J Oral Maxillofac Surg 62:1535-1544, 2004 Maxillary Sinus and Ridge Augmentations Using a Surface-Derived Autogenous Bone Graft Michael Peleg, DMD,* Arun K. Garg, DMD,† Craig M. Misch, DDS, MDS,‡ and Ziv Mazor, DMD§ Purpose: The purpose of this article is to describe a new technique and the anatomic sites for cutting and harvesting bone for grafting applications. A handheld instrument is described that cuts and collects thin shavings of bone from cortical surfaces. Materials and Methods: This study included 193 consecutive patients who needed bone augmenta- tion and simultaneous implant placement in the severely atrophic posterier maxilla and in the anterior maxilla with acquired defect of alveolar bone as a result of local trauma. A total of 477 implants were placed. Clinical criteria for evaluation at time of implant exposure included stability in all directions, crestal bone resorption, and any reported pain of discomfort. Results: There were no failures of the anterior maxilla group, and no signs of bone resorption were noted at the second stage surgery or during the follow-up. During initial and late healing, there was no dehiscence of the soft tissue flaps and no membranes were exposed. Core biopsies typically showed immature, newly formed bone and, on average, 27% to 36% vital bone. Conclusion: From this research, it appears that excellent implant success rates can be achieved in grafted sinuses or ridges when a locally harvested autogenous bone graft with a ribbon geometry is used. © 2004 American Association of Oral and Maxillofacial Surgeons J Oral Maxillofac Surg 62:1535-1544, 2004 The reconstruction of bone in the maxillofacial region has become prevalent with the expanded use of os- seointegrated implant-supported prosthetics. Autoge- nous bone continues to be the “gold standard” for bone grafting applications. 1-7 However, the use of intraoral autogenous particulate bone has been lim- ited because of time constraints, donor site morbidity, and a limited number of intraoral sites available for harvesting particulate bone. An important goal of the clinician is to provide these bone grafts for dental implant placement in such a way as to minimize donor site morbidity, to minimize costs, and to mini- mize the patient’s perceived complexity of the pro- cedure. To address these problems, clinicians have turned to alternative sources of graft material such as allogenic, xenogenic, and alloplastic materials. 8 Al- though these sources are more convenient, the pre- dictability of healing and long-term capabilities for remodeling are questionable because normal lamellar bone is not the same as for autogenous bone. 9-11 However, when these materials are used, their suc- cess and predictability can be increased with the addition of autogenous bone to create a composite graft. 8,12-15 Traditional approaches to harvesting bone in- traorally involve the removal of blocks or sections of bone through the use of trephines, saws, burs, and osteotomes. The symphysis and lateral body of the mandible are the most common sites available for harvesting blocks of bone. 7,16 Most other intraoral sites are not candidates for harvesting blocks of bone because of their proximity to tooth roots, neural structures, and the thin bones overlying the maxillary sinus and nasal antrum. The harvested bone graft has been used as blocks by some 17 but is most often rendered into a particulate form by means of rongeurs *Assistant Professor of Surgery, Division of Oral/Maxillofacial Surgery, University of Miami School of Medicine, Miami, FL. †Professor of Surgery, Division of Oral/Maxillofacial Surgery, University of Miami School of Medicine, Miami, FL. ‡Private Practice, Sarasota, FL; and Clinical Associate Profes- sor, Department of Implant Dentistry, New York University, New York, NY. §Private Practice, Ra’nana, Israel. Address correspondence and reprint requests to Dr Peleg: Divi- sion of Oral/Maxillofacial Surgery, University of Miami School of Medicine, ACC-East Building, D-44, 1611 NW 12th Ave, Miami, FL 33136; e-mail: [email protected] © 2004 American Association of Oral and Maxillofacial Surgeons 0278-2391/04/6212-0016$30.00/0 doi:10.1016/j.joms.2004.06.048 1535

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Thsnbiiahc
S
U
s
N
s
M
3
©
0
d
J Oral Maxillofac Surg62:1535-1544, 2004
Maxillary Sinus and Ridge AugmentationsUsing a Surface-Derived Autogenous
Bone GraftMichael Peleg, DMD,* Arun K. Garg, DMD,†
Craig M. Misch, DDS, MDS,‡ and Ziv Mazor, DMD§
Purpose: The purpose of this article is to describe a new technique and the anatomic sites for cuttingand harvesting bone for grafting applications. A handheld instrument is described that cuts and collectsthin shavings of bone from cortical surfaces.
Materials and Methods: This study included 193 consecutive patients who needed bone augmenta-tion and simultaneous implant placement in the severely atrophic posterier maxilla and in the anteriormaxilla with acquired defect of alveolar bone as a result of local trauma. A total of 477 implants wereplaced. Clinical criteria for evaluation at time of implant exposure included stability in all directions,crestal bone resorption, and any reported pain of discomfort.
Results: There were no failures of the anterior maxilla group, and no signs of bone resorption werenoted at the second stage surgery or during the follow-up. During initial and late healing, there was nodehiscence of the soft tissue flaps and no membranes were exposed. Core biopsies typically showedimmature, newly formed bone and, on average, 27% to 36% vital bone.
Conclusion: From this research, it appears that excellent implant success rates can be achieved ingrafted sinuses or ridges when a locally harvested autogenous bone graft with a ribbon geometry is used.© 2004 American Association of Oral and Maxillofacial Surgeons
J Oral Maxillofac Surg 62:1535-1544, 2004idmctatdrbHcag
tbomhsbssb
he reconstruction of bone in the maxillofacial regionas become prevalent with the expanded use of os-eointegrated implant-supported prosthetics. Autoge-ous bone continues to be the “gold standard” forone grafting applications.1-7 However, the use of
ntraoral autogenous particulate bone has been lim-ted because of time constraints, donor site morbidity,nd a limited number of intraoral sites available forarvesting particulate bone. An important goal of thelinician is to provide these bone grafts for dental
*Assistant Professor of Surgery, Division of Oral/Maxillofacial
urgery, University of Miami School of Medicine, Miami, FL.
†Professor of Surgery, Division of Oral/Maxillofacial Surgery,
niversity of Miami School of Medicine, Miami, FL.
‡Private Practice, Sarasota, FL; and Clinical Associate Profes-
or, Department of Implant Dentistry, New York University,
ew York, NY.
§Private Practice, Ra’nana, Israel.
Address correspondence and reprint requests to Dr Peleg: Divi-
ion of Oral/Maxillofacial Surgery, University of Miami School of
edicine, ACC-East Building, D-44, 1611 NW 12th Ave, Miami, FL
3136; e-mail: [email protected]
2004 American Association of Oral and Maxillofacial Surgeons
278-2391/04/6212-0016$30.00/0
roi:10.1016/j.joms.2004.06.048
1535
mplant placement in such a way as to minimizeonor site morbidity, to minimize costs, and to mini-ize the patient’s perceived complexity of the pro-
edure. To address these problems, clinicians haveurned to alternative sources of graft material such asllogenic, xenogenic, and alloplastic materials.8 Al-hough these sources are more convenient, the pre-ictability of healing and long-term capabilities foremodeling are questionable because normal lamellarone is not the same as for autogenous bone.9-11
owever, when these materials are used, their suc-ess and predictability can be increased with theddition of autogenous bone to create a compositeraft.8,12-15
Traditional approaches to harvesting bone in-raorally involve the removal of blocks or sections ofone through the use of trephines, saws, burs, andsteotomes. The symphysis and lateral body of theandible are the most common sites available forarvesting blocks of bone.7,16 Most other intraoralites are not candidates for harvesting blocks of boneecause of their proximity to tooth roots, neuraltructures, and the thin bones overlying the maxillaryinus and nasal antrum. The harvested bone graft haseen used as blocks by some17 but is most often
endered into a particulate form by means of rongeurs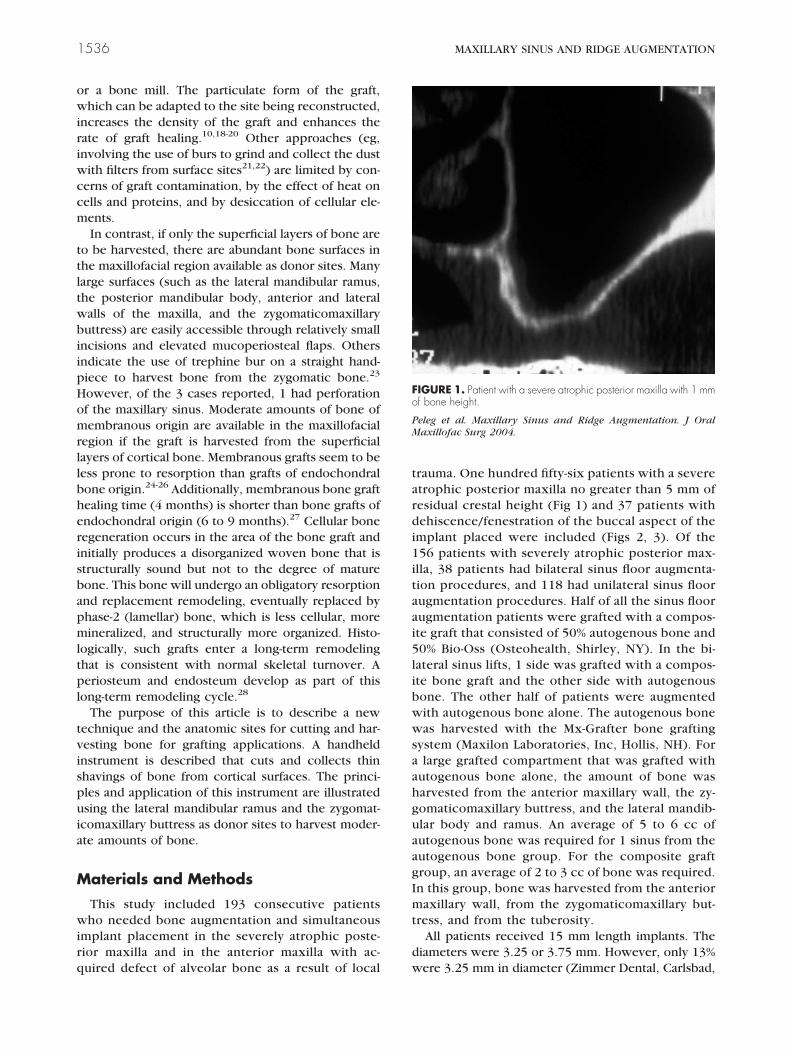
owiriwccm
ttltwbiipHomrllbherisbapmltpl
tvispuia
M
wirq
tardi1itaai5libwwsaahguaagImt
d
Fo
PM
1536 MAXILLARY SINUS AND RIDGE AUGMENTATION
r a bone mill. The particulate form of the graft,hich can be adapted to the site being reconstructed,
ncreases the density of the graft and enhances theate of graft healing.10,18-20 Other approaches (eg,nvolving the use of burs to grind and collect the dust
ith filters from surface sites21,22) are limited by con-erns of graft contamination, by the effect of heat onells and proteins, and by desiccation of cellular ele-ents.In contrast, if only the superficial layers of bone are
o be harvested, there are abundant bone surfaces inhe maxillofacial region available as donor sites. Manyarge surfaces (such as the lateral mandibular ramus,he posterior mandibular body, anterior and lateralalls of the maxilla, and the zygomaticomaxillaryuttress) are easily accessible through relatively small
ncisions and elevated mucoperiosteal flaps. Othersndicate the use of trephine bur on a straight hand-iece to harvest bone from the zygomatic bone.23
owever, of the 3 cases reported, 1 had perforationf the maxillary sinus. Moderate amounts of bone ofembranous origin are available in the maxillofacial
egion if the graft is harvested from the superficialayers of cortical bone. Membranous grafts seem to beess prone to resorption than grafts of endochondralone origin.24-26 Additionally, membranous bone graftealing time (4 months) is shorter than bone grafts ofndochondral origin (6 to 9 months).27 Cellular boneegeneration occurs in the area of the bone graft andnitially produces a disorganized woven bone that istructurally sound but not to the degree of matureone. This bone will undergo an obligatory resorptionnd replacement remodeling, eventually replaced byhase-2 (lamellar) bone, which is less cellular, moreineralized, and structurally more organized. Histo-
ogically, such grafts enter a long-term remodelinghat is consistent with normal skeletal turnover. Aeriosteum and endosteum develop as part of this
ong-term remodeling cycle.28
The purpose of this article is to describe a newechnique and the anatomic sites for cutting and har-esting bone for grafting applications. A handheldnstrument is described that cuts and collects thinhavings of bone from cortical surfaces. The princi-les and application of this instrument are illustratedsing the lateral mandibular ramus and the zygomat-
comaxillary buttress as donor sites to harvest moder-te amounts of bone.
aterials and Methods
This study included 193 consecutive patientsho needed bone augmentation and simultaneous
mplant placement in the severely atrophic poste-ior maxilla and in the anterior maxilla with ac-
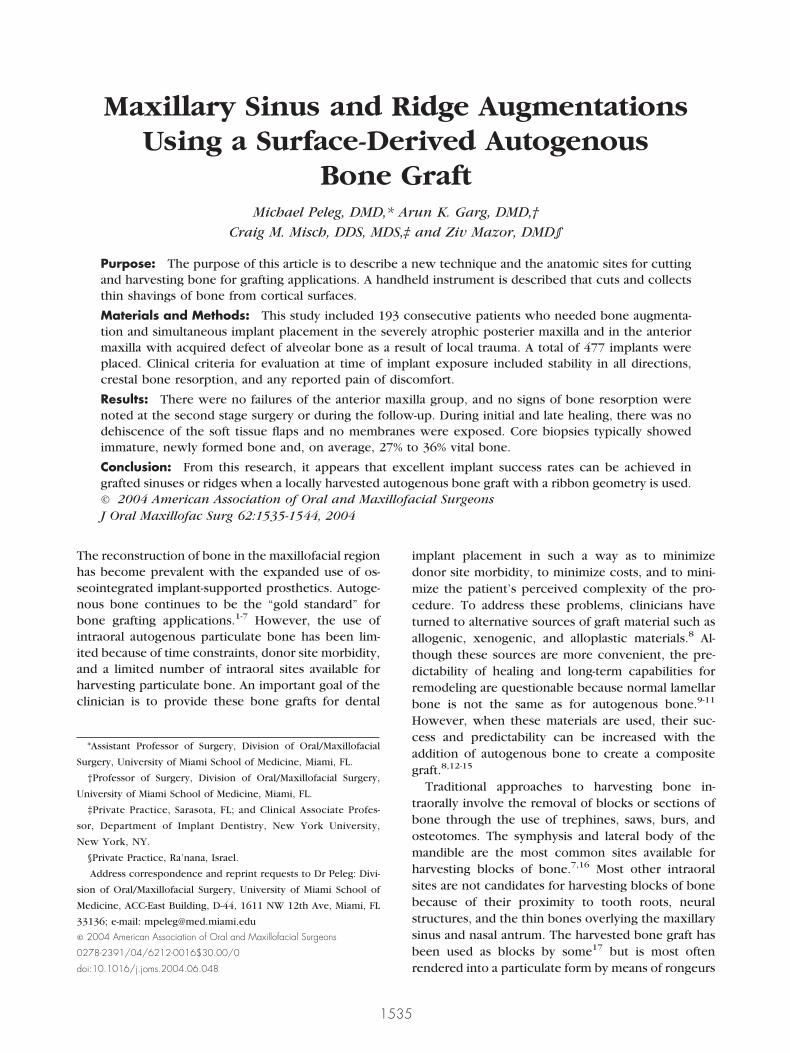
uired defect of alveolar bone as a result of local wrauma. One hundred fifty-six patients with a severetrophic posterior maxilla no greater than 5 mm ofesidual crestal height (Fig 1) and 37 patients withehiscence/fenestration of the buccal aspect of the
mplant placed were included (Figs 2, 3). Of the56 patients with severely atrophic posterior max-
lla, 38 patients had bilateral sinus floor augmenta-ion procedures, and 118 had unilateral sinus floorugmentation procedures. Half of all the sinus floorugmentation patients were grafted with a compos-te graft that consisted of 50% autogenous bone and0% Bio-Oss (Osteohealth, Shirley, NY). In the bi-
ateral sinus lifts, 1 side was grafted with a compos-te bone graft and the other side with autogenousone. The other half of patients were augmentedith autogenous bone alone. The autogenous boneas harvested with the Mx-Grafter bone grafting
ystem (Maxilon Laboratories, Inc, Hollis, NH). Forlarge grafted compartment that was grafted with
utogenous bone alone, the amount of bone wasarvested from the anterior maxillary wall, the zy-omaticomaxillary buttress, and the lateral mandib-lar body and ramus. An average of 5 to 6 cc ofutogenous bone was required for 1 sinus from theutogenous bone group. For the composite graftroup, an average of 2 to 3 cc of bone was required.n this group, bone was harvested from the anterioraxillary wall, from the zygomaticomaxillary but-
ress, and from the tuberosity.All patients received 15 mm length implants. The
iameters were 3.25 or 3.75 mm. However, only 13%
IGURE 1. Patient with a severe atrophic posterior maxilla with 1 mmf bone height.
eleg et al. Maxillary Sinus and Ridge Augmentation. J Oralaxillofac Surg 2004.
ere 3.25 mm in diameter (Zimmer Dental, Carlsbad,
Cflet
drcatmfoidtip(Dpgwmagf
P xillofac
Fp
PM
PELEG ET AL 1537
A). A total of 436 implants were placed in the sinusoor augmentation group. In 28 patients of the bilat-ral and 18 of the unilateral sinus augmentation (aotal of 38.9%), the procedures were performed un-
FIGURE 2. A, Dehiscence/fenestration of the buccal aspect of
eleg et al. Maxillary Sinus and Ridge Augmentation. J Oral Ma
IGURE 3. Dehiscence/fenestrations of the buccal aspect of implantslaced in position of 2 left maxillary incisors.
releg et al. Maxillary Sinus and Ridge Augmentation. J Oralaxillofac Surg 2004.
er intravenous sedation and local anesthesia. For theemainder of the patients treated in this study, surgi-al treatment was performed under local anesthesialone. For 37 patients with dehiscence/fenestration ofhe buccal aspect of the implant placed in the anterioraxilla, the autogenous bone graft was harvested
rom the zygomaticomaxillary buttress or the tuber-sity with an average of 1 to 1.5 cc required. The
mplant length for this group was 15 mm while theiameter was 3.75 or 3.25 mm (Zimmer Dental). Aotal of 41 implants were placed in the anterior max-lla group. For all bone grafts and for the 477 implantslaced in this study, a resorbable membraneBioMend Extend; Zimmer Dental) or Lyophilizedura Mater (University of Miami tissue bank)29 waslaced over the graft according to the principle ofuided bone regeneration. A second-stage surgeryas performed 4 to 8 months after implant place-ent. Before implant exposure, patients were evalu-
ted radiographically. Panoramic and periapical radio-raphs and computed tomography scans were usedor assessment of the newly formed bone and its close
mber 8. B, Dehiscence on buccal aspect with implant in place.
Surg 2004.
tooth nu
elation to the implants. Clinical criteria for evaluation
adp
fgfiipn
atap
S
c5
1538 MAXILLARY SINUS AND RIDGE AUGMENTATION
t time of implant exposure included stability in allirections, crestal bone resorption, and any reportedain or discomfort.For the anterior maxilla alveolar bone dehiscence/
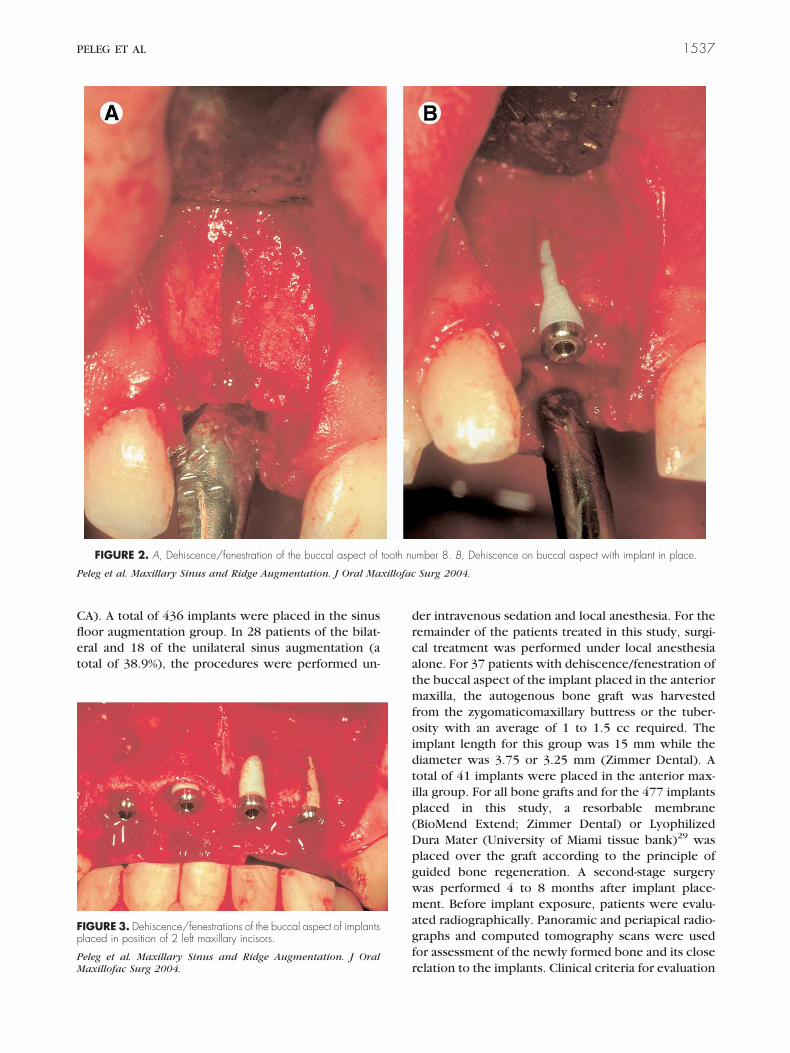
enestration group, panoramic and periapical radio-raphs were taken at second stage surgery and forollow-up. The new bone formation was assessed clin-cally at the second stage surgery (Fig 4). A crestalncision was used for this purpose rather than aunch technique. Implants were placed simulta-
eously with the grafting procedure in all cases. To wssess the new bone formation, core biopsies wereaken from the lateral window at 4 to 5 months for theutogenous bone and at 7 to 8 months for the com-osite bone graft.
urgical Technique
The instrument’s hardened hollow ground blade isurved, and when held at an angle of approximately° to 50° to the bone surface, it makes a point contact
IGURE 4. A, Dehiscence of buccal one third of implant. B, Crestalcision at stage II surgery for evaluation of bone formation. C, Radio-raphic evaluation of the area at 3 years follow-up.
eleg et al. Maxillary Sinus and Ridge Augmentation. J Oralaxillofac Surg 2004.
Fing
PM
ith the relatively flat bone surface. With light down-

wspmrsbipTaos
fogratai
ss5wzrttwzictt
ltar3taweriIaclpilrivos
cscsciobm5Rt
Fe
PM
PELEG ET AL 1539
ard pressure, forces much greater than the tensiletrength of bone are generated, enabling the blade toenetrate the bone surface. As the blade penetratesore deeply into the surface, it reaches an equilib-
ium depth that is a function of the downward pres-ure, of the surface area of the bone engaging thelade edge, and of the bone tensile strength. As the
nstrument is pulled, the blade maintains its depth andlanes a shaving of bone from the cortical surface.he curved shaving passes through a narrow aperturedjacent to the blade edge and flows into the handlef the instrument, where it can be collected andtored.
The most convenient bone-harvesting site can berom areas adjacent to the recipient site. For amountsf bone up to 2 to 3 cc as needed for the compositeraft group in the sinus floor augmentation, the ante-ior maxillary wall, the zygomaticomaxillary buttress,nd the tuberosity donor sites are accessed throughhe same full-thickness mucoperiosteal flap either bycrestal incision (in cases of edentulous ridge) or by
ntra-sulcular incision.In this case, the minimum donor site surface area
hould be approximately 10 mm � 15 mm and acces-ible with the instrument at an angle between 5° and0°. In sinus augmentation procedures, the buccalindow is mainly prepared with the grafter. For the
ygomaticomaxillary buttress harvest, the flap isaised superiorly to the point at which the origin ofhe masseter muscle is visualized at its junction withhe zygomatic process of the maxilla. This flap designill expose the entire buttress (Fig 5). Access to the
ygomaticomaxillary buttress can also be gained by anncision made through the alveolar mucosa about 5m above the mucogingival junction, starting be-ween the first and second molars and proceeding to
FIGURE 5. Harvesting bone from the zygomaticomaxillary buttress.
eleg et al. Maxillary Sinus and Ridge Augmentation. J Oralaxillofac Surg 2004.
he first premolar area.PM
The lateral aspect of the mandibular body and theateral mandibular ramus donor sites is accessedhrough an incision over the external oblique ridge inmanner similar to the approach for oblique vertical
amus osteotomy. The incision, approximately 2.5 to.0 cm long, extends into the free mucosa from thehird molar to the first molar region, and verticallylong the external oblique ridge. Local anestheticith vasoconstrictor (lidocaine 2% with 1:100,000
pinephrine) is infiltrated along the external obliqueidge, the lateral aspect of the mandibular ramus, andnferolaterally in the molar region of the mandible.nfiltration of the periosteum and a mandibular blockre required for sufficient anesthesia. To facilitatelosure, a cuff of at least 2 to 3 mm of free mucosaateral to the attached gingiva is preserved. It is im-ortant to stay lateral with the incision to allow the
nstrument to achieve the proper cutting angles to theateral mandible. A Minnesota, Langenback, or verticalamus osteotomy retractor for the mandibular ramuss used to retract the tissues laterally and provide goodisibility. This technique provides the instrument’sptimal 15° to 20° cutting angle to the lateral boneurface.
Initially, dipping the instrument into saline lubri-ates it. The instrument cuts shavings from the boneurface with an elliptical raking motion, with 1 to 2m strokes at an angle of 5° to 50° to the boneurface. The semicircular blade cuts flat, convex, andoncave bone surfaces. As the bone shavings flownto the handle, the instrument is occasionally tappedn a table surface to advance the bone into the cham-er. The instrument storage chamber holds approxi-ately 2 cc of graft material. Typically, approximatelyto 10 minutes are required to harvest 2 cc of bone.outinely, 4 cc of graft material can be harvested from
he lateral ramus site, and the instrument will stay
IGURE 6. Graft is stored in the handle of the instrument until deliv-red to the recipient site.
eleg et al. Maxillary Sinus and Ridge Augmentation. J Oralaxillofac Surg 2004.

sb
sw
ptmdaaetobmsdt
ulvftptwtu
pfaft3fltwwshapmari1edta
R
ahsmcdatbaaabzwSiM
wawwsvddif
Fb
PM
1540 MAXILLARY SINUS AND RIDGE AUGMENTATION
harp for harvesting a total of approximately 8 cc ofone.If a graft of more than 2 cc is required, the bone
havings are emptied into a sterile bowl and coveredith a moist, lint-free sponge.After irrigation, suctioning, and inspection of the
erimeter of the flap for remnants, an attempt is madeo invert wound edges by using interrupted verticalattress sutures to optimize healing and minimize
ehiscence. The recipient site should be prepared toccept the bone graft. This process includes removingny soft tissue remnants and the preparation of fen-strations in the bone surface. An alternative is to usehe grafting instrument to plane a thin layer of boneff the recipient site surface to open and expose theone’s blood vessels. This technique helps to pro-ote revascularization of the graft and provides a
ource of osteoprogenitor cells that line the en-osteum and vascular channels of the Haversian sys-ems and Volkmann’s canals.
The graft is stored in the handle of the instrumentntil delivered to the recipient site (Fig 6). The blade
ock is released and the integrated plunger is ad-anced to consolidate the graft and to move it to theorward end of the chamber. The blade is then re-racted to gain access to the graft. The instrumentrovides a convenient carrier to deliver the graft tohe recipient site. The hoop-shaped blade also cutshen drawn in a lateral motion, helpful for accessing
he medial and lateral aspects of the anterior mandib-lar ramus.The flap can be pulled over the site, and, with
alpation through the flap, the contour can beormed. After the periosteum has been released tochieve a tension-free closure, the flap is positionedor closure either with tooth forceps or a temporaryraction suture. The flap is then held in place for 20 to0 seconds with gentle pressure, thus assisting theap to adhere to the graft and taking much of theension off the closure line. The closure should beater tight with slight outward eversion of theound edges, accomplished with a vertical mattress
uture. Ice application and a semiupright positionelp to reduce swelling. Pressure with moist gauze ispplied directly over the site for about 1 hour toromote attachment of the flap and to minimize he-atoma formation. Postoperative care should includesemiupright position and ice to both the donor and
ecipient sites for 24 hours. Broad-spectrum antibiot-cs are commonly given as an initial preoperative dose
hour before the procedure and for 10 days postop-ratively. An oral antiseptic rinse, such as chlorhexi-ine gluconate, is started on the seventh postopera-ive day. In most patients, NSAIDs can provide
dequate comfort. gesults
In our 156 sinus floor augmentation proceduresnd 37 alveolar augmentations, none of the patientsad any complication related to the bone harvestingite and technique. A minimum of 1 cc and a maxi-um of 5 cc of bone were harvested for these pro-
edures. For the unilateral sinus floor grafting proce-ures, where only autogenous bone was used, anverage of 4 to 5 ccs were harvested. An average of 2o 3 ccs of bone graft was harvested for the compositeone group, and 1 to 1.5 ccs were the averagemounts of bone harvested for the anterior maxillalveolar bone dehiscence/fenestration. Between 10nd 15 minutes were required to harvest 4 to 5 cc ofone from the lateral mandibular body and ramus,ygomaticomaxillary buttress, and lateral maxillaryall. No nerve injuries, dental injuries, or tears of the
chneiderian membrane were noted from the harvest-ng procedure in any of these cases. An average of 1
x-Grafter bone grafting system was used per side.Patient follow-up has ranged from 8 to 24 months,ith an average of 16 months. For the sinus floor
ugmentation group, computed tomography scansere taken at the second stage surgery. All implantsere successful as per the Albrektsson criteria30 of
uccess and were fully surrounded by bone as re-ealed by computed tomography scan (Fig 7). Allonor sites for the bone healed without immediate orelayed complications. At the second stage surgery, 2
mplants from the autogenous group and 1 implantrom the composite bone graft group failed to inte-
IGURE 7. Implants were successful and were fully surrounded byone as revealed by computed tomography scan.
eleg et al. Maxillary Sinus and Ridge Augmentation. J Oralaxillofac Surg 2004.
rate. There were no signs of infection during the
hpei
gt8cenb
D
dttccpafttF
secato
FgGb
PELEG ET AL 1541
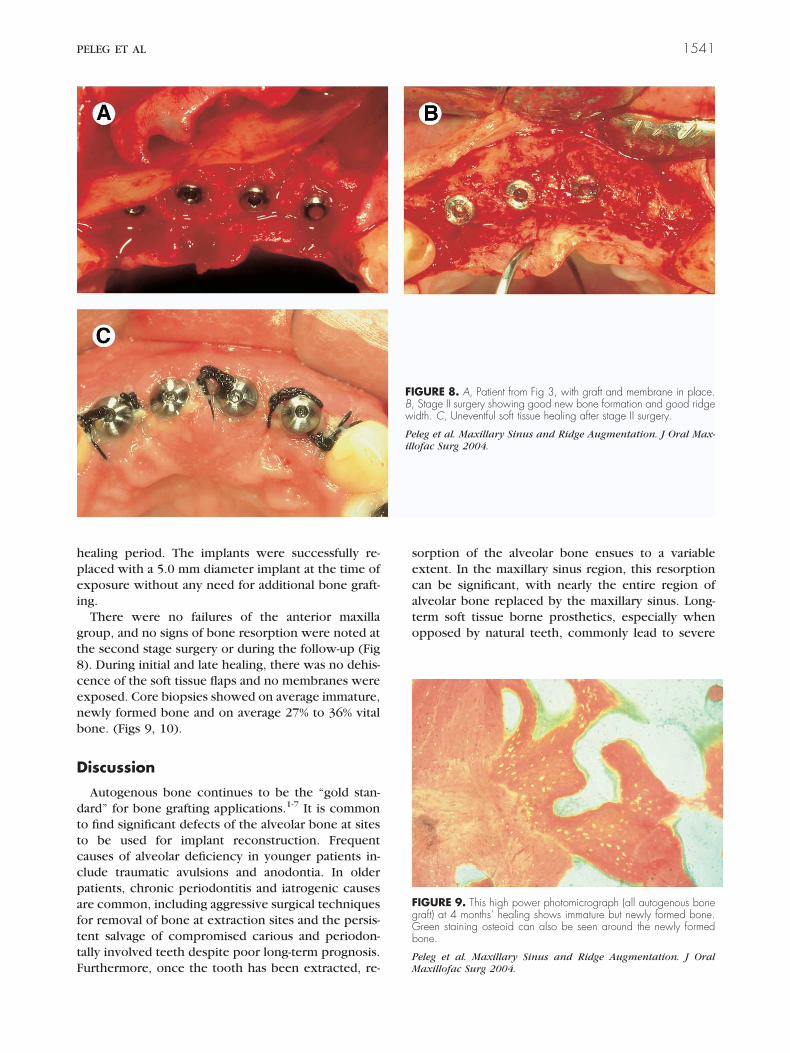
ealing period. The implants were successfully re-laced with a 5.0 mm diameter implant at the time ofxposure without any need for additional bone graft-ng.
There were no failures of the anterior maxillaroup, and no signs of bone resorption were noted athe second stage surgery or during the follow-up (Fig). During initial and late healing, there was no dehis-ence of the soft tissue flaps and no membranes werexposed. Core biopsies showed on average immature,ewly formed bone and on average 27% to 36% vitalone. (Figs 9, 10).
iscussion
Autogenous bone continues to be the “gold stan-ard” for bone grafting applications.1-7 It is commono find significant defects of the alveolar bone at siteso be used for implant reconstruction. Frequentauses of alveolar deficiency in younger patients in-lude traumatic avulsions and anodontia. In olderatients, chronic periodontitis and iatrogenic causesre common, including aggressive surgical techniquesor removal of bone at extraction sites and the persis-ent salvage of compromised carious and periodon-ally involved teeth despite poor long-term prognosis.
urthermore, once the tooth has been extracted, re-PM
orption of the alveolar bone ensues to a variablextent. In the maxillary sinus region, this resorptionan be significant, with nearly the entire region oflveolar bone replaced by the maxillary sinus. Long-erm soft tissue borne prosthetics, especially whenpposed by natural teeth, commonly lead to severe
GURE 8. A, Patient from Fig 3, with graft and membrane in place.Stage II surgery showing good new bone formation and good ridge
idth. C, Uneventful soft tissue healing after stage II surgery.
leg et al. Maxillary Sinus and Ridge Augmentation. J Oral Max-ofac Surg 2004.
IGURE 9. This high power photomicrograph (all autogenous boneraft) at 4 months’ healing shows immature but newly formed bone.reen staining osteoid can also be seen around the newly formedone.
FIB,w
Peill
eleg et al. Maxillary Sinus and Ridge Augmentation. J Oralaxillofac Surg 2004.

aeci
pomcplba
inraoNcanhg
icmtssrTds
tacwheisdha
vbhbcdcs5iclmdr
hearhdcfipatgbiplmbsipmmflts
FecT
PM
1542 MAXILLARY SINUS AND RIDGE AUGMENTATION
trophy. Clearly, alveolar bone is present to providendosseous support for teeth. Alveolar bone can beonserved by re-establishing endosseous loading us-ng osseointegrated implants.
Most patients undergo implant therapy as an out-atient procedure, which uses local anesthesia withr without sedation. This option helps not only toinimize patient costs for procedures frequently not
overed by insurance but also to lessen the patient’serception of the complexity of the procedure. One
imiting factor in the treatment of patients requiringone grafts has been how to acquire an adequatemount of bone in a minimally invasive manner.
The bone supporting a functional osseointegratedmplant should be viable lamellar bone capable oformal remodeling in response to the biomechanicalequirements of the site. Autogenous bone continuess a preferred solution for reconstruction of the alve-lus in preparation for osseointegrated implants.18-20
onautogenous preparations are still being used be-ause of limitations in acquiring adequate amounts ofutogenous bone or simply because of the conve-ience of using packaged preparations. However,ealing and remodeling of these nonautogenousrafts is less predictable.9-11
There are many accessible bone surfaces availablen the maxillofacial region. Large areas of periosteuman be elevated in this region without disruptingajor muscle attachments or neurovascular struc-
ures. However, only a limited number of intraoralites are available for harvesting of bone (eg, theymphysis) in the traditional surgical technique ofemoving blocks or sections of bone or cores of bone.his technique has been limited by difficulties such asonor site morbidity, close anatomic relation to vital
IGURE 10. This high power photomicrograph (Bio-Oss and autog-nous bone) at 7 months’ healing shows a piece of Bio-Oss in theenter surrounded by actively growing trabeculae of cancellous bone.he green-staining osteoid rims around the trabeculae.
eleg et al. Maxillary Sinus and Ridge Augmentation. J Oralaxillofac Surg 2004.
tructure (eg, tooth roots, neural structures, and the h
hin bones overlying the maxillary sinus and nasalntrum), management of the patient, and the relativeomplexity of the procedure. Typically, bone is cutith power-driven instruments, either by drillingoles or creating an osteotomy or trephine bur. Chis-ls and osteotomes are used to make or complete cutsn areas that are not easily accessible or that are notafe for power-driven tools. Usually, intravenous se-ation or general anesthesia is required for the bone-arvesting procedure, and narcotic pain medicationsre needed postoperatively.
Although dermatomes are commonly used to har-est sheets of skin, there was no equivalent to harvestone. The Mx-Grafter bone grafting system is a hand-eld instrument that planes ribbon-like shavings ofone from cortical surfaces. In addition, it directlyollects the bone shavings, stores them, and thenelivers them to the recipient site. The curved bladean plane shavings from flat, convex, and concaveurface donor sites. Working angles between 5° and0° enable the instrument to cut bone from most
ntraoral bone surfaces. The blade, shaped in a semi-ircular loop, can cut by being drawn straight back oraterally. The small, streamlined profile of the instru-
ent’s nose provides access to constricted areas un-er the soft tissue flaps. Several similar devices haveecently appeared on the market.
The matrix of ribbon-like bone shavings and bloodas a mortar-like consistency that enables it to beasily handled and positioned. It can be molded withny flat surface instrument, such as a plugger or cu-ette, and it stays where positioned. This form of graftas more consistency than other materials that areifficult to keep in place, such as pellets, dust, orhip-like particles. Bone planed off the cortical sur-ace forms narrow, ribbon-like shavings. As the bones harvested, blood from the cut bone surface is alsoassively collected and mixes with the bone to formmoldable composite matrix. The graft volume sub-
ended by the 3-dimensional ribbon-like elements isreatly expanded by this process in comparison to theone’s volume at the donor site. This process is sim-
lar to the increase in volume seen when a woodlane removes a very thin layer of wood with the
arge volume of shavings that results. This compositeatrix of ribbon-like shavings, with the patient’s
lood occupying the interconnecting porosity, haseveral potential advantages to promote a rapid heal-ng response.31 Because only a thin layer of bone islaned from the surface, the defect and subsequentorbidity at the donor site are minimized, and onlyinimal blood oozing is noted. The graft is kind to the
ap with no sharp edges, and the flap seems to adhereo this bone-blood matrix. Adherence of the flap as-ists in taking the tension off the incision line and
elps to minimize the chance of wound dehiscence.
Iw
mbfTetscqew
mgagh
maapcodcmm
uceeiTtrfatuhhv
pogwdaba
5rapta
R
1
1
1
1
1
1
PELEG ET AL 1543
n all 193 patients treated in this study, there was noound dehiscence.Typically, hard bone rapidly dulls cutting instru-ents with narrow inclusion angles, such as scalpel
lades. The apparent hardness of the bone and there-ore the rate of bone harvest varied between patients.his variance may have been a function of bone min-ral content (about 76% mineral), the orientation ofhe lamellar structure, or other unidentifiable effectsuch as is seen with long-term treatment with tetra-ycline. The blade edge dulls prematurely if it fre-uently strikes against the sides of the teeth. How-ver, an average of 1 Mx-Grafter bone grafting systemas used per side to collect 4 cc of bone.The grafts can also be mixed with bone substituteaterials such as Bio-Oss to expand the volume of
raft material; furthermore, platelet-rich plasma canlso be added to the graft matrix to enhance therowth factors in the graft and to further improve theandling characteristics.The use of the cortical surface as a source of graftaterial greatly increases the number of intraoral sites
vailable for harvesting bone. Many intraoral sites areccessed through relatively small incisions to the sub-eriosteal plane, developing mucoperiosteal flaps thatan be raised easily and safely to expose large surfacesf bone. Such sites are not constrained by concerns ofeeper elements, such as tooth roots and neurovas-ular structures. Furthermore, patient morbidity isinimized if only a small thickness of bone is re-oved passively from the donor surface.The shavings are collected passively without the
se of suction, greatly minimizing the chance of graftontamination. The potential for cell survival is alsonhanced by the minimal cutting temperatures gen-rated with a manual instrument and also by no des-ccation of the graft with a suction collection process.he bone is already in a particulate form, thus saving
ime from a secondary operation with a bone mill orongeurs. The high porosity of cortical bone in theorm of these curved ribbon-like shavings should en-ble the graft to be revascularized much more rapidlyhan cortical blocks, similar to that seen with partic-late preparations. Success rates may have been soigh because of the high surface area of the bone graftarvested in this manner. Minimal trauma to the har-ested bone may also have been a factor.From this research, it appears that excellent im-
lant success rates can be achieved in grafted sinusesr ridges when a locally harvested autogenous boneraft with a ribbon geometry is used. It also appearshen a composite bone graft is used in the sinus forental implants, with at least 50% autogenous bone inribbon geometry, similar implant success rates cane achieved as with 100% autogenous bone graft. It
lso appears that a composite bone graft consisting of0% autogenous bone can provide excellent successates for implant support. This can avoid distant ordditional graft donor sites. Further research is inrogress to fully understand the unique properties ofhis high surface area graft with expanded volumend interconnecting porosity.
eferences1. Marx RE, Saunders TM: Reconstruction and rehabilitation of
cancer patients, in Fonseca RJ, Davis WH (eds): ReconstructivePre-Prosthetic Oral and Maxillofacial Surgery. Philadelphia, PA,Saunders, 1986, pp 347-426
2. Springfield DS: Autogenous bone grafts: Nonvascular and vas-cular. Orthopedics 15:1237, 1992
3. Schneider U: Autogenous bone cell transplantation. Orthopade27:143, 1988
4. Fleming JE Jr, Cornell CN, Muschler GF: Bone cells and matri-ces in orthopedic tissue engineering. Orthop Clin North Am31:357, 2000
5. Moy PK, Lundgren S, Ralph EN: Maxillary sinus augmentationhistomorphometric analysis of graft materials for maxillary si-nus augmentation. J Oral Maxillofac Surg 51:857, 1993
6. Lorenzetti M, Mozzati M, Camapanino PP, et al: Bone augmen-tation of the inferior floor of the maxillary sinus with autoge-nous bone or composite bone grafts: A histologic-histomorpho-metric preliminary report. Int J Oral Maxillofac Implants 13:69,1998
7. Balaji SM: Management of deficient anterior maxillary alveoluswith mandibular parasymphyseal bone graft for implants. Im-plant Dent 11:363, 2002
8. Jensen OT, Shulman LB, Block MS, et al: Report of SinusConsensus Conference of 1996. Int J Oral Maxillofac Implants13:11, 1998 (suppl)
9. Yildirim M, Spiekermann H, Biesterfeld S, et al: Maxillary sinusaugmentation using xenogenic bone substitute material Bio-Oss in combination with venous blood. A histologic and histo-morphometric study in human. Clin Oral Implants Res 11:217,2000
0. Lundgren S, Moy P, Johansson C, et al: Augmentation of themaxillary sinus floor with particulated mandible: A histologicand histomorphometric study. Int J Oral Maxillofac Implants11:760, 1996
1. Landi L, Pretel RW, Hakimi NM, et al: Maxillary sinus floorelevation using a combination of DFDB and bovine-derivedporous hydroxyapatite: A preliminary histologic and histomor-phometric report. Int J Periodont Restorative Dent 20:575,2000
2. Hurzeler MB, Quinones CR, Kirsch A, et al: Maxillary sinusaugmentation using different grafting materials and dental im-plant in monkeys. Part 3. Evaluation of autogenous bone com-bined with porous hydroxyapatite. Clin Oral Implants Res8:401, 1997
3. An HS, Lynch K, Toth J: Prospective comparison of autograftvs. allograft for adult posterolateral lumbar spine fusion: Dif-ferences among freeze dried, frozen, and mixed grafts. J SpinalDisord 8:131, 1995
4. Boeck-Neto RJ, Gabrielli M, Lia R, et al: Histomorphometricalanalysis of bone formed after maxillary sinus floor augmenta-tion by grafting with a combination of autogenous bone anddemineralized freeze-dried bone allograft or hydroxyapatite. JPeriodontol 73:266, 2002
5. Maiorana C, Redemagi M, Rabagliati M, et al: Treatment ofmaxillary ridge resorption by sinus augmentation with iliaccancellous bone, an organic bovine bone, and endosseousimplants: A clinical and histologic report. Int J Oral Maxillofac
Implants 15:873, 2000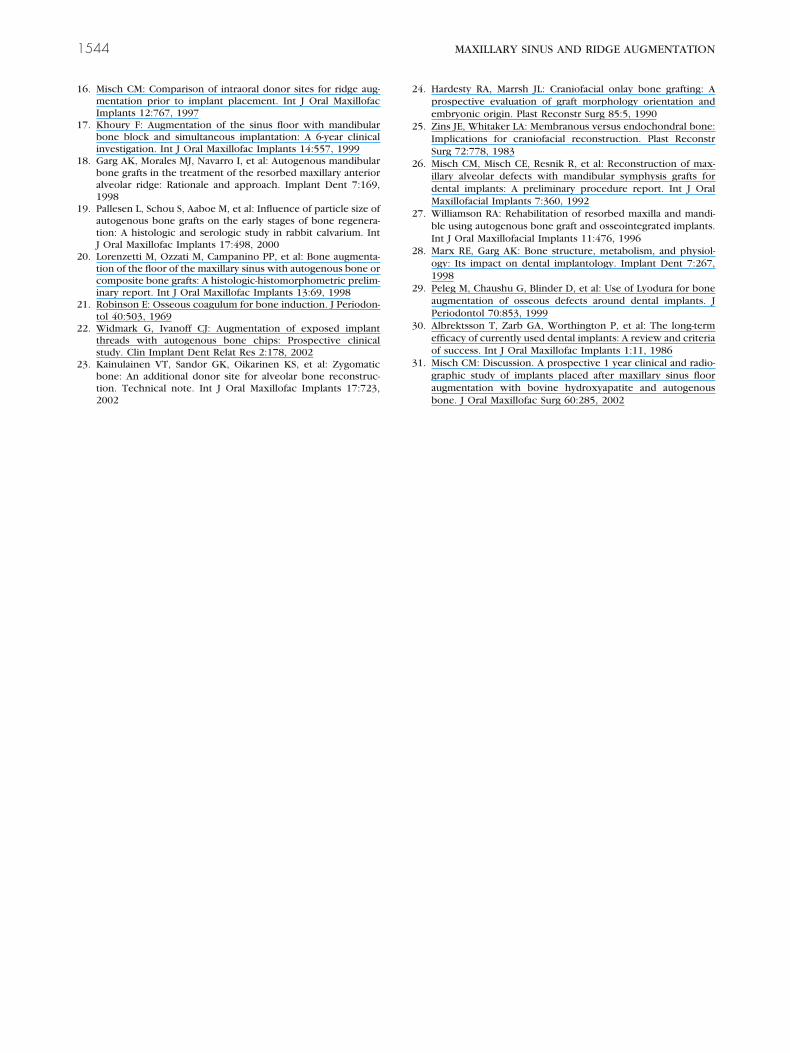
1
1
1
1
2
2
2
2
2
2
2
2
2
2
3
3
1544 MAXILLARY SINUS AND RIDGE AUGMENTATION
6. Misch CM: Comparison of intraoral donor sites for ridge aug-mentation prior to implant placement. Int J Oral MaxillofacImplants 12:767, 1997
7. Khoury F: Augmentation of the sinus floor with mandibularbone block and simultaneous implantation: A 6-year clinicalinvestigation. Int J Oral Maxillofac Implants 14:557, 1999
8. Garg AK, Morales MJ, Navarro I, et al: Autogenous mandibularbone grafts in the treatment of the resorbed maxillary anterioralveolar ridge: Rationale and approach. Implant Dent 7:169,1998
9. Pallesen L, Schou S, Aaboe M, et al: Influence of particle size ofautogenous bone grafts on the early stages of bone regenera-tion: A histologic and serologic study in rabbit calvarium. IntJ Oral Maxillofac Implants 17:498, 2000
0. Lorenzetti M, Ozzati M, Campanino PP, et al: Bone augmenta-tion of the floor of the maxillary sinus with autogenous bone orcomposite bone grafts: A histologic-histomorphometric prelim-inary report. Int J Oral Maxillofac Implants 13:69, 1998
1. Robinson E: Osseous coagulum for bone induction. J Periodon-tol 40:503, 1969
2. Widmark G, Ivanoff CJ: Augmentation of exposed implantthreads with autogenous bone chips: Prospective clinicalstudy. Clin Implant Dent Relat Res 2:178, 2002
3. Kainulainen VT, Sandor GK, Oikarinen KS, et al: Zygomaticbone: An additional donor site for alveolar bone reconstruc-tion. Technical note. Int J Oral Maxillofac Implants 17:723,
20024. Hardesty RA, Marrsh JL: Craniofacial onlay bone grafting: Aprospective evaluation of graft morphology orientation andembryonic origin. Plast Reconstr Surg 85:5, 1990
5. Zins JE, Whitaker LA: Membranous versus endochondral bone:Implications for craniofacial reconstruction. Plast ReconstrSurg 72:778, 1983
6. Misch CM, Misch CE, Resnik R, et al: Reconstruction of max-illary alveolar defects with mandibular symphysis grafts fordental implants: A preliminary procedure report. Int J OralMaxillofacial Implants 7:360, 1992
7. Williamson RA: Rehabilitation of resorbed maxilla and mandi-ble using autogenous bone graft and osseointegrated implants.Int J Oral Maxillofacial Implants 11:476, 1996
8. Marx RE, Garg AK: Bone structure, metabolism, and physiol-ogy: Its impact on dental implantology. Implant Dent 7:267,1998
9. Peleg M, Chaushu G, Blinder D, et al: Use of Lyodura for boneaugmentation of osseous defects around dental implants. JPeriodontol 70:853, 1999
0. Albrektsson T, Zarb GA, Worthington P, et al: The long-termefficacy of currently used dental implants: A review and criteriaof success. Int J Oral Maxillofac Implants 1:11, 1986
1. Misch CM: Discussion. A prospective 1 year clinical and radio-graphic study of implants placed after maxillary sinus flooraugmentation with bovine hydroxyapatite and autogenous
bone. J Oral Maxillofac Surg 60:285, 2002
Related Documents








![Microsurgical Reconstruction of Maxillary Defects€¦ · A hemi-maxillary obturator prosthesis. Edgerton and Zovickian [4] reviewed early attempts at autogenous reconstruction of](https://static.cupdf.com/doc/110x72/6061293c9557b67db91ec84c/microsurgical-reconstruction-of-maxillary-defects-a-hemi-maxillary-obturator-prosthesis.jpg)


