ANEMIA Department of Clinical Microscopy Faculty of Associated Medical Sciences, Chiang Mai University PRASIT CHANARAT, M.S.(Clin.Path) PC

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

ANEMIA
Department of Clinical Microscopy
Faculty of Associated Medical Sciences, Chiang Mai University
PRASIT CHANARAT, M.S.(Clin.Path)
PC

ANEMIASymptoms : Pallor Jaundice Fatique Palpitation Dyspnea Virtigo Peptic ulcer Glossitis Dysphagia etc
PC
Classification of Anemia I. Etiologic Classification 1. Impaired RBC production 2. Excessive destruction 3. Blood lossII. Morphologic Classification 1. Macrocytic anemia 2. Microcytic hypochromic anemia 3. Normochromic normocytic anemiaIII. Kinetic ClassificationIV. Physiologic Classification PC

Impaired RBC Production1. Abnormal bone marrow 1.1 Aplastic anemia 1.2 Myelophthisis : Myeloficrosis, Leukemia, Cancer metastasis 2. Essential factors deficiency 2.1 Deficiency anemia : Fe, Vit. B12, Folic acid, etc 2.2 Anemia in renal disease : Erythropoietin3. Stimulation factor deficiency 3.1 Anemia in chronic disease 3.2 Anemia in hypopituitarism 3.3 Anemia in hypothyroidism
PC

Excessive Destruction of RBC(cont.)
Hemolytic anemia
1. Intracorpuscular defect
1.1 Membrane : Hereditary spherocytosis
Hereditary ovalocytosis, etc.
1.2 Enzyme : G-6PD deficiency, PK def., etc.
1.3 Hemoglobin : Thalassemia, Hemoglobino- pathies
PC

Excessive Destruction of RBC
2. Extracorpuscular defect
2.1 Mechanical : March hemolytic anemia
MAHA (Microangiopathic HA)
2.2 Chemical/Physical
2.3 Infection : Clostridium tetani
2.4 Antibodies : HTR, SLE
2.5 Hypersplenism
PC

Blood Loss
1. Acute blood loss : Accident, GI bleeding
2. Chronic blood loss : Hypermenorrhea
Parasitic infestation
PC
Macrocytic Anemia MCV > 94 MCHC > 311. Megaloblastic dyspoiesis 1.1 Vit. B12 deficiency : Pernicious anemia 1.2 Folic acid deficiency : Nutritional megaloblas- tic anemia, Sprue, Other malabsorption 1.3 Inborn errors of metabolism : Orotic aciduria, etc. 1.4 Abnormal DNA synthesis : Chemotherapy, Anticonvulsant, Oral contraceptives
PC
Macrocytic Anemia MCV > 94 MCHC > 312. Non-Megaloblastic dyspoiesis 2.1 Increased erythropoiesis : Hemolytic anemia response to hemorrhage 2.2 Increased membrane surface area : Hepatic disease, Obstructive jaundice, Post-
splenectomy 2.3 Idiopathic : Hypothyroidism, Hypoplastic and Aplastic anemia
PC
Microcytic Hypochromic Anemia MCV < 80 MCHC < 311. Fe deficiency anemia : Chronic blood loss, Inadequate diet, Malabsorption, Increased demand, etc.2. Abnormal globin synthesis : Thalassemia with or without Hemoglobinopathies3. Abnormal porphyrin and heme synthesis : Pyridoxine responsive anemia, etc.4. Other abnormal Fe metabolism :
PC
Normocytic Normochromic Anemia MCV 82 - 92 MCHC > 301. Blood loss2. Increased plasma volume : Pregnancy, Overhydration3. Hemolytic anemia : depend on each cause4. Hypoplastic marrow : Aplastic anemia, RBC aplasia5. Infiltrate BM : Leukemia, Multiple myeloma, Myelofibrosis, etc.6. Abnormal endocrine : Hypothyroidism, Adrenal insufficiency, etc.7. Kidney disease / Liver disease / Cirrhosis
PC
Kinetic Classification of Anemia
1. Insufficient erythropoiesis
Stem cells , Hypoplastic marrow, Infiltrated BM
2. Ineffective erythropoiesis
- Megaloblastic anemia
- Thalassemia
- Sideroblastic anemia
3. Uncompensated hemolytic disease with continued
bleeding
PC
Physiologic Classification of Anemia
1. RPI (Reticulocyte Production Index) < 2
(Ineffective erythropoiesis)
1.1 Hypoproliferative anemia
1.2 Maturation disorder
2. RPI > 3 (Effective erythropoiesis
2.1 Hemolytic anemia
2.2 Blood loss anemia
PC

Physiologic Classification of Anemia
1. RPI (Reticulocyte Production Index) < 2
(Ineffective erythropoiesis)
1.1 Hypoproliferative anemia
(normocytic normochromic, N/N)
- Hypoplastic anemia - Idiopathic/ Chemical/ Infectious / Drug --> Maturation arrest
- Myelophthisic anemia (Marrow infiltration)
- Refractory anemia (Dysmyelopoietic syndrome)
PC
1.1.1 N/N and normal RDW
a) BM failure
b) Decrease marrow stimulation
- Endocrine disease
- Anemia of chronic disease
- Renal disease
1.1.2 Abnormal RBC morphology & RDW
a) Oval macrocyte :- Refractory dysmyelo- poietic
b) Dacrocytes/ tear drops :- Myelophthisic
PC
Physiologic Class. of Anemia RPI < 2
1.2 Maturation disorder 1.2.1 Microcytic, high RDW a) Siderblastic (Microcytic dimorphic RBC) b) Fe def. (Microcytic hypochromic RBC) 1.2.2 Microcytic, normal RDW a) Heterozygous, thalassemia syndrome
b) Anemia of chronic disease 1.2.3 Macrocytic a) Liver disease b) Folate def. c) Vit. B12 def. d) Hemolytic anemia (Normocyte
polychromasia)PC
Physiologic Class. of Anemia RPI < 2

Physiologic Classification of Anemia
2. RPI > 3
(Effective erythropoiesis)
2.1 Hemolytic anemia
- Intrinsic hereditary disorder - Extrinsic acquired disorder
2.2 Blood loss
- Acute blood loss
- Chronic blood loss (without treatment --> micro-
cytic, hypochromic anemia)PC

Evaluation of AnemiaA. Hematologic
1. Hematocrit (VPRC preferred)
2. Hemoglobin concentration
3. RBC indices : MCV, MCH, MCHC
4. Leukocyte count
5. Reticulocyte count
6. Platelet count
7. ESR (Erythrocyte sedimentation rate)
8. Stained blood smear : RBC morphologyPC

Evaluation of AnemiaB. Urine analysis 1. Appearance : Color, pH, Clarity, sp gr 2. Test for protein, Bence Jones protein 3. Bilirubin, Uribilinogen 4. Occult blood 5. Microscopic examination C. Stool 1. Appearance : Color, consistency 2. Occult blood 3. Examination for ova, parasites
PC
Evaluation of AnemiaD. Serum or Plasma 1. BUN 2. Creatinine, if urea N is abnormal 3. Bilirubin : Direct, indirect 4. Protein 5. SI (Serum iron), TIBC (Total iron binding capacity)E. Special tests in hematology Hb typing / Ham acid test / Coombs’ test, G-6PD, Ferritin
, Sucrose test, Autohemolysis test, Haptoglobin, etc.
PC
DDx of Common Anemia in Thailand
1. Acute anemia
1.1 Acute blood loss
BP , Pulse --> Acute hemorrhage
1.2 No acute blood loss• Jaundice, hemoglobinuria --> G-6-PD def.• Jaundice, No hemoglobinuria --> AIHA (NCNC), HS
(Spherocycyte), hemoglobin H disease (HCMC) • Jaundice, fever --> Malaria• No jaundice --> G-6-PD def., Hb H, Acute leukemia
PC
Hb < 9-10 gm/dL
DDx of Common Anemia in Thailand
2. Chronic anemia
2.1 No hepatosplenomegaly • No petichiae and purpura --> Fe def. Anemia, anemia
of chronic disease, folate def.• Petichiae & purpura --> ITP + Fe def., Acute leukemia
(Blast cell), Aplastic anemia• Chronic disease --> Chronic renal failure, rheumatoid
arthritis, infective endocarditis, hypothyroidism, etc.
PC
Hb < 9-10 gm/dL
DDx of Common Anemia in Thailand
2. Chronic anemia
2.2 Hepatosplenomegaly• Mongoloid face --> Thalassemia• No Mongoloid face with lymphadenopathy --> DDx
Acute leukemia, lymphoma, TB lymph node• Liver disease
PC
Hb < 9-10 gm/dL
Mechanisms of Anemia
Production Disorders:Hematopoietic Cell Damage
-Drugs, Radiation, Infections, ToxinsFactor Deficiency
-Iron (Heme Synthesis)-Vitamin B12 (DNA Synthesis)
-Folate (DNA Synthesis)
Mechanisms of Anemia
Survival Disorders:Blood Loss - External or InternalRed blood Cell Destruction -Hemolytic Anemias

Anemia
Manifestations - Cause & ChronicityNonspecific Signs and Symptoms
Weakness, Malaise, FatigueCNS hypoxia - Headaches, Faintness,
Dimness of VisionSkin Pallor, Thinning and InelasticityNail BrittlenessAngina Pectoralis (if ASCVD)

Production Disorder - Iron Deficiency
Most Common Nutritional DeficiencyRequired in Hemoglobin Synthesis
Heme + Globin Chains = HemoglobinOccurs in RBC Cytoplasm
Hypochromic Microcytic Anemia
Iron Metabolism
Iron is Absorbed Primarily in Duodenum
- 25% of Heme-Bound Iron (Red Meat)
- 1-2% of Non-Heme IronBody Losses of Iron are Limited
- 1-2 mg/Day By Epithelial Cell SheddingMucosal Block - Maintains Balance
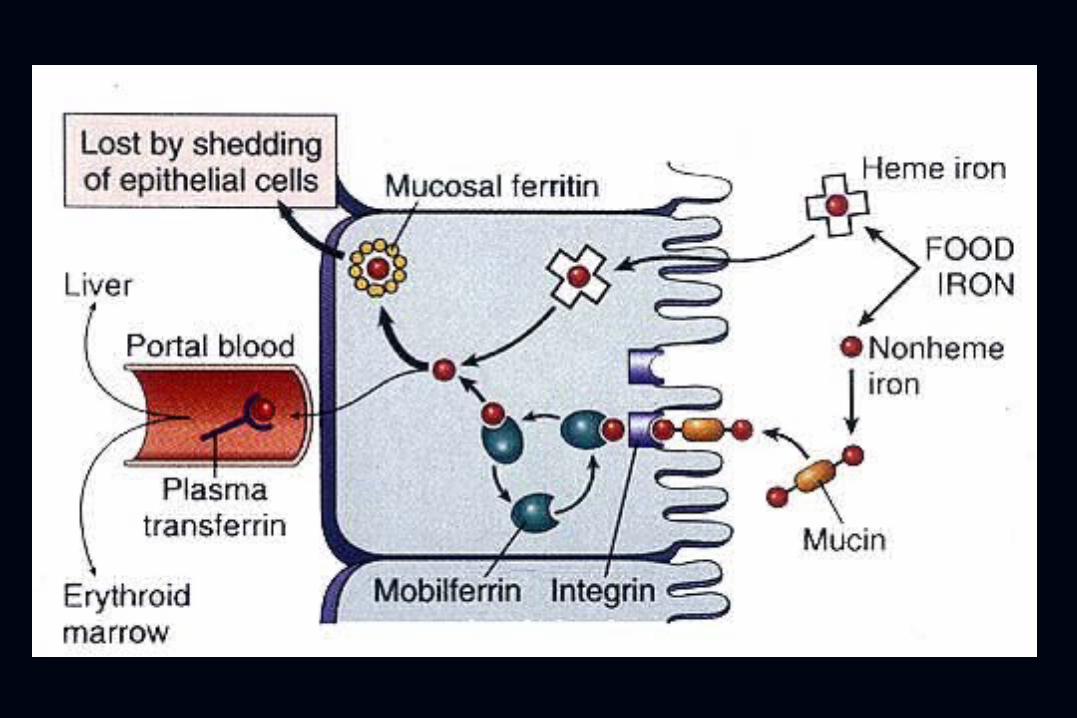
Transferrin
Transport Protein For Iron In Blood
Fully Saturated Transferrin = TIBC
300 - 350ug/dl Fe
Normal Transferrin - 1/3 Filled With Iron
100 - 120ug/dl Fe (Serum Iron)

Iron Storage
Ferritin - Protein Iron Complex *Found In All Tissues*BM, Liver (Transferrin)*Spleen (RBC Breakdown)
Hemosiderin - Breakdown Product ofFerritin
Development of Iron Deficiency
Depletion of Stores Serum Ferritin
Stainable BM Iron
Transferrin ( TIBC) Serum Fe
Transferrin Saturation Hemoglobin, Myoglobin, Fe Proteins

Iron Deficiency Anemia Laboratory Findings
Hypochromic Microcytic Anemia
( RBC Count, MCV)
Serum Ferritin Levels
Transferrin Saturation
( Serum Fe, Transferrin)

Causes of Iron Deficiency
External Blood Loss - Most CommonFemale Genital TractGastrointestinal Tract
Demand - Infancy, PregnancyDietary Deficiency - Rare
(Vegetarian Diets) Intestinal Malabsorption Syndrome
Iron DeficiencyClinical Manifestations
Anemia - Non-Specific FindingsKoilonychiaPlummer-Vinson Syndrome
-Hypochromic Microcytic Anemia-Atrophic Glossitis-Esophageal Webs (Dysphagia)
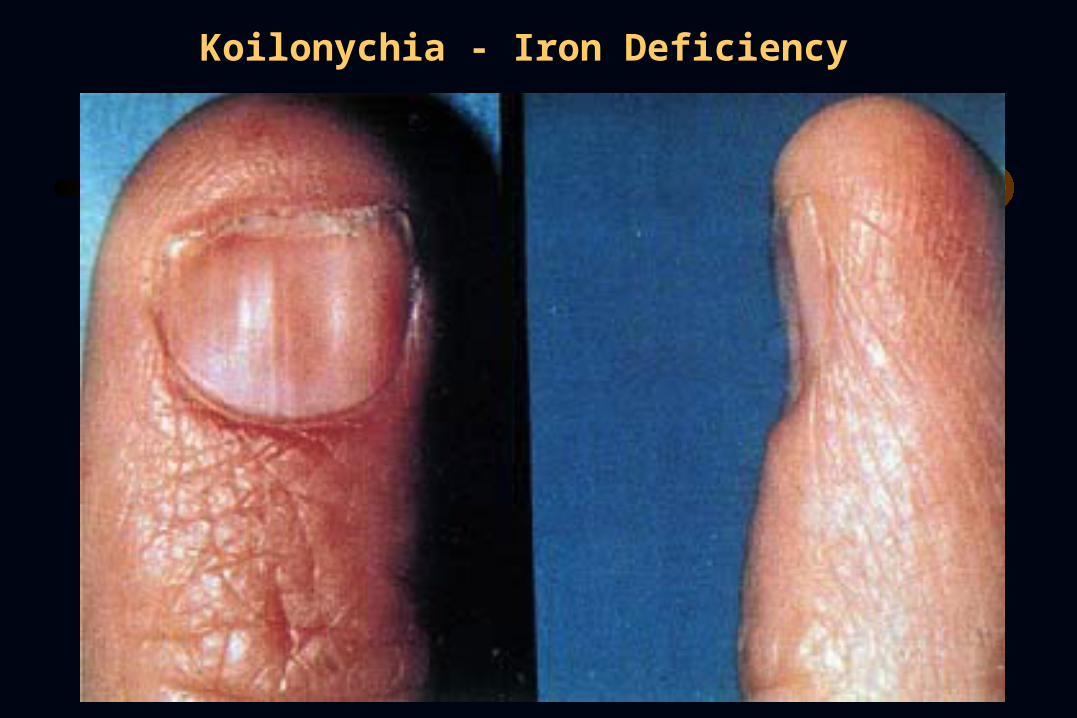
Koilonychia - Iron DeficiencyKoilonychia - Iron Deficiency
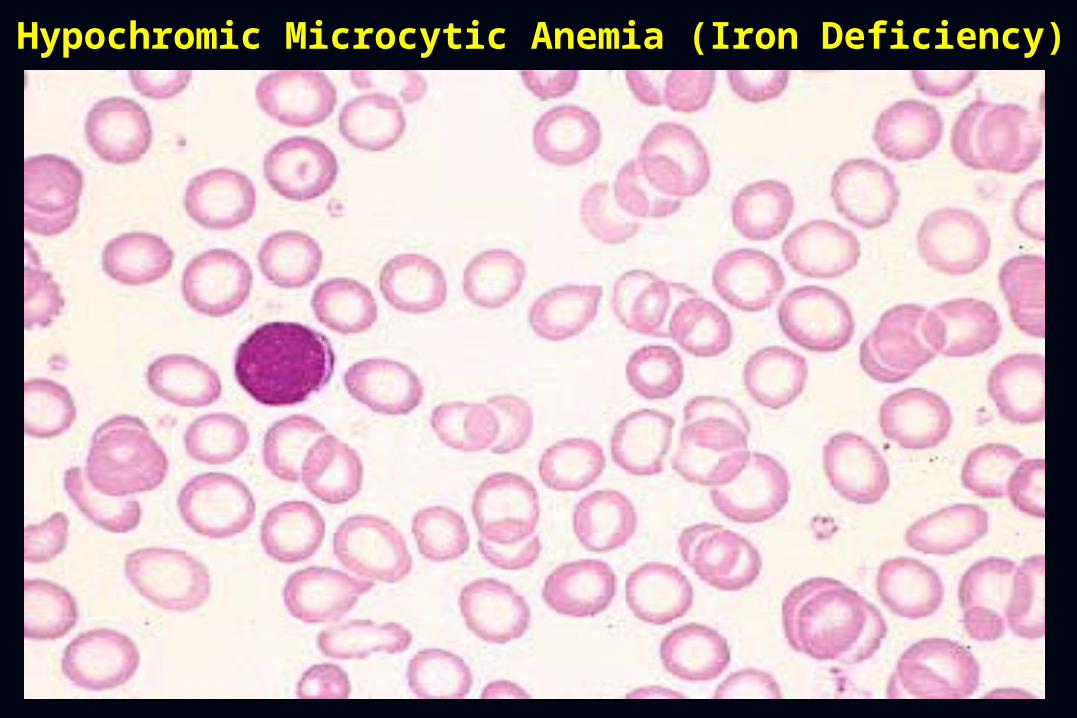
Hypochromic Microcytic Anemia (Iron Deficiency)Hypochromic Microcytic Anemia (Iron Deficiency)
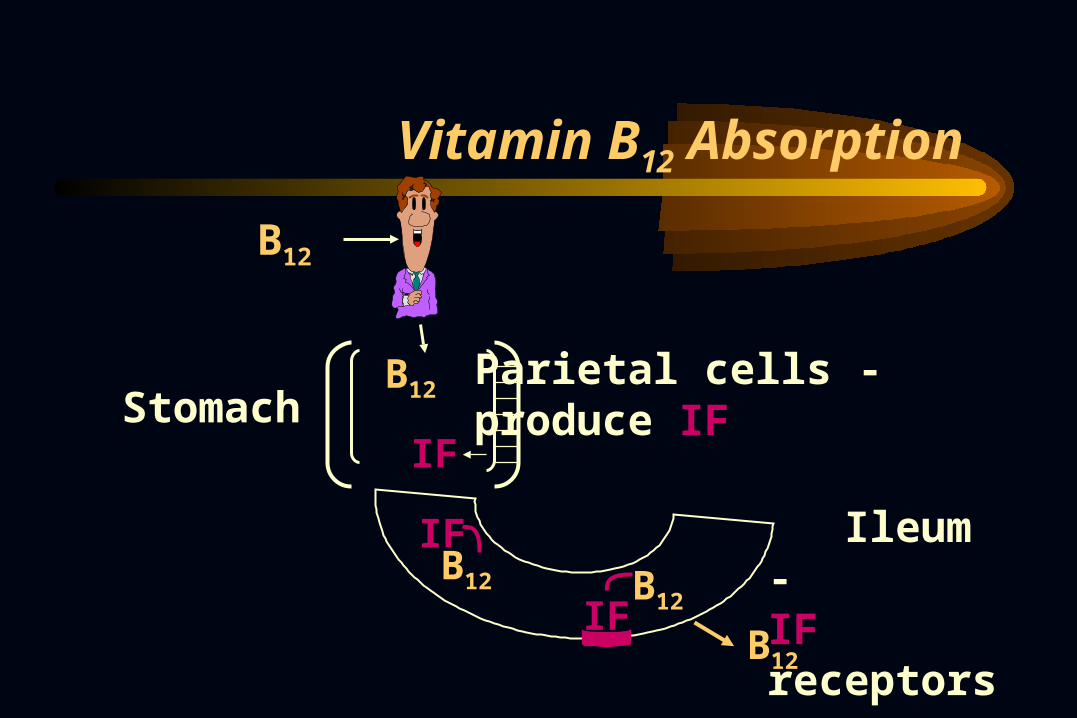
Vitamin B12 Absorption
Parietal cells - produce IF
IF
B12
B12
B12
IF
Stomach
IF
Ileum -IF receptorsB12
B12

Vitamin B12 Deficiency
Western World - Pernicious Anemia
Autoantibodies (Serum and Gastric)
IF Function Gastric
Production
IF ParietalCell
IFB12
Production Disorder - Vitamin B12 or Folate Deficiency
Megaloblastic Anemias
Impaired DNA Synthesis (Nucleus)
Function - Transfer of Carbon Groups
Affects All Rapidly Dividing Cells
-Mouth - Atrophic Glossitis
-GI tract - Intestinal Malabsorption
Megaloblastic AnemiaPeripheral Blood
RBCs - Large Oval Macroovalocytes - MCV > 100u3
Anemia Due To Ineffective Hematopoiesis- Autohemolysis of Megaloblasts(Circulating Large RBCs Destroyed)
Hypersegmented Neutrophils Thrombocytopenia, Neutropenia (Severe)

Macroovalocytes and Hypersegmented NeutrophilMacroovalocytes and Hypersegmented Neutrophil

Vitamin B12 Deficiency - Cause
Western World - Pernicious AnemiaAutoimmune Disorder -Autoantibodies to IF and Parietal Cells
-Chronic Atrophic Gastritis -Achlorhydria - Absent HCL Incidence of Other Autoimmune
Disorders
Vitamin B12 Deficiency
Additional Causes: Inadequate Diet - Rare (>20yr Stores)
-Foods Containing Animal Protein-Microorganisms Synthesize-Stored in Liver, Reabsorbed in Bile
Gastrectomy, Ileal ResectionMalabsorption States, Gastric AtrophyDiphyllobothrium Latum - Fish Tapeworm
Megaloblastic Anemia - Bone Marrow
Nuclear- Cytoplasmic Asynchrony:Erythroid Series (Hallmark Changes)
-Megaloblasts
-Erythroid HyperplasiaMyeloid SeriesMegakaryocytic Series - (Infrequent)
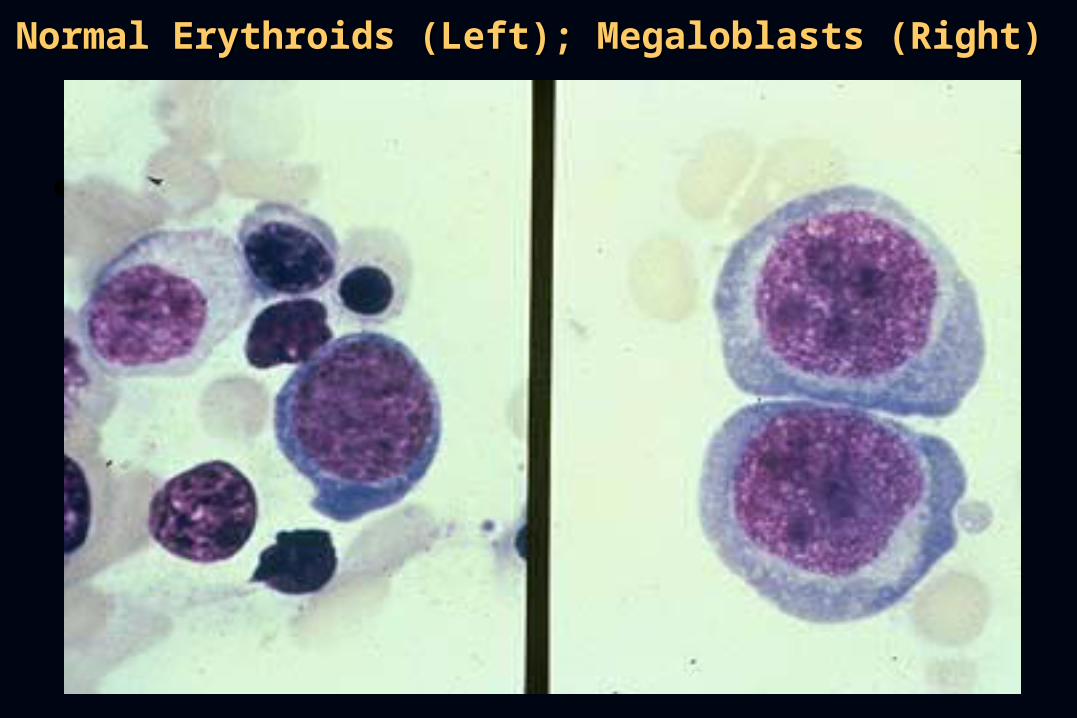
Normal Erythroids (Left); Megaloblasts (Right)Normal Erythroids (Left); Megaloblasts (Right)

B12 and Folate in DNA Synthesis
ThymidylateSynthetase
DNA
FH4 (Folate)
dTMP
N5 - Methyl FH4
Methyl Cobalamin
Cobalamin (Vitamin B12)
dUMP

Vitamin B12 Deficiency
Clinical - Similar to Folate Deficiency But Demyelinating Neurologic Disorder- Affects Both Sensory and Motor Tracts- Lack of Correlation With Anemia
Parenteral B12 - Improves Anemia, +/- Resolution of Neurologic Symptoms
Caution! Anemia of B12 Deficiency Also Improves With Folate Supplementation

Vitamin B12 Deficiency
Laboratory Findings:Low Serum Vitamin B12 LevelsNormal RBC Folate LevelsAbnormal Schilling Test - Impaired
Absorption of Radioactive Vitamin B12 Correctable by Addition of IF
Anti-Intrinsic Factor Antibodies (Anti-Parietal Antibodies Less Sensitive)

Causes of Folate Deficiency
Dietary Deprivation - Widely Distributed in Foods (Uncooked Vegetables, Fruits, Liver)- Limited Body Stores (Wks-Months) - Chronic Alcoholics, Elderly, Indigent
Malabsorption (Upper 1/3 Intestine)- Intestinal Disease (Sprue, Celiac Dx)- Chronic Drugs (Dilantin)
Folate Deficiency
Increased Requirements - Pregnancy Impaired Utilization - Folic Acid
Antagonists (Chemotherapy Drugs)Laboratory Findings:Red Blood Cell Folate - Reflects Tissue
Content of Folate Throughout BodySerum Folate - Levels Fluctuate Based on
Recent Intake, Do Not Reflect Stores
Anemia of Chronic Disease
Normochromic Normocytic Anemia(or Hypochromic Microcytic)
Chronic Disorders (Inflammation or Tissue Necrosis)
-Chronic Microbial Illnesses-Chronic Immune Disorders-Neoplasms
Often TIBC, Ferritin

Anemia of Chronic Disease
Defect
Storage Iron
IL-1
TNF IFN
Erythroid Precursors
(Insufficient Erythropoietin)

Bone Marrow Storage Iron (Blue)Bone Marrow Storage Iron (Blue)

Hematopoietic Cell DamageAplastic Anemia
Bone Marrow Aplasia (Lack of Cells)Failure of Multipotent Stem Cell
- T-cell Mediated Suppression or- Genetic Damage
Bone Marrow - Markedly HypocellularPeripheral Blood - Pancytopenia
- Normochromic Normocytic RBCs
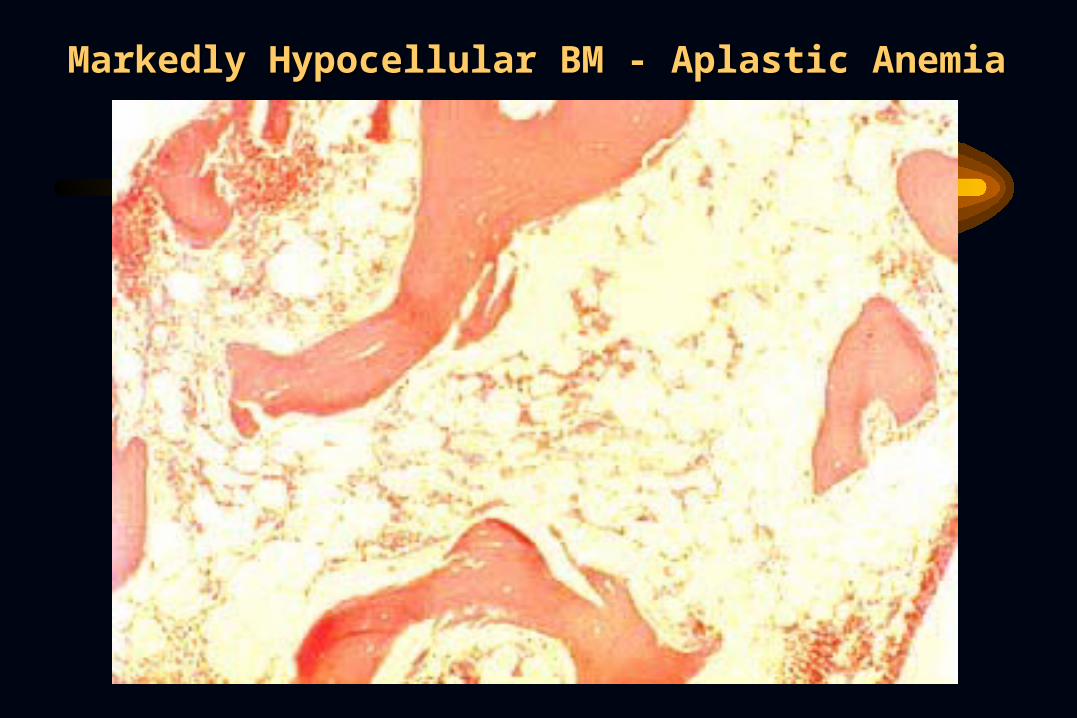
Markedly Hypocellular BM - Aplastic AnemiaMarkedly Hypocellular BM - Aplastic Anemia
Aplastic Anemia
Causes of Stem Cell Failure Idiopathic (>50%) - Poor Prognosis
Especially If < 40 Years OldWhole Body IrradiationViral Infections - Most Common
After Non-A/Non-B HepatitisChemical Agents and Drugs -
Reversible and Non-Reversible

Myelophthisic Anemia
BM Replacement BM failure:Metastatic Carcinoma Most CommonDestruction By Non-Neoplastic Process
is Less Common i.e. Fibrosis, InfectionPeripheral Blood Cytopenias, Immature
Circulating Cells

Breast Cancer Replacing BMBreast Cancer Replacing BM
ANEMIA
PC
Related Documents











