ORIGINAL PAPER Ketrina A. Sly Terry J. Lewin Vaughan J. Carr Agatha M. Conrad Martin Cohen Srinivasan Tirupati Philip B. Ward Tim Coombs Measuring observed mental state in acute psychiatric inpatients Received: 12 June 2008 / Accepted: 24 July 2008 / Published online: 23 August 2008 j Abstract Background Relationships within acute psychiatric units between patient-level experiences and events and fluctuations in mental state have rarely been examined. Aim Data from a multi-centre service evaluation (11 units, 5,546 admissions) were used to examine mental state patterns and associa- tions with clinical characteristics, events and adverse incidents. Method During the 12-month evaluation period, nursing staff completed shift-level ratings using a new rating scale, the observed mental state (OMS) scale, which assessed active psychopathology (emotional distress, disinhibition, psychosis, cogni- tive impairment) and withdrawal (45,885 sets of day/ afternoon shift ratings). Results The OMS scale performed satisfactorily and is worth considering elsewhere (e.g., active psychopathology: internal consistency, a = 0.72; short-term stability, r = 0.72; sensitivity to change, adjusted standardised differ- ence, ASD = 0.71). Levels of active psychopathology were much higher on shifts in which reportable (ASD = 1.47) and less serious aggression occurred (ASD = 1.44), compared with other shifts in which pro re nata medications were also administered (ASD = 0.76), suggesting that medication usage often followed these events, and possibly that agitation and distress levels either rose rapidly or went initially unnoticed on these shifts. Although mental state im- proved steadily across the admission, one-fifth of the patients with schizophrenia received OMS psychosis ratings in the moderate to severe range during the days prior to discharge. Conclusions Observed mental state ratings were strongly linked with diagnosis and reflected key events and incidents. Routine recording using the OMS scale may assist clinical decision- making and evaluation in acute psychiatric units. j Key words aggression – inpatients – mental disorders – observation – psychiatric status rating scales Introduction Short-term hospitalisation for acute psychiatric dis- orders is a necessary component of mental health services, but change in service provision models to- wards more community-based care has been accom- panied by an increase in illness severity among presentations to hospital [10, 13]. In addition to higher rates of disruptive patients, there have been reports of overcrowding, bed availability pressures, increased patient turnover and assault rates [39], with loss of experienced mental health staff [32]. The higher thresholds now required for hospital admission [24] parallel the observed increase in illness severity among inpatients. In clinical practice, admission decisions are often centred on an assessment of the immediate risk of harm to self or others [1, 13, 24, 41], severity of K.A. Sly T.J. Lewin (&) V.J. Carr A.M. Conrad M. Cohen S. Tirupati Centre for Brain and Mental Health Research Hunter New England Mental Health University of Newcastle P.O. Box 833 Newcastle (NSW) 2300, Australia Tel.: +61-2/4924-6643 Fax: +61-2/4924-6608 E-Mail: [email protected] T.J. Lewin V.J. Carr M. Cohen S. Tirupati P.B. Ward Schizophrenia Research Institute Darlinghurst, Sydney (NSW), Australia P.B. Ward Schizophrenia Research Unit School of Psychiatry, University of NSW (Liverpool Hospital) Liverpool (NSW), Australia T. Coombs Australian Mental Health Outcomes and Classification Network NSW Institute of Psychiatry Parramatta BC (NSW), Australia Soc Psychiatry Psychiatr Epidemiol (2009) 44:151–161 DOI 10.1007/s00127-008-0427-9 SPPE 427

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
ORIGINAL PAPER
Ketrina A. Sly Æ Terry J. Lewin Æ Vaughan J. Carr Æ Agatha M. Conrad Æ Martin CohenSrinivasan Tirupati Æ Philip B. Ward Æ Tim Coombs
Measuring observed mental state in acute psychiatric inpatients
Received: 12 June 2008 / Accepted: 24 July 2008 / Published online: 23 August 2008
j Abstract Background Relationships within acutepsychiatric units between patient-level experiencesand events and fluctuations in mental state haverarely been examined. Aim Data from a multi-centreservice evaluation (11 units, 5,546 admissions) wereused to examine mental state patterns and associa-tions with clinical characteristics, events and adverseincidents. Method During the 12-month evaluationperiod, nursing staff completed shift-level ratingsusing a new rating scale, the observed mental state(OMS) scale, which assessed active psychopathology(emotional distress, disinhibition, psychosis, cogni-tive impairment) and withdrawal (45,885 sets of day/afternoon shift ratings). Results The OMS scaleperformed satisfactorily and is worth consideringelsewhere (e.g., active psychopathology: internalconsistency, a = 0.72; short-term stability, r = 0.72;sensitivity to change, adjusted standardised differ-
ence, ASD = 0.71). Levels of active psychopathologywere much higher on shifts in which reportable(ASD = 1.47) and less serious aggression occurred(ASD = 1.44), compared with other shifts in whichpro re nata medications were also administered(ASD = 0.76), suggesting that medication usage oftenfollowed these events, and possibly that agitation anddistress levels either rose rapidly or went initiallyunnoticed on these shifts. Although mental state im-proved steadily across the admission, one-fifth of thepatients with schizophrenia received OMS psychosisratings in the moderate to severe range during thedays prior to discharge. Conclusions Observed mentalstate ratings were strongly linked with diagnosis andreflected key events and incidents. Routine recordingusing the OMS scale may assist clinical decision-making and evaluation in acute psychiatric units.
j Key words aggression – inpatients – mentaldisorders – observation – psychiatric status ratingscales
Introduction
Short-term hospitalisation for acute psychiatric dis-orders is a necessary component of mental healthservices, but change in service provision models to-wards more community-based care has been accom-panied by an increase in illness severity amongpresentations to hospital [10, 13]. In addition to higherrates of disruptive patients, there have been reports ofovercrowding, bed availability pressures, increasedpatient turnover and assault rates [39], with loss ofexperienced mental health staff [32]. The higherthresholds now required for hospital admission [24]parallel the observed increase in illness severity amonginpatients. In clinical practice, admission decisions areoften centred on an assessment of the immediate riskof harm to self or others [1, 13, 24, 41], severity of
K.A. Sly Æ T.J. Lewin (&) Æ V.J. CarrA.M. Conrad Æ M. Cohen Æ S. TirupatiCentre for Brain and Mental Health ResearchHunter New England Mental HealthUniversity of NewcastleP.O. Box 833Newcastle (NSW) 2300, AustraliaTel.: +61-2/4924-6643Fax: +61-2/4924-6608E-Mail: [email protected]
T.J. Lewin Æ V.J. Carr Æ M. Cohen Æ S. Tirupati Æ P.B. WardSchizophrenia Research InstituteDarlinghurst, Sydney (NSW), Australia
P.B. WardSchizophrenia Research UnitSchool of Psychiatry, University of NSW(Liverpool Hospital)Liverpool (NSW), Australia
T. CoombsAustralian Mental Health Outcomes and Classification NetworkNSW Institute of PsychiatryParramatta BC (NSW), Australia
Soc Psychiatry Psychiatr Epidemiol (2009) 44:151–161 DOI 10.1007/s00127-008-0427-9SP
PE
427

psychosis or depression [41], or the need for intensiveassessment or observation [1, 6].
j Mental state during acute admissions
Assessment and monitoring of mental state is essen-tial in the management of psychiatric illness, and aroutine task of clinicians in acute settings. However,few studies document mental state changes acrossthe course of an admission and their relationship toother patient factors and events. Studies of inpatientfacilities often report high-risk patients needingcontainment and medication re-instatement, admittedinvoluntarily, mainly with psychotic or severe mooddisorders and a history of previous hospitalisation[1, 38, 42]. Admissions of patients with psychoticdisorders have been associated with higher symptomlevels, recent suicide attempts or self-harm, personaldisability, medication status, and alcohol consump-tion [8]. In terms of illness severity, substantialimprovements across the course of hospitalisationhave been documented using the global assessmentof functioning (GAF) scale [30], the brief psychiat-ric rating scale (BPRS) [21], and measures of insight[31].
j Factors potentially linked to mental state changes
Inter-relationships have been observed between keypatient and admission factors associated with acutepsychiatric hospitalisation, such as legal status onadmission, diagnosis, aggression, length of stay andearly re-admission [9]. However, the extent to whichthese factors impact on or are linked to mental statechanges is less clear. Aggressive behaviour tends to benoted within the first few days [5, 38] to a week ofadmission [4, 15], with increased likelihood in bipolardisorder [5], psychoses [5, 15], personality [33] andsubstance use disorders [5, 11, 33], and amongthose with previous admissions or previous violentbehaviour [14]. Patient, environment and communi-cation factors each play a role in aggression, withpsychopathology and distorted cognitions thought tobe exacerbated by setting and communication factors[28]. Cognitive impairment and increased levels ofdisability are predictive of extended hospitalisation[3, 18, 19]. Current mental state is also associatedwith length of stay, positive symptoms, psychologi-cal discomfort on admission [18] and treatmentresistant symptoms [1], all predictive of extendedstay. Symptom severity has been shown to be a reli-able indicator of length of stay [22]. Re-admissionwithin 30 days has also been linked to: previoushospitalisation [26, 37]; impaired self-care onadmission [23]; thought disorder and self-neglect ondischarge [37]; and instability in the 5 days beforedischarge [26], suggesting a strong association withmental state.
j Measurement of inpatient mental state and events
A comprehensive measurement of mental state typi-cally requires the application of standardised instru-ments by experienced clinicians, often using a mixtureof interview and self-report instruments (e.g., BPRS[40]; PANSS [20]; and GAF [2]). While these instru-ments are suitable for periodic assessments, they arenot appropriate for capturing more frequent mentalstate fluctuations within inpatient units, either becauseof inherent measurement contamination problemsassociated with repeated re-administration in a shorttime frame, or unacceptable burdens placed on patientsand clinical staff. In contrast, observation-based ap-proaches, whilst less comprehensive, are less intrusive,and may provide a useful snapshot for assessing mentalstate and measuring change, particularly where there isa reasonable sample of behaviour to observe (e.g., an 8hour nursing shift). Unfortunately, existing observa-tional measures (e.g., [17, 34]) are too detailed forroutine high-frequency usage. For the current project,we sought to use a much simpler instrument to docu-ment nurses’ shift-by-shift observations and, therefore,developed a measurement strategy that could easily beincorporated by a large number of nurses into theireveryday practice, and which required minimal train-ing or experience with standardised assessments. Theshift-based logs that were devised had the advantage ofproviding a single strategy for recording mental stateobservations and for noting other events (e.g., visitors,therapy attendance, and adverse incidents).
j Purpose of this paper
We were commissioned to undertake a multi-centreservice evaluation project to document and evaluatekey features of acute psychiatric inpatient care,including patient characteristics, adverse incidents,and short-term outcomes, as well as associations be-tween these variables and clinical and setting factors.Opportunities also arose within the project to examineshift-to-shift fluctuations in mental state and thecharacteristics of the units’ social environment. Theinitial project report [9] detailed rates of adverseinpatient incidents and other admission-level out-comes and associations. The goals of the currentpaper are twofold: (1) to describe the observationalmethods used to record fluctuations in mental state andreport profiles across the course of the admission,including associations with diagnosis; and (2) toexamine relationships between mental state andpatient-level experiences and events.
Methods
j Data sources and participants
Data for the 11 participating psychiatric units were collected from abroad array of sources, which are detailed in a Data Resources
152

Guide available from the authors, together with the main measuresused and an examination of potential data reporting biases. Theparticipating units comprised of all the acute inpatient units fromthree New South Wales catchment-based area health services andincluded eight general psychiatric units, two high dependencyunits, and one specialised unit for patients with comorbid sub-stance abuse, totalling over 74,000 bed days for the year, with anaverage occupancy rate of 88.4%.
The main data sources could be aggregated in a variety of ways(e.g., unit-level, admission-level or shift-level analyses). Shifts werelabelled by their approximate starting times (day: 7 am; afternoon:3 pm; night: 11 pm). For the analyses reported here, two main data-sets were used: an admission-level dataset, the Health InformationExchange (HIE); and a patient-level events dataset. Formal approvalfrom regional ethics committees was not required as this was a serviceevaluation project in which the primary data were routine observa-tions and ratings by clinicians within the participating services.
j Admission-level data collection
There were 5,546 admissions recorded in the HIE during the 12-month evaluation period (by 2,210 male and 1,667 female patients).For the current analyses, the main variables extracted from the HIEwere: gender and age; legal status on admission (i.e., voluntary orinvoluntary); and primary ICD-10 discharge diagnosis, which wascollapsed into seven sub-groups (schizophrenia or related, bipolar,depression, adjustment, personality, drug or alcohol, and ‘other’disorders). Two outcome variables were also derived, length ofhospital stay and early re-admission status (i.e., unplanned re-admission within 28 days of the index admission).
j Patient-level events data collection
Patient daily logs (PDLs)
At the end of each shift the nurse assigned to each patient completed aPDL, which contained ten ratings: nursing observation/care levels;contacts with mental health staff and visitors; periods of authorised orunauthorised leave; participation in structured therapy programs;usage of pro re nata (PRN) medications; legal status changes; usage ofnon-prescribed substances; ratings of aggressive/assaultive incidents;and mental state scale completion status. Up to three aggressiveincidents per patient per shift could be rated using Morrison’s eight-level hierarchy [27]. Incidents rated 5–8 (i.e., verbal threats or de-mands without a plan to inflict harm) were regarded as less serious,while those rated 1–4 (i.e., involving physical contact or a definiteintention to inflict harm) were regarded as serious or reportable [29]in that they typically required the completion of a more detailedincident report form, as per hospital policy.
Observed mental state (OMS) ratings
In the absence of suitable alternatives, the OMS scale was developedas a short observational measure of current mental state. Each ofthe five domains assessed (emotional distress, withdrawal, disin-hibition, psychosis, and cognitive impairment) included a briefdescription of the relevant behaviours or signs to be considered,followed by a simple Likert scale for rating the patient’s typicalmental state during the shift—0, unaffected; 1, mildly affected; 2,moderately affected; or 3, severely affected. A rating of 9 was givenwhen mental state could not be evaluated (e.g., patient asleep). Thechoice of OMS domains, descriptors, scales and layout was basedprimarily on consensus meetings with experienced acute care cli-nicians. There was insufficient time or resources within the projectto undertake extensive scale development and validation. More-over, given the project demands and the numbers of nursing staffinvolved, it was essential that the OMS scale was acceptable, easy tocomplete, required minimal training, and could be used on mul-tiple occasions to provide a shift-by-shift mental state profile. The
OMS scale was printed on the back of the PDL, in the 1-week-to-a-page format shown in the ‘‘Appendix’’. A user guide was developedand is included in the Data Resources Guide available from theauthors. Several hundred nurses would have completed OMS rat-ings during the audit year as there were approximately 55 nursesper shift across the participating units.
Subsets of the patient-level events data
Since the primary focus of the current analyses was on fluctua-tions between shifts, and associations with patient-level events, wereplicated the small subset of HIE variables within each record ofthe patient-level events dataset. The overall PDL dataset contained86,688 records from a subset of 3,211 (57.9%) HIE admissions.However, 6.8% of records had incomplete OMS ratings, while77.5% of night shift and 8.5% of day/afternoon shift ratings werecoded as ‘unable to assess’ (e.g., patient asleep or absent). Con-sequently, three PDL subsets were identified for different analyses:an ‘on admission’ subset comprising all day/afternoon shift re-cords from the first 2 days; an ‘admission vs. discharge’ subsetcomprising OMS ratings from day/afternoon shifts on the first 2vs. the last 2 days of admission; and an ‘overall OMS’ subset thatincluded only day/afternoon shift records with complete OMSratings.
j Statistical analyses
Data analysis techniques primarily involved SPSS statistical soft-ware (Version 14.0; SPSS, Chicago, IL, USA). Chi-square tests wereused to assess simple associations between categorical variables,while binary logistic regressions were employed when other factorswere also taken into account, with adjusted odds ratios (AORs) asthe preferred reporting metric. Analysis of co-variance (ANCOVA)-based techniques were typically used to assess group differences onthe continuous variables, and patterns of change across the courseof the admission, with Scheffe follow-up comparisons, as required.Considering the relatively large sample sizes, and as a partialcontrol for the number of statistical tests, the threshold for sig-nificance was set at P < 0.001. For several analyses, adjustedstandardised differences (ASDs) are also reported (e.g., the mag-nitude of the change between admission and discharge, afteradjusting for the selected covariates, and expressed in effect sizeunits—using as a reference value the grand standard deviation ofratings for each OMS domain).
Results
j Sample biases and characteristics
An analysis of PDL completion rates revealed mod-erate associations with discharge diagnosis, length ofstay, and selected unit characteristics. The overallPDL completion rate was 42.3%. Higher completionrates were obtained for patients with bipolar disorder,compared to the ‘other disorders’ category (44.0 vs.35.9%), suggesting that nursing staff were more likelyto notice the behaviours of these patients, who alsodisplayed increased rates of less serious aggression[9]. Nursing staff were also less likely to completePDLs for patients hospitalised for 2 days or less, rel-ative to the other length of stay subgroups (33.6 vs.43.0%). In addition, unit characteristics accounted forapproximately 17.0% of the variance in PDL com-pletion rates, with units with more beds, higher
153
occupancy, and less experienced nursing staffrecording lower completion rates.
Based on PDLs completed within the first 2 days, thesample was predominantly male (56.4%), with the fol-lowing age distribution: under 25, 19.2%; 25–39, 45.7%;40–54, 23.9%; and >54 years, 11.2%. Legal status wasevenly distributed (51.7% involuntary), while length ofstay averaged 15.50 days (SD = 19.56, median = 9days). Schizophrenia (36.1%) was the most frequentprimary diagnosis, followed by depression (17.4%),bipolar (15.0%), drug/alcohol (10.7%), adjustment(7.9%), personality (6.0%), and other disorders (6.8%).Almost all patients received some form of therapeuticcontact each shift from nursing staff (97.0%), with lessfrequent contacts from medical staff (29.7%) and alliedhealth staff (2.5%). Approximately one-fifth of PDLsrecorded PRN medication usage (21.5%) or attendanceof visitors (21.3%), while participation in structuredtherapy programs was extremely low (3.1%). The like-lihood of a reportable (0.6%) or less serious aggressiveincident (4.0%), or an absconding incident (1.4%)occurring was relatively low for any given patient onany given shift during the first 2 days.
j Mental state scale (OMS) characteristics
There was a relatively high endorsement rate for theOMS ‘unaffected’ category (i.e., 59.3% across all ratings).In effect, the nursing staff viewed the behaviours ofindividual patients against the general backdrop of ex-pected behaviours within an acute inpatient setting, ra-ther than rating in terms of absolute levels ofpsychopathology, often scoring the patient on only oneof the five domains. For example, during the first 2 days,27.6% of OMS psychosis ratings were in the moderate tosevere range, followed by 27.4% for emotional distress,20.5% for withdrawal, 14.6% for disinhibition, and10.1% for cognitive impairment. Overall, 51.4% of PDLscompleted on admission recorded at least one mentalstate domain in the moderate to severe range, with ahigher proportion among involuntary patients (61.3 vs.40.7%; v2
(1) = 190.45, P < 0.001). The correspondingrate during the 2 days prior to discharge was 24.5%.
To better understand the properties of the OMSscale, a series of factor analyses was conducted(n = 45,491 day/afternoon shift records). Both prod-uct-moment and polychoric correlations were used asinput to principal component analyses, with obliquerotations. Polychoric correlations were examined be-cause of the distributional characteristics of the OMSand to allow for the possibility that the response scalehad ordinal rather than interval features. However,both analyses produced similar two-factor solutions,accounting for 69.1 and 78.1% of the variance,respectively. The emotional distress, disinhibition,psychosis and cognitive impairment ratings hadcomparable loadings on the first factor, and wereaveraged to form an ‘active psychopathology’ score.Withdrawal was the primary scale loading on the
second factor and was retained as a single item factor.The overall correlation between active psychopathol-ogy and withdrawal was 0.18 (P < 0.001). The internalconsistency (Cronbach alpha) coefficient for activepsychopathology was 0.72. The reliability of the OMSratings was examined across adjacent days, from days1 to 3 following admission (n = 3,851 sets of pairedratings). Significant correlations (P < 0.001) betweenadjacent days, while controlling for variance due tounit, were obtained for the five domains and activepsychopathology (average correlations: emotionaldistress, 0.57; disinhibition, 0.67; psychosis, 0.74;cognitive impairment, 0.66; active psychopathology,0.72; and withdrawal, 0.62).
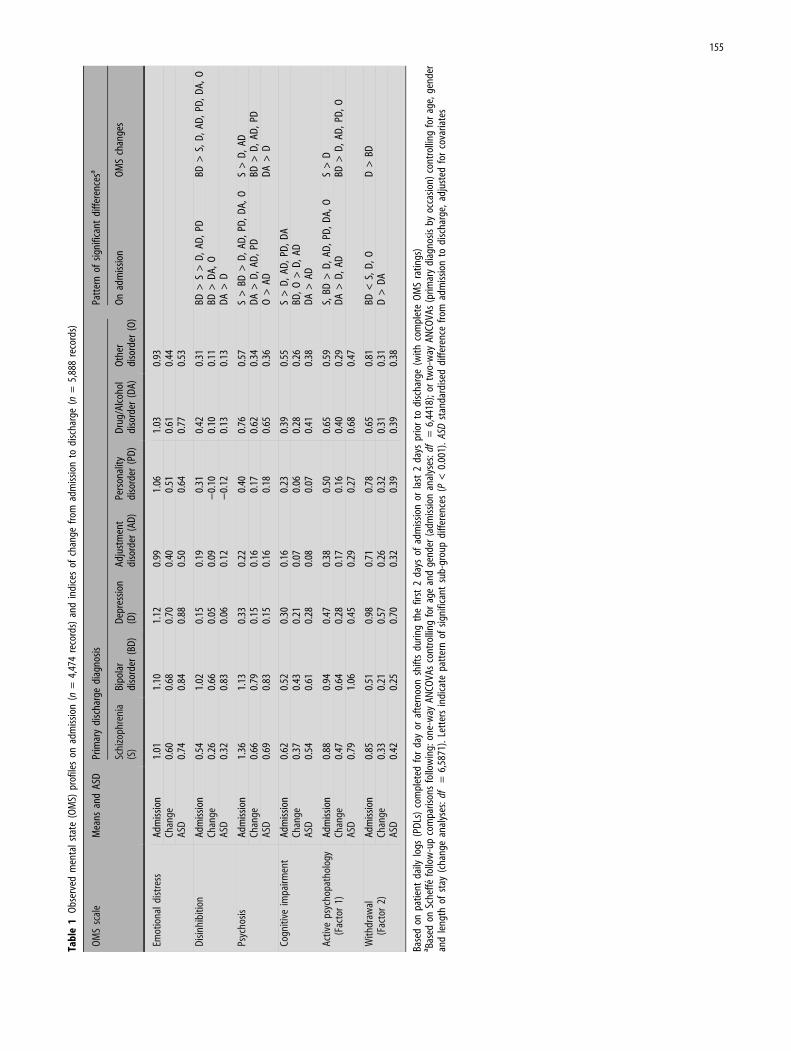
j Mental state profiles on admission
Gender and age were significantly associated with OMSratings on admission. Males were typically rated lower onemotional distress [0.96 vs. 1.14, F(1,4464) = 46.09,P < 0.001] and higher on the psychosis domain [0.94 vs.0.78, F(1,4383) = 27.23, P < 0.001]. Age group was asso-ciated with cognitive impairment [F(3,4404) = 27.15,P < 0.001], Scheffe follow-up tests revealing that pa-tients over 54 years scored higher on cognitive impair-ment than each of the younger groups (0.72 vs. 0.42).Table 1 presents a breakdown of OMS profiles by pri-mary discharge diagnosis. One-way ANCOVAs, con-trolling for age and gender, were used to examinedifferences in OMS admission profiles across diagnosticgroups. These revealed significant diagnostic associa-tions for all OMS domains except emotional distress:disinhibition [F(6,4446) = 89.49, P < 0.001]; psychosis[F(6,4376) = 166.93, P < 0.001]; cognitive impairment[F(6,4399) = 38.60, P < 0.001]; active psychopathology[F(6,4418) = 84.85, P < 0.001]; and withdrawal [F(6,4448) =22.57, P < 0.001]. Although there were no significantdifferences between diagnostic groups in emotionaldistress, the majority of patients (70.5%) exhibitedsome signs of emotional distress (i.e., OMS ratings > 0).
The second last column of Table 1 summarizes theOMS subgroup differences on admission, based onScheffe follow-up comparisons. These profiles weregenerally consistent with expectations. For example,patients with bipolar disorder displayed signifi-cantly higher levels of disinhibition than the othersubgroups, while patients with schizophrenia alsodiffered on this domain from those with depression,adjustment or personality disorders. In addition, pa-tients with a drug or alcohol disorder were moredisinhibited than those with depression. Patients withschizophrenia or bipolar disorder had the highestpsychosis scores on admission, with patients withdrug or alcohol disorders having the third highestpsychosis ratings, significantly higher than those withdepression, personality or adjustment disorders. Asshown in Table 1, cognitive impairment ratings ten-ded to be comparable for those with schizophrenia,bipolar and ‘other’ disorders, but lower among the
154
Tab
le1
Obs
erve
dm
enta
lst
ate
(OM
S)pr
ofile
son
adm
issi
on(n
=4,
474
reco
rds)
and
indi
ces
ofch
ange
from
adm
issi
onto
disc
harg
e(n
=5,
888
reco
rds)
OM
Ssc
ale
Mea
nsan
dAS
DPr
imar
ydi
scha
rge
diag
nosi
sPa
tter
nof
sign
ifica
ntdi
ffer
ence
sa
Schi
zoph
reni
a(S
)Bi
pola
rdi
sord
er(B
D)
Dep
ress
ion
(D)
Adju
stm
ent
diso
rder
(AD
)Pe
rson
ality
diso
rder
(PD
)D
rug/
Alco
hol
diso
rder
(DA)
Oth
erdi
sord
er(O
)O
nad
mis
sion
OM
Sch
ange
s
Emot
iona
ldi
stre
ssAd
mis
sion
1.01
1.10
1.12
0.99
1.06
1.03
0.93
Chan
ge0.
600.
680.
700.
400.
510.
610.
44AS
D0.
740.
840.
880.
500.
640.
770.
53
Dis
inhi
bitio
nAd
mis
sion
0.54
1.02
0.15
0.19
0.31
0.42
0.31
BD>
S>
D,
AD,
PDBD
>S,
D,
AD,
PD,
DA,
OCh
ange
0.26
0.66
0.05
0.09
)0.
100.
100.
11BD
>D
A,O
ASD
0.32
0.83
0.06
0.12
)0.
120.
130.
13D
A>
D
Psyc
hosi
sAd
mis
sion
1.36
1.13
0.33
0.22
0.40
0.76
0.57
S>
BD>
D,
AD,
PD,
DA,
OS
>D
,AD
Chan
ge0.
660.
790.
150.
160.
170.
620.
34D
A>
D,
AD,
PDBD
>D
,AD
,PD
ASD
0.69
0.83
0.15
0.16
0.18
0.65
0.36
O>
ADD
A>
D
Cogn
itive
impa
irmen
tAd
mis
sion
0.62
0.52
0.30
0.16
0.23
0.39
0.55
S>
D,
AD,
PD,
DA
Chan
ge0.
370.
430.
210.
070.
060.
280.
26BD
,O
>D
,AD
ASD
0.54
0.61
0.28
0.08
0.07
0.41
0.38
DA
>AD
Activ
eps
ycho
path
olog
y(F
acto
r1)
Adm
issi
on0.
880.
940.
470.
380.
500.
650.
59S,
BD>
D,
AD,
PD,
DA,
OS
>D
Chan
ge0.
470.
640.
280.
170.
160.
400.
29D
A>
D,
ADBD
>D
,AD
,PD
,O
ASD
0.79
1.06
0.45
0.29
0.27
0.68
0.47
With
draw
al(F
acto
r2)
Adm
issi
on0.
850.
510.
980.
710.
780.
650.
81BD
<S,
D,
OD
>BD
Chan
ge0.
330.
210.
570.
260.
320.
310.
31D
>D
AAS
D0.
420.
250.
700.
320.
390.
390.
38
Base
don
patie
ntda
ilylo
gs(P
DLs
)co
mpl
eted
for
day
oraf
tern
oon
shift
sdu
ring
the
first
2da
ysof
adm
issi
onor
last
2da
yspr
ior
todi
scha
rge
(with
com
plet
eO
MS
ratin
gs)
a Base
don
Sche
ffe
follo
w-u
pco
mpa
rison
sfo
llow
ing:
one-
way
ANCO
VAs
cont
rolli
ngfo
rag
ean
dge
nder
(adm
issi
onan
alys
es:d
f=
6,44
18);
ortw
o-w
ayAN
COVA
s(p
rimar
ydi
agno
sis
byoc
casi
on)
cont
rolli
ngfo
rag
e,ge
nder
and
leng
thof
stay
(cha
nge
anal
yses
:df
=6,
5871
).Le
tter
sin
dica
tepa
tter
nof
sign
ifica
ntsu
b-gr
oup
diff
eren
ces
(P<
0.00
1).
ASD
stan
dard
ised
diff
eren
cefr
omad
mis
sion
todi
scha
rge,
adju
sted
for
cova
riate
s
155

remaining diagnostic groups. Overall, patients with adiagnosis of schizophrenia or bipolar disorder hadhigher levels of active psychopathology, while thosewith bipolar disorder were also the least withdrawn.We also examined overall relationships betweenmental state ratings on admission, concurrent PRNmedication usage, and length of stay. Severity of OMSratings was associated with PRN administration[v2
(1) = 255.50, P < 0.001], with 32.0% of patientshaving an OMS rating in the moderate to severe rangereceiving PRN medication, compared to 12.1% per shiftamong those with less severe ratings. Patients withmore severe OMS ratings on admission also had longerhospital stays [17.95 vs. 12.87 days, F(1,4474) = 51.22,P < 0.001, controlling for age and gender].
j Mental state changes
Our primary analyses of relationships between mentalstate changes and diagnosis were based on two blocksof day/afternoon shift ratings (i.e., the first 2 vs. thelast 2 days of admission, n = 5,888 records). Conse-quently, brief admissions were excluded from theseanalyses (i.e., up to 3 days). Table 1 also reports meanOMS change profiles for each diagnostic subgroupand ASDs from admission to discharge (i.e., ‘Admis-sion’ minus ‘Discharge’, adjusted for the covariates).In this instance, two-way ANCOVAs (diagnosis byoccasion) were conducted, controlling for age, genderand length of stay. There were significant main effectsfor occasion, with scores on all OMS domainsreducing significantly: emotional distress, change =0.60, ASD = 0.76, F(1,5905) = 74.65, P < 0.001; disin-hibition, change = 0.25, ASD = 0.33, F(1,5905) = 46.08,P < 0.001; psychosis, change = 0.53, ASD = 0.56,F(1,5815) = 207.02, P < 0.001; cognitive impairment,change = 0.30, ASD = 0.45, F(1,5843) = 115.15, P <0.001; active psychopathology, change = 0.42, ASD =0.71, F(1,5871) = 1682.07, P < 0.001; and withdrawal,change = 0.34, ASD = 0.42, F(1,5905) = 160.4, P < 0.001.
The right-hand column of Table 1 details sub-group differences in change profiles, based onScheffe follow-up tests subsequent to significantoverall diagnosis by occasion interaction effects. Foremotional distress, there was no evidence of differ-ential changes in mental state by diagnosis, with anoverall ASD of 0.76 and standardised reductions of0.50 or greater for all diagnostic groups. For disin-hibition, patients with bipolar disorder had thelargest reduction (ASD = 0.83), which was signifi-cantly different from the other diagnostic groups.Three of the diagnostic groups (bipolar, schizo-phrenia, and drug/alcohol disorders) displayedstandardised reductions on the psychosis domain of0.65 or greater, with substantially smaller changesamong those with depression, adjustment or per-sonality disorder. However, many patients withschizophrenia continued to exhibit signs of psycho-sis, with 19.8% receiving OMS ratings in the mod-
erate to severe range at discharge (vs. 41.0% onadmission), compared with an average of 4.7% forall remaining diagnoses (vs. 17.7% on admission).
While the schizophrenia and bipolar disordergroups displayed reductions in cognitive impairment(with ASDs > 0.50), none of the follow-up compari-sons revealed significant differences. The largestimprovement in active psychopathology was for bipo-lar disorder (ASD = 1.06), which was significantlydifferent from depression, adjustment, personality and‘other’ disorders. The schizophrenia and drug/alcoholdisorders groups also experienced substantial reduc-tions in active psychopathology, with the schizophre-nia group differing significantly from those withdepression. The largest change on the withdrawaldomain was for patients with depression (ASD = 0.70),who differed significantly from the group with the leastchange (bipolar disorder, ASD = 0.25). In addition,there were no significant OMS differences at dischargebetween patients with and without a subsequent earlyreadmission (after controlling for age and gender), norany differences in OMS severity profiles.
Although the primary emphasis within our OMSanalyses was on associations with patient-level fac-tors and events, contextual factors such as unitcharacteristics and practices are also likely to beimportant. However, disentangling the relative con-tributions of patient and setting factors is not aneasy task. For example, approximately 7.9% of thevariance in active psychopathology ratings wasassociated with mental health unit differences(across the 11 units), although most of this (7.0%)was attributable to unit type (i.e., high dependencyvs. general vs. specialised; as opposed to individualdifferences between units), which presumably re-flects a mixture of patient characteristics, treatmentneeds, availability and practices. Figure 1 illustratesthese differences in active psychopathology profiles,as well as the improvements that typically occurprior to discharge.
0.00
0.25
0.50
0.75
1.00
1.25
1.50
> 28Days till discharge
Mea
n ac
tive
psy
chop
atho
logy
High dependencyGeneralSpecialised
Unit type:
0–12–78–1415–2122–28
Fig. 1 Changes in OMS active psychopathology ratings across days tilldischarge by unit type (n = 46,107 records from day and afternoon shifts)
156
j Inter-relationships between mental stateand shift-level events and incidents
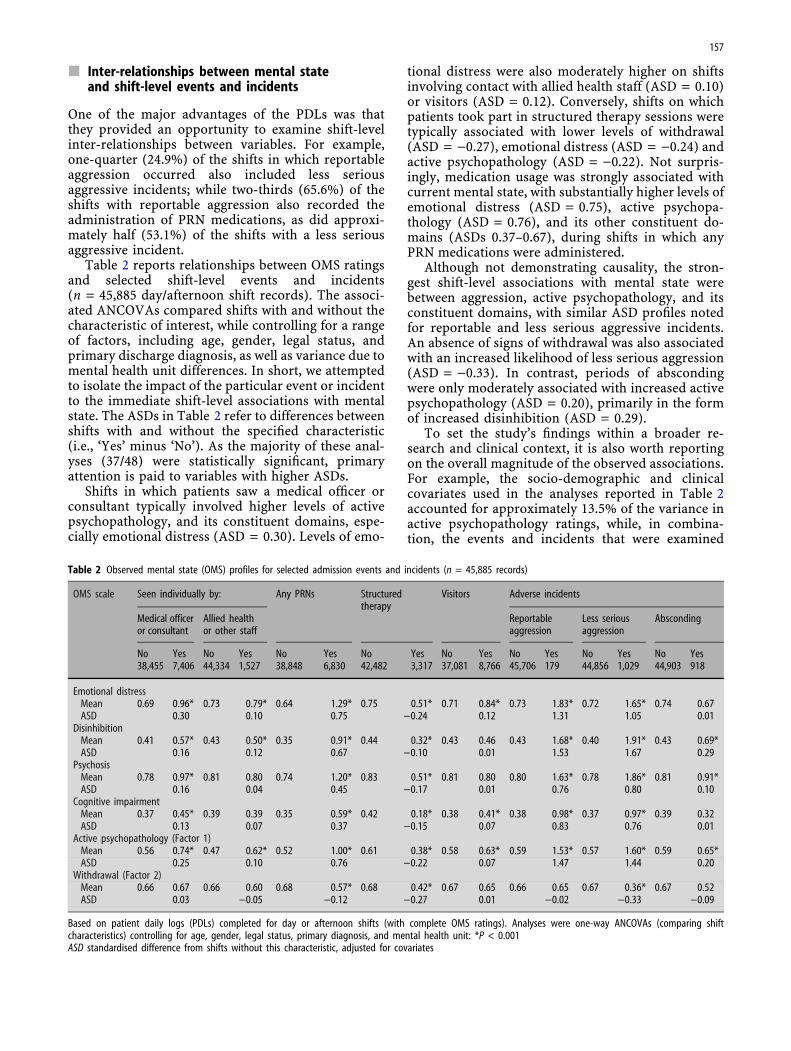
One of the major advantages of the PDLs was thatthey provided an opportunity to examine shift-levelinter-relationships between variables. For example,one-quarter (24.9%) of the shifts in which reportableaggression occurred also included less seriousaggressive incidents; while two-thirds (65.6%) of theshifts with reportable aggression also recorded theadministration of PRN medications, as did approxi-mately half (53.1%) of the shifts with a less seriousaggressive incident.
Table 2 reports relationships between OMS ratingsand selected shift-level events and incidents(n = 45,885 day/afternoon shift records). The associ-ated ANCOVAs compared shifts with and without thecharacteristic of interest, while controlling for a rangeof factors, including age, gender, legal status, andprimary discharge diagnosis, as well as variance due tomental health unit differences. In short, we attemptedto isolate the impact of the particular event or incidentto the immediate shift-level associations with mentalstate. The ASDs in Table 2 refer to differences betweenshifts with and without the specified characteristic(i.e., ‘Yes’ minus ‘No’). As the majority of these anal-yses (37/48) were statistically significant, primaryattention is paid to variables with higher ASDs.
Shifts in which patients saw a medical officer orconsultant typically involved higher levels of activepsychopathology, and its constituent domains, espe-cially emotional distress (ASD = 0.30). Levels of emo-
tional distress were also moderately higher on shiftsinvolving contact with allied health staff (ASD = 0.10)or visitors (ASD = 0.12). Conversely, shifts on whichpatients took part in structured therapy sessions weretypically associated with lower levels of withdrawal(ASD = )0.27), emotional distress (ASD = )0.24) andactive psychopathology (ASD = )0.22). Not surpris-ingly, medication usage was strongly associated withcurrent mental state, with substantially higher levels ofemotional distress (ASD = 0.75), active psychopa-thology (ASD = 0.76), and its other constituent do-mains (ASDs 0.37–0.67), during shifts in which anyPRN medications were administered.
Although not demonstrating causality, the stron-gest shift-level associations with mental state werebetween aggression, active psychopathology, and itsconstituent domains, with similar ASD profiles notedfor reportable and less serious aggressive incidents.An absence of signs of withdrawal was also associatedwith an increased likelihood of less serious aggression(ASD = )0.33). In contrast, periods of abscondingwere only moderately associated with increased activepsychopathology (ASD = 0.20), primarily in the formof increased disinhibition (ASD = 0.29).
To set the study’s findings within a broader re-search and clinical context, it is also worth reportingon the overall magnitude of the observed associations.For example, the socio-demographic and clinicalcovariates used in the analyses reported in Table 2accounted for approximately 13.5% of the variance inactive psychopathology ratings, while, in combina-tion, the events and incidents that were examined
Table 2 Observed mental state (OMS) profiles for selected admission events and incidents (n = 45,885 records)
OMS scale Seen individually by: Any PRNs Structuredtherapy
Visitors Adverse incidents
Medical officeror consultant
Allied healthor other staff
Reportableaggression
Less seriousaggression
Absconding
No Yes No Yes No Yes No Yes No Yes No Yes No Yes No Yes38,455 7,406 44,334 1,527 38,848 6,830 42,482 3,317 37,081 8,766 45,706 179 44,856 1,029 44,903 918
Emotional distressMean 0.69 0.96* 0.73 0.79* 0.64 1.29* 0.75 0.51* 0.71 0.84* 0.73 1.83* 0.72 1.65* 0.74 0.67ASD 0.30 0.10 0.75 )0.24 0.12 1.31 1.05 0.01
DisinhibitionMean 0.41 0.57* 0.43 0.50* 0.35 0.91* 0.44 0.32* 0.43 0.46 0.43 1.68* 0.40 1.91* 0.43 0.69*ASD 0.16 0.12 0.67 )0.10 0.01 1.53 1.67 0.29
PsychosisMean 0.78 0.97* 0.81 0.80 0.74 1.20* 0.83 0.51* 0.81 0.80 0.80 1.63* 0.78 1.86* 0.81 0.91*ASD 0.16 0.04 0.45 )0.17 0.01 0.76 0.80 0.10
Cognitive impairmentMean 0.37 0.45* 0.39 0.39 0.35 0.59* 0.42 0.18* 0.38 0.41* 0.38 0.98* 0.37 0.97* 0.39 0.32ASD 0.13 0.07 0.37 )0.15 0.07 0.83 0.76 0.01
Active psychopathology (Factor 1)Mean 0.56 0.74* 0.47 0.62* 0.52 1.00* 0.61 0.38* 0.58 0.63* 0.59 1.53* 0.57 1.60* 0.59 0.65*ASD 0.25 0.10 0.76 )0.22 0.07 1.47 1.44 0.20
Withdrawal (Factor 2)Mean 0.66 0.67 0.66 0.60 0.68 0.57* 0.68 0.42* 0.67 0.65 0.66 0.65 0.67 0.36* 0.67 0.52ASD 0.03 )0.05 )0.12 )0.27 0.01 )0.02 )0.33 )0.09
Based on patient daily logs (PDLs) completed for day or afternoon shifts (with complete OMS ratings). Analyses were one-way ANCOVAs (comparing shiftcharacteristics) controlling for age, gender, legal status, primary diagnosis, and mental health unit: *P < 0.001ASD standardised difference from shifts without this characteristic, adjusted for covariates
157
contributed an additional 10.7%, bringing the totalexplained variance to 24.2%. Thus, while the observedassociations are worth knowing about, most of thevariance in active psychopathology ratings wasunexplained, and presumably associated with indi-vidual differences and other illness, treatment,recovery and setting factors that were not assessed.
Discussion
j Patterns of events and incidents recordedin the shift-based logs
The socio-demographic and clinical characteristics ofthe current sample are consistent with other acuteinpatient studies [10, 37, 38, 42]. Comparisons be-tween the event and incident rates on admission andthe overall counts reported in Table 2 provide insightinto the changing demands across the course of theadmission. For example, 29.7% of patients per shiftwere seen by medical staff during the first 2 days,compared to an overall rate of 16.1%. A similar patternwas observed for PRN medication (21.5 vs. 15.0%).The rate of less serious aggression was higher onadmission, compared to the overall rate per patientper shift (4.0 vs. 2.2%). Only slightly elevated rates ofreportable aggressive incidents were observed onadmission, compared to overall (0.6 vs. 0.4%), whilethe corresponding rates for absconding were slightlylower on admission (1.4 vs. 2.0%). However, theaccumulation of these incidents across the course ofhospitalisation produced a different picture [9],revealing unacceptably high admission-level rates ofreportable aggressive incidents (11.2%), less seriousaggressive incidents (15.0%), and absconding (15.7%).
j Review of observational measures
Of necessity, the shift-based logs had to be brief,suitable for routine usage, and capable of capturingkey patient-level events and incidents, as well as coreaspects of current mental state. While clinicians aretrained to attend to changes in mental state, it doesnot necessarily follow that these are systematicallyrecorded. Here the focus was on the systematicrecording of patient-level events and behavioursacross multiple shifts, by a range of different nurseobservers. Hence, the accuracy of any given ratingmay be lower (e.g., because a particular event was notobserved), but the overall validity of the set ofobservations may be acceptable, given the timeframeover which events and behaviours are observed andtheir relevance to everyday treatment decisions.
While the psychometric properties of the OMS scalewere not formally evaluated, the findings suggest thatthe scale has adequate properties and is worth con-sidering in future studies. For example, the activepsychopathology factor demonstrated: acceptable
internal consistency (0.72); short-term stability(r = 0.72 across adjacent days); sensitivity to change(ASD = 0.71); and evidence of concurrent validity,including associations with PRN medication (ASD =0.76), reportable (ASD = 1.47) and less serious
aggression (ASD = 1.44). Mental state profiles for thedifferent diagnostic groups were strongly consistentwith expectations and showed characteristic changepatterns, providing further support for the scale’sconcurrent validity. Likewise, patients with more se-vere OMS ratings on admission had hospital stays thataveraged 5 days longer, supporting the scale’s dis-criminant validity. However, a lower threshold foridentifying and reporting psychopathology would bedesirable, to increase the proportion of ‘affected’ rat-ings. This could be achieved with more comprehensivetraining, including regular discussions with nursingstaff about the number and/or severity of the signs orbehaviours required for each level on the OMS scale.
j Mental state profiles
The mental state profiles identified in the current studywere internally coherent and broadly consistent withexpectations based on the research literature andclinical experience [21, 30]. However, during the daysprior to discharge, one-fifth of the patients withschizophrenia (19.8%) continued to receive psychosisratings in the moderate to severe range, reflecting thechronicity associated with this illness. Since OMSchange profiles would be expected to vary acrossdiagnostic groups, it may be difficult to compare indi-vidual’s day-to-day rates of improvement. Fortunately,the emotional distress ratings appear to provide auseful global index of current distress. Mean emotionaldistress scores were highest on admission (1.04, SD =0.86) and displayed substantial improvement
(ASD = 0.76). Moreover, there were no differences inemotional distress between the diagnostic groups onadmission and comparable rates of improvement wereobserved (see Table 1). In short, most patients weredistressed on admission and improved substantially bydischarge. Emotional distress ratings also strongly re-flected the shift-level events and incidents that wererecorded on the PDLs (see Table 2).
While none of the individual findings was ‘unex-pected’, the constellation of associations identified inthe current study adds to the research base aboutacute psychiatric inpatient services and providessome useful insight into the nature and timing of thepressures and demands facing patients and staff. Forexample, after controlling for socio-demographic, le-gal status, diagnostic and mental health unit differ-ences, there were still strong shift-level associationsbetween current mental state, aggression, and usageof PRN medications (see Table 2). Shifts on which anyPRN medications were administered had a mean ac-tive psychopathology score of 1.00, whereas theaverage rating for shifts involving less serious
158

aggression was 1.60. Moreover, all of the mental statedomains contributing to active psychopathology werestrongly associated with shift-level reportable and lessserious aggression (ASDs > 0.75), suggesting thatinstances of aggressive behaviour typically occurredwhen overall severity of psychopathology and distresslevels were high. Furthermore, since the implicitmental state threshold for PRN administration waslower than that associated with aggressive episodes(and the majority of shifts involving aggression alsorecorded PRNs), it is likely that medication was oftenadministered subsequent to the aggressive inci-dent—and, therefore, that the buildup in psychopa-thology levels and distress was either rapid, unnoticedand/or unattended to by staff.
A recent Australian study revealed that 83.8% ofinpatients received at least one PRN medication duringtheir admission, with patient agitation the most com-mon reason for administration [35]. Other researchershave also noted that post-incident PRN medicationmay comprise part of the containment strategy for‘angry-absconders’ [7]. There have also been calls forthe development of national, best practice guidelineson PRN administration, as well as a greater emphasis onnon-pharmacological psychotherapeutic interventionswithin inpatient units [16].
Structured therapy participation was associatedwith lower levels of emotional distress, active psy-chopathology and withdrawal, and reduced rates ofless serious aggression and absconding. However, itcould simply be the case that such activities weregenerally not offered to, or accepted by, patients untiltheir levels of emotional distress and active psycho-pathology had reduced to a level compatible withgroup participation. A further examination of thepossible positive contribution of structured therapyand other unit activities is clearly warranted.
Our study has replicated several of the previouslyobserved associations between mental state andaggression (e.g., [38]). Fluctuations in acute symptomsare likely to be more strongly linked to aggression thanis clinical diagnosis, associated with periods of exac-erbation and remission [4, 12, 25], with particularclusters of symptoms increasing or decreasing the riskof violence [36]. However, in the present study, asubstantial proportion of the variance in currentmental state was not explained by the factors exam-ined, suggesting that we still have a lot to learn aboutthe determinants and correlates of mental state inacute inpatient settings, adding weight to the use ofroutine monitoring (using scales such as the OMS).
j Limitations
The main limitations of this project were: naturalisticclinical data were collated across multiple inpatientunits, which varied in their unit policies and reportingpractices; more comprehensive training protocolswere desirable, to increase completion rates for the
shift-based logs and to better standardise the ratingthresholds for the mental state scales; the primarydata were observational, focused on short-termoutcomes, and were not cross-referenced againstother sources; and data were not collected on thesequencing of particular events and incidents withinshifts. The current analyses also focused on primarydischarge diagnosis, however, our previous paperreports detailed admission-level analyses of relation-ships between multiple diagnostic assignments andadverse incidents [9]. The layout of the log sheets alsopermitted ready access to previous ratings, whichcould have been reduced through the use of com-puterised forms. In addition, electronic data entrywould have provided a useful opportunity forgraphical feedback to clinicians, such as OMS profilesheets showing changes since admission, possiblyincluding trajectories for prototypical patients.
Conclusions
Routine use of the OMS scale by nursing staff appearsto provide a useful adjunct to other clinical assess-ments, including a snapshot of each patient’s currentmental state, a way of tracking progress over time anda means for monitoring short-term impacts of inter-vention, as well as broader impacts of setting or ser-vice level changes (e.g., programs to reduce theoverall level of environmental stress during the acutephase of hospitalisation). The OMS score profiles re-flect diagnosis and bear relationships to aggression,use of PRN medication and absconding, suggestingthat the scale may be useful in helping to plan orinitiate interventions and prevent adverse events.Serious aggressive incidents, although intermittent innature, do not appear to arise in isolation but againsta background of heightened levels of less seriousaggressive behaviour and increased overall severity ofpsychopathology on the units. Therefore, such back-ground levels of aggression and disturbed behaviourrequire careful monitoring, judicious managementdecisions and accessibility to appropriate therapeuticresources, in order to reduce the likelihood of seriousadverse outcomes on inpatient units. As the averagestay is around 2 weeks, routine recording of mentalstate may also assist decisions about when to switchthe focus of inpatient treatment from crisis manage-ment to targeted interventions that could aid thetransition to community-based management.
j Acknowledgments This project was sponsored by the Centre forMental Health (NSW Department of Health and Aged Care, Syd-ney) and received considerable ongoing support from the threeparticipating health services (Hunter, Illawarra, and South WesternSydney). We would like to formally acknowledge the assistancereceived from the nursing, medical, allied health and administrativestaff within those services. Additional acknowledgments have beenprovided previously [9].
159
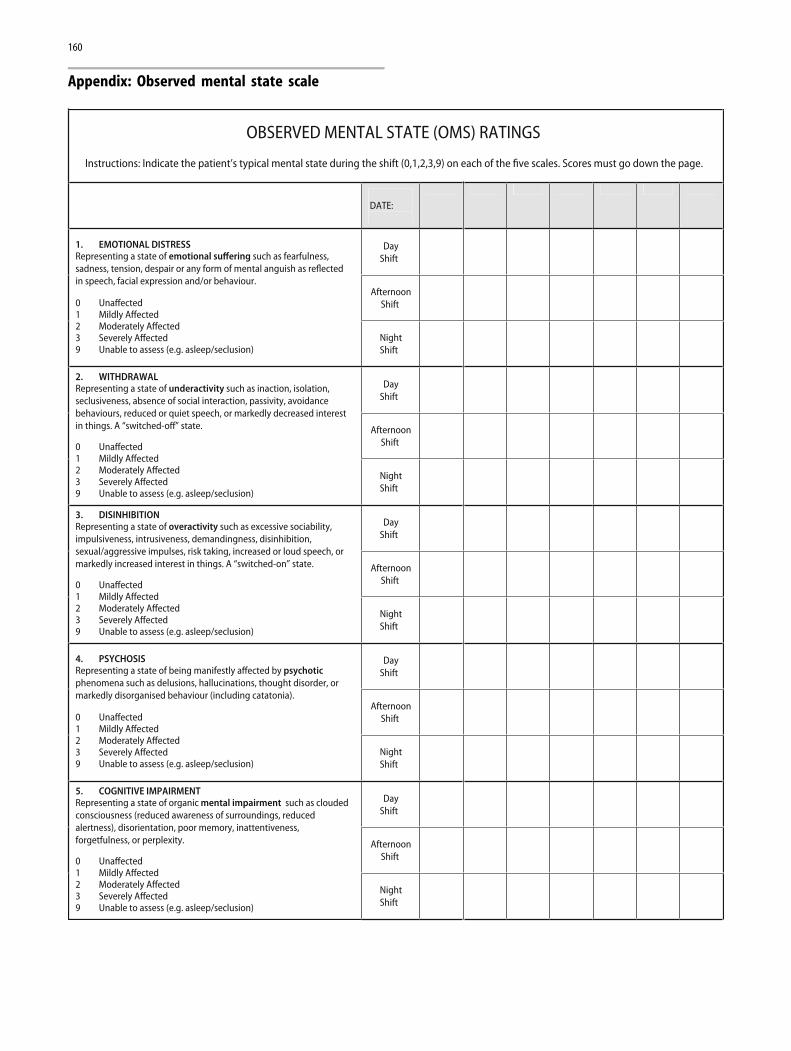
OBSERVED MENTAL STATE (OMS) RATINGS
Instructions: Indicate the patient’s typical mental state during the shift (0,1,2,3,9) on each of the five scales. Scores must go down the page.
DATE:
DayShift
AfternoonShift
1. EMOTIONAL DISTRESSRepresenting a state of emotional suffering such as fearfulness,sadness, tension, despair or any form of mental anguish as reflectedin speech, facial expression and/or behaviour.
0 Unaffected 1 Mildly Affected 2 Moderately Affected 3 Severely Affected 9 Unable to assess (e.g. asleep/seclusion)
NightShift
DayShift
AfternoonShift
2. WITHDRAWAL Representing a state of underactivity such as inaction, isolation,seclusiveness, absence of social interaction, passivity, avoidancebehaviours, reduced or quiet speech, or markedly decreased interestin things. A “switched-off” state.
0 Unaffected 1 Mildly Affected 2 Moderately Affected 3 Severely Affected 9 Unable to assess (e.g. asleep/seclusion)
NightShift
DayShift
AfternoonShift
3. DISINHIBITION Representing a state of overactivity such as excessive sociability,impulsiveness, intrusiveness, demandingness, disinhibition,sexual/aggressive impulses, risk taking, increased or loud speech, ormarkedly increased interest in things. A “switched-on” state.
0 Unaffected 1 Mildly Affected 2 Moderately Affected 3 Severely Affected 9 Unable to assess (e.g. asleep/seclusion)
NightShift
DayShift
AfternoonShift
4. PSYCHOSIS Representing a state of being manifestly affected by psychoticphenomena such as delusions, hallucinations, thought disorder, ormarkedly disorganised behaviour (including catatonia).
0 Unaffected 1 Mildly Affected 2 Moderately Affected 3 Severely Affected 9 Unable to assess (e.g. asleep/seclusion)
NightShift
DayShift
AfternoonShift
5. COGNITIVE IMPAIRMENT Representing a state of organic mental impairment such as cloudedconsciousness (reduced awareness of surroundings, reducedalertness), disorientation, poor memory, inattentiveness,forgetfulness, or perplexity.
0 Unaffected 1 Mildly Affected 2 Moderately Affected 3 Severely Affected 9 Unable to assess (e.g. asleep/seclusion)
NightShift
Appendix: Observed mental state scale
160
References
1. Abas M, Vanderpyl J, Prou TL, Kydd R, Emery B, Foliaki SA(2003) Psychiatric hospitalization: reasons for admission andalternatives to admission in South Auckland, New Zealand.Aust N Z J Psychiatry 37:620–625
2. American Psychiatric Association (1994) Diagnostic and sta-tistical manual for mental disorders (DSM-IV). AmericanPsychiatric Press, Washington
3. Anderson SW, Crist AJ, Payne N (2004) Predicting inpatientlength of stay with the expanded version of the Brief PsychiatricRating Scale (version 4.0). Psychiatr Serv 55:77–79
4. Arango C, Barba AC, Gonzalez-Salvador T, Ordonez C (1999)Violence in Inpatients with schizophrenia: a prospective study.Schizophr Bull 25:493–503
5. Barlow K, Grenyer B, Ilkiw-Lavalle OI (2000) Prevalence andprecipitants of aggression in psychiatric units. Aust N Z JPsychiatry 34:967–974
6. Bowers L (2005) Reasons for admission and their implicationsfor the nature of acute psychiatric nursing. J Psychiatr MentHealth Nurs 12:231–236
7. Bowers L, Simpson A, Alexander J (2003) Patient-staff conflict:results of a survey on acute psychiatric wards. Soc PsychiatryPsychiatr Epidemiol 38:402–408
8. Carr VJ, Johnston PJ, Lewin TJ, Rajkumar S, Carter GL, Issa-kidis C (2003) Patterns of service use among persons withschizophrenia and other psychotic disorders. Psychiatr Serv54:226–235
9. Carr VJ, Lewin TJ, Sly KA, Conrad A, Tirupati S, Cohen M,Ward PB, Coombs T (2008) Adverse incidents in acute psy-chiatric inpatient units: rates, correlates and pressures. Aust NZ J Psychiatry 42:267–282
10. Farnham FR, James D (2000) Patients’ attitudes to psychiatrichospital admission. Lancet 355:594
11. Flannery RB Jr, Stevens V, Juliano J, Walker AP (2000) Pastviolence and substance use disorder and subsequent violencetowards others: six year analysis of the Assaulted Staff ActionProgram (ASAP). Int J Emerg Ment Health 2:241–247
12. Fresan A, Apiquian R, de la Fuente-Sandoval C, Loyzaga C,Garcia-Anaya M, Meyenberg N, Nicolini H (2005) Violentbehavior in schizophrenic patients: relationship with clinicalsymptoms. Aggress Behav 31:511–520
13. George L, Durbin J, Sheldon T, Goering P (2002) Patient andcontextual factors related to the decision to hospitalize patientsfrom emergency psychiatric services. Psychiatr Serv 53:1586–1591
14. Grassi L, Biancosino B, Marmai L, Kotrotsiou V, Zanchi P,Peron L, Marangoni C, Vanni A, Barbui C (2006) Violence inpsychiatric units: a 7-year Italian study of persistently assaul-tive patients. Soc Psychiatry Psychiatr Epidemiol 41:698–703
15. Grassi L, Peron L, Marangoni C, Zanchi P, Vanni A (2001)Characteristics of violent behaviour in acute psychiatricin-patients: a 5-year Italian study. Acta Psychiatr Scand104:273–279
16. Hilton MF, Whiteford HA (2008) Pro re nata medication forpsychiatric inpatients: time to act. Aust N Z J Psychiatry42:555–564
17. Honigfeld R, Roderic D, Klett JC (1966) NOSIE-30 a treatmentsensitive ward behavior scale. Psychol Rep 19:180–182
18. Hopko DR, Lachar D, Bailley SE, Varner RV (2001) Assessingpredictive factors for extended hospitalization at acute psy-chiatric admission. Psychiatr Serv 52:1367–1373
19. Kato K, Galynker II, Miner CR, Rosenblum JL (1995) Cognitiveimpairment in psychiatric patients and length of hospital stay.Compr Psychiatry 36:213–217
20. Kay SR, Opler L, Fiszbein A (1992) The positive and negativesyndrome scale (PANSS) for schizophrenia manual. MultiHealth Systems, Toronto
21. Lieberman PB, McPhetres WB, Elliot B, Egerter E, Wiitala S(1993) Dimensions and predictors of change during brief psy-chiatric hospitalisation. Gen Hosp Psychiatry 15:316–324
22. Lyons JS (1998) The severity and acuity of psychiatric illness sca-les—adult version. The Psychological Corporation, San Antonio
23. Lyons JS, O’Mahoney MT, Miller SI, Neme J, Kabat J, Miller F(1997) Predicting readmission to the psychiatric hospital in amanaged care environment: implications for quality indicators.Am J Psychiatry 154:337–340
24. Lyons JS, Stutesman J, Neme J, Vessey JT, O’Mahoney MT,Camper HJ (1997) Predicting psychiatric emergency admis-sions and hospital outcome. Med Care 35:792–800
25. McNiel DE, Binder RL (1994) The relationship between acutepsychiatric symptoms, diagnosis, and short-term risk of vio-lence. Hosp Community Psychiatry 45:133–137
26. Monnelly EP (1997) Instability before discharge and previouspsychiatric admissions as predictors of early readmission.Psychiatr Serv 48:1584–1586
27. Morrison EF (1992) A hierarchy of aggressive and violentbehaviours among psychiatric inpatients. Hosp CommunityPsychiatry 43:505–506
28. Nijman HL, aCampo JM, Ravelli DP, Merckelbach HL (1999) Atentative model of aggression on inpatient psychiatric wards.Psychiatr Serv 50:832–834
29. Owen C, Tarantello C, Jones M, Tennant C (1998) Violence andaggression in psychiatric units. Psychiatr Serv 49:1452–1457
30. Page AC, Hooke GR, Rutherford EM (2001) Measuring mentalhealth outcomes in a private psychiatric clinic: health of thenation outcome scales and medical outcomes short form SF-36.Aust N Z J Psychiatry 35:377–381
31. Sajatovic M, Rosch DS, Sivec HJ, Sultana D, Smith DA, AlamirS, Buckley P, Bingham CR (2002) Insight into illness and atti-tudes toward medications among inpatients with schizophre-nia. Psychiatr Serv 53:1319–1321
32. Samarasekera U (2007) Staffing issues affecting care on acutepsychiatric wards. Lancet 370:119–120
33. Soliman AE, Reza H (2001) Risk factors and correlates of vio-lence among acutely ill adult psychiatric inpatients. PsychiatrServ 52:75–80
34. Squier RW (1995) An acute psychiatric rating scale for theclinical assessment of functionally disturbed inpatients. ActaPsychiatr Scand 91:402–409
35. Stein-Parbury J, Reid K, Smith N, Mouhanna D, Lamont F(2008) Use of pro re nata medications in acute inpatient care.Aust N Z J Psychiatry 42:283–292
36. Swanson JW, Swartz MS, Van Dorn RA, Elbogen EB, WagnerHR, Rosenheck RA, Stroup TS, McEvoy JP, Lieberman JA(2006) A national study of violent behavior in persons withschizophrenia. Arch Gen Psychiatry 63:490–499
37. Swett C (1995) Symptom severity and number of previouspsychiatric admissions as predictors of readmission. PsychiatrServ 46:482–485
38. Swett C, Mills T (1997) Use of the NOSIE to predict assaultsamong acute psychiatric patients. Nurses’ observational scalefor inpatient evaluation. Psychiatr Serv 48:1177–1180
39. Synder W (1994) Hospital downsizing and increased frequencyof assaults on staff. Hosp Community Psychiatry 45:378–380
40. Ventura J, Lukoff D, Nuechterlein KH, Liberman RP, Green MF,Shaner A (1993) Brief psychiatric rating scale (BPRS), expandedversion (4.0): scales, anchor points and administration manual.UCLA Department of Psychiatry and Biobehavioural Sciences,West Los Angeles VA Medical Center: Clinical Research Centerfor Schizophrenia and Psychiatric Rehabilitation, Los Angeles
41. Way BB, Banks S (2001) Clinical factors related to admissionand release decisions in psychiatric emergency services. Psy-chiatr Serv 52:214–218
42. Wynaden D, McGowan S, Chapman R, Castle D, Lau P,Headford C, Finn M (2001) Types of patients in a psychiatricintensive care unit. Aust N Z J Psychiatry 35:841–845
161
Related Documents











