The lipid-lowering therapy in patients with high risk of cardiovascular complications and with liver diseases Professor Sergey MARTSEVICH National Research Center for Preventive Medicine Moscow, Russia Vienna, April 22, 2015

Martsevich lipid-lovering therapy 2015 Vienna
Jul 20, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

The lipid-lowering therapy in patients with high risk of
cardiovascular complications and with liver diseases
Professor Sergey MARTSEVICH National Research Center for Preventive Medicine
Moscow, Russia
Vienna, April 22, 2015

Disclosures
• Research Support – PRO.MED.CS Praha a.s.
• Speaker Honoraria - PRO.MED.CS Praha a.s.

Background
• Cardiovascular diseases (CVD) remain the main cause of mortality in all developed countries.
• Hyperlipidaemia is one of the most significant CVD risk factors; its correction plays important role in reduction of CVD morbidity and mortality.
• According to recent Clinical Guidelines, target cholesterol (CH) levels become more and more low.
• To achieve target CH levels, intensive hypolipidemic therapy (preferably statins) is usually required.


Recommendations for treatment targets for LDL-C, ESC 2011
In patients at VERY HIGH CV risk LDL-C goal is < 1.8 mmol/l
In patients at HIGH CV risk LDL-C goal is < 2.5 mmol/l
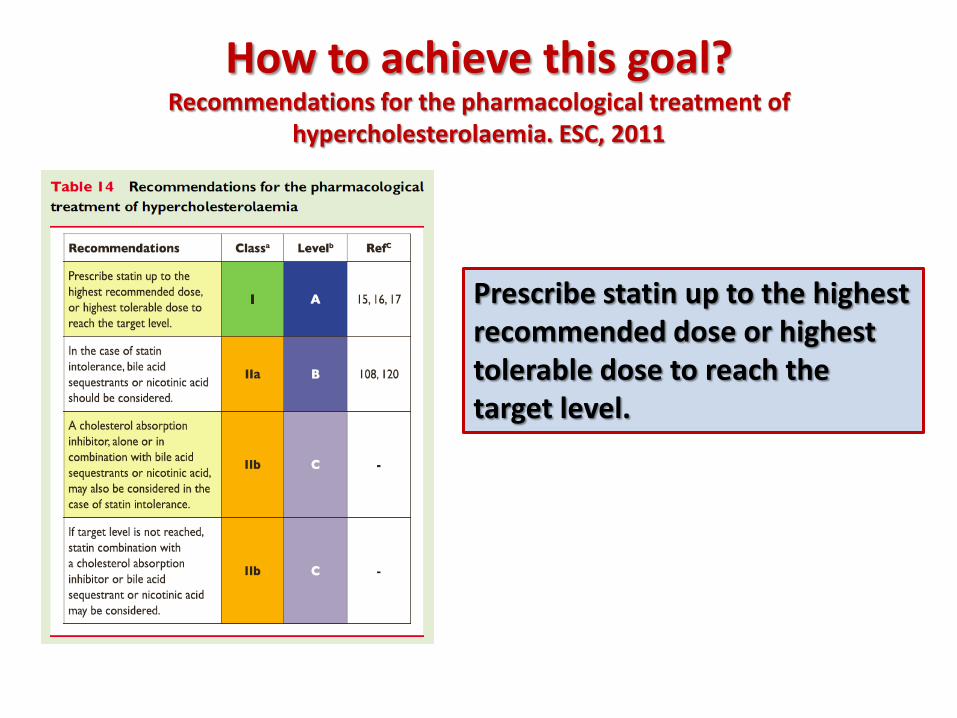
How to achieve this goal? Recommendations for the pharmacological treatment of
hypercholesterolaemia. ESC, 2011
Prescribe statin up to the highest recommended dose or highest tolerable dose to reach the target level.
Hypolipidemic therapy – evidence and reality
• Statins are the mainstay of the modern lipid-lowering therapy since they are the only group of drugs which have evident efficacy in reducing the risk of CV morbidity and mortality in different cardiovascular diseases.
• However, only a minor part of patients who really need statins receive them in real clinical practice.


Medications Percent of administration
Antiplatalets 5,7%
Statins 0,7%
Diuretics 9,9%
ACE-inhibitors 26,8%
Beta-blockers 10,2%
Angiotensin receptror blockers 1,8%
Calcium antagonists 7,6%
Oral anticoagulants (n=252 AF) 2,3%
Medical therapy prior to stroke (n=960). LIS-2 Registry data (Liubertsy, Moscow Region)
86% of patients already had AH, 21% - DM, у 26% -AF, 21% - had previous stroke, 13% - previous MI.

The other part of the problem: Even in those patients who receive statins, target LDL-CH levels
are rarely achieved
Why statin dose was not increased ?
31
87
% of target CH-LDL levels
Yes
No
• Statin safety data
0
20
40
60
80
100
120
140
160
180
No
Yes
Only in ¼ of high CV-risk patients target CH-LDL levels were achieved
“PROFILE” OUTPATIENT REGISRTRY data, Moscow, 2014

The situation with statin administration is much more complicated in patients with concomitant diseases
• What do we know about statin administration in CVD patients with concomitant
– liver diseases
– renal diseases
– muscle diseases
– In elderly patients
– …….

The situation with statin administration is much more complicated in patients with concomitant diseases
• What do we know about statin administration in CVD patients with concomitant
– liver diseases
– renal diseases
– muscle diseases
– In elderly patients
– …….
• Statins and the liver – Although liver toxicity has been a concern since
their initial introduction, several clinical studies has shown that statins are generally safe to use for prevention of coronary disease and death, even in the setting of chronic liver disease…

Statins and liver toxicity
• However, statin treatment is associated with some hepatic adverse effects, the most common of which is an asymptomatic and usually transient elevation of serum aminotransferase levels that often occurs in the first 12 weeks of therapy.
• This effect is dose-dependent.
• This finding is generally not correlated with histopathological changes and is not an indicator of liver injury.
• Clinically important statin-related hepatotoxicity is an extremely rare adverse effect.

Statins and liver toxicity

It should be pointed out that most of randomised trials excluded patients with transaminase levels more than 1-2 times the upper limit of normal, so the safety of statins in these people has not been systemically assessed.

Monitoring liver and muscle enzymes, ESC Guidelines, 2011
Current Clinical Guidelines propose for the physician a strict algorithm for management of abnormal liver enzymes before and during statin treatment…
In some situations, which are not rare, physician has to stop statin therapy or to reduce the dose despite high CV risk….

Furthermore,
• Official documents contain some restrictions on the use of statins in patients with liver diseases…

CONTRAINDICATIONS TO STATINS
http://www.accessdata.fda.gov/drugsatfda_docs/label/2009/020702s057lbl.pdf

CONTRAINDICATIONS TO ATORVASTATIN
http://www.accessdata.fda.gov/drugsatfda_docs/label/2009/020702s057lbl.pdf
Patients who have persistent AST>3 ULN increase, reduction of dose or withdrawal of atorvastatin is recommended.
Atorvastatin should be used with caution in patients who consume substantial quantities of alcohol and/or have a history of liver disease.
Active liver disease or unexplained persistent elevations of serum transaminases.

• Despite the fact that these adverse effects are reversed after treatment withdrawal, many patients with an indication for statins refuse therapy because of concerns about muscle or liver toxicity.
• This may represent a significant barrier to maximizing cardiovascular risk reduction for many patients with dislipidemia.
What are the consequences….

Moreover,
• A substantial part of physicians are afraid of prescribing statins to such patients, even in case of high CV risk….
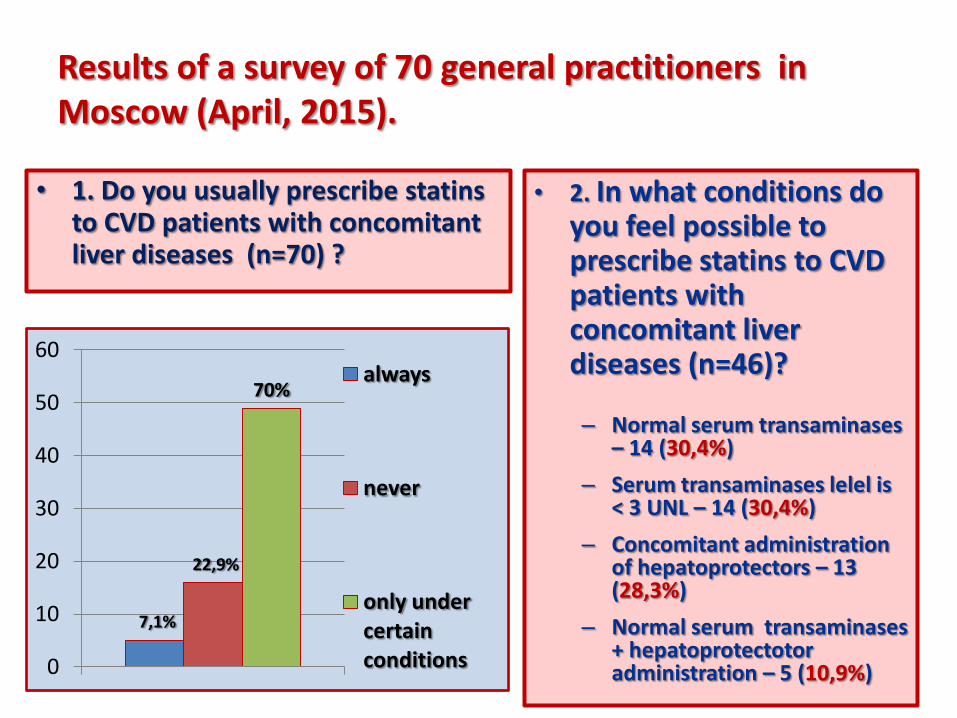
Results of a survey of 70 general practitioners in Moscow (April, 2015).
• 1. Do you usually prescribe statins to CVD patients with concomitant liver diseases (n=70) ?
• 2. In what conditions do you feel possible to prescribe statins to CVD patients with concomitant liver diseases (n=46)?
– Normal serum transaminases – 14 (30,4%)
– Serum transaminases lelel is < 3 UNL – 14 (30,4%)
– Concomitant administration of hepatoprotectors – 13 (28,3%)
– Normal serum transaminases + hepatoprotectotor administration – 5 (10,9%)
7,1%
22,9%
70%
0
10
20
30
40
50
60 always
never
only under certain conditions
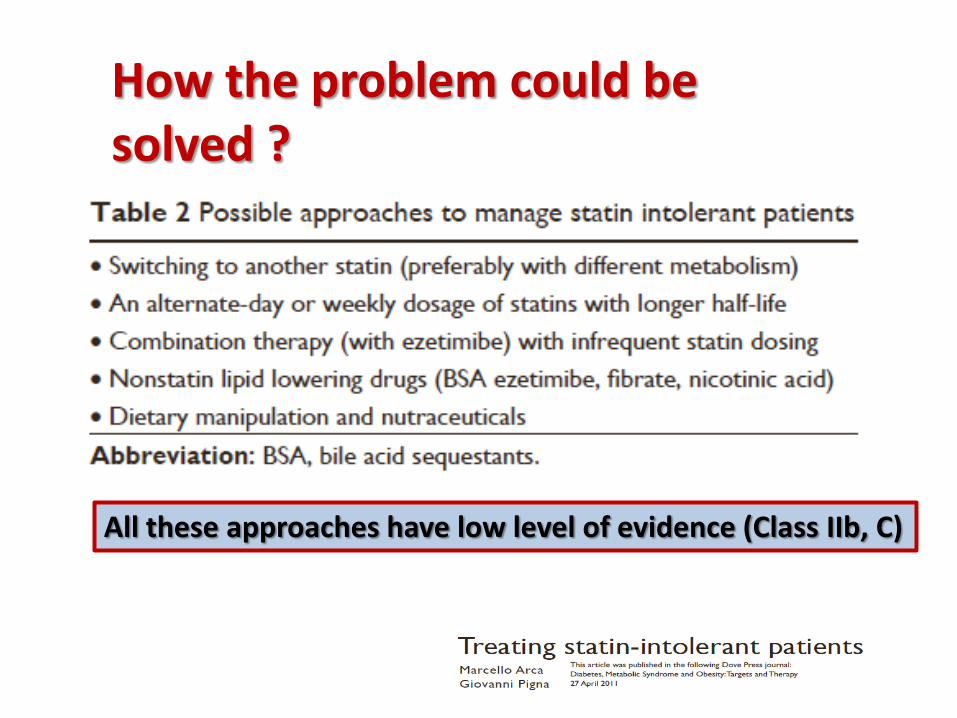
All these approaches have low level of evidence (Class IIb, C)
How the problem could be solved ?

Treating statin intolerant patients
• Combination therapy is the most reasonable approach, since it permits to reduce statin dose and ideally to diminish statin side-effects…
• Different hypolipedemic drugs can be combined with statins, however, many of them are not safe when combined with statins or not sufficiently effective….

Ursodeoxycolic acid has lipid-lowering effect

Effect of ursodeoxycholic acid combined with statins in hypercholesterolemia treatment: a prospective clinical trial • Gabezas Gelabert R. Rev Clin Esp 2004; 204:632-635.
• Random prospective clinical trial in 48 patients with primary family hypercholesterolemia nonrespondent to simvastetin or atorvastatin treatment.
• Simvastatin 20 mg/day + UDCA 300 mg/day yielded significantly greater reduction of LDL-CH than simvastatin 40 mg/day.
• Addition of atorvastatin 20 mg/day to UDCA 300 mg/day was more effective than atorvastatin 40 mg in LDL-CH reduction.
•The results of this study show that combination therapy with low doses of statins and UDCA is effective in patients initially nonrespondent to low doses of statins.

Assessment of influence of ursodeoxyholic acid on the efficacy and safety of statin
administration in patients with liver diseases “RACURS”
National Society for evidence-based pharmacotherapy
Russia

Study background:
Statins are the background of modern hypolipidemic therapy and are indicated to the majority of patients with high CV risk.
Long-term statin therapy is generally safe and well-tolerated. The most significant statin side-effects are myopathy and liver enzymes elevation.
Liver toxicity has been a concern since initial statin introduction, however, several clinical trials have shown that these drugs are safe for the prevention of CAD and death, even in patients with chronic liver disease.
Despite these facts, some official restrictions do exist concerning safety of long-term statin administration in patients with some functional liver disturbances.
Ursodeoxycholic acid (UDCA) can potentially enhance the efficacy of statins and reduce their influence on hepatic transaminases. However, no studies have addressed this problem.

• To assess efficacy and safety of combined
administration of statins and UDCA in patients
with hуperlipidemia and high CV risk, who have
concomitant liver diseases.
Study aim:
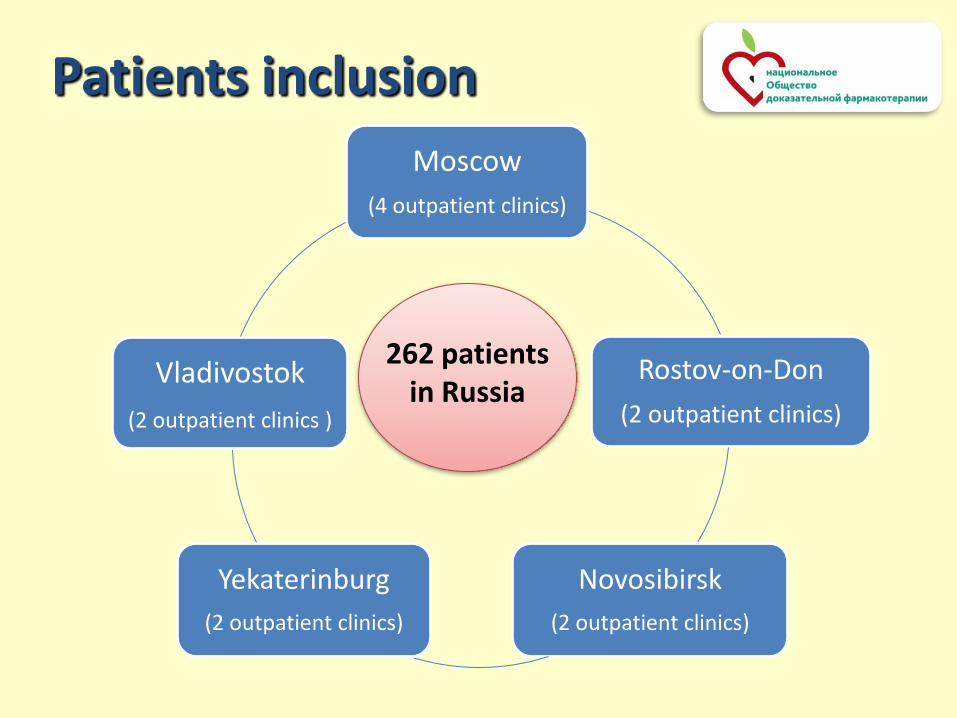
Moscow
(4 outpatient clinics)
Rostov-on-Don
(2 outpatient clinics)
Novosibirsk
(2 outpatient clinics)
Yekaterinburg
(2 outpatient clinics)
Vladivostok
(2 outpatient clinics )
262 patients in Russia
Patients inclusion

RACURS – observational registry-based study
• Every physician who took part in the study, included all consecutive patients who fulfilled inclusion criteria and recommended to add UCDA to statin therapy . All prescriptions were made in accordance with official recommendations for the use of study drugs.
• A special questionnaire was designed to assess actual compliance to the study drugs.

Ethical problems
• The study protocol was approved by Local Ethical Committee of the National Research Center for Preventive Medicine.
• All the patients gave written informed consent to participate in the study.
INCLISION CRITERIA
• Men and women > 18 years;
• Confirmed cardiovascular or cerebrovascular diseases of atherosclerotic origin or/and diabetes mellitus;
• Confirmed diagnosis of liver disease and/or laboratory abnormalities, typical for liver diseases.

Exclusion criteria
• Official contraindications to prescribe any of the study drugs (statins, UDCA);
• Acute liver diseases;
• Decompensated liver cirrhosis;
• Unstable coronary artery disease, decompensated chronic heart failure;
• Chronic renal failure;
• Patient’s refusal to participate in the study.

Patients who fulfill inclusion criteria
Received statins
Did not receive statins
M0-1
M0
M1
M3 M6
Study design:
Follow-up 6 months
UDCA recommended
Administration of statins

• Clinical evaluation – all visits.
• Blood pressure, heart rate - all visits.
• Laboratory data - serum transaminases, CK, bilirubin, glucose, lipids - all visits.
• Special questionnaire (adherence assessment) - all visits.
METHODS

Efficacy and safety assessment:
• Efficacy was assessed by reducing of CH-LDL levels and by reaching target CH-LDL levels.
• Safety was assessed by clinical status, serum transaminase and CK level dynamics, serum bilirubin level dynamics.

Patients’ characteristics (n=262)
• Included 127 men and 135 women
Data Age (years) 59,9 ± 8,7 31 - 86
BMI(kg/m2) 29,3 ± 4,8 18,7 - 49,7
Obesity 36,1% of patients with BMI > 30 kg/m2
Arterial hypertension 60,4%
Smoking status Do not smoke – 192 (75%), smoke – 61 (24%),
no data –2 (1%)
Allergy 7,5%

Cardiovascular diseases and/or DM
Condition N m/w %
Prior angioplasty 47 37/10 18,4
Prior myocardial infarction 73 50/23 28,6
Positive exercise test 88 58/33 34,5
Positive CA/scintigraphy 77 55/22 30,1
Peripheral atherosclerosis 111 53/58 43,5
Diabetes mellitus 112 68/44 43,9
Prior stroke or TIA 23 10/13 9,0

Liver diseases
Condition N m/f %
Non-alcoholic fatty liver disease
156 79/77 61,2
Сholelithiasis uncompicated 76 30/46 29,8
Postcholecystectomical syndrome
30 11/19 11,8
Chronic viral hepatitis 18 17/1 7,1
Biliary dyskinesia 84 42/42 32,9
Gilbert's Syndrome 3 1/2 1,2

Statin administration prior to study inclusion
184; 70%
78; 30%
received statins did not receive statins
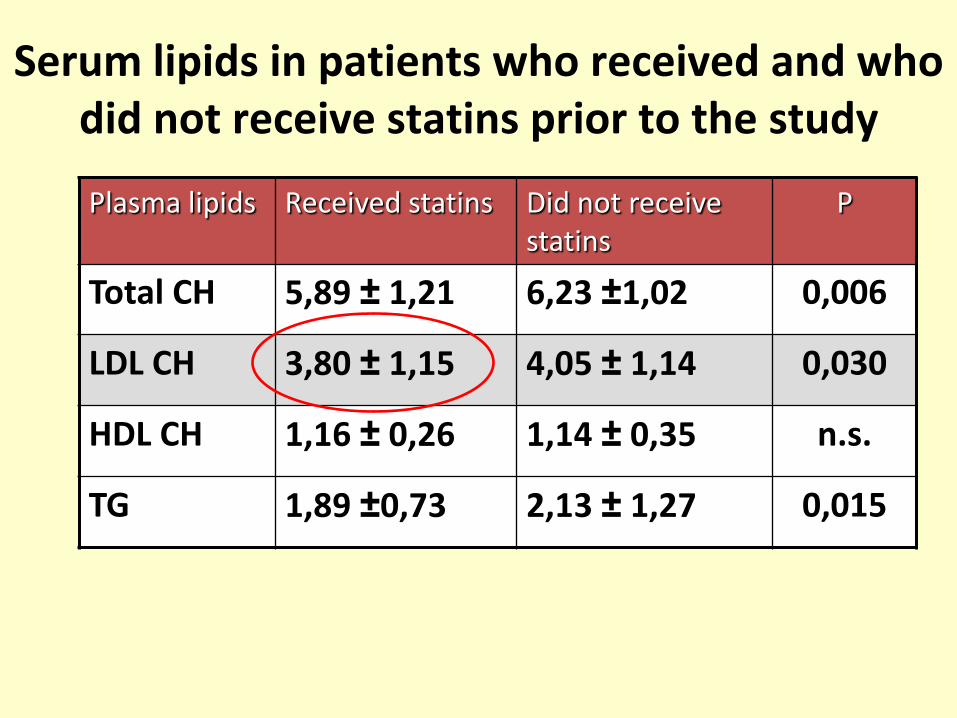
Serum lipids in patients who received and who did not receive statins prior to the study
Plasma lipids Received statins Did not receive statins
Р
Total CH 5,89 ± 1,21 6,23 ±1,02 0,006
LDL CH 3,80 ± 1,15 4,05 ± 1,14 0,030
HDL CH 1,16 ± 0,26 1,14 ± 0,35 n.s.
TG 1,89 ±0,73 2,13 ± 1,27 0,015

Study results

Serum lipid dynamics – all patients (n=262)
5,9 4,9 4,3
6,2 5,1
0
2
4
6
8
baseline 1 month 3 months 6 months
with statin without statin
3,8 2,9
2,3
4,1 3,2
0
1
2
3
4
5
baseline 1 month 3 months 6 months
Total cholesterol, mmol/l
LDL-CH, mmol/l
***
***

Laboratory data before study initiation and at the end of study – all patients (n=262)
0
40
80
120
baseline after 6 months
U/l mkmol/l

Real compliance to UDCA
• The main reason for noncompliance – high cost of UDCA
At the end of the study 62 patients (23%) din not take UDCA
219 204
179
43
19 19 32
43
0
50
100
150
200
250
1 month 3 months 6 months
administered not administered withdrawals no data
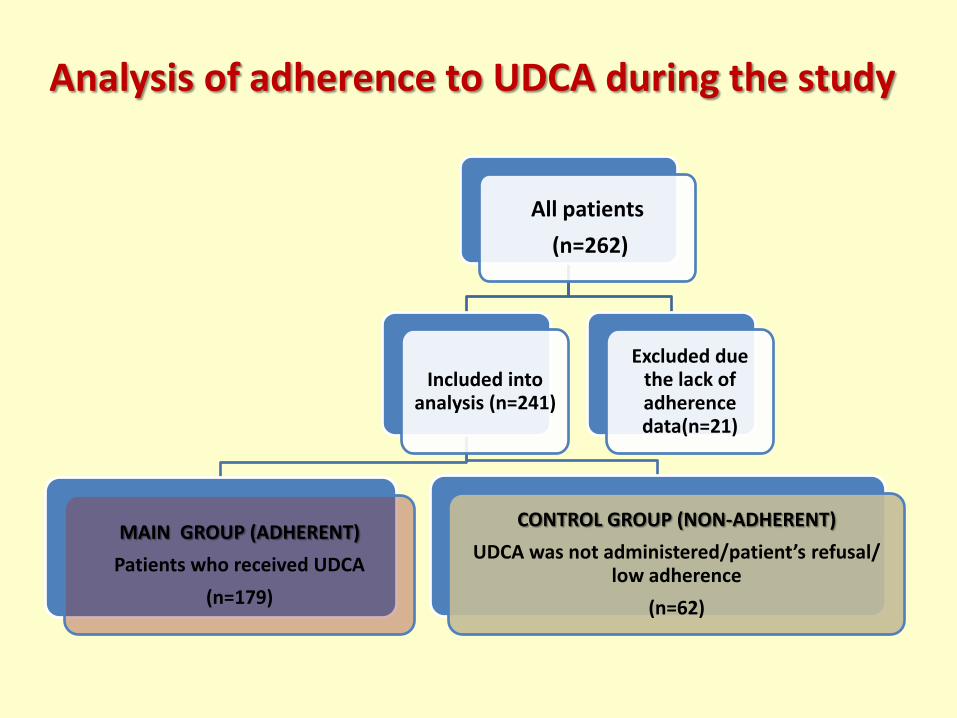
Analysis of adherence to UDCA during the study
All patients
(n=262)
Included into analysis (n=241)
MAIN GROUP (ADHERENT)
Patients who received UDCA
(n=179)
CONTROL GROUP (NON-ADHERENT)
UDCA was not administered/patient’s refusal/ low adherence
(n=62)
Excluded due the lack of adherence data(n=21)

STUDY RESULTS ANALYSIS
ALL PATIENTS (n=262)
INCLUDED INTO ANALYSIS (n=241)
MAIN GROUP
TOOK UDCA
(n=179)
CONTROL GROUP
UDCA not administered/patient’s refusal/ low adherence
(n=52)
EXCLUDED DUE TO THE LACK OF
ADHERENCE DATA (n=21)
PROPENSITY SCORE MATCHING
MAIN GROUP after propensity score matching
(n=52)

Patients who took UDCA (n=52)
Patients who did not take UDCA (n=52)
p<0,05
Age 61,6 (6) 60,8 ± 7,7 NS
Waist sirc. 98(12) 97(10) NS
BMI 28,2 (5,3) 28,9 (5,1) NS
ALT 23 (28,9) 26 (18) NS
AST 25,9 (19,2) 26 (11) NS
CH total 6 (1,5) 6,3 (1,6) NS
LDL-CH 3,9 (1,48) 4,1 (1,8) NS
TG 1,9 (0,5) 1,9 (1,09) NS
CK 106 (71) 135 (52) NS
Bilirubin 12,7 (9,6) 12 (5,3) NS
Propensity score – matching: patients who took and who did not take UDCA. Initial data.
Patients who took UDCA (n=52)
Patients, who did not take UDCA (n=52)
p<0,05
ALT 20 (11,1) 24 (10,5) NS
AST 22 (10) 24 (7) NS
CH total 4,0 (0,85) 4,52 (0,68) p<0,05
LDL-CH 1,92 (0,73) 2,6 (0,7) p<0,05
TG 1,2 (0,56) 1,3(0,64) NS
CK 105 (72) 126 (50) NS
Bilirubin 12,2 (7,2) 10,9 (6,5) NS
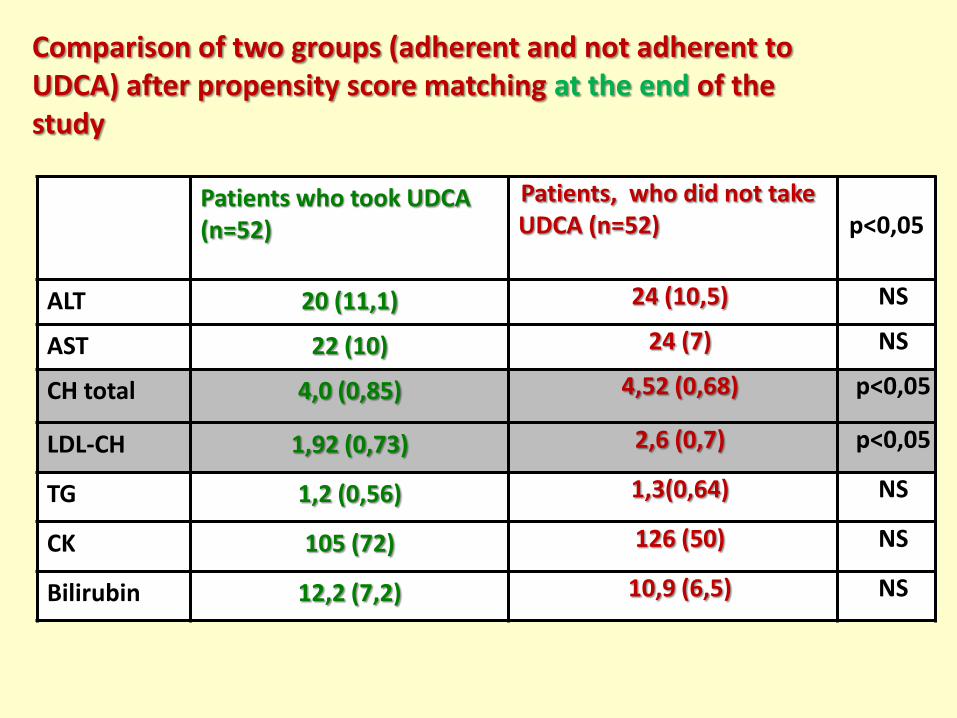
Comparison of two groups (adherent and not adherent to UDCA) after propensity score matching at the end of the study

Patients who took UDCA (n=52)
Patients, who did not take UDCA (n=52)
p<0,05
ALT 20 (11,1) 24 (10,5) NS
AST 22 (10) 24 (7) NS
CH total 4,0 (0,85) 4,52 (0,68) p<0,05
LDL-CH 1,92 (0,73) 2,6 (0,7) p<0,05
TG 1,2 (0,56) 1,3(0,64) NS
CK 105 (72) 126 (50) NS
Bilirubin 12,2 (7,2) 10,9 (6,5) NS
Comparison of two groups (adherent and not adherent to UDCA) after propensity score matching at the end of the study

Achievement of target CH-LDL levels (<1,8 mmol/l) at the end of study in the two groups of patients
35%
100%
0
10
20
30
40
50
60
with UDCA without UDCA
1,8 or more <1,8 mmol/l
n = 52 Χ2 = 21,77; р<0,01
65%
Conclusions (1)
• 1. RACURS study, performed in terms of specially designed registry, demonstrated possibility and safety of combined administration of statins and UDCA in patients with high cardiovascular risk and concomitant liver diseases.
• 2. High adherence to UDCA was revealed.
• 3. Decrease in lipids levels (total CH and CH-LDL) by the end of 6-months therapy can be explained by ability of UDCA to potentiate statins hypolipidemic activity or by its own hypolipidemic action.
Conclusions (2)
• 4. The lack of increase of serum transaminases and bilirubin at the end of 6-months treatment period may be the consequence of hepatoprotective activity of UDCA.
• 5. Combined administration of statins and UDCA is a promising approach to treat hyperlipidemia in statin intolerant patients which should be checked in a special controlled study.
Thank you for your attention !
Related Documents