Maternal and Child Health Services Title V Block Grant SUPPORTING DOCUMENT #3 Program Activities: Women/Maternal and Perinatal/Infant

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Maternal and Child Health Services Title V Block Grant SUPPORTING DOCUMENT #3
Program Activities:
Women/Maternal and Perinatal/Infant
SUPPORTING DOCUMENT #3: Program Activities – Women/Maternal and Perinatal/Infant
WOMEN/MATERNAL HEALTH Well-Woman Visit Toolkit ...................................................................................................4
A toolkit for community stakeholders, partners, and providers to use and adapt to expand access and care for women across the lifespan through the well-woman visit.
• Well-Woman Visit Toolkit: For Communities .......................................................... 5 • Well-Woman Visit Toolkit: For Providers ................................................................ 14 • Preparing for Your Well-Woman Visit Checklist..................................................... 29 • Well-Woman Infographic ........................................................................................ 32
Kansas Maternal Mortality Report & Activities .................................................................33 Information pertaining to the findings from the Kansas Maternal Mortality Review Committee (KMMRC) and related activities. Contents include:
• Kansas Maternal Mortality Report Highlights ....................................................... 34 • Pregnancy-Associated Death Infographic ............................................................. 36 • Pregnancy-Related Death Infographic .................................................................. 41 • Severe Maternal Morbidity Infographic ................................................................. 45 • Severe Maternal Morbidity Poster ......................................................................... 49 • KMMRC Member Roster ........................................................................................ 50
The full Maternal Mortality Report is available online at: https://kmmrc.org/reports/
Family Planning Life Plan ..................................................................................................51 A workbook to assist women with family planning and identifying pregnancy intentions and desires.
PERINATAL/INFANT HEALTH Kansas Perinatal Quality Collaborative (KPQC) ................................................................79
Outlines initiatives and activities led by the KPQC. Contents include:
• KPQC Overview ........................................................................................................ 80 • Fourth Trimester Initiative Overview ...................................................................... 81 • Maternal Warning Signs Initiative Kickoff Webinar .............................................. 82
Maternal Warning Signs Patient Education Toolkit ..........................................................83 A toolkit is to offer a comprehensive selection of patient education materials to providers, across all sectors and settings, to ensure consistent messaging about the warning signs of trouble for pregnant and postpartum women. Contents include:
• Guidance on Use of Patient Education Resources ............................................... 84 • Signs and Symptoms of Preterm Labor ................................................................ 86 • Know the Warning Signs: Count the Kicks ............................................................ 88 • Urgent Maternal Warning Signs ............................................................................. 90 • Depression & Anxiety Resources ........................................................................... 96 • Post-Birth Warning Signs ........................................................................................ 100
Kansas Perinatal Community Collaboratives (KPCC) .......................................................102 Information regarding the KPCC and Becoming a Mom® efforts. Contents include:
• KPCC Infographic .................................................................................................... 103 • Becoming a Mom® Overview and Impact .............................................................. 106
The full 2019 Becoming a Mom Annual Report is available online at: https://www.kdheks.gov/c-f/perinatal_program_impact.htm
PERINATAL BEHVAIORAL HEALTH Perinatal Mental Health Toolkit .........................................................................................107
This infographic shares information about a toolkit to provide education, guidance, and resources for patients and providers related to screening and treatment for perinatal mood and anxiety disorders (PMAD).
The toolkit is available online at: https://www.kdheks.gov/c-f/mental_health_integration.htm
Screening, Brief Intervention, and Referral to Treatment (SBIRT) Toolkit .......................109 This infographic shares information about a toolkit to provide education, guidance, and resources related to screening and treatment for perinatal substance use disorders for patients and providers.:
The toolkit is available online at: https://www.kdheks.gov/c-f/SBIRT_Toolkit.htm
Perinatal Support Group Guidebook .................................................................................111 A guide to provide information and guidance for those looking to start a perinatal support group.
The full Guidebook is available online at: https://www.kdheks.gov/c-f/integration_toolkits/Perinatal_Support_Group_Guidebook.pdf
Well-Woman Visit Toolkit
A toolkit for community stakeholders, partners, and providers to use and adapt to expand access and care for women across
the lifespan through the well-woman visit.
SECTION CONTENTS
• Well-Woman Visit Toolkit: For Communities .......................................................... 5 • Well-Woman Visit Toolkit: For Providers ................................................................ 14 • Preparing for Your Well-Woman Visit Checklist..................................................... 29 • Well-Woman Infographic ........................................................................................ 32
Kansas Department of Health and Environment BUREAU OF FAMILY HEALTH | 1000 SW JACKSON, SUITE 220 TOPEKA, KS 66612
Well-Woman Visit Toolkit: For Communities EVERY WOMAN. EVERY TIME.
1 | P a g e
Table of Contents Toolkit Overview .................................................................................................................................................. 2
The Importance of the Well-Woman Visit........................................................................................................... 2
Definition ..................................................................................................................................................... 2
Statement of Need in Kansas...................................................................................................................... 3
How Communities Can Help ................................................................................................................................ 3
Addressing Barriers.......................................................................................................................................... 3
Resources ............................................................................................................................................................. 6
Patient Resources ............................................................................................................................................ 6
Health Equity and Social Care ......................................................................................................................... 7
Mental Health and Substance Use .................................................................................................................. 7
Support for Service Providers ......................................................................................................................... 7
Raising Awareness................................................................................................................................................ 8
Campaigns and Promotional Tools ................................................................................................................. 8
Sample Social Media Posts .............................................................................................................................. 8
2 | P a g e
Toolkit Overview This toolkit supplement was developed by the Kansas Department of Health and Environment (KDHE)1 for communities to utilize as a guide to expand access and care for women across the lifespan through the well-woman visit. KDHE is committed to assisting communities as they work to improve health outcomes and address barriers to services that impact the health of women in Kansas.
The content of this toolkit was developed from a number of reliable and trusted sources, including the American College of Obstetricians and Gynecologists’ (ACOG) Women’s Preventive Services Initiative (WPSI), CityMatCH, and the University of Illinois School of Public Health’ (UIC-SPH) Well-Woman Project, among others.
This toolkit resource is a guide for community stakeholders and partners (allied professionals, community leaders, policymakers, etc.) to use and adapt to meet the unique needs of communities across the state. As preventive services evolve into more comprehensive, integrated and holistic endeavors, it is important to acknowledge that a single provider alone cannot address all medical and social care needs of individuals. This toolkit serves as a starting place, and for many a continuation of efforts, to ensure the provision of consistent, quality medical care while building community systems that foster long-term and sustainable health outcomes for women and families.
The Importance of the Well-Woman Visit Definition The Title V Maternal and Child Health Services Block Grant to States Program Guidance2 defines the well-woman visit as the following:
A well-woman or preconception visit provides a critical opportunity to receive recommended clinical preventive services, including screening, counseling, and immunizations, which can lead to appropriate identification, treatment, and prevention of disease to optimize the health of women before, between, and beyond potential pregnancies. For example, screening and management of chronic conditions such as diabetes, and counseling to achieve a healthy weight and smoking cessation, can be advanced within a well woman visit. This can promote women's health prior to and between pregnancies and improve subsequent maternal and postpartum outcomes. The annual well-woman visit has been endorsed by ACOG and was also identified among the women's preventive services required by the Affordable Care Act (ACA) to be covered by private insurance plans without cost-sharing.2
1 This project is supported by the Kansas Department of Health and Environment with funding through the Health Resources and Services Administration (HRSA), U.S. Department of Health and Human Services (HHS) Title V Maternal and Child Health Services Block Grant #B04MC31488 2 Health Resources and Services Administration. 2014. Title V Maternal and Child Health Services Block Grant to States Program: Guidance and Forms for the Title V Application/Annual Report, p. 66.
3 | P a g e
Statement of Need in Kansas Women across the lifecycle, throughout Kansas, are seeing declines in health outcomes. Obesity-related medical care costs [alone] in the United States, in 2008 dollars, were an estimated $147 billion.3 According to the United Health Foundation’s America’s Health Rankings, over the past 30 years Kansas has dropped from the 12th healthiest state in 1990 to the 29th healthiest state in 2019.4
• The percentage of women receiving a well-woman visit in Kansas decreased to 62.9% while the national rate rose to 66.8%.5
• Between 2016 and 2019 excessive drinking among women ages 18-44 in Kansas increased 28% from 14.9% to 19.1%.6
• A total of 30.8% of women in Kansas were obese, above the national average of 27.4%.7 • After nearly two decades of declines in cardiovascular deaths, Kansas is experiencing an increase in
cardiovascular deaths among women greater than that of the national average at 218.3 per 100,000 deaths.8
Uncontrolled chronic disease contributes to high-risk pregnancy and poor birth outcomes, including low birthweight and preterm birth, which rose nearly 9% in Kansas between 2016 and 2019.9 In addition, the severe maternal morbidity (SMM) rate among delivery hospitalizations in Kansas has steadily increased in recent years, from 54.6 in 2016 to 61.9 per 10,000 delivery hospitalizations in 2019, a 13.4% increase.
How Communities Can Help Healthy women are a cornerstone of healthy communities. We all have a stake in supporting women and increasing access to screening and prevention services. In this section community partners, allied professionals, policymakers and leaders will find resources to help communities support women and increase access and awareness around the importance of the well-woman visit.
Addressing Barriers The Well-Woman Project, a joint effort of the University of Illinois School of Public Health (UIC-SPH) and CityMatCH, conducted listening sessions with 156 women in eight cities across the country in the spring of 2016 and gathered over 100 additional stories that were shared through the Well-Woman Project website. After analysis, 13 barriers were identified along with a list of responses, recommendations and resources for each. To review the barriers and proposed solutions in their entirety, visit the Well-Woman Project website, https://www.citymatchlearning.org/well-woman/index.php. Below are a list of community-related barriers
3 Finkelstein EA1, Trogdon JG, Cohen JW, Dietz W. Annual medical spending attributable to obesity: payer-and service-specific estimates. Health Aff (Millwood). 2009 Sep-Oct;28(5):w822-31. doi: 10.1377/hlthaff.28.5.w822. 4 https://www.americashealthrankings.org/explore/annual/state/KS 5 CDC, Behavioral Risk Factor Surveillance System, 2019 6 CDC, Behavioral Risk Factor Surveillance System, 2019 7 CDC, Behavioral Risk Factor Surveillance System, 2019 8 CDC, Behavioral Risk Factor Surveillance System, 2019 9 CDC, Behavioral Risk Factor Surveillance System, 2019
4 | P a g e
and recommendations to address these obstacles, including recommendations derived from the Kansas Maternal and Child Health Needs Assessment.
1. Women in many cities reported long distances to providers, as well as no available parking, unreliable and unsafe public transportation when traveling with small children (i.e., no room for car seats, strollers), and unreliable and not woman-friendly transportation services (i.e., van services).
CityMatCH Recommendations:
• Encourage large health systems and FQHCs to explore partnerships with ride-sharing organizations for patient transportation.
• Work with city Department of Transportation to explore and develop plans to provide child-friendly public transportation.
• Work with large health system and FQHCs to encourage provision of free parking vouchers or free/discounted bus/train cards to attend appointments; development of play areas or supervised childcare facilities in health clinics/provider's offices.
KDHE Recommendations:
Access to safe and reliable public transportation is a barrier to service in both rural and urban areas of Kansas. KDHE encourages collaboration between local and state leaders and stakeholders to expand access to broadband and free wireless service that can be utilized by clients to obtain care via telehealth.
2. Some women reported being frequently unable to take their children to their appointments due to a lack of child-friendly clinics and/or being unable to obtain childcare in order to attend their health care appointments.
CityMatCH Recommendations:
• Work with city Department of Transportation to explore and develop plans to provide child-friendly public transportation.
• Work with large health system and FQHCs to encourage: provision of free parking vouchers or free/discounted bus/train cards to attend appointments; development of play areas or supervised childcare facilities in health clinics/provider's offices.
KDHE Recommendations:
• Encourage partnerships between area agencies, like the YMCA or other child care providers, to offer on-site child care one day a month and promote the service through social media, and other advertising channels to encourage women with young children to schedule their well-visit appointments.
• Fund and promote preventive care-only hours on Saturdays when other caregivers like spouses or other family members may be available to watch young children during the mother’s appointment.
• Encourage area child care providers to seek out collaborative funding opportunities to offer hours that are extended beyond traditional hours and/or available on weekends.
5 | P a g e
3. Women discussed having jobs that did not offer paid sick time, personal days, or vacation time which resulted in losing pay to see a health care provider. Women also discussed being unable to make traditional office hour appointments due to their inability to take time off during the day.
CityMatCH Recommendations:
• As needed, create a city-wide task force to include key stakeholders to consider adoption of paid sick leave for both public and private employees.
• Develop policy and educational materials focused on city-specific sick and personal leave policies.
KDHE Recommendations:
• Fund and promote child care providers to extend their hours beyond traditional times and ensure they work collaboratively with the health department and align with their office hours.
• Encourage businesses and local government entities to partner with health care navigators who can serve as resource referrals for human resource department professionals working with, or supporting, pregnant or postpartum employees.
4. Women discussed being at long distances from family members and having little to no local support network to draw upon to help with family-related tasks which increased stress and reduced their ability to be healthy or to seek health care.
CityMatCH Recommendations:
• Explore development of a cadre of women's health peer advocates who can be present at women's appointments and advertise their availability through mobile technology.
• Work with health systems, FQHCs, and other stakeholders to increase "group" approaches to care for specific types of care.
KDHE Recommendations:
• Support and promote area social groups that foster a sense of community, including neighborhood associations, faith-based organizations, Ag Extension meetings and groups such as parent support groups and public health programs such as Becoming A Mom.
• Utilize social media and online meeting platforms, like Zoom, to facilitate online meetings in addition/in place of in-person gatherings.
5. Many women serve in a multitude of roles, many of them involving caretaking. Women described the “second shift” and the competing demands of their work, family, and home duties which often prevent them from being healthy and seeking care.
CityMatCH Recommendations:
• As needed, create a city-wide task force to include key stakeholders to consider adoption of paid sick leave for both public and private employees.
• Develop policy and educational materials focused on city-specific sick and personal leave policies.
6 | P a g e
KDHE Recommendations:
• Gather area partners (afterschool programming, youth recreation, etc.) and create monthly, free ‘Parents Night Out’ events that provide free programming and child care for several hours in the evening – allowing women to rest, take care of themselves, and recharge or attend necessary appointments.
• Use social media and other advertising channels to regularly address the importance of receiving physical and mental health care.
6. Women described family and cultural barriers, specifically with respect to accessing sexual and mental health services. These perceptions and beliefs affected how frequently women sought care; some women documented using “home remedies” and self-care outside of formal medical settings to avoid seeing a provider.
CityMatCH Recommendations:
• Explore approaches to: development of a women-centered, consumer-driven mechanism to enable reviews of provider; enable women to have their health histories available on personal "apps" so that providers can readily access this information.
• Partner with major health systems to develop and offer training to increase cultural competency/humility of the clinical workforce.
KDHE Recommendations:
• Use social media and other advertising channels to frequently address the importance of receiving physical and mental health care. Ensure that the images as well as the messaging are reflective of the diversity of the community you are seeking to serve. Conduct focus groups with diverse members of the community to provide feedback on the messaging and be sure to include individuals of different races and ethnicities, socioeconomic status, and age.
• Provide direct access via integrated health models, where well-woman exams and mental health are provided synchronously in-office through collaboration between agencies. Immediate referrals may also be made from well-woman exams into mental health services by navigators- include transportation needs, child care, and paperwork required.
Resources The following resources can be distributed to and by community partners and allied professionals including social workers, school staff and other professionals.
Patient Resources Patient Well-Woman Visit Brochures (English and Spanish): https://www.nwlc.org/sites/default/files/final_well-womanbrochure.pdf
Youth Health Guide https://www.womenspreventivehealth.org/wellwomanchart/
My Life, My Goals: Reproductive Wellness Workbook https://www.kdheks.gov/c-f/integration_toolkits/Reproductive_Life_Plan.pdf
7 | P a g e
Kansas Crisis Hotline 1-888-END-ABUSE, provides confidential support 24/7 to victims of domestic violence, sexual assault and stalking. National Suicide Prevention Lifeline provides 24/7, free and confidential support for people in distress, prevention, and crisis resources for you or your loved ones, and best practices for professionals. Call 1-800-273-8255 or 1-888-628-9454 for Spanish. Crisis Text Line is a free, 24/7, confidential text message service for people in crisis. To reach a crisis counselor, text Kansas to 741741. Kansas Community Mental Health Centers (CMHCs) offer crisis services 24/7. Contact the CMHC for the county you are currently in for crisis services: http://www.acmhck.org/wp-content/uploads/2018/01/CommunityMentalHealthCentersofKS-Revised-1-10-18.pdf. Veterans Crisis Line offers 24/7, confidential support to veterans, service members, National Guard and Reserve members, and their family member and friends. Call 1-800-273-8255 and Press 1 or text 838255. Tobacco Cessation KS Quitline: 1.800.QUIT.NOW or KSQuit.org (online chat)
KS Parent Helpline 1-800-CHILDREN is a is a free, statewide, anonymous, information and referral service.
Health Equity and Social Care • National Academies of Science, Engineering and Medicine: “Integrating Social Care Into the Delivery
of Healthcare: Moving Upstream to Improve the Nation’s Health” https://www.nationalacademies.org/our-work/integrating-social-needs-care-into-the-delivery-of-health-care-to-improve-the-nations-health
• Diversity and Health Equity in Maternal and Child Healthcare: https://mchb.hrsa.gov/training/documents/MCH_Diversity_2016-05_RFS.pdf
• Moving to Institutional Equity: A Tool to Address Equity for Public Health Providers https://chronicdisease.org/resource/resmgr/gillan's_files/health_equity_june_2017.pdf
• LGBTQIA+ Health Education Center: https://www.lgbtqiahealtheducation.org/
Mitigating Implicit Bias in Healthcare: https://u.osu.edu/breakingbias/tools-for-mitigating-bias/
Mental Health and Substance Use • National Council on Behavioral Health https://www.thenationalcouncil.org/integrated-health-
coe/resources/ • SAMHSA-HRSA Center for Integrated Health Solutions https://www.integration.samhsa.gov/clinical-
practice/screening-tools • KDHE Mental Health Integration Toolkit https://www.kdheks.gov/c-f/mental_health_integration.htm • KDHE Screening, Brief Intervention, and Referral to Treatment Toolkit https://www.kdheks.gov/c-
f/SBIRT_Toolkit.htm
Support for Service Providers • SAMHSA’s Disaster Distress Hotline provides 24/7, 365-day-a-year crisis counseling and support to
people, including medical professionals, experiencing emotional distress related to natural or

8 | P a g e
human-caused disasters and infectious disease outbreaks. Call 1-800-985-5990 or text TalkWithUs to 66746. For Spanish speakers, call 1-800-985-5990 and press 2 or text Hablanos to 66746.
Raising Awareness Community-based organizations and local governments can assist in spreading awareness about the importance of the annual well-woman visit through a variety of ways. KDHE has created a Well-Woman Visit Promotional Flyer that can be printed and posted in exam rooms, waiting areas or distributed via social media, tabling events, etc. Below, we have provided tools such as awareness toolkits and sample media posts that can be used and adapted to meet the needs of your local community.
Campaigns and Promotional Tools These campaigns can be utilized in parts or in its entirety through social media, traditional press, and hard copy promotion.
• Well Women, Well Communities Toolkit https://www.citymatch.org/well-women-well-communities/
• #YouGoGirl, American Heart Association Well Woman Promotional Video https://www.youtube.com/watch?v=DIN-svKAKT4
• Care Women Deserve http://carewomendeserve.org/
• Women’s Health Month Toolkit http://www.kansasmch.org/womenshealthmonthtoolkit.asp
Sample Social Media Posts • Do you know how to #BeAWellWoman? Well-Woman visits are available without additional costs,
like co-pays and deductibles. Learn more about what questions you should be asking your provider at your next check-up. www.nwlc.org/wellwoman
• What kind of education and counseling can you get at your no-cost well-woman visit? #BeAWellWoman
Kansas Department of Health and Environment BUREAU OF FAMILY HEALTH | 1000 SW JACKSON, SUITE 220 | TOPEKA, KS 66612
Well-Woman Visit Toolkit: For Providers EVERY WOMAN. EVERY TIME.
1 | P a g e
Table of Contents Toolkit Overview .......................................................................................................................................................... 2
The Importance of the Well-Woman Visit................................................................................................................... 2
Definition .............................................................................................................................................................. 2
Statement of Need in Kansas ............................................................................................................................... 2
Recommended Components ............................................................................................................................... 3
Integration Plan ............................................................................................................................................................ 3
Training ................................................................................................................................................................. 4
Policy..................................................................................................................................................................... 4
Promotion and Partnerships ................................................................................................................................ 4
Clinical Recommendations ........................................................................................................................................... 5
Recommended Guidelines ................................................................................................................................... 5
Education and Counseling ............................................................................................................................................ 5
Screening Tools ............................................................................................................................................................ 6
Addressing Barriers ...................................................................................................................................................... 6
Resources ................................................................................................................................................................... 11
Clinical Guidance .................................................................................................................................................... 11
Trauma and Violence ............................................................................................................................................. 11
Health Equity and Social Care ................................................................................................................................ 12
Mental Health and Substance Use ........................................................................................................................ 12
Patient Resources ................................................................................................................................................... 12
Support Resources for Providers ........................................................................................................................... 13
Sample Policies ....................................................................................................................................................... 13
Workflows/Algorithms .......................................................................................................................................... 13
Raising Awareness...................................................................................................................................................... 13
Campaigns and Promotional Tools ........................................................................................................................ 14
Sample Social Media Posts .................................................................................................................................... 14
2 | P a g e
Toolkit Overview This toolkit was developed by the Kansas Department of Health and Environment (KDHE)1 for providers to utilize as a guide to expand access and care for women across the lifespan through the well-woman visit. KDHE is committed to assisting providers as they work to improve health outcomes and address barriers to services that impact the health of all women.
The content of this toolkit was developed from a number of reliable and trusted sources including, the American College of Obstetricians and Gynecologists’ (ACOG) Women’s Preventive Services Initiative (WPSI), CityMatCH and the University of Illinois School of Public Health’ (UIC-SPH) Well-Woman Project, among others. As preventive services evolve into more comprehensive, integrated and holistic endeavors it is important to acknowledge that a single provider alone cannot address all medical and social care needs of individuals. This toolkit serves as a starting place, and for many a continuation of efforts, to ensure the provision of consistent, quality medical care while building community systems that foster long-term and sustainable health outcomes for women and families.
Questions about the toolkit or its contents can be directed to 785.296.1300 or [email protected].
The Importance of the Well-Woman Visit Definition The Title V Maternal and Child Health Services Block Grant to States Program Guidance2 defines the well-woman visit as the following:
A well-woman or preconception visit provides a critical opportunity to receive recommended clinical preventive services, including screening, counseling, and immunizations, which can lead to appropriate identification, treatment, and prevention of disease to optimize the health of women before, between, and beyond potential pregnancies. For example, screening and management of chronic conditions such as diabetes, and counseling to achieve a healthy weight and smoking cessation, can be advanced within a well woman visit. This can promote women's health prior to and between pregnancies and improve subsequent maternal and postpartum outcomes. The annual well-woman visit has been endorsed by ACOG and was also identified among the women's preventive services required by the Affordable Care Act (ACA) to be covered by private insurance plans without cost-sharing.
Statement of Need in Kansas Throughout Kansas, women across the lifecycle are seeing declines in health outcomes. According to the United Health Foundation’s America’s Health Rankings, over the past 30 years Kansas has dropped from the 12th healthiest state in 1990 to the 29th healthiest state in 2019.3
1 This project is supported by the Kansas Department of Health and Environment with funding through the Health Resources and Services Administration (HRSA), U.S. Department of Health and Human Services (HHS) Title V Maternal and Child Health Services Block Grant #B04MC31488 2 Health Resources and Services Administration. 2014. Title V Maternal and Child Health Services Block Grant to States Program: Guidance and Forms for the Title V Application/Annual Report, p. 66. 3 https://www.americashealthrankings.org/explore/annual/state/KS
3 | P a g e
• The percentage of women receiving a well-woman visit in Kansas decreased to 62.9% while the national rate rose to 66.8%.4
• Between 2016 and 2019 excessive drinking among women ages 18-44 in Kansas increased 28% from 14.9% to 19.1%.5
• A total of 30.8% of women in Kansas were obese, above the national average of 27.4%.6 • After nearly two decades of declines in cardiovascular deaths, Kansas is experiencing an increase in
cardiovascular deaths among women greater than that of the national average at 218.3 per 100,000 deaths.7
Uncontrolled chronic disease contributes to high-risk pregnancy and poor birth outcomes, including low birthweight and preterm birth, which rose nearly 9% in Kansas between 2016 and 2019.8 In addition, the severe maternal morbidity (SMM) rate among delivery hospitalizations in Kansas has steadily increased in recent years, from 54.6 in 2016 to 61.9 per 10,000 delivery hospitalizations in 2019, a 13.4% increase.
Recommended Components KDHE wants to help providers, communities, and women make the most of the well-woman visit and ensure each exam includes screening and provision of services for the following:
- Chronic and infectious disease, including sexually transmitted infections - High body mass index (BMI) - Mental health (depression and anxiety) - Immunizations - Substance use (alcohol, narcotics, and tobacco) - Sexual and domestic violence and healthy relationships - Reproductive health, including goal-setting - Social determinants of health
It is not expected that a provider would be a subject-matter expert or specialist in each of these areas, but rather a starting point to initiate important conversations and provide appropriate resources and referrals.
It is KDHE’s expectation that every provider who serves women in the state will provide the services outlined above to every female patient. In the event they are unable to provide a recommended service, formal partnerships will be made with other providers in the community who are competent in that area. A sample Memorandum of Understanding (MOU) is provided in the ‘Resources’ section of this toolkit to facilitate conversations and connections.
Integration Plan After the passage of the ACA, women with public or private insurance throughout Kansas have coverage for well-woman visits. In the event a woman does not have insurance, she can access preventive care through clinics such
4 CDC, Behavioral Risk Factor Surveillance System, 2019 5 CDC, Behavioral Risk Factor Surveillance System, 2019 6 CDC, Behavioral Risk Factor Surveillance System, 2019 7 CDC, Behavioral Risk Factor Surveillance System, 2019 8 CDC, Behavioral Risk Factor Surveillance System, 2019
4 | P a g e
as Title X Family Planning, Federally Qualified Health Centers (FQHCs), rural health clinics, look-a-like clinics, and other local safety net settings. Fees for preventive services should no longer be a barrier to care; communities and providers can work together to ensure women receive a comprehensive well-woman visit on an annual basis. KDHE supports and encourages all providers and communities working to ensure every woman in Kansas receives this crucial component of preventive care.
Training A webinar that reviews the components of this tool and its application to well-woman services is available on KS Train, course number 1094552. We strongly encourage all staff to review both the toolkit and the webinar to guarantee all individuals who are serving women in your communities are knowledgeable about the importance of the well-woman visit as well as the components of the visit and potential barriers women may face when accessing care.
Policy Establishing agency policies that outline staff expectations related to well-woman care ensures consistent, high-quality services are provided to all clients, every time. To achieve this goal, providers are encouraged to develop a policy that includes the following (a sample policy is provided in the ‘Resources’ section of this toolkit):
- Every woman should receive preventive services and be screened to determine if she has had a well-woman visit in the past twelve months. She should be provided with education about the importance of a comprehensive annual exam, even if she is not the primary patient being seen; she should also be reminded to schedule her well-woman visit if she has not had one in the past 12 months i.e., a mother in-office for her child’s well-visit can be reminded to schedule her own appointment and provided with educational materials about the importance of the well-visit (materials provided in the ‘Resources’ section).
- Every woman who is seen for a well-woman visit should receive screening for each item noted on ACOG’s Recommendations for Well-Woman Care: https://www.womenspreventivehealth.org/wellwomanchart/ (provided below).
- Local partnerships must be in place for referrals/connections for any care that cannot be provided internally (a sample MOU is provided in the ‘Resources’ section of this toolkit).
Promotion and Partnerships As requirements and recommendations related to well-woman care expand and become increasingly holistic and comprehensive it is likely that agencies are unable to provide all of the recommended screenings or services. It is important to have partners in place within the community who can provide services that an agency is less equipped to provide.
- All agencies should work with community stakeholders (faith-based organizations, public health organizations, behavioral health organizations, etc.), committing to identifying and addressing barriers women face when accessing care. These barriers, as identified by CityMatCH and the University of Illinois, are outlined in the ‘Addressing Barriers’ section of this toolkit and the ‘For Communities’ Toolkit, found on the KDHE Integration Toolkit website. These resources can and should be used to start conversations with partners and collaborate in ways that creatively and effectively address patient and community concerns.
- Utilizing well-woman visit brochures, posters, and other promotional materials ensures women repeatedly see messaging regarding the importance of preventive care. Consistent and repeated messaging across varying services and care providers makes it more likely that individuals will take note
5 | P a g e
and take action to schedule a visit. These materials can be placed in waiting rooms as well as in exam rooms. PDF versions of these promotional items have been provided in the ‘Raising Awareness’ section of this toolkit.
Clinical Recommendations The well-woman visit is an opportunity to not only screen women for general health, infectious diseases, and cancer but also provides an opportunity to have important conversations related to mental health, reproductive wellness and planning, substance use, intimate partner violence, and other social determinants of health including access to healthy food and social supports. Within this section you will find resources and guidance to help ensure each well-woman visit provides integrated social and medical care for every woman.
Recommended Guidelines The following recommendations are provided by ACOG’s Women’s Preventive Services Initiative (WPSI) and were last updated in December 2019.
• To review ACOG’s Committee Opinion: https://www.acog.org/-/media/Committee-Opinions/Committee-on-Gynecologic-Practice/co755.pdf?dmc=1&ts=20200304T1849443462
• To download the recommendations chart: https://www.womenspreventivehealth.org/wellwomanchart/ • To access the clinical summary tables in their entirety as well as an interactive chart tool:
https://www.womenspreventivehealth.org/wellwomanchart/. • To add the WPSI shortcut to your mobile device: https://www.womenspreventivehealth.org/wp-
content/uploads/WPSI-Shirtcut-Postcard_CROP.pdf. • To review updated HRSA Guidelines for Women’s Prevention Services (as of December 2019):
https://www.hrsa.gov/womens-guidelines-2019
Education and Counseling As we see rates of mental distress9 continue to increase along with women’s mortality rates, it is imperative that providers take advantage of every opportunity to address issues related to both physical and mental health with their patients.
Education and Counseling Improves Health Outcomes10 Many of the most common causes of disease, disability, and death of women in the United States can be directly attributed to health risk behaviors. Behavioral counseling has proven to be effective in modifying behaviors and, subsequently, reducing the risk of developing certain chronic illnesses. Clinician advice targeted at lifestyle habits is associated with increased efforts by patients to change their behavior. For women in particular there is evidence of a “priming effect;” meaning that advice makes patients more attuned to additional information consistent with their provider’s recommendations. Patient education has been shown to increase the uptake of healthy behaviors, improve medication compliance and assist with disease management.
9 https://www.americashealthrankings.org/explore/annual/measure/mental_distress/state/KS 10 Well-Woman Provider Toolkit, National Women’s Law Center
6 | P a g e
Education and Counseling is Popular with Patients11 Qualitative research has shown that patients want more prevention counseling during clinical visits. Other studies have confirmed that patients expect their providers to educate them on key behaviors, including diet, exercise, and substance use. Women consider clinical settings to be appropriate for discussions of sexual health, intimate partner violence, and other sensitive topics, and they expect their provider to initiate these conversations.
Screening Tools In an effort to streamline the screening process for providers and increase the likelihood that patients receive all of the recommended screenings, KDHE is in the process of developing a comprehensive, integrated prescreening tool that will incorporate several prescreening and intervention tools into a single form. Affirmative answers will lead to more in-depth screening during the exam. Examples of screening and intervention tools that will be incorporated into the tool12:
o Substance use – National Institute on Drug Abuse (NIDA) Quick Screen: https://www.drugabuse.gov/sites/default/files/pdf/nmassist.pdf
o Behavioral health – Patient Health Questionnaire-2: https://www.apa.org/pi/about/publications/caregivers/practice-settings/assessment/tools/patient-health
o Pregnancy intention – One Key Question: https://powertodecide.org/one-key-question o Social determinants of health – American Academy of Family Physicians Social Screening Tool:
https://www.aafp.org/dam/AAFP/documents/patient_care/everyone_project/patient-short-print.pdf o Intimate partner violence and sexual violence – CUES: Evidence-Based Intervention:
https://ipvhealth.org/health-professionals/educate-providers/
The questionnaire will combine elements of other evidence-based prescreening tools to create a single form that a patient can complete prior to their well-woman visit. The provider can review the prescreening responses before the visit and be prepared to follow-up with any affirmative responses noted within the prescreen. KDHE will be providing separate toolkit sections and corresponding webinars to assist in the implementation of the tool for each of the prescreening topics with the goal of ensuring providers are prepared to have positive and effective interventions, when needed. The new prescreening tool has an anticipated launch date of July 2021 and will be available in DAISEY.
Addressing Barriers The Well-Woman Project, a joint effort of the University of Illinois School of Public Health (UIC-SPH) and CityMatCH, conducted listening sessions with 156 women in eight cities across the country in the spring of 2016 and gathered over 100 additional stories that were shared through the Well-Woman Project website. After analysis, 13 barriers were identified along with a list of responses, recommendations and resources for each. To review the barriers and proposed solutions in their entirety, visit the Well-Woman Project website,
11 Well-Woman Provider Toolkit, National Women’s Law Center 12 Note that as the tool is developed and recommendations evolve, these screening measure may be adjusted based on best practices and recommendations from Federal, State, and national partners.
7 | P a g e
https://www.citymatchlearning.org/well-woman/index.php. Below are a list of provider-related barriers and recommendations to address these obstacles.
1. Women in many cities reported long distances to providers, as well as no available parking, unreliable and unsafe public transportation when traveling with small children (i.e., no room for car seats, strollers), and unreliable and not woman-friendly transportation services (i.e., van services).
CityMatCH Recommendations:
• Encourage large health systems and FQHCs to explore partnerships with ride-sharing organizations for patient transportation.
• Work with city Department of Transportation to explore and develop plans to provide child-friendly public transportation.
• Work with large health systems and FQHCs to encourage provision of free parking vouchers or free/discounted bus/train cards to attend appointments and development of play areas or supervised childcare facilities in health clinics/provider's offices.
KDHE Recommendations:
As the COVID-19 pandemic has continued to shift the way we interact with one another, it is important to explore new options related to telehealth services and options that enable more patients to receive important preventive care despite a lack of transportation. To learn more about telehealth and preventive care, visit: https://www.womenspreventivehealth.org/implementation/telehealthfaq/faqs/.
• Consider using county vehicles to transport patients to and from appointments. • Consider budgeting grant funds for transportation vouchers with Uber Health or the public health system.
2. Women face barriers in obtaining any or low-cost insurance (e.g., issues with co-payments, deductibles, premiums) for a variety of reasons. Women avoid seeking health care because they are afraid they cannot afford the associated costs or fear going into debt/filing for bankruptcy due to medical bills. Women frequently discussed that the quality of care depended greatly on type of insurance.
CityMatCH Recommendations:
• Partner with large health systems, FQHCs, and other key stakeholders to provide women and families with access to insurance navigators on a year-round basis.
• Develop a city fund to cover uninsured women and families and/or to help women and families struggling with high deductibles for their privately obtained insurance.
• Partner with major health systems and FQHCs to sponsor "One Day" Medicaid/free care several times a year for all.
KDHE Recommendations:

8 | P a g e
Standard costs for preventive visits can be listed on an agency’s website or a website can include content explaining that an individual can call the office to learn more about service costs. Prior to offering or performing services, a provider should inquire about whether or not the patient has any concerns related to the costs of the exam or subsequent diagnostics and connect them with appropriate resources to assist the individual in identifying and signing up for a health plan if they express concerns over payment if feasible. Offer women and families assistance with finding affordable health insurance through the use of a navigator staff position who can also assist with applications for coverage such as Medicaid or the Children’s Health Insurance Plan.
• Offer a sliding fee scale based on the US poverty guidelines that slides to $0 for preventive care.
3. Barriers with providers stemmed from lack of trust or comfort; women felt they were not heard and that providers did not address their concerns. The structure of appointments (e.g., getting an appointment, actual time spent with provider) often cause women to delay or defer seeking health care services.
CityMatCH Recommendations:
• Explore approaches to: develop women-centered, consumer-driven mechanisms, such as a visit comment card, to enable reviews of a provider; enable women to have their health histories available on personal applications, such as MTCH PHR, so that providers can readily access the information.
• Partner with major health systems to develop and offer training to increase cultural competency/humility of the clinical workforce.
KDHE Recommendations:
Ensure all agency staff are knowledgeable and mindful of the importance of active listening and employ best practices related to listening skills when working with clients. Share resources and articles related to the importance of active listening with agency staff, including Active Listening Strategies and Making Time to Really Listen to Your Patients.
4. Women reported being discriminated against related to race/ethnicity, socioeconomic status, type of insurance, disability, and sexual orientation/gender.
CityMatCH Recommendations:
• Adopt and promote a Charter which delineates the components of a woman and family friendly health delivery system. The Maternal and Child Health Integrated Program provides a comprehensive toolkit which outlines the components of the Respectful Maternity Care Charter which can be referenced when developing an agency charter related to health equity.
• Engage in dialogue with large health systems and FQHCs to encourage increased availability of appointments outside of traditional hours, drop-in/walk-in appointments, more time per patient to facilitate patient-provider interaction, and an increase in the availability of on-line or telephone consultation.
KDHE Recommendations:
9 | P a g e
• As part of onboarding, all agency staff should complete training related to implicit and unconscious biases. To learn more, visit the Association of American Medical Colleges’ (AAMC) Unconscious Bias Resource page. For additional resources relating to bias, please reference the ‘Resources’ section of this toolkit.
• Adopt hiring practices that strive to create an inclusive and representative workforce that doesn’t simply represent the demographics of the community as a whole, rather the portion of the community that the agency serves. The AAMC provides resources that can assist agencies with evaluating their workforce and developing a plan to diversify hiring practices.
5. Some women lacked basic health knowledge or previous experience with primary care. Many women did not seek health care services until pregnancy for this reason.
CityMatCH Recommendations:
• Partner with health systems and other key stakeholders to support and develop health education campaigns that focus on women's understanding of the importance of their own health and health care.
• Ensure availability of city-wide Women's Health Hotline as a go-to-resource for up-to-date information on changing health and health care recommendations and guidelines. An existing hotline, such as 1-800-CHILDREN, could be utilized as long as staff are trained to address calls related to women’s health.
KDHE Recommendations:
• Partner with high school health curriculum facilitators or school-based health centers to incorporate preventive health materials into core classroom instruction and provide brochures to school nurses and other support professionals who can have them available in waiting rooms and offices that students frequent (review materials on the topic at https://www.kdheks.gov/c-f/Adolescent_Health.html). Provide preventive care outreach materials to area colleges, including community college campuses, that can be provided through their health awareness programming.
• Use health care navigators to refer every woman to a primary care physician at time of conception, to coincide with their obstetrician (if needed), and immediately after the six-week postpartum visit. Referrals for annual exams should also be completed at the time of the six week visit, to correspond with the timing of each woman’s identified needs during her pregnancy care (breastfeeding support, health screenings, mental health needs, family planning, parent supports, access to coverage/insurance, etc.).
6. The vast complexity of the health care system prevented many women from seeking care or obtaining care. Many women documented feeling overwhelmed with tasks from initiating a new insurance plan, finding providers within their network, navigating new health care facilities and systems, making appointments, and adhering to the referral requirements of their insurance policies.
CityMatCH Recommendations:
• Partner with health systems and other key stakeholders to support and develop health education campaigns that focus on women's understanding of the importance of their own health and health care.
• Ensure availability of city-wide Women's Health Hotline as a go-to-resource for up-to-date information on changing health and health care recommendations and guidelines.

10 | P a g e
KDHE Recommendations:
• Provide clear and concise language on the agency website that outlines the process for new patients, what insurance is accepted and who to contact if they have questions about cost, insurances accepted, etc.
• Pursue funding that will allow for a navigator position, or support services like Holistic Care Coordination, within the agency that will assist clients with determining what health care options are available , assist with completing applications, and address other potential barriers.
7. Women expressed fear in many contexts: fear of loss of confidentiality, fear of the content/results of the visit, fear related to lack of citizenship or immigration status, fear of being billed for services not covered or they could not afford, fear of being judged or stigmatized, and fear of invasive gynecological procedures performed by male providers.
CityMatCH Recommendations:
• Support the provision of training in trauma-informed care for providers.
KDHE Recommendations:
• As a part of onboarding, it is recommended that all staff receive training on trauma-informed care and best practices as well as information on compassion fatigue, vicarious trauma and resiliency.
• Staff that complete medical and sexual histories should be familiar with best practices when gathering this data, including the Center for Disease Control’s guide to Discussing Sexual Health With Your Patients.
8. Women discussed having jobs that did not offer paid sick time, personal days, or vacation time which resulted in losing pay to see a health care provider. Women also discussed being unable to make traditional office hour appointments due to their inability to take time off during the day.
CityMatCH Recommendations:
• Explore approaches to: develop women-centered, consumer-driven mechanisms, such as a visit comment card, to enable reviews of a provider; enable women to have their health histories available on personal applications, such as MTCH PHR, so that providers can readily access this information.
• Engage in dialogue with large health system and Federally Qualified Health Centers (FQHCs) to encourage increased availability of appointments outside of traditional hours, drop-in/walk-in appointments, more time per patient to facilitate patient-provider interaction, and an increase in the availability of on-line phone consultation.
KDHE Recommendations:
• Consider extending, or adjusting, office hours. Start by adding three hours a week in evenings, early mornings or Saturdays, and explore which hours work best for the community.
11 | P a g e
• Offer to provide on-site services like vaccinations, blood pressure checks, and mental health screenings, when feasible, to large employers in the area.
• Work with local industry/businesses to educate about the importance of maternal care in population-based outcomes, as evidence proves that supported and healthy mothers attend work at higher rate. If available, navigators can and should attend businesses/agencies/local industry meetings to offer information and serve as a referral resource for human resource directors.
9. Non-English-speaking women noted the lack of translational services, including language line services and/or bilingual staff, and materials available in languages other than English which made it difficult or undesirable for them to seek care.
CityMatCH Recommendations:
• Explore approaches to: enable reviews of provider through a women-centered, consumer-driven mechanism; enable women to have their health histories available on personal "apps" so that providers can readily access this information.
• Partner with major health systems to develop and offer training to increase cultural competency/humility of the clinical workforce.
KDHE Recommendations
• Utilize public health funding (e.g., WIC, MCH, Family Planning, Primary Care) for translation services, including translating all patient education materials and website content.
Resources The following resources for health departments and providers offer additional information and training.
Clinical Guidance Women’s Preventive Health Summary Tables https://www.womenspreventivehealth.org/wp-content/uploads/ClinicalSummaryTables.pdf
KDHE Preconception Health Guide https://www.kdheks.gov/c-f/integration_toolkits/Preconception_Health_Guide.pdf
Recommendations for Providing Quality STD Clinical Services: https://www.cdc.gov/std/qcs/default.htm
Trauma and Violence A Trauma-Informed Care Approach https://www.brighamandwomens.org/womens-health/connors-center/care-clinic/trauma-informed-care
National Health Resource Center on Domestic Violence https://www.futureswithoutviolence.org/health/national-health-resource-center-on-domestic-violence/
Building Partnerships with Domestic Violence and Sexual Assault Service Providers https://ipvhealthpartners.org/
12 | P a g e
Centers for Disease Control and Prevention, Connecting The Dots https://www.cdc.gov/features/cdc-connecting-dots/index.html
Health Equity and Social Care National Academies of Science, Engineering and Medicine: “Integrating Social Care Into the Delivery of Healthcare: Moving Upstream to Improve the Nation’s Health” https://www.nationalacademies.org/our-work/integrating-social-needs-care-into-the-delivery-of-health-care-to-improve-the-nations-health
Unconscious Bias Resources for Health Professionals https://www.aamc.org/what-we-do/mission-areas/diversity-inclusion/unconscious-bias-training
Diversity and Health Equity in Maternal and Child Healthcare https://mchb.hrsa.gov/training/documents/MCH_Diversity_2016-05_RFS.pdf
Moving to Institutional Equity: A Tool to Address Equity for Public Health Providers https://chronicdisease.org/resource/resmgr/gillan's_files/health_equity_june_2017.pdf
LGBTQIA+ Health Education Center https://www.lgbtqiahealtheducation.org/
Mitigating Implicit Bias in Healthcare https://u.osu.edu/breakingbias/tools-for-mitigating-bias/
Mental Health and Substance Use National Council on Behavioral Health https://www.thenationalcouncil.org/integrated-health-coe/resources/
SAMHSA-HRSA Center for Integrated Health Solutions https://www.integration.samhsa.gov/clinical-practice/screening-tools
KDHE Mental Health Integration Toolkit https://www.kdheks.gov/c-f/mental_health_integration.htm
KDHE Screening, Brief Intervention, and Referral to Treatment Toolkit https://www.kdheks.gov/c-f/SBIRT_Toolkit.htm
Patient Resources Patient Well-Woman Visit Brochures (English and Spanish): https://www.nwlc.org/sites/default/files/final_well-womanbrochure.pdf
Youth Health Guide https://www.womenspreventivehealth.org/wellwomanchart/
My Life, My Goals: Reproductive Wellness Workbook https://www.kdheks.gov/c-f/integration_toolkits/Reproductive_Life_Plan.pdf
Kansas Crisis Hotline 1-888-END-ABUSE, provides confidential support 24/7 to victims of domestic violence, sexual assault and stalking. National Suicide Prevention Lifeline provides 24/7, free and confidential support for people in distress, prevention, and crisis resources for you or your loved ones, and best practices for professionals. Call 1-800-273-8255 or 1-888-628-9454 for Spanish. Crisis Text Line is a free, 24/7, confidential text message service for people in crisis. To reach a crisis counselor, text Kansas to 741741.
13 | P a g e
Kansas Community Mental Health Centers (CMHCs) offer crisis services 24/7. Contact the CMHC for the county you are currently in for crisis services: http://www.acmhck.org/wp-content/uploads/2018/01/CommunityMentalHealthCentersofKS-Revised-1-10-18.pdf. Veterans Crisis Line offers 24/7, confidential support to veterans, service members, National Guard and Reserve members, and their family member and friends. Call 1-800-273-8255 and Press 1 or text 838255. Tobacco Cessation KS Quitline: 1.800.QUIT.NOW or KSQuit.org (online chat)
KS Parent Helpline 1-800-CHILDREN is a is a free, statewide, anonymous, information and referral service.
Support Resources for Providers SAMHSA Tips for Healthcare Professionals: Coping with Stress and Compassion Fatigue https://store.samhsa.gov/product/Tips-for-Healthcare-Professionals-Coping-with-Stress-and-Compassion-Fatigue/PEP20-01-01-016?referer=from_search_result
SAMHSA’s Disaster Distress Hotline provides 24/7, 365-day-a-year crisis counseling and support to people, including medical professionals, experiencing emotional distress related to natural or human-caused disasters and infectious disease outbreaks. Call 1-800-985-5990 or text TalkWithUs to 66746. For Spanish speakers, call 1-800-985-5990 and press 2 or text Hablanos to 66746.
Sample Policies Sample Release of Information for clients in intimate partner violence relationships https://www.kdheks.gov/c-f/integration_toolkits/Sample_IPV_Consent_for_Communication_with_Medical_Providers.pdf
Sample Release of Information for clients needing behavioral health or substance use treatment https://www.kdheks.gov/cf/integration_toolkits/Sample_ASSIST_Consent_for_Communication_with_Medical_Providers.pdf
Sample Agency Policy on Well-Woman Visits https://www.kdheks.gov/c-f/integration_toolkits/Sample_Agency_Well_Woman_policy.pdf
Sample Memorandum of Agreement https://www.kdheks.gov/c-f/integration_toolkits/SBIRT/07_Templates_for_Local_Use/06_sample_mou.doc
Workflows/Algorithms Alcohol, Smoking and Substance Involvement Screening Test (ASSIST) Algorithm https://www.kdheks.gov/c-f/integration_toolkits/SBIRT/06_Workflows_Algorithms/01_assist_algorithm.pdf
Crisis Intervention Workflow https://www.kdheks.gov/c-f/integration_toolkits/SBIRT/06_Workflows_Algorithms/04_crisis_intervention_workflow.pdf
Raising Awareness Community-based organizations and local governments can assist in spreading awareness about the importance of the annual well-woman visit through a variety of ways. KDHE has created a Well-Woman Visit Promotional Flyer that can be printed and posted in exam rooms, waiting areas or distributed via social media, tabling events, etc.
14 | P a g e
Below, we have provided tools such as awareness toolkits and sample media posts that can be used and adapted to meet the needs of your local community.
Campaigns and Promotional Tools These campaigns can be utilized in parts or in their entirety through social media, traditional press, and hard copy promotion and distribution.
• Well Women, Well Communities Toolkit https://www.citymatch.org/well-women-well-communities/ • #YouGoGirl, American Heart Association Well Woman Promotional Video
https://www.youtube.com/watch?v=DIN-svKAKT4 • Care Women Deserve http://carewomendeserve.org/
• Women’s Health Month Toolkit http://www.kansasmch.org/womenshealthmonthtoolkit.asp
Sample Social Media Posts • Do you know how to #BeAWellWoman? Well-Woman visits are available without additional costs, like co-
pays and deductibles. Learn more about what questions you should be asking your provider at your next check-up. www.nwlc.org/wellwoman
• What kind of education and counseling can you get with your no-cost well-woman visit? #BeAWellWoman • Well-woman visits are available without co-pays! It’s never been easier to #BeAWellWoman
1 | P a g e
Preparing for Your Well-Woman Visit This checklist can be used to help you get ready for your well-woman visit and ensure all your questions and concerns are addressed.
Why your well-woman visit is important The annual well-woman exam is an opportunity for your provider to assess the state of your current health. During this visit you can discuss concerns as well as steps that can be taken to prevent potential health issues in the future. Learn more about what topics are discussed during the annual well-woman exam (link to infographic).
Step 1: Know your family health history It is important to know your family health history prior to your well-woman visit. The Center for Disease Control and Prevention has created a tool to help you answer questions that provide insight into short and long-term health concerns that may be impacted by your family health history: https://phgkb.cdc.gov/FHH/html/index.html.
Step 2: Prepare a list of questions The well-woman visit is the perfect time to ask your provider questions about your physical and mental health. Below is a checklist that can be completed prior to your visit to make sure no topics are missed during your appointment. Remember, this is your time to ask questions! Health education and counseling are core components of your annual exam.
If you are nervous about how to bring up some of the questions listed below you can give this completed checklist to your provider so they can see what topics you would like to discuss. You can also start the conversation by saying:
“I want to be sure we talk about some things I am concerned about today. Do you mind if we go through the list I have prepared?”
The Well-Woman Exam Checklist Check the topics that you want to be sure to discuss with your provider. Feel free to write additional notes or questions in the blank space provided at the end.
Reproductive Health
I want to become pregnant in the next year (yes, no, unsure, ok either way?) How can I protect myself from sexually transmitted infections? Other: ____________________________
General Health
I am concerned about my blood pressure I am concerned about my heart and/or high cholesterol I am concerned about cancer I am concerned about diabetes I am concerned about osteoporosis I am concerned I do not get enough sleep (I have trouble falling asleep or staying asleep)
2 | P a g e
Other: ______________________________
Weight Management
I am concerned about my weight (I think I weigh too much or too little) I need guidance on how to eat healthy I have trouble getting fresh food to eat I need guidance on how to be more active Other: ______________________________
Menstrual Cycles
I have been having irregular cycles I have been having painful cycles I have excessive bleeding during my cycle Other: _______________________________
Mental Health
I have been feeling sad and/or hopeless I have been feeling anxious I easily become stressed or overwhelmed I become irritable or angry very quickly Other: ______________________________
Substance Use
I am worried that I drink too much I would like to quit smoking I want to quit using narcotics or prescription drugs Other: _____________________________
Healthy Relationships and Support Network
I feel unsafe in my relationship I feel like I don’t have control over my reproductive choices I don’t feel as though I have anyone who can help me when I am struggling Other: ______________________________
Screenings and Immunizations
Do I need a Pap test? Do I need a breast exam? Do I need a mammogram? Should I have any vaccinations? Should I be tested for sexually transmitted infections?

3 | P a g e
Additional Notes:
__________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________

SCHEDULE YOUR WELL-WOMAN VISIT TODAY!
Annual Well-Woman EXAMINATIONTop reasons why you should have an annual well-woman examination
Birth Control Cancer Screening Vaccinations Health Screening
Sexually Transmitted Infections Screening
Weight Control
Issues With Your Menstrual Period
Preconception Counseling
Questions AboutHealthy Relationships
Relationship with Drugs, Tobacco & Alcohol
Learn about choosing the right
birth control method for you.
Learn about breast cancer, colon cancer
or other types of cancer.
Get vaccinations against the flu, HPV
& more.
Get screened for high blood pressure,
diabetes, bone density & more.
Depression Screening
Depression is a common but serious illness. Your
provider will discuss symptoms, how often they occur and how
severe they are & provide resources.
Chlamydia, gonorrhea, and genital herpes are infections that spread
through sexual contact.
Concerns About Sex
Discuss what happens during intercourse,
pain during sex, hormonal changes
that change interest or response to sex or different forms of sex.
Learn about body mass index, exercise, obesity, & a healthy
diet.
Discuss premenstrual syndrome, painful
periods, your first period, heavy bleeding or irregular periods.
Your healthcare provider can discuss
options based on whether you are hoping
to become pregnant, don’t want to become
pregnant or are unsure.
Your provider can discuss your use of drugs,
alcohol or tobacco and provide resources to help
you quit or cut back.
Learn about what happens in healthy
and unhealthy relationships and resources in your
community that can help you stay safe.
Department of Healthand Environment

Kansas Maternal Mortality
Report & Activities
Information pertaining to the findings from the Kansas Maternal Mortality Review Committee (KMMRC) and related activities.
SECTION CONTENTS
• Kansas Maternal Mortality Report Highlights ....................................................... 34 • Pregnancy-Associated Death Infographic ............................................................. 36 • Pregnancy-Related Death Infographic .................................................................. 41 • Severe Maternal Morbidity Infographic ................................................................. 45 • Severe Maternal Morbidity Poster ......................................................................... 49 • KMMRC Member Roster ........................................................................................ 50
The full Maternal Mortality Report is available online at: https://kmmrc.org/reports/
Kansas Maternal Mortality Review Report Highlights The issue of maternal morbidity and mortality is complex. Severe maternal morbidity occurs nearly 100
times more frequently than maternal death. The Kansas Department of Health and Environment (KDHE)
identifies all pregnancy-associated deaths, or deaths occurring while a woman is pregnant or within a
year of pregnancy, to collect data on maternal mortality. KDHE works with the Kansas Maternal
Mortality Review Committee (KMMRC) to review cases of pregnancy-associated death. The purposes of
the review are to determine the factors contributing to maternal mortality in Kansas and identify public
health and clinical interventions to improve systems of care. The aim of the KMMRC is to better
understand the causes of maternal mortality and develop statewide recommendations to prevent future
maternal deaths, as well as determine whether the deaths were pregnancy-related (occurring due to a
pregnancy complication) and whether they were preventable.
_____________________________________________________________________________________
Severe Maternal Morbidity
During 2016-2019, of the 132,643 delivery hospitalizations of Kansas residents, 767 deliveries with one
or more severe maternal morbidities (SMM) were identified, representing a rate of 57.8 per 10,000
delivery hospitalizations. This implies that about 1 in 173 women who delivered a baby experienced
SMM.
• The top five most common indicators of SMM were acute renal failure, disseminated
intravascular coagulation, sepsis, hysterectomy, and adult/acute respiratory distress syndrome
• SMM was highest among women aged 40+ years and lowest for those aged 25-29 years
• Despite the downward trend in the SMM rate of non-Hispanic Black women during 2016- 2019,
the overall rate of SMM per 10,000 delivery hospitalizations for non-Hispanic Black women was
100.4: 58.3% higher than the rate among Hispanics (63.7), 72.2% higher than the rate among
non-Hispanic Asian/Pacific Islanders (58.3), and 87.3% higher than the rate among non-Hispanic
White women (53.6). The SMM rate for non-Hispanic Black women was significantly higher than
any other race and ethnicity.
• Compared with other deliveries, women who were on Medicaid or resided in ZIP Codes in the
lowest quartile of median income were more likely to experience SMM.
Pregnancy-Associated Deaths
Of the 75 identified deaths that occurred in Kansas (regardless of whether the person was a Kansas
resident) in 2016-2018, the KMMRC determined that 57 deaths were pregnancy-associated. This
translated to a pregnancy-associated mortality ratio (PAMR) of 50 deaths per every 100,000 live births
that occurred in Kansas. Of these deaths, the KMMRC subcategorized:
• 13 deaths (22.8%) were pregnancy-related
• 32 deaths (56.1%) were pregnancy-associated, but not-related, and
• 12 deaths (21.1%) were pregnancy-associated but unable to determine pregnancy-relatedness.
Timing of death:
• 17 deaths (29.8%) occurred during pregnancy.
• 13 deaths (22.8%) occurred within 42 days of the end of pregnancy.
• 27 deaths (47.4%) occurred 43 days to one year after the end of pregnancy.
The leading cause of death were motor vehicle crash, followed by homicide, poisoning/overdose, and
infection.
The KMMRC determinations on circumstances surrounding the pregnancy-associated deaths were:
• Obesity contributed to about one in six deaths (9 deaths, 15.8%).Substance use disorder
contributed to about one in three deaths (17 deaths, 29.8%).
Pregnancy-Related Deaths
During 2016-2018, in Kansas, approximately one in four deaths of women during or within one year of
pregnancy were determined to be pregnancy-related (13 deaths, 22.8%). This translated to a pregnancy-
related mortality ratio (PRMR) of 11 deaths per every 100,000 live births that occurred in Kansas.
Timing of death:
• 3 deaths (23.1%) occurred during pregnancy.
• 7 deaths (53.8%) occurred within 42 days of the end of pregnancy.
• 3 deaths (23.1%) occurred 43 days to one year after the end of pregnancy
The leading causes of death were cardiovascular and coronary conditions, followed by preeclampsia and
eclampsia, embolism, and infection.
Committee determinations on circumstances surrounding the pregnancy-related deaths were:
• Obesity contributed to more than half of the deaths (7 deaths, including 1 additional “probably
contributed”, 53.8%).
• Mental health conditions contributed to about one in 13 deaths (1 death, 7.7%).
• Substance use disorder contributed to nearly one in four deaths (3 deaths, 23.1%).
KMMRC Key Recommendations for Action for Pregnancy-Related Deaths
• Screen, provide brief intervention and referrals for:
o Comorbidities and chronic illness
o Intimate partner violence
o Pregnancy intention
o Mental health conditions (including postpartum anxiety and depression)
o Substance use disorder
• Increased communication and collaboration between providers, including referrals
• Patient education and empowerment
What We’re Doing About It
• Black maternal health week programming
• Focus groups for non-Hispanic Black mothers to determine barriers to care.
• First Trimester Initiation, including the Postpartum Discharge Transition, a safety bundle pilot
• Well-woman toolkit to address barriers and provider bias.
• Post-birth warning signs campaign and provider training with the Association of Women's
Health, Obstetric and Neonatal Nurses (AWHONN)
• Kansas Connecting Communities (KCC), including a Provider Consultation Line at 833-765-2004
• Pregnancy intention training (One Key Question) which includes provider bias training
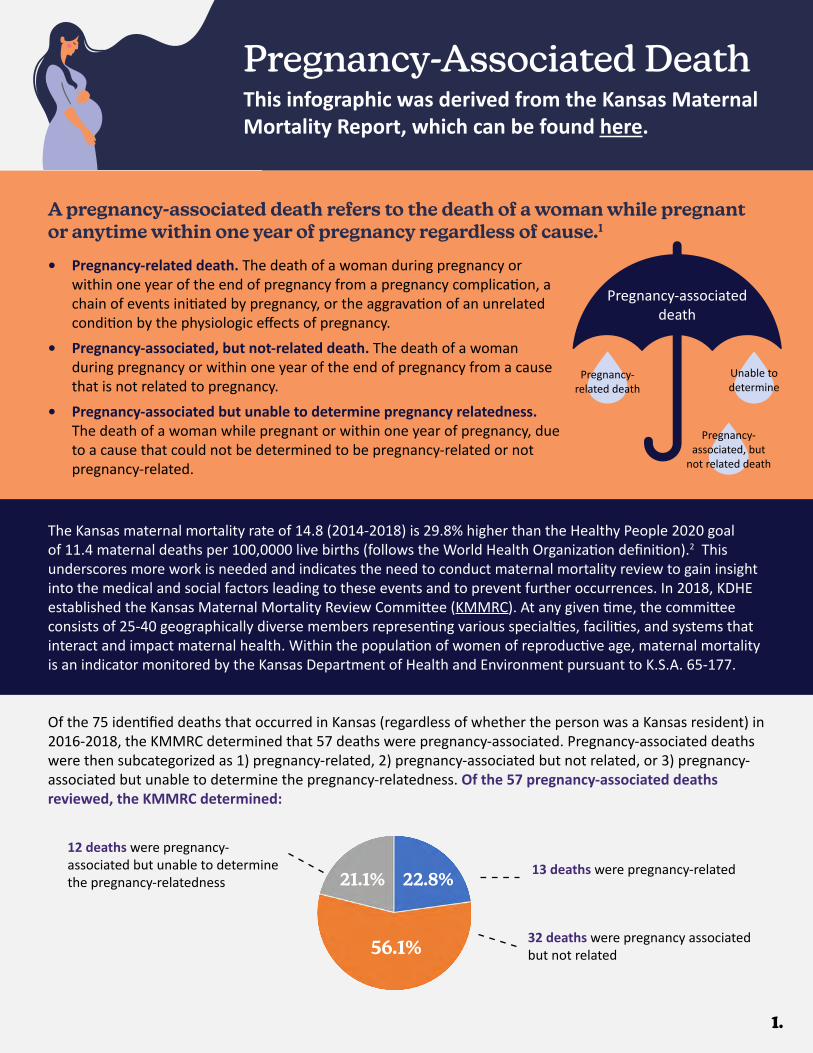
Pregnancy-Associated Death
A pregnancy-associated death refers to the death of a woman while pregnant or anytime within one year of pregnancy regardless of cause.1
Of the 75 identified deaths that occurred in Kansas (regardless of whether the person was a Kansas resident) in 2016-2018, the KMMRC determined that 57 deaths were pregnancy-associated. Pregnancy-associated deaths were then subcategorized as 1) pregnancy-related, 2) pregnancy-associated but not related, or 3) pregnancy-associated but unable to determine the pregnancy-relatedness. Of the 57 pregnancy-associated deaths reviewed, the KMMRC determined:
12 deaths were pregnancy-associated but unable to determine the pregnancy-relatedness
13 deaths were pregnancy-related
32 deaths were pregnancy associated but not related
1.
This infographic was derived from the Kansas Maternal Mortality Report, which can be found here.
56.1%
22.8%21.1%
• Pregnancy-related death. The death of a woman during pregnancy or within one year of the end of pregnancy from a pregnancy complication, a chain of events initiated by pregnancy, or the aggravation of an unrelated condition by the physiologic effects of pregnancy.
• Pregnancy-associated, but not-related death. The death of a woman during pregnancy or within one year of the end of pregnancy from a cause that is not related to pregnancy.
• Pregnancy-associated but unable to determine pregnancy relatedness. The death of a woman while pregnant or within one year of pregnancy, due to a cause that could not be determined to be pregnancy-related or not pregnancy-related.
Pregnancy-associateddeath
Pregnancy-related death
Unable to determine
Pregnancy-associated, but
not related death
The Kansas maternal mortality rate of 14.8 (2014-2018) is 29.8% higher than the Healthy People 2020 goal of 11.4 maternal deaths per 100,0000 live births (follows the World Health Organization definition).2 This underscores more work is needed and indicates the need to conduct maternal mortality review to gain insight into the medical and social factors leading to these events and to prevent further occurrences. In 2018, KDHE established the Kansas Maternal Mortality Review Committee (KMMRC). At any given time, the committee consists of 25-40 geographically diverse members representing various specialties, facilities, and systems that interact and impact maternal health. Within the population of women of reproductive age, maternal mortality is an indicator monitored by the Kansas Department of Health and Environment pursuant to K.S.A. 65-177.
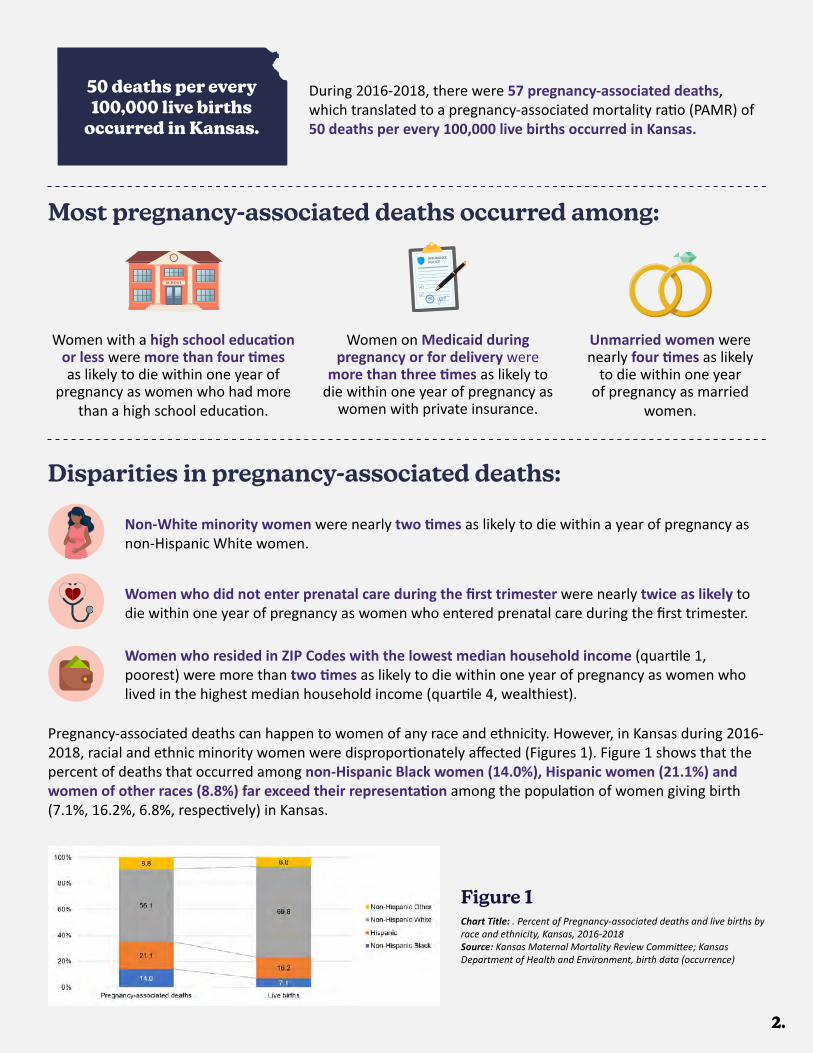
2.
Unmarried women were nearly four times as likely
to die within one year of pregnancy as married
women.
Women with a high school education or less were more than four times as likely to die within one year of
pregnancy as women who had more than a high school education.
Women on Medicaid during pregnancy or for delivery were
more than three times as likely to die within one year of pregnancy as
women with private insurance.
Non-White minority women were nearly two times as likely to die within a year of pregnancy as non-Hispanic White women.
Women who did not enter prenatal care during the first trimester were nearly twice as likely to die within one year of pregnancy as women who entered prenatal care during the first trimester.
Women who resided in ZIP Codes with the lowest median household income (quartile 1, poorest) were more than two times as likely to die within one year of pregnancy as women who lived in the highest median household income (quartile 4, wealthiest).
Most pregnancy-associated deaths occurred among:
Disparities in pregnancy-associated deaths:
Pregnancy-associated deaths can happen to women of any race and ethnicity. However, in Kansas during 2016-2018, racial and ethnic minority women were disproportionately affected (Figures 1). Figure 1 shows that the percent of deaths that occurred among non-Hispanic Black women (14.0%), Hispanic women (21.1%) and women of other races (8.8%) far exceed their representation among the population of women giving birth (7.1%, 16.2%, 6.8%, respectively) in Kansas.
Chart Title: . Percent of Pregnancy-associated deaths and live births by race and ethnicity, Kansas, 2016-2018Source: Kansas Maternal Mortality Review Committee; Kansas Department of Health and Environment, birth data (occurrence)
Figure 1
During 2016-2018, there were 57 pregnancy-associated deaths, which translated to a pregnancy-associated mortality ratio (PAMR) of 50 deaths per every 100,000 live births occurred in Kansas.
50 deaths per every 100,000 live births
occurred in Kansas.

3.
Underlying Causes of Death
It is important to understand who is most affected by pregnancy-associated death in order to target interventions and resources.3 It is important to identify the differences in pregnancy-associated deaths.
27 deaths occurred 43 days to one year after the end of pregnancy.
Timing of death:
29.8% 22.8% 47.4%
17 deaths occurredduring pregnancy.
13 deaths occurred within 42 days of the
end of pregnancy.
These data show that tracking pregnancy-associated deaths to one year postpartum is essential, rather than the traditional measure of the first 42 days, as nearly half (47.4%) of all pregnancy-associated deaths occurred after 42 days postpartum. Furthermore, in considering policy initiatives, since so many of the pregnancy-associated deaths involved health care and occurred months after parturition, these data suggest that extending Medicaid coverage for pregnant women from 60 days to 12 months postpartum, which would allow women access the care they need to address health concerns well after their pregnancy ends. This would be a first and important step toward closing gaps in access to care and improving outcomes.3 In Kansas, among non-Hispanic Black women, a greater proportion of pregnancy-associated deaths occurred during pregnancy (62.5%). If Medicaid continues in effect for one year postpartum rather than 60 days, it presents opportunities to ensure access to quality healthcare for this at-risk population, before, during, and after pregnancies, and to provide coordinated care between pregnancies to prevent pregnancy-associated deaths.4
The leading causes of death were (in order):
Motor vehicle crash Homicide Poisoning/overdose Infection19.3% (11 deaths) 14.0% (8 deaths) 10.5% (6 deaths) 8.8% (5 deaths)
• Nearly half (25 deaths, 43.9%) were related to medical causes of death, such as infection, cardiovascular and coronary conditions, embolism, or preeclampsia and eclampsia.
• About one-third (19 deaths, 33.3%) were caused by homicide, suicide, mental health conditions, or unintentional poisoning/overdose.
• The remainders were caused by motor vehicle crash and fire or burn accidents (13 deaths, 22.8%).
The combination of the underlying cause of death determined by KMMRC and the underlying cause field on the death certificate were used to categorize the type of pregnancy-associated death (Figure 2).
Underlying cause refers to the disease or injury that initiated the chain of events leading to death or the circumstances of the accident or violence which produced the fatal injury.1
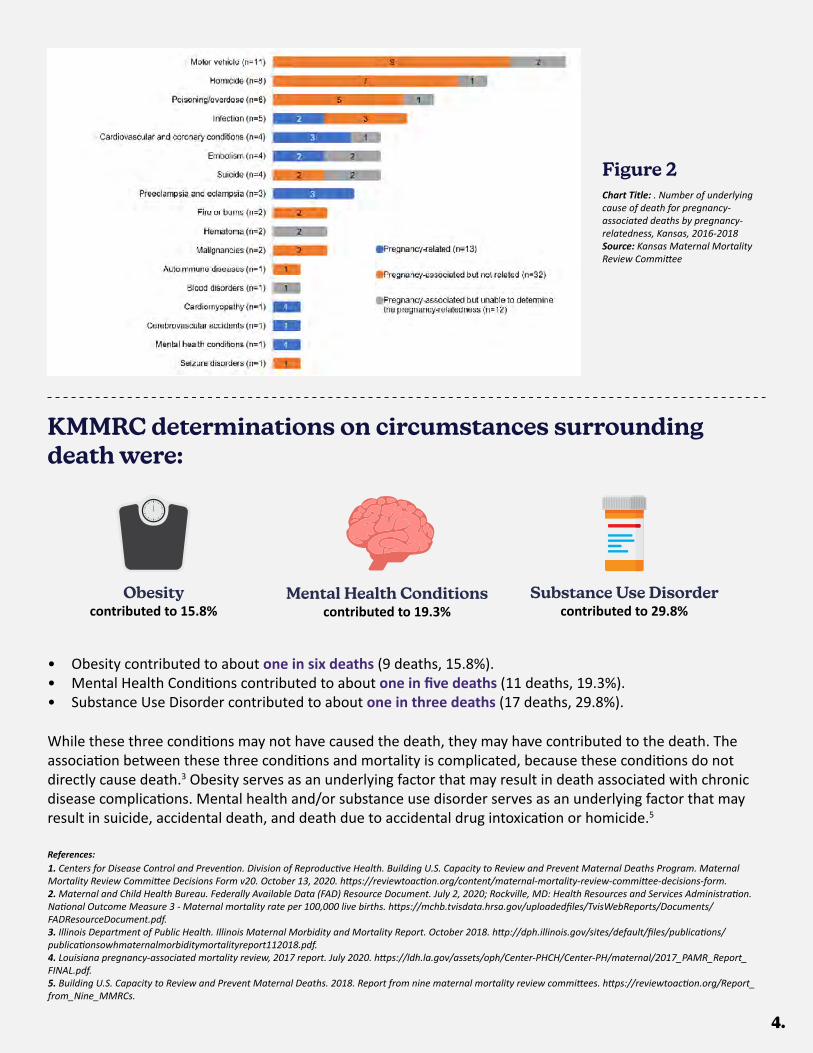
4.
• Obesity contributed to about one in six deaths (9 deaths, 15.8%). • Mental Health Conditions contributed to about one in five deaths (11 deaths, 19.3%). • Substance Use Disorder contributed to about one in three deaths (17 deaths, 29.8%).
While these three conditions may not have caused the death, they may have contributed to the death. The association between these three conditions and mortality is complicated, because these conditions do not directly cause death.3 Obesity serves as an underlying factor that may result in death associated with chronic disease complications. Mental health and/or substance use disorder serves as an underlying factor that may result in suicide, accidental death, and death due to accidental drug intoxication or homicide.5
Obesity contributed to 15.8%
Mental Health Conditionscontributed to 19.3%
Substance Use Disordercontributed to 29.8%
1. Centers for Disease Control and Prevention. Division of Reproductive Health. Building U.S. Capacity to Review and Prevent Maternal Deaths Program. Maternal Mortality Review Committee Decisions Form v20. October 13, 2020. https://reviewtoaction.org/content/maternal-mortality-review-committee-decisions-form.2. Maternal and Child Health Bureau. Federally Available Data (FAD) Resource Document. July 2, 2020; Rockville, MD: Health Resources and Services Administration. National Outcome Measure 3 - Maternal mortality rate per 100,000 live births. https://mchb.tvisdata.hrsa.gov/uploadedfiles/TvisWebReports/Documents/FADResourceDocument.pdf.3. Illinois Department of Public Health. Illinois Maternal Morbidity and Mortality Report. October 2018. http://dph.illinois.gov/sites/default/files/publications/publicationsowhmaternalmorbiditymortalityreport112018.pdf.4. Louisiana pregnancy-associated mortality review, 2017 report. July 2020. https://ldh.la.gov/assets/oph/Center-PHCH/Center-PH/maternal/2017_PAMR_Report_FINAL.pdf.5. Building U.S. Capacity to Review and Prevent Maternal Deaths. 2018. Report from nine maternal mortality review committees. https://reviewtoaction.org/Report_from_Nine_MMRCs.
Chart Title: . Number of underlying cause of death for pregnancy-associated deaths by pregnancy-relatedness, Kansas, 2016-2018Source: Kansas Maternal Mortality Review Committee
Figure 2
KMMRC determinations on circumstances surrounding death were:
References:
5.
WHAT WE’RE DOING ABOUT ITPregnancy-Associated Death
The KMMRC and KDHE Maternal and Child Health (MCH) team are closely monitoring any emerging patterns or trends identified because of case reviews.
State Perinatal Quality Collaboratives (PQCs) and MMRCs function to improve maternal and perinatal health (investing in the mother’s health leads to a healthier birth/pregnancy outcomes)• PQCs: Focus on efforts during the maternal and perinatal periods intended to improve birth outcomes and
strengthen perinatal systems of care for mothers and infants.• MMRCs: Focus on reviewing pregnancy-associated deaths to identify gaps in health services and make
actionable recommendations to prevent future deaths, improving maternal and perinatal health.• Lessons learned over time have resulted in the national recommendation (CDC) for states to intentionally
and strategically align the review efforts (MMRC) with the action/quality improvement (QI) efforts (PQC), creating a “culture of safety”.
Kansas will enroll in the Alliance for Innovation on Maternal Health (AIM) initiative when ready and implement a safety bundle pilot: Postpartum Discharge Transition, which is currently in development, in partnership with the KPQC and KMMRC (tentatively March-April 2021).• AIM is a national data-driven maternal safety and QI initiative for states and hospitals and partners from
participating states (focus on consistent obstetric practices).• AIM is based on proven implementation approaches to improving maternal safety and outcomes in the
United States.• AIM works through state teams and health systems to align national, state, and hospital level QI efforts to
improve maternal and perinatal health outcomes.• Any state can join AIM as part of a state-level PQC QI efforts/initiatives.
• Access to “Patient Safety Bundles”• Access to “Patient Safety Tools”• Access to “Education and Engagement Tools• Access to the AIM Community of States
• Fourth Trimester Initiative – KPQC Initiative based on KMMRC findings and recommendations
• The well-woman toolkit – which addresses barriers to care, including provider bias. We are working on developing supplements for the toolkit that would focus specifically on how to reach and serve Hispanic and Non-Hispanic Black women in KS
• Post-birth warning signs campaign and provider training with the Association of Women’s Health, Obstetric and Neonatal Nurses (AWHONN) (and using the CDC’s Hear Her materials)
• Pregnancy intention training (One Key Question) – which includes training on provider bias
DATA to ACTION: As of October 2019, a total of 37 pregnancy-associated deaths had been reviewed by the KMMRC. 10 (36%) of the 28 pregnancy-associated, but not-related deaths were the result of a motor vehicle crash. Frequently, the women were not wearing seat belts and were ejected from the vehicle. Deaths occured during pregnancy and the postpartum period. An action alert discussing proper seat belt use during and after pregnancy was created and disseminated. The action alert can be found at: kmmrc.org/action-alerts/.
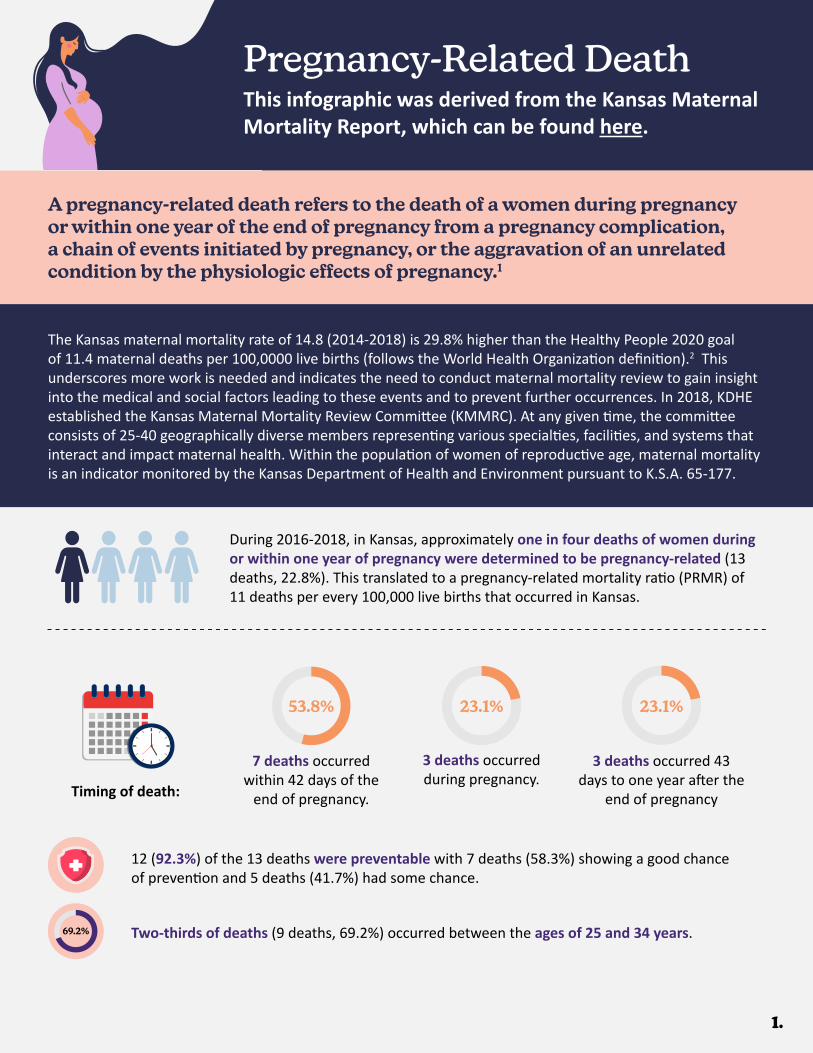
Pregnancy-Related DeathThis infographic was derived from the Kansas Maternal Mortality Report, which can be found here.
A pregnancy-related death refers to the death of a women during pregnancy or within one year of the end of pregnancy from a pregnancy complication, a chain of events initiated by pregnancy, or the aggravation of an unrelated condition by the physiologic effects of pregnancy.1
During 2016-2018, in Kansas, approximately one in four deaths of women during or within one year of pregnancy were determined to be pregnancy-related (13 deaths, 22.8%). This translated to a pregnancy-related mortality ratio (PRMR) of 11 deaths per every 100,000 live births that occurred in Kansas.
1.
7 deaths occurred within 42 days of the
end of pregnancy.
3 deaths occurred during pregnancy.
3 deaths occurred 43 days to one year after the
end of pregnancy
53.8% 23.1% 23.1%
Timing of death:
The Kansas maternal mortality rate of 14.8 (2014-2018) is 29.8% higher than the Healthy People 2020 goal of 11.4 maternal deaths per 100,0000 live births (follows the World Health Organization definition).2 This underscores more work is needed and indicates the need to conduct maternal mortality review to gain insight into the medical and social factors leading to these events and to prevent further occurrences. In 2018, KDHE established the Kansas Maternal Mortality Review Committee (KMMRC). At any given time, the committee consists of 25-40 geographically diverse members representing various specialties, facilities, and systems that interact and impact maternal health. Within the population of women of reproductive age, maternal mortality is an indicator monitored by the Kansas Department of Health and Environment pursuant to K.S.A. 65-177.
69.2%
12 (92.3%) of the 13 deaths were preventable with 7 deaths (58.3%) showing a good chance of prevention and 5 deaths (41.7%) had some chance.
Two-thirds of deaths (9 deaths, 69.2%) occurred between the ages of 25 and 34 years.

2.
Racial and ethnic minorities were disproportionately affected. About two-thirds (8 deaths, 61.5%) were racial and ethnic minorities and 5 deaths (38.5%) were non-Hispanic White women.
Obesity contributed to more than half of the deaths (7 deaths, including 1 additional probably contributed, 53.8%).
Mental health conditions contributed to about one in 13 deaths (1 death, 7.7%).
Substance use disorder contributed to nearly one in four deaths (3 deaths, 23.1%).
The distribution of underlying causes of death of pregnancy-related death by race and ethnicity varied, however, low numbers prevent strong conclusions. Pregnancy-related mortality ratio of death by race and ethnicity are not calculated because the numbers of deaths in most groups are very small. Five pregnancy-related deaths occurred in non-Hispanic White women (38.5%), three non-Hispanic Black women (23.1%), three Hispanic women (23.1%), and one involved a non-Hispanic woman of other race (15.4%). The proportion of deaths that occurred among non-Hispanic Black women (23.1%), Hispanic women (23.1%), non-Hispanic women of other races (15.4%) far exceeded their representation among the population of women giving birth (7.1%, 16.2%, 6.8%, respectively) in Kansas.
Disparities in pregnancy-related deaths:
Nearly two-thirds (8 deaths, 61.5 %) had either completed high school or general educational development (GED), or had less education than high school.
Less than half (6 deaths, 46.2 %) had private insurance; others had Medicaid, no insurance or unknown insurance status.
KMMRC determinations on circumstances surrounding death were:
Cardiovascular and coronary conditions Preeclampsia and Eclampsia Embolism Infection
The leading causes of death were (in order):
References: 1. Centers for Disease Control and Prevention. Division of Reproductive Health. Building U.S. Capacity to Review and Prevent Maternal Deaths Program. Maternal Mortality Review Committee Decisions Form v20. October 13, 2020. https://reviewtoaction.org/content/maternal-mortality-review-committee-decisions-form. 2. Maternal and Child Health Bureau. Federally Available Data (FAD) Resource Document. July 2, 2020; Rockville, MD: Health Resources and Services Administration. National Outcome Measure 3 - Maternal mortality rate per 100,000 live births. https://mchb.tvisdata.hrsa.gov/uploadedfiles/TvisWebReports/Documents/FADResourceDocument.pdf.
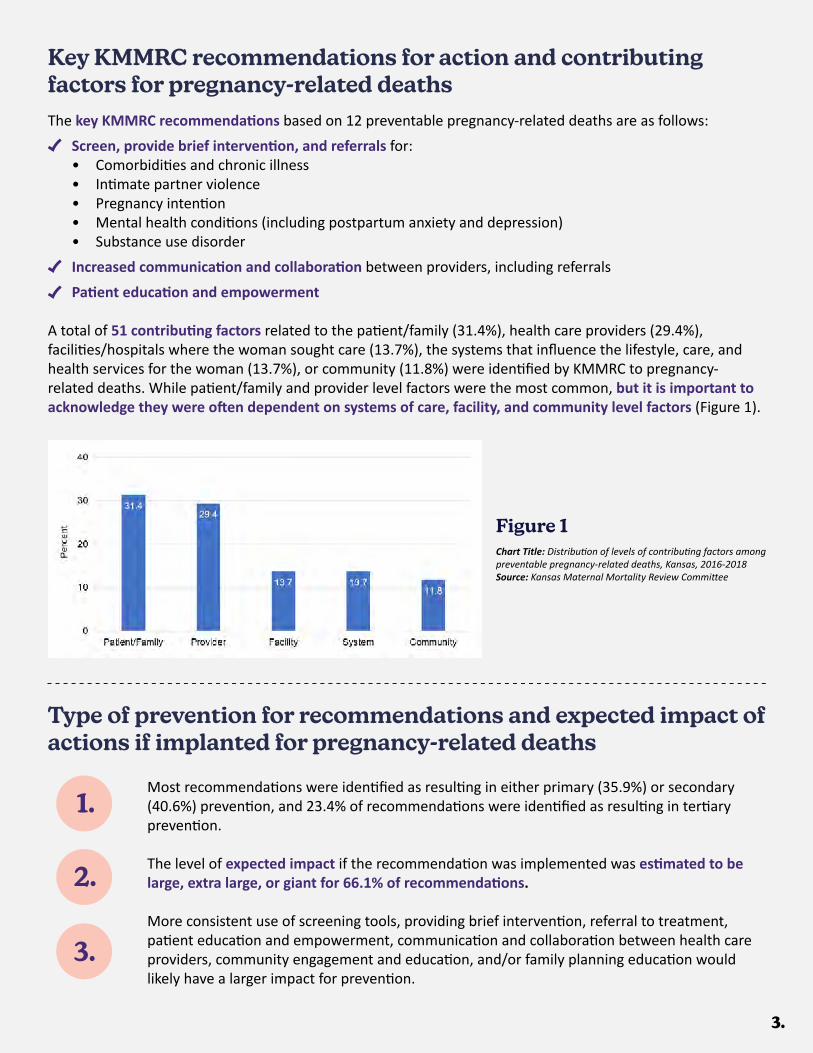
3.
Key KMMRC recommendations for action and contributing factors for pregnancy-related deathsThe key KMMRC recommendations based on 12 preventable pregnancy-related deaths are as follows:
• Screen, provide brief intervention, and referrals for:• Comorbidities and chronic illness• Intimate partner violence• Pregnancy intention• Mental health conditions (including postpartum anxiety and depression)• Substance use disorder
• Increased communication and collaboration between providers, including referrals
• Patient education and empowerment
A total of 51 contributing factors related to the patient/family (31.4%), health care providers (29.4%), facilities/hospitals where the woman sought care (13.7%), the systems that influence the lifestyle, care, and health services for the woman (13.7%), or community (11.8%) were identified by KMMRC to pregnancy-related deaths. While patient/family and provider level factors were the most common, but it is important to acknowledge they were often dependent on systems of care, facility, and community level factors (Figure 1).
Chart Title: Distribution of levels of contributing factors among preventable pregnancy-related deaths, Kansas, 2016-2018Source: Kansas Maternal Mortality Review Committee
Figure 1
Type of prevention for recommendations and expected impact of actions if implanted for pregnancy-related deaths
Most recommendations were identified as resulting in either primary (35.9%) or secondary (40.6%) prevention, and 23.4% of recommendations were identified as resulting in tertiary prevention.
The level of expected impact if the recommendation was implemented was estimated to be large, extra large, or giant for 66.1% of recommendations.
More consistent use of screening tools, providing brief intervention, referral to treatment, patient education and empowerment, communication and collaboration between health care providers, community engagement and education, and/or family planning education would likely have a larger impact for prevention.
1.
2.
3.
4.
WHAT WE’RE DOING ABOUT ITPregnancy-Related Death
The KMMRC and KDHE Maternal and Child Health (MCH) team are closely monitoring any emerging patterns or trends identified because of case reviews.
State Perinatal Quality Collaboratives (PQCs) and MMRCs function to improve maternal and perinatal health (investing in the mother’s health leads to a healthier birth/pregnancy outcomes)• PQCs: Focus on efforts during the maternal and perinatal periods intended to improve birth outcomes and
strengthen perinatal systems of care for mothers and infants.• MMRCs: Focus on reviewing pregnancy-associated deaths to identify gaps in health services and make
actionable recommendations to prevent future deaths, improving maternal and perinatal health.• Lessons learned over time have resulted in the national recommendation (CDC) for states to intentionally
and strategically align the review efforts (MMRC) with the action/quality improvement (QI) efforts (PQC), creating a “culture of safety”.
Kansas will enroll in the Alliance for Innovation on Maternal Health (AIM) initiative when ready and implement a safety bundle pilot: Postpartum Discharge Transition, which is currently in development, in partnership with the KPQC and KMMRC (tentatively March-April 2021).• AIM is a national data-driven maternal safety and QI initiative for states and hospitals and partners from
participating states (focus on consistent obstetric practices).• AIM is based on proven implementation approaches to improving maternal safety and outcomes in the
United States.• AIM works through state teams and health systems to align national, state, and hospital level QI efforts to
improve maternal and perinatal health outcomes.• Any state can join AIM as part of a state-level PQC QI efforts/initiatives.
• Access to “Patient Safety Bundles”• Access to “Patient Safety Tools”• Access to “Education and Engagement Tools”• Access to the AIM Community of States
• Fourth Trimester Initiative – KPQC Initiative based on KMMRC findings and recommendations
• The well-woman toolkit – which addresses barriers to care, including provider bias. We are working on developing supplements for the toolkit that would focus specifically on how to reach and serve Hispanic and Non-Hispanic Black women in KS
• Post-birth warning signs campaign and provider training with the Association of Women’s Health, Obstetric and Neonatal Nurses (AWHONN) (and using the CDC’s Hear Her materials)
• Pregnancy intention training (One Key Question) – which includes training on provider bias
DATA to ACTION: When deciding on the AIM bundle that fit our State’s needs best, KDHE worked in coordination with the KMMRC and KPQC to review the data and recommendations from the KMMRC. Most of the pregnancy-related deaths had recommendations involving better communication and collaboration between providers, timely referrals to specialty physicians as well as community providers, and screening for behavioral health conditions, social determinants of health, and pregnancy intentions. The AIM bundle Postpartum Discharge Transition was chosen based on these recommendations because it addresses the majority of our recommendations.
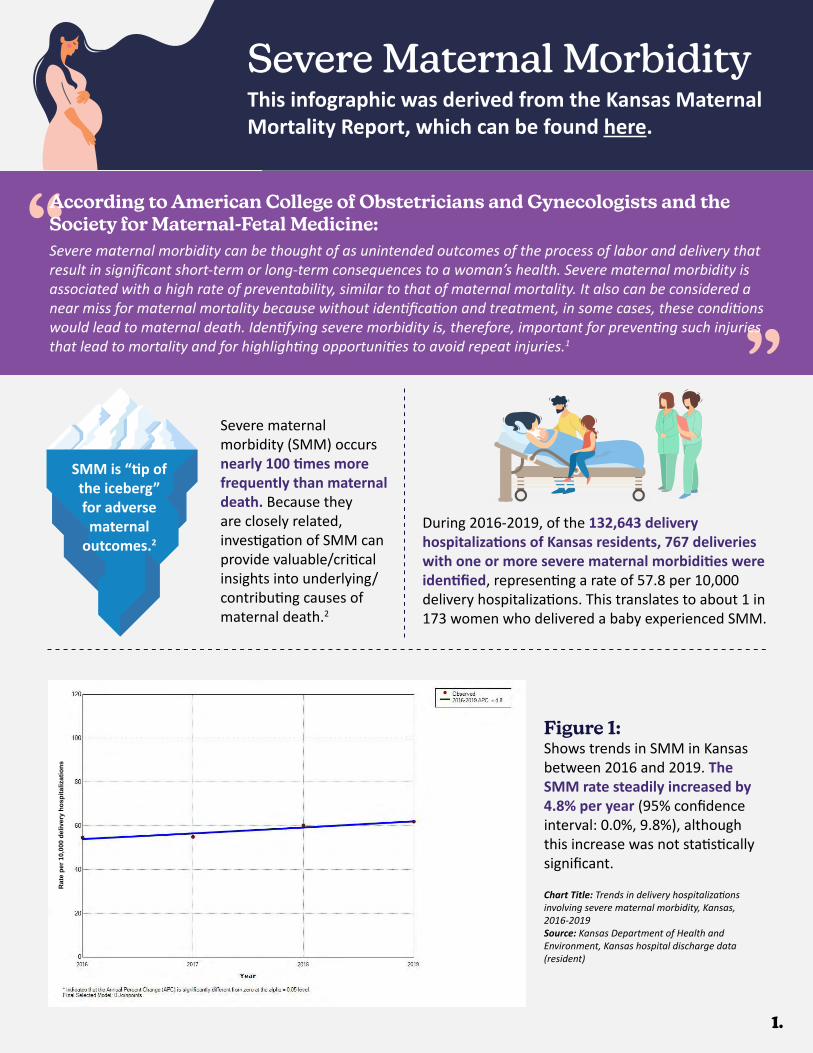
Figure 1:Shows trends in SMM in Kansas between 2016 and 2019. The SMM rate steadily increased by 4.8% per year (95% confidence interval: 0.0%, 9.8%), although this increase was not statistically significant.
SMM is “tip of the iceberg”for adversematernal
outcomes.2
Severe maternal morbidity (SMM) occurs nearly 100 times more frequently than maternal death. Because they are closely related, investigation of SMM can provide valuable/critical insights into underlying/contributing causes of maternal death.2
During 2016-2019, of the 132,643 delivery hospitalizations of Kansas residents, 767 deliveries with one or more severe maternal morbidities were identified, representing a rate of 57.8 per 10,000 delivery hospitalizations. This translates to about 1 in 173 women who delivered a baby experienced SMM.
1.
Severe Maternal MorbidityThis infographic was derived from the Kansas Maternal Mortality Report, which can be found here.
“ “
According to American College of Obstetricians and Gynecologists and the Society for Maternal-Fetal Medicine:Severe maternal morbidity can be thought of as unintended outcomes of the process of labor and delivery that result in significant short-term or long-term consequences to a woman’s health. Severe maternal morbidity is associated with a high rate of preventability, similar to that of maternal mortality. It also can be considered a near miss for maternal mortality because without identification and treatment, in some cases, these conditions would lead to maternal death. Identifying severe morbidity is, therefore, important for preventing such injuries that lead to mortality and for highlighting opportunities to avoid repeat injuries.1
Chart Title: Trends in delivery hospitalizations involving severe maternal morbidity, Kansas, 2016-2019Source: Kansas Department of Health and Environment, Kansas hospital discharge data (resident)
Rat
e pe
r 10,
000
deliv
ery
hosp
italiz
atio
ns
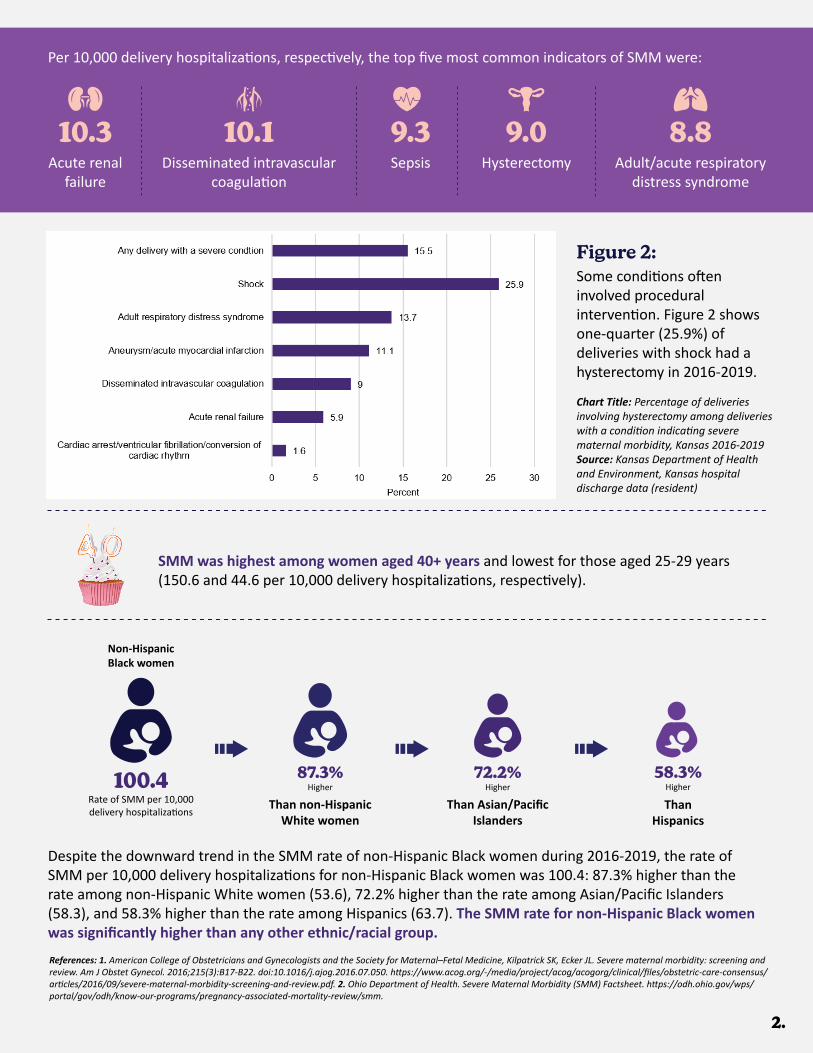
2.
Per 10,000 delivery hospitalizations, respectively, the top five most common indicators of SMM were:
Acute renal failure
Disseminated intravascular coagulation
Sepsis Hysterectomy Adult/acute respiratory distress syndrome
10.3 10.1 9.3 9.0 8.8
Figure 2:
Chart Title: Percentage of deliveries involving hysterectomy among deliveries with a condition indicating severe maternal morbidity, Kansas 2016-2019 Source: Kansas Department of Health and Environment, Kansas hospital discharge data (resident)
SMM was highest among women aged 40+ years and lowest for those aged 25-29 years (150.6 and 44.6 per 10,000 delivery hospitalizations, respectively).
Non-Hispanic Black women
100.4Rate of SMM per 10,000delivery hospitalizations
58.3%Higher
ThanHispanics
72.2%Higher
Than Asian/PacificIslanders
87.3%Higher
Than non-HispanicWhite women
References: 1. American College of Obstetricians and Gynecologists and the Society for Maternal–Fetal Medicine, Kilpatrick SK, Ecker JL. Severe maternal morbidity: screening and review. Am J Obstet Gynecol. 2016;215(3):B17-B22. doi:10.1016/j.ajog.2016.07.050. https://www.acog.org/-/media/project/acog/acogorg/clinical/files/obstetric-care-consensus/articles/2016/09/severe-maternal-morbidity-screening-and-review.pdf. 2. Ohio Department of Health. Severe Maternal Morbidity (SMM) Factsheet. https://odh.ohio.gov/wps/portal/gov/odh/know-our-programs/pregnancy-associated-mortality-review/smm.
Some conditions often involved procedural intervention. Figure 2 shows one-quarter (25.9%) of deliveries with shock had a hysterectomy in 2016-2019.
Despite the downward trend in the SMM rate of non-Hispanic Black women during 2016-2019, the rate of SMM per 10,000 delivery hospitalizations for non-Hispanic Black women was 100.4: 87.3% higher than the rate among non-Hispanic White women (53.6), 72.2% higher than the rate among Asian/Pacific Islanders (58.3), and 58.3% higher than the rate among Hispanics (63.7). The SMM rate for non-Hispanic Black women was significantly higher than any other ethnic/racial group.
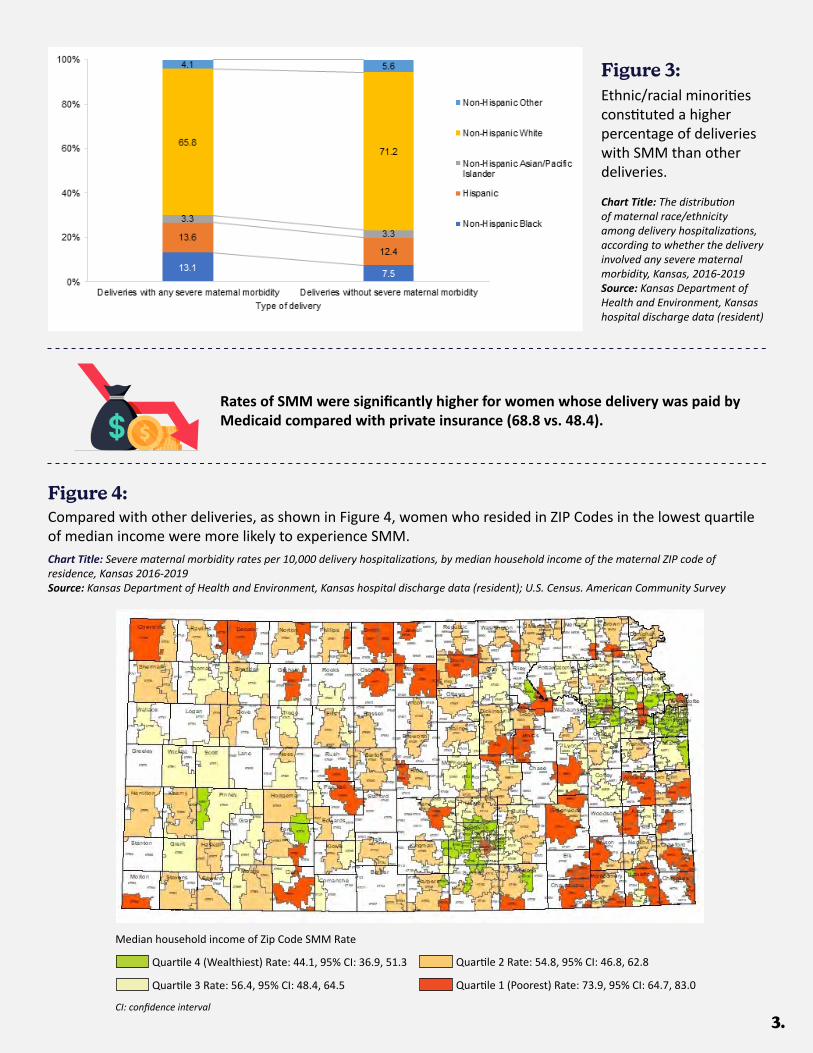
3.
Figure 3:Ethnic/racial minorities constituted a higher percentage of deliveries with SMM than other deliveries.
Figure 4:Compared with other deliveries, as shown in Figure 4, women who resided in ZIP Codes in the lowest quartile of median income were more likely to experience SMM.
Rates of SMM were significantly higher for women whose delivery was paid by Medicaid compared with private insurance (68.8 vs. 48.4).
Chart Title: The distribution of maternal race/ethnicity among delivery hospitalizations, according to whether the delivery involved any severe maternal morbidity, Kansas, 2016-2019Source: Kansas Department of Health and Environment, Kansas hospital discharge data (resident)
Chart Title: Severe maternal morbidity rates per 10,000 delivery hospitalizations, by median household income of the maternal ZIP code of residence, Kansas 2016-2019Source: Kansas Department of Health and Environment, Kansas hospital discharge data (resident); U.S. Census. American Community Survey
Median household income of Zip Code SMM Rate
Quartile 4 (Wealthiest) Rate: 44.1, 95% CI: 36.9, 51.3
Quartile 3 Rate: 56.4, 95% CI: 48.4, 64.5
Quartile 2 Rate: 54.8, 95% CI: 46.8, 62.8
Quartile 1 (Poorest) Rate: 73.9, 95% CI: 64.7, 83.0
CI: confidence interval
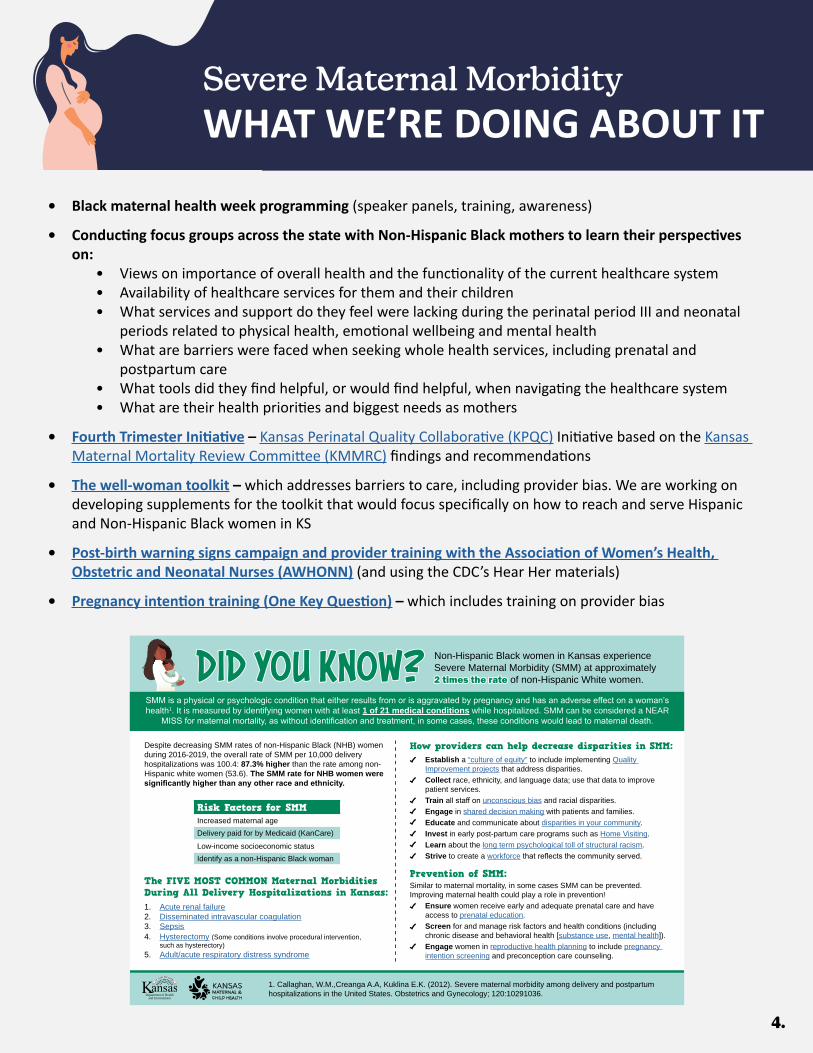
4.
• Black maternal health week programming (speaker panels, training, awareness)
• Conducting focus groups across the state with Non-Hispanic Black mothers to learn their perspectives on:
• Views on importance of overall health and the functionality of the current healthcare system• Availability of healthcare services for them and their children• What services and support do they feel were lacking during the perinatal period III and neonatal
periods related to physical health, emotional wellbeing and mental health• What are barriers were faced when seeking whole health services, including prenatal and
postpartum care• What tools did they find helpful, or would find helpful, when navigating the healthcare system• What are their health priorities and biggest needs as mothers
• Fourth Trimester Initiative – Kansas Perinatal Quality Collaborative (KPQC) Initiative based on the Kansas Maternal Mortality Review Committee (KMMRC) findings and recommendations
• The well-woman toolkit – which addresses barriers to care, including provider bias. We are working on developing supplements for the toolkit that would focus specifically on how to reach and serve Hispanic and Non-Hispanic Black women in KS
• Post-birth warning signs campaign and provider training with the Association of Women’s Health, Obstetric and Neonatal Nurses (AWHONN) (and using the CDC’s Hear Her materials)
• Pregnancy intention training (One Key Question) – which includes training on provider bias
WHAT WE’RE DOING ABOUT ITSevere Maternal Morbidity
DID YOU KNOW?DID YOU KNOW?
Department of Healthand Environment
Non-Hispanic Black women in Kansas experience Severe Maternal Morbidity (SMM) at approximately 2 times the rate2 times the rate of non-Hispanic White women.
SMM is a physical or psychologic condition that either results from or is aggravated by pregnancy and has an adverse effect on a woman’s health1. It is measured by identifying women with at least 1 of 21 medical conditions while hospitalized. SMM can be considered a NEAR
MISS for maternal mortality, as without identification and treatment, in some cases, these conditions would lead to maternal death.
Despite decreasing SMM rates of non-Hispanic Black (NHB) women during 2016-2019, the overall rate of SMM per 10,000 delivery hospitalizations was 100.4: 87.3% higher than the rate among non-Hispanic white women (53.6). The SMM rate for NHB women were significantly higher than any other race and ethnicity.
The FIVE MOST COMMON Maternal Morbidities During All Delivery Hospitalizations in Kansas: 1. Acute renal failure2. Disseminated intravascular coagulation3. Sepsis4. Hysterectomy (Some conditions involve procedural intervention,
such as hysterectory)5. Adult/acute respiratory distress syndrome
How providers can help decrease disparities in SMM:• Establish a “culture of equity” to include implementing Quality
Improvement projects that address disparities.• Collect race, ethnicity, and language data; use that data to improve
patient services.• Train all staff on unconscious bias and racial disparities.• Engage in shared decision making with patients and families.• Educate and communicate about disparities in your community.• Invest in early post-partum care programs such as Home Visiting.• Learn about the long term psychological toll of structural racism.• Strive to create a workforce that reflects the community served.
Prevention of SMM: Similar to maternal mortality, in some cases SMM can be prevented. Improving maternal health could play a role in prevention!• Ensure women receive early and adequate prenatal care and have
access to prenatal education.• Screen for and manage risk factors and health conditions (including
chronic disease and behavioral health [substance use, mental health]).• Engage women in reproductive health planning to include pregnancy
intention screening and preconception care counseling.
1. Callaghan, W.M.,Creanga A.A, Kuklina E.K. (2012). Severe maternal morbidity among delivery and postpartum hospitalizations in the United States. Obstetrics and Gynecology; 120:10291036.
Risk Factors for SMMIncreased maternal ageDelivery paid for by Medicaid (KanCare)Low-income socioeconomic statusIdentify as a non-Hispanic Black woman
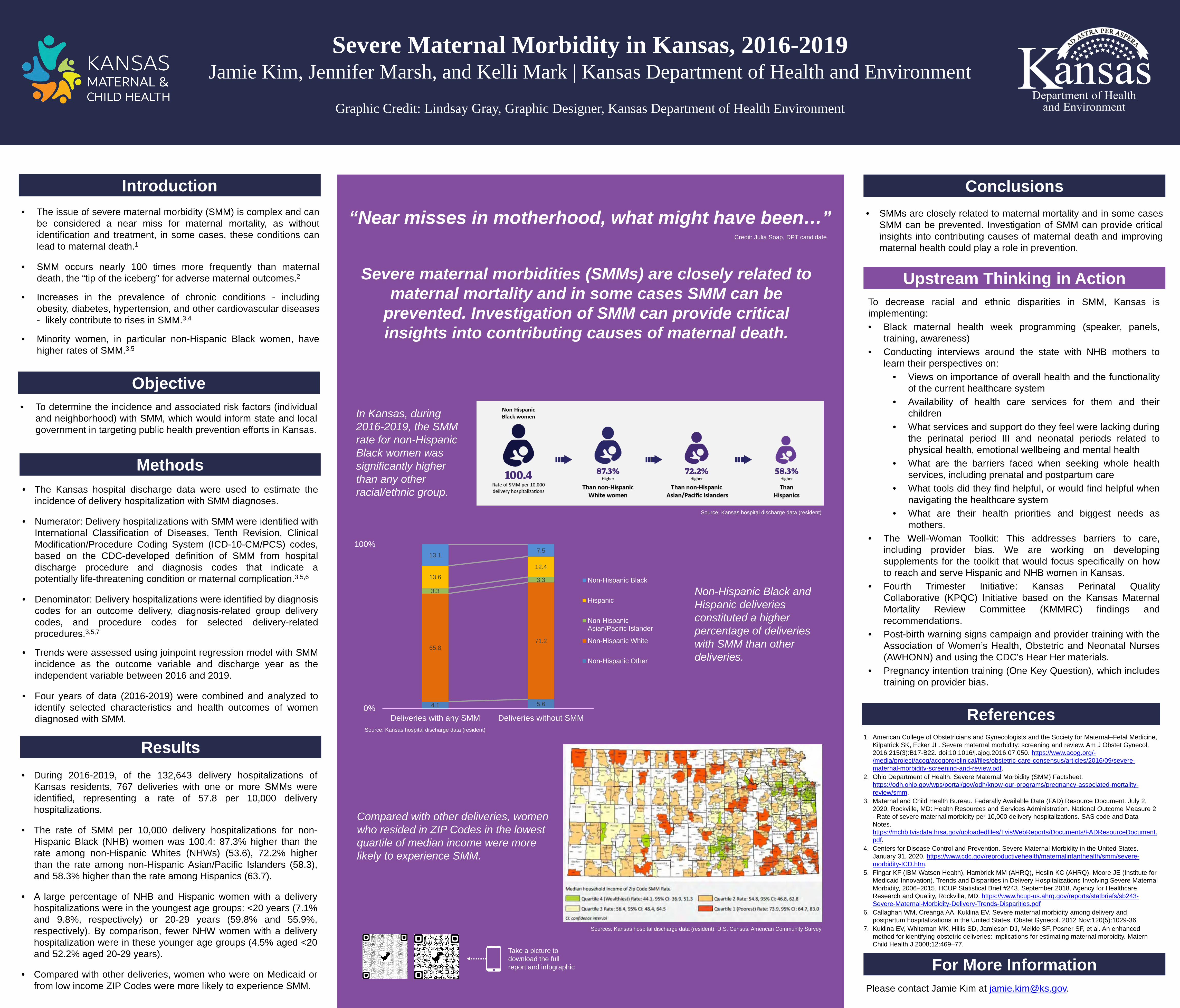
Severe Maternal Morbidity in Kansas, 2016-2019 Jamie Kim, Jennifer Marsh, and Kelli Mark | Kansas Department of Health and Environment
Graphic Credit: Lindsay Gray, Graphic Designer, Kansas Department of Health Environment
• The issue of severe maternal morbidity (SMM) is complex and canbe considered a near miss for maternal mortality, as withoutidentification and treatment, in some cases, these conditions canlead to maternal death.1
• SMM occurs nearly 100 times more frequently than maternaldeath, the “tip of the iceberg” for adverse maternal outcomes.2
• Increases in the prevalence of chronic conditions - includingobesity, diabetes, hypertension, and other cardiovascular diseases- likely contribute to rises in SMM.3,4
• Minority women, in particular non-Hispanic Black women, havehigher rates of SMM.3,5
Introduction
Objective• To determine the incidence and associated risk factors (individual
and neighborhood) with SMM, which would inform state and localgovernment in targeting public health prevention efforts in Kansas.
Methods
• SMMs are closely related to maternal mortality and in some casesSMM can be prevented. Investigation of SMM can provide criticalinsights into contributing causes of maternal death and improvingmaternal health could play a role in prevention.
• The Kansas hospital discharge data were used to estimate theincidence of delivery hospitalization with SMM diagnoses.
• Numerator: Delivery hospitalizations with SMM were identified withInternational Classification of Diseases, Tenth Revision, ClinicalModification/Procedure Coding System (ICD-10-CM/PCS) codes,based on the CDC-developed definition of SMM from hospitaldischarge procedure and diagnosis codes that indicate apotentially life-threatening condition or maternal complication.3,5,6
• Denominator: Delivery hospitalizations were identified by diagnosiscodes for an outcome delivery, diagnosis-related group deliverycodes, and procedure codes for selected delivery-relatedprocedures.3,5,7
• Trends were assessed using joinpoint regression model with SMMincidence as the outcome variable and discharge year as theindependent variable between 2016 and 2019.
• Four years of data (2016-2019) were combined and analyzed toidentify selected characteristics and health outcomes of womendiagnosed with SMM.
To decrease racial and ethnic disparities in SMM, Kansas isimplementing:• Black maternal health week programming (speaker, panels,
training, awareness)• Conducting interviews around the state with NHB mothers to
learn their perspectives on:• Views on importance of overall health and the functionality
of the current healthcare system• Availability of health care services for them and their
children• What services and support do they feel were lacking during
the perinatal period III and neonatal periods related tophysical health, emotional wellbeing and mental health
• What are the barriers faced when seeking whole healthservices, including prenatal and postpartum care
• What tools did they find helpful, or would find helpful whennavigating the healthcare system
• What are their health priorities and biggest needs asmothers.
• The Well-Woman Toolkit: This addresses barriers to care,including provider bias. We are working on developingsupplements for the toolkit that would focus specifically on howto reach and serve Hispanic and NHB women in Kansas.
• Fourth Trimester Initiative: Kansas Perinatal QualityCollaborative (KPQC) Initiative based on the Kansas MaternalMortality Review Committee (KMMRC) findings andrecommendations.
• Post-birth warning signs campaign and provider training with theAssociation of Women’s Health, Obstetric and Neonatal Nurses(AWHONN) and using the CDC’s Hear Her materials.
• Pregnancy intention training (One Key Question), which includestraining on provider bias.
Conclusions
Upstream Thinking in Action
“Near misses in motherhood, what might have been…”
In Kansas, during 2016-2019, the SMM rate for non-Hispanic Black women was significantly higher than any other racial/ethnic group.
Severe maternal morbidities (SMMs) are closely related to maternal mortality and in some cases SMM can be
prevented. Investigation of SMM can provide critical insights into contributing causes of maternal death.
Results• During 2016-2019, of the 132,643 delivery hospitalizations of
Kansas residents, 767 deliveries with one or more SMMs wereidentified, representing a rate of 57.8 per 10,000 deliveryhospitalizations.
• The rate of SMM per 10,000 delivery hospitalizations for non-Hispanic Black (NHB) women was 100.4: 87.3% higher than therate among non-Hispanic Whites (NHWs) (53.6), 72.2% higherthan the rate among non-Hispanic Asian/Pacific Islanders (58.3),and 58.3% higher than the rate among Hispanics (63.7).
• A large percentage of NHB and Hispanic women with a deliveryhospitalizations were in the youngest age groups: <20 years (7.1%and 9.8%, respectively) or 20-29 years (59.8% and 55.9%,respectively). By comparison, fewer NHW women with a deliveryhospitalization were in these younger age groups (4.5% aged <20and 52.2% aged 20-29 years).
• Compared with other deliveries, women who were on Medicaid orfrom low income ZIP Codes were more likely to experience SMM.
Non-Hispanic Black and Hispanic deliveries constituted a higher percentage of deliveries with SMM than other deliveries.
4.1 5.6
65.871.2
3.3
3.313.612.4
13.17.5
0%
100%
Deliveries with any SMM Deliveries without SMM
Non-Hispanic Black
Hispanic
Non-HispanicAsian/Pacific Islander
Non-Hispanic White
Non-Hispanic Other
References1. American College of Obstetricians and Gynecologists and the Society for Maternal–Fetal Medicine,
Kilpatrick SK, Ecker JL. Severe maternal morbidity: screening and review. Am J Obstet Gynecol. 2016;215(3):B17-B22. doi:10.1016/j.ajog.2016.07.050. https://www.acog.org/-/media/project/acog/acogorg/clinical/files/obstetric-care-consensus/articles/2016/09/severe-maternal-morbidity-screening-and-review.pdf.
2. Ohio Department of Health. Severe Maternal Morbidity (SMM) Factsheet. https://odh.ohio.gov/wps/portal/gov/odh/know-our-programs/pregnancy-associated-mortality-review/smm.
3. Maternal and Child Health Bureau. Federally Available Data (FAD) Resource Document. July 2, 2020; Rockville, MD: Health Resources and Services Administration. National Outcome Measure 2 - Rate of severe maternal morbidity per 10,000 delivery hospitalizations. SAS code and Data Notes. https://mchb.tvisdata.hrsa.gov/uploadedfiles/TvisWebReports/Documents/FADResourceDocument.pdf.
4. Centers for Disease Control and Prevention. Severe Maternal Morbidity in the United States. January 31, 2020. https://www.cdc.gov/reproductivehealth/maternalinfanthealth/smm/severe-morbidity-ICD.htm.
5. Fingar KF (IBM Watson Health), Hambrick MM (AHRQ), Heslin KC (AHRQ), Moore JE (Institute for Medicaid Innovation). Trends and Disparities in Delivery Hospitalizations Involving Severe Maternal Morbidity, 2006–2015. HCUP Statistical Brief #243. September 2018. Agency for Healthcare Research and Quality, Rockville, MD. https://www.hcup-us.ahrq.gov/reports/statbriefs/sb243-Severe-Maternal-Morbidity-Delivery-Trends-Disparities.pdf
6. Callaghan WM, Creanga AA, Kuklina EV. Severe maternal morbidity among delivery and postpartum hospitalizations in the United States. Obstet Gynecol. 2012 Nov;120(5):1029-36.
7. Kuklina EV, Whiteman MK, Hillis SD, Jamieson DJ, Meikle SF, Posner SF, et al. An enhanced method for identifying obstetric deliveries: implications for estimating maternal morbidity. Matern Child Health J 2008;12:469–77.
Take a picture to download the full report and infographic
Compared with other deliveries, women who resided in ZIP Codes in the lowest quartile of median income were more likely to experience SMM.
For More InformationPlease contact Jamie Kim at [email protected].
Credit: Julia Soap, DPT candidate
Source: Kansas hospital discharge data (resident)
Source: Kansas hospital discharge data (resident)
Sources: Kansas hospital discharge data (resident); U.S. Census. American Community Survey
KANSAS MATERNAL MORTALITY REVIEW COMMITTEE (KMMRC) MEMBER ROSTER
Kansas Department of Health and Environment (KDHE) Leadership & Staff Farah Ahmed, MPH PhD
Ashley Goss, MBA Nadyne Hagmeier Kay Haug Jamie Kim, MPH Jennifer Marsh Jill Nelson Kasey Sorell, MBA BSN RN CPC Rachel Sisson, MS Stephanie Wolf, RN BSN
*Chair **Co-Chair
Senior Vice President of Healthcare Strategy and Policy, KS Hospital Association Nurture KC OB/GYN, Saint Luke's Women’s Health South Director of Cradle Kansas City–an initiative of the Community Health Council of WY County Wichita Birth Assistance Maternal Health Program Manager, United Health Care Clinical Education Specialist, Saint Luke’s Northland Hospital Topeka Police Department Deputy Director, Wyandotte County/KC KS Unified Government Public Health Department Assistant Professor, Maternal-Fetal Medicine, Center for Advanced Fetal Care, KUMC Policy Analyst, Kansas Department of Health and Environment, Division of Health Care Finance Clinical Coordinator, Women’s Recovery Center & Options Adult Services – DCCCA, Inc. Baker University School of Nursing/Stormont Vail Hospital Health Kansas Department for Children & Families Director of Maternal Child Services & Behavioral Health Services, St. Catherine Hospital–Centura Health Director of Reintegration, Saint Francis Ministries Overland Park Police Department, Criminal Investigations Division-Special Victims Unit McCann Professor & Associate Dean for Rural Health Education, Assistant Dean and Director of Major Academic Society, Professor, Family Medicine – University of Kansas School of Medicine OB/GYN, KU Medical Center Bloom Midwifery & Lactation Services Director of Maternal Infant Health, March of Dimes Association of Community Mental Health Centers of Kansas, Inc. Professor & Chair, Department of Anesthesiology, KU School of Medicine—Wichita OB/GYN, Associates in Women’s Health, PA Director of Advocacy, Education & Rural Projects, KS Coalition Against Sexual & Domestic Violence Assistant Director, Transport & EMS Relations–Critical Care Transport, Children’s Mercy Hospital Assistant Professor KUMC Department of Preventative Medicine & Public Health Flint Hills OB/GYN—Junction City Professor, Maternal Fetal Medicine, Department of OB/GYN, University of Missouri Kansas City Patient/Consumer
Environmental Health Officer & State Epidemiologist, KDHE Deputy Secretary for Public Health, KDHE Abstractor for Maternal Mortality Review Committee, Kansas Foundation for Medical Care Director, Office of Vital Statistics; Assistant State Registrar, KDHE MCH Epidemiologist, Bureau of Family Health, KDHE Women & Maternal Health Consultant, Bureau of Family Health, KDHE Perinatal & Infant Health Consultant, Bureau of Family Health, KDHE Health Planning Consultant/KMMRC Coordinator, Bureau of Family Health, KDHE Director, Bureau of Family Health, KDHE; Kansas Title V Maternal & Child Health Director Perinatal & Infant Consultant/Nurse, Bureau of Family Health, KDHE
Rev. 12/01/2020
Karen Braman, RPh, MS Katherine Campbell, BSN RN Tara Chettiar, MD FACOG Mariah Chrans, IBCLC, PhD Deidre DeGrado, CPM Mary Sunshine-Delgado, MSN APRN Kim Dishman Donna Eubanks SGT Terrie Garrison, RN, BSN *Charles Gibbs, MD Lisa Goins, RN Donna Gorman, MS LCMFT LCAC Jeri Harvey, MSN CNL Caroline Hastings, LMSW Renee Hulett, RN MSN MHA Candace Johnson, LMSW Erin Johnson Michael Kennedy, MD Kelli Krase, MD Melinda Lavon, PhD IBCLC Elizabeth Lewis, MPA MSN WHNP-BC BSN RN Lori Marshall, LSCSW Robert S. F. McKay, MD **Randall Morgan, MD Kathy Ray, MSW Heather Scruton, MBA MSN Sharla Smith, PhD MPH Terrah Stroda, CNM John Yeast, MD MSPH Diana Zumbrunn

Family Planning Life Plan
A workbook to assist women with family planning and identifying pregnancy intentions and desires.
My Life, My GoalsFamily Planning Life Plan
A workbook to help you decide if and when to have the
healthiest pregnancy possible.
This workbook was developed through a partnership between The Kansas Department of Health and Environment, Cradle Kansas City, Vibrant Health, The Unified Government of Wyandotte County Public Health Department and March of Dimes. Review, feedback and editing was provided by the Cradle Kansas City Community Action Board. The workbook was piloted and tested by community members in Wyandotte County. The following page features a letter that was developed and written by the Cradle Kansas City Community Action Board as an introduction of the workbook to the Wyandotte County Community.
*The original workbook has been adapted for statewide use by the Kansas Department of Health and Environment and Cradle Kansas City. Funding for this project was provided by the March of Dimes.
Making choices for your life is hard. We get it, we are right there with you. If you don’t know what your future plans are, that is OK. Things change, life happens, and we can’t plan for everything. But if we have an idea of what WE WANT it is so much easier to obtain those goals.
The goal of this booklet is to help you have a conversation about your plan for the next year. A plan that you want to make as a couple or just for yourself. Part of that plan, is about whether or not you want to get pregnant this year.
What is something about yourself you are proud of?
What type of work do you like to do?
What parts of your life bring you the most joy?
What parts of your life would you like to change?
What are some of your goals for this year?
All about you, the veryremarkable you
4
Choose three positive wordsthat describe you best
I am...___________________________________________________
&
___________________________________________________
5
“Proper spacing
between children
helps your body
rebuild sufficient
nutrients”
- Maude
“Proper planning
could offer a
healthier birth
outcome”- Emily
6
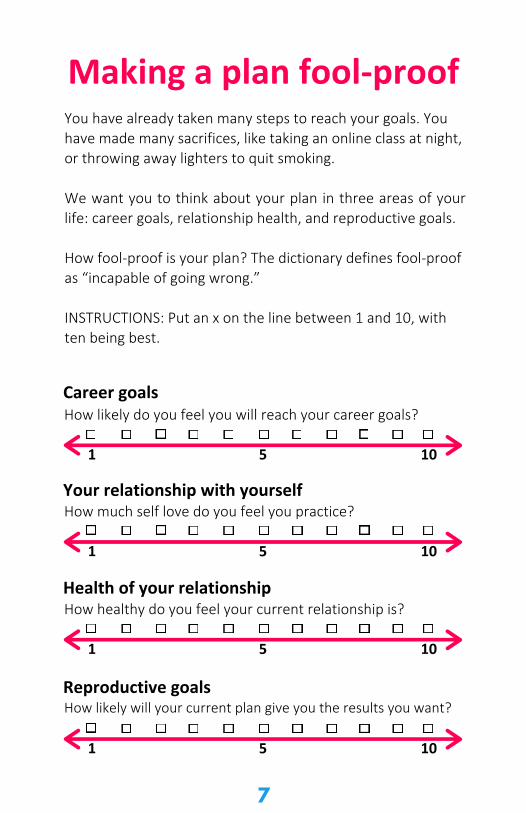
Making a plan fool-proofYou have already taken many steps to reach your goals. You have made many sacrifices, like taking an online class at night, or throwing away lighters to quit smoking.
We want you to think about your plan in three areas of your life: career goals, relationship health, and reproductive goals.
How fool-proof is your plan? The dictionary defines fool-proof as “incapable of going wrong.”
INSTRUCTIONS: Put an x on the line between 1 and 10, with ten being best.
Career goalsHow likely do you feel you will reach your career goals?
5 101
How much self love do you feel you practice?Your relationship with yourself
5 101
How healthy do you feel your current relationship is?Health of your relationship
5 101
Reproductive goalsHow likely will your current plan give you the results you want?
5 101
7
Let's reflect for a minuteWould becoming pregnant this year change
your plans or goals?
8
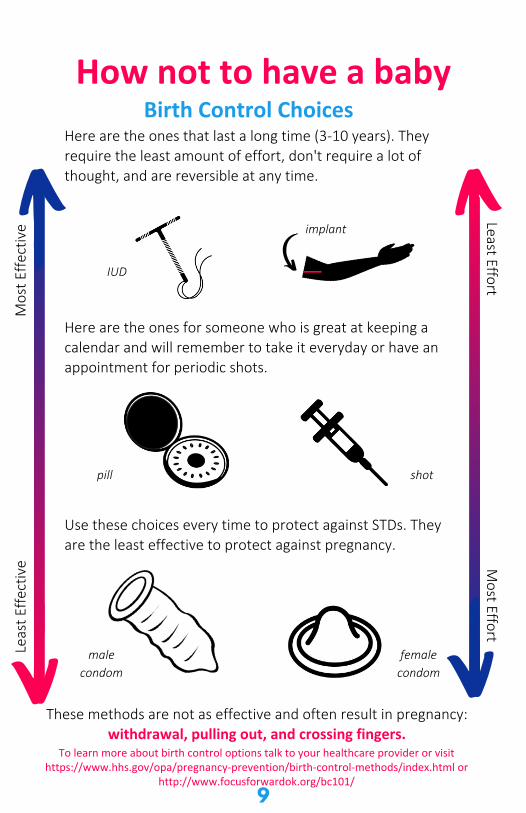
How not to have a baby
Here are the ones for someone who is great at keeping a calendar and will remember to take it everyday or have an appointment for periodic shots.
Use these choices every time to protect against STDs. Theyare the least effective to protect against pregnancy.
These methods are not as effective and often result in pregnancy: withdrawal, pulling out, and crossing fingers.
implant
IUD
pill shot
malecondom
femalecondom
Birth Control ChoicesHere are the ones that last a long time (3-10 years). They require the least amount of effort, don't require a lot of thought, and are reversible at any time.
Mos
t Effe
ctiv
eLe
ast E
ffect
ive
Least EffortM
ost Effort
9
To learn more about birth control options talk to your healthcare provider or visit https://www.hhs.gov/opa/pregnancy-prevention/birth-control-methods/index.html or
http://www.focusforwardok.org/bc101/
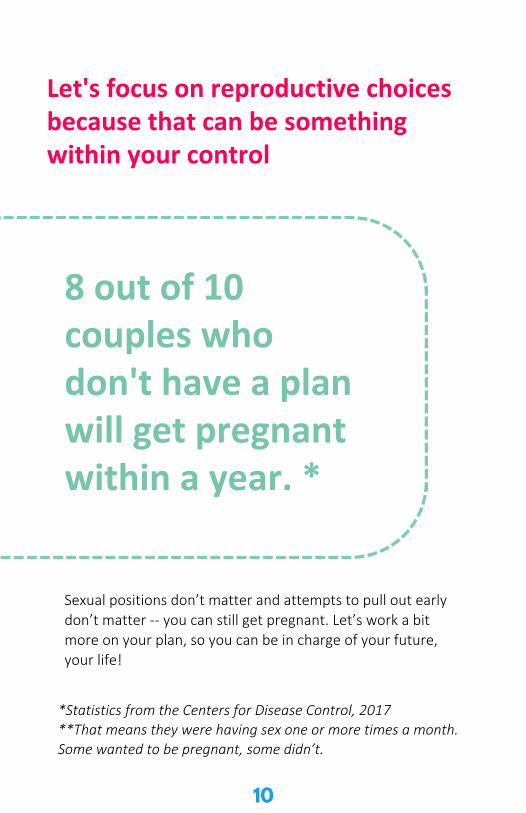
Let's focus on reproductive choices because that can be something within your control
Sexual positions don’t matter and attempts to pull out earlydon’t matter -- you can still get pregnant. Let’s work a bitmore on your plan, so you can be in charge of your future,your life!
8 out of 10couples whodon't have a planwill get pregnantwithin a year. *
*Statistics from the Centers for Disease Control, 2017**That means they were having sex one or more times a month.Some wanted to be pregnant, some didn’t.
10
Important Questions
Here's a space to jot down yourquestions and concerns.
11
Develop Your Plan
12
Do I plan to become pregnant within thenext year?
Yes, I plan to get pregnant within the next year so I will:
__________________________________________________ __________________________________________________
No, I do not plan to get pregnant within the next year so I will: __________________________________________________ __________________________________________________
I'm unsure if I want to get pregnant within the next year so I will: _________________________________________________
I'm okay either way so within the next year I will: ____________
______________________________________ __________________________________________________ To find a reproductive healthcare provider near you visit https://opa-fpclinicdb.hhs.gov/.
My Next Steps
Let's revisit your plan from page 7
After working through this booklet, would your plan stay the same or would it change?
Your plan is unique to you. You can change it any time based on how you feel, what you want, and when you want to reach your goals.
For myself this month I will do:
__________________________________________________
For my health this month I will do:
__________________________________________________
For my relationship this month I will do:
__________________________________________________
And my plan to get pregnant or not pregnant is:
__________________________________________________
13
Notes
ReflectionsHere's a space to work on yourthoughts and concerns.
and
14
Loving YourselfLet's revisit your relationship with yourself.
How much self love do you feel you practice?Health of your relationships with yourself
5 101
What is a healthy choice you have made foryourself this month? How did it make you feel?
Think about the following questions:
How likely will your current plan give you the results you want?
5 101
Thinking about the past week, how stressed were you?
5 101
What would you like that number to be?What one thing could you do to lower that number
this week?
INSTRUCTIONS: Put an x on the line between 1 and 10, with10 being best, to indicate how you feel about each question.
15
Inner health is how you feel about yourself, your relationshipsand your purpose in life. It does not mean that you will never besad or angry. Everyone will have highs and lows in life. However,
when you feel good about yourself you will be able to bounceback from sad times faster.
Here are some ways to feel good about yourself.
Love Yourself
Value who you are and what you do:
Take care of your bodyThink positivelyMake time for activities that you enjoy and that are important to youFind your strength and what makes you feel special Learn about yourself and what makes you happy or sadDecide what you want from lifeSet goals and find ways to reach themRemember, it's okay to ask for help Learn positive ways to deal with stress, such as exercise and reading
Connect with OthersBe safe in relationships Spend time with people who respect and value youSpend time with people that care and support you Help others in needThink of others and how they feelBe open to others who are different than you
For free helpCrisis TextLine: Text HOME to 741741
National Suicide Prevention Hotline: 1-800-273-8255Teen Dating Violence Hotline: Text LOVE IS to 1-866-331-9474National Sexual Assualt Hotline: 1-800-656-4673 or rainn.org
16
Health of Your RelationshipINSTRUCTIONS: Put an x on the line between 1 and 10, with
10 being best, to indicate how you feel about each questions.
How healthy do you feel your current relationship is?Health of your relationship
5 101
Take a minute to reflect on your current relationshipList the three best things about your relationship:
1.2.3.How do these make you feel?
List the three hardest things about your relationship.
1.2.3.How do these make you feel?
What one thing could you do to change this?
What one thing could your partner change do to change this?
17
Staying healthy is an everyday habit.
Think about the questions below and ask yourself:
Do I...
Get 30 minutes of physical activity everyday?See a dentist once a year and brush/floss my teeth twice a day?Get a health check-up once a year?Know my family's medical history?Have a safe place to go to, or to stay at?Have a plan to stay tobacco free?Get 6-8 hours of sleep every night?Eat fresh fruits and vegetables every day?Take a vitamin with folic acid every day?Get tested for HIV/AIDS and other Sexually Transmitted Diseases (STDs)?
If you answered yes to most of these questions you are on theroad to a healthy lifestyle.
My Next StepsIf you are planning to become pregnant, or are OK either way,now is a great time to start taking a multivitamin with folic acidonce a day.
18
Whether or not you are planning on having a familysomeday, some habits can be harmful to your overall health.
Do I...Use tobacco products?Vape or use a hookah?Drink alcohol ?Binge drink (have 4 or more alcoholic drinks at one time?Use drugs?Use medications that aren't prescribed for you?Often eat too little or too much?Go more than a week without exercise?Go to bed hungry?Feel safe at home?Have sex with more than one partner?Have sex when I do not want to?
Now may be a good time to talk with a healthcare provider about how to make changes to be healthier and feel your best.
My Next StepsTalk to a healthcare provider to reduce your health risks. Smoking or using nicotine products (including vaping or hookah), drinking alcohol, and using drugs can be harmful to your body. These substances can be very risky for a pregnancy, too. These risks can include: birth defects, brain damage, low birth weight, and prematurity. If you are looking to quit visit kanquit.org for resources.
Think sbout the questions below and ask yourself:
19
Chronic diseases, like diabetes or obesity, can have serious effects on your health. You can help change that! If you have chronic health conditions, visit with a healthcare provider regularly and follow their guidance for managing your chronic condition. Ask your healthcare provider for referrals to specialists that can help like nutritionists or counselors.
If you have a chronic condition, such as those listed below, talk with your healthcare provider to manage them safely during pregnancy.
Do I have:High blood pressureSTDs (Sexually Transmitted Diseases such as genital wartsor herpes)DiabetesHIV/AIDSAsthma Obesity Thyroid conditions SeizuresDepression or anxiety
My Next StepsIt's important to continue your medications when you become pregnant. Discussing your reproductive life plans with a health care provider can ensure you are taking the right medication for you while you are pregnant. Never stop taking medication without talking with a healthcare provider first.
Stay on top of your health by visitinga healthcare provider regularly
20
Immunizations or vaccines can help you from getting certain diseases
Make sure your vaccinations are up-to-date. Some of the most common vaccinations are listed below.
VaccinesMeasles, Mumps, RubellaHepatitis BVaricella (chicken pox) TDaP (Tetanus, Diphtheria, and Pertussis) HPV (Human Papilloma Virus) if you are 27 or youngerMeningitisInfluenza (Flu)
My Next StepsAre your vaccines up to date? Do you have access to your vaccine record? If you are unsure, contact your primary care provider and ask for your vaccination record. If you are in school they may also have a record on file they can provide.
To find out what vaccinations are right for you, check out the Centers for Disease Control and Prevention (CDC) website then talk to a healthcare provider. www.cdc.gov/features/adultimmunizations/index.html
It is important to follow CDC guidelines for vaccinations. Some vaccines have multiple doses and must be given at specific times to be effective. You can find the CDC vaccine guidelines here www.cdc.gov/vaccines/schedules.
Did you know you can get vaccines at your local health department?
21
Here are a few steps you can take to ensure you arehealthy now and in the future:
I will exercise at least 30 minutes per day, 5 or more days a week (www.getupanddosomething.org has great tips to get you started)I will do my best to eat healthy (www.myplate.gov offers great ideas for healthy eating) I will take a multivitamin with folic acid every day I will talk to my healthcare provider about my reproductive life planI will talk to my healthcare provider about the health problems that could hurt me in the future - especially if I get pregnant - such as asthma, high blood pressure, diabetes, and infectionsI will ask my parents and other family members about their own health and what problems I could inherit from them. I will be especially sure to ask if there have been any babies born too small or too soon in my family. I will get help if I feel anxious, depressed or like hurting myself (Crisis TextLine: Text HOME to 741741 or ask your health care provider for help). I will make a promise to myself to be healthy because it will make me feel good about myself.
These will help me have the best chance of having ahealthy baby when I think the time is right.
22
Notes
Reflectionsand
2323
Notes
Reflectionsand
2324
Notes
Reflectionsand
2325
Notes
Reflectionsand
2326
Department of Health and Environment
��I:. KANSAS M-• ... Al MATERNAL & •Jl"'9' CHILD HEALTH
VI BRAN Thea Ith jj il=i ii 133@¼♦
Public Health Prevent. Promote. Protect.
MARCH OF DIMES
CHC Community Health Counc1l of Wyandotte County
Kansas Perinatal Quality
Collaborative (KPQC)
Outlines initiatives and activities led by the KPQC.
SECTION CONTENTS
• KPQC Overview ........................................................................................................ 80 • Fourth Trimester Initiative Overview ...................................................................... 81 • Maternal Warning Signs Initiative Kickoff Webinar .............................................. 82

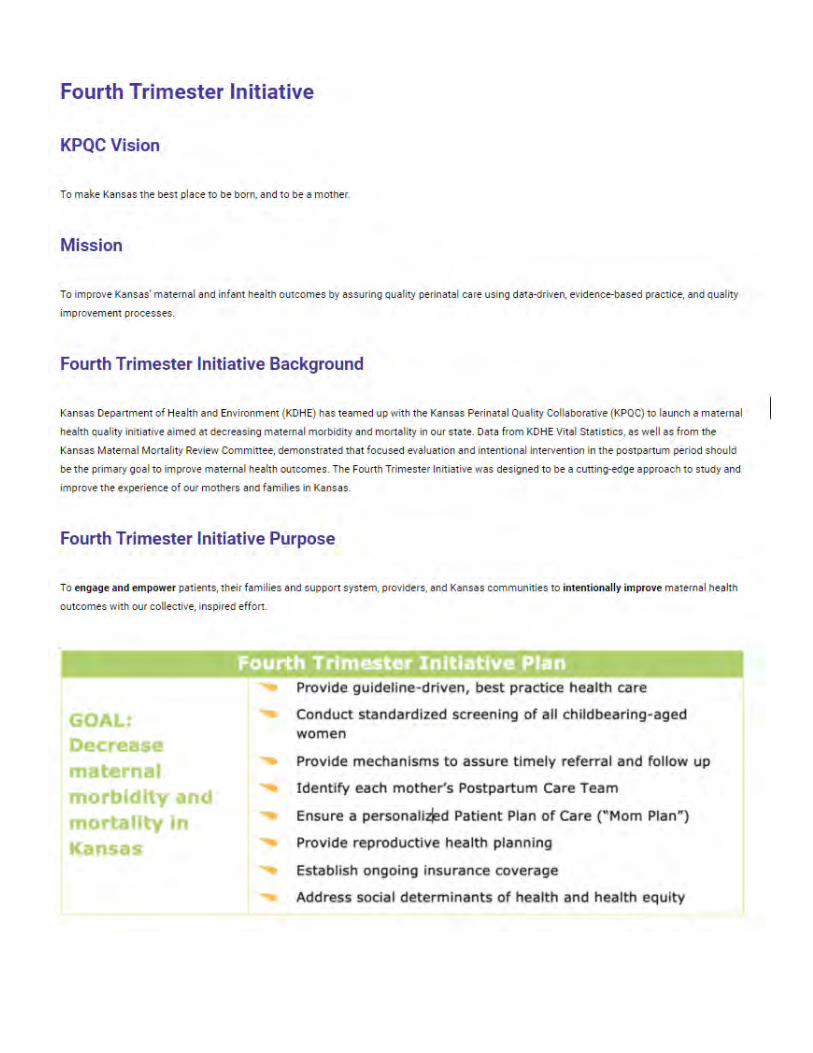
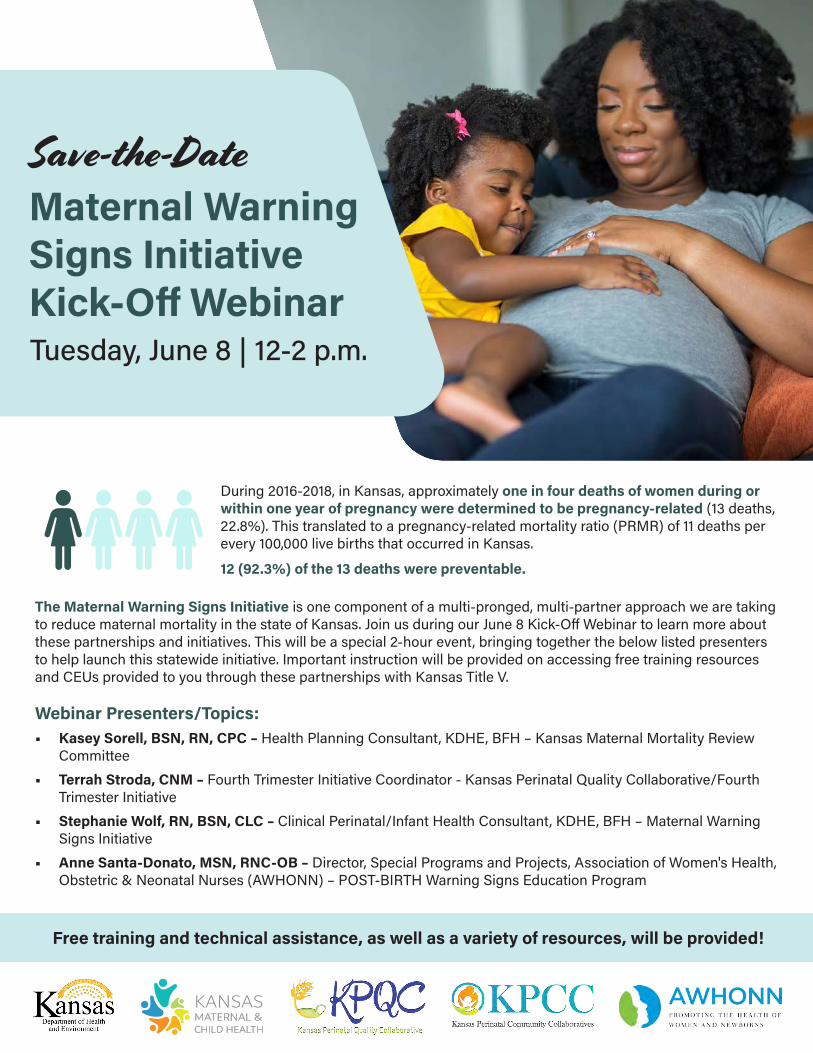
Tuesday, June 8 | 12-2 p.m.
Save-the-DateMaternal Warning Signs Initiative Kick-Off Webinar
Free training and technical assistance, as well as a variety of resources, will be provided!
During 2016-2018, in Kansas, approximately one in four deaths of women during or within one year of pregnancy were determined to be pregnancy-related (13 deaths, 22.8%). This translated to a pregnancy-related mortality ratio (PRMR) of 11 deaths per every 100,000 live births that occurred in Kansas.
12 (92.3%) of the 13 deaths were preventable.
The Maternal Warning Signs Initiative is one component of a multi-pronged, multi-partner approach we are taking to reduce maternal mortality in the state of Kansas. Join us during our June 8 Kick-Off Webinar to learn more about these partnerships and initiatives. This will be a special 2-hour event, bringing together the below listed presenters to help launch this statewide initiative. Important instruction will be provided on accessing free training resources and CEUs provided to you through these partnerships with Kansas Title V.
Webinar Presenters/Topics:• Kasey Sorell, BSN, RN, CPC – Health Planning Consultant, KDHE, BFH – Kansas Maternal Mortality Review
Committee
• Terrah Stroda, CNM – Fourth Trimester Initiative Coordinator - Kansas Perinatal Quality Collaborative/Fourth Trimester Initiative
• Stephanie Wolf, RN, BSN, CLC – Clinical Perinatal/Infant Health Consultant, KDHE, BFH – Maternal Warning Signs Initiative
• Anne Santa-Donato, MSN, RNC-OB – Director, Special Programs and Projects, Association of Women's Health, Obstetric & Neonatal Nurses (AWHONN) – POST-BIRTH Warning Signs Education Program
Maternal Warning Signs Patient Education Toolkit
A toolkit is to offer a comprehensive selection of patient education materials to providers, across all sectors and settings, to ensure consistent messaging about the warning signs of trouble for pregnant and postpartum women.
SECTION CONTENTS
• Guidance on Use of Patient Education Resources ............................................... 84 • Signs and Symptoms of Preterm Labor ................................................................ 86 • Know the Warning Signs: Count the Kicks ............................................................ 88 • Urgent Maternal Warning Signs ............................................................................. 90 • Depression & Anxiety Resources ........................................................................... 96 • Post-Birth Warning Signs ........................................................................................ 100
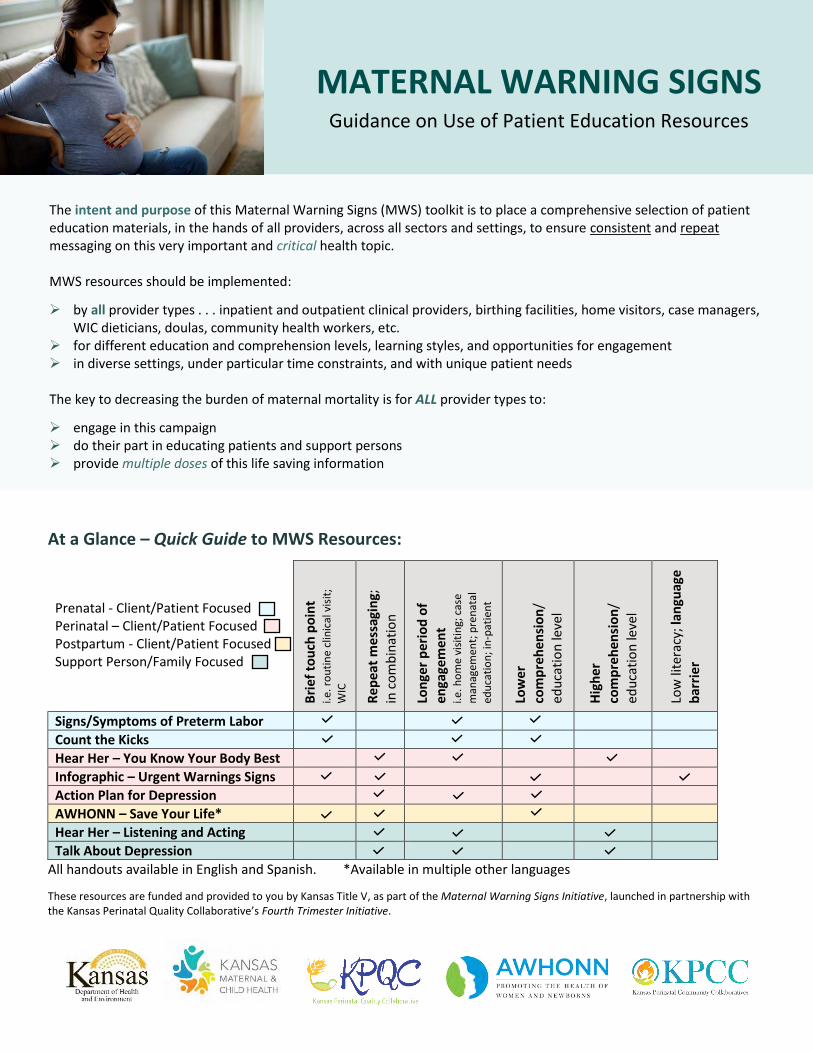
At a Glance – Quick Guide to MWS Resources:
Prenatal - Client/Patient Focused Perinatal – Client/Patient Focused Postpartum - Client/Patient Focused Support Person/Family Focused
Bri
ef t
ou
ch p
oin
t
i.e. r
ou
tin
e cl
inic
al v
isit
;
WIC
Re
pe
at m
ess
agin
g;
in c
om
bin
atio
n
Lon
ger
per
iod
of
enga
gem
en
t i.e
. ho
me
visi
tin
g; c
ase
man
agem
ent;
pre
nat
al
edu
cati
on
; in
-pat
ien
t
Low
er
com
pre
hen
sio
n/
edu
cati
on
leve
l
Hig
he
r co
mp
reh
ensi
on
/
edu
cati
on
leve
l
Low
lite
racy
; lan
guag
e
bar
rie
r
Signs/Symptoms of Preterm Labor
Count the Kicks
Hear Her – You Know Your Body Best
Infographic – Urgent Warnings Signs
Action Plan for Depression
AWHONN – Save Your Life*
Hear Her – Listening and Acting
Talk About Depression
All handouts available in English and Spanish. *Available in multiple other languages
These resources are funded and provided to you by Kansas Title V, as part of the Maternal Warning Signs Initiative, launched in partnership with the Kansas Perinatal Quality Collaborative’s Fourth Trimester Initiative.
MATERNAL WARNING SIGNS Guidance on Use of Patient Education Resources
The intent and purpose of this Maternal Warning Signs (MWS) toolkit is to place a comprehensive selection of patient education materials, in the hands of all providers, across all sectors and settings, to ensure consistent and repeat messaging on this very important and critical health topic. MWS resources should be implemented:
➢ by all provider types . . . inpatient and outpatient clinical providers, birthing facilities, home visitors, case managers, WIC dieticians, doulas, community health workers, etc.
➢ for different education and comprehension levels, learning styles, and opportunities for engagement ➢ in diverse settings, under particular time constraints, and with unique patient needs
The key to decreasing the burden of maternal mortality is for ALL provider types to:
➢ engage in this campaign ➢ do their part in educating patients and support persons ➢ provide multiple doses of this life saving information
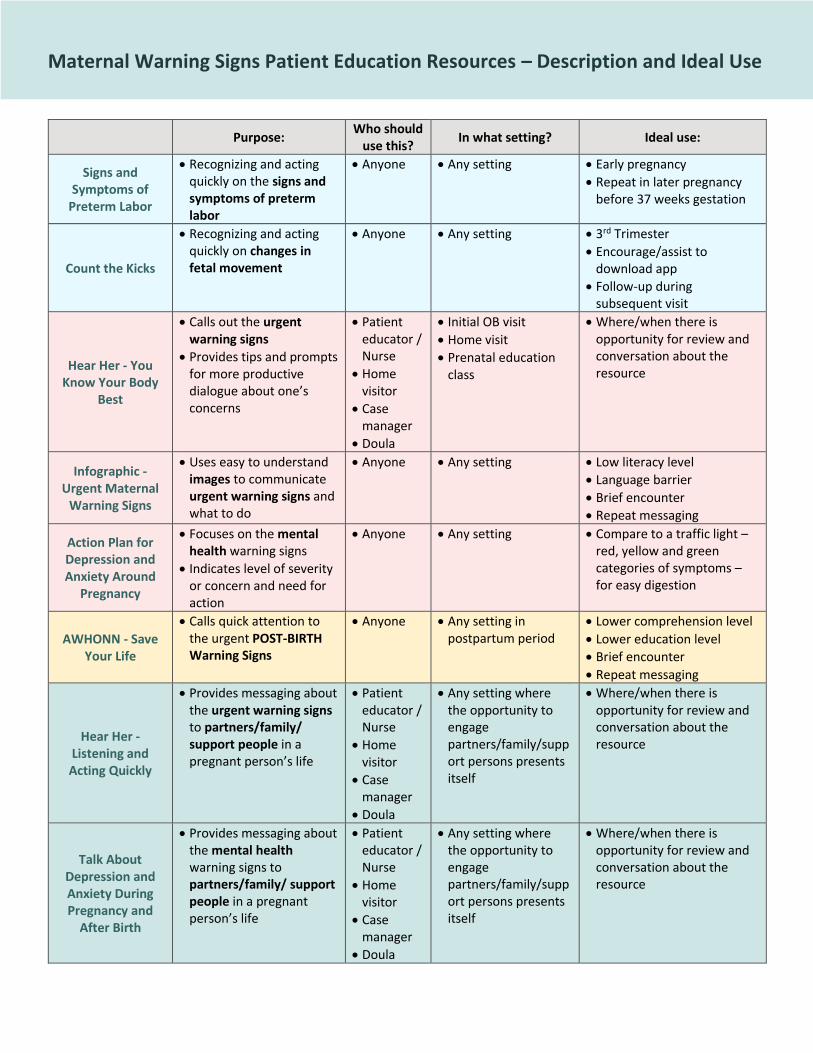
Maternal Warning Signs Patient Education Resources – Description and Ideal Use
Purpose:
Who should use this?
In what setting? Ideal use:
Signs and Symptoms of
Preterm Labor
• Recognizing and acting quickly on the signs and symptoms of preterm labor
• Anyone • Any setting • Early pregnancy
• Repeat in later pregnancy before 37 weeks gestation
Count the Kicks
• Recognizing and acting quickly on changes in fetal movement
• Anyone • Any setting • 3rd Trimester
• Encourage/assist to download app
• Follow-up during subsequent visit
Hear Her - You Know Your Body
Best
• Calls out the urgent warning signs
• Provides tips and prompts for more productive dialogue about one’s concerns
• Patient educator / Nurse
• Home visitor
• Case manager
• Doula
• Initial OB visit
• Home visit
• Prenatal education class
• Where/when there is opportunity for review and conversation about the resource
Infographic - Urgent Maternal
Warning Signs
• Uses easy to understand images to communicate urgent warning signs and what to do
• Anyone • Any setting • Low literacy level
• Language barrier
• Brief encounter
• Repeat messaging
Action Plan for Depression and Anxiety Around
Pregnancy
• Focuses on the mental health warning signs
• Indicates level of severity or concern and need for action
• Anyone • Any setting • Compare to a traffic light – red, yellow and green categories of symptoms – for easy digestion
AWHONN - Save Your Life
• Calls quick attention to the urgent POST-BIRTH Warning Signs
• Anyone • Any setting in postpartum period
• Lower comprehension level
• Lower education level
• Brief encounter
• Repeat messaging
Hear Her - Listening and Acting Quickly
• Provides messaging about the urgent warning signs to partners/family/ support people in a pregnant person’s life
• Patient educator / Nurse
• Home visitor
• Case manager
• Doula
• Any setting where the opportunity to engage partners/family/support persons presents itself
• Where/when there is opportunity for review and conversation about the resource
Talk About Depression and Anxiety During Pregnancy and
After Birth
• Provides messaging about the mental health warning signs to partners/family/ support people in a pregnant person’s life
• Patient educator / Nurse
• Home visitor
• Case manager
• Doula
• Any setting where the opportunity to engage partners/family/support persons presents itself
• Where/when there is opportunity for review and conversation about the resource
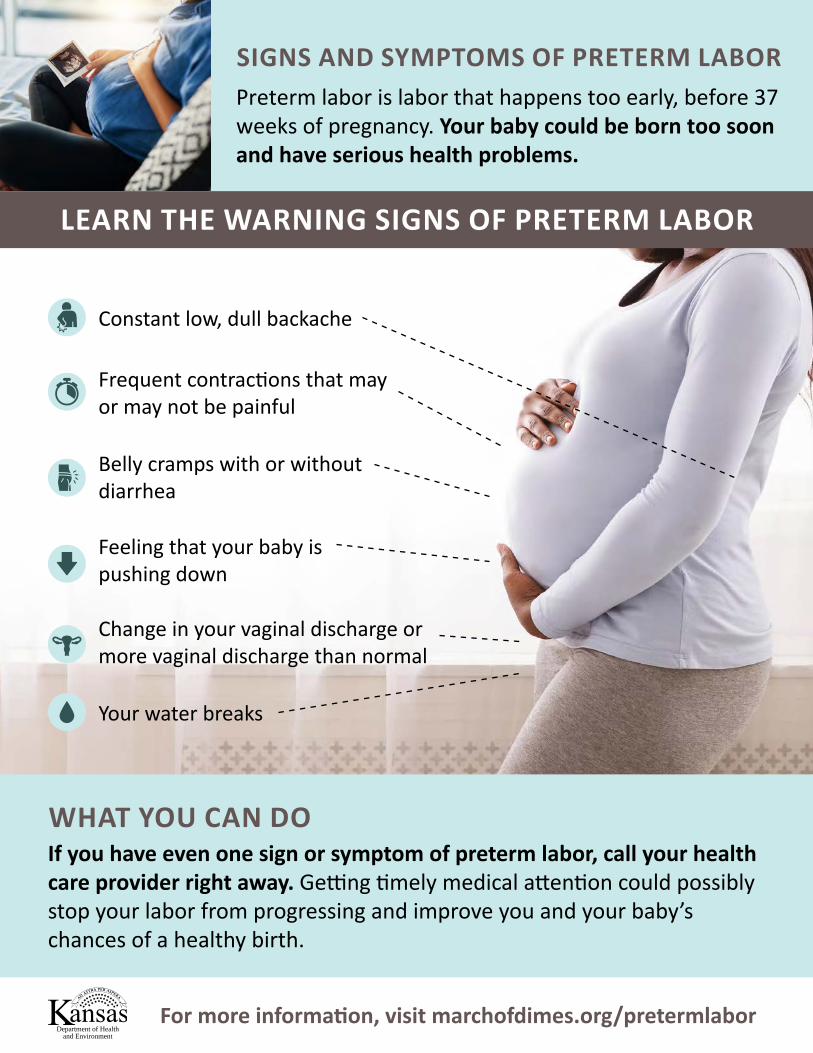
SIGNS AND SYMPTOMS OF PRETERM LABORPreterm labor is labor that happens too early, before 37 weeks of pregnancy. Your baby could be born too soon and have serious health problems.
LEARN THE WARNING SIGNS OF PRETERM LABOR
WHAT YOU CAN DOIf you have even one sign or symptom of preterm labor, call your health care provider right away. Getting timely medical attention could possibly stop your labor from progressing and improve you and your baby’s chances of a healthy birth.
Frequent contractions that may or may not be painful
Constant low, dull backache
Belly cramps with or without diarrhea
Feeling that your baby is pushing down
Change in your vaginal discharge or more vaginal discharge than normal
Your water breaks
Department of Healthand Environment
For more information, visit marchofdimes.org/pretermlabor
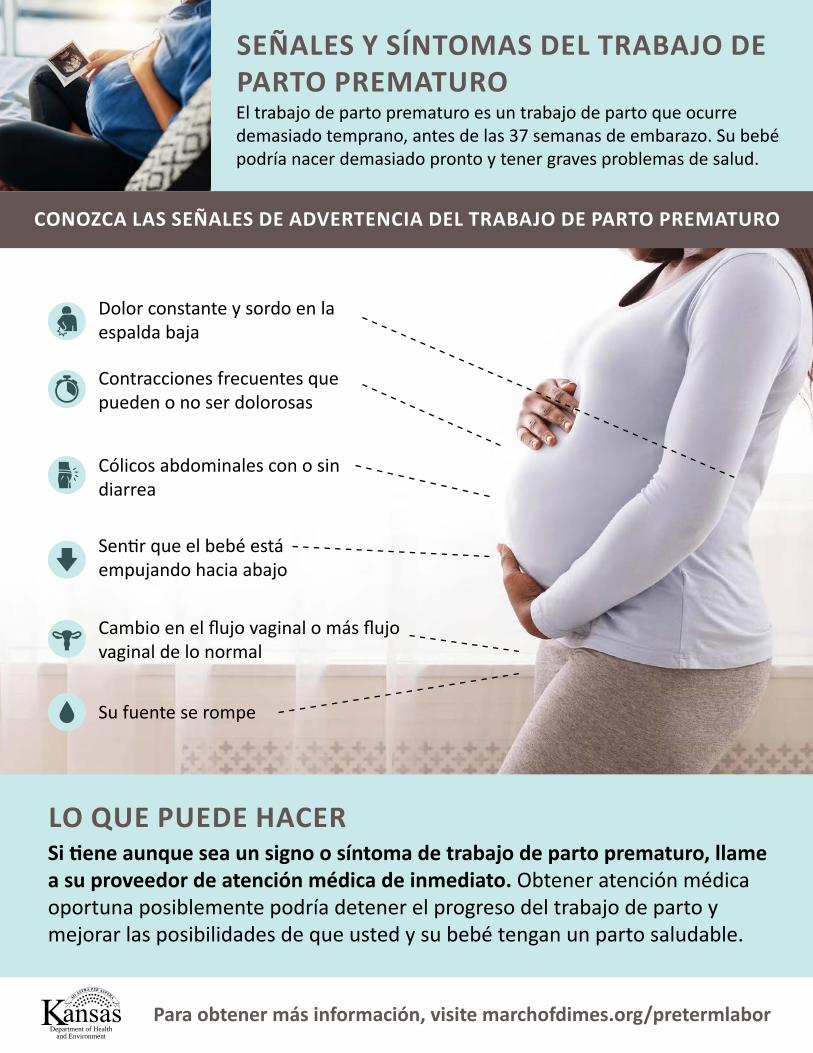
SEÑALES Y SÍNTOMAS DEL TRABAJO DE PARTO PREMATUROEl trabajo de parto prematuro es un trabajo de parto que ocurre demasiado temprano, antes de las 37 semanas de embarazo. Su bebé podría nacer demasiado pronto y tener graves problemas de salud.
CONOZCA LAS SEÑALES DE ADVERTENCIA DEL TRABAJO DE PARTO PREMATURO
LO QUE PUEDE HACERSi tiene aunque sea un signo o síntoma de trabajo de parto prematuro, llame a su proveedor de atención médica de inmediato. Obtener atención médica oportuna posiblemente podría detener el progreso del trabajo de parto y mejorar las posibilidades de que usted y su bebé tengan un parto saludable.
Contracciones frecuentes que pueden o no ser dolorosas
Dolor constante y sordo en la espalda baja
Cólicos abdominales con o sin diarrea
Sentir que el bebé está empujando hacia abajo
Cambio en el flujo vaginal o más flujo vaginal de lo normal
Su fuente se rompe
Department of Healthand Environment
Para obtener más información, visite marchofdimes.org/pretermlabor
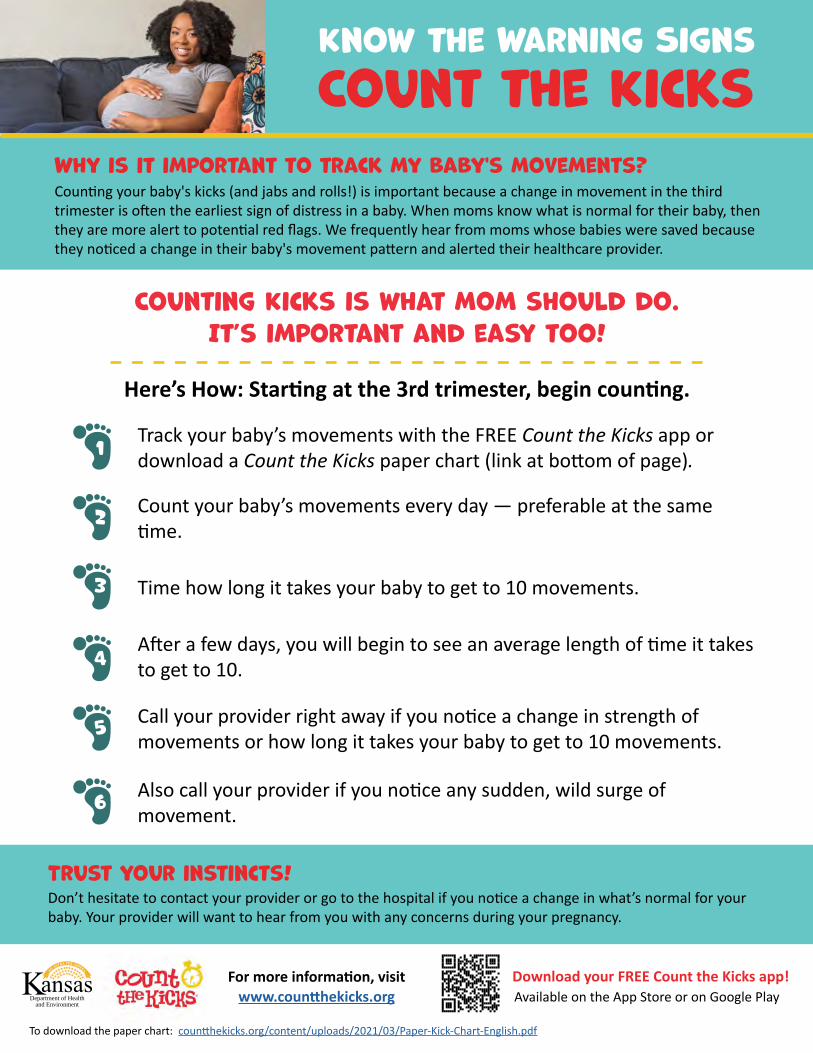
Know the Warning Signs Count the Kicks
Why is it important to track my baby's movements? Counting your baby's kicks (and jabs and rolls!) is important because a change in movement in the third trimester is often the earliest sign of distress in a baby. When moms know what is normal for their baby, then they are more alert to potential red flags. We frequently hear from moms whose babies were saved because they noticed a change in their baby's movement pattern and alerted their healthcare provider.
Counting Kicks is what mom should do.It’s important and easy too!
Here’s How: Starting at the 3rd trimester, begin counting.
Track your baby’s movements with the FREE Count the Kicks app or download a Count the Kicks paper chart (link at bottom of page).
Count your baby’s movements every day — preferable at the same time.
Time how long it takes your baby to get to 10 movements.
After a few days, you will begin to see an average length of time it takes to get to 10.
Call your provider right away if you notice a change in strength of movements or how long it takes your baby to get to 10 movements.
1
Trust your instincts!Don’t hesitate to contact your provider or go to the hospital if you notice a change in what’s normal for your baby. Your provider will want to hear from you with any concerns during your pregnancy.
Download your FREE Count the Kicks app!Available on the App Store or on Google Play
For more information, visit www.countthekicks.orgDepartment of Health
and Environment
To download the paper chart: countthekicks.org/content/uploads/2021/03/Paper-Kick-Chart-English.pdf
Also call your provider if you notice any sudden, wild surge of movement.
2
3
4
5
6
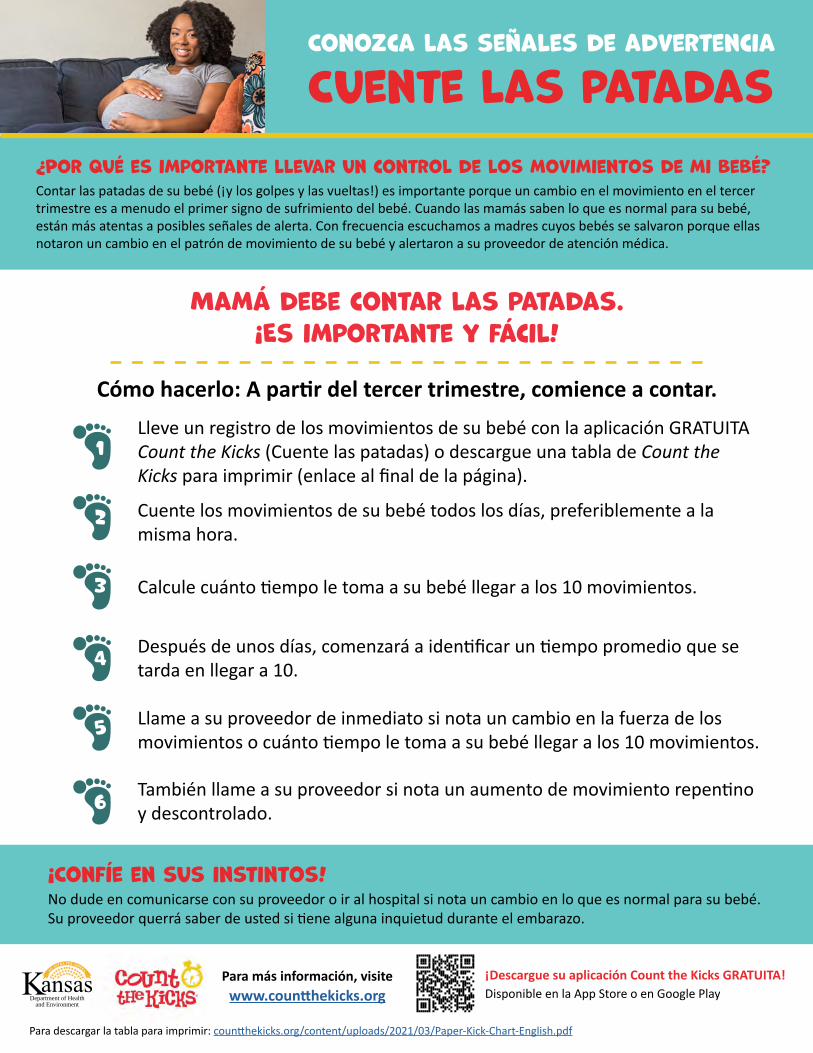
Conozca las señales de advertencia
Cuente las patadas¿Por qué es importante llevar un control de los movimientos de mi bebé?Contar las patadas de su bebé (¡y los golpes y las vueltas!) es importante porque un cambio en el movimiento en el tercer trimestre es a menudo el primer signo de sufrimiento del bebé. Cuando las mamás saben lo que es normal para su bebé, están más atentas a posibles señales de alerta. Con frecuencia escuchamos a madres cuyos bebés se salvaron porque ellas notaron un cambio en el patrón de movimiento de su bebé y alertaron a su proveedor de atención médica.
Mamá debe contar las patadas.¡Es importante y fácil!
Cómo hacerlo: A partir del tercer trimestre, comience a contar.Lleve un registro de los movimientos de su bebé con la aplicación GRATUITA Count the Kicks (Cuente las patadas) o descargue una tabla de Count the Kicks para imprimir (enlace al final de la página).
Cuente los movimientos de su bebé todos los días, preferiblemente a la misma hora.
Calcule cuánto tiempo le toma a su bebé llegar a los 10 movimientos.
Después de unos días, comenzará a identificar un tiempo promedio que se tarda en llegar a 10.
Llame a su proveedor de inmediato si nota un cambio en la fuerza de los movimientos o cuánto tiempo le toma a su bebé llegar a los 10 movimientos.
1
¡Confíe en sus instintos!No dude en comunicarse con su proveedor o ir al hospital si nota un cambio en lo que es normal para su bebé. Su proveedor querrá saber de usted si tiene alguna inquietud durante el embarazo.
¡Descargue su aplicación Count the Kicks GRATUITA!Disponible en la App Store o en Google Play
Para más información, visite www.countthekicks.orgDepartment of Health
and Environment
Para descargar la tabla para imprimir: countthekicks.org/content/uploads/2021/03/Paper-Kick-Chart-English.pdf
También llame a su proveedor si nota un aumento de movimiento repentino y descontrolado.
2
3
4
5
6
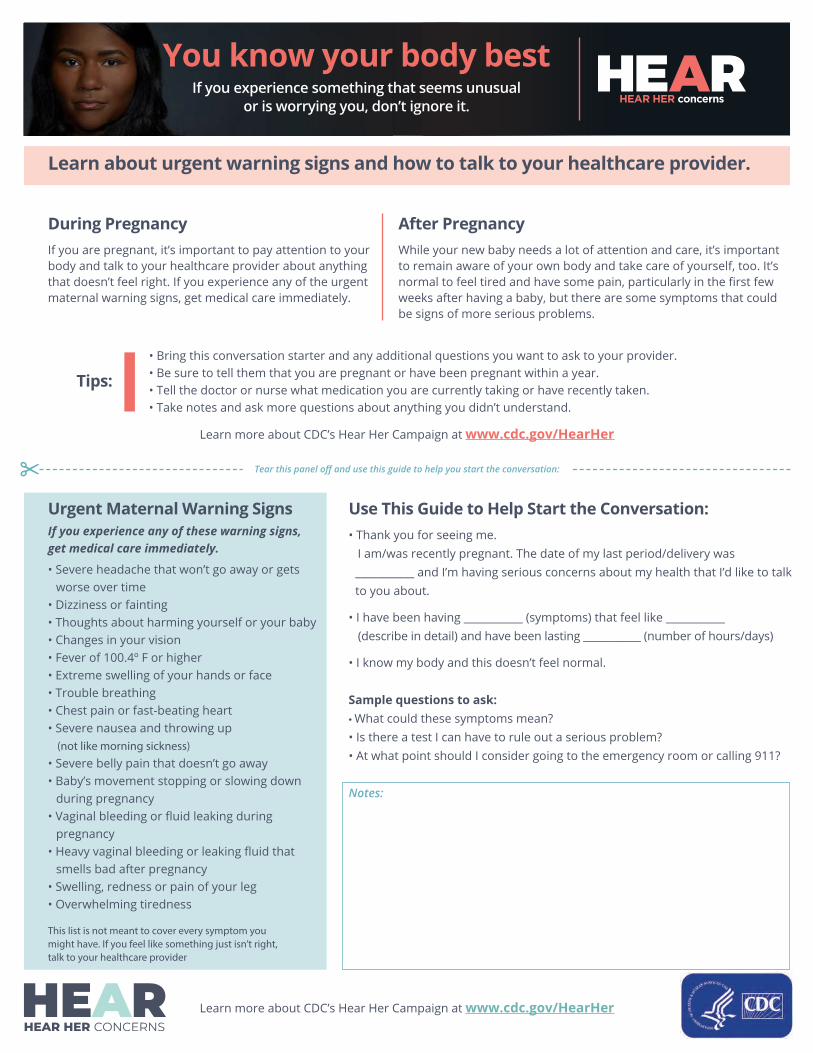
You know your body best If you experience something that seems unusual
or is worrying you, don’t ignore it.
Learn about urgent warning signs and how to talk to your healthcare provider.
During Pregnancy If you are pregnant, it’s important to pay attention to your body and talk to your healthcare provider about anything that doesn’t feel right. If you experience any of the urgent maternal warning signs, get medical care immediately.
After Pregnancy While your new baby needs a lot of attention and care, it’s important to remain aware of your own body and take care of yourself, too. It’s normal to feel tired and have some pain, particularly in the first few weeks after having a baby, but there are some symptoms that could be signs of more serious problems.
Tips: • Bring this conversation starter and any additional questions you want to ask to your provider.• Be sure to tell them that you are pregnant or have been pregnant within a year.• Tell the doctor or nurse what medication you are currently taking or have recently taken.• Take notes and ask more questions about anything you didn’t understand.
Learn more about CDC’s Hear Her Campaign at www.cdc.gov/HearHer
Tear this panel off and use this guide to help you start the conversation:
Urgent Maternal Warning Signs If you experience any of these warning signs, get medical care immediately.
• Severe headache that won’t go away or getsworse over time
• Dizziness or fainting• Thoughts about harming yourself or your baby• Changes in your vision• Fever of 100.4º F or higher• Extreme swelling of your hands or face• Trouble breathing• Chest pain or fast-beating heart• Severe nausea and throwing up
(not like morning sickness) • Severe belly pain that doesn’t go away• Baby’s movement stopping or slowing down
during pregnancy• Vaginal bleeding or fluid leaking during
pregnancy• Heavy vaginal bleeding or leaking fluid that
smells bad after pregnancy• Swelling, redness or pain of your leg• Overwhelming tiredness
This list is not meant to cover every symptom you might have. If you feel like something just isn’t right, talk to your healthcare provider
Use This Guide to Help Start the Conversation: • Thank you for seeing me.
I am/was recently pregnant. The date of my last period/delivery was___________ and I’m having serious concerns about my health that I’d like to talkto you about.
• I have been having ___________ (symptoms) that feel like ___________(describe in detail) and have been lasting ___________ (number of hours/days)
• I know my body and this doesn’t feel normal.
Sample questions to ask: • What could these symptoms mean?• Is there a test I can have to rule out a serious problem?• At what point should I consider going to the emergency room or calling 911?
Notes:
Learn more about CDC’s Hear Her Campaign at www.cdc.gov/HearHer
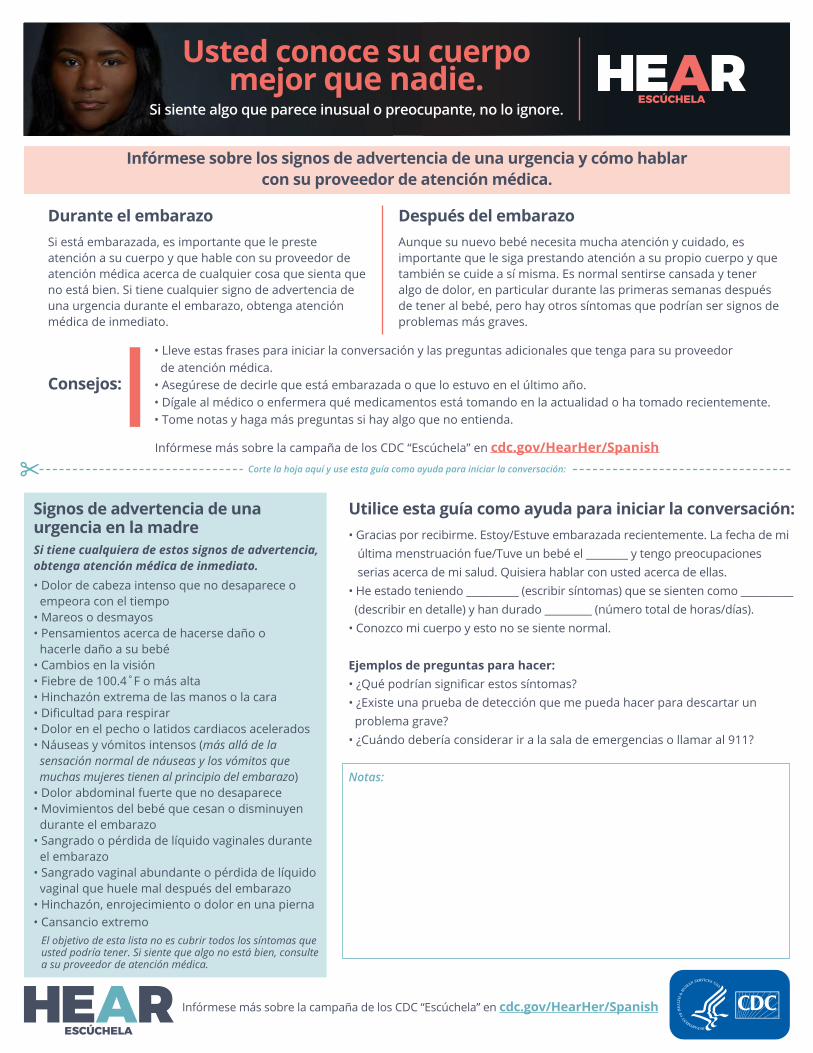
Infórmese sobre los signos de advertencia de una urgencia y cómo hablar con su proveedor de atención médica.
Si está embarazada, es importante que le preste atención a su cuerpo y que hable con su proveedor de atención médica acerca de cualquier cosa que sienta que no está bien. Si tiene cualquier signo de advertencia de una urgencia durante el embarazo, obtenga atención médica de inmediato.
Durante el embarazoAunque su nuevo bebé necesita mucha atención y cuidado, es importante que le siga prestando atención a su propio cuerpo y que también se cuide a sí misma. Es normal sentirse cansada y tener algo de dolor, en particular durante las primeras semanas después de tener al bebé, pero hay otros síntomas que podrían ser signos de problemas más graves.
Después del embarazo
• Lleve estas frases para iniciar la conversación y las preguntas adicionales que tenga para su proveedor de atención médica.
• Asegúrese de decirle que está embarazada o que lo estuvo en el último año.• Dígale al médico o enfermera qué medicamentos está tomando en la actualidad o ha tomado recientemente.• Tome notas y haga más preguntas si hay algo que no entienda.
Consejos:
Signos de advertencia de una urgencia en la madre • Gracias por recibirme. Estoy/Estuve embarazada recientemente. La fecha de mi
última menstruación fue/Tuve un bebé el ________ y tengo preocupaciones serias acerca de mi salud. Quisiera hablar con usted acerca de ellas. • He estado teniendo __________ (escribir síntomas) que se sienten como __________ (describir en detalle) y han durado _________ (número total de horas/días). • Conozco mi cuerpo y esto no se siente normal.
Ejemplos de preguntas para hacer:• ¿Qué podrían significar estos síntomas?• ¿Existe una prueba de detección que me pueda hacer para descartar un problema grave?
• ¿Cuándo debería considerar ir a la sala de emergencias o llamar al 911?
Notas:
Utilice esta guía como ayuda para iniciar la conversación:
Corte la hoja aquí y use esta guía como ayuda para iniciar la conversación:
El objetivo de esta lista no es cubrir todos los síntomas que usted podría tener. Si siente que algo no está bien, consulte a su proveedor de atención médica.
Infórmese más sobre la campaña de los CDC “Escúchela” en cdc.gov/HearHer/Spanish
• Dolor de cabeza intenso que no desaparece o empeora con el tiempo
• Mareos o desmayos• Pensamientos acerca de hacerse daño o
hacerle daño a su bebé • Cambios en la visión• Fiebre de 100.4˚F o más alta• Hinchazón extrema de las manos o la cara• Dificultad para respirar• Dolor en el pecho o latidos cardiacos acelerados• Náuseas y vómitos intensos (más allá de la
sensación normal de náuseas y los vómitos que muchas mujeres tienen al principio del embarazo)
• Dolor abdominal fuerte que no desaparece• Movimientos del bebé que cesan o disminuyen durante el embarazo • Sangrado o pérdida de líquido vaginales durante el embarazo
• Sangrado vaginal abundante o pérdida de líquido vaginal que huele mal después del embarazo
• Hinchazón, enrojecimiento o dolor en una pierna• Cansancio extremo
Usted conoce su cuerpo mejor que nadie.
Si siente algo que parece inusual o preocupante, no lo ignore.
Si tiene cualquiera de estos signos de advertencia, obtenga atención médica de inmediato.
Infórmese más sobre la campaña de los CDC “Escúchela” en cdc.gov/HearHer/Spanish

Listening and Acting Quickly
could help save her life
Urgent Maternal Warning Signs
This list is not meant to cover every symptom a woman might experience during or after pregnancy. Learn more about urgent maternal warning signs at cdc.gov/HearHer.
•
•
•
•
•
•
•
•
•
•
•
•
•
•
•
Severe headache that won’t go away or gets worse over time
Dizziness or fainting
Thoughts about harming yourself or your baby
Changes in your vision
Fever of 100.4º F or higher
Extreme swelling of your hands or face
Trouble breathing
Chest pain or fast-beating heart
Severe nausea and throwing up (not like morning sickness)
Severe belly pain that doesn’t go away
Baby’s movement stopping or slowing down during pregnancy
Vaginal bleeding or fluid leaking during pregnancy
Heavy vaginal bleeding or fluid leaking that smells bad after
pregnancy
Swelling, redness or pain of your leg
Overwhelming tiredness
If someone who is pregnant or was pregnant within the last year has any of these symptoms, she should get medical care immediately.
If a pregnant or recently pregnant woman expresses concerns about any symptoms she is having, take the time to Hear Her. Listening and acting quickly could help save her life.
•
•
•
•
•
•
Learn the urgent maternal warning signs.
Listen to her concerns.
Encourage her to seek medical help. If something doesn’t feel right, she should reach out to her provider. If she is experiencing an urgent maternal warning sign, she should get medical care right away. Be sure that she says she is pregnant or was pregnant within the last year.
Offer to go with her to get medical care and help her ask questions. Visit https://www.cdc.gov/hearher/pregnant-postpartum-women/index.html#talk.
Take notes and help her talk to a healthcare provider to get the support she needs.
Support her through follow-up care.
How Can You Help?
Pregnancy complications can happen up to a year after birth. If your loved one shares that something doesn’t feel right, support her to get the care and answers she may need. Learn the urgent warning signs that need immediate medical attention. Here are some talking points to help with the conversation:
•
•
•
It’s hard to tell what’s normal with everything that’schanging right now. It’s better to check if there’sanything you are worried about.
It’s important that we share this information withyour doctor and make sure everything is okay.
I am here for you. Let’s talk to a healthcare providerto get you the care you need.
During Pregnancy •
•
•
It’s normal to feel tired and have some pain after giving birth,but you know your body best. If something is worrying you, youshould talk to your doctor.
Although your new baby needs a lot of attention and care, it’simportant to take care of yourself, too.
You are not alone. I hear you. Let’s talk to a healthcare providerto get you the care you need.
After Pregnancy
Hear Her
If you need additional support, don’t be afraid to ask for help.
Learn more about CDC’s Hear Her Campaign at www.cdc.gov/HearHer.
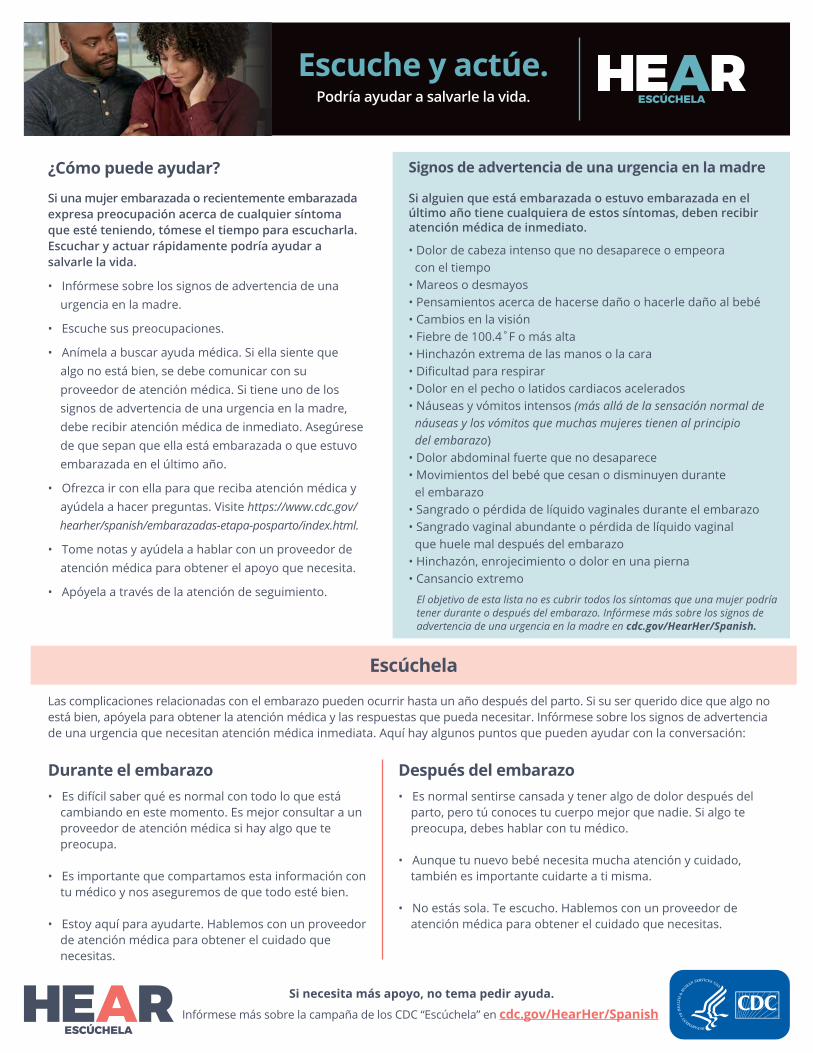
Escuche y actúe. Podría ayudar a salvarle la vida.
Signos de advertencia de una urgencia en la madre
El objetivo de esta lista no es cubrir todos los síntomas que una mujer podría tener durante o después del embarazo. Infórmese más sobre los signos de advertencia de una urgencia en la madre en cdc.gov/HearHer/Spanish.
• Dolor de cabeza intenso que no desaparece o empeora con el tiempo
• Mareos o desmayos• Pensamientos acerca de hacerse daño o hacerle daño al bebé• Cambios en la visión• Fiebre de 100.4˚F o más alta• Hinchazón extrema de las manos o la cara• Dificultad para respirar• Dolor en el pecho o latidos cardiacos acelerados• Náuseas y vómitos intensos (más allá de la sensación normal de náuseas y los vómitos que muchas mujeres tienen al principio del embarazo)
• Dolor abdominal fuerte que no desaparece• Movimientos del bebé que cesan o disminuyen durante el embarazo
• Sangrado o pérdida de líquido vaginales durante el embarazo• Sangrado vaginal abundante o pérdida de líquido vaginal
que huele mal después del embarazo • Hinchazón, enrojecimiento o dolor en una pierna• Cansancio extremo
Si alguien que está embarazada o estuvo embarazada en el último año tiene cualquiera de estos síntomas, deben recibir atención médica de inmediato.
Si una mujer embarazada o recientemente embarazada expresa preocupación acerca de cualquier síntoma que esté teniendo, tómese el tiempo para escucharla. Escuchar y actuar rápidamente podría ayudar a salvarle la vida.
• Infórmese sobre los signos de advertencia de una urgencia en la madre.
• Escuche sus preocupaciones.
• Anímela a buscar ayuda médica. Si ella siente que algo no está bien, se debe comunicar con su proveedor de atención médica. Si tiene uno de los signos de advertencia de una urgencia en la madre, debe recibir atención médica de inmediato. Asegúrese de que sepan que ella está embarazada o que estuvo embarazada en el último año.
• Ofrezca ir con ella para que reciba atención médica y ayúdela a hacer preguntas. Visite https://www.cdc.gov/ hearher/spanish/embarazadas-etapa-posparto/index.html.
• Tome notas y ayúdela a hablar con un proveedor de atención médica para obtener el apoyo que necesita.
• Apóyela a través de la atención de seguimiento.
¿Cómo puede ayudar?
Las complicaciones relacionadas con el embarazo pueden ocurrir hasta un año después del parto. Si su ser querido dice que algo no está bien, apóyela para obtener la atención médica y las respuestas que pueda necesitar. Infórmese sobre los signos de advertencia de una urgencia que necesitan atención médica inmediata. Aquí hay algunos puntos que pueden ayudar con la conversación:
• Es difícil saber qué es normal con todo lo que está cambiando en este momento. Es mejor consultar a un proveedor de atención médica si hay algo que te preocupa.
• Es importante que compartamos esta información con tu médico y nos aseguremos de que todo esté bien.
• Estoy aquí para ayudarte. Hablemos con un proveedor de atención médica para obtener el cuidado que necesitas.
Durante el embarazo• Es normal sentirse cansada y tener algo de dolor después del
parto, pero tú conoces tu cuerpo mejor que nadie. Si algo te preocupa, debes hablar con tu médico.
• Aunque tu nuevo bebé necesita mucha atención y cuidado, también es importante cuidarte a ti misma.
• No estás sola. Te escucho. Hablemos con un proveedor de atención médica para obtener el cuidado que necesitas.
Después del embarazo
Escúchela
Si necesita más apoyo, no tema pedir ayuda.
Infórmese más sobre la campaña de los CDC “Escúchela” en cdc.gov/HearHer/Spanish

URGENT MATERNAL WARNING SIGNS
Call 911 if you have:
Troublebreathing
Chest pain or fast-beating heart
Call your healthcare provider if you have:(If you can’t reach your healthcare provider, call 911 or go to an emergency room)
Headache that won’t go away,
dizziness or fainting
Thoughts of hurting yourself or your baby
Changes inyour vision
Fever
Severe belly pain that doesn’t go away
Severe nausea and throwing up (not like
morning sickness)
Baby’s movements stopping or
slowing
Vaginal bleeding or fluid leaking during
pregnancy
Vaginal bleeding soaking through more than 1 pad/
hour after pregnancy
Swelling, redness, or pain of your leg
Extreme swelling ofyour hands or face
Overwhelmingtiredness
Seizures
Incision that isnot healing
If you can't reach your provider, go to the emergency room. Remember to say that you're pregnant or have been pregnant within the last year. Learn more: safehealthcareforeverywoman.org/urgentmaternalwarningsigns
This resource has been adapted with permission from the American College of Obstetricians and Gynecologists, Council on Patient Safety in Women’s Health Care; Urgent Maternal Warning Signs, V1 May 2020
Department of Healthand Environment
Feeling intenseanxiety
Feelings of depression or having little interest
in things
Scary or upsetting thoughts that won’t
go away
If you have any of these symptoms during or after pregnancy, contact your health care provider and get help right away.

SEÑALES MATERNAS DE ADVERTENCIA URGENTES
Llame al 911 si tiene:
Dificultadpara respirar
Dolor de pecho o latidos de corazón acelerados
Llame a su proveedor de atención médica si tiene:(si no puede comunicarse con su proveedor de atención médica, llame al 911 o vaya a una sala de emergencias)
Dolor de cabeza que no desaparece, mareos o desmayos
Pensamientos de hacerse daño a sí
misma o a su bebé
Cambios dela vista
Fiebre
Dolor de estómago intenso que no desaparece.
Náuseas intensas y vómito (no como las náuseas matutinas)
Los movimientos del bebé se detienen o
disminuyen
Sangrado vaginal o pérdida de fluido
durante el embarazo
Sangrado vaginal que empapa más de 1 toalla
sanitaria/hora después del embarazo
Hinchazón, enrojecimiento o dolor en la pierna
Hinchazón extrema de las manos o la cara
Cansancioagobiante
Convulsiones
Incisión queno sana
Si no puede comunicarse con su proveedor, vaya a la sala de emergencias. Recuerde decir que está embarazada o ha estado embarazada durante el último año. Más información: safehealthcareforeverywoman.org/urgentmaternalwarningsigns
Este recurso ha sido adaptado con permiso del Colegio Estadounidense de Obstet-ras y Ginecólogos, Consejo de Seguridad del Paciente en el Cuidado de la Salud de la Mujer; Señales maternas de advertencia urgentes, V1 Mayo de 2020
Department of Healthand Environment
Sensación deansiedad intensa
Sentimientos de depresión o poco
interés en las cosas
Pensamientos aterradores o
perturbadores que no desaparecen
Si tiene alguno de estos síntomas durante o después del embarazo, comuníquese con su proveedor de atención médica y obtenga ayuda de inmediato.
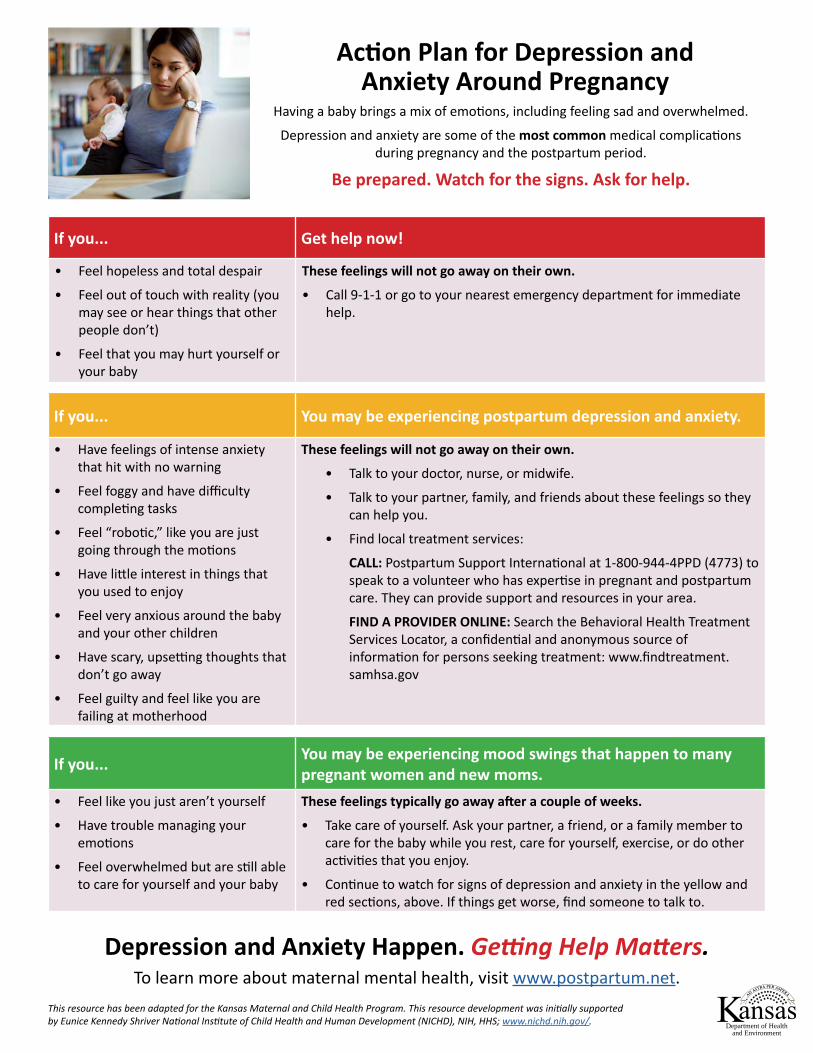
Action Plan for Depression and Anxiety Around Pregnancy
Having a baby brings a mix of emotions, including feeling sad and overwhelmed.
Depression and anxiety are some of the most common medical complications during pregnancy and the postpartum period.
Be prepared. Watch for the signs. Ask for help.
If you... You may be experiencing mood swings that happen to many pregnant women and new moms.
• Feel like you just aren’t yourself
• Have trouble managing youremotions
• Feel overwhelmed but are still ableto care for yourself and your baby
These feelings typically go away after a couple of weeks.
• Take care of yourself. Ask your partner, a friend, or a family member tocare for the baby while you rest, care for yourself, exercise, or do otheractivities that you enjoy.
• Continue to watch for signs of depression and anxiety in the yellow andred sections, above. If things get worse, find someone to talk to.
If you... You may be experiencing postpartum depression and anxiety.
• Have feelings of intense anxietythat hit with no warning
• Feel foggy and have difficultycompleting tasks
• Feel “robotic,” like you are justgoing through the motions
• Have little interest in things thatyou used to enjoy
• Feel very anxious around the babyand your other children
• Have scary, upsetting thoughts thatdon’t go away
• Feel guilty and feel like you arefailing at motherhood
These feelings will not go away on their own.
• Talk to your doctor, nurse, or midwife.
• Talk to your partner, family, and friends about these feelings so theycan help you.
• Find local treatment services:
CALL: Postpartum Support International at 1-800-944-4PPD (4773) tospeak to a volunteer who has expertise in pregnant and postpartumcare. They can provide support and resources in your area.
FIND A PROVIDER ONLINE: Search the Behavioral Health TreatmentServices Locator, a confidential and anonymous source ofinformation for persons seeking treatment: www.findtreatment.samhsa.gov
If you... Get help now!
• Feel hopeless and total despair
• Feel out of touch with reality (youmay see or hear things that otherpeople don’t)
• Feel that you may hurt yourself oryour baby
These feelings will not go away on their own.
• Call 9-1-1 or go to your nearest emergency department for immediatehelp.
Depression and Anxiety Happen. Getting Help Matters.To learn more about maternal mental health, visit www.postpartum.net.
This resource has been adapted for the Kansas Maternal and Child Health Program. This resource development was initially supported by Eunice Kennedy Shriver National Institute of Child Health and Human Development (NICHD), NIH, HHS; www.nichd.nih.gov/.
Department of Healthand Environment
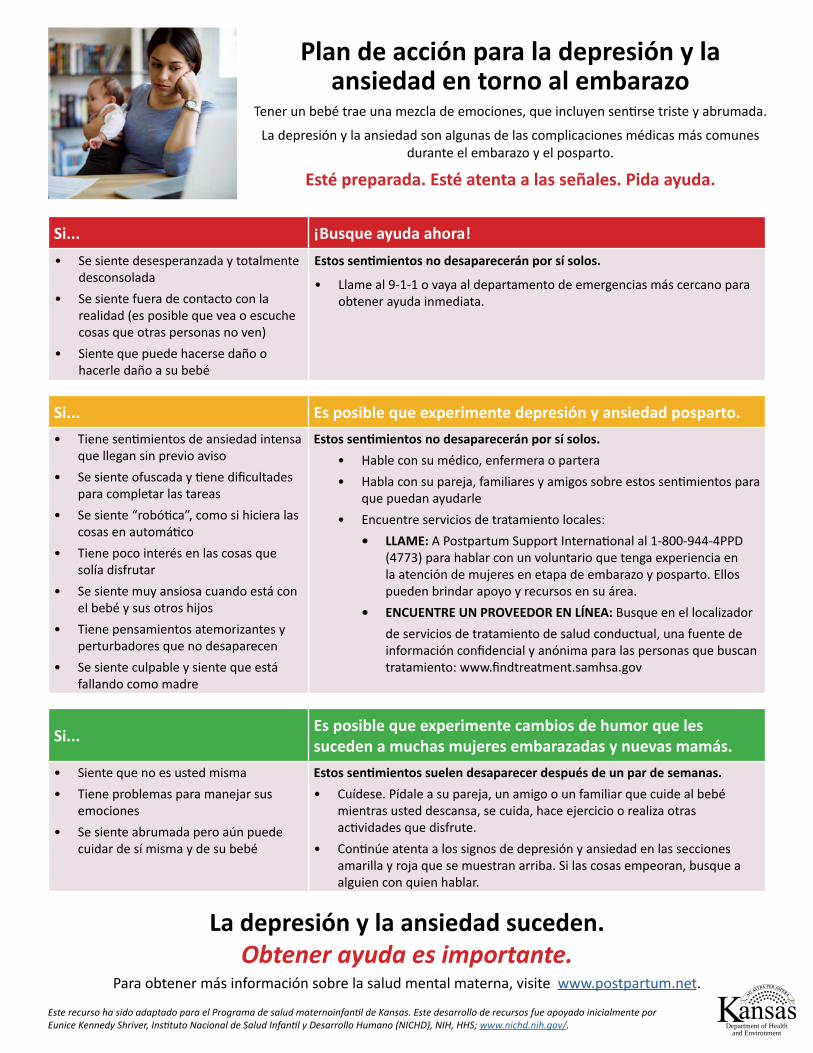
Plan de acción para la depresión y la ansiedad en torno al embarazo
Tener un bebé trae una mezcla de emociones, que incluyen sentirse triste y abrumada.
La depresión y la ansiedad son algunas de las complicaciones médicas más comunes durante el embarazo y el posparto.
Esté preparada. Esté atenta a las señales. Pida ayuda.
Si... Es posible que experimente cambios de humor que les suceden a muchas mujeres embarazadas y nuevas mamás.
• Siente que no es usted misma• Tiene problemas para manejar sus
emociones• Se siente abrumada pero aún puede
cuidar de sí misma y de su bebé
Estos sentimientos suelen desaparecer después de un par de semanas.• Cuídese. Pídale a su pareja, un amigo o un familiar que cuide al bebé
mientras usted descansa, se cuida, hace ejercicio o realiza otras actividades que disfrute.
• Continúe atenta a los signos de depresión y ansiedad en las secciones amarilla y roja que se muestran arriba. Si las cosas empeoran, busque a alguien con quien hablar.
Si... Es posible que experimente depresión y ansiedad posparto.• Tiene sentimientos de ansiedad intensa
que llegan sin previo aviso• Se siente ofuscada y tiene dificultades
para completar las tareas• Se siente “robótica”, como si hiciera las
cosas en automático• Tiene poco interés en las cosas que
solía disfrutar• Se siente muy ansiosa cuando está con
el bebé y sus otros hijos• Tiene pensamientos atemorizantes y
perturbadores que no desaparecen• Se siente culpable y siente que está
fallando como madre
Estos sentimientos no desaparecerán por sí solos.• Hable con su médico, enfermera o partera• Habla con su pareja, familiares y amigos sobre estos sentimientos para
que puedan ayudarle• Encuentre servicios de tratamiento locales:
• LLAME: A Postpartum Support International al 1-800-944-4PPD (4773) para hablar con un voluntario que tenga experiencia en la atención de mujeres en etapa de embarazo y posparto. Ellos pueden brindar apoyo y recursos en su área.
• ENCUENTRE UN PROVEEDOR EN LÍNEA: Busque en el localizador de servicios de tratamiento de salud conductual, una fuente de información confidencial y anónima para las personas que buscan tratamiento: www.findtreatment.samhsa.gov
Si... ¡Busque ayuda ahora!• Se siente desesperanzada y totalmente
desconsolada• Se siente fuera de contacto con la
realidad (es posible que vea o escuche cosas que otras personas no ven)
• Siente que puede hacerse daño o hacerle daño a su bebé
Estos sentimientos no desaparecerán por sí solos.
• Llame al 9-1-1 o vaya al departamento de emergencias más cercano para obtener ayuda inmediata.
La depresión y la ansiedad suceden.Obtener ayuda es importante.
Para obtener más información sobre la salud mental materna, visite www.postpartum.net.
Este recurso ha sido adaptado para el Programa de salud maternoinfantil de Kansas. Este desarrollo de recursos fue apoyado inicialmente por Eunice Kennedy Shriver, Instituto Nacional de Salud Infantil y Desarrollo Humano (NICHD), NIH, HHS; www.nichd.nih.gov/. Department of Health
and Environment

Talk About Depression & Anxiety During Pregnancy & After Birth
Pregnancy and a new baby can bring a mix of emotions—excitement and joy, but also sadness, stress and feeling overwhelmed. When these feelings get in the way of your partner taking care of herself or the baby—that could be a sign that she’s dealing with deeper emotions of
depression or anxiety, feelings that many pregnant women and new moms experience.
Left untreated, symptoms and suffering can worsen.
With the right care and support, however, moms can feel better. Below are some ways to help support your partner during this time.
Be prepared. Watch for the signs. Offer help.
LISTEN: Open the line of communication.• “I know everyone is focused on the baby, but I want to hear about you.”• “I notice you are having trouble sleeping, even when the baby sleeps. What’s on your mind?”• “I know a new baby is stressful, but I’m worried about you. You don’t seem like yourself. Tell me how you are feeling.”• “I really want to know how you’re feeling, and I will listen to you.”
OFFER INSIGHT: Let her know that she’s not alone and you are here to help. • “Let’s go online and see what kind of information we can find out about this.” Visit www.postpartum.net.
• “Would you like me to make an appointment so you can talk with someone?” Support her while she calls her health care provider or contacts the Postpartum Support HelpLine: 1-800-944-4773.
• “I’m very concerned about you.” Call the National Suicide Prevention Lifeline together at 1-800-273-TALK (8255) for free and confidential emotional support—they talk about more than suicide.
OFFER TO HELP: Ask her to let you help her reach out for assistance. • “Can I watch the baby while you get some rest or go see your friends?”
• “How can I help? I can take on more around the house like making meals, cleaning, or going grocery shopping.”
• ”I am here for you no matter what. Let’s schedule some alone time together, just you and me.”
Learn the Signs of Depression and Anxiety You may be the first to see signs of depression and anxiety in your partner while she is pregnant and after she has the baby.
Learn to recognize the signs and, if you do see them, urge her to talk with her health care provider.
DOES SHE: • Seem to get extremely anxious, sad, or angry without
warning?• Seem foggy and have trouble completing tasks?• Show little interest in things she used to enjoy?• Seem “robotic,” like she is just going through the motions?
DO YOU: • Notice she has trouble sleeping?• Notice she checks things and performs tasks repeatedly?• Get concerned she cannot care for herself or the baby?• Think she might hurt herself or the baby?
Depression and Anxiety Happen. Getting Help Matters.To learn more about maternal mental health, visit www.postpartum.net. Also learn about Paternal Perinatal Depression by visiting www.kdheks.gov/c-f/integration_toolkits/Paternal_PPD_Brochure_for_Families_online.pdf.
This resource has been adapted for the Kansas Maternal and Child Health Program. This resource development was initially supported by Eunice Kennedy Shriver National Institute of Child Health and Human Development (NICHD), NIH, HHS; https://www.nichd.nih.gov/.
Department of Healthand Environment

Hable sobre la depresión y la ansiedad durante el embarazo y después del parto
El embarazo y el nacimiento de un bebé pueden traer una combinación de emociones: ilusión y alegría, pero también tristeza, estrés y agobio. Cuando estos sentimientos se interponen en el camino de su pareja y le impiden cuidar de sí misma o del bebé, eso podría ser una señal de que está lidiando con emociones más profundas de depresión o ansiedad, sentimientos que experimentan muchas mujeres embarazadas y
nuevas mamás.
Si no se tratan, los síntomas y el sufrimiento pueden empeorar.
Sin embargo, con el cuidado y el apoyo adecuados, las mamás pueden sentirse mejor. A continuación, se muestran algunas formas de ayudar a apoyar a su pareja durante este tiempo.
Esté preparado. Esté atento a las señales. Ofrezca ayuda.
ESCUCHE: Abra la línea de comunicación.• “Sé que todos están enfocados en el bebé, pero quiero que me hables de ti”.• “Me doy cuenta de que tienes problemas para dormir, incluso cuando el bebé duerme. ¿Qué piensas?”• “Sé que un bebé recién nacido es estresante, pero me preocupo por ti. Te veo distinta. Dime cómo te sientes”.• “De verdad quiero saber cómo te sientes y te escucharé”.
OFREZCA PERSPECTIVA: Hágale saber que no está sola y que usted está aquí para ayudar. • “Entremos a internet y veamos qué tipo de información podemos encontrar sobre esto”. Visite www.postpartum.net.
• “¿Te gustaría que programe una cita para que puedas hablar con alguien?” Apóyela mientras llama a su proveedor de atención médica o se comunica con la Línea de ayuda de apoyo posparto: 1-800-944-4773.
• “Estoy muy preocupado(a) por ti”. Llame a la Línea Nacional de Prevención del Suicidio al 1-800-273-TALK (8255) para obtener apoyo emocional gratuito y confidencial; ahí se habla de más que suicidio.
OFREZCA AYUDA: Pídale que le permita ayudarle a pedir asistencia. • “¿Puedo cuidar al bebé mientras descansas un poco o vas a ver a tus amigos?”
• “¿Cómo puedo ayudar? Puedo hacer más cosas de la casa, como preparar comidas, limpiar o ir de compras”.
• “Estoy aquí para ti pase lo que pase. Programemos un tiempo a solas juntos, solo tú y yo”.
Conozca los signos de depresión y ansiedadUsted puede ser el primero en ver signos de depresión y ansiedad en su pareja mientras ella está embarazada y después de
tener al bebé. Aprenda a reconocer las señales y, si las ve, anímela a que hable con su proveedor de atención médica.
ELLA:• ¿Parece ponerse extremadamente ansiosa, triste o enojada
sin previo aviso?• ¿Parece ofuscada y tiene problemas para completar las
tareas?• ¿Muestra poco interés en las cosas que solía disfrutar?• ¿Parece “robótica”, como si hiciera las cosas en automático?
USTED:• ¿Nota que ella tiene problemas para dormir?• ¿Nota que ella revisa las cosas y realiza tareas
repetidamente?• ¿Se preocupa de que no pueda cuidar de sí misma o del
bebé?• ¿Cree que podría hacerse daño a sí misma o al bebé?
La depresión y la ansiedad suceden. Obtener ayuda es importante.Para obtener más información sobre la salud mental materna, visite www.postpartum.net. Aprenda también sobre la depresión perinatal paterna visitando www.kdheks.gov/c-f/integration_toolkits/Paternal_PPD_Brochure_for_Families_online.pdf.
Este recurso ha sido adaptado para el Programa de salud maternoinfantil de Kansas. Este desarrollo de recursos fue apoyado inicialmente por Eunice Kennedy Shriver, Instituto Nacional de Salud Infantil y Desarrollo Humano (NICHD), NIH, HHS; https://www.nichd.nih.gov/.
Department of Healthand Environment
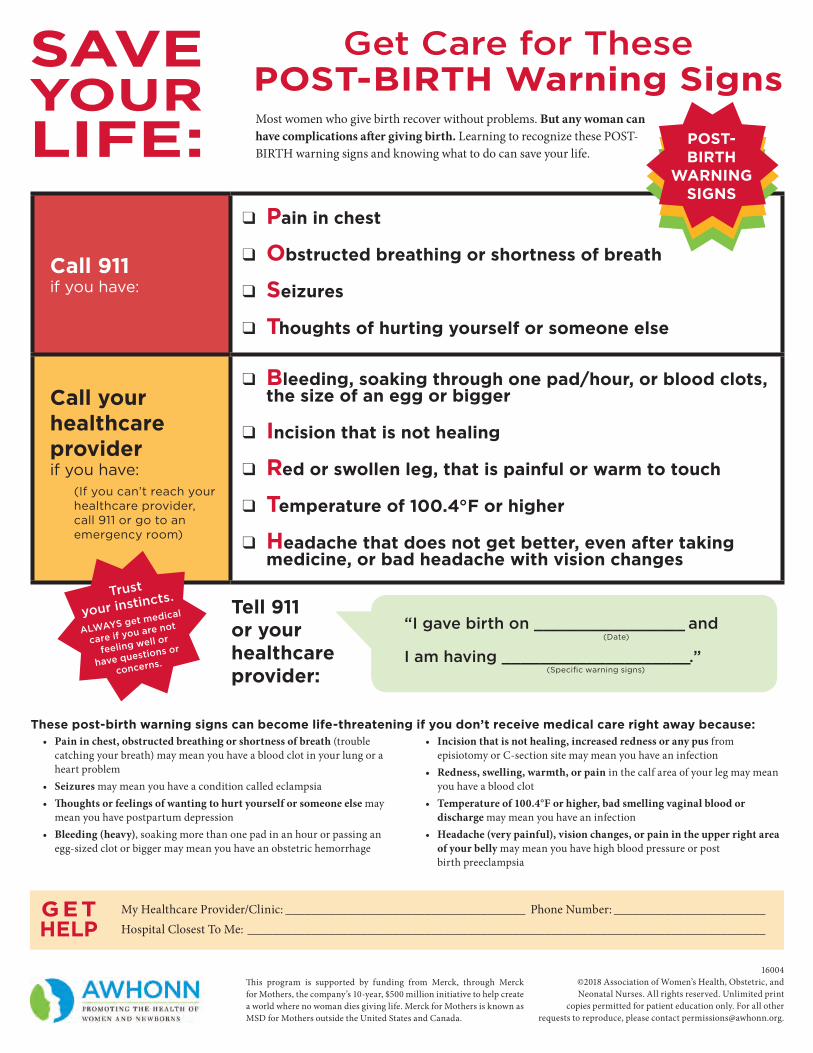
Call 911if you have:
q Pain in chest
q Obstructed breathing or shortness of breath
q Seizures
q Thoughts of hurting yourself or someone else
Call your healthcare provider if you have:
(If you can’t reach your healthcare provider, call 911 or go to an emergency room)
q Bleeding, soaking through one pad/hour, or blood clots,the size of an egg or bigger
q Incision that is not healing
q Red or swollen leg, that is painful or warm to touch
q Temperature of 100.4°F or higher
q Headache that does not get better, even after takingmedicine, or bad headache with vision changes
These post-birth warning signs can become life-threatening if you don’t receive medical care right away because:• Pain in chest, obstructed breathing or shortness of breath (trouble
catching your breath) may mean you have a blood clot in your lung or a heart problem
• Seizures may mean you have a condition called eclampsia• Thoughts or feelings of wanting to hurt yourself or someone else may
mean you have postpartum depression• Bleeding (heavy), soaking more than one pad in an hour or passing an
egg-sized clot or bigger may mean you have an obstetric hemorrhage
• Incision that is not healing, increased redness or any pus from episiotomy or C-section site may mean you have an infection
• Redness, swelling, warmth, or pain in the calf area of your leg may mean you have a blood clot
• Temperature of 100.4°F or higher, bad smelling vaginal blood or discharge may mean you have an infection
• Headache (very painful), vision changes, or pain in the upper right area of your belly may mean you have high blood pressure or post birth preeclampsia
My Healthcare Provider/Clinic: ______________________________________ Phone Number: ________________________Hospital Closest To Me: __________________________________________________________________________________
GETHELP
16004 ©2018 Association of Women’s Health, Obstetric, and Neonatal Nurses. All rights reserved. Unlimited print
copies permitted for patient education only. For all other requests to reproduce, please contact [email protected].
Tell 911 or your healthcare provider:
“I gave birth on ________________ and
I am having ____________________.”
(Date)
(Specific warning signs)
SAVE YOUR LIFE:
Get Care for These POST-BIRTH Warning SignsMost women who give birth recover without problems. But any woman can have complications after giving birth. Learning to recognize these POST-BIRTH warning signs and knowing what to do can save your life.
Trust
your instincts.
ALWAYS get medical
care if you are not
feeling well or
have questions or
concerns.
POST- BIRTH
WARNINGSIGNS
This program is supported by funding from Merck, through Merck for Mothers, the company’s 10-year, $500 million initiative to help create a world where no woman dies giving life. Merck for Mothers is known as MSD for Mothers outside the United States and Canada.
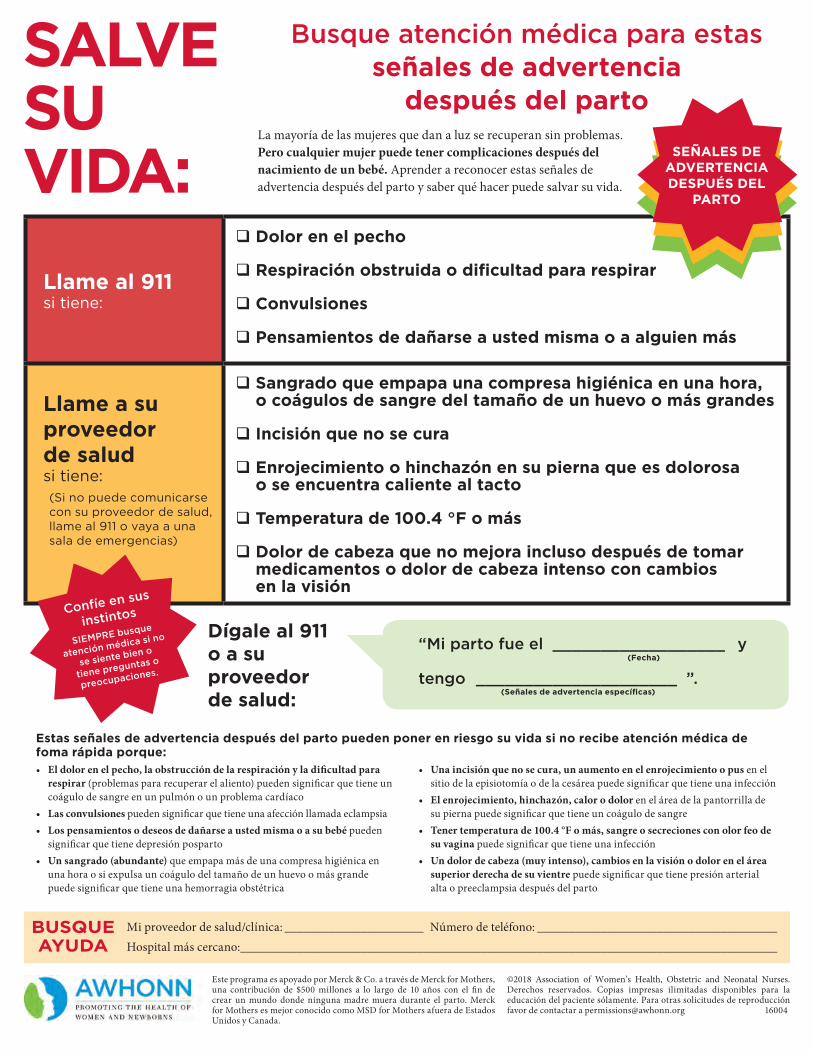
SALVE SU VIDA:
Mi proveedor de salud/clínica: ______________________ Número de teléfono: ______________________________________Hospital más cercano: _____________________________________________________________________________________
BUSQUE AYUDA
Este programa es apoyado por Merck & Co. a través de Merck for Mothers, una contribución de $500 millones a lo largo de 10 años con el fin de crear un mundo donde ninguna madre muera durante el parto. Merck for Mothers es mejor conocido como MSD for Mothers afuera de Estados Unidos y Canada.
©2018 Association of Women’s Health, Obstetric and Neonatal Nurses. Derechos reservados. Copias impresas ilimitadas disponibles para la educación del paciente sólamente. Para otras solicitudes de reproducción favor de contactar a [email protected] 16004
Busque atención médica para estasseñales de advertencia
después del partoLa mayoría de las mujeres que dan a luz se recuperan sin problemas. Pero cualquier mujer puede tener complicaciones después del nacimiento de un bebé. Aprender a reconocer estas señales de advertencia después del parto y saber qué hacer puede salvar su vida.
Llame al 911si tiene:
Dolor en el pecho
Respiración obstruida o dificultad para respirar
Convulsiones
Pensamientos de dañarse a usted misma o a alguien más
Llame a su proveedor de salud si tiene:(Si no puede comunicarse con su proveedor de salud, llame al 911 o vaya a una sala de emergencias)
Sangrado que empapa una compresa higiénica en una hora,o coágulos de sangre del tamaño de un huevo o más grandes
Incisión que no se cura
Enrojecimiento o hinchazón en su pierna que es dolorosao se encuentra caliente al tacto
Temperatura de 100.4 °F o más
Dolor de cabeza que no mejora incluso después de tomarmedicamentos o dolor de cabeza intenso con cambiosen la visión
Estas señales de advertencia después del parto pueden poner en riesgo su vida si no recibe atención médica de foma rápida porque:• El dolor en el pecho, la obstrucción de la respiración y la dificultad para
respirar (problemas para recuperar el aliento) pueden significar que tiene un coágulo de sangre en un pulmón o un problema cardíaco
• Las convulsiones pueden significar que tiene una afección llamada eclampsia• Los pensamientos o deseos de dañarse a usted misma o a su bebé pueden
significar que tiene depresión posparto• Un sangrado (abundante) que empapa más de una compresa higiénica en
una hora o si expulsa un coágulo del tamaño de un huevo o más grande puede significar que tiene una hemorragia obstétrica
• Una incisión que no se cura, un aumento en el enrojecimiento o pus en el sitio de la episiotomía o de la cesárea puede significar que tiene una infección
• El enrojecimiento, hinchazón, calor o dolor en el área de la pantorrilla de su pierna puede significar que tiene un coágulo de sangre
• Tener temperatura de 100.4 °F o más, sangre o secreciones con olor feo de su vagina puede significar que tiene una infección
• Un dolor de cabeza (muy intenso), cambios en la visión o dolor en el área superior derecha de su vientre puede significar que tiene presión arterial alta o preeclampsia después del parto
Dígale al 911o a suproveedorde salud:
“Mi parto fue el __________________ y
tengo _____________________ ”.(Fecha)
Confíe en sus
instintos
SIEMPRE busque
atención médica si no
se siente bien o
tiene preguntas o
preocupaciones.
SEÑALES DE ADVERTENCIA DESPUÉS DEL
PARTO
(Señales de advertencia específicas)
Kansas Perinatal
Community Collaboratives (KPCC)
Information regarding the KPCC and Becoming a Mom® efforts.
SECTION CONTENTS
• KPCC Infographic .................................................................................................... 103 • Becoming a Mom® Overview and Impact .............................................................. 106
The full 2019 Becoming a Mom Annual Report is available online at: https://www.kdheks.gov/c-f/perinatal_program_impact.htm

The Kansas Department of Health and Environment (KDHE) Bureau of Family Health (BFH) has been working diligently with state and local partners since 2014 to strengthen and support the implementation of the Kansas Perinatal Community Collaborative (KPCC) model across the state of Kansas. This highly successful model has proven that through collaboration and implementation of targeted interventions, improved maternal and child health outcomes can be achieved.
KPCC Employs a Three-Pronged Approach:KPCC Employs a Three-Pronged Approach:
+Perinatal Care
Perinatal Education
Perinatal Support = Improved Maternal &
Child Health Outcomes+KPCC Core Partners:KPCC Core Partners:
Health Sector Education Sector Business Sector Non-Profit Sector Other• Health Depts.• FQHCs• Hospitals• Private Providers
• Insurance Providers
• Early Childhood Education
• Early Childhood Coordinating Councils
• Home Visiting• Early Intervention
• Major Employers
• Local Retailers• Financial Institutions
• March of Dimes• United Way• Health Foundations
• Service Organizations
• Faith-Based• Transportation• Housing• Food/Nutrition• Child Care• Emergency Services
Partnerships
ProgressMeasurement
PatientSupport
PublicEngagement
ProviderInitiatives
5 P’s Approach to Improved Outcomes: 5 P’s Approach to Improved Outcomes:Within a Collective Impact framework, the KPCC Model utilizes the March of Dimes’ coined 5 P’s approach, where partnerships and collaborations are key to success and improved outcomes.
Through partnerships and public engagement, public and provider education creates awareness that increases patient support through implementation of evidence-based initiatives, leading to improved
progress measurement around: early access to care; comprehensive care coordination; knowledge and behavior change, which ultimately
leads to improved maternal and child health outcomes.
For more information, visit kdheks.gov/c-f/perinatal_community_collaboratives.htm
Department of Healthand Environment
KPCC ModelKPCC ModelImpact:Impact:
Significantly lower pre-term birth rate among KPCC births (6.4%)2 compared to Kansas births (9.7%)1
Significant drop in infant mortality rates in the two longest running KPCC sites(11.9 to 5.2 and 9.0 to 5.9; 2005-2009 to 2015-2019)2Sources: 1 KDHE, BEPHI; 2 KDHE, BFH
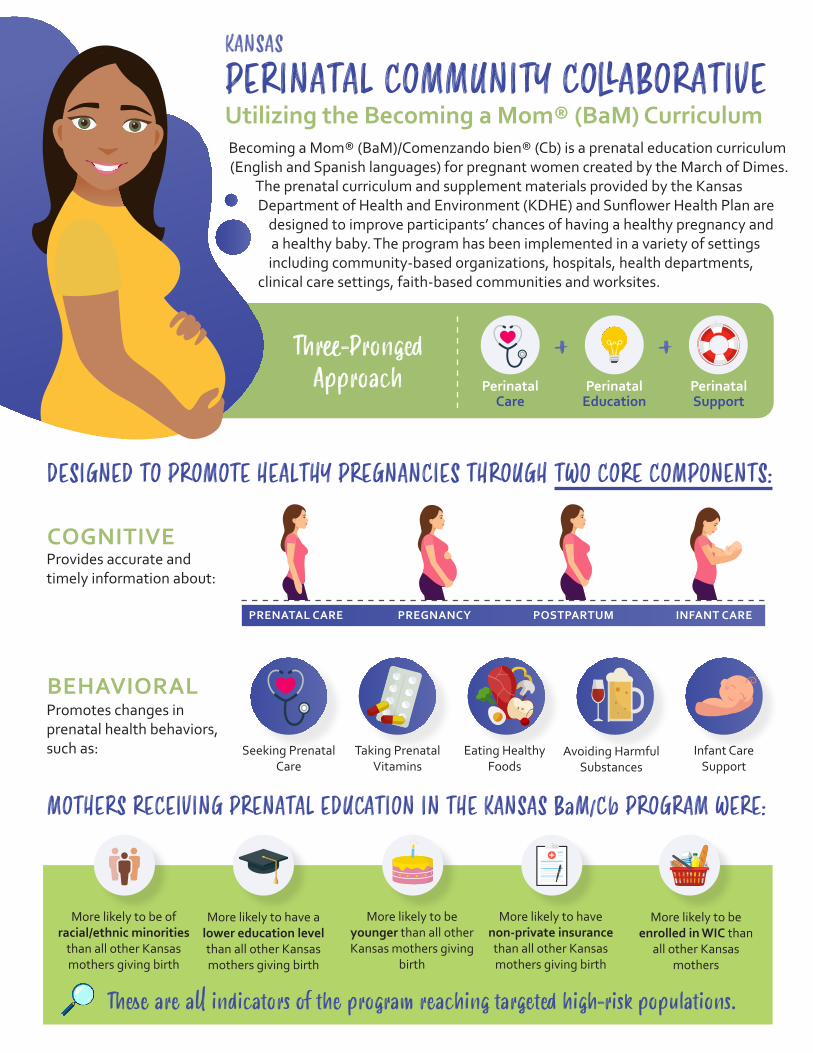
PERINATAL COMMUNITY COLLABORATIVEUtilizing the Becoming a Mom® (BaM) CurriculumBecoming a Mom® (BaM)/Comenzando bien® (Cb) is a prenatal education curriculum (English and Spanish languages) for pregnant women created by the March of Dimes.
The prenatal curriculum and supplement materials provided by the Kansas Department of Health and Environment (KDHE) and Sunflower Health Plan are
designed to improve participants’ chances of having a healthy pregnancy and a healthy baby. The program has been implemented in a variety of settings including community-based organizations, hospitals, health departments,
clinical care settings, faith-based communities and worksites.
KANSAS
Three-Pronged Approach
+ +Perinatal
Care Perinatal
EducationPerinatal Support
DESIGNED TO PROMOTE HEALTHY PREGNANCIES THROUGH TWO CORE COMPONENTS:
COGNITIVEProvides accurate and timely information about:
PRENATAL CARE PREGNANCY POSTPARTUM INFANT CARE
BEHAVIORALPromotes changes in prenatal health behaviors, such as: Infant Care
SupportSeeking Prenatal
Care Taking Prenatal
Vitamins Eating Healthy
FoodsAvoiding Harmful
Substances
MOTHERS RECEIVING PRENATAL EDUCATION IN THE KANSAS BaM/Cb PROGRAM WERE:
More likely to be of racial/ethnic minorities
than all other Kansas mothers giving birth
More likely to have a lower education level than all other Kansas mothers giving birth
More likely to be younger than all other Kansas mothers giving
birth
More likely to be enrolled in WIC than
all other Kansas mothers
More likely to have non-private insurance than all other Kansas mothers giving birth
These are all indicators of the program reaching targeted high-risk populations.
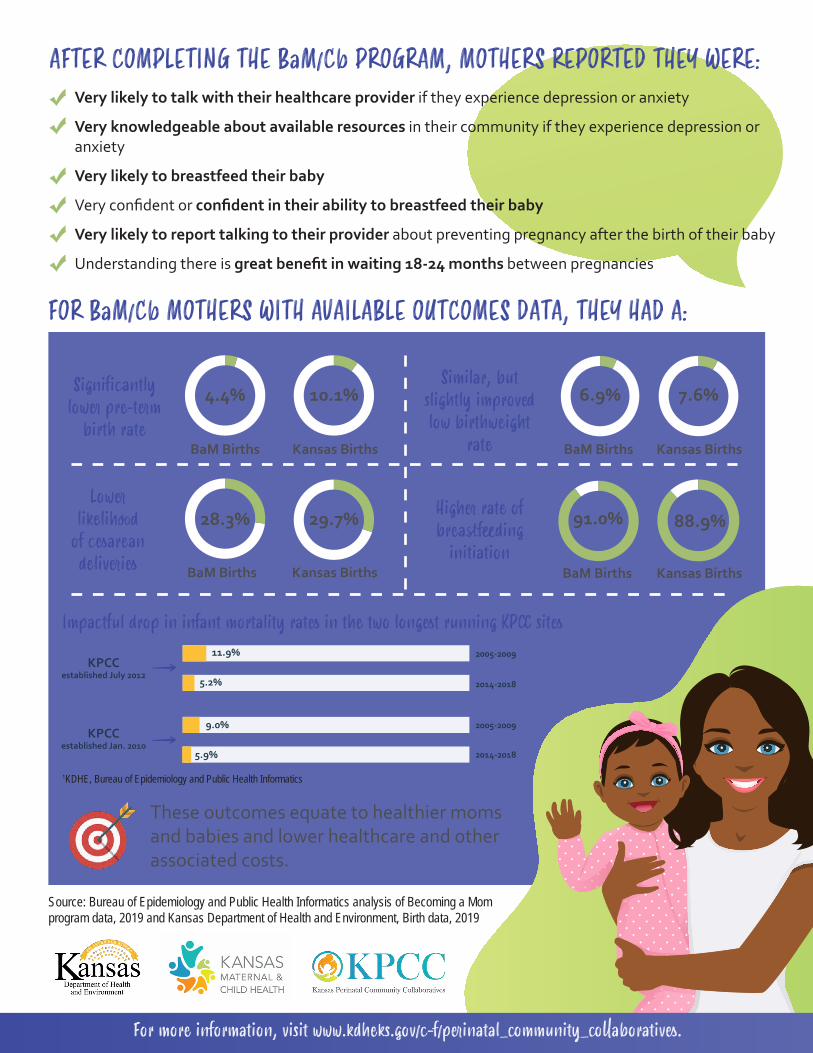
AFTER COMPLETING THE BaM/Cb PROGRAM, MOTHERS REPORTED THEY WERE:Very likely to talk with their healthcare provider if they experience depression or anxiety
Very knowledgeable about available resources in their community if they experience depression or anxiety
Very likely to breastfeed their baby
Very confident or confident in their ability to breastfeed their baby
Very likely to report talking to their provider about preventing pregnancy after the birth of their baby
Understanding there is great benefit in waiting 18-24 months between pregnancies
FOR BaM/Cb MOTHERS WITH AVAILABLE OUTCOMES DATA, THEY HAD A:
Significantly lower pre-term
birth rate
Similar, but slightly improved low birthweight
rate
Lower likelihood
of cesarean deliveries
Higher rate of breastfeeding
initiation
4.4% 10.1%
BaM Births Kansas Births
6.9% 7.6%
BaM Births Kansas Births
BaM Births Kansas Births
28.3% 29.7% 91.0% 88.9%
BaM Births Kansas Births
These outcomes equate to healthier moms and babies and lower healthcare and other associated costs.
For more information, visit www.kdheks.gov/c-f/perinatal_community_collaboratives.
Source: Bureau of Epidemiology and Public Health Informatics analysis of Becoming a Mom program data, 2019 and Kansas Department of Health and Environment, Birth data, 2019
Impactful drop in infant mortality rates in the two longest running KPCC sites
1KDHE, Bureau of Epidemiology and Public Health Informatics
KPCCestablished July 2012
KPCCestablished Jan. 2010
11.9%
5.2%
9.0%
5.9%
2005-2009
2014-2018
2005-2009
2014-2018
Kansas Perinatal Community Collaboratives Utilizing the March of Dimes Becoming a Mom® Curriculum
Becoming a Mom/Comenzando bien® is a prenatal education curriculum (English and Spanish languages) for pregnant women created by the March of Dimes. In Kansas, the curriculum has been integrated into a comprehensive community collaborative model supported and promoted by the Kansas Chapter of the March of Dimes and the Kansas Department of Health & Environment (KDHE) Maternal and Child Health (MCH) program. The prenatal curriculum and supplement materials provided by KDHE is designed to improve participants’ chances of having a healthy pregnancy and a healthy baby. The curriculum is delivered by trained facilitators in a group setting that serves as a source of social support for pregnant women by allowing them the opportunity to connect with other mothers in a similar situation. The program has been implemented in a variety of settings including community-based organizations, hospitals, health departments, clinical care settings, faith-based communities and worksites. The collaborative model and Becoming a Mom® curriculum result in a holistic approach to caring for the family by pairing education and support with clinical prenatal care. This model helps women enhance their well-being and leads to improved outcomes.
In Kansas, this incentive-based program consists of six two-hour sessions that are designed to promote healthy pregnancies through two core components: • Cognitive: provides accurate and timely information about prenatal care, pregnancy, postpartum and infant care. • Behavioral: promotes changes in prenatal health behaviors such as seeking prenatal care, taking prenatal vitamins and
eating healthy foods as well as other health behaviors such as breastfeeding and placing baby on its back to sleep.
During 2019, 1,336 pre-surveys and 901 post-surveys were collected from women enrolled in Becoming a Mom® prenatal education sessions across ten sites in Kansas. A total of 717 participants completed birth outcome cards, reporting birth outcomes and behavior changes. The evaluation revealed the following:
• Significantly lower preterm birth rate (4.4%) than for Kansas births in general (10.1%) • Similar, but slightly improved low birthweight rate (6.9%) compared to Kansas births in general (7.4%) • Lower likelihood of cesarean deliveries (28.3%) compared to Kansas births in general (29.7%) • Statistically significant improvement in likelihood of participant talking to her provider if she is experiencing depression
and/or anxiety during or after her pregnancy, as well as improved knowledge of available mental health resources in her community.
• Statistically significant increase in the number of participants reporting plans to breastfeed, confidence in her ability to breastfeed, and knowledge of available resources for breastfeeding support.
• Significantly greater knowledge in the benefits of a full-term pregnancy, back to sleep position, as well as an increase in knowledge of healthy pregnancy spacing.
• Statistically significant gain in the number of women able to correctly identify the signs and symptoms of preterm labor, what to do if experiencing symptoms of preterm labor, and symptoms that are normal to experience in the postpartum period.
• 90.4% reported breastfeeding initiation rate among participants, compared to 88.9% state rate. • 98.3% rated their overall experience with the program as positive (13.4% - Good, 84.9% - Excellent). • 99.8% reported learning from the program (23.8 % - “some” information, 76.0% - “a lot” of information) • 94.4% reported the program provided them with social support.
Success has demonstrated that group prenatal education can impact birth outcomes, enhance participant’s social support, and create behavior change. Participants gain social support and serve as mentors for each other. Adding to the impact is the community collaborative backbone that is a basis for program delivery at the community level. It is believed that this spirit of collaboration across agencies and programs is contributing to a much greater collective impact than any one agency working in isolation could do on its own. As testimony to this, we have seen the Infant Mortality Rate (IMR) in the two counties of our longest running community collaboratives significantly decrease since the inception of their local perinatal community collaboratives. The Saline County IMR decreased significantly from 10.1 (95% CI 7.2-13.7) in 2004-2008 to 5.9 (95% CI 3.6-9.1) in 2015-2019. The Geary County IMR decreased significantly from 11.9 (95% CI 8.6-16.0) in 2005-2009 to 5.2 (95% CI 3.4-7.7) in 2015-2019*.
“Source: Kansas Vital Statistics 2004-2008, 2005-2009 and 2015-2019 Updated June 2021
Perinatal Mental
Health Toolkit
This infographic shares information about a toolkit to provide education, guidance, and resources for patients and providers related to screening and
treatment for perinatal mood and anxiety disorders (PMAD).
The toolkit is available online at
https://www.kdheks.gov/c-f/mental_health_integration.htm

PROVIDERRESOURCES
Links to online trainings...
Professional recommendations on mental health screening in
perinatal period ...
Treatment options/guidelines ...
Other PMAD-centered toolkits
ALGORITHMSPMAD Screening
workflow...
Crisis Intervention protocol
SCREENINGTOOLS
Edinburgh PostnatalDepression Scale
...Supplemental stress
quiz
PATIENTRESOURCES
(English and Spanish)Patient links for online support
...Resources related to identifying
and treating PMAD ...
Websites and videos
PERINATALMENTAL HEALTH INTEGRATION
TOOLKITRESOURCES AND TOOLS TO ASSIST IN SCREENINGFOR PERINATAL MOOD AND ANXIETY DISORDERS
15–20% OF WOMEN feel moderate to severe depression or anxiety during the periods of pregnancy and/or postpartum (ACOG, 2010).
Find the toolkit here: www.kdheks.gov/c-f/mental_health_integration.htmFor more information, contact Kansas Department of Health and Environment,
Bureau of Family Health Behavioral Health Consultant at 785-296-1327
This toolkit provides education, guidance, and resources for patients and providers related to screening and treatment for perinatal mood and anxiety disorders (PMAD) .
INSIDE THE TOOLKIT
TEMPLATESFOR LOCAL USE
Mental health resource directory...
Sample Model Policy for PMAD screening
...Consent for Communication
and Refusal of Transport forms
The Kansas Connecting Communities project is supported by the Health Resources and Services Administration (HRSA) of the U.S. Department of Health and Human Services (HHS) as part of an award totaling $3,245,698 with no percentage financed with non-governmental sources. The contents are those of the author(s) and do not necessarily represent the official views of, nor an endorsement, by HRSA, HHS, or the U.S. Government. For more information, please visit HRSA.gov.

Screening, Brief Intervention, and
Referral to Treatment (SBIRT) Toolkit
This infographic shares information about a toolkit to provide education, guidance, and resources related to screening and treatment for perinatal
substance use disorders for patients and providers.
The toolkit is available online at:
https://www.kdheks.gov/c-f/SBIRT_Toolkit.htm

PROVIDERRESOURCES
SBIRT training slide decks...
Professional recommendations on screening during
perinatal period...
Additional helpful resources (websites, reference
sheets, pocket cards)
WORKFLOWS& ALGORITHM
ASSIT Alogrithm...
SBIRT Workflow...
Referral Access Point Workflow
PATIENTRESOURCES
(English and Spanish)Patient links for online support
...Resources related to specific drug use during pregnancy
...Websites and
video
SCREENING, BRIEF INTERVENTION,AND REFERRAL TO TREATMENT (SBIRT)
TOOLKITPROVIDER RESOURCES AND TOOLS TO ASSIST IN SCREENING
FOR PERINATAL SUBSTANCE USE DISORDERS
YOU CAN MAKE A DIFFERENCE! Evidence suggests that asking about alcohol and substance use may result in behavior change and asking in detail may increase women’s awareness of their actual consumption and may lead to modified behavior.
Find the toolkit here: www.kdhe.ks.gov/c-f/SBIRT_Toolkit.htmFor more information, contact Kansas Department of Health and Environment,
Bureau of Family Health Behavioral Health Consultant at 785-296-1327
SBIRT is an evidence-based practice used to identify, reduce, and prevent problematic use, abuse, and dependence on alcohol and recreational drugs. This toolkit provides education, guidance, and resources
related to screening and treatment for perinatal substance use disorders for patients and providers.
INSIDE THE TOOLKIT
TEMPLATESFOR LOCAL USE
Substance use resource directory...
Policy model for implementing SUD screening
...Consent for Communication
and Refusal of Transport forms
The Kansas Connecting Communities project is supported by the Health Resources and Services Administration (HRSA) of the U.S. Department of Health and Human Services (HHS) as part of an award totaling $3,245,698 with no percentage financed with non-governmental sources. The contents are those of the author(s) and do not necessarily represent the official views of, nor an endorsement, by HRSA, HHS, or the U.S. Government. For more information, please visit HRSA.gov.
SCREENINGTOOLS
Alcohol, Smoking, and Substance Involvement
Screening Test (ASSIST)

Perinatal Support Group Guidebook
A guide to provide information and guidance for those looking to start a perinatal support group.
The cover page, forward, and acknowledgements were included. The remainder of the Guidebook is available online at:
www.kdheks.gov/c-f/integration_toolkits/ Perinatal_Support_Group_Guidebook.pdf
Perinatal Support Group Guidebook
Provided by: Kansas Department of Health and Environment (KDHE)1000 SW Jackson St, Topeka, KS 66612
Developed by: WSU Community Engagement InstituteWICHITA STATE UNIVERSITY | 1845 N. FAIRMOUNT, WICHITA, KS 67260
1 | P a g e
ACKNOWLEDGMENTS This guidebook was prepared by the staff of Wichita State University Community Engagement Institute, led by Ellen Walker and Teresa Cornejo, with contributions from the Kansas Chapter of Postpartum Support International. Additional thanks are extended to Kansas Department of Health and Environment, Kansas Title V, and Kansas Connecting Communities staff members who provided additional content, helped to edit, and designed the report.
Wichita State University Community Engagement Institute administers Kansas Support Group Services, a website that helps people connect with peers, support groups and support resources available locally, statewide, and nationally. The website includes information on support groups and resources that can be important on the journey of parenthood
and includes topics specific to perinatal mental health and substance use, as well as general physical and mental health, self-care, recovery, and much more. This database is available 24/7 and is searchable by location or specific topic. It also contains a “toolbox” of resources for anyone--peer or providers--wishing to start or maintain a support group. WSU Community Engagement Institute staff are available to help provide more information and resources, as well as provide technical support for group development as needed. For more information, visit the website at: www.supportgroupsinkansas.org, or contact us at [email protected] or 800-445-0116.
Development of this guidebook was funded by Kansas Connecting Communities (KCC), a federally funded cooperative agreement administered by the Kansas Department of Health and Environment. KCC aims to support the improvement of maternal health outcomes across the state through increased provider capacity for the early
identification and intervention for perinatal mental health and substance use disorders. KCC works with a variety of stakeholders and partners, including Wichita State University Community Engagement Institute and Kansas Chapter of Postpartum Support International, to support professional development and continuing education for providers to better address and integrate best practices in the screening, referral, and treatment for perinatal behavioral health disorders. This includes access to training and technical assistance with expert consultants and the development of new community-based resources, such as this guidebook. Providers and stakeholders wanting to learn more about professional resources as well as the state-level work addressing perinatal behavioral health are encouraged to reach out to [email protected] for more information.
The KCC project is supported by the Health Resources and Services Administration (HRSA) of the U.S. Department of Health and Human Services (HHS) as part of an award totaling $3,245,698 with no percentage financed with non-governmental sources. The contents do not necessarily represent the official views of, nor an endorsement, by HRSA, HHS, or the U.S. Government. For more information, please visit HRSA.gov.

2 | P a g e
FOREWORD Up to 20% of mothers experience perinatal mood and anxiety disorders, making this the most common complication of pregnancy and childbirth—above preterm delivery, gestational diabetes or hypertension. Fathers are also at risk of increased anxiety and depression surrounding the birth of a child, at a 10% prevalence rate. In addition to depression and anxiety, perinatal mood and anxiety disorders include adjustment disorders, obsessive compulsive disorders, post-traumatic stress disorder, postpartum psychosis and bipolar disorders. The causes of perinatal mood and anxiety disorders are complex and multi-faceted. These include a combination of biological and psychosocial risk factors, ranging
from hormonal changes to the stress of a major life transition and inadequate support. Although perinatal mood and anxiety disorders impact parents of all socioeconomic backgrounds, the rate of perinatal mood and anxiety disorders almost doubles among low-income parents and people of color.
Untreated perinatal mood and anxiety disorders can have lifelong negative impacts on child development, individual well-being, and family function. Fortunately, effective evidence-based treatment is available and has been shown to mitigate the adverse impact of perinatal mood and anxiety disorders. These evidence-based treatments include individual therapy, couple/family therapy, medication management, group therapy, and peer support groups.
The struggle to access affordable health care is very real and experienced all too often by low-income parents. In a recent dissertation study on perinatal mood and anxiety disorders in Kansas, one mother shared, “After the twins were born and after I was out of the hospital six weeks postpartum my insurance ended because I was getting it through [Medicaid]. So, I didn’t have the money to continue going [to therapy] … I thought about maybe trying another medication [but] I wouldn’t have been able to pay for it, so I didn’t want to start on it and then have to stop it because it can become worse if you suddenly stop the medicine.” This mother was still experiencing severe depression and anxiety three years after childbirth, which also impacted her ability to reenter the workforce. Peer support groups decrease isolation and stigma and provide validation, support, and perspective. Research indicates that participating in peer support options may prevent or decrease the impact of postpartum depression. Offering accessible peer support groups to perinatal families provides a lifeline in the transition to parenthood.
The Kansas Chapter of Postpartum Support International is dedicated to promoting awareness, prevention, and treatment of mental health issues related to childbearing in Kansas. We are committed to serving and advocating for families experiencing or at risk for perinatal mental health conditions across all races, ethnicities, gender, religions, sexuality, and income-level. We are pleased to endorse this guide, created by Wichita State University Community Engagement Institute, as a foundation for offering peer support. We also recognize that peer support strategies must be tailored to local communities, cultures, and populations. Supporting people experiencing perinatal mental health complications and facilitating support groups that are trauma-informed and responsive requires additional training; thus, in addition to the tips and strategies offered in this guide, we encourage support group leaders to seek additional training in perinatal mental health and support group facilitation through a reputable organization, such as Postpartum Support International, 2020 Mom, or GPS Group Peer Support©. We also encourage support group leaders to reach out to each other and the Kansas Chapter of Postpartum Support International to troubleshoot barriers, share strategies, and support each other as you provide this vital service. For more information, or to connect with the Kansas Chapter of Postpartum Support International, visit: www.psichapters.com/ks.
Related Documents











