CHAPTER 12 MATRILINEAL STRUCTURES AND PATRIARCHAL VALUES: WOMEN’S HEALTH ON LIHIR, PAPUA NEW GUINEA Martha Macintyre Improvements in the status and health of women are often assumed to accompany the economic development process in Pacific nations. In Papua New Guinea, resource-extraction industries, especially mining and logging, are the major ways that people in rural areas are incorporated into the processes of modernization. For the women of Lihir, in New Ireland Province (see figure 12.1), where a large gold mine has been in production since mid-1997, the changes in their everyday lives have been dramatic and swift. The benefits and the damaging effects of these changes on social status and health are in some respects easily identified. Research over the period from 1994— before the mine—to 1999 has provided evidence from which to draw conclusions. A baseline study of the health of the population (Taufa et al. 1994) and a detailed social 269

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
CHAPTER 12
MATRILINEAL STRUCTURES AND PATRIARCHAL VALUES:
WOMEN’S HEALTH ON LIHIR, PAPUA NEW GUINEA
Martha Macintyre
Improvements in the status and health of women are often
assumed to accompany the economic development process in
Pacific nations. In Papua New Guinea, resource-extraction
industries, especially mining and logging, are the major
ways that people in rural areas are incorporated into the
processes of modernization. For the women of Lihir, in
New Ireland Province (see figure 12.1), where a large
gold mine has been in production since mid-1997, the
changes in their everyday lives have been dramatic and
swift. The benefits and the damaging effects of these
changes on social status and health are in some respects
easily identified. Research over the period from 1994—
before the mine—to 1999 has provided evidence from which
to draw conclusions. A baseline study of the health of
the population (Taufa et al. 1994) and a detailed social
269
270
mapping study (Burton 1995–2001) illuminate issues of
health and demographic change. But the relationships
between the observable changes and the social and
cultural forces that influence and affect them are not
easily identified, as material transformations are
mediated through cultural ideologies and practices.
<Figure 12.1>
Some transformations are novel, introduced by the
mining company and the state. Some are attributable to
cultural globalization and the fact that Lihirians have
suddenly been linked to a wider world—industrially and
through improved transport and communications. Some are
effects of greater wealth as the monetary benefits of
gold production permeate the island community. Women’s
lives are changing and even five years into the mining
project there are discernible improvements in living
standards. As if to demonstrate the accuracy of analyses
that attribute the low rates of education for girls to
the burden of subsistence agriculture on women (Avalos
271
1994), enrolments and retention rates of girls at schools
have been rising since 1997. Changes in women’s health
are less evident and while many beneficial changes are
underway, there are also detrimental effects, such as the
increase in domestic violence, which are in many respects
hidden from scrutiny.
ANTHROPOLOGY AND PUBLIC HEALTH: WOMEN’S HEALTH AND
WOMEN’S STATUS
The relationship between anthropology and public health,
as disciplines within the academic domain and as
integrated elements in strategies for improving health in
developing countries, has strengthened during the 1990s.
As political debates about global inequalities and
oppression have incorporated the discourses of culture
and difference, in order to explain disparities and
conflicts, anthropological understandings of culture have
been incorporated into public health debates. The failure
of primary health care initiatives in some communities
and their success in others is conventionally explained
in terms of cultural difference, for instance,
understandings of the cultural construction of sexuality
272
in particular groups and communities are integrated into
public health policies on AIDS prevention and family
planning.
Public health analyses deal with populations and
groups, the level of generality paralleling that of
anthropology. Public health studies dealing with cultural
factors often hark back to theories of social and
cultural determinism that underpinned functionalist
theories which informed anthropological studies in the
1960s. While public health and epidemiology have been
criticized from within for their concentration on
“generic methods for the measurement of disease
occurrence” (Farmer et al. 1996, 243) and relative
neglect of social contexts, even when these are
considered, a strange dehumanizing reductionism seems to
creep in, so that being female, or poor or black, become
“risk factors.” The emphasis on statistical demonstration
of causal relationships constrains studies so that
specific factors are identified and analyzed in relation
to each other and to the prevalence, for instance, of
disease, while the reasons for these causal relationships
273
or the sociocultural mechanisms at work remain obscure.
As public health inquiry concentrates on the material
effects of sociocultural systems it invokes alternatively
some of the functionalism of British social anthropology
following Malinowski and a cultural determinism
reminiscent of Mead and Benedict. The discovery of
demographic or epidemiological patterns in public health
studies provokes questions about the functions of
particular social arrangements or cultural understandings
that might account for crucial differences between groups
that in many respects are apparently similar. The work of
John and Pat Caldwell in India has consistently
incorporated anthropological analysis to this end, and
their correlation of familial ideologies with the health
status of women from different states in India (Caldwell
and Caldwell 1994, 339–71) provides both the inspiration
and point of departure for this chapter.
Caldwell and Caldwell observe that studies of health
in Third World countries reveal differentials in
mortality that cannot be attributed to either economic
disparities or unequal access to medical services (1994,
274
340). The clustering of those countries whose female
mortality rates are relatively high concentrates “along
an east-west axis from the Mediterranean to the Arabian
Sea, precisely the origin of the most rigid patrilineal
and patriarchal society” (340). Their discussion of
regions of excess female mortality and the correlation of
these patterns with particular types of family structure
and gender ideologies demonstrates clear relationships
between patrilineal/patriarchal societies and lower
female health status. They acknowledge that the
mechanisms, which discriminate against females (of all
ages) in such societies, are complex, often covert and
not explicitly directed toward generating female ill
health.
Within anthropology, theoretical concerns with
difference and the poststructuralist criticisms of
materialism and universalist criteria have moved debates
away from comparative studies that have any underlying
principle of relative measurement. But as public health
has become a global concern, the problems are necessarily
posed in terms of universal objectives and ideals of
275
improvement that assume fundamental similarities between
populations and cultures. The broad-brush comparative
approach of international public health studies that sets
goals for immunization levels, or sanitation, or
reduction in rates of infant and maternal mortality, has
generic human subjects at its center. In this context the
health of women in one population is legitimately
compared with that of another, and social, economic, or
cultural factors that might determine that difference are
invoked as part of the knowledge necessary to effect
change. Caldwell and Caldwell make comparisons of Third
World mortality rates that clearly demonstrate their
argument about “patriarchy and patriliny” in a broad
sense. But within anthropology the meaning of
“patriarchy” and the complexities of familial systems
associated with various forms of descent reckoning have
been subjected to intense scrutiny. Moreover, ideas about
the “status” or “value” of women have been similarly
destabilized as feminist and postcolonial scholars have
questioned the Eurocentrism of the “values” attached to
276
theoretical studies of gender relations in developing
countries (Lepowsky 1993; Lutkehaus 1995; Weiner 1976).
Where once “patriarchy” might have seemed
unproblematic, a term to designate power relations within
social formations (from the family to the State) that
privileged men and their interests over women, feminist
and poststructuralist anthropology has required that
differences and variations be acknowledged.
“Patriarchies” with various forms might exist and be
examined, but the generic term no longer can be applied
uncritically. Caldwell and Caldwell (1994) use the term
in the sense that has been applied to “Eurasian”
societies by Jack Goody (1976) and others—societies based
on agricultural economies with familial hierarchies where
the dominance of an individual older male “is achieved by
having the husband much older than the wife” (Caldwell
and Caldwell 1994, 344). Their argument is supported by
statistical comparisons of adult and child health within
India, which show that variations cannot be explained by
other factors, such as relative poverty.
277
Development and health studies of the Pacific region
also assume global categories that facilitate measurement
and comparison between nations and populations. Much of
the development literature on women infers aims that are
uncritically “progressive” and emancipatory: improved
health and education; greater participation in all levels
of government; the removal of discriminatory practices
that impede women’s access to justice; improved economic
status and living standards (Avalos 1994). The research
undertaken to account for gender disadvantage and
disparity assumes the desirability of these aims and
seeks material explanations for differences; cultural
explanations are invoked as “second order” answers to
otherwise inexplicable variation. Concepts such as
“patriarchy” are then reintroduced.
Papua New Guinean health statistics raise questions
that are similar to those of Caldwell about India. When
compared with other Pacific nations, many of which are
less economically developed, the health of women in Papua
New Guinea (PNG) is poor and the rate of infant mortality
extraordinarily high. For example, the neighboring
278
Melanesian nation, the Solomon Islands, is poorer, has a
much lower rate of adult literacy (22 percent as opposed
to 52 percent in PNG) and faces similar problems of
transport and communications that limit access to health
services. Yet, people there have a higher life expectancy
at birth (Solomon Is. 62 years, PNG 56 years) and there
is a lower infant mortality rate, with Solomon Islands
estimates currently 44 per 1,000, compared with PNG at 67
per 1,000 in some studies (Brouwer et al. 1998, 29) and
82 per 1,000 in others (National Statistical Office
1991). In PNG women’s life expectancy is 51.4 years,
making it the lowest in the Pacific. Analysis of causes
of death for women between the ages of 15 and 44 years
revealed that 29 percent of deaths were from obstetric
causes (Brouwer et al. 1998, 30). Women’s differential
access to health services and poorer health generally is
also indicated by the otherwise inexplicable masculine
bias in the population. With 111 males for every 100
females (one of the highest differentials in the world)
and no substantial evidence for any systematic female
279
infanticide, Papua New Guinea’s women appear to be “at
risk” throughout their lives.
But statistical information for Papua New Guinea is
unreliable. Collection of data presents enormous
logistical problems and the funding cuts to Health,
National Planning, and other government services over the
past decade mean that figures are in many respects
problematic for any analysis. But the disparities on
Lihir are supported by good statistical evidence.
In this context, a re-examination of issues of
women’s relative status and value has new relevance. The
differences between men’s health and women’s health in
Papua New Guinea demand explanation precisely because the
disparities systematically disadvantage women. They are
also expressive of differences in power over the
processes of change occurring in all aspects of life—in
economic development, in government, and in everyday
existence. The societies that Caldwell and Caldwell
(1994, following Goody 1976) identify as patriarchal are
patrilineal, with institutional structures, such as land
ownership, inheritance, and political authority, that
280
favor male interests over female. In PNG, communities in
which matrilineal systems of descent, land ownership, and
authority might appear to be more equitable, women are no
healthier (see Lepowsky 1993; Macintyre 1987; Modjeska
1982; Nash 1974). Indeed, the patterns of health and
illness show distinct similarities with the patrilineal,
patriarchal societies described by Caldwell and Caldwell
(1994). Lihir, in New Ireland Province, is one such
place.
MATERNAL AND CHILD HEALTH ON LIHIR
The available information on the health of women on Lihir
suggests that they are in most respects typical of the
rural female population in PNG. Malaria is endemic and
there are several villages where filariasis is common.
These mosquito-borne diseases affect people regardless of
gender, but malaria in women specifically contributes to
the high levels of anemia observed in mothers (Taufa et
al. 1994; Dickson 1994). Both women and men suffer from a
range of respiratory infections and tuberculosis which is
widespread and generally undiagnosed until it is
advanced, when people present at hospitals. In one survey
281
conducted in two villages on Lihir in 1995, the medical
team found that 80 percent of people had positive
responses to Mantoux tests. While this is not necessarily
evidence of affliction, the medical superintendent
believed that the rate of infection was extremely high
(M. Golding, pers. comm.).
When confronted by numbers showing that too many
women are anemic, suffering from malaria, or dying in
childbirth, it is easy to see the solutions as either
medical or matters of health education. In observing
women’s lives in villages on Lihir, the problems specific
to women’s health are more complex and not attributable
to either lack of knowledge or absence of services.
Moreover, changes associated with the mining development,
while undoubtedly improving health services and material
standards of living, create new inequalities and have
social effects that reduce women’s health.
Statistical information on birth rates is scant. One
reliable survey of nine villages in 1991 found 38.2 per
1,000 (Dickson 1994) and the current rate is estimated at
34 per 1,000, although this is perhaps too low due to
282
underreporting of births outside hospitals and medical
centers. In a small survey in four villages I found that
of 28 births in one year, 8 had occurred in villages and
were therefore unrecorded. The total fertility rate is
estimated at 4.5, comparable with the national rural
figure of 5.00 (Kowal 1999). Certainly, the most casual
observation of households affirms that Lihirian women can
expect to have at least four or five children in their
lives.
WOMEN’S KNOWLEDGE OF HEALTH ISSUES
Since 1995 I have regularly discussed health matters with
Lihirian women and have conducted two formal surveys (in
1995 and 1999) of fifty mothers, in order to gauge health
education needs and awareness of medically identified
health problems of women and children. Three of the
topics regularly investigated are anemia, care of women
during pregnancy and birth, and ideas about being
healthy.
ANEMIA, OR SOT BLUT
The overwhelming majority of women recognize the pidgin
term sot blut, having been told about it by a nurse during
283
antenatal care. Their explanations are conceptual and
experiential and two-thirds consistently explained causes
that are based on biomedical information. The most common
understanding of the term sot blut (lit., short blood) is
that the body has insufficient blood—a condition variously
attributed to excessive loss of blood during birth,
depletion of the mother’s blood to the fetus, and falling
pregnant soon after a birth, before the body has time to
“fill up” with blood again. Only a few educated women
described it as a deficiency in the blood, and not many
are aware that malaria can exacerbate or cause anemia.
Half the women described it in terms of their experiences
—the symptoms being extreme lethargy, weakness in the
legs, pallor, and dizziness. Over two-thirds identified
eating greens (kumu) as a way of both treating and
preventing anemia and some mentioned the need for other
iron-rich foods. Adequate rest, bush medicines, and
spacing of pregnancies were also viewed as ways of
avoiding the problem.
While the definitions of anemia do not conform to
biomedical models, Lihirian women display a high level of
284
awareness of important causes and treatments. They often
sound as if they were repeating the health messages they
have heard from the clinics. Detailed knowledge of
preventive measures has increased over the past five
years, testifying to the efficacy of the health education
programs conducted under the auspices of the mining
company. Half of the women interviewed (mostly those
between 20 and 30 years) identified medications
obtainable from the hospital and a few knew of treatment
by transfusion. They were able to recognize symptoms in
themselves and others and knew how to respond in ways
that are appropriate. But few women do so.
Given the role of nutrition in improving women’s
health and the fact that the health transition in
developing countries often includes dietary innovations
that have adverse effects on health, such as increased
consumption of saturated fats, sugar, and refined foods,
the gap between understanding and practice is alarming
(cf. Pollock this volume). Customary consumption of
greens is limited mainly because people believe that they
constitute a garnish to starchy staples, so “eating
285
greens” may involve quantities as small as one
tablespoon. Eating greens in large quantities is thus
viewed as somewhat eccentric, rather like emptying a
whole bottle of ketchup on one’s meal. At present,
families who purchase food from stores limit themselves
to rice and tinned fish and those who have more money buy
take-away foods that consist mainly of white flour fried
in palm oil or dripping. The supermarket stocks a wide
range of foods to cater for the expatriate families—and
while this is expensive, it is no more so than the
convenience foods. The food of the wealthy Lihirians now
is the food of the poor in industrialized countries—
floury deep-fried convenience food laden with sugar or
salt—that is valued for the feeling of satiation it
brings. Problems such as obesity, diabetes, hypertension,
and cardiovascular diseases are currently the subject of
education campaigns aimed at prevention, but have no
discernible effect on eating habits.
Most women consider store foods unhealthy yet appear
to accept the changes as inevitable. The prestige value
of buying ready-cooked food dominates, in part because
286
the idea of modernity or “development” is constructed in
terms of not having to engage in heavy work and being
able to buy, rather than make, food, clothing, and
household items. Thus, the economies of buying the
ingredients for “fast foods” and preparing them at home
are rejected as signs of relative poverty.
PREGNANCY AND BIRTH
The maternal and child health team regularly visits
villages and all women attend for antenatal checks by the
medical staff. All women mention “eating good food” and
“having rest” as crucial to maintaining health during
pregnancy. In 1991 about 50 percent of women gave birth
in the mission hospital. Now almost all women prefer to
give birth in hospital and the majority of women do so.
In the 1995 survey, 29 women had all their children in
hospital, 11 had all in the village, and 10 had
experienced births at both places. In the 1999 survey, 36
had all in hospital, 8 had all in the villages, and 6 in
both sites. In conversations with women of all ages the
ideal birth was represented as taking place in hospital
under medical supervision with analgesia available.
287
Questions about length of stay were invariably
interpreted subjectively. Women considered their current
circumstances and so limited their hypothetical stay to
one or two days. When asked how long they would stay if
they knew that their gardens were being cared for and
family being fed each day, the time stretched to five
days. The most common reasons given for choosing to give
birth in hospital were the availability of medical
assistance, access to medication for pain, and fear of
obstetric difficulty. Several women who delivered in the
village mentioned that the labor progressed too quickly
for them to travel. The most common reasons for not going
to hospital were lack of transport and lack of money. The
mission hospital charges 7 kina (US$2) per day and women
can stay as long as they want (usually one week); the
hospital at the mining township charges 21 kina (US$6)
per day. As the weekly income for a person working at the
mine rarely exceeds 200 kina (US$57.50), this represents
a considerable amount of money, even for wage-earning
families. There are additional costs in going to
288
hospital, as then women have to buy clothing for the
baby.
The minority of women who preferred to remain in the
village to give birth included some who did not want to
be examined (especially by a man, although there are no
male midwives and the male doctor is called only in
emergencies) or did not like taking medication. Some
women did not like the hospital environment. These
personal preferences did not appear to correlate with any
other defining characteristics, such as age or level of
education. Most women from both groups mentioned the
problems of childcare as a major obstacle and one of the
reasons for not seeking medical attention when
experiencing problems during pregnancy.
RECOGNIZING HEALTH AND ILLNESS
As health status and measurements of health utilized in
public health studies are uncompromisingly biomedical in
their criteria, most awareness campaigns assume the self-
evidence of shared views of health improvements and ideal
health. The failure of some campaigns (notably
nutritional education) in Papua New Guinea inspired
289
investigation of local understandings of “being healthy.”
The term helt ‘health’ in Tok Pisin is widely used by
those who have had primary education, but most women use
strongpela ‘strength, health’ when referring to physical
well-being. Women most commonly emphasize high energy
levels and feelings of calmness or happiness and personal
autonomy as the way they feel well.
Inquiries about the time in their lives that they
have felt most healthy revealed the ways that the
experience of motherhood is constituted negatively. By
this, most women were referring to the period when they
were bearing children, breastfeeding, and bringing up
children who were at primary school. Of the fifty mothers
surveyed in 1995, only one nominated her current state as
healthy. In 1999 the result was similar. The vast
majority of women nominated the time that they were young
adults, before their first pregnancy, as the time of
greatest health. The ways in which they explained their
healthy state throw light on the ways that women perceive
the pressures of marriage and maternity as deleterious to
their health:
290
Taim mi stap nating, mi no marit yet, mi stap strongpela. Becos mi no gat man mi
ken tingting long givim kaikai, mi kaikai tasol ‘When I was just myself,
unmarried, then I was healthy. Because I didn’t have a husband
to worry about feeding, I just fed myself’.
Mi inap long ple na go raun long poroman na mekim sampela wok olsem laik
bilong mi inap long mekim ‘I could just play and go around with my
friends and work as I pleased’.
One woman who said that she felt healthiest after she
weaned her last child described the change thus:
Mi kaikai bilong mi, mi wokabaut olgeta samting bilong mi yet, mi fil olsem pri. Skin
bilong mi i senis bekos kaikai i halipim bodi bilong mi ‘I ate for myself, I
walked about doing things for myself, I felt free. My skin
changed because the food was sustaining my body’.1
While it is often assumed that motherhood in Papua
New Guinean communities confers status and value, giving
them powers of influence and authority, few women present
this as their own experience. In discussions of the times
of greatest happiness and physical well-being, women of 1Notes
? The Tok Pisin term “skin” usually refers to the body as
well as its surface. The speaker here was differentiating
between skin and body and so used the English word
“body.”
291
all ages suggested that motherhood, especially the period
when a woman had small children, was the time that they
felt least well and were most likely to feel unhappy,
linking ideas of health and happiness to freedom and
autonomous action. While a few suggested that they were
happiest and healthiest when they had no
responsibilities, most expressed this in terms of the
freedom to decide, without any coercive pressure, when to
work. Several women described the time before marriage as
one where they could work for long periods without being
exhausted and could grow their own food and give it to
their families, thus pleasing their married sisters and
mothers. Having food to bestow as they pleased gave them
status with other women and, most of all, they felt no
compulsion to do so: “Sapos mi no laik, bai mi no givim kaikai long ol.
Ol ino ken paitim mi ‘If I didn’t feel like it, then I
wouldn’t feed them. Nobody could hit me’.”
Marriage was thus represented as a time when a woman
lost control over her own life. Motherhood is defined as
labor and little attention was given in narratives to
biological processes or birth events. Most particularly,
292
a mother’s obligation to feed others meant that she had
no choice about work. This perception of women’s lack of
autonomy over their bodies in marriage was a recurrent
theme, stated quite clearly by one woman who worked at
the mine. She had three children and had never married.
In explaining to me that this was by choice, she said:
Why would I marry? Now I can work for myself, pay my
children’s school fees, give my sisters and mother money. I
don’t have to work hard all day in the garden or get beaten
by a husband who wants his food or wants to sleep with me
when he is drunk. I can go to my garden on my days off, or
help my mother. I am happy like this.
WOMEN’S WORK AS A DEBILITATING FACTOR
Lihirian women, like many other women in rural Papua New
Guinea, produce most of the food consumed by their
families and their pigs. Although some men do work in
gardens, they are in a minority and they draw on the
labor of women to do much of the day-to-day maintenance.
Between 1995 and 1999 I observed the daily routines of
women in two villages. Women between the ages of eighteen
and fifty-five worked extremely long hours each day. In
the months prior to the yam harvest, most women spent
293
between four and six hours in their gardens and the
majority went to work in the garden four or five days a
week. Collecting water was a major daily task in both
places. Some women spent up to three hours each day
fetching water in buckets and other receptacles. In the
village where a tank had been installed the time was
reduced by two-thirds. Women walked to streams to wash
dishes and clothes most days. In addition they fetched
firewood, cleaned the hamlet area and their homes, washed
clothes, prepared all meals, and cared for their
children. The two tasks that were shared with men fairly
regularly were the feeding of pigs and childcare. Girls
assisted with all tasks, but especially by fetching water
and caring for young children, often in the company of
their mothers.
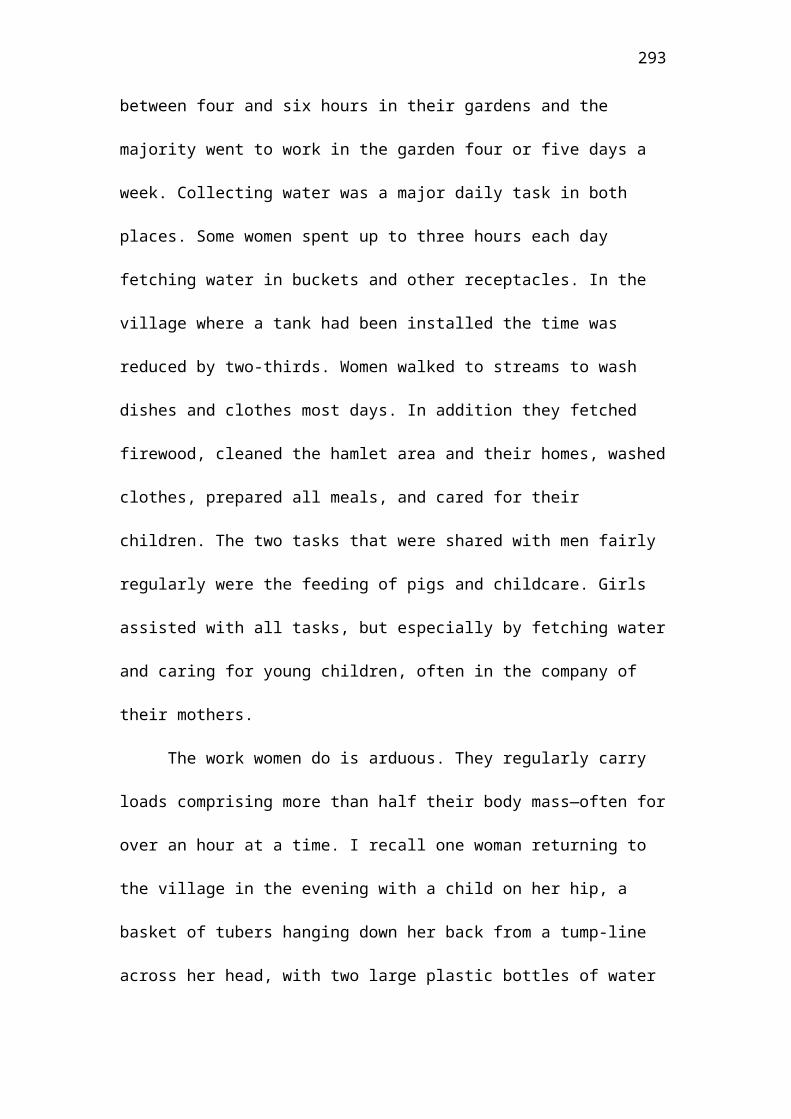
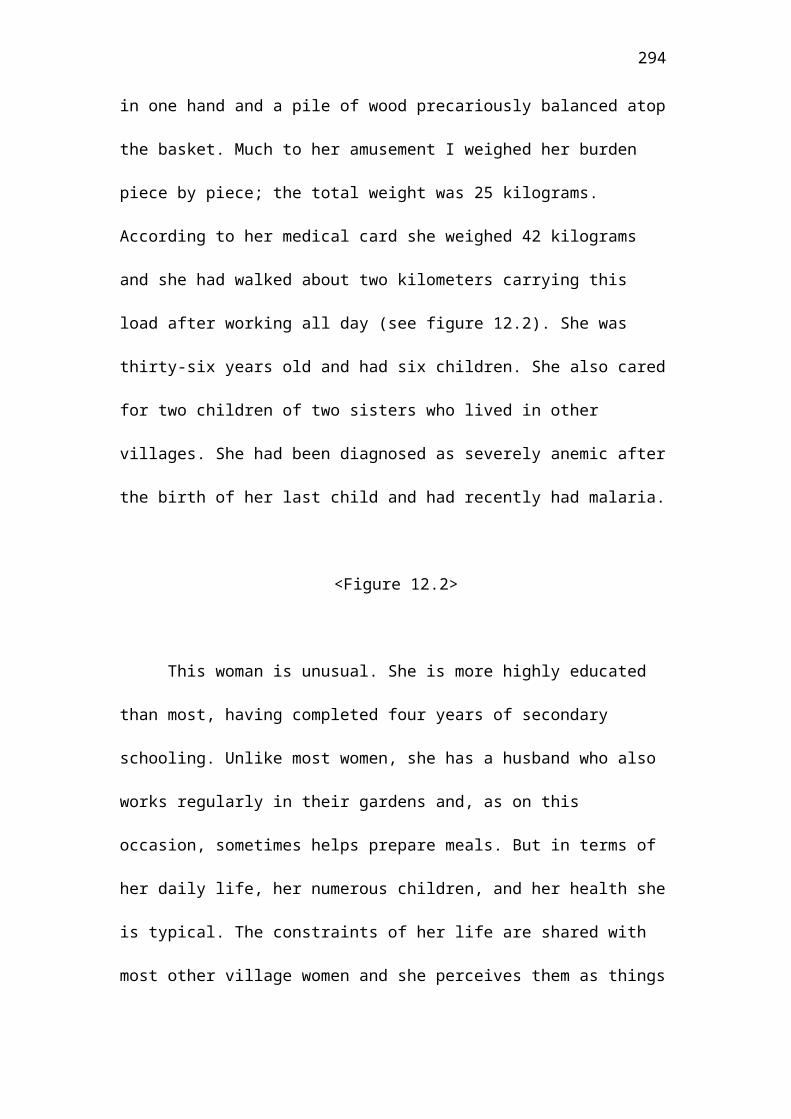
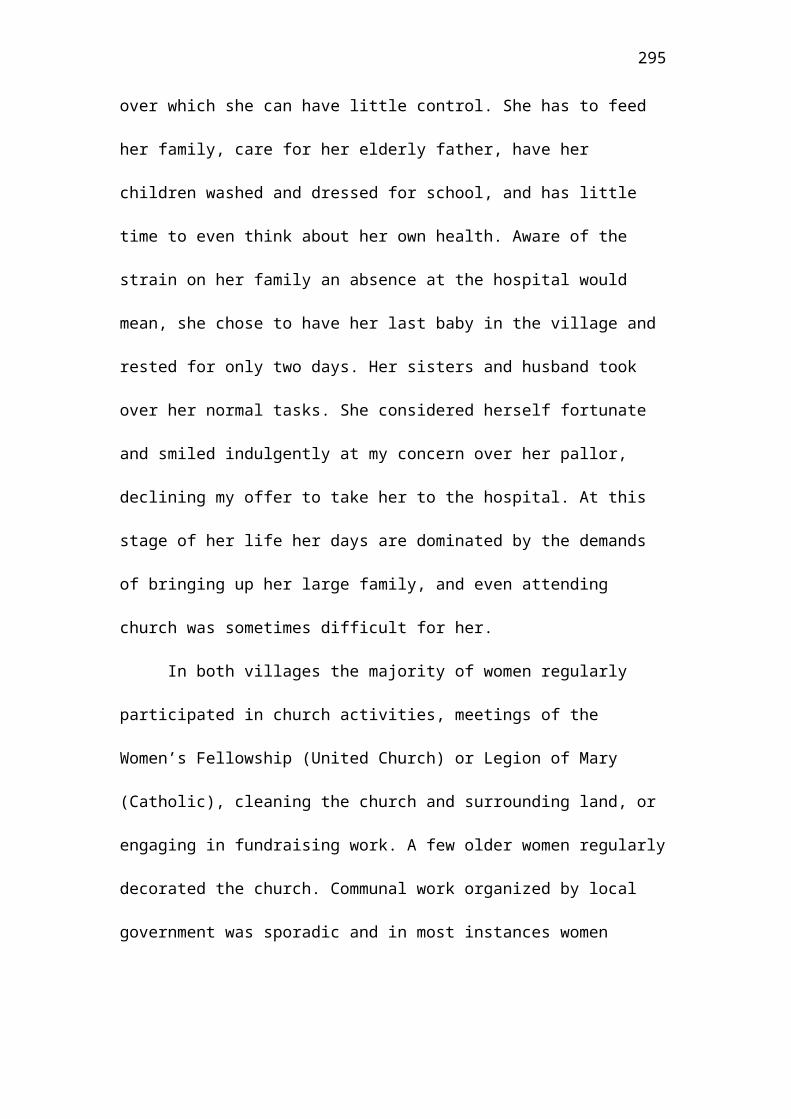
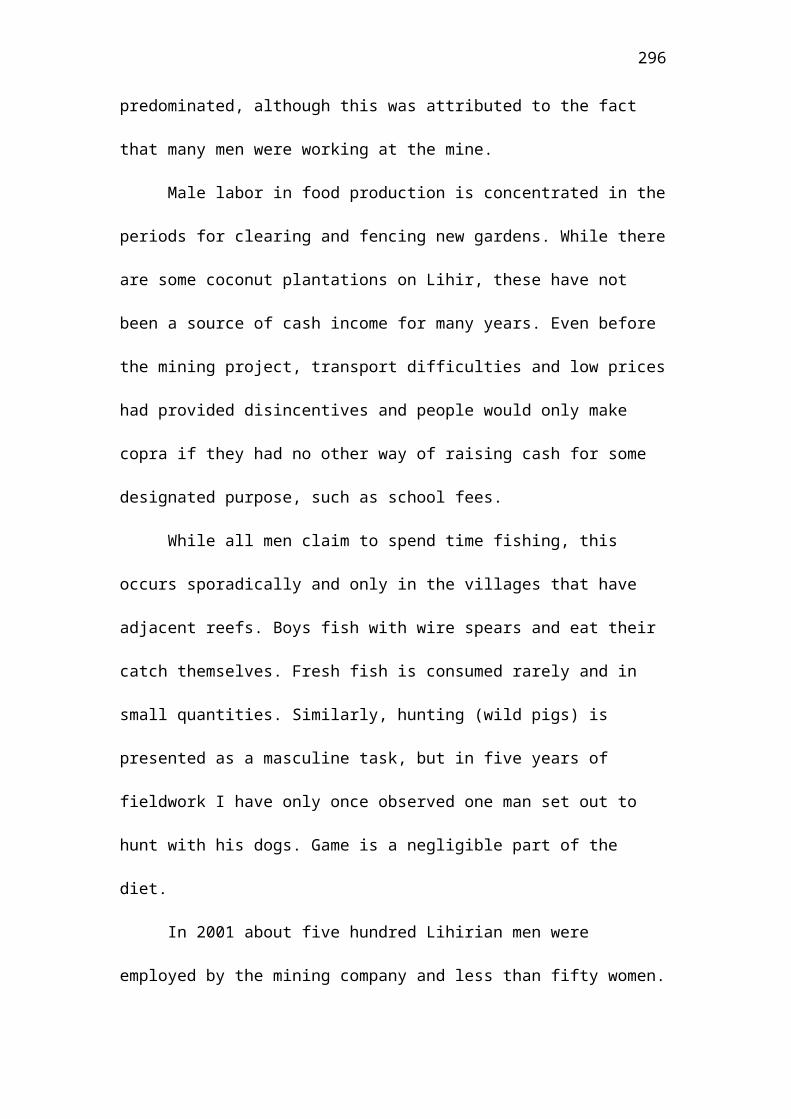
The work women do is arduous. They regularly carry
loads comprising more than half their body mass—often for
over an hour at a time. I recall one woman returning to
the village in the evening with a child on her hip, a
basket of tubers hanging down her back from a tump-line
across her head, with two large plastic bottles of water
294
in one hand and a pile of wood precariously balanced atop
the basket. Much to her amusement I weighed her burden
piece by piece; the total weight was 25 kilograms.
According to her medical card she weighed 42 kilograms
and she had walked about two kilometers carrying this
load after working all day (see figure 12.2). She was
thirty-six years old and had six children. She also cared
for two children of two sisters who lived in other
villages. She had been diagnosed as severely anemic after
the birth of her last child and had recently had malaria.
<Figure 12.2>
This woman is unusual. She is more highly educated
than most, having completed four years of secondary
schooling. Unlike most women, she has a husband who also
works regularly in their gardens and, as on this
occasion, sometimes helps prepare meals. But in terms of
her daily life, her numerous children, and her health she
is typical. The constraints of her life are shared with
most other village women and she perceives them as things
295
over which she can have little control. She has to feed
her family, care for her elderly father, have her
children washed and dressed for school, and has little
time to even think about her own health. Aware of the
strain on her family an absence at the hospital would
mean, she chose to have her last baby in the village and
rested for only two days. Her sisters and husband took
over her normal tasks. She considered herself fortunate
and smiled indulgently at my concern over her pallor,
declining my offer to take her to the hospital. At this
stage of her life her days are dominated by the demands
of bringing up her large family, and even attending
church was sometimes difficult for her.
In both villages the majority of women regularly
participated in church activities, meetings of the
Women’s Fellowship (United Church) or Legion of Mary
(Catholic), cleaning the church and surrounding land, or
engaging in fundraising work. A few older women regularly
decorated the church. Communal work organized by local
government was sporadic and in most instances women
296
predominated, although this was attributed to the fact
that many men were working at the mine.
Male labor in food production is concentrated in the
periods for clearing and fencing new gardens. While there
are some coconut plantations on Lihir, these have not
been a source of cash income for many years. Even before
the mining project, transport difficulties and low prices
had provided disincentives and people would only make
copra if they had no other way of raising cash for some
designated purpose, such as school fees.
While all men claim to spend time fishing, this
occurs sporadically and only in the villages that have
adjacent reefs. Boys fish with wire spears and eat their
catch themselves. Fresh fish is consumed rarely and in
small quantities. Similarly, hunting (wild pigs) is
presented as a masculine task, but in five years of
fieldwork I have only once observed one man set out to
hunt with his dogs. Game is a negligible part of the
diet.
In 2001 about five hundred Lihirian men were
employed by the mining company and less than fifty women.
297
The company that supplies catering and cleaning services
at the mining camp regularly employs over one hundred
women. The men are of the age group that would in the
past have done most of the heavy work in clearing
gardens. Since the construction phase of the mine women
in most villages claim that they have to work harder in
subsistence activities, even doing tasks, such as mending
fences, that would have been done by men in the past.
They observe that fewer men assist in garden clearing,
resulting in reduced fallow periods, depleted soil
fertility, and lower crop yields. There is a marked
difference between villages in the mine-affected areas
that have received benefits, such as reticulated water
and household tanks, and those (the majority) where the
mining company has no obligation to provide such
amenities. As these tend to be the villages with higher
levels of employment, where people buy rice and tinned
fish to supplement garden food, it is likely that changes
in women’s work will become increasingly obvious. At
present, however, women often perceive the dietary
changes as necessary because of their increased
298
obligations to work on communal tasks formerly done by
men and to compensate for the lack of male input into
subsistence production. Nobody interviewed believed that
the mining project had altered work patterns in ways that
had decreased their workloads.
There are a few women—those who have benefited from
large compensation payments for the land leased to the
mining company—who are now much more dependent on bought
food. Husbands rarely give wives control over money, as
most men consider their wages to be personal income. Men
buy food at the supermarket and bring it home, only
giving money for extra purchases at a local trade store
when requested specifically. In the annual surveys on
expenditure, of the 130 men surveyed, only two gave their
wives more than half their earnings. Most men (70
percent) spent over half their wages on beer and gave
more money to fathers and brothers than they did to their
wives. Conversely, women who earned money gave larger
amounts to the church (20 percent of weekly wage), spent
most of it on food and clothing for their families, and
regularly gave small amounts to their mothers and sisters
299
(who spent their money similarly). The customary division
of labor and its benefits are thus being maintained in
the distribution of female cash earnings, while the money
earned by men is used in ways that are novel and
contribute comparatively little to the subsistence of the
family. This pattern was most marked in the construction
phase of the mine, when people tended to view wages (and
all money) as a kind of windfall. As the project
progresses and workforce participation stabilizes it is
likely that male employees who do not assist with garden
work will be increasingly forced into the role of
breadwinners. At present, however, the traditional role
of women as breadwinners continues.
Arguments about the benefits of income-generating
development projects for women or female employment
stress that maternal altruism also means improvements in
child health (but see Basu and Basu 1991). On Lihir few
women are able to participate because of the demands of
subsistence work. These demands are real, but they are
reinforced by husbands who are often hostile to any
action that expresses female autonomy. Men are reluctant
300
to allow women to work in activities that take them away
from the confines of hamlet and garden, claiming that
they are neglecting their duties and possibly making
assignations with lovers. Similarly, if a woman who is
not obviously very ill attempts to visit the clinic
alone, she is accused of either having other intentions
or of going to get contraception in order to conduct an
illicit love affair. Jealousy or suspicious accusation is
one of the main ways by which men control women’s bodies.
The acceptance of imposed constraints is expressive of
the pervasive view of male sexuality as aggressive and of
sex as the locus of male entitlement. The demands and
restrictions that men impose on wives and the threat of
violence, if these are ignored or defied, are major
factors in limiting women’s choices about work and
health.
VIOLENCE AND WOMEN’S HEALTH
The health impacts of domestic violence worldwide are
well documented (e.g., Astbury 1999), with the two most
common being injury and depression. Women on Lihir rarely
seek treatment for an injury and would usually feel too
301
ashamed to explain that it was caused by their husbands
beating them. While they are quite willing to discuss the
problem as pervasive, even implying that they experience
violence personally, the wounds or scars are hidden from
view. In Papua New Guinea there is little data on mental
health generally and psychiatric service provision is
non-existent in most areas. There is almost no
information about the mental health of the female
population (Gillett 1990, 45). Nonetheless, women
themselves observe that many of those whom they consider
mentally ill (there is no specific notion of
“depression”) have been subjected to violence. Three
women whom I know well appear to me to suffer from mental
illness. One was raped as a schoolgirl and the others are
married to men who beat them regularly. The nurses whom I
interviewed suggested that women who left their marital
homes to visit sisters or family in other villages often
did so because they were depressed and unable to cope
with the stress of remaining with a violent husband.
Violence against women certainly has direct impacts on
health, most of which remain undiagnosed, unrecorded and
302
untreated on Lihir. The transference of blame to the
wives, their internalization of shame, and the absence of
sanctions against violence in marriage all indicate the
ways that the demeaning use of force by men against women
is symbolic of a hierarchy of relative social value and
status as members of a group. Parents may beat children,
and husbands may beat wives. The resort to violence is
acceptable when it is directed toward an inferior who has
affronted or denied the prerogatives of a superior.
Perhaps more than any other factor, the cultural
acceptance of domestic violence against women is
indicative of the “naturalization” of male dominance over
women. On Lihir both men and women generally accept that
men, as husbands or elders, can legitimately beat women
(see also Dinnen and Ley 2000; Toft 1985). This reveals
the deeply entrenched subordination of women. Interviews
with men reveal a sense of entitlement as regards their
control over women’s work, fertility, and sexuality.
Although some older men regarded the breakdown of
postpartum sexual taboos as reflecting badly on male lack
of restraint, even they were not prepared to uphold the
303
right of a wife to refuse her husband’s sexual access. A
very small minority of men regarded it as excessive to
beat a wife who had not prepared his meal at the end of
the day, but over the five years of research I have found
only three men who believe that wife-beating is always
unjustifiable. The vast majority claim that bride-price
confers the right to punish a wife who is not performing her
duties as defined by her husband (see also Mackenzie-Reur
this volume on Vanuatu).
This is in many respects a surprising finding, given
that Lihir is a matrilineal society in which marriage
exchanges are ideally balanced. The ideology of male
dominance resides in the exchange being construed as
between men of each lineage with the “gift” of the
alliance being symbolized in the payment to the groom’s
family and the “purchase” of the woman’s wifely and
maternal capacities in the counterprestation.
RETHINKING PAPUA NEW GUINEAN “PATRIARCHY”—STRUCTURE AND
CULTURE
The health of women on Lihir is compromised by
inequalities comparable to those of the northern Indian
304
women Caldwell and Caldwell (1994) perceive as being
deleteriously affected by patriarchal structures. The
structures they stress as crucial are institutional—
systems of identity and descent reckoning, patterns of
property ownership and inheritance. On Lihir, kinship is
structured matrilineally, land and inheritance patterns
are matrilineal, and most married women live in their own
clan villages. These structures do not support a culture
that values women’s bodies or supports their welfare in
ways that mean their health is any better than women
elsewhere in Melanesia. They offer no protection from
violence and no system of customary justice that demands
punishment or compensation for injury.
Culturally, Lihirians seem to share some of the
values surrounding gender attributes that are common in
those Mediterranean societies that Goody (1976)
describes. There is a sentimental idealization of women
as mothers that is mainly expressed rhetorically by adult
sons, often about deceased mothers. The everyday practice
of the Catholic faith on Lihir is predominantly a female
activity with an emphasis on maternal self-sacrifice,
305
long-suffering devotion to familial responsibilities, and
selfless care for others that verges on Mariolatry (see
figure 12.3). In every village, shrines to the Blessed
Virgin are maintained and regularly decorated. Elderly
men and women of all ages worship at these shrines,
offering flowers and daily prayers. Men ostentatiously
participate in feast-days or rituals, such as the
procession of the statue of the Virgin Mary, but these
dramatic public events provide a backdrop for displays of
lineage prestige rather than masculine piety (see figure
12.4).
<Figures 12.3 and 12.4>
In secular activities too, women’s roles are rarely
central. Women’s role in traditional feasts is subsumed
by the men of their households and lineages, as the men’s
house is the focal point for distribution of the foods
that women have produced and prepared. As producers of
food and rearers of pigs they are acknowledged within
their households, but, unlike the men who distribute,
306
their contributions do not confer the prestige and public
status that men accrue through hosting feasts.
In some matrilineal societies the stress on female
transmission of identity does seem to support an
ideological system that values female work, sexuality,
and fecundity as both corporeal and spiritual aspects of
female personhood. On Lihir, women’s labor, sexuality,
and fertility are conceptually abstracted from the person
in a variety of contexts. Women’s fertility and women’s
labor are explicitly acquired in bride-wealth exchanges
and, on the basis of these, men can control them in the
interests of their lineages. The maternal qualities that
are sentimentally valued on Lihir (bearing numerous
children, working hard to feed them, and producing large
quantities of food for feasts) are precisely those that
are acquired by a man’s lineage (see figure 12.5). Women
who perform these tasks “selflessly” are admired and
respected, those who do not are deemed inadequate.
Refusal to conform to male expectations is not regarded
as a form of resistance, but as a failure of capacity.
Thus, women who leave their husbands or have children
307
outside marriage, or do not grow yams for feasts, have
low status within their families. Their “failure to
conform” is viewed as shameful personal inadequacy. Most
unmarried mothers work extremely hard to feed their
children and to make contributions to lineage feasts or
other projects. But lacking a husband as their public
representative, they are often incorporated into lineage
activities as if they were adolescents, “lowly” workers
whose labor is controlled by a father, brother, or
occasionally a mother.
Preliminary investigations suggest that women who
have lower social standing also have poorer health. The
exceptions to this pattern are those few who have taken
jobs that allow them to exercise economic power
autonomously and whose incomes are sufficiently high for
them to be able to rear their children without any male
assistance. They remove themselves from the system in
various ways and then participate on their own terms as
individuals.
<Figure 12.5>
308
CONCLUSION
Anthropological studies of gender relations in Papua New
Guinea have generally stressed the ways that social
distinctions provide the institutional basis for
cooperation and integration in production and
reproduction within a specific community. Ideas such “sex
antagonism”, “status,” “inequalities,” and “patriarchy”
were eschewed as having little analytical utility as they
constituted comparisons that affronted the ideal of
cultural integrity.2 Most of the studies that presented
gender relations as systems of complementarity and
aspects of a benign, self-sustaining sociality are
written from the perspective of a perpetual subsistence-
based economy.
Industrial developments, such as mining projects,
disrupt that apparent complementarity by introducing new
forms of wealth, new ways of achieving status, and
alternative means of gaining political prestige and
power. Men benefit from these changes and women are 2 For example, see the debates around Marilyn Strathern’s
The Gender of the Gift (1988).
309
excluded and disadvantaged. The anthropological studies
that Caldwell and Caldwell (1994) draw on to present
their arguments about structural determinants of women’s
poor health did not examine the cultural ideologies that
devalue women in relation to men, nor did they explore
issues of violence against women. These topics are often
avoided because the implied criticisms are perceived as
ethnocentric. Violence against women occurs in most
societies and responses to it as a social problem demand
that the theoretical dismissal of patriarchy be
reconsidered. Feminist interpretations that assumed an
autonomous subject (arguing that women’s positive
conceptions of themselves and their bodies refuted the
arguments about pervasive patriarchal institutions)
ignored the suffering of women and their inability to
effect change.
Economic development projects and concomitant
government service provision provide the context for
examination of inequalities within and between
communities in terms other than the hermetic analytical
categories that are employed in anthropological studies
310
of single communities. Issues such as gender inequality
attain new salience and significance as simple
investigations of health, education and employment
patterns reveal inequities and disadvantages that
unequivocally reflect a hierarchy of economic and
political advantage based on sex. Women in Papua New
Guinea have poor health because their health is not
valued in itself and because the value of women is lower
than that of men. On Lihir, the health status of women
reflects the complex ways that patriarchal values work
during a period of dramatic social change. The
“traditional” structures of a matrilineally organized
economy—with land, property relations and social identity
conferred through the maternal line—were sustained within
an uncompromising patriarchal praxis that rendered women
subordinate. The patriarchal structures defined by Goody
(1976) and identified by Caldwell and Caldwell (1994) as
determinants in the poor health of women in northern
India might reinforce gender ideologies that place low
value on women. But it is the values rather than the
structures that are invoked to justify continued
311
discrimination during periods of social and economic
change. Patriarchy is remarkably flexible and adaptable;
it appears to be able to thrive in stable and unstable
environments and to sustain the interests of men over
women even when these might appear disadvantageous to the
society as a whole. Patriarchy is hegemonic in Papua New
Guinea and so the recognition of the poor health status
of women by external analysts at present serves to
reinforce ideas about female inferiority, frailty and
marginality rather than to galvanize governments into
remedial actions.
As an integral element in ideologies of
complementarity that exclude women from legal and
political action, patriarchal values can be obscured by
sentimental valuations of femaleness that affirm the
value that women have as producers and reproducers. Their
relatively poor health status can be seen then as
accidental. In the context of industrialization and
economic development, the continued poor health of women
requires explanation and the scrutiny of the issue
exposes the patriarchal foundations of gender
312
“complementarity.” The material disadvantages that women
suffer are then revealed as originating in those
traditions that consistently denied women’s interests as
people by privileging the value of men over women,
enshrining these values in those institutions that give
men power over women’s bodies.
Related Documents











