MDR/XDR Tuberculosis and Atypical Mycobacterial Disease Increasing Role for Surgery, Relearning Old Lessons John D. Mitchell, M.D. Professor and Chief Section of General Thoracic Surgery Davis Endowed Chair in Thoracic Surgery University of Colorado School of Medicine Consultant, National Jewish Health

MDR/XDR Tuberculosis and Atypical Mycobacterial Disease MDR/XDR Tuberculosis and Atypical Mycobacterial Disease Increasing Role for Surgery, Relearning.
Dec 22, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

MDR/XDR Tuberculosis and Atypical Mycobacterial Disease
Increasing Role for Surgery, Relearning Old Lessons
John D. Mitchell, M.D.Professor and ChiefSection of General Thoracic SurgeryDavis Endowed Chair in Thoracic SurgeryUniversity of Colorado School of MedicineConsultant, National Jewish Health
AATS Postgraduate Course, April 26th, 2015

No relevant financial relationships to disclose.


Case Presentation: XDR+ Tuberculosis
History• 38 yo male Armenian immigrant• Lived in Russia 2001-2005; last visit 4 years prior• No known history in Russian Prison System• Ankylosing Spondylitis, prior GSW to abdomen• Alcoholic, smoker 1.5 packs/day• History of recurrent pneumonias, AFB (-)• July 2013: Started on Remicade for AS, INH for LTBI• Dec 2013: Fevers, productive cough; AFB (+)• Diagnosed with drug resistant TB

Case Presentation: XDR+ Tuberculosis
Initial Drug Regimen• PZA 1500 mg po qday • Moxifloxacin 600 mg po qday• PAS 4 gm po bid • Linezolid 600 mg po qday• Ethionamide 250 mg qAM, 500 mg qPM• Cycloserine 250 mg po bid• Capreomycin 750 mg (12 mg/kg) IV qMon-Fri• Meropenem 2 gm IV q8h• Augmentin 500 mg po bid










Case Presentation: XDR+ Tuberculosis
Drug Sensitivity Testing (CDC)

Case Presentation: XDR+ Tuberculosis
Revised Drug Regimen• Linezolid 600 mg IV q24h• Cycloserine 250 mg po bid• Imipenem 1 gm IV q12h• Moxifloxacin 800 mg IV q24h• PAS 6 gm po bid• Bedaquiline 400 mg po qday• Clofazimine 100 mg po qday

Case Presentation: XDR+ Tuberculosis
Treatment Course• Eventually rendered sputum culture (-)• Significant medication toxicities• Debilitated, malnourished
What is the role of surgery in this patient?


Mycobacterium TuberculosisGeneral Principles
• Up to one-third of world’s population infected with mycobacterium tuberculosis
• Typical treatment regimens for drug-sensitive TB last 6 to 9 months– INH, rifampin, PZA, ethambutol– Duration and specific regimen depend on pattern of disease
and drug sensitivities, speed of culture conversion
• Chemotherapy usually curative; use of surgery rare

Worldwide Drug-Sensitive TB Treatment Success
2012

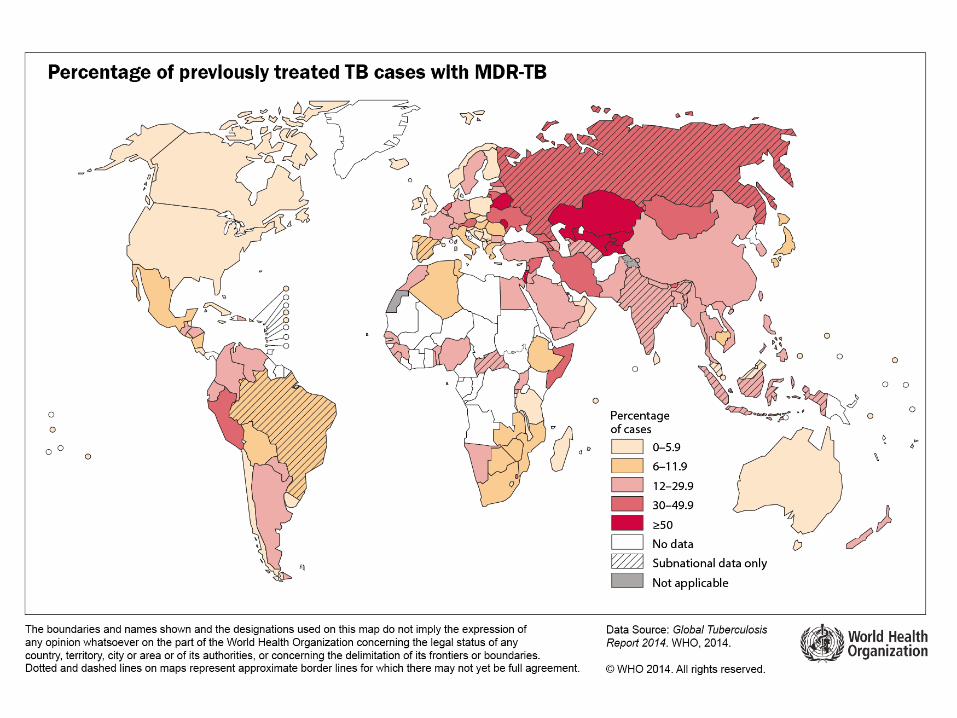
Worldwide Incidence of TuberculosisDecember, 2013
WHO Global Tuberculosis Report 2014. http://www.who.int/tb/publications/global_report/en/index.html
Estimated number of cases,
2013
Estimated number of
deaths, 2013 1.1 million*(1.0–1.3 million)
9.0 million(8.6–9.4 million)
480,000 (350,000-610,000)
All forms of TB
Multidrug-resistant TB
HIV-associated TB 1.1 million (1.0–1.2 million)
360,000(310,000–410,000)
* Excluding deaths attributed to HIV/TB
210,000(130,000–290,000)

Multidrug and Extensively Drug Resistant Tuberculosis
Drug Susceptible Any DrugResistance
MDR-TB XDR- TB
Resistance to at least isoniazid and rifampin (MDR) plus resistance to fluoroquinolones and one of the second-line injectable drugs (amikacin, kanamycin, or capreomycin)
9 million TB cases



New Diagnostic Tests for MDRTBXpert MTB/RIF Assay
• Automated PCR test that detects TB and rifampin resistance
• 2 hour turn around time
• Allows Point of Care diagnosis, treatment
• Funded by Gates Foundation, NIH
Designing a Treatment Regimen for MDRTB
General Principles• Early DR-TB detection/prompt initiation of therapy
• Regimens should be based on:• the history of drugs taken by the patient• drugs and regimens used in the country and• the prevalence of resistance
• Regimens should consist ≥ 4 effective drugs
• When possible, once daily dosing is recommended
• Drug dosage should be determined by body weight
WHO Guidelines for the Programmatic Management of Drug-Resistant TB2008

Worldwide MDRTB Treatment Success
2009
WHO Global Tuberculosis Report 2012. http://www.who.int/tb/publications/global_report/en/index.html


Worldwide XDRTB Treatment Success
2011
WHO Global Tuberculosis Report 2014. http://www.who.int/tb/publications/global_report/en/index.html

Drug Resistant TuberculosisPredictors of Success and Failure
• Use of pyrazinamide and/or ethambutol, if susceptible
• Use of a fluoroquinolone• Use of > 5 drugs• Sputum conversion by 2 mos• Surgical resection
• Previous therapy• Number of drugs resistant• Resistance to FQN• Resistance to capreomycin• Presence of cavitation• Low BMI• HIV infection• Poor adherence• Positive cultures at 2-3 mos• XDR-TB
Success Failure

Surgery for MDR-TB, XDR-TBFactors favoring Surgery
• A pattern of drug-resistance so extensive that it compromises the likelihood of medical cure
• Localized lung damage (cavitation, destroyed lung) that might be a focus of persistent disease and/or further acquired resistance
• Allergies or intolerance to essential medications that might afford cure
• Lack of access to curative chemotherapy
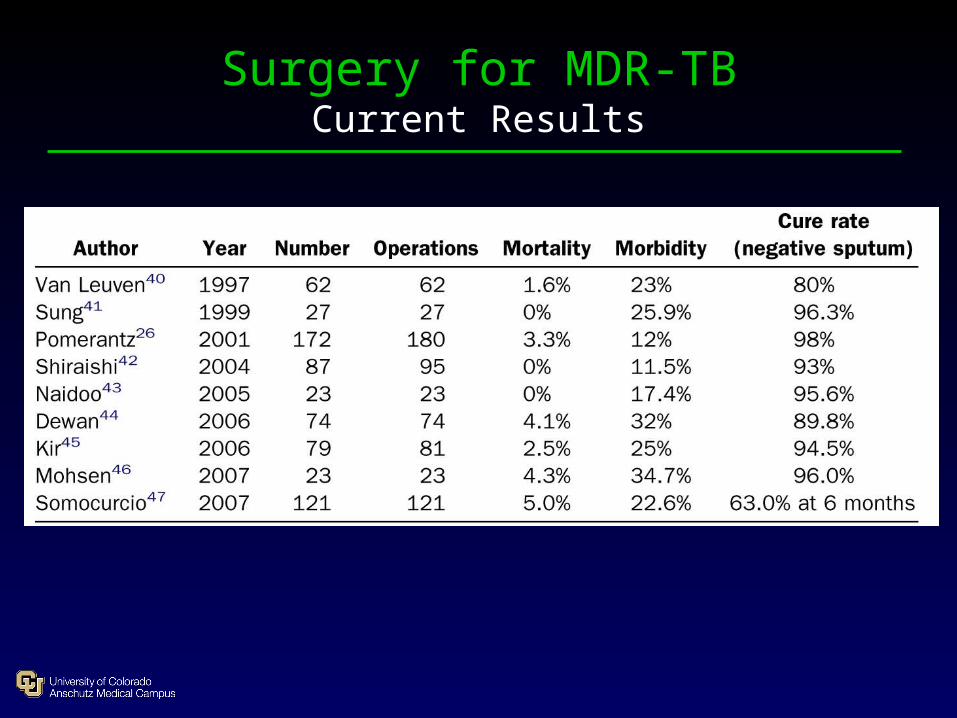
Surgery for MDR-TBCurrent Results

Surgery for MDR-TBCurrent Results
Xu HB, et al. J Antimicrob Chemother 2011; 66: 1687–1695

Role of Surgery in MDR-TBNJH Experience
Odds Ratios for Individual Variables
Drug resistance (#)
Current drug suscept. (#)
Surgery done
FQN used
Non-extensive disease
Unfavorable Favorable
-1 -0.5 0 0.5 1 1.5 2
p<0.0001
p=0.0004
p=0.0008
p=0.02
p=0.48
log OR
Chan ED, et al. AJRCCM 2004:169:1103

Surgery for MDR/XDR-TBRepublic of Georgia
Vashiakidze S et al. Ann Thorac Surg 2013;95:1892

Nontuberculous Mycobacteria (NTM)
• AKA: Atypical mycobacteria
Environmental mycobacteria (EM)
Mycobacteria other than tuberculosis (MOTT)
• Found in water, soils, food, on surfaces• Resistant to chlorination, disinfectants• Not obligate pathogens• No person to person disease transmission

Nontuberculous MycobacteriaComparison with Tuberculosis
TBNTM
AFB (+)
Person to person transmission
Reportable disease
Incidence increasing in US
Significant drug resistance seen
Nontuberculous MycobacteriaCommon NTM Species
• Slow growing mycobacteria– M. avium complex (MAC)– M. kansasii– M. xenopi– M. simiae
• Rapid growing mycobacteria– M. abscessus– M. fortuitum– M. chelonae

Nontuberculous MycobacteriaCommon NTM Species
• Slow growing mycobacteria– M. avium complex (MAC)– M. kansasii– M. xenopi– M. simiae
• Rapid growing mycobacteria– M. abscessus– M. fortuitum– M. chelonae

Nontuberculous MycobacteriaTherapy
• Therapy directed in part by susceptibility testing, and should be continued 12 months after Culture (-)
• MAC: macrolide, rifampin, ethambutol, ± amikacin• M kansasii: rifampin, ethambutol, INH ± macrolide• M abscessus: macrolide, amikacin, cefoxitin, imipenum
• Indications for surgery include persistent, focal (cavitary or bronchiectatic) parenchymal disease after antimicrobial treatment

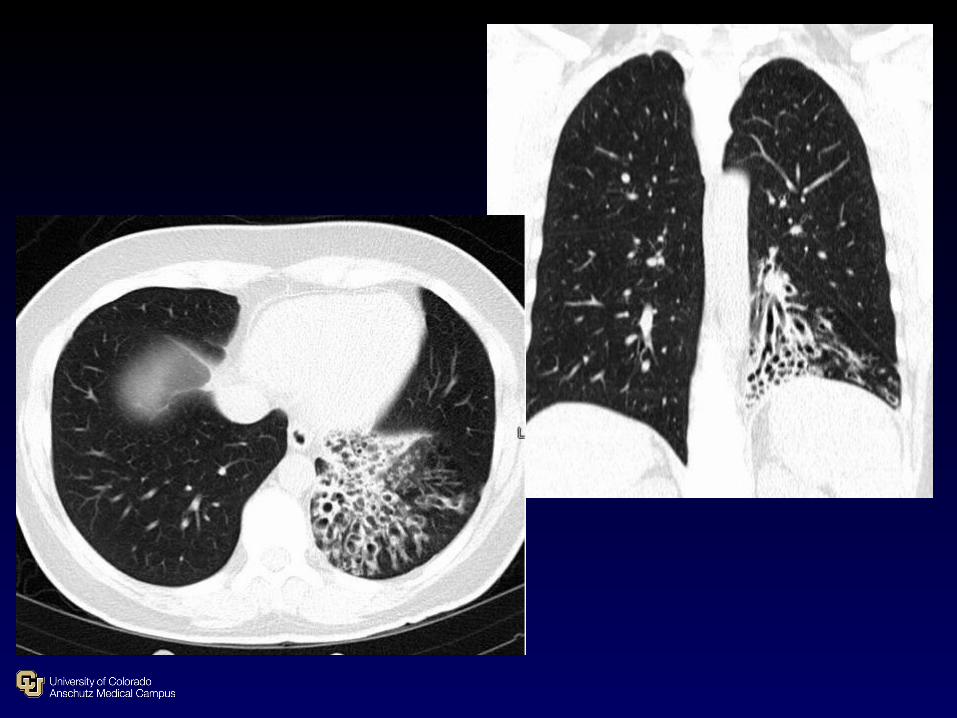
Surgery for Pulmonary NTM Disease Presentation
• Middle-aged females, thin, Caucasian, nonsmokers, right middle lobe / lingular disease
• Isolated large, thick-walled cavitary disease.
• Elderly men, smokers, ETOH abuse, underlying COPD. Resembles TB, may progress to complete lung destruction.

Surgery for Pulmonary NTM Disease Presentation
• Middle-aged females, thin, Caucasian, nonsmokers, right middle lobe / lingular disease
• Isolated large, thick-walled cavitary disease.
• Elderly men, smokers, ETOH abuse, underlying COPD. Resembles TB, may progress to complete lung destruction.

Surgery for Pulmonary NTM Disease Presentation
• Middle-aged females, thin, Caucasian, nonsmokers, right middle lobe / lingular disease
• Isolated large, thick-walled cavitary disease.
• Elderly men, smokers, ETOH abuse, underlying COPD. Resembles TB, may progress to complete lung destruction.

Surgery for Pulmonary NTM DiseaseResults of Surgical Therapy
• Corpe, 1981: 131 cases, mortality 6.9%, BPF 5.3%, 93% sputum conversion rate
• Nelson, 1998: 28 cases, mortality 7.1%, BPF 3.6%, complication rate 32%, 88% sputum conversion rate
• Shiraishi, 2002: 21 cases, mortality 0%, complication rate 29%, sputum conversion 100% → 90% at 2 years
• Mitchell, 2008: 265 cases, mortality 2.6%, complication rate 18%, BPF 4.2%, 87% sputum conversion rate

Pro
ced
ure
s
0
50
100
150
1983-1990 1991-2000 2001-
2
4
6
8
10
% M
ortality Rate
Mitchell JD et al Ann Thor Surg 2008;85(6):1887

Surgery for Pulmonary NTM Disease BPF after Pneumonectomy
Shiraishi, 2010: MDR-TB vs. NTM pneumonectomy• No operative mortality
• MDR-TB: 22 patients (7 right, 15 left)– Male 72%, Sputum negative 63%– BPF rate 4.5% (1 right)
• NTM: 11 patients (7 right, 4 left)– Female 72%, Sputum negative 9%– BPF rate 45% (4 right, 1 left)
Shiraishi Y et al. ICVTS 2010;11:429

Lung ResectionInfectious vs. Malignant Lung Disease
• Adhesions• Hypertrophied bronchial circulation• Lymphadenopathy• Dissection in hilum / around vessels• Avoid spillage from cavities• Space vs. no space• Buttressing bronchial stump• Send cultures!• Anatomic complete resection is the goal






Surgery for MDR-TB, XDR-TBSummary
• Surgical resection in MDR/XDR TB and NTM disease may lead to improved outcomes in selected cases
• Lung resection and muscle flap use often possible using modern minimally invasive techniques
• Coordination of care best approached in multidisciplinary environment
• Resection for infectious lung disease differs from resection for cancer: experience counts
Related Documents











