Measuring the Patient Experience in a Medical Home QI/PCMH Roundtable March 14, 2013, Seattle, WA

Measuring the Patient Experience in a Medical Home QI/PCMH Roundtable March 14, 2013, Seattle, WA.
Dec 15, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Measuring the Patient Experience in a Medical Home
QI/PCMH Roundtable
March 14, 2013, Seattle, WA

Radical Patient Centeredness
• (1) “The needs of the patient come first.”– Mayo Clinic
• (2) “Nothing about me without me.”– IHI
• (3) “Every patient is the only patient.”– Harvard Community Health Plan Hospital

Why Focus on Patient-Centered Interactions?
• Without a deliberate focus on integrating the patient’s perspective and the patient and families desires/goals, practice changes may create efficiency, but miss entirely the changes that would have come from patients’ experience of care.
• Without involving patients and family members in quality improvement, we are only guessing at what they want and need.

The “big ASK”: routinely asking patients about their experience of care to guide teams in the improvement and redesign aspects of achieving patient-centered medical home-ness
Methods to capture our patients’ experiences
• Regularly host focus groups• Have patient representatives on the improvement team• Ask patients about their experience at the point of service• Routinely conduct patient surveys and review the results
immediately

Radical Patient Centeredness
A never-ending inquiry to those we serve:
• “What do you want and need?”
• “What is your way?”
• “How am I doing at meeting your needs?”
• “How could I do that better?”
• “How can I help you?”

Patient-centered care as a quality dimension.
• Ask the following question at the end of most interactions:
“Is there anything at all that could have gone better today from your point of view in the care you experienced?”
And then, listen and learn.
• For quantitative ratings, ask patients to rate on a 1–5 scale disagreement to agreement with the assertion:
“They gave me all the care I needed and wanted, exactly when and how I needed and wanted it.” Seek 5s and study the low raters.
L. Gordon Moore, MD

Data for Improvement, Accountability, Research
Aspect Improvement Accountability Research
Aim Improvement of care
Comparison, choice, reassurance
New knowledge
Test Observability
Test observations Evaluate current performance; no test
Test blinded
Bias & Sample Size
Consistent bias – just enough data
Measure and adjust to reduce bias – 100% of data
Design to eliminate bias – just in case data
Flexibility of hypothesis
Improvement of care
No hypothesis Fixed hypothesis
Testing strategy Sequential tests No tests 1 test
Is change an improvement?
Run or control charts
No change focus Hypothesis tests (F-test, T-test, Chi-squared, P-value)
Confidentiality of data
Only used by those involved in improvement
Available for public consumption
Identities protectedTammy Fisher, MPH
Director, Quality & Performance Improvement
San Francisco Health Plan
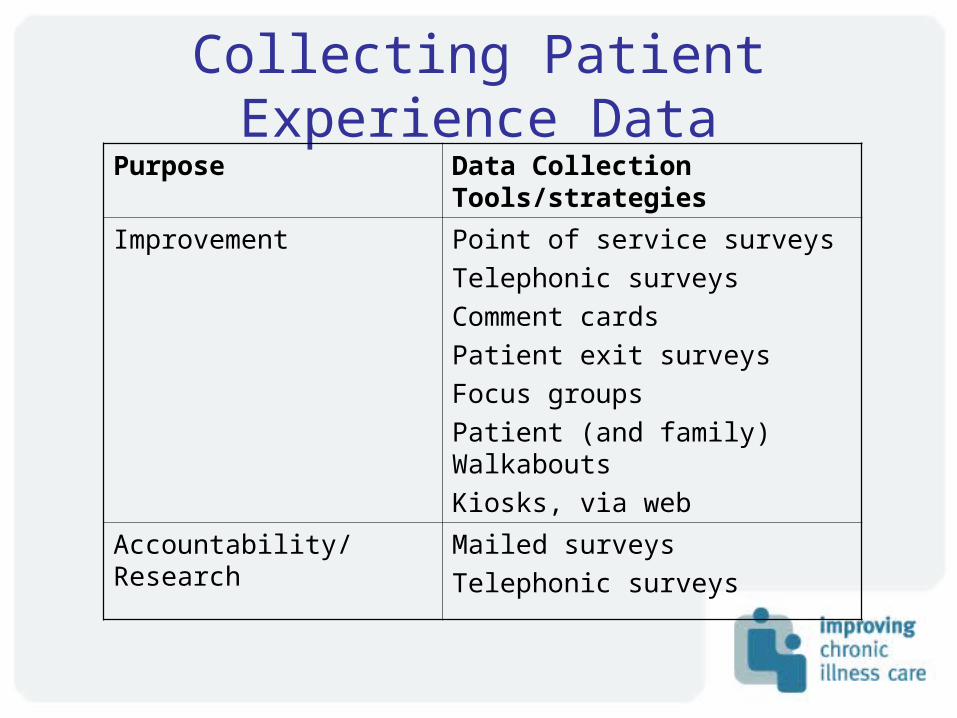
Collecting Patient Experience DataPurpose Data Collection
Tools/strategies
Improvement Point of service surveys
Telephonic surveys
Comment cards
Patient exit surveys
Focus groups
Patient (and family) Walkabouts
Kiosks, via web
Accountability/Research Mailed surveys
Telephonic surveys

Common Reasons for Using an Existing Instrument
• So normative comparisons can be made (benchmarking)
• To replicate or maintain continuity with previous studies
• Existing measure is state-of-the-art
• The time and expense of developing new measure is prohibitive

Examples of Existing Patient Experience Surveys
• CAHPS (consumer assessments of health plans survey)– http://www.cahps.ahrq.gov
• PCAT (primary care assessment tool)– http://www.jhsph.edu/pcpc/pca_tools.html– Cassady CE et al., Pediatrics (J Ambul Pediatr Assoc) 2000;105:998-
1003.• ACES (ambulatory care experience survey)
– http://160.109.101.132/icrhps/resprog/thi/aces.asp– Safran DG et al., Medical Care. 1998. 36 (5):728-739.
• IPC (interpersonal processes of care): – Stewart et al., Health Serv Res. 2007 June; 42(3 Pt 1): 1235–1256.
• PACIC (patient assessment of chronic illness care):– http://www.improvingchroniccare.org/index.php?p=PACIC_Survey&s=36– Glasgow RE, et al., Med Care 2005; 43(5):436-44

Approaches to measuring patient experience with care
• Patient surveysPatient surveys– Proprietary toolsProprietary tools– Public domain instruments (CAHPS)Public domain instruments (CAHPS)
• Focus groups and interviewsFocus groups and interviews
• WalkthroughsWalkthroughs
• ““Mystery shopping”: participant Mystery shopping”: participant observation by trained informantsobservation by trained informants
• Web-based user-generated reviewsWeb-based user-generated reviews

Sampling Issues• Patient populationPatient population
– General population General population – Specific subgroups (e.g., chronic illness)Specific subgroups (e.g., chronic illness)
• TimeframeTimeframe– Visit-basedVisit-based– Over the prior 6 or 12 monthsOver the prior 6 or 12 months
• FrequencyFrequency– Annual monitoringAnnual monitoring– Continuous sampling for improvementContinuous sampling for improvement
• Sample sizeSample size– Internal use for improvementInternal use for improvement– External use for public reporting, P4PExternal use for public reporting, P4P

Traditional Data Collection Modes
• Mail administrationMail administration– 3 waves of mailing (initial mail, postcard 3 waves of mailing (initial mail, postcard
reminder, second mail)reminder, second mail)
• Telephone administrationTelephone administration– At least 6 attempts across different days of At least 6 attempts across different days of
the week and times of daythe week and times of day
• Mixed mail and telephone administrationMixed mail and telephone administration– Boost mail survey response by adding Boost mail survey response by adding
telephone administrationtelephone administration

Alternative Modes• Internet/WebInternet/Web
– Email distributionEmail distribution– Web response optionWeb response option
• Interactive Voice Response (IVR)Interactive Voice Response (IVR)– Touchtone IVRTouchtone IVR– Active Voice IVRActive Voice IVR
• In-office distributionIn-office distribution– Paper surveyPaper survey
• Mail returnMail return• Internet returnsInternet returns• Drop box on siteDrop box on site
– Kiosk or other electronic modesKiosk or other electronic modes

Comparison of Mail, Web, and IVR ModesMailMail WebWeb Web + Web +
MailMailIVRIVR IVR + IVR +
MailMail
Response RatesResponse Rates 50.8%50.8% 18.4%18.4% 48.6%48.6% 34.7%34.7% 53.7%53.7%
Respondent Respondent Characteristics*Characteristics*
YoungerYounger
More edMore ed
HealthierHealthier
Less edLess ed
Less Less ethnicethnic
More useMore use
Survey Scores*Survey Scores*
(adjusted and (adjusted and unadjusted)unadjusted)
SameSame SameSame LowerLower LowerLower
Total CostsTotal Costs
(per completed (per completed response)response)
$5.19$5.19 $13.94$13.94 $8.01$8.01 $9.04$9.04 $8.06$8.06
Rodriguez, et al. Evaluating Patients’ Experiences with Individual Physicians. Medical Care. Vol. 44, No. 2, February 2006.

Cultural Competence Missing from CAHPS
• Communication: – Use of complementary and alternative medicine – Respect for Patient Preferences/Shared Decision-
making: Empathy and emotional support– Linguistic Competency: Access to language services;
Health literacy aspects – Experiences Leading to Trust/Distrust: Level of trust,
caring, truth-telling– Experiences of Discrimination: Due to race/ethnicity,
insurance, language, etc.

Point of Service – Good for measuring the effect of changes
tested– Focus on meaningful measures – Document collection methodology; train staff
collecting information– Collect “just enough” data – Have at least 15 completed surveys – Easy to develop reports – Data collection is burdensome!
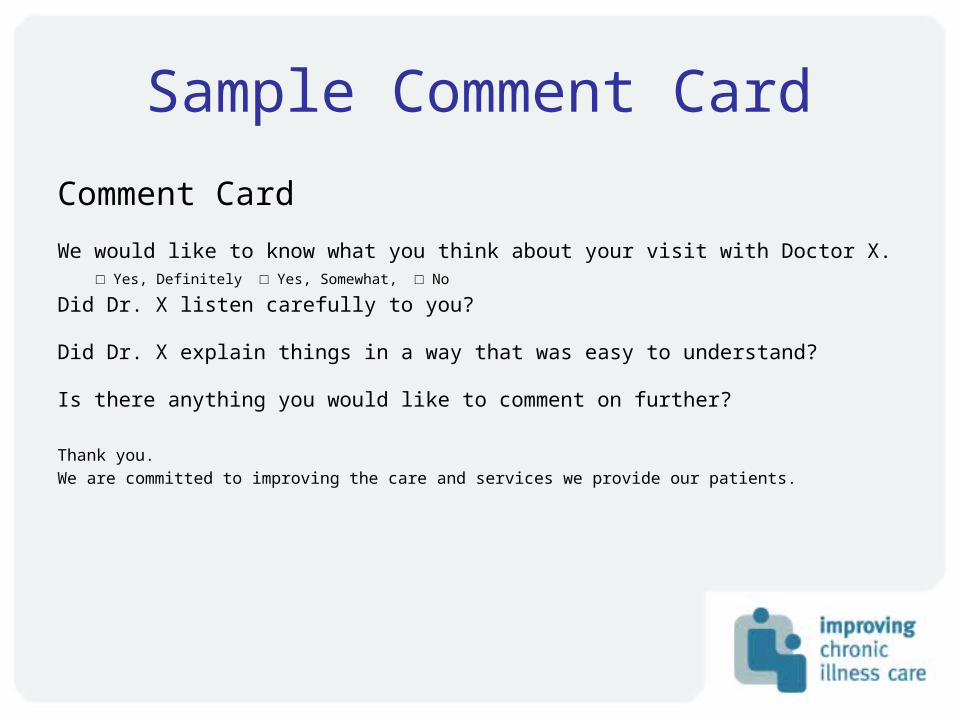
Sample Comment Card
Comment Card
We would like to know what you think about your visit with Doctor X. □ Yes, Definitely □ Yes, Somewhat, □ No
Did Dr. X listen carefully to you?
Did Dr. X explain things in a way that was easy to understand?
Is there anything you would like to comment on further?
Thank you.
We are committed to improving the care and services we provide our patients.

Telephonic Surveys
Good for measuring the effect of changes • More rapid feedback than mailed surveys• Typically less expensive• Outside vendors do it and provide reports • Easy to manipulate data for reporting • Less frequent – monthly data at best

Patient Exit Interviews
• Rapid feedback on changes tested• Not burdensome to collect data• Uncover new issues which may go unreported in
surveys• Requires translation of information into
actionable behaviors • Providers “see” the feedback • Include 3-5 questions, mix of specific measures
and open ended questions• Receptionist or non-clinic member obtains
feedback (HP or IPA staff)

What is patient-centered care?““Health care that establishes a Health care that establishes a
partnership among practitioners, partnership among practitioners, patients, and their familiespatients, and their families…to ensure …to ensure that decisions that decisions respect patients’ wants, respect patients’ wants,
needs, and preferencesneeds, and preferences and that and that patients have the patients have the education and education and
supportsupport they need to they need to make decisions make decisions and participateand participate in their own care.”in their own care.”
Institute of Medicine. Envisioning the National Health Care Quality Report. Washington, DC: National Academy Press: 2001.


Self-management Support Stepsto Build Skills and Confidence
Adequate for majority of population
Basic Skills
Goal SettingAction PlanningProblem Solving
Advanced Skills & Techniques
Motivational Interviewing
Uncomplicated Depression
Group Interactions
Training others in Basics
Expert Skills & Techniques
Ex: Cognitive Behavioral Therapy
Dialectical Behavioral Therapy
Addresses special situations
Necessary for special populations (Addictions, MH)
Source: Connie Davis. RNP

The CareSouth Carolina Elements of SMS in the Stepped Model
• Care Teams with roles and responsibilities for SMS throughout the team
• Care Managers for higher levels of need
• Standardization of group and individual learning needs
• Patient focus groups for re-design



Reliability Data for SMG Set
0102030405060708090
100
Jan
Feb
Mar
ch AprM
ayJu
ne
% SMG Set

THE PATIENT PARTNER PROJECTBetsy Stapleton, FNP & Jessica
Osborne-Stafsnes

“The process of becoming an intelligent partner in the health process can be hard for people.”
-- Toni M.

• Humboldt County AF4Q Alliance; Part of RWJF’s “Aligning Forces for Quality”
• Humboldt Focus: to generate meaningful opportunities for patient engagement in healthcare improvement, delivery, and design.
About Aligning Forces Humboldt
www.aligningforceshumboldt.org

Patient Engagement in Humboldt County, Ca
HDNIPA participates in the IHI
“Quality Allies” Project
2005-2006
2007AF4Q initiative begins,
citing patient engagement
as a key driver of quality improvement
Implementation of the Chronic
Disease Self-Management Program (CDSMP)
2008
2009HDNIPA adopts collaborative
model to improve
primary care called:
Primary Care Renewal (PCR);
10 PCP practices participate
CDSMP leaders act as faculty at PCR
meeting to discuss the patient
perspective of living with a
chronic health condition
2009
2011PCR 2.0 launches with an emphasis
on PCMH.Recruitment of a “patient partner” team member is a
requirement of participation.
Significant infrastructure is built to support
this effort.
PCR 3.0 kicks-off.Practices must
recruit two patient partners to participate.
Patients participate in
collaborative and office
improvement meetings.
2012
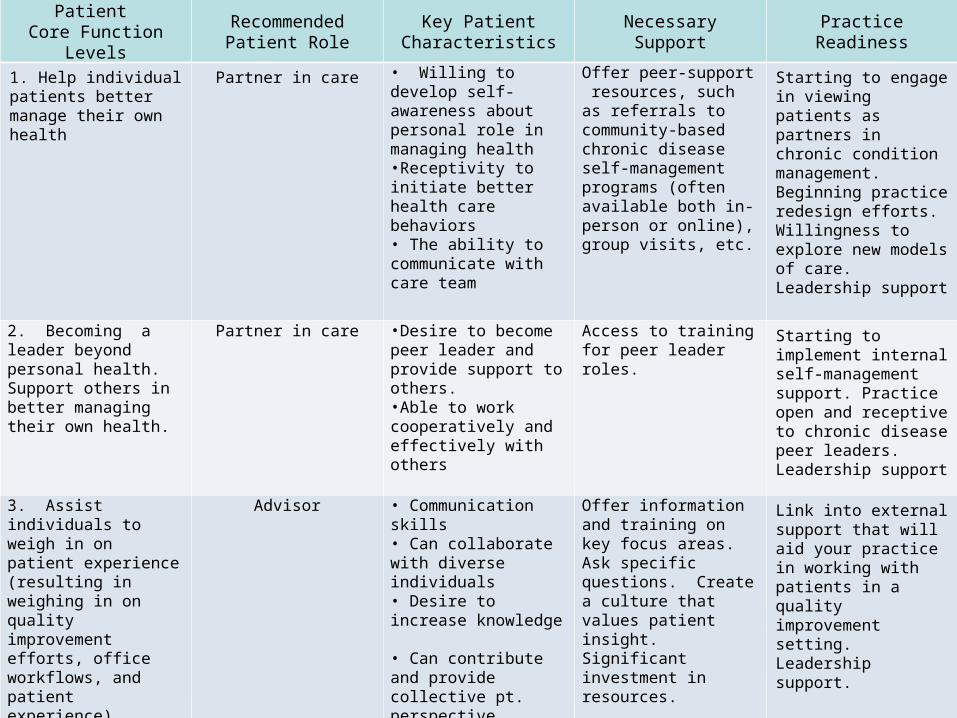
Patient Core Function Levels
Recommended Patient Role
Key Patient Characteristics
Necessary Support Practice Readiness
1. Help individual patients better manage their own health
Partner in care • Willing to develop self-awareness about personal role in managing health•Receptivity to initiate better health care behaviors• The ability to communicate with care team
Offer peer-support resources, such as referrals to community-based chronic disease self-management programs (often available both in-person or online), group visits, etc.
Starting to engage in viewing patients as partners in chronic condition management. Beginning practice redesign efforts. Willingness to explore new models of care. Leadership support
2. Becoming a leader beyond personal health. Support others in better managing their own health.
Partner in care •Desire to become peer leader and provide support to others.•Able to work cooperatively and effectively with others
Access to training for peer leader roles.
Starting to implement internal self-management support. Practice open and receptive to chronic disease peer leaders. Leadership support
3. Assist individuals to weigh in on patient experience (resulting in weighing in on quality improvement efforts, office workflows, and patient experience).
Advisor • Communication skills• Can collaborate with diverse individuals • Desire to increase knowledge • Can contribute and provide collective pt. perspective comfortably• Focused on improving care related to the team goals
Offer information and training on key focus areas. Ask specific questions. Create a culture that values patient insight. Significant investment in resources.
Link into external support that will aid your practice in working with patients in a quality improvement setting. Leadership support.
4. Foster and support champion patients as equal core members of committees that drive redesign efforts at the highest levels
Advisor and Champion •Skills listed above and:•Can articulate pt. insight and bring pt. feedback to the forefront • Functions in a fast-paced and technical setting• Problem-solves in inclusive ways
Create roles for a patient/patient advocate on committees. Solicit patient feedback. Offer educational and training opportunities. Significant investment in resources.
Link into external support that will aid your practice in working with patients in a quality improvement setting.Leadership support.
(Stapleton & Osborne-Stafsnes, 2011)
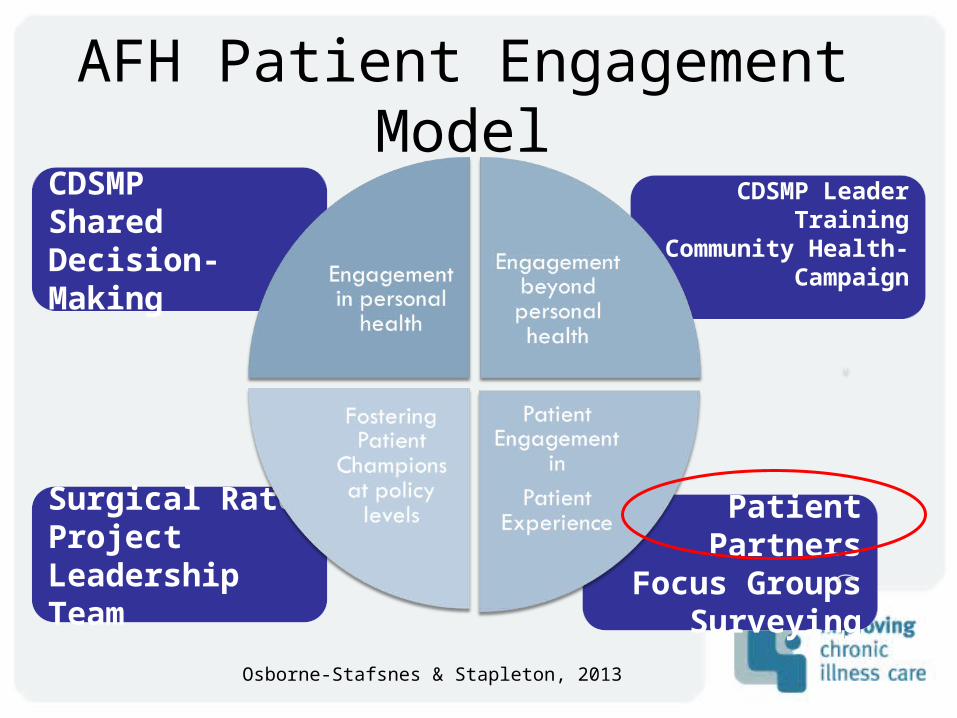
CDSMPShared Decision- Making
AFH Patient Engagement Model
Patient Partners
Focus GroupsSurveying
Surgical RateProjectLeadership Team
CDSMP Leader Training
Community Health- Campaign
Osborne-Stafsnes & Stapleton, 2013

The Patient Partner Project
“Practices often struggle with the 'fires' of the day , making it difficult to focus on larger constructs such as patient-centered care. The participation of Patient Partners on practice improvement teams keeps the importance of improving patient care at the forefront of discussion.”– Rosemary DenOuden, Chief Operating Officer, HDNIPA
Primary Care Renewal
QI collaborative •10 Practices/20 Patient Partners •Collaborative meetings every two months•Practice meetings 2X/month•Each team is assigned a practice coach
•Patient Partners receive
training and support
• Ambassadors and
advocates Share insights and feedback
explicitly
focused on collaborative topics

Conceptual Framework
Stapleton & Osborne-Stafsnes for AFH, 2013

Collaborative Coaching Model
Stapleton & Osborne-Stafsnes for AFH, 2013
Practice CoachesPatient Partner Project Managers
Practice TeamPatient Partners
Effective QI Team
Collaborative Meetings
Techniques
• Standing agenda item
that starts meeting and
sets tone
• Prep patient for
presentation
• Vary presentation mode
to keep interest
• Evaluate
Patient Partner Meetings
• Introduce meeting topics and curriculum• Practice updates, brainstorming, and problem-solving• Sharing of “best-practices”• Capture patient recommendations and perspective on meeting subjects.

Team Meetings• Patients attend one “practice improvement” meeting at their office each month.
• Some offices have standing agenda items specifically for their patient partners.
• Patients offer insight and work on projects specific to the practice.Sample Projects:
•Practice brochure
• Patient-friendly
language
• Practice ombudsman
• Testing patient portals
• Process development

Challenges“As a consumer
we are often treated like we
don't know anything or the
staff
doesn’t want us involved.
They feel that staff can
represent the consumer
instead of us consumers.”
Osborne-Stafsnes & Stapleton, 2013

Addressing Challenges

Whose Home Is It?
Providing Medical Care Patient Experience
Practice
HomeDoing BusinessQI
Practice Redesign
Medical
Home
(Stapleton, 2012)
•Patient’s Home•Patient-centered
• Staff uses comprehensible
language•Ultimately, patient is in
control
• Provider/Staff home
• Office-centered• Patient
Partners learned “Medicalese”•Ultimately,
Provider/Staff are in control

Recognizing Success
“They keep our focus centered where it should be: on the patients.”
-- Participating Clinician

Recognizing Success
• Focus Groups
• Surgical Rate Project
• Empanelment
• Process Development
• Backlog reduction
“They keep our focus centered where it should be: on the patients.”
-- Participating Clinician
Foundational Engagement Elements
1. Didactic orientation and
training
2. Clear role expectations and
focus
3. Structured solicitation of
input
4. Transparent and continuing
feedback loop
An Observation: Success occurs more often when patient activation level, staff activation level, and complexity of the project align.

Tools in PCI Implementation Guidehttp://www.safetynetmedicalhome.org/practice-
transformation/implementation-guides
Thank you!
Related Documents











