MATERNAL AND FETAL REPRESENTATIONS, DIMENSIONS OF PERSONALITY, AND PRENATAL ATTACHMENT IN WOMEN HOSPITALIZED WITH HIGH RISK PREGNANCY APPROVED BY SUPERVISORY COMMITTEE Chair: H. M. Evans, Ph.D. Wayne H. Denton, M.D., Ph.D. Sandra Pitts, Ph.D. Richard Robinson, Ph.D. C. Allen Stringer, M.D.

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
MATERNAL AND FETAL REPRESENTATIONS, DIMENSIONS OF
PERSONALITY, AND PRENATAL ATTACHMENT IN WOMEN HOSPITALIZED
WITH HIGH RISK PREGNANCY
APPROVED BY SUPERVISORY COMMITTEE
Chair: H. M. Evans, Ph.D.
Wayne H. Denton, M.D., Ph.D.
Sandra Pitts, Ph.D.
Richard Robinson, Ph.D.
C. Allen Stringer, M.D.

DEDICATION
To mothers and babies everywhere, including mine,
and to David.

MATERNAL AND FETAL REPRESENTATIONS, DIMENSIONS OF PERSONALITY,
AND PRENATAL ATTACHMENT IN WOMEN HOSPITALIZED
WITH HIGH RISK PREGNANCY
by
ANNA RACHEL BRANDON
DISSERTATION
Presented to the Faculty of the Graduate School of Biomedical Sciences
The University of Texas Southwestern Medical Center at Dallas
In Partial Fulfillment of the Requirements
For the Degree of
DOCTOR OF PHILOSOPHY
The University of Texas Southwestern Medical Center at Dallas
Dallas, Texas
June 2006

Copyright
by
Anna Rachel Brandon, 2006
All Rights Reserved
ACKNOWLEDGMENTS
Dr. Monty Evans told me the idea for research at Baylor on attachment was
conceived in a conversation he and Dr. Allen Stringer had after an inspiring presentation by
Dr. Linda Mayes a few years ago. When it became time for them to implement the project, I
happened to be a graduate student in the right place at the right time. I am ever grateful for
the trust they had in me, and for their continued support throughout the project.
I approached the dissertation process with the traditional angst, but each member of
this committee has done their utmost to help me through it. Together, Dr. Evans and Dr.
Sandy Pitts have been my “secure base,” continually encouraging me to stretch academically
and clinically. Dr. Evans’ office door was always open to me, and his confidence in me took
over when my own confidence failed. Dr. Pitts poured over articles to help me develop my
research questions, and tirelessly scored ORI’s so we would have two raters. She has also
modeled for me an amazing ability to laugh, even in the most stressful times. Dr. Richard
Robinson generously plowed into a project already in action, helped us make the necessary
corrections, and patiently guided me through the statistical mazes I had been dreading. Dr.
Wayne Denton was always understanding and ever encouraging, and never minded my
bouncing between his important Couples project and my work at Baylor. Dr. Stringer not
only made available the Baylor population for our work, but made possible my additional
training at Yale to ensure a high-quality project. I cannot conceive of any better team of
advocates and collaborators.
My classmates, Paula Miltenberger and Dana Broussard, have made significant
contributions to this work as well. Paula took the lead as the work was initiated here at
Baylor, and continued to invest in the project even while on bedrest during her own
complicated pregnancy. Dana joined us in the midst of chaos, rolled up her sleeves, and was
ever alert to new ways to streamline our operations or minimize data loss. We three could
never have kept up with the volume of work without three amazing volunteers. Daria Dato
was a key team member as we began planning the project, and continued to work through our
first six months of data collection, always willing to take on any task we needed done. Missy
Heusinger and Georgina Rangel also played valuable roles in the data collection and day-to-
day needs of our research. I am grateful to all of them.
On a personal front, my husband David has become the neighborhood hero. He did
the laundry, the shopping, the housework, and guarded my time with vigilance. David
seemed to always know when I could work a little harder, and when I needed to stop. He
believed I could do this work, and he placed its importance over his own needs. If a
dissertation could have a “producer,” he would be mine. All five of our children have
supported my continued education, even though it meant I could not always be there for them
in the way I would have liked to be. And my three beautiful grandchildren are too young to
know what this is that has kept me cloistered in the back of our home for so long, but they’ve
been there to lift my spirits or make me take a break.
Aside from the valuable education I have received, my life is richer for knowing and
working with all of these people.

MATERNAL AND FETAL REPRESENTATIONS, DIMENSIONS OF PERSONALITY,
AND PRENATAL ATTACHMENT IN WOMEN HOSPITALIZED
WITH HIGH RISK PREGNANCY
Publication No.
Anna Rachel Brandon, Ph.D.
The University of Texas Southwestern Medical Center at Dallas, 2006
H. M. Evans, Ph.D.
The present study investigated the effects of self-criticism, dependency, object representation, and risk upon maternal antenatal attachment in women hospitalized during pregnancy with high risk of maternal or fetal demise. Ninety-one women completed the Depressive Experiences Questionnaire (Blatt, D’Affliti, and Quinlan, 1976), the Object Relations Inventory (Blatt et al.,1992), the Maternal Antenatal Attachment Scale (Condon, 1973), the Edinburgh Postpartum Depression Scale (Cox, Holden, and Sagovsky, 1987) and the Center for Epidemiological Studies Depression Scale (Unauthored, 1999) within the first three days of hospital admission. No relationship was indicated between maternal representations and antenatal fetal attachment, nor was there a correlation between maternal representation and fetal representation. Self-critical mothers significantly scored lower in the measure of antenatal attachment quality and endorsed a higher number of depressive symptoms. Mothers hospitalized because of maternal risk were not significantly different in their reports of attachment than were mothers hospitalized because of fetal risk, and no significant differences were found across severity of risk factors as evaluated by the Hobel Risk Assessment. Consistent with previous research, depressive symptomatology was associated with a lower quality of maternal antenatal attachment overall. Results suggest that maternal narratives may not be significantly linked with reported antenatal attachment and depressive symptoms have a stronger association with reductions of antenatal attachment than dependent or self-critical tendencies.
vii

TABLE OF CONTENTS List of Definitions 2 Chapter One: Introduction 4 History of Attachment Theory 4 The Conceptualization of Prenatal Attachment 8 The Measure of Prenatal Attachment 12 Criticism of the MFA Construct 16 The Relevance of Prenatal Attachment 18 Purpose of the Study 23 Chapter Two: Review of the Literature 25 Search Methods 26 Internal Working Models 26
Background 26 Integration of Theory 29 MFA and Object Representation 31
The Contribution of Personality 39 The Impact of Risk 46 Conclusion of Review 54 Rationale 54 Aims 56
Hypotheses 56 Primary Hypotheses 56 Secondary Hypotheses 57 Chapter Three: Methodology 59 Participants 59 Methods and Procedures 59 Measures 60 Chapter Four: Results 66 Demographic Information 66 Overview of Statistical Analyses 68 Chapter Five: Conclusions and Recommendations 84 Characteristics of the Sample 85 Discussion of Findings 89 Theoretical Implications 100 Clinical Implications 100 Limitations and Future Directions 102 Conclusion 105
viii

PRIOR PUBLICATIONS
Brandon, A. R.; Pitts, S.; Robinson, R.; Stringer, C.A. (2006). “Preliminary findings on the
associations of object representation and personality with prenatal attachment during high-
risk pregnancy.” Presented at the Winter 2006 Meeting of the American Psychoanalytic
Association, New York City.
Denton, W. & Brandon, A. R. (2006). Couple therapy in presence of mental disorders. Journal of
Couple and Relationship Therapy, In Press.
McCullough, M. M.; Orsulak, P.; Brandon, A.; & Akers, L. (2005). Rumination, fear and cortisol:
An in vivo study of interpersonal transgressions. Health Psychology, In Press.
ix

LIST OF FIGURES
Figure 1 108 Levels of Mother Narrative Conceptual Level Across Low, Medium, and High Quality of Attachment Scores
Figure 2 109
Levels of Mother Narrative Conceptual Level Across Low, Medium, and High Intensity of Attachment Scores
Figure 3 110
Quality of Attachment and Mother Narrative Conceptual Level Figure 4 111
Intensity of Attachment and Mother Narrative Conceptual Level Figure 5 112
Global Attachment and Mother Narrative Conceptual Level Figure 6 113
Distribution of Levels of ORI Narrative Conceptual Level Figure 7 114
Attachment Style Based on Below and Above Means of MAAS Quality and Intensity Factors Figure 8 115
Distributions of ORI Conceptual Levels of Mother Narrative Across DEQ Self-Criticism Scores Figure 9 116
Distributions of ORI Conceptual levels of Mother Narrative Across DEQ Dependency Scores Figure 10 117 Type of Risk and MAAS Global Attachment Scores Figure 11 118 Type of Risk and MAAS Intensity of Attachment
x

LIST OF TABLES
Table One 119 Demographic Characteristics of Total Sample Table Two 122 Pregnancy Characteristics of Sample Table Three 123 Psychiatric Characteristics of Sample Table Four 124 Means and Standard Deviations of Measures Table Five 126 Means and Standard Deviations of the Object Relations Inventory Mother Narrative for Global Attachment Above and Below the Mean Table Six 127 Means and Standard Deviations of the Object Relations Inventory Mother Narrative for Global Attachment by Standard Deviation Table Seven 128 95% Confidence Intervals of Pairwise Differences in Mean Changes Of Attachment Quality (MAAS) by Conceptual Level of ORI Mother Narrative Table Eight 129 95% Confidence Intervals of Pairwise Differences in Mean Changes Of Attachment Intensity (MAAS) by Conceptual Level of ORI Mother Narrative Table Nine 130 Frequency Distribution of Conceptual Levels of Mother and Baby Narrative Table Ten 131 Spearman’s rho Correlations for Conceptual Level and Attachment Table Eleven 132 Two-Way Contingency Table of Levels of Object Representation Of Mother and Quality of Attachment Above and Below the Mean
xi

Table Twelve 133 Two-Way Contingency Table of Levels of Object Representation Of Mother and Quality of Attachment by Standard Deviation Table Thirteen 134 Two-Way Contingency Table of Levels of Object Representation Of Mother and Intensity of Attachment Above and Below the Mean Table Fourteen 135 Two-Way Contingency Table of Levels of Object Representation Of Mother and Intensity of Attachment by Standard Deviation Table Fifteen 136 Means and Standard Deviations on Dimensions of the Object Relations Inventory for Global Attachment Above and Below the Mean Table Sixteen 137 Means and Standard Deviations on Dimensions of the Object Relations Inventory for Global Attachment by Standard Deviation Table Seventeen 138 Spearman’s rho Correlations for Object Representations of Mother and Baby Narratives Table Eighteen 139 Two-Way Contingency Table of ORI Conceptual Level of Mother Narrative by Baby Narrative Table Nineteen 140 Pearson Product-Moment Correlations of Dependency, Self-Criticism, and Maternal Antenatal Attachment Table Twenty 141 Two-Way Contingency Table of Self-Criticism (Low, Average, and High) and Antenatal Attachment Style Table Twenty-one 142 Two-Way Contingency Table of Self-Criticism (Above and Below the Mean) and Antenatal Attachment Style Table Twenty-two ` 143 Two-Way Contingency Table of Dependency (Low, Average, and High) and Antenatal Attachment Style
xii

Table Twenty-three 144 Two-Way Contingency Table of Dependency (Above and Below the Mean) and Antenatal Attachment Style Table Twenty-four 145 Two-Way Contingency Table of Self-Criticism (Low, Average, and High) and Conceptual Level of Mother Narrative Table Twenty-five 146 Two-Way Contingency Table of Dependency (Low, Average, and High) and Conceptual Level of Mother Narrative Table Twenty-six 147 Two-Way Contingency Table of Object Representation and Self- Critical Characteristics (Below the Mean and Above the Mean) Table Twenty-seven 148 Two-Way Contingency Table of Object Representation and Dependent Characteristics (Below the Mean and Above the Mean) Table Twenty-eight 149 Hobel Risk Assessment Factors Identified as Fetal Table Twenty-nine 150 Hobel Risk Assessment Factors Identified as Maternal Table Thirty 151 Means and Standard Deviations of MAAS Global Antenatal Attachment Scores Across Three Types of Risk Table Thirty-one 152 Means and Standard Deviations of MAAS Global Antenatal Attachment Scores Across Two Types of Risk Table Thirty-two 153 95% Confidence Intervals of Pairwise Differences in Mean Changes MAAS Attachment Intensity by Type of Risk Table Thirty-three 154 Two-Way Contingency Table of Three Risk Types and Antenatal Attachment (MAAS)
xiii

Table Thirty-four 155 Two-Way Contingency Table of Three Risk Types and Maternal Antenatal Attachment Table Thirty-five 156 Pearson Product-Moment Correlations for Severity of Risk and Maternal Antenatal Attachment Table Thirty-six 157 95% Confidence Intervals of Pairwise Differences in Mean Changes MAAS Attachment Intensity by Level of Risk Table Thirty-seven 158 Pearson Product-Moment Correlations for Gestational Age and Antenatal Attachment Table Thirty-eight 159 Pearson Product-Moment Correlations for Depressive Symptoms, Attachment, and Risk Table Thirty-nine 160 Correlations Between Major Demographic Variables, Depressive Symptoms (EPDS), and Antenatal Attachment (MAAS) Table Forty 161 95% Confidence Intervals of Pairwise Differences in Means of EPDS (Depressive Symptoms) Table Forty-one 162 Chi-Square Comparison of EPDS Depressive Symptomatology and MAAS Antenatal Attachment Style Table Forty-two 163 Sample Means and Standard Deviations of Standard and Three Alternate Versions of Scoring of the Depressive Experiences Questionnaire Table Forty-three 164 Sample Intercorrelations of Four Scoring Methods of the Depressive Experiences Questionnaire
xiv
Table Forty-four 165 Pearson Product-Moment Correlations of DEQ Dependency, DEQ Self-Criticism, and MAAS Antenatal Attachment Using the McGill Scoring Method Table Forty-five 166 Pearson Product-Moment Correlations of DEQ Dependency and Relatedness with MAAS Antenatal Attachment Table Forty-six 167 Pearson Product-Moment Correlations of MAAS Antenatal Attachment And Rude & Burnham’s Needy and Connectedness DEQ Scoring Method Table Forty-seven 168 Linear Regression Analyses of Dependency and Self-Criticism Scores Predicting MAAS Global Attachment Score Table Forty-eight 169 Spearman’s rho Correlation of ORI Baby Narrative and Gestational Age (Weeks) Table Forty-nine 170 Comparison of Most Common Risk Factors Table Fifty 171 Comparison of the ORI and MAAS Means and Standard Deviations from Two Samples Table Fifty-one 172 Comparisons of Correlations for ORI Mother Narrative and Maternal Antenatal Attachment in Two Samples
xv

LIST OF APPENDICES
Appendix A: IRB Approval 175 Appendix B: Letter of Consent 176 Appendix C: Measures 177 CES-D 178 DEQ 179 EPDS 183 MAAS 185 Chart Review (Hobel) 192 ORI-Mother 194 ORI-Baby 195 Bibliography 196
xvi

LIST OF DEFINITIONS Antenatal—period of gestation also referred to as “prenatal” and “antepartum.”
Antepartum—period of gestation, also referred to as “antenatal” and “prenatal.” Antepartum depression—in this discussion, refers to the onset of a major depressive episode or minor depression during pregnancy. External validity—the extent to which a study’s conclusions can be applied to populations and settings outside those of the study itself. Incidence—the percentage of the population with an illness episode that begins within a given period of time (e.g., during pregnancy or within the first 3 months following delivery). Internal Working Model (IWM)—dynamic mental representations or “templates” constructed by infants of their interpersonal world that shape expectations, responses, and interpretations of interpersonal behavior Major depressive disorder—a type of mood disorder characterized by one or more major depressive episodes. The Diagnostic and Statistical Manual, version IV, Text Revision, (DSM-IV-TR) defines a major depressive episode as a period of at least 2 weeks during which an individual experiences daily disturbance in mood (intense feelings of sadness), or loss of interest in activities that have been pleasurable in the past, and at least four of eight symptoms: (1) hypersomnia or hyposomnia, (2) changes in appetite or loss/gain of weight, (3) psychomotor agitation or retardation, (4) loss of energy (fatigue), (5) feelings of worthlessness or excessive guilt, (6) problems with concentration, (7) loss of interest in sex, and (8) recurrent suicidal thoughts or suicidal attempt. These symptoms must be present most of the day and nearly every day during the 2-week episode, must cause clinically significant distress or impairment in functioning, and must not be the result of the direct physiologic effects of a substance or a general medical condition. Major depressive disorder is not diagnosed if symptoms are attributable to an acute grief reaction; however, it is diagnosed after an acute grief reaction if the syndrome persists for two months or longer. It is not diagnosed if there is a history of manic, hypomanic, mixed episodes, or schizophrenia. Minor depressive disorder—a subthreshold diagnosis with a number of definitions (also referred to as minor depression). This term usually describes one or more episodes of depression lasting two weeks or longer but with fewer symptoms than required for major depressive disorder diagnosis. Multigravida--a pregnant woman who has carried a previous fetus to viability, regardless of outcome.
1

Multipara—a woman who has carried more than one fetus to viability, regardless of whether the offspring were born alive. Multiparity is the condition of having carried one or more fetuses to viability, and multiparous describes a woman who has borne more than one child. Object Representation—A psychoanalytic term referring to the internal mental representational aspects of a significant other person, incorporating both realistic and fantasied characteristics of the relationship. Perinatal—during pregnancy (also referred to as prenatal) and 12 months following delivery. Period Prevalence—the percentage of the population with depression over a specific period of time (e.g., during pregnancy or from delivery to the end of the first six weeks, the first three months, or the first year, etc.). Postnatal—period of time following birth referring to the infant Postpartum—period of time following birth referring to the mother lasting from parturition to 12 months after delivery. Postpartum depression—the DSM-IV-TR defines this as a specific type of major depressive disorder that has an onset of a major depressive episode within 4 weeks after delivery. In this discussion, the term will be expanded to include minor depression. Point Prevalence—the percentage of the population with depression at a given point in time Prenatal—the period of pregnancy from conception to parturition. Primagravida—A woman during her first pregnancy. Primapara—A woman who has been delivered of one infant of at least 20 weeks gestation regardless of its viability, and primaparous describes a woman in the period of time surrounding her first pregnancy. Puerperium—the 6-week period following delivery. Reliability—the extent to which a test, inventory, or scale is consistent in its evaluation of the same individuals Screening instrument—a measure or test utilized to identify an individual with respect to likelihood of having a specific disorder. A screen itself does not provide a diagnosis, however, when positive, indicates that further investigation is necessary to confirm (or disconfirm) the presence of the disorder.
2
Sensitivity—the ability of a measure or test to correctly identify those with a syndrome, calculated as the percentage of true positive values compared to false negative values. Specificity—the ability of a measure or test to correctly identify those who do not have a syndrome, calculated as the percentage of true negative values compared to false positive values. Validity—the extent to which a test, inventory, or scale measures what it is supposed to measure.
3
CHAPTER ONE Introduction
HISTORY OF ATTACHMENT THEORY
John Bowlby, a young volunteer at a school for maladjusted children, was moved by
his experiences with two young boys—one isolated and distant, the other anxious and
clinging (Ainsworth, 1968). Since neither child had a stable mother figure, he wondered if
early family relationships had profound effects upon the personality development of children.
His curiosity and desire to explore this idea, coupled with his rigorous scientific training at
the University of Cambridge, led to a reevaluation of career goals and the decision to become
a child psychiatrist (Bretherton, 1992; Senn, 1977). Subsequent work led to his formulation
of the basic tenets of what is known today as “attachment theory,” a synthesis of elements
from ethology, cybernetics, information processing, developmental psychology, and
psychoanalysis. Bowlby’s original work focused on the infant’s biological need for a
secure early attachment to the mother and the mother’s response, a major conclusion being
that a maturing child’s mental health fundamentally required that “the infant and young child
should experience a warm, intimate, and continuous relationship with his mother (or
permanent mother substitute) in which both find satisfaction and enjoyment” (Fonagy,
2001a; Bowlby, 1951; Bowlby, 1969).
Bowlby conceptualized the attachment system as an evolutionary set of behaviors
related to those of exploration, fear, affection, and caregiving. Regulation of this system,
Bowlby reasoned, was solely biological; he posited that the infant’s primary goal was to
maintain a certain degree of physical proximity to the mother for survival. Bowlby later 4

added to his stance that attachment would include psychological goals on the part of the
developing child and mother, but his insistence that attachment was an independent
behavioral system and not related to unconscious drives was a solid wedge between his
theory and the psychoanalytic theories of his training. Even though this assumption
separated him from the analytic community, key researchers such as Mary Ainsworth, James
Robertson, Rudolph Schaffer, and Christopher Heinicke aligned with him to flesh out the
theory of attachment that is understood today.
Ainsworth, in particular, believed that the infant’s contribution to the attachment
process was more than biological and included his or her own internal appraisal of the
mother’s behaviors (Ainsworth, Blehar, Waters, & Wall, 1978). The “Strange Situation,” a
20-minute laboratory test developed by Ainsworth, was the first attempt to scientifically
capture the activation of attachment system behaviors between mother and child (Ainsworth
et al., 1978). One-year-old children were exposed to two brief separations from their
mothers; the responses of both mother and baby were recorded and became the basis for a
categorical system of attachment that is still in use today. Most of the children in this study
responded to their mothers’ absence with some distress but, at her return, were rather quickly
comforted and returned to their play. These babies were thought to be “securely attached.”
About 25 percent of the babies responded to mother’s return with indifference, a category
named “insecure—anxious avoidant.” Another 15 percent sought proximity to their mothers
but displayed little or no relief from their distress when reunited. This style was also
regarded as insecure, but called “anxious resistant.” The discovery that physical separation
alone could not account fully for infant response took attachment research to a new level.
5
Ainsworth and Bowlby persevered in their investigation of the idea that cognitive
mechanisms underpinned the behavioral components of the attachment system. Bowlby
coined the term “internal working model” to describe a process of mental representation that
the preverbal infant developed of his primary caregiver. In his historical work, Attachment
and Loss: Volume I, Attachment, Bowlby described a child’s “internal world” in this way:
Starting, we may suppose, towards the end of his first year, and probably especially actively during his second and third when he acquires the powerful and extraordinary gift of language, a child is busy constructing working models of how the physical world may be expected to behave, how his mother and other significant persons may be expected to behave, how he himself may be expected to behave, and how each interacts with all the others. Within the framework of these working models he evaluates his situation and makes his plans. And within the framework of the working models of his mother and himself he evaluates special aspects of his situation and makes his attachment plans (1969; pg. 354).
Using this concept, Ainsworth’s infants must have had distinct internal representations of
their mothers and of what separation from her meant. What went unmentioned in
Ainsworth’s original study was her ability to anticipate each infant’s attachment style based
on observations of maternal behavior. Her years of home observations in Uganda had caused
her to suspect a predictive link might exist between maternal responsiveness and security of
infant attachment (Ainsworth & Marvin, 1995). Ainsworth and colleagues subsequently
introduced the concept of “sensitivity” to describe the type of caregiving she found that
correlated with secure attachment on the part of the infant (Ainsworth, Bell, & Stayton,
1974). Mothers who exhibited sensitive caregiving behavior were those able to (a) attune to
infant’s signals with attentiveness, (b) appropriately interpret the signals, (c) respond
appropriately to the signals, and (d) react promptly, in a time period that did not provoke
excessive frustration for the child. Highlighting that central to the internal working model
was the expected availability and response of the attachment figure injected an importance
6

into the actions of the maternal part of the dyad that the previous systemic view of
attachment behaviors had not (Sroufe & Waters, 1977; Bowlby, 1973). Bowlby continued
to refine his approach, further hypothesizing that a child’s internal working model of self
takes a complementary position to the representation the infant has of his caregiver. In the
most primary form of this collaboration, the child evolves a representation of how acceptable
or unacceptable he is by how he feels his caregiver views him. More complex forms of this
transaction appear all through life in self-other relationships (Fonagy, 2001b).
Those who followed Bowlby and his fellow pioneers of theory moved beyond infancy
and began exploring attachment through the internal worlds of young children (Main,
Kaplan, & Cassidy, 1985), adolescents (Kobak & Sceery, 1988), and adults (George, Kaplan,
& Main, 1985). The Adult Attachment Inventory (AAI), developed by George et al.,
consists of a series of open-ended probing questions designed to elicit as many details as
possible about the individual’s childhood attachment experiences and personal evaluations of
the effects those early events have on current life functioning (George et al., 1985). This
enabled researchers to compare adult and child attachment within the same theoretical
framework and categorization strategy. The next wave of research divided adult attachment
into two distinct perspectives: parenting and romantic relationships (Bartholomew & Shaver,
1998; Hazan & Shaver, 1987; Bartholomew & Horowitz, 1991). Moving from the
behavioral level to the representational level allowed the exploration of how early attachment
experiences were remembered by adults as well as how these memories might act as
templates for interpersonal relationships (Main et al., 1985). This has broadened the
application of attachment theory to all stages of life, including an empathic understanding of
7

the emotional significance of death and dying (Kubler-Ross, 1969). In each vein of research,
behavioral, emotional, and cognitive markers have been identified to enable the measurement
of attachment and, since Ainsworth’s first measure, numerous objective and projective
instruments have been developed for examining childhood, adolescent, and adult attachment.
THE CONCEPTUALIZATION OF PRENATAL ATTACHMENT
It is only fitting that theoretical analyses of the experience of pregnancy largely began
with women theorists. Deutch, Bibring, and Benedeck explained prenatal attachment in
psychodynamic terms as a process in which a pregnant woman’s libidinal energy was
cathected into the fetus (Deutch, 1945; Bibring, 1959; Bibring, Dwyer, Huntington, &
Valenstein, 1961; Benedek, 1959; Benedek, 1958). They hypothesized that the fetus
becomes more human to the woman as pregnancy progresses, and eventually the fetus
becomes loved both as an extension of self and as an independent object. While this was
fascinating material, one of the first empirical suggestions that there was some prenatal
connection between mother and fetus came from Kennell and Klaus’ observations of the
intense grief exhibited by mothers of infants who died during birth (Kennell, Slyter, & Klaus,
1970). This team found maternal grief uninfluenced by whether or not the mothers had any
physical contact with the babies after delivery. Additional work by Klaus and others drew
attention to the deleterious effects of early separation between mother and neonate and
introduced ways of enhancing early postnatal attachment (Klaus et al., 1972). These new
ideas launched scientific inquiry by a few key individuals, bringing about the formulation of
the construct of prenatal attachment within both medical and psychological communities.
8

Rubin, a nurse specializing in maternity care doing doctoral work at the University of
Chicago, led the way as she explored women’s attainment of the maternal role, concluding
that the immediate bond between postpartum mother and neonate was a consequence of
prenatal processes (Rubin, 1967; Rubin, 1975). Rubin identified four specific tasks the
women she observed navigated before childbirth: (1) Seeking safe passage for self and baby,
(2) ensuring that the baby is accepted by significant others, (c) binding-in to the fetus, and (4)
giving of herself. These tasks formed a framework for early investigation of the
psychological experience of pregnancy.
Meanwhile, a perinatal epidemiologist in Australia interviewed 30 primagravidas
(first pregnancies) at various time points throughout the three trimesters of pregnancy and
found they were able to conceptualize their babies in an increasingly human way over the
passage of time (Lumley, 1972). The introduction of ultrasound during pregnancy inspired
her to examine the impact on maternal bonding of a visual image of the fetus (Lumley,
1980). Lumley’s findings suggested this early view of the fetus enhanced a mother’s ability
to differentiate it as a “little person.” Her next project was one of the first empirical
longitudinal studies of prenatal attachment. Through the use of simple tape-recorded
interviews at 5 time points before and after childbirth, she attempted to capture first-time
parents’ attitudes of their fetus. She conceptualized attachment as being an “established
relationship with the fetus in imagination,” a point at which mothers thought of their babies
as a “real person” (Lumley, 1982). Lumley reported this phenomenon in 30% of her subjects
in the first trimester, 63% in the second trimester and, by 36 weeks gestation, in 92%. She
9

interpreted delayed attachment as being related to unpleasant symptoms of pregnancy and
lack of interest or support on the part of husbands.
Leifer, a psychologist at the Illinois Institute of Technology, was the author of a
monograph reporting findings from a study of 19 primigravidas on the psychological changes
observed during the course of gestation (Leifer, 1977). She concluded that, while pregnancy
was a time of emotional upheaval and rapid role change, it was also a time of developmental
maturation. Leifer introduced the element of personality into the psychological state of
pregnancy, concluding the degree of personality integration achieved during the first months
of pregnancy could predict psychological growth throughout the rest of pregnancy and into
early motherhood.
While early formations of prenatal attachment came from the psychoanalytic
approach, the study of the concept was carried on in earnest by nurses, often in the process of
graduate work. Mecca Cranley, for example, wrote the first literature review of the subject
as her dissertation, proposing a multidimensional model composed of six aspects of
maternal-fetal attachment she had identified from her research: Differentiation of Self from
Fetus, Interaction with the Fetus, Attributing Characteristics to the Fetus, Giving of Self,
Role Taking, and Nesting (Cranley, 1979). Cranley is also credited with the first formal
definition of the construct of maternal-fetal attachment (MFA): “The extent to which women
engage in behaviors that represent an affiliation and interaction with their unborn child”
(Cranley, 1981).
Muller, a researcher who utilized Cranley’s construct of maternal fetal attachment,
ultimately found this strategy of conceptualizing the phenomenon focused on behaviors to
10

the exclusion of the thoughts and fantasies which also revealed the growing affiliation
between mother and fetus (Muller, 1993). In her dissertation work, she redefined prenatal
attachment as “the unique relationship that develops between a woman and her unborn fetus.
These feelings are not dependent on the feelings the woman has about herself as a pregnant
person or her perception of herself as a mother” (Muller, 1990). An Australian researcher,
John Condon, also found Cranley’s work insufficient in the description of MFA. He went
back to adult attachment theory and proposed Bretherton’s broad view of attachment as an
“emotional tie” or “psychological bond” to a specific object was not only applicable to MFA
but added coherence to the construct (Condon, 1993; Bretherton, 1985). Condon suggested
that antenatal attachment contained the core experience of love, and could be described as a
developing relationship in which the mother seeks “to know, to be with, to avoid separation
or loss, to protect, and to identify and gratify the needs of her fetus.” He later formally
defined prenatal attachment as simply “the emotional tie or bond which normally develops
between the pregnant parent and her unborn child” (Condon & Corkindale, 1997). Now
there were three definitions to the developing construct of prenatal attachment that did not
have much in common.
The most recent conceptualization of prenatal attachment has attempted to combine
these behavioral, cognitive, and emotional approaches with this working definition: “Prenatal
attachment is an abstract concept, representing the affiliative relationship between a parent
and fetus, which is potentially present before pregnancy, is related to cognitive and emotional
abilities to conceptualize another human being, and develops within an ecological system”
11

(Doan & Zimerman, 2003). However, no consistent use of any of these four definitions of
the construct has been noted in recent research.
THE MEASURE OF PRENATAL ATTACHMENT
Cranley developed the first antenatal attachment scale, the Maternal Fetal Attachment
Scale (MFAS), using the six aspects she had conceptualized in her dissertation work
(Differentiation of Self from Fetus, Interaction with the Fetus, Attributing Characteristics to
the Fetus, Giving of Self, Role Taking, and Nesting; Cranley, 1981; Cranley, 1979). She
asked clinicians and childbirth educators to identify statements made by their patients that
implied MFA; the resulting 37 items were then administered to 71 pregnant women between
35 and 40 weeks gestation. Due to a lack of statistical reliability, she eliminated the Nesting
aspect after this pilot of the scale. The resulting 24-item instrument yielded five subscales
and one global measure of maternal-fetal attachment. Having an instrument pushed MFA
research ahead quickly; most previous studies had been qualitative with small samples. The
MFAS gave the field a quantitative measure appropriate for cross-sectional studies of larger
samples (Grace, 1989) and, 25 years after its development, continues to be the instrument
used most frequently by nurse researchers in prenatal studies (Beck, 1999b).
Muller’s personal research utilizing the MFAS and her subsequent 1992 literature
review found no consistent results; in fact, findings were often either inconclusive or
contradictory (Muller & Ferketich, 1992; Muller, 1992). She began to entertain doubt that
Cranley’s five subscales truly captured prenatal attachment, and even wondered if MFA
could be viewed in such a multidimensional fashion (Muller & Ferketich, 1993). Another
12

research team also questioned the theoretical base of the MFAS, as well as its reliability and
validity (Mercer, Ferketich, May, DeJoseph, & Sollid, 1988). The Mercer team made data
from a study on antepartum stress available to Muller, and she conducted a secondary
analysis of the interviews with those participants (Mercer, Ferketich, DeJoseph, May, &
Sollid, 1988). Her findings indicated only three of Cranley’s subscales corresponded with
the categories generated by the interview data, and two (Giving of Self and Interaction with
the Fetus) did not correspond at all (Muller et al., 1992; Beck, 1999a). As Muller suspected,
Cranley’s items were not capturing certain emotional elements Muller documented from the
open-ended interviews of women in the Mercer et al. study (1988). Mercer participants often
made statements about their unborn babies using words like “hope,” “wish,” and “imagine;”
they seemed to be expressing feelings rather than just engaging in behaviors. This analysis
led to the development of a new scale, the Prenatal Attachment Inventory (PAI; Muller,
1990). The 29 items of this instrument were designed to measure affectionate attachment or
the personal relationship that develops during pregnancy between mother and fetus. The
construction reflected Muller’s disagreement with a multidimensional view of MFA and
contained no subscales, providing only a global score. Muller’s intent was for this scale to
emphasize affiliation, exclude behavioral measures, and stand as an adjunct to Cranley’s
MFAS, with the goal of increasing agreement across studies (Muller, 1993). Muller also
conceptualized a new model of attachment in pregnancy, postulating that an expectant
mother’s early experiences with her primary caregiver led to the development of internal
representations, which then influenced subsequent attachments to family, partner, and
13
friends. Ultimately this process enabled a woman to adapt to pregnancy and attach to her
fetus.
Muller’s claim that the MFA construct was unidimensional and her assertion that the
PAI yielded only one global measure was challenged some years later by a research team
with a sample of 171 Swedish women in their third trimester of pregnancy (Siddiqui,
Hagglof, & Eisemann, 1999). Their analysis revealed an underlying dimensional structure
with five identifiable factors representing recurrent themes that accounted for 53.9% of the
variance: Affection, differentiation of self from fetus, interaction, sharing pleasure, and
fantasy. The team proposed that Muller’s measure actually supported a multidimensional
construct of MFA, pointing out several possible explanations for the disagreement. Their
most convincing argument was that Muller’s work had been conducted on women at various
points in their pregnancy, anywhere between 14 and 40 weeks of gestation, while the
Siddiqui et al. team administered the PAI during the third trimester only (between the 36th
and 40th week of gestation). Since literature was abundant with recent findings strongly
indicating that MFA increased through the course of the pregnancy (Cranley, 1981; Grace,
1989; Lerum & LoBiondo-Wood, 1989), Muller’s data was confounded by this variation
(Siddiqui et al., 1999).
The newest instrument on the MFA scene was developed in Australia by John
Condon (Condon, 1993; Condon & Corkindale, 1998). Condon believed that the existing
instruments inadequately differentiated the attitude toward the fetus from the attitude toward
the state of pregnancy and motherhood. He included 19 items in his Maternal Antenatal
Attachment Scale (MAAS), focusing exclusively on thoughts and feelings about the baby
14

and ignoring attitudes about the physical state of pregnancy or the maternal role. Two
factors, “quality” and “intensity,” were generated. “Quality” described the affective
experiences the mother reported, such as closeness/distance, tenderness/irritation,
positive/negative, joyful/unpleasant anticipation, and a vivid/vague internalized
representation of the fetus as a real person. “Intensity” referred to the amount of time she
spent thinking about, talking to, dreaming about, or tactilely interacting with the fetus.
Condon mapped these two factors as perpendicular continuums, forming four quadrants of
attachment style.
One other scale, the Prenatal Maternal Attachment Scale, is mentioned in the
literature, however, only one published study in addition to the initial methodological study
has reported its use (Fowles, 1996; LoBiondo-Wood & Vito-O'Rourke, 1990). 29 items are
designed to be administered at any time during pregnancy, and 10 additional items are
completed only after quickening is experienced.
Of these described instruments, Cranley’s MFAS and Condon’s MAAS are the two
most commonly used measures (Laxton-Kane & Slade, 2002). While it is beyond the scope
of this discussion, it also must be noted that both Cranley and Condon have constructed
paternal adaptations of their measures, hypothesizing that there may be a complementary
paternal-fetal attachment process (Weaver & Cranley, 1983; Condon, 2005). No doubt these
multiple approaches to capturing the attachment process have stimulated the increased
attention and empirical research devoted to MFA, with particular curiosity concerning
relationships between the nature of such attachment and the mother’s early parenting
experiences, her cognitive capacity to develop an internal working model of her fetus, her
15
own adult attachment style, her level of social support, and links to perinatal depression,
anxiety, and postnatal attachment (Cannella, 2005).
CRITICISM OF THE MFA CONSTRUCT
Bowlby’s original theory was built on the premise of reciprocal elements in the
attachment system. Since prenatal attachment can only be investigated through one part
(mother) of this system, some feel that attachment cannot be measured antenatally with any
validity. In addition, the concept of prenatal attachment requires a view of the motivation of
security counter to the original theory of the attachment system. Infant and adult attachment
in the Bowlbian sense had the goal of security seeking; attachment behaviors were triggered
by distress and fear of separation from the attachment figure. In maternal antenatal
attachment the mother provides (or may feel responsible for providing) security for the fetus.
It has been proposed that prenatal attachment is more appropriately viewed as an “emotional
bond” that bears similarities to attachment but is not the same as traditional infant and adult
attachment (Pollock & Percy, 1999). Along this line of thinking, it has been suggested that
prenatal attachment inventories are no more than attitude measures that may be confounded
by social desirability and adjustment (Waters, 2005).
That pre- and post-birth attachments may require different conceptual frameworks is
inarguable; nevertheless, their interrelationship is visible in the consistent attention the
Bowlbian contingent gives to the mother’s own cognitive representations of caregiving and
by viewing the feelings and behaviors related to this internal working model as critical to her
contribution as an attachment figure for her infant. The possibility there is a convergence
16
between MFA and mother-infant attachment is illustrated by the association found between
measures of prenatal attachment and the following: Postnatal attachment style categorization
(Muller, 1996b), parental behavior before and after birth (Condon et al., 1997; Pollock &
Percy, 1999), maternal feelings for the neonate after delivery (Leifer, 1977), feeding behavior
and maternal sensitivity to an infant’s cues, (Fuller, 1990), and postnatal maternal
involvement with the infant (Siddiqui, Hagglof, & Eisemann, 2000). This author suggests
that, in the absence of the infant’s contribution to the matrix (appearance, temperament, etc.),
measuring prenatal attachment may provide an avenue for a purer investigation of factors
that are solely maternal, such as the mother’s own personality, attachment style, and mental
representations of her own early caregiving experiences.
In addition, the issue of reciprocity may be less important if the expectant mother
assigns reciprocity to the fetus in terms of movement and activity. A literature review of
prenatal attachment found that quickening, or discernable fetal movement, was consistently
found to be positively correlated with attachment as measured by questionnaires (Muller,
1992). In one randomized controlled observational study of a sample of 213 women with
uncomplicated pregnancies, fetal movement counting resulted in a statistically significant
increase in total attachment scores on the Cranley scale of maternal-fetal attachment (Mikhail
et al., 1991). Zeanah et al. reported that mothers with higher levels of prenatal attachment
perceived more movement from their fetus’ than those with lower attachment (Zeanah, Carr,
& Wolk, 1990). Additionally, an exploratory study of 26 couples proposed four levels of
parental awareness during the third trimester of pregnancy, one of which was “awareness of
infant interactive ability” (Stainton, 1990). Some participants described their infants as
17

actively participating in communication with them by moving toward abdominal stroking,
extending a limb, or increasing/decreasing activity when certain voices were present.
Lastly, fetal perceptions in utero are largely unknown. Some theorists have
hypothesized that intrauterine experience appears to leave “dim residues” that influence later
preference for open versus closed spaces (Balint, 1959), sleeping positions, and sensory
sensitivities (Piontelli, 1987; Piontelli, 1988). Neonatal research has found that newborns
can recognize their mother on the basis of visual cues alone (Bushnell, Sai, & Mullin, 1989),
by voice (Fifer, 2002), and by odor (Porter, Winberg, & Varendi, 2005). In one older trial,
neonates could produce either the mother’s voice or the voice of another female by sucking
on a nonnutritive nipple in different ways (DeCasper & Fifer, 1980). It is not inconceivable
that, beyond our measurement ability, some intrauterine fetal phenomenon complementary to
MFA takes place. Therefore, without disregarding the issues raised concerning the validity
of prenatal attachment measures, the literature available supports their use in further research
(Beck, 1999c).
THE RELEVANCE OF PRENATAL ATTACHMENT
Bowlby and colleagues illustrated how critical responsive and sensitive caregiving is
for the psychological health of humans from infancy through development, and the
contributions of the others described in this discussion have strongly suggested mothers
develop caregiving capacity through a variety of prenatal processes. As a result, from a
clinical standpoint, the concept of antenatal attachment has facilitated an understanding of
the pregnancy period, as well as an understanding of the emotional cost of the loss of a fetus
18

(Laxton-Kane et al., 2002; Stainton, 1990a; Boyce & Condon, 2000; Condon, 1986; Frost &
Condon, 1996). However, refinements of the theoretical construct tested via hypotheses in
correlational, comparative, and longitudinal designs are sorely needed (Cannella, 2005).
Along with increased empirical knowledge comes responsibility to investigate ways to
identify mothers at risk for poor attachment and interventions that can adequately prepare
women for motherhood. Women unsure of their attachment may respond to appropriate
interventions, and women unaware of or unconcerned about their attachment to their fetus
may benefit from education and motivation (Shieh, Kravitz, & Wang, 2001). While some
interventions promoting prenatal attachment have been introduced, there is much more to be
learned about the concept of attachment, what facilitates its growth, and what prevents or
stifles it (Carter-Jessop, 1981; Carson & Virden, 1984; Mikhail et al., 1991; Cranley, 1992).
Studies of the use of MFA to predict postnatal mother-infant attachment are
inconclusive in light of inconsistent research and the few available longitudinal studies.
Modest correlations have been found between an unpublished measure of attachment and
maternal feelings of attachment 24 hours after delivery (Reading, Cox, Sledmere, &
Campbell, 1984), prenatal psychological functioning and postnatal attachment (Leifer, 1980),
MFAS scores and postnatal maternal interaction (Fuller, 1990), Prenatal Attachment
Inventory (PAI) scores and the Maternal Attachment Inventory (an attitude-based postnatal
measure) (Muller, 1996a), PAI scores and postnatal maternal involvement (Siddiqui &
Hagglof, 2000), MFA and maternal competence (Mercer & Ferketich, 1994), and MFA and
mutuality in family relationships and infant mood (White, Wilson, Elander, & Persson,
1999). These longitudinal studies describing contributors to secure attachment are clinically
19

significant, but also demonstrate how much more work needs to be done in order for a
complete understanding of the impact of MFA quality on the next generation.
A generational quality to attachment is suggested by a benchmark study conducted in
Great Britain with a sample of 100 primagravidas (Fonagy, Steele, & Steele, 1991). On the
basis of AAI classifications given to expectant parents during the last trimester of pregnancy,
the research team was able to predict the Strange Situation category of infant attachment to
parent when the child was 1 year of age. The correlation between parents and babies styles
in the “secure” and “insecure” categories was robust (r = 0.75). This suggests that a parent’s
state of mind in regard to attachment has an enormous effect upon the quality of attachment
of their child (this is not to suggest that significant life events during the first year of life do
not have an effect). These findings stimulated many replication studies with the same link
between secure mothers and secure babies, and insecure mothers and insecure babies
(Levine, Tuber, Slade, & Ward, 1991; Mikulincer & Florian, 1999; Priel & Besser, 2000b).
The implication that we might be able to target families at risk for insecure attachment
provides a new venue for developing interventions to break vicious cycles and foster
healthier attachment.
Attachment theory has also provided another way of conceptualizing the vulnerability
to or etiology of psychopathology. By the publication of his second volume in the
Attachment and Loss series, Bowlby was hypothesizing links between insecure attachment
and particular psychopathologies, such as phobias (Bowlby, 1973). Later prospective studies
by a plethora of researchers have connected insecure attachment with conduct disorders,
parental depression, parental schizophrenia, borderline personality disorder, adolescent
20

suicidal acting-out, and vulnerability to psychopathology in childhood (Brisch, 2002). As
research on attachment disorders continues, new importance is ascribed to early identification
and intervention. Inge Bretherton aptly applies one of Freud’s statements:
So long as we trace the development from its final outcome backwards, the chain of events appears continuous, and we feel we have gained an insight which is completely satisfactory or even exhaustive. But if we proceed in the reverse way, if we start from the premises inferred from the analysis and try to follow these up to the final results, then we no longer get the impression of an inevitable sequence of events which could not have otherwise been determined (Bretherton, 1992; Freud, 1955).
It is an estimable goal to have enough knowledge about the role of MFA to “proceed in the
reverse way,” and endeavor to make the “inevitable sequence of events” in incomplete
mother-child attachment not so inevitable.
Poor attachment has not surprisingly been associated with the painful topic of fetal
and child abuse. A study in England with a sample of 40 women referred by Social Services
departments suggested that “negative preoccupied” antenatal attachment (as measured by the
Maternal Antenatal Attachment Scale) was predictive of an increased likelihood of
symptoms of anxiety, mood disturbance, and depression, self-reported irritation with the
fetus, and even fetal abuse (Pollock & Percy, 1999). Other researchers have looked at the
association between insecure attachment in mothers and the incidence of child abuse and
found positive correlations (Moncher, 1996). Contrastingly, strong MFA has been associated
with positive health practices during pregnancy, such as abstinence from tobacco, alcohol,
and illegal drugs, obtaining prenatal care, healthy diet and sleep habits, adequate exercise,
use of seat belts, and learning about pregnancy, childbirth, and infant care (Lindgren, 2001;
Lindgren, 2003).
21

Quality of attachment has also been associated with the perinatal mental health of the
mother. Weak attachment and negative maternal attitude have been associated with
postpartum anxiety (Blumberg, 1980; Gaffney, 1989) and depression (Condon et al., 1997;
Lindgren, 2001). On the other hand, strong attachment was found to be a moderator of the
vulnerability to postpartum depression in one sample of women in Israel (Priel & Besser,
1999). Personality vulnerability factors to depression were measured, and highly self-critical
women reported less depression when strongly attached to the fetus during pregnancy.
However, as reported in one integrative review, associations between attachment and
psychosocial variables have been disappointing (Cannella, 2005). Methods used across
studies have been inconsistent, psychometric properties of all instruments have not been
consistently valid and reliable, and the relationships investigated were exploratory rather than
theoretical. It was concluded that correlational studies utilizing theory-driven variables are
necessary for more significant findings.
An important factor for consideration is the large gap in existing research with
diverse populations. Psychometric data of current prenatal attachment measures has largely
been established using samples of low-risk, middle-class, American, Caucasian pregnant
women (Shieh et al., 2001). An increasing number of samples of women with high-risk
pregnancies (defined in this work as “fetal anomaly and/or the presence of a chronic disease
or pregnancy-induced disease threatening maternal or fetal health and carrying an increased
chance of mortality for either mother or fetus”) are being included in research, but only a few
published studies have included risk serious enough to require hospitalization (Penticuff,
1982). The reliability and validity of the existing tools for high-risk women is unknown, as
22
are the consequences of risk on parental adaptation and patterns of attachment. In addition to
the health/mortality concerns, high risk pregnancies include the significant possibility of fetal
anomaly and/or extreme prematurity. Extreme prematurity has been associated with a higher
incidence of insecure attachment; ongoing longitudinal work is examining this further, taking
into consideration the neurobiological risk factors (Brisch, 2002).
Finally, the children of societies everywhere deserve mothers (and fathers) prepared
for the awesome challenge of loving and training new humans. Five decades of research has
emphasized that caregiver response is the central element in how a child understands self and
others. John Bowlby expressed this most cogently:
Just as children are absolutely dependent on their parents for sustenance, so in all but the most primitive communities, are parents, especially their mothers, dependent on a greater society for economic provision. If a community values its children it must cherish their parents (Bowlby, 1951).
PURPOSE OF THE STUDY
In line with the recommendations of the works cited, this research will undertake a
theory-driven approach to the study of attachment in a sample of women hospitalized with
high-risk pregnancies. The purpose of this study is to investigate the influence of an
expectant mother’s personality style, her maternal object representations, and her ability to
develop an internal representation of her fetus upon the quality and intensity of maternal fetal
attachment. The exploration of the power of object representation and personality to predict
prenatal attachment in the context of hospitalization during high-risk pregnancy would have
relevance in both intervention and standard of care for such mothers. Since this is a highly
23

specialized sample of individuals, it is expected that other variables may have predictive
value. Prior depressive episodes, current levels of depression, type and severity of maternal-
fetal risk, as well as gestational age of the fetus at the onset of complications will be taken
into account.
The construct of MFA discussed in this work will be identified as suggested by Doan
and Zimmerman: “Prenatal attachment is an abstract concept, representing the affiliative
relationship between a parent and fetus, which is potentially present before pregnancy, is
related to cognitive and emotional abilities to conceptualize another human being, and
develops within an ecological system” (2003). Working on the assumption that MFA exists,
instruments developed from the psychodynamic approach will be employed to examine the
cognitive and emotional abilities of an expectant mother to conceptualize her own mother as
well as her fetus. Additionally, in view of the proposition that emotional factors preexisting
pregnancy are important potential determinants of prenatal attachment (Doan et al., 2003;
Mikulincer et al., 1999), the contribution of personality variables will be examined (Blatt,
Shahar, & Zuroff, 2001; Priel et al., 1999). The “ecological system” in this work will consist
of the situation of hospitalization due to high maternal or fetal risk, defined earlier as an
increased probability of fetal anomaly, compromises of maternal or fetal health, or maternal
or fetal demise. The literature review has been conducted consistent with these factors of
interest.
24

CHAPTER TWO
Review of the Literature
Since Cranley’s creation of a measure for her theoretical construct of maternal-fetal
attachment (MFA), there have been approximately 50 published studies incorporating some
measure of antenatal attachment in the research. The psychosocial variables examined have
included social support, interpersonal relationships, self-esteem/self-concept/sense of
mastery/efficacy, anxiety, depression, stress, and coping styles. Demographic characteristics
such as parity, age, level of education, and ethnicity have been incorporated into hypotheses
or analyzed post hoc. Biological variables such as previous substance abuse, maternal health
history, previous perinatal deaths, and maternal/fetal health outcomes have also been
correlated to attachment, and some studies have divided their sample by the presence or
absence of maternal-fetal risk. A few studies have concentrated on women with some level
of this risk, and even fewer have focused exclusively on women with risk severe enough to
require hospitalization. To date, there have been no examinations of the possible
relationships between personality style, object representations, severity of risk, and
attachment within a hospitalized population. However, there are bodies of research that
contribute significantly to our understanding of these factors in other contexts and with other
populations.
25
SEARCH METHODS
Relevant MFA studies published from 1981 (publication date of the Maternal Fetal
Attachment Scale) through 2005 were located through the use of various databases, including
Medline, Psychological Information, and Cumulative Index to Nursing and Allied Health
Literature. An ancestry approach (tracking research cited in studies reviewed) was also
employed to ensure the review of any articles missed in the database search. Dissertations
were excluded, as were articles written in languages other than English. The keywords used
were prenatal attachment, antenatal attachment, MFA, maternal-fetal attachment, internal
working model, object representation, mental representation, prenatal object relations,
personality, and high risk pregnancy. Abstracts of all articles supplied in the database
searches were reviewed to identify studies relevant to this review. Studies that incorporated
measures and discussions central to prenatal attachment, object representation, and
personality characteristics were all considered relevant. While this study is confined to
women who are hospitalized, studies that included non-hospitalized women were included in
light of the paucity of research with the hospitalized population. The studies reviewed are
categorized by their contribution to the understanding of the relationship of attachment to
object representation, personality, and risk.
INTERNAL WORKING MODELS AND OBJECT REPRESENTATION
Background
Bowlby’s premise of internal working models is reminiscent of the concept of object
representation proposed by Melanie Klein, from the very psychoanalytic approach that
26

Bowlby questioned. However, his concept of the “internal working model” has been
attributed to the psychologist and philosopher Kenneth Craik and his 1943 work, The Nature
of Explanation (Bretherton, 1992). Craik proposed that the human mind built “mental
models” of reality that were utilized to anticipate events and produce action. This internal
representational paradigm fit well with Bowlby’s belief that some cognitive mechanism was
at work with the biological system of attachment, for notice his connection in Attachment
and Loss Volume I: Attachment:
“If an individual is to draw up a plan to achieve a set-goal not only must he have some sort of working model of his environment, but he must have also some working knowledge of his own behavioural skills and potentialities… Henceforward the two working models each individual must have are referred to respectively as his environmental model and his organismic model… The environmental and organismic models described here as necessary parts of a sophisticated biological control system are, of course, none other than the ‘internal worlds’ of traditional psychoanalytic theory seen in a new perspective” (p.82).
The “new perspective” in this case had several facets. First, Bowlby held that these models
were based on real experience. Psychopathology resulted because a model “might become
totally out-of-date, or because it is only half revised and therefore remains half out-of-date, or
else because it is full of inconsistencies and confusions” but not because of unconscious
drives that generated fantasies that became internal representations (Bowlby, 1969). Second,
Bowlby pulled from the work of Spitz and Piaget to support his proposal that infants before
the age of nine months were not aware of the human characteristics of the “object;” in fact,
an infant could not even perceive of the “object” as having any permanence. He favored
Spitz’ term, “pre-object relation,” as well as Spitz’ idea that a smiling infant was responding
to a “visual gestalt signal,” not relating to a human. This fit in nicely with Bowlby’s thesis
that the five responses which made up attachment behavior—sucking, clinging, following,
crying, and smiling—were behavior patterns specific to man in much the same way that each 27
species in the animal world was endowed with its own peculiar repertoires of behavior.
Third, Bowlby also differentiated his term “instinctual response” from the usage of the term
“instinct” in psychoanalytic terms. Whereas psychoanalytic instinct referred to a
motivational drive, Bowlby’s term referred to an “observable pattern of behavior” that served
the evolutionary purpose of survival (Bowlby, 1986). Bowlby believed that during
maturation these early behavior patterns would move between various states of latency and
activity, being used in “fresh combinations.” Even the infantile behaviors like crying and
clinging would re-emerge in situations of danger, illness, or helplessness. Stress and
uncertainty could compromise adult-acquired defenses and infantile internal working models
would serve as defaults to guide behavior.
On the other hand, Melanie Klein’s conceptualization of “internal objects” (“object”
referring to a significant person in an emotional relationship) came from the psychoanalytic
view that Bowlby believed needed a “new perspective.” Klein extended Freud’s role of
fantasy as a specific mental process provoked by frustration to that of an elaborate collection
of unconscious images and knowledge that are the core of all mental processes. Klein
theorized that the child’s mental life is filled with fantasy as he establishes a complex set of
internalized object representations based on his experiences with primary caregivers. These
fantasies and anxieties concerning the internal objects become the underlying basis for an
individual’s behavior, emotions, and sense of self. Like Freud, she fueled these fantasies
with hypothesized libidinal drives and oedipal conflicts; unlike Freud, the drives are
essentially psychological forces always directed toward objects. Kleinian internal objects are
largely fabrications of the child’s unconscious drives and wishes inspired by the child’s
28

experience with real others (Greenberg & Mitchell, 1983). This drive model was integral to
the discussions of the psychological processes in pregnancy conducted by the earliest
psychoanalysts (Deutch, 1945; Benedek, 1959; Bibring, 1959).
Another contrast between attachment theory and object relations theory is how
research for each of these models was conducted. In the psychoanalytic world, investigations
of object representation were usually based on clinical case studies. Since quantitative
research was not an appropriate venue for exploring abstract conceptualizations of drive
theories, most writings were of clinical experiences with patients, often quite ill individuals.
Attachment theory, on the other hand, essentially came from work and study with normal
children and adults. The influence of ethological and biological research on these theorists
propelled them into empirical based research methods that had far greater generalizability
than the case-study driven work of the psychoanalysts.
Integration of Theory
For decades differences like these between attachment theorists and psychoanalytical
object-relational theorists prevented them from engaging in collaborative dialogue. In recent
years, there has been movement toward an integration of ideas made possible by several
changes. Peter Fonagy outlines these as: 1) A trend in attachment theory to move focus from
infant behavior and external determinants to greater interest in internal representations in
both infant and parent; 2) growing importance for observational and empirical research in the
psychoanalytic community, due to an awareness of the shortage of models that are both
scientifically acceptable and relevant to clinicians; 3) an openness between theoreticians to
integrated approaches and new ideas; and 4) the realization on the part of attachment
29

theorists that without growth through the integration of other approaches the attachment
model would remain stunted in terms of providing value to clinical work, enriching research,
and developing new theory (Fonagy, 2001a). Integrating Bowlby’s internal working model
with object representation is such an example of this new landscape.
Today’s understanding of internal working models is an amalgam of the contributions
of Bowlby, Ainsworth, Bretherton, Mulholland, Crittenden, Main, and Sroufe (Fonagy,
2001a). Fonagy depicts their composite description of the internal working model as an
evolution of four basic components: 1) Expectations based on transactions with and
interactive attributes of the primary caregiver created in the first year, 2) event
representations generated by general and specific memories of attachment-related
experiences, 3) autobiographical memories by which specific events are connected and
contribute to an ongoing personal narrative, and 4) the resulting inferential understanding of
the psychological characteristics of others and self (p. 14). Moving past the strict
interpretations of an internal working model as an imprint of historical relational
interchanges and an object representation as an elaborate concoction of libidinal-driven
fantasy allows a fresh paradigm: Mental representations and internal working models can be
described as reflections of reality-based early experiences with caregivers that are colored by
internal perceptions and transformations (Priel & Besser, 2001). Not ignoring the gap
between attachment and object relational theories, it has been proposed that these two
concepts overlap in a fashion that allows the quality of mothers’ mental representations to
predict the mother-infant attachment (Levine et al., 1991). This reconciliation of approaches
30
has inspired new forays in research with clinical relevance, particularly in the discussion of
MFA.
MFA and Object Representation
Attachment
Bowlby himself believed that the transition of a woman to motherhood mobilized the
same “forces” that had in early infancy and childhood attached her to her own mother (1986).
Some years later, Rubin restated this in her early discussion of the tasks required to fully
attain the maternal role, reporting “Mother was a major prototype and was the most
significant contributor of subject’s set of anticipations in becoming a mother” (Rubin, 1967).
If the participant’s mother was deceased, she was either interjected into the interviews in the
form of memory, or augmented by an aunt, mother-in-law, grandmother, or a person of the
mother’s generation who may have had a maternal relationship with the subject. Rubin
likened this to the “binding-in” task with the fetus, stating that her subjects seemed to also be
“binding-in” again with the mother or mother substitute. In cases where the expectant
mother was separated from her mother by distance, Rubin found that often there was an
actual or “wished-for” trip that seemed almost like a “pilgrimage.”
While not specifically looking at MFA, the Fonagy, Steele, and Steele (1991)
research appears to be the first that empirically explored the association between adult and
infant attachment style in a prospective manner beginning in pregnancy. In this longitudinal
study, the Adult Attachment Interview (AAI) was administered to 100 primagravidas in their
last trimester of pregnancy. At 12 months postpartum, the mothers and infants were assessed
in the Strange Situation exercise. An impressive 75% of mothers categorized as secure had
31
securely attached children; 73% of mothers classified in one of the insecure descriptions had
insecurely attached children. A second finding relevant to the discussion of object
representation in internal working models is that the quality of those relationships could be
measured by the expectant mother’s ability to articulate a complex representation of the
expectant mother’s relationships with her parents. These women were able to:
“fluently convey a global representation (whether favorable or unfavorable) of what her relationship to each parent was like during her childhood…she demonstrates an understanding of her own personal development that includes an awareness of the multiple motives (conscious and perhaps unconscious) that guided her parents’ behavior toward her…there are no significantly distorting mental processes at work (pg. 901).
These robust findings were not totally unexpected; Mary Main, one of the developers
of the AAI, had herself wondered if adult attachment interviews might have something to say
about the mechanism behind the intergenerational cycle of child abuse (Main & Goldwyn,
1984). In a study of 30 normal, non-abusive women whose children had 4 years earlier
participated in an Ainsworth Strange Situation study, Main found that a mother’s experience
of her own mother as rejecting was related to her rejection of her own infant. In addition,
these women also revealed systematic cognitive distortions, such as idealization of the
rejecting parent, difficulty in remembering childhood, and incoherency in discussing their
attachment to their mother. Main found one exception: Women who could coherently
describe their rejection by their mothers, expressing resentment and anger, did not exhibit the
same avoidant behavior toward their own infants. Evidently, the differences in attachment
patterns in these children and women were also related to important cognitive differences, as
illustrated by the degree of cohesion and consistency the adults were able to utilize in their
narratives (Main et al., 1985).
32
Integrating Main’s findings, Fonagy’s team hypothesized that internal working
models become activated by certain expectations or events, influencing attachment-related
cognitions and behaviors that may be best thought of as “attachment states” (Fonagy et al.,
1991). These are distinct from the internal working model which, along with personality
traits, predisposes individuals to feelings and behaviors. Their recommendation was that
models of attachment could be informed by the examination of representational processes
that influence attachment-related emotions, thoughts, and behaviors.
The AAI and the Strange Situation have been paired in research repeatedly since the
Main and Fonagy studies, with findings suggesting that attachment classifications are stable
even across three generations (Zeanah et al., 1993; Benoit & Parker, 1994). Meanwhile,
interest in MFA began increasing in the field of study devoted to child and adolescent mental
health. A pair of child psychiatrists introduced the Working Model of the Child Interview
(WMCI), a measure designed to evoke mothers’ internal representations of their infants.
Modeled after the AAI, this one-hour structured interview categorically scored a caregiver’s
perceptions and subjective experience of their child. Qualitative, content, and affective
features of the narrative result in the assignment of one of three classifications: Balanced,
disengaged, or distorted. “Balanced” responses convey relatively rich details about the
infant, including both positive and negative characteristics of the infant or the mother-infant
relationship. “Disengaged” narratives are cool, distant, or indifferent descriptions that
implied the infant’s experience was either unrecognized or disregarded; descriptions are
unelaborated, giving the sense that the caregiver does not truly know the child. “Distorted”
representations are internally inconsistent, confusing, unrealistic, and divulge a lack of
33
insight concerning the impact of parenting upon the infant. In two independent
investigations with samples of mothers and their 12-month-old infants, they found that the
mothers’ WMCI classifications were significantly correlated to their infants’ attachment
classifications according to the Strange Situation. Narratives classified as “balanced” were
associated with secure infants, “disengaged” with insecure-avoidant babies, and “distorted”
with insecure-resistant children. Benoit et al. replicated the study with 96 expectant mothers
in the third trimester of pregnancy (Benoit, Parker, & Zeanah, 1997). When the WMCI was
repeated one year later concurrent with the Strange Situation, not only were WMCI
classifications significantly stable over time for the mothers, but the pregnancy WMCI
results predicted infant Strange Situation classifications in 74% of the cases. Concordance
between 12-month WMCI and Strange Situation classification was 73%. The authors felt
that this association could have major implications for early identification of high-risk
parent-infant relationships.
Only two other research teams to date have published empirical studies of the
relationship between MFA and object representations. Levine et al., working with a sample
of 42 pregnant adolescents, hypothesized that object representation during pregnancy could
be a predictor of infant attachment style (1991). The AAI was administered before childbirth
and the Strange Situation was conducted when the 42 infants were 15-months-old. The
quality of object representation was measured by the application of the Krohn Object
Representation Scale for Dreams to the responses of the AAI. The Krohn measure is an 8-
point scale that assesses hierarchical levels of an individual’s maturity of object-
representation and capacity for interpersonal relatedness (Krohn & Mayman, 1974).
34

Originally developed for use with dream analysis, it has been used in a similar way with the
responses of a Rorschach administration; however, there is no information as to its reliability
and validity in the application of it to the AAI. While the method has been questioned (Priel
et al., 2001), this research team did find mothers’ attachment style and object representations
highly correlated, and also found that both were significantly correlated with infant’s
attachment style as categorized at 15 months of age. However, the extent to which these
findings are generalizable is questionable in light of the fifteen-year mean age of this
population. Even considering individual variation in the development of mental
representations, this process is usually viewed as unfolding gradually through maturation to
adulthood and subject to disruption by developmental demands that are age-inappropriate
(Blatt, 1974).
Overlapping Models
What exactly has been measured in this body of research? Since the AAI has formed
the basis for these analyses, is the discussion so far one of internal working models or of
object representation? While the two concepts are related, they are not identical, and as such,
may not have the same contribution to MFA. Internal working models might be described as
templates of relationships (Main et al., 1985). In contrast, object representations reflect the
internal transformations of early relationship patterns, thereby guiding the use of and
affecting the organization of those templates (Fonagy et al., 1991). The AAI was designed
to elucidate early patterns of reality-based attachment relationships and the participant is
asked to reflect on what those mean to him or her currently. The WCMI was constructed on
the same theoretical base; their correspondence is perhaps not surprising. The findings of
35

these analyses may certainly be revealing what sort of template an individual is describing,
but an understanding of what links internal working models with antenatal or maternal-infant
attachment continues to be elusive for these researchers. Some theorists, following Main’s
concept of maternal sensitivity, have assumed that maternal responsivity/sensitivity mediates
maternal attachment and infant security (van Ijzendoorn, 1995). This assumption has not
been proven, however, and other attachment theorists point to analyses of discordant mother-
infant dyads and counter that sensitivity is more accurately thought of as a moderator that can
block an attachment state of mind, as when a mother with an insecure attachment style is
found to have a secure infant (Atkinson et al., 2005). Therefore, if the interest is in what
activates a template or internal working model perhaps another form of measurement is
needed.
With this in mind, Priel and Besser of Ben-Gurion University in Israel formulated and
tested their hypothesis that a pregnant woman’s antenatal attachment and internal working
models would be mediated by the expectant mother’s internal representation of her own
mother on a sample of 120 first-time mothers in the third trimester of a low-risk pregnancy
(2001). Their strategy was to utilize operationalizations of internal working models and
object representations that corresponded to Bartholomew & Horowitz’ conceptualization of
adult attachment and Blatt and colleagues’ means of identifying object representations,
instead of the traditional Ainsworth/Main constructs of adult attachment and internal working
models (Bartholomew et al., 1991; Blatt, Chevron, Quinlan, Schaffer, & Wein, 1992a). The
Bartholomew and Horowitz conceptual development was an outgrowth of Hazan and
Shaver’s application of George and Main’s attachment categories of the AAI to the romantic
36

attachment that develops between adults (Hazan et al., 1987; George et al., 1985). As a
result of noticing a difference in the motivations behind avoidance when exhibited by
dismissive behavior (George and Main’s category) as opposed to fearful behavior (Hazan and
Shaver’s category), Bartholomew & Horowitz hypothesized a classification of adult
attachment that is defined by the positivity of the internal working models of self and other.
Four dimensions of positivity/negativity of self/other could explain four models of
attachment: secure (positive self/positive other), preoccupied (negative self/positive other),
dismissing (positive self/negative other), and fearful (negative self/negative other). The
measure that resulted from this exploration, the Relationship Questionnaire (RQ), contained
four paragraphs, each describing a particular attachment pattern. Participants were first
asked to identify which is most descriptive of self, and secondly to indicate on a 5-point scale
the extent to which each of the four paragraphs are like self. Object representation in the
Priel and Besser study was evaluated using the Object Relations Inventory (ORI), an open-
ended description of mother that is analyzed across six dimensions: Benevolence,
punitiveness, ambition, ambivalence, complexity, and conceptual level (Blatt et al., 1992a).
These measures were then compared with MFA as measured by the Condon measure of
MFA quality and intensity (MFAS; Condon, 1993). Several findings of interest emerged in
this work: (1) Participants classified as “secure” on the adult attachment measure had
maternal representations that were more benevolent and ambitious and less punitive and
ambivalent than the representations of the three “insecure” groups (preoccupied, fearful, and
dismissing). The secure group’s representations were also significantly more complex and
displayed a higher conceptual level, a skill that statistically declined from the secure group to
37

the insecure-fearful and from the fearful to the insecure-preoccupied. (Conceptual
development on the ORI is established by assessing the range of ways in which the “other” is
experienced as described in the narrative. Five conceptual levels, Sensorimotor
Preoperational, Concrete-Perceptual, External Iconic, Internal Iconic, and Conceptual
Development are used as anchor points in the scoring.) The insecure-dismissive group
generated the least conceptually developed maternal representations (all differences
significant at p < .001). Significant effects were also found between the four attachment
groups and the quality and intensity of MFA, with preoccupied participants scoring
significantly lower on both dimensions. They concluded this work supported the hypothesis
that internal working models and object representation coexist, particularly since maternal
representation was found to “fully mediate the association between internal working models
and antenatal ties to their babies.”
Using a different measurement for maternal parental representations, Priel and Besser
in another study investigated adult attachment styles, early relationships, antenatal
attachment, and perceptions of infant temperament in first-time mothers (2000). In a
longitudinal study of 115 mothers of healthy babies that began in pregnancy, the team found
that mothers who experienced their own mothers as supportive and non-intrusive were not
only secure, but reported higher MFA and perceived their 4-month-old infants as having an
“easier” temperament than those women with less positive maternal experiences. In this
study, the adult attachment category was derived from Bartholomew and Horowitz’ system
and antenatal attachment was measured with Condon’s MAAS. Maternal relationships were
analyzed using the Parental Bonding Instrument, a 25-item self-report measure of
38
participants’ memories of parental behaviors and attitudes (Parker, Tulping, & Brown, 1979).
Once more, they seemed to identify an association between mothers’ representations of their
own caregivers, mothers’ romantic attachment style, and antenatal attachment.
Priel and Besser’s travel to their conclusions may have taken a different avenue than
the Fonagy group, but they are nevertheless concordant. Fonagy et al. recognized that
attachment states might be activated by an overall organization of mental structures, not
purely by quality of early attachment experience (1991). Perhaps Priel and Besser have
introduced a rationale for the 25% discordant mother-infant dyads in the Fonagy study.
Missing from the knowledge at this point is what a mother’s object representation of
her fetus would be. Recall that earlier research described expectant mothers as able to
describe their fetus in human terms and as separate from self in an increasingly coherent way
as pregnancy progressed (Lumley, 1982; Stainton, 1990). The WCMI is a valuable tool for
insight into parental attitudes of their child, but perhaps more descriptive of the “baby
template” than of a developing mental representation of their fetus. It is the goal of this
research to investigate object representation in the fashion of Priel and Besser. In addition to
examining mental representations an expectant woman expresses of her mother, an ORI
analysis of the expectant mother’s conceptualization of her unborn child will also be
introduced.
THE CONTRIBUTION OF PERSONALITY
Although the earliest explorations into the experience of pregnancy promoted it as a
psychological process (Benedek, 1958; Bibring et al., 1961; Rubin, 1975; Rubin, 1967;
39
Leifer, 1977), and pregnancy is undoubtedly one of the most important periods of a woman’s
adult life, the contribution of personality to MFA has not been widely explored. It has been
suggested that the associations among personality, stress, and the development of close
relationships should be considered in future discussions of attachment (Mikulincer et al.,
1999). While infant temperament has been explored (Lorensen, Wilson, & White, 2004),
other than examining the relationship of self-esteem with MFA (Curry, 1987; Cranley, 1981;
Gaffney, 1989; Kemp & Page, 1987; Koniak-Griffin, 1988), relatively few studies have
incorporated personality measures in the analyses, and one research team has produced most
of the literature available (Pollock & Percy, 1999; Besser & Priel, 2003a; Besser & Priel,
2003b; Reading et al., 1984; Priel et al., 1999; Priel & Besser, 2000a). Two of these studies
do not contribute much value to this discussion because of the limited information supplied
and the measures used. When Pollock and Percy investigated hypotheses regarding variables
that might be related to self-reported risk of harming one’s fetus in their study of pregnant
women referred by Social Services for psychological evaluation (1999), they employed the
Millon Clinical Multiaxial Inventory-2 (MCMI-2). This self-report measure of personality
was designed to examine dimensions of personality disorder, which facilitated their
investigation of the relationship of borderline personality dimensions and adult attachment
(Millon, 1987). Not only are the results questionable in terms of generalizability to a non-
forensic population, the MCMI-2 was developed to measure psychopathology, not
dimensions of normal personality. Reading et al. reported administering the Eysenk
personality measure but do not report findings (1984).
40
Attachment and Personality in Adult Research
Attachment has been connected to personality style in normal adult populations
(Zuroff & Fitzpatrick, 1995; Morrison, Urquiza, & Goodlin-Jones, 1998), and extensively
explored in relation to psychopathology (Brisch, 2002; Fonagy, 2001b; Blatt, Auerbach, &
Levy, 1997). Quality of attachment has also been associated with perinatal depression
(Mercer et al., 1988; Condon et al., 1997), and individuals with certain personality
characteristics have been observed to be associated with or vulnerable to perinatal depression
(Besser et al., 2003a; Besser et al., 2003b; Steinberg & Bellavance, 1999; Besser et al.,
2003a; Priel et al., 1999; Priel et al., 2000a).
Undoubtedly, cavalierly associating attachment with general personality factors or
associating it with personality dimensions to the exclusion of other important components of
relationship functioning would be counterproductive (Griffin & Bartholomew, 1994).
However, the growing integration of internal working models and object representation and
their association to attachment theory, developmental psychology, social psychology, and
cognitive science has had a major impact on personality assessment (Blatt, Auerbach, &
Lindgren, 1997). Recognition of the centrality of these mental templates and structures to
personality organization and the difficulty of direct measurement has awakened new interest
in the use of projective devices, such as the Rorshach, the Thematic Apperception Test, and
the Krohn Object Representation Scale for Dreams, particularly in the search for new ways
of understanding intractable psychopathology.
Summarizing personality research or even developing any singular approach to
personality is not possible in this discussion, but one particular understanding blends with the
41
experience of pregnancy in an almost seamless manner. Theorists have stated that the
evolution of the capacity for mutuality, or for reciprocal, satisfying, intimate relationships
with others, accompanied by a positive, realistic, and differentiated sense of self, is central to
the human formation of individual personality (Feldman & Blatt, 1996). This interactive,
reciprocal nature (or tension) of the dynamic processes of individuation and relatedness has
often been conceptualized. These have been referred to as: Surrender and autonomy
(Angyal, 1941), moving toward, against, or away from others (Horney, 1945), connectedness
(ocnophilic) and self-sufficiency (philobatic) tendencies (Balint, 1959), communion and
agency (Bakan, 1966), intimacy and autonomy (Shor & Sanville, 1978), sociotropy and
autonomy (Beck, 1983; Beck, Epstein, Harrison, & Emery, 1983) and introjective (self-
critical) and anaclitic (dependent) (Blatt et al., 2001). Correspondingly, the transition to
parenthood for both parents but more specifically the mother, has been painted by many as a
unique, developmental period in which issues of individuation or self-definition, and
mutuality or relatedness are paramount (Diamond, Blatt, Stayner, & Kaslow, 1995; Doan et
al., 2003; Leifer, 1977; Rubin, 1967; White et al., 1999). Therefore, looking at dimensions
of personality that explicate the transition of motherhood in relation to individuation or
mutuality seems most relevant to the relationship between personality and MFA.
Dependency and Self-Criticism
Based upon a history of work with depressed individuals, Blatt and colleagues
proposed a theoretical model of personality development that took into consideration the
state of development of an individual’s concepts of self and other (Blatt et al., 1997; Blatt et
al., 2001; Blatt, D'Affliti, & Quinlan, 1976). Personality in this model develops along two
42

basic trajectories: 1) a line of relatedness to others that incorporates the capacity to form
mature, mutually satisfying relationships, and 2) a line of self-definition that involves
developing an integrated, realistic, positive and differentiated identity. These two
dimensions, termed “anaclitic” and “introjective” respectively, develop throughout life, each
dependent upon the other for growth. In psychologically healthy individuals, these two
dimensions are balanced, interactive, and mutually facilitating; an overemphasis of one
and/or the defensive avoidance of the other results in various degrees of psychological
discomfort or disorder. An exaggerated need for and dependence upon others can result in
psychopathologies such as anaclitic (empty or loss-based) depression, dependent personality
disorder, and borderline personality disorder. In contrast, an overemphasis on autonomy and
self-worth can contribute to disorders such as obsessive-compulsive personality disorder,
paranoia, narcissism, and introjective (guilt or failure-based) depression. This two-
dimensional model has been particularly useful in diagnosing and treating depression (Blatt,
1974; Blatt et al., 1976; Blatt & Zuroff, 1992b) and is interestingly similar to Bowlby’s
descriptions of depressed individuals who were either anxiously attached or compulsively
self-reliant (Bowlby, 1980).
Based upon a review of clinical literature, Blatt, D’Afflitti, and Quinlan constructed a
measure containing 66 statements that were not direct symptomatic expressions of depression
but reflected experiences frequently reported by depressed individuals (1976). The items in
the Depressive Experiences Questionnaire (DEQ) encompassed issues such as negative or
distorted sense of self or others, dependency, helplessness, egocentricity, fear of loss,
ambivalence, self-blame, guilt, loss of autonomy, and disruptions in family relationships.
43
Participants rated these items on a 7-point scale indicating agreement or disagreement with
the experience. Statistical analyses of the measure revealed three factors, dependency, self-
criticism, and efficacy (sense of confidence about one’s resources and capacities). A
considerable body of research in the last thirty years has demonstrated its reliability and
validity in a number of populations, including perinatal women (Besser et al., 2003a; Besser
et al., 2003b; Blatt et al., 1976; Blatt, 2004; Blatt, Zohar, Quinlan, & Zuroff, 1995; Blatt,
Schaffer, Bers, & Quinlan, 1992; Blatt et al., 1992a; Bacchiochi, Bagby, Cristi, & Watson,
2003; Bagby, Parker, Joffe, & Buis, 1994; Zuroff, Quinlan, & Blatt, 1990; Priel et al., 1999;
Priel et al., 2000a).
With the aid of the DEQ, research has found parallels between adult attachment styles
(secure, anxious, dismissive, fearful) and Blatt’s dimensions of personality (Zuroff et al.,
1995). Dependent (anaclitic) individuals suffer deep longings to be loved and protected, but
lack confidence that those needs will be met, fearing abandonment in their interpersonal
relationships (Blatt et al., 1992b). Self-critical (introjective) individuals are preoccupied
with constant self-scrutiny, fear being disapproved and criticized, and expect to lose the
approval and acceptance of significant others. When applied to attachment theory, Zuroff
and Fitzpatrick found that both anaclitic and introjective individuals exhibited insecure
attachment styles (1994). Dependent individuals were preoccupied with losing emotional
support from others, and introjective individuals structured relationships to remain at a
distance, perhaps protecting themselves from being hurt but becoming vulnerable to
depression as a result of dissatisfying relationships that lacked intimacy. Imbalances in
these personality styles have also been associated with various problems in social-personal
44

adjustment, including early parent-child relationships (Koestner, Zuroff, & Powers, 1991;
McCranie & Bass, 1984).
Relevant to this topic are three studies focused upon samples of pregnant women
(Besser et al., 2003b; Priel et al., 1999; Priel et al., 2000a). A prospective study of 73
primagravidas in the third trimester of pregnancy tested the hypothesis that dependency and
self-criticism could be vulnerability factors to postpartum depressive symptoms. In addition
to finding that self-criticism measured in pregnancy was significantly predictive of
postpartum depressive symptomatology at eight weeks postpartum, results also indicated that
those introjective participants who were strongly attached to the fetus during pregnancy (as
measured by the Condon instrument) had a lower risk for depression. Dependency was not
associated with depressive symptoms in this study. Priel and Besser suggested that, based on
these findings, implementation of more open and ideographic approaches to the measurement
of personality might allow a more sophisticated evaluation of antenatal attachment. This
might also allow a way to understand the confusion concerning the insecurely attached
mothers with secure infants from the earlier cited findings (Fonagy et al., 1991; Main et al.,
1984).
Another study with a sample of 120 primagravidas explored potential relationships
between personality tendencies, frequency of depressive symptoms, and perceptions of social
support (Priel et al., 2000a). Results revealed depressive symptoms in both highly anaclitic
and highly introjective women seemed to be mediated by a distinct attitude toward and style
of negotiating social support. Self-criticism was found to reduce the perception of available
support while dependency seemed to increase this perception. The conclusion was that
45
personality tendencies do have an effect on perceptions of social support and, indirectly, an
influence on depressive symptoms. This same team then underwent a third look at the
impact of anaclitic and introjective personality tendencies in relation to coping styles in
pregnant women (Besser et al., 2003b). With a sample of 146 women in their first
pregnancies, coping style also emerged as a moderator to trait vulnerability to depression.
The body of research contributed by Priel and Besser encourages further evaluation of
plausible differences between MFA processes among dependent and self-critical mothers.
Development of transactional models would allow focus to shift from simplistic direct
relationships to mutual effects of mental representation, personality variables, and the
demands of the pregnancy experience upon MFA. The variety of measures available today
also enables research teams to quantitatively measure abstract constructs such as object
representation.
THE IMPACT OF RISK
Over a million pregnant women a year are identified as being at high-risk for
maternal or fetal complications, approximately 700,000 of which are treated with bed rest
(Lumley, 2003). When the threat to maternal or fetal health is emergent, hospitalization is
required for intensive monitoring, with the aim of prolonging the pregnancy until the balance
of risk for maternal and fetal safety weighs the uterine environment unsafe to continue. Two
types of high-risk pregnant women have been described: Those with chronic illnesses that
predispose them to risk during pregnancy, and those who are faced with an unanticipated
complication that arises in what has been a normal pregnancy (Heaman, 1998). Maternal
46
risks include the hypertension spectrum (chronic hypertension/preeclampsia/eclampsia),
gestational diabetes (or pre-existing diabetes), severe anemia, and cardio-pulmonary disease
(Hobel, Hyvarinen, Okada, & Oh, 1973). Separate fetal risks include fetal anomaly,
premature rupture of membranes, placenta previa, placental abruption, and premature birth.
Preterm birth, defined by the World Health Organization as any birth occurring
between 20 and 37 weeks of gestation, is the major clinical problem most associated with
fetal demise and childhood disability (Lumley, 2003). Although only 6-10% births are
considered preterm, those births account for more than 60% of all perinatal deaths and nearly
50% of long-term neurological disability (Logghe & Walker, 2004; Wood, Marlow,
Costeloe, Gibson, & Wilkinson, 2000). While advances in neonatal care have increased the
survival rate of premature births, there are marked differences in the probability of survival
according to gestational age, with births from 20 to 27 weeks at the most severe risk for
demise or disability (Lumley, 2003). Rates for neonatal survival before 24 weeks of
gestation are extremely low; at 34 weeks, the survival rate is similar to that of full-term
gestation. Risk factors for preterm birth include previous preterm births, multiple births,
maternal age greater than 35 or less than 15, maternal weight greater than 200 or less than
100 pounds, history of abortion (spontaneous and/or elected), and poor maternal health
practices, such as smoking and substance abuse.
Obstetric Risk and Perinatal Mental Health
What past research has strongly suggested is that high-risk pregnancy alone, without
required hospitalization, is associated with increased rates of depression and anxiety (Kurki,
Hiilesmaa, Raitasalo, Mattila, & Ylikorkala, 2000). Studies focusing on hospitalized women
47

have identified higher levels of anxiety and depression, lower self-esteem, less positive
expectations for their experience of childbirth, and less optimal family functioning than
found in non-hospitalized women (Heaman, 1992; Maloni, Park, Anthony, & Musil, 2005;
Maloni & Park, 2005; Maloni, Kane, Suen, & Wang, 2002; Maloni & Kasper, 1991; Mercer
& Ferketich, 1988; Heaman, Beaton, Gupton, & Sloan, 1992; White & Ritchie, 1984;
Leichtentritt, Blumenthal, Elyassi, & Rotmensch, 2005; Mercer et al., 1994), and negative
affect during pregnancy has been associated with adverse obstetric and neonatal outcomes
(Kurki et al., 2000). Maloni et al. found that dysphoria (a composite of anxiety, depression,
and hostility) was highest upon hospital admission and was significantly greater for those
with the highest Hobel Risk Assessment scores (2002). Another finding was that gestational
age at birth was significantly correlated with postpartum dysphoria. Priel and Besser also
found increased levels of postpartum depression in a selected group of high-risk pregnant
women whose pregnancies ended well (Besser, Priel, & Wiznitzer, 2002), lending to the
hypothesis that these women may have postponed maternal bonding, which is considered a
protective factor against the vulnerability to depression (Priel et al., 1999). Gupton et al.
points out the quandary that exists with the multiple findings available: Stress and anxiety are
associated with increased risk of preterm birth and low birth weight, psychosocial factors
such as depression, anxiety, and low self-esteem have been shown to be associated with
higher incidences of poor health practices, and women experiencing a high-risk pregnancy
have higher levels of stress and anxiety, but how these factors are all related is basically
unknown (Gupton, Heaman, & Cheung, 2001). The preponderance of evidence suggests that
women with complicated pregnancies suffer from symptoms of anxiety and depression as
48

they experience threats to self and fetus and feel a loss of control. Little is known about how
long these symptoms last, whether they continue into the postpartum period, and how or if
they affect the attachment process.
Issues Specific to High-Risk Pregnancies
The first discussion of the psychological implications in high-risk pregnancy was
published in 1982 by Joy Penticuff, who provided the definition of high-risk commonly used
today. Using the theory of development during pregnancy proposed by Rubin and others, she
outlined five important issues high-risk couples face in their adaptation to pregnancy and
parenthood. Penticuff’s first point is that in uncomplicated pregnancy, ambivalence
regarding the changing roles and addition of a child to the family is usually resolved by the
end of the first trimester. However, this resolution of ambivalence can be compromised
when negative physical signs indicate danger to the fetus. When parents are informed that
there is possibility that the baby may not survive or may be born with disability, the
ambivalence toward the pregnancy is intensified. The contrasting feelings change—instead
of resolving the transitional issues of becoming a mother, the feelings become a mixture of
intense desire for a healthy baby and the fear that the baby will not live or will be damaged.
Secondly, with the possibility of a fetus that may never live, or may live but be
disabled, parents may find it hard to allow the natural growth of attachment to the baby. Fear
of disappointment and loss may thwart the normal trajectory of increasing MFA. For
hospitalized women, this danger is salient with the omnipresent fetal monitor, daily physician
visits, physical symptoms, periodic hospital tests, and separation from home and family.
49

Signs of an uncomplicated pregnancy (e.g. weight gain, appearance of the pregnancy
to others, unrestricted activity level) contribute to the sense of adequacy an expectant mother
develops through the gestational period. In high-risk pregnancy, there may be negative signs
instead, such as poor weight gain, bleeding, contractions, and prescribed bed rest that
threaten her sense that she will be able to achieve successful pregnancy and childbirth.
Feelings of threat, isolation, and a loss of control may thwart the development of maternal
adequacy and spill over into a continuing sense of inadequacy when the baby is born.
Penticuff believed women with high-risk were especially vulnerable to feelings of self-blame
and failure.
The fourth issue targeted the impairment of traditional nesting behaviors. In normal
pregnancy, the last trimester is typically spent acquiring the necessities for infant care,
selecting and preparing the layette, and decorating the nursery. Friends and family plan baby
showers, and the atmosphere is one of excitement and joy. When complications occur, all
these activities are suddenly curtailed (or may never take place), the prevailing atmosphere
becomes one of anxiety, and friends and family members are not sure what to do or say.
Finally, the very expectations of labor and delivery change. While there is always
some element of anxiety in approaching the birth experience, certain positive expectations
are in place. Couples participate in birthing classes, tour labor and delivery facilities,
imagine what seeing their baby for the first time will be like, and mothers consider breast-
feeding. Complications change all these expectations—labor and delivery are uncertain.
There may be no time for classes and tours, no choice to breastfeed an extremely premature
50
neonate, and couples must prepare themselves for the possibility of an emergency delivery
and the risk their child will not survive.
In summary, high-risk pregnancy sends an expectant mother into a state of “limbo,” a
place of uncertainty accompanied by an overwhelming sense of vulnerability, with a
realization of the loss of control and the need to surrender autonomy. “Others” take on new
significance, from the medical professionals who bring the good and the bad news, to the
husbands, friends, and families who bring food and stories of the outside world; dependency
is somewhat forced upon a high-risk mother. Since Bowlby held that the attachment system
was found to be most strongly activated under conditions of distress such as fatigue, illness,
or fear, this environment seems ideal for an investigation of attachment (Bowlby, 1973).
Previous Research with Hospitalized Populations
Only three studies of MFA have been conducted using samples that included
hospitalized women. The earliest publication reported findings on a prospective, descriptive,
correlational study of 75 women hospitalized with complications in their third trimester of
pregnancy (Curry, 1987). Curry wondered if social support and self-concept could be
intervening variables between maternal behavior and maternal history of stress. She also
wanted to take the opportunity to summarize the feelings these hospitalized women had
regarding their pregnancies and babies. Although she was unable to support her hypothesis
concerning intervening variables, there were several findings pertinent to this discussion.
There was a significant positive correlation between Cranley’s MFAS scale and the self-
concept measure Curry employed, indicating that women with high measures of self-concept
also reported high MFA. Curry hypothesized this supported a profile of women with poor
51

self-concept, perhaps as a result of inadequate mothering, who then were vulnerable to
negative effects from a high-risk pregnancy. This hypothesis was later supported by Priel
and Besser’s study of the association between introjective women and postpartum depression
in uncomplicated pregnancy (1999). Secondly, women who reported better relationships
with their mothers also scored higher in the MFAS, supporting both attachment and object
relations theories of the developments during pregnancy. However, without specific
measures of mental representation that conclusion could not be made. Curry believed that
future research using grounded theory and qualitative methods would continue to broaden the
understanding of women’s feelings in high-risk pregnancy, enable identification of women
vulnerable to negative psychological effects from the risk, and develop interventions aimed
at improving self-concept in these women.
The other two research teams investigating MFA in hospitalized women were led by
Mercer, an early spokeswoman for nurses concerned with expectant mothers at risk (Mercer,
1977; Mercer, 1983). The first study of expectant couples included 153 high-risk
hospitalized women (75 mates) and 218 low-risk women (147 mates) in the third trimester of
pregnancy (Mercer et al., 1988). Mercer expected to find no effects upon maternal or
paternal attachment (measured by Cranley’s MFAS and PFAS) of the variables social
support, self-esteem, sense of mastery, general health, marital relationship, family
functioning, life experiences, anxiety, depression, early relationships with parental figures, or
readiness for pregnancy. All measures used were self-report questionnaires, and the ability
of some to relatively capture the variable of interest is unclear. For example, in evaluating
early relationships with parental figures, Mercer et al. used a single question with a 5-point
52

Likert-type scale. It is doubtful that this would have the same predictive power of a more
comprehensive tool. While their statistical analyses did not find significance, there were
interesting trends that are informative. 25% of high-risk women conveyed worry, anxiety,
and concern compared to 8% of low-risk subjects; 11% of high-risk women reported loving
or talking to their fetus compared with 18% of low-risk subjects; only 23% of high-risk
women expressed being curious about and anticipating birth, in contrast to 48% of the low-
risk subject. The study also suffered from a 41% refusal rate of the high-risk women at the
facility from which the sample was drawn, among which 70% were not Caucasian. In
addition, the authors themselves considered that the measures utilized may not be accurately
capturing the parameters of the MFA construct.
Six years later, Mercer led another team comparing 121 high-risk women and 182
low-risk women at 5 time points: Antenatal (hospitalization for the high-risk group),
postpartal hospitalization, 1, 4, and 8 months postpartum. The hypotheses this time were that
high-risk women would report lower maternal role competence than low-risk women, and
that there would be a significant relationship between maternal competence and maternal
attachment from postpartal to 8 months postpartum. Hypothesis one was rejected, as no
significant differences were found in the maternal role competence of either group over time.
However, self-esteem and mastery were consistent predictors of maternal competence for
both groups. Fetal attachment was a consistent predictor of competence only in the high-risk
group, suggesting to the authors that perhaps these women had been sensitized to the value
they placed on safely delivering their babies. Depression also explained more variance in the
reported maternal competence of the high-risk group at 1 month postpartum, and continued
53

to have an effect on scores through the last time point. State anxiety was a major predictor to
maternal competence for both groups, but only at the postpartal time point. Although fewer
measures were used with this study, the ones used were identical to those in the previous
study, making it difficult to determine if the findings were consistent because they are
meaningful or because the measures were the same as those previously used.
CONCLUSION OF REVIEW
A study of the MFA construct in a sample of hospitalized women would add value to
the body of research that is available and perhaps begin addressing previously unanswered
questions. Viewing the high-risk population as an avenue to better understand the process of
attachment has merit from both attachment and object relational theoretical approaches, for
this group of individuals is in the exact climate Bowlby believed activated attachment
emotions, cognitions, and behaviors. Gaining an understanding of how mental
representations may motivate those reactions could refine our understanding of MFA, help
identify those with compromised attachment systems, and inspire interventions aimed at
causal mechanisms instead of symptoms. And an understanding of personality tendencies
may help tie the mechanisms of attachment and object representation together in a manner
that exposes or explains associations as well as individual differences.
RATIONALE FOR THIS RESEARCH
Findings in the literature have been inconsistent regarding the implications of risk on
maternal-fetal attachment (MFA), and there is a paucity of research investigating the impact
of hospitalization on the development of this attachment. Reviews of extant published
54
studies have consistently pointed out the necessity for additional correlational research to be
conducted with this population for two specific scientific reasons: Existing MFA measures
have not been validated outside the population of low-risk pregnant women, and there is a
need for increased knowledge regarding the construct of prenatal attachment and the
contributions of object representation and personality. This study would provide an
investigation of both.
Indirect benefit of this work could be realized as well. If women at risk for weak
attachment can be identified before childbirth, then future longitudinal study of interventions
would be justifiable and important. Successful development of interventions would require a
more refined understanding of MFA across populations (Cranley, 1992). Since strong MFA
has been linked with positive health practices during pregnancy, enhancing attachment has
the potential of reducing perinatal risk and improving the health of perinatal women and their
infants. Although findings are inconsistent, there is some suggestion that strong MFA is a
protective factor against postpartum depression; prenatal interventions with women at risk
for this tragic illness are important for mothers and babies. Current work in Germany is
suggesting that prenatal interventions do improve the sensitivity of mothers at risk for poor
caregiving (Brisch, 2002) and past research in the U.S. has proposed simple interventions
nurses can employ with women to enhance attachment (Carter-Jessop, 1981). Sound, theory-
driven studies are a necessary foundation for any of this work.
55
AIMS OF THE STUDY
The primary goals of this dissertation research are: 1) To investigate to what extent
maternal and fetal representations influence an expectant mother’s ability to form attachment
with her fetus in the uncertainty of maternal and/or fetal risk factors significant enough to
require hospitalization, and 2) to explore the association between personality, object
representation, and MFA.
Secondarily, interrelationships between object representation, personality, type of
risk, severity of risk, gestational age of fetus at time of onset of complications, and
depression will be analyzed.
HYPOTHESES
Primary Hypotheses
Hypothesis One
It is hypothesized that, in a hospitalized sample of high-risk pregnant women, those
participants expressing complex, highly integrated conceptual levels of representation of
their own mothers (as evaluated by the Conceptual Level scale of the Object Relations
Inventory) will report both a higher quality and greater intensity of attachment (as measured
by the Maternal Antenatal Attachment Scale) to their unborn babies than those whose
maternal representations are less highly developed.
56
Hypothesis Two
It is also expected that those individuals who are able to articulate more complex
representations of their mothers will also be able to do so of their babies (as evaluated by the
Conceptual Level scale of the Object Relations Inventory).
Hypothesis Three
Dependency (as identified on the Depressive Experiences Questionnaire) is expected
to be more highly associated with anxious/ambivalent prenatal attachment (as categorized
from the Maternal Antenatal Attachment Scale) while self-criticism (as identified on the
Depressive Experiences Questionnaire) is expected to be more highly associated with a
positive quality of attachment but low preoccupation (as categorized from the Maternal
Antenatal Attachment Scale).
Hypothesis Four
In addition, it is predicted that women with a self-critical personality style will
convey object representations of a higher conceptual level (as evaluated by the Object
Relations Inventory) and report a higher quality of attachment than women with a dependent
style.
Secondary Hypotheses
Hypothesis Five
Since some risks are to mother and others to fetus within high risk pregnancy, the
relationship between maternal representation/fetal representation (as evaluated by the Object
Relations Inventory) and attachment (as measured by the Maternal Antenatal Attachment
Scale) is suspected to be influenced by the type of risk described to the participant by her
57
physician. Risk in this study will be categorized as primarily maternal or primarily fetal.
Severity of risk will also be taken into account, stratifying risk as low, medium, and high,
based on the physician’s diagnosis and the Hobel Risk Assessment score. Specifically, it is
expected that fetal risk will be associated with a higher global score of the Maternal
Antenatal Attachment Scale than maternal risk.
Hypothesis Six
It is also expected that the intensity subscale scores of this measure will be higher in
patients with identified fetal risk.
Hypothesis Seven
It is also expected that gestational age of the fetus at time of onset of complications
will be positively correlated with the global attachment score.
58
CHAPTER THREE
METHODOLOGY
PARTICIPANTS
Participants were a sample of women with maternal and/or fetal risk severe enough to
require admission to the antenatal unit of Baylor University Medical Center. The antepartum
unit often receives patients who are admitted for less than 24 hours, making complete data
collection on all new admits unfeasible. In order to minimize missing data, participation in
the study was limited to women admitted to the antenatal unit of Baylor University Medical
Center with the expectation of a hospitalization longer than 72 hours. Women who were
actively psychotic, suicidal, or homicidal were excluded from the research, as were any with
cognitive impairment.
METHODS AND PROCEDURES
The study coordinator reviewed the antenatal unit’s daily log of admissions and
discharges from the floor. Information from the charge nurse regarding the proposed length
of stay determined if new admissions were solicited for the study. Patients expected to
remain in the unit for at least 72 hours were approached in their hospital rooms and the
project was introduced as a study of women’s experiences during hospitalization for
complications of pregnancy. After obtaining consent (Appendix A), a member of the
research team obtained demographic information, explained the self-report measures, and left
59

the packet with the patient for completion, arranging to return for it at a designated time. The
investigator also reviewed medical records to obtain relevant medical information including
gestational age and factors of mother/baby risk. To ensure confidentiality, each mother was
assigned a participant number and all study materials bore only that identifying number. The
consent forms were kept locked in a separate file from the measures.
MEASURES
The Center for Epidemiological Studies—Depression Scale (CES-D) was developed
as a screening instrument to detect depression in nonclinical populations. Because the items
tap few physiological symptoms (appetite, sleep, energy level, fatigue), it is well suited for
the prenatal population, in view of those symptoms being commonly associated with
pregnancy and less specific for depression (Unauthored, 1999; Beeghly et al., 2002; Besser et
al., 2002; Marcus, Flynn, Blow, & Barry, 2003). The 20 items cover the previous 7 days and
are rated on a 4-point scale. A total score is derived from summing the ratings; the score of
16 has been used as the standard cutoff point to determine distress in community samples as
well as with an obstetric population. Good internal consistency has been reported
(Cronbach’s alpha = .88-.91) in studies with perinatal women (Beeghly et al., 2002). A
threshold score of 16 or more in this study dictated the administration of The Structured
Clinical Interview for DSM-IV Axis I Disorders (SCID-I) to review symptoms and establish
or rule out the diagnosis of depression.
The Depressive Experiences Questionnaire (DEQ) was specifically developed for
assessing dependency and self-criticism, and accomplishes this by assessing a broad range of
feelings about the self and others without overlapping with the actual clinical symptoms of
60

depression (Blatt et al., 1976). This self-report questionnaire is comprised of 66 items
inquiring about the nature of an individual’s experience of depression, and requires
approximately 15 minutes for administration. Participants identify the extent to which each
item is true on a 7-point scale ranging from (1) “strongly disagree” to (7) “strongly agree.”
Negative scores indicate low involvement on that particular factor. Subscales of the factors
are also rated and yield scaled scores. Three primary factors, Dependency (interpersonal),
Self-Criticism (self-definitional), and Efficacy are analyzed. Dependency elicits concerns
about abandonment, separation, loss, and feeling unloved. Self-Criticism reflects worries of
failure, guilt, self-definition, and unreasonably high expectations. Efficacy concerns pride,
self-confidence, self-satisfaction, and strength. Since efficacy has not been found to be a risk
factor for attachment or depression, the Efficacy scores will not be used in this study. The
mean for each factor is 0, and the standard deviation is +1/-1. Psychometric properties of
the scales are reportedly satisfactory; internal consistencies are high (Cronbach alphas > .75)
and test-retest reliabilities at 12 months are similarly high (r = .79) (Zuroff, Igreja, &
Mongrain, 1990). High convergent, construct, and discriminant validity has also been
reported (Blatt et al., 1992b). Women were designated “dependent” (anaclitic) or “self-
critical” (introjective), if their score deviated from the sample mean by one standard
deviation.
The Edinburgh Depression Scale (EPDS) is a 10-item, multiple-choice self-report
scale developed specifically for the screening and assessment of perinatal depression. The
most common tool reported in previous studies (Gaynes et al., 2005), it covers the common
symptoms of depression but excludes somatic symptoms such as fatigue and changes in
61
appetite, which occur naturally in pregnancy and would not discriminate depressed women
from non-depressed women. It takes less than five minutes to complete and has been widely
used in research and clinical practice. The split-half reliability of the EPDS has been
reported to be .88 and the standardized α coefficient 0.87 (Cox & Holden, 2003b). Scores on
this scale range from 0-30; higher scores indicate more depressive symptoms. A threshold
score of 11 or higher in this study dictated the administration of The Structured Clinical
Interview for DSM-IV Axis I Disorders (SCID-I) to review symptoms and establish or rule
out the diagnosis of depression.
The Maternal Antenatal Attachment Scale (MAAS) is a self-report questionnaire
designed to capture the developing attachment of mother to fetus (Condon et al., 1997;
Condon, 1993). Nineteen items, requiring less than 10 minutes for completion, yield data
clustered in two factors: “Quality” assesses positive emotions and thoughts regarding
closeness, tenderness, the desire to know and see the baby, as well as vivid internal
representations of the baby; “Intensity” measures the mothers’ preoccupation about the baby,
including the amount of time spent thinking about and talking to it. Prenatal attachment as
measured in this instrument has been found to fall in four quadrants, each depicting an
attachment style: strong/healthy, positive affective/low preoccupation,
uninvolved/ambivalent, and anxious, ambivalent, or affectless preoccupation. Responses are
identified on a 5-point Likert-type scale, with higher values indicating greater antenatal
attachment. In item analysis, the 19 items were reported to have an internal consistency of α
= .818.
62
The Object Relations Inventory is a method developed by Blatt and colleagues for
assessment of basic dimensions of object representations (Blatt et al., 1992a). The
participant is asked to write a description of mother and fetus. The scoring procedure
includes 12 qualitative dimensions and scores of ambivalence, complexity and conceptual
level. The 12 dimensions are Likert-style ratings of perceived personal qualities of the parent
or subject of reference: affectionate, ambitious, malevolent-benevolent, cold-warm, degree of
constructive involvement, intellectual, judgmental, negative-positive ideal, nurturant,
punitive, successful, and weak-strong. The 7-point scales are anchored at 1 = “Little” and 7 =
“Very.” A score of 9 indicates that the quality is not mentioned in the narrative and cannot
be evaluated. These 12 items produce 3 factors—Benevolent, Punitive, and Ambitious.
Ambivalence, the degree to which opposite or inconsistent feelings are expressed, is rated by
the coder on a 5-point scale anchored at 1 = “none,” 3 = “moderate,” and 5 = “large.”
Complexity refers to verbal fluency and is rated on a 7-point scale according to the length of
the description. The final score, Conceptual Level, is a five-level evaluation based on the
developmental concepts of Piaget, Werner, and others. Level One, Sensorimotor
Preoperational, is a personal, subjectively focused description that identifies the individual
primarily in terms of his/her satisfying or disappointing the subject. The second level,
Concrete-Perceptual, refers to narratives that describe the person literally, concretely,
according to external characteristics or physical properties. External Iconic, Level Three,
focuses on the person as a separate entity, describing activities and attributes that are
uniquely the person’s and not related to the subject’s gratification or frustration. Internal
Iconic, the fourth level, is coded when the description that conveys the internal state of the
63

person in such a way that the reader can empathize with the person’s experience of reality, as
the subject has done in the narrative. Conceptual Representation is the highest level and is
judged on the basis of a cohesive integration of a wide range of levels on which the person is
understood and experienced. These five levels are represented on the scale on 9 points, one
for each level and one between levels to reflect narratives that may include elements from
both levels. In the assessment of maternal representations, this open-ended instrument has
been found to be reliable (Bornstein, Galley, & Leone, 1986; Fishler, Sperling, & Carr, 1990)
and it has been utilized in a recent study of expectant mothers (Priel et al., 2001). The
inclusion of the description of the fetus was novel, as there have been no published studies in
which the instrument was used for this purpose. Coding was done by two raters, and
interrater reliability was monitored throughout the course of data gathering.
Pregnancy risk was assessed with a revision of the Hobel Risk Assessment, an
instrument assigning prescribed scores to 126 medical and obstetric risk factors of mother
and neonate (Hobel et al., 1973; Hobel, Youkeles, & Forsythe, 1979). From the original
instrument, 36 factors are intrapartum (during delivery) and 35 factors are neonatal (assessed
after the birth of the infant); these factors will not be evaluated in this study. All original
items have weighted scores based on their association with mortality, and previous studies
have fixed the score of >10 as indicative of high risk. Four additional items were added that,
while not included in the original instrument, account for a large percentage of antenatal
hospital admissions. These are premature rupture of the membrane, primary dysfunctional
labor, placenta previa, and abruption placentae. The Principal Investigator of the study, John
Rosnes, M.D., assigned weighted scores to these four items. Dr. Rosnes also categorized the
64

nature of each Hobel item as primarily maternal or primarily fetal. While the chief interest
was in maternal versus fetal risk, an additional curiosity was the possible relationship
between level of risk and attachment. An analysis of risk was conducted stratifying risk into
3 categories: 1-4 = “Low risk,” 5-10 = “Medium risk,” and >10 = “High risk.”
65
CHAPTER FOUR
RESULTS
DEMOGRAPHIC INFORMATION
Unlike most previous studies utilizing largely Caucasian, middle-class, married
women, this project enjoyed a richly diverse sample. Table 1 provides the demographic
information for the sample. The sample consisted of 91 women, ranging in age from 17 to 44
years, with a mean age of 27.01 (SD = 6.44). Fifty-four percent (N = 49) were Caucasian,
33% were African American (N = 30), 11% were Hispanic (N = 10), and 2% were Asian (N
= 2). Forty-nine percent of the participants were married (N = 49), 32% were single (N =
29), 10% were living with a partner (N = 9), and 3% were separated from their husbands (N =
3). The average number of children at home was 1.02, with a range of 0 to 6 children (SD =
1.45). Eleven per cent of the sample did not complete high school (N = 10), however 25%
completed high school or had completed a General Educational Development test (N = 23),
33% received some college education (N = 30), and 26% had obtained an undergraduate or
graduate college degree (N = 24). Thirty percent had an annual household income below
$26, 000 (N = 27), 16.5% reported income of $26,000--$40,000 annually (N = 15), 16.5%
reported $41,000--$65,000 (N = 15), and 29% reported earnings of more than $65,000 a year
(N = 26). Government funds (Medicaid) covered 43% (N = 15), 48% were covered by a
private insurance plan (N = 44), and 3.3% had no coverage at the time of their admission to
Baylor (N = 3).
66

Pregnancy Characteristics
Although almost one-third of the sample was experiencing a first pregnancy (N = 29),
24% had been pregnant before (N = 22), and 44 % (N = 39) had history of at least two
previous pregnancies (Table 2). Four percent (N = 4) had suffered delivering a stillborn
baby, 27% had history of miscarriage (N = 24), and 37% had history of obstetric
complications (N = 34). Almost half of the patients were in their third trimester at onset of
obstetric complications (N = 42), but 11% (N = 10) were in their first trimester and 37% in
their second (N = 34).
Psychiatric Characteristics
As Table 3 reveals, slightly more than three-quarters of the participants denied any
history of psychiatric disturbance, hospitalization, psychotropic treatment, or counseling (N =
69), but 7% reported a history of depression (N = 6), 7% reported a history of anxiety
disorder (N = 6), 3% had been treated for both depression and anxiety (N = 3), and one
participant suffered from bipolar disorder. However, when screened for depression, 36% (N
= 33), endorsed depressive symptoms on the Center for Epidemiologic Studies- Depression
scale (CES-D; score exceeded the threshold of 16 for possible mood disorder) and 42% (N =
38), endorsed depressive symptoms on the Edinburgh Postpartum Depression Scale (EPDS).
Although 35 Structured Clinical Interviews were administered, only three patients met the
criteria for Major Depressive Disorder (six met criteria for one of the anxiety disorders).
Seventy-seven percent (N = 70), of the participants denied a familial history of psychiatric
disturbance, but 18% (N = 16), reported family history of mood, anxiety, or substance-use
disorders.
67
Nature of Obstetric Risk
There was significant variance in the severity of risk across participants in the sample
(Table 4). The mean revised Hobel Assessment score was 18.35 (SD = 9.62), with a range of
5 to 45 points. Twenty-five percent of the patients fell between 10 and 15 points of severity.
Classifying risk as “maternal” or “fetal” was not problematic; however, 42% (N = 38) of the
sample met criteria for both types of risk. This would occur, for example, when a participant
would carry the diagnosis of toxemia (severe gestational hypertension) and would also have a
history of a stillbirth and/or a premature delivery. In nine of these instances (21%), the dual
risk was due to a multiple pregnancy.
OVERVIEW OF STATISTICAL ANALYSES
Primary Hypotheses
Hypothesis One
Participants who expressed an integrated understanding of their mother’s
characteristics, qualities, and aspirations in the Object Relations Inventory (ORI) narrative
were expected to also report a higher quality and greater intensity of attachment, as evaluated
by two factors of the Maternal Antenatal Attachment Scale (MAAS). The ORI narratives are
scored on six dimensions: Benevolence, Punitiveness, Ambition, Length, Ambivalence, and
Conceptual Level. The subject’s responses on the MAAS yield a global score of attachment
as well as scores on two orthogonal factors: Quality, describing positive affect regarding the
fetus, and Intensity, reflecting the amount of time the expectant mother reports being
preoccupied with thoughts about the fetus. A one-way multivariate analysis of variance
68
(MANOVA) was conducted to determine the effect of the six dimensions of the ORI upon
the MAAS global score of attachment. The scores were separated into two levels, above and
below the mean (M = 81.5, Table 4), in the first analysis. No significant differences were
found among the dimensions for attachment, Wilks’ Λ = .899, F (6, 32) = .601, p = .728.
The multivariate η² based on Wilks’ Λ was nonsignificant, .101. Table 5 contains the means
and the standard deviations on the dependent variables for the six groups. A second
MANOVA was conducted, dividing the Global score into three groups: Lowest through -.99
sd below the mean, -1 sd through 1 sd, and 1.01 sd through the highest score. This further
stratification was also nonsignificant, Wilks’ Λ = .620, F (12, 62) = 1.393, p = .193, η² = .212
(Table 6).
A one-way analysis of variance was conducted to evaluate the relationship between
Conceptual Level of the mother narrative and the Quality of attachment score from the
MAAS. The 95% confidence intervals for the multiple comparisons, as well as the means
and standard deviations for the four Conceptual Levels, are reported in Table 7. The
independent variable, Conceptual Level of the narrative, included four levels: “Sensorimotor-
Preoperational,” “Concrete,” “External Iconic,” and “Internal Iconic” (no narratives
contained the necessary elements for the highest level, “Conceptual Level”). The dependent
variable was the Quality of Attachment score from the MAAS. The ANOVA was
nonsignificant, F (3, 79) = .434, p = .729. Figure 1 displays the distribution of the sample.
The analysis was repeated using the attachment Intensity score from the MAAS as the
dependent variable, with similar results: F (3, 77) = 1.35, p = .265 (Table 8; Figure 2). A
significant issue in the interpretation of the preceding analyses is the uneven distribution of
69

the sample across the Conceptual Level dimension of the ORI (Table 9). In view of this
limitation, several other analytical strategies were employed.
Correlation coefficients were computed among the Quality of Attachment factor, the
Intensity of Attachment factor, and only the Conceptual Level of the mother narrative (Table
10). Since the Conceptual Level score is ordinal, Spearman’s rho was computed for this
comparison. The results of the correlational analysis were nonsignificant (.02 for Quality
and -.210 for Intensity). See Figures 3 through 5 for distributions of Conceptual Level across
the MAAS Quality, Intensity, and Global scores.
In the following analysis, the ORI scores for Conceptual Level were collapsed into
two groups: Participants with narratives in the Sensorimotor-Preoperational and Concrete
levels were combined and those with narratives in the External and Internal Iconic level were
combined. A two-way contingency table analysis was conducted to assess whether there
were differences in the Quality of Attachment factor between the two levels of narratives
(Table 11). The Quality scores were divided above and below the mean and, once more, test
results were nonsignificant: Pearson χ² (1, N = 83) = .855, p = .465. A second analysis was
undertaken, forming three groups of attachment scores: “Low,” lowest through -.6,
“Average,” -.5 through .5, and “High,” .6 through the highest score (Table 12). (Since there
were no scores greater than +1 standard deviation from the mean it was necessary to choose
.5 as the point for analysis.) The test statistic changed slightly: Pearson χ² (2, N = 83) = .111,
p = .946 and, once again, the problem of unbalanced distribution across the groups of
attachment calls for caution in interpretation.
70

These two analyses were repeated exploring the relationship between MAAS
Intensity of Attachment scores and Conceptual Level of the mother narrative. The first two-
way contingency table analyzed two levels of object representation Conceptual Level,
Preoperational/Concrete and External/Internal Iconic, and two levels of Intensity, above and
below the mean. Table 13 displays the nonsignificant results: Pearson χ² (1, N = 81) = .173,
p = .727. The second analysis repeated the stratification of Conceptual Level and also
stratified Intensity into three levels: “Low” (lowest through -.6), “Average” (-.5 through .5),
and “High” (.6 through the highest score). These nonsignificant findings appear in Table 14:
Pearson χ² (1, N = 81) = 2.04, p = .361. In light of these findings, no further analyses were
performed. The results suggest that the participants’ mental representations of their mothers
were not related to the quality or intensity of antenatal attachment as evaluated by the
MAAS.
Hypothesis Two
Originally, it was also proposed that these same analytic procedures would be carried
out with participants’ narratives about their fetuses. However, in scoring the narratives it
became apparent that the twelve characteristics from which the Benevolent, Punitive, and
Ambitious dimensions are derived were not appropriate for a narrative about an unborn baby.
Three dimensions, Ambivalence, Length, and Conceptual Level, were retained for analysis,
and a MANOVA was conducted with these dimensions and the MAAS Global Attachment
score (once again divided into an “Above the Mean” group and a “Below the Mean” group).
A significant difference between the groups was found, Wilks’ Λ = .843, F (3, 81) = 5.031, p
= .003, η² = .157. Means and standard deviations are contained in Table 15. Analyses of
71

variances (ANOVA) on each dimension were conducted as follow-up test to the MANOVA.
The ANOVA on the Ambivalence dimension was significant, F (1, 83) = 11.12, p = .001, η²
= .118, while the ANOVAs on the Length, F (1,83) = .026, p = .873, and Conceptual Level,
F (1, 83) = .003, p = .958, were nonsignificant. When subjected to the same second analyses
with the Global Attachment score categorized in three levels, the significance remained;
Wilks’ Λ = .769, F (6, 160) = 3.735, p = .002, η² = .123 (Table 16). In the follow-up
ANOVAs on each dimension, the statistic on Ambivalence increased in significance, F (2,
82) = 8.52, p = .000, η² = .172. Baby narrative Conceptual Level and Length remained
nonsignificant. These findings suggest that mothers who express ambivalent feelings about
their babies have slightly lower Global scores of antenatal attachment.
It was hypothesized that women who could articulate more complex representations
of their mothers would also be able to do so of their babies, as evaluated by the Conceptual
Level dimension of the ORI. Taking into consideration the ordinal quality of the measures, a
Spearman’s rho analysis was performed and no significant association between the
Conceptual Levels of the two narratives was suggested, r = .068, p = .55. Figure 6 illustrates
the distributions of Conceptual Levels of the two narratives. Two other dimensions of the
two narratives, Ambivalence and Length, were also compared. The results of the
correlational analyses presented in Table 17 show that 8 out of the 15 correlations were
statistically significant, ranging from r = .27 to r = .72. All significant correlations were
related to Ambivalence or Length, one of which was associated with Conceptual Level. The
findings seem to suggest that women who express ambivalence toward their mothers also
express it of their babies, and these narratives tend to be more fluent than those in which no
72

ambivalence is scored. The length of the baby narrative was positively associated with the
Conceptual Level of the baby narrative, perhaps not surprising in that higher Conceptual
Levels would require greater articulation.
Two bi-level variables were created by collapsing the Conceptual Levels of mother
and baby narratives into two categories, Preoperational/Concrete and External/Internal
Iconic. A two-way contingency table analysis was conducted to evaluate whether there were
associations between these broader categories of representation. The results of the test were
nonsignificant, Pearson χ² (1, N = 82) = .206, p = .695 (Table 18). Although the two
narratives may resemble one another in terms of Ambivalence and Length, the findings do
not support any association on the dimension of Conceptual Level.
Hypothesis Three
According to Condon’s model of antenatal attachment, expectant parents resided in
one of four quadrants of attachment style, estimated by the scores on the Quality and
Intensity factors (Condon, 1993). The final stated expectations of the primary hypotheses
were that dependent tendencies would be more highly associated with an anxious, ambivalent
style of prenatal attachment as conceptualized in the fourth quadrant of the MAAS
Attachment Style paradigm. Self-critical tendencies, as identified by scores above the mean
on the Depressive Experiences Questionnaire (DEQ) were expected to be more highly
associated with a high quality of attachment but an avoidant style (second quadrant).
Blatt’s original scoring method of the DEQ (raw scores are transformed into z scores,
weighted according to the factor they are most highly correlated, and summed) was
employed for these analyses (Blatt et al., 1976). Means and standard deviations of the DEQ
73
are located in Table 4. First, a Pearson’s product-moment correlation was performed
between the DEQ z scores for dependency and self-criticism and the MAAS Global, Quality,
and Intensity of Attachment scores (Table 19). The self-critical scale of the DEQ was
negatively correlated with the MAAS Quality of Attachment factor (N = 91; r = -.366, p <
.000), but analysis revealed no significant association between the self-critical scale and the
MAAS Intensity of Attachment factor. Dependency was not found to correlate with either
the quality or intensity of attachment.
In the next analyses, participants were identified by one of Condon’s quadrants
according to their scores on the Quality and Intensity factors of the MAAS. Following
Condon’s theoretical framework, four categories were established: Quadrant One, high
Quality and high Intensity (strong, secure) ; Quadrant Two, high Quality and low Intensity
(avoidant); Quadrant Three, low Quality and low Intensity (withdrawn); and Quadrant Four,
low Quality and High Intensity (anxious, ambivalent). Quality and Intensity were rated
“high” when above the mean of the sample and “low” when below the mean. Figure 7
portrays the distribution of the sample according to Condon’s formulation. In order to
identify highly dependent or highly self-critical individuals from the DEQ scores, it had been
proposed that the sample be divided into individuals within and outside of two standard
deviations of the mean. After the data were collected, it became apparent that this strategy
was not the best way to analyze the data because of the homogeneity of the scores.
Therefore, differences of greater or less than one standard deviation on the DEQ scores
established three categories of the Self-critical style (M = -.93, SD = 1.01) and Dependent
style (M = -.53, SD = .90). (Categories were “Low” < -1 standard deviation from the mean,
74

“Average” > -1 but < 1 standard deviation from the mean, and “High” > 1 standard deviation
from the mean. A contingency table analysis was then conducted to investigate whether
pregnant women who are more self-critical reported a higher quality of attachment but a
lower intensity (Quadrant Two). A Pearson χ² analysis was nonsignificant, (6, N = 91) =
5.714, p = .456. However, the sample size was not large enough to afford a valid
interpretation (Table 20). Therefore, the Self-Criticism factor was condensed to two levels,
below and above the mean (M = -.93). The sample still lacked power, however the Pearson
χ² was significant, (3, N = 91) = 8.93, p = .03, η² = .21 (Table 21). Nevertheless, a look at the
sample reveals that those individuals who are more self-critical are less likely to reside in the
Avoidant quadrant than in the other three. It is unlikely, even with greater power, the
hypothesis would be supported.
The same approach was attempted with Dependency scores. In this sample, so few
participants scored in the average range of DEQ Dependency that the resulting Pearson chi-
square analysis cannot be interpreted (Table 22). The second analysis, identifying subjects as
above or below the mean on the Dependency factor, improved the distribution of the sample,
but those who endorse dependent statements do not appear to have a clear preference for any
of Condon’s four quadrants (Table 23). Although the analyses are somewhat underpowered,
these findings suggest that women who are more self-critical report a lower quality of
attachment and trend toward the third (withdrawn) and fourth (anxious ambivalent) quadrant
attachment styles in Condon’s model. There appear to be no significant differences in the
level of attachment intensity such women report. On the other hand, the attachment scores of
women who are more dependent do not to fit clearly into any of the Condon quadrants.
75

Hypothesis Four
It was further expected that women with a self-critical personality style would convey
object representations of a higher Conceptual Level and report a higher quality of attachment
than women with a dependent style. Once again, the distribution of the sample across the
categories did not allow for a valid analysis of four Conceptual Levels of the narrative by
self-criticism or dependency in three categories, Low, Average, and High (Tables 24 and 25).
Even when stratifying the narrative Conceptual Level into two levels
(Preoperational/Concrete and External/Internal Iconic) and the DEQ Dependency and Self-
Critical factors above and below the mean (Tables 26 and 27; Figures 8 and 9), the sample
does not distribute as expected, and is not significant. For the Self-Critical model, the
Pearson χ² (1, N = 83) = 1.51, p = .272; for the Dependent model, the Pearson χ² (1, N = 83)
= 1.32, p .284. However, the data trend toward a refutation of the original hypothesis.
Secondary Hypotheses
Hypothesis Five
The secondary hypotheses are to be viewed as exploratory. Firstly, it was
hypothesized that fetal representation and attachment might be influenced by the type of risk
(maternal, fetal, or combined) described to the patient by her obstetrician. A one-way
analysis of covariance (ANCOVA) was conducted. The independent variable, Conceptual
Level of the ORI, included two levels: Preoperational/Concrete and External/Internal Iconic.
The dependent variable was the MAAS Global attachment score and the covariate was risk.
The ANCOVA was non significant, F (1, 82) = .05, MSE = 2.49, p = .823. Holding risk
76
constant, there was no relationship between Conceptual Level of the baby narrative and the
Global attachment score.
Secondly, it was expected that those mothers identified as being hospitalized for
significant risk of fetal demise would report higher antenatal attachment, as indicated by the
global score of the MAAS, than mothers hospitalized because of significant maternal risk
factors. The risk factors of the revised Hobel scale as identified primarily “fetal” or
“maternal” are listed in Tables 28 and 29. A one-way analysis of variance was conducted to
evaluate the relationship between type of risk and attachment. The independent variable,
type of risk, included three levels: fetal, maternal, and both fetal and maternal. The
dependent variable was the change in the Global score of the MAAS. The ANOVA was
nonsignificant, F (2, 90) = .436, p = .648. The means and standard deviations for the three
types of risk are reported in Table 30 and portrayed in Figure 11. Since the third group
incorporates fetal risk, the three groups were combined into two groups, maternal and
fetal/combined maternal-fetal. Another one-way analysis of variance was conducted and was
also nonsignificant, F (1, 90) = .04, p = .841. The means and standard deviations for the two
groups are reported in Table 31. These results suggest that the type of obstetric risk has little
association with mental representation or reported attachment.
Hypothesis Six
It was expected that mothers with identified fetal risk would report a greater intensity
of antenatal attachment. First, a one-way analysis of variance was performed with the
MAAS Intensity score as the dependent variable and type of risk the independent variable
(means, standard deviations, and pairwise comparisons appear in Table 32). The ANOVA
77

was nonsignificant, F (2, 86) = 1.239, p = .295. A two-way contingency table analysis was
then conducted with three levels of risk, maternal, fetal, and fetal-maternal, and two levels of
Intensity, above and below the mean (N = 89, M = 30.71, SD = 4.88). Fetal risk and intensity
of attachment were nonsignificantly related, Pearson χ² (2, 89) = 1.36, p = .506 (Table 33).
The MAAS Quality factor and Global score were also analyzed in this manner, with no
significant findings (Table 33). The analyses were repeated collapsing risk into two
categories, maternal and fetal/combined maternal-fetal. The results remained nonsignificant,
Pearson χ² (1, 89) = .048, p = 1.00 (Table 34). A Pearson’s product-moment correlation was
performed for risk severity (represented as the sum of Hobel weighted risk items) and the
three MAAS scores (Quality, Intensity, and Global). Table 35 reports the values. A one-way
analysis of variance was also executed placing the MAAS Intensity score as the dependent
variable and the level of risk as the independent variable (means, standard deviations, and
pairwise comparisons appear in Table 36). The statistic, F (2, 86) = 1.25, p = .293, was
nonsignificant. From these analyses, there does not appear to be a significant relationship
between type of risk or level of risk severity and intensity of attachment as measured by the
MAAS.
Hypothesis Seven
It was hypothesized that older gestational age of the fetus (calculated in weeks) at the
time of admission to the antenatal unit would be positively correlated with the Global
attachment score of the MAAS. A Pearson’s product-moment correlation was employed to
assess this relationship and was also nonsignificant, so this hypothesis is disproved. Table 37
reports the correlations and probabilities.
78
Depression and Attachment
As reviewed earlier, depression and antenatal attachment have been linked by
numerous previously published studies. The data from this population support those
findings. Both screening measures, the Edinburgh Postpartum Depression Scale (EPDS) and
the Center for Epidemiologic Studies-Depression scale (CES-D) were negatively correlated
with the Quality of Attachment factor from the MAAS (Table 36). The screening measures
do not have a significant correlation with the Intensity factor, and only the EPDS is
significantly correlated with the Global score.
In order to examine this association more closely, a univariate analysis of variance
was conducted with the EPDS score as the dependent variable and attachment style as the
independent variable. The F ratio was significant, 8.693 (3, 87), p = .000, and the
relationship strong, as assessed by η², with the Quality of Attachment score accounting for
23% of the variance of the dependent variable. Post-hoc tests were performed to evaluate
pairwise differences among the means (Table 40). There was a significant difference in the
means between the groups that reside in the High Quality quadrants of Condon’s attachment
style framework. Those participants who were above the mean on the Quality factor reported
fewer depressive symptoms than those who were below the mean and in the two Low Quality
quadrants of the model. A second analysis confirmed the findings, Pearson χ² (3, 91) =
21.339, p = .000. This relationship was stronger than that reported in the ANOVA (η² = .39).
79
Exploratory Analyses
DEQ: As some have been concerned with the use of factor-derived scale scores in the
original scoring system of the DEQ, several analyses were run on the variables of interest
utilizing other scoring procedures of the instrument (Bagby et al., 1994; Rude & Burham,
1995; Santor, Zuroff, & Fielding, 1997a; Blatt et al., 1995). Bagby et al. proposed a
shortened scale in which items with excellent fit to the two-factor model (Dependency and
Self-Criticism) were isolated (1994). Blatt and colleagues identified two “facets” of the
Dependency factor that suggested two different levels of interpersonal functioning:
“Dependence,” derived from items that endorsed feelings of helplessness, broad
apprehensions about rejection or fears of separation and loss not related to a specific
individual, and “Relatedness,” the product of items that consider feelings about the loss or
loneliness that might occur as the result of disruption in a relationship with a particular
significant person (1995). Rude and Burnham theorized that dependency was not entirely
pathological, and that the Dependency scale of the DEQ could be divided into the subscales
“Connectedness” and “Neediness” (1995). Connectedness referred to healthy valuing of
relationships and neediness applied to the pathological anxiety concerning rejection and loss.
Santor et al. introduced a shortened instrument that utilizes the preferred unit-weighted
composite scoring system yet preserves the orthogonality of the factors found in the original
scoring system (1997).
First, Pearson’s product-moment intercorrelations were computed for the sample
across all four scoring systems. Table 42 reports the means and standard deviations for the
sample and Table 43 reports the intercorrelations. As would be expected, the scoring
80
systems are highly correlated; out of 28 correlations, 14 exceed r =.60, and only 5 are
nonsignificant. Note both the original scoring and the McGill scoring of the Self-Criticism
factor are not associated significantly with Rude & Burnham’s “Connectedness” aspect of
Dependency but are moderately associated with the “Neediness,” the less healthy aspect of
interpersonal functioning.
Second, Pearson product-moment correlations between MAAS attachment scores and
the three revised scoring system were conducted (Tables 44-46). The Self-Critical factor, as
scored in the McGill system, is negatively related with Quality (r = -.339, p < .01). Blatt’s
revised subscale of Dependency, Relatedness, is negatively associated with Quality (r = -
.241, p < .05) and Rude & Burnham’s subscale, Neediness, is also negatively associated with
Quality (r =-.242, p < .05).
Finally, a series of regression analyses were then conducted to compare to what
extent each scoring method of dependency and self-criticism scores could predict the MAAS
Global Attachment score. The predictors were the eight scores (original, McGill, Blatt
revised, and Rude and Burnham revised), and the criterion variable was the overall measure
of attachment provided by the MAAS. Out of four analyses, no linear combination of
dependency and self-criticism scores proved to be significantly related to the attachment
index. Table 47 contains reports the results.
Gestational age: Other investigators, as cited in the literature review, have found
relationships between attachment and gestational age, particularly after quickening. No such
relationship was found in this population in a Pearson product-moment correlation of
81
gestational age (weeks) and MAAS Global Attachment score (r = .135, p = .203), Quality of
Attachment (r = .08, p =.45), or Intensity of Attachment (r = .157, p .142).
Object Relations Inventory: The use of the Object Relations Inventory in assessing
the maternal-fetal relationship is as yet unpublished. To explore a possible relationship
between the baby narrative and gestational age, a Spearman’s rho correlation was conducted
and no significant associations were found (Table 48). Multivariate analyses of variance
were also conducted on the Length, Ambivalence, and Conceptual Level dimensions of the
mother and baby narratives across ethnicity, with nonsignificant results: Wilks’ Λ = .77, F
(18, 204) = 1.09, p = .368. Pearson’s product-moment correlations were performed between
age and the above dimensions. All correlations were nonsignificant with the exception of
ambivalence in the mother narrative, r = .230, p <.05. Within this sample, younger women
revealed more ambivalent feelings in the narratives about their mothers than did older
participants.
Another analysis explored the possibility of a relationship between the baby narrative
and having other children. A Pearson’s product-moment correlation was conducted between
“number of children at home” and the Conceptual Level of the ORI. There was no
significance: r = -.054, p = .627.
Maternal Antenatal Attachment Scale: Table 39 reports an interesting positive
correlation between age and Quality of attachment (r = .29, p < .01). This finding suggests
that older women report a higher quality of attachment than do their younger colleagues. A
second exploration investigated parity, however a two-way contingency table found no
82

significant difference in Global attachment scores of multiparous women and primagravidas,
Pearson χ² (1, 88) = 2.69, p = .10.
83

CHAPTER FIVE
Conclusions and Recommendations
The purpose of the present investigation was to delineate the convergence of
personality, object representation, and antenatal attachment in the context of significant
maternal or fetal risk. Previous research in general populations has associated depression
with the personality tendencies of dependency and self-criticism, and also with lower levels
of development in object representation. As these relationships have been investigated in
women during the perinatal period, findings have suggested that not only are there
relationships between personality, object representation, and depression, but depression often
impinges upon the natural process of maternal attachment to baby (Priel et al., 2001).
Depression and attachment seem to have a reciprocal relationship, for other research has
suggested that strong antenatal attachment acts as a protective factor against postpartum
depression (Priel et al., 1999). Most prior research has focused on uncomplicated
pregnancies in a Caucasian, middle-class, married population, however studies that have
included women with elevated obstetric risk have suggested that such risk may be both a
moderate predictor of postpartum depression and a risk factor for healthy antenatal
attachment. This study attempted to assess the variables of personality, object representation,
and maternal/fetal risk with the expectation they would have heuristic value in predicting
antenatal attachment and clinical value in identifying those women at risk for postpartum
84
depression. The knowledge of significant risk in the hospital environment was expected to
interact with these other factors by increasing the level of attachment to the fetus that
hospitalized women report.
CHARACTERISTICS OF THE SAMPLE
Demographic Qualities
In addition to their hospitalization, the 91 women who participated in this research
were quite different from the sample groups of previous studies. Almost half of the
participants were not Caucasian, however the percentage of Caucasian patients who
participated in the research is congruent with the general population of the Dallas area
(53.8% versus 59.1%). The sample percentage of Hispanic patients is slightly smaller (11%
versus 35.6%) and the number of African American patients is slightly higher (33% versus
20.3%) than the Dallas demographic (2004 Dallas Community Census). Previous research
done in this country has been done with samples that were predominantly Caucasian: Studies
utilizing high risk samples like those of Gupton (77.9%) and Maloni (94%) have to this date
underrepresented other ethnicities (Gupton et al., 2001; Maloni, Brezinski-Tomasi, &
Johnson, 2001).
Participants’ average age was 27 years, with a range of 17 to 44. This sample was
slightly younger than other research with high risk populations (Gupton reported a mean age
of 29.27 and Maloni reported 31.2) as well as with samples of women with uncomplicated
pregnancy (Zimmerman and Doan reported 30.06 and Lindgren reported 29.5) (Zimerman &
Doan, 2003; Lindgren, 2001).
85

Socioeconomic status was balanced: 24% reported less than $25, 000 in household
income, 35% reported between $26,000 and $65,000, and 29% exceeded $66,000 annually.
In comparison to Gupton’s sample, this group is somewhat wealthier (Maloni did not report
income). Educational attainment was also well represented. Eleven percent of the sample
did not finish high school, but 25% graduated or received a GED, 33% had some college, and
26% had an undergraduate/graduate degree. Ninety-four percent of Maloni’s sample had
some college (Gupton did not report education), but this is not representative of the Dallas
demographic. According to the 2004 Dallas Community Survey, 76% of Dallas County
residents 25 years and older are High school graduates and 28% have a Bachelor’s degree or
higher. The 91 women included in this research represent the area population fairly well.
According to Cornell University New Service, out-of-wedlock births accounted for
one-third of all U. S. births in 2003, exactly the same ratio of unmarried participants in this
study (Lang, 2005). Sixty-five percent were married or were cohabiting. This also
distinguishes the sample from previous psychosocial studies, as most of the participants in
other samples have been married (Gupton, 85.6%; Maloni, 92.1%).
Pregnancy-Related Qualities
Another distinctive quality of this sample is the range of new mothers to primaparous
mothers. Thirty-two percent of the sample was experiencing a first pregnancy, 24.4% were
experiencing their second, 22% their third, and 21.6% had a range of four to seven previous
pregnancies. Fifty-three percent of Gupton’s participants were pregnant for the first time,
and Lindgren reported her sample as being 41% primaparous. Maloni, in her discussion of
the impact of bed rest upon the families of her participants, reported that 45 of the 89 women
86
had other children. In this sample, 54.9% of the women had at least one child at home (33%
had two children, and 15% had from three to six children in the household).
Psychiatric Qualities
Although psychiatric illness was not a specific interest in this study, it is of interest to
compare the prevalence rates of depression and anxiety published in the Diagnostic and
Statistical Manual of Mental Disorders with the rates found in this sample of women (2000).
Almost seven percent of the sample had history of being diagnosed with depression (point
prevalence in community samples is 5-9%), and the same number reported receiving a
diagnosis of one of the anxiety disorders (one-year prevalence rate in community samples is
5%). Three percent reported a dual diagnosis (community rates are around 10%), and one
participant had previously been diagnosed with bipolar disorder (lifetime prevalence
approximately 0.5%). Almost 42% of the women scored at or over the threshold (score of
11) of the Edinburgh Postpartum Depression Scale (EPDS), and 44% scored at or over the
threshold (score of 16) on the Center for Epidemiologic Studies-Depression scale (CES-D)
provoking the administration of the Structured Clinical Interview for Diagnosis of Axis-I
Disorders (SCID). Yet of these administrations, although two participants fully met the
criteria for a dual diagnosis of Major Depressive Disorder and Generalized Anxiety Disorder,
none met the criteria for a diagnosis of depression alone. Although it is beyond the scope of
this discussion, this is a common finding due to the difficulty of choosing a threshold score
on depression screening instruments with the acceptable balance of specificity and sensitivity
(Austin & Lumley, 2003; Cox & Holden, 2003a). In Austin and Lumley’s review article of
antenatal screening research, four out of sixteen published studies reported similarly high
87
percentages of subjects exceeding the threshold. One possible explanation for the
discrepancy between positive screenings for depression and negative diagnoses in this
sample pertains to the DSM-IV criteria for Major Depressive Disorder. The EPDS instructs
the subject to answer the questions based on how she has felt over the last seven days,
however the DSM-IV criteria require that the depressive symptoms have been in place for
most of the day over the previous two-week period. The participants in this study completed
the questionnaire within the first 72 hours of hospitalization; the clinical interviews were
usually administered at a later point, dependant upon patient and research investigator
availability. Often patients would report that they had been upset initially upon
hospitalization but were “feeling better now that things have settled down.”
Varieties of Obstetric Risk
The Hobel Risk Asssessment system includes 51 antenatal maternal and fetal risk
factors (Tables 28 and 29). Its design was to enable an assessment of prematurity probability
(Hobel et al., 1973). However, the original instrument did not include in the prenatal
inventory four conditions that often present in hospital admission for obstetric risk:
Premature rupture of the membranes, preterm labor, placenta previa, and placental abruption.
In this study, these four common diagnoses were included in the risk assessment, and
weighted for severity by the Principal Investigator of the study, obstetrician John Rosnes.
Three studies provide interesting comparisons of common risks (Table 49). Perhaps
Gupton’s study is the most similar in context, for it included 105 women hospitalized for
more than 48 hours. Maloni’s study sample consisted of 89 women prescribed antepartum
bed rest in the hospital or at home, and participants in Besser’s study were not hospitalized.
88
However, there are significant differences across these three samples, testifying to the
difficulty of comparing this sample with others in the population.
DISCUSSION OF FINDINGS
Maternal Object Representation and Maternal Antenatal Attachment
A previous investigation found significant associations between antenatal attachment
and object representation (Priel et al., 2001), but the data from this sample does not support a
relationship between the two constructs. Multiple statistical analyses, both parametric and
nonparametric, were employed manipulating the sample in several configurations and all
failed to reach significance. Contrary to the hypotheses, it is intriguing that the MANOVA
procedures examining the Maternal Antenatal Attachment Scale (MAAS) scores of Quality,
Intensity, and Global attachment across the Conceptual Levels of the narratives consistently
associated lower attachment scores to the participants rated the highest in developmental
level on the Object Relations Inventory (ORI) narratives. This nonsignificant trend is an
example of the hazard of sampling error, for only eight subjects fell in the lower two levels
of development (Sensorimotor/preoperational and Concrete) in the mother narrative as
opposed to 75 found in the two higher levels of development (External and Internal Iconic).
Although the sample reached the stated minimum of 90 subjects, the power was insufficient
for confidently detecting differences in some analyses, particularly those involving the six
dimensions of the ORI. Nevertheless, this study was an effective pilot in terms of exploring
trends or signals.
89
Priel and Besser employed both the ORI and the MAAS in a study of 120 Israeli
women with uncomplicated pregnancies and a mean age of 25.21 (SD = 3.50; Priel et al.,
2001). Table 50 displays a comparison of the ORI and MAAS means and standard
deviations from their sample with those of this work. The statistics of the two samples
overlap in each score with the exception of “Punitive.” In regard to the attachment measure,
the Quality score means are within one point of one another, while the Baylor sample
Intensity means exceed those of the Israeli sample by three points. Priel and Besser were
able to report significant correlations between each ORI dimension and Quality of
attachment, as well as a significant correlation between Conceptual Level and Intensity of
attachment. Table 51 compares the correlations of the two samples. A primary difference
between the two samples is the presence of obstetric risk in the Baylor subjects, but the
differences in findings are more likely a product of discrepant sample sizes (the Israeli study
included 120 participants, 45% more than the Baylor sample).
In the absence of relationships between the ORI dimensions and the MAAS scales,
there are some interesting relationships within the ORI. One rather strong association found
in the mother narrative is that between the characteristics of Ambivalence and Length (r =
.40, p = .000). The scoring manual of the ORI directs Ambivalence to be evaluated by the
degree to which the subject relates opposing feelings about the “other,” or expressing
confused, mixed feelings. Length is evaluated by counting the lines in the narrative. In
taking a look at the specific narratives with high ambivalence scores, it clearly takes more
fluency for the subject to express the confusion. One narrative demonstrates this vividly:
My mother just turned 44 years old this month. She is also the mother of ten children, but if it weren’t for abortion and miscarriges (sic) she would probably
90
have 25 kids. She had me at the age of 16 and I was raised by my grandmother. My mother has never really had a job for a long time but she is very educated. She as attained several different degrees and not once put one to use. I sometimes believe that she has multiple personalities but she does have a good heart and you just have to know her to love her.
Ambivalence is also strongly negatively related to Benevolence (r = -.41, p = .000) and has
an even stronger positive correlation with the Punitive descriptive (r = .66, p = .000), further
explaining the nature of confusing feelings about the other.
Object Representation of Mother and Baby
One adventure of this study has been the exploration of the ORI narrative of the fetus.
The assumption was that women who had the capability of expressing complex highly
developed narratives about their mother would be able to do the same about their unborn
child. This was to be evaluated by a comparison of the Conceptual Levels of the two
narratives. This proved to be difficult in data collection, for few narratives about babies
could meet the criteria for the higher conceptual levels. Describing the fetus in
preoperational symbiotic language, concrete literal terms, or by fetal movement and activity
was dominant. Attributing thoughts, feelings, values, or understanding the baby on a wide
range of levels was less often noted. (See Table 9 for the frequencies of Conceptual Levels
in both narratives.) There was no significant association between this characteristic of the
two narratives. However, there were associations in the other dimensions of the scale. The
Conceptual Level of the baby narrative was associated with the length of the mother
narrative. Additionally, the length of the baby narrative was positively correlated with length
of the mother narrative (r = .720, p = .000), and ambivalence in both narratives. As pointed
out in the previous section, some scoring requires the subject to write more about the person,
91

so these relationships of length may be more functional than psychologically revealing. The
ORI has been validated in a number of populations and has no reports of level of education
biasing the narratives, but an analysis of this sample was performed for confirmation. A two-
way contingency table analysis failed to find significant differences in either the baby or
mother narratives according to educational level.
Another consideration is whether the baby narrative is actually capturing the mother’s
internal representation of her baby or her ability to imagine her baby. This would not be
contradictory to the theoretical stance that object representations differ from internal working
models in the respect that they introduce wish and fantasy into the mental representation of
the relationship. The fantasies of pregnant women have been alluded to in other antenatal
research; in fact, the absence of antenatal fantasy has been considered dysfunctional (Cohen,
1979; Grace, 1989; Cranley, 1981; Leifer, 1977). In one investigation, 184 pregnant women
were asked, “Please write a few sentences about what you expect your baby to be like”
(Sorenson & Schuelke, 1999). The responses were analyzed by a series of iterations that
ultimately identified ten major themes: Appearance, psychological traits, gender, behavior,
normalization, deification, role relations, impact on parents, spiritual, and ambiguity.
Findings indicated that fantasies tended to develop across gestational age and differed
between multiparas and primigravidas, with multiparous women seeming to be significantly
influenced by their older child. In investigation of this sample, however, no differences in
Conceptual Level of the ORI were found between women who had children at home and
first-time mothers.
92

Dependency, Self-Criticism, and Antenatal Attachment
In studies of romantic attachment in adult samples, dependency has been associated
with an anxious-ambivalent style and self-criticism with a fearful, avoidant style (Besser et
al., 2003a) (Zuroff et al., 1995). Similar findings resulted from research conducted with a
sample of women in uncomplicated pregnancy (Priel et al., 1999). Therefore, it was
expected that dependency in this sample would be related to Condon’s anxious ambivalent
antenatal attachment style (low quality, high intensity) and that self-criticism would be
associated to the avoidant antenatal attachment style (high quality, low intensity; Condon,
1993). A larger sample may have produced significance; however, the trend suggests that the
hypothesis would be disproved even in a larger sample. Those scoring over the mean of the
sample for dependency were fairly equally distributed throughout the four attachment styles.
Out of 39 individuals who scored above the mean for self-criticism, only three resided in the
Avoidant quadrant, whereas the other 36 participants were fairly evenly distributed across the
remaining three antenatal attachment styles.
A question that appears in this analysis is the suitability of the MAAS for this type of
exploration. First, it is possible that the Quality and Intensity scales of the MAAS are not
sufficiently orthogonal to produce the four theorized styles. Second, some of Condon’s
predictions regarding the scale are not confirmed in the sample. For example, he proposed
that multiparous women may be overrepresented in the second quadrant, Avoidant, due to a
lack of time in “attachment mode.” Analyses in this study found no differences between
multiparous and nulliparous women.
93

Self-Criticism, Dependency, and Object Representation
It was predicted that women with a self-critical style would convey maternal object
representations of a higher conceptual level and report a higher quality of antenatal
attachment than women with a dependent style. Only eight subjects responded with
narratives in the lower two conceptual levels opposed to 75 who were rated in the higher two
conceptual levels. Although the differences were not significant, it is noteworthy that
dependent and self-critical styles in the two-way contingency tables (Tables 26 and 27) are
exactly opposite in their placement. Those who are less self-critical tend to provide
narratives of higher conceptual levels, whereas those who are more dependent express
maternal representations of a higher level.
Also, the self-critical type failed to report a higher quality of attachment than the
dependent type. Self-criticism was, in fact, significantly negatively associated with Quality
of attachment (r = -.37, p <.000). This result is interesting in relation to Priel and Besser’s
finding that highly self-critical subjects’ risk for depression was lowered if they became
strongly attached to the fetus during pregnancy. If self-criticism is associated with a lower
quality of antenatal attachment, but attachment can reduce vulnerability to postpartum
depression, an interesting paradox exists.
Risk and Attachment
Previous research has been equivocal concerning the impact of risk on maternal fetal
attachment. Findings from this sample are not ambiguous—they are simply negative. A
number of statistical analyses investigating both type of risk (maternal, fetal, or combined)
and level of risk (low, medium, and high, calculated by the mean of the Hobel Risk
94
Assessment scores of the sample) failed to find any significant relationships between risk,
attachment, and object representation in this sample. Ruling out measurement error, it is
possible that the level or type of risk is not strong enough to affect differences in antenatal
attachment in the women in this sample (Cannella, 2005).
Depression
Both screening measures, the CES-D and the EPDS, were significantly correlated
with the Quality scale of the MAAS. However, only the EPDS was significantly associated
with the Global score, and neither instrument was associated with the Intensity scale. It
would be interesting in future research to investigate any potential associations between the
Intensity of Attachment factor and screening instruments designed for the spectrum of
anxiety disorders. Both screening instruments were significantly correlated with the
Dependency and Self-Criticism scales of the DEQ. However, neither instrument was
associated with the severity of risk.
Exploring the attachment styles of mothers who scored above and below the threshold
for possible depression on the EPDS depression instrument exposed an interesting and
significant relationship between depressive symptomatology and attachment quality. Table
41 portrays mothers over the threshold score of 11 as residing in the third (withdrawn) and
fourth (anxious ambivalent) quadrants of Condon’s model. This is consistent with previous
research referring to the tendency for depressed mothers to be withdrawn from their infants,
at great cost to the child (Dawson, Klinger, Panagiotides, Hill, & Spieker, 1992; Murray,
1992).
95
Alternate Scoring Methods for the DEQ
As mentioned in the results, psychometricians have concerns regarding the standard
scoring system utilized for the DEQ (Santor et al., 1997a; Bagby et al., 1994). In addition, a
growing movement within the domain of feminist psychology has questioned the assumption
of dependency as a maladaptive style of interpersonal relatedness (Rude et al., 1995).
Several theorists, Blatt and the fellow authors of the DEQ included, have suggested that the
Dependency scale might actually be composed of two subscales, a “healthy” one and an
“unhealthy” one. This has led to revisions of the scoring system and new subscales of
“Relatedness” and “Dependency” (Blatt et al., 1995; Bacchiochi et al., 2003) and
“Connectedness and Neediness” (Rude et al., 1995). Advocates of this stance believe this
distinction between the psychologically adaptive maintenance of close, reciprocal
relationships and the pathological fearful, helpless, and clinging approach to others may
explain why often those who score highly in Dependency are less vulnerable to depression
(McBride, Zuroff, Bacchiochi, & Bagby, 2006; Besser, Flett, & Davis, 2003; Zuroff et al.,
1995). As seen in Table 43, the samples’ DEQ scores were calculated by each method and
then compared for associations. Of note are the positive correlations between the two Self-
Criticism scores and Rude and Burnham’s Neediness subscale, and the lack of association
between the Self-Criticism scores and the Connectedness subscale. The difference, while
still significant, is not so striking when comparing Blatt’s subscales, Dependency and
Relatedness, with the standard scales. This generates the question of what is being measured,
personality tendencies or a vulnerability to depression that transcends self-criticism or
dependency?
96
When testing the other scoring methods for associations with attachment, there are
significant findings. The McGill scoring system produces the same negative correlation
between Self-Criticism and Quality of attachment (r = -.339, p < .001), as the standard scale
(r = -.336, p <.000), and correlations between Dependency, Intensity of attachment, and
Global attachment are all nonsignificant. Blatt et al’s subscale Relatedness (the healthy,
mature form of dependency) has a significant negative association with the Quality of
Attachment factor (r = -.24, p = .02). Adding to the confusion, Rude and Burnham’s
Neediness (the unhealthy, pathological type of dependency), has the exact same significant
negative association with Quality of attachment (r =-.24, p =.02). It is difficult to
understand why both the healthy and unhealthy forms of dependency would be negatively
correlated with attachment quality. This might be instrument error, or some piece of the
Dependency construct might be relating in an underlying fashion to the attachment measure.
When all eight scores are subjected to a linear regression with the Global attachment
score, all fail to reach significance. The standard scoring system and the McGill scoring
system are slightly more powerful than the subscales of the Dependency factor, no doubt
because of the inclusion of the Self-Criticism factor. Although it is possible that a larger
sample size would drive some of these analyses into significance, it appears that the
relationship of self-critical and dependent tendencies with attachment is far less important
than the relationship between depression and attachment. The Self-Critical and Dependent
factors of the DEQ may be more valuable in identifying risk factors for postpartum
depression than in identifying risk factors for low or poor quality attachment.
97

Gestational Age and Attachment
Since previous research has suggested that attachment grows with gestational age, it
was surprising that gestational age was not associated with the level of attachment reported
by the participants. A common observation across studies has been that fetal movement is a
trigger for increased antenatal attachment, and all subjects in this sample had experienced
quickening (Mikhail et al., 1991; Reading et al., 1984). This may have rendered the analyses
useless. However, one narrative underscores the individual nature of antenatal bonding:
“…I must say that he wasn’t planned. Me and his father were not trying to get pregnant, but it happened so quickly my eyes didn’t have time to blink.
I didn’t bond with him until I was almost 5 months pregnant. At this time, that’s when the secret about me being pregnant was finally out of the bag to my family and everybody I hid it from…”
Another confounding issue with this research is that all participants had received at
least one sonogram, many of them three-dimensional, and had pictures of the fetus at
bedside. The impact upon antenatal attachment of viewing the fetus through sonogram has
been under investigation although findings have been inconclusive (Reading et al., 1984;
Righetti, Dell'Avanzo, Grigio, & Nicolini, 2005).
Exploring Fetal Object Representation
In addition to testing the hypotheses, a few other questions were asked. Joy Penticuff
highlighted the developmental resolution of ambivalence toward a new member of the family
that occurs over the course of pregnancy (Penticuff, 1982). It was supposed that this
ambivalence was intensified in mothers with higher obstetric risks. However, in all the
analyses of risk, no significant association was found between the Ambivalence dimension of
the ORI and risk. There was a significant association between Ambivalence in the mother
98

narrative and Ambivalence in the baby narrative, suggesting that these conflicting feelings
may be more a characteristic of the mother rather than of a particular mental representation.
In addition, Ambivalence was negatively correlated with the Global attachment score,
implying that this characteristic has implications for antenatal attachment.
Other analyses tested for relationships between the ORI dimensions, ethnicity and
age, with no significant differences found in the narratives. The ability to convey complex
information about mother or baby does not seem to be related to factors outside the process
of mental representation.
A final curiosity about the fetal narrative had to do with the theories behind internal
working models and mental representations. If these are activated during infancy and are
primarily associated with caregiver relationships (and later to romantic attachment figures),
perhaps there is a distinctly different model or representation a mother constructs of her
child. This model and representation may be focused on caregiving, instead of care
“receiving.” If so, multiparous women might have a certain facility with the mental
representation of their baby that nulliparous women, with no previous model or
representation of a baby, do not possess. This was not borne out statistically and, although
the sample size was adequate for the chi-square analysis, there were no significant
differences in the Conceptual Level of the fetal narratives according to parity.
99

Maternal Antenatal Attachment Scale
The positive correlation between age and the Quality of attachment factor was
moderately strong (r = .292, p = .005). It appears that older mothers may have more positive
thoughts about their babies than younger ones, although there is no difference in their level of
preoccupation with the fetus. It has also been stated that multiparous women spend less time
in “attachment mode” because of caregiving responsibilities for other children. However,
this was unsupported in the sample, as there were no differences in attachment scores
between first-time mothers and those with children at home.
THEORETICAL IMPLICATIONS
While this study did not find the proposed relationships between personality
characteristics, mental representation, and attachment, the limitations of the sample size warn
against premature conclusions. This work did, however, contribute to the ongoing dialogue
regarding the construct of antenatal attachment and its associations. In addition, it provided a
valuable, diverse sample of hospitalized women who enabled research to ask old questions in
a new context.
CLINICAL IMPLICATIONS
Even though the construct of antenatal attachment remains elusive, this research also
adds value to the growing investigation into the insidious link between depression and
attachment. Whether depressed mothers suffer from impaired attachment or a mother’s
inability to attach to a baby contributes to a vulnerability to depression remains to be seen.
100

These findings support all those before that point to the necessity of identifying, targeting,
and intervening where possible to enhance maternal-fetal attachment and treat perinatal
depression.
The idea that self-critical tendencies are a detractor of attachment as well as a strong
contributor to depressive symptomatology is not new, but this research has broadened its
application to the population of women with high-risk pregnancy. In fact, self-criticism may
be a salient contributor in this population in view of the tendency for women with high-risk
to look inward for a causal relationship between something they did or did not do and the
complications. The findings in this research, consistent with those of the Priel and Besser
team in Israel, suggest that pregnant women who are self-critical are vulnerable to depressive
feelings and may benefit from interventions that expose these tendencies. In addition, since
self-criticism also impacts antenatal attachment, interventions that enhance attachment to the
fetus may be indicated.
Although cognitive-behavioral and interpersonal approaches with postpartum
depression have been empirically studied (Dennis, 2004), only one reference was found that
suggests treating childbearing depression from an attachment theory framework (Whiffen &
Johnson, 2006). This case example illustrated how Emotionally Focused Marital Therapy, a
manualized psychotherapy based upon attachment theory, could be employed in treating
postpartum depression. Social support has been found to be protective against perinatal
depression (Priel et al., 2000a), so targeting depression from a “couples” standpoint would be
ideal for enhancing attachment and encouraging partner support. This could be even more
critical in women with obstetric risks. Hospitalization separates them from their partners,
101
increases the partner burden in terms of household, family, and financial responsibilities, and
sets in place a fertile environment for partner blame and discord. Progressive hospitals have
added group therapy to antepartum unit care for psychosocial support with equivocal results
(Dennis, 2004). Perhaps focusing on the marital dyad would be more effective in the
prevention of perinatal depression. Interventions that highlight emotional expression and
foster understanding of each spouse’s needs and childbearing fears could be operationalized
in group sessions, similar to childbirth classes, or in the hospital room privately.
LIMITATIONS AND FUTURE DIRECTIONS
The study shared two common limitations to research of this sort. Self-report
measures are often the only practical way to approach cross-sectional research. In the battery
of measures for this study, other than the ORI, the questionnaires were all forced choice
Likert-type instruments. Future research might include other forms of data gathering, such as
structured interviews or family reports. In addition, although the instruments utilized in this
study are considered to be reliable and valid, more research is needed to assess the extent to
which they genuinely evaluate these particular constructs of personality, mental
representation, and attachment.
A possible limitation for this work specifically has to do with the method of
administration of the ORI. Because this investigation was a small piece of a larger study
including a number of measures, it was decided to include the ORI in the questionnaire
packet. Although study personnel conscientiously explained to the participants to “take five
minutes and write a description of your mother and the baby you are carrying,” the packets
102
were left for completion and in some cases the narratives were either skipped (five of the 91
subjects did not complete either the mother or the baby narrative and an additional three did
not complete the mother narrative) or so short that some of the descriptive qualities were by
necessity scored as “missing.” Future studies of this sort might consider conducting the ORI
in more of an interview fashion. Initial remarks could be recorded and probing questions
asked if additional information is needed.
Rating the fetal narratives according to the standard scoring system was not possible,
as explained earlier, because the descriptives were inappropriate in application to a fetus
(Affectionate, Ambitious, Malevolent/Benevolent, Cold-Warm, Constructive Involvement,
Intellectual, Judgmental, Negative/Positive Ideal, Nurturant, Punitive, Successful, and
Strength). However, the narratives did often contain the themes Condon posits are found in
human attachment: the desire to know, the desire to be with, the desire to protect, and the
desire to prevent loss or separation. They also reflected the themes found in the earlier cited
research on antenatal fantasies: Appearance, psychological traits, gender, behavior,
normalization, deification, role relations, impact on parents, spiritual, and ambiguity
(Sorenson & Schuelke, 1999). An intriguing future exploration might involve the use of the
ORI with a specialized rating system for the fetus utilizing these previously noted themes.
Diverse samples are both desirable and problematic. Participants in this sample
covered a broad range of age, previous pregnancy experiences, cultural backgrounds,
educational levels, and socioeconomic factors. Some were from the Dallas Metroplex, a
sprawling urban environment, and others had spent their lives in small rural communities
103

well outside city life. They represent the diversity of the state of Texas fairly, however the
experience of obstetric risk is distinct from individual to individual.
The women who agreed to participate knew they were taking part in research
investigating emotions during hospitalization, so the sample may have been biased by this
knowledge. Even though all subjects were approached within 72 hours of hospitalization,
not all completed the instruments in a timely manner. Some completed quickly, others may
have taken several days. In addition, due to HIPAA regulations, it was not possible to gather
data about those who declined to participate in the research. An observation from other work
has been that those who do not participate may not do so because they are depressed. This
possibility may impair the generalizability of the findings.
Since risk was not found to have significance in these findings, a number of avenues
of investigation would be elucidating. One calls for evaluating the woman’s perspective of
the risk, in terms of both severity and the necessity of behavioral alterations. A second
approach would entail an examination of the coping resources and social support systems of
women who are hospitalized. These variables may moderate the additional stress of obstetric
risk and hospitalization. Hospitalization itself plays the part of a social support system—a
valuable look at this variable might include a population of women with complications who
are prescribed bed-rest at home. Thirdly, there has been some suggestion that depression
may be related to specific obstetric risks, such as preeclampsia (Kurki et al., 2000). A larger
sample size would permit an investigation of the impact of specific risk factors upon
attachment and depression.
104
Since no causal inferences can be made from studies like this one, longitudinal
research on women from this population would be of great value. There are many
unanswered questions concerning perinatal mental health and mother child relationships that
can only be addressed by research covering longer time periods.
Continuing the investigation into the association between attachment and depression
is vital. As observed in this research, attachment has a stronger relationship with depressive
symptoms than many other elements in the context of complicated pregnancy. In light of the
difficult decision in prenatal screening for depression of whether to increase sensitivity and
lose specificity, resulting in large numbers of false positive screenings, or decrease sensitivity
and gain specificity, risking missing depression entirely, perhaps attachment measures such
as the MAAS and personality measures such as the DEQ could supplement traditional
instruments, increasing sensitivity and specificity in the screening process. Obstetricians,
pediatricians, nurses, and social workers are in a place of advantage for intervention with
hospitalized pregnant women identified as being at risk for depression. Multidisciplinary
teams that include psychologists and psychotherapists would afford intervention at the
earliest point possible, before the baby is born.
CONCLUSION
Women who are hospitalized with high-risk pregnancy are admitted with a host of
individual needs and concerns. Some are trying desperately to hang on to a longed-for
pregnancy, some are anxious about how their family will fare in day-to-day life without
them, and others are content to stay in the care of professionals during an uncertain time.
105

They have idiosyncratic histories. Some women in this study had experienced successful,
uncomplicated pregnancies previously, while others had buried stillborns. Because Baylor
Hospital draws a diverse geographical population, women from rural farming communities
were in rooms next to women who had never been outside the city of Dallas. And in the way
of society, some patients had visitors every day and a room full of flowers while others slept
all day in darkened rooms. What they all had in common was one (or both) of two questions:
“Will my baby make it to viability? Will my baby be born OK?”
One goal of this research was to take a closer look at perinatal depression by way of
attachment. These findings agreed with other studies that have consistently pointed to the
relationship between attachment and depression. Also apparent from this work is just how
well antenatal attachment eludes theorists and clinicians alike. It was thought that exploring
this concept in the context of risk and uncertainty would contribute to the shared
understanding of what psychodynamic forces contribute to this primordial phenomenon of
mother-baby love. Attachment was slippery even in this perfect Bowlbian environment.
What did emerge clear and strong was that women report strong attachment to their fetuses
regardless of what gestational age they are, regardless of what type of mother they had
themselves, and regardless of the risk carrying this baby poses to their own life. Women who
are sad are not as sure of this attachment, but it is there, nonetheless. Women who are self-
critical may be afraid they cannot live up to the demands of mothering, but they are attached
too. These mothers just need a little help.
The continued exploration of antenatal attachment is a worthy venture, but the next
step is to take what is known and make application to intervention. The findings of this study
106

add in a small way to the growing body of knowledge that will help develop interventions
specific to impaired maternal attachment and perinatal mood disorders.
107

Figure 1 Levels of Mother Narrative Conceptual Level Across Low, Medium, and High Quality of Attachment Scores
3.002.001.00
MAAS Low, Medium, and High Quality of Attachment
30
20
10
0
ORI Mother
51Development
73
Cou
nt
Note: ORI = Object Relations Inventory 1 = Preoperational 3 = Concrete 5 = External Iconic 7 = Internal Iconic MAAS = Maternal Antenatal Attachment Scale Low = Lowest score through -.6 SD Medium = -.5 - .5 SD High = .5 through highest score
108
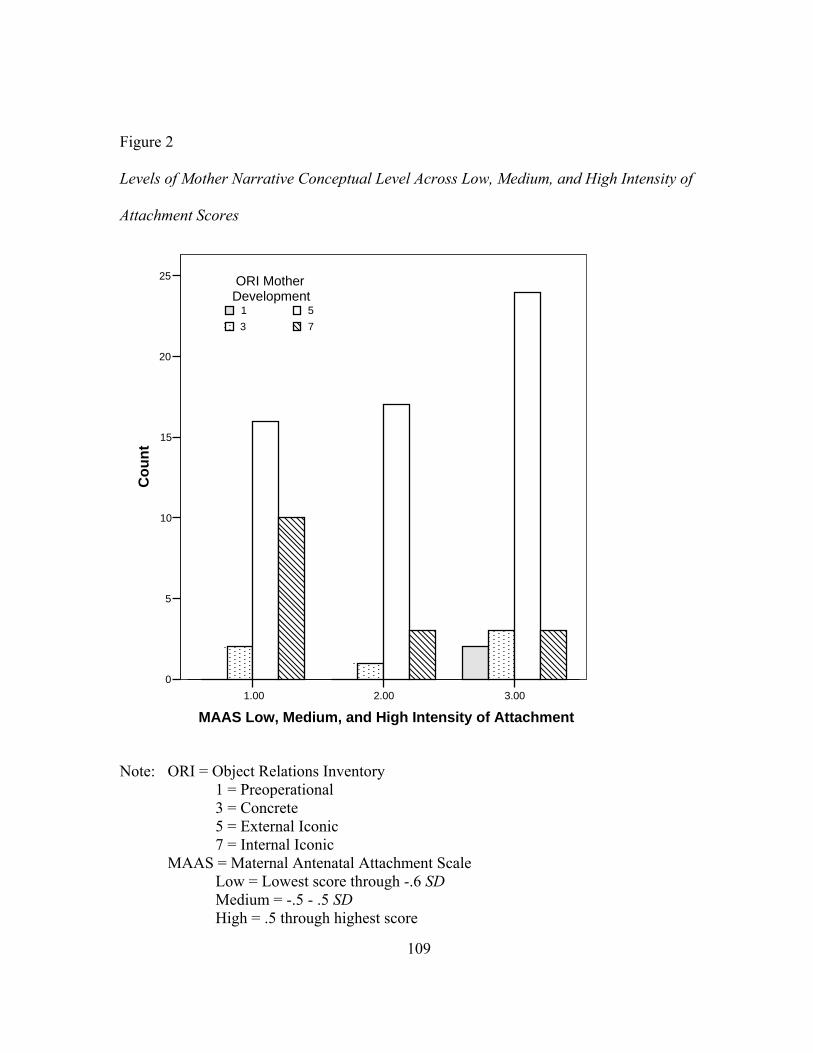
Figure 2 Levels of Mother Narrative Conceptual Level Across Low, Medium, and High Intensity of Attachment Scores
3.002.00
25
20
15
10
5
1.00
MA and High Intensity of Attachment
0
AS Low, Medium,
Cou
nt
75
31
ORI MotherDevelopment
ote:
5 = External Iconic 7 = Internal Iconic MAAS = Maternal Antenatal Attachment Scale Low = Lowest score through -.6 SD Medium = -.5 - .5 SD High = .5 through highest score
N ORI = Object Relations Inventory 1 = Preoperational 3 = Concrete
109

Figure 3 Quality of Attachment and Mother Narrative Conceptual Level
7531
ORI Mother Narrative Levels of Development
50
48
46
44
42
40
38
36
MA
AS
Qua
lity
of A
ttach
men
t
Note: MAAS = Maternal Antenatal Attachment Scale ORI = Object Relations Inventory 1 = Preoperational 3= Concrete 5 = External Iconic 7 = Internal Iconic
110

Figure 4 Intensity of Attachment and Mother Narrative Conceptual Level
7531
ORI Mother Narrative Levels of Development
40
35
30
25
20
15
MA
AS
Inte
nsity
of A
ttach
men
t
Note: MAAS = Maternal Antenatal Attachment Scale ORI = Object Relations Inventory 1 = Preoperational 3= Concrete 5 = External Iconic 7 = Internal Iconic
111
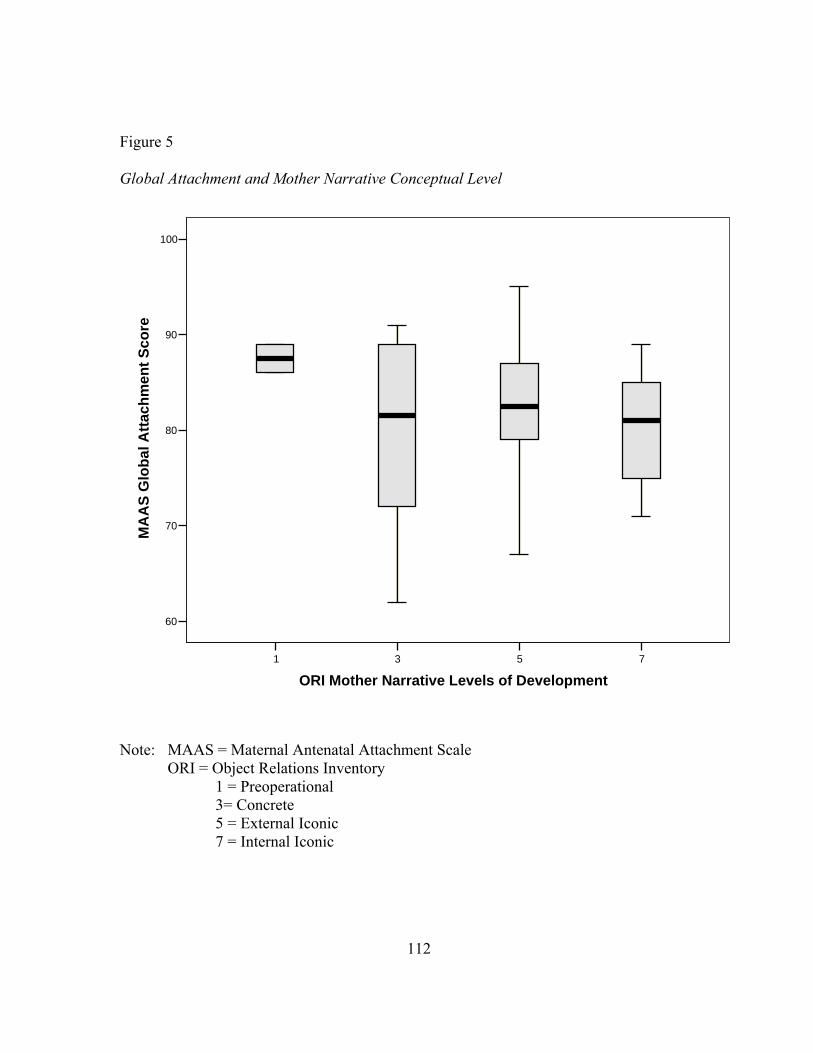
Figure 5 Global Attachment and Mother Narrative Conceptual Level
7531
ORI Mother Narrative Levels of Development
100
90
80
70
60
MA
AS
Glo
bal A
ttach
men
t Sco
re
Note: MAAS = Maternal Antenatal Attachment Scale ORI = Object Relations Inventory 1 = Preoperational 3= Concrete 5 = External Iconic 7 = Internal Iconic
112

Figure 6 Distribution of Levels of ORI Narrative Conceptual Level
7531
ORI Baby Narrative Levels of Development
30
25
20
15
10
5
0
Cou
nt
75
31
ORI Mother NarrativeDevelopment
Note: ORI = Object Relations Inventory 1 = Preoperational 3 = Concrete 5 = External Iconic 7 = Internal Iconic
113
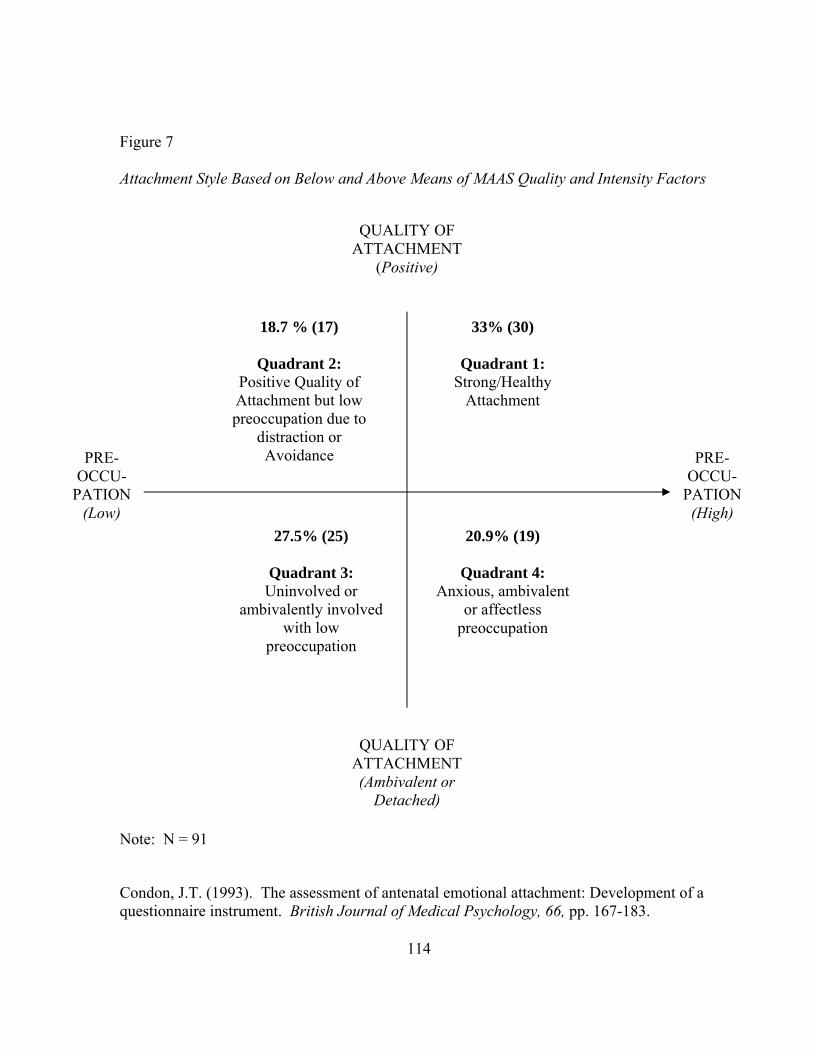
Figure 7 Attachment Style Based on Below and Above Means of MAAS Quality and Intensity Factors
Note: N = 91
QUALITY OF ATTACHMENT
(Positive)
PRE-OCCU-
PATION (Low)
PRE-
PoAtpre
QS
am
Condon, J.T. (1993).questionnaire instrum
18.7 % (17)
Quadrant 2: sitive Quality of
tachment but low occupation due todistraction or Avoidance
QUALITY OF ATTACHMENT (Ambivalent or
Detached)
27.5
QuadUninv
bivalenwit
preocc
QAnx
p
The assessment of antenatal emoent. British Journal of Medical
114
33% (30)
uadrant 1: trong/Healthy Attachment
OCCU-PATION (High)
20.9% (19)
uadrant 4: ious, ambivalent or affectless reoccupation
% (25)
rant 3: olved or tly involved h low upation
tional attachment: Development of a Psychology, 66, pp. 167-183.
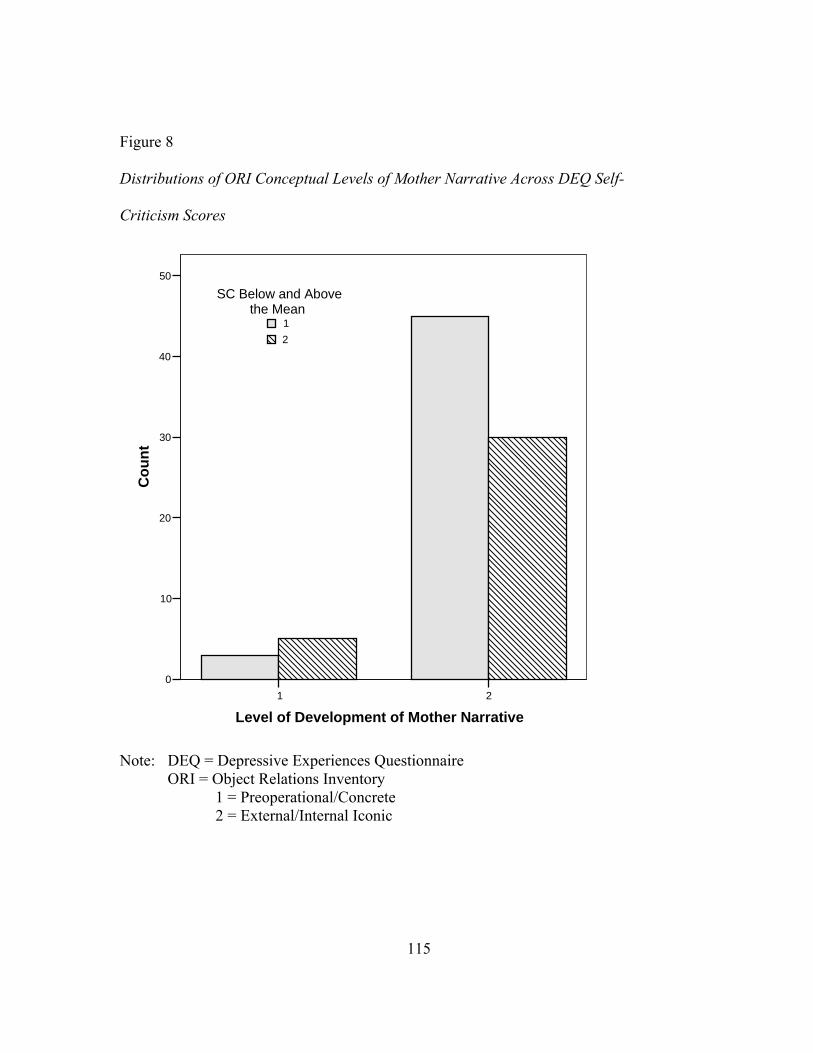
Figure 8 Distributions of ORI Conceptual Levels of Mother Narrative Across DEQ Self- Criticism Scores
21
Level of Development of Mother Narrative
50
40
30
20
10
0
Cou
nt
21
SC Below and Abovethe Mean
Note: DEQ = Depressive Experiences Questionnaire ORI = Object Relations Inventory 1 = Preoperational/Concrete 2 = External/Internal Iconic
115

Figure 9 Distributions of ORI Conceptual Levels of Mother Narrative Across DEQ Dependency Scores
21
Level of Development of Mother Narrative
50
40
30
20
10
0
C
1
Depend Below andAbove Mean
2
ount
Note: DEQ = Depressive Experiences Questionnaire ORI = Object Relations Inventory 1 = Preoperational/Concrete 2 = External/Internal Iconic
116

Figure 10 Type of Risk and MAAS Global Attachment Scores
BothFetalMaternal
Maternal, Fetal, or Combined Obstetric Risk
100
90
80
70
60
MA
AS
Glo
bal A
ttach
men
t Sco
re
Note: MAAS = Maternal Antenatal Attachment Scale
117

Figure 11 Type of Risk and MAAS Intensity of Attachment
3.002.001.00
Attachment Intensity Level
25
20
15
10
5
0
Cou
nt
BothFetalMaternal
Maternal or Fetal
Note: MAAS = Maternal Antenatal Attachment Scale
118
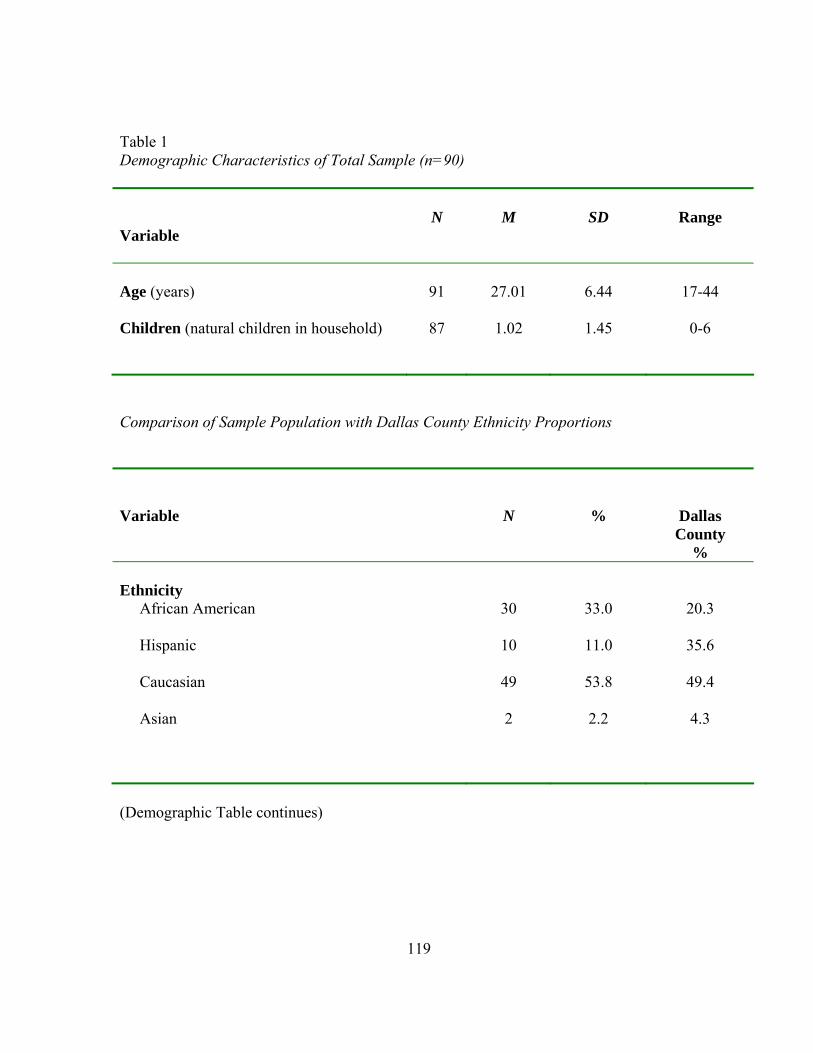
Table 1 Demographic Characteristics of Total Sample (n=90)
Variable
N
M
SD
Range
Age (years)
91
27.01
6.44
17-44
Children (natural children in household)
87 1.02 1.45 0-6
Comparison of Sample Population with Dallas County Ethnicity Proportions Variable
N
%
Dallas County
% Ethnicity
African American
30 33.0 20.3
Hispanic
10 11.0 35.6
Caucasian
49 53.8 49.4
Asian
2 2.2 4.3
(Demographic Table continues)
119
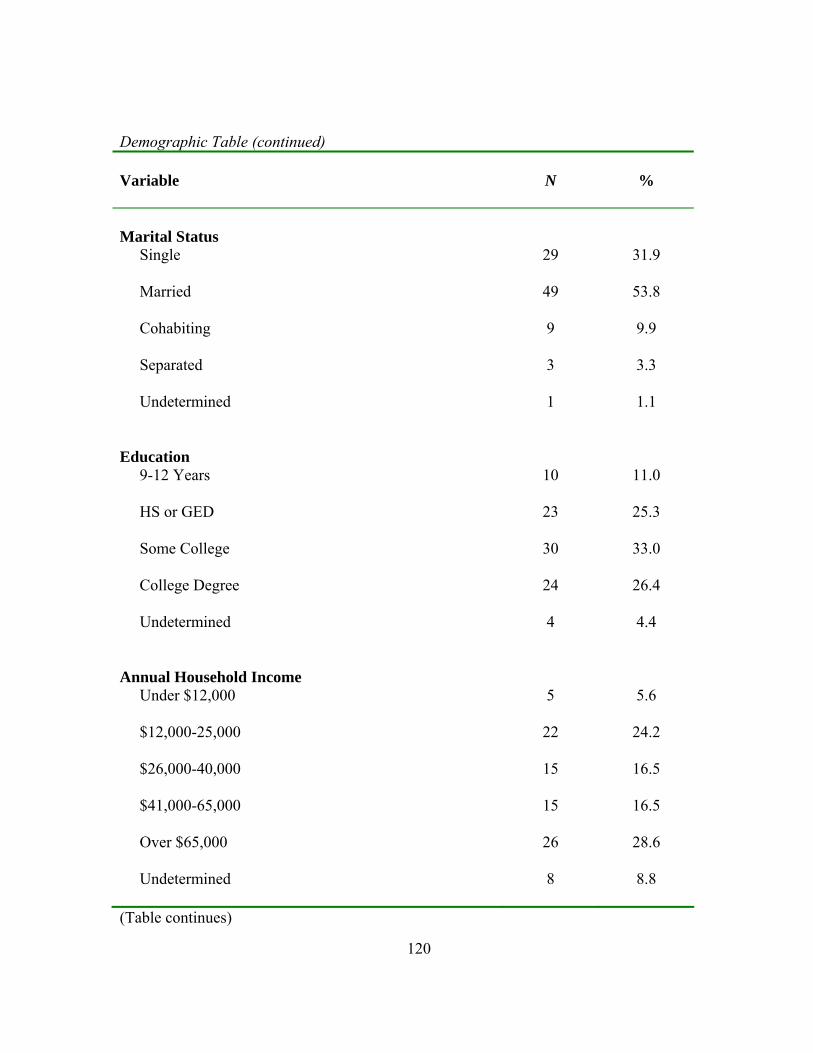
Demographic Table (continued) Variable
N
%
Marital Status
Single
29 31.9
Married
49 53.8
Cohabiting
9 9.9
Separated
3 3.3
Undetermined
1 1.1
Education 9-12 Years
10 11.0
HS or GED
23 25.3
Some College
30 33.0
College Degree
24 26.4
Undetermined
4 4.4
Annual Household Income Under $12,000
5 5.6
$12,000-25,000
22 24.2
$26,000-40,000
15 16.5
$41,000-65,000
15 16.5
Over $65,000
26 28.6
Undetermined 8 8.8
(Table continues)
120

(Demographic Table continued) Variable
N
%
Biological Children at Home
None 41 45.1
One 30 33.0
Two 6 6.6
Three 4 4.4
Four 3 3.3
Five 1 1.1
Six 3 3.3
Undetermined 3 3.4
Note: N = 91
121
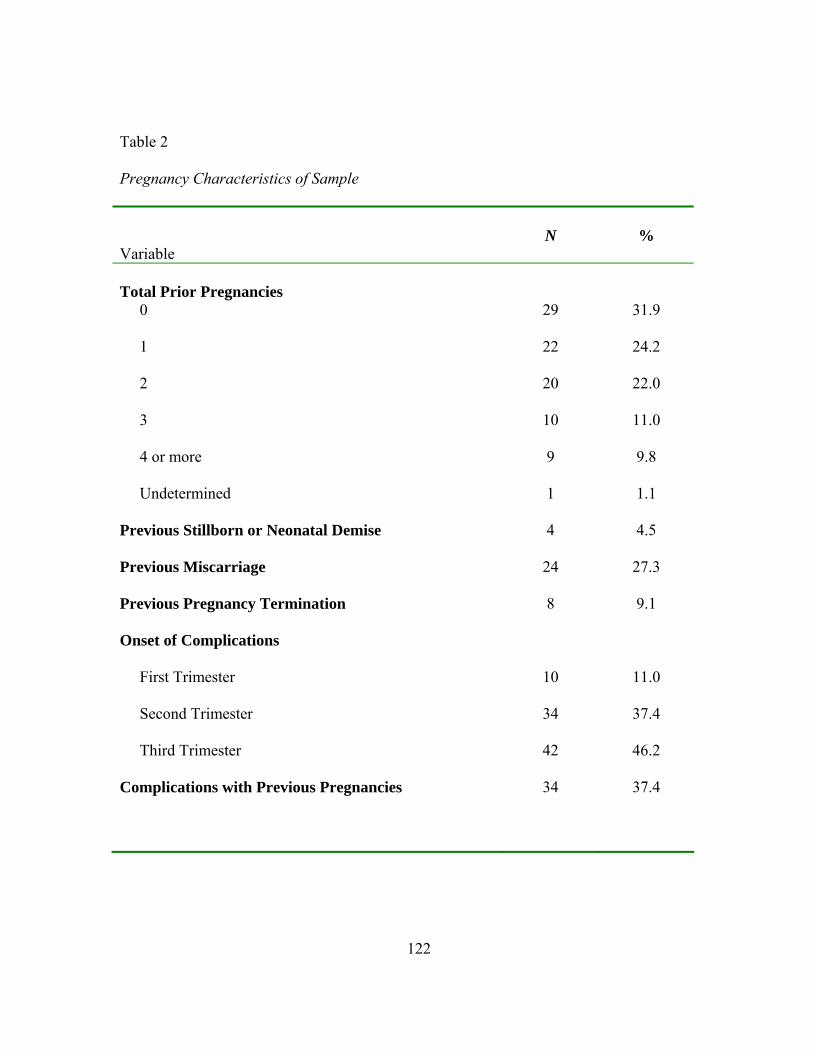
Table 2
Pregnancy Characteristics of Sample
Variable
N
%
Total Prior Pregnancies
0
29 31.9
1
22 24.2
2
20 22.0
3
10 11.0
4 or more
9 9.8
Undetermined
1 1.1
Previous Stillborn or Neonatal Demise
4 4.5
Previous Miscarriage
24 27.3
Previous Pregnancy Termination 8 9.1
Onset of Complications
First Trimester 10 11.0
Second Trimester 34 37.4
Third Trimester 42 46.2
Complications with Previous Pregnancies 34 37.4
122

Table 3 Psychiatric Characteristics of Sample
Variable
N
%
Previous Psychiatric History
Depression 6 6.6
Anxiety 6 6.6
Comorbid Depression and Anxiety 3 3.3
Bipolar Disorder 1 1.1
Undetermined 6 6.6
Positive Screening for Depression at Admission
CES-D (score > 16) 33 36.3
EPDS (score > 11) 38 41.8
Positive Diagnosis on SCID
Mood Disorder 0 0
Anxiety Disorder 5 5.5
Comorbid Mood and Anxiety Disorders 2 2.2
Family History of Psychiatric Illness 16 17.6
Note: EPDS = Edinburgh Postpartum Depression Scale CES-D = Center for Epidemiological Studies-Depression
SCID = Structured Clinical Interview for the Diagnosis of DSM-IV Axis One Disorders
123

Table 4
Means and Standard Deviations of Measures
Measure
N
M
SD
Range
Depressive Symptoms (Screening Measures) EPDS (Depression suggested at > 11)
91
9.46
5.54
0-22
CES-D (Depression suggested at > 16)
75 15.88 10.37 0-37
Personality(DEQ) Dependent Characteristics
91
-.53
.90
-2.60-1.21
Self-Critical Characteristics
91 -.93 1.01 -2.92-2.25
Antenatal Attachment (MAAS) Global Attachment Score
91
81.49
7.13
61-95
Quality of Attachment Factor
91 46.01 3.48 33-50
Intensity of Attachment Factor
89 30.71 4.88 17-40
Object Representation of Mother (ORI) Benevolent Qualities
81
4.11
1.54
.63-7.88
Punitive Nature
81 1.49 1.42 .33-6.33
Ambitious Characteristics
39 3.53 1.69 .50-7.00
Ambivalent Feelings about Mother
83 1.83 1.3 1-5
Length of Narrative
83 2.41 1.54 1-7
Conceptual Level of Narrative
83 5.17 1.22 1-7
(Table continues)
124
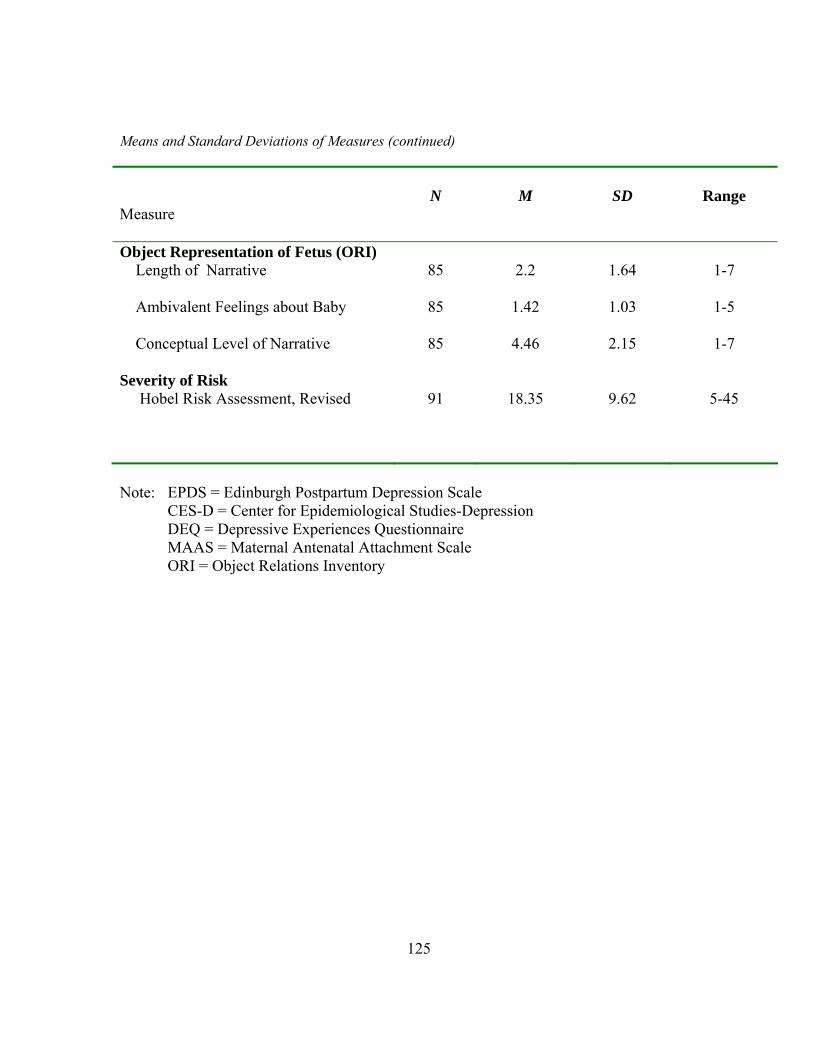
125
Means and Standard Deviations of Measures (continued) Measure
N
M
SD
Range
Object Representation of Fetus (ORI) Length of Narrative
85
2.2
1.64
1-7
Ambivalent Feelings about Baby
85 1.42 1.03 1-5
Conceptual Level of Narrative
85 4.46 2.15 1-7
Severity of Risk Hobel Risk Assessment, Revised
91
18.35
9.62
5-45
Note: EPDS = Edinburgh Postpartum Depression Scale
CES-D = Center for Epidemiological Studies-Depression DEQ = Depressive Experiences Questionnaire MAAS = Maternal Antenatal Attachment Scale ORI = Object Relations Inventory

Table 5 Means and Standard Deviations on Dimensions of the Object Relations Inventory Mother Narrative for Global Attachment Above and Below the Mean
Mother Narrative
Benevolent
Punitive
Ambitious
Length
Ambivalence
Conceptual
Level MAAS Global Attachment Score (M = 81.5)
M SD
M SD
M
SD M
SD M
SD M
SD
Below the Mean 4.38
2.11 1.81
1.65
3.43
1.70 2.79
1.85 2.43
1.79 5.57
1.22
Above the Mean 4.27
1.20 1.72
1.61
3.58
1.72 2.28
1.28 1.88
1.24 5.08
.91
Note: N = 83 MAAS = Maternal Antenatal Attachment Scale
126
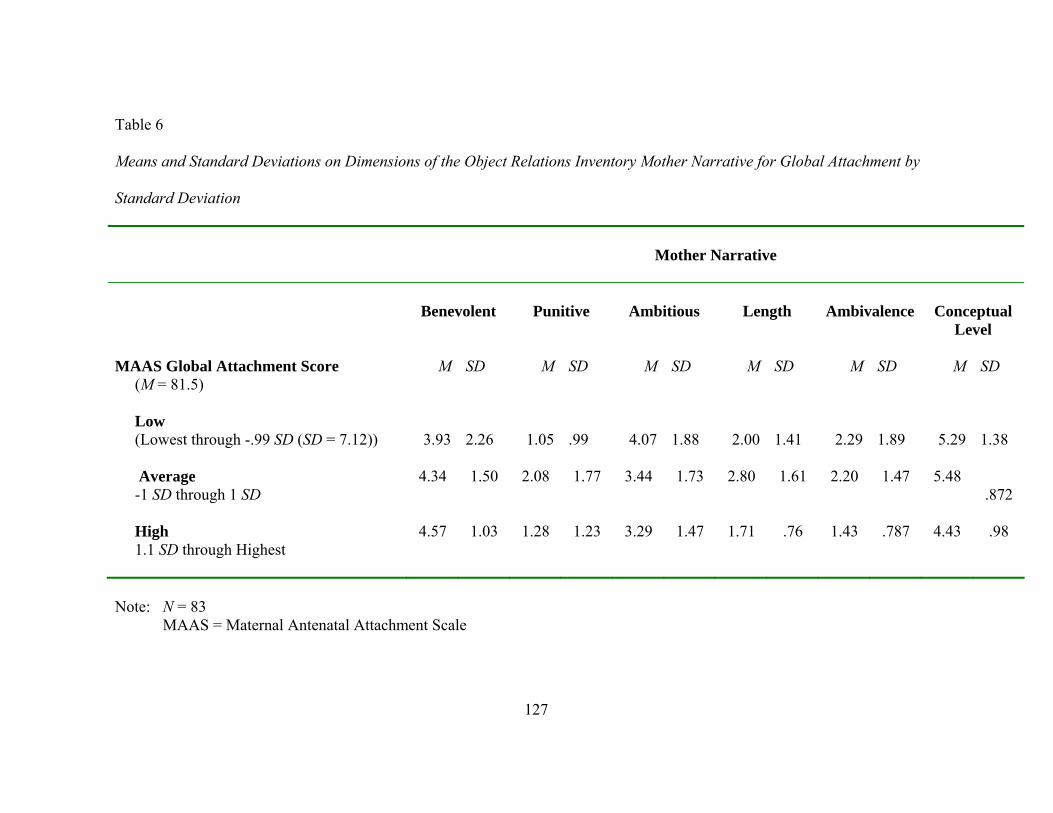
Table 6 Means and Standard Deviations on Dimensions of the Object Relations Inventory Mother Narrative for Global Attachment by Standard Deviation
Mother Narrative
Benevolent
Punitive
Ambitious
Length
Ambivalence
Conceptual
Level MAAS Global Attachment Score (M = 81.5)
M SD
M SD M
SD M
SD M
SD M
SD
Low (Lowest through -.99 SD (SD = 7.12))
3.93 2.26 1.05
.99 4.07
1.88 2.00
1.41 2.29
1.89 5.29
1.38
Average -1 SD through 1 SD
4.34 1.50 2.08 1.77 3.44 1.73 2.80 1.61 2.20 1.47 5.48.872
High 1.1 SD through Highest
4.57 1.03 1.28 1.23 3.29 1.47 1.71 .76 1.43 .787 4.43 .98
Note: N = 83 MAAS = Maternal Antenatal Attachment Scale
127

Table 7 95% Confidence Intervals of Pairwise Differences in Mean Changes of Attachment Quality (MAAS) by Conceptual Level of ORI Mother Narrative
M
SD
Pre- operational
Concrete
External Iconic
Pre-operational 47.00
2.83 Concrete 44.67 4.08 -41.93 to 37.26
External Iconic 46.16 3.37 -46.41 to 44.72
-4.76 to 7.73
Internal Iconic 46.18 2.74 -45.46 to 43.82
-4.91 to 7.93 -2.21 to 2.26
Note: N = 83 MAAS = Maternal AntenatalAttachment Scale ORI = Object Relations Inventory
128

Table 8 95% Confidence Intervals of Pairwise Differences in Mean Changes of Attachment Intensity (MAAS) by Conceptual Level of ORI Mother Narrative
M
SD
Pre- operational
Concrete
External Iconic
Pre-operational 30.67
4.91 Concrete 30.17 6.74 -5.33 to 2.80
External Iconic 31.32 4.97 -4.46 to .82
.87 to 2.83
Internal Iconic 29.06 4.11 -6.44 to 1.14
-1.10 to 2.94 -1.97 to 1.22
Note: N = 81 MAAS = Maternal AntenatalAttachment Scale ORI = Object Relations Inventory
129

130
Table 9 Frequency Distribution of Conceptual Levels of Mother and Baby Narratives (ORI)
Mother Narrative
Baby Narrative
N
Percent
Cumulative
Percent
N
Percent
Cumulative
Percent
Sensorimotor 2
2.4 2.4 18 21.2 21.2 Concrete 6 7.2 9.6 9 10.6 31.8 External Iconic 58 69.9 79.5 36 42.4 74.1 Internal Iconic 17 20.5 100.0 22 25.9 100.0 Total
83 100.0 85 100.0
Note: ORI = Object Relations Inventory

131
Table 10 Spearman’s rho Correlations for Conceptual Level and Attachment
ORI
Conceptual Conceptual
Level Mother
MAAS Quality
MAAS
Intensity
Conceptual Level of Mother
X
.023 N = 83
-.210 N= 81
Quality of Attachment Factor
X
X
.379** N = 89
Intensity of Attachment Factor
X X X
Note: MAAS = Maternal Antenatal Attachment Scale
ORI = Object Relations Inventory ** p < .01
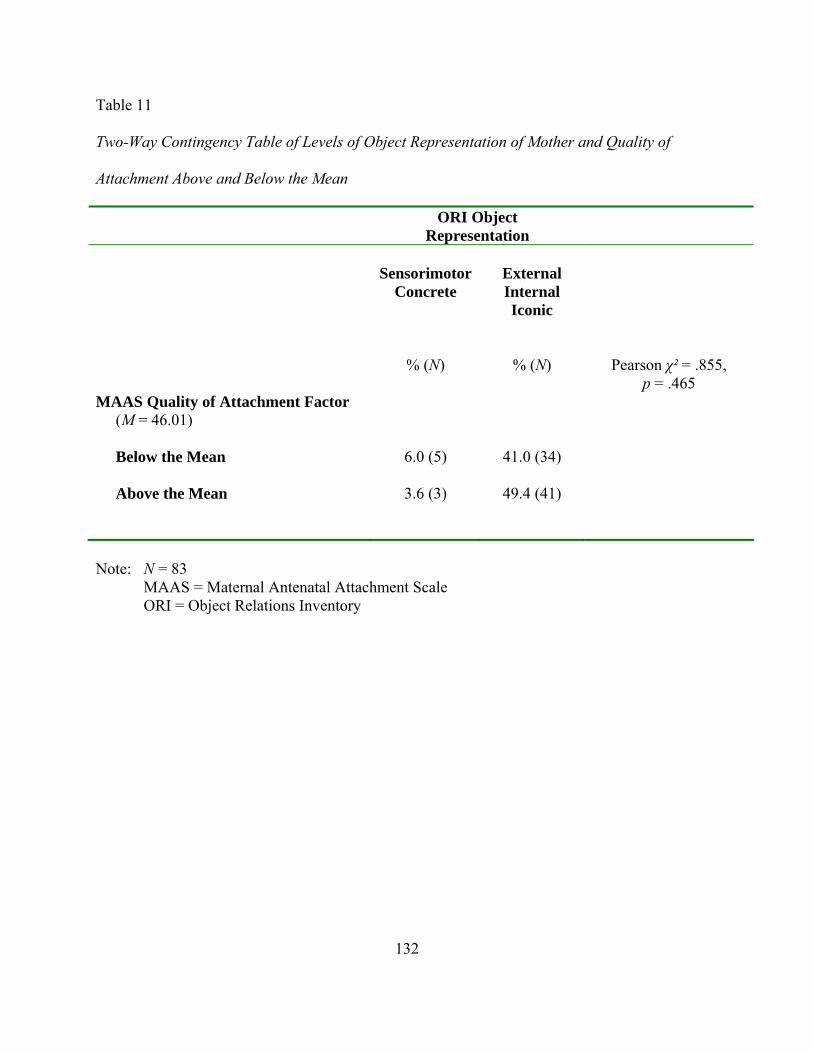
132
Table 11 Two-Way Contingency Table of Levels of Object Representation of Mother and Quality of Attachment Above and Below the Mean ORI Object
Representation
Sensorimotor
Concrete
External Internal Iconic
% (N) % (N) Pearson χ² = .855, p = .465
MAAS Quality of Attachment Factor (M = 46.01)
Below the Mean
6.0 (5) 41.0 (34)
Above the Mean
3.6 (3) 49.4 (41)
Note: N = 83
MAAS = Maternal Antenatal Attachment Scale ORI = Object Relations Inventory
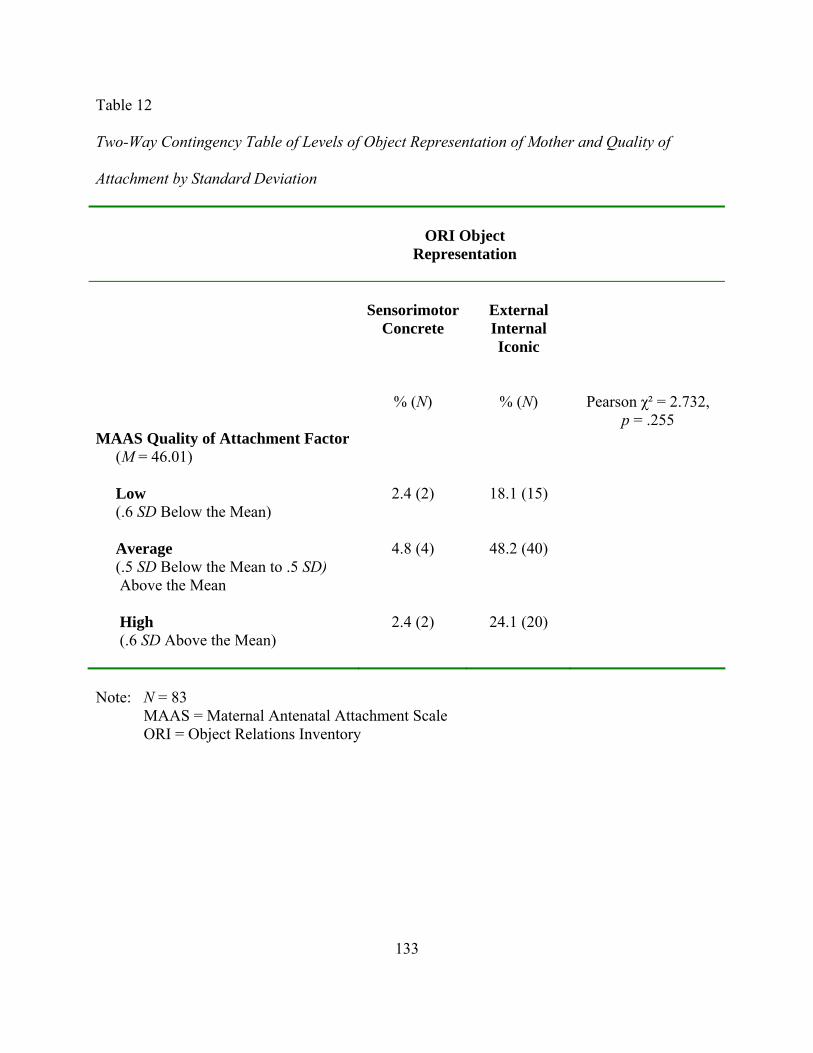
133
Table 12 Two-Way Contingency Table of Levels of Object Representation of Mother and Quality of Attachment by Standard Deviation
ORI Object Representation
Sensorimotor
Concrete
External Internal Iconic
% (N) % (N) Pearson χ² = 2.732, p = .255
MAAS Quality of Attachment Factor (M = 46.01)
Low (.6 SD Below the Mean)
2.4 (2) 18.1 (15)
Average (.5 SD Below the Mean to .5 SD) Above the Mean
4.8 (4) 48.2 (40)
High (.6 SD Above the Mean)
2.4 (2) 24.1 (20)
Note: N = 83
MAAS = Maternal Antenatal Attachment Scale ORI = Object Relations Inventory
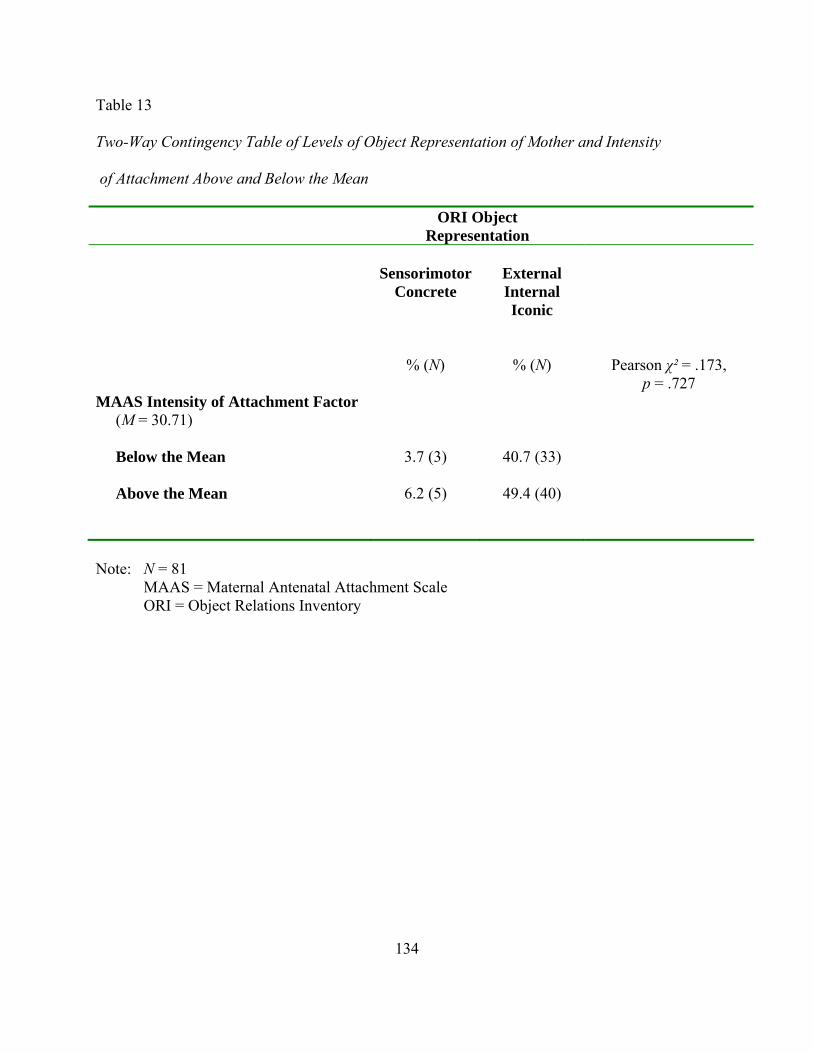
134
Table 13 Two-Way Contingency Table of Levels of Object Representation of Mother and Intensity of Attachment Above and Below the Mean ORI Object
Representation
Sensorimotor
Concrete
External Internal Iconic
% (N) % (N) Pearson χ² = .173, p = .727
MAAS Intensity of Attachment Factor (M = 30.71)
Below the Mean
3.7 (3) 40.7 (33)
Above the Mean
6.2 (5) 49.4 (40)
Note: N = 81
MAAS = Maternal Antenatal Attachment Scale ORI = Object Relations Inventory
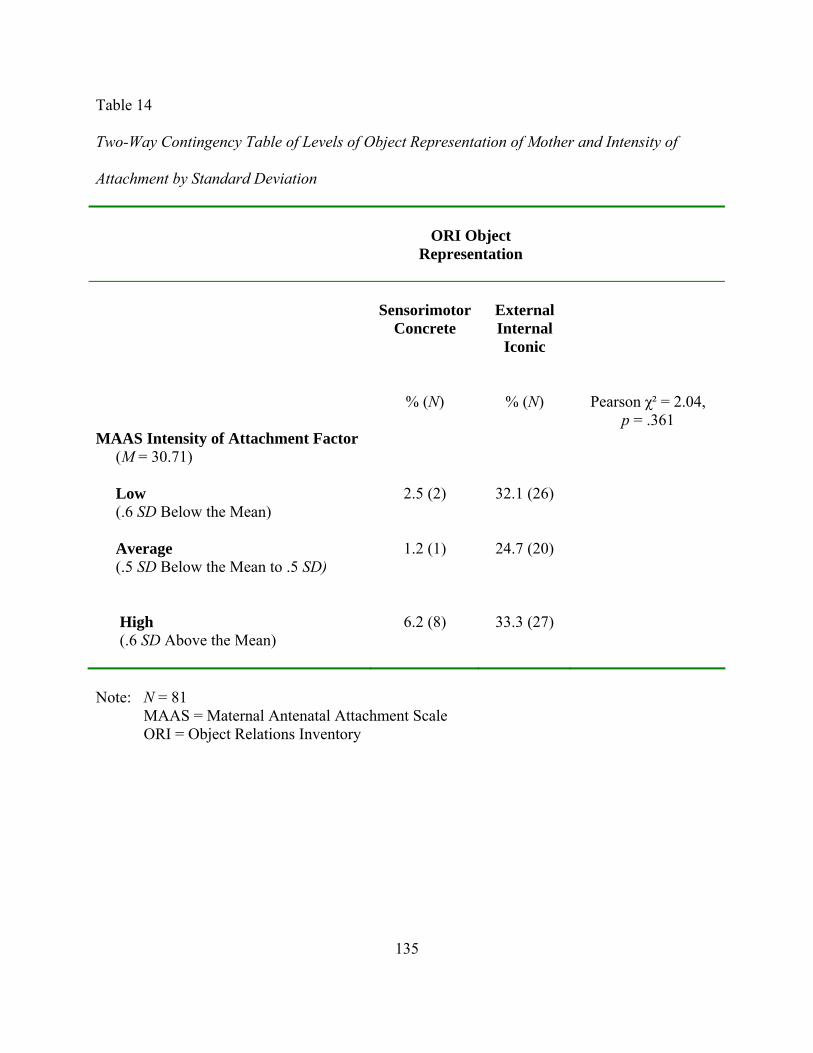
135
Table 14 Two-Way Contingency Table of Levels of Object Representation of Mother and Intensity of Attachment by Standard Deviation
ORI Object Representation
Sensorimotor
Concrete
External Internal Iconic
% (N) % (N) Pearson χ² = 2.04, p = .361
MAAS Intensity of Attachment Factor (M = 30.71)
Low (.6 SD Below the Mean)
2.5 (2) 32.1 (26)
Average (.5 SD Below the Mean to .5 SD)
1.2 (1) 24.7 (20)
High (.6 SD Above the Mean)
6.2 (8) 33.3 (27)
Note: N = 81
MAAS = Maternal Antenatal Attachment Scale ORI = Object Relations Inventory
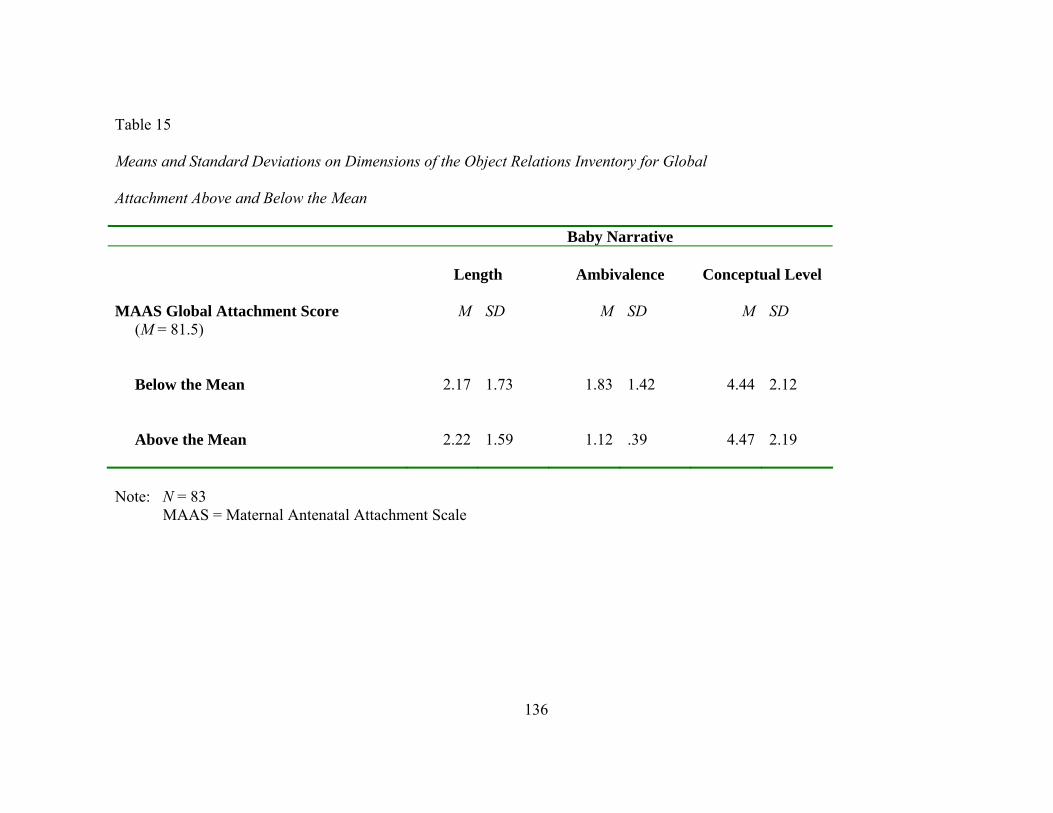
Table 15 Means and Standard Deviations on Dimensions of the Object Relations Inventory for Global Attachment Above and Below the Mean Baby Narrative
Length
Ambivalence
Conceptual Level MAAS Global Attachment Score (M = 81.5)
M
SD
M SD
M SD
Below the Mean
2.17
1.73
1.83
1.42 4.44
2.12
Above the Mean
2.22
1.59
1.12
.39 4.47
2.19
Note: N = 83
MAAS = Maternal Antenatal Attachment Scale
136

Table 16 Means and Standard Deviations on Dimensions of the ORI for Global Attachment by Standard Deviation Baby Narrative
Length
Ambivalence
Conceptual Level MAAS Global Attachment Score (M = 81.5)
M
SD
M
SD
M SD
Low (.6 SD Below the Mean)
2.05 1.76 2.14 1.67 4.18 2.11
Average (.5 SD Below the Mean to .5 SD)
2.22 1.62 1.22 .540 4.50 2.16
High (.6 SD Above the Mean)
2.30 1.61 1.11 .424 4.63 2.22
Note: N = 83
MAAS = Maternal Antenatal Attachment Scale
137

138
Table 17 Spearman’s rho Correlations for Object Representations of Mother and Baby Narratives
ORI Dimensions
Mother
Ambivalence
Mother Length
Mother
Conceptual Level
Baby
Ambivalence
Baby Length
Baby
Conceptual Conceptual
Level
Ambivalent Feelings about Mother
X .403***N = 82
.102 N = 82
.458*** N = 81
.401** N = 81
.065 N = 81
Length of Narrative about Mother
X
X .171N = 83
.184 N = 82
.720*** N = 82
.270** N = 82
Conceptual Level of Mother
X X X .310**N = 82
.307** N = 83
.068 N = 82
Ambivalent Feelings about Baby
X X X X .355**N = 85
-.170 N = 85
Length of Narrative about Baby
X X X X X .127N = 82
Conceptual Level of Baby
X X X X X X
Note: ORI = Object Relations Inventory * p < .05; ** p < .01; *** p < .001

139
Table 18 Two-Way Contingency Table of ORI Conceptual Level of Mother Narrative by Baby Narrative
Baby Narrative
Mother Narrative
Sensorimotor Concrete
External/ Internal Iconic
% (N) % (N) Pearson χ² (1, 82) = .206 p = .70
Sensorimotor/ Concrete
3.7 (3) 26.8 (22)
External/Internal Iconic
6.1 (5) 63.4 (52)
Note: N = 83 ORI = Object Relations Inventory
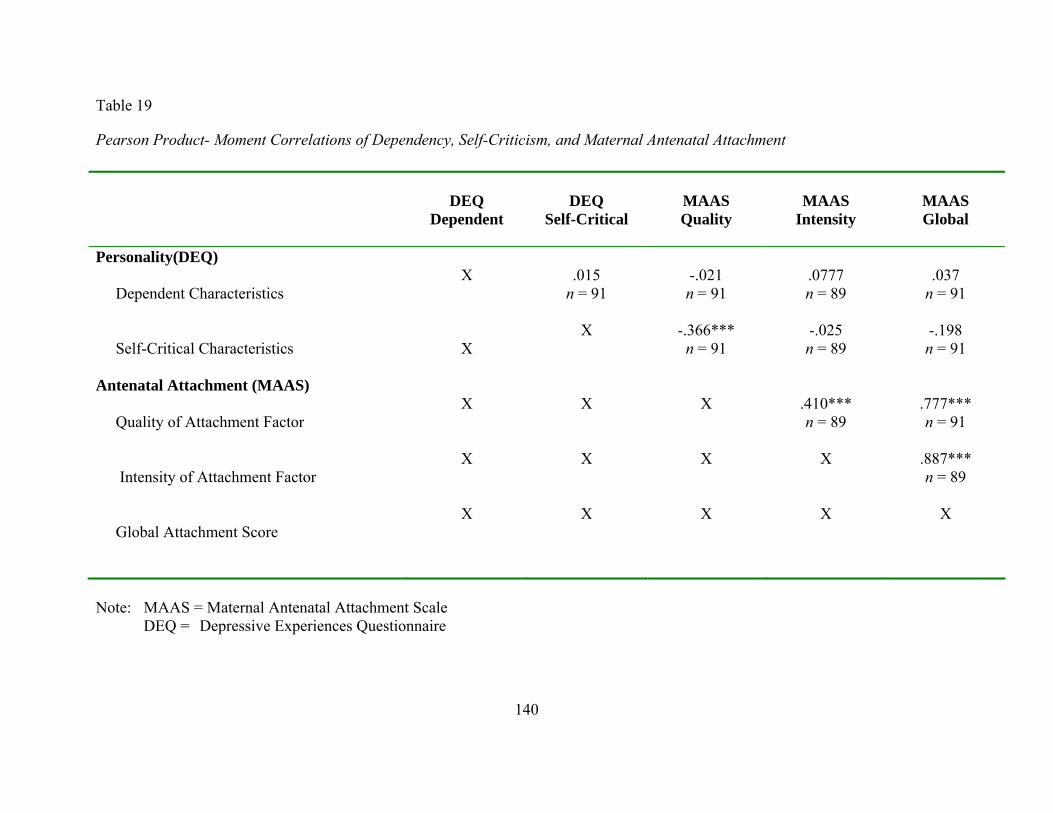
Table 19
Pearson Product- Moment Correlations of Dependency, Self-Criticism, and Maternal Antenatal Attachment
DEQ
Dependent
DEQ
Self-Critical
MAAS Quality
MAAS
Intensity
MAAS Global
Personality(DEQ) Dependent Characteristics
X
.015n = 91
-.021 n = 91
.0777 n = 89
.037 n = 91
Self-Critical Characteristics
X
X -.366***n = 91
-.025 n = 89
-.198 n = 91
Antenatal Attachment (MAAS) Quality of Attachment Factor
X X X .410***n = 89
.777*** n = 91
Intensity of Attachment Factor
X X X X .887***n = 89
Global Attachment Score
X X X X X
Note: MAAS = Maternal Antenatal Attachment Scale DEQ = Depressive Experiences Questionnaire
140
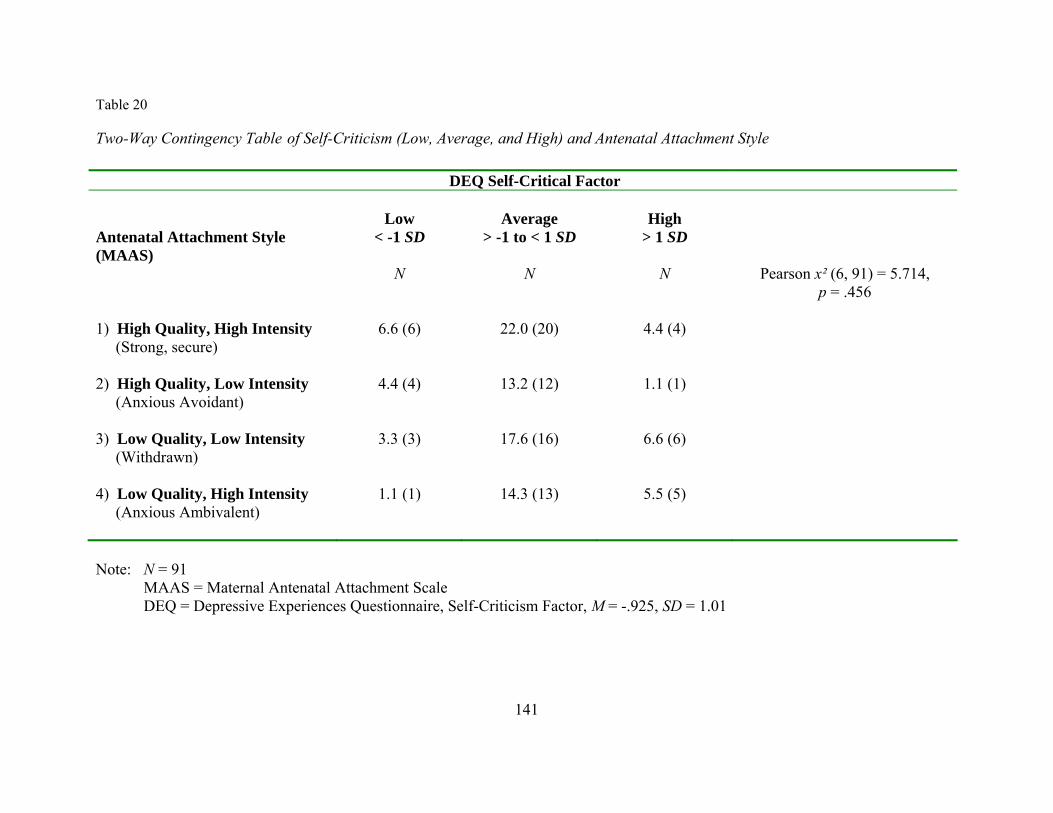
Table 20
Two-Way Contingency Table of Self-Criticism (Low, Average, and High) and Antenatal Attachment Style DEQ Self-Critical Factor Antenatal Attachment Style (MAAS)
Low
< -1 SD
Average
> -1 to < 1 SD
High
> 1 SD
N N N Pearson x² (6, 91) = 5.714, p = .456
1) High Quality, High Intensity (Strong, secure)
6.6 (6)
22.0 (20)
4.4 (4)
2) High Quality, Low Intensity (Anxious Avoidant)
4.4 (4)
13.2 (12)
1.1 (1)
3) Low Quality, Low Intensity (Withdrawn)
3.3 (3)
17.6 (16)
6.6 (6)
4) Low Quality, High Intensity (Anxious Ambivalent)
1.1 (1)
14.3 (13)
5.5 (5)
Note: N = 91
MAAS = Maternal Antenatal Attachment Scale DEQ = Depressive Experiences Questionnaire, Self-Criticism Factor, M = -.925, SD = 1.01
141

Table 21
Two-Way Contingency Table of Self-Criticism (Above the Mean and Below the Mean) and Antenatal Attachment Style
DEQ Self-Critical Factor
Antenatal Attachment Style (MAAS)
Below the Mean
Above the Mean
N N Pearson x² (3, 91) = 8.932, p = .03 1) High Quality, High Intensity (Strong, secure)
20.9 (19)
12.1 (11)
2) High Quality, Low Intensity (Anxious Avoidant)
15.4 (14)
3.3 (3)
3) Low Quality, Low Intensity (Withdrawn)
13.2 (12)
14.3 (13)
4) Low Quality, High Intensity (Anxious Ambivalent)
7.7 (7)
13.2 (12)
Note: N = 91
MAAS = Maternal Antenatal Attachment Scale DEQ = Depressive Experiences Questionnaire, Self-Criticism Factor, M = -.925, SD = 1.01
142

Table 22 Two-Way Contingency Table of Dependency (Low, Average, and High) and Antenatal Attachment Style
DEQ Dependent Factor
Antenatal Attachment Style (MAAS)
Low
< -1 SD
Average
> -1 to < 1 SD
High
> 1 SD
N N N Pearson x² (6, 91) = 10.412, p = .108
1) High Quality, High Intensity (Strong, secure)
19.8 (18)
1.1 (1)
12.1 (11)
2) High Quality, Low Intensity (Anxious Avoidant)
8.8 (8)
2.2 (2)
7.7 (7)
3) Low Quality, Low Intensity (Withdrawn)
16.5 (15)
0
11.0 (10)
4) Low Quality, High Intensity (Anxious Ambivalent)
6.6 (6)
0
14.3 (13)
Note: N = 91
MAAS = Maternal Antenatal Attachment Scale DEQ = Depressive Experiences Questionnaire, Dependency Factor, M = -.53, SD = .90
143
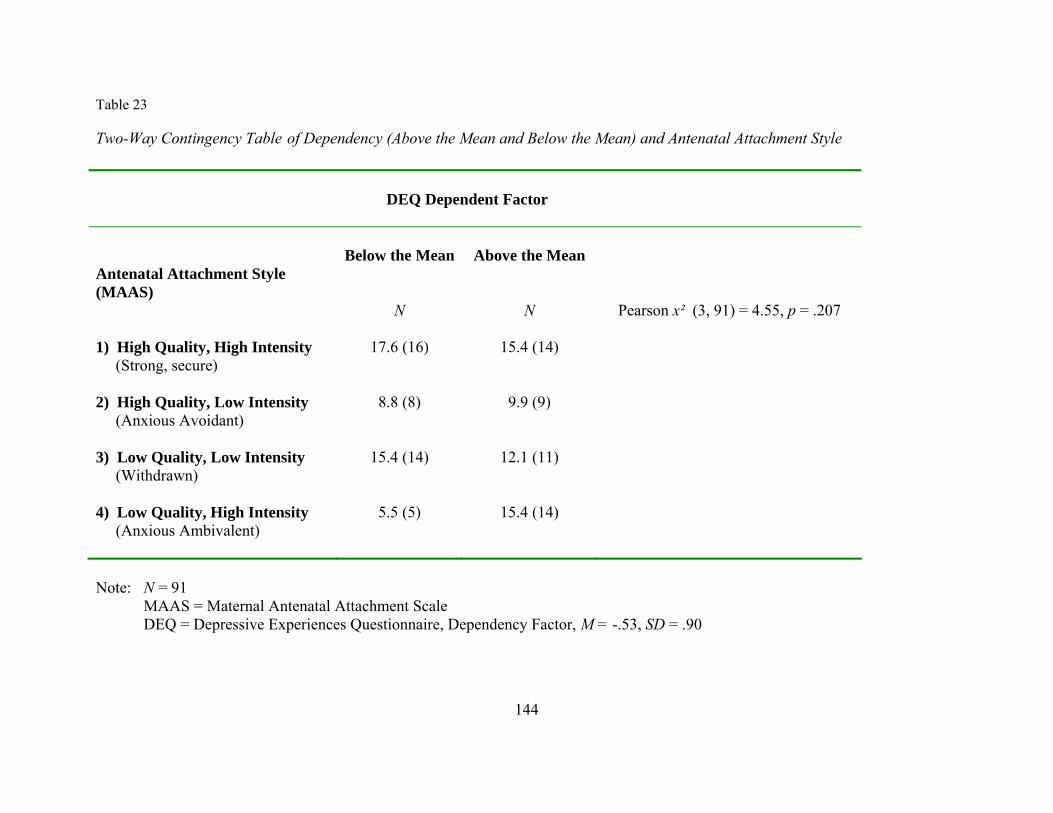
Table 23
Two-Way Contingency Table of Dependency (Above the Mean and Below the Mean) and Antenatal Attachment Style
DEQ Dependent Factor
Antenatal Attachment Style (MAAS)
Below the Mean
Above the Mean
N N Pearson x² (3, 91) = 4.55, p = .207 1) High Quality, High Intensity (Strong, secure)
17.6 (16)
15.4 (14)
2) High Quality, Low Intensity (Anxious Avoidant)
8.8 (8)
9.9 (9)
3) Low Quality, Low Intensity (Withdrawn)
15.4 (14)
12.1 (11)
4) Low Quality, High Intensity (Anxious Ambivalent)
5.5 (5)
15.4 (14)
Note: N = 91
MAAS = Maternal Antenatal Attachment Scale DEQ = Depressive Experiences Questionnaire, Dependency Factor, M = -.53, SD = .90
144

Table 24
Two-Way Contingency Table of Self-Criticism (Low, Average, and High) and Conceptual Level of Mother Narrative
DEQ Self-Critical Factor
ORI Mother Narrative Conceptual Level
Low
< -1 SD
Average
> -1 to < 1 SD
High
> 1 SD
% (N) % (N) % (N) Pearson x² (6, 83) = 4.763, p = .575
Sensorimotor
1.2 (1) 1.2 (1) 0
Concrete
1.2 (1) 4.8 (4) 1.2 (1)
External Iconic
9.6 (8) 50.6 (42) 9.6 (8)
Internal Iconic
3.6 (3) 10.8 (9) 6.0 (5)
Note: N = 83
ORI = Object Relations Inventory DEQ = Depressive Experiences Questionnaire, Self-Criticism Factor, M = -.925, SD = 1.01
145

Table 25
Two-Way Contingency Table of Dependency (Low, Average, and High) and Conceptual Level of Mother Narrative
DEQ Dependent Factor
ORI Mother Narrative Conceptual Level
Low
< -1 SD
Average
> -1 to < 1 SD
High
> 1 SD
N N N Pearson x² (6, 83) = 7.47, p = .28
Sensorimotor
1.2 (1) 0 1.2 (1)
Concrete
6.0 (5) 0 1.2 (1)
External Iconic
33.7 (28) 1.2 (1) 34.9 (29)
Internal Iconic
7.2 (6) 2.4 (2) 10.8 (9)
Note: N = 83
ORI = Object Relations Inventory DEQ = Depressive Experiences Questionnaire, Dependency Factor, M = -.53, SD = .90
146
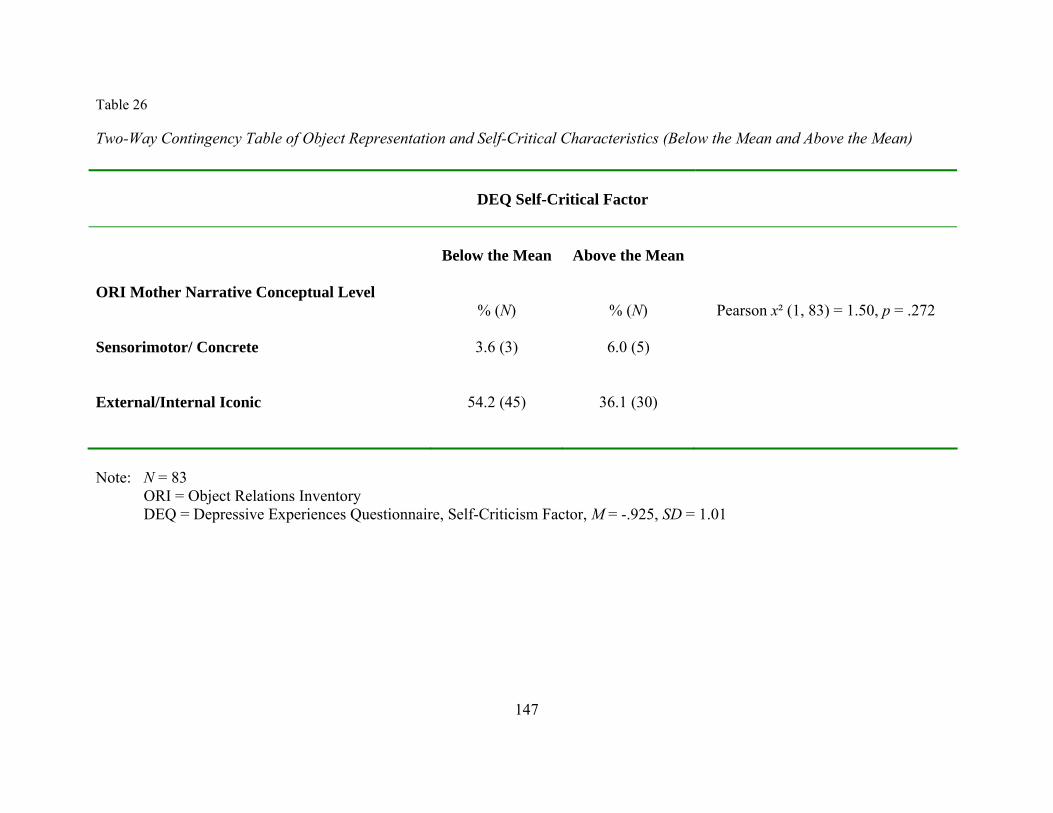
Table 26
Two-Way Contingency Table of Object Representation and Self-Critical Characteristics (Below the Mean and Above the Mean)
DEQ Self-Critical Factor
ORI Mother Narrative Conceptual Level
Below the Mean
Above the Mean
% (N) % (N) Pearson x² (1, 83) = 1.50, p = .272 Sensorimotor/ Concrete
3.6 (3)
6.0 (5)
External/Internal Iconic
54.2 (45)
36.1 (30)
Note: N = 83
ORI = Object Relations Inventory DEQ = Depressive Experiences Questionnaire, Self-Criticism Factor, M = -.925, SD = 1.01
147

148
Table 27
Two-Way Contingency Table of Object Representation and Dependent Characteristics (Below the Mean and Above the Mean)
DEQ Dependent Factor
ORI Mother Narrative Conceptual Level
Below the Mean
Above the Mean
% (N) % (N) Pearson x² (1, 83) = 1.32, p = .284 Sensorimotor/ Concrete
6.0 (5)
3.6 (3)
External/Internal Iconic
37.3 (31)
53.0 (44)
Note: N = 83
ORI = Object Relations Inventory DEQ = Depressive Experiences Questionnaire, Dependency Factor, M = -.53, SD = .90

149
Table 28 Hobel Risk Assessment Factors Identified as Fetal Previous fetal exchange transfusion for Rh Prevous premature infant Previous neonatal death Fetal anomalies Incompetent cervix Polyhydramnios Multiple pregnancy Viral disease Rh sensitization only Vaginal spotting Alcohol (moderate) Premature rupture of membrane (PROM)* Primary dysfunctional labor (PTL)*
* Items added as revision of scale

150
Table 29 Hobel Risk Assessment Factors Identified as Maternal Moderate to severe toxemia
Chronic Hypertension
Moderate to severe renal disease
Severe heart disease, Class II-IV
History of eclampsia
History of pyelitis
Class I heart disease
Mild toxemia
Acute pyelonephritis
History of cystitis
Acute cystitis
History of toxemia
Diabetes > Class A-II
Previous endocrine ablation
Thyroid disease
Prediabetes (A-I)
Family history of diabetes
Previous stillbirth
(Table continues)
151
(Maternal Risk Items continued) Post-term > 42 weeks
Previous cesarean section
Habitual abortion
Infant > 10 pounds
Multiparity > 5
Epilepsy
Uterine malformation
Abnormal fetal position
Small pelvis
Abnormal cervical cytology
Sickle cell disease
Age > 35 or < 15
Positive serology
Severe anemia (< 9 Gm. Hgb)
Excessive use of drugs
History of TB or PPD > 10 mm.
Weight < 100 or > 200 pounds
Pulmonary disease
Flu syndrome (severe)
(Table continues)
152
(Maternal Risk Items continued) Mild anemia (9-10.9 Gm. Hgb)
Smoking > 1 pack/day
Emotional problem
Placenta previa*
Abruptio placentae*
* Items added for revision of scale
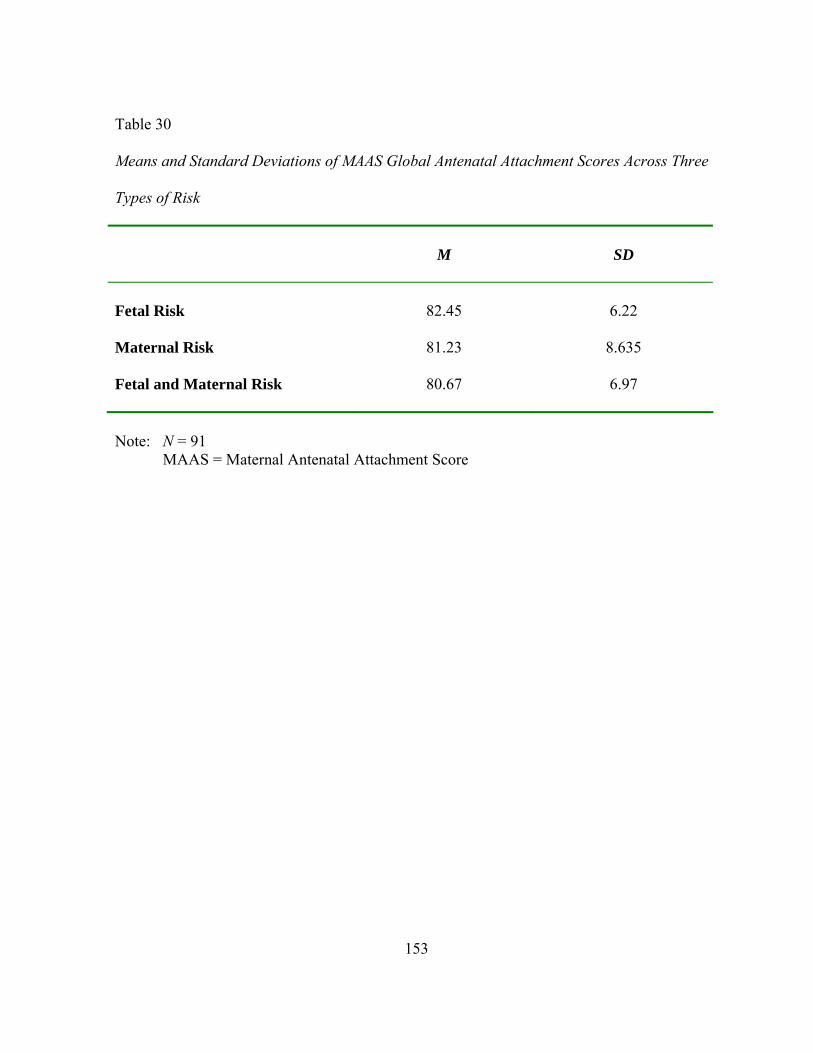
153
Table 30
Means and Standard Deviations of MAAS Global Antenatal Attachment Scores Across Three
Types of Risk
M
SD
Fetal Risk
82.45
6.22
Maternal Risk 81.23 8.635 Fetal and Maternal Risk
80.67 6.97
Note: N = 91 MAAS = Maternal Antenatal Attachment Score
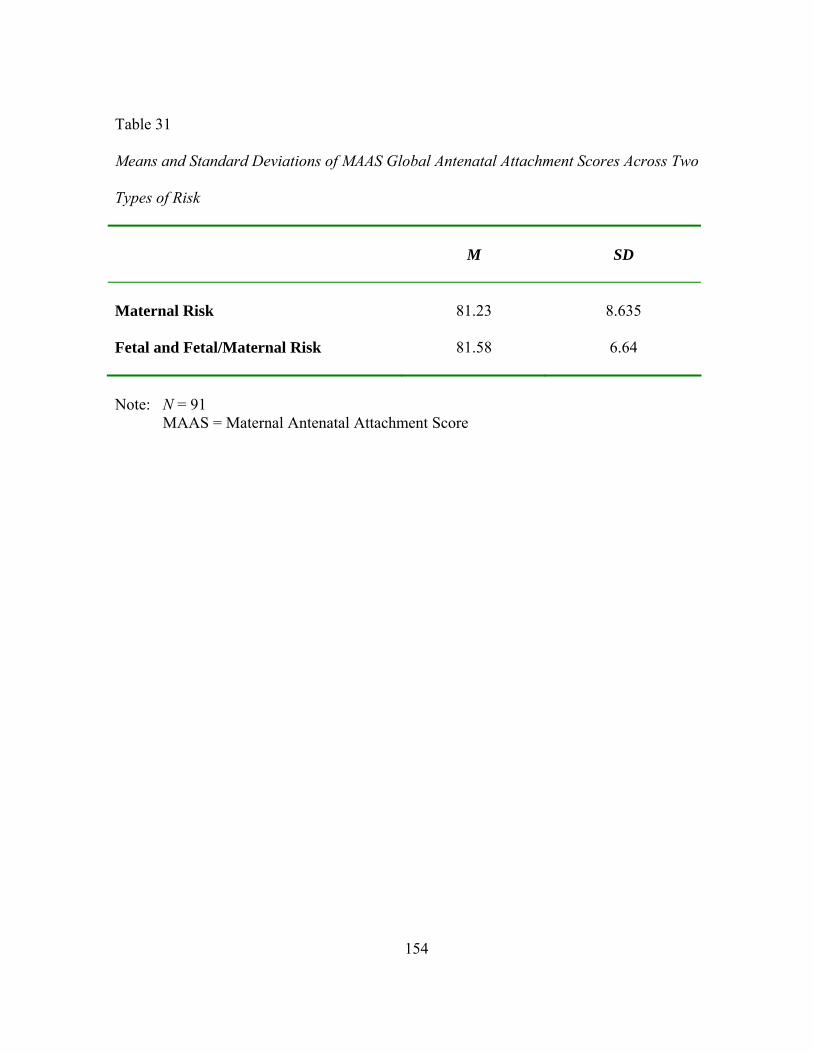
154
Table 31
Means and Standard Deviations of MAAS Global Antenatal Attachment Scores Across Two
Types of Risk
M
SD
Maternal Risk 81.23 8.635 Fetal and Fetal/Maternal Risk
81.58 6.64
Note: N = 91 MAAS = Maternal Antenatal Attachment Score

155
Table 32 95% Confidence Intervals of Pairwise Differences in Mean Changes of MAAS Attachment Intensity by Type of Risk
M
SD
Maternal
Fetal Maternal 30.52 5.45 Fetal 31.23 5.26 -3.12 to 4.54 Combined 30.39 4.31 -3.59 to 3.33 -3.76 to 2.08 Note: N = 89
MAAS = Maternal Antenatal Attachment Scale

156
Table 33
Two-Way Contingency Table of Three Risk Types and Antenatal Attachment (MAAS)
Maternal
Risk
Fetal Risk
Fetal/Maternal
Risk
% (N) % (N) % (N) Quality of Attachment Factor N = 91
Pearson x² (1, 91) = .39, p = .823
Above the mean score (46)
11.0 (10) 29.7 (27) 5.5 (5)
Below the mean score (46)
14.3 (13) 35.2 (32) 4.4 (4)
Intensity of Attachment Factor N = 89
Pearson x² (1, 89) = 1.36, p = .506
Above the mean score (31)
9.0 (8) 31.5 (28) 4.5 (4)
Below the mean score (31)
16.9 (15) 32.6 (29) 5.6 (5)
Global Attachment Score N = 89
Pearson x² (1, 89) = 2.245, p = .325
Above the mean score (81)
7.7 (7) 29.7 (27) 5.5 (5)
Below the mean score (81)
17.6 (16) 35.2 (32) 4.4 (4)
Note: MAAS = Maternal Antenatal Attachment Scale
Risk factors of revised Hobel assessment were categorized by the maternal-fetal medicine specialist, John Rosnes, M.D.

157
Table 34
Two-Way Contingency Table of Two Risk Types and Maternal Antenatal Attachment
Maternal
Risk
Fetal/Combined
Risk
Antenatal Attachment (MAAS)
% (n) % (n)
Quality of Attachment Factor N = 91
Pearson x² (1, 91) = 2.39,
p = .121 Above the mean score (46)
16.5 (15) 37.4 (34)
Below the mean score (46)
7.7 (7) 38.5 (35)
Intensity of Attachment Factor N = 89
Pearson x² (1, 89) = .048,
p = .826 Above the mean score (31)
13.5 (12) 34.8 (31)
Below the mean score (31)
10.1 (9) 34.8 (31)
Global Attachment Score N = 89
Pearson x² (1, 89) = .045,
p = .832 Above the mean score (81)
14.3 (13) 42.9 (39)
Below the mean score (81)
9.9 (9) 33.0 (30)
Note: MAAS = Maternal Antenatal Attachment Scale
Risk factors of revised Hobel assessment were categorized by the maternal-fetal medicine specialist, John Rosnes, M.D.
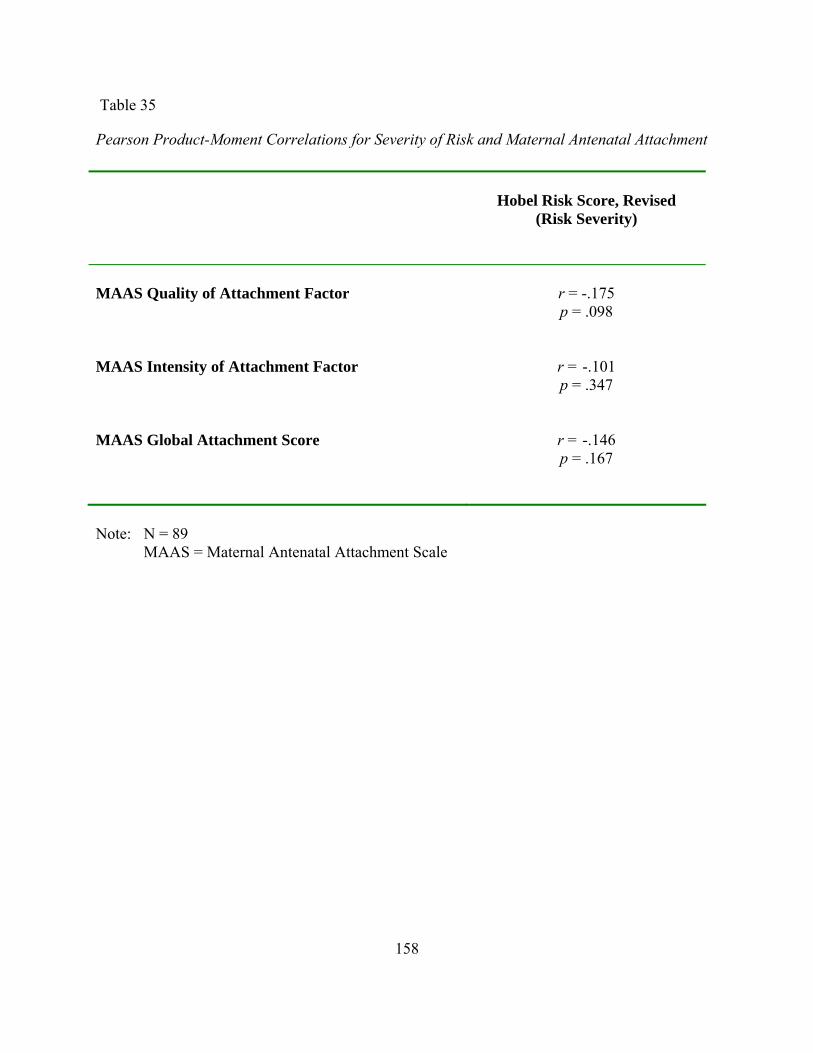
158
Table 35
Pearson Product-Moment Correlations for Severity of Risk and Maternal Antenatal Attachment
Hobel Risk Score, Revised
(Risk Severity)
MAAS Quality of Attachment Factor
r = -.175 p = .098
MAAS Intensity of Attachment Factor
r = -.101 p = .347
MAAS Global Attachment Score
r = -.146 p = .167
Note: N = 89
MAAS = Maternal Antenatal Attachment Scale
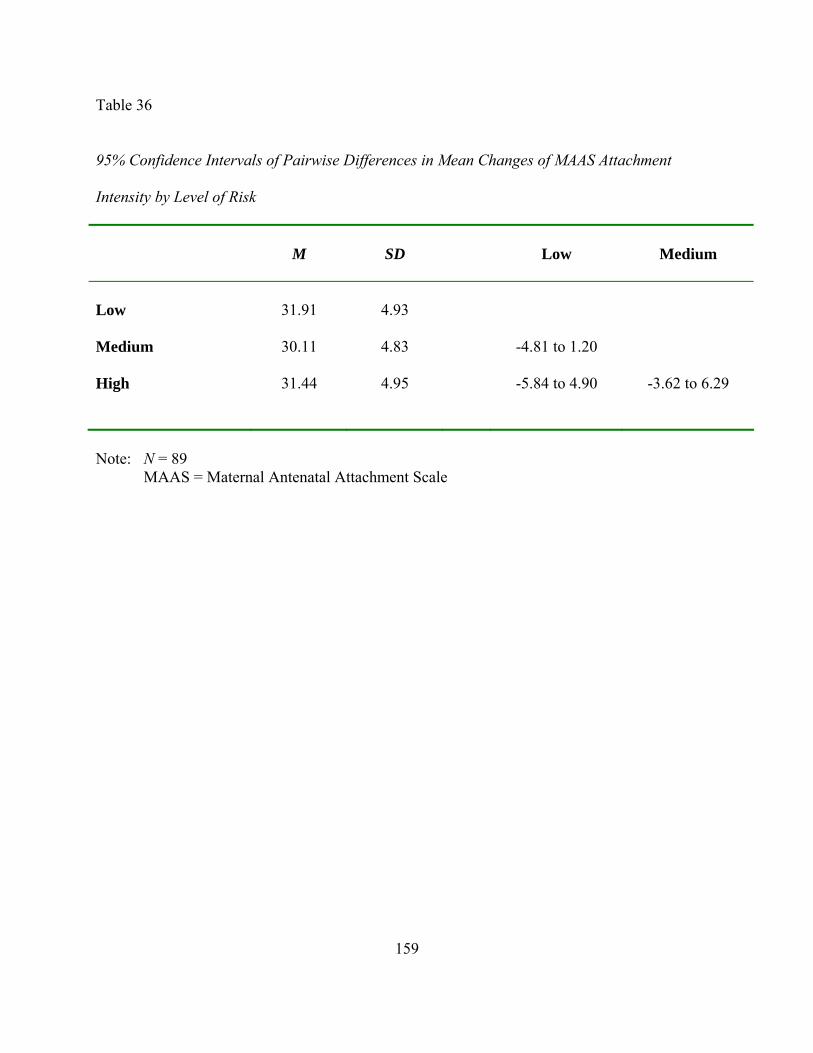
159
Table 36 95% Confidence Intervals of Pairwise Differences in Mean Changes of MAAS Attachment Intensity by Level of Risk
M
SD
Low
Medium
Low 31.91 4.93 Medium 30.11 4.83 -4.81 to 1.20 High 31.44 4.95 -5.84 to 4.90 -3.62 to 6.29
Note: N = 89
MAAS = Maternal Antenatal Attachment Scale
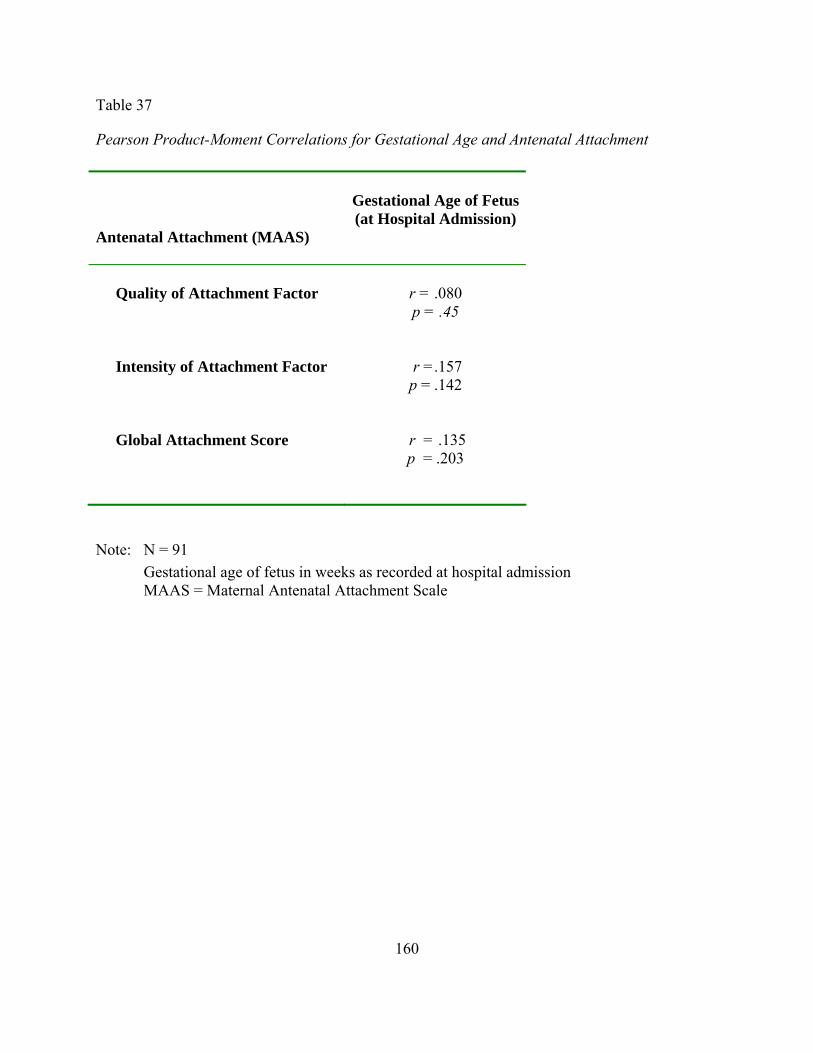
160
Table 37
Pearson Product-Moment Correlations for Gestational Age and Antenatal Attachment Antenatal Attachment (MAAS)
Gestational Age of Fetus(at Hospital Admission)
Quality of Attachment Factor
r = .080 p = .45
Intensity of Attachment Factor
r =.157 p = .142
Global Attachment Score
r = .135 p = .203
Note: N = 91 Gestational age of fetus in weeks as recorded at hospital admission MAAS = Maternal Antenatal Attachment Scale
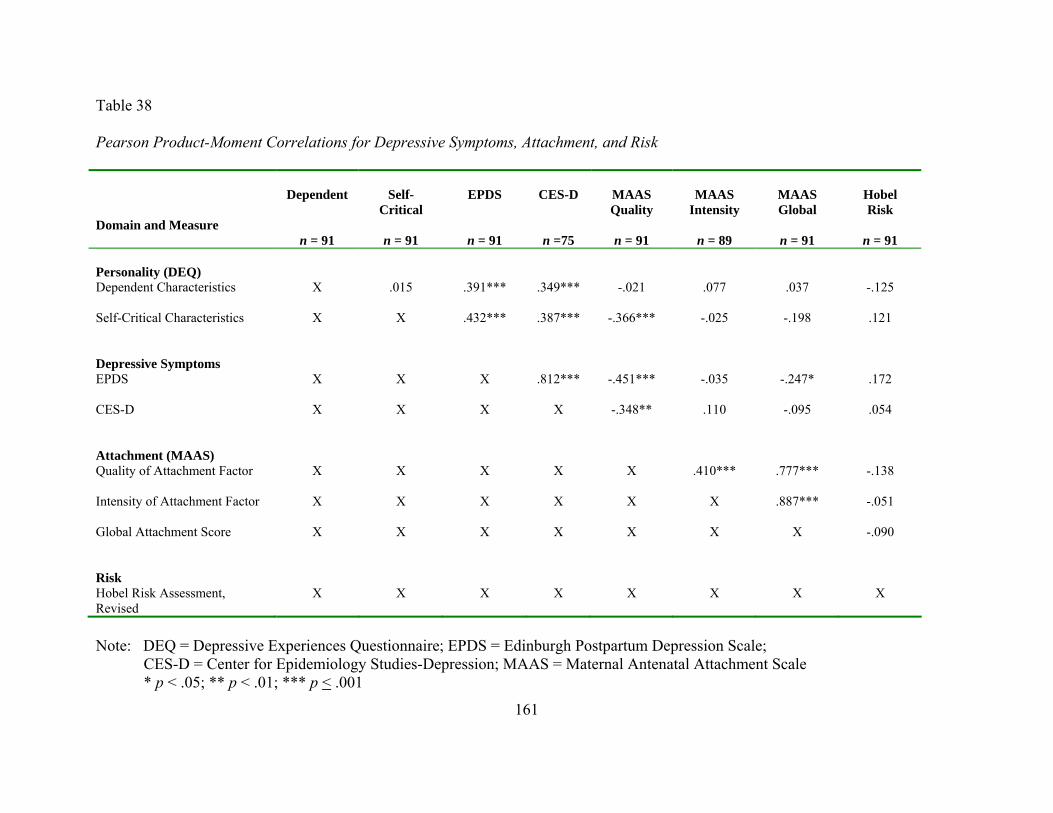
Table 38
Pearson Product-Moment Correlations for Depressive Symptoms, Attachment, and Risk
Domain and Measure
Dependent
n = 91
Self-
Critical
n = 91
EPDS
n = 91
CES-D
n =75
MAAS Quality
n = 91
MAAS
Intensity
n = 89
MAAS Global
n = 91
Hobel Risk
n = 91
Personality (DEQ)
Dependent Characteristics
X
.015 .391*** .349*** -.021 .077 .037 -.125
Self-Critical Characteristics
X X .432*** .387*** -.366*** -.025 -.198 .121
Depressive Symptoms EPDS
X X X .812*** -.451*** -.035 -.247* .172
CES-D X X X X -.348** .110 -.095 .054
Attachment (MAAS) Quality of Attachment Factor
X X X X X .410*** .777*** -.138
Intensity of Attachment Factor
X X X X X X .887*** -.051
Global Attachment Score X X X X X X X -.090
Risk Hobel Risk Assessment, Revised
X X X X X X X X
Note: DEQ = Depressive Experiences Questionnaire; EPDS = Edinburgh Postpartum Depression Scale;
CES-D = Center for Epidemiology Studies-Depression; MAAS = Maternal Antenatal Attachment Scale * p < .05; ** p < .01; *** p < .001
161
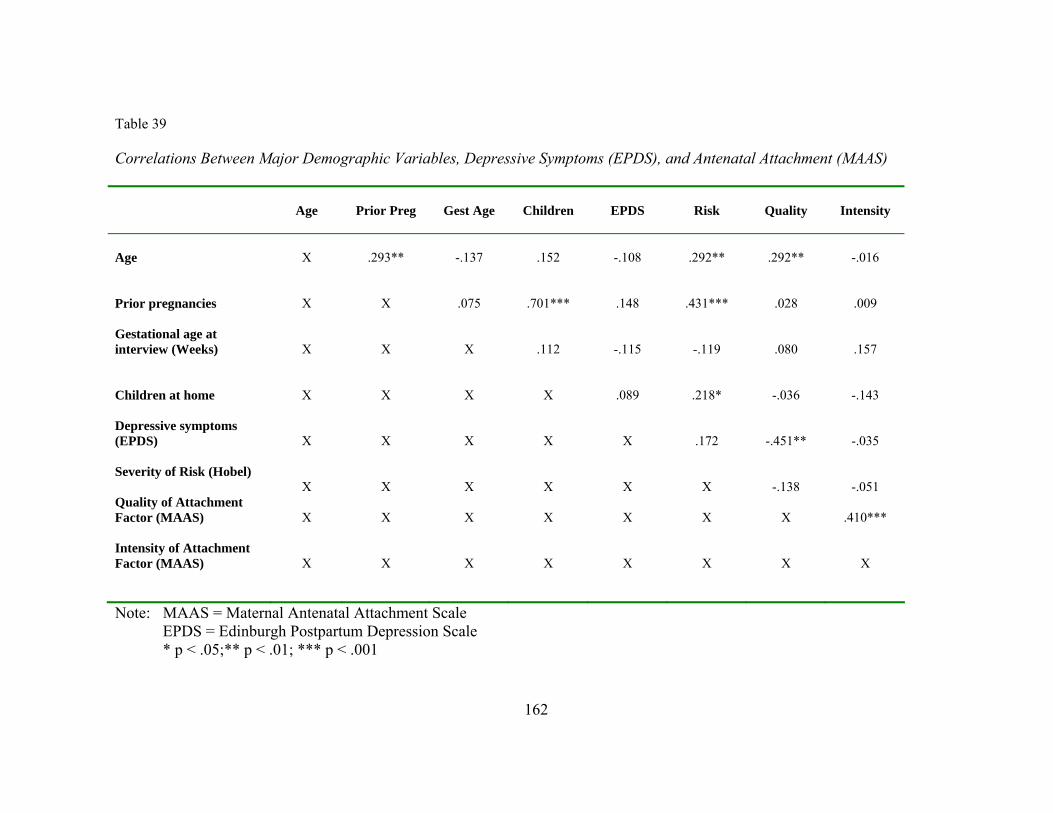
Table 39 Correlations Between Major Demographic Variables, Depressive Symptoms (EPDS), and Antenatal Attachment (MAAS)
Age
Prior Preg
Gest Age
Children
EPDS
Risk
Quality
Intensity
Age
X
.293**
-.137
.152
-.108
.292**
.292**
-.016
Prior pregnancies
X
X
.075
.701***
.148
.431***
.028
.009
Gestational age at interview (Weeks)
X
X
X
.112
-.115
-.119
.080
.157
Children at home
X
X
X
X
.089
.218*
-.036
-.143
Depressive symptoms (EPDS)
X
X
X
X
X
.172
-.451**
-.035
Severity of Risk (Hobel)
X
X
X
X
X
X
-.138
-.051
Quality of Attachment Factor (MAAS)
X
X
X
X
X
X
X
.410***
Intensity of Attachment Factor (MAAS)
X
X
X
X
X
X
X
X
Note: MAAS = Maternal Antenatal Attachment Scale EPDS = Edinburgh Postpartum Depression Scale
* p < .05;** p < .01; *** p < .001
162

163
Table 40 95% Confidence Intervals of Pairwise Differences in Means of EPDS (Depressive Symptoms) Depressive Symptoms
HighQuality
High Intensity (Strong Secure)
High Quality
Low Intensity
(Avoidant)
Low Quality
Low Intensity
(Withdrawn)
M SD 1) High Quality, High Intensity (Strong, secure)
7.13
5.41
2) High Quality, Low Intensity (Anxious Avoidant)
6.53
4.53
-4.74 to 3.53
3) Low Quality, Low Intensity (Withdrawn)
12.40
4.14
1.74 to 8.80*
1.98 to 9.76*
4) Low Quality, High Intensity (Anxious Ambivalent)
11.89
5.47
.31 to 9.21*
.63 to 10.10*
-4.72 to 3.71
Note: EPDS = Edinburgh Postpartum Depression Scale MAAS = Maternal Antenatal Attachment Scale
An asterisk indicates tht the 95% confidence interval does not contain zero, and therefore the difference in means is significant at the .95 significance using Dunnett’s C procedure.

164
Table 41 Chi-Square Comparison of EPDS Depressive Symptomatology and MAAS Antenatal Attachment Style
EPDS Below Threshold
EPDS
Above Threshold
Antenatal Attachment Style % (N) % (N) 1) High Quality, High Intensity (Strong, secure)
26.4 (24)
6.6 (6)
χ² = 21.339, p = .000
2) High Quality, Low Intensity (Anxious Avoidant)
15.4 (14)
3.3 (3)
3) Low Quality, Low Intensity (Withdrawn)
7.7 (7)
19.8 (18)
4) Low Quality, High Intensity (Anxious Ambivalent)
8.8 (8)
12.1 (11)
Note: EPDS = Edinburgh Postpartum Depression Scale (Threshold for screening > 11) MAAS = Maternal Antenatal Attachment Scale
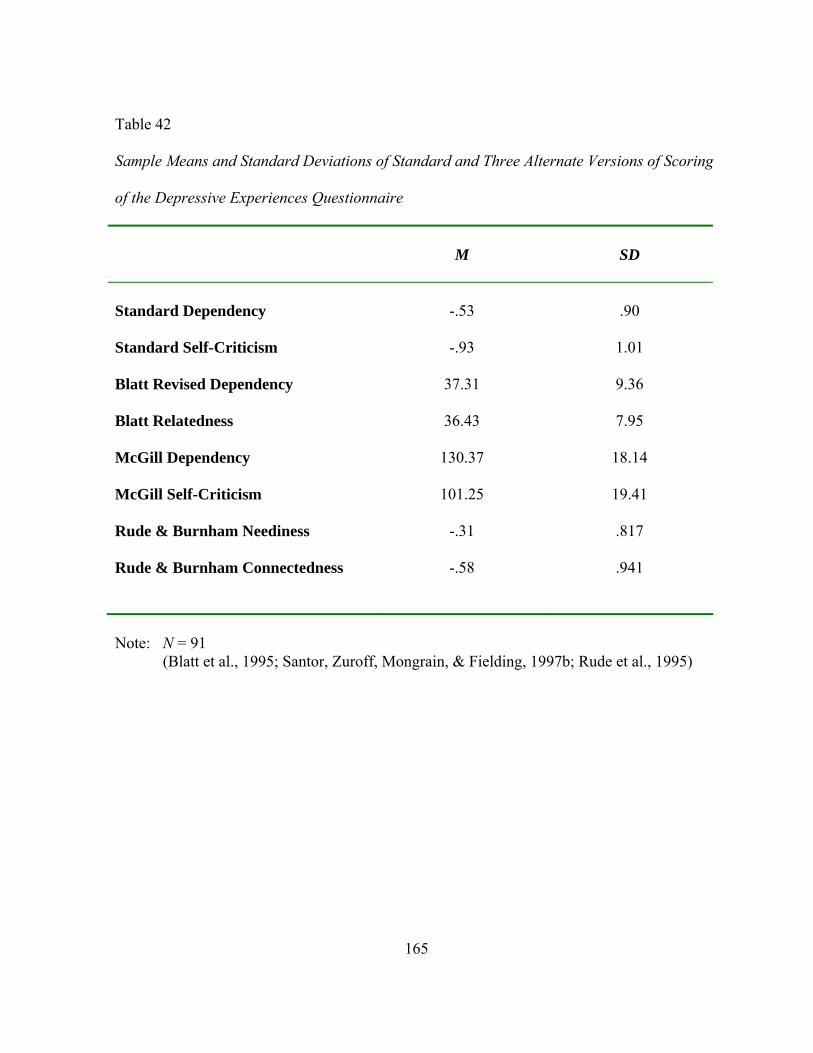
165
Table 42 Sample Means and Standard Deviations of Standard and Three Alternate Versions of Scoring of the Depressive Experiences Questionnaire
M
SD
Standard Dependency
-.53
.90
Standard Self-Criticism -.93 1.01
Blatt Revised Dependency 37.31 9.36
Blatt Relatedness 36.43 7.95
McGill Dependency 130.37 18.14
McGill Self-Criticism 101.25 19.41
Rude & Burnham Neediness -.31 .817
Rude & Burnham Connectedness -.58 .941
Note: N = 91 (Blatt et al., 1995; Santor, Zuroff, Mongrain, & Fielding, 1997b; Rude et al., 1995)
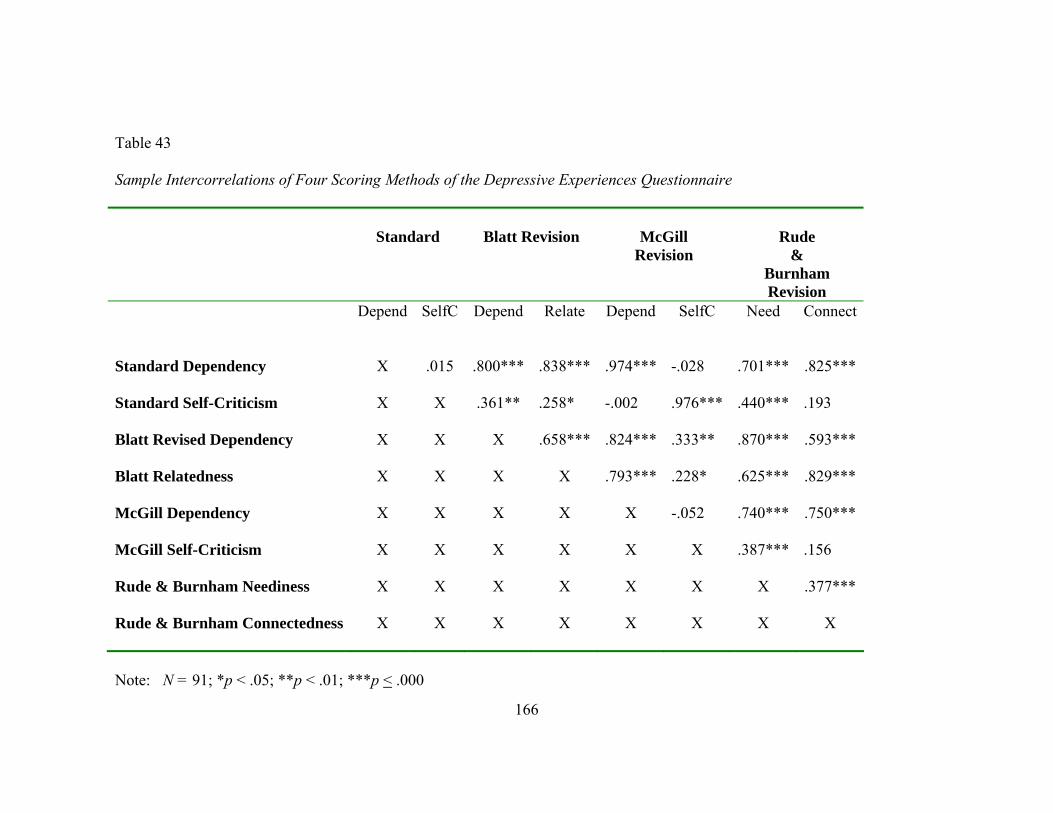
Table 43 Sample Intercorrelations of Four Scoring Methods of the Depressive Experiences Questionnaire
Standard
Blatt Revision
McGill Revision
Rude
& Burnham Revision
Depend SelfC Depend Relate Depend SelfC Need Connect
Standard Dependency
X
.015
.800***
.838***
.974***
-.028
.701***
.825***
Standard Self-Criticism X
X .361** .258* -.002 .976*** .440*** .193
Blatt Revised Dependency X X X .658*** .824*** .333** .870*** .593***
Blatt Relatedness X X X X .793*** .228* .625*** .829***
McGill Dependency X X X X X -.052 .740*** .750***
McGill Self-Criticism X X X X X X .387*** .156
Rude & Burnham Neediness X X X X X X X .377***
Rude & Burnham Connectedness X X X X X X X X
Note: N = 91; *p < .05; **p < .01; ***p < .000
166

Table 44
Pearson Product-Moment Correlations of DEQ Dependency, DEQ Self-Criticism, and MAAS Antenatal Attachment Using the
McGill Scoring Method
McGill
Dependent
McGill
Self-Critical
MAAS Quality
MAAS
Intensity
MAAS Global
Personality(DEQ) Dependent Characteristics
X
-.052
N = 91
-.060
N = 91
.057
N = 89
.004
N = 91 Self-Critical Characteristics
X
X
-.339** N = 91
-.049
N = 89
-.201
N = 91 Note: N = 91
MAAS = Maternal Antenatal Attachment Scale McGill = Revised Scoring of the Depressive Experiences Questionnaire (Santor et al., 1997b) **p < .01; ***p < .000
167

Table 45
Pearson Product- Moment Correlations of DEQ Dependency and Relatedness with MAAS Antenatal Attachment
Blatt Dependency
Blatt
Relatedness
MAAS Quality
MAAS
Intensity
MAAS Global
Personality(DEQ) Dependence (Immature)
X
.658*
-.194
.019
-.085
Relatedness (Mature)
X
X
-.241*
-.003
-.132
Note: N = 91
DEQ = Depressive Experiences Questionnaire Revised Scoring Method (Blatt et al., 1995) MAAS = Maternal Antenatal Attachment Scale * p < .05; *** p < .000
168

Table 46 Pearson Product Moment Correlations of MAAS Antenatal Attachment and Rude & Burnham’s Needy and Connectedness DEQ Scoring Method
Rude & Burnham Neediness
Rude & Burnham
Connectedness
MAAS Quality
MAAS
Intensity
MAAS Global
Personality(DEQ) Neediness (Unhealthy)
X
.377***
-.242*
.036
-.095
Connectedness (Healthy)
X
X
-.048
.041
-.004
Note: N = 91
DEQ = Depressive Experiences Questionnaire Revised Scoring Method (Rude & Burnham, 1995) * = p < .05; *** p < .000
169

170
Table 47 Linear Regression Analyses of Dependency and Self-Criticism Scores Predicting MAAS Global Attachment Score
95% CI
F (2, 88)
p
R²
Adj. R²
Standard Scoring
Dependency -1.32 to 1.96 Self-Criticism
-2.86 to .064
1.87
.16
.04
.019
McGill Scoring
Dependency -.08 to .08 Self-Criticism
-.15 to .002
1.86
.16
.04
.019
Blatt Subscales
Dependency -.37 to .13 Relatedness
-.21 to .22
.78
.46
.02
-.005
Rude & Burnham
Neediness -2.94 to 1.03 Connected
-1.44 to 2.01
.457
.63
.01
-.01
Note: N = 89

171
Table 48 Spearman’s rho Correlation of ORI Baby Narrative and Gestational Age (Weeks)
ORI Baby Narrative
Conceptual Level Length Ambivalence Conceptual Level X X X Length .127 X X Ambivalence -.170 .355** X Gestational Age (Weeks) -.114 .060 -.038
Note: N = 85
ORI = Object Relations Inventory ** = p = .001

172
Table 49 Comparison of Most Common Risk Factors
Baylor Sample Maloni Sample
Besser Sample
Gupton Sample*
N % N
% N
%
N %
Preterm Labor
40
43.95 41 46.06 X X X 20
Placenta Previa
3 3.29 7 7.86 X X X 20
Incompetent Cervix
29 31.87 6 6.74 X X X X
Cervical Abnormality
2 2.19 5 5.61 X X X X
Pregnancy-Induced Hypertension
18 19.78 3 3.3 X X X 18
Premature Rupture of Membranes
16 17.58 2 2.2 X X X 17
Other X X X 28.23 X X X 25
Diabetes
5 5.49 X X 146 100% X X
Total
91 ** 89 100 146 100% 105 100
Note: *Gupton did not include exact N per condition ** Percentages exceed 100% in view of dual or multiple diagnoses (Maloni et al., 2001; Besser et al., 2002; Gupton et al., 2001)

Table 50 Comparison of the ORI and MAAS Means and Standard Deviations from Two Samples
Baylor Sample
Israeli Sample
M SD M
SD
Object Representations (Mother)
Benevolent
4.11 1.54 4.62 1.20
Punitive
1.49 1.42 3.97 1.07
Ambitious
3.53 1.69 3.90 1.18
Ambivalent
1.83 1.30 2.61 1.32
Conceptual Level
5.17 1.22 5.34 2.08
Antenatal Attachment
Quality
46.01 3.48 45.21 4.24
Intensity
30.71 4.88 27.72 4.96
Note: Baylor Sample: Object Relations Inventory (ORI) N = 83
Maternal Antenatal Attachment Scale (MAAS) N = 91 Israeli Sample: N = 120 (Priel et al., 2001)
173

Table 51 Comparisons of Correlations for ORI Mother Narrative and Maternal Antenatal Attachment in Two Samples Baylor Sample
N = 83 Israeli Sample
N = 120 Quality Intensity Quality Intensity Object Representations (Mother)
Benevolent
.174 .045 .33*** .07
Punitive
-.020 -.154 -.23*** -.16
Ambitious
-.218 .043 .39*** .12
Ambivalent
-.130 -.168 -.29** -.11
Conceptual Level
.040 -.176 .42*** .19*
Note: **p <.01; ***p <.001 Israeli Sample (Priel et al., 2001)
174

APPENDIX A Baylor Internal Review Board Approval
175

APPENDIX B Letter of Consent
176

APPENDIX C
MEASURES
177

CENTER FOR EPIDEMIOLOGIC STUDIES—DEPRESSION SCALE (CES-D) Below is a list of some ways you may have felt or behaved. Please indicate how often you have felt this way during the last week by checking the appropriate space. Durin r
the
of a
days)
M
Time (5-7
1. I was bothered by things that usually don’t bother me.
0 1 3
2. I d ing; my appetite was poor.
0 1 2 3
3. I felt that I could not shake off the blues even with
0 1 2 3
4. I felt I was just as good as other people.
0 1 2 3
5. I had as do
0 1
6. I felt depressed.
0 1 2 3
7. I felt that everything I did was an effort.
0 1 2 3
8. I felt hopeful about the future.
0 1 2 3
9. I thou t my life had been a failure.
0 1 2 3
10. I f
0 1 2 3
11. My sleep was restless.
0 1 2 3
12. I was happy.
0 1 3
13. I talke
0 1 3
14. I f
0 1 2 3
15. People were unfriendly.
0 1 2 3
16. I enjoyed life.
0 1 2 3
17 I had
0 1
18. I felt sad. 0 1 2 3
19 felt liked me.
0 1
20. I could not get going. 0 1 2 3
g the past week: Rarely onone oftime (less than 1 day)
Some or alittlethe time (1-2 days)
Occasionally or
Moderate amount ofTime (3-4
ost or all of the
days)
2
id not feel like eat
help from my family or friends.
trouble keeping my mind on what I wing.
2 3
gh
elt fearful.
2
d less than usual.
elt lonely.
2
. crying spells. 2 3
. I that people dis 2 3
178

DEPRESSIVE EXPERIENCE UESTIONN E (DEQ)
Listed below er of statements concerning personal characteristics and traits. Read each item and decide u agree or disagree and to what extent. If you strongly agree
S Q AIR
are a numbwhether yo , circle7; if you
strongly disagree, circle 1; The midpoint, if you are neutral or undecided, is 4.
Strongly Strongly Disagree Agree
1. I set my personal goals and standards as high
as possible. 1 2 3 4 5 6 7
2. Without s pport from others who are close to me, I would be helpless. 1 2 3 4 5 6 7
3. I tend to isfied with my current plans and goals,
rat th 1 2 3 4 5 6 7
4. Sometimes I feel very big, and other times I feel v small. 2 3 5 6 7
5. When I am closely involved with someone, I never feel jealous. 1 2 3 4 5 6 7
6. I urgently need things that only other people
can provide. 1 2 3 4 5 6 7
7. I often find that I don't live up to my own standards or ideals. 1 2 3 4 5 6 7
8. I feel I am always making full use of my potential
abilities. 1 2 3 4 5 6 7 9. The lack of permanence in human relationships
doesn't bother me. 1 2 3 4 5 6 7 10. If I fail to live up to expectations, I feel unworthy. 1 2 3 4 5 6 7 11. Many times I feel helpless. 1 2 3 4 5 6 7 12. I seldom worry about being criticized for things
I have said or done. 1 2 3 4 5 6 7
13. There is a considerable difference between how I am now and how I would like to be. 1 2 3 4 5 6 7
14. I enjoy sharp competition with others. 1 2 3 4 5 6 7 15. I feel I have many responsibilities that I must meet. 1 2 3 4 5 6 7 16. There are times when I feel "empty" inside. 1 2 3 4 5 6 7 17. I tend not to be satisfied with what I have. 1 2 3 4 5 6 7 Copyright: Sidney J. Blatt, Ph.D., Joseph P. D'Afflitti, Ph.D., Donald M. Quinlan, Ph.D., 1979.
u
be sather an striving for higher goals.
ery 1 4
179

19. I become frightened when I feel alone. 1 2 3 4 5 6 7 20. I would feel like I'd be losing an important part
of myself if I lost a very close friend. 1 2 3 4 5 6 7
2 1 2 3 4 5 6 7
22. I have difficulty breaking off a relationship
1 2 3 4 5 6 7 23. I often think about the danger of losing someone
1 2 3 4 5 6 7
25.
1 2 3 4 5 6 7 26. I am not very concerned with how other people
1 2 3 4 5 6 7 27.
ejection. 1 2 3 4 5 6 7
29. It's important for my family that I succeed. 1 2 3 4 5 6 7
30. Often, I feel I have disappointed others. 1 2 3 4 5 6 7
lo . 1 2 3 4 5 6 7
t )
sts friend 1 2 3 4 5 6 7
lati nship. 1 2 3 4 5 6 7
are times when I feel extremely good about myself and other times
3 4 5 6 7
18. I don't care whether or not I live up to what other people expect of me. 1 2 3 4 5 6 7
1. People will accept me no matter how many mistakes
I have made.
that is making me unhappy.
who is close to me. 1 2 3 4 5 6 7
24. Other people have high expectations of me.
When I am with others, I tend to devalue or "undersell" myself.
respond to me.
No matter how close a relationship between two people is, there is always a large amount of uncertainty and conflict. 1 2 3 4 5 6 7
28. I am very sensitive to others for signs of r
31. If someone makes me angry, I let him (her) know
how I feel. 1 2 3 4 5 6 7
32. I constantly try, and very often go out of my way, to please or help people I am c se to
33. I have many inner resources (abilities, s rengths . 1 2 3 4 5 6 7
34. I find it very difficult to say "No" to the reque of s. 35. I never really feel secure in a close re o
. The way I feel about myself frequently varies: there36
when I see only the bad in me and feel like a total failure 1 2
180
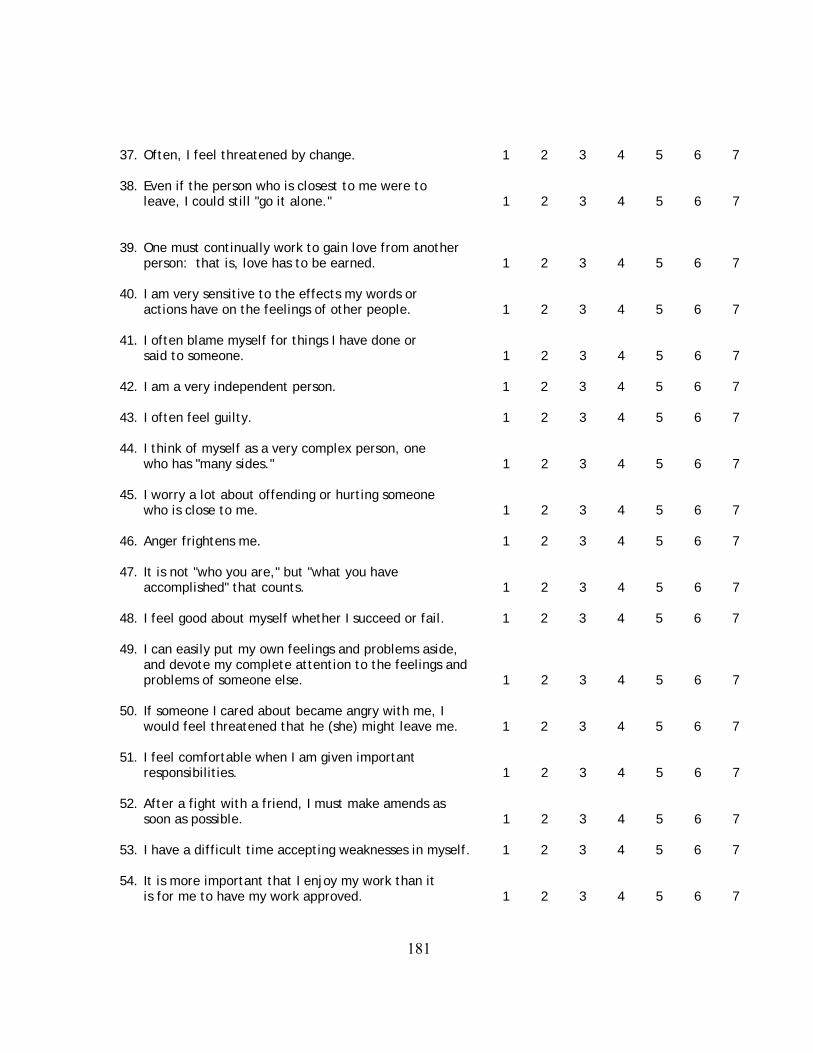
7. Often, I feel threatened by change. 1 2 3 4 5 6 7
o
leave, I could still "go it alone." 1 2 3 4 5 6 7
her
.
gs e le
1 2 3 4 5 6 7 3. I often feel guilty. 1 2 3 4 5 6 7
4. I think of myself as a very complex person, one 1 2 3 4 5 6 7
5. I worry a lot about offending or hurting someone
1 2 3 4 5 6 7 6. Anger frightens me. 1 2 3 4 5 6 7
47.accomplished" that counts. 1 2 3 4 5 6 7
8. I feel good about myself whether I succeed or fail. 1 2 3 4 5 6 7
9. I can easily put my own feelings and problems aside,
problems of someone else. 1 2 3 4 5 6 7
50.would feel threatened that he (she) might leave me. 1 2 3 4 5 6 7
51. rtant responsibilities. 1 2 3 4 5 6 7
2. After a fight with a friend, I must make amends as
s .
1 2 3 4 5 6 7
3
38. Even if the person who is closest t me were to
39. One must continually work to gain love from anotperson: that is, love has to be earned 1 2 3 4 5 6 7
40. I am very sensitive to the effects my words or
actions have on the feelin of oth r peop . 1 2 3 4 5 6 7 41. I often blame myself for things I have done or
said to someone. 1 2 3 4 5 6 7 42. I am a very independent person.
4 4
who has "many sides."
4who is close to me.
4
It is not "who you are," but "what you have
4 4
and devote my complete attention to the feelings and
If someone I cared about became angry with me, I
I feel comfortable when I am given impo
5
soon as possible. 1 2 3 4 5 6 7 53. I have a difficult time accepting weaknesses in my elf 1 2 3 4 5 6 7 54. It is more important that I enjoy my work than it
is for me to have my work approved.
181

55. After an argument, I feel very lonely. 1 2 3 4 5 6 7
56. In my relationships with others, I am very concerned 1 2 3 4 5 6 7
57. rarely think about my family. 1 2 3 4 5 6 7
me vary:
when I feel all-loving towards that person. 1 2 3 4 5 6 7
59. those around me. 1 2 3 4 5 6 7
60. " l.
ys m
1 2 3 4 5 6 7 4. I tend to be very critical of myself. 1 2 3 4 5 6 7
65. l
ar o
about what they can give to me.
I
58. Very frequently, my feelings toward someone close tothere are times when I feel completely angry and other times
What I do and say has a very strong impact on
I sometimes feel that I am specia " 1 2 3 4 5 6 7
61. I grew up in an extremely close family. 1 2 3 4 5 6 7 62. I am very satisfied with m elf and my accomplish ents. 1 2 3 4 5 6 7 63. I want many things from someone I am close to.
6
Being alone doesn't bother me at a l. 1 2 3 4 5 6 7 66. I very frequently compare myself to stand ds or g als. 1 2 3 4 5 6 7
182
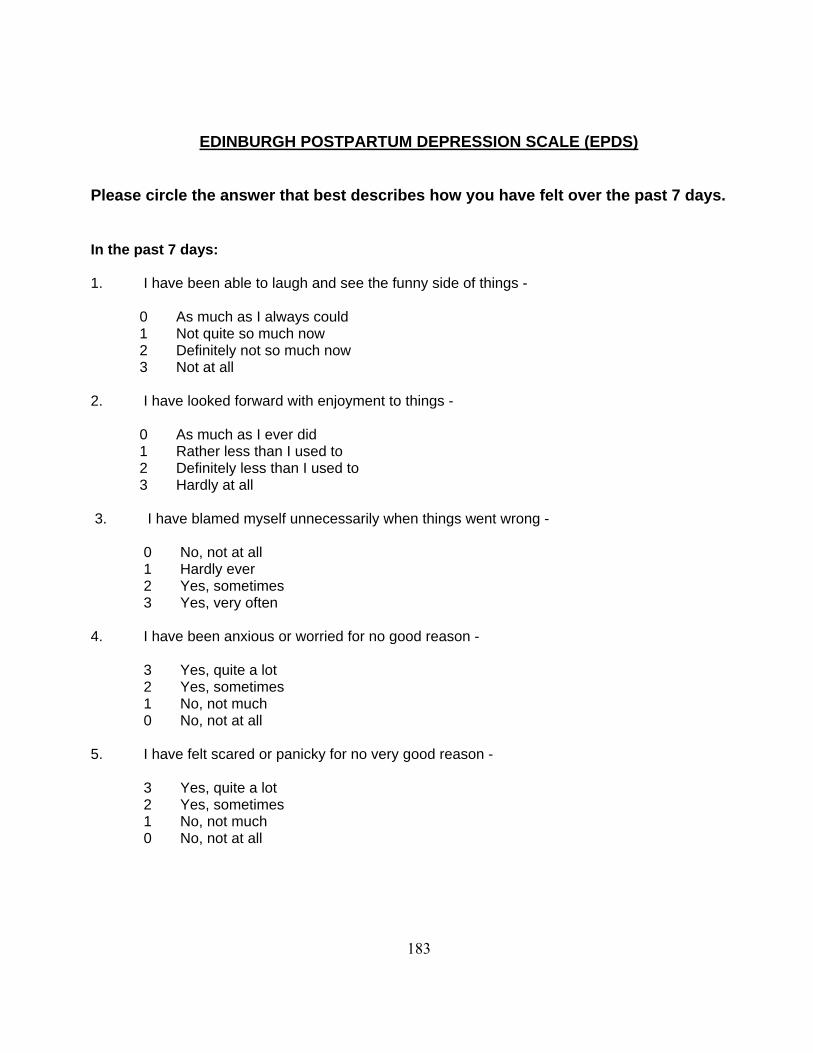
EDINBURGH POSTPARTUM DEPRESSION SCALE (EPDS)
Please circle the answ how you have felt over the past 7 days. er that best describes In the past 7 days: 1. ny sid of thin - I have been able to laugh and see the fun e gs 0 ys As much as I alwa could 1 Not quite so much now 2 Definitely not so much now 3 Not at all
2. I have looked forward with enjoyment to things - 0 As much as I ever did 1 Rather less than I used to 2 Definitely less than I used to 3 Hardly at all 3. I ha ent wrong - ve blamed myself unnecessarily when things w 0 No, not at all 1 Hardly ever 2 Yes, sometimes 3 Yes, very often 4. I have been anxious or worried for no good reason - 3 Yes, quite a lot 2 Yes, sometimes 1 No, not much 0 No, not at all 5. I have felt scared or panicky for no very good reason - 3 Yes, quite a lot 2 Yes, sometimes 1 No, not much 0 No, not at all
183
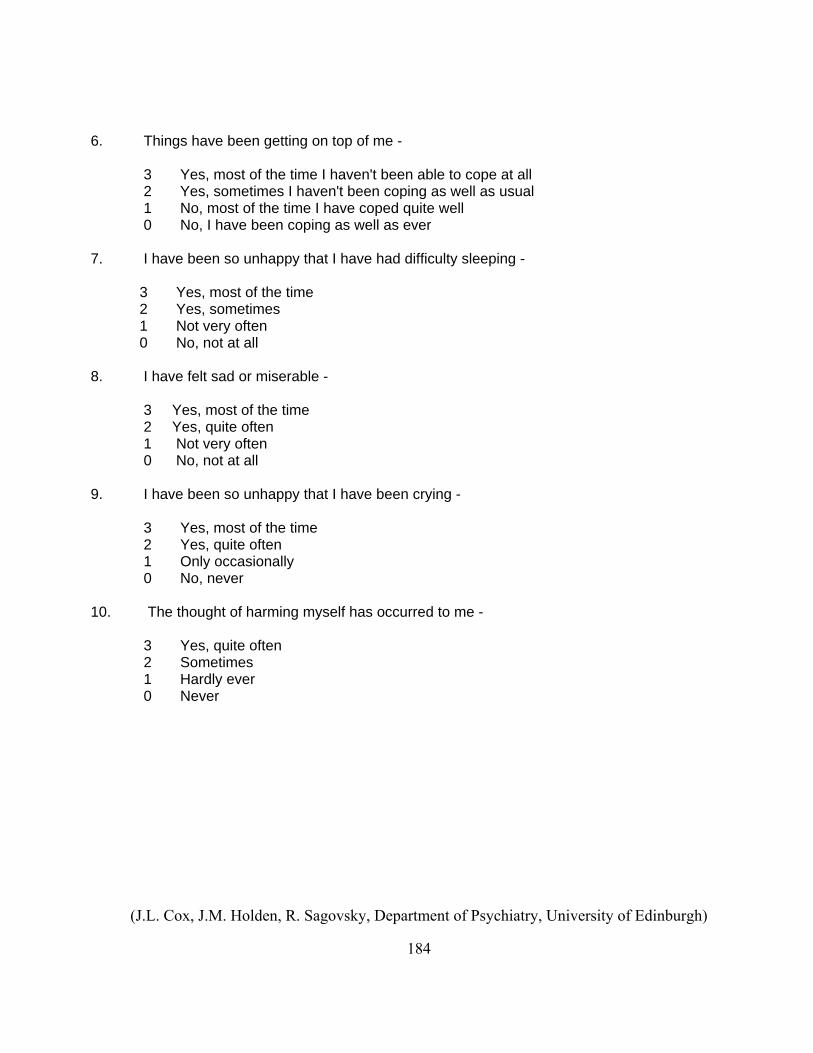
6. Things have been getting on top of me - 3 Yes, most of the time I haven't been able to cope at all 2 Yes, sometimes I haven't been coping as well as usual 1 No, most of the time I have coped quite well 0 No, I have been coping as well as ever
7. I have been so unhappy that I have had difficulty sleeping - 3 Yes, most of the time 2 Yes, sometimes 1 Not very often 0 No, not at all
8. I have felt sad or m erable - is 3 Yes, most of the time 2 Yes, quite often 1 Not very often 0 No, not at all
9. I have been so unhappy that I have been crying - 3 Yes, most of the time 2 Yes, quite often 1 Only occasionally 0 No, never
10. The thought of harming myself has occurred to me - 3 Yes, quite often 2 Sometimes 1 Hardly ever 0 Never
(J.L. Cox, J.M. Holden, R. Sagovsky, Department of Psychiatry, University of Edinburgh)
184

MATERNAL ANTENATAL ATTACHMENT SCALE (MAAS)
These questions are about your thoughts and feelings about the developing baby. Please tick one box only in answer to each question. 1) Over the past two weeks I have thought about, or been preoccupied with the baby inside me:
Almost all the time
Very fre uq ently
Frequently
Occasionally
Not at all 2) Over the past two weeks when I have spoken about, or thought about the baby inside me I got
emotional feelings which were:
Very weak or non-existent
Fairly weak
In between strong and weak
Fairly strong
Very strong 3) Over the past two weeks my feelings about the baby inside me have been:
Very positive
Mainly positive
Mixed positive and negative
Mainly negative
Very negative
185
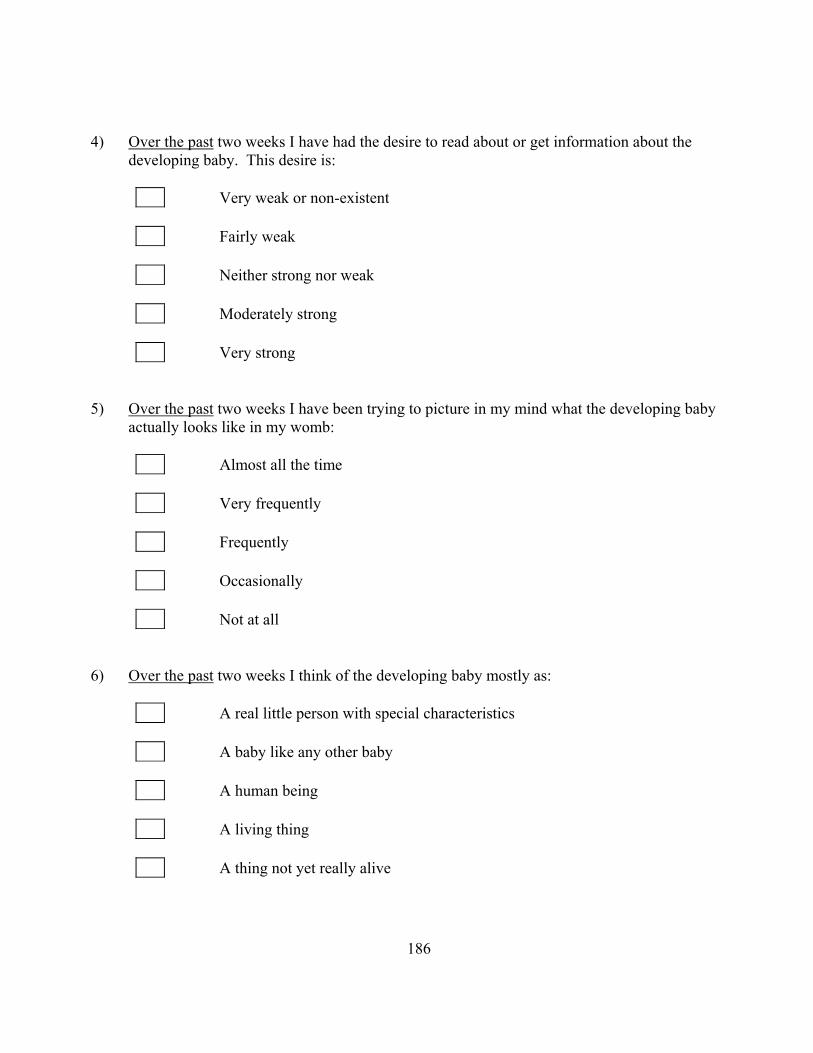
4) Over the past two weeks I have had the desire to read about or get information about the developing baby. This desire is:
Very weak or non-existent
Fairly weak
Neither strong nor weak
Moderately strong
Very strong
5) O r tve he past two weeks I have been trying to picture in my mind what the developing baby
actually looks like in my womb:
Almost all the time
Very frequently
Frequently
Occasionally
Not at all 6) Over the past two weeks I think of the developing baby mostly as:
A real little person with special characteristics
A baby like any other baby
A human being
A living thing
A thing not yet really alive
186

7) Over the past two weeks I have felt that the baby inside me is dependent on me for its well-being:
Totally
A great deal
Moderately
Slightly
Not at all 8) Over the past two weeks I have found myself talking to my baby when I am alone:
Not at all
Occasionally
Frequently
Very frequently
Almost all the time I am alone 9) Over the past two weeks when I think about (or talk to) my baby inside me, my thoughts:
Are always tender and loving
Are mostly tender and loving
Are a mixture of both tenderness and irritation
Contain a fair bit of irritation
Contain a lot of irritation
187
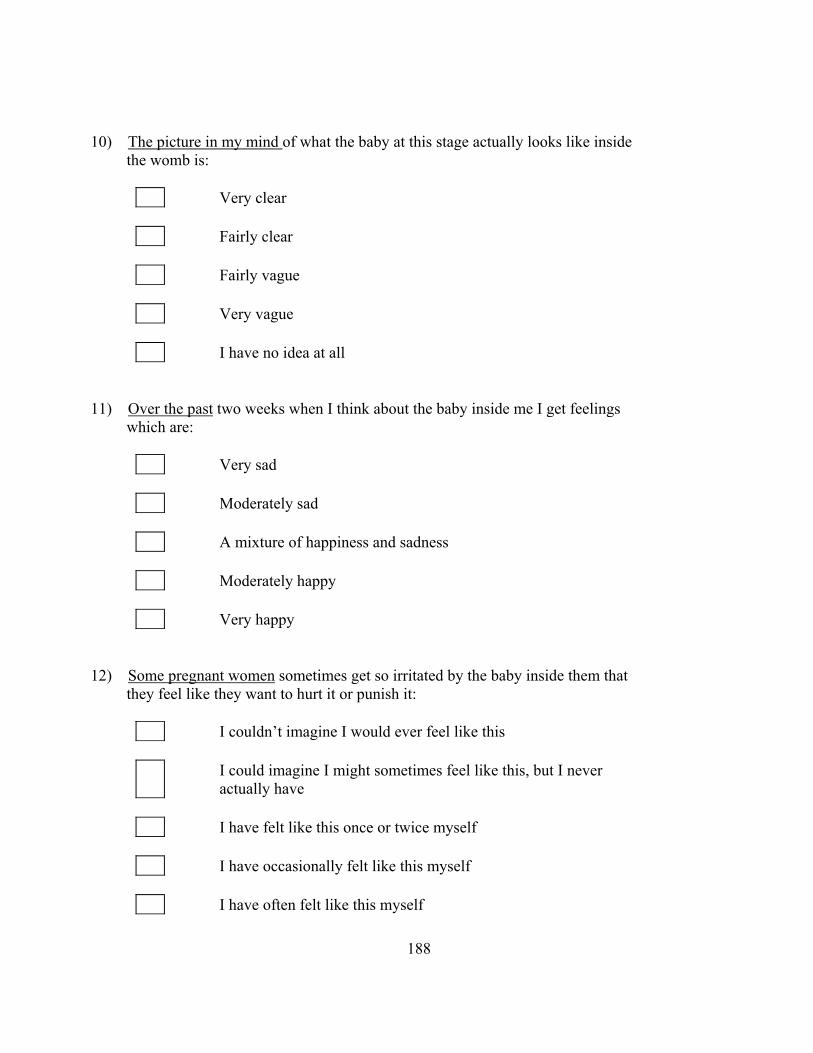
10) The picture in my mind of what the baby at this stage actually looks like inside the womb is:
Very clear
Fairly clear
Fairly vague
Very vague
I have no idea at all 11) Over the past two weeks when I think about the baby inside me I get feelings which are:
Very sad
Moderately sad
A mixture of happiness and sadness
Moderately happy
Very happy 12) Some pregnant women sometimes get so irritated by the baby inside them that they feel like they want to hurt it or punish it:
I couldn’t imagine I would ever feel like this
I could imagine I might sometimes feel like this, but I never actually have
I have felt like this once or twice myself
I have occasionally felt like this myself
I have often felt like this myself
188
13) Over the past two weeks I have felt:
Very emotionally distant from my baby
Moderately emotionally distant from my baby
Not particularly emotionally close to my baby
Moderately close emotionally to my baby
Very close emotionally to my baby 14) Over the past two weeks I have taken care with what I eat to make sure the baby gets a good diet:
Not at all
Once or twice when I ate
Occasionally when I ate
Quite often when I ate
Every time I ate 15) When I first see my baby after the birth I expect I will feel:
Intense affection
Mostly affection
Dislike about one or two aspects of the baby
Dislike about quite a few aspects of the baby
Mostly dislike
189

16) When my baby is born I would like to hold the baby:
Immediately
After it has been wrapped in a blanket
After it has been washed
After a few hours for things to settle down
The next day 17) Over the past two weeks I have had dreams about the pregnancy or baby:
Not at all
Occasionally
Frequently
Very frequently
Almost every night 18) Over the past two weeks I have found myself feeling, or rubbing with my hand, the outside of my stomach where the baby is:
A lot of times each day
At least once per day
Occasionally
Once only
Not at all
190

19) If the pregnancy was lost at this time (due to miscarriage or other accidental event) without any pain or injury to myself, I expect I would feel:
Very pleased
Moderately pleased
Neutral (i.e. neither sad nor pleased, or mixed feelings)
Moderately sad
Very sad
Copywrite JT Condon Dept. Psychiatry Flinders Medical Centre, South Australia
191

Chart Review Participant number Obstetrician of record Birthdate Ethnicity Af Am Asian Caucasian Latino Other Marital Status Single Married Separated Divorced Widowed CohabitingTotal Pregnancies (Prior) Full Term (Prior) Premature (Prior) Abortions induced Abortions spontaneous Ectopics Multiple births (Prior) Living Stillborn List any interventions that have been initiated or ordered by the doctor: HOBEL RISK ASSESSMENT--PRENATAL yes no Moderate to severe toxemia 10 0 Chronic Hypertension 10 0 Moderate to severe renal disease 10 0 Severe heart disease, Class II-IV 10 0 History of eclampsia 5 0 History of pyelitis 5 0 Class I heart disease 5 0 Mild toxemia 5 0 Acute pyelonephritis 5 0 History of cystitis 1 0 Acute cystitis 1 0 History of toxemia 1 0 Diabetes > Class A-II 10 0 Previous endocrine ablation 10 0 Thyroid disease 5 0 Prediabetes (A-I) 5 0 Family history of diabetes 1 0
192
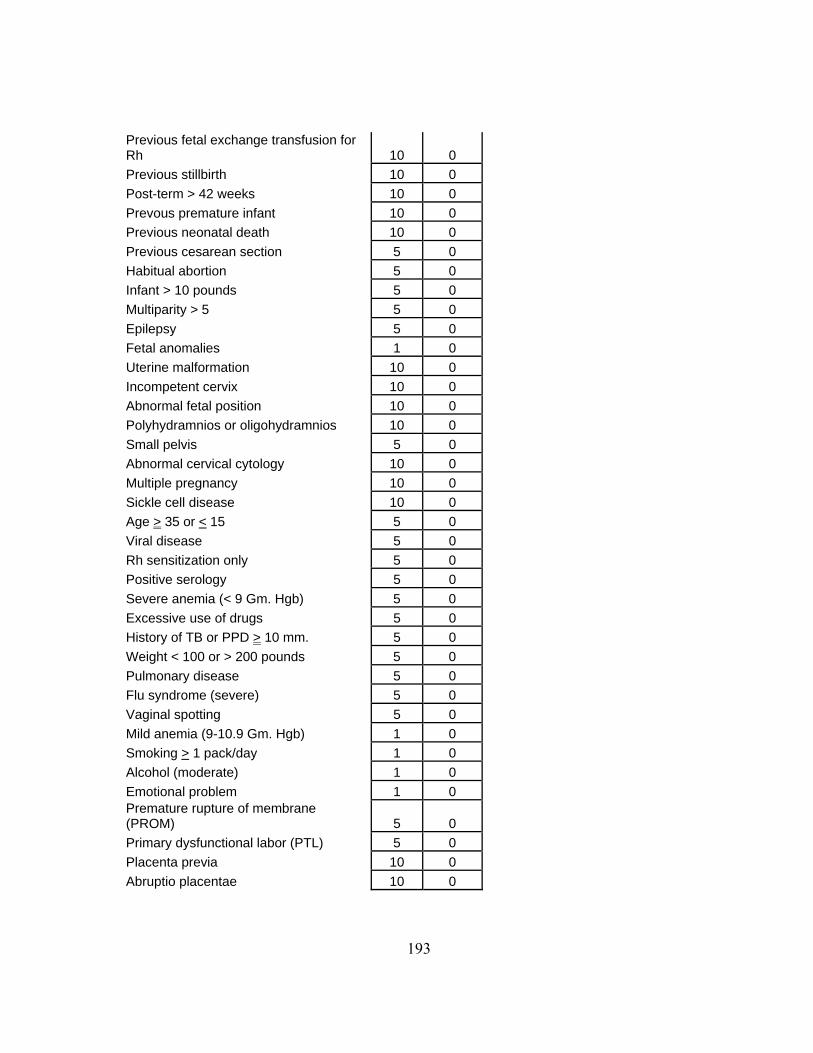
Previous fetal exchange transfusion for Rh 10 0 Previous stillbirth 10 0 Post-term > 42 weeks 10 0 Prevous premature infant 10 0 Previous neonatal death 10 0 Previous cesarean section 5 0 Habitual abortion 5 0 Infant > 10 pounds 5 0 Multiparity > 5 5 0 Epilepsy 5 0 Fetal anomalies 1 0 Uterine malformation 10 0 Incompetent cervix 10 0 Abnormal fetal position 10 0 Polyhydramnios or oligohydramnios 10 0 Small pelvis 5 0 Abnormal cervical cytology 10 0 Multiple pregnancy 10 0 Sickle cell disease 10 0 Age > 35 or < 15 5 0 Viral disease 5 0 Rh sensitization only 5 0 Positive serology 5 0 Severe anemia (< 9 Gm. Hgb) 5 0 Excessive use of drugs 5 0 History of TB or PPD > 10 mm. 5 0 Weight < 100 or > 200 pounds 5 0 Pulmonary disease 5 0 Flu syndrome (severe) 5 0 Vaginal spotting 5 0 Mild anemia (9-10.9 Gm. Hgb) 1 0 Smoking > 1 pack/day 1 0 Alcohol (moderate) 1 0 Emotional problem 1 0 Premature rupture of membrane (PROM) 5 0 Primary dysfunctional labor (PTL) 5 0 Placenta previa 10 0 Abruptio placentae 10 0
193
OBJECT RELATIONS INVENTORY (ORI)
DESCRIBE YOUR MOTHER.
194
OBJECT RELATIONS INVENTORY (ORI)
DESCRIBE THE BABY YOU ARE CARRYING.
195
BIBLIOGRAPHY
Diagnostic and Statistical Manual of Mental Disorders—IV--TR (2000).
Washington, DC: American Psychiatric Association.
Ainsworth, M. D. S. (1968). Citation for the G. Stanley hall Award to John
Bowlby. Unpublished manuscript.
Ainsworth, M. D. S., Bell, S. M., & Stayton, D. J. (1974). Infant-mother
attachment and social development: "Socialization" as a product of reciprocal
responsiveness to signals. In M. P. M. Richards (Ed.), The integration of a child into a
social world (pp. 99-135). New York: Cambridge University Press
Ainsworth, M. D. S., Blehar, M. C., Waters, E., & Wall, S. (1978). Patterns of
attachment: A psychological study of the Strange Situation. Hillsdale, NJ: Erlbaum.
Ainsworth, M. D. S. & Marvin, R. S. (1995). On the shaping of attachment theory
and research: An interview with Mary D. S. Ainsworth (Fall 1994). Monographs of the
Society for Research in Child Development, 60, -21.
Angyal, A. (1941). Foundations for a science of personality. New York: Viking
Press.
Atkinson, L., Goldberg, S., Raval, V., Pederson, D., Benoit, D., Moran, G. et al.
(2005). On the Relation Between Maternal State of Mind and Sensitivity in the Prediction
of Infant Attachment Security. Developmental Psychology, 41, 42-53.
196

Austin, M. P. & Lumley, J. (2003). Antenatal screening for postnatal depression:
A systematic review. Acta Psychiatrica Scandinavia, 107, 10-17.
Bacchiochi, J. R., Bagby, R. M., Cristi, C., & Watson, J. (2003). Validation of
connectedness and neediness as dimensions of the dependency construct. Cognitive
Therapy & Research, 27, 233-242.
Bagby, R. M., Parker, J. D., Joffe, R. T., & Buis, T. (1994). Reconstruction and
validation of the Depressive Experiences Questionnaire. Assessment, 1, 59-68.
Bakan, D. (1966). The duality of human existence: An essay on psychology and
religion. Chicago: Rand McNally.
Balint, M. (1959). Thrills and regressions. London: Hogarth Press.
Bartholomew, K. & Horowitz, L. M. (1991). Attachment styles among young
adults: A test of a four-category model. Journal of Personality and Social Psychology,
61, 226-243.
Bartholomew, K. & Shaver, P. (1998). Methods of assessing adult attachment: Do
they converge? In J. A. Simpson & W. S. Roles (Eds.), Attachment Theory and Close
Relationships (pp. 25-45). New York: Guilford
Beck, A. T. (1983). Cognitive therapy of depression: New perspectives. In P. J.
Clayton & J. E. Barrett (Eds.), Treatment of depression: Old controversies and new
approaches. New York: Raven Press
197

Beck, A. T., Epstein, N., Harrison, R. P., and Emery, G. (1983). Development of
the sociotropy autonomy scale: A measure of personality factors in psychopathology.
Unpublished manuscript.
Beck, C. T. (1999a). Available instruments for research on prenatal attachment
and adaptation to pregnancy. MCN, American Journal of Maternal Child Nursing, 24, 25-
32.
Beck, C. T. (1999c). Available instruments for research on prenatal attachment
and adaptation to pregnancy. MCN, American Journal of Maternal Child Nursing, 24, 25-
32.
Beck, C. T. (1999b). Available instruments for research on prenatal attachment
and adaptation to pregnancy. MCN, American Journal of Maternal Child Nursing, 24, 25-
32.
Beeghly, M., Weinberg, M., Olson, K., Kernan, H., Riley, J., & Tronick, E.
(2002). Stability and change in level of maternal depressive symptomatology during the
first postpartum year. Journal of Affective Disorders, 71, 169.
Benedek, T. (1959). Parenthood as a developmental phase: A contribution to the
libido theory. Journal of the American Psychoanalytic Association, 7, 389-417.
Benedek, T. (1958). Psychological aspects of pregnancy and parent-child
relationships. In S. Liebman (Ed.), (pp. 1-16). Oxford, England: Lippincott.
198

Benoit, D., Parker, K. C., & Zeanah, C. H. (1997). Mothers' representations of
their infants assessed prenatally: stability and association with infants' attachment
classifications. Journal of Child Psychology & Psychiatry & Allied Disciplines,
38(3):307-13.
Benoit, D. & Parker, K. C. H. (1994). Stability and transmission of attachment
across three generations. Child Development, 65, 1444-1456.
Besser, A. & Priel, B. (2003a). A multisource approach to self-critical
vulnerability to depression: The moderating role of attachment. Journal of Personality,
71, 515-555.
Besser, A., Flett, G. L., & Davis, R. A. (2003). Self-criticism, dependency,
silencing the self, and loneliness: A test of a mediational model. Personality & Individual
Differences, 35, 1735-1752.
Besser, A. & Priel, B. (2003b). Trait vulnerability and coping strategies in the
transition to motherhood. Current Psychology: Developmental, Learning, Personality,
Social, 22, 57-72.
Besser, A., Priel, B., & Wiznitzer, A. (2002). Childbearing depressive
symptomatology in high-risk pregnancies: The roles of working models and social
support. Personal Relationships, 9, 395-413.
199
Bibring, G. L. (1959). Some considerations of the psychological processes in
pregnancy. Psychoanalytic Study of the Child, 14, 113-121.
Bibring, G. L., Dwyer, T. F., Huntington, D. S., & Valenstein, A. F. (1961). A
study of the psychological processes in pregnancy and of the earliest mother-child
relationship. Psychoanalytic Study of the Child, 16, 9-72.
Blatt, S., Auerbach, J. S., & Lindgren, K. (1997). Mental representations in
personality development, psychopathology, and the therapeutic process. Review of
General Psychology, 1, 351-374.
Blatt, S., Chevron, S. E., Quinlan, D. M., Schaffer, C. E., and Wein, S. (1992a).
The assessment of qualitative and structural dimensions of object representations.
Unpublished manuscript.
Blatt, S. J. (1974). Levels of object representation in anaclitic and introjective
depression. The Psychoanalytic Study of the Child, 24, 107-157.
Blatt, S. J., Auerbach, J. S., & Levy, K. N. (1997). Mental representations in
personality development, psychopathology, and the therapeutic process. Review of
General Psychology, 1, 351-374.
Blatt, S. J., D'Affliti, J. P., & Quinlan, D. M. (1976). Experiences of depression in
normal young adults. Journal of Abnormal Psychology, 85, 383-389.
200

Blatt, S. J., Shahar, G., & Zuroff, D. C. (2001). Anaclitic (sociotropic) and
introjective (autonomous) dimensions. Psychotherapy, 38, 449-454.
Blatt, S. J. & Zuroff, D. C. (1992b). Interpersonal relatedness and self-definition:
Two prototypes for depression. Clinical Psychology Review, 12, 527-562.
Blatt, S. J. (2004). Measurement of anaclitic and introjective depressive
experiences. In Experiences of depression: Theoretical, clinical, and research
perspectives (pp. 91-123). Washington, DC: American Psychological Association
Blatt, S. J., Schaffer, C. E., Bers, S. A., & Quinlan, D. M. (1992). Psychometric
properties of the Depressive Experiences Questionnaire for adolescents. Journal of
Personality Assessment, 59, 82-98.
Blatt, S. J., Zohar, A. H., Quinlan, D. M., & Zuroff, D. C. (1995). Subscales
within the dependency factor of the Depressive Experiences Questionnaire. Journal of
Personality Assessment, 64, 319-339.
Blumberg, N. L. (1980). Effects of neonatal risk, maternal attitude, and cognitive
style on early postpartum adjustment. Journal of Abnormal Psychology, 89, 139-150.
Bornstein, R. F., Galley, D. J., & Leone, D. R. (1986). Parental representations
and orality. Journal of Personality Assessment, 50, 80-89.
Bowlby, J. (1969). Attachment and Loss Volume I: Attachment. New York: Basic
Books, Inc.
201

Bowlby, J. (1973). Attachment and Loss Volume II: Separation: Anxiety and
Anger. New York: Basic Books, Inc.
Bowlby, J. (1980). Attachment and Loss Volume III: Loss, Sadness, and
Depression. New York: Basic Books, Inc.
Bowlby, J. (1951). Maternal care and mental health. Bulletin of the World Health
Organization, 3, 355-533.
Bowlby, J. (1986). The nature of the child's tie to his mother. In P. Buckley (Ed.),
Essential papers on object relations (pp. 153-199). New York: New York University
Press. (Original work published 1958).
Boyce, P. & Condon, J. (2000). Traumatic childbirth and the role of debriefing. In
J. P. Wilson & B. Raphael (Eds.), Psychological debriefing: Theory, practice and
evidence (pp. 272-280). New York: Cambridge University Press.
Bretherton, I. (1992). The Origins of Attachment Theory: John Bowlby and Mary
Ainsworth. Developmental Psychology, 28, 759-775.
Bretherton, I. (1985). Attachment theory: Retrospect and prospect. In I.
Bretherton & E. Waters (Eds.), Growing Points of Attachment Theory and Research.
Monographs of the Society for Research in Child Development (pp. 3-35).
Brisch, K. H. (2002). Treating attachment disorders. New York: Guilford Press.
202

Bushnell, I. W., Sai, F., & Mullin, J. T. (1989). Neonatal recognition of the
mother's face. British Journal of Developmental Psychology, 7, 3-15.
Cannella, B. L. (2005). Maternal-fetal attachment: an integrative review. Journal
of Advanced Nursing.50(1):60-8.
Carson, K. & Virden, S. (1984). Can prenatal teaching promote maternal
attachment? Practicing nurses test Carter-Jessop's prenatal attachment intervention.
Health Care for Women International, 5(5-6):355-69.
Carter-Jessop, L. (1981). Promoting maternal attachment through prenatal
intervention. MCN, American Journal of Maternal Child Nursing, 6, 107-112.
Cohen, R. L. (1979). Maladaption to pregnancy. Seminars in Perinatology, 3, 15-
24.
Condon, J. T. (1993). The assessment of antenatal emotional attachment:
Development of a questionnaire instrument. British Journal of Medical Psychology, 66,
167-183.
Condon, J. T. (2005). Personal Communication.
Condon, J. T. & Corkindale, C. (1997). The correlates of antenatal attachment in
pregnant women. British Journal of Medical Psychology, 70, 359-372.
203

Condon, J. T. (1986). Management of established pathological grief reaction after
stillbirth. American Journal of Psychiatry, 143, 987-992.
Condon, J. T. & Corkindale, C. J. (1998). The assessment of parent-to-infant
attachment: Development of a self-report questionnaire instrument. Journal of
Reproductive and Infant Psychology, 16, -76.
Cox, J. & Holden, J. (2003a). Perinatal mental health: A guide to the Edinburgh
Postnatal Depression Scale (EPDS). London: Royal College of Psychiatrists.
Cox, J. & Holden, J. (2003b). The origins and development of the Edinburgh
Postnatal Depression Scale. In Perinatal Mental Health (pp. 15-20). London: Royal
College of Psychiatrists.
Cranley, M. S. (1992). A critical review of prenatal attachment research.
Scholarly Inquiry for Nursing Practice, 6, 23-26.
Cranley, M. S. (1979). The impact of perceived stress and social support on
maternal-fetal attachment in the third trimester. University of Wisconsin, Madison, WI.
Cranley, M. S. (1981). Development of a tool for the measurement of maternal
attachment during pregnancy. Nursing Research, 30, 281-284.
Curry, M. A. (1987). Maternal behavior of hospitalized pregnant women. Journal
of Psychosomatic Obstetrics & Gynecology, 7, 165-182.
204

Dawson, G., Klinger, L. G., Panagiotides, H., Hill, D., & Spieker, S. (1992).
Frontal lobe activity and affective behavior of infants of mothers with depressive
symptoms. Child Development, 63, 725-737.
DeCasper, A. J. & Fifer, W. P. (1980). Of human bonding: Newborns prefer their
mothers' voices. Science, 208, 1174-1176.
Dennis, C. L. (2004). Preventing postpartum depression part II: A critical review
of nonbiological interventions. Canadian Journal of Psychiatry, 49, 526-538.
Deutch, H. (1945). The psychology of women. New York: Grune & Stratton.
Diamond, D., Blatt, S. J., Stayner, D. A., and Kaslow, N. (1995). Differentiation-
relatedness of self and object representations. Unpublished manuscript.
Doan, H. M. & Zimerman, A. (2003). Conceptualizing prenatal attachment:
Toward a multidimensional view. Journal of Prenatal & Perinatal Psychology & Health,
18, 109-129.
Feldman, R. & Blatt, S. J. (1996). Precursors of relatedness and self-definition in
mother-infant interaction. In J. M. Masling & R. F. Bornstein (Eds.), Psychoanalytic
perspectives on developmental psychology (pp. 1-42). Washington, D.C.: American
Psychological Association.
205

Fifer, W. P. (2002). The fetus, the newborn, and the mother's voice. In J. Gomes-
Pedro, J. K. Nugent, J. G. Young, & T. B. Brazelton (Eds.), The infant and the family in
the twenty-first century (pp. 79-85). New York: Brunner-Routledge.
Fishler, P. H., Sperling, M. B., & Carr, A. C. (1990). Assessment of adult
relatedness: A review of empirical findings from object relations and attachment theories.
Journal of Personality Assessment, 55, 520.
Fonagy, P. (2001b). Attachment theory and psychoanalysis. New York: Other
Press.
Fonagy, P. (2001a). Introduction to attachment theory. In Attachment Theory and
Psychoanalysis (pp. 5-18). New York: Other Press.
Fonagy, P., Steele, H., & Steele, M. (1991). Maternal representations of
attachment during pregnancy predict the organization of infant-mother attachment at one
year of age. Child Development, 62, 891-905.
Fowles, E. (1996). Relationships among prenatal maternal attachment, presence
of postnatal depressive symptoms, and maternal role attainment. Journal of Society of
Perinatal Nursing, 1, 75-82.
Freud, S. (1955). The psychogenesis of a case of homosexuality in a woman
(1920). In J. Strachey (Ed.), The standard edition of the complete psychological works of
Sigmund Freud (pp. 145-172). London: Hogarth Press. (Original work published 1920.)
206

Frost, M. & Condon, J. T. (1996). The psychological sequelae of miscarriage: A
critical review of the literature. Australian and New Zealand Journal of Psychiatry, 30,
54-62.
Fuller, J. R. (1990). Early patterns of maternal attachment. Health Care for
Women International, 11, 433-446.
Gaffney, K. F. (1989). Maternal-fetal attachment in relation to self-concept and
anxiety. Journal of Perinatology, 13, 453-460.
Gaynes, B. N., Gavin, N., Meltzer-Brody, S., Lohr, K. N., Swinson, T.,
Gartlehner, G. et al. (2005). Perinatal depression: Prevalence, screening accuracy and
screening outcomes (Evidence Report/Technology Assessment No. 119). Rockville, MD:
Agency for Healthcare Research and Quality.
George, C., Kaplan, N., and Main, M. (1985). The attachment interview for
adults. Unpublished manuscript.
Grace, J. T. (1989). Development of maternal-fetal attachment during pregnancy.
Nursing Research, 38, 228-232.
Greenberg, J. R. & Mitchell, S. A. (1983). Object relations in psychoanalytic
theory. Cambridge, MA: Harvard University Press.
207

Griffin, D. W. & Bartholomew, K. (1994). Models of the self and other:
Fundamental dimensions underlying measures of adult attachment. Journal of
Personality and Social Psychology, 67, 430-445.
Gupton, A., Heaman, M., & Cheung, L. W. (2001). Complicated and
uncomplicated pregnancies: women's perception of risk. JOGNN: Journal of Obstetric,
Gynecologic, and Neonatal Nursing, 30, 192-201.
Hazan, C. & Shaver, P. (1987). Romantic love conceptualized as an attachment
process. Journal of Personality and Social Psychology, 52, 511-524.
Heaman, M. (1998). Psychosocial impact of high-risk pregnancy: Hospital and
home care. Clinical Obstetrics and Gynecology, 41, 626-639.
Heaman, M. (1992). Stressful life events, social support, and mood disturbance in
hospitalized and non-hospitalized women with pregnancy-induced hypertension.
Canadian Journal of Nursing Research, 24, 23-37.
Heaman, M., Beaton, J., Gupton, A., & Sloan, J. (1992). A comparison of
childbirth expectations in high-risk and low-risk pregnant women. Clinical Nursing
Research, 1, 252-265.
Hobel, C. J., Hyvarinen, M. A., Okada, D. M., & Oh, W. (1973). Prenatal and
intrapartum high-risk screening: I. Prediction of the high-risk neonate. American Journal
of Obstetrics and Gynecology, 117, 1-9.
208

Hobel, C. J., Youkeles, L., & Forsythe, A. (1979). Prenatal and intrapartum high-
risk screening: II. Prediction of prematurity. American Journal of Obstetrics and
Gynecology, 135, 1051-1056.
Horney, K. (1945). Our Inner Conflicts. New York: Norton.
Kemp, V. H. & Page, C. (1987). Maternal self-esteem and prenatal attachment in
high-risk pregnancy. Maternal-Child Nursing Journal.16(3):195-206.
Kennell, J. H., Slyter, H., & Klaus, M. H. (1970). The mourning response of
parents to the death of a newborn infant. New England Journal of Medicine, 283(7):344-
9.
Klaus, M. H., Jerauld, R., Kreger, N. C., McAlpine, W., Steffa, M., & Kennel, J.
H. (1972). Maternal attachment: Importance of the first post-partum days. New England
Journal of Medicine, 286(9):460-3.
Kobak, R. R. & Sceery, A. (1988). Attachment in late adolescence: Working
models, affect regulation, and representations of self and others. Child Development, 59,
135-146.
Koestner, R., Zuroff, D. C., & Powers, T. A. (1991). Family origins of adolescent
self-criticism and its continuity into adulthood. Journal of Abnormal Psychology, 100,
191-197.
209

Koniak-Griffin, D. (1988). The relationship between social support, self-esteem,
and maternal-fetal attachment in adolescents. Research in Nursing & Health, 11(4):269-
78.
Krohn, A. & Mayman, M. (1974). Object representations in dreams and projective
tests. Bulletin of the Menninger Clinic, 38, 445-466.
Kubler-Ross, E. (1969). On death and dying. New York: Macmillan.
Kurki, T., Hiilesmaa, V., Raitasalo, R., Mattila, H., & Ylikorkala, O. (2000).
Depression and anxiety in early pregnancy and risk for preeclampsia. Obstetrics and
Gynecology, 95, 487-490.
Lang, S. S. (2005). Unwed mothers' prospects for marrying well, or at all, are
greatly diminished, Cornell study finds. Cornell News Service [On-line]. Available:
http://www.news.cornell.edu/stories/Sept05/moms.marriage.ssl.html
Laxton-Kane, M. & Slade, P. (2002). The role of maternal prenatal attachment in
a woman's experience of pregnancy and implications for the process of care. Journal of
Reproductive and Infant Psychology, 20, 253-266.
Leichtentritt, R. D., Blumenthal, N., Elyassi, A., & Rotmensch, S. (2005). High
risk pregnancy and hospitalization: The women's voices. Health and Social Work, 30, 39-
47.
210

Leifer, M. (1980). Psychological effects of motherhood: A study of first
pregnancy. New York: Praeger.
Leifer, M. (1977). Psychological changes accompanying pregnancy and
motherhood. Genetic Psychology Monographs, 95, 55-96.
Lerum, C. W. & LoBiondo-Wood, G. (1989). The relationship of maternal age,
quickening, and physical symptoms of pregnancy to the development of maternal-fetal
attachment. Birth, 16, 13-17.
Levine, L. V., Tuber, S. B., Slade, A., & Ward, M. J. (1991). Mothers' mental
representations and their relationship to mother-infant attachment. Bulletin of the
Menninger Clinic, 55, 454-470.
Lindgren, K. (2001). Relationships among maternal-fetal attachment, prenatal
depression, and health practices in pregnancy. Research in Nursing and Health, 24, 203-
217.
Lindgren, K. (2003). A comparison of pregnancy health practices of women in
inner-city and small urban communities. Journal of Obstetric, Gynecologic, and
Neonatal Nursing, 32, 313-321.
LoBiondo-Wood, G. & Vito-O'Rourke, K. (1990). The prenatal maternal
attachment scale: A methodological study. Paper presented at NAACOG's Research
Conference: Denver, CO.
211

Logghe, H. & Walker, J. J. (2004). Towards improved neonatal outcome: Future
strategies. Seminars in Fetal & Neonatal Medicine, 9, 491-498.
Lorensen, M., Wilson, M. E., & White, M. A. (2004). Norwegian families:
transition to parenthood. Health Care for Women International, 25, 334-348.
Lumley, J. (2003). Defining the problem: The epidemiology of preterm birth.
BJOG: An International Journal of Obstetrics and Gynecology, 110, 3-7.
Lumley, J. M. (1972). The development of maternal-foetal bonding in first
pregnancy. Basle: Karger.
Lumley, J. M. (1980). Through a glass darkly: Ultrasound and prenatal bonding.
Birth, 17, 214-217.
Lumley, J. M. (1982). Attitudes to the fetus among primigravidae. Australian
Pediatric Journal, 18, 106-109.
Main, M. & Goldwyn, R. (1984). Predicting rejection of her infant from mother's
representation of her own experience: Implications for the abused-abusing
intergenerational cycle. Child abuse and neglect, 8, 203-217.
Main, M., Kaplan, N., & Cassidy, J. (1985). Security in infancy, childhood, and
adulthood: A move to the level of representation. Monographs of the Society for
Research in Child Development, 50, 66-104.
212

Maloni, J. A., Brezinski-Tomasi, J. E., & Johnson, L. A. (2001). Antepartum bed
rest: effect upon the family. JOGNN: Journal of Obstetric, Gynecologic, and Neonatal
Nursing, 30, 165-173.
Maloni, J. A., Kane, J. H., Suen, L., & Wang, K. K. (2002). Dysphoria among
high-risk pregnant hospitalized women on bed rest: a longitudinal study. Nursing
Research, 51, 92-99.
Maloni, J. A. & Kasper, C. E. (1991). Physical and psychosocial effects of
antepartum hospital bedrest: a review of the literature. Image: Journal of Nursing
Scholarship, 23, 187-192.
Maloni, J. A. & Park, S. (2005). Postpartum symptoms after antepartum bed rest.
JOGNN: Journal of Obstetric, Gynecologic, and Neonatal Nursing, 34, 163-171.
Maloni, J. A., Park, S., Anthony, M. K., & Musil, C. M. (2005). Measurement of
antepartum depressive symptoms during high-risk pregnancy. Research in Nursing &
Health, 28, 16-26.
Marcus, S. M., Flynn, H. A., Blow, F. C., & Barry, K. L. (2003). Depressive
symptoms among pregnant women screened in obstetrics settings. Journal of Women's
Health, 12, 373-380.
213
McBride, C., Zuroff, D. C., Bacchiochi, J., & Bagby, R. M. (2006). Depressive
experiences questionnaire: Does it measure maladaptive and adaptive forms of
dependency? Social Behavior and Personality, 34, 1-16.
McCranie, E. W. & Bass, J. D. (1984). Childhood family antecedents of
dependency and self-criticism: Implications for depression. Journal of Abnormal
Psychology, 93, 3-8.
Mercer, R. T. (1977). Nursing Care for Parents at Risk. Thorofare, N.J.: C.B.
Slack.
Mercer, R. T. (1983). Parent-infant attachment. In K. Kowalski & B. Jennings
(Eds.), Women's Health, Vol. 2 (pp. 17-42). New York: Grune & Stratton.
Mercer, R. T. & Ferketich, S. L. (1988). Stress and social support as predictors of
anxiety and depression during pregnancy. Advances in Nursing Science, 10, 26-39.
Mercer, R. T., Ferketich, S., DeJoseph, J., May, K., & Sollid, D. (1988). Effect of
stress on family functioning during pregnancy. Nursing Research, 37, 268-275.
Mercer, R. T., Ferketich, S., May, K., DeJoseph, J., & Sollid, D. (1988). Further
exploration of maternal and paternal fetal attachment. Research in Nursing & Health, 11,
269-278.
Mercer, R. T. & Ferketich, S. L. (1994). Predictors of maternal role competence
by risk status. Nursing Research, 43, 38-43.
214

Mikhail, M. S., Freda, M. C., Merkatz, R. B., Polizzotto, R., Mazloom, E., &
Merkatz, I. R. (1991). The effect of fetal movement counting on maternal attachment to
fetus. American Journal of Obstetrics & Gynecology, 165, 988-991.
Mikulincer, M. & Florian, V. (1999). Maternal-fetal bonding, coping strategies,
and mental health during pregnancy--the contribution of attachment style. Journal of
Social and Clinical Psychology, 18, 255-276.
Millon, T. (1987). Manual for the MCMI-2. Minneapolis, MN: National
Computer Systems.
Moncher, F. J. (1996). The relationship of maternal adult attachment style and
risk of physical child abuse. Journal of Interpersonal Violence, 11, 335-350.
Morrison, T. L., Urquiza, A. J., & Goodlin-Jones, B. (1998). Depressive
experience and romantic relationships in young adulthood. Psychological Reports, 82,
339-349.
Muller, M. E. (1996). Prenatal and postnatal attachment: a modest correlation.
Journal of Obstetric, Gynecologic, & Neonatal Nursing, 25, 161-166.
Muller, M. E. (1992). A critical review of prenatal attachment research. Scholarly
Inquiry for Nursing Practice, 6, 5-22.
Muller, M. E. & Ferketich, S. (1993). Factor analysis of the Maternal Fetal
Attachment Scale. Nursing Research, 42, 144-147.
215

Muller, M. E. & Ferketich, S. (1992). Assessing the validity of the dimensions of
prenatal attachment. Maternal-Child Nursing Journal., 20, 1-10.
Muller, M. E. (1990). The development and testing of the Muller Prenatal
Attachment Inventory.
Muller, M. E. (1993). Development of the prenatal attachment inventory. Western
Journal of Nursing Research, 15, 199-215.
Murray, L. (1992). The impact of postnatal depression on infant development.
Journal of Child Psychology and Psychiatry, 33, 543-561.
Parker, G., Tulping, H., & Brown, L. B. (1979). A parental attachment
instrument. British Journal of Medical Psychology, 52, 1-10.
Penticuff, J. H. (1982). Psychologic implications in high-risk pregnancy. Nursing
Clinics of North America.17(1):69-78.
Piontelli, A. (1987). Infant observation from before birth. International Journal of
Psychoanalysis, 68, 453-463.
Piontelli, A. (1988). Prenatal life reflected in the analysis of a psychotic girl at age
two. Psychoanalytic Study of the Child, 38, 337-351.
Pollock, P. H. & Percy, A. (1999b). Maternal antenatal attachment style and
potential fetal abuse. Child Abuse & Neglect, 23, 1345-1357.
216
Pollock, P. H. & Percy, A. (1999). Maternal antenatal attachment style and
potential fetal abuse. Child Abuse & Neglect, 23, 1345-1357.
Porter, R. H., Winberg, J., & Varendi, H. (2005). Prenatal Preparation for Early
Postnatal Olfactory Learning. In B. Hopkins & S. P. Johnson (Eds.), Prenatal
development of postnatal functions (pp. 103-129). Westport, CT: Praeger
Publishers/Greenwood Publishing Group, Inc.
Priel, B. & Besser, A. (2001). Bridging the gap between attachment and object
relations theories: A study of the transition to motherhood. British Journal of Medical
Psychology, 74, 85-100.
Priel, B. & Besser, A. (1999). Vulnerability to postpartum depressive
symptomatology: Dependency, self-criticism and the moderating role of antenatal
attachment. Journal of Social and Clinical Psychology, 18, 240-253.
Priel, B. & Besser, A. (2000a). Dependency and self-criticism among first-time
mothers: The roles of global and specific support. Journal of Social and Clinical
Psychology, 19, 437-450.
Priel, B. & Besser, A. (2000b). Adult attachment styles, early relationships,
antenatal attachment, and perceptions of infant temperament: A study of first-time
mothers.
217

Reading, A. E., Cox, D. N., Sledmere, C. M., & Campbell, S. (1984).
Psychological changes over the course of pregnancy: A study of attitudes toward the
futus/neonate. Health Psychology, 3, 211-221.
Righetti, P. L., Dell'Avanzo, M., Grigio, M., & Nicolini, U. (2005).
Maternal/paternal antenatal attachment and fourth-dimensional ultrasound technique: a
preliminary report. British Journal of Psychology, 96, 129-137.
Rubin, R. (1967a). Attainment of the maternal role: Part I. Processes. Nursing
Research, 16, 237-245.
Rubin, R. (1967b). Attainment of the maternal role: Part II. Models and referrants.
Nursing Research, 16, 342-346.
Rubin, R. (1975). Maternal tasks in pregnancy. Maternal Child Nursing Journal,
4, 143-153.
Rude, S. S. & Burham, B. L. (1995). Connectedness and neediness: Factors of the
DEQ and SAS dependency scales. Cognitive Therapy & Research, 19, 323-340.
Santor, D. A., Zuroff, D. C., & Fielding, A. (1997a). Analysis and revision of the
Depressive Experiences Questionnaire: Examining scale performance as a function of
scale length. Journal of Personality Assessment, 69, 163.
218
Santor, D. A., Zuroff, D. C., Mongrain, M., & Fielding, A. (1997b). Validating
the McGill revision of the Depressive Experiences Questionnaire. Journal of Personality
Assessment, 69, 164-182.
Senn, M. J. E. (1977). Interview with John Bowlby. Unpublished manuscript.
Shieh, C., Kravitz, M., & Wang, H. H. (2001). What do we know about maternal-
fetal attachment? Kaohsiung Journal of Medical Science, 17, 448-454.
Shor, J. & Sanville, J. (1978). Illusions in loving: A psychoanalytic approach to
intimacy and autonomy. Los Angelis: Double Helix.
Siddiqui, A. & Hagglof, B. (2000). Does maternal prenatal attachment predict
postnatal mother-infant interaction? Early Human Development, 59, 13-25.
Siddiqui, A., Hagglof, B., & Eisemann, M. (1999). An exploration of prenatal
attachment in Swedish expectant women. Journal of Reproductive and Infant
Psychology, 17, 369-380.
Siddiqui, A., Hagglof, B., & Eisemann, M. (2000). Own memories of upbringing
as a determinant of prenatal attachment in expectant women. Journal of Reproductive
and Infant Psychology, 18, 67-74.
Sorenson, D. S. & Schuelke, P. (1999). Fantasies of the unborn among pregnant
women. The American Journal of Maternal/Child Nursing, 24, 92-97.
219

Sroufe, L. A. & Waters, E. (1977). Attachment as an organizational construct.
Child Development, 48, 1184-1199.
Stainton, M. C. (1990). Parents' awareness of their unborn infant in the third
trimester. Birth, 17(2):92-6.
Steinberg, S. I. & Bellavance, F. (1999). Characteristics and treatment of women
with antenatal and postpartum depression. International Journal of Psychiatry in
Medicine, 29, 209-233.
Unauthored (1999). NICHD Early Child Care Research Network. Developmental
Psychology, 35, 1297.
van Ijzendoorn, M. H. (1995). Adult attachment representations, parental
responsiveness, and infant attachment: A meta-analysis on the predictive validity of the
Adult Attachment Interview. Psychological Bulletin, 117, 387-403.
Waters, E. (2005). Personal Communication.
Weaver, R. H. & Cranley, M. S. (1983). An exploration of paternal-fetal
attachment behavior. Nursing Research, 32, 68-72.
Whiffen, V. E. & Johnson, S. M. (2006). An attachment theory framework for the
treatment of childbearing depression. Clinical Psychology: Science and Practice, 5, 478-
492.
220
White, M. & Ritchie, J. (1984). Psychological stressors in antepartum
hospitalization: Reports from pregnant women. Maternal-Child Nursing Journal, 13, 47-
56.
White, M. A., Wilson, M. E., Elander, G., & Persson, B. (1999). The Swedish
family: Transition to parenthood. Journal of Advanced Nursing, 13, 171-176.
Wood, N. S., Marlow, N., Costeloe, K., Gibson, A. T., & Wilkinson, A. R.
(2000). Neurological and developmental disability after extremely preterm birth. New
England Journal of Medicine, 343, 378-384.
Zeanah, C. H., Benoit, D., Barton, M., Regan, C., Hirshberg, L. M., & Lipsitt, L.
P. (1993). Representations of attachment in mothers and their one-year-old infants.
Journal of the American Academy of Child & Adolescent Psychiatry, 32(2):278-86.
Zeanah, C. H., Carr, S., & Wolk, S. (1990). Fetal movements and the imagined
baby of pregnancy: Are they related? Journal of Reproductive and Infant Psychology, 8,
23-26.
Zimerman, A. & Doan, H. M. (2003). Prenatal attachment and other feelings and
thoughts during pregnancy in three groups of pregnant women. Journal of Prenatal &
Perinatal Psychology & Health, 18 (2), 131-148.
Zuroff, D. C. & Fitzpatrick, D. K. (1995). Depressive personality styles:
Implications for adult attachment. Personality and Individual Differences, 18, 253-265.
221

Zuroff, D. C., Igreja, I., & Mongrain, M. (1990). Dysfunctional attitudes,
dependency, and self-criticism as predictors of depressive mood states: A 12-month
longitudinal study. Cognitive Therapy & Research, 14, 326.
Zuroff, D. C., Quinlan, D. M., & Blatt, S. J. (1990). Psychometric properties of
the Depressive Experiences Questionnaire in a college population. Journal of Personality
Assessment, 55, 65-72.
222

VITAE Anna Rachel Brandon was born in Cleveland, Ohio, to Ronald and Barbara Coleman. She
completed High School in Brownwood, Texas in 1973. She married and relocated to California
where her daughters, Rachel and Sarah, were born. She returned to Texas in 1981, living in San
Antonio, where her son, David, was born. In 1991, she relocated her textile sales agency to the
Dallas International Apparel Mart. She began attending Mountain View College part-time,
completing an Associate of Arts degree in Business in 1999. She was accepted to Southern
Methodist University and, in 2001, she graduated Summa cum laude with dual degrees in
Business Administration and Psychology. In August 2002, she entered the Graduate School of
Biomedical Sciences at the University of Texas Health Science Center at Dallas.
Permanent Address: 3211 Rosedale Ave. Dallas, TX 75205
Related Documents