Management of GIST Management of GIST Dr Kwan Ming Wa Dr Kwan Ming Wa Tuen Mun Hospital Tuen Mun Hospital

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Management of GISTManagement of GIST
Dr Kwan Ming WaDr Kwan Ming Wa
Tuen Mun HospitalTuen Mun Hospital

ContentsContents
Mainly concern aboutMainly concern about OncogensisOncogensis Surgical treatmentSurgical treatment Targeted therapyTargeted therapy

IntroductionIntroduction
GIST GIST the most common Sarcoma of the GI tractthe most common Sarcoma of the GI tract derived from the Interstitial cells of Cajalderived from the Interstitial cells of Cajal
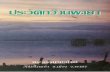
Oncogenesis of GISTOncogenesis of GIST
Gene expression
Gene expression
Signal-Transduction ATP ADP
Signal-Transduction ATP ADP
Plasma MembranePlasma MembraneSignal
MoleculeSignal
Molecule
KIT Receptor
KIT Receptor
Earl W. Sutherland (Nobel Prize – 1971)
Mutated KIT receptor become autonomous Mutated KIT receptor become autonomous and cell proliferation become uncontrolledand cell proliferation become uncontrolledMutated KIT receptor become autonomous Mutated KIT receptor become autonomous and cell proliferation become uncontrolledand cell proliferation become uncontrolled

Understanding of the oncogenesis Understanding of the oncogenesis is the key to is the key to
the advances of diagnosis and the advances of diagnosis and targeted therapytargeted therapy

Differentiation of GIST from Differentiation of GIST from smooth muscle tumoursmooth muscle tumour
KITKIT CD34CD34 DesminDesmin
GISTGIST ++ 60-70%60-70% rarerare
Smooth muscle Smooth muscle tumourtumour
__ 10-15%10-15% ++
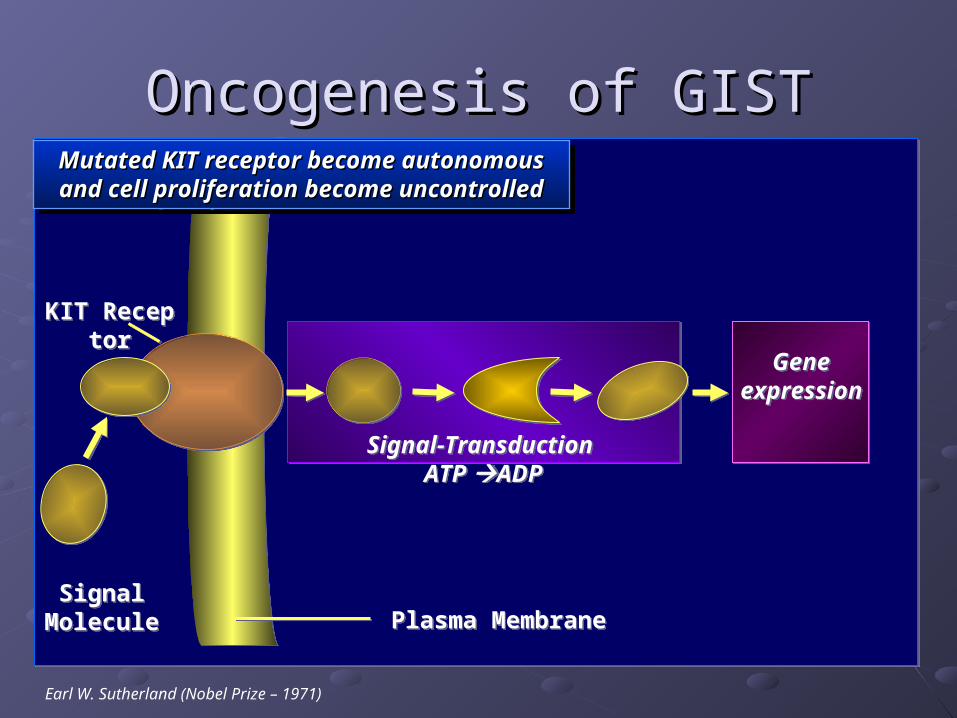
Targeted therapy (Glivec)Targeted therapy (Glivec)
Gene expression
Gene expression
ATP ADPATP ADP
Plasma MembranePlasma Membrane
Autonomous
KIT Receptor
Autonomous
KIT Receptor
Competitive inhibition of Tyrosine KinaseCompetitive inhibition of Tyrosine KinaseCompetitive inhibition of Tyrosine KinaseCompetitive inhibition of Tyrosine Kinase

Clinical features of GISTClinical features of GIST
Incidence Incidence Worldwide 10-20/ millionWorldwide 10-20/ million Tuen Mun ~13 cases/ year Tuen Mun ~13 cases/ year
Median age at 60Median age at 60
Sex ratio 1:1Sex ratio 1:1

Location of GISTLocation of GIST
SiteSite worldwideworldwide Tuen MunTuen Mun
stomachstomach 40-60 %40-60 % 55%55%
Small intestineSmall intestine 20-40%20-40% 29%29%
Colon and Colon and rectumrectum 5-15%5-15% 8%8%
esophagusesophagus <5%<5% 2%2%
othersothers 5-7%5-7% 7%7%
PresentationPresentation
GI Bleeding GI Bleeding the most common presenting symptomthe most common presenting symptom
Mass effect Mass effect when tumour is large enoughwhen tumour is large enough
Small GIST Small GIST Usually found incidentallyUsually found incidentally

Symptoms related to gastric GIST Symptoms related to gastric GIST in TuenMunin TuenMun
Others11.1%
Asymptomatic3.7%
Abdominal Mass3.7%
Abdominal Pain
18.5%Anaemia
7.4%Haematemesis
11.1%
Malaena44.4%
Preoperative biopsyPreoperative biopsyNot advocatedNot advocated
GIST is highly vascular and friableGIST is highly vascular and friable Risk of bleedingRisk of bleeding Risk tumour ruptureRisk tumour rupture Risk tumour dissemination and early recurrenceRisk tumour dissemination and early recurrence

Imaging for diagnosis and stagingImaging for diagnosis and staging
CT scan, endoscopy and EUS are commonly CT scan, endoscopy and EUS are commonly used to diagnose GISTused to diagnose GIST A well circumscribed, vascular mass associated with A well circumscribed, vascular mass associated with
stomach/ intestinestomach/ intestine
Staging primary GIST Staging primary GIST CT scan and CXR is sufficientCT scan and CXR is sufficient metastasis is usually confined to peritoneum and the metastasis is usually confined to peritoneum and the
liverliver
For complicated disease, PET-CTFor complicated disease, PET-CT Recurrent disease/ extraperitoneal metastasisRecurrent disease/ extraperitoneal metastasis

SurgerySurgery
The primary treatment for resectable GISTThe primary treatment for resectable GIST
The goal is complete resection of the The goal is complete resection of the mass without disruption of the mass without disruption of the pseudocapsulepseudocapsule

GIST generally displace rather than GIST generally displace rather than infiltrating the surrounding structureinfiltrating the surrounding structure
Achieving negative margin is usually Achieving negative margin is usually possiblepossible

Dissection of lymph node Dissection of lymph node does notdoes not
prolong survival or delay recurrenceprolong survival or delay recurrence
Connolly EM, Br J Surg 2003Connolly EM, Br J Surg 2003Sammiian L, Am Surg 2004Sammiian L, Am Surg 2004

Type of operation for gastric GIST Type of operation for gastric GIST in Tuen Munin Tuen Mun
19
3 32
0
2
4
6
8
10
12
14
16
18
20
No. of Patients
Laparotomy+wedgeexcision
Laparoscopicwedge excision
Partial gastrectomy Total gastrectomy
Types of Operation

Outcome of gastric GIST resection Outcome of gastric GIST resection in TMHin TMH

Outcome after complete resectionOutcome after complete resection
5yr survival (overall) : 48-65%5yr survival (overall) : 48-65%
Poor outcome is associated with Poor outcome is associated with Big tumour size (>5cm)Big tumour size (>5cm) High mitotic figure (>5/50HPF)High mitotic figure (>5/50HPF)

Example of excising a big GISTExample of excising a big GIST
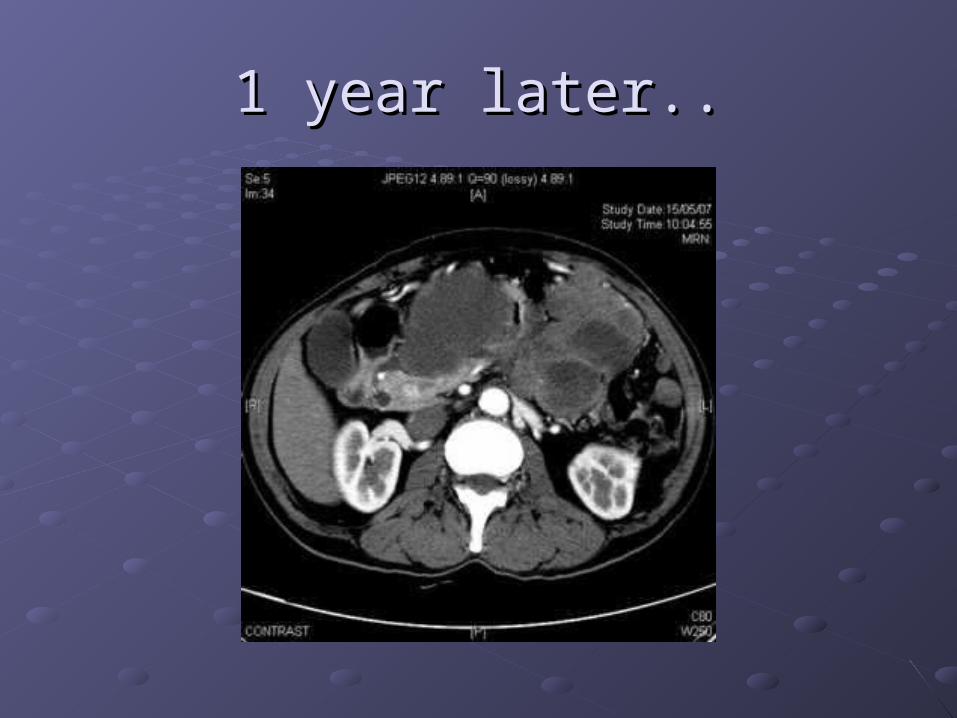
1 year later..1 year later..

Conventional adjuvant therapyConventional adjuvant therapy
Chemotherapy: refractoryChemotherapy: refractory
Radiotherapy: limited useRadiotherapy: limited use

Targeted therapyTargeted therapy
Evidence of benefit inEvidence of benefit in Treatment of advanced GISTTreatment of advanced GIST As adjuvant to primary tumour resectionAs adjuvant to primary tumour resection

Advanced GIST treated with GlivecAdvanced GIST treated with Glivec
U.S./ U.S./ Finland Finland study study (n=147)(n=147)
EORTC EORTC study (n=36)study (n=36)
Partial Partial responseresponse
54%54% 69%69%
Stable Stable diseasedisease
28%28% 19%19%
progressionprogression 14%14% 11%11%

ACOSOG Z9001:ACOSOG Z9001: A randomized, double blind A randomized, double blind study of adjuvant Glivec versus placebo following study of adjuvant Glivec versus placebo following resection of primary GISTresection of primary GIST
10 years or until death
Design:
Primary GIST
(≥ 3 cm)
Placebo x 1 year
Glivec 400mg x 1 year
RecurrenceGlivec 400mg
(or 800mg) x 2 years
FOLLOW
Complete Gross Resection

Data monitoring committee evaluated data on >600 pts with Data monitoring committee evaluated data on >600 pts with complete resection of primary GISTcomplete resection of primary GIST
At 1 year follow-up, 97% of patients on Glivec arm were free of At 1 year follow-up, 97% of patients on Glivec arm were free of recurrence compared with 83% of patients on placebo arm recurrence compared with 83% of patients on placebo arm
Approximately 65% less likely to experience recurrence within two Approximately 65% less likely to experience recurrence within two yearsyears
All patients will be unblinded, and patients in the placebo arm will be All patients will be unblinded, and patients in the placebo arm will be offered 1 year of Glivecoffered 1 year of Glivec
ACOSOG Trial Prematurely Stopped ACOSOG Trial Prematurely Stopped Due to Superior Rates of Due to Superior Rates of RRecurrence Free Survival (RFS) ecurrence Free Survival (RFS)
with Glivecwith Glivec
Available at: http://www.cancer.gov/newscenter/pressreleases/GISTtrial
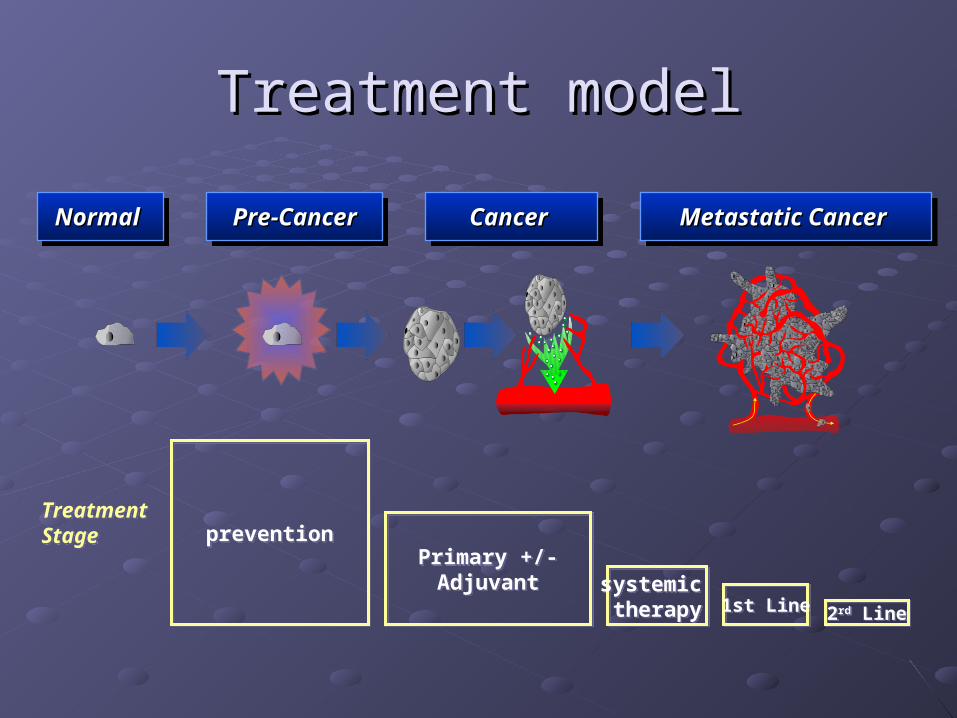
Treatment modelTreatment model
Normal Normal Normal Normal Pre-CancerPre-CancerPre-CancerPre-Cancer Metastatic Cancer Metastatic Cancer Metastatic Cancer Metastatic Cancer Cancer Cancer Cancer Cancer
preventionpreventionPrimary +/-Adjuvant
Primary +/-Adjuvant systemic
therapysystemic therapy 1st Line1st Line 2rd Line2rd Line
TreatmentStageTreatmentStage

ThankyouThankyou
Related Documents