Journal of Child and Family Studies, Vol. 6, 1997, pp. 177-190 Measuring Child Mental Health Status for Services Research Sheny Glied, Ph.D., 1,10 Christina W. Hoven, Dr.PH., 2 A. Bowen Garrett, Ph.D., 3 Robert E. Moore, Dr.PH., 4 Philip Leaf, Ph.D., 5 Hector R. Bird, M.D., 6 Sherryl Goodman, Ph.D., 7 Darrel Regier, M.D, M.RH., 8 and Margarita Alegria, Ph.D. 9 Epidemiological studies of the prevalence of mental health disorders typically contain multiple measures of mental health, using different instruments and different informants (child, parent, and interviewer). We used the Methods for the Epidemiology of Child and Adolescents Mental Disorder (MECA) study of U.S. youth to assess the effects of employing a range of these measures in mental health services research. We examined the effect of including various measures of mental health status in regressions of income on mental health service use. The estimated effect of income on service use varied widely, depending on the measure of mental health status used. Some measures of mental health status have little explanatory power in service use regressions. Measures of mental health status based on parental assessment of impairment 1Assistant Professor, Division of Health Policy and Management, Columbia School of Public Health and Department of Economics, New York, NY. 2Assistant Professor, Epidemiology in Psychiatry, Columbia University - NYS Psychiatric Institute, New York, NY. 3Robert Wood Johnson Foundation Scholar in Health Policy Research, University of California, Berkeley, Berkeley, CA. 4Assistant Professor, Epidemiology in Psychiatry, Columbia University - NYS Psychiatric Institute, New York, NY. 5Professor, Department of Mental Hygiene, Johns Hopkins University, Baltimore, MD. 6Professor, Psychiatry, Columbia University - NYS Psychiatric Institute, New York, NY. 7Professor, Department of Psychology, Emory University, Atlanta, GA. 8Associate Director, Epidemiology and Health Policy Research, National Institute of Mental Health, Rockville, MD. 9Associate Professor, School of Public Health, University of Puerto Rico, San Juan, PR. 10Correspondence should be directed to Sherry Glied, Division of Health Policy and Management, Columbia School of Public Health, 600 West 168th St, 6th Floor, New York, NY 10032. 177 1062-1024/97««00>177$12.5<M> C 1997 Human Sciences Press, Inc.

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Journal of Child and Family Studies, Vol. 6, 1997, pp. 177-190
Measuring Child Mental Health Status forServices Research
Sheny Glied, Ph.D.,1,10 Christina W. Hoven, Dr.PH.,2 A. Bowen Garrett,Ph.D.,3 Robert E. Moore, Dr.PH.,4 Philip Leaf, Ph.D.,5 Hector R. Bird,M.D.,6 Sherryl Goodman, Ph.D.,7 Darrel Regier, M.D, M.RH.,8 andMargarita Alegria, Ph.D.9
Epidemiological studies of the prevalence of mental health disorders typicallycontain multiple measures of mental health, using different instruments anddifferent informants (child, parent, and interviewer). We used the Methods forthe Epidemiology of Child and Adolescents Mental Disorder (MECA) studyof U.S. youth to assess the effects of employing a range of these measures inmental health services research. We examined the effect of including variousmeasures of mental health status in regressions of income on mental healthservice use. The estimated effect of income on service use varied widely,depending on the measure of mental health status used. Some measures ofmental health status have little explanatory power in service use regressions.Measures of mental health status based on parental assessment of impairment
1Assistant Professor, Division of Health Policy and Management, Columbia School of PublicHealth and Department of Economics, New York, NY.2Assistant Professor, Epidemiology in Psychiatry, Columbia University - NYS PsychiatricInstitute, New York, NY.3Robert Wood Johnson Foundation Scholar in Health Policy Research, University ofCalifornia, Berkeley, Berkeley, CA.4Assistant Professor, Epidemiology in Psychiatry, Columbia University - NYS PsychiatricInstitute, New York, NY.5Professor, Department of Mental Hygiene, Johns Hopkins University, Baltimore, MD.6Professor, Psychiatry, Columbia University - NYS Psychiatric Institute, New York, NY.7Professor, Department of Psychology, Emory University, Atlanta, GA.8Associate Director, Epidemiology and Health Policy Research, National Institute of MentalHealth, Rockville, MD.9Associate Professor, School of Public Health, University of Puerto Rico, San Juan, PR.
10Correspondence should be directed to Sherry Glied, Division of Health Policy andManagement, Columbia School of Public Health, 600 West 168th St, 6th Floor, New York,NY 10032.
177
1062-1024/97««00>177$12.5<M> C 1997 Human Sciences Press, Inc.

or need, such as the Columbia Impairment Scale, are less costly to collectand also have good explanatory power, but are more strongly correlated withincome. The Non-Clinician Child Global Assessment Scale (NC-CGAS)performs best in terms of explanatory power and correlation with income.Higher income parents appeared to judge behaviors differently from lowerincome parents, so analyses based on measures derived from parental reportmay lead to an understatement of the effect of income on service use.
Mental health researchers and policy makers need to understand theeffects of socioeconomic variables, such as household income, insurance,and education on service use. Measures of mental health status are in-cluded in many analyses to control for differences in the characteristics ofthe population that bias estimates of the true effects of socioeconomic vari-ables on mental health service use. From this perspective, ideal measuresof mental health status should not reflect differences in how informantswith different socioeconomic characteristics assess symptoms. If measuresof mental health also capture socioeconomic characteristics, it becomes dif-ficult to distinguish the independent effect of these socioeconomic variableson mental health service use. In policy analysis, this makes it harder toexamine how an exogeneous change, such as an increase in wages or in-come, would affect mental health service use. Use of these measures willprovide a lower bound estimate of the potential impact of a policy changeon mental health service use.
Research on adult mental and physical health illustrates how the useof different measures of health and mental health status can lead to dif-ferent interpretations of the relationship between socioeconomiccharacteristics and service use. Frank and Gertler (1991) discussed the useof various types of mental health status measures in earnings equations ofadults. They found the estimated effects of socioeconomic variables on serv-ice use varied significantly depending on the measure of mental healthemployed. Similarly, Bound (1991), discussed how self-reported measuresof physical health may exaggerate the importance of health in retirementdecisions, a result that might be explained if people use health to ration-alize retirement for other reasons.
The National Institute of Mental Health's 1992 Methods for theEpidemiology of Children and Adolescents Mental Disorders (MECA) studyof 1285 child-adult pairs, in three sites, in the mainland U.S. and in PuertoRico provides an opportunity to examine the appropriateness of a rangeof measures of youth mental health status in services research (Lahey etal., 1996; Leaf et al., 1996; Shaffer et al., 1996). The MECA study, which
died et al.178
KEY WORDS: service use; child psychopatnology; measurement; impairment; socioeconomicstatus.

was a methodological study designed to inform the ongoing longitudinalstudy of youth (UNO-CCAP), contains multiple measures of mental health,using different instruments and different informants. An understanding ofthe properties of these measures for services research is also important toprovide guidance to the analysis of other surveys that use shorter, less com-prehensive instruments.
The purpose of this study was to assess the usefulness of the variousMECA measures of mental health status for services research. We did thisby examining how including each measure of mental health status in a mul-tivariate analysis affects the measured effect of income on mental healthservice use. Youth obtain mental health services through physicians andspecialty mental health providers as well as through the school system. Weexploited the fact that household income is likely to have a relativelysmaller effect on the use of school-based services than on the use of non-school-based services to strengthen our results about overall service use.
WHY MIGHT MEASURES MATTER?
There are many ways that measures of child mental health, derivedfrom survey responses, may be affected by a respondent's socioeconomiccharacteristics. Behavior that some parents find normal may indicate a dis-order to other parents. Parents and other informants may differ in theirability to recognize child mental health problems and differences in theirattitudes toward such problems may also affect their responses. For exam-ple, a parent might under-report service need if the parent fears thatadmitting that their child has a mental health problem would lead to a lossof private insurance coverage or would reflect poorly on the quality of par-enting.
These kinds of bias are types of misspecification bias that arise fromusing a proxy variable, such as measured mental health status, in place ofactual mental health status. We illustrate the effect of misspecification biasusing income as the socioeconomic variable of interest. If the youth's truemental health status were known, we could estimate the independent effectof income on service use as the b\ in the following multivariate regression:
Measuring Mental Health Status 179
As the example above suggests, proxy measures of mental health may com-bine respondent perceptions (or other unobserved characteristics) with truemental health status. If these perceptions or characteristics are related toincome, using the proxy measure to control for mental health status can
Here, g1 measures the relationship of the discrepancy between the true andproxy measures to income.
If we could measure g1, we would be able to assess directly the extentof bias from each measure of mental health. Because we cannot measuregi directly, we use three indirect methods to evaluate the mental healthmeasures in the MECA study. A good measure should be able to explainsignificant variation in mental health service use. Our first test is to lookat the amount of variation in service use explained using each measure.This is not a sufficient condition, however, because the measure that ex-plains the most variation may produce biased estimates of the effect ofsocioeconomic variables on use. A good measure should also produce em-pirical results, that conform to a priori hypotheses. Our second test is toexamine the effect of income on office-based service use. We expect incometo have a positive (enabling) effect on the use of some mental health serv-ices, particularly services provided by specialists in offices or outpatientdepartments. Similarly, our third test is to examine the effect of incomeon school-based service use. We expect income to have less effect on theuse of school-based services because use of these services is mediatedthrough a third-party (the school) and does not, in principle, depend onfamily income.
MEASURES OF MENTAL HEALTH STATUS IN THE MECA STUDY
Data used in this study are derived from the National Institute of Men-tal Health's (NIMH's) Methods for the Epidemiology of Children andAdolescents Mental Disorders (MECA) Study. This study was conducted in1992 and consisted of a total of N = 1285 pairs of youth (9-17 years ofage) and a parent/guardian who were drawn from four geographic areashi the United States: (a) Hamden, East Haven and West Haven, Connecti-cut (N = 314); (b) DeKalb, Rockdale and Henry Counties, Georgia (N =299); (c) Westchester County, New York (N = 360); and (d) San Juan,Puerto Rico (N = 312). For sampling methods and interview proceduresof the MECA data, see Lahey et al., 1996. Our analysis excludes data for
Glied et at.180
where g1 is given by the following equation:
induce misspecification bias on the estimates of b1. The form of this biasis
Puerto Rico because the distribution of income lies so far below that forthe other three sites (median of $13,000 in Puerto Rico and $50,000 in theother sites) and because patterns of service availability and service use arequite different at that site.
The MECA study collected a range of measures of mental healthstatus including data on child psychopathology, impairment, child and par-ent-reported need for services, and life events in the preceding year (ameasure of the potential need for mental health services).
Child Psychopathology
NIMH's Diagnostic Interview Schedule for Children (DISC, version2.3) was used to assess six-month prevalence (one year prevalence for con-duct disorder) of major child and adolescent psychiatric disorders (Shafferet al., 1996). The DISC is a highly structured diagnostic instrument de-signed for administration by non-clinicians that was administered to bothstudy children and adult informants. Based on computer algorithms thatconform to standard psychiatric criteria (DSM-III-R), diagnoses were gen-erated combining information from the parent and child (Cohen, Velez,Kohn et al 1987).
Child Functional Impairment
Two measures of child functional impairment were collected in MECA.The Non-Clinician Child Global Assessment Scale (NC-CGAS), based onan assessment made by a non-clinician interviewer, is designed to capturethe lowest level of functioning of a subject during the preceding six months(Bird et al., 1987, 1990, in press; Shaffer et al., 1984). Scores range from1 (severely impaired and in need of immediate psychiatric hospitalization)to 100 (functioning at the very highest level). For each decile of scores,there are symptom and behavior anchors to guide the rating. For example,if a child was scored at 65, this child is categorized as having some prob-lems, that is, most people who do not know the child very well would notnotice the problems, but people who do know her or him would be con-cerned. In determining the overall NC-CGAS scores, the interviewer (whohas already administered a 3-hour interview to the child) synthesizes allavailable relevant data about the child's social and psychological function-ing. Psychometric data indicate that the CGAS possesses excellenttest-retest reliability and adequate to good discriminant and concurrent va-lidity (Bird et al., in press).
Measuring Mental Health Status 181
The Columbia Impairment Scale (CIS) is a 13-item measure that re-flects parents responses to questions about four major areas of functioningincluding symptoms, school problems, home problems, and peer problemsand is scored on a metric from 0 (no problem) to 4 (a very bad problem).The internal consistency reliability estimate for the scale is excellent (alphafor parent report = .88; alpha for youth report = .83). The CIS also pos-sesses excellent test-retest reliability and evidence for construct andpredictive validity (Bird et al., in press).
Parent and Child Reported Need for Services
All study children and the interviewed parent or guardian were askedabout the child's need for mental health services. Parents were asked: "Doyou think your child needs any kind of help for emotional or behavioralproblems, or for the use of alcohol or drugs?" Children were asked whetherthey had needed to see someone about an emotional or behavioral problemin the preceding 12 months.
Service Use and Risk Factors
Parents were asked about their child's use of and need for mentalhealth services (Leaf et al., 1996). The child was also asked about his orher experience with generally stressful life events in the previous year (e.g.,parents divorced). Life events have been shown to predict service useamong adults (Brown, 1993; Greenley, 1984, Sherbourne, 1988). We usedthree measures of service use in the preceding year: (a) any mental healthservice use (including school, outpatient, specialist office, social worker, andother sites); (b) use of services in a mental health specialists' office or ina psychiatric outpatient facility, and (c) use of services in school only, thatis, without use elsewhere.
Income
Survey respondents selected their level of income from a classificationof 23 income categories. We used the midpoint income level of each cate-gory as our income measure and defined income in thousands. For the topcategory (income > $100,000), we set income equal to 100 and included a"top-code" variable to indicate that the income response was top-coded.
Glied et al.182

EMPIRICAL METHOD
We examined alternative specifications of mental health service useregressions using a set of demographic variables, income, and the followingseven measures of mental health status: a) no measure of mental health;b) Non-Clinician Child Global Assessment Scale (NC-CGAS); c) ColumbiaImpairment Scale (CIS); d) the count of DSM-III-R symptoms (DSM-IIIR); e) the parent's report of need for mental health services for thechild (parent report); f) the child's report of need for mental health services(child report); and g) the number of stressful life events (EVENTS). Weestimated the parameters of each specification using a probit model andcomputed marginal effects and standard errors from the probit coefficients.The analysis was repeated using school-based and non-school-based serv-ices as dependent variables.
Because symptoms and impairment are likely to affect service usealong wide ranges of the continuum, we used scaled measures rather thanbinary variables based on cutoff-values in our analyses. Manning, Ne-whouse, and Ware (1982) suggested that scaled measures should be usedin the estimation of the demand for health services when they possess thedesirable properties of variability, symmetry, reliability, and validity in orderto capture the continuum of states of mental health. We controlled forpotential site-effects in these analyses by including a fixed effect for theGeorgia and New York sites. As additional controls for the use of childmental health services, we included age, sex, and an interaction term forage and sex. It is known that young boys are referred for services at higherrates than young girls (Burns, 1991). The interaction term was includedbecause there is a reversal of the sex ratio for certain disorders beginningat puberty, where girls are increasingly classified with depression and anxi-ety relative to boys, whereas older male adolescents report greatersubstance use problems (Brandenburg, Friedman, & Silver, 1990; Links,Boyle, & Offord, 1989). We also control for the child's family type (e.g.,single parent households).
RESULTS
Summary statistics for the sample we analyzed are presented in Table1. Seventeen percent of children in the sample had used some type of men-tal health service in the past year. Six percent used office-based services,often in addition to school-based services, and seven percent used school-based services exclusively. Forty percent met DISC diagnostic criteria forany psychiatric disorder (these diagnoses are based on symptoms only, with-
Measuring Mental Health Status 183
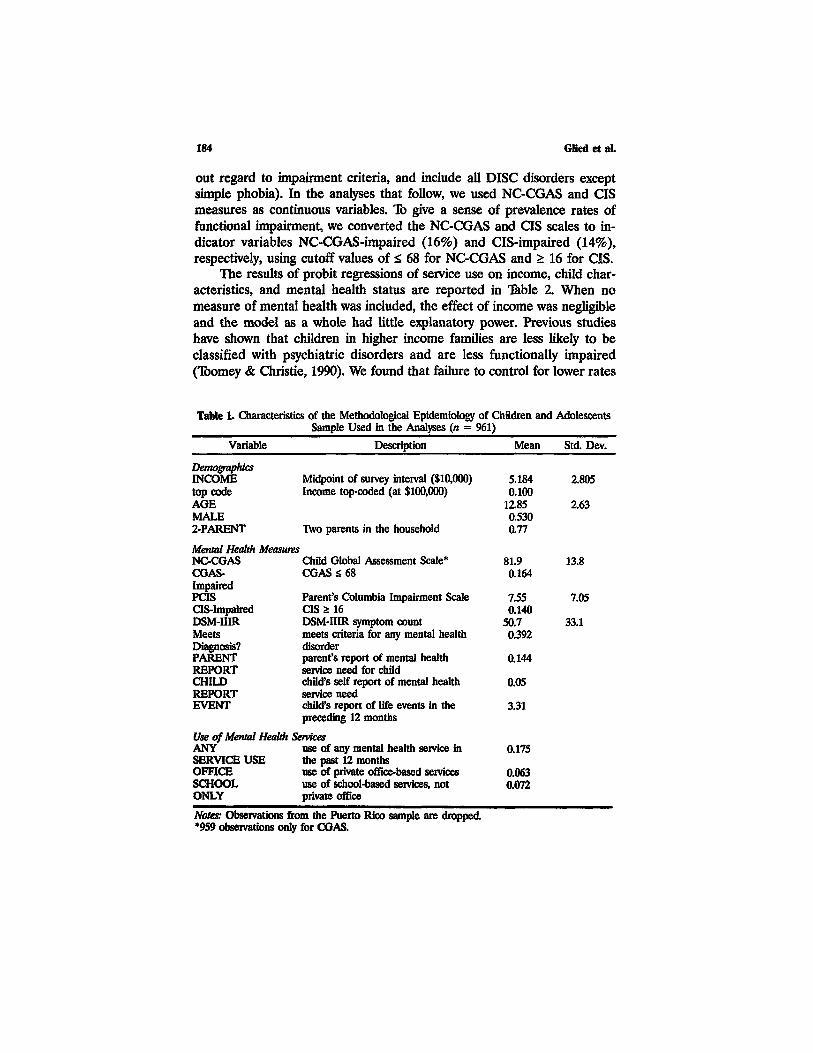
out regard to impairment criteria, and include all DISC disorders exceptsimple phobia). In the analyses that follow, we used NC-CGAS and CISmeasures as continuous variables. To give a sense of prevalence rates offunctional impairment, we converted the NC-CGAS and CIS scales to in-dicator variables NC-CGAS-impaired (16%) and CIS-impaired (14%),respectively, using cutoff values of < 68 for NC-CGAS and > 16 for CIS.
The results of probit regressions of service use on income, child char-acteristics, and mental health status are reported in Table 2. When nomeasure of mental health was included, the effect of income was negligibleand the model as a whole had little explanatory power. Previous studieshave shown that children in higher income families are less likely to beclassified with psychiatric disorders and are less functionally impaired(Toomey & Christie, 1990). We found that failure to control for lower rates
Table 1. Characteristics of the Methodological Epidemiology of Children and AdolescentsSample Used in the Analyses (n = 961)
Variable
DemographicsINCOMEtop codeAGEMALE2-PARENT
Description
Midpoint of survey interval ($10,000)Income top-coded (at $100,000)
Two parents in the household
Mean
5.1840.100
12.850.5300.77
Std. Dev.
2.805
2.63
Mental Health MeasuresNC-CGASCGAS-ImpairedpasCIS-ImpairedDSM-IIIRMeetsDiagnosis?PARENTREPORTCHILDREPORTEVENT
Child Global Assessment Scale*CGAS S 68
Parent's Columbia Impairment ScaleCIS Z 16DSM-IIIR symptom countmeets criteria for any mental healthdisorderparent's report of mental healthservice need for childchild's self report of mental healthservice needchild's report of life events in thepreceding 12 months
Use of Mental Health ServicesANYSERVICE USEOFFICESCHOOLONLY
use of any mental health service inthe past 12 monthsuse of private office-based servicesuse of school-based services, notprivate office
81.90.164
7.550.140
50.70.392
0.144
0.05
3.31
0.175
0.0630.072
13.8
7.05
33.1
Notes: Observations from the Puerto Rico sample are dropped*959 observations only for CGAS.
Glied et al.184

Table 2. Probit Regressions of Service Use on Income and Child Characteristics,Controlling for Various Measures of Mental Health Status
Mental Health PARENT CHILDMeasure (none) NC-CGAS CIS DSM-IIIR REPORT REPORT EVENT
N
INCOME
Top Code
AGE
MALE
AGE*MALE
2 PARENT
GEORGIA
NEW YORK
NC-CGAS
asDSM-IIIR
PARENT
CHILDREPORTEVENT
CONSTANT
Pseudo R2
961
0.002(0.006)0.014
(0.053)0.009
(0.007)0.227
(0.116)-0.016(0.009)-0.130(0.036)0.001
(0.031)0.008
(0.031)
—
—
—0.169
(0.014)0.025
959
0.012(0.005)0.007
(0.049)-0.000(0.006)0.120
(0.110)-0.008(0.009)-0.069(0.033)0.028
(0.031)0.032
(0.030)-0.010(0.000)
—
—
—
—
—0.128
(0.034)0.230
961
0.007(0.005)0.004
(0.048)0.003
(0.006)0.201
(0.111)-0.015(0.009)-0.089(0.034)0.010
(0.029)0.032
(0.030)
—
0.020(0.002)
—
—
—_
0.131(0.024)0.219
961
0.010(0.006)-0.008(0.047)0.002
(0.007)0.199
(0.112)-0.013(0.009)-0.095(0.034)-0.005(0.029)0.040
(0.031)
—_
0.003(0.000)
—
—_
0.144(0.025)0.136
961
0.006(0.006)0.015
(0.052)0.003
(0.007)0.118
(0.116)-0.008(0.009)-0.028(0.032)0.001
(0.030)0.006
(0.031)
—_
—0.562
(0.044)
—_
0.140(0.019)0.232
961
0.002(0.006)0.016
(0.054)0.007
(0.007)0.221
(0.116)-0.015(0.009)-0.130(0.036)-0.003(0.031)0.008
(0.031)
—
—
—
—
0.106(0.069)
—0.168(0.014)0.028
961
0.005(0.006)0.005
(0.052)0.006
(0.007)0.238
(0.115)-0.017(0.009)-0.118(0.036)-0.008(0.030)0.012
(0.031)
—
—_
—
—0.014
(0.004)0.166
(0.016)0.038
Notes: Reported coefficients are marginal effects computed from probit coefficients. Standarderrors computed for the marginal effects are in parentheses.
of mental disorders in higher income families led to the result that higherincome did not appear to enable families to access services more readily.All measures of mental health status (except child reported need and lifeevents) had significant effects on service use. In all cases, the income effectwas small. The marginal effect of an additional $10,000 in income was toincrease service use by between 0.2% and 1.2%, depending on the measureof mental health status used. Our results are consistent with those of other
Measuring Mental Health Status 185
186 Glied et al.
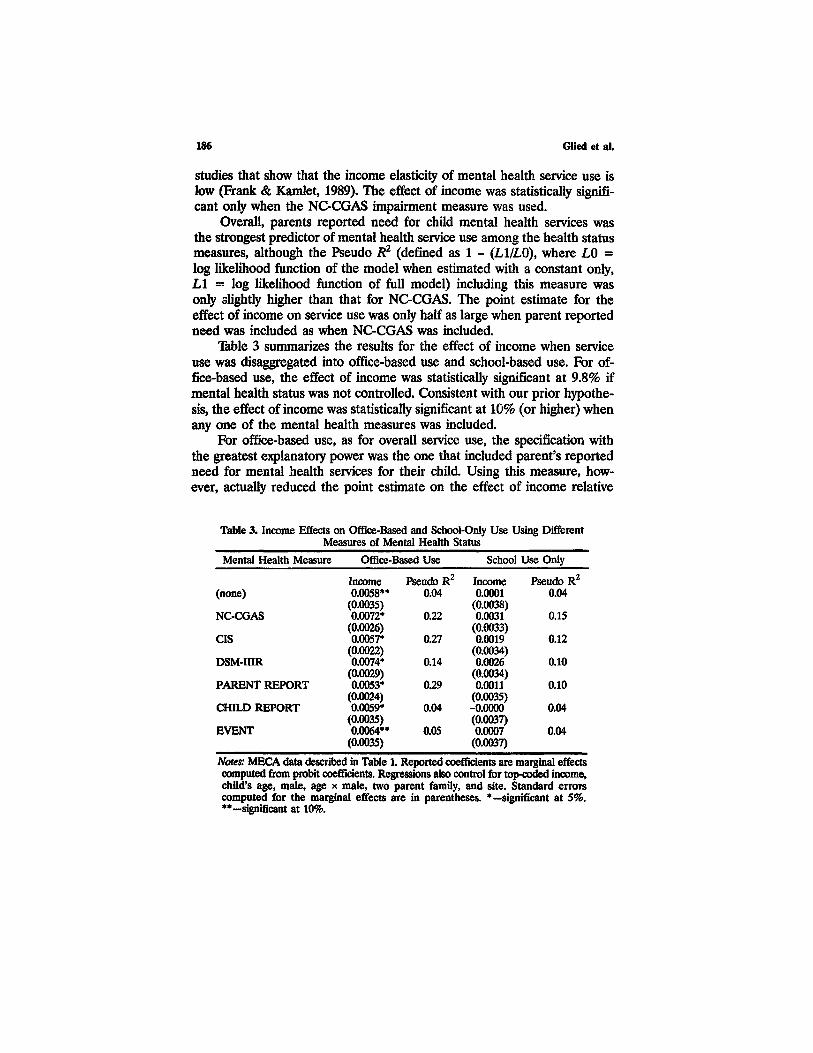
studies that show that the income elasticity of mental health service use islow (Frank & Kamlet, 1989). The effect of income was statistically signifi-cant only when the NC-CGAS impairment measure was used.
Overall, parents reported need for child mental health services wasthe strongest predictor of mental health service use among the health statusmeasures, although the Pseudo R2 (defined as 1 - (Ll/LO), where LO =log likelihood function of the model when estimated with a constant only,L1 = log likelihood function of full model) including this measure wasonly slightly higher than that for NC-CGAS. The point estimate for theeffect of income on service use was only half as large when parent reportedneed was included as when NC-CGAS was included.
Table 3 summarizes the results for the effect of income when serviceuse was disaggregated into office-based use and school-based use. For of-fice-based use, the effect of income was statistically significant at 9.8% ifmental health status was not controlled. Consistent with our prior hypothe-sis, the effect of income was statistically significant at 10% (or higher) whenany one of the mental health measures was included.
For office-based use, as for overall service use, the specification withthe greatest explanatory power was the one that included parent's reportedneed for mental health services for their child. Using this measure, how-ever, actually reduced the point estimate on the effect of income relative
Table 3. Income Effects on Office-Based and School-Only Use Using DifferentMeasures of Mental Health Status
Mental Health Measure Office-Based Use
Income(none)
NC-CGAS
CIS
DSM-IIIR
PARENT REPORT
CHILD REPORT
EVENT
0.0058**(0.0035)0.0072*
(0.0026)0.0057*
(0.0022)0.0074*
(0.0029)0.0053*
(0.0024)0.0059*
(0.0035)0.0064**
(0.0035)
Pseudo R2
0.04
0.22
0.27
0.14
0.29
0.04
0.05
School Use Only
Income0.0001
(0.0038)0.0031
(0.0033)0.0019
(0.0034)0.0026
(0.0034)0.0011
(0.0035)-0.0000(0.0037)0.0007
(0.0037)
Pseudo R2
0.04
0.15
0.12
0.10
0.10
0.04
0.04
Notes: MECA data described in Table 1. Reported coefficients are marginal effectscomputed from probit coefficients. Regressions also control for top-coded income,child's age, male, age x male, two parent family, and site. Standard errorscomputed for the marginal effects are in parentheses. *— significant at 5%.**— significant at 10%.

to the case where no mental health measure was included. This occurredbecause parent's reported need for mental health services was positivelycorrelated with income. The effect of income was highest when a measureof mental health status, based on number of DISC symptoms, was includedin the analysis. In this specification, the effect of income was almost 40percent greater than in the specification using parent's report of need (al-though the difference was not statistically significant).
The fourth and fifth column of Table 3 shows the results of the analysisusing school-based service use. Consistent with our prior hypothesis, in-come had a much smaller effect on the use of school-based services andthe effect was not statistically significant. The effect of income was greatestwhen mental health status was measured using the NC-CGAS and theDSM-IIIR diagnosis measure but in neither case did the estimate approachstatistical significance. The NC-CGAS had the most explanatory poweramong these specifications. In general, the explanatory power of the school-based service use models was lower than the office-based service usemodels.
Table 4 ranks the health status measures by their performance on thethree criteria described above. The NC-CGAS functional impairment meas-ure and the diagnosis-based symptom measure (DSM-IIIR) scored wellunder two of the three criteria and acceptably on the third. They explaineda considerable share of variation in child mental health service use, allowedincome to explain some of the variation in office-based service use, anddid not lead to significant estimated effects of income on school-based use.Parent's report of need and impairment measured by the parent (ColumbiaImpairment Scale) did well in terms of explaining variation in service use,but tended to eliminate the explanatory power of income for both officeand school-based use. In terms of expressions (2) and (3), the downwardbias indicated that, for these measures, g\ < 0. Given two families withidentical children, parents in higher income families are more likely to re-
Table 4. Ranking of Mental Health Status Measures According to Three Criteria
Variation Explained Magnitude of Income Effect on Service Use(Pseudo R2) for All
Service Use
PARENT REPORTNC-CGASCISDSM-IIIREVENTCHILD REPORTnone
Office Use
DSM-IIIRNC-CGASEVENTCHILD REPORTnoneCISPARENT REPORT
School Only
NC-CGASDSM-IIIRCISPARENT REPORTEVENTnoneCHILD REPORT
Measuring Mental Health Status 187

port impairment and a need for services. Measures of child-reported lifeevents and child-reported need did not explain much variation in serviceuse and did not change the estimated effects of income, relative to notincluding controls for mental health status at all.
CONCLUSION
We have shown that the use of different measures of mental healthstatus may lead to different estimates of the effects of socioeconomic vari-ables on child mental health service use. Measures based on interviewerassessments of impairment or diagnosis (such as the DISC or NC-CGAS)will likely yield relatively unbiased estimates of the impact of changes insocioeconomic characteristics on mental health service use. These meas-ures, however, are costly and time-consuming to collect. Less costlymeasures, based on respondent perceptions of need or impairment, how-ever, may introduce more substantial biases. The interpretation placed onthe results of any analysis should be informed by the characteristics of themeasures used.
Socioeconomic status appears to affect the way that parents assess achild's behavior. Measures of mental health status that rely on parentalperceptions of a child's condition, such as parent's report of need and theColumbia Impairment Scale, incorporate within them some socioeconomiccharacteristics. In analyses of service use that employ these measures, theimpact of socioeconomic characteristics will be captured, in part, by thecoefficients on the mental health measures themselves. Thus, use of thesemeasures will yield lower-bound estimates of the effect of socioeconomiccharacteristics on child mental health service use. Programs that affect par-ticipants' socioeconomic circumstances, such as income support programs,may lead to larger increases in service use than would be predicted on thebasis of models that use parental reported need as a measure of mentalhealth status.
ACKNOWLEDGMENTS
Data analysis was funded by NIMH Grant No. R01 MH52698-01. Wewould like to thank the original MECA collaborators for the use of thesedata. The MECA Program is an epidemiologic methodology study per-formed by four independent research teams in collaboration with staff ofthe Division of Clinical Research, which was reorganized in 1992 with com-ponents now in the Division of Epidemiology and Services Research andthe Division of Clinical and Treatment Research, of the NIMH, Rockville,
Glied et al.188
MD. The NIMH Principal Collaborators are Darrel A. Regier, MD, MPH,Ben Z. Locke, MSPH, Peter S. Jensen, MD, William E. Narrow, MD,MPH, Donald S. Rae, MA, John E. Richters, PhD, Karen H. Bourdon,MA, and Margaret T Roper, MS. The NIMH Project Officer was WilliamJ. Huber. The Principal Investigators and Coinvestigators from the foursites are as follows: Emory University, Atlanta, Georgia, UOI MH46725:Mina K. Dulcan, MD, Benjamin B. Lahey, PhD; Donna J. Brogan, PhD,Sherryl Goodman, PhD, and Elaine W Flagg, PhD; Research Foundationfor Mental Health at New York State Psychiatric Institute (Columbia Uni-versity), New York, NY, UOI MH46718: Hector R. Bird, MD, DavidShaffer, MD, Myrna Weissman, PhD, Patricia Cohen, PhD, Denise Kandel,PhD, Christina Hoven, DrPH, Mark Davies, MPH, Madelyn S. Gould,PhD, and Agnes Whitaker, MD; Yale University, New Haven, Connecticut,UOI MH46717: Mary Schwab-Stone, MD, Philip J. Leaf, PhD, Sarah Hor-witz, PhD, and Judith H. Lichtman, MPH; University of Puerto Rico, SanJuan, Puerto Rico, UOI MH46732: Glorisa Canino, PhD, Maritza Rubio-Stipec, MA, Milagros Bravo, PhD, Margarita Alegria, PhD, Julio Ribera,PhD, Sara Huertas, MD, Michael Woodbury, MD, and Jose Bauermeister.Computer analysis for this study was supported by Mental Health ResearchGrant MH30906.
REFERENCES
Bird, H. R., Canino, G., Rubio-Stipec, M., & Ribera, J. C. (1987). Further measures of thepsychometric properties of the Children's Global Assessment Scale. Archives of GeneralPsychiatry, 44, 821-824.
Bird, H. R., Yager, T. J., Staghezza, B., Gould, M. S., Canino, G., & Rubio-Stipec, M. (1990).Impairment in the epidemiological measurement of childhood psychopathology in thecommunity, Journal of the American Academy of Child and Adolescent Psychiatry, 29,796-803.
Bird, H. R., Schwab-Stone, M., Andrews, H., Goodman, S. H., Dulcan, M., Rubio-Stipec, M.,Moore, R. E, Chiang, P.-H., Canino, G., Fisher, P., Hoven, C. W., Gould, M. S., &Richters, J. (In Press). Global measures of impairment for epidemiologic and clinical usewith children and adolescents. Journal of Methods in Psychiatric Research.
Bound, J. (1991). Self-reported versus objective measures of health in retirement models.Journal of Human Resources, 26, 106-138.
Brandenburg, N., Friedman, R. M, & Silver, S. E. (1990). The epidemiology of childhoodpsychiatric disorders: prevalence findings from recent studies. Journal of the AmericanAcademy of Child and Adolescent Psychiatry, 29, 76-83.
Brown, G. M. (1993). Life events and affective disorder: Replications and limitations.Psychosomatic Medicine, 55, 248-259.
Burns, B. J. (1991). Mental health service use by adolescents in the 1970s and 1980s. Journalof the American Academy of Child and Adolescent Psychiatry 30, 144-149.
Cohen, P., Velez, N., Kohn, M., Schwab-Stone, M., & Johnson, J. (1987). Child psychiatricdiagnosis by computer algorithms: Theoretical issues and empirical tests. Journal of theAmerican Academy of Child and Adolescent Psychiatry, 26, 631-638.
Measuring Mental Health Status 189

Frank, R., & Gertler, P. (1991). An assessment of measurement error bias for estimating theeffect of mental distress on income Journal of Human Resources, 26, 154-164.
Frank, R. & Kamlet, M. (1989). Determining provider choice for the treatment of mentaldisorder: The role of health and mental health status. Health Services Research, 24, 83-103.
Greenley, J. R. (1984). Social factors, mental illness, and psychiatric care: recent advancesfrom a sociological perspective. Hospital and Community Psychiatry, 35, 813-820.
Jensen, P., Roper, M., Fisher, P., Piacentini, J., Canino, G., Richters, J., Rubio-Stipic, M.,Dulcan, M., Goodman, S., Davies, M., Rae D., Shaffer, D., Bird, H., Lahey, B., &Schwab-Stone, M. (1995). Test-retest reliability of the diagnostic interview schedule forchildren (DISC 2. 1): Parent, child, and combined informant algorithms. Archives ofGeneral Psychiatry, 52, 61-71.
Lahey, B. B., Flagg, E. W., Bird, H. R., Schwab-Stone, M., Canino, G., Dulcan, M. K., Leaf,P. J., Davies, M., Brogan, D., Bourdon, K., Horwitz, S. M., Rubio-Stipec, M., Freeman,D. H., Lichtman, J., Shaffer, D., Goodman, S. H., Narrow, W. E., Weissman, M. M.,Kandel, D. B., Jensen, P. S., Richters, J. E., & Regier, D. A. (1996) The NIMH Methodsfor the epidemiology of child and adolescent mental disorders (meca) study: Backgroundand methodology. Journal of the American Academy of Child and Adolescent Psychiatry,35, 855-864.
Leaf, P. J., Alegria, M., Cohen, P., Goodman, S. H., Horwitz, S. M., Hoven, C. W., Narrow,W. E., Vaden-Kianan, M. & Regier, D. A. (1996). Mental health service use in thecommunity and schools: Results from the four community MECA study. Journal of theAmerican Academy of Child and Adolescent Psychiatry, 35, 889-897.
Links, P. S., Boyle, M. H., & Offord, D. R. (1989). The prevalence of emotional disorder hichildren. Journal of Nervous and Mental Disease, 177, 85-91.
Manning, W., Newhouse, J., & Ware, J. (1982). The status of health in demand estimation:or beyond excellent, good, fair, poor. In V. Fuchs (Ed.) Economic aspects of health (pp.143-184). Chicago: National Bureau of Economic Research and University of ChicagoPress.
Shaffa, D., Gould, M., Brasic, J., Ambrosini, P., Fisher, P, Bird, H., & Auwahlia, S. (1984).A children's global assessment scale (C-GAS). Archives of General Psychiatry, 40, 228-231.
Shaffa, D., Fisher, P., Dulcan, M., Davies, M., Piacentini, J., Schwab-Stone, M., Lahey, B. B.,Bourdon, K., Jensen, P., Bird, H. R., Canino, G., & Regier, D. A. (1996). The secondversion of the NIMH diagnostic interview schedule for children (DISC-2): Description,acceptability, prevalence and the relationship to measures of impairment andcharacteristics of measures of onset and impairment in the MECA Study. Journal of theAmerican Academy of Child and Adolescent Psychiatry, 35, 865-877.
Schwab-Stone, M. E., Shaffa, D., Dulcan, M. K., Jensen, P. S., Fisher, M. S., Bird, H. R.,Goodman, S. H., Lahey, B. B., Lichtman, J. H., Canino, G., Rubio-Stipec, M. & Rae,D. S. (1996). Criterion validity of the NIMH diagnostic interview schedule for childrenversion 2. 3 (DISC-2. 3). Journal of the American Academy of Child and AdolescentPsychiatry, 35, 878-888.
Shaboume, C. D. (1988). The role of social support and life events stress in use of mentalhealth services. Social Science and Medicine, 27, 1393-1400.
Toomey, B. G., & Christie, D. J. (1990). Social stressors in childhood: Poverty, discrimination,and catastrophic events. In L. E. Arnold (Ed.) Childhood stress (pp. 424-456). NY: Wiley.
Glied et al.190
Related Documents











