aggression to internalising problems. This could indicate that previously identified
developmental cascades and mediating relations are potentially not due to within-person
processes but could have been the result of between-person confounding. In fact, the
comparison of results with a standard CLPM in the current study also showed that when
conflating within- and between-person effects, some of the hypothesised mediators were
indeed identified as significant. Nevertheless, there has also been some research showing
evidence for externalising-internalising and ADHD-internalising cascades when
appropriately accounting for between-person effects (Flouri et al., 2019; Murray, Caye, et al.,
2020; Murray, Eisner, & Ribeaud, 2016; Oh et al., 2020). However, these studies account for
MEDIATORS IN DEVELOPMENTAL CASCADES17
only a minority of studies and more research using appropriate statistical tools are needed to
evaluate developmental cascades and their potential mediators.
The current study offered some evidence for developmental cascades from ADHD
symptoms to internalising and externalising problems; however, these cascades were not
robust across informants. A number of previous studies have highlighted that teacher and
parent-reports are limited in their agreement on children’s psychosocial development (e.g.
Cheng et al., 2018) with cross-informant correlation having been shown to average .25 for
internalising problems, 30 for externalising problems (De Los Reyes, 2013) and range
from .09 to .52 for ADHD symptoms (Narad et al., 2015). Cross-informant correlations in the
present study showed a pattern in line with these findings (.11 to .22 for internalising
problems,.19 to .23 for externalising problems, .36 to .42 for ADHD symptoms). The large
inconsistencies between the teacher- and parent-reported ALT-SR reported here further
highlight the need for future research to include multiple informants when investigating the
development of mental health problems in children. One potential reason for the discrepancy
found in the current study could be that parents and teachers observe children in different
context with some difficulties likely being tied to specific environments. For instance,
previous research has indicated that inattentive ADHD symptoms are primarily noticeable in
the school context (Murray, Ribeaud, et al., 2019). Another reason for the observed
discrepancy could relate to the fact the questionnaire items in the parent-reported SBQ were
presented in a randomised order whereas they were presented in the same order to all
teachers. This would have addressed potential item position effects in the parents but not
teachers.
One of the developmental relations identified consistently across both time intervals
in both teacher- and parent-reported models was cascades from academic achievement to
parental involvement with higher academic achievement being predictive of less parental
MEDIATORS IN DEVELOPMENTAL CASCADES18
involvement at later time points. We also identified a significant negative developmental
cascade from parental involvement to academic achievement across both models, suggesting
that these two domains share reciprocal relations in later childhood. While a large body of
literature has investigated cascades from parental involvement to academic achievement,
finding evidence for negative, positive and null associations (for a review see Boonk,
Gijselaers, Ritzen, & Brand-Gruwel, 2018), cascades in the other direction have not been
extensively investigated yet. The results of the current study suggest that children who
performed well in school, might need less parental support later as is reflected in less parental
involvement. These findings need to be replicated in future studies.
Even though we found little evidence for longitudinal effects of peer problems,
academic achievement and parental involvement on childhood mental health problems, we
identified significant concurrent relations between all domains of psychosocial functioning
and these factors at multiple time points. This indicates that mental health problems are often
accompanied by peer problems, academic underachievement and a lack of parental
involvement; however, any directional effects between these variables are potentially at a
shorter timescale then it was possible to evaluate in the current study.
Strengths and Limitations
The key strength of this study is that we used a method suitable of overcoming the
main limitation of previous studies investigating the dual failure model, that is an ALT-SR,
which allowed us to clearly separate within- from between-person effects (Curran et al.,
2014). In addition, while most previous studies focused on one focal mediator and two
domains of psychosocial functioning, we jointly modelled internalising, externalising and
ADHD symptom cascades and potential mediators, thus, capturing the most commonly
occurring and co-occurring conditions in childhood within one comprehensive model. We
MEDIATORS IN DEVELOPMENTAL CASCADES19
were also able to investigate the studied cascades using both parent- and teacher-reported
data on children’s psychosocial development, hence, providing a more complete picture of
their development than when only using a single-informant approach.
However, the current study also has to be interpreted in light of some limitations.
First, the included measures on peer problems and academic achievement were relatively
brief. In particular, the measure on academic achievement consisted of only two items that
were based on a teacher comparing students’ performance on mathematics and language
skills to other students. Consequently, it does not provide an objective indication of a child’s
academic achievement. Ideally, future studies should replicate the current study using
standardised assessments of children’s educational attainment. In addition, it is possible that
the lack of identified longitudinal relations between peer problems and internalising
difficulties is due to the fact that only specific aspects of peer problems are related to the
development of internalising difficulties (e.g. bullying victimisation) (Roy et al., 2015).
However, the measure included in the current study was only a very general measure of peer
problems, focusing on whether the child had any negative social roles in the classroom, and
did not allow for detailed investigations of individual factors. Furthermore, we only
investigated one specific aspect of parenting behaviours, that is parental involvement. Other
dimensions of parenting behaviours, such as harsh parenting, could also be a potential linking
factor in the development of mental health problems and should therefore be investigated in
future research. Also, at some of the included time points, the measures of peer problems and
parental involvement had slightly lower reliability than desired as indicated by Cronbach’s
alphas below .70 which could have impacted our results. Finally, another main limitation of
the current study is that we used time intervals of two years to investigate developmental
cascades. As the results of concurrent relations have shown, most domains were related
within the same time point, thus, shorter time lags could have potentially provided different
MEDIATORS IN DEVELOPMENTAL CASCADES20
results as these cascades might act over shorter periods (M. P. Eisner & Malti, 2015). Future
studies should address this limitation by employing shorter time intervals to the study of
mediating factors in developmental cascades of mental health problems (Dormann & Griffin,
2015). In particular, experience sampling methods could be a useful approach to gain insights
into the short term relations between internalising problems, externalising problems, ADHD
symptoms and social and academic failure (Verhagen, Hasmi, Drukker, van Os, & Delespaul,
2016). This could provide valuable clarification on which difficulties act as antecedents to
other difficulties and consequently inform interventions. Finally, while ALT-SRs address
between-person confounds that tend to be stable over time they are vulnerable to time-
varying confounding. Future evaluations that can account for these and other complementary
work using, for example, causal inference frameworks such as mendelian randomisation or
matching-based methods could provide further insights into which mental health and
psychosocial issues have a causal impact on others during development.
Conclusion
In conclusion, findings of the current study do not provide support for the dual failure
model, neither for the original hypothesised mediating role of peer problems and academic
underachievement nor for parental involvement as an additional potential mediator. Since this
is one of only few studies appropriately disentangling within- from between-person effects
when investigating mediating factors in developmental cascade models, further research is
needed to re-evaluate the empirical evidence for the dual failure model. The results of the
current study do however highlight that peer problems, academic underachievement and lack
of parental involvement are associated with worse psychosocial development within the same
time points, thus these factors might still represent valuable intervention targets in children
suffering from psychosocial difficulties.
MEDIATORS IN DEVELOPMENTAL CASCADES21
References
Aboobaker, S., Jangam, K. V., Sagar, K. J. V., Amaresha, A. C., & Jose, A. (2019).
Predictors of emotional and behavioral problems among Indian adolescents: A clinic-
based study. Asian Journal of Psychiatry, 39, 104–109.
https://doi.org/10.1016/j.ajp.2018.12.002
Barry, T. D. S., Lyman, R. D., & Klinger, L. G. (2002). Academic underachievement and
Attention-Deficit/Hyperactivity Disorder: The negative impact of symptom severity on
school performance. Journal of School Psychology, 40(3), 259–283.
https://doi.org/10.1016/S0022-4405(02)00100-0
Beauchaine, T. P., & McNulty, T. (2013). Comorbidities and continuities as ontogenic
processes: Toward a developmental spectrum model of externalizing psychopathology.
Development and Psychopathology, 25(4 PART 2), 1505–1528. https://doi.org/10.1017/
S0954579413000746
Berry, D., & Willoughby, M. T. (2017, July 1). On the Practical Interpretability of Cross-
Lagged Panel Models: Rethinking a Developmental Workhorse. Child Development,
Vol. 88, pp. 1186–1206. Blackwell Publishing Inc. https://doi.org/10.1111/cdev.12660
Biederman, J. (2004). Impact of Comorbidity in Adults With Attention-Deficit/Hyperactivity
Disorder. The Journal of Clinical Psychiatry, 65(suppl 3), 3–7.
Boonk, L., Gijselaers, H. J. M., Ritzen, H., & Brand-Gruwel, S. (2018). A review of the
relationship between parental involvement indicators and academic achievement.
Educational Research Review, 24, 10–30. https://doi.org/10.1016/j.edurev.2018.02.001
Capaldi, D. M. (1992). Co-occurrence of conduct problems and depressive symptoms in early
adolescent boys: II. A 2-year follow-up at Grade 8. Development and Psychopathology,
4(1), 125–144. https://doi.org/10.1017/S0954579400005605
Cheng, S., Keyes, K. M., Bitfoi, A., Carta, M. G., Koç, C., Goelitz, D., … Kovess-Masfety,
MEDIATORS IN DEVELOPMENTAL CASCADES22
V. (2018). Understanding parent–teacher agreement of the Strengths and Difficulties
Questionnaire (SDQ): Comparison across seven European countries. International
Journal of Methods in Psychiatric Research, 27(1). https://doi.org/10.1002/mpr.1589
Curran, P. J., Howard, A. L., Bainter, S. A., Lane, S. T., & McGinley, J. S. (2014). The
separation of between-person and within-person components of individual change over
time: A latent curve model with structured residuals. Journal of Consulting and Clinical
Psychology, 82(5), 879–894. https://doi.org/10.1037/a0035297
De Los Reyes, A. (2013). Strategic objectives for improving understanding of informant
discrepancies in developmental psychopathology research. Development and
Psychopathology, 25(3), 669–682. https://doi.org/10.1017/S0954579413000096
De Los Reyes, A., Augenstein, T. M., Wang, M., Thomas, S. A., Drabick, D. A. G., Burgers,
D. E., & Rabinowitz, J. (2015). The validity of the multi-informant approach to
assessing child and adolescent mental health. Psychological Bulletin, 141(4), 858–900.
https://doi.org/10.1037/a0038498
Diamantopoulou, S., Henricsson, L., & Rydell, A.-M. (2005). ADHD symptoms and peer
relations of children in a community sample: Examining associated problems, self-
perceptions, and gender differences. International Journal of Behavioral Development,
29(5), 388–398. https://doi.org/10.1177/01650250500172756
Dormann, C., & Griffin, M. A. (2015). Optimal time lags in panel studies. Psychological
Methods, 20(4), 489–505. https://doi.org/10.1037/met0000041
Eisner, M. P., & Malti, T. (2015). Aggressive and Violent Behavior. In Handbook of Child
Psychology and Developmental Science (pp. 1–48). John Wiley & Sons, Inc.
https://doi.org/10.1002/9781118963418.childpsy319
Eisner, M., & Ribeaud, D. (2005). A Randomised Field Experiment to Prevent Violence -
The Zurich Intervention and Prevention Project at Schools, ZIPPS. European Journal of
MEDIATORS IN DEVELOPMENTAL CASCADES23
Crime, Criminal Law and Criminal Justice, 13. Retrieved from
https://heinonline.org/HOL/Page?handle=hein.journals/eccc13&id=31&div=&collection
=
Eisner, M., & Ribeaud, D. (2007). Conducting a Criminological Survey in a Culturally
Diverse Context. European Journal of Criminology, 4(3), 271–298.
https://doi.org/10.1177/1477370807077183
Eisner, N. L., Murray, A. L., Eisner, M., & Ribeaud, D. (2019). A practical guide to the
analysis of non-response and attrition in longitudinal research using a real data example.
International Journal of Behavioral Development, 43(1), 24–34.
https://doi.org/10.1177/0165025418797004
Enders, C. K. (2001). The performance of the full information maximum likelihood estimator
in multiple regression models with missing data. Educational and Psychological
Measurement, 61(5), 713–740. https://doi.org/10.1177/00131640121971482
Evans, S. C., & Fite, P. J. (2019). Dual Pathways from Reactive Aggression to Depressive
Symptoms in Children: Further Examination of the Failure Model. Journal of Abnormal
Child Psychology, 47(1), 85–97. https://doi.org/10.1007/s10802-018-0426-6
Flouri, E., Papachristou, E., Midouhas, E., Ploubidis, G. B., Lewis, G., & Joshi, H. (2019).
Developmental cascades of internalising symptoms, externalising problems and
cognitive ability from early childhood to middle adolescence. European Psychiatry, 57,
61–69. https://doi.org/10.1016/j.eurpsy.2018.12.005
Ghandour, R. M., Sherman, L. J., Vladutiu, C. J., Ali, M. M., Lynch, S. E., Bitsko, R. H., &
Blumberg, S. J. (2019). Prevalence and Treatment of Depression, Anxiety, and Conduct
Problems in US Children. Journal of Pediatrics, 206, 256-267.e3.
https://doi.org/10.1016/j.jpeds.2018.09.021
Gnanavel, S., Sharma, P., Kaushal, P., & Hussain, S. (2019, September 1). Attention deficit
MEDIATORS IN DEVELOPMENTAL CASCADES24
hyperactivity disorder and comorbidity: A review of literature. World Journal of
Clinical Cases, Vol. 7, pp. 2420–2426. Baishideng Publishing Group Co. https://doi.org/
10.12998/wjcc.v7.i17.2420
Hawes, D. J., Dadds, M. R., Frost, A. D. J., & Russell, A. (2013). Parenting practices and
prospective levels of hyperactivity/inattention across early- and middle-childhood.
Journal of Psychopathology and Behavioral Assessment, 35(3), 273–282. https://doi.org/
10.1007/s10862-013-9341-x
Humphreys, K. L., Katz, S. J., Lee, S. S., Hammen, C., Brennan, P. A., & Najman, J. M.
(2013). The association of ADHD and depression: Mediation by peer problems and
parent-child difficulties in two complementary samples. Journal of Abnormal
Psychology, 122(3), 854–867. https://doi.org/10.1037/a0033895
Kelly, E. V., Newton, N. C., Stapinski, L. A., Slade, T., Barrett, E. L., Conrod, P. J., &
Teesson, M. (2015). Suicidality, internalizing problems and externalizing problems
among adolescent bullies, victims and bully-victims. Preventive Medicine, 73, 100–105.
https://doi.org/10.1016/j.ypmed.2015.01.020
Kirkhaug, B., Drugli, M. B., Klöckner, C. A., & Mørch, W.-T. (2013). Association between
parental involvement in school and child conduct, social, and internalizing problems:
teacher report. Educational Research and Evaluation, 19(4), 346–361.
https://doi.org/10.1080/13803611.2013.771893
Kline, R. B. (2005). Principles and Practice of Structural Equation Modeling, Second
Edition. Guilford Publications. Retrieved from https://books.google.at/books?
id=EkMVZUxZrgIC
MacKinnon, D. P., Warsi, G., & Dwyer, J. H. (1995). A Simulation Study of Mediated Effect
Measures. Multivariate Behavioral Research, 30(1), 41–62.
https://doi.org/10.1207/s15327906mbr3001_3
MEDIATORS IN DEVELOPMENTAL CASCADES25
Masten, A. S., & Cicchetti, D. (2010, August). Developmental cascades. Development and
Psychopathology, Vol. 22, pp. 491–495. Dev Psychopathol.
https://doi.org/10.1017/S0954579410000222
McKee, L., Colletti, C., Rakow, A., Jones, D. J., & Forehand, R. (2008, June). Parenting and
child externalizing behaviors: Are the associations specific or diffuse? Aggression and
Violent Behavior, Vol. 13, pp. 201–215. NIH Public Access.
https://doi.org/10.1016/j.avb.2008.03.005
Murray, A. L., Booth, T., Ribeaud, D., & Eisner, M. (2018). Disagreeing about development:
An analysis of parent teacher agreement in ADHD symptom trajectories across the ‐
elementary school years. International Journal of Methods in Psychiatric Research,
27(3). https://doi.org/10.1002/mpr.1723
Murray, A. L., Caye, A., McKenzie, K., Auyeung, B., Murray, G., Ribeaud, D., … Eisner, M.
(2020). Reciprocal Developmental Relations Between ADHD and Anxiety in
Adolescence: A Within-Person Longitudinal Analysis of Commonly Co-Occurring
Symptoms. Journal of Attention Disorders, 108705472090833.
https://doi.org/10.1177/1087054720908333
Murray, A. L., Eisner, M., Obsuth, I., & Ribeaud, D. (2017). Situating violent ideations
within the landscape of mental health: Associations between violent ideations and
dimensions of mental health. Psychiatry Research, 249, 70–77.
https://doi.org/10.1016/j.psychres.2017.01.005
Murray, A. L., Eisner, M., & Ribeaud, D. (2016). The Development of the General Factor of
Psychopathology ‘p Factor’ Through Childhood and Adolescence. Journal of Abnormal
Child Psychology, 44(8), 1573–1586. https://doi.org/10.1007/s10802-016-0132-1
Murray, A. L., Eisner, M., & Ribeaud, D. (2019). Can the social behavior questionnaire help
meet the need for dimensional, transdiagnostic measures of childhood and adolescent
MEDIATORS IN DEVELOPMENTAL CASCADES26
psychopathology? European Journal of Psychological Assessment, 35(5), 674–679.
https://doi.org/10.1027/1015-5759/a000442
Murray, A. L., Eisner, M., & Ribeaud, D. (2020). Within person analysis of developmental ‐
cascades between externalising and internalising problems. Journal of Child Psychology
and Psychiatry, 61(6), 681–688. https://doi.org/10.1111/jcpp.13150
Murray, A. L., Obsuth, I., Speyer, L., Murray, G., McKenzie, K., Eisner, M., & Ribeaud, D.
(2021). Developmental Cascades from Aggression to Internalizing Problems via Peer
and Teacher Relationships from Early to Middle Adolescence. Journal of Youth and
Adolescence. https://doi.org/10.1007/s10964-021-01396-1
Murray, A. L., Ribeaud, D., Eisner, M., Murray, G., & McKenzie, K. (2019). Should We
Subtype ADHD According to the Context in Which Symptoms Occur? Criterion
Validity of Recognising Context-Based ADHD Presentations. Child Psychiatry and
Human Development, 50(2), 308–320. https://doi.org/10.1007/s10578-018-0842-4
Murray, A. L., Zych, I., Ribeaud, D., & Eisner, M. (2020). Developmental relations between
ADHD symptoms and bullying perpetration and victimization in adolescence.
Aggressive Behavior. https://doi.org/10.1002/ab.21930
Muthén, L. K., & Muthén, B. (2018). Mplus. The Comprehensive Modelling Program for
Applied Researchers: User’s Guide, 5.
Narad, M. E., Garner, A. A., Peugh, J. L., Tamm, L., Antonini, T. N., Kingery, K. M., …
Epstein, J. N. (2015). Parent-teacher agreement on ADHD symptoms across
development. Psychological Assessment, 27(1), 239–248.
https://doi.org/10.1037/a0037864
Obsuth, I., Murray, A. L., Di Folco, S., Ribeaud, D., & Eisner, M. (2020). Patterns of
Homotypic and Heterotypic Continuity Between ADHD Symptoms, Externalising and
Internalising Problems from Age 7 to 15. Journal of Abnormal Child Psychology, 48(2),
MEDIATORS IN DEVELOPMENTAL CASCADES27
223–236. https://doi.org/10.1007/s10802-019-00592-9
Oh, Y., Greenberg, M. T., Willoughby, M. T., Vernon-Feagans, L., Blair, C. B., Burchinal,
M. R., … Mills-Koonce, W. R. (2020). Examining Longitudinal Associations between
Externalizing and Internalizing Behavior Problems at Within- and Between-Child
Levels. Journal of Abnormal Child Psychology, 48(4), 467–480. https://doi.org/10.1007/
s10802-019-00614-6
Patterson, G. R. (2002). The early development of coercive family process. In Antisocial
behavior in children and adolescents: A developmental analysis and model for
intervention. (pp. 25–44). American Psychological Association.
https://doi.org/10.1037/10468-002
Poirier, M., Temcheff, C. E., Déry, M., Toupin, J., Verlaan, P., & Lemelin, J.-P. (2019). The
Role of Academic Skills in the Evolution of Conduct Problems and Depressive
Symptoms Among Children With and Without Early Clinically Significant Conduct
Problems. The Journal of Early Adolescence, 39(3), 340–370.
https://doi.org/10.1177/0272431618757679
Powell, V., Riglin, L., Hammerton, G., Eyre, O., Martin, J., Anney, R., … Rice, F. (2020).
What explains the link between childhood ADHD and adolescent depression?
Investigating the role of peer relationships and academic attainment. European Child
and Adolescent Psychiatry, 29(11), 1581–1591. https://doi.org/10.1007/s00787-019-
01463-w
Reale, L., Bartoli, B., Cartabia, M., Zanetti, M., Costantino, M. A., Canevini, M. P., … Rossi,
G. (2017). Comorbidity prevalence and treatment outcome in children and adolescents
with ADHD. European Child and Adolescent Psychiatry, 26(12), 1443–1457.
https://doi.org/10.1007/s00787-017-1005-z
Roy, A., Hartman, C. A., Veenstra, R., & Oldehinkel, A. J. (2015). Peer dislike and
MEDIATORS IN DEVELOPMENTAL CASCADES28
victimisation in pathways from ADHD symptoms to depression. European Child and
Adolescent Psychiatry, 24(8), 887–895. https://doi.org/10.1007/s00787-014-0633-9
Sevincok, D., Ozbay, H. C., Ozbek, M. M., Tunagur, M. T., & Aksu, H. (2020). ADHD
symptoms in relation to internalizing and externalizing symptoms in children: the
mediating role of sluggish cognitive tempo. Nordic Journal of Psychiatry, 74(4), 265–
272. https://doi.org/10.1080/08039488.2019.1697746
Shelton, K. K., Frick, P. J., & Wootton, J. (1996). Assessment of parenting practices in
families of elementary school-age children. Journal of Clinical Child Psychology, 25(3),
317–329. https://doi.org/10.1207/s15374424jccp2503_8
Sibley, M. H., Pelham, W. E., Molina, B. S. G., Gnagy, E. M., Waschbusch, D. A., Biswas,
A., … Karch, K. M. (2011). The delinquency outcomes of boys with ADHD with and
without comorbidity. Journal of Abnormal Child Psychology, 39(1), 21–32.
https://doi.org/10.1007/s10802-010-9443-9
Theule, J., Wiener, J., Tannock, R., & Jenkins, J. M. (2013). Parenting Stress in Families of
Children With ADHD. Journal of Emotional and Behavioral Disorders, 21(1), 3–17.
https://doi.org/10.1177/1063426610387433
Tremblay, R. E., Loeber, R., Gagnon, C., Charlebois, P., Larivée, S., & LeBlanc, M. (1991).
Disruptive boys with stable and unstable high fighting behavior patterns during junior
elementary school. Journal of Abnormal Child Psychology, 19(3), 285–300.
https://doi.org/10.1007/BF00911232
van Lier, P. A. C., Vitaro, F., Barker, E. D., Brendgen, M., Tremblay, R. E., & Boivin, M.
(2012). Peer victimization, poor academic achievement, and the link between childhood
externalizing and internalizing problems. Child Development, 83(5), 1775–1788. https://
doi.org/10.1111/j.1467-8624.2012.01802.x
Verhagen, S. J. W., Hasmi, L., Drukker, M., van Os, J., & Delespaul, P. A. E. G. (2016). Use
MEDIATORS IN DEVELOPMENTAL CASCADES29
of the experience sampling method in the context of clinical trials. Evidence-Based
Mental Health, 19(3), 86–89. https://doi.org/10.1136/ebmental-2016-102418
Wang, M.-T., & Sheikh-Khalil, S. (2014). Does Parental Involvement Matter for Student
Achievement and Mental Health in High School? Child Development, 85(2), 610–625.
https://doi.org/10.1111/cdev.12153
Wertz, J., Zavos, H., Matthews, T., Harvey, K., Hunt, A., Pariante, C. M., & Arseneault, L.
(2015). Why some children with externalising problems develop internalising
symptoms: Testing two pathways in a genetically sensitive cohort study. Journal of
Child Psychology and Psychiatry and Allied Disciplines, 56(7), 738–746. https://doi.org/
10.1111/jcpp.12333
WHO. (2018). WHO | Child and adolescent mental health. WHO. Retrieved from
http://www.who.int/mental_health/maternal-child/child_adolescent/en/
MEDIATORS IN DEVELOPMENTAL CASCADES30
Table 1. Descriptive statistics
N Mea
n
SD Min Max Rang
e
Ske
w
Kurtosis
Age 7 internalising (teacher) 1302 1.86 0.76 1.00 5.00 4.00 0.99 0.72
Age 9 internalising (teacher) 1281 1.84 0.74 1.00 5.00 4.00 0.85 0.41
Age 11 internalising (teacher) 1034 1.90 0.76 1.00 5.00 4.00 0.91 0.41
Age 7 internalising (parent) 1201 1.61 0.49 1.00 3.86 2.86 1.08 1.36
Age 9 internalising (parent) 1166 1.78 0.53 1.00 3.71 2.71 0.69 0.29
Age 11 internalising (parent) 1064 1.84 0.57 1.00 4.29 3.29 0.83 0.93
Age 7 ADHD symptoms (teacher) 1299 2.24 0.99 1.00 5.00 4.00 0.61 -0.43
Age 9 ADHD symptoms (teacher) 1281 2.06 0.95 1.00 5.00 4.00 0.84 0.12
Age 11 ADHD symptoms
(teacher)
1053 2.07 0.99 1.00 5.00 4.00 0.84 -0.09
Age 7 ADHD symptoms (parent) 1186 2.20 0.67 1.00 4.75 3.75 0.48 0.04
Age 9 ADHD symptoms (parent) 1155 2.29 0.70 1.00 4.75 3.75 0.44 0.11
Age 11 ADHD symptoms (parent) 1062 2.26 0.72 1.00 4.75 3.75 0.50 0.02
Age 7 externalising (teacher) 1263 1.48 0.57 1.00 4.35 3.35 1.73 3.02
Age 9 externalising (teacher) 1240 1.48 0.56 1.00 4.00 3.00 1.68 3.07
Age 11 externalising (teacher) 1039 1.40 0.52 1.00 4.06 3.06 1.84 3.44
Age 7 externalising (parent) 1087 1.58 0.37 1.00 3.71 2.71 0.87 1.61
Age 9 externalising (parent) 1102 1.63 0.38 1.00 3.18 2.18 0.63 0.33
Age 11 externalising (parent) 1022 1.59 0.39 1.00 3.53 2.53 0.91 1.36
Age 7 peer problems 1321 1.68 0.62 1.00 4.00 3.00 1.20 1.16
Age 9 peer problems 1285 1.68 0.67 1.00 4.50 3.50 1.23 1.11
Age 11 peer problems 1057 1.72 0.67 1.00 4.50 3.50 1.12 0.68
Age 7 academic achievement 1338 3.23 1.01 1.00 5.00 4.00 -0.15 -0.49
Age 9 academic achievement 1279 3.21 1.01 1.00 5.00 4.00 -0.15 -0.35
Age 11 academic achievement 1061 3.28 1.19 1.00 5.00 4.00 -0.18 -0.94
Age 7 parental involvement 1229 3.19 0.42 1.50 4.00 2.50 -0.46 0.12
Age 9 parental involvement 1180 3.08 0.41 1.10 4.00 2.90 -0.39 0.32
Age 11 parental involvement 1072 3.02 0.43 1.20 4.00 2.80 -0.19 0.15
Table 2. Indirect effects
(a) Parent-reported ALT-SR β SE p CIlower CIupper
MEDIATORS IN DEVELOPMENTAL CASCADES31
Age 7 externalising to age 11 internalising
via age 9 academic achievement 0.007 0.010 .278 -0.008 0.038
via age 9 peer problems 0.006 0.009 .464 -0.009 0.030
via age 9 parental involvement -0.000 0.005 .923 -0.021 0.014
sum of indirect effect 0.013 0.014 .365 -0.018 0.059
Age 7 ADHD to age 11 internalising
via age 9 academic achievement 0.007 0.011 .501 -0.009 0.056
via age 9 peer problems -0.002 0.004 .620 -0.014 0.007
via age 9 parental involvement 0.000 0.001 .958 -0.012 0.014
sum of indirect effect 0.005 0.011 .642 -0.018 0.058
Age 7 ADHD to age 11 externalising
via age 9 academic achievement 0.019 0.018 .278 -0.004 0.091
via age 9 peer problems 0.002 0.005 .641 -0.007 0.016
via age 9 parental involvement 0.000 0.001 .923 -0.012 0.019
sum of indirect effect 0.021 0.018 .232 -0.007 0.099
(b) Teacher-reported ALT-SR β SE p CIlower CIupper
Age 7 externalising to age 11 internalising
via age 9 academic achievement -0.000 0.004 .771 -0.014 0.011
via age 9 peer problems 0.001 0.003 .825 -0.009 0.013
via age 9 parental involvement 0.005 0.008 .474 -0.007 0.025
sum of indirect effect 0.005 0.009 .599 -0.014 0.032
Age 7 ADHD to age 11 internalising
via age 9 academic achievement 0.000 0.012 .985 -0.013 0.013
via age 9 peer problems 0.005 0.007 .442 -0.008 0.022
via age 9 parental involvement -0.012 0.011 .274 -0.038 0.009
sum of indirect effect -0.007 0.014 .620 -0.040 0.024
Age 7 ADHD to age 11 externalising
via age 9 academic achievement 0.000 0.008 .985 -0.024 0.032
via age 9 peer problems 0.006 0.008 .455 -0.022 0.014
via age 9 parental involvement 0.017 0.020 .403 -0.009 0.073
sum of indirect effect 0.011 0.023 .629 -0.025 0.075
Note. Confidence Intervals (CIs) are based on 1000 bootstrapped samples using standard
maximum likelihood estimation
MEDIATORS IN DEVELOPMENTAL CASCADES 32
Table 3. Residual correlations
(a) Parent-reported ALT-SR
Age 7 Age 9 Age 11
1. 2. 3. 4. 5. 6. 1. 2. 3. 4. 5. 6. 1. 2. 3. 4. 5. 6.
1. Internalising problems - - -2. Externalising problems .03 - .32* - .32* -3. ADHD symptoms .56* .09 - .50* .40* - .48* .29* -4. Peer problems -.10 -.09 -.10 - -.05 -.06 -.04 - .10* .13* .04 -5. Academic achievement .02 .05 .08 -.10 - .03 .22* .05 -.07 - -.01 -.12* -.22* -.21* -6. Parental involvement -.07 .03 -.11 .07 .01 - -.21* -.07 -.18* .13* -.36* - -.09* -.22* -.06 .01 -.06 -
(a) Teacher-reported ALT-SR
1. Internalising problems - - -2. Externalising problems .37* - .43* - .36* -3. ADHD symptoms .32* .46* - .44* .53* - .33* .45* -4. Peer problems .35* .54* .34* - .34* .45* .32* - .47* .45* .31* -5. Academic achievement -.08 -.07 -.17* -.13* - -.16* -.06 -.10 -.11 - -.28* -.24* -.40* -.19* -6. Parental involvement -.03 .04 .06 .07 -.02 - .10 .13 .15* .13* -.42* - -.09* -.03 -.01 .01 -.06 -
Note. *Significant at p<.05
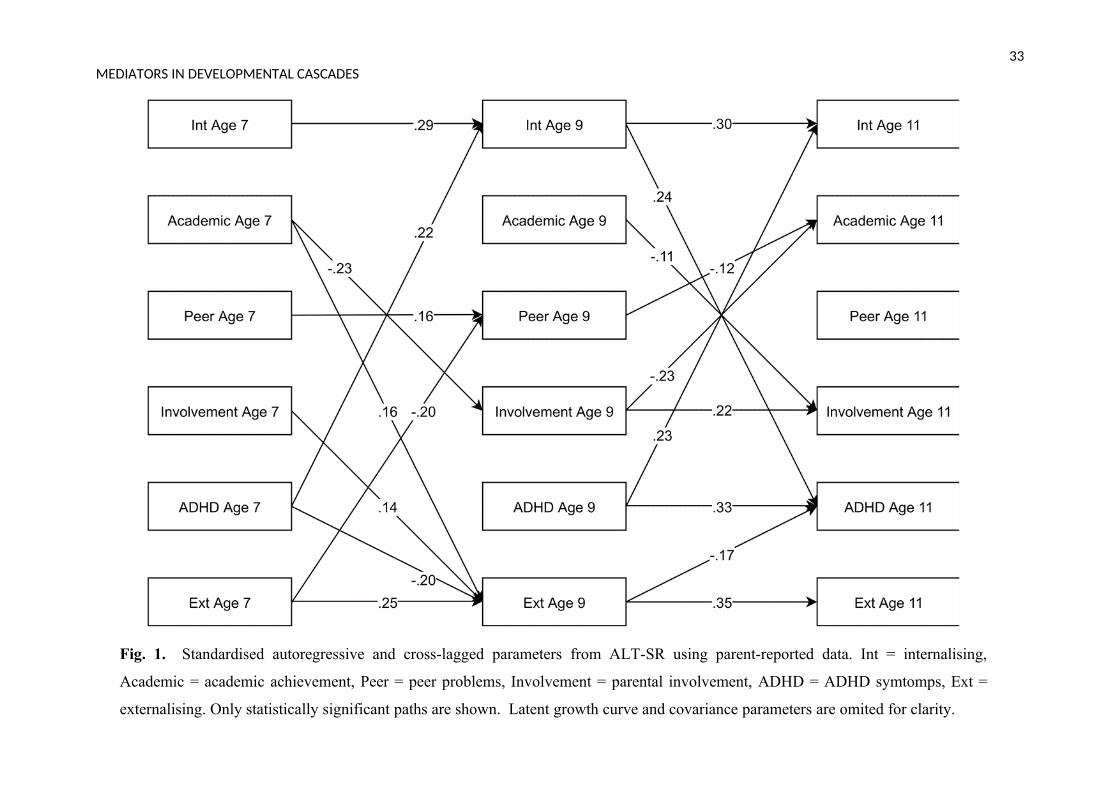
Fig. 1. Standardised autoregressive and cross-lagged parameters from ALT-SR using parent-reported data. Int = internalising,
Academic = academic achievement, Peer = peer problems, Involvement = parental involvement, ADHD = ADHD symtomps, Ext =
externalising. Only statistically significant paths are shown. Latent growth curve and covariance parameters are omited for clarity.
33MEDIATORS IN DEVELOPMENTAL CASCADES
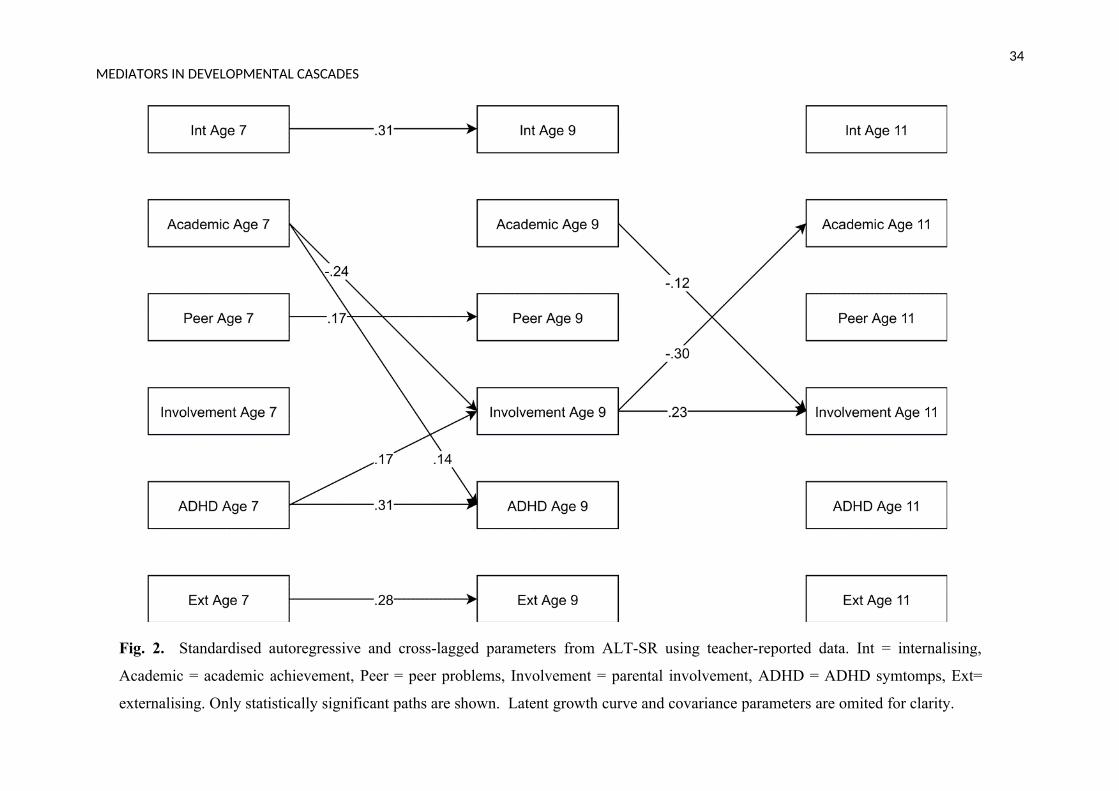
Fig. 2. Standardised autoregressive and cross-lagged parameters from ALT-SR using teacher-reported data. Int = internalising,
Academic = academic achievement, Peer = peer problems, Involvement = parental involvement, ADHD = ADHD symtomps, Ext=
externalising. Only statistically significant paths are shown. Latent growth curve and covariance parameters are omited for clarity.
34MEDIATORS IN DEVELOPMENTAL CASCADES
35MEDIATORS IN DEVELOPMENTAL CASCADES
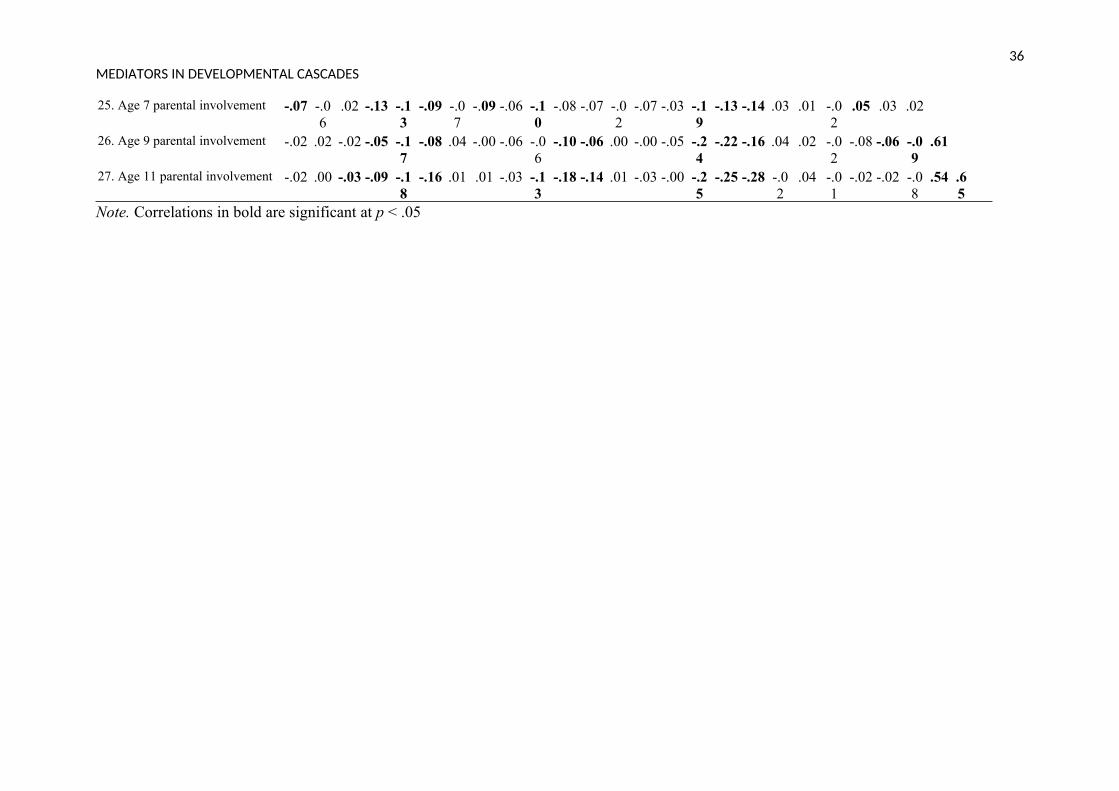
Supplementary Materials
Table S1. Correlation matrix of observed variables1. 2. 3. 4. 5. 6. 7. 8. 9. 10. 11. 12. 13. 14. 15. 16. 17. 18. 19. 20. 21. 22. 23. 24. 25. 26. 27.
1. Age 7 internalising (teacher)2. Age 9 internalising (teacher) .503. Age 11 internalising (teacher) .24 .264. Age 7 internalising (parent) .11 .03 .045. Age 9 internalising (parent) .07 .12 .12 .536. Age 11 internalising (parent) .06 .10 .22 .43 .557. Age 7 ADHD (teacher) .40 .28 .20 .05 .07 .128. Age 9 ADHD (teacher) .26 .45 .13 -.03 .02 .06 .659. Age 11 ADHD (teacher) .21 .22 .37 -.00 .09 .12 .53 .5310. Age 7 ADHD (parent) .11 .09 .15 .38 .29 .28 .36 .27 .3111. Age 9 ADHD (parent) .08 .12 .18 .26 .39 .33 .33 .34 .36 .6512. Age 11 ADHD (parent) .09 .17 .18 .18 .29 .45 .34 .36 .42 .61 .6913. Age 7 externalising (teacher) .37 .28 .12 .05 .02 .03 .63 .49 .41 .26 .19 .2314. Age 9 externalising (teacher) .24 .41 .08 -.03 .01 .06 .45 .69 .37 .16 .21 .24 .5915. Age 11 externalising (teacher) .06 .10 .33 -.02 .02 .02 .31 .30 .59 .14 .14 .18 .39 .3316. Age 7 externalising (parent) -.01 -.0
2.02 .37 .24 .26 .15 .16 .13 .47 .40 .35 .19 .14 .15
17. Age 9 externalising (parent) -.01 .05 .11 .25 .35 .30 .15 .18 .15 .37 .53 .39 .12 .17 .16 .6718. Age 11 externalising (parent) .01 .08 .11 .22 .27 .38 .16 .19 .20 .35 .44 .47 .15 .21 .23 .58 .7519. Age 7 peer problems .37 .25 .17 .08 .05 .09 .41 .29 .25 .19 .14 .20 .57 .36 .21 .07 .05 .1220. Age 9 peer problems .27 .46 .18 .01 .11 .10 .37 .42 .30 .19 .16 .19 .38 .52 .19 .02 .08 .12 .4521. Age 11 peer problems .17 .18 .54 .07 .07 .15 .23 .20 .39 .25 .15 .21 .26 .22 .55 .16 .14 .21 .20 .2322. Age 7 academic achievement -.21 -.1
3-.11 -.07 -.0
5-.10 -.3
7-.24 -.26 -.1
5-.17 -.18 -.1
7-.11 -.04 .05 .09 .03 -.2
6-.19 -.0
923. Age 9 academic achievement -.16 -.2
3-.15 -.02 -.0
9-.09 -.2
6-.28 -.26 -.0
9-.14 -.14 -.0
8-.10 .02 .10 .06 .06 -.0
7-.19 -.1
1.56
24. Age 11 academic achievement
-.17 -.15
-.28 .02 -.03
-.07 -.32
-.28 -.42 -.14
-.17 -.24 -.17
-.14 -.11 .10 .09 .05 -.16
-.18 -.17
.58 .59
36MEDIATORS IN DEVELOPMENTAL CASCADES
25. Age 7 parental involvement -.07 -.06
.02 -.13 -.13
-.09 -.07
-.09 -.06 -.10
-.08 -.07 -.02
-.07 -.03 -.19
-.13 -.14 .03 .01 -.02
.05 .03 .02
26. Age 9 parental involvement -.02 .02 -.02 -.05 -.17
-.08 .04 -.00 -.06 -.06
-.10 -.06 .00 -.00 -.05 -.24
-.22 -.16 .04 .02 -.02
-.08 -.06 -.09
.61
27. Age 11 parental involvement -.02 .00 -.03 -.09 -.18
-.16 .01 .01 -.03 -.13
-.18 -.14 .01 -.03 -.00 -.25
-.25 -.28 -.02
.04 -.01
-.02 -.02 -.08
.54 .65
Note. Correlations in bold are significant at p < .05
MEDIATORS IN DEVELOPMENTAL CASCADES37
Table S2. Standardised autoregressive and cross-lagged parameters for the parent-reported ALT-SR
Parameter Estimate SE p
Age 11 internalising on age 9 internalising 0.303 0.067 <.001*Age 11 internalising on age 9 externalising -0.051 0.066 .438Age 11 internalising on age 9 ADHD 0.234 0.073 .001*Age 11 internalising on age 9 peer problems -0.032 0.041 .429Age 11 internalising on age 9 academic achievement 0.040 0.049 .411Age 11 internalising on age 9 parental involvement 0.003 0.050 .948Age 11 internalising on age 7 externalising -0.028 0.060 .636Age 11 internalising on age 7 ADHD 0.141 0.074 .055Age 11 externalising on age 9 internalising 0.016 0.081 .842Age 11 externalising on age 9 externalising 0.354 0.084 <.001*Age 11 externalising on age 9 ADHD -0.007 0.084 .930Age 11 externalising on age 9 peer problems 0.039 0.050 .440Age 11 externalising on age 9 academic achievement 0.108 0.057 .057Age 11 externalising on age 9 parental involvement 0.011 0.066 .863Age 11 externalising on age 7 ADHD -0.169 0.087 .053Age 11 ADHD on age 9 internalising 0.241 0.084 .004*Age 11 ADHD on age 9 externalising -0.172 0.063 .007*Age 11 ADHD on age 9 ADHD 0.325 0.086 <.001*Age 11 ADHD on age 9 peer problems 0.000 0.049 .994Age 11 ADHD on age 9 academic achievement 0.004 0.050 .942Age 11 ADHD on age 9 parental involvement -0.011 0.061 .861Age 11 peer problems on age 9 internalising 0.005 0.073 .949Age 11 peer problems on age 9 externalising -0.010 0.072 .892Age 11 peer problems on age 9 ADHD -0.049 0.070 .484Age 11 peer problems on age 9 peer problems 0.023 0.056 .686Age 11 peer problems on age 9 academic achievement -0.015 0.051 .764Age 11 peer problems on age 9 parental involvement 0.033 0.062 .596Age 11 academic achievement on age 9 internalising 0.049 0.079 .536Age 11 academic achievement on age 9 externalising 0.098 0.073 .180Age 11 academic achievement on age 9 ADHD -0.129 0.075 .086Age 11 academic achievement on age 9 peer problems -0.120 0.049 .015*Age 11 academic achievement on age 9 academic achievement 0.030 0.057 .596Age 11 academic achievement on age 9 parental involvement -0.231 0.064 <.001*Age 11 parental involvement on age 9 internalising -0.062 0.072 .383Age 11 parental involvement on age 9 externalising 0.030 0.064 .640Age 11 parental involvement on age 9 ADHD -0.109 0.073 .134Age 11 parental involvement on age 9 peer problems 0.007 0.053 .890Age 11 parental involvement on age 9 academic achievement -0.111 0.054 .039*
MEDIATORS IN DEVELOPMENTAL CASCADES38
Age 11 parental involvement on age 9 parental involvement 0.216 0.076 .005*Age 9 internalising on age 7 internalising 0.287 0.105 .006*Age 9 internalising on age 7 externalising -0.107 0.086 .213Age 9 internalising on age 7 ADHD 0.223 0.088 .011*Age 9 internalising on age 7 peer problems -0.031 0.057 .583Age 9 internalising on age 7 academic achievement 0.036 0.066 .588Age 9 internalising on age 7 parental involvement -0.029 0.060 .629Age 9 externalising on age 7 internalising -0.025 0.092 .786Age 9 externalising on age 7 externalising 0.252 0.091 .005*Age 9 externalising on age 7 ADHD -0.199 0.097 .039*Age 9 externalising on age 7 peer problems -0.117 0.063 .064Age 9 externalising on age 7 academic achievement 0.156 0.073 .033*Age 9 externalising on age 7 parental involvement 0.133 0.066 .044*Age 9 ADHD on age 7 internalising 0.212 0.112 .058Age 9 ADHD on age 7 externalising -0.028 0.085 .740Age 9 ADHD on age 7 ADHD 0.192 0.099 .054Age 9 ADHD on age 7 peer problems -0.034 0.060 .566Age 9 ADHD on age 7 academic achievement 0.029 0.074 .689Age 9 ADHD on age 7 parental involvement 0.000 0.063 .999Age 9 peer problems on age 7 internalising -0.116 0.083 .163Age 9 peer problems on age 7 externalising -0.196 0.071 .005*Age 9 peer problems on age 7 ADHD 0.055 0.077 .472Age 9 peer problems on age 7 peer problems 0.163 0.063 .009*Age 9 peer problems on age 7 academic achievement -0.011 0.059 .850Age 9 peer problems on age 7 parental involvement 0.071 0.060 .239Age 9 academic achievement on age 7 internalising 0.001 0.104 .989Age 9 academic achievement on age 7 externalising 0.170 0.100 .091Age 9 academic achievement on age 7 ADHD 0.177 0.122 .146Age 9 academic achievement on age 7 peer problems 0.089 0.073 .222Age 9 academic achievement on age 7 academic achievement -0.058 0.117 .619Age 9 academic achievement on age 7 parental involvement -0.074 0.085 .385Age 9 parental involvement on age 7 internalising 0.028 0.094 .766Age 9 parental involvement on age 7 externalising -0.095 0.080 .237Age 9 parental involvement on age 7 ADHD -0.010 0.101 .921Age 9 parental involvement on age 7 peer problems 0.119 0.065 .067Age 9 parental involvement on age 7 academic achievement -0.225 0.073 .002*Age 9 parental involvement on age 7 parental involvement 0.121 0.088 .170
Note. *Significant at p<.05.
MEDIATORS IN DEVELOPMENTAL CASCADES39
Table S3. Standardised autoregressive and cross-lagged parameters for the teacher-reported ALT-SR
Parameter Estimate SE P
Age 11 internalising on age 9 internalising 0.038 0.077 .620Age 11 internalising on age 9 externalising -0.093 0.077 .230Age 11 internalising on age 9 ADHD 0.011 0.082 .889Age 11 internalising on age 9 peer problems 0.051 0.062 .412Age 11 internalising on age 9 academic achievement -0.050 0.051 .321Age 11 internalising on age 9 parental involvement -0.075 0.062 .226Age 11 internalising on age 7 externalising 0.029 0.056 .605Age 11 internalising on age 7 ADHD 0.035 0.066 .594Age 11 externalising on age 9 internalising 0.219 0.122 .073Age 11 externalising on age 9 externalising -0.142 0.149 .342Age 11 externalising on age 9 ADHD -0.065 0.108 .546Age 11 externalising on age 9 peer problems -0.054 0.075 .470Age 11 externalising on age 9 academic achievement 0.146 0.075 .052Age 11 externalising on age 9 parental involvement 0.100 0.102 .324Age 11 externalising on age 7 ADHD -0.137 0.077 .077Age 11 ADHD on age 9 internalising 0.072 0.103 .481Age 11 ADHD on age 9 externalising -0.120 0.102 .243Age 11 ADHD on age 9 ADHD 0.080 0.104 .437Age 11 ADHD on age 9 peer problems 0.109 0.066 .100Age 11 ADHD on age 9 academic achievement 0.019 0.057 .739Age 11 ADHD on age 9 parental involvement 0.040 0.074 .582Age 11 peer problems on age 9 internalising 0.068 0.071 .339Age 11 peer problems on age 9 externalising -0.070 0.078 .365Age 11 peer problems on age 9 ADHD 0.033 0.071 .640Age 11 peer problems on age 9 peer problems 0.027 0.059 .643Age 11 peer problems on age 9 academic achievement -0.005 0.052 .929Age 11 peer problems on age 9 parental involvement 0.056 0.060 .354Age 11 academic achievement on age 9 internalising 0.005 0.071 .941Age 11 academic achievement on age 9 externalising -0.019 0.078 .810Age 11 academic achievement on age 9 ADHD -0.043 0.078 .579Age 11 academic achievement on age 9 peer problems -0.080 0.058 .166Age 11 academic achievement on age 9 academic achievement 0.000 0.062 .996Age 11 academic achievement on age 9 parental involvement -0.298 0.068 <.001*Age 11 parental involvement on age 9 internalising -0.030 0.064 .642Age 11 parental involvement on age 9 externalising -0.105 0.071 .142Age 11 parental involvement on age 9 ADHD 0.117 0.066 .076Age 11 parental involvement on age 9 peer problems 0.019 0.059 .742Age 11 parental involvement on age 9 academic achievement -0.124 0.053 .020*
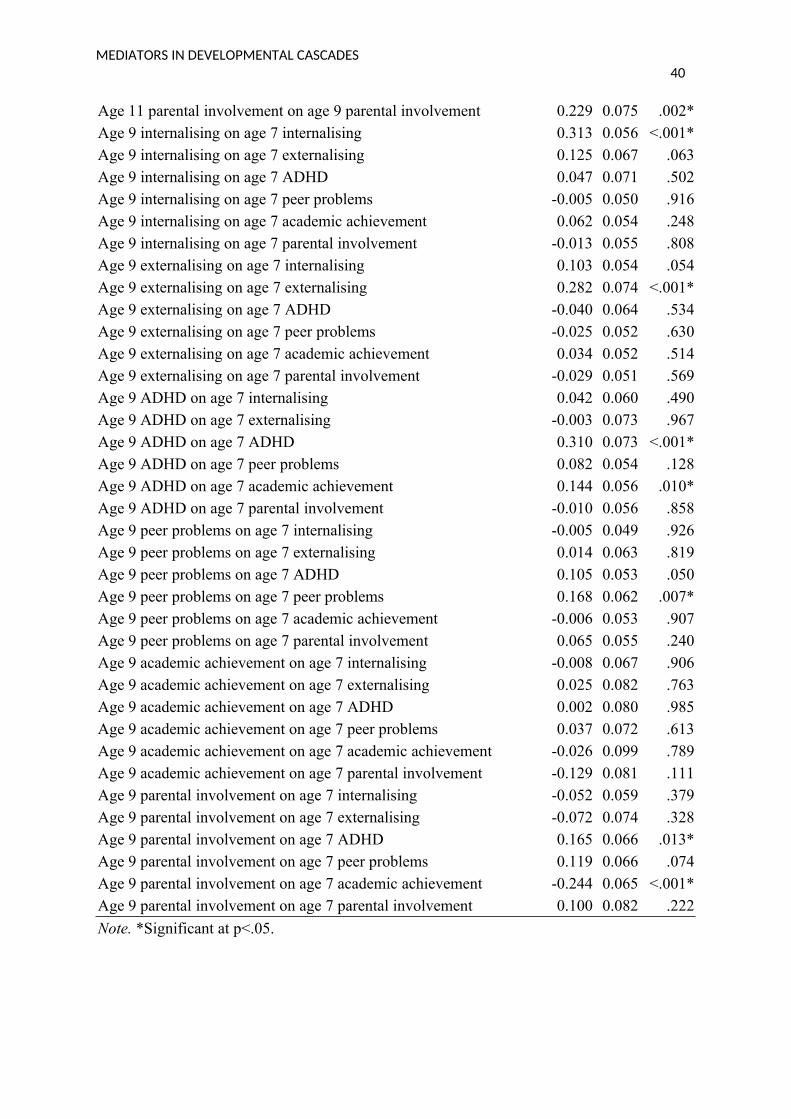
MEDIATORS IN DEVELOPMENTAL CASCADES40
Age 11 parental involvement on age 9 parental involvement 0.229 0.075 .002*Age 9 internalising on age 7 internalising 0.313 0.056 <.001*Age 9 internalising on age 7 externalising 0.125 0.067 .063Age 9 internalising on age 7 ADHD 0.047 0.071 .502Age 9 internalising on age 7 peer problems -0.005 0.050 .916Age 9 internalising on age 7 academic achievement 0.062 0.054 .248Age 9 internalising on age 7 parental involvement -0.013 0.055 .808Age 9 externalising on age 7 internalising 0.103 0.054 .054Age 9 externalising on age 7 externalising 0.282 0.074 <.001*Age 9 externalising on age 7 ADHD -0.040 0.064 .534Age 9 externalising on age 7 peer problems -0.025 0.052 .630Age 9 externalising on age 7 academic achievement 0.034 0.052 .514Age 9 externalising on age 7 parental involvement -0.029 0.051 .569Age 9 ADHD on age 7 internalising 0.042 0.060 .490Age 9 ADHD on age 7 externalising -0.003 0.073 .967Age 9 ADHD on age 7 ADHD 0.310 0.073 <.001*Age 9 ADHD on age 7 peer problems 0.082 0.054 .128Age 9 ADHD on age 7 academic achievement 0.144 0.056 .010*Age 9 ADHD on age 7 parental involvement -0.010 0.056 .858Age 9 peer problems on age 7 internalising -0.005 0.049 .926Age 9 peer problems on age 7 externalising 0.014 0.063 .819Age 9 peer problems on age 7 ADHD 0.105 0.053 .050Age 9 peer problems on age 7 peer problems 0.168 0.062 .007*Age 9 peer problems on age 7 academic achievement -0.006 0.053 .907Age 9 peer problems on age 7 parental involvement 0.065 0.055 .240Age 9 academic achievement on age 7 internalising -0.008 0.067 .906Age 9 academic achievement on age 7 externalising 0.025 0.082 .763Age 9 academic achievement on age 7 ADHD 0.002 0.080 .985Age 9 academic achievement on age 7 peer problems 0.037 0.072 .613Age 9 academic achievement on age 7 academic achievement -0.026 0.099 .789Age 9 academic achievement on age 7 parental involvement -0.129 0.081 .111Age 9 parental involvement on age 7 internalising -0.052 0.059 .379Age 9 parental involvement on age 7 externalising -0.072 0.074 .328Age 9 parental involvement on age 7 ADHD 0.165 0.066 .013*Age 9 parental involvement on age 7 peer problems 0.119 0.066 .074Age 9 parental involvement on age 7 academic achievement -0.244 0.065 <.001*Age 9 parental involvement on age 7 parental involvement 0.100 0.082 .222
Note. *Significant at p<.05.
Related Documents