-
7/31/2019 Management of Hyperglycemia in Type 2_1.
1/45
Management of Hyperglycemia in Type 2Diabetes: A Patient-Centered Approach
Position Statement of the American Diabetes Association (ADA) and
the European Association for the Study of Diabetes (EASD)
-
7/31/2019 Management of Hyperglycemia in Type 2_1.
2/45
Writing Group
American Diabetes Association
Richard M. Bergenstal MDIntl Diabetes Center, Minneapolis, MN
John B. Buse MD, PhDUniversity of North Carolina, Chapel Hill, NC
Anne L. Peters MDUniv. of Southern California, Los Angeles, CA
Richard Wender MD
Thomas Jefferson University, Philadelphia, PA
Silvio E. Inzucchi MD (co-chair)Yale University, New Haven, CT
European Assoc. for the Study of Diabetes
Michaela Diamant MD, PhDVU University, Amsterdam, The Netherlands
Ele Ferrannini MDUniversity of Pisa, Pisa, Italy
Michael Nauck MDDiabeteszentrum, Bad Lauterberg, Germany
Apostolos Tsapas MD, PhD
Aristotle University, Thessaloniki, Greece
David R. Matthews MD, DPhil (co-chair)Oxford University, Oxford, UK
-
7/31/2019 Management of Hyperglycemia in Type 2_1.
3/45
ADA-EASD Position Statement: Management of
Hyperglycemia in T2DM: A Patient-Centered Approach
1. PATIENT-CENTERED APPROACH
2. BACKGROUND
Epidemiology and health care impact
Relationship of glycemic control to outcomes Overview of the pathogenesis of Type 2 diabetes
3. ANTI-HYPERGLYCEMIC THERAPY
Glycemic targets Therapeutic options
- Lifestyle
- Oral agents & non-insulin injectables
- InsulinDiabetes Care, Diabetologia. 19 April 2012 [Epub ahead of print]
-
7/31/2019 Management of Hyperglycemia in Type 2_1.
4/45
3. ANTIHYPERGLYCEMIC THERAPY Implementation Strategies
- Initial drug therapy
- Advancing to dual combination therapy
- Advancing to triple combination therapy
- Transitions to and titrations of insulin
4. OTHER CONSIDERATIONS Age
Weight
Sex/racial/ethnic/genetic differences Comorbidities (Coronary artery disease, Heart failure,
Chronic kidney disease, Liver dysfunction, Hypoglycemia)
5. FUTURE DIRECTIONS / RESEARCH NEEDS
ADA-EASD Position Statement: Management of
Hyperglycemia in T2DM: A Patient-Centered Approach
Diabetes Care, Diabetologia. 19 April 2012 [Epub ahead of print]
-
7/31/2019 Management of Hyperglycemia in Type 2_1.
5/45
ADA-EASD Position Statement: Management of
Hyperglycemia in T2DM
1. Patient-Centered Approach
...providing care that is respectful of and responsive to
individual patient preferences, needs, and values - ensuringthat patient values guide all clinical decisions.
Gauge patients preferred level of involvement.
Explore, where possible, therapeutic choices.
Utilize decision aids.
Shared decision making final decisions re: lifestyle choicesultimately lies with the patient.
Diabetes Care, Diabetologia. 19 April 2012 [Epub ahead of print]
-
7/31/2019 Management of Hyperglycemia in Type 2_1.
6/45
ADA-EASD Position Statement: Management of
Hyperglycemia in T2DM
2. BACKGROUND
Epidemiology and health care impact
Diabetes Care, Diabetologia. 19 April 2012 [Epub ahead of print]
-
7/31/2019 Management of Hyperglycemia in Type 2_1.
7/45
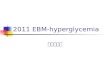
Age-adjusted Percentage of U.S. Adults with
Obesity or Diagnosed DiabetesObesity (BMI 30 kg/m2)
Diabetes
1994
1994
2000
2000
No Data 26.0%
No Data 9.0%
CDCs Division of Diabetes Translation. National Diabetes Surveillance System available
at http://www.cdc.gov/diabetes/statistics
2009
2009
OBE
SITY
OOBBEE
SSIITTYY
DIAB
ETES
DDIIAABB
EETTEESS
-
7/31/2019 Management of Hyperglycemia in Type 2_1.
8/45
The Diabetes Epidemic: Global Projections,
20102030
IDF. Diabetes Atlas 5th Ed. 2011
-
7/31/2019 Management of Hyperglycemia in Type 2_1.
9/45
ADA-EASD Position Statement: Management of
Hyperglycemia in T2DM
2. BACKGROUND
Relationship of glycemic control to outcomes
Diabetes Care, Diabetologia. 19 April 2012 [Epub ahead of print]
-
7/31/2019 Management of Hyperglycemia in Type 2_1.
10/45
Impact of Intensive Therapy for Diabetes:
Summary of Major Clinical TrialsStudy Microvasc CVD Mortality
UKPDS
DCCT / EDIC*
ACCORD ADVANCE
VADT
Long Term Follow-up
Initial Trial
* in T1DM
Kendall DM,Kendall DM, BergenstalBergenstal RM.RM. International Diabetes Center 2009International Diabetes Center 2009
UK Prospective Diabetes Study (UKPDS) Group.Lancet1998;352:854.Holman RR et al.N Engl J Med. 2008;359:1577. DCCT Research Group. N Engl J Med 1993;329;977.
Nathan DM et al.N Engl J Med. 2005;353:2643. Gerstein HC et al.N Engl J Med. 2008;358:2545.Patel A et al. N Engl J Med 2008;358:2560. Duckworth W et al. N Engl J Med 2009;360:129. (erratum:Moritz T.N Engl J Med2009;361:1024)
-
7/31/2019 Management of Hyperglycemia in Type 2_1.
11/45
ADA-EASD Position Statement: Management of
Hyperglycemia in T2DM
2. BACKGROUND
Overview of the pathogenesis of T2DM- Insulin secretory dysfunction
-Insulin resistance (muscle, fat, liver)
-Increased endogenous glucose production
-Deranged adipocyte biology
-Decreased incretin effect
Diabetes Care, Diabetologia. 19 April 2012 [Epub ahead of print]
-
7/31/2019 Management of Hyperglycemia in Type 2_1.
12/45
++++++++
peripheralglucoseuptake
hepatic
glucoseproduction
pancreaticinsulinsecretion
pancreatic
glucagonsecretion
Main Pathophysiological Defects in T2DM
gutcarbohydratedelivery &
absorption
incretineffect
HYPERGLYCEMIAHYPERGLYCEMIAHYPERGLYCEMIAHYPERGLYCEMIAHYPERGLYCEMIAHYPERGLYCEMIAHYPERGLYCEMIAHYPERGLYCEMIA
?
Adapted from: Inzucchi SE, Sherwin RS in: Cecil Medicine 2011
-
7/31/2019 Management of Hyperglycemia in Type 2_1.
13/45
ADA-EASD Position Statement: Management of
Hyperglycemia in T2DM
3. ANTI-HYPERGLYCEMIC THERAPY
Glycemic targets
- HbA1c < 7.0% (mean PG 150-160 mg/dl [8.3-8.9 mmol/l])
- Pre-prandial PG
-
7/31/2019 Management of Hyperglycemia in Type 2_1.
14/45
Figure 1 Diabetes Care, Diabetologia. 19 April 2012 [Epub ahead of print](Adapted with permission from: Ismail-Beigi F, et al.Ann Intern Med2011;154:554)
-
7/31/2019 Management of Hyperglycemia in Type 2_1.
15/45
ADA-EASD Position Statement: Management of
Hyperglycemia in T2DM
3. ANTI-HYPERGLYCEMIC THERAPY
Therapeutic options: Lifestyle
- Weight optimization
- Healthy diet
- Increased activity level
Diabetes Care, Diabetologia. 19 April 2012 [Epub ahead of print]
-
7/31/2019 Management of Hyperglycemia in Type 2_1.
16/45
ADA-EASD Position Statement: Management of
Hyperglycemia in T2DM
3. ANTI-HYPERGLYCEMIC THERAPY
Therapeutic options:Oral agents & non-insulin injectables
- Metformin
- Sulfonylureas
- Thiazolidinediones
- DPP-4 inhibitors- GLP-1 receptor agonists
- Meglitinides
- -glucosidase inhibitors
- Bile acid sequestrants
- Dopamine-2 agonists- Amylin mimetics
Diabetes Care, Diabetologia. 19 April 2012 [Epub ahead of print]
-
7/31/2019 Management of Hyperglycemia in Type 2_1.
17/45
ClassClass MechanismMechanism AdvantagesAdvantages DisadvantagesDisadvantages CostCost
Biguanides Activates AMP-kinase
Hepatic glucoseproduction
Extensive experience
No hypoglycemia Weight neutral
? CVD
Gastrointestinal
Lactic acidosis B-12 deficiency
Contraindications
Low
SUs /
Meglitinides
Closes KATP channels
Insulin secretion Extensive experience
Microvasc. risk Hypoglycemia
Weight gain
Low durability
? Ischemic
preconditioning
Low
TZDs PPAR- activator
insulin sensitivity
No hypoglycemia
Durability TGs, HDL-C ? CVD (pio)
Weight gain
Edema / heart failure Bone fractures
? MI (rosi) ? Bladder ca (pio)
High
-GIs Inhibits glucosidase
Slows carbohydrate
absorption
No hypoglycemia
Nonsystemic
Post-prandial glucose ? CVD events
Gastrointestinal
Dosing frequency
Modest A1c
Mod.
Table 1. Properties of anti-hyperglycemic agents Diabetes Care, Diabetologia. 19 April 2012 [Epub ahead of print]
-
7/31/2019 Management of Hyperglycemia in Type 2_1.
18/45
ClassClass MechanismMechanism AdvantagesAdvantages DisadvantagesDisadvantages CostCost
DPP-4
inhibitors
Inhibits DPP-4
Increases GLP-1, GIP
No hypoglycemia
Well tolerated
Modest A1c
? Pancreatitis Urticaria
High
GLP-1
receptor
agonists
Activates GLP-1 R
Insulin, glucagon gastric emptying satiety
Weight loss
No hypoglycemia
? Beta cell mass
? CV protection
GI
? Pancreatitis
Medullary ca
Injectable
High
Amylin
mimetics
Activates amylin
receptor
glucagon
gastric emptying satiety
Weight loss
PPG GI
Modest A1c Injectable
Hypo w/ insulin Dosing frequency
High
Bile acid
sequestrants
Bind bile acids
Hepatic glucoseproduction
No hypoglycemia
Nonsystemic
Post-prandial glucose CVD events
GI
Modest A1c Dosing frequency
High
Dopamine-2
agonists
Activates DA receptor
Modulates hypothalamic
control of metabolism
insulin sensitivity
No hypoglyemia
? CVD events Modest A1c Dizziness/syncope
Nausea
Fatigue
High
Table 1. Properties of anti-hyperglycemic agents Diabetes Care, Diabetologia. 19 April 2012 [Epub ahead of print]
-
7/31/2019 Management of Hyperglycemia in Type 2_1.
19/45
ClassClass MechanismMechanism AdvantagesAdvantages DisadvantagesDisadvantages CostCost
Insulin Activates insulin
receptor peripheral glucoseuptake
Universally
effective Unlimited efficacy
Microvascularrisk
Hypoglycemia
Weight gain ? Mitogenicity
Injectable
Training
requirements
Stigma
Variable
Table 1. Properties of anti-hyperglycemic agents Diabetes Care, Diabetologia. 19 April 2012 [Epub ahead of print]
-
7/31/2019 Management of Hyperglycemia in Type 2_1.
20/45
ADA-EASD Position Statement: Management of
Hyperglycemia in T2DM
3. ANTI-HYPERGLYCEMIC THERAPY
Therapeutic options: Insulin
- Neutral protamine Hagedorn (NPH)
- Regular
- Basal analogues (glargine, detemir)
- Rapid analogues (lispro, aspart, glulisine)
- Pre-mixed varieties
Diabetes Care, Diabetologia. 19 April 2012 [Epub ahead of print]
-
7/31/2019 Management of Hyperglycemia in Type 2_1.
21/45
ADA-EASD Position Statement: Management of
Hyperglycemia in T2DM
Long (Detemir)
Rapid (Lispro, Aspart, Glulisine)
Hours
Long (Glargine)
0 2 4 6 8 10 12 14 16 18 20 22 24
Short (Regular)
Hours after injection
Insulinl
ev
el
3. ANTI-HYPERGLYCEMIC THERAPY
Therapeutic options: Insulin
Intermediate (NPH)
-
7/31/2019 Management of Hyperglycemia in Type 2_1.
22/45
ADA-EASD Position Statement: Management of
Hyperglycemia in T2DM
3. ANTI-HYPERGLYCEMIC THERAPY
Implementation strategies:
- Initial therapy
- Advancing to dual combination therapy
- Advancing to triple combination therapy
- Transitions to & titrations of insulin
Diabetes Care, Diabetologia. 19 April 2012 [Epub ahead of print]
-
7/31/2019 Management of Hyperglycemia in Type 2_1.
23/45
T2DM Antihyperglycemic Therapy: General RecommendationsDiabetes Care, Diabetologia. 19 April 2012
[Epub ahead of print]
-
7/31/2019 Management of Hyperglycemia in Type 2_1.
24/45
T2DM Antihyperglycemic Therapy: General RecommendationsDiabetes Care, Diabetologia. 19 April 2012
[Epub ahead of print]
T2DM Ant yperg ycem cnt yperg ycem c T erapy: Genera Recommen at onserapy: enera ecommen at ons
-
7/31/2019 Management of Hyperglycemia in Type 2_1.
25/45
T2DM Ant yperg ycem cnt yperg ycem c T erapy: Genera Recommen at onserapy: enera ecommen at ons
Di bete C reDiabetes Care Di bet l iDiabetolo ia.. 1919 A ril 201A ril 201 E ubE ub ahead of rintahead of rint
-
7/31/2019 Management of Hyperglycemia in Type 2_1.
26/45
Diabetes Care, Diabetologia.
19 April 2012 [Epub ahead of print]
I li St t i i T2DMI li St t i i T2DM
-
7/31/2019 Management of Hyperglycemia in Type 2_1.
27/45
Insulin Strategies in T2DMInsulin Strategies in T2DM
Diabetes Care,Diabetes Care,DiabetologiaDiabetologia.. 1919 April 2012 [April 2012 [EpubEpub ahead of print]ahead of print]
ADA EASD P iti St t t M t f
-
7/31/2019 Management of Hyperglycemia in Type 2_1.
28/45
ADA-EASD Position Statement: Management of
Hyperglycemia in T2DM
4. OTHER CONSIDERATIONS
Age
WeightSex / racial / ethnic / genetic differences
Comorbidities
- Coronary artery disease- Heart Failure
- Chronic kidney disease
- Liver dysfunction- Hypoglycemia
Diabetes Care, Diabetologia. 19 April 2012 [Epub ahead of print]
ADA EASD Position Statement: Management of
-
7/31/2019 Management of Hyperglycemia in Type 2_1.
29/45
ADA-EASD Position Statement: Management of
Hyperglycemia in T2DM
4. OTHER CONSIDERATIONS
Age: Older adults
- Reduced life expectancy- Higher CVD burden
- Reduced GFR
- At risk for adverse events from polypharmacy
- More likely to be compromised from hypoglycemia
Less ambitious targets
HbA1c
-
7/31/2019 Management of Hyperglycemia in Type 2_1.
30/45
ADA-EASD Position Statement: Management of
Hyperglycemia in T2DM
4. OTHER CONSIDERATIONS
Weight
- Majority of T2DM patients overweight / obese- Intensive lifestyle program
- Metformin
- GLP-1 receptor agonists- ? Bariatric surgery
- Consider LADA in lean patients
Diabetes Care, Diabetologia. 19 April 2012 [Epub ahead of print]
T2DM AntiT2DM Anti--hyperglycemic Therapy: General Recommendationshyperglycemic Therapy: General Recommendations
-
7/31/2019 Management of Hyperglycemia in Type 2_1.
31/45
T2DM AntiT2DM Anti hyperglycemic Therapy: General Recommendationshyperglycemic Therapy: General Recommendations
Diabetes Care,Diabetes Care,DiabetologiaDiabetologia.. 1919 April 2012April 2012
[[EpubEpub ahead of print]ahead of print]
Adapted Recommendations: When Goal is to Avoid Weight GainAdapted Recommendations: When Goal is to Avoid Weight Gain
-
7/31/2019 Management of Hyperglycemia in Type 2_1.
32/45
Adapted Recommendations: When Goal is to Avoid Weight Gainp g
Diabetes Care,Diabetes Care,DiabetologiaDiabetologia.. 1919 April 2012April 2012
[[EpubEpub ahead of print]ahead of print]
ADA-EASD Position Statement: Management of
-
7/31/2019 Management of Hyperglycemia in Type 2_1.
33/45
ADA EASD Position Statement: Management of
Hyperglycemia in T2DM
4. OTHER CONSIDERATIONS
Sex/ethnic/racial/genetic differences
- Little is known- MODY & other monogenic forms of diabetes
- Latinos: more insulin resistance
- East Asians: more beta cell dysfunction- Gender may drive concerns about adverse effects (e.g.,
bone loss from TZDs)
Diabetes Care, Diabetologia. 19 April 2012 [Epub ahead of print]
ADA-EASD Position Statement: Management of
-
7/31/2019 Management of Hyperglycemia in Type 2_1.
34/45
ADA EASD Position Statement: Management of
Hyperglycemia in T2DM
4. OTHER CONSIDERATIONS
Comorbidities
- Coronary Disease
- Heart Failure
- Renal disease
- Liver dysfunction
- Hypoglycemia
Metformin: CVD benefit (UKPDS)
Avoid hypoglycemia
? SUs & ischemic preconditioning
? Pioglitazone & CVD events
? Effects of incretin-basedtherapies
Diabetes Care, Diabetologia. 19 April 2012 [Epub ahead of print]
ADA-EASD Position Statement: Management of
-
7/31/2019 Management of Hyperglycemia in Type 2_1.
35/45
g
Hyperglycemia in T2DM
4. OTHER CONSIDERATIONS
Comorbidities
- Coronary Disease
- Heart Failure
- Renal disease
- Liver dysfunction
- Hypoglycemia
Metformin: May use unless
condition is unstable or severe
Avoid TZDs
? Effects of incretin-basedtherapies
Diabetes Care, Diabetologia. 19 April 2012 [Epub ahead of print]
ADA-EASD Position Statement: Management of
-
7/31/2019 Management of Hyperglycemia in Type 2_1.
36/45
g
Hyperglycemia in T2DM
4. OTHER CONSIDERATIONS
Comorbidities
- Coronary Disease
- Heart Failure
- Renal disease
- Liver dysfunction
- Hypoglycemia
Increased risk of hypoglycemia
Metformin & lactic acidosis
US: stop @SCr 1.5 (1.4
women)
UK: dose @GFR
-
7/31/2019 Management of Hyperglycemia in Type 2_1.
37/45
Hyperglycemia in T2DM
4. OTHER CONSIDERATIONS
Comorbidities
- Coronary Disease
- Heart Failure
- Renal disease
- Liver dysfunction
- Hypoglycemia
Most drugs not tested in advancedliver disease
Pioglitazone may help steatosis
Insulin best option if disease severe
Diabetes Care, Diabetologia. 19 April 2012 [Epub ahead of print]
ADA-EASD Position Statement: Management of
-
7/31/2019 Management of Hyperglycemia in Type 2_1.
38/45
Hyperglycemia in T2DM
4. OTHER CONSIDERATIONS
Comorbidities
- Coronary Disease
- Heart Failure
- Renal disease
- Liver dysfunction
- Hypoglycemia Emerging concerns regarding
association with increased
mortality Proper drug selection in the
hypoglycemia prone
Diabetes Care, Diabetologia. 19 April 2012 [Epub ahead of print]
T2DM AntiT2DM Anti--hyperglycemic Therapy: General Recommendationshyperglycemic Therapy: General Recommendations
-
7/31/2019 Management of Hyperglycemia in Type 2_1.
39/45
Diabetes Care,Diabetes Care,DiabetologiaDiabetologia.. 1919 April 2012April 2012
[[EpubEpub ahead of print]ahead of print]
Adapted Recommendations: When Goal is to Avoid HypoglycemiaAdapted Recommendations: When Goal is to Avoid Hypoglycemia
-
7/31/2019 Management of Hyperglycemia in Type 2_1.
40/45
Diabetes Care,Diabetes Care,DiabetologiaDiabetologia.. 1919 April 2012April 2012
[[EpubEpub ahead of print]ahead of print]
Adapted Recommendations: When Goal is to Minimize CostsAdapted Recommendations: When Goal is to Minimize Costs
-
7/31/2019 Management of Hyperglycemia in Type 2_1.
41/45
Diabetes Care, Diabetologia. 19 April 2012
[Epub ahead of print]
Guidelines for Glycemic BP & Lipid Control
-
7/31/2019 Management of Hyperglycemia in Type 2_1.
42/45
Guidelines for Glycemic, BP, & Lipid Control
American Diabetes Assoc. Goals
HbA1C < 7.0% (individualization)
Preprandialglucose 70-130 mg/dL (3.9-7.2 mmol/l)
Postprandialglucose
< 180 mg/dL
Blood pressure < 130/80 mmHg
Lipids
LDL: < 100 mg/dL (2.59 mmol/l)
< 70 mg/dL (1.81 mmol/l) (with overt CVD)
HDL: > 40 mg/dL (1.04 mmol/l)
> 50 mg/dL (1.30 mmol/l)
TG: < 150 mg/dL (1.69 mmol/l)
ADA.Diabetes Care. 2012;35:S11-63HDL = high-density lipoprotein; LDL = low-density
lipoprotein; PG = plasma glucose; TG = triglycerides.
ADA-EASD Position Statement: Management of
Hyperglycemia in T2DM
-
7/31/2019 Management of Hyperglycemia in Type 2_1.
43/45
Hyperglycemia in T2DM
4. FUTURE DIRECTIONS / RESEARCH NEEDS
Comparative effectiveness research
Focus on important clinical outcomes
Contributions of genomic research
Perpetual need for clinical judgment!
Diabetes Care, Diabetologia. 19 April 2012 [Epub ahead of print]
ADA-EASD Position Statement: Management of
Hyperglycemia in T2DM
-
7/31/2019 Management of Hyperglycemia in Type 2_1.
44/45
Hyperglycemia in T2DM
KEY POINTS Glycemic targets & BG-lowering therapies must individualizedindividualized..
Diet, exercise, & educationDiet, exercise, & education: foundation of any T2DM therapy
program
Unless contraindicated, metforminmetformin = optimal 1st-line drug.
After metformin, data are limited.
Combination therapyCombination therapywith 1-2
other oral / injectable agents is reasonable; minimize side effects.
Ultimately, many patients will require insulininsulin therapy alone / in
combination with other agents to maintain BG control.
All treatment decisions should be made in conjunction with theAll treatment decisions should be made in conjunction with the
patientpatient (focus on preferences, needs & values.)
Comprehensive CV risk reductionCV risk reduction - a major focus of therapy.Di bete C reDiabetes Care Di bet l iDiabetolo ia.. 1919 A ril 2012A ril 2012 E ubE ub ahead of rintahead of rint
ADA-EASD Position Statement: Management of
Hyperglycemia in T2DM
-
7/31/2019 Management of Hyperglycemia in Type 2_1.
45/45
Hyperglycemia in T2DM
Invited Reviewers
Professional Practice Committee, American Diabetes Association
Panel for Overseeing Guidelines and Statements, European Association for the Study of Diabetes
American Association of Diabetes Educators
The Endocrine SocietyAmerican College of Physicians
James Best, The University of Melbourne, AU
Henk Bilo,Isala Clinics, Zwolle, NL
John Boltri, Wayne State University, Detroit, MI
Thomas Buchanan, Univ of So California, LA, CAPaul Callaway, University of Kansas,Wichita, KS
Bernard Charbonnel, University of Nantes, France
Stephen Colagiuri, The University of Sydney, AS
Samuel Dagogo-Jack, Univ of Tenn, Memphis, TN
Margo Farber,Detroit Medical Center, Detroit, MI
Cynthia Fritschi, University of Illinois, Chicago, IL
Rowan Hillson,Hillingdon Hospital, Uxbridge, U.K.
Faramarz Ismail-Beigi, CWR Univ, Cleveland, OH
Devan Kansagara, Oregon H&S Univ, Portland, OR
Ilias Migdalis, NIMTS Hospital,Athens, Greece
Donna Miller, Univ of So California, LA, CA
Robert Ratner,MedStar/Georgetown Univ, DC
Julio Rosenstock,Dallas Diab/Endo Ctr, Dallas, TX
Guntram Schernthaner,Rudolfstiftung Hosp, Vienna, AT
Robert Sherwin, Yale University, New Haven, CT
Jay Skyler, University of Miami, Miami, FL
Geralyn Spollett, Yale University,New Haven, CT
Ellie Strock,Intl Diabetes Center, Minneapolis, MN
Agathocles Tsatsoulis, University of Ioannina, GR
Andrew Wolf, Univ of Virginia Charlottesville, VA
Bernard Zinman, University of Toronto, CA