Management of Types III and IV Acetabular Deficiencies With the Longitudinal Oblong Revision Cup Antonio Herrera, PhD, A ´ ngelAntonio Martı´nez, MD, Jorge Cuenca, MD, and Vicente Canales, MD Abstract: Thirty-five longitudinal oblong revision (LOR) cups were used to reconstruct 29 type III and 6 type IV acetabular defects. Intraoperatively, we considered that cup contact was complete when we achieved a continuous contact between the cup periphery and the acetabular rim. When there were areas with a lack of contact, we considered that the contact was partial or incomplete. All patients were followed up for 4 to 8 years (mean = 6.3 years). At the latest follow-up, 30 cups were stable (85.8%) and 5 had migrated (14.2%). We found a significant relation between incomplete cup contact with the acetabular rim and subsequent failure ( P = .042). The abduction angle was significantly increased in the group of unstable cups ( P = .032) because of the migration of the acetabular component that became more vertical. Pain, limp, use of walking aids, functional level, and limb-length discrepancy significantly improved postoperatively ( P b .0001). The Harris hip score improved from a mean preoperative score of 37 points to that of 79 points ( P b .01). This implant showed satisfactory stability at early to midterm follow-up. Key words: acetabular defect, hip arthroplasty, longitudinal oblong revision cup. n 2006 Elsevier Inc. All rights reserved. The reconstruction management of major acetabu- lar bone defects remains a challenging problem in revision total hip arthroplasty. Standard porous-coated hemispherical cups have provided excellent results in acetabula that have an intact rim of bone [1-7]. Oversized hemispherical cups that convert a deficient acetabulum into a hemisphere with an intact rim of bone have also given good results [8]. However, if an acetabular defect is large, stan- dard or oversized hemispherical cups may not allow achieving enough stability. In such cases, several options for reconstruction have been used, including structural bone grafting [9-12], impacted morcellized cancellous bone grafting and cement [13-15], antiprotrusio cages or reinforcement rings [16-22], oblong [23-26] or bilobed [27-29] cups inserted without cement, and stemmed cups [30]. The use of large structural allografts has not given uniformly good results. The long-term fail- ure rate reported has oscillated between 13% and 50% [9-12]. Antiprotrusio cages and reinforcement rings have provided a midterm rate of success that has oscillated between 80% and 90% [16-22]. Bilobed oblong porous-coated acetabular com- ponents have been reported to have a midterm loosening rate between 0% and 24% [27-29]. There are few reports about the use of oblong but not bilobed porous-coated components. Early ex- perience was very limited, with some short series reported [24-26]. The Journal of Arthroplasty Vol. 21 No. 6 2006 857 From the Service of Orthopedic and Trauma Surgery, Miguel Servet University Hospital, Zaragoza, Spain. Submitted June 14, 2004; accepted August 5, 2005. No benefits or funds were received in support of the study. Reprint requests: Antonio Herrera, PhD, Avda Cesa ´ reo Alierta n815, 48B, 50008 Zaragoza, Spain. n 2006 Elsevier Inc. All rights reserved. 0883-5403/06/1906-0004$32.00/0 doi:10.1016/j.arth.2005.08.026

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

The Journal of Arthroplasty Vol. 21 No. 6 2006
Management of Types III and IV Acetabular
Deficiencies With the Longitudinal Oblong
Revision Cup
Antonio Herrera, PhD, Angel Antonio Martınez, MD,Jorge Cuenca, MD, and Vicente Canales, MD
From the Service oUniversity Hospital, Z
Submitted June 1No benefits or fuReprint requests:
n815, 48B, 50008 Zan 2006 Elsevier I0883-5403/06/19doi:10.1016/j.arth
Abstract: Thirty-five longitudinal oblong revision (LOR) cups were used to
reconstruct 29 type III and 6 type IV acetabular defects. Intraoperatively, we
considered that cup contact was complete when we achieved a continuous contact
between the cup periphery and the acetabular rim. When there were areas with a
lack of contact, we considered that the contact was partial or incomplete. All patients
were followed up for 4 to 8 years (mean = 6.3 years). At the latest follow-up, 30 cups
were stable (85.8%) and 5 had migrated (14.2%). We found a significant relation
between incomplete cup contact with the acetabular rim and subsequent failure
( P = .042). The abduction angle was significantly increased in the group of unstable
cups ( P = .032) because of the migration of the acetabular component that became
more vertical. Pain, limp, use of walking aids, functional level, and limb-length
discrepancy significantly improved postoperatively ( P b .0001). The Harris hip score
improved from a mean preoperative score of 37 points to that of 79 points ( P b .01).
This implant showed satisfactory stability at early to midterm follow-up. Key words:
acetabular defect, hip arthroplasty, longitudinal oblong revision cup.
n 2006 Elsevier Inc. All rights reserved.
The reconstruction management of major acetabu-
lar bone defects remains a challenging problem in
revision total hip arthroplasty.
Standard porous-coated hemispherical cups have
provided excellent results in acetabula that have an
intact rim of bone [1-7].
Oversized hemispherical cups that convert a
deficient acetabulum into a hemisphere with an
intact rim of bone have also given good results [8].
However, if an acetabular defect is large, stan-
dard or oversized hemispherical cups may not
allow achieving enough stability. In such cases,
857
f Orthopedic and Trauma Surgery, Miguel Servetaragoza, Spain.4, 2004; accepted August 5, 2005.
nds were received in support of the study.Antonio Herrera, PhD, Avda Cesareo Aliertaragoza, Spain.nc. All rights reserved.06-0004$32.00/0.2005.08.026
several options for reconstruction have been used,
including structural bone grafting [9-12], impacted
morcellized cancellous bone grafting and cement
[13-15], antiprotrusio cages or reinforcement rings
[16-22], oblong [23-26] or bilobed [27-29] cups
inserted without cement, and stemmed cups [30].
The use of large structural allografts has not
given uniformly good results. The long-term fail-
ure rate reported has oscillated between 13% and
50% [9-12].
Antiprotrusio cages and reinforcement rings
have provided a midterm rate of success that has
oscillated between 80% and 90% [16-22].
Bilobed oblong porous-coated acetabular com-
ponents have been reported to have a midterm
loosening rate between 0% and 24% [27-29].
There are few reports about the use of oblong but
not bilobed porous-coated components. Early ex-
perience was very limited, with some short series
reported [24-26].

858 The Journal of Arthroplasty Vol. 21 No. 6 September 2006
A long series has been published by Kfster et al
[23], reporting a favorable midterm result in 98%
of cases.
A partially hydroxyapatite-coated stemmed ace-
tabular cup with morcellized allograft has been
used by Badhe and Howard [30] in the manage-
ment of severe acetabular deficiencies. Early results
have shown encouraging restoration of bone stock,
with no case of aseptic loosening.
The purpose of our study was to evaluate the
results of using a longitudinal oblong revision
(LOR) cup in the management of types III and IV
acetabular defects.
Materials and Methods
Patients
Between January 1995 and October 2000, 35 pa-
tients (22 men [63%] and 13 women [37%]) under-
went acetabular reconstruction using an LOR
component. Their mean age was 63.8 years (range =
36-79 years).
The indications for LOR cup implantation were
aseptic loosening in 31 patients (88.6%), dysplasia
of the hip because of congenital subluxation that
caused a dysplastic hip with a defect in the superior
aspect of the acetabulum in 1 patient (3%), and
reimplantation after resection arthroplasty in
3 patients (8.6%).
The prerevision acetabular bone deficiency
was categorized according to the classification of
D’Antonio et al [31]. There were 29 type III (83%)
and 6 type IV (17%) defects. The follow-up period
ranged from 4 to 8 years (mean = 6.3 years), except
for the 2 cases that failed 1 year postoperatively and
required a new revision.
All cases were operated by the same group of
surgeons who used this cup. Other surgeons in our
center used other techniques, such as morcellized
cancellous bone grafting and cement as well as
reinforcement rings.
Revision Cup
The LOR cup (Allopro Sulzer, Winterthur, Swit-
zerland) consists of a titanium shell and a polyeth-
ylene inlay. It has an oblong shape with the
superoinferior dimension greater than the antero-
posterior dimension. The transverse diameter ranges
from 52 to 72 mm, in 4-mm steps. There are 2 shells
available for each transverse diameter, 1 elongated
by 6 mm and another 1 by 12 mm longitudinally.
Two rows of holes are arranged parallel to the outer
rim of the shell to take the titanium screws. The
polyethylene inlay has the articular surface central-
ly positioned in the 6-mm longitudinally elongated
sockets and central or 6 mm caudally displaced in
the 12-mm elongated sockets.
Operative Technique
A posterolateral approach was used in 28 cases
(80%) and an anterolateral approach was in
7 (20%). The acetabulum was prepared with
spherical reamers by which the longitudinal
dimension of the acetabulum was widened, re-
moving protrusions of the bony bed. The ante-
roposterior diameter of the acetabulum was
preserved. Defects were filled with bone chips in
all cases. Structural allografts were used in 2 cases.
Morcellized allograft was added in all cases. We
considered that cup contact was complete when
intraoperatively we achieved a continuous contact
between the cup periphery and the acetabular rim.
When there were areas with a lack of contact, we
considered that the contact was partial or incom-
plete. Cup contact with the acetabular rim was
considered complete in 30 cases (85.7%) and
partial in 5 (14.3%), with a lack of contact of
20% in 3 cases and of 30% in 2 cases in which
structural allograft was added. An average of
3.8 screws (range = 2-7) was used for fixation.
Usually the best screw fixation was obtained
superiorly, but additional stabilization can be
achieved by placing further screws in the pubis
and ischium. The polyethylene inlay had the
articular surface centrally positioned in 18 cases
(51.4%) and eccentrically in 17 (48.6%). Of the
35 hips, 19 had loose femoral components, which
were revised; 13 had well-fixed femoral compo-
nents (5 cemented and 8 cementless), which were
not revised; and 3 had a resection arthroplasty and
had no femoral component. Of the 19 hips in
which a femoral component was implanted, 8 were
implanted with an anatomical revision stem with
hydroxyapatite coating (Howmedica, Rutherford,
NJ) and 11 were with a straight revision stem with
hydroxyapatite coating (DePuy, Warsaw, Ind). A
28-mm head size was used in all the patients.
Postoperatively, protected weight bearing for
3 months with bilateral crutches was allowed,
except for patients with type IV defect, who were
advised non–weight bearing for 3 months.
Radiographic Assessment
Anteroposterior and lateral radiographs were
made before surgery and immediately after sur-
gery, at 3 months, at 6 months, at 1 year, and then
at 1-year intervals.
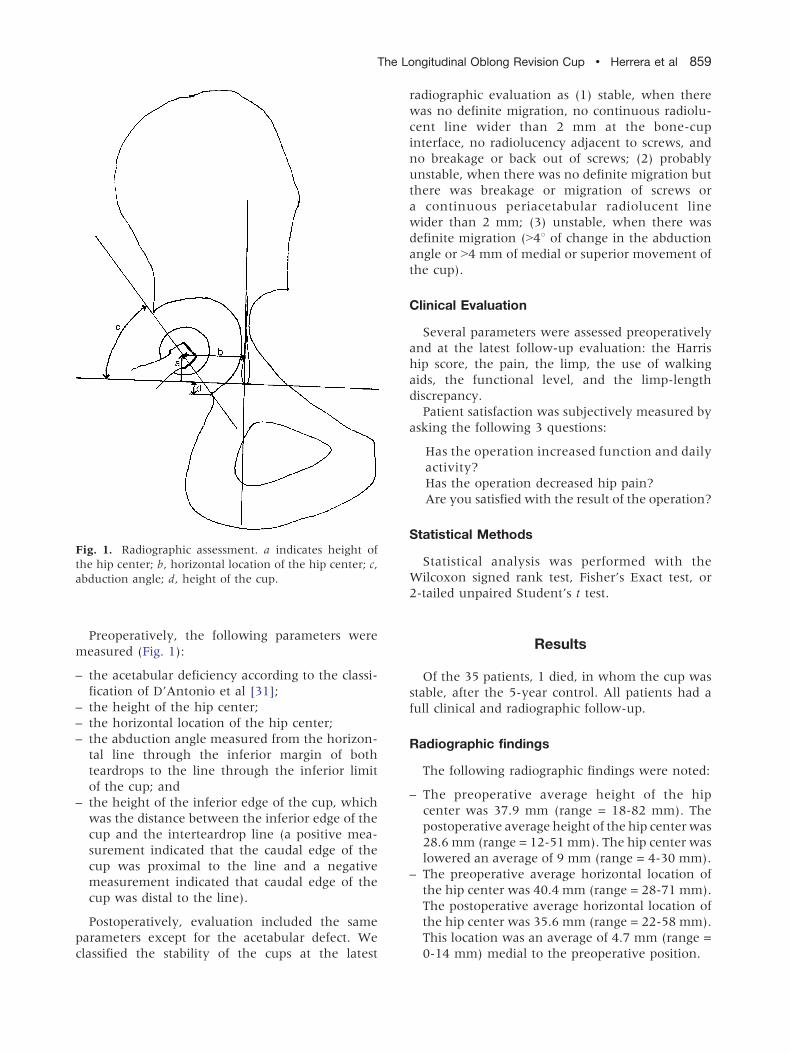
Fig. 1. Radiographic assessment. a indicates height of
the hip center; b, horizontal location of the hip center; c,
abduction angle; d, height of the cup.
The Longitudinal Oblong Revision Cup ! Herrera et al 859
Preoperatively, the following parameters were
measured (Fig. 1):
– the acetabular deficiency according to the classi-
fication of D’Antonio et al [31];
– the height of the hip center;
– the horizontal location of the hip center;
– the abduction angle measured from the horizon-
tal line through the inferior margin of both
teardrops to the line through the inferior limit
of the cup; and
– the height of the inferior edge of the cup, which
was the distance between the inferior edge of the
cup and the interteardrop line (a positive mea-
surement indicated that the caudal edge of the
cup was proximal to the line and a negative
measurement indicated that caudal edge of the
cup was distal to the line).
Postoperatively, evaluation included the same
parameters except for the acetabular defect. We
classified the stability of the cups at the latest
radiographic evaluation as (1) stable, when there
was no definite migration, no continuous radiolu-
cent line wider than 2 mm at the bone-cup
interface, no radiolucency adjacent to screws, and
no breakage or back out of screws; (2) probably
unstable, when there was no definite migration but
there was breakage or migration of screws or
a continuous periacetabular radiolucent line
wider than 2 mm; (3) unstable, when there was
definite migration (N48 of change in the abduction
angle or N4 mm of medial or superior movement of
the cup).
Clinical Evaluation
Several parameters were assessed preoperatively
and at the latest follow-up evaluation: the Harris
hip score, the pain, the limp, the use of walking
aids, the functional level, and the limp-length
discrepancy.
Patient satisfaction was subjectively measured by
asking the following 3 questions:
Has the operation increased function and daily
activity?
Has the operation decreased hip pain?
Are you satisfied with the result of the operation?
Statistical Methods
Statistical analysis was performed with the
Wilcoxon signed rank test, Fisher’s Exact test, or
2-tailed unpaired Student’s t test.
Results
Of the 35 patients, 1 died, in whom the cup was
stable, after the 5-year control. All patients had a
full clinical and radiographic follow-up.
Radiographic findings
The following radiographic findings were noted:
– The preoperative average height of the hip
center was 37.9 mm (range = 18-82 mm). The
postoperative average height of the hip center was
28.6 mm (range = 12-51 mm). The hip center was
lowered an average of 9 mm (range = 4-30 mm).
– The preoperative average horizontal location of
the hip center was 40.4 mm (range = 28-71 mm).
The postoperative average horizontal location of
the hip center was 35.6 mm (range = 22-58 mm).
This location was an average of 4.7 mm (range =
0-14 mm) medial to the preoperative position.
860 The Journal of Arthroplasty Vol. 21 No. 6 September 2006
– The preoperative average abduction angle was
55.78 (range = 208-1148). The postoperative
average abduction angle was 49.28 (range =
308-728). The abduction angle was decreased an
average of 6.48 (range = 08-428).– The preoperative average location of the inferior
edge of the cup was 9.3 mm (range = �7 to
42 mm). The postoperative average location of
the inferior edge of the cup was �2.4 mm
(range = �13 to 26 mm). This edge went down
an average of 11 mm (range = 0-18 mm).
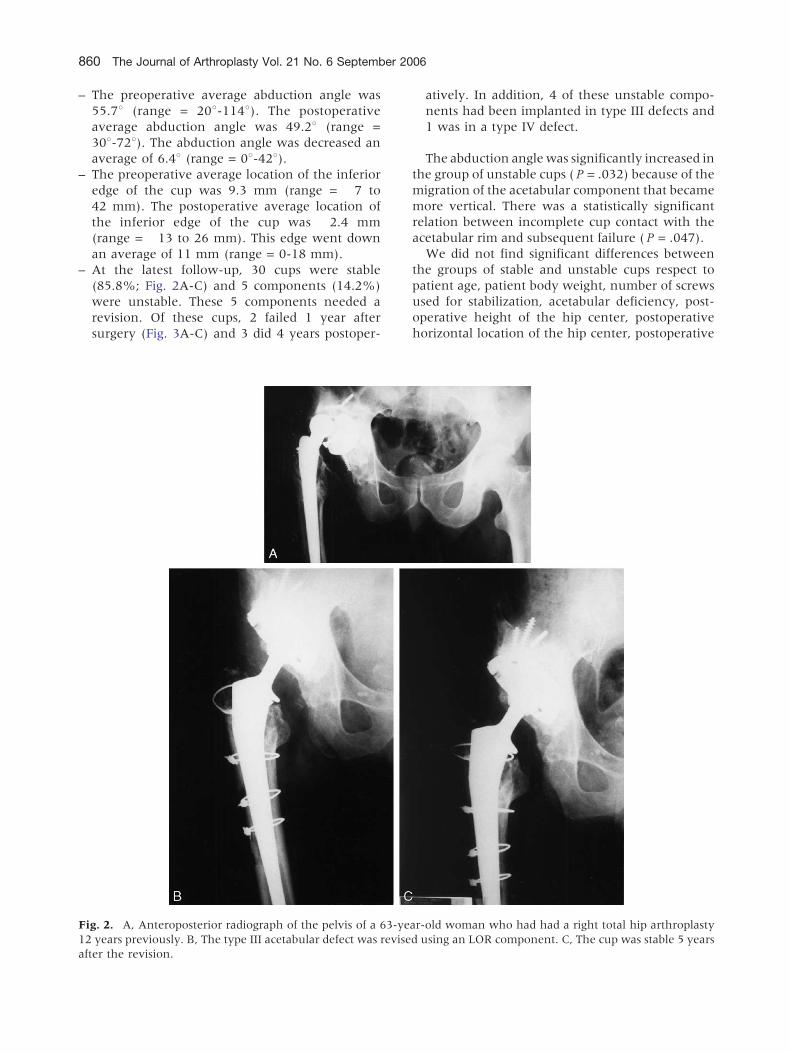
– At the latest follow-up, 30 cups were stable
(85.8%; Fig. 2A-C) and 5 components (14.2%)
were unstable. These 5 components needed a
revision. Of these cups, 2 failed 1 year after
surgery (Fig. 3A-C) and 3 did 4 years postoper-
Fig. 2. A, Anteroposterior radiograph of the pelvis of a 63-ye
12 years previously. B, The type III acetabular defect was revise
after the revision.
atively. In addition, 4 of these unstable compo-
nents had been implanted in type III defects and
1 was in a type IV defect.
The abduction angle was significantly increased in
the group of unstable cups ( P = .032) because of the
migration of the acetabular component that became
more vertical. There was a statistically significant
relation between incomplete cup contact with the
acetabular rim and subsequent failure ( P = .047).
We did not find significant differences between
the groups of stable and unstable cups respect to
patient age, patient body weight, number of screws
used for stabilization, acetabular deficiency, post-
operative height of the hip center, postoperative
horizontal location of the hip center, postoperative
ar-old woman who had had a right total hip arthroplasty
d using an LOR component. C, The cup was stable 5 years
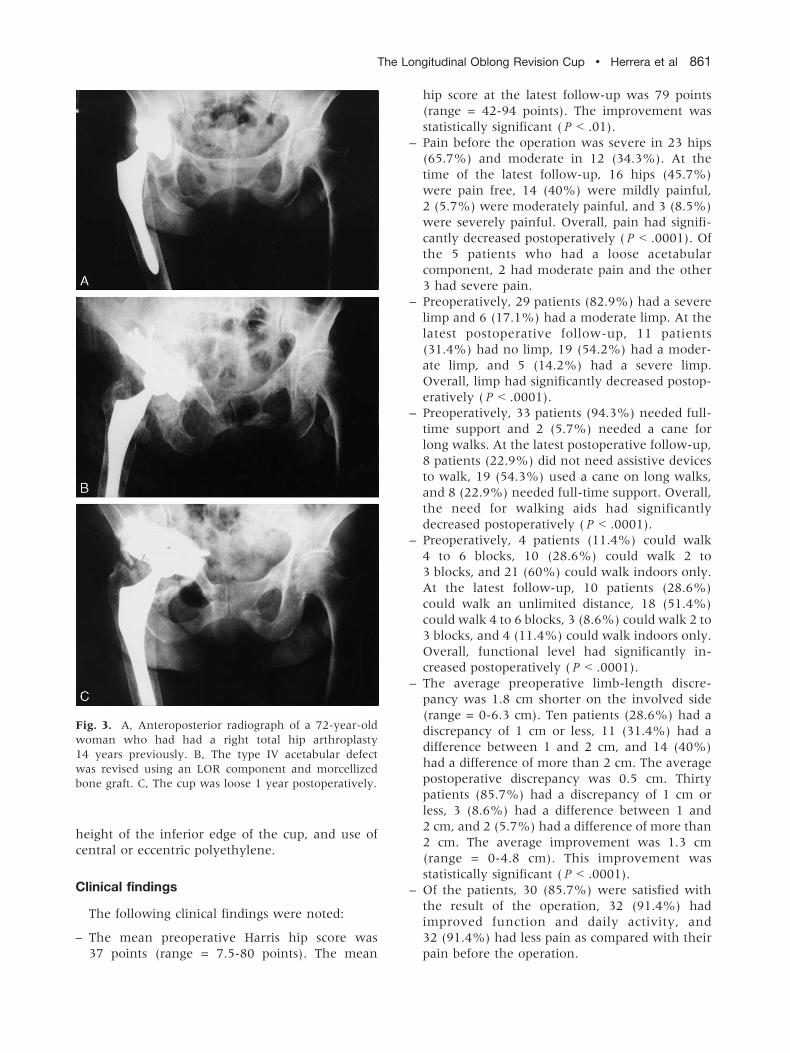
Fig. 3. A, Anteroposterior radiograph of a 72-year-old
woman who had had a right total hip arthroplasty
14 years previously. B, The type IV acetabular defect
was revised using an LOR component and morcellized
bone graft. C, The cup was loose 1 year postoperatively.
The Longitudinal Oblong Revision Cup ! Herrera et al 861
height of the inferior edge of the cup, and use of
central or eccentric polyethylene.
Clinical findings
The following clinical findings were noted:
– The mean preoperative Harris hip score was
37 points (range = 7.5-80 points). The mean
hip score at the latest follow-up was 79 points
(range = 42-94 points). The improvement was
statistically significant ( P b .01).
– Pain before the operation was severe in 23 hips
(65.7%) and moderate in 12 (34.3%). At the
time of the latest follow-up, 16 hips (45.7%)
were pain free, 14 (40%) were mildly painful,
2 (5.7%) were moderately painful, and 3 (8.5%)
were severely painful. Overall, pain had signifi-
cantly decreased postoperatively ( P b .0001). Of
the 5 patients who had a loose acetabular
component, 2 had moderate pain and the other
3 had severe pain.
– Preoperatively, 29 patients (82.9%) had a severe
limp and 6 (17.1%) had a moderate limp. At the
latest postoperative follow-up, 11 patients
(31.4%) had no limp, 19 (54.2%) had a moder-
ate limp, and 5 (14.2%) had a severe limp.
Overall, limp had significantly decreased postop-
eratively ( P b .0001).
– Preoperatively, 33 patients (94.3%) needed full-
time support and 2 (5.7%) needed a cane for
long walks. At the latest postoperative follow-up,
8 patients (22.9%) did not need assistive devices
to walk, 19 (54.3%) used a cane on long walks,
and 8 (22.9%) needed full-time support. Overall,
the need for walking aids had significantly
decreased postoperatively ( P b .0001).
– Preoperatively, 4 patients (11.4%) could walk
4 to 6 blocks, 10 (28.6%) could walk 2 to
3 blocks, and 21 (60%) could walk indoors only.
At the latest follow-up, 10 patients (28.6%)
could walk an unlimited distance, 18 (51.4%)
could walk 4 to 6 blocks, 3 (8.6%) could walk 2 to
3 blocks, and 4 (11.4%) could walk indoors only.
Overall, functional level had significantly in-
creased postoperatively ( P b .0001).
– The average preoperative limb-length discre-
pancy was 1.8 cm shorter on the involved side
(range = 0-6.3 cm). Ten patients (28.6%) had a
discrepancy of 1 cm or less, 11 (31.4%) had a
difference between 1 and 2 cm, and 14 (40%)
had a difference of more than 2 cm. The average
postoperative discrepancy was 0.5 cm. Thirty
patients (85.7%) had a discrepancy of 1 cm or
less, 3 (8.6%) had a difference between 1 and
2 cm, and 2 (5.7%) had a difference of more than
2 cm. The average improvement was 1.3 cm
(range = 0-4.8 cm). This improvement was
statistically significant ( P b .0001).
– Of the patients, 30 (85.7%) were satisfied with
the result of the operation, 32 (91.4%) had
improved function and daily activity, and
32 (91.4%) had less pain as compared with their
pain before the operation.
862 The Journal of Arthroplasty Vol. 21 No. 6 September 2006
Complications
There were 3 intraoperative femoral fractures
around the tip of the stem that were treated with
internal fixation.
A total of 3 patients had sciatic nerve palsies, 1
of which resolved completely and 2 persisted,
consequently requiring the patients to use an
ankle-foot orthosis.
There were 2 cases of deep venous thrombosis,
2 cases of late femoral fractures (1 of them treated
surgically and the other with rest and a thigh
orthosis), 2 cases of early dislocation that had no
additional dislocation after an initial closed reduc-
tion, 1 case of late dislocation that did not recur
after closed reduction, and 4 cases of heterotopic
ossifications that caused a moderate limitation of
joint mobility.
A total of 5 patients required cup revision because
of cup failure, 2 of them 1 year after surgery and the
3 remaining 4 years postoperatively.
There was one case of superficial wound in-
fection that was treated by debridement and anti-
biotic therapy.
There was no case of pulmonary embolism.
Discussion
Several technical approaches have been used to
overcome the difficulties in revising failed acetab-
ular components.
Minor defects can usually be managed with
standard implants. In larger defects, there are
several alternatives. The use of structural allog-
rafts is controversial. The failure rate has ranged
from 13% to 47%, and acetabular failure has in-
creased significantly with longer follow-up eva-
luation [9-12].
Acetabular reconstruction with impacted morcel-
lized cancellous bone autograft and a cemented cup
has been proven to provide a good long-term
result, with a survival rate of 94% [13-15].
Reinforcement rings and structural or morcel-
lized bone graft have been used successfully to
manage severe segmental or combined defects
where there is limited host bone available to
provide cup support [16-22]. Reported failure rates
have oscillated between 10% and 50%. The best
results have been obtained in cavitary deficiencies;
the worst, in combined defects.
Cementless acetabular components have been
used with satisfactory results [1-7], but their
problem is that it is not possible to obtain a good
fixation in large defects without using allografts.
The best results have been obtained in hips with
a bone defect of less than 30%; the worst, when the
bone defect was greater than 50% and a structural
bone graft was used to stabilize the prosthesis [2].
Large hemispherical cementless components
fixed with screws have been used successfully in
large defects [8], but the complication rate was
high (dislocation, late infection, trochanteric
osteotomy nonunion).
An important problem in revision arthroplasty is
that when we try to convert an oblong defect to a
hemisphere to insert an uncemented hemispheric
component, usually of extra large size, the required
reaming can damage the bone stock of the anterior
and posterior columns of the acetabulum. An
alternative option of reconstruction that avoids
large allografts or excessive reaming is the use of
porous-coated oblong acetabular implants. There
are 2 types of oblong cups: the bilobed oblong
acetabular component and the LOR cup.
The theoretical advantages of these cups are an
increased surface contact area between the porous
component and native host acetabular bone,
the avoidance of structural bone grafts, and the
potential to normalize the center of rotation. The
main disadvantage is the lack of bone stock
restoration. There are few published clinical results
about these cups.
Bilobed oblong acetabular cups have been used
by several authors [27-29]. DeBoer and Christie
[29] and Berry et al [27] reported good results at
early to midterm follow-up. They recommend this
implant for large superolateral bone deficiencies.
Chen et al [28] reported an early rate of loosening
of 24%. They believe that this device is indicated in
an oblong-shaped acetabular defect, with an intact
medial wall of the acetabulum, when a surgeon
wants to correct an elevated hip center.
Longitudinal oblong revision cups have been
used by Sutherland [24-26] and by Kfster et al
[23]. Initial series were very small [24-26]. The
largest series was published by Kfster et al [23],
who reported favorable results in 98 acetabular
revisions at midterm follow-up, with a success
rate of 98%. In this series, there were 21%
segmental deficiencies, 42% cavitary defects, 32%
combined defects, and 5% pelvic discontinuities.
This could explain these excellent results, because
the primary stability of the cup usually is very
good in segmental or cavitary defects. In our
series, the LOR cup was used in types III and IV
defects. Our loosening rate was higher than that
of Kfster et al [23], but they reported that all cup
migrations observed in their series occurred in
major defects.

The Longitudinal Oblong Revision Cup ! Herrera et al 863
We think that the LOR socket is suitable to be
used in types III and IV defects. In type IV defects,
the possibility of obtaining fixation with screws
in the ilium, pubis, and ischium allows achieving
an acceptable stabilization of the pelvic discontinu-
ity. Owing to the oblong shape of the defect, the
form of this cup allows better contact with the
remaining bone and loads distribution than if it
were hemispherical. However, we think that the
stability of the reconstruction could be improved by
treating pelvic discontinuities with plate fixation
before reconstructing the defect with the LOR cup
in type IV defects.
Oblong cups are designed to restore the position
of the hip center. In our series, we did not find
a significant relationship between the postoperative
height of the hip center and the outcome. We
found that an increased postoperative abduction
angle and an incomplete contact of the cup with the
acetabular rim significantly worsened the outcome.
Schutzer and Harris [32] have recommended using
a high hip center technique by means of a standard
small hemispherical cup screwed high on the ilium
to bypass the acetabular defect and gain stability on
healthy host bone. However, Yoder et al [33] noted
that cups placed in a nonanatomical, superolateral
position had a significantly higher femoral compo-
nent loosening rate compared with those placed in
an anatomical position.
The midterm clinical and radiographic results
using the LOR cup in our series of patients with
types III and IV defects have been encouraging. The
longitudinal oblong form of the cup obviates the
need for bulky structural allografts to fill the
superior defect or the need for excessive reaming
to obtain a hemispheric acetabulum. The initial
anchorage of the implant was achieved by means of
the contact of the cup with the acetabular rim and
the added screw fixation.
References
1. Chareancholvanich K, Tanchuling A, Seki T, et al.
Cementless acetabular revision for aseptic failure of
cemented hip arthroplasty. Clin Orthop 1999;
361:140.
2. Garcıa-Cimbrelo E. Porous-coated cementless acetab-
ular cups in revision surgery. A 6- to 11-year follow-
up study. J Arthroplasty 1999;14:397.
3. Lawrence JM, Engh CA, Macalino GE, et al. Outcome
of revision hip arthroplasty done without cement.
J Bone Joint Surg Am 1994;76-A:965.
4. Moskal JT, Danisa OA, Shaffrey CI. Isolated revision
acetabuloplasty using a porous-coated cementless
acetabular component. A 3- to 9-year follow-up
study. J Arthroplasty 1997;12:719.
5. Silverton CD, Rosenberg AG, Sheinkop MB, et al.
Revision total hip arthroplasty using a cementless
acetabular component. Clin Orthop 1995;319:201.
6. Woolson ST, Adamson GJ. Acetabular revision using
a bone-ingrowth total hip component in patients
who have acetabular bone stock deficiency.
J Arthroplasty 1996;11:661.
7. Jones CP, Lachiewicz PF. Factors influencing the
longer-term survival of uncemented acetabular com-
ponents used in total hip revisions. J Bone Joint Surg
Am 2004;86-A:342.
8. Dearborn JT, Harris WH. Acetabular revision arthro-
plasty using so-called jumbo cementless components.
An average 7-year follow-up study. J Arthroplasty
2000;15:8.
9. Avci S, Connors N, Petty W. 2- to 10-year follow-up
study of acetabular revisions using allograft bone to
repair bone defects. J Arthroplasty 1998;13:61.
10. Lee BP, Cabanela ME, Wallrichs SL, et al. Bone-graft
augmentation for acetabular deficiencies in total hip
arthroplasty. J Arthroplasty 1997;12:503.
11. Morand F, Clarac JP, Gayet LE, et al. Reconstruction
cotyloRdienne par allogreffe osseuse dans les revisions
de prothese totale de hanche. Rev Chir Orthop 1998;
84:154.
12. Stiehl JB, Saluja R, Diener T. Reconstruction of
major column defects and pelvic discontinuity in
revision total hip arthroplasty. J Arthroplasty 2000;
15:849.
13. Schreurs BW, van Tienen TG, Buma P, et al.
Favorable results of acetabular reconstruction with
impacted morsellized bone grafts in patients younger
than 50 years. A 10- to 18-year follow-up study of
34 cemented total hip arthroplasties. Acta Orthop
Scand 2001;72:120.
14. Slooff TJJH, Buma P, Gardeniers JWM, et al.
Revision of the acetabular component: bone packing.
In: Callaghan JJ, Rosenberg AG, Rubash HE, editors.
The adult hip, vol. 2. Philadelphia: Lippincott-Raven
Publishers; 1998. p. 1449.
15. Welten MLM, Schreurs BW, Buma P, et al. Acetab-
ular reconstruction with impacted morcellized can-
cellous bone autograft and cemented primary total
hip arthroplasty. A 10- to 17-year follow-up study.
J Arthroplasty 2000;15:819.
16. Brady OH, Masri BA, Garbuz DS, et al. Perspectives
on modern orthopaedics: use of reconstruction rings
for the management of acetabular bone loss during
revision hip surgery. J Am Acad Orthop Surg
1999;7:1.
17. Gill TJ, Sledge JB, Mqller ME. The management of
severe acetabular bone loss using structural allograft
and acetabular reinforcement devices. J Arthroplasty
2000;15:1.
18. Kerboull M, Hamadouche M, Kerboull L. The Ker-
boull acetabular reinforcement device in major ace-
tabular reconstructions. Clin Orthop 2000;378:155.
864 The Journal of Arthroplasty Vol. 21 No. 6 September 2006
19. Massin P, Tanaka C, Huten D, et al. Traitement des
descellements acetabulaires aseptiques par recon-
struction associant greffe osseuse et anneau de
Mqller. Analyse actuarielle sur 11 ans. Rev Chir
Orthop 1998;84:51.20. Saleh KJ, Jaroszynski G, Woodgate I, et al. Revision
total hip arthroplasty with the use of structural
acetabular allograft and reconstruction ring. A case
series with a 10 year average follow-up. J Arthro-
plasty 2000;15:951.
21. Van der Linde M, Tonino A. Acetabular revision with
impacted grafting and a reinforcement ring. Acta
Orthop Scand 2001;72:221.
22. Wachtl SW, Jung M, Jakob RP, et al. The Burch-
Schneider antiprotrusio cage in acetabular revision
surgery. A mean follow-up of 12 years. J Arthro-
plasty 2000;15:959.
23. Kfster G, Willert HG, Kfhler HP, et al. An oblong
revision cup for large acetabular defects. J Arthro-
plasty 1998;13:559.
24. Sutherland CJ. Early experience with eccentric
acetabular components in revision total hip arthro-
plasty. Am J Orthop 1996;25:284.
25. Sutherland CJ. Treatment of type III acetabular
deficiencies in revision total hip arthroplasty without
structural bone-graft. J Arthroplasty 1996;11:91.
26. Sutherland CJ. Management of type III acetabular
deficiencies in revision total hip arthroplasty without
structural bone-graft. J South Orthop Assoc 1998;
7:36.
27. Berry DJ, Sutherland CJ, Trousdale RT, et al. Bilobed
oblong porous coated acetabular components in
revision total hip arthroplasty. Clin Orthop 2000;
371:154.
28. Chen WM, Engh Jr CA, Hopper RH, et al. Acetabular
revision with use of a bilobed component inserted
without cement in patients who have acetabular
bone-stock deficiency. J Bone Joint Surg (Am) 2000;
82-A:197.
29. DeBoer DK, Christie MJ. Reconstruction of the
deficient acetabulum with an oblong prosthesis.
J Arthroplasty 1998;13:674.
30. Badhe NP, Howard PW. Partially hydroxyapatite-
coated stemmed acetabular cup and nonstructural
bone-graft in the management of severe acetabular
deficiency. J Arthroplasty 2000;15:63.
31. D’Antonio JA, Capello WN, Borden LS, et al.
Classification and management of acetabular abnor-
malities in total hip arthroplasty. Clin Orthop 1989;
243:126.
32. Schutzer SF, Harris WH. High placement of porous-
coated acetabular components in complex total hip
arthroplasty. J Arthroplasty 1994;9:359.
33. Yoder SA, Brand RA, Pedersen DR, et al. Total hip
acetabular position affects component loosening
rates. Clin Orthop 1988;228:79.
Related Documents











