Mechanical ventilation Mechanical ventilation versus CPAP versus CPAP -what are the pros and -what are the pros and cons? cons? Anne Greenough Anne Greenough Professor of Neonatology & Clinical Professor of Neonatology & Clinical Respiratory Physiology Respiratory Physiology Division of Asthma, Allergy and Lung Division of Asthma, Allergy and Lung Biology Biology King’s College, London, School of Medicine King’s College, London, School of Medicine

Mechanical ventilation versus CPAP -what are the pros and cons? Anne Greenough Professor of Neonatology & Clinical Respiratory Physiology Division of Asthma,
Dec 22, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Mechanical ventilation versus CPAPMechanical ventilation versus CPAP-what are the pros and cons? -what are the pros and cons?
Anne GreenoughAnne GreenoughProfessor of Neonatology & Clinical Respiratory PhysiologyProfessor of Neonatology & Clinical Respiratory Physiology
Division of Asthma, Allergy and Lung BiologyDivision of Asthma, Allergy and Lung BiologyKing’s College, London, School of MedicineKing’s College, London, School of Medicine

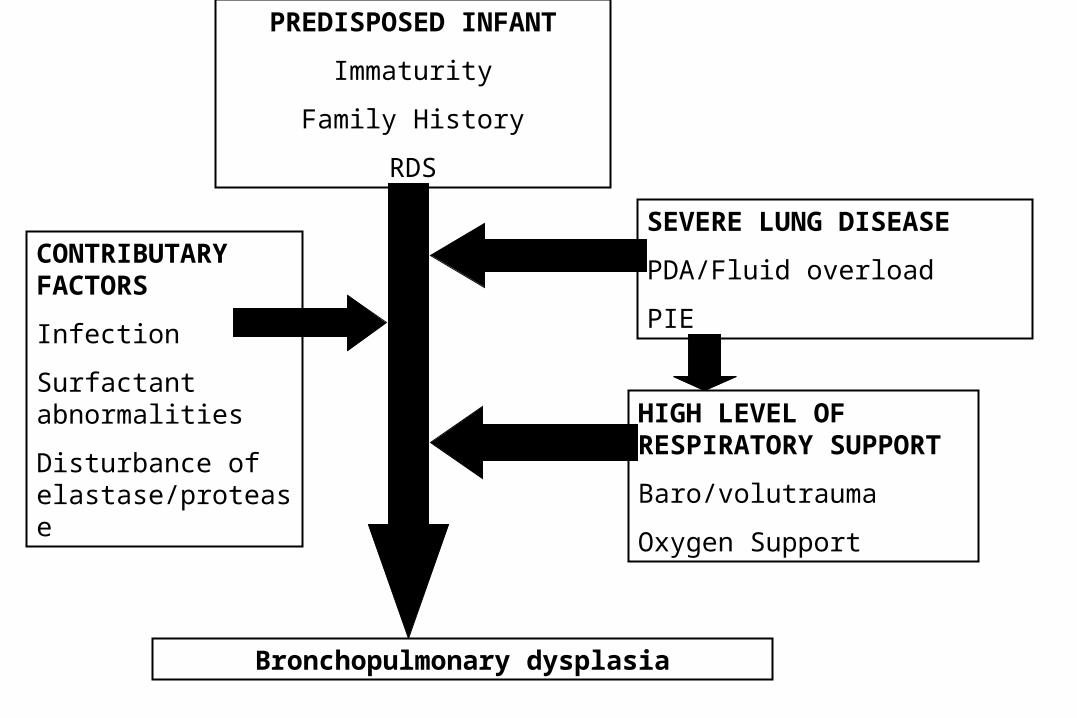
PREDISPOSED INFANT
Immaturity
Family History
RDS
SEVERE LUNG DISEASE
PDA/Fluid overload
PIE
HIGH LEVEL OF RESPIRATORY SUPPORT
Baro/volutrauma
Oxygen Support
Bronchopulmonary dysplasia
CONTRIBUTARY FACTORS
Infection
Surfactant abnormalities
Disturbance of elastase/protease

Which ventilation strategy?Which ventilation strategy?
Strategies to reduce the likelihood of baro/volutrauma:Strategies to reduce the likelihood of baro/volutrauma:
(i) Avoidance of intubation and mechanical ventilation(i) Avoidance of intubation and mechanical ventilation - nasal continuous positive airways pressure - nasal continuous positive airways pressure
(nCPAP)(nCPAP)(ii) Respiratory support working synergistically with the (ii) Respiratory support working synergistically with the infant’s respiratory effortsinfant’s respiratory efforts - patient triggered ventilation- patient triggered ventilation(iii)(iii) Minimisation of excessive “tidal” volumes Minimisation of excessive “tidal” volumes
- volume targeted ventilation- volume targeted ventilation - high frequency oscillation- high frequency oscillation

Early nCPAPEarly nCPAP
• Reduced incidence of intubation and mechanical Reduced incidence of intubation and mechanical ventilation ventilation
Jacobsen 1993, Poets 1996, Gitterman 1997Jacobsen 1993, Poets 1996, Gitterman 1997• Eight centre comparison, the centre with the lowest Eight centre comparison, the centre with the lowest
occurrence of BPD used CPAP in preference to IPPVoccurrence of BPD used CPAP in preference to IPPV
- avoided hyperventilation and muscle relaxants- avoided hyperventilation and muscle relaxants
- used permissive hypercapnia- used permissive hypercapnia
-- one individual supervised ventilatory careone individual supervised ventilatory care
Avery 1987Avery 1987
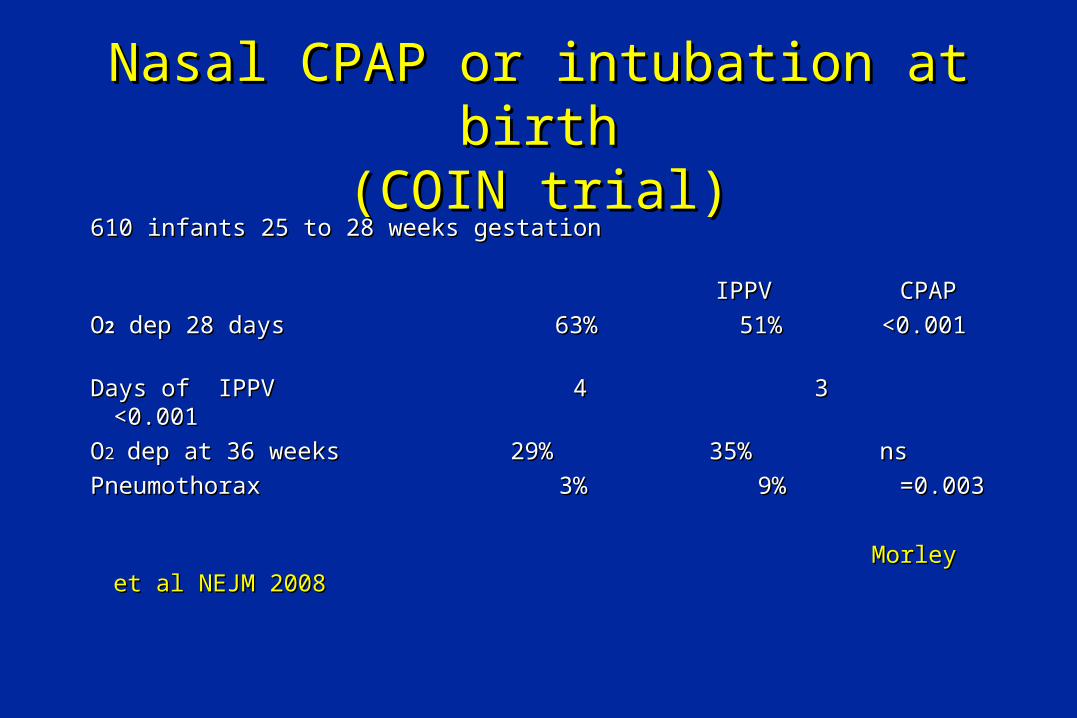
Nasal CPAP or intubation at birthNasal CPAP or intubation at birth(COIN trial)(COIN trial)
610 infants 25 to 28 weeks gestation 610 infants 25 to 28 weeks gestation
IPPV CPAPIPPV CPAP
OO22 dep 28 days 63% 51% <0.001 dep 28 days 63% 51% <0.001
Days of IPPV 4 3 <0.001Days of IPPV 4 3 <0.001
OO22 dep at 36 weeks 29% 35% nsdep at 36 weeks 29% 35% ns
Pneumothorax 3% 9% =0.003Pneumothorax 3% 9% =0.003
Morley et al NEJM 2008Morley et al NEJM 2008

Early surfactant and extubation to CPAPEarly surfactant and extubation to CPAPversus selective surfactant and IPPVversus selective surfactant and IPPV
Meta-analysis of six trials demonstrated CPAP:Meta-analysis of six trials demonstrated CPAP:
Reduced BPD 0.51(0.26-0.99)Reduced BPD 0.51(0.26-0.99)
Reduced need for IPPV 0.67 (0.57-0.79)Reduced need for IPPV 0.67 (0.57-0.79)
Reduced airleaks 0.52 (0.28,0.96)Reduced airleaks 0.52 (0.28,0.96)
Surfactant 1.62 (1.41,1.86)Surfactant 1.62 (1.41,1.86)
Stevens et al Cochrane 2007Stevens et al Cochrane 2007
But early versus selective surfactant reduces airleaks and But early versus selective surfactant reduces airleaks and BPD/death and improves survivalBPD/death and improves survival
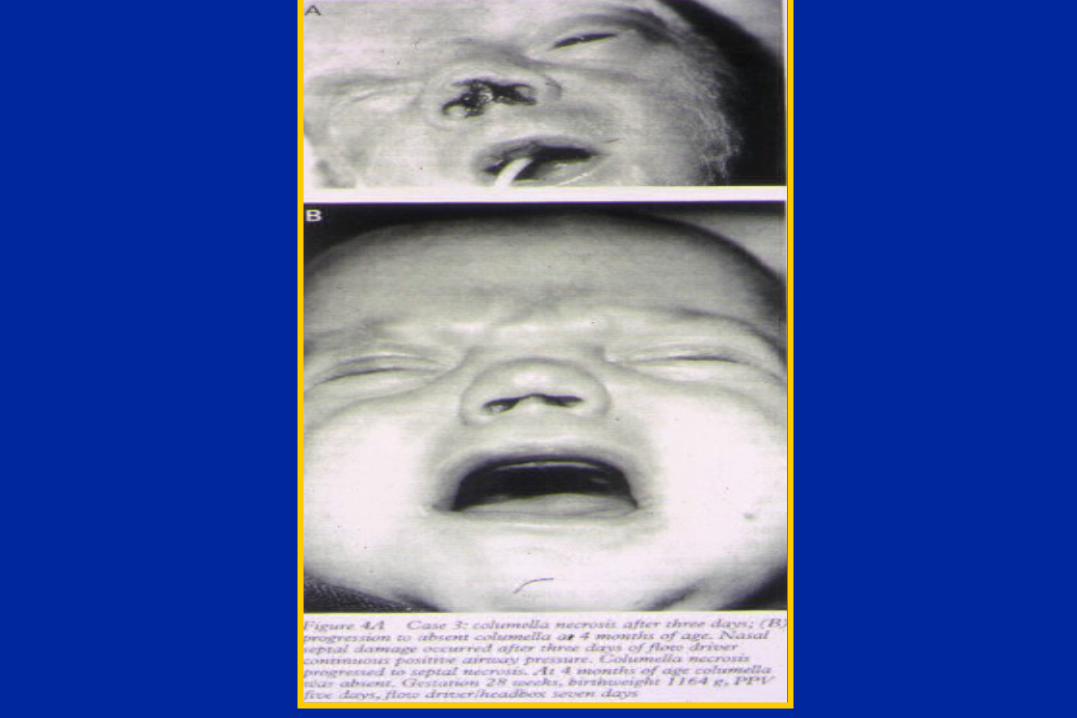

Nasal traumaNasal trauma
• 20% infants on dual prongs affected20% infants on dual prongs affected Robertson et al ADC 1996Robertson et al ADC 1996• 40 infants randomised nasaopharyngeal tube or binasal prong 40 infants randomised nasaopharyngeal tube or binasal prong - similar trauma incidence - similar trauma incidence Buettiker et al Intens Care Med 2004 Buettiker et al Intens Care Med 2004 • 89 infants randomised to binasal prong or mask 89 infants randomised to binasal prong or mask -no significant difference in nasal trauma incidence-no significant difference in nasal trauma incidence - nasal injury (32%) related to CPAP duration- nasal injury (32%) related to CPAP duration Yong et al ADC 2005Yong et al ADC 2005
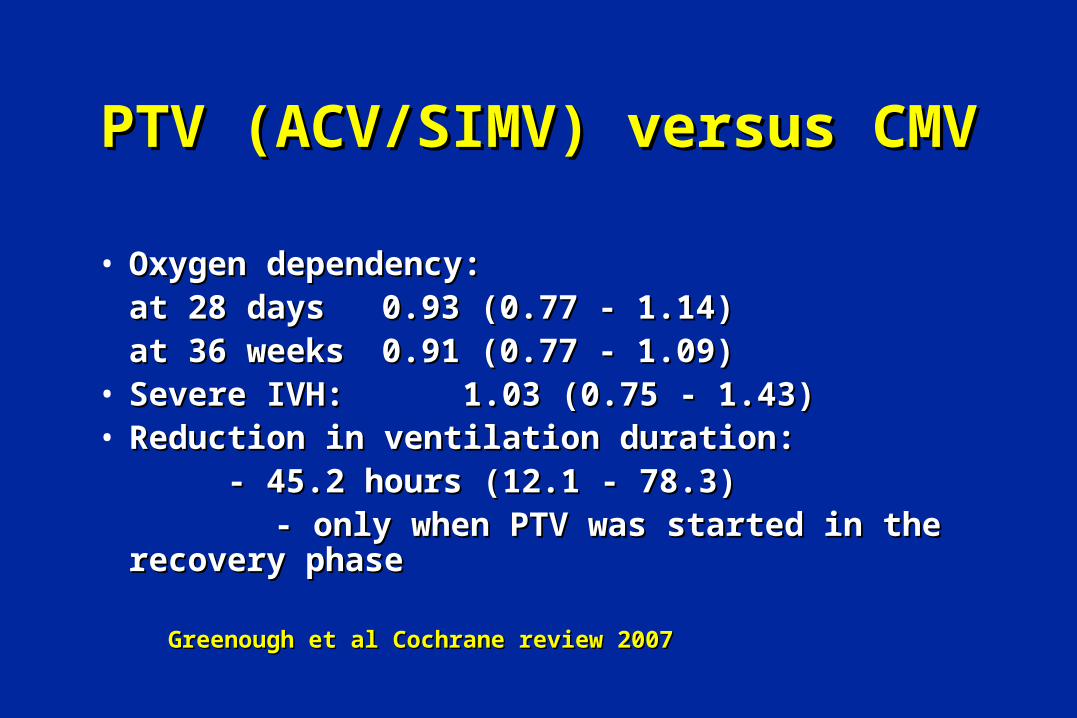
PTV (ACV/SIMV) versus CMVPTV (ACV/SIMV) versus CMV
• Oxygen dependency:Oxygen dependency:at 28 days at 28 days 0.93 (0.77 - 1.14)0.93 (0.77 - 1.14)at 36 weeksat 36 weeks 0.91 (0.77 - 1.09)0.91 (0.77 - 1.09)
• Severe IVH: 1.03 (0.75 - 1.43)Severe IVH: 1.03 (0.75 - 1.43)• Reduction in ventilation duration:Reduction in ventilation duration:
- 45.2 hours (12.1 - 78.3)- 45.2 hours (12.1 - 78.3) - only when PTV was started in the recovery phase - only when PTV was started in the recovery phase Greenough et al Cochrane review 2007Greenough et al Cochrane review 2007
Pressure support (PS)Pressure support (PS)
• Infant triggers an inflation which is pressure supported Infant triggers an inflation which is pressure supported at a preset levelat a preset level
• The beginning and end of inflation are triggered by the The beginning and end of inflation are triggered by the start and end of inspirationstart and end of inspiration
• Inflation is terminated when the inspiratory flow is Inflation is terminated when the inspiratory flow is reduced to a certain levelreduced to a certain level
-- 15% maximum flow (Draeger Babylog 2000 - PSV)15% maximum flow (Draeger Babylog 2000 - PSV)
-- 5-25% maximum flow (Bird VIP - termination 5-25% maximum flow (Bird VIP - termination sensitivity)sensitivity)

Randomised trial of SIMV versus Randomised trial of SIMV versus SIMV and pressure support (PS)SIMV and pressure support (PS)
• 107 infants birthweight 500-1000gms >one week107 infants birthweight 500-1000gms >one week• PS group SIMV rate reduced by 10bpm and PS PS group SIMV rate reduced by 10bpm and PS
added at 30-50% of the PIP-PEEPadded at 30-50% of the PIP-PEEP• PIP decreased to PaCO2 and Vt: 3 and 5 ml/kg PIP decreased to PaCO2 and Vt: 3 and 5 ml/kg • SIMV reduced to keep between 40-65mmHgSIMV reduced to keep between 40-65mmHg
Reyes et al Pediatr 2006Reyes et al Pediatr 2006

Randomised trial SIMV versus Randomised trial SIMV versus SIMV + PSSIMV + PS
all infants 700-1000all infants 700-1000 SIMV PS p SIMV PS pSIMV PS p SIMV PS pAge at finalAge at finalextubation (days) 44 35 .91 29 24 .366extubation (days) 44 35 .91 29 24 .366IPPV (days) 34 22 .18 25 15 .118IPPV (days) 34 22 .18 25 15 .118IPPV 28 days (%) 69 47 IPPV 28 days (%) 69 47 .04 .04 53 30 .116 53 30 .116OO22 at 36wks (%) 48 33 .21 58 38 .142 at 36wks (%) 48 33 .21 58 38 .142
OO2 2 ((days)days) 72 49 .11 86 58 72 49 .11 86 58 .034.034

Work of breathing during SIMV Work of breathing during SIMV with and without pressure supportwith and without pressure support
20 infants mean gestational age 31 weeks, being 20 infants mean gestational age 31 weeks, being weaned from mechanical ventilationweaned from mechanical ventilation
SIMV SIMV + PS pSIMV SIMV + PS pPTP 141 (93) 112 (85) <0.001PTP 141 (93) 112 (85) <0.001PaOPaO2 8.6 (2.6) 8.5 (1.8) 0.782 8.6 (2.6) 8.5 (1.8) 0.78
PaCOPaCO22 5.9 (1.3) 6.0 (1.6) 0.55 5.9 (1.3) 6.0 (1.6) 0.55Resp rate 64 (13) 55 (11) 0.001Resp rate 64 (13) 55 (11) 0.001 Patel et al ADC 2009Patel et al ADC 2009

Volume targeted ventilationVolume targeted ventilation
• No significant reduction in death or death and BPDNo significant reduction in death or death and BPD• Reduced duration of ventilation 2.39 daysReduced duration of ventilation 2.39 days• Reduced pneumothoraces RR 0.23Reduced pneumothoraces RR 0.23• Reduced 3-4 ICH RR 0.32Reduced 3-4 ICH RR 0.32• 4 trials identified – 178 infants4 trials identified – 178 infants
McCallion et al Cochrane database 2005McCallion et al Cochrane database 2005
Volume targeted ventilationVolume targeted ventilation
• Volume supportVolume support – desired volume is selected, the duration of – desired volume is selected, the duration of inflation depends on the time taken for the volume to be deliveredinflation depends on the time taken for the volume to be delivered
Bird VIPBird VIP• Volume limitedVolume limited – pressure support for any inflation is aborted if – pressure support for any inflation is aborted if
the measured volume exceeds the preset upper limitthe measured volume exceeds the preset upper limit SLE 5000, Bearcub 750SLE 5000, Bearcub 750• Volume guaranteeVolume guarantee – preset expiratory tidal volume is delivered, – preset expiratory tidal volume is delivered,
but the preset Ti determines the duration of inflationbut the preset Ti determines the duration of inflation Draeger BabylogDraeger Babylog• Volume controlledVolume controlled – constant flow during inspiration – the – constant flow during inspiration – the
required volume is delivered over the Tirequired volume is delivered over the Ti StephanieStephanie

Delivery depends on ventilator type Delivery depends on ventilator type
• Draeger positive pressure plateauDraeger positive pressure plateau• Stephanie pressure increasing till Ti terminationStephanie pressure increasing till Ti termination• SLE and VIP Bird inflation terminating when the volume SLE and VIP Bird inflation terminating when the volume
was deliveredwas delivered• At the same settings – different MAP delivery At the same settings – different MAP delivery
Sharma et al Acta Ped 2006Sharma et al Acta Ped 2006
Impact of VG on COImpact of VG on CO22 tensions tensions
• Randomised trial of 40 infants 27 weeks Randomised trial of 40 infants 27 weeks gestationgestation
• SIMV +/-VG 4mls/kgSIMV +/-VG 4mls/kg
• In infants > 25weeks VG halved the In infants > 25weeks VG halved the incidence of hypocarbiaincidence of hypocarbia
• Ineffective in infants <26 weeks GAIneffective in infants <26 weeks GA
Cheema et al EHD 2006Cheema et al EHD 2006

Volume controlled vs pressure limitedVolume controlled vs pressure limited
• Randomised trial - 90 infants BW 600 to 1500gms, GA Randomised trial - 90 infants BW 600 to 1500gms, GA 24 –32 wks24 –32 wks
• Bird VIP, volume controlled (VC) or pressure limited Bird VIP, volume controlled (VC) or pressure limited • Success criteria oxygenation/MAP reached at 23 hrs VC Success criteria oxygenation/MAP reached at 23 hrs VC
versus 33 hrs (p=0.15) (BW<1000gms p=0.03)versus 33 hrs (p=0.15) (BW<1000gms p=0.03)• No significant differences in other outcomesNo significant differences in other outcomes Singh et al J Pediatr 2006Singh et al J Pediatr 2006• VT 4-6mls/kg VT 4-6mls/kg

VG level and work of breathingVG level and work of breathing
20 infants mean GA 28 weeks (10 ACV; 10 SIMV)20 infants mean GA 28 weeks (10 ACV; 10 SIMV)
PTP levels at VG levels of 4, 5 and 6 mls/kgPTP levels at VG levels of 4, 5 and 6 mls/kg
VG level ACV SIMV VG level ACV SIMV
0 144 (47) 173 (88)0 144 (47) 173 (88)
4 203 (82) 237 (100) 4 203 (82) 237 (100)
5 168 (59) 180 (78)5 168 (59) 180 (78)
6 135 (47) 147 (51)6 135 (47) 147 (51)
Patel et al Pediatr 2009Patel et al Pediatr 2009

Prophylactic HFOProphylactic HFO
13 published prophylactic trials ( < 12 hours) 13 published prophylactic trials ( < 12 hours) • BPD at 36 weeks PMA or discharge in survivorsBPD at 36 weeks PMA or discharge in survivors RR 0.88 (0.79 – 0.99)RR 0.88 (0.79 – 0.99)• Death by 36 weeks PCADeath by 36 weeks PCA RR 0.98 (0.83 – 1.16)RR 0.98 (0.83 – 1.16)• Death or BPD at 36 weeks PMA or dischargeDeath or BPD at 36 weeks PMA or discharge RR 0.92 (0.85-1.00)RR 0.92 (0.85-1.00)• Pulmonary airleak RR 1.14 (1.00-1.29)Pulmonary airleak RR 1.14 (1.00-1.29)• 3-4 IVH RR 1.11 (0.95-1.1.3)3-4 IVH RR 1.11 (0.95-1.1.3)• PVL RR 1.10 (0.84-1.44)PVL RR 1.10 (0.84-1.44)

UKOS TrialUKOS Trial• Infants between 23 weeks and 28 +6 weeks gestational Infants between 23 weeks and 28 +6 weeks gestational
age, CMV or HFOV within 60 minutes of birthage, CMV or HFOV within 60 minutes of birth
CMVCMV HFOHFO
nn 397397 400400
DiedDied 26%26% 25%25%
Survived OSurvived O22
dependant at 36 weeksdependant at 36 weeks 41%41% 41%41%
AirleakAirleak 18%18% 16%16%
Cerebral abnormalityCerebral abnormality 25%25% 17%17%
Johnson et al NEJM 2002Johnson et al NEJM 2002

Pulmonary function at one year Pulmonary function at one year
Means and 95% CI of the differences in the means:Means and 95% CI of the differences in the means:
CMV HFOV (95%CI diff)CMV HFOV (95%CI diff)
Respiratory rate (bpm) 31.2 33.9 (-6.1,0.7)Respiratory rate (bpm) 31.2 33.9 (-6.1,0.7)
TGV (mls/kg) 26.9 26.5 (-2.5,3.4)TGV (mls/kg) 26.9 26.5 (-2.5,3.4)
FRC (mls/kg) 24.1 23.5 (-2.1,3.2)FRC (mls/kg) 24.1 23.5 (-2.1,3.2)
FRC:TGV 0.90 0.90 (-0.06,0.06)FRC:TGV 0.90 0.90 (-0.06,0.06)
Resistance (cmHResistance (cmH22O/l/s) 33 34 (-8,6) O/l/s) 33 34 (-8,6)
Thomas et al ARJCCM 2003Thomas et al ARJCCM 2003
908070605040
2
1
0
-1
-2
-3
-4
-5
V’ m
axF
RC
z-s
core
Crown-heel length (cm)
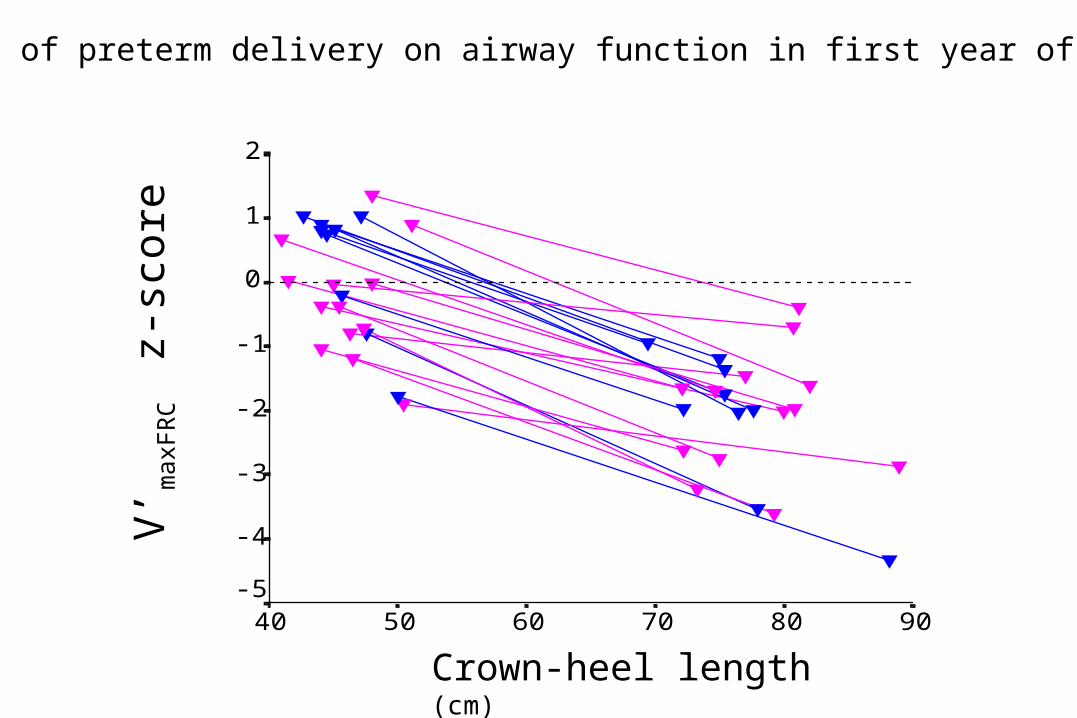
Effect of preterm delivery on airway function in first year of life
Worsening V’Worsening V’maxFRC in infants with BPDmaxFRC in infants with BPD
• 36 infants mean birthweight 837 (152) gms and 36 infants mean birthweight 837 (152) gms and gestational age 26.8 (1.7) gmsgestational age 26.8 (1.7) gms
• BW < 1250gms, IPPV>7 days, BPDBW < 1250gms, IPPV>7 days, BPD• Initial ventilation: IPPV or HFOV in the youngest and Initial ventilation: IPPV or HFOV in the youngest and
smallest infantssmallest infants• Evaluated at 6 and 12 monthsEvaluated at 6 and 12 months• Maximum flow at functional residual capacityMaximum flow at functional residual capacity (V’(V’maxFRCmaxFRC)) Hofhuis et al AJRCCM 2002Hofhuis et al AJRCCM 2002


Mechanical ventilation versus CPAPMechanical ventilation versus CPAP
Current evidence:Current evidence:• High volume HFO reduces BPD, but whether it High volume HFO reduces BPD, but whether it
improves long term lung function requires follow-up improves long term lung function requires follow-up of infants entered into RCTs of infants entered into RCTs
• Weaning is best by modes supporting every breath Weaning is best by modes supporting every breath
– –whether ACV or PSV is better merits testingwhether ACV or PSV is better merits testing• Severe respiratory distress – a trial of rescue HFOV Severe respiratory distress – a trial of rescue HFOV
with long term outcomes is neededwith long term outcomes is needed• CPAP as the preferred mode?CPAP as the preferred mode?
Related Documents











