MANTOUX DR. FIROZ A HAKKIM PG- 1 ST YR CHEST MEDICINE

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

MANTOUX
DR. FIROZ A HAKKIMPG- 1ST YR CHEST MEDICINE

TUBERCULIN SKIN TEST
Detect infection with tubercle bacilli
Low technology
In expensive
Easy to administer, read

Based on – infection with mycobacterium tuberculosis produces sensitivity to certain components called sensitins, which are contained in culture extracts called tuberculins

Used among children for detection of tuberculosis infection and as a supportive tool for diagnosis of tb disease
Limited role in diagnosis of tb among adults living in areas where tb is highly endemic
Used by epidemiologists for assesment of tbsituation in community

History

Sir robert koch – produces a filtrate prepared from heat sterilized concentrated broth cultures of human tubercle bacilli
Initialy prepared for treatment of
Tb , but proved ineffective .
Subcutaneous inoculation in a patient suffering from tb resulted in local reaction at inoculation site laid foundation of its use as diagnostic aid
Was named OLD TUBERCULIN (OT)
Clement von pirquetin 1907 , observed thatTiny scratch with a little quantity of tuberculin resulted in a local reaction at the test site

Moro in 1908 announced the patch test
Tuberculin was incorporated into an ointment that was smeared onto skin , with a piece of guaze over it
Charles mantouxdeveloped the intradermal test, to be administered by injection as a measured volume ( mantoux test )

Other test – HEAF test – used a simple instrument that caused six spring loaded needles to pierce the skin with a drop of undiluted OT

TINE test – disposable multi puncture test where tuberculin was introduced into skin by puncture with four tines coated with dried tuberculin
ONLY MANTOUX TECHNIQUE WHICH ALLOWED QUANTITATIVE MEASUREMENT HAS STOOD THE TEST OF TIME, AND IS NOW THE STANDARD METHOD OF ADMINISTRATION OF TUBERCULIN SKIN TEST

Florence B. Seibert
Siebert in 1934 showed that active principle in tuberculin reaction was the protein fraction
Made a preparation from heat concentrated synthetic medium OT by precipitation with trichloroacetic acid .
It still contained lipopolysaccharides and nucleic acid
Later precipitation achieved by ammonium sulphate to obtain a preparation with less nucleic acid and polysaccharide content termed PURIFIED PROTEIN DERIVATIVE (PPD)

ONE TUBERCULIN UNIT [TU] OF PPD WAS DEFINED AS THE ACTIVITY CONTAINED IN 0.02 MICROGRAM OF PPD

•Statens serum institute , copenhagenproduced a large batch of PPD in 1952 at behest of unicef and WHO, and was designated RT23
•TWEEN 80 is added to prevent reabsorption of tuberculin to glass surface
•Seed lot of PPD RT23 is maintained by BCG VACCINE LABORATORY , GUINDY , CHENNAI.
•It is reconstituted and is supplied as ready to use preparation in isotonic buffer solution as 5ml vials, 0.1 ml corresponding to 1 TU.

Immunological basis
Individuals infected with mycobacteiumtuberculosis respond with delayed type hypersensitivity

Test site
Injection of
tuberculin
Proliferation of sensitized
T cell lymphocytes
Cytokines & chemokines
released
Lymphocytes & monocytes
attracted
Increased permeability of local blood
capillaries
INDURATION at test site

Skin changes in TST
Reaction include a delayed course reaching a peak more than 24 hrs after injection and an induration with occasional vesicilation and necrosis
Delayed type hypersensitivity reaction peaks by 48 to 96 hours, with an area of erythmatousinduration

Standard tuberculin skin test
Standard test employs a single batch tuberculin ie PPD RT – 23
Dose – 0.02 microgram [ 1 TU ] of PPD RT -23 in 0.1 ml of the diluent with Tween 80
2 TU of PPD RT – 23 is now recomended as the standard dose , based on a series of studies conducted in india
It demonstrated equal sensitivity for 1 TU & 2TU in detecting true infection with mycobacterium tuberculosis.
Available in 1TU/0.1ml, 2TU/0.1ml, 5TU/0.1ml and 10TU/0.1ml strengths.

1TU/0.1ml5TU/0.1ml

Earlier special glass syringes with a platinum needle was preferred for injection.
These days disposable tuberculin syringes (1ml) are preferred.

Glass syringe 1 ml Plastic syringe

Storage
Tuberculin vials – stored at 2-8 ° C and used before expiry period
Avoid exposure to sunlight and heat
Never freeze or keep at temp exceeding 20°C
Vial once used may be re- used within a maximum of 48 hrs

Administration Administerd 2-4 inches
below the elbow joint
Place the forearm palm side up on a firm well lit surface
Select an area free of barriers ( scars, sores ) to placing and reading
Clean the area with an alcohol swab
Check expiry date on vial and ensure vial contains tuberculin (5TU per 0.1ml)
Use a single dose tuberculin syringe with a ¼ to ½ inch 27 gauge needle with a short bevel
Fill the syringe with 0.1 ml of tuberculin
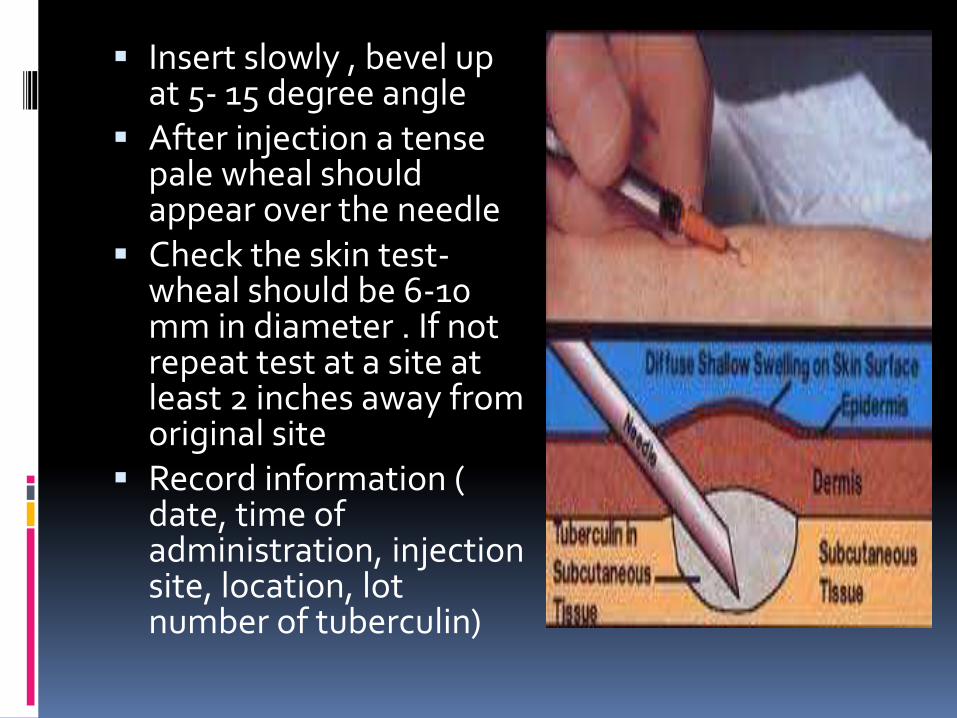
Insert slowly , bevel up at 5- 15 degree angle
After injection a tense pale wheal should appear over the needle
Check the skin test-wheal should be 6-10 mm in diameter . If not repeat test at a site at least 2 inches away from original site
Record information ( date, time of administration, injection site, location, lot number of tuberculin)



Educate the patient on the possible reactions to the TST (e.g., mild itching, swelling, irritation).
Instruct patient not to rub, scratch or put an adhesive bandage or lotion on the test site.
Schedule reading date and explain the importance of the patient returning for reading in 48 to 72 hours.
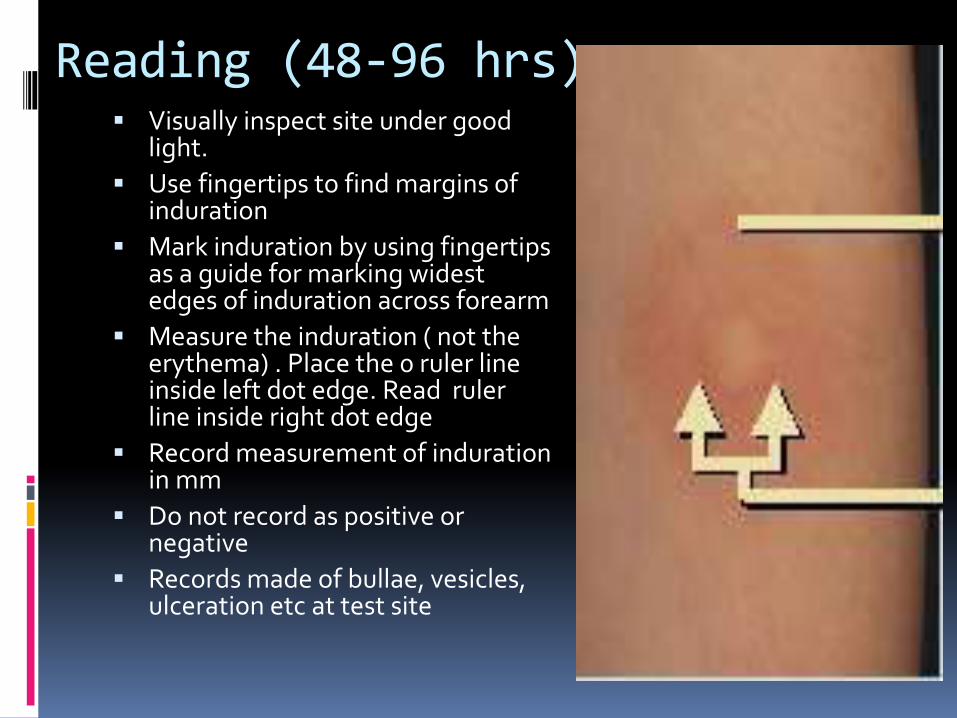
Reading (48-96 hrs) Visually inspect site under good
light.
Use fingertips to find margins of induration
Mark induration by using fingertips as a guide for marking widest edges of induration across forearm
Measure the induration ( not the erythema) . Place the 0 ruler line inside left dot edge. Read ruler line inside right dot edge
Record measurement of indurationin mm
Do not record as positive or negative
Records made of bullae, vesicles, ulceration etc at test site



Interpretation• Signifies reaction with tubercle
bacilli, irrespective of BCG vaccination status
Size of induration15 mm & above
• Cross sensitivity induced by environmental mycobacteria
• BCG induced sensitivity
• Infection with mycobacterium tuberculosis
Size of induration10-14 mm
• Cross sensitivity by environmental mycobacteria/ BCG vaccination/ infection with tubercle bacilli in the presence of immunosuppresive conditions
Size of induration5-9 mm
• Indicates absence of any type of mycobacterial infection except in individuals with severe degree of immunosuppression
Size of indurationless than 5 mm

Adverse effects
Some atopic individuals, develop an urticarialwheal, which may dissapear within minutes.
Occurence of such an allergic reaction does not signify the presence of TB.
Systemic allergic reactions seldom occur
Formation of vesicles, bullae, lymphangitis, ulceration or necrosis in a proportion of children indicates high degree of tuberculin sensitivity.


Skin sensitivity to tuberculin
Persons with sensitivity to tuberculin are called ‘Reactors’.
Not all reactors are infected with tubercle bacilli.
Sensitivity to tuberculin may oocur due to
infection with environmental mycobacteria
BCG Vaccination
Infection with Mycobacterium tuberculosis

Infection with environmental mycobacteria
Sensitivity induced by them cross-reacts with tuberculin and is known as ‘Non Specific Sensitivity’ (NSS).
sensitivity induced by these results in smaller reactions.
Distinction from true infection is not always very clear.
Highly prevalent in most parts of India.

BCG Vaccination
Sensitivity may vary from very weak to about the same level as natural infection.
Depends on strength of vaccine used, handling, administration, and time interval between vaccination and testing.
Generally peaks at 10 weeks then begin to wane.
Under UIP in India, a reduced dose of 0.05 ml of Danish 1331 strain is administered.

About 70% of children upto 9 yrs of age with a BCG scar elicited either no rection or <10mm to 1 TU PPD with Tween 80.
It may be inferred that the BCG induced sensitivity is generally weaker than that of infection with tubercle bacilli.
Weak sensitivity does not imply that vaccination is ineffective.

Infection with Mycobacterium tuberculosis
Most individuals harbouring TB infection usually elicit a larger reaction to tuberculin
The probability of true positives increases as the reaction size increases
Probability is also increased in the presence of history of contact with a sputum smear positive case of TB.

False positive reactions
Infection with environmental mycobacteria.
BCG vaccination.
Repeat testing.
Testing with high dose of tuberculin.
Reading errors.
Needle injury.
False negative reactions
Non significant reaction does not always exclude the presence of TB infection or disease.
Most common reasons being :
Improper storage
Poor technique
Other reasons :
Immunosupression
Disseminated TB
Undernutrition

Hodgkin’s
Malignancy
Sarcoidosis
HIV – AIDS
Vaccination with live virus vaccines
Acute viral infections
Window period
Infants < 3months ( immature immune system)
Old age
Cutaneous anergy
Supression due to live virus vaccines appears after 48 hrs of vaccination and start waning 4-6 wks later.
Anergy
Anergy refers to failure to mount a full immune response against a target.
Term ‘ANERGY’ was coined by Von Pirquet
Commonly used antigens for anergy panel contain trychophyton, candida , etc
Anergic patients are more likely than immunologically intact patients to present with noncavitory TB.
In sarcoidosis patients, anergy to tuberculin can be restored by concurrent administration of hydrocortisone.
This paradoxical reaction presumably also occurs in TB patients who have been desensitized for tuberculin.

Reversion, Conversion and Booster Phenomenon
Reversion:
In elderly & many adults, significant reactions to tuberculin declines with age.
Estimated to occur at a rate of 5% per yr.
Attributed to waning of CMI or loss of lymphocyte blastogenic capacity in elderly.
Booster phenomenon
Boosting of the size of the second test by the small amount of tuberculin injected for the first test.
Results from ‘recall’ of the sensitivity.
To avoid this, repeat test should be given at a different site within one week of the first test.
Boosting effect was observed when test repeated after 2 months ,not when repeated after 18 months.
Conversion Simple tuberculin conversion from a non
significant reaction at first test to a significant reaction at a subsequent test.
Larger increase in reaction size (10mm or more) correlates better with the risk of developing TB.
Other causes can be boosting effect, infection with environmental mycobacteria in the intervening period.
For detection of new infections, there should be a significant increase in reaction size (14mm or more) in the subsequent test, one-and-half to 3 yrs apart.

Interpretation in HIV patients
All HIV seropositive individuals should be assessed for active TB.
Once active TB is excluded, TST is done as soon as possible.
Reliability of TST decreases as CD4+ T-Cell count diminishes, espp. To < 200/cmm.
As the prob. of significant induration indicative of TB infection is significantly lower in HIV-infected persons, a lower cut-off point is advised.
Irrespective of the test results, patients with evidence of old healed TB in CXR or past H/O active TB and a significant reation to TST may be considered infected for all practical purposes.
TST should never be the sole criteria for diagnosing TB.

Interpretation in sarcoidosis
TST in patients with sarcoidosis has a high specificity but poor sensitivity for TB.
A –ve TST in general poulation is a sensitive test for sarcoidosis.
A +ve TST in patients suspected of havinsarcoidosis is a specific test for TB, and is an absolute indication for a thorough work-up for TB.

Epidemiological use
Tuberculin surveys are carried out among young children as the results obtained reflect relatively recent situation.
Prevalence and Average Annual Risk of Infection (ARI) are calculated.
ARI is defined as the avg. prob. of acquiring new TB infection over the course of one year.
ARI reflects the overall impact of TB prevalence in a community and the efficiency of TB control activities.

Newer tuberculins
Further attempts are being made to develop newer, more species-specific tuberculins.
One of the improvisations is to avoid heating to prevent protein denaturation of PPD.
Electrophoresis and Chromatography.
T-1327 and T-1456 are under progress.
Interferon gamma release assays ( IGRA)
In vitro assays that detect the presence of CMI towards M. tb-specific antigens.
These include the early secretory antigenic target-6 (ESAT-6), culture filtrate protein 10 (CFP-10), and the TB7.7 antigens.
The antigens in IGRAs are absent in most of NTM as well as in BCG strains.

Available methods :
Quantiferon- TB Gold assay (ELISA based)
Quantiferon- TB Gold IN Tube assay(ELISA based)
T-SPOT TB assay (ELISPOT based)

Advantages of IGRA’s
Higher specificity then TST.
Less cross reactivity with BCG vaccination and NTM infection
Less inter-reader variations.
No boosting phenomenon.
Fewer patient visits.

Disadvantages of IGRA’s
A negative IGRA does not rule out active TB or LTBI.
IGRAs are not able to differentiate LTBI from active TB.
In high-TB incidence countries, there is no added value in using IGRAs to diagnose LTBI, as the focus of prevention and control is to identify and treat active cases.
In presence of immunosuppression, a –veIGRA should not preclude further investigations or treatment if clinical suspicion is high.
Technically more demanding.
Higher cost.

Conclusion
Tuberculin test have stood the test of time and is still widely used for over a century for
detecting the infection with TB and when used wisely, has promising results.
For now, it is probably a good strategy to keep both IGRA’s and TST on the LTBI diagnostic
menu, and select the appropriate test based on population, purpose of testing and the
available resources.

REFERENCES
SHARMA
TOMANS
INTERNET

Related Documents











