
MANAGEMENT OF PROSTATE CA
Jul 16, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Introduction:
Prostate is accessory gland made up of fibromuscular stroma .
• Main function : to produce seminal fluid which nourishes the sperms after ejaculation. (30 % of seminal fluid)
• Avg. size 4 x 3 x 2cms
• Avg. weight:8g
Epidemiology:
2nd most common cancer in men- 29% of all male cancers
2nd leading cause of cancer death in men in western world
World wide incidence- 25.3 per lakh (Vera Nelson, RRCR, vol. 175, 2007)
Higher incidence –Scandinavia, North America, Australia, western and northern Europe
Low incidence- Asian countries
India- 4% of all male cancers
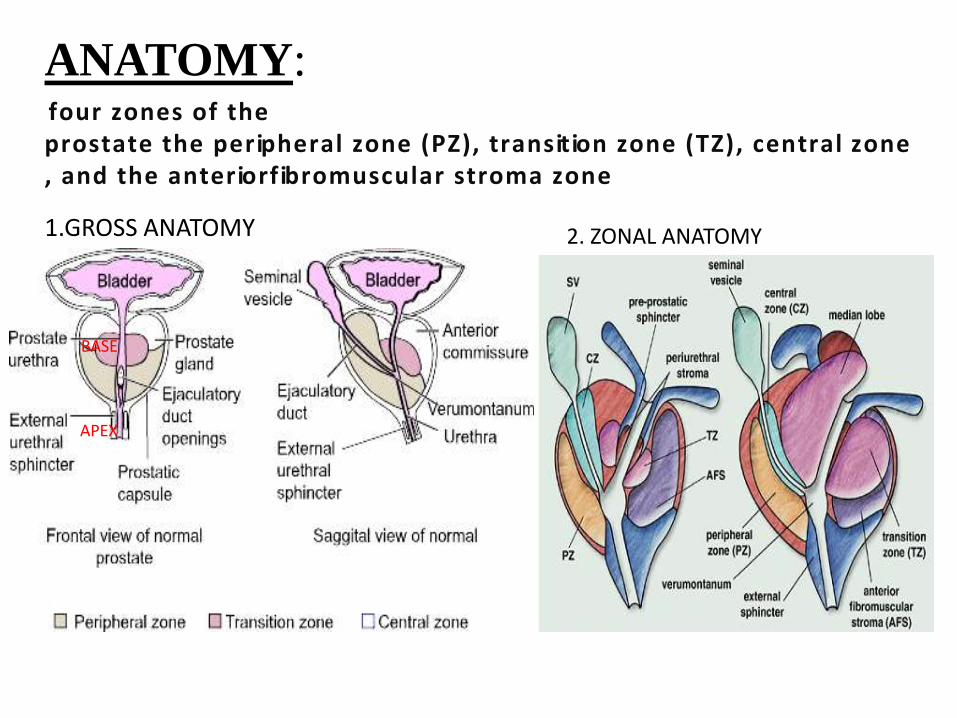
ANATOMY:f o u r z o n e s o f t h ep r o s t a t e t h e p e r ip h e r a l z o n e ( P Z ) , t r a n s it io n z o n e ( T Z ) , c e n t r a l zo n e , a n d t h e a n t e r io r f ib r o m u s c u l a r s t r o m a z o n e
1.GROSS ANATOMY
BASE
APEX
2. ZONAL ANATOMY

.• Proximity to Rectum & U. Bladder: Denonvilliers fascia
• Blood supply:Inferior vesicalMid rectalInternal pudendal
• Lymphatics:Internal iliac nodesSacral nodesPartly external iliac nodes• Nervous supply:Neurovascular bundle
Lies on either side of the prostate on the rectumDerived from the pelvic plexus - Important for erectile function

• Adenocarcinoma 95% - peripheral acinar glands
• Other Histologic Subtypes
– Periurethral duct carcinoma
– transitional cell carcinoma
– Ductal adenocarcinoma
– Neuroendocrine tumors
– Mucinous carcinoma
– Sarcomatoid carcinoma
– Endometrioid tumors
– Adenoid cystic carcinoma
– Sarcomas (leiomyosarcoma, rhabdomyosarcoma, or
fibrosarcoma)
– Carcinosarcoma
– Primary lymphoma
Pathology:

• Early state (organ confined)
– Asymptomatic
• Locally advanced
– Obstructive voiding symptoms
• Hesitancy
• Intermittent urinary stream
• Decreased force of stream
– May have growth into the urethra or bladder neck
– Hematuria
– Hematospermia
Increased PSA level
DRE
TRUS 10-18
cores from base , mid and apex
b/l & additional cores from
midline & lateral peripheral
zone.
• Difficult to detect < 1 cm
tumor
• No specific characteristics to
diff. BPH & malignancy
• T2 &T3 lesions -60%
sensitivity (Rifkin et al.)
If clinically indicated by obstructive
symptoms then separately TZ biopsy
may be taken.
Clinical presentations:
Metastasis :
– Most commonly to bone (frequently asymptomatic)
• Can cause severe and unremitting pain
– Bone metastasis
• Can result in pathologic fractures or
• Spinal cord compression• MC sites of metastasis
– Vertebral column- 74%– Ribs- 70%– Pelvis- 60%– Femora- 44%– Shoulder girdle-41%--Visceral metastases (rare)
– Can develop pulmonary, hepatic, pleural, peritoneal, and central nervous system metastases late in the natural history or after hormonal therapies fail.
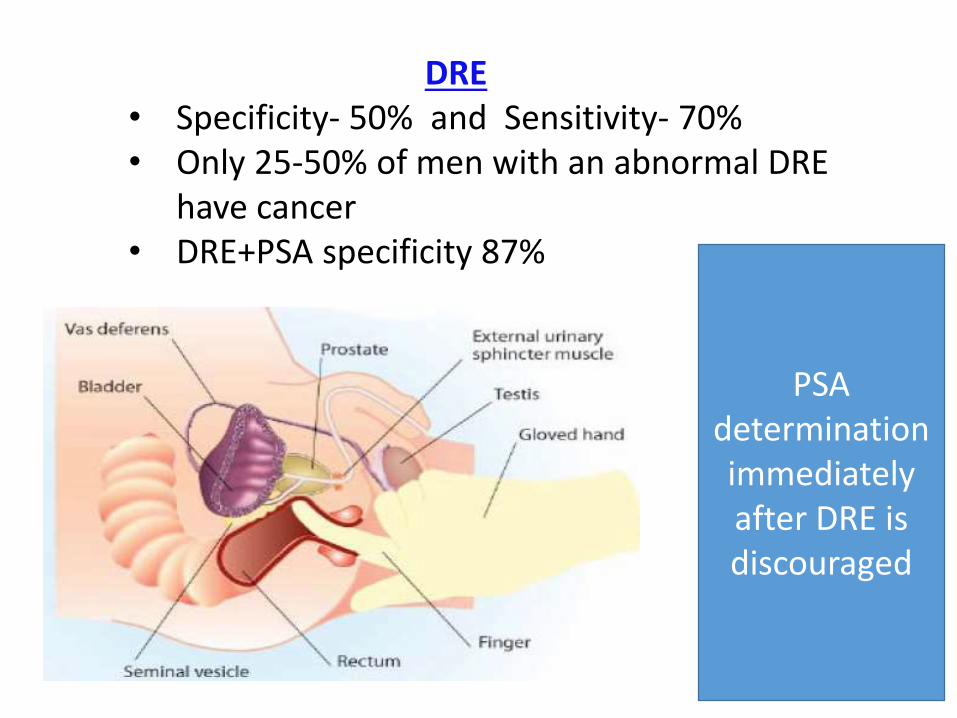
DRE• Specificity- 50% and Sensitivity- 70%• Only 25-50% of men with an abnormal DRE
have cancer• DRE+PSA specificity 87%
PSA determination immediately after DRE is discouraged

PSA:• Identified from prostatic tissue by wang et al. in 1979
• Found also in serum of ca prostate patients.
• Immensely valuable in screening for prostatic ca.( established by two landmark
screening trials—European randomized study of screening for prostate cancer
(ERSPC) & us based lung,colorectal and ovarian(PLCO) screening trials.)-----on
basis of it AMERICAN UROLOGICAL ASSOCIATION recommends DRE
and PSA screening over the age of 40 years if their life expectancy is > 10
years.
• helps in detection of disease confined to prostate before DRE palpable
disease / obstructive features.
• 70% of cancers detected by PSA screening are confined to prostate and 40 %
cancers detected by PSA are not palpable.
• The half-life of PSA is around 2.2–3.2 days, and reaches its lowest level 2–3
weeks after radical prostatectomy (RP).
• PSA>4 ng/ml is suspicious for cancer.( positive predictive value is 31%-54%)
• Caution: it is also detected by immunohistocheical techniques in pancreas ,
salivary gland and in woman, in conditions like prostatitis, BPH/increased
prostate volumes, DRE, prostatic calculi, TRUS,TURP.
• A greater yield is found if coupled with USG &DRE.
PSA density (PSAD):
More than 80% of men with high serum PSA levels have values of between 4 and 10
ng/mL. These high PSA levels are usually due to a high prevalence of benign
prostate hyperplasia (BPH). The PSAD was introduced particularly for men with
normal DRE and PSA levels of 4–10 ng/mL in order to differentiate between BPH
and prostate cancer.
• The PSAD is calculated by dividing the serum PSA level by the prostate volume,
as measured by TRUS.
• The threshold level of 0.15 or above indicates prostate cancer, while 0.15 or below
indicates benign disease.
• The main problems with the PSAD are errors in prostate volume measurement
using TRUS, changes in the epithelial–stromal ratio of the prostate, and changes in
PSA with age.
PSA velocity(PSAV): the change in PSA level over time. At least three values are
taken in an interval of 6 months.The upper limit for the
PSAV is taken to be 0.75
ng/mL/year; a value above
this limit is considered to be
a tumor-specific marker
• Free PSA: men with prostate cancer with normal to enlarged gland has
lower free psa value than in BPH patients.at Washington university a ratio of free to total PSA ≤0.2 was most likely
associated with prostate cancer and a ratio of ≤0.15 was associated with higher
gleason score and poorer prognosis
• PSA doubling time (PSADT):Which measures the exponential increase In
serum PSA over time, Reflecting a relative change.
• PCA3 marker
PCA3 is an increasingly studied new biomarker that is detectable in urine sediments
obtained after three strokes of prostatic massage during DRE. The costly Progensa
urine test for PCA3 is now commercially available. The PCA3 score increases
with PCa volume, but there is conflicting data about whether the PCA3 score
independently predicts the Gleason score, and its use as a monitoring tool in active
surveillance has not been confirmed.
The main current indication for the PCA3 urine test may be to determine whether
a man needs a repeat biopsy after an initially negative biopsy outcome, but its cost-
effectiveness remains to be shown.
Primary role
• Size determination of the gland
• Assess pelvic LN metastasis
• Treatment planning in RT
Features:
• Loss of periprostatic fat planes
• Bladder base deformity
• Obliteration of the normal angle
b/w the SV and post. aspect of
UB
LN involvement
Abnormality in size
Sensitivity 25%
Reserved for patients with higher
PSA values (>20-25 ng/ml)
CT guided FNAC
Limitation of CT:• Lacks the soft tissue
resolution needed to detect
intraprostatic anatomic
changes due to primary
tumor , capsular extension or
SVI because the neoplasm
usually has the same
attenuation as the normal
prostate gland
• Can't detect microscopic
disease
• False Positive- Artifact of
Bx and plane b/w SV and
UB base may be obscured
by rectal distension
CT SCAN

MRI (ENDORECTAL COIL)Prostate: A focal, peripheral region of decreased signal intensity surrounded by a normal(high intensity) peripheral zone
• T1-weighted imaging : is used to detect lymph node involvement and bone metastases. Post biopsy hge is appreciable in T1 images.
• T2-weighted imaging : provides superb delineation of the prostate anatomy and tumor localization.(AXIAL &CORONAL images)
• Endorectal surface coil MRI- accuracy of 54-72% staging the primary and detects SVI and ECE
Vas deferens &seminal vesicles- both axial &corornal images whereas
neurovascular bundles better delineated in coronal images.
ECE – focal ,irregular capsular bulge asymmetry or invasion of the nv bundles &
obliteration of rectoprostatic angle.
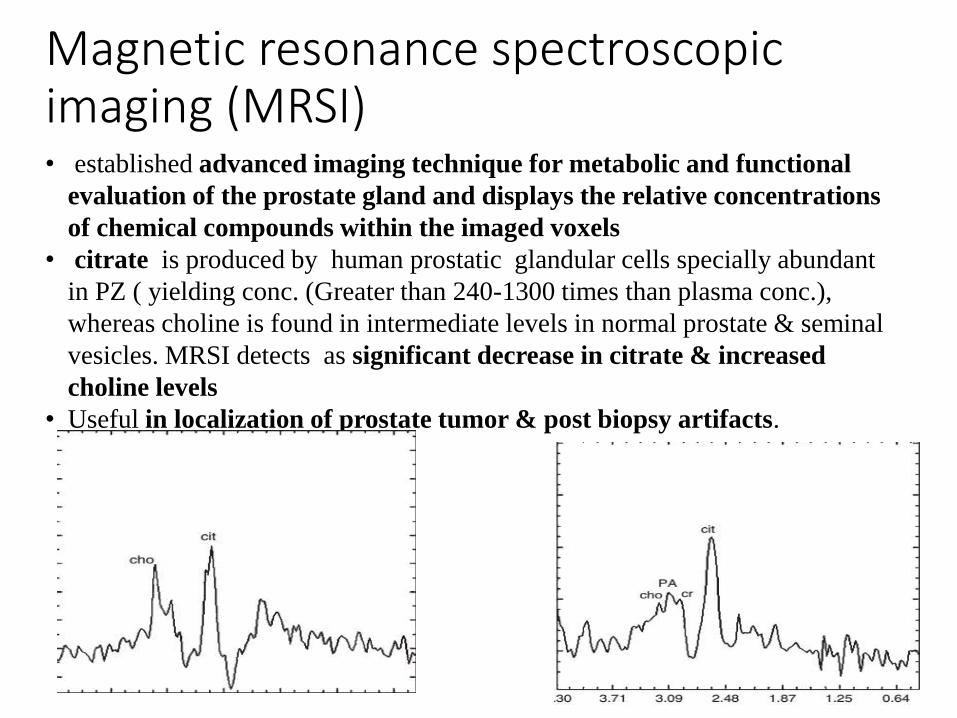
Magnetic resonance spectroscopic imaging (MRSI)• established advanced imaging technique for metabolic and functional
evaluation of the prostate gland and displays the relative concentrations
of chemical compounds within the imaged voxels
• citrate is produced by human prostatic glandular cells specially abundant
in PZ ( yielding conc. (Greater than 240-1300 times than plasma conc.),
whereas choline is found in intermediate levels in normal prostate & seminal
vesicles. MRSI detects as significant decrease in citrate & increased
choline levels
• Useful in localization of prostate tumor & post biopsy artifacts.
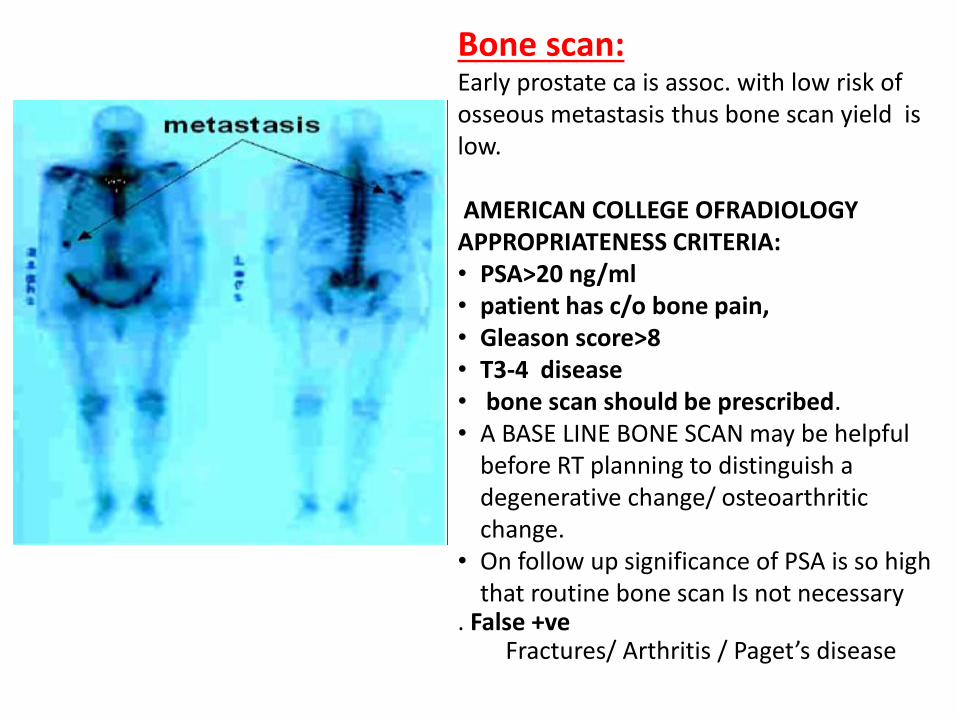
Bone scan: Early prostate ca is assoc. with low risk of osseous metastasis thus bone scan yield is low.
AMERICAN COLLEGE OFRADIOLOGY APPROPRIATENESS CRITERIA:• PSA>20 ng/ml• patient has c/o bone pain, • Gleason score>8• T3-4 disease• bone scan should be prescribed.• A BASE LINE BONE SCAN may be helpful
before RT planning to distinguish a degenerative change/ osteoarthritic change.
• On follow up significance of PSA is so high that routine bone scan Is not necessary
. False +veFractures/ Arthritis / Paget’s disease

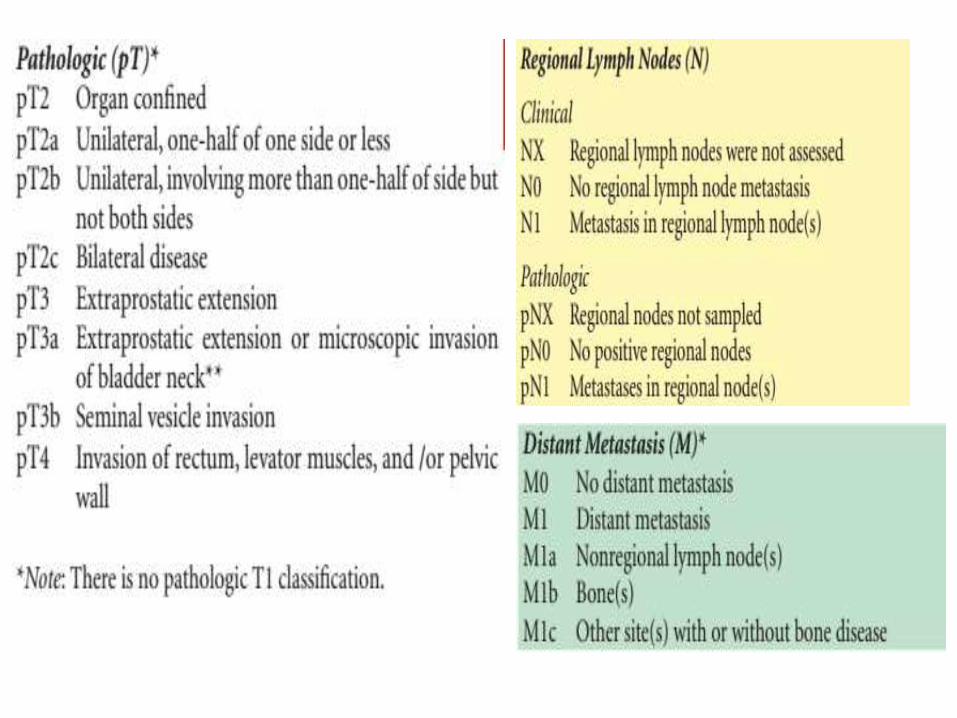
Invasion into the prostatic apex or into (but not beyond) the prostatic capsule is classified not as T3 but as T2.
S
T
A
G
I
N
G
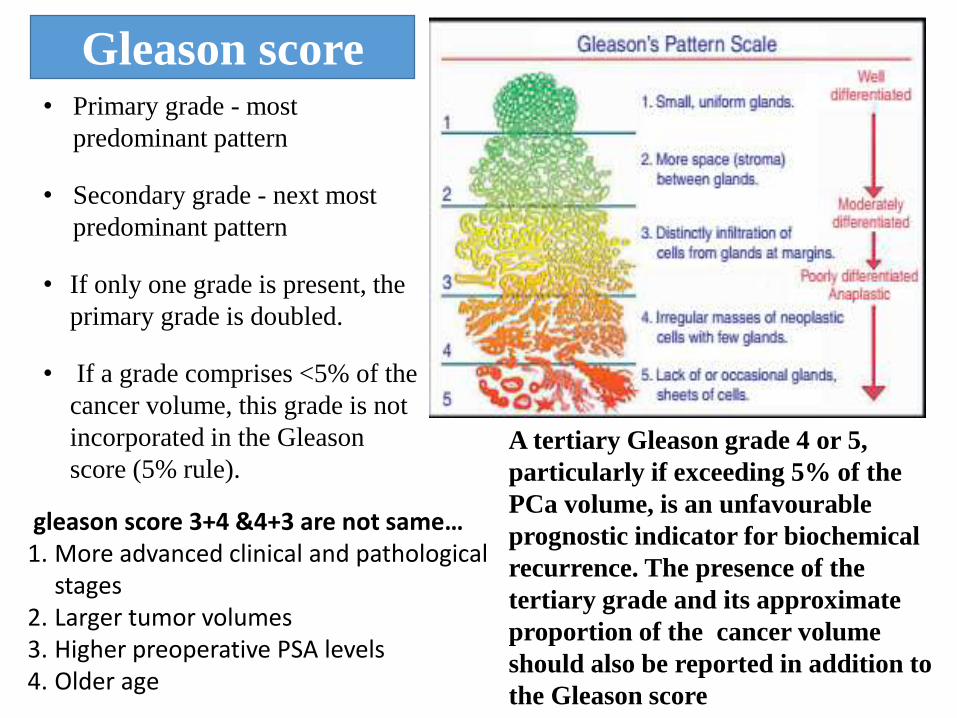
gleason score 3+4 &4+3 are not same…1. More advanced clinical and pathological
stages 2. Larger tumor volumes3. Higher preoperative PSA levels 4. Older age
• Primary grade - most
predominant pattern
• Secondary grade - next most
predominant pattern
• If only one grade is present, the
primary grade is doubled.
• If a grade comprises <5% of the
cancer volume, this grade is not
incorporated in the Gleason
score (5% rule).
Gleason score
A tertiary Gleason grade 4 or 5,
particularly if exceeding 5% of the
PCa volume, is an unfavourable
prognostic indicator for biochemical
recurrence. The presence of the
tertiary grade and its approximate
proportion of the cancer volume
should also be reported in addition to
the Gleason score
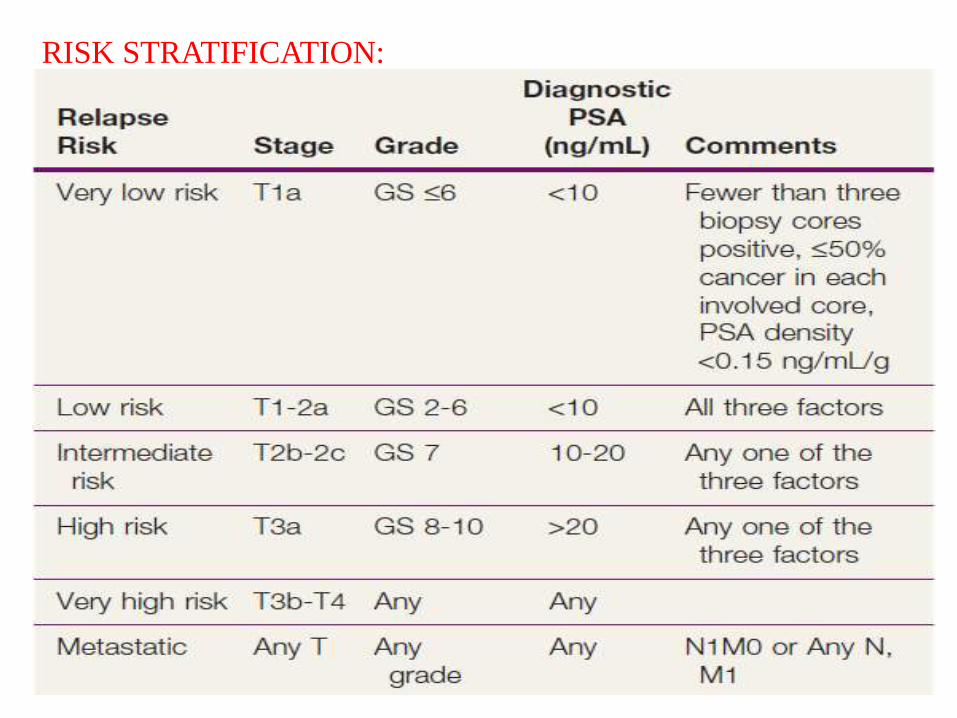
RISK STRATIFICATION:
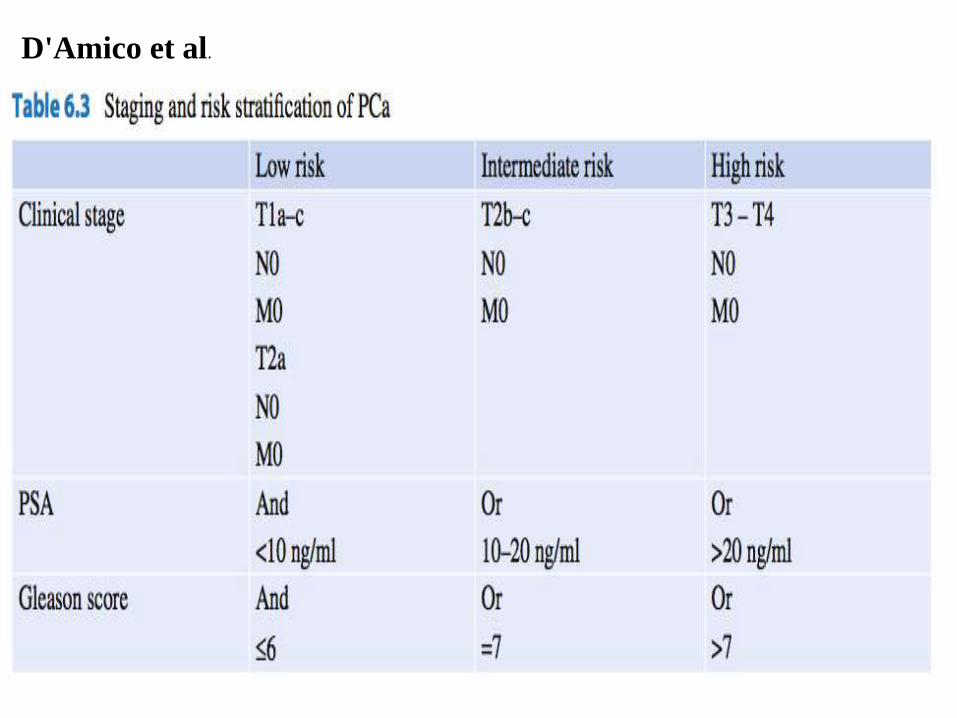
D'Amico et al.

Treatment:
Optimal management of ca prostate is very controversial
Some points must be take into consideration:
• natural history of disease
• prognostic significance of diagnosis
• potential therapeutic benefit of various modalities
• immediate and late treatment sequel.
• Life expectancy (estimated using the Social Security Administration
tables, available at: http://www.ssa.gov.)
• QOL
Various modalities used are:
• Watchful waiting/ active surveillance
• Radical prostatectomy
• Adjuvant therapy –radiotherapy /hormonal
• Upfront radiotherapy (brachytherapy/IMRT/IGRT)
• Chemotherapy
• Targated therapy

Watchful waiting:
It means no active treatment until a patient developes a symptomatic disease
progression, at that time hormonal therapy is initiated.
(goal: limit morbidity from disease and therapy)
Recently concept has changed to “active surveillance with delayed selective
intervention” assumes the risk posed by a given cancer can be assessed with
some degree of certainty and that delayed treatment will be as curative as
immediate treatment.
Long term follow up from watchful waiting shows risk of progression
accelerates over time., so AS patients must accept frequent &detailed regular
evaluation for as long as they are healthy and young enough to be candidate for
definitive therapy.

Total:407 men
239(59%) 103(25%) 65(16%)
AS Definitive treatment
Lost f/u
CARTER ET AL.-PROSPECTIVE LONGITUDINAL SURVEILLANCE PROGRAM:
407 MEN,CLINICAL stage-T1c (SMALL VOLUME CANCER)
Median age -65.7 yrs(45.8-81.5 yrs) & median f/u-2.8 yrs.(.4-12.5 yrs)
CHECK UP semiannual total & free PSA, DRE, annual surveillance
prostate examination
Treatment was recommended if there was findings of adverse
pathologic features on annual surveillance biopsy exam.
( GS>4/5,>2 cores +ve,>50% of any core involving with cancer)
Conclusion:
Small volume,
low grade
disease- careful
monitoring may
be a rational
alternative to
immediate radical
therapy for all.
53(51%) underwent radical prostatectomy,of which 20% men has has
pathological disease T2,GS≥4+3,+ve margin,stage pT3N0(extraprostatic
extension), node +ve, stage higher than pT3a
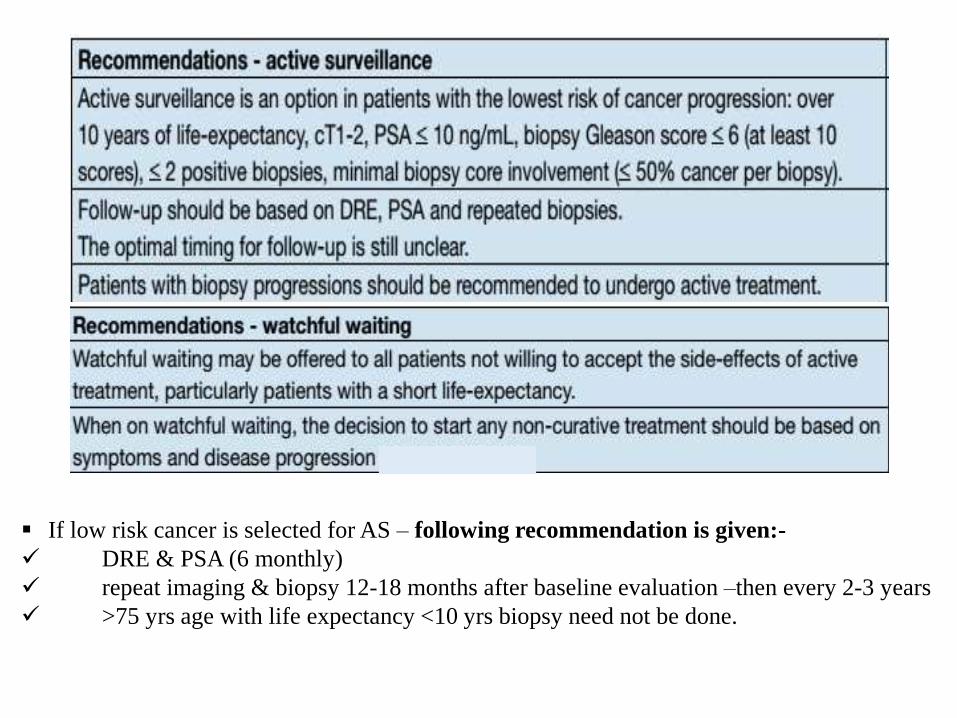
If low risk cancer is selected for AS – following recommendation is given:-
DRE & PSA (6 monthly)
repeat imaging & biopsy 12-18 months after baseline evaluation –then every 2-3 years
>75 yrs age with life expectancy <10 yrs biopsy need not be done.
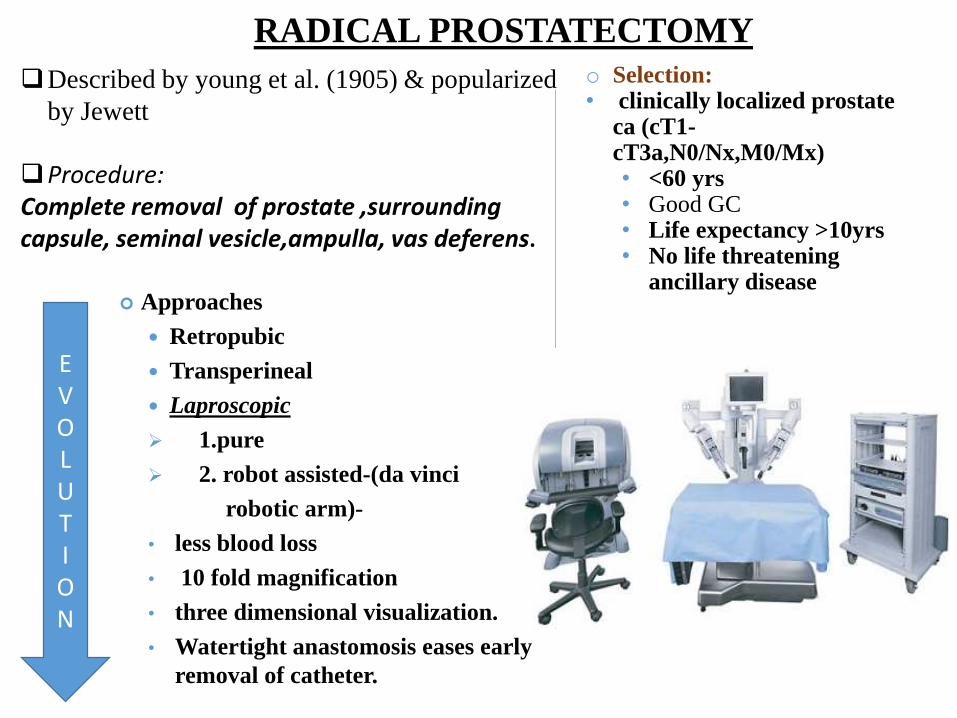
RADICAL PROSTATECTOMY
Described by young et al. (1905) & popularized
by Jewett
Procedure: Complete removal of prostate ,surrounding capsule, seminal vesicle,ampulla, vas deferens.
Approaches
Retropubic
Transperineal
Laproscopic
1.pure
2. robot assisted-(da vinci
robotic arm)-
• less blood loss
• 10 fold magnification
• three dimensional visualization.
• Watertight anastomosis eases early
removal of catheter.
o Selection:• clinically localized prostate
ca (cT1-cT3a,N0/Nx,M0/Mx)• <60 yrs• Good GC• Life expectancy >10yrs• No life threatening
ancillary disease
EVOLUTION

WATCHFUL WAITING RADICAL
PROSTATECTOMY
RR 348 (AS) 347 (RP)
0.56 (CI-0.36-0.88)
DEATH 50 30
0.6 (CI-0.42-0.86)
METS LOWER RISK OF METASTASIS
Cumulative probability of developing metastatic disease
10 yrs after diagnosis 25% in conservatively managed
patients.
Cancer specific mortality 25% in the WW patients.
Absolute & statistically significant increase in OS at 10
yrs for patients in surgery arm.
SCANDINAVIAN
TRIAL
695 men with clinically localized cancer prostate
RP vs. watchful waiting with systematic treatment deferred until disease progresses.
Patient selection for pelvic lymph node dissection:
o Definitely men with pelvic node involvement fare poorly. So controversy persists about
PND.
o Low risk disease(stage T1c, pSA≤10 ng/ml, GS≤6) Pelvic node involvement chance <5
%.
o But this underestimates the risk since the data are based on limited LN involvement (
external iliac nodes only)
o LN dissection: excision of fibrofatty tissue & lymphatic tissue between bifurcation of
common iliac artery superiorly to the femoral canal inferiorly and to pelvic sidewall
laterally. Posteriorly to obturator nv.
o Extended LN: conventional LN with posteriorly obturator vessels and iliac vein.
BADER et al.
a p r o s p e c t ive s t u d y o f t h e a n a t o m ic e x t e n t o f p e l vic n o d a l in vo l ve m e n t in a
c o h o r t o f 3 6 5 m e n w h o u n d e r w e n t a n e x t e n d e d l y m p h n o d e d is s e c t ion a n d
r a d ic a l p r o s t a t e c t o m y . T h is s t u d y in c l u d e d m e n w it h c l in ic a l l y o r g a n –
Conf in e d d is e a s e o n t h e b a s is o f a C T s c a n & b o n e s c a n . 1 9 % o f n o d e -p o s it
ive m e n h a d in vo l ve d n o d e s t h a t w e r e e x c l u s ive l y f o u n d in t h e in t e r -n a l i l ia c
r e g io n , s u g g e s t in g t h a t t h e l y m p h a t ic d r a in a g e o f p r o s t a t e c a n c e r is va r ia b l e
L A R G E R E T R O S P E C T IVE S T U D Y(J O H N S H O P K IN S )
• limited( n = 1 , 8 6 5 ) o r e x t e n d e d ( n = 2 , 1 3 5 ) n o d e d is s e c t io n s----no adjuvant therapy/ hormonal
therapy-----A s e x p e c t e d , t h e e x t e n d e d d is s e c t io n g r o u p h a d m o r e l y m p h n o d e s
r e t r ie ve d t h a n t h e l im it e d g r o u p ( 1 1 . 6 vs . 8 . 9 n o d e s ; p < 0 . 0 0 0 1 )---- in vo l ve d n o d e s
w a s a l s o s ig n if ic a n t l y h ig h e r in t h e e x t e n d e d d is s e c t io n g r o u p ( 3 . 3 % vs . 1 . 2 % ; p
< 0 . 0 0 0 1 ) .
• p a t ie n t s w it h G l e a s o n s c o r e 7 o r 8 t o 1 0 w e r e c o n s id e r e d , t h e d if f e r e n c e w a s
e ve n m o r e s t r ik in g ( 8 . 2 % vs . 2 . 4 % a n d 2 3 . 2 % vs . 8 . 9 % , r e s p e c t ive l y ).
• T h e r e w a s a t r e n d in f a vo r o f t h e e x t e n d e d d is s e c t io n g r o u p f o r 5 -y e a r
b io c h e m ic a l r e c u r r e n c e -f r e e s u r viva l ( 3 4 . 4 % vs . 1 6 . 5 % ; p = 0 . 0 7 ) ,s u g g e s t in g a
t h e r a p e u t ic b e n e f it o f e x t e n d e d d is s e c t io n in l o w vo l u m e d is e a s e
Current practice : to restrict PLND at time of RP to men with a
≥ 2% risk of positive nodes according to a contemporary
nomogram.
Nomogram limitations:
• mostly they are made of data depending on limited node dissections.
• recently nomograms by BRIGANTI ET AL. helps to address, by studying
extended lymph node dissections to predict pelvic nodal involvement,
exclusive nonobturator nodal mets and ideal nodal yield for accurate
determination.
• Previously ROACH ET AL. formula sill held relevance ( validated by
3000 patients cohort) and has an accuracy of 80%.

• Partin nomograms : pathologic stage (organ confined, ECE,
seminal vesicle invasion, or LN involvement) based on T stage, GS,
and pretreatment PSA
• Roach formulas: estimate pathologic stage based on original
Partin data
1. ECE = 3/2 × PSA + 10 × (GS-3)
2. Seminal vesicle involvement = PSA + 10 × (GS-6)
3. LN involvement = 2/3 × PSA + 10 × (GS-6)
• Kattan nomograms are computerized and predict primarily
PSA recurrence, but some also predict PFS as well as prostate
cancer specific mortality after RP, 3DCRT, or brachytherapy.
• Brignanti nomograms: (using extended LN dissection)
show higher rates and support importance of obtaining larger #
of LN (e.g., 28 to detect 90%) to improve chance of detecting
involvement
Role of NOMOGRAMS.
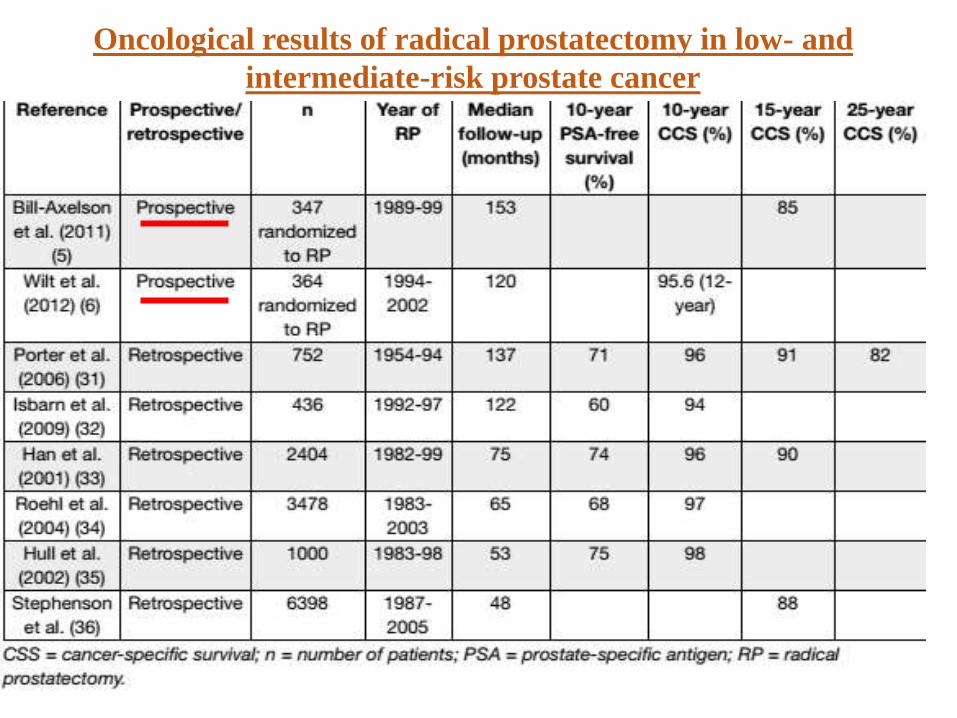
Oncological results of radical prostatectomy in low- and
intermediate-risk prostate cancer
Cancer Control with Radical Prostatectomy
Low-risk prostate cancer: cT1-T2a, Gleason score <6 and prostate-specific antigen
< 10 ng/mL
• two randomized trials comparing retropubic RP VS. watchful waiting (WW) in
localized PCa.
• SPCG-4 study: the survival benefit associated with RP was similar before and
after 9 years of follow-up and was also observed in men with low-risk PCa, and
was confined to men < 65 years of age.
• PIVOT trial: a preplanned subgroup analysis of men with low-risk tumours showed
that RP did not significantly reduce all-cause mortality.
Stage T1a-T1b prostate cancer:
• T1a-T1b PCa is found incidentally in 4-16% of patients surgically treated for benign
prostatic obstruction without any clinical suspicion of PCa.
• Levels of PSA before and after TURP increase the accuracy in estimating the need for
active management
• The decision to offer RP in cases of incidental cancer should be based upon the
estimated probability of clinical progression compared to the relative risk of
therapy and potential benefit to survival. In patients with a longer life expectancy,
especially for poorly differentiated tumours, RP should be considered.

Stage T1c and T2a prostate cancer:
• Clinically unapparent tumour identified by needle biopsy because of an elevated PSA
(cT1c) has become the most prevalent type of PCa. most reports stress that cT1c
tumours are often significant with up to 30% of cT1c tumours being locally advanced
at final histopathological analysis .
• The major challenge is how to recognize those tumours that need RP.
• Partin tables may help to improve the selection of patients
• If only one or a few cores are invaded and the percentage of invasion in one core is
limited, the PCa is more likely to be an insignificant cancer, particularly if the
lesion has a low Gleason score. It might therefore be reasonable to propose active
monitoring.
• In stage T2a patients with a 10-year life expectancy, RP is one of the recommended
standard treatments, as 35-55% of these patients will show disease progression
after 5 years if not treated.
• If active monitoring is proposed for low-grade T2 cancer, it should be remembered that
pre-operative assessment of tumour grade by needle biopsy is often unreliable .
• Extended pelvic lymph node dissection (eLND) is not necessary in low-risk PCa
because the risk for positive lymph nodes does not exceed 5%
Intermediate-risk, localized prostate cancer: cT2b-T2c or
Gleason score = 7 or prostate-specific antigen 10-20 ng/mL:
• Radical prostatectomy is one of the recommended standard treatments for
patients with intermediate risk PCa and a life expectancy of > 10 years.
• A policy of active monitoring has been proposed for some selected patients with
intermediate-risk localized tumours, but when the tumour is palpable or visible
on imaging and clinically confined to the prostate, disease progression can be
expected in most longterm survivors. Stage T2b cancer will progress in > 70%
of patients within 5 years.
• Bill-Axelson et al & Wilt et al. showed a significant reduction in disease-
specific mortality in favour of RP.

High-risk localized and locally advanced prostate cancer: cT3a or Gleason score
8-10 or prostate-specific antigen > 20 ng/mL:
Patients classified with high-risk PCa are at an increased risk of PSA failure, the need
for secondary therapy, metastatic progression and death from PCa. Nevertheless, not all
high-risk PCa patients have a uniformly poor prognosis after RP.
• There is no consensus regarding the optimal treatment of men with high-risk Pca.
• Management decisions should be made after all treatments have been discussed by a
multidisciplinary team (including urologists, radiation oncologists, medical
oncologists and radiologists), and after the balance of benefits and side effects of
each therapy modality has been considered by the patient with regard to their own
individual circumstances.
• Provided that the tumour is not fixed to the pelvic wall, or that there is no invasion
of the urethral sphincter, RP is a reasonable first step in selected patients with a low
tumour volume
• Extended LND should be performed in all high-risk PCa cases, because the estimated
risk for positive lymph nodes is 15-40%.
Locally advanced prostate cancer: cT3a:
The surgical treatment of clinical stage T3 PCa has traditionally been discouraged,
mainly because patients have an increased risk of positive surgical margins and
lymph node metastases and/or distant relapse

o Monothrerapy is not suitable for high risk cancer. In a study, among 4,708
patients undergoing RP, high-risk patients were identified based on eight
existing definitions which is as follows----
GS 8-10
PSA pre op>20
1992 TNM T3
PSA>20/T2c/GS>8
Nomo 5 yrPFP<50%
PSA>20/T3/GS>8
PSA>15/T2b/GS>8
PSAv>2ng/ml/yr
These results
suggest that
patients
diagnosed with
high-risk
cancers by
current
definitions do
not have a
uniformly poor
prognosis after
RP.
in patients with low and intermediate risk localized PCa (cT1a-T2b and GS 2-7 and PSA < 20 ng/mL) and life-expectancy > 10 years
Optional
Selected patients with low-volume, high-risk, localized PCa (cT3a or GS 8-10 or PSA > 20 ng/ mL), often in a multimodality setting
Highly selected patients with very-high-risk, localized PCa (cT3b-T4 N0 or any T N1) in the context of multimodality treatment.
Nerve-sparing surgery may be attempted in pre-operatively potent patients with low risk for extracapsular disease (T1c, GS < 7 and PSA < 10 ng/mL, or refer to Partin tables/nomograms)
Multiparametric MRI can help in deciding when to perform nerve-sparing procedures in intermediate- and high-risk disease
Recommendations for radical prostatectomy and eLND in low,
intermediate- and high-risk prostate cancer:
Complications:
• Erectile dysfunction (20-100%): depends mainly on the
quality of the nerve-sparing procedure. Even if NVB is spared,
elongation (neurotmesis) of the nerve occurs and re-enervation
will take about 8–9 months. Depending on age, the recovery is
about 60–75% for patients under 60, dropping to 45–50%
for patients over 65.
• Urinary Incontinence (4-70%)- the most disabling
complication. Pelvic floor exercises,if started before surgery,
are helpful.
• Stricture (0-12%)
• Bleeding
• Mortality (<1%)

Adjuvant
Radical
Palliative
EBRT- Conventional / Conformal
Brachytherapy
Types:
Adjuvant RT:
Indications:
Immediate- after RP with positive Sx margins,
SVI, poorly diff. ca (GS 8-10), LN mets
Delayed- ↑PSA level with no e/o distant mets,
clinically local recurrence and LN mets

50GY/25# f/b 10Gy/5# boost conventional


A LIMITATION OF THESE TRIAL: • PSA assay is now ultrasensitive, which can detect a PSA <0.01ng/ml. As an
example, ARO trial defned undetectable pSA lvel <0.1ng/ml, of which 59%
has PSA >.03-.1ng/ml.
• Thus a significant proportion of these enrolled has a measurable disease &
later received salvage RT.
• It has given rise to skepticism that active surveillance with PSA or early
initiation of RT when PSA showing upward trend has shown equivalent /better
results.
• there may be biochemical control and distant metastasis free survival(SWOG-
8794) may be compromised by waiting long time to intervene. KING et al
showed that every 0.1ng/ml increment in post op PSA there is an estimated
4% reduction in biochemical control.
The EORTC 22911,SWOG 8794, & ARO 96-02/AUO 09/95 provide consistent level 1 evidence that adjuvant Rt is
better than expectant management in terms of biochemical control, at an acceptable toxicity costs.
Adjuvant versus Salvage Radiotherapy
f in d in g s f r o m E O R T C 2 2 9 1 1 , S WO G 8 7 9 4 , a n d A R O 9 6 -0 2 / A U O 0 9 / 9 5 s t r o n g l y a d vo c a t e f o r t h e u s e o f A R T . Y e t n o n e o f t h e s e t r ia l s a d d r e s s t h e c o n c e p t o f e a r l y s a l va g e r a d io t h e r a p y g ive n w h e n t h e P S A is s t i l l l o w. S t e p h e n s o n e t a l . ( 1 1 8 ) r e p o r t e d o n t h e o u t c o m e s a n d p r o g n o s t ic
f a c t o r s o f 5 0 1 m e n w h o h a d s a l va g e r a d io t h e r a p y a f t e r a b io c h e m ic a l r e c u r r e n c e , developed a nomogram which includes PSA, PSADT, GS,ECE,LN metastasis,neoadjuvant hormones, RT dose SVI with PSA progression.
RADICALS is very important MRC led phase III trial two by three factorial
design trial.
It will question two issues:
Timing of RT(adj. RT/ early salvage RT – early biochemical failure is defined as
two consequetive rise in PSA & final PSA >0.1/ three consequetive rise in PSA)
Addition of hormone therapy to improve outcome.

PORT DOSE:Adjuvant 60-64 Gy & salvage 66-70
Gy is the current practice.
trial N=patients dose 5 yr biocem. RFS
DFS
Cozzarini et al 334 <70.2Gy vs70.2Gy
83%vs71%(p<0.001)
94%vs88%(p=0.005)
valicentti et al. 86 55-70.2 Gy 3 yrs PSA control better in >61.5 Gy arm(52 patients)-91% vs. 57%,p=0.01). Similar findings in the group >64.8 Gy.(pre RT PSA =0.2-2ng/ml) –(79%vs33%,p=0.02)


CONVENTIONAL EBRT PORTALS
• Field size :
• Superior border-L5-S1
• Inferior border- 1.5-2 cm distal to junction of prostatic and membranous urethra (lower border of ischialtuberosity)
• Lateral border- 1.5-2 cm lateral to bony pelvis
• Common iliac LN treated by 18X15 cm field
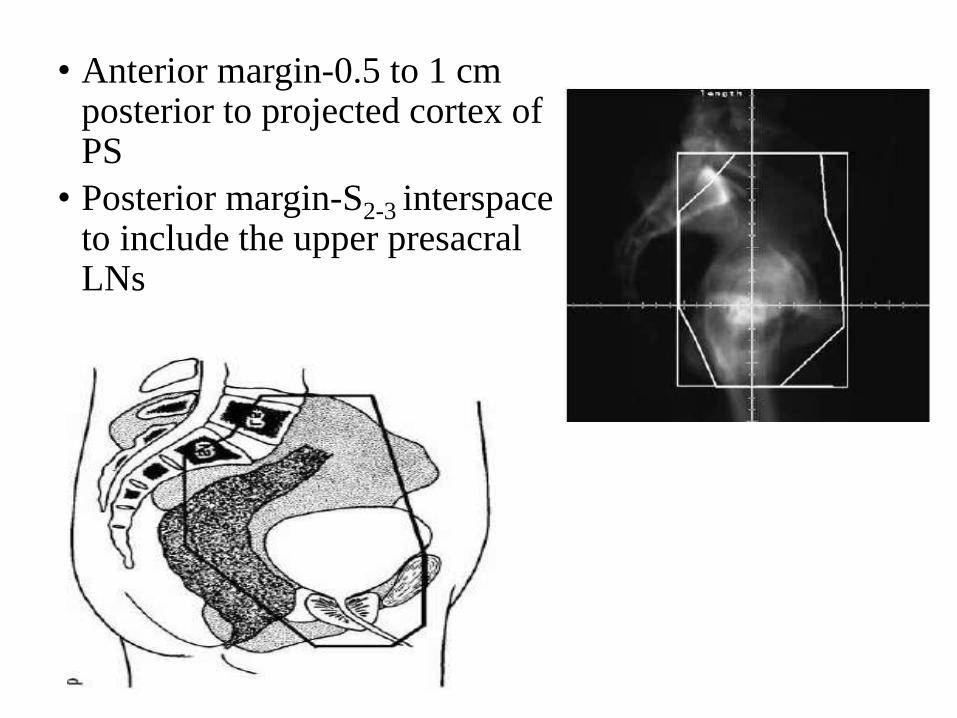
• Anterior margin-0.5 to 1 cm posterior to projected cortex of PS
• Posterior margin-S2-3 interspace to include the upper presacral LNs
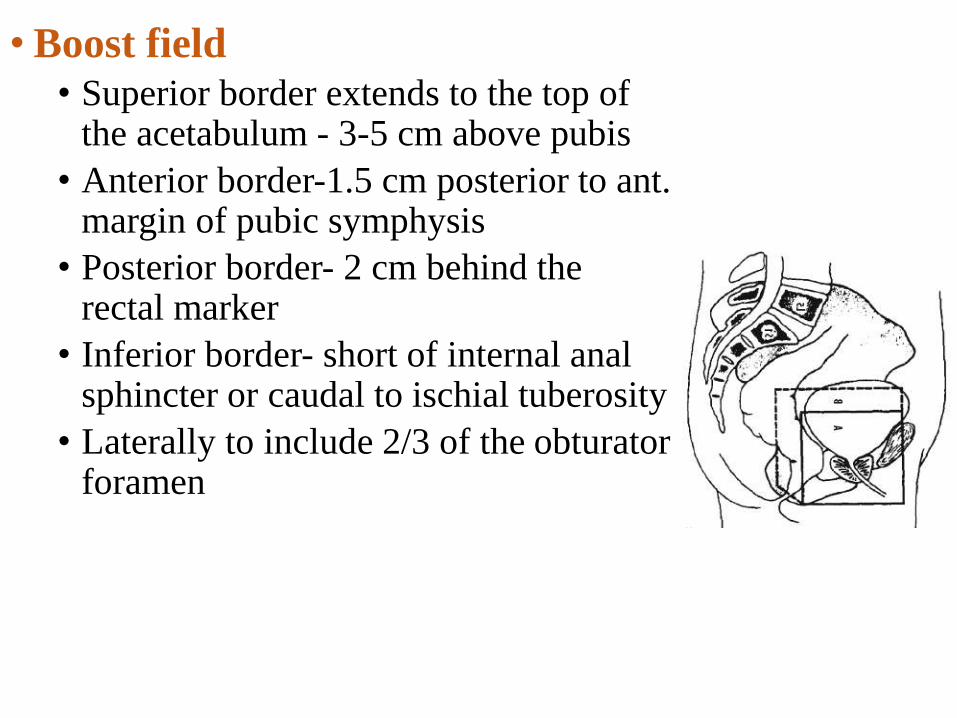
• Boost field
• Superior border extends to the top of the acetabulum - 3-5 cm above pubis
• Anterior border-1.5 cm posterior to ant. margin of pubic symphysis
• Posterior border- 2 cm behind the rectal marker
• Inferior border- short of internal anal sphincter or caudal to ischial tuberosity
• Laterally to include 2/3 of the obturatorforamen

CONFORMAL RT - 3DCRT
• CT-based images referenced to a reproducible patient position are used to localize the prostate and normal organs and to generate high-resolution 3D reconstructions of the patient
• Treatment field directions are selected using BEV techniques and the fields are shaped to conform to the patient's CT-defined target volume, thereby minimizing the volume of normal tissue irradiated
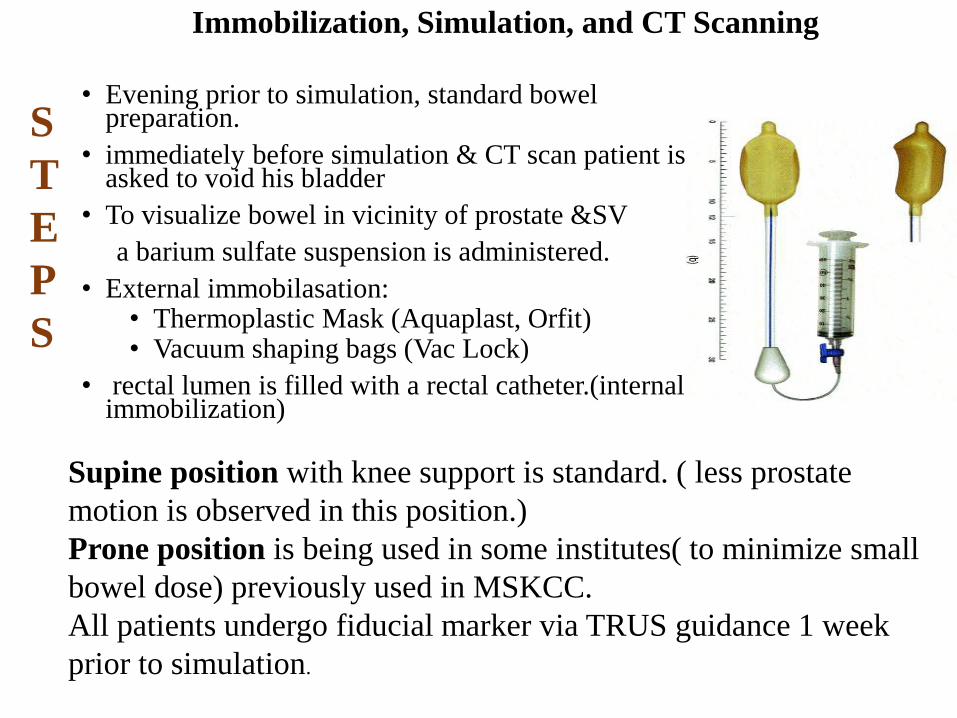
Immobilization, Simulation, and CT Scanning
• Evening prior to simulation, standard bowel preparation.
• immediately before simulation & CT scan patient is asked to void his bladder
• To visualize bowel in vicinity of prostate &SV
a barium sulfate suspension is administered.
• External immobilasation:• Thermoplastic Mask (Aquaplast, Orfit)• Vacuum shaping bags (Vac Lock)
• rectal lumen is filled with a rectal catheter.(internal immobilization)
S
T
E
P
S
Supine position with knee support is standard. ( less prostate
motion is observed in this position.)
Prone position is being used in some institutes( to minimize small
bowel dose) previously used in MSKCC.
All patients undergo fiducial marker via TRUS guidance 1 week
prior to simulation.
CT scan is taken around 20-30 cm around prostate with a slice spacing of 3 mm with the use of CT data a virtual simulation is performed using digitally reconstructed radiographs too localize the treatment area.
Isocenter placed according to anatomic landmarks near the center of the prostate gland: midline, at the caudal aspect, and ~ 5 cm posterior to the symphysis pubis.
The trianglution point for isocentre are then tattoed along with an additional tattoo aong the sagittal line , aprox. 10 cm superior to the isocentre.
To ensure the reproducible leg position to symphysis pubis, tattoos are placed on the back of legs at midshaft level,& the distance between the tattoos is recorded for future references.
• CTV=PROSTATE +SV
• PTV=CTV+MARGIN FOR SET UP ERROR +INTERFRACTIONAL+INTRAFRACTIONAL ORGAN MOTION.
At MSKCC a 1 cm margin is added to CTV except posteriorly at rectal interface 0.6 cm margin is added.
• OAR: Normal tissue is identified inner & outer walls of rectum & bladder femoral heads ,outer skin surface. Portions of small bowel / sigmoid bowel within 1 cm of PTV also contoured.
• The central 1 cm diameter of prostate is also considered for dosimetricconsideration in high dose IMRT planning.
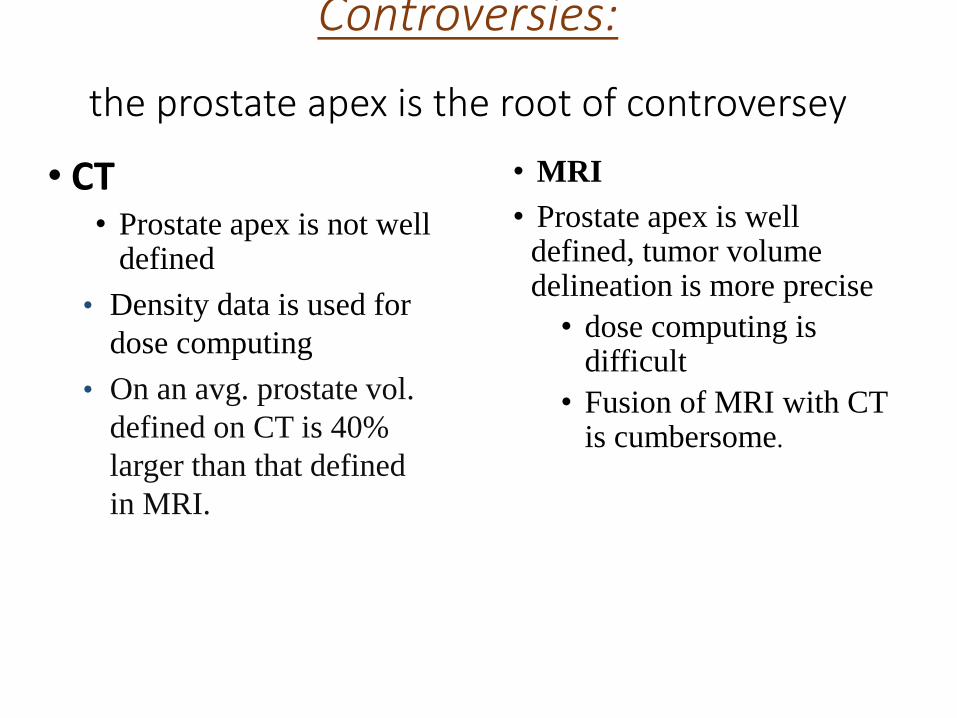
Controversies:
the prostate apex is the root of controversey
• CT• Prostate apex is not well
defined
• Density data is used for
dose computing
• On an avg. prostate vol.
defined on CT is 40%
larger than that defined
in MRI.is not well defined
• MRI
• Prostate apex is well defined, tumor volume delineation is more precise
• dose computing is difficult
• Fusion of MRI with CT is cumbersome.
• Urethrography at the time of simulation as a method to accurately localize the apex has been advocated by some and extensively studied .
• Algan et al. reviewed the location of the prostate apex in 17 patients for whom MRI scan, retrograde urethrogram & CT of the pelvis were obtained for 3D treatment planning. The location of the prostatic apex as determined by urethrogram alone was on an avg. 5.8 mm caudad to the location on MRI, whereas the location of the prostatic apex as determined by CT/Urethrogram was 3.1 mm caudad to that on MR.
• if the prostatic apex is defined as 12 mm instead of 10 mm above the urethrogram tip(junction of membranous and & prostaicurethra) the difference between the urethrogram and MRI location of Prostatic apex is removed.
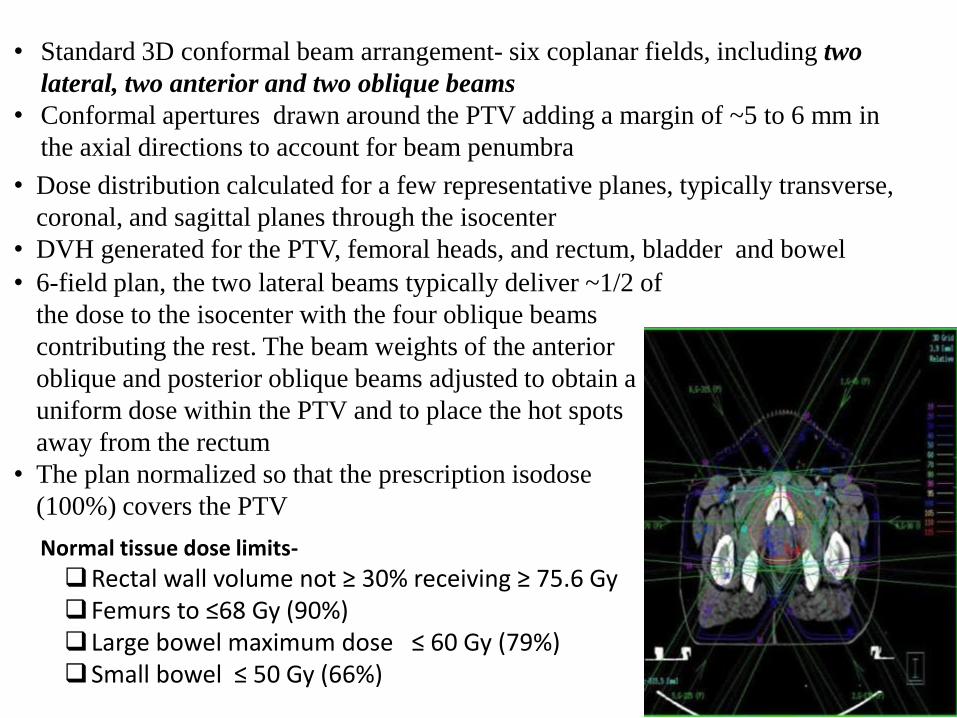
• Standard 3D conformal beam arrangement- six coplanar fields, including two
lateral, two anterior and two oblique beams
• Conformal apertures drawn around the PTV adding a margin of ~5 to 6 mm in
the axial directions to account for beam penumbra
• Dose distribution calculated for a few representative planes, typically transverse,
coronal, and sagittal planes through the isocenter
• DVH generated for the PTV, femoral heads, and rectum, bladder and bowel
• 6-field plan, the two lateral beams typically deliver ~1/2 of
the dose to the isocenter with the four oblique beams
contributing the rest. The beam weights of the anterior
oblique and posterior oblique beams adjusted to obtain a
uniform dose within the PTV and to place the hot spots
away from the rectum
• The plan normalized so that the prescription isodose
(100%) covers the PTV
Normal tissue dose limits-
Rectal wall volume not ≥ 30% receiving ≥ 75.6 Gy Femurs to ≤68 Gy (90%)Large bowel maximum dose ≤ 60 Gy (79%) Small bowel ≤ 50 Gy (66%)
IMRT
• It is a recent refinement of 3DCRT.
• Delivery of an IMRT: intensity pattern requires a computer-controlled beam-shaping apparatus on the linear accelerator known as MLC which consists of many small individually moving leaves or fingers that can create arbitrary beam shapes
• Static mode - “STEP AND SHOOT” which consists of multiple small, irregularly shaped fields delivered in sequence
• Dynamic mode - Dynamic multileaf collimation with the leaves moving during treatment to create the required irregular intensity patterns
• Defining dose ‘Constraints’ or ‘Objectives’ for the target and normal tissues, which describe the desired dose distribution in IMRT planning

I NTEN SI TY - MODULATED RADI ATION THERAPY FOR PROSTATE CANCER
GTV a d e n o c a r c i n o m a o f t h e p r o s t a t e i s n o t v i s u a l i z e d w e l l a n d t h e r ef o r e i s n o t c o n t o u r e d s e p a r a t e l y .
TARGET LOW RISK INTERMEDIATE RISK HIG RISK
CTV1 PROSTAE +/-PROXIMAL SEMINAL VESICLES(74GY)
PROSTATE +PROX. SEMINAL VESICLE(76-78GY)
PROSTATE=GROSS ETRACAPSULAR DISEASE &PROX.SEMINL VESICAL(76-78GY)
CTV2 -- DISTAL SEMINAL VESICALS(56 GY)
DISTAL SEMINAL VESICLES AND LN(56 GY)
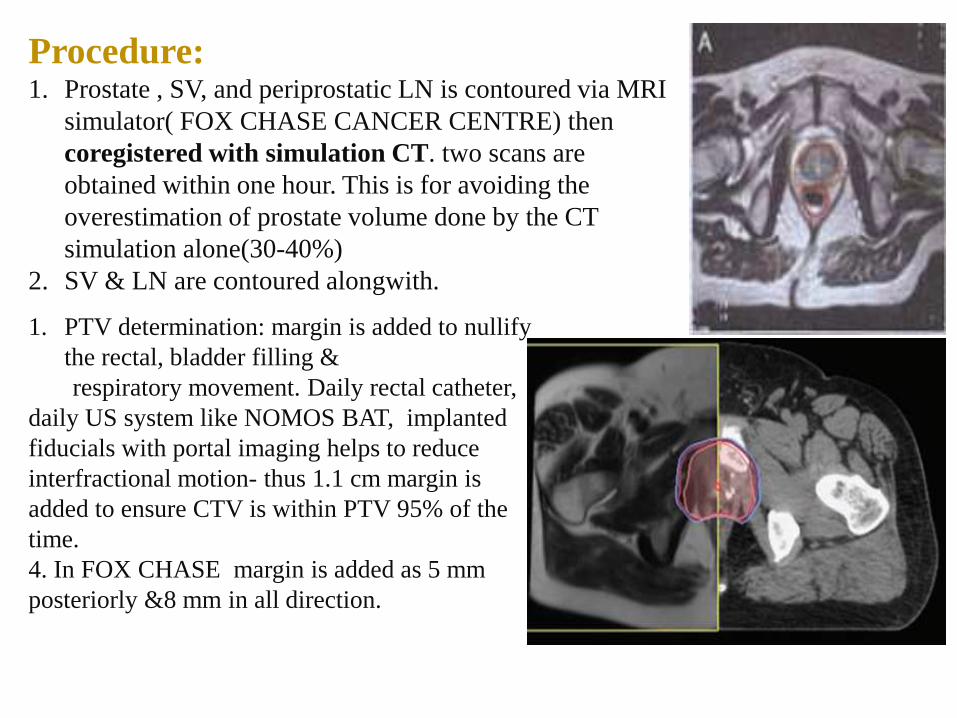
Procedure:1. Prostate , SV, and periprostatic LN is contoured via MRI
simulator( FOX CHASE CANCER CENTRE) then
coregistered with simulation CT. two scans are
obtained within one hour. This is for avoiding the
overestimation of prostate volume done by the CT
simulation alone(30-40%)
2. SV & LN are contoured alongwith.
1. PTV determination: margin is added to nullify
the rectal, bladder filling &
respiratory movement. Daily rectal catheter,
daily US system like NOMOS BAT, implanted
fiducials with portal imaging helps to reduce
interfractional motion- thus 1.1 cm margin is
added to ensure CTV is within PTV 95% of the
time.
4. In FOX CHASE margin is added as 5 mm
posteriorly &8 mm in all direction.

NORMAL TISSUE
DELINEATION:Entire rectum From ischial tuberosiy to upto
sigmoid colon is contoured with rectum empty.
At FOX CHASE patient is treated with bladder
half empty. It is because the US system is used for
daily localization as well as it reduces the bladder
dose. Bladder is contoured completely.
urethra , penile bulb or neurovascular bundle is
not contoured separately
NORMAL TISSUE DOSE CONSTRAINTS:The constarints used in FOXCHASE :
• rectum V 65≤ 17% / V 40≤ 35%
• bladder wall V65 ≤ 25% V40 ≤50%
• Femoral head V50 ≤10%
I n a d d i t i o n t o D V H a n a l y s e s , a s l i c e - b y - s l i c e ( a x i a l a n d s a g i t t a l)
a n a l y s i s o f t h e i s o d o s e l i n e s i s e s s e n t i a l t o e n s u r e t h a t t h e 9 0 %
i s o d o s e l i n e f a l l s w i t h i n t h e h a l f w i d t h m a r g i n o f t h e r e c t u m &
t h e 5 0 % i s o d o s e l i n e f a l l s w i t h i n t h e f u l l - w i d t h o f t h e r e c t u m on
a l l a x i a l s l i c e s.
ROLE OF IGRT
1. In the era of dose escalation and IMRT , set up errors became critical.
2. Thus following are new issues emerging:
a. inter and intra fractional motion of prostate .
b. Bony markers : is it sufficient for positional adjustment?
Schallenkamp et al. determined the movement of prostate as SI-9.1 mm/AP-
16.3mm/RL-15.2 mm
3. Use of fiducial gold markers and daily EPID is a strategy to improve the
planning system.
4. With a daily localization protocol, with a fiducial marker margin can be
reduced to 2.7mm(SI),2.9mm(AP),2.8 mm(RL) respectively
5. Interfractional 3D displacement of prostate and bony anatomy were 5.6
&4.4 prior to localization,2.8 &4.4 mm After post localization system.---thus
bony landmarks is not sufficient for accurate localization of the gland.
New systems invented:• CBCT-it is for online correction and it allows for soft tissue matching.
Invasive procedure can be avoided.
• Electromagnetic transponders: ( Calypso medical technology, Seattle):

• There have been no randomized studies comparing radical prostatectomy (RP)
with either external-beam radiotherapy (EBRT) or brachytherapy for localized
prostate cancer (PCa)
• Radiotherapy continues to be an important and valid alternative to surgery
alone for curative therapy.
• Intensity-modulated radiotherapy (IMRT), with or without image-guided
radiotherapy (IGRT), is the gold standard for EBRT
In addition to external irradiation, transperineal low-dose or high-dose rate
brachytherapy are widely used.
In localized and locally advanced PCa, several randomized phase III trials conducted
by the Radiation Therapy Oncology Group (RTOG) and European Organization for
Research and Treatment of Cancer (EORTC) have established the indications for the
combination of external irradiation and androgen deprivation therapy (ADT).
Thus issue are1. potential of RT in low risk vs. intermediate & high risk
disease.2. Dose escalation3. Addition of hormonal therapy ( in form of neoadjuvant/concurrent/adjuvant HT)& its duration

Outcome with EBRT in Low risk disease:
KUBAN ET AL. –large multi institutional study- 4,839 patients
T1-T2 ca- treated with EBRT from 1986 to 1995
70% treated with conventional EBRT , and rest by3DCRT
median f/u -6.3 yrs.
no ADT used
prescription dose:60-78 GY
overall 8 yr PSA
CONTROL rate:
PSA :0-4 80
4-9.9 60
10-20 40
>20 34
Higher
prescription dose
is associated with
significant
decrease in PSA
relapse but this is
more pronounced
in intermediate
and high risk
disease.
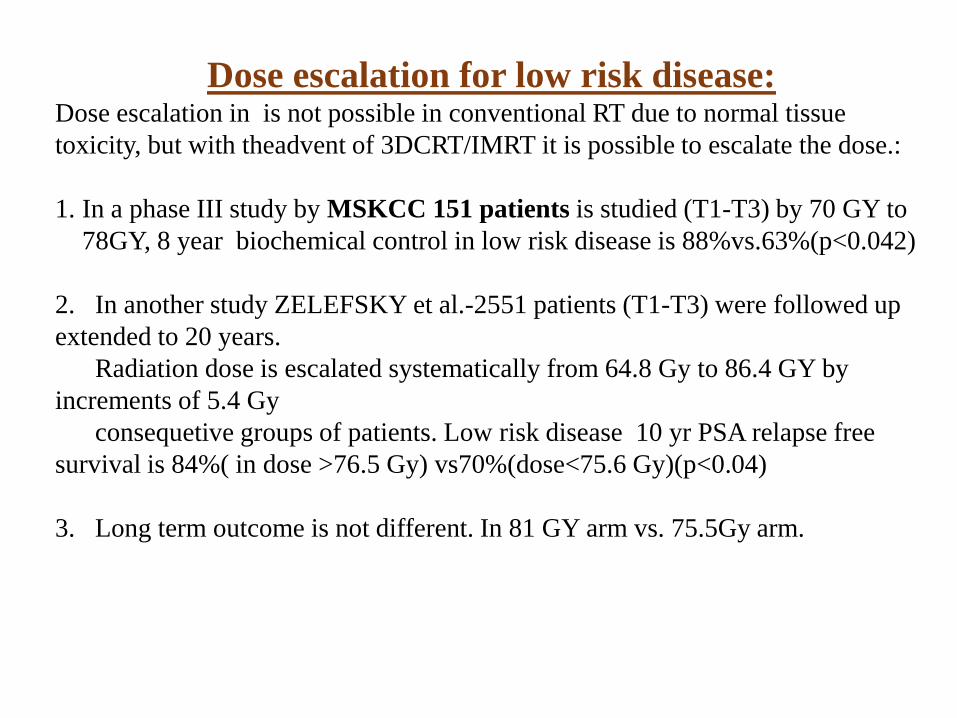
Dose escalation for low risk disease:Dose escalation in is not possible in conventional RT due to normal tissue
toxicity, but with theadvent of 3DCRT/IMRT it is possible to escalate the dose.:
1. In a phase III study by MSKCC 151 patients is studied (T1-T3) by 70 GY to
78GY, 8 year biochemical control in low risk disease is 88%vs.63%(p<0.042)
2. In another study ZELEFSKY et al.-2551 patients (T1-T3) were followed up
extended to 20 years.
Radiation dose is escalated systematically from 64.8 Gy to 86.4 GY by
increments of 5.4 Gy
consequetive groups of patients. Low risk disease 10 yr PSA relapse free
survival is 84%( in dose >76.5 Gy) vs70%(dose<75.6 Gy)(p<0.04)
3. Long term outcome is not different. In 81 GY arm vs. 75.5Gy arm.
Low
risk
disease
dose
escalati
on
trials

MD ANDERSON PROG-9509 MRC CKV096-10 GETUG06
Plan procedure
Conventional 3DCRT f/b proton
Conventional f/b conformal
3dcrt 3DCRT
DOSE 70 VS. 78 With ConformalBoost
50.4Gy f/b19.8Gy eqvs.28.8GY eq proton
64Gy vs.74 Gy 68Gy vs.78Gy 70GY vs.80Gy
HORMONE
NO ADT No ADT NADT-3-6months
Permitted acc. To doctors
Not used
MEDIAN F/U
9 YRS 8.9 yrs 63 months 70 months 61 months
5 yrbiochemical control
Superior(11% difference)
Results in favor of dose escalation
10 YR PSA Control
74%VS.43% 68%vs.82.6%
GU toxicity
same Same 80Gy arm
OS No difference No difference

MDANDERSON
PROG-9509 MRC CKV096-10
GETUG06 ZELEFSKY ET AL. PHASE I/II
Plan procedure
Conventional 3DCRT f/b proton Conventional f/b conformal
3dcrt 3DCRT 3DCRT/IMRT
DOSE 70 VS. 78 With ConformalBoost
50.4Gy f/b19.8Gy eqvs.28.8GY eqproton
64Gy vs.74 Gy
68Gy vs.78Gy
70GY vs.80Gy
66Gy VS.864Gy
HORMONE NO ADT NADT-3-6months
Permitted acc. To doctors
Not used NADT
MEDIAN F/U
9 YRS 63 months 70 months
61 months 6.6YRS
5 yrbiochemical control
superior HIGH RISK GROUP
10 YR PSA Control
74%VS.43% 68%vs.82.6%
GU toxicity same Same 80Gy arm URETHRAL STRICTURE1.5%/GRADE 2 13%
OS No difference No difference
Despite of using hormone in MRC & CKV096-10 study even using
hormones does not nullify the use of high dose.
Recently a RTOG trial 0815 has been started to evaluate addition of 6
month androgen blockade with dose escalation RT (45 Gy to prostate
and SV)by either 3DCRT /IMRT combined low dose rate (110 Gy iodine
125/100 GY Pd 103) brachytherapy boost or high dose brachytherapy
boost 10.5Gy/#such 2#.
RT dose to Prostate should be 70-75 Gy in low-risk pts and 75-80 Gy in intermediate and high-risk pts are appropriate for tumor control.
RT dose to Pelvic LN should be 45 Gy for elective LN radiation and 55-60 Gy for involved LN in pts with high-risk group.
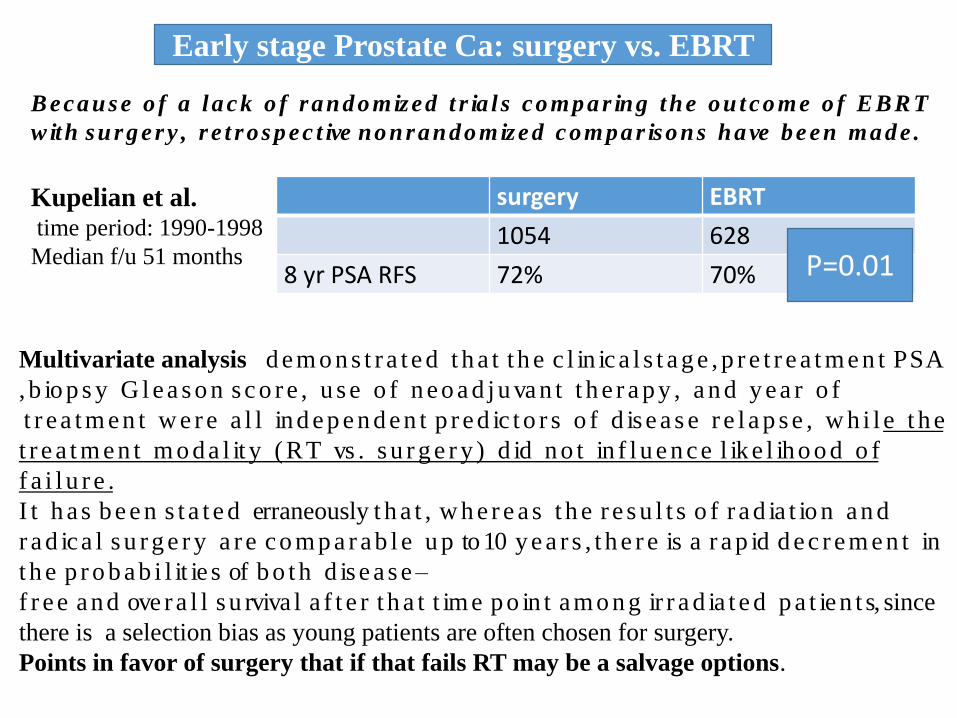
Early stage Prostate Ca: surgery vs. EBRT
surgery EBRT
1054 628
8 yr PSA RFS 72% 70%
Kupelian et al.time period: 1990-1998
Median f/u 51 months P=0.01
Multivariate analysis d e m o n s t r a t e d t h a t t h e c l in ic a l s t a g e , p r e t r e a t m e n t P S A
, b io p s y G l e a s o n s c o r e , u s e o f n e o a d j u va n t t h e r a p y , a n d y e a r o f
t r e a t m e n t w e r e a l l in d e p e n d e n t p r e d ic t o r s o f d is e a s e r e l a p s e , w h i l e t h e
t r e a t m e n t m o d a l it y ( R T vs . s u r g e r y ) d id n o t in f l u e n c e l ik e l ih o o d o f
f a i l u r e .
I t h a s b e e n s t a t e d erraneously t h a t , w h e r e a s t h e r e s u l t s o f r a d ia t io n a n d
r a d ic a l s u r g e r y a r e c o m p a r a b l e u p to 10 y e a r s , t h e r e is a r a p id d e c r e m e n t in
t h e p r o b a b i l it ie s of b o t h d is e a s e –
f r e e a n d ove r a l l s u rviva l a f t e r t h a t t im e p o in t a m o n g ir r a d ia t e d p a t ie n t s, since
there is a selection bias as young patients are often chosen for surgery.
Points in favor of surgery that if that fails RT may be a salvage options.
B e c a u s e o f a l a c k o f r a n d o m iz e d t r ia l s c o m p a r in g t h e o u t c o m e o f E BR T
w it h s u r g e r y , r e t r o s p e c t ive n o n r a n d o m iz e d c o m p a r is o n s h a ve b e e n m a d e .
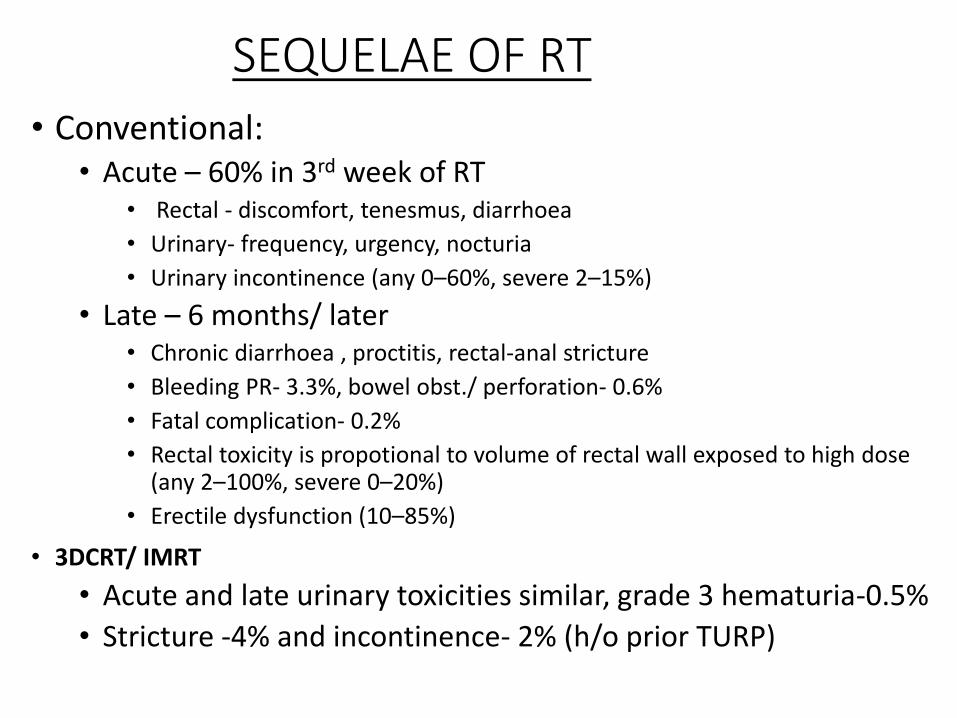
SEQUELAE OF RT
• Conventional:• Acute – 60% in 3rd week of RT
• Rectal - discomfort, tenesmus, diarrhoea
• Urinary- frequency, urgency, nocturia
• Urinary incontinence (any 0–60%, severe 2–15%)
• Late – 6 months/ later • Chronic diarrhoea , proctitis, rectal-anal stricture
• Bleeding PR- 3.3%, bowel obst./ perforation- 0.6%
• Fatal complication- 0.2%
• Rectal toxicity is propotional to volume of rectal wall exposed to high dose (any 2–100%, severe 0–20%)
• Erectile dysfunction (10–85%)
• 3DCRT/ IMRT
• Acute and late urinary toxicities similar, grade 3 hematuria-0.5%
• Stricture -4% and incontinence- 2% (h/o prior TURP)


PROSTATE SEED IMPLANTS:
Mainly plays a role in early stage cancers either alone /as after EBRT.
Types: 1. temporary (gold-198)
2.permanent(iodine-125,pd-103)
Permanent implants: 1980 onwards trans perineal approach is
taken.(advantage: TRUS, OPD basis, spinal anaesthesia is required.)
General Inclusion Criteria:
• Life expectancy > 5 years
• Clinical stage -T1b-T2c and selected
T3
• Gleason score -2-10
• PSA -In almost all cases, a PSA ≤50
ng/mL
• No pathologic evidence of pelvic
lymph node involvement
• No distant metastases
Exclusion Criteria:
• Relative contraindications:
o Severe urinary irritative/obstructive
symptomatology
o Extensive TURP defect
o Substantial median lobe hyperplasia
o Prostate dimensions larger than the grid (i.e., >
60 mm in width and > 50 mm in height)
o Severe pubic arch interference
o Gross seminal vesicle involvement
o Prior pelvic radiotherapy
o Inflammatory bowel disease
o Pathologic involvement of pelvic lymph nodes• Absolute contraindications:
o Distant metastases
o Life expectancy < 5 years
Patient Selection Criteria:
• Monotherapy:
o Clinical stage T1b-T2b and Gleason score ≤6 and PSA ≤10 ng/mL
o Seleced higher risk patients
o Salvage of selected radiation therapy failures
• Boost:
o ≥clinical stage T2c and/or Gleason score ≥7 and/or PSA > 10 ng/mL
• Special clinical situations:
o Inadequate information exists to recommend supplemental XRT
based on perineural invasion, percent positive biopsies and/or MRI-
detected extracapsular penetration

IODINE125 PALLADIUM103
T1/2 (days) 59.4 16.97
Energy(keV) 27.4 21
Form Seeds Seeds
Implant type Permanent Permanent
Dose rate 7 19
Meanactivity/seed
0.42 1.3
Monotherapy dose
145Gy mPD 125Gy mPD
+EBRT dose 110Gy mPD 100Gy mPD
TVL(mm) Pb 0.01 0.03
• A randomized trial
shows no different
between two arms
using two different
isotopes.
• Pd induced radiation
prostatitis is higher than
I 125 but it also recover
sooner than that.
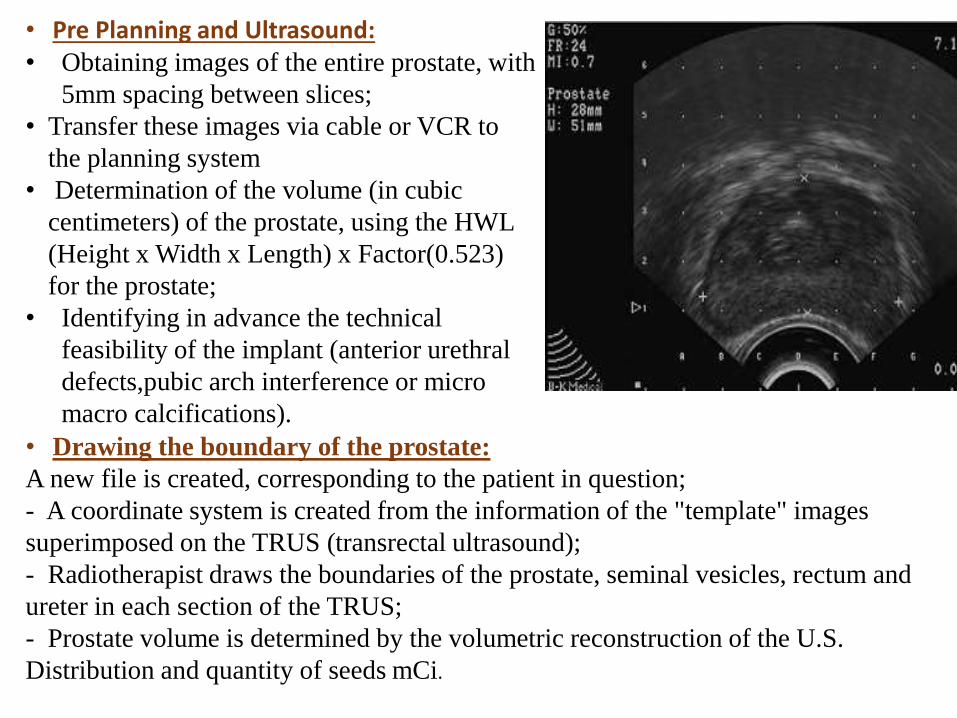
• Pre Planning and Ultrasound:• Obtaining images of the entire prostate, with
5mm spacing between slices;
• Transfer these images via cable or VCR to
the planning system
• Determination of the volume (in cubic
centimeters) of the prostate, using the HWL
(Height x Width x Length) x Factor(0.523)
for the prostate;
• Identifying in advance the technical
feasibility of the implant (anterior urethral
defects,pubic arch interference or micro
macro calcifications).
• Drawing the boundary of the prostate:
A new file is created, corresponding to the patient in question;
- A coordinate system is created from the information of the "template" images
superimposed on the TRUS (transrectal ultrasound);
- Radiotherapist draws the boundaries of the prostate, seminal vesicles, rectum and
ureter in each section of the TRUS;
- Prostate volume is determined by the volumetric reconstruction of the U.S.
Distribution and quantity of seeds mCi.
• Preparation of material for the implant:The charge physicist needs to control and verify the seeds that reach for each patient.
It is recommended that the physicist verify at least 10% of the batch using a well
chamber and the measure has a limit of 5% difference between the measured activity
and the certificate.
• Standards for sterilization of seeds:The seeds are sterilized in an autoclave system the temperature of 121 centigrade
and a pressure of 15 psi for 15 to 30 minutes, or the temperature of 133 Centigrade
and pressure of 30 psi for about 3 minutes (“flash”).
- After sterilization, using Geiger monitor to check radioactivity inside of the
autoclave.
• Positioning the patient on the table:supine and lithotomy position with legs flexed according to the survey pre-planning.
• Anesthesia, monitoring and premedication

Images of the prostate via ultrasound - Choose the largest cross section of the prostate, by transrectal ultrasound, as the target volume. - Transrectal ultrasound images has a 5 mm separation of each other, and each image is overlap with the image developed by the planning system. It is used to call this planing image as a TEMPLATE IMAGE. - Transfer images to the planning system identifying the prostate, urethra and rectum. - Revaluate of prostate volume and calculating the number of seeds and needles.
Insertion of needles and seeds - Insertion of the needles is by the urologist, according to the shape and size of the prostate and activity of the seeds under the guidance of radiotherapist. - Identify of each needle in the template and each length to be loaded; - Insert of two needles, via trans perineum, approximately 1 to 1.2 cm in the direction of the urethra after 4 and 8 hours as stabilizers.

Put the needle on the edge first and place them top to bottom. - Check the positioning of each needle with sagittal images of the ultrasound. - The needles placed in the periphery are spaced between 0.5 to 1.0 cm and 0.5 cm inside the periphery of the prostate. The typical number of needles in the periphery is 9 to12 needles. - The needles placed in the "Line 1" (the lowest) are separated by 1.0 cm and about 0.5 cm from the anterior rectal wall mucosa. - The needles in the central region of the prostate are placed at least 1.0 cm apart from the urethra. The typical number of needles in the central region is 3 to 5. - The standard distribution of the loads is 75% -80% of the total activity in the periphery and 20% -25% in the center.
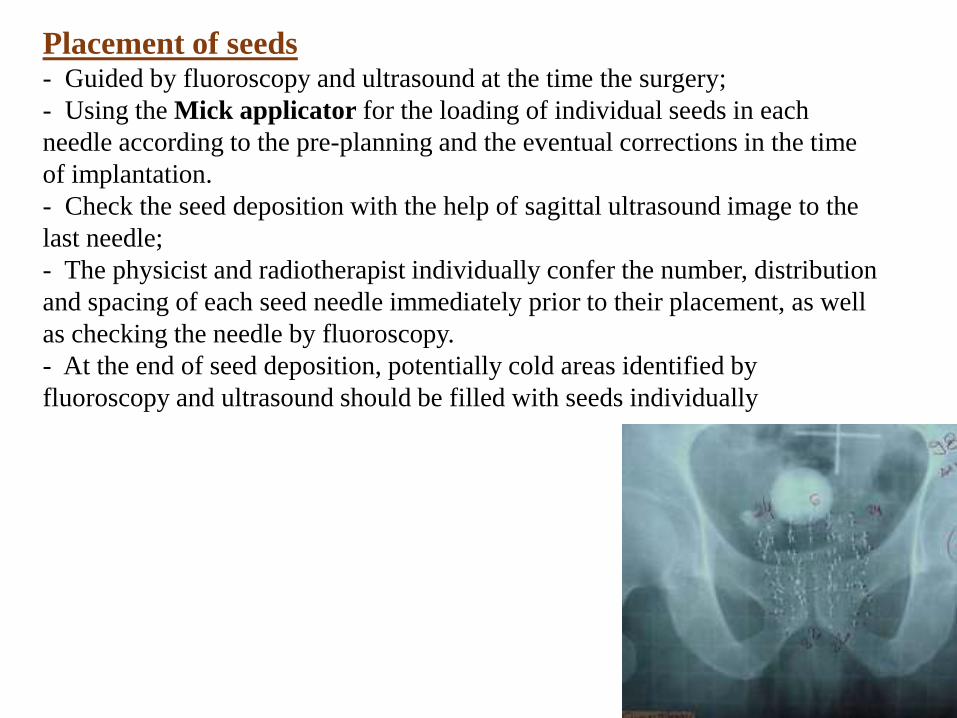
Placement of seeds - Guided by fluoroscopy and ultrasound at the time the surgery;
- Using the Mick applicator for the loading of individual seeds in each
needle according to the pre-planning and the eventual corrections in the time
of implantation.
- Check the seed deposition with the help of sagittal ultrasound image to the
last needle;
- The physicist and radiotherapist individually confer the number, distribution
and spacing of each seed needle immediately prior to their placement, as well
as checking the needle by fluoroscopy.
- At the end of seed deposition, potentially cold areas identified by
fluoroscopy and ultrasound should be filled with seeds individually
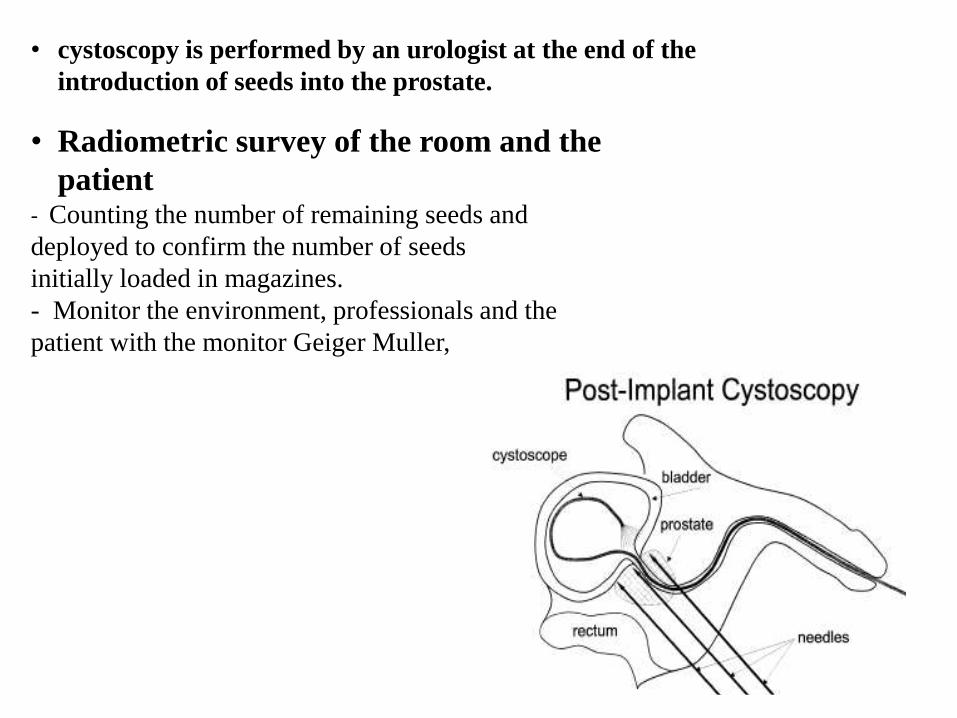
• cystoscopy is performed by an urologist at the end of the
introduction of seeds into the prostate.
• Radiometric survey of the room and the
patient - Counting the number of remaining seeds and
deployed to confirm the number of seeds
initially loaded in magazines.
- Monitor the environment, professionals and the
patient with the monitor Geiger Muller,
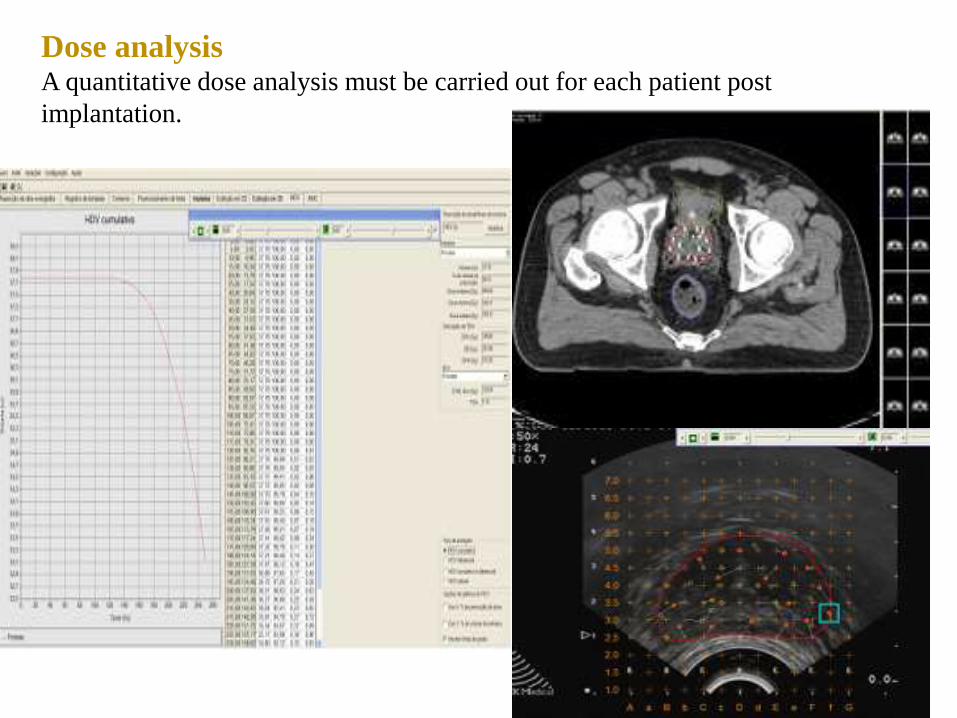
Dose analysis A quantitative dose analysis must be carried out for each patient post
implantation.
Prescribed dose 1. The recommended prescription doses for Iodine-125 are 145 Gy and 110 Gy for
monotherapy and boost implants, respectively.
2.The prescription of minimum peripheral dose (mPD) is intended to cover the CTV,
and is the reference dose for the treatment.
3.X-ray CT examination is performed immediately after implant and 3 to 5 weeks
after.
4.The patient is scanned in a supine position usually with bladder contrasting. Slices with
thickness of 3 mm or less are acquired from 2 cm cephalad to the base of the gland to
2 cm caudad to the apex.
5.All of the seeds used in the implant should be encompassed in the scan.
6.ETVs (-Evaluation Treatment Volume) are determined from this scan, as the location of
the urethra and the rectum.
7.Due to the difficulty in CT visualization of the urethra, use of Foley catheterization is
strongly recommended.
8. The urethra and the rectum contours are drawn as the outer surface of the Foley
catheter and the rectal wall, respectively.
9. The CT images are used to create a post-implant treatment plan (post plan). An AP
or anterior oblique pelvic radiograph is used to verify the number of sources and this will
be recorded.
10. A surview chest CT image is obtained to check any pulmonary migration of the
source.
Post-Treatment Evaluation• Biochemical assessment:
Serial PSA determinations – baseline at 3-6 months and then every 6
months and/or as per institutional protocol
• Physical examination: Role of routine DRE is controversial
• Quality of Life: Urinary, bowel, and sexual function should be
prospectively assessed
• Post-Treatment Biopsy: Should be reserved for protocol settings or in
clinical situations where salvage local therapy is being considered
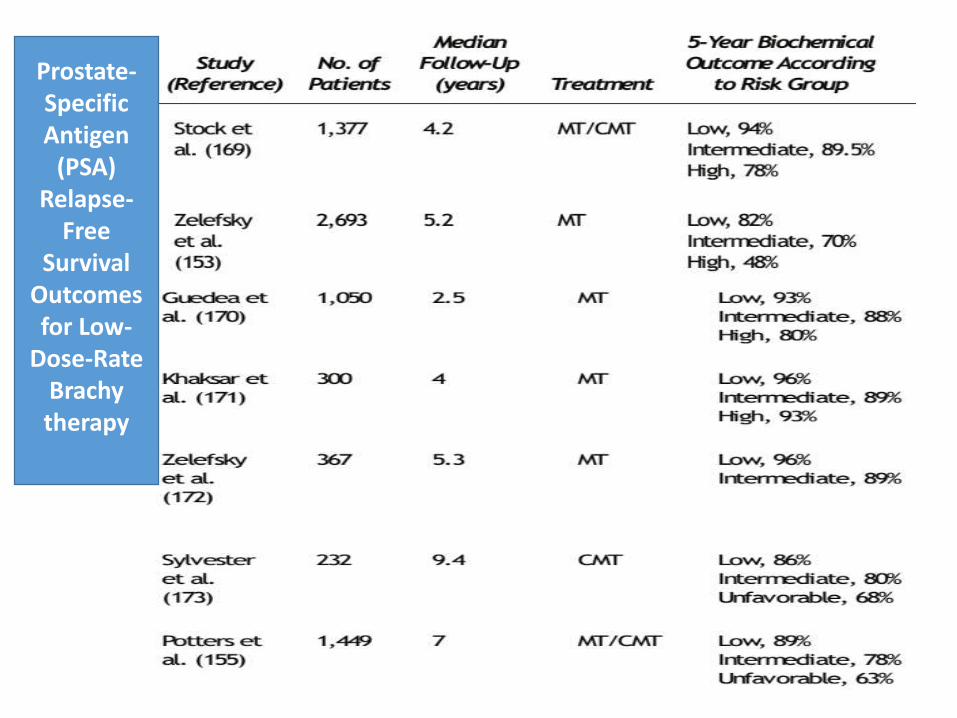
Prostate-Specific Antigen
(PSA) Relapse-
Free Survival
Outcomes for Low-
Dose-Rate Brachytherapy

General Inclusion Criteria: • Clinical Stage T1-T3b and selected T4
• Gleason score 2-10
• PSA No upper limit, but in almost all cases, patient does not
have documented distant metastasis (TxN0M0)
Exclusion Criteria: Relative Contraindications • Severe urinary obstructive symptoms • Extensive TURP defect or TURP within 6 month • Collagen vascular disease
Absolute Contraindications • Unable to undergo anesthesia (general, spinal, epidural, or local) • Unable to lay flat
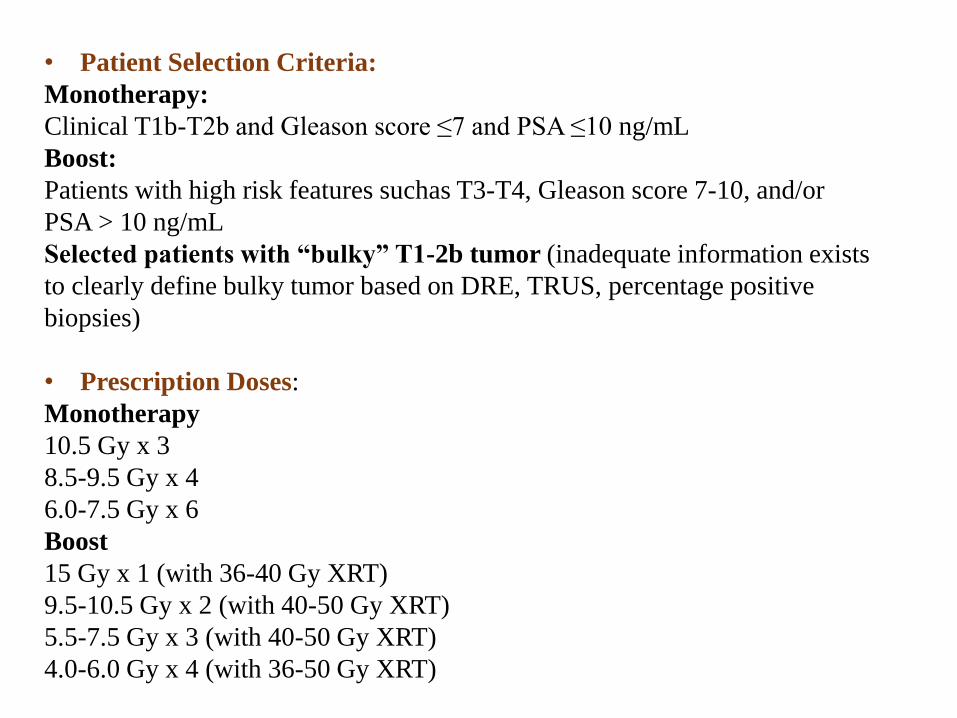
• Patient Selection Criteria:
Monotherapy:
Clinical T1b-T2b and Gleason score ≤7 and PSA ≤10 ng/mL
Boost:
Patients with high risk features suchas T3-T4, Gleason score 7-10, and/or
PSA > 10 ng/mL
Selected patients with “bulky” T1-2b tumor (inadequate information exists
to clearly define bulky tumor based on DRE, TRUS, percentage positive
biopsies)
• Prescription Doses:
Monotherapy
10.5 Gy x 3
8.5-9.5 Gy x 4
6.0-7.5 Gy x 6
Boost
15 Gy x 1 (with 36-40 Gy XRT)
9.5-10.5 Gy x 2 (with 40-50 Gy XRT)
5.5-7.5 Gy x 3 (with 40-50 Gy XRT)
4.0-6.0 Gy x 4 (with 36-50 Gy XRT)

HDR brachytherapy implants are template-based and performed under general or spinal
anesthesia with the patient in lithotomy position, similar to LDR. Comparatively, HDR has a
number of patient- and target-specific advantages over LDR therapy.
They are summarized below:
(1) overall treatment time reduction
(2) HDR -improved accuracy of needle placement and radiation dose distribution
through the use of intraoperative optimization software
(3) modulation of dwell times as well as the dwell positions for precise and
accurate 3D spatial dose coverage.
(4) This “dose sculpting” capability of HDR eliminates inherent dose
inhomogeneities for potentially increased tumor control while limiting OAR doses,
and thus toxicities.
(5) From a radiobiology perspective, HDR may be favored as treatment delivery over
a period of minutes, instead of weeks to months, does not allow malignant cells to
repopulate, advance through the cell cycle, or recover from sublethal damage.
Likewise, studies showed that if prostate cancer alpha/beta is low, in the range of 1.2–
4, HDR biological effectiveness is higher than with LDR or EBRT.
(6) single radioactive source --minimizing costs.
(7)From a radiation safety perspective, in patients do not need to follow special
precautions such as limiting distance or duration of contact with another individual,
children, or pregnant women as is necessary with LDR patients.

MECHANISMS OF ANDROGEN AXIS BLOCKADE
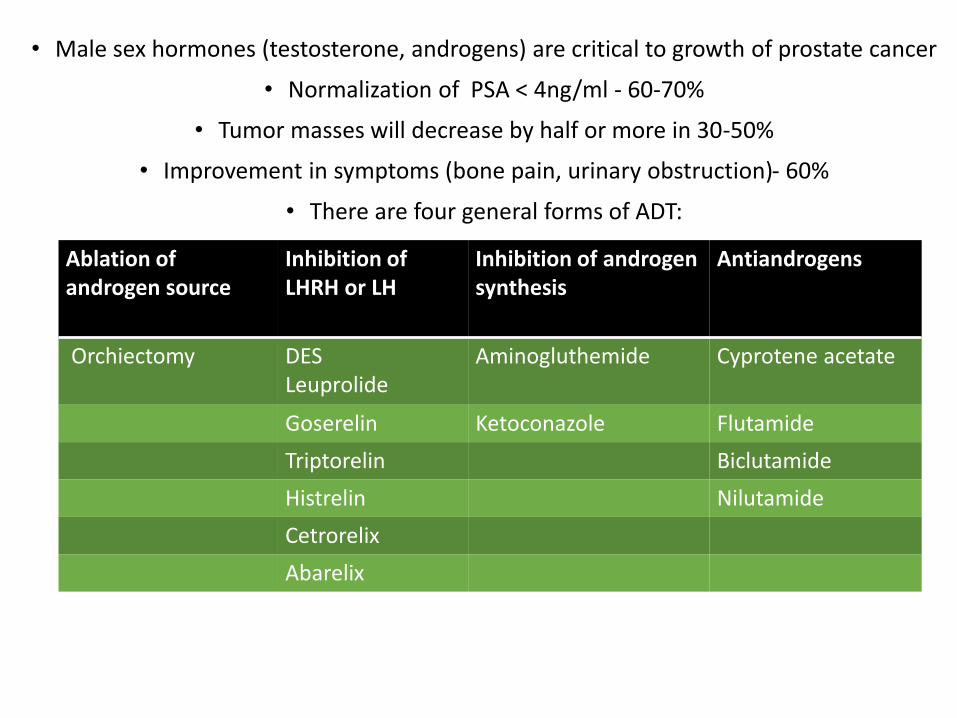
• Male sex hormones (testosterone, androgens) are critical to growth of prostate cancer
• Normalization of PSA < 4ng/ml - 60-70%
• Tumor masses will decrease by half or more in 30-50%
• Improvement in symptoms (bone pain, urinary obstruction)- 60%
• There are four general forms of ADT:
Ablation of androgen source
Inhibition of LHRH or LH
Inhibition of androgen synthesis
Antiandrogens
Orchiectomy DESLeuprolide
Aminogluthemide Cyprotene acetate
Goserelin Ketoconazole Flutamide
Triptorelin Biclutamide
Histrelin Nilutamide
Cetrorelix
Abarelix
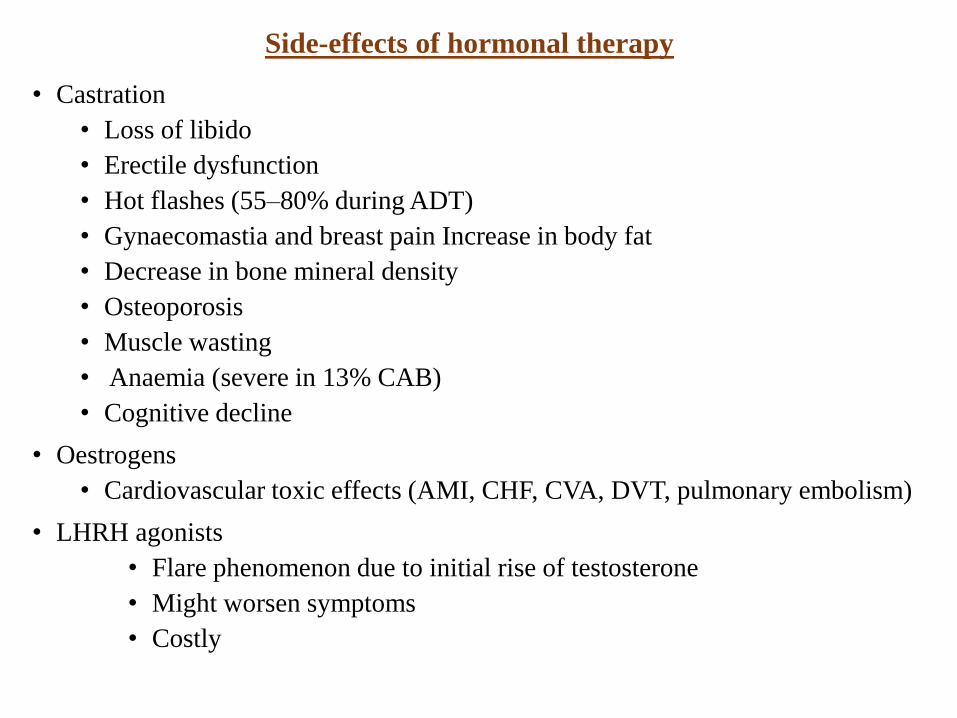
Side-effects of hormonal therapy
• Castration
• Loss of libido
• Erectile dysfunction
• Hot flashes (55–80% during ADT)
• Gynaecomastia and breast pain Increase in body fat
• Decrease in bone mineral density
• Osteoporosis
• Muscle wasting
• Anaemia (severe in 13% CAB)
• Cognitive decline
• Oestrogens
• Cardiovascular toxic effects (AMI, CHF, CVA, DVT, pulmonary embolism)
• LHRH agonists
• Flare phenomenon due to initial rise of testosterone
• Might worsen symptoms
• Costly
• NEOADJUVANT OR ADJUVANT HORMONE THERAPY PLUS RADIOTHERAPY
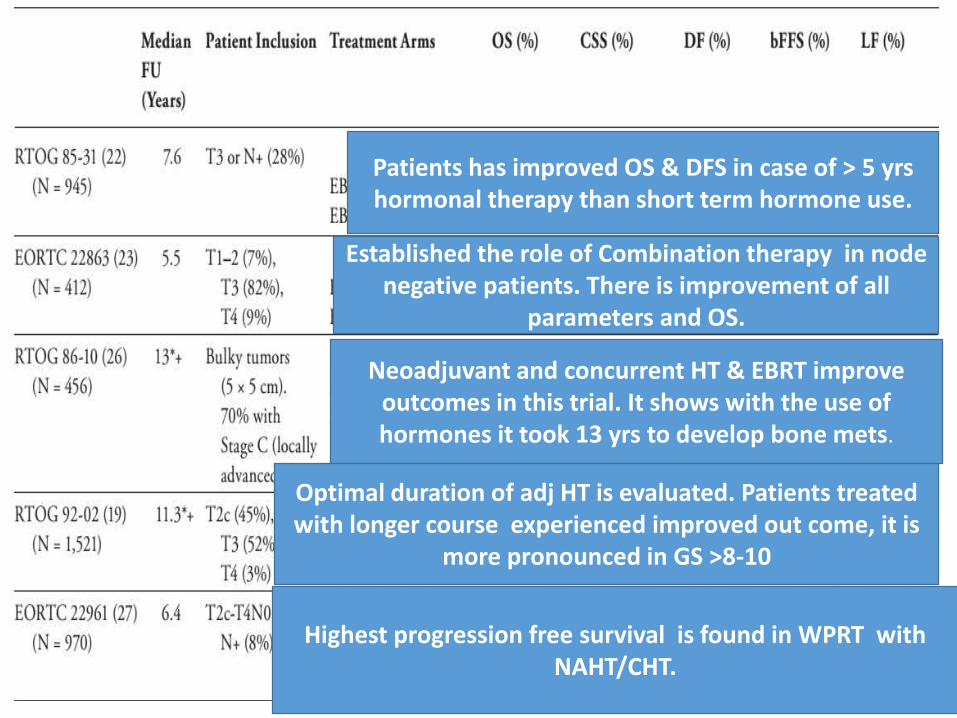
Patients has improved OS & DFS in case of > 5 yrshormonal therapy than short term hormone use.
Established the role of Combination therapy in node negative patients. There is improvement of all
parameters and OS.
Neoadjuvant and concurrent HT & EBRT improve outcomes in this trial. It shows with the use of hormones it took 13 yrs to develop bone mets.
Optimal duration of adj HT is evaluated. Patients treated with longer course experienced improved out come, it is
more pronounced in GS >8-10
Highest progression free survival is found in WPRT with NAHT/CHT.

TRIALS N STAGE NADT ADT OS PCS
TROG 818 T2b-T4N0M0
3 MONTHS VS.6 MONTHS
- IMPROVED
IMPROVED
RTOG9413
1554 T2c-T4 4 MONTHS 4+ 24 MONTHS
ONLY IN GS>8-10
IMPROVED
Duration of adjuvant or neoadjuvant ADT in combination with RT
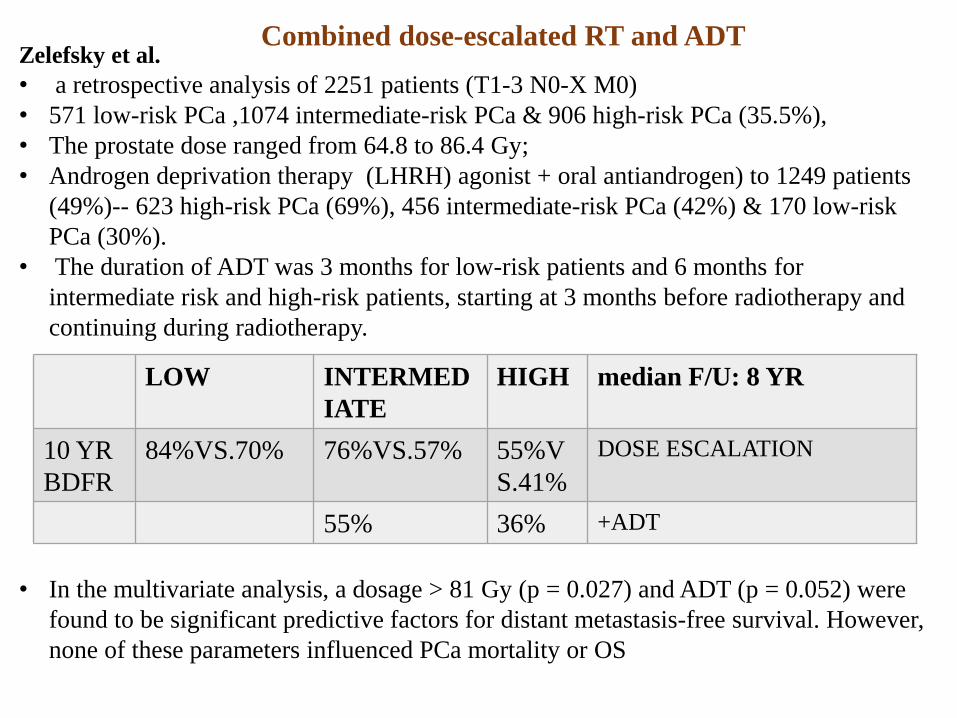
Zelefsky et al.
• a retrospective analysis of 2251 patients (T1-3 N0-X M0)
• 571 low-risk PCa ,1074 intermediate-risk PCa & 906 high-risk PCa (35.5%),
• The prostate dose ranged from 64.8 to 86.4 Gy;
• Androgen deprivation therapy (LHRH) agonist + oral antiandrogen) to 1249 patients
(49%)-- 623 high-risk PCa (69%), 456 intermediate-risk PCa (42%) & 170 low-risk
PCa (30%).
• The duration of ADT was 3 months for low-risk patients and 6 months for
intermediate risk and high-risk patients, starting at 3 months before radiotherapy and
continuing during radiotherapy.
• In the multivariate analysis, a dosage > 81 Gy (p = 0.027) and ADT (p = 0.052) were
found to be significant predictive factors for distant metastasis-free survival. However,
none of these parameters influenced PCa mortality or OS
LOW INTERMED
IATE
HIGH median F/U: 8 YR
10 YR
BDFR
84%VS.70% 76%VS.57% 55%V
S.41%
DOSE ESCALATION
55% 36% +ADT
Combined dose-escalated RT and ADT
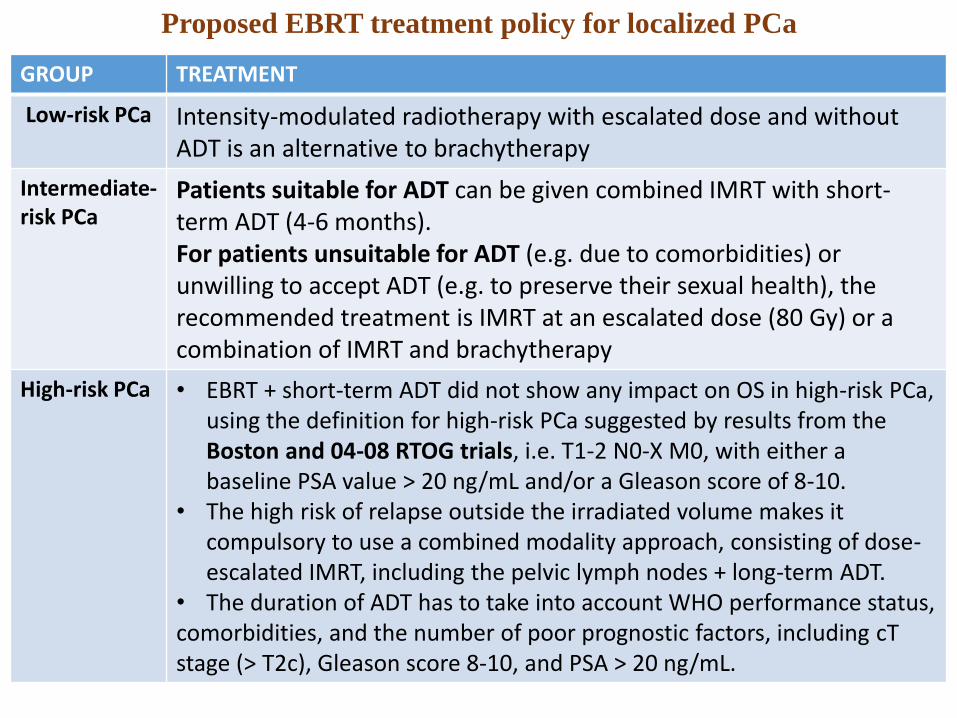
Proposed EBRT treatment policy for localized PCa
GROUP TREATMENT
Low-risk PCa Intensity-modulated radiotherapy with escalated dose and without ADT is an alternative to brachytherapy
Intermediate-risk PCa
Patients suitable for ADT can be given combined IMRT with short-term ADT (4-6 months).For patients unsuitable for ADT (e.g. due to comorbidities) or unwilling to accept ADT (e.g. to preserve their sexual health), the recommended treatment is IMRT at an escalated dose (80 Gy) or a combination of IMRT and brachytherapy
High-risk PCa • EBRT + short-term ADT did not show any impact on OS in high-risk PCa, using the definition for high-risk PCa suggested by results from the Boston and 04-08 RTOG trials, i.e. T1-2 N0-X M0, with either a baseline PSA value > 20 ng/mL and/or a Gleason score of 8-10.
• The high risk of relapse outside the irradiated volume makes it compulsory to use a combined modality approach, consisting of dose-escalated IMRT, including the pelvic lymph nodes + long-term ADT.
• The duration of ADT has to take into account WHO performance status, comorbidities, and the number of poor prognostic factors, including cTstage (> T2c), Gleason score 8-10, and PSA > 20 ng/mL.

The role of radiotherapy in locally advanced PCa: T3-4 N0, M0
The results of radiotherapy alone are very poor.
three trials have established that, in locally advanced disease, radiotherapy is
effective and that combined radiotherapy + ADT is clearly superior to ADT alone
NO. STAGE T/t PCSM OS DFS METS.DFS
LOCOREGIONAL PFS
MRCPR3-PR07
1057 T34/T2,PSA>20/GS>8
Lifelong ADT±RT
DECREASE BY 46%
GETUG 273 T3-T4/Pt3N0m0
-Lifelong ADT±RT
NA SIGNIFICAT IMPROVEMENT.
SFUO3/SPCG7
439 23.9%VS.11..9%
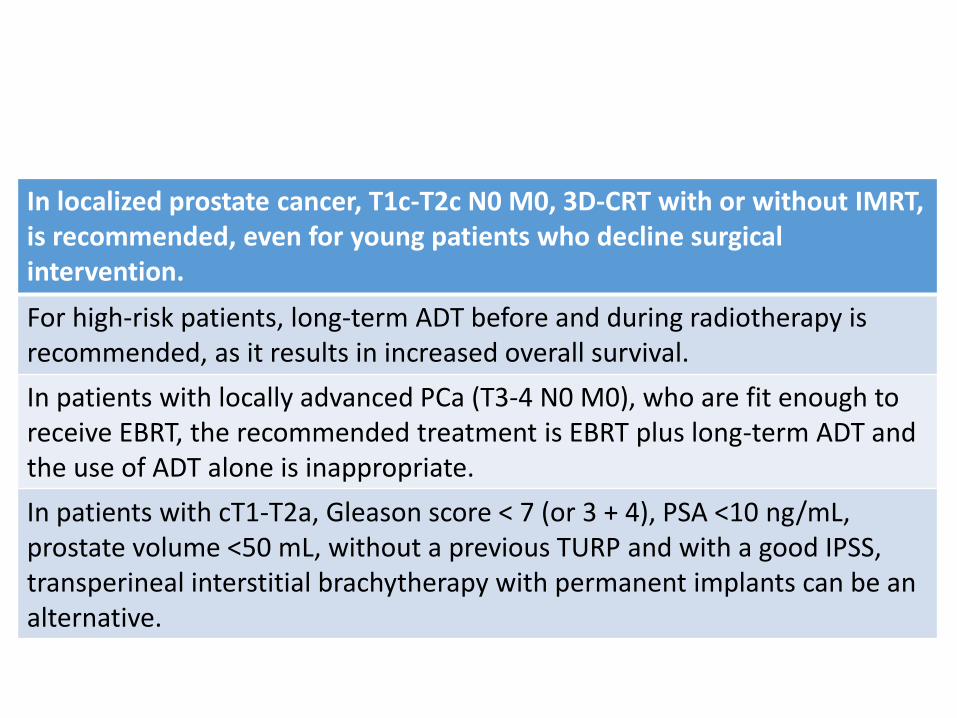
In localized prostate cancer, T1c-T2c N0 M0, 3D-CRT with or without IMRT, is recommended, even for young patients who decline surgical intervention.
For high-risk patients, long-term ADT before and during radiotherapy is recommended, as it results in increased overall survival.
In patients with locally advanced PCa (T3-4 N0 M0), who are fit enough to receive EBRT, the recommended treatment is EBRT plus long-term ADT and the use of ADT alone is inappropriate.
In patients with cT1-T2a, Gleason score < 7 (or 3 + 4), PSA <10 ng/mL, prostate volume <50 mL, without a previous TURP and with a good IPSS, transperineal interstitial brachytherapy with permanent implants can be an alternative.

in patients with pathological tumour stage T3 N0 M0, immediate post-operative external irradiation after RP may improve the biochemical and clinical disease-free survival, with the highest impact in cases of positive margins.
In patients with locally advanced PCa T3-4 N0 M0, concomitant and adjuvant hormonal therapy for a total duration of 3 years, with external-beam irradiation for patients with WHO 0-2 performance status, is recommended, as it improves the overall survival
In a subset of patients with T2c-T3 N0-X and a Gleason score of 2-6, short-term ADT before and during radiotherapy can be recommended, as it may favourably influence the overall survival.
In patients with very high-risk PCa c-pN1 M0, with no severe comorbidity, pelvic external irradiation and immediate long-term adjuvant hormonal treatment is recommended, as it may improve the overall survival, disease-specific failure rate, metastatic failure rate, and biochemical control.
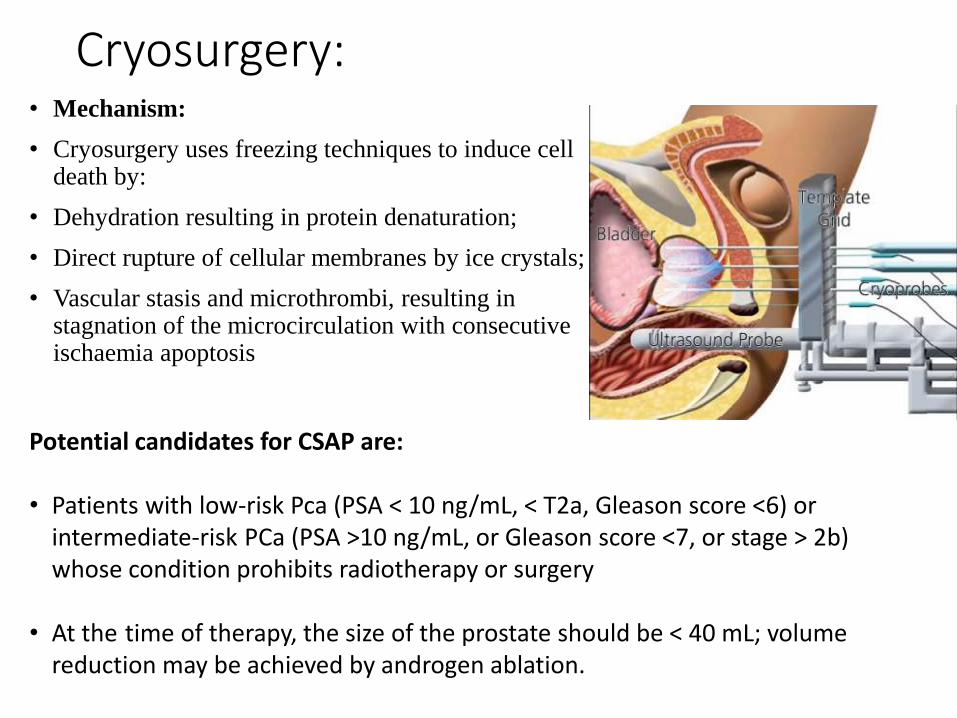
Cryosurgery:• Mechanism:
• Cryosurgery uses freezing techniques to induce cell death by:
• Dehydration resulting in protein denaturation;
• Direct rupture of cellular membranes by ice crystals;
• Vascular stasis and microthrombi, resulting in stagnation of the microcirculation with consecutive ischaemia apoptosis
Potential candidates for CSAP are:
• Patients with low-risk Pca (PSA < 10 ng/mL, < T2a, Gleason score <6) or intermediate-risk PCa (PSA >10 ng/mL, or Gleason score <7, or stage > 2b) whose condition prohibits radiotherapy or surgery
• At the time of therapy, the size of the prostate should be < 40 mL; volume reduction may be achieved by androgen ablation.
• According to a recent meta-analysis of 566 cryosurgery-related publications, there were no controlled trials,survival data or validated biochemical surrogate end-points available for analysis In a randomized comparison between whole-gland cryotherapy and external-beam radiotherapy,
• no difference in 36 months of disease progression was observed at 100 months follow-up.
• Men in both arms of the study received three to six months of neoadjuvant androgen ablative therapy.
complication rates described in third generation cryosurgery include
tissue sloughing in about 3%, incontinence in 4.4%, pelvic pain in 1.4% and
urinary retention in about 2%
• Freezing of the prostate is
ensured by the placement of 12-
15 x 17 gauge cryoneedles under
TRUS guidance.
• placement of thermosensors at
the level of the external sphincter
and bladder neck, and insertion
of a urethral warmer.
• Two freeze-thaw cycles are used
under TRUS guidance, resulting
in a temperature of -40°C in the
mid-gland and at the neurovascular
bundle.
STEPS
RESULTS

High-Intensity Focused Ultrasound
1. High-intensity focused ultrasound (HIFU) is a local ablative technology that
causes tissue damage through focused ultrasound generating intense heat in
targeted areas
2. It is now being used in Europe for the treatment of both primary and salvage
prostate cancers.
in a study of salvage HIFU series in 71 patients with radiorecurrent disease, Gelet et
al. reported progression-free survival rates ranging from 14% (for high-risk patients) to
78% for low-risk patient & at a mean follow-up of nearly 15 months, the 30-month
actuarial survival (negative biopsy and absence of BCR) was 38%
Complications:
1.Prolonged urinary retention secondary to edema
2.urethral sloughing - the most common complications following primary HIFU
treatment
3. rectourethral fistulas, the most devastating of all treatment-related complications-
treated by rectal cooling device
4. urinary incontinence- preservation of a 5-mm apical margin is done to prevent this.
Metastatic prostate cancer:Fundamental principles first articled by Charles huggins et al in 1941( through orchiectomy / estrogens induces dramatic remissions)1980: discovery of LHRH by Andrew Schally
Then sustained release LHRH became preferred choices in treating prostate cancer.
P r o g n o s is in m e t a s t a t ic p r o s t a t e c a n c e r is c l e a r l y d e p e n d e n t o n th e
e x t e n t o f d is e a s e & kinetics of disease.
M IN IM A L D IS E A S E h a s b e e n d e f in e d a s in vo l ve m e n t c o n f in e d t o t h e a x ia l
s k e l e t o n ( p e l vis a n d / o r s p in e ) a n d / o r l y m p h n o d e s ; m e d ia n p r o g r e s s io n - f r e e
su r viva l w a s 4 6 m o n t h s a n d o ve r a l l s u r viva l w a s 5 1 m o n t h s .
E X T E N S IVE D IS E A S E in vo l ve s t h e vis c e r a a n d / o r a p p e n d ic u l a r s k e l e t o n ( l o n
g b o n e s , s k u l l , r ib s p l u s o r m in u s a x ia l s k e l e t o n )
m e d ia n p r o g r e s s io n - f r e e s u r viva l w a s 1 6 m o n t h s a n d o ve r a l l s u r viva l wa s 2 7 . 5
m o n t h s
Adverse prognostic finding:PSA nadir after ADT Haemoglobin
Bone Pain Alkaline Phosphatase
GS high PFS
Extensive disease
Painful bony mets:
1.External-beam radiation therapy:
20Gy/5# & 30 Gy/10# & 8Gy single fraction
↓ pain/ stabilizes bone/ ↓ chances of pathological #
2. bisphosphonates:
3. RANKL inhibitors: denosumab
Castration-resistant prostate cancer:Synonyms: hormone refractory prostate cancer / androgen independentdefn.: Castrate serum testosterone < 50 ng/ml or 1.7 nmol/L plus either: Biochemical failure: Three consecutive rises of PSA, 1 week apart, resulting in two 50% increases over the nadir, with PSA > 2 ng/mL.Pre PSA era it is simply presented as features of weight loss/ metastatic symtoms.Post PSA era virtually all patients are asympomatic, with only rise in PSA level.
MECHANISM: Geller et al. noted more than 2 decades ago that concentrations of
dihydrotestosterone may not be fully suppressed in postorchiectomy patients. sufficient quantity of prostatic tissue androgens may be present to stimulate the AR.
Up-regulation in the androgen synthesis pathway enzymes are clearly demonstrated in various prostate model systems after castration
the concept of androgen synthesis directly occurring in CRPC cells is clearly plausible (but remains to be proven).
.
The sequencing of therapeutic options for patients with CRPC typically involves using secondary hormonal manipulations for as long they are found to be effective in halting disease progression.
Management:• the first issue in treating a patient who has progressed on ADT is to determine whether
or not serum testosterone is castrate. (arbitrarily been set < 50 ng/dL). • LHRH analogues are not fully absorbed or active. These patients will have elevated
levels of testosterone despite appropriately administered LHRH agonist therapy• Patients with progressive prostate cancer despite castrate levels of testosterone should
continue to have LHRH agonist therapies. One retrospective analysis demonstrated improved survival in association with continued LHRH agonist administration. No prospective randomized trials have examined this issue
Secondary hormonal therapies:• responsive to secondary hormonal manipulations such as
antiandrogen withdrawal, adrenal cortical suppression, glucocorticoids, or estrogens. Attempts to manage CRPC with secondary and or tertiary hormonal manipulations are commonly employed despite the absence of randomized prospective trials demonstrating a survival benefit.
Withdrawal responses (e.g., antiandrogens, megestrolacetate):
• This clinical entity was first recognized in 1993. withdrawal responses begin within a few weeks after the medication has been discontinued. Bicalutamide is an exception; this agent has a long terminal serum half-life and withdrawal response may not be observed for 6 to 8 weeks after discontinuation.
Antiandrogen administration (flutamide, bicalutamide, nilutamide)

• Adrenal suppressants (ketoconazole, aminoglutethimide): ketoconazole
(600 to 1,200 mg/day) plus low-dose glucocorticoids may reduce PSA by
50% or more in up to 71% of patients
• Glucocorticoids (e.g., dexamethasone, prednisone): may provide palliative
as well as PSA responses. Tannock et al.387 showed improvement in
symptoms of 33% of cases treated with low-dose prednisone (10 mg/day).
Dexamethasone has had PSA declines of more than 50% reported in up to
59% of patients.Prednisone has been used at oral dosages of 10 to 20 mg/day
and dexamethasone in oral doses of 0.5 to 2 mg/day.
• Estrogens (e.g., DES, fosfestrol, estramustine.): palliative effects.
DES at oral doses of 1 to 3 mg/day is associated with PSA declines in
approximately 24% to 42% of patients. Estramustine has estrogenic actions.
• Bisphosphonates (zoledronate): Zoledronate is the only FDA-approved
bisphosphonate for CRPC with bone metastases. Randomized trials of
zoledronate demonstrate that 4 mg intravenously every 3 to 4 weeks reduces
skeletal related events (defined as pathologic fractures, radiation to bone,
spinal cord compression, and/or surgery to bone) by 25%. Denosumab is
also being tested in metastasis prevention, but datas are yet to mature.

• Bone-seeking radiopharmaceuticals (samarium-153-EDTMP, strontium-89):
Three radiopharmaceuticals are currently FDA-approved for the palliative treatment of painful bone metastases1. phosphorus-32 2.strontium-89 3.samarium-153-EDTMP.
Myelosuppression is the predominate toxicity associated with all of the bone seeking radioisotopes.
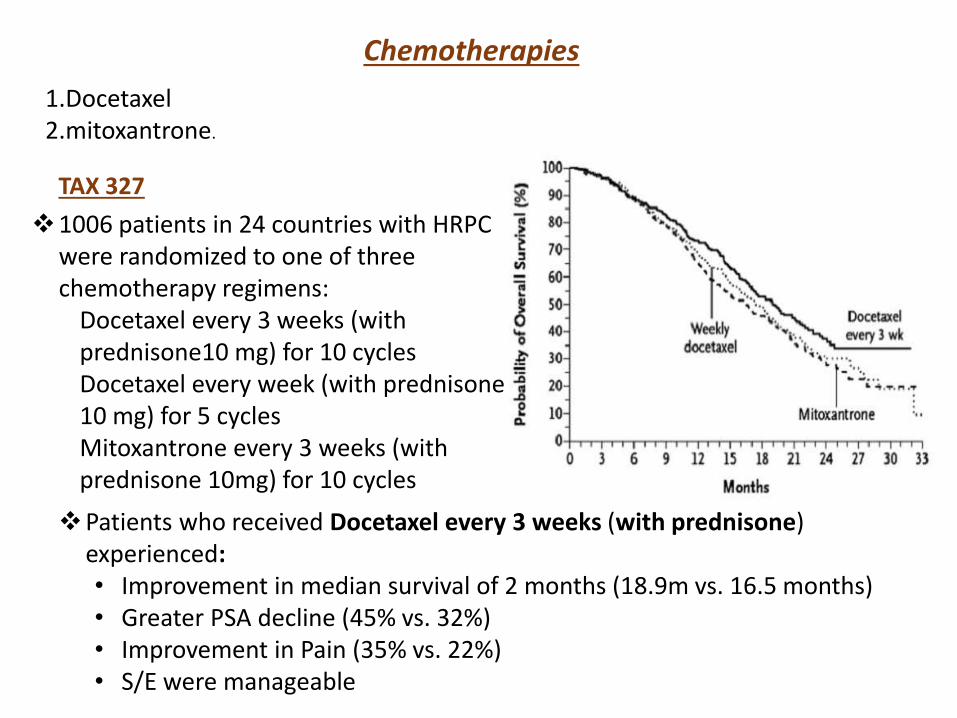
Chemotherapies
1.Docetaxel2.mitoxantrone.
TAX 327
1006 patients in 24 countries with HRPC were randomized to one of three chemotherapy regimens:
Docetaxel every 3 weeks (with prednisone10 mg) for 10 cyclesDocetaxel every week (with prednisone 10 mg) for 5 cyclesMitoxantrone every 3 weeks (with prednisone 10mg) for 10 cycles
Patients who received Docetaxel every 3 weeks (with prednisone) experienced:• Improvement in median survival of 2 months (18.9m vs. 16.5 months)• Greater PSA decline (45% vs. 32%)• Improvement in Pain (35% vs. 22%)• S/E were manageable
SWOG 9916
N=770 men
Dose used: Docetaxel (60mg/m2) & estramustine(280 mg orally 3
times daily from days 1 through 5) vs. mitoxantrone(12mg/m2) and
95 mg twice daily)
overall survival favored docetaxel (18.9 months compared with 16
months for mitoxantrone).
20% reduction in mortality in docetaxel &estramustine arm
Median time to progression significantly superior in the same
arm(6.3 vs.3.2 months)
Results Of SWOG & TAX 327 Confirms The Efficacy Of Docetaxel.
But Only Question Is That Only 2 Months Survival Increment Is By
Use Of Docetaxel.

Salvage treatment after first-line docetaxelAll patients who receive docetaxel-based chemotherapy for CRPC will progress, thus, there
have been many clinical trials investigating the role of salvage chemotherapy.
Several groups have used second-line intermittent docetaxel re-treatment in patients who
had clearly responded to first-line docetaxel.
Newer drugs:
• Cabazitaxel
1. a taxane derivative
2. Positive results have been published from, phase III trial (TROPIC trial)
comparing cabazitaxel + prednisone vs. mitoxantrone + prednisone in 755
patients with CRPC, who had progressed after or during docetaxel-based
chemotherapy .
3. An OS benefit (15.1 vs. 12.7 months, p < 0.0001) was observed in the
cabazitaxel arm. As well as PFS (2.8 vs. 1.4 months, p < 0.000).
4. Treatment-associated WHO grade 3/4 side effects developed significantly
more often in the cabazitaxel arm, particularly neutropenia and sepsis.
Enzalutamide :
• a novel anti-androgen that blocks AR binding, nuclear translocation
and transcription.
• Enzalutamide is used as a once-daily oral treatment.
• AFFIRM study in 2012 randomized 1,199 patients with metastatic
CRPC in a 2/1 fashion between enzalutamide or placebo. (The
patients had progressed after docetaxel treatment).
• After a median follow-up of 14.4 months, the median survival in
the enzalutamide group was 18.4 months compared to 13.6 months
in the placebo arm (HR: 0.63, p < 0.001). This led to the
recommendation that the study be halted and unblinded.
• The benefit was observed irrespective of age, baseline pain
intensity, and type of progression.
Abiraterone acetate
• CYP17 inhibitor.
• It is used once daily combined with prednisone twice daily (10 mg/ day).
• large phase III COU-AA-301 trial used a total of 1,195 patients with metastatic
CRPC were randomised in a 1/1 fashion between abiraterone acetate or placebo,
In patients with progressive disease after docetaxel therapy the median survival
in the abiraterone group was 15.8 months compared to 11.2 months in the placebo
arm (HR: 0.74, p < 0.001).
• The benefit was observed irrespective of age, baseline pain intensity, and type of
progression.
• most common grade 3/4 side effects did not differ significantly but
mineralocorticoid-related side effects were more frequent in the abiraterone
group, mainly grade 1/2 (fluid retention, oedema or hypokalaemia).
• As of today, the choice between third-line hormonal treatment
(using enzalutamide or abiraterone) or second line
chemotherapy (cabazitaxel) remains unclear with no clear
decision-making findings published.

Phase 2 trials of docetaxel + atrasentan/
bevacizumab/bortezomid/capecitabine/calcitriol/thalidomide
have been completed.
Randomized phase 2 trial of thalidomide/docetaxel
Phase 2 trial of docetaxel/calcitriol (ASCENT) strongly favoring survival benefit.
Mature results are anticipated within the next 3 to 5 years.
SPARC: phase III, randomized, placebo-controlled trial uses Satraplatin: novel
oral platinum compound Associated with significant PFS improvements in
chemotherapy-naive patients with hormone-refractory prostate cancer.
Immunologic TherapiesSipuleucel-T is a product freshly prepared for each treatment course consisting of
leukapheresed mononuclear cells pulsed ex vivo with a GM-CSF/prostatic acid phosphatase fusion protein. Patients are cytopheresed and dendritic cell precursors isolated prior to fusion protein exposure. Two small randomized phase 3 trials have been conducted with Sipuleucel-T, 9901 and 9902A.
Anti CTLA-4 antibody is in clinical trialPROSTVAC-VF TRICOM VACCINE has reported phase 2 data & further studies will ensue.
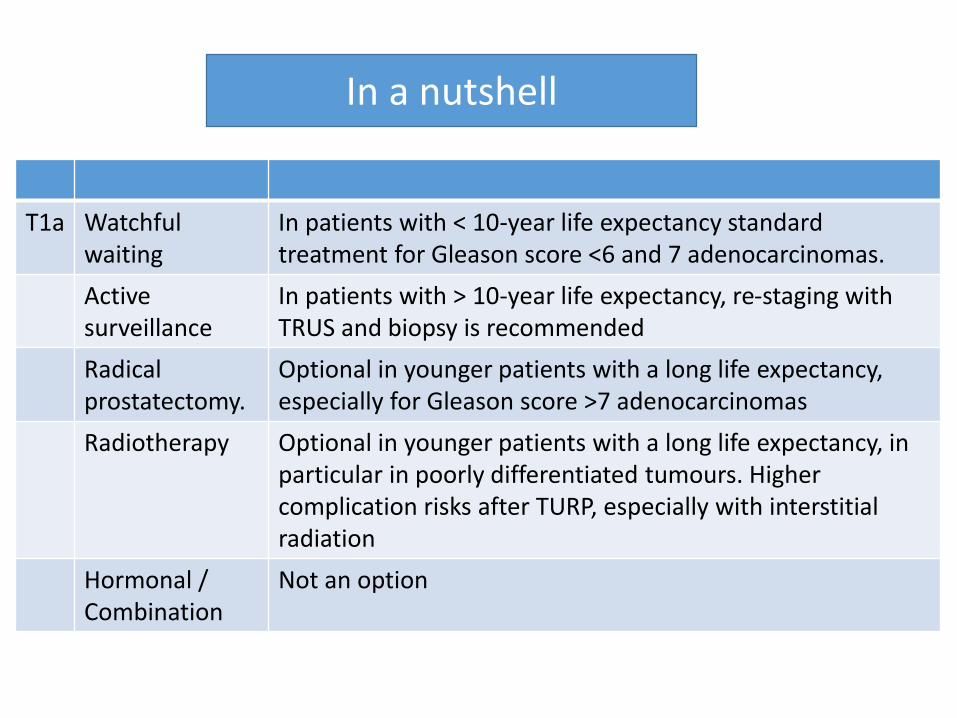
T1a Watchful waiting
In patients with < 10-year life expectancy standard treatment for Gleason score <6 and 7 adenocarcinomas.
Active surveillance
In patients with > 10-year life expectancy, re-staging with TRUS and biopsy is recommended
Radical prostatectomy.
Optional in younger patients with a long life expectancy, especially for Gleason score >7 adenocarcinomas
Radiotherapy Optional in younger patients with a long life expectancy, in particular in poorly differentiated tumours. Highercomplication risks after TURP, especially with interstitial radiation
Hormonal /Combination
Not an option
In a nutshell

T1b-T2b
Watchful waiting Patients with a life expectancy < 10 years.
Active surveillance
• Treatment option in patients with cT1c-cT2a, PSA < 10 ng/mL, biopsy Gleason score <6, <2 biopsies positive, <50% cancer involvement of each biopsy.
• Patients with a life expectancy > 10 years once they are informed about the lack of survival data beyond 10 years.
• Patients who do not accept treatment-related complications.

T1a-T2c
Watchful waiting
Patients with life expectancy < 10 years and Gleason score ≤ 7.
RP • Optional in patients with pT1a PCa.• Standard treatment for patients with a life expectancy > 10
years who accept treatment-related complications.
RT • Patients with a life expectancy > 10 years who accept treatmentrelated complications.
• Patients with contraindications for surgery.• Unfit patients with 5-10 years of life expectancy and poorly differentiated tumours
BRACHY Low-dose rate brachytherapy can be considered for low risk PCapatients with a prostate volume <50 mL and an IPSS <12
Hormone • Symptomatic patients, who need palliation of symptoms, unfit for curative treatment.
• Anti-androgens are associated with a poorer outcome compared to ‘watchful waiting’ and are not recommended.
Combination
• For high-risk patients, neoadjuvant hormonal treatment and concomitant hormonal therapy plus radiotherapy results in increased overall survival.
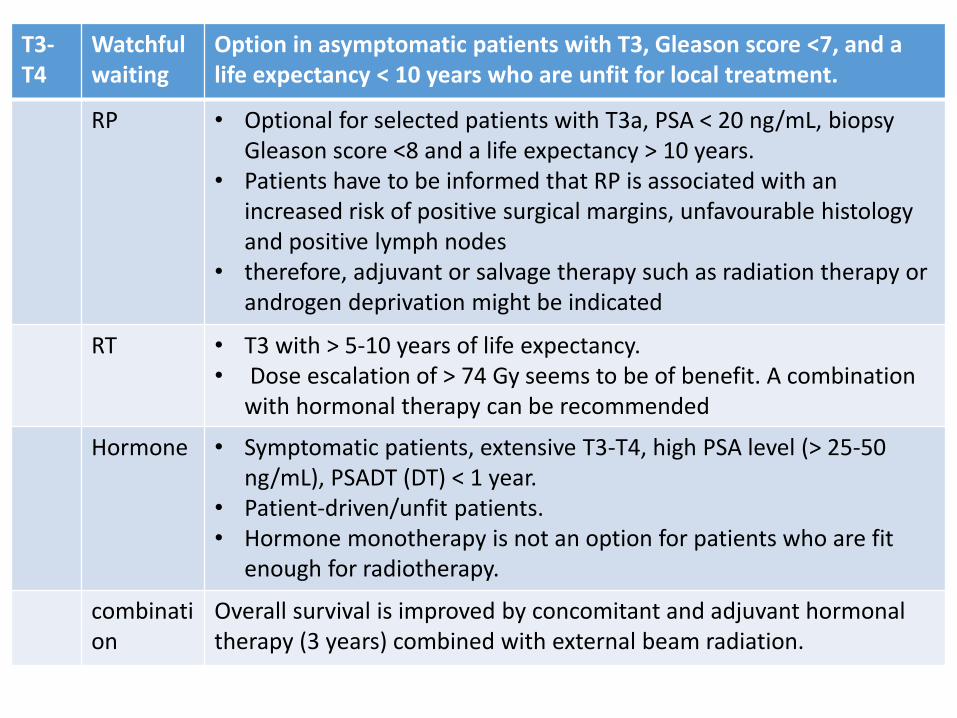
T3-T4
Watchful waiting
Option in asymptomatic patients with T3, Gleason score <7, and a life expectancy < 10 years who are unfit for local treatment.
RP • Optional for selected patients with T3a, PSA < 20 ng/mL, biopsy Gleason score <8 and a life expectancy > 10 years.
• Patients have to be informed that RP is associated with an increased risk of positive surgical margins, unfavourable histology and positive lymph nodes
• therefore, adjuvant or salvage therapy such as radiation therapy or androgen deprivation might be indicated
RT • T3 with > 5-10 years of life expectancy.• Dose escalation of > 74 Gy seems to be of benefit. A combination
with hormonal therapy can be recommended
Hormone • Symptomatic patients, extensive T3-T4, high PSA level (> 25-50 ng/mL), PSADT (DT) < 1 year.
• Patient-driven/unfit patients.• Hormone monotherapy is not an option for patients who are fit
enough for radiotherapy.
combination
Overall survival is improved by concomitant and adjuvant hormonal therapy (3 years) combined with external beam radiation.

N+, M0 Watchful waiting
Asymptomatic patients. Patient-driven (PSA < 20-50 ng/mL), PSADT > 12 months. Requires very close follow-up
RP Optional for highly selected patients with a life expectancy of > 10 years as part of a multimodal treatment approach
Radiotherapy
Optional in highly selected patients with a life expectancy of > 10 years, combination therapy with adjuvant androgen deprivation for 3 years is mandatory.
Hormone
Standard treatment after extended node dissection if > 2 positive nodes (irrespective of the local treatment: surgery or radiotherapy). Hormonal therapy should only be used as monotherapy in patients who are unfit for any type of local therapy
Combination
No standard option. Patient-driven
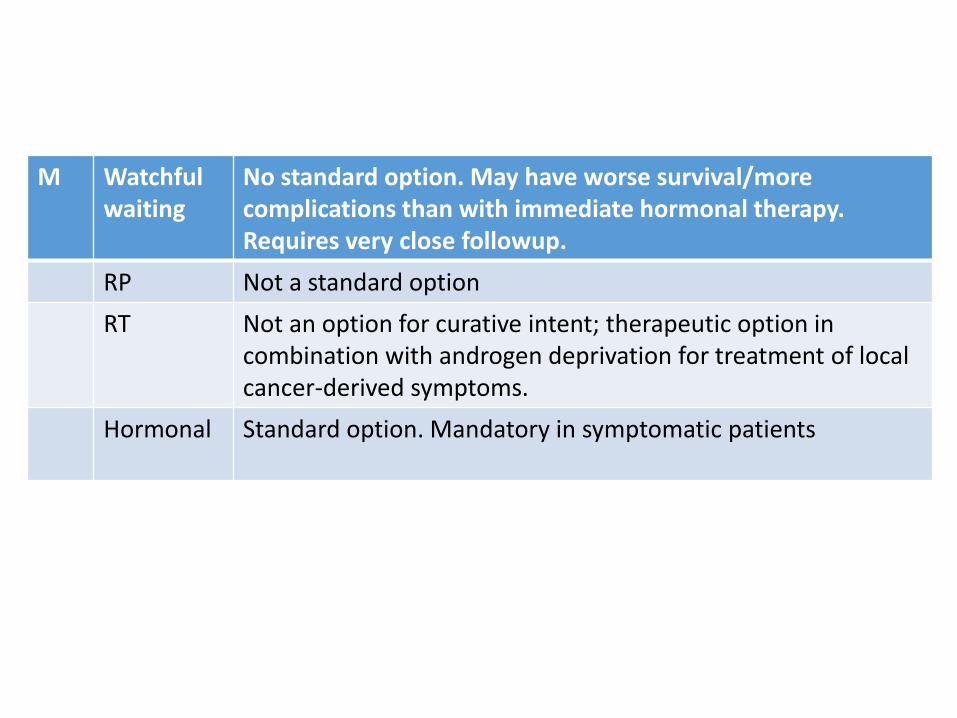
M Watchful waiting
No standard option. May have worse survival/more complications than with immediate hormonal therapy. Requires very close followup.
RP Not a standard option
RT Not an option for curative intent; therapeutic option in combination with androgen deprivation for treatment of local cancer-derived symptoms.
Hormonal Standard option. Mandatory in symptomatic patients
Related Documents











