Mapping Cognitive and Motivational Domains Across Levels of Analysis: Challenges and Opportunities for Target Specification Robert M Bilder, PhD Michael E. Tennenbaum Family Professor, and Chief of Medical Psychology – Neuropsychology, UCLA Jane & Terry Semel Institute for Neuroscience & Human Behavior, Stewart & Lynda Resnick Neuropsychiatric Hospital, Departments of Psychiatry & Biobehavioral Sciences and Psychology David Geffen School of Medicine at UCLA, and College of Letters & Science at UCLA

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Mapping Cognitive and Motivational Domains Across Levels
of Analysis: Challenges and Opportunities
for Target Specification
Robert M Bilder, PhD Michael E. Tennenbaum Family Professor, and
Chief of Medical Psychology – Neuropsychology, UCLA Jane & Terry Semel Institute for Neuroscience & Human Behavior,
Stewart & Lynda Resnick Neuropsychiatric Hospital, Departments of Psychiatry & Biobehavioral Sciences and Psychology
David Geffen School of Medicine at UCLA, and College of Letters & Science at UCLA

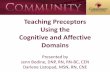
Rzhetsky et al 2009 “genetic overlap” derived from 1.5M medical records

Mapping Research Domains Impact of the NIMH Research Domains Criteria (RDoC) Initiative
• RDoC – offers new dimensions to move psychiatry beyond current diagnostic taxonomy and towards rational therapies
• Consensus meetings generated lists of elements at different levels of analysis
• Challenges: defining the true causal paths that lead from level to level (genome to syndrome)
• Opportunities: defining targets of treatment aligned with biological and psychological science

RDoC Levels of Analysis
• Personality, symptoms
Self-reports
• Rating scales, cognitive assessments
Behavior
• MRI, EEG, MEG, psychophysiology
Physiology
• Neuroanatomic nodes; imaging, basic
Circuits
• Cell physiology
Cells
• Genetics, expression, proteomics
Molecules


RDoC Matrix Specification: Expectancy/Reward Prediction Error

RDoC Working Memory Matrix

Unit of Analysis Active
Maintenance Flexible
Updating Limited Capacity
Interference Control
Genes
NRG1/Neuregulin DISC1
DTNBP1/Dysbindin
BDNF COMT DRD2 DAT1
Molecules
Dopamine X X X X D1 X X X (gain) X D2 X X ? X
Glutamate X X X X NMDA X
AMPA ? GABA X ? X X
A ? B ?
Cells
Pyramidal X Distinct Types of
Inhibitory Neurons X X
Parvalbumin X Calbindin X
Calretinin Medium Spiny Neurons (Basal
Ganglia) X
Circuits
Key Circuit: PFC-Parietal-Cingulate-Dorsal Thalamus-Dorsal Striatum
DLPFC X X VLPFC X X
Dorsal Striatum X Dorsal Parietal X
Inferior Parietal X X
MD & VA Thalamus (by virtue of their role in
circuit) X ?

Unit of Analysis Active
Maintenance Flexible
Updating Limited Capacity
Interference Control
Behavior and Paradigms
N-Back X X (?) X X (if you include non-target lures)
Delayed Match to Sample
X --- X X (if you use repeated items, or delay
period interference)
Delayed Match to Non-Sample
X --- X X (if you use repeated items, or delay
period interference)
Sequence Encoding and Reproduction
X --- X ---
Sternberg Item Recognition (including
recent negative variations)
X
X (recent negative
task increases
demand on updating)
X X (if you use repeated items, recent
negative variation)
Complex Span Tasks X X X X
Letter Memory/Running Memory
X X (?) X X (?)
Letter Number Sequencing
X X X X
Simple Span Tasks (may be more appropriate for
developmental populations, in adults
may not capture all key elements of WM)
X --- X X (if you use concurrent interference,
as in Digit Span Distraction)
Change Detection Tasks X --- X ---
Keep Track Task X X X X
AX-CPT/DPX X X X ---
Self-Ordered Pointing X X (?) X X

Is there a better way?

chronic stress depressed
mood self-reproach insomnia fatigue concentration
Borsboom & Cramer 2013 Annual Rev Psychology
Classic (psychometric) approach
Network (causal modeling) approach

“In sum, not only do we not know that symptoms are caused by mental disorders, but it is in fact extremely unlikely that they are. As a result, the hypothesis that such disorders are the proper entities to steer the organization of research, diagnosis, and treatment is, at best, awaiting scientific justification.”
Borsboom & Cramer 2013 Annual Rev Psychology

What are the proper entities?





Can we link those to real behavior in human1 patients2?
1homo sapiens 2with real-life problems

RO1MH082795, and Consortium for Neuropsychiatric Phenomics (UL1DE019580, PL1MH083271, RL1LM009833)

Architectures for cognitive ontology development
The Cognitive Atlas is conceptualized as a related set of maps. A given map may contain sets of related concepts, quantitative models of literature association, annotated effect size statistics, raw data, summaries of voting, and qualitative free-text inputs. For cognitive concepts (e.g., the “phonological buffer”) there are associated cognitive concepts, and a “test” layer comprising objective indicators of the concepts
RO1MH082795, and Consortium for Neuropsychiatric Phenomics (UL1DE019580, PL1MH083271, RL1LM009833)

It might be argued that the task of the psychologist, the task of understanding behavior and reducing the vagaries of human thought to a mechanical process of cause and effect, is a more difficult one than that of any other scientist. (D. O. Hebb, 1949, p. xi)
Consortium for Neuropsychiatric Phenomics (UL1DE019580, PL1MH083271, RL1LM009833)


Managing assertions about brain-behavior relations using a neural circuit description framework
Bilder, Howe & Sabb, 2013 Journal of Abnormal Psychology

Models to Validate Circuit Constructs
Multi-Level Assays of Working Memory and Psychopathology: R01 MH101478

Validating Cognitive Markers of Circuit-Level Constructs
Multi-Level Assays of Working Memory and Psychopathology: R01 MH101478

Mapping to Functional Status Do symptoms or diagnosis add useful prediction over basic
measures of circuit, cognitive or neuropsychological measures?
Disability
(WHODAS 2.0)
Cognitive
(8 indicators)
Neuropsych
(5 indicators)
Circuit
(5 fMRI, 3 sMRI/
DTI, 6 EEG
indicators)
Symptom
(CIDI, DSM-CC,
BPRS, PROMIS)
Diagnosis
(DSM-V)
To avoid extreme group bias, sampling strategy is agnostic to diagnosis, and comprises two groups: - Care-seeking - Not Care-seeking
Diagnoses assigned after enrollment, as one of the dependent variables under study
Multi-Level Assays of Working Memory and Psychopathology: R01 MH101478

Matching Measurements to Samples
The statistical power for a given rating scale may be reduced if it is applied in a mixed population (e.g., PANSS in SZ+BP). A new endpoint (e.g., ‘g’ from bifactor model) may show greater invariance across samples, and thus increase power.
Ariana Anderson, supported by Janssen R&D/UCLA Pharmacogenomics Research Collaboration

Conclusions
• RDoC “matrix” implies causal links across multiple levels from genome to syndrome
• Causal models can help specify what to measure and how to measure
• Validation can proceed directly to function if the functions and populations are well defined
• New paradigm: specify models of dimensions and targets without disease entity assumption
• Caveat: new models must be explicit

Many thanks!
http://www.semel.ucla.edu/creativity http://www.phenomics.ucla.edu
Consortium for Neuropsychiatric Phenomics investigators (52) including PI’s: Freimer, Cannon, London, Jentsch, Parker, Evans Cognitive Atlas investigators including: Poldrack, Toga, van Horn, Sabb RDoC WM investigators including: Rissman, Loo, Bearden, Gitlin, Makeig Janssen R&D/UCLA team including: Anderson, Salvadore, Chung, Wilcox, Savitz, Alphs, Wang, Li
Related Documents