MASTOIDECTOMY - DR. DHIRENDRA V. PATIL M.S. (ENT) J.N.M.C., Aligarh Muslim University

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

MASTOIDECTOMY
- DR. DHIRENDRA V. PATILM.S. (ENT)
J.N.M.C., Aligarh Muslim University

HISTORY
The first scholarly treatise on mastoid surgery for suppurative disease was by ‘Schwartze’ in 1873.
The procedure he described was a ‘cortical mastoidectomy’ with limited exenteration of mastoid air cells.
In1890, Zaufal described removing the superior and posterior canal wall, tympanic membrane, and lateral ossicular chain, a procedure now known as the ‘radical mastoidectomy’.

This procedure was modified by Bondy, who recognized that disease limited to the pars flaccida could simply be exteriorized, leaving the uninvolved middle ear alone. His description of the “modified radical mastoidectomy” or “Bondy procedure” in 1910 represented one of the first reports addressing hearing function.

Interest in hearing preservation and restoration gained further attention after Lempert introduced the fenestration operation in 1938, and Zollner and Wullsteindescribed tympanoplasty techniques in early1950s.
Lempert popularized the use of a drill and loupe magnification in the 1920s.

During the next decade, Jansen, Sheehy, and others extended these principles of restoring function and maintaining normal anatomy with the introduction of the intact canal wall mastoidectomy with facial recess approach.
With the advent of CWU mastoidectomy, disease control as well as preservation of anatomy and function became a reality.

The first postauricular incision was introduced in 1853 by Sir Willium Wilde of Dublin.

INTRODUCTION
Descriptions of chronic and suppurativeinfections of the mastoid have been discovered dating back to ancient Greece.
Prior to the advent of surgery and antibiotics, morbidity from acute mastoiditis was considerable.
Mastoid surgery has evolved from simple trephination for acute infection, to the canalwall preserving mastoidectomy employed by inost otologists today.

Chronic otitis media, with or without cholesteatoma, is one of the more common indications for performing a mastoidectomy.
Mastoidectomy permits access to remove cholesteatoma matrix or diseased air cells in chronic otitis media.

CWU mastoidectomy is used as a standard approach for
1. Cochlear implantation,
2. Excision of tumors, and
3. Surgery for vertigo.
However, the primary role of CWU mastoidectomy is in the control of chronic otitismedia, with and without cholesteatoma.

CLASSIFICATIONS
Traditionally, classified as :
1. Simple (cortical, complete) mastoidectomy
2. Modified radical mastoidectomy
3. Radical mastoidectomy
A fourth procedure, Tympanomastoidectomy , combines the simple mastoidectomy with a middle-ear procedure, maintaining the posterior and superior canal walls.

Depending on the fact whether postero-superior canal is removed or not,
1. Canal Wall Up mastoidectomy
2. Canal Wall Down mastoidectomy.

SUBCLASSIFICATION (M.Tos)
CANAL WALL UP (CWU) CANAL WALL DOWN (CWD)
1. Simple/ cortical/ complete/ Schwartze’s mastoidectomy
1. Atticotomy
2. Classic Intact Canal Wall Mastoidectomy/ Combined Approach Tympanoplasty (CAT)
2. Atticoantrotomy
3. Radical Mastoidectomy
4. Modified Radical Mastoidectomy/ bondy’sProcedure
5. Retrograde Mastoidectomy
Depending upon the mastoid cavity,
1. Open Technique
2. Closed Technique

CLASSIFICATION IN RELATION TO REMOVAL OF THE BONY EAR CANAL WALL AND OBLITERATION
OF CAVITY

ANATOMICAL CONSIDERATIONS

The temporal bone consists of four parts: squamous, tympanic, mastoid, and petrous(Figs.)
Important surface landmarks on the mastoid include the temporal line, which extends posteriorly from the zygomatic root and is the insertion site for the temporalis muscle.


The suprameatal spine of Henle is a small bony protuberance extending superficially from the posterior and superior bony EAC.
Posterior to the suprameatal spine, a group of small holes is seen, described as the cribriform area.
Small vessels pass through these foramina to the mucosa of the underlying antrum in infants, and it’s here that a subperiosteal abscess forms in cases of acute coalescent mastoiditis.
This cribriform area lies within Macewen’striangle, an imaginary triangle defined by three lines-
1. Temporal line
2. Line formed by the superior and posterior margins of the external bony meatus (This line goes through the suprameatal spine)
3. Line drawn perpendiular to the first line and tangential to the second.



Mastoid antrum lies around 1.25 cm to 1.5 cm deep from the surface of Macewen’s triangle.
Cymba concha is the soft tissue anatomical landmark for the mastoid antrum.


Facial Bridge is that portion of posterosuperior bony meatal wall that bridges over the notch of Rivinus and overlies the ossicles.
Facial Ridge is that part of the bony meatalwall which houses the posterior bend and vertical segment of facial nerve.
Anterior Buttress is the point at which the posterior bony canal wall meets the tegmen.

DIAGRAM TO SHOW FACIAL RIDGE, BRIDGE, ANTERIOR AND POSTERIOR BUTTRES

Posterior buttress marks the meeting of the posterior canal wall and the floor of the EAC lateral to the facial nerve.
Its removal causes the floor of EAC to slope off gently into the mastoid tip.




Citelli’s angle (Sinodural angle)- is an angle between the sigmoid sinus and middle fossadural plate.
Solid angle is an area where three bony semicircular canals meet.
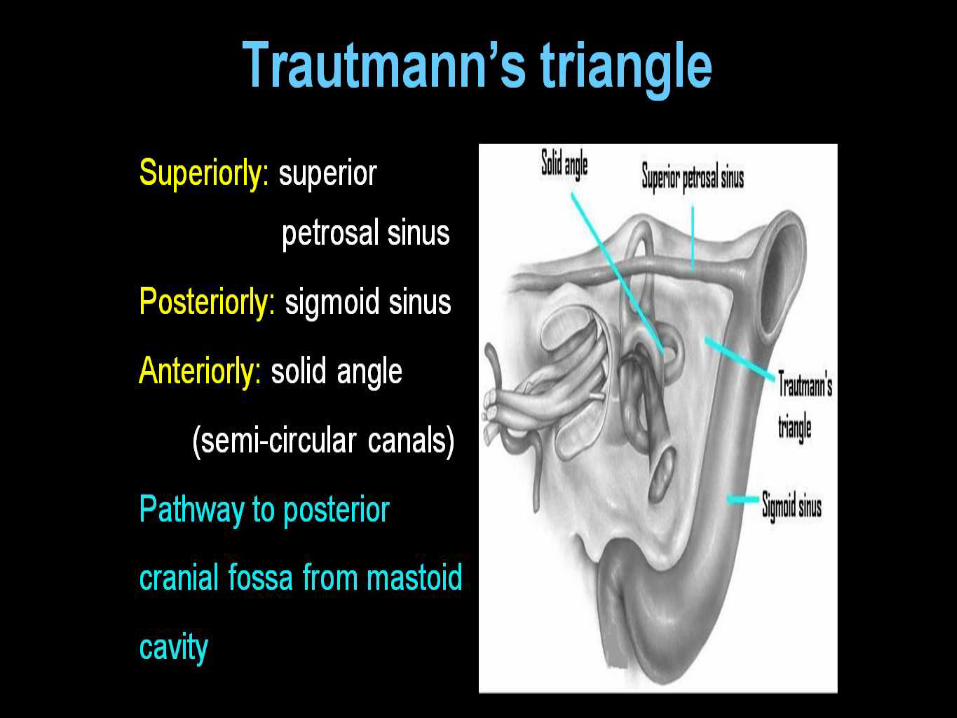
Trautmann’s triangle is bounded by bony labyrinth (solid angle) anteriorly, sigmoid sinus posteriorly and dura superiorly.

Donaldson’s line is a line passing through the horizontal semicircular canal and bisects the posterior semicircular canal.
This line is a landmark for the endolymphatic sac.


DEFINITIONS

APPROACHES And ROUTES
The term ‘Approach’ means the method of access to the middle ear through the soft tissues.
eg. Endaural approach, Retroauricularapproach.
The term ‘Route’ means the method of access to the middle ear through the bone.
eg. Transcortical route, Transmeatal Route.


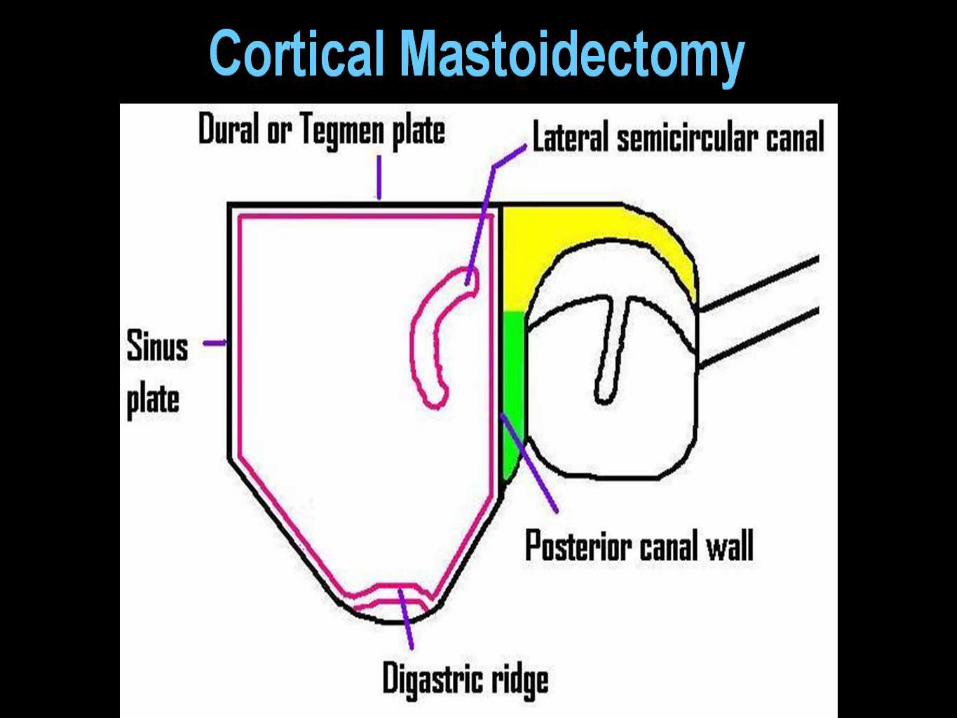
CORTICAL MASTOIDECTOMY
CORTICAL MASTOIDECTOMY (Schwartze 1873) is a transcortical opening of the mastoid cells and the antrum.
It is the initial stage of any transmastoidsurgery of the
1)middle ear 2)inner ear, 3) facial nerve, 4)endolymphatic sac, 5) labyrinth, 6) I.A.C and 7) skull base.



SIMPLE MASTOIDECTOMY – This term is usually used when mastoidectomy is done for drainage of a mastoid abscess.

COMBINED APPROACH TYMPANOPLASTY
(CAT)/ CLASSIC INTACT CANAL WALL
MASTOIDECTOMY
CAT consists of a large mastoidectomy with an intact but thin bony ear canal wall and a posterior atticotympanotomy.
The intact canal wall technique is performed in two stages.
The first operation is performed to remove all cholesteatoma and repair the tympanic membrane.

Six months later, the second operation is performed to inspect the mastoid and middle ear for residual or recurrent cholesteatoma and to improve hearing by ossicular reconstruction.
STEPS OF CAT
1. Cortical mastoidectomy
2. Anterior Tympanotomy : via tympanomeatalflap
3. Posterior Tympanotomy: via facial recess approach
4. Tympanoplasty



DEFINITIONS
ATTICOTOMY (EPITYMPANOTOMY)- denotes opening of the attic, performed through the transmeatal route.


ATTICOANTROTOMY- is an extension of the atticotomy in a posterior direction through the transmeatal route, in which lateral attic and aditus walls are removed, and the antrum is entered.
It can be performed through the transcorticalroute, but is usually performed through a transmeatal route.

BONDY’S OPERATION – An atticoantrotomy is called as Bondy’s operation if the tympanic cavity is not entered.
The lateral part of the cholesteatoma is removed (fig) and the medial part is left in place (fig), marsupialising the cholesteatoma.
If the tympanic cavity is entered, it is NOT described as BONDY’S operation but as an atticoantrotomy or conservative radical operation.



MODIFIED RADICAL MASTOIDECTOMY
Classically, modified radical mastoidectomyrefers to the Bondy procedure, in which disease limited to the epitympanum is simply exteriorized by removing portions of the adjacent superior or posterior canal wall.
But, Frequently, the term modified radical mastoidectomy is used interchangeably with canal wall down mastoidectomy.

A primary feature of the modified radical procedure is complete removal of the posterior canal wall, the major reason for failure of the Bondy procedure.
MRM is an effective method to manage cholesteatoma in a ‘single-stage’ approach (Unlike CAT).
MRM is a surgical procedure where the disease process is eradicated from the middle ear cleft;followed by converting the mastoid cavity, middle ear and EAC into a single, smooth, self-cleansing cavity exteriorised through EAC.

RADICAL MASTOIDECTOMY
Radical mastoidectomy is a canal wall down mastoidectomy performed to eradicate disease from middle ear cleft in which mastoid cavity, tympanum and EAC are converted into a common cavity exteriorised through the EAC, wherein the structures of tympanic cavity (remnants of the incus and malleus, and the drum remnant) are removed.

In ‘Classical Radical Cavity’, closure of the eustachian tube is performed.
But, closure of the eustachian tube is NOT essential for the term ‘Classical Radical Operation’.


INDICATIONS

INDICATIONS OF CORTICAL MASTOIDECTOMY
1) Coalescent Mastoiditis and Masked Mastoiditis.
2) CSOM TTD Active Refractory to antibiotics.
3) Secretory otitis media Refractory to antibiotics.
4) Approach to:
-Endolymphatic sac surgery.
-Facial nerve decompression.
-Vestibulo cochlear nerve section.
-Translabyrinthine Approach for CP angle.
-Cochlear implant surgery.
-Combined Approach Tympanoplasty.

Indications For MRM
Absolute Indications (Shambaugh):
1. Unresectable disease
2. Unreconstructable Posterior canal wall
3. Failure of first stage CWU procedure because of poor E T function.
4. Inadequate Patient Follow up.

Relative Indications (Shambaugh):
1. Disease in only hearing ear or in a dead ear.
2. Medical illness
3. Severe otologic or CNS complications
4. Neoplasms
5. Poor E T function.

CONTRAINDICATIONS
1. Chronic otitis media without cholesteatoma
2. Acute otitis media with coalescent mastoiditis,
3. persistent secretory otitis media, or
4. Chronic allergic otitis media.
5. Tuberculous otitis media.

Indications For Radical Mastoidectomy (shambaugh)
1. Unresectable cholesteatoma extending down the Eustachian tube or into the petrous apex
2. Promontory cochlear fistula caused by cholesteatoma
3. Chronic perilabyrinthine osteitis or cholesteatoma that cannot be removed and must be cleaned or inspected periodically
4. Resection of temporal bone neoplasms with periodic monitoring

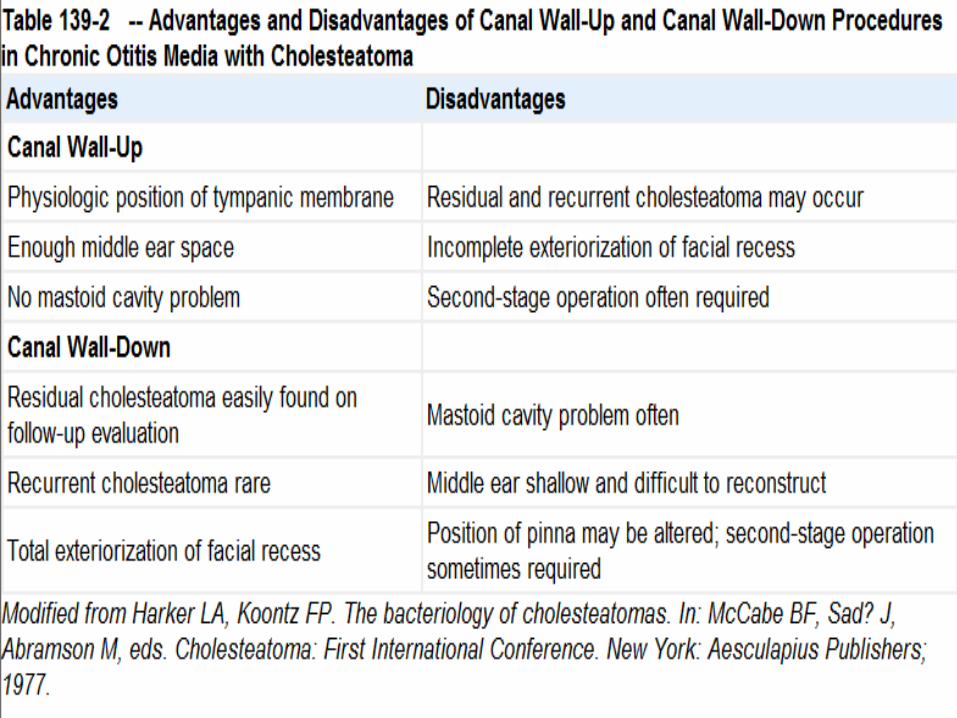
CWU Vs CWD
The choice for preserving or removing the posterior wall of the EAC, ie, CWU versus CWD mastoidectomy, has been extensively debated.
Preservation of the canal wall is preferred.
The decision to remove the wall is most often made during surgery, when the extent of the disease is fully appreciated.

Intraoperative findings that may be indications for a CWD procedure include
-labyrinthine fistula,
-unresectable disease on the facial nerve or stapes footplate,
-a low-lying tegmen that limits access to the attic,
-unresectable sinus tympani disease,
-and an unreconstructable posterior canal wall defect.

Removal of the canal wall does not improve access to the sinus tympani.
Rarely, our preoperative evaluation may result in the decision to take down the canal wall.
1.Obvious posterior wall erosion,
2.larger labyrinthine fistula on CT scan,
3.elderly or infirmed patients in which second look is unadvisable.

4. Occasionally with disease in an only hearing ear, are preoperative conditions that may warrant a CWD procedure.

OPERATIVE TECHNIQUES(CWU)
Preparation-
General anesthesia without paralytic agents and with continuous facial nerve Monitoring.
Tragus and postauricular skin are injected with 1% lidocaine with epinephrine (1: 100,000) to provide hemostasis and local anesthesia.
“Pre-scrub" the ear and the entire side of the head, including hair, with betadine.

The surgical site is
then prepped and draped in sterile fashion.

INCISION
The postauricular incision is made from helical rim to mastoid tip, approximately 1 cm posterior to the sulcus.
Care is taken to avoid making the incision in the sulcus as this can make closure more difficult.

A T-shaped incision is made in the mastoid periosteum to expose the mastoid cortex
An incision is made along the linea temporalis, to the level of the underlying bone.
A second periosteal incision is made perpendicular to the linea temporalis and is carried down to the mastoid tip.

.

Using the Lempert elevator, the periosteum is elevated superiorly over the tegmen, posteriorly over the sigmoid sinus, and anteriorlyto the level of the EAC meatus.

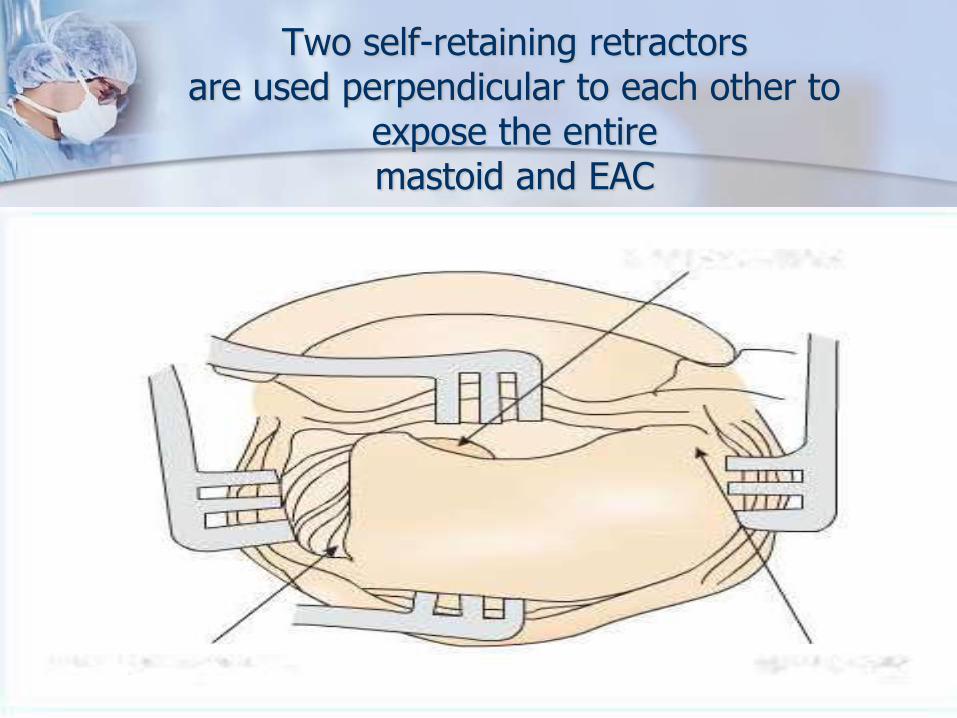
Two self-retaining retractorsare used perpendicular to each other to
expose the entiremastoid and EAC
Middle Ear Dissection
Some authors (shambaugh) prefer to begin with middle ear dissection prior to mastoidectomy to control middle ear disease and ascertain the state of the ossicular chain.
Ossicular erosion may allow for removal of the incus and malleus to protect the stapes and footplate from injury prior to dissection of the attic.
The tympanomeatal flap is elevated anteriorlyand is carefully dissected free from the ossicular chain.
Cholesteatoma, if present, is gently dissected from the middle ear to expose the ossicles and facial nerve.

Cholesteatoma or granulation tissue is dissected free from the ossicles, leaving the ossicular chain intact if possible.
If preservation of the ossicular chain is not possible, separation of the incudostapedial joint is performed early to prevent injury to the stapes or inner ear.

Canalplasty
Often middle ear dissection and postoperative follow-up is facilitated by canalplasty, which is performed at the onset of the procedure.
Using a 2-mm diamond burr, excess tympanic bone at the tympanomastoid and tympanosquamous suture lines is removed.
Often removal of this small amount of bone greatly improves the exposure, ensuring better disease resection and graft placement.

Extreme care must be taken when drilling in postrior-inferior quadrant of the canal as this is the area of the canal where the facial nerve is at most risk to injury.
A canalplasty should always be done first as it defines the anterior limit of your mastoidectomy .

Completed canalplasty with entire annulus visible

Mastoidectomy
BASICS:
Mastoidectomy is conducted with the visualization afforded by the
1. Binocular-operating microscope
2. High-speed drill, and
3. Suction-irrigation.


a) cutting bur b)cutting diamond bur (note the course texture) c) a diamond bur.

Cutting burrs are efficient at removing large amounts of bone in a small amount of time.
Diamond burrs are very good at delicate dissection around important structures, thinning the bone off the sigmoid sinus, tegmen, facial nerve, and opening the facial recess.
During the mastoidectomy, larger burrs are used first and the burr size is sequentially decreased as the areas of dissection get narrower.
The largest burr possible should always be used as it is less likely to inadvertently penetrate an underlying structure and is yet more efficient for bone removal.
The surgeon must always be aware of what the back of the burr may be touching.

Drilling tips
Avoid keyhole surgery; work through a wide space
The tip of the drill should always be visible
Never drill behind edges of bone
Drilling should always be parallel to any structure you are trying to preserve e.g. facial nerve, sigmoid sinus
When drilling deeper in the mastoid cavity the burr needs to be lengthened

One cannot lengthen a cutting burr as this will cause the drill to jump with the risk of injuring structures
Therefore if it is necessary to lengthen the burr, then change to a rough diamond or diamond burr.

Effective use of the suction irrigator is important for safe and effective drilling.
Appropriate irrigation is necessary
1. to clear bone dust from the field of dissection,
2. to prevent excessive heat transfer to underlying structures (especially the facial nerve), and
3. to maintain a clean cutting surface on the bur.

Canal-Wall-Up Mastoidectomy
Initial dissection involves using a 5- or 6-mm cutting burr and removing bone along the lineatemporalis to identify the underlying tegmen.

The surgeon should look for the emergence of a pink hue under the bone as it is thinned over the tegmen, accompanied by a change (more "tinny") in the sound of the burr.
Once located, the surface of the tegmen is followed medially toward the antrum.
The middle fossa dura is always delineated as it is the superior extent of the dissection.

After identification of the tegmen, cortical bone is removed behind the EAC, keeping the posterior wall of the EAC thin, but intact.
A key landmark in performing mastoid surgery is the antrum with the dome of the horizontal semicircular canal (HSCC) along its floor. The ease of locating the antrum depends largely on the degree of mastoid pneumatization.

Three key principles assist this part of the dissection:
1.saucerization,
2.identification of the tegmen plate, and
3.thinning the posterior canal wall.
The deepest dissection is at the point where the initial cortical bone cuts intersect, but widely saucerizing toward the tegmen and especially posteriorly (from the sinodural angle to the mastoid tip) as the antrum is approached is essential.
As the bone over the sigmoid sinus is thinned, a bluish hue will become apparent beneath the bone, accompanied by a change in the sound of the burr.

With the tegmen, sigmoid sinus, and posterior canal wall identified, the antrum can now be dissected, following the tegmen anteriorly.
Koerner's septum, the embryologic remnant of the fusion plane between the petrous and the squamous bones is often encountered next. After penetrating Koerner's septum, the antrumis uncovered and the surgeon can identify the lateral semicircular canal.


In patients with CSOM, the antrum may be observed with cholesteatoma, granulation tissue, or edematous mucosa, obscuring the lateral semicircular canal and making its identification more difficult.

The next step is attic dissection, which is performed by following the tegmen anteriorlyand by thinning the canal wall posteriorly and superiorly.
Care is taken to avoid drilling a hole in the bony canal wall.
Rotating the operating bed toward the surgeon affords simultameous viewing of the canal and the mastoid.

Drilling out the zygomatic root and opening the attic is often better accomplished with a 3-mm cutting burr and a smaller suction irrigator.
The tegmen is carefully followed and usually dips inferiorly as the epitympanum is approached from posterior to anterior.
The attic air cells are opened completely, fully exposing any epitympanic disease.
Granulation and cholesteatoma can now be removed from the canal or attic vantage points.
The cog is a flat, thin, bony projection from the tegmen, in the parasagittal plane, that appears to have a semicircle cut out of the inferior border. (Cog: bony ridge hanging from tegmen tympani lies 1 mm above & posterior to cochleariform process.)
Located directly superior to the cochleariformprocess, with the tensor tympani tendon it creates a small, roughly round aperture that opens into the anterior epitympanum.
If it is not specifically identified and removed, significant disease may be left in the anterior attic.
Preserving facial nerve function is paramount in ear surgery.

Except for simple mastoidectomy, it is always safer to define the location of facial nerve than simply to avoid it.
In intact canal wall mastoidectomy (or when a cochlear implant is placed), the space between the facial nerve and the chorda tympani nerve—the facial recess—provides access into the middle ear (Fig.)



In canal wall down approaches, identifying the facial nerve allows the surgeon to lower the facial ridge appropriately, creating a more care-free cavity.

The most important landmarks for the facial nerve are the
1. HSCC,
2. The short process of the incus,
3. The posterior bony external auditory canal
4. The digastric ridge.
The genu and proximal portion of the mastoid segment of the facial nerve lie anterior and just medial to the dome of the HSCC.

The mastoid segment of the facial nerve also lies medial to the plane of the short process of the incus at the base of the posterior canal wall.
Removing air cells from the posterior bony canal wall until it is only a few millimeters thick is essential.

If the canal wall is not thinned appropriately, a wall of air cells continues to cover the facial nerve, and the dissection is carried too far posteriorly, potentially exposing the posterior side of the facial nerve to injury.
After locating the antrum, a diamond bur is used to open the aditus ad antrum, which leads into the epitympanic space.


The short process of the incus is exposed. With this landmark visible, a larger cutting bur or coarse diamond bur removes bone over the area of the facial nerve, with continued thinning of the posterior bony canal wall as the dissection is carried medially.
When the plane of the short process of the incus is reached, it is anticipated that the facial nerve will be 1 to 2 mm deeper, and the bur type is changed to a fine diamond

Strokes are made in a longitudinal direction, paralleling the course of the facial nerve.
Dehiscences of the mastoid portion of the fallopian canal, even in the presence of mastoid disease, are infrequent.
This is in contradistinction to the tympanic segment of the facial nerve, where congenital and disease-mediated dehiscences are common.

Appropriately thinning the canal wall often exposes the chorda tympani nerve, which can be distinguished from the facial nerve by size and course of direction.
If disease is limited to the antrum,its not needed to uncover the vertical segment of the facial nerve to determine its location.
Opening the Facial Recess
The facial recess is a triangular-shaped area bordered by the facial nerve posteriorly, the incus buttress superiorly, and chorda tympani nerve anterolaterally (Figure).
Access to the mesotympanum can be gained by removing the bone in the facial recess.


For additional exposure, the facial recess can be extended inferiorly by sacrificing the chorda tympani nerve
The entire mesotympanum and hypotympanum can usually be accessed through the mastoid by the extended facial recess approach (figure).


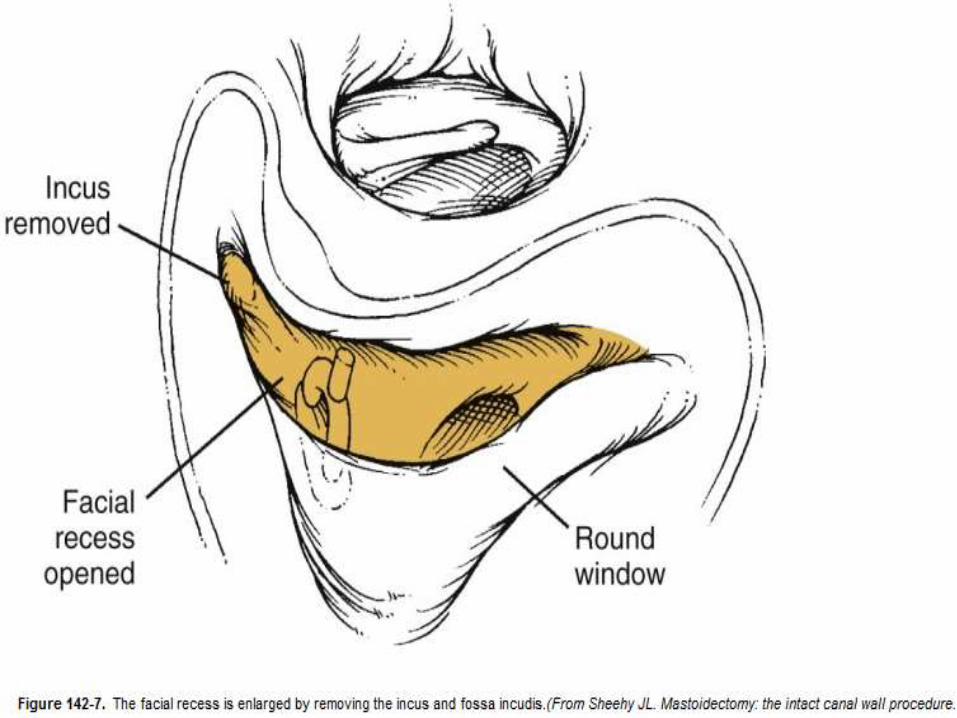
In chronic ear surgery, the long process of the incus has been eroded, and that ossicle is removed.
In such cases, the fossa incudis is taken down, connecting the facial recess with the aditus ad antrum, providing wide exposure over the HSCC and the genu of the facial nerve into the epitympanum (Fig).

Opening the Epitympanum
In intact canal wall mastoid surgery, it is frequently necessary to expose the epitympanum.
Cholesteatoma can track medially to the heads of the ossicles and extend into the anterior epitympanic space, also termed the supratubalrecess. Opening the epitympanum is much easier if there is discontinuity of the ossicularchain (e.g., eroded long process of the incus).

In such cases, the incus remnant and the head of the malleus are removed, providing good access into the anterior aspect of the epitympanum.
It is important to appreciate the anatomic relationships of the facial nerve within the epitympanic space.

As the nerve is traced anteriorly from the mastoid genu to the geniculateganglion, it takes a slightly medial course. It passes superior to the oval window and cochleariform process (Fig.).

The facial nerve in the floor of the anterior epitympanic space can be dehiscent, especially if extensive cholesteatoma involves this region (Fig.).


Dissection of Cholesteatoma
Before dissecting the cholesteatoma sac from the mastoid bone, the sac should be opened and its contents should be evacuated, leaving the matrix in place.
The consistency of cholesteatoma matrix is quite variable, ranging from a relatively thick and well defined capsule to loose squamousdebris without any visible capsule.

CLOSURE
Upon complete removal of disease, the ear canal and mastoid cavity are irrigated extensively with antibiotic-containing saline solution to remove any bone dust and remaining squamous debris.
The self-retaining retractors are removed and the vascular strip skin flap is unfurled and placed back into the ear canal.
The postauricular incision is closed in two layers.

The incision is covered in antibiotic ointment and a Glasscock ear dressing (Otomed) is applied.

Canal Wall Down Mastoidectomy

Many of the disadvantages of a canal wall down procedure can be minimized with proper creation of the mastoid cavity.
Crucial components of the procedure include the following:
1.Aggressively saucerizing the cavity
2.Eliminating irregularities within the cavity (e.g., deep recess and bony overhangs)
3.Removing the posterior bony canal wall to the level of the facial nerve
4.Creating a large meatus.
Saucerization decreases the depth and the size of the mastoid cavity.
The cortical edges of the cavity are taken down to the approximate level of the tegmen superiorly, sigmoid sinus posteriorly, and digastric ridge inferiorly (Fig.).


All mastoid air cells should be removed with exposure of the middle fossa and posterior fossa dural plates, the sigmoid sinus, digastricridge, and bony canal wall (Figure 31-lE).

Cholesteatoma and granulations filling the central mastoid tract can be removed at this time.
The vertical segment of the facial nerve should now be identified, followed by opening of the facial recess (Figure 31-lF).


The posterior canal wall can now be safely taken down with a rongeur and the facial ridge can be lowered until a thin layer of bone remains over the vertical segment of the facial nerve (Figure 31-IG)


The inferior canal wall must be drilled away until the inferior canal wall and mastoid tip are confluent, with no bony overhang to obscure the mastoid tip.
The sinus tympani is the most difficult region to investigate. If disease extends into this region, and if the stapes is absent, the pyramidal

eminence can be removed with a small diamond bur.
At this point, the cavity should be smooth-walled and free of active disease (Figure 31-lH).


Meatoplasty:
One percent lidocaine with 1:100,000 epinephrine is infiltrated into the conchal bowl.
With a finger in the conchal bowl, a semilunar incision is made into the cartilage posteriorly until the knife tip is felt through the anterior skin.
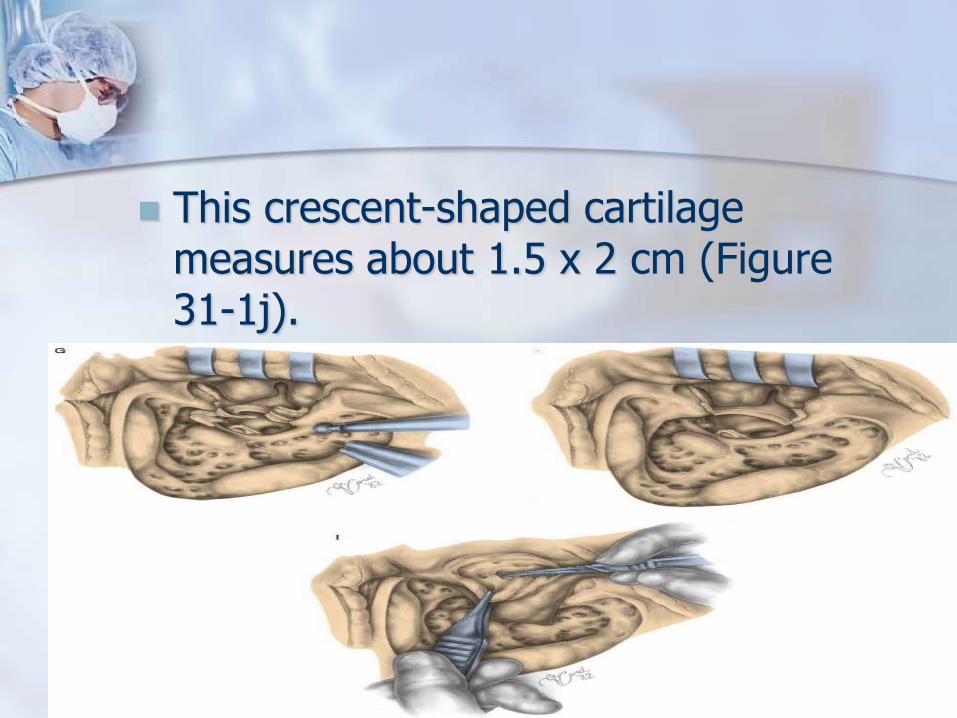
This crescent-shaped cartilage measures about 1.5 x 2 cm (Figure 31-1j).




COMPLICATIONS
Trauma to Dura
Horizontal Semicircular Fistula
Trauma to Facial Nerve
Sigmoid Sinus and Jugular Bulb Injury.
TRAUMA TO DURA
A dural tear or significant abrasion with herniation of arachnoid tissue with or without a cerebrospinal fluid leak requires REPAIR.
Best repaired with a layered closure using soft tissue such as fascia or perichondriumcombined with a more rigid support material such as bone or cartilage.
Broad-spectrum antibiotics.

Firmly packing the mastoid (or epitympanum) with absorbable gelatin sponge (Gelfoam) (with or without fibrin glue) can be used to support the repair.

Horizontal Semicircular Fistula
Should always be considered when performing chronic ear surgery
A flattened HSCC dome suggests labyrinthine erosion.
In such cases, the cholesteatoma sac is opened, the desquamated epithelium is removed, and the matrix is left intact over the canal.

If an actual erosion into the fluid space of the HSCC is encountered or suspected during palpation, the cholesteatoma matrix should be left in place.
When all other disease is removed, several options are possible:
1) remove all matrix, and cover the defect with soft tissue or bone wax;
2) perform a canal wall down procedure, and allow the matrix to remain in place as part of the mastoid cavity; or

Or
3) perform an intact canal wall procedure and leave the matrix in place to be removed at a second stage when the ear is sterile.
-Broad-spectrum antibiotic and steroids should be considered if the canal has been entered.

Iatrogenic injury to the HSCC requires immediate closure- bone wax/soft tissue.
INJURY TO FACIAL NERVE
Identification, rather than avoidance, of this structure is fundamental for Mastoidectomyprocedure.


Sigmoid Sinus and Jugular Bulb Injury
Sigmoid sinus and jugular bulb are characterized by variable anatomy.
This fact places these structures at risk for inadvertent injury.
Injury to these low-pressure, but high-volume, venous structures is initially treated with digital pressure.
For small tears-bone wax.
For larger rents-cellulose-type surgical packing.

Related Documents


![[PPT]PowerPoint Presentation - The Medical Post | Trusting · Web view2011/02/12 · Dr. Vishal Sharma Schwartze’s Cortical Mastoidectomy Middle ear cleft (Right) Cortical Mastoidectomy](https://static.cupdf.com/doc/110x72/5aac7bf87f8b9a8d678cf81c/pptpowerpoint-presentation-the-medical-post-trusting-view20110212dr.jpg)








