42 Journal of Dental Research and Review ● Jan-Apr 2014 ● Vol. 1 ● Issue 1 Introduction T he global incidence of oral cancer is 5,00,000 cases per year with mortality of 2,70,000 cases per year. The incidence of oral cancer in India is 40% among all cancers and about 1,00,000 patients suffer from oral cancer in any year. Oral cancer is responsible for 7% of all cancer deaths in males and 3% in females. [1] The recent protocol for management of oral cancer includes multimodal therapy, such as surgery with radiotherapy and/or chemotherapy. Radiation therapy is one of the major treatment modalities for the management of oral malignancies. Like with any treatment modality, even radiation therapy is associated with various complications. A long‑term side effect of radiotherapy that is also the most serious is osteoradionecrosis. [2,3] Literature reveals many terminologies to represent the same disease, such as radiation osteitis, radio‑osteonecrosis, radiation osteomyelitis, osteomyelitis of irradiated bone, osteonecrosis, radio‑osteomyelitis, septic osteoradionecrosis, and post‑radiotherapy osteonecrosis. [4] This review focuses on the general information on maxillofacial osteoradionecrosis for general practitioners. Historical perspective In 1922, Regaud published the first report about osteoradionecrosis of jaws after radiotherapy. [4] In 1926, further description of osteoradionecrosis was given by Ewing under the name Radiation Osteitis. [5] In 1970, Meyer classified osteoradionecrosis as one special type of osteomyelitis. In 1975, Mainous advocated the use of hyperbaric oxygen therapy (HBO) for late radiation tissue injury. In 1983, Robert Marx proposed the hypoxic, hypocellular, and hypovascular theory as a new way of understanding the pathophysiology of osteoradionecrosis. In 1992, Harris introduced the use of Ultrasound as one of the modes to treat osteoradionecrosis. [6] In 1998, Marx gave the 30/10 protocol that was employed in the treatment of established osteoradionecrosis. In 2004, Delanian and Lefaix put forward a new theory named radiation‑induced fibrosis that accounts for the damage to normal tissues, including bone after radiotherapy. [7] Definitions In literature, osteoradionecrosis has been defined in many ways [Table 1]. [8,9] However, the authors feel that the definition given by Wong, Wood, and McLean (1997) [8] is the most appropriate and complete: “A slow‑healing radiation‑induced ischemic necrosis of bone with associated soft tissue necrosis of variable extent occurring in the absence of local primary tumour necrosis, recurrence, or metastatic disease that may or may not: i. Be superinfected (and accompanied by fistulation or cellulitis) ii. End in pathologic fracture iii. Resolve without surgery, hyperbaric oxygen therapy or both.” Maxillofacial osteoradionecrosis Amit T. Suryawanshi, S. N. Santhosh Kumar, R. S. Dolas, Ruchi Khindria, Vivek Pawar, Manju Singh Review Article Access this article online Quick Response Code: Website: www.jdrr.org DOI: 10.4103/2348-3172.126171 How to cite this article: Suryawanshi AT, Kumar SS, Dolas RS, Khindria R, Pawar V, Singh M. Maxillofacial osteoradionecrosis. J Dent Res Rev 2014;1:42-9. ABSTRACT Osteoradionecrosis is a severe and delayed radiation‑induced injury, characterized by bone tissue necrosis and failure to heal. Cases of osteoradionecrosis present to the clinician with features of pain, drainage, and fistulation of the mucosa or skin related to exposed bone in the previously irradiated area. The tumour size and location, radiation dose, occurrence of local trauma, dental extractions, infection, immune defects, and malnutrition are predisposing factors. A better understanding of risk factors leading to the development osteoradionecrosis and of the underlying pathophysiology may improve the ability of the clinician to prevent the occurrence and help improve the prognosis of this complication. Although the frequency of osteoradionecrosis has declined since the introduction of newer methods of radiotherapy, this review focuses on the etiology, pathophysiology, clinical features, radiological features, diagnosis, and treatment modalities including the newer modalities. KEY WORDS: Jaws, management, osteoradionecrosis, physiopathology, risk factors Department of Oral and Maxillofacial Surgery, DPU, Dr. D. Y. Patil Dental College and Hospital, Pimpri, Pune, Maharashtra, India Address for correspondence: Dr. Amit Suryawanshi, E‑mail: amitsuryawanshi999 @gmail.com [Downloaded free from http://www.jdrr.org on Wednesday, September 09, 2015, IP: 14.140.125.38]

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

42 Journal of Dental Research and Review ● Jan-Apr 2014 ● Vol. 1 ● Issue 1
Introduction
T he global incidence of oral cancer is 5,00,000 cases per year with mortality of 2,70,000 cases per year. The
incidence of oral cancer in India is 40% among all cancers and about 1,00,000 patients suffer from oral cancer in any year. Oral cancer is responsible for 7% of all cancer deaths in males and 3% in females.[1]
The recent protocol for management of oral cancer includes multimodal therapy, such as surgery with radiotherapy and/or chemotherapy. Radiation therapy is one of the major treatment modalities for the management of oral malignancies. Like with any treatment modality, even radiation therapy is associated with various complications. A long‑term side effect of radiotherapy that is also the most serious is osteoradionecrosis.[2,3] Literature reveals many terminologies to represent the same disease, such as radiation osteitis, radio‑osteonecrosis, radiation osteomyelitis, osteomyelitis of irradiated bone, osteonecrosis, radio‑osteomyelitis, septic osteoradionecrosis, and post‑radiotherapy osteonecrosis.[4]
This review focuses on the general information on maxillofacial osteoradionecrosis for general practitioners.
Historical perspective
In 1922, Regaud published the first report about osteoradionecrosis of jaws after radiotherapy.[4] In 1926, further description of osteoradionecrosis was given by Ewing under the name Radiation Osteitis.[5] In 1970, Meyer classified osteoradionecrosis as one special type of osteomyelitis. In 1975, Mainous advocated the use of hyperbaric oxygen therapy (HBO) for late radiation tissue injury. In 1983, Robert Marx proposed the hypoxic, hypocellular, and hypovascular theory as a new way of understanding the pathophysiology of osteoradionecrosis. In 1992, Harris introduced the use of Ultrasound as one of the modes to treat osteoradionecrosis.[6] In 1998, Marx gave the 30/10 protocol that was employed in the treatment of established osteoradionecrosis. In 2004, Delanian and Lefaix put forward a new theory named radiation‑induced fibrosis that accounts for the damage to normal tissues, including bone after radiotherapy.[7]
Definitions
In literature, osteoradionecrosis has been defined in many ways [Table 1].[8,9] However, the authors feel that the definition given by Wong, Wood, and McLean (1997)[8] is the most appropriate and complete:
“A slow‑healing radiation‑induced ischemic necrosis of bone with associated soft tissue necrosis of variable extent occurring in the absence of local primary tumour necrosis, recurrence, or metastatic disease that may or may not:i. Be superinfected (and accompanied by fistulation or cellulitis)ii. End in pathologic fractureiii. Resolve without surgery, hyperbaric oxygen therapy or both.”
Maxillofacial osteoradionecrosisAmit T. Suryawanshi, S. N. Santhosh Kumar, R. S. Dolas, Ruchi Khindria, Vivek Pawar, Manju Singh
Review Article
Access this article onlineQuick Response Code:
Website:
www.jdrr.org
DOI:
10.4103/2348-3172.126171
How to cite this article: Suryawanshi AT, Kumar SS, Dolas RS, Khindria R, Pawar V, Singh M. Maxillofacial osteoradionecrosis. J Dent Res Rev 2014;1:42-9.
ABSTRACTOsteoradionecrosis is a severe and delayed radiation‑induced injury, characterized by bone tissue necrosis and failure to heal. Cases of osteoradionecrosis present to the clinician with features of pain, drainage, and fistulation of the mucosa or skin related to exposed bone in the previously irradiated area. The tumour size and location, radiation dose, occurrence of local trauma, dental extractions, infection, immune defects, and malnutrition are predisposing factors. A better understanding of risk factors leading to the development osteoradionecrosis and of the underlying pathophysiology may improve the ability of the clinician to prevent the occurrence and help improve the prognosis of this complication. Although the frequency of osteoradionecrosis has declined since the introduction of newer methods of radiotherapy, this review focuses on the etiology, pathophysiology, clinical features, radiological features, diagnosis, and treatment modalities including the newer modalities.
KEY WORDS: Jaws, management, osteoradionecrosis, physiopathology, risk factors
Department of Oral and Maxillofacial Surgery, DPU, Dr. D. Y. Patil Dental College and Hospital, Pimpri, Pune, Maharashtra, India
Address for correspondence: Dr. Amit Suryawanshi, E‑mail: amitsuryawanshi999 @gmail.com
[Downloaded free from http://www.jdrr.org on Wednesday, September 09, 2015, IP: 14.140.125.38]
Suryawanshi, et al.: Maxillofacial osteoradionecrosis
Journal of Dental Research and Review ● Jan-Apr 2014 ● Vol. 1 ● Issue 1 43
• Marx’sHypoxic,hypocellular,andhypovasculartheory[20]
• Delanian’sRadiation‑inducedfibroatrophictheory.[21]
Meyer’s radiation, trauma, and infection theory
In 1970, in an excellent monograph on infectious disease of the jaws, Meyer defined the classic triad of osteoradionecrosis as radiation, trauma, and infection [Figure 1].[19] Meyer portrayed that the trauma provided the portal for invasion by oral microbiological floraintotheunderlyingirradiatedbone.Meyer’stheorylastedfor a decade and became the foundation for the popular use of antibiotics with surgery to treat osteoradionecrosis.[19]
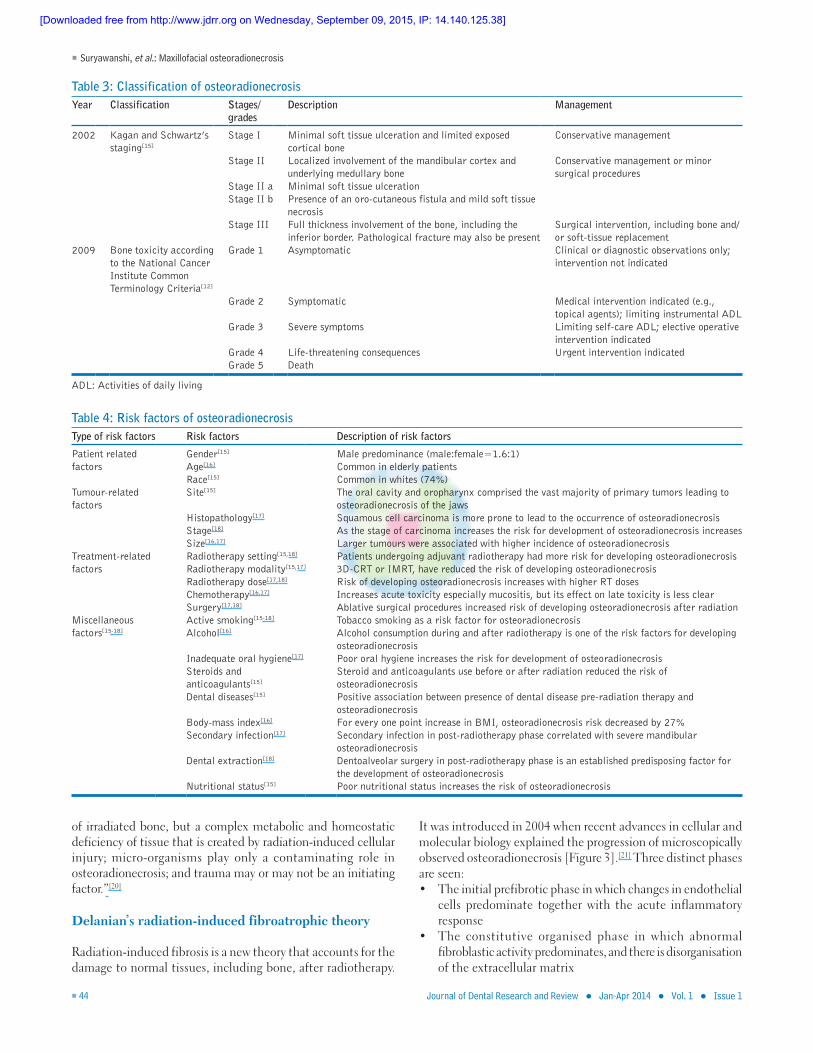
Marx’s hypoxic, hypocellular, and hypovascular theory
Robert E Marx in his landmark study noted that there was no injury before the onset of osteoradionecrosis in 35% of his cases. He also found that composite irradiated tissues were more hypoxic than those that had not been irradiated [Figure 2].[20] Marx concluded that “Osteoradionecrosis is not a primary infection
Table 2: Classification systems of osteoradionecrosisYear Authors Basis for classification
1983 Coffin’s classification[10] Based on the extent of involvementMinor and Major
1983 Marx classification[8] Based on time period between radiation therapy and occurrence of osteoradionecrosisType I-III
1983 Marx staging[8] Based on the treatment modalities involved along with HBO therapyStage I-III
1986 Morton and simpson’s Classification[11]
Based on the duration of occurrence of osteoradionecrosisMinor, Moderate and Major
1987 Epstein’s stages[10] Based on the progress of the diseaseStage I-III
1995 Late effects of normal tissue/ Somatic objective management analytic (SOMA) scale[12]
Based on subjective symptoms and objective signs of osteoradionecrosisGrade 1-4
1997 Clayman’s classification[13]
Based on the presence/absence of soft tissue break downType I and II
1998 Radiation therapy oncology group scoring[12]
Based on the severity of bone morbidityGrade 0-5
2000 Store and Boysen’s staging[11]
Based on the extent of involvement of soft and hard tissuesStage 0-3
2002 Kagan and Schwartz’s staging[14]
Based on the clinical assessment and physical findings of osteoradionecrosisStage I-III
2003 Notani et al’s Classification[12]
For mandibular osteoradionecrosis after clinical examination and orthopantogramClass I-III
2009 National cancer institute common terminology criteria (version-IV)[12]
Based on clinical presentation of osteoradionecrosisGrade 1-5
LENT: Late effects of normal tissue, SOMA: Somatic objective management analytic
Classification and staging systems
There have been several staging or scoring systems that have been proposed. These systems are based on response to HBO therapy, degree of bone damage, clinical–radiological findings, length of bone exposure through the overlying skin or mucosa, and treatment needed [Tables 2 and 3].[8‑15]
Risk factors
The existing articles in literature fail to give an exact etiology for osteoradionecrosis. The etiology of osteoradionecrosis is considered to be multifactorial. These factors may increase the risk of the patient for development of osteoradionecrosis. The factors are classified into four groups as shown in Table 4.[15‑18]
Pathophysiology
The pathophysiology of osteoradionecrosis is not very clear till date. However, literature reveals three theories that have been put forward since 1970, as mentioned in the following:• Meyer’sRadiation,traumaandinfectiontheory[19]
Table 1: Definitions of osteoradionecrosisYear Author(s) Definition
1983 Marx[8] An area of exposed bone greater than 1 cm in a field of irradiation that had failed to show any evidence of healing for at least 6 months
1983 BeumerIII, Harrison, Sanders and Kurrasch[9]
An exposure of bone of the maxilla or mandible within the radiation treatment volume persisting for more than 3 months or longer
1986 Morton and Simpson[9] A loss of soft tissue integrity and exposure of radiation damaged bone
1987 Marx and Johnson[9] An exposure of nonvital irradiated bone, which fails to heal without intervention
1987 Epstein, Rea, Wong, Spinelli and Stevenson-Moore[9]
An ulceration or necrosis of the mucous membrane (In the absence of recurrent or metastatic disease), with exposure of necrotic bone for more than 3 months
1989 Widmark, Sagne and Heikel[9]
A non healing mucous or cutaneous ulcer with denuded bone, lasting for more than 3 months
1990 Koka, Deo, Lusinichi, Roland and Schwaab[9]
A persistent ulceration with exposure of devitalised bone, cellulitis, fistula and a pathologic mandibular fracture. Patients tumour free at primary site
1992 Harris[9] Exposed and necrotic bone associated with ulcerated or necrotic surrounding soft tissue which persists for greater 3 months in an area that had been previously irradiated (not caused by tumor recurrence)
1993 Mirante and Urken et al.[9]
A loss of viable bone resulting from radiation therapy
1995 Van Merkesteyn, Bakker and Borgmeijer-Hoelen[9]
A bone and soft tissue necrosis of 6 months duration excluding radiation-induced periodontal breakdown
[Downloaded free from http://www.jdrr.org on Wednesday, September 09, 2015, IP: 14.140.125.38]
Suryawanshi, et al.: Maxillofacial osteoradionecrosis
44 Journal of Dental Research and Review ● Jan-Apr 2014 ● Vol. 1 ● Issue 1
of irradiated bone, but a complex metabolic and homeostatic deficiency of tissue that is created by radiation‑induced cellular injury; micro‑organisms play only a contaminating role in osteoradionecrosis; and trauma may or may not be an initiating factor.”[20]
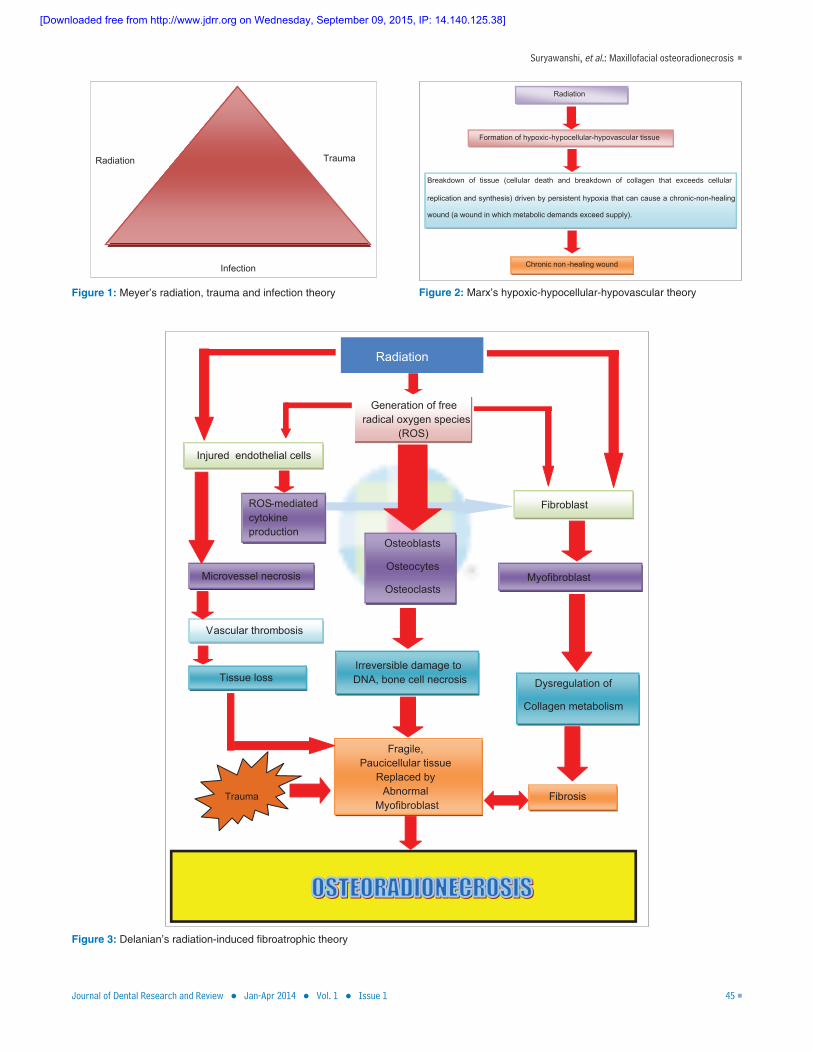
Delanian’s radiation‑induced fibroatrophic theory
Radiation‑induced fibrosis is a new theory that accounts for the damage to normal tissues, including bone, after radiotherapy.
It was introduced in 2004 when recent advances in cellular and molecular biology explained the progression of microscopically observed osteoradionecrosis [Figure 3].[21] Three distinct phases are seen:• Theinitialprefibroticphaseinwhichchangesinendothelial
cells predominate together with the acute inflammatory response
• The constitutive organised phase in which abnormalfibroblastic activity predominates, and there is disorganisation of the extracellular matrix
Table 3: Classification of osteoradionecrosisYear Classification Stages/
gradesDescription Management
2002 Kagan and Schwartz’s staging[15]
Stage I Minimal soft tissue ulceration and limited exposed cortical bone
Conservative management
Stage II Localized involvement of the mandibular cortex and underlying medullary bone
Conservative management or minor surgical procedures
Stage II a Minimal soft tissue ulcerationStage II b Presence of an oro-cutaneous fistula and mild soft tissue
necrosisStage III Full thickness involvement of the bone, including the
inferior border. Pathological fracture may also be presentSurgical intervention, including bone and/or soft-tissue replacement
2009 Bone toxicity according to the National Cancer Institute Common Terminology Criteria[12]
Grade 1 Asymptomatic Clinical or diagnostic observations only; intervention not indicated
Grade 2 Symptomatic Medical intervention indicated (e.g., topical agents); limiting instrumental ADL
Grade 3 Severe symptoms Limiting self-care ADL; elective operative intervention indicated
Grade 4 Life-threatening consequences Urgent intervention indicatedGrade 5 Death
ADL: Activities of daily living
Table 4: Risk factors of osteoradionecrosisType of risk factors Risk factors Description of risk factors
Patient related factors
Gender[15] Male predominance (male:female=1.6:1)Age[16] Common in elderly patientsRace[15] Common in whites (74%)
Tumour-related factors
Site[15] The oral cavity and oropharynx comprised the vast majority of primary tumors leading to osteoradionecrosis of the jaws
Histopathology[17] Squamous cell carcinoma is more prone to lead to the occurrence of osteoradionecrosisStage[18] As the stage of carcinoma increases the risk for development of osteoradionecrosis increasesSize[16,17] Larger tumours were associated with higher incidence of osteoradionecrosis
Treatment-related factors
Radiotherapy setting[15,18] Patients undergoing adjuvant radiotherapy had more risk for developing osteoradionecrosisRadiotherapy modality[15,17] 3D-CRT or IMRT, have reduced the risk of developing osteoradionecrosisRadiotherapy dose[17,18] Risk of developing osteoradionecrosis increases with higher RT dosesChemotherapy[16,17] Increases acute toxicity especially mucositis, but its effect on late toxicity is less clearSurgery[17,18] Ablative surgical procedures increased risk of developing osteoradionecrosis after radiation
Miscellaneous factors[15-18]
Active smoking[15-18] Tobacco smoking as a risk factor for osteoradionecrosisAlcohol[16] Alcohol consumption during and after radiotherapy is one of the risk factors for developing
osteoradionecrosisInadequate oral hygiene[17] Poor oral hygiene increases the risk for development of osteoradionecrosisSteroids and anticoagulants[15]
Steroid and anticoagulants use before or after radiation reduced the risk of osteoradionecrosis
Dental diseases[15] Positive association between presence of dental disease pre-radiation therapy and osteoradionecrosis
Body-mass index[16] For every one point increase in BMI, osteoradionecrosis risk decreased by 27%Secondary infection[17] Secondary infection in post-radiotherapy phase correlated with severe mandibular
osteoradionecrosisDental extraction[18] Dentoalveolar surgery in post-radiotherapy phase is an established predisposing factor for
the development of osteoradionecrosisNutritional status[15] Poor nutritional status increases the risk of osteoradionecrosis
[Downloaded free from http://www.jdrr.org on Wednesday, September 09, 2015, IP: 14.140.125.38]
Suryawanshi, et al.: Maxillofacial osteoradionecrosis
Journal of Dental Research and Review ● Jan-Apr 2014 ● Vol. 1 ● Issue 1 45
Figure 3: Delanian’s radiation-induced fibroatrophic theory
Figure 1: Meyer’s radiation, trauma and infection theory Figure 2: Marx’s hypoxic-hypocellular-hypovascular theory
[Downloaded free from http://www.jdrr.org on Wednesday, September 09, 2015, IP: 14.140.125.38]
Suryawanshi, et al.: Maxillofacial osteoradionecrosis
46 Journal of Dental Research and Review ● Jan-Apr 2014 ● Vol. 1 ● Issue 1
• The late fibroatrophic phase, when attempted tissueremodelling occurs with the formation of fragile healed tissues that carry a serious inherent risk of late reactivated inflammation in the event of local injury.[10]
Microbiology
Osteoradionecrosis was earlier attributed to secondary infection in the traumatized irradiated tissue following the nonhealing wounds and exposed bone. However, this was challenged by Robert Marx in 1983.[20] The detailed description of various microorganisms detected in osteoradionecrosis is given in Table 5.[8,22‑27] Further studies on bacterial flora associated with osteoradionecrosis are required, which may contribute to a more precise use of antibiotics.
Clinical features
The incidence of osteoradionecrosis varies from 0.95% to 35% as shown in Table 6.[28‑36] The patient is usually asymptomatic. Pain and evidence of exposed bone are the most common chief complaints. Trismus, fetor oris, and elevated body temperature are usually present during the initial period although acute infection is usually not present. Other clinical features of osteoradionecrosis are swelling, nonresolving painful mucosal ulcer, dysgeusia, dysguesia, xerostomia, food impaction, malocclusion, telangiectasia, orocutaneous fistula, and missing hair follicles. The tissues surrounding the bone may be indurated. Surface texture changes such as cutaneous flaking and keratinisation may be present. Surface colour changes may also be seen. Pathologic fracture of the jaws may be evident in severe cases. Rarely, Deep cellulitis of face and neck may be present.[28]
Radiological features
The presence of osteoradionecrosis cannot always be diagnosed radiographically and often clinically obvious signs of exposed necrotic may not be accompanied by significant radiologic changes.
Plain radiography shows an ill‑defined cortical destruction without sequestration. The periphery may be ill‑defined as in osteomyelitis. Bone pattern can be granular. Scattered regions of radiolucency may be seen, with or without central sequestra. The most common effect on surrounding bone is stimulation of sclerosis.
Computed tomography plays an important role in diagnosis of osteoradionecrosis since it is hard tissue lesion. Anterior–posterior and supero–inferior extent of the osteolytic lesion is best judged with CT scans comparatively. Hence, from diagnostic purpose to the surgical intervention, CT is recommended as far as osteoradionecrosis is concerned.[29]
MRI reveals development of new heterogeneous signal within the marrow of an irradiated area (intermediate or low T1 signal, intermediate or high T2 signal). Adjacent muscles may appear oedematous and show intense enhancement, which can be
difficult to differentiate from recurrent tumour if bone changes are not visible on CT.[28]
PET scan is helpful to differentiate between osteoradionecrosis and recurrent tumour.[28]
Radionuclide bone scanning with technetium methylene diphosphonate (99mTc‑MDP) can identify pathophysiologic
Table 5: Microbiology of osteoradionecrosisYear Author(s) Microorganisms isolated
1983 Marx[8] Surface contaminants2005 Store and
Olsen[22]
Polymicrobial bacterial infection-rods, spirochetes and cocci. Rods were the predominant
2005 Støre, Eribe and Olsen[22]
Porphyromonas gingivalisActinomyces species
2006 Hansen, Wagner, Kirkpatrick and Kunkel[23]
Actinomyces species
2007 Nason and Chole[24]
50% of the oral and 80% of the intestinal indigenous bacterial flora consist of uncultured phylotypes
2005 Aas, Paster, Stokes, Olsen and Dewhirst[25]
FirmicutesActinobacteriaProteobacteriaFusobacteria-Fusobacterium nucleatumSpirochaetesBacteroidetesCampylobacter gracilisStreptococcus intermediusPeptostreptococcus sp. oral clone FG014Uncultured bacterium clone RL178Prevotella spp
1988 Calhoun, Shapiro, Stiernberg, Calhoun and Mader[26]
Streptococcus sp.Bacteroides sp.Lactobacillus sp.Eubacterium sp.Klebsiella sp.Actinomyces
2006 Kjetil Pedersen[27]
Treponema sppPorphyromonas gingivalis
Table 6: Incidence of osteoradionecrosisYear Author(s) Incidence (%)
1972 Carl, Schaaf, Chen, and Tak Yee[28] 41972 Daley, Drane, and Mc Comb[29] 221974 Wang[30] 171976 Bedwinck[31] 141980 Murray, Herson, Daly, and
Zimmerman[32]
19
1995 Constantino, Friedman and Steinberg[33]
5 to 15
1997 Epstein and van der Meij et al.[34] 5 to 151997 Clayman[35] Before 1968-11.8
After 1968-5.42000 Thorn, Sand Hansen, Specht and
Bastholt[36]
5 to 15
2003 Vissink, Jansma, Spijkervet, Burlage and Coppes[37]
2.6 to 22
2004 Reuther, Schuster, Mende, and Kübler[38]
1 to 37.5
2006 Wahl[39] 3 to 3.5
[Downloaded free from http://www.jdrr.org on Wednesday, September 09, 2015, IP: 14.140.125.38]
Suryawanshi, et al.: Maxillofacial osteoradionecrosis
Journal of Dental Research and Review ● Jan-Apr 2014 ● Vol. 1 ● Issue 1 47
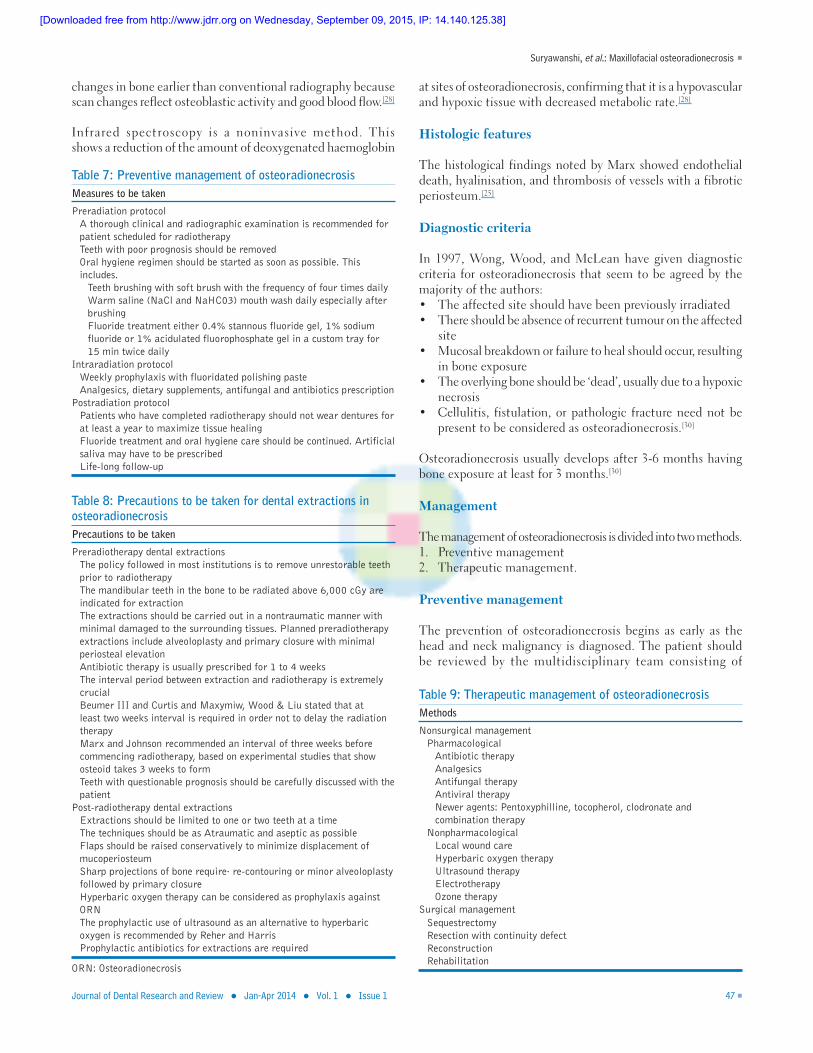
Table 7: Preventive management of osteoradionecrosisMeasures to be taken
Preradiation protocolA thorough clinical and radiographic examination is recommended for patient scheduled for radiotherapyTeeth with poor prognosis should be removedOral hygiene regimen should be started as soon as possible. This includes.
Teeth brushing with soft brush with the frequency of four times dailyWarm saline (NaCl and NaHC03) mouth wash daily especially after brushingFluoride treatment either 0.4% stannous fluoride gel, 1% sodium fluoride or 1% acidulated fluorophosphate gel in a custom tray for 15 min twice daily
Intraradiation protocolWeekly prophylaxis with fluoridated polishing pasteAnalgesics, dietary supplements, antifungal and antibiotics prescription
Postradiation protocolPatients who have completed radiotherapy should not wear dentures for at least a year to maximize tissue healingFluoride treatment and oral hygiene care should be continued. Artificial saliva may have to be prescribedLife-long follow-up
Table 8: Precautions to be taken for dental extractions in osteoradionecrosisPrecautions to be taken
Preradiotherapy dental extractionsThe policy followed in most institutions is to remove unrestorable teeth prior to radiotherapyThe mandibular teeth in the bone to be radiated above 6,000 cGy are indicated for extractionThe extractions should be carried out in a nontraumatic manner with minimal damaged to the surrounding tissues. Planned preradiotherapy extractions include alveoloplasty and primary closure with minimal periosteal elevationAntibiotic therapy is usually prescribed for 1 to 4 weeksThe interval period between extraction and radiotherapy is extremely crucialBeumer III and Curtis and Maxymiw, Wood & Liu stated that at least two weeks interval is required in order not to delay the radiation therapyMarx and Johnson recommended an interval of three weeks before commencing radiotherapy, based on experimental studies that show osteoid takes 3 weeks to formTeeth with questionable prognosis should be carefully discussed with the patient
Post-radiotherapy dental extractionsExtractions should be limited to one or two teeth at a timeThe techniques should be as Atraumatic and aseptic as possibleFlaps should be raised conservatively to minimize displacement of mucoperiosteumSharp projections of bone require· re-contouring or minor alveoloplasty followed by primary closureHyperbaric oxygen therapy can be considered as prophylaxis against ORNThe prophylactic use of ultrasound as an alternative to hyperbaric oxygen is recommended by Reher and HarrisProphylactic antibiotics for extractions are required
ORN: Osteoradionecrosis
changes in bone earlier than conventional radiography because scan changes reflect osteoblastic activity and good blood flow.[28]
Infrared spectroscopy is a noninvasive method. This shows a reduction of the amount of deoxygenated haemoglobin
at sites of osteoradionecrosis, confirming that it is a hypovascular and hypoxic tissue with decreased metabolic rate.[28]
Histologic features
The histological findings noted by Marx showed endothelial death, hyalinisation, and thrombosis of vessels with a fibrotic periosteum.[25]
Diagnostic criteria
In 1997, Wong, Wood, and McLean have given diagnostic criteria for osteoradionecrosis that seem to be agreed by the majority of the authors:• Theaffectedsiteshouldhavebeenpreviouslyirradiated• Thereshouldbeabsenceofrecurrenttumourontheaffected
site• Mucosalbreakdownorfailuretohealshouldoccur,resulting
in bone exposure• Theoverlyingboneshouldbe‘dead’,usuallyduetoahypoxic
necrosis• Cellulitis, fistulation, orpathologic fractureneednotbe
present to be considered as osteoradionecrosis.[30]
Osteoradionecrosis usually develops after 3‑6 months having bone exposure at least for 3 months.[30]
Management
The management of osteoradionecrosis is divided into two methods.1. Preventive management2. Therapeutic management.
Preventive management
The prevention of osteoradionecrosis begins as early as the head and neck malignancy is diagnosed. The patient should be reviewed by the multidisciplinary team consisting of
Table 9: Therapeutic management of osteoradionecrosisMethods
Nonsurgical managementPharmacological
Antibiotic therapyAnalgesicsAntifungal therapyAntiviral therapyNewer agents: Pentoxyphilline, tocopherol, clodronate and combination therapy
NonpharmacologicalLocal wound careHyperbaric oxygen therapyUltrasound therapyElectrotherapyOzone therapy
Surgical managementSequestrectomyResection with continuity defectReconstructionRehabilitation
[Downloaded free from http://www.jdrr.org on Wednesday, September 09, 2015, IP: 14.140.125.38]
Suryawanshi, et al.: Maxillofacial osteoradionecrosis
48 Journal of Dental Research and Review ● Jan-Apr 2014 ● Vol. 1 ● Issue 1
a dentist/oral and maxillofacial surgeon. The measures taken toprevent osteoradionecrosis, as perDonoff’s protocol, arementioned in Table 7.[37] The precautions that are to be taken during dental extraction are summarized in Table 8.[38]
Therapeutic management
The nonsurgical and surgical management with a note on recent medications are summarized in Table 9.[39]
Conclusion
Osteoradionecrosis can be a cruel blow to patients and their families who have been enduring radiotherapy for the treatment of cancer. Prevention of osteoradionecrosis by regular follow‑up and early diagnosis should be the goal of every health care professional managing head and neck cancer patients. Improved radiotherapy protocols, multidisciplinary preventive care and reconstructive surgery can help to improve the quality of life of patients suffering from osteoradionecrosis.
References
1. Peter S. Essentials of preventive and community dentistry, 4th edition. New Delhi, India:Arya Medi Publishing House; 2006.
2. Peterson DE, Doerr W, Hovan A. Osteoradionecrosis in cancer patients: The evidence base for treatment-dependent frequency, current management strategies, and future studies. Support Care Cancer 2010;18:1089-98.
3. Silverman S Jr: Complications of treatment. In: Silverman S Jr, ed.: Oral Cancer. 5th ed. Hamilton, Canada: BC Decker Inc, 2003, pp 113-28.
4. Lyons A, Ghazali N. osteoradionecrosis of the jaws: current understanding of its pathophysiology and treatment. Br J Oral Maxillofac Surg 2008;46:653-60.
5. Murray CG, Herson J, Daly TE, Zimmerman S Radiation necrosis of the mandible: A 10 year study. Part II. Dental factors; onset, duration and management of necrosis. Int J Radiat Oncol Biol Phys 1980b;6:549-53.
6. Kluth EV, Jain PR, Stuchell RN, Frich JC Jr. A study of factors contributing to the development of osteoradionecrosis of the jaws. J Prosthet Dent 1988;59:194-201.
7. Granström G, Fagerberg-Mohlin B, Fomander J. Aspects on the management of patients with osteoradionecrosis after therapy of head and neck cancer. XVIIIth Annual Meeting of EUBS, 1992a. pp. 163-9.
8. Marx RE. A new concept in the treatment of osteoradionecrosis. J Oral Maxillofac Surg 1983;41:351.
9. Reher P. Evidence for the use of ultrasound therapy for the management of mandibular osteoradionecrosis. Doctorate Thesis, University of London; 1999.
10. Beumer J 3rd, Curtis T, Harrison RE. Radiation therapy of the oral cavity: sequelae and management, Part 1. Head Neck Surg 1979a;1:301-12.
11. MacDougall RH, Orr JA, Kerr GR, Duncan W. Fast neuron treatment for squamous cell carcinoma of the head and neck: final report of Edinburgh randomised trial. Br Med J 1990;301:1241-2.
12. Chen A. Introduction to NCI-Common Toxicity Criteria Adverse Event Objectives (CTCAE). National Cancer Institute, US department of health and human services (Version-IV, 2009). Available at http://www.google.co.in/url?sa=t&rct=j&q=&esrc=s&source=web&cd=5&ved=0CEsQFjAE&url=http%3A%2F%2Fwww.calgb.org%2FPublic%2Fmeetings%2Fpresentations%2F2009%2Fsummer_group%2Fcra_committee%2F04_CTCAE-Chen_062009.pdf&ei=9HviUsiMNcnsrAe-i4CQBA&usg=AFQjCNGQkQkTQYZb80P1aVckaODaXlEddA&sig2=_vINN3E3AlywFikjK6BraQ&bvm=bv.59930103,d.bmk) [Last accessed on 2013 Dec 15].
13. Meghji S. Bone remodelling. Br Dent J 1992;172:235-42.14. Van Merkesteyn JP, Bakker DJ, Borgmeijer-Hoelen AM. Hyperbaric
oxygen treatment of osteoradionecrosis of the mandible: experience in 29 patients. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 1995;80:12-6.
15. Regaud C (1922a) Sur la necrose des os attenté par un processus cancereux et traites par les radiaions. Compt Rend Soc Biol 1992a;87:427.
16. Hutchinson IL, Colpe M, Delpy DT, Richardson CE, Harris M. The investigation of osteoradionecrosis of the mandible by near infrared spectroscopy. Br J Oral Maxillofac Surg 1990;28:150-4.
17. Tong AC, Leung AC, Cheng JC, Sham J. Incidence of complicated healing and osteoradionecrosis following tooth extraction in patients receiving radiotherapy for treatment of nasopharyngeal carcinoma. Aust Dent J 1999;44:187-94.
18. Oh HK, Chambers MS, Garden AS, Wong PF, Martin JW. Risk of osteoradionecrosis after extraction of impacted third molars in irradiated head and neck cancer patients. J Oral Maxillofac Surg 2004;62:139-44.
19. Meyer I. Infectious diseases of the jaws. J Oral Surg 1970;28:17-26.20. Marx RE. Osteoradionecrosis: A new concept of its pathophysiology.
J Oral Maxillofac Surg 1983a;41:283-8.21. Delanian S, Lefaix JL. The radiation-induced fibroatrophic process:
Therapeutic perspective via thantioxidant pathway. Radiother Oncol 2004;73:119-31.
22. Store G, Eribe ERK, Olsen I. DNA-DNA hybridization demonstrates multiple bacteria in osteoradionecrosis. Int J Oral Maxillofac Surg 2005;34:193-6.
23. Hansen T, Kunkel M, Weber A, James Kirkpatrick C.Osteonecrosis of the jaws in patients treated with bisphosphonates - histomorphologic analysis in comparison with infected osteoradionecrosis. J Oral Pathol Med 2006 Mar;35:155-60.
24. Nason R, Chole RA. Bacterial biofilms may explain chronicity in osteoradionecrosis of the temporal bone. Otol Neurotol 2007;28:1026-8.
25. Aas JA, Paster BJ, Stokes LN, Olsen I, Dewhirst FE.Defining the normal bacterial flora of the oral cavity. J Clin Microbiol 2005;43:5721-32.
26. Calhoun KH, Shapiro RD, Stiernberg CM, Calhoun JH, Mader JT. Osteomyelitis of the mandible. Arch Otolaryngol Head Neck Surg. 1988;114:1157-62.
27. Aas JA, Reime L, Pedersen K, Eribe ER, Abesha-Belay E, Støre G, et al. Osteoradionecrosis contains a wide variety of cultivable and noncultivable bacteria. J Oral Microbiol 2010;2. doi: 10.3402/jom.v2i0.5072.
28. Chrcanovic BR, Reher P, Sousa AA, Harris M. Osteoradionecrosis of the jaws – a current overview – Part 1. Physiopathology and risk and predisposing factors. J Oral Maxillofac Surg 2010;14:3-16.
29. Al-Nawas B, Duschner H, Grötz KA. Early cellular alterations in bone after radiation therapy and its relation to osteoradionecrosis. J Oral Maxillofac Surg 2004;62:1045.
30. Wang, Schaaf, Chen. Dental extractions in irradiated head and neck patient: a retrospective analysis of Memorial Sloan-Kettering Cancer Center protocols, criteria and end results. J Oral Maxillofac Surg 1974;61:1123-31.
31. Bedwinck, Hutchinson IL. Complications of radiotherapy in the head and neck: an orofacial surgeon's view. In: Tobias JS, Thomas PRM (eds) Current radiation oncology. Arnold, London, 1976. pp 144-77.
32. Thorn JJ, Hansen HS, Specht L, Bastholt L. Osteoradionecrosis of the jaws: Clinical characteristics and relation to the field of irradiation. J Oral Maxillofac Surg 2000;58:1088-93.
33. Hutchison IL, Cope M, Delpy DT, Richardson CE, Harris M. The investigation of osteoradionecrosis of the mandible by near infrared spectroscopy. Br J Oral Maxillofac Surg 1995;28:150-4.
34. van der Meij, Beumer J 3rd, Harrison R, Sanders B, Kurrasch M. Preradiation dental extractions and the incidence of bone necrosis. Head Neck Surg 1997;5:514-21.
35. Harris M. The conservative management of osteoradionecrosis of the mandible with ultrasound therapy. Br J Oral Maxillofac Surg 1997;30:313-8.
36. Morrish RB Jr, Chan E, Silverman S Jr, Meyer J, Fu KK, Greenspan D. Osteonecrosis in patients irradiated for head and neck carcinoma. Cancer 1981;47:1980-3.
37. Tong AC, Leung AC, Cheng JC, Sham J. Incidence of complicated healing and osteoradionecrosis following tooth extraction in patients
[Downloaded free from http://www.jdrr.org on Wednesday, September 09, 2015, IP: 14.140.125.38]
Suryawanshi, et al.: Maxillofacial osteoradionecrosis
Journal of Dental Research and Review ● Jan-Apr 2014 ● Vol. 1 ● Issue 1 49
receiving radiotherapy for treatment of nasopharyngeal carcinoma. Aust Dent J 1999;44:187-94.
38. Ramli R, Ngeow WC, Rahman RA, Chai WL. Managing complications of radiation therapy in head and neck cancer patients: Part IV. Management of osteoradionecrosis. Singapore Dent J 2006;28:11-5.
39. Vanderpuye V, Goldson A. Osteoradionecrosis of the mandible. J Natl Med Assoc 2000;92:579-84.
Source of Support: Nil, Conflict of Interest: None declared.
Staying in touch with the journal
1) Table of Contents (TOC) email alert Receive an email alert containing the TOC when a new complete issue of the journal is made available online. To register for TOC alerts go to
www.jdrr.org/signup.asp.
2) RSS feeds Really Simple Syndication (RSS) helps you to get alerts on new publication right on your desktop without going to the journal’s website.
You need a software (e.g. RSSReader, Feed Demon, FeedReader, My Yahoo!, NewsGator and NewzCrawler) to get advantage of this tool. RSS feeds can also be read through FireFox or Microsoft Outlook 2007. Once any of these small (and mostly free) software is installed, add www.jdrr.org/rssfeed.asp as one of the feeds.
[Downloaded free from http://www.jdrr.org on Wednesday, September 09, 2015, IP: 14.140.125.38]
Related Documents











