Masochism: On how to like pain Abraham Sapién Córdoba Master’s thesis Cogmaster M2 ENS, EHESS, Paris V Institut Jean Nicod 4 th June 2013

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Masochism:
On how to like pain
Abraham Sapién Córdoba
Master’s thesis
Cogmaster M2
ENS, EHESS, Paris V
Institut Jean Nicod
4th June 2013
2
Originality declaration:
In the present study I propose a new model that gives account of our different
interactions with pain. More importantly, the current study addresses the relationship
between pain and masochism. In comparison to other models, the model here presented
studies pain as part of a wider spectrum that considers our interaction with pleasant and
unpleasant phenomena.
Contribution declaration:
Given the theoretical approach of the present study, the final product is the result of the
collaboration between my advisor, Frédérique de Vignemont, and myself.

3
Acknowledgements
From the general to the particular, I would like to thank people in three levels. First, I
would like to thank all the people and institutions that supported and welcomed me to
come study in France. Second, I deeply thank all the people that have discussed with me
about the nature of pain and I would also like to thank the ones who have devoted their
own research to understand pain, without this input not only my project, but research in
general, would be impossible. Third, I would like to particularly thank Frédérique de
Vignemont for her sharp mind and help.

4
Introduction
“Whip me”, I begged, “whip me without mercy.”
Wanda swung the whip, and hit me twice. “Are you satisfied now?”
“No.”
“Seriously, no?”
“Whip me, I beg you, it is a joy to me”
Sacher-Masoch, Venus in Furs, (1870).
The main motivation of this research is to have a better understanding of the sensation
of pain, or “physical pain”, by using masochism as a case study. The main characteristic
of masochism is that, in contradiction to the usual behavior in presence of pain,
masochists pursue pain. The standard abhorrent nature of pain has already been
questioned by other medical cases where patients do not present the usual avoidance
behavior in presence of pain. Broadly, in all these cases patients tend to have no
reaction, although they claim that they feel pain. However, the fact that masochists have
the complete opposite behavior arises many questions concerning the nature of pain and
its relationship with pleasure. That is, in order to understand masochism, we need to
understand pain as part of a wider spectrum that also includes our relationship with
pleasant phenomena.
In this research I will address two main issues in relation to pain, one from the medical
sciences and the other concerning the current discussion in philosophy. The first one is
related with medical cases and experimental models, which support that a descriptive
and an evaluative dimension constitute pain; although we usually experience pain as a
whole, there is good evidence that we can experience these two aspects of pain
separately and that they also correspond to different areas of the nervous system. The
second issue is related to the nature of pain. More particularly, one needs to clarify the
notion of unpleasantness in pain and that the intimate relation between the sensation and
avoidance behavior, which is not encountered in other kinds of perception.

5
In this sense, in the present research I do not tackle other questions concerning the
physiological or theoretical nature of pain. For instance, I do not carry any sort of
experiments concerning pain or masochism and I do not address the discussion about
the nature of pain in representational terms. The current study proposes a theoretical and
cognitive approach that pursues to shed light on the diverse interactions that we can
have with pain. More precisely, thanks to the medical models of pain and the
philosophical discussion on it, I will propose a model that provides a coherent solution
to masochism and to our general interaction with pleasant and unpleasant sensations.
Finally, if we reconsider our interactions with pain and pleasure, I argue, we are all
masochists, at least to a certain degree.
6
Part I.
Do they really like it?
In this first part, I clarify why masochism is an interesting case study for pain. To do so
I proceed in three sections. First, I elucidate on why masochism is usually considered as
a problematic case for pain. Second, I offer a first possible answer in order to show that
masochism is not really problematic; this solution is based on the medical definitions of
both pain and masochism. Third, I will present a second possible answer, which
proposes to explain that, in masochism, pain is merely a means for an end. Finally, I
will show that even if both attempts are useful to get a better understanding about the
nature of pain and our interaction with it, these solutions are insufficient to clarify the
relationship between pain and masochism.
1. Masochist contradiction
1.1. Necessary unpleasantness
The usual contradiction between pain and masochism has the following structure:
1) Pain is unpleasant
2) We dislike unpleasant things
3) Masochists like pain
4) So, masochists like and dislike the same thing!
In other words, what is interesting about masochism is that it seems to be the only
situation where people have a complete opposite behavior in the presence of pain:
masochists seek pain. Since pain is paradigmatically an unpleasant sensation, it seems
contradictory that masochist like pain. So, in order to enter the discussion between pain
and masochism, there are two questions that we have to address: 1) is pain necessarily
unpleasant? And 2) do masochists really like pain?

7
We can start by the first question. That is, we usually think masochists cannot like pain
because pain is unpleasant, but are we completely sure that pain is unpleasant? George
Pitcher (1970) concludes that it is. To tackle this question, he develops a dialogue
between two counter parties: on one corner the Affirmativist, who claims that pain is
necessarily unpleasant, and on the other side the Negativist, who argues the opposite.
According to the Negativist, the usual unpleasantness of pain can be dismissed in three
different ways: 1) by special conditioning, e.g., fakirs that have normal pain receptors
but who have trained themselves to stand pain, and pavlovian animals that can be
conditioned to give themselves electric shocks for food; 2) by medical procedures, e.g.,
cases of lobotomy where people affirm that they still have the sensation of pain,
although it is no longer unpleasant; or 3) by unusual desires, such as masochism. In all
these cases, the Negativist argues, people (or animals) are experiencing pain but it is not
unpleasant and, therefore, pain is not necessarily so.
On the contrary, the Affirmativist answers back by saying that these cases do no imply
that pain has lost its unpleasantness. In fact, it can be the case that pain is still in itself
unpleasant; pain may appear surrounded by elements that make the situation less
disagreeable or even pleasant. For the Affirmativist pain in masochism is like olives in
paella: although you may not like olives in themselves, since they are constitutive of
paella, you like them when they are part of the dish. You may not like olives, but you
like paella as a whole, even if it must have olives.
In this way, the Affirmativist could claim that pain is still in itself unpleasant, although
fakirs learn how to control it, lobotomy patients stop minding it, and masochists like it
as part of a whole situation. Following the pain-olive analogy, in the same way that
olives have an intrinsic way they taste, pains have and intrinsic unpleasant way they
feel. In this sense, it is as if the fakir learns how to control his reaction to olives in his
paella, lobotomy patients stop minding the flavor of olives, and masochists desire olives
because they like them as part of the whole paella experience.
Since both the Negativist and the Affirmativist have no further reasons on why one
should interpret the former cases in their way, Pitcher concludes that all the former
cases can be explained with the help of empirical studies. Namely, he claims that if the
Melzack-Wall (1965) Gate Theory is correct, then all the cases can be explained and,
therefore, pain is necessarily unpleasant.
8
Nevertheless, there are some problems about Pitcher’s view. For example, Pitcher never
clarifies what he understands by “unpleasant”. In the first two type of cases advanced by
the Negativist, the unpleasantness appears to be reduced to behavior, and in the third it
seems to be described in terms of desires. That is, the fact that fakirs, lobotomy patients,
and pablovian animals do not react as if they were in pain, makes the Negativist
conclude that their chronic pains, the bed of nails, and the electric shocks must not be
hurting them. In addition, this does not fit very well with the third case, where
unpleasantness in masochism can be dissolved by unusual desires.
Moreover, according to Stephen J. Noren and Arlis Davis (1974), Pitcher does not
really have a case against the necessary unpleasantness of pain. They claim that his
argument is fallacious and that empirical studies are irrelevant for the philosophical
problem of whether or not pain is unpleasant. They argue that Pitcher relies importantly
in assuming that the Gate Theory is true. Pitcher assumes such theory and then derives
that, in all the counter examples of unpleasant pain, “the gate of the person or animal is
closed, or nearly closed” (Pitcher, 1970, p. 491).
Noren and Davis point out two problems about Pitcher’s conclusion: 1) it cannot be
simply derived from the fact that there is such gate that, in these particular difficult
cases, the gate is actually closed or nearly closed, further empirical corroboration should
be presented in order to accept it; and 2) the fact that the gate is partially closed does not
imply that there is no pain and that pain is not unpleasant, probably the pain can be
mitigated by an almost-closed gate, but that does not imply that such sensation is not
unpleasant.
In summary, it is very difficult to avoid getting lost in the discussion about the
necessary unpleasant nature of pain, mainly because it is not clear what exactly
“unpleasant” means. The most distinctive feature between masochism and the rest of the
pain cases previously discussed is that, in contrast to pablovian animals, fakirs, or
lobotomy patients, where we are not sure how to determine if their pain is or not
unpleasant, masochism is the only case where we have to determine exactly the
opposite, i.e., if their pain is pleasant.

9
2. Medical definitions
2.1 Pain definition
So, if masochists like pain, we can explore what we actually mean by “pain”. The
traditional, and highly problematic, definition of pain is well rephrased by Dennett
(1978). He proposes an intuitive characterization of pain, where pain is constituted of
two properties:
(I) Pain experiences are essentially painful, awful, abhorrent, so that it is a logical
impossibility to have an affectively neutral pain experience
(II) A subject's access to her pain experiences is essentially privileged or infallible or
incorrigible
Dennett (1978) discusses a clinical case called “reactive dissociation” (RD). This is a
peculiar condition where people affirm to have painful experiences that are not
unpleasant. They claim to have the sensation of pain, although they are not bothered by
it. Finally, Dennett claims that there is a contradiction in this conception of pain and
that, given that contradictory terms cannot refer to an on object, we should abandon this
definition and replace it for whatever neurosciences find pain can be.
Following Dennett’s advice, we may take a look at different medical definitions of pain.
One canonical version of pain is the definition proposed by the International
Association for the Study of Pain (IASP), “an unpleasant sensory and emotional
experience associated with actual or potential tissue damage, or described in terms of
such damage”. However, this definition seems to agree quite well with the definition
that Dennett showed to be wrong. That is, in accordance to I), pain is always unpleasant,
and similarly to II), it does not matter what the situation is, if someone says she is in
pain, we take it as true.1
1 I believe we consider ourselves infallible about our own pain probably because we represent pain in our
bodies, in contrast to other perceptions such visual perception, where we represent shapes and colors “out
there”. That is, our degree of certainty depends on how internal or external the representation is.
10
In fact, not only does the IASP definition encounters problems with RD, there are
several medical cases that put into question the unpleasant nature of pain. The common
feature of these cases is that whereas people claim that they feel pain, they also say that
pain does not bother them. Such claims suggest that, in fact, the sensory dimension of
pain can be dissociated from its evaluative-motivational one. It is well know that certain
surgical procedures, pain syndromes, and drugs can “remove” the unpleasantness of
pain. Among these cases, there seems to be different levels of indifference:
First, there are the patients that are not bothered by their pain sometimes; for example,
patients who had undergone prefrontal lobotomy, cingulotomy, or patients treated with
morphine who react normally to momentarily painful stimulation, although they have a
neutral reaction to persistent or chronic pain. Second, there are the patients that are
never bothered by their pain; people with pain asymbolia claim that they can recognize
their experiences as painful, although they do not react in presence of painpricks, small
cuts, or burns. Third, people who do not seem to feel pain at all; people with congenital
insensitivity to pain do not show any responses to usual painful stimuli but, in contrast
to pain asymbolia, they do not report to actually feel the pain sensation.2
In face of these problematic cases of pain, where people claim that their pain is not
unpleasant, various medical models have proposed that there is dissociation between the
sensorial and the affective-motivational aspect of pain. For example, Melzack and Wall
(1965) proposed the Gate Control Theory of Pain. This theory establishes that pain can
be modulated through a gate that impedes the unpleasantness of pain to be processed
and, therefore, leaves the pain sensation intact. In more recent studies Melzack (1996,
1999) proposed that pain is processed in a “neuromatrix”; in this matrix, pain
processing is importantly dependent on psychological aspects that explain the different
interactions that people have with pain. Further, Schnitzler & Ploner (2000) have
studied several brain regions that are associated with pain processing in a “pain matrix”;
this matrix includes the SI and SII somatosensory cortex, the insula, and the anterior
cingulated cortex (ACC), and the last two components are considered to be importantly
involved in the affective-motivational aspect of pain.
2 For a precise bibliography on these conditions see Aydede (2006), “Introduction: A Crtitical and quasi-
Historical Essay on Theories of Pain”.
11
Other example of theories that have proposed that pain has multiple factors is Fields
(1999). He suggested that two levels of processing compose pain: first, “algeosity”,
which refers the way pain feels like, the specific sensation that differentiates it from
other sensations such as tickles; second, “secondary unpleasantness”, that refers to a
higher order process that constitutes the motivational aspect of pain. Also Price (2000)
has made emphasis in the affective subjective dimension of pain. He has conducted
several experiments in order to show that pain is constituted of different levels that are
closely related. According to Price and coll. (2006), pain is constituted of three
dimensions. First, the sensory dimension refers to way pain feels like, which can be
separable from the second level, the immediate affection, which is what Price usually
calls “unpleasantness”, and the third level, the secondary affective, that is associated
with long lasting periods of pain and emotional states such as rumination.
In summary, several models have suggested that two dimensions compose pain. On the
one hand, there is a purely descriptive dimension of pain, which informs about the
presence of tissue damage, from now on I will refer to this as nociception. On the other
hand, there is an evaluative dimension, which is associated with the unpleasantness of
pain and our motivation to avoid such damage,3 from now on I will call this dimension
algeosity.
Now, considering that pain is the combination of these two dimensions, what can we
say about the two former questions in relation to pain and masochism? First, is pain
necessarily unpleasant? The answer is no, if we consider that nociception suffices for
something to be pain. Following this idea, we would admit that RD patients, people
treated with morphine, lobotomy and cingulotomy patients, and pain asymbolia patients
do feel pain because they still have nociception, although their algeosity can be
diminished or even completely absent. On the contrary, the answer is yes, pain is
necessarily unpleasant, if we consider that pain is constituted of nociception and
algeosity. In this sense, if there are people who only have nociception and no algeosity,
then we must conclude that what they feel is not really pain.
Regarding the second question, do masochist really like pain? We could answer, “yes,
masochists like pain”, in the sense that they like their nociception. However, this does
3 I will address this relation between evaluations and motivation in more detail in Part II.
12
not give a straightforward answer of how that could be, i.e., how someone could like
stimuli that is usually considered as negative. Even if we accept the distinction between
the descriptive and the evaluative dimension of pain, this gives neither an explanation of
what constitutes a negative evaluation of pain, nor a solution of how such evaluation
can turn into being positive. In other words, we could try to explain what is happening
to masochistic Tomas by claiming that he has a different interaction with nociception,
i.e., his nociception becomes pleasant. But how can we explain this if we do not know
what we mean by “pleasant” or “unpleasant”? How could we explain that, for
masochists, their pain evaluation is inversed?4
2.2 Masochism definitions
Now, with a clearer understanding of what we mean by pain, i.e., the combination of
nociception and algeosity, we can start to find out what exactly we mean by
“masochism”. I think there is a crucial question in order to understand masochism: do
masochists like every instance of pain or they only like it in very specific
circumstances? The fact that Tomas actually likes pain does not imply that he likes
every instance of it; if Tomas claims to be a masochist, that does not mean he keeps on
pinching himself all day long just for the pleasure of it. If he goes to the doctor because
he has a terrible toothache, then we could argue two things: i) that his pain system is not
so different from others’ because he can have usual nociception and algeosity and ii)
that context may affect on pain.
If pain is unpleasant, it seems contradictory to enjoy pain, yet we can analyze if
masochism is really (or mainly) constituted by the fact that people like their pain. We
can begin by an intuitive version of masochism. For instance, Tomas sincerely believes:
(α) he is having a pain experience and; (β) his pain experience is pleasant. This is
contradictory with conceptions of pain such as Dennett’s (1978) and the IASP definition
of pain. But we could also compare Tomas’ sincere masochist affirmations (α) and (β)
with pain conceived as composed by nociception and algeosity.
4 Since this is a crucial issue, I will devote an entire section in Part II.
13
In this sense, there are various things that can be questioned. Let us start with (α), is
Tomas’ pain experience really composed of nociception and algeosity? Could it be that
he calls his experience “pain” even if there is just nociception? We could imagine that,
since he is not aware of the dissociation between nociception and algeosity, he calls his
experience “pain”, because it feels like it in the descriptive sense, but not because he has
the a negative evaluation of it. Now, what about (β)? What does Tomas mean when he
says his experience is pleasant? Is it pleasant because of they way it feels, because he
wants it, because he seeks for it? That is, we could argue that when Tomas says he likes
pain, what he actually has in mind is that he likes nociception; Tomas does not mean he
likes algeosity, which would be more difficult to make sense.
Similarly to what we did in analyzing different versions of pain, we can also take a look
into the medical definitions of masochism. For example, the American Psychiatric
Association DSM-V (1999) proposes the following criteria for Sexual Masochism:
A. Over a period of at least six months, recurrent, intense sexually arousing
fantasies, sexual urges, or behaviors involving the act of being humiliated,
beaten, bound, or otherwise made to suffer.
B. The fantasies, sexual urges, or behaviors cause clinically significant distress
or impairment in social, occupational, or other important areas of functioning.
C. Specify if: with Asphyxiophilia (Sexually Aroused by Asphyxiation)
Further, we can also consider the ICD-10 Classification of Mental and Behavior
Disorders Diagnostic criteria for research (World Health Organization, 1993) for
Sadomasochism:
A. The general criteria for disorders of sexual preference (F65) must be met.5
B. There is preference for sexual activity, as recipient (masochism) or provider
(sadism), or both, which involves at least6 one of the following:
5 F65 Disorders of sexual preference: G1. The individual experiences recurrent intense sexual urges and
fantasies involving unusual objects of activities. G2. The individual either acts on the urges or is
markedly distressed by them. G3. The preference has been present for at least 6months. 6 My emphasis.
14
(1) pain; (2) humiliation; (3) bondage.
C. The sadomasochistic activity is the most important source of stimulation or is
necessary for sexual gratification.
I believe there are three remarkable things about these medical definitions of
masochism. The first one, these definitions do not necessarily consider that to be a
masochist one must have a preference for pain, i.e., it is sufficient to like humiliation
and/or bondage to be a masochist; if Tomas is a masochist he must have “at least” one
of these three practices. The second one, the unpleasant activities that constitute
masochism are considered to be a problematic and they have to be used for at least six
months; that is, if Tomas uses any of these practices but he is happy about it, or he has
been only doing it less that six months, then he would not be considered to be a
masochist. Third, these definitions do not specify why activities such as being
humiliated, beaten, bound, burned, and so are considered as unpleasant, or why
masochists engage in them if they are so.
What I am trying to point out is that, if we strictly consider these medical definitions of
masochism, then there is no necessary dilemma between pain and masochism. This is
because of two reasons: 1) it could be that Tomas, somehow, actually likes pain, but he
has not being doing it for long time and that does not cause him any problems, then he
would no be considered a masochist or 2) if Tomas likes being humiliated as part of his
sexual practices, this is problematic for him, and it has been happening for a long time,
then Tomas would be considered to be a masochist, although his masochism has
nothing to do with pain.
Nevertheless, the puzzle is still out there. One the one hand, we could try to explain
masochism by claiming that sometimes masochists have a different interaction with
their nociception, but we still have no clue of how that could be. On the other hand, we
could say that according to the medical conception of masochism, being a masochist
does not necessarily entail that you like pain; although this does not solve the matter
because there are instances of masochism where it seems like you could like it.

15
3. Pain as a means
3.1 Means vs. Ends
Another alternative to give sense of why masochists undertake pain is to notice that pain
can be the means for something else or it could be an end on its own; so, we could
argue, in masochism pain is a means for something else that is valuable. On the one
hand, there are situations where we accept to feel pain as a means, e.g., if we are very
sick, we may want to get the cure even if we know it is going to be very painful, i.e., our
nociception will be accompanied with a high degree of algeosity. This shows that the
fact that Tomas behaves in favor of receiving pain does not imply that he likes it, what
he actually wants is to stop being ill. On the other hand, if Tomas wants to feel pain just
because he wants to experience it, then this seems problematic. It is more difficult to
explain why someone would like to experience nociception and algeosity for
themselves.
In fact, we could argue that the two medicals definitions of masochism previously
discussed suggest that pain is a means for achieving sexual satisfaction. The DSM-V
claims that masochists have “sexual urges, or behaviors involving the act of being
humiliated, beaten, bound”, but the fact that they have such urges and behaviors does
not imply that they like the pain in itself. Moreover, the ICD-10 classification
establishes that “the sadomasochistic activity […] is necessary for sexual gratification”,
but the activities involving pain, submission, humiliation, etc. are not considered to be
gratifying by themselves. In other words, we could say that masochists need such
unpleasant activities to find sexual satisfaction, which is a valuable end.
In fact, there are people who have taken this position in order to explain masochistic
behavior. According to Goldstein (1983), masochists desire to experience pain because
it represents a way of self-punishment. If we consider that “pain” is equivalent to
“unwanted thing”, it seems absurd that someone wants to experience pain. However, we
can desire pain pains as means, and this does not entail any logical contradiction.
Goldstein considers that “masochists often view their pain as a deserved punishment,
and this is a clue to their thinking” (Goldstein, 1983, p. 221). In other words, masochists
desire to experience pain because they consider that inflicting pain to themselves is the

16
means to achieve their punishment. Finally, in Goldstein’s opinion, it is crucial to take
into account that masochism is a perversion, and, at least to a certain extent, the desire
to experience pain as self-punishment is irrational.
Other authors share the view that masochists do not really like pain for itself. For
example, according to Pitcher (1970, p. 485.), masochists mistakenly think they like
pain:
It seems implausible to say that he likes the pains of the whipstrokes and the
cigarette burns. Even if he thinks he does like or want them, it is
overwhelmingly likely that he is the victim of an illusion or of self-deception
or whatever. What he really wants is something quite different —the
humiliation that being whipped or burned entails, or the sexual gratification
that is to follow. Since for the masochist the pain is an essential precondition of
these desirable things, he might naturally be expected to think —wrongly—
that it is the pain he desires. He does not like the pain: he only thinks he does.
Nagel (1986, p. 156-157) also considers that one may pursue pain “as means to some
end or […] backed up by dark reasons like guilt or sexual masochism”. Moreover,
Rachels (2000) argues that masochists cannot like to suffer severe pain; the claim that
masochists pursue pain, may be true, but pursuing pain does not imply that they have “a
favorable emotional attitude towards pain itself, considered merely as a feeling, and
seek its continuation for that reason”. Rachels considers that masochists dislike pain,
but like the pleasure or gratification that accompanies it. Again, what is contradictory is
to have a positive attitude towards pain, by desiring, pursuing, or engaging in painful
activities only because people want to experience pain, which they also consider
unpleasant. So, if pain in masochism is merely a means, then there is no contradiction.
3.2 Painful Rituals
Thanks to this means-and-end distinction, other interesting pain cases can be analyzed.
For example, people undertake some ritual initiations that include pain; we could also
explain that people put themselves in such unpleasant situations because pain has a
mediated value. That is, people submit themselves to processes that imply pain and
humiliation because thanks to them they will obtain, for instance, a new higher social
status.

17
There has been research which focuses on torture and pain inflection in ritual initiations.
For example, for Clastres (1973), an important difference between torture and rituals is
that, whereas there seems to be no way in which the victim of torture wants to suffer
pain, in rituals there is a certain acceptance from people who go through the painful
activities. Ritual initiations, although painful and sometimes denigrating, entail other
positive values such as courage, wisdom, manhood, and so. Although pain infliction is
constitutive for torture and initiations rituals, there is a crucial characteristic that makes
them different: whereas the objective of torture is to go beyond the bearable limits of
pain, in ritual initiations suffering intervenes in a way that it is still beneath a tolerable
threshold (Houseman, 1996).
Torture and painful initiations have important divergences and they use pain with a
quite different purpose. Given the general abhorrent nature of pain, it is easier to figure
out why it is used in torture. That is to say, if Tomas is being tortured, it is not because
he wants to be tortured, and the objective of the torturer is to makes Tomas confess or to
make him suffer. In torture there is no valuable thing to be obtained, at least not from
the perspective of the one being tortured. In contrast, in ritual pain, as it also occurs in
masochism, there is certain complicity and acceptance of pain.
For instance, there are initiations where men have to pass through an important amount
of pain in order to obtain the new social status of adulthood. Lemaire (2008) discusses
the initiation process in Côte d’Ivoire. The initiation, broadly, consists in seven years
where men have to perform intense farming and agricultural labors that entail pain.
During their initiation, they also have to be isolated and during the seven first days of
their initiation they have to overcome several painful tests. This is an example, as many
initiation rituals, where part of the challenge is to defeat the difficulties constituted by
painful tasks. Once people have concluded the process, they are inserted in a new higher
social category. Finally, this shows that pain can be conceived as the means: sometimes
for sexual satisfaction, and in other cases for achieving adulthood.

18
4. So, do they really like it?
Up until now, there are two ways of answering this question. The first answer is that
masochists do not really like pain. Strictly according to the medical definitions of
masochism, if Tomas only uses humiliation as part of his sexual practices, he can be
considered to be a masochist without claiming to enjoy pain under any circumstance.
Further, we could argue that masochists do not really like pain on itself, what they
really like is something else that they will obtain through pain.
Nevertheless, these answers still leave many things unexplained. For example, the first
one does not tell us anything about the cases where masochists do use pain as part of
their sexual practices, and the second does not exclude the possibility that pain can be
an end. That is to say, even if these answers give us a better understanding of the
different interactions that we may have with pain, they do not explain neither how
masochists could find pleasure in using pain nor why pain could not be something that
we may want to experience as an end.
So, do masochists really like pain? I think they do, and I think so for two reasons:
First, if pain is part of their sexual experience, we cannot clearly differentiate between
time T1 when the unpleasant pain is inflicted and then time T2 when pleasure starts. In
masochism both things are part of the same experience. In contrast to ritual pain, in
masochism we cannot make a clearly distinction between unpleasant means and a
pleasant end because the two things are part of the same experience.
Second, and more importantly, since we usually do not differentiate nociception from
algeosity, we could explain that masochist can interact in different ways with
nociception. We think that masochists cannot like pain because we have in mind that no
one can like algeosity, which is what we usually call “unpleasantness”, but not because
we could not like nociception, which, in principle, we could. The fact both dimensions
of pain are usually experienced as a whole does not imply that it has to be that way. For
example, cases such as pain asymbolia suggests that nociception can be experienced
without algeosity. So, what masochists really like is their nociception, but we still have
to explain how.

19
Part II.
How do they like it?
In this second part, I address the relationship between unpleasantness and pain. First, I
tackle the different interpretations of what the unpleasantness of pain stands for, and
how we can explain that, given that pain is unpleasant, we tend to avoid it. Second,
given the different possible interpretations of unpleasantness, I propose a pertinent
equivalent for a theory of pleasure. This is especially important in the case of
masochism since not only do they not experience unpleasantness, but they also
experience pleasantness. Third, I propose a model that recovers the definitions of pain
proposed by the medical studies and includes the philosophical discussion on the nature
of unpleasantness. Finally this model is capable if explaining how masochists may find
pain pleasant.
1. Unpleasantness
1.1 Kinds of algeosity
As we saw in the previous section, it is rather difficult, if not impossible, to work on
pain as a paradigmatic unpleasant sensation without establishing what we mean by
“unpleasant”. In accordance with the previous section, by “unpleasantness” we mean
the evaluative and motivational dimension of pain; so, from now on, I will consider
“unpleasantness” and “algeosity” as interchangeable terms. Similarly, when we consider
something to be “painful”, I believe that what we have in mind is that it is unpleasant,
i.e., that it has algeosity. This, for instance, explains why it does not appear as
particularly shocking to say “painful pain” because we are talking about nociception
with algeosity.
Everyone agrees that pain typically entails algeosity, this is why cases such as
masochism or pain asymbolia are so shocking: they put into question that pain is
necessarily algeostic. But, why do these cases put that in question? One may answer:
because masochists and pain asymbolics do not have the expected behavior to
20
nociceptive stimulation. But this does not really explain much since we cannot presume
that algeosity can be reduced to behavior. In addition, if we have the intuition that
algeosity is something you feel, and not something you do, then behavior can only be an
indicator or a result of algeosity, but not constitute it.
Philosophers have offered different theories in order to account for the unpleasantness
of pain, i.e., for the algeostic nociception. One of the more recurrent alternatives is to
think that unpleasantness can be explained in terms of body damage. However, as one
may notice, it is different to say that unpleasantness is the result of body damage and to
say that unpleasantness can be reduced to such damage. For example, if we accept that
unpleasantness is necessarily caused by body damage, then we have to deal with the
difficulty that not every unpleasant thing is caused by a body representation; things such
as boredom or dissapointment are unpleasant yet do not seem to clearly represent any
body damage.
We could also argue that unpleasantness consists in the subject believing the she has
body damage. However, this account also has to face the difficulty that in various
intuitive cases of pain, people do not believe they have an injury in their bodies, they
believe they are in pain. For instance, let us analyze the sentence “I believe I have an
injury in my hand” for a phantom limb patient. Clearly a phantom limb patient does not
believe this: she knows there is no injury in her hand because she knows she has no
hand.
Furthermore, when we think in representational terms about pain, we take pain as a
whole, without noticing that it can be decomposed into subtler layers. If we see a red
apple, we can differentiate its shape from its color, even if we perceive them as one
unity. Similarly, even if we experience pain as one event, we can decompose it into
nociception and algeosity. That is to say, when we say that pain is the representation of
body damage, are we taking about nociception, algeosity, or both? Because, it seems to
me, it is not the same to represent that something is occurring in our body, to represent
that that thing is bad.
Another alternative, leaving the representational issue aside, is to explain
unpleasantness in terms of dislike. For example, for Richard J. Hall (1989) the dislike is
a separate mental state from the sensation, and this can explain that you dislike pain for
two main reasons: either 1) you learn to dislike it based on life-experience associations
21
or 2) it is the result of an innate evolutionary adaptation. According to his first
approach, the main reason why we dislike pain is because it is associated with tissue
damage, i.e., nociception seems to be a much more efficient method to know about
body damage that, say, visual perception: whereas you may not see that you have a
wound, you can feel it. Following this idea, the fact our dislike of nociception is part of
an innate mechanism does not imply that we necessarily dislike it. The dislike of
nociception is merely contingent; it is an arbitrary fact that such specific sensation has
been associated with body damage.
If we explain unpleasantness in terms of dislike, we could presume that the degree of
the former depends on the degree of the latter. The algeosity of your nociception
depends on it being disliked and its degree on how much you dislike it. However, it is
not very clear that there is a correlation between these two things. Rachels (2000) offers
the following example: if you expect to be burnt, you close your eyes and, instead of
being burnt, someone puts an ice on your skin, he concludes, you dislike the experience
although it is not necessarily very unpleasant. However, it seems to me that Rachels is
begging the question. Opposite to what he thinks, one could say that actually it was very
unpleasant to feel that ice.
What I believe that the real problem for understanding algeosity in terms of dislike is
that we have two options, we can either think that 1) the dislike is what constitutes
algeosity or think that 2) dislike is a different mental state. If we take the first way, then
the natural question comes: what does it mean to dislike something? And it can be
tempting to give the circular answer: we dislike something because it is unpleasant.
Then, if we take the second way, we are not explaining algeosity; the dislike we usually
have of nociception comes from the fact that it has a certain degree of algeosity, so the
notion of dislike does not shed any light. Again, we dislike things because they are
unpleasant, and not the other way around.
22
1.2 Motivating pain
Another possibility to explain algeosity is to define it by our motivation to stop it.
Indeed, one of the interesting things about pain perception is that we tend to evade it.
Even if there are cases that put this into question, there is something about pain that
motivates us to avoid it. If Tomas is cooking and he accidentally touches the pan with
his elbow, he will instantaneously move his elbow back. In contrast to other sorts of
perception such as visual perception, we could explain that the algeosity of pain is
explained by our motivation to stay away from it; whereas pain perception has
algeosity, visual perception does not, and this explain why we do not have a tendency to
avoid colors as we tend to avoid nociceptive stimuli.
In more recent years, a renewed interest on unpleasantness took place. People like Klein
(2007; 2010; 2011), Hall (2008), and Martinez (2010) have defended that the
unpleasantness of pain, at least partially, can be understood as “imperative commands”.
These commands explain our behavior towards pain. Broadly speaking, this view
proposes that whereas the function of general perception, like visual perception, is to
inform us about facts of the world the world, there are other kinds of perception that
command us things. For example, hunger commands us to eat, thirst to drink, and itch
to scratch. In the case of pain, and more precisely, the unpleasantness of pain commands
us to do something. This command is considered to carry the biological function of
maintaining our bodies healthy and intact. So what differentiates pain perception to, say,
visual perception is that whereas the former has an imperative content, the latter has an
indicative one.
Klein (2007) points out that when we think about pain, we usually state it in terms of
“My B hurts” or “I have a pain in my B”, instead of putting in terms of an action such
as “It hurts when I A” or “My B hurts when I A”. Based on this, he proposes that the
painfulness of pain consists of a command that tells us not to do the action that is
hurting us. For instance, if you have an injury in your ankle, the command would tell
you “stop putting height on it!”. This view makes emphasis that pain is not really about
informing about body damage, and there are several reason to think so: 1) pain is not
always caused by body damage, 2) pain is not a reliable source of information about
body damage, and 3) it does not seem like the biological reason of pain is only to
inform us but rather to make us do something about it.
23
Bain (2011) argues that this imperative view is insufficient to explain on what consists
the nature of pain and that it does not even clarify why we have the tendency to avoid
pain. The “hedomotive challenge”, according to Bain, is to explain why we react in
order to avoid pain; for the “imperativists”, it is because there is a command that tells us
to do so; for Bain, the notion of command is insufficient for explaining such
hedomotive aspect. Bain offers five different arguments against imperativism:
1. Hedomotive claims: it is not clear exactly what the commands tell us to do, nor that
every single instance of pain shares the same command, e.g. it is difficult to find the
shared command between menstrual cramps and a burned finger. Moreover, if, as Klein
proposes, the commands tell you to stop doing something, this cannot explain situations
when you are in pain but you are not doing anything. Moreover, there are commands
that tell you to do something, e.g., to take a pain killer.
2. Urges: although imperativism proposes that unpleasantness can be understood as a
command, it could be also understood as an urge to do something, which is not
necessarily a command. In other words, not all commands are urges and not all urges
are commands. For example, someone may command you to do sit down, but that does
no imply that you will have the urge do it. Imperativists could argue that, indeed,
commands are urges, but, according to Bain, this seems too ad hockery, and, in this
sense, the extrapolation of the word “command” from a linguistic context does not seem
to illuminate “unpleasantness”.
3. Unpleasantness: it is no very clear why a command constitutes unpleasantness. That
is to say, there are two broad ways in which we can explain unpleasantness through
commands: a) the command constitutes the pain’s unpleasantness, or b) the command is
part of or may cause unpleasantness. Whereas Klein embraces the first option, Hall
seems to take the second weaker version. For Bain, it is straightforward clear that the
constitutive version is wrong, this can be seen in well-known cases such as pain
asymbolia, where people claim to have pain but no particular motivation to stop it.
Grahek (2007) also presents this counter example for imperativism, where people who
suffer such condition are shockingly indifferent to their pain.7
7 More recently, Klein (2011) proposes a different way to understand pain asymbolia. He considers that
“asymbolics lacked a fundamental capacity to care about the integrity of their body”, and they do it
24
4. Reasons: another (apparent) advantage of the imperativist view is that it provides
reasons for avoiding pain; the action of taking your finger away from the flame has a
reason, i.e., there is a command issued by a pain module that “tells” you to take it away.
The module knows best. However, Bain has a counter example for this: imagine that
you know that something will not cause you injury, e.g., the light beam of a lamp on
your hand, but your pain module is malfunctioning and it commands you to avoid the
light because it is extremely unpleasant. According to Bain, this is a case that the pain
command fails to illuminate.
5. Intensity: we can explain that some pains are more intense than other because there is
a stronger command that tells us to stop some behavior. Nonetheless, the imperativists
theory does not clarify what makes a command stronger than other. Further, if a
command is stronger because it prevents you from an even more unpleasant situation,
then the notions becomes circular. That is, we cannot explain unpleasantness by using
the notion of command that presupposes the notion of unpleasantness.
Another possibility would be to explain than a stronger command consists in warning
that there is higher risk of injury, but in this case then commands would not be really
concerned for unpleasantness. One more option could be to say that stronger commands
inform you about how much attention the unpleasantness will grab, but then commands
would be about grabbing instead of unpleasantness.
In summary, there have been various attempts that try to explain the nature of pain,
considering that unpleasantness is in the core of it. An important attempt has been to
explain (or reduce) unpleasantness as the representation on body damage, although this
account fails for two main reasons: 1) it fails to explain why when we experience
unpleasantness in pain, or in other situations, we do not experience it as body damage,
and 2) it fails to illustrate why we usually avoid such unpleasantness. In the face of such
problems, Bain (2012) proposes another alternative: evaluations.
because they suffer a depersonalization syndrome; this, he argues, fits with a “modest version of
motivationalism”, which considers that pains may fail to motivate, but only in situations where the agent
is severely impaired.

25
A subjects’s being in unpleasant pain consist in his (i) undergoing an experience (the pain)
that represents a disturbance of a certain sort, and (ii) that same experience additionally
representing the disturbance as bad for him in the bodily sense.
Bain claims that this approach to pain has the advantage that (i) considers a
representational state that can be either true or false, because unpleasant pain represent
that disturbance, and (ii) gives an explanation for the motivational dimension of
unpleasantness: we avoid pain because it represents something that is bad. Evaluations,
constructed as body-directed, Bain argues, can give a reason for behavior. In this view
unpleasantness is bad in itself, because it represents something that is bad for the body.
One of the main features of this view is that the representation is bad in itself, and this is
what motivates us to act and not the other way around. Unpleasant things are not bad
because we avoid them; we avoid them because they are unpleasant. This may seem like
a little difference, but it makes a big difference.
However, Bain’s evaluativist theory does not address the degree issue either.8 He does
not explain why, if unpleasantness depends on a representation of something that is bad
for the body, some body disturbances would be represented as worse than others.
Maybe, if we accept that pain has a biological function of keeping our bodies intact and
safe, as Klein had considered, then this would complement Bain’s proposal. Namely,
this could shed light on why third-degree burns are more unpleasant than superficial
ones, because the former are represented as worse. Although, this still does not explain,
for example, why menstrual cramps can be so painful for some women and very light
for some other, that is, why should in one case menstruation be represented as a worse
body disturbance?
8 I prefer to use “degree” when it comes to unpleasantness rather than “intensity”. I believe that the
former captures better the qualitative aspect of it.
26
2. Pleasant vs. Unpleasant
Most of the theories that focused on the unpleasantness of pain try to address this issue
without an equivalent theory of pleasantness. However, can we really have a theory of
unpleasantness with total lack of a theory of pleasantness? I think there are two reasons
why we cannot:
First, cases like masochism demand a clearer understanding about what we mean by
pleasant and unpleasant. Explaining masochistic behavior based on “masked desires”
that drive masochists to hurt themselves does not really solve the puzzle. Even if
masochists had such desires, we would still have to explain how these desires drive
masochists to seek something pleasant, if pain is just a means for sexual pleasure or
self-punishment, what is the common feature between these two things? Someone may
say, “that they are pleasant”, but that is exactly what these explanations are missing.
Moreover, it is not clear that masochism can be really explained by means and ends, in
contrast to pain in rituals or medical cures, the pleasure and displeasure in masochism
are not two clearly separate experiences.
Second, experiences are categorized in a range that contrasts unpleasantness and
pleasantness. If we simply focus on one side of the spectrum, it seems like we have an
incomplete model. Further, odd cases of pain put into question that the same sensation
is attached to the same degree of unpleasantness or pleasantness. The exact same stimuli
can even be judge in opposite ways depending on the point of reference. For example,
the exact same environmental temperature can be judged as cold or warm depending on
where it is experienced: 20 Celsius degrees can be cold where it is always sunny, but
could also be considered as warm after a long snowy winter.
2.1 Nociception vs. Placiception
Strangely, and I believe this contributes importantly to the confusion about
unpleasantness, we use the word “pain” in ambiguous ways. We use it for bodily
sensations such as headaches, menstrual cramps, sunburns, and broken ankles, but
sometimes we can also use it to refer to emotional suffering, e.g., when we consider that
27
disappointment or grief can be painful. Moreover, when we think about the opposite of
pain, “pleasure”, it can also refers to “physical pleasure”, broadly refereeing to pleasure
that we perceive as in our body, such as orgasm and sunbathes or “emotional pleasure”
such as joy or the fulfillment to having accomplished a goal. I believe this ambiguous
use of “pain” is related to the fact that, since nociception is accompanied by algeosity,
then we use “pain” and “unpleasant” indifferently. On the other hand, we use “pleasure”
to generally refer to pleasant things, which can be bodily experiences, like a caress, or
more emotional, such as fulfillment.
In order to avoid these vague uses of “pain” and “pleasure”, from now on I will use
“nociception” and “placiception”. Nociception, as I mentioned before, refers to the
bodily sensory aspect of things such as headaches, burns, cramps, and broken ankles,
and placiception to caress, the warm feeling in the skin when we take sunbathes,
orgasm, and so on. Although, nociception is usually unpleasant, and placiception is
usually pleasant, I consider that this is just a contingent fact about those experiences.
This, in fact, is supported by cases where we consider that nociception is not evidently
unpleasant, like pain asymbolia or masochism, and by people who do not like to be
caressed or touch and who avoid to experience placiception.
In this way, since the sensory aspect of experience can be distinguished from its
evaluative-motivational one, there is no reason why this would not be valid for bodily
sensation that we usually consider pleasurable. On the one hand, cases such as morphine
patients, lobotomy patients, and pain asymbolia, confirm that nociception does not
always have the same degree unpleasantness; and, on the other hand, there are also
situations where our interaction with placiception can be variable, e.g., a caress could be
very pleasant or unpleasant depending on the person from who we receive it, and an
orgasm could be judged as something we should avoid experiencing given our beliefs or
the context where we find ourselves. Furthermore, as Bain (2012) points out, a one-year
orgasm may become quite annoying and unpleasant.
28
2.2 Algeosity vs. Hedonisity
Now, in order to get a better grasp of what happens in masochism and in the variety of
sensory experiences, we can try to find an equivalent of algeosity on the other side of
the spectrum. Among the approaches to pain unpleasantness, very few have considered
what the equivalent would be in terms of usually hedonistic sensations. In several of the
medical studies of pain, they seem to consider that behavior and verbal reports are
sufficient for attributing algeosity to nociception. Besides the several issues that a
behaviorist approach entails in order to explain algeosity, we could consider which
would be the behavioral equivalent of hedonisity. From now on I will consider
“pleasantness” and “hedonisity” as interchangeable terms. For example, if we saw that
people try to maintain certain stimuli, and smiled when it is present, we could think that
it is an indicator of hedonisity. However, given all the problems that behaviorism has in
order to explain what constitutes unpleasantness, it may not be a very good option for
explaining pleasantness either.
Another important attempt to explain the unpleasantness of pain is to put it in
representational terms, and we could try to find its equivalent in terms of pleasantness.
So, for example, in the way we try to explain unpleasantness as the representation of
body damage, then pleasantness should be the representation of some body benefit.
Nevertheless this is problematic: sometimes unpleasantness does not represent body
damage, like disappointment, and sometimes pleasantness does not represent body
benefits, like fulfillment.
In order to avoid this kind of problems, we could focus on the unpleasantness of
nociception and the pleasantness of placiception. By doing this, it makes more sense
that such unpleasantness and pleasantness are a representation of something related to
our bodies. For instance, this could explain why burning ourselves is usually unpleasant
because it entails some body damage, whereas a sunbath is something pleasant because
it entails some body benefit. However, this does not solve all instances of body
sensations, e.g., this does not shed much light on why menstrual cramps can be so
unpleasant or orgasms could be so pleasant. That is, menstrual cramps are not clearly
29
damaging for women’s body, nor is it obvious than an orgasm entails something good
strictly in terms of our body.9
More importantly, the mere fact that we get a representation of something occurring in
our bodies does not have any answer of why such representations drive us to act, why
do we put our finger away from the flame and why we go out and sit on the grass once
the winter is over? Again, the fact that we perceive something different in our body,
does not entail any clue on why such modification moves us to act. The imperative view
tried to give and answer to this. In Hall’s (2008) words, “if it itches, scratch it!”. If we
accepted the imperative view for algeosity, then, we could try to explain hedonisity in
terms of commands too.
So, if we took this option, we could say that hedonisity is, if not constitutively at least to
some degree, a command to maintain our bodies safe and intact. That is, in contrast to
avoidance-behavior commands for unpleasantness, as Klein (2007) proposes,
pleasantness would be explained in terms of seek-behavior commands. Nevertheless, as
Bain argues, there are many aspects that the imperative view does not explain and, more
importantly, it cannot clarify why such commands would move us to act in order to
avoid unpleasantness and seek pleasantness: the fact that we receive a command does
not imply that we will follow it.
One last option is that algeosity and hedonisity are intrinsic properties of nociception
and placiception. That is, these properties of experience do not depend and are not
reduced in other terms such as behavior, dislike, urges, inclinations, commands, and so.
Rachels (2000), for instance, advocates to this view for unpleasantness, he considers
that it is a property that supervenes on the pain experience. However, if unpleasantness
and pleasantness are mere supervenient properties, then we still have to explain why
they motivate actions. How can those supervinient properties have a causal role? This
way of intrinsically conceiving such properties seem to have problems answering to the
hedomotive challenge, i.e., illuminating why we tend to something in the presence of
nociception and placiception.
9 Orgasms may be interpreted as benefit at the level of the survival of the species. However, I do not
believe this is a prima facie benefit for your body.
30
Following Bain (2012)’s evaluativist theory, we could say that pleasantness and
unpleasantness are, respectively, intrinsically good (or bad) for people who
experiencing them. They are so because they represent something good (or bad) in the
bodily sense and this is what explains that they make us act. We avoid them because
they are bad and we seek them because they are good. If Bain’s proposal manages to
give an account of algeostic nociception, then it could be a suitable baseline for
explaining hedonistic placiception:
A subjects’s being in a hedonistic placiception consists in his (i) undergoing an experience
(the placiception) that represents a disturbance of a certain sort, and (ii) that same
experience additionally representing the disturbance as good for him in the bodily sense.
Following this idea, placiception is hedonistic because it represents something good for
the body. This could explain, for instance, why we find pleasure in eating sugar or why
we like to take long sunbathes; because, in a general sense, they are good for our bodies.
However, we may still have to clarify what exactly constitutes a good disturbance of the
body. For example, in contrast to sugar, it may not be very clear how an orgasm could
be good for the body. Orgasms may be disturbances, but that does not mean they are
good. Maybe they are so in the sense that they allow the transmission of our genes, but
that is not strictly speaking something good for our own bodies, but rather for our
species. Further, as I mentioned before, Bain’s new proposal does not address the
degree of unpleasantness, so, similarly, there is still no explanation for the degree
pleasantness either.
2.3 High vs. low
I believe that there is an important feature about nociception and placiception that has
not be highlighted: we do not always react with the same aversion or acceptance to
similar stimuli. For example, if you accidentally touch hot water, even if you do not get
hurt, your hand immediately moves back as a reflex; in opposition, when people go to
an almost boiling jacuzzi, they enter it and stay there for a long time. In contrast, the
caress of a beloved person can be very nice, whereas if the same stimulus is receive by
someone we dislike or in an inappropriate situation, it could be quite bothersome. How
could we give an account of this? I think it is because algeosity and hedonisity have
different levels of processing.

31
In the low level, we could find the stereotypical innate reactions to nociception and
placiception. For example, when we accidentally touch something hot, our body
immediately reacts by putting distance between our bodies and the hot object, or if we
are jumping and we twist our ankle, we immediately stop moving. I believe this kind of
immediate reactions is what the imperativists had in mind when they proposed that there
was a command that made you avoid pain. However, they did not considered that a)
nociception is not always unpleasant and b) that we do not always follow a command.
Nonetheless, it is true that we have typical reactions to typical painful-stimuli. In other
words, we usually avoid nociceptive stimuli because it is usually algeostic.
As Hall first (1989) suggested, those stereotypical reactions could be explained by
either 1) the fact that you learn to react in such way based on life-experience
associations or 2) it is the result of an innate evolutionary adaptation. This also fits with
Pitcher’s (1970) Negativists intuition about fakirs, lobotomy patients, and pavlovian
animals, i.e., that those usual reactions may disappear because, I would say, the low-
level algeosity processing can be altered. It is a contingent fact that boiling water and
broken ankles produce nociception that we find algeostic because, contingently, it is
represented as bad for us. We could imagine that if soft light beams damaged our skin,
we would have learned or evolutionarily adapted to find light beams unpleasant. If, for
example, perceiving red color would be represented as bad for our eyes, then we would
1) learn to avoid it based on life-experience or 2) we would adapt to instantaneously
avoid it.
This low-level immediate reaction, I claim, recovers the intuition of the imperative
view, i.e., that there is a sort of strong impulse to avoid whatever is causing nociception.
However, we do not have to explain such impulse in terms of commands; the reason
why we act in order to avoid unpleasant stimuli is, as Bain (2012) points out, because
we represented it as a disturbance that is bad for our body, and, I would add, we
represent it that way either by learning or by adaptation. Moreover, this can also explain
that not only adult humans are capable of experiencing algeostic nociception, the innate
mechanisms that allow us to detect unpleasantness are probably shared with human
babies and with many animals too, allowing them to be experience unpleasant
nociception, at least in the low-level of it.
32
This could also give account of the fact we do not always react in the same way to the
same stimulus, even if we feel the same sensation. For instance, plavovian dogs modify
their low-level algeosity by their training, i.e., they associate the nociception produced
by electrical shocks to food rewarding; further, in pain asymbolia patients, we could
explain that their low-level algeosity processing is importantly, if not completely,
damaged, which explains why they still feel nociception but they do not react in order to
avoid it because they lack low-level algeosity.
Accordingly, we find all sorts of examples of things we do in order to avoid something
that is bad for our bodies, e.g., hunger motivates us to find something to eat, and even if
you try to hold you breath, your respiratory system starts working again even if you do
not want to. In this sense, we could explain that there is a low-level module of algeosity
that avoids harm for you body and, in the case of hedonisity, it seeks things that are
good for it.
Added to this, I propose, there is another is high-level of algeosity and hedonisity. This,
I believe, recovers the intuition of the theories that have tried to put unpleasantness in
terms of desires, beliefs, attention, and so on. In fact, as I will discuss in the next
section, several of these psychological factors seem to importantly influence the
algeosity of our nociception. But we may wonder, how is it possible that higher-level
motivates us to act? My answer is that, broadly and in a similar way that the low-low
level works, when we represent something as bad and therefore unpleasant, this gives us
a reason to have avoidance-behavior; on the contrary, when we represent something as
good, i.e., pleasant, then this motivates seek-behavior. The main difference is that this
higher-level does not have to represent things in bodily terms.
In fact, I believe that this higher-level explains algeostic and hedonistic states that
constantly troubled the previous theories of unpleasantness. For instance, when we
think of disappointment and fulfillment as examples of unpleasant and pleasant
experiences, it is not very clear that they represent any kind of tissue injury. However,
we could explain that they entail something bad and good in psychological terms. That
is to say, when we compare disappointment to broken ankles, we compare them because
they are algeostic, not because both phenomena feel in the same way in bodily terms.
Similarly, the fulfillment of accomplishing our goals and entering a jacuzzi are
hedonistc experiences, even if they clearly do not feel in the same in our skin.

33
I presume that this higher psychological level mainly, or at least evidently, belongs to
adult humans. Whereas the lower level explains why we can find more stereotypical
behavior in dogs and cats that in humans, the combinations of both can shed light on the
complexity of our interaction with bodily sensations. For example, this can explain that
whereas the caress of a beloved person is hedonistic in both levels, when an unknown
person touches us, the same stimulus may be represented as something bad; it is bad
because of our associations and by the fact that it is represented as something bad in
terms of beliefs and expectations. That is to say, if you think is going to be bad, then it
is actually worse and if you think it is good for you, then it does feel better.
3. So, how do they like it?
Masochists may pursue pain as an end, but how could we explain that this is possible?
My answer is that if we consider that 1) a descriptive sensory dimension and an
evaluative-motivational one compose pain, and 2) that the latter can be importantly
influenced by our high-level psychological representations, then we can explain that
masochists represent nociception as hedonistic. In other words, people burn or cut
themselves because training or associations can mitigate their low-level of algeosity
and, more importantly, their high-level may be inversed to hedonisity since they
consider that such cuts and burns are good for them.
Similarly, things such as orgasm, which are paradigmatically pleasant, may be
unpleasant. If we conceive an orgasm as something that we should feel guilty about,
although it may be represented with a certain degree of low-level hedonisity, it may
have a high degree of high-level algeosity. Moreover, the fact that these phenomena are
importantly influenced by the high-level explains why we do not see masochistic
behavior or auto-control of sexual impulses in animals.

34
Part III.
Can anybody like it?
In this third part, I propose a model that gives an account of masochism, our general
interaction with pain phenomena, and pain modulation. First, I summarize such model, I
explain how it accounts for various pleasant and unpleasant experiences, and precisely
how it sheds light on masochism. Second, I discuss several examples of pain
modulation that can also be explained with this model. Pain modulation supports the
influence of cognition, i.e., high-level processing, on pain perception. Third, I finally
conclude that, given the possible interaction that we may have with pain, anybody could
be, in principle, a masochist.
1. Pain = nociception + low-level algeosity + high-level
algeosity
1.1 Pain model
In summary, I propose that what we usually consider as pain, is actually the
combination three different things. First, there is the descriptive sensory aspect of it,
what I call nociception; this is what we normally recognized as a physical pain, which is
a sensation normally localized in some part of our bodies and that we identify in
experiences such as headaches, stomachaches, broken and twisted ankles, cramps,
burns, cuts, electrical shocks, etc. Second, added to such sensory content, there is the
low-level of algeosity, this is the representation of something bad in bodily terms, the
fact that it is bodily-bad gives us a reason to avoid it, and this is the result of
associations and innate evolutionary mechanisms. Third, there is a high-level algeosity,
which represents something as psychologically bad for us; similarly, the representation
of something being psychologically bad gives us a reason to avoid it, although such
35
actions depend on other competing desires and motivations.10 Presumably, this level is
more developed in humans, and also sheds light on unpleasant experiences that do not
clearly represent things in body terms.
In addition, this model is coherent with several medical studies. If we reconsidered the
three dimensions of pain proposed by Price et al. (2006), the sensory dimension, would
be the equivalent to nociception, the immediate affection, would correspond to the low-
level of processing of algeosity, and the secondary affective, would be equivalent to
high-level processing of algeosity. Moreover, regarding Schnitzler & Ploner’s (2000)
studies, I would presume that whereas the SI and SII somatosensory cortex are related
with nociception and probably low-level processing, the insula and the anterior
cingulated cortex may correspond to the higher psychological level of algeosity.
Further, concerning this high-level of processing, Melzack’s neuromatrix (1996, 1999)
considers that there is a very important psychological aspect that explains the
interaction that people have with pain.
One of the important differences between the current model and the medical models of
pain is that it considers an equivalent for pleasurable experiences. What we usually
conceive as a pleasant sensation is composed by three dimensions: placiception, low-
level hedonisity, and high-level hedonisity. Furthermore, the current model
distinguishes evaluations from motivation: the reason why we act is because we
represent stimuli as algeostic or hedonistic. Finally, this model also allows us to
understand experiences that do not represent things in clear body terms. Based on these
distinctions, we can categorize several unpleasant and pleasant phenomena:
10 This could explain why during depressive states people cannot easily find the motivation to get out of
their negative situation. That is, even if they represent something as bad and they would prefer to stop
felling depressed, there are other competing beliefs and desire that impede them to do something about it.
36
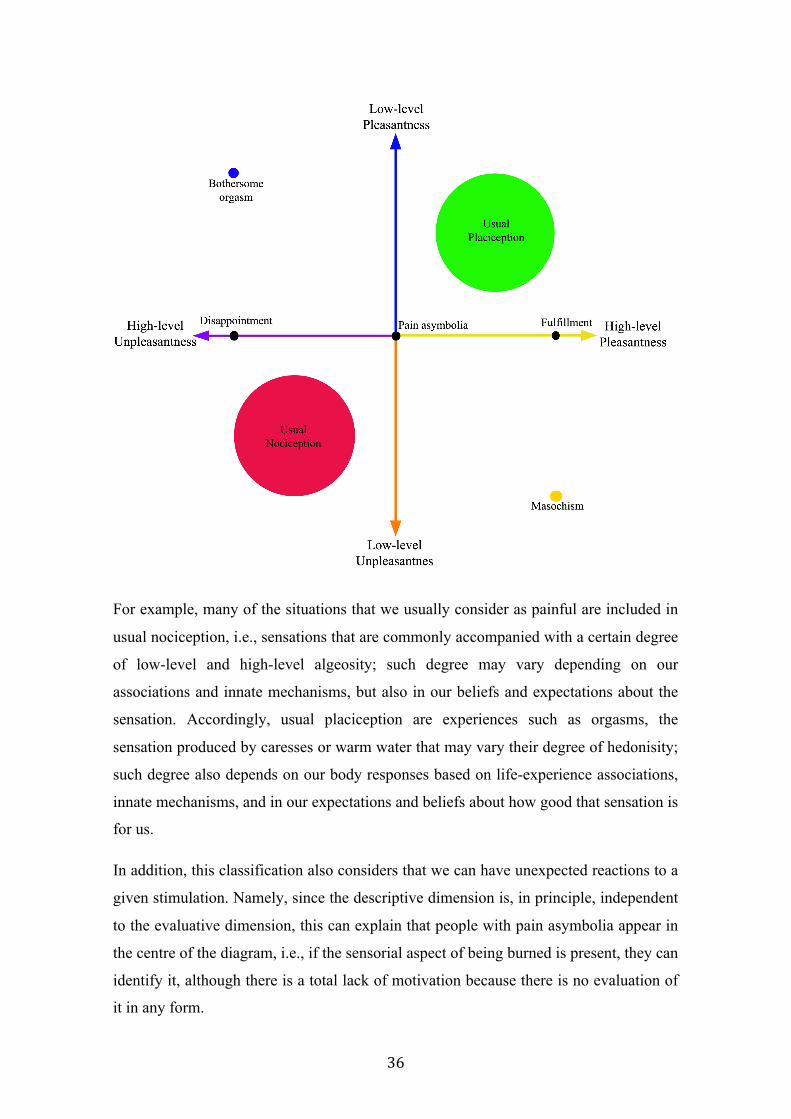
For example, many of the situations that we usually consider as painful are included in
usual nociception, i.e., sensations that are commonly accompanied with a certain degree
of low-level and high-level algeosity; such degree may vary depending on our
associations and innate mechanisms, but also in our beliefs and expectations about the
sensation. Accordingly, usual placiception are experiences such as orgasms, the
sensation produced by caresses or warm water that may vary their degree of hedonisity;
such degree also depends on our body responses based on life-experience associations,
innate mechanisms, and in our expectations and beliefs about how good that sensation is
for us.
In addition, this classification also considers that we can have unexpected reactions to a
given stimulation. Namely, since the descriptive dimension is, in principle, independent
to the evaluative dimension, this can explain that people with pain asymbolia appear in
the centre of the diagram, i.e., if the sensorial aspect of being burned is present, they can
identify it, although there is a total lack of motivation because there is no evaluation of
it in any form.
37
Lastly, and in contrast to previous models of pain, we can have a place to accommodate
other unpleasant phenomena such as disappointment, unfulfillment, frustration, defeat
or pleasant experiences such as fulfillment, achievement, contentment and so on. These
kind or experiences are not clear body experiences. Even if someone may say that
disappointment is somehow in her chest, it is not comparable to burns or cuts that can be
easily detected in your hand or you feet, e.g., it would be odd to have a disappointed
ear. Similarly, things such as fulfillment cannot be experienced in a very specific part of
our bodies; there is no such thing as fulfilled fingers. For these sort of unpleasant
experiences, we can say that it has an important high-level algeosity, even if it is not
accompanied of a body representation, and for the pleasant ones, we could explain them
as high-level hedonisity with no low-level representation.
So, in conclusion, this model has several advantages: 1) it recovers the intuition from
the medical models concerning different levels of pain processing; 2) it solves the
hedomotive challenge by considering that unpleasantness and pleasantness are
motivating because they represent things as bad or good; 3) it proposes a correspondent
theory of pleasure; 4) it gives an account of the degree of unpleasantness and
pleasantness, since something can be more unpleasant or pleasant if both dimensions are
present; 5) it enters the possibility of explaining unpleasantness and pleasantness for
other situations that are not clear body representations; and 6) it offers an answer not
only for masochism, but also to many other normal and pathological interactions with
pain.
1.2 Masochism: hedonistic nociception
Now, in face of a model of pain that distinguishes nociception from placiception, low-
level and high-level algeosity and hedonisity, what can we say about masochism? Let us
remember that, if Tomas is masochist in a way that is relevant to the discussion about
pain perception, it is because he finds pleasure in the sensation that he identifies as pain.
It is a relevant case of masochism if, say, Tomas likes to spill hot wax in his skin
because he finds pleasure in the sensation produced by such hot wax, al least under
certain circumstances. To explain how Tomas engages in such an unexpected way with
pain, there are three different possible paths of explanation:
38
Either a), something different happens regarding his nociception. That is, there is
something in his body that is different from the rest of the people; Tomas’ masochist
nervous system is pre-wired in a way that explains why he has different thresholds and
reactions to pain. There is something about his nociception that does not allow him to
process stimuli properly. For example, recent studies (Pollok, et al., 2010) claim that
masochists, in contrast to controls, have increased pain thresholds and a positive
evaluation of painful laser stimulation.
However, this path cannot lead us to the answer. Let us remember that nociception has
nothing to do with liking or disliking. Even if nociception may work differently in
Tomas, this could only tell us if Tomas is capable of perceiving the raw descriptive
dimension of pain. If Tomas is capable of detecting that there is melting wax on his
skin, then this means that his nociceptors are working correctly. So, since nociception is
not concerned with the fact that Tomas finds his sensation pleasant or unpleasant, then
if something different occurs in masochistic experiences should not be, in principle, at
this dimension of pain processing.
Or could be b), there is something different in Tomas’ low-level processing. That is to
say, the stereotypical innate responses that we have towards pain are different for him,
either by conditioning or by the way his anatomy is organized. I think here lays part of
the answer. As we stayed before, the unpleasantness of pain can be modified by life
experiences, learning, and conditioning, this explain why dogs can be trained to stop
minding electrical shocks. So, similarly, this could also explain Pollok and coll.’s
results. Namely, Tomas has a higher pain threshold; he is less susceptible to algeosity
because he has gotten used to it.
In fact, there are two possibilities about how the low-level of processing could be
different in Tomas. It could be either that 1) he processes nociception as low-level
hedonisity, and therefore, we should expect that he likes and seeks most body damages:
he seeks to be burned constantly by all sort of means and he may even like other
instances of nociception such as broken ankles. The other alternative is to that 2) in
presence of nociception Tomas’ low-level is still algeostic, but it may be slightly
decreased by his habits or his anatomy.
Lastly, it could be that c) there is something different concerning his high-level
processing. I believe here lays the key to explain such unexpected behavior to stimuli

39
such as melting wax. That is, Tomas has different beliefs, memories, and expectations
that represent the hot wax as good for him. One of the main features about masochism
is that not only are masochists less bothered by nociception that the rest of the
population, they like that nociception. In contrast to people who seek nociception for
obtaining something else, like a new social status or avoid more suffering, the difficulty
of masochism rests in the fact that they like that nociception. So, my answer is that
Tomas seeks to be burned with hot wax because, at least under certain contexts, because
his nociception is represented with high-level hedonisity.
In this sense, probably his nociception works adequately, so he knows when he
accidentally cuts or burns himself while cooking in the kitchen; his low-level algeosity
might be slightly modified concerning light burns because he has gotten used to them,
so he has a low-level degree of algeosity when he is burned by hot wax; but most
importantly, his beliefs about his nociception related with wax burns are very positive.
This results in a high degree of high-level hedonisity, which explain why he likes it and,
therefore, why he engages in such practices. He actually likes pain sometimes.

40
2. Pain Modulation
2. 1 Types of modulation
We can start thinking about a particular pain case mentioned by Valerie Gray
Hardcastle (1999, p. 13). Mathieu Formet-Savoie was a gifted cellist who was
diagnosed with cancer at an early age and had to stop playing music because of this.
The relevant thing about this situation concerning pain is that Mathieu generally refused
any kind of medication to reduce his physical and emotional suffering. He preferred to
deal with it by refocusing his creative energy into writing about his experiences; he
considered himself to be surrounded by a healthy supporting environment, which is
unusual for people who share his medical condition. He died at age thirteen soon after
he published his life’s work Le cancer à 11 ans. What is intriguing about the way he
managed his pain is that it suggests that at least some part of it may depend in our
intellectual capacities to deal with it. Indeed, in recent years several studies have shown
that there are cognitive variables that modulate pain perception. In particular, attention
and emotion play a key role for pain modulation (Villemure and Bushbell, 2002).
For example, several experiments show that attention can influence on pain perception.
Bantick and coll. (2002) gave noxious thermal stimuli to subjects while they had to
perform a stroop task. Interestingly, the authors found that when the task was more
difficult, people reported feeling less pain. Likewise, Pud and Shapir (2006) also
attenuated pain perception by simultaneously giving noxious heat stimulation, auditory
stimulation, and a cognitive task. They found that pain rating was highest when heat
stimulation was presented alone, and that pain rating was attenuated when passive
auditory stimulation was added.
Emotions are also related to pain perception. For example, several studies support that
chronic pain patients are likely to develop depression. However, even if it may seem
more intuitive that long-lasting periods of pain can lead to negative emotional states,
there is also evidence for the reverse causal relationship: being in a negative mood can
also increase pain. For example, Bras et al. (2010) claim that chronic stress disorders
may lead to increase sensibility: patients find unpleasant some stimuli that are not
usually considered as so.
41
It has also been shown that pain can also be attenuated by mindfulness, i.e., by having
an “empty mind”. Gard et al. (2009) measured three different variables (pain intensity,
unpleasantness, and anticipatory anxiety) in two groups, one that was trained in
meditation and one that was not. They proportioned noxious stimuli to the subjects
while meditating and in a cognitively neutral situation. In contrast to this neutral setting,
all subjects reported less pain while they were in a state of mindfulness. Further, ratings
were significantly lower for people who were used to meditate.
Another interesting example of pain modulation is hypnosis. Rainville and coll. (1999)
conducted three experiments showing that pain can be modulated by hypnotizing
subjects. During the first experiment, they put subjects under noxious stimuli and after
hypnosis they repeatedly told them that their sensation was of “well-being” and
“surprisingly pleasant”; in the second experiment, they did something similar but told
them that their sensation was of “discomfort” and “surprisingly unpleasant”; in the last
experiment they told subjects that their pain would be more intense and they used words
such as “burning”, “acking”, and “stinging” to emphasize the sensorial aspect of pain.
After the first two tests, they concluded that the degree of unpleasantness could be both
increased and decreased thank to hypnosis; similarly to previously conducted tests
(Rainville and coll., 1992), their results suggest that: 1) as the result of hypnotic
suggestion, people may consider the same intensity of noxious stimuli as more or less
unpleasant, and 2) they can also consider as equally unpleasant different intensities of
noxious stimuli. In addition, based on their in third experiment, what they call “pain
intensity”, could also be modified. Additionally, their results suggest that there is a
correlation between hypnotic susceptibility and pain modulation.
One last example of pain modulation is the placebo and nocebo effects. Nir and coll.
(2011) showed that people’s appreciation of the degree of unpleasantness could be
decreased with a placebo or increased with a nocebo. They administered painful thermal
stimuli to one placebo and nocebo group (and to its correspondent control groups); the
placebo group was told that they would receive a cream that diminished pain and the
nocebo group a cream that, of course, would augment their pain. As expected, people
reported that their pain was less unpleasant with a placebo and more unpleasant with a
nocebo, in comparison to their respective controls. These results point out that pain

42
perception is not merely based in the external stimuli and emphasize the relevance of
endogenous analgesia in humans.
In summary, all the previous mentioned authors agree that there is pain modulation. In
most of the cases it seems like such modulation is due to a high-order cognitive skill,
such as performing a stroop task, by having negative emotions and expectations, by
empting our minds, or by changing our beliefs about the nature of the sensation with
hypnosis. However, it is neither clear which is the most effective way to modulate pain,
nor how it is possible that our cognition modifies the unpleasantness of our experiences.
2. 2 Levels of modulation
Among the cultures and individuals people have different reactions towards pain. There
is no conclusive data that show different pain thresholds in different ethnic categories.
Nonetheless, it has been shown that culture modulates how people respond to pain.
Zborowski (1952) described how Americans from different origins (Italian, Jewish,
Irish, and “Old American”) react in different ways in relation to painful stimuli. What
could explain that these different groups have different reactions to the same stimuli? It
could be either that 1) they have different pain receptors so some of them perceive the
same nociceptive stimulation in different ways, or 2) they experience pain in different
ways because of their different cultural background. I believe the latter is the correct
answer. If an ethnic group considers pain as more unpleasant than other is because its
cultural practices lead people to represent nociception as worse in the bodily and/or
psychological sense.
In this way, we can explain the various cases of pain modulation. In the examples where
attention gets modified by focusing on a cognitive task, or by being distracted by
auditory stimulation, algeosity may decrease because the higher-level representation of
pain gets oriented into other stimuli. Further, in the case of mindfulness, the reason why
people who are trained in meditation report less unpleasant pain is because, by “empting
their mind”, they manage to have no high-level representation of their pain. They say
that pain is less unpleasant because their nociception is not represented as bad.
Moreover, they also probably know how to control their low-level algeosity as a result
of their training to rest in uncomfortable positions for long periods of time.
43
In addition, this also fits with the fact that negative emotions and chronic stress makes
people more susceptible to pain. That is to say, the fact that we represent nociceptive
stimuli as bad for us, because we are stressed or depressed, can indeed augment the
degree of algeosity that we experience. Similarly, for pain modulation through
hypnosis, we could explain that people find the same stimulus as more or less
unpleasant because they represent it as better or worse, but they represent it as such
because of what they believe. How susceptible they are to change the way they
represent their nociception rests upon how susceptible they are to hypnosis. In other
words, how susceptible they are to modify their high-level representation of such
stimuli as good or bad for them.
Lastly, in the case of the nocebo and placebo effects, we could explain something
similar. This kind of modulation clearly has nothing to do with a modification in the
evaluative low-level. That main difference between taking a placebo and a real
painkiller is that we think that both are going to take our pain away but only one has the
capacity to directly affect our body mechanisms. In the experiments previously
discussed, the fact that people believe that a cream will change their degree of
unpleasantness is what renders their nociception more or less unpleasant.

44
3. So, can anybody like it?
Yes, anybody can like pain. However, not everyone likes pain. That is to say, even if we
usually represent nociception as bad, this does not mean that nociception is necessarily
unpleasant. The exact same stimuli can be represented in different ways. There are good
evolutionary reasons why nociception is most of the time represented as bad, which
explains our usual avoidance behavior. Nonetheless, we can change the way we
represent nociception.
Interestingly, the changes in our evaluative representations can work in both directions,
not only can things change their degree of unpleasantness but also of pleasantness.
People, in principle, are capable of representing nociception as good. Pain cognitive
modulation is an example of how changes in our high-level evaluative representations
result in changes in the degree of algeosity. For masochism, this modulation goes
further: people represent their nociception as high-level hedonistic. So, as long as
someone is capable of representing their nociception as hedonistic, that person would
have motivations to seek for it, and would be a masochist.
45
Conclusion
The main purpose of this research was to make sense of masochists’ seek for pain.
Since we usually avoid unpleasant things and seek for pleasant ones, and given that pain
is conceived as paradigmatically unpleasant, it seems odd that someone engages in
painful activities just for the pleasure of it. In other words, if pain is unpleasant, it seems
to be nonsense to desire pain as an end. In order to figure out this puzzle I decompose
the discussion into three parts.
In the first part, I clarified why we think that pain is problematic for masochism and
why masochism is different from other controversial pain cases. I analyzed two
different ways in which we could explain that pain is not really a problem for
masochism:
1) Based on the analysis on the medical definitions, pain and masochism are not
necessarily contradictory. On the one hand, according to medical explanations of pain,
we could explain that masochists have the same descriptive experience of pain and a
positive evaluation; however, these theories do no explain how such evaluation may
become positive. On the other hand, strictly according to the medical definitions of
masochism, someone can be a masochist and have a completely normal interaction with
pain; nevertheless, this still leaves unexplained why some masochists could have such
odd interaction with pain.
2) The second possible way to answer is by claiming that pain is only a means for a
valuable end. Namely, pain in masochism is somehow similar to receiving a painful
antidote in order to feel better when we are sick or to be part of a painful ritual initiation
that will give us access to a higher social status. However, in contrast to these situations
in which pain is an unpleasant means for a valuable end, pain in masochism cannot be
clearly dissociated into means and end. Masochism is a situation were people find
pleasure in a sensation that is usually unpleasant. Masochists may pursue pain as an
end.
In the second part, using an evaluativist approach to explain the unpleasantness of pain,
I offered an equivalent theory of pleasantness. This theory broadly postulates that in the
46
same way that we avoid pain because we represent it as something bad in the bodily
sense, we tend to seek for pleasant sensations because there are stimuli that we represent
as good in the bodily sense. I propose a model that incorporates i) the medical models of
pain, where pain is understood as composed of different levels of processing, ii) the
philosophical discussion concerning the unpleasant nature of pain and our usual
tendency to avoid it, and iii) a theory of sensations that includes the spectrum varying
from unpleasant to pleasant phenomena. This model proposes that the phenomenology
of sensations is dependent on three dimensions: 1) the purely descriptive sensorial
dimension; 2) a low-level evaluative dimension, which represents stimuli as good or
bad in the bodily sense; and 3) high-level evaluative dimension, which represents
stimuli as good or bad in the psychological sense. Finally, I claim, masochists are able
to find pleasure in pain in the sense that their nociception is represented as positive, and
therefore pleasant, mainly in the high-level evaluative dimension.
Finally, in the third part, I used such model to concretely account for masochism and
give a coherent organization and predictions to several normal and pathological cases of
pain. Cases of masochism in which people seek for pain as an end could be explained
in the following way: 1) their sensorial descriptive level works adequately, which
explains why they can detect cuts and burns normally; 2) their low-level evaluative
dimension represent the stimuli as bad in the bodily sense, although it can be attenuated,
e.g., by conditioning; and 3) their high level evaluative dimension represents the stimuli
as good, which explains masochists’ behavior to seek for cuts and burns. In other
words, masochists may seek pain as an end in the sense that the same descriptive
sensation associated with pain can be, as a whole, evaluated as good and, therefore,
pleasant. In addition, this is coherent with many studies that report that pain can be
modulated by our cognition. That is, the fact that we cognitively represent stimuli as
good or bad does alter how it feels and how we react to it.

47
References:
American Psychiatric Association, (1994), DSM-IV Diagnostic and statistical manual of metal health disorders (4th ed), Wasington DC: Author.
Aydede, M., (2006), Pain: New Essays on Its Nature and the Methodology of Its Study. M. Aydede, Ed. Cambridge, Mass.: MIT Press.
Bain, D., (2011), "The Imperative View of Pain", Journal of Consciousness Studies, vol. 18, no. 9-10: 164-85.
Bain, D., (2012), “What makes pains unpleasant?”, Philosophical Studies. doi:10.1007/s11098-012-0049-7
Bantick, S. J., Wise, R. G., Ploghaus, A., Clare, S., Smith, S. M., & Tracey, I., (2002), “Imaging how attention modulates pain in humans using functional MRI”, Brain : a journal of neurology, 125(Pt 2): 310–9.
Bras, M., Loncar, Z., Gregurek, R., Milunovic, V., Boban, M. & Djordjevic, V., (2010), “Chronic low back pain in chronic combat related to posttraumatic stress disorder”, European Psychiatry, Volume 25, Supplement 1: 478.
Clastres, P., (1973), "De la torture dans les sociétés primitives", L’Homme 13 (3) : 114-120.
Dennett, D. C., (1978), “Why You Can't Make a Computer that Feels Pain”, in: Brainstorms. Cambridge, MA: MIT Press: 190-229.
Fields, H.L., (1999), “Pain: an unpleasant topic”, Pain, Suppl. 6: 61-69.
Gard, T., Ho, B. K., Sack, A. T., Hempel, H., Lazar, S. W., Vaitl, D., & Ott, U.,(2011). “Pain Attenuation through Mindfulness is Associated with Decreased Cognitive Control and Increased Sensory Processing in the Brain”, Cerebral Cortex: 1–11.
Goldstein, I., (1983), “Pain and Masochism”, Journal of Value Inquiry 17 (3): 219-223.
Hall, R. J., (1989), "Are Pains Necessarily Unpleasant?", Philosophy and Phenomenological Research, 49(4): 643–659
Hall, R. J.,(2008), “If it itches, scratch!”, Australian Journal of Philosophy, 86 (4): 525-535.
Hardcastle, V. G. (1999). The Myth of Pain. Cambridge, Massachusetts: MIT Press.
Houseman, M., (1996), “Quelques configurations relationnelles de la douleur”, in F. Hérituer De la violence II, Paris, Editions Odile Jacob, 1999: 77-112.
IASP, (1986), “Pain Terms: A List with Definitions and Notes of Usage”, International Association for he Study of Pain, Supplement 3: 216-221.
Klein, C., (2007), “An imperative theory of pains”, Journal of Philosophy, 104 (10): 517-532.
Klein, C., (2010), “Response to Tumulty on pain and imperatives”, Journal of Philosophy, 107 (10): 554–557.
Klein, C., (2011), “What Pain Asymbolia Really Shows”, (Forthcoming publication).
Lemaire, M., (2008), “Le doute et la douleur: Initiations et affects en pays sénoufo (Côte d’Ivoire)”, Systèmes de pensée en Afrique noire, 18: 193-218.
48
Martínez, M, (2011), “Imperative content and the painfulness of pain”. Phenom Cogn Sci, (10): 67–90.
Melzack, R. (1999). “From the gate to the neuromatrix”, Pain, 6(1): 121–126.
Melzack, R., (1996), “Gate control theory”, Pain Forum, 5(1): 128–138.
Melzack, R., & Wall, P. D., (1965), “Pain Mechanism: a New Theory”. Science. Washington, D.C.; 150: 971-979.
Nagel, T., (1986), The View from Nowhere, Oxford University Press.
Nir, R., Yarnitsky, D., Honigman, L., & Granot, M., (2012), “Cognitive manipulation targeted at decreasing the conditioning pain perception reduces the efficacy of conditioned pain modulation”, Pain, 153(1): 170-176.
Noren, Stephen J & Davis, A., (1974), “Pitcher on the awfulness of pain”, Tradition, 25(2): 117-123.
Pitcher, G., (1970), "The Awfulness of Pain.", The Journal of Philosophy, 67(14): 481–492.
Pollok B, et al., (2010), “Differential Effects of Painful and Non-Painful Stimulation on Tactile Processing in Fibromyalgia Syndrome and Subjects with Masochistic Behaviour”, Plos one, 5,(12).
Price, D.D., (2000), “Psychological and Neural Mechanism of the Affective Dimension of Pain”, Science 288(9): 1769-72.
Price, D. D., Verne, G. N., & Schwartz, J. M. (2006). Plasticity in brain processing and modulation of pain. Progress in Brain Research, 157: 333–353.
Pud, D., & Sapir, S., (2006), “The effects of noxious heat , auditory stimulation , a cognitive task , and time on task on pain perception and performance accuracy in healthy volunteers : A new experimental model”, Pain, 120: 155–160.
Rachels, S., (2000), "Is Unpleasantness Intrinsic to Unpleasant Experiences?", Philosophical Studies, 99: 187–210.
Schnitzler, a, & Ploner, M., (2000). “Neurophysiology and functional neuroanatomy of pain perception”, Journal of clinical neurophysiology : official publication of the American Electroencephalographic Society, 17(6): 592–603.
Villemure, C., & Bushnell, M. C., (2002), “Cognitive modulation of pain: how do attention and emotion influence pain processing?”, Pain, 95(3): 195–9.
W.H.O, (1992), ICD-10, Mental and Behavioral Disorders, 10th International Classification of Diseases. Clinical Descriptions and Diagnoses. World Health Organization.on, D.C.; 150: 971- 979.
Zborowski, M., (1952), “Cultural components in responses to a pain”. Journal of Social Issues, 8, I: 6-30.
Related Documents











![Flesh for fantasy: the future of sado- masochism and ... · masochism and performance ... sadomasochism in Coldness and Cruelty [1969 (Eng. tr. 1971)]. Deleuze's primary aim with](https://static.cupdf.com/doc/110x72/5ac2289d7f8b9ac6688e34e1/flesh-for-fantasy-the-future-of-sado-masochism-and-and-performance-sadomasochism.jpg)