
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript


OVERT DIABETESOVERT DIABETES

Classic signs/ symptoms of DM + RBS >200 mg/dl FBS ≥126 mg/dl 2 hr PPBS ≥200 mg/dl

PRE-CONCEPTIONAL CAREPRECONCEPTIONAL COUNSELING
Good glycaemic control before pregnancy can reduce (but not eliminate) the risk of adverse pregnancy outcomes
Regular glucose monitoring Diet, body weight and exercise Weight reduction if BMI > 27 kg/m2 The importance of planning of pregnancy and the role of contraception
Folic acid (5 mg/day) until 12 weeks of gestation to reduce the risk of NTD
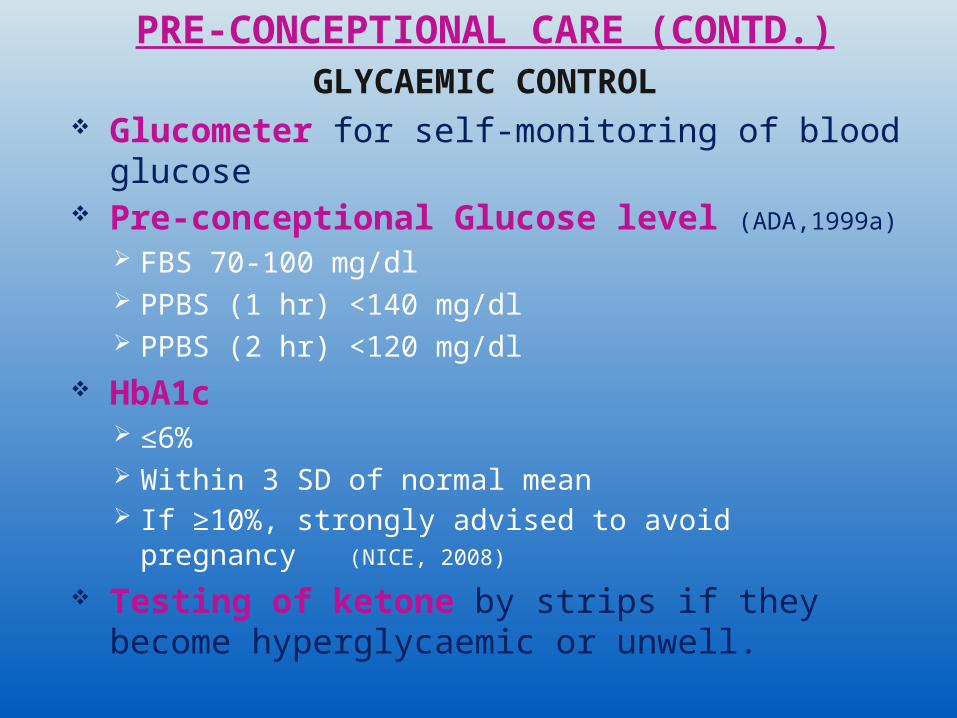
PRE-CONCEPTIONAL CARE (CONTD.)GLYCAEMIC CONTROL
Glucometer for self-monitoring of blood glucose
Pre-conceptional Glucose level (ADA,1999a) FBS 70-100 mg/dl PPBS (1 hr) <140 mg/dl PPBS (2 hr) <120 mg/dl
HbA1c ≤6% Within 3 SD of normal mean If ≥10%, strongly advised to avoid pregnancy (NICE, 2008)
Testing of ketone by strips if they become hyperglycaemic or unwell.
PRE-CONCEPTIONAL CARE (CONTD.)DRUGS (NICE, 2008)
Metformin- can be used in the pre-conception period and during pregnancy, when the likely benefits from improved glycaemic control outweigh the potential for harm
All other OHAs- should be discontinued before pregnancy except Glyburide
Aspart & Lispro insulin- no adverse effects in pregnancy
NPH insulin- the first choice for long-acting insulin in pregnancy
ACE inhibitors and ARBs- discontinued before conception or as soon as pregnancy is confirmed
Statins- discontinued before pregnancy or as soon as pregnancy is confirmed
PRE-CONCEPTIONAL CARE (CONTD.)RETINAL ASSESSMENT (NICE, 2008)
Done at the first appointment Thereafter annually, if no diabetic
retinopathy is found By digital imaging with mydriasis
using tropicamide Women should defer rapid optimisation
of glycaemic control until after retinal assessment and treatment have been completed
PRE-CONCEPTIONAL CARE (CONTD.)RENAL ASSESSMENT (NICE, 2008)
Includes measurement of microalbuminuria before pregnancy
Referral to a nephrologist should be considered before discontinuing contraception if Serum creatinine ≥120 µmol/LEstimated GFR <45 ml/min/1.73 m2

MANAGEMENT IN FIRST TRIMESTERDIETARY MANAGEMENT
3 meals and 3 snacks per day
Consistent timing with food intakeTo facilitate insulin dosage & avoid hypoglycaemia
Specially for NPH + Regular insulinNot so rigorous for Glargine + Aspart/ Lispro

MANAGEMENT IN FIRST TRIMESTER (CONTD.)
INSULIN THERAPY Mainstay of management in type I DM To cover Basal needs (Basal Insulin)- Intermediate/ Long acting Insulin-
To suppress hepatic neoglucogenesis
between meals & during fasting
PP rise of sugar (Prandial Insulin)- Short acting Insulin
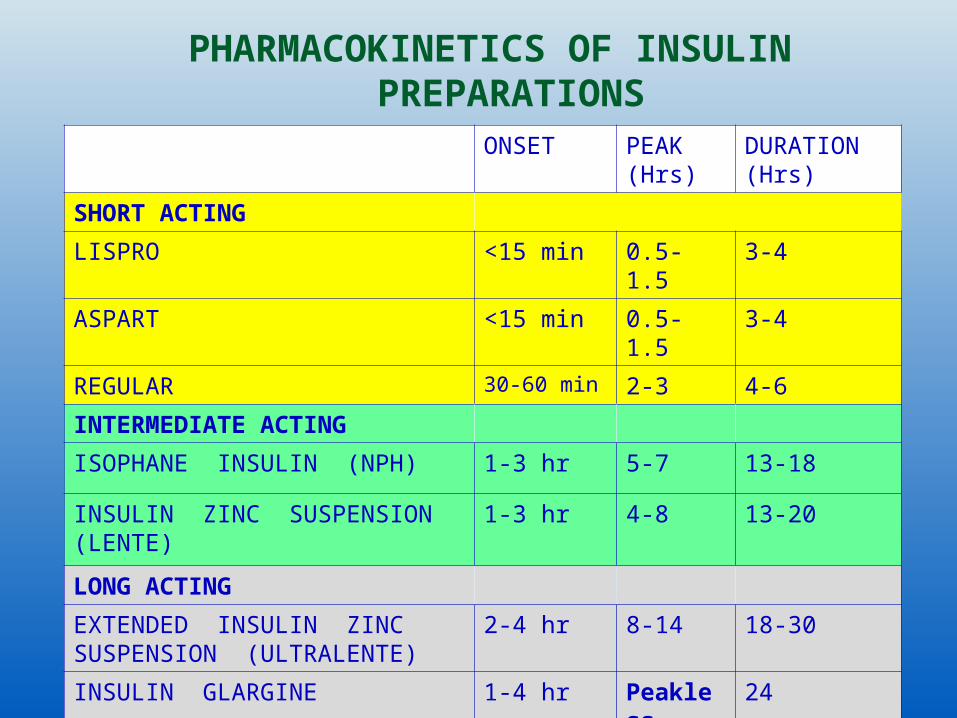
PHARMACOKINETICS OF INSULIN PREPARATIONS
ONSET PEAK (Hrs)
DURATION (Hrs)
SHORT ACTINGLISPRO <15 min 0.5-
1.53-4
ASPART <15 min 0.5-1.5
3-4
REGULAR 30-60 min 2-3 4-6INTERMEDIATE ACTINGISOPHANE INSULIN (NPH) 1-3 hr 5-7 13-18
INSULIN ZINC SUSPENSION (LENTE)
1-3 hr 4-8 13-20
LONG ACTINGEXTENDED INSULIN ZINC SUSPENSION (ULTRALENTE)
2-4 hr 8-14 18-30
INSULIN GLARGINE 1-4 hr Peakless
24

INSULIN THERAPY (CONTD.)I.Multiple daily SC injections Total daily requirement
0.6 U/kg current weight- 1st trimester0.7 U/kg current weight- 2nd trimester0.9 U/kg current weight- 3rd trimester
Regular + NPH – commonly used 4/6 at breakfast (2/3 NPH, 1/3 Regular) 1/6 before dinner- Regular 1/6 at bed time- NPH To be administered >30 min before meal Mid-morning & mid-afternoon snacks necessary to avoid hypoglycaemia
Glargine + Lispro/ Aspart- Mimics physiological system Less rigorous timing of meals But Inj Lispro necessary before each meals

INSULIN THERAPY (CONTD.)II.Subcutaneous insulin infusion pump
Only for those women who are highly motivated, where multiple daily injections are ineffective & no disabling hypoglycaemia
Needs strict asepsisNeeds less Insulin (0.3-0.5 U/kg)
III. Inhaled Insulin Not well studied in pregnancy Needs PFT monitoring
INSULIN THERAPY (CONTD.) Insulin: Carbohydrate ratio:
One method to calculate prandinal Insulin
How many grams of CHO is covered by 1 U Regular Insulin
Insulin : CHO = 500/ total daily requirement
Typically in the range of 10-15 Insulin Sensitivity Factor Estimated drop in blood glucose per unit of Regular Insulin
Equal to 1500/ total daily requirement Amount of supplemental Insulin needed = difference between actual and desired blood glucose/ sensitivity factor
Useful to make sliding scale

MANAGEMENT IN FIRST TRIMESTER (CONTD.)
BLOOD SUGAR MONITORING Self-monitoring of capillary blood glucose (CBG) Finger-prick method using a Glucometer
Noninvasive- by Iontophoresis Goals of glucose control (ACOG, 2005)
Fasting ≤ 95 mg/dlPremeal ≤ 100 mg/dl1 Hr PP ≤ 140 mg/dl2 Hr PP ≤ 120 mg/dl02.00- 06.00 AM ≥ 60 mg/dlMean (Average) 100 mg/dlHbA1c ≤ 6 %

BLOOD SUGAR MONITORING (CONTD.) Blood Sugar should be measured in fasting, 1 hr before meals and at bed time (NICE, 2008)
Rotine use of HbA1C in 2nd and 3rd trimester is not recommended (NICE, 2008)
Ketone should be measured if women feel unwell or hyperglycaemic
MANAGEMENT IN SECOND TRIMESTER Congenital anomaly detection
Vaginal probe USG at 10-14 weeks to detect NTD & Nuchal tranlucency
MSAFP (values lower in DM) at 16-20 weeks to detect NTD
Detailed sonographic examination at 18-20 weeks
Fetal echocardiography for the four-chamber view of the fetal heart and outflow tracts at 20-22 weeks
Individualized glycaemic control Insulin requirement increases after 24 weeks
Dietary management continues Regular antenatal visits

MANAGEMENT IN THIRD TRIMESTER Insulin and dietary control continues Fetal monitoring Ultrasound monitoring Fetal growth and amniotic fluid
volume Every 4 weeks from 28 to 36 weeks Routine monitoring of fetal well-being Not recommended before 38 weeks Indications of monitoring of fetal well-
being From 28 weeks
Women at risk of IUGR (macrovascular disease and/or nephropathy)
Unstable DM Women requiring >100 U insulin/day

MANAGEMENT IN LABOUR Decision for delivery
To be taken at 36 weeks- Induction vs CS
Discussion with patient, keeping respect to her decision
CS often for macrosomia in White class B and C
DM is not a contraindication to VBAC Timing of delivery
Stable DM- at 38 weeksUnstable DM- as soon as fetal lung maturity is attained
MANAGEMENT IN LABOUR (CONTD.) Preterm labour
β-mimetics are to be avoidedNifedipine is preferred drug<32 weeks, intrauterine infections to be excluded
Steroids for lung maturity are not contraindicated
Needs additional insulin Close monitoring
Labour management IVF & insulin for glycaemic control Careful monitoring
MANAGEMENT IN PUERPERIUM CBG should be regularly monitored Often patient needs no insulin in 1st 24 hr
Start with ½ to 2/3 of pre-delivery doses of insulin
Breastfeeding should be encouraged Risk of hypoglycaemia during breast feeding
Infections promptly detected and treated Contraceptive advices
IUCD does not increase infection rate Hormonal contraceptives are avoided in vascular disease
Puerperal sterilisation, if suitable Counseling regarding future pregnancy


INSULIN RESISTANCE Impaired metabolic response to endogenous or exogenous insulin (ADA)
Peak insulin levels in 3 hr GTT (µU/ml) <100- normal 100-150- mild resistance 150-300- moderate resistance >300- severe resistance
FBS (mg/dl) : fasting insulin (µU/ml) <4.5
C-peptide assay Glucose-clamp technique
METABOLIC SYNDROME Also called syndrome X, Insulin
Resistance syndrome or Deadly Quartet NCEPATP III definition- At least three of the following FBS ≥110 mg/dl Abdominal obesity (waist
circumference >35 inch. In women, >40 inch in men)
Triglycerides >150 mg/dl; HDL <50 mg/dl in women, <40 mg/dl in men BP ≥ 130/85 mm Hg
MANAGEMENT IN PREGNANCYDIETARY MANAGEMENT
Like GDM To maintain a calorie intake adequate for pregnancy but with minimum weight gain
Ideal weight gainNormal weight 25-35 lbOverweight 15-25 lbObese 11-20 lb
Underweight 28-40 lb

MANAGEMENT IN PREGNANCY (CONTD.)GLYBURIDE
Normal weight/ moderately obese Good β-cell functions Duration of DM <5 years
MANAGEMENT IN PREGNANCY (CONTD.)INSULIN THERAPY
Glyburide + NPH insulin at bed time (to suppress hepatic neoglucogenesis to lower FBS)
Or Glargine in the morning (less hypoglycaemia)
Starting dose is 20 U SC usually If CBG values are still elevated, the dose may be ↑ by 5 U every 5 days until adequate control is obtained

MANAGEMENT IN PREGNANCY (CONTD.)
BLOOD SUGAR MONITORING
Self-monitoring of CBG HbA1C Fructosamine <2.6 µmol/L

MANAGEMENT OF LABOUR AND PUERPERIUM
Similar to GDM

DIABETIC NEPHROPATHY Especially in type I Hypertension & proteinuria Risk of Preeclampsia and preterm labour, IUGR
Renal assessment to be done in the first ANC visit
Referral to a nephrologist - if Serum creatinine ≥120 µmol/L Total protein excretion >2 g/day
Estimated GFR should not be used in pregnancy
Thromboprophylaxis should be considered- If proteinuria >5 g/day (macroalbuminuria)
DIABETIC RETINOPATHY (DR)
Both in type I & type II DM Pregnancy worsens retinopathy Acute rigorous metabolic control worsens retinopathy
Slows down progression of retinopathy in long term
Insulin Lispro may worsen retinopathy (?)
Retinopathy is associated with reduced fetal growth
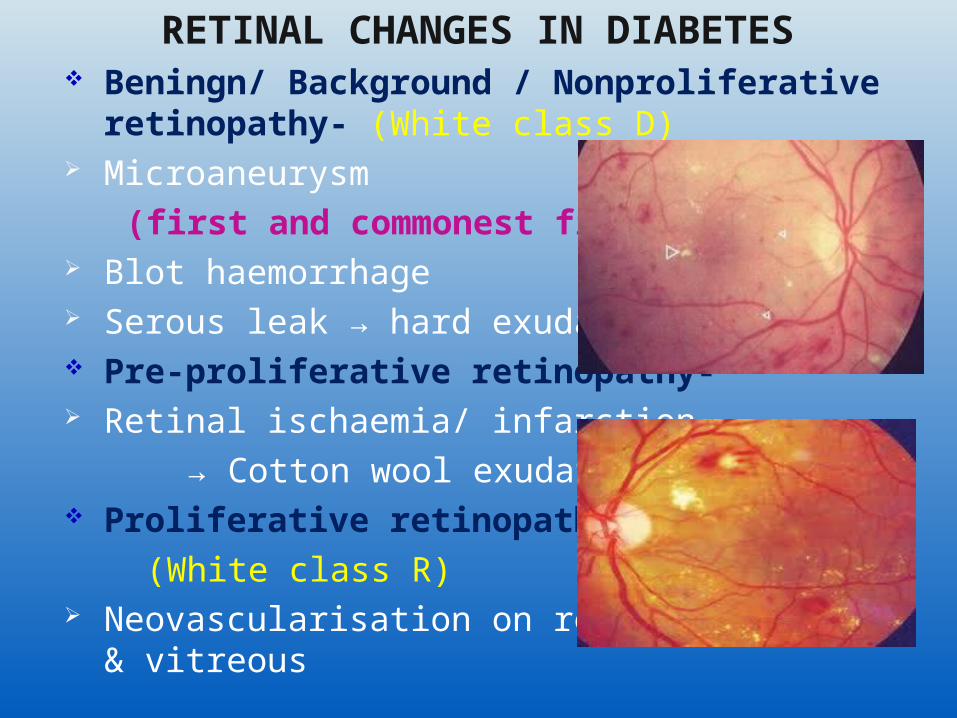
RETINAL CHANGES IN DIABETES Beningn/ Background / Nonproliferative retinopathy- (White class D)
Microaneurysm (first and commonest finding) Blot haemorrhage Serous leak → hard exudates Pre-proliferative retinopathy- Retinal ischaemia/ infarction → Cotton wool exudates Proliferative retinopathy- (White class R) Neovascularisation on retinal surface & vitreous
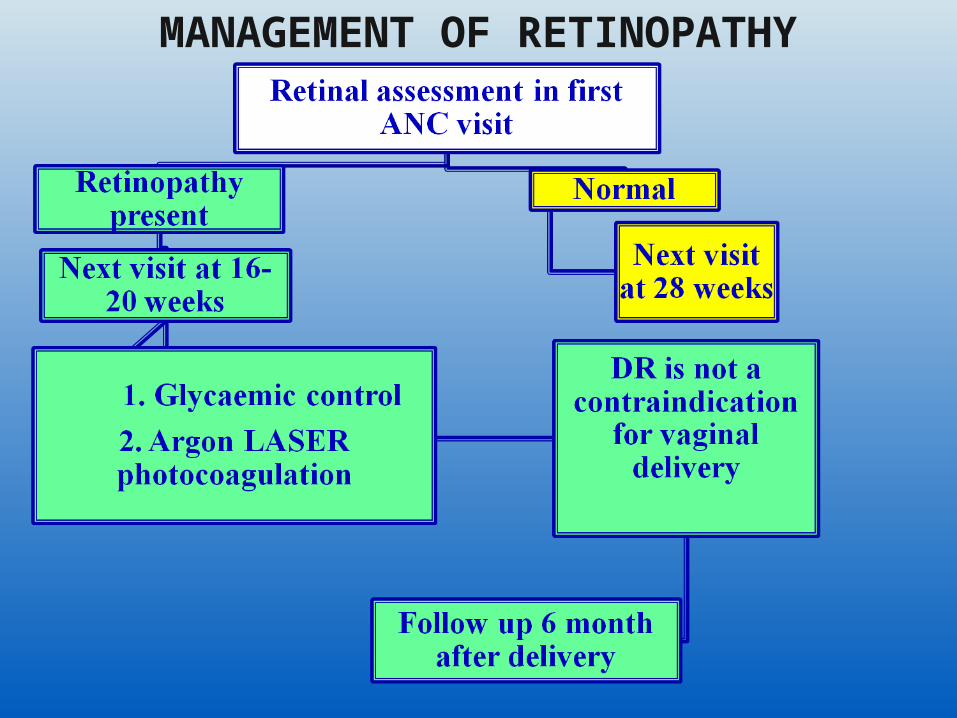
MANAGEMENT OF RETINOPATHY

DIABETIC NEUROPATHY
Peripheral sensory-motor neuropathy- uncommon in pregnancy
DIABETIC GASTROPATHY- More troublesome in pregnancy Nausea, vomiting, nutritional problems
Difficult glucose control Needs Metoclopramide, H2 receptor blockers, Erythromycin or Intermittent gastric intubation
INFECTIONS Urinary tract infections
Associated with preterm labourMay cause pyelonephritisScreening and treatment of asymptomatic bacteruria to be done
Respiratory tract infections Vulvovaginal infections Puerperal pelvic infections Wound infections after Caesarean Section
Needs prompt diagnosis and treatment with antibiotics
DIABETIC KETOACIDOSIS (DKA) Most serious complication Affects 1% of diabetic pregnancies Fetal loss 20% Unique to type I DM Precipitating factors
Hyperemesis gravidarum Noncompliance to insulin therapy Tocolytics, corticosteroids
Pregnant women usually develop DKA at lower level of glucose than nonpregnant individuals
DIAGNOSIS OF DKA
Blood glucose >250 mg/dl usually Ketone bodies in urine & plasma Arterial pH <7.3 Serum bicarbonate <15 mEq/L
MANAGEMENT OF DKA(ACOG 2005)
Laboratory assessmentABG, glucose, ketones, eletrolytes every 1-2 hr
InsulinIV loading 0.2-0.4 U/KgIV maintenance 2-10 U/hr
FluidsIsotonic NaCl1 L in 1st hr500-1000 ml/hr for next 2-4 hr250 ml/hr until 80% replacedTotal replacement in 1st 12 hrs of 4-6 L

MANAGEMENT OF DKA (CONTD.) Glucose
When CBG <250 mg/dl, 5%DNS infusion
PotassiumIf initially normal/ low- 15-20 mEq/ hr
If elevated, wait, until it becomes normal, then 20-30 mEq/ L IV solution
Bicarbonate If pH < 7.1, add 1 amp (44 mEq) to 1 Lit of 0.45% NS

HYPEROSMOLAR NONKETOTIC COMA
Peculiar to type II DM Severe hyperglycaemia (>600 mg/dl) Serum hyperosmolarity (>320 mOsm/L) No ketonaemia Management- Aggressive fluid therapy to combat severe dehydration
Insulin PotassiumRarely seen in pregnancy
HYPOGLYCAEMIA Especially occurs in 1st trimester with type I DM
Peak incidence at 10-15 weeks Significant hypoglycaemia occurs when CBG values are less than 35 mg/dl
Woman should know symptoms of hypoglycaemia
ManagementOral glucoseIf unconscious- 20 ml of 50% dextrose, followed by 10% dextrose drip
If severe, injection Glucagon 1 mg IM/ SC

FASTING HYPERGLYCAEMIASOMOGYI’S PHENOMENON
High fasting blood sugar & C/O nightmares/ nocturnal sweating
Nocturnal hypoglycaemia (01.00- 05.00 AM) → exaggerated counter-regulatory response
Treatment is to DECREASE the night dose of intermediate/ long acting insulin
DAWN PHENOMENON High fasting blood sugar in absence of
nocturnal hypoglycaemia Cause not known exactly Treatment is to INCREASE the night dose
of intermediate/ long acting insulin

THANK YOUTHANK YOU
Related Documents











