Management of Head and Neck Cutaneous Squamous Cell Carcinoma Resident: Eugene Son, MD Faculty Mentor: Susan D. McCammon , MD. FACS The University of Texas Medical Branch Department of Otolaryngology Grand Rounds Presentation May 29, 2014 Series Editor: Francis B. Quinn, Jr., MD, FACS – Archivist: Melinda Stoner Quinn, MSICS

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Management of Head and Neck Cutaneous Squamous Cell Carcinoma
Resident: Eugene Son, MD
Faculty Mentor: Susan D. McCammon, MD. FACS
The University of Texas Medical Branch
Department of Otolaryngology
Grand Rounds Presentation
May 29, 2014
Series Editor: Francis B. Quinn, Jr., MD, FACS – Archivist: Melinda Stoner Quinn, MSICS

Overview
• Anatomy• Skin anatomy
• Lymphatic drainage
• Clinical evaluation
• Differential diagnosis
• Screening and prevention
• Carcinogenesis
• Histopathology
• Staging and prognosis
• Treatment• Primary Surgery
• Locoregional metastasis
• Cervical involvement
• Parotid involvement
• SLNB
• Other modalities
• Radiation therapy
• Chemotherapy

Skin AnatomyComponents:
1. Epidermis
2. Dermis

Epidermis
Layers:
• Stratum corneum
• Stratum granulosum
• Stratum spinosum
• Stratum basale• mitotic
• IMAGE
Image Source: http://missinglink.ucsf.edu/lm/dermatologyglossary/epidermis.html

Epidermis
• Melanocytes• Melanin pigment
• Neural crest origin
• Langerhans cells• Dendritic histiotic cells
• Type of APC
• Class II MHC antigens
• Neuroendocrine cells• Merkel cells
• Pressure sense for light touch

Fitzpatrick’s Classification

Skin Components
Basement Membrane
• Dermoepidermal junction
• Layers:• Lamina lucida
• Lamina densa
Dermis
• Fibroblast
• Collagen (70%):• Type I (85%)
• Type III (15%)
• Layers:• Papillary
• Reticular
Lymphatic Drainage

Lymphatic Drainage
Source: Pathak I, et al. Do nodal metastases from cutaneous melanoma of the head and neck follow a clinically predictable pattern? Head & Neck 2001:785-790.

Source: Vauterin TJ, et al. Patterns of lymph node spread of cutaneous squamous cell carcinoma of the head and neck. Head & Neck 2005: 785-91.
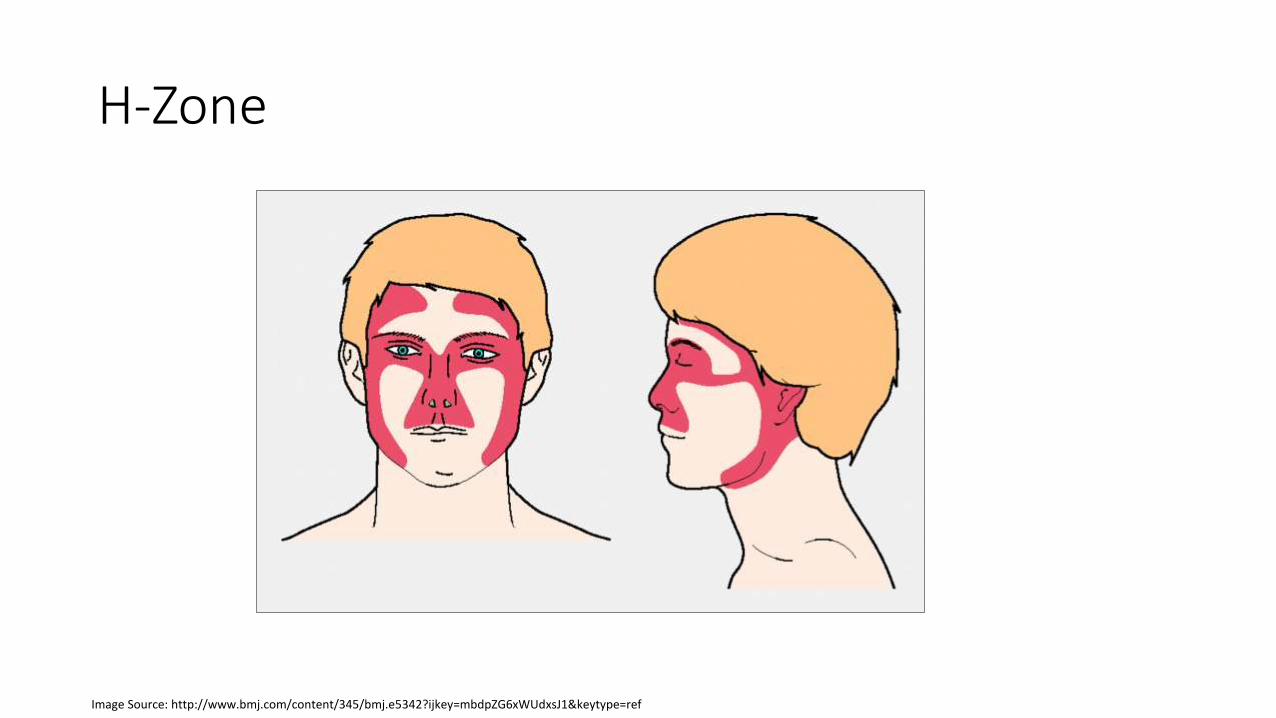
H-Zone
Image Source: http://www.bmj.com/content/345/bmj.e5342?ijkey=mbdpZG6xWUdxsJ1&keytype=ref

Clinical Evaluation

Epidemiology
• 20-25% of NMSC (2nd most common)
• Annual Incidence• Australia – 300 per 100,000• USA – 35-150 per 100,000
• 70,000 new cases annually• 4,000 die from cSCC annually
• Central Europe – 16 per 100,000• Northern Europe – 10 per 100,000• Singapore – 2.2 per 100,000
• Incidence increasing• Population factors• Social factors
Image Source: http://www.bookequals.com/2010/05/19/jersey-shore-quote-book/

Host and Environmental Risk Factors
• Ultraviolet radiation (UVA, UVB)
• Male sex
• Increasing age
• Natural blonde or red hair color
• Blue eyes
• Fitzpatrick grade I/II
• Living closer to equator
• Exposure to ionizing radiation
• Immunosuppression
• Cigarette smoking
• Trauma, burns (Marjolin’s ulcers), chronic ulcers
• Exposure to: coal tar, pitch, creosote, arsenic, paraffin, mustard gas
Image Source: http://www.aad.org/dermatology-a-to-z/diseases-and-treatments/q---t/squamous-cell-carcinoma

Genetic and Molecular factors
• Xeroderma pigmentosum (XP)
• Albinism
• Human papilloma virus (HPV)
• Epidermodysplasia verruciformis
• Mutations in: p53, p21, c-Ha-ras, K-ras
History
• Key Historical Questions:• How long has lesion been present?
• How has it changed?
• What is concerning about lesion?
• Other lesions?
• Painful?
• Bleed?
• Parathesias?
• Fomication?
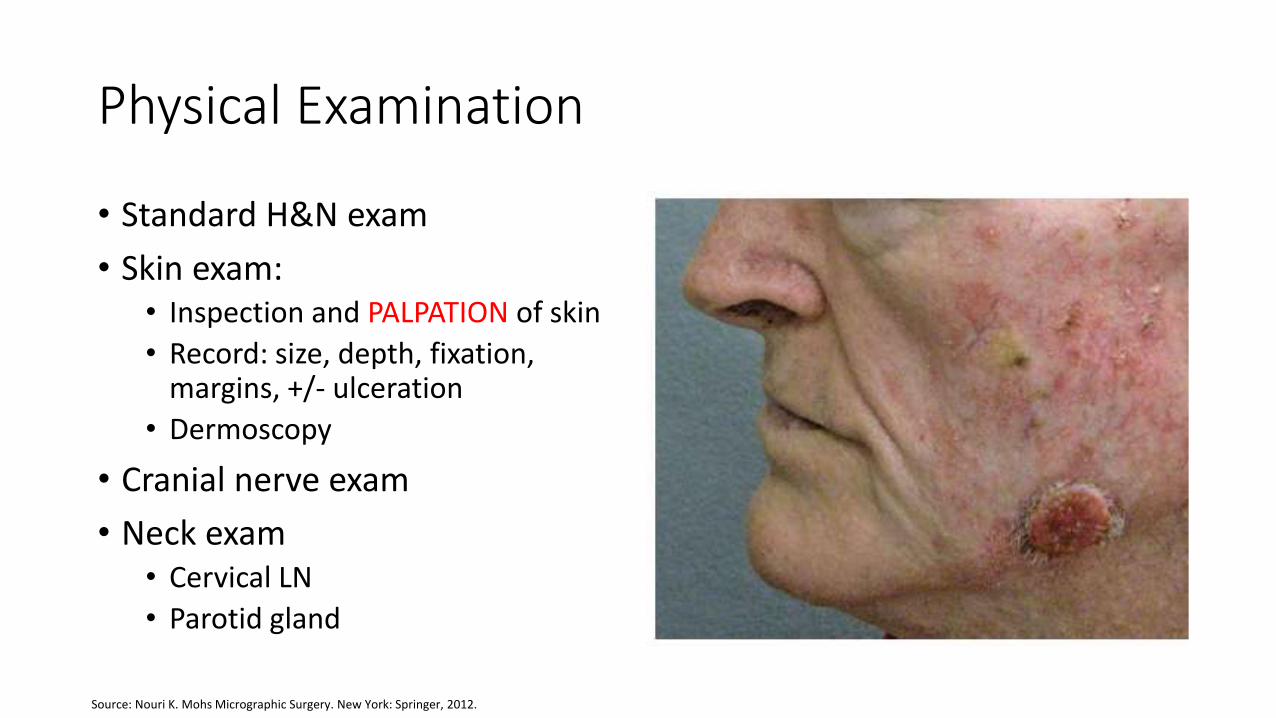
Physical Examination
• Standard H&N exam
• Skin exam:• Inspection and PALPATION of skin
• Record: size, depth, fixation, margins, +/- ulceration
• Dermoscopy
• Cranial nerve exam
• Neck exam• Cervical LN
• Parotid gland
Source: Nouri K. Mohs Micrographic Surgery. New York: Springer, 2012.
Biopsy
• Pathologic diagnosis
• Tumor depth, ulceration, mitotic rate, vascular or perineural invasion (PNI)
• Types:• Excisional full-thickness biopsy
• Punch biopsy
• Avoid: shave biopsy, FNA, partial thickness
Imaging
• For advanced or aggressive tumors
• CXR
• CT with contrast of neck
• MRI
• Ultrasound
• PET-CT
Differential Diagnosis

Differential of Skin Lesion
Benign Lesions
• Keratoacanthoma
• Actinic keratosis
• Seborrheic keratosis
• Pseudoepitheliomatoushyperplasia
• Pilar tumor
Common Malignant Tumors
• BCC
• SCC
• MM
• MCC

Mesenchymal neoplasms
Mesenchymal neoplasms• Fibrohistiocytic proliferations
• Dermtofibroma• Dermatofibrosarcoma protuberans• Atypical fibroxanthoma• Malignant fibrous histiocytoma
• Vascular tumors• Kaposi sarcoma
• HHV-8, Mediterranean, HIV, OTR, Dorfman bodies
• Angiosarcoma
• Smooth muscle and neural tumors• Leiomyosarcoma• Malignant peripheral nerve sheath
tumor• NF-2
• Granular cell tumor (Abrikossofftumor)
• 70% intra-oral
Malignant adnexal neoplasms
• Follicular neoplasms• Trichilemmal carcinoma• Malignant pilar tumor
• Eccrine tumor• Porocarcinoma• Hidradenocarcinoma• Microcystic adnexal
carcinoma• Malignant mixed tumor • Mucinous carcinoma
• Sebaceous neoplasms• Sebaceous adenoma• Sebaceous epithelioma• Sebaceous carcinoma
Malignant adnexal neoplasms
• Cutaneous lymphoid hyperplasia
• Angiolymphoidhyperplasia with eosinophilia
• Primary cutaneous B-cell lymphomas
• Primary cutaneous T-cell lymphomas• Mycosis fungoides –
most common• Sezary Syndrome

Screening and Prevention Source: http://myfortlauderdalebeach.com/wp-content/uploads/skin-cancer-month.jpg

Screening Recommendations
• USPSTF (US Preventative Services Task Force)• Does not recommend routine skin cancer screening
by PCP or patient.• Evidence is insufficient
• AADSCSP (American Academy of Dermatology’s Skin Cancer Screening Program)• Dermatologist skin screening can find melanoma in
earlier stages in SEER
• ACS (American Cancer Society)• Total skin screening for 20 yo and older
• AAD (American Academy of Dermatology)• Free yearly screening program
Image Source: http://localtvwghp.files.wordpress.com/2012/04/ap-skin-cancer-screening-20.jpg

Screening
• Self-Screening Examination (SSE)• ABCD - asymmetry, border
irregularity, color variation, diameter
• E - evolving
• Physician screening• Dermatoscopy
• High-resolution photography
• Confocal scanning laser microscopy (CSLM)
Image Source: http://www.dermatologist.gr/en/dermoscopy/

Screening Candidates
• Phenotype
• Ultraviolet radiation (UVR)
• Ionizing radiation
• Precursor lesions
• Personal history of previous SCC
• Genetic syndromes
• Immunosuppression
Image Source: http://www.pinterest.com/pin/528328600005760028/

Question
• How many times increased risk dose an immunocompromised patient s/p solid organ transplant have versus a healthy individual?
a) 5 times increased risk
b) 10 times increased risk
c) 100 times increased risk
d) 1000 times increased risk
e) No increased risk

Immunosuppression
• One of the most important risk factors for developing SCC.
• Common causes:• Solid organ transplantation
• Lymphoma (esp NHL) and leukemia (esp CLL)
• HIV
• 65-250 times increased risk in solid OTR.• Also greater risk of recurrence and metastasis.
• 10-18% with nodal metastases in NHL/CLL.
• HIV has 5 x increased risk.

Prevention
• Photoprotection• UV protective clothing• Avoiding sun at peak hours• Wearing sunscreen
• Education • Harm of tanning• Genetic education
• Pre-cursor lesion management (AK, SCCis)• Cryotherapy • 5-fluorouracil (5-FU)• Imiquimod• COX inhibitors• Oral isotretinoin• Topical retinoids• Photodynamic therapy (PDT)

• UVC does not reach earth’s surface• UVB causes cancer – does not go past derma-epidermal junction• UVA causes cancer, aging – longer wavelength allows deeper penetration to dermis.

Sunscreen
Source: Environmental Protection Agency. The Burning Facts. Sept 2006.

Medical Therapy
• 5-fluorouracil (5-FU)
• Imiquimod
• COX inhibitors
• Oral isotretinoin
• Topical retinoids
Source: Nouri K. Mohs Micrographic Surgery. New York: Springer, 2012.

Photodynamic Therapy (PDT)
• Photosensitizing drug + oxygen + light• Photosensitizer accumulates in tumor cells then exposed to light
• ROS results in necrosis and apoptosis, vascular compromise and inflammatory damage
• Photosensitizers• Given IV, po, or topical
• Porfimer Sodium
• 5-Aminolevulinic acid (5-ALA)• Combines forms protophyrin
• Methyl aminolevulinic acid (MAL)• More lipophilic for better penetration

PDT
• Light• Nonpulsed monochromatic coherent light
• Broad band, incoherent light sources
• Light emitting diodes (LED)
• Argon pumped-dye laser
• Indications• AK
• SCC in situ
• SCC (not optimal, <50% response rate)
Image Source: http://bjtpms.en.made-in-china.com/product/XMrEYSvhXqUL/China-Table-LED-Photodynamic-Therapy-PDT-Light-Therapy-Beauty-Machine-L2-.html

Carcinogenesis
Image Source: http://blogs.scientificamerican.com/observations/2010/07/25/subatomic-sunscreen-how-light-particles-can-repair-uv-damaged-dna/

Associated Lesions
• SCC arises from keratinocyte.
• Actinic keratosis• Red-to-tan macules or scales• 0.075-0.096% malignant degeneration rate per year (10-20% over 10-25
years)
• SCC in situ (Bowen’s disease)• Erythematous plaques, patches or papules• 3% precede development of SCC by many years
• Invasive SCC• Enlarging or non-healing sore• Firm erythematous lesion with elevated borders and central ulceration

Mutagenesis
• UVB (293 nm)
• 2 types of UVB “signature mutations”1. Cyclobutane pyrimidine dimers
2. Pyrimidine (6-4) pyrimidine photoproducts
• 90% of human cutaneous SCC have these mutations in the p53 suppressor gene
• Indirect DNA damage• Both UVA and UVB activate ROS
UV-induced Immunosuppression
• UVR plays critical role in suppressing secondary immune reactions and suppressing memory response.
• UVR:• Suppresses contact hypersensitivity
• Suppresses Th1-driven immune reactions
• Suppresses induction of complement fixing antibodies
• Suppresses immune response to cellular pathogens.

Epidermal UV Photoreceptors
1. DNA
2. Trans-urocanic acid (UCA)
3. Membrane lipids

Cellular Targets
Skin Targets
1. Langerhans cells
2. Keratinocytes
3. Mast cells
Regulatory Cell Targets
1. T regulatory cells
2. Natural killer cells
3. B cells

Histopathology

Actinic Keratosis (AK)
Source: Rapini RP. Practical Dermatopathology. Elsevier, 2012.

AK Variants
• Hyperplastic AK
• Pigmented AK
• Acantholytic AK
• Lichenoid AK

SCC in situ
Source: Rapini RP. Practical Dermatopathology. Elsevier, 2012.

SCC
• One of the main features: BM/dermal invasion
• Histologic grading• Well-differentiated
• Moderately differentiated
• Poorly differentiated
• Undifferentiated
• Immunohistochemical (IHC) markers• + cytokeratin 5 and 6 (CK5/6)
• + p63

SCC, Well-differentiated
Source: Rapini RP. Practical Dermatopathology. Elsevier, 2012.

SCC, Poorly Differentiated
Source: Rapini RP. Practical Dermatopathology. Elsevier, 2012.
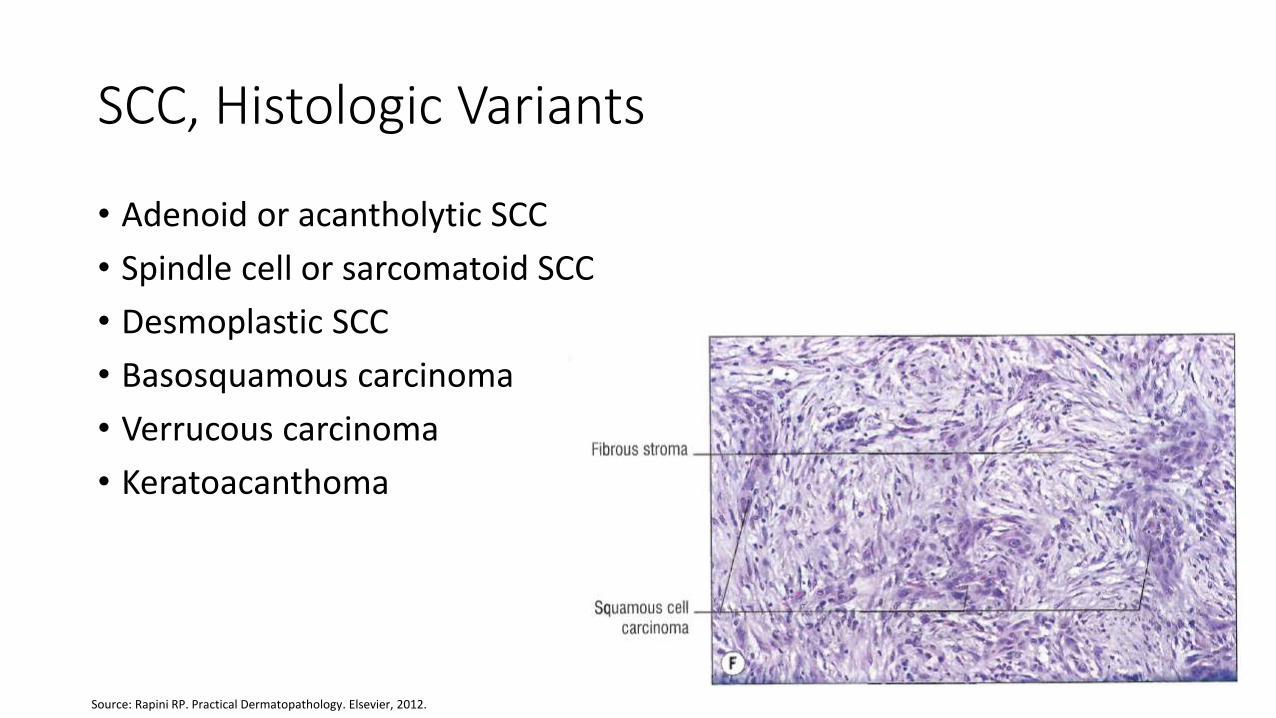
SCC, Histologic Variants
• Adenoid or acantholytic SCC
• Spindle cell or sarcomatoid SCC
• Desmoplastic SCC
• Basosquamous carcinoma
• Verrucous carcinoma
• Keratoacanthoma
Source: Rapini RP. Practical Dermatopathology. Elsevier, 2012.

Keratoacanthoma
Source: Rapini RP. Practical Dermatopathology. Elsevier, 2012.

PNI
Source: Rapini RP. Practical Dermatopathology. Elsevier, 2012.

Staging and Prognosis

Question
Based on the AJCC Cancer Staging Manual 6th Ed, stage the following patient: 50 yo M with 1 cm in diameter lesion on right cheek. Biopsy shows SCC with poor differentiation and perinerual invasion. There is a 2.5 cm lymph node in left level II. No evidence of metastasis.
a) T1N1M0
b) T2N1M0
c) T1N2M0
d) T2N2M0

Old Staging
American Joint Committee on Cancer (AJCC), Cancer Staging Manual tumor, node, metastasis (TNM) system. 6th Ed. 2002.
• T0, Tis• T1 - 2 cm or less
• T2 – more than 2 cm, less than 5 cm
• T3 – more than 5 cm
• T4 – invades deep extradermal structures• Cartilage, muscle, bone
• N0 or N1
• M0 or M1
AJCC Cancer Staging Manual 6th Edition. New York: Springer, 2002.

Question
Based on the AJCC Cancer Staging Manual 7th Ed, stage the following patient: 50 yo M with 1 cm in diameter lesion on right cheek. Biopsy shows SCC with poor differentiation and perinerual invasion. There is a 2.5 cm lymph node in left level II. No evidence of metastasis.
a) T1N1M0
b) T2N1M0
c) T1N2M0
d) T2N2M0

Current Staging
American Joint Committee on Cancer (AJCC), Cancer Staging Manual tumor, node, metastasis (TNM) system. 7th Ed. 2010.
• T stage based on high-risk features• Depth/Invasion
• 2 mm or greater thickness, Clark level 4 or greater, PNI
• Anatomic location• Ear, non-hair-bearing lip
• Differentiation• Poorly or un- differentiated
• N and M stage same as UADT SCC staging.
AJCC Cancer Staging Manual 7th Edition. New York: Springer, 2010.

Source: Weber RS, Moore BA. Cutaneous Malignancy of the Head and Neck: A Multidisciplinary Approach. San Diego: Plural Publishing, 2011.

Clark and Breslow Levels
Source: Cummings, CW. Otolaryngology, Head and Neck Surgery. Ed. 5. Mosby, 2010.

Staging made easy…
• Stage 0 – CIS
• Stage 1 – T1
• Stage 2 – T2
• Stage 3 – T3 or N1
• Stage 4 – T4 or N2 or M1

Tumor (T)
• Horizontal size not used anymore.
• Brantsch et al landmark study with 615 pts. • 14/90 pts (16%) with >6 mm thick tumors had LN mets.
• 0 pts with <2 mm thick tumors had LN mets.
• Kraus et al • 1/3 of pts (33%) with SCC have >4 mm thickness but they account for >80% of
lesions with LN mets.
• Breuninger et al study with 500 pts.• 0% pts with <2 mm had LN mets
• 20% pts with >5 mm had LN mets.
Brantsch KD, et al. Analysis of risk factors determining prognosis of cutaneous squamous-cell carcinoma: a prospective study. Lancet Oncol 2008;9:713-20.Kraus DH, et al. Regional lymph node metastasis from cutaneous squamous cell carcinoma. Arch Otolaryngol Head and Neck Surg 1998;124:582-7.

Tumor (T)
• Australian study• 46% of pts with nodal mets had moderately or poorly differentiated tumors
• 12% of pts with nodal mets had well-differentiated tumors
• Goepfert reported tumors with PNI had 47% local recurrence rate and 34.8% metastasis rate.
• Other factors not accounted for:• Recurrent lesions
• 32% and 45% of recurrent lip and ear SCC had LN mets.
• Immunosuppression
Weber RS, Moore BA. Cutaneous Malignancy of the Head and Neck: A Multidisciplinary Approach. San Diego: Plural Publishing, 2011.

Nodal Metastasis
• Low risk SCC has 3-5% LN mets.
• Tertiary H&N cancer centers have 10-15% LN mets.
• Parotid most frequent site for mets
• 70-80% will have both parotid and cervical LN mets vs. 20-30% with only cervical LN mets.
• Over 70% of mets occur within 1 yr of treatment of primary lesion.

Nodal Metastasis
• Prior editions of AJCC consisted of Nx, N0, N1
• O’Brien et al came up with parotid+neck staging in 2002.
Source: O’Brien CJ, et al. Significance of clinical stage, extent of surgery, and pathologic findings in metastatic cutaneous squamous carcinoma of the parotid gland. Head Neck 2002:417-22.

Prognosis
• Majority cured with single modality.
• ~10% develop local recurrence.
• ~5% develop nodal mets.
• Southwell et al. study with 49 pts with metastatic SCC.• 9 had significant immunosuppression
• Recurrence rate of 56%
• 0% survival at 2 yrs vs. 87% survival in immunocompetent
Southwell KE, et al. Effects of immunocompromised on metastatic cutaneous squamous cell carcinoma in the parotid and neck. Head Neck 2006:244-8.

Westmead Hospital Group
• Study with 4-factor prognostic scoring system• ITEM (weight of Y/N):
• Immunosuppression (1.8/0)
• Treatment – multimodal (-1.8) vs single (0)
• ECS (4.8/0)
• +Margins (1/0)
• Ranges: 2.6 or less, greater than 2.6 to 3, greater than 3• 5 yr survival: 6%, 24%, 56%
• These factors most important in metastatic cutaneous SCC prognosis.
Southwell KE, et al. Effects of immunocompromised on metastatic cutaneous squamous cell carcinoma in the parotid and neck. Head Neck 2006:244-8.

Treatment

Treatment
• Surgical management
• Management of locoregional metastasis
• Other modalities• Radiation therapy
• Chemotherapy
• Topical medical treatment
• Photodynamic therapy
• Current research

Surgical ManagementStandard surgical excision
Moh’s micrographic surgery

Surgical Excision
• Wide local excision (WLE)• Cure rate 90-95%
• Margins• 4 mm will give > 95% cure rate for low risk lesions.
• NCCN guideline recommends 4-6 mm surgical margin.
• Intraoperative frozen sectioning (bread-loafing)
• May need to include underlying fat, muscle, bone.
Image Source: http://skincancersurgery.co.uk/Info/MinorSurgery.html
Moh’s Surgery
• Developed in 1983 by Dr. Frederic Mohs.
• Surgeon is also the pathologist
• Technique• Surgical removal of tumor.
• Cryostat and H&E staining
• Positive margins are marked and targeted for excision.
• Serial “pie pan” is excised and the whole margin is looked over.• As opposed to frozen sectioning in the OR or “bread loafing.”
• Up to 99% cure rate.

Image Source: http://www.dailymail.co.uk/health/article-2414954/The-paper-pencil-cure-skin-cancer-Surgery-99-cent-success-rate-scarring-treatments.html

Management of Locoregional Metastasis

The N0 Neck
• Controversial topic.
• Most SCC will not metastasize.• Aggressive SCC:
• Recurrent lesions, >2 cm in size, rapid growth, near eyes or lips, poor differentiation, desmoplastic and spindle cell subtypes of SCC, invasion into subcutaneous tissue, PNI, lymphovascular invasion
• Options:• Watchful waiting• Neck dissection• SLNB• +/- XRT

Elective Neck Dissection
• Face, scalp, anterior to half of EAC• Superficial parotidectomy + Levels II through IV
• Posterior to half of EAC• Levels II through V
• Lips, midface• Levels I through III
• Consider bilateral in midline lesions

Sentinel Lymph Node Biopsy (SLNB)
• Advantages• Minimally invasive• Cost-effective• Avoid morbidity with neck dissection
• Disadvantage• False negative
• More accepted in melanoma.
• Studies have shown high negative predictive value but limited to small sample size and short follow-up.

SLNB
• Systematic review of cSCCHN SLNB in Nov 2013.• 73 pts from 11 pubs with median 21.5 mo f/up
• At least 1 SLN identified in 100%• 13.5% (n=10) had +SLN
• 4.8% (n=3) failed regionally after –SLN.
• Pooled data:• 77% sensitivity
• 100% specificity
• 95.2% NPV
Ahmed MM, et al. Utility of head and neck cutaneous squamous cell carcinoma sentinel node biopsy: A systemic review. Otolaryngol – Head & Neck Surg 2013;150(2):180-7.

Parotid Gland Metastasis
• Superficial parotidectomy alone recommended for parotid nodal disease or parotid capsule invasion with intact facial nerve.
• No evidence suggests total parotidectomy (vs. superficial) improves locoregional control.
• Superficial parotidectomy with adjuvant XRT is adequate for mets to parotid with microscopic residual disease involving facial nerve and normal facial function.
• Weakness of facial nerve or temporal bone invasion requires radical parotidectomy with sacrifice of involved branches and likely temporal bone resection.

Prognostic Indicators
• Chart review of pts with cSCCHN s/p parotidectomy (2003-12), 2014.• 218 pts identified
• 49% had new primary lesion• 51% had recurrence• 91% had concurrent neck dissection
• Parotid and cervical LN status• 52% had +parotid LN• 28% had +cervical LN• 18% had both positive• 44% had both negative• 33% had only +parotid LN• 5% had only +cervical LN
• Overall survival• 2- and 5-yr survival was 0.71 and 0.58• Overall 5-yr survival lower for recurrent (0.49) vs new primary (0.69)• Overall 5-yr survival lower with cervical LN status: 0.47 vs. 0.62• No overall survival difference by: parotid involvement, margin status, PNI, FN sacrifice, type of
parotidectomy, +/- adjuvant radiation therapy
Sweeny L, et al. Head and neck cutaneous squamous cell carcinoma requiring parotidectomy: prognostic indicators and treatment selection. Otolaryngology-Head & Neck Surg 2014;150(4):610-7.

N+ Neck
• If clinically or radiographically evident nodal disease.
• At least the upper neck should be addressed if parotidectomy performed.

Anatomic Considerations
• Forehead and scalp• Frontozygomatic area can have supraorbital nerve or frontal nerve branch
involvement• Consider involvement of frontal sinus. • Neurosurgeon needed for calvarium, dura involvement.
• Periorbital• No consensus on margin but recommend 5 mm by large Australian series.• Lid margin needs full thickness excision.• Medial canthus lesions may involve lacrimal system which then would need
removal of drainage system• Orbital exenteration• Ophthalmologist needed

Auricular and Periauricular
• 10-16% with LN mets (vs. 0.5-5% all cSCCHN)• Consider involvement of TMJ, EAC, temporal bone• Auriculectomy
• When most of auricle involved.
• Lateral temporal bone resection• Bony canal involvement
• Weak FN or macroscopic involvement• Radical parotidectomy
• SCC of external ear with neck disease• 2 and 5 yr survival was 65% and 46%• 2 or more nodes dropped survival from 57% to 14%.
• ECS in 93% of these pts.

Reconstruction
• “Reconstructive ladder”
• Delay until margins are confirmed to be negative.
Image Source: Nouri K. Mohs Micrographic Surgery. New York: Springer, 2012.

Other TherapiesRadiation Therapy
Chemotherapy
Targeted Therapies
Image Source: http://www.dvucancercare.com/preparing/

Radiotherapy Alone
• Surgery usually preferred method for primary lesion• Avoid in younger pts.
• Unacceptable long term cosmetic result
• More relevant to older pts.• Limited life expectancy
• Higher risk of perioperative complication.
• Regional LN mets• RT alone only in:
• Tumor extent makes unresectable
• Poor medical condition

Adjuvant Radiation Therapy
• Indications:• > 4 cm or recurrent tumors, aggressive histology, PNI, close or positive margins,
multiple positive nodes, ECS.
• Improves local control, disease-specific survival, overall survival in cases of PNI• Evidence for pathological PNI vs. clinically-evident/radiographic PNI• Australian study by Jackson et al. on SCC+BCC:
• Path PNI – 90% local control at 5 yrs• Clinical or radiographic PNI – 57% local control at 5 yrs
• General recommendation• Above indications for P+ and/or N+.• In P+ and N0, irradiate entire ipsilateral neck for high risk of subclinical disease.
Jackson JE, et al. Radiotherapy for perineural invasion in cutaneous head and neck carcinomas: toward a risk-adapted treatment approach. Head Neck 2009:604-10.

MDA Practice for Locoregional LN
• Cervical LN• 1 node without ECS
• Primary surgery alone, no XRT
• 2+ nodes or ECS• Postop XRT
• Parotid LN• Parotid node
• Parotidectomy + adjuvant XRT
• Parotid node fixed with possible unresectability• High dose pre-op XRT (6000-7000 cGy)
Weber RS, Moore BA. Cutaneous Malignancy of the Head and Neck: A Multidisciplinary Approach. San Diego: Plural Publishing, 2011.

XRT Techniques
• Primary Lesion• Orthovoltage RT
• Early SCC • Advantages: maximum dose at skin, bolus not required, smaller fields can be used, shielding
of eyes easier, less expensive• Disadvantages: higher dose to deeper tissue/bone/cartilage
• Electron beam• Scalp to reduce underlying brain dose
• High energy XR or photon• Advanced SCC with deep invasion
• Covers deep extent. Bolus used.
• IMRT• May also be used for primary lesion to reduce dose to surrounding structures
• Parotid and Neck – en face mixed beam of x-rays and high-energy electrons.

Chemotherapy
• Combined with XRT as adjuvant therapy.
• Candidates:• Positive margins, multiple positive nodes, ECS
• Promising data with cisplatin, carboplatin, cetuximab.• Most data extrapolated from mucosal SCC of UADT.
• Retrospective cohort with pts with stage III/IV SCC with high risk features of 2+ LN, +margins, or ECS. • N – 61, 27 had adjuvant XRT vs. 34 had adjuvant XRT+chemo• Median recurrence-free survivals 15.4 and 40.3 mo• No difference in overall survival
Tanvetyanon T, et al. Postoperative concurrent chemotherapy and radiotherapy for high-risk cutaneous squamous cell carcinoma of the head and neck. Head Neck 2014; epub ahead of print.

Targeted Therapy
• EGFR inhibition• Rationale
• Ligand and receptor expression correlate with outcome• EGFR accelerates oncogenic signaling• Highly overexpressed in SCC
• Cetuximab used in mucosal H&N SCC.• EGFR Tyrosine kinase inhibitor
• Gefitinib• Erlotinib
• mTOR inhibiton• Sirolimus• Everolimus

Targeted Therapy
MDA prospective phase II study (Lewis et al.)
• Gefitinib as neoadjuvant chemotherapy for aggressive cSCCHN• 22 evaluated for response to therapy
• CR in 18.2%• No cancer found in n=3 in resulting surgical excision
• PR in 27.3%
• Overall 45.5% response rate
• Toxicity also evaluated• 13/22 had grade 2 toxicities
• 4/13 also had grade 3 toxicities
Lewis CM, et al. A phase II study of gefitinib for aggressive cutaneous squamous cell carcinoma of the head and neck. Clin Cancer Res 2012;18:1435-46.
Targeted Therapy
Sirolimus as a de novo therapy in OTR.
• 1st prospective randomized trial of sirolimus in renal transplant pts. • Sirolimus group (16)
• 1 new skin cancer
• Control group (17)• 8 new NMSC
• Benefits:• Delayed development of premalignancies
• Induced regression of pre-existing lesions
• Decelerate incidence of new skin cancers

Follow-up
• Local disease• q3-6 mo for 2 yr
• q6-12 mo for 3 yr
• q12 mo for life
• Regional disease• q1-3 mo for 1 yr
• q2-4 mo for 1 yr
• q4-6 mo for 3 yr
• q6-12 for life

Conclusion
• As the incidence of cSCCHN is rising, the responsibility is with the physician to help prevent and cure this treatable disease.
• Primary surgical excision usually provides cure as a single modality.
• The physician must be cognizant of features of aggressive cSCCHNwhich can metastasize locoregionally.• Addressing the lymph node basins while considering other modalities
including XRT and chemotherapy must be taken into account to prolong a disease free life of the patient.
• SLNB has promising data but more research needs to be done before it becomes standard of care.

Bibliography
Ahmed MM, et al. Utility of head and neck cutaneous squamous cell carcinoma sentinel node biopsy: A systemic review. Otolaryngol – Head & Neck Surg 2013;150(2):180-7.
AJCC Cancer Staging Manual 6th Edition. New York: Springer, 2002.
AJCC Cancer Staging Manual 7th Edition. New York: Springer, 2010.
Brantsch KD, et al. Analysis of risk factors determining prognosis of cutaneous squamous-cell carcinoma: a prospective study. Lancet Oncol 2008;9:713-20.
Byers R, et al. Squamous carcinoma of the external ear. Amer J Surg 1983;146:447-50.
Cummings, CW. Otolaryngology, Head and Neck Surgery. Ed. 5. Mosby, 2010.
Environmental Protection Agency. The Burning Facts. Sept 2006.
Kraus DH, et al. Regional lymph node metastasis from cutaneous squamous cell carcinoma. Arch Otolaryngol Head and Neck Surg 1998;124:582-7.
Jackson JE, et al. Radiotherapy for perineural invasion in cutaneous head and neck carcinomas: toward a risk-adapted treatment approach. Head Neck 2009:604-10.
Lardaro T, et al. Improvements in the staging of cutaneous squamous-cell carcinoma in the 7th edition of the AJCC Cancer Staging Manual. Ann Surg Oncol 2010;17:1979-80.
Leblanc KG, et al. The role of sirolimus in the prevention of cutaneous squamous cell carcinoma in organ transplant recipients. Amer Soc Derm Surg 2011;37:744-9.
Lewis CM, et al. A phase II study of gefitinib for aggressive cutaneous squamous cell carcinoma of the head and neck. Clin Cancer Res 2012;18:1435-46.
Nouri K. Mohs Micrographic Surgery. New York: Springer, 2012.
O’Brien CJ, et al. Incidence of cervical node involvement in metastatic cutaneous malignancy involving the parotid gland. Head Neck 2001:744-8.
O’Brien CJ, et al. Significance of clinical stage, extent of surgery, and pathologic findings in metastatic cutaneous squamous carcinoma of the parotid gland. Head Neck 2002:417-22.
Oddone N, et al. Metastatic cutaneous squamous cell carcinoma of the head and neck. Cancer 2009:1883-91.
Pathak I, et al. Do nodal metastases from cutaneous melanoma of the head and neck follow a clinically predictable pattern? Head & Neck 2001:785-790.
Rapini RP. Practical Dermatopathology. Elsevier, 2012.
Southwell KE, et al. Effects of immunocompromised on metastatic cutaneous squamous cell carcinoma in the parotid and neck. Head Neck 2006:244-8.
Sweeny L, et al. Head and neck cutaneous squamous cell carcinoma requiring parotidectomy: prognostic indicators and treatment selection. Otolaryngology-Head & Neck Surg 2014;150(4):610-7.
Tanvetyanon T, et al. Postoperative concurrent chemotherapy and radiotherapy for high-risk cutaneous squamous cell carcinoma of the head and neck. Head Neck 2014; epub ahead of print.
Vauterin TJ, et al. Patterns of lymph node spread of cutaneous squamous cell carcinoma of the head and neck. Head & Neck 2005: 785-91.
Weber RS, Moore BA. Cutaneous Malignancy of the Head and Neck: A Multidisciplinary Approach. San Diego: Plural Publishing, 2011.
Related Documents











