Assessment of Medical Radioactive Waste Management in Hospitals: | Richard Okot i ASSESSMENT OF MEDICAL RADIOACTIVE WASTE MANAGEMENT IN HOSPITALS Richard Okot BSc- Environmental Science, Management and Technology P/O BOX 1, Kyambogo University Kampala Uganda [email protected] +256-784848542 +256-754267894 Supervisor Mrs. Pamela Lawino Okori Lecturer Kyambogo university Chemistry Department Faculty of Science MSc – environmental science & technology PGDS – Environmental Impact Assessment; Limnology & Wetland Ecology BSc – Botany & Zoology; BST – Chemistry [email protected]

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Assessment of Medical Radioactive Waste Management in Hospitals: | Richard Okot
i
ASSESSMENT OF MEDICAL RADIOACTIVE WASTE
MANAGEMENT IN HOSPITALS
Richard Okot
BSc- Environmental Science, Management and Technology
P/O BOX 1, Kyambogo University
Kampala Uganda
+256-784848542
+256-754267894
Supervisor
Mrs. Pamela Lawino Okori
Lecturer Kyambogo university
Chemistry Department Faculty of Science
MSc – environmental science & technology
PGDS – Environmental Impact Assessment; Limnology & Wetland Ecology
BSc – Botany & Zoology;
BST – Chemistry
Assessment of Medical Radioactive Waste Management in Hospitals: | Richard Okot
ii
DEDICATION
This research report is dedicated to my parents Mr. and Ms. Obita, who supported me financially,
morally and spiritually. Your advice, solidarity and relentless efforts to this course made me reach
this academic level.
MAY GOD BLESS YOU.
Assessment of Medical Radioactive Waste Management in Hospitals: | Richard Okot
iii
ACKNOWLEDGEMENT
I would like to first give and praise to the Almighty God, without Him this truly would not have
been. Thanks for Your love and abundant gift of life.
I thank Mrs. Pamela .L. Okori for her invaluable academic supervision and enthusiasm throughout
this report, as well as for the support and confidence she gave me from every meeting and point of
contact that occurred from start to finish.
My gratitude goes to my dad Mr. Valeriano Obita and my mum Mrs. Leorina Obita, and all my
family members (Margret, Scovia, Nancy and Jane: brothers David, Ivan and Kenneth) without
whose love, financial support and wisdom I could not have been where I am today.
Thanks must also go to the people who agreed to undertake the surveys, without which the study
would have seriously been compromised.
I am grateful to all my former lectures of Chemistry Department, Kyambogo University, for their
academic guidance and guidance that facilitated me through my study.
Finally, thanks must go to all my course mates (Angela Nsaali, Helen brain, Auma Charoline, Lagu
Richard, and Ogwang Norbert) and friends (Opio Kenneth, Wampande Mika, Namanya Ernest,
Kibikyabo Festo, Discharch Musa) for their continual support and enthusiasm towards this study.
May the almighty God bless you all.
Assessment of Medical Radioactive Waste Management in Hospitals: | Richard Okot
iv
ABSTRACT
The high generation rate of medical radioactive waste in Uganda is a proof that medical waste
management in Uganda is problematic. Based on a case study undertaken at Hospitals within
Kampala, this research looked in to the various issues in the field of medical radioactive waste
management. It explores the staff‘s perception towards the medical radioactive waste management
and aims to examine the knowledge level, attitude and role of health care workers towards the
medical radioactive waste management. The study looks in to the various medical radioactive
waste treatment technologies available and chooses the best available technology for the on-site
treatment of the waste.
In Uganda, there has been an emerging concern regarding medical radioactive waste management
and the enforcement of international and national regulations requiring health care establishment
to ensure that such waste is handled without any adverse effects to the human health and the
environment (Ugandan Ministry of Environment and Forests, 1998). According to the Ministry of
Health (2009), the current medical radioactive waste management system in Uganda is inadequate
both at public and private level. The actual amount of medical radioactive wastes generated in
Ugandan hospitals is not known and even trying to estimate it would be problematic (Wekoy,
2005). In addition, there is insufficient capacity and research data on medical radioactive waste
generation, separation, storage, treatment and final disposal mechanisms in Uganda. Therefore,
this study tried to provide a glimpse of how radioactive wastes are being handled at various
hospitals.
The study used 10 respondents and simple random sampling was used for the study. Data sources
were both primary and secondary. The data collection methods included; interviews,
questionnaires, secondary data, observation and photography. The captured data was presented in
graphic form like pie-chats, bar graph and percentages were generated. The research study found
out that, much of the wastes collected consisted of solid radioactive wastes followed by liquid and
lastly gaseous wastes and they were of low level according to their categorization. The radioactive
wastes generated were mostly used gloves, syringes, items used by hospitalised patients after
radiation therapy, protective clothing, masks, filters, overshoes, towels, hand tools, contaminated
water and effluent, body fluids, discarded liquid radiopharmaceuticals, and liquid-patient

Assessment of Medical Radioactive Waste Management in Hospitals: | Richard Okot
v
excretion. These wastes are collected from the different departments of hospitals into one place,
separated to different categories, some treated and others transported to the KCCA treatment plant
after they have piled up. Much of the wastes after segregation are stored on the KCCA containers
awaiting transportation to the Municipal treatment plant and the remaining, mostly with highly
radioactive materials are incinerated or treated from within the hospitals.
In conclusion, it was established that much of the radioactive wastes produced by hospitals were
in forms which included; solids, liquids and gases. These wastes are segregated and then deposited
at either the KCCA container or incinerated or in temporary plastic dustbins within the hospitals
which were then further transferred to the Municipal waste treatment plant at Kiteezi in Wakiso
district. Much of the radioactive wastes produced are low level waste. Some high level wastes
produced were incinerated at the hospital premises to reduce their effect to the environment and
the staff involved in the garbage collection process.
Assessment of Medical Radioactive Waste Management in Hospitals: | Richard Okot
vi
TABLE OF CONTENTS
DEDICATION ................................................................................................................................ ii
ACKNOWLEDGEMENT ............................................................................................................. iii
ABSTRACT ................................................................................................................................... iv
TABLE OF CONTENTS ............................................................................................................... vi
LIST OF FIGURES ....................................................................................................................... ix
ABBREVIATION AND ACCRONYMS ..................................................................................... xi
OPERATIONAL DEFINITION OF TERMS .............................................................................. xii
CHAPTER ONE: INTRODUCTION ......................................................................................... 1
1.1 Global perspective of radioactive waste generation and management ..................................... 1
1.1.1 Radioactive waste generation in developed countries........................................................ 1
1.1.2 Radioactive waste generation in developing countries ...................................................... 1
1.1.3 Strategies for radioactive waste management .................................................................... 2
1.2 The application of nuclear medicine in hospitals ..................................................................... 3
1.3 Effects of mismanaging medical radioactive wastes in the environment ................................. 5
1.4 Statement of the Problem .......................................................................................................... 5
1.5 Significance of the study ........................................................................................................... 6
1.6 Objectives of the study.............................................................................................................. 7
1.6.1 General objective................................................................................................................ 7
1.6.2 Specific objectives.............................................................................................................. 7
1.7 Research questions .................................................................................................................... 7
1.8 Expected outcome ..................................................................................................................... 8
1.9 Scope of the study ..................................................................................................................... 8
1.9.1 Time scope ......................................................................................................................... 8
1.9.2 Geographical scope ............................................................................................................ 8
CHAPTER TWO: LITERATURE REVIEW .......................................................................... 10
2.1 Introduction ............................................................................................................................. 10
2.2 Definitions of terms and concepts ........................................................................................... 10
2.3 The main health care wastes generated in health care establishments .................................... 11
2.4 Classification of radioactive wastes ........................................................................................ 12
2.5 Management options for medical radioactive wastes ............................................................. 13
2.5.1 Segregation, temporal storage and transportation ............................................................ 13
Assessment of Medical Radioactive Waste Management in Hospitals: | Richard Okot
vii
2.5.2 Dilute and Disperse .......................................................................................................... 14
2.5.3 Delay and Decay .............................................................................................................. 14
2.5.4 Concentrate and Contain .................................................................................................. 14
2.5.5 Incineration....................................................................................................................... 15
2.6 Policy and legal frameworks for radioactive waste management ........................................... 16
2.6.1 The Basel Convention ...................................................................................................... 16
2.6.2 Convention on Nuclear Safety ......................................................................................... 17
2.6.3 International Commission on Radiological Protection (ICRP) ........................................ 17
2.6.4 OECD Nuclear Energy Agency (OECD NEA)................................................................ 17
2.6.5 The Constitution of the Republic of Uganda (1995) ........................................................ 17
2.6.6 The National Environment Act CAP 153 ........................................................................ 17
2.7 Institutional frameworks for radioactive wastes management................................................ 18
2.7.1 Ministry of Water Lands and Environment...................................................................... 18
CHAPTER THREE: METHODOLOGY ................................................................................ 19
3.1 Introduction ............................................................................................................................. 19
3.2 Description of study area ........................................................................................................ 19
3.2.1 Climate of the study area .................................................................................................. 19
3.2.2 Population of the study area ............................................................................................. 20
3.2.3 Geology of the study Area ............................................................................................... 20
3.2.4 Soils of the study Area ..................................................................................................... 20
3.3 Research design ...................................................................................................................... 20
3.3.1 Methods of Data collection .............................................................................................. 20
3.3.1.1 Key informant interviews ....................................................................................... 20
3.3.1.2 Questionnaires......................................................................................................... 21
3.3.1.3 Secondary data ........................................................................................................... 21
3.3.1.4 Observation ............................................................................................................. 21
3.3.1.5 Photography. .............................................................................................................. 21
3.4 Sample size and Selection criteria .......................................................................................... 21
3.5 Data Analysis and interpretation ............................................................................................. 22
3.6 Dissemination of the results .................................................................................................... 22
3.7 Ethical consideration ............................................................................................................... 22
3.8 Limitations of the study .......................................................................................................... 22
Assessment of Medical Radioactive Waste Management in Hospitals: | Richard Okot
viii
CHAPTER FOUR: DATA ANALYSIS AND RESULTS ....................................................... 24
4.1 INTRODUCTION .................................................................................................................. 24
4.2 Demographic characteristics of the respondents..................................................................... 24
4.2.1 Age distribution of the respondents ................................................................................. 24
4.2.2 Education level of respondents ........................................................................................ 25
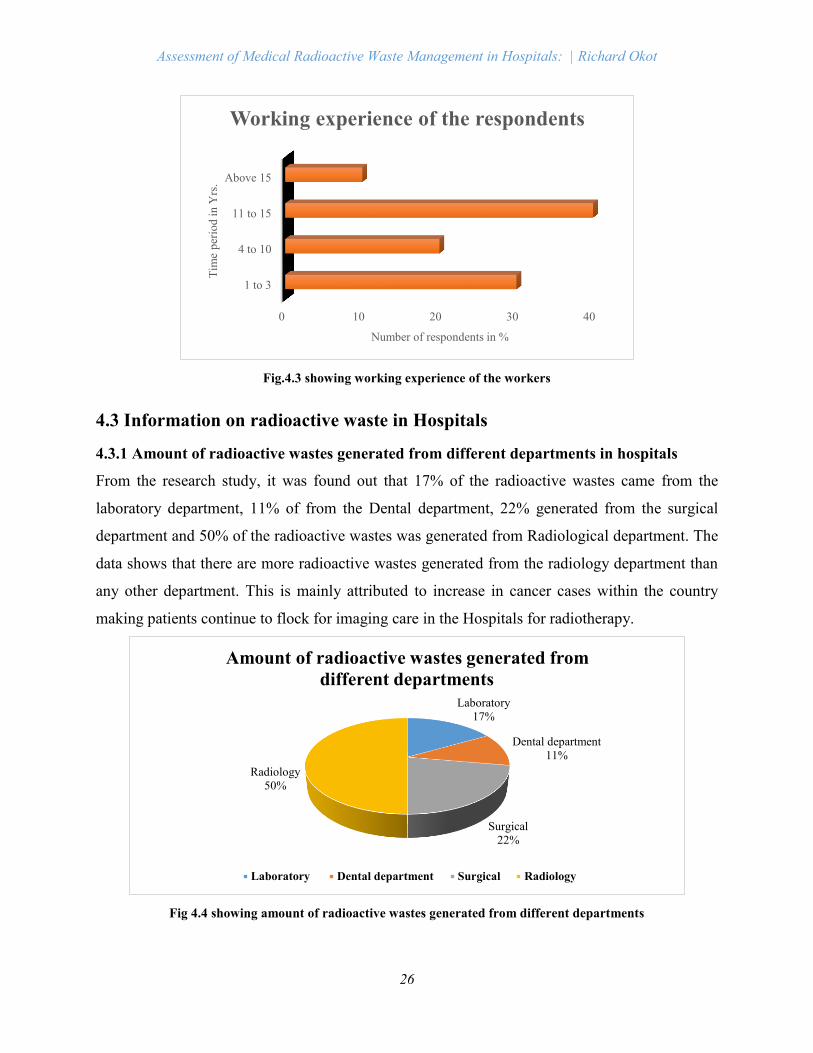
4.2.3 Working experience of the respondents ........................................................................... 25
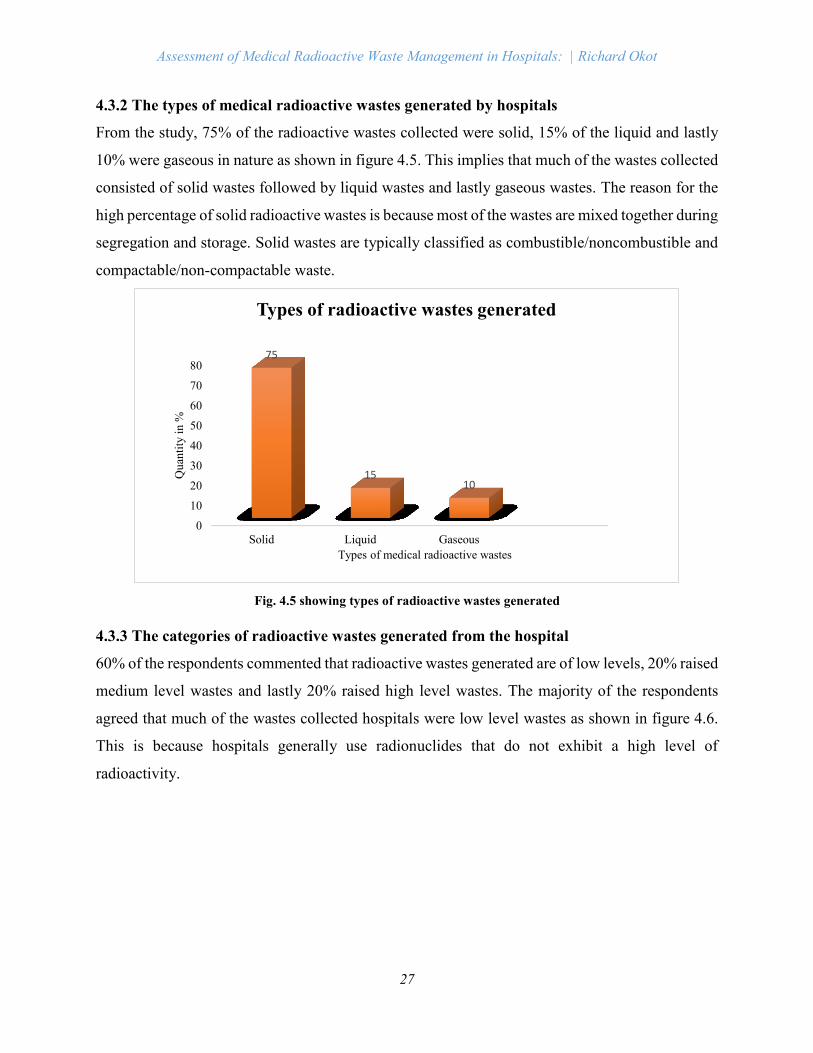
4.3 Information on radioactive waste in Hospitals ....................................................................... 26
4.3.1 Amount of radioactive wastes generated from different departments of hospitals .......... 26
4.3.2 The types of medical radioactive wastes generated by hospitals ..................................... 27
4.3.3 The categories of radioactive wastes generated from hospitals ....................................... 27
4.4 Radioactive waste management in Hospitals .......................................................................... 28
4.4.1 Segregation of the radioactive wastes .............................................................................. 28
4.4.2 Storage of the radioactive wastes ..................................................................................... 28
4.4.3 Radioactive waste disposal............................................................................................... 29
4.4.4 Whether there are various method available for radioactive waste management ............ 29
4.4.5 Whether there is a special department handling waste management activity .................. 29
4.4.6 Whether there is any alternative method/ idea of disposing waste other than the one
practiced. ................................................................................................................................... 30
4.5 Personnel involved in the management of hospital wastes ..................................................... 30
4.5.1 Number of personnel involved in the management of radioactive wastes in hospitals ... 30
4.5.2 Level of knowledge of the dangers of radioactive wastes on the environment ............... 30
4.5.3 Training given to the waste management staff ................................................................. 31
CHAPTER 5: DISCUSSION ..................................................................................................... 32
5.1 Introduction ............................................................................................................................. 32
5.2 Kinds of medical radioactive wastes generated from hospitals .............................................. 32
5.3 Current radioactive waste management practice within hospitals .......................................... 32
5.4 Knowledge and awareness of the dangers of radioactive wastes on the environment by the
workers .......................................................................................................................................... 34
5.5 Alternatives for radioactive waste disposal and selection of best available Technology ....... 35
CHAPTER SIX: CONCLUSIONS AND RECOMMENDATIONS ...................................... 38
6.1 Introduction ............................................................................................................................. 38
6.2 Conclusion .............................................................................................................................. 38
6.3 Recommendations ................................................................................................................... 39
Assessment of Medical Radioactive Waste Management in Hospitals: | Richard Okot
ix
REFERENCES ............................................................................................................................. 41
APPENDIX I: QUESTIONAIRE ................................................................................................. 43
LIST OF FIGURES
Figure 4.1: Age of the respondents………………………………………………………………22
Figure 4.2: Educational Level……………………………………………………………………23
Figure 4.3: Working experience of the respondents…….……………………………………….23
Figure 4.4: Amount of radioactive wastes generated from different Department……………….24
Figure 4.5: Types of radioactive wastes generated………………………………………………25
Figure 4.6: The categories of the radioactive wastes generated………………………………….26
Figure 4.7: Whether there are other better materials to dispose waste other than those made out of
plastic…………………………………………………………………………………………….27
Figure 4.8: Number pf personnel involved in waste management…….………………………….28
LIST OF TABLE
Table 1.1: shows the list of commonly used radionuclide in nuclear medicine…..........................3
LIST OF PLATES
Plate 1.1 showing radioactive waste disposal facility at El Cabril……………………….……….3
Plate 2.1 showing vial wastes generated by hospitals……………………….……….…………..11
Plate 2.2 showing empty plastics generated by hospitals………………………………………..11
Plate 2.3 showing containers used for temporal storage of the wastes………..…………………14
Plate 2.4 showing storage facility for low level radioactive wastes.......................................…...15
Plate 2.5 showing an incinerator being operated within hospitals establishment…….………….16
Plate 5.1 showing personal wearing PPEs……………………………………………………….36
Assessment of Medical Radioactive Waste Management in Hospitals: | Richard Okot
xi
ABBREVIATION AND ACCRONYMS
DNA : Deoxyribonucleic Acid
EPA : Environment Protection Agency
EPA : Environmental Protection Agency
HCW : Health Care Waste
HCW : Health Care Wastes
HCWM : Health Care Wastes Management
IAEA : International Atomic Energy Agency
ICRP : International Commission on Radiological Protection
KBq : Kilo Becquerel
KCCA : Kampala City Council Authority
LDC : Low Developed Countries
LDCs : Least developed countries
LLW : Low Level Wastes
MOH : Ministry Of Health
NASA : National Aeronautics and Space Administration
NEMA : National Environment Management Authority
NHMRC : National Health and Medical Research Council
OECD : Organisation for Economic Co-Operation and Development
PVC : Polyvinyl Chloride
Sv : Sievert
UK : United Kingdom
WHO : World Health Organisation
WMR : Waste Management Report
Assessment of Medical Radioactive Waste Management in Hospitals: | Richard Okot
xii
OPERATIONAL DEFINITION OF TERMS
Alpha particle. This is a particle consisting of two protons plus two neutrons and is emitted by a
radionuclide. Alpha particles can be stopped by a piece of paper and are only a concern when
alpha-emitting isotopes are taken into the body.
Becquerel. Unit of radioactivity (Standard International unit). One Becquerel equals one
radioactive disintegration per second.
Beta particle. An electron emitted by the nucleus of a radionuclide. The electric charge may be
positive, in which case the beta particle is called a positron. Beta particles have a short range in air
and even shorter range in more dense material.
Gamma ray. A very high frequency form of electromagnetic radiation that consists of photons
emitted by radioactive elements. Gamma rays can injure and destroy body cells and tissue,
especially cell nuclei.
Gray. One gray is the absorption of one joule of radiation energy by one kilogram of matter, and
is a physical measure of radiation energy absorbed only.
Half-life (T½). This is the time it takes for the amount of a material to be reduced by half. In the
case of radioactive materials, the physical half-life is the time for the isotope to decay to half its
activity.
Hypothyroidism. An underactive thyroid gland; a glandular disorder resulting from insufficient
production of thyroid hormones
Iodine. The radioisotope 131I is often used in nuclear medicine for both imaging and treatment.
Photomultiplier tubes. These are devices used extensively in nuclear medicine to detect gamma
rays (although other devices may also be used).
Radioactivity. This is the spontaneous emission of radiation from unstable atoms. Radionuclides
lose particles for example alpha or beta and energy through radioactive decay.
Assessment of Medical Radioactive Waste Management in Hospitals: | Richard Okot
xiii
Radioisotope/Radionuclide. These are atoms with an unstable number of neutrons that
disintegrate, releasing rays of subatomic particles.
Radiopharmaceutical. These are pharmaceuticals consisting of radioactive compounds used in
radiation therapy. They are also used to examine the function of specific body organs.
Sievert (Sv). This is the unit of measure for the radiation dose equivalent for biological tissues,
and allows for the biological effect on different tissues – as sensitivity will vary with the type of
particle and the tissue.
Technetium. A chemical element with atomic number 43. Technetium was discovered in 1937 at
the University of California at Berkeley by Enrico Fermi and Carlo Perrier. Its chemistry allows
easy labelling of many pharmaceuticals.
X-ray. Photons or electromagnetic radiation produced by the de-excitation of bound atomic
electrons. The energy of an x-ray is equivalent to the difference in energy of the initial and final
atomic state minus the binding energy of the electron.
Assessment of Medical Radioactive Waste Management in Hospitals: | Richard Okot
1
CHAPTER ONE: INTRODUCTION
1.1 Global perspective of radioactive waste generation and management
1.1.1 Radioactive waste generation in developed countries
Annually, nuclear power generation facilities worldwide produce about 200,000 m3 of low- and
intermediate-level radioactive waste, and about 10,000 m3 of high-level waste including used fuel
designated as waste (INSC, 2002). In the OECD countries, some 300 million tonnes of toxic wastes
are produced each year, but conditioned radioactive wastes amount to only 81,000 m3 per year this
imply that only 1% is treated. In the UK for instance, the total amount of radioactive waste
generated is about 4.7 million m3 with 1 million m3 already disposed of these radioactive wastes,
94% falls into the low-level radioactive waste category and 6% (290,000 m3) is in the intermediate-
level radioactive waste category, and less than 0.1% is classed as high-level waste. Although the
volume of High Level Waste is relatively small, it contains about 95% of the total inventory of
radioactivity.
Since the 1960s, more than 200,000 tons of spent fuel have been produced by 400 reactors in 30
countries, and every year 10,000 tons are added with the debate over the management of
radioactive wastes continues with no satisfactory solutions. In 1998, evidence emerged that
radioactive waste from 80 scrapped nuclear submarines in the area of the northern Russian naval
port of Murmansk had begun leaking into the sea (Edwards, 1998). Further quantities of wastes
were generated by the dismantling old weapons, including 50 tonnes of plutonium in United States,
(Curtis, 1994). The global plutonium stockpile is estimated at 1,100 tonnes and growing rapidly
(Panofsky et al., 1994). According to the European Union, at the end of 2004, there was 647,000
m3 of radioactive waste of which 26% was classified as very low-level waste and about 1% as
highly active waste. However estimates of additional radioactive waste and spent fuel likely to be
generated by Member States between 2004 and 2020 were made in 2008. The figure for
radioactive waste being 1,772,300 m3, of which approximately 25% was to be very low-level
waste and 0.1% was to be high level waste.
1.1.2 Radioactive waste management in developing countries
Medical radioactive waste management is one of the leading problems facing African countries
and other developing countries of the world (Glenn and Garwal, 1999). Waste generated in the

Assessment of Medical Radioactive Waste Management in Hospitals: | Richard Okot
2
course of the health care activities carries higher potential for infection and injury than any other
type of waste (Virenter, 2007). The medical waste problem is increasing mainly because of the
rapid demographic development, urban expansion coupled with inadequate resources and
insufficient management capacity.
In most developing countries, nuclear power plants are not the focal point of radioactive waste
generation because only about 7% of the world's installed nuclear power capacity exist in
developing countries which include in Asia, Latin America, and the Mediterranean region. At the
present time, developing countries are mostly concerned with the management of nuclear wastes
generated from medical centres, research institutes, industrial facilities, and mining operations. In
certain instances, management of such wastes has lapsed causing serious accidents due to radiation
source mismanagement resulting in fatalities to the public in Mexico (1962), Algeria (1978), and
Morocco (1984) (K.T. Thomas, 2002).
1.1.3 Strategies for radioactive waste management
Radioactive wastes are a potential risk to health and the environment due to their radiological and
chemical properties. Although there are different categories and types of radioactive waste and
accordingly different kinds of risks, there is a common basic principle for their management:
radioactive waste shall be managed in a manner that protects human health and the environment,
now and in the future without imposing undue burdens on future generations, (IAEA, 2006). Due
to the long timescales involved, the implementation of this principle is especially relevant when
considering HLW.
Disposal in near-surface facilities
Radioactive wastes that decay to harmless levels within time spans ranging from some decades to
a few centuries8 are typically disposed of in engineered near-surface structures that can be
designed to remain stable and intact as long as the wastes remain a hazard. (IAEA, 1999; IAEA,
2002c). Near surface disposal of wastes in trenches is generally applied to wastes that contain
mainly short-lived radioisotopes and, potentially, low concentrations of long-lived radioisotopes.
The use of trenches may be especially cost effective when disposing of large volumes of low
activity wastes and/or large items of decommissioning waste. Long-term safety may be provided
Assessment of Medical Radioactive Waste Management in Hospitals: | Richard Okot
3
largely by a combination of natural site conditions, the engineered disposal system and the waste
form. Designs to minimize plant and animal intrusion may also be employed.
Deep disposal in geological formations
Deep geological disposal of radioactive waste is generally considered the most appropriate
approach for high-level waste and spent nuclear fuel where it is necessary to isolate them from the
biosphere for many thousands years. The overall objective of deep disposal is thus to isolate the
wastes from the biosphere until such time as natural processes of decay and dilution prevent any
radionuclide from returning in concentrations sufficient to pose an unacceptable hazard. Clearly,
many processes of mobilization, transport, retardation, retention, dilution, re-concentration,
etcetera, need to be accounted for in evaluating whether this aim can be met, for a range of possible
scenarios of future evolution of the disposal system. Geological disposal is based on the multi-
barrier approach, whereby the engineered barriers and geological environment around the solid
waste act together to provide a variety of “safety functions” that control any eventual releases of
radioactivity from the repository and their movement through the rock.
Plate 1.1 Showing radioactive waste disposal facility at El Cabril
1.2 The application of nuclear medicine in hospitals
The incorporation of radionuclides in a chemical compound provides it with unique properties
such as specific biological affinity. When used in medicine these compounds are referred to as
Assessment of Medical Radioactive Waste Management in Hospitals: | Richard Okot
4
radiopharmaceuticals and its use in life science is extensive (Gregory choppin et al, 2001).
Radionuclides used in medicine include the radioisotopes of iodine, gallium, thallium and
technetium, amongst others. The physical characteristics of each are different and the selection of
a particular radionuclide relates directly with its intended clinical use, that is, whether a diagnostic
or therapeutic result is desired and it’s used to gain information that aids in a patient's diagnosis,
therapy and prognosis (AIM, 2007).
Clinical diagnostic imaging is a general term applied to non-destructive photographic techniques
of investigating the gross internal structure of any object (McGraw-Hill Encyclopaedia, 2005).
The procedures are diverse and span a wide spectrum ranging from X-ray based examinations to
sound, radionuclide and magnet based investigations (AIM, 2007). It is used to exclude disease,
to prove the existence of a pathological process, to assist in the planning of treatment or to follow
the course of a disease already diagnosed and/or treated. WHO estimates that simple X-ray and
ultrasound examination either singly or in combination, are all that is necessary to confirm a
diagnosis in approximately two thirds of patients who need diagnostic imaging (WHO, 2007).
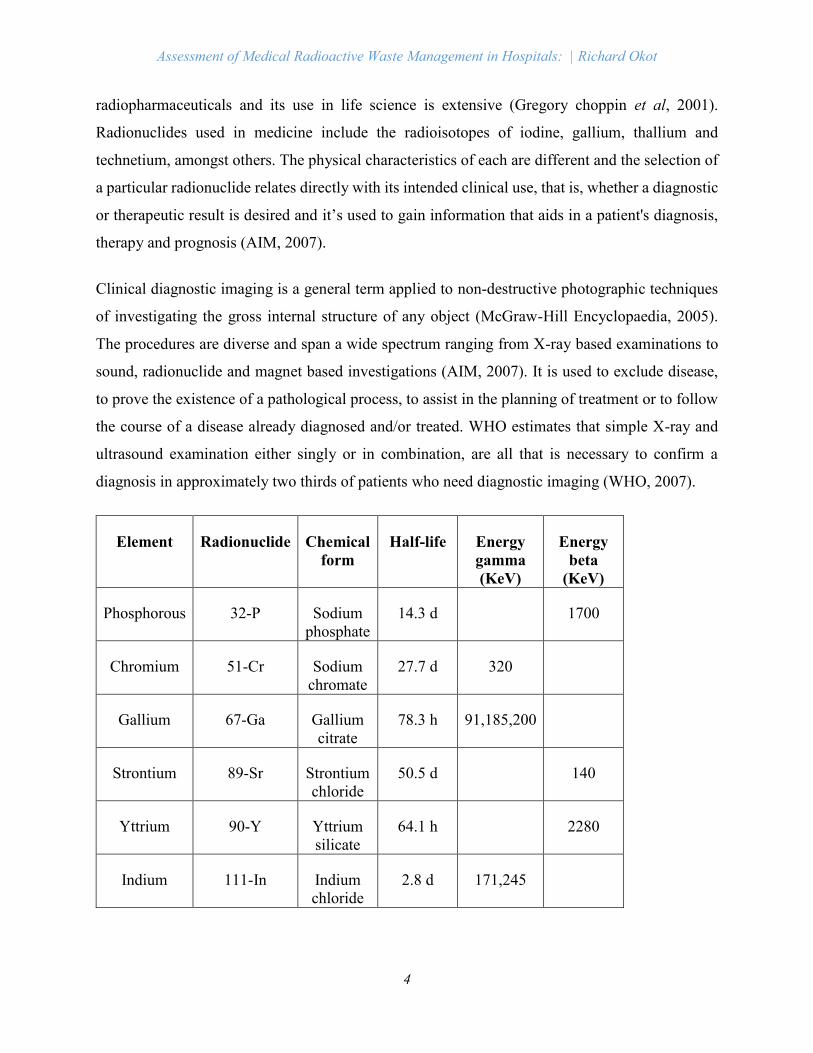
Element Radionuclide Chemical
form
Half-life Energy
gamma
(KeV)
Energy
beta
(KeV)
Phosphorous 32-P Sodium
phosphate
14.3 d 1700
Chromium 51-Cr Sodium
chromate
27.7 d 320
Gallium 67-Ga Gallium
citrate
78.3 h 91,185,200
Strontium 89-Sr Strontium
chloride
50.5 d 140
Yttrium 90-Y Yttrium
silicate
64.1 h 2280
Indium 111-In Indium
chloride
2.8 d 171,245
Assessment of Medical Radioactive Waste Management in Hospitals: | Richard Okot
5
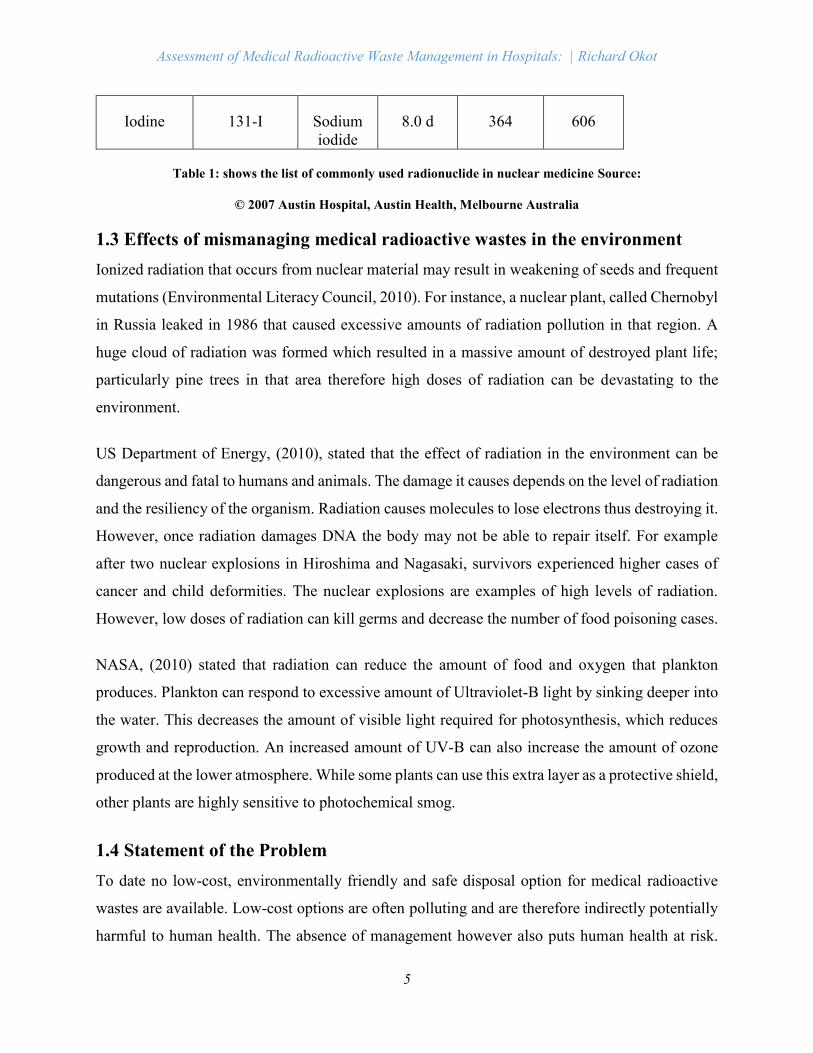
Iodine 131-I Sodium
iodide
8.0 d 364 606
Table 1: shows the list of commonly used radionuclide in nuclear medicine Source:
© 2007 Austin Hospital, Austin Health, Melbourne Australia
1.3 Effects of mismanaging medical radioactive wastes in the environment
Ionized radiation that occurs from nuclear material may result in weakening of seeds and frequent
mutations (Environmental Literacy Council, 2010). For instance, a nuclear plant, called Chernobyl
in Russia leaked in 1986 that caused excessive amounts of radiation pollution in that region. A
huge cloud of radiation was formed which resulted in a massive amount of destroyed plant life;
particularly pine trees in that area therefore high doses of radiation can be devastating to the
environment.
US Department of Energy, (2010), stated that the effect of radiation in the environment can be
dangerous and fatal to humans and animals. The damage it causes depends on the level of radiation
and the resiliency of the organism. Radiation causes molecules to lose electrons thus destroying it.
However, once radiation damages DNA the body may not be able to repair itself. For example
after two nuclear explosions in Hiroshima and Nagasaki, survivors experienced higher cases of
cancer and child deformities. The nuclear explosions are examples of high levels of radiation.
However, low doses of radiation can kill germs and decrease the number of food poisoning cases.
NASA, (2010) stated that radiation can reduce the amount of food and oxygen that plankton
produces. Plankton can respond to excessive amount of Ultraviolet-B light by sinking deeper into
the water. This decreases the amount of visible light required for photosynthesis, which reduces
growth and reproduction. An increased amount of UV-B can also increase the amount of ozone
produced at the lower atmosphere. While some plants can use this extra layer as a protective shield,
other plants are highly sensitive to photochemical smog.
1.4 Statement of the Problem
To date no low-cost, environmentally friendly and safe disposal option for medical radioactive
wastes are available. Low-cost options are often polluting and are therefore indirectly potentially
harmful to human health. The absence of management however also puts human health at risk.

Assessment of Medical Radioactive Waste Management in Hospitals: | Richard Okot
6
Significant improvements can however be achieved by management options such as purchase
policies, and isolation and proper treatment of key segments of the waste. According to the
Ministry of Health (2009), the current medical radioactive waste management system in Uganda
is inadequate both at public and private level. The actual amount of medical radioactive wastes
generated in Ugandan hospitals is not known and even trying to estimate it would be problematic
(Wekoy, 2005) and this is mainly attributed to insufficient capacity and research data on medical
radioactive waste generation, separation, storage, treatment and final disposal mechanisms.
In Uganda, the percentage of public health facilities equipped with diagnostic imaging machines
was 73.6% in 2004 (MOH Uganda, 2004) and the national coverage with x-ray and ultrasound
machines among private health providers was 8% and 11% respectively (Mandelli et al., 2005).
Despite this relatively high national coverage with imaging services, patients continue to flock for
imaging care in Kampala. However, the influx leads to congestion of the diagnostic imaging
departments in the national referral hospital at Mulago. Congestion affects the quality of care, the
timeliness of releasing results, and the rate of radioactive generation in hospitals and as a result
there is a likelihood that all the radioactive wastes generated will end up in the environment.
Therefore, this study will try to provide a glimpse of how much radioactive wastes is being
generated, the dangers it causes in the environment. The data to be gathered in this study will
provide technocrats with information relating to how medical radioactive wastes should be
managed.
1.5 Significance of the study
Health care institutions are responsible for delivery of patient care services and in the process of
delivering this, wastes comprising radioactive nuclides are generated. Poor handling of the medical
radioactive materials potentially exposes health care workers, waste handlers and the community
at large to radiation effects. Once these wastes are not properly managed, they end up into the
environment. Once in the environment, they can remain active for hours or several months and if
the radionuclides get into air, water supplies, and soil, they enter into food chains thus causing
various illnesses which include among others hypothyroidism in newly borne babies which is a
consequence of exposure to iodine, alteration of an organisms’ DNA thus leading to mutations,
cancer which is considered a primary health effect from radiation exposure, changes in blood
Assessment of Medical Radioactive Waste Management in Hospitals: | Richard Okot
7
chemistry and also cause some adverse effects to other living organisms (plants and animals) thus
reducing biodiversity.
The conclusions generated from the study will help generate more information to the already
existing body of knowledge in the area of medical radioactive waste management and to Hospitals
in particular. Also the research findings will enlighten the decision makers like NEMA,
Environment Officers, and KCCA of the gaps existing in the radioactive waste management. These
findings will help in drafting appropriate guidelines on the management of the wastes and create
awareness to the people concerned of the dangers of poor radioactive waste management so that
there would be a joint effort to solve the problem at hand.
1.6 Objectives of the study
1.6.1 General objective
To investigate the current use of medical radionuclides and generation, collection, storage,
transportation and disposal of the medical radioactive wastes generated from the different
departments of hospitals.
1.6.2 Specific objectives
1. To determine the kinds of medical radioactive wastes generated from different departments
of hospitals.
2. To determine information on the current collection, storage, transportation, treatment and
disposal of the medical radioactive wastes from hospitals.
3. To assess knowledge and awareness of the dangers of radioactive wastes on the
environment.
4. To identify the possible recommendations to archive proper medical radioactive waste
management.
1.7 Research questions
1. What are the kinds of medical radioactive wastes generated from the various departments
of hospitals?
2. How are the medical radioactive wastes collected, stored, transported, treated, and disposed
of?
Assessment of Medical Radioactive Waste Management in Hospitals: | Richard Okot
8
3. Are the people involved in the radioactive wastes management have knowledge and
awareness about the dangers of radioactive wastes to the environment?
4. What are the possible recommendations for medical radioactive waste management in
hospitals?
1.8 Expected outcome
1. The types and categories of the medical radioactive wastes generated from the various
departments of hospitals would have been determined.
2. The current method used in collection, storage, transportation, treatment and disposal of
the medical radioactive wastes would have been assessed.
3. The level of knowledge and awareness of the dangers of medical radioactive wastes on the
environment would have been evaluated.
4. Possible recommendations for proper medical radioactive waste management would have
been identified.
1.9 Scope of the study
The focus of this research was to assess the management of medical radioactive wastes emanating
from various hospitals within Kampala Uganda. The study will focused on 10 hospitals in a bid to
assess the management of medical radioactive wastes and the study was both quantitative and
qualitative in nature.
The study reviewed documents, reports and collected data from hospitals. The data collected were
used to estimate the extent of the medical radioactive waste management.
1.9.1 Time scope
The study took four months starting from April to July 2014. This period was sufficiently enough
to carry out baseline survey, collect relevant literature and carry out data collection for six weeks.
Sampling and analysis of assessment of the medical radioactive waste management in the hospital,
submission and approval of the study report.
Geographical scope
The study was conducted in 10 Hospitals located in Kampala District, the capital of Uganda and
the largest city in the country. The district is bordered by Wakiso District to the south, the west
Assessment of Medical Radioactive Waste Management in Hospitals: | Richard Okot
9
and the north and by Kira Municipality to the east. The coordinates of the district are: 00 19N, 32
35E.

Assessment of Medical Radioactive Waste Management in Hospitals: | Richard Okot
10
CHAPTER TWO: LITERATURE REVIEW
2.1 Introduction
This chapter presents a review of available literature to assess the objectives of the study. It consists
definitions of terms, classification of radioactive wastes, management options for radioactive
wastes, policy and legal frameworks on radioactive waste management and institution
arrangements concerning the radioactive waste management
2.2 Definitions of terms and concepts
Waste is a man-made substance in a given time and places which in its actual structure and state
is not useful to the owner or is an output without an owner and purpose. In other words, waste is
anything that we no longer need. It is also commonly referred to as rubbish, trash, garbage, refuse,
effluents and “unwanted, or unusable materials”. (Zake J: 2007). Medical waste is the waste
generated by hospitals, healthcare establishments, medical laboratories and research facilities
during the process of diagnosis, treatment, and associated medical research. Medical radioactive
wastes may be in the form of liquid, solid and gaseous which may be comprising of sharps, tissues,
cytotoxic drugs, genotoxic chemicals, pharmaceutical, heavy stained bandages, and other
discarded materials during the provision of healthcare, (Visvanathan, 2006). According to NHMRC
(1999), radioactive wastes are materials contaminated with radio-isotopes, which arises from the medical
or research use of radionuclides. It is produced, for example during nuclear medicine, radio-immune assay
and bacteriological procedures, and may be in a solid, liquid or gaseous form.
In the past few years, the world concern over the disposal and management of medical radioactive
waste has markedly increased. Medical waste newsletter (2005) cited improper handling, transport
and disposal of medical waste removed during surgery, autopsy and other medical procedures
along California beaches which violate the state laws regarding potentially infectious medical
wastes. A report by the ministry of territory development, water and environment, (www.
arabicnews.com) showed that morocco generates over 38000 tons of medical waste per year;
12000 of which is hazardous. The report indicates that hardly this kind of waste is getting more
complex because it contains biologically non degradable substances.
Assessment of Medical Radioactive Waste Management in Hospitals: | Richard Okot
11
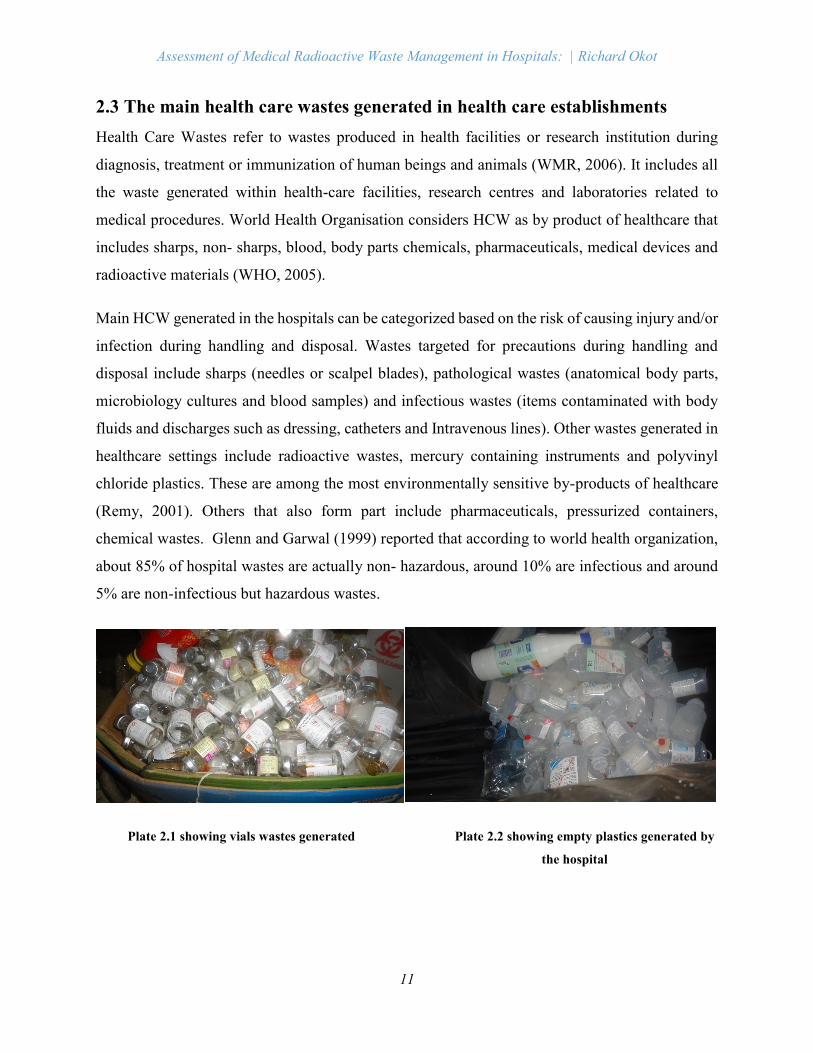
2.3 The main health care wastes generated in health care establishments
Health Care Wastes refer to wastes produced in health facilities or research institution during
diagnosis, treatment or immunization of human beings and animals (WMR, 2006). It includes all
the waste generated within health-care facilities, research centres and laboratories related to
medical procedures. World Health Organisation considers HCW as by product of healthcare that
includes sharps, non- sharps, blood, body parts chemicals, pharmaceuticals, medical devices and
radioactive materials (WHO, 2005).
Main HCW generated in the hospitals can be categorized based on the risk of causing injury and/or
infection during handling and disposal. Wastes targeted for precautions during handling and
disposal include sharps (needles or scalpel blades), pathological wastes (anatomical body parts,
microbiology cultures and blood samples) and infectious wastes (items contaminated with body
fluids and discharges such as dressing, catheters and Intravenous lines). Other wastes generated in
healthcare settings include radioactive wastes, mercury containing instruments and polyvinyl
chloride plastics. These are among the most environmentally sensitive by-products of healthcare
(Remy, 2001). Others that also form part include pharmaceuticals, pressurized containers,
chemical wastes. Glenn and Garwal (1999) reported that according to world health organization,
about 85% of hospital wastes are actually non- hazardous, around 10% are infectious and around
5% are non-infectious but hazardous wastes.
Plate 2.1 showing vials wastes generated Plate 2.2 showing empty plastics generated by
the hospital
Assessment of Medical Radioactive Waste Management in Hospitals: | Richard Okot
12
2.4 Classification of radioactive wastes
Several classifications are possible when describing radioactive waste. These include physical
state (since radioactive waste can be solid, liquid or gaseous) as well as isotopic content and
concentration. The types of radiation (alpha, beta and gamma) emitted by the prevailing
radioisotopes in the waste is another basis for classification that defines the necessary degree of
shielding. Another form of classification relates to the half-life of the predominant radionuclides
of a given waste.
The system adopted by IAEA, which is the most internationally accepted, combines the type of
radiation emitted, the activity of the waste and its half-life to present an easy method of
classification based on the main following categories: (IAEA, 1994).
i. Exempt waste (EW): excluded from regulatory controls because radiological hazards are
negligible.
ii. Low- and intermediate-level waste (LILW): radioactivity levels are above those for exempt
waste and thermal power below about 2 kW/m3; IAEA recognizes two sub-categories of
LILW:
Short-lived waste (LILW-SL): primarily contains short-lived radionuclides, with long lived
radionuclide (including long-lived alpha emitter) concentrations restricted to an overall
average of 400 Bq/g per waste package;
Long-lived waste (LILW-LL): contains long-lived radionuclide concentrations that exceed
limits for short-lived waste.
iii. High-level waste (HLW): contains sufficient concentration of radionuclides to produce
heat generation greater than 2 kW/m3; the typical activity levels are in the range of 5x104
to 5x 105 TBq/m3.
There are three exceptions to some radioactive waste classification schemes that correspond to the
following materials:
Mining and milling wastes: residues left from mining and extraction of uranium and other
raw materials that contain naturally occurring radionuclides;
Assessment of Medical Radioactive Waste Management in Hospitals: | Richard Okot
13
Environmental contamination: radioactively contaminated environmental media, such as
soil and groundwater;
Spent nuclear fuel (fuel that is removed from a reactor when its irradiation and energy
output has reached its designed level) is considered as either a resource (as it still contains
unused uranium and usable plutonium) or a waste depending on which management
strategy a country is using.
2.5 Management options for medical radioactive wastes
Literature reviews on waste disposal/ waste treatment technologies are rather contradictory. Some
of the most common technologies for the management of radioactive wastes include segregation,
temporal storage, dilute and disperse, delay and decay, incineration, and transportation to a secured
landfill. According to previous studies (Park and Jeong, 2001; Lee et al., 2004), about 49–60% of
medical waste is treated by various incinerations, 20–37% by autoclave sterilization, and 4–5% by
other methods.
2.5.1 Segregation, temporal storage and transportation
Handling, segregation, storage, transportation and final disposal are vital steps for safe and
scientific management of medical radioactive wastes in any establishment (Acharya and Singh
Meeta, 2000). Peter Ikome Kuwoh Muchungong, (2011), reported in his PhD research on
environmental exposure and public health impacts of clinical waste treatment and disposal in
Cameroon that thorough segregation and temporal storage of clinical waste in to its infectious and
non- infectious components is an important process in any efficient HCWM. According to peter,
the process guarantees reduction in the amount of radioactive waste requiring special treatment
and curbs potential occupational and operational risks to health care employees and by extension,
the general public. Peter further stressed that, despite these merits, the process of segregation is
overwhelmed with challenges that are pretty obvious in health care settings in the developing
world.
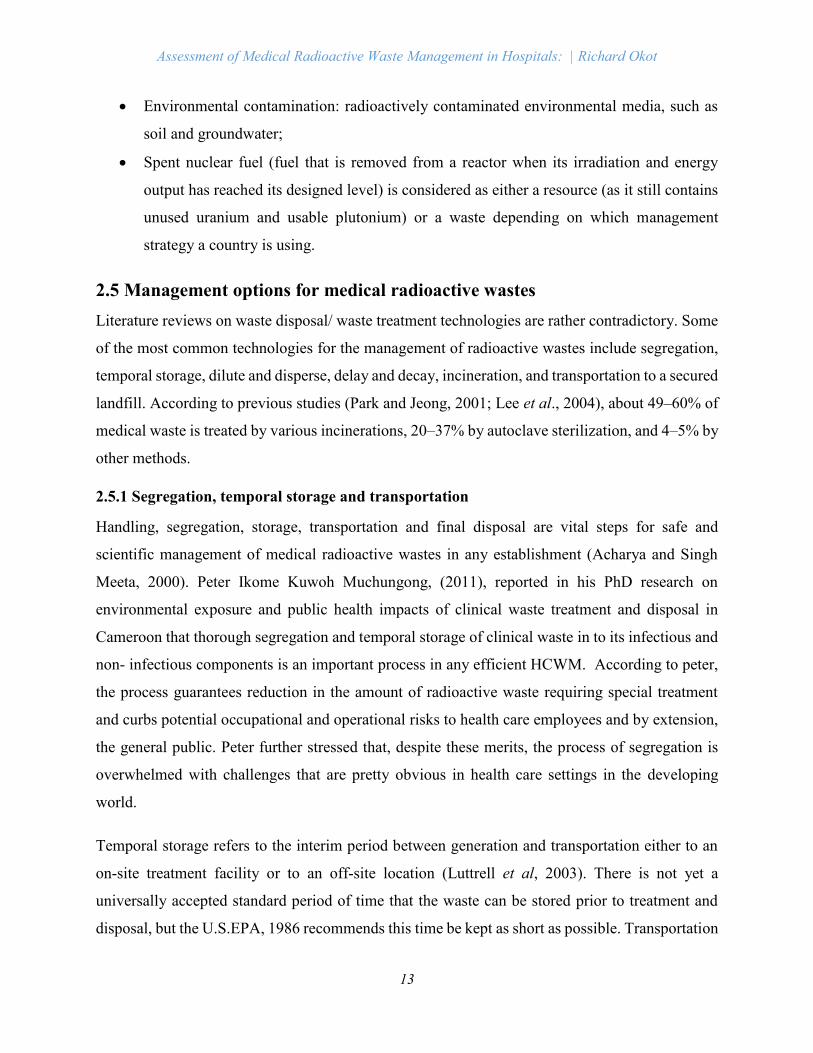
Temporal storage refers to the interim period between generation and transportation either to an
on-site treatment facility or to an off-site location (Luttrell et al, 2003). There is not yet a
universally accepted standard period of time that the waste can be stored prior to treatment and
disposal, but the U.S.EPA, 1986 recommends this time be kept as short as possible. Transportation
Assessment of Medical Radioactive Waste Management in Hospitals: | Richard Okot
14
of clinical waste involves an on-site treatment or disposal facility or removal from a source of
generation to an on-site temporal storage facility before eventual transportation to an off-site
treatment and disposal facility.
Plate2.3 showing containers sed for temporal starge of the wastes
2.5.2 Dilute and Disperse
Low activity solid particle may be disposed of as ordinary hospital waste provided the activity of
the article does not exceed 1.35 microcuries or the overall package concentration does not exceed
135 microcuries / m3. Coker et al, (2009) stated that liquid radioactive waste with activity less
than microcuries level can be disposed of into the sanitary sewerage system with adequate flushing
with water following the disposal (Patil and Shekdar,2001). However, the maximum limit of total
discharge of liquid radioactive material into sanitary sewerage system should not exceed the
prescribed limits.
2.5.3 Delay and Decay
Radioactive wastes from the medical sector does not present a significant long term waste
management problem when compared to wastes generated from nuclear fuel cycle operations
(Remy, 2001). The storage room should be properly ventilated with an exhaust system conducted
through a duct line to a roof top exit. Biomedical radioactive wastes typically contain low energy
and emitters and is generally of low total and specific activity.
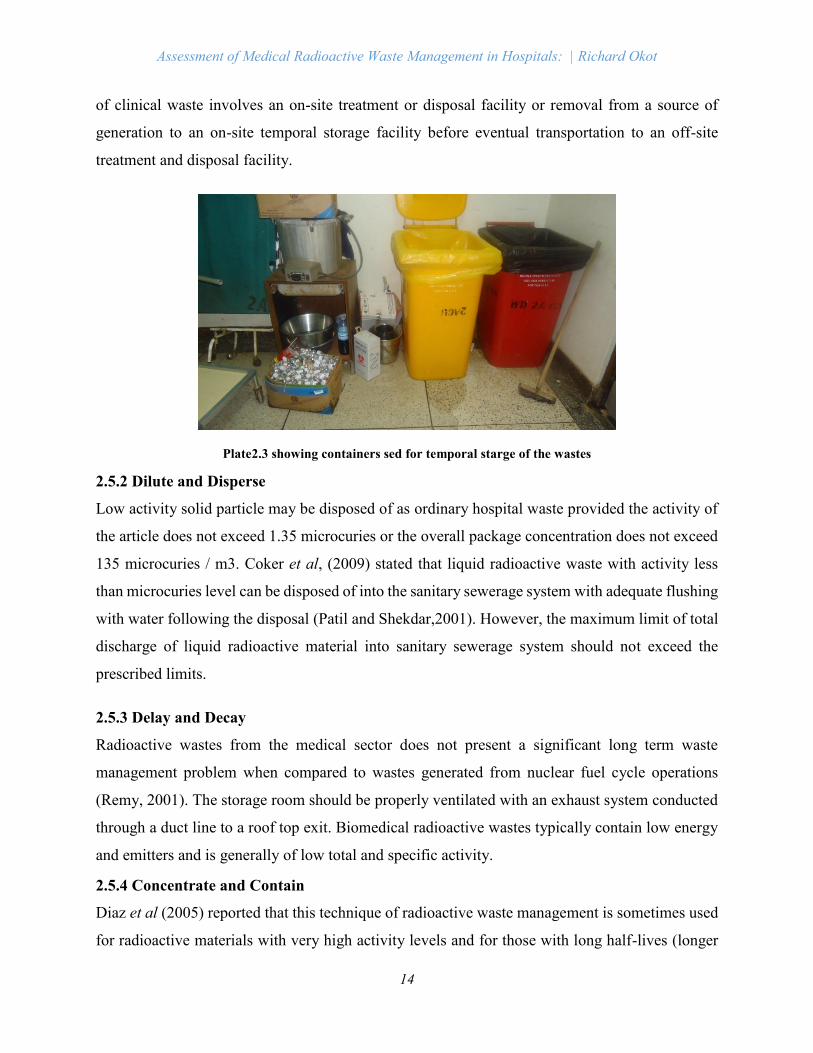
2.5.4 Concentrate and Contain
Diaz et al (2005) reported that this technique of radioactive waste management is sometimes used
for radioactive materials with very high activity levels and for those with long half-lives (longer
Assessment of Medical Radioactive Waste Management in Hospitals: | Richard Okot
15
than a month). Their disposal by delay and decay method is impractical because of longer storage
period, particularly if space availability is limited. Radioactive waste is collected in suitably
designed and labelled containers and then buried in exclusive burial sites approved by the
competent authority (Glenn and Garwal, 1999). In day-to-day work of a hospital, we do not come
across radioactive waste of this nature and as such, this method of radioactive waste disposal is
rarely used.
Plate 2.4 Storage of low level waste (LLW) at ANSTO
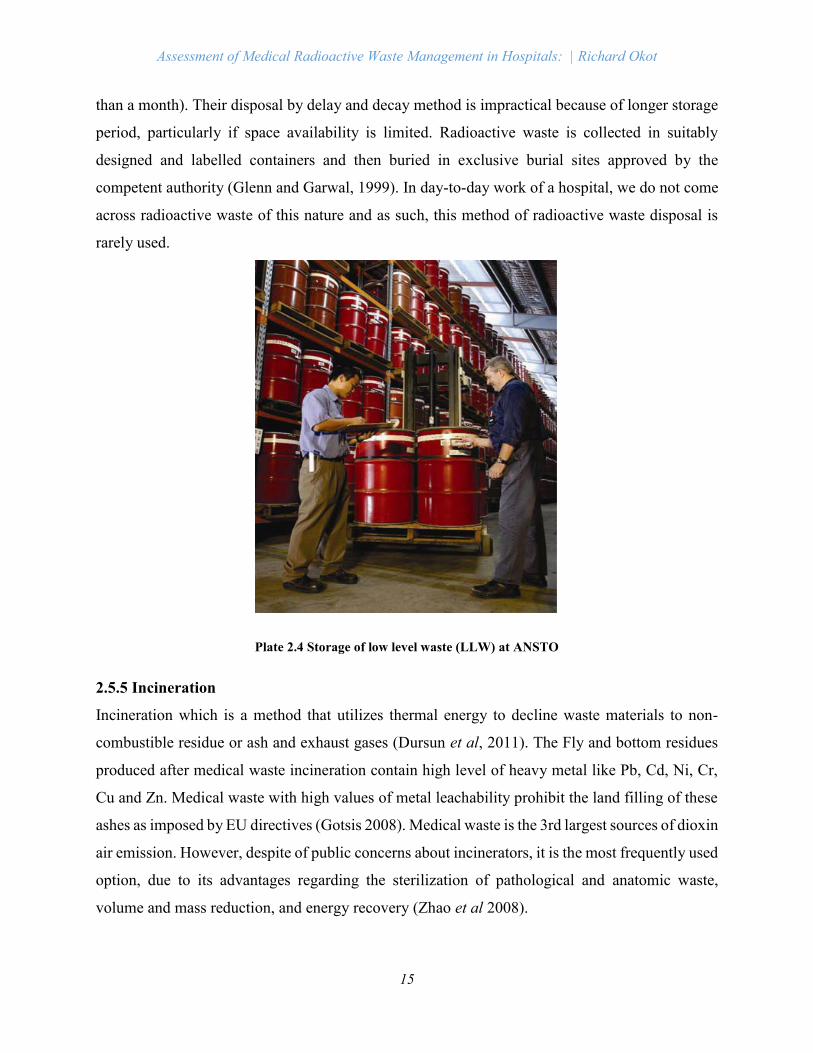
2.5.5 Incineration
Incineration which is a method that utilizes thermal energy to decline waste materials to non-
combustible residue or ash and exhaust gases (Dursun et al, 2011). The Fly and bottom residues
produced after medical waste incineration contain high level of heavy metal like Pb, Cd, Ni, Cr,
Cu and Zn. Medical waste with high values of metal leachability prohibit the land filling of these
ashes as imposed by EU directives (Gotsis 2008). Medical waste is the 3rd largest sources of dioxin
air emission. However, despite of public concerns about incinerators, it is the most frequently used
option, due to its advantages regarding the sterilization of pathological and anatomic waste,
volume and mass reduction, and energy recovery (Zhao et al 2008).
Assessment of Medical Radioactive Waste Management in Hospitals: | Richard Okot
16
Plate 2.5 showing an incinerator being operated within the hospital establishment
The criteria used in evaluating technological options considers environmental, health and
economic factors (Batterman 2004). The best technology for the medical waste treatment can be
different for different hospitals. It may depend on the local conditions and the requirement of the
hospital. However WHO gives a list of factors to guide the selection of best technology for treating
medical waste (Pruss 1999). They are; disinfection efficiency, volume and mass reduction,
quantity of wastes for treatment, infrastructure requirements, options available for final disposal,
operation and maintenance consideration, location and surroundings of the treatment site and
disposal facility, and public acceptability hence, it can be interpreted from the literature that,
medical waste management is an area of high concern due to the high generation of medical waste,
improper segregation and also due contradictory views about the various technologies. Medical
waste management is an area which needs more research and study to gear it towards sustainability.
2.6 Policy and legal frameworks for radioactive waste management
2.6.1 The Basel Convention
Basel Convention is an international treaty that was designed to reduce the movements of
hazardous waste between nations, and specifically to prevent transfer of hazardous waste from
developed to less developed countries. The Convention is also intended to minimize the amount
and toxicity of wastes generated, to ensure their environmentally sound management as closely as
Assessment of Medical Radioactive Waste Management in Hospitals: | Richard Okot
17
possible to the source of generation, and to assist LDCs in environmentally sound management of
the hazardous and other wastes they generate.
2.6.2 Convention on Nuclear Safety
The Convention on Nuclear Safety was designed to create awareness on the importance to the
international community of ensuring that the use of nuclear energy is safe, well regulated and
environmentally sound. It was adopted on 17 June 1994 by a Diplomatic Conference convened by
the IAEA at its Headquarters from 14 to 17 June 1994 and was opened for signature on 20
September 1994.
2.6.3 International Commission on Radiological Protection (ICRP)
This body was founded in 1928, under the then name of “International X-ray and Radium
Protection Committee.” ICRP is an international advisory body providing recommendations and
guidance on radiation protection. The secretariat of this body is located in Sweden.
2.6.4 OECD Nuclear Energy Agency (OECD NEA)
The NEA is an agency of the OECD. Membership currently consists of all European Union
member countries as well as Australia, Canada, Japan, Republic of Korea, Mexico and the US.
The primary objective of NEA is to promote co-operation among the governments of its
participating countries in furthering the development of nuclear power as a safe, environmentally
acceptable and economic energy source.
2.6.5 The Constitution of the Republic of Uganda (1995)
The Uganda Constitution of 1995, Articles 39 and 41 provide that everyone has a duty to maintain
and enjoy a sound environment. Every person in Uganda has a right to a clean and healthy
environment and as such can bring action for any pollution or disposal of wastes. It states that
government will promote development, utilization and public awareness of the need to manage
land, air and water resources in a balanced and sustainable manner for present and future
generations.
2.6.6 The National Environment Act CAP 153
Section 5 provides for a person who owns or controls a facility or premises, which generate waste,
to minimize the waste generated by adopting cleaner production methods. Subsection l (b) (i):
Assessment of Medical Radioactive Waste Management in Hospitals: | Richard Okot
18
identifying and eliminating potential negative impacts of the product/waste, (c): incorporating
environmental concerns in the design and disposal of a product.
2.6.7 The Local Governments Act, 1997
This act provides for a district-based system of local governments. This system provides for elected
councils that have both legislative and executive powers. Thus the district councils play an
important role in land administration, land surveying, physical planning, and management of
forests, wetlands, environment and sanitation services that are not the responsibility of the central
government.
2.7 Institutional frameworks for radioactive wastes management
2.7.1 Ministry of Water Lands and Environment
The ministry is the institution responsible for the formulation of policies that govern environmental
management in Uganda hence responsible for environmental issues in the country.
2.7.2 National Environment Management Authority
This is the principal agency in Uganda responsible for the management of environment and is
charged with the coordination, supervision and monitoring of all activities related to environmental
management.
2.7.3 Kampala City Council Authority
Though NEMA is charged with the coordination of sectoral environmental issues, KCCA ensures
that the collection, transportation and disposal of radioactive wastes are done in line with the legal
guidelines provided.
Assessment of Medical Radioactive Waste Management in Hospitals: | Richard Okot
19
CHAPTER THREE: METHODOLOGY
3.1 Introduction
This chapter covered the description of study area, research design, sample size and selection
criteria, data analysis and presentation, dissemination of results, ethical consideration and
limitations the study.
3.2 Description of study area
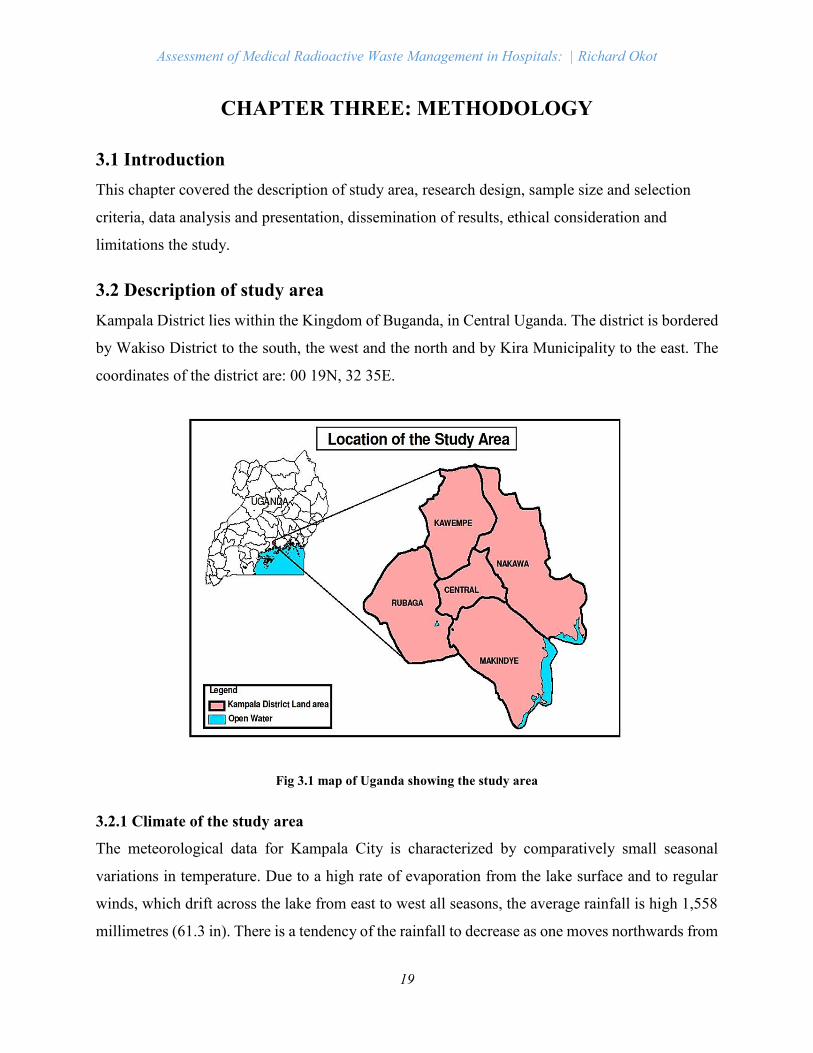
Kampala District lies within the Kingdom of Buganda, in Central Uganda. The district is bordered
by Wakiso District to the south, the west and the north and by Kira Municipality to the east. The
coordinates of the district are: 00 19N, 32 35E.
Fig 3.1 map of Uganda showing the study area
3.2.1 Climate of the study area
The meteorological data for Kampala City is characterized by comparatively small seasonal
variations in temperature. Due to a high rate of evaporation from the lake surface and to regular
winds, which drift across the lake from east to west all seasons, the average rainfall is high 1,558
millimetres (61.3 in). There is a tendency of the rainfall to decrease as one moves northwards from
Assessment of Medical Radioactive Waste Management in Hospitals: | Richard Okot
20
the lake shores. The rain falls in 160 to 170 days each year, with two peaks from March to May
and from October to November.
3.2.2 Population of the study area
The 2002 census put the population of Kampala at 1,189,100 people, the Uganda Bureau of
Statistics estimated the population of Kampala at 1,597,900 in 2010. In 2011, the city’s population
was estimated at approximately 1,659,600.
3.2.3 Geology of the study Area
The general geology of the landfill area consists of Basement complex system of rocks of the
Precambrian age. The lithology is mainly undifferentiated gneiss and migmitites (geological map
of central Uganda, 1974). Characteristic to these rocks in the tropical environment, insitu
weathering generally results in the development of a layer of weathered material referred to as
regolith. In general the regolith is the potential aquifer and the permeability varies according to the
clay content.
3.2.5 Soils of the study Area
The area has alluvial soil consisting of top black loamy soil underlain by the reddish brown ferrate
soils. Close to the valley, there exist alluvial sediments consisting of coarse quartz grains that grade
into fine grains. Granite gneiss is completely weathered sometimes with relict foliation observed
at a depth of 6.0m. In some places, the gneisses has become kaolinite. Pneumatisation of the
gneisses is notable in the north of the project area.
3.3 Research design
3.3.1 Methods of Data collection
During the study, both qualitative and quantitative methods of data collection were used because
qualitative methods involve the use of words rather than numbers; while quantitative methods
involve the collection of numerical data in order to explain, predict and control phenomena of
interest. These methods included, administering questionnaire, interviewing and observation.
3.3.1.1 Key informant interviews
The purpose of the interview with the waste management officer at Hospitals was to collect the
primary data and background information about the waste management practices at the hospital.
The data and information collected formed the basis for this research. An interview protocol was
Assessment of Medical Radioactive Waste Management in Hospitals: | Richard Okot
21
initially developed to cover qualitative data collection that included interview technique, sampling,
ethical issues and data analysis.
3.3.1.2 Questionnaires
The questionnaires were designed for the study and it comprised of sections like; the demography
were the respondent’s working experience, educational level, among others will be asked. The
questionnaire also consisted of questions both open and closed in which exhausted the research
objectives and question. The method gave the respondents enough time to reflect, concentrate and
at times consult.
3.3.1.3 Secondary data
The researcher will get information from the study of documents about waste management; these
documents will include the publications, annual reports of the ministry of health, periodicals,
journals, magazines and other literature written by different knowledgeable scholars. This data
could be government or non-governmental / private statistics. The data will help the researcher
with the starting point for additional research.
3.3.1.4 Observation
An initial walk over the site was undertaken to become familiar with the layout and internal
activities in hospitals. The observation were carried out two times during the month of June to
July. The observations were carried along with the waste management team while they were
collecting medical waste from the wards. The following were some of the activities observed
during the research study;
3.3.1.5 Photography.
This was employed in collection of data aspects including facilities such as the waste bins, and the
disposal sites and incineration facilities available at hospitals.
3.4 Sample size and Selection criteria
The sample size comprised of 10 hospitals from different divisions in Kampala. During the study,
non-probability sampling procedure where purposive and quota sampling techniques was
employed. This is because, in purposive/judgmental sampling, the researcher purposively chooses
respondents who, in his opinion, are thought to be relevant to the research topic. Whereas in quota
sampling instead of dividing the population into strata and randomly choosing of respondents, the
Assessment of Medical Radioactive Waste Management in Hospitals: | Richard Okot
22
researcher sets a ‘quota’ of respondents to be chosen in specific population groups, by defining the
basis of choice ( gender, education, status, etc.) and this still be used in determining size.
3.5 Data Analysis and interpretation
Data analysis was done manually and where possible using Microsoft Excel Spreadsheets
identifying areas of emphasis according to themes and the responses summarized in a narrative
form as a presentation of the major findings of the study. The data was presented in graphic forms
like pie-chats, bar graph and percentages were be generated. At the end of it all, it was from the
results of analysis that the data was interpreted and discussions obtained in relation to phenomenon
of medical radioactive waste management.
3.6 Dissemination of the results
After the researcher was done with analysing the data, he distributed the findings to the areas /
offices that were helpful during data collection exercise. For instance, NEMA and Nakawa
Division Health inspectors to enable them update their information and to discover the gaps
existing in radioactive waste management. The university retained a copy of the approved research
report for academic reference and the researcher retained his copy.
3.7 Ethical consideration
An introduction letter from the university was obtained prior to the study and it was presented to
respective authorities at Hospital to be allowed to carry out research in the area. The names of the
respondents were not included in the report and at the same time explanations were given in regards
to the purpose of research to the respondents.
3.8 Limitations of the study
Availability of data was a real issue for the research due to which certain areas of waste
management like emissions from the incinerators were not considered.
The results are subjected to the reliability on the response of health care workers on the
questions in the survey
The researcher was not allowed to conduct the waste audit due to health and safety risk
associated with the medical waste.

Assessment of Medical Radioactive Waste Management in Hospitals: | Richard Okot
23
The cost benefit analysis of the on-site incineration is not done as the feasibility study of
the on-site incinerator is expected as the follow up of this research.
Assessment of Medical Radioactive Waste Management in Hospitals: | Richard Okot
24
CHAPTER FOUR: DATA ANALYSIS AND RESULTS
4.1 INTRODUCTION
This chapter reveals the analysis and results on the investigation of the current generation,
collection, storage, transportation and disposal of the medical radioactive wastes generated from
the different departments in hospitals.
4.2 Demographic characteristics of the respondents
The first aspect of the study deals with the personal information of the respondents which includes;
age, level of education, and working experience of the respondents
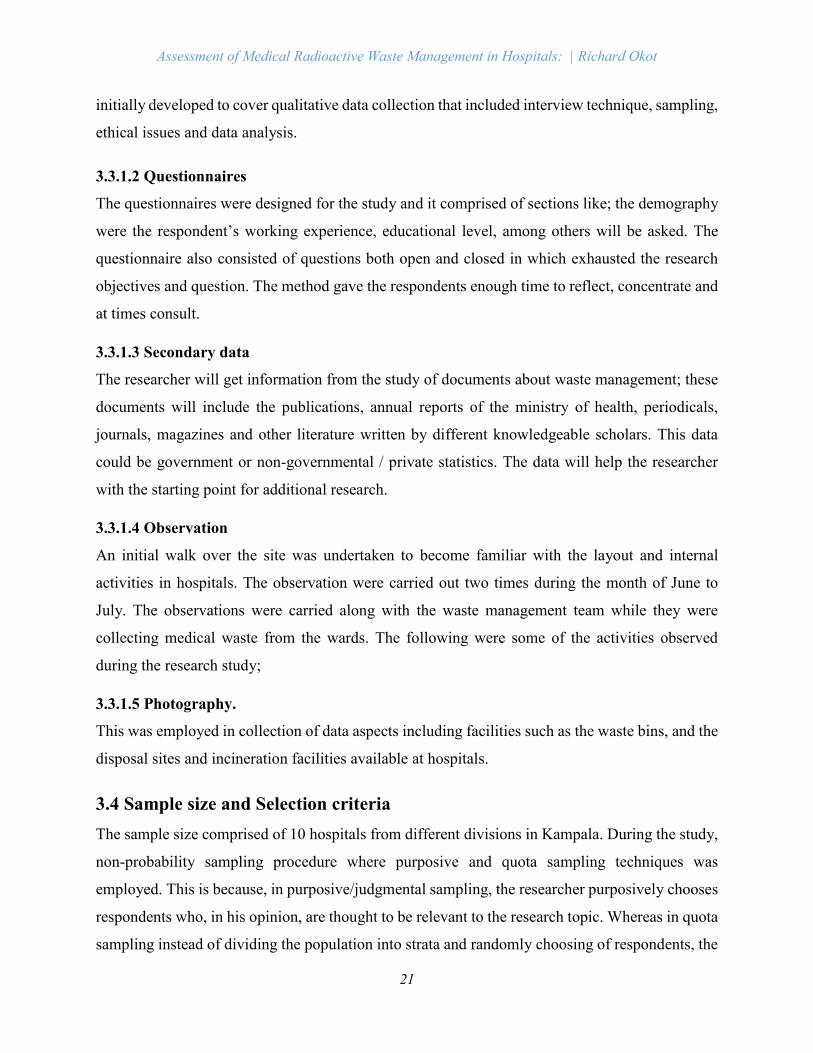
4.2.1 Age distribution of the respondents
Figure 4.1 showing age of the respondents.
From the figure above, it was found out that 20% of the respondents were in the age bracket of 21-
30, 30% in the range of 31-40, 40% within the range 41-50 and lastly 10% were above 50. Figure
4.1 reveals that the proportion of respondents above than 40years of age is 50% percent of the total
population interviewed. Higher age groups has an advantage in that they are seen keener about
improving the waste management practices whereas most of the employees among younger age
group had the “I don‘t care” attitude towards waste management.
0
5
10
15
20
25
30
35
40
21-30 31-40 41-50 Above 50
Per
cen
tag
e
Age Group
Percentage age distribution of respondents
Assessment of Medical Radioactive Waste Management in Hospitals: | Richard Okot
25
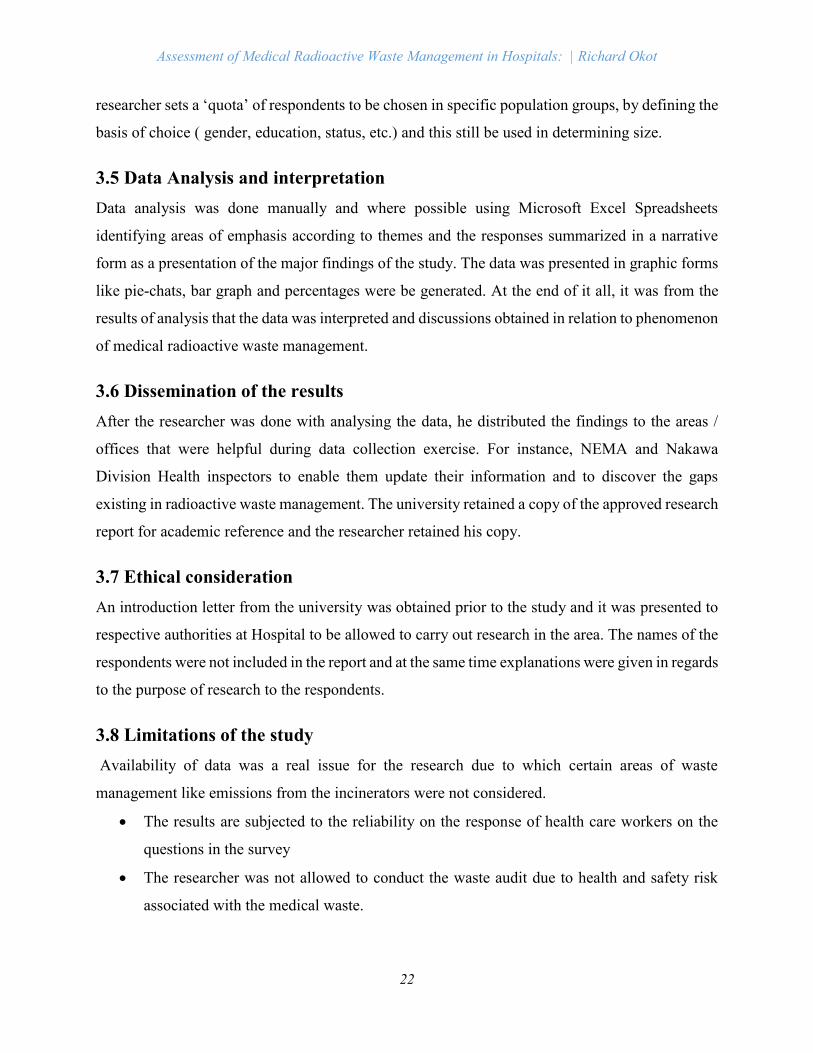
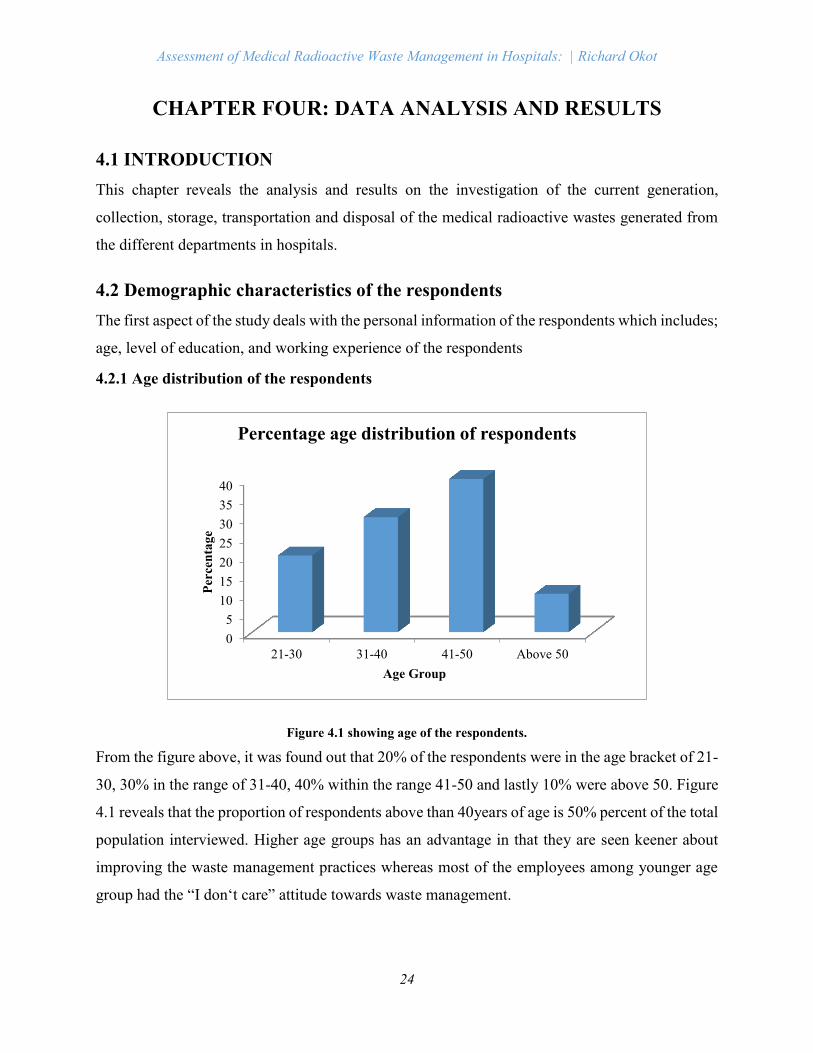
4.2.2 Education level of respondents
From the study, it was found out that all the respondents had attained some level of education. Of
this, 10% were of secondary level, 20% were of diploma level, 40% were bachelor holders and
30% were certificate holders as shown in figure 4.2. From the study it was found that respondents
who had attained higher level of education had more knowledge on better ways managing the
radioactive wastes than their counterparts who had attained low levels of education. Education is
very paramount for the development of any waste management strategy for an organisation
because attainment of education is strongly associated with decision-making and promotes
development.
Figure 4.2: Educational Level
4.2.3 Working experience of the respondents
It was found out from the study that 30% of the respondents had worked for less than 3years, 20%
between 4-10years, 40% between 11-15years and 10% had worked at the hospitals for more than
15years as shown in figure 4.3 above. The following data revealed from the data presented 40%
of the respondents had a working experience of 11-15 years which shows a higher number of
experienced people working on the department of the waste management which promotes proper
radioactive waste management.
10
30
20
40
0
5
10
15
20
25
30
35
40
45
Secondary. Certificate Diploma B.Sc. degree
Per
cen
tag
e
Education Levels
Education Levels of Respondents
Assessment of Medical Radioactive Waste Management in Hospitals: | Richard Okot
26
Fig.4.3 showing working experience of the workers
4.3 Information on radioactive waste in Hospitals
4.3.1 Amount of radioactive wastes generated from different departments in hospitals
From the research study, it was found out that 17% of the radioactive wastes came from the
laboratory department, 11% of from the Dental department, 22% generated from the surgical
department and 50% of the radioactive wastes was generated from Radiological department. The
data shows that there are more radioactive wastes generated from the radiology department than
any other department. This is mainly attributed to increase in cancer cases within the country
making patients continue to flock for imaging care in the Hospitals for radiotherapy.
Fig 4.4 showing amount of radioactive wastes generated from different departments
0 10 20 30 40
1 to 3
4 to 10
11 to 15
Above 15
Number of respondents in %
Tim
e p
erio
d i
n Y
rs.
Working experience of the respondents
Laboratory
17%
Dental department
11%
Surgical
22%
Radiology
50%
Amount of radioactive wastes generated from
different departments
Laboratory Dental department Surgical Radiology
Assessment of Medical Radioactive Waste Management in Hospitals: | Richard Okot
27
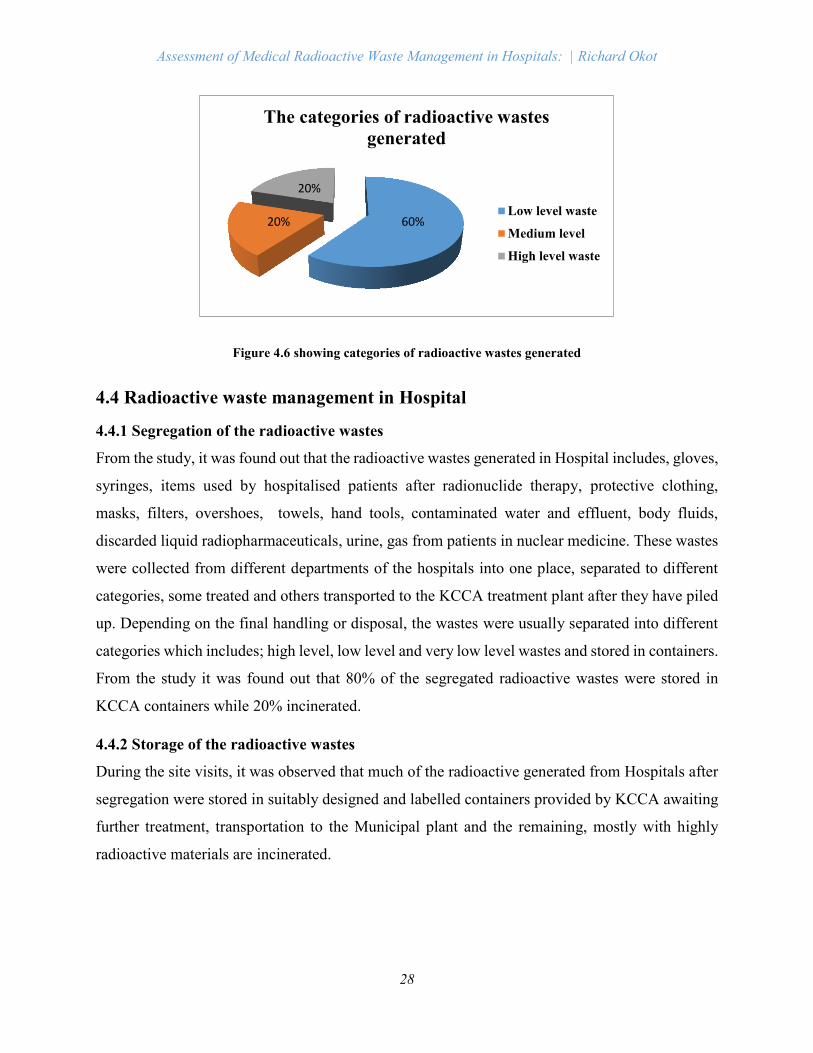
4.3.2 The types of medical radioactive wastes generated by hospitals
From the study, 75% of the radioactive wastes collected were solid, 15% of the liquid and lastly
10% were gaseous in nature as shown in figure 4.5. This implies that much of the wastes collected
consisted of solid wastes followed by liquid wastes and lastly gaseous wastes. The reason for the
high percentage of solid radioactive wastes is because most of the wastes are mixed together during
segregation and storage. Solid wastes are typically classified as combustible/noncombustible and
compactable/non-compactable waste.
Fig. 4.5 showing types of radioactive wastes generated
4.3.3 The categories of radioactive wastes generated from the hospital
60% of the respondents commented that radioactive wastes generated are of low levels, 20% raised
medium level wastes and lastly 20% raised high level wastes. The majority of the respondents
agreed that much of the wastes collected hospitals were low level wastes as shown in figure 4.6.
This is because hospitals generally use radionuclides that do not exhibit a high level of
radioactivity.
0
10
20
30
40
50
60
70
80
Solid Liquid Gaseous
75
1510
Qu
anti
ty i
n %
Types of medical radioactive wastes
Types of radioactive wastes generated
Assessment of Medical Radioactive Waste Management in Hospitals: | Richard Okot
28
Figure 4.6 showing categories of radioactive wastes generated
4.4 Radioactive waste management in Hospital
4.4.1 Segregation of the radioactive wastes
From the study, it was found out that the radioactive wastes generated in Hospital includes, gloves,
syringes, items used by hospitalised patients after radionuclide therapy, protective clothing,
masks, filters, overshoes, towels, hand tools, contaminated water and effluent, body fluids,
discarded liquid radiopharmaceuticals, urine, gas from patients in nuclear medicine. These wastes
were collected from different departments of the hospitals into one place, separated to different
categories, some treated and others transported to the KCCA treatment plant after they have piled
up. Depending on the final handling or disposal, the wastes were usually separated into different
categories which includes; high level, low level and very low level wastes and stored in containers.
From the study it was found out that 80% of the segregated radioactive wastes were stored in
KCCA containers while 20% incinerated.
4.4.2 Storage of the radioactive wastes
During the site visits, it was observed that much of the radioactive generated from Hospitals after
segregation were stored in suitably designed and labelled containers provided by KCCA awaiting
further treatment, transportation to the Municipal plant and the remaining, mostly with highly
radioactive materials are incinerated.
60%20%
20%
The categories of radioactive wastes
generated
Low level waste
Medium level
High level waste
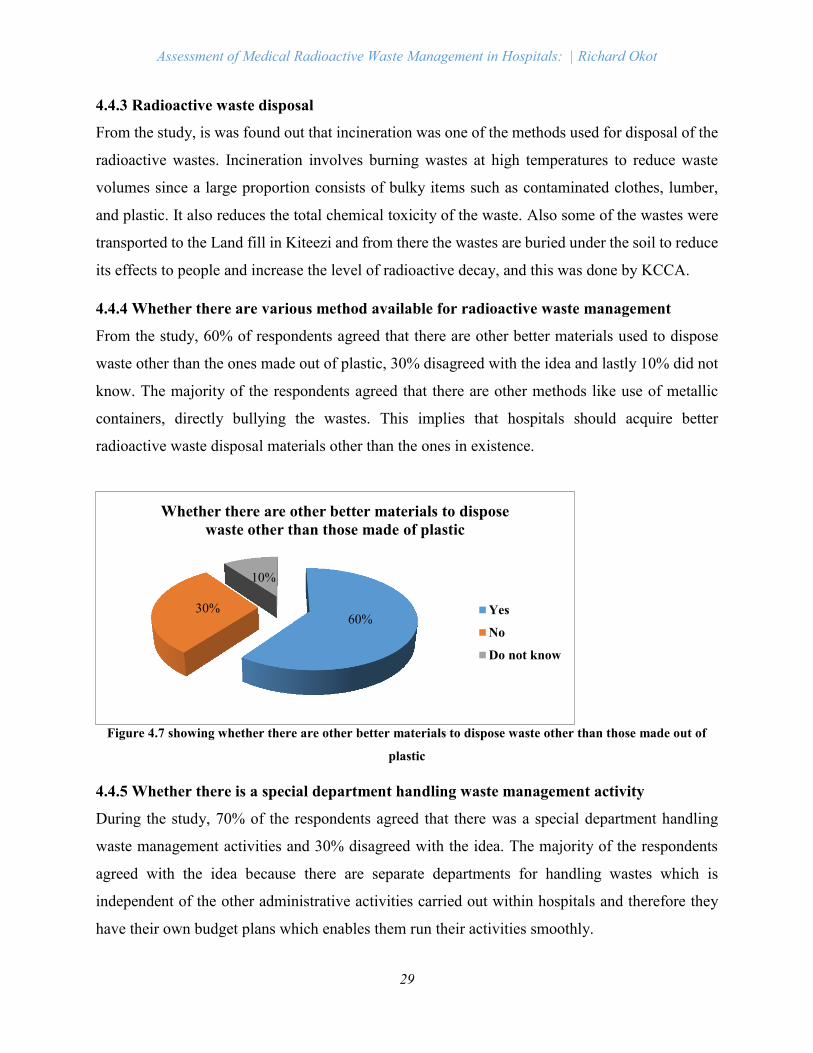
Assessment of Medical Radioactive Waste Management in Hospitals: | Richard Okot
29
4.4.3 Radioactive waste disposal
From the study, is was found out that incineration was one of the methods used for disposal of the
radioactive wastes. Incineration involves burning wastes at high temperatures to reduce waste
volumes since a large proportion consists of bulky items such as contaminated clothes, lumber,
and plastic. It also reduces the total chemical toxicity of the waste. Also some of the wastes were
transported to the Land fill in Kiteezi and from there the wastes are buried under the soil to reduce
its effects to people and increase the level of radioactive decay, and this was done by KCCA.
4.4.4 Whether there are various method available for radioactive waste management
From the study, 60% of respondents agreed that there are other better materials used to dispose
waste other than the ones made out of plastic, 30% disagreed with the idea and lastly 10% did not
know. The majority of the respondents agreed that there are other methods like use of metallic
containers, directly bullying the wastes. This implies that hospitals should acquire better
radioactive waste disposal materials other than the ones in existence.
Figure 4.7 showing whether there are other better materials to dispose waste other than those made out of
plastic
4.4.5 Whether there is a special department handling waste management activity
During the study, 70% of the respondents agreed that there was a special department handling
waste management activities and 30% disagreed with the idea. The majority of the respondents
agreed with the idea because there are separate departments for handling wastes which is
independent of the other administrative activities carried out within hospitals and therefore they
have their own budget plans which enables them run their activities smoothly.
60%30%
10%
Whether there are other better materials to dispose
waste other than those made of plastic
Yes
No
Do not know
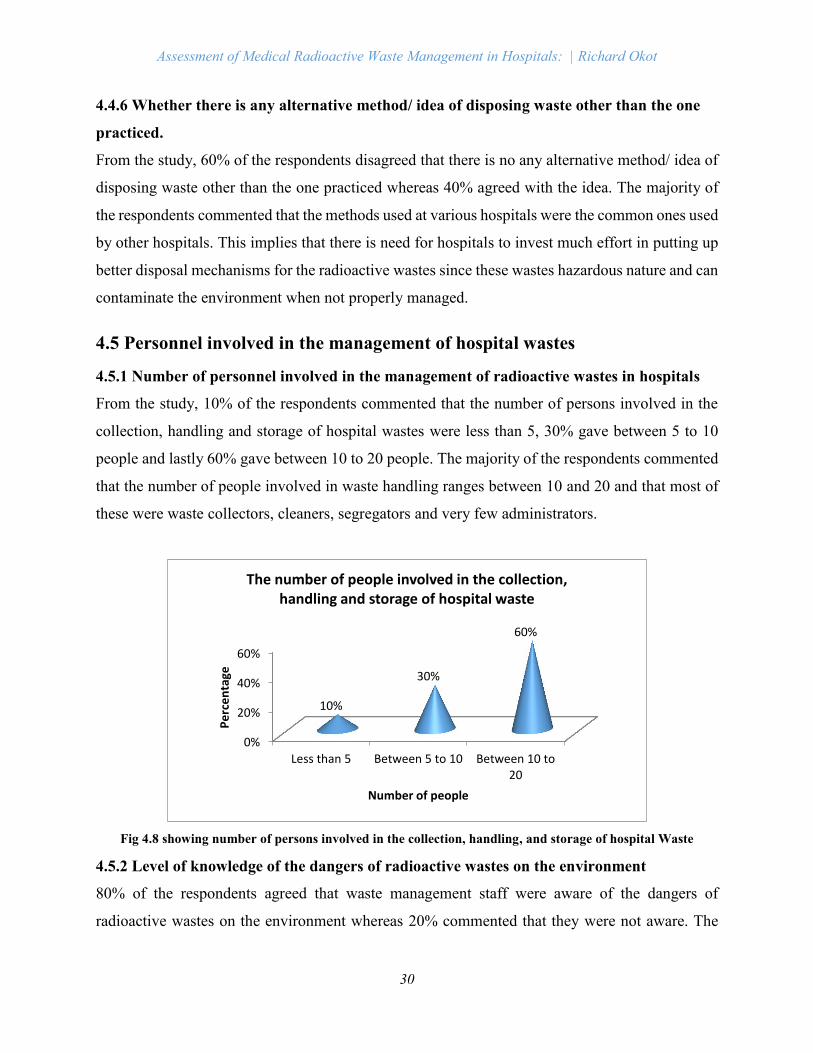
Assessment of Medical Radioactive Waste Management in Hospitals: | Richard Okot
30
4.4.6 Whether there is any alternative method/ idea of disposing waste other than the one
practiced.
From the study, 60% of the respondents disagreed that there is no any alternative method/ idea of
disposing waste other than the one practiced whereas 40% agreed with the idea. The majority of
the respondents commented that the methods used at various hospitals were the common ones used
by other hospitals. This implies that there is need for hospitals to invest much effort in putting up
better disposal mechanisms for the radioactive wastes since these wastes hazardous nature and can
contaminate the environment when not properly managed.
4.5 Personnel involved in the management of hospital wastes
4.5.1 Number of personnel involved in the management of radioactive wastes in hospitals
From the study, 10% of the respondents commented that the number of persons involved in the
collection, handling and storage of hospital wastes were less than 5, 30% gave between 5 to 10
people and lastly 60% gave between 10 to 20 people. The majority of the respondents commented
that the number of people involved in waste handling ranges between 10 and 20 and that most of
these were waste collectors, cleaners, segregators and very few administrators.
Fig 4.8 showing number of persons involved in the collection, handling, and storage of hospital Waste
4.5.2 Level of knowledge of the dangers of radioactive wastes on the environment
80% of the respondents agreed that waste management staff were aware of the dangers of
radioactive wastes on the environment whereas 20% commented that they were not aware. The
0%
20%
40%
60%
Less than 5 Between 5 to 10 Between 10 to20
10%
30%
60%
Pe
rce
nta
ge
Number of people
The number of people involved in the collection, handling and storage of hospital waste
Assessment of Medical Radioactive Waste Management in Hospitals: | Richard Okot
31
majority of the respondents agreed with the idea because the staff members were informed about
the challenges involved during the training period after recruitment.
4.5.3 Training given to the waste management staff
It was found out that 90% of the waste management staff had received whereas 10% disagreed
with the idea. The majority of the respondents agreed with the idea and it was found out that formal
training was provided for the duration mostly ranging between 3 to 5 days depending on the level
of understanding of the people being trained.
Assessment of Medical Radioactive Waste Management in Hospitals: | Richard Okot
32
CHAPTER 5: DISCUSSION
5.1 Introduction
This chapter presents a discussion of results obtained as present in chapter four. The presentation
of the discussions is in line with the study objectives.
5.2 Kinds of medical radioactive wastes generated from the hospital
Different radionuclides were found to be in use in hospitals to exclude disease, prove the existence
of a pathological process, assist in the planning of treatment or to follow the course of a disease
already diagnosed and/or treated and these included the radioisotopes of iodine, gallium, thallium
and technetium, amongst others as shown in Table 1.1. The increased use of radionuclides were
mainly attributed to increase in cancer cases within the country making patients flock for imaging
care. However, this influx lead to congestion of the diagnostic imaging departments leading to an
increase in the rate of radioactive wastes generation. It was established from the study that the
radioactive wastes produced from the Hospitals were in forms which included; solids (75%),
liquids (15%) and gases (10%) as shown in figure 4.5
Once these wastes are exposed to the environment, they can remain active for hours or several
months and if the radionuclides are to get into air, soil and water supplies accessible by both
animals and humans, these resources can become contaminated. In human exposure to radiations
that are 5 Sievert are usually fatal. Newly borne babies exposed to iodine may suffer from
hypothyroidism. Other living organisms may also experience adverse effects of radiation thus
causing alteration in DNA sequence which can subsequently lead to both low crop and animal
productivity. Although the dose produced through this indirect exposure is much smaller than a
direct exposure dose, there is a greater potential for a larger population to be exposed henceforth
proper disposal is essential to ensure protection of health and safety of the public and the quality
of the environment including, air, water supplies, and soil.
5.3 Current radioactive waste management practice within the hospitals
The management of the radioactive wastes in the various hospitals were mainly divided into six
different steps: pre-treatment (collection and handling), conditioning, storage, treatment,
transportation and disposal. For practical reasons the wastes were divided into solid, liquid and
Assessment of Medical Radioactive Waste Management in Hospitals: | Richard Okot
33
gaseous form to enable easy handling. The solid radioactive waste generated by the hospitals
included cover papers, gloves, empty vials and syringes, radionuclide generators, items used by
hospitalised patients after radionuclide therapy, sealed sources used in therapy, sealed sources used
for the calibration of instruments, and other biological waste. In the liquid waste category residues
of radionuclides, patient excreta, liquid scintillation solutions, and in the gaseous waste exhausted
gas from patients in in the radiology department were found out.
Depending on the final handling or disposal, the wastes were divided into different categories. One
category where the wastes would end up in a public waste treatment system with or without
incineration, the next where would be poured out in the public sewage system, and the third where
it was disposed of in a national disposal plant (Kiteezi). The following were some of the special
situations of radioactive waste management in the Hospitals observed during the course of the
study.
Pre-treatment. The thorough pre-treatment of the waste the most important step towards
a rational (both practical and economical) and safe handling of the waste. It includes steps
such as collection, segregation, chemical adjustment and decontamination. The segregation
is crucial and it was done taking into account the different aspects of the waste with a clear
view of the final treatment and/or disposal. The segregation of wastes into appropriate
categories took place during the waste collection.
Conditioning. This includes those operations that produce a waste package suitable for
handling, transportation, storage and/or disposal. It may include the conversion of the waste
to a solid waste form, enclosure of the waste in containers and, if necessary, providing an
over pack.
Storage. Interim storage of radioactive waste may be needed in different stages of the
waste management process. For many of the wastes generated in hospitals, storage for
decay is a useful option because the radionuclides have short half-lives. This can be done
in hospitals and may include some treatment of the wastes to ensure safe storage. After a
sufficient storage time, the final step, disposal as exempt waste, can also be performed at
the hospitals. Other types of waste containing radionuclides with longer half-lives must be
transferred to a special waste treatment, storage and disposal facility outside the hospitals.
Assessment of Medical Radioactive Waste Management in Hospitals: | Richard Okot
34
Transportation. During transportation, safety management included appropriate
packaging, labelling, transportation of documents including sender, retriever, content of
the waste, categorisation, and information to possible rescue personnel. The packages and
containers were strong enough to ensure a safe, sometimes rough, handling.
Disposal. There were mainly two approaches to the disposal of radioactive waste from the
hospitals. One was "dilute and disperse" and the other was "confine and contain". By the
"dilute and disperse" concept, radioactive material, in aqueous or gaseous form, were
released into the environment in such a way that the material was diluted and distributed
over a large volume so that the final concentration of radionuclides is acceptably low. In
the "confine and contain" approach, the waste was collected and converted into a form such
that, when placed in a repository, it will retain the radionuclides until the activity was
decayed, or at least will ensure that the leakage of radionuclides from the repository does
not give rise to unacceptable concentrations anywhere in the environment. This approach
was used for longer-lived solid radioactive waste.
The radioactive wastes generated were safely managed because of the hazardous nature it possess
to human health and the environment. Through good practices in the production and use of
radionuclides, the amount of wastes were significantly reduced but not fully eliminated. It was
noted during the study that full compliance with all relevant regulations were considered and
planned for in the early stages of radioactive waste management.
5.4 Knowledge and awareness of the dangers of radioactive wastes on the
environment by the workers
Due to hazardous nature of the medical radioactive wastes, poor disposal practices have sparked
concern regarding the impact it possess on public health and the environment. Lack of sufficient
knowledge of the associated risks is a strong factor contributing to inadequate disposal practices.
From the study, knowledge, and awareness status concerning the dangers radioactive wastes on
the environment by the workers was examined. More than 95% of the workers were found out to
have proper knowledge about the hazardous components of medical waste which is an essential
component in radioactive waste management therefore it was easy for them to segregate the wastes
into various medical waste categories which made handling easier. A positive attitude was also
shown by Hospital employees towards the training on proper medical waste management and

Assessment of Medical Radioactive Waste Management in Hospitals: | Richard Okot
35
improving the current waste management practice and this enabled them acquire the action
competences or skills of environment- in order to be able to identify and anticipate environmental
problems and work with others to resolve, minimize and prevent them. However from the study,
it was found out that about 55% of the workers surveyed had not attended training in past 12
months and this affected the the level of consistency in the managerial practice of radioactive waste
management since they lacked skills, knowledge and values concerning current management of
the waste and this impacts on practices of appropriate waste disposal.
On the aspect of personal protection, workers were observed using protective equipments such as
overalls and mouth masks during the handling of the wastes which showed a level of awareness
towards the hazardous nature of the wastes being handled but the hospital administrations should
provide the workers with complete protective ware in order to limit the chances of them being
exposed to radiations during the management process.
Plate 5.1 showing personnel wearing PPEs (overalls and mouth masks)
5.5 Alternatives for radioactive waste disposal and selection of best available
Technology
The use of radioactive materials for medical uses, brings with it the question of waste management
policy. Most countries using nuclear power have well developed strategies for radioactive wastes
and there are many similarities between the programmes of different countries. The study shows
that the incinerator is the best available technology for the on-site treatment of medical radioactive.

Assessment of Medical Radioactive Waste Management in Hospitals: | Richard Okot
36
As discussed in the literature none of the above mentioned technologies seemed to be
environmental friendly or pollution free. But the study shows that a modern incinerator seems to
be the best available option for the hospitals. Incinerator seem to be the most favourable treatment
technology due to the advantages like waste reduction and can be used for all types of waste.
Incinerator will continue to be the favourable treatment technology unless and until we develop a
technology which can treat all types of medical waste so in the meantime alternatives for
radioactive waste management that can be taken up by the institution include; dilute and disperse,
concentrate and contain, Delay and decay. The first two methods are advantageous in that they can
be used in the treatment of non-radioactive wastes whereas delay and decay is unique to radioactive
wastes management.
Vitrification. This involves stabilisation of the wastes into a form which will neither react
nor degrade for extended periods of time. The waste is mixed with sugar and the calcined.
Calcination involves passing the waste through a heated rotating tube so that water is
evaporated from the waste and de-nitrate the fission products to assist the stability of the
glass produced.
Ion exchange. Here ferric hydroxide is used to remove radioactive metals from aqueos
mixtures. After the radioisotopes are absorbed onto the ferric hydroxide, the resulting
sludge can be placed in a metal drum being mixed cement to form a solid waste form.
Space Disposal. Of all disposal methods of radioactive wastes, this method has the greatest
potential to isolate the wastes permanently from the biosphere. Although it is technically
possible, its costs would be very high. Studies have indicated that the number of flights
required to transport high volume of radioactive waste would be impractical; space disposal
could be feasible only for very small volume of reprocessed high-level wastes. The risk of
catastrophic accidents is estimated to be about one per cent per flight, and thus that the
radiological risk of disposal in space is higher than for geological disposal.
Ice Sheet Disposal. Disposal of radioactive wastes in ice sheets has also been suggested in
the past and at first sight appears to be feasible, however, it has not been extensively
researched. The idea has the advantage of placing the waste in a slowly changing
environment devoid of living organisms. Canadian glaciers are too small for this method,
so ice sheets in Greenland or the Antarctic would have to be employed. Correspondingly,

Assessment of Medical Radioactive Waste Management in Hospitals: | Richard Okot
37
the wastes would have to be transported over great distances. Moreover, treaty obligations
preclude disposal in the Antarctic.
Assessment of Medical Radioactive Waste Management in Hospitals: | Richard Okot
38
CHAPTER SIX: CONCLUSIONS AND RECOMMENDATIONS
6.1 Introduction
This chapter presents the conclusions and the recommendation of the study.
6.2 Conclusion
The overall goal of this research was to investigate the current use of medical radionuclides and
generation, collection, storage, transportation and disposal of the medical radioactive wastes
generated from the different departments in Hospitals. The four general objectives of this research
were to:
1. To determine the kinds of medical radioactive wastes generated from different departments
of the hospitals.
2. To determine information on the current collection, storage, transportation, treatment and
disposal of the medical radioactive wastes from the hospitals.
3. To assess knowledge and awareness of the dangers of radioactive wastes on the
environment.
4. To identify the possible recommendations to archive proper medical radioactive waste
management
From the study, it was established that much of the radioactive wastes produced at Hospitals were
in forms which included; solids (75%), liquids (15%) and gases (10%) as shown in figure 4.5.
These wastes were segregated and then stored in the KCCA container or in temporary plastic
dustbins around the hospitals. The wastes were further transferred once in a day and usually in the
morning hours to the Municipal waste disposal plant at Kiteezi in Wakiso district. Much of the
radioactive wastes produced were low level waste of these some were incinerated at the hospital
premises as a means of disposal to reduce their effect to the environment and the staff involved in
the garbage collection process. It was also discovered that most of the staff involved in waste
handling had knowledge concerning the dangers of radioactive wastes and trained in the different
ways of protecting themselves.
Assessment of Medical Radioactive Waste Management in Hospitals: | Richard Okot
39
This study by no means provides a synthesis of all the available information on the radioactive
waste management system in hospitals and proscribing detailed plans for appropriate waste
reduction projects is beyond the scope of this study. Further research should be done to address
specific issues within the sector, and requirements for appropriate waste reduction technologies;
and further work should be conducted to develop targets and objectives for long-term waste
reduction strategies.
The value of the present research exists in its utility to the hospital authorities involved in waste
management. The findings can be used to facilitate more effective and appropriate radioactive
waste management programs like waste reduction initiatives, by capitalizing on the incentives
while strategically reducing the barriers or taking action to transform them into incentives.
6.3 Recommendations
In response to the conclusions presented, the following recommendations are provided for
improving the management of medical radioactive wastes in hospitals. The recommendations are
specific to each stakeholder that should be involved in the strategic planning of the specific
interventions. The recommendations are based on the synthesis of information gathered in the
research findings, in-depth interviews, available literature, as well as on the author’s experience
while carrying out site visits.
Similar studies should be conducted in other hospitals in Uganda in order to develop unique
solutions based on the prevailing radioactive waste management.
Review of the waste management policies should be done so that it focuses not only on the
waste minimization strategies but should also contain strategies to encourage greater
engagement and to change the intended behaviour to a more sustainable behaviour.
The waste manager should consult with the staffs and a consensus should be made on the
location of waste bins.
The employees should be highly encouraged to inform the waste management team
whenever they have put wrong waste in wrong bin.
Proper consideration of record, track and monitoring for the waste generation pattern for
each wards.
Assessment of Medical Radioactive Waste Management in Hospitals: | Richard Okot
40
The management of hospitals should allocate enough funds to the department responsible
for handling radioactive wastes so as to purchase modern gadgets for use.
The staff members involved in handling wastes should be provided with protective wears
such as overalls, gloves and gumboots.
Hospitals should provide periodic training to its staff members involved in handling
radioactive wastes.
Specific designs and engineering courses should be developed and introduced in higher
institutions of learning so as to enhance the science of radioactive waste management.
Responsible authorities like the KCCA, NEMA should ensure the sustainability of
radioactive wastes management systems by improving the effectiveness of collection and
recycling system.
Enforcement of rules and regulations regarding waste disposal should be taken as a serious
issue by the government.
Assessment of Medical Radioactive Waste Management in Hospitals: | Richard Okot
41
REFERENCES
1. AERB Safety Code for Nuclear Medicine Laboratories (SC/MED 4) Appendix 511. 1989.
pp. 47–49.
2. Cherry SR, Sorenson JA, Phelps ME. Physics on Nuclear Medicine. 3rd Edition. Saunders;
Philadelphia, Pennsylvania: 1980.
3. Classification of Radioactive Waste, a Safety Guide. A Publication in the Radioactive
wastes Programme. Safety Series No. 111-G-1.1, IAEA 1994.
4. CoRWM Implementation Working Group, Draft Discussion Paper on Implementation,
CoRWM Document Number 1703.1, 2006.
5. CoRWM, Managing our Radioactive Waste Safely: CoRWM's Recommendations to
Government, CoRWM Document Number 700, 2006.
6. Defra News Release, Government Welcomes CoRWM's Package of Measures for Long
Term Management of Radioactive Waste, July 2006.
7. Department of Environment, Office of the Deputy Prime Minister, Scottish Executive and
Welsh Assembly Government, a Practical Guide to the Strategic Environmental
Assessment Directive, 2005.
8. Department of the Environment, Department for Environment, Food and Rural Affairs, the
National Assembly of Wales, and the Scottish Executive, Managing Radioactive Waste
Safely: Proposals for Developing a Policy for Managing Radioactive Waste in the UK,
2001.
9. Establishing and National System for Radioactive Waste Management, Safety Series No.
111-S-1, Vienna 1995.
10. Govida Rajan KN. BARC; Mumbai: 2002. Basic Safety Standards. Accredition
Programme for Nuclear Medicine Technologists in Radiation Safety; pp. 8.1–8.9.
11. ICRP Recommendations of the International Commission on Radiological Protection. Brit
J Radiol. 1995 ;( Suppl 6)
12. Kinni KS. Planning of Nuclear Medicine Laboratories for Diagnostic and Therapeutic
Procedures. Indian J Nuclear Med. 1998; 13(4):165–192.
13. Kishore J, Goel P, Sagar B, Joshi TK. Awareness about biomedical waste management and
infection control among dentists of a teaching hospital in New Delhi. Indian
Assessment of Medical Radioactive Waste Management in Hospitals: | Richard Okot
42
14. Murthy BKS. BARC; Mumbai: 2000. Operational limits. Training workshop on Radiation
Safety in Nuclear Medicine and RSO Certification Examination; pp. 6.1–6.6.
15. Nagalakshmi B. BARC; Mumbai: 2000. Radioactive waste disposal with special reference
to Nuclear Medicine Laboratories; pp. 16.1–16.4. Training workshop on Radiation Safety
in Nuclear Medicine and RSO Certification Examination.
16. Narang RS, Manchanda A, Singh S, Verma N, Padda S. Awareness of biomedical waste
management among dental professionals and auxiliary staff in Amritsar, India. Oral Health
and Dental Management. 2012; 11: 162-168.
17. ODPM, Sustainability Appraisal of Regional Spatial Strategies and Local Development
Documents, 2005.
18. Radiation Protection for Medical and Allied Health Personnel 1989. NCRP Report No 105.
19. Rao PH. Report: Hospital waste management-awareness and practices: A study of three
states in India. Waste Management and Research. 2008; 26: 297-303.
20. Sharma S. Awareness about bio-medical waste management among health care personnel
of some important medical centers in Agra. International Journal of Environmental.
21. Sudhakar V, Chandrashekhar J. Dental health care waste disposal among private dental
practices in Bangalore.
22. Tabish SA. Hospital Infection Control: Conceptual Framework. Academia Publishers;
2005. Ecohealth: Management of Biomedical Waste; pp. 139–145.
23. The Nuclear Decommissioning Authority, Managing Radioactive Waste Safely: A Review
of International Experience of Partnerships, 2007.
24. The Principles of Radioactive Waste Management, Safety Series No. 111-F, IAEA, Vienna
1995.
25. The Radiation protection Rules (RPR) 1971, under Section 30 of The Atomic Energy Act,
1962.
Assessment of Medical Radioactive Waste Management in Hospitals: | Richard Okot
43
APPENDIX I: QUESTIONAIRE
This questionnaire has been designed to assess the medical radioactive wastes management in
Hospitals, Kampala city. Therefore it seeks to request for your assistance in answering questions.
Your response will provide data for research and will be highly confidential and will strictly be
used for this study only.
Dear respondents,
Instructions
Please put a tick in the appropriate box in every question or give your own opinion in the spaces
provided.
PART ONE: BIO-DATA
Typology Category
Typology Characteristics
Response.
Age (Years)
21-30
31-40
41-50
50+
Education level.
Secondary
Diploma
B.Sc. degree
Graduate studies
Working experience (Years)
1-3
4-10
11-15
15+
Assessment of Medical Radioactive Waste Management in Hospitals: | Richard Okot
44
PART 2: INFORMATION ON RADIOACTIVE WASTE IN HOSPITAL
a) Amount of radioactive wastes generated in different departments of the hospital.
Department. Average waste collected per
day (approximately in kg)
Material used for collection of
waste for disposal
(approximately in kg)
Laboratory.
Radiology department
Dental.
Surgical ward
b) Pleases let me know on the quantities of the types of medical radioactive wastes
generated by your hospital
Type of radioactive wastes
generated.
Average waste collected
per day (approximately in
kg)
Solid
Liquid
Gaseous
c) Categories of the radioactive wastes generated.
Category. Response.
Low level waste
Medium level
High level waste
Assessment of Medical Radioactive Waste Management in Hospitals: | Richard Okot
45
PART 3: RADIOACTIVE WASTE MANAGEMENT IN HOSPITAL
i. Describe briefly what happens between segregation (if any) and final disposal of Medical
Radioactive waste
................................................................................................................................................
....................................................................................................................................
ii. Where is the segregated waste stored while awaiting removal from the hospital or disposal?
Describe
................................................................................................................................................
................................................................................................................................................
............
iii. Describe briefly the final disposal of segregated waste (taken to municipal landfill, buried
on hospital grounds, incinerated, open burned, etc.).
................................................................................................................................................
................................................................................................................................................
............
iv. Where do you dispose the waste? Please mention the location
................................................................................................................................................
................................................................................................................................................
............
v. Do you think there are other better materials to dispose waste other than those made out of
plastic?
................................................................................................................................................
................................................................................................................................................
............
vi. Is there any special department handling waste management activity?
Yes No
vii. Do you suggest any alternative method/ idea of disposing waste other than that is practiced
now?
................................................................................................................................................
...........................................................................................................................
Assessment of Medical Radioactive Waste Management in Hospitals: | Richard Okot
46
PART 4: PERSONNEL INVOLVED IN THE MANAGEMENT OF HOSPITAL
WASTES.
i. Indicate the number of persons involved in the collection, handling, and storage of hospital
Waste
................................................................................................................................................
.........................................................................................................................
ii. Are the waste management staff aware of the dangers of radioactive wastes on the
environment?
Yes No
iii. Are instructions/training given to newly hired waste management staff?
Yes No
iv. If yes, what type of training and of what duration?
................................................................................................................................................
....................................................................................................................................
***THANK YOU ***
Related Documents











