Belly Basics: “Mapping Out” Prenatal Care Susanna Magee, MD MPH

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Belly Basics: “Mapping Out” Prenatal Care
Susanna Magee, MD MPH
Objectives
• Become familiar with the general
components of prenatal care
• Be able to recognize high risk conditions,
not necessarily treat them
• Develop ability to use our Centricity
prenatal care map as a tool to administer
and improve prenatal care
• Understand the importance of appropriate
documentation

First Trimester Objectives • Risk Assessment
– Intake visit with nurse, social worker and nutritionist
– History and Physical
– Intake labs including CF, Tay Sachs, MaterniT21 or Harmony where appropriate
• Health Promotion – Begin Prenatal vitamins/DHA/folate
– Counseling and Education, Immunizations
• Pregnancy Dating – Ultrasound for uncertain dating – Counsel on genetic screening options

History
• Review intake notes from
nurse, social worker, and
nutritionist (*L)
• Review patient
medical/surgical history
• Review past OB history
noting type of delivery,
gestational age, labor
duration, weight of infant,
maternal/infant
complications

History
• Paternal/Family History including h/o
congenital anomalies
• Medication Allergies/Anesthesia reactions
• Gyn Hx: Abnormal Pap Smears, cryo or
LEEP procedures
• Create Problem List, review and update
each visit
– where does this go? (*L)

Physical Exam
• Thorough head to toe exam
– Vitals
– General – obese? flat affect?
– Thyroid
– Breast exam
– CV - is there need for echo (pathologic) or is this just a flow murmur?
– Abdomen- scars
– Baseline reflexes
– Pelvic and Pelvimetry • Lost art

Physical
• Pelvimetry:
– Inlet = Obstetrical (true)
conjugate which is distance
from sacral promontory to
superior aspect of pubic
symphysis (10-12 cm).
– Mid = distance between
ischial spines (>10cm), note
sacral concavity and
inclination
– Outlet = pubic arch,
distance between ischial
tuberosities (8cm), coccyx

Physical
• DOCUMENT COMPLETE PHYSICAL
EXAM (*L)
First Trimester Labs
• Baseline CBC - check for anemia
• Blood Type ? Need for Rhogam – presence of D antigen on RBC means Rh+,
absence of D antigen means Rh -
• Antibody Screen - checks for antibodies against major and minor antigens on maternal RBC membrane – anti D antibodies means isoimmunization in
Rh( -) women
– Review other major/minor antigens like Kell/Duffy etc
– Pathologic vs. Non-pathologic
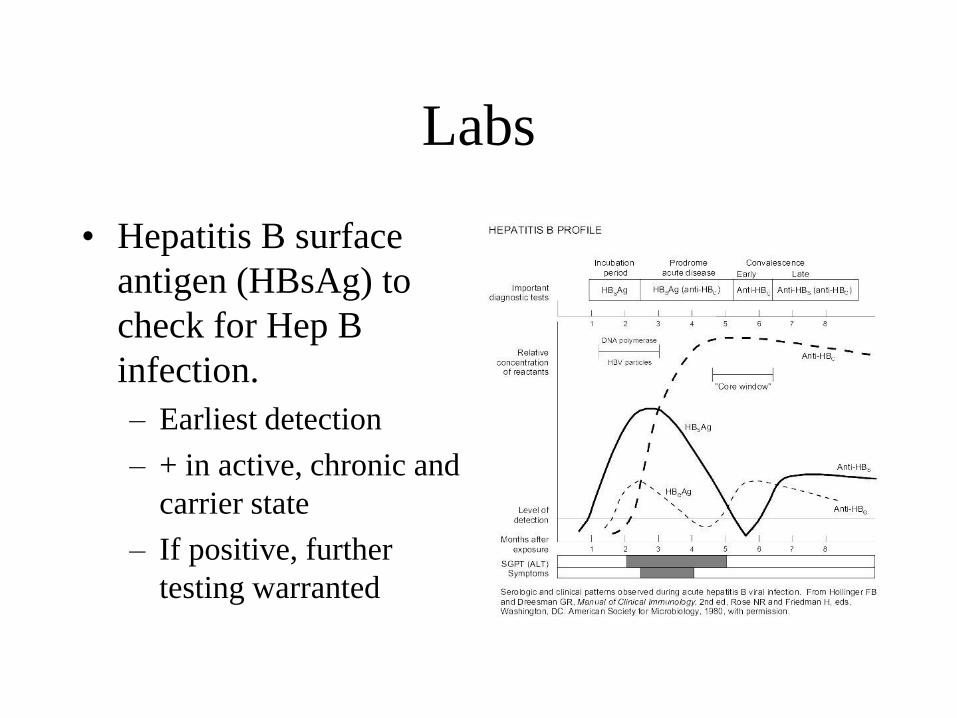
Labs
• Hepatitis B surface
antigen (HBsAg) to
check for Hep B
infection.
– Earliest detection
– + in active, chronic and
carrier state
– If positive, further
testing warranted

Labs
• Urine C & S
– Higher risk for UTI
– Remember to treat asymptomatic bacteriuria in
pregnancy.
• Controversy: how many colonies are bacteriuria
• Always get repeat UA/C&S as TOC after treatment
– Any GBS = prophylaxis in labor against GBS
– 2 UTIs or 1 pyelonephritis buys prophylaxis
against repeat infection

Labs
• Rubella antibody
• Syphilis screen (RPR, STS, VDRL)
– If positive, obtain confirmatory FTA-ABS
qualitative.
– If FTA-ABS positive, obtain quantitative
screening titer (RPR) and treat accordingly with
PCN
– Follow titers of RPR q 4-6 weeks
– Treat as indicated
Labs
• PAP, GC, Chlamydia, Wet mount (if
indicated) done at initial OB exam
– History of PTB/symptomatic d/c: wet mount
• HIV - All pregnant women should be
counseled and offered test. If patient
declines, document
• +/- Obtain Hgb electrophoresis
Labs
• For high risk patients, place PPD and read
in 48-72 hours. If positive (review
guidelines), check CXR.
– no need to delay xray
– If PPD+, CXR - : INH for 9 mo postpartum
(TB clinic starts about 3 months pp)
– Do not attribute +PPD to childhood BCG
vaccination
• Quantiferron gold

Labs
• Obtain intake 1 hour non fasting 50 g
glucose screen:
– history of abnormal glucose value or gestational
diabetes
– consider if multiple historical risk factors • family history
• prior macrosomia
• obesity
• congenital anomaly
• IUFD
Labs
• Toxoplasmosis, Varicella, CMV,
Parvovirus, HCV, HSV titers not routinely
recommended.
• Obtain UTOX in high risk patients,
especially if they present late for care,
frequently miss appointments or admit to
drug use.
– Follow up + UTOX at least q trimester
Vaccinations
• May give Hepatitis B, TdaP, and Influenza during pregnancy. – May start hepatitis series at intake.
– TdaP best given 28-36 week window to confer passive immunity to infant
– Influenza vaccine indicated for all pregnant woman regardless of gestational age during flu season (Oct - Mar)

Pregnancy Dating (more in the second trimester)
• Naegele’s Rule: EDD = FDLMP + 7d - 3m
• LMP
• Uterine size at intake
• Conception
• Ultrasound findings
• hCG levels

Pregnancy dating
LMP and u/s correlation
• 0-9 weeks +/- 4 days
• 10-13 weeks +/- 7 days
• 14+ weeks +/- 10 days
Counseling and Education
• Monthly visits
• Encourage breastfeeding right from initial
visit
– Definitively by 20 weeks
• Ensure safe environment/confirm supports
– Volunteer doula program
– Group visits
• Substance abuse counseling
Second trimester
Cruising along...

Second Trimester
• Definition: 12-24 weeks
• At and around 23-24 weeks, viability issues
– Importance of accurate dating
• Prenatal visits are typically every 4 weeks
Second Trimester
• 3 issues:
– Housekeeping
– Completing genetic
screening tests
– Establish dating
Housekeeping
Is the BTL signed and faxed to WOOD 2?
H and P done?
Intake?
Labs documented?
Is your name listed as provider?
Are previous deliveries entered?
Problem list updated?
Dating finalized?

Screening
• Discuss genetic testing with your patient
and DOCUMENT pt’s decision.
– What are the five screening tests?
– When should they be offered?
Prenatal Screening Tests
• Maternal serum markers and / or u/s findings to help
identify patients at risk for fetal malformations and
chromosomal abnormalities.
• Quad test includes a-fetoprotein (MSAFP), inhibin A,
unconjugated estradiol (uE3) and human chorionic
gonadotropin (hCG)
• AFP (most studied) is a protein made by the yolk sac, fetal
GI tract and fetal liver. Peaks in amniotic fluid by 12-14
weeks, detectable in maternal serum by 15-18 weeks
• Defect in fetal skin or fetal bleeding increases AFP in
amniotic fluid and therefore maternal serum

Prenatal Screening Tests

AFP
High levels, > 2.0 MoM (Multiples of the Mean)
may indicate the following:
neural tube defects, abdominal wall defects, impending fetal death,
multiple gestation, ectopic pregnancy, maternal hepatitis, herpes
infection, Rh disease, and fetal growth restriction
Low levels, < 0.25 MoM
• Suspect chromosomal abnormality
– primarily Down’s Syndrome (5%), molar pregnancy or
fetal demise

Genetic Screening
• MPSS
– MaterniT21
– Harmony
• Abnl ultrasound finding
• AMA
• H/O Trisomy in previous pregnancy
• Abnormal integrated screening


History of Spontaneous Preterm Birth
17 P
• Efficacy of Progesterone • 36.3 treatment vs. 54.9 % placebo delivered at < 37
weeks
• 20.6 vs 30.7% at < 35 weeks
• 11.4 vs 19% at < 32 weeks
– lower risk NEC, IVH and need for O2
– Most follow cervical length rather than screen
with FFN
History of Preterm Birth
FFN vs. cervical length
• FFN
– 22 and 34 and 6
– intact membranes
– < 3 cm dilation
– no intercourse or cervical manipulation within 24 hours
– fFn first--before other samples or manual cervical check
– high negative predictive value
• 1/1000 change delivery in 7 days if neg
• + predictive value poor, but as many as 14% will deliver within 2 weeks
Preterm Birth
• The incidental short cervix
– Vaginal progesterone
Third Trimester The homestretch
Third Trimester
• Definition: 24 weeks (viability) and beyond
• Number of Prenatal Visits
– Monthly until 28-32 weeks, then biweekly
visits at 32-34 weeks, and weekly after 36
weeks
• Continued Risk Assessment
– Domestic violence, symptoms of depression,
excessive weight gain, etc.

Third Trimester
Counseling/Visits
• 24-34 weeks – Repeat Risk Assessment…Update Problem List
• Consider influenza/hepatitis B vaccine
– Suggest prenatal classes / teaching ultrasound /
handouts
– Discuss breastfeeding, +/- circumcision, contraception
plans, home preparation, identify labor support
– Confirm fetal presentation
– Review dating
• VBAC-counseling high risk appointment at 32-34 weeks
• RCS-34 weeks
• BTL consents at 28 weeks FOR ALL PATIENTS

Third Trimester Labs
• Ensure previous trimester labs are complete
and documented!
• 26-28 weeks: 1 hour glucose screen (GDS2) • Order 3 hour screen (after the patient has followed a
high carb diet for 3 days) if 1 hour is > 130 (Carpenter &
Coustan)
– Repeat H & H
– Repeat STS in high risk women
– Repeat HIV GC Chlam in high risk women
• Defined by ACOG as all under age 25…..


Third Trimester Labs
• If pt. Rh -, time to order Antibody Titers
and give Rhogam (with 26-28 week labs)
– Order Rho Studies (on red lab sheet, check
Type and Screen, and Rho box)
– Lab will test maternal sample for anti-D Ab
• standard is 300 mcg
– Mom has 10 days to come in for shot
• If they miss, need to repeat the Rho studies to be
sure the dose of Rhogam is correct

Third Trimester Labs
– Standard dose Rhogam
is 300 mg, which
covers a 15 ml or less
mix of maternal fetal
blood.
– Rh Immunoglobulin
(Rhogam) is good for
12 weeks

Rh Special Situations
• If patient has vaginal bleeding in pregnancy
and is known to be Rh-, she should have
Rho studies and receive Rhogam
• If she presents days after the bleeding
occurred, then order Rho studies to see if
she has already produced anti-D Antibody
• If she has not, then give Rhogam – If she already had made anti-D Ab, then its too late to
give the Rhogam
Third Trimester Labs
• 35-40 weeks
– GBS vaginal rectal screen is recommended by
ACOG and AAFP for all pregnant patients at
35-37 weeks gestation
– Swab is considered interpretable for up to 5
weeks • If positive, PCN in labor
• If low risk PCN allergy: Ancef
• If high risk PCN allergy: sensitivities must be done to Clinda Erythromycin,
and Vancomycin
• If patient had GBS in urine during pregnancy, then requires Prophylactic Rx in
labor and no need vag/rectal swab
• Document your results and treatment plan
Third Trimester Labs
• You’re now at 40 weeks….what tests do
you recommend?
Third Trimester Labs
• Answer: NONE!
– No postdates testing is needed until pregnant
woman reaches 41 weeks unless there is some
other indication
• Decreased fetal movement
• Leaking fluid...
• What test should be done at 41 weeks?
Third Trimester Labs
• Answer: Best Evidence weighing cost
benefit ratio is for NST/AFI, otherwise
known as modified BPP
– Provides an immediate evaluation of fetal well-
being (NST) and uteroplacental function (AFI)
– What is an abnormal test?
• If NST abnormal (non-reactive, presence of deep or
prolonged variable decelerations, presence of late
decelerations)
• If AFI < 5 (5-8 considered low normal and will
require repeating in 2 days)

Third Trimester Labs
• What is the evidence?
– Has not been studied in a randomized
prospective fashion
– Miller et al 1996--largest and most respected
study
• Retrospective series of 15,482 high and low risk
pregnancies in which 56,617 MBPP’s were
performed as the initial fetal surveillance test

Miller et al, continued
• Positive Predictive Value (diagnostic accuracy of
an abnormal test to predict a compromised fetus)
– When applied to low risk conditions, the
positive predictive value is not very good
• Negative Predictive Value (diagnostic accuracy of
a normal test result to predict a healthy fetus)
– Comparable to the use of the BPP or CST, and
is much higher than the NST alone)
Miller et al, continued
• Evidence to date suggests that using NST
AFI together at 41 weeks, 41.5 weeks and
42 weeks results in a 50% decrease in the
rate of fetal demise after a normal test result
– 0.8 fetal deaths per 1000 versus 1.9 fetal deaths
in 1000)
• Note number of tragic outcomes very small
• There is no evidence to suggest that testing be done
before 41 weeks

Postdates….uggh!
• What do we do with this information?
– Once patient approaching 41.0 weeks, need to
discuss induction plan
– Plan should be documented and begin at 41+
weeks +/- and reviewed with the attending on
call
• “Stripping membranes”
– Some evidence that stripping at 37 weeks (term) prevents
the need for postdates management
How to determine ripening vs.
induction
• Bishop’s scoring
– Help assess the need for cervical ripening vs. straight
induction with oxytocin
– See form next page
Third Trimester Review
• Utilize the Prenatal Care Map
• Document Labs and Relevant Information
on the Problem List
• Your MCH Faculty are always available
– If they don’t know the answer, they’ll find it
out! Then everyone learns.
– Utilize OB Floor Preceptors in a Pinch

GET HELP
• Please precept your EDC
• Please precept your bimanuals/pelvimetry
• Please review your EDC and your labs each visit
• Print an OB Summary every trimester to be sure it is properly filled out
• If there are items not populating the care map contact Cathy Masterson.

ENJOY THIS EXPERIENCE
• Your hands may be the first ones to ever touch another
human being, even before their parents…
Related Documents











