1 Ministry of higher Education And scientific Research Collage of maisan university Department of dentistary Gradution progect Manegment and Etiology of Dental cross bite APROGECT SUBMITTED TO THE MAISAN UNIVERCITY COLLEGE DEPARTMENT OF DENTISTARY IN PARTIAL FULFILLMENT OF THE REQUIRMENT FOR THE B.SC IN DENTISTARY BY:_ Tuqa saleem Mareim radhi Ban kareem Supervised by:_ Salam raad abd alwahab Younis mohemmed D.h 1439 2018 A.H

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

1
Ministry of higher Education
And scientific Research
Collage of maisan university
Department of dentistary
Gradution progect
Manegment and Etiology of Dental cross bite
APROGECT SUBMITTED TO THE MAISAN
UNIVERCITY COLLEGE DEPARTMENT OF DENTISTARY
IN PARTIAL FULFILLMENT OF THE REQUIRMENT FOR
THE B.SC IN DENTISTARY
BY:_
Tuqa saleem
Mareim radhi
Ban kareem
Supervised by:_
Salam raad abd alwahab
Younis mohemmed
D.h 1439 2018A.H

2
Crossbite :_is a form of malocclusion where a tooth (or teeth) has a
More bucal or lingual position (that is, the tooth is either closer to the
cheek or to the tongue) than its corresponding antagonist tooth in the upp
er or lower dental arch. In other words or
crossbite:_ is a lateral misalignment of the dental arches.
Buccal crossbite: the buccal cusps of the lower teeth occlude buccal
to the buccal cusps of the upper teeth.
Lingual crossbite: the buccal cusps of the lower teeth occlude lingual
to the lingual cusps of the upper teeth. This is also known as a
scissors bite.
Aetiology
A variety of factors acting either singly or in combination can lead to the
development of a crossbite.
1 -Local causes
1-The most common local cause is crowding where one or two teeth are
displaced from the arch. For example, a crossbite of an upper lateral
incisor often arises owing to lack of space between the upper central incis
or and the deciduous canine, which forces the lateral incisor to erupt
palatally and in linguo-occlusion with the opposing teeth. Posteriorly,
early loss of a second deciduous molar in a crowded mouth may result in
forward movement of the upper fi rst permanent molar, forcing the second

3
premolar to erupt palatally. Also
2- retention of a primary tooth can deflect the eruption of the permanent s
uccessor leading to a crossbite.
2 Skeletal:_ Generally, the greater the number of teeth in crossbite, the
greater is the skeletal component of the aetiology. A crossbite of the buccal
segments may be due purely to a mismatch in the relative width of the
arches, or to an anteroposterior discrepancy, which results in a wider
part of one arch occluding with a narrower part of the opposing jaw.
For this reason buccal crossbites of an entire buccal segment are most
commonly associated with Class III malocclusions_ and lingual
crossbites are associated with Class II malocclusions. Anterior
crossbites are associated with Class III skeletal patterns. Crossbites can
also be associated with true skeletal asymmetry and/or asymmetric
mandibular growth.
3-Soft tissues :_A posterior crossbite is often associated with a
digit-sucking habit, as the position of the tongue is lowered and a negative
pressure is generated intra-orally.
4 -Rarer causes:_ These include cleft lip and palate, where growth in t
he width of the upper arch is restrained by the scar tissue of the cleft repai
r. Trauma to, or pathology of, the temporomandibular joints can lead to re
striction of growth of the mandible on one side, leading to
asymmetryection.

4
Types of cross bite:
1_Anterior crossbite:_
An anterior crossbite can be referred as negative overjet, and is typical of
class III skeletal relations (prognathism).
a-Primary/mixed dentitions
An anterior crossbite in a child with baby teeth or mixed dentition may ha
ppen due to either dental misalignment or skeletal misalignment. Dental
causes may be due to displacement of one or two teeth, where skeletal
causes involve either mandibular hyperplasia, maxillary hypoplasia or
combination of both.
b-Dental crossbite
An anterior crossbite due to dental component involves displacement of
either maxillary central or lateral incisors lingual to their original erupting
positions. This may happen due to delayed eruption of the primary teeth
leading to permanent teeth moving lingual to their primary predecessors.
This will lead to anterior crossbite where upon biting, upper teeth are
behind the lower front teeth and may involve few or all frontal incisors. In
this type of crossbite, the maxillary and mandibular proportions are
normal to each other and to the cranial base. Another reason that may lead
to a dental crossbite is crowding in the maxillary arch. Permanent teeth
will tend to erupt lingual to the primary teeth in presence of crowding.
Side-effects caused by dental crossbite can be increased recession on the
buccal of lower incisors and higher chance of inflammation in the same
area. Another term for an anterior crossbite due to dental interferences is
Pseudo Class III Crossbite or Malocclusion.

5
c-Single tooth crossbite
Single tooth crossbites can occur due to uneruption of a primary teeth in a
timely manner which causes permanent tooth to erupt in a different
eruption pattern which is lingual to the primary tooth. Single tooth
crossbites are often fixed by using a finger-spring based appliances This
type of spring can be attached to a removable appliance which is used by
patient every day to correct the tooth position.
d-Skeletal crossbite
An anterior crossbite due to skeletal reasons will involve a deficient maxill
a and a more hyperplastic or overgrown mandible. People with this type of
crossbite will have dental compensation which involves proclined
maxillary incisors and retroclined mandibular incisors. A proper
diagnosis can be made by having a person bite into their centric relation
will show mandibular incisors ahead of the maxillary incisors, which will s
how the skeletal discrepancy between the two jaws
2-Posterior crossbite
Bjork defined posterior crossbite as a malocclusion where the buccal cusps
of canine, premolar and molar of upper teeth occlude lingually to the
buccal cusps of canine, premolar and molar of lower teeth. Posterior cross
bite is often correlated to a narrow maxilla and upper dental arch.
A posterior crossbite can be :_
1- unilateral
2- bilateral
3- single-tooth or entire segment crossbite.
Posterior crossbite has been reported to occur between 7–23% of the
population. The most common type of posterior crossbite to occur is the

6
unilateral crossbite which occurs in 80% to 97% of the posterior crossbite
cases Posterior crossbites also occur most commonly in primary and
mixed dentition. This type of crossbite usually presents with a functional
shift of the mandible towards the side of the crossbite. Posterior crossbite
can occur due to: either skeletal, Dentalor functional abnormalities
One of the common reasons for development of posterior
Crossbite
* is the size difference between maxilla and mandible, where maxilla is
smaller than mandible Posterior crossbite can result due to
Upper Airway Obstruction where people with "adenoid faces" who have
trouble breathing through their nose. They have an open bite
malocclusion and present with development of posterior crossbite.
*Prolong digit or suckling habits which can lead to constriction of maxilla
posteriorly
*Prolong pacifier use (beyond age 4)
a--Unilateral posterior crossbite
Unilateral crossbite involves one side of the arch. The most common cause
of unilateral crossbite is a narrow maxillary dental arch. This can happen
due to habits such as digit sucking, prolonged use of pacifier or upper
airway obstruction. Due to the discrepancy between the maxillary and
mandibular arch, neuromuscular guidance of the mandible causes mandibl
e to shift towards the side of the crossbiteThis is also known as Functional
mandibular shift. This shift can become structural if left untreated for a
long time during growth, leading to skeletal asymmetries. Unilateral
crossbites can present with following features in a child
*Lower midline deviation to the crossbite side

7
*Class 2 Subdivision relationships .
B_Bilateral buccal crossbite:_
Bilateral crossbites are more likely to be associated with a
skeletal discrepancy, either in the anteroposterior or transverse
dimension, or in both
C_ Bilateral lingual crossbite (scissors bite)
Again, this crossbite is typically associated with an underlying skeletal
discrepancy, often a Class II malocclusion with the upper arch further
forward relative to the lower so that the lower buccal teeth occlude with
a wider segment of the upper arch.
Crossbite Treatment
Achild with posterior crossbite should be treated immediately if the child
shifts his mandible on closing which is often seen in a unilateral crossbite
as mentioned above. The best age to treat a child with crossbite is in their
mixed dentition when their palatal sutures have not fused to each other.
Palatal expansion allows more space in an arch to relieve crowding and
correct posterior crossbite. The correction can include any type of palatal
expanders that will expand the palate which resolves the narrow
constriction of the maxilla.There are several therapies that can be used to
correct a posterior crossbite:
-braces
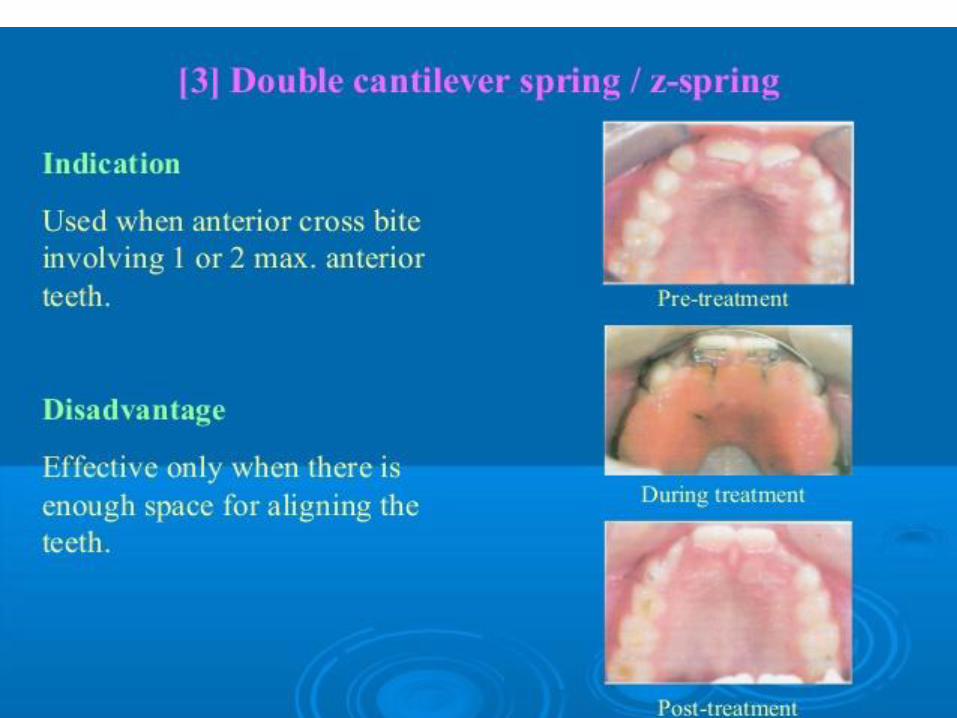
- 'Z' spring or cantilever spring,
- quad helix,-

8
- removable plates, -clear aligner therapy
-or a Delaire mask.
The correct therapy should be decided by the orthodontist depending on
the type and severity of the crossbite.
One of the keys in diagnosing the anterior crossbite due to skeletal vs
dental causes is diagnosing a CR-CO shift in a patient. An adolescent presen
ting with anterior crossbite may be positioning their mandible forward
into centric occlusion (CO) due to the dental interferences. Thus finding
their occlusion in centric relation (CR) is key in diagnosis. For anterior
crossbite
- if their CO matches their CR then the patient truly has a skeletal compone
nt to their crossbite.
-If the CR shows a less severe class 3 malocclusion or teeth not in anterior
crossbite, this may mean that their anterior crossbite results due to dental
interferences.
* * Goal to treat unilateral crossbites should definitely include removal of
occlusal interferences and elimination of the functional shift. Treating
posterior crossbites early may help prevent the occurrence of
Temporomandibular joint pathology.
**Unilateral crossbites can also be diagnosed and treated properly by
using a Deprogramming splint. This splint has flat occlusal surface which
causes the muscles to deprogram themselves and establish new sensory
engrams. When the splint is removed, a proper centric relation bite can be
diagnosed from the bite.

9
Self-correction
Literature states that very few crossbites tend to self-correct which often
justify the treatment approach of correcting these bites as early as
possible. Only 0–9% of crossbites self-correct. Lindner et al. reported that i
n a 50% of crossbites were corrected in 76 four year old children.
Treatment of anterior crossbite
The following factors should be considered.
• What type of movement is required? If bodily or apical movement is
required then fi xed appliances are indicated; however, if in the mixed
dentition tipping movements will suffi ce, a removable appliance can
be considered.
• How much overbite is expected at the end of treatment? For treatment
to be successful there must be some overbite present to retain the correctd
incisor position. However, when planning treatment it should be
remembered that proclination of an upper incisor will result in a reductin
of overbite compared with the pre-treatment position
• Is reciprocal movement of the opposing tooth/teeth required?
In the mixed dentition, provided that there is suffi cient overbite and
tilting movements will suffi ce, treatment can often be accomplished more
readily with a removable appliance. The appliance should incorporate
good anterior retention to counteract the displacing eff ect of the active
element (where two or more teeth are to be proclined, a screw appliance
may circumvent this problem) and buccal capping just thick enough to free
the occlusion with the opposing arch . Otherwise it may
be advisable to wait until the permanent dentition is established and
comprehensive fi xed appliance treatment can be carried out
. If there will be insufficient overbite to retain the corrected incisor(s),

10
then consideration should be given to moving the lower incisors lingually
within the
confines of the soft tissue envelope in order to try and increase overbite.
If the upper arch is crowded, the upper lateral incisor often erupts in
a palatal position relative to the arch.
Treatment of posterior crossbite
Treatment in mixed dentition and perminent
It is important to consider the aetiology of this feature before embarking
on treatment. For example, is the crossbite due to
A_displacement of one tooth from the arch, in which case correction will
inolve aligning this tooth
-or is reciprocal movement of two or more opposing teeth
required? Also, if there is a skeletal component, will it be possible to
compensate for this by tooth movement? The inclination of the aff ected
teeth should also be evaluated. Upper arch expansion is more likely to
be stable if the teeth to be moved were initially tilted palatally.
Even when fixed appliances are used, expansion of the upper buccal
segment teeth will result in some tipping down of the palatal cusps
. This has the effect of hinging the mandible downwards leading
to an increase in lower face height, which may be undesirable in patients
who already have an increased lower facial height and/or reduced
overbite.
*If expansion is indicated in these patients, fixed appliances are
required to apply buccal root torque to the buccal segment teeth in order
to try and resist this tendency, perhaps with high-pull headgear as well.
Recent work has indicated that transverse problems which are amenable

11
to orthodontic correction are best treated in the pre-pubertal
growth spurt. But the actual timing of treatment will depend upon other
features of the malocclusion.
As expansion will create additional space, it may be advisable to
defer a decision regarding extractions until after the expansion phase
has been completed.
b-Where a crossbite is due to skeletal asymmetry then a thorough
assessment is required to determine the aetiology and contribution of
both the maxilla and mandible to the presenting features. Correction
will require a combined approach involving orthognathic surgery once
growth has slowed to adult levels.
Interestingly, a Cochrane review on this topic reported that due to a
paucity of good quality evidence the authors were not able to make
recommendations
treatment of deciduous crossbit
*regarding treatment of crossbite in the mixed and permanent
dentitions. However, they did find that removal of premature
contacts in the deciduous dentition was eff ective in preventing posterior
crossbites being perpetuated into mixed/permanent dentition. Further
more, when grinding alone was not eff ective an URA could be used
to expand the upper arch to reduce the risk of the crossbite persisting.
Some typee of appliance used
1- The quadhelix appliance
The quadhelix is a very effi cient fi xed slow expansion appliance
. The quadhelix appliance can also be adjusted to give more
expansion anteriorly or posteriorly as required and can also be used to
de-rotate rotated molar teeth. When active expansion is complete it can
be made passive to aid retention of the expansion.

12
A quadhelix is fabricated in 1 mm stainless steel wire and attached
to the teeth by bands cemented to a molar tooth on each side. Preformed
types are available which slot into palatal attachments welded
onto bands on the molars and can be readily removed by the operator
for adjustment. However, the appliance can also be custom-made in a
laboratory. The usual activation is about half a tooth width each side.
Over-expansion can occur readily if the appliance is overactivated, and
therefore its use should be limited to those who are experienced with
fi xed appliances.
*A tri-helix has only one anterior coil and is therefore less effi cient. Its
use is limited to cases with narrow and/or high palatal vaults, for example
in cleft lip and palate patients.
2- Rapid maxillary expansion (RME)
This upper appliance incorporates a Hyrax screw (similar to the type
used for expansion in removable appliances) soldered to bands, usually
to both a premolar and molar tooth on both sides. The screw is
turned twice daily, resulting in expansion of the order of 0.2–0.5 mm/
day, usually over an active treatment period of 2 weeks .
The large force generated is designed to open the midline suture
and expand the upper arch by skeletal expansion rather than by
movement of the teeth. For this reason some advocate limiting this
approach to patients in their early teens before the suture fuses, or
cleft palate patients where it can be utilized to expand the cleft segments
by stretching the scar tissue. If considering this approach it is
advisable to check that there is adequate buccal supporting bone and
soft tissues.

13
Once expansion is complete the appliance is left in situ as a retainer,
usually for several months. Bony infi ll of the expanded suture has
been demonstrated but on removing the appliance approximately 50
percent of the expansion gained is lost, and for this reason some
overexpansion is indicated. This appliance should only be used by the
experienced clinician.
Surgically assisted RME (SARPE) is gaining acceptance, however
claims of reduced periodontal support loss (compared with conventional
expansion) and improved nasal airfl ow are unsubstantiated.
This approach involves surgically cutting the mid-palatal suture prior to
expansion
14
REFFRENCE:_
CONTEMPORARY ORTHODONTICS(proffit 2013 )
TEXTBOOK OF ORTHONTICS (singh 2007 )
AN INTRODCTION TO ORTHODONTICS(michelle 2003 )
TEXTBOOK OF ORTHONTICS(foster 1990 )
ORTHODONTICS TREATMENT MECHANICS AND THE
PREADJUSTED APPLAINCE(BENNETT 1992 )






























Related Documents











