Mediastinum Anatomy & Physiology PA 481 C Tony Serino, Ph.D. Biology Department Misericordia Univ.

Mediastinum Anatomy & Physiology PA 481 C Tony Serino, Ph.D. Biology Department Misericordia Univ.
Dec 29, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Mediastinum
Anatomy & Physiology PA 481 C
Tony Serino, Ph.D.
Biology Department
Misericordia Univ.

Mediastinum
Anterior
Superior
Middle
Posterior
Superior and anterior are continuous with each other; both may bereferred to as the superior mediastinum

Superior Mediastinum
Great Vessels of the Heart
Aortic arch
Transverse thoracic plane

Remnant of Ductus arteriosus
Ligamentumarteriosum

Usual Aortic Arch Pattern
65% of all people
RS
BT
LS
LCRC

Aortic Arch Variations
27% one BT withboth CC exiting 5%
1.2% two BT
left vert. a.

SVC
BC BC
SVC
Vagus
Phrenic

Pulmonary Arteries and Veins

Trachea and Primary bronchi

Structure Order
BC
Aorta PA
Trachea

Esophagus• Function: Deglutition• Two sphincters: upper
and lower esophageal sphincters (lower is physiological only)
• Retropleural position (therefore, covered by adventitia)
• Mucosa: stratified squamous with many mucus glands (esophageal glands)
• Muscularis: changes from skeletal to smooth muscle

Esophagus Histology

Thymus Gland• Bilobed organ that is largest in children, but begins to regress sharply at the onset of puberty (around age 11)
• It is the site of T-cell lymphocyte production and produces hormones (such as, thymosin) that modifies their physiology

General Circulatory System
1. Cardiovascular– Consists of a closed
system of vessels which transport blood
– Two circuits: Systemic and Pulmonary
– Arteries move blood away from the heart
– Veins move blood toward the heart

General Circulatory System2. Lymphvascular –
moves lymph– Consist of blind end
tubes which collect interstitial fluid (now called lymph) and returns it to circulation
– The lymph is cleaned before returned to the blood vessels

Heart Development

Fetal Circulation

Selected Heart Defects

Heart as a Dual Pump
• Cardiac muscle arranged as whorls that squeeze the blood
• Twin pumps: systemic and pulmonary
• Four chambers: 2 atria and 2 ventricles

Cardiac Muscle Cells

Cardiac Muscle Depolarization

Conductance of Ions during Depolarization

Heart: Location

Heart in Relation to other Organs

Layers of the Heart and Pericardium

Heart: Anterior ViewTransverse Pericardial sinus

Heart: Posterior View
Oblique Pericardial sinus

Heart: Internal Anatomy

Differences in Ventricular Wall

Coronary Artery Schematic
(LAD)

Most Common Coronary Arterial Pattern
Fig. 1.51
Ant. Desc. a. (LAD)
Post. Desc. a.
R. Marginal a.
L. Marginal a.
Circumflex a.

Coronary Variation
15% LCA dominant
Single CA
Most people right dominant.
Circumflex from right aortic sinus
(4% have an accessory coronary artery)
(note: which branch gives rise to posterior descending a.determines dominance)

Fig. 12.66b

Fig. 12.66c

Fig. 12.66d


Coronary Vein Schematic

Coronary Veins
Fig. 1.52
Coronary sinus
Great Cardiac v.
Small Cardiac v. Middle Cardiac v.
Ant. Cardiac veins

Major Cardiac Valves

aortic valve (SL)AV (tricuspid)
Heart Valves
sinus
Nodule (corpara aranti)
cusps

Fig. 12.07b

Diastole: Period of Ventricular Filling

Systole: Isovolumetric Contraction

Systole: Ventricular Ejection

Diastole: Isovolumetric Relaxation

Conduction System of Heart

Pacemaker Potential


ECG and electrical changes

Normal ECG

ECG
Normal Sinus Rhythm
Junctional Rhythm (AV node rhythm)

Second Degree Heart Block
Ventricular Fibrillation (V-fib)

Heart Sounds
• “Lub-dub”• Sound associated with
valve closing producing turbulent blood flow

Cardiac Cycle
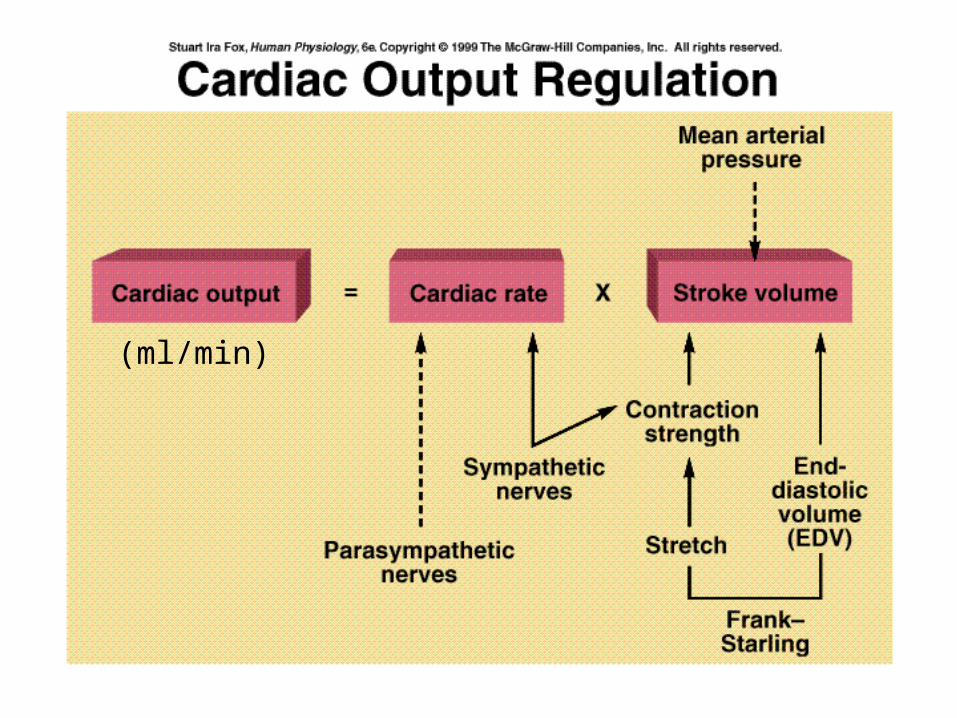
(ml/min)

Factors Affecting SV• Stroke Volume (SV) =
End Diastolic Volume – End Systolic Volume• SV = EDV – ESV (ml/beat)• EDV affected by:
– Venous return which is dependent on venous tone, skeletal muscle pumps, etc.
• ESV– As the heart fills it is stretched which allows for better overlap of
the contractile proteins which will affect the force of contraction and the ESV (Starling’s Law of the Heart)
– Increasing the force of contraction at any EDV will decrease the ESV and increase the SV (sympathetic stimulation and epinephrine)


Sympathetic Stimulation
• Leads to increase HR• Increases in Ca++
release from SR, increase Ca++ through membrane and increase myosin crossbridge cycling
• Increases force of contraction

Heart Rate Control• Sinus Rhythm = normal SA node control• Autonomic Activity
– Sympathetic (thoracic trunk) = accelerator (induces tachycardia)
– Parasympathetic (vagus n.)= brake (induces bradycardia)
• Hormones– epinephrine
• Drugs-caffeine, nicotine, atropine, etc.

Posterior Mediastinum
Thoracic aorta
Sympathetic trunk
Vagus n.
Azygous v.
Trachea
Esophagus
Phrenic n.
Intercostal a., v., & n.
Hemiazygous v.
Lung root
Thoracic duct

Small Aortic Branches
Bronchial a.
Intercostals
Coronary
Esophageal

Azygous vein
Hemiazygous v.

Nerves of Post. Mediastinum

Thoracic Duct
Related Documents