Measurement of the buccolingual inclination of teeth: Manual technique vs 3-dimensional software Mahtab Nouri, a Amir Hossein Abdi, b Arash Farzan, c Faraneh Mokhtarpour, d and AliReza Akbarzadeh Baghban e Tehran and Babol, Iran Introduction: In this study, we aimed to measure the inclination of teeth on dental casts by a manual technique with the tooth inclination protractor (TIP; MBI, Newport, United Kingdom) and a newly designed 3-dimensional (3D) software program. The correlation of the 2 techniques was evaluated, and the reliability of each technique was assessed separately. Methods: This study was conducted on 36 dental casts of normal, well-aligned Class I occlusions; we assessed 432 teeth. All casts had a normal Class I occlusion. After determining the facial axis of the clinical crown and the facial axis points on the dental casts, we measured the inclinations of the incisors and posterior teeth up to the first molars in each dental arch relative to Andrews' occlusal plane and the posterior occlusal plane using the TIP. Moreover, the casts were scanned by a structured- light 3D scanner. The inclination of teeth relative to the occlusal plane was determined using the new software. To assess the reliability, measurements of all teeth from 15 casts were repeated twice by the 2 methods. Intraclass correlation coefficient and Dahlberg's formula were used for calculation of correlation and reliability. Results: Overall, the 2 techniques were not significantly different in the measurements of the inclinations of the teeth in both jaws. The ranges of Dahlberg's formula were 3.1 to 5.8 for the maxilla and 3.3 to 5.9 for the mandible. The overall correlation of the 2 techniques according to the intraclass cor- relation coefficient was 0.91. For calculation of reliability, the intraclass correlation coefficients for the TIP and the 3D method were 0.73 and 0.82, respectively. Conclusions: The TIP and the 3D software showed a high correlation for measurement of the inclinations of maxillary and mandibular teeth relative to the occlusal plane. Also, the reproducibility of the measurements in each method was high. (Am J Orthod Dentofacial Orthop 2014;146:522-9) T he inclination of anterior teeth is an extremely important factor in smile esthetics. It has been introduced as 1 of the 6 keys of occlusion by An- drews. 1 Moreover, it is a fundamental parameter in determination of the prescription of preadjusted ortho- dontic appliances. 2 Two issues are important for the measurement of tooth inclination: the measurement tool and the defined landmarks. Several tools have been used for this purpose: cephalometric angular measurements, 3,4 conveyor and compass on dental casts, 5 the tooth inclination protractor (TIP; MBI, New- port, United Kingdom) on the casts 6 or intraorally, 7 and 3-dimensional (3D) methods including angular mea- surements on 3D cast models 8-14 or cone-beam computed tomography (CBCT). 15,16 An accurate error- free technique for this purpose has yet to be found. However, the TIP has been demonstrated to be an inex- pensive, easy-to-use, noninvasive, and reliable method a Associate professor, Dentofacial Deformities Research Center, Research Institute of Dental Sciences, and Department of Orthodontics, School of Dentistry, Shahid Beheshti University of Medical Sciences, Tehran, Iran. b Research assistant, Computer Engineering Department, Sharif University of Technology, and School of Dentistry, Shahid Beheshti University of Medical Sci- ences, Tehran, Iran. c Postgraduate student, Department of Orthodontics, Dental Research Center, Research Institute of Dental Sciences, Shahid Beheshti University of Medical Sciences, Tehran, Iran. d Postgraduate student, Department of Operative Dentistry, School of Dentistry, Babol University of Medical Sciences, Babol, Iran. e Associate professor, Department of Basic Sciences, School of Rehabilitation, Shahid Beheshti University of Medical Sciences, Tehran, Iran. All authors have completed and submitted the ICMJE Form for Disclosure of Potential Conflicts of Interest, and none were reported. This study was based on an undergraduate thesis by Faraneh Mokhtarpour and supervised by Mahtab Nouri at the Dental School of Shahid Beheshti University of Medical Sciences. It was funded by the Dentofacial Deformity Research Center, Research Institute of Dental Sciences, Shahid Beheshti University of Medical Sciences, grant no. 419/326. Address correspondence to: Arash Farzan, Department of Orthodontics, School of Dentistry, Shahid Beheshti University of Medical Sciences, Tehran, Iran; e-mail, [email protected]. Submitted, February 2014; revised and accepted, June 2014. 0889-5406/$36.00 Copyright Ó 2014 by the American Association of Orthodontists. http://dx.doi.org/10.1016/j.ajodo.2014.06.018 522 TECHNO BYTES

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
TECHNO BYTES
Measurement of the buccolingual inclinationof teeth: Manual technique vs 3-dimensionalsoftware
Mahtab Nouri,a Amir Hossein Abdi,b Arash Farzan,c Faraneh Mokhtarpour,d and AliReza Akbarzadeh Baghbane
Tehran and Babol, Iran
aAssoof DeBehesbReseTechnencescPostgReseaSciendPostBaboleAssoShahi
522
Introduction: In this study, we aimed to measure the inclination of teeth on dental casts by amanual techniquewith the tooth inclination protractor (TIP; MBI, Newport, United Kingdom) and a newly designed 3-dimensional(3D) software program. The correlation of the 2 techniques was evaluated, and the reliability of each techniquewas assessed separately. Methods: This study was conducted on 36 dental casts of normal, well-alignedClass I occlusions; we assessed 432 teeth. All casts had a normal Class I occlusion. After determining thefacial axis of the clinical crown and the facial axis points on the dental casts, we measured the inclinationsof the incisors and posterior teeth up to the first molars in each dental arch relative to Andrews' occlusalplane and the posterior occlusal plane using the TIP. Moreover, the casts were scanned by a structured-light 3D scanner. The inclination of teeth relative to the occlusal plane was determined using the newsoftware. To assess the reliability, measurements of all teeth from 15 casts were repeated twice by the 2methods. Intraclass correlation coefficient and Dahlberg's formula were used for calculation of correlationand reliability. Results: Overall, the 2 techniques were not significantly different in the measurements ofthe inclinations of the teeth in both jaws. The ranges of Dahlberg's formula were 3.1� to 5.8� for the maxillaand 3.3� to 5.9� for the mandible. The overall correlation of the 2 techniques according to the intraclass cor-relation coefficient was 0.91. For calculation of reliability, the intraclass correlation coefficients for the TIPand the 3D method were 0.73 and 0.82, respectively. Conclusions: The TIP and the 3D software showeda high correlation for measurement of the inclinations of maxillary and mandibular teeth relative to the occlusalplane. Also, the reproducibility of the measurements in each method was high. (Am J Orthod DentofacialOrthop 2014;146:522-9)
The inclination of anterior teeth is an extremelyimportant factor in smile esthetics. It has beenintroduced as 1 of the 6 keys of occlusion by An-
drews.1 Moreover, it is a fundamental parameter indetermination of the prescription of preadjusted ortho-dontic appliances.2 Two issues are important for themeasurement of tooth inclination: the measurementtool and the defined landmarks. Several tools havebeen used for this purpose: cephalometric angular
ciate professor, Dentofacial Deformities Research Center, Research Institutental Sciences, and Department of Orthodontics, School of Dentistry, Shahidhti University of Medical Sciences, Tehran, Iran.arch assistant, Computer Engineering Department, Sharif University ofology, and School of Dentistry, Shahid Beheshti University of Medical Sci-, Tehran, Iran.raduate student, Department of Orthodontics, Dental Research Center,rch Institute of Dental Sciences, Shahid Beheshti University of Medicalces, Tehran, Iran.graduate student, Department of Operative Dentistry, School of Dentistry,University of Medical Sciences, Babol, Iran.ciate professor, Department of Basic Sciences, School of Rehabilitation,d Beheshti University of Medical Sciences, Tehran, Iran.
measurements,3,4 conveyor and compass on dentalcasts,5 the tooth inclination protractor (TIP; MBI, New-port, United Kingdom) on the casts6 or intraorally,7 and3-dimensional (3D) methods including angular mea-surements on 3D cast models8-14 or cone-beamcomputed tomography (CBCT).15,16 An accurate error-free technique for this purpose has yet to be found.However, the TIP has been demonstrated to be an inex-pensive, easy-to-use, noninvasive, and reliable method
All authors have completed and submitted the ICMJE Form for Disclosure ofPotential Conflicts of Interest, and none were reported.This study was based on an undergraduate thesis by Faraneh Mokhtarpour andsupervised by Mahtab Nouri at the Dental School of Shahid Beheshti Universityof Medical Sciences. It was funded by the Dentofacial Deformity ResearchCenter, Research Institute of Dental Sciences, Shahid Beheshti University ofMedical Sciences, grant no. 419/326.Address correspondence to: Arash Farzan, Department of Orthodontics, Schoolof Dentistry, Shahid Beheshti University of Medical Sciences, Tehran, Iran;e-mail, [email protected], February 2014; revised and accepted, June 2014.0889-5406/$36.00Copyright � 2014 by the American Association of Orthodontists.http://dx.doi.org/10.1016/j.ajodo.2014.06.018

Nouri et al 523
for measuring incisor crown inclination.6,7 Moreover, 3Dtechniques have high reliability and accuracy for suchangular measurements.10,14
Landmarks used for measuring tooth inclinations aredifferent in lateral cephalograms, cast measurements,3D models, and 3D imaging (CBCT). In 2-dimensionaland 3D radiographic techniques, the long axis of thetooth has been used3,4,16; in cast-based or intraoralmeasurements, the facial axis of the clinical crown hasbeen used.5 Moreover, different horizontal referenceplanes have been used in various studies. Cephalometricmethods use palatal, mandibular, and occlusal refer-ence planes.3,4 Andrews1 used an occlusal plane thatwas approximated with a plastic template. This tem-plate was in contact with the anterior and posteriorteeth.5,17 He used this method for measuring toothinclination represented by tip and torque. Ross et al18
introduced the posterior occlusal plane for measuringthe inclination of posterior teeth. This plane wastangent with the most occlusal cusp points in both firstmolars, and 1 or 2 premolars. Richmond et al6 used theirown invented device, the TIP, with an occlusal planesimilar to that of Andrews. In the 3D cast-basedmethods and radiography, different reference planeshave been used.14,16 Overall, changes in the horizontalreference plane compromise the validity of differentmethods for measuring tooth inclinations (relative toone another, or at different treatment phases).However, this plane might have a minimal impact onreliability.6
At present, modern 3D digital technologies makesuch measurements easily possible in a short time andwith high accuracy. Furthermore, software programshave been developed for 3D analysis of dental castsused for diagnosis of discrepancies, treatment planning,and evaluation of changes as a result of treatment. Thesesoftware programs have the potential for measuring all 6keys of ideal occlusion suggested by Andrews.11,14
Several manufacturers, such as Orthocad,19 Ortho-proof,20 and O3DM,14 have introduced commercial soft-ware programs for analyzing digital models andmeasuring linear and angular parameters on 3D models.
Considering all the above, in this study we had thefollowing objectives: (1) to measure the inclinations ofthe incisors, canines, premolars, and first molars ondental casts using the TIP and a 3D software developedat Shahid Beheshti Dental School in Tehran, Iran; (2) toassess the correlations of the 2 techniques and the dis-crepancies between measurements; and (3) to assessthe reliability of the 2 techniques.
The null hypothesis of the study was that no signifi-cant correlation exists between measurements madewith the TIP and the computer software.
American Journal of Orthodontics and Dentofacial Orthoped
MATERIAL AND METHODS
This study was conducted on 36 dental casts ofnormal and well-aligned Class I occlusions (432 teeth).The buccolingual inclinations of the incisors, canines,premolars, and first molars (12 teeth in each cast) weremeasured by the TIP and a 3D laser scanner. Thesenormal-occlusion casts were selected from the cast ar-chives of Qazvin Dental School in Qazvin, Iran, usingconvenience sampling.
We used the following tools. The TIP was used tomeasure the inclinations of the anterior teeth, premolars,andmolars on the dental casts and in the mouth: this de-vice has a horizontal plane, a conveyor, and a rod forcontact with the labial surfaces of the teeth formeasuring the axial inclination of the tooth crown. Astructured-light 3D scanner (Maestro3D Desktop Scan-ner; AGE Solutions, Pontedera, Italy) was used for the3D scanning of the dental casts with 10-mm readability.
The measurement technique was the following. First,the locations of the facial axis points were marked oneach tooth with a fine-tip pencil (diameter, 0.5 mm) ac-cording to the method of Andrews.1
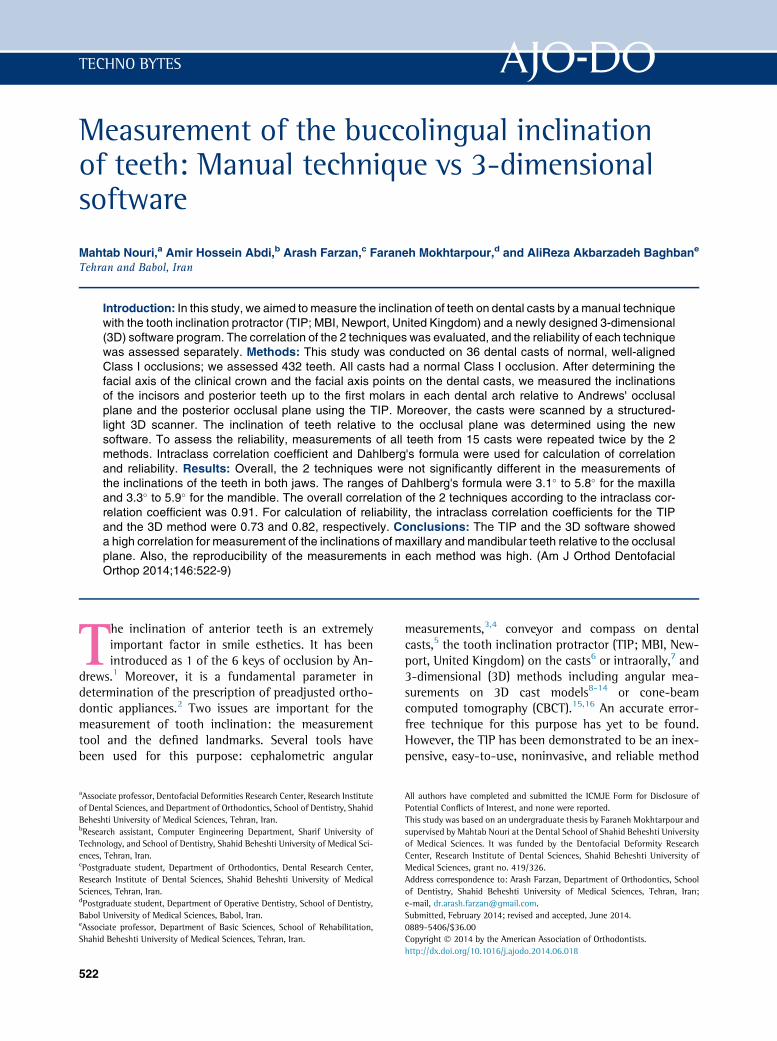
For measuring the inclinations of the anterior teethwith the TIP, the horizontal plane of the device wasplaced in contact with the occlusal plane, as describedby Andrews.5 Then, the axial inclination of the crownwas recorded by contacting the vertical rod with thecrown surface and reading the degree displayed by theconveyor (Fig 1, A and B).
For measuring the inclinations of the canines, pre-molars, and first molars, the posterior occlusal planewas used as described by Ross et al,18 and the axial incli-nation of teeth was measured as described for the ante-rior teeth. Because of the TIP's structure, using theocclusal plane, including the contact points with all in-cisors, was not possible in all cases when measuring theinclinations of the canines, premolars, and molars (Fig 1,C and D).
For the 3D measurements, all casts were digitizedby the 3D scanner, and their 3D models were saved instereolithography format.
A simulator software program for 3D measurementwas developed at the Orthodontic Department of ShahidBeheshti Dental School in Iran by 1 of the authors(A.H.A.), a dentist who also has a master's degree in com-puter science (artificial intelligence). This software hasthe following capabilities: display of 3D point clouds,triangulation of the point cloud and production of theobject's surface, measurement of distances betweenpoints in a virtual model, definition of occlusal andsagittal planes, measurement of the inclination of eachtooth, and superimposition of 2 dental models based
ics October 2014 � Vol 146 � Issue 4
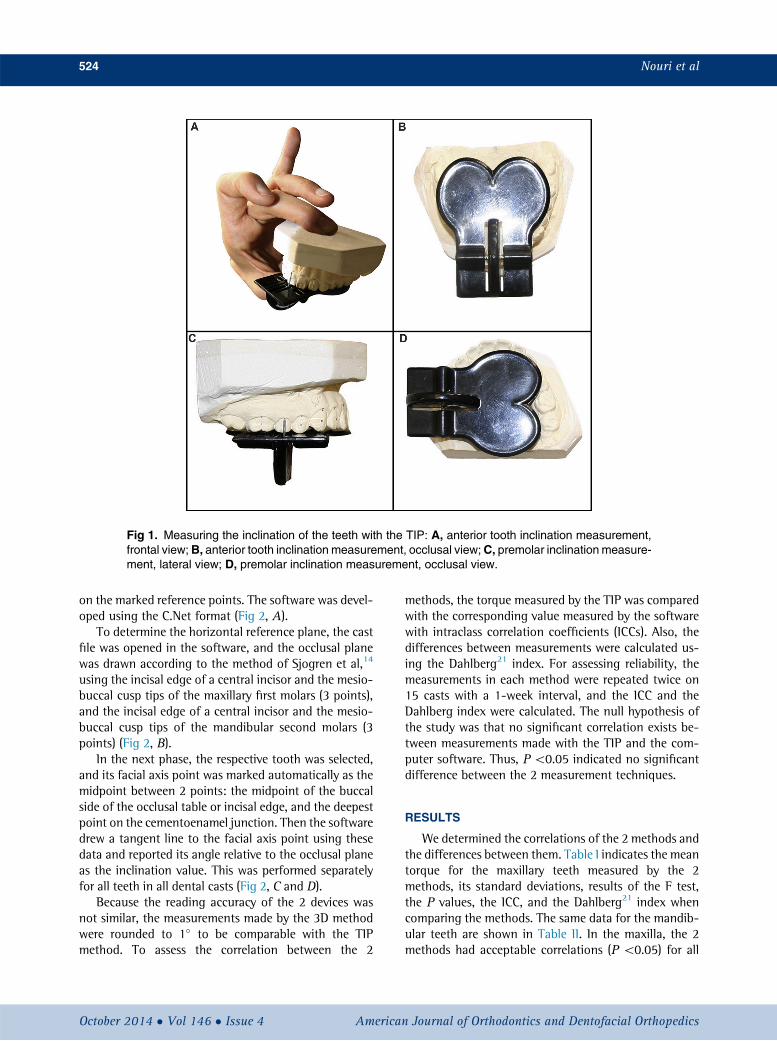
Fig 1. Measuring the inclination of the teeth with the TIP: A, anterior tooth inclination measurement,frontal view;B, anterior tooth inclination measurement, occlusal view;C, premolar inclination measure-ment, lateral view; D, premolar inclination measurement, occlusal view.
524 Nouri et al
on the marked reference points. The software was devel-oped using the C.Net format (Fig 2, A).
To determine the horizontal reference plane, the castfile was opened in the software, and the occlusal planewas drawn according to the method of Sjogren et al,14
using the incisal edge of a central incisor and the mesio-buccal cusp tips of the maxillary first molars (3 points),and the incisal edge of a central incisor and the mesio-buccal cusp tips of the mandibular second molars (3points) (Fig 2, B).
In the next phase, the respective tooth was selected,and its facial axis point was marked automatically as themidpoint between 2 points: the midpoint of the buccalside of the occlusal table or incisal edge, and the deepestpoint on the cementoenamel junction. Then the softwaredrew a tangent line to the facial axis point using thesedata and reported its angle relative to the occlusal planeas the inclination value. This was performed separatelyfor all teeth in all dental casts (Fig 2, C and D).
Because the reading accuracy of the 2 devices wasnot similar, the measurements made by the 3D methodwere rounded to 1� to be comparable with the TIPmethod. To assess the correlation between the 2
October 2014 � Vol 146 � Issue 4 American
methods, the torque measured by the TIP was comparedwith the corresponding value measured by the softwarewith intraclass correlation coefficients (ICCs). Also, thedifferences between measurements were calculated us-ing the Dahlberg21 index. For assessing reliability, themeasurements in each method were repeated twice on15 casts with a 1-week interval, and the ICC and theDahlberg index were calculated. The null hypothesis ofthe study was that no significant correlation exists be-tween measurements made with the TIP and the com-puter software. Thus, P\0.05 indicated no significantdifference between the 2 measurement techniques.
RESULTS
We determined the correlations of the 2 methods andthe differences between them. Table I indicates the meantorque for the maxillary teeth measured by the 2methods, its standard deviations, results of the F test,the P values, the ICC, and the Dahlberg21 index whencomparing the methods. The same data for the mandib-ular teeth are shown in Table II. In the maxilla, the 2methods had acceptable correlations (P \0.05) for all
Journal of Orthodontics and Dentofacial Orthopedics
Fig 2. The programmed software in the Shahid Beheshti University orthodontic department:A, generalview of the software; B, selecting the horizontal reference plane; C, 3 points were selected: facial axispoint, its corresponding points on the occlusal or incisal surface and the cervical surface; D, the soft-ware obtained the tangent line at the facial axis point using the reference points and reported its anglerelative to the occlusal plane as the inclination value.
Table I. Mean torque values (degrees) for the maxillary teeth measured by the TIP and the 3D software
Tooth
Maxillary right Maxillary left
6 5 4 3 2 1 1 2 3 4 5 63DMean �10.5 �10.9 �7.5 �4.8 10.6 10.5 8.6 8.2 �5.9 �8.8 �12.9 �9.8SD 4.8 6.4 7.6 7.4 5.7 6.1 4.4 7.6 5.7 8.5 7.6 3.5
TIPMean �11.1 �13.7 �11.8 �5.4 8.2 7.1 6.7 4.4 �6.6 �12.4 �14.1 �10.9SD 6.7 5.1 4.2 5.7 4.1 6.2 6.0 5.9 4.7 5.7 7.3 6.3
F 3.547 5.376 2.320 5.692 3.049 3.900 5.548 2.227 3.141 2.973 4.446 3.501P value 0.006 0.001 0.046 0.000 0.014 0.004 0.000 0.054 0.012 0.015 0.002 0.007ICC (r) 0.727 0.771 0.492 0.830 0.636 0.689 0.796 0.507 0.690 0.622 0.779 0.721Dahlberg 3.8 3.7 5.6 3.5 3.8 4.5 3.1 5.8 3.6 5.6 4.5 4.5
P values less than 0.05 indicate no statistical significance considering the null hypothesis of negative correlation between the 2 methods.6, First molar; 5, second premolar; 4, fist premolar; 3, canine; 2, lateral incisor; 1, central incisor.
Nouri et al 525
teeth. Also, according to the Dahlberg index, the differ-ences in measurements ranged from 3.1� (left centralincisor) to 5.8� (left lateral incisor).
In the mandible, the 2 methods had acceptable corre-lations for all teeth (P\0.05). Furthermore, the differ-ences in measurements according to the Dahlberg21
index ranged from 3.3� (left central incisor) to 5.9�
(left lateral incisor).Overall, the differences in measurements between the
2methods were insignificant. The total correlation coeffi-cient between the TIP and the software was 0.91, and thetotal numeric difference in measurements was 4.4�.
American Journal of Orthodontics and Dentofacial Orthoped
For reliability, the ICC values were 0.73 and 0.82 forrepeated measurements made by the TIP and the soft-ware on the 15 casts, respectively.
The Dahlberg21 index values for repeated measure-ments made by the TIP and the software on the 15 castswere 1.5� to 4� and 1.2� to 3.6�, respectively. The detailsregarding the ICC and the Dahlberg index for the TIP andthe 3D software are given in Tables III and IV.
DISCUSSION
In this study, the buccolingual inclinations of inci-sors, canines, premolars, and first molars in 36 dental
ics October 2014 � Vol 146 � Issue 4
Table III. ICC values and the Dahlberg index for the TIP method in the 2 time measurements
Tooth
6 5 4 3 2 1 1 2 3 4 5 6ICC 0.91 0.78 0.8 0.63 0.71 0.71 0.74 0.7 0.39 0.71 0.83 0.96Dahlberg 4 1.9 1.9 2.6 2.2 3 2.1 3.4 2.8 2.5 1.5 2.6
These values indicate the reproducibility of the measurements.6, First molar; 5, second premolar; 4, fist premolar; 3, canine; 2, lateral incisor; 1, central incisor.
Table II. Mean torque values (degrees) for the mandibular teeth measured by the 2 methods
Tooth
Mandibular right Mandibular left
6 5 4 3 2 1 1 2 3 4 5 63DMean �36.1 �25.4 �18.2 �10.3 1.8 7.9 6.4 3.6 �9.2 �21 �27.4 �32.9SD 4.9 7.5 6.9 6.0 8.0 8.0 7.7 7.8 7.7 6.4 8.9 5.8
TIPMean �35.3 �24.9 �20.3 �11.5 0.7 3.9 3.2 0.2 �11.3 �23.1 �28.2 �33.4SD 5.8 6.5 6.0 6.9 5.7 6.2 6.7 6.3 7.7 8.9 7.1 6.1
F 5.585 2.633 2.045 6.739 5.971 10.405 4.035 7.934 8.754 2.470 6.031 3.603P value 0.001 0.027 0.075 0.000 0.000 0.000 0.003 0.000 0.000 0.035 0.000 0.009ICC (r) 0.757 0.633 0.505 0.850 0.835 0.843 0.719 0.827 0.873 0.593 0.839 0.734Dahlberg 3.6 5.1 5.3 3.3 3.7 4.1 4.9 4 3.7 5.9 4.2 3.8
P values less than 0.05 indicate no statistical significance considering the null hypothesis of negative correlation between the 2 methods.6, First molar; 5, second premolar; 4, fist premolar; 3, canine; 2, lateral incisor; 1, central incisor.
Table IV. ICC values and the Dahlberg index for the 3D software in the 2 time measurements
Tooth
6 5 4 3 2 1 1 2 3 4 5 6ICC 0.6 0.86 0.89 0.9 0.92 0.95 0.96 0.72 0.85 0.91 0.68 0.64Dahlberg 3.6 2.4 3.1 2.7 1.2 1.6 2.1 2.2 2.4 3 1.9 2.9
These values indicate the reproducibility of the measurements.6, First molar; 5, second premolar; 4, fist premolar; 3, canine; 2, lateral incisor; 1, central incisor.
526 Nouri et al
casts of normal Class I occlusions were determined by amanual technique with the TIP and a 3D method using anewly developed software after scanning with astructured-light 3D scanner with 10-mm precision. Thecorrelations between the 2 techniques and the reliabilityof each method were evaluated.
The coronal landmarks used in the 2 methods wereequal, and the facial axis points were used for this pur-pose. However, the horizontal reference planes weredifferent. In the TIP method, an occlusal plane tangentto the molars and incisors was constructed for the inci-sors. Nevertheless, use of this plane was difficult becauseof the small horizontal plane of the device. When we re-corded the inclinations of posterior teeth (canines, pre-molars, and first molars), contact was not possible withall incisors. Thus, the posterior occlusal plane was usedfor these teeth.18 In the 3D measurement software, a
October 2014 � Vol 146 � Issue 4 American
plane similar to that suggested by Andrews5,17 andapplied by Sjogren et al14 was used. It is obvious thatthe difference in the horizontal reference planes causesa systematic difference between the recorded inclina-tions of the 2 methods. However, it seems that the over-all effect of this issue is small and not great enough tocause statistically significant differences between the 2methods.
The numeric differences for the incisors (with thesame horizontal reference plane in both techniques)and the posterior teeth (with different horizontal refer-ence planes in the 2 methods) were not significant either(the Dahlberg21 index ranged between 3.1� and 5.8� forthe maxillary incisors and between 3.5� and 5.6� for allother posterior maxillary teeth). These ranges were 3.7�
to 4.9� for the mandibular incisors and 3.3� to 5.9� forall other posterior mandibular teeth. However, this
Journal of Orthodontics and Dentofacial Orthopedics

Nouri et al 527
finding does not indicate the clinical insignificance ofthe horizontal reference plane for the measurement ac-curacy of the inclination of tooth crowns. A fixed hori-zontal reference plane is important, especially for themeasurement of alterations in tooth inclinations afterorthodontic treatment.10 Costalos et al9 evaluated thecorrelations between the OrthoCad and the manualtechnique in the measurements of the American Boardof Orthodontics' objective grading system criteria. Theyobserved a statistically significant difference whenmeasuring alignment and buccolingual inclination ofthe teeth between the plaster and digital models. More-over, in a similar study, Okunami et al13 excluded thebuccolingual inclination of the teeth from the compari-son of the 2 methods because they believed that Ortho-Cad was not capable of measuring this index accordingto American Board of Orthodontics' criteria. This issue isprobably due to the different methods of assessment ofthe buccolingual inclination relative to a horizontal linepassing through the corresponding cusp tip. Thus, whenrecording the buccolingual inclination in the manualand 3D methods, using a reference plane instead ofthe line connecting the corresponding cusp tips in-creases the similarity of the 2 techniques. Furthermore,Kodaka et al12 compared the inclination of tooth crownsaccording to the method of Andrews,5,17 using a 3D laserscanner and Octane (Silicon Graphics) software with themanual technique and a conveyor in their study. Theyfound no significant difference in the mean value ofthe 2 methods; however, the variance of the 3Dmethod was higher than the manual technique.
For assessing the reliability of the TIP device in ourstudy, the measurements were repeated twice on 15casts with a 1-week interval. The lowest ICC value be-longed to a canine (0.39). This finding is probably attrib-utable to the labial surface morphology and the largeangle at the incisal and cervical thirds of this surfacerelative to the facial axis point. Furthermore, the levelof the canine tip, which is the highest relative to theocclusal plane, causes fluctuations in the stability ofthe occlusal plane when one is reading the inclinationson the TIP. In this situation, we have fewer contactpoints on the occlusal plane. The reliability for deter-mining the inclination of incisors was 0.72, which isclose to the rate reported by Richmond et al (0.82).6
To the best of our knowledge, no data are available inthe literature regarding the accuracy of the TIP formeasuring the inclinations of canines, premolars, andmolars. However, the manual for this device claimsthat it can be used for measuring the inclinations of pos-terior teeth. Investigators should be aware of the differ-ence between reference occlusal planes in measuring theinclinations of incisors and canines or posterior teeth,
American Journal of Orthodontics and Dentofacial Orthoped
because this device lacks contact with all anterior teethwhile measuring the inclinations of canines and poste-rior teeth. In this study, the ICC for measuring the reli-ability of the TIP for premolars and first molars rangedbetween 0.71 and 0.96, and the Dahlberg21 index rangedfrom 1.5� to 4�. These values were different from therates reported by Shu et al,22 who used a device similarto the TIP with the posterior occlusal plane (the ICCand the Dahlberg index in their study were 0.993 to0.929 and 1.622� to 0.719�, respectively). However,these differences were not clinically significant.
Overall, the reliability of the 3D method for anteriorteeth was higher than for posterior teeth (ICC values,0.88, 0.76, and 0.87 for incisors, canines, and posteriorteeth, respectively). The ICC value between the 2 mea-surements with this device was 0.82 for all teeth, andthe Dahlberg21 index ranged between 1.2� and 3.6�.Thus, the reliability of the 3D method for measurementof inclination was slightly better than the manual tech-nique. This finding agrees with the results of Costaloset al,9 who compared the OrthoCad and the conventionaltechnique for measurement of the American Board ofOrthodontics' objective grading system indexes. The reli-ability of the 3D method used in our study was slightlyless than that of the 3D method used by Kodakaet al12 (ICC, 0.98; Dahlberg index, 0.15�). Moreover,the lower reliability of the measurement of molar incli-nation in our study agreed with the reports of by Se-bata,23 Chiashi et al,8 and Kodaka et al.
In the literature, various techniques have been usedfor the measurement of axial inclinations of teeth, andvariable landmarks have been used. Traditionally, lateralcephalograms were used to measure the inclination ofthe incisors. This technique provided the crown-rootinclination relative to a horizontal reference plane(palatal, occlusal, or mandibular). However, the mistakesin registering the landmarks to assess the inclination ofeach tooth, or using the occlusal plane as the reference,and the ionizing beam radiation are among the short-comings of this technique.3,4,24,25 In dental cast-basedmethods, some of these drawbacks have been obviated.
Andrews5,17 tried to determine the tooth crowninclination, considering the facial axis of the clinicalcrown and the occlusal plane that passes through theanterior and posterior teeth. He used a glass sheet, aconveyor, and a compass for this purpose and aimedto determine the norm of tooth crown inclinations.However, his technique was both time-consuming andrelatively difficult.
The TIP was first introduced for the measurement ofthe inclination of incisors on a dental cast.6 Previousstudies have demonstrated that the TIP is a simple, inex-pensive, and reliable tool for the assessment of tooth
ics October 2014 � Vol 146 � Issue 4

528 Nouri et al
inclination.6,7 Such advantages were determiningfactors for its use for measuring tooth inclinations ondental casts in our study. However, it has someinherent deficiencies regarding the validity of themeasurements, especially in the case of an inordinateocclusal plane (eg, deep curve of Spee, severe curve ofWilson, canted occlusal plane, malposed teeth, oropen-bite malocclusion).6,7 We used casts of normalClass I occlusions because our main objective in thisstudy was to compare the 2 devices for their axialinclination measurements capabilities. Richmond et al6
reported correlations of 0.77 and 0.59 for the inclina-tions of the maxillary and mandibular incisors, respec-tively, between their invented technique and lateralcephalometry. Also, they showed that the TIP consis-tently underestimated the maxillary incisor inclinationby 10.46� compared with lateral cephalometry, but itoverestimated the inclination of mandibular incisors.In a similar study, Ghahferokhi et al7 demonstratedthat the TIP underestimated the inclination of incisorcrowns by an average of 14� relative to the maxillaryplane on lateral cephalometry. However, the TIP calcu-lated the inclination of mandibular incisor crowns rela-tive to the mandibular plane, similar to the value inlateral cephalometry. In our study, the agreement indexvalues between our 2 methods were 0.657 and 0.806,respectively, for measurement of the inclinations of themaxillary and mandibular incisors. Moreover, the 3Dsoftware overestimated the inclinations of maxillaryand mandibular teeth by 2.875� and 2.925�, respec-tively. Although in this study the inclination of the inci-sors in lateral cephalometry was not measured,considering the differences between our study resultsand those of Richmond et al, we can assume that the3D software generally tends to report the inclination ofmaxillary incisors closer and that of mandibular incisorsfarther than the values measured on lateral cephalom-etry compared with the TIP. Meanwhile, when interpret-ing these results, it should be taken into account that thehorizontal reference plane used in the 3D method wasslightly different from the one used in the TIP.3,4,6,24
On the other hand, considering the popularity ofCBCT because of its lower costs and radiation doses,it is now possible to accurately assess the crown androot 3 dimensionally.15 Shewinvanakitkul et al16
measured the inclination of the mandibular caninesand the first molars using CBCT, with the mandibularplane as the reference plane. The reliability of this tech-nique was reported to be excellent (.0.94). In general,in studies assessing tooth inclinations on the casts, theocclusal plane was used, and in radiographic studies,skeletal planes have been used. Considering the changeof occlusal plane during orthodontic treatment, this
October 2014 � Vol 146 � Issue 4 American
plane does not have enough stability to be used as areference plane for measuring tooth inclination.Furthermore, use of radiographic techniques such asCBCT has 2 drawbacks: exposure to the ionizing beamand feasibility of application.
Overall, since the standard deviations of the measure-ments for all teeth were greater than the differences be-tween the measurements made with the 2 methods and,also, greater than the reliability of each technique alone,it seems that both the TIP and the 3D software have clin-ically acceptable accuracy for measuring the inclinationsof teeth.
CONCLUSIONS
A high correlation (r 5 0.91) was found between theTIP device and our 3D method for crown inclinationmeasurements. The overall difference between the 2methods was 4.4�. The reliability of measurements inthe 3D method was higher than that with the TIP device(ICC values, 0.82 vs 0.73, respectively).
ACKNOWLEDGMENT
We thank all the persons who collaborated in thisstudy for their scientific and financial support.
REFERENCES
1. Andrews LF. The six keys to normal occlusion. Am J Orthod 1972;62:296-309.
2. Andrews LF. The straight-wire appliance, origin, controversy, com-mentary. J Clin Orthod 1976;10:99-114.
3. Baumrind S, Frantz RC. The reliability of head film measurements:1. Landmark identification. Am J Orthod 1971;60:111-27.
4. Baumrind S, Frantz RC. The reliability of head film measurements:2. Conventional angular and linear measures. Am J Orthod 1971;60:505-17.
5. Andrews LF. Straight wire: the concept and appliance. San Diego:LA Wells; 1989.
6. Richmond S, Klufas ML, Sywanyk M. Assessing incisor inclination:a non-invasive technique. Eur J Orthod 1998;20:721-6.
7. Ghahferokhi AE, Elias L, Jonsson S, Rolfe B, Richmond S. Criticalassessment of a device to measure incisor crown inclination. AmJ Orthod Dentofacial Orthop 2002;121:185-91.
8. Chiashi M, Aria K, Nakahara R. Measurement method of three-dimensional crown inclination—the effect of differences in bracketbase area on the analysis of crown inclination. OrthodWaves 2004;63:186-92.
9. Costalos PA, Sarraf K, Cangialosi TJ, Efstratiadis S. Evaluation ofthe accuracy of digital model analysis for the American Board ofOrthodontics objective grading system for dental casts. Am J Or-thod Dentofacial Orthop 2005;128:624-9.
10. Ferrario VF, Sforza C, Colombo A, Ciusa V, Serrao G. Three-dimensional inclination of the dental axes in healthy permanentdentitions—a cross-sectional study in a normal population. AngleOrthod 2001;71:257-64.
11. Fukagawa H, Motegi E, Fuma A, Nomura M, Kano M, Sueishi K,et al. Tooth inclination in elderly with many remaining teethobserved by 3-D imaging. Bull Tokyo Dent Coll 2010;51:69-76.
Journal of Orthodontics and Dentofacial Orthopedics

Nouri et al 529
12. Kodaka K, Nishii Y, Sakurai Y, Nojima K, Sueishi K. Crown inclina-tion measured by laser scanner. Orthod Waves 2010;69:8-12.
13. Okunami TR, Kusnoto B, BeGole E, Evans CA, Sadowsky C,Fadavi S. Assessing the American Board of Orthodontics objectivegrading system: digital vs plaster dental casts. Am J Orthod Den-tofacial Orthop 2007;131:51-6.
14. Sjogren AP, Lindgren JE, Huggare JA. Orthodontic study cast anal-ysis—reproducibility of recordings and agreement between con-ventional and 3D virtual measurements. J Digit Imaging 2010;23:482-92.
15. German DS, German J. Cone-beam volumetric imaging: a two-minute drill. J Clin Orthod 2010;44:253-65.
16. Shewinvanakitkul W, Hans MG, Narendran S, Palomo JM.Measuring buccolingual inclination of mandibular canines andfirst molars using CBCT. Orthod Craniofac Res 2011;14:168-74.
17. Andrews LF. Straight wire. Basi teoriche e applicazioni pratiche.Milan, Italy: Elsevier Masson; 1993.
18. Ross VA, Isaacson RJ, Germane N, Rubenstein LK. Influence ofvertical growth pattern on faciolingual inclinations and treat-
American Journal of Orthodontics and Dentofacial Orthoped
ment mechanics. Am J Orthod Dentofacial Orthop 1990;98:422-9.
19. Marcel TJ. Three-dimensional on-screen virtual models. Am J Or-thod Dentofacial Orthop 2001;119:666-8.
20. Favero L, Terrazzani C, Favero V, Stellini E, Cocilovo F. Virtualstudy models: a comparison of modular application systems.Prog Orthod 2009;10:16-25.
21. Dahlberg G. Statistical methods for medical and biological stu-dents. New York: Interscience Publications; 1940.
22. Shu R, Han X, Wang Y, Xu H, Ai D, Wang L, et al. Comparison ofarch width, alveolar width and buccolingual inclination of teethbetween Class II division 1 malocclusion and Class I occlusion.Angle Orthod 2013;83:246-52.
23. Sebata E. An orthodontic study of teeth and dental arch form onthe Japanese normal occlusions. Shikwa Gakuho 1980;80:945-69.
24. Houston W. The analysis of errors in orthodontic measurements.Am J Orthod 1983;83:382-90.
25. Wall B, Kendall G. Collective doses and risks from dental radiologyin Great Britain. Br J Radiol 1983;56:511-6.
ics October 2014 � Vol 146 � Issue 4
Related Documents











