REVIEW Management of Primary Pulmonary Artery Sarcomas Shanda H. Blackmon, MD, MPH, David C. Rice, MMB, BCh, Arlene M. Correa, PhD, Reza Mehran, MD, Joe B. Putnam, MD, W. Roy Smythe, MD, Jon-Cecil Walkes, MD, Garrett L. Walsh, MD, Cesar Moran, MD, Harsh Singh, MD, Ara A. Vaporciyan, MD, and Michael Reardon, MD The Methodist Hospital Department of Surgery, The Methodist DeBakey Heart Center, The University of Texas MD Anderson Cancer Center, Houston, Texas; Christchurch, Canterbury, New Zealand; and Weill Medical College of Cornell University, New York, New York The objective of this review is to determine the outcome of patients with sarcomas involving the main pulmonary artery, pulmonic valve, or right ventricular outflow tract. Survival data were analyzed using an aggregate series derived from the published literature in conjunction with a current series. Median survival was 36.5 20.2 months for patients undergoing an attempt at curative resection compared with 11 3 months for those under- going incomplete resection. Median survival was 24.7 8.5 months for patients undergoing multimodality treat- ment compared with 8.0 1.7 months for patients having single-modality therapy. A complete review of diagnosis, evaluation, treatment, and surveillance of primary pul- monary artery sarcomas follows. (Ann Thorac Surg 2009;87:977– 84) © 2009 by The Society of Thoracic Surgeons P rimary pulmonary artery (PA) sarcomas are uncom- mon tumors. The first published case was reported in 1923 from an autopsy by Mandelstamm [1], and since then, fewer than 250 patients with primary PA sarcoma have been described. For a subclassification of PA sarco- mas, please refer to Table 1 [2– 4]. Patients with PA sarcoma often present with dyspnea, cough, hemoptysis, or chest pain. Because these symp- toms sometimes mimic pulmonary emboli, patients are often initially treated with anticoagulation therapy. Clin- ical data that aid in the differentiation between these two diagnoses include fever, elevated erythrocyte sedimenta- tion rate, anemia, weight loss, absence of a procoagulant state, and a lack of history for deep venous thrombosis [5]. PA sarcomas can be evaluated by a variety of imaging modalities, but a contrast computed tomography (CT) scan is usually standard. The results of chemotherapy management alone are suboptimal [6], and there is no established treatment regimen. Survival for this disease is often reported in weeks instead of months or years. Interventions reported for PA sarcomas range from palliative stenting, pneumo- nectomy, debulking, and endarterectomy to excision with or without pneumonectomy and with or without recon- struction of the PA. If complete resection is achieved, the entire right ventricular outflow tract or main PA trunk may require excision. Owing to the extensive operation required to achieve a complete resection, the paucity of clinical data indicating benefit, and the frequent lack of preoperative tissue diagnoses, aggressive resections are infrequently per- formed or reported. Our institutional experience with extended resections for cardiac tumors has led us to adopt an aggressive approach to these tumors in selected patients [7–9]. We report a review of the literature, including our cumulative experience to date, along with treatment guidelines derived from the combined groups separated by treatment type. Methods A literature search of Ovid/Medline was performed us- ing the terms “sarcoma,” “pulmonary artery,” “surgery,” and/or “chemotherapy,” and/or “radiation therapy.” The search was limited to English articles about humans in the past 17 years. Each article was screened for central primary PA sarcomas as the diagnosis for each patient. Patients with lung parenchymal disease were included as long as their primary tumor was a central primary PA sarcoma. The analysis only included PA sarcomas under- going treatment such as chemotherapy, anticoagulation therapy, stenting, or surgery. Autopsy reports or diag- nostic reports with no discussion of patient treatment were excluded. The article search identified 60 patients. The case reports of patients from these articles were tabulated in a standard form to allow comparison against the current study group. The last date of reported survival was considered the last date of contact. The patients were recorded as dead or alive on the last date of contact for calculation of survival. Statistical analysis included calculation of mean and median age, survival, and disease-free interval. Kaplan- Address correspondence to Dr Blackmon, 6550 Fannin St, Smith Tower Ste 1661, Houston, TX 77030; e-mail: [email protected]. © 2009 by The Society of Thoracic Surgeons 0003-4975/09/$36.00 Published by Elsevier Inc doi:10.1016/j.athoracsur.2008.08.018 REVIEW

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

MSSRGaTCN
ToaSdwmr
Pithm
ctoidts[ms
srwfnosem
cb
AS
©P
REVIEW
anagement of Primary Pulmonary Arteryarcomas
handa H. Blackmon, MD, MPH, David C. Rice, MMB, BCh, Arlene M. Correa, PhD,eza Mehran, MD, Joe B. Putnam, MD, W. Roy Smythe, MD, Jon-Cecil Walkes, MD,arrett L. Walsh, MD, Cesar Moran, MD, Harsh Singh, MD, Ara A. Vaporciyan, MD,
nd Michael Reardon, MDhe Methodist Hospital Department of Surgery, The Methodist DeBakey Heart Center, The University of Texas MD Andersonancer Center, Houston, Texas; Christchurch, Canterbury, New Zealand; and Weill Medical College of Cornell University,
ew York, New Yorkg8msem
he objective of this review is to determine the outcomef patients with sarcomas involving the main pulmonaryrtery, pulmonic valve, or right ventricular outflow tract.urvival data were analyzed using an aggregate serieserived from the published literature in conjunctionith a current series. Median survival was 36.5 � 20.2onths for patients undergoing an attempt at curative
esection compared with 11 � 3 months for those under-
dfeapits
M
AiastpPlsgtnw
rsscrc
mddress correspondence to Dr Blackmon, 6550 Fannin St, Smith Towerte 1661, Houston, TX 77030; e-mail: [email protected].
2009 by The Society of Thoracic Surgeonsublished by Elsevier Inc
oing incomplete resection. Median survival was 24.7 �.5 months for patients undergoing multimodality treat-ent compared with 8.0 � 1.7 months for patients having
ingle-modality therapy. A complete review of diagnosis,valuation, treatment, and surveillance of primary pul-onary artery sarcomas follows.
(Ann Thorac Surg 2009;87:977–84)
© 2009 by The Society of Thoracic SurgeonsREV
IEW
rimary pulmonary artery (PA) sarcomas are uncom-mon tumors. The first published case was reported
n 1923 from an autopsy by Mandelstamm [1], and sincehen, fewer than 250 patients with primary PA sarcomaave been described. For a subclassification of PA sarco-as, please refer to Table 1 [2–4].Patients with PA sarcoma often present with dyspnea,
ough, hemoptysis, or chest pain. Because these symp-oms sometimes mimic pulmonary emboli, patients areften initially treated with anticoagulation therapy. Clin-
cal data that aid in the differentiation between these twoiagnoses include fever, elevated erythrocyte sedimenta-
ion rate, anemia, weight loss, absence of a procoagulanttate, and a lack of history for deep venous thrombosis5]. PA sarcomas can be evaluated by a variety of imaging
odalities, but a contrast computed tomography (CT)can is usually standard.
The results of chemotherapy management alone areuboptimal [6], and there is no established treatmentegimen. Survival for this disease is often reported ineeks instead of months or years. Interventions reported
or PA sarcomas range from palliative stenting, pneumo-ectomy, debulking, and endarterectomy to excision withr without pneumonectomy and with or without recon-truction of the PA. If complete resection is achieved, thentire right ventricular outflow tract or main PA trunkay require excision.Owing to the extensive operation required to achieve a
omplete resection, the paucity of clinical data indicatingenefit, and the frequent lack of preoperative tissue
iagnoses, aggressive resections are infrequently per-ormed or reported. Our institutional experience withxtended resections for cardiac tumors has led us todopt an aggressive approach to these tumors in selectedatients [7–9]. We report a review of the literature,
ncluding our cumulative experience to date, along withreatment guidelines derived from the combined groupseparated by treatment type.
ethods
literature search of Ovid/Medline was performed us-ng the terms “sarcoma,” “pulmonary artery,” “surgery,”nd/or “chemotherapy,” and/or “radiation therapy.” Theearch was limited to English articles about humans inhe past 17 years. Each article was screened for centralrimary PA sarcomas as the diagnosis for each patient.atients with lung parenchymal disease were included as
ong as their primary tumor was a central primary PAarcoma. The analysis only included PA sarcomas under-oing treatment such as chemotherapy, anticoagulationherapy, stenting, or surgery. Autopsy reports or diag-ostic reports with no discussion of patient treatmentere excluded.The article search identified 60 patients. The case
eports of patients from these articles were tabulated in atandard form to allow comparison against the currenttudy group. The last date of reported survival wasonsidered the last date of contact. The patients wereecorded as dead or alive on the last date of contact foralculation of survival.
Statistical analysis included calculation of mean and
edian age, survival, and disease-free interval. Kaplan-0003-4975/09/$36.00doi:10.1016/j.athoracsur.2008.08.018

Mw
dcdTturtt
appi
SPctitmilnfintelcphmn
IPp
picucsrfidt
lesetgpnct
deosataoiwe
PMsoc[totom
PMvsrrIp(T1
TS
a
978 REVIEW BLACKMON ET AL Ann Thorac SurgMANAGEMENT OF PA SARCOMAS 2009;87:977–84
REV
IEW
eier survival curves were calculated using SPSS soft-are (SPSS Inc, Chicago, IL).Current patients were identified from an institutional
atabase queried for the terms “pulmonary artery sar-oma,” “surgery,” and “chemotherapy.” The pathologyepartment database was also queried for PA specimens.he results of the two queries were reviewed to obtain
he final list of 8 patients with primary PA sarcomasndergoing surgical therapy with curative intent. A ret-ospective medical record review in conjunction withelephone interviews was performed on all patients iden-ified from this search.
Institutional Review Board approval was obtained forll patient queries, and consent was waived for the 8atients included in the current analysis. Since 2005, allatient data have been collected prospectively for an
nstitutional PA sarcoma database.
ymptoms and Signsatients with PA sarcomas present with a variety ofardiopulmonary complaints. A complete list of symp-oms in study patients is compiled in Table 2. Lungnvolvement is present in about 50% of patients [3]. Theypical duration of symptoms before diagnosis is 3 to 12
onths, usually because of initial misdiagnosis. Thenitial differential diagnosis includes pulmonary embo-us, pulmonary hypertension, congenital pulmonary ste-osis, fibrosing mediastinitis, or lung tumor. Clinicalndings include right ventricular dysfunction, pulmo-ary hypertension, and pulmonary insufficiency. A sys-
olic ejection murmur is often noted. Evidence from ourxperience and that of others shows that patients witharge pulmonary emboli, constitutional symptoms, un-haracteristic CT scans for thrombus, and especiallyatients with lesions refractory to anticoagulation shouldave further evaluation to diagnose primary PA sarco-as at the earliest stage possible. A recommended diag-
osis and treatment algorithm is presented in Figure 1.
magingA sarcomas can be evaluated by computed tomogra-
able 1. Subclassifications of Primary Pulmonary Arteryarcomasa
● Undifferentiated● Rhabdomyosarcoma● Osteogenic sarcoma● Angiosarcoma● Fibrosarcoma● Malignant mesenchymoma● Myxosarcoma● Chondrosarcoma● Osteosarcoma● Malignant fibrous histiocytoma● Liposarcoma● Unclassified leiomyosarcomas
References 2–4.
hy/computed tomography angiography (CT/CTA) scan, p
ositron-emission tomography scan, magnetic resonancemaging (MRI) and angiography, transesophageal echo-ardiography, intravascular ultrasound, and intracardiacltrasound. Findings on CT scan differentiating PA sar-omas from pulmonary emboli include hyperdense le-ions with nonhomogenous attenuation from hemor-hage, beaded peripheral PAs, contiguously soft tissue–lled PAs with the entire lumen occupied, vascularistention from tumor growth, distal oligemia, and ex-
ravascular spread [27, 35, 45, 46].The CT scans in all of our patients showed hyperdense
esions and vascular distention when the tumor filled thentire PA (Fig 2). We also found MRI to be even morepecific for identifying PA sarcomas, because the tumornhances with gadolinium contrast more than blandhrombus (Fig 3) [21, 46–51]. This feature also makesadolinium-enhanced MRI helpful for monitoring suchatients after resection if an intraluminal abnormality isoted. The degree of enhancement has been shown toorrelate with the degree of tumor differentiation, con-ent of myxoid matrix, and associated thrombus [23].
Angiographic findings include polyploid filling defects,efects that move with the cardiac cycle, pressure gradi-nts across the mass, and tumor neovascularity identifiedn bronchial arteriography [48, 52]. Intravascular ultra-ound and transesophageal echocardiography imagesre helpful in determining the extent of involvement ofhe pulmonic valve [53–56]. Because tumor is more met-bolically active than thrombus, findings from fluorode-xyglucose-positron emission tomography (FDG-PET)
nclude increased uptake within the tumor [57, 58], whichas noted in one of our patients who underwent PET
valuation (Fig 2).
athophysiologyost of these tumors are noted to arise from the dorsal
urface of the main pulmonary trunk [4] and the intimalr subintimal surface [59, 60] as multipotential mesen-hymal cells of the muscle anlage of the bulbus cordis46]. The pulmonic valve is involved about 30% of theime [4]. A significant amount of intraluminal extension isften noted before any extension outside the lumen ofhe vessel, as our study also found. The lung peripheryften becomes involved from emboli, infarction, andetastases [61].
athologyoran and colleagues [3] recently reported longer sur-
ival associated with leiomyosarcoma and worse progno-is with rhabdomyosarcoma. With few cases available foreview, other reports in the literature have not corrobo-ated this histologic correlation with survival [5, 15, 21, 62].mmunohistochemical staining of the tumor is routinelyerformed for desmin, cytokeratin, vimentin, and actin
smooth muscle specific and muscle specific) [3, 18].hese tumors also over-express mdm2 and have gains of2q13–14 [3, 24]. Expression of apoptosis-related proteins,
53, and DNA fragmentation are also noted to occur [28].
TWpaowtOprdaAmpi
pwttas
TEmuiasm
T
P
P
P
P
P
P
P
P
P
a
Ac(Ippls
979Ann Thorac Surg REVIEW BLACKMON ET AL2009;87:977–84 MANAGEMENT OF PA SARCOMAS
REV
IEW
reatment Results From Review of the Literaturee reviewed 77 patients from the past 17 years of
ublished data. Survival was not reported for 11 patients,nd thus their data were recorded as missing. Some typef multimodality treatment was initiated in 20 patients,hich consisted of two of the three following interven-
ions: chemotherapy, radiation therapy, or operation.nly one type of intervention was commenced in 28atients, consisting of operation alone, chemotherapy, oradiation therapy. Reports for 12 patients did not includeata about whether the patients received additional ther-py, and thus their data were recorded as missing.ttempted curative resections were done in 25 patients,uch like all of the patients in our current series. A more
alliative type of resection was done in 24 patients,
able 2. The Methodist Hospital-MD Anderson Cancer Cente
atientAge,
Gender Symptoms Site, Pathology Th
atient 1 69 M C/D PV, MPA, LPA Adj: GTAngiosarcoma
atient 2 22 F C/D, pain MPA, LPA, LL, LPv, Neo: A/HG sarcoma Adj: Dac
atient 3 62 F C/D MPA, RPA, Adj: A/ISpindle cell
sarcoma
atient 4 73 M C/D MPA, LPA, LL Neo: XRAngiosarcoma Adj: A/I
atient 5 72 M C/D MPA, BPA, RL Neo: A/
HG intimal Adj: G,atient 6 49 M C/D MPA, LL Adj: A/I
HG leiomyosarcomaatient 7 44 M C/D PV, BPA, MPA Adj: A/I
Unspecifiedsarcoma
atient 8 54 M C/D 1. LPA, LL Adj: A/I2. LL SBRT3. Brain4. PV, MPA, RPA
Leiomyosarcoma
All patients had cardiopulmonary bypass and median sternotomy.
/I � Adriamycin/ifosfamide; A � alive; Adj � adjuvant; Bisplatin; CABG � coronary artery bypass grafting; C/D � coughDuPont, Wilmington, DE) used for reconstruction; G � gemcitabinfosfamide; HG � high grade; IL-2 � interleukin 2; L � leuulmonary artery; LPv � left pulmonary vein; M/F � male/femulmonary artery; Peri � pericardium used for reconstruction; P
ung; RP � right pneumonectomy; RPA � right pulmonary artery;tereotactic body radiation therapy; T � Taxane; XRT � radiation th
ncluding tumor debulking, thromboendarterectomy, or t
alliative pneumonectomy. Recorded data for 11 patientsere not appropriate to determine what type of resec-
ion, if any, was performed. Patient data from our litera-ure review are summarized in Table 3 [5, 10–44]. Meannd 5-year survival was 18 � 3.5 months and 18.5% in theeries of historical patients (Fig 4).
reatment Results From Current Seriesight patients underwent resection combined with che-otherapy or radiation therapy. Patients who were eval-
ated but did not undergo an operation are not includedn this review. Patients were prospectively followed up,nd data were recorded in our multi-institutional PAarcoma database. The group comprised 7 men, andean patient age was 54 years. All of the patients from
mary Pulmonary Artery Sarcoma Resections, 1999–2006
y Procedurea Recurrence
VitalSurvival,
mon
H-recon LPA, RP None A, 29
2; G, C 1. BC, H-recon MPA LP Distant A, 802. Dist. recurrence
resectionI 1. Peri-recon RPA Local & distant D, 24
2. Local re-resectionRPLT & Rmetatarsectomies
Gy 1. H-recon RPA None A, 30CABG �3, LP
1. CABG � 1, recon withallograft RV-PAconduit 27-mmDacron interposition
None A, 23
1. Peri-recon BPA Lpneumonectomy
Distant D, 70
1. H-recon RVOTthrombectomy RPA
Local D, 19
1. DP-LPA closed local Local & distant A, 92. L PLT, LP3. Brain resection4. Re-do MS, H recon
RVOT/RPA
bilateral clamshell; BPA � bilateral pulmonary arteries; C �dyspnea; D � dead; Dac � dacarbazine; DP � Dacron patch
H-recon � homograft used for reconstruction; HDI � High doserin; LL � left lung; LP � left pneumonectomy; LPA � left
MPA � main pulmonary artery; Neo � neoadjuvant; PA �posterolateral thoracotomy; PV � pulmonary valve; RL � right� right ventricle; RVOT � right ventricular outflow tract; SBRT �
.
r Pri
erap
I, IL-
, HD
T 20
I
T
C �ande;covoale;
LT �RV
erapy
he current series presented with a cough and dyspnea,
agT
wecliP
p
Frpsn
FcmAparceicpm
Fsct
980 REVIEW BLACKMON ET AL Ann Thorac SurgMANAGEMENT OF PA SARCOMAS 2009;87:977–84
REV
IEW
nd only 1 patient complained of pain. Patient demo-raphic data from our current series are summarized inable 2.
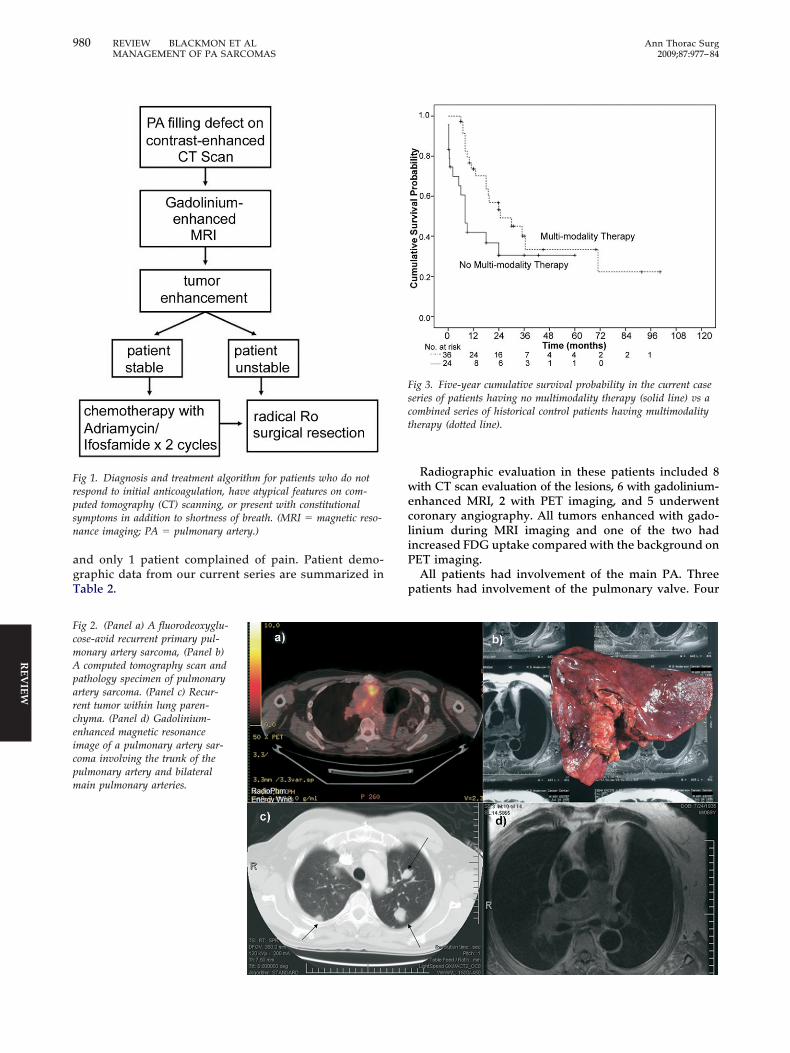
ig 1. Diagnosis and treatment algorithm for patients who do notespond to initial anticoagulation, have atypical features on com-uted tomography (CT) scanning, or present with constitutionalymptoms in addition to shortness of breath. (MRI � magnetic reso-ance imaging; PA � pulmonary artery.)
ig 2. (Panel a) A fluorodeoxyglu-ose-avid recurrent primary pul-onary artery sarcoma, (Panel b)computed tomography scan and
athology specimen of pulmonaryrtery sarcoma. (Panel c) Recur-ent tumor within lung paren-hyma. (Panel d) Gadolinium-nhanced magnetic resonancemage of a pulmonary artery sar-oma involving the trunk of theulmonary artery and bilateralain pulmonary arteries.
Radiographic evaluation in these patients included 8ith CT scan evaluation of the lesions, 6 with gadolinium-
nhanced MRI, 2 with PET imaging, and 5 underwentoronary angiography. All tumors enhanced with gado-inium during MRI imaging and one of the two hadncreased FDG uptake compared with the background onET imaging.All patients had involvement of the main PA. Three
atients had involvement of the pulmonary valve. Four
ig 3. Five-year cumulative survival probability in the current caseeries of patients having no multimodality therapy (solid line) vs aombined series of historical control patients having multimodalityherapy (dotted line).
ptlsg
pF3ciw
atSthb
a5s
TWc3capthspwosth
TTlausasacct
Fsc
Fstlt
TRf
a
981Ann Thorac Surg REVIEW BLACKMON ET AL2009;87:977–84 MANAGEMENT OF PA SARCOMAS
REV
IEW
atients had extensive lung involvement on one side ofhe chest. Two patients had angiosarcomas, 2 hadeiomyosarcomas, and 1 patient each had a high-gradearcoma (undifferentiated), spindle cell sarcoma, high-rade intimal sarcoma, or unspecified sarcoma.All patients underwent median sternotomy and cardio-
ulmonary bypass for at least one of their procedures.ive patients had homograft replacement of the main PA,required pulmonic valve replacement, and 5 underwent
oncomitant pneumonectomy. Local recurrence resultedn four repeat resections. The 30-day or hospital mortalityas zero.Two patients underwent neoadjuvant chemotherapy,
nd 6 patients underwent adjuvant chemotherapy. Theherapy regimens ranged from Adriamycin (Pharmacia.p.A, Milan, Italy) plus ifosfamide to gemcitabine plus
axane or dacarbazine regimens, and not enough patientsad one type of chemotherapy regimen to determine anyenefit. Sites of distant recurrence included the pancreas,
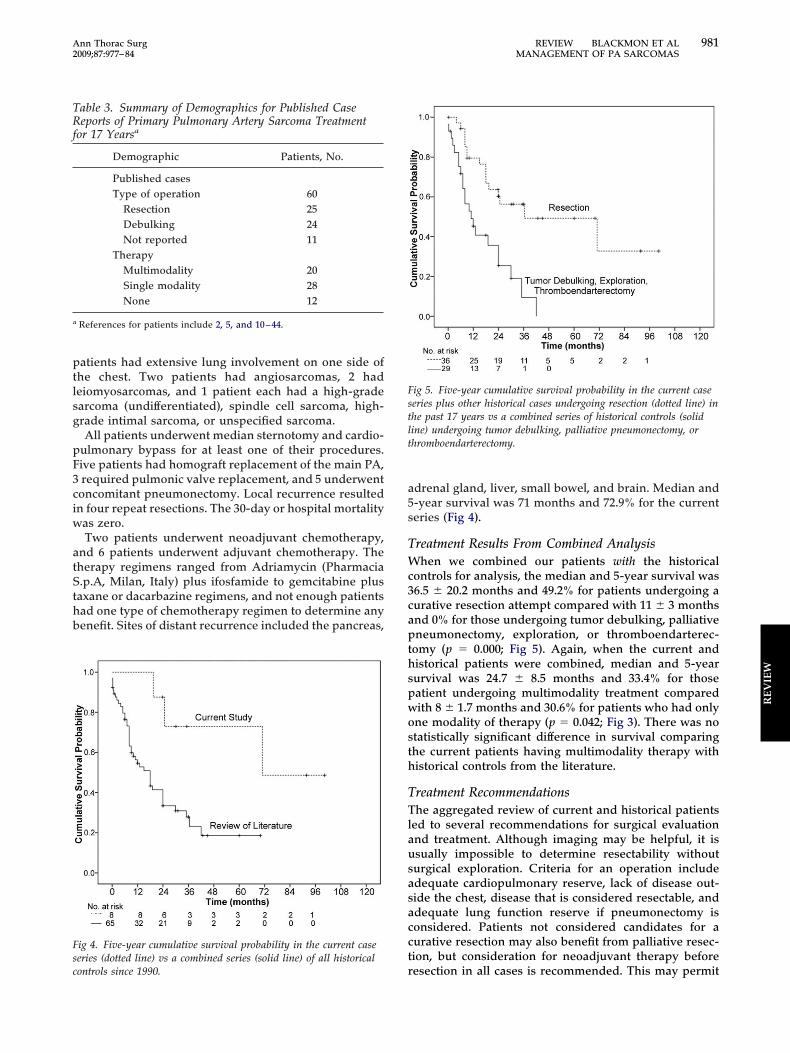
ig 4. Five-year cumulative survival probability in the current caseeries (dotted line) vs a combined series (solid line) of all historical
able 3. Summary of Demographics for Published Caseeports of Primary Pulmonary Artery Sarcoma Treatment
or 17 Yearsa
Demographic Patients, No.
Published casesType of operation 60
Resection 25Debulking 24Not reported 11
TherapyMultimodality 20Single modality 28None 12
References for patients include 2, 5, and 10–44.
rontrols since 1990.
drenal gland, liver, small bowel, and brain. Median and-year survival was 71 months and 72.9% for the currenteries (Fig 4).
reatment Results From Combined Analysishen we combined our patients with the historical
ontrols for analysis, the median and 5-year survival was6.5 � 20.2 months and 49.2% for patients undergoing aurative resection attempt compared with 11 � 3 monthsnd 0% for those undergoing tumor debulking, palliativeneumonectomy, exploration, or thromboendarterec-
omy (p � 0.000; Fig 5). Again, when the current andistorical patients were combined, median and 5-yearurvival was 24.7 � 8.5 months and 33.4% for thoseatient undergoing multimodality treatment comparedith 8 � 1.7 months and 30.6% for patients who had onlyne modality of therapy (p � 0.042; Fig 3). There was notatistically significant difference in survival comparinghe current patients having multimodality therapy withistorical controls from the literature.
reatment Recommendationshe aggregated review of current and historical patients
ed to several recommendations for surgical evaluationnd treatment. Although imaging may be helpful, it issually impossible to determine resectability withouturgical exploration. Criteria for an operation includedequate cardiopulmonary reserve, lack of disease out-ide the chest, disease that is considered resectable, anddequate lung function reserve if pneumonectomy isonsidered. Patients not considered candidates for aurative resection may also benefit from palliative resec-ion, but consideration for neoadjuvant therapy before
ig 5. Five-year cumulative survival probability in the current caseeries plus other historical cases undergoing resection (dotted line) inhe past 17 years vs a combined series of historical controls (solidine) undergoing tumor debulking, palliative pneumonectomy, orhromboendarterectomy.
esection in all cases is recommended. This may permit

tnim
mcmarartatrb
tstot
b[cte
tUstmvsccaWpaphittp
SAbtpsbtmttpaadoacss
pm
FsM
TA
SS
SS
982 REVIEW BLACKMON ET AL Ann Thorac SurgMANAGEMENT OF PA SARCOMAS 2009;87:977–84
REV
IEW
umor shrinkage, enhance resectability, and potentiallyeutralize micrometastatic disease. For an algorithm for
nitial evaluation of the patient with an intrapulmonaryass, please refer to Figure 1.Resection of the full extent of the tumor is recom-ended. Frozen specimen analysis is useful to determine
ompleteness of radial, proximal, and distal resectionargins. If excision of the pulmonic valve is necessary for
n Ro resection, then a homograft can be used foreconstruction. All patients should have at the minimum
CT scan to evaluate the extent of tumor and planesection. Intraoperative frozen specimens can be ob-ained to confirm malignancy. Intraoperative transesoph-geal echocardiography is routinely used in our institu-ion. Patients may benefit from resection even if a Ro
esection cannot be achieved, but local recurrence shoulde expected.The survival difference we have noted between pa-
ients undergoing complete resection vs incomplete re-ection, stenting, or palliative pneumonectomy leads uso recommend complete excision when possible. Bewaref lung infarcts: The parenchyma may appear to haveumor involvement and instead have necrosis from em-
ig 6. Recommended schedule for primary pulmonary artery (PA)arcoma postoperative evaluation. (CT � computed tomography;
pRI � magnetic resonance imaging.)
olization and lack of collateral blood supply to the lobe2]. For cases that appear equivocal, transvenous suctionatheter biopsy can be helpful [2]. We also noted a trendoward decreased survival in patients presenting witharly lung parenchymal recurrence.Surgical resection combined with neoadjuvant chemo-
herapy remains the therapy of choice for PA sarcomas.nfortunately, many patients are not hemodynamically
table to undergo such therapy and will have adjuvantherapy instead. After reviewing 13 pathologic speci-
ens, Burke and colleagues [15] reported a mean sur-ival of 23 months. With resection alone, the meanurvival ranges from a few days to 60 months [6, 18] in theurrent literature (Table 2). There appears to be noonsensus regarding the benefit of adjuvant chemother-py, with some in favor [5, 13, 20] and some against [48].
hen a preoperative diagnosis can be made and theatient is stable, most agree to the clinical benefit neo-djuvant chemotherapy offers [20]. In the current review,atients undergoing a bimodality regimen appeared toave prolonged survival compared with those undergo-
ng a single modality treatment regimen. On the basis ofhese data, our preference is to deliver neoadjuvant chemo-herapy to patients who are stable and adjuvant therapy toatients who will not tolerate waiting for resection.
urveillancefter resection, patients should have regular follow-upy a complete history, physical examination, and con-
rast-enhanced CT scan to detect early recurrence. Thoseatients with an intraluminal filling defect should haveubsequent gadolinium-enhanced MRI to differentiateetween tumor and thrombus. If thrombus is detected,
hey should remain on an anticoagulation therapy regi-en until the defect resolves. If there is no resolution,
hen tumor should again be suspected and repeat resec-ion should be considered. Please refer to Figure 6 for aostoperative evaluation algorithm that was developedt our own institution to eliminate unnecessary antico-gulation therapy for patients with new filling defectsue to tumor recurrence after initial resection. Becausene of our own patients was initially treated with antico-gulation therapy before being referred back to ourenter for repeat resection of a recurrent tumor, we haveubsequently followed this algorithm for postoperativeurveillance.
Owing the rarity of this type and location of tumor, norospective trials have evaluated these treatment regi-ens. Patients undergoing evaluation with a diagnosis of
able 4. Proposed Staging System for Primary Pulmonaryrtery Sarcomas
tage I Tumor limited to the main pulmonary arterytage II Tumor involving one lung plus a main pulmonary
arterytage III Bilateral lung involvementtage IV Extrathoracic spread
rimary PA sarcoma have the opportunity to be included

intddiIcmstp
C
P2srvdjmtw8ara
R
1
1
1
1
1
1
1
1
1
1
2
2
2
2
2
2
2
2
2
2
3
3
3
3
3
983Ann Thorac Surg REVIEW BLACKMON ET AL2009;87:977–84 MANAGEMENT OF PA SARCOMAS
REV
IEW
n our International Tumor Registry so that these smallumbers of patients can be tracked to ensure optimal
herapy can be determined. We used the limited survivalata recorded by our own institution and others toevelop a proposed PA sarcoma staging system (Table 4),
n which stage I tumors are limited to the main PA, stageI tumors involve 1 lung plus a main PA, stage III tumorsonstitute bilateral lung involvement, and stage IV tu-ors present with extrathoracic spread. This staging
ystem would require further validation by an Interna-ional Tumor Registry with larger numbers of patientser category to test validation.
omment
rimary PA sarcomas are rare tumors, with fewer than50 cases reported. Although surgical resection is thetandard of care, radical complete resection is rarelyeported for tumors involving the main PA, pulmonicalve, or right ventricular outflow tract. In patients un-ergoing PA resection instead of thrombectomy, in con-
unction with chemotherapy, our series reports a longedian survival of 71 months. This improved survival is
hought to be due to two factors: aggressive resectionith a curative intent and multimodality therapy. Of thepatients in the current series, 5 are still living and 3
ppear to have no evidence of disease to date. Radical PAesection in conjunction with chemotherapy is both safend appears to improve survival.
eferences
1. Mandelstamm M. Uber primare Neubildungen des Herzens.Virchows Arch 1923;245:43–54.
2. Miura S, Meirmanov S, Nakashima M, et al. Intimal sarcomaof the pulmonary artery: report of an autopsy case. PatholRes Pract 2005;201:469–74.
3. Huo L, Moran CA, Fuller GN, Gladish G, Suster S. Pulmo-nary artery sarcoma: a clinicopathologic and immunohisto-chemical study of 12 cases. Am J Clin Pathol 2006;125:419–24.
4. Nonomura A, Kurumaya H, Kono N, et al. Primary pulmo-nary artery sarcoma. Report of two autopsy cases studied byimmunohistochemistry and electron microscopy, and reviewof 110 cases reported in the literature. Acta Pathol Jpn1988;38:883–96.
5. Anderson MB, Kriett JM, Kapelanski DP, et al. Primarypulmonary artery sarcoma: a report of six cases. Ann ThoracSurg 1995;59:1487–90.
6. Kruger I, Borowski A, Horst M, et al. Symptoms, diagnosis,and therapy of primary sarcomas of the pulmonary artery.Thorac Cardiovasc Surg 1990;38:91–5.
7. Reardon MJ, Malaisrie SC, Walkes JC, et al. Cardiac auto-transplantation for primary cardiac tumors. Ann ThoracSurg 2006;82:645–50.
8. Reardon MJ, Walkes JC, Benjamin R. Therapy insight: ma-lignant primary cardiac tumors. Nat Clin Pract CardiovascMed 2006;3:548–53.
9. Reardon MJ, Walkes JC, Defelice CA, Wojciechowski Z.Cardiac autotransplantation for surgical resection of a pri-mary malignant left ventricular tumor. Tex Heart Inst J2006;33:495–7.
0. Redmond ML, Shepard JW, Gaffey TA, Payne WS. Primarypulmonary artery sarcoma. A method of resection. Chest1990;98:752–3.
1. Varriale P, Chryssos B. Pulmonary artery sarcoma: anothercause of sudden death. Clin Cardiol 1991;14:160–4.
2. Hiroshima K, Uruma T, Ishibashi M, Ohwada H, Hayashi Y.A case of primary sarcoma of the pulmonary artery. ActaPathol Jpn 1992;42:755–9.
3. Head HD, Flam MS, John MJ, Lipnik SS, Slater DL, StewartRD. Long-term palliation of pulmonary artery sarcoma byradical excision and adjuvant therapy. Ann Thorac Surg1992;53:332–4.
4. Ramp U, Gerharz CD, Iversen S, Schweden F, Steppling H,Gabbert HE. Sarcoma of the pulmonary artery: report of twocases and a review of the literature. J Cancer Res Clin Oncol1992;118:551–6.
5. Burke AP, Virmani R. Sarcomas of the great vessels: aclinicopathologic study. Cancer 1993;71:1761–73.
6. Tanaka I, Masuda R, Inoue M, et al. Primary pulmonaryartery sarcoma. Thorac Cardiovasc Surgeon 1994;42:64–8.
7. Salamat SM, Landy HJ, O’Sullivan MJ. Pulmonary arterysarcoma in a pregnant woman: report of a case. ObstetGynecol 1994;84:668–9.
8. Johansson L, Carlen B. Sarcoma of the pulmonary artery:report of four cases with electron microscopic and immuno-histochemical examinations, and review of the literature.Virchows Arch 1994;424:217–24.
9. Goldblum JR, Rice TW. Epithelioid angiosarcoma of thepulmonary artery. Hum Pathol 1995;26:1275–7.
0. Zerkowski HR, Hofmann HS, Gybels I, et al. Primary sar-coma of pulmonary artery and valve: multimodality treat-ment by chemotherapy and homograft replacement. J Tho-rac Cardiovasc Surg 1996;112:1122–4.
1. Parish JM, Rosenow EC III, Swensen SJ, et al. Pulmonaryartery sarcoma: clinical features. Chest 1996;110:1480–8.
2. Akomea-Agyin C, Dussek JE, Anderson DR, Hartley RB.Pulmonary artery sarcoma mimicking pulmonary embolism:successful surgical intervention. Ann Thorac Surg 1996;61:1536–8.
3. Kacl GM, Bruder E, Pfammatter T, Follath F, Salomon F,Debatin JF. Primary angiosarcoma of the pulmonary arteries:dynamic contrast-enhanced MRI. J Comput Assist Tomogr1998;22:687–91.
4. Bode-Lesniewska B, Zhao J, Speel EJ, et al. Gains of 12q13–14and over expression of mdm2 are frequent findings inintimal sarcomas of the pulmonary artery. Virchows Arch2001;438:57–65.
5. Simpson WL, Mendelson DS. Pulmonary artery and aorticsarcomas: cross-sectional imaging. J Thorac Imaging 2000;15:290–4.
6. Tanaka H, Hasegawa S, Egi K, Tachou H, Saitoh F,Sunamori M. Successful radical resection of a leiomyosar-coma of the pulmonary trunk. J Thorac Cardiovasc Surg2001;122:1039 – 40.
7. Dennie CJ, Veinot JP, McCormack DG, Rubens FD. Intimalsarcoma of the pulmonary arteries seen as a mosaic patternof lung attenuation on high-resolution CT. AJR Am J Roet-genol 2002;178:1208–10.
8. Gaumann A, Tews DS, Mayer E, et al. Expression of apop-tosis-related proteins, p53, and DNA fragmentation in sar-comas of the pulmonary artery. Cancer 2001;92:1237–44.
9. Govender D, Pillay S, Right pulmonary artery sarcoma,Pathology 2001;33:243–5.
0. Mattoo A, Fedullo PF, Kapelanski D, Ilowite JS. Pulmonaryartery sarcoma: a case report of surgical cure and 5-yearfollow-up. Chest 2002;122:745–7.
1. Tschirch FT, Del Grande F, Marincek B, et al. Angiosarcomaof the pulmonary trunk mimicking pulmonary thromboem-bolic disease. A case report, Acta Radiol 2003;44:504–7.
2. Kotooka N, Nagaya N, Tanaka R. Pulmonary artery sarcoma.Heart 2003;89:1388.
3. Totaro M, Miraldi F, Ghiribelli C, et al. Cardiac angiosar-coma arising from pulmonary artery: endovascular treat-ment. Ann Thorac Surg 2004;78:1468–70.
4. Tsunezuka Y, Oda M, Takahashi M, Minato H, Watanabe G.Primary chondromatous osteosarcoma of the pulmonary
artery. Ann Thorac Surg 2004;77:331–4.
3
3
3
3
3
4
4
4
4
4
4
4
4
4
4
5
5
5
5
5
5
5
5
5
5
6
6
6
984 REVIEW BLACKMON ET AL Ann Thorac SurgMANAGEMENT OF PA SARCOMAS 2009;87:977–84
REV
IEW
5. Choi EY, Yoon YW, Kwon HM, et al. A case of pulmonaryartery intimal sarcoma diagnosed with multislice CT scanwith 3D reconstruction. Yonsei Med J 2004;45:547.
6. Choong KC, Lawton JS, Moon MR, Damiano RJ. Failure ofmedical therapy for pulmonary thromboembolic disease:beware the unsuspected primary sarcoma of the pulmonaryartery, J Thorac Cardiovasc Surg 2004;128:763–5.
7. Park BJ, Bacchetta M, Bains MS, et al. Surgical managementof thoracic malignancies invading the heart or great vessels.Ann Thorac Surg 2004;78:1024–30.
8. Funabashi N, Komuro I. Images in clinical medicine. Heart-shaped tumor in pulmonary trunk. N Engl J Med 2005;10;352:608.
9. Uchida A, Tabata M, Kiura K, et al. Successful treatment ofpulmonary artery sarcoma by a two-drug combination che-motherapy consisting of ifosfamide and epirubicin. JpnJ Clin Oncol 2005;35:417–9.
0. Widera E, Sulica R. Pulmonary artery sarcoma misdiagnosedas chronic thromboembolic pulmonary hypertension. MtSinai J 2005;72:360–4.
1. Furest I, Marín M, Escribano P, Gómez MA, Cortinac J,Blanquer R. Intimal sarcoma of the pulmonary artery: a rarecause of pulmonary hypertension. Arch Bronconeumol 2006;42:148–50.
2. Maruo A, Okita Y, Okada K, Yamashita T, Tobe S, TanimuraN. Surgical experience for the pulmonary artery sarcoma.Ann Thorac Surg 2006;82:2014–6.
3. Komanapalli C, Alsoufi B, Shen I, Slater M. Recurrentpulmonary artery sarcoma. J Card Surg 2006;21:587–9.
4. Heid F, Guth S, Mayer E, et al. Extracorporal circulation andcardiac arrest in an awake patient: a safe approach for singlelung pulmonary artery stenting? Ann Thorac Surg 2006;82:746–7.
5. Yi ES. Tumors of the pulmonary vasculature. Cardiol Clin2004;22:431–40.
6. Kauczor HU. Pulmonary artery sarcoma mimicking chronicthromboembolic disease: computed tomography and mag-netic resonance imaging findings. Cardiovasc Intervent Ra-diol 1994;17:185–9.
7. Riedel B, Lim J, Brauer K, Shaw A, Reardon M, Rice D.Diagnosis and management of persistent pulmonary throm-boembolism. J Cardiothorac Vasc Anesth 2006;20:616–9.
8. Cox JE, Chiles C, Aquino SL, et al. Pulmonary artery sarco-mas: a review of clinical and radiologic features. J Comput
Assist Tomogr 1997;21:750–5.9. Smith WS, Lesar MS, Travis WD, et al. MR and CT findingsin pulmonary artery sarcoma. J Comput Assist Tomogr1989;13:906–9.
0. Weinreb JC, Davis SD, Berkmen YM, Isom W, Naidich DP.Pulmonary artery sarcoma: evaluation using Gd-DTPA.J Comput Assist Tomogr 1990;14:647–9.
1. Rafal RB, Nichols JN, Markisz JA. Pulmonary artery sarcoma:diagnosis and postoperative follow-up with gadolinium-diethylenetriamine pentaacetic acid– enhanced magneticresonance imaging. Mayo Clin Proc 1995;70:173–6.
2. Schermoly M. Pulmonary artery sarcoma—unusual pulmo-nary angiographic finding—a case report. Angiology 1987;38:617–21.
3. Ricou F, Nicod P, Moser KM, et al. Catheter-based intravas-cular ultrasound imaging of chronic thromboembolic pul-monary disease. Am J Cardiol 1991;76:749–52.
4. Pandian NG, Weintraub A, Kreis A, et al. Intracardiac,intravascular, two-dimensional, high frequency ultrasoundimaging of pulmonary and its branches in humans andanimals. Circulation 1990;81:2007–12.
5. Okano Y, Satoh T, Tatewaki T, et al. Pulmonary arterysarcoma diagnosed using intravascular ultrasound images.Thorax 1999;54:748–9.
6. Esakof DD, Schneider AT, Pandian NG, et al. Delineation ofpulmonary artery sarcoma with multiplane and panoramictransesophageal echocardiography. J Am Soc Echocardiogr1993;6:619–23.
7. Chong S, Kim TS, Kim BT, Cho EY, Kim J. Pulmonaryartery sarcoma mimicking pulmonary thromboembolism:integrated FDG PET/CT. AJR Am J Roetgenol 2007;188:1691–3.
8. Thurer RL, Thorsen A, Parker A, Karp DD. FDG imaging of apulmonary artery sarcoma. Ann Thorac Surg 2000;70:1414–5.
9. Baker PB, Goodwin RA. Pulmonary artery sarcomas: a re-view and report of a case. Arch Pathol Lab Med 1985;109:35–9.
0. Shmookler BM, Marsh HB, Roberts WC. Primary sarcoma ofthe pulmonary trunk and/or right or left main pulmonaryartery. A rare cause of obstruction to right ventricularoutflow; report on two patients and analysis of 35 previouslydescribed patients. Am J Med 1977;63:263–72.
1. Moffat RE, Chang CH, Slaven JE. Roentgen considerationsin primary pulmonary artery sarcomas. Radiology 1972;104:283–8.
2. Mayer E, Kriegsmann J, Gaumann A, et al. Surgical treat-ment of pulmonary artery sarcoma. J Thorac Cardiovasc
Surg 2001;121:77–82.
Related Documents











