MANAGEMENT OF HYPERTENSION Focus on CCB & JNC VIII dr. ANDI SULISTYO HARIBOWO, SpPD INTERNIST

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
MANAGEMENT OF HYPERTENSION
Focus on CCB & JNC VIII
dr. ANDI SULISTYO HARIBOWO, SpPD
INTERNIST

CURRICULUM VITAENama : dr. Andi Sulistyo Haribowo, SpPD
TTL : Malang, 28 Mei 1978
Alamat : Jl. Ters. Sigura-gura C-15 Malang
Phone : 08123591692
Pendidikan Tinggi:
- Sarjana Kedokteran, FKUB Malang, 1999
- Dokter Umum, FKUB Malang, 2002
- Dokter Spesialis Penyakit Dalam, FKUB/Pengurus BesarPerhimpunan Dokter Spesialis Penyakit Dalam Indonesia (PB PAPDI), 2010
Pengalaman kerja:
- Dokter Klinik 24 jam di Pasuruan dan Sidoarjo (2002-2003)
- Dokter Kontrak RSU Ngudi Waluyo, Wlingi, Blitar (2002-2003)
- Dokter PTT Depkes RI Brigade Siaga Bencana (2003-2004)
- Dokter PNS Kota Malang (2004-sekarang) RSUD Kota Malang
- Program Studi Pendidikan Dokter Spesialis Penyakit Dalam(PPDS) RSSA (2006-2010)
- Dokter SpPD di RSU Mitra Delima dan RSU Prasetya Husada KabMalang (2010-sekarang)
- Dosen Luar Biasa FK Universitas Islam Malang (2010-sekarang)

Measurement blood pressure
Persons seated quietly for at least 5 minutes in a chair , with feet on the floor, and arm supported at heart level.
Caffeine, exercise, and smoking should be avoided for at least 30 minutes prior to measurement.
An appropriately sized cuff (cuff bladder encircling at least 80 percent of the arm) should be used to ensure accuracy.
At least two measurements should be made and the average recorded.
For manual determinations,palpated radial pulse obliteration pressure
should be used to estimate SBP—the cuff should then be inflated 20–30 mmHg above this level
The cuff deflation rate for auscultatory readings should be 2 mmHg per second.
SBP is the point at which the first of two or more Korotkoff sounds is heard (onset of phase 1), and the disappearance of Korotkoff sound (onset of phase 5) is used to define DBP.


30/9/2549 CVD S&S Med 4
Blood pressure measurement

30/9/2549 CVD S&S Med 4
Korotkoff sound in BP measurement

Persistent elevation of arterial blood pressure (BP)
~72 million Americans (31%) have BP > 140/90 mmHg
RISKESDAS 2013 25,8% in Indonesia
Most patients asymptomatic
Increasing prevalence with aging of population and epidemic of overweight/obesity

28
3842
47 49 49
55
38
0
20
40
60
Italy Sweden England Spain Finland Germany
Adults aged 35–64 years (data are age- and sex-adjusted), except* (adults aged ≥ 30 years)
Hypertension defined as BP 140/90 mmHg or on treatment
Wolf-Maier et al. JAMA. 2003;289:23632369; Sekikawa, Hayakawa. J Hum Hypertens. 2004; 2004;18:911–912.
Pre
vale
nce o
f hypert
ensio
n (
%)
US Japan*
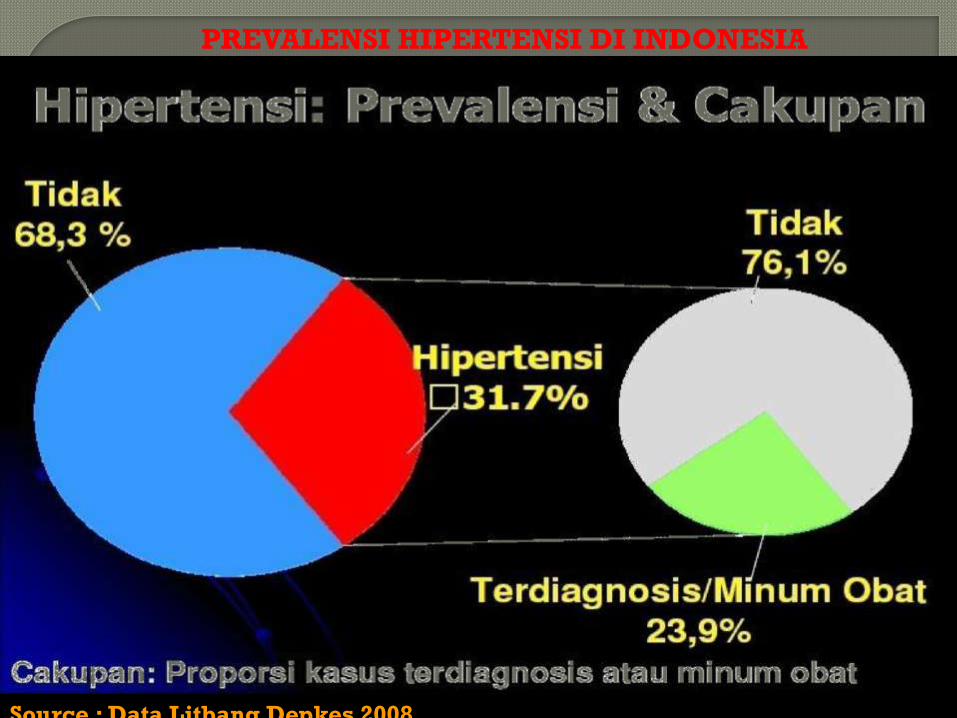
PREVALENSI HIPERTENSI DI INDONESIA
Source : Data Litbang Depkes 2008

H. + Komplikasi
H. + Keluhan +
Pengobatan tak baik
H. + Keluhan +
Pengobatan baik
H. Tanpa keluhan
Normotensi
Border line
FENOMENA GUNUNG ES

1970 - 1975 1975 - 1980 1980 - 1985 1985 - 1990
Aware (%) 51 64 73 84
Treated (%) 36 34 56 73
Control (%) 16 20 34 55
HIPERTENSION, AWARENESS,
TREATMENT, AND CONTROL RATES

Hypertension:
A Risk Factor for Cardiovascular Disease
9.5
3.3 2.45.0
2.03.5
2.1
45.5
21.3
12.4
6.2
9.97.3
13.9
6.3
22.7
0
5
10
15
20
25
30
35
40
45
50
Man Woman Man Woman Man Woman Man Woman
Normotensive
Hypertensive
Ratio
Risk: 2.0 2.2 3.8 2.6 2.0 3.7 4.0 3.0
Kannel WB. JAMA 1996;275:1571-1576
Coronary
diseaseStroke
Peripheral artery
disease
Cardiac
failure
Bie
nn
ial a
ge
-ad
jus
ted
ra
te
pe
r 1
,00
0 s
ub
jec
ts



*Individuals aged 40-69 years, starting at blood pressure 115/75 mm Hg.CV, cardiovascular; DBP, diastolic blood pressure; SBP, systolic blood pressure.Chobanian AV et al. JAMA. 2003;289(19):2560-2572.Lewington S et al. Lancet. 2002;360(9349):1903-1913.
Kematian akibat Kardiovaskular Meningkat Dua Kali
Lipat tiap Peningkatan
20-mm Hg TDS atau 10-mmHg TDD*
Cardiovascular
mortality
risk
SBP/DBP (mm Hg)
0
1
2
3
4
5
6
7
8
115/75 135/85 155/95 175/105
2x
4x
8x

Penurunan Tekanan Darah sebesar 2 mm Hg
Menurunkan Resiko Kardiovaskular hingga 10%
Meta-analysis of 61 prospective, observational studies
1 million adults
12.7 million person-years
Prospective Studies Collaboration. Lancet. 2002;360:1903-1913.
2 mm Hg
decrease in
mean SBP 10% reduction
in risk of stroke
mortality
7% reduction
in risk of CHD
mortality


JNC 7 blood pressure classification
in adults aged ≥18 years
BP
Classification
SBP
(mm HG)
DBP
(mm HG)
Normal <120 and <80
Prehypertension 120-139 or 80-89
Stage 1
hypertension140-159 or 90-99
Stage 2
hypertension160 or 100
National Heart, Lung, and Blood Institute. JNC 7 Express. The Seventh Report of the Joint National Committee on
the Prevention, Detection, Evaluation and Treatment of High Blood Pressure. 2003.



Lifestyle Modification
Modification Approximate SBP reduction
(range)
Weight reduction 5–20 mmHg/10 kg weight loss
Adopt eating plan 8–14 mmHg
sodium reduction 2–8 mmHg
Physical activity 4–9 mmHg
Moderation of
alcohol consumption
2–4 mmHg

Multiple antihypertensive agents
are needed to achieve target BP
AASK MAP <92
Target BP (mmHg)
Number of antihypertensive agents
1
UKPDS DBP <85
ABCD DBP <75
MDRD MAP <92
HOT DBP <80
Trial 2 3 4
DBP, diastolic blood pressure; MAP, mean arterial pressure;
SBP, systolic blood pressure
IDNT SBP <135/DBP <85
ALLHAT SBP <140/DBP <90
1) Bakris GL, et al. Am J Kidney Dis 2000;36:646-661; 2) Lewis EJ, et al. N Engl J Med 2001;345:851-860;
3) Cushman WC, et al. J Clin Hypertens 2002;4:393-404

Combining drugs is better than high
dose monotherapy in BP control
Wald et al. Am J Med 2009;122:290–300
Conclusions from a meta-analysis comparing combination antihypertensive therapy with monotherapy in
over 11,000 patients from 42 trials
‘The extra BP reduction from combining drugs from 2 different classes is
approximately 5 times greater than doubling the dose of 1 drug’
?

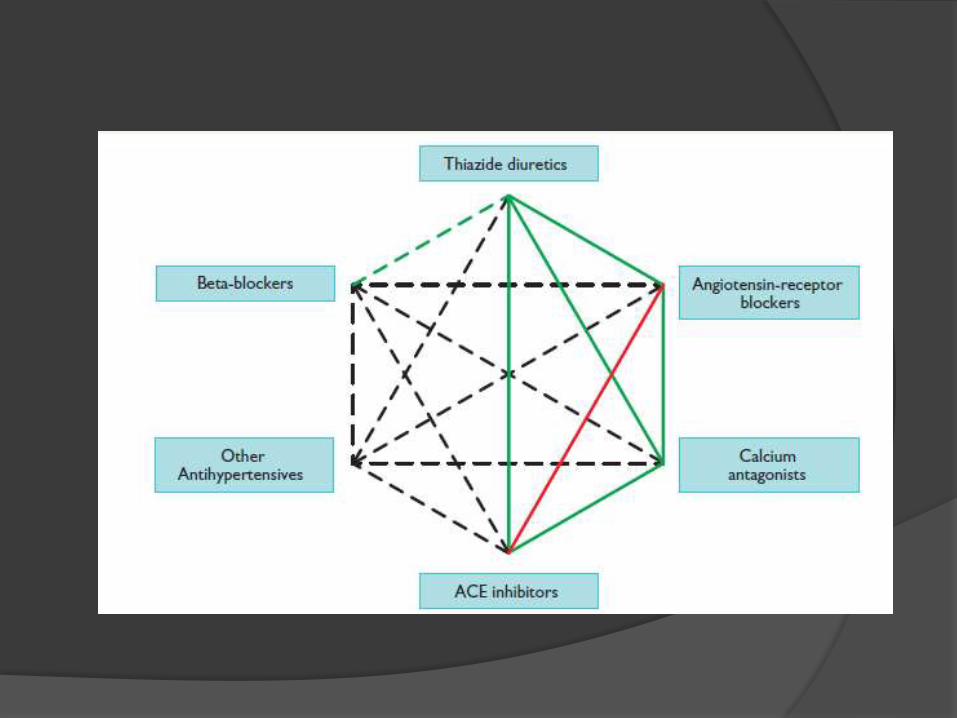
2013 ESH-ESC Guideline for Arterial
Hypertension: Choice of Antihypertensive Drugs
Mancia et al. ESH/ESC Guidelines July 2013, Journal of Hypertension : Vol. 31: Nu.7;1285-1357

James PA et al. JAMA 2014;311:507–20;
JNC 8:
Hypertension Management Algorithm



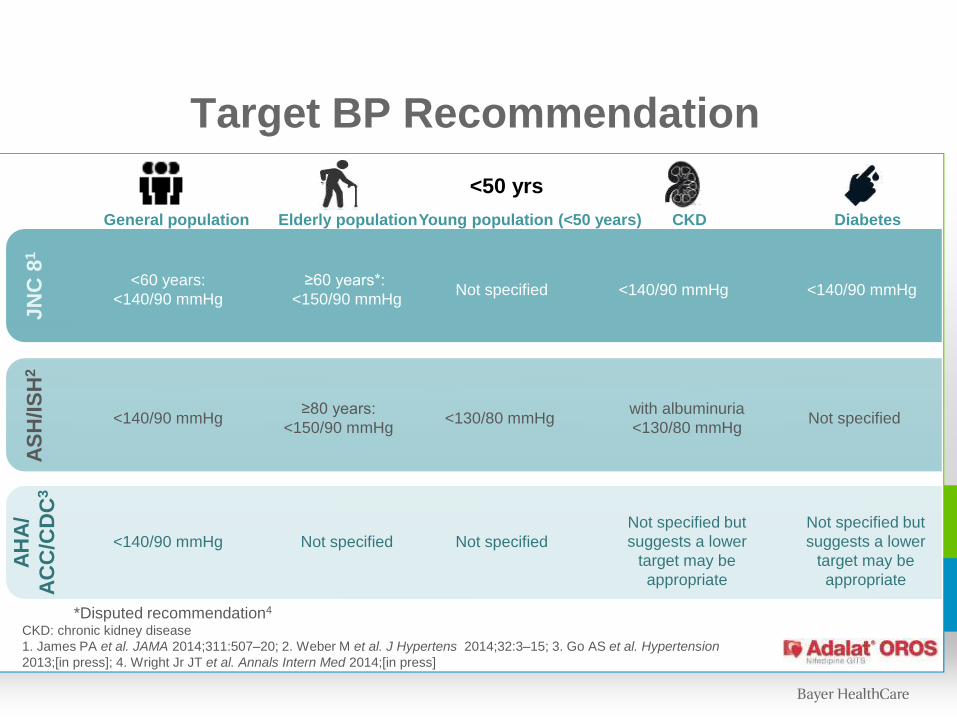
Target BP Recommendation
CKD: chronic kidney disease
1. James PA et al. JAMA 2014;311:507–20; 2. Weber M et al. J Hypertens 2014;32:3–15; 3. Go AS et al. Hypertension
2013;[in press]; 4. Wright Jr JT et al. Annals Intern Med 2014;[in press]
≥80 years:
<150/90 mmHg
≥60 years*:
<150/90 mmHg
Not specified
<60 years:
<140/90 mmHg
<140/90 mmHg
<140/90 mmHg
Not specified
Not specified
<130/80 mmHg
<140/90 mmHg
Not specified but
suggests a lower
target may be
appropriate
with albuminuria
<130/80 mmHg
<140/90 mmHg
Not specified
Not specified but
suggests a lower
target may be
appropriate
General population Elderly populationYoung population (<50 years) CKD Diabetes
<50 yrs
JN
C 8
1A
SH
/IS
H2
AH
A/
AC
C/C
DC
3
*Disputed recommendation4

Treatment Algorithm for Adults with Systolic-Diastolic
Hypertension without another compelling indication
TARGET <140/90 mmHg
Beta-blocker
Long-actingDHP-CCBARBThiazide ACE-I
INITIAL TREATMENT AND MONOTHERAPY
Alpha-blocker
as initial
monotherapy
Lifestyle modification
therapy
2003 Canadian Hypertension Education Program Recommendations.

1950
1960
1970
1980
Diuretics
Beta blockers
CCBs
1-blockers
ACE-inhibitors 1990
2010AT1-antagonists
DRI
Reserpin (1949)
HCT (1958)
Verapamil (1963)
Furosemide (1964)
Propanolol (1965)
Nifedipin (1975)
Prazosin (1977)
Captopril (1981)
Losartan (1995)
Development of Antihypertensive Drugs
Aliskiren (2005)
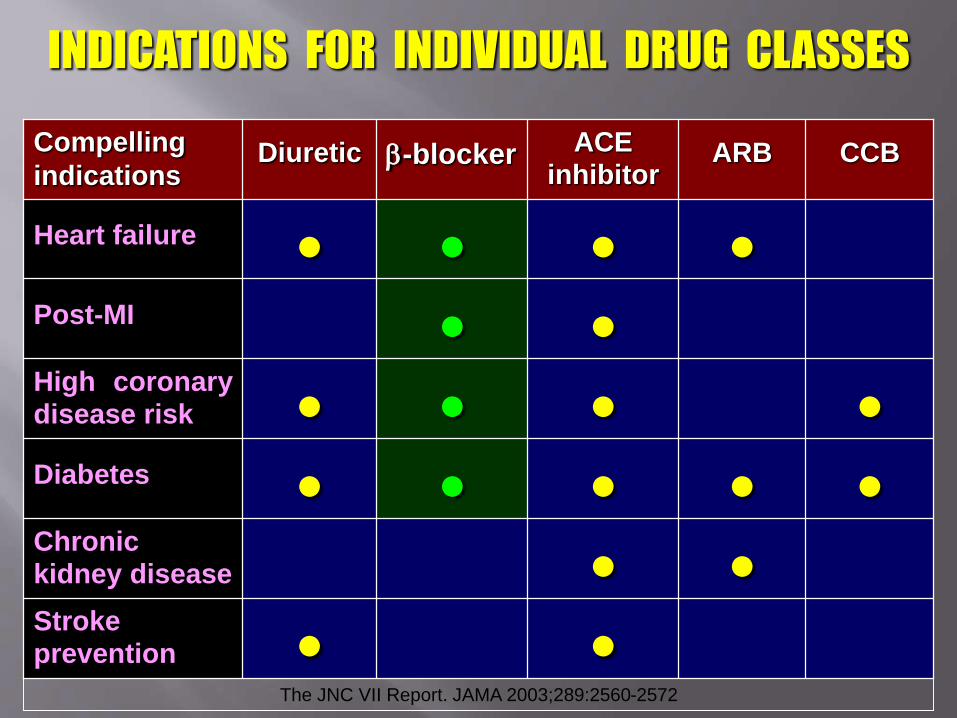
INDICATIONS FOR INDIVIDUAL DRUG CLASSES
••Strokeprevention
••Chronickidney disease
•••••Diabetes
••••High coronarydisease risk
••Post-MI
••••Heart failure
CCBARBACE inhibitor
-blockerDiureticCompelling
indications
The JNC VII Report. JAMA 2003;289:2560-2572


INDICATIONS FOR INDIVIDUAL DRUG CLASSES
••Strokeprevention
••Chronickidney disease
•••••Diabetes
••••High coronarydisease risk
••Post-MI
••••Heart failure
CCBARBACE inhibitor
-blockerDiureticCompelling
indications
The JNC VII Report. JAMA 2003;289:2560-2572


Dihydropyridine :
1. Nifedipin
2. Amlodipin
Non Dihydropyridine :
1. Diltiazem
2. Verapamil

CCB HR AV & SA node
Myocardial Contractility
Peripheral Contractility
CO CBF
Nifedipine - -
Amlodipin - -
Diltiazem V
Verapamil V
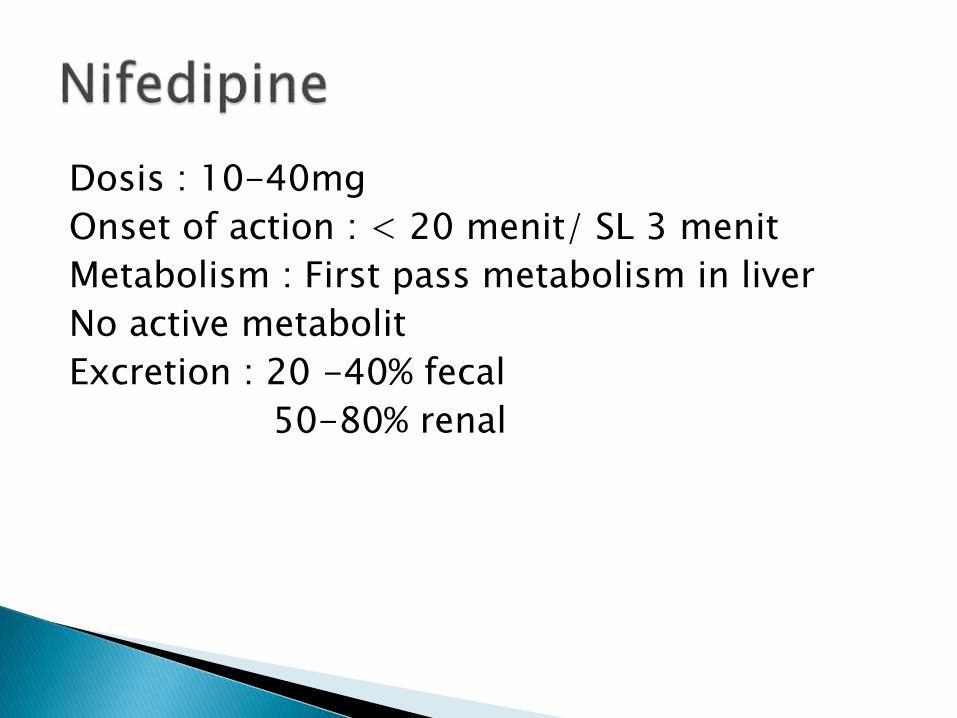
Dosis : 10-40mg
Onset of action : < 20 menit/ SL 3 menit
Metabolism : First pass metabolism in liver
No active metabolit
Excretion : 20 -40% fecal
50-80% renal

Acute neurohormonal effects on blood
pressure homeostasis
Heart rate and cardiac output
Perfusion
Sodium and water retention
Blood pressure
RAA SNS

Mengapa Harus Adalat® OROS?

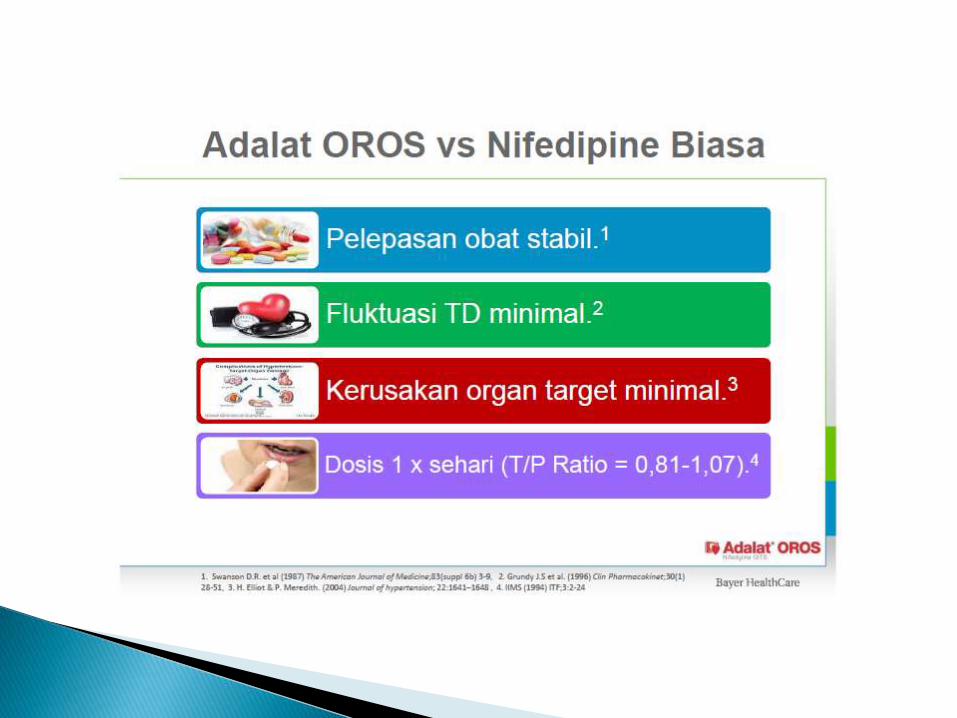

Dihydropiridine (DHP) CCBs
DHP CCBs : nifedipine & amlodipine
Nifedipine is widely used to treat angina and
hypertension.
Short-acting formulations of nifedipine possibly
harmful. Thus..
Long-acting Nifedipine : GITS / OROS
BHS, Drug Classes, CCBs, Dec 2008
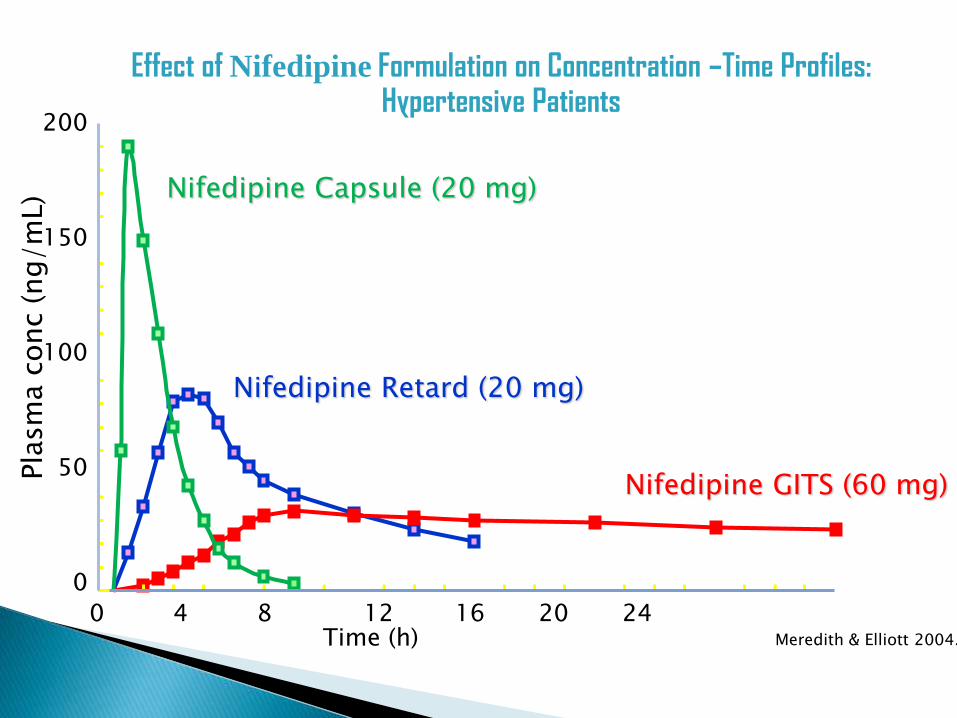
Nifedipine Retard (20 mg)
Nifedipine GITS (60 mg)
Nifedipine Capsule (20 mg)
200
150
100
50
0
Pla
sm
a c
onc
(ng/m
L)
Effect of Nifedipine Formulation on Concentration –Time Profiles: Hypertensive Patients
Meredith & Elliott 2004.
0 4 8 12 16 20 24Time (h)

Nifedipine GITS (60 mg)
Nifedipine Retard (20 mg)
Nifedipine Capsule (20 mg)
50
40
30
20
10
0
-10
Heart
Rate
(beats
/m
in)
Effect of Nifedipine Formulation on Heart Rate Responses: Hypertensive Patients
Meredith & Elliott 2004.
0 4 8 12 16 20 24Time (h)


Pla
sm
a N
ora
dre
naline (pg/m
l)
0 1 2 3 94 5 7 86Time (h)
200
300
400
500
200
300
400
500
amlodipine
Nifedipine GITS
Efek peningkatan kadar plasma Noradrenalin pada pasien setelahpenggunaan Adalat OROS vs Amlodipine
de Champlain et al 1998
1st dose steady state

0.3
0.2
0.1
0
-0.1
-0.2
Chnge in Q
OL r
esponsiv
enes improves
worsen
OverallQOL
Mental Health Index Psychological
Well-Being
PsychologicalDistress
Perceived Health
amlodipine nifedipine GITS
* p<0.05 versus amlodipine
**
Change from Baseline in Quality of Life Summary Scales for Patients Taking Nifedipine GITS or Amlodipine
Testa et al 1998

Incidence of Peripheral Edema
Julius, et. al., VALUE trial, Lancet, June 2004Brown, et. al., INSIGHT study, Lancet 2000
28 %32.9 %
0
10
20
30
40
NifedipineGITS
Amlodipine
VALUE Study(vs. Valsartan)
INSIGHT Study(vs. Thiazide)
Perc
enta
ge o
f Patients
w
ith E
dem
a
Most common side effect of CCBs
Greater incidence in DHPs than non-DHPs (due to its greater vascular selectivity)



THANK YOU !!!
Related Documents











