MCGILL UNIVERSITY INTERDISCIPLINARY DISCHARGE PLANNING ROUNDS: IMPACT ON TIMING OF SOCIAL WORK INTERVENTION, LENGTH OF' STAY AND READMISSION A Thesls Submltted to the School of Social Work F clculty of Graduate Studies and Research In PartIal Fui f 11lment of the Requirements for The Master's Degree in Social Work by (c) Iryna M. Dulka Montreal, September 1993

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

MCGILL UNIVERSITY
INTERDISCIPLINARY DISCHARGE PLANNING ROUNDS: IMPACT ON TIMING OF SOCIAL WORK INTERVENTION,
LENGTH OF' STAY AND READMISSION
A Thesls Submltted to the School of Social Work
F clculty of Graduate Studies and Research
In PartIal Fui f 11lment of the Requirements
for
The Master's Degree in Social Work
by (c) Iryna M. Dulka
Montreal, September 1993

MCGILL UNIVERSITY
INTERDISCIPLINARY DISCHARGE PLANNING ROUNDS: IMIPACT ON OUTCOMES
A THESIS SUSMITTED TO THE SCHOOL OF SOCIAL WORK
FACULTY OF GRADUATE STUDIES AND RESEARCH
IN PARTIAL FULFILLMENT OF THE REQUIREMENTS
FOR
THE MASTER'S DEGREe:: IN SOCIAL WORK
SY (c) IRYNA M. DULKA
MONTREAL, OCTOBER 1993

ABBTRACT
This study examlned th~ effect of Interdlsclpllnary
discharge planning rounds on timing of social work
lnterventlon, length of stay (LOS), and readmlSSlons for
pat lents aged 55 and over. Data sources were the medlcal
charts of 449 pat lents
corresponding 28 day perlods
the lmplementatlon of rounds)
Planning Commlttee minutes
dl schar'ged durlng two
(one before and one after
supplemented by Dlscharge
(OPCM)
four key lnformants. No slgn 1 f 1.cant
and lntervlews wlth
dlfferences ln the
tlming of social work Intervention, LOS, or readmlsslons
were found between the two sampi es. Qualltatlve resœarch
revealed that essentlal components were elther mlsslng
(physlclan partlclpatlon),
(famlly participation) ln
or not
rc)unds,
unJ. forml y
and that
lnc 1 uded
staff felt
that rounds lmproved communication amcng th~ dlsclpllnes
and contr lbuted
and
to Improved
pOSth03p 1 tal
e'fflC Jency in plc1lnnlng
se,"vlces. hosp 1 tal
hlghllght the need ta furthE!r 'study
T"e!:.e f 1 nd 1 ngs
al1 asp~cts of the
to Identlfy factors complex dlscharge planning
that would reduce LOS and readmlsslons.

Cette étude a porté sur l'Impact de séances multldlsclpllnaires
de planification des congés sur 1 e moment chOisi pour les
lnterventions sociales, la durée du séJour et la fréquence de
réhospltallsatlon chez des patients âgés de sOixante-cinq ans et
plus. Les dOllnées ont été t ll'"ées de troIs sources dl fférentes, SOlt:
les dossiers médicaux de 449 patients qUI ont reçu leur cong~ dU
cours de l'une de deux périodes correspondantes de 28 Jours (la
première avant la mise oeuvr~ des séances de planiflcatlon et la
seconde, après), les procés-verbaux des séances du comité de
planification des congés et, enfin, les lnformations obtenues lors
d'entrevues avec quatre Informateurs clés. On n'a démontré aucune
différence significative entre les deux échantillons en c~ qUI
concernp le moment de l'lnterventlon sociale, la durée du séjour et
de réhospltallsation. Une évaluation qualitative a la fréquence
révélé, d'une part, que des élément!! essentiels manqua lent
(partiCipation des médecins> ou n'avaient pas été Inclus de façon
systématique
1 a famille)
séances
dans les séances
et, d'autre part,
de plan! hCiltlon
multldlsclpllnaires (pilrtlclpation de
que le personnel trouvait que les
favorisalent les échanges
interdiSCiplinaires et une planification plus efficace des services
hospitaliers et posthospitallers. En conclusion, ces résultats
soulignent que l'on dOit mener des études plus approfondies sur tous
hi
...... _--------------------- ------ -

les aspects du processus complexe qu'est la planIfIcatIon du congé,
si l'on souhalte ldentlfler les facteurs qUl permettraient de rédulre
la durée du séJour et la fréquence de réhospltallsatlon.
iv
ACKNOWLEDGEMENTS
My Slncere thanks are extended to my thesls advlsor, Sydney Duder, for stlmulatlng my lnterest ln research, for her patlence, unwaverlng enthuslasm and her expertIse. l want to thank Lllly Katofsky, who flrst encouraged me to conduct research on thlS partlcular subJect, who gave of her tlme for consultations, and who made lt possible for me to acqulre the data used ln thlS study.
Thanks to Dr. MoraleJo, at St. Mary's HospItal, for permIssIon to conduct thlS study, and to the very helpful staff ln the MedIcal Records Department. l am also Indebted to the four people who made tlme ln their very busy schedules to be Intervlewed, and whose contributions are so valuable to thlS study.
To my payents--my earllest teachers, thank you for glvlng me the love of learnlng and YOUr support. l also want to thank my brother for hlS reassurances, and my frlend, Marsha, for her encouragement and for agreelng to do my share of dlshes throughout my thesls-wrltlng perlod.
v

TABLE OF CONTENTS
ACKNOWLEDGEMENTS v
LIST OF TABLES VIIl
LIST OF fIGURES lX
1. INTRODUCTION
1.1 Focus of the Study . . . . . . . . . . 1
1.2 Case MlX Groups .• 3
1.3 Discharge Planning . . . . . . . 5
1.4 Health Care, Hospltallzatlon, and Older Patients • • • • • • 6
1.5 Length of Stay, Delayed Dlscharges, and Readmissions • • • • • • • 8
1.5.1 Pat lent S~tlsfactlon and
1. S. 2 1.5.3
1.5.4
Partlclpatlon Pat lent Follow-Up Other D1SC~aYge Plannlng
Obstacles ..• Dlscharge Planning Audlt •
1.6 Information Retrleval for Research Purposes •
1.7 Interdisclpllndry Olscharge Plannlng
11 12
13 15
15
at the Hospltal • • • • • • • • 16 1.7.1 Tradltlonal Procedure .... 1/ 1.7.2 Revised Discharge Plannlng
Protocol . . . . . . .. 18
1.8 Study DeSign 19
VI

2. METHODOLOGY
Sample •.•••.•• Data Collectlon. • .• Data and Chart Problems •
2.1 2.2 2.3 2.4 AnalYS1S •...•••.•.••••.
2.4.1 Data from Medical Charts •••• 2.4.2 Data from Dlscharge Plannlng
Commlttee MInutes ••••.• 2.4.3 Data from Interviews ••••
3. FINDINGS
3. 1 Descrlptlon of the Sdmple · · · · · · · 3.2 Ef fec ts of the Dlscharge Planning Rounds . . · · · · · · · · · · · · · 3.3 COlltrolllng for Demographlc and
Illness-Related Varlables · · · 3.3. 1 Path Analyses · · · · · 3.4 DPC MInutes and Interviews · · · · · · 3.4.1 Attend:once at Rounds · · · · 3.4.2 Reasor.~ for Delayed u1scharges · 3.4.3 Physlc Hm Partlclpatlon · · · · 3.4.4 Patient Part1c1patlon · · · 3.4.5 Dlscharge Planning Form · · · · 3.4.6 Increased Workloads · · · · 3.4.7 Beneflts Derived from Rounds
3.4.8 Recordlng Problems · · · · · 4. DISCUSSION
4.1 Key Flnd1ngs · · · · · · · · · · · · · 4.2 Llmltat10ns of the Study · · · · · · · 4.3 Impl1cat 10ns · · · · · · · · · · · · · 4.3.1 Impllcatlons for Research · · · 4.3.2 Impl1cat1ons for Pract1ce · · · APPENDIX 1. Data Collectlon Instrument
APPENDIX 2. Recod1ng Var1ables
REFERENCE LIST
Vil
21 22 23 24 24
29 30
32
36
41 45
49 49 49 54 56 57 58 61 62
65 67 68 68 71
7S
78
81

LIST O~ TABLES
1. Demographie Variables, by Year 33
2. Status Prlor to Hospltallzatlon, by Year 35
3. Admission Informatlon, by Year 37
4. Hospltallzatlon and Dlscharge Information, by Year . 38
5. Outcome Variables, by Year 40
6. Predlctors of Year to Year Change: Stepwlse Regressions 42
7. Predlctors of Year to Year Change: Block Regression 44
V1l1

LIST OF" F"IGURES
1. Relatlonshlp Between Variables:
Causal Model • • • • • • . . . . . 27
2. Predictors of Social Work Interventlon:
Path Diagram · . . . . . . . . . . . 46
3. Predlctors of Length of Stay:
Path Dlagram · . . . . . . . . . . . . . 48
4. Predictors of Readmissions:
Path Diagram · . . . . . . . . . . . . . 50
ix

1. INTRODUCTION
1.1 (oeu. of the Study
CurY"ent
hospltals, the
care system,
lntroduclng
economlc condltlons
largest lnstltutlons wlthln
ta provlde hlgh-quallty
effectlve cost-contalnment
compelllng
the heal th
care whlle
strategles
(Edwards, Rell ey, Morls & Doody, 11313 1; FaY"ren, 1991 ;
Navak, 1988; Taylor, 19131). Proposed changes ln health
care flnanclng, comblned wlth the recognlzed detrlmental
effects of lnstltutlonallzlng aIder persons, have been
plvotal ln motlvatlng health care professlonals to become
more effective and effiCient ln enabllng patients to
return to,
and health.
and malntaln, thelr optlmum standard of llfe
stemmlng from the drIve for lncreased efflclency
and effectlveness, some hosp 1 tal sare
lnterdisclplinary dlscharge planning rounds.
lmplementlng
On February
4, 1991, lnterdlsclpllnary dlscharge plannlng rounds were
lnstltuted on every medlcal and surglcal unit of the 414
bed, acute care, university-afflilated hospltal (from now
on referred ta as the Hospltal) WhlCh served as the
settlng for thlS study.

2
The rounds were seen as a way to streamllne the
process by WhlCh patIents' progress, and thelr needs upon
dlscharge, could be Identlfled, monltored, dlscussed and
planned for (L. Katofsky, Dlrector of SocIal SerVIces,
personal communlcatlon, January 18, 1993). Moreover, at
the Hosp 1 tal' s Discharge PlannIng Commlttee's (OPC)
Oc t :>ber 19, 1991 meetIng, was reported that the
Canadlan HOspItal Management Research Instltute (CHMRl)l,
had establlshed the Hospltal's average length of stay
(LOS) across seven serVlces for the prevlous year, as
5200 days above the natIonal norm. The development of
dlscharge plannIng rounds was therefore regarded as
t1mely, as the longer stays had caused man y d1ff1cult1es
ln terms of bed d1stributlon and hosp1tal resource
allocat lon.
The purpose of th1S study was to establlsh whether
Interdisclpllnary d1scharge plannIng rounds contr1bute to
changes ln the t1m1ng of soc lai work 1ntervent 10n, to
shorter LOS, and to fewer readm1ss10ns for pat lents aged
65 and over. The rat10nale for th1S study grew from
earl1er stud1es Wh1Ch found that 1nterdlsc1pllnary
dlscharge plannlng rounds reduce hospltal1zation costs,
CHMRI 1S a Canad1an, company that special l,es ln 1nformat1on serV1ces.
federally chartered independent pat1ent-spec1f1c health related

3
Increase qualltyof care, and provlde optImum patient
care post-hospltallza~lon, thus reduclng the llkellhood
of readmlSSlons (Berkman, Camplon, Swagerty & Goldman,
1983; Edwards et al., 1991; Hauser, Robinson, Powers &
Laubacher, 1991; Thllverls, 1990).
Berkman et al. (1983) studled the effects of the
development of a Gerlatrlc Consultation Team (GCT> WhlCh
met tWlce weekly to dlSCUSS patlents' needs upon
dlscharge, and to provlde follow-up assessments of
patients' progress postdlscharge. Thelr results
Indicated a slgnlflcantly longer LOS, although they were
able to llnk better quallty of service dellvery,
Increased utlllzatlon of soclal health services, and a
reductlon of recurrent early readmlsslons, to the work of
the GCT. Wertheimer and Klelnman's (1990) study of
interdlSClpllnary dlscharge planning, however, found no
dlfferences ln LOS between patients whose dlscharges were
planned ln an InterdlSClpllnary settlng, and those whose
discharges were planned ln the tradltlonal way.
1.2 C ••• "lx Group.
Diagnostic Related Groups <DRGs) were developed ln
the
and
Unlted States to
meanlngful groups
could be est ab Il shed.
categorlze patients
on WhlCh standard
Into relevant
fundlng rates
These groups are based on

4
dlscharge dlagnosls, utillzation of hospltal-based
services and length of huspltal staY--In other words,
standard hospltal "products"
Ho f f man, 1985 ) •
(Botz ~ Devereux, 1991 ;
In 1983, CHMRI Introduced Case MIX Groups (CMGs)
WhlCh were modeled on DRGs, as a means of organlzlng
dlscharge Information wlth regard to patient lilness and
hospltallzatlon to make It possible for hospltals to
monitor and manage resource utillzation more effectlvely
(De Groot, McDonald, Peabody & Sheppard, 1992). CMGs are
now belng utillzed in certain segments of the Canadlan
health c~re system, as a fundlng mechanlsm ln response to
demands for Increased accountablilty (Botz ~ Devereux,
1991>. In Canada, thlS means that ultlmately aIl
hospltal budgets will no longer be determined by the
actual workload ~elated to a patlent's hospltallzation,
but on the expected workload correspondlng to the
patlent's asslgned CMG category (Botz & Devereux, 1991).
CMGs were Introduced at the Hospital ln November
1991 for the pur pose
to CHMRI. At the
Hospltal's management
budgetary purposes
of reporting cllnlcal patient data
tlme, It was expected that the
of CMGs would be evaluated for
and to see how the Hospltal's
performance compared wlth that of other similar patient

groups
Social
1993) •
ln other hospltals
SerVlces, personal
1.3 Di.charge planniDQ
5
commun 1 C at Hm,
The dlscharge plannlng process must
Dl rec tor of
January 18,
Include the
ldentlficatlon of patlents who may be at r15k upon
dlscharge, and the assessment of thelr SOC lai and health
care needs, ln order to plan and co-ordlnate the serVices
and supports that they wlil need at dlscharge (Berkman,
Mlilar, Holmes ~ Bonander, 1990). Dl~charge plannlng lS
cruclal to quallty patlent care, and actlve partlclpatlon
of ail health care provlders lnvolved ln a patlent'5 care
lS essentlal to the success of the dlscharge plannlng
process (Blumenfield, 1986; Hauser et: al., 1991; Jesse ~
Doyle, 1984; Wacker, Kundrat Sc Keith, 1(391).
In a social work context, dlscharge planning 15
defined as the process in WhlCh SCCldl workers counsel
patients and thelr famliles ln relatlon to SOC lai and
envlronmental dlfflcultles assoclated wlth lliness,
hospltallzatlon, and posthospltal Cdre (Berkman, Mlilar,
Holmes ~ Bonander, 1990). AlI thlS lS sald to contrlbute
to the reductlon in LOS and readmlsslons, as patient,
patlent's famlly, and communlty resources gather an
understandlng of the patlent's health deflclts and health

care needs at dlscharge <Berkman et al., 1990).
Marchette and Holloman < 1986), however, ln thel r
study of 500 patIents at a medlcal center (average age 72
years) found that pat lents who recelved soc lai work
InterventIon for dlscharge plannIng stayed ln hospltal
7.6 days longer than pat lents who had no contact wlth
soc laI workers. They explalned that the longer LOS for
pat lents who had contact wlth soc lai workers was because
they were probably fraller and ln poorer health; these
were the pat lents who needed more postdlscharge
aSslstance, or who were not returnlng to thelr homes, and
therefore needed assIstance wlth the placement process.
1.4 H.alth Car •• Ho.pttaltzatton. and 01d.r Patt.nt.
Lengthy or unnecessarlly prolonged hospltallzatlons
have been described as a serlOUS problem in the medical
care of the elderly (Alexander, 1990; Berkman et a1.,
1983; Johnson & Fethke, 1985). Regardless of a patlent's
age, however, hospltallzation is often dlfflcult to
adJust to because of the unusual routIne, uncomfortable
procedures, and loss of prlvacy, self-esteem, and
lndlvlduallty; these losses can 1 ead to a radIcal
alteratlon of role and self-lmage (Berkman et al., 1983;
Blumenfleld,
1983).
1983; John~on & F"ethke, 1985; Malllck,

7
older population, as ln ~ounger Among the
population groups, gender, dge and SOClo-economlC status
govern how one percelves the need for, and th~ d@llvery
of, heülth and social servlces <Slmmons, 198&; UJlffiotO,
1988). Ethnlclty or culture also provldes an Important
basls for assesslng pat lent needs, bath durlng
hospltallzatlon and dlscharge planning <Henkle
Kennerly, 1990; UJlmoto p 1988).
The stress of hOspltallzatlon, If comblned wlth
grievlng over a recent
partial oy complete 1055
loss, or fear
of independence,
of permanent,
may render a
person's usual coplng mechanlsms Ineffectlve (Johnson &
Pethke, 19B5). There IS a also a growlng body of
llteratu~e that exposes the latrogenlc effects of
medlcall~atlon and
IlllCh, 1975; Klnes,
the Importance of
hOspltallzatlon (Alexander, 1990;
1989). AlI these elements underllne
reducing and ellmlnatlng, whenever
posslble, unnecessarlly prolonged hospltal stays for
older patients.
Currently, a comblnatlon of new tec~nologies and
pharmacologies make the ellmlnatlon of hospltallzatlon
possible ln certain cases; for example, more of certain
surglcal
baSls.
procedures are performed on
As a result, a hlgher proportion
an out-pat lent
of the patients

8
over-65, who are belng hospltallzed today are serlously
111 and have potentlally greater psychosocIal needs
related to thelr Illness (Peterson, 1987),
1.5 Length of St.V, Delayed Discharges, and Readmissions
Delayed dlscharges have been the focus of several
studles of hospltallzed elderly. A delayed dlschar~e is
deflned as the perlod of tlme past the date the patIent
lS consldered medlcally ready for dlscharge, and the date
that the patlent lS actually dlscharged. Delayed
dlscharges are a burden on hospltal resources, and can be
especially hard for older patIents and ~helr
(talcone, Bolda & Crawford Leak, 1991).
Studies have been conducted ln an
determlne which hOSpl tal admlssion and
famliles
ef fort to
discharge
procedures are most effectIve ln lmprovlng pat lent
satlsfactlon and well-belng, and ln controlllng health
care costs related to hospltal readmlsslons (Farren,
1991; Hauser et al., 1991; Jackson, 1990; WertheImer Sc
Klelnman, 1990). Hauser et al. (1991> found that the
development of an Interdlsclpllnary team, where members
worked together to provlde comprehenSIve evaluatlon and
treatment plans to pat lents who no longer requlred acute
medlcal care, resulted in a 1.4 day decrease ln average
LOS and also lmproved dlscharge status. Berkman et al.

9
(1990), Marchette and Holloman (1986), and Naylor (1990b)
found that pat lent LOS can be reduced, rehospltallzatlons
prevented, and optlmal patIent outcomes attalned, through
the Implementatlon of effectIve and tlmely hospItal
dlscharge plannIng.
Marchette and Holloman (1986) found that pat lents
admltted from thelr own home, but discharged to a nurslng
home, had hospltal stays that were 10 to 12 days longer
than other pat lents. Schrager et al. (1978) Ident 1 fled
several factors contrlbutlng to delayed patIent
discharges and longer LOS: late referrals from medlClnej
incomplete referral or transfer forms from medIclne,
nurslng or thelr afflilated professlons; unavallablilty
of posthospital dlscharge beds, and unantlclpated changes
ln, or deterloratlon of, the patlent's medlcal status.
Kennedy, Neldllnger & Scrogglns (1987) found that
comprehenslve dlscharge plannIng for pat lents aged over
75 resulted ln LOS that were two days shorter for
patients ln the treatment group when compared to the
control group. Farren <1991> also found that discharge
plannIng lmplemented wlthln 24 hours of hospltallzatlon,
resulted ln a two day decrease ln LOS for pat lents ln the
experlmental group who had been systematlcally admltted
Into the study. Falcone et al. <1991> however, reported

10
that pat lent age, race and need for heavy care were
factors ln delayed dlscharges; unavallabliltyof post
hospltal beds was not a signlflcant predlctor of delayed
dIscharge.
In thelr experlmental study, Kennedy et al. (1987)
found that pat lents who had recelved comprehenslve
dlscharge plannIng were readmltted an average of 11.2
days later than pat lents ln the control group. Wlmberly
and Blazyk (1989) concluded that poorer and older
patlents had more frequent and eariler readmlsslons.
They found that pat lents Wlth lncomes hoverlng close to
the poverty llne were less llkely to benefit from home
dellvered meais and collectlve or communlty meals and
outlngs, and were more prone to hardshIp as a resuit of
thelr Inablilty to pay for prIv~te servlces whIle on
waItIng llsts for government SUbsldized serVIces.
Jackson (1990) found that patlents at greatest risk
for readmlsslon were those who received the most
communlty based homecare servlces, llved aione, had the
greatest number of medlcal and nurslng diagnoses, and
were the frallest, though not necessarlly the oldest,
patlents. The decllne of physlcal actlvity that often
results from lengthy hospltai stays has aiso been Ilnked
to early readmisSlons (Berkman & Abrams, 1986).

1 1
Vlctor and Vetter (1985) found that readmlsslons
were not related to patients's socIal 01'" demogl'"aprllC
charac ter lSt lCS, but were a result of relapses and
bre~kdowns ln the pat lents' orlglnal medical cond I t lons.
They also found that pat lents' own pel'"Ceptlons of
readlness for dlscharge Influenced whether 01'" not they
were readmitted. Werthelmer and Klelnman (1990) agreed
wlth these flndlngs, and stated that pOOl'" dlscharge
plannlng lS not necessarlly to blame for readmlsslons.
1.S.1 Pati.nt Satisfaction and Participation
Hosp 1 tal admlnlstrators al'"e paylng more attent10n
to patlents' satlsfactlon wlth care (Berkman, Bedell,
Parker, McCarthy & Rosenbaum, 1988; Kennedy et al., 1987;
Moher, Welnberg, Hanlon & Runnalls, 1992) . Among the
outcome measures, patIent satlsfactlon lS lmportant when
to determlne whether the ObJectIves of new
patlent-centered procedures are belng met
Hedrlck et al., 1991).
(Dake, 1984;
Pat lent oplnlons about thelr hospltal care have
been found to lnfluence thelr Vlew of the health care
system, and to determlne thelr partlclpatlon ln plans for
p05t-hospital care. Pat lent satlsfactlon 15 seen as
havlng a dlrect posltlve .mpact on enhanced patIent
compllance, WhlCh ln turn affects h osp 1 t aIl z a t Ion

outcomes (Courts, 1988) •
12
It lS prlmarlly among older
patients that elevatlon ln health status, and lncreased
pat lent s~tlsfactlon, are Ilnked wlth effective dlscharge
planning procedures (Haddock, 1991).
Increased p~tlent lnvolvement dlscharge
planning, especlally soon after admission, has been
found to be effective ln decreaslng LOS and lncreaslng
patient and patient famlly satisfaction. Where pat lents
and famliles agree ta partlclpate, thelr lnvolvement
enhances thelr knowledge of hospltal procedures whlch ln
turn promotes a greater sense of control and contrlbutes
to lmproved patient well-belng, a greater sense of self-
responslblilty, and lncreased confidence for recovery
(Abramson, 1990; Farren, 1991; Wac ker et al. 1991).
1.~.2 Patient ~ollow-up
Muenchow and Carlson (1985), eVldence
that
Ar cord lng t 0
the planned contlnulty of care was provlded, and
that patients returned to the most lndependent level of
care possible, are the two outcomes that most eff~ctlvely
measure success of the dlscharge planning process.
Jackson (1990), and Jones, Densen and Brown ( 1989) ,
confirm the need for the contlnuous assessment of the
dlscharged patlent's potentlally changlng needs.

13
Jones et al. (1989) found that many discharged
pat lents were unaware of the community serV1ces ava1lable
to them, and that no one had talked wlth them about
communlty serVIces wh1le they were hospltallzed. Follow-
up lS crucIal; ev en patlents whose health care needs have
been met may have unresolved llmltatlons that are
physlcal, soclal, or envlronmental ln nature, WhlCh place
them at r1sk for poor dlscharge outcomes, such as the
decllne ln health and well-belng,
readmlsS10n (BI~menfleld & Rosenberg,
Klelnman, 1990).
and consequent
1988; Werthelmer &
1.S.3 Other Di.charge Planning Ob.tacl ••
The goal of d1scharge planning for older pat lents
should be the preventlon of unnecessary, premature, and
avoldable hospltal readmlSSlons CNaylor, 1990a) . What
would be consldered efflclent and effectlve hospltal
dlscharges by pat lents and hospltal staff may, however,
requlre more than the plannlng for a safe and stable
trans1t1on from hospltal to posthospltal destlnatlon
(Werthelmer & Klelnman, 1990),
Any organlzatlon made up of lndlVlduals wlth
varlous capaGllltles and personal phllosophles must face
the lssue of multIple loyaltles; loyaltles to the
organlzatlon, to the posltlon held, and to the professlon

14
(Etzlonl, 1964; Ker foot
MacDonald Walsh ~ Paplle
St Kelly,
D'Day, 1981).
1985; McKeehan,
The tImIng and
clrcumstances
c ar~ led out,
ln WhlCh dlscharge plannIng tasks must be
comblned wlth the lnte~dlsclpllnary
Impl1catlons, cont~lbute to the complex1ty of the
hospltal d1scha~ge plannIng process (P~octo~ St Mo~~ow-
Howell, 1990) • However, Mohe~ et al. (1992), a~gue
that discha~ge planning, wlth ltS
potent1al for expedlent discha~ges, can not only have a
posItIve Impact on patients but can also gene~ate
posltlve feelings among the profess10nals lnvolved.
Impo~tant
med lcal sta f f,
to consider lS that membe~s of the
held
for
p~lma~lly the physlcians, a~e
accountable fo~ dete~mlnlng patIent ~eadlness
discharge (Procto~ L Horrow-Howell, 1990) . We~theimer
and Klelnman (1990) , ln p~esentlng a model for
lnte~dlsclpllna~y dlscha~ge planning found that, Wl thout
physlc~an partIcIpation on t~aditlonal ~ounds, the
discharge plannlng teams could not conduct p~oductlve and
effectlve discha~ge plannIng.
F'u~thermo~e, a
being
greate~
in need ldent 1 hed as
discharge plans translates lnto
number of patients
of inte~disc Ipl inary
inc~eased wo~kloads fo~
the p~ofesslonals involved. Often, the implementatlon of

15
procedures WhlCh result ln lncreased workloads LS not
coupled wlth increases ln staff. If not addressed,
increased workloads could create resentment ~mong the
professlonals affected, and could also Interfere wlth the
delivery of serVlces. Another factor to conslder in
interdisclpllnary dlscharge planning lS that ln hospltals
as in many other settlngs, professlonals are often heard
complainlng about the number of meetings they must
attend, and about the reams of paperwork for WhlCh they
are responsible. Professlonals often state that tlme
spent on paperwork and meetings lS tlme taken away from
clients (Ml1ner, 1980).
I.S.4 Di.charg. Planning Audit
Jesse and Doyle (1984) developed and studled an
audit in an acute care hospltal.
ident 1 fy and
shortcomings,
solve problems
and contrlbuted
The audit served to
rel ated to discharge
to Interdlsclpllnary
teamwork essential for discharge planning. Thliveris
(1990), ln a study of a Canadlan general hospltal, also
found that a hospltal-wlde dlscharge planning program,
that Included an audit, improved hospltal and communlty
resource utllizatlon.
1.6 In'gr.at'on R.tr'wv.l 'or R .... rcb Purpo ...
Problems wlth incomplete assessment forms have been

16
ldentlfled ln several studles of
(Cake, 1984; Hagan Hennessy" Shen,
dlscharge plannIng
1986; Jesse & Doyle,
1984). Some studles of dlfferent models of dlscharge
plannlng have hlghllghted the need for accuracy ln the
screenlng process, and have pOlnted to screenlng
procedures WhlCh fall to accurately examlne or record
patient posthospltal needs (Iglehart, 1990). The varying
needs and objectives of dlfferent health care
professlonals, ln terms of what each Vlews and records as
relevant and essentlal InformatIon, have been clted as
generally problematlc for researchers trylng to conduct
patient-centered studles (Hagan Hennessy & Shen, 1986;
Iglehart, 1990). ror example, patients may not routinely
be asked about their flnanclal situation, even though
studles show that the limltatlons experienced by patients
who are poor contribute to the llkelihood of unsuccessful
discharges (Wimberly " Blazyk, 1989).
1.7 Intwrdl.,lpllnary DlwebarAw planninA at thw HO.Dit.1
The idea of weekly lnterdisclplinary dlscharge
plannIng rounds was concelved at the Hospital ln rebruary
1989, malnly ln response to severe overcrowding of the
Hospltal's emergency room. These rounds were seen as a
way of maklng the dlscharge process more effective
through the lmproved identification of patients who would
requlre transfers to rehabilitatlon institutions,

17
referrals to Local Communlty Health and Social Service
Center~ (CLSCs), or who would need other dlscharge
planning ~nterventlons CL. Katofsky, Olrector of Social
Services. personal communication, January 18, 1993).
1.7.1 Tradition.1 Procedure
The Hospital's tradltlonal dlscharge planning
procedure lncluded a system whereby a team composed of
the liaison nurse, the geriatrlc nurse consultant, and
the director of the SOCial Work Department, would meet
wlth the head nurse of each unit to reVlew the patients
on that unit. Although this system was valuable ln
identifying and planning for patients ready for
discharge, lt had one main disadvantage--each of the
eight unlts were visited once per month.
In terms of SOCial work lnvolvement, patients could
be referred to the SOCial Work Department by the
physiclan or nurse in charge, or at tlmes the patient or
patient's family would request SOCial work assistance.
The danger of not havlng a weekly reVlew of patient
progress was that a patlent's condition could deterlorate
later ln the hospltallzatlon, or referrals would not be
tlmely, making a successful discharge more dlfflcult to
plan (OPCM, March 1, 1991).

18
1.7.2 R.vi •• d Di.charg. Planning Protocol
Weekly lnterdlsclpllnary dlscharge planning rounds
were lnstltuted on every medlcal and surglcal unit of the
Hospital on February 4, 1991. Discharge planning became
the responslbllity of the Interdisclpllnary dlscharge
planning teams of each unit; these were comprised ot
representatlves trom nurslng, nurslng liaison services,
rehabliitation and social work services, and were led by
the head nurses of each of the elght units. While
representatlves trom medlclne dld not attend the rounds,
communication was expected to flow between the physicians
and the head nurses (St. Mary's Hospital Center, 1991b).
ln conJunction with the development of the
dlscharge planning rounds, a Discharge Planning Committee
(OPC) was tormed. Members included representatives from
Nursing, Social Work, Rehabilitation Services, Liaison,
Gerlatrics, Hospital Administration, and Famlly Medicine.
who lnitlally met at least SIX tlmes a year, and later,
on a monthly baSIS (DPCM, October 4, 1991), to ensure
conslstency ln the ë~pllcation of the Oischarge Planning
Model, and to coordinate and monitor the actlvlties of
each of the teams (St. Mary's Hospital Center, 1991b).
An Important dlfference between the traditional
system and the gUldelines establlshed for the new

19
InterdlSClplinary dlscharge plannlng rounds, was that
with rounds, prlntouts of patient names were prepared and
dlstrlbuted each week prlor to rounds, ln order that each
discipline could come prepared wlth an update of the
patients that they were followlng and that had been
dlscussed the previous week (St. Mary's Hospltal Center,
1991b). ThlS new dlscharge tool--the llst of patient
names--was used to gUlde
planning (DPCM, May 3, 1991).
dlScusSlon for dlscharge
Through rounds, attendlng members of the Social
Work Department could ldentify pat lents who would
potentially beneflt from SOCial work lnterventlon.
Social workers became engaged ln a more actlve role in
the ldentlflcation of, and planning for, patients' needs
durlng hospltalization and at dlscharge (L. Katofsky,
Director of Social Services, personal communlcatlon,
January 18, 1993).
1.8 Study D •• ign
ThlS
comparison
examlne
pl~nning
study was
of patient
the ~ffects
rounds on
deslgned
outcomes.
as a year-to-year
The purpose was to
of lnterdlsciplinary dlscharge
the tlming of SOCial work
lnterventlons, LOS, and readmisslon rates, as compared to
the hospital's traditl0nal general dlscharge plannlng

20
procedure.
A comparlson of lnformatlon ln the medlcal charts
of pat lents dlscharged durlng two correspondlng perlods,
one before and one after the lntroductlon of rounds, was
made. Because no m~tchlng or randomizatlon was posslble,
the analysls was deslgned to control
dlfferences ln demographlc variables
for year-to-year
<e.g., gender,
relIgion, age, b1rthplace, marital and employment status,
and Ilv1ng sltuat10n), and ln slckness-related variables
<e.g., functlonal status, type and nature of admlssion,
dlagnosls, and expected LOS) that had been found ln other
studles to affect outcomes.

2:L
2. t1ETHODOLOGV
2.1 Sampi.
The data were collected from the medlcal charts of
two groups of pat lents (N=449) aged 65 and over, who were
dlscharged durlng two correspond1ng 28 days perlods ln
1990 and 1992, that lS, one year before and one year
after the lmplementatlon of Interdlsclpllnary dlscharge
planning rounds. A retrospectlve reVlew of the data was
conducted and a comparlson deslgn was used for analysls.
In 1990, 212 pat lents aged 55 and over were
discharged between January 28 and February 24; 237
patients were discharged durlng the correspondlng perlod
in 1992 (February 9 to March 7).
pat ients, 395
el iminat lng the
remalned
char"Cs of
in the
those who
Of the total 449
study sample after
durlng
hospltalizatlon, or whose hospltallzatlons had been
classified as long terme Long-term patlents are those
who have been ldentlfled by the1r treatlng physlclan as
unable to return to the settlng from WhlCh they were
adm 1 t t ed (i. e. , own home, home of a relative, or foster
home), and who no longer requlre active medlcal treatment
or attention (St. Mary's Hospltal Center, t991a).

22
2.2 Data Collection
The medlcal charts were examlned to determlne
dlfferences ln tlmlng of soclal work lnterventlon, LOS
and readmlsslon rates between the two groups. As 1 t was
difflcult to establlsh from the medlcal charts whether
any lndivldual pat lent had been discussed durlng
dlscharge plannlng rounds, the overall statlstlcs for
each sample were compared to determlne lf there were
signiflcant dlfferences between the two samples.
Medical, nurslng and admisslon records ln the
charts were revlewed for socio-demographlc data such as
age at admission, gender, marltal status, functional
status, Ilvlng situation, recent maJor life events, pre-
and post-hospitallzatl0n homecare services, health
status, LOS, and readmisslons. Social work notes that
were ln the charts were revlewed for eVldence of tlmlng
of soc laI work Interventions and for addltional
psychosoclal lnformation (see Appendlx 1).
Detalls of the hospltallzatlon itself were limited
to type of admission (emergency, semi- or non-emergency),
the maln diagnosis, pat lent compllancy
hospltallzatlon, admlsslon and discharge dates,
destln.tlon and the reason for, and tlming
readmisslon or return to emergency room.
during
dlscharge
of, any

23
Upon admission to hospltal, a patlent's main
diagnosis may not always be eVldent, and may only be
determlned after approprlate medlcal tests are conducted.
The computerlzed prlntouts of the physlclans' records
were therefore studled to determlne the ~aln dlagnosls
and CMG for each patlent (Appendl~ 2), and to establlsh
whether the hospltallzatlon was medlcal or surglcal ln
nature.
2.3 Da'a and 'Char' proble ••
The information ln the medical charts was recorded
by different professionals (e.g., nurses, phySIC lans,
occupatlonal theraplsts, soc lai workers, and physlcal
therapists) on varlOUS hospltal forms, maklng lt
sometimes hard to locate the necessary pertinent
infOrmation. Handwrlting was at tlmes difflcult to
decipher, and
Proh 1 e F"orm,
certain hospltal forms, such as the Patient
were often Incomplete or contalned
informatlon that was not helpful ln determlnlng the
patlent's
discharge.
si tuat ion
Important
before hospltallzation and after
Information was elther mlsslng or
not easlly found ln the charts; for example, patients
were not routinely asked about their flnanclal situation.
For the question related to the liVing Situation of
the patlent before hospltallzatlon, the response often

24
recorded was that the patlent 11ved ln an apartment or
house; the lnformatlon lmportant for effectlve dlscharge
plannlng lS whether the patient lives alone or w1th a
slgnlflcant dependent or lndependent other. Al so, ln 275
of the total of 395 charts, the questlon about maJor Ilfe
changes was not answered; thlS lnformatlon lS crltlcal ln
plann1ng hospltal dlscharges for aIl patients, especlally
older pat lents.
2." Analy.'.
2 .... 1 Data from Medical Chart.
The focus of the analysls was to compare t1mlng of
SOCial work lnterventlons, LOS, and readmlSSlon rates,
before and after the lntroductlon the
lnterdlSClpllnary dlscharge plannlng rounds,
of
that 1 s,
between the 1990 and 1992 sampI es. The deslgn was a
year-to-year comparlson; thlS procedure was lntroduced
because there was no posslblilty of havlng randomly
asslgned sampI es.
The flrst step ln the analysls was ta establlsh the
equlvalence of the samples based on aIl of the control
varlables--"that the treatment and comparlson groups are
sa slmllar on measures belleved related ta the outcome
that they can be vlewed àS equlvalent except for the
treatment (and aIl unmeasured varlables)" (Julnes Sc Mohr,

25
1989, p. 635) . The control varlables Included those
whlch descrlbed the patlent's sItuatIon pr 10r to
hosp1tal1zat1on, that 1S, the demographlc, functlonal
status, and slckness~related variables. Nominal
(categor1cal) var1ables were crosstabulated by year, and
chl-square tests of slgnlflcance calculated. Mean values
of cont1nuously-scaled var1ables, such as age, wel'"e
calculated for the two sampI es, and t-tests of
sign1f1cance p~rformed.
The second step in the analyris was to make a
direct compar1son of the three dependent (outcome)
var1ables for the two years. For LOS thls was done by
calculat1ng me an days for the two years, with at-test
for slgnif1cant d1fference; for tlmlng of social work
intervent10n and readm1ss1on, by crosstabulat1on and
~alculatlon of chl-square (see Appendix 2).
The thlrd step, for each of the three dependent
var1ables, was to determlne the effect of year,
controll1ng for relevant demographlc and slckness-related
variables. Th1S was c10ne by multlple regresslon
analYSls, in three steps:
1. Backward stepwlse regress10ns uSlng aIl of the demographic and lilness-related varlables, were performed to establ1sh a short 11St of pred1ctors that appeared to have a slgn1flcant effect on each dependent variable; thlS was done wlthout year as a variable. Each of the three stepwlse procedlJres

26
was termlnated at the step that Ylelded the maxImum adJusted R 2. 2. Block regresslons were then performed for dependent varlable to examIne the effect of when added to the best model obtalned ln stepwIse regYeSSlon.
each year the
3. ThIS was followed by a path analysls to examIne patterns of causatlon among the control varIables (demographlc, functlonal status and slcknessrelated) that were expected to have an effect on the three dependent varIables.
ThIS procedure followed the recommendat1ons of Julnes and
Mohr (1986):
Once the declslon lS made that the groups are "equlvalent" on the bas1s of a no-d1fference f1nd1ng, the 1nformat1on from the control var1ables lS typ1cally d1scarded. Thls d1sregard of valuable 1nformat1on lS unn~cessary and unfortunate •••• 1t lS best to use th1S 1nformatlon about d1fferences ln the analys1s •••• for example, as lndependent varIables ln a mult1ple regress10n equatlon (p. 636).
1 lS a graph1c presentatIon, of the
hypotheses about relatlonshlps between the control and
dependent varIables, that gU1ded the analysIs. The
causal model examIned postulates that gender, age, and
llvlng sltuat10n affect pat1ent's funct lonal status
(degree of physlcal ab1llty or lmpa1rment), Wh1Ch
1nfluences the type (emergency, semi-uygent or non-
urgent) and nature (medlcal or surg1cal) of admIssIon,
and dlagnosls, and that these ln turn have an effect on
the t1mlng of soc1al work InterventIon, LOS, and
readm1SS1on. Whether or not 1nterd1sclpl1nary d1scharge
plannlng rounds had an lmpact on the outcome varlables

Figure l.--Relationship Between Variables: Causal Model
Interdlsciplinary discharge planning rounds
Age
Gender
I~ivin~ ~SltuatJon 1 1
Hypothesis
Control variables
Type of admission
(emergency or Dot)
-1l> r=0nal l----t> l'Nature.of C~ __ --l: admissIon
(Medicall surgical)
i
iDiagnosis
Outcome SW mtervention
Length ofstay
Readnllsslon
1\) --..J

28
was the focus of thlS study.
To make the regresslon analysis possible,
data had to be manlpulated:
certain
1. Tlme ta Readmlsslon: Data collection occurred
three months after the latest possible dlscharge date for
the 1992 Sample, therefore the longest possIble tlme
lapse between dlscharge and readmlsslon for the 1992
Sample was 90 days. The timing of the data collection
thus allowed for a smaller number of readmisslons from
the 1992 Sample than from the 1990 Sample. To make the
samples comparable, a
Tlme to r.admlsslon
new ordinal
was recoded
variable was created.
into categories; a
patient who was not readmitted in the available tlme was
coded ln the last category together with readmissions
over 90 days after dlscharge.
are glven ln Appendlx 2.
Details of the procedure
2. Social work Intervention: The problem here was
to find a way to deal statistically with patients who
were not referred to social work at ail; to omit them
from the analysis would represent an important 10s5 of
information. Agaln values were recoded to form an
ordinal scale, with patients who did not recelve social
work Intervention grouped wlth patients who were referred
to social work 90 days after admIssion CAppendix 2).

29
3. Diagnosis (Expected LOS): A maJor technlcal
problem was presented by the fact that the maln
determinant of LOS lS the nature of the patlent's
illness. A way had to be found of controlli.ng for
diagnosls ln the year-to-year comparlson. Th 1 S ~Jas done
by using standard CMG classlflcatlons to establlsh an
expected LOS (days) for each patlent, based on that
patient's dlagnosis (see Appendlx 2).
4. Sever a 1 ot her variables (e.g., funct ional
status, type and nature of admission) also had to be
recoded for use in the regresslon analyses (Appendlx 2).
Ali data were analyzed utillsing the Statistlcal
Package for the Social Sciences (SPSS).
2.4.2 Data fro. Di.charg. Planning Ca..ttt .. "inut ••
Qualitative research methods were a1so incorporated
into this study. Wh.n it was discovered that there were
no slgnlfic.nt dlfferences, ln the expected dlrect7.on,
in the timing of soc lai work lntervention, LOS, and
readmlsslon rates between the 1990
sect ions 3. 1 to
dlscharge
undertaken,
Committee
planning
through
minutes
3.3 below), an
process at
a reVlew of
(OPCM), to
and 1992 samp1es (see
examlnation of the
the Hospi.tal was
Discharge
look for
Planning
possible

30
explanations. ror thlS study, the mInutes of the ope
meetings from Oecember 1990 to October 1992 were studled
to better understand the actual procedures and effects of
the dlscharge plannIng rounds.
ThIS procedure follows the recommendations of other
researchers. Knafl and Howard (1984) , suggest that
to studies qualitatIve research "serves as an adjunct
that are primarlly quantitative ln nature"
Wilson (1985) stated, "Quai itat ive anecdotes
(p. 18) •
are often
used to answer 'why' and 'how' questions associated with
quantltat1ve study findings" (p. 399). Also, Steckler
(1989) found qualitative methods useful ln identlfying
the presence of a Type III error, defined as the "failure
to implement a programmatic intervention completely or
adequately" Cp. 118).
2.4.3 Data fra. Int.rvl.w.
According to Berg (1989), "the interview is an
especially effect1ve method of collecting information for
certain types of research questions". Also, Berg stated
that "particularly when investigators are interested in
understanding the perceptions of partic1pants, or
learning how partIcIpants come to attach certain meanings
to phenomena or events, interviewing becomes a use fui
means of access" (p. 19).

31
An Interview gUIde, WhlCh lncluded categories that
emerged from the study of OPC mlnutes, was developed and
used for semistructured lntervlews wlth four members of
Hospital staff (a physiclan, a nurse, and two social
workers> who were selected on the basls of the followlng
criteria:
1. They were ail working at the Hospital durlng 1990 and 1992.
2. They either attended the weekly discharge planning rounds regularly or particlpated in discussions at the DPC meetings; the social workers participated at both, whlle the physlclan attended only DPC meetings and the nurse attended only rounds.
3. They ail had direct contact wlth patients. The nurse and one of the social workers held supervisory positIons; the physlclan was a senior administrator.
The four one-hour interviews were audio recorded,
transcribed, and content analyzed. The data gathered
from the content of the interviews was then organlzed and
lncorporated with related findings from the study of the
OPC minutes. Ali four key lnformants contributed inslght
lnto how some disciplines regarded the rounds, changlng
patient attitudes, and also into the inconslstencies in
discharge planning procedures.

32
3. Finding.
3.1 D •• çription of 'hM Sampl.
The study sample comprlsed the medlcal charts of
395 dlscharged medlcal and surglcal, acute care patlents
aged 65 and over: 182 pat lents in 1990, (before discharge
plannlng rounds) and 213 pat lents in 1992 (after the
rounds were establlshed). Table 1 shows demographic
varlables; the 1990 and 1992 Samples were slmllar in most
respects, with mean ages of 77.9 and 78.3 respectlvely.
The only slgnificant difference between samples was ln
livlng arrangements; a signiflcantly hlgher percentage of
pat lents ln the 1992 Sample were admitted from a
sheltered environment, such as a nurslng home or foster
home.
Table 2 shows status prlor to hospitalizatl0n, by
year. There were tWQ slgnificant differences: the 1992
Sample had more patients recelvlng homecare services
before hospltalizatlon than did the 1990 Sample. AIso, a
higher percentage of p,ltients in the 1992 Sample had
experienced recent 11fe changes prior to
hospltallzatlon. Information about such 11fe changes was
av.ilable trom 94 patient charts in the 1992 Sample,
compared to only 23 charts for the 1990 Sample.

33
Table 1.--Demographlc Varlabies, by Vear
1990 Sampie (n=192) 1992 Sample (n=213) ri ('l.) tf ('l.)
&llnd.r Male 66 36.7 73 34.3 remale 114 63.3 140 65.7 Misslng 2 0
Ag. Cat-vory 65-74 63 35.2 B3 39.2 75-84 B6 48.0 81 38.2 85 and over 30 16.8 48 22.6 Missing 3 1
Plac. of BArth Quebec 83 45.9 115 54.5 Other Canadian
province 19 10.5 19 9.0 Great Bntain 5 2.8 8 3.8 Eastern Europe 33 18.2 25 11.8 Other European
country 11 6.1 16 7.6 w.stern ASla and
Arab countries 5 2.8 6 2.8 C.ribbean 2 1.1 3 1.4 Other countrles 23 12.7 19 9.0 Missing 1 2
Civil atatu. Wido~ed, dlvorced
separated 95 54.9 96 46.6 Single 16 9.2 30 14.6 Marned 62 35.8 BO 38.8 Mis.lng 9 7
bic atatu. Not employed 163 94.8 192 93.2 Elllployed 9 5.2 14 6.8 Missing 10 7

34
Table 1.--Continued
1990 Salllple (n=182> 1992 Sample (n=213> ri (X> ri (X>
Occupation Engaged in whlln Ellploy.d Servlce-related 44 24.4 40 19.1 Professlonal 12 6.7 13 6.2 Sales 6 3.3 10 4.8 Managelllent or
admlOlstrat ion 13 7.2 11 5.3 Not indlcated 105 58.3 135 64.6 Misslng 2 4
Living Arrang...,tl
Wlth lnd.pendent slgnl ficant
other 83 46.1 86 40.6 WI th dependent
signi ficant other 10 5.6 11 5.2
Lives alone 67 37.2 66 31.1 LIves in
shelt.r.d setting 12 6.7 38 17.9
Not clear 8 4.4 11 5.2 MIssing 2 1
Religion CathollC 95 53.4 115 54.0 Protestant 32 18.0 31 14.6 Jewlsh 27 15.2 42 19.7 Christian Orthodox 15 8.4 13 6.1 Buddhlst or
Moslell 1 .6 3 1.4 Not lndicated 8 4.5 9 4.2 Missing 5 0
Note. Percentages lIIay not always add to 100 due to rounding .'fech.
1 Chi-square (4, n= 392> = 11.57, Q<.05.

35
Table 2.--Status Prlor to Hospltallzatlon, by Year
1990 Sample (n=182) 1992 Sample (n=213) N (ï.) N (ï.>
FunetionAl statu. (Di.abU iU .. >
None lndlcated 64 36.2 63 30.0 Hearlng/vlsual 24 13.5 23 11.0 Moblilty problems 25 14.1 56 26.7 Incontinent 5 2.8 1 .5
Unusual behaVlour 1 4 2.3 5 2.4 Alcohol/drug abuse 3 1.7 4 1.9 Multlele eroblems
Two of the above 34 19.2 40 19.0 More than two 11 6.2 15 7.1 More than thn?e 7 4.0 3 1.4
Servie .. rec:.i v.J None lndlcated 118 65.2 96 45.1 Not appllcable 10 5.5 34 16.0 One service 8 4.4 29 13.6 More then one 17 9.4 41 19.2 Services recelved--type
and number unknown 28 15.5 13 6. 1 Mlsslng 1 0
Yicti .. of Abu .. Ves 10 5.5 12 5.6 No 171 '94.5 201 '94.4 Mlsslng 1 0
Ev..,ta/Olang.J Not lndlcated 158 87.3 117 55.5 No 6 3.3 65 30.8 Ves 17 9.4 29 13.7 T:z:ee of change
Loss of fr lendl relative 6 3.3 10 4.7
Move to a 'home' 4 2.2 6 2.8 Other change 7 3.'9 13 6.2 Mlsslng 1 2
Note. Percentages may not always add to 100 due to roundlng effects.
Includes confusion and forgetfulness.
2 Chi-Square (4, n = 394) = 40.36, 2<.0001.
3 Chi-Square (4, ~ - 392) = 56.38, ~<.0001.
36
Table 3 shows admIssIon Information by year, and
Table 4 shows hospltallzation and dlscharge Information.
The two samples were slmllar in type of admISSIon,
preVlous admIssIon history, and nature of admiSSIon
(medlcal or surglcal). No slgnlflcant dlfferences were
found between years ln expected LOS (1990 and 1992 means
were 8.92 and 8.63 respectlvely), or ln the number of
patIents referred to as non-compilant ln the medical
charts (Table 4).
A slgnlficantly higher percentage of patients in
1992 than ln 1990, howrver, were dlscharged to sheltered
settings, such as foster homes or nursing homes (more
were also admltted from these--see Table 1), returned to
Emergency for reasons related to their previous
hospltalizatlons, and recelved homecare se~vices after
dlscharge. The dlfferences between the two samples is
more a reflection of the patients' lncoming status, than
of dlscharge plannIng outcomes.
3.2 EfflCt. of the Di.charg_ Planning Roynd.
Table 5 shows a comparison of outcome variables
for the two years. Mean length of tlme before patients
recelved socIal work intervention was slmilar; in 1990,
soclal work lnterventlon began an average 8.27 days after
admlssion, and ln 1992, 8.91 days. Mean LOS was lower

Table 3.--Admission
Type of Ad.t •• ion Emergency Se/lli-emergency Non-emergency t1lsslng
PrllYiaus Ad.issians rirst admission to
Hospltal Admitted frOftl long
term care 1
Readmi Ued 2 within 1 week SII .. e di Agnos i 5
3
Other dlagnosis R.admitt~ wi~hin
1 IIOnth Salle diagnosls Other diagnosis
Readmitted within 1 v.ar
Sa ... diagnosis Other diagnosis
Readmitted after 1
No Adllission informatlon
Hissinv
Natur. of Ad.issian Hedical Surgiea1 Hissing
37
Information, by Vear
1990 Sample
this
yeilr
ri
109 8
52 13
69
2
4 0
6 1
26 9
58
2 3
100 72 10
(n=182) ('1.)
64.5 4.7
30.8
39.0
1. 1
2.3 0.0
3.4 6.6
14.7 5.1
32.8
1.1
58.1 41.9
1992 Sampi e t'!
149 12 42 10
5B
0
4 1
7 5
37 21 74
3 3
129 76 B
1 Classi fication ehangltd frOfll long ter,. to aeuh care.
(n=213) (%)
73.4 5.9
20.7
27.6
0.0
1.9 .5
3.3 2.4
17.6 10.0 35.2
1.4
62.9 37.1
2 Read/llitted after being dlscharged fra. the s ... Hospital 1ess than one week ago.
3 Current diagnosis was related to the dlagnos15 durlng previous hospitalizatlon.

38
Table 4.--Hospitallzatlon and Discharge InformatIon, by Vear
1990 Sample (n=182) 1992 Sample (nz 2t3) ri (Y.) ri (Yo)
ExpllC tlKl LOS ~ 2 days 22 12.8 21 10.2 3 - 5 days 3S 20.3 39 18.9 6 - 8 days 38 22.1 51 24.8 9 - 12 days 42 24.4 58 28.2 13 - 17 days IS 8.7 21 10.2 18 - 24 days 16 9.3 13 6.3 25 - 30 days 2 1.2 3 1.5 31 - 35 days 2 1.2 0 0.0 1"I1ss1ng 10 7
Prabl_ Pat i..,t COIllpI iant 164 90.6 195 91.5 Not conpllant with:
Hospital routine 7 3.9 10 4.7 Other aspect of
hOSpl talization 7 3.9 4 1.9 r10re th.n one
aspect of hospit.l iz.tion 3 1.7 4 1.9
l"Iisslng 1 0
o..t inat iont
With independant signl hc.nt other 79 43.9 73 34.4
Wi th dependant slgni ficant other 6 3.3 8 3.8
Ho"e alone 50 27.8 47 22.2 To sheltered
settlng 40 22.2 68 32.1 Not clear 5 2.8 16 7.5 Mlsslng 2 1

39
Table 4.--Contlnued
1990 Sample (n=182) 1992 Sample (n=213)
t! (%) ri (%)
Servie .. r.c:.iv.d Aft.r discharge 2 None lndlcated 84 45.4 74 34.7 Not applicable 37 20.4 G5 31.0 One serVlce 11 5.1 17 8.0 More than one 12 5.6 28 13. 1 Recelved serVices,
but nature/number of services not Indlcated 37 20.4 28 13. 1
Mlsslng 0
Days between diKharg. and r.turn to .-rg."cy ward ~ 28 days 3 1.7 9 4.3 Between 29 and
89 days 5 2.8 8 3.8 Not returned
Wl th ln 90 days 173 95.6 193 91.9 Mlsslng 1 3
Why baek in .. rg."cy ward Same reason3 38 38.1 11 64.7
Other reason 13 61.9 6 35.3
Not returned Wlthln 90 days 161 196
Note. Percentages may not always add to 100 because of roundlng effects.
1 Chi-square (4, !l = 392) = 11.10. Q<.05 2 Chi-square (4, ~ = 394) = 15.23, ~<.005 3 Presentlng problem related to prevlous hospltallzatlon.
-------- - --

40
Table 5.--0utcome VarIables, by Year
8. W. int.rvention No Yes
~ 10 days 11 - 19 days 20 - 89 days Mlsslng
Actu.l LOS ~ 2 days 3 - 5 days 6 - 8 days 9 - 12 days 13 - 17 days 18 - 24 days 25 - 30 days 31 - 35 days > 35 days M1SSlOg
Days bet.,..., discharge and r.ad.ission 1 ~ 28 days Between 29 and ~ 90 days Mlss1ng
Why r •• d.1i tt~ Same reason 2 Other reason Not readmltted
89
1990 Sample (n=182) ri (1.)
151 30
20 5 5 1
11 47 34 27 15 12 8 4
19 5
12 28
141 1
51
40 91
83.4 16.6
11. 1 2.8 2.8
6.2 26.6 19.2 15.3 8.5 6.8 4.5 2.3
10.7
6.6 15.5 77.9
56.0 44.0
1992 Sample (n=213) ri (1.)
167 46
34 5 7 0
25 40 25 26 23 25 12 6
28 3
29 21
162 1
34 21
158
78.4 21.6
16.0 2.3 3.3
11.9 19.0 11..9 12.4 11.0 11.9 5.7 2.9
13.3
13.7 9.9
76.4
61.8 38.2
Note. Percentages may not always add to 100 because of roundlng effects. 1 Chi-square (2, !! .- 393) = 7.10, .9.<.05 2 Presentlng problem related to prevlous hospltallzation.

41
for the 1992 Sample (17.71 days) than for the 1990
Sample (20.27 days), thaugh thlS dlfference was not
slgn1ficant. T-tests showed no slgnlflcant dlfference
(cutaff for readmlss10n belng 90 days, see Appendlx 2)
between the 1990 Sample and the 1992 Sample ln overall
numbers of days between dlscharge and readmlsslon (means
of 36.63 and 31.82 respectlvely). There was, however, a
Slgn 1 f 1cant dlfference ln the readm1sslon patterns
between years; ln 1992 there was a hlgher number of
readmlSS10ns wlthln 28 days of dlscharge, but a lower
number of readmlss10ns between 29 and 89 days.
3.3 Control1ing for D,moaraDhic and Illn ••• -R.lat.d yariabl ••
Table 6 shows the results of the stepwlse multlple
regresslon analysls for the best models wlthout year.
For aIl three dependent varlables (soc laI work
interventlon, LOS and readmlsslon), the same llst of
Independent varlables was lncluded ln the analys1s: age
(years), gender, funct 10nal status (degree of ablilty or
dl sab 11 1 t Y ) , type of admlssl0n (emergency, seml-urgent,
non-urgent), nature of adm1sslon (medlcal or surglcal),
and expected LOS (days). The var1able for living
sltuation had been dlscarded fram the analysls because of
1tS weak relat10nshlp ta the outcome varlables and ItS
m1ss1ng values. The var1ables that were found to be

42
'~I, 6.-",14lcto" of y,., to y,., Ch .. ,,: St.,vl" '.",sslonl
o.,Ift.t Vlrl.bl, P"dlcton 1 I,t. t t
.l!!ùo hp,ct'd -.07 -." -3.57 (.0005 Soc 1.1 Mor' l.n,th of Int,n.nt 10ft' Shy
runction.1 -.!9 -.29 -5.72 (.0001 St.tlll
ror Entlr, RQd.11 r~2, 347' K 26.01, t(.OOOI , = .131 AdJlIst .. ,2 = .126
llft,th of St.y Ex,tet .. 1.77 .30 5.81 (,0001 'dl,l) llft,tll of
Sta)' rUllet ionl. 7.1' .13 2.54 .OH4 St.tlll
'"e of 3.16 -.10 -1." .0531 AII.IlIlon
'or Ellti ri 110ft Il '13, 343' • Il.7', t(.OOOI , • .141 AIIj,.tH ,2 •• 134
!iJLlt .... ", .20 .14 2.67 (.01 III .. illilll' h,tet .. .01 .10 1.12 .07
llllttil If St.)'
,,,. of .10 • 13 2 •• .02 ... illion
ror E.ta" ... 1 '(3, 346) ~ 5.01, tC.OI ,2 •• M2 "JtI.tH ,2 • .034
• Or.I •• 1 lui" (lit ""'11 2). 1 l" Ilot ,_ Il i. '.1. 7 lltellll. 1 .. lMitiOll1 vlri.ln ",. Il''' -
I0Il vi'" III.illl VI.ItI.

43
signlficant for each of the three dependent variables are
shown ln Table 6.
Table 6 shows a slgnlflcant negatlve aSSOCiation
between timing of SOCial work intervention and the
variables for expected LOS and functlonal status; thlS
indlcates a shorter period of tlme between admisslon and
SOC laI work Intervention for patients who had longer
expeeted LOS (that IS, more serlOUS dlagnosis) and who
were most di5abled.
The slgnl fleant
variables expeeted LOS
that longer hospltal
relatlonships between LOS and the
and funetlonal status indieate
stays are assoclated wlth more
serious diagnosls and wlth poorer funetional status; the
negative coefficient for type of admission denotes that
emergency admissions tend to stay ln hospital longer.
For the dependent variable timing of r~admlsslon,
Table 6 shows that male patients with shorter expected
LOS (le5s serl0US diagnosis>, and who tended to have been
elasslfied as emergency admiSSions, were found to have
the shortest time between dlscharge and readmlsslon
Append i x 2),
(see
Table 7 shows the results of the block regreBsion5

44
, .... 7.--".dlcto'l of Y'I' to y,., Ch.ng': Iloc' R""slion
, dt Il,,n ,2 f , SqIlU' Squlr'
Il.t IOdtl vithout Y'I' 212.72 2 106.36 .134 29.02 (.0001
fa .. to (E.ptet •• LOS S .... (fllnction.l St.tlll Int.rvtflt IOftt
lm. Ln L !J1 dU. L11 .li
'ohl bplllntd 217.32 3 72.44 .137 19.7' (.0001 llIl'u.1 1,::69.83 374 3." .863
rohl 1,587.14 377
IIIt 104.1 v.thout Y • ., 54,320 3 Il,107 .140 18.82 (.0001
Lllltii {(1,te'M LOS .f Sta, (fllCtiOftII StatMI ela,l' (T" •• f 1 •• ilIIOl
!w. L.llZ. L wu. dU. L..ti JI.
'otal (l'Iii .... SS,437 4 13,15' .143 14.41 (.1001 Ils 1 l1li 1 331,750 345 962 .157
:~hl .7,117 349
IIIt .... 1 vitll .. t Y •• , '.430 3 2.143 .041 4.97 .002
ra .. t. (€l,Kt" lOS fI'HiliiOftI ( ..... ,
(T". of ... ils'"
!!IL a !. JI!. am hA ~
'otal (1,1 ..... 7.010 4 1.153 .044 4.07 .003 Inl •• 1 150.747 350 .431 .956
'ohl 157.151 3S4
1 Or .... 1 .. rl.lIl. (III "'1ft'1I 2'.

4S
for each outcome variable; flrst the best model wlthout
year (Table G), and then the addltlon of year as a
predictor.
the three
Year effect was not slgnlflcant for any of
dependent varlables. Improvement ln
(percentage of var lance explalned) was less than 1% ln
ail three cases. Also, overall ~ values were very low
for aIl three models; variance explalned varled trom a
hlgh of 14.3% (LOS) to a low of 4.4;' (readmlsslon).
These low percentages
factors, not measured in
suggest that other lmportant
thlS study, affected LOS and the
timing of socIal work intervention and readmlsslons.
3.3.1 Path Analy ...
ror aIl three dependent varIables, age, ger.der,
functional status, type of admlsslon <emergency, semi-
urgent or non-urgent) and expected LOS, were lncluded ln
the model--for only the slgnlflcant paths
(~<.05) are shown in the following figures. Two
variables included ln rlgure 1 were not lneluded ln the
mOdel--living sltuatlon, beeause of dat. problems (s.e
page 23) and no slgnlflcant relatlonshlp wlth the outcome
variables, and nature of admlssion (medlcal or surgieal),
because lt was found to have weak relatlonships wlth both
lndependent and outcome variables.
rigure 2 shows th. results of the path analysis for

Figure 2.--Predictors of Social Work Intervention: Path Diagram
1 Age nmm_-l .14· Expected (years) l------------j[!» length of stay
- (days)
\~~-~ . . 25··· .11·
-.27···
-.15·· Timeto social work intervention
FWlctional status
O=okay l=disabled 2=very
I----------------!h,~·
(dayscode) 1=<4 2=5-10 3=11-20 4=21-35 5=36-50 6=51 .. 89 7=>89
·p<.05 ··p<.OJ
···p<.OOl
disabled
N=352; numbers are beta coefficients
.a (J"I

47
timlng of soc lal work lntervent lon.
lndividual relatlonshlps are as expected.
Most of the
We can see
that funct lonal status had a very signlflcant negatlve
impact on the tlmlng of soc lai work Intervention, and
aiso somewhat of an effect on expected LOS. Th 15 means
that a patlent wlth serious dlsabllitles was llkely to
recelve soc lai work lnterventlon closer to the tlme of
admission than a patient who was not dlsabled, and that
those more dlsabled had more serlOUS dlagnosls (longer
LOS) • Age had no dlrect effect on tlmlng of social work
interventlon, but a strong lndirect effect through
functional
disabled) ,
(diagnosis) •
status (older people tended to be more
and a weaker effect through expected LOS
The negatlve relatlonshlp between expected
LOS and social work intervention lndlcates that pat lents
with greater expected LOS (more serious dlagnosls) had
earlier social work Intervention.
Again in ~lgure 3, age had no direct effect on
actual LOS, but a slgnlflcant lndlrect effect through
functional status, expected LOS (dlagnosls), and type of
admlssion--older people tended to be more dlsabled, have
more serl0US lilnesses, and more emergency admiSSions,
aIl of WhlCh were assoclated wlth longer stays ln
hospital.
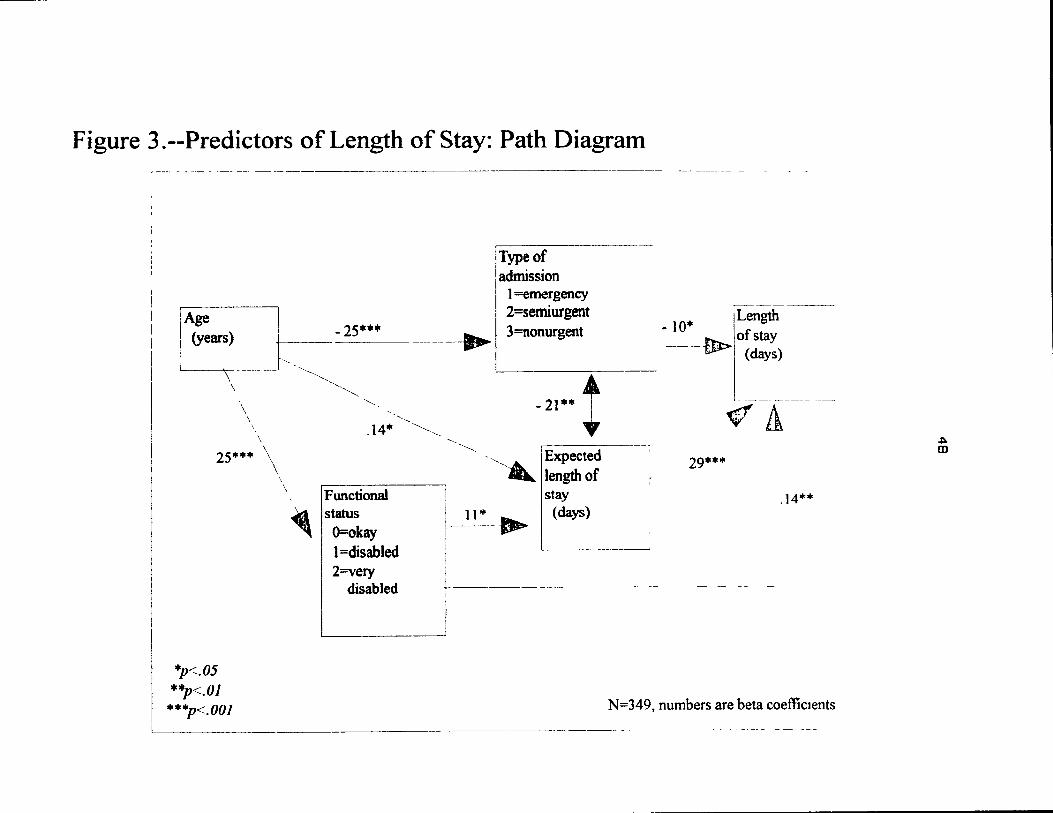
Figure 3.--Predictors of Length of Stay: Path Diagram
[Age
1 (years)
L . \
\ ,
\ \
\ \
25 ...... • \
·p<.05 ··p<.OJ
·*"'p<.OOJ
".
\
- 25··· _._-
---",~,~~
~
'-,
.14·
Functional status
O=okay l=disabled 2=very
disabled
~
•
il Type of admission
1 =emergency 2=semiurgent 3=nonurgent
-21** t '------ "".1 Expected
.... lengthof stay
Il''' .. 1 (days)
1 Length - la'" jofstay --- -- tll> (days)
'- ---- ----- ---
~11
29· ... •
.14**
- -- ~- -- - - ---
N=349, numbers are beta coefficIents
------------- -- ------- -~ ---
.:. m

49
~lgure 4 demonstrates that agaln there was no
direct age effect on readmlsslon, but a slgnlflcant
IndIrect negatlve effect through type of admIssion. Here
there was also a gender effect--males tended to be
readmltted after a shorter Interval than females.
3.4 ppe "inut •• and Int.ryi.w.
3.4.1 Att.udanc. at Rounds
Attendance at the rounds was lnitlally a problem,
due to the confllctlng schedules of team members <DPCM
May 3, 1991>. ThIS was resolved as everyone became
accustomed to the ldea of weekly rounds, and the tlmlng
of rounds was modified to fit team members' schedules.
Once the dlscharge planning rounds were held accordlng to
plan, and well attended, several factors were hlghllghted
by the DPC as possible contrlbutors to delayed dlscharges
and readmissions.
The DPe subcommlttee on research presented a report
(August 16, 1991), defining factors contributlng to
discharge delays:
1. Delay in consultatlons/assessments 2. Breakdown ln team communications 3. ~amily breakdown 4. Inadequate communlty resources S. Inadequate finances [patients'] 6. Waitlng for rehabllltation or convAlescent car ••

Figure 4.--Predictors of Readmission: Path Diagram - -- - -----------
,---- ----, ITyp~ o~ :Days to
: readmission
l
'Age 1 - 25*** ! (years) r-~--"
i adnllsslon .13 * 1=emergency ~~_ ~ 1 1=<28
~I 2=semiurgent 3=nonurgent
Gender -~~-------1 =male 1 ~ _______ ------ -~----- .13 *
I _______ ~-
1 2=female r 1 1
, 2=28-89 3=>89
__ - V -~
-~
*p<:.05 ***p<.OOl N=352~ numbers are beta coefficients
(JI
o

51
Two other dlscharge problems were ldentlfled ln
specifiC relation to orthopedic transfers (DPCM, Apr1l
10, 1992):
1. Delay ln receivlng medical summarles from orthopedlcs and lnaccuracy of lnformatlon.
2. Rehabllltatlon and convalescent facllltles wlll not accept incontlnent or confused patients.
Problematlc orthopedlc transfers were agaln dlscussed ln
June 1992, at Wh1Ch t1me the Chalr of the DPC stated that
she would meet wlth the Dlrector of Professlonal SerVlces
to discuss "the delay ln medlcal dlscharge summarles •.••
[whichl has created a backlog ln the transfer of
orthoped ic pat ients to other f ac ill t les".
On delayed discharges, one of the soc1al workers
interviewed stated:
1 think 1nternally we have our own problems w1th processlng the papers, sometimes the physlclans are fairly slow processors, sometlmes [pat lent] needs are not be1ng Identifled as qUlckly as posslble.
The same soc lai worker added however, that "there 15 much
less last mlnute or last day calls for [homel help than
there used to be".
The nurse provided an important perspect1ve on the
new type of patient that is belng admltted to hospltal:
Along wlth your urge to become eff1clent, consumers have become much more knowledgeable about thelr partlcular rlghts, and so they have more demands than they ever had. They come ln, and after two minutes on the nursing unit, [they say] they want a
52
soc1al worker, they want a convalescent bed, want, they want, they want.
they
And 1f they [patient's chlldrenJ have a parent who is ln a good functl0nal foster home, lS d01ng very weIl but who happens to phys1cally deterlorate temporarl1y wlth a partlcular condltl0n, and lf healed or cured could very weIl go back there [the foster homeJ ..•• but the faml1y from the mlnute of adm1ss10n here closed the bed ln the foster home and now wants thelr parent placed ln a chronlc care facll1ty because they know that lt 1S aval1able-they know that lt eXlsts.
We have many more [chlldren of patlentsJ com1ng to us saylng "my mother or father can't leave [the hospltall and should go up to the gerlatrlc floor-the 7th floor" •••• 1 ask them how they know that we have a gerlatrlc floor, and they s~y that they know that every hospital has a long-term unlt. So you get a lot of thlS much more so than you ever did.
The consumer is definitely more aware, and that can certalnly create a llttle blt of a dichotomy because you're focused ln from a health care perspectlve to be efficient and to get people out of the hospltal, and yet the consumer is coming to you with his or her own agenda.
In additlon to the factors contributlng to delayed
dlscharges mentioned above, WhlCh include both hospltal
procedures and changes in patient or patlent-family
attitudes, the nurse speculated about why patients,
speclflcally olde~ patients, might ln some way contrlbute
to delayed dlscharges:
Demographlcally and sociologlcally the reality lS that many old people are very lonely, that lS the blggest thing in the world that you notlce when you look after old people. They are dylng of loneliness and so when they come lnto a setting where they are nurtured, where th~y are fed, where they are loved, where they are given activities, where they can talk to people, they don't want to go home. Would you?

53
1 wouldn't say they sabotage conscl0usly •.•• they'll come up at the last minute with a reason why they can't leave. There lS such a need for geriatrlc day hospitals and geriatric day centers where people can go to be together .... (we have] isolated lonely peopl~ who are gett1ng depressed, that lS why they are gettlng slck--they get depressed, they don't eat, they don't talk to anybody for days. It lS very sad, and that's why 1 thlnk there lS such a large number of older people ln hospltals, ln lnst1tutlons ••• on the other hand in aIl falrness, there are a lot of people of that age, and that generatlon that are not comfortable when they are ln groups.
The physlclan Interviewed produced a prlntout of
flgures received from CHMRI WhlCh showed total LOS for
aIl medlcal and surglcal patients dlscharged durlng the
1989/1990 fiscal year (~ = 5,866), WhlCh lncluded the
1990 Sample ln this study, and the 1991/1992 fiscal year
(~ = 6,535), which Included thlS study's 1992 Sample.
For th~ medlcal patients dlscharged durlng the 1991/1992
fiscal year (48Y. of ail patients) there had been a 7.1
day decrease ln overall LOS from the 1989/1990 perlod
(38.2% medlcal patients). The correspondlng percent ages
of medlcal patlents lncluded ln thlS study were 58.1Y.
(1990 Sample) and 62.9Y. (1992 Sample); there was a much
higher percentage of medlcal admlsslons for the aIder
patients whose medlcal charts were examlned for thlS
study.

54
The physlclan dld pOlnt out that older medlcal
patients are the ones that have the most dlscharge
pY'oblems--thls was stated ln relatl0n to the LOS
dlfferences between aIl of pat lents dlscharged from the
Hospltal and those whose LOS was examlned foY' thlS study.
The physlclan however, added:
There lS also a blt of artlflClallty (ln the LOS numbersJ because up untll 1990/1991 we used the emeY'gency room dlfferently than we use It now. The patient would [ln the pastl come in and would not be admltted rlght away, tests would be done whlle he was stlll ln emergency. Then we had a Y'eal CY'lSlS ln 1990/1991 wlth the closlng of beds ..•. so now If we aY'e not sure whetheY' the pat lent has to be admltted or not--we admlt hlm. We no longer say that If we're not sUY'e we should hold hlm (ln emeY'gencyl. What that (change ln pY'ocedurel dld was that we admltted man y patients Into the Hospltal, whose LOS, had we admltted them befoY'e, would have been 2 to 3 days. The numbers are slgnlficant .••• also mOY'e surgerles aY'e done on an outpatlent basls.
ThlS change ln procedure lS Y'eflected ln Table 5, which
shows more patients ln the less than 2 day LOS category
ln 1992 than ln 1990. The second soc lai wOY'ker commented
on the change ln admlsslon procedure: "This policyof
admltt1ng the patient when in doubt 15 more humane and
contrlbutes to quallty of care".
3.4.3 Phy.ician Participation
There was some discussion at DPe meetings that
physlclans weY'e not attendlng the dischaY'ge planning
rounds. The Director of PY'ofessional Services reported

55
(DPCM, January 11, 1991) that:
the He dlscussed the model of rounds wlth Department Chlefs [Physlclansl at thelr quarterly meeting and [stated] that thlS was vlewed posltlvely by them. He also commented that he would encourage physlclan partlclpatlon at the rounds conslderlng the Importance of thelr role ln dlscharge planning.
Lack of medlcal Input was agaln dlscussed at the
Commlttee's June 14, 1991 meeting, where the absence of
physlclans was described as the 'mlsslng llnk' ln rounds,
and was still unresolved several months later.
The Issue of physiclan partlclpatlon was
presented at a commlttee meeting several months later
(DPCM, October, 1992):
The medlcal Input has to be Sollclted elther before or after the rounds. This Ilmlts the effectlveness of the rounds. The Umbrella Bed Management Commlttee suggested that the service chlefs be lnvlted to the DPC meeting to dIS~USS the absence of direct medlcal Input on the dlscharge plannlng rounds.
AIl the informants referred to the loglstlcal
problems lnvolved ln trylng to get physlclans to
particlpate at rounds. A SOCial worker sald:
The practlcal fact lS that we're deallng wlth 30 patients who could have 10 doctors--doctors are not gOlng to stand around waltlng for Dr. A. to have hlS say and then Dr. C. talk about hlS pat lent. l'm very happy wlth the way the head nurses coyer
the head nurse Will get ln touch wlth the physlclan, and thlS acts as an impetus to get the patient on to the next step ln the treatment.
The physlclan dlscussed the problem of loglstlCS but also

56
presented the following reasons for the absence of
physlcians at rounds:
For one thlng the physlcians are not geared to thlnk that the rounds are ail that lmportant ..•• There lS thlS terrlble thlng that happens ln medlClne where three orthopedlC patIents wlll have three d1fferent orthopedie surgeons, there 1S 50
much fragmentatIon among physlclans, whereas nurses and perhaps soc1al workers work mainly on the same floors.
The nurse put forth the followlng perspect1ve on
physlClan partIcIpatIon at rounds:
1 flnd that the fam1ly mediclne physlc1ans, who have graduated recently, and whose focus is more in terms of famlly-centered care and a more holistic perspectlve on medicine, ln general have more respect for a mult1dlsClplinary approach. 1 think perhaps they are used to it, they have been tralned that way and 50 they see the benefit of 1t, whereas some of the phys1clans who have specla11zed have a 11ttle blt of dlff1culty. 1 suppose in a way they feel 1t'S a b1t of a power struggle--they feel that they are the ones who should be in charge of admissions and discharges, and Cfeel thatl "who are these other people who are sort of gatekeeping?"-if you will.
3.4.4 Pati.nt Participation
The intervlews revealed inconsistent practiees at
discharge plannlng rounds in relation to patient and
family partlc1pation at round~. One social worker said:
If you wanted to speak to a particular family you probably could at beg1nning or end of rounds. 1 have never seen 1t happen--because of problems of loglstics and confident1ality--you couldn't have them sitting there listenlng to other people's storles, of course you could parachute them in--it could be done, particularly 1f you wanted them to see all the dlsclpllnes at once.

57
The nurse, however, descrlbed how patient and
family participation lS handled on her unit:
What we usually do IS walt untll the end of the rounds and then we focus ln on one partlcular family or patient situation. ThiS lS ve~y routine, we have a lot of famlly meetlngs--3 o~ 4 a week. Ali the people lnvolved ln the direct or lndlrect care of the patient, Includlng pastoral serVices, are asked to attend; thlS lS where you wlll often get your physlclan attendlng for a partlcular pat ient dlScussion. These meet Ings an~ occurr Ing more frequently since the Initiation of dlscharge planning rounds.
She went on to explain why some health care professl0nals
may not be as keen on rounds that lnclude pat lents and
thelr famll ies:
1 happen to have a very big Interest ln thlS; 1 think it's a very productive way to solve problems and doesn't glve anybody an autocratlc power base to make decHtions. It helps familles to see that these Chealth care professionalsl are the people that are 100king after thelr mother, thelr father, their husband, and that lt IS not Just the doctor, or its not Just the nurse, but that thure are a lot of people lnvolved.
3.4.S Dl.charge Planning For.
ln an effort to further Improve discharge planning
procedures, a form was created and clrculated at the
beglnning of 1991. The form was to be a tool used for
the purpose of summarlzlng and communlcatlng dlsch~rge
informat ion to team members, espec lally InformatIon
concerning high-risk patients, and for promoting
communicat Ion between the physiclans and other
disciplines (DPCM, December, 1990; January, 1991; March,

58
1991).
Under-utlllzatlon of the discharge plann1ng form
was reported at the DPC's May 1991 meetlng; at the June
1991 meeting lt was revealed that the form was for the
most part belng Ignored. utillzatlon of the form dld not
lmprove, and as a result, the OPC agreed to discontlnue
lts use (OPCM, June 5, 1992). One soc lai worker's view
of the form's fallure:
Vou only use a th1ng that you need to use--that glves you something. If you are getting the lnformat10n you need by talk1ng to people around the table rat rounds] ••• then you do not need a form on whlch to transmit 1nformation.
The nurse agreed wlth the social worker's Vlew of the
discharge plannlng form:
The structure of the form Itself left a lot to be desired •••• lt was set up to repeat a lot of informatIon that was already in other places and people are not lnterested today, nor do they have tlme for repetitlon.
3.4.6 Incr ••• ed Worklo.d.
The Ilkel1hood of increased workloads was a concern
of the Oepartment of Social Work (St. Mary's Hospital
Center, November 14, 1990) ln presenting a proposaI for
weekly interdlsClpllnary discharge planning rounds:
Rounds may generate more work than our present complement of staff can handle. It is a risk that we must undertake in order to achieve our objectives to lmprove the system of dlscharge planning wlthln the hospital; to decrease the average LOS and most importantly to improve the

S9
opportunltles for successful discharge and return of the patient to hlS or her home.
Since the Introduction of the rounds, aIl
disciplines Involved had, desplte their enthuslasm,
reported Increased workloads (DPCM, March 1, 1991):
Commlttee members stated that thlS may be due to the newness of the proJect. The ldentlflcatlon of high-rlsk patients should become moye streamllned as everyone becomes more famlilar wlth the dlscharge planning process.
Increased volume of work was dlscussed agaln at the June
14, 1991 meeting of the OPC:
Liaison nurslng reported the highest number of CLSC referrals ever in Perlod 2, 1991. The total number of referrals was 6S (22 gerlatrlc patients) as compared to 49 (15 gerlatrlc patients), for the same period last year. Physlotherapy reported that there had not been a signlflcant Increase ln the number of ln-patient referrals but that referrals are more appropriate.
While they acknowledged that more work was belng
generated, the informants revealed that they had a very
positive attitude toward rounds; thlS positive attitude
was however, not reflected ln the minutes of the OPC. A
social worker spoke of how rounds lmproved her workload:
1 think what happened IS
referrals, not aIl of them open cases. It looked llke [referrals] because we would same day.
that we dld gat more worked out to be big
we were gettlng more get them aIl ln the
They [rounds] are an Investment ln tlme; picture of what the whole unit lS llke, ldea from other disciplines how you can own work. My work lS more comfortable organized because of rounds.
you get a you gat an
pace your and better

60
The same SOC lai woyker stated that "The moye lnslght you
have the more actIon you are gOlng to take" and added,
"You have an lncreased workload but you also have a
better pat lent plan, and you also have more competence
for dlscharge plannlng--so the benefits outwelgh the
deficlts.
Another socIal woyker IndIcated that her review of
a number of charts revealed that in some instances where
socIal workers were not involved, lt was because the
pat lent had retuyned home, the liaIson nurse havlng
arranged for the approprlate homecare servIces; also,
thlS soc lai worker added, Il The geYlatrlc nurse checks It
out [patlent's situatlon] and finds a complex family
situation, and then lnvolves SocIal Work ••• this may be
• more appYOprlate use of disCIplines".
Although ~hlS study dld not find a signiflcant
difference between the samples in the number of patients
ti,,..t recel ved social woYk InterventIon, ln absolute
numbeys 16 more patIents were seen by social woYkers ln
1992 than ln 1990 (Table 5). As there were thyee social
workers asslgned to the patients from which the both
samples weye drawn, each social woYker would have had an
additlonal 5.3 patIents added to thelr caseload dUYlng
the 28 day perlod studied ln 1992; thlS incyease could

61
certainly have an effect on workload.
As reported above, aIl of the lnformants that
attended rounds, when asked about increased workloads,
reported beneflts that the disclpllnes Involved ln the
rounds experlenced, both collectlvely and Indlvldually.
other beneflts were also reported by one of the social
workers:
Maybe we are gettlng lnto more of a position of power from the rounds--wlth the rounds It 1S no longer Just one Indlvldual meekly comlng up to the doctor and saylng "excuse me, but do you thlnk that ••• ?" Now you can come out of rounds and say "The team wants ta know ••• , or, have you ordered that brace for this patient yet?". We can almost tell them [doctorsl what we want.
It [rounds] has created a lot more frlendllness and colleglality between the dlsclpllnes, It 0lve. us more of a chance to slt together, there i5 better communicatlon, and 1 llke It.
Also the head nurse has become much member. 1 remember when 1 was worklng hospltal several years ago, and the there were llke queens. They are now approachable, much eaSler to work wlth.
more a team at another head nurses
much more
The nurse also descrlbed posltlve aspects of rounds:
1 flnd It very good for the patients, 1 flnd It very good for us--I flnd it's a great way to help us plan our care better. The nurses flnd that thls [rounds] is where they can go to find resources. Whereas before they were gOlng to books, now they are gOlng ta the SOCial worker directly or to the occupational theraplst or to the physlotheraplst directly •••• 1 thlnk that more than anythlng else it glves each diSCipline much greater respect for the role of the other.

62
Problems with information about patient admission
recorded by nurses were addressed at the October 1992
meeting of the OPC:
Wrong InformatIon about where the patient came from lS at tlmes collected because some nurses are not famlilar wlth the difference in the levels of care requlred for foster homes and Centres d'accueil, for example.... SocIal Work CdepartmentJ lS avallable to attend nursing meetings to explain these dlfferences.
On problems wlth recording and misslng InformatIon, a
soci.l worker stated:
1 thlnk lt depends a lot on the service, for my own servIce 1 am qUlte satlsfled as the recording is really quite good, but 1 was replacing on another floor .nd the form [Patient Profile Forml was almost blank. The nurses that 1 work wlth seem to hav~ been sensltized to the importance of fully and accurately completing the forms--I don't know how it happened, it couid be the head nurse's Influence on the nurslng staff.
The second socIal worker remarked that any improvements
in the recordlng and gathering of patient Information may
be the resuit of the disciplines' sensitizatlon to this
problem at the rounds.
According to the physic ian interviewed, "the best
writers are usuaIIy nurses--they are very good at writing
reports and physicians are generally terrible". The
nurse revealed that measures h.d been taken to reduce
delayed patIent discharges which resulted from missing
info~m~tion on referral forms:

63
One of the big problems ln trylng to get pat lents to convalescent faclllt1es was that people ~ere forgettlng thlS form or that forme AlI lt took was sitting down and redes1gn1ng an envelope that lS very functlonal and very useful, and 1 belleve that the same thlng can happen wlth the dlscharge plann1ng forme
The nurse also commented speclflcally about the Patient
Profile Form w~ich had been a poor source of Information
for thlS study:
The form leaves a lot to be deSlred ln terms of where we are today ln nurslng. The form was developed 7 or 8 years ago, and was based on a model of nursing called 'Henderson's Model' WhlCh is a good model of nurslng but very task orlent@d. With the changes that have come through now, especially wlth Bill 120, where the patient and the famlly Are really being focused on, and the whole perspective of medlclne ln g@neral lS becomlng broader and more hollStlC, we have to change our method of doing pat lent assessments.
There has been a very actlve commlttee struck to look at the whole lssue of the Patient Profile Forms more focused on f.mllies. 50 for example, the question on 11vlng situation would be mueh broader ln this new Pat lent Profile Form.
Ali of ab ove pOlnts seem to provlde eVldenee that
interdiseiplinary discharge plannlng rounds were not
viewed in the same way by aIl the diSCiplInes, that ln
fAet, procedures related to dlseharge plannlng were not
being lmplemented unlformly durlng the perlod under study
in the following respects:
1. Attendance at rounds was lnltlally problematlc, as team members got used to incorporating the rounds lnto their sehedules, and until the scheduled tlmes for rounds were modlfled to conform to members' various tlme constralnts.

64
2. Physicians were plannlng rounds; nor were important.
not did
attending they thlnk
the dlscharge that rounds
3. Dlscharge plannlng summary frrms, whlch may have enhanced communIcatIon about dlscharges, especlally wlth physlclans, were nct used.
4. There contlnued to be processlng of lnformatlon dlscharge planning summarles.
some such
delays as the
in the medlcal
5. No measures were taken to find out whether dlsclpllnes experlenced lncreased workloads.
6. There were vary1ng degrees of experlenced by the different teams, recordlng of patient informatIon.
problems wlth the
7. Evidence provided by lnformants lndicates that there was no consistency ln the application of interdisclpllnary dlscharge planning procedures utlllzed by the dlfferent dlscharge plannlng teams (eg., familyand patient participation, physician part ic lpat ion).
Other important factors that can affect discharge
outcomes were 41150 lntroduced~
1. Patients and thelr familles are adopting more of a consumer's approach to health care (i.e., making more demands and belng better informed of what is aval1able to them).
2. Changes ln hospital procedure, such as the change in admlsslons P011CY, were seen to have a deflnlte impact on dlscharge outcomes such as overall LOS.
3. That hospital can sometlmes be seen as a by lonely, dlsadvantaged older patients; patients may be reluctant to be discharged.
haven these

65
4. Diacussion
4.1 Key (i"dings
There were no slgnlficant differences ln patient
outcomes between 1990 (the year before the introduction
of discharge planning rounds) and 1992 (the year after
di.charge planning rounds were lntroduced). No emplrlcal
eV1dence was found to suggest that the 1mplementatlon of
interdisclplinary dlscharge planning rounds decreased
patient length of stay and readm1ss10ns, or improved the
timing of social work InterventIon. ThiS supports the
findings of Wertheimer and Klelnman (1990) who also found
no differences ln LOS between pat lents whose d1scharges
were plAnned in the interdlsclplinary d1scharge settlng
And those whose dlscharges were planned ln the
tradltional way. Contrary to commonly held beliefs that
equate older age with increas~d utllizatlon of hospltal
resources, no signlflcant direct effect of age on any of
the three outcome variables was found. Age did
lndlrectly affect LOS through functlonal status, type of
admission, and diagnosis; age alone, however, dld not
influence LOS.
The DPC minutes and interViews provlde considerable
~vidence that the specifie procedures introdueed to

66
enhance, or found to be effectlve ln other studles of,
lnterdlsclpllnary dlscharge planning, were not ln fact
followed (physiclans not attendlng rounds, no eVldence of
patient follow-up after dlscharge). Lack of physlclan
partlclpatlon at rounds, or thelr lack of support or
understandlng of rounds could be seen as a factor
contrlbutlng to the no-dlfference flndlngs
Other problems wlth dlscharge planning
of thlS study.
continued to
pers lSt,
planning
problems,
report) ,
such as recurrent delays ln medical dlscharge
summarles, patient-Information recordlng
no evidence of (other than one lnformant's
or standard procedure for, patient or pat lent
famlly lnvolvement. Furthermore, slnce the inception of
discharge pl.nnlng rounds, some of the diSCiplines
reported lncreased workloads, posslbly a combinat ion of
more meetings to attend, and more work wlth patients and
lssue needs to be studled ln thelr familles; thlS
relation to ltS Impact on effective dlscharge planning.
Several pOSitive aspects of rounds were reported
during interViews wlth the four key informants; these
inc 1 uded lncreased
colleglallty among
work ef f ic lency
the disciplines.
and
The
lmproved
positive
comments made by the lnformants about rounds support
l'toher et al.' s (1992) study, wh lch found that the t lmel y
and approprlate dlscharges, which could result from

67
interdisclplinary dlscharge plannlng, can also generate
positive feelings among the profess10nals 1nvolved ln
pat lent care.
4.2 Limitation. of th. StudV
There were several problems w1th the retrleval of
informatlon from the pat lent charts. Important
Informat10n, such as pat1ents' llv1ng arrangements,
ethniclty, and lncome levels, was often mlsslng. Also,
there was a slgnlflcant dlfference ln whether or not
patients' recent maJor life changes or events were
recorded; th1S question was answered s1gnlflcantly more
times in the Patient Profile Forms of the 1992 Sample.
Also, lt was difficult to determ1ne whether or not
.n indivldua\ patient had been dlscussed at rounds;
because of thlS, only the overall d1fferences ln the
outcomes for each sample could be studled. In fact a
number of patients ln 1992 may not actually have been
dlscussed, or needed to be dlscussed, at rounds at ail.
It was also Impossible to establlsh whether the
professionals directly Involved ln a partlcular patlent's
care had any Input Into the Interdlsclpllnary dlscharge
planning diSCUSSions
planning form been
additlonal useful
for that patient. Had the dlscharge
successful, lt could have provlded
lnformatlon about pat lent outcomes

68
followlng dlscharge dlScusslons, and about whether or not
speclflc pat lents had been dlscussed at rounds.
This study dld not establlsh whether there was a
dlfference between the two samples l~ the tlming of
medlcal referrals, ln the orderlng of tests, or of other
lnterventlons that
delays ln any
could affect dlscharge. We know that
of these Impede dlscharges, if the
dlscharge date hinges on referrals; therefore the study
of the tlmlng of any lnterventlons affectlng dlscharge
must be carefully analyzed. An experlmental study,
Incorporatlng lnformatlon about the tlmlng of referrals
and the orderlng of tests, could provlde more Information
about predlctors for hospltal discharge outcomes that
include LOS and readmlss10ns.
4.3 Implic.tiQ'~
4.3.1 Implic.tion. for R .... rch
An experlmental controlled study, rather than a
retrospectlve study such as thlS one, would mOre
effectlvely allow for comparlsons between patients that
received dlscharge plannlng ln the traditlonal way, and
those who were dlscussed at lnterdlsclpllnary dlscharge
plannlng rounds. Such a study could to some extent
repllcate tarren's (1991) study ln which systematlc
sampllng was used to select subjects. In a study of

effects of 1nterdlsclpllnary dlscharge planning rounds,
patients ln the experlmental group would be dlscussed at
rounds, whereas the control group's dlscharges would be
handled ln the tradltlonal way.
A questlonnalre to each patlent, and hlS or her
famlly, would result ln more complete responses to the
questions related to soclo-demographlc lnformatlon,
as living arrangements, lncome and educatlon levels,
such
and
ethnlclty;
admission
thlS lnformatlon
whenever pOSSible.
could
A
be gathered at
questlonnalre
admlnlstered ln thlS way would be more rellôble and could
provlde better
predlct hospitai
readmlsslons.
Information on variables
dlscharge outcomes, such
This me'chod of gatherlng
that mlght
as LOS and
informatlon
would aiso ensure more accurate follow up ln relatlon to
mortailty, readmlsslon to another hospltal, and placement
after returnlng to the communlty.
Important lnformatlon related to pat lent outcomes,
such as patient satisfaction wlth treatment, must be
studled, as hospltal admlnlstrators are beglnnlng to pay
more attention to the 1mportance of pat lents'
satisfaction wlth care, and to whether new pat 1ent
centered procedures are belng lmplemented successfully.
Information perta1n1ng to whether or not d1scharge plans

70
were implemented, and an accurate d~scriptlon of the
sett1ng to WhlCh the pat1ent has been d1scharged, could
be also be gathered after discharge from hospital.
There was no eVldence ln the pat lent charts that
patients' ethnlcity, culture or f1nanCial status were
given speclAI attentIon. Hospltallzatlons need to be
exam1ned to determine what influences length of stay and
readmlss10ns--ls more 1nvolved than pat1ent's diagnosls
and actual state of health? Do ethnlcity, re11gi0us
bellefs, and outlook toward health and Il1ness, combined
with pat1ent's age, and social and financial situation,
for example, requlre speclal attention ln view of their
Impact on length of stay and readmission rates? If yes,
then efforts could be made to incorporate procedures that
would do m~re to recognlze and respect soclo-demographic
d1fference among patients wlth the alm of improving
he<h and social servIce delivery.
As thlS study did not find any evidence of patIent
follow-up, future studies could determine whether LOS and
readmlssl0ns are llnked to the absence of patlent follow
up. Patlent satlsfacti0n with care could also measured
to flnd out whether patient compllance and well-being can
Influence LOS and yeadmlssions.

71
Finally, ln a large Institution such as a hospltal,
medical or adminlstratlve procedures are belng constantly
lmproved, and new procedures lntroduced (e.g., the change
ln the Hospltal's admlsslons pOII~y referred to earller).
For thlS reason, any study that examInes a specIfie
hospltal procedure must control for changes ln other
procedures WhlCh
lndirectly on
facliitate the
could have an effect elther dlreetly or
outcomes; an experlmental study would
control of the Impact of such changes on
outcomes.
4.3.2 I~ltc.tton. for Practtc.
The findings of thls study indicate the need to
conduct an lntenslve audit of the hospltal dlscharge
plAnning process to determlne whether comparable
interd1sc1pl1nary d1scharge planning procedures are being
fuliy implemented throughout the Hospital, and what, If
any, aspects of the dlscharge plann1ng process need to be
modifled in arder to attaln positive patient outcomes.
The form that was deslgned to chronlcle plans for
discharge was abandoned due to under-utlllzatl0n; as lt
could be an 1mportant tool for dlscnarge planning, the
reason for its demise needs to be carefully examlned.
Th1s tool,
summarize
or another mechanlsm that would clearly
and record the varlous dlSC1pllnes'

72
InterventIons related to dlscharge plans, could enhance
lnterdlsclpllnary communIcatIon, hospltal efflclency and
pat lent outcomes. Such a tool would also be very
valuable for audIt and research purposes.
Furthermore, at the t ime of th IS study, the
HospItal did not have a method of
followlng-up patIents after dlscharge.
systematically
It IS essential
as studles have to have follow-up procedures ln place,
conf Iymed
discharge,
that assessments of
reduce recurrent
patIents' progress post-
readmlsslons. Such
procedur~s could monItor the implementation of discharge
plan~, as weil as measure patIents' satIsfaction wlth
care; thls could glve eVldence as to whether new patient
centered procedures are successfully being implemented.
be present at discussions at
rounds;
Physlcians should
however If this contInues to be a logistic
could be impossibl1lty, then a
deslgnated to attend
med lcal
.... ounds,
representatlve
to address any med ical
Issues that arIse. Studles have shown that lt IS VItal
for physlclans to partlclpate ln any effort that would
make health care dellvery more effiCIent and effectIve
through shortened LOS and reduced readmlsslons;
partIcipation of ail health care provlde .... s Involved in a
pat lI!nt' scare IS essentlal to the success of the

73
discharge planning process.
Not only can these rounds not really be called
interdisclpllnary when the physlclan does not
partlclpate, but there was no eV1dence ln the charts that
another key component of the dlScuss10ns, the patient,
was present when he or she could have b~en lncluded.
Patient Involvement ln
ln several studles
dlscharge planning has been found
to be synonymous wlth poslt1ve
discharge outcomes, lncludlng decreased LOS and
readmlsslons. While patients and the1r familles were to
some extent Involved ln the discharge plans (comments of
key informants indlcated 1nconslstent patlent and patient
family participation patterns>, a pOllcy of earller and
increased patient and family Involvement should be set ln
motion, with clear recorded eVldence of such lnvolvement.
As a result of the data collect10n undertaken for
thlS study,
ln format Ion
it was found that the record-keeplng, and
gatherlng, spec 1 flcall y on the Pat lent
Profile Form, was Incomplete; there had, however, been
some improvement
Patient Prohle
ln
Forms
the recordlng
of the Year 2
clear, complete and accurate bas1c
of lnformat Ion on
patients. Havlng
Information about
patients would not only be more efficient, but would also
facliitate research of patlent-related Issues.

74
The proposed changes ln health care financlng, and
the harmful effects of unnecessarlly Instltutlonallzlng
older persons, are motlvatlng health care professlonals
to become more focused on attalnlng pOSItIve dlscharge
outcomes. Along wlth other health care dIscIplines,
SOCIal workers have an Important role in enhanclng
patIent well-belng by ensurlng that patients' needs are
met both during and followlng hospltallzatlon. Social
workers also have a responslbillty to improve the system
wlthin whlch they work. SOCIal workers who navigate the
health care system to provlde optimal services, should
strlve to Implement procedures which could make servIce
dellvery more approprlate, as weIl as effective and
effiCIent. An Interdiscipllnary discharge planning
proce5S, such as the one studled here, puts hospltal
SOCIal workers in a pOSItion to meet their
responsibilltles.
Especlally ln relation to older populatIon groups,
however, SOCIal workers need to focus on factors that can
influence health and well-being, such as psychosocial and
socio-economic characteristics. In working to lmprove
the status of older people generally, and speciflcally of
older marglnallzed Indlviduals, SOCIal workers ln health
care settlngs can begln to make a difference in terms of
'effectIve and effIcIent' hospital resource utlllzatlon.

APPENDIX 1
IIfor. DPI Chlrt nulb.n
Data Recording In.tru •• nt ~fter OPR
1. Id.ntifiution nulb.r: 2. Ty,. of .d.ilsion 3 ••• tionIlUy 4. I.II,iOll 5. DOl ,. &tn~tr 7. lirthpl.c. 8. A4lisslon Info t. OcCl,lp.tiOft
10. IIor' St"tlll II. D.t. of .~.isSIOft 12. Civil ItltuS 13. Dots p.tillt IlV' •••••
N •• :
0-------------1---------------2-----------4-----------5----------,------------7--------8------,-.1011. vitll ind., V"'PII'. ,,,idlllC' ,,,. ho.I.II' lunin, not n.'.
(Ollft hOilI ,.I.tivil ,.lltiv.' (folt." v/r.l.tiv. sh.ltl' 11011 iR~IC.tld .,U f,i ... ~ f,itn~ Illier'.) (CMIII Il.'.,U .IOft.
14. ,ri., to hOlpit,liz.tion, v.s ,.tient 1. visu.lly I.,.i, .. 'R' ",.,ing 11P.1,1d? 2. ,,"s. v/,"ul.tiOR? 3. vilM.ll, ilPli, .. 0' h."iRI ilPlir,~? 4. incOIItinlftt? 5. for"tfull conful~/inlpp'op'i.tl ~.h.vlou, 7. ~i~ ,.ti .. t .~" .lcohol/~ru,.' O. nonl of th. ,~ov. 1. 1Or' th.n 2 of th. Ibov. (10'011')
t. "'1 thln 3 of th •• bov. (IOrtvo)
15. "Iliry Itdiell ~ilgno.is .t 1 •• iSlion l.cl,~iovllcul.r diliiSI 2. CliC" 3.r.lpi,.to,y '11111. 4.dilbetfl 5 •• rthritil/~Oft. ln jury Ite 6·"YI ... 7.confuliOll 1 IIftt.1 illftlSS 8.111".1 '''Ylie,1 ~.t.rior.tIOft '.oth" ___________ ('Plcity)

76
APPENDIX 1 - CONTINUED
1'.Op".tlon whil. in hosplt.l
17. Dotl ,.tilftt h.v •• soei.l IUp,o,t Syltll
Il. Any "Clftt l'Jor lif •• v.ntl?
., yfl 2) no
l) yes 2) no 3) n. i.
O-----~I-------------2-----------3---------4-----------5-----------------,----------7-----1---no d •• th 0' ciOi' IOVt to vietl' of r.ti'fllnt IOV. o, clol' IOV. to ntu n.i. 1011
fntnd/"hhvt -ur'-rll- crl.ln.1 .ct "lltiv,/frilnd c Uy/cOUltry of .ut •
20 •• 1 th.r. lIy indic.tion t~l' 'hl ,.tilft' lIy b. "llId? if Y'I, 'y whOl?
0-----1-----2----3----------4---------------5--------,-----------7---------1-ni llOUIi 101 dlU,ht., .th.r ,.I.tlv. (f,itnd) n'llh'ou, 1.lf oth'f
21. Il th". 'Iy lndic.tion th.t th. ,.tilftt il not co.,lilftt? If Y'I, Il wh.t v.y?
0----1--------2------------3----------4---------5-----------6-------7---------no IIdlc.tion hOlpit.1 cDllUnity dl.t h •• lth .idl oth., IOr. th.n 01.
rOlti.. If,vicli
•• yfl 2. no 3. n.i.
22. M.I ,.tllftt ,.c,ivint '011 htl,? ,rio, to hos,it.IIZ.tIOft? _____
O.nOl' indic.t .. viii p.tilftt 'tc.iv, I.'VIC.I ,ost hOlpltIIIZ.tIOft _____
0.101. indle.tld 1. ,"IOft.1 c.r •• llilt.nc.: h.l, vith 'lldint. ,.thin" dr'llint, tOII.tl." """'1(', IIdIC.tions, nU"ln, c"', bld tr.nl'.r, vhttlch.lr tr.nl'.', Iftd Mlh.,.
2. hou.th,ld 'iiiitanc.: y.r' c.,., llUld'" •• 1 ".,,,.hon, hOUItvork, Iftd t.l.,hOl •• llilt.nc.
3. cOllUnlty .llllt.ne.: h.l, vith tr.nl",t.tlon,lh",int .nd .".ndl, h.n.l.l, lOI." Iftd "rlon.l bUlinill.
1.'''101.1 Clrt
2.houlthold '1Iiitanc.
3.cOIIUIity .llilt.nc.

77
APPENDI X 1 - CONTINlED
22. UI. ,atilftt rec.ivin, hOit h.I,? (continut~)
prior to hospitllizltion' _____ viii pltitnt rtCtlVt strvicis post hO'pltlllzltlon ____ __
4. psyChosOCll1 15si5tlnc'l .upport vith tlltphone chlck-up Ind c.,lniongip 5. Y", 'ut vhich Ind hov 'Iny not ,plcifild 6. tvo of Ibove 7. lOri thln 2 of IboVI 8. lOri thln thrll of IboVI 9. n.l.
23. What VIS di5chlr" ~estinltion ?
4.psycho.ocill IS51stance
5.wh i cil and hov .111 Y not 6. tllO of ibov. 7. IOre t~1n 2 of .bove 8. lOri thln threl of IboVI 9. n.a.
0---------1-----------2-----------3-------4------------5-----------6-----------7--------8 --------1101. vith iA4., v/d.,tnd. oth.r rtlidenc.' r'5i~tn(l. hoatl.5.' not 1.1. n.l. rthl'.
(ovn hOlt reiativil rliitivel hosp. fOiter/nursing v/rel. shell.r cl.ar IPU friend friMd Ilonl
24. Dit. of l.t .ocial var. cORsult
25. Dit. di,ehlrg.d
26. Dite of rlld.i,sion
27. llllOft for r.ld.iI5aon
1. '1" or r.llt.d dal,nosi, 2. Inothlr dilfRosis or eon~ltion
21. lit. rlturnld to El bIt not Idlitt"
29 •• ,Uon
1. 5111 or rehted ~i .. nOlis 2. Ilot~lr dil,nosi. or condition

78
APPENDIX - 2
1. Timing of social work lnt.rv.ntlon variabl ••
Inltially the variable for soclal work Intervention represented the tlme (days) that lapsed between the day of patient's admission, and the day that a written request for SOCial work intervention was made. If no such request was made, but eVldence of SOCial work Intervention eXlsted ln the pat lent chart, then the date of the flrst wrltten social work note was used to calculate the timing of social work Intervention. If no eVldence of SOCial work Intervention was founa in the chart, then category 7 was recorded for the SOCial work lnterventlon variable. An ordinal scale was created to refl@ct the possibilitles in terms of soc lai work lnterventlon:
1- ~ 4 days 2. 5 - 10 days 3. 11 - 20 days 4. 21 - 35 dillys S. 36 SO days 6. 51 - 89 days 7. ~ 90 days.
2. TiMing of R •• dMission Calculatlng the number of days between discharge
And reAdmisslon (readmission variable) was done by subtracting the dlschillrge date from date of readmissl~n. However, the greatest number of days possible ln the 1992 SiIlmple was 90 because of the tlmlng of the data collectlon. To ensure an equltable comparison of these varIables for both samples, the followlng ordinal scale was developed for both:
1. ~ 28 days 1 2. between 29 and 89 days 3. ~ 90 days.
I Th1S t lme fame was chosen to conform to the Hospital's deflnition of an early readmission.

79
APPENDIX 2 CONT1 NUED
3. Controlling for Diagno.i.
There are currently 553 CMGs; the speclflc CMG that a patient lS asslgned depends on dlagnosls, hosp1tal procedures requlred durlng hospltallzatlon and, for certain diagnoses, age and any med1cal compllcat1ons.
Pat lent Information lS coded ln the Hospltal's Medical Records Department and then matched wlth the appropriate CMG number. For example, ln 1992, a patient aged over 70 who was dlagnosed wlth cellulitls, and who suffered complications related to thlS condition was categorized lnto CMG number 451. The correspondlng Canadian 1992 database mean LOS for thls CMG lS 10.3 days; thlS LOS then becomes the length of t1me (number of days) that a person ass1gned CMG number 451 lS expected to stay in hospital.
3.2 C"G Calcul.tlon for thl. 8tudy
A problem arose when it was noticed that the CMG classification numbers for most dlagnoses ln 1990 were changed ln 1992. In order to have cons1stency, and to be able to draw comparlsons based on slmllar diagnostic grouplngs, the CMG numbers for 1990 were matched to the CMG numbers correspondlng to the same d1agnoses ln 1992.
Once the main dlagnosls and CMG number for each patient was establlshed, the expected LOS (days>, based on the CHMRI's database mean, was recorded. It was learned, however, that due to medlcal and technologleal advancements, expected LOS may have decreased wlth tlme. A conservatlve strategy was adopted to compare the sampIes' expected LOS; had thlS not been done, shorter expected LOS for the 1992 would have been antlclpated.
To make the comparlson of the two years' expeeted mean length of stay possible, as the whole pOint of thlS was to control for dlagnosls, each 1990 CMG category's expected LOS was averaged wlth the correspondlng 1992 expected LOS - thlS resulted ln a new expected LOS (days) for each CMG ln both years. Aiso for the pur pose of thlS study, the expected LOS day5 were rounded off.

80
APPENDIX 2 - CONTINUED
4. Categorie. u •• d for oth.r variable. ln regr ... lon ••
Vayiable Name
Gendey
LIvIng Situation
Type of Admission
Natuye of Admission
Categories
1-male 2=female
O=with signiflcant other l=lives alone 2=in a sheltered enVlronment
O=okay 1=dlsabled 2=veyy disabled
1=emergency 2=semi-urgent 3=non-urgent
l=medlcal 2=surglcal

81
REFERENCE LIST
Abramson, J. S. Cllnlcal process.
(1990). Enhanclng patient paytlclpatlon: strategles ln the dlsch .• rge plannIng
Social Work ln Hedlth Care, ~ (4), 53-69.
Alexander, T. (1990, June/July). The elderly ln acute care: A llterature reVlew. Dlmenslons, 27-33.
Berg, B. B. (1989>. Qualltatlve Research Methods. Needham Helghts, Mass.: Allyn and Bacon.
Berkman, B., le Abrams, R. (1986). Factors related to hospltal readmlsslon of elderly cardlac patIents. SOCial Work, ~(2), 99-103.
Berkman, B., Bedell, D., Parker, E., McCarthy, L., Rosenbaum, C. (1988). Preadmlsslon screenlng: An efflcacy study. SOCial Work ln Health Care, ~(3), 35-50.
Berkman, B., Camplon, E. W., Swagerty, E., le Goldman, M. (1983, Spring). Gerlatric consultatlon team: Alternate approach to SOCial work d1scharge plan n 1 n g • J=o;::u:..:.r...:.n..:;a::..:,l_..::o=-.:..f _...::G:::e::.:r:.....::::o::..:n~t~0~1~0:::i9L.:l~c""'"a~I_..::S::=.;0=c~1...::a:...!I~-:::::W:.::o~r....:k~, 5(3), 77-88.
Berkman, B., Mlilar, S., Holmes, W., le Bonander, E. (1990, February). Scr@enlng eld@r cardlac patlents to ldentlfy need for SOCial work serVlces. Health and Soc laI Work, 64-72.
Blumenfleld, S. and a91ng: Journal of 60.
(1983, F"all/Wlnter). The hospltal center A challenge for the SOCial worker.
Gerontologlcal Soc lai Work, ~(1,2), 35-
Blumenfleld, S. (1986, F"ebruary). Dlscharge Chang@s for hospltal SOC lai work ln a care cllmate. QRB, 51-54.
plannlng: new health
Blumenfield, S., Ic Rosenberg, G. (1988). Towards a network of soc lai health services: Redeflnlng dlscharge plannl~g and expandlng the soc lai work domaln. Soc laI Work ln Health Car@, ~(4), 31-48.

82
Botz, C. K., Sc Devereux, J. (1991). Impact of case mlX fundlng (CMGs and RIWs) on medlcal soclal work. In P. A. Taylor & J. Devereux (Eds.>, Soclal work adminlstratlve Dractlce ln health care settlnrra (pp.87-95). Toronto: Canadlan Scholars' Press.
Courts, N. F. (1988, March-Aprll). A patIent satlsfactlon sur vey for a rehabliltatlon unlt. Rehabliitatlon Nurslng, ~(2), 79-81.
Dake, N. (1984, DecemberL dlscharge plannlng ln 566-570.
Nurslng responslbllltles a communlty hospltal.
for QRB,
De Gro~tl L., McDonald, J. R., Peabody, L., & Sheppard, L. (1992, Septembey 22). Casemlx systems and hospltal soc la: work: A consensus conference. Paper presented ln conJunctlon wlth the 1992 CASWAHF conference, Ottawa, Ontarlo.
Edwards, J., Relley, P., Moris, A. M., (1991). An analysls of the quallty and of the dl~charge plannIng process. Nurslng Quallty Assurance, ~(2), 17-27.
& Doody, J. effectlveness Journal of
Etzionl, A. (1964). Modern Organlzatlons. Englewood Cllffs, New Jersey: Prentlce-Hall Inc.
Falcone, D., Bolda, E., Sc Crawford Leak, S., wlth the asslstance of Ensley, D., Moore, C., Sc Starkman, A. <1991, August). Waltlng for placement: An exploratory analysls of determlnants of delayed dlscharges of elderly hospltal patIents. HSR: Health Servlces Research, 26(3), 339-374.
Farren, E. A. (1991, January-February,). Effects of dlscharge plannIng on length of hOspltal Nurslng EconomlcS, ~(l), 25-30,63.
early stay.
Flelds, G. (1978, Fall). Ed 1 t or lal.S =-==o;.::c:...:l:..:a=-=-I_...::W~o~r..:;:k'---!.H...l.:e=-=a,-=l...::t:...:.h..!. Care, 1., 5-6.
Haddock, K. S. (1991>. Characterlstlcs of effectIve dlscharge planning programs for the frail elderly. Journal of Gerontologlcal Nurslng, !Z.(7), 10-14.
Hagan Hennessy, C., & Shen, Sources of "unrellabl11t y " assessment of the elderly. 178-192.
J • K • M. ( 1 986, Ap r 11 ) • ln multldl~cipllnary team EvaluatIon Revlew, 10(2),

83
Hauser, 8., RobInson, J., Powers, J., & Laubacher, M. A. (1991, May). The evaluatlon of an Intermedlate -aregerlatrlc evaluatlon unIt ln a veterans admInIstratIon hospitai. Southern Medlc~l Journal, 84(5), 597-602.
HedrIck, S., Barrand, N., Deyo, R., Haber, P., James, K., Metter, J., Mor, V., Scanlon, W., Weissert, W., & WIllIams, M. (1991). Working group recommendatlons: Measuring outcomes of care ln gerIatrlc evaluatlon and management unlts. Journal of the American Gerlatrlc SOCIety, 39, 485-525.
Henkle, J. O., & K2nnerly, S. M. ( 1990) . Cultural dlversIty: a nurslng care.
resource ln plannIng and Implementlng PublIC Health Nurslng, l(3), 145-149.
Hoffman, F. M. (1985>. Dlagnosls-related gro...lps: Fears and reaiities. In E. McClelland, K. Kelly, & K.C. Buckwalter (Eds.), C0ntlnulty of care: Advanclng the concept of dlscharge plannIng (pp.l05-l15). Orlando: Grune & 5tratton Inc./ Harcourt 8race Jovanovlch.
Iglehart, A. P. (1990, November). Discharge plannIng: professionai perspectIves versus organizational effects. Health and SOCIal Work, ~(4), 301-308.
1 1 11 ch, I. (1 97 El LM :..:..:e:.:d::...:.l.;:::;c..::a:..:l,--N~e:..:.m:.:.;e=s:..::l,-,s::..·::.., __ T,-,h...;..:e---=E:..;x""pc::.:..r-=o::..lp=-=-r...:;l-=a=-t::...;.l.::oc:..n~o~f Health. New York: Pantheon.
Jackson, M. F. (1990). Use of community support serVICes by elderly patIents discharged from general medlcal and geriatric medicai wards. J~o~u~r~n~a~I~~o~f~.~A~d~v~a~n~c~e~d
Nurslng, ~, 167-175.
Jesse, W. F., & Doyle, B. J. (1984, December). plannIng: USlng audit to Identlfy areas Improvement. QRB, 552-555.
Dlscharge that need
Johnson, N., & Fethke, C. C. (1985). Postdischargf> outcomes and care plannIng for the hospltallzed elderly. In Continulty of care: Advanclng the concept of dlscharge plannIng (pp.231-240). Orlando: Grune & Stratton Inc./ Harcourt Brace Jovanovlch.
Jones, E. W., Densen, P. M., & Brown, S. D. (1989, December). Posthospitai needs of elderly people at home: Findings from an elght-month follow-up study. HSR: Health SerVIces Research, 24(5), 643-664.

84
Julnes, G., St Mohr, L .B. <1989, December). Analysls of no-dlfference flndlngs ln pvaluatlon research. Evaluation Revlew, ~(6), 628-655.
Kennedy, L., Neldllnger, S., &c Scrogglns, K. (198?). Effectlve comprehenslve dlscharge plannIng for hospltallzed elderly. The Gerontologlst, 27<5>, 577-580.
Kerfoot, K. M., &c Kelly, K. (1985), Factors Influenclng Management Strategies Related to Olseharge PlannIng Programs. In E. McClelland, K. Kelly, &c K.C. Buckwalter (Eds.>, Contlnulty of Care: Advanclng the Concept of Dlscharge Planning (pp. 135-148). Orlando: Grune St Stratton Inc./ Harcourt Brace Jovanovlch.
Kines, M. (1989, September). Gerlatrle assessment and long-tern rehablll tat lon work. Olmenslons, (28-31).
Knafl, K. A., St Howard, M. J. (1984). Interpretlng and reportlng qualItatIve research. Research ln Nurslng ~nd Health, 7, 17-24.
Mallick, M. O. (1982, Fall/Winter). Understandlng lllness and aglng. Journal of Gerontologlcal Social Work, S( 1! 2), 113-126.
Marchette, L" 8t Holloman, F. (1986, Mareh). Length of stay: Signlficant variables. JONA, ~(3), 12-19.
McKeehan, K.M., MacDonald Walsh, C., &c Paplle D'Day, J. (1981). Management of multldlSclpllnary communlcat ion in discharge plannIng. In. K. M. McKeehan (Ed.), Continulng Carel A multldlsclpllnary ,approach to dlscharge planning (pp.al-91)' St. LOUIS, Missouri: The C.V. Mosby Company.
Mechanic, D. (1976). The Growth of Bureaucratlc MedICIne: An Ingulry into the Dvnamlcs of Pattent Behavlour and the Organlzation of Medical Care. New York: John Wlley St Sons.
Mllner Jr., M. (1980). Unegual Care: A Case Studyof Interorganlzatlonal Relatlons ln Health Care. New York: Columbia University Press.
MOher, D., Weinberg, A., Hanlon, R., &c Runnalls, K. (1992, February 15). Effects of medlcal team coordinator on length of hospltal stay. Canadlan Medical Association Journal, 146(4), 511-515.

85
Muenchow, J. D., Sc Carlson, B. B. (1985>. Evaluatlng programs of dlscharge plannlng. Contlnulty of care: Advanclng th~ concept of dlscharge plannlng (pp.149-159). Orlando: Grune & Stratton Inc./ Harcourt Brace Jovanovlch.
Naylor, M. L. (1990a, May/June>. Comprehenslve dlscharge planning for hospltallzed elderly: A pilot study. Nurslng Research, 39(3), 156-161.
Naylor, M. D. (1990b). Special feature--An example of a research grant appllcation: Comprehensive dlscharge planning for the elderly. Research ln Nurslng Sc Health, 13, 327-347.
NO'/ak, M. (1988). Health care. In Aglng and Canadlan soclety: a Canadlan perspective (pp.1S1-169). Scarborough, Ontario: Nelson Canada.
Peterson, K. J. (1987). Changlng needs of patients and familles ln the acute care hospital: Implications for social work practlce. Soci~l Work ln Health Care, ~(2), 1-13.
Proctor, E. 1<., & Morrow-Howell, N. (1990, F"ebruary). Complications in dlscharge planning wlth medicare patients. Health and Social Work, 45-54.
St. Mary's HOspital Center. (1990-1992). Minutes of the Dlscharge Planning Commlttee Meetings. Montreal: author.
St. Mary's Hospital Center. (1990, Nov 14). Proposal for weekly cardex rounds. Department of SOCial Work: Pilot ProJect. Montreal: author.
St. Mary's Hospital Center. (1991a, June 1). Declarlng patients long term. Department of Admlnlstratlon: Policy/Standard and Procedures. Montreal: author.
St. Mary's Hospital Center. (1991b, August 16). GUldellnes for Discharge Planning Teams. Montreal: author.
Slmmons, W. J. (1986, F"ebruary). Planning for discharge wlth the elderly. QRB, 68-71
Steckler, A. (1989). The use methods to test internaI work site health promotion Health Professions, ~(2),
of qualitative evaluation valldity: An example in a program. Evaluation &c the 115-133.

86
Taylor, P.A. <1991>. Old battles--new front lers: dlrectlon of health care ln the 21st century Impllcatlons for social work. In P. A. Taylor ~ J. Devereux (Eds.), Social work administrative practlce ln health care settlngs (pp.1-8). Toronto: Canadlan Scholars' Press.
Thllverls, M. (February, 1990), A hospltalwlde dlscharge plannlng program. Dlmenslons, 38-39.
UJlmoto, K. V. (1988), Aglng, ethnlclty, and health. In B. S. Solarla ~ H. D. Dlcklnson (Eds.), Soclology of health care ln Canada (p~.220-243). Toronto: Harcourt Brace Jovanovlch Canada, Inc.
V 1 C t or , C. R. , readmlsslon Age 1 ng, 1.1..,
~ Vetter, N. J. of the elderly to
37-42.
(1985) . The earl y hospltal. 6g~ and
Wacker, R. R., Kundrat, M. A., ~ Keith, P. M. (1991, June). What do dlscharge planners plan: Impllcatlons for older medlcare patlents. Journal of Applled Gerontology, ~(2), 197-207.
Wertheimer, D. S., & Klelnman, L. S. (1990). A model for interdlsclplinary dlscharge plannlng ln a unlverslty hospltal. The Gerontologlst, 30(6), 837-840.
Wilson, H. S. (1985). The craft of qualltatlve analysls: From ~bservation to explanatlons. In H. S. Wilson (Ed.), Research ln Nurslng (pp.394-428). Menlo Park, Ca.: Addlson-Wesley.
Wllson, P. A. (1984). The expandlng role of soc laI workers in coordlnation of health care services. In Lurie, A., ~ Rosenberg, G. (Eds.), Soc laI work adminlstratlon in health care (pp.281-292). New York: The Haworth Press.
Wlmberly, E. T., ~ Slazyk, S. (1989, November). Monltorlng patient outcome followln~ dlscharge: A computerized gerlatrlc case-management system. Health and Soc laI Work, 269-276.
Related Documents











