MAXIMIZE TODAY PREPARE FOR TOMORROW BRADLEY GLICK, D.O., FAOCD DAVID GRICE, D.O., FAOCD PROGRAM CHAIRS 2012 American Osteopathic College of Dermatology Annual Meeting San Diego, California October 6-10, 2012

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
MaxiMize Today
PrePare for ToMorrow
Bradley Glick, d.o., faocddavid Grice, d.o., faocd
ProGraM chairs
2012Amer ican Osteopath ic
Co l lege o f Dermato logyAnnua l Meet ing
San D iego , Ca l i fo rn iaOctober 6 -10 , 2012

3
FACULTYBradley Glick, D.O., FAOCDAOCD President
Dr. Brad P. Glick, is a Board Certified Dermatologist practicing in Margate and Wellington, Florida. He performs a blend of dermatologic and cosmetic/aesthetic services.
He graduated from Emory University with a B.A. in chemistry and received his M.P.H. at Emory University School of Public Health. He earned his medical D.O. degree with honors at Nova Southeastern University. His internship in internal medicine was performed at Humana South Broward Hospital and his residency in dermatology was performed at Wellington
Regional Medical Center Palm Beach County Public Health Unit and Greater Miami Skin and Laser Center at Mount Sinai Medical Center which included Cutaneous and Laser Surgery.
Dr. Glick is a Diplomate of the American Osteopathic Board of Dermatology, American Osteopathic Board of Family Practice and National Board of Osteopathic Medical Examiners. He held staff positions at University of Florida College of Medicine, Nova Southeastern University College of Osteopathic Medicine, Northwest Medical Center, University Hospital and Medical Center, Coral Springs Medical Center and Mount Sinai Medical Center. Dr. Glick has been the author of numerous publications including journal articles and textbook chapters. He is a guest lecturer for the Novartis and Merz Pharmaceutical Speakers Bureaus and has received numerous honors during his career and was recently elected Program Chairman of the Broward County Dermatologic Society.
David Grice, D.O., FAOCDAOCD President-Elect
Dr. Grice is a Board Certified dermatologist and a fellow of the American Osteopathic College of Dermatology. He has been in dermatology practice since 1996 serving Grand Prairie now for over 14 years. He is a 1989 graduate of the Texas College of Osteopathic Medicine. Dr. Grice completed a one-year internship and a year of internal medicine at Dallas/Fort Worth Medical Center in Grand Prairie, where he also completed a three-year dermatology residency.
Education Undergraduate: Pearland High School Pearland, Texas 1976 -1980 Graduate: St. Mary’s University San Antonio, Texas BA 1980 -1984
Medical School TCOM Fort Worth, Texas D.O. 1985 -1989 Residency: Dallas/Fort Worth Medical Center Grand Prairie, Texas 1993 -1996
Board Certifications/Associations AOBD - 1996 AOCD, AOA, TOMA, AAD Dallas/Fort Worth Dermatologic Society Texas Dermatological Association Texas Medical Association Dallas County Medical Association
4
Gregory Papadeas, D.O., FAOCD
Dr. Papadeas is a Denver native. He is board certified in dermatology and an active member of the American Academy of Dermatology. He attended Cherry Creek High School. After completing his undergraduate degree at San Diego State University, he furthered his studies in Europe while playing competitive basketball. Dr. Papadeas earned his medical degree at the Philadelphia College of Osteopathic Medicine and his dermatology training was completed at Ohio University, Grandview Hospital and Medical Center. He is past-president of the Colorado Dermatological Society and The American Osteopathic College of Dermatology.
Daniel Siegel, MD, AAD President
Dr. Siegel attended Rensselaer Polytechnic Institute where he received his magna cum laude undergraduate education as part of a combined six year biomedical program with Albany Medical College from which he received his Doctor of Medicine Degree in 1981.
Daniel Mark Siegel, M.D. has been practicing Mohs surgery since completing his Fellowship in Mohs Micrographic Surgery and Dermatologic Surgery at the Baylor College of Medicine in Houston, Texas in 1986.
Currently, he is Clinical Professor of Dermatology at the State University of New York at Downstate School of Medicine where he teaches residents, medical students and Fellows; directs the American College of Graduate Medical Education approved Procedural Dermatology Fellowship and the American College of Mohs Surgery training program and spends part of his week at both the Brooklyn Veterans Administration Hospital and SUNY Downstate.
Victoria Werth, M.D.
Victoria Werth was initially on the full-time staff at NYU until 1989, at which time she joined the dermatology faculty at the University of Pennsylvania. She has been at Penn since 1989, and has clinical and research interests in medical dermatology. This includes caring for patients with autoimmune blistering and connective tissue diseases, as well as research into the cause of photo-exacerbated skin diseases such as lupus erythematosus and dermatomyositis. She also is conducting a multicenter trial looking at the role of dapsone as a steroid-sparing agent in pemphigus vulgaris. She co-founded the Medical Dermatology Society and spearheaded an effort to have a 5-year combined residency program in internal medicine and dermatology.
Disclosure Attestation:Consultant for Pfizer, Medimmune, Lups Foundation of America, Stiefel, Sanofi, Rigel, CelgeneLicensing: Lupus Foundation, Amgen, Celgene, NovartisGrants: Celgene, Amgen
Brian Kim, M.D.
EducationB.S.: Haverford College 2001M.D.:University of Washington 2007Internship: University of Washington 2008
Disclosure Attestation: None listed
5
Emily Chu, M.D., Ph.D
EducationB.S., M.S., Yale University 1999Ph.D., University of Pennsylvania 2005M.D., University of Pennsylvania 2006
Disclosure Attestation: None listed
Michael Ming, M.D., M.S.C.E.
EducationMedical School: Harvard Medical SchoolInternship: Massachusetts General HospitalResidency: Harvard UniversityFellowship: University of California/San Francisco
Disclosure Attestation: None listed
Fred Ghali, MD
Dr. Ghali has completed advanced training to become a pediatric dermatologist. He is board-certified in Pediatric Dermatology, General Pediatrics, and General Dermatology. He is an active fellow in both the American Academy of Dermatology and the American Academy of Pediatrics.
Upon completion of his dermatology residency, he served a brief interim as a Clinical Instructor in the Department of Dermatology at the University of Texas Medical School at
Houston. His next position was the Chief of Pediatric Dermatology (1999-2001), Cook Children’s Medical Center, Ft. Worth.
In 2001, Dr. Ghali founded Pediatric Dermatology of North Texas, PA, a private practice clinic providing dermatologic care exclusively for pediatric and adolescent patients. Located in Grapevine, his office offers a central location for families in the Metroplex. In addition to his private practice, Dr. Ghali serves as Clinical Assistant Professor of Dermatology at UT Southwestern Medical School in Dallas. He invests much of his time educating dermatology residents in Pediatric Dermatology.
EducationB.S. (Biology), Dallas Baptist University; Dallas, TX, 1989.M.D., UT Southwestern Medical School; Dallas, TX, 1993.Pediatrics Residency, UT Southwestern/Children’s Medical Center; Dallas, TX, 1996.Dermatology Residency, University of North Carolina at Chapel Hill; Chapel, Hill, NC, 1999.
Disclosure Attestation:Speaker, consultant, Advisory Board: Galderma Labs; Promius; Top MD, Inc.Research: Astellas; Top MD, Inc.Investor: Top MD, Inc.
6
Melinda Greenfield, D.O., FAOCD
Melinda F. Greenfield is a board certified dermatologist specializing in the diagnosis and treatment of the skin, hair and nails. Her additional areas of expertise include cutaneous surgery, Botox, Fillers, leg vein treatment (sclerotherapy) and other cosmetic procedures.
She is an Associate Clinical Professor at the Georgia Campus of the Philadelphia College of Osteopathic Medicine and the Georgia Health Sciences University (Medical College of
Georgia). She is on the board of the Dougherty County Medical Society, as well as the Georgia Osteopathic Medical Association and will be president of the Georgia Osteopathic Medical Association for the 2011-2012 term. She is also an Associate Editor of The Journal of the American Osteopathic College of Dermatology.
Dr. Greenfield received her Bachelor of Science degree from the University of Maryland, and received her medical degree with honors from Nova Southeastern University in Ft. Lauderdale, Florida. She completed a year of internal medicine at Sinai Hospital of Baltimore prior to her three year dermatology residency at St. Barnabas Hospital in Bronx, New York.
Disclosure Attestation: None listed
Stephen Purcell, D.O., FAOCD
Dr. Purcell is a graduate of Muhlenberg College and Chicago College of Osteopathic Medicine. He completed his dermatology residency program at Lackland Air Force Base in San Antonio, Texas. He served eight years on active duty as a physician in the Air Force. He received his license in New York in 1981 and in Pennsylvania in 1988. Dr. Purcell returned to the east coast in 1988 to begin practicing dermatology in Allentown and Pottsville. He is certified by the American Board of Dermatology and the American Osteopathic Board of Dermatology. In addition, he received a certificate of special competency in dermatopathology from the American Osteopathic Association. Dr. Purcell’s medical articles have been
published in several dermatologic journals. He has lectured at national, regional, and local medical meetings. Dr. Purcell is Chief of the Division of Dermatology at Lehigh Valley Health Network and Program Director of Lehigh Valley Health Network and Philadelphia College of Osteopathic Medicine Dermatology Residency Program. He is also Chairman of the Division of Dermatology at Philadelphia College of Osteopathic Medicine. Dr. Purcell is Chairman of the American Osteopathic Board of Dermatology
Disclosure Attestation: None listed
Michael Morgan, M.D.
EducationB.A., Rollins College 1985M.D., University of South Florida College of Medicine 1989Internship, University of South Florida 1990Residency (Anatomic/Clinical Pathology), University of South Florida 1994Fellowship (Dermatopathology), University of Oklahoma 1995
Residency (Dermatology), University of Oklahoma 1996
Disclosure Attestation: None listed
7
Anthony Dixon, M.D.
Dr. Dixon graduated Medical School from The University of Melbourne in 1982.
His interest in skin cancer dates from his junior resident days in 1983-1985. An ophthalmologist with a special interest in skin cancer on the eyelids taught Dr. Dixon the beginnings of management of skin cancer and the complexity of its treatment. His first experiences and training revolved around eyelid and nose skin cancers.
His interest, training and skills have developed since that time. He has a particular interest in large and/or difficult tumors in awkward areas of the face. A host of repair and reconstruction techniques are employed to close defects remaining after skin cancers are excised.
From a rural surgical background, now Dr. Dixon is exclusively focused on this important sub specialty area. It had been described as the area where dermatology and plastic surgery merge.
Dr. Dixon is involved in advanced post graduate skin cancer management training. He runs comprehensive training programs to assist doctors in their skills managing skin cancer. He is also involved in cutting edge research in skin cancer management. In particular, Dr. Dixon is involved in progressing new techniques in reconstruction following tumor excision.
His Ph.D. studies pertained to research on the complications of skin cancer surgery and their risk factors.
These original studies have been published in the major international journals, including the British Journal of Surgery, Dermatologic Surgery, British Journal of Dermatology, British Medical Journal, Journal of American Academy of Dermatology and the Journal of Plastic Reconstructive and Aesthetic Surgery.
Disclosure Attestation:Stock/Bond Holdings: Allmedic Pty. Ltd.
Steven Grekin, D.O., FAOCD
Dr. Steven Grekin has made it his personal and professional mission to help his patients put their best face forward. Years of research at the International Skin Rejuvenation Institute in Paris, France, and Quebec, Canada, have led Dr. Grekin to understand the secrets to younger, smoother, more radiant skin. He now brings these secrets to his patients in America.
Respected here and abroad as an expert in cosmetic dermatology, Dr. Grekin comes from a long line of physicians-six are dermatologists. He has participated in international teaching and training courses, and is an internationally recognized lecturer in his field.
Guided by cutting-edge principles of modern dermatology, natural medicine, and the highest quality medical care, Dr. Grekin offers his patients an elegant, intelligent program distinguished by its unique flexibility to restore every skin type to its youthful, natural best!
His family has been providing health care in the United States for almost 100 years. Dr. Grekin is committed to helping patients from all over the world. He now offers his programs on-line, so that he may reach out and help as many people as he can put their best face forward.
Disclosure Attestation: None listed
8
Peter Saitta, D.O
EducationB.A., New York University 2003D.O., University of Medicine and Dentistry of New Jersey School of Osteopathic Medicine 2008Internship, Richmond Heights Medical Center 2009Residency, Oakwood Southshore Healthcare System 2012
Disclosure Attestation: None listed
Francisca Kartono, D.O., FAOCD
EducationB.S., UCLA 2003D.O, Western University of Health Sciences 2007Residency, Botsford General Hospital 2011Fellowship, Ohio State University Wexner Medical Center 2012
Disclosure Attestation: Subinvestigator/Clinical Trials: Abbott, Johnson & Johnson, Celgene
Robert Greenberg, M.D.Trained at UCSF Medical Center, Dr. Greenberg has become a leader in his field using the most up to date therapies for the treatment of medical dermatology. Dr. Greenberg has participated in many studies involving Psoriasis, Eczema, Acne and Rosacea.
Dr. Greenberg frequently lectures on the topics of Psoriasis, Inflammatory Skin disorders, Acne and Rosacea. Using an interactive technique with his attendees, he has become a popular spokesperson for the companies that he represents through lectures, roundtables and CME
programs.
Dr. Greenberg uses his expertise and clinical experience to educate his colleagues on disease states and therapeutic options. His expert opinion is highly valued, particularly with the use of Combination Therapies, Phototherapy, Biologic Therapy, Traditional Systemic Therapies and Topical Medications. Dr. Greenberg has become a major referral source for difficult to treat patients in the Bay Area.
Disclosure Attestation:Speaker/Advisor: Abbott, Amgen, Centocor, Galderma, Medicis, Leo, Onset, Ranbaxy, Promius, Allergan, Bayer
Joseph Jorizzo, M.D.
EducationAB Boston University 1972 MD Boston University School of Medicine 1975 Internship Internal Medicine North Carolina Mem Hosp 1976Residency Dermatology North Carolina Mem Hosp 1979
Clinical Specialties
Rheumatologic/Immunodermatology, Allergic Skin Disease, Nail Disease, Skin Care, Skin and Systemic Disease, Dermatology (general), Pediatric Dermatology, Phototherapy, Skin Cancer
9
Angela McKinney, D.O. Botsford Hospital/McLaren-Oakland, Pontiac, MI
Alma AcMoody, D.O. Summa Western Reserve Hospital, Cuyahoga Falls, OH
Keith Robinson, D.O. Summa Western Reserve Hospital, Cuyahoga Falls, OH
Stephen Weis, D.O. UNTHSC/TCOM, Fort Worth, TX
Paul Aanderud, D.O. Oakwood Southshore Medical Center, Warren, MI
Peter Knabel, D.O. Northeast Regional Medical Center, Kirksville, MO
Grace Kim, D.O. Valley Hospital Medical Center, Las Vegas, NV
Mari Batta, D.O. Alta Dermatology, Mesa, AZ
Jeremy Bingham, D.O. Advanced Desert Dermatology, Peoria, AZ
Helia Eragi, D.O. Pacific Hospital, Torrance, CA
Tatyana Groysman, D.O. PCOM/Lehigh Valley Health Network, Allentown, PA
Mounir Wassef, D.O. Columbia Hospital, West Palm Beach, FL
Alison Himes, D.O. O’Blenness Hospital, Dublin, OH
Sanjosh Singh, D.O. St. John’s Episcopal Hospital, Lindenhurst, NY
Charlotte Noorollah, D.O. St. John’s Episcopal Hospital, Lindenhurst, NY
James B. Young, D.O. St. Joseph Mercy Health System, Clinton Twp., MI
Heather Orkwis, D.O. St. Joseph Mercy Health System, Clinton Twp., MI
Libby Rhee, D.O. St. Barnabas Hospital, Bronx, NY
Blakely Richardson, D.O. University Hospitals, Cleveland, OH
Ashley Kittridge, D.O. University Hospitals, Cleveland, OH
Ellecia Cook, D.O. Largo Medical Center, Port Richey, FL
RESIDENT FACULTY
10
ACCREDITATION The American Osteopathic College of Dermatology is accredited by the American Osteopathic Association to award con-tinuing medical education to physicians. This activity has been planned and implemented in accordance with the Policies of the Council on Continuing Medical Education of the AOA.
MEETING OBJECTIVES: The 2012 Annual Meeting will provide a diversified CME program focusing on the art and science of Dermatology. Infor-mation will be presented through lectures and scientific paper presentations. Attendees will be updated on a broad range of new developments in dermatology and acquire a better understanding of advances in medical and surgical therapies. They will also gain greater insight into current trends in practice management as well as financial and medical/legal chal-lenges facing today’s clinician.
It is expected that attendees of this meeting will increase diagnostic skills in a wide range of dermatology as well as derma-topathology. In addition to increased diagnostic competence, enhanced concepts of therapy and treatment in dermatologic care will be taken back for implementation in everyday practice. The overall result being improved physician/provider per-formance and increased positive patient outcomes.
NEEDS ASSESMENTS The program was developed based upon the needs of physicians within the association identified through:
• A program evaluation/survey provided to meeting participants at both our annual and midyear meeting, • Recommendations received through the mail, email, or by phone, • Recommendations from previous program chair, • New advances in dermatologic treatment identified in major publications or research studies. • The Board of Trustees also meets to discuss previous conferences and to provide additional topics and potential
speaker contacts.
FACULTY DISCLOSURE As a sponsor accredited by the AOA, it is the policy of the AOCD to require the disclosure of anyone who is in a position to control the content of an educational activity. All relevant financial relationships with any commercial interests and/or manufacturers must be disclosed.
DISCLOSURE of COMMERCIAL SUPPORT of CME As you undoubtedly know from the national media, there has been much discussion concerning the relationships between CME sponsors, faculty and commercial companies providing support of CME.
Both the American Osteopathic Association and the Committee on Continuing Medical Education have adopted regula-tions for ethical actions in this area which the American Osteopathic College of Dermatology endorse and have adopted for all our educational activities.
Please be assured that having an affiliation with a company does not imply in any way that something is wrong or improp-er; however, we want to inform attendees that such a relationship exists.
Should you have any questions regarding the facilities, handouts, program content, or concerns about CME compliance with the AOA “Uniform Guidelines,” feel free to contact the AOCD representative:
Marsha A. Wise, B.S. Executive Director P.O. Box 7525 Kirksville, MO 63501 660-665-2184 800-449-2623
Unresolved issues regarding compliance with the AOA “Uniform Guidelines” can be brought to the attention of the AOA Division of CME by calling:
800-621-1773, extension 8262 or by writing:
AOA CME Office 142 East Ontario Street
Chicago, IL 60611
11
All Events to take place in the San Diego Convention Center unless otherwise noted.
7:00 am - 8:00 am AOCD Registration
8:00 am - 8:30 am CLIA – Proficiency Tests Gregory Papadeas, D.O., FAOCD
8:30 am - 9:00 am Daniel Siegel, MD, AAD President
9:00 am - 12:00 am 2nd Annual University of Pennsylvania Symposium
9:00 am - 9:45 am Update in Autoimmune Skin Disease Victoria Werth, M.D. University of Pennsylvania Health System
9:45 am - 10:30 am Atopic Dermatitis Brian Kim, M.D. University of Pennsylvania Health System
10:30 am - 11:15 am Newer Drug Reactions Emily Chu, M.D., Ph.D. University of Pennsylvania Health System
11:15 am - 12:00 pm Issues in Melanoma Michael Ming, M.D., M.S.C.E. University of Pennsylvania Health System
12:00 pm - 1:00 pm Lunch on your own
1:00 pm - 2:00 pm Novel Topical Dermatologic Treatments for the Pediatric Patient Fred Ghali, M.D. Pediatric Dermatology of North Texas, PA, Grapevine, TX
2:00 pm - 3:00 pm Cosmeceuticals Steven Grekin, D.O., FAOCD
3:00 pm - 3:15 pm Break
3:15 pm - 5:00 pm AOCD General Business Meeting
6:00 pm - 9:00 pm Presidential Celebration (Ticketed Event) San Diego Marriott
MONDAY, OCTOBER 8, 2012
12
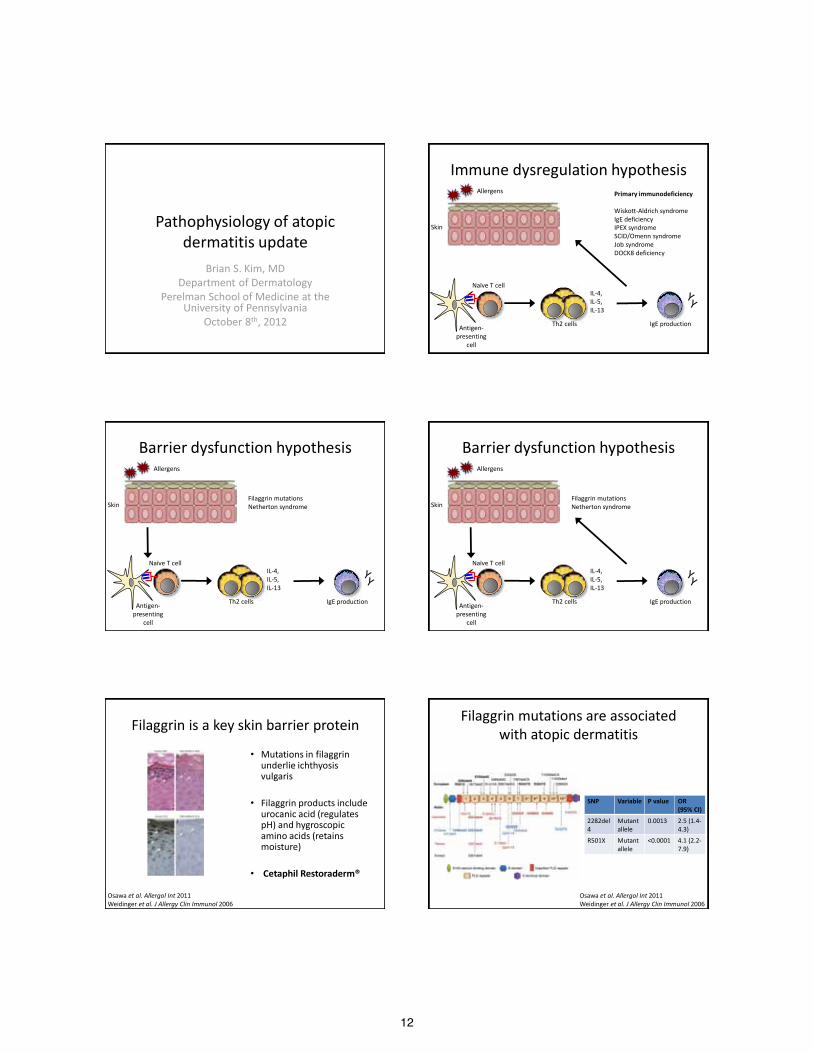
Pathophysiology of atopic dermatitis update
Brian S. Kim, MD Department of Dermatology
Perelman School of Medicine at the University of Pennsylvania
October 8th, 2012
Immune dysregulation hypothesis
IL-4, IL-5, IL-13
Th2 cells
Naïve T cell
Antigen-presenting
cell
IgE production
Allergens
Skin
Primary immunodeficiency Wiskott-Aldrich syndrome IgE deficiency IPEX syndrome SCID/Omenn syndrome Job syndrome DOCK8 deficiency
Barrier dysfunction hypothesis
IL-4, IL-5, IL-13
Th2 cells IgE production
Allergens
Skin Filaggrin mutations Netherton syndrome
Naïve T cell
Antigen-presenting
cell
Barrier dysfunction hypothesis
IL-4, IL-5, IL-13
Th2 cells IgE production
Allergens
Skin Filaggrin mutations Netherton syndrome
Naïve T cell
Antigen-presenting
cell
Filaggrin is a key skin barrier protein
• Mutations in filaggrin underlie ichthyosis vulgaris
• Filaggrin products include urocanic acid (regulates pH) and hygroscopic amino acids (retains moisture)
• Cetaphil Restoraderm®
Osawa et al. Allergol Int 2011 Weidinger et al. J Allergy Clin Immunol 2006
Filaggrin mutations are associated with atopic dermatitis
Osawa et al. Allergol Int 2011 Weidinger et al. J Allergy Clin Immunol 2006
SNP Variable P value OR (95% CI)
2282del4
Mutant allele
0.0013 2.5 (1.4-4.3)
R501X Mutant allele
<0.0001 4.1 (2.2-7.9)
13
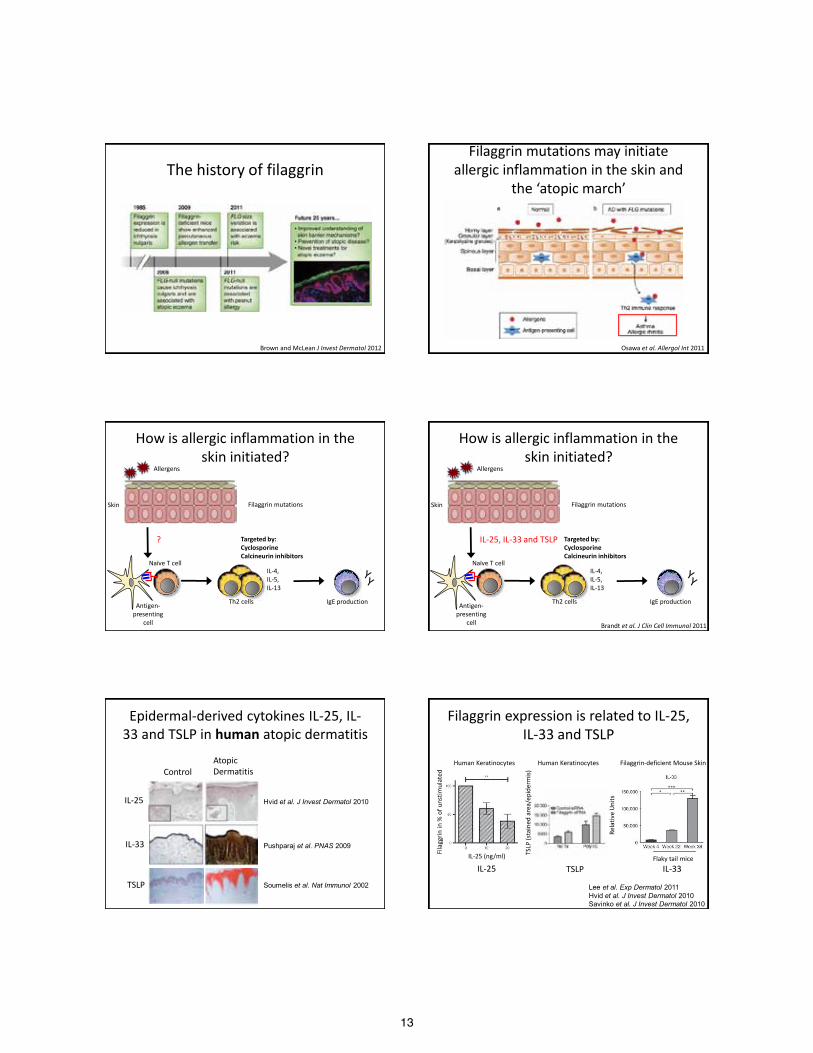
The history of filaggrin
Brown and McLean J Invest Dermatol 2012
Filaggrin mutations may initiate allergic inflammation in the skin and
the ‘atopic march’
Osawa et al. Allergol Int 2011
How is allergic inflammation in the skin initiated?
IL-4, IL-5, IL-13
Th2 cells IgE production
Allergens
Skin Filaggrin mutations
? Targeted by: Cyclosporine Calcineurin inhibitors
Naïve T cell
Antigen-presenting
cell
How is allergic inflammation in the skin initiated?
IL-4, IL-5, IL-13
Th2 cells IgE production
Allergens
Skin Filaggrin mutations
IL-25, IL-33 and TSLP
Brandt et al. J Clin Cell Immunol 2011
Targeted by: Cyclosporine Calcineurin inhibitors
Naïve T cell
Antigen-presenting
cell
Epidermal-derived cytokines IL-25, IL-33 and TSLP in human atopic dermatitis
Control Atopic Dermatitis
IL-25
IL-33
TSLP Soumelis et al. Nat Immunol 2002
Hvid et al. J Invest Dermatol 2010
Pushparaj et al. PNAS 2009
Filaggrin expression is related to IL-25, IL-33 and TSLP
Lee et al. Exp Dermatol 2011 Hvid et al. J Invest Dermatol 2010 Savinko et al. J Invest Dermatol 2010
Human Keratinocytes Human Keratinocytes Filaggrin-deficient Mouse Skin
IL-25 TSLP IL-33
Fila
ggrin
in %
of u
nstim
ulat
ed
IL-25 (ng/ml) TSLP
(sta
ined
are
a/ep
ider
mis)
Rela
tive
Uni
ts
Flaky tail mice
14
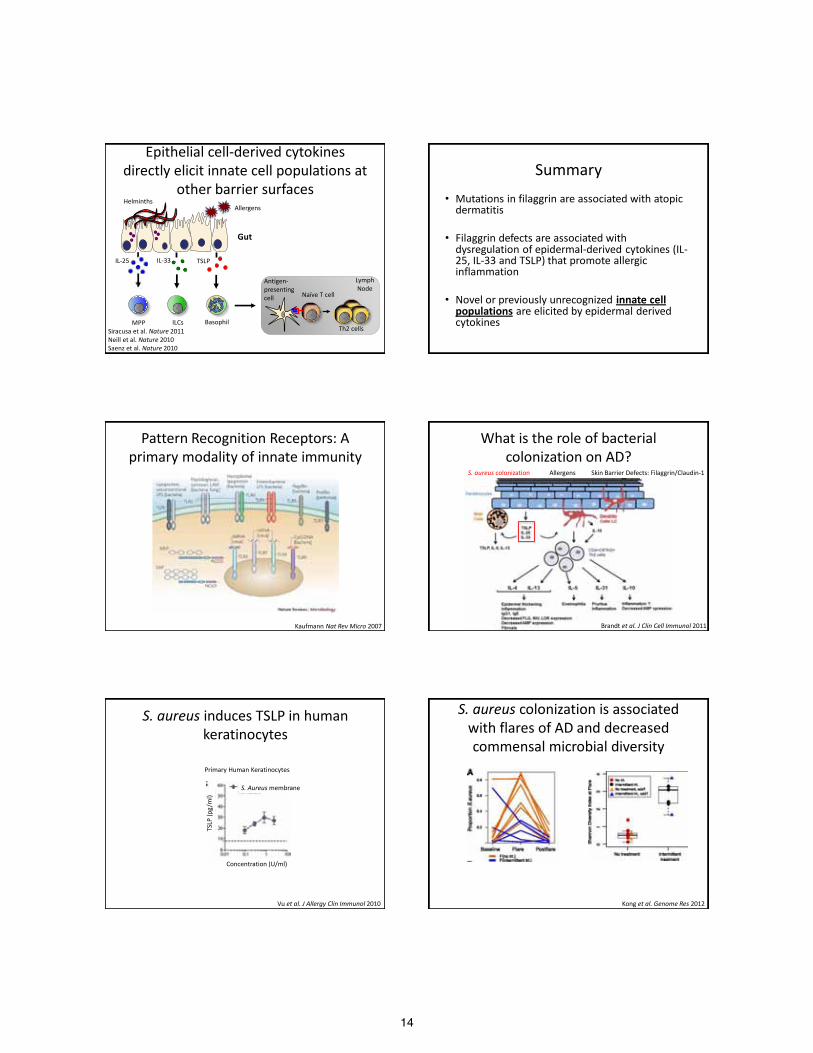
Epithelial cell-derived cytokines directly elicit innate cell populations at
other barrier surfaces Allergens
Gut
Th2 cells
Lymph Node
ILCs MPP
IL-33 IL-25
Siracusa et al. Nature 2011 Neill et al. Nature 2010 Saenz et al. Nature 2010
Basophil
TSLP
Helminths
Antigen- presenting cell Naïve T cell
Summary • Mutations in filaggrin are associated with atopic
dermatitis
• Filaggrin defects are associated with dysregulation of epidermal-derived cytokines (IL-25, IL-33 and TSLP) that promote allergic inflammation
• Novel or previously unrecognized innate cell populations are elicited by epidermal derived cytokines
Pattern Recognition Receptors: A primary modality of innate immunity
Kaufmann Nat Rev Micro 2007
What is the role of bacterial colonization on AD?
Brandt et al. J Clin Cell Immunol 2011
S. aureus colonization Allergens Skin Barrier Defects: Filaggrin/Claudin-1
S. aureus induces TSLP in human keratinocytes
Primary Human Keratinocytes
Vu et al. J Allergy Clin Immunol 2010
Concentration (U/ml)
S. Aureus membrane
TSLP
(pg/
ml)
S. aureus colonization is associated with flares of AD and decreased commensal microbial diversity
Kong et al. Genome Res 2012
15
Depletion of commensal bacteria enhances allergic inflammation
March 2012
Summary
• S. aureus may enhance allergic inflammation via epidermal cell-derived cytokines such as TSLP
• S. aureus is associated with flares of atopic dermatitis
• Commensal bacterial diversity is associated with improved atopic dermatitis
Pathogen vs. Commensal
Commensals
Pathogens
What is the role of skin bacteria?
• Does short-term antimicrobial therapy work because of S. aureus-targeted therapy?
• Is there a role for “probiotic” therapy?
Topical bleach baths and intranasal mupirocin improves eczema severity
%BS
A
EASI
Sco
re
Huang et al. Pediatrics 2009
Months Months
What is the role of (commensal) fungi?
16
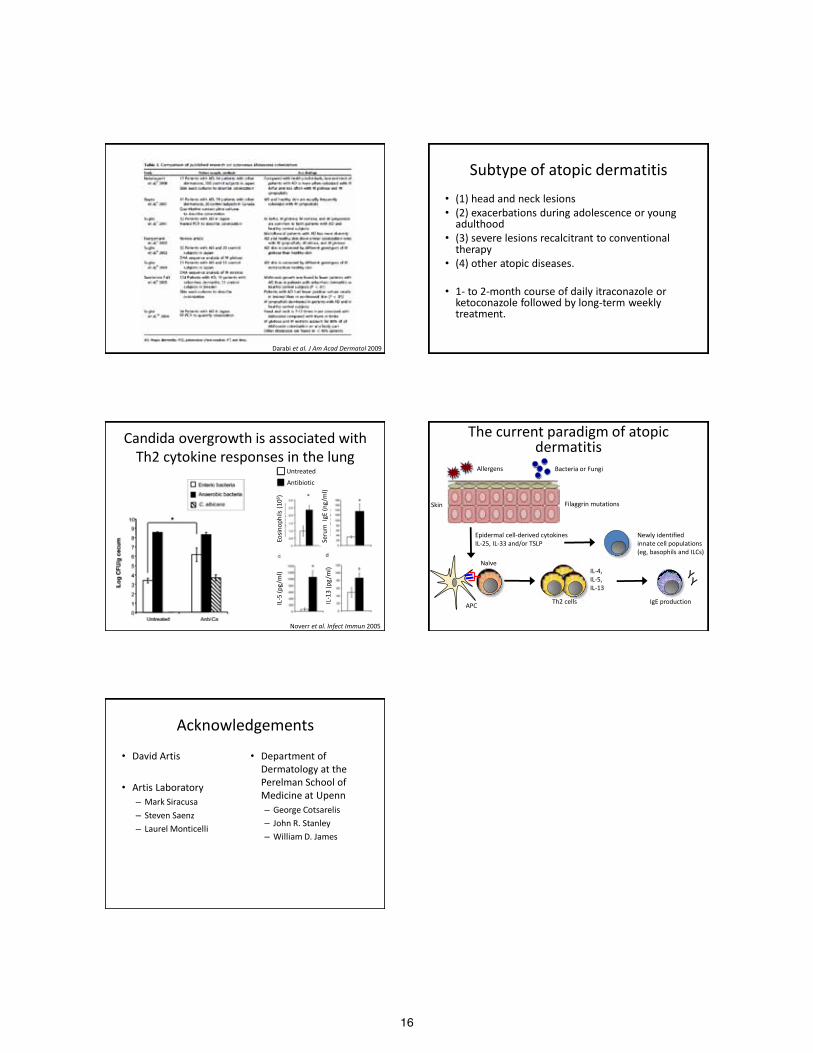
Darabi et al. J Am Acad Dermatol 2009
Subtype of atopic dermatitis • (1) head and neck lesions • (2) exacerbations during adolescence or young
adulthood • (3) severe lesions recalcitrant to conventional
therapy • (4) other atopic diseases.
• 1- to 2-month course of daily itraconazole or
ketoconazole followed by long-term weekly treatment.
Candida overgrowth is associated with Th2 cytokine responses in the lung
Noverr et al. Infect Immun 2005
Antibiotic
Untreated
Eosin
ophi
ls (1
06 )
Seru
m I
gE (n
g/m
l)
IL-5
(pg/
ml)
IL-1
3 (p
g/m
l)
The current paradigm of atopic dermatitis
IL-4, IL-5, IL-13
Th2 cells
Naïve
APC IgE production
Allergens
Skin Filaggrin mutations
Bacteria or Fungi
Epidermal cell-derived cytokines IL-25, IL-33 and/or TSLP
Newly identified innate cell populations (eg, basophils and ILCs)
Acknowledgements
• David Artis
• Artis Laboratory – Mark Siracusa – Steven Saenz – Laurel Monticelli
• Department of Dermatology at the Perelman School of Medicine at Upenn – George Cotsarelis – John R. Stanley – William D. James
17
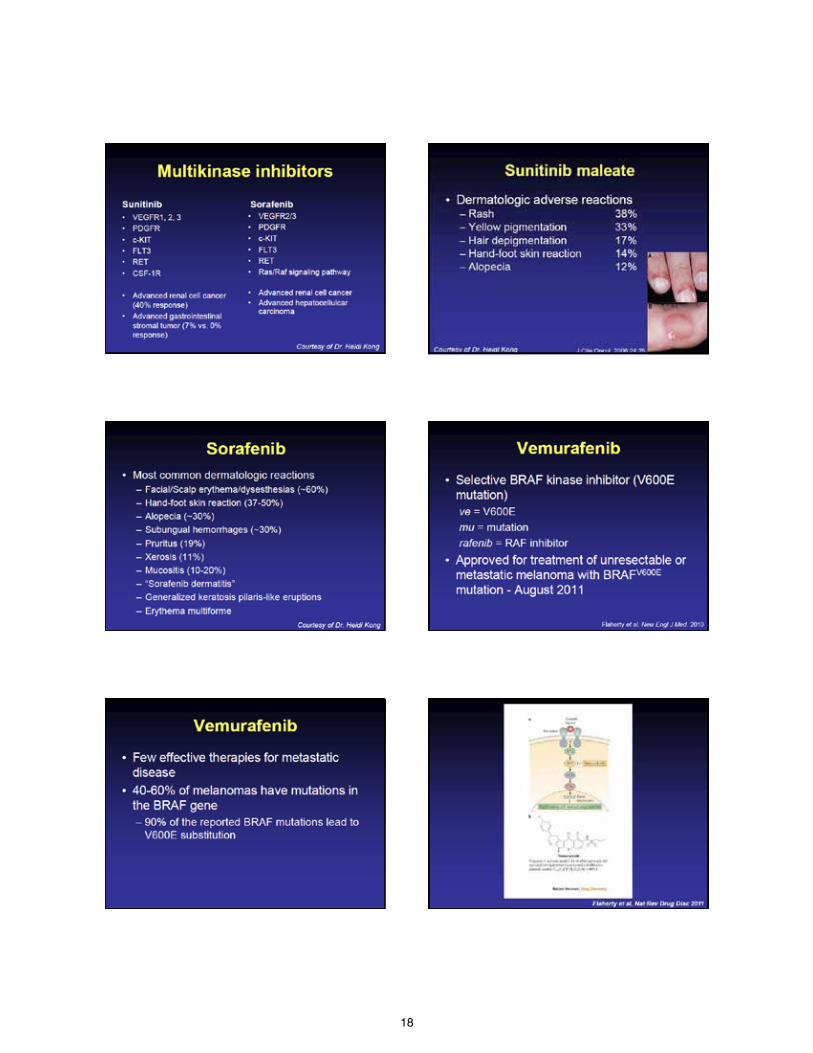
18
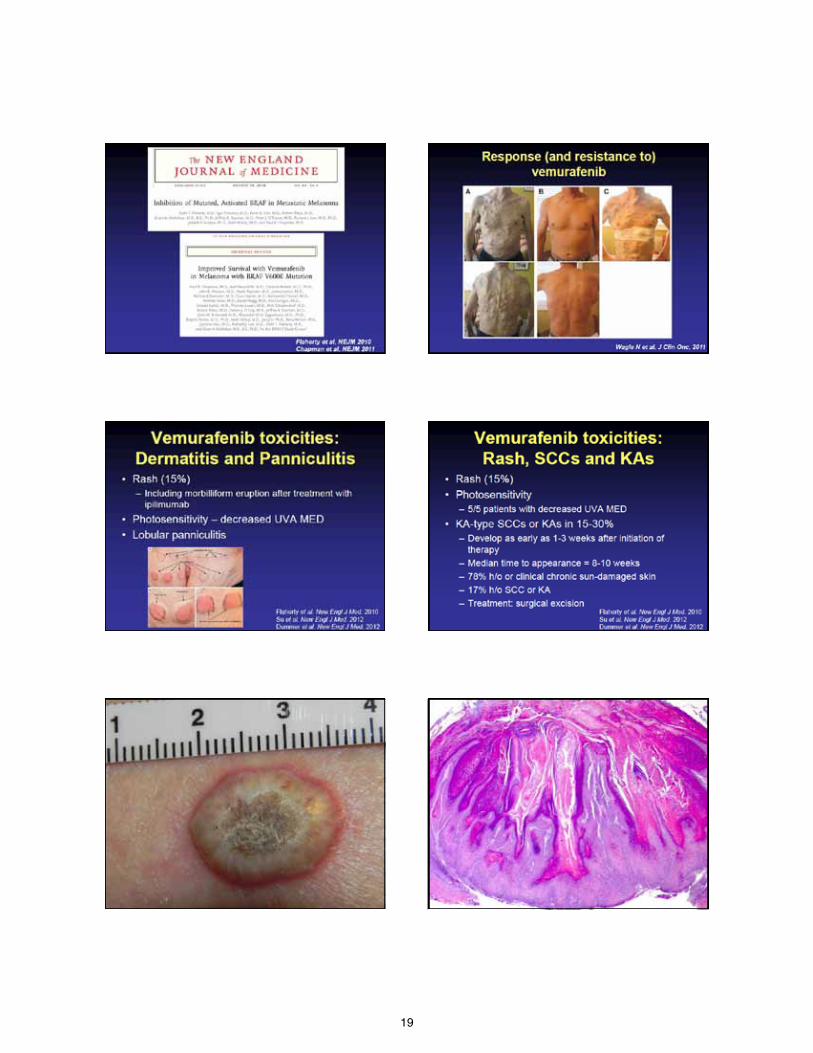
19
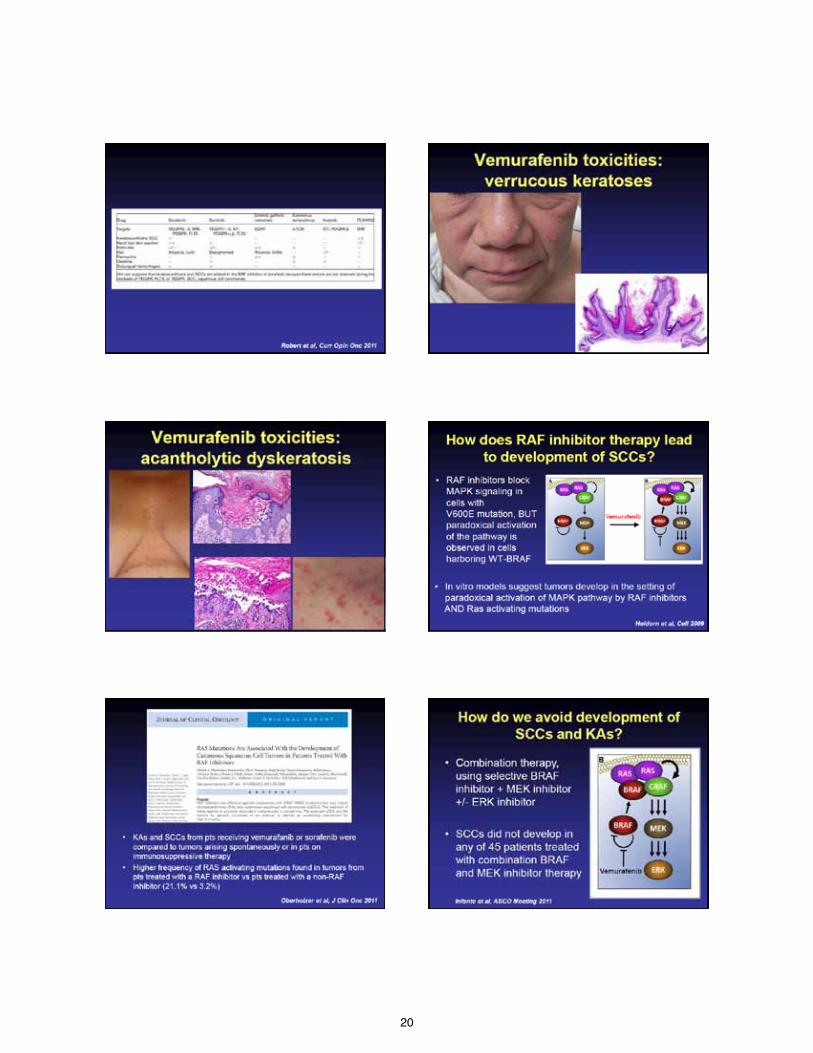
20

21
22
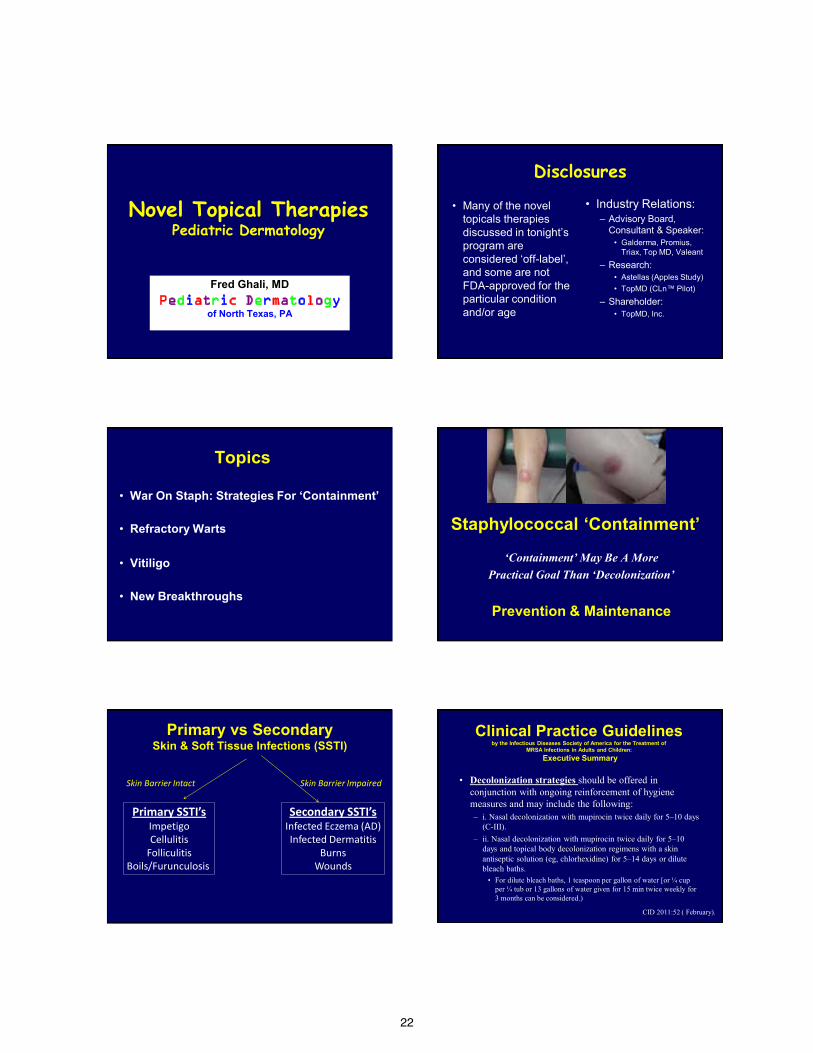
Novel Topical Therapies Pediatric Dermatology
Fred Ghali, MD Pediatric Dermatology
of North Texas, PA
Disclosures
• Many of the novel topicals therapies discussed in tonight’s program are considered ‘off-label’, and some are not FDA-approved for the particular condition and/or age
• Industry Relations: – Advisory Board,
Consultant & Speaker: • Galderma, Promius,
Triax, Top MD, Valeant
– Research: • Astellas (Apples Study) • TopMD (CLn™ Pilot)
– Shareholder: • TopMD, Inc.
Topics
• War On Staph: Strategies For ‘Containment’
• Refractory Warts
• Vitiligo
• New Breakthroughs
Staphylococcal ‘Containment’
‘Containment’ May Be A More Practical Goal Than ‘Decolonization’
Prevention & Maintenance Primary vs Secondary
Skin & Soft Tissue Infections (SSTI)
Primary SSTI’s Impetigo Cellulitis
Folliculitis Boils/Furunculosis
Secondary SSTI’s Infected Eczema (AD) Infected Dermatitis
Burns Wounds
Skin Barrier Intact Skin Barrier Impaired
Clinical Practice Guidelines by the Infectious Diseases Society of America for the Treatment of
MRSA Infections in Adults and Children: Executive Summary
• Decolonization strategies should be offered in conjunction with ongoing reinforcement of hygiene measures and may include the following: – i. Nasal decolonization with mupirocin twice daily for 5–10 days
(C-III). – ii. Nasal decolonization with mupirocin twice daily for 5–10
days and topical body decolonization regimens with a skin antiseptic solution (eg, chlorhexidine) for 5–14 days or dilute bleach baths. • For dilute bleach baths, 1 teaspoon per gallon of water [or ¼ cup
per ¼ tub or 13 gallons of water given for 15 min twice weekly for 3 months can be considered.)
CID 2011:52 ( February).
23
‘Biocide’ Resistance (Cross Resistance Becoming An Issue)
• Because biocides tend to act concurrently on multiple sites within the microorganism, resistance is often mediated by non-specific means.
• Most Mentioned: – Triclosan – Benzalkonium chloride
• Report of linked to oxacillin resistance in Staphylococcus aureus. (Akimitsu et al)
• Mechanisms: – Decreased cell wall
permeability • Decreases biocide reaching
the cell
– Efflux pumps – Change in biofilm – Induction of genes
(Plasmid-generated) – Enzymatic transformation
Scientific Committee on Emerging and Newly Identified Health Risks SCENIHR. Assessment of the Antibiotic Resistance Effects of Biocides, 2009 report
Resistance To Topicals
• Resistance rates to topical therapies such as mupirocin and fusidic acid are increasing and have been reported
• Mupirocin resistance rates among S. aureus isolates in SSTI documented – US: 5.2% (SENTRY
Antimicrobial Surveillance Program 2000)
– Multiple reports worldwide
Oranje AP et al.. Dermatology 2007;215:331–340. Simor AE et al. Antimicrob Agents Chemother 2007;51: 3880–3886. Deshpande et al. l Infect Dis 2002;42:283–290. SENTRY Antimicrobial Surveillance Program Upton A, et al. . J Antimicrob Chemother 2003;51:613–617.
History of Bleach Dakin’s Solution
• Developed by English chemist, Henry Drysdale Dakin, and French surgeon, Alexis Carrel, after a long search for an ideal wound antiseptic
• Prepared by passing chlorine into a solution of sodium hydroxide
• Used in WW I as a wound
antiseptic
• Dakin’s solution is highly diluted antiseptic
– Sodium hypochlorite 0.5% • Sometimes this higher % can be cytotoxic
– Boric acid 4% – This higher % of sodium hypochlorite can
be cytotoxic to tissues
• References in the literature show that a sodium hypochlorite (Dakin’s) solution diluted to 0.005% is bactericidal while being non-cytotoxic to fibroblasts. – More dilute variations of Dakin’s
solution marketed by Century Pharmaceuticals
Mechanisms of Bleach (HOCL)
• Reacts with DNA, RNA, fatty acids, cholesterol, lipids, proteins
• Additionally, the increased pH is harmful to cells
• Specifics: – 1) Reaction with protein
sulfhydryl groups1
– 2) reaction with protein amino groups (chloramination-AA decompose)1
– 3) oxidative unfolding and aggregation of proteins (heat shock protein 33)2
1) Estrela et al, Braz Dent J, 2002:13: 113-117; 2) Winter et al., Cell, 2008; 135:691-701
Bleach Dilutions (6%)
Sodium Cups Bathtub (40-60 gallon) Hypochlorite (%) 0.009% (90 ppm) ¼ cup ¼ tub 0.019% (190 ppm) ½ cup ¼ tub 0.005% (50 ppm) ¼ cup ½ tub 0.009% (90 ppm) ½ cup ½ tub 0.005% (50 ppm) ½ cup Full tub
References: Bathtub: 40-60 gallons; 1 gallon = 128 oz, 40 gallons = 5120 oz; 1 cup = 8 oz Swimming pool reference: 3 parts per million (available chlorine)
8-10 minutes, 2-3 times/wk Infant tub: 1-2 tsp/gallon Rinse after
Product Indication Availability NaOCL Diluted Dakins Mechanically cleanse OTC (510K) 0.0125% (Di-Dak-Sol®) and debride open wounds Aurstat® Gel Abrasions Rx (510K) KIT 0.002% lacerations, irritations Atrapro™ HydroGel Pain, burning, itching Rx (510K) * with various dermatoses *(also HOCL)
Atrapro™ Spray Management of Rx (510K) 0.004% wounds (also 0.003% HOCL)
CLn® BodyWash Clean and relieve Cosmetic 0.0061% dryness/flaking of skin
Commercially Available Products (Sodium hypochlorite)
* = Present only to ‘preserve’ hydrogel
24
S. Aureus & AD
S. aureus & AD • AD skin found to deficient
in antimicrobial peptides – Decreased levels of
cathelicidins are thought to be due to IL-4, which is increased in atopics
• S. aureus • Eczema herpeticum
• Superantigens of S. aureus
cause T-cell dysfunction – Also increased IgE Ab
• S. aureus Colonization: – ~ 10% carrier state in non-
atopic patients – Much higher in atopic
patients • Lesional (~40-93%) • Non-lesional (~40-76%) • Nares (~40-79%)
Leyden et al (Br J Dermatol 1974) Balma-Mena et al. Int J Dermatol. 2011:682-8.
MRSA in Atopics Colonization vs Infection
• Colonization: (cross-sectional studies)
– 16% MRSA (7/43 patients), 80% were colonized with S. aureus (43 ⁄ 54)1 (Philly)
– 1 case/200 MRSA; 62% colonization of S. aureus (Canada)
– 13.5% MRSA 57% (57/100) colonized with S. aureus (Sri Lanka)
– 31% (24 /168) were MRSA 78/168, overall 46% healthy children with AD colonized with S. aureus, and (Taiwan)
• Infection : – Same prior study showed 60%
MRSA (12/20) (Taiwan) – 11/78 isolates of SSTI’s (14.1%)
from atopics were MRSA, significantly lower than 44% in general peds population (658 /1482)
• Colonization and infection are on a continuum – My experience:
• Mild-mod: 20% • Mod-severe: 44% • Severe plus: 50%
1Suh et el., Pediatric Dermatol Vol. 25 No. 5 528–534, 2008 2Balma-Mena et al. Int J Dermatol. 2011:682-8. 3 Tang et al., Pediatr Int. 2011 Jun;53(3):363-7. 4 Matiz et al., Pediatr Dermatol. 2011 Jan-Feb;28(1):6-11
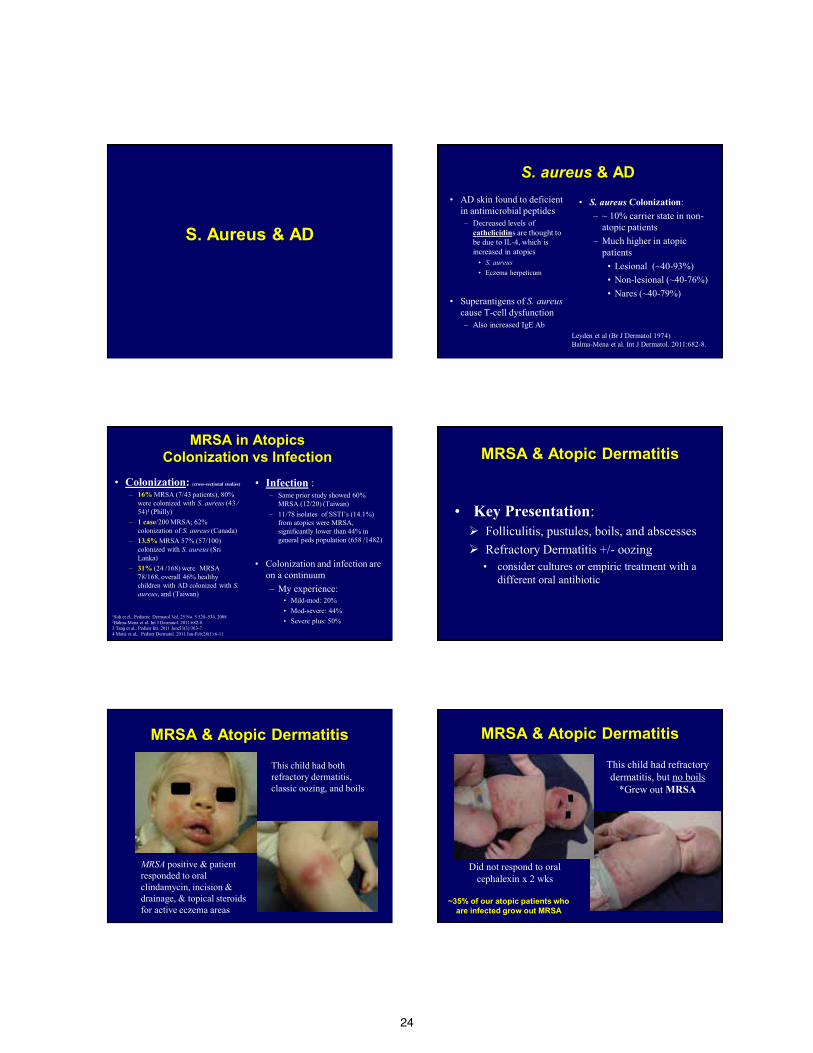
MRSA & Atopic Dermatitis
• Key Presentation: Folliculitis, pustules, boils, and abscesses Refractory Dermatitis +/- oozing
• consider cultures or empiric treatment with a different oral antibiotic
MRSA & Atopic Dermatitis
MRSA positive & patient responded to oral clindamycin, incision & drainage, & topical steroids for active eczema areas
This child had both refractory dermatitis, classic oozing, and boils
MRSA & Atopic Dermatitis
This child had refractory dermatitis, but no boils
*Grew out MRSA
Did not respond to oral cephalexin x 2 wks
~35% of our atopic patients who are infected grow out MRSA
25
Sodium Hypochlorite (Bleach) Baths: A Potential Measure to Reduce the Incidence of Recurrent, Cutaneous Staphylococcus aureus Superinfection among Susceptible Populations
John Browning, MD1, Moise Levy, MD1,2, Alexandra Rousseau, MD1, Raphael Rousseau, MD1,
Sheldon Kaplan, MD2, and Denise Metry, MD1,2
Departments of Dermatology1 and Pediatrics2, Baylor College of Medicine and Texas Children’s Hospital, Houston, TX
INTRODUCTION
PATIENTS AND METHODS
RESULTS
DISCUSSION AND CONCLUSION
Table 2. Decrease in MRSA and MSSA superinfections in patients with atopic dermatitis after starting sodium hypochlorite baths and intranasal mupirocin.
REFERENCES
Patients with atopic dermatitis (AD) are more susceptible to cutaneous superinfection due to an impaired skin barrier that is both inherent and secondary to pruritus-induced excoriations. In turn, secondary infection further exacerbates the inflammatory process of AD (Figures 1 and 2).
Greater than 90% of AD patients harbor large numbers of Staphylococcus aureus bacteria, which can be cultured not only from eczematous plaques, but also from clinically normal skin, the anterior nares, and subungual spaces. While in the past these S. aureus strains have been primarily susceptible to methicillin (MSSA), increasing numbers of resistant staphylococcal strains (MRSA) are being identified in healthy patients without any risk factors: so-called “community-acquired” MRSA (CA-MRSA). A dramatic rise in such infections has been increasingly reported from our and other institutions, and has been reflected in our pediatric dermatology population, particularly patients with AD (Table 1).
Recurrent cutaneous superinfection with S. aureus is problematic, and to our knowledge, no standard treatment recommendations exist. Along with other authors, we have observed the resolution of cutaneous infection, both when an oral antibiotic was given to which the organism was later found to be non-susceptible, and even in the absence of any treatment. Given these observations, along with known concerns regarding antibiotic overuse and increasing bacterial resistance patterns, we have tended to reserve systemic antibiotics for patients with evidence of more widespread cutaneous infection and/or those with systemic symptoms. Accordingly, we have also sought alternative measures to reduce patient susceptibility to recurrent cutaneous staphylococcal superinfection.
Beginning in May of 2002, we implemented “anti-Staphylococcal measures” among patients and their household members with a history of cutaneous superinfection. These measures combine the use of intranasal mupirocin (pea-sized amount of mupirocin ointment applied to the anterior nares twice daily for 7 days a month for 6 months) with sodium hypochlorite baths (2 teaspoons of 6% sodium hypochlorite household bleach per gallon of bath water or ¼ cup per full tub of water, twice weekly for 6 months) (Figure 3).
Sodium hypochlorite has been used to prevent bacterial skin infections among burn patients, as well as those with epidermolysis bullosa. In one study, concentrations of 0.25%, 0.025%, and 0.0125% sodium hypochlorite were investigated. Concentrations as low as 0.0125% were found to be bactericidal to gram positive organisms without causing tissue toxicity (Heggers, et al). A second study found sodium hypochlorite concentrations as low as 0.01% to be bactericidal against S. aureus (Rutala, et al). Our recommended dilution yields a similar concentration of sodium hypochlorite (2 tsp per gallon compared to 1.6 tsp/gallon necessary to achieve a .0125% dilution, compared to .06 tsp per gallon in a normally chlorinated swimming pool).
Sodium hypochlorite is bactericidal due to a direct effect on the bacteria cells and thus carries no risk for increased resistance. Thus, the effect of sodium hypochlorite on S. aureus is similar to that of benzoyl peroxide on Propionibacterium acnes.
Potential risks of sodium hypochlorite, particularly among the AD population, include irritation and xerosis, although we have found this modality to be well-tolerated by our patients. We recommend rinsing with clean water followed by immediate emollient application, and reassuring families who can be anxious about the use of “bleach” that the recommended dilution is low. While other antiseptic products are certainly available, sodium hypochlorite is a readily accessible, inexpensive and well-tolerated option. Although prospective, controlled studies are greatly needed, we believe that the additional use of sodium hypochlorite baths, in combination with intranasal mupirocin, may be an effective measure towards reducing the incidence of recurrent staphylococcal cutaneous superinfection, including MRSA, among susceptible populations.
In an IRB-approved retrospective chart review performed on
243 children clinically diagnosed with AD who were seen in our outpatient dermatology clinics between January 1999 and October 2002, we observed a dramatic decrease in culture confirmed
staphylococcal skin infections concomitant with implementation of these measures (Figure). In continuing these preventative measures, we observed a decrease from 60 cases of staphylococcal infections a year (August 2001 – July 2002) to 6 cases a year (August 2003 – July 2004).
1. Purcell K, Fergie J. Epidemic of community-acquired methicillin-resistant Staphylococcus aureus infections: a 14-year study at Driscoll Children’s Hospital. Arch Pediatr Adolesc Med. 2005;159(10):980-5.
2. Kaplan SL, Hulten KG, Gonzalez BE, et al. Three-year surveillance of community-acquired Staphylococcus aureus infections in children. Clin Infect Dis 2005; 40:1785-1791.
3. Heggers JP, et al. Bactericidal and wound-heali ng properties of sodium hypochlorite solutions: the 1991 Lindberg Award. J Burn Care Rehabil 1991; 12(5):420-
4. McGuire, Joseph. Personal communication.
5. Rutala WA, Cole EC, Thomann CA, Weber DJ. Stability and bactericidal activity of chlorine solutions. Infect Cont Hosp Epi 1998; 19(5):323-7.
Figure 1. Eczematous patches along the anterior neck, superinfected with CA-MRSA.
Figure 2. Child with atopic dermatitis who developed a cutaneous abscess from CA-MRSA superinfection.
Table 1. Identification of community-acquired MRSA infections at Texas Children’s Hospital between August 2001 and December 2003
Figure 3. “Anti-Staphylococcal measures” implemented in May 2002.
0
20
40
60
80
100
120
140
160
180
200
8 10 12 2 4 6 8 10 12 2 4 6 8 10 12
MSSA MRSA
Application of mupirocin (Bactroban ®) to the anterior nares twice a day for 7 days every month for 6 months.
Bathing in water with sodium hypochlorite (2 tsp per gallon of water or ¼ cup per full tub of water) twice a week for 6 months.
0
2
4
6
8
10
12
04/99
-06/99
07/99
-09/99
10/99
-12/99
01/00
-03/00
04/00
-06/00
07/00
-09/00
10/00
-12/00
01/01
-03/01
04/01
-06/01
07/01
-09/01
10/01
-12/01
01/02
-03/02
04/02
-06/02
07/02
-09/02
10/02
-12/02
Nu
mb
er
of
ca
se
s
MSSAMRSAOther
Startpoint of mupirocin prophylaxisand sodium hypochlorite baths
Treatment of Staph Colonization Huang et al. Pediatrics 2009; May 808-814
• Double-blind, placebo-controlled, ~25 patients for follow-up
• Chronic use of dilute bleach baths with intermittent intranasal application of mupirocin ointment decreased the clinical severity of atopic dermatitis in patients with clinical signs of secondary bacterial infections.
• Patients with atopic dermatitis do not seem to have increased susceptibility to infection or colonization with resistant strains of S aureus. –I DISAGREE (35% TX)
• The mean EASI scores for the head and neck did not decrease for patients in the treatment group, whereas scores for other body sites (submerged in the dilute bleach baths) decreased at 1 and 3 months, in comparison with placebo-treated patients.
Reserve for Clinically Infected • F.J. Bath-Hextall; Interventions to Reduce Staphylococcus
aureus in the Management of Atopic Eczema: An Updated Cochrane Review. Br J Derm 2010.
• Conclusions:
– We failed to find any evidence that commonly used anti-staphylococcal interventions are clinically helpful in people with eczema that is not clinically infected.
– Their continued use should be questioned in such situations, until better and longer-term studies show clear evidence of clinical benefit.
What about infection-prone patients?? Colonization vs Infection –Sometimes A Slippery Slope
CLn® Body Wash
• Indication: – Clean and relieve
dryness/flaking of skin
• Available as cosmetic product – In-office dispensing – Web site (www.clnwash.com)
• Passed All Basic Testing:
– Epiocular™; Repeat insult patch test; US/Euro Antimicrobial Effectiveness Test
• Kill Rates S. aureus: • 98% kill rate at 2 min • 99.9 at 3 and 5 min
• Studies: – Completed Pilot Study
• 18 moderate-severe atopics (submitted for publication)
– Planned: • 50 patient multi-center study
in moderate-severe atopics • 20 patient single-center
comparative study for hand eczema (investigator-initiated)
• 30 patient acne pilot study
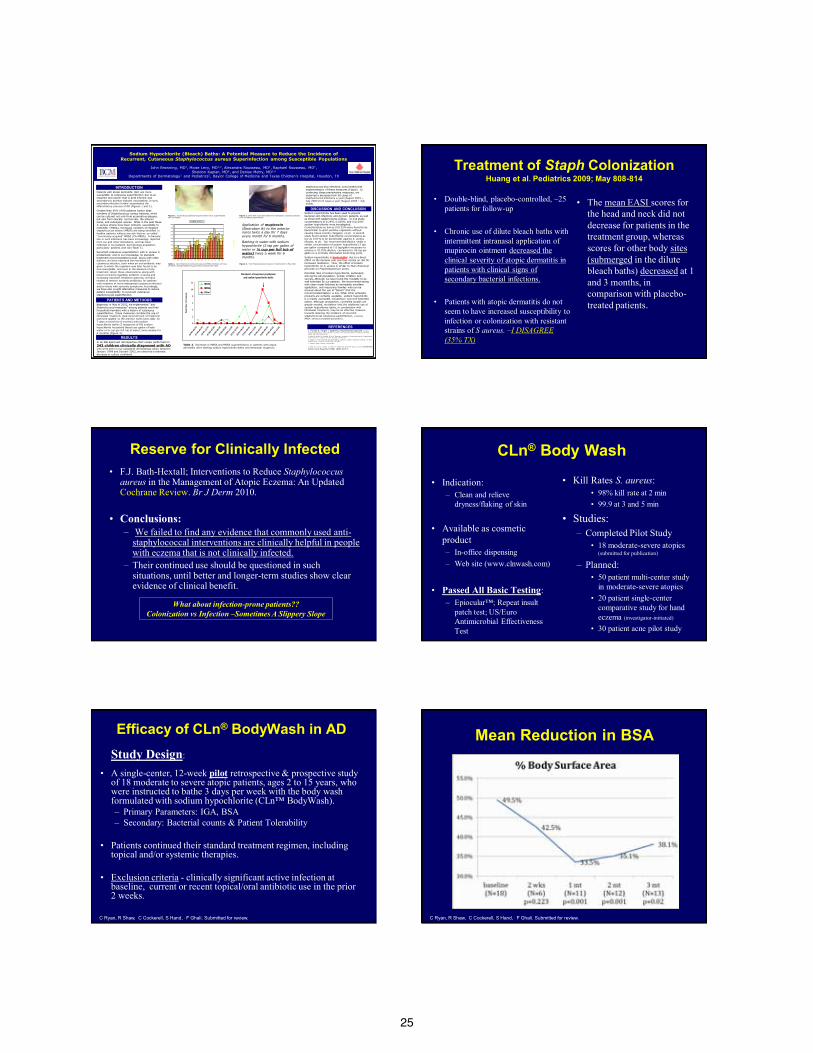
Efficacy of CLn® BodyWash in AD Study Design:
• A single-center, 12-week pilot retrospective & prospective study of 18 moderate to severe atopic patients, ages 2 to 15 years, who were instructed to bathe 3 days per week with the body wash formulated with sodium hypochlorite (CLn™ BodyWash). – Primary Parameters: IGA, BSA – Secondary: Bacterial counts & Patient Tolerability
• Patients continued their standard treatment regimen, including
topical and/or systemic therapies.
• Exclusion criteria - clinically significant active infection at baseline, current or recent topical/oral antibiotic use in the prior 2 weeks.
C Ryan, R Shaw, C Cockerell, S Hand, , F Ghali. Submitted for review.
Mean Reduction in BSA
C Ryan, R Shaw, C Cockerell, S Hand, , F Ghali. Submitted for review.

26
Mean Change In IGA
C Ryan, R Shaw, C Cockerell, S Hand, , F Ghali. Submitted for review.
Case (7) Baseline
6 weeks
2 weeks
10 weeks
Case (11)
Baseline 8 weeks
Results: CLn® BodyWash
• Changes in BSA and IGA showed statistically significant results.
• Adverse Events: – 3 reported burning/stinging
• Tolerability:
– CLn Body Wash™ was well-tolerated and overall patient preference was statistically significant over the traditional bleach baths.
• Bacteriology: – Decreasing trend in
quantitative S. aureus counts; statistically significant at 1 month • MRSA colonization rate
44%, higher than in other studies
• Conclusions:
– Similar to traditional bleach baths, this study supports the adjunctive use of CLn® BodyWash in AD.
C Ryan, R Shaw, C Cockerell, S Hand, , F Ghali. Submitted for review.
‘Containment’ Maintenance Strategies
Primary Staph (SSTI’s)
Secondary Staph SSTI’s
Chlorhexidine Antimicrobial Soaps
Sodium Hypochlorite
(Bleach) Topical
Antibiotics
Topical Antibiotics
Sodium Hypochlorite
(Bleach)
Refractory Warts
Topical Contact Immunotherapy

27
Be Cautious!!
‘Ring Warts’
Cantharadin Outpatient & In-Office Cryo
Cantharadin
• Extract of blister beetle
• Not FDA approved – But is included under the
Bulk Substance Act for compounding to physicians or ordered from Canada
• I use only for warts on the
palms/soles
• Advantage: – Painless procedure
• Two Major Forms: (Both mixed in collodion)
– Cantharadin 0.7% – Cantharadin Plus is
my preference for small (<5 mm) warts (plantar/plantar) • Cantharadin 1% • Podophyllin 5% • Salicylic acid 30%
Ring Warts & Cantharadin
• Very common occurrence, especially on dorsal surfaces of the skin
• I tend to use only for warts located on the palms/soles – Will not use on the fingers,
cuticles, face, or other areas – This will translate to very
little development of ring warts
Ring wart
In-Office
Ring Warts OTC, Histofreeze/Verruca-Freeze • There is a very high risk of ring
warts with ‘over-freezing” Hook-m Horns
Ring wart
Topical Contact Sensitization • General Principle
– In-office application to a skin site (usually the arm) to induce contact allergy (sensitization)
– At home patients use a lower concentration painted on warts to induce immune response • Advancing 3x/wk…4x/wk…daily
• Squaric acid is more popular w/ pedi derms
– DNCB not used much in peds b/c of mutagenic potential
• Side effects: – Contact dermatitis
• At sensitization site, wart site, possible id reaction
Squaric Acid My Experience
Step 1: Sensitize w/ 2% in the office
– On upper arm Step 2: Apply weaker % at home
– After ~ 2 wks, pt applies 0.4% at home to the warts
Step 3: Recheck in the office
– If no response in 2 mos, double strength
At Home
Expected erythema around warts

28
Squaric Acid My Experience
• “Recall” Phenomena – Appears at original
sensitization site – When the patient
begins applying the weaker % of sq acid onto the treated warts
– It does mean they are truly sensitized
• Its presence does correlate well with a good response – But its absence does not
translate into a failure as the majority of responders do not demonstrate this reaction
At Home Squaric Acid My Experience
• I avoid use on the face/neck/groin
• ~ 70% effective – Seems to work best
against plantar warts – Duration: 2-4 months
2 months later 0.4%
Squaric Acid Case Examples
• Advantages – Non-painful – May combine w/ other
treatments – Ease of sensitization in
most patients – Lack of mutagenicity – Scarcity in common
human environments 3 mos later (0.4%)
Side Effects-Contact Dermatitis
• May occur at the sensitization site or any applied site – Less likely can develop
“Auto-eczema”/ “id”
• Treatment: – Decrease applications – Potent topical steroid or
oral steroid if severe
At Home
Case Example
Baseline S/P Squaric acid 0.6% x 2 mos
When It Fails… And Your Back Is Against The Wall
• May do 1-1.5% outpt protocol – Must be extra-
careful!!
• Or apply 2% in-office & return in 2 wks
Before
This patient failed 0.4%…0.8%..but responded to 1.5%
After
29
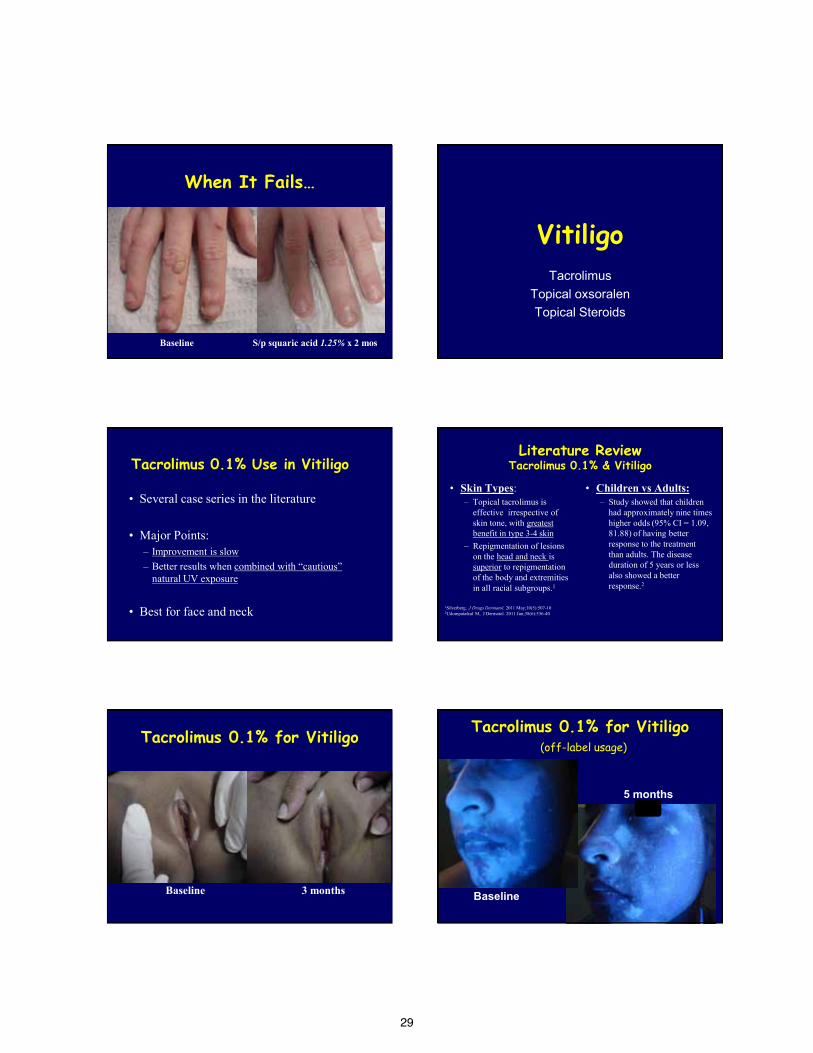
When It Fails…
Baseline S/p squaric acid 1.25% x 2 mos
Vitiligo Tacrolimus
Topical oxsoralen Topical Steroids
Tacrolimus 0.1% Use in Vitiligo
• Several case series in the literature
• Major Points: – Improvement is slow – Better results when combined with “cautious”
natural UV exposure • Best for face and neck
Literature Review Tacrolimus 0.1% & Vitiligo
• Skin Types: – Topical tacrolimus is
effective irrespective of skin tone, with greatest benefit in type 3-4 skin
– Repigmentation of lesions on the head and neck is superior to repigmentation of the body and extremities in all racial subgroups.1
• Children vs Adults: – Study showed that children
had approximately nine times higher odds (95% CI = 1.09, 81.88) of having better response to the treatment than adults. The disease duration of 5 years or less also showed a better response.2
1Silverberg, J Drugs Dermatol. 2011 May;10(5):507-10 2Udompataikul M, J Dermatol. 2011 Jun;38(6):536-40
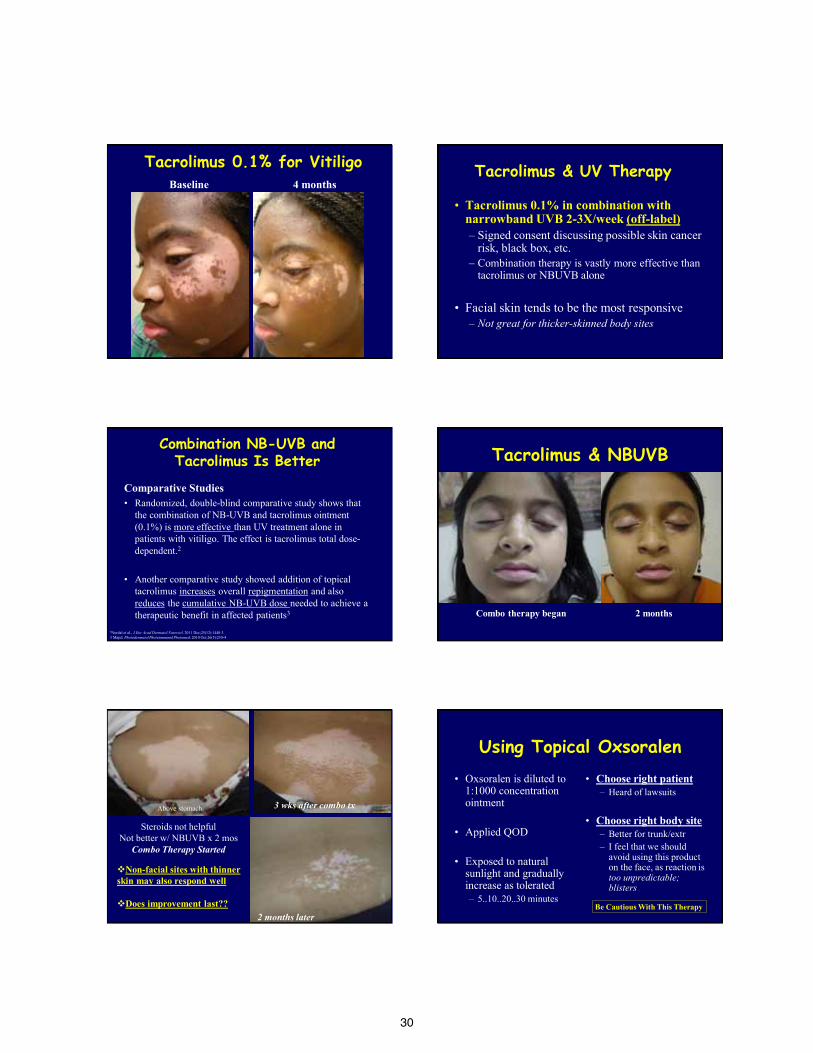
Tacrolimus 0.1% for Vitiligo
Baseline 3 months
Tacrolimus 0.1% for Vitiligo (off-label usage)
Baseline
5 months
30
Tacrolimus 0.1% for Vitiligo Baseline 4 months
Tacrolimus & UV Therapy
• Tacrolimus 0.1% in combination with narrowband UVB 2-3X/week (off-label) – Signed consent discussing possible skin cancer
risk, black box, etc. – Combination therapy is vastly more effective than
tacrolimus or NBUVB alone
• Facial skin tends to be the most responsive – Not great for thicker-skinned body sites
Combination NB-UVB and Tacrolimus Is Better
Comparative Studies • Randomized, double-blind comparative study shows that
the combination of NB-UVB and tacrolimus ointment (0.1%) is more effective than UV treatment alone in patients with vitiligo. The effect is tacrolimus total dose-dependent.2
• Another comparative study showed addition of topical tacrolimus increases overall repigmentation and also reduces the cumulative NB-UVB dose needed to achieve a therapeutic benefit in affected patients3
2Nordal et al., J Eur Acad Dermatol Venereol. 2011 Dec;25(12):1440-3 3 Majid. Photodermatol Photoimmunol Photomed. 2010 Oct;26(5):230-4
Combo therapy began 2 months
Tacrolimus & NBUVB
Steroids not helpful Not better w/ NBUVB x 2 mos
Combo Therapy Started
3 wks after combo tx
2 months later
Above stomach
Non-facial sites with thinner skin may also respond well
Does improvement last??
Using Topical Oxsoralen • Oxsoralen is diluted to
1:1000 concentration ointment
• Applied QOD
• Exposed to natural sunlight and gradually increase as tolerated – 5..10..20..30 minutes
• Choose right patient – Heard of lawsuits
• Choose right body site
– Better for trunk/extr – I feel that we should
avoid using this product on the face, as reaction is too unpredictable; blisters
Be Cautious With This Therapy
31
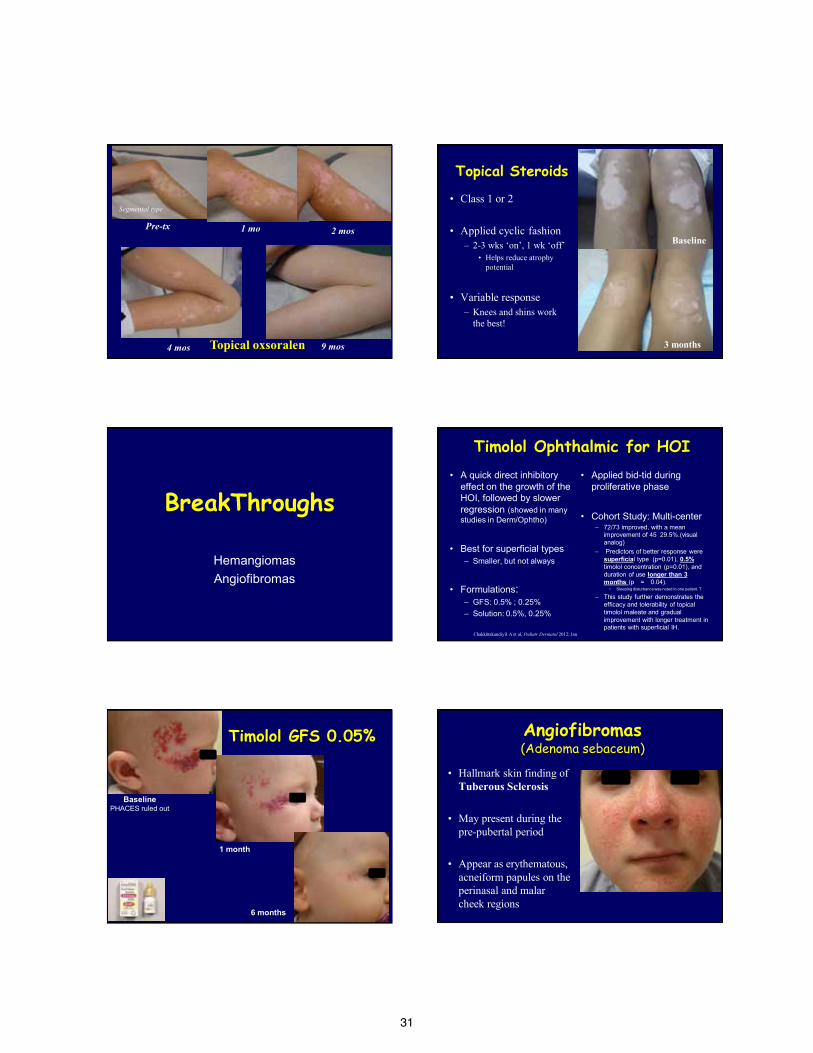
Pre-tx 1 mo 2 mos
4 mos 9 mos Topical oxsoralen
Segmental type
Topical Steroids
• Class 1 or 2
• Applied cyclic fashion – 2-3 wks ‘on’, 1 wk ‘off’
• Helps reduce atrophy potential
• Variable response
– Knees and shins work the best! 3 months
Baseline
BreakThroughs
Hemangiomas Angiofibromas
Timolol Ophthalmic for HOI
• A quick direct inhibitory effect on the growth of the HOI, followed by slower regression (showed in many studies in Derm/Ophtho)
• Best for superficial types
– Smaller, but not always
• Formulations: – GFS: 0.5% ; 0.25% – Solution: 0.5%, 0.25%
• Applied bid-tid during proliferative phase
• Cohort Study: Multi-center – 72/73 improved, with a mean
improvement of 45
29.5%.(visual analog)
– Predictors of better response were superficial type (p=0.01), 0.5% timolol concentration (p=0.01), and duration of use longer than 3 months (p = 0.04).
• Sleeping disturbance was noted in one patient. T
– This study further demonstrates the efficacy and tolerability of topical timolol maleate and gradual improvement with longer treatment in patients with superficial IH.
Chakkittakandiyil A et al, Pediatr Dermatol 2012; Jan
Timolol GFS 0.05%
Baseline PHACES ruled out
1 month
6 months
Angiofibromas (Adenoma sebaceum)
• Hallmark skin finding of Tuberous Sclerosis
• May present during the pre-pubertal period
• Appear as erythematous, acneiform papules on the perinasal and malar cheek regions
32
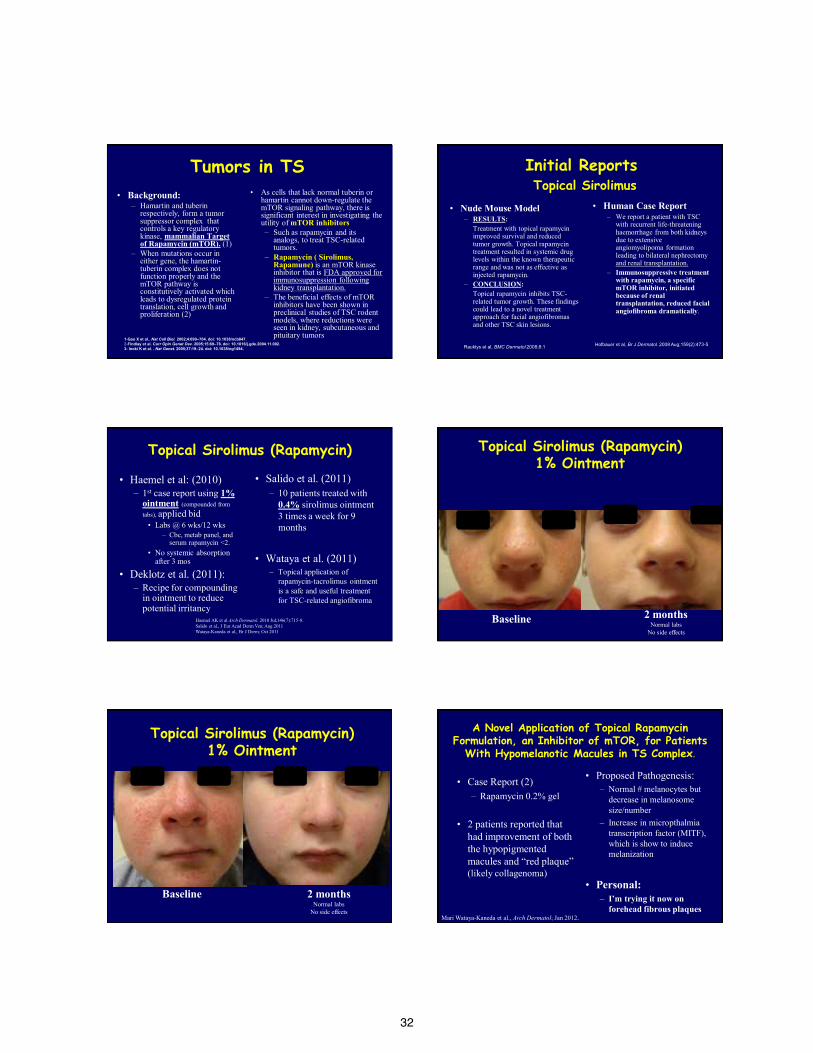
Tumors in TS • Background:
– Hamartin and tuberin respectively, form a tumor suppressor complex that controls a key regulatory kinase, mammalian Target of Rapamycin (mTOR). (1)
– When mutations occur in either gene, the hamartin-tuberin complex does not function properly and the mTOR pathway is constitutively activated which leads to dysregulated protein translation, cell growth and proliferation (2)
• As cells that lack normal tuberin or hamartin cannot down-regulate the mTOR signaling pathway, there is significant interest in investigating the utility of mTOR inhibitors – Such as rapamycin and its
analogs, to treat TSC-related tumors.
– Rapamycin ( Sirolimus, Rapamune) is an mTOR kinase inhibitor that is FDA approved for immunosuppression following kidney transplantation.
– The beneficial effects of mTOR inhibitors have been shown in preclinical studies of TSC rodent models, where reductions were seen in kidney, subcutaneous and pituitary tumors
1-Gao X et al.. Nat Cell Biol. 2002;4:699–704. doi: 10.1038/ncb847. 2-Findlay et al. Curr Opin Genet Dev. 2005;15:69–76. doi: 10.1016/j.gde.2004.11.002. 3- Inoki K et al. . Nat Genet. 2005;37:19–24. doi: 10.1038/ng1494.
Initial Reports Topical Sirolimus
• Nude Mouse Model – RESULTS: Treatment with topical rapamycin
improved survival and reduced tumor growth. Topical rapamycin treatment resulted in systemic drug levels within the known therapeutic range and was not as effective as injected rapamycin.
– CONCLUSION: Topical rapamycin inhibits TSC-
related tumor growth. These findings could lead to a novel treatment approach for facial angiofibromas and other TSC skin lesions.
• Human Case Report – We report a patient with TSC
with recurrent life-threatening haemorrhage from both kidneys due to extensive angiomyolipoma formation leading to bilateral nephrectomy and renal transplantation.
– Immunosuppressive treatment with rapamycin, a specific mTOR inhibitor, initiated because of renal transplantation, reduced facial angiofibroma dramatically.
Rauktys et al, BMC Dermatol 2008;8:1 Hofbauer et al, Br J Dermatol. 2008 Aug;159(2):473-5
Topical Sirolimus (Rapamycin)
• Haemel et al: (2010) – 1st case report using 1%
ointment (compounded from tabs), applied bid • Labs @ 6 wks/12 wks
– Cbc, metab panel, and serum rapamycin <2.
• No systemic absorption after 3 mos
• Deklotz et al. (2011): – Recipe for compounding
in ointment to reduce potential irritancy
• Salido et al. (2011) – 10 patients treated with
0.4% sirolimus ointment 3 times a week for 9 months
• Wataya et al. (2011)
– Topical application of rapamycin-tacrolimus ointment is a safe and useful treatment for TSC-related angiofibroma
Haemel AK et al Arch Dermatol. 2010 Jul;146(7):715-8. Salido et al., J Eur Acad Derm Ven; Aug 2011 Wataya-Kaneda et al., Br J Derm; Oct 2011
Topical Sirolimus (Rapamycin) 1% Ointment
Baseline 2 months Normal labs
No side effects
Topical Sirolimus (Rapamycin) 1% Ointment
Baseline 2 months Normal labs
No side effects
A Novel Application of Topical Rapamycin Formulation, an Inhibitor of mTOR, for Patients
With Hypomelanotic Macules in TS Complex.
• Case Report (2) – Rapamycin 0.2% gel
• 2 patients reported that
had improvement of both the hypopigmented macules and “red plaque” (likely collagenoma)
• Proposed Pathogenesis: – Normal # melanocytes but
decrease in melanosome size/number
– Increase in micropthalmia transcription factor (MITF), which is show to induce melanization
• Personal:
– I’m trying it now on forehead fibrous plaques
Mari Wataya-Kaneda et al., Arch Dermatol; Jan 2012.

33
Review • War On Staph: Strategies For ‘Containment’
– Role of sodium hypochlorite
• Refractory Warts: Topical Immunotherapy
• Vitiligo: Location-dependent topical options
• New Breakthroughs – Timolol; Sirolimus
34
1
Cosmeceuticals Steven Grekin, DO, FAOCD
Program Director Oakwood Southshore Medical Center
2
Financial Disclosures None to report pertaining to this topic
3
Objectives Evaluate the definition “cosmeceutical” Examine the evidence regarding the efficacy of
common ingredients Discuss the relevance to everyday clinical
practice
4
Why is this an important topic for our profession?
We live in a society that believes in holding onto youthfulness, despite an aging population with increased life expectancy.
Skin is the organ that most vividly
gives away our age!
5
Unfortunately, as we age we accumulate damage to the skin over time and lose the youthful quality to our skin. This is seen in the development of rhytides, lentigines, telangiectasias, and dyschromia.
Many are willing to trade wealth for youth, which has resulted in a demand for the development and manufacturing of high-end, anti-aging products.
This search for youthfulness has resulted in the establishment and growth of the cosmeceutical industry.
Brandt FS, Cazzaniga A, Hann M. Cosmeceuticals: current trends and market analysis. Semin Cutan Med Surg. 2011;30(3):141-3. Giacomoni PU. Advancement in skin aging: the future cosmeceuticals. Clin Dermatol. 26(4):364-6. Martin KI, Glaser DA. Cosmeceuticals: the new medicine of beauty. Mo Med. 108(1):60-3.
6
Aging defined… Chronological aging vs. photoaging and the overlap… It is important to understand that chronological aging is
defined primarily by the passage of time, while photoaging is defined by the accumulation of damage to the skin from UV irradiation.
Of course, an overlap exists and even sun protected skin ages with time, but is usually thinner, more evenly pigmented, laxer, and more finely lined than chronologically aged skin with superimposed photodamage.
Fisher, GJ, Kang S, et. al. Mechanisms of photoaging and chronological aging. Archives of Dermatology. 2002; 138:1462-1470
35
7
The big business of the cosmeceutical market…
Consumers, many of which are our patients, spend billions of dollars on cosmetics and cosmeceutical products each year!
Cosmeceuticals are one of the fastest growing segments of the personal care industry.
Cosmeceuticals provide patients with an alternative to surgical procedures and prescriptions, often times at a lower cost.
Sachdev M, Friedman A. Cosmeceuticals in day-to-day clinical practice. J Drugs Dermatol. 2010;9(5 Suppl ODAC Conf Pt 1):s62-6.] Newburger AE. Cosmeceuticals: myths and misconceptions. Clin Dermatol. 27(5):446-52.
8
The Smart Consumer Our patients are savvy, searching the internet and
exploring magazines for products that will make them look better, younger… and they expect results!
Patients come to us for our “expert opinion.” This makes it extremely important that we understand
the products that our patients are bringing to us to evaluate.
Often times these are products we are selling to patients in our own office!
9
Dr. Albert Kligman first popularized the term
“Cosmeceutical” in 1984 to describe a unique category of products somewhere on the continuum between drugs and cosmetics. These products are expected to have both cosmetic and therapeutic or physiologic benefits.
Brandt FS, Cazzaniga A, Hann M. Cosmeceuticals: current trends and market analysis. Semin Cutan Med Surg. 2011;30(3):141-3. Rivers JK. The role of cosmeceuticals in antiaging therapy. Skin Therapy Lett. 13(8):5-9. Kligman D. Cosmeceuticals. Dermatol Clin. 2000;18(4):609-15.
10
The Federal Food, Drug, and Cosmetic Act - 1930
The law defines cosmetics as "articles intended to be rubbed, poured, sprinkled, or sprayed on, introduced into, or otherwise applied to the human body...for cleansing, beautifying, promoting attractiveness, or altering the appearance"
[FD&C Act, sec. 201(i)]
Rivers JK. The role of cosmeceuticals in antiaging therapy. Skin Therapy Lett. 13(8):5-9. Kligman D. Cosmeceuticals. Dermatol Clin. 2000;18(4):609-15. http://www.fda.gov/regulatoryinformation/legislation/federalfooddrugandcosmeticactfdcact/default.htm Accessed 8-29-2012
11
The Federal Food, Drug, and Cosmetic Act - 1930
This includes: skin moisturizers, perfumes, lipsticks, fingernail polishes, eye and facial makeup, shampoos, hair colors, and deodorants, as well as any substance intended for use as a component of a cosmetic product.
http://www.fda.gov/Cosmetics/GuidanceComplianceRegulatoryInformation/ucm074201.htm 12
The Federal Food, Drug, and Cosmetic Act - 1930
The law defines drugs as "articles intended for use in the diagnosis, cure, mitigation, treatment, or prevention of disease and intended to affect the structure or any function of the body . . . "
[FD&C Act, sec. 201(g)(1)]
36
13
Stratum Corneum: The Gatekeeper
The disconnect with these definitions is that the laws were created when the strateum corneum (SC) was thought to be an inert and complete barrier to the deeper layers of the epidermis.
It is now known that the SC is quite complex and dynamic, providing primary control over the permeation of topical compounds.
Verma P, Pathak K. Therapeutic and cosmeceutical potential of ethosomes: An overview. J Adv Pharm Technol Res. 2010;1(3):274-82. Menon GK, Cleary GW, Lane ME. The structure and function of the stratum corneum. Int J Pharm. 2012;435(1):3-9.
14
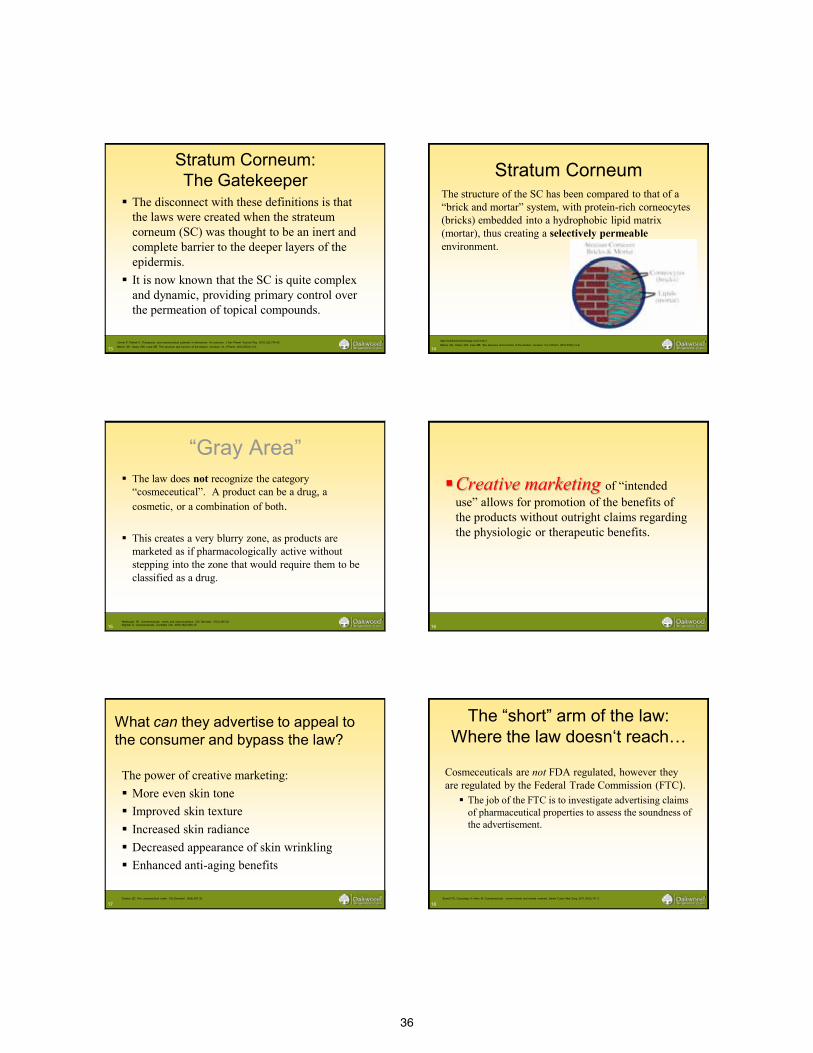
Stratum Corneum The structure of the SC has been compared to that of a
“brick and mortar” system, with protein-rich corneocytes (bricks) embedded into a hydrophobic lipid matrix (mortar), thus creating a selectively permeable environment.
http://nutritionforskinbeauty.com/?cat=1 Menon GK, Cleary GW, Lane ME. The structure and function of the stratum corneum. Int J Pharm. 2012;435(1):3-9.
15
“Gray Area” The law does not recognize the category
“cosmeceutical”. A product can be a drug, a cosmetic, or a combination of both.
This creates a very blurry zone, as products are marketed as if pharmacologically active without stepping into the zone that would require them to be classified as a drug.
Newburger AE. Cosmeceuticals: myths and misconceptions. Clin Dermatol. 27(5):446-52. Kligman D. Cosmeceuticals. Dermatol Clin. 2000;18(4):609-15.
16
Creative marketing of “intended use” allows for promotion of the benefits of the products without outright claims regarding the physiologic or therapeutic benefits.
17
What can they advertise to appeal to the consumer and bypass the law?
The power of creative marketing: More even skin tone Improved skin texture Increased skin radiance Decreased appearance of skin wrinkling Enhanced anti-aging benefits Draelos ZD. The cosmeceutical realm. Clin Dermatol. 26(6):627-32. 18
The “short” arm of the law: Where the law doesn‘t reach…
Cosmeceuticals are not FDA regulated, however they are regulated by the Federal Trade Commission (FTC).
The job of the FTC is to investigate advertising claims of pharmaceutical properties to assess the soundness of the advertisement.
Brandt FS, Cazzaniga A, Hann M. Cosmeceuticals: current trends and market analysis. Semin Cutan Med Surg. 2011;30(3):141-3.
37
19
Are they safe? The FDA has provided guidelines for cosmetic good
manufacturing practice (GMP) to ensure against adulterated or mislabeled products, but no regulations exist.
In contrast, the law requires strict adherence to GMP requirements for drugs, and there are regulations specifying minimum current GMP requirements
However, the FDA may conduct research on cosmetic products and ingredients to address safety concerns
http://www.fda.gov/Cosmetics/GuidanceComplianceRegulatoryInformation/ucm074201.htm
20
Do they really work? Efficacy is usually tested using the final formulation, making it
challenging to separate out the effect of an individual ingredient.
Most (not all) cosmeceuticals are made from ingredients that already have a proven safety record in the cosmetic market.
New, raw ingredients generally undergo extensive animal testing to determine if the ingredient is appropriate for human use.
Draelos ZD. The cosmeceutical realm. Clin Dermatol. 26(6):627-32.
21
The “Catch 22”
Invasive evaluations of the effect of the product on the skin cannot be performed, because this would indicate that, in fact, the product has pharmacological effects rather than cosmetic benefits. How is the efficacy of a cosmeceutical tested?
Draelos ZD. Cosmeceuticals: undefined, unclassified, and unregulated. Clin Dermatol. 27(5):431-4..
22
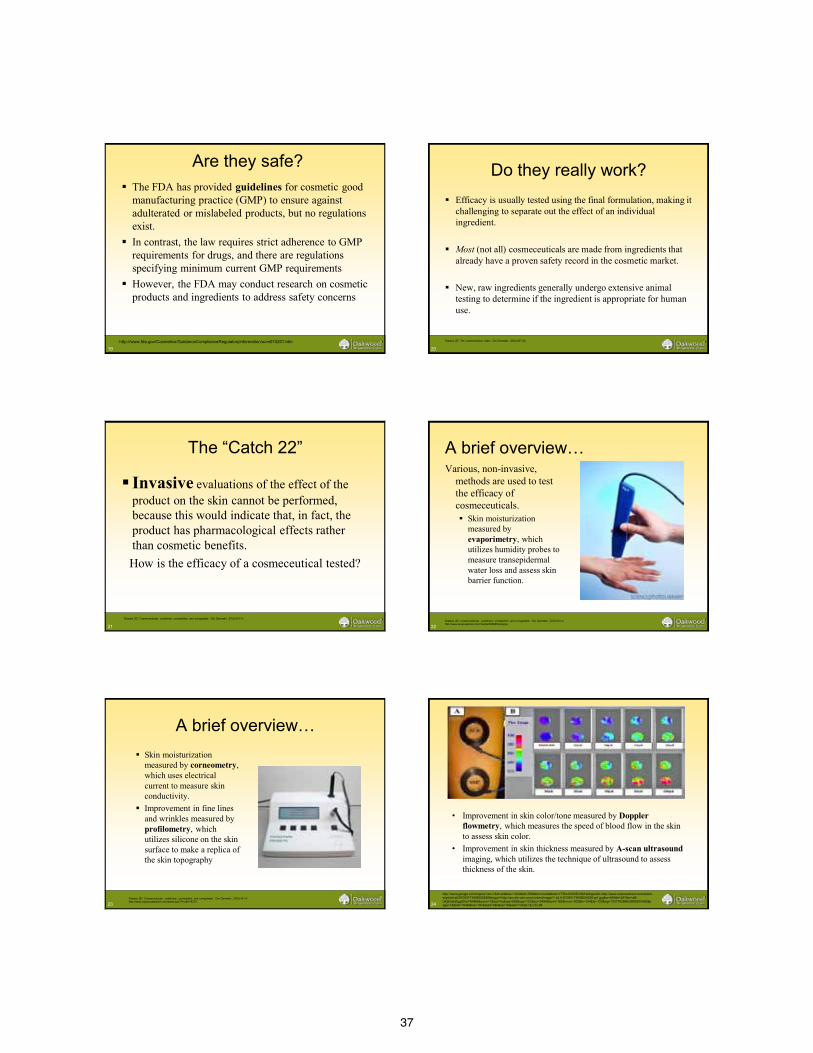
A brief overview… Various, non-invasive,
methods are used to test the efficacy of cosmeceuticals. Skin moisturization
measured by evaporimetry, which utilizes humidity probes to measure transepidermal water loss and assess skin barrier function.
Draelos ZD. Cosmeceuticals: undefined, unclassified, and unregulated. Clin Dermatol. 27(5):431-4. http://www.sciencephoto.com/media/296686/enlarge
23
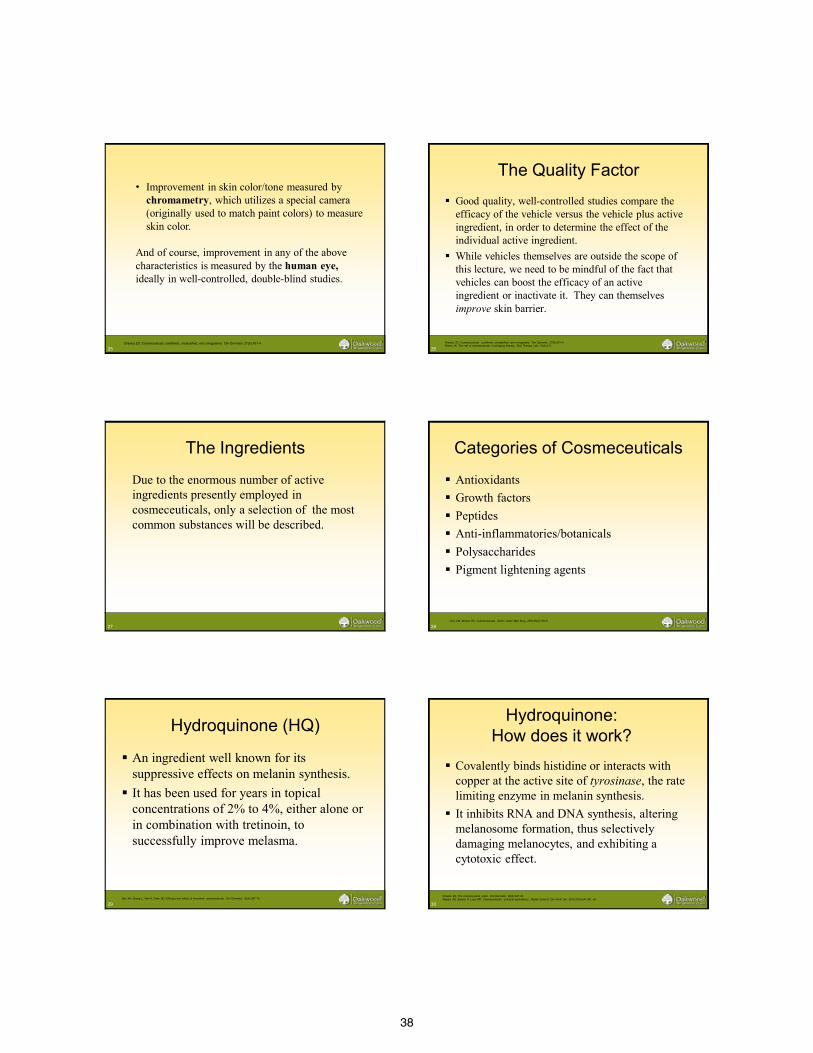
A brief overview… Skin moisturization
measured by corneometry, which uses electrical current to measure skin conductivity.
Improvement in fine lines and wrinkles measured by profilometry, which utilizes silicone on the skin surface to make a replica of the skin topography
Draelos ZD. Cosmeceuticals: undefined, unclassified, and unregulated. Clin Dermatol. 27(5):431-4. http://www.surplussalesline.com/detail.asp?ProdID=8373 24
• Improvement in skin color/tone measured by Doppler flowmetry, which measures the speed of blood flow in the skin to assess skin color.
• Improvement in skin thickness measured by A-scan ultrasound imaging, which utilizes the technique of ultrasound to assess thickness of the skin.
http://www.google.com/imgres?um=1&hl=en&biw=1024&bih=506&tbm=isch&tbnid=YFRm10IS6E2t3M:&imgrefurl=http://www.sciencedirect.com/science/article/pii/S1050173808000236&imgurl=http://ars.els-cdn.com/content/image/1-s2.0-S1050173808000236-gr1.jpg&w=546&h=297&ei=al8-UKj2GsHZqgGKwYH4BA&zoom=1&iact=hc&vpx=553&vpy=121&dur=3494&hovh=165&hovw=305&tx=164&ty=123&sig=103776399020605810590&page=1&tbnh=104&tbnw=191&start=0&ndsp=10&ved=1t:429,r:8,s:0,i:98
38
25
• Improvement in skin color/tone measured by chromametry, which utilizes a special camera (originally used to match paint colors) to measure skin color.
And of course, improvement in any of the above characteristics is measured by the human eye, ideally in well-controlled, double-blind studies.
Draelos ZD. Cosmeceuticals: undefined, unclassified, and unregulated. Clin Dermatol. 27(5):431-4
26
The Quality Factor Good quality, well-controlled studies compare the
efficacy of the vehicle versus the vehicle plus active ingredient, in order to determine the effect of the individual active ingredient.
While vehicles themselves are outside the scope of this lecture, we need to be mindful of the fact that vehicles can boost the efficacy of an active ingredient or inactivate it. They can themselves improve skin barrier.
Draelos ZD. Cosmeceuticals: undefined, unclassified, and unregulated. Clin Dermatol. 27(5):431-4. Rivers JK. The role of cosmeceuticals in antiaging therapy. Skin Therapy Lett. 13(8):5-9.
27
The Ingredients
Due to the enormous number of active ingredients presently employed in cosmeceuticals, only a selection of the most common substances will be described.
28
Categories of Cosmeceuticals
Antioxidants Growth factors Peptides Anti-inflammatories/botanicals Polysaccharides Pigment lightening agents
Choi CM, Berson DS. Cosmeceuticals. Semin Cutan Med Surg. 2006;25(3):163-8
29
Hydroquinone (HQ)
An ingredient well known for its suppressive effects on melanin synthesis.
It has been used for years in topical concentrations of 2% to 4%, either alone or in combination with tretinoin, to successfully improve melasma.
Gao XH, Zhang L, Wei H, Chen HD. Efficacy and safety of innovative cosmeceuticals. Clin Dermatol. 26(4):367-74. 30
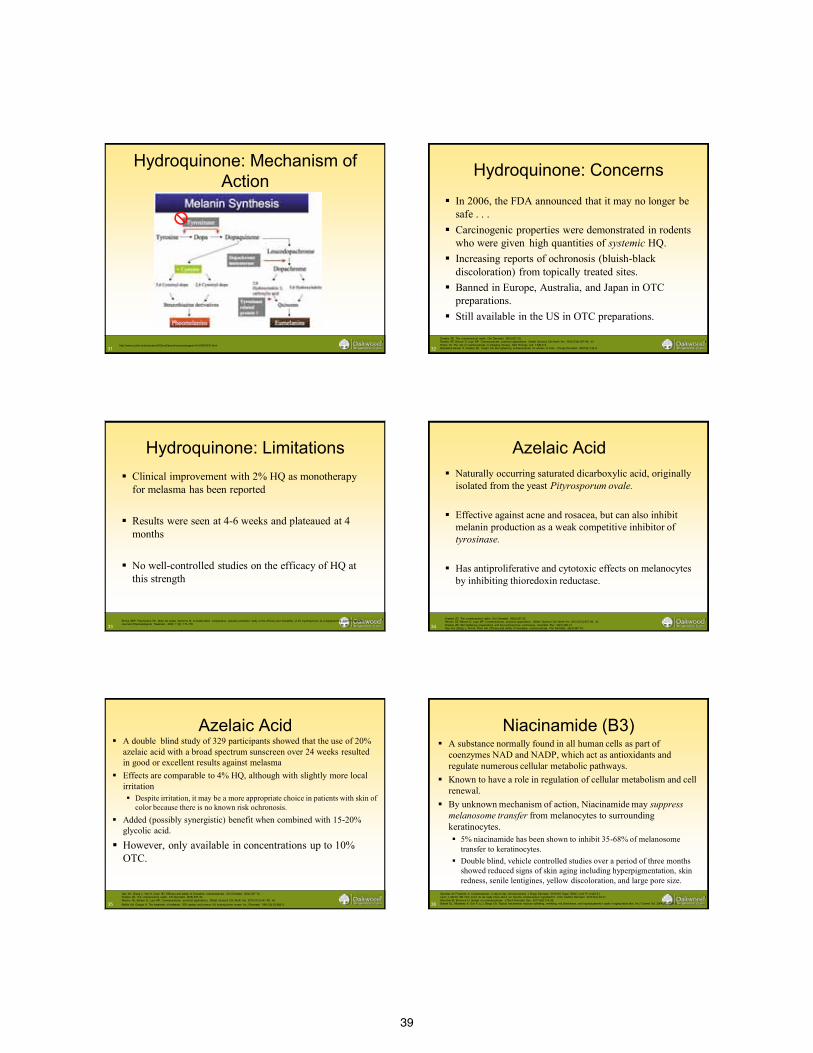
Hydroquinone: How does it work?
Covalently binds histidine or interacts with copper at the active site of tyrosinase, the rate limiting enzyme in melanin synthesis.
It inhibits RNA and DNA synthesis, altering melanosome formation, thus selectively damaging melanocytes, and exhibiting a cytotoxic effect.
Draelos ZD. The cosmeceutical realm. Clin Dermatol. 26(6):627-32. Reszko AE, Berson D, Lupo MP. Cosmeceuticals: practical applications. Obstet Gynecol Clin North Am. 2010;37(4):547-69, viii.
39
31 http://www.oculist.net/downaton502/prof/ebook/duanes/pages/v4/ch038/001f.html
Hydroquinone: Mechanism of Action
32
Hydroquinone: Concerns In 2006, the FDA announced that it may no longer be
safe . . . Carcinogenic properties were demonstrated in rodents
who were given high quantities of systemic HQ. Increasing reports of ochronosis (bluish-black
discoloration) from topically treated sites. Banned in Europe, Australia, and Japan in OTC
preparations. Still available in the US in OTC preparations.
Draelos ZD. The cosmeceutical realm. Clin Dermatol. 26(6):627-32. Reszko AE, Berson D, Lupo MP. Cosmeceuticals: practical applications. Obstet Gynecol Clin North Am. 2010;37(4):547-69, viii. Rivers JK. The role of cosmeceuticals in antiaging therapy. Skin Therapy Lett. 13(8):5-9. Badreshia-bansal S, Draelos ZD. Insight into skin lightening cosmeceuticals for women of color. J Drugs Dermatol. 2007;6(1):32-9.
33
Hydroquinone: Limitations Clinical improvement with 2% HQ as monotherapy
for melasma has been reported
Results were seen at 4-6 weeks and plateaued at 4 months
No well-controlled studies on the efficacy of HQ at this strength
Ennes SBP, Paschoalick RC, Mota De Avelar Alchorne M. A double-blind, comparative, placebo-controlled study of the efficacy and tolerability of 4% hydroquinone as a depigmenting agent in melasma. Journal of Dermatological Treatment. 2000; 11(3): 173-179.
34
Azelaic Acid Naturally occurring saturated dicarboxylic acid, originally
isolated from the yeast Pityrosporum ovale.
Effective against acne and rosacea, but can also inhibit melanin production as a weak competitive inhibitor of tyrosinase.
Has antiproliferative and cytotoxic effects on melanocytes by inhibiting thioredoxin reductase.
Draelos ZD. The cosmeceutical realm. Clin Dermatol. 26(6):627-32. Reszko AE, Berson D, Lupo MP. Cosmeceuticals: practical applications. Obstet Gynecol Clin North Am. 2010;37(4):547-69, viii. Draelos ZD. Skin lightening preparations and the hydroquinone controversy. Dermatol Ther. 20(5):308-13. Gao XH, Zhang L, Wei H, Chen HD. Efficacy and safety of innovative cosmeceuticals. Clin Dermatol. 26(4):367-74.
35
Azelaic Acid A double blind study of 329 participants showed that the use of 20%
azelaic acid with a broad spectrum sunscreen over 24 weeks resulted in good or excellent results against melasma
Effects are comparable to 4% HQ, although with slightly more local irritation Despite irritation, it may be a more appropriate choice in patients with skin of
color because there is no known risk ochronosis. Added (possibly synergistic) benefit when combined with 15-20%
glycolic acid.
However, only available in concentrations up to 10% OTC.
Gao XH, Zhang L, Wei H, Chen HD. Efficacy and safety of innovative cosmeceuticals. Clin Dermatol. 26(4):367-74. Draelos ZD. The cosmeceutical realm. Clin Dermatol. 26(6):627-32. Reszko AE, Berson D, Lupo MP. Cosmeceuticals: practical applications. Obstet Gynecol Clin North Am. 2010;37(4):547-69, viii. Baliña LM, Graupe K. The treatment of melasma. 20% azelaic acid versus 4% hydroquinone cream. Int J Dermatol. 1991;30(12):893-5.
36
Niacinamide (B3) A substance normally found in all human cells as part of
coenzymes NAD and NADP, which act as antioxidants and regulate numerous cellular metabolic pathways.
Known to have a role in regulation of cellular metabolism and cell renewal.
By unknown mechanism of action, Niacinamide may suppress melanosome transfer from melanocytes to surrounding keratinocytes. 5% niacinamide has been shown to inhibit 35-68% of melanosome
transfer to keratinocytes. Double blind, vehicle controlled studies over a period of three months
showed reduced signs of skin aging including hyperpigmentation, skin redness, senile lentigines, yellow discoloration, and large pore size.
Sachdev M, Friedman A. Cosmeceuticals in day-to-day clinical practice. J Drugs Dermatol. 2010;9(5 Suppl ODAC Conf Pt 1):s62-6.] Levin J, Momin SB. How much do we really know about our favorite cosmeceutical ingredients? J Clin Aesthet Dermatol. 2010;3(2):22-41. Kerscher M, Buntrock H. Update on cosmeceuticals. J Dtsch Dermatol Ges. 2011;9(4):314-26. Bissett DL, Miyamoto K, Sun P, Li J, Berge CA. Topical niacinamide reduces yellowing, wrinkling, red blotchiness, and hyperpigmented spots in aging facial skin. Int J Cosmet Sci. 2004;26(5):231-8.
40
37
Niacinamide (B3)… Beyond Pigment Modification
Has also showed promising improvement of skin barrier, skin elasticity, as well as fine lines and wrinkles. A randomized, double-blind study on 50 white
females, who applied 5% niacinamide twice daily for 12 weeks had improvement in fine lines, wrinkles, pigmentation, and skin elasticity.
Sold in concentrations of up to 5%. Has a very good tolerability profile.
Kerscher M, Buntrock H. Update on cosmeceuticals. J Dtsch Dermatol Ges. 2011;9(4):314-26. Bissett DL, Miyamoto K, Sun P, Li J, Berge CA. Topical niacinamide reduces yellowing, wrinkling, red blotchiness, and hyperpigmented spots in aging facial skin. Int J Cosmet Sci. 2004;26(5):231-8. 38
Antioxidants: Vitamin E
Vitamin E (α-tocopherol) is considered a lipophillic antioxidant, protecting cells from free radical induced lipid peroxidation and physically blocking UVR.
Sachdev M, Friedman A. Cosmeceuticals in day-to-day clinical practice. J Drugs Dermatol. 2010;9(5 Suppl ODAC Conf Pt 1):s62-6.] Reszko AE, Berson D, Lupo MP. Cosmeceuticals: practical applications. Obstet Gynecol Clin North Am. 2010;37(4):547-69, viii.
39
Vitamin E Found in countless skin care products in concentrations
of 2-20%. In the form of α-tocopherol, the most active form,
topical Vitamin E has been noted to improve the wrinkling and hyperpigmentation caused by free radicals and also have a photoprotective effect. A double-blinded, randomized, and vehicle controlled study on
10 subjects by Zhai et al. demonstrated decreased UV-induced erythema and inflammatory skin damage with the application of a topical vitamin E emulsion.
Excellent tolerability.
Kerscher M, Buntrock H. Update on cosmeceuticals. J Dtsch Dermatol Ges. 2011;9(4):314-26. Martin KI, Glaser DA. Cosmeceuticals: the new medicine of beauty. Mo Med. 108(1):60-3.
40
Antioxidants: Vitamin C Vitamin C (L-ascorbic acid) functions as a free
radical scavenger, which allows it to extinguish reactive species and protect cells from oxidative stress.
Has been shown to play a role in many factors of anti-aging, including promotion of collagen synthesis, and skin lightening.
Sachdev M, Friedman A. Cosmeceuticals in day-to-day clinical practice. J Drugs Dermatol. 2010;9(5 Suppl ODAC Conf Pt 1):s62-6.] Reszko AE, Berson D, Lupo MP. Cosmeceuticals: practical applications. Obstet Gynecol Clin North Am. 2010;37(4):547-69, viii.
41
Vitamin C and Pigment Studies evaluating improvement in
hyperpigmentation have shown promising results. In a split-faced clinical trial, 16 women with
melasma were treated with a nightly application of 5% ascorbic acid cream on one side, and 4% HQ on the opposite side for 16 weeks.
Both sides showed excellent results, with no statistical difference in outcome. Topical ascorbic acid was well tolerated, with much lower rates of side effects vs. HQ.
Reszko AE, Berson D, Lupo MP. Cosmeceuticals: practical applications. Obstet Gynecol Clin North Am. 2010;37(4):547-69, viii. Espinal-perez LE, Moncada B, Castanedo-cazares JP. A double-blind randomized trial of 5% ascorbic acid vs. 4% hydroquinone in melasma. Int J Dermatol. 2004;43(8):604-7.
42
Vitamin C and Rhytides A double-blind, split-face, vehicle controlled
study by Fitzpatrick et. al, of 10 subjects utilizing a vitamin C complex of ascorbic acid and provitamin C demonstrated significant improvement in wrinkling when used topically for 12 weeks.
Biopsies showed increased Grenz zone collagen, as well as increased staining for mRNA for type I collagen!
Fitzpatrick RE, Rostan EF. Double-blind, half-face study comparing topical vitamin C and vehicle for rejuvenation of photodamage. Dermatol Surg. 2002;28(3):231-6.
41
43
Vitamins C and E Vitamins C and E have been shown to act
synergistically to provide antioxidant protection from UVR when combined with ferulic acid Improved chemical stability of the vitamin C and
vitamin E Doubled photoprotection of skin from 4-fold to
approximately 8-fold as measured by MED and histological sunburn cell count on weanling white Yorkshire pig skin.
Lin FH, Lin JY, Gupta RD, et al. Ferulic acid stabilizes a solution of vitamins C and E and doubles its photoprotection of skin. J Invest Dermatol. 2005;125(4):826-32.
44
Retinoids Compounds with the basic core structure of
Vitamin A and its oxidized metabolites, or synthetic compounds that share similar mechanisms of action as naturally occurring retinoids. Forms:
Retinol (Vit A alcohol) Retinal (Vit A aldehyde) Retinoic acid (Vit A acid)
Reszko AE, Berson D, Lupo MP. Cosmeceuticals: practical applications. Obstet Gynecol Clin North Am. 2010;37(4):547-69, viii. Gao XH, Zhang L, Wei H, Chen HD. Efficacy and safety of innovative cosmeceuticals. Clin Dermatol. 26(4):367-74.
45
Retinoids
In the skin, retinol is reversibly oxidized into retinaldehyde (retinal), which is in turn irreversibly oxidized to retinoic acid, which is the biologically active form of Vitamin A.
Topical cosmeceuticals containing retinol and retinal theoretically work because once absorbed they are metabolized to retinoic acid, which induces pharmacological activity.
Levin J, Momin SB. How much do we really know about our favorite cosmeceutical ingredients? J Clin Aesthet Dermatol. 2010;3(2):22-41.
46
Retinoids: The Limitation Unfortunately, only a
small amount of retinol and retinal can be converted by the skin, accounting for the increased efficacy seen with prescription preparations containing retinoic acid.
Draelos ZD. The cosmeceutical realm. Clin Dermatol. 26(6):627-32.
http://www.advancedskintech.com/GCScience.htm
47
Retinoids: The workhorse? One of the most studied ingredients in cosmeceuticals. An effective topical treatment for photoaging, acne, and
numerous dermatological disorders. Tretinoin is considered to be one of the most potent
compounds available for treating the signs of aging and/or photodamaged skin, however side effects such as burning and scaling can limits its use and acceptance.
Retinol is available OTC and is considered the “gold standard” cosmeceutical in anti-aging. Less irritating to the skin with better tolerability than prescription
tretinoin.
Rivers JK. The role of cosmeceuticals in antiaging therapy. Skin Therapy Lett. 13(8):5-9. Levin J, Momin SB. How much do we really know about our favorite cosmeceutical ingredients? J Clin Aesthet Dermatol. 2010;3(2):22-41. Kerscher M, Buntrock H. Update on cosmeceuticals. J Dtsch Dermatol Ges. 2011;9(4):314-26. 48
Retinoids and Pigmentation Retinoids effectively reduce pigment by dispersing
melanosomes, interfering with melanocyte-keratinocyte pigment transfer, and accelerating epidermal turnover and subsequently, pigment loss.
Additionally, retinoids may inhibit melanogenesis by inhibiting tyrosinase and DOPAchrome conversion factor.
All-trans-retinoic acid (tretinoin) inhibits melanin synthesis through down regulation of tryrosinase and tyrosinase-related protein 1(TRP-1) expression in melanocytes. Reszko AE, Berson D, Lupo MP. Cosmeceuticals: practical applications. Obstet Gynecol Clin North Am. 2010;37(4):547-69, viii.
Gao XH, Zhang L, Wei H, Chen HD. Efficacy and safety of innovative cosmeceuticals. Clin Dermatol. 26(4):367-74.
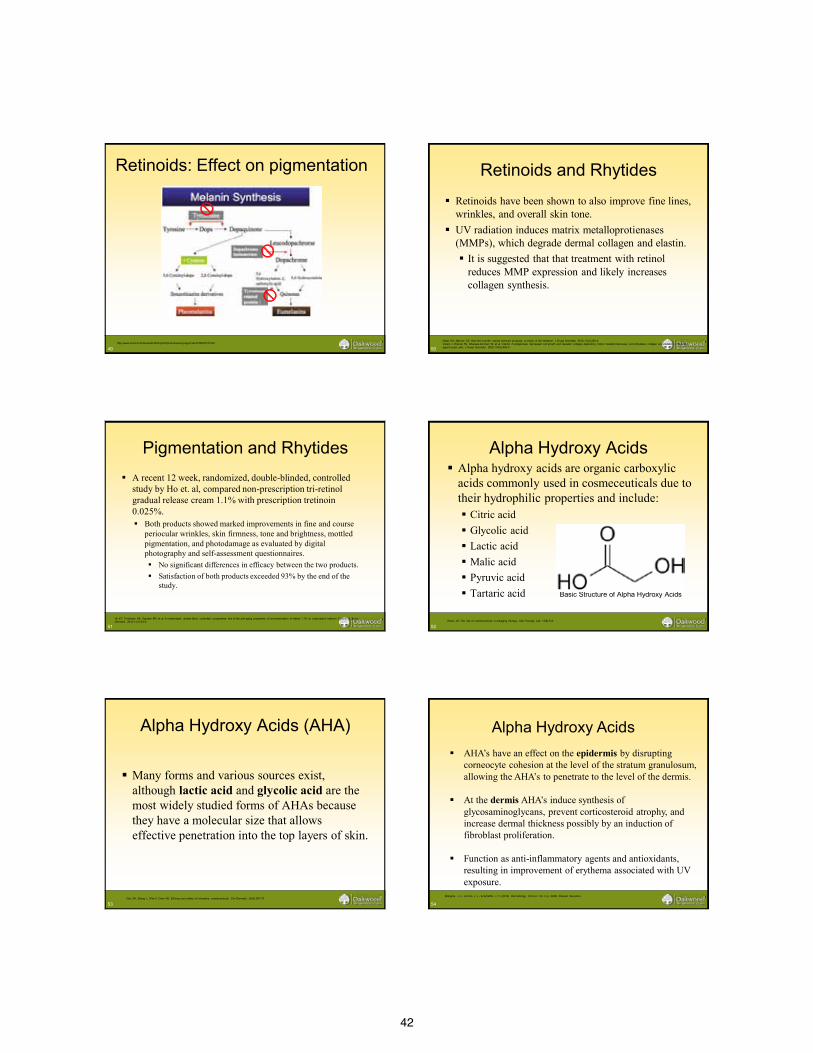
42
49
http://www.oculist.net/downaton502/prof/ebook/duanes/pages/v4/ch038/001f.html
Retinoids: Effect on pigmentation
50
Retinoids and Rhytides Retinoids have been shown to also improve fine lines,
wrinkles, and overall skin tone. UV radiation induces matrix metalloprotienases
(MMPs), which degrade dermal collagen and elastin. It is suggested that that treatment with retinol
reduces MMP expression and likely increases collagen synthesis.
Nolan KA, Marmur ES. Over-the-counter topical skincare products: a review of the literature. J Drugs Dermatol. 2012;11(2):220-4. Varani J, Warner RL, Gharaee-kermani M, et al. Vitamin A antagonizes decreased cell growth and elevated collagen-degrading matrix metalloproteinases and stimulates collagen accumulation in naturally. aged human skin. J Invest Dermatol. 2000;114(3):480-6
51
Pigmentation and Rhytides A recent 12 week, randomized, double-blinded, controlled
study by Ho et. al, compared non-prescription tri-retinol gradual release cream 1.1% with prescription tretinoin 0.025%. Both products showed marked improvements in fine and course
periocular wrinkles, skin firmness, tone and brightness, mottled pigmentation, and photodamage as evaluated by digital photography and self-assessment questionnaires. No significant differences in efficacy between the two products. Satisfaction of both products exceeded 93% by the end of the
study.
Ho ET, Trookman NS, Sperber BR, et al. A randomized, double-blind, controlled comparative trial of the anti-aging properties of non-prescription tri-retinol 1.1% vs. prescription tretinoin 0.025%. J Drugs Dermatol. 2012;11(1):64-9. 52
Alpha Hydroxy Acids Alpha hydroxy acids are organic carboxylic
acids commonly used in cosmeceuticals due to their hydrophilic properties and include: Citric acid Glycolic acid Lactic acid Malic acid Pyruvic acid Tartaric acid Basic Structure of Alpha Hydroxy Acids
Rivers JK. The role of cosmeceuticals in antiaging therapy. Skin Therapy Lett. 13(8):5-9.
53
Alpha Hydroxy Acids (AHA)
Many forms and various sources exist,
although lactic acid and glycolic acid are the most widely studied forms of AHAs because they have a molecular size that allows effective penetration into the top layers of skin.
Gao XH, Zhang L, Wei H, Chen HD. Efficacy and safety of innovative cosmeceuticals. Clin Dermatol. 26(4):367-74.
54
AHA’s have an effect on the epidermis by disrupting corneocyte cohesion at the level of the stratum granulosum, allowing the AHA’s to penetrate to the level of the dermis. At the dermis AHA’s induce synthesis of glycosaminoglycans, prevent corticosteroid atrophy, and increase dermal thickness possibly by an induction of fibroblast proliferation. Function as anti-inflammatory agents and antioxidants, resulting in improvement of erythema associated with UV exposure.
Alpha Hydroxy Acids
Bolognia, J. L., Jorizzo, J. L., & Schaffer, J. V. (2012). Dermatology. (3rd ed., Vol. 2, p. 2488). Elsevier Saunders.
43
55
Alpha Hydroxy Acids
OTC products must have less than a 10 percent concentration.
A 22 week, double-blind, vehicle-controlled study evaluating 8% glycolic acid and 8% L-lactic acid creams showed marked improvement in photodamaged skin.
Stiller MJ, Bartolone J, Stern R, et al. Topical 8% glycolic acid and 8% L-lactic acid creams for the treatment of photodamaged skin. A double-blind vehicle-controlled clinical trial. Arch Dermatol. 1996;132(6):631-6. 56
Alpha Hydroxy Acids
Side effects including redness, swelling, blistering, burning, itching, discoloration, and increased photosensitivity are related to the pH and concentration of AHA, vehicles used, and frequency of application.
Gao XH, Zhang L, Wei H, Chen HD. Efficacy and safety of innovative cosmeceuticals. Clin Dermatol. 26(4):367-74.
57
Soy Soy-derived products
are believed to have a range of dermatologic benefits, from depigmentation to prevention of photodamage and photoaging.
Levin J, Momin SB. How much do we really know about our favorite cosmeceutical ingredients? J Clin Aesthet Dermatol. 2010;3(2):22-41. Kerscher M, Buntrock H. Update on cosmeceuticals. J Dtsch Dermatol Ges. 2011;9(4):314-26. Leyden J, Wallo W. The mechanism of action and clinical benefits of soy for the treatment of hyperpigmentation. Int J Dermatol. 2011;50(4):470-7. 58
Soy When evaluating topical soy-containing
products, it is important to know which active ingredient(s) are within, so that the desired effect may be achieved.
Soy compounds, namely isoflavones and serine protease inhibitors (soybean trypsin inhibitor (STI) and Bowman-Birk protease inhibitor (BBI)), have been studied for their potential benefits in human skin.
Leyden J, Wallo W. The mechanism of action and clinical benefits of soy for the treatment of hyperpigmentation. Int J Dermatol. 2011;50(4):470-7.
59
Soy: Serine Protease Inhibitors Improve pigmentation. Stems from the ability of STI and BBI to inhibit
keratinocyte protease-activated receptor 2 (PAR-2), thereby decreasing transfer of melanosomes to keratinocytes.
Products containing STI have demonstrated significant reductions in post-inflammatory hyperpigmentation, desquamation, and erythema following UV-exposure.
Leyden J, Wallo W. The mechanism of action and clinical benefits of soy for the treatment of hyperpigmentation. Int J Dermatol. 2011;50(4):470-7. Liu J-C, Seiberg M, Miller J, et al. Soy: potential applications in skin care. Poster presented at: 59th Annual Meeting of the American Academy of Dermatology, Washington DC, March 60
STI
http://aac.asm.org/content/53/5/1760/F1.expansion
Soy: Serine Protease Inhibitors
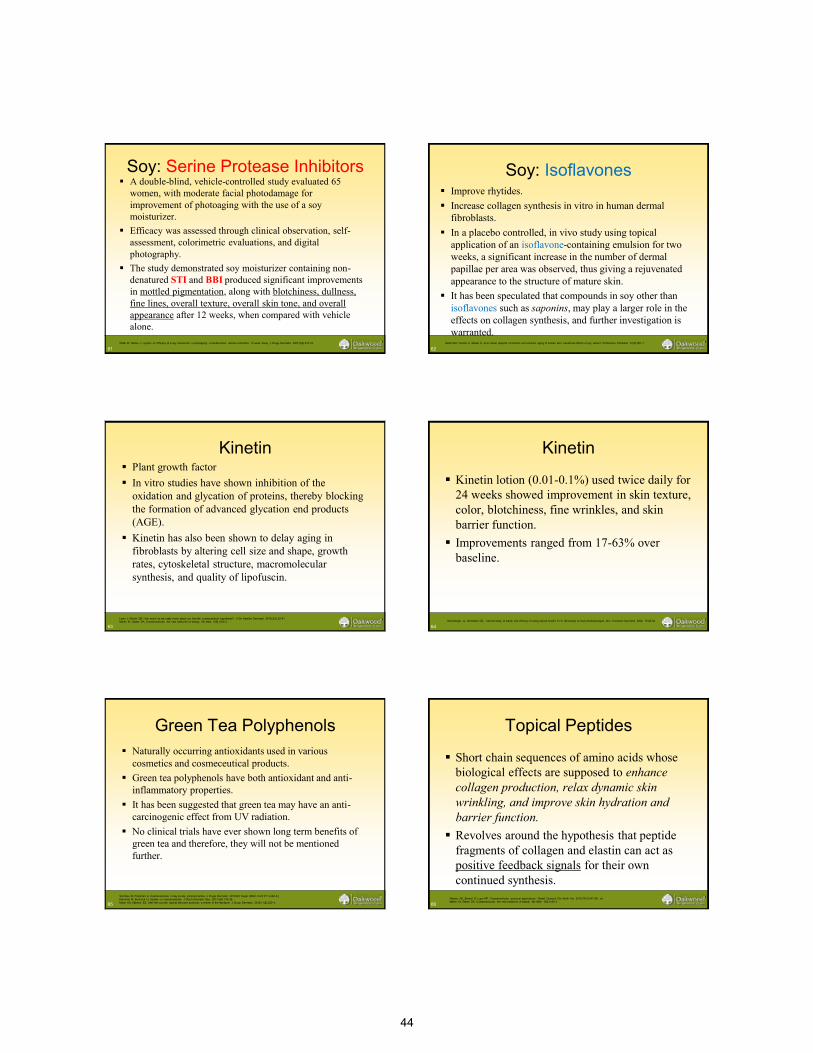
44
61
Soy: Serine Protease Inhibitors A double-blind, vehicle-controlled study evaluated 65
women, with moderate facial photodamage for improvement of photoaging with the use of a soy moisturizer.
Efficacy was assessed through clinical observation, self-assessment, colorimetric evaluations, and digital photography.
The study demonstrated soy moisturizer containing non-denatured STI and BBI produced significant improvements in mottled pigmentation, along with blotchiness, dullness, fine lines, overall texture, overall skin tone, and overall appearance after 12 weeks, when compared with vehicle alone.
Wallo W, Nebus J, Leyden JJ. Efficacy of a soy moisturizer in photoaging: a double-blind, vehicle-controlled, 12-week study. J Drugs Dermatol. 2007;6(9):917-22.
62
Soy: Isoflavones Improve rhytides. Increase collagen synthesis in vitro in human dermal
fibroblasts. In a placebo controlled, in vivo study using topical
application of an isoflavone-containing emulsion for two weeks, a significant increase in the number of dermal papillae per area was observed, thus giving a rejuvenated appearance to the structure of mature skin.
It has been speculated that compounds in soy other than isoflavones such as saponins, may play a larger role in the effects on collagen synthesis, and further investigation is warranted.
Südel KM, Venzke K, Mielke H, et al. Novel aspects of intrinsic and extrinsic aging of human skin: beneficial effects of soy extract. Photochem Photobiol. 81(3):581-7.
63
Kinetin Plant growth factor In vitro studies have shown inhibition of the
oxidation and glycation of proteins, thereby blocking the formation of advanced glycation end products (AGE).
Kinetin has also been shown to delay aging in fibroblasts by altering cell size and shape, growth rates, cytoskeletal structure, macromolecular synthesis, and quality of lipofuscin.
Levin J, Momin SB. How much do we really know about our favorite cosmeceutical ingredients? J Clin Aesthet Dermatol. 2010;3(2):22-41. Martin KI, Glaser DA. Cosmeceuticals: the new medicine of beauty. Mo Med. 108(1):60-3.
64
Kinetin
Kinetin lotion (0.01-0.1%) used twice daily for 24 weeks showed improvement in skin texture, color, blotchiness, fine wrinkles, and skin barrier function.
Improvements ranged from 17-63% over baseline.
McCullough JL, Weinstein GD. Clinical study of safety and efficacy of using topical kinetin 0.1% (Kinerase) to treat photodamaged skin. Cosmetic Dermatol. 2002; 15:29-32.
65
Green Tea Polyphenols Naturally occurring antioxidants used in various
cosmetics and cosmeceutical products. Green tea polyphenols have both antioxidant and anti-
inflammatory properties. It has been suggested that green tea may have an anti-
carcinogenic effect from UV radiation. No clinical trials have ever shown long term benefits of
green tea and therefore, they will not be mentioned further.
Sachdev M, Friedman A. Cosmeceuticals in day-to-day clinical practice. J Drugs Dermatol. 2010;9(5 Suppl ODAC Conf Pt 1):s62-6.] Kerscher M, Buntrock H. Update on cosmeceuticals. J Dtsch Dermatol Ges. 2011;9(4):314-26. Nolan KA, Marmur ES. Over-the-counter topical skincare products: a review of the literature. J Drugs Dermatol. 2012;11(2):220-4.
66
Topical Peptides
Short chain sequences of amino acids whose biological effects are supposed to enhance collagen production, relax dynamic skin wrinkling, and improve skin hydration and barrier function.
Revolves around the hypothesis that peptide fragments of collagen and elastin can act as positive feedback signals for their own continued synthesis.
Reszko AE, Berson D, Lupo MP. Cosmeceuticals: practical applications. Obstet Gynecol Clin North Am. 2010;37(4):547-69, viii. Martin KI, Glaser DA. Cosmeceuticals: the new medicine of beauty. Mo Med. 108(1):60-3.
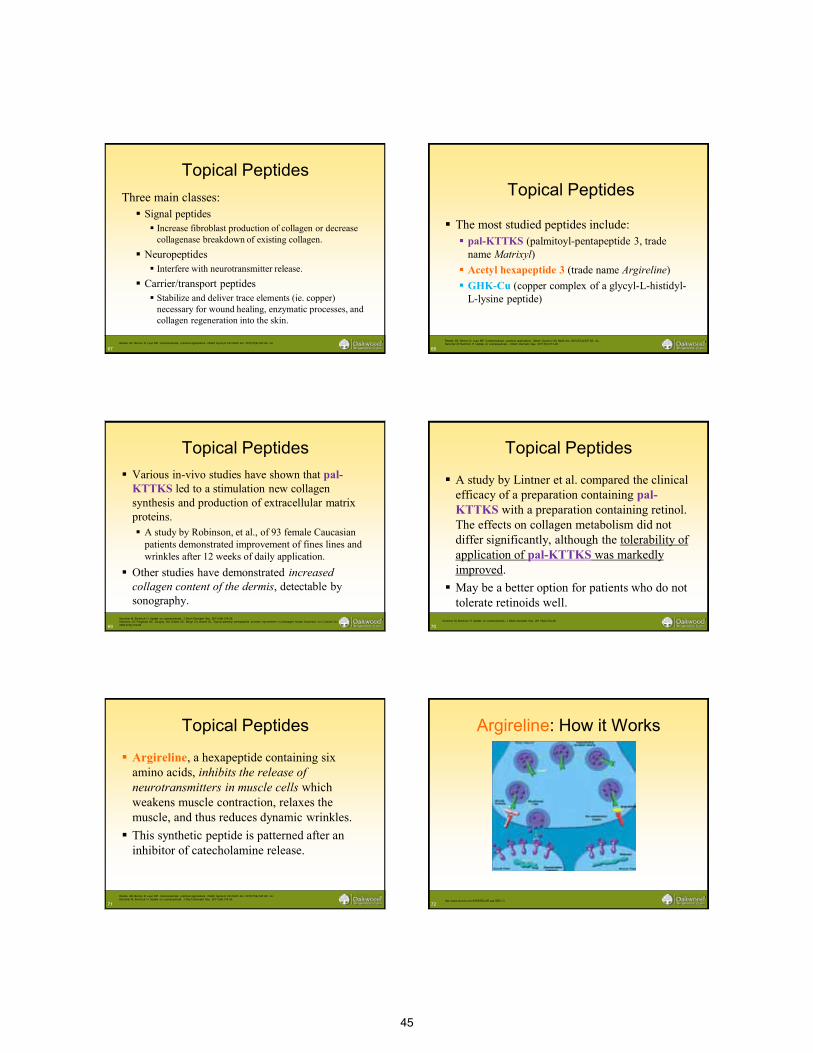
45
67
Topical Peptides Three main classes:
Signal peptides Increase fibroblast production of collagen or decrease
collagenase breakdown of existing collagen. Neuropeptides
Interfere with neurotransmitter release. Carrier/transport peptides
Stabilize and deliver trace elements (ie. copper) necessary for wound healing, enzymatic processes, and collagen regeneration into the skin.
Reszko AE, Berson D, Lupo MP. Cosmeceuticals: practical applications. Obstet Gynecol Clin North Am. 2010;37(4):547-69, viii.
68
Topical Peptides
The most studied peptides include: pal-KTTKS (palmitoyl-pentapeptide 3, trade
name Matrixyl) Acetyl hexapeptide 3 (trade name Argireline) GHK-Cu (copper complex of a glycyl-L-histidyl-
L-lysine peptide)
Reszko AE, Berson D, Lupo MP. Cosmeceuticals: practical applications. Obstet Gynecol Clin North Am. 2010;37(4):547-69, viii.. Kerscher M, Buntrock H. Update on cosmeceuticals. J Dtsch Dermatol Ges. 2011;9(4):314-26.
69
Topical Peptides Various in-vivo studies have shown that pal-
KTTKS led to a stimulation new collagen synthesis and production of extracellular matrix proteins. A study by Robinson, et al., of 93 female Caucasian
patients demonstrated improvement of fines lines and wrinkles after 12 weeks of daily application.
Other studies have demonstrated increased collagen content of the dermis, detectable by sonography.
Kerscher M, Buntrock H. Update on cosmeceuticals. J Dtsch Dermatol Ges. 2011;9(4):314-26. Robinson LR, Fitzgerald NC, Doughty DG, Dawes NC, Berge CA, Bissett DL. Topical palmitoyl pentapeptide provides improvement in photoaged human facial skin. Int J Cosmet Sci. 2005;27(3):155-60.
70
Topical Peptides
A study by Lintner et al. compared the clinical efficacy of a preparation containing pal-KTTKS with a preparation containing retinol. The effects on collagen metabolism did not differ significantly, although the tolerability of application of pal-KTTKS was markedly improved.
May be a better option for patients who do not tolerate retinoids well.
Kerscher M, Buntrock H. Update on cosmeceuticals. J Dtsch Dermatol Ges. 2011;9(4):314-26.
71
Topical Peptides
Argireline, a hexapeptide containing six amino acids, inhibits the release of neurotransmitters in muscle cells which weakens muscle contraction, relaxes the muscle, and thus reduces dynamic wrinkles.
This synthetic peptide is patterned after an inhibitor of catecholamine release.
Reszko AE, Berson D, Lupo MP. Cosmeceuticals: practical applications. Obstet Gynecol Clin North Am. 2010;37(4):547-69, viii.. Kerscher M, Buntrock H. Update on cosmeceuticals. J Dtsch Dermatol Ges. 2011;9(4):314-26.
72 http://www.revoris.com/ARGIRELINE.asp?SEC=3
Argireline: How it Works
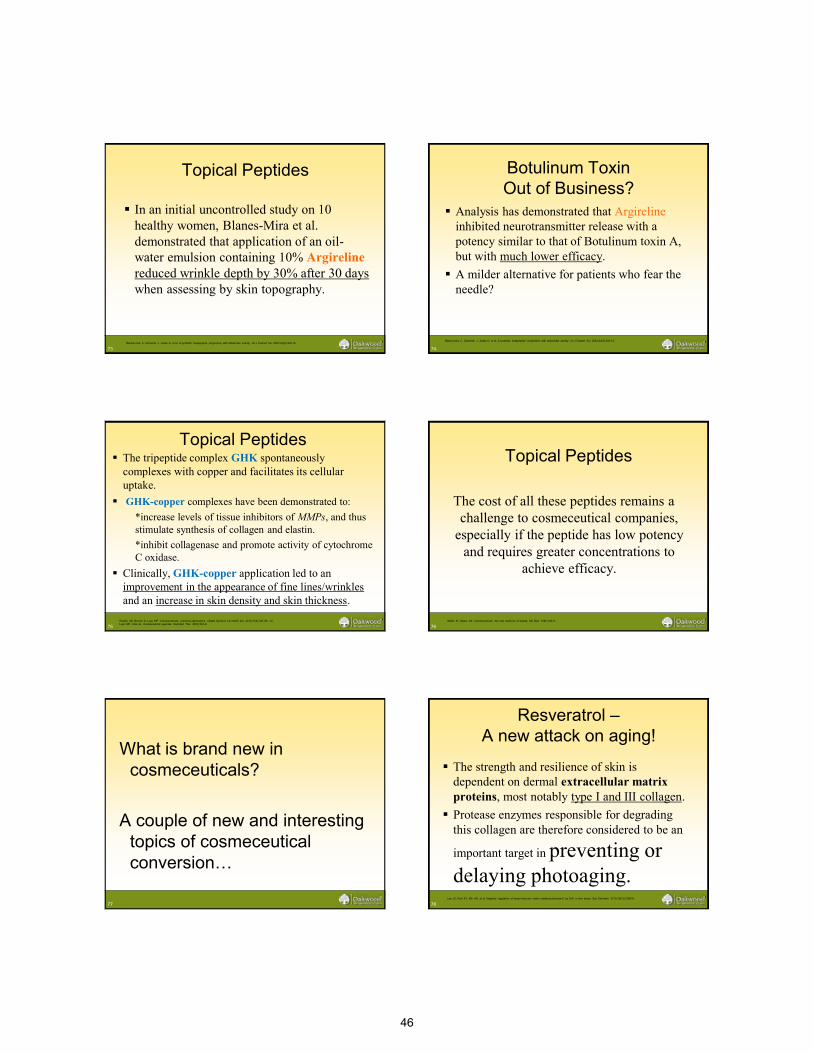
46
73
Topical Peptides
In an initial uncontrolled study on 10 healthy women, Blanes-Mira et al. demonstrated that application of an oil-water emulsion containing 10% Argireline reduced wrinkle depth by 30% after 30 days when assessing by skin topography.
Blanes-mira C, Clemente J, Jodas G, et al. A synthetic hexapeptide (Argireline) with antiwrinkle activity. Int J Cosmet Sci. 2002;24(5):303-10.
74
Botulinum Toxin Out of Business?
Analysis has demonstrated that Argireline inhibited neurotransmitter release with a potency similar to that of Botulinum toxin A, but with much lower efficacy.
A milder alternative for patients who fear the needle?
Blanes-mira C, Clemente J, Jodas G, et al. A synthetic hexapeptide (Argireline) with antiwrinkle activity. Int J Cosmet Sci. 2002;24(5):303-10.
75
Topical Peptides The tripeptide complex GHK spontaneously
complexes with copper and facilitates its cellular uptake.
GHK-copper complexes have been demonstrated to: *increase levels of tissue inhibitors of MMPs, and thus
stimulate synthesis of collagen and elastin. *inhibit collagenase and promote activity of cytochrome
C oxidase. Clinically, GHK-copper application led to an
improvement in the appearance of fine lines/wrinkles and an increase in skin density and skin thickness.
Reszko AE, Berson D, Lupo MP. Cosmeceuticals: practical applications. Obstet Gynecol Clin North Am. 2010;37(4):547-69, viii. Lupo MP, Cole AL. Cosmeceutical peptides. Dermatol Ther. 20(5):343-9.
76
Topical Peptides
The cost of all these peptides remains a challenge to cosmeceutical companies,
especially if the peptide has low potency and requires greater concentrations to
achieve efficacy.
Martin KI, Glaser DA. Cosmeceuticals: the new medicine of beauty. Mo Med. 108(1):60-3.
77
What is brand new in cosmeceuticals?
A couple of new and interesting
topics of cosmeceutical conversion…
78
Resveratrol – A new attack on aging!
The strength and resilience of skin is dependent on dermal extracellular matrix proteins, most notably type I and III collagen.
Protease enzymes responsible for degrading this collagen are therefore considered to be an
important target in preventing or delaying photoaging.
Lee JS, Park KY, Min HG, et al. Negative regulation of stress-induced matrix metalloproteinase-9 by Sirt1 in skin tissue. Exp Dermatol. 2010;19(12):1060-6.
47
79
Resveratrol – What is it?
A polyphenolic antioxidant with diverse biological effects found in high concentrations in grapes and red wine.
Farris PK. Innovative cosmeceuticals: sirtuin activators and anti-glycation compounds. Semin Cutan Med Surg. 2011;30(3):163-6
80
Resveratrol – To preserve and prevent…
Has been shown to down regulate transcription factors involved in photoaging, and suppress expression of MMP-1 and MMP-3 in dermal fibroblasts, which may prove valuable in preserving dermal collagen
http://www.mdidea.com/products/herbextract/resveratrol/data07.html http://www.deltalabsusa.com/product_resveratrol.php
81
Resveratrol: Preservation of collagen
A study by Lee et al. using a mouse skin model revealed that resveratrol pretreatment prior to UV exposure was able to reduce collagen degradation by UVR stress.
Lee JS, Park KY, Min HG, et al. Negative regulation of stress-induced matrix metalloproteinase-9 by Sirt1 in skin tissue. Exp Dermatol. 2010;19(12):1060-6. 82
Resveratrol – the future?
Objective clinical studies confirming these benefits are lacking, however the science behind resveratrol is plentiful and promising.
Studies to evaluate the efficacy of synthetic derivatives of resveratrol are currently underway.
Farris PK. Innovative cosmeceuticals: sirtuin activators and anti-glycation compounds. Semin Cutan Med Surg. 2011;30(3):163-6.
83
Sebum Regulation
Independent from environmental factors, the oily appearance of skin may be due, in part, to overproduction of sebum, controlled by the enzyme 5-alpha-reductase.
Squalene, a proposed marker of human sebum, is reported to favor comedo formation.
Vogelgesang B, Abdul-malak N, Reymermier C, Altobelli C, Saget J. On the effects of a plant extract of Orthosiphon stamineus on sebum-related skin imperfections. Int J Cosmet Sci. 2011;33(1):44-52.
84
Sebum and Botanicals
In a recent French study evaluating the effects of various botanical ingredients on oily skin, a potent extract from the orthosiphon stamineus leaf, or “java tea” plant, effectively decreased 5-alpha reductase activity in human skin.
Squalene synthesis was also noted to be significantly reduced.
Vogelgesang B, Abdul-malak N, Reymermier C, Altobelli C, Saget J. On the effects of a plant extract of Orthosiphon stamineus on sebum-related skin imperfections. Int J Cosmet Sci. 2011;33(1):44-52.
48
85
Botanicals buffer the shine…
After 28 days of using a 2% extract twice daily on the whole face, 80% patients self-reported their complexion was more even, 100% said their skin was more radiant, and 92% described their skin texture improved.
A study in Thai women with similar results was produced by the same authors.
Vogelgesang B, Abdul-malak N, Reymermier C, Altobelli C, Saget J. On the effects of a plant extract of Orthosiphon stamineus on sebum-related skin imperfections. Int J Cosmet Sci. 2011;33(1):44-52. 86
Cellulite = old skin?
Although cellulite can be present in women of all ages, it may be regarded as a form of skin aging, as the characteristic “cottage cheese” appearance is partly due to a weakening of the dermis.
Non-invasive approaches to treat cellulite, which target both fat breakdown and dermal restrengthening, have been studied.
Badreshia-bansal S, Draelos ZD. Insight into skin lightening cosmeceuticals for women of color. J Drugs Dermatol. 2007;6(1):32-9.
87
Cosmetic Ingredients as Anticellulites
Ingredients studied to be effective against cellulite: Retinoid
Stimulates collagen production by “aged” fibroblasts, inhibits conversion of pre-adipocytes to mature adipocytes.
Algae extract Stimulates fibroblasts to produce pro-collagen I at even
greater levels than retinoid. Conjugated linoleic acid (CLA)
Prevents triacylglycerol accumulation in adipocytes. Glaucine
Encourages lipolysis in adipocytes.
Vogelgesang B, Abdul-malak N, Reymermier C, Altobelli C, Saget J. On the effects of a plant extract of Orthosiphon stamineus on sebum-related skin imperfections. Int J Cosmet Sci. 2011;33(1):44-52. 88
The “cosmeceutical cocktail”
A topical combination of the previously described ingredients in a study by Al-Bader et al. was reported to yield a synergistic increase in glycerol release, suggesting that combinations of cosmeceuticals can act as a powerful mixture to stimulate fat breakdown.
Badreshia-bansal S, Draelos ZD. Insight into skin lightening cosmeceuticals for women of color. J Drugs Dermatol. 2007;6(1):32-9.
89
Anticellulites – the “cosmeceutical cocktail”
Clinically significant improvement in the appearance of cellulite on the thigh was observed, when treated with creams containing a mixture of retinoid, algae extract, CLA, and glaucine, over the course of 12 weeks.
Badreshia-bansal S, Draelos ZD. Insight into skin lightening cosmeceuticals for women of color. J Drugs Dermatol. 2007;6(1):32-9.
90
What’s the take home?
49
91
How to have the conversation with your patients:
Most importantly, we, as the physician and the “expert opinion” need to stay up to date on this rapidly expanding and evolving field of cosmetic medicine and the “newest, latest, and greatest” products coming out on the market.
Education is key, for yourself, and for your patients.
Kligman D. Cosmeceuticals. Dermatol Clin. 2000;18(4):609-15.
92
Dr. Kligman’s Rules: When evaluating a cosmeceutical product, be able to
logically assess… whether the product is actually able to penetrate
the stratum corneum to the level of the desired target.
whether the product can do what it claims to do at the desired target.
whether there are peer-reviewed, double-blinded, placebo-controlled, statistically significant clinical trials regarding the efficacy of the product.
Kligman D. Cosmeceuticals. Dermatol Clin. 2000;18(4):609-15.
93
The Bottom Line: Limitations
Unfortunately, many of the studies that we have regarding these products are small.
More importantly, as mentioned before, the claims regarding what these products can REALLY do in-vivo is limited by these products being labeled as cosmeceuticals.
94
The Bottom Line: What we know works!
More importantly, however, we must not forget to stress the importance of daily…
SUNSCREEN MOISTURIZER
95
SUNSCREEN is the most biologically active antiaging ingredient in skin care products!!
80% of the formulations of OTC skin care
products primarily MOISTURIZERS (petrolatum, dimethicone, or glycerin) with added ingredients to support marketing claims
Draelos ZD. Active agents in common skin care products. Plast Reconstr Surg. 2010 Feb; 125(2):719-24.
96
References: 1. Sachdev M, Friedman A. Cosmeceuticals in day-to-day clinical practice. J Drugs Dermatol. 2010;9(5 Suppl ODAC Conf Pt 1):s62-6.] 2. Newburger AE. Cosmeceuticals: myths and misconceptions. Clin Dermatol. 27(5):446-52. 3. Green JB, Metelitsa AI. Introduction. Cosmeceuticals: current trends and market analysis. Semin Cutan Med Surg. 2011;30(3):139-40. 4. Draelos ZD. The cosmeceutical realm. Clin Dermatol. 26(6):627-32. 5. Draelos ZD. Cosmeceuticals: undefined, unclassified, and unregulated. Clin Dermatol. 27(5):431-4. 6. Brandt FS, Cazzaniga A, Hann M. Cosmeceuticals: current trends and market analysis. Semin Cutan Med Surg. 2011;30(3):141-3. 7. Reszko AE, Berson D, Lupo MP. Cosmeceuticals: practical applications. Obstet Gynecol Clin North Am. 2010;37(4):547-69, viii. 8. Rivers JK. The role of cosmeceuticals in antiaging therapy. Skin Therapy Lett. 13(8):5-9. 9. Kligman D. Cosmeceuticals. Dermatol Clin. 2000;18(4):609-15. 10. Levin J, Momin SB. How much do we really know about our favorite cosmeceutical ingredients? J Clin Aesthet Dermatol. 2010;3(2):22-41. 11. Kerscher M, Buntrock H. Update on cosmeceuticals. J Dtsch Dermatol Ges. 2011;9(4):314-26. 12. Gao XH, Zhang L, Wei H, Chen HD. Efficacy and safety of innovative cosmeceuticals. Clin Dermatol. 26(4):367-74. 13. Smirnova MH. A will to youth: The woman's anti-aging elixir. Soc Sci Med. 2012; 14. Lupo M, Jacob L. Cosmeceuticals used in conjunction with laser resurfacing. Semin Cutan Med Surg. 2011;30(3):156-62. 15. Lintner K, Mas-chamberlin C, Mondon P, Peschard O, Lamy L. Cosmeceuticals and active ingredients. Clin Dermatol. 27(5):461-8. 16. Giacomoni PU. Advancement in skin aging: the future cosmeceuticals. Clin Dermatol. 26(4):364-6. 17. Amer M, Maged M. Cosmeceuticals versus pharmaceuticals. Clin Dermatol. 27(5):428-30 18. Konda S, Geria AN, Halder RM. New horizons in treating disorders of hyperpigmentation in skin of color. Semin Cutan Med Surg. 2012;31(2):133-9. 19. Vogelgesang B, Abdul-malak N, Reymermier C, Altobelli C, Saget J. On the effects of a plant extract of Orthosiphon stamineus on sebum-related skin
imperfections. Int J Cosmet Sci. 2011;33(1):44-52. 20. Hunt KJ, Hung SK, Ernst E. Botanical extracts as anti-aging preparations for the skin: a systematic review. Drugs Aging. 2010;27(12):973-85. 21. Leyden J, Wallo W. The mechanism of action and clinical benefits of soy for the treatment of hyperpigmentation. Int J Dermatol. 2011;50(4):470-7. 22. Martin KI, Glaser DA. Cosmeceuticals: the new medicine of beauty. Mo Med. 108(1):60-3. 23. Lee JS, Park KY, Min HG, et al. Negative regulation of stress-induced matrix metalloproteinase-9 by Sirt1 in skin tissue. Exp Dermatol. 2010;19(12):1060-6. 24. Farris PK. Innovative cosmeceuticals: sirtuin activators and anti-glycation compounds. Semin Cutan Med Surg. 2011;30(3):163-6. 25. Badreshia-bansal S, Draelos ZD. Insight into skin lightening cosmeceuticals for women of color. J Drugs Dermatol. 2007;6(1):32-9.
50
97
26. Draelos ZD. Skin lightening preparations and the hydroquinone controversy. Dermatol Ther. 20(5):308-13. 27. Baliña LM, Graupe K. The treatment of melasma. 20% azelaic acid versus 4% hydroquinone cream. Int J Dermatol. 1991;30(12):893-5. 28. Bissett DL, Miyamoto K, Sun P, Li J, Berge CA. Topical niacinamide reduces yellowing, wrinkling, red blotchiness, and hyperpigmented spots in aging
facial skin. Int J Cosmet Sci. 2004;26(5):231-8. 29. Bissett DL. Common cosmeceuticals. Clin Dermatol. 27(5):435-45. 30. Gehring W. Nicotinic acid/niacinamide and the skin. J Cosmet Dermatol. 2004;3(2):88-93. 31. Bissett DL, Oblong JE, Berge CA. Niacinamide: A B vitamin that improves aging facial skin appearance. Dermatol Surg. 2005;31(7 Pt 2):860-5. 32. Espinal-perez LE, Moncada B, Castanedo-cazares JP. A double-blind randomized trial of 5% ascorbic acid vs. 4% hydroquinone in melasma. Int J
Dermatol. 2004;43(8):604-7. 33. Farris PK. Topical vitamin C: a useful agent for treating photoaging and other dermatologic conditions. Dermatol Surg. 2005;31(7 Pt 2):814-7. 34. Nolan KA, Marmur ES. Over-the-counter topical skincare products: a review of the literature. J Drugs Dermatol. 2012;11(2):220-4. 35. Varani J, Warner RL, Gharaee-kermani M, et al. Vitamin A antagonizes decreased cell growth and elevated collagen-degrading matrix metalloproteinases
and stimulates collagen accumulation in naturally aged human skin. J Invest Dermatol. 2000;114(3):480-6. 36. Kafi R, Kwak HS, Schumacher WE, et al. Improvement of naturally aged skin with vitamin A (retinol). Arch Dermatol. 2007;143(5):606-12. 37. Stiller MJ, Bartolone J, Stern R, et al. Topical 8% glycolic acid and 8% L-lactic acid creams for the treatment of photodamaged skin. A double-blind
vehicle-controlled clinical trial. Arch Dermatol. 1996;132(6):631-6. 38. Wallo W, Nebus J, Leyden JJ. Efficacy of a soy moisturizer in photoaging: a double-blind, vehicle-controlled, 12-week study. J Drugs Dermatol.
2007;6(9):917-22. 39. Liu J-C, Seiberg M, Miller J, et al. Soy: potential applications in skin care. Poster presented at: 59th Annual Meeting of the American Academy of
Dermatology, Washington DC, March 2001 40. Dreher F, Gabard B, Schwindt DA, Maibach HI. Topical melatonin in combination with vitamins E and C protects skin from ultraviolet-induced erythema:
a human study in vivo. Br J Dermatol. 1998;139(2):332-9. 41. Südel KM, Venzke K, Mielke H, et al. Novel aspects of intrinsic and extrinsic aging of human skin: beneficial effects of soy extract. Photochem Photobiol.
81(3):581-7. 42. Ho ET, Trookman NS, Sperber BR, et al. A randomized, double-blind, controlled comparative trial of the anti-aging properties of non-prescription tri-
retinol 1.1% vs. prescription tretinoin 0.025%. J Drugs Dermatol. 2012;11(1):64-9. 43. Zhai H, Behnam S, Villarama CD, Arens-corell M, Choi MJ, Maibach HI. Evaluation of the antioxidant capacity and preventive effects of a topical
emulsion and its vehicle control on the skin response to UV exposure. Skin Pharmacol Physiol. 18(6):288-93. 44. Fitzpatrick RE, Rostan EF. Double-blind, half-face study comparing topical vitamin C and vehicle for rejuvenation of photodamage. Dermatol Surg.
2002;28(3):231-6. 45. Lin FH, Lin JY, Gupta RD, et al. Ferulic acid stabilizes a solution of vitamins C and E and doubles its photoprotection of skin. J Invest Dermatol.
2005;125(4):826-32. 46. Blanes-mira C, Clemente J, Jodas G, et al. A synthetic hexapeptide (Argireline) with antiwrinkle activity. Int J Cosmet Sci. 2002;24(5):303-10. 47. Robinson LR, Fitzgerald NC, Doughty DG, Dawes NC, Berge CA, Bissett DL. Topical palmitoyl pentapeptide provides improvement in photoaged human
facial skin. Int J Cosmet Sci. 2005;27(3):155-60. 48. Lupo MP, Cole AL. Cosmeceutical peptides. Dermatol Ther. 20(5):343-9.
98
49. Verma P, Pathak K. Therapeutic and cosmeceutical potential of ethosomes: An overview. J Adv Pharm Technol Res. 2010;1(3):274-82 50. Bariya SH, Gohel MC, Mehta TA, Sharma OP. Microneedles: an emerging transdermal drug delivery system. J Pharm Pharmacol. 2012;64(1):11-29. 51. Menon GK, Cleary GW, Lane ME. The structure and function of the stratum corneum. Int J Pharm. 2012;435(1):3-9. 52. Choi CM, Berson DS. Cosmeceuticals. Semin Cutan Med Surg. 2006;25(3):163-8. 53. Ennes SBP, Paschoalick RC, Mota De Avelar Alchorne M. A double-blind, comparative, placebo-controlled study of the efficacy and tolerability of 4%
hydroquinone as a depigmenting agent in melasma. Journal of Dermatological Treatment. 2000; 11(3): 173-179 54. Bolognia, J. L., Jorizzo, J. L., & Schaffer, J. V. (2012). Dermatology. (3rd ed., Vol. 2, p. 2488). Elsevier Saunders. 55. McCullough JL, Weinstein GD. Clinical study of safety and efficacy of using topical kinetin 0.1% (Kinerase) to treat photodamaged skin. Cosmetic
Dermatol. 2002; 15:29-32. 56. Fisher, GJ, Kang S, et. al. Mechanisms of photoaging and chronological aging. Archives of Dermatology. 2002; 138:1462-1470. 57. Draelos ZD. Active agents in common skin care products. Plast Reconstr Surg. 2010 Feb; 125(2):719-24.
99
Images
1. http://www.oculist.net/downaton502/prof/ebook/duanes/pages/v4/ch038/001f.html 2. http://www.globalskinatlas.com/imagedetail.cfm?TopLevelid=2296&ImageID=5117&did=218 3. http://www.azelaic-acid.com/en/azelaic-acid-component/azelaic-acid/index.php 4. http://www.chemspider.com/Chemical-Structure.2179.html 5. http://www.infohealthz.org/thearticle-Antioxidant-vitamins.html 6. http://www.sciencedirect.com/science/article/pii/S0278691598000623 7. http://home.caregroup.org/clinical/altmed/interactions/Nutrients/Vitamin_E.htm 8. http://course1.winona.edu/sberg/495/Papers/DH-paper.htm 9. http://www.sciencedirect.com/science/article/pii/S1574334906160044 10. http://www.advancedskintech.com/GCScience.htm 11. http://swiftcraftymonkey.blogspot.com/2010/02/alpha-hydroxy-acids.html 12. http://aac.asm.org/content/53/5/1760/F1.expansion 13. http://www.medik8.com/en/pretox/pretox_infin8.html 14. http://www.mdidea.com/products/herbextract/resveratrol/data07.html 15. http://www.deltalabsusa.com/product_resveratrol.php 16. http://www.sciencephoto.com/media/296686/enlarge 17. http://www.surplussalesline.com/detail.asp?ProdID=8373 18. http://nutritionforskinbeauty.com/?cat=1
51
6:30 am AOCD Registration
6:45 am - 8:00 am Great Cases from Osteopathic Institutions Cindy Hoffman, D.O., FAOCD Moderator
8:00 am Tats, Holes, and Landscapes: The Curious History of Body Art, Piercings, and Personal Grooming Melinda Greenfield, D.O. Albany Dermatology Center, Albany, GA
9:00 am Interesting and Unusual Dermatologic Cases Stephen Purcell, D.O., FAOCD Advanced Dermatology Associates, Allentown, PA
10:00 am Break
10:15 am - 12:00 pm Dermpath Review Michael Morgan, M.D.
12:00 pm - 1:00 pm Lunch on your own
1:00 pm PDT for Skin Cancers and Actinic Damage: Australian & Global Experience Anthony Dixon, M.D.
2:00 pm Alopecia Neoplastica Heralding a Diagnosis of Breast Cancer Mounir Wassef, D.O. Columbia Hospital, West Palm Beach, FL
2:20 pm Merkel Cell Carcinoma: A Case and Review Alison Himes, D.O. O’Blenness Hospital, Dublin, OH
2:40 pm Morphea Associated with Celiac Disease Sanjosh Singh, D.O. St. John’s Episcopal Hospital, Lindenhurst, NY
3:00 pm Linear Psoriasis in Lines of Blaschko Charlotte Noorollah, D.O. St. John’s Episcopal Hospital, Lindenhurst, NY
TUESDAY, OCTOBER 9, 2012
52
3:20 pm Break
4:00 pm Parry-Romberg Syndrome Case Series James B. Young, D.O. St. Joseph Mercy Health System, Clinton Twp., MI
4:20 pm Muckle Wells Syndrome: A Cold Case Report Heather Orkwis, D.O. St. Joseph Mercy Health System, Clinton Twp., MI
4:40 pm A Curious Case of Cutaneous Angiokeratomas Libby Rhee, D.O. St. Barnabas Hospital, Bronx, NY
5:00 pm Gender as an Age-Specific Modifier for Ulcerated Malignant Melanomas Blakely Richardson, D.O. University Hospitals, Cleveland, OH
5:20 pm Diagnostic Tests for Bullous Pemphigoid Ashley Kittridge, D.O. University Hospitals, Cleveland, OH
5:40 pm Diagnosing HIV: Our Role as Dermatologists Ellecia Cook, D.O. Largo Medical Center, Port Richey, FL
6:00 pm End of Day
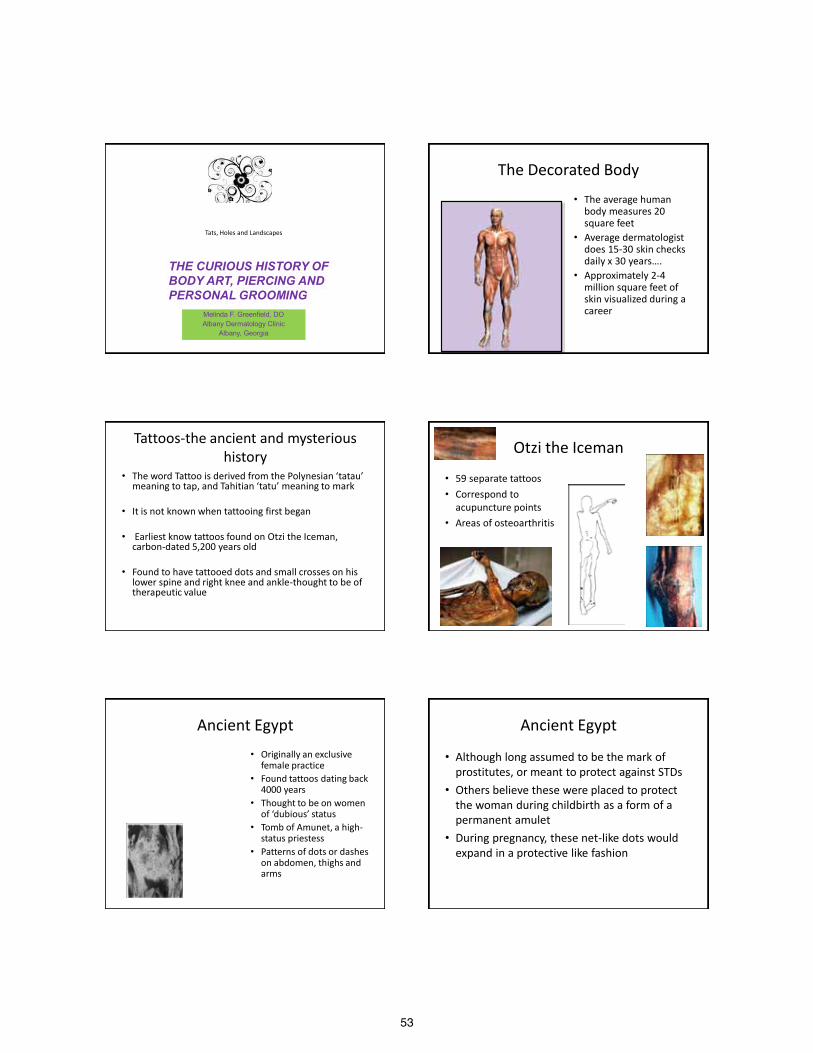
53
Tats, Holes and Landscapes
Melinda F. Greenfield, DO Albany Dermatology Clinic
Albany, Georgia
THE CURIOUS HISTORY OF BODY ART, PIERCING AND PERSONAL GROOMING
The Decorated Body
• The average human body measures 20 square feet
• Average dermatologist does 15-30 skin checks daily x 30 years….
• Approximately 2-4 million square feet of skin visualized during a career
Tattoos-the ancient and mysterious history
• The word Tattoo is derived from the Polynesian ‘tatau’ meaning to tap, and Tahitian ‘tatu’ meaning to mark
• It is not known when tattooing first began
• Earliest know tattoos found on Otzi the Iceman, carbon-dated 5,200 years old
• Found to have tattooed dots and small crosses on his lower spine and right knee and ankle-thought to be of therapeutic value
Otzi the Iceman
• 59 separate tattoos • Correspond to
acupuncture points • Areas of osteoarthritis
Ancient Egypt • Originally an exclusive
female practice • Found tattoos dating back
4000 years • Thought to be on women
of ‘dubious’ status • Tomb of Amunet, a high-
status priestess • Patterns of dots or dashes
on abdomen, thighs and arms
Ancient Egypt
• Although long assumed to be the mark of prostitutes, or meant to protect against STDs
• Others believe these were placed to protect the woman during childbirth as a form of a permanent amulet
• During pregnancy, these net-like dots would expand in a protective like fashion
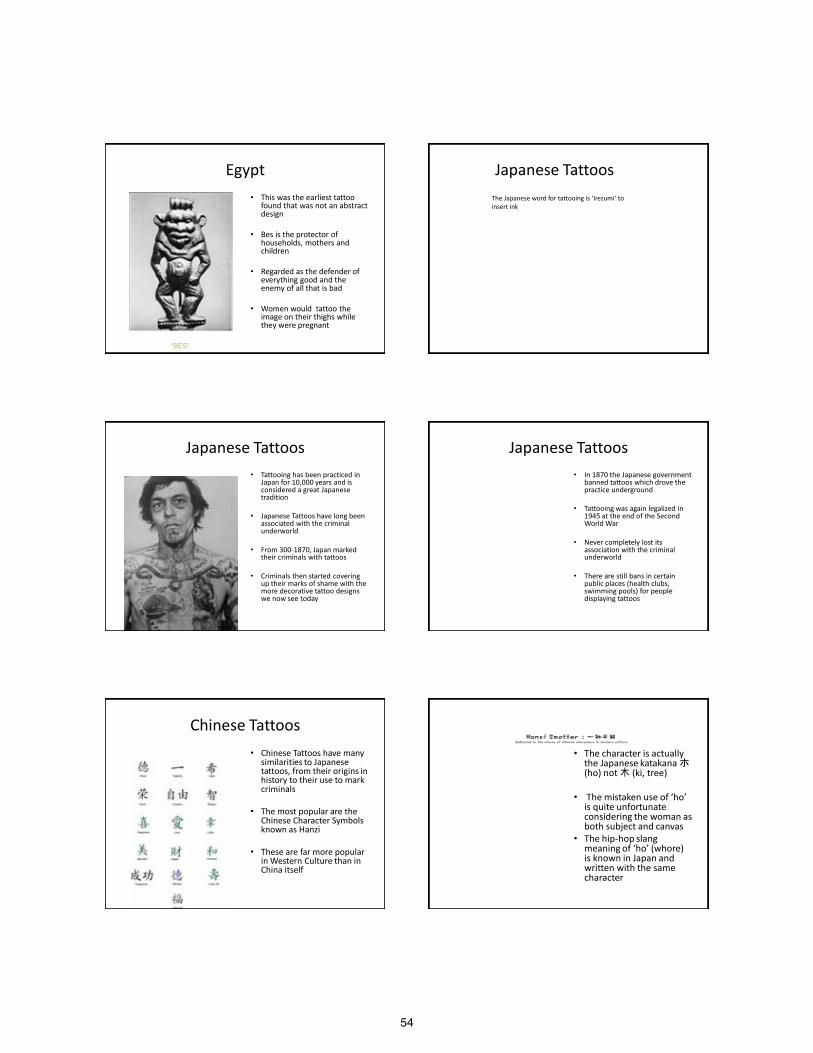
54
Egypt • This was the earliest tattoo
found that was not an abstract design
• Bes is the protector of households, mothers and children
• Regarded as the defender of everything good and the enemy of all that is bad
• Women would tattoo the image on their thighs while they were pregnant
“BES”
Japanese Tattoos The Japanese word for tattooing is ‘Irezumi‘ to insert ink
Japanese Tattoos • Tattooing has been practiced in
Japan for 10,000 years and is considered a great Japanese tradition
• Japanese Tattoos have long been associated with the criminal underworld
• From 300-1870, Japan marked their criminals with tattoos
• Criminals then started covering up their marks of shame with the more decorative tattoo designs we now see today
Japanese Tattoos • In 1870 the Japanese government
banned tattoos which drove the practice underground
• Tattooing was again legalized in 1945 at the end of the Second World War
• Never completely lost its association with the criminal underworld
• There are still bans in certain public places (health clubs, swimming pools) for people displaying tattoos
Chinese Tattoos • Chinese Tattoos have many
similarities to Japanese tattoos, from their origins in history to their use to mark criminals
• The most popular are the Chinese Character Symbols known as Hanzi
• These are far more popular in Western Culture than in China itself
• The character is actually the Japanese katakana ホ (ho) not 木 (ki, tree)
• The mistaken use of ‘ho’ is quite unfortunate considering the woman as both subject and canvas
• The hip-hop slang meaning of ‘ho’ (whore) is known in Japan and written with the same character
55
Chinese Tattoos
• According to the Hanzi smatter site all of these tattoos are complete gibberish
Other Ancient Cultures
• Native Americans- Cree (A.D. 1475)- Extensive facial and body tattoos
• Polynesian- Highly elaborate geometric designs that sometimes covered the entire body
• Maori culture of New Zealand tattooed on their faces, concentrated around the nose and lips
Bridging the gap from Ancient to Today
• With the rise of Christianity in Europe, tattooing faded out
• Sailors, however, continued to circle the globe and return home with the art of the various tribes and regions that were encountered
• Some sailors got a tattoo with every voyage: • Lighthouse= guide a sailor home • Turtle= indicated crossing of the equator • Dragon= crossing of the international date line • Anchor= sailed the Atlantic
Who gets tattoos? • 2006 article in JAAD, 500 random calls were placed to
individuals 18-50 years of age • Questions were asked regarding tattoos and piercings: • 24% had tattoos, 14% piercings • Tattooing was equally common in both sexes, body piercing
was more common in women • Common associations with tattoos: lack of religious
affiliation, extended jail time, previous drinking and drug use
• Complications with piercings included: broken teeth, and increases in jewelry allergies
• Most common location of a tattoo in men: arm; women: ankle
Who gets tattoos? • A 2012 Harris survey interviewed 2016 adults and found that 21%
have at least one tattoo
• Age was a major factor: only 11% of 50-64 year olds are inked while a whopping 38% of those in their 30’s report tattoos
• Women are more likely than men to have tattoos 23% vs 19%
• 86% of those in this survey say they have never regretted their decision, 30% say it makes them feel sexy
• Among the un-tattooed, 45% say that a person with a tattoo is actually less sexy
Regulations on tattoo parlors • No federal regulations
• NM, ND, DC- unregulated
states
• Regulated states forbid tattoos or piercings on a minor
• CO, FL, ID, LA minors can be tattooed if they have signed parental permission
56
Regulations • Restricts artist from tattooing any person who is jaundice, or any part of
the skin that appears inflamed, or has a rash, boils or infection
• Patrons must be sober and in good general health
• Must be a separate area for tattooing and have a clean bathroom
• Artist must wear gloves, wash hands and arms, and use a different needle for each patron
• Equipment must be sterilized in an autoclave
• Infections must be reported to the local health department within 48 hours
Regulations • Regulated states require that tattoo parlors obtain permits before
opening
• Permits require an official inspection by the health department
• Unregulated states require no permit or inspection
• Georgia is a regulated state, prohibits tattooing within 1" of eye; tattooing of minors is prohibited; licensure required by department of health
• www.aaatattoodirectory.com to check your state
Safe Body Art Act- California
• Bill aiming to make it safer to get inked up in CA was introduced for the 3rd time after being twice vetoed by Gov. Schwartzenegger
• He stated that ‘overregulation’ is driving business out of California
History of Piercing • Nose piercing was first recorded in the Middle East ~ 4,000 years
ago
• It was mentioned in the bible in Genesis: • Abraham requested that his servant find a wife for his son, Isaac.
The servant found Rebekah and one of the gifts he gave her was a ‘golden earring’. The original Hebrew word used was Shanf, which translates as ‘nose-ring’
• This is still followed in nomadic tribes in Africa
• The size of the ring denotes the wealth of the family, and is ‘security’ for the wife in case of divorce
Nose Piercing • Brought to India in the 16th
century
• In India a stud is worn in the left nostril, sometimes joined by a chain to the ear
• Left side is most common
• In Ayurvedic medicine the nose is associated with the female reproductive organs, piercing is supposed to make childbirth easier and lessen menstrual pain
Nose Piercings
• In the west, nose piercing first appeared among hippies who traveled to India in the late 60’s
• It was later adopted by the punk movement of the 70’s as a sign of rebellion
57
Ear Lobe Piercing • Oldest mummified body dates back to over 5,000
years, was found to have pierced ears with hole that were enlarged to 7-11mm
• Ears were pierced for magical purposes • Primitive tribes believed that demons entered the
body through the ear and because demons and spirits are repelled by metal, ear piercing prevents them from entering the body
• Sailors would pierce their ears so that if their body washed up somewhere it would pay for a Christian burial
Lip Piercing • Piercing of the lips is widely practiced throughout the
world
• Among the Dogon Tribe of Mali, lip piercing was done for religious purposes
• They believe that the world was created by their ancestor spirit "Noomi" weaving thread through her teeth, but instead of thread out came speech
• Lips are either pierced with a ring or a labret, which consists of a pin of wood, ivory, metal, or even crystals
Genital Piercing • The Prince Albert
• Named after Queen Victoria’s husband (19th century)
• Albert had his penis pierced with a ring called a ‘dressing ring’ so he could manipulate his privates to prevent an unseemly bulge when he wore tight trousers
Landscapes
Pubic Hair: Who is Shaving?? • Poll taken by Leipzig psychologist published in 2009 stated that 50%
of women between the ages of 18-25 admit to shaving their pubic hair, and 25% of men either shave or trim
• Article goes on to state that “it used to be only women or gay men in the ‘depilation studio’ but nowadays no man needs to feel ashamed when ordering the standard selection of ‘back, crack and sack’”
• In a study commissioned by Wilkinson, 61.9% of women want men to shave their pubic hair, and the men in the study supposedly stated that “unshaved women have fewer sex prospects”
Our Award Winning betty™ products are specially formulated color dyes for the hair down there. In just a few years, we have hundreds of thousands of happy customers using betty to naturally match their hair above, cover gray or just for fun! Whether you're a blonde (be a true blonde now!), radiant auburn, rich brunette, raven black or want to try hot pink for fun, our easy to use no-drip formula gives you the perfect finishing touch.
Matching the carpet to the drapes
58
Art history of Pubic Hair • In ancient Egyptian art, female pubic
hair is indicated in the form of painted triangles
• In medieval and classical European art, it was very rarely depicted, and male pubic hair was often omitted
• The same was true in much Indian art, and in other Eastern portrayals of the nude
• In 16th century southern Europe Michelangelo showed the male David with stylized pubic hair, but female bodies remained hairless below the head
• Michelangelo’s male nudes on the Sistine chapel ceiling display no pubic hair
1540 “Eve”
Art History
• Francisco Goya’s The Nude Maja ca. 1800, has been considered as the first European painting to show woman's pubic hair, though others had hinted at it
• The painting was considered quite pornographic at the time
Art History • Before the twentieth century, fine-art paintings and
sculpture in the Western tradition usually depicted women without pubic hair
• John Ruskin, the famous author, artist, and art critic, was apparently accustomed to these depictions and unaware of the actual appearance of nude women
• On his wedding night, he was allegedly so shocked by his discovery of his wife Effie's pubic hair that he rejected her, and the marriage was legally annulled
Pubic Hair in Society • Among the upper class in 19th
century Victorian Britain, pubic hair from one's lover was frequently collected as a souvenir
• The curls were worn like cockades in men's hats as potency talismans, or exchanged among lovers as tokens of affection
• The museum of St. Andrews University in Scotland has in its collection a snuff box full of pubic hair of one of King George IV's mistresses
Removal of Pubic Hair • Trimming or removing pubic hair is a custom in many cultures
• In Islamic societies removing the pubic hair is a religiously endorsed
practice, and is as important as cleaning the teeth, nostrils and removing armpit hair
• It is generally recommended: Both men and women should remove armpit and pubic hair at least every 40 days
• For men a beard is desirable
• Women can remove 'unnatural' facial hair but should not reshape eyebrows for reasons of vanity
History of Hair Removal • Europeans have been
generally accepting of body hair, except for a short period in the Middle Ages when returning Crusaders made the Arabic idea of total body depilation for women fashionable
• The Hanafi branch of Islam, which includes the Sunni Turks, demands that every part of the body be free from hair
59
History of hair removal • In Japan there is a long
tradition of fastidiousness in matters of personal hygiene.
• There have been several Japanese studies of laser depilation and the technique seems widespread.
• The main difference between Japanese and Western practice is that waxing is less commonly used and 'sandpaper' friction strips are particularly popular
Sikh • The Sikh religion forbids
cutting or shaving any bodily hair
• Orthodox Sikhs always carry a dagger with them, lest someone try to force them to do something against their religion
• The dagger is considered one of the five "outer badges"
• The others are wearing hair and beard unshorn; wearing a turban; wearing knee-length pants; and wearing a steel bracelet on the right wrist
The Bikini • The bikini was created in 1946 by Louis Reard • It wasn’t until the ‘sexual revolution’ in the 1960’s that
America could accept the bikini • It was, in fact, banned from the Mrs. World pageant • In the 1970s the string bikini became popular in Brazil • Bloomingdale’s first shipment of 150 string bikinis in
1974 sold out in less than 2 weeks • With the increase in popularity so became the increase
in pressure to remove pubic hair in order to wear the latest fashion
Shaving trends • With the ease of access
modern day pornography and in the increase in popularity of ‘shaved styles’, more adults and teens are jumping on the bandwagon
• Along with this trend comes issues such as folliculitis, infected cysts, contact dermatitis, and other issues we couldn’t even begin to imagine
• As physicians we need to be prepared to address the issues and be open to these new trends
60
Interesting and Unusual Dermatologic Cases
Stephen M. Purcell, D.O.
San Diego
2012
Objectives
■ Present several clinical and clinical-histopathological cases
■ Emphasize interesting or unusual aspect of the case
■ Offer a pearl of wisdom for your edification
Case #1
Case • HPI: 10 year old previously healthy Hispanic female. Developed fever (104o) on
6/22 accompanied by myalgias, abdominal pain, headache, minor epistaxis, oral ulcers. 2 days later, became confused/unconscious. Developed tonic-clonic seizures.
• PMHx: Recurrent oral ulcers, headaches, seasonal allergies, constipation, tonsillectomy
• Social Hx: Had been swimming in a lake 1 week prior to becoming ill. No sick
contacts. No hx of animal bites. • ROS: (-) N/V, (-) diarrhea, (-) conjunctival injection, (-) lymphadenopathy, • (-) muscle weakness, (-) arthralgias • Gen: Sedated, intubated
• Skin: No abnormal skin findings
Studies • CBC:
– WBC: 8.8 – Hgb: 8.3 – Platelets: 226
• BMP: WNL • Blood Cx: (-) • Urine Cx: >100,000 non-lactose fermenting G(-) rods • O & P stool: (-) • Tox Screen: (+) BZD • Lyme, HSV1, HSV2, EBV, Enterovirus, CMV, VZV, Arbovirus, West Nile
Virus: Negative • CSF: Glucose, protein WNL • C-ANCA, P-ANCA: WNL
Plan
• Imp: 10 year old female with encephalopathy, refractory seizures of unknown etiology.
• Dermatology consult:
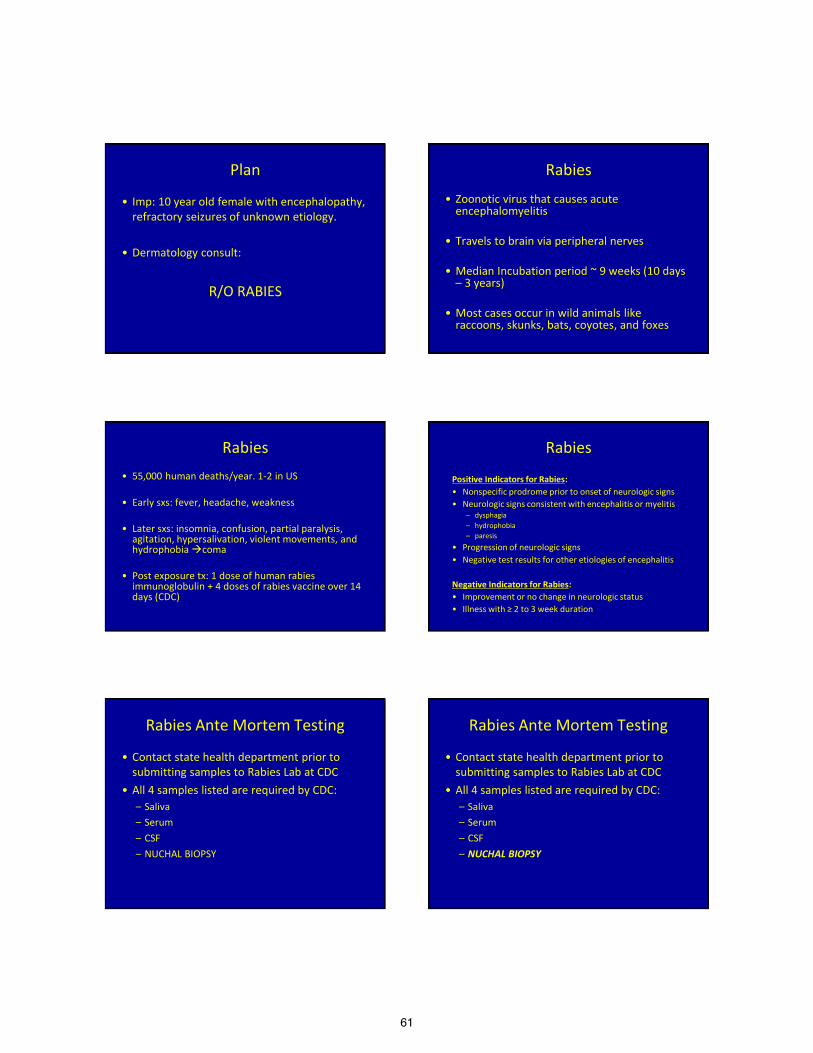
61
Plan
• Imp: 10 year old female with encephalopathy, refractory seizures of unknown etiology.
• Dermatology consult:
R/O RABIES
Rabies
• Zoonotic virus that causes acute encephalomyelitis
• Travels to brain via peripheral nerves
• Median Incubation period ~ 9 weeks (10 days – 3 years)
• Most cases occur in wild animals like raccoons, skunks, bats, coyotes, and foxes
Rabies • 55,000 human deaths/year. 1-2 in US
• Early sxs: fever, headache, weakness
• Later sxs: insomnia, confusion, partial paralysis,
agitation, hypersalivation, violent movements, and hydrophobia coma
• Post exposure tx: 1 dose of human rabies immunoglobulin + 4 doses of rabies vaccine over 14 days (CDC)
Rabies Positive Indicators for Rabies: • Nonspecific prodrome prior to onset of neurologic signs • Neurologic signs consistent with encephalitis or myelitis
– dysphagia – hydrophobia – paresis
• Progression of neurologic signs • Negative test results for other etiologies of encephalitis Negative Indicators for Rabies: • Improvement or no change in neurologic status • Illness with ≥ 2 to 3 week duration
Rabies Ante Mortem Testing
• Contact state health department prior to submitting samples to Rabies Lab at CDC
• All 4 samples listed are required by CDC: – Saliva – Serum – CSF – NUCHAL BIOPSY
Rabies Ante Mortem Testing
• Contact state health department prior to submitting samples to Rabies Lab at CDC
• All 4 samples listed are required by CDC: – Saliva – Serum – CSF – NUCHAL BIOPSY
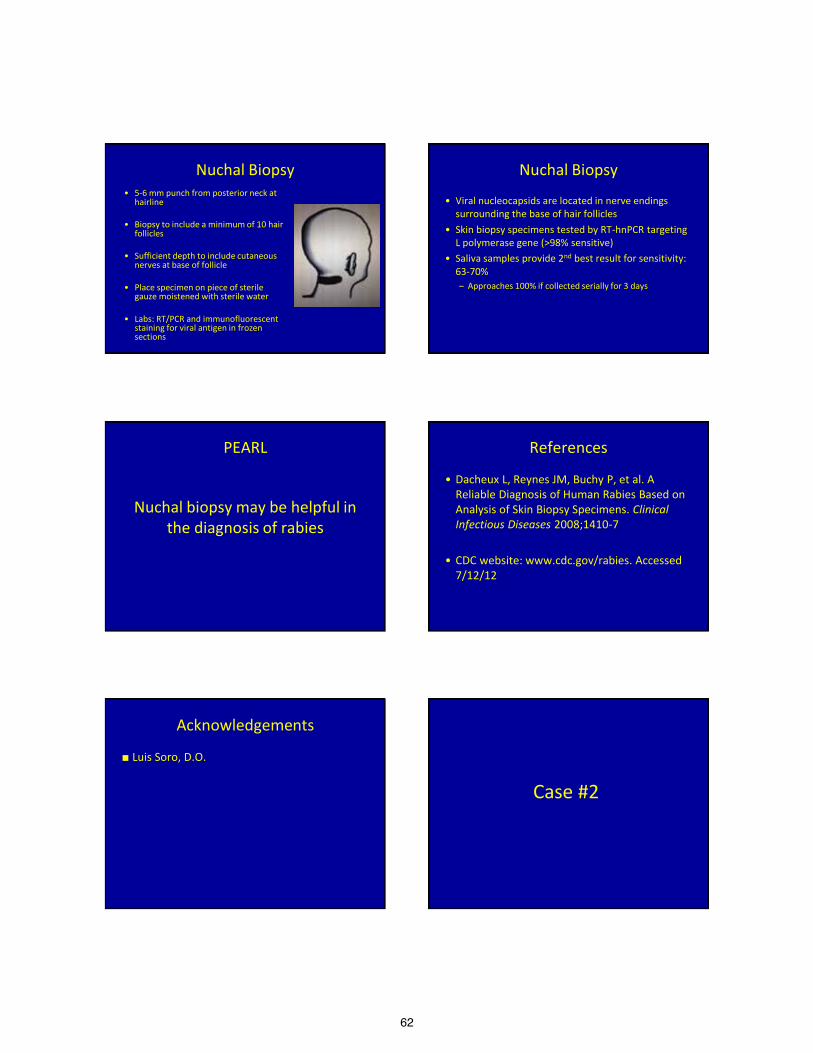
62
Nuchal Biopsy • 5-6 mm punch from posterior neck at
hairline • Biopsy to include a minimum of 10 hair
follicles • Sufficient depth to include cutaneous
nerves at base of follicle • Place specimen on piece of sterile
gauze moistened with sterile water • Labs: RT/PCR and immunofluorescent
staining for viral antigen in frozen sections
Nuchal Biopsy
• Viral nucleocapsids are located in nerve endings surrounding the base of hair follicles
• Skin biopsy specimens tested by RT-hnPCR targeting L polymerase gene (>98% sensitive)
• Saliva samples provide 2nd best result for sensitivity: 63-70% – Approaches 100% if collected serially for 3 days
PEARL
Nuchal biopsy may be helpful in
the diagnosis of rabies
References
• Dacheux L, Reynes JM, Buchy P, et al. A Reliable Diagnosis of Human Rabies Based on Analysis of Skin Biopsy Specimens. Clinical Infectious Diseases 2008;1410-7
• CDC website: www.cdc.gov/rabies. Accessed
7/12/12
Acknowledgements
■ Luis Soro, D.O.
Case #2
63
Case • A 47 year male was diagnosed with basal cell nevus
syndrome at age 18 based on the findings of odontogenic keratocysts, calcification of the falx cerebri and palmar pits.
• At age 33 he began to develop multiple basal cell carcinomas requiring numerous surgeries including Mohs and curettage and electrodesiccation.
Case • In May of 2010, the patient enrolled in a trial of GDC-
0449, an oral drug that inhibits Hedgehog pathway signaling.
• The 18 month trial ended in November of 2011.
• The patient experieinced significant side effects including recalcitrant nausea and loss of taste resulting in weight loss of 25 pounds. Additionally, he experieinced abdominal pain, diarrhea, fatigue and generalized alopecia.
Case • His symptoms resolved after discontinuation of the
trial, suggesting he was not in the placebo arm.
• His existing basal cell carcinoma tumors resolved and he has not developed any new tumors since.
• Interestingly, his palmar pits disappeared.
GDC-0449
• Vismodegib (ErivedgeTM) • First drug approved by the U.S.
Food and Drug Administration • Indication
– Metastatic BCC – Locally advanced BCC that has
recurred following surgery – Those who are not candidates for
surgery or radiation
http://www.globalpharmasectornews.com/wp-content/uploads/2012/02/Erivedge.jpg
64
Sonic Hedgehog Signaling (SHH) Pathway Inhibitors
• Majority of sporadic BCCs have mutations in genes encoding patched 1 (PTCH1) or smoothened (SMO)
SHH pathway Loss-of-PTCH1 mutation Inhibition of smoothened (SMO) signaling by GDC-0449
N Engl J Med. 2009 Sep 17;361(12):1164-72. PMID: 19726763
Vismodegib Efficacy • Evaluated in a single multicenter clinical study • 96 patients with locally advanced or metastatic
BCC • 21% carried a diagnosis of BCNS • Metastatic disease
– 30% partial response • Locally advanced disease
– 21% complete response – 22% partial response
Vismodegib Activity in Patients with Locally Advanced BCC
60-year-old man with BCNS with lesions of the posterior scalp at baseline and after 5 months 41-year-old woman with facial lesions at baseline and after 2 months
N Engl J Med. 2009 Sep 17;361(12):1164-72. PMID: 19726763
Vismodegib in BCNS ■ Phase II clinical trial ■ Incidence of new BCCs after 8 months
– Vismodegib arm - 0.07 cancers per month – Control arm - 1.74 cancers per month
■ 25-fold reduction in the rate of new BCCs ■ Existing tumors decreased in size within
the first month ■ Clearance of palmar and plantar pits and
odontogenic keratocysts ■ No tumor resistance observed
Vismodegib Side Effect Profile
■ Taste loss (83%) ■ Muscle spasms (70%) ■ Alopecia (50%) ■ Weight loss ■ Fatigue ■ Arthralgias
■ Diarrhea ■ Decreased appetite ■ Constipation ■ Nausea ■ Vomiting
Vismodegib Therapy
■ All side effects reversed 1 month after discontinuation
■ After stopping therapy, tumors did not return to baseline size or increase in number during the next 6 months
■ Intermittent regimen with the aim of minimizing side effects – 3 months on therapy, 2 months off
65
PEARL
Vismodogib (Erivedge) may be
beneficial in patients with BCNS or those with unresectable BCC
References • De Smaele E, Ferretti E, Gulino A. Vismodegib, a small-molecule inhibitor of the hedgehog pathway
for the treatment of advanced cancers. Curr Opin Investig Drugs 2010;11:707-718 • Dlugosz AA, Talpaz M. Following the hedgehog to new cancer therapies. N Engl J Med
2009;17;361(12):1202-5 • ErivedgeTM [package insert]. South San Francisco, CA: Genentech USA, Inc; 2012 • Göppner D, Leverkus M. Basal cell carcinoma: from the molecular understanding of the
pathogenesis to targeted therapy of progressive disease. J Skin Cancer 2011;2011:650258 • Gupta S, Takebe N, LoRusso P. Targeting the Hedgehog pathway in cancer. Ther Adv Med Oncol
2010;2:237-250 • Jancin B. AAD: Oral Vismodegib Promising for Basal Cell Nevus Syndrome. Skin & Allergy News
Digital Network February 7, 2011 <www.skinandallergynews.com/news/medical-dermatology/single-article/aad-oral-vismodegib-promising-for-basal-cell-nevus-syndrome/545d88a3f3.html>
• Scare H, Kalthoff F, Meingassner JG, et al. Topical treatment of Basal cell carcinomas in nevoid Basal cell carcinoma syndrome with a smoothened inhibitor. J Invest Dermatol 2011;131(8):1735-4
• Von Hoff DD, LoRusso PM, Rudin CM, Reddy JC, Yauch RL, Tibes R, Weiss GJ, Borad MJ, Hann CL, Brahmer JR, Mackey HM, Lum BL, Darbonne WC, Marsters JC Jr, de Sauvage FJ, Low JA. Inhibition of the hedgehog pathway in advanced basal-cell carcinoma. N Engl J Med 2009 Sep 17;361(12):1164-72. PMID: 19726763
Acknowledgements
■ Tatyana Groysman, D.O. ■ Steven A. Oberlender, M.D.
Case #3
Case • HPI: 35 y.o. female with intermittent pruritic urticarial eruption on the chest and
back. Associated symptoms include headaches, fevers, debilitating fatigue, joint pain and swelling, eye redness and blurred vision. Triggers include cold weather, exercise, fatigue, and stress. Patient noted significant association between symptoms and cutaneous surgery.
• Medical Hx: Basal cell nevus syndrome (BCNS) • Family Hx: Mother has BCNS, daughter does not have BCNS but has same
symptoms as described above. • Labs: CBC, CMP, TSH, ESR and thyroid auto-antibodies all WNL.
• Histopathology: dermal edema and sparse perivascular lymphocytic infiltrate
consistent with the clinical diagnosis of urticaria
4x Back
66
40x Back
7A
7B
Diagnosis:
Muckle-Wells Syndrome in a patient with
Basal Cell Nevus Syndrome
Muckle-Wells Syndrome • Muckle-Wells syndrome (MWS) is a cryopyrin associated periodic
syndrome (CAPS), which is a rare group of cytokine disorders.
• Common to all CAPS are recurrent episodes of multisystem inflammation with recurrent urticaria that begins in infancy or childhood.
• The three phenotypes of CAPS are: – Neonatal-onset multisystem inflammatory disease (NOMID) – MWS – Familial cold auto-inflammatory syndrome
Muckle-Wells Syndrome • MWS is rare and symptoms may overlap with other
conditions leading to a delay in diagnosis.
• Symptoms may arise spontaneously without provocation or be triggered by cold, stress or exercise.
• In our patient, her symptoms were triggered by cutaneous surgery.
• A review of the literature failed to reveal an association between MWS and BCNS.

67
Muckle-Wells Syndrome • MWS results from a gain-of-function gene mutation
of the NLRP3 gene coding for cryopyrin.
• Results in the formation of an intracellular complex known as an inflammasome.
• Defects in the inflammasome lead to overproduction of interleukin-1 (IL-1) which lead to the inflammatory symptoms.
Muckle-Wells Syndrome • Therapy of MWS is directed toward inhibition of IL-1
production.
• Anakinra – a recombinant human IL-1 receptor antagonist
• Canakinumab – an IL-1B antibody
• Rilonacept – a dimeric fusion protein that fuses the Fc portion of IgG1
PEARL
IL-1 inhibitors such as anakinra
may be helpful in the treatment of MWS
References
• Kanazawa N, Furukawa F. Autoinflammatory syndromes with a dermatological perspective. The Journal of Dermatology 2007;34:601-618.
• Newell L, August S, Foria V, Godfrey K. Lifelong urticarial and multiple unexplained systemic symptoms. Clin and Exper Derm 2011;36:431-433.
• Yu JR, Leslie KS. Cryopyrin-Associated Periodic Syndrome: An update on diagnosis and treatment response Curr Allergy Asthma Rep 2011;11:12-20.
Acknowledgements
■ Marie Lewars, D.O. ■ Joseph Laskas, D.O.
Case #4
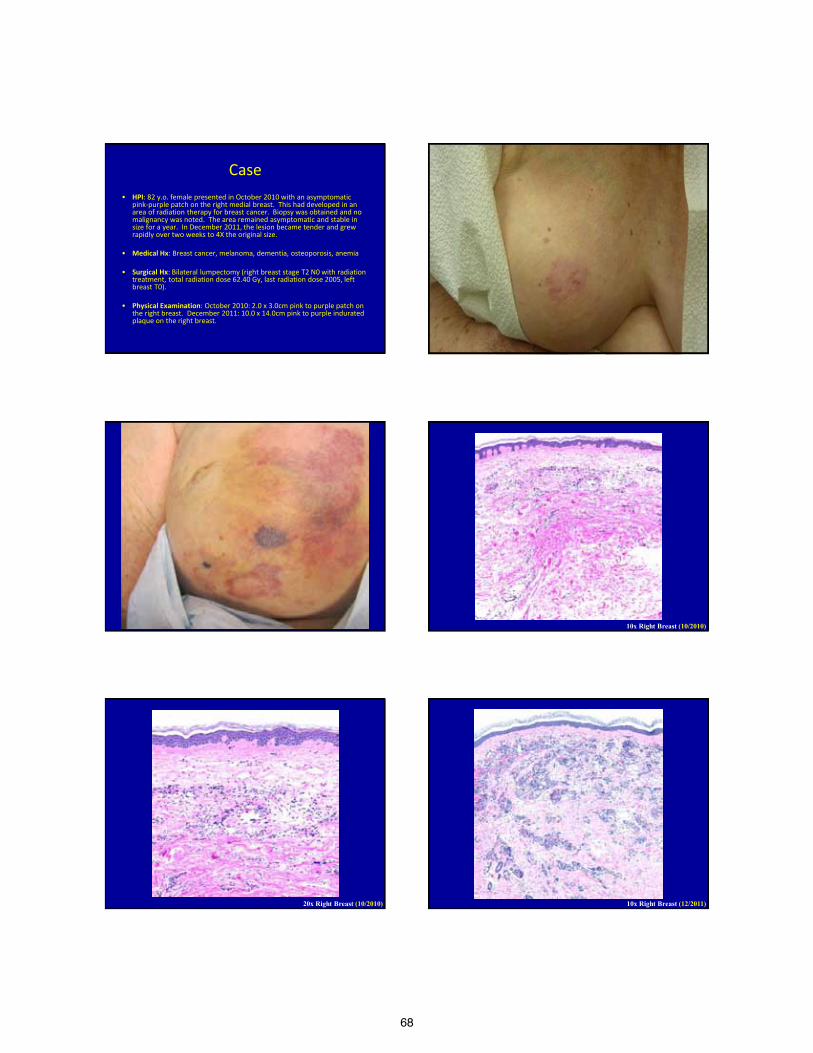
68
Case • HPI: 82 y.o. female presented in October 2010 with an asymptomatic
pink-purple patch on the right medial breast. This had developed in an area of radiation therapy for breast cancer. Biopsy was obtained and no malignancy was noted. The area remained asymptomatic and stable in size for a year. In December 2011, the lesion became tender and grew rapidly over two weeks to 4X the original size.
• Medical Hx: Breast cancer, melanoma, dementia, osteoporosis, anemia • Surgical Hx: Bilateral lumpectomy (right breast stage T2 N0 with radiation
treatment, total radiation dose 62.40 Gy, last radiation dose 2005, left breast T0).
• Physical Examination: October 2010: 2.0 x 3.0cm pink to purple patch on
the right breast. December 2011: 10.0 x 14.0cm pink to purple indurated plaque on the right breast.
10x Right Breast (10/2010)
20x Right Breast (10/2010) 10x Right Breast (12/2011)
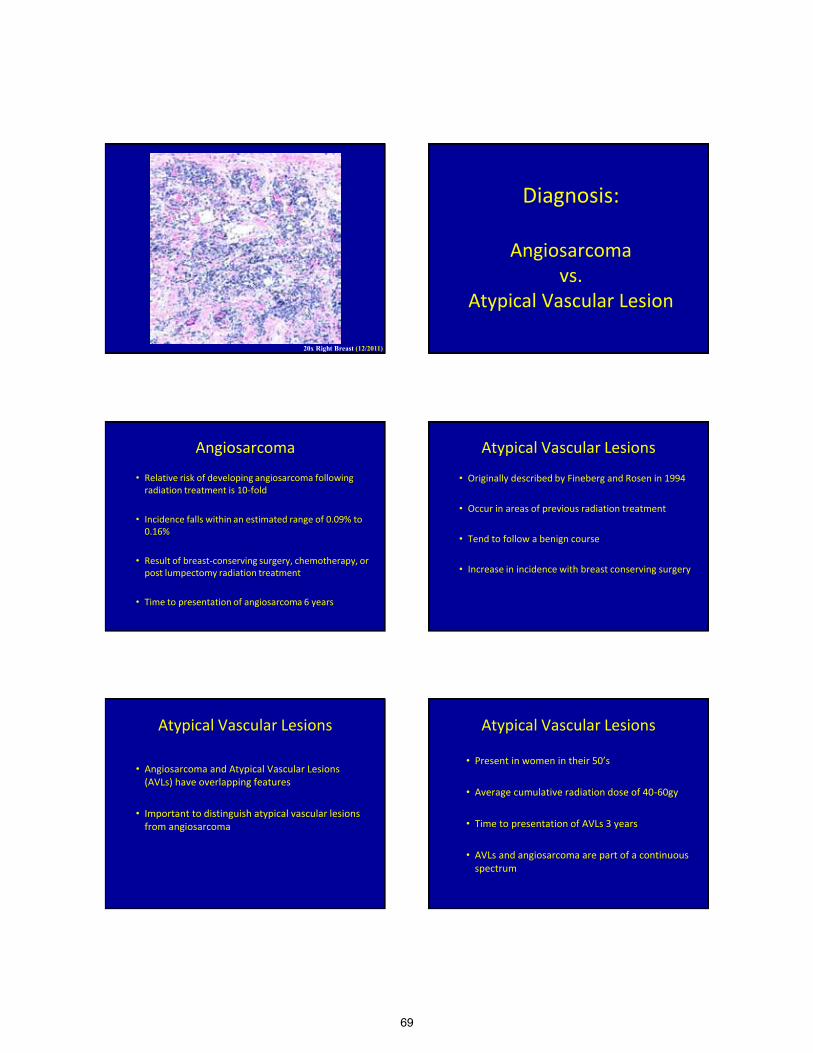
69
20x Right Breast (12/2011)
Diagnosis:
Angiosarcoma vs.
Atypical Vascular Lesion
Angiosarcoma
• Relative risk of developing angiosarcoma following radiation treatment is 10-fold
• Incidence falls within an estimated range of 0.09% to 0.16%
• Result of breast-conserving surgery, chemotherapy, or post lumpectomy radiation treatment
• Time to presentation of angiosarcoma 6 years
Atypical Vascular Lesions
• Originally described by Fineberg and Rosen in 1994
• Occur in areas of previous radiation treatment
• Tend to follow a benign course
• Increase in incidence with breast conserving surgery
Atypical Vascular Lesions
• Angiosarcoma and Atypical Vascular Lesions (AVLs) have overlapping features
• Important to distinguish atypical vascular lesions from angiosarcoma
Atypical Vascular Lesions
• Present in women in their 50’s
• Average cumulative radiation dose of 40-60gy
• Time to presentation of AVLs 3 years
• AVLs and angiosarcoma are part of a continuous spectrum
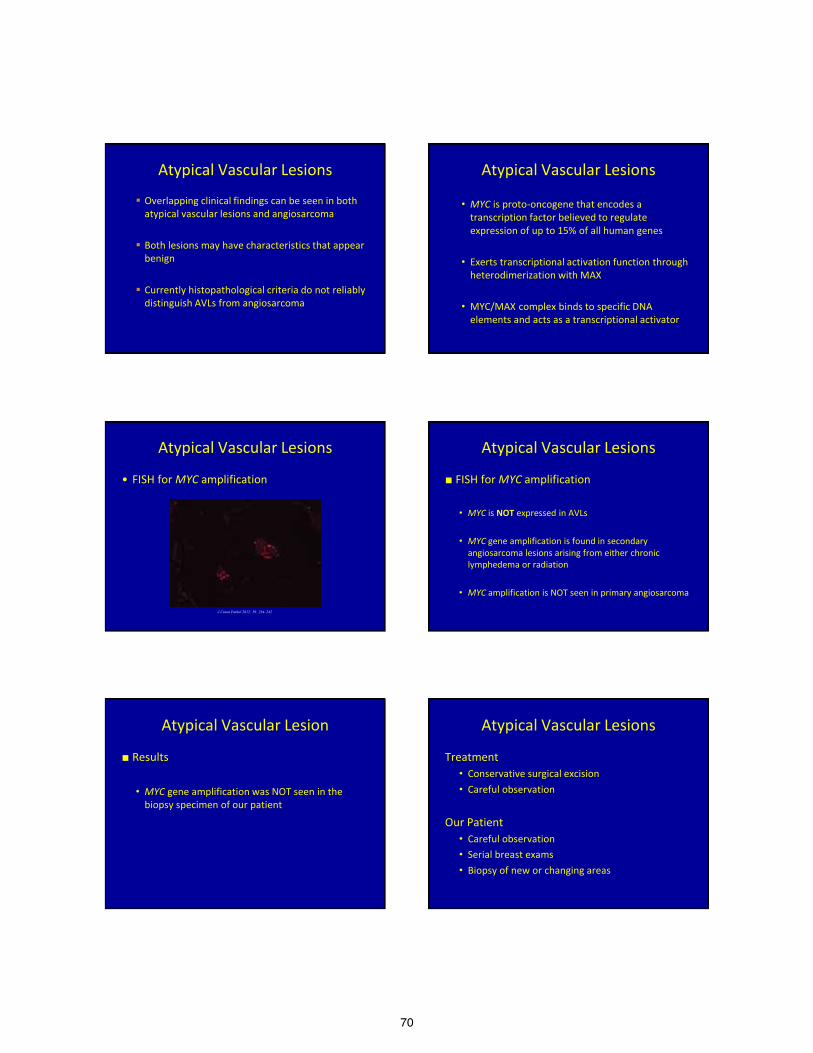
70
Atypical Vascular Lesions
Overlapping clinical findings can be seen in both atypical vascular lesions and angiosarcoma
Both lesions may have characteristics that appear benign
Currently histopathological criteria do not reliably distinguish AVLs from angiosarcoma
Atypical Vascular Lesions
• MYC is proto-oncogene that encodes a transcription factor believed to regulate expression of up to 15% of all human genes
• Exerts transcriptional activation function through heterodimerization with MAX
• MYC/MAX complex binds to specific DNA elements and acts as a transcriptional activator
Atypical Vascular Lesions
• FISH for MYC amplification
J Cutan Pathol 2012: 39: 234–242
Atypical Vascular Lesions
■ FISH for MYC amplification • MYC is NOT expressed in AVLs
• MYC gene amplification is found in secondary
angiosarcoma lesions arising from either chronic lymphedema or radiation
• MYC amplification is NOT seen in primary angiosarcoma
Atypical Vascular Lesion
■ Results • MYC gene amplification was NOT seen in the
biopsy specimen of our patient
Atypical Vascular Lesions
Treatment • Conservative surgical excision • Careful observation
Our Patient • Careful observation • Serial breast exams • Biopsy of new or changing areas
71
PEARLS
• Differentiation of AVLs and angiosarcoma can be difficult
• Many different overlapping features suggest a lesional spectrum
• FISH for MYC amplification may be used as an adjunct to distinguish lesions
References • Brenn T, Fletcher C. Radiation-associated cutaneous atypical vascular lesions and angiosarcoma: clinicopathologic analysis of 42 cases. Am. J. Surg. Pathol. 2005; 29:983-966. • Brenn T, Fletcher C. Postradiation vascular proliferations: an increasing problem. Histopathology. 2006;48:106-114. • Patton K, Deyrup A, Weiss S. Atypical vascular lesions after surgery and radiation of the breast: a clinicopathologic study of 32 cases analyzing histologic heterogeneity and association with angiosarcoma. Am. J. Pathol. 2008;32:943-950. • Fernandez A, Sun Y, Tubbs R, Goldblum J, Billings S. FISH for myc amplification and anti myc immunohistochemistry: useful diagnostic tools in the assessment of secondary angiosarcoma and atypical vascular lesion proliferations. J Cutan Pathol. 2012;29:234-
242 • Bolognia J, Jorizzo J, Rapini R. Dermatology 2nd edition. Elsevier/Mosby 2007.
Acknowledgements
■ Christian Oram, D.O.
72
Photodynamic therapy in skin cancer
The experience in Australia and elsewhere
Anthony Dixon PhD MB BS FACRRM
Conflicts of interest • Allmedic ® – ALA PDT supplier
– Shareholding granted on trial start • We donated this to charity • Externally managed
– Manager decided to donate all income • To child obesity research
• Dixon family cannot – Make decisions on shareholding – Benefit from shareholding
PDT for invasive SCC
• Unacceptable • All studies terrible outcomes
• Nice summary of collated data: • Braathen J A A D Jan 2007 • (All authors paid by Galderma)
PDT for Bowens Disease
• 4 studies reviewed • 225, 40, 19 and 16 patients • Around 90% clearance rate
• Comparable with cryotherapy • ? Better cosmesis • Braathen J A A D Jan 2007
PDT for superficial BCC
• 12 studies reviewed • Patient numbers: 147 118, 80, 80, 55, 47, 39,
38, 37, 32, 23, 6
• Clearance rates around 90%
• Recurrence rates 18 – 38% !! • Braathen J A A D Jan 2007
ALA PDT Vs Surgery – nodular BCC
• RCT 85 PDT Vs 88 Excision • 3 year follow up
• Failure rates: – 2.3% Surgery (3 mm margin) – 30% PDT p<0.001
• PDT not good enough for nodular BCC • Mosterd BJD Sep 2008
73
ALA PDT for nodular BCC
• “High and sustained efficacy . . . “ ??? • 60 BCCs on 44 patients
– Curette prior to PDT – 10 year follow up
• 75% response – failures all within 3 years • Cosmesis “good” or “excellent” in 91%
• Christensen BJD June 2012 • Is this actually a good result ? ? ?
Recurrence after treating BCCs • 90 patients with 157 BCCs • Recurrence rates observed:
– 7% at 3 months – 19% at 6 months – 27% at 12 months – 31% at 24 months
• Worse if patients > 60 years 35% Vs 19% • Worse if BCC nodular 28% Vs 13% Spfcl • Lindberg-Larsen 2012 Act Derm-Ven
Our photodynamic therapy trial
• Our trial of PDT for actinic keratoses
• I was approached – By Allmedic Pty. Ltd. ® – Lead an industry initiated & sponsored RCT – Their newly marketed PDT – For face actinic field damage
– March 2008
Field damage RCT
• Inclusion criteria: – Previous invasive skin cancer on face
• Randomized controlled trial • 6 centres across Australia • Face treated with field Allmedic ALA ®
– Versus observation
Protocol details
• Intervention patients: • 2 treatments with Allmedic ALA ®
– (aminolevulonic acid)
• 2 weeks apart • All patients followed up for 2 years + • Any suspicious lesions biopsied • Any cancers excised
Trial end point • Does treatment with field PDT
–Reduce future risk of skin cancer?
• Concept was: –If future cancer risk clearly reduced –Then face PDT should follow
• Excision of cancer from face
74
Severe adverse events
• 5 of the 34 intervention patients • & the control who had PDT
• Total 6 out 35 = 17%
% of trial patients developing one or more new skin cancers on face – 3 year follow up
0
5
10
15
20
25
30
35
40
Intervention Control
InterventionControl
%
All new cancers were BCCs or SCCs
Except for two patients who had PDT
Kaplan Meier Curve
Complex face surgery pain versus PDT
0
5
10
15
20
25
30
35
40
45
No pain Minimal Paracetamol Strong tabs Severe Worst ever
Large face Surgery PDT
Highly significant P < 0.0001 Mann Whitney U
% Kruskal Wallace Test 0
1
2
3
4
5
6
7
PDT N=34 Major face N=68 All face N=170 All sites N=563
OpenHighLowClose
Pain score ordinal 1 to 6
75
FDA much tougher
• I think some Australian doctors
• Would be in serious legal trouble • If they were doing same in USA
• Australia needs to toughen up • TGA needs to have power to act • Australians need to be protected
PDT and langerhans cells? • When PDT used to treat BCCS • Epidermal langerhans cells sharply reduced • Effect sustained 24 hours
• Is this effecting anti tumour responses?
• Could this explain high recurrence rates
– When PDT used to treat cancers? • Evangelou BJD May 2012
Sentinel node
Activated Dendritic cell
T lymphocyte
Barnetson 2004 Clin & Exp Derm Kalb 2012 ## J Immunology
Mechanism of action - imiquimod
## Have their own cytotoxic properties
Langerhan’s cell dysfunction
• Does this in part explain • Why PDT has shown:
• Very high recurrence rates –When treating cancer
• Lack of cancer prevention –When treating actinic damage
That’s all folks
Anthony Dixon PhD MB BS
FACRRM
Special thanks to: • Jason Mazzurco DO • Lloyd Cleaver DO • Howard Steinman MD • Stuart Anderson MD • Ken Harvey MD • John Dixon MD
- For their totally unpaid contributions and advice towards our clinical trial on Allmedic ® PDT
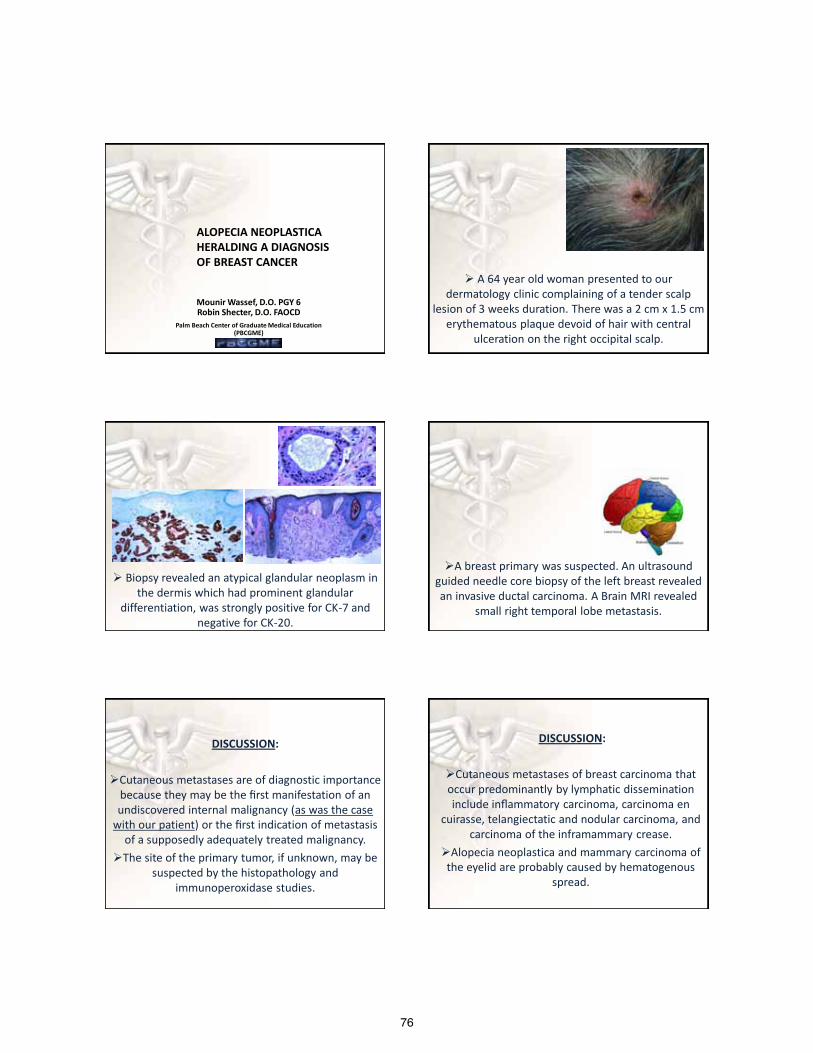
76
Mounir Wassef, D.O. PGY 6 Robin Shecter, D.O. FAOCD
Palm Beach Center of Graduate Medical Education (PBCGME)
ALOPECIA NEOPLASTICA HERALDING A DIAGNOSIS OF BREAST CANCER
A 64 year old woman presented to our dermatology clinic complaining of a tender scalp
lesion of 3 weeks duration. There was a 2 cm x 1.5 cm erythematous plaque devoid of hair with central
ulceration on the right occipital scalp.
Biopsy revealed an atypical glandular neoplasm in the dermis which had prominent glandular
differentiation, was strongly positive for CK-7 and negative for CK-20.
A breast primary was suspected. An ultrasound guided needle core biopsy of the left breast revealed an invasive ductal carcinoma. A Brain MRI revealed
small right temporal lobe metastasis.
DISCUSSION:
Cutaneous metastases are of diagnostic importance because they may be the first manifestation of an undiscovered internal malignancy (as was the case
with our patient) or the first indication of metastasis of a supposedly adequately treated malignancy.
The site of the primary tumor, if unknown, may be suspected by the histopathology and
immunoperoxidase studies.
DISCUSSION:
Cutaneous metastases of breast carcinoma that occur predominantly by lymphatic dissemination include inflammatory carcinoma, carcinoma en
cuirasse, telangiectatic and nodular carcinoma, and carcinoma of the inframammary crease.
Alopecia neoplastica and mammary carcinoma of the eyelid are probably caused by hematogenous
spread.
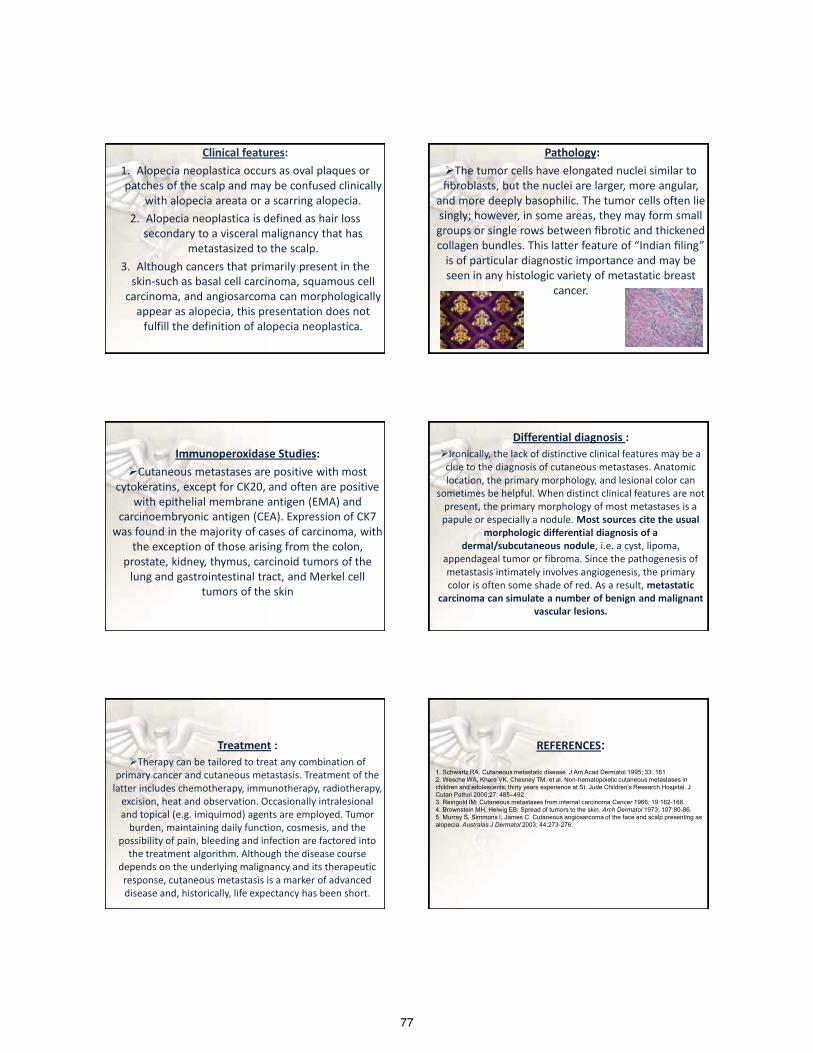
77
Clinical features: 1. Alopecia neoplastica occurs as oval plaques or patches of the scalp and may be confused clinically
with alopecia areata or a scarring alopecia. 2. Alopecia neoplastica is defined as hair loss
secondary to a visceral malignancy that has metastasized to the scalp.
3. Although cancers that primarily present in the skin-such as basal cell carcinoma, squamous cell
carcinoma, and angiosarcoma can morphologically appear as alopecia, this presentation does not
fulfill the definition of alopecia neoplastica.
Pathology: The tumor cells have elongated nuclei similar to fibroblasts, but the nuclei are larger, more angular,
and more deeply basophilic. The tumor cells often lie singly; however, in some areas, they may form small groups or single rows between fibrotic and thickened collagen bundles. This latter feature of “Indian filing”
is of particular diagnostic importance and may be seen in any histologic variety of metastatic breast
cancer.
Immunoperoxidase Studies: Cutaneous metastases are positive with most
cytokeratins, except for CK20, and often are positive with epithelial membrane antigen (EMA) and
carcinoembryonic antigen (CEA). Expression of CK7 was found in the majority of cases of carcinoma, with
the exception of those arising from the colon, prostate, kidney, thymus, carcinoid tumors of the
lung and gastrointestinal tract, and Merkel cell tumors of the skin
Differential diagnosis : Ironically, the lack of distinctive clinical features may be a
clue to the diagnosis of cutaneous metastases. Anatomic location, the primary morphology, and lesional color can
sometimes be helpful. When distinct clinical features are not present, the primary morphology of most metastases is a papule or especially a nodule. Most sources cite the usual
morphologic differential diagnosis of a dermal/subcutaneous nodule, i.e. a cyst, lipoma,
appendageal tumor or fibroma. Since the pathogenesis of metastasis intimately involves angiogenesis, the primary color is often some shade of red. As a result, metastatic
carcinoma can simulate a number of benign and malignant vascular lesions.
Treatment : Therapy can be tailored to treat any combination of
primary cancer and cutaneous metastasis. Treatment of the latter includes chemotherapy, immunotherapy, radiotherapy,
excision, heat and observation. Occasionally intralesional and topical (e.g. imiquimod) agents are employed. Tumor
burden, maintaining daily function, cosmesis, and the possibility of pain, bleeding and infection are factored into
the treatment algorithm. Although the disease course depends on the underlying malignancy and its therapeutic response, cutaneous metastasis is a marker of advanced disease and, historically, life expectancy has been short.
REFERENCES:
1. Schwartz RA. Cutaneous metastatic disease. J Am Acad Dermatol 1995; 33: 161 2. Wesche WA, Khare VK, Chesney TM, et al. Non-hematopoietic cutaneous metastases in children and adolescents: thirty years experience at St. Jude Children’s Research Hospital. J Cutan Pathol 2000;27: 485–492 3. Reingold IM: Cutaneous metastases from internal carcinoma Cancer 1966; 19:162-168. 4. Brownstein MH, Helwig EB: Spread of tumors to the skin. Arch Dermatol 1973; 107:80-86. 5. Murray S, Simmons I, James C. Cutaneous angiosarcoma of the face and scalp presenting as alopecia. Australas J Dermatol 2003; 44:273-276.
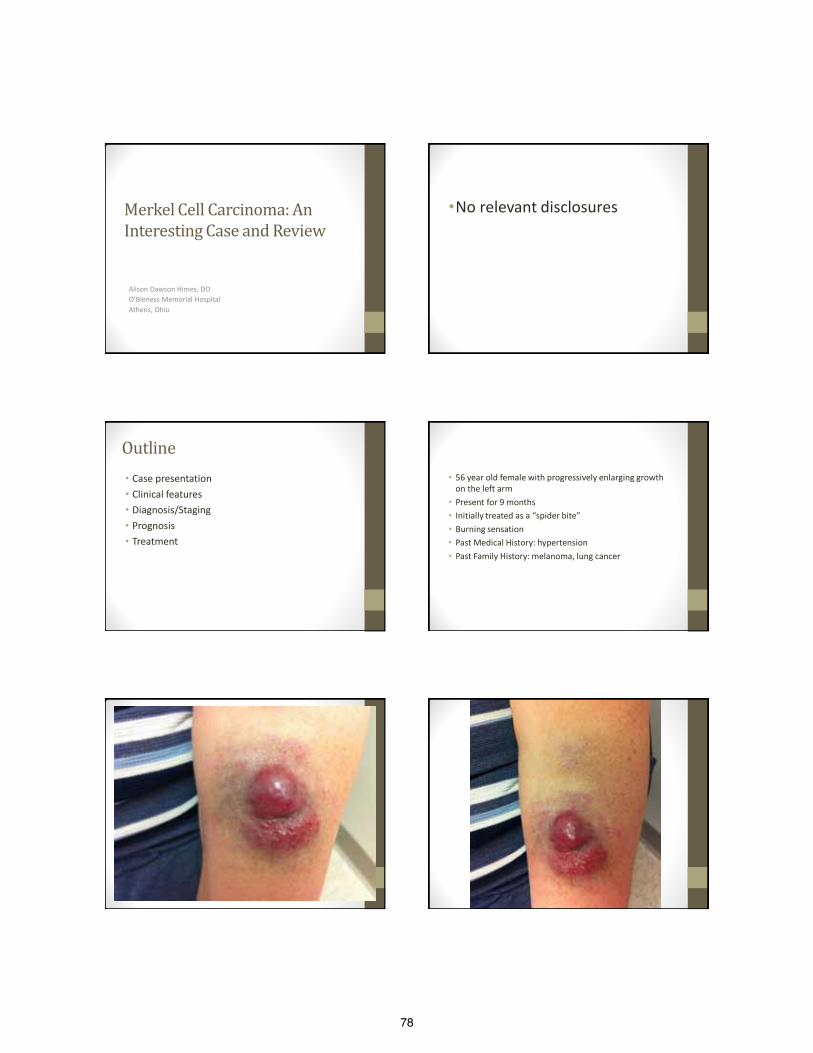
78
Merkel Cell Carcinoma: An Interesting Case and Review
Alison Dawson Himes, DO O’Bleness Memorial Hospital Athens, Ohio
•No relevant disclosures
Outline • Case presentation • Clinical features • Diagnosis/Staging • Prognosis • Treatment
• 56 year old female with progressively enlarging growth on the left arm
• Present for 9 months • Initially treated as a “spider bite” • Burning sensation • Past Medical History: hypertension • Past Family History: melanoma, lung cancer
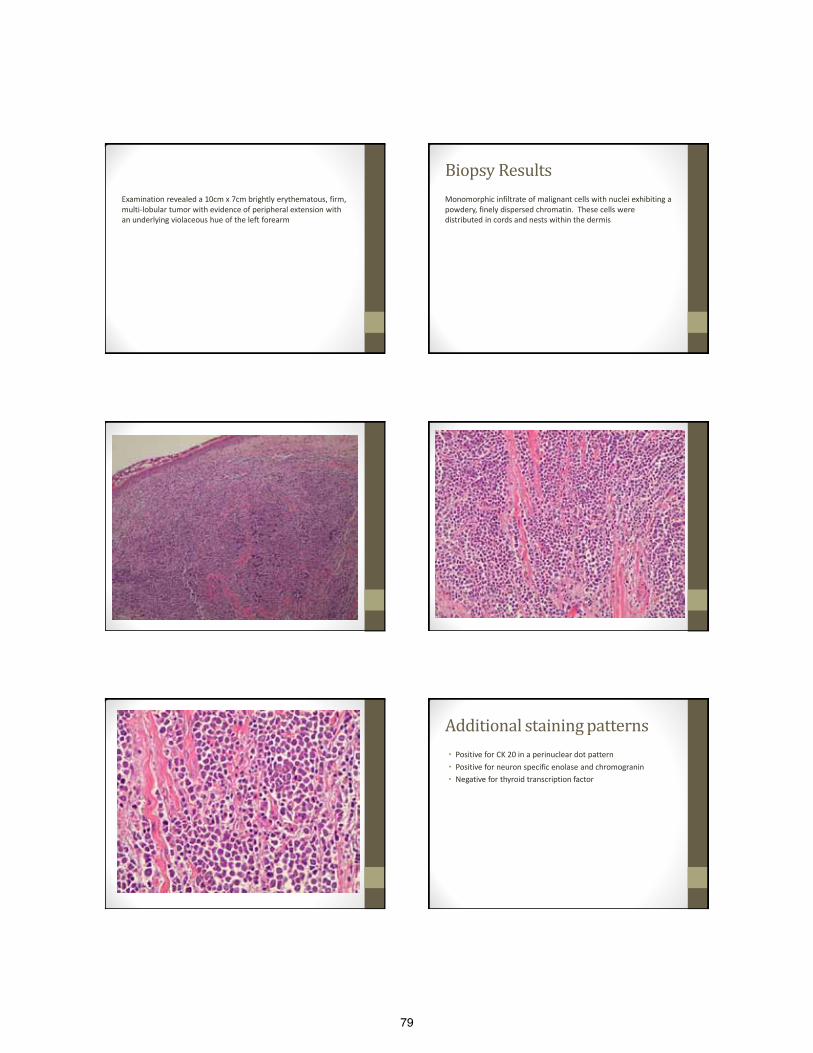
79
Examination revealed a 10cm x 7cm brightly erythematous, firm, multi-lobular tumor with evidence of peripheral extension with an underlying violaceous hue of the left forearm
Biopsy Results Monomorphic infiltrate of malignant cells with nuclei exhibiting a powdery, finely dispersed chromatin. These cells were distributed in cords and nests within the dermis
Additional staining patterns • Positive for CK 20 in a perinuclear dot pattern • Positive for neuron specific enolase and chromogranin • Negative for thyroid transcription factor
80
• Consistent with primary Merkel Cell Carcinoma • Chest and Pelvic CT scans showed no evidence of metastatic disease • Underwent radical resection and sentinel lymph node biopsy. • Evidence of lymphovascular invasion and positive left axillary
sentinel lymph node • Axillary dissection showed 2/39 positive nodes • Had external beam radiotherapy • Stage IIIa: T3, N1a, M0 • 1 year later no evidence of recurrence
Why is MCC important? • More lethal than melanoma
- 30-33% mortality (about 15% for melanoma) • Incidence is increasing
- Quadrupled since 1986 • Approximately 1500 cases a year
Merkel Cells • Discovered in 1875 by Frederick Merkel • High density on fingertips and lips • Mechanoreceptor- essential for touch • 1972 Toker described 5 cases of “trabecular carcinoma of the
skin” • 1978 Tang and Toker discovered dense core granules on EM
that were typical of Merkel cells • 1980 the name Merkel Cell Carcinoma was applied to this
tumor
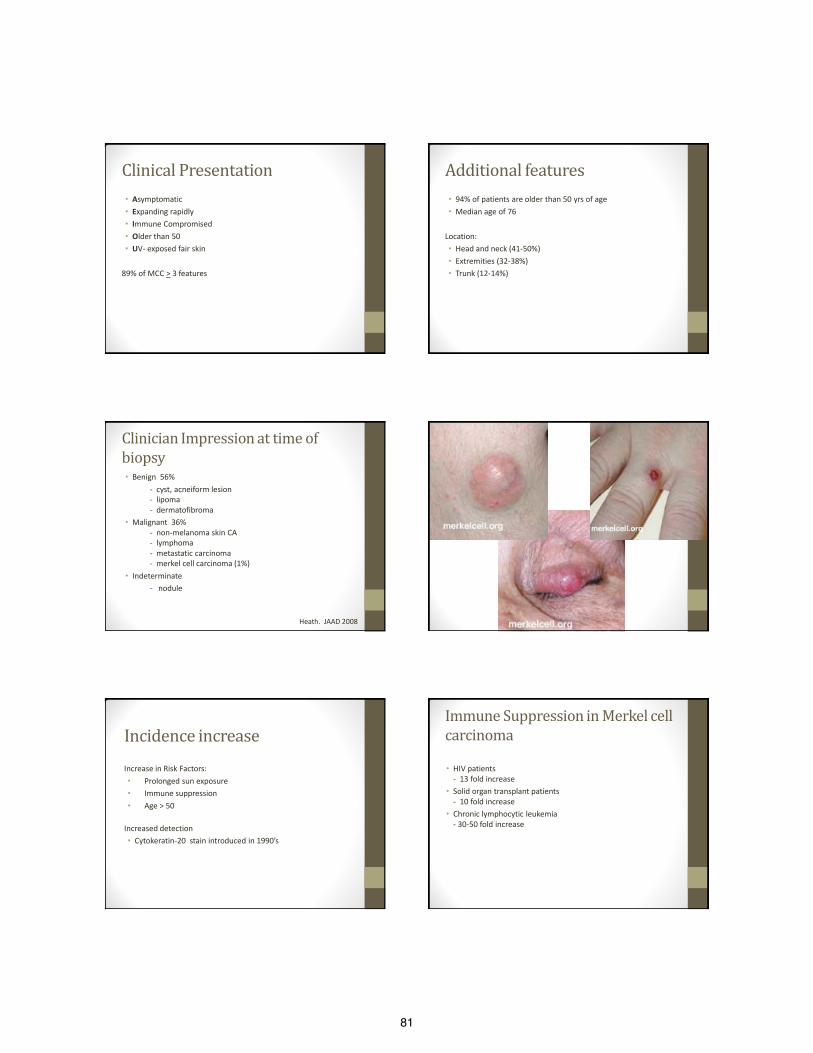
81
Clinical Presentation • Asymptomatic • Expanding rapidly • Immune Compromised • Older than 50 • UV- exposed fair skin
89% of MCC > 3 features
Additional features • 94% of patients are older than 50 yrs of age • Median age of 76
Location: • Head and neck (41-50%) • Extremities (32-38%) • Trunk (12-14%)
Clinician Impression at time of biopsy • Benign 56%
- cyst, acneiform lesion - lipoma - dermatofibroma • Malignant 36%
- non-melanoma skin CA - lymphoma - metastatic carcinoma - merkel cell carcinoma (1%)
• Indeterminate - nodule Heath. JAAD 2008
Incidence increase Increase in Risk Factors: • Prolonged sun exposure • Immune suppression • Age > 50
Increased detection • Cytokeratin-20 stain introduced in 1990’s
Immune Suppression in Merkel cell carcinoma • HIV patients
- 13 fold increase • Solid organ transplant patients
- 10 fold increase • Chronic lymphocytic leukemia
- 30-50 fold increase
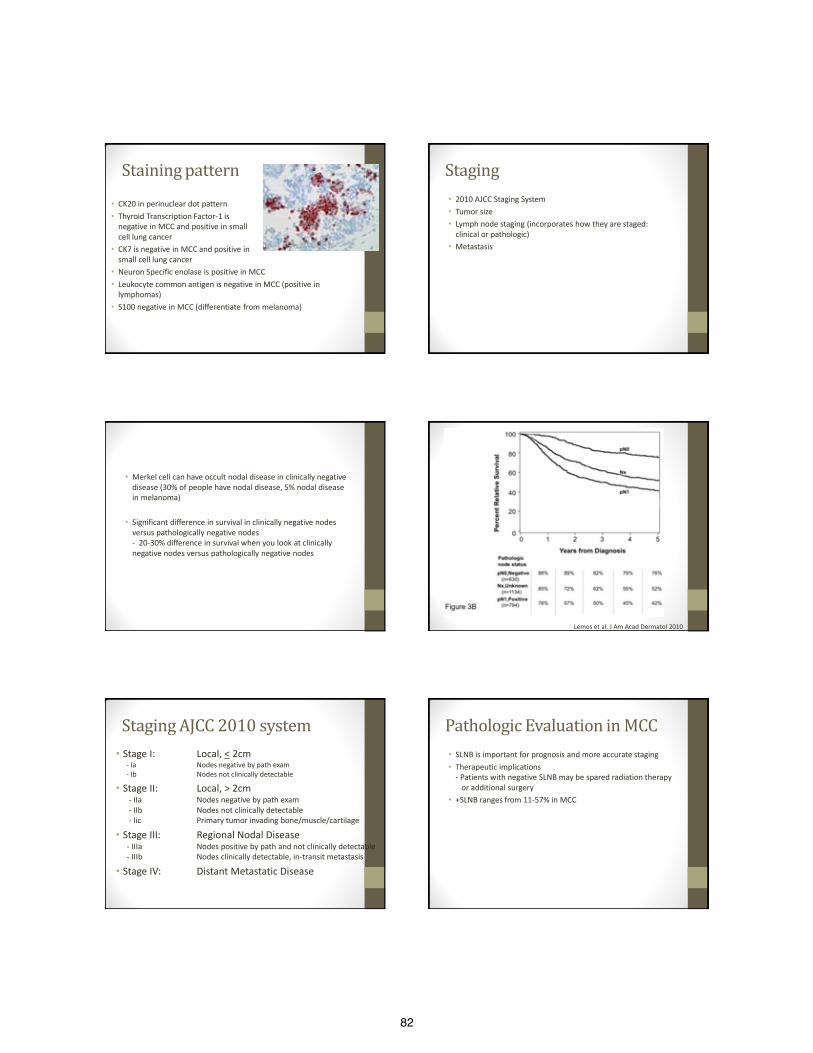
82
Staining pattern • CK20 in perinuclear dot pattern • Thyroid Transcription Factor-1 is
negative in MCC and positive in small cell lung cancer
• CK7 is negative in MCC and positive in small cell lung cancer
• Neuron Specific enolase is positive in MCC • Leukocyte common antigen is negative in MCC (positive in
lymphomas) • S100 negative in MCC (differentiate from melanoma)
Staging • 2010 AJCC Staging System • Tumor size • Lymph node staging (incorporates how they are staged:
clinical or pathologic) • Metastasis
• Merkel cell can have occult nodal disease in clinically negative disease (30% of people have nodal disease, 5% nodal disease in melanoma)
• Significant difference in survival in clinically negative nodes versus pathologically negative nodes - 20-30% difference in survival when you look at clinically negative nodes versus pathologically negative nodes
Lemos et al. J Am Acad Dermatol 2010
Staging AJCC 2010 system • Stage I: Local, < 2cm
- Ia Nodes negative by path exam - Ib Nodes not clinically detectable
• Stage II: Local, > 2cm - IIa Nodes negative by path exam - IIb Nodes not clinically detectable - Iic Primary tumor invading bone/muscle/cartilage
• Stage III: Regional Nodal Disease - IIIa Nodes positive by path and not clinically detectable - IIIb Nodes clinically detectable, in-transit metastasis
• Stage IV: Distant Metastatic Disease
Pathologic Evaluation in MCC • SLNB is important for prognosis and more accurate staging • Therapeutic implications
- Patients with negative SLNB may be spared radiation therapy or additional surgery
• +SLNB ranges from 11-57% in MCC
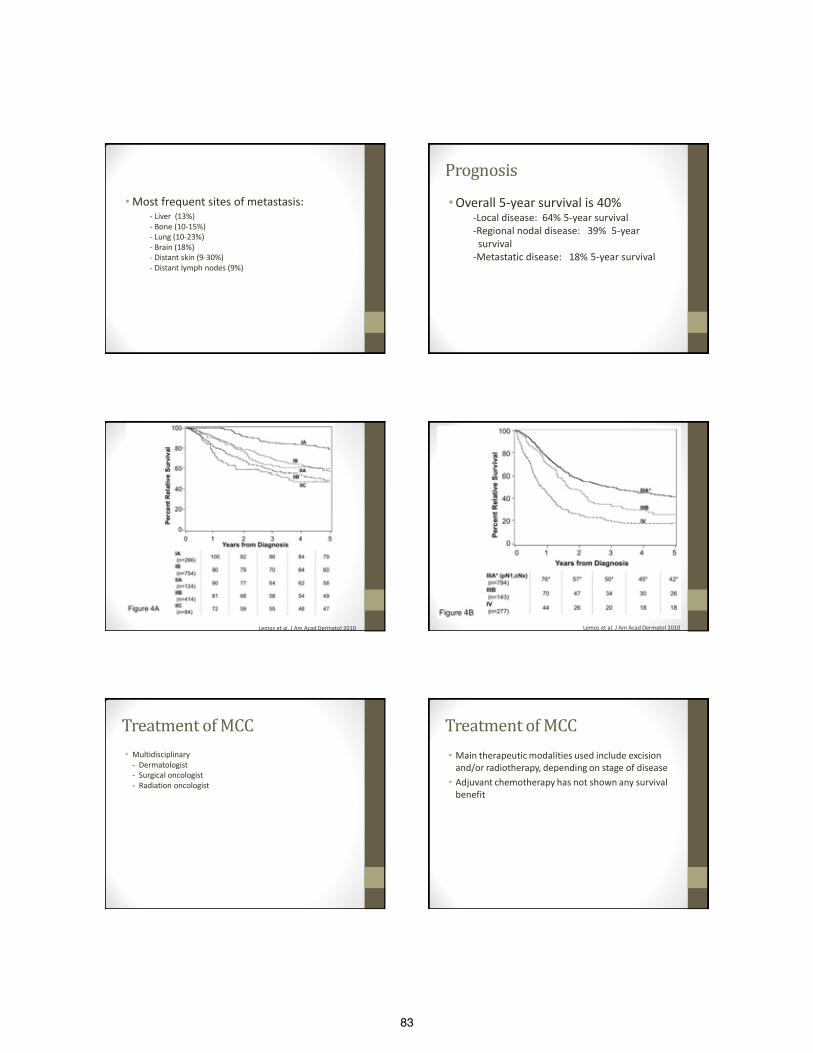
83
• Most frequent sites of metastasis: - Liver (13%) - Bone (10-15%) - Lung (10-23%) - Brain (18%) - Distant skin (9-30%) - Distant lymph nodes (9%)
Prognosis • Overall 5-year survival is 40%
-Local disease: 64% 5-year survival -Regional nodal disease: 39% 5-year survival -Metastatic disease: 18% 5-year survival
Lemos et al. J Am Acad Dermatol 2010
Lemos et al. J Am Acad Dermatol 2010
Treatment of MCC • Multidisciplinary
- Dermatologist - Surgical oncologist - Radiation oncologist
Treatment of MCC • Main therapeutic modalities used include excision
and/or radiotherapy, depending on stage of disease • Adjuvant chemotherapy has not shown any survival
benefit
84
Localized Disease with Clinically Negative nodes
• SLN biopsy and local excision of primary tumor ◦ If SLN positive: perform node dissection and/or radiation therapy. May also consider adjuvant chemotherapy ◦ If SLN negative: Consider observation or radiation therapy
• In head and neck cases where SLN is not performed, consider radiation therapy to primary site, nodal beds, and in-transit lymphatics
Clinically Positive Lymph Nodes
• Perform Fine Needle Aspiration with appropriate Immunopanel ◦ FNA positive: Clinically indicated imaging studies → If no evidence of distant metastatic disease: node dissection and/or radiation therapy. May consider adjuvant chemo ◦ FNA negative: Perform open biopsy of Lymph node → If open biopsy positive treat as above → If open biopsy negative, follow clinical negative nodal pathway
Metastatic disease • Multidisciplinary tumor board consultation • Consider any of the following therapies or combinations
of: ◦ Surgery ◦ Radiation therapy ◦ Chemotherapy
Excision of Merkel Cell • 1-2 cm margins to investing fascia of muscle or pericranium
with clear pathologic margins • Mohs technique • Modified Mohs (final margin for permanent section
assessment) • CCPDMA- Complete circumferential and peripheral deep
margin assessment
Chemotherapy in Merkel Cell • Local disease: not recommended
• Regional disease: not routinely recommended
◦ Cisplatin + etoposide ◦ Carboplatin + etoposide
• Disseminated disease: ◦ Cisplatin + etoposide ◦ Carboplatin + etoposide ◦ Topotecan ◦ Cyclophosphamide, doxorubicin, and vincristine
Follow up • Complete skin examination with lymph node
evaluation performed: ◦ Every 3-6 months for the first 2 years ◦ Annually thereafter
85
Take Home Points • MCC is an aggressive, potentially fatal neuroendocrine
carcinoma of skin • Upon presentation, it often has a benign appearance to the
physician • Remember AEIOU: Asymptomatic, Expanding rapidly, Immune
compromised, Older than 50, UV-exposed skin • Sentinel lymph node biopsy is important in
staging/determining prognosis • Excision with narrow but clear margins (carried out at the time
of SLNB) followed by adjuvant radiation therapy is a reasonable approach to management.
References • Toker C. Trabecular carcinoma of the skin. Arch of Dermatol. 1972;105:107–110. • Hodgson NC. Merkel cell carcinoma: changing incidence trends. J Surg Oncol 2005;89(1):1-4. • Kaae J, Hansen AV, Biggar RJ, Boyd HA, Moore PS, Wohlfahrt J, et al. Merkel Cell Carcinoma: Incidence, Mortality, and Risk of Other
Cancers. J Natl Cancer Inst. 2010;102:793-801. doi:10.1093/jnci/djq120 [Pub Med] • Mott RT, Smoller BR, Morgan MB. Merkel cell carcinoma: a clinicopathologic study with prognostic implications. J Cutan Pathol.
2004;31:217–23. • Heath M, Jaimes N, Lemos B, et al. Clinical characteristics of MCC at diagnosis in 195 patients: the AIEOU features. J Am Acad Dermatol.
2008;58:375–81. • Nicolaidou, E, Mikrova A, Antoniou C, Katsambas, AD. Advances in Merkel cell carcinoma pathogenesis and management: a recently
discovered virus, a new international consensus staging system and new diagnostic codes. British Journal of Dermatol. 2011;166:16-21. • Engels EA, Frisch M, Goedert JJ et al. Merkel cell carcinoma and HIV infection. Lancet 2002; 359:497-8 • Feng H, Shuda M, Chang Y, Moore PS. Clonal integration of a polyomavirus in human Merkel cell carcinoma. Science 2008; 319;1096-
100. • Wong HH, Wang J. Merkel cell carcinoma. Arch Pathol Lab Med 2010; 134:1711-16. • Bichakjian, CK, Lowe, L, Lao CD et al. Merkel cell carcinoma: critical review with guidelines for multidisciplinary management. Cancer
2007; 110:1-12. • Kontochristopoulos GJ, Stavropoulous PG, Krasagakis K et al. Differentiation between Merkel cell carcinoma and malignant melanoma:
an immunohistochemical study. Dermatology 2000; 201:123-6. • Lemos BD, Storer BE, Iyer JG et al. Pathologic nodal evaluation improves prognostic accuracy in Merkel cell carcinoma: analysis of 5823
cases as the basis of the first consensus staging system. J Am Acad Dermatol 2010; 63:751-61. • Gupta SG, Wang LC, Penas PF, Gellenthin M, Lee SJ, Nghiem P. Sentinal lymph node biopsy for evaluation and treatment of patients with
Merkel cell carcinoma: The Dana-Farber experience and meta-analysis of the literature. Arch Dermatol 2006; 142(6):685-90. • National Comprehensive Cancer Network. Clinical Practice Guidelines in Oncology. Merkel Cell Carcinoma. V.1. Fort Washington,
PA:NCCN, 2010. • Medina-Franco H, Urist MM, Fiveash J et al. Multimodality treatment of Merkel cell carcinoma: case series and literature review of 1024
cases. Ann Surg Oncol 2001;8:204-8. • Mortier L, Mirabel X, Fournier C, Piette F, Lartigau E. Radiotherapy alone for primary Merkel cell carcinoma. Arch Dermatol.
2003;139:1587-90. • Maza S, Trefzer U, Hofmann M et al. Impact of sentinal lymph node biopsy in patients with Merkel cell carcinoma: results of a
prospective study and review of the literature. Eur J Nucl Med Mol Imaging 2006; 33:433-40. • Mojica P, Smith D, Ellenhorn JDI. Adjuvant radiation therapy is associated with improved survival in Merkel cell carcinoma of the skin. J
Clin Oncol 2007; 25:1043-7. • National Comprehensive Cancer Network. Clinical Practice Guidelines in Oncology. Merkel Cell Carcinoma. V.1.2012 Fort Washington,
PA: NCCN, 2012.
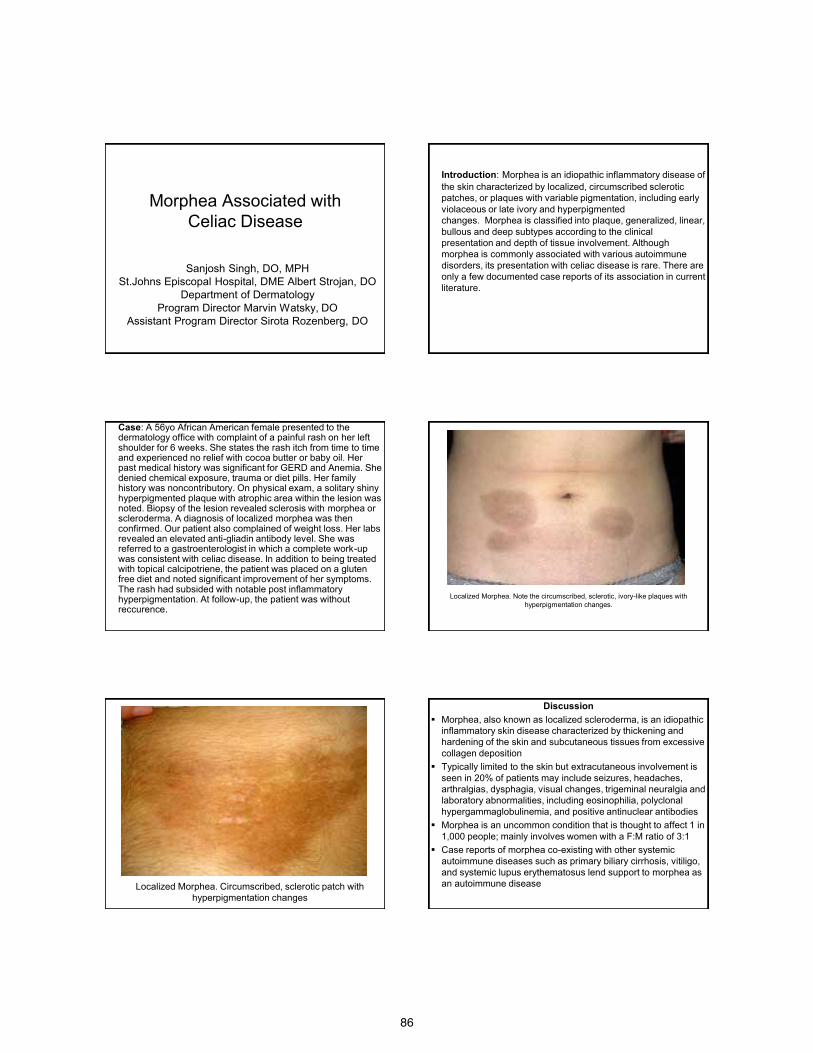
86
Morphea Associated with Celiac Disease
Sanjosh Singh, DO, MPH St.Johns Episcopal Hospital, DME Albert Strojan, DO
Department of Dermatology Program Director Marvin Watsky, DO
Assistant Program Director Sirota Rozenberg, DO
Introduction: Morphea is an idiopathic inflammatory disease of the skin characterized by localized, circumscribed sclerotic patches, or plaques with variable pigmentation, including early violaceous or late ivory and hyperpigmented changes. Morphea is classified into plaque, generalized, linear, bullous and deep subtypes according to the clinical presentation and depth of tissue involvement. Although morphea is commonly associated with various autoimmune disorders, its presentation with celiac disease is rare. There are only a few documented case reports of its association in current literature.
Case: A 56yo African American female presented to the dermatology office with complaint of a painful rash on her left shoulder for 6 weeks. She states the rash itch from time to time and experienced no relief with cocoa butter or baby oil. Her past medical history was significant for GERD and Anemia. She denied chemical exposure, trauma or diet pills. Her family history was noncontributory. On physical exam, a solitary shiny hyperpigmented plaque with atrophic area within the lesion was noted. Biopsy of the lesion revealed sclerosis with morphea or scleroderma. A diagnosis of localized morphea was then confirmed. Our patient also complained of weight loss. Her labs revealed an elevated anti-gliadin antibody level. She was referred to a gastroenterologist in which a complete work-up was consistent with celiac disease. In addition to being treated with topical calcipotriene, the patient was placed on a gluten free diet and noted significant improvement of her symptoms. The rash had subsided with notable post inflammatory hyperpigmentation. At follow-up, the patient was without reccurence.
Localized Morphea. Note the circumscribed, sclerotic, ivory-like plaques with hyperpigmentation changes.
Localized Morphea. Circumscribed, sclerotic patch with hyperpigmentation changes
Discussion Morphea, also known as localized scleroderma, is an idiopathic
inflammatory skin disease characterized by thickening and hardening of the skin and subcutaneous tissues from excessive collagen deposition
Typically limited to the skin but extracutaneous involvement is seen in 20% of patients may include seizures, headaches, arthralgias, dysphagia, visual changes, trigeminal neuralgia and laboratory abnormalities, including eosinophilia, polyclonal hypergammaglobulinemia, and positive antinuclear antibodies
Morphea is an uncommon condition that is thought to affect 1 in 1,000 people; mainly involves women with a F:M ratio of 3:1
Case reports of morphea co-existing with other systemic autoimmune diseases such as primary biliary cirrhosis, vitiligo, and systemic lupus erythematosus lend support to morphea as an autoimmune disease
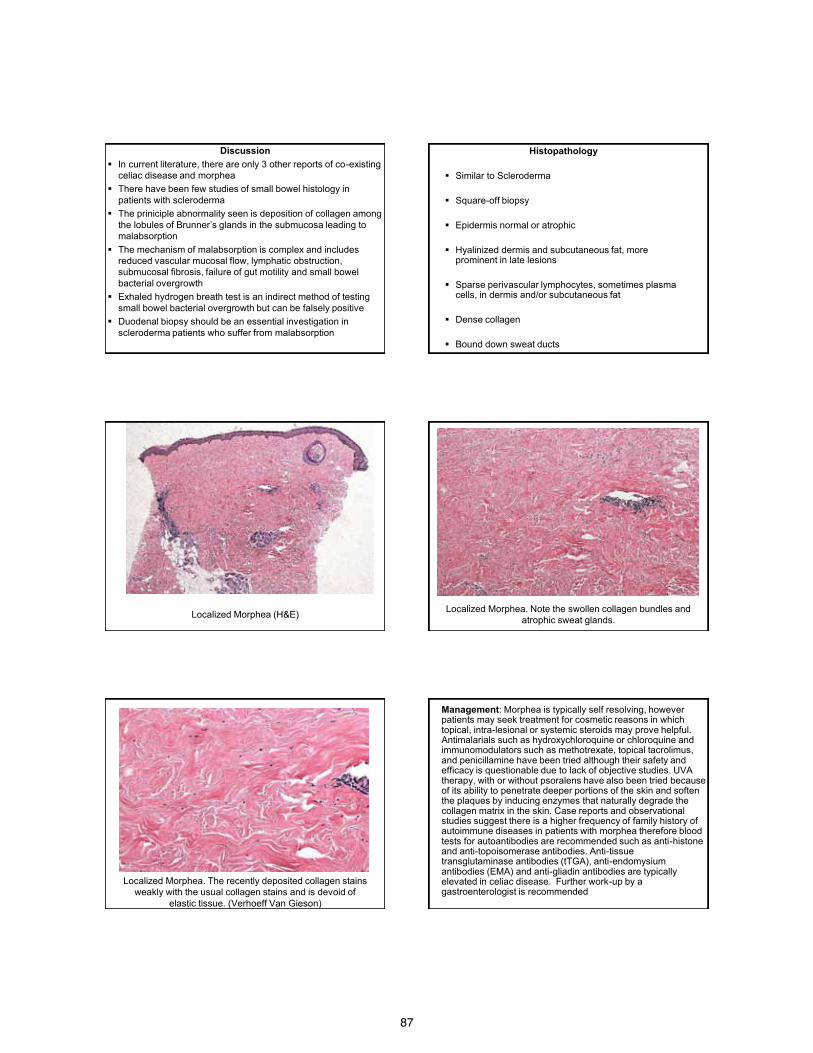
87
Discussion In current literature, there are only 3 other reports of co-existing
celiac disease and morphea There have been few studies of small bowel histology in
patients with scleroderma The priniciple abnormality seen is deposition of collagen among
the lobules of Brunner’s glands in the submucosa leading to malabsorption
The mechanism of malabsorption is complex and includes reduced vascular mucosal flow, lymphatic obstruction, submucosal fibrosis, failure of gut motility and small bowel bacterial overgrowth
Exhaled hydrogen breath test is an indirect method of testing small bowel bacterial overgrowth but can be falsely positive
Duodenal biopsy should be an essential investigation in scleroderma patients who suffer from malabsorption
Histopathology
Similar to Scleroderma Square-off biopsy
Epidermis normal or atrophic
Hyalinized dermis and subcutaneous fat, more
prominent in late lesions
Sparse perivascular lymphocytes, sometimes plasma cells, in dermis and/or subcutaneous fat
Dense collagen
Bound down sweat ducts
Localized Morphea (H&E) Localized Morphea. Note the swollen collagen bundles and atrophic sweat glands.
Localized Morphea. The recently deposited collagen stains weakly with the usual collagen stains and is devoid of
elastic tissue. (Verhoeff Van Gieson)
Management: Morphea is typically self resolving, however patients may seek treatment for cosmetic reasons in which topical, intra-lesional or systemic steroids may prove helpful. Antimalarials such as hydroxychloroquine or chloroquine and immunomodulators such as methotrexate, topical tacrolimus, and penicillamine have been tried although their safety and efficacy is questionable due to lack of objective studies. UVA therapy, with or without psoralens have also been tried because of its ability to penetrate deeper portions of the skin and soften the plaques by inducing enzymes that naturally degrade the collagen matrix in the skin. Case reports and observational studies suggest there is a higher frequency of family history of autoimmune diseases in patients with morphea therefore blood tests for autoantibodies are recommended such as anti-histone and anti-topoisomerase antibodies. Anti-tissue transglutaminase antibodies (tTGA), anti-endomysium antibodies (EMA) and anti-gliadin antibodies are typically elevated in celiac disease. Further work-up by a gastroenterologist is recommended

88
References
1) Firoz E et al. Morphea, Diabete Mellitus Type 1, and Celiac Disease: Case Report and Review of the Literature. Pediatric Dermatology. 2010 Vol. 27 No.1 48-52
2) James WD, Berger TG, Elston DM. Andrews’ Diseases of the Skin Clinical Dermatology. 10th Ed. Philadelphia, PA: Elsevier Inc Publisher, 2006. pg.171-175
3) JL Bolognia, JL Jorizzo, RP Rapini. Dermatology. 2nd Ed. Spain: Elsevier Limited Publisher, 2003. pg. 1469-76
4) Marguerie C et al. Malabsorption caused by celiac disease in patients who have scleroderma. Br J Rheumatol. 1995 Sep;34(9):858-61
5) Rapini RP. Practical Dermatopathology. 1st Ed. Philadelphia, PA: Elsevier Inc Publisher, 2005. pg.132
6) Sheehan NJ, Stanton-King K. Co-existent celiac disease and scleroderma. Br J Rheumatol. 1996 Aug;35(8):807

89
Psoriasis in Lines of Blaschko
Charlotte Noorollah DO St Johns Episcopal Hospital, South Shore
Far Rockaway New York Program Directors: Marvin Watsky DO, Suzanne Sirota
Rozenberg DO
Case Presentation
• A 17-year-old female presented with a 3-month history of an eruption limited to her right arm, shoulder and chest
• She admitted to mild itching but denied pain, or constitutional symptoms
• Review of systems was non-contributory
Case Presentation
• PMHX: Non-Contributory • PSHX: Non-Contributory • Family Hx: She denied any personal or family
history of psoriasis • She was not on any medications prior to the onset
of the rash
Case Presentation
Case Presentation
• Differential diagnosis at the time of presentation included:
• Psoriasis • Inflammatory linear verrucous epidermal nevus
(ILVEN) • Linear lichen planus
Histopathology
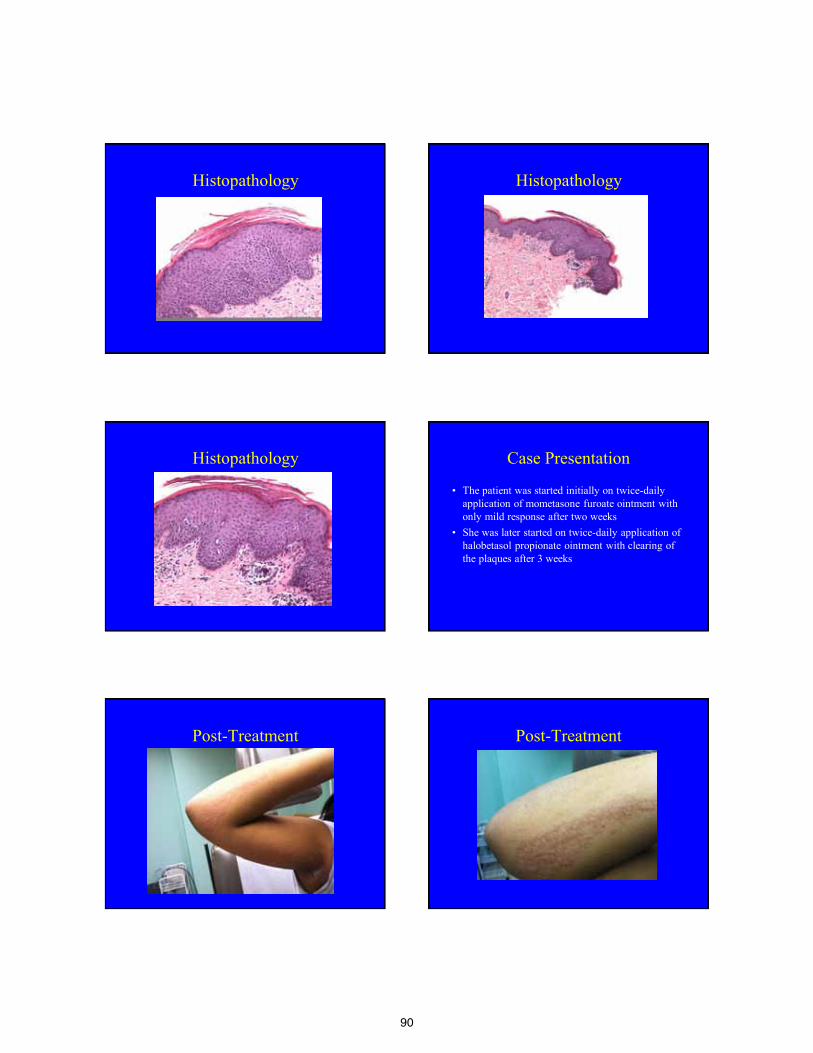
90
Histopathology Histopathology
Histopathology Case Presentation
• The patient was started initially on twice-daily application of mometasone furoate ointment with only mild response after two weeks
• She was later started on twice-daily application of halobetasol propionate ointment with clearing of the plaques after 3 weeks
Post-Treatment Post-Treatment
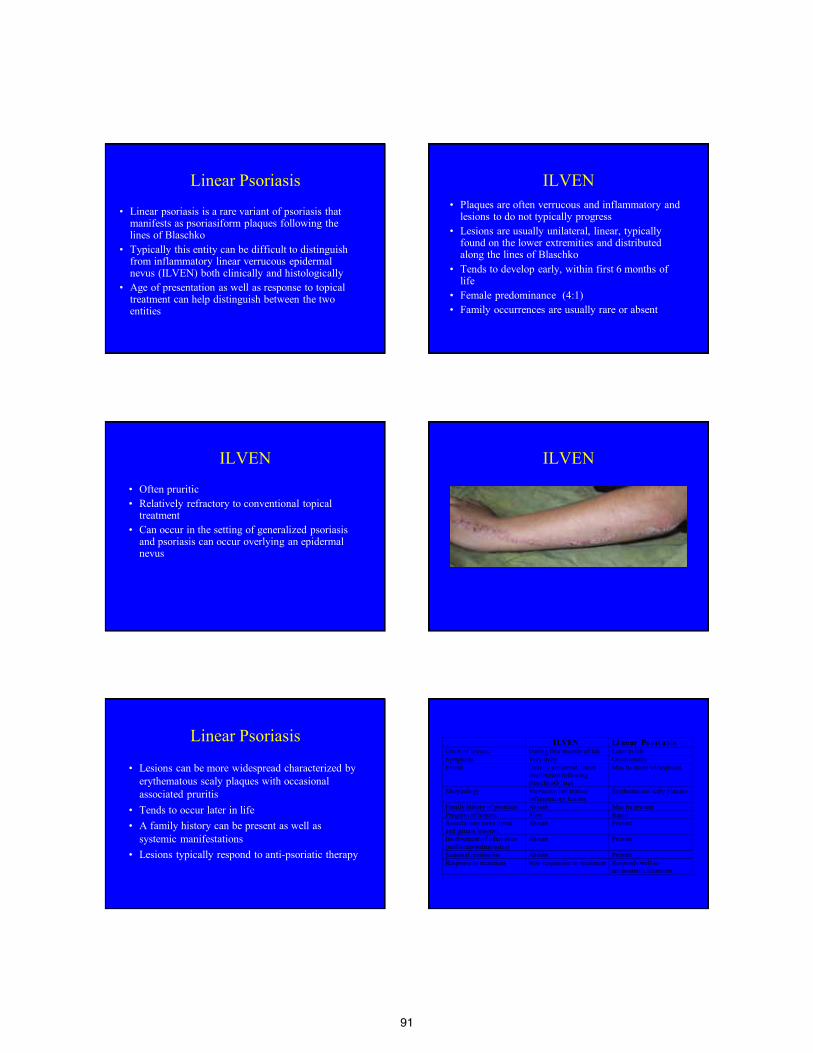
91
Linear Psoriasis
• Linear psoriasis is a rare variant of psoriasis that manifests as psoriasiform plaques following the lines of Blaschko
• Typically this entity can be difficult to distinguish from inflammatory linear verrucous epidermal nevus (ILVEN) both clinically and histologically
• Age of presentation as well as response to topical treatment can help distinguish between the two entities
ILVEN
• Plaques are often verrucous and inflammatory and lesions to do not typically progress
• Lesions are usually unilateral, linear, typically found on the lower extremities and distributed along the lines of Blaschko
• Tends to develop early, within first 6 months of life
• Female predominance (4:1) • Family occurrences are usually rare or absent
ILVEN
• Often pruritic • Relatively refractory to conventional topical
treatment • Can occur in the setting of generalized psoriasis
and psoriasis can occur overlying an epidermal nevus
ILVEN
•
Linear Psoriasis
• Lesions can be more widespread characterized by erythematous scaly plaques with occasional associated pruritis
• Tends to occur later in life • A family history can be present as well as
systemic manifestations • Lesions typically respond to anti-psoriatic therapy
ILVEN Li near Ps ori asis Onset of lesions During first months of life Later in life Symptoms Very itchy Occasionally Extent Usually unilateral, linear
distribution following BlaschkoÕs lines
May be more widespread
Morphology Verrucous infiltrative inflammatory lesions
Erythematous scaly plaques
Family history of psoriasis Absent May be present Progress of lesions Slow Rapid Associations (sore throat and guttate lesions)
Absent Present
Involvement of other sites (nail/scalp/palms/soles)
Absent Present
Seasonal remissions Absent Present Response to treatment Non-responsive to treatment Responds well to
antipsoriatic treatment
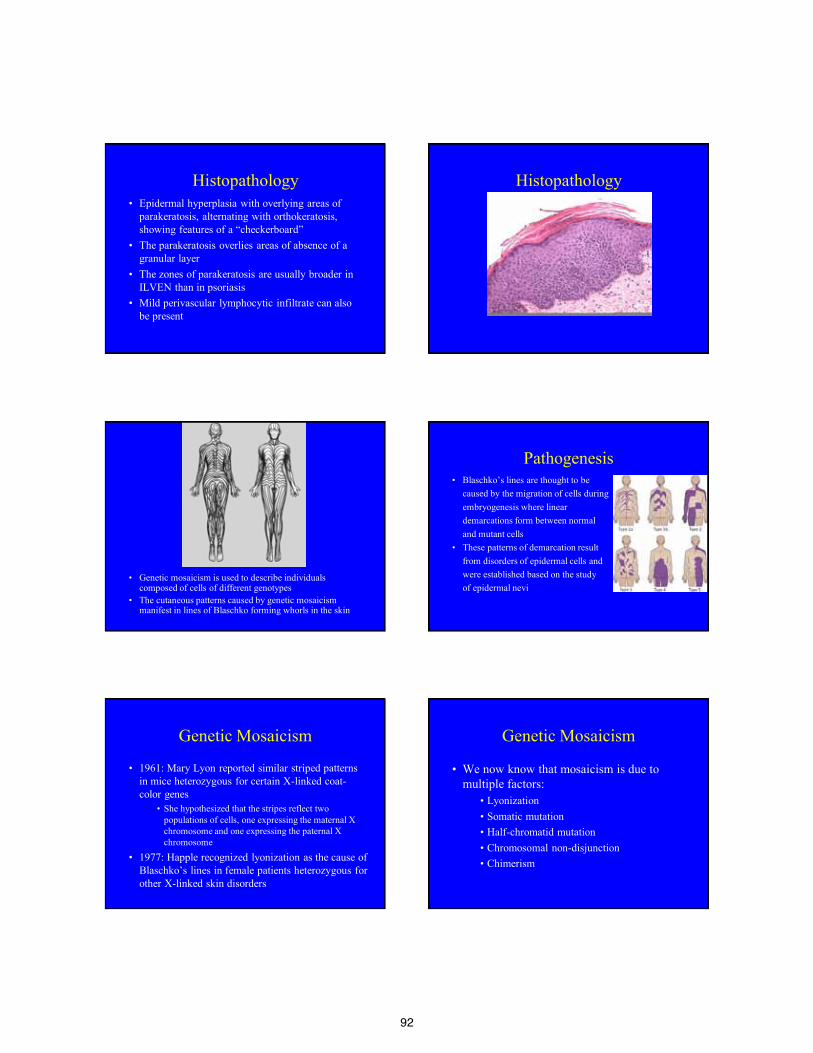
92
Histopathology • Epidermal hyperplasia with overlying areas of
parakeratosis, alternating with orthokeratosis, showing features of a “checkerboard”
• The parakeratosis overlies areas of absence of a granular layer
• The zones of parakeratosis are usually broader in ILVEN than in psoriasis
• Mild perivascular lymphocytic infiltrate can also be present
Histopathology
• Genetic mosaicism is used to describe individuals composed of cells of different genotypes
• The cutaneous patterns caused by genetic mosaicism manifest in lines of Blaschko forming whorls in the skin
Pathogenesis • Blaschko’s lines are thought to be caused by the migration of cells during embryogenesis where linear demarcations form between normal and mutant cells • These patterns of demarcation result from disorders of epidermal cells and were established based on the study of epidermal nevi
Genetic Mosaicism
• 1961: Mary Lyon reported similar striped patterns in mice heterozygous for certain X-linked coat-color genes
• She hypothesized that the stripes reflect two populations of cells, one expressing the maternal X chromosome and one expressing the paternal X chromosome
• 1977: Happle recognized lyonization as the cause of Blaschko’s lines in female patients heterozygous for other X-linked skin disorders
Genetic Mosaicism
• We now know that mosaicism is due to multiple factors:
• Lyonization • Somatic mutation • Half-chromatid mutation • Chromosomal non-disjunction • Chimerism

93
Cutaneous Mosaicism
• Cutaneous manifestations are determined by cell migration which is dependent on the stage of development at which mosaicism occurs
• The earlier the mutation, the more widely distributed the mosaic clone and the longer the lines of migration
Cutaneous Mosaicism
• Embryonic keratinocytes: move outwards from the neural crest and proliferate forming a continuous line and cutaneous patterns form based on cell migration and surface remodeling
• Melanoblasts: move outwards by single cell migration and proliferate at or before birth locally in the skin
Pathogenesis
• It is thought that that a linear clone of psoriasis is characterized by a susceptibility mutation that gives rise to the clinically linear appearance of the lesions
Pathogenesis
• Linear psoriasis is a multifactorial inflammatory disorder with autosomal dominant or polygenic inheritance
• ILVEN is a presumed autosomal dominant lethal disorder “rescued” by mosaicism and thus never seen in a generalized form
Immunohistochemistry
• Keratin 10 and Ki-67 positive nuclei are markers for epidermal differentiation
• There tends to be a lower expression of Keratin 10 in psoriasis as compared to those levels found in ILVEN
• Reduced number of Ki-67 positive nuclei in ILVEN as compared to psoriasis
94
Immunohistochemistry
• Assessment of elastase-positive cells can also be helpful in differentiating between ILVEN and linear psoriasis
Immunohistochemistry • De Jong et al sought to assess inflammation, proliferation
and keratinization in ILVEN and linear psoriasis by using immunohistochemical studies
• In ILVEN, they observed: • Low occurrence of elastase-positive cells (PMN) • Focal staining pattern of Ks8.2 (anti-keratin 16) • Homogeneous pattern distribution of RKSE60 (anti-
keratin 10)
• In psoriasis: • Occurrence of elastase-positive cells were more
substantial
Role of T Lymphocytes • Psoriasis is a disorder activated by T lymphocyte
production • Visser et al sought to analyze T lymphocyte
subsets to help distinguish between ILVEN and psoriasis
• They compared the number and composition of the T lymphocyte infiltrate of patients with ILVEN without any associated psoriasis and those with psoriasis
Role of T Lymphocytes
• The authors found that T-cell subsets important in the pathogenesis of psoriasis are reduced in ILVEN as compared to psoriasis; specifically CD8, CD45RO, CD2, CD94, and CD161
Human leukocyte antigen • Human leukocyte antigen (HLA) Cw6 A2 has
been found to be associated with linear psoriasis • Magalhaes et al described two cases of linear
psoriasis in Brazilian children with specific HLA class I-associated alleles
• They proposed that the HLA class I allele findings in patients with linear psoriasis differ from those in early onset psoriasis
Human leukocyte antigen
• Differences suggest that linear psoriatic lesions may represent cellular mosaicism where cells within those areas react differently due to chromosomal differences from their surrounding cells
95
Treatment • Typical treatment options for linear psoriasis are
the same as those used for generalized psoriasis including:
• Topical steroid treatment • Keratolytics • Calcipotriol • Narrow-band ultraviolet B phototherapy
Treatment
• Systemic agents such as Acitretin, Methotrexate, or TNF inhibitors can be helpful for long-standing or refractory cases
Conclusion
• Psoriasis occurring in a blaschkoid distribution is a rare entity
• Distinguishing it from ILVEN both clinically and histologically can often be difficult
• Later onset of presentation and response to anti-psoriatic treatment can often help the clinician to differentiate between the two conditions
References • Purohit S, Kanodia S, Shukla SR. Linear Psoriasis. Indian J Dermatology and Leprology. 2006 Sep-
Oct;72(5):398. • Li, Wei, and Xiao Yong Man. "Linear Psoriasis." Canadian Medical Association Journal 184.7
(2012): 789. Print. • Weedon, David, Geoffrey Strutton, Adam I. Rubin, and David Weedon. Weedon's Skin Pathology.
3rd ed. [Edinburgh]: Churchill Livingstone/Elsevier, 2010. Print. • De Jong, EM, Rulo, HF and PCM Van De Kerkhof. "Inflammatory Linear Verrucous Epidermal
Nevus (ILVEN) Versus Linear Psoriasis." Arch Derm Venereol 71.4 (1991): 343-46. Print. • Saraswat, Abir, Kamaldeep Sandhu, Rajeev Shukla, and Sanjeev Handa. "Unilateral Linear Psoriasis
with Palmoplantar, Nail, and Scalp Involvement." Pediatric Dermatology 21.1 (2004): 70-73. Print. • Bolognia, Jean, Joseph L. Jorizzo, and Ronald P. Rapini. Dermatology. 2nd ed. Vol. One. [St. Louis,
Mo.]: Mosby/Elsevier, 2008. Print. • Busam, KJ. "Tumors of the Epidermis." Dermatopathology. [Philadelphia]: Saunders/Elsevier, 333-
38. 2010. Print. • Barnhill, Raymond L. Dermatopathology. 3rd ed. New York: McGraw-Hill Medical, 2010. Print. • Brinca, Ana, F. Santiago, and D. Serra. "Linear Psoriasis - A Case Report." Case Reports in
Dermatology 3 (2011): 8-12. UK Pubmed Central. Web. • Chien, Peter, Karla Rosenman, and Wang Cheung. "Linear Psoriasis." Dermatology Online Journal
4th ser. 15.8 (2009): Web. • Vissers, W. H., L. Muys, and P. E. Erp. "Immunohistochemical Differentiation between
Inflammatory Linear Verrucous Epidermal Nevus (ILVEN) and Psoriasis." European Journal of Dermatology 14.4 (2004): 216-20. Print.
• Magalhaes, RF, et al. Linear Psoriasis in Brazilian children and HLA haplotypes. Journal European Academy of Dermatology and Venerology. 2007; 21:1439. Print
• Raza N, Iqbal P, Anwer J. 填nilateral Psoriass along Blaschko Lines�. Journal Aub Med Coll Abottabad. 2005 Jan-Mar;17(1):87-8.
THANK YOU
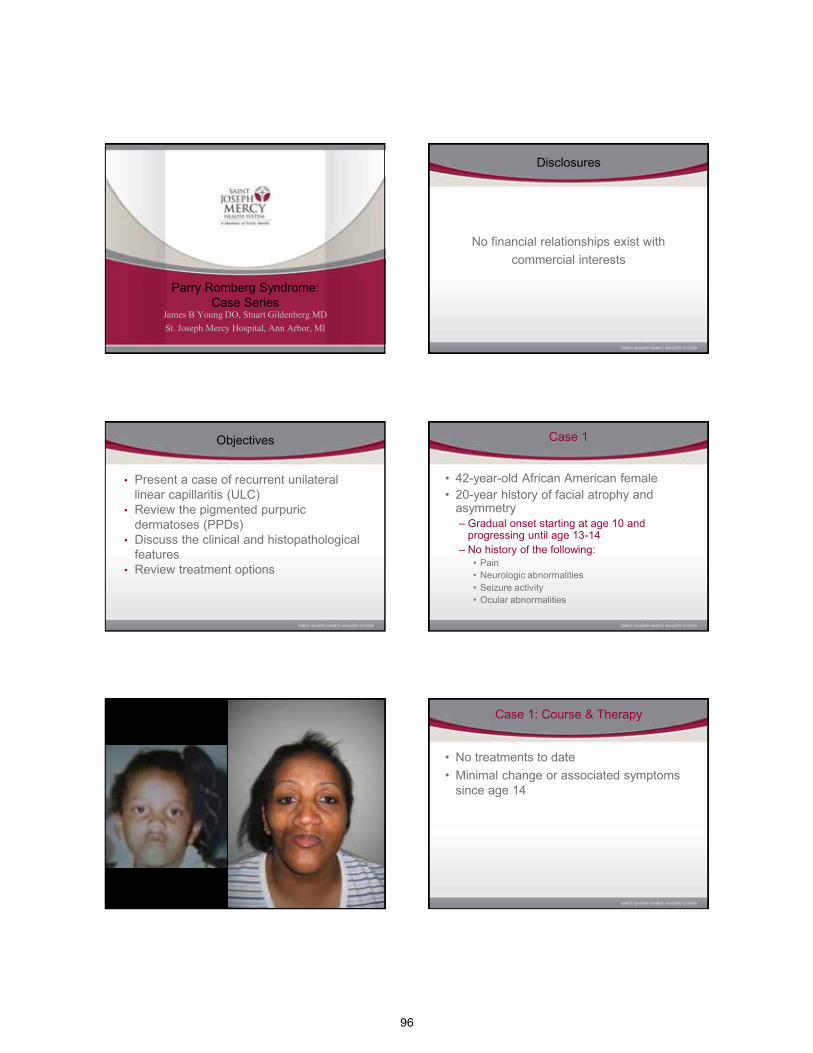
96
Parry Romberg Syndrome: Case Series
James B Young DO, Stuart Gildenberg MD St. Joseph Mercy Hospital, Ann Arbor, MI
AOCD Annual Meeting Wednesday, November 2, 2011
Disclosures
No financial relationships exist with commercial interests
Objectives
• Present a case of recurrent unilateral linear capillaritis (ULC)
• Review the pigmented purpuric dermatoses (PPDs)
• Discuss the clinical and histopathological features
• Review treatment options
Case 1
• 42-year-old African American female • 20-year history of facial atrophy and
asymmetry – Gradual onset starting at age 10 and
progressing until age 13-14 – No history of the following:
• Pain • Neurologic abnormalities • Seizure activity • Ocular abnormalities
Case 1: Course & Therapy
• No treatments to date • Minimal change or associated symptoms
since age 14
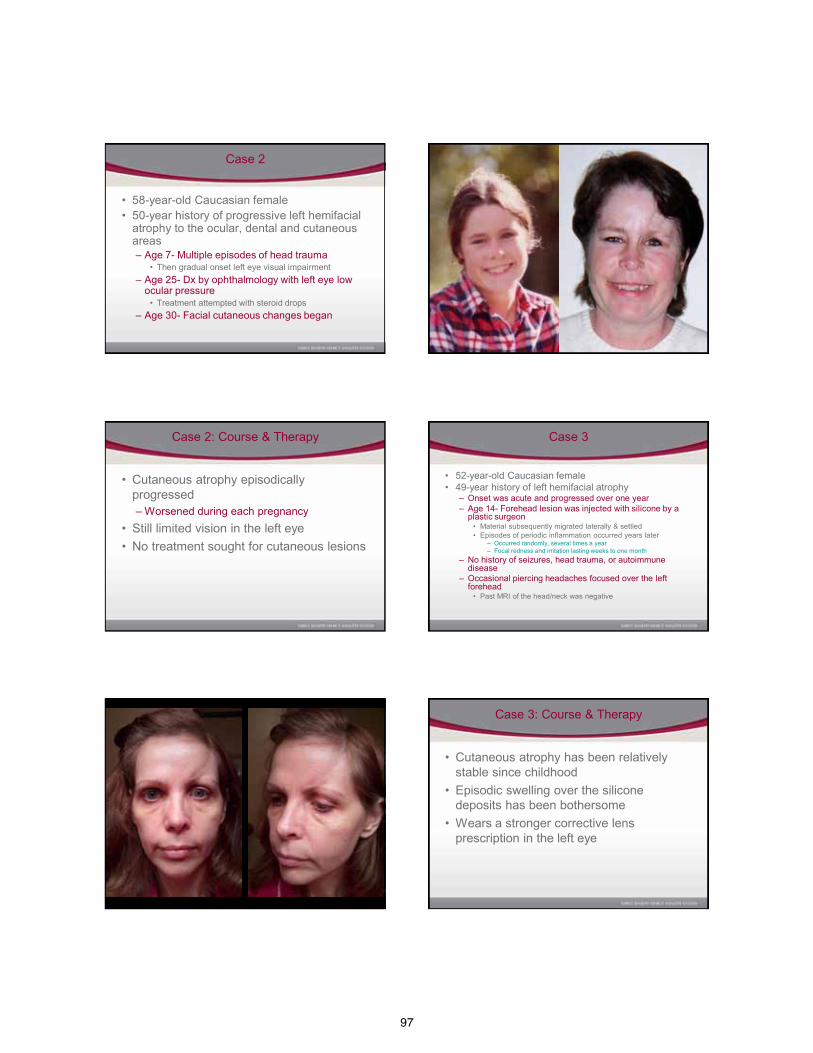
97
Case 2
• 58-year-old Caucasian female • 50-year history of progressive left hemifacial
atrophy to the ocular, dental and cutaneous areas – Age 7- Multiple episodes of head trauma
• Then gradual onset left eye visual impairment – Age 25- Dx by ophthalmology with left eye low
ocular pressure • Treatment attempted with steroid drops
– Age 30- Facial cutaneous changes began
Case 2: Course & Therapy
• Cutaneous atrophy episodically progressed – Worsened during each pregnancy
• Still limited vision in the left eye • No treatment sought for cutaneous lesions
Case 3
• 52-year-old Caucasian female • 49-year history of left hemifacial atrophy
– Onset was acute and progressed over one year – Age 14- Forehead lesion was injected with silicone by a
plastic surgeon • Material subsequently migrated laterally & settled • Episodes of periodic inflammation occurred years later
– Occurred randomly, several times a year – Focal redness and irritation lasting weeks to one month
– No history of seizures, head trauma, or autoimmune disease
– Occasional piercing headaches focused over the left forehead
• Past MRI of the head/neck was negative
Case 3: Course & Therapy
• Cutaneous atrophy has been relatively stable since childhood
• Episodic swelling over the silicone deposits has been bothersome
• Wears a stronger corrective lens prescription in the left eye
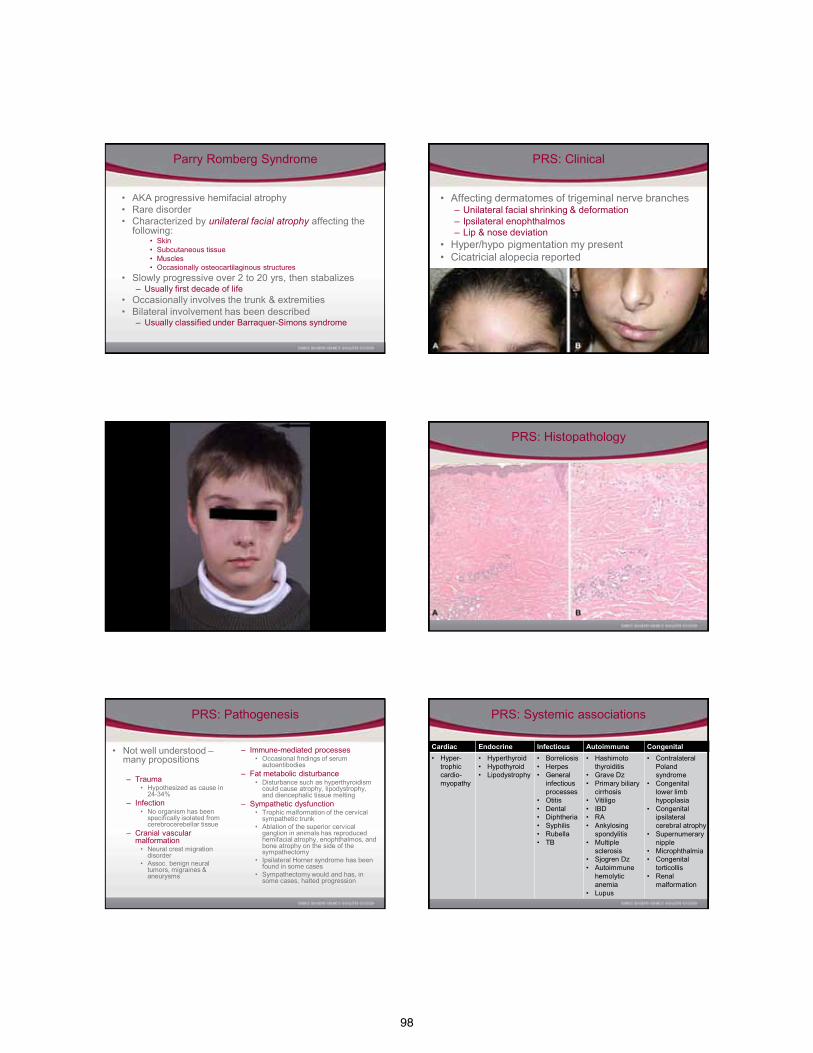
98
Parry Romberg Syndrome
• AKA progressive hemifacial atrophy • Rare disorder • Characterized by unilateral facial atrophy affecting the
following: • Skin • Subcutaneous tissue • Muscles • Occasionally osteocartilaginous structures
• Slowly progressive over 2 to 20 yrs, then stabalizes – Usually first decade of life
• Occasionally involves the trunk & extremities • Bilateral involvement has been described
– Usually classified under Barraquer-Simons syndrome
PRS: Clinical
• Affecting dermatomes of trigeminal nerve branches – Unilateral facial shrinking & deformation – Ipsilateral enophthalmos – Lip & nose deviation
• Hyper/hypo pigmentation my present • Cicatricial alopecia reported
PRS: Histopathology
PRS: Pathogenesis
• Not well understood – many propositions
– Trauma
• Hypothesized as cause in 24-34%
– Infection • No organism has been
specifically isolated from cerebrocerebellar tissue
– Cranial vascular malformation
• Neural crest migration disorder
• Assoc. benign neural tumors, migraines & aneurysms
– Immune-mediated processes • Occasional findings of serum
autoantibodies – Fat metabolic disturbance
• Disturbance such as hyperthyroidism could cause atrophy, lipodystrophy, and diencephalic tissue melting
– Sympathetic dysfunction • Trophic malformation of the cervical
sympathetic trunk • Ablation of the superior cervical
ganglion in animals has reproduced hemifacial atrophy, enophthalmos, and bone atrophy on the side of the sympathectomy
• Ipsilateral Horner syndrome has been found in some cases
• Sympathectomy would and has, in some cases, halted progression
PRS: Systemic associations
Cardiac Endocrine Infectious Autoimmune Congenital • Hyper-
trophic cardio-myopathy
• Hyperthyroid • Hypothyroid • Lipodystrophy
• Borreliosis • Herpes • General
infectious processes
• Otitis • Dental • Diphtheria • Syphilis • Rubella • TB
• Hashimoto thyroiditis
• Grave Dz • Primary biliary
cirrhosis • Vitiligo • IBD • RA • Ankylosing
spondylitis • Multiple
sclerosis • Sjogren Dz • Autoimmune
hemolytic anemia
• Lupus
• Contralateral Poland syndrome
• Congenital lower limb hypoplasia
• Congenital ipsilateral cerebral atrophy
• Supernumerary nipple
• Microphthalmia • Congenital
torticollis • Renal
malformation
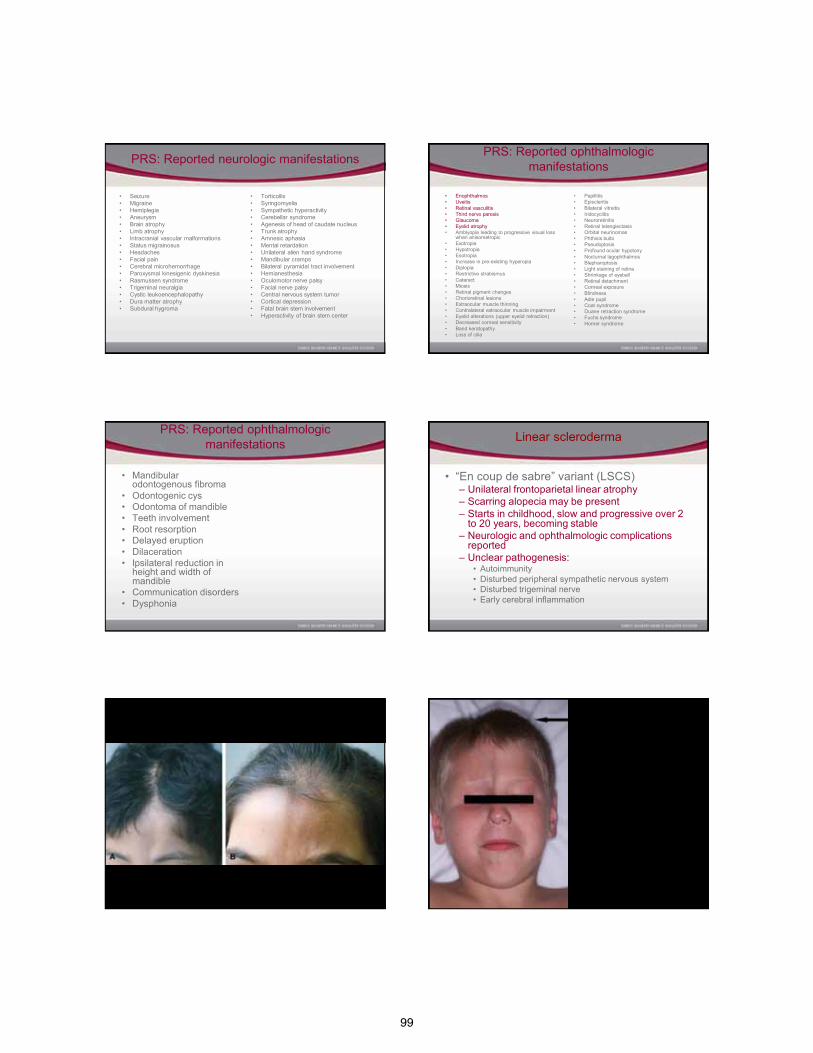
99
PRS: Reported neurologic manifestations
• Seizure • Migraine • Hemiplegia • Aneurysm • Brain atrophy • Limb atrophy • Intracranial vascular malformations • Status migrainosus • Headaches • Facial pain • Cerebral microhemorrhage • Paroxysmal kinesigenic dyskinesia • Rasmussen syndrome • Trigeminal neuralgia • Cystic leukoencephalopathy • Dura matter atrophy • Subdural hygroma
• Torticollis • Syringomyelia • Sympathetic hyperactivity • Cerebellar syndrome • Agenesis of head of caudate nucleus • Trunk atrophy • Amnesic aphasia • Mental retardation • Unilateral alien hand syndrome • Mandibular cramps • Bilateral pyramidal tract involvement • Hemianesthesia • Oculomotor nerve palsy • Facial nerve palsy • Central nervous system tumor • Cortical depression • Fatal brain stem involvement • Hyperactivity of brain stem center
PRS: Reported ophthalmologic manifestations
• Enophthalmos • Uveitis • Retinal vasculitis • Third nerve paresis • Glaucoma • Eyelid atrophy • Amblyopia leading to progressive visual loss
when anisometropic • Exotropia • Hypotropia • Esotropia • Increase in pre-existing hyperopia • Diplopia • Restrictive strabismus • Cataract • Miosis • Retinal pigment changes • Chorioretinal lesions • Extraocular muscle thinning • Contralateral extraocular muscle impairment • Eyelid alterations (upper eyelid retraction) • Decreased corneal sensitivity • Band keratopathy • Loss of cilia
• Papillitis • Episcleritis • Bilateral vitreitis • Iridocyclitis • Neuroretinitis • Retinal telangiectasis • Orbital neurinomas • Phthisis bulbi • Pseudoptosis • Profound ocular hypotony • Nocturnal lagophthalmos • Blepharoptosis • Light staining of retina • Shrinkage of eyeball • Retinal detachment • Corneal exposure • Blindness • Adie pupil • Coat syndrome • Duane retraction syndrome • Fuchs syndrome • Horner syndrome
PRS: Reported ophthalmologic manifestations
• Mandibular odontogenous fibroma
• Odontogenic cys • Odontoma of mandible • Teeth involvement • Root resorption • Delayed eruption • Dilaceration • Ipsilateral reduction in
height and width of mandible
• Communication disorders • Dysphonia
Linear scleroderma
• “En coup de sabre” variant (LSCS) – Unilateral frontoparietal linear atrophy – Scarring alopecia may be present – Starts in childhood, slow and progressive over 2
to 20 years, becoming stable – Neurologic and ophthalmologic complications
reported – Unclear pathogenesis:
• Autoimmunity • Disturbed peripheral sympathetic nervous system • Disturbed trigeminal nerve • Early cerebral inflammation
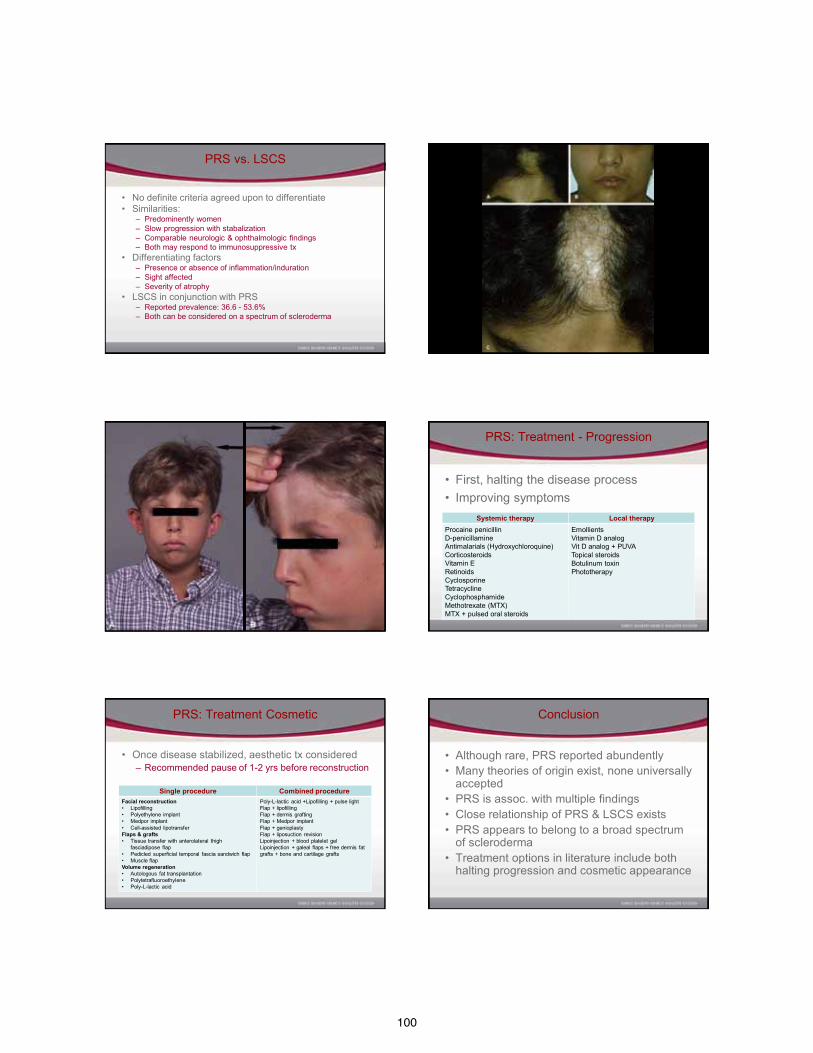
100
PRS vs. LSCS
• No definite criteria agreed upon to differentiate • Similarities:
– Predominently women – Slow progression with stabalization – Comparable neurologic & ophthalmologic findings – Both may respond to immunosuppressive tx
• Differentiating factors – Presence or absence of inflammation/induration – Sight affected – Severity of atrophy
• LSCS in conjunction with PRS – Reported prevalence: 36.6 - 53.6% – Both can be considered on a spectrum of scleroderma
PRS: Treatment - Progression
• First, halting the disease process • Improving symptoms
Systemic therapy Local therapy Procaine penicillin D-penicillamine Antimalarials (Hydroxychloroquine) Corticosteroids Vitamin E Retinoids Cyclosporine Tetracycline Cyclophosphamide Methotrexate (MTX) MTX + pulsed oral steroids
Emollients Vitamin D analog Vit D analog + PUVA Topical steroids Botulinum toxin Phototherapy
PRS: Treatment Cosmetic
• Once disease stabilized, aesthetic tx considered – Recommended pause of 1-2 yrs before reconstruction
Single procedure Combined procedure Facial reconstruction • Lipofilling • Polyethylene implant • Medpor implant • Cell-assisted lipotransfer Flaps & grafts • Tissue transfer with anterolateral thigh
fasciadipose flap • Pedicled superficial temporal fascia sandwich flap • Muscle flap Volume regeneration • Autologous fat transplantation • Polytetrafluoroethylene • Poly-L-lactic acid
Poly-L-lactic acid +Lipofilling + pulse light Flap + lipofilling Flap + dermis grafting Flap + Medpor implant Flap + genioplasty Flap + liposuction revision Lipoinjection + blood platelet gel Lipoinjection + galeal flaps + free dermis fat grafts + bone and cartilage grafts
Conclusion
• Although rare, PRS reported abundently • Many theories of origin exist, none universally
accepted • PRS is assoc. with multiple findings • Close relationship of PRS & LSCS exists • PRS appears to belong to a broad spectrum
of scleroderma • Treatment options in literature include both
halting progression and cosmetic appearance

101
References
1. El-Kehdy J, Abbas O, Rubiez N. A review of Parry-Romberg syndrome. J Am Acad Dermatol. 2012 Mar 7. [Epub ahead of print]
2. Gulati S, Jain V, Garg G. Parry Romberg syndrome. Indian J Pediatr. 2006;73:448–449. 3. A. Duymaz, F.E. Karabekmez, M. Keskin, Z. Tosun. Parry-Romberg syndrome: facial
atrophy and its relationship with other regions of the body. Ann Plast Surg, 63 (2009), pp. 457–461
4. Stone J. Parry-Romberg syndrome. Practical Neurology. 2006;6:185–188. 5. Lazaridou E, Giannopoulou C, et al. Parry-Romberg Syndrome. J Dermatol Case Rep.
2012 Nov: 4(2):30-32. 6. Tollefson MM, Witman PM. En coup de sabre morphea and Parry-Romberg syndrome: a
retrospective review of 54 patients. J Am Acad Dermatol. 2007;56:257–263. 7. Kreuter A, Altmeyer P, Gambichler T. Treatment of localized scleroderma depends on
the clinical subtype. Br J Dermatol. 2007;156:1363–1365. 8. Weibel L, Sampaio MC, Visentin MT, Howell KJ, Woo P, Harper JI. Evaluation of
methotrexate and corticosteroids for the treatment of localized scleroderma (morphoea) in children. Br J Dermatol. 2006;155:1013–1020.
9. Cervelli V, Gentile P. Use of cell fat mixed with platelet gel in progressive hemifacial atrophy. Aesthetic Plast Surg. 2009 Jan;33(1):22-7.
102
Muckle-Wells Syndrome: A Cold Case Diagnosis
Heather Kiraly Orkwis DO, James Ramirez MD, Anthony Baron MD, Stuart Gildenberg MD
St. Joseph Mercy Hospital
October 9, 2012
Disclosures
No financial relationships exist with commercial interests
Objectives
• Present a case of Muckle-Wells Syndrome
• Discuss the clinical and histopathological features
• Review the Cryopyrin Associated Periodic Syndromes
• Identify current treatment options
History
• 25-year-old Caucasian male – Recurrent fevers – Urticaria from infancy – Sensorineural hearing loss – Arthralgias – Myalgias – Abdominal pain
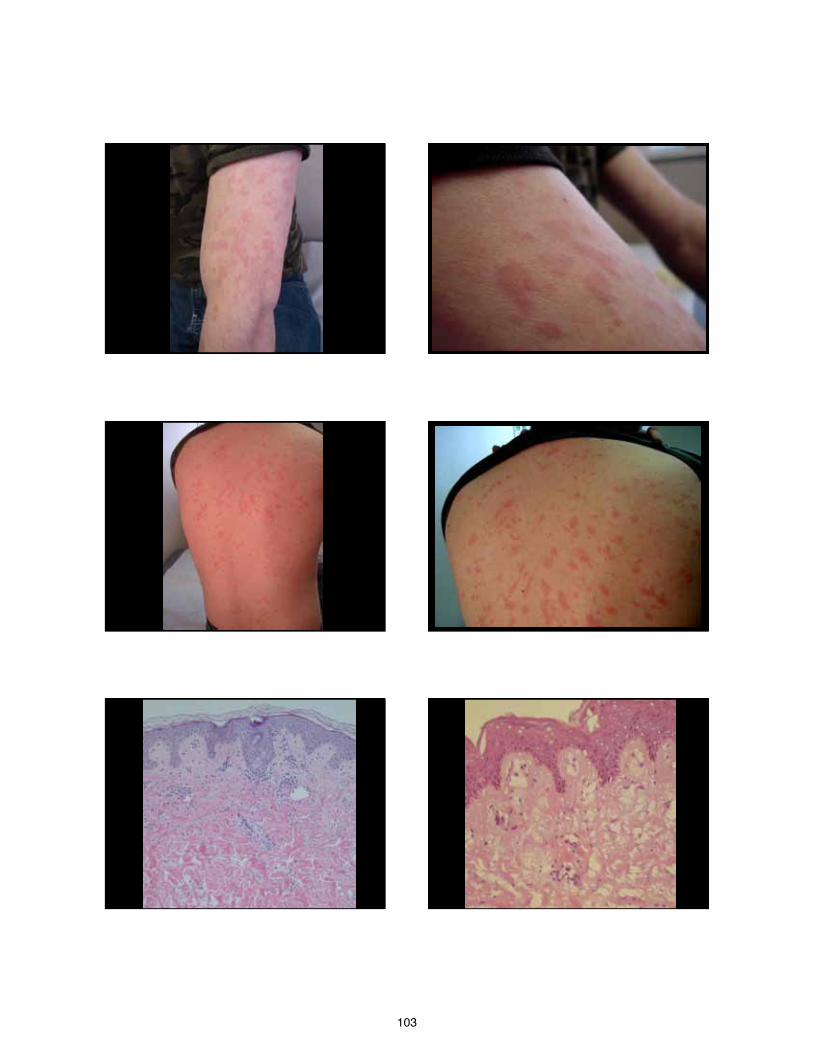
103
104
Laboratory
• CBC • CMP • Complement levels • ANA • UA • ESR • CRP
Further Evaluation
• NIH – Genetic and Rare Diseases Center
• Vision and hearing evaluations • Genetic analysis
–NLRP3 gene (CIAS1)
Diagnosis
Muckle-Wells Syndrome
Cryopyrin Associated Periodic Syndromes (CAPS)
• Muckle-Wells Syndrome
• Familial Cold Autoinflammatory Syndrome
• Neonatal Onset Multisystem Inflammatory Disease
Muckle-Wells Syndrome
• Autosomal Dominant – NLRP3 gene (CIAS1) •Chromosome 1q44
–Cryopyrin
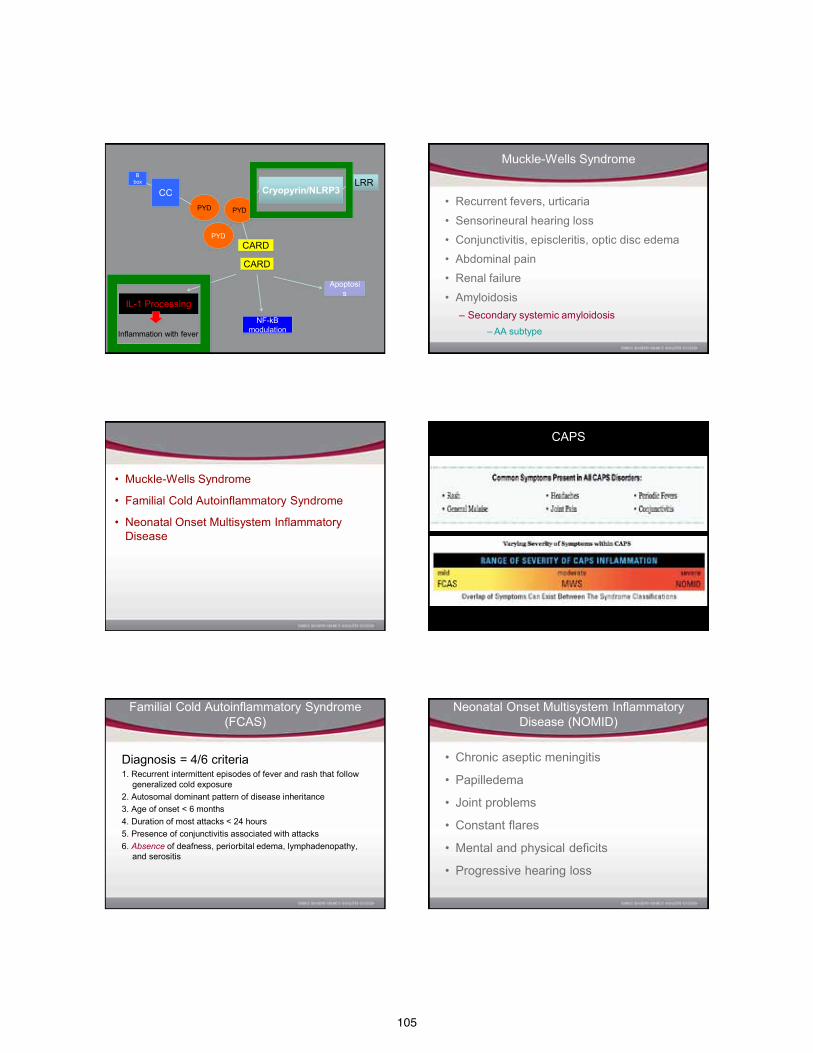
105
Inflammation with fever
Cryopyrin/NLRP3 LRR
PYD
PYD PYD
CARD
CARD
CC
B box
IL-1 Processing
NF-kB modulation
Apoptosis
Muckle-Wells Syndrome
• Recurrent fevers, urticaria • Sensorineural hearing loss • Conjunctivitis, episcleritis, optic disc edema • Abdominal pain • Renal failure • Amyloidosis
– Secondary systemic amyloidosis – AA subtype
Cryopyrin Associated Periodic Syndromes (CAPS)
• Muckle-Wells Syndrome
• Familial Cold Autoinflammatory Syndrome
• Neonatal Onset Multisystem Inflammatory Disease
CAPS
Familial Cold Autoinflammatory Syndrome (FCAS)
Diagnosis = 4/6 criteria 1. Recurrent intermittent episodes of fever and rash that follow
generalized cold exposure 2. Autosomal dominant pattern of disease inheritance 3. Age of onset < 6 months 4. Duration of most attacks < 24 hours 5. Presence of conjunctivitis associated with attacks 6. Absence of deafness, periorbital edema, lymphadenopathy,
and serositis
Neonatal Onset Multisystem Inflammatory Disease (NOMID)
• Chronic aseptic meningitis
• Papilledema
• Joint problems
• Constant flares
• Mental and physical deficits
• Progressive hearing loss
106
IL-1 Receptor Antagonists
Treatment of MWS
• Surveillance – Amyloidosis – Hearing loss
• IL-1 receptor antagonists
– Anakinra, Canakinumab, Rilonacept
Summary: CAPS
• Muckle-Wells Syndrome
• Familial Cold Autoinflammatory Syndrome
• Neonatal Onset Multisystem Inflammatory Disease
Patient Support
• NIH Rare Diseases Center http://rarediseases.info.nih.gov
• National Organization for Rare Disorders www.rarediseases.org
• Clinical trials www.clinicaltrials.gov
• NOMID Alliance www.nomidalliance.org
• Facebook www.facebook.com/pages/Cryopyrin-associated-periodic-syndrome
References
1. Kazushi Izawa, et al. Detection of Base Substitution-Type Somatic Mosaicism of the NLRP3 Gene with >99.9% Statistical Confidence by Massively Parallel Sequencing DNA Res first published online January 24, 2012 doi:10.1093/dnares/dsr047.
2. Kümmerle-Deschner, J. B., Tyrrell, P. N., Reess, F., Kötter, I., Lohse, P., Girschick, H., Huemer, C., Horneff, G., Haas, J.-P., Koitschev, A., Deuter, C. and Benseler, S. M. (2010), “Risk factors for severe Muckle-Wells syndrome.” Arthritis & Rheumatism, 62: 3783–3791.
3. Maksimovic, L., et al. "New CIAS1 Mutation and Anakinra Efficacy in Overlapping of Muckle-Wells and Familial Cold Autoinflammatory Syndromes." Rheumatology 47.3 (2008): 309-10.
4. Kuemmerle-Deschner, Jasmin, et al. Anakinra in the Treatment of Muckle-Wells Syndrome - A Series of Four Cases, 2005. COS Conference Papers Index.
5. Hoffman, Hal M., et al. "Mutation of a New Gene Encoding a Putative Pyrin-Like Protein Causes Familial Cold Autoinflammatory Syndrome and Muckle-Wells Syndrome." Nature genetics 29.3 (2001): 301-5.
6. Hoffman HM. Familial Cold Autoinflammatory Syndrome, Orphanet Encyclopedia. February 2005: http://www.orpha.net/data/patho/GB/uk-FCAS.pdf.
7. Lachmann, HJ., and Hawkins, PN Developments in the scientific and clinical understanding of autoinflammatory disorders Arthritis Research & Therapy 2009, 11:212doi:10.1186/ar2579.
8. Goldbach-Mansky R, Dailey NJ, Canna SW, et al. Neonatal-onset multisystem inflammatory disease responsive to interleukin-1β inhibition. N Engl J Med 2006;355:581-92.
9. NOMID Alliance. http://www.nomidalliance.org.
107
When Seemingly pathognomonic is actually a mystery
AOCD – Annual Meeting 2012
Libby Rhee, DO Harleen Sidhu, MD Robert Phelps, MD
Cindy Hoffman, DO
No conflicts of interests to disclose.
History of Present illness
• 24 year old female with a complaint of the sudden appearance of red-to-purple papules on the abdomen, left flank, buttocks, and right upper arm, which were progressing over the past three years.
• Lesions start as pink-to-red pinpoint macules and papules that eventually enlarge into firm violaceous papules.
• Newest lesions were on her right upper arm.
• Asymptomatic for the most part, however, they bleed easily and profusely with minor trauma.
History of Present illness
• Denied any childhood illnesses; relatively healthy.
• No family members with similar complaints/findings.
• Review of systems: Admitted to increased fatigue, intermittent arthralgias, severe
bouts of “shooting pain,” which started when she was 14 years old, paresthesias, periodic episodes of dizziness, and significant weight gain during the last three years.
Denied headaches, vision changes, changes in appetite, diarrhea, hyper- or hypohydrosis, abdominal pain, chest pain, or bone pain.
Other History
• Past medical history: Asthma, seasonal allergies
• Past surgical history: None
• Family history: Non-contributory
• Social history: Married with a healthy 3-year old daughter. Works as health care aide. Denied tobacco, etoh, drugs.
• Medications: Allegra, singular, nasonex, calcium, acidophilus, acai, folic acid
• Allergies: Shellfish
PHYSICAL EXAM
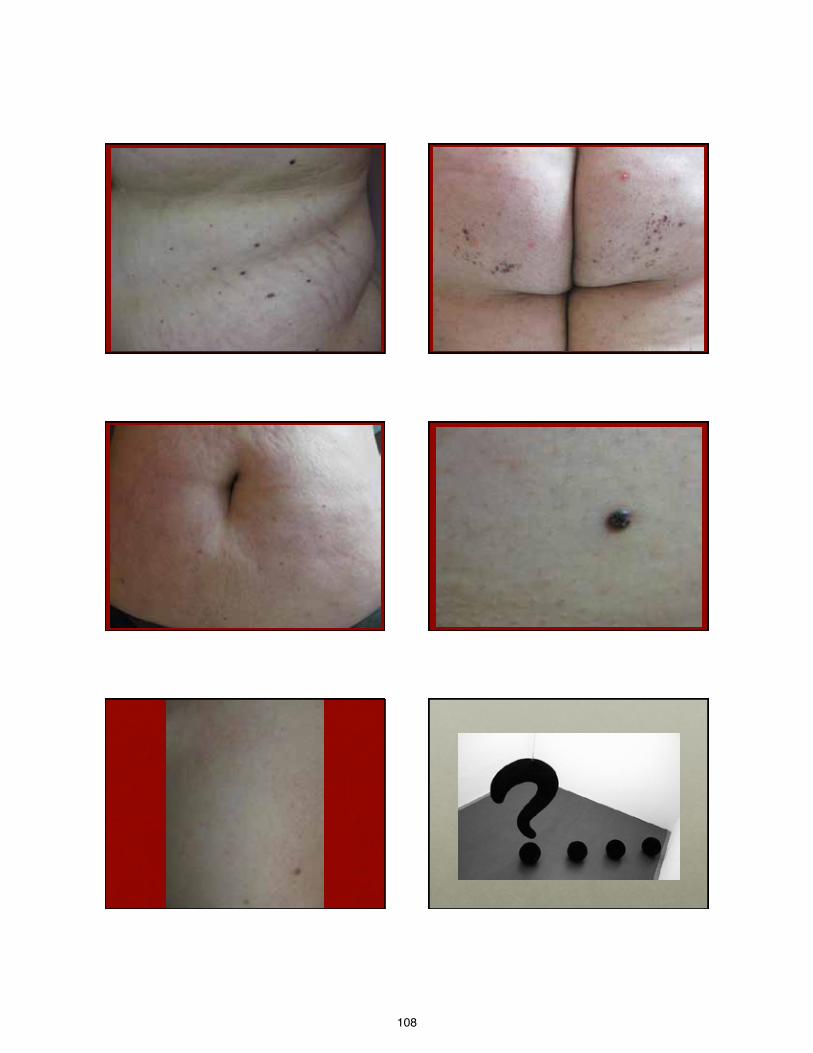
108
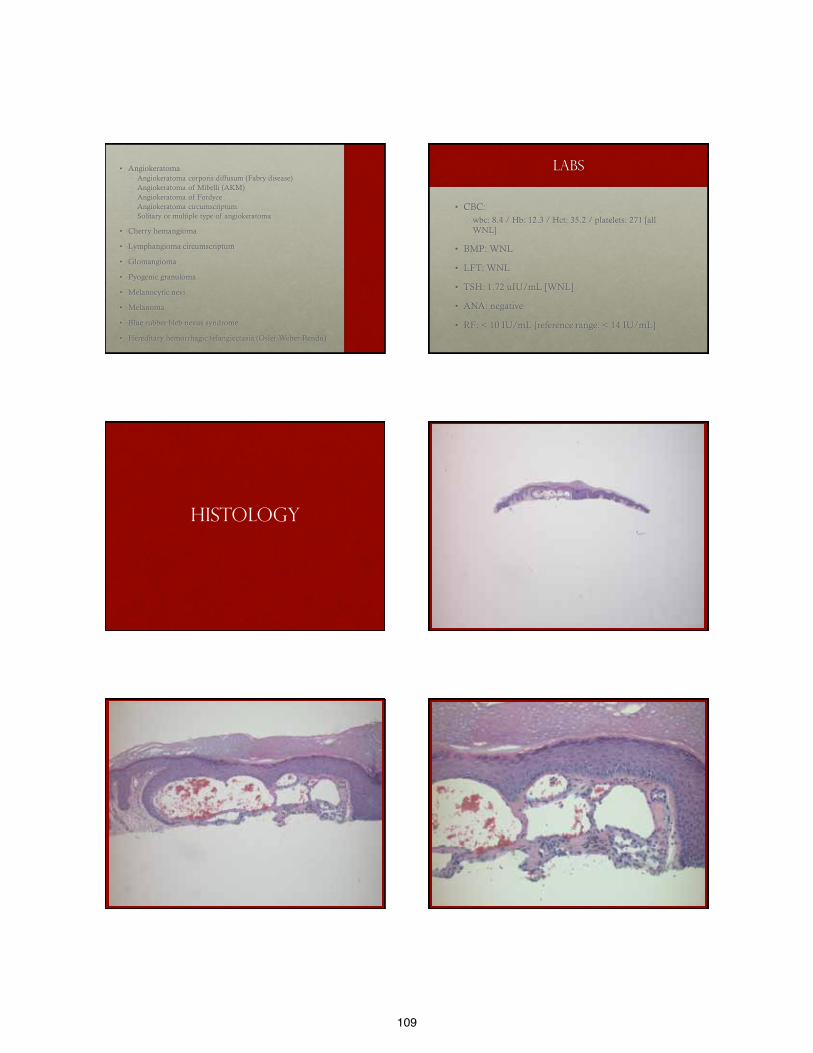
109
• Angiokeratoma Angiokeratoma corporis diffusum (Fabry disease) Angiokeratoma of Mibelli (AKM) Angiokeratoma of Fordyce Angiokeratoma circumscriptum Solitary or multiple type of angiokeratoma
• Cherry hemangioma
• Lymphangioma circumscriptum
• Glomangioma
• Pyogenic granuloma
• Melanocytic nevi
• Melanoma
• Blue rubber bleb nevus syndrome
• Hereditary hemorrhagic telangiectasia (Osler-Weber-Rendu)
Labs
• CBC: wbc: 8.4 / Hb: 12.3 / Hct: 35.2 / platelets: 271 [all
WNL]
• BMP: WNL
• LFT: WNL
• TSH: 1.72 uIU/mL [WNL]
• ANA: negative
• RF: < 10 IU/mL [reference range: < 14 IU/mL]
HISTOLOGY
110
Further work up
• Serum alpha-galactosidase A: WNL 54.4 nmol/hr/mg p [28-80]
• Urine/Plasma GL-3: WNL
• Electron microscopy: No evidence of lysosomal storage disease (zebra-like inclusion bodies)
• Cytogenic analysis: Normal female karyotype
• Genetic mutation analysis/DNA sequencing: negative for alpha-GLA allelic mutations
• Eye exam: normal No corneal or lenticular opacities on slit lamp examination Vision, eye pressure, visual fields, pupillary examination, motility,
and fundoscopic examination all normal
ANGIOKERATOMA CORPORIS DIFFUSUM Sine Fabry?
Angiokeratomas
• Well-circumscribed vascular lesions consisting of superficial vascular ectasia and hyperkeratosis.
• Five variants: Solitary or multiple angiokeratomas Angiokeratomas of scrotum or vulva (aka, angiokeratoma of
Fordyce) Angiokeratoma of Mibelli (AKM) Angiokeratoma circumscriptum Angiokeratoma corporis diffusum (ACD)
• Result from ectatic dilation of pre-existing vessels in the papillary dermis Angiokeratoma circumscriptum capillary–lymphatic
malformation
Solitary or multiple angiokeratomas
• Small, warty, black papule on the lower extremities, but may occur anywhere on the body.
• Thought to result from injury or trauma to or chronic irritation of the venule wall in the papillary dermis.
• Solitary lesions may be confused with melanoma.
Angiokeratomas of fordyce
• Typically asymptomatic 2-to-5mm, red to black in color, may be single or multiple, and arise along superficial vessels.
• Most common in older age groups but may occur as early as the 2nd/3rd decade.
• Scrotum >> penile shaft, labia majora, inner thighs, lower abdomen.
• May be associated with thrombophlebitis, varicoceles and inguinal hernias.
• Vulvar lesions may be associated with vulvar varicosities, hemorrhoids, OCPs, or increased venous pressure during pregnancy.
Angiokeratoma of Mibelli
• Usually develop between the ages of 10 and 15 years.
• Dorsal and lateral aspects of the fingers and toes.
• Sometimes on the dorsa of the hands and feet and rarely on the elbows and knees.
• May be associated with chilblains and acrocyanosis.
• Rarely, ulceration of the fingertips may occur.
• There is a familial predisposition and the disorder may be transmitted in an autosomal dominant fashion with variable penetrance.
111
Angiokeratoma circumscriptum
• Least frequent variant of angiokeratomas.
• Capillary-lymphatic malformations.
• 3:1 female predominance.
• Commonly present at birth or develop during infancy/childhood as either a plaque of multiple discrete papules or hyperkeratotic papules and nodules that often become confluent.
• Trunk, arms or legs; unilateral in most patients.
• Rare manifestation of angiokeratoma circumscriptum naeviforme, on the neck.
Angiokeratoma corporis diffusum
• Characterized by the development of multiple, often clustered angiokeratomas, usually in a bathing trunk distribution.
• Lesions vary in number (only a few to many) and usually begin to appear during late childhood or adolescence.
• Most commonly associated with Fabry disease, which results from a deficiency of the lysosomal enzyme α-galactosidase A.
• Accumulation of the neutral glycolipid ceramide trihexidose within lysosomes of multiple cell types.
Pathology
• Marked dilatation of the papillary dermal vessels in association with an acanthotic, variably hyperkeratotic epidermis.
• Elongated rete ridges may partially or completely enclose vascular channels, and a collarette may be present.
• Fabry disease vacuoles can be detected in endothelial cells and pericytes.
• The amount of glycolipid is small and may be difficult to detect in routinely prepared sections. Deposits are PAS-positive and Sudan black-positive.
They can also be demonstrated by electron microscopy.
Fabry Disease
• Progressive and life-threatening; affects both males and females.
• X-linked recessive lysosomal storage disorder resulting from a deficiency of α-galactosidase A. GLA gene; > 370 different mutations Systemic deposition of glycosphingolipids, predominantly
globotriaosylceramide and galabiosylceramide.
• Clinical manifestations result primarily from the accumulation of glycosphingolipids in vascular endothelium.
• Affects ~1/40,000 males; all ethnicities.
• Female heterozygotes are also less frequently affected, usually with milder, late-onset forms compared to male hemizygotes.
Fabry Disease
• Skin, kidneys, heart, and nervous system primarily affected.
• Cardinal clinical features - first two-to-three decades of life: Pain and paresthesias of the extremities (with onset often
during childhood or adolescence).
Multiple angiokeratomas of the skin and mucous membranes.
Hypohidrosis.
Characteristic corneal and lenticular opacities.
• Progressive renal insufficiency develops.
• Coronary insufficiency and cerebrovascular disease.
Fabry Disease
• Angiokeratomas may be one of the earliest manifestations.
• Appear in almost all affected male patients and approximately 30% of heterozygous females.
• Lesions classically develop slowly as individual punctate, dark-red to blue–black macules or slightly elevated papules that do not blanch and may become slightly keratotic as they enlarge.
• Angiokeratomas tend to be clustered between the umbilicus and the knees in Fabry disease but can be present anywhere.
• Oral mucosa and conjunctival involvement is common.
• Anhidrosis/hypohidrosis is an early and almost constant feature.
112
Fabry Disease
• In the skin, there is evidence of lipid storage in the endothelium, pericytes and smooth muscle of capillaries, venules and arterioles, and arrector pili muscles.
• Lipid accumulation may also be observed in sweat gland epithelium and perineural cells. Ultrastructural examination of eccrine sweat glands reveals
characteristic cytoplasmic inclusions within the secretory coil, coiled duct and basal cells of the straight duct.
Inclusions are also seen in the unmyelinated axons innervating the sweat glands.
Fabry Disease
• Definitive diagnosis of Fabry disease is established by demonstration of α-galactosidase A deficiency in plasma or leukocytes.
• Polarizing microscopy of urine reveals birefringent lipid globules (‘Maltese crosses’).
Fabry Disease Testing Algorithm*
Other lysosomal Storage disorders
• Although most commonly seen in association with Fabry disease, it is important to recognize that angiokeratomas are not unique to this disorder.
• They are also observed in a number of other lysosomal storage disorders.
Fabry Disease - Treatment
• Oral phenytoin, gabapentin or carbamazepine can be very beneficial in treating the debilitating limb pain.
• End-stage renal disease has historically been treated with dialysis and renal transplantation.
• Enzyme replacement therapy is now available for Fabry disease and is administered biweekly by intravenous infusion. Agalsidase alfa (Replagal®; Transkaryotic Therapies,
Cambridge, MA, USA)
Agalsidase beta (Fabrazyme®; Genzyme Corporation, Cambridge, MA, USA)
Cutaneous variant of ACD
• 33 year old male with idiopathic type of ACD.
• 10 previously reported cases of ACD with “normal” enzyme function.
• No systemic disease or dysmorphic facies characteristic of glycoprotein metabolism enzyme deficiencies.
• The pathogenesis of these angiokeratomas in the absence of enzyme deficiency, such as in this case, is unclear.
• It may represent a partial deficiency or enzyme mosaicism.
Arch Dermatol. 2006;142:615-618
113
Treatment
• No treatment is necessary if only cutaneous lesions
• Cryotherapy
• Electrocautery
• Laser therapy: • 578-nm copper vapor laser • Argon laser • Flashlamp-pumped pulse dye laser • 532-nm KTP laser
• Surgical excision
References
Jean L. Bolognia MD and Joseph L. Jorizzo MD, Dermatology e-dition, 2nd Ed: Text with Continually Updated Online Reference, 2-Volume Set, 2008. Accessed via www.expertconsult.com 10/01/11.
Tarabuso AL. Fabry Disease. Skinmed. 2011 May-Jun;9(3):173-7.
Germain DP. Fabry Disease. Orphanet J Rare Dis. 2010 Nov 22;5:30.
Sodaifi M, Aghaei S, Monabati A. Cutaneous variant of angiokeratoma corporis diffusum associated with angiokeratoma circumscriptum. Dermatology Online Journal, 2004 10 (1): 20
Kelly E, Kelly B. Angiokeratoma Corporis Diffusum in a Patient With No Recognizable Enzyme Abnormalities. Arch Dermatol. 2006 May;142(5):615-8.
Schaefer RM, Tylki-Szymańska A, Hilz MJ. Enzyme replacement therapy for Fabry disease: a systematic review of available evidence. Drugs. 2009 Nov 12;69(16):2179-205.
Fabry Disease Testing Algorithm*. Mayo Foundation for Medical Education and Research (MFMER). Accessed via www.mayomedicallaboratories.com/media/articles/algorithms/fabrydisease.pdf 10/04/11.
Poetke M, Philipp C, Berlien HP. Flashlamp-Pumped Pulsed Dye Laser for Hemangiomas in Infancy. Arch Dermatol. 2000 May;136(5):628-32.
Thank you!
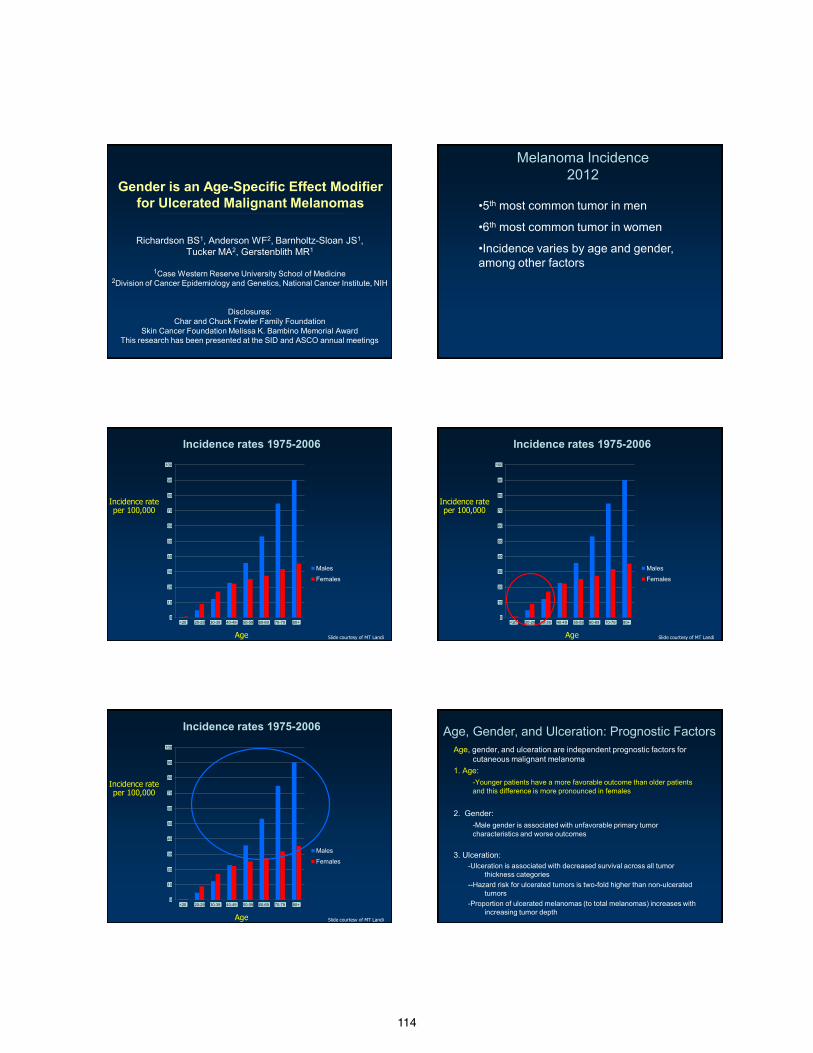
114
Gender is an Age-Specific Effect Modifier for Ulcerated Malignant Melanomas
Richardson BS1, Anderson WF2, Barnholtz-Sloan JS1, Tucker MA2, Gerstenblith MR1
1Case Western Reserve University School of Medicine
2Division of Cancer Epidemiology and Genetics, National Cancer Institute, NIH
Disclosures: Char and Chuck Fowler Family Foundation
Skin Cancer Foundation Melissa K. Bambino Memorial Award This research has been presented at the SID and ASCO annual meetings
Melanoma Incidence 2012
•5th most common tumor in men
•6th most common tumor in women
•Incidence varies by age and gender, among other factors
0
10
20
30
40
50
60
70
80
90
100
<20 20-29 30-39 40-49 50-59 60-69 70-79 80+
Males
Females
Incidence rates 1975-2006
Age
Incidence rate per 100,000
Slide courtesy of MT Landi
0
10
20
30
40
50
60
70
80
90
100
<20 20-29 30-39 40-49 50-59 60-69 70-79 80+
Males
Females
Incidence rates 1975-2006
Age
Incidence rate per 100,000
Slide courtesy of MT Landi
0
10
20
30
40
50
60
70
80
90
100
<20 20-29 30-39 40-49 50-59 60-69 70-79 80+
Males
Females
Incidence rates 1975-2006
Age
Incidence rate per 100,000
Slide courtesy of MT Landi
Age, gender, and ulceration are independent prognostic factors for cutaneous malignant melanoma
1. Age: -Younger patients have a more favorable outcome than older patients
and this difference is more pronounced in females 2. Gender: -Male gender is associated with unfavorable primary tumor
characteristics and worse outcomes 3. Ulceration:
-Ulceration is associated with decreased survival across all tumor thickness categories
--Hazard risk for ulcerated tumors is two-fold higher than non-ulcerated tumors
-Proportion of ulcerated melanomas (to total melanomas) increases with increasing tumor depth
Age, Gender, and Ulceration: Prognostic Factors
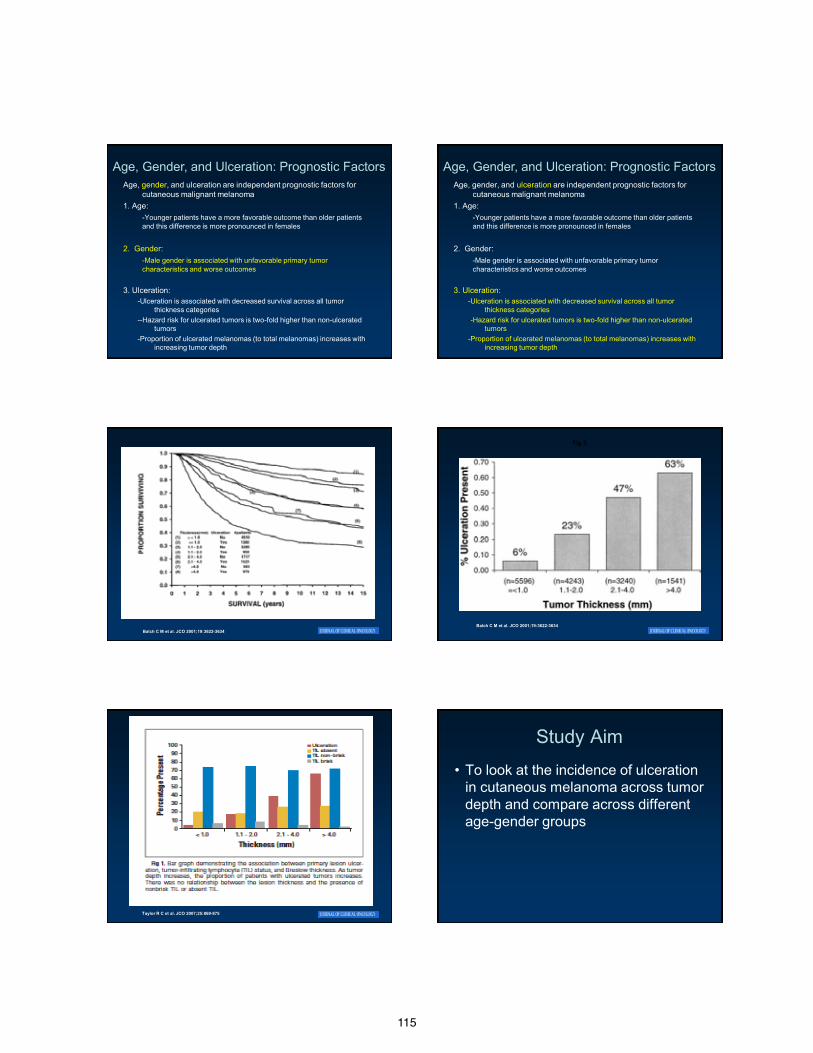
115
Age, gender, and ulceration are independent prognostic factors for cutaneous malignant melanoma
1. Age: -Younger patients have a more favorable outcome than older patients
and this difference is more pronounced in females 2. Gender: -Male gender is associated with unfavorable primary tumor
characteristics and worse outcomes 3. Ulceration:
-Ulceration is associated with decreased survival across all tumor thickness categories
--Hazard risk for ulcerated tumors is two-fold higher than non-ulcerated tumors
-Proportion of ulcerated melanomas (to total melanomas) increases with increasing tumor depth
Age, Gender, and Ulceration: Prognostic Factors Age, gender, and ulceration are independent prognostic factors for
cutaneous malignant melanoma 1. Age: -Younger patients have a more favorable outcome than older patients
and this difference is more pronounced in females 2. Gender: -Male gender is associated with unfavorable primary tumor
characteristics and worse outcomes 3. Ulceration:
-Ulceration is associated with decreased survival across all tumor thickness categories
--Hazard risk for ulcerated tumors is two-fold higher than non-ulcerated tumors
-Proportion of ulcerated melanomas (to total melanomas) increases with increasing tumor depth
Age, Gender, and Ulceration: Prognostic Factors
Balch C M et al. JCO 2001;19:3622-3634
Fig 3.
Balch C M et al. JCO 2001;19:3622-3634
Taylor R C et al. JCO 2007;25:869-875
Study Aim
• To look at the incidence of ulceration in cutaneous melanoma across tumor depth and compare across different age-gender groups
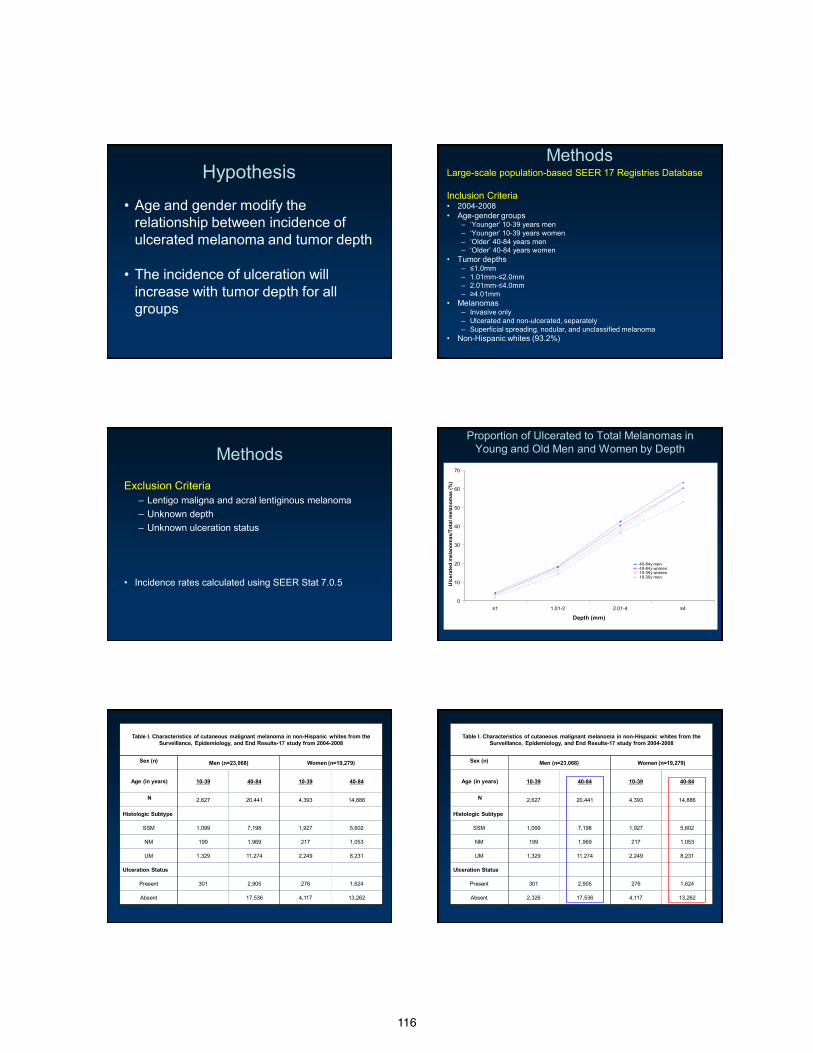
116
Hypothesis
• Age and gender modify the relationship between incidence of ulcerated melanoma and tumor depth
• The incidence of ulceration will increase with tumor depth for all groups
Methods Large-scale population-based SEER 17 Registries Database Inclusion Criteria • 2004-2008 • Age-gender groups
– ‘Younger’ 10-39 years men – ‘Younger’ 10-39 years women – ‘Older’ 40-84 years men – ‘Older’ 40-84 years women
• Tumor depths – ≤1.0mm – 1.01mm-≤2.0mm – 2.01mm-≤4.0mm – ≥4.01mm
• Melanomas – Invasive only – Ulcerated and non-ulcerated, separately – Superficial spreading, nodular, and unclassified melanoma
• Non-Hispanic whites (93.2%)
Methods
Exclusion Criteria – Lentigo maligna and acral lentiginous melanoma – Unknown depth – Unknown ulceration status
• Incidence rates calculated using SEER Stat 7.0.5
Proportion of Ulcerated to Total Melanomas in Young and Old Men and Women by Depth
0
10
20
30
40
50
60
70
≤1 1.01-2 2.01-4 ≥4
Depth (mm)
Ulc
erat
ed m
elan
omas
/Tot
al m
elan
omas
(%)
40-84y men40-84y women10-39y women10-39y men
Table I. Characteristics of cutaneous malignant melanoma in non-Hispanic whites from the Surveillance, Epidemiology, and End Results-17 study from 2004-2008
Sex (n) Men (n=23,068) Women (n=19,279)
Age (in years) 10-39 40-84 10-39 40-84
N 2,627 20,441 4,393 14,886
Histologic Subtype
SSM 1,099 7,198 1,927 5,602
NM 199 1,969 217 1,053
UM 1,329 11,274 2,249 8,231
Ulceration Status
Present 301 2,905 276 1,624
Absent 17,536 4,117 13,262
Table I. Characteristics of cutaneous malignant melanoma in non-Hispanic whites from the Surveillance, Epidemiology, and End Results-17 study from 2004-2008
Sex (n) Men (n=23,068) Women (n=19,279)
Age (in years) 10-39 40-84 10-39 40-84
N 2,627 20,441 4,393 14,886
Histologic Subtype
SSM 1,099 7,198 1,927 5,602
NM 199 1,969 217 1,053
UM 1,329 11,274 2,249 8,231
Ulceration Status
Present 301 2,905 276 1,624
Absent 2,326 17,536 4,117 13,262
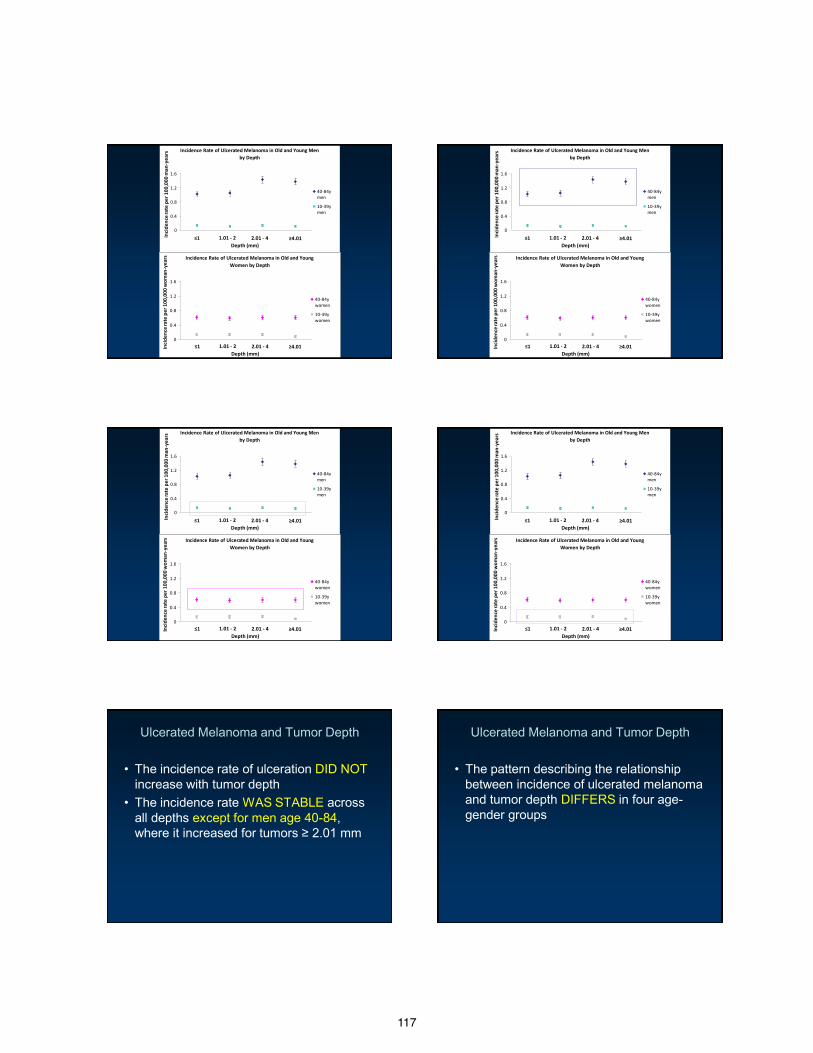
117
Incidence Rate of Ulcerated Melanoma in Old and Young Men by Depth
0
0.4
0.8
1.2
1.6
≤ 1 1.01 - 2 2.01 - 4 ≥ 4
40-84ymen
10-39ymen
≤1 1.01 - 2 2.01 - 4 ≥4.01 Depth (mm)
Inci
denc
e ra
te p
er 1
00,0
00 m
an-y
ears
Incidence Rate of Ulcerated Melanoma in Old and Young Women by Depth
0
0.4
0.8
1.2
1.6
≤ 1 1.01 - 2 2.01 - 4 ≥ 4
40-84ywomen
10-39ywomen
≤1 1.01 - 2 2.01 - 4 ≥4.01 Depth (mm)
Inci
denc
e ra
te p
er 1
00,0
00 w
oman
-yea
rs
Incidence Rate of Ulcerated Melanoma in Old and Young Men by Depth
0
0.4
0.8
1.2
1.6
≤ 1 1.01 - 2 2.01 - 4 ≥ 4
40-84ymen
10-39ymen
≤1 1.01 - 2 2.01 - 4 ≥4.01 Depth (mm)
Inci
denc
e ra
te p
er 1
00,0
00 m
an-y
ears
Incidence Rate of Ulcerated Melanoma in Old and Young Women by Depth
0
0.4
0.8
1.2
1.6
≤ 1 1.01 - 2 2.01 - 4 ≥ 4
40-84ywomen
10-39ywomen
≤1 1.01 - 2 2.01 - 4 ≥4.01 Depth (mm)
Inci
denc
e ra
te p
er 1
00,0
00 w
oman
-yea
rs
Incidence Rate of Ulcerated Melanoma in Old and Young Men by Depth
0
0.4
0.8
1.2
1.6
≤ 1 1.01 - 2 2.01 - 4 ≥ 4
40-84ymen
10-39ymen
≤1 1.01 - 2 2.01 - 4 ≥4.01 Depth (mm)
Inci
denc
e ra
te p
er 1
00,0
00 m
an-y
ears
Incidence Rate of Ulcerated Melanoma in Old and Young Women by Depth
0
0.4
0.8
1.2
1.6
≤ 1 1.01 - 2 2.01 - 4 ≥ 4
40-84ywomen
10-39ywomen
≤1 1.01 - 2 2.01 - 4 ≥4.01 Depth (mm)
Inci
denc
e ra
te p
er 1
00,0
00 w
oman
-yea
rs
Incidence Rate of Ulcerated Melanoma in Old and Young Men by Depth
0
0.4
0.8
1.2
1.6
≤ 1 1.01 - 2 2.01 - 4 ≥ 4
40-84ymen
10-39ymen
≤1 1.01 - 2 2.01 - 4 ≥4.01 Depth (mm)
Inci
denc
e ra
te p
er 1
00,0
00 m
an-y
ears
Incidence Rate of Ulcerated Melanoma in Old and Young Women by Depth
0
0.4
0.8
1.2
1.6
≤ 1 1.01 - 2 2.01 - 4 ≥ 4
40-84ywomen
10-39ywomen
≤1 1.01 - 2 2.01 - 4 ≥4.01 Depth (mm)
Inci
denc
e ra
te p
er 1
00,0
00 w
oman
-yea
rs
Ulcerated Melanoma and Tumor Depth
• The incidence rate of ulceration DID NOT increase with tumor depth
• The incidence rate WAS STABLE across all depths except for men age 40-84, where it increased for tumors ≥ 2.01 mm
Ulcerated Melanoma and Tumor Depth
• The pattern describing the relationship between incidence of ulcerated melanoma and tumor depth DIFFERS in four age-gender groups
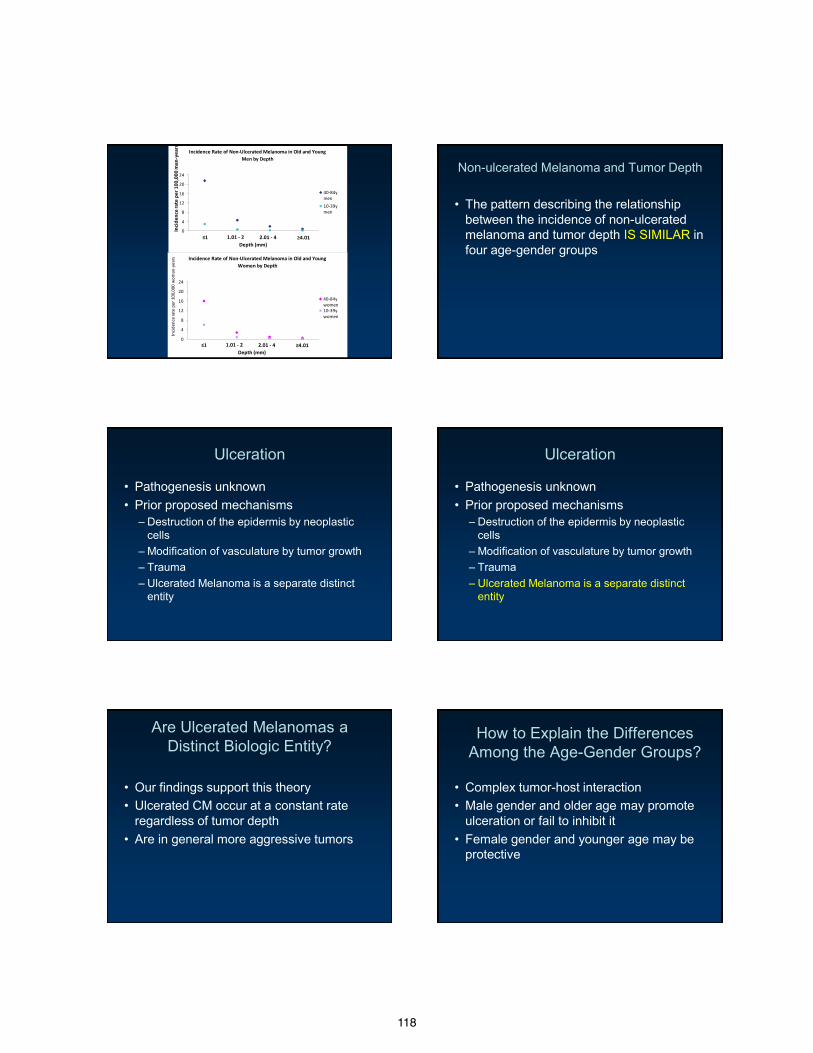
118
Incidence Rate of Non-Ulcerated Melanoma in Old and Young Women by Depth
0
4
8
12
16
20
24
≤ 1 1.01 - 2 2.01 - 4 ≥ 4
40-84ywomen10-39ywomen
Inci
denc
e rat
e pe
r 100
,000
wom
an-y
ears
≤1 1.01 - 2 2.01 - 4 ≥4.01 Depth (mm)
Incidence Rate of Non-Ulcerated Melanoma in Old and Young Men by Depth
0
4
8
12
16
20
24
≤ 1 1.01 - 2 2.01 - 4 ≥ 4
40-84ymen10-39ymen
≤1 1.01 - 2 2.01 - 4 ≥4.01 Depth (mm)
Inci
denc
e ra
te p
er 1
00,0
00 m
an-y
ears
Non-ulcerated Melanoma and Tumor Depth
• The pattern describing the relationship between the incidence of non-ulcerated melanoma and tumor depth IS SIMILAR in four age-gender groups
Ulceration
• Pathogenesis unknown • Prior proposed mechanisms
– Destruction of the epidermis by neoplastic cells
– Modification of vasculature by tumor growth – Trauma – Ulcerated Melanoma is a separate distinct
entity
Ulceration
• Pathogenesis unknown • Prior proposed mechanisms
– Destruction of the epidermis by neoplastic cells
– Modification of vasculature by tumor growth – Trauma – Ulcerated Melanoma is a separate distinct
entity
Are Ulcerated Melanomas a Distinct Biologic Entity?
• Our findings support this theory • Ulcerated CM occur at a constant rate
regardless of tumor depth • Are in general more aggressive tumors
How to Explain the Differences Among the Age-Gender Groups?
• Complex tumor-host interaction • Male gender and older age may promote
ulceration or fail to inhibit it • Female gender and younger age may be
protective
119
Incidence of Ulceration in Thin Tumors
• The consistent rate of ulceration, even in
thin tumors is interesting
• We cannot exclude the possibility that our findings are not real
• Future studies needed
Study Limitations
• Inaccurate coding in SEER
• Variation in experience and interpretation of tumor ulceration vs traumatic ulceration among a variety dermatopathologists and general pathologists
Summary
• Older age at diagnosis in both men and women is associated with higher incidence rates of ulcerated and non-ulcerated melanomas
• Highest incidence rates for both occur in men at each depth Age and gender effects seen on incidence for both ulcerated and non-ulcerated melanomas
Summary
• The proportion of ulcerated to non-ulcerated tumors increased across tumor depth
• We expected that the incidence of ulceration would also increase across tumor depth
• THIS WAS NOT THE CASE
• The incidence rate of ulceration remained stable for all groups, except men 40-84, where is increased for tumors ≥ 2.01 mm
Summary
• The stable incidence rate of ulceration across depth with the
decrease in incidence rate across depth for non-ulcerated tumors explain the increase in proportion across tumor depth
Conclusions
• The incidence of ulcerated melanomas are stable across tumor depth, except for men age 40-84
• Supports the hypothesis that ulcerated melanomas are a distinct biologic entity, which occur at a constant rate, regardless of tumor depth
• Supports the hypothesis that there is a complex tumor-host interaction where male gender and older age appear to promote or fail to inhibit ulcerated CM
• Future studies are needed to verify our findings and further understand ulcerated melanoma and tumor-host interactions
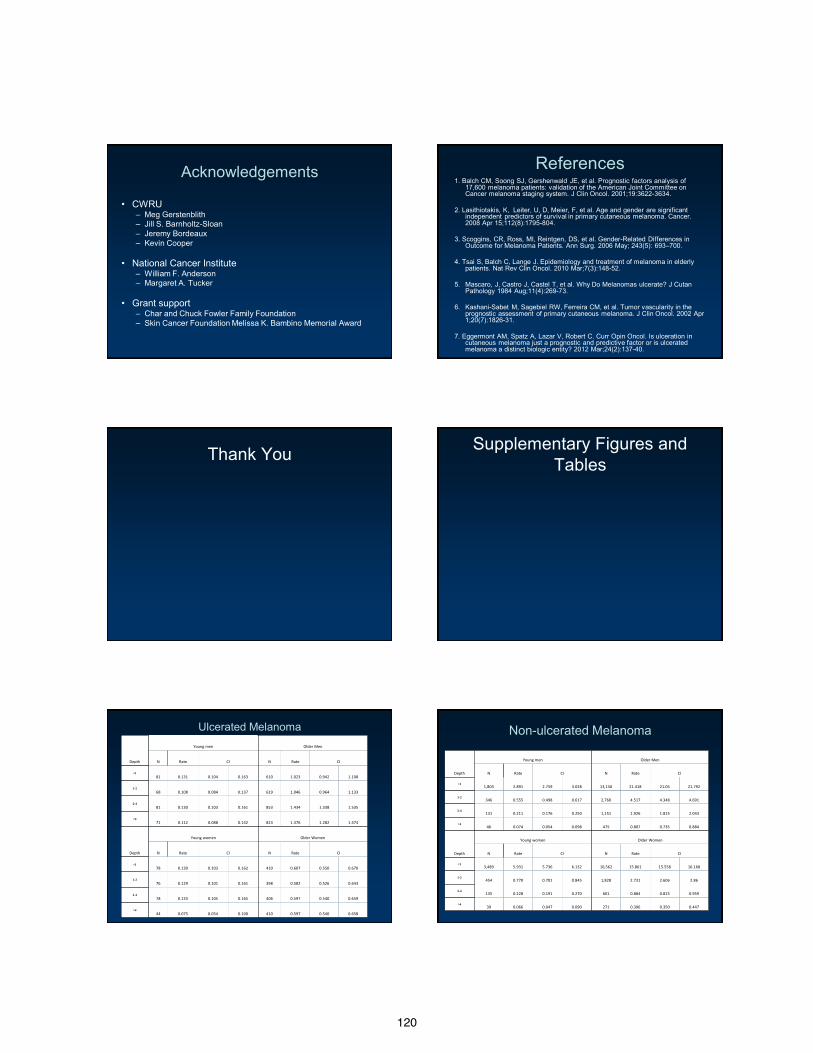
120
Acknowledgements
• CWRU – Meg Gerstenblith – Jill S. Barnholtz-Sloan – Jeremy Bordeaux – Kevin Cooper
• National Cancer Institute
– William F. Anderson – Margaret A. Tucker
• Grant support
– Char and Chuck Fowler Family Foundation – Skin Cancer Foundation Melissa K. Bambino Memorial Award
References 1. Balch CM, Soong SJ, Gershenwald JE, et al. Prognostic factors analysis of
17,600 melanoma patients: validation of the American Joint Committee on Cancer melanoma staging system. J Clin Oncol. 2001;19:3622-3634.
2. Lasithiotakis, K, Leiter, U, D, Meier, F, et al. Age and gender are significant
independent predictors of survival in primary cutaneous melanoma. Cancer. 2008 Apr 15;112(8):1795-804.
3. Scoggins, CR, Ross, MI, Reintgen, DS, et al. Gender-Related Differences in
Outcome for Melanoma Patients. Ann Surg. 2006 May; 243(5): 693–700. 4. Tsai S, Balch C, Lange J. Epidemiology and treatment of melanoma in elderly
patients. Nat Rev Clin Oncol. 2010 Mar;7(3):148-52. 5. Mascaro, J, Castro J, Castel T, et al. Why Do Melanomas ulcerate? J Cutan
Pathology 1984 Aug;11(4):269-73.
6. Kashani-Sabet M, Sagebiel RW, Ferreira CM, et al. Tumor vascularity in the prognostic assessment of primary cutaneous melanoma. J Clin Oncol. 2002 Apr 1;20(7):1826-31.
7. Eggermont AM, Spatz A, Lazar V, Robert C. Curr Opin Oncol. Is ulceration in
cutaneous melanoma just a prognostic and predictive factor or is ulcerated melanoma a distinct biologic entity? 2012 Mar;24(2):137-40.
Thank You Supplementary Figures and Tables
Depth
Young men Older Men
N Rate CI N Rate CI
<1 81 0.131 0.104 0.163 610 1.023 0.942 1.108
1-2 68 0.108 0.084 0.137 619 1.046 0.964 1.133
2-4 81 0.130 0.103 0.161 853 1.434 1.338 1.535
>4 71 0.112 0.088 0.142 823 1.376 1.282 1.474
Depth
Young women Older Women
N Rate CI N Rate CI
<1 78 0.130 0.103 0.162 410 0.607 0.550 0.670
1-2 76 0.129 0.101 0.161 398 0.582 0.526 0.643
2-4 78 0.133 0.105 0.165 406 0.597 0.540 0.659
>4 44 0.075 0.054 0.100 410 0.597 0.540 0.658
Ulcerated Melanoma Non-ulcerated Melanoma
Depth
Young men Older Men
N Rate CI N Rate CI
<1 1,803 2.891 2.759 3.028 13,150 21.418 21.05 21.792
1-2 346 0.555 0.498 0.617 2,760 4.517 4.348 4.691
2-4 131 0.211 0.176 0.250 1,151 1.926 1.815 2.043
>4 46 0.074 0.054 0.098 475 0.807 0.735 0.884
Depth
Young women Older Women
N Rate CI N Rate CI
<1 3,489 5.931 5.736 6.132 10,562 15.861 15.558 16.168
1-2 454 0.770 0.701 0.845 1,828 2.731 2.606 2.86
2-4 135 0.228 0.191 0.270 601 0.884 0.815 0.959
>4 39 0.066 0.047 0.090 271 0.396 0.350 0.447
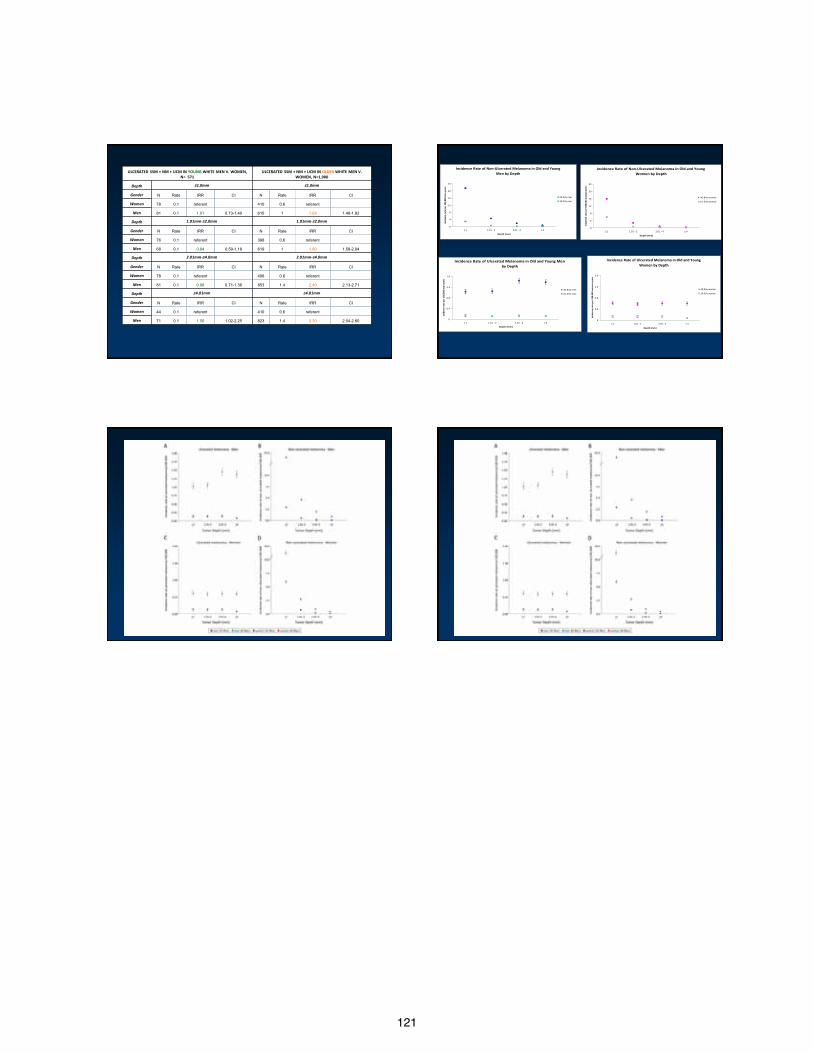
121
ULCERATED SSM + NM + UCM IN YOUNG WHITE MEN V. WOMEN, N= 571
ULCERATED SSM + NM + UCM IN OLDER WHITE MEN V. WOMEN, N=1,900
Depth ≤1.0mm ≤1.0mm
Gender N Rate IRR CI N Rate IRR CI
Women 78 0.1 referent 410 0.6 referent
Men 81 0.1 1.01 0.73-1.40 610 1 1.68 1.48-1.92
Depth 1.01mm-≤2.0mm 1.01mm-≤2.0mm
Gender N Rate IRR CI N Rate IRR CI
Women 76 0.1 referent 398 0.6 referent
Men 68 0.1 0.84 0.59-1.18 619 1 1.80 1.58-2.04
Depth 2.01mm-≤4.0mm 2.01mm-≤4.0mm
Gender N Rate IRR CI N Rate IRR CI
Women 78 0.1 referent 406 0.6 referent
Men 81 0.1 0.98 0.71-1.36 853 1.4 2.40 2.13-2.71
Depth ≥4.01mm ≥4.01mm
Gender N Rate IRR CI N Rate IRR CI
Women 44 0.1 referent 410 0.6 referent
Men 71 0.1 1.50 1.02-2.25 823 1.4 2.30 2.04-2.60
Incidence Rate of Ulcerated Melanoma in Old and Young Men by Depth
0
0.4
0.8
1.2
1.6
≤ 1 1.01 - 2 2.01 - 4 ≥ 4
Depth (mm)
Incid
ence
rate
per
100
,000
man
-yea
rs
40-84y men
10-39y men
Incidence Rate of Ulcerated Melanoma in Old and Young Women by Depth
0
0.4
0.8
1.2
1.6
≤ 1 1.01 - 2 2.01 - 4 ≥ 4
Depth (mm)
Incid
ence
rate
per
100
,000
wom
an-y
ears
40-84y women
10-39y women
Incidence Rate of Non-Ulcerated Melanoma in Old and Young Men by Depth
0
4
8
12
16
20
24
≤ 1 1.01 - 2 2.01 - 4 ≥ 4
Depth (mm)
Incid
ence
rate
per
100
,000
man
-yea
rs
40-84y men
10-39y men
Incidence Rate of Non-Ulcerated Melanoma in Old and Young Women by Depth
0
4
8
12
16
20
24
≤ 1 1.01 - 2 2.01 - 4 ≥ 4
Depth (mm)
Incid
ence
rate
per
100
,000
wom
an-y
ears
40-84y women
10-39y women
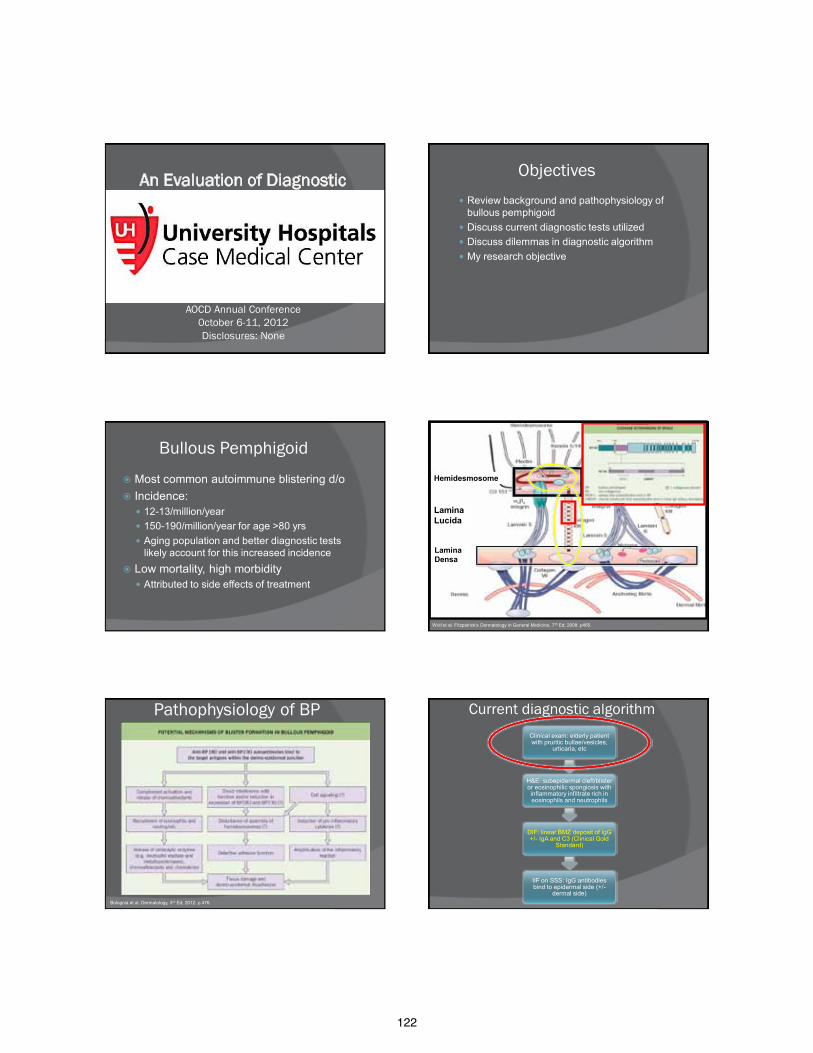
122
An Evaluation of Diagnostic Tests in Bullous Pemphigoid
Ashley Kittridge, DO University Hospitals Case Medical Center, PGY4
AOCD Annual Conference 0ctober 6-11, 2012 Disclosures: None
Objectives Review background and pathophysiology of
bullous pemphigoid Discuss current diagnostic tests utilized Discuss dilemmas in diagnostic algorithm My research objective
Bullous Pemphigoid
Most common autoimmune blistering d/o Incidence: 12-13/million/year 150-190/million/year for age >80 yrs Aging population and better diagnostic tests
likely account for this increased incidence Low mortality, high morbidity Attributed to side effects of treatment
Hemidesmosome
Lamina Densa
Lamina Lucida
Wolf et al. Fitzpatrick’s Dermatology in General Medicine, 7th Ed; 2008: p455.
Pathophysiology of BP
Antibodies to hemidesmosomal proteins BP180 (BPAG2/Collagen XVII) BP230 (BPAG1) BP180- NC16A Epitopes outside NC16A domain
Cause a cascade of events Compliment activation Defective adhesion function Induction of cytokines and amplification of
inflammatory reaction Bolognia et al. Dermatology, 3rd Ed; 2012: p 476.
Current diagnostic algorithm Clinical exam: elderly patient with pruritic bullae/vesicles,
urticaria, etc
H&E: subepidermal cleft/blister or eosinophilic spongiosis with inflammatory infiltrate rich in eosinophils and neutrophils
DIF: linear BMZ deposit of IgG +/- IgA and C3 (Clinical Gold
Standard)
IIF on SSS: IgG antibodies bind to epidermal side (+/-
dermal side)
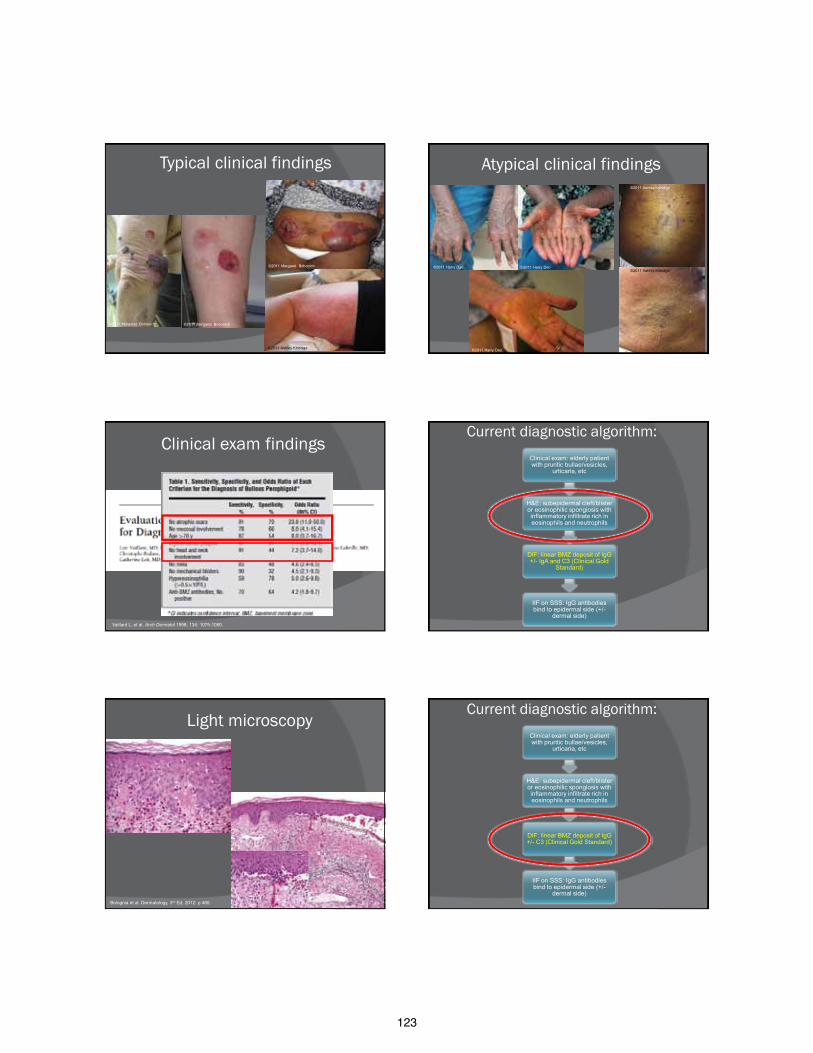
123
Typical clinical findings
©2011 Margaret Bobonich
©2011 Margaret Bobonich
©2011 Ashley Kittridge
©2011 Margaret Bobonich
Atypical clinical findings ©2011 Ashley Kittridge
©2011 Harry Dao ©2011 Ashley Kittridge
©2011 Harry Dao
©2011 Harry Dao
Clinical exam findings
Vaillant L, et al. Arch Dermatol 1998; 134: 1075-1080.
Current diagnostic algorithm: Clinical exam: elderly patient with pruritic bullae/vesicles,
urticaria, etc
H&E: subepidermal cleft/blister or eosinophilic spongiosis with inflammatory infiltrate rich in eosinophils and neutrophils
DIF: linear BMZ deposit of IgG +/- IgA and C3 (Clinical Gold
Standard)
IIF on SSS: IgG antibodies bind to epidermal side (+/-
dermal side)
Light microscopy
Bolognia et al. Dermatology, 3rd Ed; 2012: p 480.
Current diagnostic algorithm: Clinical exam: elderly patient with pruritic bullae/vesicles,
urticaria, etc
H&E: subepidermal cleft/blister or eosinophilic spongiosis with inflammatory infiltrate rich in eosinophils and neutrophils
DIF: linear BMZ deposit of IgG +/- C3 (Clinical Gold Standard)
IIF on SSS: IgG antibodies bind to epidermal side (+/-
dermal side)
124
Direct Immunofluorescence
Chan et al. Experimental Dermatol 2003; 28: 651-6.
Current diagnostic algorithm: Clinical exam: elderly patient with pruritic bullae/vesicles,
urticaria, etc
H&E: subepidermal cleft/blister or eosinophilic spongiosis with inflammatory infiltrate rich in eosinophils and neutrophils
DIF: linear BMZ deposit of IgG +/- IgA and C3 (Clinical Gold
Standard)
IIF on SSS: IgG antibodies bind to epidermal side (+/-
dermal side)
Indirect Immunofluorescence
Bolognia et al. Dermatology, 3rd Ed; 2012: p 480. Kasperkiewicz M, et al. Autoimmunity 2012; 45(1):55-70.
ELISA in the diagnosis of BP
Commercial kit for BP180 NC16a and BP230 NC16a domain Less operator/interlab variability than
previous assays Quantitative study Sensitivity: (BP180 + BP230) > BP180 > BP230
Zillikens D et al. J Invest Dermatol 1997; 109(5): 679-83. Di Zezo et al. Clin Dermatol 2012; 30: 3-16.
125
Roussel A, et al. Arch Dermatol 2011; 147(3): 293-8. Charneux J, et al. Arch Dermatol 2011; 147(3): 286-291.
ELISA vs IIF
Current diagnostic algorithm Clinical exam: elderly patient with pruritic bullae/vesicles,
urticaria, etc
H&E: subepidermal cleft/blister or eosinophilic spongiosis with inflammatory infiltrate rich in eosinophils and neutrophils
DIF: linear BMZ deposit of IgG +/- IgA and C3 (Clinical Gold
Standard)
IIF on SSS: IgG antibodies bind to epidermal side (+/-
dermal side)
Where does ELISA fit?
Why is ELISA underused? Performance gap? Resource gap? Knowledge gap?
Where does ELISA fit into the diagnostic algorithm of BP?
Chan L. Arch Dermatol 2011; 147(3): 291-2.
Dilemmas in current diagnostic
algorithm…in summary
ELISA BP180-NC16A +/- BP 230 • Standardized test • Sensitive and specific • Quantitative • Cheaper • NOT commonly used
IIF on SSS • Operator variability, not standardized • 10-15% no detectable circulating antibodies • False positives reported • High cost
DIF • Operator variability, not standardized • Does not distinguish between other subepidermal blistering disorders • False negatives • High cost
H & E • Not specific nor diagnostic
Clinical exam • Variable
My research objective Compare the sensitivities and specificities
of clinical exam findings, DIF, IIF on SSS and ELISA (BP180-NC16A & BP230) in the diagnosis of BP
Identify the combination of findings with highest sensitivity and specificity
Further clarify the role of ELISA in the dx of BP
Cost analysis of each combination of studies
Identify new cost-effective diagnostic algorithm
126
Hypothesis/Proposed diagnostic Algorithm:
Clinical exam (>2 criteria): age >70, no scarring, no mucosal
involvement, no H&N involvement, presence of urticaria/bullae
Perform ELISA BP180-NC16A &
BP230
Consider new diagnosis Treat
Perform ELISA BP180-NC16A
Perform ELISA BP230
Consider new diagnosis Treat
Treat
Methods
IRB approved study Prospectively enrolling patients Inclusion criteria:
• +IIF on SSS OR +ELISA BP180-NC16A/230
AND • All must have:
• Clinical findings documented
• H&E • DIF • IIF • ELISA BP180-NC16A &
BP230
Clinical findings: • No scarring • No head and neck
involvement • No oral involvement • Age > 70 years old • Urticaria/bullae
Positive H&E = Eosinophilic and/or neutrophilic infiltrate +/-spongiosis, sub- or intraepidermal blister
Positive DIF = linear IgG and/or C3 at BMZ
Positive IIF = IgG on epidermal side SSS
Positive ELISA = ≥ 9 U/mL
…. Any Questions?
76 charts reviewed
20 patients met inclusion criteria
All met clinical criteria
All met H&E criteria
16 patients +ELISA
6 patients +ELISA BP180
alone
2 patients +ELISA BP230
alone
8 patients +ELISA (BP180
& BP230)
16 patients +IIF (IgG on
epidermal side of SSS)
15 patients +DIF (linear IgG +/- C3)
44 patients did not meet inclusion criteria
9 patients with some data still
pending 3 patients with
MMP
2 patients +BP230 …. Any Questions?
127
Study/Year Test Specificity Sensitivity Comparison
Chan et al, 2003 N=23
DIF 91% IIF 96% Immunoblot (BP180 + BP230) 100%
ELISA BP180-NC16A 96%
Barnadas et al, 2008 N=28
ELISA BP180-NC16A 96% 92%
IIF 96% 74% Giovanni et al, 2008 N=49
BP230 71% BP180 NC16A 90%
BP180 non NC16A domain 96%
BP180 + BP230 100%
IIF vs ELISA (BP180 + BP230) ELISA superior
IIIF vs ELISA BP180 IIF superior
Tampoia et al, 2009 N=38
ELISA BP180 98.8% 90% ELISA BP230 98.8% 60%
Atzori et al, 2008 N=19
ELISA BP180 95%
Sitaru et al, 2007 N=118
ELISA BP180 NC16A tetramer 97.8% 89.8%
ELISA BP180 NC16A MBL 94.8% 89%
Thoma-Uszynski et al, 2004 N=127
ELISA BP180 94% 95.3% ELISA BP230 95.3% 81.5%
Feng et al, 2008 N=20
ELISA BP180 NC16a 19/20 pts + and levels correlated with dz activity
Kobayashi et al, 2002 N=64
ELISA BP180 NC16a 98.9% 84.4%
Zillikens et al, 1997 N=50
ELISA BP180NC16a 99.9% 94%
Sano et al, 2008 DIF 55.6%

128
Ellecia Cook, DO, PGY-4
Program Director: Richard Miller, DO, FAOCD
No Financial Disclosures
OBJECTIVES
• Basic overview of HIV • Present 10 cases of cutaneous
manifestations of HIV • Review 6 atypical presentations of
dermatologic conditions in HIV patients
INTRODUCTION
• 40 Million infected Worldwide • 5 Million new infections per year worldwide • Leading cause of death in Africa • Fourth leading cause of death worldwide
INTRODUCTION • Enveloped RNA virus • Lentivirus genus, Retroviridae family • HIV-1: West Africa
• HIV-2: United States and Europe
INTRODUCTION • > 90% develop dermatologic disorders • Cutaneous disease is often initial
manifestation of undiagnosed HIV • Dermatologists play a key role in
diagnosing HIV
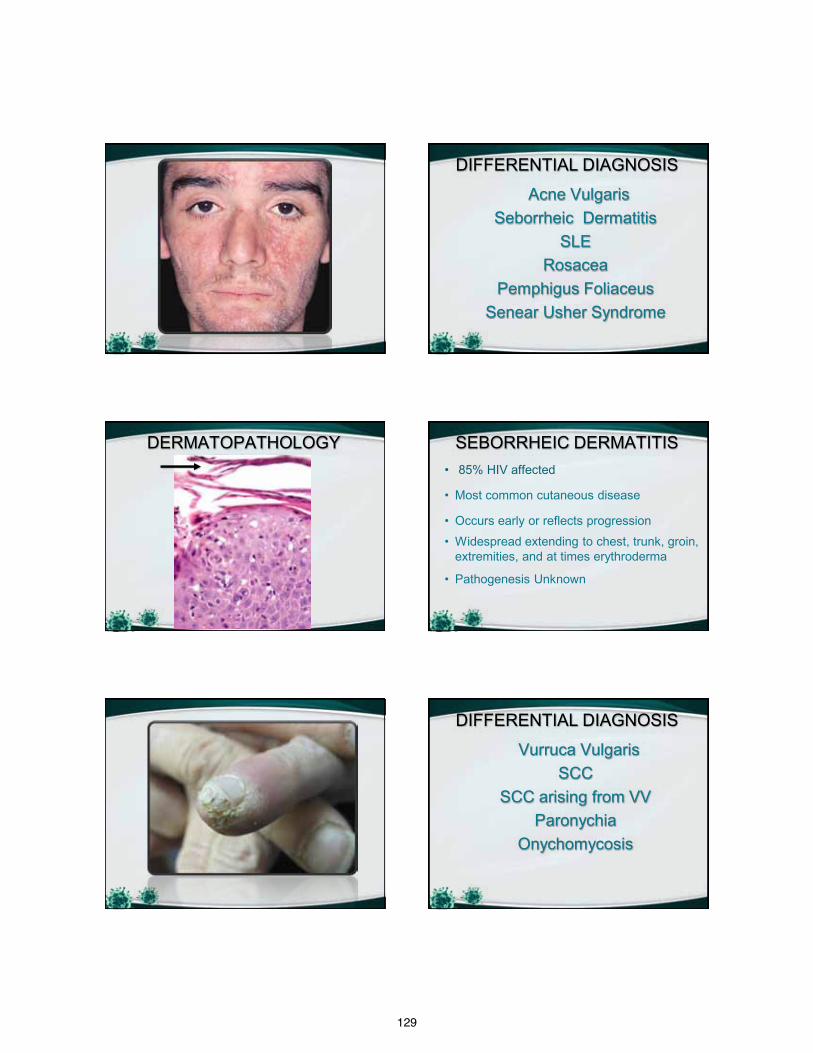
129
DIFFERENTIAL DIAGNOSIS
Acne Vulgaris Seborrheic Dermatitis
SLE Rosacea
Pemphigus Foliaceus Senear Usher Syndrome
DERMATOPATHOLOGY SEBORRHEIC DERMATITIS • 85% HIV affected
• Most common cutaneous disease
• Occurs early or reflects progression
• Widespread extending to chest, trunk, groin, extremities, and at times erythroderma
• Pathogenesis Unknown
DIFFERENTIAL DIAGNOSIS
Vurruca Vulgaris SCC
SCC arising from VV Paronychia
Onychomycosis

130
DERMATOPATHOLOGY SQUAMOUS CELL CARCINOMA arising from
VERRUCA VULGARIS • HPV 16 • High risk HPV serotypes • Aggressive squamous cell carcinomas • Prompt diagnosis and aggressive
treatment required
DIFFERENTIAL DIAGNOSIS
Scabies Infestation Psoriasis
Arthropod Assault Contact Dermatitis Atopic Dermatitis
Seborrheic Dermatitis
DERMATOPATHOLOGY SCABIES INFESTATION • Most common ectoparasitic skin infestation
• Burrows are less apparent
• Ears, face, and scalp involvement
• Crusted scabies – Generalized with thousands-millions of mites
• Scrape hyponychium for protected mites
• Bacteremia and fatal septicemia reported
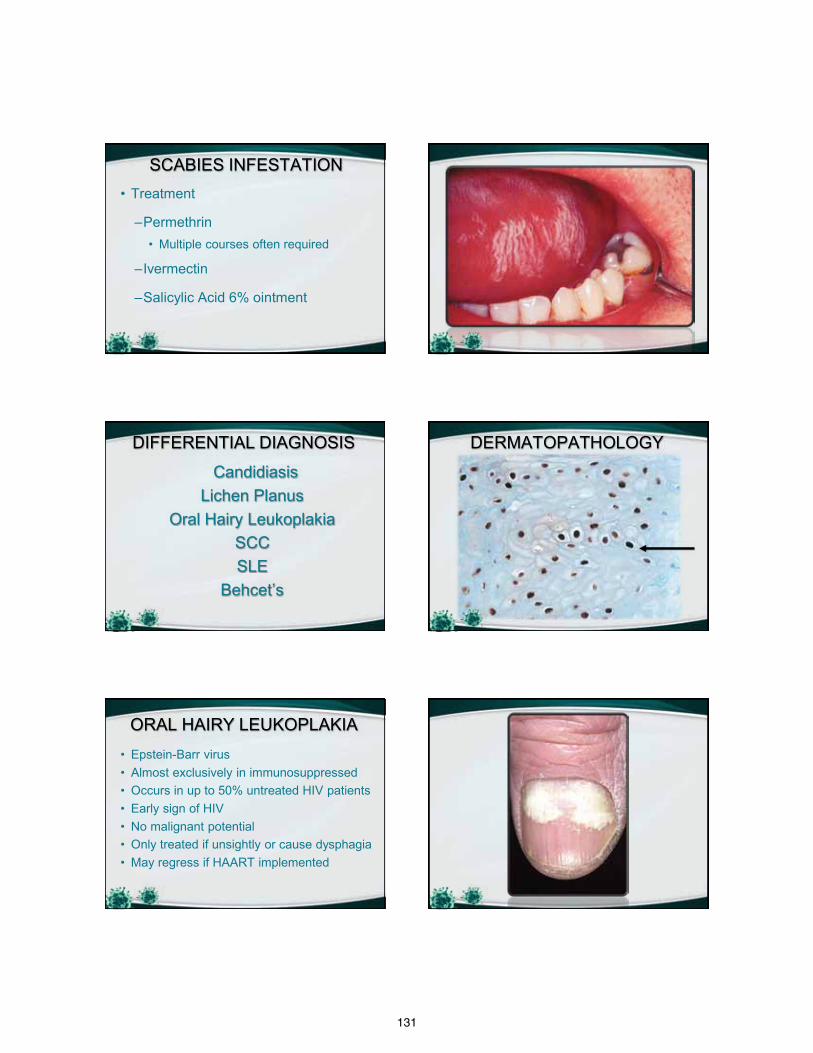
131
SCABIES INFESTATION • Treatment
–Permethrin • Multiple courses often required
–Ivermectin
–Salicylic Acid 6% ointment
DIFFERENTIAL DIAGNOSIS
Candidiasis Lichen Planus
Oral Hairy Leukoplakia SCC SLE
Behcet’s
DERMATOPATHOLOGY
• Epstein-Barr virus • Almost exclusively in immunosuppressed • Occurs in up to 50% untreated HIV patients • Early sign of HIV • No malignant potential • Only treated if unsightly or cause dysphagia • May regress if HAART implemented
ORAL HAIRY LEUKOPLAKIA
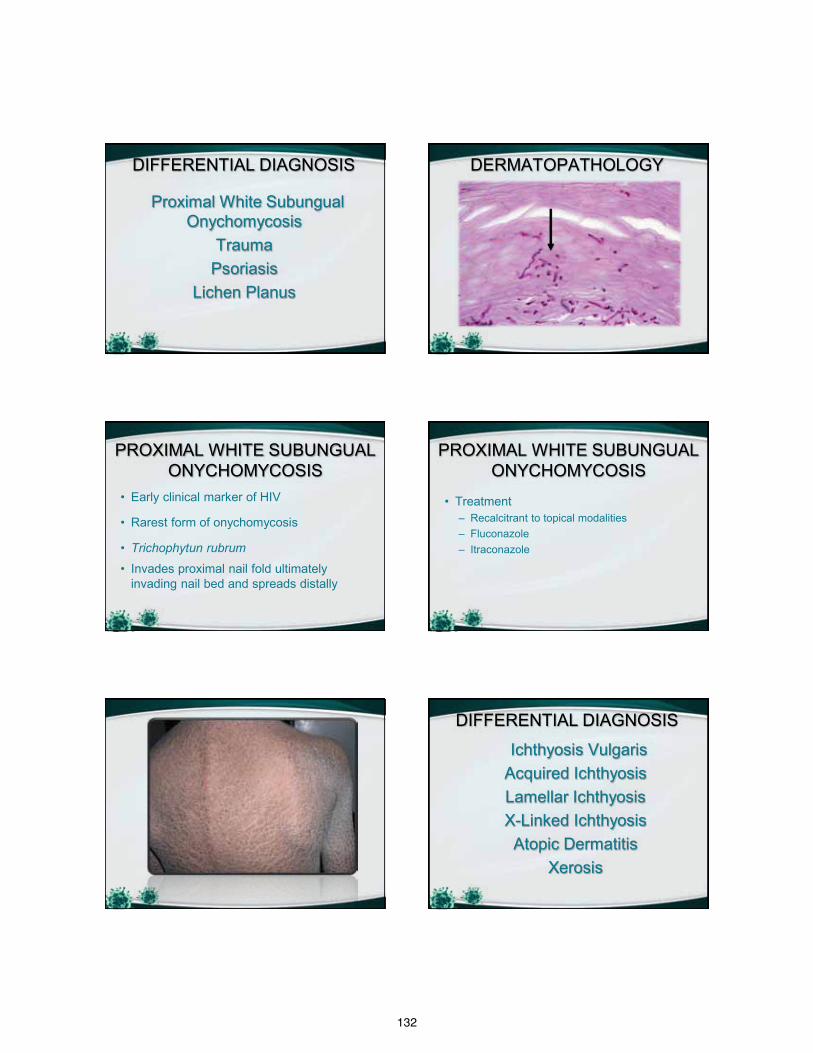
132
DIFFERENTIAL DIAGNOSIS
Proximal White Subungual Onychomycosis
Trauma Psoriasis
Lichen Planus
DERMATOPATHOLOGY
• Early clinical marker of HIV
• Rarest form of onychomycosis
• Trichophytun rubrum
• Invades proximal nail fold ultimately invading nail bed and spreads distally
PROXIMAL WHITE SUBUNGUAL ONYCHOMYCOSIS
• Treatment – Recalcitrant to topical modalities – Fluconazole – Itraconazole
PROXIMAL WHITE SUBUNGUAL ONYCHOMYCOSIS
DIFFERENTIAL DIAGNOSIS
Ichthyosis Vulgaris Acquired Ichthyosis Lamellar Ichthyosis X-Linked Ichthyosis Atopic Dermatitis
Xerosis
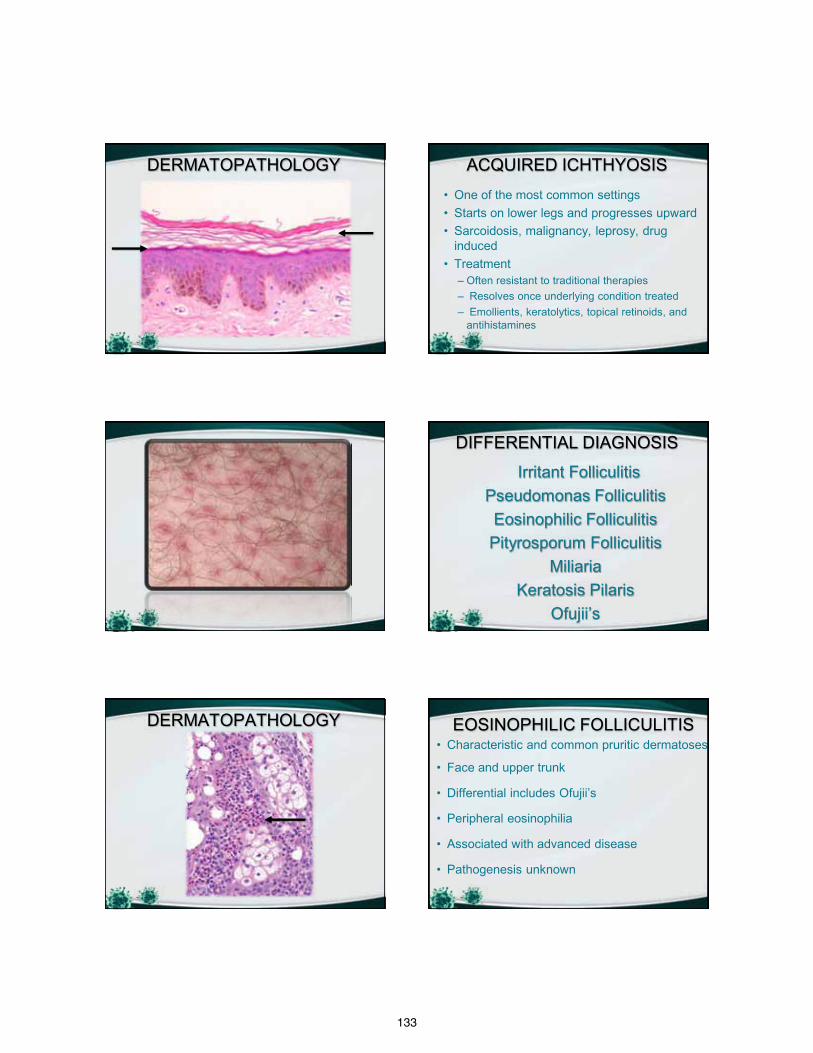
133
DERMATOPATHOLOGY • One of the most common settings • Starts on lower legs and progresses upward • Sarcoidosis, malignancy, leprosy, drug
induced • Treatment
– Often resistant to traditional therapies – Resolves once underlying condition treated – Emollients, keratolytics, topical retinoids, and
antihistamines
ACQUIRED ICHTHYOSIS
DIFFERENTIAL DIAGNOSIS
Irritant Folliculitis Pseudomonas Folliculitis Eosinophilic Folliculitis Pityrosporum Folliculitis
Miliaria Keratosis Pilaris
Ofujii’s
DERMATOPATHOLOGY EOSINOPHILIC FOLLICULITIS • Characteristic and common pruritic dermatoses
• Face and upper trunk
• Differential includes Ofujii’s
• Peripheral eosinophilia
• Associated with advanced disease
• Pathogenesis unknown
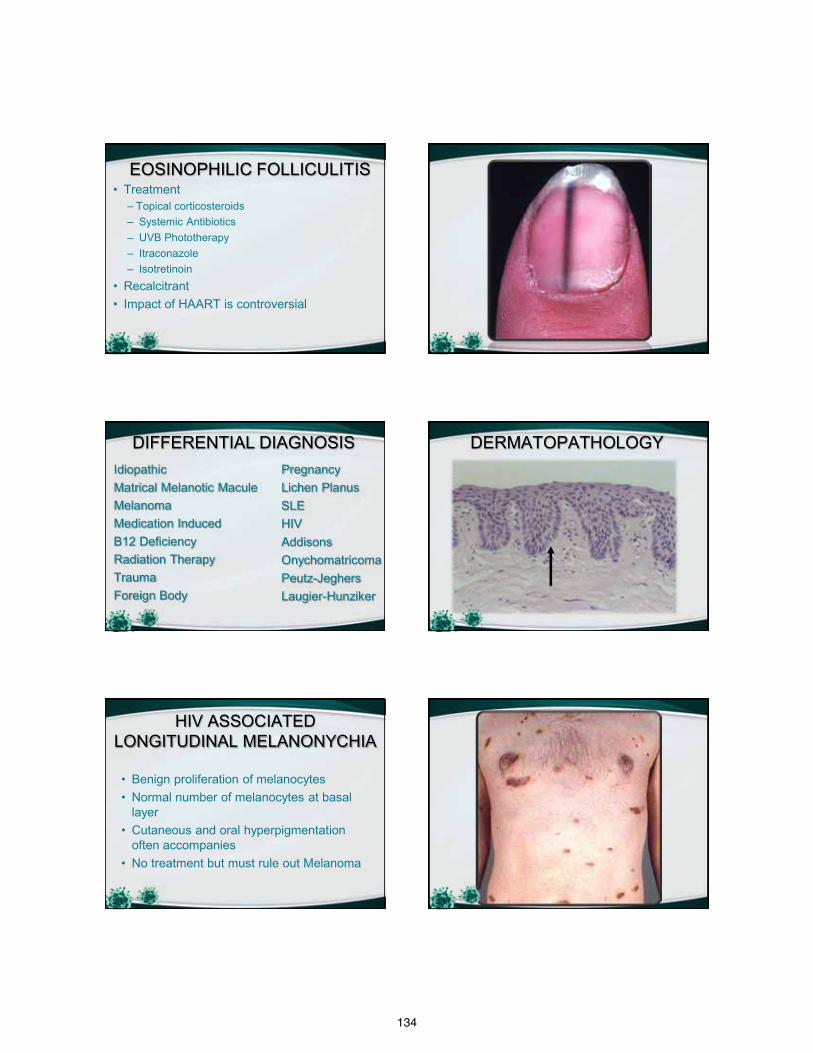
134
EOSINOPHILIC FOLLICULITIS • Treatment
– Topical corticosteroids – Systemic Antibiotics – UVB Phototherapy – Itraconazole – Isotretinoin
• Recalcitrant • Impact of HAART is controversial
DIFFERENTIAL DIAGNOSIS Idiopathic Matrical Melanotic Macule Melanoma Medication Induced B12 Deficiency Radiation Therapy Trauma Foreign Body
Pregnancy Lichen Planus SLE HIV Addisons Onychomatricoma Peutz-Jeghers Laugier-Hunziker
DERMATOPATHOLOGY
• Benign proliferation of melanocytes • Normal number of melanocytes at basal
layer • Cutaneous and oral hyperpigmentation
often accompanies • No treatment but must rule out Melanoma
HIV ASSOCIATED LONGITUDINAL MELANONYCHIA
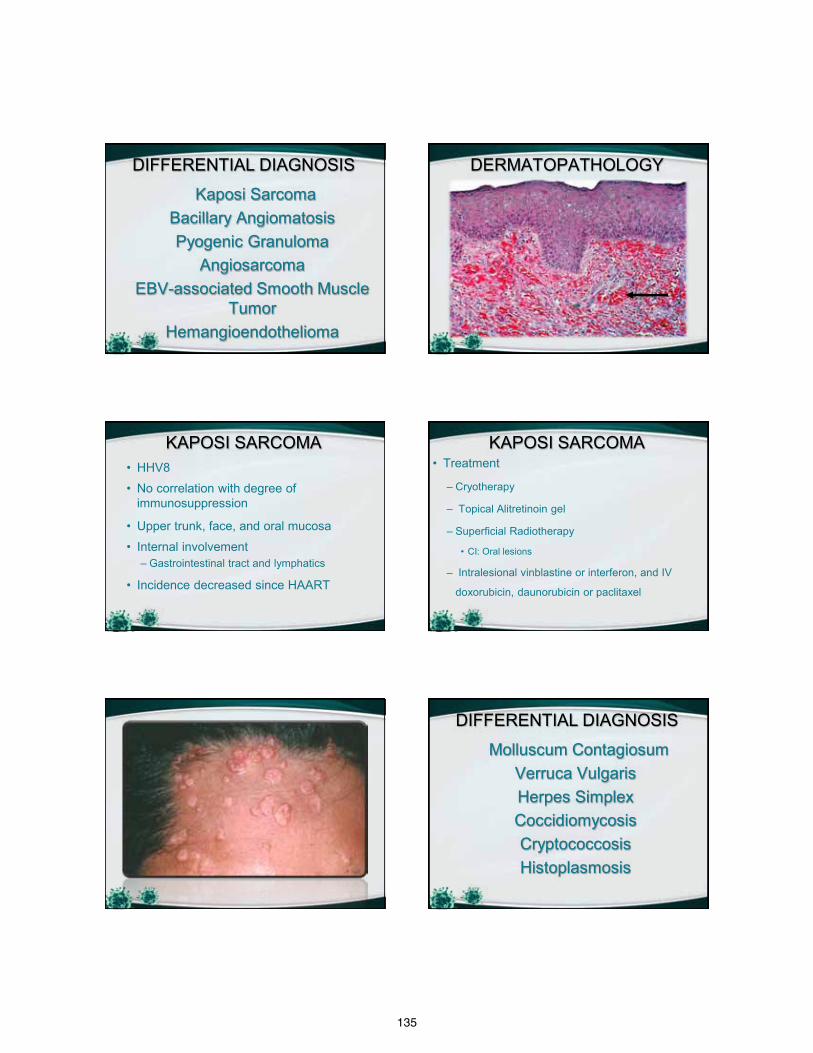
135
DIFFERENTIAL DIAGNOSIS
Kaposi Sarcoma Bacillary Angiomatosis Pyogenic Granuloma
Angiosarcoma EBV-associated Smooth Muscle
Tumor Hemangioendothelioma
DERMATOPATHOLOGY
• HHV8
• No correlation with degree of immunosuppression
• Upper trunk, face, and oral mucosa
• Internal involvement – Gastrointestinal tract and lymphatics
• Incidence decreased since HAART
KAPOSI SARCOMA • Treatment
– Cryotherapy
– Topical Alitretinoin gel
– Superficial Radiotherapy
• CI: Oral lesions
– Intralesional vinblastine or interferon, and IV
doxorubicin, daunorubicin or paclitaxel
KAPOSI SARCOMA
DIFFERENTIAL DIAGNOSIS
Molluscum Contagiosum Verruca Vulgaris Herpes Simplex Coccidiomycosis Cryptococcosis Histoplasmosis
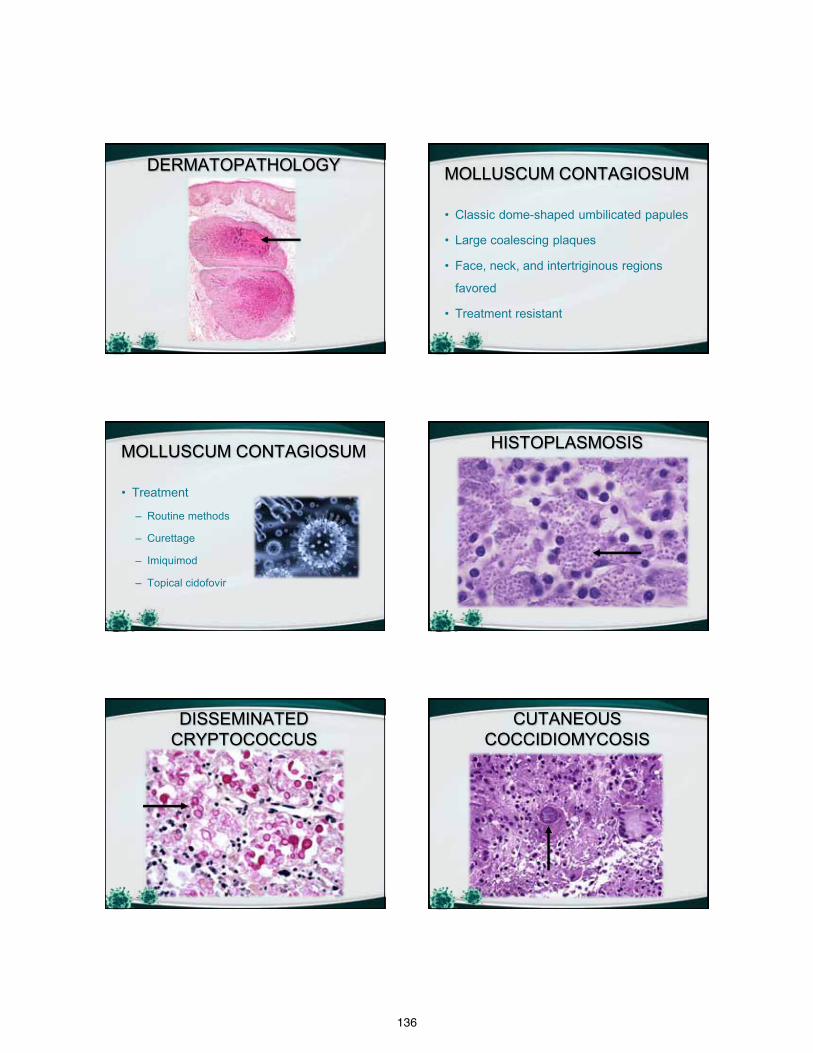
136
DERMATOPATHOLOGY MOLLUSCUM CONTAGIOSUM
• Classic dome-shaped umbilicated papules
• Large coalescing plaques
• Face, neck, and intertriginous regions
favored
• Treatment resistant
MOLLUSCUM CONTAGIOSUM
• Treatment
– Routine methods
– Curettage
– Imiquimod
– Topical cidofovir
HISTOPLASMOSIS
DISSEMINATED CRYPTOCOCCUS
CUTANEOUS COCCIDIOMYCOSIS
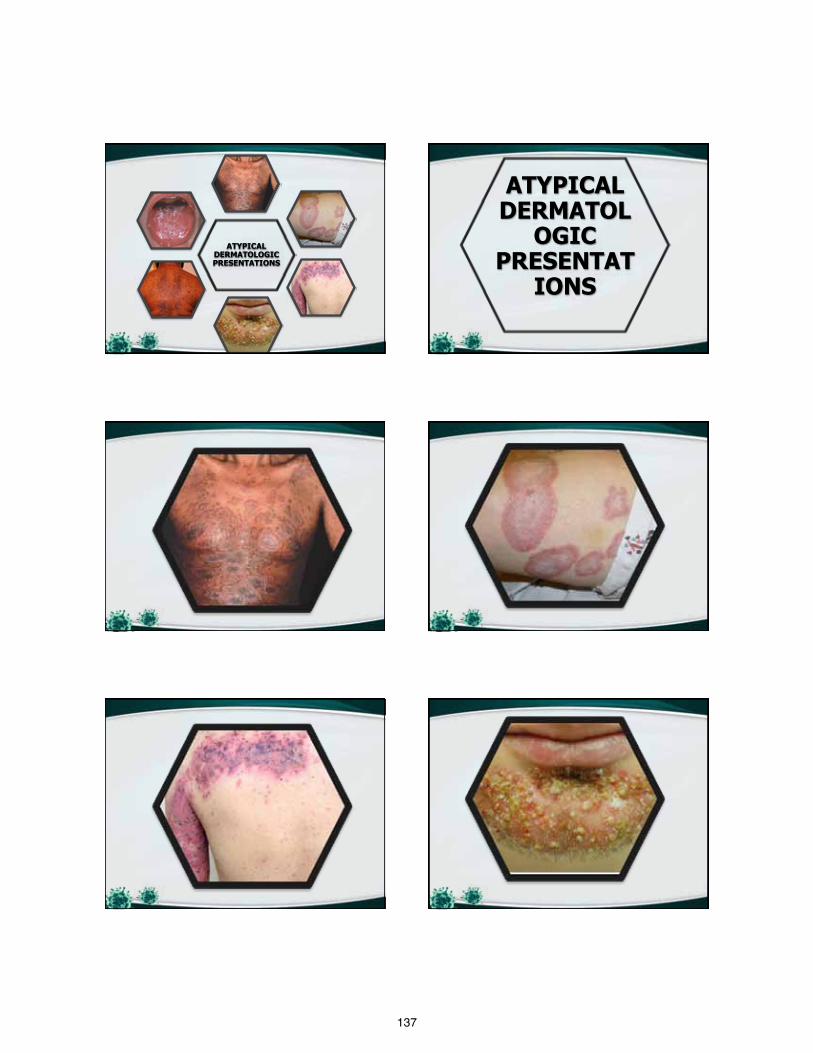
137
ATYPICAL DERMATOLOGIC PRESENTATIONS
ATYPICAL DERMATOL
OGIC PRESENTAT
IONS
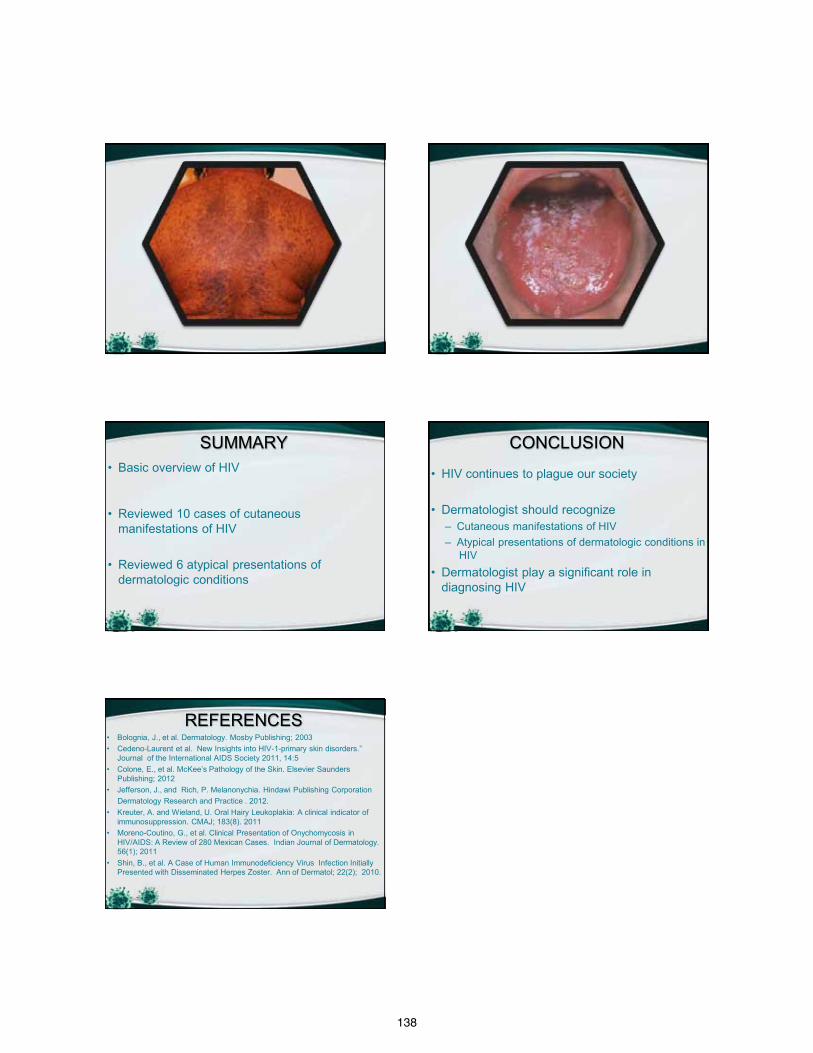
138
SUMMARY • Basic overview of HIV
• Reviewed 10 cases of cutaneous manifestations of HIV
• Reviewed 6 atypical presentations of
dermatologic conditions
CONCLUSION
• HIV continues to plague our society • Dermatologist should recognize
– Cutaneous manifestations of HIV – Atypical presentations of dermatologic conditions in
HIV • Dermatologist play a significant role in
diagnosing HIV
REFERENCES • Bolognia, J., et al. Dermatology. Mosby Publishing; 2003 • Cedeno-Laurent et al. New Insights into HIV-1-primary skin disorders.”
Journal of the International AIDS Society 2011, 14:5 • Colone, E., et al. McKee’s Pathology of the Skin. Elsevier Saunders
Publishing; 2012 • Jefferson, J., and Rich, P. Melanonychia. Hindawi Publishing Corporation Dermatology Research and Practice . 2012. • Kreuter, A. and Wieland, U. Oral Hairy Leukoplakia: A clinical indicator of
immunosuppression. CMAJ; 183(8). 2011 • Moreno-Coutino, G., et al. Clinical Presentation of Onychomycosis in
HIV/AIDS: A Review of 280 Mexican Cases. Indian Journal of Dermatology. 56(1); 2011
• Shin, B., et al. A Case of Human Immunodeficiency Virus Infection Initially Presented with Disseminated Herpes Zoster. Ann of Dermatol; 22(2); 2010.
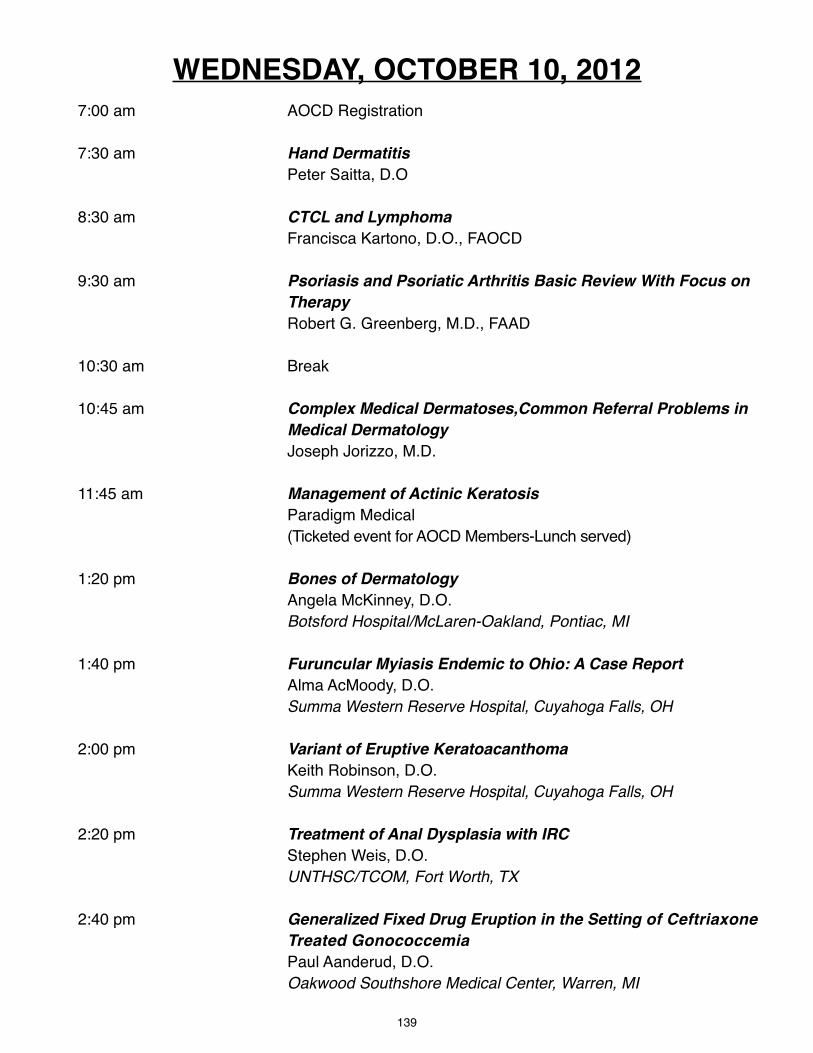
139
7:00 am AOCD Registration
7:30 am Hand Dermatitis Peter Saitta, D.O
8:30 am CTCL and Lymphoma Francisca Kartono, D.O., FAOCD
9:30 am Psoriasis and Psoriatic Arthritis Basic Review With Focus on Therapy Robert G. Greenberg, M.D., FAAD
10:30 am Break
10:45 am Complex Medical Dermatoses,Common Referral Problems in Medical Dermatology Joseph Jorizzo, M.D.
11:45 am Management of Actinic Keratosis Paradigm Medical (Ticketed event for AOCD Members-Lunch served)
1:20 pm Bones of Dermatology Angela McKinney, D.O. Botsford Hospital/McLaren-Oakland, Pontiac, MI
1:40 pm Furuncular Myiasis Endemic to Ohio: A Case Report Alma AcMoody, D.O. Summa Western Reserve Hospital, Cuyahoga Falls, OH
2:00 pm Variant of Eruptive Keratoacanthoma Keith Robinson, D.O. Summa Western Reserve Hospital, Cuyahoga Falls, OH
2:20 pm Treatment of Anal Dysplasia with IRC Stephen Weis, D.O. UNTHSC/TCOM, Fort Worth, TX
2:40 pm Generalized Fixed Drug Eruption in the Setting of Ceftriaxone Treated Gonococcemia Paul Aanderud, D.O. Oakwood Southshore Medical Center, Warren, MI
WEDNESDAY, OCTOBER 10, 2012
140
3:00 pm Break
3:20 pm Arbor Cutis: Hyperkeratotic Plaque Secondary to the Use of Imiquimod Peter Knabel, D.O. Northeast Regional Medical Center, Kirksville, MO
3:40 pm Oral Spironolactone in Post-Teenage Acne in Females Grace Kim, D.O. Valley Hospital Medical Center, Las Vegas, NV
4:00 pm Acne Scar Lysing Mari Batta, D.O. Alta Dermatology, Mesa, AZ
4:20 pm Adalimumab for the Treatment of Pityriasis Rubra Pilaris with an Overview of Disease Classification Jeremy Bingham, D.O. Advanced Desert Dermatology, Peoria, AZ
4:40 pm Primary Mucinous Carcinoma of Skin Helia Eragi, D.O. Pacific Hospital, Torrance, CA
5:00 pm Hereditary Disorders of Cornification Tatyana Groysman, D.O. PCOM/Lehigh Valley Health Network, Allentown, PA
5:20 pm End of Meeting
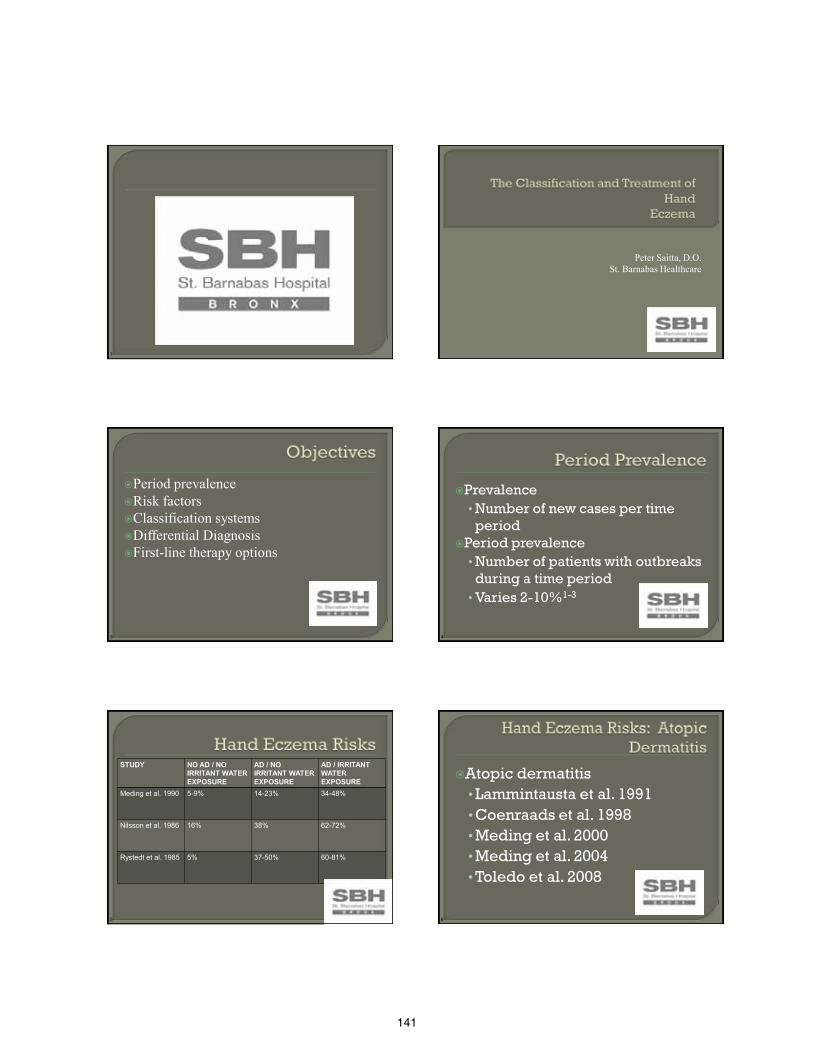
141
1
Peter Saitta, D.O. St. Barnabas Healthcare
3
Period prevalence Risk factors Classification systems Differential Diagnosis First-line therapy options
4
Prevalence •Number of new cases per time period
Period prevalence •Number of patients with outbreaks during a time period •Varies 2-10%1-3
5
STUDY NO AD / NO IRRITANT WATER EXPOSURE
AD / NO IRRITANT WATER EXPOSURE
AD / IRRITANT WATER EXPOSURE
Meding et al. 1990 5-9% 14-23% 34-48%
Nilsson et al. 1986 16% 38% 62-72%
Rystedt et al. 1985 5% 37-50% 60-81%
6
Atopic dermatitis •Lammintausta et al. 1991 •Coenraads et al. 1998 •Meding et al. 2000 •Meding et al. 2004 •Toledo et al. 2008
142
7
Allergic rhinitis/asthma increases risk of hand eczema •But not more than atopic dermatitis4
8
Female gender increased risk
• Coenraads et al. 1983 • Kavli et al. 1984 • Lantinga et al. 1984 • Bryld et al. 2000 • Yngveson et al. 2000 • Meding et al. 2001 • Mortz et al. 2001 • Dickel et al. 2002
9
Meding et al.5
• Wet work in 19-29 year-olds • 37.5% of women occupationally exposed • 18.2% of men
Learbek et al.6 • Private exposures
10
STUDY TYPE OF STUDY
STUDY POPULATION
INCIDENCE (PER 100)
Lantinga et al. 1984
Retrospective General Population
7.9
Uter et al. 1994 Prospective Hairdressers 152
Smit et al. 1994 Prospective Hairdressers Nurses
328 145
Brisman et al. 1998
Retrospective Bakers M: 16.7 F:34.4
Uter et al. 1998 Prospective Office workers 41
Funke et al. 2001 Prospective Industrial Factory Workers
47
11
SUPPORT RISK NEGATE RISK
Edman et al. Montnemery et al. Linneberg et al.
Lerbeack et al. Berndt et al
12
ACD7
Delay onset of treatment8
Atopic Dermatitis9
Greater area of involved skin10
> 1 year of duration8
143
13
Etiology Morphology •No clear link between morphology and etiology11
•Question the need of morphological classification system
14
Irritant contact dermatitis Allergic contact dermatitis Atopic dermatitis •80%
Idiopathic •20%
15
Irritant Contact Dermatitis11
•Most common Wet work Water Mechanic / Machinery oils Detergents Tight-fitting gloves Friction
16
Wet hands or glove wearing > 2 cumulative hours daily11,12
Greater than 20 hand washes daily12
17
Allergic Contact Dermatitis • Way more common in occupational exposures vs. private
exposures (Hobby)11
• “Hand eczema that spreads”13 Protein Contact Dermatitis
• RARE • Latex • Food proteins • Burning, stinging and itching seconds to minutes after contact14
Systemic Contact Dermatitis
• VERY RARE • Specific definition11 Positive patch test Ingest an oral version Vesicular hand/foot rash
18
Atopic dermatitis Other genetic
• Filaggrin null mutations15,16 • Twin studies show that MZ twin individuals having a
co-twin with hand eczema had an increased risk of hand eczema compared with DZ twins6 Atopic dermatitis adjusted
Idiopathic CHE 20%11
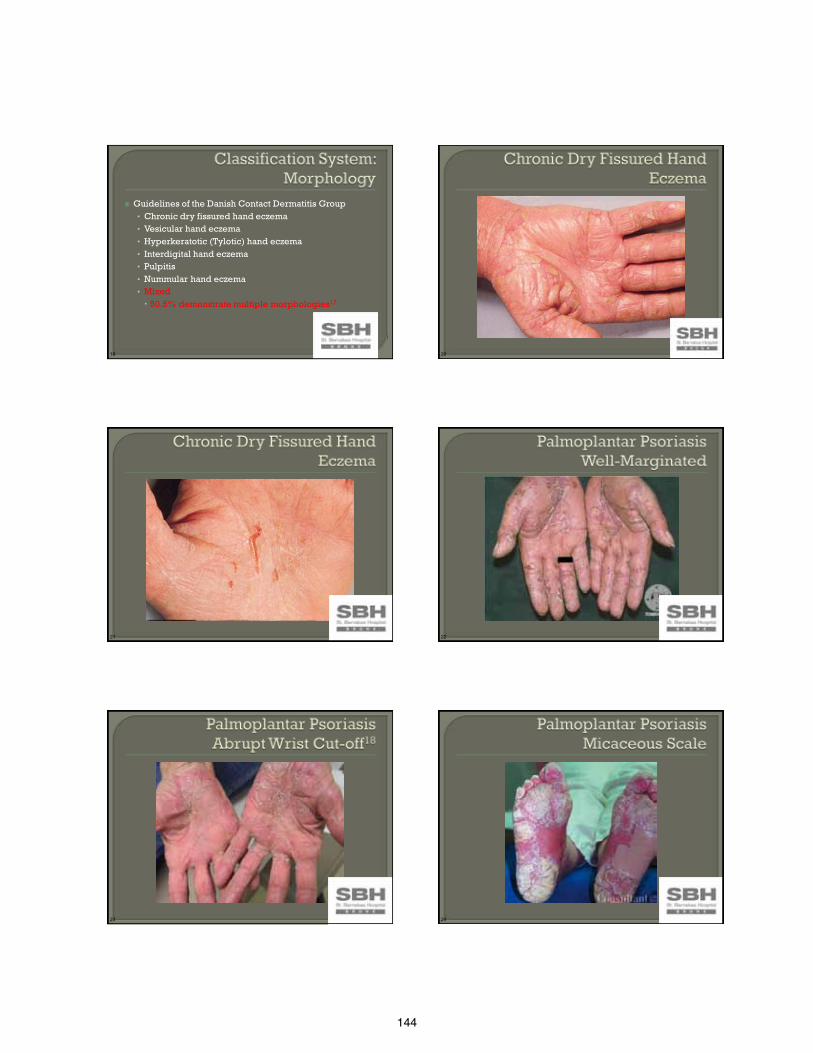
144
19
Guidelines of the Danish Contact Dermatitis Group • Chronic dry fissured hand eczema • Vesicular hand eczema • Hyperkeratotic (Tylotic) hand eczema • Interdigital hand eczema • Pulpitis • Nummular hand eczema • Mixed 50.5% demonstrate multiple morphologies17
20
21 22
23 24

145
25
Frequency based on location19
• 1. Generalized Plaque – 49.3% • 2. Localized Plaque – 16.9% • 3. Guttate – 12.8% • 4. Arthropathic – 7.7% • 5. Palmoplantar – 7.5% • 6. Pustular – 3.1% • 7. Other – 2.7%
26
Intermittent20
• Intensely pruritic • Palms/soles, nail, and sides of fingers • Attacks between 1 and 10 months
Two historical descriptions Pompholyx Dyshidrosis
27
Frequency of location20 • 1. Hands alone – 46.8% • 2. Feet alone – 24.1% • 3. Hands and feet – 15.6% • 4. Nail apparatus – 13.5%
28
Anatomic Location20 Fungi Positive Hands 1.2% Feet 47.8% Epidermophyton interdigitale 100% of feet cases
29
Lane et al.21
• 25% of any location positive fungal infection Pitche et al.22
• 10% of any location positive fungal infection Guillet et al.23
• 15.8% of any location with T. rubrum or candida infection
30
Always check the feet • Foot involvement is rare • 47.8% dermatophyte infection
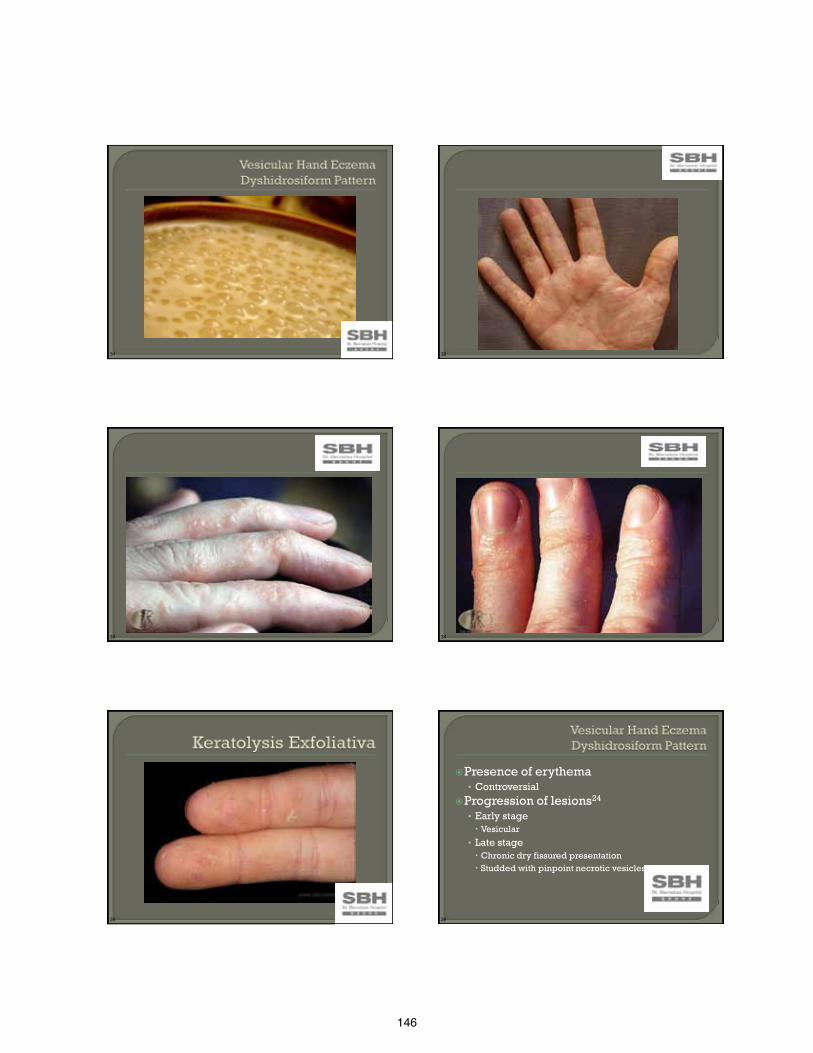
146
31 32
33 34
35 36
Presence of erythema • Controversial
Progression of lesions24 • Early stage Vesicular
• Late stage Chronic dry fissured presentation Studded with pinpoint necrotic vesicles
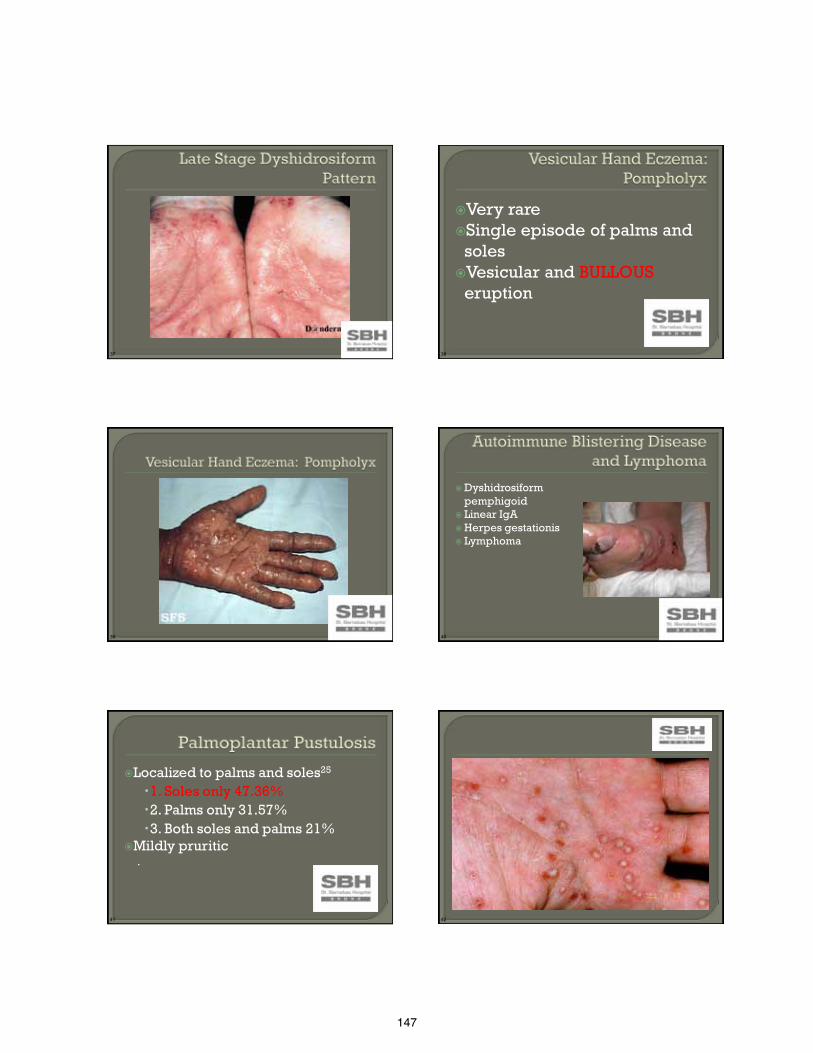
147
37 38
Very rare Single episode of palms and
soles Vesicular and BULLOUS
eruption
39 40
Dyshidrosiform pemphigoid
Linear IgA Herpes gestationis Lymphoma
41
Localized to palms and soles25 1. Soles only 47.36% 2. Palms only 31.57% 3. Both soles and palms 21%
Mildly pruritic .
42

148
43 44
Middle-aged men NEVER VESICLES
45 46
47 48
Dominant hand Site for the start of irritant hand
dermatitis26,27
149
49 50
51 52
53 54
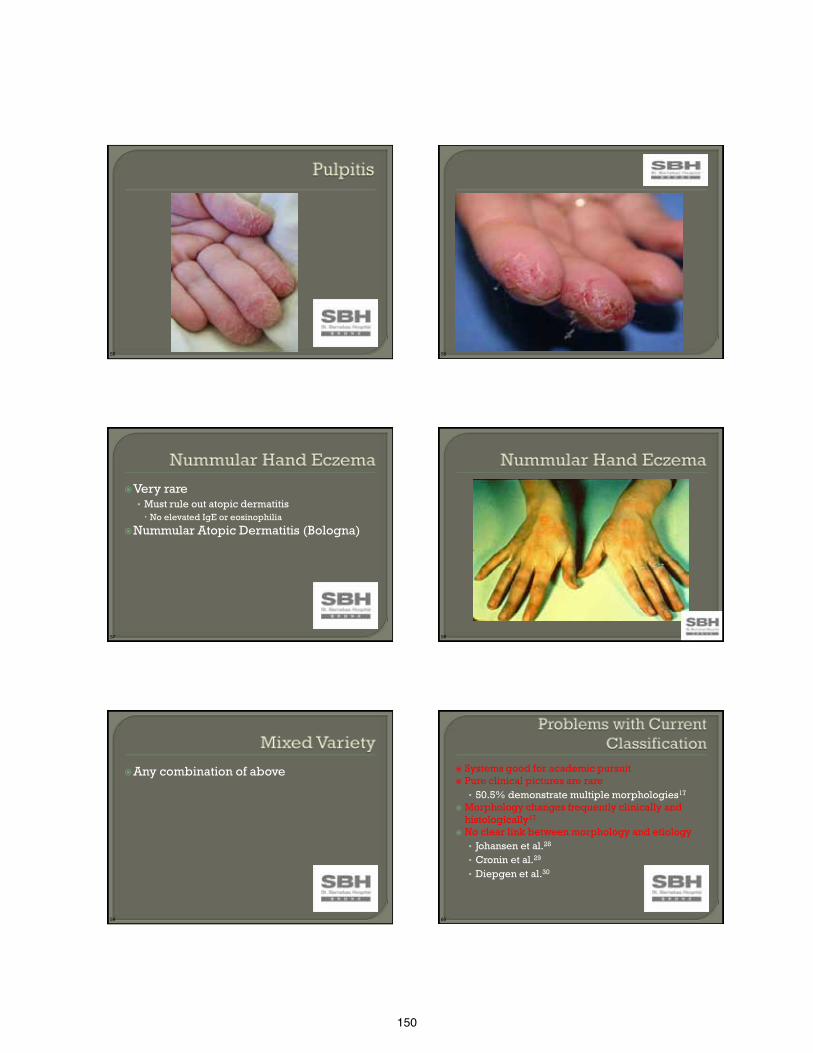
150
55 56
57
Very rare • Must rule out atopic dermatitis No elevated IgE or eosinophilia
Nummular Atopic Dermatitis (Bologna)
58
59
Any combination of above
60
Systems good for academic pursuit Pure clinical pictures are rare
• 50.5% demonstrate multiple morphologies17 Morphology changes frequently clinically and
histologically17 No clear link between morphology and etiology
• Johansen et al.28 • Cronin et al.29 • Diepgen et al.30

151
61
Eczematous reactive process • Acute – vesicles/bullae/erythema • Subacute – scaling/erythema • Chronic – scaling/erythema/lichenification
62
CHECK THE FEET CHECK THE FEET CHECK THE FEET
63
Palmoplantar Psoriasis Palmoplantar Pustulosis
Scabies Erythema Multiforme
Lichen Planus Id reactions
Keratolysis exfoliativa Palmoplantar keratoderma
Autoimmune blistering diseases Lymphoma
Erosio Interdigitalis Blastomycetica
64
Hand Eczema Evaluation Irritant, Atopic, Allergic What do you do for work? Do you touch liquids routinely at work? How many times a day do you wash your
hands? Do you wear gloves and touch food at
work? Do you have childhood eczema, allergies,
or asthma?
65
Standard Series • Toledo et al. • Linberg et al. • Menne et al.
Worker’s Compensation
Irritant contact dermatitis31-33
21% with positive patch test34 • 30% relevant • Nickel (100%)
ACD worse prognosis7
66
#1 Treatment is the same • #2 Blow them up • Faster clearance initially lowers risk of chronicity43
• #3 And then juice em • Systemic and topical steroids35
One episode – 38.4%
Intermittent non-cyclic – 30.8% Intermittent cyclic-28.5% Chronic – 2.3% Patients perceive systemic agents as powerful
#4 Don’t stop treatment if it gets better
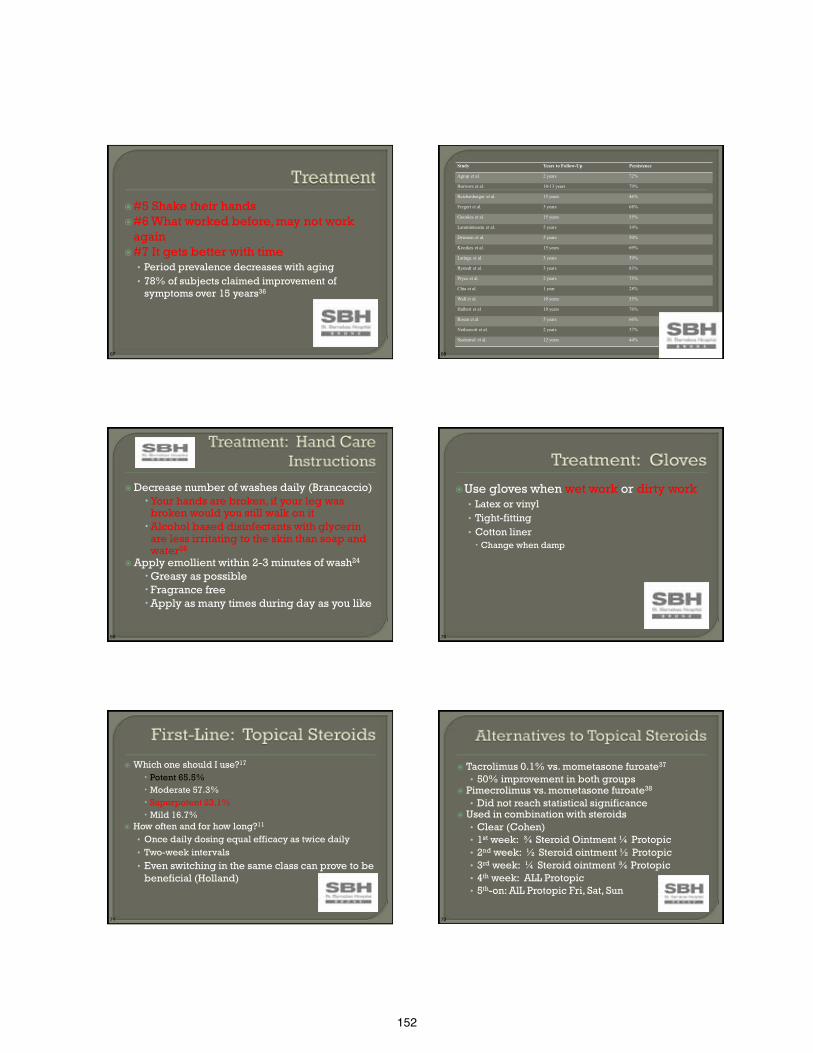
152
67
#5 Shake their hands #6 What worked before, may not work
again #7 It gets better with time
• Period prevalence decreases with aging • 78% of subjects claimed improvement of
symptoms over 15 years36
68
Study Years to Follow-Up Persistence
Agrup et al. 2 years 72%
Burrows et al. 10-13 years 79%
Reichenberger et al. 15 years 46%
Fregert et al. 3 years 68%
Gooskes et al. 15 years 55%
Lammintausta et al. 5 years 34%
Driessen et al. 5 years 50%
Keczkes et al. 15 years 69%
Latinga et al. 3 years 59%
Rystedt et al. 3 years 83%
Pryce et al. 2 years 75%
Chia et al. 1 year 28%
Wall et al. 10 years 55%
Halbert et al 10 years 76%
Rosen et al 5 years 66%
Nethercott et al. 2 years 37%
Susitaival et al. 12 years 44%
69
Decrease number of washes daily (Brancaccio) Your hands are broken, if your leg was
broken would you still walk on it Alcohol based disinfectants with glycerin
are less irritating to the skin than soap and water26
Apply emollient within 2-3 minutes of wash24
Greasy as possible Fragrance free Apply as many times during day as you like
70
Use gloves when wet work or dirty work • Latex or vinyl • Tight-fitting • Cotton liner Change when damp
71
Which one should I use?17
Potent 65.5% Moderate 57.3% Superpotent 23.1% Mild 16.7%
How often and for how long?11
• Once daily dosing equal efficacy as twice daily • Two-week intervals
• Even switching in the same class can prove to be beneficial (Holland)
72
Tacrolimus 0.1% vs. mometasone furoate37 • 50% improvement in both groups
Pimecrolimus vs. mometasone furoate38
• Did not reach statistical significance
Used in combination with steroids • Clear (Cohen) • 1st week: ¾ Steroid Ointment ¼ Protopic • 2nd week: ½ Steroid ointment ½ Protopic • 3rd week: ¼ Steroid ointment ¾ Protopic • 4th week: ALL Protopic • 5th-on: AlL Protopic Fri, Sat, Sun
153
73
First Blow • Prednisone 40-60mg daily initial dose and taper
between 3-4 weeks39
• Intramuscular Kenalog 40-80mg40 Limit 4 shots per year (Wolverton)
Second Blow • Prednisolone 30mg daily for 3 days at onset of
eruptions41 • Prednisone 40-60mg x 1 dose on day 1 of the
eruption23
74
S. aureus • Systemic antibiotics superior to topicals24
75
Botulinum toxin A42
• Left versus right study • Vesicular hand dermatitis only • 100 units plus topical steroids
Botulinum toxin43 • Left versus right study • Vesicular hand dermatitis only • 162 units of botox but no steroids
76
UVA >>> NBUVB >>> UVB52
• Apoptosis of lymphocytes through reactive oxygen species and FAS ligand
• Increase in IL-10 inhibition of interferon –gamma. Efficacy PUVA53,54
• Systemic = Topical = Bath • Bath with least side effect Decreased UVA doses due to uniform absorption Phototoxicity risk disappears after 2 hours Sunblock and gloves
• High dose UVA-1 Max single dose of 130J/cm2 Cumulative dose 1720J/cm2 As effective as cream puva52
Reduction in pruritus in first week55
77
Azathioprine 100-150mg daily44
Methotrexate 15-25mg weekly45
Mycophenolate mofetil 2g/day46
Cyclosporine 2.5mg/kg/day47
Etanercept 25mg twice weekly48
78
Approved Europe • Indicated for chronic hand eczema refractory to
topical and systemic steroids • Not for vesicular hand dermatitis
Panagonist RXR, RAR Retinoid Adverse Events
• Headache, mucocutaneous dryness, elevated liver enzymes, elevated blood lipid levels, teratogenicity
No combination studies
154
79
Alitretinoin 30mg daily49 • Median time to clear hands is 12 weeks
Placebo, Alitretinoin 10mg, 20mg, 40mg daily doses for 12 weeks50 • 70% reduction in 50%
Alitretinoin 10mg, 30mg daily for 24 weeks51 • 100% reduction in 48% • More response with 30mg
80
Grenz ray • Energy less than 20kv • Deposited on skin surface
Superficial radiation therapy • Energy 50-150kv • 5mm depth of penetration
Megavoltage electron/photon beam therapy • Measured by a Gray
81
Period prevalence • 2-10%
Risk factors • Atopic dermatitis, allergic rhinitis/asthma, occupation, wet irritant
exposure Classification systems
• Etiology and morphology • Not practical day-to-day clinic
Differential Diagnosis • Check the feet
First-line therapy options • Blow em up and then juice em
82
1. Kavli et al. Hand dermatoses in Tromso. Contact Dermatitis. 1984;10:174-177. 2. Coenraads P et al. Prevalence of eczema and other dermatoses of the hands and arms in the Netherlands. Association with age and occupation. Clin Exp Dermatol. 1983;9:495-503. 3. Goh et al. Occupational dermatoses in Singapore. Contact Dermatitis. 1984;11:288-293. 4. Meding et al. Hand eczema in Swedish adults – changes in prevalence between 1983-1996. 5. Meding B etl a. Incidence of Hand Eczema – a population based retrospective study. J Invest Deramtol. 122;873-877.2004. 6. Lerbeak et al. Incidence of hand eczema in a population-based twin cohort: genetic and environmental risk factors. Br J Dermatol.2007;552-557. 7. Cahill et al. The prognosis of occupational contact dermatitis in 2004. Contact Dermatitis. 2004;51:219-226. 8. Veien N et al. Hand eczema:causes, course, and prognosis. Contact Dermatitis. 2008;58:330-4. 9. Toledo et al. Patch testing in children with hand eczema. Contact Dermatitis. 65;213-219. 10.Meding B et al. Fifteen-year follow-up of hand eczema: predictive factors. J Invest Dermatol. 2005;124:893-7. 11. Menne T et al. Hand eczema guidelines based on the Danish guidelines for the diagnosis and treatment of hand eczema. Contact Dermatitis 65;3-12. 12. Coenraads P et al. Risk for hand eczema in employees with past or present atopic dermatitis. Ach Occup Environ Health. 1998;71:7-13. 13. Molin et al. Diagnosing chronic hand eczema by an algorithm: a tool for classification in clinical practice. Clin and Exp Dermatol. 36;595-601. 14. Janssens V et al. Protein contact dermatitis: myth or reality? Br J Dermatol. 1995; 132:1-6. 15.Thyssen J et al. Filaggrin null mutations increase the risk and persistence of hand eczema in subjects with atopic dermatitis: results from a general population study. Br J Dermatol.
2010;115-120. 16.Molin S et al. Filaggrin mutations may confer susceptibility to chronic allergic and irritant hand dermatitis. Br J Deramtol. 2009;801-7. 17.Apfelbacher C et al. CARPE: a registry project of the German Dermatological Society for the characterization and care of chronic hand eczema. JDDG;2011:682-688. 18. Kumar et al. Palmoplantar lesions in psoriasis: a study of 3065 patients. Acta Derm Venerol. 82;192-195. 19. Sampogna et al. Prevalence of symptoms experienced by patients with different clinical types of psoriasis. Br J Dermatol. 2004;151:594-599. 20. Tibor B et al. Pompholyx on the hands and feet. Its etiology, pathogenesis, and specific vaccine therapy. Mycopath et Mycol applicata. 1974;53:25-44. 21. Lane et al. Dermatoses of the hands. JAMA. 128;987-993. 22. Guillet M et al. A-year causative study of pomphylox in 120 patients. Arch Dermatol. 2007;143:12:1504-8. 23. Storrs et al. Acute and recurrent vesicular hand dermatitis not pompholyx or dyshidrosis. Arch Dmeratol. 2007;143-5. 24. Brady M et al. Hands and feet that blister and peel: dyshidrosis. J Ped Health Care. 1993;7:37-8. 25. Brunasso A et al. Can we really separate plamoplantar pustulosis from psoriasis? JEADV 2010;24:611-624. 26.Kampf G et al. Prevention of irritant contact dermatitis among health care workers by using evidence-based hand hygience practices: a review. Ind health. 2007;645-652. 27.Schwanitz H et al. Interdigital dermatitis; sentinel skin damage in hairdressers. Br J Dermatol. 2000;1011-1012. 28. Johansen et al. Classification of hand eczema: clinical and etiological types. Based on the guideline of the Danish Contact Dermatitis Group. Contact Dermatitis. 65;13-21. 29. Cronin E. Clinical pattern of hand eczema in women. Contact Dermatitis. 1985;13:153-161. 30. Diepgen T etl al. European Environmental contact dermatitis research group. Hand eczema multicentre study of the etiology and morphology of hand eczema. Br J Dermatol.
2009;160:353-358. 31. Veien N et al. Hand eczema: causes, course and prognosis 1. Contact Dermatitis 2008;58:330-334. 32. Lantinga H et al. Prevalence, incidence and course of eczema on the hands and forearms in a sample of the general population. Contact Dermatitis. 1984;10:135-139. 33. Agner T. Hand eczema. Contact Dermatitis. 4th edition. Forsch PI. Berlin. Springer. 2006;pp335-344. 34. Beattie PE et al. Which dhildren should we patch test? Clin Exp Dermatol 2006;32:6-11. 35. Apfelbacher C et al. Occurrence and prognosis of hand eczema in the care industry: results from the PACO follow-up study (PACO II). Contact Dermatitis. 2008;58:322-329. 36. Meding et al. Fifteen-year follow up of hand eczema: persistence and cosequences. Br J Dermatol. 2005;152:975-980. 37. Schnopp C et al. Topical tacrolimus and mometasone furoate in treatment of dyshidrotic palmar eczema: a randomized, observer-blinded trial. J Am Acad Dermatol. 2002;46:73-7.
83
38. Belsito D et al. Multicenter Investigator group: pimecrolimus cream 1%: a potential new treatment for chronic hand dermatitis. Cutis. 2004;73(1):31-8. 39.Wollin U et al. Pharmacotherapy of pompholyx. Exper Opin Pharmaother 2004;5(7)1517-22. 40.Boettget et al. Increased vagal modulation in atopic dermatitis. J Dermatol Sci 2009;53(1):55-9. 41. Veien N. Acute and recurrent vesicular hand dermatitis. Dermatol Clin. 2009;337-353. 42. Wollina et al. Adjuvant botulinum toxin A in dyshidrotic hand eczema: controlled prospective pilot study with left-right comparison. J Eur Acad Dermatol
Venereol 2002;16:40-2. 43.Bansal C et al. Novel cutaneous uses for botulinum toxin type A. J Cosmet Dermtol. 2006;5(3):268-72. 44. Sceerri L et al. Azathioprine in dermatological practice: an overview with special emphasis on its use in non-bullous inflammatory dermatoses. Adv Exp Med
Biol 1999;455:343-8. 45.Egan et al. Low-dose oral methotrexate treatment for recalcitrant palmoplantar pompholyx. J am Acd Dmeratol. 1999;40(4)612-14. 46. Pickenacker A et al. Dyshidrotic eczema treated with mycophenolate mofetil. Arch Dermatol. 1998;134(3):378-9. 47. Reitamo S et al. Cyclosporin A in the treatment of chronic dermatitis of the hands. Br J Dermatol. 1994;130(1):75-8. 48. Ogden S. Recalcitrant hand pomphylox; variable response to etanercept. Cli and Exp Dermatol. 31; 129-156. 49. Bissonnette R et al. Successful retreatment with alitretinoin in patients with relapsed chronic hand eczema. Br J Dermatol. 2010;162:420-26. 50. Ruzicka et al. Oral alitretinoin (9-cis-retinoic acid) therapy for chronic hand eczema dermatitis in patient refractory to stand therapy: results of a randomized,
double-blind, placebo-controlled, multicenter trial. Arch Dermatol. 2004;140(12):1453-9. 51. Ruzicka et al. Efficacy and safety of oral alitretinoin (9-cis-retinoic acid_ in patients with severe chronic hand eczema refractory to topical coriticosteroids:
restuls of a randomized double blind, placebo controlled, multicentre trial. Br j Dermatol. 2008;158:808-817. 52. Krutman J. Phototherapy for atopic dermatitis. Clin Exp Deramtol. 2000;25(7):552-8. 53.Grattan C et al. Comparison of topical PUVA with UVA for chronic vesicular hand eczema. Acta Derm Venerol. 1991;71:118-22. 54.Petering H et al. Comparison of locatlized high-dose UVA2 versus topical cream psorlenUVA for treatment of chronic vesicular dyshidrotic eczema. J Am Acad
Dermatol. 2004;68-72. 55. UVA1 Irradiation is effective in ttreatment of chronic vesicular dyshidrotic hand eczema. Acta Derm Venerol 56. ansen G. Grenz rays:adequate or antiquated? J Deramtol Surg Oncol 1978;4:627-9.
155
The Ohio State University Comprehensive Cancer Center – Arthur G. James Cancer Hospital and Richard J. Solove Research Institute 1
Approaching Primary Cutaneous Lymphomas from a (General) Dermatologist’s Perspective
2012 AOCD Annual Meeting
October 10, 2012
Francisca Kartono, DO Ohio State University Medical Center
Department of Dermatology Assistant Clinical Professor
The Ohio State University Comprehensive Cancer Center – Arthur G. James Cancer Hospital and Richard J. Solove Research Institute
Disclosures
Subinvestigator for clinical trials for Abbott, Amgen, Celgene and Janssen
I have no relevant conflicts of interest pertaining to this topic
The Ohio State University Comprehensive Cancer Center – Arthur G. James Cancer Hospital and Richard J. Solove Research Institute
Objectives Classification of Primary Cutaneous Lymphomas
Cutaneous T-cell lymphomas Mycosis fungoides / Sezary
Cutaneous B-cell lymphomas
Treatment approach
Community dermatologist’s perspective Multidisciplinary approach ( Derm, Onc, Rads, PCP)
Patient support : a team approach
The Ohio State University Comprehensive Cancer Center – Arthur G. James Cancer Hospital and Richard J. Solove Research Institute
Cutaneous lymphoproliferative disease
Primary Cutaneous lymphoproliferative diseases Secondary Cutaneous involvement from a nodal or
systemic lymphoma
A constellation of morphologic, immunologic, genetic, and clinical criteria.
Behavior is distinct from nodal lymphomas Anatomic locations with distinct behavior T- cell and B cell lymphomas
The Ohio State University Comprehensive Cancer Center – Arthur G. James Cancer Hospital and Richard J. Solove Research Institute
CTCL
5
The Ohio State University Comprehensive Cancer Center – Arthur G. James Cancer Hospital and Richard J. Solove Research Institute
Immunopathogenesis (S Whittaker, Semin Oncol 2006)
Skin T cells in immunosurveillance Skin – homing malignant T cell in MF:
CD4+ T helper cells Th2 >Th1 predominance in disease progression Malignant T cell clonality
Defects in pro and anti-apoptotic signals Genomic and epigenetic changes Defects in TCR and cytokine signaling Constitutive activation STAT/NFKB/AP1 Large cell transformation Genomic instability
6
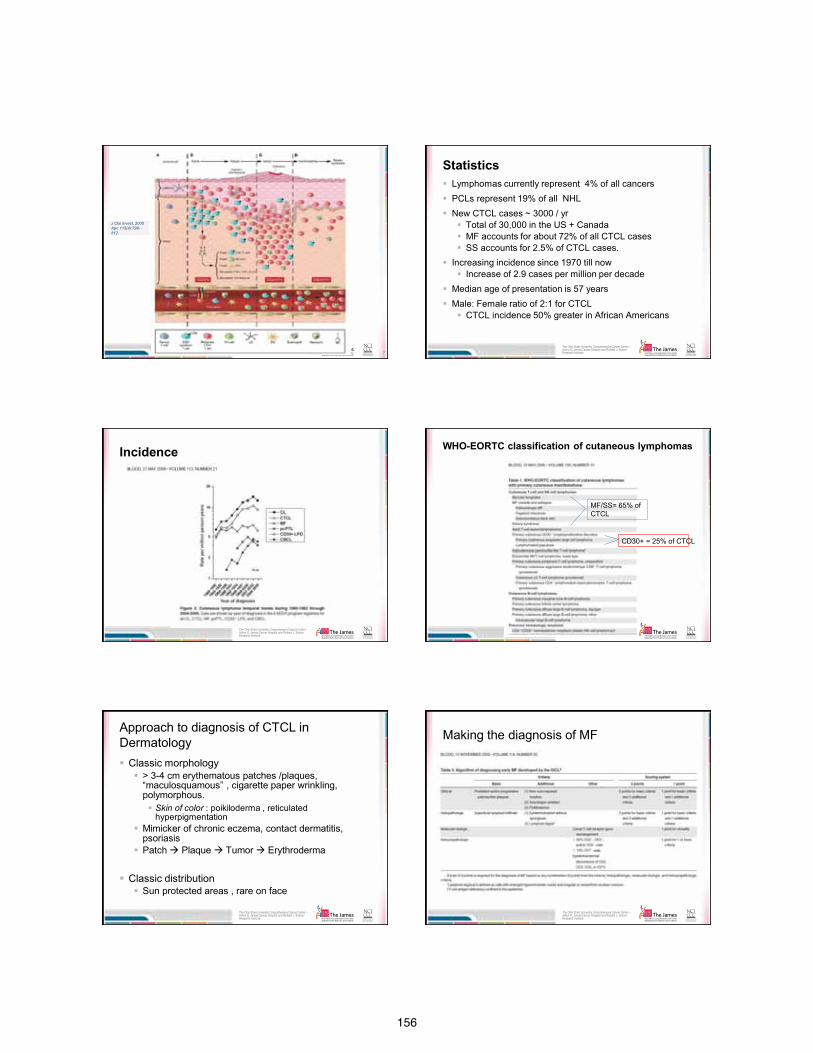
156
The Ohio State University Comprehensive Cancer Center – Arthur G. James Cancer Hospital and Richard J. Solove Research Institute 7
J Clin Invest. 2005 Apr; 115(4):798-812.
The Ohio State University Comprehensive Cancer Center – Arthur G. James Cancer Hospital and Richard J. Solove Research Institute
Statistics Lymphomas currently represent 4% of all cancers PCLs represent 19% of all NHL New CTCL cases ~ 3000 / yr
Total of 30,000 in the US + Canada MF accounts for about 72% of all CTCL cases SS accounts for 2.5% of CTCL cases.
Increasing incidence since 1970 till now Increase of 2.9 cases per million per decade
Median age of presentation is 57 years Male: Female ratio of 2:1 for CTCL
CTCL incidence 50% greater in African Americans
The Ohio State University Comprehensive Cancer Center – Arthur G. James Cancer Hospital and Richard J. Solove Research Institute
Incidence
The Ohio State University Comprehensive Cancer Center – Arthur G. James Cancer Hospital and Richard J. Solove Research Institute
WHO-EORTC classification of cutaneous lymphomas
MF/SS= 65% of CTCL
CD30+ = 25% of CTCL
The Ohio State University Comprehensive Cancer Center – Arthur G. James Cancer Hospital and Richard J. Solove Research Institute
Approach to diagnosis of CTCL in Dermatology Classic morphology
> 3-4 cm erythematous patches /plaques, “maculosquamous” , cigarette paper wrinkling, polymorphous. Skin of color : poikiloderma , reticulated
hyperpigmentation Mimicker of chronic eczema, contact dermatitis,
psoriasis Patch Plaque Tumor Erythroderma
Classic distribution Sun protected areas , rare on face
The Ohio State University Comprehensive Cancer Center – Arthur G. James Cancer Hospital and Richard J. Solove Research Institute
Making the diagnosis of MF
157
The Ohio State University Comprehensive Cancer Center – Arthur G. James Cancer Hospital and Richard J. Solove Research Institute
Pathology
13 The Ohio State University Comprehensive Cancer Center – Arthur G. James Cancer Hospital and Richard J. Solove Research Institute
Pathology Immunophenotyping IHC on paraffin or fresh tissue using antibodies that
can react with cell surface/ cytoplasmic markers IHC: CD 3, 5, 7, CD4/8 Flow cytometry
Immunogenotyping (PCR) TCR gene rearrangement : clonality
The Ohio State University Comprehensive Cancer Center – Arthur G. James Cancer Hospital and Richard J. Solove Research Institute
Workup
Suspect MF 2 skin biopsies, different sites
Off therapy Dermatopathologist to review If indicated:
Immunophenotyping Molecular studies ( TCR)
CLINICOPATHOLOGIC CORRELATION FOR FINAL INTERPRETATION
15
The Ohio State University Comprehensive Cancer Center – Arthur G. James Cancer Hospital and Richard J. Solove Research Institute
Staging
The Ohio State University Comprehensive Cancer Center – Arthur G. James Cancer Hospital and Richard J. Solove Research Institute
B2
The Ohio State University Comprehensive Cancer Center – Arthur G. James Cancer Hospital and Richard J. Solove Research Institute
CTCL patient visit
Complete history and physical exam of skin Assessment of lymph nodes
Cervical Axillary Inguinal >1.5 cm palpable nodes will need imaging workup. No need to blindly biopsy unpalpable nodes
Imaging:
CXR / nodal ultrasound staging PET/CT
Labs: periodic CBC and Sezary cell count .
CMP, LDH, TCR (tissue or blood) Flow cytometry (blood) in place of Sezary count
158
The Ohio State University Comprehensive Cancer Center – Arthur G. James Cancer Hospital and Richard J. Solove Research Institute
Treatment approach
General/community dermatologists Manage early stage CTCL
Tertiary care referral for advanced disease Clinical trials
Several principles in treatment:
Skin-directed-therapies first Loop-back mechanism of treatment options Combination therapy not monotherapy SUPPORTIVE CARE: improve QoL for patients
The Ohio State University Comprehensive Cancer Center – Arthur G. James Cancer Hospital and Richard J. Solove Research Institute
Skin directed therapies
Nitrogen Mustard Topical steroids Topical bexarotene Tazarotene / topical retinoids Imiquimod Tacrolimus **
Phototherapy PUVA/UVB:
Good combos: PUVA + po retinoid PUVA + interferon
The Ohio State University Comprehensive Cancer Center – Arthur G. James Cancer Hospital and Richard J. Solove Research Institute
Local or TSEB
Total Skin Electron Beam Therapy
Stanford protocol “RESET” button. Can repeat it 2-3 times over a lifetime Response is great, but may need to be bridged to a
maintenance regimen. TSEB response may be short-lived.
3,600 cGy in small fractions three times a week for approximately 10 week
The Ohio State University Comprehensive Cancer Center – Arthur G. James Cancer Hospital and Richard J. Solove Research Institute
The Ohio State University Comprehensive Cancer Center – Arthur G. James Cancer Hospital and Richard J. Solove Research Institute
Systemic Therapy Biologic response modifiers
IFN, retinoids, dinileukin diftitox
Histone Deacetylase Inhibitors Romidepsin, vorinostat,
Immunotherapy alemtuzumab
ECP Clinical trial agents Chemotherapy
Does not treat CTCL appropriately as first line tx. CHOP, Gemcitabine, Liposomal doxorubicin MTX, praletrexate
The Ohio State University Comprehensive Cancer Center – Arthur G. James Cancer Hospital and Richard J. Solove Research Institute
Allogeneic HSCT
Graft vs lymphoma effect Lifetime expectation of transformed MF /SS ( ~2.5
years). Allogeneic HSCT
Relapse rate 39%, time to relapse was 50 Days. Difficult to time properly as the skin may not clear
sufficiently
Duvic et al. J Clin Oncol 28(14):2365-72
159
The Ohio State University Comprehensive Cancer Center – Arthur G. James Cancer Hospital and Richard J. Solove Research Institute
Primary Cutaneous B cell Lymphomas
25 The Ohio State University Comprehensive Cancer Center – Arthur G. James Cancer Hospital and Richard J. Solove Research Institute
Primary cutaneous B cell lymphomas: Mostly indolent
Different from their systemic/ nodal counterparts Confined to the skin at presentation Complete staging procedures are negative ( 6
months after initial workup) Cerroni L, Signoretti S, Hofler G, et al. Primary cutaneous marginal zone B-cell lymphoma: a recently described entity of low-grade malignant cutaneous
B-cell lymphoma. Am J Surg Pathol 1997;21:1307-15.
20-25% of all cutaneous lymphomas Evolving classification
WHO-EORTC classification since 2005 , revised 2007, 2008
No standardized guidelines for care !
The Ohio State University Comprehensive Cancer Center – Arthur G. James Cancer Hospital and Richard J. Solove Research Institute
Epidemiology
SEER data from 16 registries representing ~26% of US population
2001-2005 total of 1105 cases pCBCL
CBCL: non Hispanic whites had highest IR ( vs Af Am in
CTCL) M>F IRR= 1.72 Metropolitan locations vs non metropolitan locations Head and neck
The Ohio State University Comprehensive Cancer Center –
Arthur G. James Cancer Hospital and Richard J. Solove Research Institute
The Ohio State University Comprehensive Cancer Center – Arthur G. James Cancer Hospital and Richard J. Solove Research Institute
EORTC WHO This particular study of n=556
Old Classification
The Ohio State University Comprehensive Cancer Center – Arthur G. James Cancer Hospital and Richard J. Solove Research Institute
Classification
WHO-EORTC Classification
Behavior B cell lymphoma type Indolent Marginal zone Indolent Follicle Center Intermediate Diffuse large B cell, other Agressive Diffuse large B cell , leg type
Blood 2005; 105: 3768-85
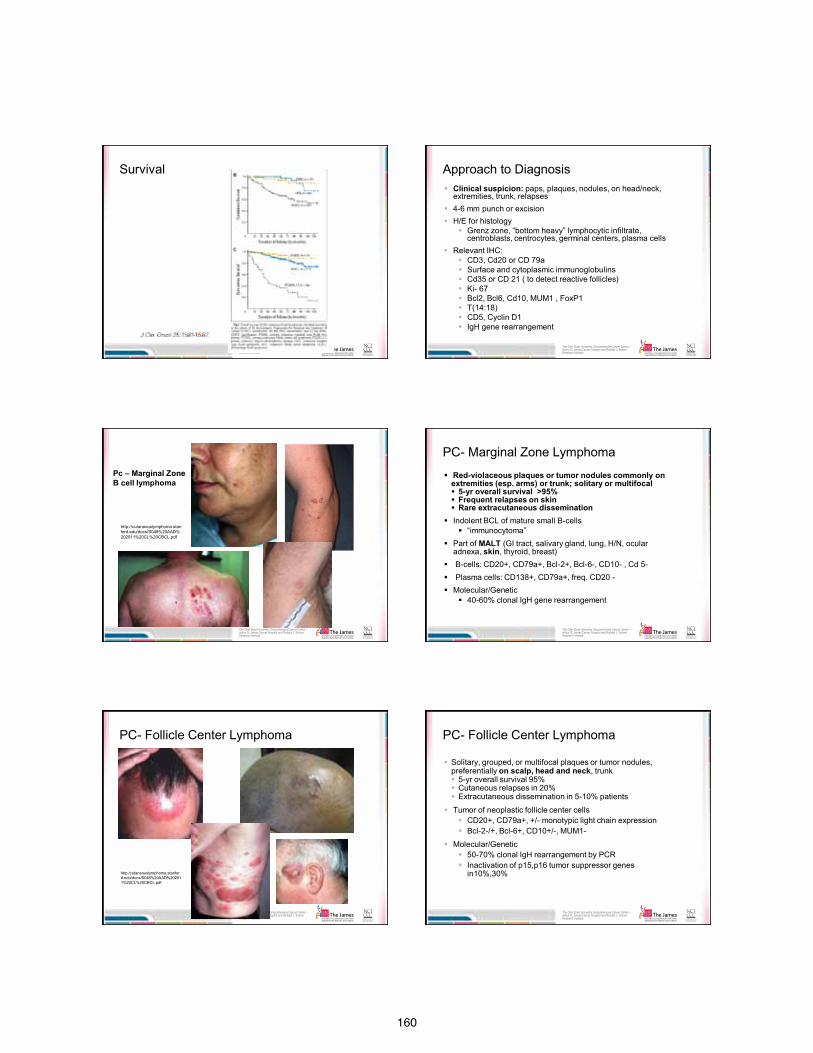
160
The Ohio State University Comprehensive Cancer Center – Arthur G. James Cancer Hospital and Richard J. Solove Research Institute
Survival
The Ohio State University Comprehensive Cancer Center – Arthur G. James Cancer Hospital and Richard J. Solove Research Institute
Approach to Diagnosis Clinical suspicion: paps, plaques, nodules, on head/neck,
extremities, trunk, relapses 4-6 mm punch or excision H/E for histology
Grenz zone, “bottom heavy” lymphocytic infiltrate, centroblasts, centrocytes, germinal centers, plasma cells
Relevant IHC: CD3, Cd20 or CD 79a Surface and cytoplasmic immunoglobulins Cd35 or CD 21 ( to detect reactive follicles) Ki- 67 Bcl2, Bcl6, Cd10, MUM1 , FoxP1 T(14:18) CD5, Cyclin D1 IgH gene rearrangement
The Ohio State University Comprehensive Cancer Center – Arthur G. James Cancer Hospital and Richard J. Solove Research Institute
Pc – Marginal Zone B cell lymphoma
http://cutaneouslymphoma.stanford.edu/docs/S048%20AAD%202011%20CL%20CBCL.pdf
The Ohio State University Comprehensive Cancer Center – Arthur G. James Cancer Hospital and Richard J. Solove Research Institute
PC- Marginal Zone Lymphoma
Red-violaceous plaques or tumor nodules commonly on extremities (esp. arms) or trunk; solitary or multifocal 5-yr overall survival >95% Frequent relapses on skin Rare extracutaneous dissemination
Indolent BCL of mature small B-cells “immunocytoma”
Part of MALT (GI tract, salivary gland, lung, H/N, ocular adnexa, skin, thyroid, breast)
B-cells: CD20+, CD79a+, Bcl-2+, Bcl-6-, CD10- , Cd 5- Plasma cells: CD138+, CD79a+, freq. CD20 - Molecular/Genetic
40-60% clonal IgH gene rearrangement
The Ohio State University Comprehensive Cancer Center – Arthur G. James Cancer Hospital and Richard J. Solove Research Institute
PC- Follicle Center Lymphoma
http:/cutaneouslymphoma.stanford.edu/docs/S048%20AAD%202011%20CL%20CBCL.pdf
The Ohio State University Comprehensive Cancer Center – Arthur G. James Cancer Hospital and Richard J. Solove Research Institute
PC- Follicle Center Lymphoma
Solitary, grouped, or multifocal plaques or tumor nodules, preferentially on scalp, head and neck, trunk 5-yr overall survival 95% Cutaneous relapses in 20% Extracutaneous dissemination in 5-10% patients
Tumor of neoplastic follicle center cells CD20+, CD79a+, +/- monotypic light chain expression Bcl-2-/+, Bcl-6+, CD10+/-, MUM1-
Molecular/Genetic 50-70% clonal IgH rearrangement by PCR Inactivation of p15,p16 tumor suppressor genes
in10%,30%
161
The Ohio State University Comprehensive Cancer Center – Arthur G. James Cancer Hospital and Richard J. Solove Research Institute
Primary Cutaneous Large B-cell Lymphoma , Leg- type
The Ohio State University Comprehensive Cancer Center – Arthur G. James Cancer Hospital and Richard J. Solove Research Institute
Primary Cutaneous Large B-cell Lymphoma , Leg- type
Common in elderly Rapidly growing red-violaceous tumors,
most commonly on leg, but can affect non-leg site 5-yr OS 35-50%
CD20+, CD79a+, monotypic light chain expression Bcl-2+ +, Bcl-6+/-, CD10-, MUM1+, FOXP1+,
IgM+,IgD+/-– Lack t(14;18) despite strong Bcl-2 Inactivation of p15, p16 in Frequent clonal IgH gene rearrangement by PCR
The Ohio State University Comprehensive Cancer Center – Arthur G. James Cancer Hospital and Richard J. Solove Research Institute
Classification
The Ohio State University Comprehensive Cancer Center – Arthur G. James Cancer Hospital and Richard J. Solove Research Institute
NCCN TNM classification
Staging
The Ohio State University Comprehensive Cancer Center – Arthur G. James Cancer Hospital and Richard J. Solove Research Institute
Staging procedures ISCL/EORTC Recommendations for Staging Evaluation in
Cutaneous Lymphomas other than MF/SS, Blood 2007;110:479-484
Complete history and review of systems
Trauma, bugbite B symptoms
Thorough physical examination
Labs: CBC, CMP, LDH, beta2 microglobulin
SPEP : monoclonal gammopathy flow cytometry of peripheral blood ( esp. if lymphocytosis
present) No need to look for Borrelia in US
The Ohio State University Comprehensive Cancer Center – Arthur G. James Cancer Hospital and Richard J. Solove Research Institute
Borrelia link not demonstrated in US cases
162
The Ohio State University Comprehensive Cancer Center – Arthur G. James Cancer Hospital and Richard J. Solove Research Institute
Imaging
Imaging studies– CT neck, chest, abdomen & pelvis w/ contrast alone or with whole body FDG-PET
Whole body integrated PET/CT as alternative
LNs > 1.0 cm in short axis and /or have significantly increased PET activity should be sampled for tissue examination (an excisional bx is preferable whenever possible)
The Ohio State University Comprehensive Cancer Center – Arthur G. James Cancer Hospital and Richard J. Solove Research Institute
On Bone Marrow Biopsy …
Senff NJ, et al . Br J Haematol. 2008; 28: 502-507.
11% ( 22/193) of patients with FCL present in the skin have BM involvement In 9/22, this was the ONLY sign of extrcutaneous dz
OS 44% DSS 63% in BM+ pts OS 84% DSS 95% in FCL pts without extracutaneous dz
2/ 82 MZL patients had extracutaneous involvement of BM.
Conclusion: No consensus on BMB currently. Still essential part of workup until proven otherwise
The Ohio State University Comprehensive Cancer Center – Arthur G. James Cancer Hospital and Richard J. Solove Research Institute
NCCN Guidelines
US Treatment Guidelines in PCBCL NCCN practice guidelines for available since 2009
www.nccn.org First available standard of care treatment guideline
in cutaneous lymphoma Help with insurance pre-auth and reimbursement
The Ohio State University Comprehensive Cancer Center – Arthur G. James Cancer Hospital and Richard J. Solove Research Institute
Management of PCBCL
MZL/FCl ( indolent) DLBCL leg type (Aggressive)
Solitary / Regional Generalized Solitary Multiple -Observation
-ILK -Excision -Topicals: NM, imiquimod, retinoids -XRT -Clinical trials
-Observation -Topicals -RT + sx -Biologics: Rituximab, IFN, retinoids -Chemotherapy -Clinical trials
RT ( caution) RCHOP+- IFRT Clinical trials
RCHOP +- IFRT Clinical trials
The Ohio State University Comprehensive Cancer Center – Arthur G. James Cancer Hospital and Richard J. Solove Research Institute
In summary
Indolent (FCL/MZL) vs. aggressive (DLBCL leg-type) Do not over treat Management driven by symptom Local tx for localized disease Rituximab only if generalized disease present and
symptomatic 40-60% relapse rate post initial therapy, regardless of tx type
Do not under treat aggressive cases Utilize NCCN practice guidelines Clinical trial for advanced cases and new targeted
therapies
The Ohio State University Comprehensive Cancer Center – Arthur G. James Cancer Hospital and Richard J. Solove Research Institute
Patient Support
http://www.clfoundation.org
48
163
Robert G. Greenberg, M.D., F.A.A.D. Robert G. Greenberg, M.D., Dermatologist – San Ramon, CA
As many as 7.5 million Americans have psoriasis
Common, chronic, inflammatory disease of skin and joints
Auto-immune disease caused by both genetic and environmental influences
Plaque psoriasis is the most common form
Guttate: Small, red, individual spots on skin. Usually appears on trunk and limbs.
Inverse: Found in skin folds. Lesions are very red and usually lack scale.
Pustular: White pustules surrounded by red skin.
Erythrodermic: Fiery redness on large areas of skin. Often accompanied by severe itching and pain.
Scalp Elbows/knees Lower back Navel Hands/feet
Pitting Peeling Discoloration Lifting up from the
nail bed Ridging
PsoriasisGenetic
Predisposition
TriggersTrauma, infection,
drugs, stress
Skin cell proliferationInflammation
Itch
Immune Dysregulation
Image courtesy of Kelly Cordoro, MD, UCSF
Current view of psoriasis
164
1. Psoriasis trigger is delivered to draining lymph nodes
2. Activation of T-cells
3. T-cells move from lymph nodes into the skin
4. T –cells release of inflammatory factors in the skin
5. Inflammatory factors trigger: rapid production of skin cells, widen blood vessels and, stimulate itch nerves
1.
2.
3.
4.
5.
Current view of psoriasis Psoriasis skin
But known triggers may include: Emotional stress Infection (strep) Injury to the skin (includes tattoo, piercing) Weather (cold, dry) Certain kinds of drugs (lithium, some beta blockers)
Key findings from the Psoriasis Foundation ◦ 28% have another chronic, inflammatory disease ◦ 59% suffer from physical pain from their psoriasis ◦ 63% said psoriasis negatively impacts their overall
well being ◦ 71% said they feel “helpless” and 73% said they feel
“angry” or “frustrated”
Results based on 6 years of summarized data from nearly 5,000 survey participants with psoriasis and/or psoriatic arthritis.
Treating psoriasis
Psoriasis is chronic and requires lifelong treatment
No single treatment works for everyone Switching treatments is common Many treatment options are available for
psoriasis and psoriatic arthritis Combination treatment is common
165
Localized disease <5% body surface area
Widespread disease >5% body surface
area Psoriatic arthritis Vulnerable areas
o Palms/soles o Genital area
biologics cyclosporine methotrexate retinoids
Over the counter topical treatments Salicylic acid, other keratolytics Low dose corticosteroids Tar preparations Moisturizers and other oils, salt or oatmeal bath
Prescription topical treatments: Mid-to-high strength corticosteroids Vitamin D analogs Combination corticosteroids and vitamin D Anti-inflammatory agents Retinoids (tazorac) Anthralin Intralesional corticosteroids
Calcitriol (Vectical®) Vitamin D Non-steroidal Twice-daily application Comes in ointment form
Calcipotriene and betamethasone dipropionate (Taclonex®) Vitamin D + topical corticosteroid Once-daily application Comes in ointment and a scalp solution
166
Light therapy Excimer (ultraviolet light B) laser treatment Pulse-dye laser treatment
Phototherapy Ultraviolet light B (UVB) o Broadband o Narrowband
PUVA (drug psoralen plus ultraviolet light A) Home light boxes
Traditional systemics Cyclosporine Methotrexate Acitretin (brand name Soriatane®) Sulfasalazine Hydroxyurea
Protein-based drug derived from
living cells cultured in a laboratory
Given through injection or intravenous (IV) infusion
First biologic drug approved for psoriasis was Alefacept in 2003
Biologics for psoriatic disease target a specific protein, rather than the entire immune system
Biological medications or biologics
*Alefacept (Amevive®): 20-25% Etanercept (Enbrel®): 40-50% Adalimumab (Humira®): 60-
70% Infliximab (Remicade®): 75-
80% Ustekinumab (Stelara®): 65-
75%
020406080
100FDA approved for psoriasis
*Alefacept (Amevive) was voluntarily discontinued November 16, 2011. National Psoriasis Foundation, presented at the American Academy of Dermatology in February 2007
39% of psoriasis patients with severe disease are not receiving any treatment
57% of psoriasis patients with severe disease are being treated with topical therapy alone
167
Effectiveness of the treatment Potential side effects and long-term risks Type of psoriasis Other health conditions—possible drug
interactions Disease severity—physical and psychosocial Ease of treatment application—patient
adherence Pregnancy considerations Insurance coverage/out-of-pocket costs
Psoriasis Treatment Pipeline
PSORIASIS
627 clinical trials for Psoriasis registered with ClinicalTrials.gov o 103 ongoing “interventional” trials o testing 36 different treatments
PSORIATIC ARTHRITIS
122 Clinical trials for Psoriatic arthritis registered with ClinicalTrials.gov o 21 ongoing “interventional” trials o testing 8 different treatments
Information on clinical trials, visit: www.clincaltrials.gov or www.centerwatch.com
Oral drug - Phosphodiesterase-4 inhibitor (Celegene®)
Anti-inflammatory
Phase II results: 41% PASI75 & 44% ACR20
Recruiting for Phase III
Both psoriasis and psoriatic arthritis
Two other PDE4i in the pipeline: AN2728 (Anacor®) and MK-0873 (Merck®).
Janus kinase (JAK) inhibitor (Pfizer®) Immunosuppressive Phase II results: 67% PASI 75 Recruiting for phase III in psoriasis Other JAK inhibitors in the pipeline: ASP015K
(Astellas®), INCB18424 (Incyte®)
168
Monoclonal antibody blocks IL-17 (AIN457, LY2439821) or IL-17 receptor (AMG 827)
Phase II/III Also being developed for rheumatoid
arthritis
Monoclonal antibody blocks IL-23
Phase II Pathway is also blocked by
Stelara®
Inflammatory joint disease found in up to 30% of patients with psoriasis
Stiffness, pain, swelling and tenderness of the joints and surrounding ligaments and tendons
Early recognition, diagnosis and treatment can help prevent progressive joint involvement and damage
Skin symptoms usually appear before joint symptoms, but not always
Early diagnosis and treatment is the key to preventing long-term joint damage
Sausage digit
169
Joint damage is irreversible
Symptoms to be aware of Back pain/stiffness Pain in heel or bottom of foot Morning stiffness lasting longer than 30 minutes Generalized fatigue Reduced range of motion Swollen fingers and/or toes
There is no one test that can diagnose psoriatic arthritis
Physical exam looking for signs of psoriasis and/or psoriatic arthritis ◦ Skin, joints, reflexes and muscle strength
Other tests include ◦ X-rays or other imaging tests ◦ Blood test ◦ Other tests (e.g. sample of synovial fluid)
Ruling out other diseases or conditions Rheumatoid arthritis Gout Ankylosing spondylitis Reactive arthritis Others
Nonsteroidal anti-inflammatory drugs (NSAIDs) ◦ Over-the-counter (OTC) medications such as
aspirin and ibuprofen ◦ Prescription strength products
These will help with pain and inflammation but not with the progression of the disease.
170
Disease-modifying antirheumatic drugs (DMARDs) may relieve more severe symptoms
and attempt to slow or stop joint/tissue damage and the progression of psoriatic arthritis. Methotrexate (oral and injection) Leflunomide (oral) Sulfasalizine (oral)
Biologics approved by FDA for psoriatic arthritis: Etanercept (Enbrel®) Adalimumab (Humira®) Infliximab (Remicade®) Golimumab (Simponi®)
Etanercept (Enbrel®) Administered as a self injection once or twice weekly
Adalimumab (Humira®) Administered as a self injection with a pre-filled syringe
typically once every other week
Golimumab (Simponi®) Administered as a self injection once a month
Infliximab (Remicade®) Administered through intravenous infusion every 6 to 8
weeks
Name Sponsor Mechanism Route Development phase
Apremilast Celgene Anti-inflammatory (PDE4 inihibitor)
Oral III
Cimzia (Certolizumab)
UCB TNF blocker Injectable III
Tofacitinib Pfizer Anti-inflammatory (JAK3 inhibitor)
Oral III
Stelara (Ustekinumab)
Centocor IL-12/-23 blocker
Injectable III
Secukinumab (AIN457)
Novartis IL-17 blocker Injectable II
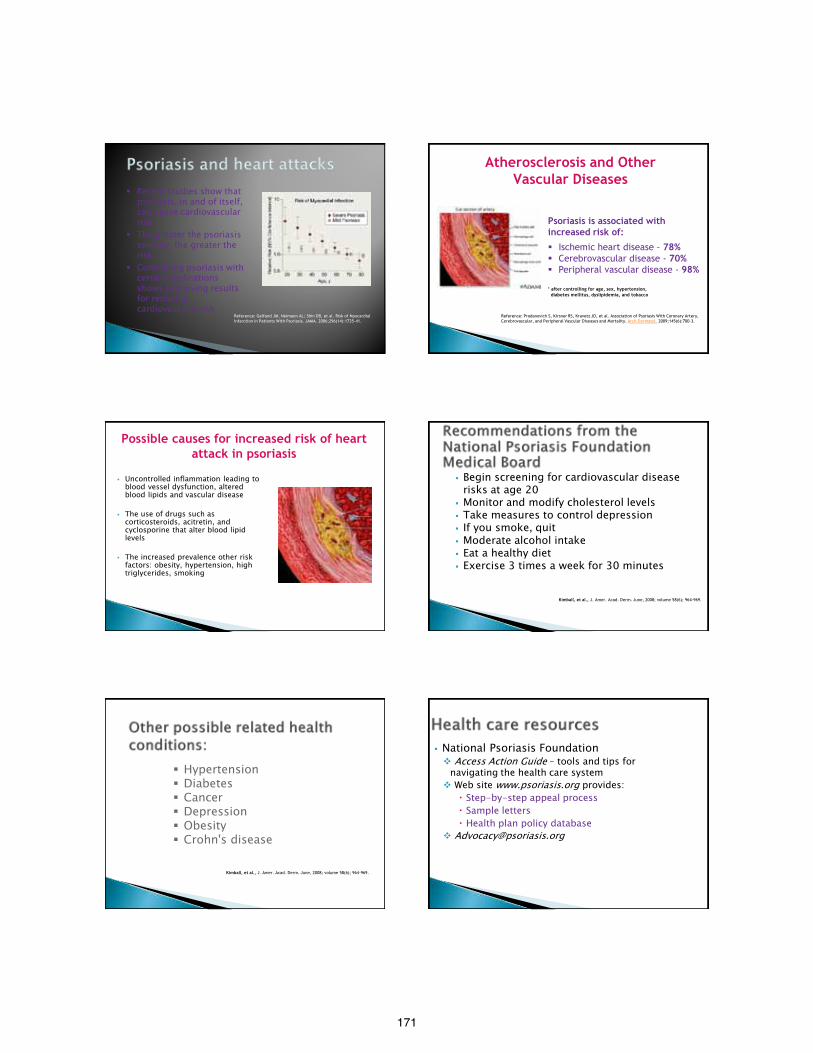
171
Recent studies show that psoriasis, in and of itself, can cause cardiovascular risk
The greater the psoriasis severity, the greater the risk
Controlling psoriasis with certain medications shows promising results for reducing cardiovascular risk
Reference: Gelfand JM, Neimann AL; Shin DB, et al. Risk of Myocardial Infarction in Patients With Psoriasis. JAMA. 2006;296(14):1735-41.
Psoriasis is associated with increased risk of:
Ischemic heart disease - 78% Cerebrovascular disease - 70% Peripheral vascular disease - 98% * after controlling for age, sex, hypertension, diabetes mellitus, dyslipidemia, and tobacco
Atherosclerosis and Other Vascular Diseases
Reference: Prodanovich S, Kirsner RS, Kravetz JD, et al. Association of Psoriasis With Coronary Artery, Cerebrovascular, and Peripheral Vascular Diseases and Mortality. Arch Dermatol. 2009;145(6):700-3.
Uncontrolled inflammation leading to blood vessel dysfunction, altered blood lipids and vascular disease
The use of drugs such as corticosteroids, acitretin, and cyclosporine that alter blood lipid levels
The increased prevalence other risk factors: obesity, hypertension, high triglycerides, smoking
Possible causes for increased risk of heart attack in psoriasis
Begin screening for cardiovascular disease risks at age 20
Monitor and modify cholesterol levels Take measures to control depression If you smoke, quit Moderate alcohol intake Eat a healthy diet Exercise 3 times a week for 30 minutes
Kimball, et al., J. Amer. Acad. Derm. June, 2008; volume 58(6); 964-969.
Hypertension Diabetes Cancer Depression Obesity Crohn's disease
Kimball, et al., J. Amer. Acad. Derm. June, 2008; volume 58(6); 964-969.
National Psoriasis Foundation Access Action Guide – tools and tips for
navigating the health care system Web site www.psoriasis.org provides:
Step-by-step appeal process Sample letters Health plan policy database
172
National Psoriasis Foundation Provides support with health insurance appeals Assists with disability claims Offers assistance with discrimination cases Provides a list of corporate, government and non-profit financial resources
Questions for Dr. Greenberg
173
The Bones of Dermatology
Angela McKinney, D.O. Botsford Dermatology Residency Program
Objectives
• Provide an informative case presentation on SAPHO syndrome
• Review various dermatologic conditions with associated skeletal findings.
• Ensure prompt diagnosis and proper disease management
• To offer board relevant pearls for residents and attending physicians for their recertification exams
History of present illness • 16 year old previously healthy Caucasian male
• 2 month history of increased acne severity
• 3 week history of bilateral ankle pain, that progressed to involve his left hip and left shoulder
• Extreme worsening of his pain led to an in-patient hospital evaluation
Face
Chest Upper Back
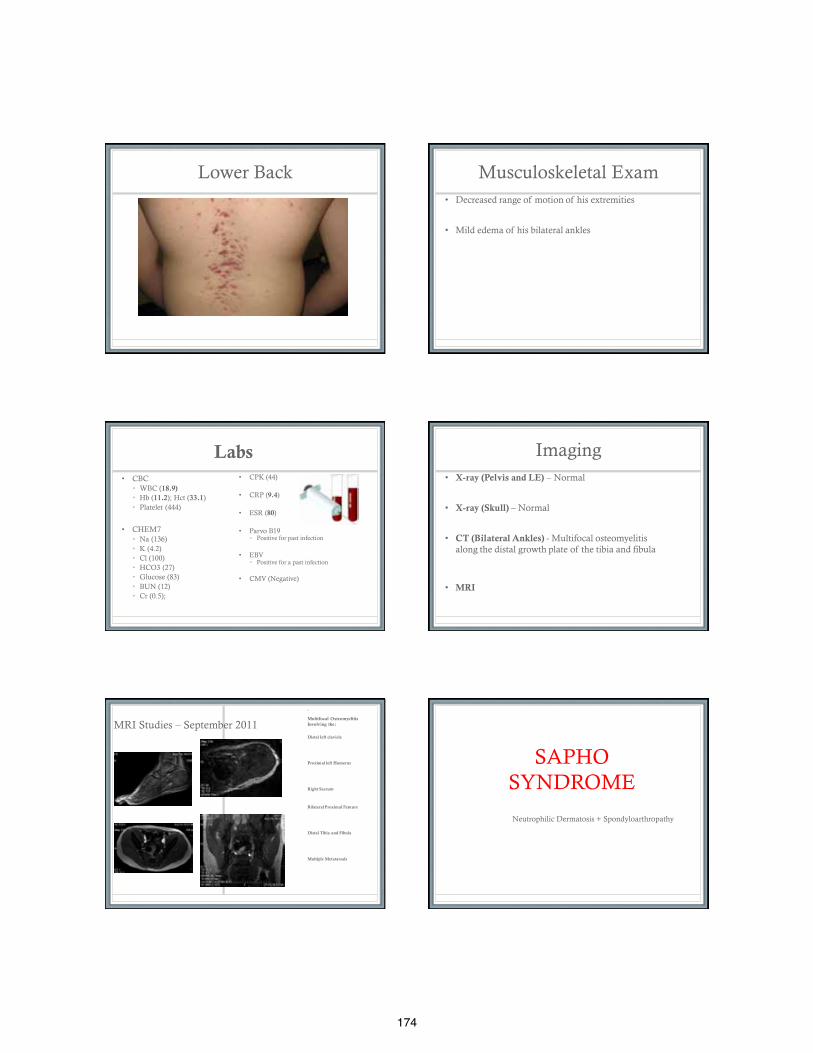
174
Lower Back Musculoskeletal Exam • Decreased range of motion of his extremities
• Mild edema of his bilateral ankles
Labs • CBC
• WBC (18.9) • Hb (11.2); Hct (33.1) • Platelet (444)
• CHEM7 • Na (136) • K (4.2) • Cl (100) • HCO3 (27) • Glucose (83) • BUN (12) • Cr (0.5);
• CPK (44)
• CRP (9.4)
• ESR (80)
• Parvo B19 • Positive for past infection
• EBV • Positive for a past infection
• CMV (Negative)
Imaging • X-ray (Pelvis and LE) – Normal
• X-ray (Skull) – Normal
• CT (Bilateral Ankles) - Multifocal osteomyelitis along the distal growth plate of the tibia and fibula
• MRI
MRI Studies – September 2011
•
Multifocal Osteomyelitis Involving the:
Distal left clavicle
Proximal left Humerus
Right Sacrum
Bilateral Proximal Femurs
Distal Tibia and Fibula
Multiple Metatarsals
SAPHO SYNDROME
Neutrophilic Dermatosis + Spondyloarthropathy
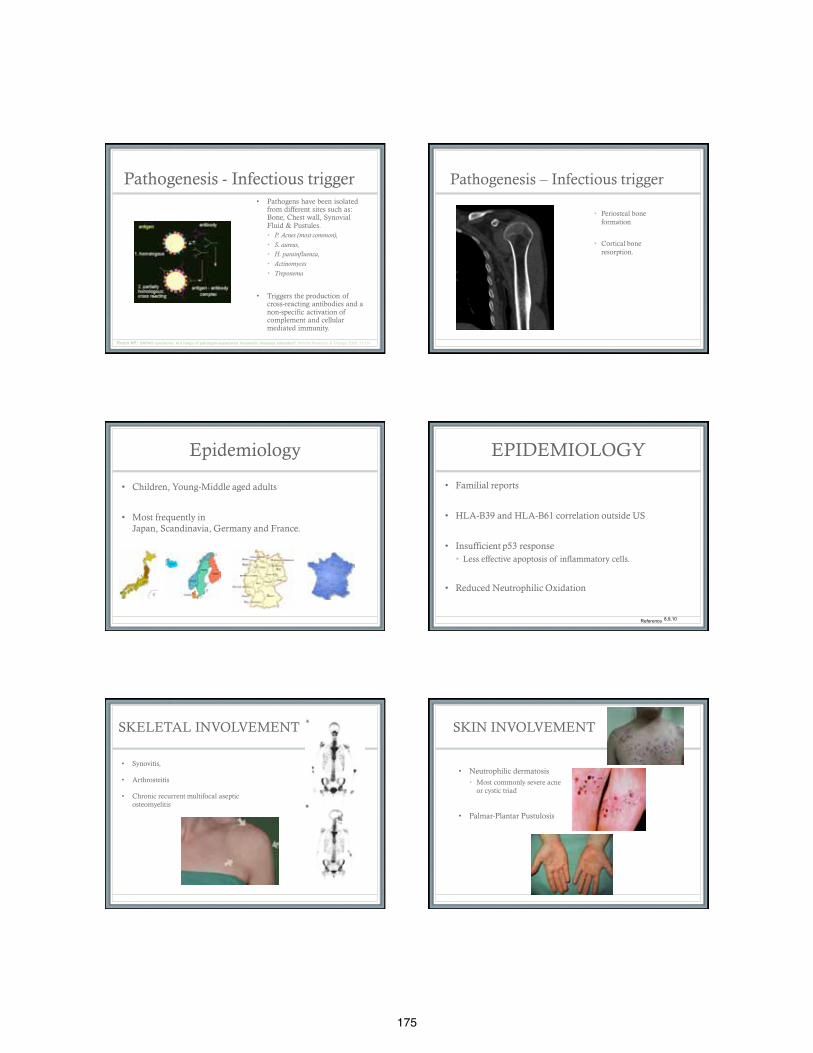
175
Pathogenesis - Infectious trigger
• Pathogens have been isolated from different sites such as: Bone, Chest wall, Synovial Fluid & Pustules. • P. Acnes (most common), • S. aureus, • H. parainfluenza, • Actinomyces • Treponema
• Triggers the production of cross-reacting antibodies and a non-specific activation of complement and cellular mediated immunity.
Rozin AP: SAPHO syndrome: Is a range of pathogen-associated rheumatic diseases extended? Arthritis Research & Therapy 2009, 11:131
Pathogenesis – Infectious trigger
• • Periosteal bone formation
• Cortical bone resorption.
Epidemiology
• Children, Young-Middle aged adults
• Most frequently in Japan, Scandinavia, Germany and France.
EPIDEMIOLOGY
• Familial reports
• HLA-B39 and HLA-B61 correlation outside US
• Insufficient p53 response • Less effective apoptosis of inflammatory cells.
• Reduced Neutrophilic Oxidation
Reference 8,9,10
SKELETAL INVOLVEMENT
• Synovitis,
• Arthrosteitis
• Chronic recurrent multifocal aseptic osteomyelitis
SKIN INVOLVEMENT
• Neutrophilic dermatosis • Most commonly severe acne
or cystic triad
• Palmar-Plantar Pustulosis
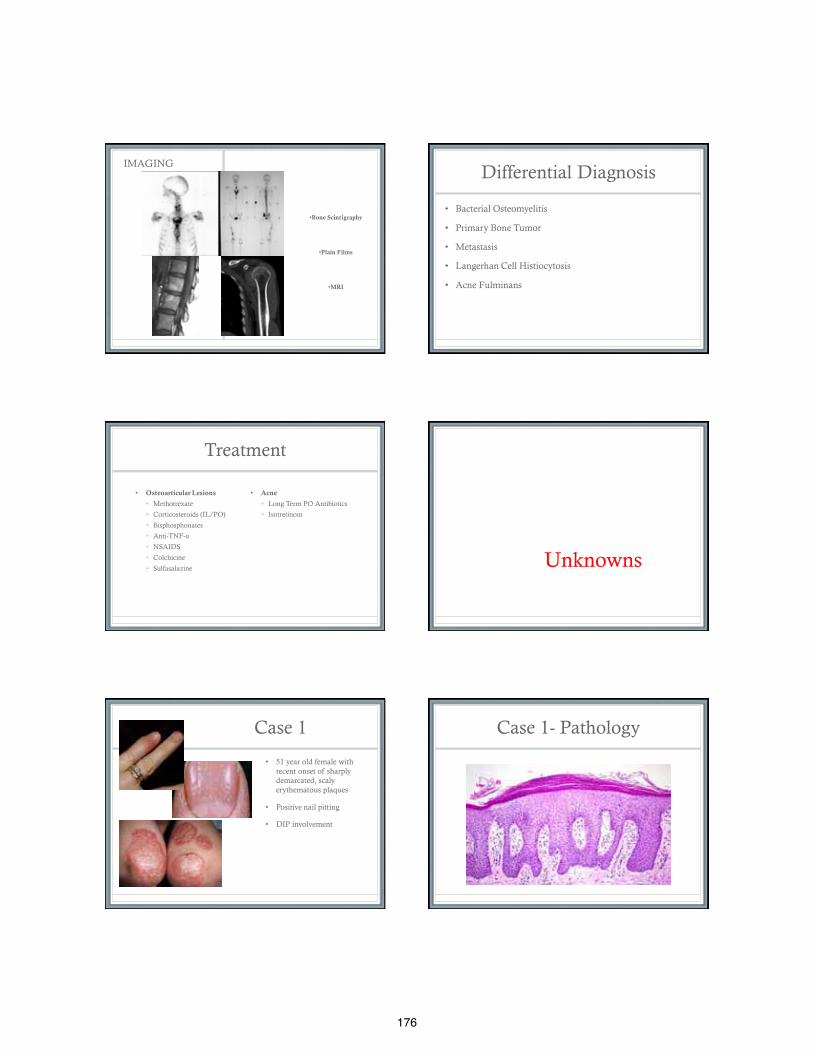
176
IMAGING
•Bone Scintigraphy
•Plain Films
•MRI
Differential Diagnosis
• Bacterial Osteomyelitis
• Primary Bone Tumor
• Metastasis
• Langerhan Cell Histiocytosis
• Acne Fulminans
Treatment
• Osteoarticular Lesions
• Methotrexate
• Corticosteroids (IL/PO)
• Bisphosphonates
• Anti-TNF-α
• NSAIDS
• Colchicine
• Sulfasalazine
• Acne
• Long Term PO Antibiotics
• Isotretinoin
Unknowns
Case 1
• 51 year old female with recent onset of sharply demarcated, scaly erythematous plaques
• Positive nail pitting
• DIP involvement
Case 1- Pathology
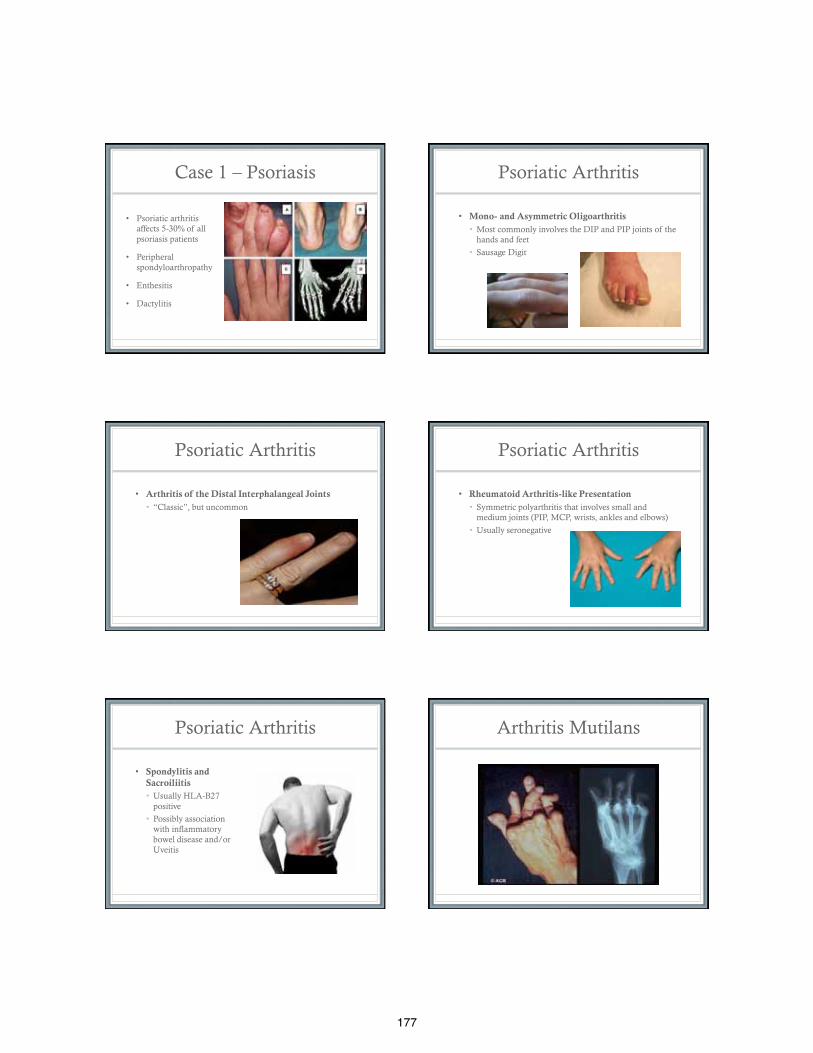
177
Case 1 – Psoriasis
• Psoriatic arthritis affects 5-30% of all psoriasis patients
• Peripheral spondyloarthropathy
• Enthesitis
• Dactylitis
Psoriatic Arthritis
• Mono- and Asymmetric Oligoarthritis • Most commonly involves the DIP and PIP joints of the
hands and feet
• Sausage Digit
Psoriatic Arthritis
• Arthritis of the Distal Interphalangeal Joints • “Classic”, but uncommon
Psoriatic Arthritis
• Rheumatoid Arthritis-like Presentation • Symmetric polyarthritis that involves small and
medium joints (PIP, MCP, wrists, ankles and elbows)
• Usually seronegative
Psoriatic Arthritis
• Spondylitis and Sacroiliitis • Usually HLA-B27
positive
• Possibly association with inflammatory bowel disease and/or Uveitis
Arthritis Mutilans
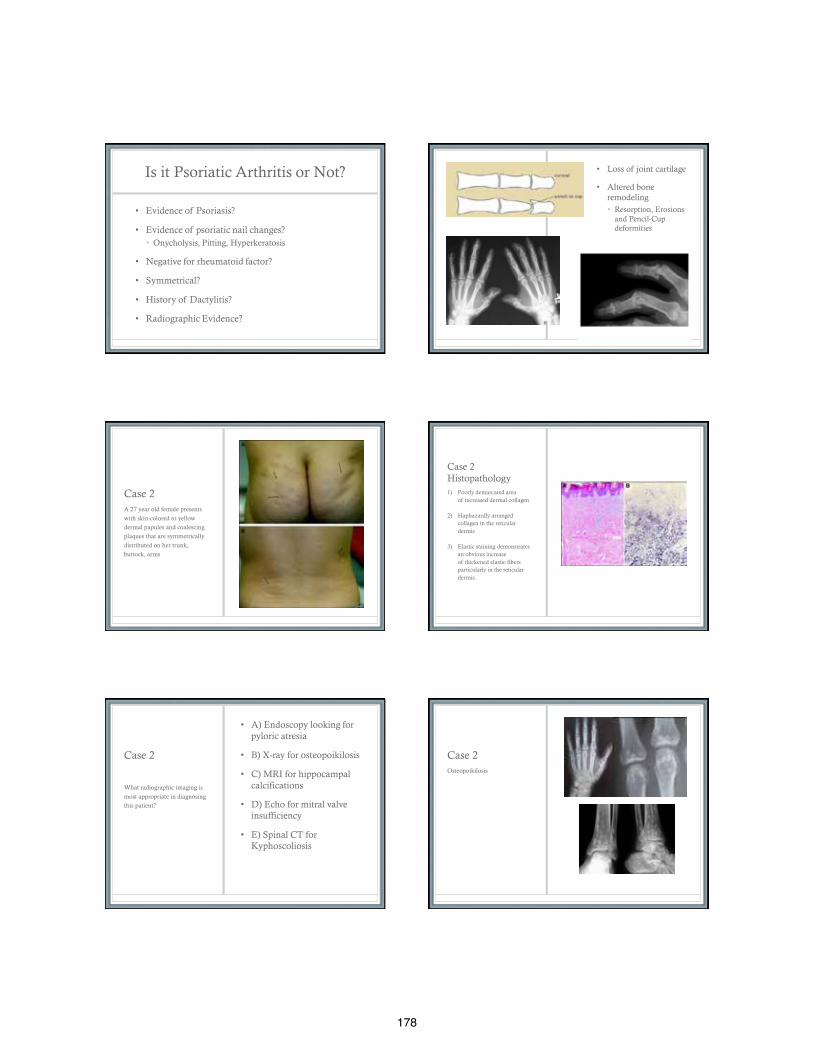
178
Is it Psoriatic Arthritis or Not?
• Evidence of Psoriasis?
• Evidence of psoriatic nail changes? • Onycholysis, Pitting, Hyperkeratosis
• Negative for rheumatoid factor?
• Symmetrical?
• History of Dactylitis?
• Radiographic Evidence?
• Loss of joint cartilage
• Altered bone remodeling • Resorption, Erosions
and Pencil-Cup deformities
Case 2 A 27 year old female presents
with skin-colored to yellow
dermal papules and coalescing
plaques that are symmetrically
distributed on her trunk,
buttock, arms
Case 2 Histopathology 1) Poorly demarcated area
of increased dermal collagen
2) Haphazardly arranged collagen in the reticular dermis
3) Elastic staining demonstrates an obvious increase of thickened elastic fibers particularly in the reticular dermis.
Case 2
• A) Endoscopy looking for pyloric atresia
• B) X-ray for osteopoikilosis
• C) MRI for hippocampal calcifications
• D) Echo for mitral valve insufficiency
• E) Spinal CT for Kyphoscoliosis
What radiographic imaging is
most appropriate in diagnosing
this patient?
Case 2 Osteopoikilosis
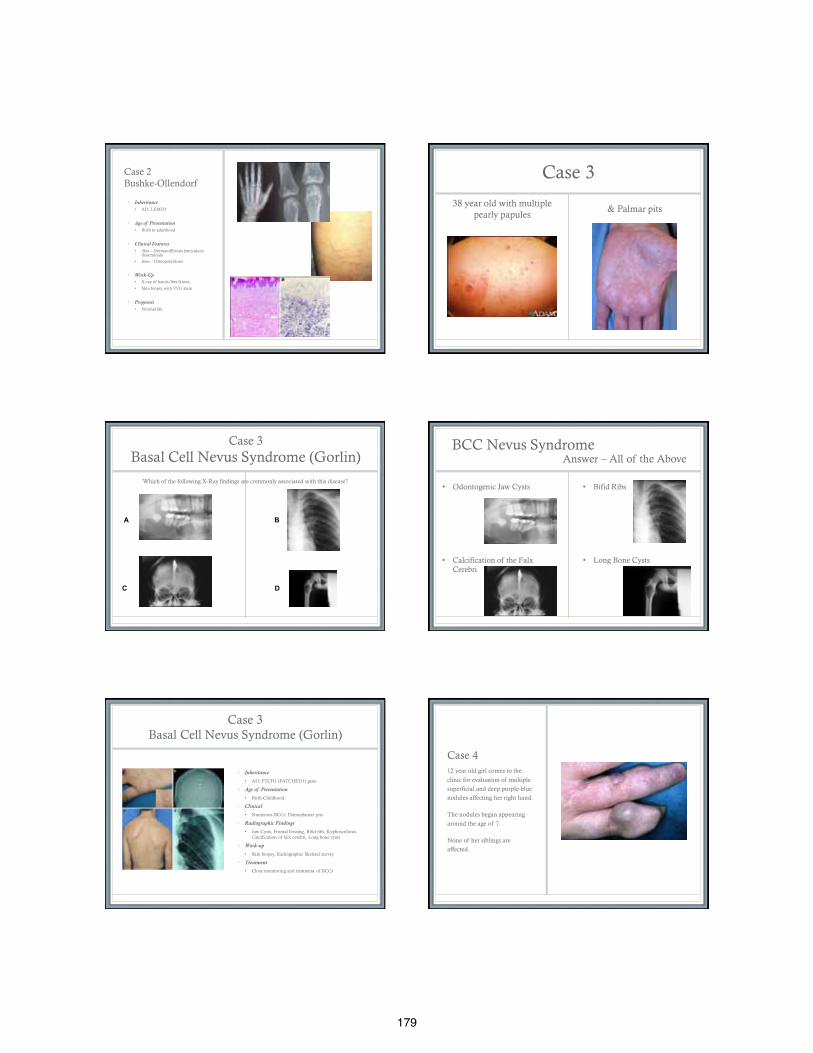
179
Case 2 Bushke-Ollendorf
• Inheritance • AD, LEMD3
• Age of Presentation
• Birth to adulthood
• Clinical Features
• Skin – Dermatofibrosis lenticularis disseminata
• Bone – Osteopoikolosis
• Work-Up
• X-ray of hands/feet/knees,
• Skin biopsy with VVG stain
• Prognosis
• Normal life
Case 3
38 year old with multiple pearly papules
& Palmar pits
Case 3 Basal Cell Nevus Syndrome (Gorlin)
Which of the following X-Ray findings are commonly associated with this disease?
A B
C D
BCC Nevus Syndrome Answer – All of the Above
• Odontogenic Jaw Cysts
• Calcification of the Falx Cerebri
• Bifid Ribs
• Long Bone Cysts
Case 3 Basal Cell Nevus Syndrome (Gorlin)
• Inheritance
• AD; PTCH1 (PATCHED1) gene
• Age of Presentation
• Birth-Childhood
• Clinical
• Numerous BCCs; Palmoplantar pits
• Radiographic Findings
• Jaw Cysts, Frontal bossing, Bifid ribs, Kyphoscoliosis. Calcification of falx cerebri, Long bone cysts
• Work-up
• Skin biopsy, Radiographic Skeletal survey
• Treatment
• Close monitoring and treatment of BCCs
Case 4 12 year old girl comes to the
clinic for evaluation of multiple
superficial and deep purple-blue
nodules affecting her right hand.
The nodules began appearing
around the age of 7.
None of her siblings are
affected.
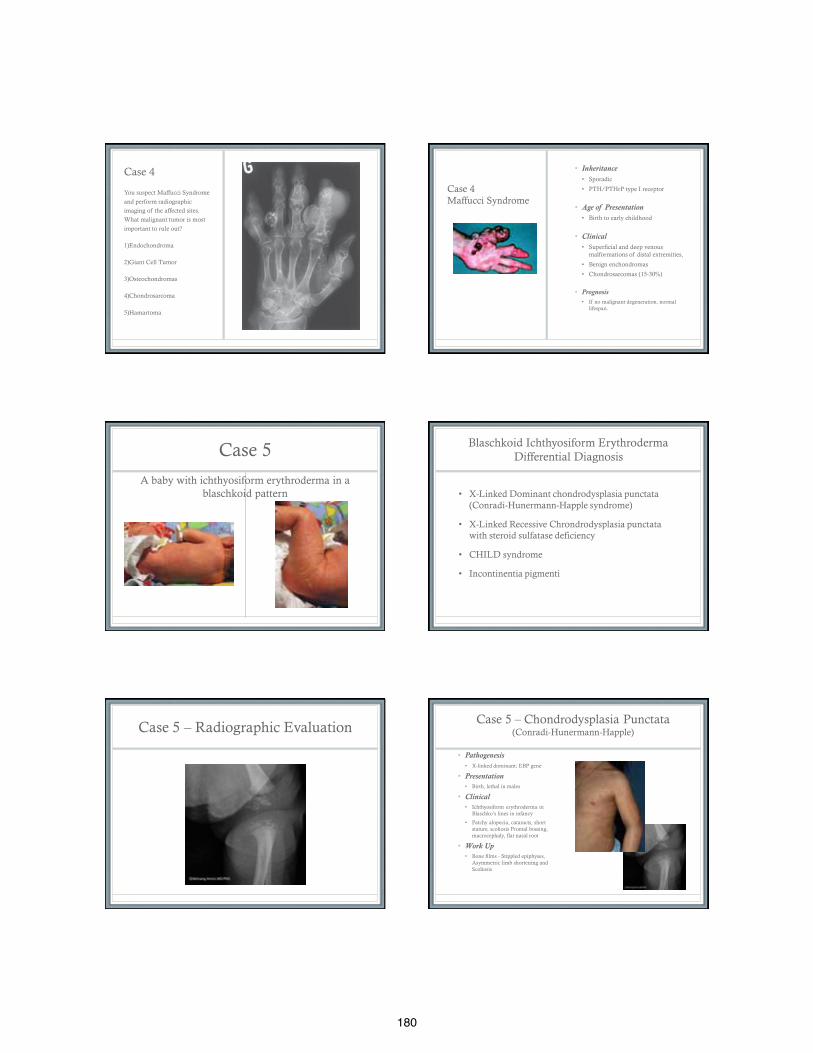
180
Case 4
You suspect Maffucci Syndrome
and perform radiographic
imaging of the affected sites.
What malignant tumor is most
important to rule out?
1)Endochondroma
2)Giant Cell Tumor
3)Osteochondromas
4)Chondrosarcoma
5)Hamartoma
Case 4 Maffucci Syndrome
• Inheritance • Sporadic
• PTH/PTHrP type I receptor
• Age of Presentation • Birth to early childhood
• Clinical • Superficial and deep venous
malformations of distal extremities,
• Benign enchondromas
• Chondrosarcomas (15-30%)
• Prognosis • If no malignant degeneration, normal
lifespan.
Case 5
A baby with ichthyosiform erythroderma in a blaschkoid pattern
Blaschkoid Ichthyosiform Erythroderma Differential Diagnosis
• X-Linked Dominant chondrodysplasia punctata (Conradi-Hunermann-Happle syndrome)
• X-Linked Recessive Chrondrodysplasia punctata with steroid sulfatase deficiency
• CHILD syndrome
• Incontinentia pigmenti
Case 5 – Radiographic Evaluation Case 5 – Chondrodysplasia Punctata
(Conradi-Hunermann-Happle)
• Pathogenesis
• X-linked dominant; EBP gene
• Presentation • Birth, lethal in males
• Clinical • Ichthyosiform erythroderma in
Blaschko’s lines in infancy
• Patchy alopecia, cataracts, short stature, scoliosis Frontal bossing, macrocephaly, flat nasal root
• Work Up • Bone films - Stippled epiphyses,
Asymmetric limb shortening and Scoliosis
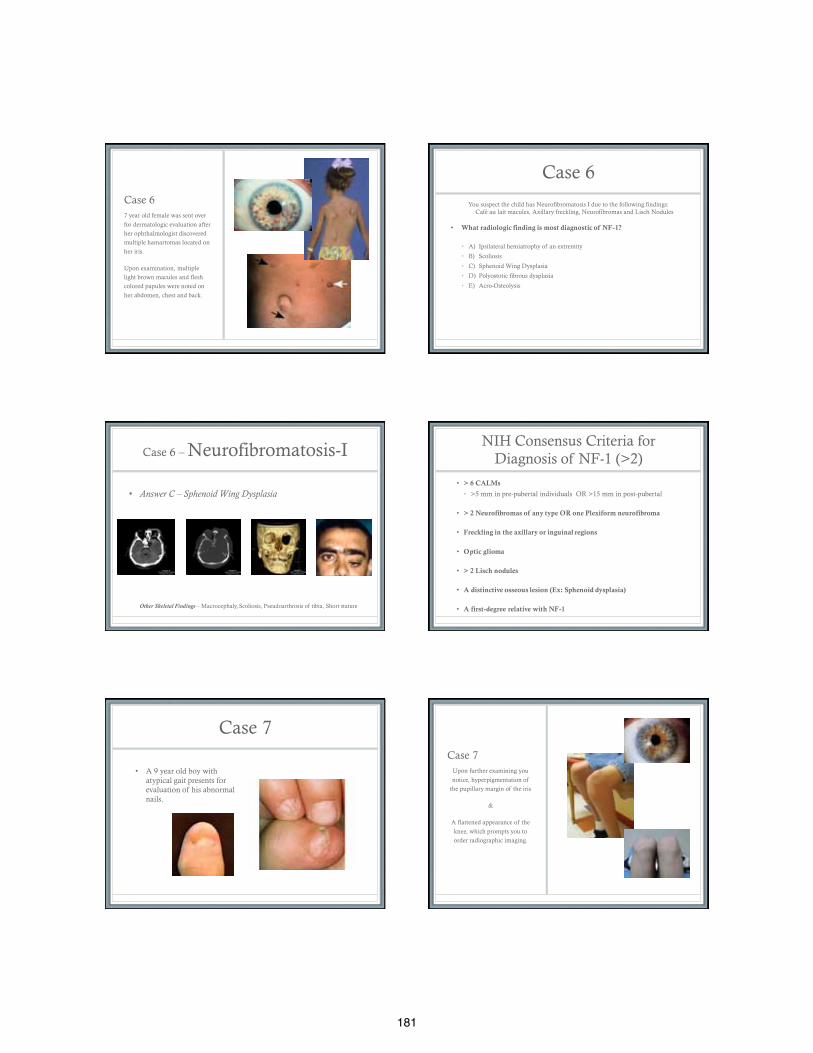
181
Case 6 7 year old female was sent over
for dermatologic evaluation after
her ophthalmologist discovered
multiple hamartomas located on
her iris.
Upon examination, multiple
light brown macules and flesh
colored papules were noted on
her abdomen, chest and back.
Case 6
You suspect the child has Neurofibromatosis I due to the following findings: Café au lait macules, Axillary freckling, Neurofibromas and Lisch Nodules
• What radiologic finding is most diagnostic of NF-1?
• A) Ipsilateral hemiatrophy of an extremity
• B) Scoliosis
• C) Sphenoid Wing Dysplasia
• D) Polyostotic fibrous dysplasia
• E) Acro-Osteolysis
Case 6 – Neurofibromatosis-I
• Answer C – Sphenoid Wing Dysplasia Other Skeletal Findings – Macrocephaly, Scoliosis, Pseudoarthrosis of tibia, Short stature
NIH Consensus Criteria for Diagnosis of NF-1 (>2)
• > 6 CALMs
• >5 mm in pre-pubertal individuals OR >15 mm in post-pubertal
• > 2 Neurofibromas of any type OR one Plexiform neurofibroma
• Freckling in the axillary or inguinal regions
• Optic glioma
• > 2 Lisch nodules
• A distinctive osseous lesion (Ex: Sphenoid dysplasia)
• A first-degree relative with NF-1
Case 7
• A 9 year old boy with atypical gait presents for evaluation of his abnormal nails.
Case 7 Upon further examining you
notice, hyperpigmentation of
the pupillary margin of the iris
&
A flattened appearance of the
knee, which prompts you to
order radiographic imaging.
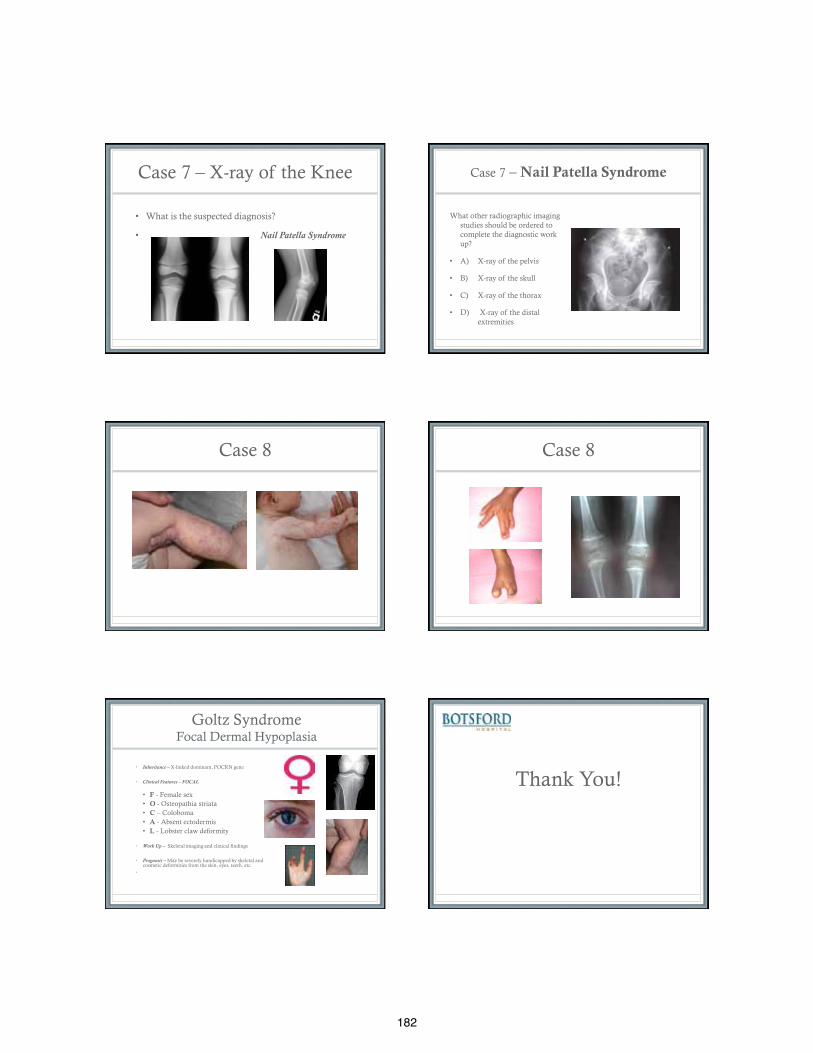
182
Case 7 – X-ray of the Knee
• What is the suspected diagnosis?
• Nail Patella Syndrome
Case 7 – Nail Patella Syndrome
What other radiographic imaging studies should be ordered to complete the diagnostic work up?
• A) X-ray of the pelvis
• B) X-ray of the skull
• C) X-ray of the thorax
• D) X-ray of the distal extremities
Case 8 Case 8
Goltz Syndrome Focal Dermal Hypoplasia
• Inheritance – X-linked dominant, POCRN gene
• Clinical Features – FOCAL
• F - Female sex • O - Osteopathia striata • C – Coloboma • A - Absent ectodermis • L - Lobster claw deformity
• Work Up – Skeletal imaging and clinical findings
• Prognosis – May be severely handicapped by skeletal and
cosmetic deformities from the skin, eyes, teeth, etc. •
Thank You!

183
References
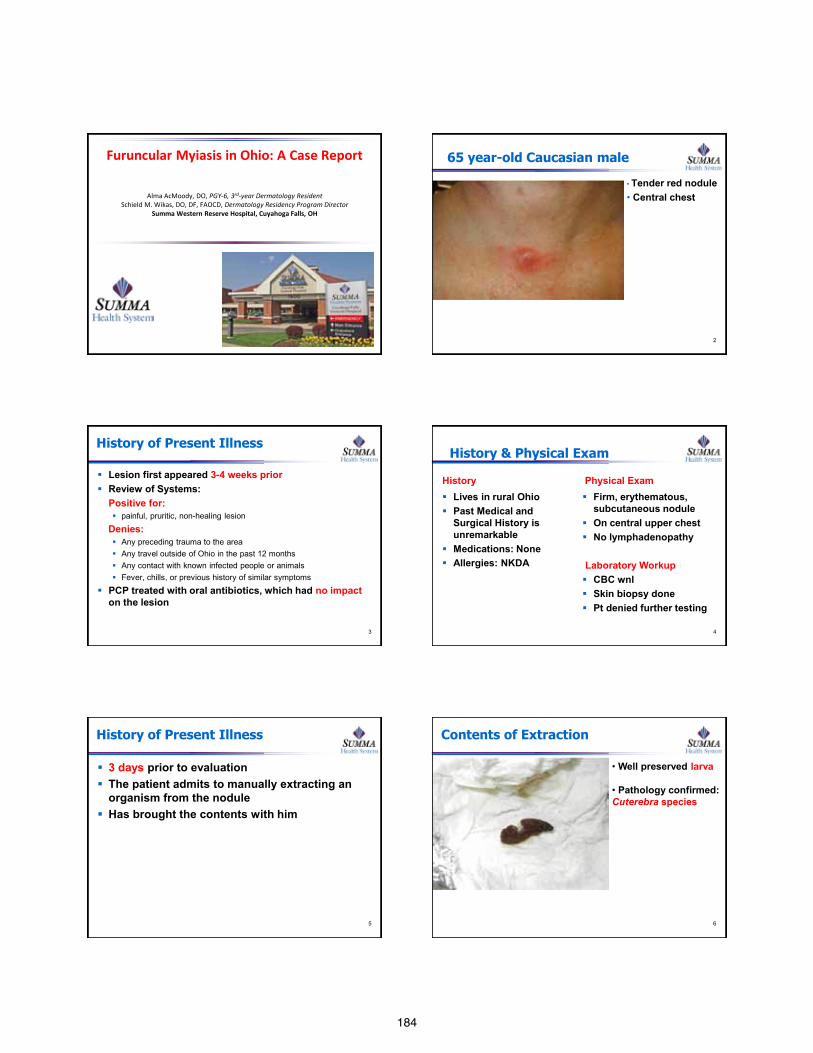
184
Furuncular Myiasis in Ohio: A Case Report
Alma AcMoody, DO, PGY-6, 3rd-year Dermatology Resident Schield M. Wikas, DO, DF, FAOCD, Dermatology Residency Program Director
Summa Western Reserve Hospital, Cuyahoga Falls, OH
65 year-old Caucasian male
• Tender red nodule • Central chest
2
History of Present Illness
Lesion first appeared 3-4 weeks prior Review of Systems: Positive for:
painful, pruritic, non-healing lesion
Denies: Any preceding trauma to the area Any travel outside of Ohio in the past 12 months Any contact with known infected people or animals Fever, chills, or previous history of similar symptoms
PCP treated with oral antibiotics, which had no impact on the lesion
3
History & Physical Exam
History Lives in rural Ohio Past Medical and
Surgical History is unremarkable
Medications: None Allergies: NKDA
Physical Exam Firm, erythematous,
subcutaneous nodule On central upper chest No lymphadenopathy Laboratory Workup CBC wnl Skin biopsy done Pt denied further testing
4
History of Present Illness
3 days prior to evaluation The patient admits to manually extracting an
organism from the nodule Has brought the contents with him
5
Contents of Extraction
6
• Well preserved larva
• Pathology confirmed: Cuterebra species
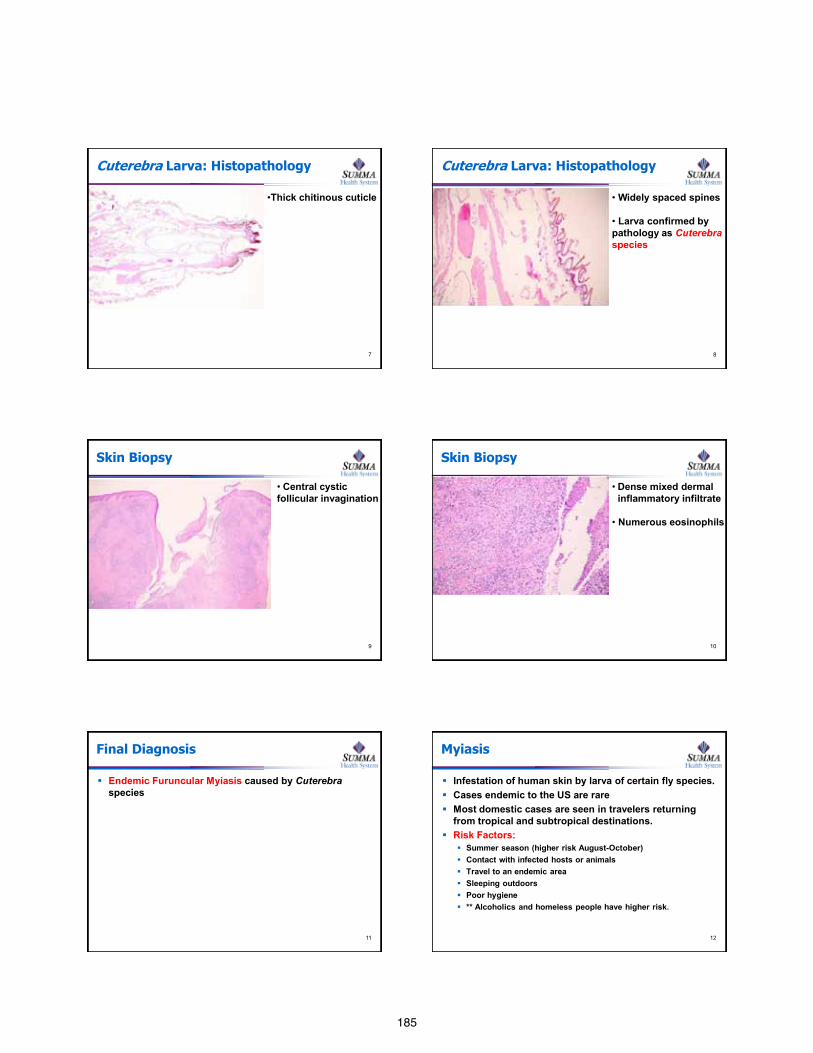
185
Cuterebra Larva: Histopathology
7
•Thick chitinous cuticle
Cuterebra Larva: Histopathology
8
• Widely spaced spines
• Larva confirmed by pathology as Cuterebra species
Skin Biopsy
9
• Central cystic follicular invagination
Skin Biopsy
10
• Dense mixed dermal inflammatory infiltrate
• Numerous eosinophils
Final Diagnosis
Endemic Furuncular Myiasis caused by Cuterebra species
11
Myiasis
Infestation of human skin by larva of certain fly species. Cases endemic to the US are rare Most domestic cases are seen in travelers returning
from tropical and subtropical destinations. Risk Factors:
Summer season (higher risk August-October) Contact with infected hosts or animals Travel to an endemic area Sleeping outdoors Poor hygiene ** Alcoholics and homeless people have higher risk.
12
186
Myiasis
3 forms of cutaneous myiasis: 1. Furuncular: larva burrow directly into the dermis (most common) 2. Wound: Larva infestation in open wounds. 3. Migratory: Human infestation from infected animals
Furuncular myiasis Boil-like lesions with central punctum Serosanguinous discharge Painful and pruritic
Systemic manifestations can include: Fever and regional lymphadenopathy Blood workup can show leukocytosis and eosinophilia
13
Treatment Options
Occlusion Deprives the larva of oxygen May kill the larva Induces it to move upward in search of air
Manual Removal Surgical excision Manual pressure to squeeze out the larva
Antiparasitics Ivermectin
Our patient had complete resolution with oral
Ivermectin 18mg 14
Conclusion
Consider cutaneous myiasis: Non-healing pruritic nodules with a central opening Patient feels movement or sees something in the lesion When presumed bacterial infections do not respond to
antibiotic therapy. High risk patients: poor hygiene, sleeping outdoors Patients with recent travel to tropical and sub-tropical
locations
15
References
1. McGraw TA et al. Cutaneous Myiasis. JAAD 2008; 58:907-926. 2. Baird JK et al. North American Cuterebrid Myiasis. JAAD 1989; 21:763. 3. Plotinsky RN et al. Short report: Cuterebra Cutaneous Myiasis, New
Hampshire, 2004. Am J Trop Med Hyg 2007; 76:596-597. 4. Helm TN et al. Furuncular Myiasis: A Case Report. Cutis 2010; 86: 85-86.
16
Questions and Comments.
Thank you for your attention.
17
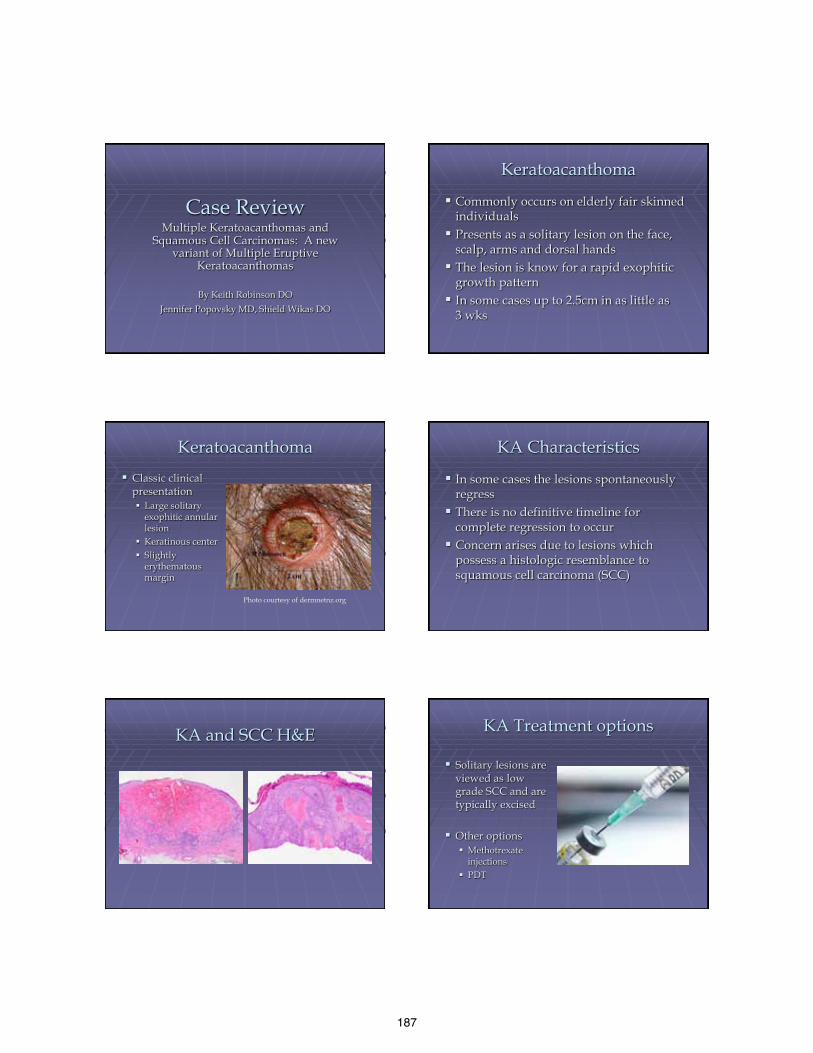
187
Case Review Multiple Keratoacanthomas and
Squamous Cell Carcinomas: A new variant of Multiple Eruptive
Keratoacanthomas
By Keith Robinson DO Jennifer Popovsky MD, Shield Wikas DO
Keratoacanthoma
Commonly occurs on elderly fair skinned individuals
Presents as a solitary lesion on the face, scalp, arms and dorsal hands
The lesion is know for a rapid exophitic growth pattern
In some cases up to 2.5cm in as little as 3 wks
Keratoacanthoma Classic clinical
presentation Large solitary
exophitic annular lesion
Keratinous center Slightly
erythematous margin
Photo courtesy of dermnetnz.org
KA Characteristics
In some cases the lesions spontaneously regress
There is no definitive timeline for complete regression to occur
Concern arises due to lesions which possess a histologic resemblance to squamous cell carcinoma (SCC)
KA and SCC H&E KA Treatment options
Solitary lesions are viewed as low grade SCC and are typically excised
Other options Methotrexate
injections PDT
188
Multi/Eruptive Keratoacanthomas
Three variants currently discussed in the literature
Each has a subtle variance in size, distribution, and inheritance pattern
I. Grzybowski II. Ferguson Smith III. Witten & Zak
Grzybowski Variant
Noted for its smaller more numerous lesions
Patients may develop thousands of pruritic small 2 to 7mm flesh colored papules
Lesions resemble milia and are commonly found on the palms, soles, and mucosal membranes
Has the tendency to regress spontaneously
Grzybowki Variant
No known etiology for this particular variant of multiple eruptive keratoacanthomas
Courtesy of dermnetnz.org
Ferguson Smith Also know as multiple self-healing
squamous epithilioma Noted for larger less numerous lesions
typically found on sun exposed skin and sites of trauma
Lesions have been known to grow upwards of 3cm in diameter
Autosomal dominant inheritance pattern, which typically develops in adolescence
Ferguson Smith
Genetic defect is located on a region of the 9q22 chromosome.
High through-put sequencing identified, 11 distinct mutations in the transforming growth factor beta receptor 1 gene (TGFβR1)
Identified in 18 predominantly Scottish kindreds [1]
Ferguson Smith
Typically the lesions spontaneously resolve in two to three weeks on average
189
Witten & Zak
Display both larger and miliary-type lesions with associated ulcerative and destructive tumors [2]
Case Review
54 year old healthy female developed multiple KAs on her lower extremities as well as a her upper extremities
Multiple lesions developed over six months
No family history Significant history of sunbathing
Past Medical History
Asthma/Allergies Depression
Medications
Prednisone intermittent Inhaled Corticosteroids Montelukast Anithistamines
Initial Presentation
October 2010
Location: Right calf Pathology results: Invasive SCC Treatment: Complete excision with clear
margins E&M: Primary dermatologist
Erupting Lesions March 2011
Lesions: 2 right shin Pathology results: SCC Treatment: Simple excision
Complications Delayed healing with the development of new
lesions around the excision site which clinically appeared to be KAs
Surgical treatment
June of 2011 Pt referred to a plastic surgeon due to
increased lesion size New lesions were diagnosed as invasive SCC Split thickness grafts harvested from the
thighs and placed on the shins. Grafts healed well, however the pt continued
to develop new lesions in close proximity
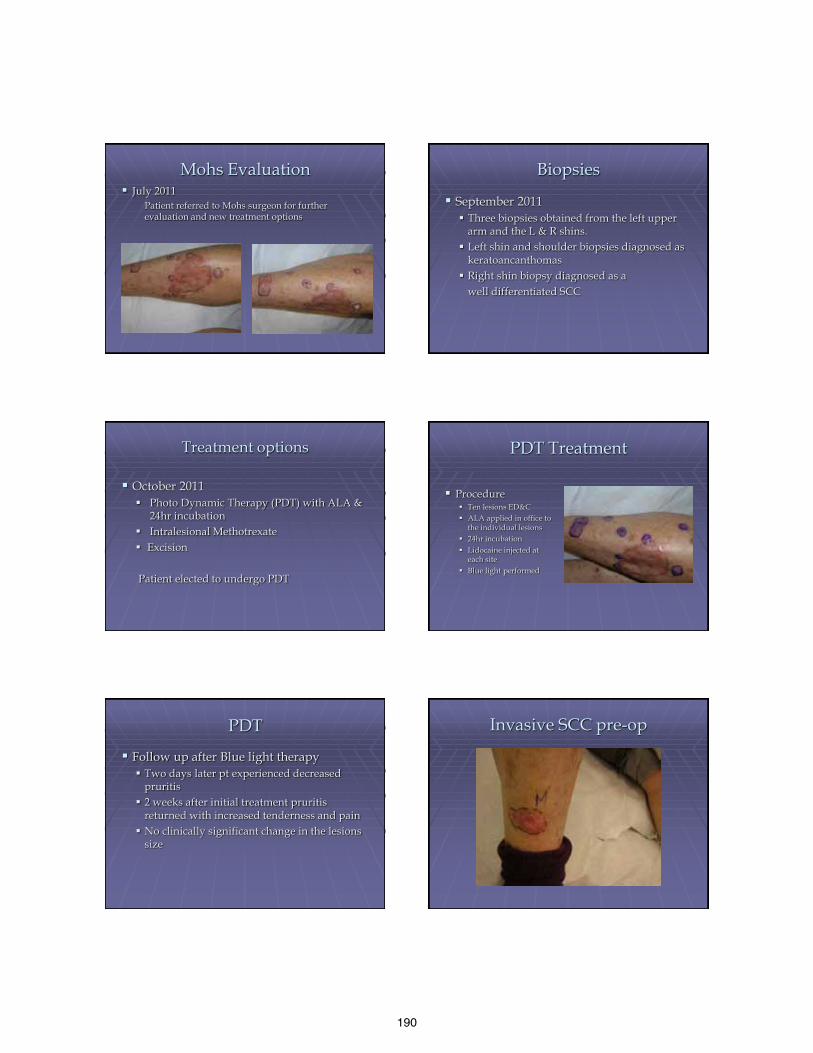
190
Mohs Evaluation July 2011
Patient referred to Mohs surgeon for further evaluation and new treatment options
Biopsies
September 2011 Three biopsies obtained from the left upper
arm and the L & R shins. Left shin and shoulder biopsies diagnosed as
keratoancanthomas Right shin biopsy diagnosed as a well differentiated SCC
Treatment options
October 2011 Photo Dynamic Therapy (PDT) with ALA &
24hr incubation Intralesional Methotrexate Excision Patient elected to undergo PDT
PDT Treatment Procedure
Ten lesions ED&C ALA applied in office to
the individual lesions 24hr incubation Lidocaine injected at
each site Blue light performed
PDT
Follow up after Blue light therapy Two days later pt experienced decreased
pruritis 2 weeks after initial treatment pruritis
returned with increased tenderness and pain No clinically significant change in the lesions
size
Invasive SCC pre-op

191
Invasive SCC excision
December 2011 Mohs resection of SCC
on R shin due to poor response to PDT
Invasive SCC post-op
12 wk follow up after excision of SCC and graft placement
Intralesional Methotrexate
February 2012 Baseline CBC, CMP, and LFTs obtained Intralesional methotrexate injections started Initial treatment 2cc of 12.5mg/cc solution
totaling 25mg Methotrexate was injected equally into 5
lesions
Methotrexate treatment
2 week Follow up No appreciable change in lesion size Patient did complain of mild nausea which
was relieved with famotidine Due to the nausea and increased fatigue,
methotrexate was not administered Labs were rechecked.
Methotrexate treatment
March 2012 Follow up Labs obtained were determined to be normal 4wks s/p injections subjective improvement
noted Injections were continued q2wks
Treatment Results
June 2012 Significant
improvement noted after 12wks
Complete resolution of some lesions and regression of others
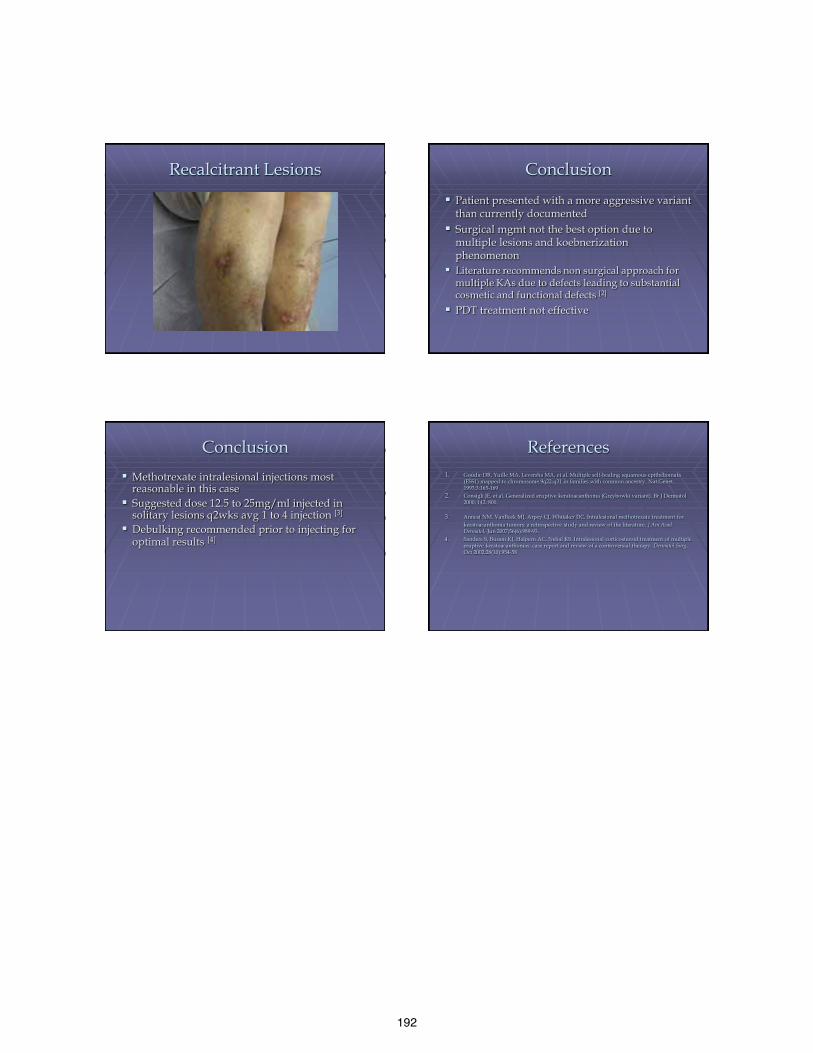
192
Recalcitrant Lesions Conclusion Patient presented with a more aggressive variant
than currently documented Surgical mgmt not the best option due to
multiple lesions and koebnerization phenomenon
Literature recommends non surgical approach for multiple KAs due to defects leading to substantial cosmetic and functional defects [2]
PDT treatment not effective
Conclusion Methotrexate intralesional injections most
reasonable in this case Suggested dose 12.5 to 25mg/ml injected in
solitary lesions q2wks avg 1 to 4 injection [3]
Debulking recommended prior to injecting for optimal results [4]
References 1. Goudie DR, Yuille MA, Leversha MA, et al. Multiple self-healing squamous epitheliomata
(ESS1) mapped to chromosome 9q22-q31 in families with common ancestry. Nat Genet. 1993;3:165-169
2. Consigli JE, et al. Generalized eruptive keratoacanthoma (Grzybowki variant). Br J Dermatol 2000; 142: 800.
3. Annest NM, VanBeek MJ, Arpey CJ, Whitaker DC. Intralesional methotrexate treatment for keratoacanthoma tumors: a retrospective study and review of the literature. J Am Acad
Dermatol. Jun 2007;56(6):989-93. 4. Sanders S, Busam KJ, Halpern AC, Nehal KS. Intralesional corticosteroid treatment of multiple
eruptive keratoacanthomas: case report and review of a controversial therapy. Dermatol Surg. Oct 2002;28(10):954-58
193
Treatment if anal dysplasia with infrared coagulation
Stephen Weis, DO Joseph Susa, DO
S. Robert Harla, DO, FAOCD UNTHSC
Presentation Outline
Anal cancer and anal HPV epidemiology Discuss how to screen for anal cancer Demonstrate the appearance of the anal
canal during high resolution anoscopy and during infrared coagulation
Outcome of treatment program in HIV clinic
HPV- related anogenital disease Condylomata High-grade squamous dysplasia Bowen disease of perineum, perianal area,
and vulva Invasive squamous cell carcinoma-field HPV-related anogenital disease tends to be
more prevalent in HIV-infected persons, more advanced at diagnosis, and more recalcitrant to standard therapies
HIV Care
As a result of the benefits of HAART, there are now more people in the United States living with HIV infection than ever before.[18] Our expanded expertise in treating HIV infection and its complications has shifted the spectrum of diseases in HIV-infected persons
Incidence of anal cancer /100,000
1.061.26
1.61.39
1.691.84
2.042.06
0
0.5
1
1.5
2
2.5
1973-79 1980-86 1987-1993 1994-2000
MenWomen
Daling JR. Cancer 101:281-8; 2004
Incidence of anal cancer
Anal Cancer Population: 2/100,000 Anal Cancer MSM: 35/100,000 Anal cancer MSM + HIV: 70-90/100,000 Cervical Cancer before 40-50/100,000 Cervical cancer currently 8/100,000
Daling JR. NEJM 317:973-7; 1987 Goedert JJ. Lancet 351:1833-9;1998 Daling JR. Cancer 101:281-8; 2004 Bower et al. JAIDS 2004;37:1563-1565

194
HPV is double stranded DNA virus (>100 subtypes)
Oncogenic HPV types- Cause Cancer 16, 18, 31, 33, 35 39, 45, 51, 52, 56, 58, 70 Non-Oncogenic HPV Types-Cause warts 6, 11, 42, 43, 44
Veruca Vulgaris HPV types 2, 4
Anogenital Cancer HPV types 16,18 Potential Cofactors for HPV
Progression Infections: Chlamydia, HSV-2 coinfection Diet: Vitamins A, C, E, folic acid Hormonal: Parity, oral contraceptive use Immunogenetics: HLA type Smoking Host factors: Immune response (HIV) HPV related: Type, variants, viral load
Pinto AP. Natural History of Cervical Neoplasia. Clinic Obster Gyncol 2000;43:352-362
Ryan D et al. N Engl J Med 2000;342:792-800
Anatomy of the Anus Cervical cancer as model for Anal Cancer
Cervical and Anal Cancer frequently arise in transformation zone where columnar epithelium changes to squamous
Both strongly associated with oncogenic HPV strains Both associated with squamous intraepithelial
lesions after HPV infections (SIL) Cervical HSIL Cervical CA Anal HSIL are suspected Anal CA
Frisch M et al, NEJM, 1997;337:1350-8. Palefsky Joel. Multiple publications
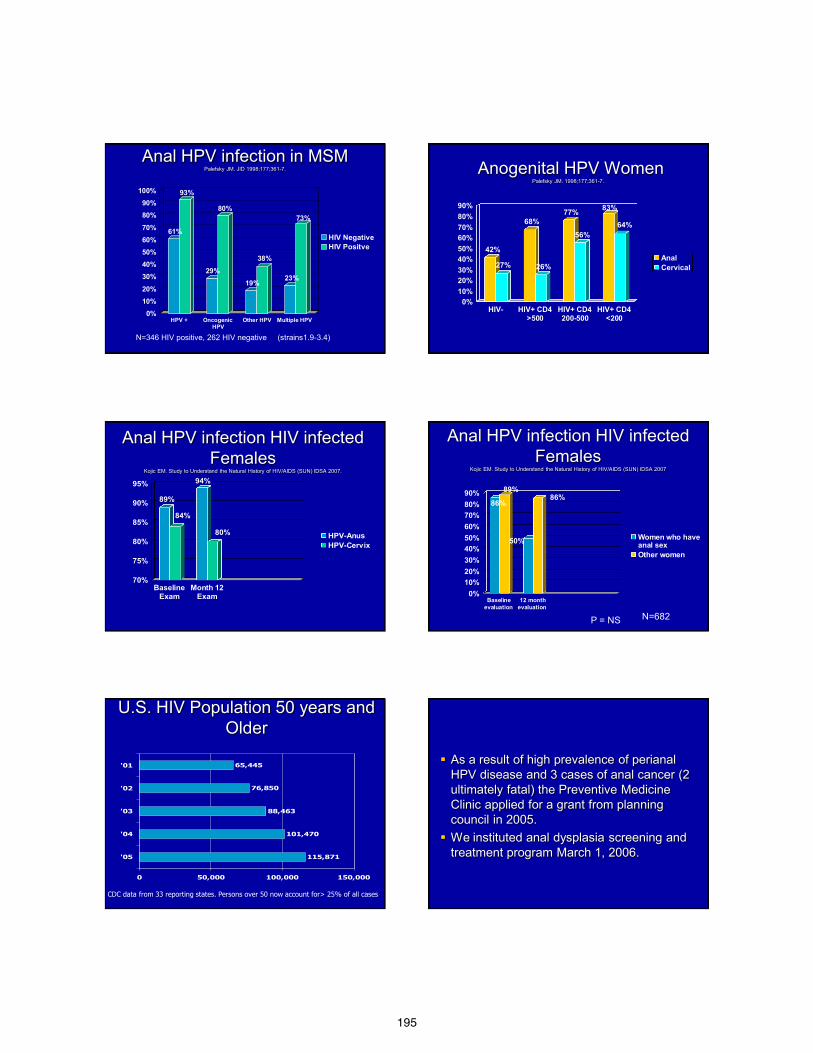
195
Anal HPV infection in MSM Palefsky JM. JID 1998;177;361-7.
61%
93%
29%
80%
19%
38%
23%
73%
0%10%20%
30%40%50%60%70%
80%90%
100%
HPV + OncogenicHPV
Other HPV Multiple HPV
HIV NegativeHIV Positve
N=346 HIV positive, 262 HIV negative (strains1.9-3.4)
Anogenital HPV Women Palefsky JM. 1998;177;361-7.
42%
27%
68%
26%
77%
56%
83%
64%
0%10%20%30%40%50%60%70%80%90%
HIV- HIV+ CD4>500
HIV+ CD4200-500
HIV+ CD4<200
AnalCervical
89%
84%
94%
80%
70%
75%
80%
85%
90%
95%
BaselineExam
Month 12Exam
HPV-AnusHPV-Cervix
Anal HPV infection HIV infected Females
Kojic EM. Study to Understand the Natural History of HIV/AIDS (SUN) IDSA 2007.
Anal HPV infection HIV infected Females
Kojic EM. Study to Understand the Natural History of HIV/AIDS (SUN) IDSA 2007
86%
89%
50%
86%
0%10%20%30%40%50%60%70%80%90%
Baselineevaluation
12 monthevaluation
Women who haveanal sexOther women
P = NS N=682
U.S. HIV Population 50 years and Older
115,871
101,470
88,463
76,850
65,445
0 50,000 100,000 150,000
'05
'04
'03
'02
'01
CDC data from 33 reporting states. Persons over 50 now account for> 25% of all cases
As a result of high prevalence of perianal HPV disease and 3 cases of anal cancer (2 ultimately fatal) the Preventive Medicine Clinic applied for a grant from planning council in 2005.
We instituted anal dysplasia screening and treatment program March 1, 2006.
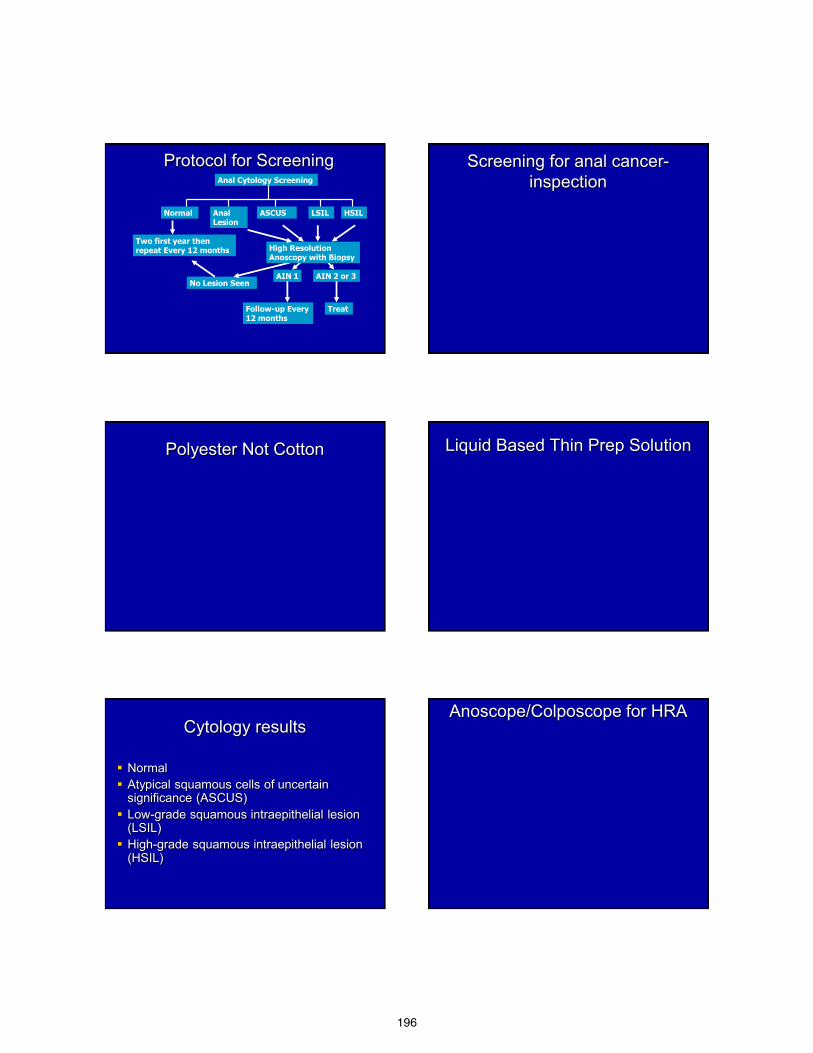
196
Protocol for Screening Anal Cytology Screening
Two first year then repeat Every 12 months
AIN 1
Follow-up Every 12 months
AIN 2 or 3
Treat
No Lesion Seen
High Resolution Anoscopy with Biopsy
Normal ASCUS HSIL LSIL Anal Lesion
Screening for anal cancer-inspection
Polyester Not Cotton Liquid Based Thin Prep Solution
Cytology results
Normal Atypical squamous cells of uncertain
significance (ASCUS) Low-grade squamous intraepithelial lesion
(LSIL) High-grade squamous intraepithelial lesion
(HSIL)
Anoscope/Colposcope for HRA
197
Anal Biopsy AIN-1
AIN-1 AIN-3
Relatively normal transformation zone High Grade dysplasia 16X
198
High Grade dysplasia 16X
Weis, SE. et al Dis Colon Rec 2012. In press
HGAIN that was treated infrared
coagulation (N=98)
74% no HGAIN (High Grade) detectable on biopsy
26% still had HGAIN None had cancer After additional IRC treatment 87% had no HGAIN detectable on biopsy
Weis, SE et al Dis Colon Rec 2012. In press
High Grade AIN (HGAIN)
Not Treated (N=42)
5 % (N=2) no HGAIN detectable on biopsy 88% (N=38) still had HGAIN 5% (N=2) had developed anal cancer
Weis, SE et al Dis Colon Rec 2012. In press
History of “Asymptomatic” after procedure
Sits on stool 5 times a day. With Loperamide goes same number of times but is stool is harder. Feels like he needs to go frequently often only passes gas. Has had for several years. Thinks multiple stools a day is “normal” for people with HIV!
Has anal pain for 2 years. Comes and goes. Believes it is “just a hemorrhoid”. Uses preparation H chronically.
Sometimes has bleeding after anal sex.
History after procedure “Plenty of itching” in anal canal. Scratches
inside anal canal with fingernails. Has “normal anal sex only.” Never used
dildos or did fisting. Does not recall any particular sexual
episode that was unusually painful. No history of herpes, syphilis, or warts. He
was certain his problem was only hemorrhoids.
199
“Asymptomatic” male
2 biopsies of large anal wart biopsies both showed AIN-2
3 biopsies borders of anal ulceration-AIN 2 Biopsy of base shows “nonspecific
ulceration”. No evidence of herpes or CMV with special stains
“Asymptomatic” male
Had bleeding and some pain for 5 days after procedure.
Went to work every day. Now is truly an “Asymptomatic male”
Anus is skin. High grade anal dysplasia is histologically squamous cell cancer in situ Anal cytology is similar in cost and takes the
same amount of time as a full body skin exam High resolution anoscopy is another way to
take a skin biopsy. Infrared coagulation of high grade dysplasia is
similar procedure to electrodessication and curettage of SCC-IS
It is low morbidity, low cost outpatient procedure.
What clinicians do • These data do not exist for most situations • There are not expert guidelines for every situations • What do clinicians do when they have an evolving
problem and there is no data? • That’s why we go to medical school, do residencies
and fellowships. Not just to become technically proficient but to be able to be flexible and work with our patients to create solutions for problems with the best with the available information.
• That is why they call it medical practice and is one of the reasons that we come together in journal clubs to share ideas and opinions to help us deal with indecision tomorrow in our exam rooms.
200
I Blame the Drugs PAUL AANDERUD, DO
Oakwood Hospital Healthcare System, Trenton, Michigan
Drug Adverse Reactions
• Common occurrence
• Variable morphology – Urticarial – Morbilliform – Hypersensitivity syndrome – Lichenoid dermatitis – Vasculitis – Fixed drug eruption (FDE) – Many more
Fixed drug Eruptions
• Underdiagnosed
– We now believe Fixed Drug Eruptions account for 20% of all cutaneous drug eruptions
• Polypharmacy makes diagnosis difficult
– The average patient is taking multiple drugs and over the counter supplements
Pathophysiology • Thought to be caused by an antibody-dependent, cell-
mediated cytotoxic response • CD8+ effector/memory T cells play an important role in
reactivation of lesions with re-exposure to the offending drug
• The offending drug is thought to function as a hapten that preferentially binds to basal keratinocytes, leading to an inflammatory response
• Cytokines such as TNF-alpha up-regulates intercellular adhesion molecule-1 (ICAM1) and this in turn helps T cells migrate to the site of injury. TNF-alpha and INF-gamma continue tissue destruction
Fixed drug Eruptions
• Multiple Types of FDE mentioned in the literature – Pigmenting fixed drug eruption – Generalized or multiple fixed drug eruption – Linear fixed drug eruption – Wandering fixed drug eruption – Nonpigmenting fixed drug eruption – Bullous fixed drug eruption – Eczematous fixed drug eruption – Urticarial fixed drug eruption – Erythema dyschromicum perstans–like fixed drug
eruption – Psoriasiform – Cellulitislike eruption
Unique Case
• Chief Complaint
A 22-year-old African American female
presented to the emergency department with complaints of chills, fever, nausea, myalgia, arthralgia, and a tender rash on the hands for 2 weeks
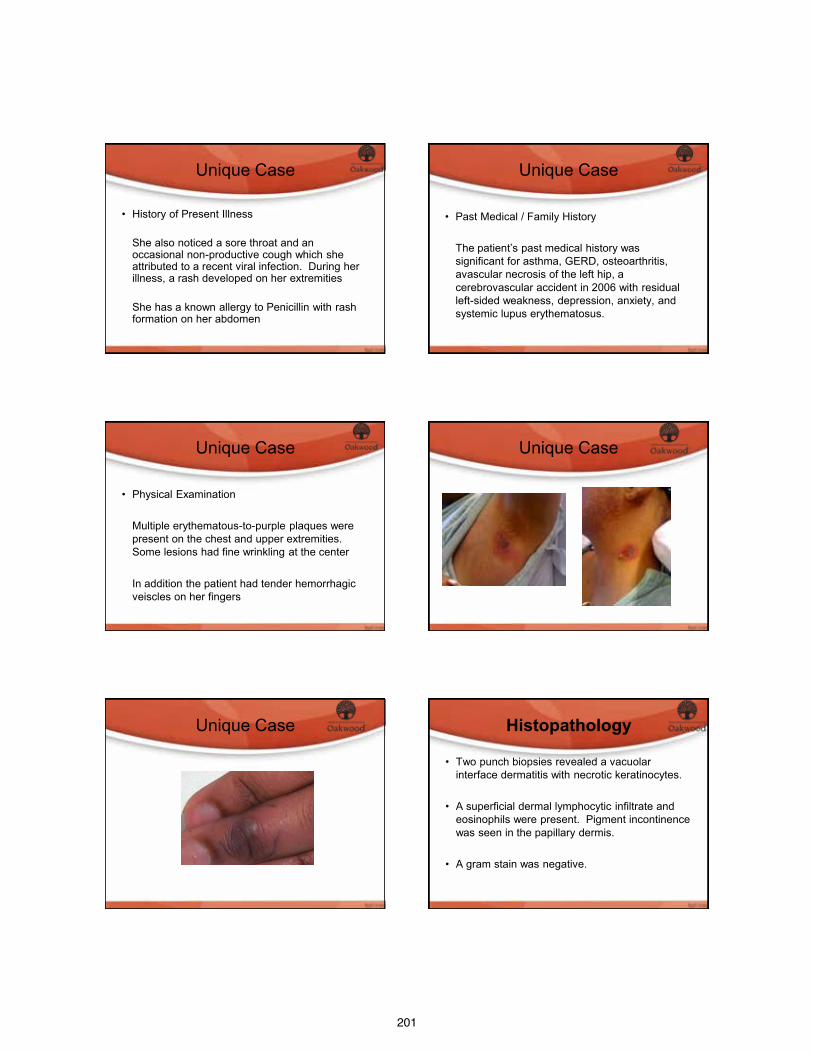
201
Unique Case
• History of Present Illness She also noticed a sore throat and an
occasional non-productive cough which she attributed to a recent viral infection. During her illness, a rash developed on her extremities
She has a known allergy to Penicillin with rash
formation on her abdomen
Unique Case
• Past Medical / Family History
The patient’s past medical history was
significant for asthma, GERD, osteoarthritis, avascular necrosis of the left hip, a cerebrovascular accident in 2006 with residual left-sided weakness, depression, anxiety, and systemic lupus erythematosus.
Unique Case
• Physical Examination Multiple erythematous-to-purple plaques were
present on the chest and upper extremities. Some lesions had fine wrinkling at the center
In addition the patient had tender hemorrhagic veiscles on her fingers
Unique Case
Unique Case Histopathology • Two punch biopsies revealed a vacuolar
interface dermatitis with necrotic keratinocytes.
• A superficial dermal lymphocytic infiltrate and eosinophils were present. Pigment incontinence was seen in the papillary dermis.
• A gram stain was negative.
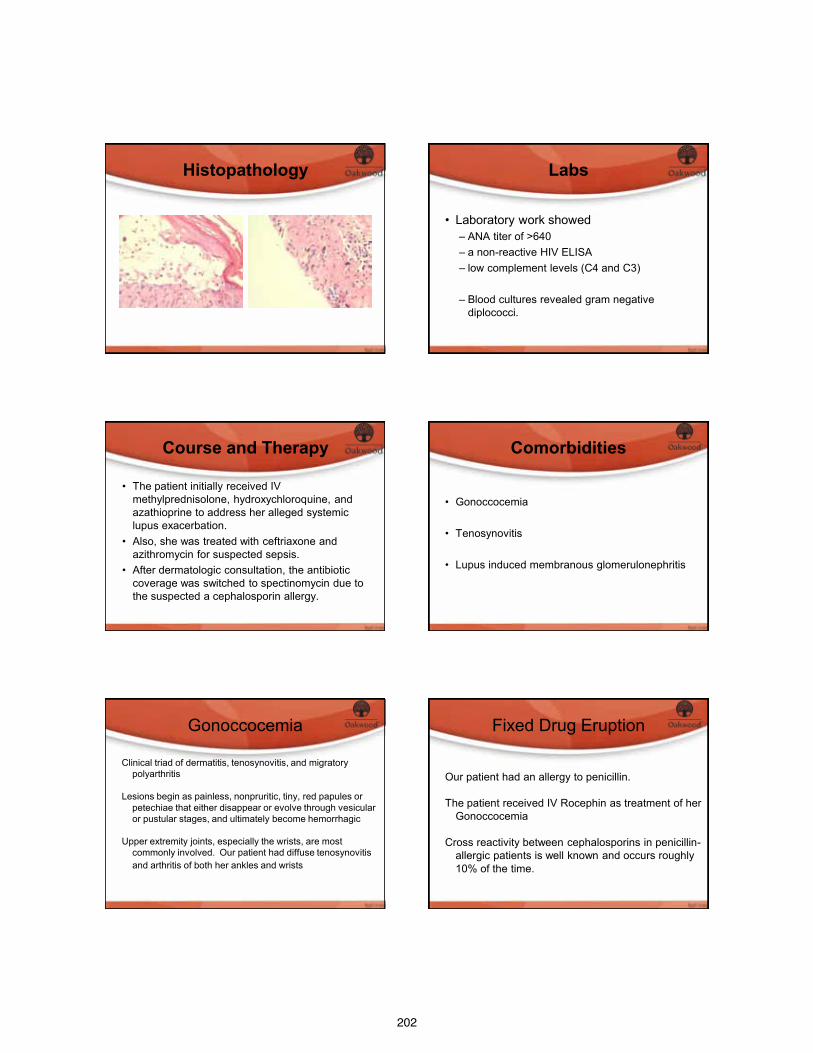
202
Histopathology Labs
• Laboratory work showed
– ANA titer of >640 – a non-reactive HIV ELISA – low complement levels (C4 and C3)
– Blood cultures revealed gram negative
diplococci.
Course and Therapy
• The patient initially received IV methylprednisolone, hydroxychloroquine, and azathioprine to address her alleged systemic lupus exacerbation.
• Also, she was treated with ceftriaxone and azithromycin for suspected sepsis.
• After dermatologic consultation, the antibiotic coverage was switched to spectinomycin due to the suspected a cephalosporin allergy.
Comorbidities
• Gonoccocemia
• Tenosynovitis
• Lupus induced membranous glomerulonephritis
Gonoccocemia
Clinical triad of dermatitis, tenosynovitis, and migratory polyarthritis
Lesions begin as painless, nonpruritic, tiny, red papules or
petechiae that either disappear or evolve through vesicular or pustular stages, and ultimately become hemorrhagic
Upper extremity joints, especially the wrists, are most
commonly involved. Our patient had diffuse tenosynovitis and arthritis of both her ankles and wrists
Fixed Drug Eruption
Our patient had an allergy to penicillin. The patient received IV Rocephin as treatment of her
Gonoccocemia Cross reactivity between cephalosporins in penicillin-
allergic patients is well known and occurs roughly 10% of the time.
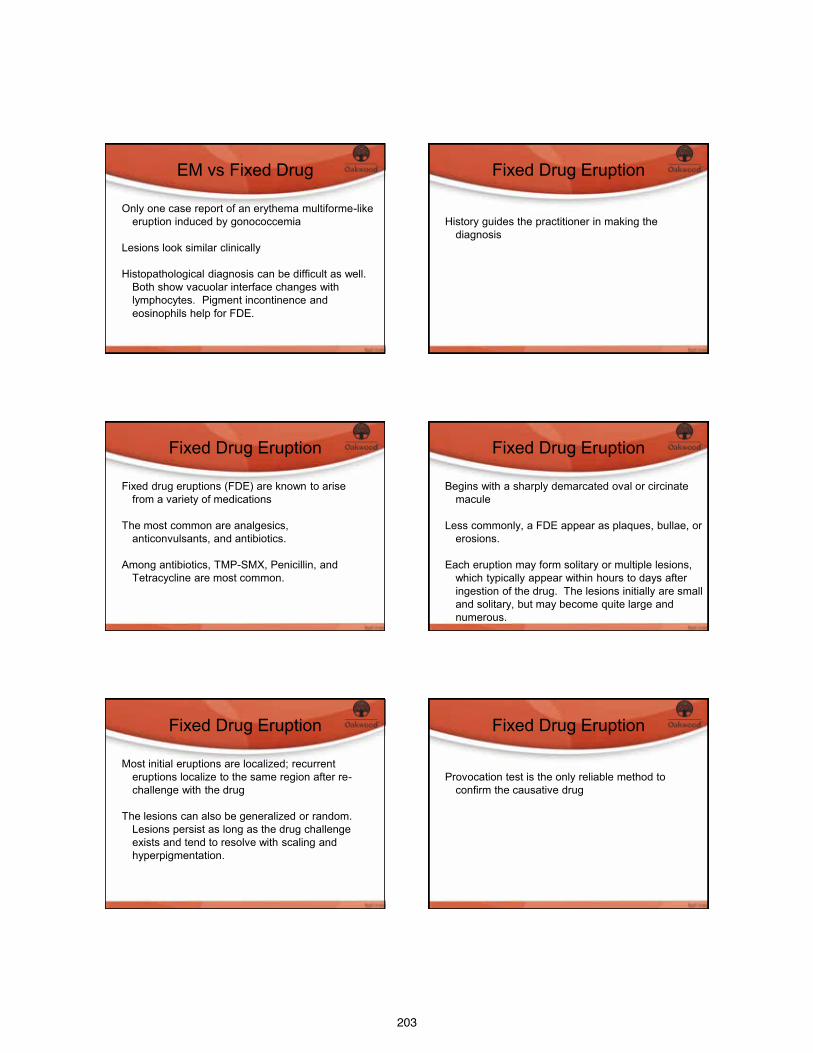
203
EM vs Fixed Drug
Only one case report of an erythema multiforme-like eruption induced by gonococcemia
Lesions look similar clinically Histopathological diagnosis can be difficult as well.
Both show vacuolar interface changes with lymphocytes. Pigment incontinence and eosinophils help for FDE.
Fixed Drug Eruption
History guides the practitioner in making the
diagnosis
Fixed Drug Eruption
Fixed drug eruptions (FDE) are known to arise from a variety of medications
The most common are analgesics,
anticonvulsants, and antibiotics. Among antibiotics, TMP-SMX, Penicillin, and
Tetracycline are most common.
Fixed Drug Eruption
Begins with a sharply demarcated oval or circinate macule
Less commonly, a FDE appear as plaques, bullae, or
erosions. Each eruption may form solitary or multiple lesions,
which typically appear within hours to days after ingestion of the drug. The lesions initially are small and solitary, but may become quite large and numerous.
Fixed Drug Eruption
Most initial eruptions are localized; recurrent eruptions localize to the same region after re-challenge with the drug
The lesions can also be generalized or random.
Lesions persist as long as the drug challenge exists and tend to resolve with scaling and hyperpigmentation.
Fixed Drug Eruption
Provocation test is the only reliable method to
confirm the causative drug
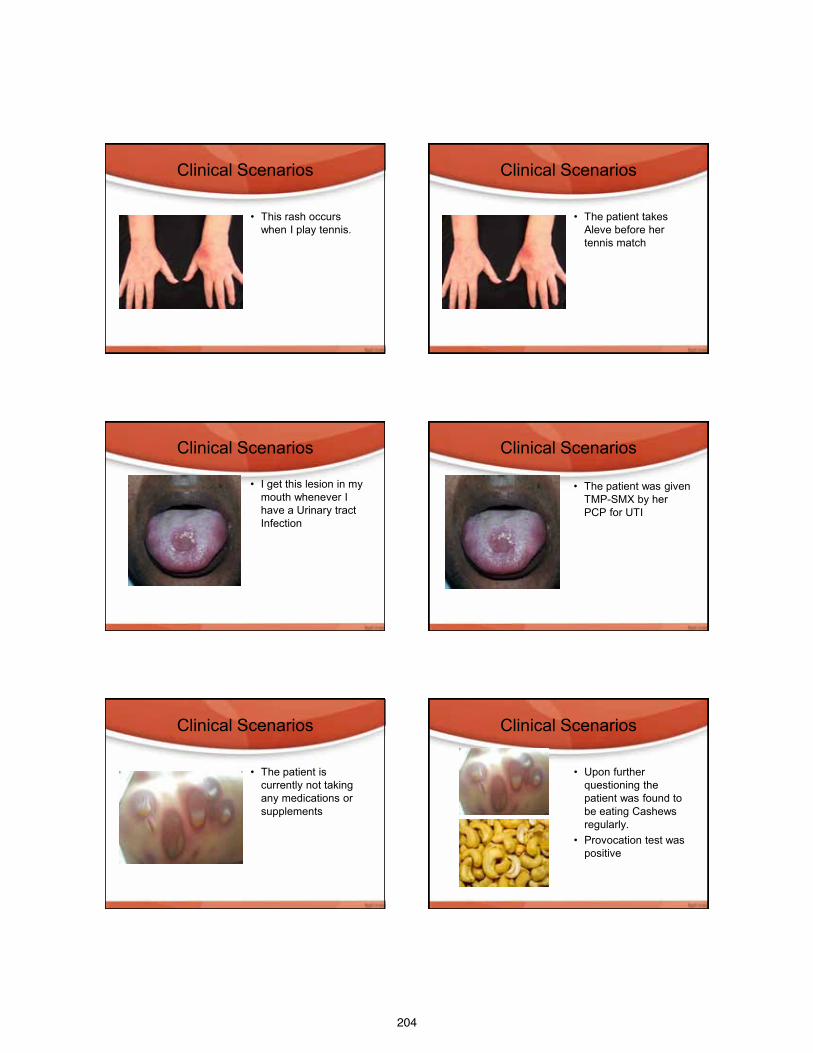
204
Clinical Scenarios
• This rash occurs
when I play tennis.
Clinical Scenarios
• The patient takes
Aleve before her tennis match
Clinical Scenarios
• I get this lesion in my mouth whenever I have a Urinary tract Infection
Clinical Scenarios
• The patient was given TMP-SMX by her PCP for UTI
Clinical Scenarios
• The patient is
currently not taking any medications or supplements
Clinical Scenarios
• Upon further
questioning the patient was found to be eating Cashews regularly.
• Provocation test was positive
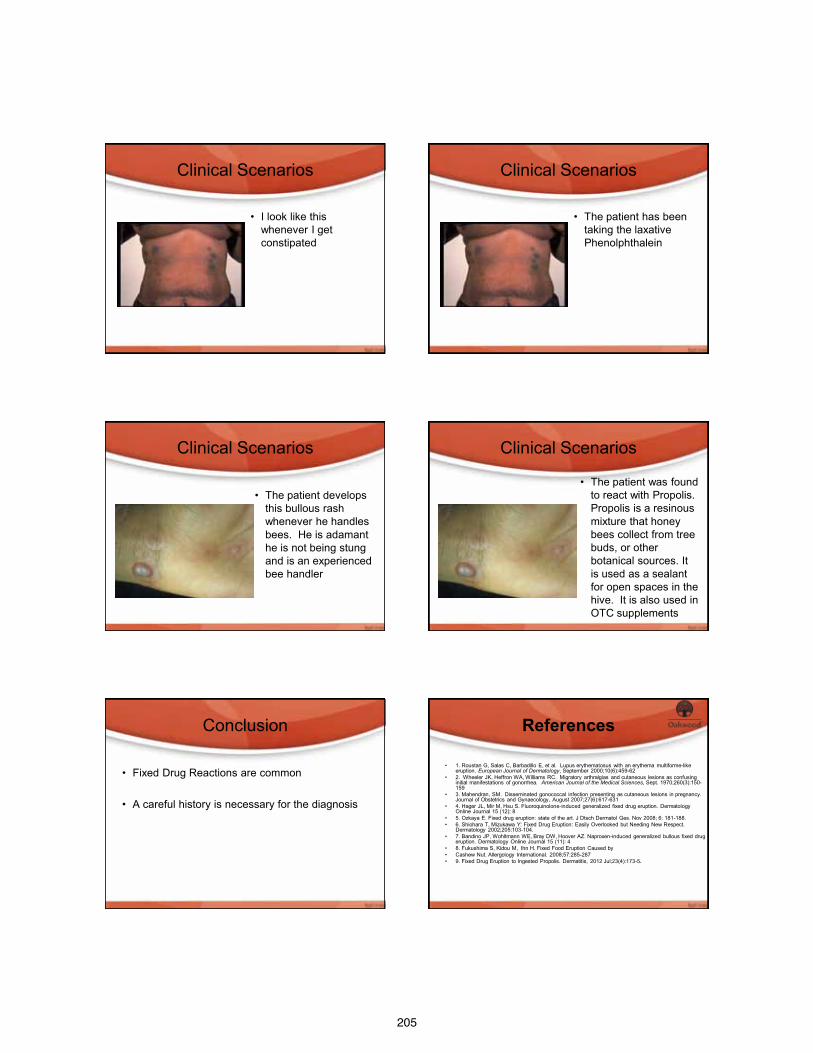
205
Clinical Scenarios
• I look like this
whenever I get constipated
Clinical Scenarios
• The patient has been
taking the laxative Phenolphthalein
Clinical Scenarios
• The patient develops
this bullous rash whenever he handles bees. He is adamant he is not being stung and is an experienced bee handler
Clinical Scenarios
• The patient was found to react with Propolis. Propolis is a resinous mixture that honey bees collect from tree buds, or other botanical sources. It is used as a sealant for open spaces in the hive. It is also used in OTC supplements
Conclusion
• Fixed Drug Reactions are common
• A careful history is necessary for the diagnosis
References • 1. Roustan G, Salas C, Barbadillo E, et al. Lupus erythematosus with an erythema multiforme-like
eruption. European Journal of Dermatology, September 2000;10(6):459-62 • 2. Wheeler JK, Heffron WA, Williams RC. Migratory arthralgias and cutaneous lesions as confusing
initial manifestations of gonorrhea. American Journal of the Medical Sciences, Sept. 1970;260(3):150-159
• 3. Mahendran, SM. Disseminated gonococcal infection presenting as cutaneous lesions in pregnancy. Journal of Obstetrics and Gynaecology, August 2007;27(6):617-631
• 4. Hager JL, Mir M, Hsu S. Fluoroquinolone-induced generalized fixed drug eruption. Dermatology Online Journal 15 (12): 8
• 5. Ozkaya E. Fixed drug eruption: state of the art. J Dtsch Dermatol Ges. Nov 2008; 6: 181-188. • 6. Shiohara T, Mizukawa Y: Fixed Drug Eruption: Easily Overlooked but Needing New Respect.
Dermatology 2002;205:103-104. • 7. Bandino JP, Wohltmann WE, Bray DW, Hoover AZ. Naproxen-induced generalized bullous fixed drug
eruption. Dermatology Online Journal 15 (11): 4 • 8. Fukushima S, Kidou M, Ihn H. Fixed Food Eruption Caused by • Cashew Nut. Allergology International. 2008;57:285-287 • 9. Fixed Drug Eruption to Ingested Propolis. Dermatitis, 2012 Jul;23(4):173-5.
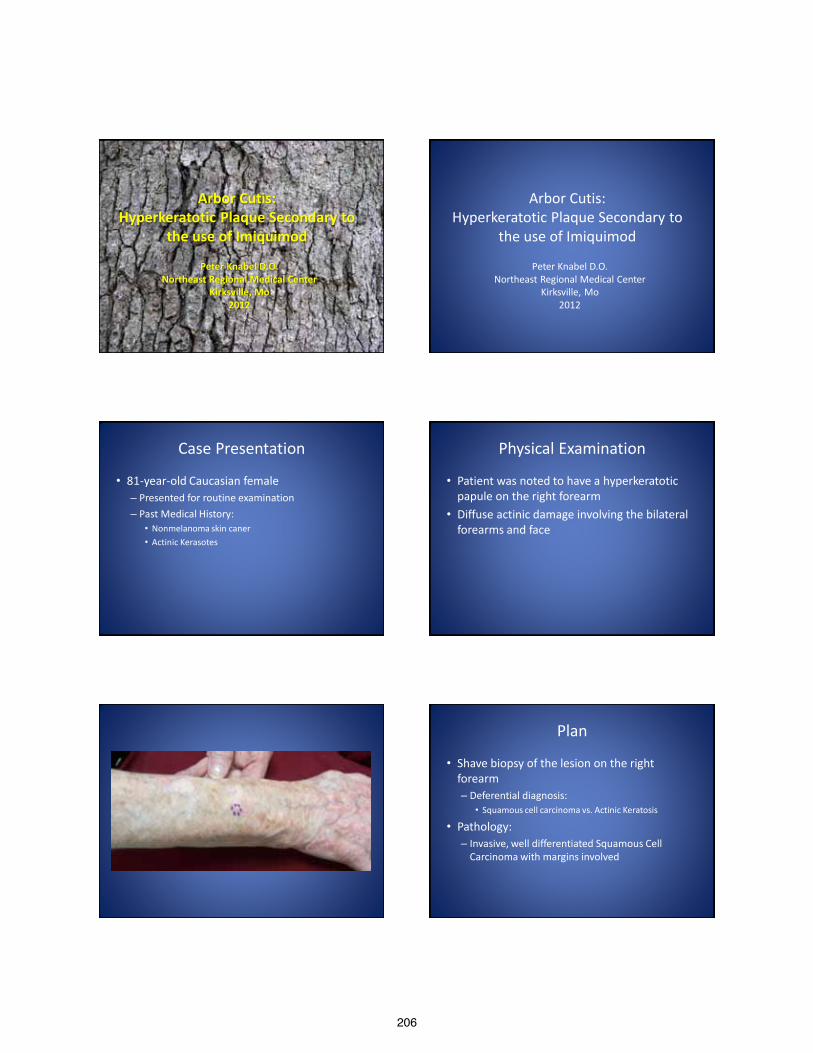
206
Arbor Cutis: Hyperkeratotic Plaque Secondary to
the use of Imiquimod
Peter Knabel D.O. Northeast Regional Medical Center
Kirksville, Mo 2012
Arbor Cutis: Hyperkeratotic Plaque Secondary to
the use of Imiquimod
Peter Knabel D.O. Northeast Regional Medical Center
Kirksville, Mo 2012
Case Presentation
• 81-year-old Caucasian female – Presented for routine examination – Past Medical History:
• Nonmelanoma skin caner • Actinic Kerasotes
Physical Examination
• Patient was noted to have a hyperkeratotic papule on the right forearm
• Diffuse actinic damage involving the bilateral forearms and face
Plan
• Shave biopsy of the lesion on the right forearm – Deferential diagnosis:
• Squamous cell carcinoma vs. Actinic Keratosis
• Pathology: – Invasive, well differentiated Squamous Cell
Carcinoma with margins involved
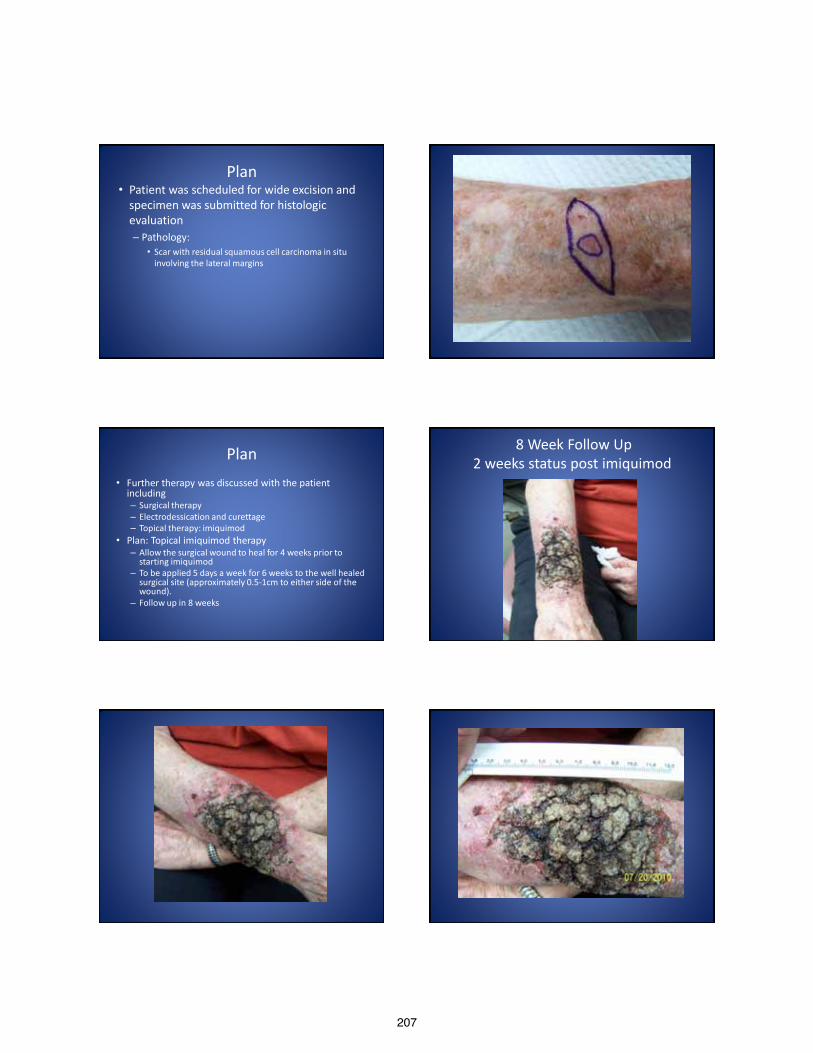
207
Plan • Patient was scheduled for wide excision and
specimen was submitted for histologic evaluation – Pathology:
• Scar with residual squamous cell carcinoma in situ involving the lateral margins
Plan • Further therapy was discussed with the patient
including – Surgical therapy – Electrodessication and curettage – Topical therapy: imiquimod
• Plan: Topical imiquimod therapy – Allow the surgical wound to heal for 4 weeks prior to
starting imiquimod – To be applied 5 days a week for 6 weeks to the well healed
surgical site (approximately 0.5-1cm to either side of the wound).
– Follow up in 8 weeks
8 Week Follow Up 2 weeks status post imiquimod
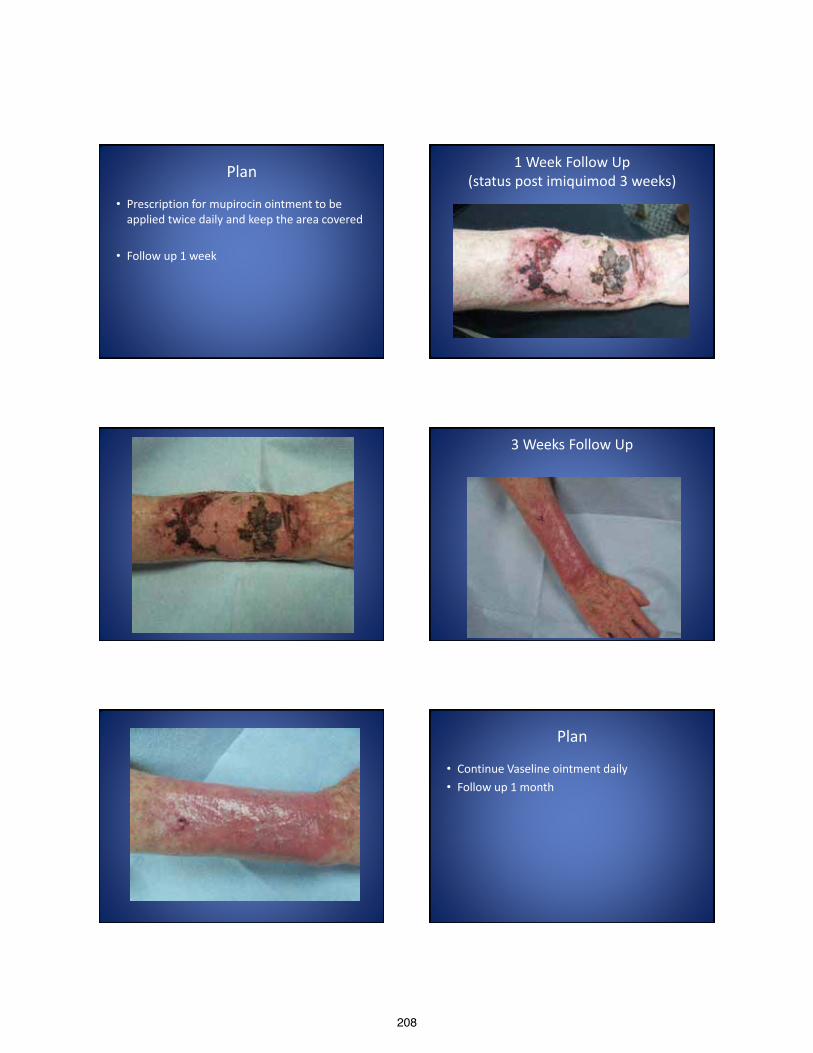
208
Plan
• Prescription for mupirocin ointment to be applied twice daily and keep the area covered
• Follow up 1 week
1 Week Follow Up (status post imiquimod 3 weeks)
3 Weeks Follow Up
Plan
• Continue Vaseline ointment daily • Follow up 1 month

209
1 Month Follow Up
Plan
• Prescription for triamcinolone 0.1% ointment to apply twice daily to the affected areas on the right forearm
• Follow up in 3 month
3 Month Follow Up
Discussion
• Imiquimod – Aldara 5% – Zyclara 2.5%, 3.75% – Belongs to the class of imidazoquinolones – FDA approved for:
• Superficial Basal Cell Carcinoma • Actinic Keratoses • Condyloma Accuminata
– Half-life 1 day – Immune response modifier

210
The Immune System
• The human immune system consists of two components that function synergistically – Innate Immune System – Acquired Immune System
• Humoral • Cellular
The Innate Immune System
• Frist line defense against pathogens • Physical and chemical barriers
– Skin – Cellular barriers – phagocytes – Molecular pattern based reactions
• Toll-like receptors – Activate phagocytes and tissue dendritic cells in response to
pathogens – Facilitates initiation of the acquired immune response – Toll-like receptor 7 specific to imiquimod
• Interferon • Complement
The Innate Immune System
• Specialized cells – produce cytokines – Leukocytes – Granular Cells
• Basophils, Mast cells, Eosinophils, and Neutrophils
– Monocytes – Macrophages
• Natural Killer Cells
The Acquired Immune System • Unique to vertebrates • Composed of the Humoral and Cellular responses • Humoral – B cell mediated
– Antibodies – Immunoglobulins
• Cellular (cell mediated response) – T cell medicated process – T cell types:
• CD4+ – helper T cells • CD8+ – cytotoxic T cells
– T cells • Cooperate with B cells to enhance production of antibodies • Release cytokines – activate and signal B cells • Monocytes/macrophage migration and activation • Cytotoxic effects
Imiquimod
• Activates (Innate) – Monocytes, macrophages, and dendritic cells
• Via binding to Toll-Like Receptor 7 – Secretion of pro-inflammatory cytokines
• Interferon alpha (IFN-α) • Tumor necrosis factor alpha (TNF- α) • Interleukin-12 (IL-12)
– Cytokines • Interleukins 1, 6, 8, and 10 • Favors a Th-1 response
Imiquimod • Activation of T-helper cells
– Th-1 • Interferon-gamma (INF-ɣ)
– Stimulates cellular immunity – Inhibits Th-2 type cytokines
• Stimulates cytotoxic T lymphocytes • Activation of Langerhans cells
– Major antigen presenting cells within the epidermis – Activation of T cells
• Antiangiogenesis – Increased levels of IL-10 and IL-12 – Mediates production of INF-ɣ
211
Imiquimod
• Enhanced cell-mediated immunity – Long term protection – Prolonged tumor clearance via the adaptive
immunity to recognize carcinogenic antigens – Field Effect
Side Effects
• Local cutaneous reactions – Erythema, inflammation, flaking, pruritus, pain,
edema, erosions, ulcerations, vesicles, desquamation, drainage, hypo/hyperpigmentation, and scabbing or crusting
• Systemic reactions – Headache, fatigue, myalgia, nausea, and influenza-like
symptoms • Rarer reactions
– Vitiligo-like depigmentation, erythema multiforme, alopecia, pemphigus foliaceus, psoriasis, and a lupus erythematosus-like reaction
Inflammation
• Severity of the reaction – Better results?
• Caution
– Topical Steroids
Clearance Rates
• No one recommended treatment – Strength (2.5%, 3.75% or 5%) – Duration (weeks) – Dosing (twice daily, daily, 5 days a week, 3 days a
weeks) – Occlusion
Clearance Rates
• Actinic Keratoses: 25%-85% • Squamous Cell Carcinoma In-situ: 73-88% • Superficial Basal Cell Carcinoma: 50-100% • Nodular Basal Cell Carcinoma: 50-100% • Lentigo maligna: 66-100%
• Surgical Excision remains gold standard
Conclusion • Surgery is still considered the Gold Standard for treatment of
cutaneous carcinomas • Imiquimod
– Surgery is not an option… • Location • Disfiguring/cosmesis • Size of lesion • Age of patient
• Close follow-up is necessary – No histologic proof of clearance – Field biopsies
• Potential skip areas • Affective • Accurate
• Ant-aging affect
212
Conclusion
Thank you
References 1. David CV, Nguyen H, Goldenbery G. Imiquimod: A Review of Off Label Clinical Applications. J of Drugs in Dermatology 2011; 10: 1300-1306 2. Garland SM. Imiquimod. Infectious Diseases 2003; 16: 85-89 3. Desai T, Chen CL, Desai A, Kirby W. Basic Pharmacology of Topical Imiquimod, 5-Fluorouracil, and Diclofenac for the Dermatologic Surgeon. Dermatol Surg 2012; 38:97-103. 4. Urosevic M, Dummer R. Role of Imiquimod in Skin Cancer Treatment. Am J Clin Dermatology 2004; 5(6): 453-458. 5. Trying S, Conant M, Marini M, et al. Imiquimod; an international update on therapeutic uses in dermatology. International Journal of Dermatology 2002; 41: 810-816 6. Amini S, Viera MH, Valins W, et al. Nonsurgical Innovations in the Treatment of Nonmelanoma Skin Cancer. J of Clinical and Aesthetic Dermatology 2010; 3(6): 20-34. 7. Ridky TW. Nonmelanoma Skin Cancer. J Am Acad Dermatology 2007; 57: 484-501. 8. Hanke CW, Beer KR, Stockfleth E, et al. Imiquimod 2.5% and 3.75% for the treatment of actinic keratosis: Results of two placebo-controlled studies of daily application to the face and
balding scalp for two 3 week cycles. J Am Acad Dermatology 2010; 62: 573-581. 9. Zeichner JA, Stern DWK, Uliasz A, et al. Placebo-controlled, double blind, randomized pilot study of imiquimod 5% cream applied once per week for 6 months for the treatment of
actinic keratosis. J Am Acad Dermatology 2009; 60: 59-62 10. Wagstaff AJ, Perry CM. Topical Imiquimod: A review of its uses in the management of anogenital warts, actinic keratosis, basal cell carcinoma and other skin lesions. Drugs 2007; 15:
2187-2210 11. Shimizu I, Cruz A, Chang KH, et al. Treatment of Squamous Cell Carcinoma in Situ: A Review. Dermatol Surg 2011; 37: 1394-1411. 12. Patel GK, Goodwin R, Chawla M, et al. Imiquimod 5% cream monotherapy for cutaneous squamous cell carcinoma in situ (Bowen’s disease): A randomized, double-blind, placebo-
controlled trial. J Am Acad Dermatol 2006 Jun; 54(6): 1025-32. 13. Eigentler RK, Kamin A, Weide BM, et al. A phase III, randomized, open label study to evaluate the safety and efficacy of imiquimod 5% cream applied thrice weekly for 8 and 12 weeks
in the treatment of low risk nodular basal cell carcinoma. J Am Acad Dermatol 2007 Oct; 57(4); 616-621. 14. Lacarrubba F, Nasca MR, Micali G. Advances in the use of topical imiquimod to treat dermatologic disorders. Therapeutics and Clinical Risk Management 2008; 4(1): 87-97 15. Raasch B. Management of superficial basal cell carcinoma: a focus on imiquimod. Clinical, Cosmetic, and Investigational Dermatology 2009; 2: 65-75. 16. Junkins-Hopkins JM. Imiquimod use in the treatment of lentigo maligna. Dialogues in Dermatology. J Am Acad Dermatology 2009 Nov; 61(5): 865-867. 17. Woodmansee CS, McCall MW. Recurrence of Lentigo Maligna and Development of Invasive Melanoma after Treatment of Lentigo Maligna with Imiquimod. Dermatol Surg 2009; 35:
1286-1289. 18. Nagore E, et al. Imiquimod para el tratamiento del lentigo maligna. Actas Dermosifiliogr 2011; 102: 559-62. 19. Sriprakash K, Godbolt A. Vitiligo-like depigmentation induced by imiquimod treatment of superficial basal cell carcinoma. Australasian Journal of Dermatology 2009; 50: 211-213. 20. Garcia-Apra M, Rodriquez-Vazquez M, et al. Erythema Multiforme Due to 5% imiquimod cream. Actas Dermosifiliogr 2010; 101(6): 551-571. 21. Conde J, David K, Ntuen E, et al. A case of imiquimod-induced alopecia. Journal of Dermatological Treatment 2010; 21: 122-124. 22. Sebaratnam DF, Martin LK, Rubin AI, et al. Reversible relapse of pemphigus foliaceus triggered by topical imiquimod suggests that Toll-like receptor 7 inhibitors may be useful
treatments for pemphigus. Clinical and Experimental Dermatology 2010; 36: 91-100. 23. Patel U, Mark NM, Machler BC, et al. Imiquimod 5% cream induced psoriasis: a case report, summary of the literature and mechanism. British Association of Dermatologists 2011;
164: 665-683. 24. Rajan N, Langtry JAA. Generalized exacerbation of psoriasis associated with imiquimod cream treatment of superficial basal cell carcinomas. Clinical and Experimental Dermatology
2005; 31: 129-156. 25. Fanti PA, Dilca E, Vaccari S, et al. Generalized psoriasis induced by topical treatment of actinic keratosis with imiquimod. International Journal of Dermatology 2006; 45: 1464-1465. 26. Chan MP, Zimarowski MJ. Lupus Erythematosus-Like Reaction in Imiquimod – Treated Skin: A Report of 2 Cases. Am J Dermatopathol 2011 July; 33(5): 523-527. 27. Caperton C, Berman B. Safety, efficacy, and patient acceptability of imiquimod for topical treatment of actinic keratosis. Clinical, cosmetic, and Investigational Dermatology 2011; 4:
35-40.
213
Grace K. Kim D.O. Valley Hospital Medical Center
PGY IV
I have no disclosures
Indications for spironolactone therapy Expected response time Guidelines for laboratory monitoring Side effects of spironolactone therapy The origin of the black box warning
◦ Poor candidates for therapy Benefits of combination (i.e. antibiotics, oral
contraceptives) therapy
Aldosterone antagonist used as a potassium sparing diuretic
Anti-androgenic effects discovered when being used to treat hypertension in women with polycystic ovarian syndrome (PCOS)
Now used for women with hormonal pattern acne vulgaris (AV) and inhibits sebaceous activity
Off label: inflammatory, tender, deep seated papules, located on the lower half of the face and anterior lateral neck region.
↓5-alpha reductase activity via ↑clearance of testosterone
↑level of steroid hormone binding globulin (SHBG) ↓circulating free testosterone more bound
Overall ↑estrogenic state gynecomastia, decreased libido
Local action competing with dihydrotestosterone (DHT) for cutaneous androgen receptors and inhibit testosterone
Physiological effects ◦ androgenic alopecia,
hirsutism, excess sebum and acne vulgaris
Fig 1 C19 steroid metabolism
Changes observed in both ends of the spectrum of acne onset Acne is starting earlier…and starting later Acne is starting earlier…and hanging around longer
Definitions of Pediatric acne (birth to 11 years)* Neonatal acne Birth through 4 weeks of age Infantile acne 1 month through 12 months of age Mid-childhood acne >1 year through 6 years of age Preadolescent acne >7 years through 11 years of
age Adolescent acne 12 years to adulthood
Definitions of Post-adolescent acne in females#
Late-onset acne >age 25 years *Mancini A, et al. Semin Cutan Med Surg 2011;30:S2-S5. #Goulden V, et al. Br J Dermatol 1997;136:66-70; Cunliffe W, et al. Br Med J 1979;26:931-35; Goulden V, et al. J Am Acad Dermatol 1999;41:577-80.
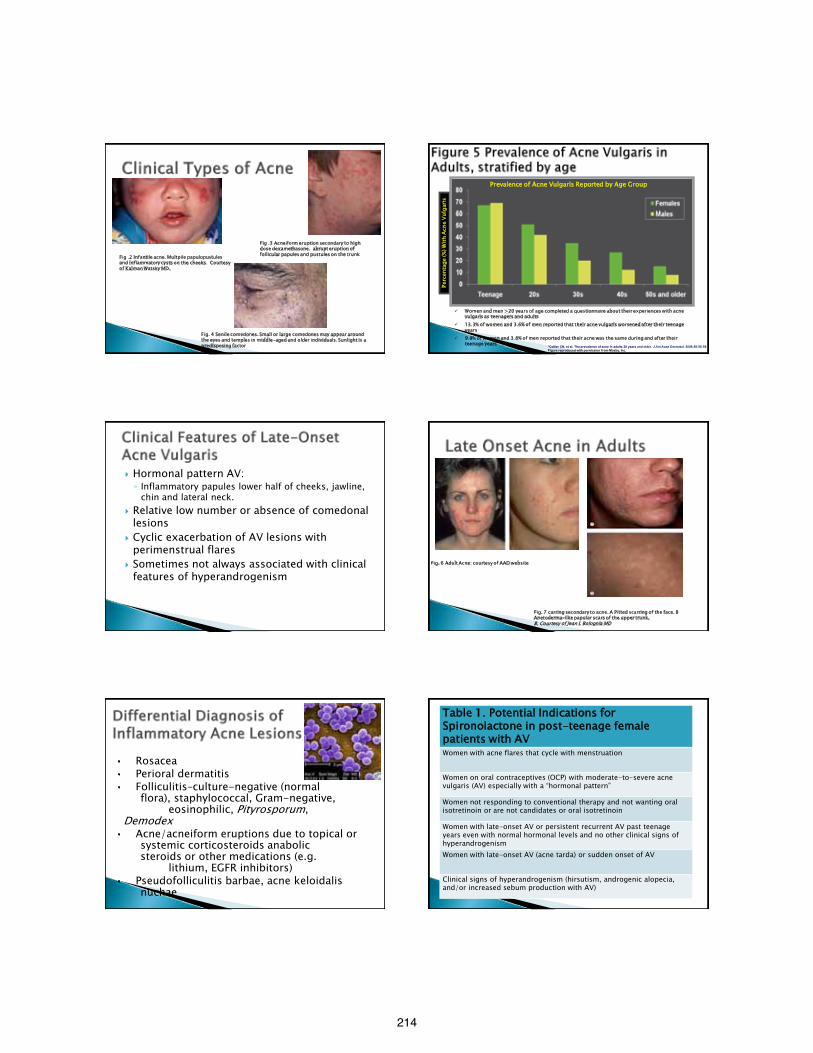
214
Fig .2 Infantile acne. Multpile papulopustules and inflammatory cysts on the cheeks. Courtesy of Kalman Watsky MD.
Fig .3 Acneiform eruption secondary to high dose dexamethasone. abrupt eruption of follicular papules and pustules on the trunk
Fig. 4 Senile comedones. Small or large comedones may appear around the eyes and temples in middle-aged and older individuals. Sunlight is a predisposing factor
Perc
enta
ge (%
) With
Acn
e Vu
lgar
is
8 *Collier CN, et al. The prevalence of acne in adults 20 years and older. J Am Acad Dermatol. 2008;58:56-59. Figure reproduced with permission from Mosby, Inc.
Women and men >20 years of age completed a questionnaire about their experiences with acne vulgaris as teenagers and adults
13.3% of women and 3.6% of men reported that their acne vulgaris worsened after their teenage years
9.8% of women and 3.8% of men reported that their acne was the same during and after their teenage years
Prevalence of Acne Vulgaris Reported by Age Group
Hormonal pattern AV: ◦ Inflammatory papules lower half of cheeks, jawline,
chin and lateral neck. Relative low number or absence of comedonal
lesions Cyclic exacerbation of AV lesions with
perimenstrual flares Sometimes not always associated with clinical
features of hyperandrogenism
Fig. 7 carring secondary to acne. A Pitted scarring of the face. B Anetoderma-like papular scars of the upper trunk. B, Courtesy of Jean L Bolognia MD
Fig. 6 Adult Acne: courtesy of AAD website
• Rosacea • Perioral dermatitis • Folliculitis–culture-negative (normal
flora), staphylococcal, Gram-negative, eosinophilic, Pityrosporum, Demodex • Acne/acneiform eruptions due to topical or
systemic corticosteroids anabolic steroids or other medications (e.g. lithium, EGFR inhibitors) • Pseudofolliculitis barbae, acne keloidalis
nuchae
Table 1. Potential Indications for Spironolactone in post-teenage female patients with AV Women with acne flares that cycle with menstruation
Women on oral contraceptives (OCP) with moderate-to-severe acne vulgaris (AV) especially with a “hormonal pattern”
Women not responding to conventional therapy and not wanting oral isotretinoin or are not candidates or oral isotretinoin
Women with late-onset AV or persistent recurrent AV past teenage years even with normal hormonal levels and no other clinical signs of hyperandrogenism Women with late-onset AV (acne tarda) or sudden onset of AV
Clinical signs of hyperandrogenism (hirsutism, androgenic alopecia, and/or increased sebum production with AV)
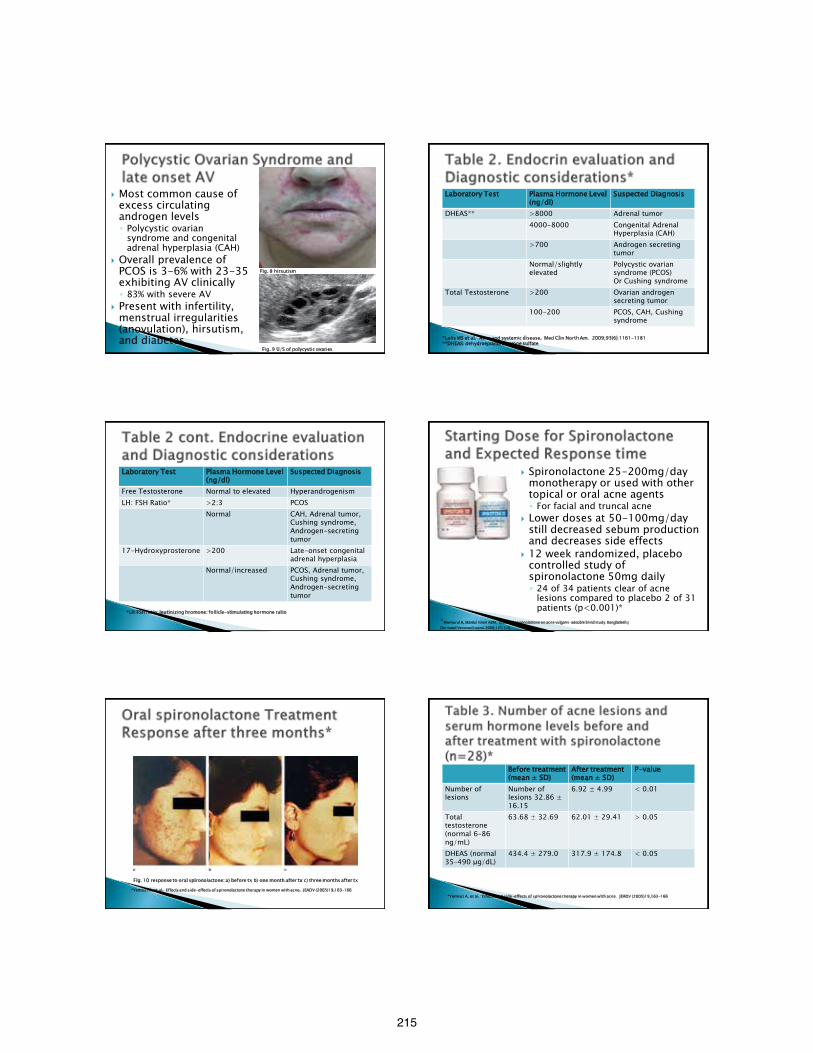
215
Most common cause of excess circulating androgen levels ◦ Polycystic ovarian
syndrome and congenital adrenal hyperplasia (CAH)
Overall prevalence of PCOS is 3-6% with 23-35 exhibiting AV clinically ◦ 83% with severe AV
Present with infertility, menstrual irregularities (anovulation), hirsutism, and diabetes
Fig. 8 hirsutism
Fig. 9 U/S of polycystic ovaries
Laboratory Test Plasma Hormone Level (ng/dl)
Suspected Diagnosis
DHEAS** >8000 Adrenal tumor 4000-8000 Congenital Adrenal
Hyperplasia (CAH) >700 Androgen secreting
tumor Normal/slightly elevated
Polycystic ovarian syndrome (PCOS) Or Cushing syndrome
Total Testosterone >200 Ovarian androgen secreting tumor
100-200 PCOS, CAH, Cushing syndrome
*Lolis MS et al. Acne and systemic disease. Med Clin North Am. 2009;93(6):1161-1181 **DHEAS: dehydroepiandrosterone sulfate
Laboratory Test Plasma Hormone Level (ng/dl)
Suspected Diagnosis
Free Testosterone Normal to elevated Hyperandrogenism LH: FSH Ratio* >2:3 PCOS
Normal CAH, Adrenal tumor, Cushing syndrome, Androgen-secreting tumor
17-Hydroxyprosterone >200 Late-onset congenital adrenal hyperplasia
Normal/increased PCOS, Adrenal tumor, Cushing syndrome, Androgen-secreting tumor
*LH:FSH ratio: leutinizing hromone: follicle-stimulating hormone ratio
Spironolactone 25-200mg/day monotherapy or used with other topical or oral acne agents ◦ For facial and truncal acne
Lower doses at 50-100mg/day still decreased sebum production and decreases side effects
12 week randomized, placebo controlled study of spironolactone 50mg daily ◦ 24 of 34 patients clear of acne
lesions compared to placebo 2 of 31 patients (p<0.001)*
*Mansurul A, Maidul Islam AZM. Effect of spironolactone on acne vulgaris-adouble blind study. Bangladesh J Dermatol Venereol Leprol.2000;171:1-4
Fig. 10 response to oral spironolactone: a) before tx b) one month after tx c) three months after tx
*Yemisci A, et al. Effects and side-effects of spironolactone therapy in women with acne. JEADV (2005)19,163–166
Before treatment (mean ± SD)
After treatment (mean ± SD)
P-value
Number of lesions
Number of lesions 32.86 ± 16.15
6.92 ± 4.99 < 0.01
Total testosterone (normal 6–86 ng/mL)
63.68 ± 32.69 62.01 ± 29.41 > 0.05
DHEAS (normal 35–490 μg/dL)
434.4 ± 279.0 317.9 ± 174.8 < 0.05
*Yemisci A, et al. Effects and side-effects of spironolactone therapy in women with acne. JEADV (2005)19,163–166
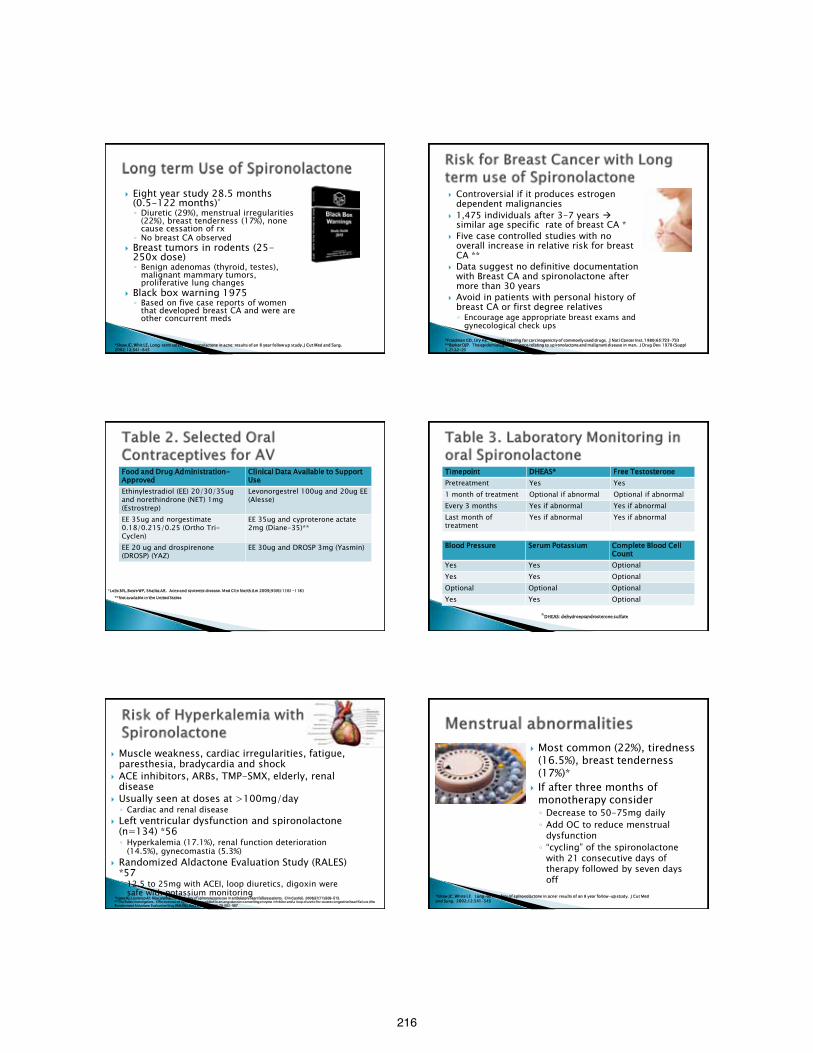
216
Eight year study 28.5 months (0.5-122 months)* ◦ Diuretic (29%), menstrual irregularities
(22%), breast tenderness (17%), none cause cessation of rx
◦ No breast CA observed Breast tumors in rodents (25-
250x dose) ◦ Benign adenomas (thyroid, testes),
malignant mammary tumors, proliferative lung changes
Black box warning 1975 ◦ Based on five case reports of women
that developed breast CA and were are other concurrent meds
*Shaw JC, Whit LE, Long-term safety of spironolactone in acne: results of an 8 year follow up study. J Cut Med and Surg. 2002;12:541-545
Controversial if it produces estrogen dependent malignancies
1,475 individuals after 3-7 years similar age specific rate of breast CA *
Five case controlled studies with no overall increase in relative risk for breast CA **
Data suggest no definitive documentation with Breast CA and spironolactone after more than 30 years
Avoid in patients with personal history of breast CA or first degree relatives ◦ Encourage age appropriate breast exams and
gynecological check ups *Friedman GD, Ury HK. Initial Screening for carcinogenicity of commonly used drugs. J Natl Cancer Inst. 1980;65:723-733 **Barker DJP. The epidemiological evidence relating to spironolactone and malignant disease in man. J Drug Dev. 1978 ( Suppl 1.2):22-25
Food and Drug Administration-Approved
Clinical Data Available to Support Use
Ethinylestradiol (EE) 20/30/35ug and norethindrone (NET) 1mg (Estrostrep)
Levonorgestrel 100ug and 20ug EE (Alesse)
EE 35ug and norgestimate 0.18/0.215/0.25 (Ortho Tri-Cyclen)
EE 35ug and cyproterone actate 2mg (Diane-35)**
EE 20 ug and drospirenone (DROSP) (YAZ)
EE 30ug and DROSP 3mg (Yasmin)
**Not available in the United States *Lolis MS, Bowe WP, Shalita AR. Acne and systemic disease. Med Clin North Am 2009;93(6):1161-1181
Timepoint DHEAS* Free Testosterone Pretreatment Yes Yes 1 month of treatment Optional if abnormal Optional if abnormal Every 3 months Yes if abnormal Yes if abnormal Last month of treatment
Yes if abnormal Yes if abnormal
Blood Pressure Serum Potassium Complete Blood Cell Count
Yes Yes Optional Yes Yes Optional Optional Optional Optional Yes Yes Optional
*DHEAS: dehydroepiandrosterone sulfate
Muscle weakness, cardiac irregularities, fatigue, paresthesia, bradycardia and shock
ACE inhibitors, ARBs, TMP-SMX, elderly, renal disease
Usually seen at doses at >100mg/day ◦ Cardiac and renal disease
Left ventricular dysfunction and spironolactone (n=134) *56 ◦ Hyperkalemia (17.1%), renal function deterioration
(14.5%), gynecomastia (5.3%) Randomized Aldactone Evaluation Study (RALES)
*57 ◦ 12.5 to 25mg with ACEI, loop diuretics, digoxin were
safe with potassium monitoring *Lopes RJ, Lourenco AP, Mascarenhas J et al. Safety of spironolactone use in ambulatory heart failure patients. Clin Cardiol. 2008;31(11):509-513. **The Rales investigators. Effectiveness of spironolactone added to an angiotensin-converting enzyme inhibitor and a loop diuretic for severe congestive heart failure (the Randomized Aldactone Evaluation Stuy [RALES]). Am J Cardiol. 1996;78:902-907
Most common (22%), tiredness (16.5%), breast tenderness (17%)*
If after three months of monotherapy consider ◦ Decrease to 50-75mg daily ◦ Add OC to reduce menstrual
dysfunction ◦ “cycling” of the spironolactone
with 21 consecutive days of therapy followed by seven days off *Shaw JC, White LE. Long-term safety of spironolactone in acne: results of an 8 year follow-up study. J Cut Med
and Surg. 2002;12:541-545
217
Drugs Side effects Diuretics and Potassium sparing drugs
Hyperkalemia
ACE inhibitors Hyperkalemia Barbiturates, alcohol, and narcotics Orthostatic Hypotension Corticosteroids or adrenocorticotropin hormone (ACTH)
Electrolyte depletion, hypokalemia
Digoxin Elevated serum levels of digoxin Non-depolarizing neuromuscular blocking agents
Potentiated with spironolactone use
*Aldactazide (sprionolactone with hydrochlorothiazide) tablets [package insert]. Chicago, IL: Searle; 2003
Should be avoided in pregnancy category C
Male fetus: masculinization occurs after 6 weeks and if drug d/c early, risk is negligible
Currently, no links with congenital defects and no well controlled studies with pregnancy
Case reports of two developed healthy males after high dose tx ◦ spironolactone (200-400mg) and K
supplements maternal Bartter syndrome*
*Groves TD, Corenblum B. Spironolactone therapy during human pregnancy. Am J Ostet Gynecol. 1995;172(5):1655-1656.
skjef
Monotherapy or in combination with other agents ◦ OC (reduces side effects and risk of preg) and antibiotics ◦ Other topical acne agents
Women with hormonal pattern acne, PCOS, or hyperandrogenism state
Women with normal circulating androgen levels but with late onset acne can benefit
Recalcitrant cases, resistant to conventional treatment ◦ Many times it is a myth that it will “run its course”
Spironolactone should be considered as an armamentarium for women with adult acne ◦ Avoid in pts wanting to get pregnant ◦ Avoid in pts with breast CA risk
1.Goulden V, Clark SM, Cunliffe WJ. Post-adolescent acne: a review of clinical features. Br J of Dermatol. 1997;136:66-70. 2. Collier CN, Harper JC, Cantrell WC. The prevalence of acne in adults 20 years and older. J Am Acad Dermatol. 2008;58:56-9. 3. Cunliffe W, Gould D. Prevalence of facial acne vulgaris in late adolescence and in adults. Br Med J. 1979;26:931-5. 4. Stoll S, Shalita AR, Webster GF. The effect of menstrual cycle on acne. J Am Acad Dermatol. 2001;45:957-60. 5. Thiboutot D. Acne: hormonal concepts and therapy. Clin Dermatol. 2004;22:419-28 6. Akamatsu H, Zouboulis CC, Orfanos CE. Spironolactone directly inhibits proliferation of cultured human faciall sebocytes and acts antagonistically to testosterone and 5-alpha-dihidrotestosterone in vitro. J Invest Dermatol. 1993;100:660-62. 7. Thiboutot D, Chen W. Update and future of hormonal therapy in acne. Dermatology. 2003;206:57-67. 8. Goodfellow A, Alaghband-Zadeh J, Carter G et al. Oral spironolactone improve acne vulgaris and reduced sebum excretion. Br J Dermatol 1984;111:124-5. 9. Shaw JC, White LE. Long-term safety of spironolacone in acne: results of an 8 year followup study. J of Cut Med and Surg. 2002;12:541-45. 10. Barker DJP. The epidemiological evidence relating to spironolactone and malignant disease in man. J Drug Dev. 1978;1(Suppl1. 2):22-25. 11. Shaw JC. Hormonal therapies in acne. Exper Opin Pharmacother. 2003;3(7):865-74. 12. Lolis MS, Bowe WP, Shalita AR. Acne and systemic disease. Med Clin North Am. 2009;93(6):1161-81.
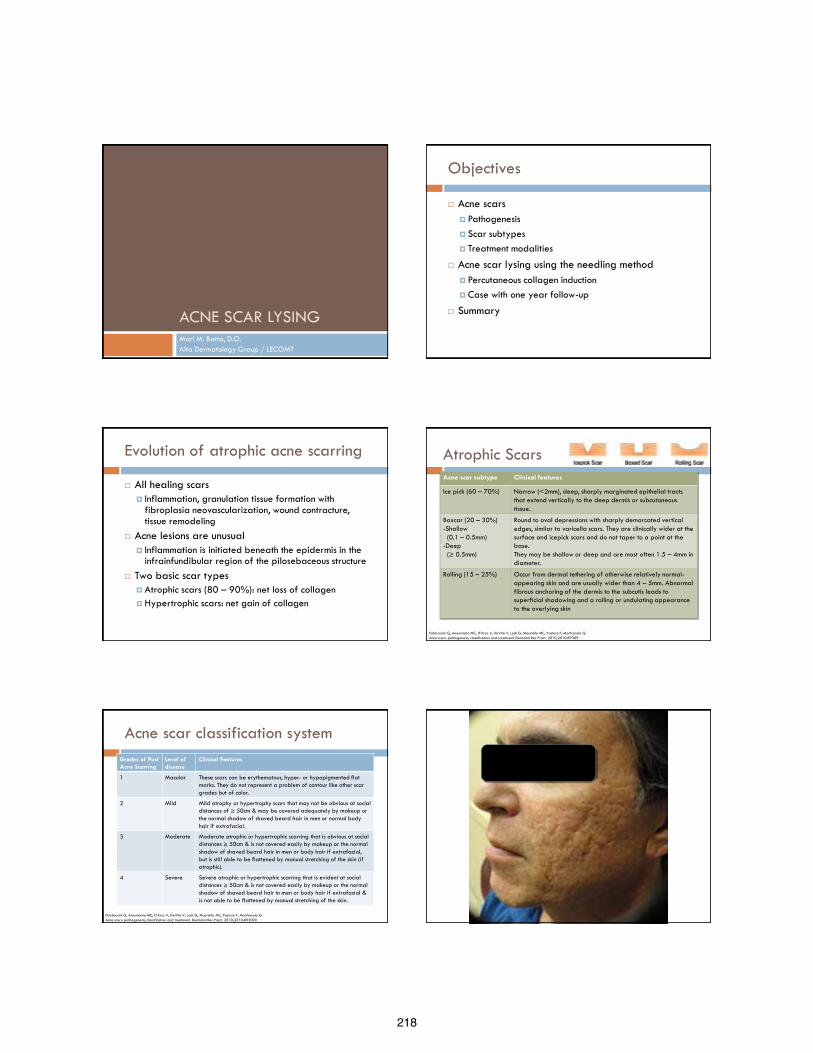
218
ACNE SCAR LYSING Mari M. Batta, D.O. Alta Dermatology Group / LECOMT
Objectives
Acne scars Pathogenesis Scar subtypes Treatment modalities
Acne scar lysing using the needling method Percutaneous collagen induction Case with one year follow-up
Summary
Evolution of atrophic acne scarring
All healing scars Inflammation, granulation tissue formation with
fibroplasia neovascularization, wound contracture, tissue remodeling
Acne lesions are unusual Inflammation is initiated beneath the epidermis in the
infrainfundibular region of the pilosebaceous structure Two basic scar types Atrophic scars (80 – 90%): net loss of collagen Hypertrophic scars: net gain of collagen
Atrophic Scars Acne scar subtype Clinical features
Ice pick (60 – 70%) Narrow (<2mm), deep, sharply marginated epithelial tracts that extend vertically to the deep dermis or subcutaneous tissue.
Boxcar (20 – 30%) -Shallow (0.1 – 0.5mm) -Deep (≥ 0.5mm)
Round to oval depressions with sharply demarcated vertical edges, similar to varicella scars. They are clinically wider at the surface and icepick scars and do not taper to a point at the base. They may be shallow or deep and are most often 1.5 – 4mm in diameter.
Rolling (15 – 25%) Occur from dermal tethering of otherwise relatively normal-appearing skin and are usually wider than 4 – 5mm. Abnormal fibrous anchoring of the dermis to the subcutis leads to superficial shadowing and a rolling or undulating appearance to the overlying skin
Fabbrocini G, Annunziata MC, D’Arco V, DeVita V, Lodi G, Mauriello MC, Pastore F, Monfrecola G. Acne scars: pathogenesis, classification and treatment. Dermatol Res Pract. 2010;2010:89309
Acne scar classification system Grades of Post Acne Scarring
Level of disease
Clinical Features
1 Macular These scars can be erythematous, hyper- or hypopigmented flat marks. They do not represent a problem of contour like other scar grades but of color.
2 Mild Mild atrophy or hypertrophy scars that may not be obvious at social distances of ≥ 50cm & may be covered adequately by makeup or the normal shadow of shaved beard hair in men or normal body hair if extrafacial.
3 Moderate Moderate atrophic or hypertrophic scarring that is obvious at social distances ≥ 50cm & is not covered easily by makeup or the normal shadow of shaved beard hair in men or body hair if extrafacial, but is still able to be flattened by manual stretching of the skin (if atrophic).
4 Severe Severe atrophic or hypertrophic scarring that is evident at social distances ≥ 50cm & is not covered easily by makeup or the normal shadow of shaved beard hair in men or body hair if extrafacial & is not able to be flattened by manual stretching of the skin.
Fabbrocini G, Annunziata MC, D’Arco V, DeVita V, Lodi G, Mauriello MC, Pastore F, Monfrecola G. Acne scars: pathogenesis, classification and treatment. Dermatol Res Pract. 2010;2010:893090
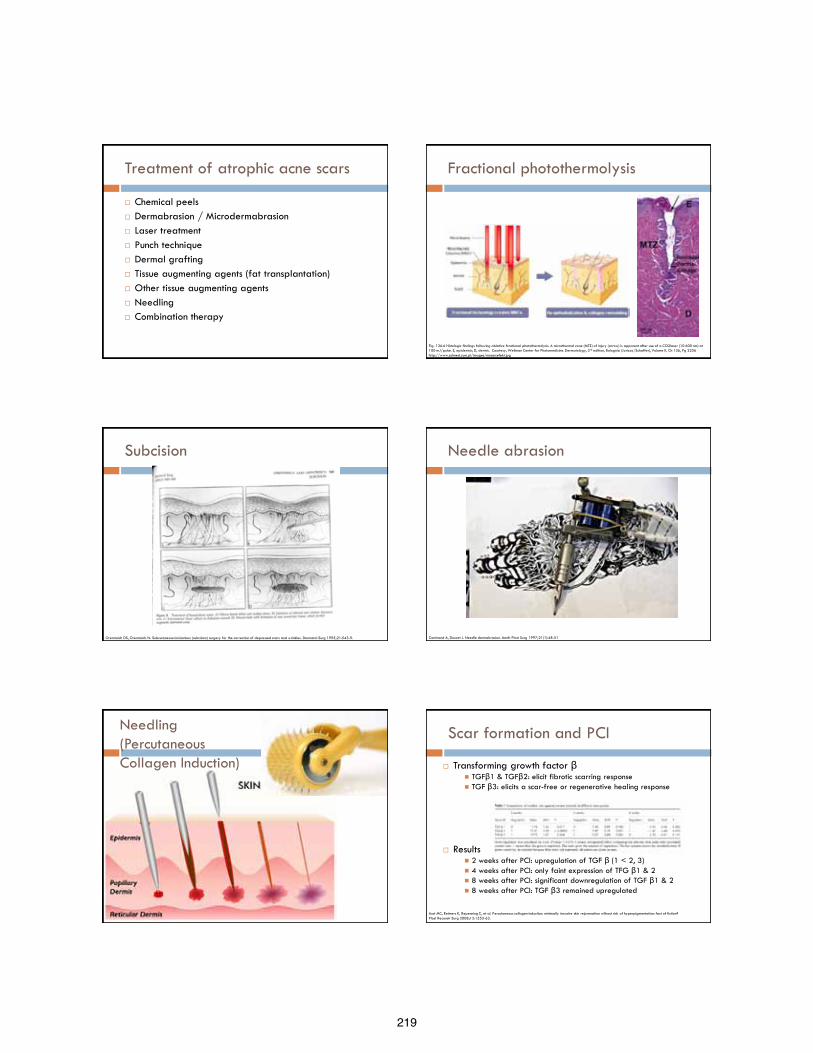
219
Treatment of atrophic acne scars
Chemical peels Dermabrasion / Microdermabrasion Laser treatment Punch technique Dermal grafting Tissue augmenting agents (fat transplantation) Other tissue augmenting agents Needling Combination therapy
Fractional photothermolysis
Fig. 136.6 Histologic findings following ablative fractional photothermolysis. A microthermal zone (MTZ) of injury (arrow) is apparent after use of a CO2laser (10 600 nm) at 100 mJ/pulse. E, epidermis; D, dermis. Courtesy, Wellman Center for Photomedicine. Dermatology, 3rd edition, Bolognia (Jorizzo/Schaffer), Volume II, Ch 136, Pg 2256 http://www.solmed.com.pl/images/mosaicefekt.jpg
Subcision
Orentreich DS, Orentreich N. Subcutaneous incisionless (subcision) surgery for the correction of depressed scars and wrinkles. Dermatol Surg 1995;21:543-9.
Needle abrasion
Camirand A, Doucet J. Needle dermabrasion. Aesth Plast Surg 1997;21(1):48-51
Needling (Percutaneous Collagen Induction)
Scar formation and PCI
Transforming growth factor β TGFβ1 & TGFβ2: elicit fibrotic scarring response TGF β3: elicits a scar-free or regenerative healing response
Results 2 weeks after PCI: upregulation of TGF β (1 < 2, 3) 4 weeks after PCI: only faint expression of TFG β1 & 2 8 weeks after PCI: significant downregulation of TGF β1 & 2 8 weeks after PCI: TGF β3 remained upregulated
Aust MC, Reimers K, Repenning C, et al. Percutaneous collagen induction: minimally invasive skin rejuvenation without risk of hyperpigmentation: fact of fiction? Plast Reconstr Surg 2008;12:1553-63.
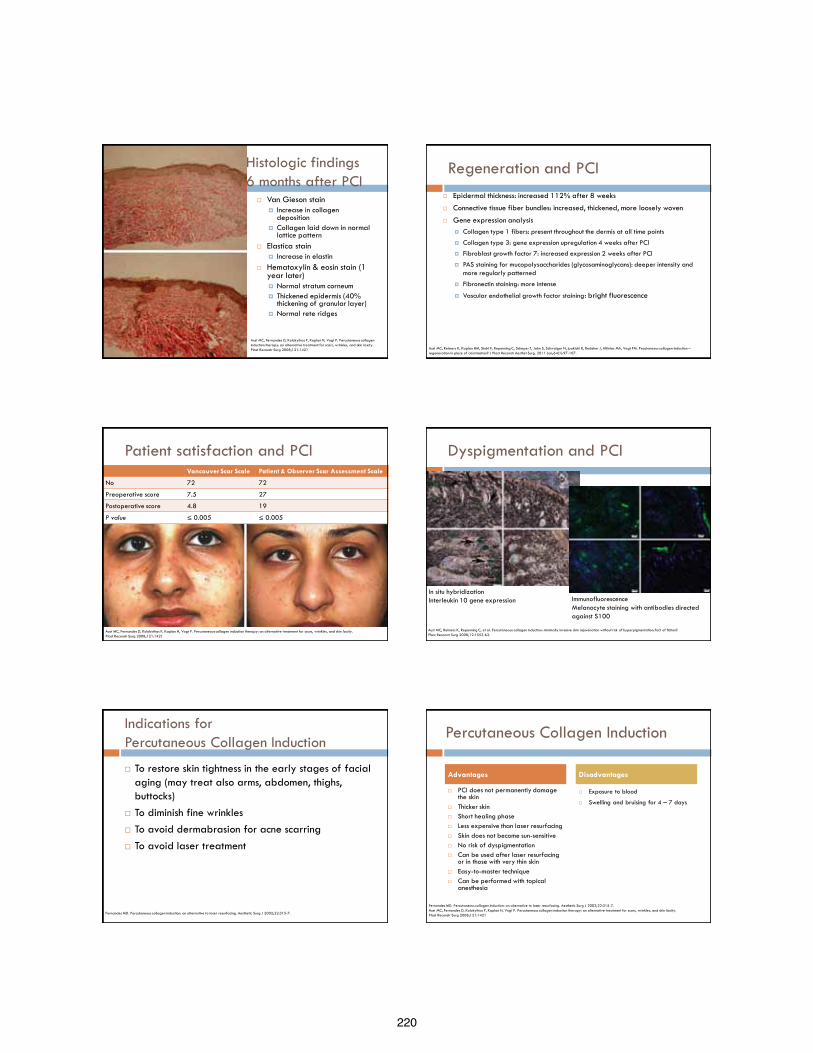
220
Histologic findings 6 months after PCI
Van Gieson stain Increase in collagen
deposition Collagen laid down in normal
lattice pattern Elastica stain
Increase in elastin Hematoxylin & eosin stain (1
year later) Normal stratum corneum Thickened epidermis (40%
thickening of granular layer) Normal rete ridges
Aust MC, Fernandes D, Kolokythas P, Kaplan H, Vogt P. Percutaneous collagen Induction therapy: an alternative treatment for scars, wrinkles, and skin laxity. Plast Reconstr Surg 2008;121:1421
Regeneration and PCI Epidermal thickness: increased 112% after 8 weeks
Connective tissue fiber bundles: increased, thickened, more loosely woven
Gene expression analysis Collagen type 1 fibers: present throughout the dermis at all time points
Collagen type 3: gene expression upregulation 4 weeks after PCI
Fibroblast growth factor 7: increased expression 2 weeks after PCI
PAS staining for mucopolysaccharides (glycosaminoglycans): deeper intensity and more regularly patterned
Fibronectin staining: more intense
Vascular endothelial growth factor staining: bright fluorescence
Aust MC, Reimers K, Kaplan HM, Stahl F, Repenning C, Scheper T, Jahn S, Schwaiger N, Ipaktchi R, Redeker J, Altintas MA, Vogt PM. Pecutaneous collagen induction – regeneration in place of cicatrisation? J Plast Reconstr Aesthet Surg. 2011 Jan;64(1):97-107.
Patient satisfaction and PCI Vancouver Scar Scale Patient & Observer Scar Assessment Scale
No 72 72
Preoperative score 7.5 27
Postoperative score 4.8 19
P value ≤ 0.005 ≤ 0.005
Aust MC, Fernandes D, Kolokythas P, Kaplan H, Vogt P. Percutaneous collagen induction therapy: an alternative treatment for scars, wrinkles, and skin laxity. Plast Reconstr Surg 2008;121:1421
Dyspigmentation and PCI
Aust MC, Reimers K, Repenning C, et al. Percutaneous collagen induction: minimally invasive skin rejuvenation without risk of hyperpigmentation: fact of fiction? Plast Reconstr Surg 2008;12:1553-63.
In situ hybridization Interleukin 10 gene expression Immunofluorescence
Melanocyte staining with antibodies directed against S100
Indications for Percutaneous Collagen Induction
To restore skin tightness in the early stages of facial aging (may treat also arms, abdomen, thighs, buttocks)
To diminish fine wrinkles To avoid dermabrasion for acne scarring To avoid laser treatment
Fernandes MD. Percutaneous collagen induction: an alternative to laser resurfacing. Aesthetic Surg J 2002;22:315-7.
Percutaneous Collagen Induction
PCI does not permanently damage the skin
Thicker skin Short healing phase Less expensive than laser resurfacing Skin does not become sun-sensitive No risk of dyspigmentation Can be used after laser resurfacing
or in those with very thin skin Easy-to-master technique Can be performed with topical
anesthesia
Exposure to blood
Swelling and bruising for 4 – 7 days
Advantages Disadvantages
Fernandes MD. Percutaneous collagen induction: an alternative to laser resurfacing. Aesthetic Surg J 2002;22:315-7. Aust MC, Fernandes D, Kolokythas P, Kaplan H, Vogt P. Percutaneous collagen induction therapy: an alternative treatment for scars, wrinkles, and skin laxity. Plast Reconstr Surg 2008;121:1421
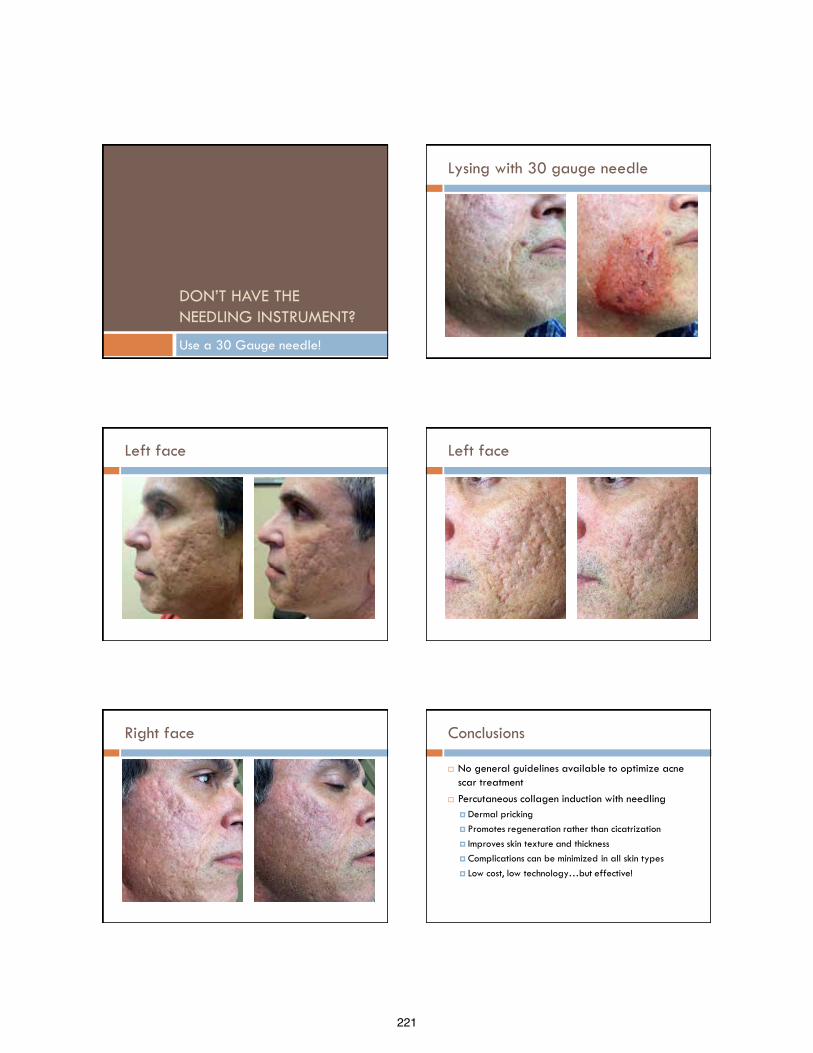
221
DON’T HAVE THE NEEDLING INSTRUMENT?
Use a 30 Gauge needle!
Lysing with 30 gauge needle
Left face Left face
Right face Conclusions
No general guidelines available to optimize acne scar treatment
Percutaneous collagen induction with needling Dermal pricking Promotes regeneration rather than cicatrization Improves skin texture and thickness Complications can be minimized in all skin types Low cost, low technology…but effective!
222
References Khunger N, Bhardwaj D, Khunger M. Evaluation of CROSS technique with 100% TCA in the management of ice pick acne scars in darker skin types. J Cosmet Dermatol.
2011 Mar;10(1):51-7.
Lee JW, Kim BJ, Kim MN, Lee CK. Treatment of acne scars using subdermal minimal surgery technology. Dermatol Surg. 2010 Aug;36(8):1281-7.
Manuskiatti W, Triwongwaranat D, Varothai S, Eimpunth S, Wanitphakdeedecha R. Efficacy and safety of a carbon-dioxide ablative fractional resurfacing device for treatment of atrophic acne scars in Asians. J Am Acad Dermatol. 2010 Aug;63(2):274-83.
Fabbrocini G, Annunziata MC, D’Arco V, DeVita V, Lodi G, Mauriello MC, Pastore F, Monfrecola G. Acne scars: pathogenesis, classification and treatment. Dermatol Res Pract. 2010;2010:893090
Fabbrocini G, Fardella N, Monfrecola A, Proietti I, Innocenzi D. Acne scarring treatment using skin needling. Clin Exp Dermatol. 2009 Dec;34(8):874-9.
Cooper JS, Lee BT. Treatment of facial scarring: lasers, filler, and nonoperative techniques. Facial Plast Surg. 2009 Dec;25(5):311-5.
Rivera AE. Acne scarring: a review and current treatment modalities. J Am Acad Dermatol. 2008 Oct;59(4):659-76.
Khunger N; IADVL Task Force. Standard guidelines of care for acne surgery. Indian J Dermatol Venereol Leprol. 2008 Jan;74 Suppl:S61-7.
Alam M, Omura N, Kaminer MS. Subcision for acne scarring: technique and outcomes in 40 patients. Dermatol Surg. 2005 Mar;31(3):310-7.
Jacob CI, Dover JS, Kaminer MS. Acne scarring: a classification system and review of treatment options. J Am Acad Dermatol. 2001 Jul;45(1):109-17.
Goodman GJ. Management of post-acne scarring. What are the options for treatment? Am J Clin Dermatol. 2000 Jan-Feb;1(1):3-17.
Fernandes MD. Percutaneous collagen induction: an alternative to laser resurfacing. Aesthetic Surg J 2002;22:315-7.
Camirand A, Doucet J. Needle dermabrasion. Aesth Plast Surg 1997;21(1):48-51.
Orentreich DS, Orentreich N. Subcutaneous incisionless (subcision) surgery for the correction of depressed scars and wrinkles. Dermatol Surg 1995;21:543-9.
Aust MC, Fernandes D, Kolokythas P, Kaplan H, Vogt P. Percutaneous collagen induction therapy: an alternative treatment for scars, wrinkles, and skin laxity. Plast Reconstr Surg 2008;121:1421
Aust MC, Reimers K, Repenning C, Stahl F, Jahn S, Guggenheim M, Schwaiger N, Gohritz A, Vogt PM. Percutaneous collagen induction: minimally invasive skin rejuvenation without risk of hyperpigmentation: fact of fiction? Plast Reconstr Surg 2008;12:1553-63.
Aust MC, Reimers K, Kaplan HM, Stahl F, Repenning C, Scheper T, Jahn S, Schwaiger N, Ipaktchi R, Redeker J, Altintas MA, Vogt PM. Pecutaneous collagen induction – regeneration in place of cicatrisation? J Plast Reconstr Aesthet Surg. 2011 Jan;64(1):97-107.
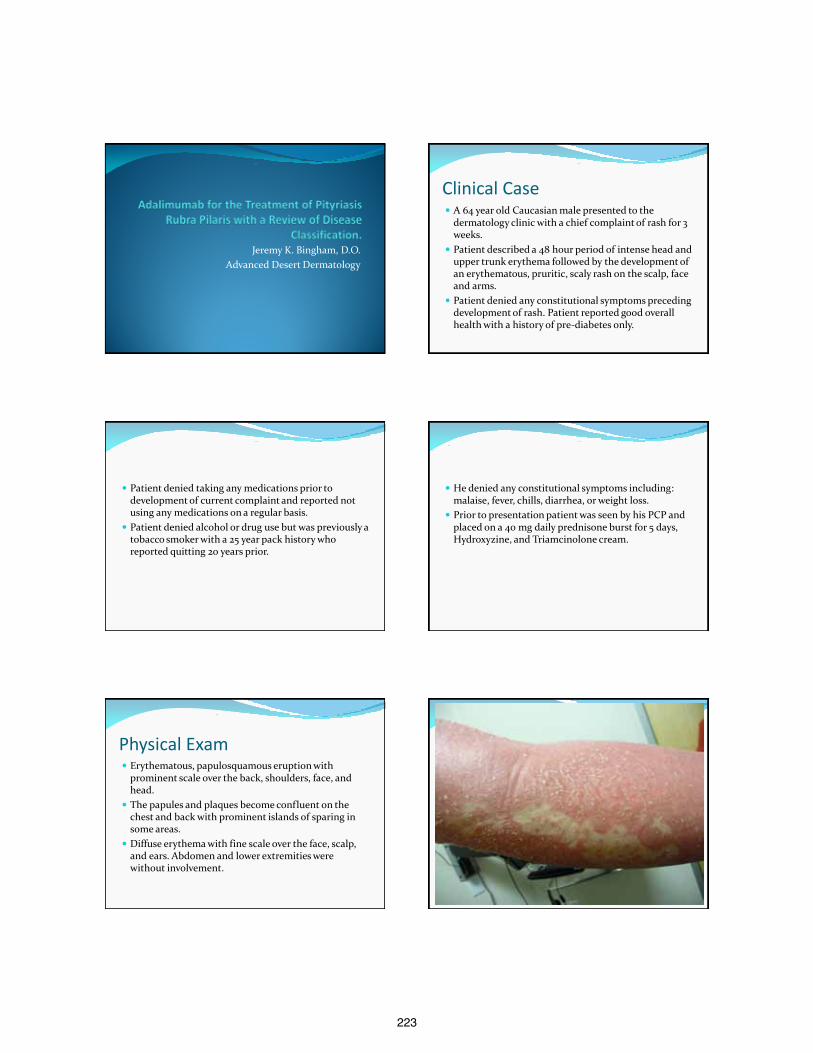
223
Jeremy K. Bingham, D.O. Advanced Desert Dermatology
Clinical Case A 64 year old Caucasian male presented to the
dermatology clinic with a chief complaint of rash for 3 weeks.
Patient described a 48 hour period of intense head and upper trunk erythema followed by the development of an erythematous, pruritic, scaly rash on the scalp, face and arms.
Patient denied any constitutional symptoms preceding development of rash. Patient reported good overall health with a history of pre-diabetes only.
Patient denied taking any medications prior to development of current complaint and reported not using any medications on a regular basis.
Patient denied alcohol or drug use but was previously a tobacco smoker with a 25 year pack history who reported quitting 20 years prior.
He denied any constitutional symptoms including: malaise, fever, chills, diarrhea, or weight loss.
Prior to presentation patient was seen by his PCP and placed on a 40 mg daily prednisone burst for 5 days, Hydroxyzine, and Triamcinolone cream.
Physical Exam Erythematous, papulosquamous eruption with
prominent scale over the back, shoulders, face, and head.
The papules and plaques become confluent on the chest and back with prominent islands of sparing in some areas.
Diffuse erythema with fine scale over the face, scalp, and ears. Abdomen and lower extremities were without involvement.
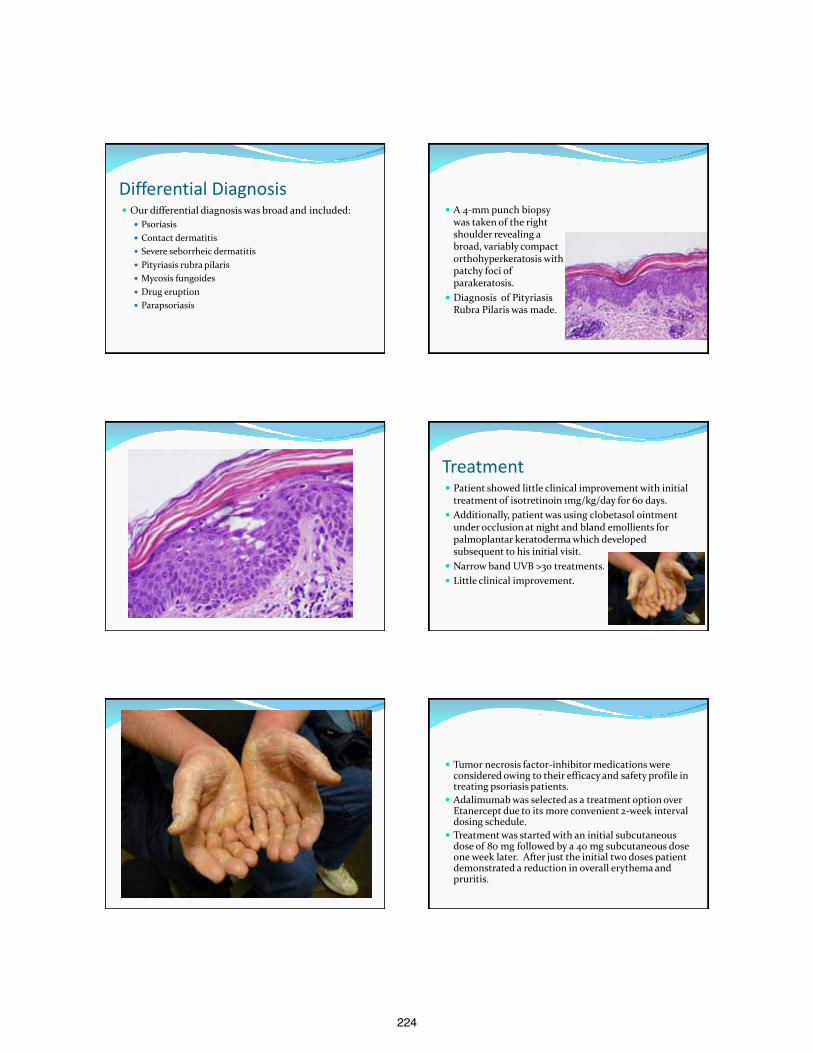
224
Differential Diagnosis Our differential diagnosis was broad and included:
Psoriasis Contact dermatitis Severe seborrheic dermatitis Pityriasis rubra pilaris Mycosis fungoides Drug eruption Parapsoriasis
A 4-mm punch biopsy was taken of the right shoulder revealing a broad, variably compact orthohyperkeratosis with patchy foci of parakeratosis.
Diagnosis of Pityriasis Rubra Pilaris was made.
Treatment Patient showed little clinical improvement with initial
treatment of isotretinoin 1mg/kg/day for 60 days. Additionally, patient was using clobetasol ointment
under occlusion at night and bland emollients for palmoplantar keratoderma which developed subsequent to his initial visit.
Narrow band UVB >30 treatments. Little clinical improvement.
Tumor necrosis factor-inhibitor medications were considered owing to their efficacy and safety profile in treating psoriasis patients.
Adalimumab was selected as a treatment option over Etanercept due to its more convenient 2-week interval dosing schedule.
Treatment was started with an initial subcutaneous dose of 80 mg followed by a 40 mg subcutaneous dose one week later. After just the initial two doses patient demonstrated a reduction in overall erythema and pruritis.
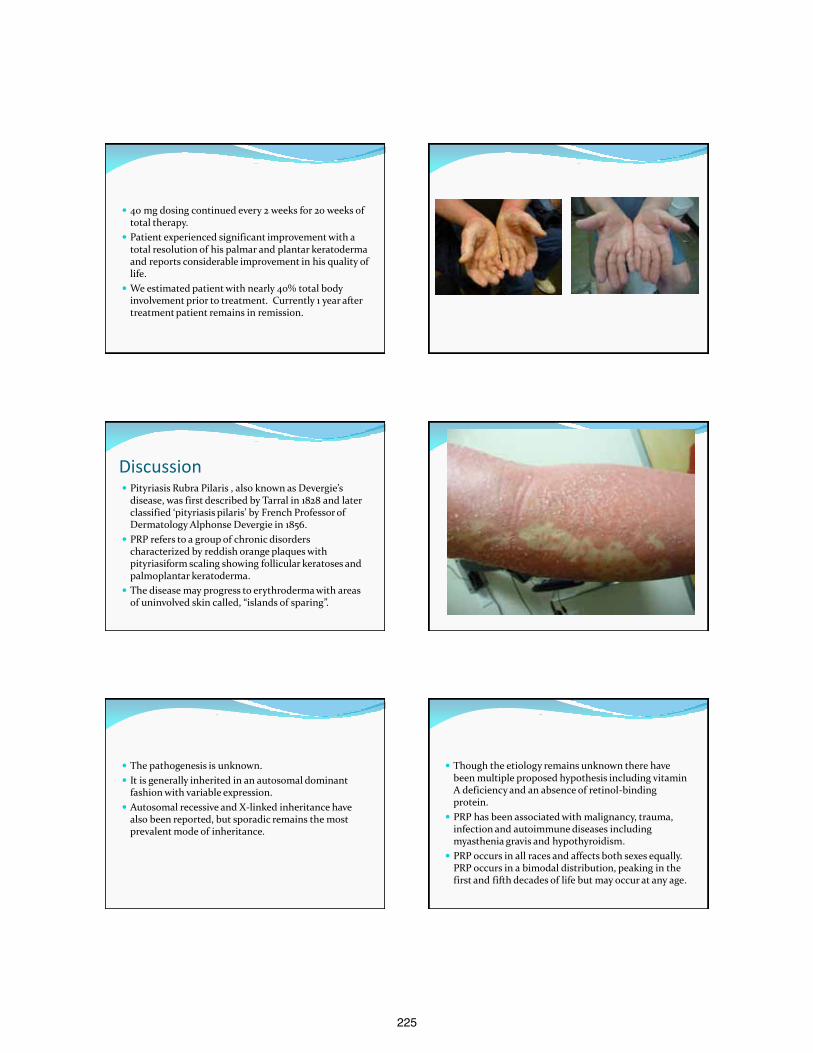
225
40 mg dosing continued every 2 weeks for 20 weeks of total therapy.
Patient experienced significant improvement with a total resolution of his palmar and plantar keratoderma and reports considerable improvement in his quality of life.
We estimated patient with nearly 40% total body involvement prior to treatment. Currently 1 year after treatment patient remains in remission.
Discussion Pityriasis Rubra Pilaris , also known as Devergie’s
disease, was first described by Tarral in 1828 and later classified ‘pityriasis pilaris’ by French Professor of Dermatology Alphonse Devergie in 1856.
PRP refers to a group of chronic disorders characterized by reddish orange plaques with pityriasiform scaling showing follicular keratoses and palmoplantar keratoderma.
The disease may progress to erythroderma with areas of uninvolved skin called, “islands of sparing”.
The pathogenesis is unknown. It is generally inherited in an autosomal dominant
fashion with variable expression. Autosomal recessive and X-linked inheritance have
also been reported, but sporadic remains the most prevalent mode of inheritance.
Though the etiology remains unknown there have been multiple proposed hypothesis including vitamin A deficiency and an absence of retinol-binding protein.
PRP has been associated with malignancy, trauma, infection and autoimmune diseases including myasthenia gravis and hypothyroidism.
PRP occurs in all races and affects both sexes equally. PRP occurs in a bimodal distribution, peaking in the first and fifth decades of life but may occur at any age.
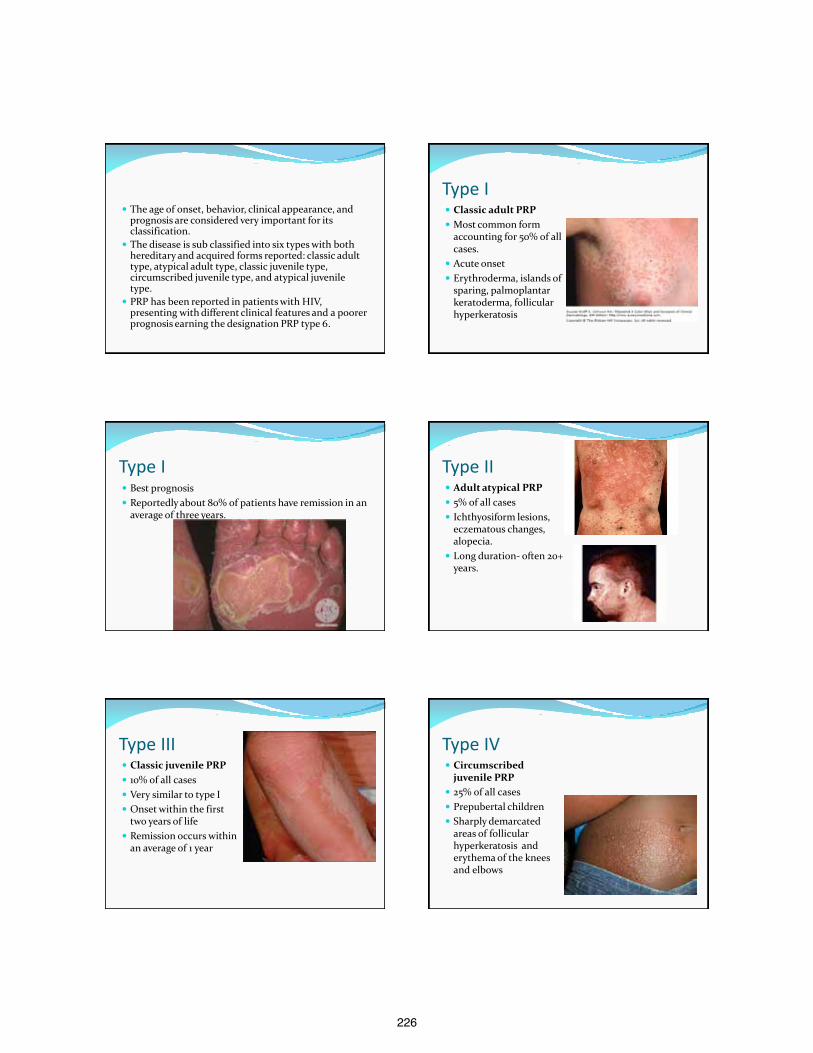
226
The age of onset, behavior, clinical appearance, and prognosis are considered very important for its classification.
The disease is sub classified into six types with both hereditary and acquired forms reported: classic adult type, atypical adult type, classic juvenile type, circumscribed juvenile type, and atypical juvenile type.
PRP has been reported in patients with HIV, presenting with different clinical features and a poorer prognosis earning the designation PRP type 6.
Type I Classic adult PRP Most common form
accounting for 50% of all cases.
Acute onset Erythroderma, islands of
sparing, palmoplantar keratoderma, follicular hyperkeratosis
Type I Best prognosis Reportedly about 80% of patients have remission in an
average of three years.
Type II Adult atypical PRP 5% of all cases Ichthyosiform lesions,
eczematous changes, alopecia.
Long duration- often 20+ years.
Type III Classic juvenile PRP 10% of all cases Very similar to type I Onset within the first
two years of life Remission occurs within
an average of 1 year
Type IV Circumscribed
juvenile PRP 25% of all cases Prepubertal children Sharply demarcated
areas of follicular hyperkeratosis and erythema of the knees and elbows
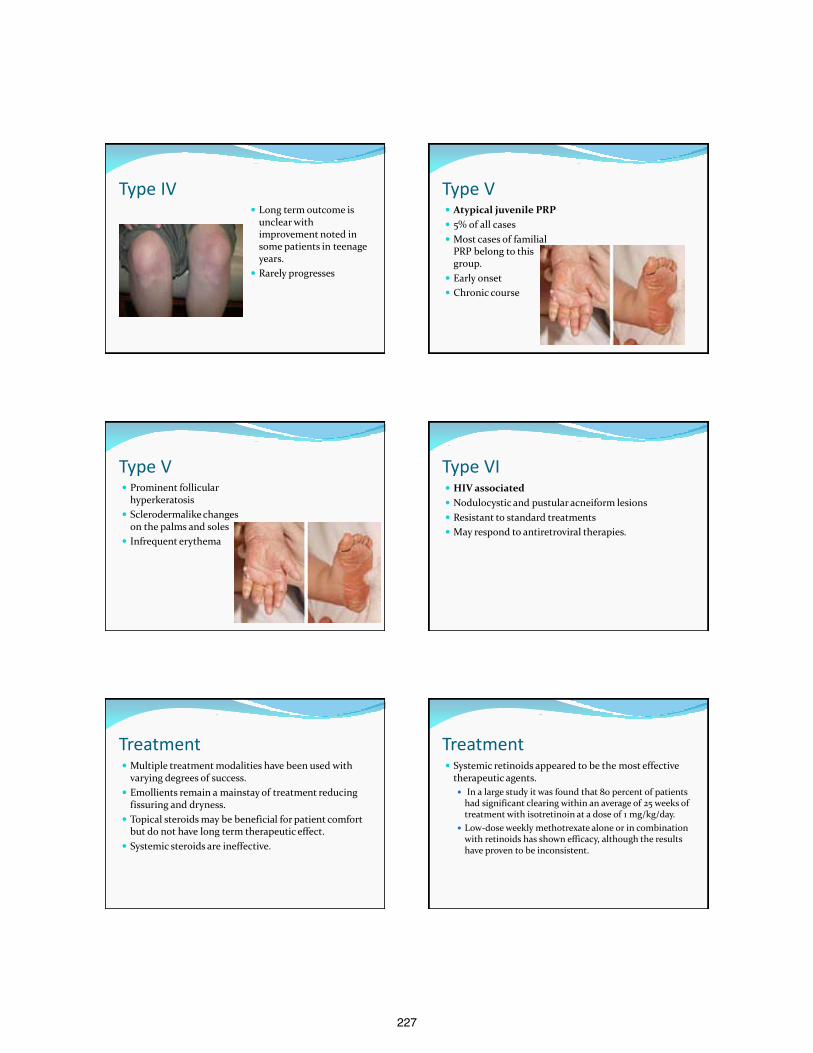
227
Type IV Long term outcome is
unclear with improvement noted in some patients in teenage years.
Rarely progresses
Type V Atypical juvenile PRP 5% of all cases Most cases of familial
PRP belong to this group.
Early onset Chronic course
Type V Prominent follicular
hyperkeratosis Sclerodermalike changes
on the palms and soles Infrequent erythema
Type VI HIV associated Nodulocystic and pustular acneiform lesions Resistant to standard treatments May respond to antiretroviral therapies.
Treatment Multiple treatment modalities have been used with
varying degrees of success. Emollients remain a mainstay of treatment reducing
fissuring and dryness. Topical steroids may be beneficial for patient comfort
but do not have long term therapeutic effect. Systemic steroids are ineffective.
Treatment Systemic retinoids appeared to be the most effective
therapeutic agents.
In a large study it was found that 80 percent of patients had significant clearing within an average of 25 weeks of treatment with isotretinoin at a dose of 1 mg/kg/day.
Low-dose weekly methotrexate alone or in combination with retinoids has shown efficacy, although the results have proven to be inconsistent.
228
An extensive side effect profile of the oral retinoids including xerotic skin, hyperlipidemia, ocular sicca, and teratogenic potential has provided an impetus in finding a safer, more convenient treatment option.
Treatment with cyclosporine, azathioprine, PUVA, and mycophenolate mofetil, have all been reported with variable degrees of success.
Newer biologic therapy has shown promise in the treatment of PRP.
Tumor necrosis factor (TNF)-alpha inhibitors, first licensed for clinical use in 1998, is one class of biologic agent.
TNF represents an important cytokine involved in normal inflammatory and immune responses.
Elevated levels of TNF have been found in psoriatic plaque and in the synovial fluid of both psoriatic and rheumatoid arthritis. Not surprisingly, given the clinical and histological overlap with psoriasis, up regulation of TNF- alpha has been detected in punch biopsies of PRP lesions
In 2009, Walling and Swick were the first to publish the use of Adalimumab in PRP treatment.
They reported a dramatic and rapid response in a 72 year male patient with a near complete resolution of PRP eruption after 8 weeks of monotherapy.
Adalimumab is a recombinant human IgG1 monoclonal antibody specific for human TNF.
Adalimumab binds specifically to TNF-alpha and blocks its interaction with p55 and p75 cell surface receptors, preventing the action of TNF on TNF receptors 1 and 2.
The release of pro-inflammatory cytokines by macrophages and keratinocytes is prevented, and the production of acute phase proteins by hepatocytes is inhibited.
Inflammation and hyperproliferation of keratinocytes are key features of PRP
Additional recent case reports have been published with encouraging findings showing prolonged efficacy with maintenance Adalimumab dosing.
Given the safety profile of Adalimumab and its convenient bi-monthly dosing it is anticipated that additional reportings will be published on its successful use in PRP patients.
Thank you.
229
References REFERENCES 1. Klein A, Landthaler M, Karrer S. Pityriasis Rubra Pilaris: A Review of Diagnosis and Treatment. Am J Clin Dermatol 2010; 0 (0): 0-0 1175-
0561. 2. Sehgal VN, Srivastava G, Dogra S. Adult onset pityriasis rubra pilaris. Indian J Dermatol Venereol Leprol 2008; 74: 311-21. 3. Griffiths WAD. Pityriasis rubra pilaris. Clin Exp Dermatol 1980; 5: 105-12. 4. Miralles ES, Nunez M, Se Las Heras ME, et al. Pityriasis rubra pilaris and human immunodeficiency virus infection. Br J Dermatol 1995;
133: 990-3. 5. Vasher M, Smithberger E, Lien MH, Fenske NA. Familial pityriasis rubra pilaris: report of a family and therapeutic response to etanercept.
J Drugs Dermatol. 2010; 9: 844-50. 6. Chan H, Liu FT, Naguwa S. A review of pityriasis rubra pilaris and rheumatologic associations. Clin Dev Immunol 2004; 11: 57-60. 7. Seghal VN, Jain MK, Mathur RP. Pityriasis rubra pilaris in Indians. Br J Dermatol 1989; 121: 821-22. 8. Weller R, Hunter J, Savin J et al. Clinical Dermatology, 75-77. Fourth Edition. Blackwell publishing, 2008. 9. Bolognia J, Jorizzo J, Rapini R. Dermatology. Second Edition: Elsevier, 2008. 10. Lu R, George SJ, Hsu S. Pityriasis rubra pilaris: failure of combination treatment with acitretin and infliximab. Dermatol Online J 2006;
12:18. 11. Martinez Calixto LE, Suresh L, Matsumura E, et al. Oral pityriasis rubra pilaris. Oral Sur Oral Med Oral Pathol Oral Radiol Endod 2006;
101: 604-7. 12. Champion A. Pityiriasis rubra pilaris in Disorders of Keratinization: Follicular Keratosis. Textbook of Dermatology. Fifth Edition.
Blackwell Scientific, 1992. 13. Van de Kerkhof PCM, Steijlen PM. Topical treatment of pityriasis rubra pilaris with calcipotriol. Br J Dermatol 1994; 130: 675-8.
References 14. Dickens CH. Treatment of classic pityriasis rubra pilaris. J Am Acad Dermatol. 1994; 31:997-9. 15. Clayton BD, Jorizzo JL, Hitchcock MG, et al. Adult pityriasis rubra pilaris: a 10 year case series. J Am Acad Dermatol.
1997;36:959-64. 16. Albert MR, Mackool BT. Pityriasis rubra pilaris. Int J Dermatol. 1999;38:1-11. 17. Zhang Y, Zhou Y, Ball N, Su M, Xu J, Zheng Z. Type I pityriasis rubra pilaris: upregulation of tumor necrosis factoe a
and response to adalimumab therapy. J Cutan Med Surg. 2010;14(4):185-188 18. Müller H, Gattringer C, Zelger B, et al. Infliximab monotherapy as first-line treatment for adult onset pityriasis
rubra pilaris: case report and review of the literature on biologic therapy. J Am Acad Dermatol 2008; 59(suppl 5):S65–S70.
19. Seckin D, Tula E, Ergun T. Successful use of etanercept in type I pityriasis rubra pilaris. Br J Dermatol 2008; 158:642-
4. 20. Walling Hobart W, Swick Brian L. Pityriasis rubra pilaris responding rapidly to adalimumab. Arch. Dermatol.
2009;145(1):99-101. 21. Schreml S, Zeller V, Babilas P, Karrer S, Landthaler M, Szeimies RM. Pityriasis rubra pilaris successfully treated with
adalimumab. Clin Exp. Dermatol. 2010;35(7):792-793. 22. O’Kane D, Devereux CE, Walsh MY, Hoey SHE. Rapid and sustained remission of pityriasis rubra pillaris with
adalimumab treatment. Clin exp. Dermatol. 2010;35(4):e 155-e156. 23. Palacios A, Gonzalez R, Agesta N, Acebo E, Diaz-Ramon L, Gardeazabal J. Successful use of adalimumab (Humira ®)
in pityriasis rubra pilaris. J. Eur. Acad. Dermatol. Venereol. 2010;24(Suppl 4):75-76.
Type I pic 1 http://accessemergencymedicine.com/content.aspx?aid=5203019 Type I Pic 2 http://www3.dermis.net/dermisroot/en/32821/image.htm Type IV http://dermatlas.med.jhmi.edu/derm/indexDisplay.cfm?ImageID=-1125586974 http://skinworld.blogspot.com/2008/05/drug-hypersensitivity-syndrome.html Type V http://casereports.bmj.com/content/2010/bcr.11.2009.2453.full?sid=804984da-340a-4a3b-
a394-1d5c000a243f

230
Primary Mucinous Carcinoma of the skin
Helia Eragi, DO, PGY-4 10/10/12
Pacific Hospital Long Beach, California Program director: Dr. David Horowitz
Case Presentation
49 yo Asian male presented to the dermatology clinic with a clear mass on his chin.
Patient states the lesion has been there for the past two years, enlarging over the past few months.
Denies any pain or other physical complaints.
Case presentation
Review of system: negative for weight loss, fever, night sweats or other constitutional symptoms
Past medical history: none Medication: none
Case presentation
Physical exam revealed a 3.0 x 2.0 cm clear flesh colored cystic structure on the chin.
No tenderness on palpation. Lesion was initially thought to be a cyst
and was removed using an elliptical excision , during which a profuse amount of mucin was drained.
Histopathology
The histopathology revealed expansive lakes of mucin diffusely replacing the dermis and focally extending into the skeletal muscle and biopsy margins.
Extended within the lakes of mucin were islands of epithelial cells arranged in cohesive nests and forming ductal structures and focal cribriform features.
Histopathology
There were possible apocrine differentiation as well as focal peripheral palisation.
There was no definitive attachment to the overlying epidermis.
It stained positive for PAS stain and diastase resistant.
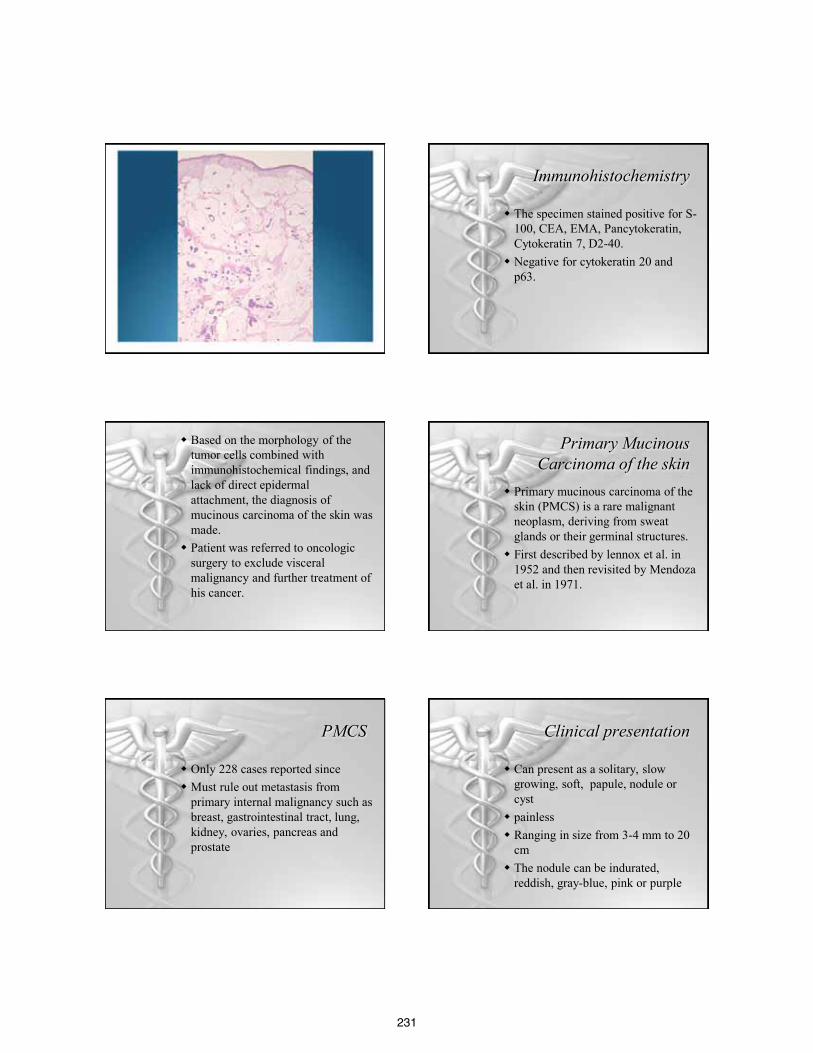
231
Immunohistochemistry
The specimen stained positive for S-100, CEA, EMA, Pancytokeratin, Cytokeratin 7, D2-40.
Negative for cytokeratin 20 and p63.
Based on the morphology of the tumor cells combined with immunohistochemical findings, and lack of direct epidermal attachment, the diagnosis of mucinous carcinoma of the skin was made.
Patient was referred to oncologic surgery to exclude visceral malignancy and further treatment of his cancer.
Primary Mucinous Carcinoma of the skin
Primary mucinous carcinoma of the skin (PMCS) is a rare malignant neoplasm, deriving from sweat glands or their germinal structures.
First described by lennox et al. in 1952 and then revisited by Mendoza et al. in 1971.
PMCS
Only 228 cases reported since Must rule out metastasis from
primary internal malignancy such as breast, gastrointestinal tract, lung, kidney, ovaries, pancreas and prostate
Clinical presentation
Can present as a solitary, slow growing, soft, papule, nodule or cyst
painless Ranging in size from 3-4 mm to 20
cm The nodule can be indurated,
reddish, gray-blue, pink or purple

232
Clinical presentation
Male> Female Predilection for white (62%) and
black (34%) Elderly, average age 62.6 y.o Head and neck, most commonly
periorbital
Pathophysiology
Variant of sweat gland carcinoma The origin thought to favor eccrine
more than apocrine differentiation
Pathophysiology
Some literature suggests that PMCS develops as a progression of abnormal apocrine or eccrine ducts similar to mucinous carcinoma of the breast, ranging from ductal hyperplasia, atypical ductal hyperplasia or ductal carinoma in situ or combination of all three
Pathophysiology
Presence of copious amount of mucin serves as a physical barrier, compressing the tumor stroma, and decreasing the rate of angiogenesis by inhibiting DNA synthesis
Thus contributes to the benign nature of this tumor and it’s low metastatic potential
Histopathology Well circumscribed dermal tumor
consisting of islands of epithelial cells surrounded by large pool of basophilic mucin
Sialomucin, stains positive with PAS, with or without diastase, hyaluronidase resistant
This mucin also stains positive with mucicarmine, alcian blue at pH 2.5 and colloidal iron
Histopathology
Epithelial cells show moderate nuclear pleomorphism
Forms glandular patterns Tumor cells are small, cuboidal and
bland May have vacuolated eosinophilic
cytoplasm Mitoses and cellular pleomorphism
rare

233
Immunohistochemistry
Tumor is positive for low molecular weight cytokeratin, CEA, EMA, S100
Some cases, estrogen and progesterone receptor and GCDFP-15 positive
Negative for CK 20- excluding metastatic colorectal carcinoma
Differential Diagnosis
Metastatic adenocarcinoma Cystic Basal cell carcinoma Hidrocystoma Epidermoid cyst Sebaceous cyst Sebaceous Carcinoma
Differential Diagnosis
Pilomatricoma Hemangioma Melanoma Squamous cell carcinoma Lipoma
Work up Since primary mucinous carcinoma of
the skin is a very rare neoplasm, a full work up to rule out metastasis from other primary internal malignancies such as breast, gastrointestinal, lung, kidney, prostate, pancreas and ovaries must be done.
The location of tumor can provide some clue to differentiate PMCS from metastasis.
Breast metastasis tends to show preference for the chest, breast and axilla and very unlikely to metastasize to the face.
Breast and gastrointestinal malignancies in particular can have very similar histopathology and immunohistochemistry.
Organ specific immunohistochemistry markers should be done
PMCS stains negative for CK20 which is a marker colonic mucinous carcinoma
PMCS stain positive for estrogen receptor, progesterone receptor and GCDFP-15.
234
Qureshi, et al. suggested that finding an in-situ component of tumor cell staining positive for p63 and CK 5/6 favors PMCS and excludes metastasis from breast.
Prognosis
PMCS has a favorable prognosis with low mortality rate and low metastatic rate of 9.6%
However, it has a high recurrence rate of 29.4%
It can be locally invasive and metastasize to regional lymph nodes, lungs, and parotid glands
Treatment
Wide local excision with at least 1 cm margin and dissection of lymph nodes.
If high grade tumor, prophylactic lymph node dissection is recommended
Treatment
Several reports suggesting success with Mohs micrographic surgery using low-molecular weight immunostaining.
PMCS not responsive to chemotherapy or radiation.
Follow up
Due to it’s high recurrence rate, patients should be followed up annually and examined for development of lymphadenapathy.
References
1. Breiting L, Christensen L, Dahlstrøm K, Breiting V, Winther JF. Primary mucinous carcinoma of the skin: a population-based study. Int J Dermatol. Mar;47(3):242-5, 2008.
2. Miyasaka M, Tanaka R, Hirabayashi K, Yamazaki A, Shinohara H, Taira H, Akamatsu T. Primary mucinous carcinoma of the skin: a case of metastasis after 10 years of disease-free interval. European Journal of Plastic Surgery. 32: 189-193, 2008.
3. Scholz IM, Hartschuh W. Primary mucinous eccrine carcinoma of the skin--a rare clinical tumor with many differential diagnoses. Journal of German Society of Dermatology. 8(6):446-8, 2010.
4. Levy G, Finkelstein A, McNiff JM. Immunohistochemical techniques to compare primary vs. metastatic mucinous carcinoma of the skin. J Cutan Pathol. 37(4):411-5, 2010.

235
5. Cecchi R, Rapicano V. Primary cutaneous mucinous carcinoma: report of two cases treated with Mohs' micrographic surgery. Australas J Dermatol. 47(3):192-4, 2006.
6. S. R. Martinez & S. E. Young : Primary Mucinous Carcinoma of the Skin: A Review . The Internet Journal of Oncology. Volume 2 Number 2, 2005.
7. Brietling LB, Christensen L, Dahlstrom K, Winther JF, Breiting VB, Kalialis LV. Primary mucinous carcinoma of the skin--a literature review. Ugeskr Laeger. 170(43):3399-402,2008.
8. Ivan D, Nash JW, Prieto VG,et al. Use of p63 expression in distinguishing primary and metastatic cutaneous adnexal neoplasms from metastatic adenocarcinoma to skin. J Cutan Pathol 34: 474–480, 2007.
9. Vodovnik A. Primary mucinous carcinoma of the skin. J Cutan Pathol 33: 61, 2006.
10. Breitling L, Dahlstrom K, Christensen L,Winther J, Breitling V. Primary mucinous carcinoma of the skin. Am J Dermatopathol 29: 595, 2007.
11. Qureshi H, Salama M, Chitale D, et al. Primary cutaneous mucinous carcinoma: presence of myoepithelial cells as a clue to the cutaneous origin. Am J Dermatopathol 26: 353, 2004.
12. Yugue ros, Patricia M.D.; Kane, William J. M.D.; Goellner, John R. M.D. Sweat Gland Carcinoma: A Clinicopathologic Analysis of an Expanded Series in a Single Institution. Plastic & Reconstructive Surgery. Issue: Volume 102(3) pp 705-710, 1998.
13. Snow SN, Reizner GT. Mucinous eccrine carcinoma of the eyelid. Cancer 1992;15:2099-104
14. UrsoC, Bondi R, Paglierani M, Salvadori A, Anichini C, Giannini A. Caricinomas of sweat glands: report of 60 cases. Arch Pathol Lab Med 2001; 125:498-505
15. Carson, HJ, Gattuso P, Raslan WF, Reddy V. Mucinous carcinoma of the eyelid. An immunohistochemical study. AM J Dermatopathol 1995; 17:494-8.
16. Balin AK, Fine RM, Golitz LE. Mucinous carcinoma. J Dermatol Surg Concol 1988;14:521-4.
17. Fukamizu H, Tomita K, Inoue K, Takigawa M. Primary
mucinous carcinoma of the skin. J Dermatol Surg Oncol 1993; 19:625-628.
18. Gupta A, Flowers FP, Lessner AM. Asymptomatic eyelid papule in a 57 year old healthy man. Arch Dermatol 2000; 136:1409-14
19. Jih MH, Friedman PM, Kimyai-Asaeli A, Golderberg LH. A rare case of fatal primary cutaneous mucinous carcinoma of scalp with multiple in transit and pulmonary metastasis. J AM Acad Dermatol. 52: 576-80, 2005.
20. Indian J Opthalmol. 2009 Mar-Apr; 57(2):150-152
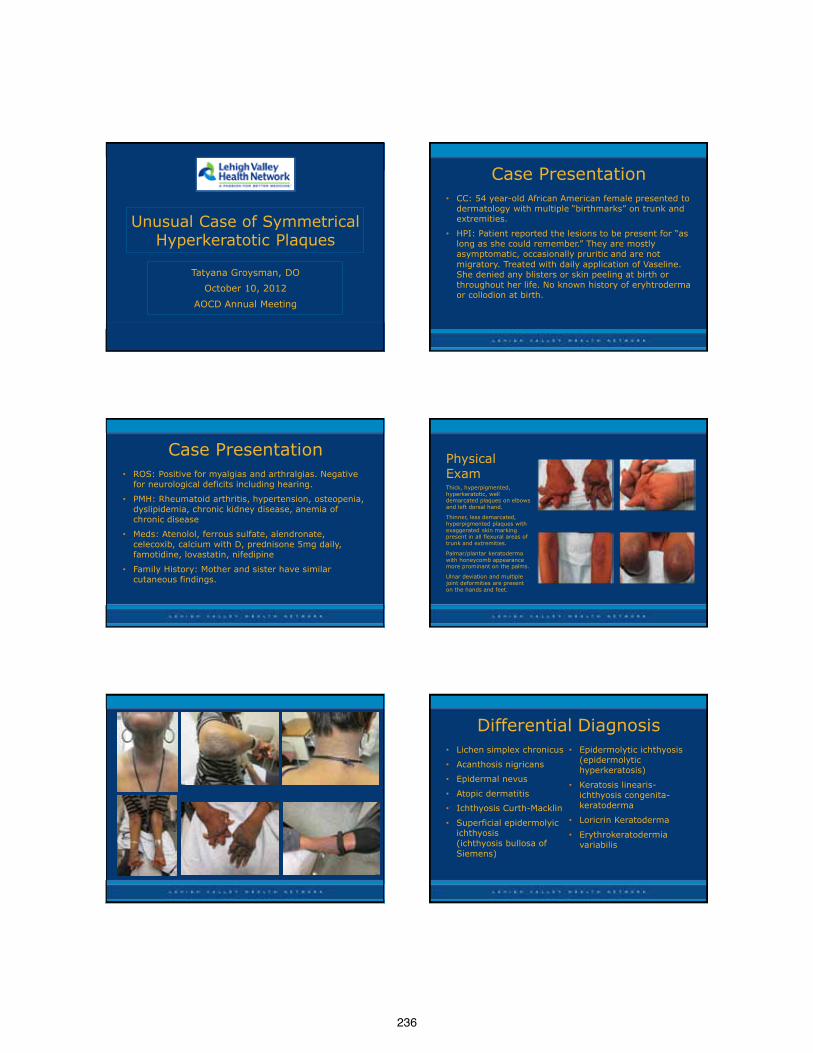
236
Unusual Case of Symmetrical Hyperkeratotic Plaques
Tatyana Groysman, DO
October 10, 2012
AOCD Annual Meeting
Case Presentation • CC: 54 year-old African American female presented to
dermatology with multiple “birthmarks” on trunk and extremities.
• HPI: Patient reported the lesions to be present for “as long as she could remember.” They are mostly asymptomatic, occasionally pruritic and are not migratory. Treated with daily application of Vaseline. She denied any blisters or skin peeling at birth or throughout her life. No known history of eryhtroderma or collodion at birth.
Case Presentation • ROS: Positive for myalgias and arthralgias. Negative
for neurological deficits including hearing.
• PMH: Rheumatoid arthritis, hypertension, osteopenia, dyslipidemia, chronic kidney disease, anemia of chronic disease
• Meds: Atenolol, ferrous sulfate, alendronate, celecoxib, calcium with D, prednisone 5mg daily, famotidine, lovastatin, nifedipine
• Family History: Mother and sister have similar cutaneous findings.
Physical Exam Thick, hyperpigmented, hyperkeratotic, well demarcated plaques on elbows and left dorsal hand.
Thinner, less demarcated, hyperpigmented plaques with exaggerated skin marking present in all flexural areas of trunk and extremities.
Palmar/plantar keratoderma with honeycomb appearance more prominant on the palms.
Ulnar deviation and multiple joint deformities are present on the hands and feet.
Differential Diagnosis • Lichen simplex chronicus
• Acanthosis nigricans
• Epidermal nevus
• Atopic dermatitis
• Ichthyosis Curth-Macklin
• Superficial epidermolyic ichthyosis (ichthyosis bullosa of Siemens)
• Epidermolytic ichthyosis (epidermolytic hyperkeratosis)
• Keratosis linearis-ichthyosis congenita-keratoderma
• Loricrin Keratoderma
• Erythrokeratodermia variabilis
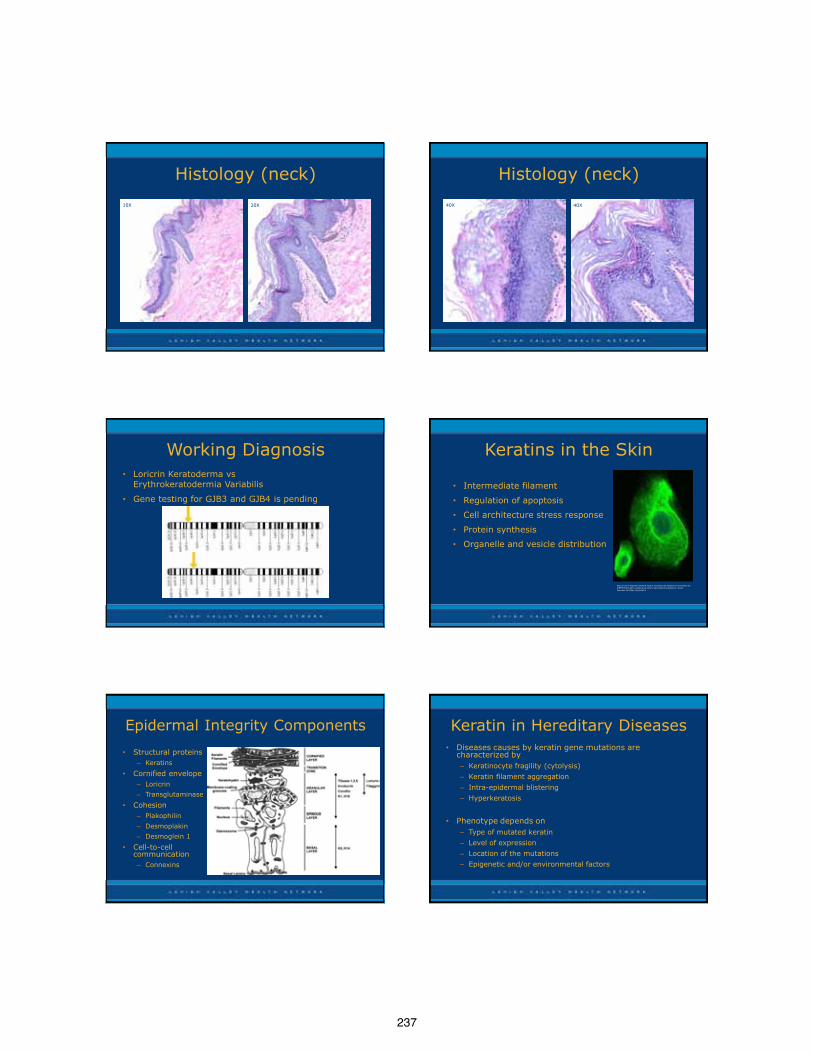
237
Histology (neck)
10X 20X
Histology (neck)
40X 40X
Working Diagnosis • Loricrin Keratoderma vs
Erythrokeratodermia Variabilis
• Gene testing for GJB3 and GJB4 is pending
Keratins in the Skin
• Intermediate filament
• Regulation of apoptosis
• Cell architecture stress response
• Protein synthesis
• Organelle and vesicle distribution
Shimomura Y, Wajid M, Kurban M, Sato N, Christiano AM. Mutations in the keratin 85 (KRT85/hHb5) gene underlie pure hair and nail ectodermal dysplasia. J Invest Dermatol. 2010 Mar;130(3):892-5.
Epidermal Integrity Components
• Structural proteins – Keratins
• Cornified envelope – Loricrin
– Transglutaminase
• Cohesion – Plakophilin
– Desmoplakin
– Desmoglein 1
• Cell-to-cell communication – Connexins
Keratin in Hereditary Diseases • Diseases causes by keratin gene mutations are
characterized by – Keratinocyte fragility (cytolysis)
– Keratin filament aggregation
– Intra-epidermal blistering
– Hyperkeratosis
• Phenotype depends on
– Type of mutated keratin
– Level of expression
– Location of the mutations
– Epigenetic and/or environmental factors
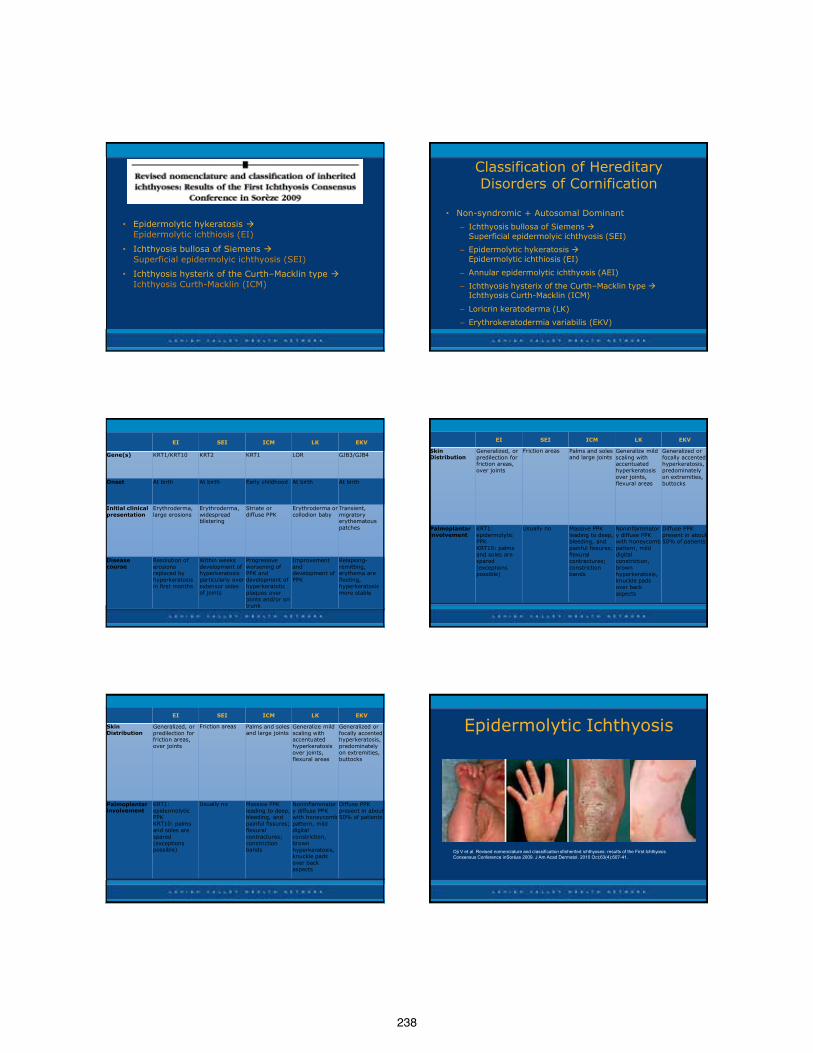
238
• Epidermolytic hykeratosis Epidermolytic ichthiosis (EI)
• Ichthyosis bullosa of Siemens Superficial epidermolyic ichthyosis (SEI)
• Ichthyosis hysterix of the Curth–Macklin type Ichthyosis Curth-Macklin (ICM)
Classification of Hereditary Disorders of Cornification
• Non-syndromic + Autosomal Dominant
– Ichthyosis bullosa of Siemens Superficial epidermolyic ichthyosis (SEI)
– Epidermolytic hykeratosis Epidermolytic ichthiosis (EI)
– Annular epidermolytic ichthyosis (AEI)
– Ichthyosis hysterix of the Curth–Macklin type Ichthyosis Curth-Macklin (ICM)
– Loricrin keratoderma (LK)
– Erythrokeratodermia variabilis (EKV)
EI SEI ICM LK EKV
Gene(s) KRT1/KRT10 KRT2 KRT1 LOR GJB3/GJB4
Onset At birth At birth Early childhood At birth At birth
Initial clinical presentation
Erythroderma, large erosions
Erythroderma, widespread blistering
Striate or diffuse PPK
Erythroderma or collodion baby
Transient, migratory erythematous patches
Disease course
Resolution of erosions replaced by hyperkeratosis in first months
Within weeks development of hyperkeratosis particularly over extensor sides of joints
Progressive worsening of PPK and development of hyperkeratotic plaques over joints and/or on trunk
Improvement and development of PPK
Relapsing-remitting, erythema are fleeting, hyperkeratosis more stable
EI SEI ICM LK EKV
Skin Distribution
Generalized, or predilection for friction areas, over joints
Friction areas Palms and soles and large joints
Generalize mild scaling with accentuated hyperkeratosis over joints, flexural areas
Generalized or focally accented hyperkeratosis, predominately on extremities, buttocks
Palmoplantar involvement
KRT1: epidermolytic PPK KRT10: palms and soles are spared (exceptions possible)
Usually no Massive PPK leading to deep, bleeding, and painful fissures; flexural contractures; constriction bands
Noninflammatory diffuse PPK with honeycomb pattern, mild digital constriction, brown hyperkeratosis, knuckle pads over back aspects
Diffuse PPK present in about 50% of patients
EI SEI ICM LK EKV
Skin Distribution
Generalized, or predilection for friction areas, over joints
Friction areas Palms and soles and large joints
Generalize mild scaling with accentuated hyperkeratosis over joints, flexural areas
Generalized or focally accented hyperkeratosis, predominately on extremities, buttocks
Palmoplantar involvement
KRT1: epidermolytic PPK KRT10: palms and soles are spared (exceptions possible)
Usually no Massive PPK leading to deep, bleeding, and painful fissures; flexural contractures; constriction bands
Noninflammatory diffuse PPK with honeycomb pattern, mild digital constriction, brown hyperkeratosis, knuckle pads over back aspects
Diffuse PPK present in about 50% of patients
Epidermolytic Ichthyosis
Oji V et al. Revised nomenclature and classification ofinherited ichthyoses: results of the First Ichthyosis Consensus Conference inSorèze 2009. J Am Acad Dermatol. 2010 Oct;63(4):607-41.
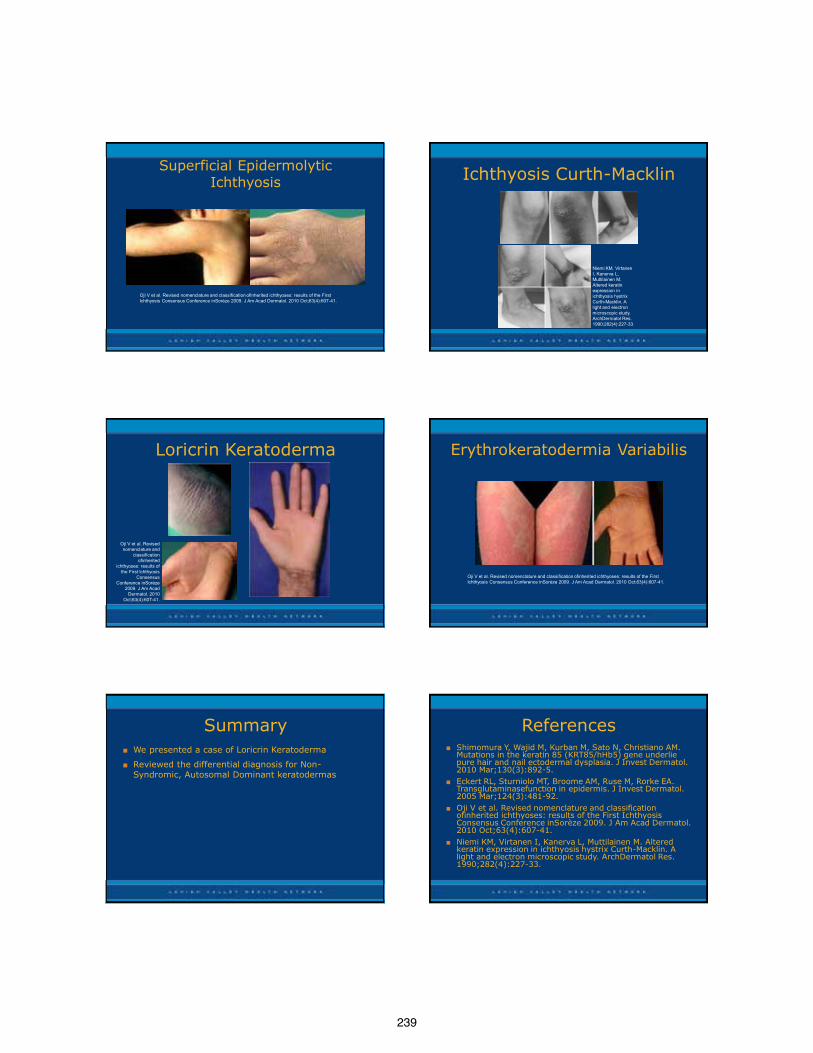
239
Superficial Epidermolytic Ichthyosis
Oji V et al. Revised nomenclature and classification ofinherited ichthyoses: results of the First Ichthyosis Consensus Conference inSorèze 2009. J Am Acad Dermatol. 2010 Oct;63(4):607-41.
Ichthyosis Curth-Macklin
Niemi KM, Virtanen I, Kanerva L, Muttilainen M. Altered keratin expression in ichthyosis hystrix Curth-Macklin. A light and electron microscopic study. ArchDermatol Res. 1990;282(4):227-33.
Loricrin Keratoderma
Oji V et al. Revised nomenclature and
classification ofinherited
ichthyoses: results of the First Ichthyosis
Consensus Conference inSorèze
2009. J Am Acad Dermatol. 2010
Oct;63(4):607-41.
Erythrokeratodermia Variabilis
Oji V et al. Revised nomenclature and classification ofinherited ichthyoses: results of the First Ichthyosis Consensus Conference inSorèze 2009. J Am Acad Dermatol. 2010 Oct;63(4):607-41.
Summary ■ We presented a case of Loricrin Keratoderma
■ Reviewed the differential diagnosis for Non-Syndromic, Autosomal Dominant keratodermas
References ■ Shimomura Y, Wajid M, Kurban M, Sato N, Christiano AM.
Mutations in the keratin 85 (KRT85/hHb5) gene underlie pure hair and nail ectodermal dysplasia. J Invest Dermatol. 2010 Mar;130(3):892-5.
■ Eckert RL, Sturniolo MT, Broome AM, Ruse M, Rorke EA. Transglutaminasefunction in epidermis. J Invest Dermatol. 2005 Mar;124(3):481-92.
■ Oji V et al. Revised nomenclature and classification ofinherited ichthyoses: results of the First Ichthyosis Consensus Conference inSorèze 2009. J Am Acad Dermatol. 2010 Oct;63(4):607-41.
■ Niemi KM, Virtanen I, Kanerva L, Muttilainen M. Altered keratin expression in ichthyosis hystrix Curth-Macklin. A light and electron microscopic study. ArchDermatol Res. 1990;282(4):227-33.
240
Acknowledgements • Tanya Ermolovich, D.O.
• Stephen M. Purcell, D.O.
• Thomas D. Griffin, M.D.
• Fellow Residents
241
RESIDENT POSTER PRESENTATIONSPorokeratotic Eccrine Ostial and Dermal Duct Nevus: A Case Report and Literature Review Nicholas Benner, D.O. O’Bleness Hospital, Dublin, OH
CREST Syndrome Mariel Bird, D.O. Oakwood Southshore Medical Center, Warren, MI
An Uncommon Cause of Purpura Fulminans: Pasteurella multocida Sepsis Lise Brown, D.O. Alta Dermatology, Mesa, AZ
Treatment of Verruca Vulgaris with Nd:YAG 1064nm Laser Winifred Chu, D.O. St. John’s Episcopal Hospital, Lindenhurst, NY
Painful Palmar Petechiae: An Atypical Presentation of Dermatitis Herpetiformis Nathan Cleaver, D.O. St. Joseph Mercy Health System, Clinton Township, MI
A Review and Update on Melanocyte Stimulating Hormone Therapy: Afamelanotide Jordan Fabrikant, D.O. NSUCOM/Larkin Community Hospital, Miami, FL
Muir-Torre syndrome: A Case Associated with an Infrequent Genetic Mutation Christina Feser, D.O. Oakwood Southshore Medical Center, Warren, MI
Linear Morphea Treated with Methotrexate and Excimer Laser Anne Hanson, D.O. St. Joseph Mercy Health System, Clinton Township, MI
Epidermolytic Hyperkeratosis Trey Haunson, D.O. LewisGale Hospital, Blacksburg, VA
An Atypical Presentation of a Common Disease in a Middle-Aged HIV Positive Male Jared Heaton, D.O. Largo Medical Center, Port Richey, FL
Cutaneous Polyarteritis Nodosa Teresa Ishak, D.O. Western University/Pacific Hospital, Long Beach, CA
Primary Dermal Melanoma: Differing Characteristics from Conventional Melanoma? Jesse Jensen, D.O. McLaren Oakland Hospital, Commerce Township, MI
Iatrogenic Kaposi’s Sarcoma Arising After Renal Transplant Immunosuppression Katherine Johnson, D.O. McLaren Oakland Hospital, Commerce Township, MI
Exaggerated insect bite-like reaction in a patient with chronic lymphocytic leukemia Holly Kanavy, D.O. St. Barnabas Hospital, Bronx, NY
Sweet’s Syndrome in Concordance with Acute Coronary Syndrome Michael Kassardjian, D.O. Western University/Pacific Hospital, Long Beach, CA
Lichen Planus Pemphigoides: Review of Treatment Options Raymond Knisley, D.O. Advanced Desert Dermatology, Peoria, AZ
Persistent Rash in a 75 Year Old Male Cathy Koger, D.O. NRMC, Kirksville, MO
Invasive Ductal Breast Carcinoma Presenting as Lipoma in a Male: A Case Report and a Review of the Literature James Landero, D.O. Wellington Regional Medical Center, Margate, FL
Metachronous Classical Kaposi Sarcoma in a Hispanic Male Tang Le, D.O. South Texas Dermatology, Houston, TX
Carcinoid Tumors and Carcinoid Syndrome: A Review From A Two-Point Perspective Katy Matthews, D.O. Columbia Hospital, West Palm Beach, FL
Sweet’s Syndrome Masquerading as Disseminated Herpes Zoster in an HIV Positive Patient Charisse McCall, D.O. St. John’s Episcopal Hospital, Lindenhurst, NY
242
Carcinoma Erysipeloides Morgan McCarty, D.O. St. Joseph Mercy Health System, Clinton Township, MI
Successful Treatment of Advanced Inoperable Basal Cell Carcinoma with Vismodegib Suzanne Horwitz, D.O. Wellington Regional Medical Center, Margate, FL
Case of a Peculiar Fungating Nose Lesion Panagiotis Mitropoulos D.O. NSUCOM/BGMC, Hollywood, FL
Multiple Sebaceous Trichofolliculomas on the Face Megan Morrison, D.O. St. Joseph Mercy Health System, Clinton Township, MI
High-Risk Cutaneous Squamous Cell Carcinoma: A Case Report and Review of Literature Julian Ngo, D.O. Largo Medical Center, Port Richey, FL
Atypical Vascular Lesion Arising in an Area of Previous Radiation Treatment on the Breast Christian Oram, D.O. PCOM, Allentown, PA
A Case of Persistent Acantholytic Dermatosis Sital Patel, D.O. University Hospitals, Cleveland, OH
Treatment of Inflammatory Linear Verrucous Epidermal Nevi with Monotherapy Topical Retinoid Ryan Pham, D.O. UNTHSC/TCOM, Fort Worth, Texas
Mohs Surgery in Patients with Immunobullous Diseases: Should Prednisone be Increased Prior to Surgery? Justin Rubin, D.O. NSUCOM/BGMC, Hollywood, FL
Potential Complications of Psoriasis Therapy: A Case Report and Review of Catastrophic Antiphospholipid Syndrome (CAPS) Nicholas Rudloff, D.O. Summa Western Reserve Hospital, Cuyahoga Falls, OH
A report of cutaneous spread of Multiple Myeloma Clayton Schiltz, D.O. Genesys Regional Medical Center, Grand Blanc, MI
McCune-Albright Syndrome Pezham Shoureshi, D.O. University Hospitals, Cleveland, OH
A Case of Classic Kaposi’s Sarcoma Treated with Electron Beam Radiation Therapy Luis Soro, D.O. PCOM, Allentown, PA
Cutaneous Metastatic Crohn’s Disease of the Leg: A Rare Case Report and Review of the Literature Brooke Walls, D.O. Largo Medical Center, Port Richey, FL
A Prominent Eruption in a Female with Myelodysplastic Syndrome Dustin Wilkes, D.O. St. Joseph Mercy Health System, Clinton Township, MI
Telangiectasia Macularis Eruptiva Perstans: A Case Report Samuel Wilson, D.O. LewisGale Hospital, Blacksburg, VA
Recalcitrant Headaches Secondary to Facial Filler Injecions Matthew Zarraga, D.O. Wellington Regional Medical Center, Margate, FL
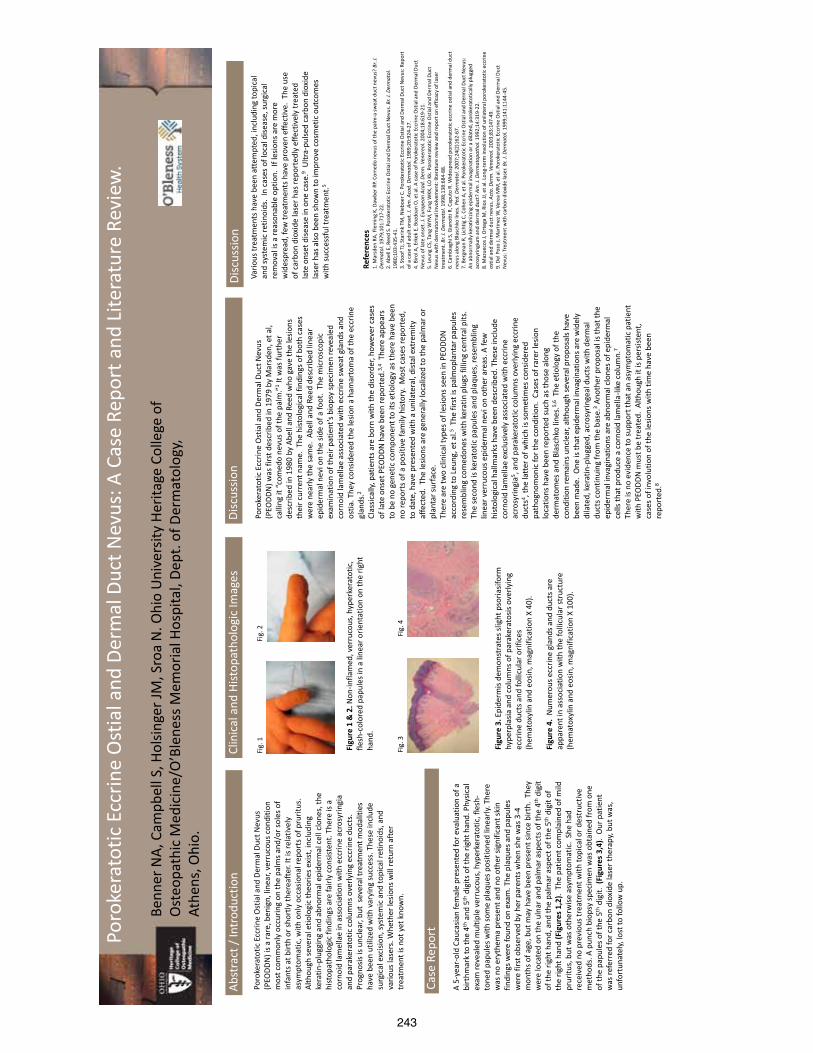
243
Refe
renc
es
1. M
arsd
en R
A, F
lem
ing
K, D
awbe
r RP.
Com
edo
nevu
s of t
he p
alm
-a sw
eat d
uct n
evus
? Br
. J.
Derm
atol
. 197
9;10
1:71
7-22
. 2.
Abe
ll E,
Ree
d S.
Por
oker
atot
ic E
ccrin
e O
stia
l and
Der
mal
Duc
t Nev
us. B
r. J.
Derm
atol
. 19
80;1
03:4
35-4
1.
3. S
toof
TJ,
Star
ink
TM, N
iebo
er C
. Por
oker
atot
ic E
ccrin
e O
stia
l and
Der
mal
Duc
t Nev
us: R
epor
t of
a c
ase
of a
dult
onse
t. J.
Am. A
cad.
Der
mat
ol. 1
989;
20:9
24-2
7.
4. B
irol A
, Erk
ek E
, Boz
doan
O, e
t al.
A ca
se o
f Por
oker
atot
ic E
ccrin
e O
stia
l and
Der
mal
Duc
t N
evus
of l
ate
onse
t. J.
Euro
pean
Aca
d. D
erm
. Ven
ereo
l. 20
04;1
8:61
9-21
. 5.
Leu
ng C
S, Ta
ng W
YM, F
ung
WKK
, LO
Kk.
Por
oker
atot
ic E
ccrin
e O
stia
l and
Der
mal
Duc
t N
evus
with
der
mat
omal
invo
lvem
ent:
liter
atur
e re
view
and
repo
rt o
n ef
ficac
y of
lase
r tr
eatm
ent.
Br. J
. Der
mat
ol. 1
998;
138:
684-
88.
6. C
ambi
aghi
S, G
iano
tti R
, Cap
uto
R. W
ides
prea
d po
roke
rato
tic e
ccrin
e os
tial a
nd d
erm
al d
uct
nevu
s alo
ng B
lasc
hko
lines
. Ped
. Der
mat
ol. 2
007;
24(2
)162
-67.
7.
Ber
gman
R, L
icht
ig C
, Coh
en A
, et a
l. Po
roke
rato
tic E
ccrin
e O
stia
l and
Der
mal
Duc
t Nev
us:
An a
bnor
mal
ly k
erat
inizi
ng e
pide
rmal
inva
gina
tion
or a
dila
ted,
por
oker
atot
ical
ly p
lugg
ed
acro
syrin
gium
and
der
mal
duc
t? A
m. J
. Der
mat
opat
hol.
1992
;14:
319-
22.
8. M
azue
cos J
, Ort
ega
M, R
ios J
J, et
al.
Long
-term
invo
lutio
n of
uni
late
ral p
orok
erat
otic
ecc
rine
ostia
l and
der
mal
duc
t nev
us. A
cta.
Der
m. V
ener
eol.
2003
;83:
147-
49.
9. D
el P
ozo
J, M
artin
ez W
, Ver
ea M
M, e
t al.
Poro
kera
totic
Ecc
rine
Ost
ial a
nd D
erm
al D
uct
Nev
us: T
reat
men
t with
carb
on d
ioxi
de la
ser.
Br. J
. Der
mat
ol. 1
999;
141:
1144
-45.
Abst
ract
/ In
trod
uctio
n
A 5-
year
-old
Cau
casia
n fe
mal
e pr
esen
ted
for e
valu
atio
n of
a
birt
hmar
k to
the
4th a
nd 5
th d
igits
of t
he ri
ght h
and.
Phy
sical
ex
am re
veal
ed m
ultip
le v
erru
cous
, hyp
erke
rato
tic, f
lesh
-to
ned
papu
les w
ith so
me
plaq
ues p
ositi
oned
line
arly.
The
re
was
no
eryt
hem
a pr
esen
t and
no
othe
r sig
nific
ant s
kin
findi
ngs w
ere
foun
d on
exa
m. T
he p
laqu
es a
nd p
apul
es
wer
e fir
st o
bser
ved
by h
er p
aren
ts w
hen
she
was
3-4
m
onth
s of a
ge, b
ut m
ay h
ave
been
pre
sent
sinc
e bi
rth.
The
y w
ere
loca
ted
on th
e ul
nar a
nd p
alm
ar a
spec
ts o
f the
4th
dig
it of
the
right
han
d, a
nd th
e pa
lmar
asp
ect o
f the
5th
dig
it of
th
e rig
ht h
and
(Fig
ures
1,2
). T
he p
atie
nt co
mpl
aine
d of
mild
pr
uritu
s, b
ut w
as o
ther
wise
asy
mpt
omat
ic.
She
had
rece
ived
no
prev
ious
trea
tmen
t with
topi
cal o
r des
truc
tive
met
hods
. A p
unch
bio
psy
spec
imen
was
obt
aine
d fr
om o
ne
of th
e pa
pule
s of t
he 5
th d
igit.
(Fi
gure
s 3,4
). O
ur p
atie
nt
was
refe
rred
for c
arbo
n di
oxid
e la
ser t
hera
py, b
ut w
as,
unfo
rtun
atel
y, lo
st to
follo
w u
p.
Case
Rep
ort
Clin
ical
and
Hist
opat
holo
gic
Imag
es
Fig.
1
Figu
re 1
& 2
. Non
-infla
med
, ver
ruco
us, h
yper
kera
totic
, fle
sh-c
olor
ed p
apul
es in
a li
near
orie
ntat
ion
on th
e rig
ht
hand
.
Fig.
2
Figu
re 3
. Epi
derm
is de
mon
stra
tes s
light
pso
riasif
orm
hy
perp
lasia
and
col
umns
of p
arak
erat
osis
over
lyin
g ec
crin
e du
cts a
nd fo
llicu
lar o
rific
es
(hem
atox
ylin
and
eos
in, m
agni
ficat
ion
X 40
). Fi
gure
4.
Num
erou
s ecc
rine
glan
ds a
nd d
ucts
are
ap
pare
nt in
ass
ocia
tion
with
the
folli
cula
r str
uctu
re
(hem
atox
ylin
and
eos
in, m
agni
ficat
ion
X 10
0).
Poro
kera
totic
Ecc
rine
Ost
ial a
nd D
erm
al D
uct N
evus
(P
EODD
N) w
as fi
rst d
escr
ibed
in 1
979
by M
arsd
en, e
t al,
calli
ng it
“com
edo
nevu
s of t
he p
alm
.”1 It w
as fu
rthe
r de
scrib
ed in
198
0 by
Abe
ll an
d Re
ed w
ho g
ave
the
lesio
ns
thei
r cur
rent
nam
e. T
he h
istol
ogic
al fi
ndin
gs o
f bot
h ca
ses
wer
e ne
arly
the
sam
e. A
bell
and
Reed
des
crib
ed li
near
ep
ider
mal
nev
i on
the
side
of a
foot
. Th
e m
icro
scop
ic
exam
inat
ion
of th
eir p
atie
nt’s
biop
sy sp
ecim
en re
veal
ed
corn
oid
lam
ella
e as
soci
ated
with
ecc
rine
swea
t gla
nds a
nd
ostia
. The
y co
nsid
ered
the
lesio
n a
ham
arto
ma
of th
e ec
crin
e gl
ands
.2
Clas
sical
ly, p
atie
nts a
re b
orn
with
the
diso
rder
, how
ever
cas
es
of la
te o
nset
PEO
DDN
hav
e be
en re
port
ed.3,
4 Th
ere
appe
ars
to b
e no
gen
etic
com
pone
nt to
its e
tiolo
gy a
s the
re h
ave
been
no
repo
rts o
f a p
ositi
ve fa
mily
hist
ory.
Mos
t cas
es re
port
ed,
to d
ate,
hav
e pr
esen
ted
with
a u
nila
tera
l, di
stal
ext
rem
ity
affe
cted
. Th
e le
sions
are
gen
eral
ly lo
caliz
ed to
the
palm
ar o
r pl
anta
r sur
face
. Th
ere
are
two
clin
ical
type
s of l
esio
ns se
en in
PEO
DDN
ac
cord
ing
to L
eung
, et a
l.5 Th
e fir
st is
pal
mop
lant
ar p
apul
es
rese
mbl
ing
com
edon
es w
ith k
erat
in p
lugs
filli
ng c
entr
al p
its.
The
seco
nd is
ker
atot
ic p
apul
es a
nd p
laqu
es, r
esem
blin
g lin
ear v
erru
cous
epi
derm
al n
evi o
n ot
her a
reas
. A fe
w
hist
olog
ical
hal
lmar
ks h
ave
been
des
crib
ed. T
hese
incl
ude
corn
oid
lam
ella
e ex
clus
ivel
y as
soci
ated
with
ecc
rine
acro
syrin
gia5 ,
and
para
kera
totic
col
umns
ove
rlyin
g ec
crin
e du
cts4 ,
the
latt
er o
f whi
ch is
som
etim
es c
onsid
ered
pa
thog
nom
onic
for t
he c
ondi
tion.
Cas
es o
f rar
er le
sion
loca
tions
hav
e be
en re
port
ed su
ch a
s tho
se a
long
de
rmat
omes
and
Bla
schk
o lin
es.5,
6 Th
e et
iolo
gy o
f the
co
nditi
on re
mai
ns u
ncle
ar, a
lthou
gh se
vera
l pro
posa
ls ha
ve
been
mad
e. O
ne is
that
epi
derm
al in
vagi
natio
ns a
re w
idel
y di
late
d, k
erat
in-p
lugg
ed, a
cros
yrin
geal
duc
ts w
ith d
erm
al
duct
s con
tinui
ng fr
om th
e ba
se.3 A
noth
er p
ropo
sal i
s tha
t the
ep
ider
mal
inva
gina
tions
are
abn
orm
al c
lone
s of e
pide
rmal
ce
lls th
at p
rodu
ce a
cor
noid
lam
ella
-like
col
umn.
7 Th
ere
is no
evi
denc
e to
supp
ort t
hat a
n as
ympt
omat
ic p
atie
nt
with
PEO
DDN
mus
t be
trea
ted.
Alth
ough
it is
per
siste
nt,
case
s of i
nvol
utio
n of
the
lesio
ns w
ith ti
me
have
bee
n re
port
ed.8
Vario
us tr
eatm
ents
hav
e be
en a
ttem
pted
, inc
ludi
ng to
pica
l an
d sy
stem
ic re
tinoi
ds.
In c
ases
of l
ocal
dise
ase,
surg
ical
re
mov
al is
a re
ason
able
opt
ion.
If l
esio
ns a
re m
ore
wid
espr
ead,
few
trea
tmen
ts h
ave
prov
en e
ffect
ive.
The
use
of
car
bon
diox
ide
lase
r has
repo
rted
ly e
ffect
ivel
y tr
eate
d la
te o
nset
dise
ase
in o
ne c
ase.
9 U
ltra-
pulse
d ca
rbon
dio
xide
la
ser h
as a
lso b
een
show
n to
impr
ove
cosm
etic
out
com
es
with
succ
essf
ul tr
eatm
ent.5
Disc
ussio
n
Poro
kera
totic
Ecc
rine
Ost
ial a
nd D
erm
al D
uct N
evus
: A C
ase
Repo
rt a
nd L
itera
ture
Rev
iew
.
Benn
er N
A, C
ampb
ell S
, Hol
singe
r JM
, Sro
a N
. Ohi
o U
nive
rsity
Her
itage
Col
lege
of
Ost
eopa
thic
Med
icin
e/O
’Ble
ness
Mem
oria
l Hos
pita
l, De
pt. o
f Der
mat
olog
y, At
hens
, Ohi
o.
Fig.
3
Fi
g. 4
Poro
kera
totic
Ecc
rine
Ost
ial a
nd D
erm
al D
uct N
evus
(P
EODD
N) i
s a ra
re, b
enig
n, li
near
, ver
ruco
us co
nditi
on
mos
t com
mon
ly o
ccur
ing
on th
e pa
lms a
nd/o
r sol
es o
f in
fant
s at b
irth
or sh
ortly
ther
eafte
r. It
is re
lativ
ely
asym
ptom
atic
, with
onl
y oc
casio
nal r
epor
ts o
f pru
ritus
. Al
thou
gh se
vera
l etio
logi
c th
eorie
s exi
st, i
nclu
ding
ke
ratin
-plu
ggin
g an
d ab
norm
al e
pide
rmal
cel
l clo
nes,
the
hist
opat
holo
gic
findi
ngs a
re fa
irly
cons
isten
t. Th
ere
is a
corn
oid
lam
ella
e in
ass
ocia
tion
with
ecc
rine
acro
syrin
gia
and
para
kera
totic
col
umns
ove
rlyin
g ec
crin
e du
cts.
Pr
ogno
sis is
unc
lear
, but
sev
eral
trea
tmen
t mod
aliti
es
have
bee
n ut
ilize
d w
ith v
aryi
ng su
cces
s. T
hese
incl
ude
surg
ical
exc
ision
, sys
tem
ic a
nd to
pica
l ret
inoi
ds, a
nd
vario
us la
sers
. Whe
ther
lesio
ns w
ill re
turn
afte
r tr
eatm
ent i
s not
yet
kno
wn.
Disc
ussio
n
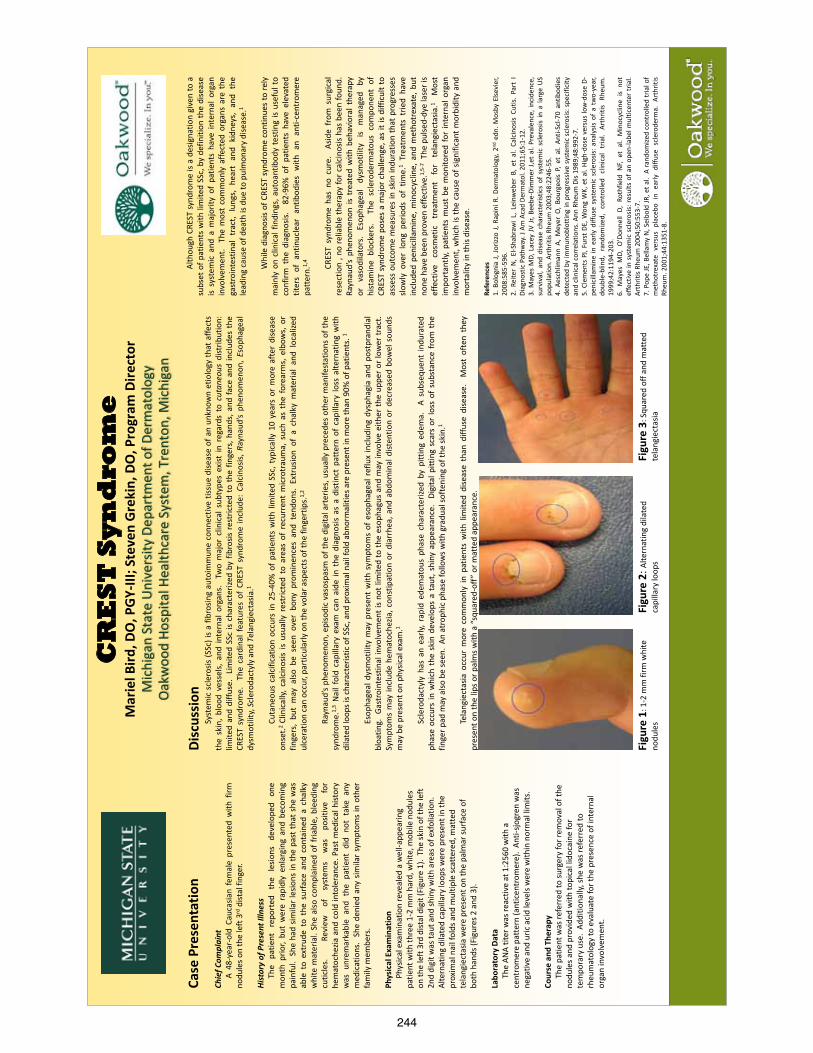
244
CR
ES
T S
yn
dro
me
M
arie
l Bird
, DO
, PGY
-III;
Stev
en G
reki
n, D
O, P
rogr
am D
irect
or
Mic
higa
n St
ate
Uni
vers
ity D
epar
tmen
t of D
erm
atol
ogy
Oak
woo
d Ho
spita
l Hea
lthca
re S
yste
m, T
rent
on, M
ichi
gan
Case
Pre
sent
atio
n Ch
ief C
ompl
aint
A 4
8-ye
ar-o
ld C
auca
sian
fem
ale
pres
ente
d w
ith f
irm
nodu
les o
n th
e le
ft 3
rd d
istal
fing
er.
Hist
ory
of P
rese
nt Il
lnes
s
The
pa
tient
re
port
ed
the
lesio
ns
deve
lope
d on
e m
onth
prio
r, bu
t w
ere
rapi
dly
enla
rgin
g an
d be
com
ing
pain
ful.
She
had
sim
ilar l
esio
ns in
the
past
that
she
was
ab
le t
o ex
trud
e to
the
sur
face
and
con
tain
ed a
cha
lky
whi
te m
ater
ial.
She
also
com
plai
ned
of fr
iabl
e, b
leed
ing
cutic
les.
Revi
ew
of
syst
ems
was
po
sitiv
e fo
r he
mat
oche
zia a
nd c
old
into
lera
nce.
Pas
t med
ical
hist
ory
was
unr
emar
kabl
e an
d th
e pa
tient
did
not
tak
e an
y m
edic
atio
ns.
She
deni
ed a
ny s
imila
r sy
mpt
oms
in o
ther
fa
mily
mem
bers
. Ph
ysic
al E
xam
inat
ion
Phy
sical
exa
min
atio
n re
veal
ed a
wel
l-app
earin
g pa
tient
with
thre
e 1-
2 m
m h
ard,
whi
te, m
obile
nod
ules
on
the
left
3rd
dist
al d
igit
(Fig
ure
1).
The
skin
of t
he le
ft
2nd
digi
t was
taut
and
shin
y w
ith a
reas
of e
xfol
iatio
n.
Alte
rnat
ing
dila
ted
capi
llary
loop
s wer
e pr
esen
t in
the
prox
imal
nai
l fol
ds a
nd m
ultip
le sc
atte
red,
mat
ted
tela
ngie
ctas
ia w
ere
pres
ent o
n th
e pa
lmar
surfa
ce o
f bo
th h
ands
(Fig
ures
2 a
nd 3
). La
bora
tory
Dat
a
The
AN
A tit
er w
as re
activ
e at
1:2
560
with
a
cent
rom
ere
patt
ern
(ant
icen
trom
ere)
. An
ti-sjo
gren
was
ne
gativ
e an
d ur
ic a
cid
leve
ls w
ere
with
in n
orm
al li
mits
. Co
urse
and
The
rapy
The
pat
ient
was
refe
rred
to su
rger
y fo
r rem
oval
of t
he
nodu
les a
nd p
rovi
ded
with
topi
cal l
idoc
aine
for
tem
pora
ry u
se.
Addi
tiona
lly, s
he w
as re
ferr
ed to
rh
eum
atol
ogy
to e
valu
ate
for t
he p
rese
nce
of in
tern
al
orga
n in
volv
emen
t.
Disc
ussi
on
Sy
stem
ic s
cler
osis
(SSc
) is
a fib
rosin
g au
toim
mun
e co
nnec
tive
tissu
e di
seas
e of
an
unkn
own
etio
logy
that
affe
cts
the
skin
, bl
ood
vess
els,
and
inte
rnal
org
ans.
Tw
o m
ajor
clin
ical
sub
type
s ex
ist in
reg
ards
to
cuta
neou
s di
strib
utio
n:
limite
d an
d di
ffuse
. Li
mite
d SS
c is
char
acte
rized
by
fibro
sis r
estr
icte
d to
the
fing
ers,
han
ds, a
nd fa
ce a
nd in
clud
es t
he
CRES
T sy
ndro
me.
Th
e ca
rdin
al f
eatu
res
of C
REST
syn
drom
e in
clud
e: C
alci
nosis
, Ray
naud
’s ph
enom
enon
, Eso
phag
eal
dysm
otili
ty, S
cler
odac
tyly
and
Tel
angi
ecta
sia.1
Cu
tane
ous
calc
ifica
tion
occu
rs in
25-
40%
of
patie
nts
with
lim
ited
SSc,
typ
ical
ly 1
0 ye
ars
or m
ore
afte
r di
seas
e on
set.2
Clin
ical
ly, c
alci
nosis
is u
sual
ly r
estr
icte
d to
are
as o
f re
curr
ent
mic
rotr
aum
a, s
uch
as t
he f
orea
rms,
elb
ows,
or
finge
rs,
but
may
also
be
seen
ove
r bo
ny p
rom
inen
ces
and
tend
ons.
Ext
rusio
n of
a c
halk
y m
ater
ial
and
loca
lized
ul
cera
tion
can
occu
r, pa
rtic
ular
ly o
n th
e vo
lar a
spec
ts o
f the
fing
ertip
s.1,
2
Ra
ynau
d’s
phen
omen
on, e
piso
dic
vaso
spas
m o
f the
dig
ital a
rter
ies,
usu
ally
pre
cede
s ot
her m
anife
stat
ions
of t
he
synd
rom
e.1,
3 N
ail f
old
capi
llary
exa
m c
an a
ide
in t
he d
iagn
osis
as a
dist
inct
pat
tern
of
capi
llary
loss
alte
rnat
ing
with
di
late
d lo
ops i
s cha
ract
erist
ic o
f SSc
, and
pro
xim
al n
ail f
old
abno
rmal
ities
are
pre
sent
in m
ore
than
90%
of p
atie
nts.
1
Esop
hage
al d
ysm
otili
ty m
ay p
rese
nt w
ith s
ympt
oms
of e
soph
agea
l ref
lux
incl
udin
g dy
spha
gia
and
post
pran
dial
bl
oatin
g. G
astr
oint
estin
al in
volv
emen
t is
not l
imite
d to
the
esop
hagu
s an
d m
ay in
volv
e ei
ther
the
uppe
r or l
ower
trac
t.
Sym
ptom
s m
ay in
clud
e he
mat
oche
zia, c
onst
ipat
ion
or d
iarr
hea,
and
abd
omin
al d
isten
tion
or d
ecre
ased
bow
el s
ound
s m
ay b
e pr
esen
t on
phys
ical
exa
m.1
Sc
lero
dact
yly
has
an e
arly,
rap
id e
dem
atou
s ph
ase
char
acte
rized
by
pitt
ing
edem
a.
A su
bseq
uent
indu
rate
d ph
ase
occu
rs in
whi
ch t
he s
kin
deve
lops
a t
aut,
shin
y ap
pear
ance
. Di
gita
l pitt
ing
scar
s or
loss
of
subs
tanc
e fr
om t
he
finge
r pad
may
also
be
seen
. An
atr
ophi
c ph
ase
follo
ws w
ith g
radu
al so
fteni
ng o
f the
skin
.1
Te
lang
iect
asia
occ
ur m
ore
com
mon
ly in
pat
ient
s w
ith li
mite
d di
seas
e th
an d
iffus
e di
seas
e.
Mos
t of
ten
they
pr
esen
t on
the
lips o
r pal
ms w
ith a
“squ
ared
-off
” or
mat
ted
appe
aran
ce.
Al
thou
gh C
REST
synd
rom
e is
a de
signa
tion
give
n to
a
subs
et o
f pat
ient
s w
ith li
mite
d SS
c, b
y de
finiti
on th
e di
seas
e is
syst
emic
and
a m
ajor
ity o
f pa
tient
s ha
ve in
tern
al o
rgan
in
volv
emen
t. T
he m
ost
com
mon
ly a
ffect
ed o
rgan
s ar
e th
e ga
stro
inte
stin
al t
ract
, lu
ngs,
hea
rt a
nd k
idne
ys,
and
the
lead
ing
caus
e of
dea
th is
due
to p
ulm
onar
y di
seas
e.1
W
hile
dia
gnos
is of
CRE
ST sy
ndro
me
cont
inue
s to
rely
m
ainl
y on
clin
ical
find
ings
, aut
oant
ibod
y te
stin
g is
usef
ul t
o co
nfirm
the
dia
gnos
is.
82-9
6% o
f pa
tient
s ha
ve e
leva
ted
titer
s of
ant
inuc
lear
ant
ibod
ies
with
an
anti-
cent
rom
ere
patt
ern.
1,4
CR
EST
synd
rom
e ha
s no
cur
e.
Asid
e fr
om s
urgi
cal
rese
ctio
n , n
o re
liabl
e th
erap
y fo
r cal
cino
sis h
as b
een
foun
d.
Rayn
aud’
s ph
enom
enon
is t
reat
ed w
ith b
ehav
iora
l the
rapy
or
va
sodi
lato
rs.
Esop
hage
al
dysm
otili
ty
is m
anag
ed
by
hist
amin
e bl
ocke
rs.
The
scl
erod
erm
atou
s co
mpo
nent
of
CRES
T sy
ndro
me
pose
s a
maj
or c
halle
nge,
as
it is
diffi
cult
to
asse
ss o
utco
me
mea
sure
s in
ski
n in
dura
tion
that
pro
gres
ses
slow
ly o
ver
long
per
iods
of
time.
1 Tr
eatm
ents
trie
d ha
ve
incl
uded
pen
icill
amin
e, m
inoc
yclin
e, a
nd m
etho
trex
ate,
but
no
ne h
ave
been
pro
ven
effe
ctiv
e.1,
5-7
The
pulse
d-dy
e la
ser i
s ef
fect
ive
cosm
etic
tr
eatm
ent
for
tela
ngie
ctas
ia.1
Mos
t im
port
antly
, pat
ient
s m
ust
be m
onito
red
for
inte
rnal
org
an
invo
lvem
ent,
whi
ch is
the
caus
e of
sig
nific
ant m
orbi
dity
and
m
orta
lity
in th
is di
seas
e.
Refe
renc
es
1. B
olog
nia
J, Jo
rizzo
J, R
apin
i R. D
erm
atol
ogy,
2nd e
dn. M
osby
Else
vier
, 20
08:5
85-5
96.
2. R
eite
r N
, El
-Sha
braw
i L,
Lei
nweb
er B
, et
al.
Calc
inos
is Cu
tis.
Part
I
Diag
nost
ic P
athw
ay. J
Am
Aca
d De
rmat
ol. 2
011;
65:1
-12.
3.
May
es M
D, L
acey
JV J
r, Be
ebe-
Dim
mer
J,et
al.
Prev
alen
ce, i
ncid
ence
, su
rviv
al, a
nd d
iseas
e ch
arac
teris
tics
of s
yste
mic
scl
eros
is in
a la
rge
US
popu
latio
n. A
rthr
itis R
heum
200
3;48
:224
6-55
. 4.
Aes
chlim
ann
A, M
eyer
O,
Bour
geoi
s P,
et
al.
Anti-
Scl-7
0 an
tibod
ies
dete
cted
by
imm
unob
lott
ing
in p
rogr
essiv
e sy
stem
ic s
cler
osis:
spe
cific
ity
and
clin
ical
cor
rela
tions
. Ann
Rhe
um D
is 19
89;4
8:99
2-7.
5.
Cle
men
ts P
J, Fu
rst D
E, W
ong
WK,
et a
l. Hi
gh-d
ose
vers
us lo
w-d
ose
D-pe
nici
llam
ine
in e
arly
diff
use
syst
emic
scl
eros
is: a
naly
sis o
f a
two-
year
, do
uble
-blin
d, r
ando
mize
d, c
ontr
olle
d cl
inic
al
tria
l. Ar
thrit
is Rh
eum
. 19
99;4
2:11
94-2
03.
6.
May
es M
D, O
’Don
nell
D, R
othf
ield
NF,
et a
l. M
inoc
yclin
e is
not
effe
ctiv
e in
sys
tem
ic s
cler
osis:
resu
lts o
f an
open
-labe
l mul
ticen
ter
tria
l. Ar
thrit
is Rh
eum
200
4;50
:553
-7.
7. P
ope
JE, B
ella
my
N, S
eibo
ld JR
, et a
l. A
rand
omize
d co
ntro
lled
tria
l of
met
hotr
exat
e ve
rsus
pla
cebo
in
early
diff
use
scle
rode
rma.
Art
hriti
s Rh
eum
. 200
1;44
:135
1-8.
Figu
re 2
: Alte
rnat
ing
dila
ted
capi
llary
loop
s Fi
gure
1: 1
-2 m
m fi
rm w
hite
no
dule
s Fi
gure
3: S
quar
ed o
ff an
d m
atte
d te
lang
iect
asia

245
TEM
PLAT
E D
ESIG
N ©
200
8
ww
w.P
oste
rPre
sent
atio
ns.c
om
An U
ncom
mon C
ause
of P
urpu
ra F
ulmina
ns: P
aste
urell
a mult
ocida
Sep
sis
Lise D
. Bro
wn D
.O.1 ,
Ther
esa C
ao D
.O.1 ,
David
Dro
ller M
.D.2 A
ngela
Com
bs, D
.O. 3 T
racy
Fav
reau
, D.O
.3
ABST
RACT
DI
SCUS
SION
(con
t’d)
DISC
USSI
ON (c
ont’d
)
CONC
LUSI
ON
1.W
yson
g A, V
enka
tesan
P. A
n app
roac
h to t
he pa
tient
with
retifo
rm pu
rpur
a. De
rmato
lol
Ther
apy.
2011
Mar
ch-A
pr; 2
4(2)
:151-
172.
2.Ch
almer
s E, C
oope
r P, F
orma
n K, G
rimley
C, K
hair K
, Minf
ord A
, Mor
gan M
, Mum
ford
AD. P
urpu
ra fu
lmina
ns: r
ecog
nition
, diag
nosis
and m
anag
emen
t. Arch
Dis
Child
2010
3.
Fran
cis R
B. A
cquir
ed pu
rpur
a fulm
inans
. Sem
in Th
romb
Hae
mosta
t 199
0 16:3
10-2
5. 4.
Nolan
J, S
inclai
r R. R
eview
of m
anag
emen
t of p
urpu
ra fu
lmina
ns an
d two
case
repo
rts.
Br J
Anae
sth. 2
001 8
6:581
-6.
5.Ga
llowa
y RE.
Mam
malia
n bite
s. J E
merg
Med
1988
;6:32
5-31
. 6.
Web
er D
J, Ha
nsen
AR.
Infec
tions
resu
lting f
rom
anim
al bit
es. In
fect D
is Cl
in No
rth A
m.
1991
;5:66
3-80
. 7.
Zurlo
JJ. P
asteu
rella
spec
ies. M
ande
ll, Do
uglas
, and
Ben
nett’s
Prin
ciples
and P
racti
ce
of Inf
ectio
us D
iseas
es. 7
th ed.
2009
Chu
rchill
Living
stone
. 8.
Web
er D
J, W
olfso
n JS,
Swa
tz MN
, Hoo
per D
C. P
asteu
rella
mult
ocida
infec
tions
. Rep
ort
of 34
case
s and
revie
w of
the lit
eratu
re. M
edici
ne. 1
984 M
ay, 6
3(3)
:133-
54.
9.Go
ldstei
n EJ.
Bite
woun
ds an
d infe
ction
. Clin
Infec
t Dis
1992
14:63
3-63
8.
10.
Fern
ande
z-Vale
ncia
JA, G
arcia
S, P
rat S
. Pas
teure
lla m
ultoc
ida se
ptic s
hock
after
a ca
t sc
ratch
in an
elde
rly ot
herw
ise he
althy
wom
an: a
case
repo
rt. A
m J E
merg
Med
. 200
8.
11.
Golds
tein E
JC, R
einha
rdt J
F, Mu
rray P
M. O
utpati
ent th
erap
y of b
ite w
ound
s: de
mogr
aphic
data,
bacte
riolog
y, an
d a pr
ospe
ctive
, ran
domi
zed t
rial o
f am
oxoc
illin/c
lavula
nic ac
id ve
rsus p
enici
llin +/
- dicl
oxac
illin.
Int J
Derm
atol 1
987;2
6:124
-7.
12
.Am
erica
n Aca
demy
of P
ediat
rics.
Pastu
rella
infec
tions
. In R
ed B
ook:
2009
Rep
ort o
f the
Comm
ittee o
n Infe
ctiou
s Dise
ases
, 28th e
d. Pi
cker
ing, L
K (E
d), A
m Ac
ad P
ed, E
lk Gr
ove
Villa
ge, Il
2009
, p. 4
93.
(for p
atien
ts 18
year
s of a
ge an
d olde
r), d
oxyc
yclin
e (for
child
ren 8
ye
ars o
f age
and o
lder),
and t
he ex
tende
d spe
ctrum
ceph
alosp
orins
su
ch as
cefix
ine or
cefpo
doxim
e, as
well
as tr
imeth
oprim
-su
lfame
thoxa
zole,
altho
ugh m
etron
idazo
le sh
ould
be ad
ded t
o the
se
antib
iotics
for a
naer
obic
cove
rage
.11 C
linica
l failu
res h
ave b
een n
oted
in pa
tients
trea
ted w
ith or
al ma
crolid
es, s
emi-s
ynthe
tic pe
nicilli
ns su
ch
as di
cloxa
cillin
, first
-gen
erati
on ce
phalo
spor
ins an
d clin
damy
cin an
d thu
s sho
uld be
avoid
ed.12
CASE
REP
ORT
A 74
year
old C
auca
sian w
oman
with
a pa
st me
dical
histor
y sign
ifican
t for
hype
rtens
ion an
d car
otid a
rtery
disea
se w
as fo
und u
nres
pons
ive in
he
r car
on a
hot s
umme
r day
. In th
e ER,
she w
as no
ted to
be
hypo
tensiv
e and
hype
rther
mic w
ith a
tempe
ratur
e of 1
07 de
gree
s Fa
hren
heit.
Her la
bs su
gges
ted sh
e was
in ea
rly di
ssem
inated
int
rava
scula
r coa
gulop
athy.
Over
her b
ack a
nd an
terior
thigh
s wer
e re
tiform
purp
ura a
nd la
rge,
hemo
rrhag
ic bu
llae (
Figur
e 1.),
as w
ell as
pe
techia
e of th
e fac
e (Fig
ure 2
.). S
he w
as pl
aced
on po
sitive
inotr
opic
supp
ort, c
ooled
to a
tempe
ratur
e of 1
02 de
gree
s, mu
ltiple
blood
cu
lture
s wer
e dra
wn, a
nd sh
e was
star
ted on
broa
d spe
ctrum
empir
ic an
tibiot
ics. T
he pa
tient
was
place
d in r
espir
atory
isolat
ion w
ith a
pres
umpti
ve di
agno
sis of
men
ingoc
occe
mia b
ased
on pr
elimi
nary
blood
cultu
res p
ositiv
e for
Gra
m ne
gativ
e coc
coba
cilli.
She a
lso
rece
ived s
ubcu
taneo
us lo
w-mo
lecula
r weig
ht he
parin
. Fur
ther h
istor
y fro
m the
patie
nt’s f
amily
reve
aled t
wo da
ys pr
ior sh
e had
been
bitte
n on
the l
eg by
her in
door
pet c
at an
d dev
elope
d cell
ulitis
(Figu
re 3.
). On
ly on
e of s
ix blo
od cu
lture
s tak
en ov
er a
perio
d of tw
o day
s sho
wed
grow
th of
pan-
sens
itive P
aste
urell
a m
ultoc
ida. A
cere
bros
pinal
fluid
analy
sis w
as no
t per
forme
d due
to se
vere
thro
mboc
ytope
nia. A
deep
tis
sue c
ultur
e fro
m the
pupu
ric fu
lmina
ns er
uptio
n on t
he th
igh w
as
nega
tive f
or gr
owth.
Immu
noglo
bulin
leve
ls an
d a se
rum
prote
in ele
ctrop
hore
sis w
ith im
muno
fixati
on w
ere o
rder
ed to
rule
out a
n un
derly
ing im
muno
defic
iency
. Whil
e the
stud
ies di
d not
demo
nstra
te a
mono
clona
l gam
mopa
thy, s
he di
d hav
e acq
uired
IgG
defic
iency
se
cond
ary t
o sep
sis an
d sub
sequ
ently
rece
ived I
VIG.
Ove
r the
fol
lowing
two w
eeks
, the p
atien
t was
wea
ned f
rom
vaso
pres
sor
supp
ort. H
er la
b valu
es no
rmali
zed,
howe
ver, s
he re
maine
d mini
mally
re
spon
sive a
nd w
as su
bseq
uentl
y tra
nsfer
red t
o a ch
ronic
venti
lator
an
d reh
abilit
ation
unit f
or se
vere
ence
phalo
pathy
attrib
uted t
o the
hy
perth
ermi
a she
had s
ustai
ned.
Unfor
tunate
ly, th
e pati
ent p
asse
d aw
ay a
month
and a
half l
ater.
CLIN
ICAL
IMAG
ES
DISC
USSI
ON 1 D
erma
tolog
y Res
ident,
Nov
a Sou
theas
tern U
niver
sity C
olleg
e of O
steop
athic
Medic
ine/B
rowa
rd G
ener
al Me
dical
Cente
r, For
t Lau
derd
ale, F
lorida
; 2 Divi
sion o
f Infec
tious
Dise
ases
, Bro
ward
Gen
eral
Medic
al Ce
nter, F
ort L
aude
rdale
, FL;
3 Co-
Prog
ram
Dire
ctor, N
ova S
outhe
aster
n Univ
ersit
y Coll
ege o
f Oste
opath
ic Me
dicine
/Bro
ward
Gen
eral
Medic
al Ce
nter D
erma
tolog
y Res
idenc
y, Fo
rt La
uder
dale,
Flor
ida
Figu
re 1.
Pur
pura
fulm
inans
of th
e bila
teral
thigh
s.
Fres
h fro
zen p
lasma
also
conta
ins pr
otein
C, bu
t in le
sser
co
ncen
tratio
ns. H
epar
in, w
hile t
heor
etica
lly in
dicate
d in p
atien
ts wi
th thr
ombo
sis (i.
e., pa
tients
in D
IC),
is lim
ited b
y the
degr
ee of
thr
ombo
cytop
enia;
a no
t unc
ommo
n find
ing in
critic
ally i
ll pati
ents.
Th
ere a
re ar
gume
nts fo
r givi
ng he
parin
befor
e clot
ting f
actor
s are
re
place
d, in
orde
r to a
void
furthe
r thr
ombo
sis.4 A
t time
s, su
rgica
l de
bride
ment
of ne
crotic
skin,
esch
aroto
mies
, and
fasc
iotom
ies m
ay
be in
dicate
d, as
well
as su
bseq
uent
skin
graft
ing. D
eep n
ecro
sis of
lim
bs or
digit
s may
be ex
tensiv
e eno
ugh t
o war
rant
ampu
tation
. Sp
ecies
of th
e gen
us P
aste
urell
a ar
e non
motile
, facu
ltativ
e ana
erob
ic,
gram
-neg
ative
cocc
obac
illi th
at inh
abit t
he or
al ca
vity a
nd
gastr
ointes
tinal
tract
of ma
ny an
imals
, with
dogs
and c
ats ha
ving
partic
ularly
high
colon
izatio
n rate
s. Th
e mos
t com
mon h
uman
isola
tes
belon
g to t
he P.
mult
ocida
grou
p. Ap
prox
imate
ly 15
% to
20%
of do
g bit
e wou
nds a
nd up
to 50
% of
cat b
ite w
ound
s bec
ome i
nfecte
d.5 M
ost
infec
tions
that
deve
lop fr
om do
g and
cat b
ites a
re p
olymi
crobia
l. In a
stu
dy of
107 s
ubjec
ts wi
th do
g and
cat b
ite in
fectio
ns, m
ixed a
erob
ic an
d ana
erob
ic inf
ectio
ns w
ere p
rese
nt in
56%
of al
l wou
nds (
dogs
: 48
%; c
ats: 6
3%).
Paste
urell
a spe
cies w
as th
e mos
t com
mon
patho
gen i
solat
ed fr
om bo
th do
g (50
%) a
nd ca
t (75
%) b
ites f
ollow
ed
by S
trept
ococ
ci (4
6% of
both
types
of bi
te inf
ectio
ns).6
Paste
urell
a spe
cies a
re fa
stidio
us an
d can
be di
fficult
to is
olate
espe
cially
from
nons
terile
spec
imen
s suc
h as s
putum
.7 In G
ram
staine
d spe
cimen
s, the
y gen
erall
y app
ear a
s a si
ngle
bacil
lus, o
ften
with
bipola
r stai
ning,
but m
ay al
so be
seen
in pa
irs or
shor
t cha
ins an
d ca
n be c
onfus
ed w
ith N
eisse
ria m
ening
itidis.
Th
e mos
t com
mon t
ypes
of in
fectio
ns ca
used
by P.
mult
ocida
are l
ocal
woun
d infe
ction
s foll
owing
anim
al bit
es or
scra
tches
. Abs
cess
es an
d ten
osyn
ovitis
are t
he m
ost fr
eque
nt co
mplic
ation
s of P
aste
urell
a soft
tis
sue i
nfecti
on, w
ith se
ptic a
rthriti
s and
oste
omye
litis b
eing l
ess
comm
on.8 O
ther s
ites o
f infec
tion,
besid
es sk
in an
d soft
tissu
e, ar
e un
comm
on an
d hav
e bee
n des
cribe
d in c
ase r
epor
ts an
d sma
ll cas
e se
ries.
Exam
ples i
nclud
e men
ingitis
, foca
l bra
in les
ions,
uppe
r and
lowe
r re
spira
tory t
ract
infec
tions
, and
intra
-abd
omina
l infec
tions
and t
ypica
lly
occu
r in pr
edisp
osed
patie
nts w
ith un
derly
ing lu
ng or
liver
dise
ase.
9 A
high p
ropo
rtion o
f pati
ents
with
comp
licati
on of
septi
c sho
ck ex
hibite
d se
rious
unde
rlying
med
ical c
ondit
ions.
A lite
ratur
e rev
iew fo
r Pa
steur
ella s
eptic
shoc
k in a
n othe
rwise
healt
hy pa
tient
yields
only
a few
case
repo
rts, w
hich d
escri
be pr
eviou
sly he
althy
indiv
iduals
who
de
velop
ed se
ptic s
hock
and D
IC.10
Spe
cific
skin
findin
gs in
cludin
g pu
rpur
a fulm
inans
wer
e not
desc
ribed
. Em
piric
antim
icrob
ial th
erap
y for
infec
ted do
g and
cat b
ite w
ound
s sh
ould
includ
e cov
erag
e aga
inst P
aste
urell
a, str
eptoc
occi,
sta
phylo
cocc
i, and
anae
robic
spec
ies. T
he co
mbina
tion o
f a pe
nicilli
n wi
th a b
eta-la
ctama
se in
hibito
r is w
idely
reco
mmen
ded f
or pa
tients
wi
th no
histo
ry of
penic
illin a
llerg
y. Ot
her o
ption
s inc
lude
levofl
oxac
in
We d
escri
be a
case
of P
aste
urell
a sep
sis co
mplic
ated b
y dis
semi
nated
intra
vasc
ular c
oagu
lopath
y with
skin
findin
gs of
purp
ura
fulmi
nans
. The
mos
t com
mon i
nfecti
ons c
ause
d by P
. mult
ocida
are
local
woun
d infe
ction
s foll
owing
anim
al bit
es or
scra
tches
. Mor
e se
vere
infec
tions
inclu
ding s
epsis
, men
ingitis
, or p
ulmon
ary d
iseas
e typ
ically
occu
r in pa
tients
with
unde
rlying
med
ical p
roble
ms. A
lite
ratur
e sea
rch re
veals
only
a han
dful o
f cas
e rep
orts
of P.
mult
ocida
se
psis
occu
rring
in pr
esum
ably
healt
hy in
dividu
als. M
anag
emen
t of
purp
ura f
ulmina
ns is
also
revie
wed.
Figu
re 3.
Pun
cture
wou
nd of
the
lower
leg f
rom
a cat
bite.
The t
erm
'retifo
rm pu
rpur
a' de
scrib
es le
sions
that
demo
nstra
te an
an
gulat
ed or
bran
ched
confi
gura
tion a
nd oc
curs
in a v
ariet
y of
disor
ders
as a
cons
eque
nce o
f disr
upted
vasc
ular f
low in
the s
kin or
su
bcuti
s due
to ve
ssel
occlu
sion.
1 Ves
sel o
cclus
ion ca
n res
ult fr
om
throm
bosis
or ve
ssel
wall d
estru
ction
. If is
chem
ia is
prolo
nged
, skin
ne
crosis
due t
o infa
rction
may
be pr
esen
t.
The t
erm
'purp
ura f
ulmina
ns' re
fers t
o wide
spre
ad re
tiform
purp
ura a
nd
occu
rs in
seve
ral c
linica
l sett
ings,
most
notab
ly in
patie
nts w
ho ar
e cri
ticall
y ill w
ith D
IC. P
urpu
ra fu
lmina
ns in
the l
atter
case
is th
ough
t to
be a
resu
lt of a
cquir
ed pr
otein
C de
ficien
cy 2 ,
and i
s mos
t com
monly
att
ribute
d to m
ening
ococ
cemi
a.
Purp
ura f
ulmina
ns in
a se
ptic p
atien
t is an
omino
us si
gn to
the
serio
usne
ss of
the u
nder
lying
cond
ition.
Repla
ceme
nt of
defic
ient
blood
comp
onen
ts wi
th fre
sh fr
ozen
plas
ma an
d clot
ting f
actor
s and
tre
ating
the u
nder
lying
caus
e are
the m
ainsta
y of th
erap
y. St
udies
with
ac
tivate
d pro
tein C
conc
entra
te ha
ve sh
own p
romi
sing r
esult
s in
reve
rsing
purp
ura f
ulmina
ns on
ce th
e pro
cess
has b
egun
.3
REFE
RENC
ES
This
case
demo
nstra
tes an
unus
ual c
ause
of p
urpu
ra fu
lmina
ns in
a pa
tient
with
Paste
urell
a sep
sis. I
t stre
sses
the i
mpor
tance
of
reco
gnizi
ng ca
t bite
s as a
poten
tial c
ause
for m
ore s
eriou
s infe
ction
s, ev
en in
seem
ingly
healt
hy in
dividu
als. P
roph
ylacti
c anti
biotic
s sho
uld
be im
pleme
nted w
ithin
24 ho
urs f
or pu
nctur
e wou
nds,
espe
cially
if the
pa
tient
has u
nder
lying
cirrh
osis.
Anti
biotic
choic
e sho
uld be
base
d on
the m
ultipl
e stud
ies de
mons
tratin
g tha
t cat
and d
og bi
te wo
unds
are
polym
icrob
ial. O
ur ca
se al
so de
mons
trates
that
in se
ptic p
atien
ts,
multip
le blo
od cu
lture
s may
be ne
cess
ary t
o ide
ntify
the cu
lprit,
given
tha
t cer
tain o
rgan
isms s
uch a
s Pas
teur
ella
mult
ocida
are f
astid
ious.
Al
thoug
h a tis
sue c
ultur
e fro
m the
bite
woun
d was
not p
erfor
med,
in re
trosp
ect, i
t may
have
been
helpf
ul sh
ould
the bl
ood c
ultur
es ha
ve
rema
ined n
egati
ve. F
urthe
rmor
e, ea
rly re
cogn
ition o
f pur
pura
fulm
inans
inf
ectio
ns m
ay tr
ansla
te int
o ear
ly im
pleme
ntatio
n of fr
esh f
roze
n pla
sma o
r pro
tein C
conc
entra
te to
halt e
volut
ion of
skin
lesion
s.
Purp
ura i
s a br
oad t
erm
used
to de
scrib
e non
blanc
hable
, he
morrh
agic
skin
lesion
s tha
t res
ult fr
om lo
cal e
xtrav
asati
on of
red
blood
cells
in th
e skin
. Plat
elet d
isord
ers o
r exc
essiv
e pre
ssur
e ap
plied
to th
e skin
may
caus
e dam
age t
o sup
erfic
ial ca
pillar
ies or
sm
all ca
liber
vess
els an
d pre
sent
as sm
all, p
urpu
ric le
sions
1 - 2
mm
in dia
meter
refer
red t
o as p
etech
iae.
DISC
USSI
ON (c
ont’d
)
Figu
re 2.
Pete
chiae
.

246
Tem
plat
e pr
ovid
ed b
y: “p
oste
rs4r
esea
rch.
com
”
Trea
tmen
t of
Ver
ruca
Vul
gari
s w
ith
Nd:
YAG
106
4nm
Las
er
Win
ifred
S. C
hu, D
.O.,
M.P
.H.
St. J
ohn’
s Ep
isco
pal H
ospi
tal-
Dep
artm
ent o
f Der
mat
olog
y- D
r. M
arvi
n W
atsk
y, D
.O.
Prog
ram
Dire
ctor
Abst
ract
C
ase P
rese
ntat
ion
V
erru
ca vu
lgaris
(com
mon w
arts)
are c
ause
d by H
PV in
fectio
n of th
e epit
helia
l tis
sues
of th
e skin
and m
ucou
s mem
bran
es. T
hey m
ay be
foun
d any
wher
e on t
he sk
in,
partic
ularly
on th
e dor
sum
of the
hand
, betw
een t
he fin
gers,
and a
roun
d the
nails
(p
eriun
gual)
. Tre
atmen
t opti
ons o
f ver
ruca
inclu
de: c
ryothe
rapy
with
liquid
nitro
gen,
salic
ylic
acid,
duct
tape,
canth
aridi
n, ble
omyc
in, su
rgica
l abla
tion,
cure
ttage
and d
esicc
ation
, 5-
Fluor
oura
cil, tr
etino
in, ci
metid
ine, im
iquim
od, in
trales
ional
immu
nothe
rapy
, and
lase
r tre
atmen
t usin
g puls
ed dy
e las
er, an
d CO2
lase
r. La
sers
such
as N
d:YAG
and K
TP 53
2nm
we
re re
porte
d to b
e effe
ctive
but th
ere i
s les
s evid
ence
for t
heir u
se. W
e pre
sent
a cas
e of a
39
year
-old
female
with
a wa
rt on
her f
inger
that
was r
esist
ant to
diffe
rent
thera
pies.
Ho
weve
r, afte
r the
use o
f four
Nd:Y
AG 1
064n
m las
er tr
eatm
ents,
the w
art w
as co
mplet
ely
destr
oyed
. This
case
illus
trates
and s
uppo
rts th
e effe
ctive
ness
of us
ing N
d:YAG
1064
nm
laser
ther
apy f
or tr
eatm
ent o
f ver
ruca
vulga
ris th
at do
not r
espo
nd to
stan
dard
ther
apy.
Ear
ly ins
titutio
n of th
is tre
atmen
t opti
on ca
n help
to pr
even
t war
t gro
wth a
nd sp
read
ing, a
nd al
low
for ea
rly di
seas
e rem
ission
.
A
39-ye
ar-o
ld Ca
ucas
ian fe
male
pres
ents
to a p
rivate
derm
atolog
y pra
ctice
with
a 2m
m, no
n-pr
uritic
, per
iungu
al, ve
rruco
us pa
pule
on he
r righ
t third
finge
r. Th
e les
ion w
as fir
st no
ticed
to be
a fle
sh-co
lored
bump
whic
h gre
w in
size o
ver t
he pa
st few
mon
ths.
A dia
gnos
is of
verru
ca vu
lgaris
was
mad
e, an
d pati
ent r
eceiv
ed m
ultipl
e tre
atmen
t ses
sions
using
liquid
nit
roge
n for
war
t des
tructi
on. H
owev
er, sh
e rep
orted
no im
prov
emen
t at h
er fo
llow-
up vi
sits
and t
he w
art r
emain
ed to
be of
the s
ame s
ize. S
ubse
quen
tly, p
atien
t was
pres
cribe
d top
ical
treatm
ents
includ
ing A
ldara
5% cr
eam,
Ver
egen
15%
ointm
ent, a
nd Z
yclar
a but
they d
id no
t sig
nifica
ntly h
elp to
decre
ase t
he si
ze of
the w
art.
At he
r ten
th vis
it to o
ur of
fice,
patie
nt be
gan t
o rec
eive N
d:YAG
1064
nmm
laser
ther
apy f
or w
art tr
eatm
ent a
t two w
eeks
inter
val.
After
the c
omple
tion o
f the f
ourth
lase
r tre
atmen
t, the
war
t was
comp
letely
destr
oyed
. HP
I: 39 y
ear-o
ld Ca
ucas
ian fe
male
pres
ents
to the
derm
atolog
y offic
e c/o
a non
-itchy
, un
painf
ul bu
mp on
her f
inger
that
has b
een i
ncre
asing
in si
ze fo
r the
past
few m
onths
. PM
H: de
nies
PS
H: de
nies
Me
ds: d
enies
Al
lergie
s: NK
DA
Socia
l Hx:
denie
s tob
acco
, alco
hol o
r illic
it dru
g use
FH
: non
-contr
ibutor
y RO
S: de
nies a
ny sy
stemi
c sym
ptoms
PE
: 2mm
flesh
-color
ed, fi
rm, h
yper
kera
totic,
verru
cous
papu
le wi
th dis
rupti
on of
norm
al fin
gerp
rint li
nes a
nd di
splay
of sm
all bl
ack d
ots (t
hrom
bose
d cap
illarie
s) on
right
midd
le thi
rd
finge
r clos
e to t
he na
il Dx
: Ver
ruca
Vulg
aris
(bas
ed up
on cl
inica
l app
eara
nce)
Ma
nage
ment:
cryo
thera
py w
ith liq
uid ni
troge
n, po
doph
yllin,
Alda
ra 5%
crea
m Qd
x8 w
ks,
Vere
gen 1
5% oi
ntmen
t Tid
x 4 w
ks, Z
yclar
a 3.75
% cr
eam
Qd x
4wks
, 4 tr
eatm
ents
with
Nd:Y
AG 10
64 nm
lase
r (2m
m sp
ot, po
wer 8
/9, 2
pass
es).
Disc
ussio
n
Figu
re 2.
Bef
ore (
left)
and A
fter (
right
) Las
er Tr
eatm
ent
Ve
rruca
vulga
ris ar
e cau
sed b
y HPV
infec
tion (
subty
pes 1
,2,4,2
7,57,
and 6
3), a
nd oc
cur
mostl
y in c
hildr
en an
d you
ng ad
ults.
The
y are
usua
lly as
ympto
matic
, and
are t
rans
mitte
d via
skin-
to-sk
in co
ntact.
Tra
uma a
nd m
acer
ation
may
facil
itate
initia
l epid
erma
l inoc
ulatio
n, an
d spr
eadin
g ma
y sub
sequ
ently
occu
r by a
utoino
culat
ion.
Comm
on w
arts
are o
ften p
rese
nt as
well
-de
marca
ted, r
ough
, har
d nod
ules o
r plaq
ues w
ith irr
egula
r sur
faces
. Diag
nosis
of v
erru
ca is
ba
sed u
pon c
linica
l app
eara
nce.
Spo
ntane
ous r
emiss
ion of
war
ts oc
curs
in up
to tw
o-thi
rds o
f pa
tients
with
in tw
o yea
rs; he
nce,
obse
rvatio
n is a
n opti
on fo
r all p
atien
ts. H
owev
er, re
curre
nce o
f ve
rruca
is co
mmon
, so i
t is be
tter a
nd ea
sier t
o tre
at a w
art w
hen i
t is sm
aller
in si
ze th
an w
ait
until
it enla
rges
or m
ultipl
e to i
nitiat
e tre
atmen
t.
Trea
tmen
t of v
erru
ca in
volve
s two
appr
oach
es: d
estru
ction
of w
art a
nd in
ducti
on of
loca
l im
mune
reac
tion w
ith im
muno
thera
py.
Destr
uctiv
e meth
ods a
re m
ost c
ommo
nly us
ed as
initia
l the
rapy
and t
hey i
nclud
e cryo
surg
ery,
electr
ocau
tery,
cure
ttage
, exc
ision
, lase
r the
rapy
. Im
muno
thera
py is
aime
d at e
licitin
g an
immu
ne re
spon
se to
HPV
whic
h may
be ac
hieve
d by
apply
ing to
pical
irrita
nt su
ch as
salic
ylic a
cid, c
antha
ridin,
trich
loroa
cetic
acid
, pod
ophy
llum
resin
, 5-
Fluor
oura
cil, o
r tre
tinoin
over
the w
art.
Thes
e com
poun
ds ca
n also
be us
ed in
comb
inatio
n or
with
a des
tructi
ve m
ethod
. Anti
viral
effec
t can
be ac
hieve
d with
bleo
mycin
and i
nterfe
ron ɑ
2b bu
t the
y are
rese
rved f
or re
calci
trant
warts
. Imi
quim
od 5%
crea
m ma
y be u
sed t
o ind
uce s
kin lo
cally
to
prod
uce a
ntivir
al cy
tokine
s. In
trales
ional
immu
nothe
rapy
with
skin
test a
ntige
ns (ie
: mum
ps,
Cand
ida, o
r Tric
hoph
yton a
ntige
ns) a
nd H
PV va
ccine
have
demo
nstra
ted su
cces
s in t
reati
ng
warts
. Les
ions t
hat h
ave f
ailed
to re
spon
d to r
outin
e offic
e mod
alitie
s are
often
succ
essfu
lly
treate
d with
lase
r the
rapy
such
as ca
rbon
diox
ide or
pulse
d dye
lase
r. Nd
:YAG
1064
nm la
ser
have
also
been
repo
rted t
o be s
ucce
ssful
in tr
eatin
g ver
ruca
, and
has r
eceiv
ed F
DA cl
eara
nce f
or
this i
ndica
tion.
The N
d:YAG
106
4nm
laser
trea
tmen
t invo
lves t
he de
liver
y of la
ser li
ght ir
radia
tion a
t wa
velen
gth 10
64nm
, whic
h allo
ws p
enetr
ation
into
deep
er an
d thic
ker t
issue
comp
aring
to sh
orter
wa
velen
gth la
sers,
and t
he la
ser u
sed i
n this
stud
y doe
s not
conta
ct the
verru
ca. T
his la
ser is
also
us
ed fo
r tre
ating
vasc
ular &
pigm
ented
lesio
ns, h
air an
d PFB
remo
val, s
kin re
juven
ation
, on
ycho
myco
sis an
d man
y othe
r aes
thetic
and m
edica
l trea
tmen
ts. A
minim
um o
f one
to tw
o tre
atmen
t ses
sions
are n
eede
d, wi
th se
ssion
s spa
ced b
etwee
n two
to th
ree w
eeks
apar
t. Tr
eatm
ent s
essio
ns us
ually
begin
using
a foc
used
lens
with
a 2m
m sp
ot un
der t
he se
ttings
of
1.5ms
pulse
dura
tion a
nd en
ergy
mod
e of 8
or 9
(fluen
ce of
255 J
/cm² t
o 287
J/cm
²). A
s in t
he
case
of ou
r pati
ent, a
total
of tw
o pas
ses o
ver t
he w
art w
ere a
pplie
d with
each
trea
tmen
t ses
sion
and p
atien
t toler
ated t
he tr
eatm
ent v
ery w
ell. U
pon t
he en
d of th
e fou
rth tr
eatm
ent s
essio
n, the
pa
tient’
s war
t was
comp
letely
destr
oyed
. Bas
ed on
the c
ase t
hat w
e hav
e jus
t pre
sente
d, we
have
de
mons
trated
the s
ucce
ss of
utiliz
ing N
d:YAG
1064
nm la
ser in
trea
ting v
erru
ca th
at ha
d fail
ed in
re
spon
ding t
o stan
dard
trea
tmen
t. Der
matol
ogist
s sho
uld co
nside
r usin
g this
lase
r the
rapy
early
in
the co
urse
of tr
eatin
g res
istan
t war
ts sin
ce it
is we
ll tole
rated
by pa
tients
, and
it pr
ovide
s tim
ely,
signif
icant
resu
lts w
hich h
elp to
bring
dise
ase r
emiss
ion.
Tabl
e I.
Refe
renc
es
Figu
re 1.
Nd:
YAG
1064
nm L
aser
Pen
etra
tion
of d
epth
– T
echn
olog
y E
volu
tion
Bour
ke J
F, Be
rth-
Jone
s J,
Hutc
hins
on P
E. C
ryot
hera
py o
f com
mon
vira
l war
ts a
t int
erva
ls of
1, 2
and
3 w
eeks
. Br
J De
rmat
ol 1
995;
132
:433
. Bu
nney
MH,
Nol
an M
W, W
illia
ms D
A. A
n as
sess
men
t of m
etho
ds o
f tre
atin
g vi
ral w
arts
by
com
para
tive
trea
tmen
t tria
ls ba
sed
on a
stan
dard
des
ign.
Br J
Der
mat
ol 1
976;
94:
667.
Fo
cht D
R, S
pice
r C, F
airc
hok
MP.
The
effi
cacy
of d
uct t
ape
vs p
lace
bo in
the
trea
tmen
t of v
erru
ca v
ulga
ris (t
he c
omm
on
war
t).
Arch
Ped
iatr
Ado
lesc
Med
200
2; 1
56:9
71.
Jam
es W
D, B
erge
r TG,
Elst
on D
M. A
ndre
w’s
Dise
ases
of t
he S
kin:
Clin
ical
Der
mat
olog
y, 10
th E
d. P
hila
delp
hia:
WB
Saun
ders
, 20
00: 4
03-4
07.
John
son
SM, R
ober
son
PK, H
orn
TD.
Intr
ales
iona
l inj
ectio
n of
mum
ps o
r Can
dida
skin
test
ant
igen
s: a
nov
el
imm
unot
hera
py fo
r war
ts.
Arch
Der
mat
ol 2
003;
20:
268.
Ro
ss B
S, L
evin
e VJ
, Neh
al K
, et a
l. Pu
lsed
dye
lase
r tre
atm
ent o
f war
ts: a
n up
date
. Der
mat
ol S
urg
1999
; 25:
377.
Sl
oan
K, H
aber
man
H, L
ynde
CW
. Ca
rbon
dio
xide
lase
r-tr
eatm
ent o
f res
istan
t ver
ruca
e vu
lgar
is: re
tros
pect
ive
anal
ysis.
J
Cuta
n M
ed S
urg.
199
8; 2
(3):1
42-5
. ht
tp:/
/ww
w.m
erck
man
uals.
com
/pro
fess
iona
l/sec
10/c
h122
/ch1
22c.
htm
l.
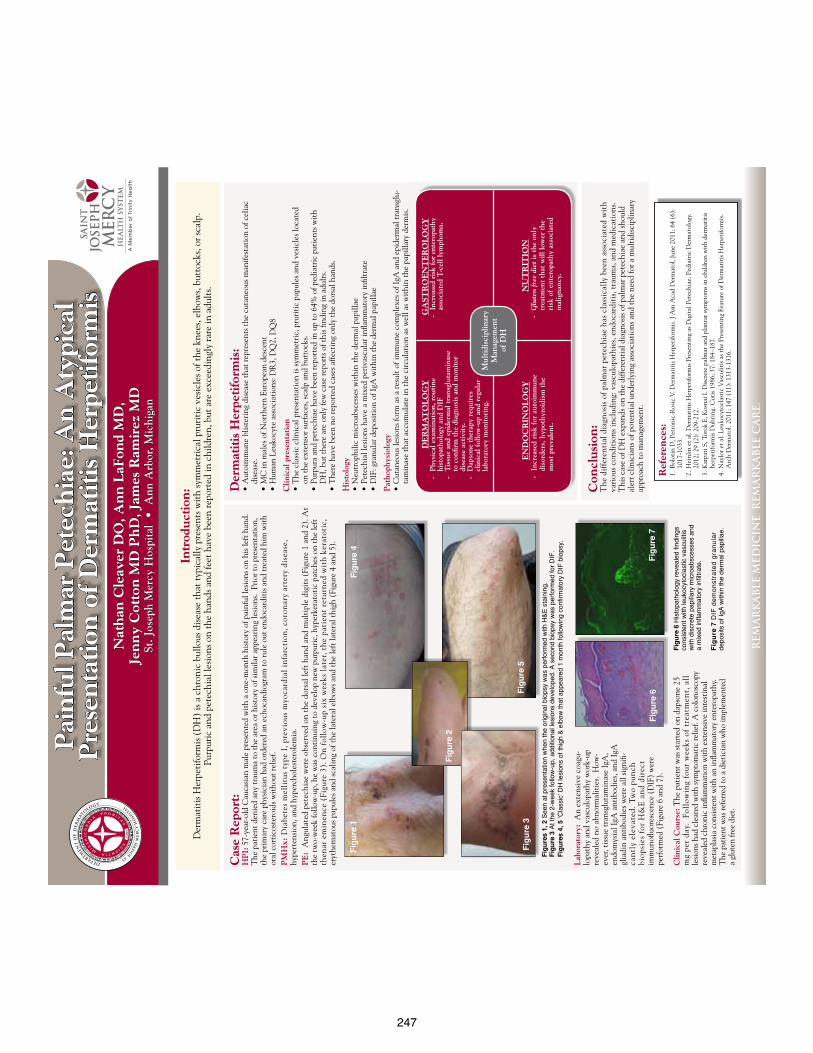
247
Pai
nfu
l Pal
mar
Pet
ech
iae:
An
Aty
pica
l P
rese
nta
tion
of
Der
mat
itis
Her
peti
form
isN
ath
an C
leav
er D
O, A
nn
LaF
ond
MD
, Je
nn
y C
otto
n M
D P
hD
, Jam
es R
amir
ez M
D
St. J
osep
h M
ercy
Hos
pita
l •
Ann
Arb
or, M
ichi
gan
REM
AR
KA
BLE
MED
ICIN
E. R
EMA
RK
AB
LE C
AR
E.
Cas
e R
epor
t:H
PI:
57-
year
-old
Cau
casi
an m
ale
pres
ente
d w
ith
a on
e-m
onth
his
tory
of p
ainf
ul le
sion
s on
his l
eft h
and.
T
he p
atie
nt d
enie
d an
y tr
aum
a to
the
area
or h
isto
ry o
f sim
ilar a
ppea
ring
lesi
ons.
Pri
or to
pre
sent
atio
n,
the
prim
ary
care
phy
sici
an h
ad o
rder
ed a
n ec
hoca
rdio
gram
to ru
le o
ut e
ndoc
ardi
tis a
nd tr
eate
d hi
m w
ith
oral
cor
tico
ster
oids
wit
hout
relie
f.
PM
Hx:
Dia
bete
s m
elli
tus
type
I, p
revi
ous
myo
card
ial
infa
rcti
on, c
oron
ary
arte
ry d
isea
se,
hype
rten
sion
, and
hyp
erch
oles
tero
lem
ia.
PE
: A
ngul
ated
pet
echi
ae w
ere
obse
rved
on
the
dors
al le
ft h
and
and
mul
tipl
e di
gits
(Fi
gure
1 a
nd 2
). A
t th
e tw
o-w
eek
follo
w-u
p, h
e w
as c
onti
nuin
g to
dev
elop
new
pur
puri
c, h
yper
kera
toti
c pa
tche
s on
the
left
th
enar
em
inen
ce (
Figu
re 3
). O
n f
ollo
w-u
p si
x w
eeks
lat
er, t
he
pati
ent
retu
rned
wit
h k
erat
otic
, er
ythe
mat
ous p
apul
es a
nd sc
alin
g of
the
late
ral e
lbow
s and
the
left
late
ral t
high
(Fi
gure
4 a
nd 5
).
Ref
eren
ces:
1.
Bol
otin
D, P
etro
nic-
Ros
ic V
. Der
mat
itis
Her
peti
form
is. J
Am
Aca
d D
erm
atol
. Jun
e 20
11; 6
4 (6
):
1017
-103
3.2.
Hei
nlin
et a
l. D
erm
atit
is H
erpe
tifo
rmis
Pre
sent
ing
as D
igit
al P
etec
hiae
. Ped
iatr
ic D
erm
atol
ogy.
20
12; 2
9 (2
): 2
09-2
12.
3. K
arpa
ti S
, Tor
ok E
, Kos
nai I
. Dis
cret
e pa
lmar
and
pla
ntar
sym
ptom
s in
child
ren
wit
h de
rmat
itis
he
rpet
iform
is D
uhri
ng. C
utis
198
6; 3
7: 1
84–1
87.
4. N
aylo
r et a
l. Le
ukoc
ytoc
last
ic V
ascu
litis
as t
he P
rese
ntin
g Fe
atur
e of
Der
mat
itis
Her
peti
form
is.
Arc
h D
erm
atol
. 201
1; 1
47 (
11):
131
3-13
16.
Figu
res
1, 2
See
n at
pre
sent
atio
n w
hen
the
orig
inal
bio
psy
was
per
form
ed w
ith H
&E s
tain
ing.
Fi
gure
3 A
t the
2-w
eek
follo
w-u
p, a
dditi
onal
lesi
ons
deve
lope
d. A
sec
ond
biop
sy w
as p
erfo
rmed
for D
IF.
Figu
res
4, 5
‘Cla
ssic
’ DH
lesi
ons
of th
igh
& el
bow
that
app
eare
d 1
mon
th fo
llow
ing
confi
rmat
ory
DIF
bio
psy.
Con
clu
sion
: T
he d
iffe
rent
ial d
iagn
osis
of p
alm
ar p
etec
hiae
has
cla
ssic
ally
bee
n as
soci
ated
wit
h
vari
ous
cond
itio
ns in
clud
ing:
vas
culo
path
ies,
end
ocar
diti
s, t
raum
a, a
nd m
edic
atio
ns.
T
his c
ase
of D
H e
xpan
ds o
n th
e di
ffere
ntia
l dia
gnos
is o
f pal
mar
pet
echi
ae a
nd sh
ould
al
ert c
linic
ians
of p
oten
tial
und
erly
ing
asso
ciat
ions
and
the
need
for a
mul
tidi
scip
linar
y ap
proa
ch to
man
agem
ent.
Intr
odu
ctio
n:
Der
mat
itis
Her
peti
form
is (
DH
) is
a c
hron
ic b
ullo
us d
isea
se th
at ty
pica
lly p
rese
nts w
ith
sym
met
rica
l pru
riti
c ve
sicl
es o
f the
kne
es, e
lbow
s, bu
ttoc
ks, o
r sca
lp.
Pu
rpur
ic a
nd p
etec
hial
lesi
ons o
n th
e ha
nds a
nd fe
et h
ave
been
repo
rted
in c
hild
ren,
but
are
exc
eedi
ngly
rare
in a
dult
s.
Lab
orat
ory:
An
exte
nsiv
e co
agu-
lopa
thy
and
vasc
ulop
athy
wor
k-up
re
veal
ed n
o ab
norm
alit
ies.
How
-ev
er, t
issu
e tr
ansg
luta
min
ase
IgA
, en
dom
ysia
l IgA
ant
ibod
ies,
and
IgA
gl
iadi
n an
tibo
dies
wer
e al
l sig
nifi-
can
tly
elev
ated
. Tw
o pu
nch
bi
opsi
es f
or H
&E
an
d di
rect
im
mun
ofluo
resc
ence
(D
IF)
wer
e pe
rfor
med
(Fi
gure
6 a
nd 7
).
Der
mat
itis
Her
peti
form
is:
• A
utoi
mm
une
blis
teri
ng d
isea
se th
at re
pres
ents
the
cuta
neou
s man
ifest
atio
n of
cel
iac
di
seas
e.
• M
C in
mal
es o
f Nor
ther
n Eu
rope
an d
esce
nt
• H
uman
Leu
kocy
te a
ssoc
iati
ons:
DR
3, D
Q2,
DQ
8
Clin
ical
pre
sent
atio
n•
The
cla
ssic
clin
ical
pre
sent
atio
n is
sym
met
ric,
pru
riti
c pa
pule
s and
ves
icle
s loc
ated
on
the
exte
nsor
surf
aces
, sca
lp a
nd b
utto
cks.
• P
urpu
ra a
nd p
etec
hiae
hav
e be
en re
port
ed in
up
to 6
4% o
f ped
iatr
ic p
atie
nts w
ith
D
H, b
ut th
ere
are
only
few
cas
e re
port
s of t
his fi
ndin
g in
adu
lts.
•
The
re h
ave
been
no
repo
rted
cas
es a
ffect
ing
only
the
dors
al h
ands
.
His
tolo
gy•
Neu
trop
hilic
mic
roab
sces
ses w
ithi
n th
e de
rmal
pap
illae
• P
etec
hial
lesi
ons h
ave
a m
ixed
per
ivas
cula
r infl
amm
ator
y in
filtr
ate
• D
IF: g
ranu
lar d
epos
itio
n of
IgA
wit
hin
the
derm
al p
apill
ae
Pat
hoph
ysio
logy
• C
utan
eous
lesi
ons f
orm
as a
resu
lt o
f im
mun
e co
mpl
exes
of I
gA a
nd e
pide
rmal
tran
sglu
-ta
min
ase
that
acc
umul
ate
in th
e ci
rcul
atio
n as
wel
l as w
ithi
n th
e pa
pilla
ry d
erm
is.
Figu
re 6
His
topa
thol
ogy
reve
aled
find
ings
co
nsis
tent
with
leuk
ocyt
ocla
stic
vas
culit
is
with
dis
cret
e pa
pilla
ry m
icro
absc
esse
s an
d
a m
ixed
infla
mm
ator
y in
filtra
te.
Figu
re 7
DIF
dem
onst
rate
d gr
anul
ar
depo
sits
of I
gA w
ithin
the
derm
al p
apilla
e.
Figu
re 1
Figu
re 2
Figu
re 3
Figu
re 4
Figu
re 5
Figu
re 6
Figu
re 7
Clin
ical
Cou
rse:
The
pat
ient
was
star
ted
on d
apso
ne 2
5 m
g pe
r da
y.
Foll
owin
g fo
ur w
eeks
of
trea
tmen
t, a
ll
lesi
ons h
ad c
lear
ed w
ith
sym
ptom
atic
relie
f. A
col
onos
copy
re
veal
ed c
hron
ic in
flam
mat
ion
wit
h ex
tens
ive
inte
stin
al
met
apla
sia
cons
iste
nt w
ith
an in
flam
mat
ory
ente
ropa
thy.
T
he p
atie
nt w
as re
ferr
ed to
a d
ieti
cian
who
impl
emen
ted
a
glut
en fr
ee d
iet.
DE
RM
AT
OL
OG
Y-
Phy
sica
l exa
min
atio
n, r
outi
ne
hi
stop
atho
logy
and
DIF
- T
issu
e an
d ep
ider
mal
tra
nsgl
utam
inas
e
to c
onfir
m t
he d
iagn
osis
and
mon
itor
dise
ase
acti
vity
. -
Dap
sone
the
rapy
req
uire
s
cl
inic
al f
ollo
w-u
p an
d re
gula
r
la
bora
tory
mon
itor
ing.
GA
STR
OE
NT
ER
OL
OG
Y
- In
crea
sed
risk
for
ente
ropa
thy
asso
ciat
ed T
-cel
l lym
phom
a.
NU
TR
ITIO
N
- G
lute
n fr
ee d
iet
is t
he o
nly
trea
tmen
t th
at w
ill lo
wer
the
risk
of
ente
ropa
thy
asso
ciat
ed
m
alig
nanc
y.
EN
DO
CR
INO
LO
GY
-
Incr
ease
d ri
sk f
or a
utoi
mm
une
diso
rder
s, h
ypot
hyro
idis
m t
he
m
ost
prev
alen
t.
Mul
tidi
scip
linar
y M
anag
emen
tof
DH
248
QU
ICK
DES
IGN
GU
IDE
(--T
HIS
SEC
TIO
N D
OES
NO
T PR
INT-
-)
Th
is P
ower
Poin
t 20
07 t
empl
ate
prod
uces
a 3
6”x6
0”
prof
essi
onal
pos
ter.
It w
ill s
ave
you
valu
able
tim
e pl
acin
g ti
tles
, su
btit
les,
tex
t, a
nd g
raph
ics.
U
se it
to
crea
te y
our
pres
enta
tion
. Th
en s
end
it t
o Po
ster
Pres
enta
tion
s.co
m f
or p
rem
ium
qua
lity,
sam
e da
y af
ford
able
pri
ntin
g.
We
prov
ide
a se
ries
of
onlin
e tu
tori
als
that
will
gui
de y
ou
thro
ugh
the
post
er d
esig
n pr
oces
s an
d an
swer
you
r po
ster
pr
oduc
tion
que
stio
ns.
Vi
ew o
ur o
nlin
e tu
tori
als
at:
htt
p://
bit.
ly/P
oste
r_cr
eati
on_h
elp
(c
opy
and
past
e th
e lin
k in
to y
our
web
bro
wse
r).
For
assi
stan
ce a
nd t
o or
der
your
pri
nted
pos
ter
call
Post
erPr
esen
tati
ons.
com
at 1.
866.
649.
3004
Obj
ect
Plac
ehol
ders
Use
the
pla
ceho
lder
s pr
ovid
ed b
elow
to
add
new
ele
men
ts
to y
our
post
er:
Dra
g a
plac
ehol
der
onto
the
pos
ter
area
, si
ze it
, an
d cl
ick
it t
o ed
it.
Sect
ion
Hea
der
plac
ehol
der
Use
sec
tion
hea
ders
to
sepa
rate
top
ics
or c
once
pts
wit
hin
your
pre
sent
atio
n.
Text
pla
ceho
lder
M
ove
this
pre
form
atte
d te
xt p
lace
hold
er t
o th
e po
ster
to
add
a ne
w b
ody
of t
ext.
Pi
ctur
e pl
aceh
olde
r M
ove
this
gra
phic
pla
ceho
lder
ont
o yo
ur p
oste
r, s
ize
it
firs
t, a
nd t
hen
clic
k it
to
add
a pi
ctur
e to
the
pos
ter.
RES
EAR
CH
PO
STER
PR
ESEN
TATI
ON
DES
IGN
© 2
011
ww
w.P
oste
rPre
sent
atio
ns.c
om
QU
ICK
TIPS
(-
-TH
IS S
ECTI
ON
DO
ES N
OT
PRIN
T--)
Th
is P
ower
Poin
t te
mpl
ate
requ
ires
bas
ic P
ower
Poin
t (v
ersi
on 2
007
or n
ewer
) sk
ills.
Bel
ow is
a li
st o
f co
mm
only
as
ked
ques
tion
s sp
ecif
ic t
o th
is t
empl
ate.
If
you
are
usi
ng a
n ol
der
vers
ion
of P
ower
Poin
t so
me
tem
plat
e fe
atur
es m
ay n
ot w
ork
prop
erly
.
Usi
ng t
he t
empl
ate
Veri
fyin
g th
e qu
alit
y of
you
r gr
aphi
cs
Go
to t
he V
IEW
men
u an
d cl
ick
on Z
OO
M t
o se
t yo
ur
pref
erre
d m
agni
fica
tion
. Th
is t
empl
ate
is a
t 50
% th
e si
ze
of t
he f
inal
pos
ter.
All
text
and
gra
phic
s w
ill b
e pr
inte
d at
20
0% t
heir
siz
e. T
o se
e w
hat
your
pos
ter
will
look
like
w
hen
prin
ted,
set
the
zoo
m t
o 20
0% a
nd e
valu
ate
the
qual
ity
of a
ll yo
ur g
raph
ics
befo
re y
ou s
ubm
it y
our
post
er
for
prin
ting
. U
sing
the
pla
ceho
lder
s To
add
tex
t to
thi
s te
mpl
ate
clic
k in
side
a p
lace
hold
er a
nd
type
in o
r pa
ste
your
tex
t. T
o m
ove
a pl
aceh
olde
r, c
lick
on
it o
nce
(to
sele
ct it
), p
lace
you
r cu
rsor
on
its
fram
e an
d yo
ur c
urso
r w
ill c
hang
e to
thi
s sy
mbo
l:
Then
, cl
ick
once
and
dra
g it
to
its
new
loca
tion
whe
re y
ou c
an r
esiz
e it
as
need
ed.
Addi
tion
al p
lace
hold
ers
can
be f
ound
on
the
left
sid
e of
thi
s te
mpl
ate.
M
odif
ying
the
layo
ut
This
tem
plat
e ha
s fo
ur
diff
eren
t co
lum
n la
yout
s.
Righ
t-cl
ick
your
mou
se
on t
he b
ackg
roun
d an
d
clic
k on
“La
yout
” to
see
th
e la
yout
opt
ions
. Th
e co
lum
ns in
the
pro
vide
d la
yout
s ar
e fi
xed
and
cann
ot
be m
oved
but
adv
ance
d us
ers
can
mod
ify
any
layo
ut b
y go
ing
to V
IEW
and
the
n SL
IDE
MAS
TER.
Im
port
ing
text
and
gra
phic
s fr
om e
xter
nal s
ourc
es
TEXT
: Pa
ste
or t
ype
your
tex
t in
to a
pre
-exi
stin
g pl
aceh
olde
r or
dra
g in
a n
ew p
lace
hold
er f
rom
the
lef
t si
de o
f th
e te
mpl
ate.
Mov
e it
any
whe
re a
s ne
eded
. PH
OTO
S: D
rag
in a
pic
ture
pla
ceho
lder
, si
ze it
fir
st,
clic
k in
it a
nd in
sert
a p
hoto
fro
m t
he m
enu.
TA
BLES
: Yo
u ca
n co
py a
nd p
aste
a t
able
fro
m a
n ex
tern
al
docu
men
t on
to t
his
post
er t
empl
ate.
To
mak
e th
e te
xt f
it
bett
er in
the
cel
ls o
f an
impo
rted
tab
le,
righ
t-cl
ick
on t
he
tabl
e, c
lick
FORM
AT S
HAP
E t
hen
clic
k on
TEX
T BO
X an
d ch
ange
the
INTE
RNAL
MAR
GIN
val
ues
to 0
.25
Mod
ifyi
ng t
he c
olor
sch
eme
To c
hang
e th
e co
lor
sche
me
of t
his
tem
plat
e go
to
the
“Des
ign”
men
u an
d cl
ick
on “
Colo
rs”.
You
can
cho
ose
from
th
e pr
ovid
e co
lor
com
bina
tion
s or
you
can
cre
ate
your
ow
n.
© 2
011
Post
erPr
esen
tatio
ns.c
om
2
117
Four
th S
tree
t , U
nit C
Ber
kele
y C
A 9
4710
pos
terp
rese
nter
@gm
ail.c
om
Stud
ent
disc
ount
s ar
e av
aila
ble
on o
ur F
aceb
ook
page
.
Go
to P
oste
rPre
sent
atio
ns.c
om a
nd c
lick
on t
he F
B ic
on.
A Re
view
and
Upd
ate
on M
elan
ocyt
e St
imul
atin
g H
orm
one
Ther
apy:
Afa
mel
anot
ide
Afam
elan
otid
e (
[Nle
4-D
-Phe
7]-a
lpha
-MSH
) is
an
anal
og o
f al
pha-
mel
anoc
yte
stim
ulat
ing
horm
one
(alp
ha-M
SH)
give
n as
a s
ubcu
tane
ous
inje
ctio
n. A
fam
elan
otid
e is
cur
rent
ly u
nder
goin
g ph
ase
II an
d III
tri
als
in E
urop
e an
d th
e U
S fo
r sk
in d
isea
ses
incl
udin
g vi
tilig
o an
d er
ythr
opoi
etic
pro
topo
rphy
ria.
Af
amel
anot
ide
is c
urre
ntly
on
the
mar
ket
in It
aly
and
Swit
zerl
and
for
pati
ents
wit
h er
ythr
opoi
etic
pro
topo
rphy
ria.
U
nreg
ulat
ed a
nalo
gs a
re b
eing
sol
d on
line
ahea
d of
for
mal
app
rova
l. T
hese
“M
elan
otan
s,”
a co
unte
rfei
t fo
rmul
atio
n, c
an b
e pu
rcha
sed
onlin
e by
the
pub
lic a
nd a
re s
elf-
inje
cted
for
tan
ning
pur
pose
s.
A so
luti
on t
o th
e di
stri
buti
on o
f co
unte
rfei
t m
edic
atio
n m
ay b
e to
app
rove
the
dru
g fo
r ta
nnin
g if
pro
ven
safe
in r
igor
ous
clin
ical
tr
ials
.
Abst
ract
Jord
an F
abrik
ant,
DO*
Kha
sha
Toul
oei,
OM
S –I
V,**
Sta
nley
E S
kopi
t DO,
MSE
, FAO
CD**
*
* 2
nd y
ear D
erm
atol
ogy
Resid
ent,
Lark
in C
omm
unity
Hos
pita
l – N
ova
Sout
heas
tern
Uni
vers
ity C
olle
ge o
f Ost
eopa
thic
Med
icine
, Dep
artm
ent o
f Der
mat
olog
y, M
iam
i, FL
**
Inte
rn, L
argo
Med
ical C
ente
r, La
rgo,
FL
**
*Der
mat
olog
y Re
siden
cy P
rogr
am D
irect
or, N
SUCO
M/L
arki
n Co
mm
unity
Hos
pita
l , S
outh
Mia
mi,
FL
Intr
oduc
tion
Afte
r su
nlig
ht e
xpos
ure,
the
ph
otos
ensi
tivi
ty o
f EP
P ca
uses
pai
n,
follo
wed
by
eryt
hem
a, e
dem
a, a
nd
crus
ting
.
Med
icat
ion
prof
ile
Poly
mor
phic
lig
ht e
rupt
ion
(PM
LE)
is a
n ac
quir
ed d
isor
der
that
is
char
acte
rize
d by
pru
riti
c pa
pule
s, s
mal
l ve
sicl
es,
and
plaq
ues
trig
gere
d by
UVR
. Th
is d
isea
se a
ffec
ts m
ainl
y pe
ople
of
nort
hern
Eur
opea
n de
scen
t w
ho h
ave
skin
rea
ctio
n fo
llow
ing
sunl
ight
exp
osur
e.
Prel
imin
ary
resu
lts
have
bee
n re
port
ed b
y fr
om a
dou
ble
blin
d,
plac
ebo
cont
rolle
d tr
ial,
whi
ch d
emon
stra
ted
that
at
day
15,
pati
ents
ha
d a
redu
ctio
n in
Phy
sici
an G
loba
l Se
veri
ty In
dex
(P=0
.077
) bu
t no
t by
da
y 12
0 (P
=0.4
48).
Afa
mel
anot
ide
is c
urre
ntly
in P
hase
III t
rial
s in
Au
stra
lia a
nd E
urop
e fo
r PM
LE (
20).
Poly
mor
phic
ligh
t eru
ptio
n
Conc
lusi
on
Thus
far
, st
udie
s in
vit
ro a
nd i
n vi
vo in
dica
te t
hat
afam
elan
otid
e is
nei
ther
tox
ic n
or c
arci
noge
nic
and,
in h
uman
s,
afam
elan
otid
e ha
s be
en s
how
n to
indu
ce p
igm
enta
ry r
espo
nse.
Add
itio
nally
, af
amel
anot
ide
redu
ces
the
toxi
c re
spon
se o
f su
nbur
ned
cells
, w
hile
it a
lso
has
the
abili
ty t
o in
duce
pig
men
tary
cha
nge
in p
atie
nts
who
hav
e po
lym
orph
ism
s of
MC1
R ge
ne.
It h
as n
ot b
een
prov
en if
alp
ha-M
SH a
nalo
gues
will
dec
reas
e th
e ri
sk o
f sk
in c
ance
r in
pe
ople
who
are
sus
cept
ible
, bu
t th
ere
is s
uffi
cien
t ev
iden
ce t
hat
alph
a-M
SH d
oes
not
caus
e m
alig
nant
tr
ansf
orm
atio
n or
unc
ontr
olle
d ce
llula
r pr
olif
erat
ion
of m
elan
ocyt
es.
Cur
rent
ly,
it h
as o
nly
been
app
rove
d in
Ita
ly
and
Swit
zerl
and
for
peop
le w
ho a
re a
fflic
ted
wit
h er
ythr
opoi
etic
pro
topo
rphy
ria
(EPP
). F
inal
ly,
the
prol
onge
d ac
ting
de
pot
form
ulat
ion
has
show
n m
inim
al a
dver
se e
ffec
ts t
hus
far.
A r
evie
w o
f th
e lit
erat
ure
reve
als
that
afa
mel
anot
ide
has
grea
t po
tent
ial
to b
e an
eff
ecti
ve a
nd s
afe
ther
apeu
tic
tool
in a
num
ber
of s
kin
dise
ases
in t
he f
utur
e, h
owev
er
furt
her
tria
ls a
re n
eede
d.
Refe
renc
es
Wit
h ul
trav
iole
t ra
diat
ion
caus
ing
skin
agi
ng a
nd s
kin
canc
er,
the
use
of m
elan
otro
pic
pept
ides
are
slo
wly
bec
omin
g m
ore
popu
lar
as c
onsu
mer
s ar
e lo
okin
g fo
r al
tern
ativ
e w
ays
to o
btai
n a
facu
ltat
ive
tan.
How
ever
, th
e pr
oduc
ts a
re
unre
gula
ted
and
can
be o
btai
ned
thro
ugh
the
inte
rnet
, gy
ms,
and
tan
ning
sal
ons.
Th
ey a
re m
arke
ted
as
‘Mel
anot
ans’
whi
ch c
an in
duce
ski
n ta
nnin
g.
Ther
e is
onl
y on
e re
gula
ted
alph
a-M
SH a
nalo
g kn
own
as a
fam
elan
otid
e ([
Nle
4-D
-Phe
7]-a
lpha
-MSH
). It
was
app
rove
d in
Ital
y in
201
0 an
d Sw
itze
rlan
d in
201
2 fo
r pa
tien
ts d
iagn
osed
wit
h er
ythr
opoi
etic
pro
topo
rphy
ria
(EPP
). T
he
trea
tmen
t pr
opos
ed is
cur
rent
ly in
tri
als
in t
he U
S fo
r EP
P an
d vi
tilig
o.
Clin
ical
tri
als
in E
urop
e an
d Au
stra
lia i
nclu
de
EPP,
pol
ymor
phic
lig
ht e
rupt
ion
(PLE
), v
itili
go,
acti
nic
kera
tose
s (A
K),
and
squa
mou
s ce
ll ca
rcin
oma
(SCC
) in
org
an
tran
spla
nt r
ecip
ient
s. T
he c
ompo
und
serv
es a
s a
phot
o pr
otec
tive
dru
g fo
r pa
tien
ts w
ho a
re m
ost
at r
isk
from
UV
and
sun
expo
sure
, an
d as
a t
hera
peut
ic o
ptio
n in
non
-seg
men
tal v
itili
go (
NSV
).
Skin
pig
men
tati
on i
s a
stro
ng c
ompo
nent
of
phot
o pr
otec
tion
. T
he e
pide
rmal
chr
omop
hore
mel
anin
act
s as
a f
ilter
to
att
enua
te u
ltra
viol
et (
UV)
ligh
t. In
crea
sed
mel
aniz
atio
n de
crea
ses
the
effe
cts
expe
rien
ced
from
ult
ravi
olet
ra
diat
ion
(UVR
) in
clud
ing
decr
ease
d su
nbur
n an
d di
rect
DN
A da
mag
e fr
om u
ltra
viol
et-B
(U
VB).
Mel
anin
abs
orbs
UVB
, U
VA a
nd v
isib
le l
ight
, pl
ayin
g a
grea
t ro
le in
pho
topr
otec
tion
. W
ith
afam
elan
otid
e’s
abili
ty t
o pr
olon
g sk
in m
elan
in
prod
ucti
on,
it c
an b
e us
ed f
or t
he p
reve
ntio
n of
ski
n di
seas
es t
hat
are
caus
ed b
y su
nlig
ht.
Alph
a m
elan
ocyt
e st
imul
atin
g ho
rmon
e (A
lpha
-MSH
) is
13
amin
o ac
ids
in le
ngth
and
is s
ynth
esiz
ed f
rom
2 s
ourc
es:
the
pitu
itar
y gl
and
and
skin
. Al
pha-
MSH
is s
ynth
esiz
ed b
y en
dopr
oteo
lyti
c de
com
posi
tion
of
prop
iom
elan
ocor
tin(
POM
C).
UVR
dam
ages
DN
A in
the
ker
atin
ocyt
e w
hich
lea
ds t
o an
incr
ease
in a
lpha
-MSH
sy
nthe
sis
and
rele
ase(
9).
D
urin
g th
e re
pair
pro
cess
, PO
MC
gene
tra
nscr
ipti
on o
ccur
s an
d th
e ge
ne p
rodu
ct a
lpha
-MSH
is s
ynth
esiz
ed.
Alph
a-M
SH b
inds
to
the
mel
anoc
orti
n-1
rece
ptor
(M
C1R)
whi
ch is
pre
sent
in d
erm
al c
ells
incl
udin
g m
elan
ocyt
es,
kera
tino
cyte
s, e
ndot
helia
l cel
ls,
skin
fib
robl
asts
and
mas
t ce
lls.
MC1
R is
not
exp
ress
ed in
mel
anoc
yte
stem
cel
ls,
or
mel
anob
last
s. W
hen
MC1
R is
sti
mul
ated
, m
elan
ogen
esis
occ
urs
by in
crea
sing
tyr
osin
ase
acti
vity
and
incr
easi
ng
mel
anoc
yte
prol
ifer
atio
n. P
hysi
olog
ic a
lpha
-MSH
, re
leas
ed f
rom
ker
atin
ocyt
es,
acts
loc
ally
on
adja
cent
mel
anoc
ytes
vi
a a
para
crin
e m
echa
nism
and
on
them
selv
es v
ia a
n au
tocr
ine
mec
hani
sm (
1-8)
.
Curr
ent
tria
ls r
evea
l tha
t th
e re
gula
ted
med
icat
ion,
afa
mel
anot
ide,
is
wel
l tol
erat
ed b
y pa
tien
ts,
wit
h na
usea
and
he
adac
hes
as p
rim
ary
side
eff
ects
. H
owev
er,
ther
e ar
e ri
sks
asso
ciat
ed w
ith
buyi
ng u
nreg
ulat
ed p
rodu
cts,
incl
udin
g th
e po
tent
ial
impu
rity
of
chem
ical
s, a
nd in
fect
ive
com
plic
atio
ns s
econ
dary
to
need
le s
hari
ng.
Ther
e ha
ve b
een
seve
ral c
ases
of
atyp
ical
rap
idly
pig
men
ting
eru
ptiv
e ne
vi f
orm
ing
from
unr
egul
ated
ver
sion
s. T
he m
ain
issu
e is
the
in
abili
ty t
o re
trie
ve in
form
atio
n on
fre
quen
cy o
f us
e an
d or
igin
of
chem
ical
s pu
rcha
sed.
The
adm
inis
trat
ion
of t
he
unre
gula
ted
med
icat
ion
can
chan
ge t
he c
linic
al p
rese
ntat
ion
of p
atie
nts
wit
h pi
gmen
ted
lesi
ons
caus
ing
atyp
ical
cl
inic
al a
nd h
isto
logi
cal
feat
ures
. It
has
bee
n as
soci
ated
wit
h ch
ange
s in
the
clin
ical
pre
sent
atio
n of
pre
-exi
stin
g ne
vi a
nd t
he d
evel
opm
ent
of n
ew n
evi.
One
cas
e of
mal
igna
nt m
elan
oma
has
been
pub
lishe
d in
a m
elan
otan
I us
er.
Mul
tipl
e st
udie
s in
dica
te t
hat
the
utili
zati
on o
f th
ese
anal
ogue
s al
ters
the
pig
men
t in
mel
anoc
ytic
les
ions
the
reby
re
duci
ng t
he a
bilit
y to
ass
ess
pati
ents
' cur
rent
lesi
ons
for
mal
igna
nt p
oten
tial
(17
-19)
.
The
MT-
1 th
at t
he p
ublic
buy
s fr
om g
yms,
tan
ning
sal
ons,
and
the
inte
rnet
is a
dif
fere
nt p
rodu
ct f
rom
the
reg
ulat
ed
afam
elan
otid
e be
ing
pres
crib
ed f
or s
tudi
es.
The
form
er is
unr
egul
ated
and
off
ered
onl
ine
for
self
-adm
inis
trat
ion,
w
here
by s
ynth
esis
, or
igin
and
for
mul
atio
n ar
e al
l unk
now
n. U
sage
of
thes
e pr
oduc
ts a
re s
tron
gly
disc
oura
ged
by
seve
ral a
genc
ies
incl
udin
g th
e U
K an
d D
anis
h go
vern
men
tal h
ealt
hcar
e ag
enci
es,
and
the
Med
icin
es a
nd H
ealt
hcar
e Re
gula
tory
Age
ncy
(MH
RA).
The
FD
A ha
s is
sued
sta
tem
ents
for
the
pub
lic t
o st
op p
urch
asin
g M
T I &
II.
Alth
ough
a
war
ning
ove
r th
eir
sale
and
use
has
bee
n is
sued
by
auth
orit
ies,
the
y ha
ve n
ot b
anne
d an
y pr
oduc
ts (
9-16
).
Sinc
e M
T1 h
as b
een
asso
ciat
ed w
ith
unre
gula
ted
prod
ucts
sol
d ov
er t
he in
tern
et a
nd a
t gy
ms,
it w
ill n
ot b
e fu
rthe
r re
ferr
ed t
o in
thi
s po
ster
. Af
amel
anot
ide
is m
ore
resi
stan
t to
enz
ymat
ic b
reak
dow
n, w
hich
incr
ease
s it
s po
tenc
y an
d al
so p
rolo
ngs
the
dura
tion
of
acti
on a
t th
e M
C1R
. In
the
ear
ly 1
990s
, in
vest
igat
ors
foun
d th
at s
ubcu
tane
ous
afam
elan
otid
e in
ject
ions
inc
reas
e sk
in p
igm
enta
tion
. Af
amel
anot
ide
indu
ces
incr
ease
s in
eum
elan
in/p
heom
elan
in
rati
o of
nor
mal
sub
ject
s w
ith
skin
typ
es I
to V
I des
pite
the
abs
ence
of
sunl
ight
exp
osur
e.
In a
dou
ble
blin
d ph
ase
I tri
al,
30 s
ubje
cts
wer
e gi
ven
0.16
mg/
kg/d
ay f
or 1
0 da
ys a
fam
elan
otid
e or
pla
cebo
. Th
e m
ain
find
ing
in t
his
stud
y w
as t
hat
mel
anin
den
sity
incr
ease
d in
pat
ient
s w
ho w
ere
trea
ted
wit
h af
amel
anot
ide.
An
ad
diti
onal
res
ult
was
tha
t U
V in
duce
d su
nbur
n ce
lls w
ere
decr
ease
d in
pat
ient
s w
ho h
ad a
ris
k fo
r U
V in
duce
d sk
in
dam
age.
Stu
dies
hav
e sh
own
that
the
odd
s ra
tio
for
skin
can
cers
dec
reas
es b
y a
fact
or o
f 2
for
ever
y pe
rcen
t in
crea
se in
mel
anin
den
sity
. Th
e fi
ndin
gs f
rom
thi
s st
udy
indi
cate
tha
t af
amel
anot
ide
can
be m
ost
bene
fici
al in
pr
otec
ting
aga
inst
UV
skin
dam
age
in f
air
skin
ned
peop
le.
Si
nce
afam
elan
otid
e do
es n
ot p
enet
rate
the
epi
derm
is,
a to
pica
l do
sage
was
not
sho
wn
to b
e ef
fica
ciou
s. H
ence
a
subc
utan
eous
rou
te w
as c
hose
n, s
ince
it’s
mor
e ef
fect
ive
for
prot
ein
and
pept
ide
base
d dr
ugs.
Init
ially
it
was
ap
plie
d su
bcut
aneo
usly
in s
alin
e so
luti
on.
Due
to
its
shor
t ha
lf-l
ife,
sal
ine
inje
ctio
ns w
ere
requ
ired
dai
ly.
Thu
s, a
su
stai
ned
cont
rolle
d re
leas
e fo
rmul
atio
n w
as c
reat
ed w
hich
has
red
uced
adv
erse
eff
ects
and
impr
oved
eff
icac
y.
Th
ese
impl
ants
, ro
ughl
y th
e si
ze o
f a
grai
n of
ric
e, w
ere
deve
lope
d to
allo
w o
ne s
ingl
e ad
min
istr
atio
n to
pro
vide
m
axim
al t
anni
ng f
or t
wo
to t
hree
mon
ths.
The
y ar
e ad
min
iste
red
by p
hysi
cian
s in
the
fat
ty t
issu
e ab
ove
the
hip
for
roug
hly
ten
days
, an
d th
e ef
fect
of
the
drug
is s
een
for
abou
t 60
day
s. In
rec
ent
tria
ls,
the
med
icat
ion
is g
iven
onc
e ev
ery
60 d
ays.
Onc
e th
e dr
ug is
pre
sent
in t
he b
ody,
it t
akes
tw
o da
ys f
or s
kin
to b
ecom
e da
rker
. C
urre
ntly
, 16
mg
of a
fam
elan
otid
e gi
ven
subc
utan
eous
ly r
esul
ts in
max
imal
tan
ning
eff
icac
y w
ith
a ha
lf-l
ife
of l
ess
than
50
min
utes
.
1. M
ahne
C.
Impl
ant
Off
ers
Tann
ing
Revo
luti
on.
2002
. Av
aila
ble
at:
http
://n
ews.
bbc.
co.u
k/1/
hi/h
ealt
h/22
3199
1.st
m (
last
acce
ssed
7 J
une
2010
).
2.
Lan
gan
EA,
Nie
Z,
Rhod
es L
E. M
elan
otro
pic
pept
ides
: m
ore
than
jus
t ‘B
arbi
e dr
ugs’
and
‘su
n-ta
n ja
bs’?
Br
J D
erm
atol
201
0; 1
63:
451–
5.
3.
Gar
be C
, Bu
ttne
r P,
Wei
sz J
et
al.
Risk
fac
tors
for
dev
elop
ing
cuta
neou
s m
elan
oma
and
crit
eria
for
iden
tify
ing
pers
ons
at r
isk:
m
ulti
cent
er c
ase–
cont
rol s
tudy
of
the
cent
ral m
alig
nant
mel
anom
a re
gist
ry o
f th
e G
erm
an D
erm
atol
ogic
al S
ocie
ty.
J In
vest
D
erm
atol
199
4; 1
02:6
95–9
.
4. B
arne
tson
RS,
Ooi
TKT
, Zh
uang
L e
t al
. [N
le4-
d-Ph
e7]-
alph
a-m
elan
ocyt
e-st
imul
atin
g ho
rmon
e si
gnif
ican
tly
incr
ease
d pi
gmen
tati
on a
nd d
ecre
ased
UV
dam
age
in f
air-
skin
ned
Cauc
asia
n vo
lunt
eers
. J
Inve
st D
erm
atol
200
6; 1
26:1
869–
78.
5.
Dor
r RT
, Er
tl G
, N
et
al.
Effe
cts
of a
sup
er p
oten
t m
elan
otro
pic
pept
ide
in c
ombi
nati
on w
ith
sola
r U
V ra
diat
ion
on t
anni
ng o
f th
e sk
in in
hum
an v
olun
teer
s. A
rch
Der
mat
ol 2
004;
140
:827
–35.
6. B
renn
er M
, H
eari
ng V
. Th
e pr
otec
tive
rol
e of
mel
anin
aga
inst
UV
dam
age
in h
uman
ski
n. P
hoto
chem
Pho
tobi
ol 2
008;
84:
539–
49.
7.
Kai
dbey
K,
Agin
P,
Sayr
e R
et a
l. P
hoto
prot
ecti
on b
y m
elan
in –
a c
ompa
riso
n of
bla
ck a
nd C
auca
sian
ski
n. J
Am
Aca
d D
erm
atol
19
79;1
:249
–60.
8. K
ollia
s N
, Sa
yre
R, Z
eise
L e
t al
. Ph
otop
rote
ctio
n by
mel
anin
. J
Phot
oche
m P
hoto
biol
B 1
991;
9:1
35–6
0.
9.
Afa
mel
anot
ide:
Mel
anoc
orti
n M
C1 r
ecep
tor
agon
ist
phot
opro
tect
ive
agen
t.E.
I. D
rugs
of
the
Futu
re 2
010
35:5
(36
5-37
2
10.
Cui,
R.,
Wui
dlun
d, H
.R.,
Feig
e, E
. et
al.
Cen
tral
rol
e of
p53
in t
he s
unta
n re
spon
se a
nd p
atho
logi
c hy
perp
igm
enta
tion
. Ce
ll 20
07,
128(
5):
853-
64
11.
ME,
Dor
r RT
. M
elan
ocor
tin
pept
ide
ther
apeu
tics
: hi
stor
ic m
ilest
ones
, cl
inic
al s
tudi
es a
nd c
omm
erci
aliz
atio
n. P
epti
des
2006
; 27
:921
–30
12.
Valv
erde
P,
Hea
ly E
, Ja
ckso
n I,
Ree
s JL
, Th
ody
AJ.
Vari
ants
of
the
mel
anoc
yte-
stim
ulat
ing
horm
one
rece
ptor
gen
e ar
e as
soci
ated
wit
h re
d ha
ir a
nd f
air
skin
in h
uman
s. N
at G
enet
199
5;11
:328
–30
13.
Spen
cer
JD,
Scha
llreu
ter
KU.
Regu
lati
on o
f pi
gmen
tati
on in
hum
an e
pide
rmal
mel
anoc
ytes
by
func
tion
al h
igh-
affi
nity
bet
a-m
elan
ocyt
e-st
imul
atin
g ho
rmon
e/m
elan
ocor
tin-
4 re
cept
or s
igna
ling.
End
ocri
nolo
gy 2
009;
150:
1250
-8
14.
Schi
oth
HB,
Chh
ajla
ni V
, M
ucen
iece
R,
et a
l. M
ajor
pha
rmac
olog
ical
dis
tinc
tion
of
the
ACTH
rec
epto
r fr
om o
ther
mel
anoc
orti
n re
cept
ors.
Lif
e Sc
i 199
6;59
:797
-801
15.
Levi
ne N
, Sh
efte
l SN
, Ey
tan
T et
al.
Indu
ctio
n of
tan
ning
by
subc
utan
eous
adm
inis
trat
ion
of a
pot
ent
synt
heti
c m
elan
otro
pin.
JA
MA
1991
; 22
6:27
30–6
16
. H
unt
G,
Kyne
S,
Wak
amat
su K
et
al.
[Nle
4-D
-Phe
7]-a
-MSH
incr
ease
s th
e eu
mel
anin
: ph
eom
elan
in r
atio
in c
ultu
red
hum
an
mel
anoc
ytes
. J
Inve
st D
erm
atol
199
5; 1
04:8
3–5
17.
Pain
e-M
urri
eta
GD
, Ta
ylor
CW
, Cu
rtis
RA,
Lop
ez M
HA,
Dor
r RT
, Jo
hnso
n CS
, et
al.
Hum
an t
umor
mod
els
in t
he s
ever
e co
mbi
ned
imm
une
defi
cien
t (s
cid)
mou
se.
Canc
er C
hem
othe
r Ph
arm
acol
199
7;40
:209
–14
18.
Crom
bie,
I.K.
Var
iati
on o
f m
elan
oma
inci
denc
e w
ith
lati
tude
in N
orth
Am
eric
a an
d Eu
rope
. Br
J C
ance
r 19
79,
40(5
):77
4-81
.
19.
Dw
yer
T, B
lizza
rd L
, As
hbol
t R,
Plu
mb
J, B
erw
ick
M,
Stan
kovi
ch J
M.
Cuta
neou
s m
elan
in d
ensi
ty o
f Ca
ucas
ians
mea
sure
d by
sp
ectr
opho
tom
etry
and
ris
k of
mal
igna
nt m
elan
oma,
bas
al c
ell c
arci
nom
a, a
nd s
quam
ous
cell
carc
inom
a of
the
ski
n. A
m J
Ep
idem
iol 2
002;
155:
614
–21
20.
Nor
weg
ian
Med
icin
es A
genc
y. L
egem
iidee
lver
ket.
adv
arer
mot
bru
kav
Mel
atoa
n 20
08.w
ww
.lef
emid
dvek
er.n
o/tr
ampl
es/i
nter
page
....
6511
10.a
spx
21.
G.
Biol
cati
, J.
C. D
eyba
ch,S
. H
anne
ken,
P.
Wils
on,
S. W
ahlin
,§ G
. Va
rigo
s,–
L. R
hode
s, C
. Au
rizi
, C.
Min
der,
B.
Coff
in,
N.
Neu
man
n, F
. D
e Ro
oij,
G.
Ross
, F.
Ste
war
t an
d E.
Min
der
A ra
ndom
ized
pha
se II
I tri
al o
f af
amel
anot
ide
(Sce
ness
e),
an a
goni
stic
a-
mel
anoc
yte
stim
ulat
ing
horm
one
anal
ogue
in t
he t
reat
men
t of
pro
topo
rphy
ria
indu
ced
phot
otox
icit
y BJ
D ,
201
1 Br
itis
h As
soci
atio
n of
Der
mat
olog
ists
201
1 16
4, p
p112
5–11
76
22
. Sa
fety
and
eff
icac
y of
an
agon
isti
c a-
mel
anoc
yte
stim
ulat
ing
horm
one
anal
ogue
, af
amel
anot
ide
(Sce
ness
e),
in t
reat
ing
pati
ents
w
ith
eryt
hrop
oiet
ic p
roto
porp
hyri
a fo
r 2.
5 co
nsec
utiv
e ye
ars
S. K
reim
, S.
Lau
tens
chla
ger
and
E. M
inde
r
23.
Hay
lett
AK,
Nie
Z,
Brow
nrig
g M
, Ta
ylor
R,
Rhod
es L
E.Sy
stem
ic p
hoto
prot
ecti
on in
sol
ar u
rtic
aria
wit
h α
-mel
anoc
yte-
stim
ulat
ing
horm
one
anal
ogue
[N
le4-
D-P
he7]
-α-M
SH.
Br J
Der
mat
ol.
2011
Feb
;164
(2):
407-
14.
doi:
10.
1111
/j.1
365-
2133
.201
0.10
104.
x 24
. Be
atti
e PE
, D
awe
RS,
Ibbo
tson
SH
et
al.
Char
acte
rist
ics
and
prog
nosi
s of
idio
path
ic s
olar
urt
icar
ia:
a co
hort
of
87 c
ases
. Ar
ch
Der
mat
ol 2
003;
139
:114
9–54
25.
Bern
hard
J,
Jaen
icke
K,
Mom
taz
TK,
Parr
ish
JA.
Ult
ravi
olet
A p
hoto
ther
apy
in t
he p
roph
ylax
is o
f so
lar
urti
cari
a. J
Am
Aca
d D
erm
atol
198
4; 1
0:29
–33
26.
Inte
rnat
iona
l Ass
ocia
tion
for
Res
earc
h on
Can
cer.
IARC
Mon
ogra
phs
on t
he E
valu
atio
n of
Car
cino
geni
c Ri
sks
to H
uman
s. V
olum
e 55
. So
lar
and
Ult
ravi
olet
Rad
iati
on.
Lyon
: In
tern
atio
nal A
ssoc
iati
on f
or R
esea
rch
on C
ance
r, 1
992.
27.
Clin
uvel
to
eval
uate
SCE
NES
SE (
afam
elan
otid
e) a
s th
erap
y in
vit
iligo
. M
elbo
urne
, Au
stra
lia:
Clin
uvel
Pha
rmac
euti
cals
Ltd
. 20
10.
Avai
labl
e fr
om:
http
://w
ww
.clin
uvel
.com
/res
ourc
es/c
msf
iles/
pdf/
2010
0825
CUV0
31Vi
tilig
o.pd
f
An e
arlie
r al
pha-
MSH
ana
logu
e, f
orm
erly
kno
wn
as m
elan
otan
-I (
MT1
), w
as c
hem
ical
ly a
lter
ed a
nd o
ptim
ized
to
its
curr
ent
form
ulat
ion
as a
fam
elan
otid
e.
It w
as f
irst
syn
thes
ized
in 1
980
and
is a
sup
er p
oten
t m
elan
ocor
tin.
Viti
ligo
is a
n ac
quir
ed p
igm
enta
ry d
isor
der
of t
he s
kin
and
muc
ous
mem
bran
es,
and
it is
cha
ract
eriz
ed b
y ci
rcum
scri
bed
depi
gmen
ted
mac
ules
and
pat
ches
. It
is a
pro
gres
sive
dis
orde
r in
whi
ch s
ome
or a
ll of
the
m
elan
ocyt
es i
n th
e af
fect
ed s
kin
are
abse
nt.
A ph
ase
II st
udy
was
con
duct
ed in
the
US
for
the
trea
tmen
t of
vit
iligo
. In
thi
s st
udy,
50%
of
pati
ents
wer
e tr
eate
d w
ith
narr
ow b
and
UVB
and
afa
mel
anot
ide,
whi
le t
he r
emai
ning
50%
wer
e tr
eate
d w
ith
narr
owba
nd U
VB a
lone
. Th
e go
al o
f th
e st
udy
was
to
dete
rmin
e if
afa
mel
anot
ide
decr
ease
d th
e to
tal
dose
of
narr
ow b
and
UVB
exp
osur
e ne
eded
, an
d ti
me
requ
ired
to
reac
tiva
te m
elan
ocyt
es i
n vi
tilig
o le
sion
s. D
ata
was
fav
orab
le in
the
21
pati
ents
rec
eivi
ng 1
6 m
g im
plan
ts.
The
maj
orit
y of
pat
ient
s in
the
stu
dy h
ad s
kin
type
s IV
– V
I and
wer
e di
agno
sed
wit
h N
SV w
ithi
n in
the
la
st 5
yea
rs.
The
data
als
o su
gges
ted
that
afa
mel
anot
ide
incr
ease
s re
pigm
enta
tion
rat
e an
d re
spon
se t
ime
follo
win
g na
rrow
ban
d U
VB e
xpos
ure
in p
atie
nts,
in
the
days
imm
edia
tely
aft
er a
dmin
istr
atio
n.
Furt
her,
afa
mel
anot
ide,
for
th
e tr
eatm
ent
of v
itili
go,
has
rece
ntly
als
o be
en a
ppro
ved
to b
e te
sted
in in
tern
atio
nal
clin
ical
tri
als
(26,
27)
.
The
eryt
hem
al f
lare
and
whe
al f
orm
atio
n ty
pica
l of
sol
ar u
rtic
aria
. It
is a
lso
acco
mpa
nied
by
prur
itus
.
Sola
r ur
tica
ria
SU is
a r
are
form
of
chro
nic
urti
cari
a th
at is
mar
ked
by p
ruri
tus,
ery
them
al f
lare
, an
d w
heal
fo
rmat
ion
wit
hin
min
utes
of
sunl
ight
exp
osur
e an
d re
solu
tion
wit
hin
a fe
w h
ours
. Fo
r th
e m
ost
part
, su
n ex
pose
d ar
eas
are
affe
cted
an
d th
e qu
alit
y of
lif
e in
pat
ient
s su
ffer
ing
from
SU
is v
ery
poor
. Se
vera
l stu
dies
hav
e be
en
cond
ucte
d w
hich
sho
w t
hat
phot
othe
rapy
can
incr
ease
tol
eran
ce in
sol
ar u
rtic
aria
wit
h m
elan
ogen
esis
pro
pose
d as
a
mec
hani
sm.
The
prob
lem
wit
h th
is t
reat
men
t is
tha
t U
V ra
diat
ion
is a
car
cino
gen
whi
ch a
lso
stim
ulat
es m
elan
in t
o re
duce
pen
etra
tion
of
UV
wav
elen
gths
, al
low
ing
for
incr
ease
d pr
otec
tion
in
sola
r ur
tica
ria.
H
ayle
tt e
t al
con
duct
ed a
n op
en l
abel
pha
se II
stu
dy o
n 5
pati
ents
wit
h so
lar
urti
cari
a by
giv
ing
them
16
mg
subc
utan
eous
impl
ant
of a
fam
elan
otid
e du
ring
the
win
ter
as a
pro
phyl
acti
c tr
eatm
ent.
The
stu
dy w
as d
one
in t
he
win
ter
to m
inim
ize
UV
radi
atio
n an
d to
pre
vent
aug
men
tati
on i
n th
e m
elan
ogen
ic r
espo
nse.
All
5 pa
tien
ts s
elec
ted
disp
laye
d po
siti
ve u
rtic
aria
l re
spon
se t
o pr
ovoc
atio
n up
on p
hoto
tes
ting
. Th
e m
elan
in d
ensi
ty in
exp
osed
and
un
expo
sed
site
s w
as a
sses
sed
in a
ll th
e pa
tien
ts o
n da
y 0,
7,
15,
30,
and
60 a
nd t
he r
esul
ts in
dica
te a
red
ucti
on in
so
lar
urti
cari
a re
spon
se o
ver
a br
oad
spec
trum
of
wav
elen
gths
. Th
eir
resu
lts
indi
cate
the
pos
sibi
lity
of
afam
elan
otid
e to
be
a pr
otec
tive
tre
atm
ent
for
pati
ents
suf
feri
ng f
rom
SU
, re
duce
d re
spon
ses
are
due
to t
he
imm
unom
odul
ator
y ef
fect
s of
[N
le4-
D-P
he7]
-alp
ha-M
SH a
nd p
hoto
pro
tect
ion
(22-
25).
Eryt
hrop
oiet
ic p
roto
porp
hyri
a (E
PP)
is c
ause
d by
an
enzy
mat
ic d
efic
ienc
y of
fer
roch
elat
ase,
due
to
an in
heri
ted
defe
ct in
the
last
ste
p of
the
hem
e bi
osyn
thes
is p
athw
ay.
Thi
s ca
uses
an
accu
mul
atio
n of
pho
tose
nsit
izin
g pr
otop
orph
yrin
IX
in t
he d
erm
is w
hich
lea
ds t
o in
crea
sed
sens
itiv
ity
to l
ight
, re
sult
ing
in p
ain
and
inca
paci
tati
ng
phot
o to
xic
reac
tion
s w
hen
expo
sed
to t
he v
isib
le s
pect
rum
. Th
e di
seas
e is
cha
ract
eriz
ed b
y se
vere
into
lera
nce
to
light
.
A ph
ase
II st
udy
was
con
duct
ed o
n 5
pati
ents
suf
feri
ng f
rom
EPP
for
mor
e th
an 4
mon
ths
who
the
n re
ceiv
ed a
su
bcut
aneo
us 2
0 m
g im
plan
t of
afa
mel
anot
ide.
Re
sult
s in
dica
ted
an in
crea
se i
n sk
in p
igm
enta
tion
and
als
o a
sign
ific
ant
incr
ease
in t
oler
ance
to
phot
o pr
ovoc
atio
n.
In a
noth
er p
hase
II t
rial
, 68
pat
ient
s w
ere
trea
ted
for
6 m
onth
s du
ring
pea
k su
nlig
ht s
easo
ns o
f sp
ring
and
sum
mer
, w
here
a s
ubse
t of
pat
ient
s w
ere
expo
sed
to l
ight
on
thei
r ba
ck a
nd h
ands
to
asse
ss t
he t
ime
and
dose
req
uire
d to
cau
se a
rea
ctio
n. P
atie
nts
who
rec
eive
d af
amel
anot
ide
wer
e ab
le t
o sp
end
mor
e ti
me
in d
irec
t su
nlig
ht,
spec
ific
ally
the
mid
dle
of t
he d
ay.
Thes
e pa
tien
ts o
n th
e m
edic
atio
n re
port
ed a
thr
eefo
ld in
crea
se in
the
am
ount
of
tim
e th
ey c
ould
spe
nd in
dir
ect
sunl
ight
.
Rece
ntly
, a
pha
se II
I, r
ando
miz
ed,
doub
le b
lind
cont
rolle
d, a
nd m
ulti
cent
er s
tudy
in E
urop
e an
d Au
stra
lia c
onsi
stin
g of
101
EPP
pat
ient
s to
ok p
lace
ove
r th
e co
urse
of
a ye
ar.
Dat
a fr
om t
he s
tudy
had
bee
n pr
esen
ted
and
dem
onst
rate
d EP
P pa
in in
tens
ity
that
was
sig
nifi
cant
ly l
ower
, an
d su
nlig
ht e
xpos
ure
tim
e th
at w
as s
igni
fica
ntly
hig
her
duri
ng
adm
inis
trat
ion
of a
fam
elan
otid
e. S
ever
al o
ther
pha
se II
I tri
als
have
sho
wn
sim
ilar
resu
lts
(21,
22)
.
ALPH
A M
ELAN
OCY
TE
STIM
ULA
TIN
G H
ORM
ON
E (A
lpha
-MSH
) M
ELAN
OG
ENES
IS
& M
ELAN
OCO
RTIN
1R
Al
pha
mel
anoc
yte
stim
ulat
ing
horm
one
(Alp
ha-M
SH)
is a
tr
idec
apep
tide
pig
men
tary
ho
rmon
e w
hich
is 1
3 am
ino
acid
s in
leng
th a
nd is
sy
nthe
size
d fr
om 2
sou
rces
: th
e pi
tuit
ary
glan
d an
d sk
in
Safe
ty a
nd m
alig
nanc
y
Vitil
igo
Sola
r Urt
icar
ia
Eryt
hrop
oiet
ic p
roto
porp
hyria
Afam
elan
otid
e in
crea
ses
mel
anin
den
sity
, (F
itzp
atri
ck t
ype
1, 2
,3)
. M
edic
atio
n is
re
leas
ed o
ver
10 d
ays,
and
mel
anin
incr
ease
s fo
r 60
day
s.
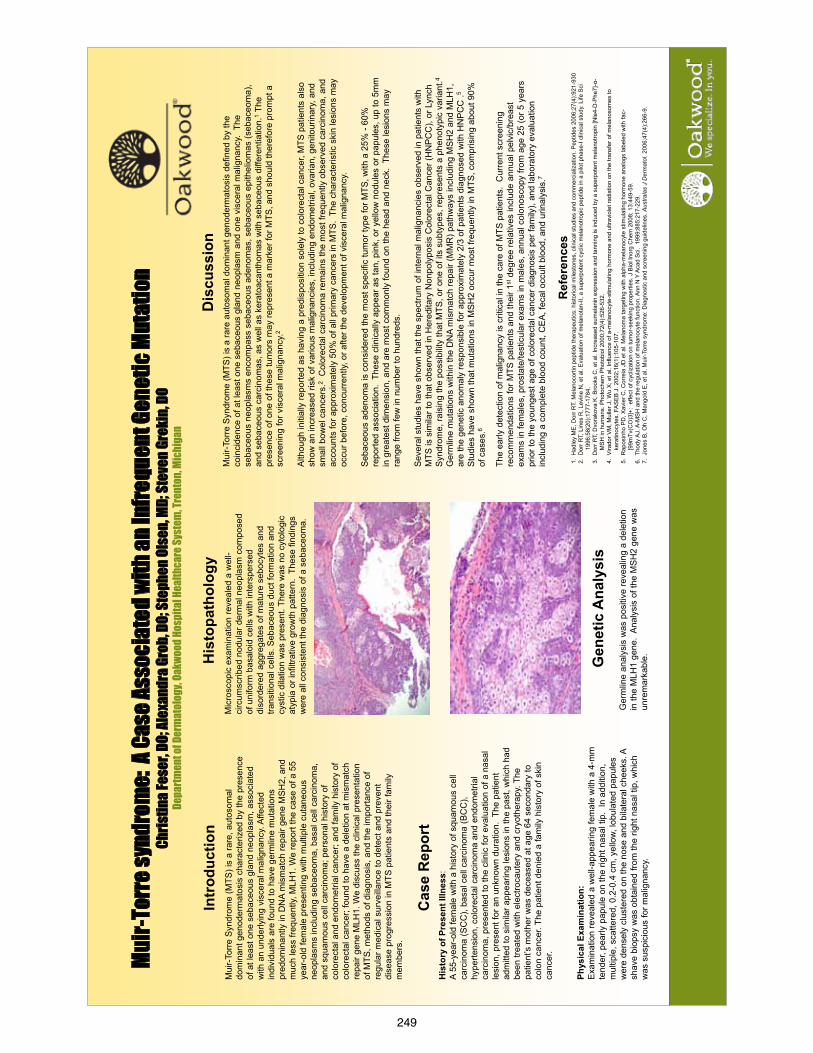
249
Muir-
Torre
synd
rom
e: A
Case
Asso
ciat
ed w
ith an
Infre
quen
t Gen
etic
Mut
atio
n Ch
ristin
a Fes
er, D
O; Al
exan
dra G
rob,
DO; S
teph
en Ol
sen,
MD; S
teve
n Gre
kin,
DO
Depa
rtmen
t of D
erm
atol
ogy,
Oakw
ood H
ospi
tal H
ealth
care
Syst
em, T
rent
on, M
ichi
gan
Dis
cuss
ion
Mui
r-To
rre
Syn
drom
e (M
TS) i
s a
rare
aut
osom
al d
omin
ant g
enod
erm
atos
is d
efin
ed b
y th
e co
inci
denc
e of
at l
east
one
seb
aceo
us g
land
neo
plas
m a
nd o
ne v
isce
ral m
alig
nanc
y. T
he
seba
ceou
s ne
opla
sms
enco
mpa
ss s
ebac
eous
ade
nom
as, s
ebac
eous
epi
thel
iom
as (s
ebac
eom
a),
and
seba
ceou
s ca
rcin
omas
, as
wel
l as
kera
toac
anth
omas
with
seb
aceo
us d
iffer
entia
tion.
1 The
pr
esen
ce o
f one
of t
hese
tum
ors
may
repr
esen
t a m
arke
r for
MTS
, and
sho
uld
ther
efor
e pr
ompt
a
scre
enin
g fo
r vis
cera
l mal
igna
ncy.
2
Alth
ough
initi
ally
repo
rted
as h
avin
g a
pred
ispo
sitio
n so
lely
to c
olor
ecta
l can
cer,
MTS
pat
ient
s al
so
show
an
incr
ease
d ris
k of
var
ious
mal
igna
ncie
s, in
clud
ing
endo
met
rial,
ovar
ian,
gen
itour
inar
y, a
nd
smal
l bow
el c
ance
rs.2
Col
orec
tal c
arci
nom
a re
mai
ns th
e m
ost f
requ
ently
obs
erve
d ca
rcin
oma,
and
ac
coun
ts fo
r app
roxi
mat
ely
50%
of a
ll pr
imar
y ca
ncer
s in
MTS
. Th
e ch
arac
teris
tic s
kin
lesi
ons
may
oc
cur b
efor
e, c
oncu
rren
tly, o
r afte
r the
dev
elop
men
t of v
isce
ral m
alig
nanc
y.
Seb
aceo
us a
deno
ma
is c
onsi
dere
d th
e m
ost s
peci
fic tu
mor
type
for M
TS, w
ith a
25%
- 60
%
repo
rted
asso
ciat
ion.
The
se c
linic
ally
app
ear a
s ta
n, p
ink,
or y
ello
w n
odul
es o
r pap
ules
, up
to 5
mm
in
gre
ates
t dim
ensi
on, a
nd a
re m
ost c
omm
only
foun
d on
the
head
and
nec
k. T
hese
lesi
ons
may
ra
nge
from
few
in n
umbe
r to
hund
reds
.
Sev
eral
stu
dies
hav
e sh
own
that
the
spec
trum
of i
nter
nal m
alig
nanc
ies
obse
rved
in p
atie
nts
with
M
TS is
sim
ilar t
o th
at o
bser
ved
in H
ered
itary
Non
poly
posi
s C
olor
ecta
l Can
cer (
HN
PCC
), or
Lyn
ch
Syn
drom
e, ra
isin
g th
e po
ssib
ility
that
MTS
, or o
ne o
f its
sub
type
s, re
pres
ents
a p
heno
typi
c va
riant
.4 G
erm
line
mut
atio
ns w
ithin
the
DN
A m
ism
atch
repa
ir (M
MR
) pat
hway
s in
clud
ing
MS
H2
and
MLH
1,
are
the
gene
tic a
nom
aly
resp
onsi
ble
for a
ppro
xim
atel
y 2/
3 of
pat
ient
s di
agno
sed
with
HN
PC
C .5
S
tudi
es h
ave
show
n th
at m
utat
ions
in M
SH
2 oc
cur m
ost f
requ
ently
in M
TS, c
ompr
isin
g ab
out 9
0%
of c
ases
.6
The
early
det
ectio
n of
mal
igna
ncy
is c
ritic
al in
the
care
of M
TS p
atie
nts.
Cur
rent
scr
eeni
ng
reco
mm
enda
tions
for M
TS p
atie
nts
and
thei
r 1st d
egre
e re
lativ
es in
clud
e an
nual
pel
vic/
brea
st
exam
s in
fem
ales
, pro
stat
e/te
stic
ular
exa
ms
in m
ales
, ann
ual c
olon
osco
py fr
om a
ge 2
5 (o
r 5 y
ears
pr
ior t
o th
e yo
unge
st a
ge o
f col
orec
tal c
ance
r dia
gnos
is p
er fa
mily
), an
d la
bora
tory
eva
luat
ion
incl
udin
g a
com
plet
e bl
ood
coun
t, C
EA,
feca
l occ
ult b
lood
, and
urin
alys
is.7
Ref
eren
ces
1. H
adle
y M
E, D
orr R
T. M
elan
ocor
tin p
eptid
e th
erap
eutic
s: h
isto
rical
mile
ston
es, c
linic
al s
tudi
es a
nd c
omm
erci
aliz
atio
n. P
eptid
es 2
006;
27(4
):921
-930
2.
Dor
r RT,
Lin
es R
, Lev
ine
N, e
t al.
Eva
luat
ion
of m
elan
otan
-II, a
sup
erpo
tent
cyc
lic m
elan
otro
pic
pept
ide
in a
pilo
t pha
se-I
clin
ical
stu
dy. L
ife S
ci
1996
;58(
20):1
777-
1784
. 3.
Dor
r RT,
Dvo
rako
va K
, Bro
oks
C, e
t al.
Incr
ease
d eu
mel
anin
exp
ress
ion
and
tann
ing
is in
duce
d by
a s
uper
pote
nt m
elan
otro
pin
[Nle
4-D
-Phe
7]-α
-M
SH
in h
uman
s. P
hoto
chem
Pho
tobi
ol 2
000;
72(4
):526
-532
. 4.
Vira
dor V
M, M
ulle
r J, W
u X
; et a
l. In
fluen
ce o
f a-m
elan
ocyt
e-st
imul
atin
g ho
rmon
e an
d ul
travi
olet
radi
atio
n on
the
trans
fer o
f mel
anos
omes
to
kera
tinoc
ytes
. FA
SE
B J
. 200
2;16
(1):1
05-1
07.
5. R
apos
inho
PD
, Xav
ier C
, Cor
reia
JD
et a
l. M
elan
oma
targ
etin
g w
ith a
lpha
-mel
anoc
yte
stim
ulat
ing
horm
one
anal
ogs
labe
led
with
fac-
[9
9mTv
(CO
)3]+
: ef
fect
of c
ycliz
atio
n on
tum
or-s
eeki
ng p
rope
rties
. J B
iol I
norg
Che
m 2
008;
13:
449-
59.
6. T
hody
AJ.
A-M
SH
and
the
regu
latio
n of
mel
anoc
yte
func
tion.
Ann
N Y
Aca
d S
ci.
1999
;885
:217
-229
. 7.
Jon
es B
, Oh
C, M
ango
ld E
, et a
l. M
uir-
Torre
syn
drom
e: D
iagn
ostic
and
scr
eeni
ng g
uide
lines
. Aus
trala
s J
Der
mat
ol. 2
006;
47(4
):266
-9.
Intr
oduc
tion
M
uir-
Torr
e S
yndr
ome
(MTS
) is
a ra
re, a
utos
omal
do
min
ant g
enod
erm
atos
is c
hara
cter
ized
by
the
pres
ence
of
at l
east
one
seb
aceo
us g
land
neo
plas
m, a
ssoc
iate
d w
ith a
n un
derly
ing
visc
eral
mal
igna
ncy.
Affe
cted
in
divi
dual
s ar
e fo
und
to h
ave
germ
line
mut
atio
ns
pred
omin
antly
in D
NA
mis
mat
ch re
pair
gene
MS
H2,
and
m
uch
less
freq
uent
ly, M
LH1.
We
repo
rt th
e ca
se o
f a 5
5 ye
ar-o
ld fe
mal
e pr
esen
ting
with
mul
tiple
cut
aneo
us
neop
lasm
s in
clud
ing
seba
ceom
a, b
asal
cel
l car
cino
ma,
an
d sq
uam
ous
cell
carc
inom
a; p
erso
nal h
isto
ry o
f co
lore
ctal
and
end
omet
rial c
ance
r; an
d fa
mily
his
tory
of
colo
rect
al c
ance
r; fo
und
to h
ave
a de
letio
n at
mis
mat
ch
repa
ir ge
ne M
LH1.
We
disc
uss
the
clin
ical
pre
sent
atio
n of
MTS
, met
hods
of d
iagn
osis
, and
the
impo
rtanc
e of
re
gula
r med
ical
sur
veilla
nce
to d
etec
t and
pre
vent
di
seas
e pr
ogre
ssio
n in
MTS
pat
ient
s an
d th
eir f
amily
m
embe
rs.
Cas
e R
epor
t H
isto
ry o
f Pre
sent
Illn
ess:
A
55-y
ear-
old
fem
ale
with
a h
isto
ry o
f squ
amou
s ce
ll ca
rcin
oma
(SC
C),
basa
l cel
l car
cino
ma
(BC
C),
hype
rtens
ion,
col
orec
tal c
arci
nom
a an
d en
dom
etria
l ca
rcin
oma,
pre
sent
ed to
the
clin
ic fo
r eva
luat
ion
of a
nas
al
lesi
on, p
rese
nt fo
r an
unkn
own
dura
tion.
The
pat
ient
ad
mitt
ed to
sim
ilar a
ppea
ring
lesi
ons
in th
e pa
st, w
hich
had
be
en tr
eate
d w
ith e
lect
roca
uter
y an
d cr
yoth
erap
y. T
he
patie
nt’s
mot
her w
as d
ecea
sed
at a
ge 6
4 se
cond
ary
to
colo
n ca
ncer
. The
pat
ient
den
ied
a fa
mily
his
tory
of s
kin
canc
er.
Phys
ical
Exa
min
atio
n:
Exa
min
atio
n re
veal
ed a
wel
l-app
earin
g fe
mal
e w
ith a
4-m
m
tend
er, p
early
pap
ule
on th
e rig
ht n
asal
tip.
In
addi
tion,
m
ultip
le, s
catte
red,
0.2
-0.4
cm
, yel
low,
lobu
late
d pa
pule
s w
ere
dens
ely
clus
tere
d on
the
nose
and
bila
tera
l che
eks.
A
shav
e bi
opsy
was
obt
aine
d fro
m th
e rig
ht n
asal
tip,
whi
ch
was
sus
pici
ous
for m
alig
nanc
y.
His
topa
thol
ogy
Mic
rosc
opic
exa
min
atio
n re
veal
ed a
wel
l-ci
rcum
scrib
ed n
odul
ar d
erm
al n
eopl
asm
com
pose
d of
uni
form
bas
aloi
d ce
lls w
ith in
ters
pers
ed
diso
rder
ed a
ggre
gate
s of
mat
ure
sebo
cyte
s an
d tra
nsiti
onal
cel
ls. S
ebac
eous
duc
t for
mat
ion
and
cyst
ic d
ilatio
n w
as p
rese
nt. T
here
was
no
cyto
logi
c at
ypia
or i
nfilt
rativ
e gr
owth
pat
tern
. Th
ese
findi
ngs
wer
e al
l con
sist
ent t
he d
iagn
osis
of a
seb
aceo
ma.
Gen
etic
Ana
lysi
s G
erm
line
anal
ysis
was
pos
itive
reve
alin
g a
dele
tion
in th
e M
LH1
gene
. A
naly
sis
of th
e M
SH
2 ge
ne w
as
unre
mar
kabl
e.
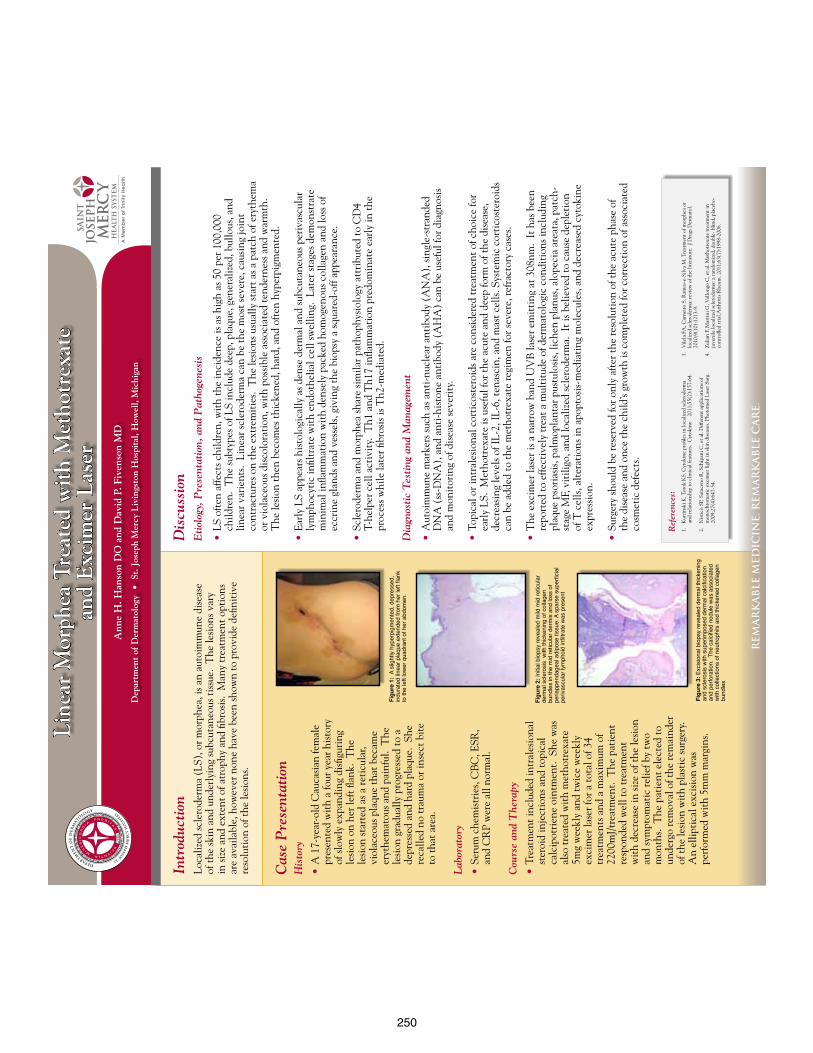
250
re
ma
rk
ab
le m
ed
icin
e. r
em
ar
ka
ble
ca
re
.
Intr
oduc
tion
Loca
lized
scle
rode
rma
(LS)
, or m
orph
ea, i
s an
auto
imm
une
dise
ase
of th
e sk
in a
nd u
nder
lyin
g su
bcut
aneo
us ti
ssue
. T
he le
sion
s var
y in
size
and
ext
ent o
f atr
ophy
and
fibr
osis
. M
any
trea
tmen
t opt
ions
ar
e av
aila
ble,
how
ever
non
e ha
ve b
een
show
n to
pro
vide
defi
niti
ve
reso
luti
on o
f the
lesi
ons.
Ref
eren
ces:
1.
Kur
zins
ki K
, Tor
ok K
S. C
ytok
ine
profi
les i
n lo
caliz
ed sc
lero
derm
a an
d re
lati
onsh
ip to
clin
ical
feat
ures
. C
ytok
ine.
20
11;5
5(2)
:157
-64.
2.
Nis
ticò
SP,
Sar
acen
o R
, Sch
ipan
i C, e
t al.
Diff
eren
t app
licat
ions
of
mon
ochr
omat
ic e
xcim
er li
ght i
n sk
in d
isea
ses.
Phot
omed
Las
er S
urg.
20
09;2
7(4)
:647
-54.
Dis
cuss
ion
Eti
olog
y, P
rese
ntat
ion,
and
Pat
hoge
nesi
s
• L
S of
ten
affe
cts c
hild
ren,
wit
h th
e in
cide
nce
is a
s hig
h as
50
per 1
00,0
00
child
ren.
The
subt
ypes
of L
S in
clud
e de
ep, p
laqu
e, g
ener
aliz
ed, b
ullo
us, a
nd
linea
r var
ient
s. L
inea
r scl
erod
erm
a ca
n be
the
mos
t sev
ere,
cau
sing
join
t co
ntra
ctur
es o
n th
e ex
trem
itie
s. T
he le
sion
s usu
ally
star
t as a
pat
ch o
f ery
them
a or
vio
lace
ous d
isco
lora
tion
, wit
h po
ssib
le a
ssoc
iate
d te
nder
ness
and
war
mth
. T
he le
sion
then
bec
omes
thic
kene
d, h
ard,
and
oft
en h
yper
pigm
ente
d.
• E
arly
LS
appe
ars h
isto
logi
cally
as d
ense
der
mal
and
subc
utan
eous
per
ivas
cula
r ly
mph
ocyt
ic in
filtr
ate
wit
h en
doth
elia
l cel
l sw
ellin
g. L
ater
stag
es d
emon
stra
te
min
imal
infla
mm
atio
n w
ith
dens
ely
pack
ed h
omog
enou
s col
lage
n an
d lo
ss o
f ec
crin
e gl
ands
and
ves
sels
, giv
ing
the
biop
sy a
squa
red-
off a
ppea
ranc
e.
• S
cler
oder
ma
and
mor
phea
shar
e si
mila
r pat
hoph
ysio
logy
att
ribu
ted
to C
D4
T-he
lper
cel
l act
ivit
y. T
h1 a
nd T
h17
infla
mm
atio
n pr
edom
inat
e ea
rly
in th
e pr
oces
s whi
le la
ter fi
bros
is is
Th2
-med
iate
d.
Dia
gnos
tic
Tes
ting
and
Man
agem
ent
• A
utoi
mm
une
mar
kers
such
as a
nti-
nucl
ear a
ntib
ody
(AN
A),
sing
le-s
tran
ded
DN
A (
ss-D
NA
), a
nd a
nti-
hist
one
anti
body
(A
HA
) ca
n be
use
ful f
or d
iagn
osis
an
d m
onit
orin
g of
dis
ease
seve
rity
.
• T
opic
al o
r int
rale
sion
al c
orti
cost
eroi
ds a
re c
onsi
dere
d tr
eatm
ent o
f cho
ice
for
earl
y LS
. M
etho
trex
ate
is u
sefu
l for
the
acut
e an
d de
ep fo
rm o
f the
dis
ease
, de
crea
sing
leve
ls o
f IL-
2, IL
-6, t
enas
cin,
and
mas
t cel
ls. S
yste
mic
cor
tico
ster
oids
ca
n be
add
ed to
the
met
hotr
exat
e re
gim
en fo
r sev
ere,
refr
acto
ry c
ases
.
• T
he e
xcim
er la
ser i
s a n
arro
w b
and
UV
B la
ser e
mit
ting
at 3
08nm
. It
has
bee
n re
port
ed to
effe
ctiv
ely
trea
t a m
ulti
tude
of d
erm
atol
ogic
con
diti
ons i
nclu
ding
pl
aque
pso
rias
is, p
alm
opla
ntar
pus
tulo
sis,
liche
n pl
anus
, alo
peci
a ar
eata
, pat
ch-
stag
e M
F, v
itili
go, a
nd lo
caliz
ed sc
lero
derm
a. I
t is b
elie
ved
to c
ause
dep
leti
on
of T
cel
ls, a
lter
atio
ns in
apo
ptos
is-m
edia
ting
mol
ecul
es, a
nd d
ecre
ased
cyt
okin
e ex
pres
sion
.
• S
urge
ry sh
ould
be
rese
rved
for o
nly
afte
r the
reso
luti
on o
f the
acu
te p
hase
of
the
dise
ase
and
once
the
child
’s gr
owth
is c
ompl
eted
for c
orre
ctio
n of
ass
ocia
ted
cosm
etic
def
ects
.
Lin
ear
Mor
phea
Tre
ated
wit
h M
etho
trex
ate
and
Exc
imer
Las
erA
nne
H. H
anso
n D
O a
nd D
avid
P. F
iven
son
MD
Dep
artm
ent
of D
erm
atol
ogy
• S
t. J
osep
h M
ercy
Liv
ings
ton
Hos
pita
l, H
owel
l, M
ichi
gan
Cas
e P
rese
ntat
ion
His
tory
• A
17-
year
-old
Cau
casi
an fe
mal
e pr
esen
ted
wit
h a
four
yea
r his
tory
of
slow
ly e
xpan
ding
dis
figur
ing
lesi
on o
n he
r lef
t flan
k. T
he
lesi
on st
arte
d as
a re
ticu
lar,
viol
aceo
us p
laqu
e th
at b
ecam
e er
ythe
mat
ous a
nd p
ainf
ul.
The
le
sion
gra
dual
ly p
rogr
esse
d to
a
depr
esse
d an
d ha
rd p
laqu
e. S
he
reca
lled
no tr
aum
a or
inse
ct b
ite
to th
at a
rea.
Lab
orat
ory
• S
erum
che
mis
trie
s, C
BC
, ESR
, an
d C
RP
wer
e al
l nor
mal
.
Cou
rse
and
The
rapy
• T
reat
men
t inc
lude
d in
tral
esio
nal
ster
oid
inje
ctio
ns a
nd to
pica
l ca
lcip
otri
ene
oint
men
t. S
he w
as
also
trea
ted
wit
h m
etho
trex
ate
5mg
wee
kly
and
twic
e w
eekl
y ex
cim
er la
ser f
or a
tota
l of 3
4 tr
eatm
ents
and
a m
axim
um o
f 22
00m
J/tr
eatm
ent.
The
pat
ient
re
spon
ded
wel
l to
trea
tmen
t w
ith
decr
ease
in si
ze o
f the
lesi
on
and
sym
ptom
atic
relie
f by
two
mon
ths.
The
pat
ient
ele
cted
to
unde
rgo
rem
oval
of t
he re
mai
nder
of
the
lesi
on w
ith
plas
tic
surg
ery.
A
n el
lipti
cal e
xcis
ion
was
pe
rfor
med
wit
h 5m
m m
argi
ns.
Figu
re 1
: A
slig
htly
hyp
erpi
gmen
ted,
dep
ress
ed,
indu
rate
d lin
ear p
laqu
e ex
tend
ed fr
om h
er le
ft fla
nk
to th
e le
ft lo
wer
qua
dran
t of h
er a
bdom
en.
Figu
re 2
: Ini
tial b
iops
y re
veal
ed m
ild m
id re
ticul
ar
derm
al s
cler
osis
with
thic
keni
ng o
f col
lage
n bu
ndle
s in
the
mid
retic
ular
der
mis
and
loss
of
peria
ppen
dage
al a
dipo
se ti
ssue
. A s
pars
e su
perfi
cial
pe
rivas
cula
r lym
phoi
d in
filtra
te w
as p
rese
nt
Figu
re 3
: Exc
isio
nal b
iops
y re
veal
ed d
erm
al th
icke
ning
an
d sc
lero
sis
with
sup
erim
pose
d de
rmal
cal
cific
atio
n an
d pe
rfora
tion.
The
cal
cifie
d no
dule
was
ass
ocia
ted
with
col
lect
ions
of n
eutro
phils
and
thic
kene
d co
llage
n bu
ndle
s
3.
Vile
la F
A, C
arne
iro
S, R
amos
-e-S
ilva
M. T
reat
men
t of m
orph
ea o
r lo
caliz
ed sc
lero
derm
a: re
view
of t
he li
tera
ture
. J D
rugs
Der
mat
ol.
2010
;9(1
0):1
213-
9.
4.
Zulia
n F,
Mar
tini
G, V
allo
ngo
C, e
t al.
Met
hotr
exat
e tr
eatm
ent i
n ju
veni
le lo
caliz
ed sc
lero
derm
a: a
rand
omiz
ed, d
oubl
e- b
lind,
pla
cebo
-co
ntro
lled
tria
l.Art
hrit
is R
heum
. 201
1;63
(7):
1998
-200
6.
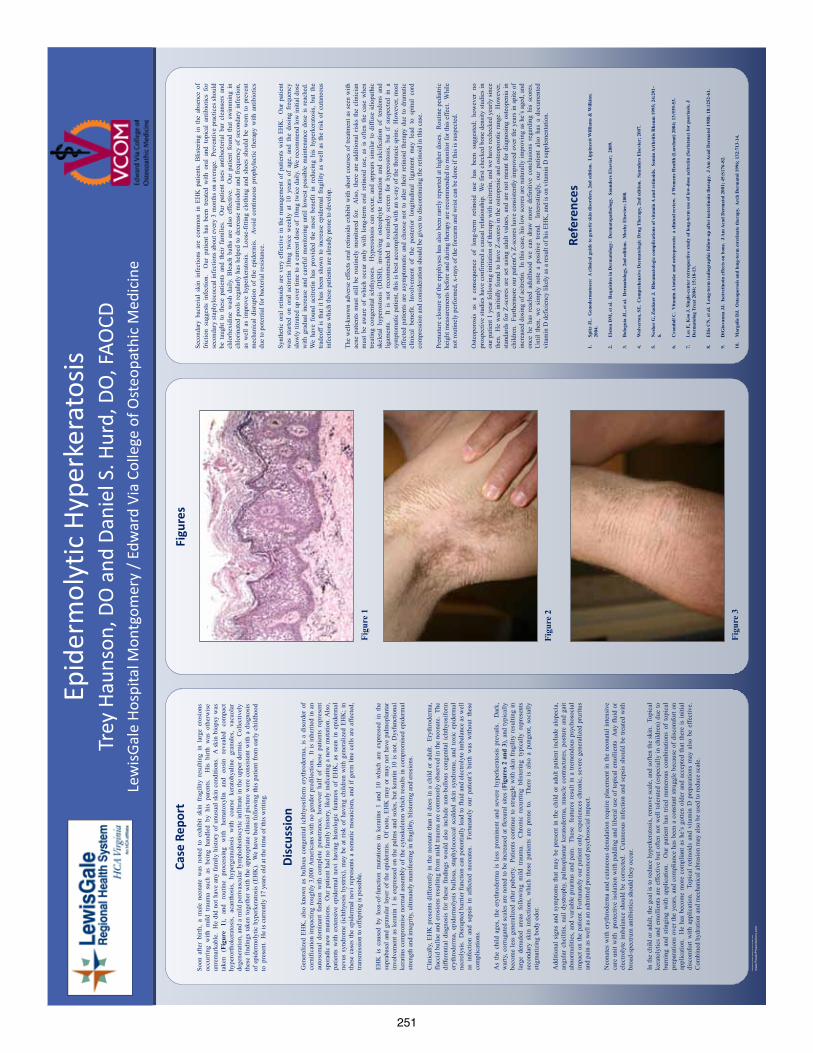
251
RES
EAR
CH
PO
STER
PR
ESEN
TATI
ON
DES
IGN
© 2
012
ww
w.P
oste
rPre
sent
atio
ns.c
om
Soon
afte
r bi
rth,
a m
ale
neon
ate
was
not
ed t
o ex
hibi
t sk
in f
ragi
lity
resu
lting
in
larg
e er
osio
ns
occu
rrin
g w
ith m
ild t
raum
a su
ch a
s be
ing
hand
led
by h
is p
aren
ts.
His
birt
h w
as o
ther
wis
e un
rem
arka
ble.
He
did
not h
ave
any
fam
ily h
isto
ry o
f unu
sual
ski
n co
nditi
ons.
A s
kin
biop
sy w
as
take
n (F
igur
e 1)
, an
d ro
utin
e pr
oces
sing
w
ith
hem
atox
ylin
an
d eo
sin
reve
aled
co
mpa
ct
hype
rorth
oker
atos
is,
acan
thos
is,
hype
rgra
nulo
sis
with
coa
rse
kera
tohy
alin
e gr
anul
es,
vacu
olar
de
gene
ratio
n, a
nd a
mild
per
ivas
cula
r lym
phoh
istio
cytic
infil
trate
in th
e up
per d
erm
is.
Col
lect
ivel
y th
ese
findi
ngs
take
n to
geth
er w
ith th
e ap
prop
riate
clin
ical
pic
ture
wer
e co
nsis
tent
with
a d
iagn
osis
of
epi
derm
olyt
ic h
yper
kera
tosi
s (E
HK
). W
e ha
ve b
een
follo
win
g th
is p
atie
nt fr
om e
arly
chi
ldho
od
to p
rese
nt.
He
is c
urre
ntly
17
year
s ol
d at
the
time
of th
is w
ritin
g.
Case
Rep
ort
Gen
eral
ized
EH
K, a
lso
know
n as
bul
lous
con
geni
tal i
chth
yosi
form
ery
thro
derm
a, is
a d
isor
der
of
corn
ifica
tion
impa
ctin
g ro
ughl
y 3,
000
Am
eric
ans
with
no
gend
er p
redi
lect
ion.
It i
s in
herit
ed in
an
auto
som
al d
omin
ant
fash
ion
with
com
plet
e pe
netra
nce,
how
ever
hal
f of
the
se p
atie
nts
repr
esen
t sp
orad
ic n
ew m
utat
ions
. O
ur p
atie
nt h
ad n
o fa
mily
his
tory
, lik
ely
indi
catin
g a
new
mut
atio
n. A
lso,
pa
tient
s w
ith e
xten
sive
epi
derm
al n
evi
havi
ng h
isto
logi
c fe
atur
es o
f EH
K,
as s
een
in e
pide
rmal
ne
vus
synd
rom
e (ic
hthy
osis
hys
trix)
, may
be
at r
isk
of h
avin
g ch
ildre
n w
ith g
ener
aliz
ed E
HK
; in
thes
e ca
ses
the
epid
erm
al n
evi r
epre
sent
s a
som
atic
mos
aici
sm, a
nd if
ger
m li
ne c
ells
are
affe
cted
, tra
nsm
issi
on to
offs
prin
g is
pos
sibl
e.
EHK
is
caus
ed b
y lo
ss-o
f-fu
nctio
n m
utat
ions
in
kera
tins
1 an
d 10
whi
ch a
re e
xpre
ssed
in
the
supr
abas
al a
nd g
ranu
lar l
ayer
of
the
epid
erm
is.
Of
note
, EH
K m
ay o
r m
ay n
ot h
ave
palm
opla
ntar
in
volv
emen
t as
kera
tin 1
is e
xpre
ssed
on
the
palm
s an
d so
les,
but k
erat
in 1
0 is
not
. Dys
func
tiona
l ke
ratin
s co
mpr
omis
e no
rmal
ass
embl
y of
the
cyto
skel
eton
whi
ch re
sults
in c
ompr
omis
ed e
pide
rmal
st
reng
th a
nd in
tegr
ity, u
ltim
atel
y m
anife
stin
g in
frag
ility
, blis
terin
g an
d er
osio
ns.
Clin
ical
ly, E
HK
pre
sent
s di
ffere
ntly
in th
e ne
onat
e th
an it
doe
s in
a c
hild
or
adul
t. E
ryth
rode
rma,
fla
ccid
bul
lae
and
eros
ions
resu
lting
from
mild
trau
ma
are
com
mon
ly o
bser
ved
in th
e ne
onat
e. T
he
diffe
rent
ial
diag
nosi
s fo
r th
ese
findi
ngs
wou
ld a
lso
incl
ude
non-
bullo
us c
onge
nita
l ic
hthy
osifo
rm
eryt
hrod
erm
a, e
pide
rmol
ysis
bul
losa
, sta
phyl
ococ
cal
scal
ded
skin
syn
drom
e, a
nd t
oxic
epi
derm
al
necr
olys
is.
Dis
rupt
ed b
arrie
r fun
ctio
n ca
n po
tent
ially
lead
to fl
uid
and
elec
troly
te im
bala
nce
as w
ell
as i
nfec
tion
and
seps
is i
n af
fect
ed n
eona
tes.
For
tuna
tely
our
patient’s
birt
h w
as w
ithou
t th
ese
com
plic
atio
ns.
As
the
child
age
s, th
e er
ythr
oder
ma
is l
ess
prom
inen
t an
d se
vere
hyp
erke
rato
sis
prev
ails
. D
ark,
w
arty
, cor
ruga
ted
scal
es a
re n
oted
to b
e in
crea
sed
at fl
exur
al s
ites
(Fig
ures
2 a
nd 3
), an
d ty
pica
lly
beco
me
less
gen
eral
ized
afte
r pub
erty
. Pa
tient
s co
ntin
ue to
stru
ggle
with
ski
n fr
agili
ty re
sulti
ng in
la
rge
denu
ded
area
s fo
llow
ing
mild
tra
uma.
C
hron
ic r
ecur
ring
blis
terin
g ty
pica
lly r
epre
sent
s se
cond
ary
skin
inf
ectio
ns,
whi
ch t
hese
pat
ient
s ar
e pr
one
to.
The
re i
s al
so a
pun
gent
, so
cial
ly
stig
mat
izin
g bo
dy o
dor.
A
dditi
onal
sig
ns a
nd s
ympt
oms
that
may
be
pres
ent i
n th
e ch
ild o
r ad
ult p
atie
nt in
clud
e al
opec
ia,
angu
lar
chei
litis
, nai
l dys
troph
y, p
alm
opla
ntar
ker
atod
erm
a, m
uscl
e co
ntra
ctur
es, p
ostu
re a
nd g
ait
abno
rmal
ities
, and
var
iabl
e pr
uritu
s an
d pa
in.
Thes
e f
eatu
res
resu
lt in
a tr
emen
dous
psy
chos
ocia
l im
pact
on
the
patie
nt. F
ortu
nate
ly o
ur p
atie
nt o
nly
expe
rienc
es c
hron
ic, s
ever
e ge
nera
lized
pru
ritus
an
d pa
in a
s wel
l as a
n ad
mitt
ed p
rono
unce
d ps
ycho
soci
al im
pact
. N
eona
tes
with
ery
thro
derm
a an
d cu
tane
ous
denu
datio
n re
quire
pla
cem
ent i
n th
e ne
onat
al in
tens
ive
care
uni
t with
pro
tect
ive
isol
atio
n w
ith p
addi
ng a
nd li
bera
l use
of t
opic
al e
mol
lient
s A
ny fl
uid
or
elec
troly
te im
bala
nce
shou
ld b
e co
rrec
ted.
C
utan
eous
infe
ctio
n an
d se
psis
sho
uld
be tr
eate
d w
ith
broa
d-sp
ectru
m a
ntib
iotic
s sho
uld
they
occ
ur.
In th
e ch
ild o
r adu
lt, th
e go
al is
to re
duce
hyp
erke
rato
sis,
rem
ove
scal
e, a
nd so
ften
the
skin
. To
pica
l ke
rato
lytic
s an
d em
ollie
nts
are
effe
ctiv
e bu
t ofte
n no
t wel
l tol
erat
ed (
espe
cial
ly in
chi
ldre
n) d
ue to
bu
rnin
g an
d st
ingi
ng w
ith a
pplic
atio
n.
Our
pat
ient
has
trie
d nu
mer
ous
com
bina
tions
of
topi
cal
prep
arat
ions
ove
r the
yea
rs, a
nd c
ompl
ianc
e ha
s be
en a
con
stan
t stru
ggle
bec
ause
of d
isco
mfo
rt on
ap
plic
atio
n.
He
has
beco
me
mor
e co
mpl
iant
as he
’s g
otte
n ol
der
and
acce
pted
that
ther
e is
initi
al
disc
omfo
rt w
ith a
pplic
atio
n.
Topi
cal r
etin
oids
and
vita
min
D p
repa
ratio
ns m
ay a
lso
be e
ffect
ive.
C
ombi
ned
hydr
atio
n an
d m
echa
nica
l abr
asio
n m
ay a
lso
be u
sed
to re
duce
scal
e.
Disc
ussi
on
Seco
ndar
y ba
cter
ial
skin
inf
ectio
ns a
re c
omm
on i
n EH
K p
atie
nts.
Blis
terin
g in
the
abs
ence
of
fric
tion
sugg
ests
inf
ectio
n.
Our
pat
ient
has
bee
n tre
ated
with
ora
l an
d to
pica
l an
tibio
tics
for
seco
ndar
y st
aphy
loco
ccal
infe
ctio
ns a
bout
eve
ry 3
mon
ths
on a
vera
ge.
Prev
entiv
e pr
actic
es sh
ould
be
tau
ght
to t
hese
pat
ient
s an
d th
eir
fam
ilies
. O
ur p
atie
nt u
ses
antib
acte
rial
bar
clea
nser
s an
d ch
lorh
exid
ine
was
h da
ily. B
leac
h ba
ths
are
also
effe
ctiv
e.
Our
pat
ient
fou
nd t
hat
swim
min
g in
ch
lorin
ated
poo
ls r
egul
arly
has
hel
ped
to d
ecre
ase
mal
odor
and
fre
quen
cy o
f se
cond
ary
infe
ctio
n,
as w
ell
as i
mpr
ove
hype
rker
atos
is.
Loos
e-fit
ting
clot
hing
and
sho
es s
houl
d be
wor
n to
pre
vent
m
echa
nica
l di
srup
tion
of t
he e
pide
rmis
. Av
oid
cont
inuo
us p
roph
ylac
tic t
hera
py w
ith a
ntib
iotic
s du
e to
pot
entia
l for
bac
teria
l res
ista
nce.
Sy
nthe
tic o
ral r
etin
oids
are
ver
y ef
fect
ive
in th
e m
anag
emen
t of
patie
nts
with
EH
K.
Our
pat
ient
w
as s
tarte
d on
ora
l ac
itret
in 1
0mg
twic
e w
eekl
y at
10
year
s of
age
, an
d th
e do
sing
fre
quen
cy
slow
ly ti
trate
d up
ove
r tim
e to
a c
urre
nt d
ose
of 1
0mg
twic
e da
ily. W
e re
com
men
d lo
w in
itial
dos
e w
ith g
radu
al i
ncre
ase
and
care
ful
mon
itorin
g un
til l
owes
t po
ssib
le m
aint
enan
ce d
ose
is r
each
ed.
We
have
fou
nd a
citre
tin h
as p
rovi
ded
the
mos
t be
nefit
in
redu
cing
his
hyp
erke
rato
sis,
but
the
trade
off
is th
at it
has
bee
n sh
own
to in
crea
se e
pide
rmal
fra
gilit
y as
wel
l as
the
risk
of c
utan
eous
in
fect
ions
whi
ch th
ese
patie
nts a
re a
lread
y pr
one
to d
evel
op.
The
wel
l-kno
wn
adve
rse
effe
cts
oral
retin
oids
exh
ibit
with
sho
rt co
urse
s of
trea
tmen
t as
seen
with
ac
ne p
atie
nts
mus
t stil
l be
rout
inel
y m
onito
red
for.
Als
o, th
ere
are
addi
tiona
l ris
ks th
e cl
inic
ian
mus
t be
aw
are
of w
hich
occ
ur o
nly
with
lon
g-te
rm o
ral
retin
oid
use,
as
is o
ften
the
case
whe
n tre
atin
g co
ngen
ital i
chth
yose
s. H
yper
osto
sis
can
occu
r, an
d ap
pear
s si
mila
r to
diff
use
idio
path
ic
skel
etal
hyp
eros
tosi
s (D
ISH
), in
volv
ing
oste
ophy
te f
orm
atio
n an
d ca
lcifi
catio
n of
ten
dons
and
lig
amen
ts.
It
is n
ot r
ecom
men
ded
to r
outin
ely
scre
en f
or h
yper
osto
sis,
but
if su
spec
ted
in a
sy
mpt
omat
ic p
atie
nt, t
his
is b
est a
ccom
plis
hed
with
an
x-ra
y of
the
thor
acic
spi
ne.
How
ever
, mos
t af
fect
ed p
atie
nts
are
asym
ptom
atic
and
cho
ose
not t
o al
ter
thei
r re
tinoi
d th
erap
y du
e to
dra
mat
ic
clin
ical
ben
efit.
Inv
olve
men
t of
the
pos
terio
r lo
ngitu
dina
l lig
amen
t m
ay l
ead
to s
pina
l co
rd
com
pres
sion
and
con
side
ratio
n sh
ould
be
give
n to
dis
cont
inui
ng th
e re
tinoi
d in
this
cas
e.
Prem
atur
e cl
osur
e of
the
epip
hyse
s ha
s als
o be
en ra
rely
repo
rted
at h
ighe
r dos
es.
Rou
tine
pedi
atric
he
ight
mea
sure
men
ts b
efor
e an
d du
ring
ther
apy
are
reco
mm
ende
d to
mon
itor f
or th
is e
ffect
. W
hile
no
t rou
tinel
y pe
rfor
med
, x-r
ays
of th
e fo
rear
m a
nd w
rist c
an b
e do
ne if
this
is su
spec
ted.
O
steo
poro
sis
as a
con
sequ
ence
of
long
-term
ret
inoi
d us
e ha
s be
en s
ugge
sted
; ho
wev
er n
o pr
ospe
ctiv
e st
udie
s ha
ve c
onfir
med
a c
ausa
l rel
atio
nshi
p. W
e fir
st c
heck
ed b
one
dens
ity s
tudi
es in
ou
r pat
ient
1 y
ear f
ollo
win
g in
itiat
ion
of th
erap
y w
ith a
citre
tin, a
nd w
e ha
ve re
chec
ked
year
ly si
nce
then
. H
e w
as in
itial
ly fo
und
to h
ave
Z-sc
ores
in th
e os
teop
enic
and
ost
eopo
rotic
rang
e. H
owev
er,
stan
dard
s fo
r Z-
scor
es a
re s
et u
sing
adu
lt va
lues
, and
are
not
mea
nt f
or d
iagn
osin
g os
teop
enia
in
child
ren.
Fur
ther
mor
e ou
r patient’s
Z-s
core
s ha
ve c
onsi
sten
tly im
prov
ed o
ver t
he y
ears
in s
pite
of
incr
ease
d do
sing
of a
citre
tin.
In th
is c
ase,
his
low
sco
res
are
natu
rally
impr
ovin
g as
he’s
aged
, and
on
ce h
e ha
s re
ache
d ad
ulth
ood
we
can
draw
mor
e de
finiti
ve c
oncl
usio
ns r
egar
ding
his
sco
res.
U
ntil
then
, w
e si
mpl
y no
te a
pos
itive
tre
nd.
Int
eres
tingl
y, o
ur p
atie
nt a
lso
has
a do
cum
ente
d vi
tam
in D
def
icie
ncy
likel
y as
a re
sult
of h
is E
HK
, and
is o
n vi
tam
in D
supp
lem
enta
tion.
Refe
renc
es
1.Sp
itz J
L.
Gen
oder
mat
oses
: A
clin
ical
gui
de to
gen
etic
skin
dis
orde
rs, 2
nd e
ditio
n. L
ippi
ncot
t Will
iam
s & W
ilkin
s;
2004
.
2.E
lsto
n D
M, e
t al.
Req
uisi
tes i
n D
erm
atol
ogy:
Der
mat
opat
holo
gy.
Saun
ders
Els
evie
r; 2
009.
3.B
olog
nia
JL, e
t al.
Der
mat
olog
y, 2
nd e
ditio
n. M
osby
Els
evie
r; 2
008.
4.W
olve
rton
, SE
. C
ompr
ehen
sive
Der
mat
olog
ic D
rug
The
rapy
, 2nd
edi
tion.
Sau
nder
s Els
evie
r; 2
007.
5.N
eshe
r G
, Zuc
kner
J.
Rhe
umat
olog
ic c
ompl
icat
ions
of v
itam
in A
and
ret
inoi
ds.
Sem
in A
rthr
itis R
heum
199
5; 2
4:29
1-6.
6.C
rand
all C
. V
itam
in A
inta
ke a
nd o
steo
poro
sis:
a c
linic
al r
evie
w.
J W
omen
s Hea
lth (L
arch
mt)
200
4; 1
3:93
9-53
.
7.L
ee E
, Koo
J. S
ingl
e-ce
nter
ret
rosp
ectiv
e st
udy
of lo
ng-t
erm
use
of l
ow-d
ose
acitr
etin
(Sor
iata
ne) f
or p
sori
asis
. J
Der
mat
olog
Tre
at 2
004;
15:
18-1
3.
8.
Elli
s CN
, et a
l. L
ong-
term
rad
iogr
aphi
c fo
llow
-up
afte
r is
otre
tinoi
n th
erap
y. J
Am
Aca
d D
erm
atol
198
8; 1
8:12
52-6
1.
9.
DiG
iova
nna
JJ.
Isot
retin
oin
effe
cts o
n bo
ne.
J A
m A
cad
Der
mat
ol 2
001;
45:
S176
-82.
10.
Mar
golis
DJ.
Ost
eopo
rosi
s and
long
-ter
m e
tret
inat
e th
erap
y. A
rch
Der
mat
ol 1
996;
132
:713
-14.
Lew
isGal
e Ho
spita
l Mon
tgom
ery
/ Edw
ard
Via
Colle
ge o
f Ost
eopa
thic
Med
icin
e
Trey
Hau
nson
, DO
and
Dan
iel S
. Hur
d, D
O, F
AOCD
Epid
erm
olyt
ic H
yper
kera
tosis
Figu
res
Figu
re 1
Figu
re 2
Figu
re 3

252
Jare
d He
aton
DO,
Larg
o Med
ical C
ente
r, La
rgo F
lorid
a
CAS
E R
EPO
RT
A 52
-year
-old
HIV
pos
itive
mal
e pre
sent
ed w
ith a
2 m
onth
hist
ory o
f a
mild
ly pr
uriti
c sca
ly er
uptio
n on h
is ch
est,
face
and
uppe
r extr
emiti
es.
He w
as re
cent
ly pr
escr
ibed
hydr
ochl
orot
hiaz
ide f
or hy
perte
nsio
n. H
is ot
her m
edica
tions
inclu
ded
lopi
navir
/rito
navir
, em
tricit
abin
e/
teno
fovir
, lans
opra
zole
, ros
uvas
tatin
, pro
met
hazin
e, a
lpra
zola
m,
dron
abin
ol, r
isper
idon
e and
lisin
opril
. He d
enie
d an
y hist
ory o
f dru
g al
lerg
ies o
r sim
ilar r
ashe
s.
Phys
ical e
xam
inat
ion
reve
aled
larg
e, p
ink,
pol
ycyc
lic, s
caly
plaq
ues o
f th
e che
st an
d up
per e
xtrem
ities
with
pro
min
ent e
ryth
ema
of th
e mal
ar
chee
ks (F
igs 1
and
2). T
he p
roxim
al n
ail f
olds
had
dila
ted,
non-
alte
rnat
ing,
vasc
ular
loop
s.
Due t
o the
mor
phol
ogy a
nd d
istrib
utio
n of t
he p
laqu
es, a
nd th
e rec
ent
addi
tion o
f hyd
roch
loro
thia
zide,
our
pat
ient
was
give
n a w
orkin
g di
agno
sis of
suba
cute
cuta
neou
s lup
us er
ythem
atos
us (S
CLE)
. Ro
utin
e blo
od w
ork a
nd b
iops
y, ho
weve
r, re
veal
ed n
o evid
ence
of
SCLE
or co
nnec
tive t
issue
diso
rder
s. Th
e bio
psy w
as co
nsist
ent w
ith a
psor
iasif
orm
spon
giot
ic de
rmat
itis.
Psor
iasis
is a
com
mon
, rec
urre
nt p
apul
osqu
amou
s ski
n dise
ase t
hat
is th
ough
t to b
e a T-
cell a
nd cy
toki
ne m
edia
ted
auto
imm
une d
isord
er
of ke
ratin
ocyte
hyp
erpr
olife
ratio
n. R
ecog
nizin
g pso
riasis
in p
atie
nts
with
HIV
may
be c
halle
ngin
g. Th
e clin
ical a
ppea
ranc
e may
mim
ic ot
her s
kin d
isord
ers a
ssoc
iate
d wi
th H
IV or
even
the c
utan
eous
ad
vers
e effe
cts f
rom
hig
hly a
ctive
antir
etro
viral
ther
apy (
HAAR
T).1
Near
ly al
l HIV
pat
ient
s will
be a
ffect
ed b
y a d
erm
atol
ogic
cond
ition
. In
fact
, it m
ay b
e the
firs
t sig
n of t
heir
HIV i
nfec
tion.
2 Th
e pre
sent
atio
n of
ps
oria
sis an
d m
any o
ther
der
mat
oses
is of
ten a
typica
l and
mor
e se
vere
in th
ese p
atie
nts.1,
3,4
Furth
erm
ore,
a va
riety
of d
erm
atol
ogic
com
plica
tions
from
HAA
RT ca
n mak
e it d
ifficu
lt to
dist
ingu
ish
psor
iasis
from
a cu
tane
ous a
dver
se ef
fect
of t
hese
med
icatio
ns.5
Psor
iasis
can o
ccur
at an
y sta
ge of
HIV
, but
usua
lly ap
pear
s lat
e in t
he
non-
term
inal
stag
e.1,6 A
dist
ingu
ishin
g fea
ture
of H
IV-a
ssoc
iate
d ps
oria
sis is
that
mul
tiple
form
s, in
cludi
ng gu
ttate
, ery
thro
derm
ic,
inve
rse,
and
acra
l pso
riasis
, can
occu
r sim
ulta
neou
sly in
the s
ame
patie
nt. In
addi
tion,
thes
e pat
ient
s may
hav
e pso
riatic
arth
ritis
which
ha
s a hi
gher
incid
ence
in th
is po
pula
tion.
1,4,
7 In
non-
HIV
indi
vidua
ls, im
mun
osup
pres
sive t
hera
py th
at d
ecre
ases
T-ce
ll cou
nts t
ypica
lly im
prov
es p
soria
sis. Ho
weve
r, wh
en C
D4 T-
cell
coun
ts d
ecre
ase i
n HIV
pat
ient
s pso
riasis
par
adox
ically
wor
sens
. Va
rious
expl
anat
ions
for t
his p
arad
ox ha
ve b
een p
ropo
sed
inclu
ding
an
incr
ease
in th
e CD8
/CD4
T-ce
ll rat
io, a
n alte
ratio
n of
infla
mm
ator
y cy
toki
nes f
rom
the c
lass
ic T h
elpe
r cel
l 1 to
the T
help
er ce
ll 2
path
way,
an in
crea
se in
inte
rfero
n-
and
supe
rant
igen
stim
ulat
ion b
y HI
V, ot
her v
iruse
s or b
acte
ria. 1,
7-9
DIS
CUSS
ION
REF
EREN
CES
1.M
orar
N, W
illis-
Owen
SA, M
aure
r T, e
t al.
HIV-
asso
ciate
d pso
riasis
: pat
hoge
nesis
, clin
ical fe
atur
es, a
nd m
anag
emen
t.
Lanc
et In
fect
Dis.
201
0;10
:470
-478
2.
Garm
an M
E, Ty
ring S
K. T
he cu
tane
ous m
anife
stat
ions
of H
IV in
fect
ion.
Der
mat
ol C
lin. 2
002;
20:1
93-2
08
3.M
orar
N, D
lova
NC,
Mos
am A
, et a
l. Cu
tane
ous m
anife
stat
ions
of H
IV in
Kwa
-Zul
u Nat
al, S
outh
Afri
ca. I
nter
natio
nal
Jour
nal o
f Der
mat
olog
y. 2
006;
45:1
006-
1007
4.
Men
on K
, Van
Voor
hees
AS,
Beb
o BF J
r, et
al.
Psor
iasis
in p
atie
nts w
ith H
IV in
fect
ion:
From
the m
edica
l boa
rd of
the
Natio
nal P
soria
sis Fo
unda
tion.
J Am
Aca
d De
rmat
ol. 2
010;
62(2
):291
-299
5.
Kong
HH,
Mye
rs S
A. C
utan
eous
effe
cts o
f hig
hly a
ctive
ant
iretro
viral
ther
apy i
n HIV
-infe
cted
patie
nts.
Der
mat
olog
ic Th
erap
y . 2
005;
18:5
8-66
6.
Mah
ajan
VK, S
harm
a NL,
Sarin
S, e
t al.
Tripl
e ant
iretro
viral
ther
apy i
mpr
oves
pso
riasis
asso
ciate
d hu
man
im
mun
odef
icien
cy vi
rus i
nfec
tion:
a cli
nico
-ther
apeu
tic ex
perie
nce.
JEA
DV. 2
008;
22:1
017-
1018
7.
Mal
lon E
, Bun
ker C
B. H
IV-A
ssoc
iate
d Pso
riasis
. AID
S PA
TIENT
CAR
E an
d STD
s. 2
000;
14(5
):239
-246
8.
Fife D
J, W
alle
r JM
, Jef
fes E
W, e
t al.
Unra
velin
g the
par
adox
es of
HIV
-ass
ocia
ted p
soria
sis: a
revie
w of
T-ce
ll sub
sets
an
d cyto
kine p
rofil
es. D
erm
atol
ogy O
nlin
e Jou
rnal
. 200
7;13
(2):4
9.
Nam
azi M
R. P
arad
oxica
l Exa
cerb
atio
n of P
soria
sis in
AID
S: P
ropo
sed E
xpla
natio
ns In
cludi
ng th
e Pot
entia
l Rol
es o
f Su
bsta
nce P
and
Gram
-Neg
ative
Bac
teria
. Aut
oim
mun
ity. 2
004;
37(1
):67-
71
FIG
URES
The m
anag
emen
t of p
soria
sis in
HIV
pos
itive
pat
ient
s can
be
chal
leng
ing a
s it t
ends
to b
e mor
e sev
ere a
nd re
calci
trant
to
treat
men
t. Th
e Nat
iona
l Pso
riasis
Foun
datio
n rec
ently
pub
lishe
d gu
idel
ines
for t
reat
men
t of p
soria
sis in
HIV
pat
ient
s. Th
e aut
hors
re
com
men
d to
pica
ls as
firs
t-lin
e the
rapy
in m
ild to
mod
erat
e di
seas
e, fo
llowe
d by
antir
etro
viral
s and
ultr
avio
let l
ight
for
mod
erat
e to s
ever
e pso
riasis
. Ora
l ret
inoi
ds sh
ould
be c
onsid
ered
se
cond
-line
for m
oder
ate t
o sev
ere d
iseas
e. Im
mun
osup
pres
sive
agen
ts in
cludi
ng hy
drox
yure
a, cy
closp
orin
e, m
etho
trexa
te a
nd
tum
or ne
cros
is fa
ctor
-α in
hibi
tors
may
be c
onsid
ered
for s
ever
e an
d re
fract
ory d
iseas
e. T
he au
thor
s rec
omm
end
close
mon
itorin
g fo
r adv
erse
even
ts es
pecia
lly w
hen u
sing i
mm
unos
uppr
essiv
e th
erap
y. M
onito
ring o
f CD4
T-ce
ll cou
nts a
nd vi
ral lo
ad in
co
ordi
natio
n with
an in
fect
ious
dise
ase s
pecia
list i
s also
ad
vised
.4
1 2
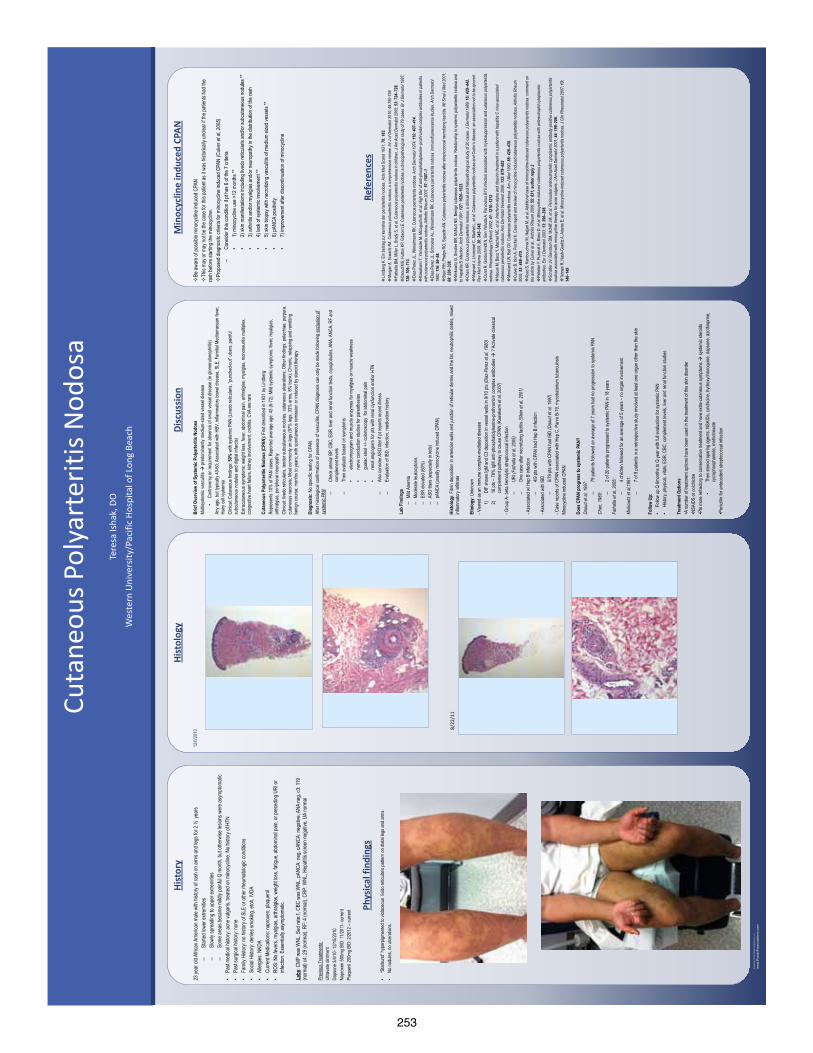
253
QU
ICK
TIPS
(-
-TH
IS S
ECTI
ON
DO
ES N
OT
PRIN
T--)
This
Pow
erPo
int
tem
plat
e re
quir
es b
asic
Pow
erPo
int
(ver
sion
200
7 or
new
er)
skill
s. B
elow
is a
list
of
com
mon
ly a
sked
que
stio
ns s
peci
fic
to t
his
tem
plat
e.
If y
ou a
re u
sing
an
olde
r ve
rsio
n of
Pow
erPo
int
som
e te
mpl
ate
feat
ures
may
not
wor
k pr
oper
ly.
U
sing
the
tem
plat
e
Veri
fyin
g th
e qu
alit
y of
you
r gr
aphi
cs
Go
to t
he V
IEW
men
u an
d cl
ick
on Z
OO
M t
o se
t yo
ur
pref
erre
d m
agni
fica
tion
. Th
is t
empl
ate
is a
t 10
0%
the
size
of
the
fina
l pos
ter.
All
text
and
gra
phic
s w
ill
be p
rint
ed a
t 10
0% t
heir
siz
e. T
o se
e w
hat
your
po
ster
will
look
like
whe
n pr
inte
d, s
et t
he z
oom
to
100%
and
eva
luat
e th
e qu
alit
y of
all
your
gra
phic
s be
fore
you
sub
mit
you
r po
ster
for
pri
ntin
g.
Usi
ng t
he p
lace
hold
ers
To a
dd t
ext
to t
his
tem
plat
e cl
ick
insi
de a
pl
aceh
olde
r an
d ty
pe in
or
past
e yo
ur t
ext.
To
mov
e a
plac
ehol
der,
clic
k on
it o
nce
(to
sele
ct it
), p
lace
yo
ur c
urso
r on
its
fram
e an
d yo
ur c
urso
r w
ill c
hang
e to
thi
s sy
mbo
l:
Then
, cl
ick
once
and
dra
g it
to
its
new
loca
tion
whe
re y
ou c
an r
esiz
e it
as
need
ed.
Addi
tion
al p
lace
hold
ers
can
be f
ound
on
the
left
si
de o
f th
is t
empl
ate.
M
odif
ying
the
layo
ut
This
tem
plat
e ha
s fo
ur
diff
eren
t co
lum
n la
yout
s.
Righ
t-cl
ick
your
mou
se
on t
he b
ackg
roun
d an
d
clic
k on
“La
yout
” to
see
th
e la
yout
opt
ions
. Th
e co
lum
ns in
the
pro
vide
d la
yout
s ar
e fi
xed
and
cann
ot b
e m
oved
but
adv
ance
d us
ers
can
mod
ify
any
layo
ut b
y go
ing
to V
IEW
and
the
n SL
IDE
MAS
TER.
Im
port
ing
text
and
gra
phic
s fr
om e
xter
nal s
ourc
es
TEXT
: Pa
ste
or t
ype
your
tex
t in
to a
pre
-exi
stin
g pl
aceh
olde
r or
dra
g in
a n
ew p
lace
hold
er f
rom
the
le
ft s
ide
of t
he t
empl
ate.
Mov
e it
any
whe
re a
s ne
eded
. PH
OTO
S: D
rag
in a
pic
ture
pla
ceho
lder
, si
ze it
fir
st,
clic
k in
it a
nd in
sert
a p
hoto
fro
m t
he m
enu.
TA
BLES
: Yo
u ca
n co
py a
nd p
aste
a t
able
fro
m a
n ex
tern
al d
ocum
ent
onto
thi
s po
ster
tem
plat
e. T
o ad
just
th
e w
ay t
he t
ext
fits
wit
hin
the
cells
of
a ta
ble
that
has
bee
n pa
sted
, ri
ght-
clic
k on
the
tab
le,
clic
k FO
RMAT
SH
APE
the
n cl
ick
on T
EXT
BOX
and
chan
ge t
he IN
TERN
AL M
ARG
IN v
alue
s to
0.2
5 M
odif
ying
the
col
or s
chem
e To
cha
nge
the
colo
r sc
hem
e of
thi
s te
mpl
ate
go t
o th
e “D
esig
n” m
enu
and
clic
k on
“Co
lors
”. Y
ou c
an
choo
se f
rom
the
pro
vide
col
or c
ombi
nati
ons
or y
ou
can
crea
te y
our
own.
QU
ICK
DES
IGN
GU
IDE
(--T
HIS
SEC
TIO
N D
OES
NO
T PR
INT-
-)
Th
is P
ower
Poin
t 20
07 t
empl
ate
prod
uces
a 3
6”x4
8”
prof
essi
onal
po
ster
. It
will
sav
e yo
u va
luab
le t
ime
plac
ing
titl
es,
subt
itle
s, t
ext,
and
gra
phic
s.
Use
it t
o cr
eate
you
r pr
esen
tati
on.
Then
sen
d it
to
Post
erPr
esen
tati
ons.
com
for
pre
miu
m q
ualit
y, s
ame
day
affo
rdab
le p
rint
ing.
W
e pr
ovid
e a
seri
es o
f on
line
tuto
rial
s th
at w
ill
guid
e yo
u th
roug
h th
e po
ster
des
ign
proc
ess
and
answ
er y
our
post
er p
rodu
ctio
n qu
esti
ons.
Vi
ew o
ur o
nlin
e tu
tori
als
at:
htt
p://
bit.
ly/P
oste
r_cr
eati
on_h
elp
(c
opy
and
past
e th
e lin
k in
to y
our
web
bro
wse
r).
For
assi
stan
ce a
nd t
o or
der
your
pri
nted
pos
ter
call
Post
erPr
esen
tati
ons.
com
at 1.
866.
649.
3004
Obj
ect
Plac
ehol
ders
Use
the
pla
ceho
lder
s pr
ovid
ed b
elow
to
add
new
el
emen
ts t
o yo
ur p
oste
r: D
rag
a pl
aceh
olde
r on
to
the
post
er a
rea,
siz
e it
, an
d cl
ick
it t
o ed
it.
Sect
ion
Hea
der
plac
ehol
der
Mov
e th
is p
refo
rmat
ted
sect
ion
head
er p
lace
hold
er
to t
he p
oste
r ar
ea t
o ad
d an
othe
r se
ctio
n he
ader
. U
se s
ecti
on h
eade
rs t
o se
para
te t
opic
s or
con
cept
s w
ithi
n yo
ur p
rese
ntat
ion.
Te
xt p
lace
hold
er
Mov
e th
is p
refo
rmat
ted
text
pla
ceho
lder
to
the
post
er t
o ad
d a
new
bod
y of
tex
t.
Pict
ure
plac
ehol
der
Mov
e th
is g
raph
ic p
lace
hold
er o
nto
your
pos
ter,
siz
e it
fir
st,
and
then
clic
k it
to
add
a pi
ctur
e to
the
po
ster
.
RES
EAR
CH
PO
STER
PR
ESEN
TATI
ON
DES
IGN
© 2
012
ww
w.P
oste
rPre
sent
atio
ns.c
om
© 2
012
Post
erPr
esen
tatio
ns.c
om
2
117
Four
th S
tree
t , U
nit C
Ber
kele
y CA
947
10
p
oste
rpre
sent
er@
gmai
l.com
St
uden
t di
scou
nts
are
avai
labl
e on
our
Fac
eboo
k pa
ge.
Go
to P
oste
rPre
sent
atio
ns.c
om a
nd c
lick
on t
he F
B ic
on.
23 ye
ar ol
d Afric
an A
meric
an m
ale w
ith hi
story
of ra
sh on
arms
and l
egs f
or 2
½ ye
ars
–St
arted
lowe
r extr
emitie
s –
Slow
ly sp
read
ing to
uppe
r extr
emitie
s –
Some
area
s bec
ame m
ildly
painf
ul Q
month
, but
other
wise
lesio
ns w
ere a
symp
tomati
c •
Past
medic
al his
tory:
acne
vulga
ris, tr
eated
on m
inocy
cline
. No h
istor
y of H
TN
•Pa
st su
rgica
l hist
ory:
none
•
Fami
ly Hi
story:
no hi
story
of SL
E or
othe
r rhe
umato
logic
cond
itions
•
Socia
l Hist
ory:
denie
s smo
king,
etoh,
IVDA
•
Aller
gies:
NKDA
•
Curre
nt Me
dicati
ons:
napr
oxen
, plaq
uenil
•
ROS:
No f
ever
s, my
algias
, arth
ralgi
as, w
eight
loss,
fatigu
e, ab
domi
nal p
ain, o
r pre
cedin
g URI
or
infec
tion.
Esse
ntiall
y asy
mptom
atic.
La
bs: C
MP w
as W
NL, S
ed ra
te:1,
CBC
was W
NL, p
ANCA
: neg
, cAN
CA: n
egati
ve, A
NA ne
g, c3
: 119
(n
orma
l) c4:
29 (n
orma
l), RF
: 4 (n
orma
l), CR
P: W
NL, H
epati
tis sc
reen
nega
tive,
UA no
rmal
Pr
eviou
s Tre
atmen
ts:
Ultra
vate
ointm
ent
Daps
one
3/4/10
- 12/1
5/201
0 Na
prox
en 5
00mg
BID
: 11/2
011-
curre
nt Pl
aque
nil 2
00mg
BID
: 2/20
12 –
curre
nt
Hist
ory
Phys
ical
find
ings
12/6/
2010
Hist
olog
y Br
ief O
verv
iew o
f Sys
tem
ic Po
lyarte
ritis
Nodo
sa
Multis
ystem
ic va
sculi
tis
pred
omina
ntly m
edium
-size
d ve
ssel
disea
se
•Co
ntrov
ersy
on re
quire
ment
for ab
senc
e of
small
vess
el dis
ease
(ie g
lomer
ulone
phriti
s) An
y age
, but
typica
lly 40
-60;
Asso
ciated
with
HBV
, infla
mmato
ry bo
wel d
iseas
e, SL
E, F
amilia
l Med
iterra
nean
feve
r, Ha
iry ce
ll leu
kemi
a Cl
inica
l: Cuta
neou
s find
ings:
50%
with
syste
mic P
AN (L
ivedo
retic
ularis
, “pu
nche
d-ou
t” ulc
ers,
painf
ul su
bcuta
neou
s nod
ules a
nd di
gital
infar
cts)
Extra
cutan
eous
symp
toms:
weigh
t loss
, feve
r, abd
omina
l pain
, arth
ralgi
as, m
yalgi
as, m
onon
euriti
s mult
iplex
, co
nges
tive
hear
t fail
ure,
kidne
y inv
olvem
ent,
orch
itis, C
VA ar
e rar
e
Cuta
neou
s Pol
yarte
ritis
Nodo
sa (C
PAN)
: Firs
t des
cribe
d in
1931
by L
indbe
rg
Repr
esen
ts 10
% o
f PAN
case
s; Re
porte
d av
erag
e ag
e: 43
(6-7
2); M
ild sy
stemi
c sym
ptoms
: feve
r, mya
lgias
, ar
thralg
ias, p
eriph
eral
neur
opath
y Cl
inica
l: live
do re
ticula
ris, te
nder
subc
utane
ous n
odule
s, cu
taneo
us u
lcera
tions
; Othe
r find
ings:
petec
hiae,
purp
ura,
cutan
eous
nec
rosis
; Mos
t com
monly
on le
gs (9
7% le
gs, 3
3% a
rms,
8% tr
unk);
Chr
onic,
relap
sing
and
remi
tting
benig
n co
urse
; mon
ths to
year
s; wi
th sp
ontan
eous
remi
ssion
or in
duce
d by
ster
oid th
erap
y
Diag
nosis
: No s
pecif
ic tes
ting
for C
PAN
After
histo
logica
l con
firmati
on o
f pre
senc
e of
vasc
ulitis
, CPA
N dia
gnos
is ca
n only
be m
ade
follow
ing e
xclus
ion o
f sy
stem
ic PA
N –Ch
eck a
rteria
l BP,
CBC,
ESR
, live
r and
rena
l func
tion
tests,
cryo
globu
lins,
ANA,
ANC
A, R
F an
d co
mplem
ent le
vels
–Th
en e
valua
te ba
sed
on sy
mptom
s:
•ele
ctrom
yogr
am a
nd m
uscle
enzy
mes f
or m
yalgi
as or
mus
cle w
eakn
ess
•ne
rve co
nduc
tion
studie
s for
pare
sthes
ias
•gu
aiac s
tool +
/- co
lonos
copy
for
abdo
mina
l pain
•
rena
l ang
iogra
m for
pts w
ith re
nal d
ysfun
ction
and
/or H
TN
–Al
so co
nside
r ASO
titer
if pt
repo
rts re
cent
illnes
s –
Evalu
ation
of IB
D, in
fectio
n, me
dicati
on h
istor
y
Lab
Find
ings
–
Mild
Anem
ia –
Mode
rate
leuko
cytos
is –
ESR
eleva
ted (6
0%)
–AS
O tite
rs (e
spec
ially
in kid
s) –
pANC
A (u
suall
y mino
cylci
ne in
duce
d CP
AN)
Hist
olog
y: Fib
rin de
posit
ion in
arter
iolar
wall
s and
junc
tion
of re
ticula
r der
mis a
nd th
e fat,
neu
troph
ilic d
ebris
, mixe
d inf
lamma
tory i
nfiltra
te
Et
iolo
gy: U
nkno
wn
- View
ed as
an im
mune
comp
lex-m
ediat
ed d
iseas
e 1)
DIF
show
s IgM
and
C3 de
posit
ion in
vess
el wa
lls in
9/10
pts
(Diaz
-Per
ez e
t al, 1
980)
2)
16 pt
s – 78
% Ig
M an
ti-pho
spha
tidyls
erine
-pro
throm
bin co
mplex
antib
odies
?
Activ
ate cl
assic
al co
mplem
ent p
athwa
y to c
ause
CPA
N (K
awak
ami e
t al, 2
007)
- G
roup
A- b
eta h
emoly
tic st
repto
cocc
al inf
ectio
n –
URI (
Fath
alla
et a
l, 200
5)
–On
e cas
e afte
r nec
rotiz
ing fa
ciitis
(Ste
in et
al, 2
001)
- A
ssoc
iated
w/ H
ep B
infec
tion
–4/9
pts w
ith C
PAN
had
Hep B
infec
tion
- A
ssoc
iated
with
IBD
–5/7
9 pts
with
CPA
N ha
d IB
D (D
aoud
et a
l, 199
7)
- Cas
e rep
orts
of CP
AN as
socia
ted w
ith H
ep C
, Par
vo B
-19,
myco
bater
ium tu
bercu
losis
Mino
cycli
ne in
duce
d CP
AN
Does
CPA
N pr
ogre
ss to
syst
emic
PAN?
Da
oud
et a
l, 199
7:
–79
patie
nts fo
llowe
d an
aver
age
of 7 y
ears
had
no pr
ogre
ssion
to sy
stemi
c PAN
Ch
en, 1
989:
–2 o
f 20 p
atien
ts pr
ogre
ssed
to sy
stemi
c PAN
in 18
year
s Fa
thall
a et
al, 2
005:
–
4 chil
dren
follo
wed
for an
aver
age
of 5 y
ears
– no o
rgan
invo
lveme
nt M
inkow
itz e
t al,1
991:
–
7 of 9
patie
nts in
a re
trosp
ectiv
e stud
y inv
olved
at le
ast o
ne o
rgan
othe
r tha
n the
skin
Fo
llow
Up:
•Fo
llow
up Q
6mon
ths to
Q ye
ar w
ith fu
ll eva
luatio
n for
syste
mic P
AN
•Hi
story,
phys
ical, v
itals,
ESR
, CBC
, com
pleme
nt lev
els, li
ver a
nd re
nal fu
nctio
n stu
dies
Trea
tmen
t Opt
ions
•A
numb
er o
f trea
tmen
t opti
ons h
ave b
een
used
in th
e tre
atmen
t of th
is sk
in dis
orde
r •N
SAID
S or
colch
icine
•P
ts mo
re re
fracto
ry to
cons
erva
tive t
reatm
ent a
nd h
ave e
xtra-
cutan
eous
symp
toms
syste
mic s
teroid
s •
Then
ster
oid sp
aring
agen
ts: N
SAID
s, co
lchici
ne, h
ydro
xych
loroq
uine,
daps
one,
azoth
ioprin
e, cy
cloph
osph
amide
, meth
otrex
ate
•Pen
icillin
for a
ntece
dent
strep
tococ
cal in
fectio
n
Disc
ussi
on
Min
ocyc
line
indu
ced
CPAN
Be
awar
e of p
ossib
le mi
nocy
cline
indu
ced C
PAN
Th
is ma
y or m
ay no
t be t
he ca
se fo
r this
patie
nt as
it wa
s hist
orica
lly un
clear
if the
patie
nts ha
d the
ra
sh be
fore s
tartin
g the
mino
cycli
ne.
Pr
opos
ed di
agno
sitc c
riteria
for m
inocy
cline
indu
ced C
PAN
(Culv
er e
t al, 2
005)
–
Cons
ider t
his co
nditio
n if p
t has
6 of
the 7
criter
ia •
1) m
inocy
cline
use >
12 m
onths
**
•2)
skin
manif
estat
ions i
nclud
ing liv
edo r
eticu
laris
and/o
r sub
cutan
eous
nodu
les **
•
3) ar
thritis
and/o
r mya
lgias
and/o
r neu
ropa
thy in
the d
istrib
ution
of th
e ras
h •
4) la
ck of
syste
mic i
nvolv
emen
t **
•5)
skin
biops
y with
necro
tizing
vasc
ulitis
of m
edium
size
d ves
sels
** •
6) pA
NCA
posit
ivity
•7)
impr
ovem
ent a
fter d
iscon
tinua
tion o
f mino
cycli
ne
Refe
renc
es
Lin
dber
g K. E
in be
itrag z
ur ke
nntni
s der
peria
rteriti
s nod
osa.
Acta
Med
Sca
nd 19
31; 7
6: 18
3.
Mor
gan A
, Scw
artz
RA. C
utan
eous
polua
rterit
is no
dosa
: a co
mpr
ehen
sive r
eivew
. Int
J of
Der
mat
ol 20
10; 4
9:75
0-75
6
Fatha
lla B
M, M
iller L
, Bra
dy S
, et a
l. Cut
aneo
us po
lyarte
ritis
nodo
sa in
child
ren.
J Am
Aca
d De
rmat
ol 20
05; 5
3: 72
4–72
8.
Daou
d MS,
Hutt
on K
P, Gi
bson
LE. C
utane
ous p
eriar
teritis
nodo
sa: a
clini
copa
tholog
ical s
tudy o
f 79 c
ases
. Br J
Der
mat
ol 19
97;
136:
706–
713.
Di
az-P
erez
JL, W
inkelm
ann R
K. C
utane
ous p
eriar
teritis
nodo
sa. A
rch
Derm
atol
1974
; 110
: 407
–414
.
Kawa
kami
T, Y
amaz
aki M
, Mizo
guch
i M, e
t al. H
igh tit
er o
f ant
i-pho
spha
tidyls
erine
–pro
thro
mbin
com
plex a
ntibo
dies i
n pa
tient
s wi
th cu
tane
ous p
olyar
terit
is no
dosa
. Arth
ritis
Rheu
m 20
07; 5
7: 15
07–1
Diaz
-Per
ez JL
, Sch
roete
r AL,
Wink
elman
n RK.
Cuta
neou
s per
iarter
itis no
dosa
: immu
noflu
ores
cenc
e stud
ies. A
rch
Derm
atol
1980
; 116
: 56–
58.
St
ein R
H, P
helps
RG,
Sap
adin
AN. C
utane
ous p
olyar
teritis
nodo
sa af
ter st
repto
cocc
al ne
crotiz
ing fa
sciiti
s. M
t Sina
i J M
ed 20
01;
68: 3
36–3
38.
Mi
nkow
itz G
, Smo
ller B
R, M
cNutt
NS.
Ben
ign cu
taneo
us po
lyarte
ritis n
odos
a. Re
lation
ship
to sy
stemi
c poly
arter
itis no
dosa
and
to he
patiti
s B in
fectio
n. Ar
ch D
erm
atol
1991
; 127
: 152
0–15
23.
Ch
en K
R. C
utane
ous p
olyar
teritis
nodo
sa: a
clini
cal a
nd hi
stopa
tholog
ical s
tudy o
f 20 c
ases
. J D
erm
atol
1989
; 16:
429–
442.
Ma
gnan
t J, L
homm
et C,
Mac
het L
, et a
l. Cut
aneo
us po
lyarte
ritis
nodo
sa an
d Cro
hn’s
disea
se: a
n as
socia
tion n
ot to
be i
gnor
ed.
Rev M
ed In
tern
e 200
9; 30
: 345
–348
.
Durst
R, G
oldsc
hmidt
N, B
en Ye
huda
A. P
arvo
virus
B19
infec
tion a
ssoc
iated
with
mye
losup
pres
sion a
nd cu
taneo
us po
lyarte
ritis
nodo
sa. R
heum
atolo
gy (O
xford
) 200
2; 41
: 121
0–12
12
Na
ouri M
, Bac
q Y, M
ache
t MC,
et a
l. Int
erfe
ron-
alpha
and r
ibavir
in tre
atm
ent in
a p
atien
t with
hep
atitis
C vi
rus-
asso
ciate
d cu
tane
ous p
eriar
terit
is no
dosa
. Ann
Der
mat
ol Ve
nere
ol 20
06; 1
33: 6
79–6
82
Mo
relan
d LW
, Ball
GV.
Cuta
neou
s poly
arter
itis no
dosa
. Am
J M
ed 19
90; 8
8: 42
6–43
0.
Culve
r B, It
kin A
, Pisc
hel K
. Cas
e rep
ort a
nd re
view
of mi
nocy
cline
-indu
ced c
utane
ous p
olyar
teritis
nodo
sa. A
rthrit
is Rh
eum
20
05; 5
3: 46
8–47
0.
Abad
S, K
ambo
uchn
er M
, Nejj
ari M
, et a
l. Add
itiona
l cas
e of
mino
cycli
ne-in
duce
d cut
aneo
us po
lyarte
ritis
nodo
sa: c
omm
ent o
n th
e arti
cle b
y Culv
er e
t al..
Arth
ritis
Rheu
m 20
06; 5
5: 83
1; au
thor
repl
y 2
Pe
lletie
r F, P
uzen
at E,
Blan
c D, e
t al. M
inocy
cline
-indu
ced c
utan
eous
polya
rterit
is no
dosa
with
ant
ineut
roph
il cyto
plasm
ic an
tibod
ies. E
ur J
Derm
atol
2003
; 13:
396–
398.
Sc
haffe
r JV,
Dav
idson
DM,
McN
iff JM
, et a
l. Per
inucle
ar an
tineu
troph
ilic cy
topla
smic
antib
ody-
posit
ive cu
tane
ous p
olyar
terit
is no
dosa
asso
ciate
d with
mino
cycli
ne th
erap
y for
acn
e vu
lgaris
. J A
m A
cad
Derm
atol
2001
; 44:
198–
206.
Te
hran
i R, N
ash-
Goeli
tz A,
Ada
ms E
, et a
l. Mino
cycli
ne-in
duce
d cu
tane
ous p
olyar
terit
is no
dosa
. J C
lin R
heum
atol
2007
; 13:
14
6–14
9
•“S
tarbu
rst” h
yper
pigme
nted
to vio
laceo
us li
vido r
eticu
laris
patte
rn o
n dist
al leg
s and
arms
•
No no
dules
, no u
lcera
tions
.
Wes
tern
Uni
vers
ity/P
acifi
c Ho
spita
l of L
ong
Beac
h
Te
resa
Isha
k, D
O
Cuta
neou
s Pol
yart
eriti
s Nod
osa
8/22
/11
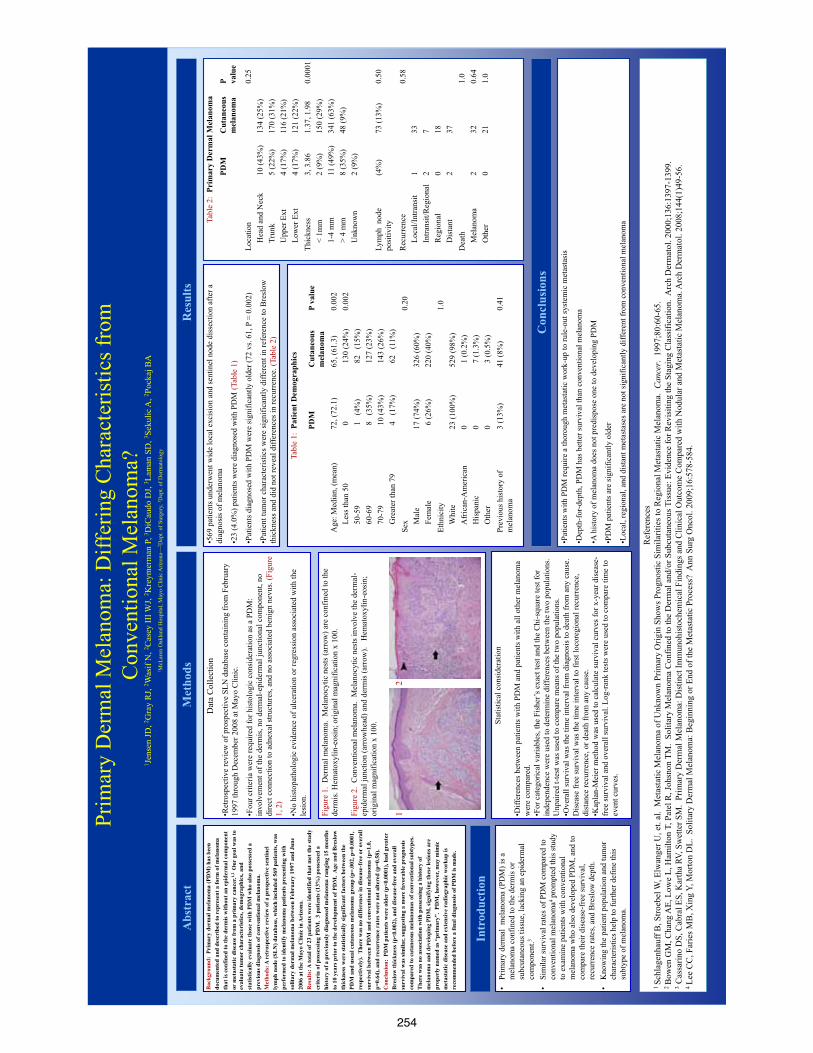
254
Tabl
e 1:
Pat
ient
Dem
ogra
phic
s
Abs
trac
t R
esul
ts
Bac
kgro
und:
Pri
mar
y de
rmal
mel
anom
a (P
DM
) has
bee
n do
cum
ente
d an
d de
scri
bed
to r
epre
sent
a fo
rm o
f mel
anom
a th
at is
con
fined
to th
e de
rmis
with
out a
n ep
ider
mal
com
pone
nt
or m
etas
tatic
dis
ease
from
a p
rim
ary
canc
er.1,
2 O
ur g
oal w
as to
ev
alua
te tu
mor
cha
ract
eris
tics,
dem
ogra
phic
s, an
d st
atis
tical
ly e
valu
ate
thos
e w
ith P
DM
who
als
o po
sses
sed
a pr
evio
us d
iagn
osis
of c
onve
ntio
nal m
elan
oma.
M
etho
ds: A
ret
rosp
ectiv
e re
view
of a
pro
spec
tive
sent
inel
ly
mph
nod
e (S
LN
) dat
abas
e, w
hich
incl
uded
569
pat
ient
s, w
as
perf
orm
ed to
iden
tify
mel
anom
a pa
tient
s pre
sent
ing
with
so
litar
y de
rmal
mel
anom
a be
twee
n Fe
brua
ry 1
997
and
June
20
06 a
t the
May
o C
linic
in A
rizo
na.
R
esul
ts: A
tota
l of 2
3 pa
tient
s wer
e id
entif
ied
that
met
the
stud
y
crite
ria
of p
osse
ssin
g PD
M.
3 pa
tient
s (13
%) p
osse
ssed
a
hist
ory
of a
pre
viou
sly
diag
nose
d m
elan
oma
rang
ing
15 m
onth
s to
10
year
s pri
or to
the
deve
lopm
ent o
f PD
M.
Age
and
Bre
slow
th
ickn
ess
wer
e st
atis
tical
ly s
igni
fican
t fac
tors
bet
wee
n th
e PD
M a
nd u
sual
cut
aneo
us m
elan
oma
grou
p (p
=.00
2, p
=0.0
001,
re
spec
tivel
y).
The
re w
as n
o di
ffer
ence
in d
isea
se-f
ree
or o
vera
ll su
rviv
al b
etw
een
PDM
and
con
vent
iona
l mel
anom
a (p
=1.0
, p=
0.64
), an
d re
curr
ence
rat
es w
ere
not a
ltere
d (p
=0.5
8).
C
oncl
usio
n: P
DM
pat
ient
s wer
e ol
der
(p<0
.000
1), h
ad g
reat
er
Bre
slow
thic
knes
s (p
<0.0
02),
and
dise
ase-
free
and
ove
rall
surv
ival
was
sim
ilar,
sugg
estin
g a
mor
e fa
vora
ble
prog
nosi
s co
mpa
red
to c
utan
eous
mel
anom
as o
f con
vent
iona
l sub
type
s.
The
re w
as n
o as
soci
atio
n w
ith p
osse
ssin
g a
hist
ory
of
mel
anom
a an
d de
velo
ping
PD
M, s
igni
fyin
g th
ese
lesi
ons a
re
prop
erly
nam
ed a
s “pr
imar
y”.
PDM
, how
ever
, may
mim
ic
met
asta
tic d
isea
se a
nd e
xten
sive
rad
iogr
aphi
c w
orku
p is
re
com
men
ded
befo
re a
fina
l dia
gnos
is o
f PD
M is
mad
e.
Intr
oduc
tion
•Pr
imar
y de
rmal
mel
anom
a (P
DM
) is a
m
elan
oma
conf
ined
to th
e de
rmis
or
subc
utan
eous
tiss
ue, l
acki
ng a
n ep
ider
mal
co
mpo
nent
.3 •
Sim
ilar s
urvi
val r
ates
of P
DM
com
pare
d to
co
nven
tiona
l mel
anom
a4 pr
ompt
ed th
is st
udy
to e
xam
ine
patie
nts w
ith c
onve
ntio
nal
mel
anom
a w
ho a
lso
deve
lope
d PD
M, a
nd to
co
mpa
re th
eir d
isea
se-f
ree
surv
ival
, re
curr
ence
rate
s, an
d B
resl
ow d
epth
. •
Kno
win
g th
e pa
tient
pop
ulat
ion
and
tum
or
char
acte
ristic
s hel
p to
furth
er d
efin
e th
is
subt
ype
of m
elan
oma.
Met
hods
Dat
a C
olle
ctio
n
•Ret
rosp
ectiv
e re
view
of p
rosp
ectiv
e SL
N d
atab
ase
cont
aini
ng fr
om F
ebru
ary
1997
thro
ugh
Dec
embe
r 200
8 at
May
o C
linic
.
•Fou
r crit
eria
wer
e re
quire
d fo
r his
tolo
gic
cons
ider
atio
n as
a P
DM
: in
volv
emen
t of t
he d
erm
is, n
o de
rmal
-epi
derm
al ju
nctio
nal c
ompo
nent
, no
dire
ct c
onne
ctio
n to
adn
exal
stru
ctur
es, a
nd n
o as
soci
ated
ben
ign
nevu
s. (F
igur
e 1,
2)
•No
hist
opat
holo
gic
evid
ence
of u
lcer
atio
n or
regr
essi
on a
ssoc
iate
d w
ith th
e le
sion
.
Figu
re 1
. D
erm
al m
elan
oma.
Mel
anoc
ytic
nes
ts (a
rrow
) are
con
fined
to th
e de
rmis
. Hem
atox
ylin
-eos
in; o
rigin
al m
agni
ficat
ion
x 10
0.
Figu
re 2
. C
onve
ntio
nal m
elan
oma.
Mel
anoc
ytic
nes
ts in
volv
e th
e de
rmal
-ep
ider
mal
junc
tion
(arr
owhe
ad) a
nd d
erm
is (a
rrow
). H
emat
oxyl
in-e
osin
; or
igin
al m
agni
ficat
ion
x 10
0.
1
2
Stat
istic
al c
onsi
dera
tion
•Diff
eren
ces b
etw
een
patie
nts w
ith P
DM
and
pat
ient
s with
all
othe
r mel
anom
a w
ere
com
pare
d.
•For
cat
egor
ical
var
iabl
es, t
he F
ishe
r’s e
xact
test
and
the
Chi
-squ
are
test
for
inde
pend
ence
wer
e us
ed to
det
erm
ine
diffe
renc
es b
etw
een
the
two
popu
latio
ns.
Unp
aire
d t-t
est w
as u
sed
to c
ompa
re m
eans
of t
he tw
o po
pula
tions
. •O
vera
ll su
rviv
al w
as th
e tim
e in
terv
al fr
om d
iagn
osis
to d
eath
from
any
cau
se.
Dis
ease
free
surv
ival
was
the
time
inte
rval
to fi
rst l
ocor
egio
nal r
ecur
renc
e,
dist
ance
recu
rren
ce, o
r dea
th fr
om a
ny c
ause
. •K
apla
n-M
eier
met
hod
was
use
d to
cal
cula
te su
rviv
al c
urve
s for
x-y
ear d
isea
se-
free
surv
ival
and
ove
rall
surv
ival
. Log
-ran
k te
sts w
ere
used
to c
ompa
re ti
me
to
even
t cur
ves.
•569
pat
ient
s und
erw
ent w
ide
loca
l exc
isio
n an
d se
ntin
el n
ode
diss
ectio
n af
ter a
di
agno
sis o
f mel
anom
a
•23
(4.0
%) p
atie
nts w
ere
diag
nose
d w
ith P
DM
(Tab
le 1
)
•Pat
ient
s dia
gnos
ed w
ith P
DM
wer
e si
gnifi
cant
ly o
lder
(72
vs. 6
1, P
= 0
.002
)
•Pat
ient
tum
or c
hara
cter
istic
s wer
e si
gnifi
cant
ly d
iffer
ent i
n re
fere
nce
to B
resl
ow
thic
knes
s and
did
not
reve
al d
iffer
ence
s in
recu
rren
ce. (
Tabl
e 2)
PDM
C
utan
eous
m
elan
oma
P va
lue
Age
: Med
ian,
(mea
n)
L
ess t
han
50
5
0-59
60-
69
7
0-79
Gre
ater
than
79
72, (
72.1
) 0
1
(4
%)
8
(35%
) 1
0 (4
3%)
4
(17%
)
65, (
61.3
) 1
30 (2
4%)
82
(15
%)
127
(23%
) 1
43 (2
6%)
62
(11
%)
0.00
2 0.
002
Sex
M
ale
F
emal
e
17 (7
4%)
6 (2
6%)
326
(60%
) 22
0 (4
0%)
0.20
Ethn
icity
Whi
te
A
fric
an-A
mer
ican
His
pani
c
Oth
er
23 (1
00%
) 0 0 0
529
(98%
) 1
(0.2
%)
7 (1
.3%
) 3
(0.5
%)
1.0
Prev
ious
his
tory
of
mel
anom
a 3
(13%
) 41
(8%
) 0.
41
Tabl
e 2:
Pri
mar
y D
erm
al M
elan
oma
PDM
C
utan
eous
m
elan
oma
P valu
e
Loca
tion
H
ead
and
Nec
k
Tru
nk
U
pper
Ext
Low
er E
xt
10 (4
3%)
5 (2
2%)
4 (1
7%)
4 (1
7%)
134
(25%
) 17
0 (3
1%)
116
(21%
) 12
1 (2
2%)
0.25
Thic
knes
s
< 1
mm
1-4
mm
> 4
mm
Unk
now
n
3, 3
.86
2 (9
%)
11 (4
9%)
8 (3
5%)
2 (9
%)
1.37
, 1.9
8 15
0 (2
9%)
341
(63%
) 48
(9%
)
0.00
01
Lym
ph n
ode
posi
tivity
(4
%)
73 (1
3%)
0.50
Rec
urre
nce
L
ocal
/Intra
nsit
In
trans
it/R
egio
nal
R
egio
nal
D
ista
nt
1 2 0 2
33
7 18
37
0.58
Dea
th
M
elan
oma
O
ther
2 0
32
21
1.0
0.64
1.
0
Con
clus
ions
•Pat
ient
s with
PD
M re
quire
a th
orou
gh m
etas
tatic
wor
k-up
to ru
le-o
ut sy
stem
ic m
etas
tasi
s
•Dep
th-f
or-d
epth
, PD
M h
as b
ette
r sur
viva
l tha
n co
nven
tiona
l mel
anom
a
•A h
isto
ry o
f mel
anom
a do
es n
ot p
redi
spos
e on
e to
dev
elop
ing
PDM
•PD
M p
atie
nts a
re si
gnifi
cant
ly o
lder
•Loc
al, r
egio
nal,
and
dist
ant m
etas
tase
s are
not
sign
ifica
ntly
diff
eren
t fro
m c
onve
ntio
nal m
elan
oma
Ref
eren
ces
1 Sc
hlag
enha
uff B
, Stro
ebel
W, E
lwan
ger U
, et.
al.
Met
asta
tic M
elan
oma
of U
nkno
wn
Prim
ary
Orig
in S
how
s Pro
gnos
tic S
imila
ritie
s to
Reg
iona
l Met
asta
tic M
elan
oma.
Can
cer.
199
7;80
:60-
65.
2 B
owen
GM
, Cha
ng A
E, L
owe
L, H
amilt
on T
, Pat
el R
, Joh
snon
TM
. So
litar
y M
elan
oma
Con
fined
to th
e D
erm
al a
nd/o
r Sub
cuta
neou
s Tis
sue:
Evi
denc
e fo
r Rev
isiti
ng th
e St
agin
g C
lass
ifica
tion.
Arc
h D
erm
atol
. 200
0;13
6:13
97-1
399.
3 C
assa
rino
DS,
Cab
ral E
S, K
arth
a RV
, Sw
ette
r SM
. Pr
imar
y D
erm
al M
elan
oma:
Dis
tinct
Imm
unoh
isto
chem
ical
Fin
ding
s and
Clin
ical
Out
com
e C
ompa
red
with
Nod
ular
and
Met
asta
tic M
elan
oma.
Arc
h D
erm
atol
. 200
8;14
4(1)
49-5
6.
4 Le
e C
C, F
arie
s MB
, Xin
g Y,
Mor
ton
DL.
Sol
itary
Der
mal
Mel
anom
a: B
egin
ning
or E
nd o
f the
Met
asta
tic P
roce
ss?
Ann
Sur
g O
ncol
. 200
9;16
:578
-584
.
Prim
ary
Der
mal
Mel
anom
a: D
iffer
ing
Cha
ract
eris
tics f
rom
C
onve
ntio
nal M
elan
oma?
1 J
ense
n JD
, 2 Gra
y R
J, 2 W
asif
N, 2 C
asey
III W
J, 2 K
reym
erm
an P
, 3 DiC
audo
DJ,
3 Lam
an S
D, 3 S
ekul
ic A
, 2 Poc
kaj B
A
1 McL
aren
Oak
land
Hos
pita
l, M
ayo
Clin
ic A
rizon
a—2 D
ept.
of S
urge
ry, 3 D
ept.
of D
erm
atol
ogy
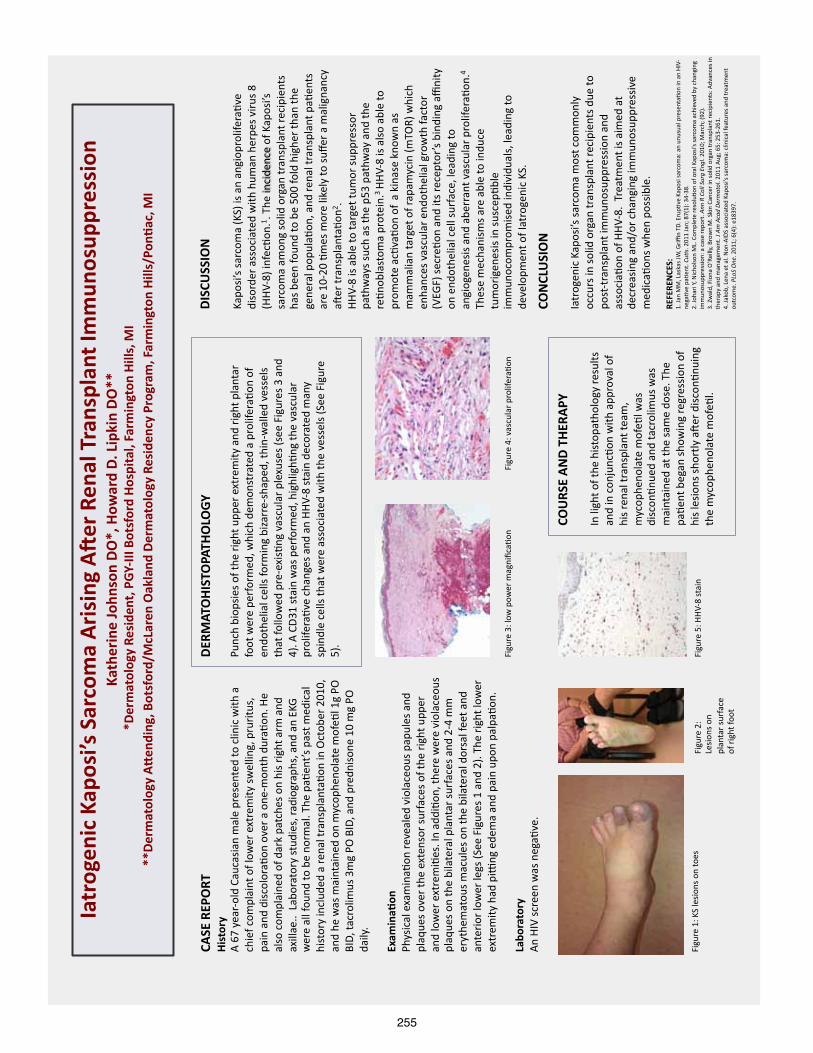
255
Iatr
ogen
ic K
apos
i’s S
arco
ma
Ari
sing
A3
er R
enal
Tra
nspl
ant I
mm
unos
uppr
essi
on
Kath
erin
e Jo
hnso
n D
O*,
How
ard
D. L
ipki
n D
O**
*
Der
mat
olog
y Re
side
nt, P
GY-‐
III B
otsf
ord
Hos
pita
l, Fa
rmin
gton
Hill
s, M
I **
Der
mat
olog
y A
Men
ding
, Bot
sfor
d/M
cLar
en O
akla
nd D
erm
atol
ogy
Resi
denc
y Pr
ogra
m, F
arm
ingt
on H
ills/
PonO
ac, M
I
CASE
REP
ORT
H
isto
ry
A 67 year-‐old Caucasian male presented to clinic with a
chief complaint of lower extremity swelling, pruritus,
pain and discolora<on over a one-‐month dura<on. He
also complained of dark patches on his right arm and
axillae.. Laboratory studies, radiographs, and an EKG
were all found to be normal. The pa<ent’s past medical
history included a renal transplanta<on in October 2010,
and he was maintained on mycophenolate mofe<l 1g PO
BID, tacrolimus 3mg PO BID, and prednisone 10 mg PO
daily.
Exam
inaO
on
Physical examina<on revealed violaceous papules and
plaques over the extensor surfaces of the right upper
and lower extremi<es. In addi<on, there were violaceous
plaques on the bilateral plantar surfaces and 2-‐4 mm
erythematous macules on the bilateral dorsal feet and
anterior lower legs (See Figures 1 and 2). The right lower
extremity had piWng edema and pain upon palpa<on.
Labo
rato
ry
An HIV screen was nega<ve.
Figure 3: low power magnifica<on
DER
MAT
OH
ISTO
PATH
OLO
GY
Punch biopsies of the right upper extremity and right plantar
foot were performed, which demonstrated a prolifera<on of
endothelial cells forming bizarre-‐shaped, thin-‐walled vessels
that followed pre-‐exis<ng vascular plexuses (see Figures 3 and
4). A CD31 stain was performed, highligh<ng the vascular
prolifera<ve changes and an HHV-‐8 stain decorated many
spindle cells that were associated with the vessels (See Figure
5).
Figure 4: vascular prolifera<on
Figure 1: KS lesions on toes
Figure 2:
Lesions on
plantar surface
of right foot
Figure 5: HHV-‐8 stain
COU
RSE
AN
D T
HER
APY
In light of the histopathology results
and in conjunc<on with approval of
his renal transplant team,
mycophenolate mofe<l was
discon<nued and tacrolimus was
maintained at the same dose. The
pa<ent began showing regression of
his lesions shortly a_er discon<nuing
the mycophenolate mofe<l.
CON
CLU
SIO
N
Iatrogenic Kaposi’s sarcoma most commonly
occurs in solid organ transplant recipients due to
post-‐transplant immunosuppression and
associa<on of HHV-‐8. Treatment is aimed at
decreasing and/or changing immunosuppressive
medica<ons when possible.
REFE
REN
CES:
1. Jan MM, Laskas JW, Griffin TD. Erup<ve Kaposi sarcoma: an unusual presenta<on in an HIV-‐
nega<ve pa<ent. Cu#
s. 2011 Jan; 87(1): 34-‐38.
2. Johari Y, Nicholson ML. Complete resolu<on of oral Kaposi’s sarcoma achieved by changing
immunosuppression: a case report. A
nn R Coll Surg Engl. 2010; March; (92).
3. Zwald, Fiona O’Reilly, Brown M. Skin Cancer in solid organ transplant recipients: Advances in
therapy and management. J Am Acad Dermatol. 2011 Aug; 65: 253-‐261.
4. Jakob, Lena et al. Non-‐AIDS associated Kaposi’s sarcoma: clinical features and treatment
outcome. PLoS One. 2011; 6(4): e18397.

256
RES
EAR
CH
PO
STER
PR
ESEN
TATI
ON
DES
IGN
© 2
011
ww
w.P
oste
rPre
sent
atio
ns.c
om
QU
ICK
TIPS
(-
-TH
IS S
ECTI
ON
DO
ES N
OT
PRIN
T--)
This
Pow
erPo
int
tem
plat
e re
quir
es b
asic
Pow
erPo
int
(ver
sion
200
7 or
new
er)
skill
s. B
elow
is a
list
of
com
mon
ly a
sked
que
stio
ns s
peci
fic
to t
his
tem
plat
e.
If y
ou a
re u
sing
an
olde
r ve
rsio
n of
Pow
erPo
int
som
e te
mpl
ate
feat
ures
may
not
wor
k pr
oper
ly.
U
sing
the
tem
plat
e
Veri
fyin
g th
e qu
alit
y of
you
r gr
aphi
cs
Go
to t
he V
IEW
men
u an
d cl
ick
on Z
OO
M t
o se
t yo
ur
pref
erre
d m
agni
fica
tion
. Th
is t
empl
ate
is a
t 10
0%
the
size
of
the
fina
l pos
ter.
All
text
and
gra
phic
s w
ill
be p
rint
ed a
t 10
0% t
heir
siz
e. T
o se
e w
hat
your
po
ster
will
look
like
whe
n pr
inte
d, s
et t
he z
oom
to
100%
and
eva
luat
e th
e qu
alit
y of
all
your
gra
phic
s be
fore
you
sub
mit
you
r po
ster
for
pri
ntin
g.
Usi
ng t
he p
lace
hold
ers
To a
dd t
ext
to t
his
tem
plat
e cl
ick
insi
de a
pl
aceh
olde
r an
d ty
pe in
or
past
e yo
ur t
ext.
To
mov
e a
plac
ehol
der,
clic
k on
it o
nce
(to
sele
ct it
), p
lace
yo
ur c
urso
r on
its
fram
e an
d yo
ur c
urso
r w
ill c
hang
e to
thi
s sy
mbo
l:
Then
, cl
ick
once
and
dra
g it
to
its
new
loca
tion
whe
re y
ou c
an r
esiz
e it
as
need
ed.
Addi
tion
al p
lace
hold
ers
can
be f
ound
on
the
left
si
de o
f th
is t
empl
ate.
M
odif
ying
the
layo
ut
This
tem
plat
e ha
s fo
ur
diff
eren
t co
lum
n la
yout
s.
Righ
t-cl
ick
your
mou
se
on t
he b
ackg
roun
d an
d
clic
k on
“La
yout
” to
see
th
e la
yout
opt
ions
. Th
e co
lum
ns in
the
pro
vide
d la
yout
s ar
e fi
xed
and
cann
ot b
e m
oved
but
adv
ance
d us
ers
can
mod
ify
any
layo
ut b
y go
ing
to V
IEW
and
the
n SL
IDE
MAS
TER.
Im
port
ing
text
and
gra
phic
s fr
om e
xter
nal s
ourc
es
TEXT
: Pa
ste
or t
ype
your
tex
t in
to a
pre
-exi
stin
g pl
aceh
olde
r or
dra
g in
a n
ew p
lace
hold
er f
rom
the
le
ft s
ide
of t
he t
empl
ate.
Mov
e it
any
whe
re a
s ne
eded
. PH
OTO
S: D
rag
in a
pic
ture
pla
ceho
lder
, si
ze it
fir
st,
clic
k in
it a
nd in
sert
a p
hoto
fro
m t
he m
enu.
TA
BLES
: Yo
u ca
n co
py a
nd p
aste
a t
able
fro
m a
n ex
tern
al d
ocum
ent
onto
thi
s po
ster
tem
plat
e. T
o ad
just
th
e w
ay t
he t
ext
fits
wit
hin
the
cells
of
a ta
ble
that
has
bee
n pa
sted
, ri
ght-
clic
k on
the
tab
le,
clic
k FO
RMAT
SH
APE
the
n cl
ick
on T
EXT
BOX
and
chan
ge t
he IN
TERN
AL M
ARG
IN v
alue
s to
0.2
5 M
odif
ying
the
col
or s
chem
e To
cha
nge
the
colo
r sc
hem
e of
thi
s te
mpl
ate
go t
o th
e “D
esig
n” m
enu
and
clic
k on
“Co
lors
”. Y
ou c
an
choo
se f
rom
the
pro
vide
col
or c
ombi
nati
ons
or y
ou
can
crea
te y
our
own.
QU
ICK
DES
IGN
GU
IDE
(--T
HIS
SEC
TIO
N D
OES
NO
T PR
INT-
-)
Th
is P
ower
Poin
t 20
07 t
empl
ate
prod
uces
a 3
6”x4
8”
prof
essi
onal
po
ster
. It
will
sav
e yo
u va
luab
le t
ime
plac
ing
titl
es,
subt
itle
s, t
ext,
and
gra
phic
s.
Use
it t
o cr
eate
you
r pr
esen
tati
on.
Then
sen
d it
to
Post
erPr
esen
tati
ons.
com
for
pre
miu
m q
ualit
y, s
ame
day
affo
rdab
le p
rint
ing.
W
e pr
ovid
e a
seri
es o
f on
line
tuto
rial
s th
at w
ill
guid
e yo
u th
roug
h th
e po
ster
des
ign
proc
ess
and
answ
er y
our
post
er p
rodu
ctio
n qu
esti
ons.
Vi
ew o
ur o
nlin
e tu
tori
als
at:
htt
p://
bit.
ly/P
oste
r_cr
eati
on_h
elp
(c
opy
and
past
e th
e lin
k in
to y
our
web
bro
wse
r).
For
assi
stan
ce a
nd t
o or
der
your
pri
nted
pos
ter
call
Post
erPr
esen
tati
ons.
com
at 1.
866.
649.
3004
Obj
ect
Plac
ehol
ders
Use
the
pla
ceho
lder
s pr
ovid
ed b
elow
to
add
new
el
emen
ts t
o yo
ur p
oste
r: D
rag
a pl
aceh
olde
r on
to
the
post
er a
rea,
siz
e it
, an
d cl
ick
it t
o ed
it.
Sect
ion
Hea
der
plac
ehol
der
Mov
e th
is p
refo
rmat
ted
sect
ion
head
er p
lace
hold
er
to t
he p
oste
r ar
ea t
o ad
d an
othe
r se
ctio
n he
ader
. U
se s
ecti
on h
eade
rs t
o se
para
te t
opic
s or
con
cept
s w
ithi
n yo
ur p
rese
ntat
ion.
Te
xt p
lace
hold
er
Mov
e th
is p
refo
rmat
ted
text
pla
ceho
lder
to
the
post
er t
o ad
d a
new
bod
y of
tex
t.
Pict
ure
plac
ehol
der
Mov
e th
is g
raph
ic p
lace
hold
er o
nto
your
pos
ter,
siz
e it
fir
st,
and
then
clic
k it
to
add
a pi
ctur
e to
the
po
ster
.
©
201
1 Po
ster
Pres
enta
tions
.com
211
7 Fo
urth
Str
eet ,
Uni
t C
B
erke
ley
CA 9
4710
pos
terp
rese
nter
@gm
ail.c
om
Stud
ent
disc
ount
s ar
e av
aila
ble
on o
ur F
aceb
ook
page
. G
o to
Pos
terP
rese
ntat
ions
.com
and
clic
k on
the
FB
icon
.
Exag
gera
ted
reac
tion
to
inse
ct b
ites
is a
rar
e ph
enom
enon
see
n in
pat
ient
s w
ith
chro
nic
lym
phoc
ytic
leuk
emia
. S
kin
lesi
ons
usua
lly a
ppea
r m
onth
s to
yea
rs a
fter
the
dia
gnos
is o
f le
ukem
ia a
nd a
re u
nrel
ated
to
the
cour
se o
f th
e di
seas
e.
We
repo
rt a
pat
ient
wit
h ch
roni
c ly
mph
ocyt
ic le
ukem
ia (
CLL)
who
pre
sent
ed w
ith
a re
curr
ent
prur
itic
pap
ulov
esic
ular
and
bu
llous
eru
ptio
n th
at w
as h
isto
logi
cally
con
sist
ent
wit
h an
exa
gger
ated
res
pons
e to
an
inse
ct b
ite.
Her
ein,
we
desc
ribe
wha
t is
kno
wn
abou
t th
is p
heno
men
on in
clud
ing
its
pres
enta
tion
, pr
opos
ed p
atho
gene
sis,
and
opt
ions
for
tre
atm
ent.
Intr
oduc
tion
A 71
yea
r-ol
d H
ispa
nic
mal
e pr
esen
ted
to t
he d
erm
atol
ogy
clin
ic w
ith
a re
curr
ent
gene
raliz
ed p
ruri
tic
erup
tion
tha
t he
bel
ieve
d to
be
the
resu
lt o
f in
sect
bit
es.
The
pat
ient
ha
d a
hist
ory
of B
-cel
l chr
onic
lym
phoc
ytic
leuk
emia
(CL
L) t
hat
was
dia
gnos
ed a
nd t
reat
ed
in 2
006
wit
h 5
cycl
es o
f ch
emot
hera
py w
ith
flud
arab
ine.
The
pat
ient
was
als
o di
agno
sed
wit
h pr
imar
y cu
tane
ous
CD30
+ an
apla
stic
lar
ge-c
ell
lym
phom
a (A
LCL)
of
the
left
thi
gh in
20
07,
for
whi
ch h
e un
derw
ent
CHO
P ch
emot
hera
py a
long
wit
h ex
cisi
on a
nd lo
cal r
adia
tion
th
erap
y w
ith
com
plet
e re
solu
tion
. A
ddit
iona
l med
ical
his
tory
incl
udes
a d
eep
vein
th
rom
bosi
s of
the
left
low
er e
xtre
mit
y fo
r w
hich
an
IVC
filt
er w
as p
lace
d. T
he p
atie
nt w
as
taki
ng n
o m
edic
atio
ns a
nd r
epor
ted
no a
llerg
ies.
So
cial
his
tory
was
non
-con
trib
utor
y.
Revi
ew o
f sy
stem
s w
as n
egat
ive
othe
r th
an t
he p
ruri
tus
asso
ciat
ed w
ith
the
rash
. T
he
pati
ent
was
und
ergo
ing
regu
lar
mon
itor
ing
by H
emat
olog
y/O
ncol
ogy
and
all r
ecen
t la
bora
tory
stu
dies
wer
e no
rmal
.
On
phys
ical
exa
min
atio
n, m
ulti
ple
papu
love
sicl
es w
ere
pres
ent
on t
he u
pper
and
low
er
extr
emit
ies.
Se
vera
l les
ions
on
the
low
er l
egs
cont
aine
d te
nse
hem
orrh
agic
bul
lae,
som
e of
w
hich
wer
e un
roof
ed,
bear
ing
an e
rode
d su
rfac
e. (
Figu
re 1
) N
ikol
sky
sign
and
Asb
oe-
Han
sen
sign
wer
e ne
gati
ve.
H
isto
path
olog
ical
exa
min
atio
n of
lesi
onal
ski
n re
veal
ed e
pide
rmal
spo
ngio
sis
and
vesi
cula
tion
wit
h su
perf
icia
l an
d de
ep p
eriv
ascu
lar
and
inte
rsti
tial
mix
ed c
ell i
nfilt
rate
wit
h ly
mph
ocyt
es a
nd e
osin
ophi
ls.
(Fig
ure
2) N
o at
ypic
al c
ells
wer
e pr
esen
t.
Dir
ect
imm
unof
luor
esce
nt s
tudi
es o
f pe
rile
sion
al s
kin
wer
e ne
gati
ve.
Tre
atm
ent
wit
h po
tent
to
pica
l ste
roid
s re
sult
ed in
sig
nifi
cant
impr
ovem
ent.
Figu
re 2
: Hist
opat
holo
gy
Figu
re 1
: Clin
ical
pre
sent
atio
n Di
scus
sion
(con
t)
Refe
renc
es
1.
Cerr
oni L
, Ze
nahl
ik P
, H
ofle
r G
, Ka
ddu
S, S
mol
le J
, Ke
rl H
. Sp
ecif
ic c
utan
eous
infi
ltra
tes
of B
-cel
l chr
onic
lym
phoc
ytic
leuk
emia
: a
clin
icop
atho
logi
c an
d pr
ogno
stic
stu
dy o
f 42
pat
ient
s. A
m J
Sur
g Pa
thol
. Au
g 19
96;2
0(8)
:100
0-10
10.
2.
Agne
w K
L, R
uchl
emer
R,
Cato
vsky
D,
Mat
utes
E,
Bunk
er C
B. C
utan
eous
fin
ding
s in
chr
onic
lym
phoc
ytic
leuk
aem
ia.
Br J
Der
mat
ol.
Jun
2004
;150
(6):
1129
-113
5.
3.
Roba
k E,
Rob
ak T
. Sk
in le
sion
s in
chr
onic
lym
phoc
ytic
leuk
emia
. Le
uk L
ymph
oma.
May
200
7;48
(5):
855-
865.
4.
W
eed
RI.
Exag
gera
ted
Del
ayed
Hyp
erse
nsit
ivit
y to
Mos
quit
o Bi
tes
in C
hron
ic L
ymph
ocyt
ic L
euke
mia
. Bl
ood.
Sep
196
5;26
:257
-268
. 5.
U
lmer
A,
Met
zler
G,
Scha
nz S
, Fi
erlb
eck
G.
Dap
sone
in t
he m
anag
emen
t of
"in
sect
bit
e-lik
e re
acti
on"
in a
pat
ient
wit
h ch
roni
c ly
mph
ocyt
ic l
euka
emia
. Br
J
Der
mat
ol.
Jan
2007
;156
(1):
172-
174.
6.
D
avis
MD
, Pe
rnic
iaro
C,
Dah
l PR,
Ran
dle
HW
, M
cEvo
y M
T, L
eife
rman
KM
. Ex
agge
rate
d ar
thro
pod-
bite
lesi
ons
in p
atie
nts
wit
h ch
roni
c ly
mph
ocyt
ic le
ukem
ia:
a cl
inic
al,
hist
opat
holo
gic,
and
imm
unop
atho
logi
c st
udy
of e
ight
pat
ient
s. J
Am
Aca
d D
erm
atol
. Ju
l 199
8;39
(1):
27-3
5.
7.
Blum
RR,
Phe
lps
RG,
Wei
H. A
rthr
opod
bit
es m
anif
esti
ng a
s re
curr
ent
bulla
e in
a p
atie
nt w
ith
chro
nic
lym
phoc
ytic
leuk
emia
. J
Cuta
n M
ed S
urg.
Jul
-Aug
20
01;5
(4):
312-
314.
8.
Co
curo
ccia
B,
Gis
ondi
P,
Gub
inel
li E,
Gir
olom
oni G
. An
itch
y ve
sicu
lobu
llous
eru
ptio
n in
a p
atie
nt w
ith
chro
nic
lym
phoc
ytic
leuk
aem
ia.
Int
J Cl
in P
ract
. D
ec
2004
;58(
12):
1177
-117
9.
9.
Smit
h KJ
, Sk
elto
n H
G,
3rd,
Vog
el P
, Ye
ager
J,
Baxt
er D
, W
agne
r KF
. Ex
agge
rate
d in
sect
bit
e re
acti
ons
in p
atie
nts
posi
tive
for
HIV
. M
ilita
ry M
edic
al C
onso
rtiu
m
for
the
Adva
ncem
ent
of R
etro
vira
l Re
sear
ch.
J A
m A
cad
Der
mat
ol.
Aug
1993
;29(
2 Pt
1):
269-
272.
10
. Ba
rzila
i A,
Shpi
ro D
, G
oldb
erg
I, e
t al
. In
sect
bit
e-lik
e re
acti
on in
pat
ient
s w
ith
hem
atol
ogic
mal
igna
nt n
eopl
asm
s. A
rch
Der
mat
ol.
Dec
199
9;13
5(12
):15
03-1
507.
11
. Ab
erer
W,
Konr
ad K
, W
olff
K.
Wel
ls' s
yndr
ome
is a
dis
tinc
tive
dis
ease
ent
ity
and
not
a hi
stol
ogic
dia
gnos
is.
J A
m A
cad
Der
mat
ol.
Jan
1988
;18(
1 Pt
1):
105-
114.
12
. Ze
eli T
, Fe
inm
esse
r M
, Se
gal R
, D
avid
M.
Inse
ct-b
ite-
like
Wel
ls' s
yndr
ome
in a
ssoc
iati
on w
ith
man
tle-
zone
lym
phom
a. B
r J
Der
mat
ol.
Sep
2006
;155
(3):
614-
616.
13
. Li
ndel
of B
, Is
lam
N,
Eklu
nd G
, Arf
ors
L. P
emph
igoi
d an
d ca
ncer
. A
rch
Der
mat
ol.
Jan
1990
;126
(1):
66-6
8.
14.
Bolo
gnia
J,
ed D
erm
atol
ogy.
2 e
d. S
t. L
ouis
: M
osby
Els
evie
r; 2
008.
15
. Te
ffer
i A,
Vard
iman
JW
. Cl
assi
fica
tion
and
dia
gnos
is o
f m
yelo
prol
ifer
ativ
e ne
opla
sms:
the
200
8 W
orld
Hea
lth
Org
aniz
atio
n cr
iter
ia a
nd p
oint
-of-
care
dia
gnos
tic
algo
rith
ms.
Leu
kem
ia.
Jan
2008
;22(
1):1
4-22
. 16
. Va
ssal
lo C
, Pa
ssam
onti
F,
Cana
nzi R
, et
al.
Exa
gger
ated
inse
ct b
ite-
like
reac
tion
in p
atie
nts
affe
cted
by
onco
haem
atol
ogic
al d
isea
ses.
Act
a D
erm
Ven
ereo
l.
2005
;85(
1):7
6-77
. 17
. W
alke
r P,
Lon
g D
, Ja
mes
C,
Mar
shm
an G
. Ex
agge
rate
d in
sect
bit
e re
acti
on e
xace
rbat
ed b
y a
pyog
enic
infe
ctio
n in
a p
atie
nt w
ith
chro
nic
lym
phoc
ytic
le
ukae
mia
. A
ustr
alas
J D
erm
atol
. Au
g 20
07;4
8(3)
:165
-169
.
Exag
gera
ted
inse
ct b
ite-
like
reac
tion
in
a p
atie
nt w
ith
chro
nic
lym
phoc
ytic
leuk
emia
St.
Barn
abas
Hos
pita
l, De
part
men
t of D
erm
atol
ogy,
Bron
x, N
Y 10
457
Pati
ents
wit
h he
mop
rolif
erat
ive
diso
rder
s, p
arti
cula
rly
CLL,
may
pre
sent
wit
h an
exa
gger
ated
re
acti
on t
o in
sect
bit
es,
and
this
dia
gnos
is s
houl
d be
con
side
red
in s
uch
pati
ents
who
pre
sent
w
ith
a no
nspe
cifi
c ra
sh.
Phy
sici
ans
shou
ld b
e co
gniz
ant
of t
he f
act
that
the
eru
ptio
n m
ay
occu
r pr
ior
to t
he d
iagn
osis
of
the
hem
atol
ogic
dis
orde
r, a
nd f
urth
er e
valu
atio
n of
the
se
pati
ents
may
be
war
rant
ed.
Skin
eru
ptio
ns a
re s
een
in a
ppro
xim
atel
y 25
% of
pat
ient
s w
ith
CLL
and
are
cate
gori
zed
as
eith
er s
peci
fic
or n
onsp
ecif
ic.
Spe
cifi
c le
sion
s ar
e de
fine
d as
tho
se w
ith
lym
phom
atou
s m
alig
nant
infi
ltra
tion
of
the
skin
, i.
e. le
ukem
ia c
utis
. N
onsp
ecif
ic le
sion
s in
clud
e th
ose
due
to a
bnor
mal
hem
atop
oies
is (
typi
cally
pre
sent
ing
as e
cchy
mos
es o
r pu
rpur
a),
infe
ctio
ns,
drug
eru
ptio
ns,
vasc
ulit
is,
graf
t ve
rsus
hos
t di
seas
e (G
VHD
), im
mun
obul
lous
dis
ease
s in
clud
ing
bullo
us p
emph
igoi
d (B
P) a
nd p
aran
eopl
asti
c pe
mph
igus
(PN
P),
and
EIBL
R.1-
3 In
ad
diti
on,
pyod
erm
a ga
ngen
osum
, er
ythe
ma
nodo
sum
, an
d Sw
eets
syn
drom
e m
ay o
ccur
as
para
neop
last
ic p
heno
men
a.3
H
eigh
tene
d re
acti
ons
to in
sect
bit
es in
ass
ocia
tion
wit
h he
mop
rolif
erat
ive
dise
ase
was
fir
st
repo
rted
by
Wee
d in
196
5 in
a p
atie
nt w
ith
CLL.
4 S
ince
the
n, t
here
hav
e be
en s
ever
al
othe
r re
port
s of
thi
s ph
enom
enon
des
crib
ed in
ass
ocia
tion
wit
h CL
L, a
s w
ell a
s in
pat
ient
s w
ith
ALL,
man
tle-
cell
and
larg
e-ce
ll ly
mph
oma,
HIV
infe
ctio
n an
d co
ngen
ital
ag
amm
agol
ubul
inem
ia.
5-9
In W
eeds
ori
gina
l des
crip
tion
, th
e re
acti
on w
as d
efin
ed b
y le
sion
s gr
eate
r th
an 2
0mm
in d
iam
eter
, ch
arac
teri
zed
by in
dura
tion
, ed
ema,
ery
them
a an
d pr
urit
us a
t th
e si
te o
f a
know
n m
osqu
ito
bite
or
evid
ence
the
reof
.4
Lesi
ons
coul
d pr
esen
t w
ith
vari
ous
mor
phol
ogie
s, in
clud
ing
mac
ules
, pa
pule
s, n
odul
es,
vesi
cles
, an
d bu
llae
up t
o 10
cm,
and
leav
e no
res
idua
l pos
t in
flam
mat
ory
hype
rpig
men
tati
on.4
, 6-
7 T
hey
are
typi
cally
re
curr
ent
and
tend
to
pers
ist.
Cl
inic
al d
iagn
osis
is o
ften
cha
lleng
ing
sinc
e m
ost
pati
ents
do
not
reca
ll an
ant
eced
ent
inse
ct b
ite.
8 T
he e
rupt
ion
can
pres
ent
any
tim
e fr
om m
onth
s to
ye
ars
afte
r th
e di
agno
sis
of le
ukem
ia,
and
in s
ome
case
s ye
ars
prio
r.8,
10
It is
not
rel
ated
to
the
cour
se o
f di
seas
e, la
bora
tory
val
ues,
or
trea
tmen
t.4,
6,
10 T
here
is s
ome
evid
ence
tha
t th
e pr
esen
ce o
f EI
BLR
in p
atie
nts
wit
h CL
L po
rten
ds a
mor
e di
smal
pro
gnos
is.
In a
stu
dy
cond
ucte
d by
Bar
zila
i et
al,
3 pa
tien
ts w
ith
CLL
and
EIBL
R de
mon
stra
ted
rapi
d pr
ogre
ssio
n of
the
ir C
LL.1
0 F
urth
erm
ore,
fat
al c
ompl
icat
ions
dev
elop
ed in
3 o
f th
e 8
pati
ents
wit
h CL
L an
d EI
BLR
desc
ribe
d by
Dav
is e
t al
.6 T
here
are
sev
eral
rep
orts
in t
he li
tera
ture
of
vesi
culo
bullo
us W
ells
syn
drom
e oc
curr
ing
in a
ssoc
iati
on w
ith
B-ce
ll ly
mph
omas
. W
hile
so
me
cons
ider
Wel
ls’
synd
rom
e a
dist
inct
clin
ical
ent
ity,
11 w
e re
gard
it a
s a
derm
al
hype
rsen
siti
vity
rea
ctio
n to
som
e tr
igge
ring
eve
nt t
hat
resu
lts
in d
egra
nula
tion
of
a la
rge
num
ber
of d
erm
al e
osin
ophi
ls.
Pot
enti
al t
rigg
ers
incl
ude
arth
ropo
d bi
tes,
vir
al in
fect
ions
, pa
rasi
tic
infe
ctio
ns,
mal
igna
ncy,
mye
lopr
olif
erat
ive
diso
rder
s, d
rugs
and
vac
cina
tion
s.12
It
is
our
bel
ief
that
rep
orts
of
Wel
ls’
synd
rom
e in
the
set
ting
of
hem
atol
ogic
mal
igna
ncy
repr
esen
t an
alt
erna
te d
escr
ipti
on o
f th
e sa
me
phen
omen
on o
bser
ved
in E
IBLR
.
Case
Pre
sent
atio
n
Holly
Kan
avy,
DO, K
asha
Toul
oei,
MSI
V, C
harle
s Gro
pper
, MD,
Dam
ian
DiCo
stan
zo, M
D, C
indy
Hof
fman
, DO
b
Disc
ussi
on
Disc
ussi
on (c
ont)
Conc
lusi
on
Disc
ussi
on (c
ont)
A B
In t
he d
iffe
rent
ial
diag
nosi
s of
ves
icul
obul
lous
eru
ptio
ns in
pat
ient
s w
ith
an u
nder
lyin
g m
alig
nanc
y, im
mun
obul
lous
dis
ease
mus
t be
con
side
red.
13
Bullo
us p
emph
igoi
d is
com
mon
ly
seen
in t
he e
lder
ly a
nd in
volv
es s
kin
of t
he g
roin
, ax
illae
, an
d fl
exor
sur
face
s of
the
for
earm
s.
Dir
ect
imm
unof
luor
esce
nce
typi
cally
rev
eals
lin
ear
depo
sits
of
IgG
and
/or
C3 a
long
the
ba
sem
ent
mem
bran
e.14
PN
P is
com
mon
ly a
ssoc
iate
d w
ith
B-ce
ll ly
mph
opro
lifer
ativ
e di
sord
ers
and
is c
hara
cter
ized
by
pain
ful
muc
osal
ulc
erat
ions
alo
ng w
ith
a po
lym
orph
ic e
rupt
ion
of t
he
trun
k, p
alm
s, a
nd s
oles
.3
Dia
gnos
is o
f PN
P re
sts
upon
dem
onst
rati
on o
f Ig
G a
nd C
3 w
ithi
n in
terc
ellu
lar
spac
es a
nd a
long
the
bas
emen
t m
embr
ane
zone
on
dire
ct im
mun
oflu
ores
cent
st
udie
s of
per
ilesi
onal
ski
n.14
Le
ukem
ia c
utis
is m
ost
com
mon
ly s
een
in m
yelo
id l
euke
mia
s an
d m
anif
ests
as
disc
rete
gro
uped
or
gene
raliz
ed,
firm
, de
ep,
red-
brow
n pa
pule
s, p
laqu
es,
or
nodu
les
that
can
man
ifes
t on
any
par
t of
the
bod
y, m
ost
com
mon
ly t
he h
ead.
H
isto
logi
c ex
amin
atio
n an
d im
mun
ohis
toch
emis
try
assa
ys c
an b
e us
ed t
o ex
clud
e th
e di
agno
sis.
Sk
in
lesi
ons
freq
uent
ly r
esol
ve w
ith
trea
tmen
t of
the
und
erly
ing
leuk
emia
.15
Cu
tane
ous
infe
ctio
ns a
re a
fre
quen
t oc
curr
ence
in p
atie
nts
wit
h CL
L du
e to
imm
unol
ogic
su
ppre
ssio
n, a
nd in
clud
e bo
th c
omm
on a
nd o
ppor
tuni
stic
pat
hoge
ns.
The
mos
t co
mm
on
infe
ctio
ns s
een
are
due
to h
erpe
s si
mpl
ex v
irus
and
her
pes
zost
er.1
M
anif
esta
tion
s of
the
se
may
be
seve
re,
diss
emin
ated
or
recu
rren
t. A
ddit
iona
lly,
papu
lar
and
nodu
lar
lesi
ons
can
occu
r at
the
sit
e of
her
pes
sim
plex
or
herp
es z
oste
r sc
ars.
1 O
ther
cut
aneo
us in
fect
ions
incl
ude
diss
emin
ated
mol
lusc
um c
onta
gios
um,
baci
llary
ang
iom
atos
is,
and
atyp
ical
myc
obac
teri
al
infe
ctio
ns.3
Sk
in s
wab
s ca
n be
con
duct
ed t
o ru
le o
ut b
acte
rial
and
fun
gal
infe
ctio
n.
The
path
ogen
esis
of
EIBL
R is
poo
rly
unde
rsto
od.
Bar
zila
i et
al p
ropo
se t
hat
sinc
e m
any
of t
he
hem
atol
ogic
mal
igna
ncie
s in
the
se p
atie
nts
are
of B
cel
l ori
gin,
the
phe
nom
enon
may
be
due
to a
cyt
okin
e im
bala
nce,
wit
h an
exc
ess
of in
terl
euki
ns 4
and
5 le
adin
g to
pro
lifer
atio
n of
m
alig
nant
B c
ells
and
alt
ered
imm
une
resp
onse
cha
ract
eriz
ed b
y eo
sino
phili
c in
filt
rati
on o
f th
e sk
in.
Bec
ause
hei
ghte
ned
inse
ct b
ite
reac
tion
s ha
ve b
een
docu
men
ted
in H
IV in
fect
ion
and
cong
enit
al a
gam
mag
olub
ulin
emia
, an
d pr
esen
t si
mila
rly
to t
hose
wit
h he
mat
olog
ic m
alig
nanc
y,
the
path
ogen
esis
may
be
attr
ibut
able
to
imm
unod
efic
ienc
y pl
us a
n im
mun
olog
ic s
tim
ulus
suc
h as
inse
ct b
ites
or
vira
l inf
ecti
on.1
0 V
assa
lo e
t al
pro
pose
an
imm
uno-
alle
rgic
mec
hani
sm,
spec
ific
ally
, an
alle
rgic
rea
ctio
n to
the
inse
ct b
ite
and
an im
pair
ed im
mun
e re
spon
se.1
6
A re
view
of
the
liter
atur
e in
dica
tes
that
EIB
LR is
res
ista
nt t
o m
ost
trea
tmen
ts.7
Alt
houg
h ou
r pa
tien
t re
spon
ded
favo
rabl
y to
top
ical
ste
roid
s, t
his
trea
tmen
t is
usu
ally
inef
fect
ive.
10
Sim
ilarl
y, t
opic
al a
nti-
prur
itic
s an
d U
VB p
hoto
ther
apy
are
rare
ly o
f an
y be
nefi
t.10
Pr
edni
sone
40
mg/
day
may
pro
vide
tra
nsie
nt r
elie
f, b
ut t
he e
rupt
ion
recu
rs o
nce
the
med
icat
ion
is
tape
red.
7-8,
10
Oth
er t
reat
men
ts t
hat
have
bee
n at
tem
pted
wit
h in
adeq
uate
res
pons
e in
clud
e an
tibi
otic
s, s
yste
mic
ant
ihis
tam
ines
, in
trav
enou
s im
mun
oglo
bulin
, ch
lora
mbu
cil,
and
in
terf
eron
alp
ha.1
0 V
aryi
ng d
egre
es o
f im
prov
emen
t ha
ve b
een
repo
rted
in p
atie
nts
wit
h CL
L un
derg
oing
che
mot
hera
py,
and
in o
ne r
epor
t, t
he e
rupt
ion
reso
lved
com
plet
ely
afte
r ef
fect
ive
trea
tmen
t of
the
und
erly
ing
ALL.
6, 1
7 T
here
is a
rep
ort
of p
atie
nt r
espo
ndin
g to
Dea
d Se
a ph
otot
hera
py i
ndic
atin
g th
e ps
oral
en U
VA t
hera
py m
ay p
rove
ben
efic
ial.
10
Dai
ly o
ral
daps
one
may
als
o be
a p
rom
isin
g tr
eatm
ent
opti
on a
s tw
o ca
se r
epor
ts h
ave
docu
men
ted
mar
ked
impr
ovem
ent.
5, 7
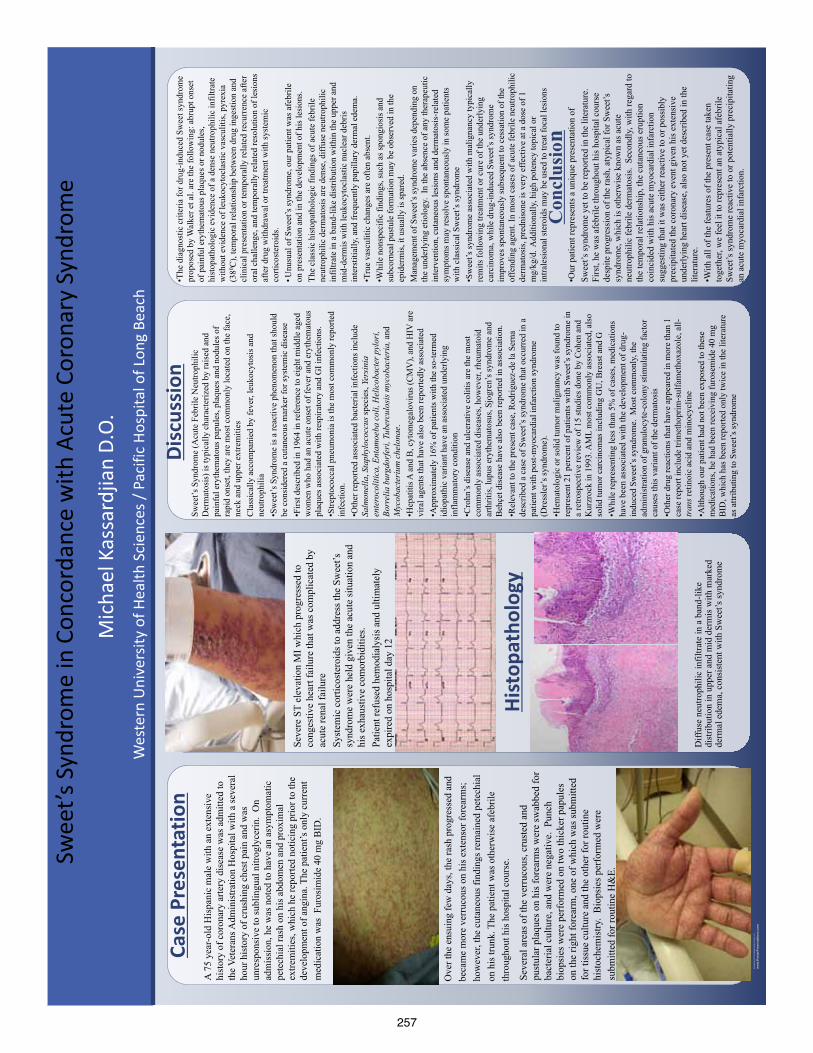
257
Q U I C K T I P S ( - - T H I S S E C T I O N D O E S N O T P R I N T - - ) T h i s P o w e r P o i n t t e m p l a t e r e q u i r e s b a s i c P o w e r P o i n t ( v e r s i o n 2 0 0 7 o r n e w e r ) s k i l l s . B e l o w i s a l i s t o f c o m m o n l y a s k e d q u e s t i o n s s p e c i f i c t o t h i s t e m p l a t e . I f y o u a r e u s i n g a n o l d e r v e r s i o n o f P o w e r P o i n t s o m e t e m p l a t e f e a t u r e s m a y n o t w o r k p r o p e r l y . U s i n g t h e t e m p l a t e V e r i f y i n g t h e q u a l i t y o f y o u r g r a p h i c s G o t o t h e V I E W m e n u a n d c l i c k o n Z O O M t o s e t y o u r p r e f e r r e d m a g n i f i c a t i o n . T h i s t e m p l a t e i s a t 1 0 0 % t h e s i z e o f t h e f i n a l p o s t e r . A l l t e x t a n d g r a p h i c s w i l l b e p r i n t e d a t 1 0 0 % t h e i r s i z e . T o s e e w h a t y o u r p o s t e r w i l l l o o k l i k e w h e n p r i n t e d , s e t t h e z o o m t o 1 0 0 % a n d e v a l u a t e t h e q u a l i t y o f a l l y o u r g r a p h i c s b e f o r e y o u s u b m i t y o u r p o s t e r f o r p r i n t i n g . U s i n g t h e p l a c e h o l d e r s T o a d d t e x t t o t h i s t e m p l a t e c l i c k i n s i d e a p l a c e h o l d e r a n d t y p e i n o r p a s t e y o u r t e x t . T o m o v e a p l a c e h o l d e r , c l i c k o n i t o n c e ( t o s e l e c t i t ) , p l a c e y o u r c u r s o r o n i t s f r a m e a n d y o u r c u r s o r w i l l c h a n g e t o t h i s s y m b o l :
T h e n , c l i c k o n c e a n d d r a g i t t o i t s n e w l o c a t i o n w h e r e y o u c a n r e s i z e i t a s n e e d e d . A d d i t i o n a l p l a c e h o l d e r s c a n b e f o u n d o n t h e l e f t s i d e o f t h i s t e m p l a t e . M o d i f y i n g t h e l a y o u t T h i s t e m p l a t e h a s f o u r d i f f e r e n t c o l u m n l a y o u t s . R i g h t - c l i c k y o u r m o u s e o n t h e b a c k g r o u n d a n d c l i c k o n “ L a y o u t ” t o s e e t h e l a y o u t o p t i o n s . T h e c o l u m n s i n t h e p r o v i d e d l a y o u t s a r e f i x e d a n d c a n n o t b e m o v e d b u t a d v a n c e d u s e r s c a n m o d i f y a n y l a y o u t b y g o i n g t o V I E W a n d t h e n S L I D E M A S T E R . I m p o r t i n g t e x t a n d g r a p h i c s f r o m e x t e r n a l s o u r c e s T E X T : P a s t e o r t y p e y o u r t e x t i n t o a p r e - e x i s t i n g p l a c e h o l d e r o r d r a g i n a n e w p l a c e h o l d e r f r o m t h e l e f t s i d e o f t h e t e m p l a t e . M o v e i t a n y w h e r e a s n e e d e d . P H O T O S : D r a g i n a p i c t u r e p l a c e h o l d e r , s i z e i t f i r s t , c l i c k i n i t a n d i n s e r t a p h o t o f r o m t h e m e n u . T A B L E S : Y o u c a n c o p y a n d p a s t e a t a b l e f r o m a n e x t e r n a l d o c u m e n t o n t o t h i s p o s t e r t e m p l a t e . T o a d j u s t t h e w a y t h e t e x t f i t s w i t h i n t h e c e l l s o f a t a b l e t h a t h a s b e e n p a s t e d , r i g h t - c l i c k o n t h e t a b l e , c l i c k F O R M A T S H A P E t h e n c l i c k o n T E X T B O X a n d c h a n g e t h e I N T E R N A L M A R G I N v a l u e s t o 0 . 2 5 M o d i f y i n g t h e c o l o r s c h e m e T o c h a n g e t h e c o l o r s c h e m e o f t h i s t e m p l a t e g o t o t h e “ D e s i g n ” m e n u a n d c l i c k o n “ C o l o r s ” . Y o u c a n c h o o s e f r o m t h e p r o v i d e c o l o r c o m b i n a t i o n s o r y o u c a n c r e a t e y o u r o w n .
QU
ICK
DES
IGN
GU
IDE
(--T
HIS
SEC
TIO
N D
OES
NO
T PR
INT-
-)
Th
is P
ower
Poin
t 20
07 t
empl
ate
prod
uces
a 3
6”x4
8”
prof
essi
onal
po
ster
. It
will
sav
e yo
u va
luab
le t
ime
plac
ing
titl
es,
subt
itle
s, t
ext,
and
gra
phic
s.
Use
it t
o cr
eate
you
r pr
esen
tati
on.
Then
sen
d it
to
Post
erPr
esen
tati
ons.
com
for
pre
miu
m q
ualit
y, s
ame
day
affo
rdab
le p
rint
ing.
W
e pr
ovid
e a
seri
es o
f on
line
tuto
rial
s th
at w
ill
guid
e yo
u th
roug
h th
e po
ster
des
ign
proc
ess
and
answ
er y
our
post
er p
rodu
ctio
n qu
esti
ons.
Vi
ew o
ur o
nlin
e tu
tori
als
at:
htt
p://
bit.
ly/P
oste
r_cr
eati
on_h
elp
(c
opy
and
past
e th
e lin
k in
to y
our
web
bro
wse
r).
For
assi
stan
ce a
nd t
o or
der
your
pri
nted
pos
ter
call
Post
erPr
esen
tati
ons.
com
at 1.
866.
649.
3004
Obj
ect
Plac
ehol
ders
Use
the
pla
ceho
lder
s pr
ovid
ed b
elow
to
add
new
el
emen
ts t
o yo
ur p
oste
r: D
rag
a pl
aceh
olde
r on
to
the
post
er a
rea,
siz
e it
, an
d cl
ick
it t
o ed
it.
Sect
ion
Hea
der
plac
ehol
der
Mov
e th
is p
refo
rmat
ted
sect
ion
head
er p
lace
hold
er
to t
he p
oste
r ar
ea t
o ad
d an
othe
r se
ctio
n he
ader
. U
se s
ecti
on h
eade
rs t
o se
para
te t
opic
s or
con
cept
s w
ithi
n yo
ur p
rese
ntat
ion.
Te
xt p
lace
hold
er
Mov
e th
is p
refo
rmat
ted
text
pla
ceho
lder
to
the
post
er t
o ad
d a
new
bod
y of
tex
t.
Pict
ure
plac
ehol
der
Mov
e th
is g
raph
ic p
lace
hold
er o
nto
your
pos
ter,
siz
e it
fir
st,
and
then
clic
k it
to
add
a pi
ctur
e to
the
po
ster
.
RES
EAR
CH
PO
STER
PR
ESEN
TATI
ON
DES
IGN
© 2
012
ww
w.P
oste
rPre
sent
atio
ns.c
om
© 2 0 1 2 P o s t e r P r e s e n t a t i o n s . c o m
2 1 1 7 F o u r t h S t r e e t , U n i t C
B e r k e l e y C A 9 4 7 1 0
p o s t e r p r e s e n t e r @ g m a i l . c o m
Stud
ent
disc
ount
s ar
e av
aila
ble
on o
ur F
aceb
ook
page
. G
o to
Pos
terP
rese
ntat
ions
.com
and
clic
k on
the
FB
icon
.
A 7
5 ye
ar-o
ld H
ispa
nic
mal
e w
ith a
n ex
tens
ive
hist
ory
of c
oron
ary
arte
ry d
isea
se w
as a
dmitt
ed to
th
e Ve
tera
ns A
dmin
istra
tion
Hos
pita
l with
a se
vera
l ho
ur h
isto
ry o
f cru
shin
g ch
est p
ain
and
was
un
resp
onsi
ve to
subl
ingu
al n
itrog
lyce
rin.
On
adm
issi
on, h
e w
as n
oted
to h
ave
an a
sym
ptom
atic
pe
tech
ial r
ash
on h
is a
bdom
en a
nd p
roxi
mal
ex
trem
ities
, whi
ch h
e re
porte
d no
ticin
g pr
ior t
o th
e de
velo
pmen
t of a
ngin
a. T
he p
atie
nt’s
onl
y cu
rren
t m
edic
atio
n w
as F
uros
imid
e 40
mg
BID
.
Case
Pre
sent
atio
n
Ove
r the
ens
uing
few
day
s, th
e ra
sh p
rogr
esse
d an
d be
cam
e m
ore
verr
ucou
s on
his e
xten
sor f
orea
rms;
ho
wev
er, t
he c
utan
eous
find
ings
rem
aine
d pe
tech
ial
on h
is tr
unk.
The
pat
ient
was
oth
erw
ise
afeb
rile
thro
ugho
ut h
is h
ospi
tal c
ours
e.
Seve
ral a
reas
of t
he v
erru
cous
, cru
sted
and
pu
stul
ar p
laqu
es o
n hi
s for
earm
s wer
e sw
abbe
d fo
r ba
cter
ial c
ultu
re, a
nd w
ere
nega
tive.
Pun
ch
biop
sies
wer
e pe
rfor
med
on
two
thic
ker p
apul
es
on th
e rig
ht fo
rear
m, o
ne o
f whi
ch w
as su
bmitt
ed
for t
issu
e cu
lture
and
the
othe
r for
rout
ine
hist
oche
mis
try.
Bio
psie
s per
form
ed w
ere
subm
itted
for r
outin
e H
&E.
Seve
re S
T el
evat
ion
MI w
hich
pro
gres
sed
to
cong
estiv
e he
art f
ailu
re th
at w
as c
ompl
icat
ed b
y ac
ute
rena
l fai
lure
Sy
stem
ic c
ortic
oste
roid
s to
addr
ess t
he S
wee
t’s
synd
rom
e w
ere
held
giv
en th
e ac
ute
situ
atio
n an
d hi
s exh
aust
ive
com
orbi
ditie
s.
Patie
nt re
fuse
d he
mod
ialy
sis a
nd u
ltim
atel
y ex
pire
d on
hos
pita
l day
12
Hist
opat
holo
gy
Con
clus
ion
•The
dia
gnos
tic c
riter
ia fo
r dru
g-in
duce
d Sw
eet s
yndr
ome
prop
osed
by
Wal
ker e
t al.
are
the
follo
win
g: a
brup
t ons
et
of p
ainf
ul e
ryth
emat
ous p
laqu
es o
r nod
ules
, hi
stop
atho
logi
c ev
iden
ce o
f a d
ense
neu
troph
ilic
infil
trate
w
ithou
t evi
denc
e of
leuk
ocyt
ocla
stic
vas
culit
is, p
yrex
ia
(380 C
), te
mpo
ral r
elat
ions
hip
betw
een
drug
inge
stio
n an
d cl
inic
al p
rese
ntat
ion
or te
mpo
rally
rela
ted
recu
rren
ce a
fter
oral
cha
lleng
e, a
nd te
mpo
rally
rela
ted
reso
lutio
n of
lesi
ons
afte
r dru
g w
ithdr
awal
or t
reat
men
t with
syst
emic
co
rtico
ster
oids
.
• Unu
sual
of S
wee
t’s sy
ndro
me,
our
pat
ient
was
afe
brile
on
pre
sent
atio
n an
d in
the
deve
lopm
ent o
f his
lesi
ons.
The
clas
sic
hist
opat
holo
gic
findi
ngs o
f acu
te fe
brile
ne
utro
phili
c de
rmat
osis
are
den
se, d
iffus
e ne
utro
phili
c in
filtra
te in
a b
and-
like
dist
ribut
ion
with
in th
e up
per a
nd
mid
-der
mis
with
leuk
ocyt
ocla
stic
nuc
lear
deb
ris
inte
rstit
ially
, and
freq
uent
ly p
apill
ary
derm
al e
dem
a.
•Tru
e va
scul
itic
chan
ges a
re o
ften
abse
nt.
•W
hile
non
spec
ific
findi
ngs,
such
as s
pong
iosi
s and
su
bcor
neal
pus
tule
form
atio
n m
ay b
e ob
serv
ed in
the
epid
erm
is, i
t usu
ally
is sp
ared
. M
anag
emen
t of S
wee
t’s sy
ndro
me
varie
s dep
endi
ng o
n th
e un
derly
ing
etio
logy
. In
the
abse
nce
of a
ny th
erap
eutic
in
terv
entio
n, c
utan
eous
lesi
ons a
nd d
erm
atos
is-r
elat
ed
sym
ptom
s may
reso
lve
spon
tane
ousl
y in
som
e pa
tient
s w
ith c
lass
ical
Sw
eet’s
synd
rom
e
•Sw
eet’s
synd
rom
e as
soci
ated
with
mal
igna
ncy
typi
cally
re
mits
follo
win
g tre
atm
ent o
r cur
e of
the
unde
rlyin
g ca
rcin
oma,
whi
le d
rug-
indu
ced
Swee
t’s sy
ndro
me
impr
oves
spon
tane
ousl
y su
bseq
uent
to c
essa
tion
of th
e of
fend
ing
agen
t. In
mos
t cas
es o
f acu
te fe
brile
neu
troph
ilic
derm
atos
is, p
redn
ison
e is
ver
y ef
fect
ive
at a
dos
e of
1
mg/
kg/d
. Add
ition
ally
, hig
h po
tenc
y to
pica
l or
intra
lesi
onal
ster
oids
may
be
used
to tr
eat f
ocal
lesi
ons
Disc
ussi
on
Swee
t’s S
yndr
ome
(Acu
te F
ebril
e N
eutro
phili
c D
erm
atos
is) i
s typ
ical
ly c
hara
cter
ized
by
rais
ed a
nd
pain
ful e
ryth
emat
ous p
apul
es, p
laqu
es a
nd n
odul
es o
f ra
pid
onse
t, th
ey a
re m
ost c
omm
only
loca
ted
on th
e fa
ce,
neck
and
upp
er e
xtre
miti
es
Cla
ssic
ally
acc
ompa
nied
by
feve
r, le
ukoc
ytos
is a
nd
neut
roph
ilia
•Sw
eet’s
Syn
drom
e is
a re
activ
e ph
enom
enon
that
shou
ld
be c
onsi
dere
d a
cuta
neou
s mar
ker f
or sy
stem
ic d
isea
se
•Firs
t des
crib
ed in
196
4 in
refe
renc
e to
eig
ht m
iddl
e ag
ed
wom
en w
ho h
ad a
n ac
ute
onse
t of f
ever
and
ery
them
atou
s pl
aque
s ass
ocia
ted
with
resp
irato
ry a
nd G
I inf
ectio
ns.
•Stre
ptoc
occa
l pne
umon
ia is
the
mos
t com
mon
ly re
porte
d in
fect
ion.
•Oth
er re
porte
d as
soci
ated
bac
teria
l inf
ectio
ns in
clud
e Sa
lmon
ella
, Sta
phyl
ococ
cus s
peci
es, Y
ersi
nia
ente
roco
litic
a, E
ntam
oeba
col
i, H
elic
obac
ter p
ylor
i, Bo
rrel
ia b
urgd
orfe
ri, T
uber
culo
sis m
ycob
acte
ria,
and
M
ycob
acte
rium
che
lona
e.
•Hep
atiti
s A a
nd B
, cyt
omeg
alov
irus (
CM
V),
and
HIV
are
vi
ral a
gent
s tha
t hav
e al
so b
een
repo
rtedl
y as
soci
ated
•A
ppro
xim
atel
y 16
% o
f pat
ient
s with
the
so-te
rmed
id
iopa
thic
var
iant
hav
e an
ass
ocia
ted
unde
rlyin
g in
flam
mat
ory
cond
ition
•C
rohn
’s d
isea
se a
nd u
lcer
ativ
e co
litis
are
the
mos
t co
mm
only
ass
ocia
ted
dise
ases
, how
ever
, rhe
umat
oid
arth
ritis
, lup
us e
ryth
emat
osus
, Sjo
gren
’s sy
ndro
me
and
Beh
çet d
isea
se h
ave
also
bee
n re
porte
d in
ass
ocia
tion.
•R
elev
ant t
o th
e pr
esen
t cas
e, R
odrig
uez-
de la
Ser
na
desc
ribed
a c
ase
of S
wee
t’s sy
ndro
me
that
occ
urre
d in
a
patie
nt w
ith p
ost-m
yoca
rdia
l inf
arct
ion
synd
rom
e (D
ress
ler’s
synd
rom
e).
•Hem
atol
ogic
or s
olid
tum
or m
alig
nanc
y w
as fo
und
to
repr
esen
t 21
perc
ent o
f pat
ient
s with
Sw
eet’s
synd
rom
e in
a
retro
spec
tive
revi
ew o
f 15
stud
ies d
one
by C
ohen
and
K
urzr
ock
in 1
993.
AM
L m
ost c
omm
only
ass
ocia
ted,
als
o so
lid tu
mor
car
cino
mas
incl
udin
g G
U, B
reas
t and
G
•Whi
le re
pres
entin
g le
ss th
an 5
% o
f cas
es, m
edic
atio
ns
have
bee
n as
soci
ated
with
the
deve
lopm
ent o
f dru
g-in
duce
d Sw
eet’s
synd
rom
e. M
ost c
omm
only
, the
ad
min
istra
tion
of g
ranu
locy
te-c
olon
y st
imul
atin
g fa
ctor
ca
uses
this
var
iant
of t
he d
erm
atos
is
•Oth
er d
rug
reac
tions
that
hav
e ap
pear
ed in
mor
e th
an 1
ca
se re
port
incl
ude
trim
etho
prim
-sul
fam
etho
xazo
le, a
ll-tr
ans r
etin
oic
acid
and
min
ocyc
line
•Alth
ough
our
pat
ient
had
not
bee
n ex
pose
d to
thes
e m
edic
atio
ns, h
e ha
d be
en re
ceiv
ing
furo
sem
ide
40 m
g B
ID, w
hich
has
bee
n re
porte
d on
ly tw
ice
in th
e lit
erat
ure
as a
ttrib
utin
g to
Sw
eet’s
synd
rom
e
•Our
pat
ient
repr
esen
ts a
uni
que
pres
enta
tion
of
Swee
t’s sy
ndro
me
yet t
o be
repo
rted
in th
e lit
erat
ure.
Fi
rst,
he w
as a
febr
ile th
roug
hout
his
hos
pita
l cou
rse
desp
ite p
rogr
essi
on o
f the
rash
, aty
pica
l for
Sw
eet’s
sy
ndro
me,
whi
ch is
oth
erw
ise
know
n as
acu
te
neut
roph
ilic
febr
ile d
erm
atos
is.
Seco
ndly
, with
rega
rd to
th
e te
mpo
ral r
elat
ions
hip,
the
cuta
neou
s eru
ptio
n co
inci
ded
with
his
acu
te m
yoca
rdia
l inf
arct
ion
sugg
estin
g th
at it
was
eith
er re
activ
e to
or p
ossi
bly
prec
ipita
ted
the
coro
nary
eve
nt g
iven
his
ext
ensi
ve
unde
rlyin
g he
art d
isea
se, a
lso
not y
et d
escr
ibed
in th
e lit
erat
ure.
•W
ith a
ll of
the
feat
ures
of t
he p
rese
nt c
ase
take
n to
geth
er, w
e fe
el it
to re
pres
ent a
n at
ypic
al a
febr
ile
Swee
t’s sy
ndro
me
reac
tive
to o
r pot
entia
lly p
reci
pita
ting
an a
cute
myo
card
ial i
nfar
ctio
n.
Diff
use
neut
roph
ilic
infil
trate
in a
ban
d-lik
e di
strib
utio
n in
upp
er a
nd m
id d
erm
is w
ith m
arke
d de
rmal
ede
ma,
con
sist
ent w
ith S
wee
t’s sy
ndro
me
Wes
tern
Uni
vers
ity o
f Hea
lth S
cien
ces /
Pac
ific
Hosp
ital o
f Lon
g Be
ach
Mic
hael
Kas
sard
jian
D.O
.
Swee
t’s S
yndr
ome
in C
onco
rdan
ce w
ith A
cute
Cor
onar
y Sy
ndro
me
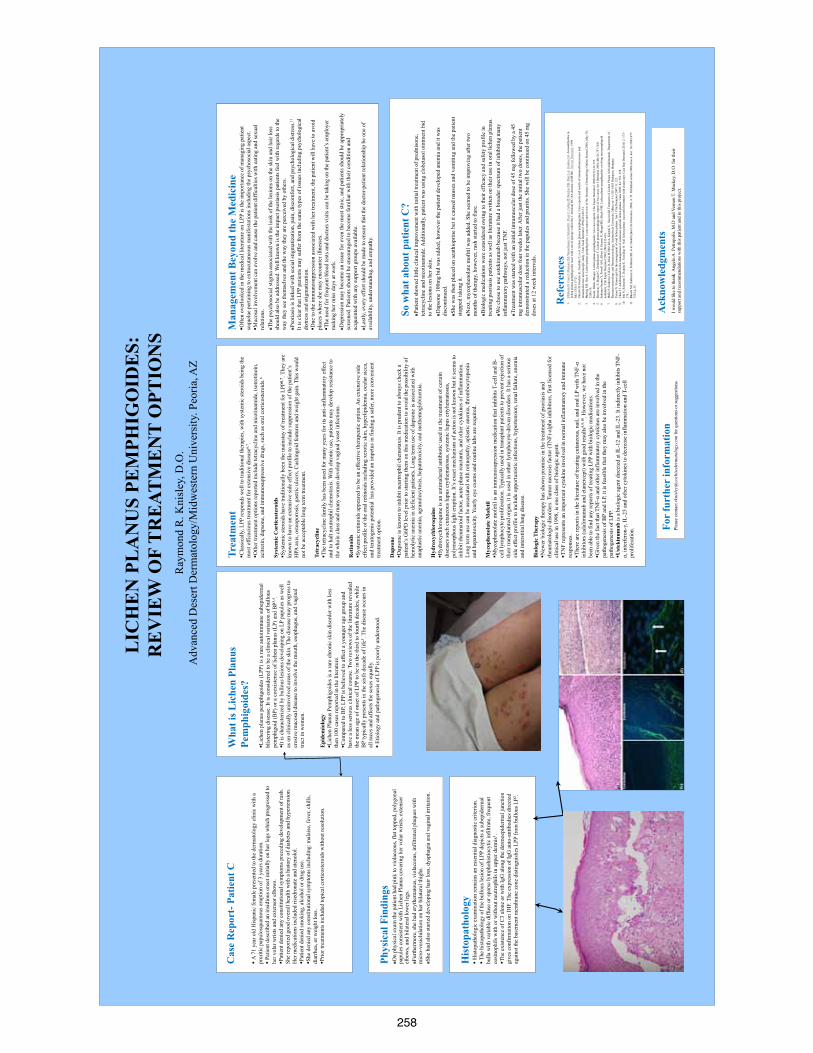
258
rrr
Wha
t is L
iche
n Pl
anus
Pe
mph
igoi
des?
L
iche
n pl
anus
pem
phig
oide
s (LP
P) is
a ra
re a
utoi
mm
une
sube
pide
rmal
bl
iste
ring
dise
ase.
It is
con
side
red
to b
e a
clin
ical
var
iatio
n of
bul
lous
pe
mph
igoi
d (B
P) o
r a c
oexi
sten
ce o
f lic
hen
plan
us (L
P) a
nd B
P3,4 .
It i
s cha
ract
eriz
ed b
y bu
llous
lesi
ons d
evel
opin
g on
LP
papu
les a
s wel
l as
on
clin
ical
ly u
ninv
olve
d ar
eas o
f the
skin
. The
dis
ease
may
pro
gres
s to
eros
ive
muc
osal
dis
ease
to in
volv
e th
e m
outh
, eso
phag
us, a
nd v
agin
al
tract
in w
omen
. E
pide
mio
logy
L
iche
n Pl
anus
Pem
phig
oide
s is a
rare
chr
onic
skin
dis
orde
r with
less
th
en 1
00 c
ases
repo
rted
in th
e lit
erat
ure.
C
ompa
red
to B
P, L
PP is
bel
ieve
d to
affe
ct a
you
nger
age
gro
up a
nd
have
a le
ss se
rious
clin
ical
cou
rse.
Tw
o re
view
s of t
he li
tera
ture
reve
aled
th
e m
ean
age
of o
nset
of L
PP to
be
in th
e th
ird to
four
th d
ecad
es, w
hile
B
P ty
pica
lly p
rese
nts i
n th
e si
xth
deca
de o
f life
5 . Th
e di
seas
e oc
curs
in
all r
aces
and
affe
cts t
he se
xes e
qual
ly.
Et
iolo
gy a
nd p
atho
gene
sis o
f LPP
is p
oorly
und
erst
ood.
Ack
now
ledg
men
ts
I wou
ld li
ke to
than
k A
ngel
o A
. Pet
ropo
lis, M
.D a
nd V
erno
n T.
Mac
key,
D.O
. for
thei
r su
ppor
t and
reco
mm
enda
tions
with
this
pat
ient
and
in th
is p
roje
ct.
Cas
e R
epor
t- P
atie
nt C
A 7
1 ye
ar o
ld H
ispa
nic
fem
ale
pres
ente
d to
the
derm
atol
ogy
clin
ic w
ith a
pr
uriti
c pa
pulo
squa
mou
s eru
ptio
n of
3 y
ears
dur
atio
n.
Pa
tient
des
crib
ed a
n in
sidi
ous o
nset
initi
ally
on
her l
egs w
hich
pro
gres
sed
to
her v
olar
wris
ts a
nd e
xten
sor e
lbow
s.
Pat
ient
den
ied
any
cons
titut
iona
l sym
ptom
s pre
cedi
ng d
evel
opm
ent o
f ras
h.
She
repo
rted
good
ove
rall
heal
th w
ith a
his
tory
of d
iabe
tes a
nd h
yper
tens
ion.
H
er m
edic
atio
ns in
clud
ed ri
sedr
onat
e an
d at
enol
ol.
Pat
ient
den
ied
smok
ing,
alc
ohol
or d
rug
use.
S
he d
enie
d an
y co
nstit
utio
nal s
ympt
oms i
nclu
ding
: mal
aise
, fev
er, c
hills
, di
arrh
ea, o
r wei
ght l
oss.
Prio
r tre
atm
ents
incl
uded
topi
cal c
ortic
oste
roid
s with
out r
esol
utio
n.
So w
hat a
bout
pat
ient
C?
Pa
tient
show
ed li
ttle
clin
ical
impr
ovem
ent w
ith in
itial
trea
tmen
t of p
redn
ison
e,
tetra
cycl
ine
and
nico
tinam
ide.
Add
ition
ally
, pat
ient
was
usi
ng c
lobe
taso
l oin
tmen
t bid
to
the
lesi
ons o
n he
r ski
n.
D
apso
ne 1
00m
g bi
d w
as a
dded
, how
ever
the
patie
nt d
evel
oped
ane
mia
and
it w
as
disc
ontin
ued.
Sh
e w
as th
en p
lace
d on
aza
thio
prin
e bu
t it c
ause
d na
usea
and
vom
iting
and
the
patie
nt
stop
ped
taki
ng it
. N
ext,
myc
ophe
nola
te m
ofiti
l was
add
ed. S
he se
emed
to b
e im
prov
ing
afte
r tw
o m
onth
s of t
hera
py, h
owev
er, r
ash
star
ted
to fl
are.
B
iolo
gic
med
icat
ions
wer
e co
nsid
ered
ow
ing
to th
eir e
ffica
cy a
nd sa
fety
pro
file
in
treat
ing
psor
iasi
s pat
ient
s as w
ell a
s lite
ratu
re w
ritte
n on
thei
r use
in o
ral l
iche
n pl
anus
. W
e ch
ose
to u
se u
stek
inum
ab b
ecau
se it
had
a b
road
er sp
ectru
m o
f inh
ibiti
ng m
any
infla
mm
ator
y pa
thw
ays,
not j
ust T
NF.
Tr
eatm
ent w
as st
arte
d w
ith a
n in
itial
intra
mus
cula
r dos
e of
45
mg
follo
wed
by
a 45
m
g in
tram
uscu
lar d
ose
four
wee
ks la
ter.
Afte
r jus
t the
initi
al tw
o do
ses,
the
patie
nt
dem
onst
rate
d a
redu
ctio
n in
the
papu
les a
nd p
rurit
is. S
he w
ill b
e co
ntin
ued
on 4
5 m
g do
ses a
t 12
wee
k in
terv
als.
Ray
mon
d R
. Kni
sley
, D.O
. A
dvan
ced
Des
ert D
erm
atol
ogy/
Mid
wes
tern
Uni
vers
ity. P
eoria
, AZ
For
furt
her
info
rmat
ion
Plea
se c
onta
ct rk
nisl
ey@
coch
isede
rmat
olog
y.com
for q
uest
ions
or s
ugge
stio
ns.
Phys
ical
Fin
ding
s O
n ph
ysic
al e
xam
the
patie
nt h
ad p
ink
to v
iola
ceou
s, fla
t top
ped,
pol
ygon
al
papu
les c
onsi
sten
t with
Lic
hen
Plan
us c
over
ing
her v
olar
wris
ts, e
xten
sor
elbo
ws,
and
bila
tera
l low
er le
gs.
Fu
rther
mor
e, sh
e ha
d er
ythe
mat
ous,
viol
aceo
us, i
nfilt
rate
d pl
aque
s with
m
icro
-ves
iclu
latio
n on
her
bila
tera
l thi
ghs.
Sh
e ha
d al
so st
arte
d de
velo
ping
hai
r los
s, dy
spha
gia
and
vagi
nal i
rrita
tion.
LIC
HE
N P
LA
NU
S PE
MPH
IGO
IDE
S:
RE
VIE
W O
F T
RE
ATM
EN
T O
PTIO
NS
Man
agem
ent B
eyon
d th
e M
edic
ine
Ofte
n ov
erlo
oked
in th
e m
edic
al li
tera
ture
on
LPP
is th
e im
porta
nce
of m
anag
ing
patie
nt
sequ
elae
per
tain
ing
to e
xtra
cuta
neou
s man
ifest
atio
ns in
clud
ing
the
psyc
hoso
cial
asp
ect.
Muc
osal
invo
lvem
ent c
an e
volv
e an
d ca
use
the
patie
nt d
iffic
ultie
s with
eat
ing
and
sexu
al
rela
tions
. Th
e ps
ycho
soci
al st
igm
a as
soci
ated
with
the
look
of t
he le
sion
s on
the
skin
and
hai
r los
s sh
ould
als
o be
add
ress
ed. W
ell k
now
n is
the
impa
ct p
soria
sis p
atie
nts f
eel w
ith re
gard
s to
the
way
they
see
them
selv
es a
nd th
e w
ay th
ey a
re p
erce
ived
by
othe
rs.
Ps
oria
sis i
s lin
ked
with
soci
al st
igm
atiz
atio
n, p
ain,
dis
com
fort,
and
psy
chol
ogic
al d
istre
ss.11
It
is c
lear
that
LPP
pat
ient
s may
suffe
r fro
m th
e sa
me
type
s of i
ssue
s inc
ludi
ng p
sych
olog
ical
di
stre
ss a
nd st
igm
atiz
atio
n.
Due
to th
e im
mun
osup
pres
sion
ass
ocia
ted
with
her
trea
tmen
t, th
e pa
tient
will
hav
e to
avo
id
plac
es w
here
she
may
enc
ount
er il
lnes
ses.
The
nee
d fo
r fre
quen
t blo
od te
sts a
nd d
octo
rs v
isits
can
be
taki
ng o
n th
e pa
tient
’s e
mpl
oyer
m
akin
g he
r mis
s day
s at w
ork.
D
epre
ssio
n m
ay b
ecom
e an
issu
e fo
r eve
n th
e m
ost s
toic
, and
pat
ient
s sho
uld
be a
ppro
pria
tely
sc
reen
ed. P
atie
nts s
houl
d be
enc
oura
ged
to b
ecom
e fa
mili
ar w
ith th
eir c
ondi
tion
and
acqu
aint
ed w
ith a
ny su
ppor
t gro
ups a
vaila
ble.
La
stly
, eve
ry e
ffort
shou
ld b
e m
ade
to e
nsur
e th
at th
e do
ctor
-pat
ient
rela
tions
hip
be o
ne o
f av
aila
bilit
y, u
nder
stan
ding
, and
em
path
y.
Trea
tmen
t C
lass
ical
ly, L
PP re
spon
ds w
ell t
o tra
ditio
nal t
hera
pies
, with
syst
emic
ster
oids
bei
ng th
e m
ost e
ffica
ciou
s tre
atm
ent f
or e
xten
sive
dis
ease
6,7 .
O
ther
trea
tmen
t opt
ions
repo
rted
incl
ude
tetra
cycl
ine
and
nico
tinam
ide,
isot
retin
oin,
ac
itret
in, d
apso
ne, a
nd im
mun
osup
pres
sive
dru
gs, s
uch
as o
ral c
ortic
oste
roid
s.6
Syst
emic
Cor
ticos
tero
ids
Sys
tem
ic st
eroi
ds h
ave
tradi
tiona
lly b
een
the
mai
nsta
y of
trea
tmen
t for
LPP
6,7 .
They
are
kn
own
to h
ave
an e
xten
sive
side
effe
ct p
rofil
e to
incl
ude
supp
ress
ion
of th
e pa
tient
’s
HPA
axi
s, os
teop
oros
is, g
astri
c ul
cers
, Cus
hing
oid
feat
ures
and
wei
ght g
ain.
Thi
s wou
ld
not b
e ac
cept
able
long
term
trea
tmen
t. Te
trac
yclin
e T
he te
tracy
clin
e fa
mily
has
bee
n us
ed fo
r man
y ye
ars f
or it
s ant
i-inf
lam
mat
ory
effe
ct
and
to h
alt n
eutro
phil
chem
otax
is. W
ith c
hron
ic u
se, p
atie
nts m
ay d
evel
op re
sist
ance
to
the
who
le c
lass
and
man
y w
omen
dev
elop
vag
inal
yea
st in
fect
ions
. R
etin
oids
S
yste
mic
retin
oids
app
eare
d to
be
an e
ffect
ive
ther
apeu
tic o
ptio
n. A
n ex
tens
ive
side
ef
fect
pro
file
of th
e or
al re
tinoi
ds in
clud
ing
xero
tic sk
in, h
yper
lipid
emia
, ocu
lar s
icca
, an
d te
rato
geni
c po
tent
ial
has p
rovi
ded
an im
petu
s in
findi
ng a
safe
r, m
ore
conv
enie
nt
treat
men
t opt
ion.
D
apso
ne
Dap
sone
is k
now
n to
inhi
bit n
eurtr
ophi
l che
mot
axis
. It i
s pru
dent
to a
lway
s che
ck a
pa
tient
’s G
6PD
leve
l prio
r to
star
ting
them
on
this
med
icat
ion
to a
void
the
poss
ibili
ty o
f he
mol
ytic
ane
mia
in d
efic
ient
pat
ient
s. Lo
ng te
rm u
se o
f dap
sone
is a
ssoc
iate
d w
ith
anap
last
ic a
nem
ia, a
gran
uloc
ytos
is, h
epat
otox
icity
, and
met
hem
oglo
bine
mia
. H
ydro
xych
loro
quin
e H
ydro
xych
loro
quin
e is
an
antim
alar
ial a
ntib
iotic
use
d in
the
treat
men
t of c
erta
in
dise
ases
such
cut
aneo
us lu
pus e
ryth
emat
osus
, sys
tem
ic lu
pus e
rtyhe
mat
osus
, po
lym
orph
ous l
ight
eru
ptio
n. It
’s e
xact
mec
hani
sm o
f act
ion
is n
ot k
now
n bu
t it s
eem
s to
inhi
bit r
heum
atoi
d fa
ctor
, acu
te p
hase
reac
tant
s, an
d ot
her c
ytok
ines
of i
nfla
mm
atio
n.
Long
term
use
can
be
asso
ciat
ed w
ith re
tinop
athy
, apl
astic
ane
mia
, thr
ombo
cyto
peni
a an
d he
pato
toxi
city
. Yea
rly e
ye e
xam
s and
rout
ine
labs
are
requ
ired.
M
ycop
heno
late
Mof
etil
Myc
ophe
nola
te m
ofet
il is
an
imm
unos
upre
ssio
n m
edic
atio
n th
at in
hibi
ts T
-cel
l and
B-
cell
lym
phoc
yte
prol
ifera
tion.
Typ
ical
ly u
sed
in tr
ansp
lant
pat
ient
s to
prev
ent r
ejec
tion
of
thei
r tra
nspl
ante
d or
gan,
it is
use
d in
oth
er ly
mph
ocyt
e-dr
iven
dis
orde
rs. I
t has
a se
rious
si
de e
ffect
pro
file
to in
clud
e op
portu
nist
ic in
fect
ions
, hyp
erte
nsio
n, re
nal f
ailu
re, a
nem
ia
and
inte
rstit
ial l
ung
dise
ase.
B
iolo
gic
The
rapy
N
ewer
bio
logi
c th
erap
y ha
s sho
wn
prom
ise
in th
e tre
atm
ent o
f pso
riasi
s and
rh
eum
atol
ogic
dis
orde
rs. T
umor
nec
rosi
s fac
tor (
TNF)
-alp
ha in
hibi
tors
, firs
t lic
ense
d fo
r cl
inic
al u
se in
199
8, is
one
cla
ss o
f bio
logi
c ag
ent.
T
NF
repr
esen
ts a
n im
porta
nt c
ytok
ine
invo
lved
in n
orm
al in
flam
mat
ory
and
imm
une
resp
onse
s.
The
re a
re re
ports
in th
e lit
erat
ure
of tr
eatin
g cu
tane
ous,
nail,
and
ora
l LP
with
TN
F-α
inhi
bito
rs (a
dalim
umab
and
eta
nerc
ept)
with
goo
d re
sults
8,9,
10. H
owev
er, w
e ha
ve n
ot
been
abl
e to
find
any
repo
rts o
f tre
atin
g LP
P w
ith b
iolo
gic
med
icat
ions
. G
iven
the
fact
that
TN
F-α
and
othe
r inf
lam
mat
ory
cyto
kine
s are
invo
lved
in th
e pa
thog
enes
is o
f BP
and
LP, i
t is f
easi
ble
that
they
may
als
o be
invo
lved
in th
e pa
thog
enes
is o
f LPP
. U
stek
inum
ab is
a b
iolo
gic
agen
t dire
cted
at I
L-12
and
IL-2
3. It
indi
rect
ly in
hibi
ts T
NF-
α, in
terf
eron
-γ, I
L-23
and
oth
er c
ytok
ines
to d
ecre
ase
infla
mm
atio
n an
d T-
cell
prol
ifera
tion.
His
topa
thol
ogy
H
isto
path
olog
ic e
xam
inat
ion
rem
ains
an
esse
ntia
l dia
gnos
tic c
riter
ion.
The
hist
opat
holo
gy o
f the
bul
lous
lesi
on o
f LPP
dep
icts
a su
bepi
derm
al
bulla
with
var
iabl
e di
ffuse
or s
pars
e ly
mph
ohis
tiocy
tic in
filtra
te, f
requ
ent
eosi
noph
ils w
ith o
r with
out n
eutro
phils
in u
pper
der
mis
1 .
The
exi
sten
ce o
f C3
alon
e or
with
IgG
alo
ng th
e de
rmoe
pide
rmal
junc
tion
give
s con
firm
atio
n on
DIF
. The
exp
ress
ion
of Ig
G a
uto-
antib
odie
s dire
cted
ag
ains
t the
bas
emen
t mem
bran
e zo
ne d
istin
guis
hes L
PP fr
om b
ullo
us L
P2 .
Ref
eren
ces
1.Zi
llike
ns D
, Cau
x F,
Mas
caro
JM, W
esse
lman
n U
, Sch
mid
t E, P
rost
C, C
alle
n JP
, Brö
cker
EB
, Dia
z LA
, Giu
dice
GJ.
Aut
oant
ibod
ies
in
liche
n pl
anus
pem
phig
oide
s rea
ct w
ith a
nov
el e
pito
pe w
ithin
the
C-te
rmin
al N
C16
A d
omai
n of
BP1
80. J
Inve
st D
erm
atol
. 199
9 Ju
l;113
(1):1
17-2
1.
2.O
koch
i H, N
ashi
ro K
, Tsu
chid
a T,
et a
l. Li
chen
pla
nus p
emph
igoi
des:
Cas
e re
ports
and
resu
lts o
f im
mun
oflo
ures
cenc
e an
d im
mun
oele
ctro
n m
icro
scop
ic s
tudy
. J A
m A
cad
Der
mat
ol 1
990;
22:6
26-3
1.
3.H
artin
g M
S, H
su S
. Lic
hen
plan
us p
emph
igoi
des:
a c
ase
repo
rt an
d re
view
of t
he li
tera
ture
. Der
mat
olog
y O
nlin
e Jo
urna
l 200
6, M
ay 3
0;
12(4
):10.
4.
Swal
e, B
lack
, Bho
gal.
Lich
en p
lanu
s pem
phig
oide
s: tw
o ca
se re
ports
. Clin
Exp
er D
erm
atol
199
8;23
(3):1
32-1
35.
5.D
emirc
ay Z
, Bay
kal C
, Dem
irkes
en C
. Lic
hen
plan
us p
emph
igoi
des:
repo
rt of
two
case
s. In
t J D
erm
atol
200
1;40
(12)
:757
-760
. 6.
Saku
ma-
Oya
ma
Y, P
owel
l AM
, Alb
ert S
, Oya
ma
N, B
hoga
l BS,
Bla
ck N
M. L
iche
n pl
anus
pem
phig
oide
s ev
olvi
ng in
to p
emph
igoi
d no
dula
ris. C
lin E
xper
Der
mat
ol 2
004
;28(
6):6
13-6
16.
7.H
olló
P, S
zako
nyi J
, Kis
s D, J
okai
H, H
orvá
th A
, Kár
páti
S. S
ucce
ssfu
l Tre
atm
ent o
f Lic
hen
Plan
us w
ith A
dalim
umab
, Dep
artm
ent o
f D
erm
atov
ener
eolo
gy a
nd D
erm
atoo
ncol
ogy,
Sem
mel
wei
s U
nive
rsity
, Már
ia st
r. 41
, HU
-108
5 B
udap
est,
Hun
gary
. 8.
Yaro
m N
. Eta
nerc
ept f
or th
e m
anag
emen
t of o
ral l
iche
n pl
anus
. Am
J C
lin D
erm
atol
200
7; 8
: 121
. 9.
Cha
o TJ
. Ada
limum
ab in
the
man
agem
ent o
f cut
aneo
us a
nd o
ral l
iche
n pl
anus
. Cut
is 2
009;
84:
352
–358
. 10
.Ir
la N
, Sch
neite
r T, H
anek
e E,
Yaw
alka
r N. N
ail l
iche
n pl
anus
: suc
cess
ful t
reat
men
t with
eta
nerc
ept.
Cas
e R
ep D
erm
atol
201
0; 2
: 173
–17
6.
11.
Bho
sle
MJ,
Kul
karn
i A, F
eldm
an S
R, e
t al.
Hea
lth Q
ual L
ife O
utco
mes
. 200
6; 4
: 35.
Pub
lishe
d on
line
2006
June
6. d
oi: 1
0.11
86/1
477-
7525
-4-3
5.
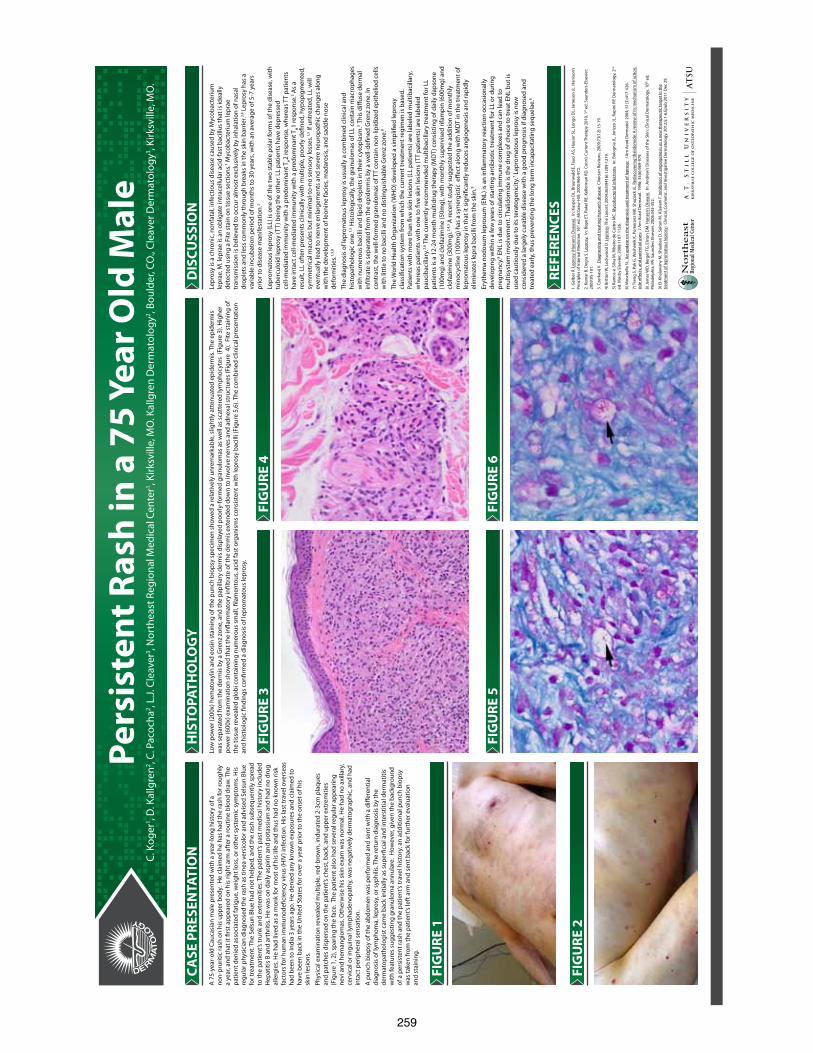
259
Pers
iste
nt R
ash
in a
75
Year
Old
Mal
eC.
Kog
er1 , D
. Kal
lgre
n2 , C. P
acoc
ha2 , L
.J. C
leav
er3 , N
orth
east
Reg
iona
l Med
ical
Cen
ter1 , K
irksv
ille,
MO
. Kal
lgre
n D
erm
atol
ogy2 , B
ould
er, C
O.,
Clea
ver D
erm
atol
ogy3 , K
irksv
ille,
MO
.
CASE
PRE
SEN
TATI
ON
FIG
URE
1
FIG
URE
3
FIG
URE
5
FIG
URE
4
FIG
URE
6
FIG
URE
2
A 7
5-ye
ar-o
ld C
auca
sian
mal
e pr
esen
ted
with
a y
ear-
long
his
tory
of a
no
n-pr
uriti
c ra
sh o
n hi
s up
per b
ody.
He
clai
med
he
has
had
the
rash
for r
ough
ly
a ye
ar, a
nd th
at it
�rs
t app
eare
d on
his
righ
t arm
aft
er a
rout
ine
bloo
d dr
aw. T
he
patie
nt d
enie
d as
soci
ated
fatig
ue, w
eigh
t los
s, or
oth
er s
yste
mic
sym
ptom
s. H
is
regu
lar p
hysi
cian
dia
gnos
ed th
e ra
sh a
s tin
ea v
ersi
colo
r and
adv
ised
Sel
sun
Blue
fo
r tre
atm
ent.
The
Sels
un B
lue
had
not h
elpe
d, a
nd th
e ra
sh s
ubse
quen
tly s
prea
d to
the
patie
nt’s
trun
k an
d ex
trem
ities
. The
pat
ient
’s pa
st m
edic
al h
isto
ry in
clud
ed
Hep
atiti
s B
and
arth
ritis
. He
was
on
daily
asp
irin
and
pota
ssiu
m a
nd h
ad n
o dr
ug
alle
rgie
s. H
e ha
d liv
ed a
s a
mon
k fo
r mos
t of h
is li
fe a
nd th
us h
ad n
o kn
own
risk
fact
ors
for h
uman
imm
unod
e�ci
ency
viru
s (H
IV) i
nfec
tion.
His
last
trav
el o
vers
eas
had
been
to In
dia
3 ye
ars
ago.
He
deni
ed a
ny k
now
n ex
posu
res
and
clai
med
to
have
bee
n ba
ck in
the
Uni
ted
Stat
es fo
r ove
r a y
ear p
rior t
o th
e on
set o
f his
skin
lesi
ons.
Phys
ical
exa
min
atio
n re
veal
ed m
ultip
le, r
ed-b
row
n, in
dura
ted
2-3c
m p
laqu
es
and
patc
hes
disp
erse
d on
the
patie
nt’s
ches
t, ba
ck, a
nd u
pper
ext
rem
ities
(F
igur
e 1,
2),
spar
ing
the
face
. The
pat
ient
als
o ha
d se
vera
l reg
ular
app
earin
g ne
vi a
nd h
eman
giom
as. O
ther
wis
e hi
s sk
in e
xam
was
nor
mal
. He
had
no a
xilla
ry,
cerv
ical
or i
ngui
nal l
ymph
aden
opat
hy, w
as n
egat
ivel
y de
rmat
ogra
phic
, and
had
in
tact
per
iphe
ral s
ensa
tion.
A p
unch
bio
psy
of th
e ab
dom
en w
as p
erfo
rmed
and
sen
t with
a d
i�er
entia
l di
agno
sis
of ly
mph
oma,
lepr
osy,
or s
yphi
lis. T
he re
turn
dia
gnos
is b
y th
e de
rmat
opat
holo
gist
cam
e ba
ck in
itial
ly a
s su
per�
cial
and
inte
rstit
ial d
erm
atiti
s w
ith fe
atur
es s
ugge
stin
g gr
anul
oma
annu
lare
. H
owev
er, g
iven
the
back
grou
nd
of a
per
sist
ent r
ash
and
the
patie
nt’s
trav
el h
isto
ry, a
n ad
ditio
nal p
unch
bio
psy
was
take
n fr
om th
e pa
tient
’s le
ft a
rm a
nd s
ent b
ack
for f
urth
er e
valu
atio
nan
d st
aini
ng.
HIS
TOPA
THO
LOG
YLo
w p
ower
(200
x) h
emat
oxyl
in a
nd e
osin
sta
inin
g of
the
punc
h bi
opsy
spe
cim
en s
how
ed a
rela
tivel
y un
rem
arka
ble,
slig
htly
att
enua
ted
epid
erm
is. T
he e
pide
rmis
w
as s
epar
ated
from
the
derm
is b
y a
Gre
nz z
one,
and
the
papi
llary
der
mis
dis
play
ed p
oorly
-form
ed g
ranu
lom
as a
s w
ell a
s sc
atte
red
lym
phoc
ytes
(Fi
gure
3).
Hig
her
pow
er (6
00x)
exa
min
atio
n sh
owed
that
the
in�a
mm
ator
y in
�ltr
ate
of th
e de
rmis
ext
ende
d do
wn
to in
volv
e ne
rves
and
adn
exal
str
uctu
res
(Fig
ure
4).
Fite
sta
inin
g of
th
e tis
sue
reve
aled
glo
bi c
onta
inin
g nu
mer
ous
smal
l, �l
amen
tous
, aci
d fa
st o
rgan
ism
s co
nsis
tent
with
lepr
osy
baci
lli (F
igur
e 5,
6). T
he c
ombi
ned
clin
ical
pre
sent
atio
n an
d hi
stio
logi
c �n
ding
s co
n�rm
ed a
dia
gnos
is o
f lep
rom
atou
s le
pros
y.
DIS
CUSS
ION
Lepr
osy
is a
chr
onic
, non
fata
l, in
fect
ious
dis
ease
cau
sed
by M
ycob
acte
rium
le
prae
. M. l
epra
e is
an
oblig
ate
intr
acel
lula
r aci
d-fa
st b
acill
us th
at is
idea
lly
dete
cted
usi
ng a
Fite
sta
in o
n tis
sue
sect
ions
.1 Myc
obac
teriu
m le
prae
tr
ansm
issi
on is
bel
ieve
d to
occ
ur a
lmos
t exc
lusi
vely
by
inha
latio
n of
nas
al
drop
lets
and
less
com
mon
ly th
roug
h br
eaks
in th
e sk
in b
arrie
r.3,4 L
epro
sy h
as a
va
riabl
e in
cuba
tion
perio
d of
mon
ths
to 3
0 ye
ars,
with
an
aver
age
of 5
-7 y
ears
pr
ior t
o di
seas
e m
anife
stat
ion.
2
Lepr
omat
ous
lepr
osy
(LL)
is o
ne o
f the
two
stab
le p
olar
form
s of
the
dise
ase,
with
tu
berc
uloi
d le
pros
y (T
T) b
eing
the
othe
r. LL
pat
ient
s ha
ve d
epre
ssed
ce
ll-m
edia
ted
imm
unity
with
a p
redo
min
ant T
H2
resp
onse
, whe
reas
TT
patie
nts
have
inta
ct c
ell-m
edia
ted
imm
unity
with
a p
redo
min
ant T
H1
resp
onse
.5 As
a re
sult,
LL
ofte
n pr
esen
ts c
linic
ally
with
mul
tiple
, poo
rly d
e�ne
d, h
ypop
igm
ente
d,
sym
met
rical
mac
ules
but
min
imal
-to-
no s
enso
ry lo
sses
.1,5 If
unt
reat
ed, L
L w
ill
even
tual
ly le
ad to
ner
ve e
nlar
gem
ents
and
sev
ere
neur
opat
hic
chan
ges
alon
g w
ith th
e de
velo
pmen
t of l
eoni
ne fa
cies
, mad
aros
is, a
nd s
addl
e no
se
defo
rmiti
es.1,
5,8
The
diag
nosi
s of
lepr
omat
ous
lepr
osy
is u
sual
ly a
com
bine
d cl
inic
al a
nd
hist
opat
holo
gic
one.
1,5
His
tolo
gica
lly, t
he g
ranu
lom
as o
f LL
cont
ain
mac
roph
ages
w
ith n
umer
ous
baci
lli a
nd li
pid
drop
lets
in th
eir c
ytop
lasm
.5 Th
is d
i�us
e de
rmal
in
�ltr
ate
is s
epar
ated
from
the
epid
erm
is b
y a
wel
l-de�
ned
Gre
nz z
one.
In
cont
rast
, the
wel
l-for
med
gra
nulo
mas
of T
T co
ntai
n no
n-lip
idiz
ed e
pith
elio
d ce
lls
with
litt
le to
no
baci
lli a
nd n
o di
stin
guis
habl
e G
renz
zon
e.8
The
Wor
ld H
ealth
Org
aniz
atio
n (W
HO
) dev
elop
ed a
sim
pli�
ed le
pros
y cl
assi
�cat
ion
syst
em fr
om w
hich
the
curr
ent t
reat
men
t reg
imen
is b
ased
. Pa
tient
s w
ith m
ore
than
�ve
ski
n le
sion
s (L
L pa
tient
s) a
re la
bele
d m
ultib
acill
ary,
w
here
as p
atie
nts
with
one
to �
ve s
kin
lesi
ons
(TT
patie
nts)
are
labe
led
pauc
ibac
illar
y.2,
6 The
cur
rent
ly re
com
men
ded
mul
tibac
illar
y tr
eatm
ent f
or L
L pa
tient
s is
a 1
2-24
mon
th m
ultid
rug
ther
apy
(MD
T) c
onsi
stin
g of
dai
ly d
apso
ne
(100
mg)
and
clo
fazi
min
e (5
0mg)
, with
mon
thly
sup
ervi
sed
rifam
pin
(600
mg)
and
cl
ofaz
imin
e (3
00m
g).2,
4,5 A
rece
nt s
tudy
sug
gest
ed th
e ad
ditio
n of
mon
thly
m
inoc
yclin
e (1
00m
g) h
as a
syn
ergi
stic
e�e
ct a
long
with
MD
T in
the
trea
tmen
t of
lepr
omat
ous
lepr
osy
in th
at it
sig
ni�c
antly
redu
ces
angi
ogen
esis
and
rapi
dly
elim
inat
es le
pra
baci
lli fr
om th
e sk
in.9
Eryt
hem
a no
dosu
m le
pros
um (E
NL)
is a
n in
�am
mat
ory
reac
tion
occa
sion
ally
de
velo
ping
with
in a
few
yea
rs o
f sta
rtin
g an
tibio
tic tr
eatm
ent f
or L
L or
dur
ing
preg
nanc
y.8 E
NL
is d
ue to
circ
ulat
ing
imm
une
com
plex
es a
nd c
an le
ad to
m
ultis
yste
m in
volv
emen
t. Th
alid
omid
e is
the
drug
of c
hoic
e to
trea
t EN
L bu
t is
used
cau
tious
ly d
ue to
its
tera
toge
nici
ty.7 L
epro
mat
ous
lepr
osy
is n
ow
cons
ider
ed a
larg
ely
cura
ble
dise
ase
with
a g
ood
prog
nosi
s if
diag
nose
d an
d tr
eate
d ea
rly, t
hus
prev
entin
g th
e lo
ng te
rm in
capa
cita
ting
sequ
elae
.6
REFE
REN
CES
1. G
elbe
r R. L
epro
sy (H
anse
n’s
Dis
ease
). In
: Kas
per D
L, B
raun
wal
d E,
Fau
ci A
S, H
ause
r SL,
Lon
go D
L, Ja
mes
on JL
. Har
rison
’s Pr
inci
ples
of I
nter
nal M
edic
ine,
16th
ed.
McG
raw
-Hill
; 200
5:96
6-97
2.
2. K
umar
B. D
egra
S. L
epro
sy.
In: B
ope
ET, R
akel
RE,
Kel
lerm
an R
D. C
onn’
s Cu
rren
t The
rapy
201
0, 1
st e
d. S
aund
ers-
Else
vier
; 20
09:9
5-10
1.
3. C
zerk
asij
V. D
iagn
osin
g an
d tr
eatin
g H
anse
n’s
dise
ase:
Clin
icia
n Re
view
s. 20
09;7
3(12
):15-
19.
4) B
ritto
n W
, Loc
kwoo
d D
. Lep
rosy
: The
Lan
cet.
2004
;363
(941
6):1
209-
1219
.
5) R
amos
-e-S
ilva
M, R
ibei
ro d
e Ca
stro
MC.
Myc
obac
teria
l Inf
ectio
ns.
In: B
olog
nia
JL, J
oriz
zo JL
, Rap
ini R
P. D
erm
atol
ogy,
2nd
ed
. Mos
by E
lsev
ier;
2008
:110
7-11
26.
6) M
osch
ella
SL.
An
upda
te o
n th
e di
agno
sis
and
trea
tmen
t of l
epro
sy:
J Am
Aca
d D
erm
atol
. 200
4; 5
1(3)
:417
-426
.
7) T
seng
S, P
ak G
, Was
heni
k K,
Pom
eran
z M
K, S
hupa
ck JL
. Red
isco
verin
g th
alid
omid
e: A
revi
ew o
f its
mec
hani
sm o
f act
ion,
si
de e
�ect
s, an
d po
tent
ial u
ses:
J A
m A
cad
Der
mat
ol. 1
996;
35(
6):9
69-9
79.
8) Ja
mes
WD
, Ber
ger T
G, E
lsto
n D
M. H
anse
n’s
Dis
ease
. In
: And
rew
’s D
isea
ses
of th
e Sk
in: C
linic
al D
erm
atol
ogy.
10th
ed.
Ph
ilade
lphi
a, P
A: S
aund
ers
Else
vier
. 200
6:34
3-35
2.
9) E
l-Kha
law
any
M, S
haab
an D
, Sul
tan
M, A
lsal
am F
. Inh
ibiti
on o
f ang
ioge
nesi
s as
a n
ew th
erap
eutic
targ
et in
the
trea
tmen
t of l
epro
mat
ous
lepr
osy:
Clin
ical
, Cos
met
ic, a
nd In
vest
igat
ive
Der
mat
olog
y. 2
012;
5:1-
6.Ep
ub 2
011
Dec
29.
260
Inva
sive
Duc
tal B
reas
t Car
cino
ma
Pres
entin
g as
Lip
oma
in a
Mal
e: A
Cas
e R
epor
t and
a
Rev
iew
of t
he L
itera
ture
Ja
mes
Lan
dero
, DO
W
ellin
gton
Reg
iona
l Med
ical
Cen
ter
Abs
trac
t D
iscu
ssio
n
App
roac
h
Cas
e R
epor
t
Pres
ente
d at
the
2012
ann
ual m
eetin
g of
the
Am
eric
an O
steo
path
ic C
olle
ge o
f Der
mat
olog
y in
San
Die
go, C
A
Bre
ast C
A in
Mal
es
Con
clus
ion
Ref
eren
ces
Mal
e br
east
can
cer,
alth
ough
a ra
re m
alig
nanc
y th
at a
ccou
nts
for
less
than
1%
of a
ll ca
ncer
s in
men
is e
asily
trea
ted
whe
n ca
ught
in
the
early
sta
ges.
We
desc
ribe
the
case
of a
76
year
old
Cau
casi
an
mal
e pa
tient
with
inva
sive
duc
tal b
reas
t car
cino
ma
who
pre
sent
ed
with
a s
impl
e br
east
lum
p co
nsis
tent
with
a c
omm
on li
pom
a ov
erly
ing
the
mal
igna
nt tu
mor
. Thi
s pa
per w
ill re
view
the
curr
ent
liter
atur
e on
epi
dem
iolo
gy, r
isk
fact
ors,
etio
logy
, diff
eren
t typ
es o
f br
east
can
cer,
clin
ical
pre
sent
atio
n, im
agin
g, d
iagn
ostic
wor
kup
and
treat
men
t. W
e st
ress
the
impo
rtanc
e of
a th
orou
gh e
valu
atio
n of
a
brea
st lu
mp
in a
ny p
erso
n, m
ale
or fe
mal
e to
avo
id u
nder
-dia
gnos
is.
We
also
sup
port
a lo
wer
thre
shol
d fo
r bio
psy
of a
ny b
reas
t lum
p,
espe
cial
ly w
ith a
his
tory
of r
ecen
t dis
cove
ry o
r gro
wth
.
Epid
emio
logy
C
urre
ntly,
mal
e br
east
car
cino
ma
acco
unts
for l
ess
than
1%
of a
ll ca
ncer
s in
men
and
is o
nly
0.7%
of a
ll br
east
can
cers
(2, 3
). M
ale
brea
st
canc
er c
ompr
ises
1%
of a
ll m
alig
nant
bre
ast c
ance
r and
lead
s to
less
than
0.1
% o
f can
cer r
elat
ed d
eath
s in
men
(14)
. The
mal
e to
fem
ale
ratio
fo
r bre
ast c
ance
r is
1:10
0 (1
). Th
e pe
ak in
cide
nce
at w
hich
age
bre
ast c
ance
r affe
cts
men
is 7
1 (6
8) a
nd u
sual
ly d
evel
ops
afte
r the
age
of 6
0 (1
6). T
he m
edia
n ag
e of
dia
gnos
is in
men
is 6
5 ye
ars
old
(23)
. Men
are
dia
gnos
ed w
ith b
reas
t can
cer l
ater
than
wom
en (6
8) b
y 5
to 1
0 ye
ars
(4).
Ther
e ha
ve b
een
case
s of
bre
ast c
ance
r occ
urrin
g in
mal
es b
etw
een
the
ages
of 1
3 an
d 32
(2, 6
8, 2
5, 2
4). M
iao
et a
l's d
ata
show
s th
at
mal
e br
east
can
cer h
as re
mai
ned
stab
le o
ver t
he la
st 3
8 ye
ars
inte
rnat
iona
lly. T
he c
urre
nt li
tera
ture
sta
tes
that
the
inci
denc
e of
bre
ast c
ance
r in
men
is 1
cas
e in
eve
ry 1
00,0
00 m
en (6
8). I
n 20
10, 1
970
case
s w
ere
diag
nose
d in
the
US
, with
390
pre
dict
ed to
die
(41)
. In
2009
, the
Uni
ted
Sta
tes
had
1900
new
dia
gnos
ed c
ases
of m
ale
brea
st c
ance
r and
440
dea
ths
(18)
. Ash
kena
zi J
ews
(57)
and
Afri
can
Am
eric
an m
en h
ave
a hi
gher
pre
vale
nce
com
pare
d to
Cau
casi
an m
en (4
3).
Wor
kup/
Imag
ing
Imag
ing
that
can
be
carr
ied
out i
nclu
de m
amm
ogra
phy,
whi
ch c
an d
etec
t if t
he le
sion
is m
alig
nant
or b
enig
n (1
,2).
Bec
ause
of t
he ra
rity
of th
e di
seas
e,
mam
mog
raph
y is
not
nee
ded
for s
cree
ning
pur
pose
s (4)
. Men
who
hav
e an
incr
ease
d ris
k of
bre
ast c
ance
r inc
ludi
ng s
trong
fam
ily h
isto
ry, B
RC
A2
posi
tive,
K
linef
elte
r syn
drom
e ar
e re
com
men
ded
to u
nder
go b
ase-
line
mam
mog
raph
y, fo
llow
ed b
y an
nual
mam
mog
raph
y an
d se
mia
nnua
l bre
ast e
xam
inat
ion(
92).
M
amm
ogra
phy
has a
sens
itivi
ty a
nd sp
ecifi
city
of 9
2% a
nd 9
0% in
mal
e br
east
can
cer,
resp
ectiv
ely
(60)
. It c
an a
lso
be u
sed
to d
iffer
entia
te b
etw
een
mal
igna
ncy
and
gyne
com
astia
(74)
. Mic
roca
lcifi
catio
ns a
re le
ss c
omm
on o
n m
amm
ogra
phy
in m
ale
brea
st c
ance
r whe
n co
mpa
red
to fe
mal
e br
east
can
cer
(74)
. Ultr
asou
nd c
an b
e us
ed fo
r nod
al in
volv
emen
t (61
). C
ore
biop
sy is
use
d fo
r def
initi
ve d
iagn
osis
(42
or 2
1), w
hich
mea
ns th
at fi
ne n
eedl
e as
pira
tion
can
also
be
used
in m
ales
as i
t is v
ery
sens
itive
and
spec
ific.
Onc
e a
lesi
on h
as b
een
conf
irmed
to b
e m
alig
nant
, the
tum
or st
age
shou
ld b
e as
sess
ed a
nd th
e tis
sue
shou
ld a
lso
be e
valu
ated
for h
orm
one
rece
ptor
sta
tus.
The
tum
or st
agin
g sh
ould
follo
w th
e Am
eric
an J
oint
Com
mitt
ee o
n C
ance
r cla
ssifi
catio
n sy
stem
, w
hich
incl
udes
tum
or si
ze, n
odal
invo
lvem
ent,
and
dist
ant m
etas
tase
s (6
3). H
isto
logi
cal t
umor
gra
ding
sho
uld
be a
sses
sed
usin
g th
e Sc
arff
Blo
om a
nd
Ric
hard
son
hist
olog
ical
sys
tem
. Im
mun
ohis
toch
emic
al a
naly
sis
shou
ld b
e do
ne a
t thi
s tim
e to
ass
ess h
orm
one
rece
ptor
sta
tus o
f est
roge
n (E
R) a
nd
prog
este
rone
rece
ptor
(PR
). M
etas
tase
s ar
e ex
amin
ed th
e sa
me
way
they
are
don
e in
fem
ale
brea
st c
ance
r: th
roug
h la
b w
ork,
che
st x
-ray
, bon
e sc
an, a
nd C
T sc
an o
f the
abd
omen
and
pel
vis (
62).
The
liter
atur
e do
es n
ot h
ave
any
reco
mm
enda
tion
for f
ollo
w u
p im
agin
g af
ter d
iagn
osis
. Our
reco
mm
enda
tions
wou
ld
be to
follo
w th
e sa
me
guid
elin
es fo
r fem
ale
brea
st c
ance
r.
We
pres
ent a
76-
year
-old
Cau
casi
an g
entle
man
who
pre
sent
ed to
our
clin
ic fo
r ev
alua
tion
of a
pai
nles
s lum
p on
his
left
brea
st th
at h
ad b
een
pres
ent f
or 6
yea
rs
with
rece
nt g
row
th o
ver t
he la
st 6
mon
ths.
The
patie
nt's
past
med
ical
his
tory
was
si
gnifi
cant
for b
asal
cel
l car
cino
ma,
hyp
erte
nsio
n an
d hy
perc
hole
ster
olem
ia. H
is
med
icat
ions
incl
ude
aten
olol
, lov
asta
tin a
nd h
ydro
chlo
roth
iazi
de. T
he p
atie
nt
repo
rted
no a
llerg
ies.
He
deni
ed sm
okin
g bu
t adm
itted
to a
lcoh
ol u
se. R
evie
w o
f sy
stem
s was
unr
emar
kabl
e. P
atie
nt d
enie
d ni
pple
retra
ctio
n, d
isch
arge
, or
ulce
ratio
n. P
hysi
cal e
xam
inat
ion
reve
aled
a w
ell-d
evel
oped
, wel
l-nou
rishe
d m
ale.
Upo
n co
mpl
ete
skin
exa
min
atio
n, th
e le
ft lo
wer
qua
dran
t of h
is le
ft br
east
re
veal
ed a
soft,
rubb
ery,
mob
ile, w
ell c
ircum
scrib
ed m
ass a
bout
2.5
cm X
2cm
in
diam
eter
. An
exci
sion
al b
iops
y of
this
mas
s was
per
form
ed w
hich
was
wel
l co
nsis
tent
clin
ical
ly w
ith a
lipo
ma.
How
ever
upo
n fu
rther
insp
ectio
n an
d pa
lpat
ion
of th
e ar
ea, a
firm
mas
s was
felt
in d
eepe
r tis
sue.
The
dec
isio
n w
as
mad
e ex
plor
e de
eper
und
erne
ath
the
fat.
We
foun
d an
irre
gula
r mas
s abo
ut 2
X
3 cm
in d
iam
eter
, ver
y fir
m a
nd n
oted
to h
ave
a gr
ay c
olor
. Th
is m
ass w
as a
lso
sent
for h
isto
logi
cal e
xam
inat
ion
and
reve
aled
a 0
.7cm
gra
de II
inva
sive
duc
tal
carc
inom
a w
ith m
icro
calc
ifica
tions
. Th
e pa
tient
did
not
exh
ibit
any
axill
ary
lym
phad
enop
athy
and
did
not
hav
e an
y br
east
dis
char
ge. T
here
wer
e no
ab
norm
aliti
es o
r mas
ses n
oted
in th
e co
ntra
late
ral c
hest
wal
l or c
ontra
late
ral
axill
a. F
ollo
win
g re
view
of t
he h
isto
path
olog
y, th
e pa
tient
was
dia
gnos
ed w
ith
brea
st d
ucta
l car
cino
ma.
A c
ompu
ted
tom
ogra
phy
was
com
plet
ed o
f his
che
st
and
abdo
men
whi
ch d
emon
stra
ted
no m
etas
tasi
s. Si
nce
his i
nitia
l vis
it, th
ere
has
been
no
evid
ence
of r
ecur
renc
e ba
sed
on m
amm
ogra
phy
take
n 3
mon
ths p
ost-
biop
sy. T
he p
atie
nt is
cur
rent
ly u
nder
stric
t sur
veill
ance
with
regu
lar c
ompl
ete
cuta
neou
s exa
ms a
nd m
amm
ogra
phy
ever
y 6
mon
ths.
This
cas
e re
port
serv
es to
ra
ise
awar
enes
s of a
ny g
row
ths p
rese
ntin
g in
the
brea
sts o
f bot
h m
ale
and
fem
ale
to e
xclu
de b
reas
t car
cino
ma
as a
n un
derly
ing
path
olog
y. W
e ex
amin
e th
e cu
rren
t lite
ratu
re su
rrou
ndin
g m
ale
brea
st c
arci
nom
a.
The
grea
test
risk
fact
or fo
r mal
e br
east
can
cer i
s Klin
efel
ter’s
syn
drom
e w
hich
incr
ease
s m
ale
brea
st c
ance
r ris
k by
50
fold
(24,
69)
. Klin
efel
ter
patie
nts h
ave
a lif
etim
e ris
k of
mal
e br
east
can
cer o
f 5%
(44)
. A fa
mily
his
tory
of b
reas
t can
cer i
n m
en h
ave
an e
stim
ated
odd
s rad
io o
f 3.9
8 fo
r de
velo
ping
bre
ast c
ance
r (49
) and
a re
lativ
e ris
k of
2.5
(59)
. G
enet
ic a
nd h
orm
onal
imba
lanc
es p
lay
a m
ajor
role
in m
ale
brea
st c
ance
r. B
RC
A2
(17)
is a
stro
ng ri
sk fa
ctor
, alth
ough
BR
CA
1 ha
s als
o be
en
repo
rted
(26-
28);
so m
en w
ho p
rese
nt w
ith b
reas
t can
cer s
houl
d ha
ve g
enet
ic c
ouns
elin
g an
d te
stin
g do
ne (7
1). C
urre
ntly
the
Nat
iona
l C
ompr
ehen
sive
Can
cer N
etw
ork
reco
mm
ends
that
pat
ient
s w
ith B
RC
A1/
2 m
utat
ions
shou
ld b
e ta
ught
how
to u
nder
go b
reas
t sel
f-ex
amin
atio
n (7
1). M
utat
ions
in C
HEK
2 (1
100d
elC
) als
o in
crea
se th
e ris
k of
mal
e br
east
can
cer b
y 10
fold
(55)
and
gen
etic
var
iant
s at
chr
omos
omes
2q3
5, 5
p12,
6q
25.1
,10q
26.1
3, a
nd 1
6q12
(70)
hav
e be
en a
ssoc
iate
d w
ith m
ale
brea
st c
ance
r.
A p
ossi
ble
etio
logy
for m
ale
brea
st c
ance
r is d
isea
se s
econ
dary
to h
orm
onal
abn
orm
aliti
es (6
8), l
ack
of a
ndro
gen(
58) i
ncre
ased
est
roge
n ex
posu
re
(3, 5
,6),
estro
gen
adm
inis
tratio
n (7
1),
or e
stro
gen
rela
ted
dise
ase
incl
udin
g bu
t not
lim
ited
to: g
ynec
omas
tia (1
5), c
irrho
sis (
29),
and
obes
ity. T
he
incr
ease
in b
reas
t can
cer i
n m
en h
as b
een
attri
bute
d to
a p
ossi
ble
incr
ease
d es
troge
n co
nver
sion
in a
dipo
se ti
ssue
(6).
Als
o, te
stic
ular
trau
ma
(68)
, co
ngen
ital i
ngui
nal h
erni
a (7
2), o
rchi
tis, o
rchi
dect
omy
(72)
Cow
den’
s dis
ease
(21)
, rad
iatio
n(68
), fa
mily
his
tory
of b
reas
t or o
varia
n ca
ncer
(44)
pr
edis
pose
to th
e pa
thol
ogy.
A
n in
crea
sed
risk
of b
reas
t can
cer h
as a
lso
been
not
ed in
pat
ient
s who
hav
e a
hist
ory
of o
ccup
atio
nal e
xpos
ure
to b
last
furn
aces
, rol
ling
mill
s, m
otor
veh
icle
man
ufac
turin
g an
d st
eel w
orks
(7).
). O
ur p
atie
nt d
id n
ot h
ave
a hi
stor
y of
pre
viou
s occ
upat
iona
l exp
osur
e. O
ther
risk
fact
ors
incl
ude
low
leve
l of p
hysi
cal a
ctiv
ity(5
6), h
isto
ry o
f bon
e fr
actu
re a
fter a
ge 4
5 (5
6).
1. T
emm
im L
, Luq
man
i YA
, Jar
alla
h M
, et a
l. E
valu
atio
n of
pro
gnos
tic fa
ctor
s in
mal
e br
east
can
cer.
Bre
ast.
2001
;10:
166–
175.
2.
Bre
ast e
nlar
gem
ent i
n yo
ung
men
not
alw
aysg
ynae
com
astia
: Bre
ast c
ance
r in
a 22
-yea
r-ol
d m
an. A
NZ
J S
urg.
200
5;75
:914
–916
. 3.
Gio
rdan
o S
H. A
revi
ew o
f the
dia
gnos
is a
nd m
anag
emen
t of m
ale
brea
st c
ance
r. O
ncol
ogis
t. 20
05; 1
0:47
1–47
9.
4. G
iord
ano
SH
, Coh
en D
S, B
uzda
r AU
, et a
l. B
reas
t car
cino
ma
in m
en: A
pop
ulat
ion-
base
d st
udy.
Can
cer.
2004
;101
:51–
57.
5. H
sing
AW
, McL
augh
lin J
K, C
occo
P, e
t al.
Ris
k fa
ctor
s fo
r mal
e br
east
can
cer (
Uni
ted
Sta
tes)
. Can
cer C
ause
s C
ontro
l. 19
98;9
:269
–275
. 6.
Gio
rdan
o S
H, B
uzda
r AU
, Hor
toba
gyi G
N. B
reas
t can
cer i
n m
en. A
nn In
tern
Med
. 200
2;13
7:67
8–68
7.
7. C
occo
P, F
iggs
L, D
osem
eci M
, et a
l. C
ase-
cont
rol s
tudy
of o
ccup
atio
nal e
xpos
ures
and
mal
e br
east
can
cer.
Occ
up E
nviro
n M
ed. 1
998;
55:5
99–6
04.
8. G
iord
ano
SH
, Per
kins
G, B
rogl
io K
, et a
l. A
djuv
ant s
yste
mic
ther
apy
for m
ale
brea
st c
arci
nom
a. C
ance
r. 20
05;1
04:2
359–
2364
. 9.
Spe
nce
RA
, Mac
Ken
zie
G, A
nder
son
JR, e
t al.
Long
-term
sur
viva
l fol
low
ing
canc
er o
f the
mal
e br
east
in N
orth
ern
Irela
nd. A
repo
rt of
81
case
s. C
ance
r. 19
85;5
5:64
8–65
2.
10. G
oss
PE
, Rei
d C
, Pin
tilie
M, e
t al.
Mal
e br
east
car
cino
ma:
A re
view
of 2
29 p
atie
nts
who
pre
sent
ed to
the
Prin
cess
Mar
gare
t Hos
pita
l dur
ing
40 y
ears
: 195
5–19
96. C
ance
r. 19
99;8
5:62
9–63
9.
11. R
ibei
ro G
G, S
win
dell
R, H
arris
M, e
t al.
A re
view
of t
he m
anag
emen
t of t
he m
ale
brea
st c
arci
nom
a ba
sed
on a
n an
alys
is o
f 420
trea
ted
case
s. B
reas
t. 19
96;5
:141
–146
. 12
. Gos
s P
E, R
eid
C, P
intil
ie M
, et a
l. M
ale
brea
st c
arci
nom
a: A
revi
ew o
f 229
pat
ient
s w
ho p
rese
nted
to th
e P
rince
ss M
arga
ret H
ospi
tal d
urin
g 40
yea
rs:1
955–
1996
. Can
cer.
1999
;85:
629–
639.
13
. Rib
eiro
G, S
win
dell
R. A
djuv
ant t
amox
ifen
for m
ale
brea
st c
ance
r (M
BC
). B
r J C
ance
r. 19
92;6
5:25
2–25
4.
14. W
iess
JR
, Moy
isch
KB
, Sw
ede
H. E
pide
myo
logy
of m
ale
brea
st c
ance
r. C
ance
r Epd
emio
l Bbi
omar
kers
Pre
v 20
05l 1
4: 2
0 - 2
6.
15. K
ahla
PB
, Cas
saro
S V
ladi
mir,
Fg
Way
ne M
G, C
amm
arat
a. B
ilate
ral s
ynch
rono
us b
reas
t can
cer i
n a
mal
e. M
s S
inai
J M
ed 2
005l
72:
120
-123
. 16
. bey
rout
e M
I, B
eyro
uti R
, Rey
rout
i R e
t al.
Bre
ast c
ance
r in
men
. Pre
sse
Med
200
7: 1
919
-192
4.
17. s
tratto
n M
R, F
ord
D, N
euha
sen
S e
t al.
Fam
ilial
mal
e br
east
can
cer i
s no
t lin
ed to
the
BR
CA
1 lo
cus
on c
hrom
osom
e 17
q. N
at G
enet
199
4l 7
: 103
-7
18. J
emal
A, S
iege
l R, W
ard
E, H
ao Y
, Xu
J, T
hun
MJ:
Can
cer s
tatis
tics.
CA
Can
cer J
Clin
200
9, 5
9:22
5-24
9.
19. G
enna
ri R
, Cur
iglia
no G
, Jer
ecze
k-Fo
ssa
BA
, Zur
rida
S, R
enne
G, I
ntra
M, G
alim
berti
V, L
uini
A, O
recc
hia
R, V
iale
G, G
oldh
risch
A, V
eron
esi U
: Mal
e br
east
can
cer:
a sp
ecia
l the
rape
utic
pro
blem
. Any
thin
g ne
w?
(Rev
iew
). In
t J
Onc
ol 2
004,
24:
663-
670.
20
. Gio
rdan
o S
H, C
ohen
DS
, Buz
dar A
U, P
erki
ns G
, Hor
toba
gyi G
N: B
reas
t car
cino
ma
in m
en: a
pop
ulat
ion-
base
d st
udy.
Can
cer 2
004,
101
:51-
57.
21. F
entim
an IS
, Fou
rque
t A, H
orto
bagy
i GN
: Mal
e br
east
can
cer.
Lanc
et 2
006,
367
:595
-604
. 22
. Cze
ne K
, Ber
gqvi
st J
, Hal
l P, B
ergh
J: H
ow to
trea
t mal
e br
east
can
cer.
Bre
ast 2
007,
16(
Sup
pl 2
):S14
7-15
4.
23. S
AM
E A
S 4
5 C
utul
i B: S
trate
gies
in tr
eatin
g m
ale
brea
st c
ance
r. E
xper
t Opi
n P
harm
acot
her
2007
, 8:1
93-2
02.
24. A
hmad
R, L
ewis
S, M
ahar
aj D
: A m
ale
patie
nt fr
om th
e W
est I
ndie
s w
ith
inva
sive
duc
tal c
arci
nom
a in
the
right
bre
ast:
A c
ase
repo
rt an
d lit
erat
ure
revi
ew. G
end
Med
201
0, 7
:179
-183
. 25
. Cha
ng H
L, K
ish
JB, S
mith
BL,
Gol
dste
in A
M: A
16-
year
-old
mal
e w
ith g
ynec
omas
tia a
nd d
ucta
l car
cino
ma
in s
itu. P
edia
tr S
urg
Int 2
008,
24:
1251
-125
3.
26. F
rank
TS
, Def
fenb
augh
AM
, Rei
d JE
, Hul
ick
M, W
ard
BE
, Lin
genf
elte
r B
, Gum
pper
KL,
Sch
oll T
, Tav
tigia
n S
V, P
russ
DR
, Crit
chfie
ld G
C: C
linic
al c
hara
cter
istic
s of
indi
vidu
als
with
ger
mlin
e m
utat
ions
in B
RC
A1
and
BR
CA
2:
anal
ysis
of 1
0,00
0 in
divi
dual
s. J
Clin
Onc
ol 2
002,
20:
1480
-149
0.
27. F
riedm
an L
S, G
ayth
er S
A, K
uros
aki T
, Gor
don
D, N
oble
B, C
asey
G, P
onde
r BA
, Ant
on-C
ulve
r H: M
utat
ion
anal
ysis
of B
RC
A1
and
BR
CA
2 in
a m
ale
brea
st c
ance
r pop
ulat
ion.
Am
J H
um G
enet
199
7, 6
0:31
3-31
9.
28. H
aral
dsso
n K
, Lom
an N
, Zha
ng Q
X, J
ohan
nsso
n O
, Ols
son
H, B
org
A: B
RC
A2
germ
-line
mut
atio
ns a
re fr
eque
nt in
mal
e br
east
can
cer p
atie
nts
with
out a
fam
ily h
isto
ry o
f the
dis
ease
. Can
cer R
es 1
998,
58:
1367
-137
1.
29. G
anly
I, T
aylo
r EW
: Bre
ast c
ance
r in
a tra
ns-s
exua
l man
rece
ivin
g ho
rmon
e re
plac
emen
t the
rapy
. Br J
Sur
g 19
95, 8
2:34
1.
30. C
olom
bo-B
enkm
ann
M, S
tern
J, H
erfa
rth C
: On
the
negl
ecte
d en
tity
of u
nila
tera
l gyn
ecom
astia
. Ann
Pla
st S
urg
2006
, 56:
346.
31
. Gom
ez-R
apos
o C
, Zam
bran
a Te
var F
, Ser
eno
Moy
ano
M, L
opez
Gom
ez M
, Cas
ado
E: M
ale
brea
st c
ance
r. C
ance
r Tre
at R
ev 2
010.
32
. Auv
inen
A, C
urtis
RE
, Ron
E: R
isk
of s
ubse
quen
t can
cer f
ollo
win
g br
east
can
cer i
n m
en. J
Nat
l Can
cer I
nst 2
002,
94:
1330
-133
2.
33. B
ruce
DM
, Hey
s S
D, P
ayne
S, M
iller
ID, E
rem
in O
: Mal
e br
east
can
cer:
clin
ico-
path
olog
ical
feat
ures
, im
mun
ocyt
oche
mic
al c
hara
cter
istic
s an
d pr
ogno
sis.
Eur
J S
urg
Onc
ol 1
996,
22:
42-4
6.
34. B
en D
hiab
T, B
ouzi
d T,
Gam
oudi
A, B
en H
asso
una
J, K
hom
si F
, Bou
ssen
H, e
t al:
Mal
e br
east
can
cer:
abou
t 123
cas
es c
olle
cted
at t
he In
stitu
te S
alah
-Aza
iz o
f Tun
is fr
om 1
979
to 1
999.
Bul
l Can
cer 2
005,
92(
3):2
81-5
. 35
. Ona
mi S
usan
, Oza
ki M
elan
ie, M
ortim
er E
Joan
ne, P
al K
umar
Sum
anta
, et a
l: M
ale
brea
st c
ance
r: A
n up
date
in d
iagn
osis
, tre
atm
ent a
nd m
olec
ular
pro
filin
g. M
atur
itas
65(2
010)
:308
-314
. 36
. Yu
E, S
uzuk
i H, Y
ounu
s J,
Elfi
ki T
, Stit
t L, Y
au G
, et a
l: Th
e Im
pact
of p
ostm
aste
ctom
y ra
diat
ion
ther
apy
on m
ale
brea
st c
ance
r pat
ient
s-A
cas
e se
ries.
Int J
Rad
iat O
ncol
Bio
l Phy
s 20
11.
37. T
unon
de
Lara
C, G
oudy
G, M
acG
roga
n G
, Dur
and
M, D
ilhuy
dy J
-M, A
vril
A, e
t al:
Mal
e br
east
can
cer:
A re
view
of 5
2 ca
ses
colle
cted
at t
he In
stitu
te
Ber
goni
e (B
orde
aux,
Fra
nce)
from
198
0 to
200
4. G
ynéc
olog
ie O
bsté
triqu
e &
Fer
tilité
200
8, 3
6:38
6-39
4.
38. G
ómez
-Rap
oso
C, Z
ambr
ana
Téva
r F, S
eren
o M
oyan
o M
, Lóp
ez G
ómez
M, C
asad
o E
, et a
l: M
ale
brea
st c
ance
r. C
ance
r Tre
atm
ent R
evie
ws
2010
. 39
. Otti
ni L
aura
, Pal
li D
omen
ico,
Riz
zo S
ergi
o, F
eder
ico
Mar
io, B
azan
Viv
iana
, Ant
onio
Rus
so, e
t al:
Mal
e br
east
can
cer.
Crit
ical
Rev
iew
s in
Onc
olog
y/H
emat
olog
y 20
10, 7
3:14
1-15
5.
40. G
entil
ini O
, Cha
gas
E, Z
urrid
a S
, et a
l. S
entin
el ly
mph
nod
e bi
opsy
in m
ale
patie
nts
with
ear
ly b
reas
t can
cer.
Onc
olog
ist 2
007;
12:5
12–5
15
41. A
mer
ican
Can
cer S
ocie
ty. (
2010
). C
ance
r fac
ts &
figu
res
2010
. Atla
nta,
GA
: Aut
hor.
Ret
rieve
d fro
m h
ttp://
ww
w.c
ance
r.org
/acs
/gro
ups/
cont
ent/@
nho/
docu
men
ts/d
ocum
ent/
acsp
c-02
4113
42
. Fen
timan
, I. S
., Fo
urqu
et, A
., &
Hor
toba
gyi,
G. N
. (20
06).
Mal
e br
east
can
cer.
Lanc
et, 3
67, 5
95-6
04.
43. A
nder
son,
W. F
., A
lthui
s, M
D.,
Brin
ton,
L. A
., &
Dev
esa,
S. S
. (20
04).
Is m
ale
brea
st c
ance
r sim
ilar o
r diff
eren
t tha
n fe
mal
e br
east
can
cer?
Bre
ast C
ance
r Res
earc
h an
d Tr
eatm
ent,
83,
77-8
6.
44. K
orde
, L. A
., Zu
jew
ski,
J. A
., K
amin
, L.,
Gio
rdan
o, S
., D
omch
ek, S
., A
nder
son,
W. F
., &
. . .
Car
doso
, F. (
2010
) Mul
tidis
cipl
inar
y m
eetin
g on
mal
e br
east
can
cer:
Sum
mar
y an
d re
sear
ch r
ecom
men
datio
ns. J
ourn
al o
f Clin
ical
O
ncol
ogy,
28, 2
114-
2122
. 45
. Cut
ili, B
. (20
07).
Stra
tegi
es in
trea
ting
mal
e br
east
can
cer.
Exp
ert O
pini
on o
n P
harm
acot
hera
py, 8
, 193
-202
. 46
. Meg
uerd
itchi
an, A
. N.,
Fala
rdea
u, M
., &
Mar
tin, G
. (20
02).
Mal
e br
east
car
cino
ma.
Can
adia
n Jo
urna
l of S
urge
ry, 4
5, 2
96-3
02.
47. A
nelli
TFM
, Ane
lli A
, Tra
n K
N, e
t al:
Tam
oxife
n ad
min
istra
tion
is a
ssoc
iate
d w
ith a
hig
h-ra
te o
f tre
atm
ent-l
imiti
ng s
ympt
oms
in m
ale
brea
st c
ance
r pat
ient
s. C
ance
r 74:
74-7
7, 1
994
48. V
isra
m H
, Kan
ji F,
Den
t SF:
End
ocrin
e th
erap
y fo
r mal
e br
east
can
cer:
Rat
es o
f tox
icity
and
adh
eren
ce. C
urr O
ncol
17:
17-2
1, 2
010
49. K
. A. R
osen
blat
t, D
. B. T
hom
as, A
. McT
iern
an e
t al.,
“Bre
ast c
ance
r in
men
: asp
ects
of f
amili
al a
ggre
gatio
n,”
Jour
nal o
f the
Nat
iona
l Can
cer I
nstit
ute,
vol
. 83,
no.
12,
pp.
849
–854
, 199
1.
50. A
lbo
D, A
mes
FC
, Hun
t KK
, Ros
s M
I, S
ingl
etar
y S
E, K
uere
r HM
. Eva
luat
ion
of ly
mph
nod
e st
atus
in m
ale
brea
st c
ance
r pat
ient
s: a
role
for s
entin
el ly
mph
nod
e bi
opsy
*. B
reas
t Can
cer R
es
Trea
t 200
3;77
:9–1
4.
51. 1
9. F
lynn
LW
, Par
k J,
Pat
il S
M, C
ody
Iii H
S, P
ort E
R. S
entin
el ly
mph
nod
e bi
opsy
is s
ucce
ssfu
l and
acc
urat
e in
mal
e br
east
car
cino
ma.
J A
m C
oll S
urg
2008
;206
:616
–21.
52
. Bou
ghey
JC
, Bed
rosi
an I,
Mer
ic-B
erns
tam
F, e
t al.
Com
para
tive
anal
ysis
of s
entin
el ly
mph
nod
e op
erat
ion
in m
ale
and
fem
ale
brea
st c
ance
r pat
ient
s. J
Am
Col
l Sur
g 20
06;2
03:4
75–8
0.
53. G
rena
der
T, G
oldb
erg
A, S
havi
t L. S
econ
d ca
ncer
s in
pat
ient
s w
ith m
ale
brea
st c
ance
r: a
liter
atur
e re
view
. J C
ance
r Sur
viv
2008
;2:7
3–8.
54
. Auv
inen
A, C
urtis
RE
, Ron
E. R
isk
of s
ubse
quen
t can
cer f
ollo
win
g br
east
can
cer i
n m
en. J
Nat
l Can
cer I
nst 2
002;
94:1
330–
2.
55. M
eije
rs-H
eijb
oer
H, v
an d
en O
uwel
and
A, K
lijn
J, W
asie
lew
ski M
, de
Sno
o A
, et a
l. (2
002)
Low
-pen
etra
nce
susc
eptib
ility
to b
reas
t can
cer d
ue to
CH
EK
2(*)
1100
delC
in n
onca
rrier
s of
BR
CA
1 or
BR
CA
2 m
utat
ions
. Nat
Gen
et 3
1:
55–5
9.
56. B
rinto
n LA
, Ric
hess
on D
A, G
iera
ch G
L, e
t al.
Pro
spec
tive
eval
uatio
n of
risk
fact
ors
for m
ale
brea
st c
ance
r. J
Nat
l Can
cer I
nst 2
008;
100:
1477
. 57
. Bre
nner
B, F
ried
G, L
evitz
ki P
, et a
l. M
ale
brea
st c
arci
nom
a in
Isra
el: h
ighe
r inc
iden
t but
pos
sibl
y pr
ogno
sis
in A
shke
nazi
Jew
s. C
ance
r 200
2;94
(8):2
128–
33.
58. T
hom
as D
B, J
imen
ez L
M, M
cTie
rnan
A, e
t al.
Bre
ast c
ance
r in
men
: ris
k fa
ctor
s w
ith h
orm
onal
impl
icat
ions
. Am
J E
pide
mio
l 199
2;13
5:73
4–48
. 59
. Ros
enbl
att K
A, T
hom
as D
B, M
cTie
rnan
A, e
t al.
Bre
ast c
ance
r in
men
: asp
ects
of f
amili
al a
ggre
gatio
n. J
Nat
l Can
cer I
nst 1
991;
83:8
49–5
4.
60. E
vans
GF,
Ant
hony
T, T
urna
ge R
H, e
t al.
The
diag
nost
ic a
ccur
acy
of m
amm
ogra
phy
in th
e ev
alua
tion
of m
ale
brea
st d
isea
se. A
m J
Sur
g 20
01;1
81:9
6–10
0.
61. C
ouch
FJ,
Far
id L
M, D
eSha
no M
L, e
t al.
BR
CA
2 ge
rmlin
e m
utat
ions
in m
ale
brea
st c
ance
r cas
es a
nd b
reas
t can
cer f
amili
es. N
at G
enet
199
6;13
:123
–5.
62. N
atio
nal C
ompr
ehen
sive
Can
cer N
etw
ork
(NC
CN
). G
uide
lines
ava
ilabl
e on
line
at w
ww
.ncc
n.or
g.
63. S
ingl
etar
y S
E, A
llred
C, A
shle
y P
, et a
l. R
evis
ion
of th
e A
mer
ican
Joi
nt C
omm
ittee
on
Can
cer s
tagi
ng s
yste
m fo
r bre
ast c
ance
r. J
Clin
Onc
ol 2
002;
20:3
628–
36.
64. G
iord
ano
SH
. A re
view
of t
he d
iagn
osis
and
man
agem
ent o
f mal
e br
east
can
cer.
Onc
olog
ist 2
005;
10:4
71–9
. 65
. Blo
om K
J, G
ovil
H, G
attu
so P
, et a
l. S
tatu
s of
HE
R-2
in m
ale
and
fem
ale
brea
st c
arci
nom
a. A
m J
Sur
g 20
01;1
82:3
89–9
2.
66. M
uir D
, Kan
than
R, K
anth
an S
C. M
ale
vers
us fe
mal
e br
east
can
cers
. A p
opul
atio
n-ba
sed
com
para
tive
imm
unoh
isto
chem
ical
ana
lysi
s. A
rch
Pat
hol L
ab M
ed 2
003;
127:
36–4
1.
67. R
udlo
wsk
i C, F
riedr
ichs
N, F
arld
l A, e
t al.
Her
-2/n
eu g
ene
ampl
ifica
tion
and
prot
ein
expr
essi
on in
prim
ary
mal
e br
east
can
cer.
Bre
ast C
ance
r Res
Tre
at 2
004;
84:2
15.
68. M
adei
ra M
, Mat
tar
A, P
asso
s R
J, M
ora
CD
, Mam
ede
LH, K
ishi
no V
H, T
orre
s TZ
, de
Sá
AF,
dos
San
tos
RE
, Geb
rim L
H.A
cas
e re
port
of m
ale
brea
st c
ance
r in
a ve
ry y
oung
pat
ient
: wha
t is
chan
ging
?Wor
ld J
Sur
g O
ncol
. 201
1 Fe
b 3;
9:16
. 69
. Har
nden
DG
, Mac
lean
N, L
angl
ands
AO
. Car
cino
ma
of th
e br
east
and
Klin
efel
ter’s
syn
drom
e. J
Med
Gen
et 1
971;
8:46
0–1.
70
. Orr
N, C
ooke
R, J
ones
M, F
letc
her O
, Dud
brid
ge F
, Chi
lcot
t-Bur
ns S
, Tom
czyk
K, B
rode
rick
P, H
ouls
ton
R, A
shw
orth
A, S
wer
dlow
A. G
enet
ic v
aria
nts
at c
hrom
osom
es 2
q35,
5p1
2, 6
q25.
1, 1
0q26
.13,
and
16q
12.1
influ
ence
the
risk
of b
reas
t can
cer i
n m
en.P
LoS
Gen
et. 2
011
Sep
;7(9
):e10
0229
0. E
pub
2011
Sep
15.
71
. Rav
i A, B
ang
H, K
arsi
f K, N
ori D
.Bre
ast C
ance
r in
Men
: Pro
gnos
tic F
acto
rs, T
reat
men
t Pat
tern
s, a
nd O
utco
me.
Am
J M
ens
Hea
lth. 2
011
Aug
10
72. O
tto F
. Mal
e br
east
can
cer -
neg
lect
ed tu
mou
r.Eur
J C
ance
r. 20
11 S
ep;4
7 S
uppl
3:S
340-
1.
73. F
idan
E, Y
ildiz
B, E
rsoz
S, O
zdem
ir F.
Bila
tera
l bre
ast c
ance
r: a
mal
e pa
tient
. Bra
tisl L
ek L
isty
. 201
1;11
2(10
):589
-90.
74
. Góm
ez-R
apos
o C
, Zam
bran
a Té
var F
, Ser
eno
Moy
ano
M, L
ópez
Góm
ez M
, Cas
ado
E. M
ale
brea
st c
ance
r. C
ance
r Tre
at R
ev. 2
010
Oct
;36(
6):4
51-7
. Epu
b 20
10 M
ar 2
. 75
. Sco
tt-C
onne
r C
E, H
ochi
mse
n P
R, M
enck
HR
, Win
ches
ter D
J. A
n an
alys
is o
f mal
e an
d fe
mal
e br
east
can
cer t
reat
men
t and
sur
viva
l am
ong
dem
ogra
phic
ally
iden
tical
pai
rs o
f pat
ient
s. S
urge
ry 1
999;
126:
775.
76
. Mac
dona
ld G
, Pal
tiel C
, Oliv
otto
IA, T
ylde
sley
S. A
com
para
tive
anal
ysis
of r
adio
ther
apy
use
and
patie
nt o
utco
me
in m
ales
and
fem
ales
with
bre
ast c
ance
r. A
nn O
ncol
200
5;16
:144
2–8.
77
. Cut
uli B
, Lac
roze
M, D
ilhuy
dy J
M, e
t al.
Mal
e br
east
can
cer:
resu
lts o
f the
trea
tmen
ts a
nd p
rogn
ostic
fact
ors
in 3
97 c
ases
. Eur
J C
ance
r 199
5;31
A:1
960–
4.
78. D
oneg
an W
L, R
edlic
h P
N, L
ang
PJ,
et a
l. C
arci
nom
a of
the
brea
st in
mal
es: a
mul
tiins
titut
iona
l sur
vey.
Can
cer 1
998;
83:4
98–5
09.
79. S
penc
e R
A, M
acK
enzi
e G
, And
erso
n JR
, et a
l. Lo
ng-te
rm s
urvi
val f
ollo
win
g ca
ncer
of t
he m
ale
brea
st in
Nor
ther
n Ire
land
. A re
port
of 8
1 ca
ses.
Can
cer
1985
;55:
648–
52.
80. E
rlich
man
C, M
urph
y K
C, E
lhak
im T
. Mal
e br
east
can
cer:
a 13
-yea
r re
view
of 8
9 pa
tient
s. J
Clin
Onc
ol 1
984;
2:90
3–9.
Sch
ucha
rt U
, See
gens
chm
iedt
MH
, Kirs
chne
r MJ,
et a
l. A
djuv
ant r
adio
ther
apy
for b
reas
t car
cino
ma
in m
en:
a 20
-yea
r cl
inic
al e
xper
ienc
e. A
m J
Clin
Onc
ol
1996
;19:
330.
81
. Sch
ucha
rt U
, See
gens
chm
iedt
MH
, Kirs
chne
r MJ,
et a
l. A
djuv
ant r
adio
ther
apy
for b
reas
t car
cino
ma
in m
en: a
20-
year
clin
ical
exp
erie
nce.
Am
J C
lin O
ncol
199
6;19
:330
. 82
. Nat
iona
l Com
preh
ensi
ve C
ance
r Net
wor
k (N
CC
N).
Gui
delin
es a
vaila
ble
onlin
e at
ww
w.n
ccn.
org.
83
. Bag
ley
CS
, Wes
ley
MN
, You
ng R
C, e
t al.
Adj
uvan
t che
mot
hera
py in
mal
es w
ith c
ance
r of t
he b
reas
t. A
m J
Clin
Onc
ol 1
987;
10:5
5–60
. 84
. Yild
irim
E, B
erbe
rogl
u U
. Mal
e br
east
can
cer:
a 22
-yea
r ex
perie
nce.
Eur
J S
urg
Onc
ol 1
998;
24:5
48–5
2 85
. Pat
el H
Z, B
uzda
r AU
, Hor
toba
gyi G
N. R
ole
of a
djuv
ant c
hem
othe
rapy
in m
ale
brea
st c
ance
r. C
ance
r 198
9;64
:158
3–5.
86
. Izq
uier
do M
A, A
lons
o C
, De
And
res
L, e
t al.
Mal
e br
east
can
cer.
Rep
ort o
f a
serie
s of
50
case
s. A
cta
Onc
ol 1
994;
33:7
67–7
1.
87. G
iord
ano
SH
, Per
kins
GH
, Bro
gio
K, e
t al.
Adj
uvan
t sys
tem
ic th
erap
y fo
r mal
e br
east
car
cino
ma.
Can
cer 2
005;
104:
2359
. 88
. Jai
yesi
mi I
A, B
uzda
r AU
, Sah
in A
A, e
t al.
Car
cino
ma
of th
e m
ale
brea
st. A
nn
Inte
rn M
ed 1
992;
117:
771–
7.
89. L
opez
M, D
i Lau
ro L
, Laz
zaro
B, e
t al.
Hor
mon
al tr
eatm
ent o
f dis
sem
inat
ed
mal
e br
east
can
cer.
Onc
olog
y 19
85;4
2:34
5–9.
90
. Kilu
k JV
, Lee
MC
, Par
k C
K, M
eade
T, M
into
n S
, Har
ris E
, Kim
J, L
aron
ga C
.Mal
e br
east
can
cer:
man
agem
ent a
nd fo
llow
-up
reco
mm
enda
tions
. Bre
ast J
. 201
1 S
ep-O
ct;1
7(5)
:503
-9. d
oi: 1
0.11
11/j.
1524
-474
1.20
11.0
1148
.x.
Epu
b 20
11 A
ug 2
9.
91. M
iao
H, V
erko
oije
n H
M, C
hia
KS
, Bou
char
dy C
, Puk
kala
E, L
arøn
ning
en S
, Mel
lem
kjæ
r L, C
zene
K, H
artm
an M
. In
cide
nce
and
Out
com
e of
Mal
e B
reas
t Can
cer:
An
Inte
rnat
iona
l Pop
ulat
ion-
Bas
ed S
tudy
. J C
lin O
ncol
. 201
1 O
ct 3
. [E
pub
ahea
d of
prin
t] 92
. Joh
anse
n Ta
ber J
A, M
oris
y LR
, Osb
ahr
AJ,
Dic
kins
on B
D. M
ale
brea
st c
ance
r: ris
k fa
ctor
s, d
iagn
osis
, and
man
agem
ent (
revi
ew).
Onc
ol R
ep 2
010;
24:1
115−
20
The
prog
nosi
s for
mal
e br
east
can
cer i
s sim
ilar t
o w
omen
, with
lym
ph n
ode
invo
lvem
ent a
nd tu
mor
size
bei
ng th
e m
ost d
eter
min
ant
prog
nost
ic fa
ctor
(4).
Sim
ilar t
o w
omen
, pro
gnos
is is
det
erm
ined
by
stag
ing
of th
e tu
mor
, alth
ough
in m
en it
is ty
pica
lly d
etec
ted
late
r in
dire
ctly
.
Mor
talit
y in
crea
ses b
y 50
% w
ith ly
mph
nod
e in
volv
emen
t (71
). If
the
tum
or m
easu
res b
etw
een
2 an
d 5
cm, m
orta
lity
incr
ease
s by
40%
(7
1). M
orta
lity
is a
lso
incr
ease
d if
the
patie
nt is
gre
ater
than
65
year
s old
(71)
, but
mal
e se
x is
a fa
vora
ble
prog
nost
ic fa
ctor
(81)
. B
ourh
afou
r et a
l's st
udy
of 1
27 c
ases
of m
ale
brea
st c
ance
r rev
eale
d m
etas
tase
s in
41 c
ases
(32%
), w
ith th
e bo
ne b
eing
the
mos
t com
mon
si
te fo
r met
asta
sis.
Cur
rent
ly, t
he 5
yea
r sur
viva
l rat
e fo
r mal
e br
east
can
cer s
tand
s at 6
0% a
nd th
e 10
yea
r sur
viva
l rat
e at
40%
(38)
. The
5
year
surv
ival
rate
bas
ed o
n st
age
is a
s fol
low
s: S
tage
I 78
%; S
tage
II 6
7%; S
tage
III 4
0%; a
nd S
tage
IV 1
9% (4
). O
f all
ethn
iciti
es,
Afr
ican
Am
eric
an m
en te
nd to
hav
e a
wor
se p
rogn
osis
(44)
. Unf
ortu
nate
ly, l
ater
det
ectio
n in
men
is a
lso
due
to m
en n
ot h
avin
g ch
ange
s in
sym
ptom
s in
brea
sts s
imila
r to
how
fem
ales
typi
cally
do
(71)
. How
ever
, mal
e pa
tient
s with
bre
ast c
ance
r hav
e a
low
er ri
sk o
f dea
th
from
bre
ast c
ance
r whe
n co
mpa
red
to fe
mal
es w
hen
adju
stin
g fo
r hig
her a
ge a
t dia
gnos
is, d
iffer
ent s
tand
ard
of tr
eatm
ent a
nd m
ore
adva
nced
stag
e at
dia
gnos
is (8
1).
Nea
rly h
alf o
f new
ly d
iagn
osed
bre
ast c
ance
rs in
men
are
dia
gnos
ed a
t sta
ge II
I or I
V (2
1), e
ven
thou
gh B
ourh
afou
r et a
l sho
wed
that
82
% o
f cas
es w
ere
diag
nose
d at
stag
e II
or I
II. T
his f
urth
er a
dds t
o th
e re
ason
why
mas
ses o
n th
e m
ale
brea
st a
re n
ot a
ggre
ssiv
ely
soug
ht
afte
r. Ea
rlier
dia
gnos
is le
ads t
o st
rong
er su
cces
s with
trea
tmen
t (68
), bu
t men
are
typi
cally
dia
gnos
ed in
itial
ly w
ith g
ynec
omas
tia c
ausi
ng
treat
men
t to
be d
elay
ed.
Th
e la
ter d
etec
tion
is m
ost l
ikel
y du
e to
bet
ter a
nd m
ore
freq
uent
scre
enin
g in
wom
en, b
ut a
lso
the
lack
of a
war
enes
s of m
ale
brea
st
canc
er c
ontri
bute
s to
it be
ing
igno
red
in m
any
case
s or b
eing
mis
take
n w
ith g
ynec
omas
tia. S
ympt
oms o
f mal
e br
east
can
cer t
ypic
ally
pr
esen
t lat
er w
hen
com
pare
d to
wom
en, w
hich
als
o ca
uses
men
to h
ave
a la
ter d
iagn
osis
and
wor
se p
rogn
osis
(5).
Ris
k Fa
ctor
s/Et
iolo
gy
Trea
tmen
t
Type
s of B
reas
t Can
cer
in M
en
90%
of m
ale
brea
st c
arci
nom
as a
re o
f an
inva
sive
type
with
the
mos
t com
mon
bei
ng in
filtra
ting
duct
al c
arci
nom
a, w
hich
acc
ount
s fo
r gre
ater
than
65
to 9
5% (1
9,20
). Pa
pilla
ry c
arci
nom
as re
pres
ents
2.6
% (6
4) o
f cas
es a
nd m
ucin
ous 1
.8%
of c
ases
(64)
. Lob
ular
car
cino
mas
repr
esen
t 1.5
% o
f ca
ses (
4). O
ther
subt
ype
incl
udin
g m
edul
lary
, muc
inou
s, tu
bula
r, an
d sq
uam
ous c
arci
nom
as h
ave
been
repo
rted
in is
olat
ed c
ase
repo
rts w
ith le
ss
freq
uenc
y in
men
com
pare
d to
wom
en. P
aget
's di
seas
e an
d in
flam
mat
ory
carc
inom
a pr
esen
t equ
ally
in m
ales
and
fem
ales
but
hav
e ra
rely
bee
n re
porte
d in
men
(34)
. M
ales
tend
to h
ave
a hi
gher
exp
ress
ion
of h
orm
one
rece
ptor
, spe
cific
ally
90%
of m
ale
brea
st c
ance
rs e
xpre
ss e
stro
gen
rece
ptor
pos
itivi
ty a
nd 8
0%
expr
ess p
roge
ster
one
rece
ptor
pos
itivi
ty (4
). Th
e de
gree
of H
er2-
neu
over
expr
essi
on in
men
is le
ss th
an w
omen
(2–1
5%) a
nd h
as b
een
docu
men
ted
in
(65-
67).
•C
linic
al P
rese
ntat
ion
The
mos
t com
mon
pre
sent
atio
n of
a m
ale
with
bre
ast c
ance
r is a
pai
nles
s pal
pabl
e lu
mp
loca
ted
suba
reol
arly
(1,2
). M
ale
patie
nts a
lso
som
etim
es
pres
ent w
ith o
ther
sym
ptom
s, in
clud
ing
nipp
le p
ain,
ble
edin
g, re
tract
ion,
ulc
erat
ion
or d
isch
arge
(21)
. Lym
phad
enop
athy
may
als
o be
pre
sent
(73)
. G
ynec
omas
tia is
pre
sent
in 6
to 3
8% o
f cas
es o
f mal
e br
east
can
cer (
30).
Mal
e br
east
can
cer t
ypic
ally
affe
cts
the
right
bre
ast w
hich
is si
mila
r to
fem
ales
(1,2
). Th
e po
ssib
ility
of a
con
trala
tera
l bre
ast c
ance
r dev
elop
ing
in m
en is
hig
her t
han
wom
en(3
1), s
peci
fical
ly 3
0 fo
ld p
ossi
bilit
y in
men
(3
2) b
ut th
e ab
solu
te ri
sk is
0.1
% p
er y
ear (
53, 5
4). T
he d
iffer
entia
l dia
gnos
is fo
r mal
e br
east
can
cer i
nclu
des b
reas
t abs
cess
, lip
oma,
gyn
ecom
astia
, m
etas
tase
s to
the
brea
st, a
nd sa
rcom
as (7
4).
Ove
rall,
the
mos
t eff
ectiv
e tre
atm
ent s
houl
d be
targ
eted
tow
ard
the
stag
e of
the
dise
ase,
the
patie
nt's
over
all h
ealth
, the
age
of d
iagn
osis
, the
pr
esen
ce o
f hor
mon
e re
cept
or H
ER2,
and
BR
CA
(71)
. C
urre
nt tr
eatm
ent r
ecom
men
datio
ns a
re n
ot b
ased
on
data
from
clin
ical
stud
ies i
n m
en b
ut
the
mos
t agr
eed
upon
stan
dard
trea
tmen
t in
the
liter
atur
e is
mod
ified
radi
cal m
aste
ctom
y w
ith a
xilla
ry ly
mph
nod
e di
ssec
tion
or se
ntin
el n
ode
lym
ph b
iops
y (S
LNB
). M
ale
patie
nts w
ho p
rese
nt w
ith a
solit
ary
tum
or w
ith n
o m
etas
tasi
s sho
uld
have
a m
odifi
ed ra
dica
l mas
tect
omy
with
ax
illar
y ly
mph
nod
e di
ssec
tion
(3, 3
5).
Sent
inel
lym
ph n
ode
biop
sy c
an b
e do
ne in
pat
ient
s with
a c
linic
ally
neg
ativ
e ax
illa
to a
void
inva
sive
ax
illar
y di
ssec
tion
(40)
. Mal
es w
ho h
ave
DC
IS sh
ould
und
ergo
lum
pect
omy
follo
wed
by
brea
st ir
radi
atio
n (7
1), w
hile
smal
ler i
nvas
ive
tum
ors
can
be tr
eate
d w
ith lu
mpe
ctom
y an
d se
ntin
el n
ode
biop
sy fo
llow
ed b
y ad
juva
nt ra
diat
ion
ther
apy
(71)
. For
loca
lly a
dvan
ced
tum
ors,
loco
re
gion
al ra
diat
ion
to c
hest
wal
l and
lym
ph n
odes
shou
ld b
e do
ne (7
1). O
vera
ll, se
ntin
el n
ode
biop
sy is
one
of t
he m
ost e
ffec
tive
way
s of
as
sess
ing
noda
l inv
olve
men
t (50
-52)
. D
ue to
the
high
pre
vale
nce
of e
stro
gen
rece
ptor
pos
itivi
ty in
mal
e br
east
can
cers
, firs
t lin
e st
anda
rd a
djuv
ant t
hera
py is
tam
oxife
n (8
). Ta
mox
ifen
has s
how
n to
impr
ove
surv
ival
and
recu
rren
ce in
mal
e br
east
can
cer a
ssoc
iate
d w
ith e
stro
gen
rece
ptor
pos
itivi
ty (4
2) a
nd m
en w
ho a
re tr
eate
d w
ith ta
mox
ifen
have
bet
ter p
rogn
osis
and
surv
ival
rate
s(9-
11).
Gos
s et a
l con
duct
ed a
stud
y of
57
patie
nts w
ho h
ad si
gnifi
cant
impr
ovem
ent w
ith
tam
oxife
n (1
2). T
amox
ifen
has b
een
effe
ctiv
e in
trea
ting
met
asta
tic m
ale
brea
st c
ance
r, w
hich
Cut
tie e
t al d
emon
stra
ted
in th
eir s
tudy
of 2
43 n
ode
posi
tive
men
and
saw
can
cer r
ates
redu
ced
from
62%
to 2
8% (2
3 or
45)
. Thi
s is a
lso
cons
iste
nt w
ith o
ther
stud
ies (
89,9
0). T
amox
ifen
com
plia
nce
in m
en h
as b
een
chal
leng
ing
due
to th
e dr
ug n
ot b
eing
tole
rate
d (4
7,48
). Fi
ve y
ears
of a
djuv
ant t
amox
ifen
is re
com
men
ded
for m
en w
ith H
R-
posi
tive
brea
st c
ance
r afte
r mas
tect
omy
is p
erfo
rmed
(75)
. Th
ere
is c
onfli
ctin
g in
form
atio
n in
term
s of w
hen
radi
atio
n sh
ould
be
give
n. M
ale
patie
nts t
ypic
ally
rece
ive
radi
atio
n m
ore
ofte
n th
an fe
mal
es,
due
to m
ore
adva
nced
stag
e w
hen
diag
nose
d (7
6,21
or 4
2). I
ndic
atio
n fo
r rad
iatio
n th
erap
y co
mes
from
the
data
from
fem
ale
brea
st c
ance
rs
whi
ch in
clud
es la
rge
tum
ors,
axill
ary
node
invo
lvem
ent,
and
an a
dvan
ced
tum
or st
age
(45)
. Som
e of
the
mor
e re
cent
lite
ratu
re is
adv
ocat
ing
for a
m
odifi
ed ra
dica
l or s
impl
e m
aste
ctom
y in
add
ition
to ra
diat
ion
ther
apy.
If a
lum
pect
omy
is p
erfo
rmed
, adj
uvan
t rad
iatio
n sh
ould
als
o be
incl
uded
(7
1), i
nclu
ding
che
st w
all r
adia
tion
(24)
. How
ever
, if l
ymph
nod
e or
pec
tora
l mus
cle
inva
sion
is p
rese
nt, r
adio
ther
apy
follo
win
g m
aste
ctom
y sh
ould
be
perf
orm
ed (7
3).
Ther
e is
als
o co
nflic
ting
info
rmat
ion
in te
rms o
f how
radi
atio
n af
fect
s mal
e br
east
can
cer.
One
stud
y sh
ows t
hat p
osto
pera
tive
radi
atio
n pr
even
ts
recu
rren
ce b
ut h
as n
o ef
fect
on
patie
nt su
rviv
al (4
6). A
djuv
ant r
adio
ther
apy
appe
ars t
o be
eff
ectiv
e in
pre
vent
ing
recu
rren
ces i
n m
ale
brea
st
canc
er, b
ut d
iffer
ence
s in
mor
talit
y ha
ve n
ot b
een
iden
tifie
d (7
7-81
). A
djuv
ant r
adio
ther
apy
is a
dvis
ed in
men
with
pos
itive
lym
ph n
odes
or
tum
or >
5 cm
or m
argi
ns p
ositi
ve (8
2).
Som
e of
the
liter
atur
e st
ates
that
adj
uvan
t che
mot
hera
py s
houl
d be
add
ed w
hen
dise
ase
is a
dvan
ced
or th
ere
is a
xilla
ry n
ode
invo
lvem
ent (
71).
Som
e ch
emot
hera
py o
ptio
ns u
sed
incl
ude
CM
F (c
yclo
phos
pham
ide,
met
hotre
xate
, and
fluo
rour
acil)
, FEC
and
EC
(37)
. Thu
s far
, no
curr
ent d
ata
exis
ts o
n th
e us
e of
tras
tuzu
mab
in m
ale
brea
st c
ance
r. A
djuv
ant c
hem
othe
rapy
is re
com
men
ded
in th
e yo
unge
r pat
ient
pop
ulat
ion,
pat
ient
s with
la
rger
tum
ors,
and
patie
nts w
ho h
ave
axill
ary
node
invo
lvem
ent (
71).
To
date
, onl
y on
e pr
ospe
ctiv
e st
udy
of a
djuv
ant c
hem
othe
rapy
has
bee
n pu
blis
hed
in p
atie
nts w
ith m
ale
brea
st c
ance
r (83
). C
hem
othe
rapy
has
bee
n sh
own
in re
trosp
ectiv
e da
ta to
dec
reas
e re
curr
ence
and
impr
ove
mor
talit
y (8
4-86
) and
it h
as b
een
show
n to
incr
ease
bot
h, 5
yea
r and
10
year
sur
viva
l rat
es (8
3, 8
7). M
en w
ith in
term
edia
te o
r hig
h ris
k br
east
ca
ncer
and
hor
mon
e re
cept
or n
egat
ive
tum
ors (
74) o
r pat
ient
s who
bec
ome
refr
acto
ry to
hor
mon
e th
erap
y sh
ould
rece
ive
adju
vant
che
mot
hera
py.
The
best
follo
w u
p is
clin
ical
ass
essm
ent a
nd se
lf-br
east
exa
min
atio
n si
nce
mos
t mal
e br
east
can
cers
pre
sent
with
a p
alpa
ble
mas
s (90
). Yo
u ca
n pl
ace
your
org
aniz
atio
ns lo
gos o
n ei
ther
side
of t
he ti
tle o
f the
pos
ter.
Inse
rt yo
ur te
xt h
ere.
Prog
nosi
s
Mal
e br
east
can
cer,
alth
ough
a ra
re c
ondi
tion
is li
kely
und
er d
iagn
osed
freq
uent
ly.
Der
mat
olog
ists
can
pl
ay a
cru
cial
role
in th
e di
agno
sis o
f thi
s tre
atab
le d
isea
se.
Der
mat
olog
ists
shou
ld in
clud
e br
east
ca
rcin
oma
in th
eir d
iffer
entia
l dia
gnos
es o
f a lu
mp
in th
e br
east
of b
oth
mal
es a
nd fe
mal
es a
like.
Cur
rent
ly
the
liter
atur
e is
lack
ing
in c
linic
al ra
ndom
ized
tria
ls o
n m
ale
brea
st c
ance
r pat
ient
s in
term
s of t
he b
est
treat
men
t and
man
agem
ent a
nd fu
rther
, the
pat
hoph
ysio
logy
of m
ale
brea
st c
ance
r is n
ot c
lear
ly u
nder
stoo
d at
pre
sent
. Man
agem
ent o
f bre
ast c
ance
r may
not
be
sole
ly in
the
hand
s of d
erm
atol
ogis
ts, t
here
fore
we
stre
ss th
e im
porta
nce
of m
aking
the
diag
nosi
s. T
his i
nclu
des s
ampl
ing
with
his
topa
thol
ogy
and
imag
ing
stud
ies a
s a m
eans
to b
ette
r pre
pare
the
patie
nt f
or sp
ecia
lists
in su
rger
y an
d on
colo
gy fo
r def
initi
ve
treat
men
t.
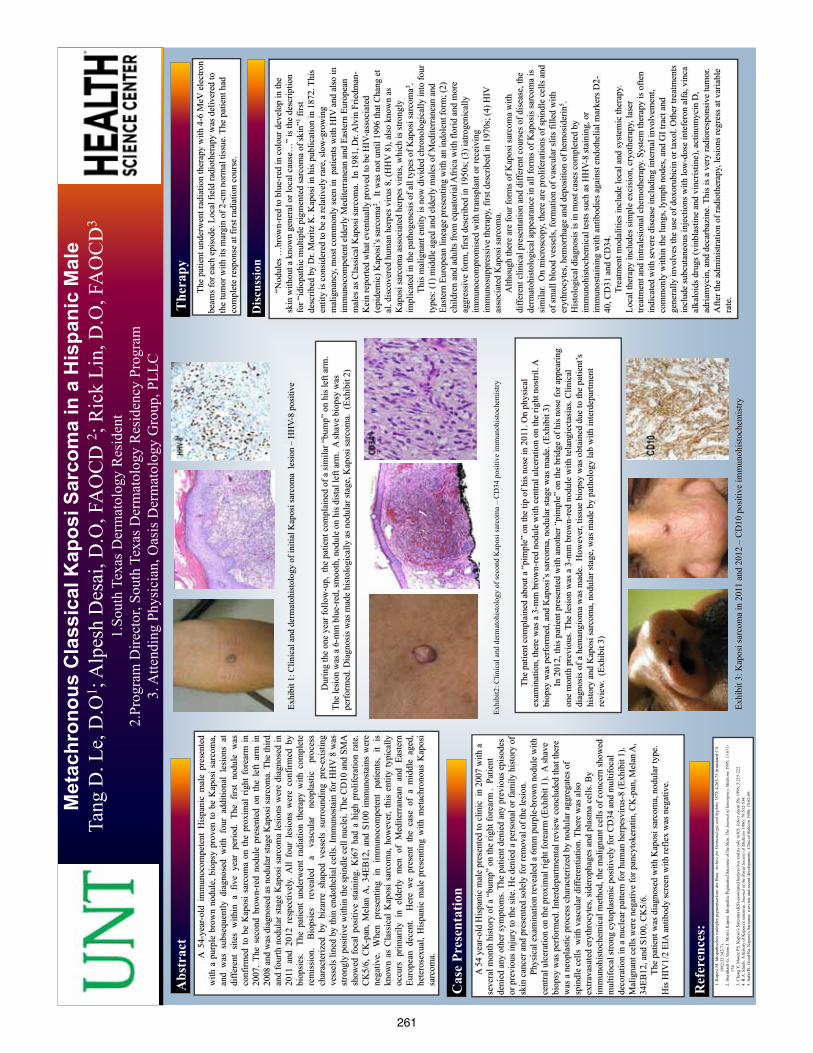
261
prin
ted
by
ww
w.po
ster
sess
ion.
com
Met
achr
onou
s C
lass
ical
Kap
osi S
arco
ma
in a
His
pani
c M
ale
Tang
D. L
e, D
.O1 ;
Alp
esh
Des
ai, D
.O, F
AO
CD
2 ; R
ick
Lin,
D.O
, FA
OC
D3
1.So
uth
Texa
s Der
mat
olog
y R
esid
ent
2.Pr
ogra
m D
irect
or, S
outh
Tex
as D
erm
atol
ogy
Res
iden
cy P
rogr
am
3. A
ttend
ing
Phys
icia
n, O
asis
Der
mat
olog
y G
roup
, PLL
C
“N
odul
es …
brow
n-re
d to
blu
e-re
d in
col
our d
evel
op in
the
skin
with
out a
kno
wn
gene
ral o
r loc
al c
ause
…”
is th
e de
scrip
tion
for “
idio
path
ic m
ultip
le p
igm
ente
d sa
rcom
a of
skin
”1 firs
t de
scrib
ed b
y D
r. M
oritz
K. K
apos
i in
his p
ublic
atio
n in
187
2. T
his
entit
y is
con
side
red
to b
e a
rela
tivel
y ra
re, s
low
-gro
win
g m
alig
nanc
y, m
ost c
omm
only
seen
in p
atie
nts w
ith H
IV a
nd a
lso
in
imm
unoc
ompe
tent
eld
erly
Med
iterr
anea
n an
d Ea
ster
n Eu
rope
an
mal
es a
s Cla
ssic
al K
apos
i sar
com
a. I
n 19
81, D
r. A
lvin
Frie
dman
-K
ein
repo
rted
wha
t eve
ntua
lly p
rove
d to
be
HIV
-ass
ocia
ted
(epi
dem
ic) K
apos
i’s sa
rcom
a2 . It
was
not
unt
il 19
96 th
at C
hang
et
al. d
isco
vere
d hu
man
her
pes v
irus 8
, (H
HV
8),
also
kno
wn
as
Kap
osi s
arco
ma
asso
ciat
ed h
erpe
s viru
s, w
hich
is st
rong
ly
impl
icat
ed in
the
path
ogen
esis
of a
ll ty
pes o
f Kap
osi s
arco
ma3 .
This
mal
igna
nt e
ntity
is n
ow d
ivid
ed c
hron
olog
ical
ly in
to fo
ur
type
s: (1
) mid
dle
aged
and
eld
erly
mal
es o
f Med
iterr
anea
n an
d Ea
ster
n Eu
rope
an li
neag
e pr
esen
ting
with
an
indo
lent
form
; (2)
ch
ildre
n an
d ad
ults
from
equ
ator
ial A
fric
a w
ith fl
orid
and
mor
e ag
gres
sive
form
, firs
t des
crib
ed in
195
0s; (
3) ia
troge
nica
lly
imm
unoc
ompr
omis
ed w
ith tr
ansp
lant
or r
ecei
ving
im
mun
osup
pres
sive
ther
apy,
firs
t des
crib
ed in
197
0s; (
4) H
IV
asso
ciat
ed K
apos
i sar
com
a.
A
lthou
gh th
ere
are
four
form
s of K
apos
i sar
com
a w
ith
diffe
rent
clin
ical
pre
sent
atio
n an
d di
ffere
nt c
ours
es o
f dis
ease
, the
de
rmat
ohis
tolo
gica
l app
eara
nce
in a
ll fo
rms o
f Kap
osis
sarc
oma
is
sim
ilar.
On
mic
rosc
opy,
ther
e ar
e pr
olife
ratio
ns o
f spi
ndle
cel
ls a
nd
of sm
all b
lood
ves
sels
, for
mat
ion
of v
ascu
lar s
lits f
illed
with
er
ythr
ocyt
es, h
emor
rhag
e an
d de
posi
tion
of h
emos
ider
in5 .
H
isto
logi
cal d
iagn
osis
is in
mos
t cas
es c
ompl
eted
by
imm
unoh
isto
chem
ical
test
s suc
h as
HH
V-8
stai
ning
, or
imm
unos
tain
ing
with
ant
ibod
ies a
gain
st e
ndot
helia
l mar
kers
D2-
40, C
D31
and
CD
34.
Tr
eatm
ent m
odal
ities
incl
ude
loca
l and
syst
emic
ther
apy.
Lo
cal t
hera
py in
clud
es si
mpl
e ex
cisi
on, c
ryot
hera
py, l
aser
tre
atm
ent a
nd in
trale
sion
al c
hem
othe
rapy
. Sys
tem
ther
apy
is o
ften
indi
cate
d w
ith se
vere
dis
ease
incl
udin
g in
tern
al in
volv
emen
t, co
mm
only
with
in th
e lu
ngs,
lym
ph n
odes
, and
GI t
ract
and
ge
nera
lly in
volv
es th
e us
e of
dox
orub
icin
or t
axol
. Oth
er tr
eatm
ents
in
clud
e su
bcut
aneo
us in
ject
ions
with
low
-dos
e in
tefe
ron
alfa
, vin
ca
alka
loid
s dru
gs (v
inbl
astin
e an
d vi
ncris
tine)
, act
inom
ycin
D,
adria
myc
in, a
nd d
ecar
bazi
ne. T
his i
s a v
ery
radi
ores
pons
ive
tum
or.
Afte
r the
adm
inis
tratio
n of
radi
othe
rapy
, les
ions
regr
ess a
t var
iabl
e ra
te.
A
54
year
-old
His
pani
c m
ale
pres
ente
d to
clin
ic i
n 20
07 w
ith a
se
vera
l mon
th h
isto
ry o
f a “
bum
p” o
n th
e rig
ht fo
rear
m .
Pat
ient
de
nied
any
oth
er sy
mpt
oms.
The
patie
nt d
enie
d an
y pr
evio
us e
piso
des
or p
revi
ous i
njur
y to
the
site
. He
deni
ed a
per
sona
l or f
amily
his
tory
of
skin
can
cer a
nd p
rese
nted
sole
ly fo
r rem
oval
of t
he le
sion
.
Phys
ical
exa
min
atio
n re
veal
ed a
6m
m p
urpl
e-br
own
nodu
le w
ith
cent
ral u
lcer
atio
n on
the
prox
imal
righ
t for
earm
(Exh
ibit
1).
A sh
ave
biop
sy w
as p
erfo
rmed
. Int
erde
partm
enta
l rev
iew
con
clud
ed th
at th
ere
was
a n
eopl
astic
pro
cess
cha
ract
eriz
ed b
y no
dula
r agg
rega
tes o
f sp
indl
e ce
lls w
ith v
ascu
lar d
iffer
entia
tion.
The
re w
as a
lso
extra
vasa
ted
eryt
hroc
ytes
, sid
erop
hage
s and
pla
sma
cells
. By
imm
unoh
isto
chem
ical
met
hod,
the
mal
igna
nt c
ells
of c
once
rn sh
owed
m
ultif
ocal
stro
ng c
ytop
lasm
ic p
ositi
vely
for C
D34
and
mul
tifoc
al
deco
ratio
n in
a n
ucle
ar p
atte
rn fo
r hum
an h
erpe
sviru
s-8
(Exh
ibit
1).
Mal
igna
nt c
ells
wer
e ne
gativ
e fo
r pan
cyto
kera
tin, C
K-p
an, M
elan
A,
34EB
12, a
nd S
100,
CK
5/6.
The
patie
nt w
as d
iagn
osed
with
Kap
osi s
arco
ma,
nod
ular
type
. H
is H
IV1/
2 EI
A a
ntib
ody
scre
en w
ith re
flex
was
neg
ativ
e.
Abs
trac
t
Cas
e Pr
esen
tatio
n
Dis
cuss
ion
D
urin
g th
e on
e ye
ar fo
llow
-up,
the
pat
ient
com
plai
ned
of a
sim
ilar “
bum
p” o
n hi
s lef
t arm
. Th
e le
sion
was
a 6
-mm
blu
e-re
d, sm
ooth
, nod
ule
on h
is d
ista
l lef
t arm
. A
shav
e bi
opsy
was
pe
rfor
med
. Dia
gnos
is w
as m
ade
hist
olog
ical
ly a
s nod
ular
stag
e, K
apos
i sar
com
a. (
Exhi
bit 2
)
Exhi
bit 1
: Clin
ical
and
der
mat
ohis
tolo
gy o
f ini
tial K
apos
i sar
com
a le
sion
– H
HV-
8 po
sitiv
e
Exhi
bit2
: Clin
ical
and
der
mat
ohis
tolo
gy o
f sec
ond
Kap
osi s
arco
ma
– C
D34
pos
itive
imm
unoh
isto
chem
istry
Th
e pa
tient
com
plai
ned
abou
t a “
pim
ple”
on
the
tip o
f his
nos
e in
201
1. O
n ph
ysic
al
exam
inat
ion,
ther
e w
as a
3-m
m b
row
n-re
d no
dule
with
cen
tral u
lcer
atio
n on
the
right
nos
tril.
A
biop
sy w
as p
erfo
rmed
, and
Kap
osi’s
sarc
oma,
nod
ular
stag
e w
as m
ade.
(Exh
ibit
3)
In
201
2, th
is p
atie
nt p
rese
nted
with
ano
ther
“pi
mpl
e” o
n th
e br
idge
of h
is n
ose
for a
ppea
ring
one
mon
th p
revi
ous.
The
lesi
on w
as a
3-m
m b
row
n-re
d no
dule
with
tela
ngie
ctas
ias.
Clin
ical
di
agno
sis o
f a h
eman
giom
a w
as m
ade.
How
ever
, tis
sue
biop
sy w
as o
btai
ned
due
to th
e pa
tient
’s
hist
ory
and
Kap
osi s
arco
ma,
nod
ular
stag
e, w
as m
ade
by p
atho
logy
lab
with
inte
rdep
artm
ent
revi
ew.
(Exh
ibit
3)
Exhi
bit 3
: Kap
osi s
arco
ma
in 2
011
and
2012
– C
D10
pos
itive
imm
unoh
isto
chem
istry
Th
e pa
tient
und
erw
ent r
adia
tion
ther
apy
with
4-6
MeV
ele
ctro
n be
ams f
or e
ach
epis
ode.
Loc
al fi
eld
radi
othe
rapy
was
del
iver
ed to
th
e tu
mor
with
its m
argi
n of
2-c
m n
orm
al ti
ssue
. The
pat
ient
had
co
mpl
ete
resp
onse
at f
irst r
adia
tion
cour
se.
The
rapy
1. K
apos
i M. I
diop
athi
sche
s mul
tiple
s pi
gmen
tsar
kom
der
Hau
t. Ar
chiv
e fu
r Der
mat
olog
ie u
nd S
yphi
lis 1
872;
4:2
65-7
3 (tr
ansl
ated
CA
19
82;3
2:34
2-7)
. 2.
Ste
rnba
ch G
, Var
on J.
Mor
itz K
apos
i: Id
iopa
thic
Pig
men
ted
Sarc
oma
of th
e Sk
in. T
he J
ourn
al o
f Em
erge
ncy
Med
icin
e 19
95; 1
3:67
1-17
4.
3. C
hang
Y, M
oore
PS.
Kap
osi’s
Sar
com
a (K
S)-a
ssoc
iate
d he
rpes
viru
s and
its r
ole
in K
S. In
fect
Age
nt D
is 1
996;
5:2
15-2
22.
4. R
.A. S
hiel
s. A
his
tory
of K
apos
i’s sa
rcom
a. J
ourn
al o
f the
Roy
al S
ocie
ty o
f Med
icin
e 19
86; 7
9:53
2-53
4.
5. S
afai
B.,
Goo
d R
a. K
apos
i’s S
arco
ma:
a re
view
and
rece
nt d
evel
opm
ents
. Clin
ical
Bul
letin
198
0; 1
0:62
-69.
A 5
4-ye
ar-o
ld i
mm
unoc
ompe
tent
His
pani
c m
ale
pres
ente
d w
ith a
pur
ple
brow
n no
dule
, bio
psy
prov
en to
be
Kap
osi s
arco
ma,
an
d w
as s
ubse
quen
tly d
iagn
osed
with
fou
r ad
ditio
nal
lesi
ons
at
diffe
rent
site
s w
ithin
a f
ive
year
per
iod.
The
firs
t no
dule
was
co
nfirm
ed to
be
Kap
osi
sarc
oma
on th
e pr
oxim
al r
ight
for
earm
in
2007
. Th
e se
cond
bro
wn-
red
nodu
le p
rese
nted
on
the
left
arm
in
2008
and
was
dia
gnos
ed a
s nod
ular
stag
e K
apos
i sar
com
a. T
he th
ird
and
four
th n
odul
ar s
tage
Kap
osi s
arco
ma
lesi
ons
wer
e di
agno
sed
in
2011
and
201
2 re
spec
tivel
y. A
ll fo
ur l
esio
ns w
ere
conf
irmed
by
biop
sies
. T
he p
atie
nt u
nder
wen
t ra
diat
ion
ther
apy
with
com
plet
e re
mis
sion
. B
iops
ies
reve
aled
a
vasc
ular
ne
opla
stic
pr
oces
s ch
arac
teriz
ed b
y bi
zarr
e sh
aped
ves
sels
sur
roun
ding
pre
-exi
stin
g ve
ssel
s lin
ed b
y th
in e
ndot
helia
l cel
ls. I
mm
unos
tain
for H
HV
8 w
as
stro
ngly
pos
itive
with
in th
e sp
indl
e ce
ll nu
clei
. The
CD
10 a
nd S
MA
sh
owed
foc
al p
ositi
ve s
tain
ing.
Ki6
7 ha
d a
high
pro
lifer
atio
n ra
te.
CK
5/6,
CK
-pan
, Mel
an A
, 34E
B12
, and
S10
0 im
mun
osta
ins
wer
e ne
gativ
e. W
hen
pres
entin
g in
im
mun
ocom
pete
nt p
atie
nts,
it is
kn
own
as C
lass
ical
Kap
osi s
arco
ma,
how
ever
, thi
s en
tity
typi
cally
oc
curs
prim
arily
in
elde
rly m
en o
f M
edite
rran
ean
and
East
ern
Euro
pean
dec
ent.
Her
e w
e pr
esen
t th
e ca
se o
f a
mid
dle
aged
, he
tero
sexu
al, H
ispa
nic
mal
e pr
esen
ting
with
met
achr
onou
s K
apos
i sa
rcom
a.
Ref
eren
ces:

262
Carc
inoi
d Tu
mor
s an
d Ca
rcin
oid
Synd
rom
eA
Rev
iew
Fro
m A
Tw
o-Po
int P
ersp
ectiv
e
Katy
Mat
thew
s, D
.O.,
Robi
n Sh
ecte
r, D
.O.,
PBCG
ME/
Der
mat
olog
y, C
olum
bia
Hos
pita
l
Palm
Bea
ch C
entr
e fo
r Gra
duat
e M
edic
al E
duca
tion
Thro
ugh
the
eyes
of a
n in
tern
ist..
..Ca
rcin
oid
tum
ors
are
low
-gra
de m
alig
nant
gas
troi
ntes
tinal
and
pul
mon
ary
neur
oend
ocrin
e tu
mor
s w
hich
con
-ta
in n
euro
secr
etor
y gr
anul
es [1
]. Th
e tu
mor
s ar
e cl
assi
�ed
acco
rdin
g to
site
of o
rigin
, and
the
secr
etor
y pr
od-
ucts
var
y ac
cord
ing
to lo
catio
n [1
]. 1.
For
egut
(eso
phag
us, s
tom
ach,
duo
denu
m, p
ancr
eas,
gallb
ladd
er, b
ronc
hus/
lung
/tra
chea
)= lo
w s
erot
onin
-se
cret
ing;
thus
rare
for c
arci
noid
syn
drom
e to
dev
elop
[1].
2. M
idgu
t (je
junu
m, i
leum
, app
endi
x, m
ecke
l's d
iver
ticul
um, a
scen
ding
/ tra
nsve
rse/
desc
endi
ng c
olon
, liv
er,
ovar
ies,
test
es)=
hig
h se
roto
nin-
secr
etin
g; th
us v
ery
com
mon
ly c
ause
car
cino
id s
yndr
ome,
esp
ecia
lly w
hen
tum
ors
met
asta
size
to li
ver [
1].
3. H
indg
ut (r
ectu
m)=
low
ser
oton
in-s
ecre
ting;
thus
rare
ly c
ause
car
cino
id s
yndr
ome
[1].
INCR
EASE
D #
OF
NEU
ROSE
CRET
ORY
GRA
NU
LES
= IN
CREA
SED
RIS
K O
F CA
RCIN
OID
SYN
DRO
ME
SO W
HAT
EXA
CTL
Y IS
CA
RCIN
OID
SYN
DRO
ME?
FLU
SHIN
G
DIA
RRH
EA
MID
GU
T CA
RCIN
OID
TU
MO
RS
(+)
WH
EEZI
NG
, PEL
LAG
RA, R
IGH
T H
EART
PU
LMO
NIC
STEN
OSI
S, T
R, C
ON
DU
CTI
ON
DEF
ECTS
[1,2
].
Carc
inoi
d tu
mor
s ca
n oc
cur i
n th
e ab
senc
e of
car
cino
id s
yndr
ome,
and
the
mea
n ag
e fo
r tum
ors
is a
ge 6
3 [1
].
The
smal
l int
estin
e, lu
ng, a
nd b
ronc
hus
are
the
mor
e co
mm
on s
ites
curr
ently
, with
the
smal
l int
estin
e (il
eum
) by
far w
inni
ng th
e #1
spo
t [1]
.
DIA
GN
OSI
S:
1. S
ERU
M C
HRO
MO
GRA
NIN
A(A
LSO
SEE
N IN
PH
EO, R
ENA
L IN
SUFF
I-CI
ENCY
, LIV
ER F
AIL
URE
, IBD
, PPI
S [4
,6})
2. U
RIN
ARY
5-H
IAA
3. U
RIN
ARY
5-H
T
4. U
RIN
ARY
5-H
TP(fo
r pat
ient
s w
ith d
opa
deca
rbox
ylas
e de
fect
{1}
5. O
CTR
EOTI
DE
SCIN
TIG
RAPH
Y
INTE
RNA
L SY
MPT
OM
S O
F CA
RCIN
OID
TU
MO
RS:
COU
GH
WH
EEZI
NG
HEM
OPT
YSIS
BRO
NCH
IAL
OBS
TRU
CTI
ON
RECU
RREN
T PN
AA
NTE
RIO
R M
EDIA
STIN
AL
THYM
IC M
ASS
GI B
LEED
ING
HSM
WIT
H N
ORM
AL
LFTS
ABD
OM
INA
L PA
INSB
O
Thro
ugh
the
eyes
of a
der
mat
olog
ist..
.1.
Cla
ssic
car
cino
id �
ush:
rapi
d on
set f
acia
l and
che
st d
eep
eryt
hem
a, fo
llow
ed b
y a
cyan
otic
hue
, som
etim
es
asso
ciat
ed w
ith p
rurit
is/e
dem
a/ la
crim
atio
n/di
arrh
ea. T
his
is s
een
in 1
0% o
f car
cino
id s
yndr
ome
with
live
r m
ets,
but i
s al
so s
een
in m
idgu
t tum
ors
(app
endi
x, s
mal
l int
estin
e, a
nd p
roxi
mal
col
on) [
1,2,
5,6]
.2.
Brig
ht s
alm
on-p
ink
red
�ush
rese
mbl
ing
phys
iolo
gic
�ush
ing:
Thi
s is
see
n in
fore
gut t
umor
s [5
,6].
3. B
right
red
prur
itic
and
patc
hy �
ush
with
whi
te p
atch
es in
term
ixed
on
face
and
nec
k: T
his
is s
een
in g
astr
ic
carc
inoi
d tu
mor
s [1
,2].
4. R
ed-p
urpl
e �u
sh, l
astin
g ho
urs-
days
, ass
ocia
ted
with
sal
ivat
ion/
la
crim
atio
n/di
apho
resi
s/di
arrh
ea/h
ypot
ensi
on: S
een
in b
ronc
hial
car
cino
id tu
mor
s [1
,2].
5. H
indg
ut tu
mor
s ar
e N
OT
usua
lly a
ssoc
iate
d w
ith �
ushi
ng [2
].
DER
MAT
OLO
GIC
MA
NIF
ESTA
TIO
NS:
FLU
SHIN
G H
YPER
HID
ROSI
SPE
LLAG
RASC
LERO
DER
MA
PHO
TOD
ERM
ATO
SIS
ACU
TE-O
NSE
T RO
SACE
A W
ITH
TEL
AN
GEC
TASI
AS
AN
D R
HIN
OPH
YMA
HYP
ERPI
GM
ENTA
TIO
NRA
YNAU
D’S
NF1
MEN
1
TREA
TMEN
T:Fi
rst l
ine
ther
apy
invo
lves
loca
lizat
ion
of tu
mor
and
sur
gica
l res
ectio
n; fo
r non
-met
asta
tic tu
mor
s, su
rger
y is
us
ually
cur
ativ
e[1]
. Pr
e-op
erat
ive
man
agem
ent i
nvol
ves
avoi
ding
pre
cipi
tant
s of
�us
hing
suc
h as
alc
ohol
, sp
icy
food
s, st
ress
, SSR
Is a
nd c
hees
e [1
]. T
here
are
a v
arie
ty o
f "sy
mpt
om re
lievi
ng" m
edic
atio
ns th
at a
re d
i-re
cted
at t
he m
ain
unde
rlyin
g sy
mpt
omat
olog
y lik
e an
ti-di
arrh
ea a
gent
s (lo
pera
mid
e), c
ombi
natio
n H
1 an
d H
2 an
tago
nist
s (d
iphe
nhyd
ram
ine,
cim
etid
ine,
and
rani
tidin
e) a
nd b
ronc
hodi
lato
rs [1
]. S
erot
onin
rece
ptor
an
tago
nist
s (m
ethy
serg
ide,
cyp
rohe
pata
dine
, and
ket
anse
rin) a
re a
lso
occa
sion
ally
use
d [1
]. C
uren
tly, t
he
mos
t com
mon
sys
tem
ic tr
eatm
ent u
tiliz
ed (e
spec
ially
with
the
synd
rom
e) a
re th
e so
mat
osta
tin a
nalo
gues
oc
treo
tide
and
lanr
eotid
e [1
]. If
met
asta
tic d
isea
se is
pre
sent
in th
e liv
er, a
com
bina
tion
of h
epat
ic a
rter
y em
boliz
atio
n (w
ith o
r with
out c
hem
othe
rape
utic
age
nts
5-FU
, adr
iam
ycin
, cis
plat
in, m
itom
ycin
) and
in
terf
eron
-alp
ha is
use
d [1
.]
THE
ROLE
OF
CHRO
MO
GRA
NIN
A IN
FO
RMAT
ION
OF
NEU
ROSE
CRET
ORY
G
RAN
ULE
S N
EJM
200
3; 3
48: F
IGU
RE 4
HA
RRIS
ON
’S P
RIN
CIPL
ES O
F IN
TERN
AL
MED
ICIN
E 16
TH E
DIT
ION
, 20
05; F
IGU
RE 3
29-1
Refe
renc
es
1.Ka
sper
DL,
Har
rison
TR.
Har
rison
's Pr
inci
ples
of I
nter
nal M
edic
ine.
ebo
ok, 1
6th
editi
on, 2
005,
222
0-22
26.
Acce
ssed
via
Nov
a So
uthe
aste
rn U
nive
rsity
libr
arie
s EB
SCO
hos
t on
4/12
/12.
2.Bo
logn
ia JL
, Jor
izzo
JL, R
apin
i RP.
Der
mat
olog
y. 2
nd e
ditio
n; v
olum
es 1
,2. E
lsev
ier 2
008.
3.W
ol�
K, G
olds
mith
LA
, Kat
z SI
, Gilc
hres
t BA
, Pal
ler A
S, L
e�el
l DJ.
Fitz
patr
ick'
s D
erm
atol
ogy
in G
ener
al M
edic
ine.
7th
edi
tion;
vol
umes
1,2
. McG
raw
Hill
200
8.4.
Taup
enot
L, H
arpe
r KL,
O'C
onne
r D. T
he C
hrom
ogra
nin-
Secr
etog
rani
n Fa
mily
. The
New
Eng
land
Jour
nal o
f Med
icin
e 20
03; 3
48: 1
134-
1149
.5.
Bell
HK,
Pos
ton
GJ,
Vora
J, W
ilson
NJE
. Cu
tane
ous
man
ifest
atio
ns o
f the
mal
igna
nt c
arci
noid
syn
drom
e. C
linic
al a
nd la
bora
tory
inve
stig
atio
ns, B
ritis
h Jo
urna
l of D
erm
atol
ogy
2005
; 152
: 71-
75.
6.Ja
bbou
r SA
. Sk
in m
anife
stat
ions
of h
orm
one-
secr
etin
g tu
mor
s. D
erm
atol
ogic
The
rapy
201
0; 2
3: 6
43-6
50.
Ther
e ar
e se
vera
l oth
er n
otew
orth
y cu
tane
ous
man
ifest
atio
ns. A
cute
-ons
et ro
sace
a, in
the
sett
ing
of th
e "3
H's:
HO
T (d
iaph
ores
is),
HTN
, HR
(tac
hyca
rdia
)" (+
) dia
rrhe
a, s
houl
d pr
ompt
one
to in
vest
igat
e fo
r car
cino
id
synd
rom
e [1
,2].
Sero
toni
n, b
eing
a v
asoa
ctiv
e su
bsta
nce,
dire
ctly
con
trib
utes
to th
e ro
sace
a [2
]. It
has
also
bee
n sh
own
that
long
-ter
m re
peat
ed �
ushi
ng c
ause
s ro
sace
a, te
lang
iect
asia
s, �x
ed e
ryth
ema,
and
ear
ly rh
i-no
phym
a [2
,5].
Patie
nts
can
also
dev
elop
scl
erod
erm
a/sc
lero
derm
oid
skin
cha
nges
, but
thes
e pr
edom
inat
ely
a�ec
t the
bila
tera
l low
er e
xtre
miti
es (r
athe
r tha
n up
per e
xtre
miti
es) w
ith a
n ab
senc
e of
rayn
aud'
s ph
e-no
men
on [2
, 5].
Di�
use
hype
rpig
men
tatio
n (d
ue to
MSH
pro
duct
ion
from
tum
or),
hype
rhid
rosi
s, an
d pr
esen
tatio
n as
a p
hoto
aggr
avat
ed d
erm
atos
is c
an a
lso
occu
r [2,
3]. N
euro
�bro
mat
osis
type
1 h
as b
een
asso
ciat
ed
with
duo
dena
l car
cino
ids,
and
up to
12%
of N
F1 p
atie
nts
deve
lop
an u
pper
GI c
arci
noid
tum
or, c
hara
cter
istic
ally
at t
he p
eri-a
mpu
lla [1
,2,7
]. Ra
rely
, pat
ient
s w
ith M
EN1
deve
lop
carc
inoi
d tu
mor
s; s
peci
�cal
ly 8
% o
f M
EN1
patie
nts
deve
lop
bron
chia
l car
cino
ids,
8% th
ymic
car
cino
ids,
and
13-3
0% o
f pat
ient
s w
ith Z
ollin
ger-
Ellis
on S
yndr
ome
and
MEN
1 ha
ve g
astr
ic c
arci
noid
s! [1
,2].
Col
umbi
a H
ospi
tal
Palm
s Wes
t Hos
pita
lSt
. Luc
ie M
edic
al C
ente
rU
nive
rsity
Hos
pita
l &
Med
ical
Cen
ter
PELL
AGRA
DER
MAT
ITIS
DEM
ENTI
A
DIA
RRH
EA
DEA
TH
TRYP
TOPH
AN
NIA
CIN
(VIT
B3)
**C
ERA
MID
ES**
SERO
TON
IN

263
Tem
plat
e pr
ovid
ed b
y: “p
oste
rs4r
esea
rch.
com
”
EPID
EMIO
LOG
Y
•Sw
eet’s
synd
rom
e is
an
unco
mm
on d
isea
se, a
bout
500
repo
rted
case
s •
Wor
ldw
ide
dist
ribut
ion,
slig
htly
hig
her i
ncid
ence
in Ja
pan
•Fe
mal
e: m
ale
ratio
= 4
:1
•Av
erag
e ag
e of
ons
et 3
0-60
yea
rs
•In
fant
s, ch
ildre
n an
d el
derly
may
als
o be
affe
cted
•
Up
to 2
0% m
ay h
ave
an in
tern
al m
alig
nanc
y (n
o se
x pr
efer
ence
in
thes
e ca
ses)
•
Dru
g-in
duce
d sw
eet’s
synd
rom
e is
mor
e co
mm
on in
wom
en (1
) ET
IOLO
GY
AN
D P
ATH
OG
ENES
IS
•Pa
thog
enes
is u
nkno
wn,
thou
ght t
o be
a h
yper
sens
itivi
ty re
actio
n.
•C
an b
e as
soci
ated
with
infe
ctio
ns, a
utoi
mm
une
dise
ases
, IB
D,
mal
igna
ncie
s (e.
g. m
yelo
geno
us le
ukem
ia),
drug
-rea
ctio
ns a
nd
preg
nanc
y, h
owev
er 5
0% o
f cas
es a
re id
iopa
thic
. (1,
2)
•So
me
of th
e dr
ugs t
hat h
ave
foun
d to
be
asso
ciat
ed in
clud
e ab
acav
ir, tr
imet
hopr
im/s
ulfa
met
hoxa
zole
, min
ocyc
line,
tetra
cycl
ine,
Al
l-tra
ns re
tinoi
c ac
id, g
ranu
locy
te c
olon
y-st
imul
atin
g fa
ctor
, le
vono
rges
trel/e
thin
yl e
stra
diol
, and
cel
ecox
ib (3
,4,5
,6).
•O
rigin
ally
swee
t’s sy
ndro
me
was
thou
ght t
o be
an
imm
une
com
plex
va
scul
itis w
ith a
ltere
d ne
utro
phil
func
tion,
how
ever
cur
rent
rese
arch
no
long
er su
ppor
ts th
is.
•A
new
theo
ry is
that
cyt
okin
es su
ch a
s IL-
1, g
ranu
locy
te c
olon
y-st
imul
atin
g fa
ctor
(G-C
SF),
gran
uloc
yte-
mac
roph
age
colo
ny-
stim
ulat
ing
fact
or (G
M-C
SF),
and
IFN
-gam
ma
are
dysr
egul
ated
ei
ther
loca
lly o
r sys
tem
ical
ly. (
1)
•A
50
year
-old
His
pani
c fe
mal
e w
as a
dmitt
ed to
the
hosp
ital w
ith
a ch
ief c
ompl
aint
of a
diff
use
pain
ful r
ash.
•
PMH
: HIV
, Gen
ital H
erpe
s •
Med
s: N
orvi
r, Ep
zico
m, R
eyat
az, B
enad
ryl,
Perc
ocet
, Pep
cid,
C
olac
e an
d C
linda
myc
in
•A
ll: N
iasp
an, P
CN
•
Surg
: Den
tal p
roce
dure
2-3
wee
ks p
rior
•Fa
m: n
onco
ntrib
utor
y •
Soc:
Occ
asio
nal E
TOH
, den
ies d
rug
abus
e, d
enie
s sm
okin
g,
perio
ds re
gula
r •
Hos
pita
l Cou
rse:
The
pat
ient
was
initi
ally
susp
ecte
d to
hav
e di
ssem
inat
ed h
erpe
s zos
ter d
ue to
a v
esic
ular
rash
not
ed b
y th
e
med
ical
team
and
her
imm
unoc
ompr
omis
ed st
atus
. Sh
e w
as
plac
ed o
n is
olat
ion
and
treat
ed w
ith a
cycl
ovir.
•
Upo
n de
rmat
olog
ic c
onsu
ltatio
n, w
e w
ere
able
to e
luci
date
a
rece
nt h
isto
ry o
f a d
enta
l pro
cedu
re fo
r whi
ch sh
e w
as
pres
crib
ed C
linda
myc
in.
In a
dditi
on, s
he c
ompl
aine
d of
feve
rs,
coug
hing
, mya
lgia
and
dia
rrhe
a fo
r one
wee
k pr
ior t
o th
e ra
sh.
She
repo
rts th
at h
er P
MD
susp
ecte
d an
influ
enza
infe
ctio
n,
pres
crib
ed o
selta
miv
ir an
d ad
min
iste
red
the
influ
enza
vac
cine
.
•O
n sk
in e
xam
ther
e w
ere
diffu
se e
ryth
emat
ous,
edem
atou
s, te
nder
pap
ules
and
pla
ques
ove
r her
che
st, b
ack,
abd
omen
, arm
s an
d le
gs.
Som
e le
sion
s had
pse
udov
esic
les a
t the
per
iphe
ry d
ue
to th
e ex
tens
ive
edem
a, e
xpla
inin
g th
e he
rpes
zos
ter d
iffer
entia
l.
(See
Fig
ures
I-II
I)
•La
bora
tory
eva
luat
ion
show
ed a
mild
ly in
crea
sed
WB
C (1
0.9)
, m
ild a
nem
ia, n
orm
al e
lect
roly
tes,
norm
al c
oagu
latio
n pr
ofile
, C
D4
coun
t of 1
90, n
egat
ive
hepa
titis
pan
el, n
onre
activ
e R
PR,
nega
tive
C.d
iff to
xin,
neg
ativ
e bl
ood
cultu
res,
elev
ated
VZV
Ig
G b
ut n
egat
ive
VZV
IgM
.
•U
pon
furth
er q
uest
ioni
ng, t
he p
atie
nt a
dmitt
ed to
a c
hild
hood
ch
icke
n po
x in
fect
ion,
con
sist
ent w
ith th
e V
ZV Ig
G.
The
nega
tive
IgM
pro
vide
d ev
iden
ce a
gain
st th
e di
agno
sis o
f di
ssem
inat
ed h
erpe
s zos
ter.
•
A p
unch
bio
psy
of th
e sk
in w
as o
btai
ned
and
the
path
olog
y w
as
cons
iste
nt w
ith S
wee
t’s sy
ndro
me.
She
was
dis
char
ged
hom
e or
al p
redn
ison
e an
d to
pica
l cor
ticos
tero
id o
intm
ent a
nd th
e co
nditi
on re
solv
ed w
ithin
6 w
eeks
.
AB
STR
AC
T
CA
SE D
ESC
RIP
TIO
N
CO
NC
LU
SIO
N
RE
FER
EN
CE
S
Swee
t’s S
yndr
ome
Mas
quer
adin
g as
Dis
sem
inat
ed H
erpe
s Zos
ter
in a
n H
IV P
ositi
ve P
atie
nt
Cha
riss
e M
cCal
l, D
O, O
GM
E-I
I D
epar
tmen
t of D
erm
atol
ogy,
St.
John
’s E
psic
opal
Hos
pita
l, Fa
r Roc
kaw
ay, N
Y
Pr
ogra
m D
irec
tor:
Mar
vin
Wat
sky,
DO
- A
ssis
tant
Pro
gram
Dir
ecto
r: S
uzan
ne S
irot
a R
ozen
berg
, DO
- D
ME
: Alb
ert S
troj
an, D
O
Logo
H
ere
We
desc
ribe
a pa
tient
with
an
unus
ual
pres
enta
tion
of a
rare
synd
rom
e in
the
setti
ng o
f a
com
plic
ated
med
ical
his
tory
. The
se fa
ctor
s lea
d to
an
initi
al m
isdi
agno
sis a
nd a
del
ay in
ap
prop
riate
trea
tmen
t. T
his c
ase
serv
es to
in
crea
se a
war
enes
s of t
his u
ncom
mon
skin
di
seas
e an
d hi
ghlig
hts t
he n
eed
for p
rom
pt
derm
atol
ogic
con
sulta
tion
in th
e ho
spita
lized
pa
tient
with
an
unus
ual r
ash,
incl
udin
g sk
in
biop
sy if
indi
cate
d.
DIS
CU
SSIO
N
1) JL
Bol
ogni
a, JL
Joriz
zo, R
P R
apin
i. D
erm
atol
ogy.
2nd
Ed.
Spa
in:
Else
vier
, 200
3. p
p 38
0-3.
2)
Rap
ini R
P. P
ract
ical
Der
mat
opat
holo
gy. 1
st E
d. P
hila
delp
hia,
PA
: El
sevi
er In
c, 2
005.
p 1
32.
3) D
el G
iudi
ce P
, Van
denb
os F
, Per
rin C
, Ber
nard
E, M
arq
L,
Del
lam
onic
a P.
Sw
eet’s
synd
rom
e fo
llow
ing
abac
avir
ther
apy.
Jour
nal o
f th
e Am
eric
an A
cade
my
of D
erm
atol
ogy.
200
4;Vo
l 51,
No
3:47
4-47
5.
4) K
han
Dur
ani B
, Jap
pe U
. Dru
g-in
duce
d Sw
eet’s
synd
rom
e in
acn
e ca
used
by
diffe
rent
tetra
cycl
ines
: cas
e re
port
and
revi
ew o
f the
lite
ratu
re.
Br J
Der
mat
ol 2
002;
147:
558-
62.
5) D
enis
e C
. Wal
ker,
MD
, Phi
lip R
. Coh
en, M
D. T
rimet
hopr
im-
sulfa
met
hoxa
zole
-ass
ocia
ted
acut
e fe
brile
neu
troph
ilic
derm
atos
is: C
ase
repo
rt an
d re
view
of d
rug-
indu
ced
Swee
t's sy
ndro
me.
Jour
nal o
f the
A
mer
ican
Aca
dem
y of
Der
mat
olog
y. 1
996;
Vol 3
4,N
o 5,
Part
2:91
8-92
3.
6) K
enne
th H
. Fye
, MD
, Eile
en C
row
ley,
MD
, PhD
, Tim
othy
G. B
erge
r, M
D, P
hilip
E. L
eBoi
t, M
D, M
. Kar
i Con
nolly
, MD
. Cel
ecox
ib-in
duce
d Sw
eet’s
synd
rom
e. J
Am
Aca
d D
erm
atol
200
1;45
:300
-2.
7) W
olff
K, J
ohns
on R
A. F
itzpa
trick
’s C
olor
Atla
s & S
ynop
sis o
f Clin
ical
D
erm
atol
ogy.
6th
Ed.
The
McG
raw
-Hill
Com
pani
es, 2
009.
pp
160-
162.
Sw
eet’s
synd
rom
e, a
lso
know
n as
acu
te fe
brile
neu
troph
ilic
derm
atos
is,
has a
n un
know
n pa
thog
enes
is.
It is
ofte
n id
iopa
thic
but
has
bee
n re
porte
d in
ass
ocia
tion
with
acu
te u
pper
resp
irato
ry in
fect
ion,
gas
troin
test
inal
in
fect
ion,
HIV
, vac
cina
tions
, med
icat
ions
, aut
oim
mun
e di
seas
es a
nd
mal
igna
ncie
s. O
ur c
ase
is in
tere
stin
g in
that
man
y of
thes
e et
iolo
gic
fact
ors w
ere
pres
ent i
mm
edia
tely
pre
cedi
ng h
er ra
sh. T
he e
xact
cau
se o
f he
r eru
ptio
n is
unk
now
n an
d m
ay h
ave
been
bro
ught
on
by th
e H
IV
infe
ctio
n, re
cent
flu-
like
illne
ss, i
nflu
enza
vac
cine
, rec
ent d
enta
l inf
ectio
n,
the
antib
iotic
s use
d to
trea
t the
den
tal i
nfec
tion
or a
com
bina
tion
of
fact
ors.
Ther
e is
a n
eed
for m
ore
rese
arch
on
the
mec
hani
sm o
f thi
s di
seas
e. T
he tw
o th
eorie
s tha
t are
cur
rent
ly b
eing
stud
ied
are
hype
rsen
sitiv
ity re
actio
n an
d dy
sreg
ulat
ion
of c
ytok
ine
secr
etio
n. T
he
pseu
dove
sicu
lar f
eatu
res o
f the
pat
ient
’s le
sion
s are
als
o a
rare
pr
esen
tatio
n, a
nd le
ad to
the
initi
al m
isdi
agno
sis a
s a d
isse
min
ated
her
pes
zost
er in
fect
ion.
Thi
s del
ay o
f acc
urat
e di
agno
sis a
nd tr
eatm
ent r
einf
orce
s th
e ne
ed fo
r ear
ly d
erm
atol
ogic
con
sulta
tion
in th
e in
patie
nt se
tting
. T
he
case
als
o re
min
ds u
s tha
t the
re sh
ould
be
a ve
ry lo
w th
resh
old
for s
kin
biop
sy, a
s it i
s min
imal
ly in
vasi
ve a
nd o
ften
inva
luab
le in
mak
ing
the
corr
ect d
iagn
osis
.
Figu
re II
I
CLI
NIC
AL
FEAT
UR
ES
•R
apid
ons
et o
f pai
nful
, brig
ht re
d, sm
ooth
, ten
der p
apul
es (2
-4m
m
in d
iam
eter
) tha
t coa
lesc
e to
form
irre
gula
r, sh
arpl
y bo
rder
ed,
edem
atou
s pla
ques
. •
The
bord
er o
f the
pla
que
may
look
as i
f com
pose
d of
ves
icle
s, m
imic
king
dis
sem
inat
ed z
oste
r inf
ectio
n as
in o
ur c
ase.
How
ever
pa
lpat
ion
reve
als t
hat t
he le
sion
s are
solid
, als
o kn
own
as
pseu
dove
sicu
latio
n, in
whi
ch in
tens
e ed
ema
give
s the
app
eara
nce
of
vesi
cula
tion.
•
Lesi
ons m
ost c
omm
only
pre
sent
on
face
, nec
k an
d up
per e
xtre
miti
es
but a
lso
on lo
wer
ext
rem
ities
whe
re le
sion
s may
be
deep
in th
e fa
t an
d m
imic
pan
nicu
litis
or e
ryth
ema
nodo
sum
. •
As t
he le
sion
s evo
lve,
cen
tral c
lear
ing
may
lead
to a
rcua
te o
r an
nula
r pat
tern
s. Ti
ny, s
uper
ficia
l pus
tule
s may
occ
ur.
•If
ass
ocia
ted
with
leuk
emia
, bul
lous
lesi
ons m
ay o
ccur
and
lesi
ons
may
mim
ic p
yode
rma
gang
reno
sum
. •
May
be
acco
mpa
nied
by
feve
r, ar
thra
lgia
and
per
iphe
ral
leuk
ocyt
osis
. (1,
7)
•D
iagn
osis
is m
ade
afte
r exc
ludi
ng in
fect
ion
in th
e sk
in le
sion
s with
sp
ecia
l sta
ins a
nd c
ultu
res.
(2)
DIA
GN
OST
IC C
RIT
ERIA
M
ajor
•
Sudd
en o
nset
of p
laqu
es, o
r ery
them
atou
s to
viol
aceo
us a
nd p
ainf
ul
nodu
les
•D
erm
al n
eutro
phili
c in
filtra
te w
ithou
t leu
kocy
tocl
astic
vas
culit
is
Min
or
•Pr
eced
ing
infe
ctio
n, v
acci
natio
n, in
flam
mat
ion
(or)
ass
ocia
ted
with
in
flam
mat
ion,
hem
opro
lifer
ativ
e di
sord
er, s
olid
tum
or o
r pre
gnan
cy
•Fe
ver a
bove
38
degr
ees C
elsi
us
•Le
ukoc
ytos
is w
ith n
eutro
phili
a, in
crea
sed
CR
P an
d ES
R
•Ex
celle
nt re
spon
se to
syst
emic
cor
ticos
tero
ids (
1)
HIS
TOPA
THO
LOG
Y (S
ee F
igur
e IV
) •
Epid
erm
al c
hang
es v
aria
ble,
som
etim
es e
pide
rmal
nec
rosi
s •
Supe
rfic
ial d
erm
al e
dem
a •
Diff
use
derm
al n
eutro
phils
, but
als
o ly
mph
ocyt
es, h
istio
cyte
s and
a
few
eos
inop
hils
•
No
true
vasc
uliti
s (no
ves
sel w
all n
ecro
sis)
•
Som
etim
es e
xtra
vasa
ted
eryt
hroc
ytes
(2)
PRO
GN
OSI
S A
ND
TR
EATM
ENT
•Sw
eet’s
synd
rom
e is
a b
enig
n co
nditi
on w
hich
, if l
eft u
ntre
ated
, may
pe
rsis
t for
wee
ks to
mon
ths.
•
Cut
aneo
us le
sion
s inv
olut
e sp
onta
neou
sly,
leav
ing
no sc
ars.
•
Rec
urre
nces
occ
ur in
app
roxi
mat
ely
30%
of p
atie
nts,
and
occu
r m
ore
ofte
n in
thos
e w
ith h
emat
olog
ic d
isor
ders
. •
The
mos
t effe
ctiv
e th
erap
y fo
r Sw
eet’s
Syn
drom
e is
ora
l pre
dnis
one
(0.5
-1m
g/kg
/day
) for
4-6
wee
ks. T
here
is p
rom
pt re
lief o
f cut
aneo
us
and
extra
cuta
neou
s man
ifest
atio
ns. I
n so
me
patie
nts,
prol
onge
d lo
w
dose
pre
dnis
one
for a
n ad
ditio
nal 2
-3 m
onth
s may
be
nece
ssar
y to
su
ppre
ss re
curr
ence
s. (1
) •
Whe
n th
e le
sion
s are
few
and
loca
lized
, top
ical
supe
rpot
ent o
r in
trale
sion
al c
ortic
oste
roid
s and
/or t
opic
al c
alci
neur
in in
hibi
tors
m
ay h
elp.
•
Maj
or a
ltern
ativ
e st
eroi
d-sp
arin
g dr
ugs a
re p
otas
sium
iodi
de,
daps
one
and
colc
hici
ne. N
on-s
tero
idal
ant
i-inf
lam
mat
ory
(e.g
. in
dom
etha
cin,
nap
roxe
n, su
linda
c) c
lofa
zim
ine,
cyc
losp
orin
e,
thal
idom
ide
and
inte
rfer
on-a
lpha
hav
e al
so b
een
repo
rted
to le
ad to
im
prov
emen
t of S
wee
t’s sy
ndro
me.
(1)
Figu
re II
Figu
re IV
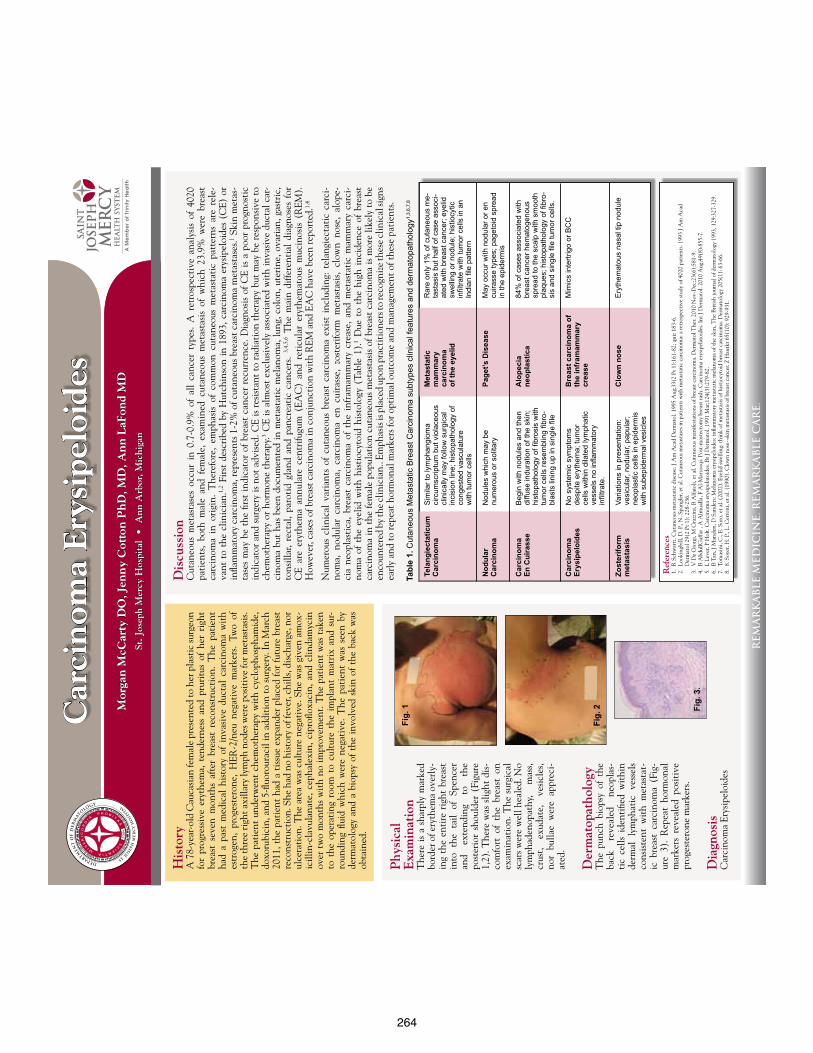
264
Car
cin
oma
Ery
sipe
loid
esM
orga
n M
cCar
ty D
O, J
enn
y C
otto
n P
hD
, MD
, An
n L
aFon
d M
D
St. J
osep
h M
ercy
Hos
pita
l •
Ann
Arb
or, M
ichi
gan
REM
AR
KA
BLE
MED
ICIN
E. R
EMA
RK
AB
LE C
AR
E.
Phy
sica
lE
xam
inat
ion
The
re i
s a
shar
ply
mar
ked
bord
er o
f ery
them
a ov
erly
-in
g th
e en
tire
rig
ht b
reas
t in
to t
he t
ail
of S
penc
er
and
exte
ndin
g to
th
e po
ster
ior
shou
lder
(Fi
gure
1,
2). T
here
was
slig
ht d
is-
com
fort
of
the
brea
st o
n ex
amin
atio
n. T
he s
urgi
cal
scar
s w
ere
wel
l hea
led.
No
lym
phad
enop
athy
, m
ass,
crus
t, ex
udat
e,
vesi
cles
, no
r bu
llae
wer
e ap
prec
i-at
ed.
Der
mat
opat
holo
gyT
he p
unch
bio
psy
of t
he
back
re
veal
ed
neop
las-
tic
cells
ide
ntifi
ed w
ithi
n de
rmal
lym
phat
ic v
esse
ls
cons
iste
nt w
ith
met
asta
t-ic
bre
ast
carc
inom
a (F
ig-
ure
3).
Rep
eat
horm
onal
m
arke
rs r
evea
led
posi
tive
pr
oges
tero
ne m
arke
rs.
Dia
gnos
isC
arci
nom
a Er
ysip
eloi
des
Tabl
e 1.
Cut
aneo
us M
etas
tatic
Bre
ast C
arci
nom
a su
btyp
es c
linic
al fe
atur
es a
nd d
erm
atop
atho
logy
1,3,
6,7,
8
His
tory
A 7
8-ye
ar-o
ld C
auca
sian
fem
ale
pres
ente
d to
her
pla
stic
surg
eon
for
prog
ress
ive
eryt
hem
a, t
ende
rnes
s an
d pr
urit
us o
f he
r ri
ght
brea
st s
even
mon
ths
afte
r br
east
rec
onst
ruct
ion.
The
pat
ient
ha
d a
past
med
ical
his
tory
of
inva
sive
duc
tal
carc
inom
a w
ith
estr
ogen
, pr
oges
tero
ne,
HER
-2/n
eu n
egat
ive
mar
kers
. Tw
o of
th
e th
ree
righ
t axi
llary
lym
ph n
odes
wer
e po
siti
ve fo
r met
asta
sis.
The
pat
ient
und
erw
ent
chem
othe
rapy
wit
h cy
clop
hosp
ham
ide,
do
xoru
bici
n, a
nd 5
-fluo
rour
acil
in a
ddit
ion
to s
urge
ry. I
n M
arch
20
11, t
he p
atie
nt h
ad a
tis
sue
expa
nder
pla
ced
for
futu
re b
reas
t re
cons
truc
tion
. She
had
no
hist
ory
of fe
ver,
chill
s, di
scha
rge,
nor
ul
cera
tion
. The
are
a w
as c
ultu
re n
egat
ive.
She
was
giv
en a
mox
-ic
illin
-cla
vula
nate
, ce
phal
exin
, ci
profl
oxac
in,
and
clin
dam
ycin
ov
er t
wo
mon
ths
wit
h no
impr
ovem
ent.
The
pat
ient
was
tak
en
to t
he o
pera
ting
roo
m t
o cu
ltur
e th
e im
plan
t m
atri
x an
d su
r-ro
undi
ng fl
uid
whi
ch w
ere
nega
tive
. T
he p
atie
nt w
as s
een
by
derm
atol
ogy
and
a bi
opsy
of
the
invo
lved
ski
n of
the
bac
k w
as
obta
ined
.
Ref
eren
ces
1. R
Sch
war
tz. C
utan
eous
met
asta
tic
dise
ase.
J A
m A
cad
Der
mat
ol. 1
995
Aug
;33(
2 Pt
1):
161-
82; q
uiz 1
83-6
.2.
Loo
king
bill,
D. P
., N
. Spa
ngle
r, et
al.
Cut
aneo
us m
etas
tase
s in
pati
ents
wit
h m
etas
tati
c ca
rcin
oma:
a re
tros
pect
ive
stud
y of
402
0 pa
tien
ts. 1
993
J Am
Aca
d
Der
mat
ol 2
9(2
Pt 1
): 2
28-2
36.
3. V
De
Gio
rgi,
M G
razz
ini,
B A
lfaio
li, e
t al.
Cut
aneo
us m
anife
stat
ions
of b
reas
t car
cino
ma.
Der
mat
ol T
her.
2010
Nov
-Dec
;23(
6):5
81-9
.4.
B A
bdul
lGaf
far ,
A A
lmua
lla, F
Al-
Mar
zooq
i. Po
st-m
aste
ctom
y br
east
rash
. Car
cino
ma
erys
ipel
atoi
des.
Int J
Der
mat
ol. 2
010
Aug
;49(
8):8
55-7
.5.
L L
ever
, P H
olt.
Car
cino
ma
erys
ipel
atoi
des.
Br J
Der
mat
ol. 1
991
Mar
;124
(3):
279-
82.
6. B
Tan
, J M
arsd
en, D
San
ders
: Mel
anom
a er
ysip
eloi
des:
infla
mm
ator
y m
etas
tati
c m
elan
oma
of th
e sk
in, T
he B
riti
sh jo
urna
l of d
erm
atol
ogy
1993
, 129
:327
-329
.7.
Tom
asin
i, C
., E.
Sor
o, e
t al.
(200
2). E
yelid
swel
ling:
thin
k of
met
asta
sis o
f his
tioc
ytoi
d br
east
car
cino
ma.
Der
mat
olog
y 20
5(1)
: 63-
66.
8. 8
. Soy
er, H
. P.,
L. C
erro
ni, e
t al.
(199
0). C
low
n no
se--
skin
met
asta
sis o
f bre
ast c
ance
r. Z
Hau
tkr 6
5(10
): 9
29-9
31.
Dis
cuss
ion
Cut
aneo
us m
etas
tase
s oc
cur
in 0
.7-0
.9%
of
all
canc
er t
ypes
. A
ret
rosp
ecti
ve a
naly
sis
of 4
020
pati
ents
, bo
th m
ale
and
fem
ale,
exa
min
ed c
utan
eous
met
asta
sis
of w
hich
23.
9% w
ere
brea
st
carc
inom
a in
ori
gin.
The
refo
re,
emph
asis
of
com
mon
cut
aneo
us m
etas
tati
c pa
tter
ns a
re r
ele-
vant
to
the
clin
icia
n.1,
2 Fi
rst
desc
ribe
d by
Hut
chin
son
in 1
893,
car
cino
ma
erys
ipel
oide
s (C
E) o
r in
flam
mat
ory
carc
inom
a, r
epre
sent
s 1-
2% o
f cut
aneo
us b
reas
t ca
rcin
oma
met
asta
ses.1 S
kin
met
as-
tase
s m
ay b
e th
e fir
st i
ndic
ator
of
brea
st c
ance
r re
curr
ence
. Dia
gnos
is o
f C
E is
a p
oor
prog
nost
ic
indi
cato
r an
d su
rger
y is
not
adv
ised
. CE
is r
esis
tant
to
radi
atio
n th
erap
y bu
t m
ay b
e re
spon
sive
to
chem
othe
rapy
or
horm
one
ther
apy.
3 CE
is a
lmos
t ex
clus
ivel
y as
soci
ated
wit
h in
vasi
ve d
ucta
l car
-ci
nom
a bu
t ha
s be
en d
ocum
ente
d in
met
asta
tic
mel
anom
a, lu
ng, c
olon
, ute
rine
, ova
rian
, gas
tric
, to
nsill
ar,
rect
al,
paro
tid
glan
d an
d pa
ncre
atic
can
cers
. 3,
4,5,
6 T
he m
ain
diffe
rent
ial
diag
nose
s fo
r C
E ar
e er
ythe
ma
annu
lare
cen
trifu
gum
(EA
C)
and
reti
cula
r er
ythe
mat
ous
muc
inos
is (
REM
).
How
ever
, cas
es o
f bre
ast c
arci
nom
a in
con
junc
tion
wit
h R
EM a
nd E
AC
hav
e be
en re
port
ed.1,
4
Num
erou
s cl
inic
al v
aria
nts
of c
utan
eous
bre
ast
carc
inom
a ex
ist
incl
udin
g: t
elan
giec
tati
c ca
rci-
nom
a, n
odul
ar c
arci
nom
a, c
arci
nom
a en
cui
rass
e, z
oste
rifo
rm m
etas
tasi
s, cl
own
nose
, al
ope-
cia
neop
last
ica,
bre
ast
carc
inom
a of
the
inf
ram
amm
ary
crea
se,
and
met
asta
tic
mam
mar
y ca
rci-
nom
a of
the
eye
lid w
ith
hist
iocy
toid
his
tolo
gy (
Tabl
e 1)
.1 D
ue t
o th
e hi
gh i
ncid
ence
of
brea
st
carc
inom
a in
the
fem
ale
popu
lati
on c
utan
eous
met
asta
sis
of b
reas
t ca
rcin
oma
is m
ore
likel
y to
be
enco
unte
red
by th
e cl
inic
ian.
. Em
phas
is is
pla
ced
upon
pra
ctit
ione
rs to
reco
gniz
e th
ese
clin
ical
sign
s ea
rly
and
to re
peat
hor
mon
al m
arke
rs fo
r opt
imal
out
com
e an
d m
anag
emen
t of t
hese
pat
ient
s.Fi
g. 1
Fig.
2 Fig.
3.
Tela
ngie
ctat
icum
C
arci
nom
a
Nod
ular
C
arci
nom
a
Car
cino
ma
En C
uira
sse
Car
cino
ma
Er
ysip
eloi
des
Zost
erifo
rm
met
asta
sis
Sim
ilar t
o ly
mph
angi
oma
ci
rcum
scrip
tum
but
vio
lace
ous
clin
ical
ly m
ay fo
llow
sur
gica
l in
cisi
on li
ne; h
isto
path
olog
y of
co
nges
ted
vasc
ulat
ure
w
ith tu
mor
cel
ls
Nod
ules
whi
ch m
ay b
e
num
erou
s or
sol
itary
Beg
in w
ith n
odul
es a
nd th
en
diffu
se in
dura
tion
of th
e sk
in;
hist
opat
holo
gy o
f fibr
osis
with
tu
mor
cel
ls re
sem
blin
g fib
ro-
blas
ts li
ning
up
in s
ingl
e fil
e
No
syst
emic
sym
ptom
s
desp
ite e
ryth
ema;
tum
or
cells
with
in d
ilate
d ly
mph
atic
ve
ssel
s no
infla
mm
ator
y
infil
trate
.
Varia
tions
in p
rese
ntat
ion:
ve
sicu
lar,
nodu
lar,
papu
lar;
neop
last
ic c
ells
in e
pide
rmis
w
ith s
ubep
ider
mal
ves
icle
s
Met
asta
tic
mam
mar
y
carc
inom
a
of th
e ey
elid
Page
t’s D
isea
se
Alo
peci
a
neop
last
ica
Bre
ast c
arci
nom
a of
th
e in
fram
amm
ary
crea
se
Clo
wn
nose
Rar
e on
ly 1
% o
f cut
aneo
us m
e-ta
stas
is b
ut h
alf o
f cas
e as
soci
-at
ed w
ith b
reas
t can
cer;
eyel
id
swel
ling
or n
odul
e; h
istio
cytic
in
filtra
te w
ith tu
mor
cel
ls in
an
Indi
an fi
le p
atte
rn
May
occ
ur w
ith n
odul
ar o
r en
cuira
sse
type
s; p
aget
oid
spre
ad
in th
e ep
ider
mis
84%
of c
ases
ass
ocia
ted
with
br
east
can
cer h
emat
ogen
ous
spre
ad to
the
scal
p w
ith s
moo
th
plaq
ues;
his
topa
thol
ogy
of fi
bro-
sis
and
sing
le fi
le tu
mor
cel
ls.
Mim
ics
inte
rtrig
o or
BC
C
Ery
them
atou
s na
sal t
ip n
odul
e
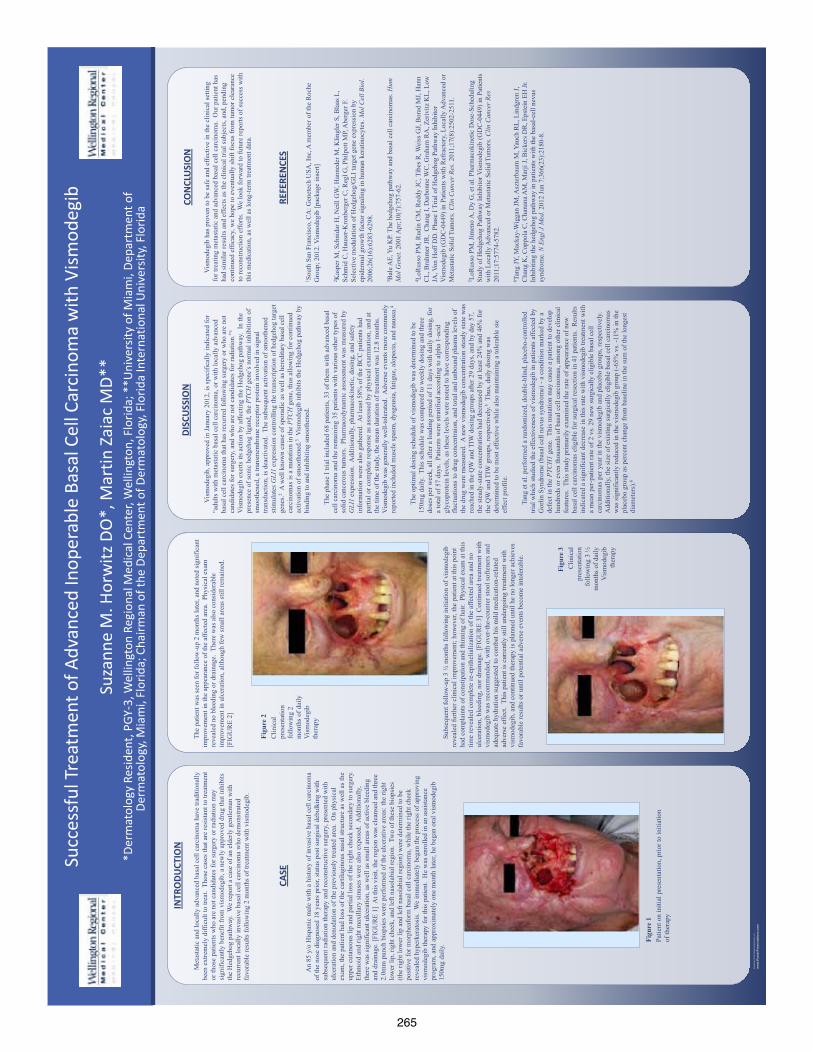
265
QU
ICK
TIPS
(-
-TH
IS S
ECTI
ON
DO
ES N
OT
PRIN
T--)
This
Pow
erPo
int
tem
plat
e re
quir
es b
asic
Pow
erPo
int
(ver
sion
200
7 or
new
er)
skill
s. B
elow
is a
list
of
com
mon
ly a
sked
que
stio
ns s
peci
fic
to t
his
tem
plat
e.
If y
ou a
re u
sing
an
olde
r ve
rsio
n of
Pow
erPo
int
som
e te
mpl
ate
feat
ures
may
not
wor
k pr
oper
ly.
U
sing
the
tem
plat
e
Veri
fyin
g th
e qu
alit
y of
you
r gr
aphi
cs
Go
to t
he V
IEW
men
u an
d cl
ick
on Z
OO
M t
o se
t yo
ur
pref
erre
d m
agni
fica
tion
. Th
is t
empl
ate
is a
t 10
0%
the
size
of
the
fina
l pos
ter.
All
text
and
gra
phic
s w
ill
be p
rint
ed a
t 10
0% t
heir
siz
e. T
o se
e w
hat
your
po
ster
will
look
like
whe
n pr
inte
d, s
et t
he z
oom
to
100%
and
eva
luat
e th
e qu
alit
y of
all
your
gra
phic
s be
fore
you
sub
mit
you
r po
ster
for
pri
ntin
g.
Usi
ng t
he p
lace
hold
ers
To a
dd t
ext
to t
his
tem
plat
e cl
ick
insi
de a
pl
aceh
olde
r an
d ty
pe in
or
past
e yo
ur t
ext.
To
mov
e a
plac
ehol
der,
clic
k on
it o
nce
(to
sele
ct it
), p
lace
yo
ur c
urso
r on
its
fram
e an
d yo
ur c
urso
r w
ill c
hang
e to
thi
s sy
mbo
l:
Then
, cl
ick
once
and
dra
g it
to
its
new
loca
tion
whe
re y
ou c
an r
esiz
e it
as
need
ed.
Addi
tion
al p
lace
hold
ers
can
be f
ound
on
the
left
si
de o
f th
is t
empl
ate.
M
odif
ying
the
layo
ut
This
tem
plat
e ha
s fo
ur
diff
eren
t co
lum
n la
yout
s.
Righ
t-cl
ick
your
mou
se
on t
he b
ackg
roun
d an
d
clic
k on
“La
yout
” to
see
th
e la
yout
opt
ions
. Th
e co
lum
ns in
the
pro
vide
d la
yout
s ar
e fi
xed
and
cann
ot b
e m
oved
but
adv
ance
d us
ers
can
mod
ify
any
layo
ut b
y go
ing
to V
IEW
and
the
n SL
IDE
MAS
TER.
Im
port
ing
text
and
gra
phic
s fr
om e
xter
nal s
ourc
es
TEXT
: Pa
ste
or t
ype
your
tex
t in
to a
pre
-exi
stin
g pl
aceh
olde
r or
dra
g in
a n
ew p
lace
hold
er f
rom
the
le
ft s
ide
of t
he t
empl
ate.
Mov
e it
any
whe
re a
s ne
eded
. PH
OTO
S: D
rag
in a
pic
ture
pla
ceho
lder
, si
ze it
fir
st,
clic
k in
it a
nd in
sert
a p
hoto
fro
m t
he m
enu.
TA
BLES
: Yo
u ca
n co
py a
nd p
aste
a t
able
fro
m a
n ex
tern
al d
ocum
ent
onto
thi
s po
ster
tem
plat
e. T
o ad
just
th
e w
ay t
he t
ext
fits
wit
hin
the
cells
of
a ta
ble
that
has
bee
n pa
sted
, ri
ght-
clic
k on
the
tab
le,
clic
k FO
RMAT
SH
APE
the
n cl
ick
on T
EXT
BOX
and
chan
ge t
he IN
TERN
AL M
ARG
IN v
alue
s to
0.2
5 M
odif
ying
the
col
or s
chem
e To
cha
nge
the
colo
r sc
hem
e of
thi
s te
mpl
ate
go t
o th
e “D
esig
n” m
enu
and
clic
k on
“Co
lors
”. Y
ou c
an
choo
se f
rom
the
pro
vide
col
or c
ombi
nati
ons
or y
ou
can
crea
te y
our
own.
QU
ICK
DES
IGN
GU
IDE
(--T
HIS
SEC
TIO
N D
OES
NO
T PR
INT-
-)
Th
is P
ower
Poin
t 20
07 t
empl
ate
prod
uces
a 3
6”x4
8”
prof
essi
onal
po
ster
. It
will
sav
e yo
u va
luab
le t
ime
plac
ing
titl
es,
subt
itle
s, t
ext,
and
gra
phic
s.
Use
it t
o cr
eate
you
r pr
esen
tati
on.
Then
sen
d it
to
Post
erPr
esen
tati
ons.
com
for
pre
miu
m q
ualit
y, s
ame
day
affo
rdab
le p
rint
ing.
W
e pr
ovid
e a
seri
es o
f on
line
tuto
rial
s th
at w
ill
guid
e yo
u th
roug
h th
e po
ster
des
ign
proc
ess
and
answ
er y
our
post
er p
rodu
ctio
n qu
esti
ons.
Vi
ew o
ur o
nlin
e tu
tori
als
at:
htt
p://
bit.
ly/P
oste
r_cr
eati
on_h
elp
(c
opy
and
past
e th
e lin
k in
to y
our
web
bro
wse
r).
For
assi
stan
ce a
nd t
o or
der
your
pri
nted
pos
ter
call
Post
erPr
esen
tati
ons.
com
at 1.
866.
649.
3004
Obj
ect
Plac
ehol
ders
Use
the
pla
ceho
lder
s pr
ovid
ed b
elow
to
add
new
el
emen
ts t
o yo
ur p
oste
r: D
rag
a pl
aceh
olde
r on
to
the
post
er a
rea,
siz
e it
, an
d cl
ick
it t
o ed
it.
Sect
ion
Hea
der
plac
ehol
der
Mov
e th
is p
refo
rmat
ted
sect
ion
head
er p
lace
hold
er
to t
he p
oste
r ar
ea t
o ad
d an
othe
r se
ctio
n he
ader
. U
se s
ecti
on h
eade
rs t
o se
para
te t
opic
s or
con
cept
s w
ithi
n yo
ur p
rese
ntat
ion.
Te
xt p
lace
hold
er
Mov
e th
is p
refo
rmat
ted
text
pla
ceho
lder
to
the
post
er t
o ad
d a
new
bod
y of
tex
t.
Pict
ure
plac
ehol
der
Mov
e th
is g
raph
ic p
lace
hold
er o
nto
your
pos
ter,
siz
e it
fir
st,
and
then
clic
k it
to
add
a pi
ctur
e to
the
po
ster
.
RES
EAR
CH
PO
STER
PR
ESEN
TATI
ON
DES
IGN
© 2
012
ww
w.P
oste
rPre
sent
atio
ns.c
om
© 2
012
Post
erPr
esen
tatio
ns.c
om
2
117
Four
th S
tree
t , U
nit C
Ber
kele
y CA
947
10
p
oste
rpre
sent
er@
gmai
l.com
St
uden
t di
scou
nts
are
avai
labl
e on
our
Fac
eboo
k pa
ge.
Go
to P
oste
rPre
sent
atio
ns.c
om a
nd c
lick
on t
he F
B ic
on.
Met
asta
tic a
nd lo
cally
adv
ance
d ba
sal c
ell c
arci
nom
a ha
ve tr
aditi
onal
ly
been
ext
rem
ely
diffi
cult
to tr
eat.
Tho
se c
ases
that
are
resi
stan
t to
treat
men
t or
thos
e pa
tient
s who
are
not
can
dida
tes
for s
urge
ry o
r rad
iatio
n m
ay
sign
ifica
ntly
ben
efit
from
vis
mod
egib
, a n
ewly
app
rove
d dr
ug th
at in
hibi
ts
the
Hed
geho
g pa
thw
ay.
We
repo
rt a
case
of a
n el
derly
gen
tlem
an w
ith
recu
rren
t loc
ally
inva
sive
bas
al c
ell c
arci
nom
a w
ho d
emon
stra
ted
favo
rabl
e re
sults
follo
win
g 2
mon
ths
of tr
eatm
ent w
ith v
ism
odeg
ib.
INTR
ODU
CTIO
N
CASE
Vis
mod
egib
, app
rove
d in
Janu
ary
2012
, is s
peci
fical
ly in
dica
ted
for
“adu
lts w
ith m
etas
tatic
bas
al c
ell c
arci
nom
a, o
r with
loca
lly a
dvan
ced
basa
l cel
l car
cino
ma
that
has
recu
rred
follo
win
g su
rger
y or
who
are
not
ca
ndid
ates
for s
urge
ry, a
nd w
ho a
re n
ot c
andi
date
s for
radi
atio
n.”1
Vis
mod
egib
exe
rts it
s act
ion
by a
ffect
ing
the
Hed
geho
g pa
thw
ay.
In th
e pr
esen
ce o
f son
ic h
edge
hog
ligan
d, th
e PT
CH
gen
e’s n
orm
al in
hibi
tion
of
smoo
then
ed, a
tran
smem
bran
e re
cept
or p
rote
in in
volv
ed in
sign
al
trans
duct
ion,
is d
eact
ivat
ed.
The
subs
eque
nt a
ctiv
atio
n of
smoo
then
ed
stim
ulat
es G
LI1
expr
essi
on c
ontro
lling
the
trans
crip
tion
of h
edge
hog
targ
et
gene
s.2 A
wel
l kno
wn
caus
e of
spor
adic
as w
ell a
s her
edita
ry b
asal
cel
l ca
rcin
omas
is a
mut
atio
n in
the
PTC
H g
ene,
thus
allo
win
g fo
r con
tinue
d ac
tivat
ion
of sm
ooth
ened
.3 V
ism
odeg
ib in
hibi
ts th
e H
edge
hog
path
way
by
bind
ing
to a
nd in
hibi
ting
smoo
then
ed.
The
pha
se I
trial
incl
uded
68
patie
nts,
33 o
f the
m w
ith a
dvan
ced
basa
l ce
ll ca
rcin
oma
and
the
rem
aini
ng 3
5 pa
tient
s with
var
ious
oth
er ty
pes o
f so
lid c
ance
rous
tum
ors.
Pha
rmac
odyn
amic
ass
essm
ent w
as m
easu
red
by
GLI
1 ex
pres
sion
. A
dditi
onal
ly, p
harm
acok
inet
ic, d
osin
g, a
nd sa
fety
in
form
atio
n w
ere
also
gat
here
d. A
t lea
st 5
8% o
f the
BC
C p
atie
nts h
ad
parti
al o
r com
plet
e re
spon
se a
s ass
esse
d by
phy
sica
l exa
min
atio
n, a
nd a
t th
e tim
e of
the
stud
y, th
e m
ean
dura
tion
of tr
eatm
ent w
as 1
2.8
mon
ths.
V
ism
odeg
ib w
as g
ener
ally
wel
l-tol
erat
ed.
Adv
erse
eve
nts m
ore
com
mon
ly
repo
rted
incl
uded
mus
cle
spas
m, d
ysge
usia
, fat
igue
, alo
peci
a, a
nd n
ause
a.4
The
opt
imal
dos
ing
sche
dule
of v
ism
odeg
ib w
as d
eter
min
ed to
be
150m
g da
ily.
This
sche
dule
was
com
pare
d to
wee
kly
dosi
ng a
nd th
ree
dose
s per
wee
k, a
ll af
ter a
load
ing
perio
d of
11
days
with
dai
ly d
osin
g, fo
r a
tota
l of 5
7 da
ys.
Patie
nts w
ere
stra
tifie
d ac
cord
ing
to a
lpha
1-a
cid
glyc
opro
tein
leve
ls, a
s the
se le
vels
wer
e no
ted
to h
ave
corr
espo
ndin
g flu
ctua
tions
to d
rug
conc
entra
ion,
and
tota
l and
unb
ound
pla
sma
leve
ls o
f th
e dr
ug w
ere
mea
sure
d. A
new
vis
mod
egib
con
cent
ratio
n st
eady
stat
e w
as
reac
hed
in th
e Q
W a
nd T
IW d
osin
g gr
oups
afte
r 29
days
, and
by
day
57,
the
stea
dy-s
tate
con
cent
ratio
n ha
d de
crea
sed
by a
t lea
st 2
4% a
nd 4
6% fo
r th
e Q
W a
nd T
IW g
roup
s, re
spec
tivel
y.5
Thus
, dai
ly d
osin
g w
as
dete
rmin
ed to
be
mos
t effe
ctiv
e w
hile
als
o m
aint
aini
ng a
tole
rabl
e si
e ef
fect
pro
file.
Tan
g et
al.
perf
orm
ed a
rand
omiz
ed, d
oubl
e-bl
ind,
pla
cebo
-con
trolle
d tri
al w
hich
stud
ied
the
effe
ctiv
enes
s of
vis
mod
egib
in p
atie
nts a
ffect
ed b
y G
orlin
Syn
drom
e (b
asal
cel
l nev
us sy
ndro
me)
- a
cond
ition
mar
ked
by a
de
fect
in th
e PT
CH
1 ge
ne.
This
mut
atio
n m
ay c
ause
a p
atie
nt to
dev
elop
hu
ndre
ds o
r eve
n th
ousa
nds o
f bas
al c
ell c
arci
nom
as, a
mon
g ot
her c
linic
al
feat
ures
. Th
is st
udy
prim
arily
exa
min
ed th
e ra
te o
f app
eara
nce
of n
ew
basa
l cel
l car
cino
mas
elig
ible
for s
urgi
cal r
esec
tion
in 4
1 pa
tient
s. R
esul
ts
indi
cate
d a
sign
ifica
nt d
ecre
ase
in th
is ra
te w
ith v
ism
odeg
ib tr
eatm
ent w
ith
a m
ean
per-p
atie
nt ra
te o
f 2 v
s. 29
new
surg
ical
ly e
ligib
le b
asal
cel
l ca
rcin
omas
per
yea
r in
the
vism
odeg
ib a
nd p
lace
bo g
roup
s, re
spec
tivel
y.
Add
ition
ally
, the
size
of e
xist
ing
surg
ical
ly e
ligib
le b
asal
cel
l car
cino
mas
w
as si
gnifi
cant
ly re
duce
d in
the
vism
odeg
ib g
roup
(-65
% v
s. -1
1% in
the
plac
ebo
grou
p as
per
cent
cha
nge
from
bas
elin
e in
the
sum
of t
he lo
nges
t di
amet
ers)
.6
DISC
USS
ION
CO
NCL
USI
ON
V
ism
odeg
ib h
as p
rove
n to
be
safe
and
effe
ctiv
e in
the
clin
ical
setti
ng
for t
reat
ing
met
asta
tic a
nd a
dvan
ced
basa
l cel
l car
cino
ma.
Our
pat
ient
has
ha
d si
mila
r res
ults
and
effe
cts
as th
e cl
inic
al tr
ial s
ubje
cts,
and,
pen
ding
co
ntin
ued
effic
acy,
we
hope
to e
vent
ually
shi
ft fo
cus f
rom
tum
or c
lear
ance
to
reco
nstru
ctio
n ef
forts
. W
e lo
ok fo
rwar
d to
futu
re re
ports
of s
ucce
ss w
ith
this
med
icat
ion,
as w
ell a
s lon
g-te
rm tr
eatm
ent d
ata.
REFE
REN
CES
1 Sou
th S
an F
ranc
isco
, CA
: Gen
etec
h U
SA, I
nc, A
mem
ber o
f the
Roc
he
Gro
up; 2
012.
Vis
mod
egib
[pac
kage
inse
rt]
2 Kas
per M
, Sch
nida
r H, N
eill
GW
, Han
nede
r M, K
lingl
er S
, Bla
as L
, Sc
hmid
C, H
ause
r-Kro
nber
ger C
, Reg
l G, P
hilp
ott M
P, A
berg
er F
. Se
lect
ive
mod
ulat
ion
of H
edge
hog/
GLI
targ
et g
ene
expr
essi
on b
y ep
ider
mal
gro
wth
fact
or s
igna
ling
in h
uman
ker
atin
ocyt
es. M
ol C
ell B
iol.
2006
;26(
16):6
283-
6298
. 3 B
ale A
E, Y
u K
P. T
he h
edge
hog
path
way
and
bas
al c
ell c
arci
nom
as. H
um
Mol
Gen
et. 2
001
Apr
;10(
7):7
57-6
2.
4 LoR
usso
PM
, Rud
in C
M, R
eddy
JC, T
ibes
R, W
eiss
GJ,
Bor
ad M
J, H
ann
CL,
Bra
hmer
JR
, C
hang
I, D
arbo
nne
WC
, Gra
ham
RA
, Zer
ivitz
KL,
Low
JA
, Von
Hof
f DD
. Pha
se I
Tria
l of H
edge
hog
Path
way
Inhi
bito
r V
ism
odeg
ib (G
DC
-044
9) in
Pat
ient
s with
Ref
ract
ory,
Loc
ally
Adv
ance
d or
M
etas
tatic
Sol
id T
umor
s. C
lin C
ance
r Res
. 201
1;17
(8):2
502-
2511
. 5 L
oRus
so P
M, J
imen
o A
, Dy
G, e
t al.
Phar
mac
okin
etic
Dos
e-Sc
hedu
ling
Stud
y of
Hed
geho
g Pa
thw
ay In
hibi
tor V
ism
odeg
ib (G
DC
-044
9) in
Pat
ient
s w
ith L
ocal
ly A
dvan
ced
or M
etas
tatic
Sol
id T
umor
s. C
lin C
ance
r Res
20
11;1
7:57
74-5
782.
6 T
ang
JY, M
acka
y-W
igga
n JM
, Asz
terb
aum
M, Y
auch
RL,
Lin
dgre
n J,
Cha
ng K
, Cop
pola
C, C
hana
na A
M, M
arji
J, B
icke
rs D
R, E
pste
in E
H Jr
. In
hibi
ting
the
hedg
ehog
pat
hway
in p
atie
nts w
ith th
e ba
sal-c
ell n
evus
sy
ndro
me.
N E
ngl J
Med
. 201
2 Ju
n 7;
366(
23):2
180-
8.
A
n 85
y/o
His
pani
c m
ale
with
a h
isto
ry o
f inv
asiv
e ba
sal c
ell c
arci
nom
a of
the
nose
dia
gnos
ed 1
8 ye
ars p
rior,
stat
us p
ost s
urgi
cal d
ebul
king
with
su
bseq
uent
radi
atio
n th
erap
y an
d re
cons
truct
ive
surg
ery,
pre
sent
ed w
ith
ulce
ratio
n an
d de
nuda
tion
of th
e pr
evio
usly
trea
ted
area
. O
n ph
ysic
al
exam
, the
pat
ient
had
loss
of t
he c
artil
agin
ous
nasa
l stru
ctur
e as
wel
l as t
he
uppe
r cut
aneo
us li
p an
d pa
rtial
loss
of t
he ri
ght c
heek
seco
ndar
y to
surg
ery.
Et
hmoi
d an
d rig
ht m
axill
ary
sinu
ses w
ere
also
exp
osed
. A
dditi
onal
ly,
ther
e w
as si
gnifi
cant
ulc
erat
ion,
as w
ell a
s sm
all a
reas
of a
ctiv
e bl
eedi
ng
and
drai
nage
. [FI
GU
RE
1] A
t thi
s vis
it, th
e re
gion
was
cle
anse
d an
d th
ree
2.0m
m p
unch
bio
psie
s wer
e pe
rfor
med
of t
he u
lcer
ativ
e ar
eas:
the
right
lo
wer
lip,
righ
t che
ek, a
nd le
ft na
sola
bial
regi
on.
Two
of th
ese
biop
sies
(th
e rig
ht lo
wer
lip
and
left
naso
labi
al re
gion
) wer
e de
term
ined
to b
e po
sitiv
e fo
r mor
phea
form
bas
al c
ell c
arci
nom
a, w
hile
the
right
che
ek
reve
aled
hyp
erke
rato
sis.
We
imm
edia
tely
beg
an th
e pr
oces
s of a
ppro
ving
vi
smod
egib
ther
apy
for t
his p
atie
nt.
He
was
enr
olle
d in
an
assi
stan
ce
prog
ram
, and
app
roxi
mat
ely
one
mon
th la
ter,
he b
egan
ora
l vis
mod
egib
15
0mg
daily
.
Figu
re 3
C
linic
al
pres
enta
tion
follo
win
g 3
½
mon
ths
of d
aily
V
ism
odeg
ib
ther
apy
S
ubse
quen
t fol
low
-up
3 ½
mon
ths f
ollo
win
g in
itiat
ion
of v
ism
odeg
ib
reve
aled
furth
er c
linic
al im
prov
emen
t; ho
wev
er, t
he p
atie
nt a
t thi
s poi
nt
had
com
plai
nts
of c
onst
ipat
ion
and
thin
ning
of h
air.
Phy
sica
l exa
m a
t thi
s tim
e re
veal
ed c
ompl
ete
re-e
pith
elia
lizat
ion
of th
e af
fect
ed a
rea
and
no
ulce
ratio
n, b
leed
ing,
nor
dra
inag
e. [F
IGU
RE
3] C
ontin
ued
treat
men
t with
vi
smod
egib
was
reco
mm
ende
d, w
ith o
ver-t
he-c
ount
er s
tool
softe
ners
and
ad
equa
te h
ydra
tion
sugg
este
d to
com
bat h
is m
ild m
edic
atio
n-re
late
d ad
vers
e ef
fect
. Th
is p
atie
nt is
cur
rent
ly st
ill u
nder
goin
g tre
atm
ent w
ith
vism
odeg
ib, a
nd c
ontin
ued
ther
apy
is p
lann
ed u
ntil
he n
o lo
nger
ach
ieve
s fa
vora
ble
resu
lts o
r unt
il po
tent
ial a
dver
se e
vent
s bec
ome
into
lera
ble.
Figu
re 2
C
linic
al
pres
enta
tion
follo
win
g 2
mon
ths
of d
aily
V
ism
odeg
ib
ther
apy
T
he p
atie
nt w
as se
en fo
r fol
low
-up
2 m
onth
s lat
er, a
nd n
oted
sign
ifica
nt
impr
ovem
ent i
n th
e ap
pear
ance
of t
he a
ffect
ed a
rea.
Phy
sica
l exa
m
reve
aled
no
blee
ding
or d
rain
age.
The
re w
as a
lso
cons
ider
able
im
prov
emen
t in
ulce
ratio
n, a
lthou
gh fe
w sm
all a
reas
still
rem
aine
d.
[FIG
UR
E 2]
Figu
re 1
Pa
tient
on
initi
al p
rese
ntat
ion,
prio
r to
initi
atio
n of
ther
apy
*Der
mat
olog
y Re
siden
t, PG
Y-3,
Wel
lingt
on R
egio
nal M
edic
al C
ente
r, W
ellin
gton
, Flo
rida;
**U
nive
rsity
of M
iam
i, De
part
men
t of
Derm
atol
ogy,
Mia
mi,
Flor
ida;
Cha
irman
of t
he D
epar
tmen
t of D
erm
atol
ogy,
Flor
ida
Inte
rnat
iona
l Uni
vers
ity, F
lorid
a
Suza
nne
M. H
orw
itz D
O*,
Mar
tin Z
aiac
MD*
*
Succ
essf
ul T
reat
men
t of A
dvan
ced
Inop
erab
le B
asal
Cel
l Car
cino
ma
with
Vism
odeg
ib
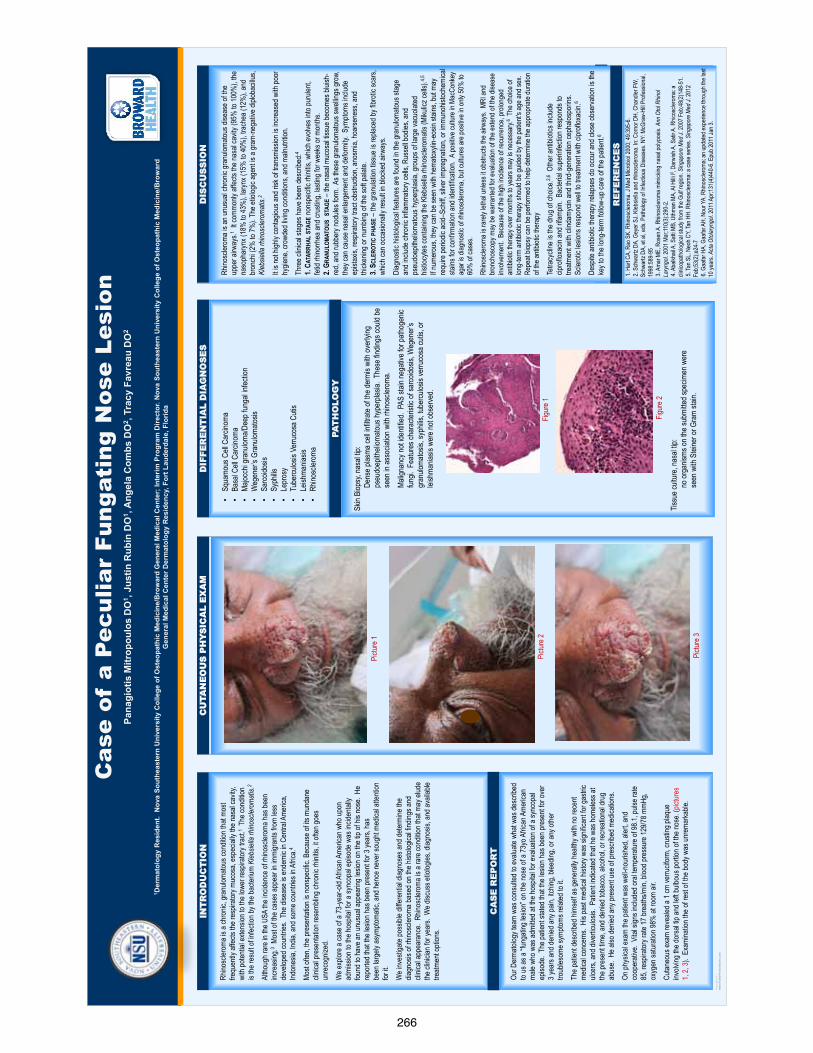
266
TEM
PLAT
E D
ESIG
N ©
200
8
ww
w.P
oste
rPre
sent
atio
ns.c
om
Cas
e of
a P
ecul
iar
Fung
atin
g N
ose
Lesi
on
Pana
giot
is M
itrop
oulo
s D
O1 ,
Just
in R
ubin
DO
1 , A
ngel
a C
ombs
DO
2 , Tr
acy
Favr
eau
DO
2
1 Der
mat
olog
y R
esid
ent.
Nov
a So
uthe
aste
rn U
nive
rsity
Col
lege
of O
steo
path
ic M
edic
ine/
Bro
war
d G
ener
al M
edic
al C
ente
r; In
terim
Pro
gram
Dire
ctor
. Nov
a So
uthe
aste
rn U
nive
rsity
Col
lege
of O
steo
path
ic M
edic
ine/
Bro
war
d G
ener
al M
edic
al C
ente
r Der
mat
olog
y R
esid
ency
, For
t Lau
derd
ale,
Flo
rida
INT
RO
DU
CT
ION
D
IFFE
RE
NT
IAL
DIA
GN
OS
ES
D
ISC
US
SIO
N
Refe
renc
es
Rhino
scler
oma i
s a ch
ronic
, gra
nulom
atous
cond
ition t
hat m
ost
frequ
ently
affec
ts the
resp
irator
y muc
osa,
espe
cially
the n
asal
cavit
y, wi
th po
tentia
l exte
nsion
to th
e low
er re
spira
tory t
ract.
1 Th
e con
dition
is
the re
sult o
f infec
tion b
y the
bacte
rium
Kleb
siella
rhino
scler
omat
is.2
Altho
ugh r
are i
n the
USA
the i
ncide
nce o
f rhin
oscle
roma
has b
een
incre
asing
.3 Mo
st of
the ca
ses a
ppea
r in im
migr
ants
from
less
deve
loped
coun
tries.
The
dise
ase i
s end
emic
in Ce
ntral
Amer
ica,
Indon
esia,
India
, and
some
coun
tries i
n Afric
a.4
Most
often
, the p
rese
ntatio
n is n
onsp
ecific
. Bec
ause
of its
mun
dane
cli
nical
pres
entat
ion re
semb
ling c
hron
ic rh
initis
, it of
ten go
es
unre
cogn
ized.
We e
xplor
e a ca
se of
a 73
-year
-old
Afric
an A
meric
an w
ho up
on
admi
ssion
to th
e hos
pital
for a
sync
opal
episo
de w
as in
ciden
tally
found
to ha
ve an
unus
ual a
ppea
ring
lesion
on th
e tip
of his
nose
. He
repo
rted t
hat th
e les
ion ha
s bee
n pre
sent
for 3
year
s, ha
s be
en la
rgely
asym
ptoma
tic, a
nd he
nce n
ever
soug
ht me
dical
atten
tion
for it.
We i
nves
tigate
poss
ible d
iffere
ntial
diagn
oses
and
deter
mine
the
diagn
osis
of rh
inosc
lerom
a ba
sed o
n the
histo
logica
l find
ings a
nd
clinic
al ap
pear
ance
. Rhin
oscle
roma
is a
rare
cond
ition t
hat m
ay el
ude
the cl
inicia
n for
year
s. W
e disc
uss e
tiolog
ies, d
iagno
sis, a
nd av
ailab
le tre
atmen
t opti
ons.
CA
SE
RE
PO
RT
Our D
erma
tolog
y tea
m wa
s con
sulte
d to e
valua
te wh
at wa
s des
cribe
d to
us as
a “fu
ngati
ng le
sion”
on th
e nos
e of a
73yo
Afric
an A
meric
an
male
who w
as ad
mitte
d at th
e hos
pital
for ev
aluati
on of
a sy
ncop
al ep
isode
. The
patie
nt sta
ted th
at the
lesio
n has
been
pres
ent fo
r ove
r 3 y
ears
and d
enied
any p
ain, it
ching
, blee
ding,
or an
y othe
r tro
ubles
ome s
ympto
ms re
lated
to it.
The p
atien
t des
cribe
d him
self a
s gen
erall
y hea
lthy w
ith no
rece
nt me
dical
conc
erns
. His
past
medic
al his
tory w
as si
gnific
ant fo
r gas
tric
ulcer
s, an
d dive
rticulo
sis. P
atien
t indic
ated t
hat h
e was
home
less a
t the
pres
ent ti
me, a
nd de
nied t
obac
co, a
lcoho
l, or r
ecre
ation
al dr
ug
abus
e. H
e also
denie
d any
pres
ent u
se of
pres
cribe
d med
icatio
ns.
On ph
ysica
l exa
m the
patie
nt wa
s well
-nou
rishe
d, ale
rt, an
d co
oper
ative
. Vita
l sign
s inc
luded
oral
tempe
ratur
e of 9
8.1, p
ulse r
ate
85, r
espir
atory
rate
17 br
eaths
/min,
bloo
d pre
ssur
e 129
/78 m
mHg,
oxyg
en sa
turati
on 98
% at
room
air.
Cutan
eous
exam
reve
aled a
1 cm
verru
cifor
m, cr
ustin
g plaq
ue
involv
ing th
e dor
sal ti
p and
left b
ulbou
s por
tion o
f the n
ose.
(pict
ures
1,
2, 3)
. Exa
mina
tion t
he of
rest
of the
body
was
unre
marka
ble.
CU
TAN
EO
US
PH
YS
ICA
L E
XA
M
Imag
e 1
Imag
e 2
Imag
e 3
•Sq
uamo
us C
ell C
arcin
oma
•Ba
sal C
ell C
arcin
oma
•Ma
jocch
i gra
nulom
a/Dee
p fun
gal in
fectio
n •
Weg
ener
’s Gr
anulo
matos
is •
Sarco
idosis
•
Syph
ilis
•Le
pros
y •
Tube
rculos
is Ve
rruco
sa C
utis
•Le
ishma
niasis
•
Rhino
scler
oma
Rhino
scler
oma i
s an u
nusu
al ch
ronic
gran
uloma
tous d
iseas
e of th
e up
per a
irway
s.1 It c
ommo
nly af
fects
the na
sal c
avity
(95%
to 10
0%),
the
naso
phar
ynx (
18%
to 43
%),
laryn
x (15
% to
40%
), tra
chea
(12%
), an
d br
onch
i (2%
to 7%
). Th
e etio
logic
agen
t is a
gram
-neg
ative
diplo
bacil
lus,
Kleb
siella
rhino
scler
omat
is.2
It is n
ot hig
hly co
ntagio
us an
d risk
of tr
ansm
ission
is in
creas
ed w
ith po
or
hygie
ne, c
rowd
ed liv
ing co
nditio
ns, a
nd m
alnutr
ition.
Thre
e clin
ical s
tages
have
been
desc
ribed
:4 1.
C ATA
RRHA
L STA
GE no
nspe
cific
rhini
tis, w
hich e
volve
s into
puru
lent,
fetid
rhino
rrhea
and c
rusti
ng, la
sting
for w
eeks
or m
onths
. 2.
G RAN
ULOM
ATOU
S ST
AGE –
the n
asal
muco
sal ti
ssue
beco
mes b
luish
-re
d, an
d rub
bery
nodu
les fo
rm. A
s the
se gr
anulo
matou
s swe
llings
grow
, the
y can
caus
e nas
al en
large
ment
and d
eform
ity. S
ympto
ms in
clude
ep
istax
is, re
spira
tory t
ract
obstr
uctio
n, an
osmi
a, ho
arse
ness
, and
thi
cken
ing or
numb
ing of
the s
oft pa
late.
3.
S CLE
ROTI
C PH
ASE –
the g
ranu
lation
tissu
e is r
eplac
ed by
fibro
tic sc
ars,
which
can o
ccas
ionall
y res
ult in
bloc
ked a
irway
s.
Diag
nosti
c hist
ologic
al fea
tures
are f
ound
in th
e gra
nulom
atous
stag
e an
d inc
lude c
hron
ic inf
lamma
tory c
ells,
Russ
ell bo
dies,
and
pseu
doep
itheli
omato
us h
yper
plasia
, gro
ups o
f larg
e vac
uolat
ed
histio
cytes
conta
ining
the K
lebsie
lla rh
inosc
lerom
atis (
Miku
licz c
ells).
4,5
If num
erou
s, the
y can
be se
en w
ith he
matox
ylin-
eosin
stain
s, bu
t may
re
quire
perio
dic ac
id–Sc
hiff, s
ilver
impr
egna
tion,
or im
muno
histoc
hemi
cal
stains
for c
onfirm
ation
and i
denti
ficati
on.
A po
sitive
cultu
re in
Mac
Conk
ey
agar
is di
agno
stic o
f rhin
oscle
roma
, but
cultu
res a
re po
sitive
in on
ly 50
% to
60
% of
case
s.
Rhino
scler
oma i
s rar
ely le
thal u
nless
it ob
struc
ts the
airw
ays.
MRI
and
bron
chos
copy
may
be w
arra
nted f
or ev
aluati
on of
the e
xtend
of th
e dise
ase
involv
emen
t. Be
caus
e of th
e high
incid
ence
of re
curre
nce,
prolo
nged
an
tibiot
ic the
rapy
over
mon
ths to
year
s may
is ne
cess
ary.6
The c
hoice
of
long-
term
antib
iotic
thera
py sh
ould
be gu
ided b
y the
patie
nt's a
ge an
d sex
. Re
peat
biops
y can
be pe
rform
ed to
help
deter
mine
the a
ppro
priat
e dur
ation
of
the an
tibiot
ic the
rapy
Tetra
cycli
ne is
the d
rug o
f cho
ice.2,6
Othe
r anti
biotic
s inc
lude
cipro
floxa
cin an
d rifa
mpin.
Bac
terial
supe
rinfec
tion r
espo
nds t
o tre
atmen
t with
clind
amyc
in an
d thir
d-ge
nera
tion c
epha
lospo
rins.
Sc
leroti
c les
ions r
espo
nd w
ell to
trea
tmen
t with
cipr
oflox
acin.
6
Desp
ite an
tibiot
ic the
rapy
relap
ses d
o occ
ur an
d clos
e obs
erva
tion i
s the
ke
y to t
he lo
ng-te
rm fo
llow-
up ca
re of
the p
atien
t.6
PAT
HO
LOG
Y
Skin
Biop
sy, n
asal
tip:
De
nse p
lasma
cell i
nfiltra
te of
the de
rmis
with
over
lying
pseu
doep
itheli
omato
us h
yper
plasia
. The
se fin
dings
could
be
se
en in
asso
ciatio
n with
rhino
scler
oma.
Ma
ligna
ncy n
ot ide
ntifie
d. P
AS st
ain ne
gativ
e for
patho
genic
fungi.
Fea
tures
char
acter
istic
of sa
rcoido
sis, W
egen
er’s
gr
anulo
matos
is, sy
philis
, tube
rculos
is ve
rruco
sa cu
tis, o
r
leish
mania
sis w
ere n
ot ob
serve
d. T
issue
cultu
re, n
asal
tip:
no
orga
nisms
on th
e sub
mitte
d spe
cimen
wer
e
seen
with
Stei
ner o
r Gra
m sta
in.
P
ictur
e 3
Pictu
re 2
Pictu
re 1
RE
FER
EN
CE
S
1. H
art C
A, R
ao S
K. R
hinos
clero
ma. J
Med
Micr
obiol
2000
; 49:3
95-6
. 2
. Sch
wartz
DA,
Gey
er S
J. Kl
ebsie
lla an
d rhin
oscle
roma
. In: C
orno
r DH,
Cha
ndler
FW
, Sc
hwar
tz DA
, et a
l, eds
. Path
ology
of In
fectio
us D
iseas
es. N
Y: M
cGra
w-Hi
ll Pro
fessio
nal,
1998
:589-
95
3. A
mar M
E, R
osen
A. R
hinos
clero
ma m
imick
ing na
sal p
olypo
sis. A
nn O
tol R
hinol
Lary
ngol.
2001
Mar
;110(
3):29
0-2.
4. A
balkh
ail A
, Satt
i MB,
Uthm
an M
A, A
l Hilli
F, D
arwi
sh A
, Sati
r A. R
hicos
clero
ma: a
cli
nicop
atholo
gical
study
from
the G
ulf re
gion.
Sing
apor
e M
ed J.
2007
Feb
;48(2
)148
-51.
5. T
an S
L, Ne
oh C
Y, Ta
n HH.
Rhin
oscle
roma
: a ca
se se
ries.
Sing
apor
e Med
J. 20
12
Feb;5
3(2)
;e24-
7 6
. Gaa
far H
A, G
aafar
AH,
Nou
r YA.
Rhin
oscle
roma
; an u
pdate
d exp
erien
ce th
roug
h the
last
10 ye
ars.
Acta
Oto
laryn
gol. 2
011 A
pr;13
1(4)
440-
6. Ep
ub 20
11 Ja
n 3.
Figu
re 2
Figu
re 1
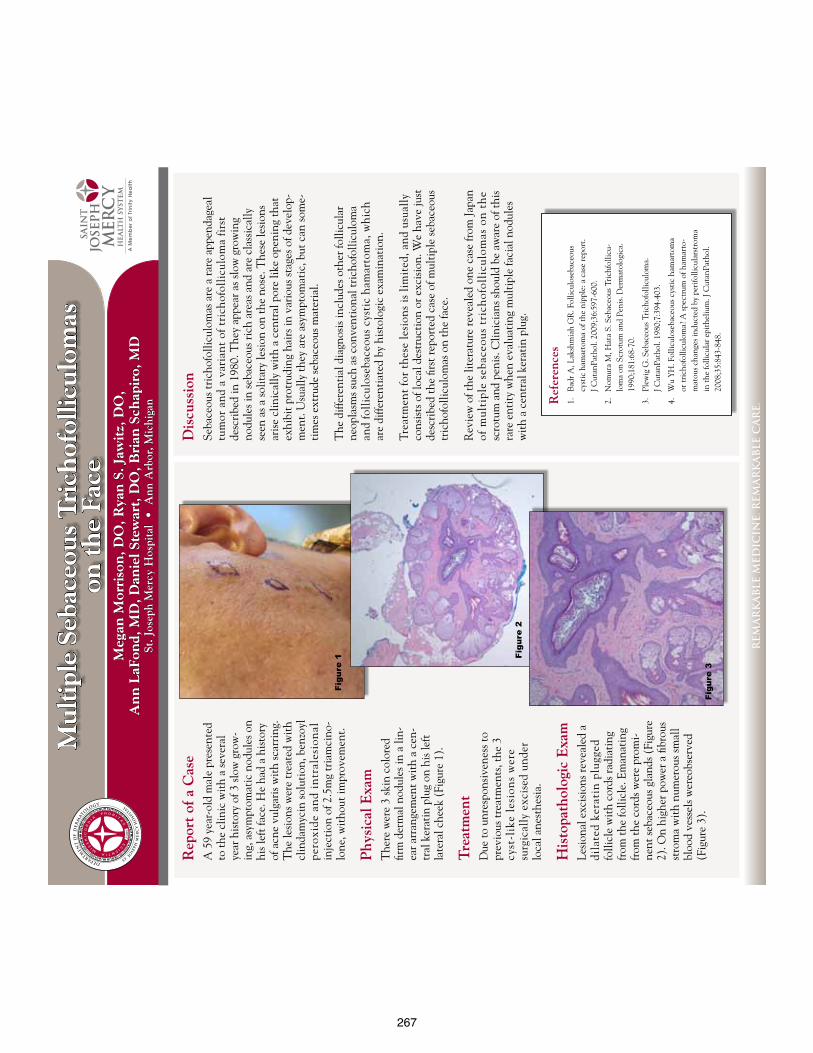
267
Mu
ltip
le S
ebac
eou
s T
rich
ofol
licu
lom
as
on t
he
Face
Meg
an M
orri
son
, DO
, Rya
n S
. Jaw
itz,
DO
, A
nn
LaF
ond,
MD
, Dan
iel S
tew
art,
DO
, Bri
an S
chap
iro,
MD
St. J
osep
h M
ercy
Hos
pita
l •
Ann
Arb
or, M
ichi
gan
REM
AR
KA
BLE
MED
ICIN
E. R
EMA
RK
AB
LE C
AR
E.
Ref
eren
ces
1.
Bad
r A, L
aksh
mia
h G
R. F
ollic
ulos
ebac
eous
cy
stic
ham
arto
ma
of th
e ni
pple
: a c
ase
repo
rt.
J Cut
anPa
thol
. 200
9;36
:597
-600
.
2.
Nom
ura
M, H
ata
S. S
ebac
eous
Tri
chfo
llicu
-lo
ma
on S
crot
um a
nd P
enis
. Der
mat
olog
ica.
19
90;1
81:6
8-70
.
3.
Plew
ig G
. Seb
aceo
us T
rich
ofol
licul
oma.
J C
utan
Path
ol. 1
980;
7:39
4-40
3.
4.
Wu
YH
. Fol
licul
oseb
aceo
us c
ysti
c ha
mar
tom
a or
tric
hofo
llicu
lom
a? A
spec
trum
of h
amar
to-
mat
ous c
hang
es in
duct
ed b
y pe
rifo
llicu
lars
trom
a in
the
folli
cula
r epi
thel
ium
. J C
utan
Path
ol.
2008
;35:
843-
848.
Dis
cuss
ion
Seba
ceou
s tri
chof
ollic
ulom
as a
re a
rare
app
enda
geal
tu
mor
and
a v
aria
nt o
f tri
chof
olli
culo
ma
firs
t
desc
ribe
d in
198
0. T
hey
appe
ar a
s slo
w g
row
ing
no
dule
s in
seba
ceou
s ric
h ar
eas a
nd a
re c
lass
ical
ly
seen
as a
solit
ary
lesi
on o
n th
e no
se. T
hese
lesi
ons
aris
e cl
inic
ally
wit
h a
cent
ral p
ore
like
open
ing
that
ex
hibi
t pro
trud
ing
hair
s in
vari
ous s
tage
s of d
evel
op-
men
t. U
sual
ly th
ey a
re a
sym
ptom
atic
, but
can
som
e-ti
mes
ext
rude
seba
ceou
s mat
eria
l.
The
diff
eren
tial
dia
gnos
is in
clud
es o
ther
folli
cula
r ne
opla
sms s
uch
as c
onve
ntio
nal t
rich
ofol
licul
oma
and
foll
icul
oseb
aceo
us c
ysti
c ha
mar
tom
a, w
hich
ar
e di
ffere
ntia
ted
by h
isto
logi
c ex
amin
atio
n.
Trea
tmen
t fo
r th
ese
lesi
ons
is li
mit
ed, a
nd u
sual
ly
cons
ists
of l
ocal
des
truc
tion
or e
xcis
ion.
We
have
just
de
scri
bed
the
first
repo
rted
cas
e of
mul
tipl
e se
bace
ous
tric
hofo
llicu
lom
as o
n th
e fa
ce.
Rev
iew
of t
he li
tera
ture
reve
aled
one
cas
e fr
om Ja
pan
of m
ulti
ple
seba
ceou
s tr
ich
ofol
licu
lom
as o
n t
he
sc
rotu
m a
nd p
enis
. Clin
icia
ns sh
ould
be
awar
e of
this
ra
re e
ntit
y w
hen
eval
uati
ng m
ulti
ple
faci
al n
odul
es
wit
h a
cent
ral k
erat
in p
lug.
Rep
ort
of a
Cas
eA
59
year
-old
mal
e pr
esen
ted
to th
e cl
inic
wit
h a
seve
ral
year
his
tory
of 3
slow
gro
w-
ing,
asy
mpt
omat
ic n
odul
es o
n hi
s lef
t fac
e. H
e ha
d a
hist
ory
of a
cne
vulg
aris
wit
h sc
arri
ng.
The
lesi
ons w
ere
trea
ted
wit
h cl
inda
myc
in so
luti
on, b
enzo
yl
pero
xide
an
d in
tral
esio
nal
in
ject
ion
of 2
.5m
g tr
iam
cino
-lo
ne, w
itho
ut im
prov
emen
t.
Phy
sica
l Exa
mT
here
wer
e 3
skin
col
ored
fir
m d
erm
al n
odul
es in
a li
n-ea
r arr
ange
men
t wit
h a
cen-
tral
ker
atin
plu
g on
his
left
la
tera
l che
ek (
Figu
re 1
).
Tre
atm
ent
Due
to u
nres
pons
iven
ess t
o pr
evio
us tr
eatm
ents
, the
3
cyst
-lik
e le
sion
s w
ere
su
rgic
ally
exc
ised
und
er
loca
l ane
sthe
sia.
His
topa
thol
ogic
Exa
mLe
sion
al e
xcis
ions
reve
aled
a
dila
ted
kera
tin
plu
gged
fo
llicl
e w
ith
cord
s rad
iati
ng
from
the
folli
cle.
Em
anat
ing
from
the
cord
s wer
e pr
omi-
nent
seba
ceou
s gla
nds (
Figu
re
2). O
n hi
gher
pow
er a
fibr
ous
stro
ma
wit
h nu
mer
ous s
mal
l bl
ood
vess
els w
ereo
bser
ved
(Fig
ure
3).
Figu
re 1 Fi
gure
2
Figu
re 3

268
Julia
n M
. Ngo
, DO,
Larg
o Med
ical C
ente
r, La
rgo,
Flor
ida
4707
CAS
E R
EPO
RT
A 39
year
old
heal
thy m
ale p
rese
nted
with
a 3-
4 ye
ar hi
stor
y of a
pr
ogre
ssive
ly en
larg
ing g
rowt
h on
the r
ight
ear.
Pas
t med
ical h
istor
y is
signi
fican
t for
dep
ress
ion,
anxie
ty. H
e den
ies a
fam
ily or
per
sona
l hi
stor
y of m
elan
oma
or no
n-m
elan
oma
skin
canc
ers.
Soc
ial h
istor
y is
posit
ive fo
r sm
okin
g for
man
y yea
rs. R
evie
w of
syst
ems i
s neg
ative
for
pain
, ten
dern
ess ,
or b
leed
ing o
f the
righ
t ear
. He d
enie
s any
co
nstit
utio
nal s
ympt
oms.
Exam
inat
ion
of th
e rig
ht ea
r rev
eals
a lar
ge 2
.7cm
X 1.
2cm
, exo
phyti
c, hy
perk
erat
otic,
ill-d
efin
ed, i
ndur
ated
pla
que (
Fig. 1
). N
o reg
iona
l lym
phad
enop
athy
is no
ted.
Hist
opat
holo
gy o
f thi
s les
ion
is
cons
isten
t with
inva
sive,
wel
l diff
eren
tiate
d sq
uam
ous c
ell
carc
inom
a.
Com
plet
e exc
ision
of th
e SCC
was
per
form
ed u
sing M
ohs
micr
ogra
phic
surg
ery.
The p
atie
nt w
as se
en m
onth
ly po
st-o
pera
tivel
y fo
r fol
low-
up an
d ha
d no
com
plica
tions
dur
ing t
he in
itial
mon
ths.
Ho
weve
r, he
miss
ed tw
o fol
low-
up ap
poin
tmen
ts 4
mon
ths a
fter h
is su
rger
y and
upo
n ret
urn,
2 cy
stic
nodu
les i
n the
pos
t-aur
icula
r reg
ion
were
note
d (F
ig. 2
). A
deno
path
y in
all o
ther
regi
ons w
ere n
egat
ive.
Hist
opat
holo
gic e
xam
inat
ion
of th
is le
sion w
as co
nsist
ent w
ith
met
asta
tic S
CC. T
he p
atie
nt w
as re
ferre
d fo
r che
mor
adio
ther
apy
follo
wed
by ri
ght n
eck d
issec
tion.
Cuta
neou
s Squ
amou
s Cel
l Car
cinom
a (C
SCC)
is th
e sec
ond
mos
t co
mm
on ty
pe of
skin
canc
er a
nd e
ach y
ear m
ore t
han
3,00
0,00
0 ca
ses a
re d
iagn
osed
wor
ldwi
de. 1 Al
thou
gh m
ost c
ases
can b
e cur
ed, a
sm
all p
erce
ntag
e can
caus
e sig
nific
ant m
orbi
dity
and
mor
talit
y.
Appr
oxim
atel
y 4%
can r
esul
t in n
odal
met
asta
sis a
nd 1
.5%
in d
eath
.1,
Give
n the
sign
ifica
nt im
pact
met
asta
tic C
SCC
can h
ave o
n pat
ient
s, it’
s im
porta
nt fo
r clin
ician
s to i
dent
ify hi
gh-ri
sk ca
ses e
arly
so
man
agem
ent c
an b
e opt
imize
d wi
th a
redu
ctio
n in m
orbi
dity
and
mor
talit
y for
thes
e pat
ient
s.
Ther
e are
no st
anda
rdize
d de
finiti
ons o
f hig
h-ris
k cut
aneo
us
squa
mou
s cel
l car
cinom
a (H
RCSC
C). D
iffer
ent s
tudi
es an
d gu
idel
ines
us
e diff
eren
t par
amet
ers i
n det
erm
inin
g HRC
SCC1,
2,4 .
Howe
ver,
amon
g the
diff
eren
t gui
delin
es in
the l
itera
ture
ther
e are
som
e wid
ely
acce
pted
par
amet
ers t
hat w
ould
aid
in id
entif
ying
high
-risk
pat
ient
s.
Thes
e fea
ture
s are
dim
ensio
ns la
rger
than
2 cm
in d
iam
eter
, thi
ckne
ss
grea
ter t
han 4
mm
, rec
urre
nt le
sion,
poo
rly d
iffer
entia
ted
tum
ors,
pres
ence
of p
erin
eura
l inva
sion,
lym
phov
ascu
lar i
nvas
ion,
loca
tion
(muc
osal
surfa
ces,
geni
talia
, “m
ask a
reas
” of
face
–ey
elid
s and
br
ows,
perio
rbita
l, lip
s, ea
rs, n
ose,
tem
ple,
pre
and
post
auric
ular
, ch
in),
imm
unos
uppr
essio
n, an
d or
gan
trans
plan
t pat
ient
s. As
you c
an
see f
rom
our
case
mul
tiple
high
-risk
feat
ures
wer
e pre
sent
in ou
r pa
tient
. On
ce it
’s de
term
ined
that
a pa
tient
has a
high
-risk
CSC
C , a
thor
ough
ph
ysica
l exa
min
atio
n sh
ould
be p
erfo
rmed
inclu
ding
dra
inin
g nod
al
basin
s1 . If n
o clin
ically
pal
pabl
e nod
es ar
e pre
sent
addi
tiona
l im
agin
g (CT
, MRI
) stu
dies
may
be p
erfo
rmed
in or
der t
o aid
in
eval
uatin
g fo
r pos
sible
subc
linica
l nod
al in
volve
men
t1 .
DIS
CUSS
ION
REF
EREN
CES
1.Le
Boeu
f NR,
Sch
mul
ts C
D. U
pdat
e on
the
Man
agem
ent o
f Hig
h-Ri
sk S
quam
ous C
ell C
arin
oma.
Se
min
Cut
an M
ed S
urg.
201
1 M
ar;3
0(1)
:26-
34
2.Pu
glia
no-M
auro
M, G
oldm
an G
. Moh
s sur
gery
is e
ffect
ive
for h
igh-
risk
cuta
neou
s squ
amou
s ce
ll ca
rcin
oma.
Der
mat
ol S
urg.
201
0 O
ct;3
6(10
):154
4-53
. 3.
Kwon
S, D
ong
ZM, W
u PC
. Sen
tinel
lym
ph n
ode
biop
sy fo
r hig
h-ris
k cu
tane
ous s
quam
ous c
ell
carc
inom
a: cl
inic
al e
xper
ienc
e an
d re
view
of l
itera
ture
. Wor
ld J
Surg
Onc
ol. 2
011
Jul 1
9;9:
80.
Revi
ew.
4.Ja
mbu
saria
-Pah
laja
ni A
, Hes
s SD,
Kat
z KA,
Ber
g D,
Sch
mul
ts C
D. U
ncer
tain
ty in
the
perio
pera
tive
man
agem
ent o
f hig
h-ris
k cu
tane
ous s
quam
ous c
ell c
arci
nom
a am
ong
Moh
s sur
geon
s. A
rch
Derm
atol
. 201
0 N
ov;1
46(1
1):1
225-
31.
5.Ve
ness
MJ,
Mor
gan
GJ, P
alm
e CE
, Geb
ski V
. Sur
gery
and
adj
uvan
t rad
ioth
erap
y in
pat
ient
s with
cu
tane
ous h
ead
and
neck
squa
mou
s cel
l car
cino
ma
met
asta
tic to
lym
ph n
odes
: com
bine
d tr
eatm
ent s
houl
d be
con
sider
ed b
est p
ract
ice.
Lar
yngo
scop
e. 2
005
May
;115
(5):8
70-5
. 6.
Mou
rouz
is C,
Boy
nton
A, G
rant
J, U
mar
T, W
ilson
A, M
acph
eson
D, P
ratt
C. C
utan
eous
hea
d an
d ne
ck S
CCs a
nd ri
sk o
f nod
al m
etas
tasis
- U
K ex
perie
nce.
J Cr
anio
max
illof
ac S
urg.
200
9 De
c;37
(8):4
43-7
. Epu
b 20
09 A
ug 2
7.
7.D'
Souz
a J,
Clar
k J.
Man
agem
ent o
f the
nec
k in
met
asta
tic c
utan
eous
squa
mou
s cel
l car
cino
ma
of
the
head
and
nec
k. C
urr O
pin
Oto
lary
ngol
Hea
d N
eck
Surg
. 201
1 Ap
r;19(
2):9
9-10
5. R
evie
w
FIG
URES
Howe
ver,
ther
e is n
o gol
d st
anda
rd fo
r rad
iolo
gic s
tagi
ng o
f CSC
C an
d se
nsiti
vity a
nd sp
ecifi
city a
re la
ckin
g1 . The
role
of se
ntin
el
lymph
node
bio
psy i
n nod
e neg
ative
HRC
SCC
patie
nts r
emai
n in
vest
igat
iona
l and
is cu
rrent
ly no
t a st
anda
rd
reco
mm
enda
tion1,
3 . How
ever
, it m
ay b
e a us
eful
tool
in th
e fut
ure
give
n ear
ly de
tect
ion
of no
dal d
iseas
e res
ults
in a
high
-cur
e rat
e (7
3%)1 .
Moh
s sur
gery
is th
e rec
omm
ende
d th
erap
y for
all H
RCSC
C an
d is
an ef
fect
ive m
onot
hera
py w
ith lo
w re
curre
nce r
ates
2 . The
re is
lim
ited
date
rega
rdin
g adj
uvan
t rad
ioth
erap
y, ex
cept
in p
atie
nts
with
per
ineu
ral in
vasio
n. In
case
of m
etas
tatic
CSC
C su
rger
y with
ad
juva
nt ra
diot
hera
py is
reco
mm
ende
d. C
hem
othe
rapy
is al
so an
op
tion.
Pa
tient
s sho
uld
be fo
llowe
d clo
sely
afte
r tre
atm
ent,
espe
cially
du
ring t
he fi
rst 2
year
s as m
ost m
etas
tasis
occ
ur d
urin
g thi
s tim
e.
1 2
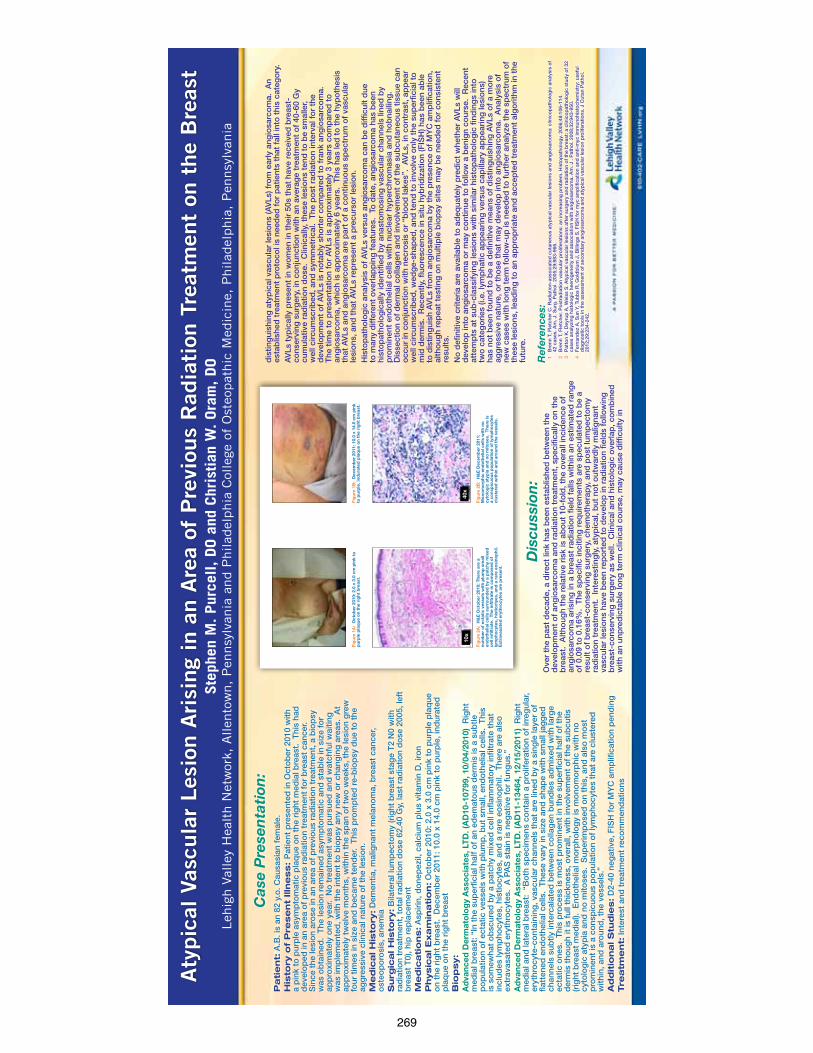
269
Aty
pic
al V
ascu
lar
Les
ion A
risi
ng
in a
n A
rea
of P
revi
ous
Rad
iati
on T
reat
men
t on
the
Bre
ast
Leh
igh V
alle
y H
ealt
h N
etw
ork,
Allen
tow
n,
Pen
nsy
lvan
ia a
nd P
hilad
elphia
Col
lege
of
Ost
eopat
hic
Med
icin
e, P
hilad
elphia
, P
ennsy
lvan
iaSte
phen
M. Pur
cell, DO a
nd C
hris
tian
W. Ora
m, DO R
efer
ence
s:1
Bre
nn T
, Fle
tche
r C
. Rad
iatio
n-as
soci
ated
cut
aneo
us a
typ
ical
vas
cula
r le
sio
ns a
nd a
ngio
sarc
om
a: c
linic
op
atho
log
ic a
naly
sis
of
42 c
ases
. Am
. J. S
urg
. Pat
hol.
2005
;29:
983-
966.
2 B
renn
T, F
letc
her.
Po
stra
dia
tion
vasc
ular
pro
lifer
atio
ns: a
n in
crea
sing
pro
ble
m. H
isto
pat
holo
gy.
200
6;48
:106
-114
.3
Pat
ton
K, D
eyru
p A
, Wei
ss S
. Aty
pic
al v
ascu
lar
lesi
ons
aft
er s
urg
ery
and
rad
iatio
n o
f th
e b
reas
t: a
clin
ico
pat
holo
gic
stu
dy
of
32
case
s an
alyz
ing
his
tolo
gic
hee
rog
enei
ty a
nd a
sso
ciat
ion
with
ang
iosa
rco
ma.
Am
. J .
Pat
hol.
2008
;32:
943-
950.
4 F
erna
ndez
A, S
un Y
, Tub
bs
R, G
old
blu
m J
, Bill
ing
s S
. FIS
H f
or
myc
am
plif
icat
ion
and
ant
i-m
yc im
mun
ohi
sto
chem
istr
y: u
sefu
l d
iag
nost
ic t
oo
ls in
the
ass
essm
ent
of
seco
ndar
y an
gio
sarc
om
a an
d a
typ
ical
vas
cula
r le
sio
n p
rolif
erat
ions
. J C
utan
Pat
hol.
2012
;29:
234-
242.
Pa
tie
nt:
A.B
. is
an 8
2 y.
o. C
ausa
sian
fem
ale.
His
tory
of
Pre
se
nt
Illn
ess:
Pat
ient
pre
sent
ed in
Oct
ob
er 2
010
with
a
pin
k to
pur
ple
asy
mp
tom
atic
pla
que
on
the
rig
ht m
edia
l bre
ast.
Thi
s ha
d
dev
elo
ped
in a
n ar
ea o
f p
revi
ous
rad
iatio
n tr
eatm
ent
for
bre
ast
canc
er.
Sin
ce t
he le
sio
n ar
ose
in a
n ar
ea o
f p
revi
ous
rad
iatio
n tr
eatm
ent,
a b
iop
sy
was
ob
tain
ed.
The
lesi
on
rem
aine
d a
sym
pto
mat
ic a
nd s
tab
le in
siz
e fo
r ap
pro
xim
atel
y o
ne y
ear.
No
tre
atm
ent
was
pur
sued
and
wat
chfu
l wai
ting
w
as im
ple
men
ted
, with
the
inte
nt t
o b
iop
sy a
ny n
ew o
r ch
ang
ing
are
as.
At
app
roxi
mat
ely
twel
ve m
ont
hs, w
ithin
the
sp
an o
f tw
o w
eeks
, the
lesi
on
gre
w
four
tim
es in
siz
e an
d b
ecam
e te
nder
. T
his
pro
mp
ted
re-
bio
psy
due
to
the
ag
gre
ssiv
e cl
inic
al n
atur
e o
f th
e le
sio
n.
M
ed
ica
l H
isto
ry:
Dem
entia
, mal
igna
nt m
elan
om
a, b
reas
t ca
ncer
, o
steo
po
rosi
s, a
nem
iaS
urg
ica
l H
isto
ry:
Bila
tera
l lum
pec
tom
y (r
ight
bre
ast
stag
e T
2 N
0 w
ith
rad
iatio
n tr
eatm
ent,
to
tal r
adia
tion
do
se 6
2.40
Gy,
last
rad
iatio
n d
ose
200
5, le
ft
bre
ast
T0)
, hip
rep
lace
men
tM
ed
ica
tio
ns:
Asp
irin
, do
nep
ezil,
cal
cium
plu
s vi
tam
in D
, iro
n P
hysic
al E
xa
min
atio
n:
Oct
ob
er 2
010:
2.0
x 3
.0 c
m p
ink
to p
urp
le p
laq
ue
on
the
rig
ht b
reas
t. D
ecem
ber
201
1: 1
0.0
x 14
.0 c
m p
ink
to p
urp
le, i
ndur
ated
p
laq
ue o
n th
e ri
ght
bre
ast
B
iop
sy:
Ad
vanc
ed D
erm
ato
log
y A
sso
ciat
es, L
TD
. (A
D10
-107
99, 1
0/04
/201
0) R
ight
m
edia
l bre
ast:
“In
the
sup
erfic
ial h
alf
of
an e
dem
ato
us d
erm
is is
a s
ubtle
p
op
ulat
ion
of
ecta
tic v
esse
ls w
ith p
lum
p, b
ut s
mal
l, en
do
thel
ial c
ells
. T
his
is s
om
ewha
t o
bsc
ured
by
a p
atch
y m
ixed
cel
l inf
lam
mat
ory
infil
trat
e th
at
incl
udes
lym
pho
cyte
s, h
istio
cyte
s, a
nd a
rar
e eo
sino
phi
l. T
here
are
als
o
extr
avas
ated
ery
thro
cyte
s. A
PA
S s
tain
is n
egat
ive
for
fung
us.”
Ad
vanc
ed D
erm
ato
log
y A
sso
ciat
es, L
TD
. (A
D11
-134
64, 1
2/15
/201
1) R
ight
m
edia
l and
late
ral b
reas
t: “
Bo
th s
pec
imen
s co
ntai
n a
pro
lifer
atio
n o
f ir
reg
ular
, er
ythr
ocy
te-c
ont
aini
ng, v
ascu
lar
chan
nels
tha
t ar
e lin
ed b
y a
sing
le la
yer
of
flatt
ened
end
oth
elia
l cel
ls.
The
se v
ary
in s
ize
and
sha
pe
with
sm
all j
agg
ed
chan
nels
sub
tly in
terc
alat
ed b
etw
een
colla
gen
bun
dle
s ad
mix
ed w
ith la
rge
ecta
tic o
nes.
Thi
s p
roce
ss is
mo
st p
rom
inen
t in
the
sup
erfic
ial h
alf
of
the
der
mis
tho
ugh
it is
ful
l thi
ckne
ss, o
vera
ll, w
ith in
volv
emen
t o
f th
e su
bcu
tis
(rig
ht b
reas
t m
edia
l). E
ndo
thel
ial m
orp
holo
gy
is m
ono
mo
rphi
c w
ith n
o
cyto
log
ic a
typ
ia a
nd n
o m
itose
s. S
uper
imp
ose
d o
n th
is, a
nd a
lso
mo
st
pro
min
ent
is a
co
nsp
icuo
us p
op
ulat
ion
of
lym
pho
cyte
s th
at a
re c
lust
ered
w
ithin
, and
aro
und
, the
ves
sels
.”A
dd
itio
na
l S
tud
ies:
D2-
40 n
egat
ive,
FIS
H f
or
MY
C a
mp
lific
atio
n p
end
ing
Tre
atm
en
t: In
tere
st a
nd t
reat
men
t re
com
men
dat
ions
Cas
e P
rese
nta
tion
:
Dis
cuss
ion
:O
ver
the
pas
t d
ecad
e, a
dire
ct li
nk h
as b
een
esta
blis
hed
bet
wee
n th
e d
evel
op
men
t o
f an
gio
sarc
om
a an
d r
adia
tion
trea
tmen
t, s
pec
ifica
lly o
n th
e b
reas
t. A
ltho
ugh
the
rela
tive
risk
is a
bo
ut 1
0-fo
ld, t
he o
vera
ll in
cid
ence
of
ang
iosa
rco
ma
aris
ing
in a
bre
ast
rad
iatio
n fie
ld f
alls
with
in a
n es
timat
ed r
ang
e o
f 0.
09 t
o 0
.16%
. T
he s
pec
ific
inci
ting
req
uire
men
ts a
re s
pec
ulat
ed t
o b
e a
resu
lt o
f b
reas
t-co
nser
ving
sur
ger
y, c
hem
oth
erap
y, a
nd p
ost
lum
pec
tom
y ra
dia
tion
trea
tmen
t. I
nter
estin
gly
, aty
pic
al, b
ut n
ot
out
war
dly
mal
igna
nt
vasc
ular
lesi
ons
hav
e b
een
rep
ort
ed t
o d
evel
op
in r
adia
tion
field
s fo
llow
ing
b
reas
t-co
nser
ving
sur
ger
y as
wel
l. C
linic
al a
nd h
isto
log
ic o
verl
ap, c
om
bin
ed
with
an
unp
red
icta
ble
long
ter
m c
linic
al c
our
se, m
ay c
ause
diff
icul
ty in
Fig
ure
1A:
Oct
ob
er 2
010:
2.0
x 3
.0 c
m p
ink
to
pur
ple
pla
que
on
the
rig
ht b
reas
t.
Fig
ure
1B:
Dec
emb
er 2
011:
10.
0 x
14.0
cm
pin
k to
pur
ple
, ind
urat
ed p
laq
ue o
n th
e ri
ght
bre
ast.
Fig
ure
2A:
H&
E O
cto
ber
201
0: T
here
are
a
num
ber
of
ecta
tic
vess
els
wit
h p
lum
p s
mal
l en
do
thel
ial c
ells
sur
roun
ded
by
a p
atch
y m
ixed
ce
ll in
filt
rate
. T
he in
filt
rate
is c
om
po
sed
of
lym
pho
cyte
s, h
isti
oct
yes,
and
a r
are
eosi
nop
hil.
E
xtra
vasa
ted
ery
thro
cyte
s ar
e p
rese
nt.
Fig
ure
2B:
H&
E D
ecem
ber
201
1:
Mo
nom
orp
hic
end
oth
elia
l cel
ls w
ith
no
cyto
log
ic a
typ
ia a
nd n
o m
ito
ses.
The
re is
a
cons
pic
uous
po
pul
atio
n o
f ly
mp
hocy
tes
clus
tere
d w
ithi
n an
d a
roun
d t
he v
esse
ls.
dis
ting
uish
ing
aty
pic
al v
ascu
lar
lesi
ons
(AV
Ls) f
rom
ear
ly a
ngio
sarc
om
a. A
n es
tab
lishe
d t
reat
men
t p
roto
col i
s ne
eded
fo
r p
atie
nts
that
fal
l int
o t
his
cate
go
ry.
AV
Ls t
ypic
ally
pre
sent
in w
om
en in
the
ir 5
0s t
hat
have
rec
eive
d b
reas
t-co
nser
ving
sur
ger
y, in
co
njun
ctio
n w
ith a
n av
erag
e tr
eatm
ent
of
40-6
0 G
y cu
mul
ativ
e ra
dia
tion
do
se.
Clin
ical
ly, t
hese
lesi
ons
ten
d t
o b
e sm
alle
r, w
ell c
ircum
scri
bed
, and
sym
met
rica
l. T
he p
ost
rad
iatio
n in
terv
al f
or
the
dev
elo
pm
ent
of
AV
Ls is
no
tab
ly s
hort
er c
om
par
ed t
o f
rank
ang
iosa
rco
ma.
T
he t
ime
to p
rese
ntat
ion
for
AV
Ls is
ap
pro
xim
atel
y 3
year
s co
mp
ared
to
an
gio
sarc
om
a, w
hich
is a
pp
roxi
mat
ely
6 ye
ars.
Thi
s ha
s le
d t
o t
he h
ypo
thes
is
that
AV
Ls a
nd a
ngio
sarc
om
a ar
e p
art
of
a co
ntin
uous
sp
ectr
um o
f va
scul
ar
lesi
ons
, and
tha
t A
VLs
rep
rese
nt a
pre
curs
or
lesi
on.
H
isto
pat
holo
gic
ana
lysi
s o
f A
VLs
ver
sus
ang
iosa
rco
ma
can
be
diff
icul
t d
ue
to m
any
diff
eren
t o
verl
app
ing
fea
ture
s. T
o d
ate,
ang
iosa
rco
ma
has
bee
n hi
sto
pat
holo
gic
ally
iden
tifie
d b
y an
asto
mo
sing
vas
cula
r ch
anne
ls li
ned
by
pro
min
ent
end
oth
elia
l cel
ls w
ith n
ucle
ar h
yper
chro
mas
ia a
nd h
ob
naili
ng.
Dis
sect
ion
of
der
mal
co
llag
en a
nd in
volv
emen
t o
f th
e su
bcu
tane
ous
tis
sue
can
occ
ur in
co
njun
ctio
n w
ith n
ecro
sis
or
“blo
od
lake
s”.
AV
Ls, i
n co
ntra
st, a
pp
ear
wel
l circ
umsc
rib
ed, w
edg
e-sh
aped
, and
ten
d t
o in
volv
e o
nly
the
sup
erfic
ial t
o
mid
der
mis
. R
ecen
tly, f
luo
resc
ence
in s
itu h
ybri
diz
atio
n (F
ISH
) has
bee
n ab
le
to d
istin
gui
sh A
VLs
fro
m a
ngio
sarc
om
a b
y th
e p
rese
nce
of
MY
C a
mp
lific
atio
n,
alth
oug
h re
pea
t te
stin
g o
n m
ultip
le b
iop
sy s
ites
may
be
need
ed f
or
cons
iste
nt
resu
lts.
N
o d
efin
itive
cri
teri
a ar
e av
aila
ble
to
ad
equa
tely
pre
dic
t w
heth
er A
VLs
will
d
evel
op
into
ang
iosa
rco
ma
or
may
co
ntin
ue t
o f
ollo
w a
ben
ign
cour
se.
Rec
ent
atte
mp
ts a
t su
b-c
lass
ifyin
g le
sio
ns w
ith s
imila
r hi
sto
pat
holo
gic
fin
din
gs
into
tw
o c
ateg
ori
es (i
.e. l
ymp
hatic
ap
pea
ring
ver
sus
cap
illar
y ap
pea
ring
lesi
ons
) ha
s no
t b
een
foun
d t
o b
e a
def
initi
ve m
eans
of
dis
ting
uish
ing
AV
Ls o
f a
mo
re
agg
ress
ive
natu
re, o
r th
ose
tha
t m
ay d
evel
op
into
ang
iosa
rco
ma.
Ana
lysi
s o
f ne
w c
ases
with
long
ter
m f
ollo
w-u
p is
nee
ded
to
fur
ther
ana
lyze
the
sp
ectr
um o
f th
ese
lesi
ons
, lea
din
g t
o a
n ap
pro
pri
ate
and
acc
epte
d t
reat
men
t al
go
rith
m in
the
fu
ture
.
40x
10x
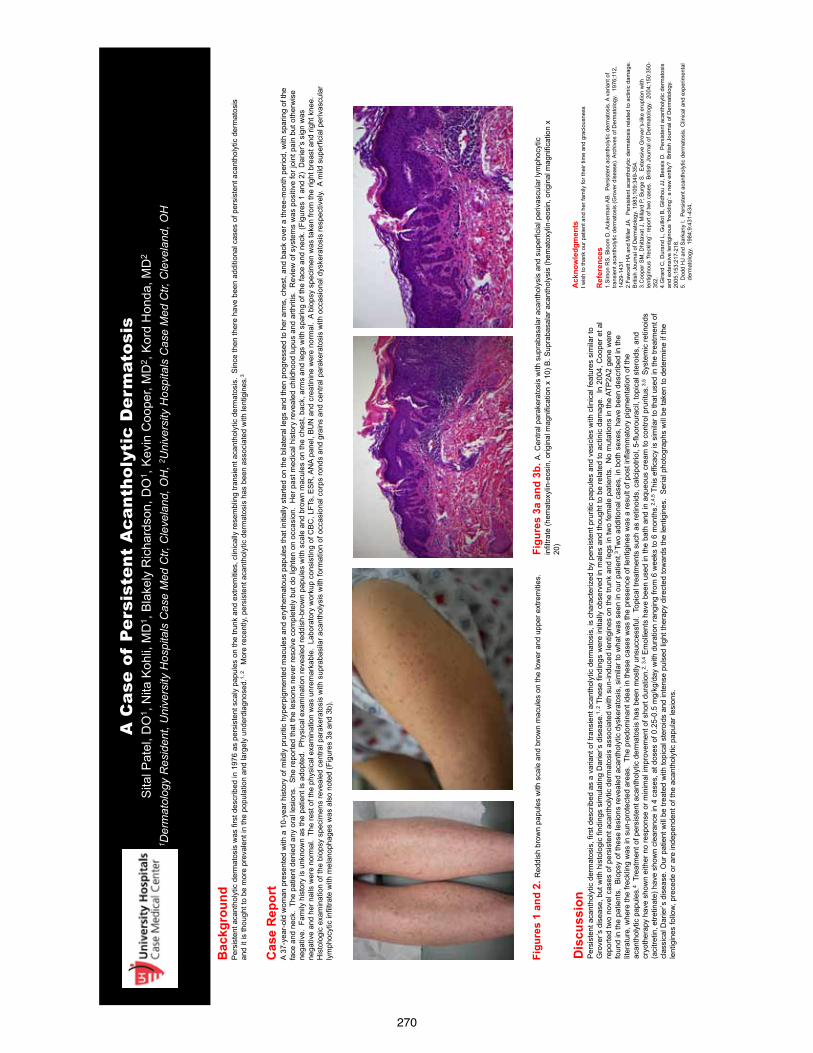
270
A
Cas
e of
Per
sist
ent
Aca
ntho
lyti
c D
erm
atos
is
Sita
l Pat
el, D
O1 ,
Nita
Koh
li, M
D1 ,
Bla
kely
Ric
hard
son,
DO
1 , K
evin
Coo
per,
MD
2 , K
ord
Hon
da, M
D2
1 Der
mat
olog
y R
esid
ent,
Uni
vers
ity H
ospi
tals
Cas
e M
ed C
tr, C
leve
land
, OH
, 2U
nive
rsity
Hos
pita
ls C
ase
Med
Ctr,
Cle
vela
nd, O
H
Bac
kgro
und
Per
sist
ent a
cant
holy
tic d
erm
atos
is w
as fi
rst d
escr
ibed
in 1
976
as p
ersi
sten
t sca
ly p
apul
es o
n th
e tru
nk a
nd e
xtre
miti
es, c
linic
ally
rese
mbl
ing
trans
ient
aca
ntho
lytic
der
mat
osis
. S
ince
then
ther
e ha
ve b
een
addi
tiona
l cas
es o
f per
sist
ent a
cant
holy
tic d
erm
atos
is
and
it is
thou
ght t
o be
mor
e pr
eval
ent i
n th
e po
pula
tion
and
larg
ely
unde
rdia
gnos
ed.1,
2
Mor
e re
cent
ly, p
ersi
sten
t aca
ntho
lytic
der
mat
osis
has
bee
n as
soci
ated
with
lent
igin
es.3
Figu
res
1 an
d 2.
Red
dish
bro
wn
papu
les
with
sca
le a
nd b
row
n m
acul
es o
n th
e lo
wer
and
upp
er e
xtre
miti
es.
Ref
eren
ces
1.S
imon
RS,
Blo
om D
, Ack
erm
an A
B. P
ersi
sten
t aca
ntho
lytic
der
mat
osis
. A v
aria
nt o
f tra
nsie
nt a
cant
holy
tic d
erm
atos
is (G
rove
r dis
ease
). A
rchi
ves
of D
erm
atol
ogy.
197
6;11
2,
1429
-143
1
2.Fa
wce
tt H
A an
d M
iller J
A.
Per
sist
ent a
cant
holy
tic d
erm
atos
is re
late
d to
act
inic
dam
age.
B
ritis
h Jo
urna
l of D
erm
atol
ogy.
198
3;10
9:34
9-35
4.
3.C
oope
r SM
, Dhi
ttava
t J, M
illard
P, B
urge
S.
Ext
ensi
ve G
rove
r’s-li
ke e
rupt
ion
with
le
ntig
inou
s ‘fr
eckl
ing’
: rep
ort o
f tw
o ca
ses.
Brit
ish
Jour
nal o
f Der
mat
olog
y. 2
004;
150:
350-
352.
4.
Gira
rd C
, Dur
and
L, G
uillo
t B, G
ildho
u JJ
, Bes
sis
D.
Per
sist
ent a
cant
holy
tic d
erm
atos
is
and
exte
nsiv
e le
ntig
inou
s ‘fr
eckl
ing’
: a n
ew e
ntity
? B
ritis
h Jo
urna
l of D
erm
atol
ogy.
20
05;1
53:2
17-2
18.
5. D
odd
HJ
and
Sar
kany
I. P
ersi
sten
t aca
ntho
lytic
der
mat
osis
. Clin
ical
and
exp
erim
enta
l
der
mat
olog
y. 1
984;
9:43
1-43
4.
Ack
now
ledg
men
ts
I wis
h to
than
k ou
r pat
ient
and
her
fam
ily fo
r the
ir tim
e an
d gr
acio
usne
ss
Dis
cuss
ion
Per
sist
ent a
cant
holy
tic d
erm
atos
is, f
irst d
escr
ibed
as
a va
riant
of t
rans
ient
aca
ntho
lytic
der
mat
osis
, is
char
acte
rized
by
pers
iste
nt p
rurit
ic p
apul
es a
nd v
esic
les
with
clin
ical
feat
ures
sim
ilar t
o G
rove
r’s d
isea
se, b
ut w
ith h
isto
logi
c fin
ding
s si
mul
atin
g D
arie
r’s d
isea
se.1,
2 T
hese
find
ings
wer
e in
itial
ly o
bser
ved
in m
ales
and
thou
ght t
o be
rela
ted
to a
ctin
ic d
amag
e. I
n 20
04, C
oope
r et a
l re
porte
d tw
o no
vel c
ases
of p
ersi
sten
t aca
ntho
lytic
der
mat
osis
ass
ocia
ted
with
sun
-indu
ced
lent
igin
es o
n th
e tru
nk a
nd le
gs in
two
fem
ale
patie
nts.
No
mut
atio
ns in
the
ATP
2A2
gene
wer
e fo
und
in th
e pa
tient
s. B
iops
y of
thes
e le
sion
s re
veal
ed a
cant
holy
tic d
yske
rato
sis,
sim
ilar t
o w
hat w
as s
een
in o
ur p
atie
nt.3
Two
addi
tiona
l cas
es, i
n bo
th s
exes
, hav
e be
en d
escr
ibed
in th
e lit
erat
ure,
whe
re th
e fre
cklin
g w
as in
sun
-pro
tect
ed a
reas
. Th
e pr
edom
inan
t ide
a in
thes
e ca
ses
was
the
pres
ence
of l
entig
ines
was
a re
sult
of p
ost i
nfla
mm
ator
y pi
gmen
tatio
n of
the
acan
thol
ytic
pap
ules
.4 T
reat
men
t of p
ersi
sten
t aca
ntho
lytic
der
mat
osis
has
bee
n m
ostly
uns
ucce
ssfu
l. T
opic
al tr
eatm
ents
suc
h as
retin
oids
, cal
cipo
triol
, 5-fl
uoro
urac
il, to
pica
l ste
roid
s, a
nd
cryo
ther
apy
have
sho
wn
eith
er n
o re
spon
se o
r min
imal
impr
ovem
ent o
f sho
rt du
ratio
n.2,
3,4 E
mol
lient
s ha
ve b
een
used
in th
e ba
th a
nd in
aqu
eous
cre
am to
con
trol p
rurit
us.3,
5 S
yste
mic
retin
oids
(a
citre
tin, e
tretin
ate)
hav
e sh
own
clea
ranc
e in
4 c
ases
, at d
oses
of 0
.25-
0.5
mg/
kg/d
ay w
ith d
urat
ion
rang
ing
from
6 w
eeks
to 6
mon
ths.
2,4,
5 Thi
s ef
ficac
y is
sim
ilar t
o th
at u
sed
in th
e tre
atm
ent o
f cl
assi
cal D
arie
r’s d
isea
se. O
ur p
atie
nt w
ill b
e tre
ated
with
topi
cal s
tero
ids
and
inte
nse
puls
ed li
ght t
hera
py d
irect
ed to
war
ds th
e le
ntig
ines
. S
eria
l pho
togr
aphs
will
be
take
n to
det
erm
ine
if th
e le
ntig
ines
follo
w, p
rece
de o
r are
inde
pend
ent o
f the
aca
ntho
lytic
pap
ular
lesi
ons.
Cas
e R
epor
t A
37-y
ear-o
ld w
oman
pre
sent
ed w
ith a
10-
year
his
tory
of m
ildly
pru
ritic
hyp
erpi
gmen
ted
mac
ules
and
ery
them
atou
s pa
pule
s th
at in
itial
ly s
tarte
d on
the
bila
tera
l leg
s an
d th
en p
rogr
esse
d to
her
arm
s, c
hest
, and
bac
k ov
er a
thre
e-m
onth
per
iod,
with
spa
ring
of th
e fa
ce a
nd n
eck.
The
pat
ient
den
ied
any
oral
lesi
ons.
She
repo
rted
that
the
lesi
ons
neve
r res
olve
com
plet
ely
but d
o lig
hten
on
occa
sion
. H
er p
ast m
edic
al h
isto
ry re
veal
ed c
hild
hood
lupu
s an
d ar
thrit
is.
Rev
iew
of s
yste
ms
was
pos
itive
for j
oint
pai
n bu
t oth
erw
ise
nega
tive.
Fam
ily h
isto
ry is
unk
now
n as
the
patie
nt is
ado
pted
. P
hysi
cal e
xam
inat
ion
reve
aled
redd
ish-
brow
n pa
pule
s w
ith s
cale
and
bro
wn
mac
ules
on
the
ches
t, ba
ck, a
rms
and
legs
with
spa
ring
of th
e fa
ce a
nd n
eck.
(Fig
ures
1 a
nd 2
) D
arie
r’s s
ign
was
ne
gativ
e an
d he
r nai
ls w
ere
norm
al.
The
rest
of t
he p
hysi
cal e
xam
inat
ion
was
unr
emar
kabl
e. L
abor
ator
y w
orku
p co
nsis
ting
of C
BC
, LFT
s, E
SR
, AN
A pa
nel,
BUN
and
cre
atin
ine
wer
e no
rmal
. A
biop
sy s
peci
men
was
take
n fro
m th
e rig
ht b
reas
t and
righ
t kne
e.
His
tolo
gic
exam
inat
ion
of th
e bi
opsy
spe
cim
ens
reve
aled
cen
tral p
arak
erat
osis
with
sup
raba
sila
r aca
ntho
lysi
s w
ith fo
rmat
ion
of o
ccas
iona
l cor
ps ro
nds
and
grai
ns a
nd c
entra
l par
aker
atos
is w
ith o
ccas
iona
l dys
kera
tosi
s re
spec
tivel
y. A
mild
sup
erfic
ial p
eriv
ascu
lar
lym
phoc
ytic
infil
trate
with
mel
anop
hage
s w
as a
lso
note
d (F
igur
es 3
a an
d 3b
).
.
Figu
res
3a a
nd 3
b. A
. Cen
tral p
arak
erat
osis
with
sup
raba
sala
r aca
ntho
lysi
s an
d su
perfi
cial
per
ivas
cula
r lym
phoc
ytic
in
filtra
te (h
emat
oxyl
in-e
osin
, orig
inal
mag
nific
atio
n x
10) B
. Sup
raba
sala
r aca
ntho
lysi
s (h
emat
oxyl
in-e
osin
, orig
inal
mag
nific
atio
n x
20)
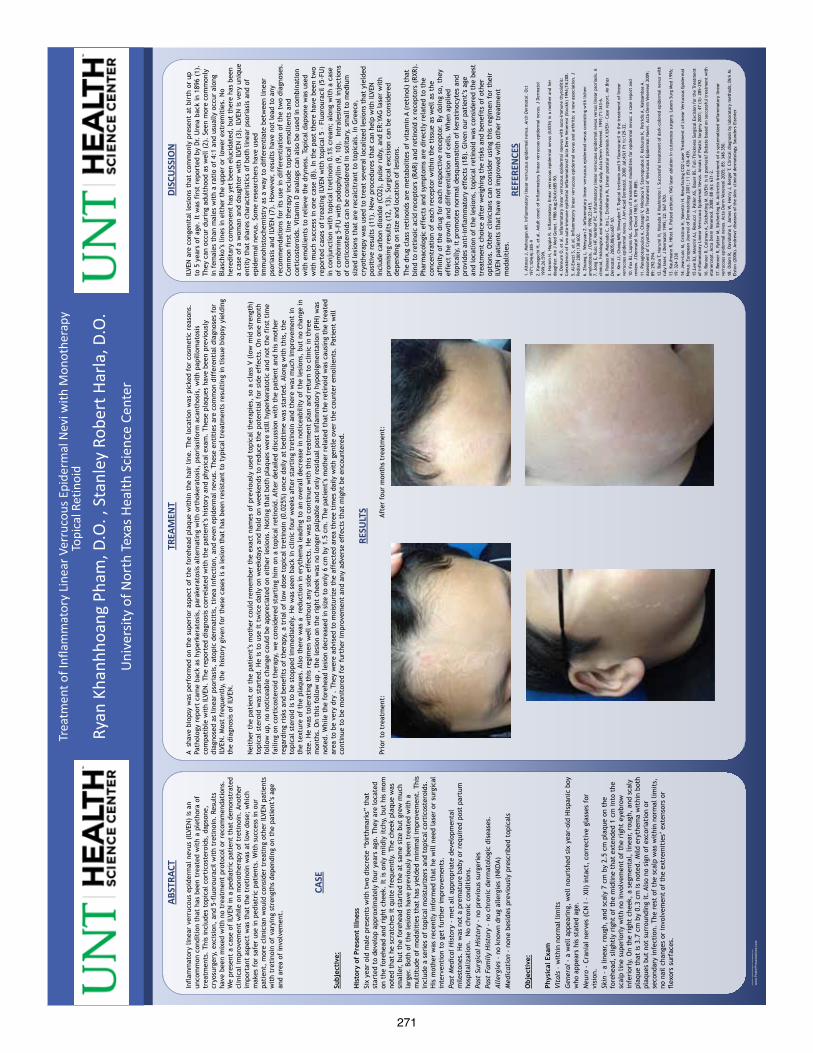
271
QU
ICK
TIPS
(-
-TH
IS S
ECTI
ON
DO
ES N
OT
PRIN
T--)
This
Pow
erPo
int
tem
plat
e re
quir
es b
asic
Pow
erPo
int
(ver
sion
200
7 or
new
er)
skill
s. B
elow
is a
list
of
com
mon
ly a
sked
que
stio
ns s
peci
fic
to t
his
tem
plat
e.
If y
ou a
re u
sing
an
olde
r ve
rsio
n of
Pow
erPo
int
som
e te
mpl
ate
feat
ures
may
not
wor
k pr
oper
ly.
U
sing
the
tem
plat
e
Veri
fyin
g th
e qu
alit
y of
you
r gr
aphi
cs
Go
to t
he V
IEW
men
u an
d cl
ick
on Z
OO
M t
o se
t yo
ur
pref
erre
d m
agni
fica
tion
. Th
is t
empl
ate
is a
t 10
0%
the
size
of
the
fina
l pos
ter.
All
text
and
gra
phic
s w
ill
be p
rint
ed a
t 10
0% t
heir
siz
e. T
o se
e w
hat
your
po
ster
will
look
like
whe
n pr
inte
d, s
et t
he z
oom
to
100%
and
eva
luat
e th
e qu
alit
y of
all
your
gra
phic
s be
fore
you
sub
mit
you
r po
ster
for
pri
ntin
g.
Usi
ng t
he p
lace
hold
ers
To a
dd t
ext
to t
his
tem
plat
e cl
ick
insi
de a
pl
aceh
olde
r an
d ty
pe in
or
past
e yo
ur t
ext.
To
mov
e a
plac
ehol
der,
clic
k on
it o
nce
(to
sele
ct it
), p
lace
yo
ur c
urso
r on
its
fram
e an
d yo
ur c
urso
r w
ill c
hang
e to
thi
s sy
mbo
l:
Then
, cl
ick
once
and
dra
g it
to
its
new
loca
tion
whe
re y
ou c
an r
esiz
e it
as
need
ed.
Addi
tion
al p
lace
hold
ers
can
be f
ound
on
the
left
si
de o
f th
is t
empl
ate.
M
odif
ying
the
layo
ut
This
tem
plat
e w
as s
peci
fica
lly d
esig
ned
for
a 48
x36
tri-
fold
pre
sent
atio
n. It
s la
yout
sho
uld
not
be
chan
ged
or it
may
not
fit
on
a st
anda
rd b
oard
. It
has
a
one
foot
col
umn
on t
he le
ft,
a 2
foot
col
umn
in
the
mid
dle
and
a 1
foot
col
umn
on t
he r
ight
. Th
e co
lum
ns in
the
pro
vide
d la
yout
are
fix
ed a
nd
cann
ot b
e m
oved
but
adv
ance
d us
ers
can
mod
ify
any
layo
ut b
y go
ing
to V
IEW
and
the
n SL
IDE
MAS
TER.
Im
port
ing
text
and
gra
phic
s fr
om e
xter
nal s
ourc
es
TEXT
: Pa
ste
or t
ype
your
tex
t in
to a
pre
-exi
stin
g pl
aceh
olde
r or
dra
g in
a n
ew p
lace
hold
er f
rom
the
le
ft s
ide
of t
he t
empl
ate.
Mov
e it
any
whe
re a
s ne
eded
. PH
OTO
S: D
rag
in a
pic
ture
pla
ceho
lder
, si
ze it
fir
st,
clic
k in
it a
nd in
sert
a p
hoto
fro
m t
he m
enu.
TA
BLES
: Yo
u ca
n co
py a
nd p
aste
a t
able
fro
m a
n ex
tern
al d
ocum
ent
onto
thi
s po
ster
tem
plat
e. T
o ad
just
th
e w
ay t
he t
ext
fits
wit
hin
the
cells
of
a ta
ble
that
has
bee
n pa
sted
, ri
ght-
clic
k on
the
tab
le,
clic
k FO
RMAT
SH
APE
the
n cl
ick
on T
EXT
BOX
and
chan
ge t
he IN
TERN
AL M
ARG
IN v
alue
s to
0.2
5 M
odif
ying
the
col
or s
chem
e To
cha
nge
the
colo
r sc
hem
e of
thi
s te
mpl
ate
go t
o th
e “D
esig
n” m
enu
and
clic
k on
“Co
lors
”. Y
ou c
an
choo
se f
rom
the
pro
vide
col
or c
ombi
nati
ons
or y
ou
can
crea
te y
our
own.
QU
ICK
DES
IGN
GU
IDE
(--T
HIS
SEC
TIO
N D
OES
NO
T PR
INT-
-)
Th
is P
ower
Poin
t 20
07 t
empl
ate
prod
uces
a 3
6”x4
8”
tri-
fold
pre
sent
atio
n p
oste
r. It
will
sav
e yo
u va
luab
le t
ime
plac
ing
titl
es,
subt
itle
s, t
ext,
and
gr
aphi
cs.
U
se it
to
crea
te y
our
pres
enta
tion
. Th
en s
end
it t
o Po
ster
Pres
enta
tion
s.co
m f
or p
rem
ium
qua
lity,
sam
e da
y af
ford
able
pri
ntin
g.
We
prov
ide
a se
ries
of
onlin
e tu
tori
als
that
will
gu
ide
you
thro
ugh
the
post
er d
esig
n pr
oces
s an
d an
swer
you
r po
ster
pro
duct
ion
ques
tion
s.
View
our
onl
ine
tuto
rial
s at
: h
ttp:
//bi
t.ly
/Pos
ter_
crea
tion
_hel
p
(cop
y an
d pa
ste
the
link
into
you
r w
eb b
row
ser)
. Fo
r as
sist
ance
and
to
orde
r yo
ur p
rint
ed p
oste
r ca
ll Po
ster
Pres
enta
tion
s.co
m a
t 1.
866.
649.
3004
Obj
ect
Plac
ehol
ders
Use
the
pla
ceho
lder
s pr
ovid
ed b
elow
to
add
new
el
emen
ts t
o yo
ur p
oste
r: D
rag
a pl
aceh
olde
r on
to
the
post
er a
rea,
siz
e it
, an
d cl
ick
it t
o ed
it.
Sect
ion
Hea
der
plac
ehol
der
Mov
e th
is p
refo
rmat
ted
sect
ion
head
er p
lace
hold
er
to t
he p
oste
r ar
ea t
o ad
d an
othe
r se
ctio
n he
ader
. U
se s
ecti
on h
eade
rs t
o se
para
te t
opic
s or
con
cept
s w
ithi
n yo
ur p
rese
ntat
ion.
Te
xt p
lace
hold
er
Mov
e th
is p
refo
rmat
ted
text
pla
ceho
lder
to
the
post
er t
o ad
d a
new
bod
y of
tex
t.
Pict
ure
plac
ehol
der
Mov
e th
is g
raph
ic p
lace
hold
er o
nto
your
pos
ter,
siz
e it
fir
st,
and
then
clic
k it
to
add
a pi
ctur
e to
the
po
ster
.
RES
EAR
CH
PO
STER
PR
ESEN
TATI
ON
DES
IGN
© 2
012
ww
w.P
oste
rPre
sent
atio
ns.c
om
© 2
012
Post
erPr
esen
tatio
ns.c
om
2
117
Four
th S
tree
t , U
nit C
Ber
kele
y CA
947
10
p
oste
rpre
sent
er@
gmai
l.com
St
uden
t di
scou
nts
are
avai
labl
e on
our
Fac
eboo
k pa
ge.
Go
to P
oste
rPre
sent
atio
ns.c
om a
nd c
lick
on t
he F
B ic
on.
Infl
amm
ator
y lin
ear
verr
ucou
s ep
ider
mal
nev
us (
ILVE
N)
is a
n un
com
mon
con
diti
on t
hat
has
been
tre
ated
wit
h a
plet
hora
of
trea
tmen
ts.
This
incl
udes
top
ical
cor
tico
ster
oids
, da
pson
e,
cryo
surg
ery,
exc
isio
n, a
nd 5
-flu
orou
raci
l wit
h tr
etin
oin.
Res
ults
ha
ve b
een
mix
ed w
ith
no t
reat
men
t pr
otoc
ol o
r re
com
men
dati
ons.
W
e pr
esen
t a
case
of
ILVE
N in
a p
edia
tric
pat
ient
tha
t de
mon
stra
ted
clin
ical
impr
ovem
ent
whi
le o
n m
onot
hera
py o
f tr
etin
oin.
Ano
ther
im
port
ant
aspe
ct w
as t
hat
the
tret
inoi
n w
as a
t lo
w d
ose;
whi
ch
mak
es f
or s
afer
use
in p
edia
tric
pat
ient
s. W
ith
succ
ess
in o
ur
pati
ent,
mor
e cl
inic
ian
wou
ld c
onsi
der
trea
ting
oth
er IL
VEN
pat
ient
s w
ith
tret
inoi
n of
var
ying
str
engt
hs d
epen
ding
on
the
pati
ent’
s ag
e an
d ar
ea o
f in
volv
emen
t.
ABST
RACT
CASE
A s
have
bio
psy
was
per
form
ed o
n th
e su
peri
or a
spec
t of
the
for
ehea
d pl
aque
wit
hin
the
hair
line
. Th
e lo
cati
on w
as p
icke
d fo
r co
smet
ic r
easo
ns.
Pa
thol
ogy
repo
rt c
ame
back
as
hype
rker
atos
is,
para
kera
tosi
s al
tern
atin
g w
ith
orth
oker
atos
is,
psor
iasi
form
aca
ntho
sis,
wit
h pa
pillo
mat
osis
co
mpa
tibl
e w
ith
ILVE
N.
The
repo
rted
dia
gnos
is c
orre
late
d w
ith
the
pati
ent’
s hi
stor
y an
d ph
ysic
al e
xam
. Th
ese
plaq
ues
have
bee
n pr
evio
usly
di
agno
sed
as li
near
pso
rias
is,
atop
ic d
erm
atit
is,
tine
a in
fect
ion,
and
eve
n ep
ider
mal
nev
us.
Thes
e en
titi
es a
re c
omm
on d
iffe
rent
ial
diag
nose
s fo
r IL
VEN
. M
ost
freq
uent
ly,
the
his
tory
giv
en f
or t
hese
cas
es is
a le
sion
tha
t ha
s be
en r
esis
tant
to
typi
cal t
reat
men
ts r
esul
ting
in t
issu
e bi
opsy
yie
ldin
g th
e di
agno
sis
of IL
VEN
.
Nei
ther
the
pat
ient
or
the
pati
ent’
s m
othe
r co
uld
rem
embe
r th
e ex
act
nam
es o
f pr
evio
usly
use
d to
pica
l the
rapi
es,
so a
cla
ss V
(lo
w m
id s
tren
gth)
to
pica
l ste
roid
was
sta
rted
. H
e is
to
use
it t
wic
e da
ily o
n w
eekd
ays
and
hold
on
wee
kend
s to
red
uce
the
pote
ntia
l for
sid
e ef
fect
s. O
n on
e m
onth
fo
llow
up,
no
noti
ceab
le c
hang
e co
uld
be a
ppre
ciat
ed o
n ei
ther
lesi
ons.
Not
ing
that
bot
h pl
aque
s w
ere
still
hyp
erke
rato
tic
and
not
the
firs
t ti
me
faili
ng o
n co
rtic
oste
roid
the
rapy
, w
e co
nsid
ered
sta
rtin
g hi
m o
n a
topi
cal r
etin
oid.
Aft
er d
etai
led
disc
ussi
on w
ith
the
pati
ent
and
his
mot
her
rega
rdin
g ri
sks
and
bene
fits
of
ther
apy,
a t
rial
of
low
dos
e to
pica
l tre
tino
in (
0.02
5%)
once
dai
ly a
t be
dtim
e w
as s
tart
ed.
Alon
g w
ith
this
, th
e to
pica
l ste
roid
is t
o be
sto
pped
imm
edia
tely
. H
e w
as s
een
back
in c
linic
fou
r w
eeks
aft
er s
tart
ing
tret
inoi
n an
d th
ere
was
muc
h im
prov
emen
t in
th
e te
xtur
e of
the
pla
ques
. Al
so t
here
was
a
redu
ctio
n in
ery
them
a le
adin
g to
an
over
all d
ecre
ase
in n
otic
eabi
lity
of t
he le
sion
s, b
ut n
o ch
ange
in
size
. H
e w
as t
oler
atin
g th
is r
egim
en w
ell w
itho
ut a
ny s
ide
effe
cts.
He
was
to
cont
inue
wit
h th
is t
reat
men
t pl
an a
nd r
etur
n to
clin
ic in
thr
ee
mon
ths.
On
this
fol
low
up
, th
e le
sion
on
the
righ
t ch
eek
was
no
long
er p
alpa
ble
and
only
res
idua
l pos
t in
flam
mat
ory
hypo
pigm
enta
tion
(PI
H)
was
no
ted.
Whi
le t
he f
oreh
ead
lesi
on d
ecre
ased
in s
ize
to o
nly
6 cm
by
1.5
cm.
The
pati
ent’
s m
othe
r re
late
d th
at t
he r
etin
oid
was
cau
sing
the
tre
ated
ar
ea t
o be
ver
y dr
y .
They
wer
e ad
vise
d to
moi
stur
ize
the
affe
cted
are
a th
ree
tim
es d
aily
wit
h ge
ntle
ove
r th
e co
unte
r em
ollie
nts.
Pat
ient
will
co
ntin
ue t
o be
mon
itor
ed f
or f
urth
er im
prov
emen
t an
d an
y ad
vers
e ef
fect
s th
at m
ight
be
enco
unte
red.
TREA
MEN
T
Prio
r to
tre
atm
ent:
A
fter
fou
r m
onth
s tr
eatm
ent:
RESU
LTS
DISC
USS
ION
REFE
REN
CES
1. A
ltm
an J
, M
ehre
gan
AH.
Infl
amm
ator
y lin
ear
verr
ucou
s ep
ider
mal
nev
us.
Arc
h D
erm
atol
. O
ct
1971
;104
(4):
385-
9 2.
Kaw
aguc
hi H
, et
al.
Adu
lt o
nset
of
infl
amm
ator
y lin
ear
verr
ucou
s ep
ider
mal
nev
us.
J D
erm
atol
19
99;2
6:59
9.
3. H
amm
H,
Hap
ple
R. In
flam
mat
ory
linea
r ve
rruc
ous
epid
erm
al n
evus
(IL
VEN
) in
a m
othe
r an
d he
r da
ught
er.
Am J
Med
Gen
et.
1986
Aug
;24(
4):6
85-9
0.
4. D
ereu
re O
, et
al.
Infl
amm
ator
y lin
ear
verr
ucou
s ep
ider
mal
nae
vus
wit
h au
to-i
mm
une
thyr
oidi
tis:
Co
exis
tenc
e of
tw
o au
to-i
mm
une
epit
helia
l in
flam
mat
ions
? Ac
ta D
erm
Ven
ereo
l (S
tock
h) 1
994;
74:2
08.
5. A
l-En
ezi
S, e
t al
. In
flam
mat
ory
linea
r ve
rruc
ous
epid
erm
al n
evus
and
art
hrit
is:
a ne
w a
ssoc
iati
on.
J Pe
diat
r 20
01;1
38:6
02.
6. Z
huan
g L,
Wen
yuan
Z.
Infl
amm
ator
y lin
ear
verr
ucou
s ep
ider
mal
nev
us c
oexi
stin
g w
ith
liche
n am
yloi
dosi
s. J
Der
mat
ol 1
996;
23:4
15.
7. J
ong
E, R
ulo
HF,
Ker
khof
PC.
Infl
amm
ator
y lin
ear
verr
ucou
s ep
ider
mal
nev
us v
ersu
s lin
ear
psor
iasi
s. A
cl
inic
al,
hist
olog
ical
and
imun
nohi
stoc
hem
ical
stu
dy.
Acta
Der
m V
ener
eol.
199
1;71
:343
-6.
8. P
aixa
o M
, M
acha
do C
, It
o L,
Eno
kiha
ra M
, Li
near
pus
tula
r ps
oria
sis
X IL
VEN
- C
ase
repo
rt.
An
Bras
D
erm
atol
. 20
05;8
0(6)
:607
-10.
9.
Ki
m J
J, C
hang
MW
, Sh
way
der
T. T
opic
al t
reti
noin
and
5-f
luor
oura
cil
in t
he t
reat
men
t of
lin
ear
verr
ucou
s ep
ider
mal
nev
us.
J Am
Aca
d D
erm
atol
. 20
00 J
ul;4
3(1
Pt 1
):12
9-32
. 10
. Fo
x BJ
, La
pins
NA.
Com
pari
son
of t
reat
men
t m
odal
itie
s fo
r ep
ider
mal
nev
us:
a ca
se r
epor
t an
d re
view
. J
Der
mat
ol S
urg
Onc
ol 1
983;
9:
879–
885.
11
. Pa
nagi
otop
oulo
s A,
Cha
sapi
V,
Nik
olao
u V,
Sta
vrop
oulo
s P,
Kaf
ouro
s K,
Pet
ridi
s A,
Kat
sam
bas
A.
Asse
ssm
ent
of C
ryot
hera
py f
or t
he T
reat
men
t of
Ver
ruco
us E
pide
rmal
Nae
vi.
Acta
Der
m V
ener
eol
2009
; 89
: 29
2-29
4.
12.
Baba
T,
Nar
umi H
, H
anad
a K
Has
him
oto
I. S
ucce
ssfu
l tre
atm
ent
of d
ark-
colo
red
epid
erm
al n
evus
wit
h ru
by la
ser.
J D
erm
atol
199
5; 2
2: 5
67–5
70.
13.
Kauf
man
n R,
Hib
st R
. Pu
lsed
erb
ium
: YA
G l
aser
abl
atio
n in
cut
aneo
us s
urge
ry.
Lase
rs S
urg
Med
199
6;
19:
324–
330
14.
Jean
-Loi
c M
, Cr
isti
na H
, Va
lent
in H
. Re
surf
acin
g CO
2 La
ser
Trea
tmen
t of
Lin
ear
Verr
ucou
s Ep
ider
mal
N
evus
. Eu
rope
an J
ourn
al o
f D
erm
atol
ogy
2001
; 11
(5)
: 43
6-43
9.
15.L
ee B
J, M
anci
ni A
J, R
enuc
ci J
, Pa
ller
AS,
Baue
r BS
. Fu
ll-Th
ickn
ess
Surg
ical
Exc
isio
n fo
r th
e Tr
eatm
ent
of In
flam
mat
ory
Line
ar V
erru
cous
Epi
derm
al N
evus
. An
nals
of
Plas
tic
Surg
ery
2001
; 47
(3)
: 28
5-29
2.
16.
Renn
er R
, Co
lsm
an A
, St
iche
rlin
g M
. IL
VEN
: is
it p
sori
asis
? D
ebat
e ba
sed
on s
ucce
ssfu
l tre
atm
ent
wit
h et
aner
cept
. Ac
ta D
erm
Ven
ereo
l. 2
008;
88
(6):
631
-2.
17.
Renn
er R
, Ry
tter
M,
Stic
herl
ing
M.
Acit
reti
n tr
eatm
ent
of a
sys
tem
atiz
ed in
flam
mat
ory
linea
r ve
rruc
ous
epid
erm
al n
evus
. Ac
ta D
erm
Ven
ereo
l 20
05;
85:
348–
350.
18
. O
dom
R,
Dav
idso
hn I,
Jam
es W
, H
enry
J,
Berg
er T
. Cl
inic
al d
iagn
osis
by
labo
rato
ry m
etho
ds;
Dir
k M
. El
ston
(20
06).
And
rew
s' di
seas
es o
f th
e sk
in:
clin
ical
der
mat
olog
y. S
aund
ers
Else
vier
Subj
ecti
ve:
His
tory
of
Pres
ent
Illne
ss
Six
year
old
mal
e pr
esen
ts w
ith
two
disc
rete
“bi
rthm
arks
” th
at
star
ted
to d
evel
op a
ppro
xim
atel
y fo
ur y
ears
ago
. Th
ey a
re lo
cate
d on
the
for
ehea
d an
d ri
ght
chee
k. It
is o
nly
mild
ly it
chy,
but
his
mom
no
ted
that
he
scra
tche
s it
qui
te f
requ
entl
y. T
he c
heek
pla
que
was
sm
alle
r, b
ut t
he f
oreh
ead
star
ted
the
at s
ame
size
but
gre
w m
uch
larg
er.
Both
of
the
lesi
ons
have
pre
viou
sly
been
tre
ated
wit
h a
mul
titu
de o
f m
odal
itie
s th
at h
as y
ield
ed m
inim
al im
prov
emen
t. T
his
incl
ude
a se
ries
of
topi
cal m
oist
uriz
ers
and
topi
cal c
orti
cost
eroi
ds.
His
mot
her
was
rec
entl
y in
form
ed t
hat
he w
ill n
eed
lase
r or
sur
gica
l in
terv
enti
on t
o ge
t fu
rthe
r im
prov
emen
ts.
Past
Med
ical
His
tory
- m
et a
ll ap
prop
riat
e de
velo
pmen
tal
mile
ston
es.
He
was
not
a p
rem
atur
e ba
by o
r re
quir
ed p
ost
part
um
hosp
ital
izat
ion.
No
chro
nic
cond
itio
ns.
Pa
st S
urgi
cal
His
tory
- n
o pr
evio
us s
urge
ries
Pa
st F
amil
y H
isto
ry –
no
chro
nic
derm
atol
ogic
dis
ease
s.
All
ergi
es –
no
know
n dr
ug a
llerg
ies
(NKD
A)
Med
icat
ion
– no
ne b
esid
es p
revi
ousl
y pr
escr
ibed
top
ical
s O
bjec
tive
: Ph
ysic
al E
xam
Vi
tals
– w
ithi
n no
rmal
lim
its
Gen
eral
- a
wel
l app
eari
ng,
wel
l nou
rish
ed s
ix y
ear-
old
His
pani
c bo
y w
ho a
ppea
rs h
is s
tate
d ag
e.
Neu
ro -
Cra
nial
ner
ves
(CN
I –
XII)
inta
ct,
corr
ecti
ve g
lass
es f
or
visi
on.
Sk
in –
a li
near
, ro
ugh,
and
sca
ly 7
cm
by
2.5
cm p
laqu
e on
the
fo
rehe
ad,
slig
htly
rig
ht o
f th
e m
idlin
e th
at e
xten
ded
1 cm
into
the
sc
alp
line
supe
rior
ly w
ith
no in
volv
emen
t of
the
rig
ht e
yebr
ow
infe
rior
ly.
On
the
righ
t ch
eek,
a s
egm
enta
l, li
near
, ro
ugh,
and
sca
ly
plaq
ue t
hat
is 3
.7 c
m b
y 0.
3 cm
is n
oted
. M
ild e
ryth
ema
wit
hin
both
pl
aque
s bu
t no
t su
rrou
ndin
g it
. Al
so n
o si
gn o
f ex
cori
atio
n or
se
cond
ary
infe
ctio
n. T
he r
est
of t
he s
calp
was
wit
hin
norm
al li
mit
s,
no n
ail c
hang
es o
r in
volv
emen
t of
the
ext
rem
itie
s’ e
xten
sors
or
flex
ors
surf
aces
.
Ryan
Kha
nhho
ang
Pham
, D.O
. , S
tanl
ey R
ober
t Har
la, D
.O.
Uni
vers
ity o
f Nor
th Te
xas H
ealth
Sci
ence
Cen
ter
ILVE
N a
re c
onge
nita
l les
ions
tha
t co
mm
only
pre
sent
at
birt
h or
up
to 5
yea
rs o
f ag
e. It
was
fir
st r
epor
ted
by D
r. U
nna
back
in 1
896
(1).
Th
ey c
an o
ccur
dur
ing
adul
thoo
d as
wel
l (2)
. Se
en m
ore
com
mon
ly
in f
emal
es t
han
mal
es w
ith
a ra
tio
of 4
:1 a
nd u
sual
ly o
ccur
alo
ng
Blas
chko
’s li
nes
in e
ithe
r th
e up
per
or lo
wer
ext
rem
itie
s. N
o he
redi
tary
com
pone
nt h
as y
et b
een
eluc
idat
ed,
but
ther
e ha
s be
en
a ca
se o
f a
wom
an a
nd d
augh
ter
wit
h IL
VEN
(3)
. IL
VEN
is v
ery
uniq
ue
enti
ty t
hat
shar
es c
hara
cter
isti
cs o
f bo
th li
near
pso
rias
is a
nd o
f ep
ider
mal
nev
us.
Som
e re
sear
cher
s ha
ve u
sed
imm
unoh
isto
chem
istr
y as
a w
ay t
o di
ffer
enti
ate
betw
een
linea
r ps
oria
sis
and
ILVE
N (
7).
How
ever
, re
sult
s ha
ve n
ot le
ad t
o an
y re
com
men
dati
ons
for
its
use
in d
iffe
rent
iati
on o
f th
e tw
o di
agno
ses.
Co
mm
on f
irst
line
the
rapy
incl
ude
topi
cal e
mol
lient
s an
d co
rtic
oste
roid
s. V
itam
in D
ana
logs
can
als
o be
use
d in
com
bina
tion
w
ith
emol
lient
s to
rel
ieve
the
dry
ness
. To
pica
l dap
sone
was
use
d w
ith
muc
h su
cces
s in
one
cas
e (8
). In
the
pas
t th
ere
have
bee
n tw
o re
port
ed c
ases
of
trea
ting
ILVE
N w
ith
topi
cal 5
– F
luor
oura
cil (
5-FU
) in
con
junc
tion
wit
h to
pica
l tre
tino
in 0
.1%
crea
m;
alon
g w
ith
a ca
se
of c
ombi
ning
5-F
U w
ith
podo
phyl
lin (
9, 1
0).
Intr
ales
iona
l in
ject
ions
of
cor
tico
ster
oids
can
be
cons
ider
ed in
sol
itar
y, s
mal
l to
med
ium
si
zed
lesi
ons
that
are
rec
alci
tran
t to
top
ical
s. In
Gre
ece,
cr
yoth
erap
y w
as u
sed
to t
reat
sev
eral
loc
aliz
ed le
sion
s th
at y
ield
ed
posi
tive
res
ults
(11
). N
ew p
roce
dure
s th
at c
an h
elp
wit
h IL
VEN
in
clud
e ca
rbon
dio
xide
(CO
2),
puls
e ru
by,
and
ER:Y
AG la
ser
wit
h pr
omis
ing
resu
lts
(12,
13)
. Su
rgic
al e
xcis
ion
can
be c
onsi
dere
d de
pend
ing
on s
ize
and
loca
tion
of
lesi
ons.
Th
e dr
ug c
lass
ret
inoi
ds a
re m
etab
olit
es o
f vi
tam
in A
(re
tino
l) t
hat
bind
to
reti
noic
aci
d re
cept
ors
(RAR
) an
d re
tino
id x
rec
epto
rs (
RXR)
. Ph
arm
acol
ogic
eff
ects
and
sym
ptom
s ar
e di
rect
ly r
elat
ed t
o th
e co
ncen
trat
ion
of e
ach
rece
ptor
wit
hin
the
tiss
ue a
s w
ell a
s th
e af
fini
ty o
f th
e dr
ug f
or e
ach
resp
ecti
ve r
ecep
tor.
By
doin
g so
, th
ey
effe
ct t
he g
row
th a
nd d
iffe
rent
iati
on o
f ce
lls.
Whe
n ap
plie
d to
pica
lly,
it p
rom
otes
nor
mal
des
quam
atio
n of
ker
atin
ocyt
es a
nd
prov
ides
ant
i-in
flam
mat
ory
effe
cts
(18)
. G
iven
our
pat
ient
’s a
ge
and
loca
tion
of
the
lesi
ons,
top
ical
ret
inoi
d w
as c
onsi
dere
d th
e be
st
trea
tmen
t ch
oice
aft
er w
eigh
ing
the
risk
s an
d be
nefi
ts o
f ot
her
opti
ons.
Oth
er c
linic
ians
can
con
side
r us
ing
this
reg
imen
for
the
ir
ILVE
N p
atie
nts
that
hav
e no
t im
prov
ed w
ith
othe
r tr
eatm
ent
mod
alit
ies.
Trea
tmen
t of I
nfla
mm
ator
y Li
near
Ver
ruco
us E
pide
rmal
Nev
i with
Mon
othe
rapy
To
pica
l Ret
inoi
d
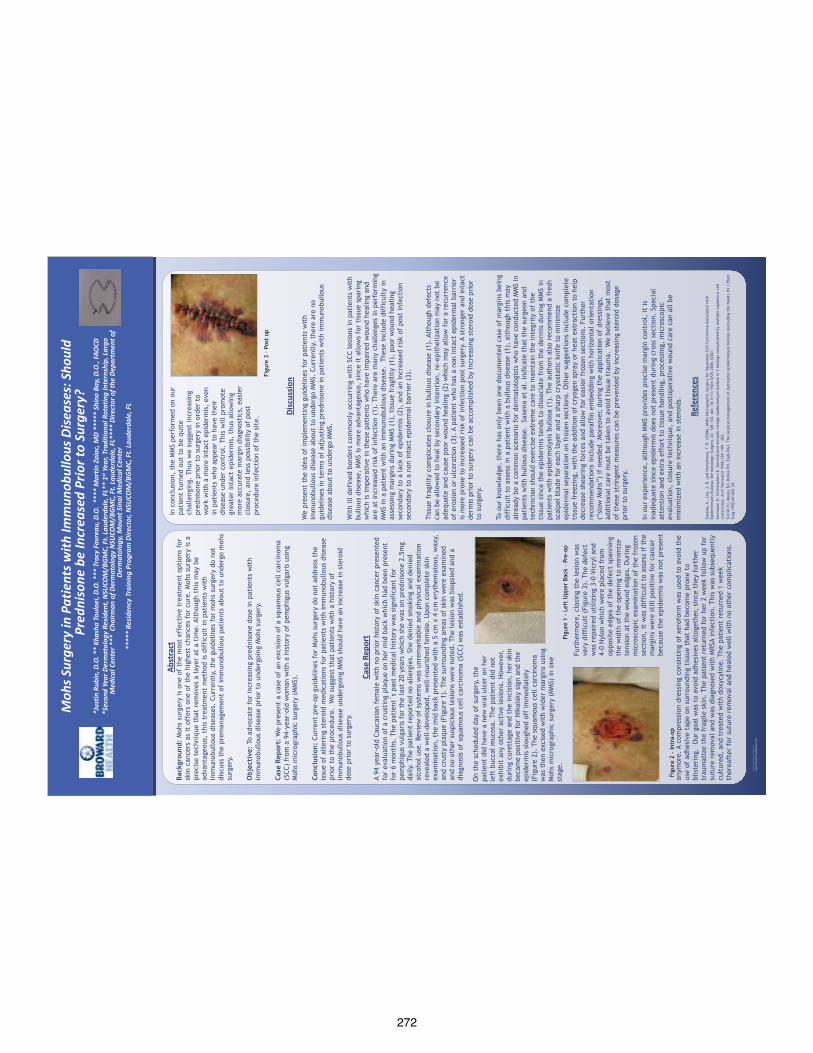
272
QU
ICK
TIPS
(-
-TH
IS S
ECTI
ON
DO
ES N
OT
PRIN
T--)
This
Pow
erPo
int
tem
plat
e re
quir
es b
asic
Pow
erPo
int
(ver
sion
200
7 or
new
er)
skill
s. B
elow
is a
list
of
com
mon
ly
aske
d qu
esti
ons
spec
ific
to
this
tem
plat
e.
If y
ou a
re u
sing
an
olde
r ve
rsio
n of
Pow
erPo
int
som
e te
mpl
ate
feat
ures
may
not
wor
k pr
oper
ly.
U
sing
the
tem
plat
e
Veri
fyin
g th
e qu
alit
y of
you
r gr
aphi
cs
Go
to t
he V
IEW
men
u an
d cl
ick
on Z
OO
M t
o se
t yo
ur
pref
erre
d m
agni
fica
tion
. Th
is t
empl
ate
is a
t 10
0% t
he s
ize
of t
he f
inal
pos
ter.
All
text
and
gra
phic
s w
ill b
e pr
inte
d at
10
0% t
heir
siz
e. T
o se
e w
hat
your
pos
ter
will
look
like
w
hen
prin
ted,
set
the
zoo
m t
o 10
0% a
nd e
valu
ate
the
qual
ity
of a
ll yo
ur g
raph
ics
befo
re y
ou s
ubm
it y
our
post
er
for
prin
ting
. U
sing
the
pla
ceho
lder
s To
add
tex
t to
thi
s te
mpl
ate
clic
k in
side
a p
lace
hold
er a
nd
type
in o
r pa
ste
your
tex
t. T
o m
ove
a pl
aceh
olde
r, c
lick
on
it o
nce
(to
sele
ct it
), p
lace
you
r cu
rsor
on
its
fram
e an
d yo
ur c
urso
r w
ill c
hang
e to
thi
s sy
mbo
l:
The
n, c
lick
once
and
dra
g it
to
its
new
loca
tion
whe
re y
ou c
an r
esiz
e it
as
need
ed.
Addi
tion
al p
lace
hold
ers
can
be f
ound
on
the
left
sid
e of
thi
s te
mpl
ate.
M
odif
ying
the
layo
ut
This
tem
plat
e ha
s fo
ur d
iffe
rent
co
lum
n la
yout
s.
Rig
ht-c
lick
your
m
ouse
on
the
back
grou
nd a
nd
clic
k on
“La
yout
” to
see
the
la
yout
opt
ions
. T
he c
olum
ns in
th
e pr
ovid
ed la
yout
s ar
e fi
xed
and
can
not
be m
oved
but
ad
vanc
ed u
sers
can
mod
ify
any
layo
ut b
y go
ing
to V
IEW
an
d th
en S
LID
E M
ASTE
R.
Impo
rtin
g te
xt a
nd g
raph
ics
from
ext
erna
l sou
rces
TE
XT:
Past
e or
typ
e yo
ur t
ext
into
a p
re-e
xist
ing
plac
ehol
der
or d
rag
in a
new
pla
ceho
lder
fro
m t
he le
ft
side
of
the
tem
plat
e. M
ove
it a
nyw
here
as
need
ed.
PHO
TOS:
Dra
g in
a p
ictu
re p
lace
hold
er,
size
it f
irst
, cl
ick
in it
and
inse
rt a
pho
to f
rom
the
men
u.
TABL
ES:
You
can
copy
and
pas
te a
tab
le f
rom
an
exte
rnal
do
cum
ent
onto
thi
s po
ster
tem
plat
e. T
o ad
just
the
way
th
e te
xt f
its
wit
hin
the
cells
of
a ta
ble
that
has
bee
n pa
sted
, ri
ght-
clic
k on
the
tab
le,
clic
k FO
RMAT
SH
APE
th
en c
lick
on T
EXT
BOX
and
chan
ge t
he IN
TERN
AL M
ARG
IN
valu
es t
o 0.
25
Mod
ifyi
ng t
he c
olor
sch
eme
To c
hang
e th
e co
lor
sche
me
of t
his
tem
plat
e go
to
the
“Des
ign”
men
u an
d cl
ick
on “
Colo
rs”.
You
can
cho
ose
from
th
e pr
ovid
e co
lor
com
bina
tion
s or
you
can
cre
ate
your
ow
n.
QU
ICK
DES
IGN
GU
IDE
(--T
HIS
SEC
TIO
N D
OES
NO
T PR
INT-
-)
Th
is P
ower
Poin
t 20
07 t
empl
ate
prod
uces
a 3
0x40
inch
pr
ofes
sion
al p
oste
r. It
will
sav
e yo
u va
luab
le t
ime
plac
ing
titl
es,
subt
itle
s, t
ext,
and
gra
phic
s.
Use
it t
o cr
eate
you
r pr
esen
tati
on.
Then
sen
d it
to
Post
erPr
esen
tati
ons.
com
for
pre
miu
m q
ualit
y, s
ame
day
affo
rdab
le p
rint
ing.
W
e pr
ovid
e a
seri
es o
f on
line
tuto
rial
s th
at w
ill g
uide
you
th
roug
h th
e po
ster
des
ign
proc
ess
and
answ
er y
our
post
er
prod
ucti
on q
uest
ions
.
View
our
onl
ine
tuto
rial
s at
: h
ttp:
//bi
t.ly
/Pos
ter_
crea
tion
_hel
p
(cop
y an
d pa
ste
the
link
into
you
r w
eb b
row
ser)
. Fo
r as
sist
ance
and
to
orde
r yo
ur p
rint
ed p
oste
r ca
ll Po
ster
Pres
enta
tion
s.co
m a
t 1.
866.
649.
3004
Obj
ect
Plac
ehol
ders
Use
the
pla
ceho
lder
s pr
ovid
ed b
elow
to
add
new
ele
men
ts
to y
our
post
er:
Dra
g a
plac
ehol
der
onto
the
pos
ter
area
, si
ze it
, an
d cl
ick
it t
o ed
it.
Sect
ion
Hea
der
plac
ehol
der
Mov
e th
is p
refo
rmat
ted
sect
ion
head
er p
lace
hold
er t
o th
e po
ster
are
a to
add
ano
ther
sec
tion
hea
der.
Use
sec
tion
he
ader
s to
sep
arat
e to
pics
or
conc
epts
wit
hin
your
pr
esen
tati
on.
Te
xt p
lace
hold
er
Mov
e th
is p
refo
rmat
ted
text
pla
ceho
lder
to
the
post
er t
o ad
d a
new
bod
y of
tex
t.
Pict
ure
plac
ehol
der
Mov
e th
is g
raph
ic p
lace
hold
er o
nto
your
pos
ter,
siz
e it
fi
rst,
and
the
n cl
ick
it t
o ad
d a
pict
ure
to t
he p
oste
r.
RES
EAR
CH
PO
STER
PR
ESEN
TATI
ON
DES
IGN
© 2
012
ww
w.P
oste
rPre
sent
atio
ns.c
om
© 2
012
Post
erPr
esen
tatio
ns.c
om
2
117
Four
th S
tree
t , U
nit C
Ber
kele
y CA
947
10
p
oste
rpre
sent
er@
gmai
l.com
St
uden
t di
scou
nts
are
avai
labl
e on
our
Fac
eboo
k pa
ge.
Go
to P
oste
rPre
sent
atio
ns.c
om a
nd c
lick
on t
he F
B ic
on.
Back
grou
nd:
Moh
s su
rger
y is
one
of
the
mos
t ef
fect
ive
trea
tmen
t op
tion
s fo
r sk
in c
ance
rs a
s it
off
ers
one
of t
he h
ighe
st c
hanc
es f
or c
ure.
Moh
s su
rger
y is
a
prec
ise
tech
niqu
e th
at r
emov
es a
laye
r at
a t
ime.
Alt
houg
h th
is m
ay b
e ad
vant
ageo
us,
this
tre
atm
ent
met
hod
is d
iffi
cult
in p
atie
nts
wit
h im
mun
obul
lous
dis
ease
s. C
urre
ntly
, th
e gu
idel
ines
for
moh
s su
rger
y do
not
di
scus
s th
e pr
eman
agem
ent
of im
mun
obul
lous
pat
ient
s ab
out
to u
nder
go m
ohs
surg
ery.
O
bjec
tive
: To
adv
ocat
e fo
r in
crea
sing
pre
dnis
one
dose
in p
atie
nts
wit
h im
mun
obul
lous
dis
ease
pri
or t
o un
derg
oing
Moh
s su
rger
y.
Case
Rep
ort:
We
pres
ent
a ca
se o
f an
exc
isio
n of
a s
quam
ous
cell
carc
inom
a (S
CC)
from
a 9
4-ye
ar-o
ld w
oman
wit
h a
hist
ory
of p
emph
igus
vul
gari
s us
ing
Moh
s m
icro
grap
hic
surg
ery
(MM
S).
Co
nclu
sion
: Cu
rren
t pr
e-op
gui
delin
es f
or M
ohs
surg
ery
do n
ot a
ddre
ss t
he
issu
e of
alt
erin
g st
eroi
d m
edic
atio
ns f
or p
atie
nts
wit
h im
mun
obul
lous
dis
ease
pr
ior
to t
he p
roce
dure
. W
e su
gges
t th
at p
atie
nts
wit
h a
hist
ory
of
imm
unob
ullo
us d
isea
se u
nder
goin
g M
MS
shou
ld h
ave
an in
crea
se in
ste
roid
do
se p
rior
to
surg
ery.
Abst
ract
Case
Rep
ort
Disc
ussi
on
We
pres
ent
the
idea
of
impl
emen
ting
gui
delin
es f
or p
atie
nts
wit
h im
mun
obul
lous
dis
ease
abo
ut t
o un
derg
o M
MS.
Cur
rent
ly,
ther
e ar
e no
gu
idel
ines
in t
erm
s of
adj
usti
ng p
redn
ison
e in
pat
ient
s w
ith
imm
unob
ullo
us
dise
ase
abou
t to
und
ergo
MM
S.
Wit
h ill
def
ined
bor
ders
com
mon
ly o
ccur
ring
wit
h SC
C le
sion
s in
pat
ient
s w
ith
bullo
us d
isea
se,
MM
S is
mor
e ad
vant
ageo
us,
sinc
e it
allo
ws
for
tiss
ue s
pari
ng
whi
ch is
impe
rati
ve i
n th
ese
pati
ents
who
hav
e im
pair
ed w
ound
hea
ling
and
are
at in
crea
sed
risk
of
infe
ctio
n (1
). T
here
are
man
y ch
alle
nges
in p
erfo
rmin
g M
MS
in a
pat
ient
wit
h an
imm
unob
ullo
us d
isea
se.
The
se in
clud
e di
ffic
ulty
in
asse
ssin
g m
argi
ns d
urin
g M
MS
(1),
tis
sue
frag
ility
(1)
, po
or w
ound
hea
ling
seco
ndar
y to
a la
ck o
f ep
ider
mis
(2)
, an
d an
incr
ease
d ri
sk o
f po
st in
fect
ion
seco
ndar
y to
a n
on in
tact
epi
derm
al b
arri
er (
3).
Tiss
ue f
ragi
lity
com
plic
ates
clo
sure
in b
ullo
us d
isea
se (
1).
Alth
ough
def
ects
ca
n be
allo
wed
to
heal
by
seco
ndar
y in
tent
ion,
re-
epit
heliz
atio
n m
ay n
ot b
e ad
equa
te a
nd c
ause
poo
r w
ound
hea
ling
(2)
whi
ch m
ay a
llow
for
a r
ecur
renc
e of
ero
sion
or
ulce
rati
on (
3).
A pa
tien
t w
ho h
as a
non
inta
ct e
pide
rmal
bar
rier
is
mor
e pr
one
to in
crea
sed
risk
of
infe
ctio
n po
st s
urge
ry.
A st
rong
er a
nd in
tact
de
rmis
pri
or t
o su
rger
y ca
n be
acc
ompl
ishe
d by
incr
easi
ng s
tero
id d
ose
prio
r to
sur
gery
.
To o
ur k
now
ledg
e, t
here
has
onl
y be
en o
ne d
ocum
ente
d ca
se o
f m
argi
ns b
eing
di
ffic
ult
to a
sses
s in
a p
atie
nt w
ith
a bu
llous
dis
ease
(1)
, al
thou
gh t
his
may
al
read
y be
a c
omm
on s
cena
rio
for
derm
atol
ogis
ts w
ho h
ave
cond
ucte
d M
MS
in
pati
ents
wit
h bu
llous
dis
ease
. S
axen
a et
al.
indi
cate
tha
t th
e su
rgeo
n an
d te
chni
cian
sho
uld
exer
cise
ext
rem
e ca
re t
o m
aint
ain
the
inte
grit
y of
the
ti
ssue
sin
ce t
he e
pide
rmis
ten
ds t
o di
ssoc
iate
fro
m t
he d
erm
is d
urin
g M
MS
in
pati
ents
wit
h ep
ider
mol
ysis
bul
losa
(1)
. Th
e au
thor
s al
so r
ecom
men
d a
fres
h sc
alpe
l bl
ade
for
each
laye
r an
d a
shar
p cr
yost
atic
kni
fe t
o m
inim
ize
epid
erm
al s
epar
atio
n on
fro
zen
sect
ions
. O
ther
sug
gest
ions
incl
ude
com
plet
e ti
ssue
fre
ezin
g, w
ith
the
addi
tion
of
cryo
gen
spra
y or
hea
t ex
trac
tion
to
help
de
crea
se s
hear
ing
forc
es a
nd a
llow
for
eas
ier
froz
en s
ecti
ons.
Fur
ther
re
com
men
dati
ons
incl
ude
para
ffin
em
bedd
ing
wit
h ho
rizo
ntal
ori
enta
tion
(“
slow
Moh
s”)
if n
eede
d. M
oreo
ver,
dur
ing
the
appl
icat
ion
of d
ress
ings
, ad
diti
onal
car
e m
ust
be t
aken
to
avoi
d ti
ssue
tra
uma.
W
e be
lieve
tha
t m
ost
of t
hese
str
inge
nt m
easu
res
can
be p
reve
nted
by
incr
easi
ng s
tero
id d
osag
e pr
ior
to s
urge
ry.
In
our
exp
erie
nce,
alt
houg
h M
MS
prov
ides
pre
cise
mar
gin
cont
rol,
it is
in
adeq
uate
sin
ce e
pide
rmis
doe
s no
t pr
esen
t du
ring
cro
ss s
ecti
on.
Spec
ial
atte
ntio
n an
d ex
tra
effo
rt t
o ti
ssue
han
dlin
g, p
roce
ssin
g, m
icro
scop
ic
eval
uati
on,
clos
ure
tech
niqu
e, a
nd p
osto
pera
tive
wou
nd c
are
can
all b
e m
inim
ized
wit
h an
incr
ease
in s
tero
ids.
Refe
renc
es
Saxe
na,
A.,
Lee,
J.
B. a
nd H
umph
reys
, T.
R.
(200
6),
Moh
s M
icro
grap
hic
Surg
ery
for
Squa
mou
s Ce
ll Ca
rcin
oma
Asso
ciat
ed w
ith
Epid
erm
olys
is B
ullo
sa.
Der
mat
olog
ic S
urge
ry,
32:
128–
134.
doi
: 10
.111
1/15
24-4
725.
2006
.320
21
Swen
sson
O,
Chri
stop
hers
E.
Gen
eral
ized
atr
ophi
c be
nign
epi
derm
olys
is b
ullo
sa i
n 2
sibl
ings
com
plic
ated
by
mul
tipl
e sq
uam
ous
cell
carc
inom
as.
Arch
Der
mat
ol 1
998;
134:
199
– 2
03.
Terr
ill P
J, M
ayou
BJ,
McK
ee P
H,
Eady
RAJ
. Th
e su
rgic
al m
anag
emen
t of
dys
trop
hic
epid
erm
olys
is b
ullo
sa (
excl
udin
g th
e ha
nd).
Br
J Pl
ast
Surg
199
2;45
:426
–34.
A 94
yea
r-ol
d Ca
ucas
ian
fem
ale
wit
h no
pri
or h
isto
ry o
f sk
in c
ance
r pr
esen
ted
for
eval
uati
on o
f a
crus
ting
pla
que
on h
er m
id b
ack
whi
ch h
ad b
een
pres
ent
for
6 m
onth
s. T
he p
atie
nt´s
pas
t m
edic
al h
isto
ry w
as s
igni
fica
nt f
or
pem
phig
us v
ulga
ris
for
the
last
20
year
s w
hich
she
was
on
pred
niso
ne 2
.5m
g da
ily.
The
pati
ent
repo
rted
no
alle
rgie
s. S
he d
enie
d sm
okin
g an
d de
nied
al
coho
l use
. Re
view
of
syst
ems
was
unr
emar
kabl
e an
d ph
ysic
al e
xam
inat
ion
reve
aled
a w
ell-
deve
lope
d, w
ell-
nour
ishe
d fe
mal
e. U
pon
com
plet
e sk
in
exam
inat
ion,
the
mid
bac
k pr
esen
ted
wit
h a
5 cm
x 4
cm
ery
them
atou
s, w
axy,
an
d cr
usty
pla
que
(Fig
ure
1).
The
surr
ound
ing
area
s of
ski
n w
ere
exam
ined
an
d no
oth
er s
uspi
ciou
s le
sion
s w
ere
note
d. T
he le
sion
was
bio
psie
d an
d a
diag
nosi
s of
squ
amou
s ce
ll ca
rcin
oma
(SCC
) w
as e
stab
lishe
d.
On
the
sche
dule
d da
y of
sur
gery
, th
e pa
tien
t di
d ha
ve a
new
ora
l ulc
er o
n he
r le
ft b
ucca
l m
ucos
a. T
he p
atie
nt d
id n
ot
exhi
bit
any
othe
r ac
tive
les
ions
. H
owev
er,
duri
ng c
uret
tage
and
the
inci
sion
, he
r sk
in
beca
me
posi
tive
for
Nik
olsk
y si
gn a
nd t
he
epid
erm
is s
loug
hed
off
imm
edia
tely
(F
igur
e 2)
. Th
e sq
uam
ous
cell
carc
inom
a w
as t
hen
exci
sed
wit
h w
ider
mar
gins
usi
ng
Moh
s m
icro
grap
hic
surg
ery
(MM
S) in
one
st
age.
In c
oncl
usio
n, t
he M
MS
perf
orm
ed o
n ou
r pa
tien
t tu
rned
out
to
be q
uite
ch
alle
ngin
g. T
hus
we
sugg
est
incr
easi
ng
pred
niso
ne p
rior
to
surg
ery
in o
rder
to
wor
k w
ith
a m
ore
inta
ct e
pide
rmis
, ev
en
in p
atie
nts
who
app
ear
to h
ave
thei
r di
seas
e un
der
cont
rol.
Thi
s w
ill p
rom
ote
grea
ter
inta
ct e
pide
rmis
, th
us a
llow
ing
mor
e ac
cura
te m
argi
n di
agno
stic
s, e
asie
r cl
osur
e, a
nd le
ss p
ossi
bilit
y of
pos
t pr
oced
ure
infe
ctio
n of
the
sit
e.
anym
ore.
A c
ompr
essi
on d
ress
ing
cons
isti
ng o
f xe
rofo
rm w
as u
sed
to a
void
the
us
e of
adh
esiv
e ta
pe o
n su
rrou
ndin
g ti
ssue
tha
t ha
d be
com
e pr
one
to
blis
teri
ng.
Our
goa
l was
to
avoi
d ad
hesi
ves
alto
geth
er,
sinc
e th
ey f
urth
er
trau
mat
ize
the
frag
ile s
kin.
The
pat
ient
ret
urne
d fo
r he
r 2
wee
k fo
llow
up
for
sutu
re r
emov
al a
nd w
as d
iagn
osed
wit
h M
RSA
infe
ctio
n. T
his
was
sub
sequ
entl
y cu
ltur
ed,
and
trea
ted
wit
h do
xycy
line.
The
pat
ient
ret
urne
d 1
wee
k th
erea
fter
for
sut
ure
rem
oval
and
hea
led
wel
l wit
h no
oth
er c
ompl
icat
ions
.
Figu
re 1
- L
eft
Upp
er B
ack
– Pr
e-op
Furt
herm
ore,
clo
sing
the
lesi
on w
as
very
dif
ficu
lt (
Figu
re 3
). T
he d
efec
t w
as r
epai
red
utili
zing
3-0
Vic
ryl a
nd
4-0
Nyl
on w
hich
wer
e pl
aced
fro
m
oppo
site
edg
es o
f th
e de
fect
spa
nnin
g th
e w
idth
of
the
open
ing
to m
inim
ize
tens
ion
at t
he w
ound
edg
es.
Dur
ing
mic
rosc
opic
exa
min
atio
n of
the
fro
zen
sect
ion,
it w
as d
iffi
cult
to
asse
ss if
the
m
argi
ns w
ere
still
pos
itiv
e fo
r ca
ncer
be
caus
e th
e ep
ider
mis
was
not
pre
sent
*Jus
tin R
ubin
, D.O
. **
Khas
ha T
oulo
ei, D
.O. *
** T
racy
Fav
reau
, D.O
. **
** M
artin
Zai
ac, M
D **
***
Shin
o Ba
y, D
.O.,
FAO
CD
*Sec
ond
Year
Der
mat
olog
y Re
side
nt, N
SUCO
M/B
GM
C, F
t. La
uder
dale
, FL*
* 1st
Yea
r, Tr
aditi
onal
Rot
atin
g In
tern
ship
, Lar
go
Med
ical
Cen
ter *
** C
hairm
an o
f Der
mat
olog
y N
SUCO
M/B
GM
C, F
t. La
uder
dale
, FL*
***
Dire
ctor
of t
he D
epar
tmen
t of
Derm
atol
ogy,
Mou
nt S
inai
Med
ical
Cen
ter
****
* Re
side
ncy
Trai
ning
Pro
gram
Dire
ctor
, NSU
COM
/BG
MC,
Ft.
Laud
erda
le, F
L
Moh
s Sur
gery
in P
atie
nts w
ith Im
mun
obul
lous
Dis
ease
s: S
houl
d Pr
edni
sone
be
Incr
ease
d Pr
ior t
o Su
rger
y?
Figu
re 2
- In
tra-
op
Figu
re 3
– P
ost
op

273
Pote
ntia
l Com
plic
atio
ns o
f Ps
oria
sis
Ther
apy:
A C
ase
Repo
rt a
nd
Revi
ew o
f Ca
tast
roph
ic A
ntip
hosp
holip
id S
yndr
ome
(CA
PS)
Nic
hola
s A
. Rud
loff
, D.O
.* an
d Sc
hiel
d M
. Wik
as, D
.O.,
DF,
FA
OCD
**O
hio
Uni
vers
ity
Colle
ge o
f O
steo
path
ic M
edic
ine
Sum
ma
Wes
tern
Res
erve
Hos
pita
l, Cu
yaho
ga F
alls
, OH
, USA
*Der
mat
olog
y Re
side
nt (P
GY-
5), S
WRH
, **D
erm
atol
ogy
Resi
denc
y Pr
ogra
m D
irec
tor,
SWRH
Cata
stro
phic
ant
ipho
spho
lipid
syn
drom
e (C
APS
) is
a ra
re c
ondi
tion
tha
t m
akes
up
a sm
all s
ubse
t of
pat
ient
s w
ith
anti
phos
phol
ipid
syn
drom
e (A
PS).
It in
volv
es a
dra
mat
ic, a
ccel
erat
ed f
orm
of
APS
whi
ch r
esul
ts in
mul
ti-o
rgan
fa
ilure
and
a h
igh
mor
talit
y ra
te. T
o da
te, n
o ca
ses
of C
APS
hav
e be
en
repo
rted
in p
atie
nts
whi
le o
n et
aner
cept
for
tre
atm
ent
of c
hron
ic p
atch
and
pl
aque
pso
rias
is v
ulga
ris.
We
desc
ribe
a 5
1-ye
ar-o
ld m
ale
who
pre
sent
ed
wit
h “fl
u-lik
e” s
ympt
oms
whi
le o
n sy
stem
ic b
iolo
gic
ther
apy,
eta
nerc
ept.
H
e de
velo
ped
rapi
d on
set
of m
ulti
ple
thro
mbo
embo
li an
d a
sequ
ence
of
life-
thre
aten
ing
even
ts; h
e w
as d
iagn
osed
wit
h CA
PS. T
his
case
rep
ort
exhi
bits
pot
enti
al r
are
com
plic
atio
ns in
the
man
agem
ent
of p
sori
asis
and
re
view
s CA
PS in
clud
ing
clin
ical
pre
sent
atio
n, m
anag
emen
t an
d di
scus
sion
.
Case
Des
crip
tion
1. V
ora
SK, A
sher
son
RA, E
rkan
D. C
atas
trop
hic
antip
hosp
holip
id s
yndr
ome.
J In
tens
ive
Care
Med
. 200
6; 2
1:14
4-15
9.2.
Ber
mas
B, e
t al.
Clin
ical
man
ifest
atio
ns o
f the
ant
ipho
spho
lipid
syn
drom
e. U
ptod
ate.
201
0; D
ate
acce
ssed
2/9
/11.
3.
Buc
ciar
elli
S, E
spin
osa
G, C
erve
ra R
. The
CAP
S Re
gist
ry: m
orbi
dity
and
mor
talit
y of
the
cata
stro
phic
ant
ipho
spho
lipid
syn
drom
e. L
upus
. 200
9;18
:905
-912
.4.
Cer
vera
R, e
t al.
Cata
stro
phic
ant
ipho
spho
lipid
syn
drom
e (C
APS)
: upd
ate
from
the
‘CAP
S Re
gist
ry.’
Lupu
s. 2
010;
19:4
12-4
18.
5. C
erve
ra R
, Esp
inos
a G,
Buc
ciar
elli
S, e
t al.
Less
ons
from
the
cata
stro
phic
ant
ipho
spho
lipid
syn
drom
e (C
APS)
reg
istr
y. A
utoi
mm
unity
Rev
iew
s 6.
200
6;81
-84.
6. A
than
azio
D, e
t al.
Chro
nic
cata
stro
phic
-lik
e an
tipho
spho
lipid
syn
drom
e: a
“sm
olde
ring”
var
iant
? Rh
eum
atol
Int.
2009
;30:
123-
125.
7. S
olte
sz P
, et a
l. Ca
tast
roph
ic a
ntip
hosp
holip
id s
yndr
ome
in c
ance
r. H
aem
atol
ogia
. 200
0;30
(4):3
03-3
11.
8. B
ayra
ktar
U, e
t al.
The
clin
ical
spe
ctru
m o
f cat
astr
ophi
c an
tipho
spho
lipid
syn
drom
e in
the
abse
nce
and
pres
ence
of l
upus
. Jou
rnal
of R
heum
atol
ogy.
200
7;34
(2):
346-
352.
9. A
sher
son
RA, e
t al.
Dis
sem
inat
ed in
trav
ascu
lar
coag
ulat
ion
in c
atas
trop
hic
antip
hosp
holip
id s
yndr
ome:
clin
ical
and
hae
mat
olog
ical
cha
ract
eris
tics
of 2
3 pa
tient
s. A
nn
Rheu
m D
is. 2
005;
64:9
43-9
46.
10.
Kim
S, e
t al.
Cata
stro
phic
ant
ipho
spho
lipid
syn
drom
e tr
igge
red
by s
epsi
s. H
SSJ.
2009
;5:6
7-72
.11
. M
agee
CC,
et a
l. Ca
se 2
-200
8: A
38-
year
-old
wom
an w
ith p
ostp
artu
m v
isua
l los
s, s
hort
ness
of b
reat
h, a
nd r
enal
failu
re. N
Eng
l J M
ed. 2
008;
358:
275-
289.
12
. As
hers
on R
A, C
erve
ra R
, de
Groo
t PG,
et a
l. Ca
tast
roph
ic a
ntip
hosp
holip
id s
yndr
ome:
inte
rnat
iona
l con
sens
us s
tate
men
t on
clas
sific
atio
n cr
iteria
and
trea
tmen
t gu
idel
ines
. Lup
us. 2
003;
12:5
30-5
34.
13.
Ashe
rson
RA,
Sho
enfe
ld Y
. The
rol
e of
infe
ctio
n in
the
path
ogen
esis
of c
atas
trop
hic
antip
hosp
holip
id s
yndr
ome-
mol
ecul
ar m
imic
ry?
Jour
nal o
f Rhe
umat
olog
y.
2000
;27(
1):2
012-
2014
.14
. Ca
npol
at N
, et a
l. A
case
of c
atas
trop
hic
antip
hosp
holip
id s
yndr
ome
in a
n ad
oles
cent
girl
with
par
vovi
rus
B19
infe
ctio
n. C
linic
al P
edia
tric
s. 2
008;
47(6
):593
-597
.15
. Id
eguc
hi H
, Ohn
o S,
Ishi
gats
ubo
Y. C
atas
trop
hic
antip
hosp
holip
id s
yndr
ome
asso
ciat
ed w
ith m
alig
nanc
ies
(cas
e re
port
and
rev
iew
of t
he li
tera
ture
). Lu
pus.
20
07;1
6:59
-64.
16.
Wes
tney
G, H
arris
NE.
Cat
astr
ophi
c an
tipho
spho
lipid
syn
drom
e in
the
inte
nsiv
e ca
re u
nit.
Crit
Care
Clin
. 200
2;18
:805
-817
.17
. As
hers
on R
. Mul
tiorg
an fa
ilure
and
ant
ipho
spho
lipid
ant
ibod
ies:
the
cata
stro
phic
ant
ipho
spho
lipid
(Ash
erso
n’s)
syn
drom
e. Im
mun
onbi
olog
y. 2
005;
210:
727-
733.
18.
Peng
o V,
et a
l. An
ti B2
-gly
copr
otei
n I a
ntib
odie
s in
a p
atie
nt w
ith c
atas
trop
hic
antip
hosp
holip
id s
yndr
ome.
Clin
ical
rhe
umat
olog
y. 1
995;
14(6
):646
-649
.19
. Er
kan
D, L
ocks
hin
MD
. New
trea
tmen
ts fo
r an
tipho
spho
lipid
syn
drom
e. R
heum
Dis
Clin
N A
m. 2
006;
32:1
29-1
48.
20.
Erka
n D
, Cer
vera
R, A
sher
son
RA. C
atas
trop
hic
antip
hosp
holip
id s
yndr
ome:
whe
re d
o w
e st
and?
Art
hriti
s an
d Rh
eum
atis
m. 2
003;
48(1
2):3
320-
3327
.21
. N
euw
elt C
M, e
t al.
Cata
stro
phic
ant
ipho
spho
lipid
syn
drom
e: r
espo
nse
to r
epea
ted
plas
map
here
sis
over
thre
e ye
ars.
Art
hriti
s an
d Rh
eum
atis
m. 1
997;
40(8
):153
4-15
39.
Refe
renc
es
Abs
trac
t
CA
PS D
iagn
ostic
Cri
teri
a:1.
Clin
ical
evi
denc
e of
mul
tiple
org
an in
volv
emen
t de
velo
ping
ove
r a v
ery
shor
t per
iod
of ti
me.
2. H
isto
path
olog
ical
evi
denc
e of
mul
tiple
smal
l ves
sel
occl
usio
ns.
3. L
abor
ator
y co
nfirm
atio
n of
the
pres
ence
of
antip
hosp
holip
id a
ntib
odie
s, us
ually
in a
hig
h tit
er.
Figu
res
Dis
cuss
ion
A 5
1-ye
ar-o
ld c
auca
sian
mal
e pr
esen
ted
to t
he o
utpa
tien
t de
rmat
olog
y cl
inic
for
rou
tine
fol
low
-up
for
chro
nic
patc
h an
d pl
aque
pso
rias
is (F
ig. 1
). U
pon
revi
ew o
f sy
stem
s, t
he p
atie
nt d
escr
ibed
“flu
-lik
e” s
ympt
oms
for
seve
ral m
onth
s in
clud
ing:
fev
er, c
hills
, nig
ht s
wea
ts, w
eakn
ess,
fat
igue
and
ar
thra
lgia
s in
his
han
ds w
ith
asso
ciat
ed s
wel
ling.
Past
med
ical
his
tory
was
sig
nific
ant
for
at le
ast
a tw
enty
-yea
r hi
stor
y of
ch
roni
c pa
tch
and
plaq
ue t
ype
psor
iasi
s vu
lgar
is.
Ther
apeu
tic
stra
tegy
co
nsis
ted
of t
opic
al t
hera
py a
nd s
yste
mic
bio
logi
c th
erap
y et
aner
cept
25m
g su
bcut
aneo
usly
tw
ice
wee
kly
for
psor
iasi
s ov
er a
ppro
xim
atel
y th
e pa
st
thre
e ye
ars.
On
init
ial p
rese
ntat
ion,
the
pat
ient
app
eare
d in
no
dist
ress
. H
e ex
hibi
ted
sign
ifica
nt b
ilate
ral a
xilla
ry ly
mph
aden
opat
hy u
pon
palp
atio
n an
d ha
d ha
nd
swel
ling
invo
lvin
g th
e m
etac
arpa
l-ph
alan
geal
join
ts a
nd p
roxi
mal
in
terp
hala
ngea
l joi
nts
of b
oth
hand
s. T
he p
atie
nt w
as o
rder
ed p
rom
pt
labo
rato
ry e
valu
atio
n an
d ch
est
radi
ogra
phy
rega
rdin
g hi
s sy
mpt
oms.
A
lso,
wit
h co
ncer
n fo
r an
und
erly
ing
mal
igna
ncy,
the
pat
ient
was
ref
erre
d to
hem
atol
ogy/
onco
logy
for
con
sult
atio
n. I
niti
al la
bs:
-Ele
vate
d rh
eum
atoi
d fa
ctor
of
443
U/m
L-E
ryth
rocy
te s
edim
enta
tion
rat
e of
22
mm
/hr.
-LFT
’s, A
NA
, ACE
, tot
al c
ompl
emen
t ac
tivi
ty (C
H50
), se
rum
cry
oglo
bulin
s an
d SP
EP w
ere
all u
nrem
arka
ble.
-P
erip
hera
l sm
ear
reve
aled
a le
ukoc
ytos
is a
nd a
thr
ombo
cyto
sis
cons
iste
nt
wit
h re
acti
ve c
hang
es.
-Che
st r
adio
grap
h sh
owed
mul
tipl
e lu
ng n
odul
es in
the
bila
tera
l upp
er
lobe
s, t
he t
wo
larg
est
mea
suri
ng 1
3.3m
m in
the
rig
ht u
pper
lobe
and
15
.2m
m in
the
left
upp
er lo
be (F
ig. 2
).
Ove
r th
e co
urse
of
the
next
day
, the
pat
ient
dev
elop
ed s
ever
e ba
ck p
ain
and
bila
tera
l leg
dis
com
fort
. He
pres
ente
d to
a lo
cal c
omm
unit
y em
erge
ncy
depa
rtm
ent
and
was
fou
nd t
o ha
ve a
bsen
t bi
late
ral l
ower
ext
rem
ity
puls
es.
Com
pute
rize
d To
mog
raph
y A
ngio
gram
(CTA
) of
the
ches
t, ab
dom
en a
nd
pelv
is w
ith
bila
tera
l low
er e
xtre
mit
y ru
n-off
s sh
owed
diff
use
arte
rial
th
rom
bi in
the
aor
ta a
nd a
sad
dle
embo
lism
at
the
aort
oilia
c bi
furc
atio
n ex
tend
ing
into
the
left
com
mon
ilia
c ar
tery
(Fig
. 3).
Add
itio
nally
, inf
arct
ions
of
the
spl
een
and
kidn
eys
wer
e no
ted
(Fig
. 4).
The
pat
ient
was
imm
edia
tely
tr
ansf
erre
d to
a t
erti
ary
care
cen
ter.
He
unde
rwen
t m
ulti
ple
proc
edur
es
incl
udin
g em
erge
nt t
hrom
boem
bole
ctom
y an
d w
as t
reat
ed f
or a
nem
ia,
leuk
ocyt
osis
, thr
ombo
cyto
peni
a, S
TEM
I, ac
ute
rena
l fai
lure
, acu
te
resp
irat
ory
failu
re w
ith
mec
hani
cal v
enti
lati
on, s
yste
mic
infla
mm
ator
y re
spon
se s
yndr
ome
(SIR
S), m
ulti
ple
arte
rial
thr
ombi
, ren
al a
nd s
plen
ic
infa
rcts
. Fu
rthe
r la
bora
tory
stu
dies
rev
eale
d an
ele
vate
d an
tica
rdio
lipin
an
tibo
dy t
iter
. H
e w
as d
iagn
osed
wit
h ca
tast
roph
ic a
ntip
hosp
holip
id
synd
rom
e (C
APS
). A
fter
a t
wen
ty d
ay h
ospi
taliz
atio
n th
e pa
tien
t w
as
disc
harg
ed h
ome
in s
tabl
e co
ndit
ion.
Cata
stro
phic
ant
ipho
spho
lipid
syn
drom
e (C
APS
) is
a ra
re, l
ife-
thre
aten
ing,
w
ides
prea
d co
agul
opat
hy c
onsi
stin
g of
rap
id o
nset
of
vasc
ular
th
rom
boem
bolis
ms
that
oft
en r
esul
ts in
dea
th.1,
2
Curr
entl
y, it
com
pris
es 1
% o
f ca
ses
of A
PS.3
Mor
talit
y ra
tes
appr
oach
50%
.3-5
Mos
t ca
ses
aris
e de
nov
o (p
rim
ary)
, wit
hout
pre
viou
s hi
stor
y of
thr
ombo
sis,
3,6
but
It c
an a
lso
be a
ssoc
iate
d w
ith
othe
r au
toim
mun
e co
ndit
ions
(s
econ
dary
), su
ch a
s sy
stem
ic lu
pus
eryt
hem
atos
us, s
yste
mic
scl
eros
is a
nd
rheu
mat
oid
arth
riti
s.6-
8
Mor
e th
an h
alf
of t
he C
APS
cas
es a
re a
ssoc
iate
d w
ith
a pr
ecip
itat
ing
even
t su
ch a
s in
fect
ions
, sur
gery
, tra
uma,
neo
plas
ms
and
othe
rs. D
iagn
osis
can
be
mad
e w
ith
crit
eria
list
ed in
Fig
ure
5.9-
17
Alm
ost
all o
rgan
sys
tem
s ca
n be
invo
lved
in t
he s
pect
rum
of
CAPS
(Fig
. 6)
The
mos
t co
mm
on la
bora
tory
tes
ting
use
d to
det
ect
anti
phos
phol
ipid
an
tibo
dies
are
the
lupu
s an
tico
agul
ant
test
, ant
icar
diol
ipin
ant
ibod
y,
enzy
me
linke
d im
mun
osor
bent
ass
ay (E
LISA
) and
ant
i-B2
-gly
copr
otei
n-I
anti
body
ELI
SA.18
,19
Trea
tmen
t re
volv
es a
roun
d ea
rly
diag
nosi
s an
d ag
gres
sive
the
rapi
es.
The
mos
t pr
oven
the
rape
utic
str
ateg
ies
incl
ude:
ant
icoa
gula
tion
, co
rtic
oste
roid
s, p
lasm
a ex
chan
ge a
nd in
trav
enou
s im
mun
oglo
bulin
.20,2
1 T
he
com
bina
tion
of
thes
e st
rate
gies
hav
e be
en a
ssoc
iate
d w
ith
reco
very
rat
es
rang
ing
from
50-
80%
.12,1
9
Our
pat
ient
sur
vive
d an
d w
as d
isch
arge
d ho
me
from
the
hos
pita
l on
day
20. A
t 6
mon
th f
ollo
w u
p th
e pa
tien
t w
as s
till
livin
g an
d hi
s lo
ng-t
erm
pr
ogno
sis
is g
ood.
Th
e ro
le o
f et
aner
cept
in c
ontr
ibut
ing
to t
he c
ompl
icat
ions
of
our
pati
ent
is
diffi
cult
to
dete
rmin
e. C
once
rn f
or a
n in
fect
ious
pro
cess
tri
gger
ing
the
casc
ade-
effec
t of
CA
PS w
as a
pos
sibi
lity.
Als
o, a
n un
derl
ying
mal
igna
ncy
was
a m
ajor
con
side
rati
on in
the
init
ial w
orku
p. E
tane
rcep
t ha
s be
en
asso
ciat
ed w
ith
both
. Ce
rtai
nly,
the
re is
an
argu
men
t fo
r a
com
plet
ely
inde
pend
ent
proc
ess
such
as
a ne
w-o
nset
rhe
umat
oid
arth
riti
s. T
he
gene
ral c
onse
nsus
am
ong
the
heal
thca
re p
rovi
ders
in t
his
spec
ific
case
was
th
at e
tane
rcep
t pl
ayed
a r
ole
in t
he d
evel
opm
ent
of C
APS
; how
ever
, no
expl
icit
evi
denc
e ex
ists
to
prov
e th
is.
Alt
houg
h th
e ex
act
prec
ipit
atin
g fa
ctor
of
CAPS
in t
his
pati
ent
is d
ifficu
lt t
o pi
npoi
nt, t
his
case
rep
ort
does
re
veal
pot
enti
al r
are
com
plic
atio
ns t
hat
may
pre
sent
in t
he m
anag
emen
t of
a
pati
ent
wit
h ps
oria
sis.
Conc
lusi
onIn
sum
mar
y, C
APS
is a
rar
e co
ndit
ion,
acc
ount
ing
for
1% o
f al
l pat
ient
s w
ith
APS
. W
e de
mon
stra
ted
a ca
se-s
tudy
invo
lvin
g a
51-y
ear-
old
mal
e w
ith
psor
iasi
s vu
lgar
is w
ho p
rese
nted
to
the
outp
atie
nt d
erm
atol
ogy
office
wit
h “fl
u-lik
e” s
ympt
oms
whi
le o
n sy
stem
ic b
iolo
gic
ther
apy,
eta
nerc
ept.
In t
he
mid
st o
f ou
r w
orku
p, t
he p
atie
nt d
evel
oped
a r
apid
ons
et o
f ex
tens
ive
thro
mbo
embo
li an
d a
sequ
ence
of
life-
thre
aten
ing
even
ts t
hat
follo
wed
. Th
e pa
tien
t w
as d
iagn
osed
wit
h CA
PS.
We
revi
ewed
thi
s ra
re v
aria
nt o
f A
PS
and
disc
usse
d th
e sc
ope
of C
APS
in r
elat
ion
to o
ur p
atie
nt’s
pre
sent
atio
n.
Figu
res
(con
t.)
Fig.
1-C
hron
ic p
atch
and
pla
que
psor
iasi
s
Fig.
2-C
hest
X-r
ay s
how
ing
mul
tipl
e lu
ng n
odul
es in
the
bi
late
ral u
pper
lobe
s
Fig.
3-C
TA im
agin
g sh
owin
g sa
ddle
em
bolu
s at
the
aor
toili
ac
bifu
rcat
ion
exte
ndin
g in
to t
he le
ft
com
mon
ilia
c ar
tery
Fig.
4-C
TA im
agin
g sh
owin
g la
rge
rena
l inf
arct
s
Fig.
5-C
APS
Dia
gnos
tic
Crit
eria
11,1
2
Fig.
6-O
rgan
sys
tem
invo
lvem
ent
in C
APS
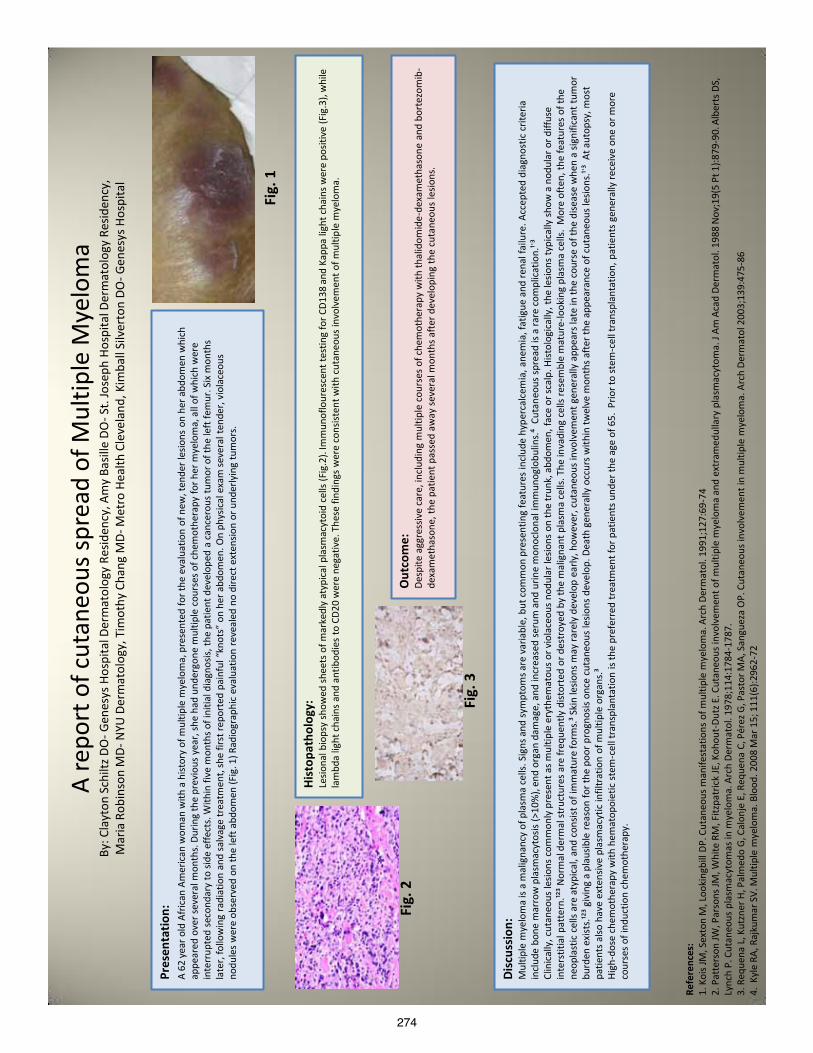
274
A re
port
of c
utan
eous
spre
ad o
f Mul
tiple
Mye
lom
a By
: Cla
yton
Sch
iltz D
O- G
enes
ys H
ospi
tal D
erm
atol
ogy
Resid
ency
, Am
y Ba
sille
DO
- St.
Jose
ph H
ospi
tal D
erm
atol
ogy
Resid
ency
, M
aria
Rob
inso
n M
D- N
YU D
erm
atol
ogy,
Tim
othy
Cha
ng M
D- M
etro
Hea
lth C
leve
land
, Kim
ball
Silv
erto
n DO
- Gen
esys
Hos
pita
l
Pres
enta
tion:
A
62 y
ear o
ld A
fric
an A
mer
ican
wom
an w
ith a
hist
ory
of m
ultip
le m
yelo
ma,
pre
sent
ed fo
r the
eva
luat
ion
of n
ew, t
ende
r les
ions
on
her a
bdom
en w
hich
ap
pear
ed o
ver s
ever
al m
onth
s. D
urin
g th
e pr
evio
us y
ear,
she
had
unde
rgon
e m
ultip
le c
ours
es o
f che
mot
hera
py fo
r her
mye
lom
a, a
ll of
whi
ch w
ere
inte
rrup
ted
seco
ndar
y to
side
effe
cts.
With
in fi
ve m
onth
s of i
nitia
l dia
gnos
is, th
e pa
tient
dev
elop
ed a
can
cero
us tu
mor
of t
he le
ft fe
mur
. Six
mon
ths
late
r, fo
llow
ing
radi
atio
n an
d sa
lvag
e tr
eatm
ent,
she
first
repo
rted
pai
nful
“kn
ots”
on
her a
bdom
en. O
n ph
ysic
al e
xam
seve
ral t
ende
r, vi
olac
eous
no
dule
s w
ere
obse
rved
on
the
left
abdo
men
(Fig
. 1) R
adio
grap
hic
eval
uatio
n re
veal
ed n
o di
rect
ext
ensio
n or
und
erly
ing
tum
ors.
Fig.
1
Hist
opat
holo
gy:
Lesio
nal b
iops
y sh
owed
shee
ts o
f mar
kedl
y at
ypic
al p
lasm
acyt
oid
cells
(Fig
.2).
Imm
unof
lour
esce
nt te
stin
g fo
r CD1
38 a
nd K
appa
ligh
t cha
ins w
ere
posit
ive
(Fig
.3),
whi
le
lam
bda
light
cha
ins
and
antib
odie
s to
CD2
0 w
ere
nega
tive.
The
se fi
ndin
gs w
ere
cons
isten
t with
cut
aneo
us in
volv
emen
t of m
ultip
le m
yelo
ma.
Out
com
e:
Desp
ite a
ggre
ssiv
e ca
re, i
nclu
ding
mul
tiple
cou
rses
of c
hem
othe
rapy
with
thal
idom
ide-
dexa
met
haso
ne a
nd b
orte
zom
ib-
dexa
met
haso
ne, t
he p
atie
nt p
asse
d aw
ay se
vera
l mon
ths a
fter d
evel
opin
g th
e cu
tane
ous
lesio
ns.
Fig.
2
Fig.
3
Disc
ussio
n:
Mul
tiple
mye
lom
a is
a m
alig
nanc
y of
pla
sma
cells
. Sig
ns a
nd sy
mpt
oms a
re v
aria
ble,
but
com
mon
pre
sent
ing
feat
ures
incl
ude
hype
rcal
cem
ia, a
nem
ia, f
atig
ue a
nd re
nal f
ailu
re. A
ccep
ted
diag
nost
ic c
riter
ia
incl
ude
bone
mar
row
pla
smac
ytos
is (>
10%
), en
d or
gan
dam
age,
and
incr
ease
d se
rum
and
urin
e m
onoc
lona
l im
mun
oglo
bulin
s.⁴
Cuta
neou
s sp
read
is a
rare
com
plic
atio
n.¹ʾ³
Cl
inic
ally
, cut
aneo
us le
sions
com
mon
ly p
rese
nt a
s mul
tiple
ery
them
atou
s or v
iola
ceou
s no
dula
r les
ions
on
the
trun
k, a
bdom
en, f
ace
or sc
alp.
Hist
olog
ical
ly, t
he le
sions
typi
cally
sho
w a
nod
ular
or d
iffus
e in
ters
titia
l pat
tern
.¹²³ N
orm
al d
erm
al st
ruct
ures
are
freq
uent
ly d
istor
ted
or d
estr
oyed
by
the
mal
igna
nt p
lasm
a ce
lls. T
he in
vadi
ng c
ells
rese
mbl
e m
atur
e-lo
okin
g pl
asm
a ce
lls.
Mor
e of
ten,
the
feat
ures
of t
he
neop
last
ic c
ells
are
atyp
ical
, and
con
sist o
f im
mat
ure
form
s.³ S
kin
lesio
ns m
ay ra
rely
dev
elop
ear
ly, h
owev
er, c
utan
eous
invo
lvem
ent g
ener
ally
app
ears
late
in th
e co
urse
of t
he d
iseas
e w
hen
a sig
nific
ant t
umor
bu
rden
exi
sts.
¹²³ g
ivin
g a
plau
sible
reas
on fo
r the
poo
r pro
gnos
is on
ce c
utan
eous
lesio
ns d
evel
op. D
eath
gen
eral
ly o
ccur
s with
in tw
elve
mon
ths a
fter t
he a
ppea
ranc
e of
cut
aneo
us le
sions
.¹ʾ³
At a
utop
sy, m
ost
patie
nts a
lso h
ave
exte
nsiv
e pl
asm
acyt
ic in
filtr
atio
n of
mul
tiple
org
ans.
³ Hi
gh-d
ose
chem
othe
rapy
with
hem
atop
oiet
ic s
tem
-cel
l tra
nspl
anta
tion
is th
e pr
efer
red
trea
tmen
t for
pat
ient
s und
er th
e ag
e of
65.
Prio
r to
stem
-cel
l tra
nspl
anta
tion,
pat
ient
s ge
nera
lly re
ceiv
e on
e or
mor
e co
urse
s of i
nduc
tion
chem
othe
rapy
.
Refe
renc
es:
1. K
ois J
M, S
exto
n M
, Loo
king
bill
DP. C
utan
eous
man
ifest
atio
ns o
f mul
tiple
mye
lom
a. A
rch
Derm
atol
. 199
1;12
7:69
-74
2. P
atte
rson
JW, P
arso
ns JM
, Whi
te R
M, F
itzpa
tric
k JE
, Koh
out-
Dutz
E. C
utan
eous
invo
lvem
ent o
f mul
tiple
mye
lom
a an
d ex
tram
edul
lary
pla
smac
ytom
a. J
Am A
cad
Derm
atol
. 198
8 N
ov;1
9(5
Pt 1
):879
-90.
Alb
erts
DS,
Ly
nch
P. C
utan
eous
pla
smac
ytom
as in
mye
lom
a. A
rch
Derm
atol
. 197
8;11
4:17
84-1
787.
3.
Req
uena
L, K
utzn
er H
, Pal
med
o G,
Cal
onje
E, R
eque
na C
, Pér
ez G
, Pas
tor M
A, S
angu
eza
OP.
Cut
aneo
us in
volv
emen
t in
mul
tiple
mye
lom
a. A
rch
Derm
atol
200
3;13
9:47
5-86
4.
Kyl
e RA
, Raj
kum
ar S
V. M
ultip
le m
yelo
ma.
Blo
od. 2
008
Mar
15;
111
(6):2
962-
72
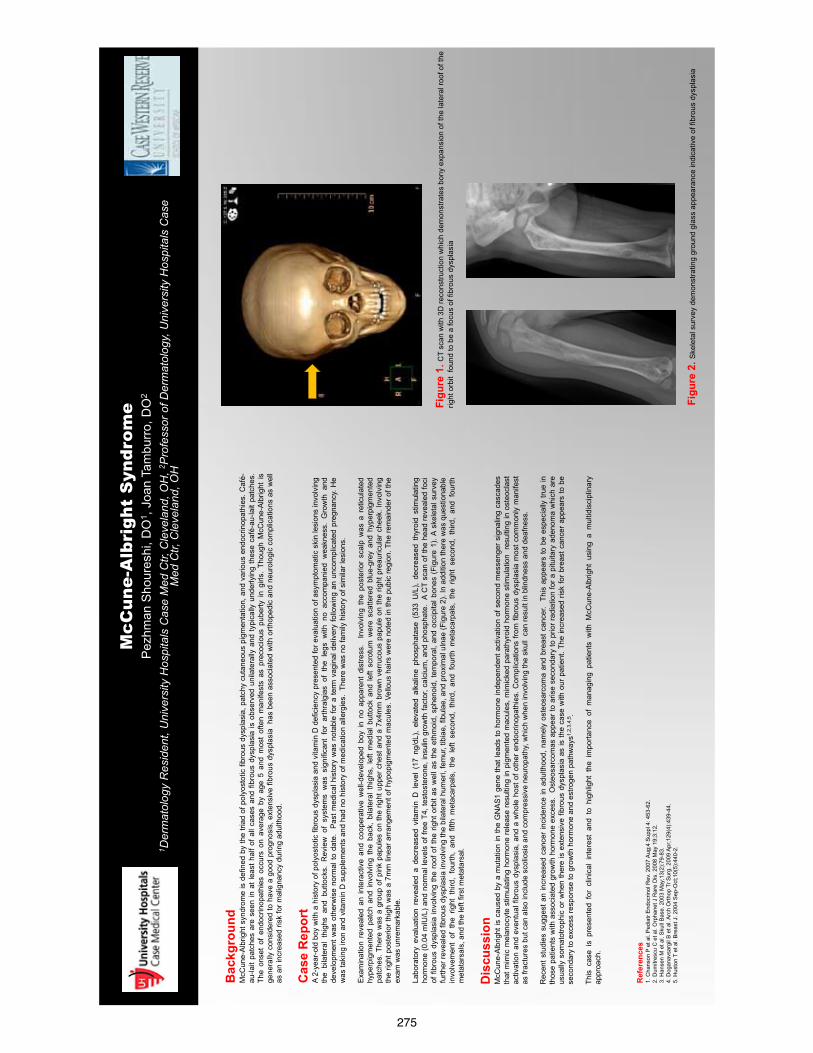
275
M
cCun
e-A
lbri
ght
Syn
drom
e P
ezhm
an S
hour
eshi
, DO
1 , Jo
an T
ambu
rro,
DO
2 1 D
erm
atol
ogy
Res
iden
t, U
nive
rsity
Hos
pita
ls C
ase
Med
Ctr,
Cle
vela
nd, O
H, 2
Pro
fess
or o
f Der
mat
olog
y, U
nive
rsity
Hos
pita
ls C
ase
Med
Ctr,
Cle
vela
nd, O
H
Bac
kgro
und
McC
une-
Alb
right
syn
drom
e is
def
ined
by
the
triad
of p
olyo
stot
ic fi
brou
s dy
spla
sia,
pat
chy
cuta
neou
s pi
gmen
tatio
n, a
nd v
ario
us e
ndoc
rinop
athi
es. C
afé-
au-la
it pa
tche
s ar
e se
en in
at l
east
hal
f of a
ll ca
ses
and
fibro
us d
yspl
asia
is o
bser
ved
unila
tera
lly a
nd ty
pica
lly u
nder
lyin
g th
ese
café
-au-
lait
patc
hes.
Th
e on
set
of e
ndoc
rinop
athi
es o
ccur
s on
ave
rage
by
age
5 an
d m
ost
ofte
n m
anife
sts
as p
reco
ciou
s pu
berty
in
girls
. Th
ough
McC
une-
Alb
right
is
gene
rally
con
side
red
to h
ave
a go
od p
rogn
osis
, ext
ensi
ve fi
brou
s dy
spla
sia
has
bee
n as
soci
ated
with
orth
oped
ic a
nd n
euro
logi
c co
mpl
icat
ions
as
wel
l as
an
incr
ease
d ris
k fo
r mal
igna
ncy
durin
g ad
ulth
ood.
Ref
eren
ces
1. C
hans
on P
et a
l. P
edia
tr E
ndoc
rinol
Rev
. 200
7 A
ug;4
Sup
pl 4
: 453
-62.
2.
Dum
itres
cu C
et a
l. O
rpha
net J
Rar
e D
is. 2
008
May
19;
3:12
. 3.
Han
sen
M e
t al.
Sku
ll B
ase.
200
3 M
ay;1
3(2)
:79-
83.
4. D
ogan
avsa
rgil
B e
t al.
Arc
h O
rthop
Tr S
urg.
200
9 A
pr;1
29(4
):439
-44.
5.
Hus
ton
T et
al.
Bre
ast J
. 200
4 S
ep-O
ct;1
0(5)
:440
-2.
Dis
cuss
ion
McC
une-
Alb
right
is c
ause
d by
a m
utat
ion
in th
e G
NA
S1
gene
that
lead
s to
hor
mon
e in
depe
nden
t act
ivat
ion
of s
econ
d m
esse
nger
sig
nalin
g ca
scad
es
that
mim
ic m
elan
ocyt
e st
imul
atin
g ho
rmon
e re
leas
e re
sulti
ng in
pig
men
ted
mac
ules
, mim
icke
d pa
rath
yroi
d ho
rmon
e st
imul
atio
n re
sulti
ng in
ost
eocl
ast
activ
atio
n an
d ev
entu
al fi
brou
s dy
spla
sia,
and
a w
hole
hos
t of o
ther
end
ocrin
opat
hies
. Com
plic
atio
ns fr
om fi
brou
s dy
spla
sia
mos
t com
mon
ly m
anife
st
as fr
actu
res
but c
an a
lso
incl
ude
scol
iosi
s an
d co
mpr
essi
ve n
euro
path
y, w
hich
whe
n in
volv
ing
the
skul
l ca
n re
sult
in b
lindn
ess
and
deaf
ness
. R
ecen
t stu
dies
sug
gest
an
incr
ease
d ca
ncer
inci
denc
e in
adu
lthoo
d, n
amel
y os
teos
arco
ma
and
brea
st c
ance
r. T
his
appe
ars
to b
e es
peci
ally
true
in
thos
e pa
tient
s w
ith a
ssoc
iate
d gr
owth
hor
mon
e ex
cess
. O
steo
sarc
omas
app
ear t
o ar
ise
seco
ndar
y to
prio
r rad
iatio
n fo
r a p
ituita
ry a
deno
ma
whi
ch a
re
usua
lly s
omat
otro
phic
or
whe
n th
ere
is e
xten
sive
fibr
ous
dysp
lasi
a as
is th
e ca
se w
ith o
ur p
atie
nt. T
he in
crea
sed
risk
for
brea
st c
ance
r app
ears
to b
e se
cond
ary
to e
xces
s re
spon
se to
gro
wth
hor
mon
e an
d es
troge
n pa
thw
ays1
,2,3
,4,5.
This
cas
e is
pre
sent
ed f
or c
linic
al i
nter
est
and
to h
ighl
ight
the
im
porta
nce
of m
anag
ing
patie
nts
with
McC
une-
Alb
right
usi
ng a
mul
tidis
cipl
inar
y ap
proa
ch.
Cas
e R
epor
t A
2-ye
ar-o
ld b
oy w
ith a
his
tory
of p
olyo
stot
ic fi
brou
s dy
spla
sia
and
vita
min
D d
efic
ienc
y pr
esen
ted
for e
valu
atio
n of
asy
mpt
omat
ic s
kin
lesi
ons
invo
lvin
g th
e bi
late
ral
thig
hs a
nd b
utto
cks.
Rev
iew
of
syst
ems
was
sig
nific
ant
for
arth
ralg
ias
of t
he l
egs
with
no
acco
mpa
nied
wea
knes
s. G
row
th a
nd
deve
lopm
ent w
as o
ther
wis
e no
rmal
to d
ate.
P
ast m
edic
al h
isto
ry w
as n
otab
le fo
r a
term
vag
inal
del
iver
y fo
llow
ing
an u
ncom
plic
ated
pre
gnan
cy. H
e w
as ta
king
iron
and
vita
min
D s
uppl
emen
ts a
nd h
ad n
o hi
stor
y of
med
icat
ion
alle
rgie
s. T
here
was
no
fam
ily h
isto
ry o
f sim
ilar l
esio
ns.
Exa
min
atio
n re
veal
ed a
n in
tera
ctiv
e an
d co
oper
ativ
e w
ell-d
evel
oped
boy
in n
o ap
pare
nt d
istre
ss.
Inv
olvi
ng t
he p
oste
rior
scal
p w
as a
ret
icul
ated
hy
perp
igm
ente
d pa
tch
and
invo
lvin
g th
e ba
ck,
bila
tera
l thi
ghs,
left
med
ial b
utto
ck a
nd le
ft sc
rotu
m w
ere
scat
tere
d bl
ue-g
rey
and
hype
rpig
men
ted
patc
hes.
The
re w
as a
gro
up o
f pin
k pa
pule
s on
the
right
upp
er c
hest
and
a 7
x4m
m b
row
n ve
rruco
us p
apul
e on
the
right
pre
auric
ular
che
ek. I
nvol
ving
th
e rig
ht p
oste
rior t
high
was
a 7
mm
line
ar a
rran
gem
ent o
f hyp
opig
men
ted
mac
ules
. Vel
lous
hai
rs w
ere
note
d in
the
pubi
c re
gion
. The
rem
aind
er o
f the
ex
am w
as u
nrem
arka
ble.
La
bora
tory
eva
luat
ion
reve
aled
a d
ecre
ased
vita
min
D l
evel
(17
ng/
dL),
elev
ated
alk
alin
e ph
osph
atas
e (5
33 U
/L),
decr
ease
d th
yroi
d st
imul
atin
g ho
rmon
e (0
.04
mIU
/L) a
nd n
orm
al le
vels
of f
ree
T4, t
esto
ster
one,
insu
lin g
row
th fa
ctor
, cal
cium
, and
pho
spha
te.
A C
T sc
an o
f the
hea
d re
veal
ed fo
ci
of fi
brou
s dy
spla
sia
invo
lvin
g th
e ro
of o
f the
rig
ht o
rbit
as w
ell a
s th
e et
hmoi
d, s
phen
oid,
tem
pora
l, an
d oc
cipi
tal b
ones
(Fi
gure
1).
A sk
elet
al s
urve
y fu
rther
reve
aled
fibr
ous
dysp
lasi
a in
volv
ing
the
bila
tera
l hum
eri,
fem
ur, t
ibia
e, fi
bula
e, a
nd p
roxi
mal
uln
ae (F
igur
e 2)
. In
addi
tion
ther
e w
as q
uest
iona
ble
invo
lvem
ent
of t
he r
ight
thi
rd,
four
th,
and
fifth
met
acar
pals
, th
e le
ft se
cond
, th
ird,
and
four
th m
etac
arpa
ls,
the
right
sec
ond,
thi
rd,
and
four
th
met
atar
sals
, and
the
left
first
met
atar
sal.
Figu
re 2
. Ske
leta
l sur
vey
dem
onst
ratin
g gr
ound
gla
ss a
ppea
ranc
e in
dica
tive
of fi
brou
s dy
spla
sia
Figu
re 1
. CT
scan
with
3D
reco
nstru
ctio
n w
hich
dem
onst
rate
s bo
ny e
xpan
sion
of t
he la
tera
l roo
f of t
he
right
orb
it fo
und
to b
e a
focu
s of
fibr
ous
dysp
lasi
a
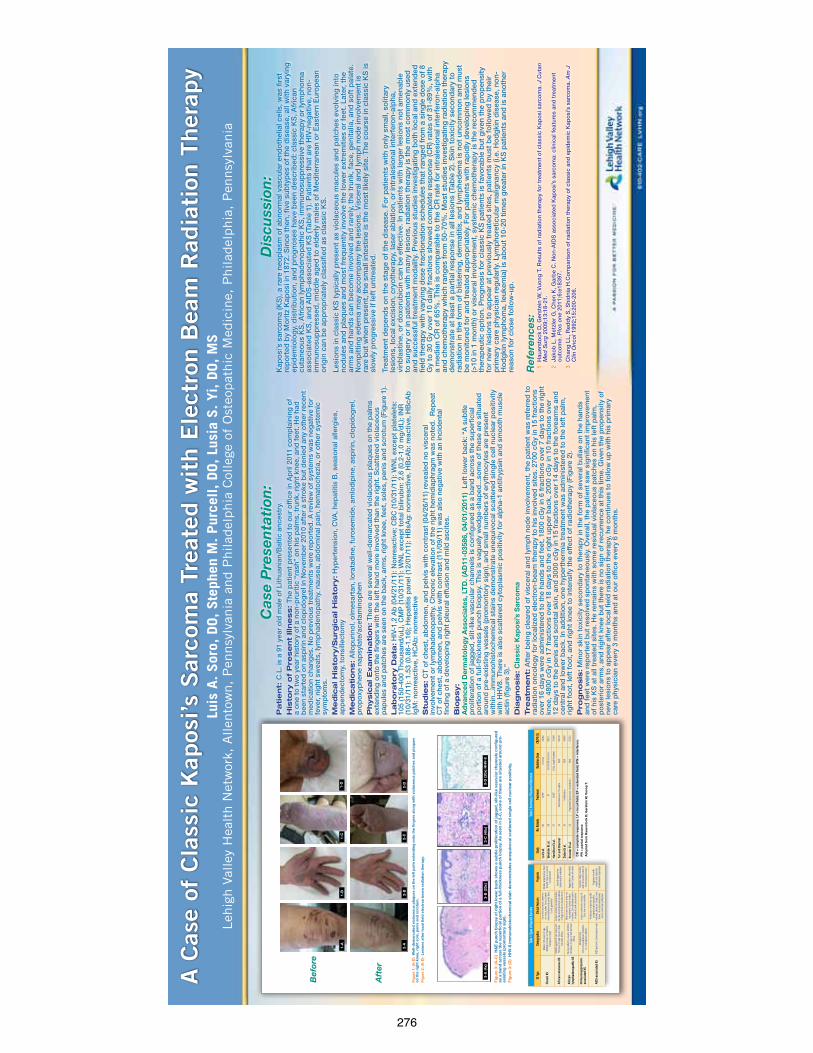
276
A C
ase
of C
lass
ic K
apos
i’s S
arco
ma
Trea
ted w
ith E
lect
ron B
eam
Rad
iati
on T
her
apy
Leh
igh V
alle
y H
ealt
h N
etw
ork,
Allen
tow
n,
Pen
nsy
lvan
ia a
nd P
hilad
elphia
Col
lege
of
Ost
eopat
hic
Med
icin
e, P
hilad
elphia
, P
ennsy
lvan
iaLu
is A
. Sor
o, D
O, Ste
phen
M. Pur
cell, DO, Lu
sia
S. Yi
, DO, M
S
Ref
eren
ces:
1 H
auer
sto
ck D
, Ger
stei
n W
, Vuo
ng T
. Res
ults
of
rad
iatio
n th
erap
y fo
r tr
eatm
ent
of
clas
sic
Kap
osi
sar
com
a. J
Cut
an
Med
Sur
g 2
009;
13:1
8-21
.
2 Ja
kob
L, M
etzl
er G
, Che
n K
, Gar
be
C. N
on-
AID
S a
sso
ciat
ed K
apo
si’s
sar
com
a: c
linic
al f
eatu
res
and
tre
atm
ent
out
com
e. P
los
one
201
1;6:
e183
97.
3 C
hang
LL,
Red
dy
S, S
hid
nia
H.C
om
par
iso
n o
f ra
dia
tion
ther
apy
of
clas
sic
and
ep
idem
ic K
apo
si’s
sar
com
a. A
m J
C
lin O
nco
l 199
2;15
:200
-206
.
Pa
tie
nt:
C.L
. is
a 91
yea
r o
ld m
ale
of
Lith
uani
an/B
altic
anc
estr
y.
His
tory
of
Pre
se
nt
Illn
ess:
The
pat
ient
pre
sent
ed t
o o
ur o
ffic
e in
Ap
ril 2
011
com
pla
inin
g o
f a
one
to
tw
o y
ear
hist
ory
of
a no
n-p
ruri
tic “
rash
” o
n hi
s p
alm
s, t
runk
, rig
ht k
nee,
and
fee
t. H
e ha
d
bee
n st
arte
d o
n as
pir
in a
nd c
lop
ido
gre
l in
No
vem
ber
201
0 af
ter
a st
roke
but
den
ied
any
oth
er r
ecen
t m
edic
atio
n ch
ang
es. N
o p
revi
ous
tre
atm
ents
wer
e re
po
rted
. A r
evie
w o
f sy
stem
s w
as n
egat
ive
for
feve
r, ni
ght
sw
eats
, lym
pha
den
op
athy
, nau
sea,
ab
do
min
al p
ain,
hem
ato
chez
ia, o
r o
ther
sys
tem
ic
sym
pto
ms.
Me
dic
al H
isto
ry/S
urg
ica
l H
isto
ry:
Hyp
erte
nsio
n, C
VA, h
epat
itis
B, s
easo
nal a
llerg
ies,
ap
pen
dec
tom
y, t
ons
illec
tom
y
Me
dic
atio
ns:
Allo
pur
ino
l, o
lmes
arta
n, lo
rata
din
e, f
uro
sem
ide,
am
lod
ipin
e, a
spir
in, c
lop
ido
gre
l, p
rop
oxy
phe
ne n
apsy
late
/ace
tam
ino
phe
n
Ph
ysic
al E
xa
min
atio
n:
The
re a
re s
ever
al w
ell-
dem
arca
ted
vio
lace
ous
pla
que
s o
n th
e p
alm
s ex
tend
ing
ont
o t
he f
ing
ers
with
the
left
han
d m
ore
invo
lved
tha
n th
e ri
ght
. Sca
tter
ed v
iola
ceo
us
pap
ules
and
pat
ches
are
see
n o
n th
e b
ack,
arm
s, r
ight
kne
e, f
eet,
so
les,
pen
is a
nd s
cro
tum
(Fig
ure
1).
La
bo
rato
ry D
ata
: H
IV-1
,2 A
b (0
4/21
/11)
: No
nrea
ctiv
e; C
BC
(10/
31/1
1): W
NL
exce
pt
pla
tele
ts:
105
(150
-400
Tho
usan
d/u
L), C
MP
(10/
31/1
1): W
NL
exce
pt
tota
l bili
rub
in: 2
.6 (0
.2-1
.0 m
g/d
L); I
NR
(1
0/31
/11)
: 1.5
3 (0
.86-
1.16
); H
epat
itis
pan
el (1
2/01
/11)
: HB
sAg
: no
nrea
ctiv
e, H
BcA
b: r
eact
ive,
HB
cAb
Ig
M: n
onr
eact
ive,
HC
Ab
: no
nrea
ctiv
e
Stu
die
s:
CT
of
ches
t, a
bd
om
en, a
nd p
elvi
s w
ith c
ont
rast
(04/
26/1
1) r
evea
led
no
vis
cera
l in
volv
emen
t o
r ly
mp
had
eno
pat
hy. C
hro
nic
elev
atio
n o
f th
e ri
ght
hem
idia
phr
agm
was
no
ted
. R
epea
t C
T o
f ch
est,
ab
do
men
, and
pel
vis
with
co
ntra
st (1
1/09
/11)
was
als
o n
egat
ive
with
an
inci
den
tal
find
ing
of
a d
evel
op
ing
rig
ht p
leur
al e
ffus
ion
and
mild
asc
ites.
Bio
psy:
Ad
vanc
ed D
erm
ato
log
y A
sso
ciat
es, L
TD
. (A
D11
-035
86, 0
4/01
/201
1) L
eft
low
er b
ack:
“A
sub
tle
pro
lifer
atio
n o
f ja
gg
ed, s
lit-l
ike
vasc
ular
cha
nnel
s is
co
nfig
ured
as
a b
and
acr
oss
the
sup
erfic
ial
po
rtio
n o
f a
full-
thic
knes
s p
unch
bio
psy
. Thi
s is
vag
uely
wed
ge-
shap
ed...
som
e o
f th
ese
are
situ
ated
ar
oun
d p
re-e
xist
ing
ves
sels
(pro
mo
nto
ry s
ign)
, and
sm
all n
umb
ers
of
eryt
hro
cyte
s ar
e p
rese
nt
with
in...
imm
uno
hist
och
emic
al s
tain
s d
emo
nstr
ate
uneq
uivo
cal s
catt
ered
sin
gle
cel
l nuc
lear
po
sitiv
ity
with
HH
V8.
The
re is
als
o s
catt
ered
cyt
op
lasm
ic p
osi
tivity
fo
r al
pha
-1 a
ntitr
ypsi
n an
d s
mo
oth
mus
cle
actin
(fig
ure
3).”
Dia
gn
osis
: C
lass
ic K
apo
si’s
Sar
com
aTre
atm
en
t: A
fter
bei
ng c
lear
ed o
f vi
scer
al a
nd ly
mp
h no
de
invo
lvem
ent,
the
pat
ient
was
ref
erre
d t
o
rad
iatio
n o
nco
log
y fo
r lo
caliz
ed e
lect
ron-
bea
m t
hera
py
to h
is in
volv
ed s
ites.
270
0 cG
y in
15
frac
tions
o
ver
16 d
ays
wer
e ad
min
iste
red
to
the
han
ds
and
fee
t, 1
800
cGy
in 6
fra
ctio
ns o
ver
7 d
ays
to t
he r
ight
kn
ee, 4
800
cGy
in 1
7 fr
actio
ns o
ver
18 d
ays
to t
he r
ight
up
per
bac
k, 2
000
cGy
in 1
0 fr
actio
ns o
ver
12 d
ays
to t
he p
enis
and
scr
ota
l ski
n, a
nd 3
000
cGy
in 1
5 fr
actio
ns o
ver
14 d
ays
to t
he f
ore
arm
s an
d
cent
ral a
nd lo
wer
bac
k. In
ad
diti
on,
one
hyp
erth
erm
ia t
reat
men
t w
as a
dm
inis
tere
d t
o t
he le
ft p
alm
, ri
ght
fo
ot,
left
fo
ot,
and
rig
ht k
nee
to in
tens
ify t
he e
ffec
t o
f ra
dio
ther
apy
(Fig
ure
2).
Pro
gn
osis
: M
ino
r sk
in t
oxi
city
sec
ond
ary
to t
hera
py
in t
he f
orm
of
seve
ral b
ulla
e o
n th
e ha
nds
and
fee
t w
ere
rep
ort
ed b
ut r
eso
lved
sp
ont
aneo
usly
. Ove
rall,
the
pat
ient
saw
sig
nific
ant
imp
rove
men
t o
f hi
s K
S a
t al
l tre
ated
site
s. H
e re
mai
ns w
ith s
om
e re
sid
ual v
iola
ceo
us p
atch
es o
n hi
s le
ft p
alm
, p
ost
erio
r ar
ms,
and
rig
ht k
nee
but
the
re is
no
sig
n o
f re
curr
ence
at
this
tim
e. G
iven
the
pro
pen
sity
of
new
lesi
ons
to
ap
pea
r af
ter
loca
l fie
ld r
adia
tion
ther
apy,
he
cont
inue
s to
fo
llow
up
with
his
pri
mar
y ca
re p
hysi
cian
eve
ry 3
mo
nths
and
at
our
off
ice
ever
y 6
mo
nths
.
Cas
e P
rese
nta
tion
:D
iscu
ssio
n:
Kap
osi
’s s
arco
ma
(KS
), a
rare
neo
pla
sm o
f ab
norm
al v
ascu
lar
end
oth
elia
l cel
ls, w
as f
irst
re
po
rted
by
Mo
ritz
Kap
osi
in 1
872.
Sin
ce t
hen,
fiv
e su
bty
pes
of
the
dis
ease
, all
with
var
ying
ep
idem
iolo
gy,
dis
trib
utio
n, a
nd p
rog
nose
s ha
ve b
een
des
crib
ed: c
lass
ic K
S, A
fric
an
cuta
neo
us K
S, A
fric
an ly
mp
had
eno
pat
hic
KS
, im
mun
osu
pp
ress
ive
ther
apy
or
lym
pho
ma
asso
ciat
ed K
S, a
nd A
IDS
-ass
oci
ated
KS
(Tab
le 1
). P
atie
nts
that
are
HIV
-neg
ativ
e, n
on-
imm
uno
sup
pre
ssed
, mid
dle
ag
ed t
o e
lder
ly m
ales
of
Med
iterr
anea
n o
r E
aste
rn E
uro
pea
n o
rig
in c
an b
e ap
pro
pri
atel
y cl
assi
fied
as
clas
sic
KS
.
Lesi
ons
in c
lass
ic K
S t
ypic
ally
pre
sent
as
vio
lace
ous
mac
ules
and
pat
ches
evo
lvin
g in
to
nod
ules
and
pla
que
s an
d m
ost
fre
que
ntly
invo
lve
the
low
er e
xtre
miti
es o
r fe
et. L
ater
, the
ar
ms
and
han
ds
can
bec
om
e in
volv
ed a
nd r
arel
y, t
he t
runk
, fac
e, g
enita
lia, a
nd s
oft
pal
ate.
N
onp
ittin
g e
dem
a m
ay a
cco
mp
any
the
lesi
ons
. Vis
cera
l and
lym
ph
nod
e in
volv
emen
t is
ra
re b
ut w
hen
pre
sent
, the
sm
all i
ntes
tine
is t
he m
ost
like
ly s
ite. T
he c
our
se in
cla
ssic
KS
is
slo
wly
pro
gre
ssiv
e if
left
unt
reat
ed.
Trea
tmen
t d
epen
ds
on
the
stag
e o
f th
e d
isea
se. F
or
pat
ient
s w
ith o
nly
smal
l, so
litar
y le
sio
ns, l
oca
l exc
isio
n, c
ryo
ther
apy,
lase
r ab
latio
n, o
r in
tral
esio
nal i
nter
fero
n-al
pha
, vi
nbla
stin
e, o
r d
oxo
rub
icin
can
be
effe
ctiv
e. In
pat
ient
s w
ith la
rger
lesi
ons
no
t am
enab
le
to s
urg
ery
or
in p
atie
nts
with
man
y le
sio
ns, r
adia
tion
ther
apy
is t
he m
ost
co
mm
onl
y us
ed
and
suc
cess
ful t
reat
men
t m
od
ality
. Pre
vio
us s
tud
ies
inve
stig
atin
g b
oth
loca
l and
ext
end
ed
field
the
rap
y w
ith v
aryi
ng d
ose
fra
ctio
natio
n sc
hed
ules
tha
t ra
nged
fro
m a
sin
gle
do
se o
f 8
Gy
to 3
0 G
y o
ver
10 d
aily
fra
ctio
ns s
how
ed c
om
ple
te r
esp
ons
e (C
R) r
ates
of
31-8
9%, w
ith
a m
edia
n C
R o
f 65
%. T
his
is c
om
par
able
to
the
CR
rat
e fo
r in
tral
esio
nal i
nter
fero
n-al
pha
an
d c
hem
oth
erap
y w
hich
ran
ges
fro
m 5
0-70
%. M
ost
stu
die
s in
vest
igat
ing
rad
iatio
n th
erap
y d
emo
nstr
ate
at le
ast
a p
artia
l res
po
nse
in a
ll le
sio
ns (T
able
2).
Ski
n to
xici
ty s
eco
ndar
y to
ra
dia
tion
in t
he f
orm
of
blis
teri
ng, d
erm
atiti
s, a
nd ly
mp
hed
ema
is n
ot
unco
mm
on
and
mus
t b
e m
oni
tore
d f
or
and
tre
ated
ap
pro
pri
atel
y. F
or
pat
ient
s w
ith r
apid
ly d
evel
op
ing
lesi
ons
(>
10 in
1 m
ont
h) o
r vi
scer
al in
volv
emen
t, s
yste
mic
che
mo
ther
apy
is t
he r
eco
mm
end
ed
ther
apeu
tic o
ptio
n. P
rog
nosi
s fo
r cl
assi
c K
S p
atie
nts
is f
avo
rab
le b
ut g
iven
the
pro
pen
sity
fo
r ne
w le
sio
ns t
o a
pp
ear
at p
revi
ous
ly t
reat
ed s
ites,
pat
ient
s m
ust
be
follo
wed
by
thei
r p
rim
ary
care
phy
sici
an r
egul
arly
. Lym
pho
retic
ular
mal
igna
ncy
(i.e.
Ho
dg
kin
dis
ease
, no
n-H
od
gki
n ly
mp
hom
a, le
ukem
ia) i
s ab
out
10-
20 t
imes
gre
ater
in K
S p
atie
nts
and
is a
noth
er
reas
on
for
clo
se f
ollo
w-u
p.
Fig
ure
1: (A
-D)
Wel
l-d
emar
cate
d v
iola
ceo
us p
laq
ues
on
the
left
pal
m e
xten
din
g o
nto
the
fing
ers
alo
ng w
ith
vio
lace
ous
pat
ches
and
pla
que
s o
n th
e ri
ght
kne
e, r
ight
so
le, p
enis
and
scr
otu
m.
Fig
ure
2: (A
-D)
Lesi
ons
aft
er lo
cal fi
eld
ele
ctro
n b
eam
rad
iati
on
ther
apy.
Fig
ure
3: (A
-C)
H&
E p
unch
bio
psy
of
rig
ht lo
wer
bac
k sh
ow
s a
sub
tle
pro
lifer
atio
n o
f ja
gg
ed, s
lit-l
ike
vasc
ular
cha
nnel
s co
nfig
ured
as
a b
and
acr
oss
the
sup
erfi
cial
po
rtio
n o
f a
full-
thic
knes
s p
unch
bio
psy
. As
seen
in 2
-C, s
om
e o
f th
ese
are
situ
ated
aro
und
pre
-ex
isti
ng v
esse
ls (p
rom
ont
ory
sig
n).
Fig
ure
3: (D
) H
HV-
8 im
mun
ohi
sto
chem
ical
sta
in d
emo
nstr
ates
une
qui
voca
l sca
tter
ed s
ing
le c
ell n
ucle
ar p
osi
tivi
ty.
Table
1: Ty
pes o
f Kap
osi’s
Sarco
ma
KS Typ
eDe
mogra
phics
Clinic
al Feat
ures
Progno
sis
Clas
sic K
SM
ales
>50
year
s of a
ge.
Med
iterra
nean
or E
aste
rn
Euro
pean
orig
in
Early
lesio
ns m
ost c
omm
on
on to
es, s
oles
. Arm
s, ha
nds
invo
lved
late
r and
rare
ly fa
ce,
trunk
, gen
italia
Slow
ly pr
ogre
ssive
. Rar
e lym
ph n
ose
or vi
scer
al
invo
lvem
ent
Afric
an cu
tane
ous K
SM
iddl
e-ag
ed A
frica
n m
ales
20-
50 ye
ars o
f age
. See
n in
Sub-
Saha
ran
Afric
a
Lesio
ns m
ostly
on
extre
miti
es.
Can
be a
ccom
pani
ed b
y ede
ma
of le
gs a
nd b
one
invo
lvem
ent
Loca
lly a
ggre
ssive
. Sy
stem
ically
indo
lent
Afric
an
lym
phad
enop
athi
c KS
Youn
g pa
tient
s, us
ually
child
ren
<10
year
s of a
ge in
Sub-
Saha
ran
Afric
a
Skin
lesio
ns lm
ay o
r may
not
be
pre
sent
. Lym
ph n
odes
in
volve
d. C
an d
evel
op le
sions
on
eye
lids a
nd co
njun
ctiva
Aggr
essiv
e, o
ften
fata
l w
ithin
2 ye
ars o
f ons
et
Imm
unos
uppr
essio
n-as
socia
ted
KSIa
troge
nica
lly
imm
unos
uppr
esse
d pa
tient
s, i.e
. tra
nspl
ant p
atien
ts
Lesio
ns si
mila
r to
class
ic KS
. Sit
es a
re m
ore
varia
ble
Varia
ble.
May
reso
lve
with
disc
ontin
uatio
n of
im
mun
osup
pres
sion
AIDS
-ass
ocia
ted
KSAI
DS p
atien
ts, h
omos
exua
l men
Viol
aceo
us m
acul
es ra
pidl
y pr
ogre
ssin
g to
pap
ules
, no
dule
s, pl
aque
s. He
ad, n
eck,
tru
nk, m
ucou
s mem
bran
es
mor
e co
mm
only
affec
ted
Prog
ress
ive w
ith
noda
l and
syst
emic
invo
lvem
ent e
xpec
ted
Table
2: Su
mmary
of Tr
eatm
ent O
utcom
es
Study
No. P
atien
tsTre
atmen
tRa
diatio
n Dose
CR/PR
(%)
Lo E
t al.
60LF
/EF
2-15
Gy
46/4
6
Wes
hler
Et a
l.28
EF30
GY/
10 fr
actio
ns89
/11
Ham
ilton
Et a
l.37
LF/E
F8
Gy, s
ingl
e fra
ction
73/N
R
Tur a
nd B
renn
er11
Subc
utan
eous
IFN-
alph
aN/
A63
/18
Zida
n Et
al.
10Vi
nbla
stine
N/A
50/4
0
Kreu
ter E
t al.
12Pe
gyla
ted,
lipos
omal
, dox
orbu
cinN/
A67
/25
CR
= c
om
ple
te r
esp
ons
e; L
F =
loca
l fiel
d; E
F =
ext
end
ed fi
eld
; IFN
= in
terf
ero
n;
PR
= p
arti
al r
esp
ons
eA
do
pte
d f
rom
Hau
erst
ock
D, G
erst
ein
W, V
uong
T.
Bef
ore
1-A
1-
B
1-C
1-
D
2-A
2-B
2-
C2-
D
3-A
(4x)
3-
B (2
0x)
3-C
(40x
) 3-
D (2
0x) H
HV-
8
Aft
er

277
Broo
ke W
alls,
DO,
Larg
o Med
ical C
ente
r, La
rgo,
Flor
ida
4640
CAS
E R
EPO
RT
A 49
-year
-old
Cau
casia
n fe
mal
e pre
sent
ed w
ith a
larg
e ten
der
plaq
ue o
n her
righ
t low
er ex
trem
ity. T
he p
laqu
e en
larg
ed
prog
ress
ively
over
the c
ours
e of 2
mon
ths a
nd w
as a
ssoc
iate
d wi
th a
n in
term
itten
t “st
ingi
ng” s
ensa
tion.
She
repo
rted
a hist
ory
of si
mila
r but
smal
ler a
nd se
lf-he
alin
g le
sions
sinc
e her
dia
gnos
is of
Cro
hn’s
dise
ase (
CD) a
t the
age
of 2
2. S
he d
enie
d an
y rec
ent
flare
of h
er ga
stro
inte
stin
al sy
mpt
oms.
Her
pas
t sur
gica
l hist
ory
was s
igni
fican
t for
2 la
rge b
owel
rese
ctio
ns a
nd 1
smal
l bow
el
rese
ctio
n se
cond
ary t
o CD
. Cur
rent
med
icatio
ns in
clude
6-
mer
capt
opur
ine
120
mg d
aily.
Ex
amin
atio
n of
her
righ
t pos
terio
r cal
f rev
eale
d a
tend
er, 1
0 x
12
cm, u
lcera
tive
plaq
ue w
ith u
nder
lying
ery
them
a (F
ig 1
). A
pun
ch
biop
sy w
as co
nsist
ent w
ith cu
tane
ous m
etas
tatic
Cro
hn’s
dise
ase.
Hist
opat
holo
gic f
indi
ngs i
nclu
ded
ulce
ratio
n ac
com
pani
ed b
y rea
ctive
hyp
erpl
asia
of t
he ep
ider
mis
and
nons
uppu
rativ
e gr
anul
omat
ous d
erm
al in
flam
mat
ion
(Fig
2).
Mul
tinuc
leat
ed fo
reig
n bo
dy-ty
pe gi
ant c
ells
were
pre
sent
. Sp
ecia
l sta
ins f
or a
cid-fa
st b
acill
i and
fung
i wer
e neg
ative
.
CD is
a ch
roni
c inf
lam
mat
ory b
owel
dise
ase w
ith a
rela
psin
g co
urse
. Extr
aint
estin
al m
anife
stat
ions
of C
D ar
e com
mon
and
ca
n in
clude
cuta
neou
s, ar
thrit
ic, o
cula
r, an
d pu
lmon
ary
invo
lvem
ent.
Cuta
neou
s les
ions
can
vary
from
a re
activ
e pr
oces
s su
ch a
s pyo
derm
a ga
ngre
nosu
m, t
o m
ucoc
utan
eous
exte
nsio
ns
in th
e ora
l muc
osa
or p
eria
nal a
rea,
and
/or n
utrit
iona
l def
icien
cy
synd
rom
es se
cond
ary t
o m
alab
sorp
tion.
3 How
ever
, one
of t
he
mos
t int
rigui
ng cu
tane
ous m
anife
stat
ions
of C
D is
cuta
neou
s m
etas
tatic
Cro
hn’s
dise
ase
(CM
CD),
a ra
re m
anife
stat
ion
invo
lving
lesio
ns th
at a
re h
istol
ogica
lly id
entic
al to
thos
e fou
nd in
th
e bow
el, s
pecif
ically
non
case
atin
g gr
anul
omat
ous
infla
mm
ator
y les
ions
, at n
on-c
ontig
uous
site
s fro
m th
e al
imen
tary
trac
t.4 CM
CD o
ccur
s mos
t com
mon
ly on
the p
osta
uricu
lar r
egio
n,
flexu
ral r
egio
ns, o
r extr
emiti
es b
ut m
ay o
ccur
on
any c
utan
eous
su
rface
. Ove
r hal
f of t
he p
atie
nts a
re fe
mal
e and
mos
t pat
ient
s ar
e bet
ween
the a
ges o
f 20-
40 ye
ars.1,
6 Clin
ically
, cut
aneo
us
lesio
ns co
nsist
of s
mal
l ery
them
atou
s pap
ules
, whi
ch m
ay
enla
rge
into
nod
ules
and
ulti
mat
ely u
lcera
te. T
he te
rm
“met
asta
tic” i
s a m
isnom
er si
nce t
hese
lesio
ns co
ntai
n th
e sam
e hi
stop
atho
logy
that
char
acte
rizes
CD
and
are n
ot sp
read
ing
hem
atog
enou
sly.
Hist
olog
ically
, CM
CD co
nsist
s of n
onca
seat
ing
gran
ulom
atou
s sk
in le
sions
that
are
loca
ted
at si
tes d
istan
t fro
m th
e ga
stro
inte
stin
al tr
act.2
DIS
CUSS
ION
REF
EREN
CES
FIG
URES
1 2
The e
tiolo
gy o
f CM
CD is
unk
nown
but
pot
entia
lly re
late
d to
an
exag
gera
ted
Th1
cell m
edia
ted
resp
onse
.5 Th1
resp
onse
s pr
oduc
e IN
F-γ,
a po
tent
chem
otac
tic m
edia
tor a
nd a
ctiva
tor
for h
istio
cyte
s. S
ome h
ave h
ypot
hesiz
ed a
bac
teria
l id ty
pe o
f re
actio
n. A
noth
er th
eory
rela
tes a
utoi
mm
une
phen
omen
on,
invo
lving
cros
s rea
ctin
g an
tibod
ies b
etwe
en th
e gut
and
skin
-ba
sed
antig
ens.6 R
ecen
t res
earc
h di
scov
ered
sim
ilarit
ies i
n tro
pom
yosin
isof
orm
s of t
he gu
t, sk
in, e
ye, a
nd jo
ints
that
may
co
ntrib
ute
to a
utoi
mm
unity
.7 Tre
atm
ent o
ptio
ns co
nsist
of im
mun
osup
pres
sive a
gent
s suc
h as
pred
niso
ne, a
zath
iopr
ine,
sulfa
sala
zine,
and
met
hotre
xate
. On
e of t
he m
ost e
ffect
ive tr
eatm
ents
repo
rted
is or
al
met
roni
dazo
le, a
lone
or i
n com
bina
tion
with
Infli
ximab
.8-9
1.Ro
thfu
ss, K
atja
S, E
duar
d F S
tang
e, K
laus
R H
errli
nger
. Extr
aint
estin
al m
anife
stat
ions
and
com
plica
tions
in
infla
mm
ator
y bow
el d
iseas
es. W
orld
J Ga
stro
ente
rol 2
006;
12(3
0):4
819-
4831
2.
Lars
en S
, Ben
dtze
n K, N
elso
n OH
. Extr
aint
estin
al m
anife
stat
ions
of i
nfla
mm
ator
y bow
el d
iseas
e: e
pide
mio
logy
, di
agno
sis, a
nd m
anag
emen
t. A
nn M
ed 2
010;
42(2
):97-
114
3.Le
ster
LU, R
apin
i RP.
Der
mat
olog
ic m
anife
stat
ions
of c
olon
ic di
sord
ers.
Cur
r Opi
n Ga
ster
oent
erol
200
9;25
(1):6
6-73
4.
Park
s, AG
, BC
Mor
son,
JS P
egum
. Cro
hn’s
Dise
ase w
ith C
utan
eous
Invo
lvem
ent.
Pro
ceed
ings
of th
e Roy
al S
ocie
ty of
M
edici
ne 1
965;
58:2
41-2
42
5.Po
dolsk
y, DK
. Inf
lam
mat
ory b
owel
dise
ase.
N E
ngl J
Med
200
2;34
7(6)
:417
-429
6.
Crow
son,
A. N
eil,
MD,
Ger
ard
J Nuo
vo, M
D, M
artin
C. M
ihm
, Jr,
MD,
and
Cynt
hia
Mag
ro, M
D. C
utan
eous
Man
ifest
atio
ns
of C
rohn
’s Di
seas
e, It
s Spe
ctru
m, a
nd It
s Pat
hoge
nesis
: Int
race
llula
r Con
sens
us B
acte
rial 1
6S rR
NA Is
Ass
ocia
ted
With
th
e Gas
troin
test
inal
But
Not
the C
utan
eous
Man
ifest
atio
ns o
f Cro
hn’s
Dise
ase.
Hum
an P
atho
logy
200
3;34
:11
7.Ge
ng X,
Bia
ncon
e L, D
ai H
H, Li
n JJ,
Yosh
izaki
N, D
asgu
pta A
, Pal
lone
F, D
as K
M. T
ropo
myo
sin is
ofor
ms i
n in
test
inal
m
ucos
a: p
rodu
ctio
n of
aut
oant
ibod
es to
trop
omyo
sin is
ofor
ms i
n ul
cera
tive c
oliti
s. G
astro
ente
rolo
gy 1
998;
114
:912
-92
2 8.
Risp
o, A
., R.
Sca
rpa,
E. D
iGiro
lam
o, A
. Coz
zolin
o, G
. Lem
bo, M
. Atte
no, T
. DeF
alco
, M. L
oPre
sti,
F. C
astig
lione
. In
flixim
ab in
the t
reat
men
t of e
xtra-
inte
stin
al m
anife
stat
ions
of C
rohn
’s Di
seas
e. S
cand
inav
ian
Jour
nal o
f Rh
eum
atol
ogy
2005
;387
-391
9.
Konr
ad, A
. and
F. S
eibo
ld. R
espo
nse o
f cut
aneo
us C
rohn
’s di
seas
e to
infli
ximab
and
met
hotre
xate
. Dig
estiv
e and
Live
r Di
seas
e 20
03;3
51-3
56
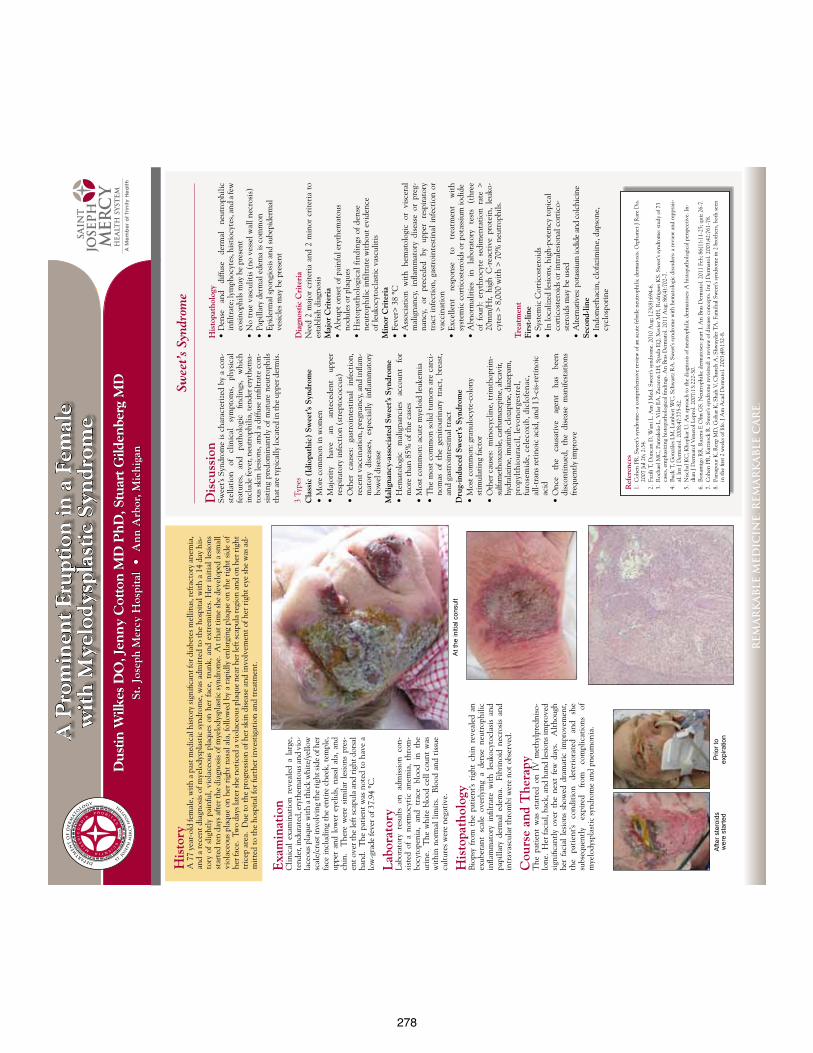
278
A P
rom
inen
t E
rupt
ion
in a
Fem
ale
wit
h M
yelo
dysp
last
ic S
yndr
ome
Du
stin
Wilk
es D
O, J
enn
y C
otto
n M
D P
hD
, Stu
art G
ilden
berg
MD
St. J
osep
h M
ercy
Hos
pita
l •
Ann
Arb
or, M
ichi
gan
REM
AR
KA
BLE
MED
ICIN
E. R
EMA
RK
AB
LE C
AR
E.
Swee
t’s S
yndr
ome
At t
he in
itial
con
sult
Afte
r ste
roid
s w
ere
star
ted
Prio
r to
expi
ratio
n
Exa
min
atio
nC
linic
al e
xam
inat
ion
reve
aled
a l
arge
, te
nder
, ind
urat
ed, e
ryth
emat
ous a
nd v
io-
lace
ous p
laqu
e w
ith
a th
ick
whi
te/y
ello
w
scal
e/cr
ust i
nvol
ving
the
righ
t sid
e of
her
fa
ce in
clud
ing
the
enti
re c
heek
, tem
ple,
up
per
and
low
er e
yelid
s, na
sal
ala,
and
ch
in.
The
re w
ere
sim
ilar
lesi
ons
pres
-en
t ove
r the
left
scap
ula
and
righ
t dor
sal
hand
. T
he p
atie
nt w
as n
oted
to
have
a
low
-gra
de fe
ver o
f 37.
94 °
C.
Lab
orat
ory
Labo
rato
ry r
esul
ts o
n ad
mis
sion
con
-si
sted
of
a no
rmoc
ytic
ane
mia
, th
rom
-bo
cyto
peni
a, a
nd t
race
blo
od i
n th
e ur
ine.
T
he w
hite
blo
od c
ell
coun
t w
as
wit
hin
norm
al li
mit
s. B
lood
and
tis
sue
cult
ures
wer
e ne
gati
ve.
His
topa
thol
ogy
Bio
psy
from
the
pat
ient
’s ri
ght
chin
rev
eale
d an
ex
uber
ant
scal
e ov
erly
ing
a de
nse
neut
roph
ilic
infla
mm
ator
y in
filtr
ate
wit
h le
ukoc
ytoc
lasi
s an
d pa
pilla
ry d
erm
al e
dem
a.
Fibr
inoi
d ne
cros
is a
nd
intr
avas
cula
r thr
ombi
wer
e no
t obs
erve
d.
Cou
rse
and
The
rapy
The
pat
ient
was
sta
rted
on
IV m
ethy
lpre
dnis
o-lo
ne.
Her
faci
al, b
ack,
and
han
d le
sion
s im
prov
ed
sign
ifica
ntly
ove
r th
e ne
xt f
ew d
ays.
Alt
houg
h he
r fa
cial
les
ions
sho
wed
dra
mat
ic i
mpr
ovem
ent,
the
pati
ent’s
co
ndit
ion
dete
rior
ated
an
d sh
e su
bseq
uent
ly
expi
red
from
co
mpl
icat
ions
of
m
yelo
dysp
last
ic sy
ndro
me
and
pneu
mon
ia.
His
tory
A 7
7 ye
ar-o
ld fe
mal
e, w
ith
a pa
st m
edic
al h
isto
ry si
gnifi
cant
for d
iabe
tes m
ellit
us, r
efra
ctor
y an
emia
, an
d a
rece
nt d
iagn
osis
of m
yelo
dysp
last
ic sy
ndro
me,
was
adm
itte
d to
the
hosp
ital
wit
h a
14 d
ay h
is-
tory
of
slig
htly
pai
nful
, vio
lace
ous
plaq
ues
on h
er f
ace,
tru
nk, a
nd e
xtre
mit
ies.
Her
ini
tial
les
ions
st
arte
d te
n da
ys a
fter
the
diag
nosi
s of m
yelo
dysp
last
ic sy
ndro
me.
At t
hat t
ime
she
deve
lope
d a
smal
l vi
olac
eous
pla
que
on h
er r
ight
nas
al a
la, f
ollo
wed
by
a ra
pidl
y en
larg
ing
plaq
ue o
n th
e ri
ght
side
of
her f
ace.
Tw
o da
ys la
ter s
he n
otic
ed a
vio
lace
ous p
laqu
e ne
ar h
er le
ft sc
apul
a re
gion
and
on
her r
ight
tr
icep
are
a. D
ue to
the
prog
ress
ion
of h
er sk
in d
isea
se a
nd in
volv
emen
t of h
er ri
ght e
ye sh
e w
as a
d-m
itte
d to
the
hosp
ital
for f
urth
er in
vest
igat
ion
and
trea
tmen
t.
Dis
cuss
ion
Swee
t’s S
yndr
ome
is c
hara
cter
ized
by
a co
n-st
ella
tion
of
cl
inic
al
sym
ptom
s, ph
ysic
al
feat
ures
, an
d pa
thol
ogic
fin
ding
s, w
hich
in
clud
e fe
ver,
neut
roph
ilia,
tend
er e
ryth
ema-
tous
ski
n le
sion
s, an
d a
diffu
se in
filtr
ate
con-
sist
ing
pred
omin
antl
y of
mat
ure
neut
roph
ils
that
are
typi
cally
loca
ted
in th
e up
per d
erm
is.
3 Ty
pes
Cla
ssic
(Id
iopa
thic
) Sw
eet’s
Syn
drom
e•
Mor
e co
mm
on in
wom
en
• M
ajor
ity
have
an
an
tece
dent
up
per
resp
irat
ory
infe
ctio
n (s
trep
toco
ccus
)•
Oth
er c
ause
s: ga
stro
inte
stin
al i
nfec
tion
, re
cent
vac
cina
tion
, pre
gnan
cy, a
nd in
flam
-m
ator
y di
seas
es,
espe
cial
ly i
nflam
mat
ory
bow
el d
isea
se
Mal
igna
ncy-
asso
ciat
ed S
wee
t’s S
yndr
ome
• H
emat
olog
ic
mal
igna
ncie
s ac
coun
t fo
r m
ore
than
85%
of t
he c
ases
• M
ost c
omm
on: a
cute
mye
loid
leuk
emia
• T
he m
ost
com
mon
sol
id t
umor
s ar
e ca
rci-
nom
as o
f th
e ge
nito
urin
ary
trac
t, br
east
, an
d ga
stro
inte
stin
al tr
act
Dru
g-in
duce
d Sw
eet’s
Syn
drom
e•
Mos
t com
mon
: gra
nulo
cyte
-col
ony
st
imul
atin
g fa
ctor
• O
ther
cau
ses:
min
ocyc
line,
trim
thop
rim
-su
lfam
etho
xazo
le, c
arba
maz
epin
e, a
bcav
ir,
hydr
alaz
ine,
imat
inib
, clo
zapi
ne, d
iaze
pam
, pr
opyl
thio
urac
il, l
evon
orge
stre
l,
furo
sem
ide,
cel
ecox
ib, d
iclo
fena
c,
all-
tran
s ret
inoi
c ac
id, a
nd 1
3-ci
s-re
tino
ic
acid
• O
nce
the
caus
ativ
e ag
ent
has
been
di
scon
tinu
ed,
the
dise
ase
man
ifest
atio
ns
freq
uent
ly im
prov
e
Ref
eren
ces
1. C
ohen
PR
. Sw
eet’s
synd
rom
e--a
com
preh
ensi
ve re
view
of a
n ac
ute
febr
ile n
eutr
ophi
lic d
erm
atos
is. O
rpha
net J
Rar
e D
is.
2007
Jul 2
6; 2
:34.
2. F
azili
T, D
unca
n D
, Wan
i L. A
m J
Med
. Sw
eet’s
synd
rom
e. 2
010
Aug
; 123
(8):
694-
6.3.
Roc
hael
MC
, Pan
tale
ão L
, Vila
r EA
, Zac
aron
LH
, Spa
da E
Q, X
avie
r MH
, Rod
rigu
es K
S. S
wee
t’s sy
ndro
me:
stud
y of
73
case
s, em
phas
izin
g hi
stop
atho
logi
cal fi
ndin
gs. A
n B
ras D
erm
atol
. 201
1 A
ug; 8
6(4)
:702
-7.
4. B
uck
T, G
onzá
les L
M, L
ambe
rt W
C, S
chw
artz
RA
. Sw
eet’s
synd
rom
e w
ith
hem
atol
ogic
dis
orde
rs: a
revi
ew a
nd re
ppra
is-
al. I
nt J
Der
mat
ol. 2
008;
47:7
75-8
2.5.
Nis
chal
KC
, Kho
pkar
U. A
n ap
roac
h to
the
diag
nosi
s of n
eutr
ophi
lic d
erm
atos
es: A
his
topa
thol
ogic
al p
ersp
ecti
ve. I
n-di
an J
Der
mat
ol V
ener
ol L
epro
l. 20
07:1
3:22
2-30
.6.
Bon
amig
o R
R, R
azer
a F,
Olm
GS.
Neu
trop
hilic
der
mat
oses
: par
t I. A
n B
ras D
erm
atol
. 201
1 Fe
b; 8
6(1)
:11-
25; q
uiz 2
6-7.
7. C
ohen
PR
, Kur
zroc
k R
. Sw
eet’s
synd
rom
e re
visi
ted:
a re
view
of d
isea
se c
once
pts.
Int J
Der
mat
ol. 2
003;
42:7
61-7
8.8.
Par
sapo
ur K
, Ree
p M
D, G
ohar
K, S
hah
V, C
hurc
h A
, Shw
ayde
r TA
. Fam
ilial
Sw
eet’s
synd
rom
e in
2 b
roth
ers,
both
seen
in
the
first
2 w
eeks
of l
ife. J
Am
Aca
d D
erm
atol
. 200
3;49
:132
-8.
His
topa
thol
ogy
• D
ense
an
d di
ffuse
de
rmal
ne
utro
phili
c in
filtr
ate;
lym
phoc
ytes
, his
tioc
ytes
, and
a fe
w
eosi
noph
ils m
ay b
e pr
esen
t•
No
true
vas
culit
is (
no v
esse
l wal
l nec
rosi
s)•
Pap
illar
y de
rmal
ede
ma
is c
omm
on
• E
pide
rmal
spon
gios
is a
nd su
bepi
derm
al
vesi
cles
may
be
pres
ent
Dia
gnos
tic
Cri
teri
aN
eed
2 m
ajor
cri
teri
a an
d 2
min
or c
rite
ria
to
esta
blis
h di
agno
sis
Maj
or C
rite
ria
• A
brup
t ons
et o
f pai
nful
ery
them
atou
s no
dule
s or p
laqu
es•
His
topa
thol
ogic
al fi
ndin
gs o
f den
se
neut
roph
ilic
infil
trat
e w
itho
ut e
vide
nce
of
leuk
ocyt
ocla
stic
vas
culit
isM
inor
Cri
teri
a•
Fev
er>
38
°C•
Ass
ocia
tion
wit
h he
mat
olog
ic o
r vi
scer
al
mal
igna
ncy,
infl
amm
ator
y di
seas
e or
pre
g-na
ncy,
or
pr
eced
ed
by
uppe
r re
spir
ator
y tr
act
infe
ctio
n, g
astr
oint
esti
nal
infe
ctio
n or
va
ccin
atio
n•
Exc
elle
nt
resp
onse
to
tr
eatm
ent
wit
h sy
stem
ic c
orti
cost
eroi
ds o
r pot
assi
um io
dide
• A
bnor
mal
itie
s in
la
bora
tory
te
sts
(thr
ee
of f
our)
: er
ythr
ocyt
e se
dim
enta
tion
rat
e >
20
mm
/Hr,
high
C-r
eact
ive
prot
ein,
leu
ko-
cyte
s > 8
,000
wit
h >
70%
neu
trop
hils
.
Tre
atm
ent
Firs
t-lin
e•
Sys
tem
ic C
orti
cost
eroi
ds•
In
loca
lized
lesi
ons,
high
-pot
ency
topi
cal
cort
icos
tero
ids o
r int
rale
sion
al c
orti
co-
ster
oids
may
be
used
• A
ltern
ativ
es: p
otas
sium
iodi
de a
nd c
olch
icin
e Se
cond
-lin
e•
Ind
omet
haci
n, c
lofa
zim
ine,
dap
sone
, cy
clos
pori
ne
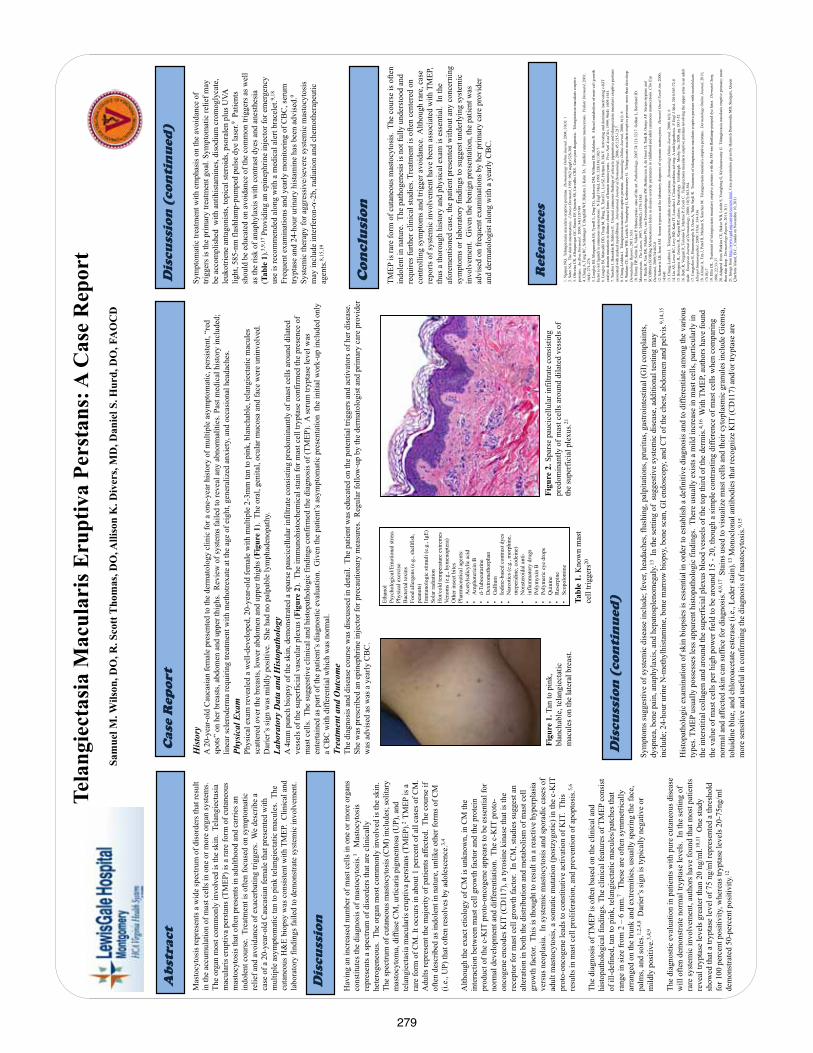
279
Hav
ing
an in
crea
sed
num
ber o
f mas
t cel
ls in
one
or m
ore
orga
ns
cons
titut
es th
e di
agno
sis o
f mas
tocy
tosi
s.1 M
asto
cyto
sis
repr
esen
ts a
spec
trum
of d
isor
ders
that
are
clin
ical
ly
hete
roge
neou
s. T
he o
rgan
mos
t com
mon
ly in
volv
ed is
the
skin
. Th
e sp
ectru
m o
f cut
aneo
us m
asto
cyto
sis (
CM
) inc
lude
s; so
litar
y m
asto
cyto
ma,
diff
use
CM
, urti
caria
pig
men
tosa
(UP)
, and
te
lang
iect
asia
mac
ular
is e
rupt
iva
pers
tans
(TM
EP).2
TM
EP is
a
rare
form
of C
M. I
t occ
urs i
n ab
out 1
per
cent
of a
ll ca
ses o
f CM
.
Adu
lts re
pres
ent t
he m
ajor
ity o
f pat
ient
s affe
cted
. Th
e co
urse
if
ofte
n de
scrib
ed a
s ind
olen
t in
natu
re, u
nlik
e ot
her f
orm
s of C
M
(i.e.
, UP)
that
ofte
n re
solv
es b
y ad
oles
cenc
e.3,
4
Alth
ough
the
exac
t etio
logy
of C
M is
unk
now
n, in
CM
the
inte
ract
ion
betw
een
mas
t cel
l gro
wth
fact
or a
nd th
e pr
otei
n pr
oduc
t of t
he c
-KIT
pro
to-o
ncog
ene
appe
ars t
o be
ess
entia
l for
no
rmal
dev
elop
men
t and
diff
eren
tiatio
n. T
he c
-KIT
pro
to-
onco
gene
enc
odes
KIT
(CD
117)
, a ty
rosi
ne k
inas
e th
at is
the
rece
ptor
for m
ast c
ell g
row
th fa
ctor
. In
CM
, stu
dies
sugg
est a
n al
tera
tion
in b
oth
the
dist
ribut
ion
and
met
abol
ism
of m
ast c
ell
grow
th fa
ctor
. Th
is is
thou
ght t
o re
sult
in a
reac
tive
hype
rpla
sia
vers
us n
eopl
asia
. In
syst
emic
mas
tocy
tosi
s and
spor
adic
cas
es o
f ad
ult m
asto
cyto
sis,
a so
mat
ic m
utat
ion
(pos
tzyg
otic
) in
the
c-K
IT
prot
o-on
coge
ne le
ads t
o co
nstit
utiv
e ac
tivat
ion
of K
IT.
This
re
sults
in m
ast c
ell p
rolif
erat
ion,
and
pre
vent
ion
of a
popt
osis
.5,6
The
diag
nosi
s of T
MEP
is o
ften
base
d on
the
clin
ical
and
hi
stop
atho
logi
cal f
indi
ngs.
The
clin
ical
feat
ures
of T
MEP
con
sist
of
ill-d
efin
ed, t
an to
pin
k, te
lang
iect
atic
mac
ules
/pat
ches
that
ra
nge
in si
ze fr
om 2
– 6
mm
.7 T
hese
are
ofte
n sy
mm
etric
ally
ar
rang
ed o
n th
e tru
nk a
nd e
xtre
miti
es, u
sual
ly sp
arin
g th
e fa
ce,
palm
s, an
d so
les.1,
2,4,
8 D
arie
r’s si
gn is
typi
cally
neg
ativ
e or
m
ildly
pos
itive
.3,4,
9
The
diag
nost
ic e
valu
atio
n in
pat
ient
s with
pur
e cu
tane
ous d
isea
se
will
ofte
n de
mon
stra
te n
orm
al tr
ypta
se le
vels
. In
the
setti
ng o
f ra
re sy
stem
ic in
volv
emen
t, au
thor
s hav
e fo
und
that
mos
t pat
ient
s re
veal
tryp
tase
leve
ls g
reat
er th
an 2
0 ng
/ml.10
,11
One
stud
y sh
owed
that
a tr
ypta
se le
vel o
f 75
ng/m
l rep
rese
nted
a th
resh
old
for 1
00 p
erce
nt p
ositi
vity
, whe
reas
tryp
tase
leve
ls 2
0-75
ng/m
l de
mon
stra
ted
50-p
erce
nt p
ositi
vity
.12
Cas
e R
epor
t
Ref
eren
ces
Mas
tocy
tosi
s rep
rese
nts a
wid
e sp
ectru
m o
f dis
orde
rs th
at re
sult
in th
e ac
cum
ulat
ion
of m
ast c
ells
in o
ne o
r mor
e or
gan
syst
ems.
Th
e or
gan
mos
t com
mon
ly in
volv
ed is
the
skin
. Te
lang
iect
asia
m
acul
aris
eru
ptiv
a pe
rsta
ns (T
MEP
) is a
rare
form
of c
utan
eous
m
asto
cyto
sis t
hat o
ften
pres
ents
in a
dulth
ood
and
carr
ies a
n in
dole
nt c
ours
e. T
reat
men
t is o
ften
focu
sed
on sy
mpt
omat
ic
relie
f and
avo
idan
ce o
f exa
cerb
atin
g tri
gger
s. W
e de
scrib
e a
case
of a
20-
year
-old
Cau
casi
an fe
mal
e th
at p
rese
nted
with
m
ultip
le a
sym
ptom
atic
tan
to p
ink
tela
ngie
ctat
ic m
acul
es.
The
cuta
neou
s H&
E bi
opsy
was
con
sist
ent w
ith T
MEP
. C
linic
al a
nd
labo
rato
ry fi
ndin
gs fa
iled
to d
emon
stra
te sy
stem
ic in
volv
emen
t.
Ab
stra
ct
.
Te
lang
iect
asia
Mac
ular
is E
rupt
iva
Pers
tans
: A C
ase
Rep
ort
Sa
mue
l M. W
ilson
, DO
, R. S
cott
Tho
mas
, DO
, Alli
son
K. D
iver
s, M
D, D
anie
l S. H
urd,
DO
, FA
OC
D
His
tory
A
20-
year
-old
Cau
casi
an fe
mal
e pr
esen
ted
to th
e de
rmat
olog
y cl
inic
for a
one
-yea
r his
tory
of m
ultip
le a
sym
ptom
atic
, per
sist
ent,
“red
sp
ots”
on
her b
reas
ts, a
bdom
en a
nd u
pper
thig
hs.
Rev
iew
of s
yste
ms f
aile
d to
reve
al a
ny a
bnor
mal
ities
. Pas
t med
ical
his
tory
incl
uded
; lin
ear s
cler
oder
ma
requ
iring
trea
tmen
t with
met
hotre
xate
at t
he a
ge o
f eig
ht, g
ener
aliz
ed a
nxie
ty, a
nd o
ccas
iona
l hea
dach
es.
Phys
ical
Exa
m
Phys
ical
exa
m re
veal
ed a
wel
l-dev
elop
ed, 2
0-ye
ar-o
ld fe
mal
e w
ith m
ultip
le 2
-3m
m ta
n to
pin
k, b
lanc
habl
e, te
lang
iect
atic
mac
ules
sc
atte
red
over
the
brea
sts,
low
er a
bdom
en a
nd u
pper
thig
hs (F
igur
e 1)
. Th
e or
al, g
enita
l, oc
ular
muc
osa
and
face
wer
e un
invo
lved
. D
arie
r’s si
gn w
as m
ildly
pos
itive
. Sh
e ha
d no
pal
pabl
e ly
mph
aden
opat
hy.
Labo
rato
ry D
ata
and
His
topa
thol
ogy
A 4
mm
pun
ch b
iops
y of
the
skin
, dem
onst
rate
d a
spar
se p
auci
cellu
lar i
nfilt
rate
con
sist
ing
pred
omin
antly
of m
ast c
ells
aro
und
dila
ted
vess
els o
f the
supe
rfic
ial v
ascu
lar p
lexu
s (Fi
gure
2).
The
imm
unoh
isto
chem
ical
stai
n fo
r mas
t cel
l try
ptas
e co
nfirm
ed th
e pr
esen
ce o
f m
ast c
ells
. Th
e su
gges
tive
clin
ical
and
his
topa
thol
ogic
find
ings
con
firm
ed th
e di
agno
sis o
f (TM
EP).
A se
rum
tryp
tase
leve
l was
en
terta
ined
as p
art o
f the
pat
ient
’s d
iagn
ostic
eva
luat
ion.
Giv
en th
e pa
tient
’s a
sym
ptom
atic
pre
sent
atio
n th
e in
itial
wor
k-up
incl
uded
onl
y a
CB
C w
ith d
iffer
entia
l whi
ch w
as n
orm
al.
Trea
tmen
t and
Out
com
e
The
diag
nosi
s and
dis
ease
cou
rse
was
dis
cuss
ed in
det
ail.
The
pat
ient
was
edu
cate
d on
the
pote
ntia
l trig
gers
and
act
ivat
ors
of h
er d
isea
se.
She
was
pre
scrib
ed a
n ep
inep
hrin
e in
ject
or fo
r pre
caut
iona
ry m
easu
res.
Reg
ular
follo
w-u
p by
the
derm
atol
ogis
t and
prim
ary
care
pro
vide
r w
as a
dvis
ed a
s was
a y
early
CB
C.
Dis
cuss
ion
Dis
cuss
ion
(co
nti
nu
ed)
1. N
guye
n N
Q.
Tela
ngie
ctas
ia m
acul
aris
eru
ptiv
e pe
rsta
ns.
Der
mat
olog
y O
nlin
e Jo
urna
l, 20
04; 1
0(3)
: 1
2. S
oter
NA
. Th
e sk
in in
mas
tocy
tosi
s. J
Inve
st D
erm
atol
, 199
1; 9
6(3
supp
l):32
S-38
S 3.
Oliv
eira
CR
, Alb
uque
rque
GC
, Sim
on E
F, Q
uine
te S
S, C
arva
lho
CR
S. C
aso
para
dia
gnos
tic.
Tela
ngie
ctas
ia m
acul
aris
eru
ptiv
e pe
rsta
ns.
An B
ras D
erm
atol
. 20
09; 8
4(1)
:87-
89
4. C
hang
A, T
ung
RC
, Sch
lesi
nger
T, B
ergf
eld
WF,
Dijk
stra
J, K
ahn
TA.
Fam
ilial
cut
aneo
us m
asto
cyto
sis.
Ped
iatr
Der
mat
ol, 2
001;
18
(4):
271-
276
5. L
ongl
ey B
J, M
orga
nrot
h G
S, T
yrre
ll L,
Din
g TG
, And
erso
n D
M, W
illia
ms
DE,
Hal
aban
R.
Alte
red
met
abol
ism
of m
ast-c
ell g
row
th
fact
or (c
-kit
ligan
d) in
cut
aneo
us m
asto
cyto
sis.
N E
ngl J
Med
, 199
3; 3
28(1
8):1
302-
7 6.
Lon
gley
BJ,
Met
calfe
DD
, Tha
rp M
, Wan
g X
, Tyr
rell
L, L
u SZ
, Hei
tjan
D, M
a Y.
Act
ivat
ing
and
dom
inan
t ina
ctiv
atin
g c-
KIT
ca
taly
tic d
omai
n m
utat
ions
in d
istin
ct c
linic
al fo
rms o
f hum
an m
asto
cyto
sis.
Pro
c N
atl A
cad
Sci,
1999
; 96(
4): 1
609-
1614
7.
Tur
chin
I, B
aran
kin
B, S
chlo
ss E
. U
nusu
al c
utan
eous
find
ings
of u
rtica
ria p
igm
ento
sa a
nd te
lang
iect
asia
mac
ular
is e
rupt
iva
pers
tans
as
soci
ated
with
mar
ked
mye
lofib
rosi
s. In
tern
atio
nal J
ourn
al o
f Der
mat
olog
y, 20
06; 4
5:12
15-1
217.
8.
Chu
ng-L
eddo
n J.
Tel
angi
ecta
sia
mac
ular
is e
rupt
ive
pers
tans
. D
erm
atol
ogy
Onl
ine
Jour
nal,
2000
; 6(1
): 6
9. W
atki
ns C
E, B
okor
WB
, Lei
cht S
, You
ngbe
rg G
, Kris
hnas
wam
y G
. Te
lang
ieca
sia
mac
ular
is e
rupt
ive
pers
tans
: mor
e th
an sk
in d
eep.
D
erm
atol
ogy
Repo
rts,
2011
; 3(1
) 10
. Hor
ny H
P, S
otla
r K, V
alen
t P. M
asto
cyto
sis:
sta
te o
f the
art.
Pat
hobi
olog
y, 2
007;
74:1
21-3
217.
Gol
kar L
, Ber
nhar
d JD
. M
asto
cyto
sis.
The
Lan
cet,
1997
; 349
(906
2):1
379-
1385
. 11
. Hei
de R
, Van
DK
, Mul
der P
G, v
an T
oore
nenb
erge
n AW
, Bei
shui
zen
A, d
e G
root
H, T
ank
B, O
ranj
e AP.
Ser
um tr
ypta
se a
nd
SCO
RM
A (S
CO
Rin
g M
Ast
ocyt
osis
) Ind
ex a
s dis
ease
seve
rity
para
met
ers i
n ch
ildho
od a
nd a
dult
cuta
neou
s mas
tocy
tosi
s. C
lin E
xp
Der
mat
ol, 2
009;
34:4
62-8
12
. Sch
war
tz L
B, I
rani
AM
. Se
rum
tryp
tase
and
the
labo
rato
ry d
iagn
osis
of s
yste
mic
mas
tocy
tosi
s. H
emat
ol O
ncol
Nor
th A
m, 2
000;
14
:641
13
. Chu
ng-L
eddo
n J.
Tel
angi
ecta
sia
mac
ular
is e
rupt
ive
pers
tans
. D
erm
atol
ogy
Onl
ine
Jour
nal,
2000
; 6(1
): 6
14. L
iu A
Y, L
owe
RC
, Lev
y B
D, K
atz
JT, L
osca
lzo
J. C
linic
al p
robl
em-s
olvi
ng. A
rash
hyp
othe
sis.
N E
ngl J
Med
, 201
0;36
3:72
-8
15. B
olog
nia
JL, J
oriz
zo JL
, Rap
ini R
P, e
dito
rs.
Der
mat
olog
y. E
dinb
urgh
: M
osby
, Inc
; 200
8; p
g 18
51-5
2 16
. Bet
ti R
, Ver
gani
R, T
olom
io E
, Mar
tino
P, C
rost
i C.
Tela
ngie
ctas
ia m
acul
aris
eru
ptiv
e pe
rsta
ns in
volv
ing
the
uppe
r arm
s in
an
adul
t m
ale.
Eur
opea
n Jo
urna
l of D
erm
atol
ogy,
200
0; 1
0(7)
:563
-564
17
. Cen
gizl
ier R
, Huc
umen
oglu
S, O
zen
A, T
ulin
Say
li R
. Tr
eatm
ent o
f tel
angi
ecta
sia
mac
ular
is e
rupt
iva
pers
tans
with
mon
telu
kast
. Al
lerg
ol Im
mun
opat
hol,
2009
; 37(
6): 3
34-3
36
18. A
ltine
r A, T
zu J,
Pat
el R
, Mee
han
S, S
anch
ez M
. Te
lang
iect
asia
mac
ular
is e
rupt
iva
pers
tans
. D
erm
atol
ogy
Onl
ine
Jour
nal,
2011
; 17
(10)
:7
19. E
llis D
L. T
reat
men
t of t
elan
giec
tasi
a m
acul
aris
eru
ptiv
e pe
rsta
ns w
ith th
e 58
5-nm
flas
hlam
p-pu
mpe
d dy
e la
ser.
Der
mat
ol S
urg,
19
96; 2
2:33
-37
20. A
dapt
ed f
rom
Wat
kins
CE,
Bok
or W
B, L
eich
t S, Y
oung
berg
G, K
rishn
asw
amy
G.
Tela
ngie
casi
a m
acul
aris
eru
ptiv
e pe
rsta
ns: m
ore
than
skin
dee
p. D
erm
atol
ogy
Repo
rts,
2011
; 3(1
) 21
. Im
age
from
http
://w
ww.
vgrd
.org
/cur
rent
/cur
rent
.htm
l, C
ase
pres
enta
tion
give
n by
Hai
mis
h D
unw
oodi
e M
D, S
kidg
ate,
Que
en
Cha
rlotte
Isla
nd, B
.C.,
Can
ada
on N
ovem
ber 1
0, 2
011
Con
clu
sion
TMEP
is ra
re fo
rm o
f cut
aneo
us m
asto
cyto
sis.
The
cou
rse
is o
ften
indo
lent
in n
atur
e. T
he p
atho
gene
sis i
s not
fully
und
erst
ood
and
requ
ires f
urth
er c
linic
al st
udie
s. Tr
eatm
ent i
s ofte
n ce
nter
ed o
n co
ntro
lling
sym
ptom
s and
trig
ger a
void
ance
. A
lthou
gh ra
re, c
ase
repo
rts o
f sys
tem
ic in
volv
emen
t hav
e be
en a
ssoc
iate
d w
ith T
MEP
, th
us a
thor
ough
his
tory
and
phy
sica
l exa
m is
ess
entia
l. In
the
afor
emen
tione
d ca
se, t
he p
atie
nt p
rese
nted
with
out a
ny c
once
rnin
g sy
mpt
oms o
r lab
orat
ory
findi
ngs t
o su
gges
t und
erly
ing
syst
emic
in
volv
emen
t. G
iven
the
beni
gn p
rese
ntat
ion,
the
patie
nt w
as
advi
sed
on fr
eque
nt e
xam
inat
ions
by
her p
rimar
y ca
re p
rovi
der
and
derm
atol
ogis
t alo
ng w
ith a
yea
rly C
BC
.
Figu
re 1
. Tan
to p
ink,
bl
anch
able
, tel
angi
ecta
tic
mac
ules
on
the
late
ral b
reas
t.
Figu
re 2
. Spa
rse
pauc
icel
lula
r inf
iltra
te c
onsi
stin
g pr
edom
inan
tly o
f mas
t cel
ls a
roun
d di
late
d ve
ssel
s of
the
supe
rfic
ial p
lexu
s.21
Sym
ptom
atic
trea
tmen
t with
em
phas
is o
n th
e av
oida
nce
of
trigg
ers i
s the
prim
ary
treat
men
t goa
l. Sy
mpt
omat
ic re
lief m
ay
be a
ccom
plis
hed
with
ant
ihis
tam
ines
, dis
odiu
m c
rom
ogly
cate
, le
ukot
riene
ant
agon
ists
, top
ical
ster
oids
, pso
rale
n pl
us U
VA
light
, 585
-nm
flas
hlam
p-pu
mpe
d pu
lse
dye
lase
r.9 Pa
tient
s sh
ould
be
educ
ated
on
avoi
danc
e of
the
com
mon
trig
gers
as w
ell
as th
e ris
k of
ana
phyl
axis
with
con
trast
dye
s and
ane
sthe
sia
(Tab
le 1
).3,9,
17 P
rovi
ding
an
epin
ephr
ine
inje
ctor
for e
mer
genc
y us
e is
reco
mm
ende
d al
ong
with
a m
edic
al a
lert
brac
elet
.9,18
Fr
eque
nt e
xam
inat
ions
and
yea
rly m
onito
ring
of C
BC
, ser
um
trypt
ase
and
24-h
our u
rinar
y hi
stam
ine
has b
een
advi
sed.
9
Syst
emic
ther
apy
for a
ggre
ssiv
e/se
vere
syst
emic
mas
tocy
tosi
s m
ay in
clud
e in
terf
eron
--2
b, ra
diat
ion
and
chem
othe
rape
utic
ag
ents
.8,15
,19
Dis
cuss
ion
(co
nti
nu
ed)
Sym
ptom
s sug
gest
ive
of sy
stem
ic d
isea
se in
clud
e; fe
ver,
head
ache
s, flu
shin
g, p
alpi
tatio
ns, p
rurit
us, g
astro
inte
stin
al (G
I) c
ompl
aint
s, dy
spne
a, b
one
pain
, ana
phyl
axis
, and
hep
atos
plen
omeg
aly.
13 I
n th
e se
tting
of
sugg
estiv
e sy
stem
ic d
isea
se, a
dditi
onal
test
ing
may
in
clud
e; 2
4-ho
ur u
rine
N-m
ethy
lhis
tam
ine,
bon
e m
arro
w b
iops
y, b
one
scan
, GI e
ndos
copy
, and
CT
of th
e ch
est,
abdo
men
and
pel
vis.
9,14
,15
His
topa
thol
ogic
exa
min
atio
n of
skin
bio
psie
s is e
ssen
tial i
n or
der t
o es
tabl
ish
a de
finiti
ve d
iagn
osis
and
to d
iffer
entia
te a
mon
g th
e va
rious
ty
pes.
TMEP
usu
ally
pos
sess
es le
ss a
ppar
ent h
isto
path
olog
ic fi
ndin
gs.
Ther
e us
ually
exi
sts a
mild
incr
ease
in m
ast c
ells
, par
ticul
arly
in
the
inte
rstit
ial c
olla
gen
and
arou
nd th
e su
perf
icia
l ple
xus b
lood
ves
sels
of t
he to
p th
ird o
f the
der
mis
.4,16
With
TM
EP, a
utho
rs h
ave
foun
d th
e va
lue
of m
ast c
ells
per
hig
h po
wer
fiel
d to
be
arou
nd 1
5 - 2
0, th
ough
a si
mpl
e co
ntra
stin
g di
ffere
nce
of m
ast c
ells
whe
n co
mpa
ring
norm
al a
nd a
ffect
ed sk
in c
an su
ffice
for d
iagn
osis
.4,9,
17 S
tain
s use
d to
vis
ualiz
e m
ast c
ells
and
thei
r cyt
opla
smic
gra
nule
s inc
lude
Gie
msa
, to
luid
ine
blue
, and
chl
oroa
ceta
te e
ster
ase
(i.e.
, Led
er st
ain)
.13 M
onoc
lona
l ant
ibod
ies t
hat r
ecog
nize
KIT
(CD
117)
and
/or t
rypt
ase
are
mor
e se
nsiti
ve a
nd u
sefu
l in
conf
irmin
g th
e di
agno
sis o
f mas
tocy
tosi
s.9,
15
Etha
nol
Psyc
holo
gica
l/Em
otio
nal s
tress
Ph
ysic
al e
xerc
ise
Bac
teria
l tox
ins
Food
alle
rgen
s (e.
g., s
hellf
ish,
pe
anut
s)
Imm
unol
ogic
stim
uli (
e.g.
, IgE
) So
lar r
adia
tion
Hot
/col
d te
mpe
ratu
re e
xtre
mes
Ve
nom
s (e.
g., h
ymen
opte
ra)
Oth
er in
sect
bite
s Ph
arm
aceu
tical
age
nts:
•
Ace
tyls
alic
ylic
aci
d •
Am
phot
eric
in B
•
d-Tu
bocu
rarin
e •
Dex
trom
etho
rpha
n •
Gal
lium
•
Iodi
ne-b
ased
con
trast
dye
s •
Nar
cotic
s (e.
g., m
orph
ine,
m
eper
idin
e, c
odei
ne)
•N
onst
eroi
dal a
nti-
infla
mm
ator
y dr
ugs
•Po
lym
yxin
B
•Po
lym
eric
eye
dro
ps
•Q
uini
ne
•R
eser
pine
•
Scop
olom
ine
Tabl
e 1.
Kno
wn
mas
t ce
ll tri
gger
s20
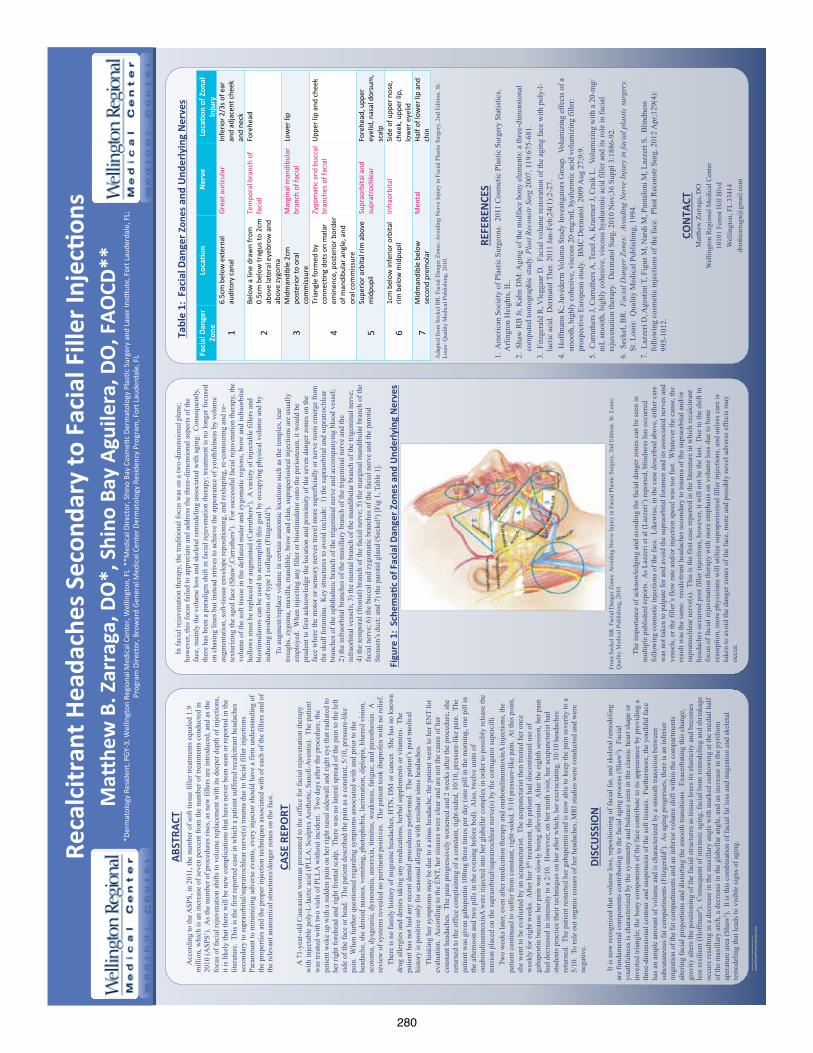
280
RES
EAR
CH
PO
STER
PR
ESEN
TATI
ON
DES
IGN
© 2
012
ww
w.P
oste
rPre
sent
atio
ns.c
om
QU
ICK
TIPS
(-
-TH
IS S
ECTI
ON
DO
ES N
OT
PRIN
T--)
This
Pow
erPo
int
tem
plat
e re
quir
es b
asic
Pow
erPo
int
(ver
sion
200
7 or
new
er)
skill
s. B
elow
is a
list
of
com
mon
ly a
sked
que
stio
ns s
peci
fic
to t
his
tem
plat
e.
If y
ou a
re u
sing
an
olde
r ve
rsio
n of
Pow
erPo
int
som
e te
mpl
ate
feat
ures
may
not
wor
k pr
oper
ly.
U
sing
the
tem
plat
e
Veri
fyin
g th
e qu
alit
y of
you
r gr
aphi
cs
Go
to t
he V
IEW
men
u an
d cl
ick
on Z
OO
M t
o se
t yo
ur
pref
erre
d m
agni
fica
tion
. Th
is t
empl
ate
is a
t 10
0%
the
size
of
the
fina
l pos
ter.
All
text
and
gra
phic
s w
ill
be p
rint
ed a
t 10
0% t
heir
siz
e. T
o se
e w
hat
your
po
ster
will
look
like
whe
n pr
inte
d, s
et t
he z
oom
to
100%
and
eva
luat
e th
e qu
alit
y of
all
your
gra
phic
s be
fore
you
sub
mit
you
r po
ster
for
pri
ntin
g.
Usi
ng t
he p
lace
hold
ers
To a
dd t
ext
to t
his
tem
plat
e cl
ick
insi
de a
pl
aceh
olde
r an
d ty
pe in
or
past
e yo
ur t
ext.
To
mov
e a
plac
ehol
der,
clic
k on
it o
nce
(to
sele
ct it
), p
lace
yo
ur c
urso
r on
its
fram
e an
d yo
ur c
urso
r w
ill c
hang
e to
thi
s sy
mbo
l:
Then
, cl
ick
once
and
dra
g it
to
its
new
loca
tion
whe
re y
ou c
an r
esiz
e it
as
need
ed.
Addi
tion
al p
lace
hold
ers
can
be f
ound
on
the
left
si
de o
f th
is t
empl
ate.
M
odif
ying
the
layo
ut
This
tem
plat
e ha
s fo
ur
diff
eren
t co
lum
n la
yout
s.
Righ
t-cl
ick
your
mou
se
on t
he b
ackg
roun
d an
d
clic
k on
“La
yout
” to
see
th
e la
yout
opt
ions
. Th
e co
lum
ns in
the
pro
vide
d la
yout
s ar
e fi
xed
and
cann
ot b
e m
oved
but
adv
ance
d us
ers
can
mod
ify
any
layo
ut b
y go
ing
to V
IEW
and
the
n SL
IDE
MAS
TER.
Im
port
ing
text
and
gra
phic
s fr
om e
xter
nal s
ourc
es
TEXT
: Pa
ste
or t
ype
your
tex
t in
to a
pre
-exi
stin
g pl
aceh
olde
r or
dra
g in
a n
ew p
lace
hold
er f
rom
the
le
ft s
ide
of t
he t
empl
ate.
Mov
e it
any
whe
re a
s ne
eded
. PH
OTO
S: D
rag
in a
pic
ture
pla
ceho
lder
, si
ze it
fir
st,
clic
k in
it a
nd in
sert
a p
hoto
fro
m t
he m
enu.
TA
BLES
: Yo
u ca
n co
py a
nd p
aste
a t
able
fro
m a
n ex
tern
al d
ocum
ent
onto
thi
s po
ster
tem
plat
e. T
o ad
just
the
way
the
tex
t fi
ts w
ithi
n th
e ce
lls o
f a
tabl
e th
at h
as b
een
past
ed,
righ
t-cl
ick
on t
he t
able
, cl
ick
FORM
AT S
HAP
E t
hen
clic
k on
TEX
T BO
X an
d ch
ange
the
INTE
RNAL
MAR
GIN
val
ues
to 0
.25
Mod
ifyi
ng t
he c
olor
sch
eme
To c
hang
e th
e co
lor
sche
me
of t
his
tem
plat
e go
to
the
“Des
ign”
men
u an
d cl
ick
on “
Colo
rs”.
You
can
ch
oose
fro
m t
he p
rovi
de c
olor
com
bina
tion
s or
you
ca
n cr
eate
you
r ow
n.
QU
ICK
DES
IGN
GU
IDE
(--T
HIS
SEC
TIO
N D
OES
NO
T PR
INT-
-)
Th
is P
ower
Poin
t 20
07 t
empl
ate
prod
uces
a 3
6”x4
8” p
rofe
ssio
nal
post
er.
It w
ill s
ave
you
valu
able
tim
e pl
acin
g ti
tles
, su
btit
les,
tex
t, a
nd
grap
hics
.
Use
it t
o cr
eate
you
r pr
esen
tati
on.
Then
sen
d it
to
Post
erPr
esen
tati
ons.
com
for
pre
miu
m q
ualit
y, s
ame
day
affo
rdab
le
prin
ting
. W
e pr
ovid
e a
seri
es o
f on
line
tuto
rial
s th
at w
ill g
uide
you
thr
ough
the
po
ster
des
ign
proc
ess
and
answ
er y
our
post
er p
rodu
ctio
n qu
esti
ons.
Vi
ew o
ur o
nlin
e tu
tori
als
at:
htt
p://
bit.
ly/P
oste
r_cr
eati
on_h
elp
(c
opy
and
past
e th
e lin
k in
to y
our
web
bro
wse
r).
For
assi
stan
ce a
nd t
o or
der
your
pri
nted
pos
ter
call
Post
erPr
esen
tati
ons.
com
at 1.
866.
649.
3004
Obj
ect
Plac
ehol
ders
Use
the
pla
ceho
lder
s pr
ovid
ed b
elow
to
add
new
ele
men
ts t
o yo
ur
post
er:
Dra
g a
plac
ehol
der
onto
the
pos
ter
area
, si
ze it
, an
d cl
ick
it t
o ed
it.
Sect
ion
Hea
der
plac
ehol
der
Mov
e th
is p
refo
rmat
ted
sect
ion
head
er p
lace
hold
er t
o th
e po
ster
are
a to
add
ano
ther
sec
tion
hea
der.
Use
sec
tion
hea
ders
to
sepa
rate
top
ics
or c
once
pts
wit
hin
your
pre
sent
atio
n.
Text
pla
ceho
lder
M
ove
this
pre
form
atte
d te
xt p
lace
hold
er t
o th
e po
ster
to
add
a ne
w
body
of
text
. Pi
ctur
e pl
aceh
olde
r M
ove
this
gra
phic
pla
ceho
lder
ont
o yo
ur p
oste
r, s
ize
it f
irst
, an
d th
en
clic
k it
to
add
a pi
ctur
e to
the
pos
ter.
© 2012 PosterPresenta.ons.com
2117 Fourth Street , Unit C
Berkeley CA 94710
posterpresenter@gm
ail.com
St
uden
t di
scou
nts
are
avai
labl
e on
our
Fac
eboo
k pa
ge.
Go
to P
oste
rPre
sent
atio
ns.c
om a
nd c
lick
on t
he F
B ic
on.
Acc
ordi
ng to
the A
SPS,
in 2
011,
the
num
ber o
f sof
t tis
sue
fille
r tre
atm
ents
equ
aled
1.9
m
illio
n, w
hich
is a
n in
crea
se o
f sev
en p
erce
nt fr
om th
e nu
mbe
r of t
reat
men
ts c
ondu
cted
in
2010
(ASP
S1 ).
As t
he n
umbe
r of p
roce
dure
s ris
es, a
s new
fille
rs a
re in
trodu
ced,
and
as t
he
focu
s of f
acia
l rej
uven
atio
n sh
ifts t
o vo
lum
e re
plac
emen
t with
its d
eepe
r dep
th o
f inj
ectio
ns,
it is
like
ly th
at th
ere
will
be
new
com
plic
atio
ns th
at h
ave
neve
r bee
n se
en o
r rep
orte
d in
the
liter
atur
e. T
his i
s the
firs
t rep
orte
d ca
se in
whi
ch a
pat
ient
suffe
red
reca
lcitr
ant h
eada
ches
se
cond
ary
to su
prao
rbita
l/sup
ratro
chle
ar n
erve
(s) t
raum
a du
e to
faci
al fi
ller i
njec
tions
. Pa
ram
ount
to m
inim
izin
g ad
vers
e ev
ents
, eve
ry in
ject
or sh
ould
hav
e a
firm
und
erst
andi
ng o
f th
e pr
oper
ties a
nd th
e pr
oper
inje
ctio
n te
chni
ques
ass
ocia
ted
with
of e
ach
of th
e fil
lers
and
of
the
rele
vant
ana
tom
ical
stru
ctur
es/d
ange
r zon
es o
n th
e fa
ce.
ABSTRA
CT
A 7
1-ye
ar-o
ld C
auca
sian
wom
an p
rese
nted
to th
e of
fice
for f
acia
l rej
uven
atio
n th
erap
y w
ith in
ject
able
pol
y-L-
lact
ic a
cid
(PLL
A; S
culp
tra A
esth
etic
, San
ofi-A
vent
is).
The
pat
ient
w
as tr
eate
d w
ith tw
o vi
als o
f PLL
A w
ithou
t inc
iden
t. T
wo
days
afte
r the
pro
cedu
re, t
he
patie
nt w
oke
up w
ith a
sudd
en p
ain
on h
er ri
ght n
asal
side
wal
l and
righ
t eye
that
radi
ated
to
her r
ight
fore
head
and
righ
t fro
ntal
scal
p. T
here
was
no
late
ral s
prea
d of
the
pain
to th
e le
ft si
de o
f the
face
or h
ead.
The
pat
ient
des
crib
ed th
e pa
in a
s a c
onst
ant,
5/10
, pre
ssur
e-lik
e pa
in.
Whe
n fu
rther
que
stio
ned
rega
rdin
g sy
mpt
oms a
ssoc
iate
d w
ith a
nd p
rior t
o th
e he
adac
he, s
he d
enie
d na
usea
, vom
iting
, pho
toph
obia
, lac
rimat
ion,
dip
lopi
a, b
lurr
ed v
isio
n,
scot
oma,
dys
geus
ia, d
ysno
smia
, ano
rexi
a, ti
nnitu
s, w
eakn
ess,
fatig
ue, a
nd p
ares
thes
ias.
A
revi
ew o
f sys
tem
s rev
eale
d no
per
tinen
t pos
itive
s. T
he p
atie
nt to
ok ib
upro
fen
with
no
relie
f.
The
re is
no
fam
ily h
isto
ry o
f mig
rain
e he
adac
hes,
HTN
, DM
or c
ance
r. S
he h
as n
o kn
own
drug
alle
rgie
s and
den
ies t
akin
g an
y m
edic
atio
ns, h
erba
l sup
plem
ents
or v
itam
ins.
The
pa
tient
has
not
had
any
rece
nt d
enta
l pro
cedu
res p
erfo
rmed
. Th
e pa
tient
’s p
ast m
edic
al
hist
ory
is p
ositi
ve o
nly
for s
easo
nal a
llerg
ies w
ith re
sulta
nt si
nus h
eada
ches
.
Thi
nkin
g he
r sym
ptom
s may
be
due
to a
sinu
s hea
dach
e, th
e pa
tient
wen
t to
her E
NT
for
eval
uatio
n. A
ccor
ding
to th
e EN
T, h
er si
nuse
s wer
e cl
ear a
nd a
re n
ot th
e ca
use
of h
er
cons
tant
hea
dach
es.
The
pain
pro
gres
sive
ly w
orse
ned
and
2 w
eeks
afte
r the
pro
cedu
re, s
he
retu
rned
to th
e of
fice
com
plai
ning
of a
con
stan
t, rig
ht-s
ided
, 10/
10, p
ress
ure-
like
pain
. Th
e pa
tient
was
giv
en g
abap
entin
100
mg
thre
e tim
es p
er d
ay (o
ne p
ill in
the
mor
ning
, one
pill
in
the
afte
rnoo
n an
d tw
o pi
lls in
the
even
ing
befo
re b
ed).
Als
o, tw
elve
uni
ts o
f on
abot
ulin
umto
xinA
wer
e in
ject
ed in
to h
er g
labe
llar c
ompl
ex in
ord
er to
pos
sibl
y re
leas
e th
e te
nsio
n pl
aced
on
the
supr
aorb
ital/s
upra
troch
lear
ner
ve(s
) by
the
corr
ugat
or su
perc
illi.
T
wo
wee
ks la
ter,
even
afte
r med
icat
ion
ther
apy
and
onab
otul
inum
toxi
nA in
ject
ions
, the
pa
tient
con
tinue
d to
suffe
r fro
m c
onst
ant,
right
-sid
ed, 5
/10
pres
sure
-like
pai
n. A
t thi
s poi
nt,
she
wen
t to
be e
valu
ated
by
an a
cupu
nctu
rist.
The
acu
punc
turis
t the
n tre
ated
her
onc
e w
eekl
y fo
r eig
ht w
eeks
. A
fter h
er 5
th tr
eatm
ent,
the
patie
nt h
ad d
isco
ntin
ued
use
of
gaba
pent
in b
ecau
se h
er p
ain
was
slow
ly b
eing
alle
viat
ed.
Afte
r the
eig
hth
sess
ion,
her
pai
n ha
d de
crea
sed
in in
tens
ity to
a 2
/10.
How
ever
, on
her n
inth
vis
it, h
er a
cupu
nctu
rist h
ad
stud
ents
pra
ctic
e th
eir t
echn
ique
s on
her a
fter w
hich
, her
exc
ruci
atin
g, 1
0/10
hea
dach
es
retu
rned
. Th
e pa
tient
rest
arte
d he
r gab
apen
tin a
nd is
now
abl
e to
kee
p th
e pa
in se
verit
y to
a
5/10
. To
rule
out
org
anic
cau
ses o
f her
hea
dach
es, M
RI s
tudi
es w
ere
cond
ucte
d an
d w
ere
nega
tive.
CASE REPORT
In
faci
al re
juve
natio
n th
erap
y, th
e tra
ditio
nal f
ocus
was
on
a tw
o-di
men
sion
al p
lane
; ho
wev
er, t
his f
ocus
faile
d to
app
reci
ate
and
addr
ess t
he th
ree-
dim
ensi
onal
asp
ects
of t
he
face
, mai
nly
the
volu
me
loss
and
skel
etal
rem
odel
ing
asso
ciat
ed w
ith a
ging
. C
onse
quen
tly,
ther
e ha
s bee
n a
para
digm
shift
in fa
cial
reju
vena
tion
ther
apy;
trea
tmen
t is n
o lo
nger
focu
sed
on c
hasi
ng li
nes b
ut in
stea
d st
rives
to a
chie
ve th
e ap
pear
ance
of y
outh
fuln
ess b
y vo
lum
e au
gmen
tatio
n, so
ft-tis
sue
enve
lope
repo
sitio
ning
, and
resh
apin
g, re
-con
tour
ing
and
re-
text
uriz
ing
the
aged
face
(Sha
w2 ,C
arru
ther
s5 ).
For s
ucce
ssfu
l fac
ial r
ejuv
enat
ion
ther
apy,
the
volu
me
of th
e so
ft tis
sue
in th
e de
flate
d m
alar
and
zyg
omat
ic re
gion
s, br
ow a
nd in
frao
rbita
l ho
llow
s mus
t be
repl
aced
or a
ugm
ente
d (C
arru
ther
s5 ).
A v
arie
ty o
f inj
ecta
ble
fille
rs a
nd
bios
timul
ator
s can
be
used
to a
ccom
plis
h th
is g
oal b
y oc
cupy
ing
phys
ical
vol
ume
and
by
indu
cing
pro
duct
ion
of ty
pe I
colla
gen
(Fitz
gera
ld3 )
.
To
augm
ent/r
epla
ce v
olum
e in
cer
tain
ana
tom
ic lo
catio
ns su
ch a
s the
tem
ples
, tea
r tro
ughs
, zyg
oma,
max
illa,
man
dibl
e, b
row
and
chi
n, su
prap
erio
stea
l inj
ectio
ns a
re u
sual
ly
empl
oyed
. W
hen
inje
ctin
g an
y fil
ler o
r bio
stim
ulat
or o
nto
the
perio
steu
m, i
t wou
ld b
e pr
uden
t to
first
ack
now
ledg
e th
e lo
catio
n an
d pr
oxim
ity o
f the
seve
n da
nger
zon
es o
n th
e fa
ce w
here
the
mot
or o
r sen
sory
ner
ves t
rave
l mor
e su
perf
icia
lly o
r ner
ve ro
ots e
mer
ge fr
om
the
skul
l for
amin
a. K
ey st
ruct
ures
to a
void
incl
ude:
1) t
he su
prao
rbita
l and
supr
atro
chle
ar
bran
ches
of t
he o
phth
alm
ic b
ranc
h of
the
trige
min
al n
erve
and
acc
ompa
nyin
g bl
ood
vess
el;
2) th
e in
frao
rbita
l bra
nche
s of t
he m
axill
ary
bran
ch o
f the
trig
emin
al n
erve
and
the
infr
aorb
ital v
esse
ls; 3
) the
men
tal b
ranc
h of
the
man
dibu
lar b
ranc
h of
the
trige
min
al n
erve
; 4)
the
tem
pora
l (fr
onta
l) br
anch
of t
he fa
cial
ner
ve; 5
) the
mar
gina
l man
dibu
lar b
ranc
h of
the
faci
al n
erve
; 6) t
he b
ucca
l and
zyg
omat
ic b
ranc
hes o
f the
faci
al n
erve
and
the
paro
tid
Sten
sen’
s duc
t; an
d 7)
the
paro
tid g
land
(Sec
kel6 )
[Fig
1, T
able
1].
The
impo
rtanc
e of
ack
now
ledg
ing
and
avoi
ding
the
faci
al d
ange
r zon
es c
an b
e se
en in
m
ultip
le p
ublis
hed
repo
rts.
As L
azze
ri et
al (
Lazz
eri7 )
repo
rted,
blin
dnes
s has
occ
urre
d fo
llow
ing
cosm
etic
inje
ctio
ns o
f the
face
. Li
kew
ise,
in th
e ca
se d
escr
ibed
abo
ve, e
ither
car
e w
as n
ot ta
ken
to p
alpa
te fo
r and
avo
id th
e su
prao
rbita
l for
amen
and
its a
ssoc
iate
d ne
rves
and
ve
ssel
s, or
the
fille
r’s fl
ow ra
te a
nd/o
r inj
ectio
n sp
eed
was
too
fast
. W
hate
ver t
he c
ause
, the
re
sult
was
the
sam
e: r
ecal
citra
nt h
eada
ches
seco
ndar
y to
trau
ma
of th
e su
prao
rbita
l and
/or
supr
atro
chle
ar n
erve
(s).
Thi
s is t
he fi
rst c
ase
repo
rted
in th
e lit
erat
ure
in w
hich
reca
lcitr
ant
head
ache
s occ
urre
d po
st fi
ller i
njec
tions
, how
ever
, it w
ill n
ot b
e th
e la
st.
Due
to th
e sh
ift in
fo
cus o
f fac
ial r
ejuv
enat
ion
ther
apy
with
mor
e em
phas
is o
n vo
lum
e lo
ss d
ue to
bon
e re
sorp
tion,
mor
e ph
ysic
ians
will
util
ize
supr
aper
iost
eal f
iller
inje
ctio
ns, a
nd u
nles
s car
e is
ta
ken
to a
void
the
dang
er z
ones
of t
he fa
ce, m
ore
and
poss
ibly
nov
el a
dver
se e
ffect
s may
oc
cur.
DISCUSSION
Table 1: Facial D
anger Z
ones and Underlying Nerves
REFERENCES
1. A
mer
ican
Soc
iety
of P
last
ic S
urge
ons.
201
1 C
osm
etic
Pla
stic
Sur
gery
Sta
tistic
s.
Arli
ngto
n H
eigh
ts, I
L.
2. S
haw
RB
Jr, K
ahn
DM
: Agi
ng o
f the
mid
face
bon
y el
emen
ts: a
thre
e-di
men
sion
al
com
pute
d to
mog
raph
ic st
udy.
Pla
st R
econ
str S
urg
2007
, 119
:675
-681
. 3.
Fitz
gera
ld R
, Vle
ggaa
r D.
Faci
al v
olum
e re
stor
atio
n of
the
agin
g fa
ce w
ith p
oly-
l-la
ctic
aci
d. D
erm
atol
The
r. 20
11 Ja
n-Fe
b;24
(1):2
-27.
4.
Hof
fman
n K
; Juv
éder
m V
olum
a St
udy
Inve
stig
ator
s Gro
up.
Volu
miz
ing
effe
cts o
f a
smoo
th, h
ighl
y co
hesi
ve, v
isco
us 2
0-m
g/m
L hy
alur
onic
aci
d vo
lum
izin
g fil
ler:
pros
pect
ive
Euro
pean
stud
y. B
MC
Der
mat
ol. 2
009
Aug
27;
9:9.
5.
Car
ruth
ers J
, Car
ruth
ers A
, Tez
el A
, Kra
emer
J, C
raik
L.
Volu
miz
ing
with
a 2
0-m
g/m
L sm
ooth
, hig
hly
cohe
sive
, vis
cous
hya
luro
nic
acid
fille
r and
its r
ole
in fa
cial
re
juve
natio
n th
erap
y. D
erm
atol
Sur
g. 2
010
Nov
;36
Supp
l 3:1
886-
92.
6. S
ecke
l, B
R.
Faci
al D
ange
r Zon
es:
Avoi
ding
Ner
ve In
jury
in fa
cial
pla
stic
surg
ery.
St
. Lou
is:
Qua
lity
Med
ical
Pub
lishi
ng, 1
994.
7.
Laz
zeri
D, A
gost
ini T
, Fig
us M
, Nar
di M
, Pan
talo
ni M
, Laz
zeri
S. B
lindn
ess
follo
win
g co
smet
ic in
ject
ions
of t
he fa
ce.
Plas
t Rec
onst
r Sur
g. 2
012
Apr
;129
(4):
995-
1012
.
CONTA
CT
Mat
thew
Zar
raga
, DO
W
ellin
gton
Reg
iona
l Med
ical
Cen
ter
1010
1 Fo
rest
Hill
Blv
d W
ellin
gton
, FL
3341
4 dr
mbz
arra
ga@
gmai
l.com
From
Sec
kel B
R. F
acia
l Dan
ger Z
ones
: Avo
idin
g N
erve
Inju
ry in
Fac
ial P
last
ic S
urge
ry, 2
nd E
ditio
n. S
t. Lo
uis:
Q
ualit
y M
edic
al P
ublis
hing
, 201
0.
Ada
pted
from
Sec
kel B
R. F
acia
l Dan
ger Z
ones
: Avo
idin
g N
erve
Inju
ry in
Fac
ial P
last
ic S
urge
ry, 2
nd E
ditio
n. S
t. Lo
uis:
Qua
lity
Med
ical
Pub
lishi
ng, 2
010.
I
t is n
ow re
cogn
ized
that
vol
ume
loss
, rep
ositi
onin
g of
faci
al fa
t, an
d sk
elet
al re
mod
elin
g ar
e fu
ndam
enta
l com
pone
nts c
ontri
butin
g to
the
faci
al a
ging
pro
cess
(Sha
w2 )
. Fa
cial
yo
uthf
ulne
ss is
cha
ract
eriz
ed b
y th
e sy
mm
etry
and
bal
ance
seen
in th
e cl
assi
c he
art s
hape
or
inve
rted
trian
gle;
the
bony
com
pone
nts o
f the
face
con
tribu
te to
its a
ppea
ranc
e by
pro
vidi
ng a
th
ree-
dim
ensi
onal
con
tour
and
susp
ensi
on o
f the
soft
tissu
es.
Furth
erm
ore,
the
yout
hful
face
ha
s an
ampl
e am
ount
of v
olum
e an
d is
cha
ract
eriz
ed b
y a
smoo
th tr
ansi
tion
betw
een
subc
utan
eous
fat c
ompa
rtmen
ts (F
itzge
rald
3 ).
As a
ging
pro
gres
ses,
ther
e is
an
infe
rior
mig
ratio
n of
the
fat c
ompa
rtmen
ts a
nd a
n in
ferio
r vol
ume
shift
with
in th
e co
mpa
rtmen
ts
alte
ring
faci
al p
ropo
rtion
s and
dis
torti
ng th
e sm
ooth
tran
sitio
ns.
Exac
erba
ting
this
cha
nge,
gr
avity
alte
rs th
e po
sitio
ning
of t
he fa
cial
stru
ctur
es a
s tis
sue
lose
s its
ela
stic
ity a
nd b
ecom
es
less
resi
lient
(Hof
fman
4 ).
Con
sequ
ent o
f int
rinsi
c ag
ing,
faci
al b
one
rem
odel
ing
and
shrin
kage
oc
curs
resu
lting
in a
dec
reas
e in
the
max
illar
y an
gle
with
mar
ked
outb
owin
g at
the
med
ial h
alf
of th
e m
axill
ary
arch
, a d
ecre
ase
in th
e gl
abel
lar a
ngle
, and
an
incr
ease
in th
e py
rifor
m
aper
atur
e ar
ea (S
haw
2 ).
It is
this
com
bina
tion
of fa
cial
fat l
oss a
nd m
igra
tion
and
skel
etal
re
mod
elin
g th
at le
ads t
o vi
sibl
e si
gns o
f agi
ng. *Dermatology Resident, PGY-‐3, Wellington Regional Medical Center, Wellington, FL **Medical Director, Shino Bay Cosme.c Dermatology Plas.c Surgery and Laser Ins.tute, Fort Lauderdale, FL;
Program Director, Broward General Medical Center Dermatology Residency Program, Fort Lauderdale, FL
MaG
hew B. Zarraga, D
O*, Shino
Bay Aguilera, D
O, FAO
CD**
Recalcitrant H
eadaches Secon
dary to
Facial Filler InjecOon
s
Facial Danger
Zone
LocaOo
n Nerve
LocaOo
n of Zon
al
Injury
1 6.5cm below external
auditory canal
Great auricular
Inferior 2/3s of ear
and adjacent cheek
and neck
2 Below a line drawn from
0.5cm below tragus to 2cm
above lateral eyebrow and
above zygoma
Temporal branch of
facial
Forehead
3 Midmandible 2cm
posterior to oral
commissure
Marginal mandibular
branch of facial
Lower lip
4
Triangle formed by
connec.ng dots on malar
eminence, posterior border
of mandibular angle, and
oral commissure
Zygoma.c and buccal
branches of facial
Upper lip and cheek
5 Superior orbital rim above
midpupil
Supraorbital and
supratrochlear
Forehead, upper
eyelid, nasal dorsum,
scalp
6 1cm below inferior orbital
rim below midpupil
Infraorbital
Side of upper nose,
cheek, upper lip,
lower eyelid
7 Midmandible below
second premolar
Mental
Half of lower lip and
chin
Figure 1: SchemaO
c of Facial D
anger Zon
es and
Und
erlying Nerves
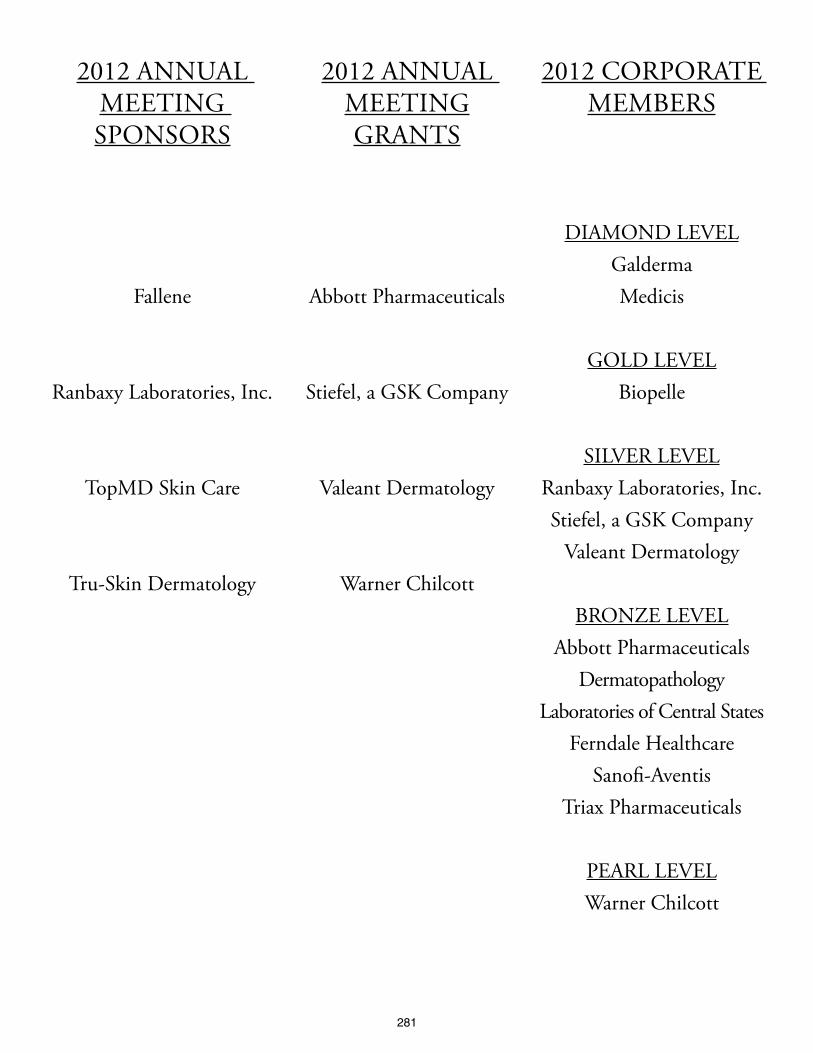
281
2012 AnnuAl Meeting SponSorS
Fallene
ranbaxy laboratories, inc.
topMD Skin Care
tru-Skin Dermatology
2012 AnnuAl MeetinggrAntS
Abbott pharmaceuticals
Stiefel, a gSK Company
Valeant Dermatology
Warner Chilcott
2012 CorporAte MeMberS
DiAMonD leVelgaldermaMedicis
golD leVelbiopelle
SilVer leVelranbaxy laboratories, inc.Stiefel, a gSK Company
Valeant Dermatology
bronZe leVelAbbott pharmaceuticals
Dermatopathology laboratories of Central States
Ferndale HealthcareSanofi-Aventis
triax pharmaceuticals
peArl leVelWarner Chilcott

Related Documents











